
Effects of guided deep breathing on breathlessness and the breathing pattern in chronic obstructive...
9
Intervention Effects of guided deep breathing on breathlessness and the breathing pattern in chronic obstructive pulmonary disease: A double-blind randomized control study Christine R. Borge a,b,1, *, Anne Marit Mengshoel a , Ernst Omenaas c , Torbjørn Moum d , Inger Ekman e , Martha P. Lein b , Ulrich Mack b , Astrid K. Wahl a a Department of Health Sciences, University of Oslo, Norway b Department of Medicine, Lovisenberg Diaconal Hospital, Oslo, Norway c Centre for Clinical Research, Haukeland University Hospital, Bergen, Norway d Department of Behavioral Sciences in Medicine, University of Oslo, Norway e Institute of Health and Care Sciences, the Sahlgrenska Academy, University of Gothenburg Sweden and Centre for Person-centered care, University of Gothenburg, Sweden 1. Introduction Chronic obstructive pulmonary disease (COPD) is demanding for the individual patient and the symptom breathlessness and impaired quality of life (QOL) [1,2] increase during the more severe stages of the disease [3]. Breathlessness is often the reason why patients with COPD seek medical help. Thus, relieving symptoms and improving QOL are important aims for patient care and treatment approaches [3]. The use of pharmacological treatments alone is not effective; thus, additional nonpharmacological approaches such as breath retraining exercises have been suggested [4]. COPD is caused by a complex array of physical changes such as chronic obstruction of the airways and destroyed alveoli. This may lead to an overload or fatigue of respiratory muscles, disturbances of gas exchange between the lung and blood and air trapping [4]. Hence, people with COPD may develop an ineffective breathing pattern in form of an insufficient ventilation, resulting in an increased respiratory rate (RR), decreased vital capacity, and decreased time on inspiration (TIN), and expiration (TEX), which are also associated with symptoms of breathlessness/dyspnea [5,6]. Diaphragmatic breathing, deep breathing, yoga breathing, and pursed-lip breathing are breathing exercises that can affect the Patient Education and Counseling xxx (2014) xxx–xxx A R T I C L E I N F O Article history: Received 26 April 2014 Received in revised form 15 August 2014 Accepted 19 October 2014 Keywords: COPD Breathlessness Quality of life Randomized control trial Self-management A B S T R A C T Objective: To investigate whether guided deep breathing using a device improves breathlessness, quality of life, and breathing pattern in moderate and severe stage of chronic obstructive pulmonary disease (COPD). Methods: In total, 150 patients participated in a double-blind randomized controlled trial in a four-week intervention and a four-month follow-up. Participants were randomized into a guided deep breathing group (GDBG), music listening group (MLG), or sitting still group (SSG). The patients’ symptom score using the St George’s Respiratory Questionnaire (SGRQ), and a Global Rating Change scale (GRC) was applied to measure breathlessness as primary outcome. The activity score and impact score of SRGQ, and breathing pattern were secondary outcomes. Results: Positive effects of the GDBG were detected in GRC scale in breathlessness at four weeks (p = 0.03) with remaining effect compared to MLG (p = 0.04), but not to SSG at four months follow-up. GDBG showed positive effect for respiratory rate (p < 0.001) at four weeks follow-up. A positive significant change (p < 0.05–0.01) was found in all groups of SGRQ symptom score. Conclusion: GDBG had a beneficial effect on respiratory pattern and breathlessness. MLG and SSG also yielded significant improvements. Practice implications: Guided deep breathing may be used as a self-management procedure. ß 2014 Elsevier Ireland Ltd. All rights reserved. * Corresponding author at: Institute of Health and Society, Department of Health Sciences, PB 1089 Blindern, 0317 Oslo, Norway. Tel.: +47 22845372; fax: +47 22845091. E-mail addresses: [email protected], [email protected] (C.R. Borge). 1 Lovisenberg Diaconal Hospital, Medical Department, 0440 Oslo, Norway. Tel.: +47 23225000. G Model PEC-4916; No. of Pages 9 Please cite this article in press as: Borge CR, et al. Effects of guided deep breathing on breathlessness and the breathing pattern in chronic obstructive pulmonary disease: A double-blind randomized control study. Patient Educ Couns (2014), http://dx.doi.org/10.1016/ j.pec.2014.10.017 Contents lists available at ScienceDirect Patient Education and Counseling jo ur n al h o mep ag e: w ww .elsevier .co m /loc ate/p ated u co u http://dx.doi.org/10.1016/j.pec.2014.10.017 0738-3991/ß 2014 Elsevier Ireland Ltd. All rights reserved.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Effects of guided deep breathing on breathlessness and the breathing pattern in chronic obstructive...

Patient Education and Counseling xxx (2014) xxx–xxx
G Model
PEC-4916; No. of Pages 9
Intervention
Effects of guided deep breathing on breathlessness and the breathingpattern in chronic obstructive pulmonary disease: A double-blindrandomized control study
Christine R. Borge a,b,1,*, Anne Marit Mengshoel a, Ernst Omenaas c, Torbjørn Moum d,Inger Ekman e, Martha P. Lein b, Ulrich Mack b, Astrid K. Wahl a
a Department of Health Sciences, University of Oslo, Norwayb Department of Medicine, Lovisenberg Diaconal Hospital, Oslo, Norwayc Centre for Clinical Research, Haukeland University Hospital, Bergen, Norwayd Department of Behavioral Sciences in Medicine, University of Oslo, Norwaye Institute of Health and Care Sciences, the Sahlgrenska Academy, University of Gothenburg Sweden and Centre for Person-centered care,
University of Gothenburg, Sweden
A R T I C L E I N F O
Article history:
Received 26 April 2014
Received in revised form 15 August 2014
Accepted 19 October 2014
Keywords:
COPD
Breathlessness
Quality of life
Randomized control trial
Self-management
A B S T R A C T
Objective: To investigate whether guided deep breathing using a device improves breathlessness, quality
of life, and breathing pattern in moderate and severe stage of chronic obstructive pulmonary disease
(COPD).
Methods: In total, 150 patients participated in a double-blind randomized controlled trial in a four-week
intervention and a four-month follow-up. Participants were randomized into a guided deep breathing
group (GDBG), music listening group (MLG), or sitting still group (SSG). The patients’ symptom score
using the St George’s Respiratory Questionnaire (SGRQ), and a Global Rating Change scale (GRC) was
applied to measure breathlessness as primary outcome. The activity score and impact score of SRGQ, and
breathing pattern were secondary outcomes.
Results: Positive effects of the GDBG were detected in GRC scale in breathlessness at four weeks
(p = 0.03) with remaining effect compared to MLG (p = 0.04), but not to SSG at four months follow-up.
GDBG showed positive effect for respiratory rate (p < 0.001) at four weeks follow-up. A positive
significant change (p < 0.05–0.01) was found in all groups of SGRQ symptom score.
Conclusion: GDBG had a beneficial effect on respiratory pattern and breathlessness. MLG and SSG also
yielded significant improvements.
Practice implications: Guided deep breathing may be used as a self-management procedure.
