
Effect of calcium and vitamin D supplementation on bone mineral density of celiac children
10
Effect of Calcium and Vitamin D Supplementation on Blood Pressure The Women’s Health Initiative Randomized Trial Karen L. Margolis, Roberta M. Ray, Linda Van Horn, JoAnn E. Manson, Matthew A. Allison, Henry R. Black, Shirley A.A. Beresford, Stephanie A. Connelly, J. David Curb, Richard H. Grimm, Jr, Theodore A. Kotchen, Lewis H. Kuller, Sylvia Wassertheil-Smoller, Cynthia A. Thomson, James C. Torner; for the Women’s Health Initiative Investigators Abstract—Experimental and epidemiological studies suggest that calcium and vitamin D supplements may lower blood pressure. We examined the effect of calcium plus vitamin D supplementation on blood pressure and the incidence of hypertension in postmenopausal women. The Women’s Health Initiative Calcium/Vitamin D Trial randomly assigned 36 282 postmenopausal women to receive 1000 mg of elemental calcium plus 400 IU of vitamin D3 daily or placebo in a double-blind fashion. Change in blood pressure and the incidence of hypertension were ascertained. Over a median follow-up time of 7 years, there was no significant difference in the mean change over time in systolic blood pressure (0.22 mm Hg; 95% CI: 0.05 to 0.49 mm Hg) and diastolic blood pressure (0.11 mm Hg; 95% CI: 0.04 to 0.27 mm Hg) between the active and placebo treatment groups. This null result was robust in analyses accounting for nonadherence to study pills and in baseline subgroups of interest, including black subjects and women with hypertension or high levels of blood pressure, with low intakes of calcium and vitamin D or low serum levels of vitamin D. In 17 122 nonhypertensive participants at baseline, the hazard ratio for incident hypertension associated with calcium/vitamin D treatment was 1.01 (95% CI: 0.96 to 1.06.) In postmenopausal women, calcium plus vitamin D3 supplementation did not reduce either blood pressure or the risk of developing hypertension over 7 years of follow-up. (Hypertension. 2008;52:847-855.) Key Words: calcium supplementation 25-hydroxyvitamin D 1 25-dihydroxyvitamin D blood pressure hypertension clinical trials T he role of calcium in the prevention and treatment of hypertension is controversial, despite decades of study. An overall healthy dietary pattern that is rich in calcium from low-fat dairy products, fruits, and vegetables has been shown to lower blood pressure substantially compared with a typical diet higher in fat and sodium and lower in calcium, magne- sium, potassium, and fiber. 1–4 However, meta-analyses 5–12 and systematic reviews 13 of the epidemiological and clinical trial evidence regarding dietary intake of calcium as a single nutrient have generally concluded that the effect on systolic blood pressure (BP) lowering is small, on the order of 2 mm Hg. The effect on diastolic BP, if any, may be even smaller. Nevertheless, at a population level, sustained BP lowering of this degree by calcium supplementation could have important benefits on cardiovascular disease. Although the relation between vitamin D and BP has been less studied, 2 small, short-term intervention studies suggest that vitamin D, either as ultraviolet light exposure or as an oral supplement, may lower BP. 14,15 In addition, the risk of incident hypertension was lower in a 4-year prospective study among men and women with higher plasma levels of 25(OH) vitamin D. 16 Animal studies have also shown that oral supplementation with vitamin D lowered BP in hypertensive rats; in this model vitamin D inhibited renin expression in the juxtaglomerular apparatus and inhibited smooth muscle proliferation. 17–20 Received April 28, 2008; first decision May 26, 2008; revision accepted September 2, 2008. From the HealthPartners Research Foundation (K.L.M.), Minneapolis, Minn; Division of Public Health Sciences (R.M.R.), Fred Hutchinson Cancer Research Center, Seattle, Wash; Department of Preventative Medicine (L.V.H.), Feinberg School of Medicine, Northwestern University, Chicago, Ill; Division of Preventive Medicine (J.E.M.), Brigham and Women’s Hospital, Harvard Medical School, Boston, Mass; Department of Family and Preventive Medicine (M.A.A.), University of California San Diego; Department of Medicine (H.R.B.), Rush Medical College, Chicago, Ill; Department of Epidemiology (S.A.A.B.), University of Washington, Seattle; Department of Preventative Medicine (S.A.C.), University of Tennessee, Memphis; Department of Geriatric Medicine (J.D.C.), University of Hawaii, Honolulu; Berman Center for Outcomes of Clinical Research (R.H.G.), Minneapolis, Minn; Department of Medicine (T.A.K.), Medical College of Wisconsin, Milwaukee; Department of Epidemiology (L.H.K.), University of Pittsburgh, Pa; Department of Epidemiology and Population Health (S.W.-S.), Albert Einstein College of Medicine, New York, NY; Department of Nutritional Sciences (C.A.T.), University of Arizona, Tuscon; and the Department of Epidemiology (J.C.T.), University of Iowa, Iowa City. Please see http://hyper.ahajournals.org for a short list of the Women’s Health Initiative investigators. Correspondence to Karen L. Margolis, HealthPartners Research Foundation, Box 1524, Mailstop 21111R, Minneapolis, MN 55440-1524. E-mail [email protected] © 2008 American Heart Association, Inc. Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.108.114991 847 Clinical Trial by guest on December 19, 2015 http://hyper.ahajournals.org/ Downloaded from