� 2014 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
Patient Education and Counseling
jo ur n al h o mep ag e: w ww .e lsev ier . co m / loc ate /p ated u co u
1. Introduction
Chronic obstructive pulmonary disease (COPD) is demanding forthe individual patient and the symptom breathlessness and impairedquality of life (QOL) [1,2] increase during the more severe stages ofthe disease [3]. Breathlessness is often the reason why patients withCOPD seek medical help. Thus, relieving symptoms and improving
* Corresponding author at: Institute of Health and Society, Department of Health
Sciences, PB 1089 Blindern, 0317 Oslo, Norway. Tel.: +47 22845372;
fax: +47 22845091.
E-mail addresses: [email protected], [email protected]
(C.R. Borge).1 Lovisenberg Diaconal Hospital, Medical Department, 0440 Oslo, Norway.
Tel.: +47 23225000.
Please cite this article in press as: Borge CR, et al. Effects of guided deepobstructive pulmonary disease: A double-blind randomized controj.pec.2014.10.017
http://dx.doi.org/10.1016/j.pec.2014.10.017
0738-3991/� 2014 Elsevier Ireland Ltd. All rights reserved.
QOL are important aims for patient care and treatment approaches[3]. The use of pharmacological treatments alone is not effective;thus, additional nonpharmacological approaches such as breathretraining exercises have been suggested [4].
COPD is caused by a complex array of physical changes such aschronic obstruction of the airways and destroyed alveoli. This maylead to an overload or fatigue of respiratory muscles, disturbances ofgas exchange between the lung and blood and air trapping[4]. Hence, people with COPD may develop an ineffective breathingpattern in form of an insufficient ventilation, resulting in anincreased respiratory rate (RR), decreased vital capacity, anddecreased time on inspiration (TIN), and expiration (TEX), whichare also associated with symptoms of breathlessness/dyspnea [5,6].
Diaphragmatic breathing, deep breathing, yoga breathing, andpursed-lip breathing are breathing exercises that can affect the
breathing on breathlessness and the breathing pattern in chronicl study. Patient Educ Couns (2014), http://dx.doi.org/10.1016/

Table 1Inclusion and exclusion criteria.
Inclusion criteria Exclusion criteria
Diagnosis of COPD in medical records
with moderate stage or severe stagea
at inclusion.
Change in medication during the last
four weeks.
MRC dyspnea scaleb�1 at inclusion. Diagnosis of cancer.
Able to read, write, and speak
Norwegian
Presently attending a pulmonary
rehabilitation course or other similar
COPD education course.
Attending a competing study.
Diagnosis of neuromuscular disease
or dementia.
Present drug abuse or alcohol abuse.
Receiving help from a pulmonary
physiotherapist.
a Moderate stage and severe stage = FVC < 70% and FEV1% � 30% and � 80% of
predicted values (FVC = forced volume capacity, FEV1 = forced expiratory volume
in 1 s).b MRC (Medical Research Council) dyspnea scale measures disabilities associated
with breathlessness using five levels (0–4), where a higher score represents more
disabilities associated with breathlessness.
C.R. Borge et al. / Patient Education and Counseling xxx (2014) xxx–xxx2
G Model
PEC-4916; No. of Pages 9
ability [7] to improve an ineffective breathing pattern, to breathedeeply and, thereby reducing breathlessness.
Studies have investigated the effects of diaphragmatic, pursed-lip breathing, and yoga breathing, but few were randomizedcontrol trials (RCTs) [8–11]. For instance, a recent systematicreview by Holland et al. [10], based on pooled data from two RCTsreports that practicing pursed lip breathing gave less breathless-ness. In the same review, one RCT on diaphragmatic breathing andone on yoga breathing showed effects on disease related QOL. Allthe said studies were rated as being of low to moderate quality andthe results were interpreted as inconsistent, indicating thatadditional high quality RCTs are required. In addition, otherinterventions such as music listening alone and in combinationwith breathing control exercises have been found to reducebreathlessness in patients with COPD [12]. In order to refinethe evidence of BCEs it is important to design breathing controltrials that control for other interventions that might reducebreathlessness.
Previous studies that employed a biofeedback device to guidethe user to breathe more deeply have reported positive effects onsymptoms [13], blood pressure [14], and QOL [13,14] in patientswith heart failure [13] and hypertension [14]. In the biofeedbackdevice a voice guides the users through air phones/plugs tellingthem to follow music tones on inspiration and expiration based onthe respiratory movement, measured with a sensor belt, whilebreathing patterns are stored in the device [15].
Such device-guided breathing control based on musical tonesand instruction has not been investigated in patients with COPDand we hypothesize that it may guide patients to breathe moredeeply and slowly and have positive effects on their breathingpattern and breathlessness.
In the present study, we performed a three-armed double-blindRCT to investigate whether subjects in the moderate and severestages of COPD reported beneficial effects on breathlessness, QOL,and their breathing pattern after a four weeks interventionprogram using device-guided breathing control and at four monthsfollow-up compared with a group who listened to music and asham control group who sat still.
2. Methods
2.1. Research design
We performed a three-armed, parallel group, double-blind,randomized RCT where the patients were in the moderate orsevere stages of COPD. The arms comprised a guided deepbreathing group (GDBG), a music listening group (MLG), and asham group sitting still (SSG).
In total, 150 patients with COPD who had been diagnosed withmoderate and severe stages of COPD according to the GlobalInitiative for Chronic Obstructive Lung Disease criteria participatedin this study [3]. The patients were enrolled between July 2011 andSeptember 2013 from outpatient units at three different hospitalsin Oslo, Norway (Hospitals A, B, and C) following similar treatmentprocedures. All the participants were offered free transportation toattend individual appointments at the main hospital A.
2.2. Recruitment
At each hospital nurses and doctors were instructed to screenfor and recruit eligible patients with moderate and severe stageCOPD. Patients were given oral and written information at eachhospital before they consented to be contacted by telephone by theresearcher or a study nurse to confirm their willingness toparticipate in the study as well as fulfilling the exclusion andinclusion criteria (Table 1).
Please cite this article in press as: Borge CR, et al. Effects of guided deepobstructive pulmonary disease: A double-blind randomized controj.pec.2014.10.017
2.3. Ethics
The study was approved by the data protection supervisor ofthe three hospitals and by the Regional Committee for MedicalResearch Ethics for Southern Norway (reference number: 2010/1521), as well as reported to the Clinical Trials government registry(ClinicalTrials.gov identifier: NCT015120043). The protocol com-plied with the Declaration of Helsinki. All participants signed awritten consent before entering the study.
2.4. Intervention
The participants were instructed orally and in writing by astudy nurse on how to use the device (RespeRate, InterCure Inc.,New York, USA; www.Resperate.com/MD) [13,15]. The device wasused for the first time at the hospital for 15 min and later at home,twice a day (i.e. morning and evening) for four weeks. When usingthe device the participants were told to sit down in a comfortablechair with few interrupting elements around them.
During the intervention, the patients used the same device tomeasure their breathing pattern, but different instructions weregiven via earphones/earplugs.
The GDBG group members used the device and receivedinstructions about how to breathe slowly based on their RR, whichwas measured by a sensor belt that was placed around the waist.The device played soft, non-rhythmic music in the background, anda voice instructed the participants to breathe out while the musicalnote lasted during expiration, whereas a new musical notefollowed during inspiration.
The MLG group members listened to the same music beingplayed in the background as the GDBG group members, but theywere not given any instructions to breathe slowly.
The SSG members only received an introductory instruction tosit down and listen to the same music for 1–2 min, but without anyinstructions about breathing or music during the at the rest of thesession.
2.5. Data collection
A questionnaire booklet covering self-reported outcomesrelated to sociodemographic variables, breathlessness, and QOLwas sent by postal mail. Participants were asked to complete thequestionnaire at home 1–2 days before attending the main projecthospital at baseline (T1), in the follow up after four weeks (T2) andfour months after baseline (T3).
breathing on breathlessness and the breathing pattern in chronicl study. Patient Educ Couns (2014), http://dx.doi.org/10.1016/
C.R. Borge et al. / Patient Education and Counseling xxx (2014) xxx–xxx 3
G Model
PEC-4916; No. of Pages 9
At T1 the questionnaire was checked for items with non-responseand physical tests (i.e. pulmonary function test, blood gas sample)were performed by the main researcher before the participants wereallocated to the assigned group. At T2 and T3 the same physical testsas baseline were performed by the main researcher who was blindedfor group assignment and the questionnaire was checked for itemswith non-response by the study nurse. The study nurse called theparticipants after two days and then subsequently once a weekduring the four weeks intervention period to obtain informationabout the RR and the quality of the measured RR. This informationwas obtained from the device guided with detailed instruction bythe study nurse. The same data collection was performed for allgroups (i.e. GDBG, MLG, SSG).
2.6. Outcomes
The primary outcome was measured in two ways: relief ofsymptoms using the St George’s Respiratory Questionnaire (SGRQ)and reported changes in breathlessness using the Global Rating ofChange scale (GRC). The secondary outcomes were scores fordiseases related to QOL (i.e., activity and impact according to theSGRQ) and the breathing pattern (i.e., TIN, TEX, and RR).
The SGRQ (four-week version) [16] comprises 50 items that yieldone total score, but it can also be divided into three subcategories:symptoms (i.e., out of breath, coughing, wheeze, and sputum),activity limitation (i.e., breathlessness during various tasks andphysical activity), and impact of the disease (i.e., how illness andbreathlessness affect social, emotional, and family life). The ranges ofthe scores were 0–100, where a high score indicated morelimitations. The SGRQ has been tested thoroughly to confirm itsreliability and validity in previous studies [17]. In the present study,Cronbach’s alpha was 0.79 for the symptom score, 0.82 for theactivity score, 0.89 for the impact score, and 0.90 for the total score.
The GRC scale was applied to assess change in breathlessness.The GRC scale was chosen because it is simple, easy to understandfor patients and gives responders the opportunity to quantify theirevaluation of improvement over time [18] with regard tobreathlessness. We asked whether the participants experienceda positive change in breathlessness after using the device for fourweeks and at the four months follow-up, on a numeric rating scaleanchored 0–10, where 0 = no change and 10 = a high degree ofchange. A similar instrument called the vertical visual analoguescale (VAS) is known to be valid for measuring dyspnea in asthmaand COPD patients [19]. The NRS and VAS are highly correlated, butNRS is recommended because it is easier to use [20].
The RespeRate breathing device used in the study [15]comprised a belt-type respiration sensor and a computerizedcontrol unit. The system analyzed and stored detailed data for thebreathing pattern variables, i.e., RR, TIN, and TEX (per minuteduring each 15-minute session), the number of sessions, and thebreath detection results for the members of all the groups.Specialized software was prepared for the MLG and the SSG groups.The measures of breathing pattern variables were available duringthe period between T1 and T2.
The lung function values (i.e., forced vital capacity (FVC), forcedexpiratory volume per second (FEV1), the ratio of FEV1/FVC = FEV%, and the vital capacity) [21] were measured byspirometry (MasterScreen Bodyplethysmography, Jaeger,Germany) and the blood gases were sampled (i.e., pressure ofoxygen (PO2) and pressure of carbon dioxide tension (PCO2) [22];Roche OMNI C, Mannheim, Germany).
2.7. Randomization
A person who was not involved in the project was responsiblefor randomizing the participants into the GDBG, MLG, and SSG
Please cite this article in press as: Borge CR, et al. Effects of guided deepobstructive pulmonary disease: A double-blind randomized controj.pec.2014.10.017
groups. Envelopes were prepared and the patients were numbered(1–120). The study was randomized with 14 blocks, with 14–16patients in each block and four to six patients in each group. First,the block was drawn. Next, a coded name from the group wasdrawn in each block and put into a sealed envelope.
2.8. Blinding
The study nurse made sure that the participants and the mainresearcher received no information about whether the participantshad been allocated to guided breathing, music, or sitting still.However, the participants were informed that the aim of theproject was to test if relaxation, silence, or breathing could changethe experience of breathlessness in people with COPD. Theparticipants were told not to discuss the content of their devicewith the main researcher and such contact with the mainresearcher was also minimized after they had received the device.An external person entered all the data in the statistical softwareand data was not analyzed before the data collection wascompleted.
2.9. Power calculation
We calculated the sample size using the main outcome variable,i.e., the symptom score according to the SGRQ, based on the effectsfound in a COPD rehabilitation study [23] where the threshold ofchange >4 [24]. We aimed for an expected effect of a difference ofeight points between groups, standard deviation (SD) of 16,significance level of 5%, and a power of 80%; thus, we estimated anecessary sample size of 150 in total, with 50 in each group. Weoversampled each group by 20 patients (total n = 210), but stoppedinclusion at n = 150 because of difficulties recruiting more patients.
2.10. Analysis
SPSS statistical package version 22 (SPSS Inc, Chicago, IL, USA)was used to perform the analyses. Descriptive analyses wereperformed for sociodemographic and clinical variables, and for thescores obtained using the questionnaires. Analysis of covariance(ANCOVA) was used to assess differential changes between groupsfrom T1 to T2 and T1 to T3, while controlling for the T1 values(General Linear Model procedure in SPSS). Paired Student’s t-testswere used to assess changes within groups from T1 to T2 and T1 toT3. Wilcoxon signed ranks test was performed when criteria ofnormally distributed variables were not met. ANOVAs were used toassess possible differences in the means between groups at T1. Weused the first measured variables from the first session and lastsession for TIN, TEX and RR in the analyses. An intention-to-treatanalysis (last carry forward) was performed (i.e. n = 8 at T2 andn = 16 at T3 for the SGRQ symptoms score, n = 12 at T3 for GRCscale). These analyses included x–y additional subjects (dependingon outcome) and revealed only marginal differences in the meanoutcomes, with identical conclusions regarding p-values to theanalyses performed as standard protocol. Thus standard protocolresults have been reported in our tables. Interaction analyses wereperformed for the main outcomes to test whether the effect of theintervention differed significantly between specific subgroups ofpatients as defined by age, gender, infection, smoking status, COPDstage, co-morbidities and living status. The interaction terms wereentered one at a time in the ANCOVAs while retaining the maineffects in the model. We calculated and interpreted effect sizesaccording to Cohen [25]. The differences within groups werecalculated by dividing the mean changes by the average SD at T1and T2, and T1 and T3, respectively, and between groups bydividing the difference of the mean changes in the experimentaland the control groups by their average SDs.
breathing on breathlessness and the breathing pattern in chronicl study. Patient Educ Couns (2014), http://dx.doi.org/10.1016/

C.R. Borge et al. / Patient Education and Counseling xxx (2014) xxx–xxx4
G Model
PEC-4916; No. of Pages 9
3. Results
3.1. Patient enrollment
Among 341 patients who were eligible, 150 patients (44%response rate) with moderate or severe stages of COPD agreed toparticipate and were randomized.