Transcript of Effect of calcium and vitamin D supplementation on bone mineral density of celiac children

Effect of Calcium and Vitamin D Supplementation onBlood Pressure
The Women’s Health Initiative Randomized Trial
Karen L. Margolis, Roberta M. Ray, Linda Van Horn, JoAnn E. Manson, Matthew A. Allison,Henry R. Black, Shirley A.A. Beresford, Stephanie A. Connelly, J. David Curb, Richard H. Grimm, Jr,
Theodore A. Kotchen, Lewis H. Kuller, Sylvia Wassertheil-Smoller, Cynthia A. Thomson,James C. Torner; for the Women’s Health Initiative Investigators
Abstract—Experimental and epidemiological studies suggest that calcium and vitamin D supplements may lower bloodpressure. We examined the effect of calcium plus vitamin D supplementation on blood pressure and the incidence ofhypertension in postmenopausal women. The Women’s Health Initiative Calcium/Vitamin D Trial randomly assigned 36 282postmenopausal women to receive 1000 mg of elemental calcium plus 400 IU of vitamin D3 daily or placebo in a double-blindfashion. Change in blood pressure and the incidence of hypertension were ascertained. Over a median follow-up time of 7years, there was no significant difference in the mean change over time in systolic blood pressure (0.22 mm Hg; 95% CI:�0.05 to 0.49 mm Hg) and diastolic blood pressure (0.11 mm Hg; 95% CI: �0.04 to 0.27 mm Hg) between the active andplacebo treatment groups. This null result was robust in analyses accounting for nonadherence to study pills and in baselinesubgroups of interest, including black subjects and women with hypertension or high levels of blood pressure, with low intakesof calcium and vitamin D or low serum levels of vitamin D. In 17 122 nonhypertensive participants at baseline, the hazardratio for incident hypertension associated with calcium/vitamin D treatment was 1.01 (95% CI: 0.96 to 1.06.) Inpostmenopausal women, calcium plus vitamin D3 supplementation did not reduce either blood pressure or the risk ofdeveloping hypertension over 7 years of follow-up. (Hypertension. 2008;52:847-855.)
Key Words: calcium supplementation � 25-hydroxyvitamin D � 1 � 25-dihydroxyvitamin D � blood pressure� hypertension � clinical trials
The role of calcium in the prevention and treatment ofhypertension is controversial, despite decades of study.
An overall healthy dietary pattern that is rich in calcium fromlow-fat dairy products, fruits, and vegetables has been shownto lower blood pressure substantially compared with a typicaldiet higher in fat and sodium and lower in calcium, magne-sium, potassium, and fiber.1–4 However, meta-analyses5–12
and systematic reviews13 of the epidemiological and clinicaltrial evidence regarding dietary intake of calcium as a singlenutrient have generally concluded that the effect on systolicblood pressure (BP) lowering is small, on the order of2 mm Hg. The effect on diastolic BP, if any, may be evensmaller. Nevertheless, at a population level, sustained BP
lowering of this degree by calcium supplementation couldhave important benefits on cardiovascular disease.
Although the relation between vitamin D and BP has beenless studied, 2 small, short-term intervention studies suggestthat vitamin D, either as ultraviolet light exposure or as anoral supplement, may lower BP.14,15 In addition, the risk ofincident hypertension was lower in a 4-year prospective studyamong men and women with higher plasma levels of 25(OH)vitamin D.16 Animal studies have also shown that oralsupplementation with vitamin D lowered BP in hypertensiverats; in this model vitamin D inhibited renin expression in thejuxtaglomerular apparatus and inhibited smooth muscleproliferation.17–20
Received April 28, 2008; first decision May 26, 2008; revision accepted September 2, 2008.From the HealthPartners Research Foundation (K.L.M.), Minneapolis, Minn; Division of Public Health Sciences (R.M.R.), Fred Hutchinson Cancer
Research Center, Seattle, Wash; Department of Preventative Medicine (L.V.H.), Feinberg School of Medicine, Northwestern University, Chicago, Ill;Division of Preventive Medicine (J.E.M.), Brigham and Women’s Hospital, Harvard Medical School, Boston, Mass; Department of Family and PreventiveMedicine (M.A.A.), University of California San Diego; Department of Medicine (H.R.B.), Rush Medical College, Chicago, Ill; Department ofEpidemiology (S.A.A.B.), University of Washington, Seattle; Department of Preventative Medicine (S.A.C.), University of Tennessee, Memphis;Department of Geriatric Medicine (J.D.C.), University of Hawaii, Honolulu; Berman Center for Outcomes of Clinical Research (R.H.G.), Minneapolis,Minn; Department of Medicine (T.A.K.), Medical College of Wisconsin, Milwaukee; Department of Epidemiology (L.H.K.), University of Pittsburgh,Pa; Department of Epidemiology and Population Health (S.W.-S.), Albert Einstein College of Medicine, New York, NY; Department of NutritionalSciences (C.A.T.), University of Arizona, Tuscon; and the Department of Epidemiology (J.C.T.), University of Iowa, Iowa City.