The randomization procedure allocated 51 patients to the GDBGgroup, 50 patients to the MLG groups, and 49 patients to the SSGgroup. During the four-week intervention, two patients dropped outfrom each of the GDBG and MLG groups, whereas three patientsdropped out from the SSG group. Four of these patients turned intheir device, but data from these were not considered in the analysis.
Seven patients in the GDBG group, eight patients in the MLGgroup, and five intheSSG groupwerelostto follow-upatfour monthsafter baseline. Four of these patients turned in their questionnaire bypostal mail. These patients received the intervention and aretherefore included in the analysis of subjective outcomes.
Fig. 1 shows further information.All the three groups used the device an equal number of times in
terms of the mean number of sessions conducted during the fourweeks: the GDBG group with a mean of 50.3 times (SD = 10.5), theMLG group with a mean of 49.2 times (SD = 11.6), and the SSGgroup with a mean of 50.8 times (SD = 10.2).
3.2. Demographic and clinical characteristics
Table 2 shows the clinical characteristics of the participants atbaseline. Predicted lung function is significantly higher in the SSGcompared to GDBG and MLG (p < 0.05). Further number of
Fig. 1. Flow diagram
Please cite this article in press as: Borge CR, et al. Effects of guided deepobstructive pulmonary disease: A double-blind randomized controj.pec.2014.10.017
comorbidities was significantly lower in the MLG compared toGDBG and SSG at T1 (p < 0.05).
3.3. Effect of deep breathing
3.3.1. Primary outcomes
There was statistically significant within-group decrease in theSGRQ symptom score (p � 0.05–0.001) in all the groups from T1 toT2, and for MLG and SSG (p � 0.05–0.001) from T1 to T3. Therewere no significant changes in the SGRQ symptom scores betweengroups from T1 to T2 and from T1 to T3.
The GRC scale for breathlessness detected a significant positivedifference with GDBG (p = 0.03) at T2. At T3 the GRC scale GDBGwas significantly different from MLG (p = 0.04), whereas therewere no significant differences when GDBG was compared to SSG(not reported in table).
No strong systematic interaction effects were found betweengroups on the primary outcome (i.e. symptom score T2 and gender(eta square = 5%), GRC scale and gender T3 (eta square = 7%)).
3.4. Secondary outcomes
For the activity score and the total SGRQ score, there were nosignificant differences between groups at T1 and no significantchanges between groups at T2 and T3. Further information isprovided in Table 3.
For the whole GDBG group, the mean percentage following theinstructions given by the device was 53.3 (SD = 23). For all groupsthere were no significant differences between groups of the sensorrecognizing the breathing pattern.
of enrollment.
breathing on breathlessness and the breathing pattern in chronicl study. Patient Educ Couns (2014), http://dx.doi.org/10.1016/

Table 2Demographic and clinical variables at baseline n = 150.
Variables All participants n = 150 Guided deep breathing
group (GDBG) n = 51
Music listening group
(MLG) n = 50
Sitting still group (SSG)
n = 49
n (%) Mean (SD) n (%) Mean (SD) n (%) Mean (SD) n (%) Mean (SD)
Age 67.4 (9.0) 67.2 (9.9) 68.4 (8.2) 66.6 (8.9)
Gender
Male 75 (50) 23 (45.1) 30 (60) 22 (44.9)
Female 75 (50) 28 (54.9) 20 (40) 27 (55.1)
Living status
Living alone 81 (57) 30 (63.8) 26 (56.5) 25 (51)
Living with someone 61 (43) 17 (36.2) 20 (43.5) 24 (49)
Education
Primary school 34 (25.6) 13 (30.2) 10 (21.3) 11 (25.6)
Vocational school 18 (13.5) 7 (16.3) 5 (10.6) 6 (14)
Secondary school 38 (28.6) 12 (27.9) 16 (34) 10 (23.3)
University < 4 years 27 (20.3) 6 (14) 11 (23.4) 10 (23.3)
University > 4 years 16 (12) 5 (11.6) 5 (10.6) 6 (14)
Smoking
Yes 60 (40.3) 23 (45.1) 15 (30.6) 22 (44.9)
No 89 (59.7) 28 (54.9) 34 (69.4) 27 (55.1)
Infection in the last four weeks
Yes 26 (17.3) 7(13.7) 9 (18) 10 (20.4)
No 124 (82.7) 44 (86.3) 41 (82) 39 (79.6)
Use of breathing exercises
Yes 55 (37.7) 21 (43.8) 17 (34) 17 (35.4)
No 91 (62.3) 27 (56.3) 33 (66) 31 (64.6)
Pulmonary function
FEV1 predicted 57.6 (17.0) 55.4 (15.1) 54.6 (18.6) 62.7 (16.2)*
RV predicted 178.4 (45.5) 182.2 (49.2) 186.4 (45.8) 166.7 (39.2)
VC predicted 84 (28.2) 82.5 (16.7) 83.2 (20.1) 86.1 (18.1)
COPD stage
Moderate stage 97 (65.1) 31 (60.8) 26 (53.1) 40 (81.6)
Severe stage 52 (34.9) 20 (39.2) 23 (46.9) 9 (18.4) **
Blood gas analysis
PO2 9.6 (1.3) 9.4 (1) 9.6 (1.4) 9.7 (1.5)
PCO2 5.3 (0.8) 5.2 (0.5) 5.4 (0.8) 5.3 (0.9)
Years with COPD 6.1 (6.1) 6.8 (6.9) 6.3 (6.4) 4.3 (1.8)
Number with comorbidity 3.9 (1.9) 4.3 (1.9) 3.1 (1.6)* 4.3 (1.8)*
* Significant difference between groups, p < 0.05 according to ANOVA.** Significant difference between groups, p < 0.01 according to Pearson Chi-Square.
C.R. Borge et al. / Patient Education and Counseling xxx (2014) xxx–xxx 5
G Model
PEC-4916; No. of Pages 9
At T1, there were significant differences between groups interms of RR, TIN, and TEX (p � 0.001), with positive effects in theGDBG group.
There were also significant changes in RR (p � 0.001) and TEX(p � 0.001) between groups from T1 to T2 at the start and at the endof sessions, with positive effects in the GDBG group. There was asignificant change for TIN end of session (p � 0.001) in favor ofGDBG, but not for TIN start of session between groups from T1 to T2.