Please see http://hyper.ahajournals.org for a short list of the Women’s Health Initiative investigators.Correspondence to Karen L. Margolis, HealthPartners Research Foundation, Box 1524, Mailstop 21111R, Minneapolis, MN 55440-1524. E-mail
[email protected]© 2008 American Heart Association, Inc.
Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.108.114991
847
Clinical Trial
by guest on December 19, 2015http://hyper.ahajournals.org/Downloaded from

Most individual trials of calcium supplementation (with orwithout vitamin D) have been relatively small, short induration, or both. Meta-analyses and reviews have called forhigh-quality, long-term studies including subgroups thatmight have greater BP lowering from calcium supplementa-tion, such as individuals with elevated BP or hypertension(especially low renin or “salt-sensitive” hypertension), blacksubjects, or those with habitual low intake of calcium orvitamin D.21–24 The Women’s Health Initiative (WHI) in-cluded a methodologically rigorous randomized, double-blind, placebo-controlled trial of dietary supplementationwith calcium plus vitamin D supplementation and long-termfollow-up. We examined the effect on BP and the incidenceof hypertension in this study of 36 282 postmenopausalwomen. Because of the large size of the trial, we were able toexamine subgroups that might have differing degrees ofbenefit.
MethodsStudy Population and InterventionBetween 1993 and 1998, postmenopausal women aged 50 to 79years were recruited at 40 US clinical centers into the WHIrandomized trials assessing the risks and benefits of hormone therapyand dietary modification.25 Participants enrolled in one or both trialswere further invited to join the calcium plus vitamin D (CaD) trial attheir first (n�33 070) or second (n�3212) annual follow-up visit.26
Women with �3 years of predicted survival, a history of kidneystone or hypercalcemia, current oral corticosteroid use, or currentcalcitriol use were excluded. The primary outcome for the CaDintervention trial was incident hip fracture, and the secondaryoutcome was colorectal cancer. Results of these analyses have beenpublished.27,28 The study protocol was approved by the institutionalreview board at each participating institution, and written informedconsent was granted by each participant before the random assign-ment into the CaD trial.
Participants were randomly assigned in a double-blind fashion toreceive 1000 mg of elemental calcium plus 400 IU of vitamin D3daily or placebo.26 Each active tablet provided 500 mg of calcium (ascalcium carbonate) and 200 IU of vitamin D3 (provided by Glaxo-SmithKline). Participants were instructed to take 2 tablets daily,preferably in divided doses with meals. Women in both the activesupplement and placebo groups were allowed to continue their ownopen-label use of calcium and vitamin D supplements as long asnonstudy use of vitamin D did not exceed 600 IU daily. The upperlimit of nonstudy vitamin D intake was raised to 1000 IU after theInstitute of Medicine released its report on the tolerable upper limitsof vitamin D intake.29 Adherence to study medication was assessedby weighing returned bottles.
BP Measurement and Ascertainmentof HypertensionBP was measured by certified staff using standardized proceduresand instruments, in the right arm, with a conventional mercurysphygmomanometer and an appropriately sized cuff, after the par-ticipant was seated and resting for 5 minutes.30 Two measurements,obtained �30 seconds apart, were performed at the WHI enrollmentvisit and at each subsequent annual visit, including the CaDenrollment visit. The average of the 2 measurements was used foranalyses. At enrollment, participants were asked whether they hadbeen diagnosed by a physician with high BP or hypertension andwhether they were taking medications for hypertension. Then, ateach semiannual contact, participants were asked, “Since the dategiven on the front of this form, has a doctor prescribed any of thefollowing pills or treatments?” The choices included “pills forhypertension.” Medication inventories were conducted at WHIenrollment, and at the first, third, sixth, and ninth annual visits. The
product or generic name of the medications on the label was enteredinto the study database and matched to the corresponding item in apharmacy database (Master Drug Data Base, Medi-Span). Drugsfrom the following classes were considered to be antihypertensiveagents: angiotensin-converting enzyme inhibitors, angiotensin recep-tor blockers, �-blockers, calcium channel blockers, diuretics, cen-trally acting antihypertensive agents, vasodilators, and combinationsof these medications. At enrollment in the WHI study, 94% ofwomen with self-reported hypertension treatment had an antihyper-tensive agent in the baseline drug inventory, and 79% with incidentself-reported hypertension treatment during the first year of the trialbrought an antihypertensive medication to the year 1 drug inventory.