Further information is provided in Table 4.
4. Discussion, limitations and conclusion
To the best of our knowledge, this is the first three-armeddouble-blind RCT to evaluate the relief of breathlessness usingnonpharmacological interventions of device guided breathing forpatients in the moderate or severe stages of COPD. We found thatall the groups (i.e., GDBG, MLG, and SSG) exhibited changes in theirsymptom scores during the four-week intervention but there wereno differences in the effects on the symptom scores between thegroups. We also detected a significant positive effect in terms of thequestion that evaluated changes in breathlessness after using thedevice and there was a positive effect on the breathing pattern inthe guided deep breathing group.
4.1. Discussion
Although, there was no significant effect for the SRGQ symptomscore, our study demonstrated that the patients in the DGBG group
Please cite this article in press as: Borge CR, et al. Effects of guided deepobstructive pulmonary disease: A double-blind randomized controj.pec.2014.10.017
were able to change their breathing pattern by breathing moreslowly, thereby decreasing their RR and they reported a perceivedchange in breathlessness for the GRC scale. An improved breathingpattern may lead to reduced sympathetic activity [26] andstrengthen the baroreflex to improve breathlessness [11]. Thebreathing patterns were improved in the GDBG members from theirfirst session until their last session, which showed that the patientsappeared to have learned how to breathe slowly. Our results mayjustify recommending guided deep breathing by use of a biofeed-back system as an appropriate self-management support procedurethat could help people with moderate and severe stage of COPD totake more control over their ineffective breathing pattern andimpairment due to breathlessness. However, we found limitedeffects on breathlessness in the GRC scale at four months follow-up,indicating that continued long-term instructions are needed in orderto achieve an optimal performance of the exercise. A device mightthen be more practical to use in a home situation and pulmonarytraining programs than guided instruction by a health person.
Although the global rating scale showed effect betweengroups, there were no differences between the groups in termsof the SGRQ symptom score. Other studies have reporteddifferences between groups using the same outcome measurein breathing control studies. For example, Katiyar et al. [27]reported a positive effect of yoga breathing according to all theSGRQ scores. In addition, Yamaguti et al. [28] detected a differencein the total SGRQ score where there was a positive effect ofdiaphragmatic breathing compared with a usual care group. Wefound that breathlessness was reduced in all of our study groups in
breathing on breathlessness and the breathing pattern in chronicl study. Patient Educ Couns (2014), http://dx.doi.org/10.1016/

Table 3Mean scores according to St George’s Respiratory Questionnaire (SGRQ) and a numerical rating scale (NRS). Differences between GDBG MLG, and SSG were tested by ANCOVA using the baseline as a covariate. Reported changes in
breathlessness, symptoms, and quality of life (QOL) were estimated at two time points.
Outcomes Group n Baseline
(T1)Mean
(SD)
After four
weeks (T2)
Mean (SD)
Cohen
between
T1 and T2
Cohen between
GDBG and MLG,
GDBG and SSG
p-value
T1–T2
(whole
model)
n Baseline
(T1)Mean
(SD)
After four
months (T3)
Mean (SD)
Cohen between
T1 and T3
Cohen between
GDBG and MLG,
and GDBG and SSG
p-value T1–T3
(whole model)
Main outcome variables
Reported change in
breathlessness after
using the device
(GRC scale)#
GDBG 46 NM 3.2 (2.9) 45 NM 2.8 (3.1)
MLG 48 NM 1.8 (2.4) 0.53 42 NM 1.5 (2.4) 0.48
SSG 45 NM 1.9 (2.9) 0.45 0.03a 43 NM 2.4 (3.2) 0.13 0.1b
Symptom score## (SRGQ) GDBG 48 57.4 (21.8) 52.1 (21.9)* 0.24 45 57.3 (22.3) 56.1 (26) 0.05
MLG 47 56.4 (21.8) 48.4 (21.1)** 0.37 �0.13 45 54.9 (24.5) 50.3 (24.5)** 0.19 �0.13
SSG 45 50.2 (24.7) 45.3 (26.6)* 0.19 0.02 0.6 42 49.8 (25.4) 46.0 (27.3)* 0.14 �0.10 0.5
Secondary outcome variables:
Activity score## (SRGQ) GDBG 47 63.5 (19.3) 63.8 (20.2) �0.02 0.2 46 63.1 (19) 63 (21) 0.01 0.1
MLG 48 64 (18.8) 62.2 (21.3) 0.09 �0.10 43 64.3 (18.7) 60.9 (21.9) 0.17 �0.15
SSG 46 56.3 (21.6) 52.8 (24.4) 0.15 �0.17 42 55.8 (21.4) 50.4 (22.9)** 0.24 �0.24
Impact score## (SRGQ) GDBG 48 40.4 (22.7)c 39.6 (23.2) 0.04 46 39.5 (22)c 39.9 (24.1) �0.02
MLG 48 37.9 (20.0) 35.4 (18.3) 0.13 �0.08 44 37.1 (19.9) 33.7 (19.5) 0.17 �0.17
SSG 45 29.3 (20.5) 28.4 (17.6) 0.05 �0.01 0.5 42 28.4 (20.4) 28.7 (17.2) �0.02 �0.01 0.2
Total score## (SRGQ) GDBG 47 49.8 (19.7) 48.5 (20.3) 0.07 46 49.4 (19.3) 49.7 (21.6) 0.00
MLG 47 48.9 (18.3) 46 (17.6)* 0.16 �0.08 43 48.4 (18.1) 44.9 (18.7)* 0.19 �0.18
SSG 46 40.3 (19.6) 38.3 (19.6)d 0.10 �0.04 0.5 41 39.8 (19.7) 37.6 (18.9) 0.11 �0.11 0.1
GDBG = guided deep breathing group; GRC = global rating change MLG = music listening group; NM = not measured; RR = respiratory rate; SSG = sitting still group; SGRQ = St George’s Respiratory Questionnaire.* Significant difference within group from baseline, p�0.05.** Significant difference within group from baseline, p�0.001.# Higher score = higher degree of positive change. Possible score from 0–10.## Higher score = higher degree of problems. Possible score from 0–100.a t-test and ANOVA between groups at T2.b t-test and ANOVA between groups at T3.c Significant difference at baseline between GDBG and SSG, p<0.05.d Non-parametric test p<0.05, t-test non significant.
C.R
. B
org
e et
al.
/ P
atien
t E
du
catio
n a
nd
Co
un
seling
xxx (2
01
4)
xxx–xxx
6 G M
od
el
PE
C-4
91
6;
No
. o
f P
ages
9
Ple
ase
cite th
is a
rticle in
pre
ss a
s: B
org
e C
R,
et
al.