CovariatesDemographic and health history data were self-reported at WHIbaseline. Dietary data were collected using a validated food fre-quency questionnaire.31 Total calcium and vitamin D intakes in-cluded both dietary and supplement sources determined from themedication and supplement inventory. Metabolic equivalent taskscores were calculated from the frequency and duration of recre-ational physical activity.32 Baseline 25-hydroxyvitamin D levelswere measured using the DiaSorin Liaison chemiluminescent immu-noassay system in a subset of CaD trial participants as part of nestedcase-control studies examining fractures, breast cancer, and colorec-tal cancer.27,28 Only participants selected as control subjects wereincluded in these biomarker analyses (n�2029).
Statistical MethodsOf 36 282 postmenopausal women enrolled in the CaD trial, 36 189had either a systolic or diastolic BP measurement at randomassignment. The primary outcome measure was BP change (annualBP measurements collected through 7 years of follow-up minusthe BP at the CaD randomization visit). All of the participants with �1BP change measurement were included in the intent-to-treat analysisusing linear repeated-measures regression modeling with an unstruc-tured covariance matrix (using SAS PROC MIXED 9.1, SASInstitute). Repeated-measures regression allows for correlationsamong responses within an individual and allows for missingresponse data. This procedure does not impute missing data or carrythe last observation forward but allows the inclusion of available datafrom individuals with missing responses by using a maximumlikelihood approach that gives valid results under missing-at-randomassumptions. Plots of longitudinal data are based on fitted meansfrom these models where both treatment assignment and time aremodeled as class variables, and treatment effect is allowed to varyover time (saturated model).
The effect of treatment on incident hypertension was examinedusing Cox proportional hazards models stratified by age and ran-domization status for other WHI trials. Incident hypertension wasdefined as self-report of medication prescribed for hypertension orany BP �140/90 mm Hg during 7 years of follow-up among 17 122women who did not have hypertension at CaD enrollment (noself-report of hypertension treatment, no antihypertensive medica-tions in inventory, and BP at all visits �140/90 mm Hg beforerandom assignment). We also examined the effect of treatment onincident prehypertension (�1 visit with BP 120 to 139/80 to89 mm Hg with no self-report of medication prescribed for hyper-tension) or hypertension during follow-up among 9416 normotensivewomen at CaD enrollment (no self-report of hypertension treatment,no antihypertensive medications in inventory, and BP �120/80 mm Hg at all prerandomization visits). For all of the analyses ofincident hypertension, women were considered at risk from entryinto the CaD trial until the date at which hypertension was deter-mined or until the last date during the follow-up period that outcomedata were available. Women who were normotensive at CaDenrollment were considered at risk for prehypertension or hyperten-sion from date of entry into the CaD trial until the first annual visitwith BP �120/80 mm Hg, a self-report of medication prescribed forhypertension, or the last date that outcome data were available.
To examine the effect of nonadherence to the active CaDsupplements or placebo, sensitivity analyses were conducted in
848 Hypertension November 2008
by guest on December 19, 2015http://hyper.ahajournals.org/Downloaded from
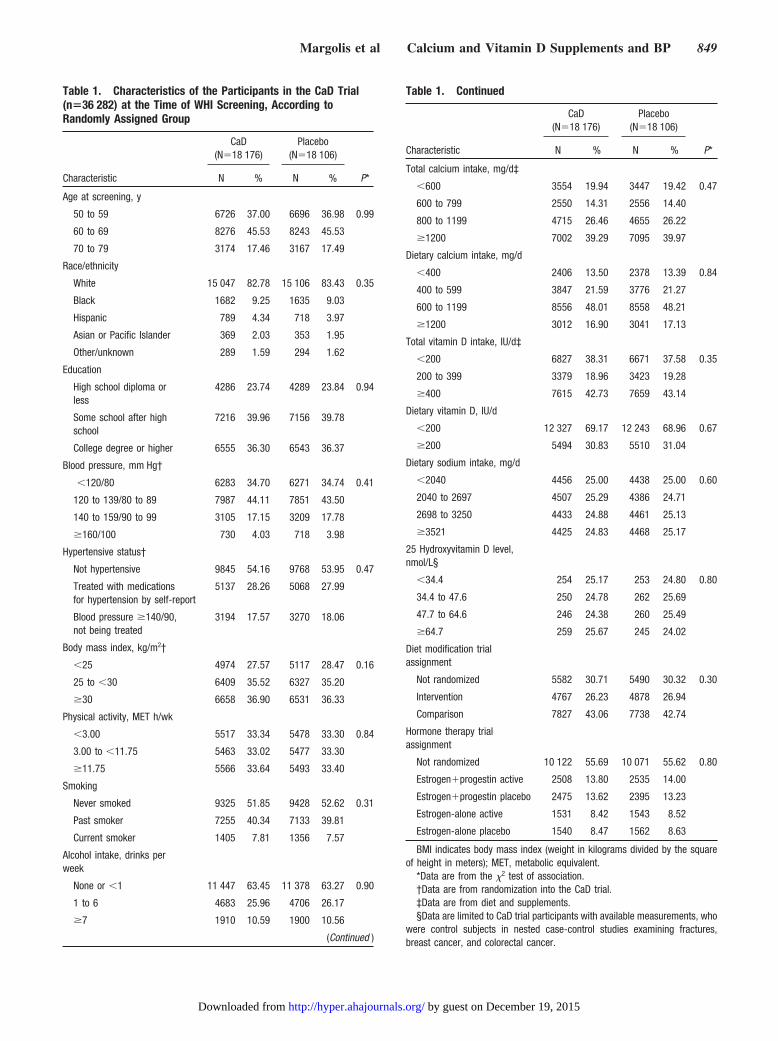
Table 1. Characteristics of the Participants in the CaD Trial(n�36 282) at the Time of WHI Screening, According toRandomly Assigned Group
Characteristic
CaD(N�18 176)
Placebo(N�18 106)
P*N % N %
Age at screening, y
50 to 59 6726 37.00 6696 36.98 0.99
60 to 69 8276 45.53 8243 45.53
70 to 79 3174 17.46 3167 17.49
Race/ethnicity
White 15 047 82.78 15 106 83.43 0.35
Black 1682 9.25 1635 9.03
Hispanic 789 4.34 718 3.97
Asian or Pacific Islander 369 2.03 353 1.95
Other/unknown 289 1.59 294 1.62
Education
High school diploma orless
4286 23.74 4289 23.84 0.94
Some school after highschool
7216 39.96 7156 39.78
College degree or higher 6555 36.30 6543 36.37
Blood pressure, mm Hg†
�120/80 6283 34.70 6271 34.74 0.41
120 to 139/80 to 89 7987 44.11 7851 43.50
140 to 159/90 to 99 3105 17.15 3209 17.78
�160/100 730 4.03 718 3.98
Hypertensive status†
Not hypertensive 9845 54.16 9768 53.95 0.47
Treated with medicationsfor hypertension by self-report
5137 28.26 5068 27.99
Blood pressure �140/90,not being treated
3194 17.57 3270 18.06
Body mass index, kg/m2†
�25 4974 27.57 5117 28.47 0.16
25 to �30 6409 35.52 6327 35.20
�30 6658 36.90 6531 36.33
Physical activity, MET h/wk
�3.00 5517 33.34 5478 33.30 0.84
3.00 to �11.75 5463 33.02 5477 33.30
�11.75 5566 33.64 5493 33.40
Smoking
Never smoked 9325 51.85 9428 52.62 0.31
Past smoker 7255 40.34 7133 39.81
Current smoker 1405 7.81 1356 7.57
Alcohol intake, drinks perweek
None or �1 11 447 63.45 11 378 63.27 0.90
1 to 6 4683 25.96 4706 26.17
�7 1910 10.59 1900 10.56
(Continued )
Table 1. Continued
Characteristic
CaD(N�18 176)
Placebo(N�18 106)
P*N % N %
Total calcium intake, mg/d‡
�600 3554 19.94 3447 19.42 0.47
600 to 799 2550 14.31 2556 14.40
800 to 1199 4715 26.46 4655 26.22
�1200 7002 39.29 7095 39.97
Dietary calcium intake, mg/d
�400 2406 13.50 2378 13.39 0.84
400 to 599 3847 21.59 3776 21.27
600 to 1199 8556 48.01 8558 48.21
�1200 3012 16.90 3041 17.13
Total vitamin D intake, IU/d‡
�200 6827 38.31 6671 37.58 0.35
200 to 399 3379 18.96 3423 19.28
�400 7615 42.73 7659 43.14
Dietary vitamin D, IU/d
�200 12 327 69.17 12 243 68.96 0.67
�200 5494 30.83 5510 31.04
Dietary sodium intake, mg/d
�2040 4456 25.00 4438 25.00 0.60
2040 to 2697 4507 25.29 4386 24.71
2698 to 3250 4433 24.88 4461 25.13
�3521 4425 24.83 4468 25.17
25 Hydroxyvitamin D level,nmol/L§
�34.4 254 25.17 253 24.80 0.80
34.4 to 47.6 250 24.78 262 25.69
47.7 to 64.6 246 24.38 260 25.49
�64.7 259 25.67 245 24.02
Diet modification trialassignment
Not randomized 5582 30.71 5490 30.32 0.30
Intervention 4767 26.23 4878 26.94
Comparison 7827 43.06 7738 42.74
Hormone therapy trialassignment
Not randomized 10 122 55.69 10 071 55.62 0.80
Estrogen�progestin active 2508 13.80 2535 14.00
Estrogen�progestin placebo 2475 13.62 2395 13.23
Estrogen-alone active 1531 8.42 1543 8.52
Estrogen-alone placebo 1540 8.47 1562 8.63
BMI indicates body mass index (weight in kilograms divided by the squareof height in meters); MET, metabolic equivalent.