Effe
cts o
f g
uid
ed
de
ep
bre
ath
ing
on
bre
ath
lessn
ess
an
d th
e b
rea
thin
g p
atte
rn in
chro
nic
ob
structiv
e p
ulm
on
ary
dise
ase
: A
do
ub
le-b
lind
ran
do
mize
d co
ntro
l stu
dy
. P
atie
nt
Ed
uc
Co
un
s (2
01
4),
http
://dx
.do
i.org
/10
.10
16
/j.p
ec.2
01
4.1
0.0
17
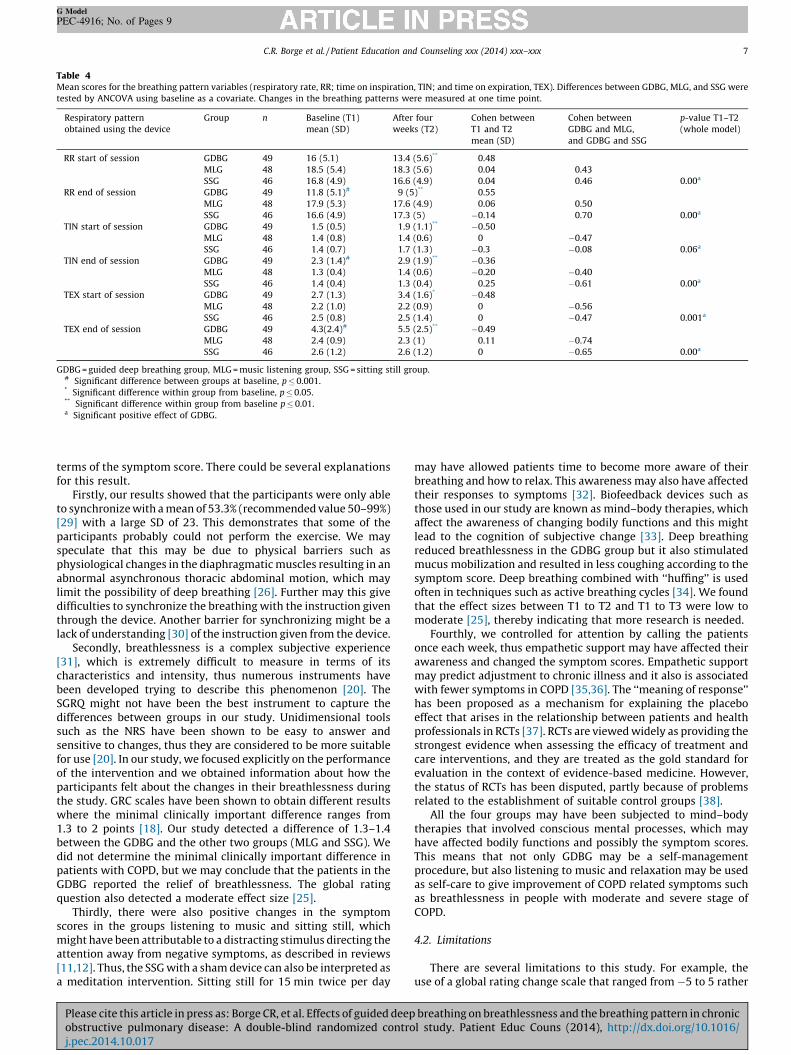
Table 4Mean scores for the breathing pattern variables (respiratory rate, RR; time on inspiration, TIN; and time on expiration, TEX). Differences between GDBG, MLG, and SSG were
tested by ANCOVA using baseline as a covariate. Changes in the breathing patterns were measured at one time point.
Respiratory pattern
obtained using the device
Group n Baseline (T1)
mean (SD)
After four
weeks (T2)
Cohen between
T1 and T2
mean (SD)
Cohen between
GDBG and MLG,
and GDBG and SSG
p-value T1–T2
(whole model)
RR start of session GDBG 49 16 (5.1) 13.4 (5.6)** 0.48
MLG 48 18.5 (5.4) 18.3 (5.6) 0.04 0.43
SSG 46 16.8 (4.9) 16.6 (4.9) 0.04 0.46 0.00a
RR end of session GDBG 49 11.8 (5.1)# 9 (5)** 0.55
MLG 48 17.9 (5.3) 17.6 (4.9) 0.06 0.50
SSG 46 16.6 (4.9) 17.3 (5) �0.14 0.70 0.00a
TIN start of session GDBG 49 1.5 (0.5) 1.9 (1.1)** �0.50
MLG 48 1.4 (0.8) 1.4 (0.6) 0 �0.47
SSG 46 1.4 (0.7) 1.7 (1.3) �0.3 �0.08 0.06a
TIN end of session GDBG 49 2.3 (1.4)# 2.9 (1.9)** �0.36
MLG 48 1.3 (0.4) 1.4 (0.6) �0.20 �0.40
SSG 46 1.4 (0.4) 1.3 (0.4) 0.25 �0.61 0.00a
TEX start of session GDBG 49 2.7 (1.3) 3.4 (1.6)* �0.48
MLG 48 2.2 (1.0) 2.2 (0.9) 0 �0.56
SSG 46 2.5 (0.8) 2.5 (1.4) 0 �0.47 0.001a
TEX end of session GDBG 49 4.3(2.4)# 5.5 (2.5)** �0.49
MLG 48 2.4 (0.9) 2.3 (1) 0.11 �0.74
SSG 46 2.6 (1.2) 2.6 (1.2) 0 �0.65 0.00a
GDBG = guided deep breathing group, MLG = music listening group, SSG = sitting still group.# Significant difference between groups at baseline, p � 0.001.* Significant difference within group from baseline, p � 0.05.** Significant difference within group from baseline p � 0.01.a Significant positive effect of GDBG.
C.R. Borge et al. / Patient Education and Counseling xxx (2014) xxx–xxx 7
G Model
PEC-4916; No. of Pages 9
terms of the symptom score. There could be several explanationsfor this result.
Firstly, our results showed that the participants were only ableto synchronize with a mean of 53.3% (recommended value 50–99%)[29] with a large SD of 23. This demonstrates that some of theparticipants probably could not perform the exercise. We mayspeculate that this may be due to physical barriers such asphysiological changes in the diaphragmatic muscles resulting in anabnormal asynchronous thoracic abdominal motion, which maylimit the possibility of deep breathing [26]. Further may this givedifficulties to synchronize the breathing with the instruction giventhrough the device. Another barrier for synchronizing might be alack of understanding [30] of the instruction given from the device.
Secondly, breathlessness is a complex subjective experience[31], which is extremely difficult to measure in terms of itscharacteristics and intensity, thus numerous instruments havebeen developed trying to describe this phenomenon [20]. TheSGRQ might not have been the best instrument to capture thedifferences between groups in our study. Unidimensional toolssuch as the NRS have been shown to be easy to answer andsensitive to changes, thus they are considered to be more suitablefor use [20]. In our study, we focused explicitly on the performanceof the intervention and we obtained information about how theparticipants felt about the changes in their breathlessness duringthe study. GRC scales have been shown to obtain different resultswhere the minimal clinically important difference ranges from1.3 to 2 points [18]. Our study detected a difference of 1.3–1.4between the GDBG and the other two groups (MLG and SSG). Wedid not determine the minimal clinically important difference inpatients with COPD, but we may conclude that the patients in theGDBG reported the relief of breathlessness. The global ratingquestion also detected a moderate effect size [25].