*Data are from the �2 test of association.†Data are from randomization into the CaD trial.‡Data are from diet and supplements.§Data are limited to CaD trial participants with available measurements, who
were control subjects in nested case-control studies examining fractures,breast cancer, and colorectal cancer.
Margolis et al Calcium and Vitamin D Supplements and BP 849
by guest on December 19, 2015http://hyper.ahajournals.org/Downloaded from
which participants were censored after their first visit at whichnonadherence was detected, defined as use of �80% of the studypills.
To assess whether the effect of CaD supplementation on BP andincident hypertension varied according to baseline risk factors, thesame models were extended, and formal tests of interactions wereperformed. These factors included demographic characteristics;other risk factors for hypertension (baseline BP, presence of hyper-tension, body mass index, and physical activity); baseline intake ofsodium, calcium, and vitamin D; and randomization status in thehormone therapy and dietary modification trials. Because 16 inter-actions with baseline characteristics were investigated, chance alonewould be expected to produce �1 statistically significant interactiontest at the 0.05 level of significance.
ResultsBaseline Characteristics, Retention, and AdherenceBetween 1995 and 2000, 36 282 women were randomlyassigned into the CaD trial: 18 176 were assigned to theactive CaD supplementation and 18 106 to placebo. Mean(SD) follow-up time was 7.0 years (1.4 years). Participantcharacteristics, described in detail in Table 1, did not differ byCaD treatment assignment. The mean age at enrollment in theWHI Trial of women included in this study was 62�7 years;83% described themselves as non-Hispanic white, 9% black,4% Hispanic, �1% American Indian, and 2% Asian/PacificIslander. Mean BP was 126/75 mm Hg, and 46% of theparticipants had evidence of hypertension (28% with self-reported antihypertensive treatment and 18% with �1 visitBP �140/90 mm Hg).
Mean (SD) dietary calcium intake was 825 mg/d (438mg/d), total calcium intake was 1150 mg/d (656 mg/d),dietary vitamin D intake was 175 IU/d (117 IU/d), and meantotal vitamin D intake was 367 IU/d (266 IU/d). The meanintake of dairy products was 1.5 servings per day, and 52% ofthe participants reported the use of calcium supplements. AtCaD enrollment, 40% of women met the current recommen-dation for 1200 mg/d of calcium intake from supplements anddiet combined.
At the termination of the trial, 1551 participants (4.3%) haddied, and 2.7% percent had withdrawn or been lost tofollow-up. In year 1, the proportion taking �80% of studymedication was 60% overall and remained stable throughyear 7, ranging between 56% and 63%, with small differencesbetween treatment groups. The mean dose of open-labelsupplemental calcium increased by �100 mg/d during thetrial from 325 mg/d at enrollment and was similar across bothtreatment groups.
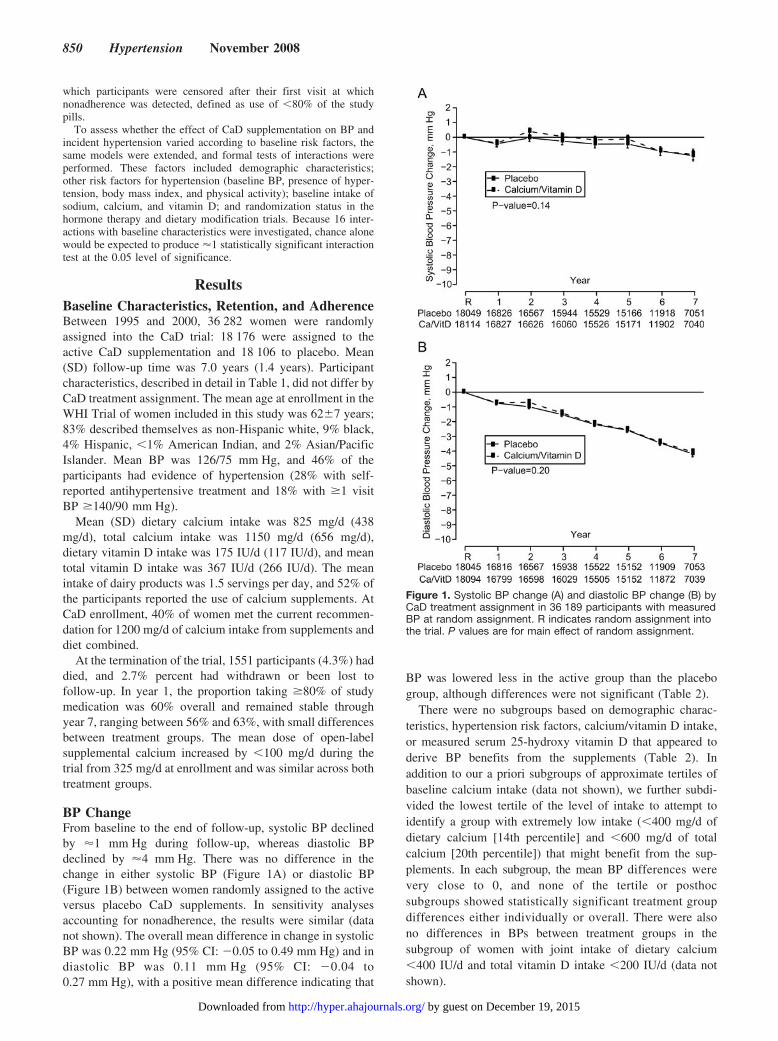
BP ChangeFrom baseline to the end of follow-up, systolic BP declinedby �1 mm Hg during follow-up, whereas diastolic BPdeclined by �4 mm Hg. There was no difference in thechange in either systolic BP (Figure 1A) or diastolic BP(Figure 1B) between women randomly assigned to the activeversus placebo CaD supplements. In sensitivity analysesaccounting for nonadherence, the results were similar (datanot shown). The overall mean difference in change in systolicBP was 0.22 mm Hg (95% CI: �0.05 to 0.49 mm Hg) and indiastolic BP was 0.11 mm Hg (95% CI: �0.04 to0.27 mm Hg), with a positive mean difference indicating that
BP was lowered less in the active group than the placebogroup, although differences were not significant (Table 2).
There were no subgroups based on demographic charac-teristics, hypertension risk factors, calcium/vitamin D intake,or measured serum 25-hydroxy vitamin D that appeared toderive BP benefits from the supplements (Table 2). Inaddition to our a priori subgroups of approximate tertiles ofbaseline calcium intake (data not shown), we further subdi-vided the lowest tertile of the level of intake to attempt toidentify a group with extremely low intake (�400 mg/d ofdietary calcium [14th percentile] and �600 mg/d of totalcalcium [20th percentile]) that might benefit from the sup-plements. In each subgroup, the mean BP differences werevery close to 0, and none of the tertile or posthocsubgroups showed statistically significant treatment groupdifferences either individually or overall. There were alsono differences in BPs between treatment groups in thesubgroup of women with joint intake of dietary calcium�400 IU/d and total vitamin D intake �200 IU/d (data notshown).
Figure 1. Systolic BP change (A) and diastolic BP change (B) byCaD treatment assignment in 36 189 participants with measuredBP at random assignment. R indicates random assignment intothe trial. P values are for main effect of random assignment.