Thirdly, there were also positive changes in the symptomscores in the groups listening to music and sitting still, whichmight have been attributable to a distracting stimulus directing theattention away from negative symptoms, as described in reviews[11,12]. Thus, the SSG with a sham device can also be interpreted asa meditation intervention. Sitting still for 15 min twice per day
Please cite this article in press as: Borge CR, et al. Effects of guided deepobstructive pulmonary disease: A double-blind randomized controj.pec.2014.10.017
may have allowed patients time to become more aware of theirbreathing and how to relax. This awareness may also have affectedtheir responses to symptoms [32]. Biofeedback devices such asthose used in our study are known as mind–body therapies, whichaffect the awareness of changing bodily functions and this mightlead to the cognition of subjective change [33]. Deep breathingreduced breathlessness in the GDBG group but it also stimulatedmucus mobilization and resulted in less coughing according to thesymptom score. Deep breathing combined with ‘‘huffing’’ is usedoften in techniques such as active breathing cycles [34]. We foundthat the effect sizes between T1 to T2 and T1 to T3 were low tomoderate [25], thereby indicating that more research is needed.
Fourthly, we controlled for attention by calling the patientsonce each week, thus empathetic support may have affected theirawareness and changed the symptom scores. Empathetic supportmay predict adjustment to chronic illness and it also is associatedwith fewer symptoms in COPD [35,36]. The ‘‘meaning of response’’has been proposed as a mechanism for explaining the placeboeffect that arises in the relationship between patients and healthprofessionals in RCTs [37]. RCTs are viewed widely as providing thestrongest evidence when assessing the efficacy of treatment andcare interventions, and they are treated as the gold standard forevaluation in the context of evidence-based medicine. However,the status of RCTs has been disputed, partly because of problemsrelated to the establishment of suitable control groups [38].
All the four groups may have been subjected to mind–bodytherapies that involved conscious mental processes, which mayhave affected bodily functions and possibly the symptom scores.This means that not only GDBG may be a self-managementprocedure, but also listening to music and relaxation may be usedas self-care to give improvement of COPD related symptoms suchas breathlessness in people with moderate and severe stage ofCOPD.
4.2. Limitations
There are several limitations to this study. For example, theuse of a global rating change scale that ranged from �5 to 5 rather
breathing on breathlessness and the breathing pattern in chronicl study. Patient Educ Couns (2014), http://dx.doi.org/10.1016/

C.R. Borge et al. / Patient Education and Counseling xxx (2014) xxx–xxx8
G Model
PEC-4916; No. of Pages 9
than 0–10 to rate breathlessness might have yielded moreinformation regarding possible negative changes [18]. Although,the participants were not informed of the group to which they hadbeen assigned, they may have suspected having been randomizedto a control group (i.e. MLG, SSG). However, since all the groupsimproved significantly on the symptoms score at the first follow-up, we believe that most of the patients were not aware of theiractual group assignment.
The study nurse checked the questionnaires for missingresponses at T2 and T3. She was also the nurse who handed thedevice to the participants at T1, thus she could have influenced theparticipants’ responses in the questionnaires. However, thequestionnaires were completed at home by the patients beforethey attended their hospital appointments and the informationgiven to the participants was stored safely. Thus, we consider thatthe study nurse could only have had a limited effect on theresponses in the questionnaires. The study nurse also called thepatients each week to investigate compliance by asking questionsabout breathing pattern read out from the device. This may havemotivated the users and clarified some questions, but it might alsohave affected the results of our study.
Out of the total of 150 patients, 7 (4.7%) failed to follow up atfour weeks and 20 (13%) patients failed to follow up at fourmonths. This percentage dropping out is less than 15%, which isrecommended as the maximum drop-out rate [39]. We aretherefore rather confident that our results are not due to adrop-out bias. However, overall our study only had a response rateof 44% which may raise questions regarding the representativenessof our sample. We have no information about non-responders, butit is likely that the reason for not participating in the study mightconcern the extra effort it would entail. The significantly higherlung function in the SSG and the lower number of comorbidities inthe MG at baseline may have marginally affected our result. In theANOVAs, those with severe stage of COPD showed slightly greaterimprovement on the GRC scale at T3 (p = 0.02, not shown in tables),but severity yielded no significant interaction terms with groups.We therefore believe that the slightly uneven distribution ofseverity across groups has not biased our results.
4.3. Conclusions
The device-guided breathing appeared to have a positive effecton the breathing patterns and perceived change of breathlessnessin COPD patients compared with a group listening to music and asham control group sitting still. However, all three approachesproduced positive changes in the symptom scores from baseline tothe post intervention assessment.
4.4. Practice implications
Our results indicate that self-care support is effective to someextent. Deep breathing with a biofeedback device may be used as aself-management procedure by COPD patients in both at home andin combination with other non-pharmacological interventions.
However, further RCTs of breathing control exercises shouldinclude comparisons with other non-pharmacological and atten-tion-based interventions.
Author contributions
CRB, AKW, AMM, TM, and IE were responsible for theconception and design of the study. CRB, MPL, and UM wereresponsible for data collection. CRB, AKW, and TM performed theanalysis. CRB, AKW, AMM, MPL, EO, TM, UM, and IE wereresponsible for writing and revising the manuscript. All authorshave approved the final article.
Please cite this article in press as: Borge CR, et al. Effects of guided deepobstructive pulmonary disease: A double-blind randomized controj.pec.2014.10.017
Funding
This project was supported financially by the Norwegian ExtraFoundation for Health and Rehabilitation through EXTRA funds, theNorwegian Nurses’ Organisation (NNO) for the pulmonary nurses inthe NNO, the Norwegian Heart and Lung Patient Organization, theUniversity of Oslo Department of Health Sciences, and the mainproject hospital; Lovisenberg Diaconal Hospital.
Competing interest
None declared.
Acknowledgments
We acknowledge the participants in the study.
References
[1] Bentsen SB, Henriksen AH, Wentzel-Larsen T, Hanestad BR, Wahl AK. Whatdetermines subjective health status in patients with chronic obstructivepulmonary disease: importance of symptoms in subjective health status ofCOPD patients. Health Qual Life Outcomes 2008;6:115.
[2] Tsiligianni I, Kocks J, Tzanakis N, Siafakas N, van der Molen T. Factors thatinfluence disease-specific quality of life or health status in patients with COPD:a review and meta-analysis of Pearson correlations. Prim Care Respir J2011;20:257–68.
[3] GOLD. Global Initiative for Chronic Obstructive Lung Disease, Globalstrategy for the diagnosis, management, and prevention of chronic obstructivepulmonary disease; 2013. Available from: hhttp://www.goldcopd.orgi[11.01.13].
[4] American Thoracic Society.. Dyspnea. Mechanisms, assessment, and manage-ment: a consensus statement. Am J Respir Crit Care Med 1999;159:321–40.
[5] Loveridge B, West P, Anthonisen NR, Kryger MH. Breathing patterns in patientswith chronic obstructive pulmonary disease. Am Rev Respir Dis1984;130:730–3.
[6] Siela D. Ineffective breathing pattern. In: Ackley BJ, Ladwig GB, editors.Nursing diagnosis handbook: an evidence-based guide to planning care. St.Louis, MO: Mosby Elsevier; 2013. p. 175–8.
[7] Gosselink R. Controlled breathing and dyspnea in patients with chronicobstructive pulmonary disease (COPD). J Rehabil Res Dev 2003;40:25–33.
[8] Dechman G, Wilson CR. Evidence underlying breathing retraining in people withstable chronic obstructive pulmonary disease. Phys Ther 2004;84:1189–97.
[9] Cahalin LP, Braga M, Matsuo Y, Hernandez ED. Efficacy of diaphragmaticbreathing in persons with chronic obstructive pulmonary disease: a reviewof the literature. J Cardiopulm Rehabil 2002;22:7–21.
[10] Holland AE, Hill CJ, Jones AY, McDonald CF. Breathing exercises for chronicobstructive pulmonary disease. Cochrane Database Syst Rev 2012;10:CD008250.
[11] Norweg A, Collins EG. Evidence for cognitive-behavioral strategies improvingdyspnea and related distress in COPD. Int J Chronic Obstr Pulm Dis 2013;8:439–451.
[12] Panigrahi A, Sohani S, Amadi C, Joshi A. Role of music in the management ofchronic obstructive pulmonary disease (COPD): a literature review. TechnolHealth Care 2014;22:53–61.
[13] Ekman I, Kjellstrom B, Falk K, Norman J, Swedberg K. Impact of device-guidedslow breathing on symptoms of chronic heart failure: a randomized, con-trolled feasibility study. Eur J Heart Fail 2011;13:1000–5.
[14] Mahtani KR, Nunan D, Heneghan CJ. Device-guided breathing exercises in thecontrol of human blood pressure: systematic review and meta-analysis. JHypertens 2012;30:852–60.
[15] Gavish B. Device-guided breathing in the home setting: technology, perfor-mance and clinical outcomes. Biol Psychol 2010;84:150–6.
[16] Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure ofhealth status for chronic airflow limitation. The St. George’s RespiratoryQuestionnaire. Am Rev Respir Dis 1992;145:1321–7.
[17] ATS. (American Thoracic Society): St. George’s Respiratory Questionnaire(SGRQ). hhttp://www.thoracic.org/assemblies/srn/questionaires/sgrq.phpi[04.26.14].
[18] Kamper SJ, Maher CG, Mackay G. Global rating of change scales: a review ofstrengths and weaknesses and considerations for design. J Man Manip Ther2009;17:163–70.
[19] Gift AG. Validation of a vertical visual analogue scale as a measure of clinicaldyspnea. Rehabil Nurs 1989;14:323–5.
[20] Bausewein C, Farquhar M, Booth S, Gysels M, Higginson IJ. Measurement ofbreathlessness in advanced disease: a systematic review. Respir Med 2007;101:399–410.
[21] Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al.Interpretative strategies for lung function tests. Eur Respir J 2005;26:948–68.
breathing on breathlessness and the breathing pattern in chronicl study. Patient Educ Couns (2014), http://dx.doi.org/10.1016/

C.R. Borge et al. / Patient Education and Counseling xxx (2014) xxx–xxx 9
G Model
PEC-4916; No. of Pages 9
[22] Hyatt RE, Scanlon PD, Nakamura M. Interpretation of pulmonary functiontests: a practical guide. third ed, Philadelphia, PA: Lippincott Williams &Wilkins; 2009.
[23] Griffiths TL, Burr ML, Campbell IA, Lewis-Jenkins V, Mullins J, Shiels K, et al.Results at 1 year of outpatient multidisciplinary pulmonary rehabilitation: arandomised controlled trial. Lancet 2000;355:362–8.
[24] Jones PW. Interpreting thresholds for a clinically significant change in healthstatus in asthma and COPD. Eur Respir J 2002;19:398–404.
[25] Cohen J. Statistical power analysis for the behavioral sciences. second ed,Hillsdale, NJ: Lawrence Erlbaum Associates; 1988.
[26] Raupach T, Bahr F, Herrmann P, Luethje L, Heusser K, Hasenfuss G, et al.Slow breathing reduces sympathoexcitation in COPD. Eur Respir J 2008;32:387–392.
[27] Katiyar SK, Bihari S. Role of pranayama in rehabilitation of COPD patients—arandomized controlled study. Indian J Allergy Asthma Immunol 2006;20:98–104.
[28] Yamaguti WP, Claudino RC, Neto AP, Chammas MC, Gomes AC, Salge JM,et al. Diaphragmatic breathing training program improves abdominalmotion during natural breathing in patients with chronic obstructivepulmonary disease: a randomized controlled trial. Arch Phys Med Rehabil2012;93:571–7.
[29] InterCure Ltd. RespeRate User Manual. hhttp://www.resperate.com/wpi. con-tent/uploads/2014/04/UserManual-english-orange.pdf. [08.14.14].
Please cite this article in press as: Borge CR, et al. Effects of guided deepobstructive pulmonary disease: A double-blind randomized controj.pec.2014.10.017
[30] Roberts NJ, Younis I, Kidd L, Partidge MR. Barriers to the implmentation of selfmanagement support in long term lung conditions. Lond J Prim Care 2012;13–25.
[31] Hayen A, Herigstad M, Pattinson KT. Understanding dyspnea as a complexindividual experience. Maturitas 2013;76:45–50.
[32] Lansing RW, Gracely RH, Banzett RB. The multiple dimensions of dyspnea:review and hypotheses. Respir Physiol Neurobiol 2009;167:53–60.
[33] Park C. Mind-body CAM interventions: current status and considerations forintegration into clinical health psychology. J Clin Psychol 2013;69:45–63.
[34] Dean E, Frownfelter D. Cardiovascular and pulmonary physical therapy evi-dence and practice. fourth ed. St. Louis, MO: Mosby Elsevier; 2006.
[35] Graydon JE, Ross E. Influence of symptoms, lung function, mood, and socialsupport on level of functioning of patients with COPD. Res Nurs Health1995;18:525–33.
[36] Ketelaars CA, Huyer Abu-Saad H, Halfens RJ, Schlosser MA, Mostert R, WoutersEF. Effects of specialized community nursing care in patients with chronicobstructive pulmonary disease. Heart Lung 1998;27:109–20.
[37] Miller FG, Colloca L, Kaptchuk TJ. The placebo effect: illness and interpersonalhealing. Perspect Biol Med 2009;52:518–39.
[38] Grossman J, Mackenzie FJ. The randomized controlled trial: gold standard, ormerely standard? Perspect Biol Med 2005;48:516–34.
[39] Herbert R, Jamtvedt G, Hagen KB, Mead J. Practical evidence-based physio-therapy. Second ed, Eidinburgh, London, New York, Oxford, Philadelphia, StLouis, Sydney, Torontor: Chrichill Livingstone Elsevier; 2014.
breathing on breathlessness and the breathing pattern in chronicl study. Patient Educ Couns (2014), http://dx.doi.org/10.1016/




