850 Hypertension November 2008
by guest on December 19, 2015http://hyper.ahajournals.org/Downloaded from
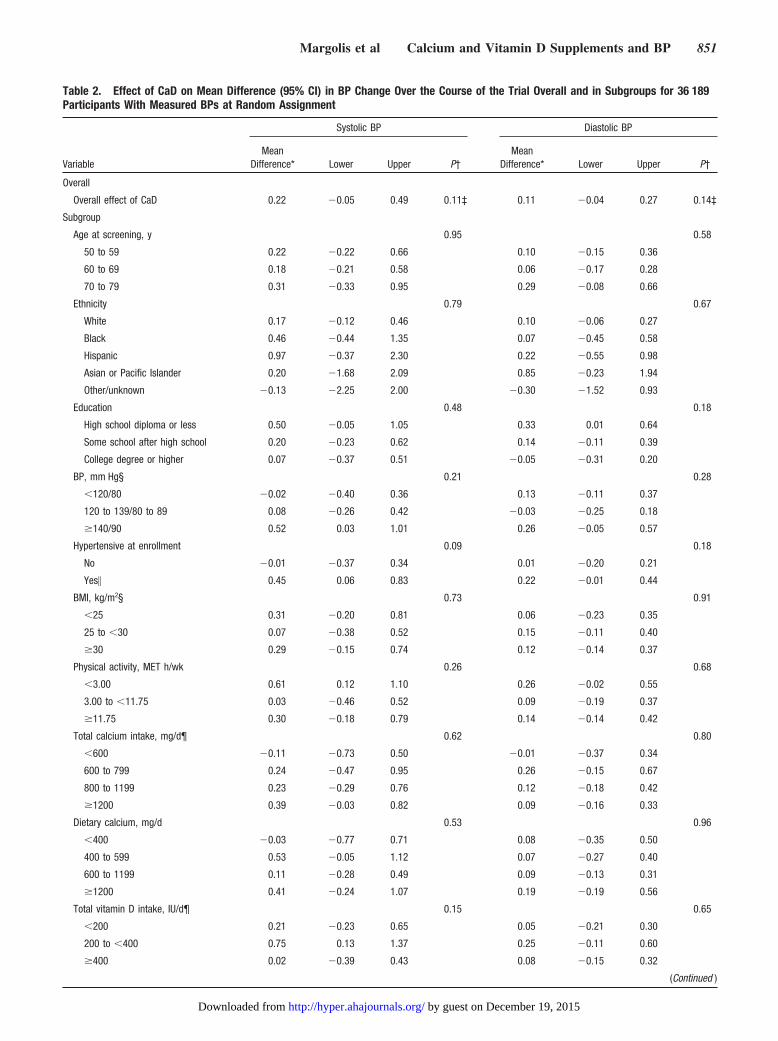
Table 2. Effect of CaD on Mean Difference (95% CI) in BP Change Over the Course of the Trial Overall and in Subgroups for 36 189Participants With Measured BPs at Random Assignment
Variable
Systolic BP Diastolic BP
MeanDifference* Lower Upper P†
MeanDifference* Lower Upper P†
Overall
Overall effect of CaD 0.22 �0.05 0.49 0.11‡ 0.11 �0.04 0.27 0.14‡
Subgroup
Age at screening, y 0.95 0.58
50 to 59 0.22 �0.22 0.66 0.10 �0.15 0.36
60 to 69 0.18 �0.21 0.58 0.06 �0.17 0.28
70 to 79 0.31 �0.33 0.95 0.29 �0.08 0.66
Ethnicity 0.79 0.67
White 0.17 �0.12 0.46 0.10 �0.06 0.27
Black 0.46 �0.44 1.35 0.07 �0.45 0.58
Hispanic 0.97 �0.37 2.30 0.22 �0.55 0.98
Asian or Pacific Islander 0.20 �1.68 2.09 0.85 �0.23 1.94
Other/unknown �0.13 �2.25 2.00 �0.30 �1.52 0.93
Education 0.48 0.18
High school diploma or less 0.50 �0.05 1.05 0.33 0.01 0.64
Some school after high school 0.20 �0.23 0.62 0.14 �0.11 0.39
College degree or higher 0.07 �0.37 0.51 �0.05 �0.31 0.20
BP, mm Hg§ 0.21 0.28
�120/80 �0.02 �0.40 0.36 0.13 �0.11 0.37
120 to 139/80 to 89 0.08 �0.26 0.42 �0.03 �0.25 0.18
�140/90 0.52 0.03 1.01 0.26 �0.05 0.57
Hypertensive at enrollment 0.09 0.18
No �0.01 �0.37 0.34 0.01 �0.20 0.21
Yes� 0.45 0.06 0.83 0.22 �0.01 0.44
BMI, kg/m2§ 0.73 0.91
�25 0.31 �0.20 0.81 0.06 �0.23 0.35
25 to �30 0.07 �0.38 0.52 0.15 �0.11 0.40
�30 0.29 �0.15 0.74 0.12 �0.14 0.37
Physical activity, MET h/wk 0.26 0.68
�3.00 0.61 0.12 1.10 0.26 �0.02 0.55
3.00 to �11.75 0.03 �0.46 0.52 0.09 �0.19 0.37
�11.75 0.30 �0.18 0.79 0.14 �0.14 0.42
Total calcium intake, mg/d¶ 0.62 0.80
�600 �0.11 �0.73 0.50 �0.01 �0.37 0.34
600 to 799 0.24 �0.47 0.95 0.26 �0.15 0.67
800 to 1199 0.23 �0.29 0.76 0.12 �0.18 0.42
�1200 0.39 �0.03 0.82 0.09 �0.16 0.33
Dietary calcium, mg/d 0.53 0.96
�400 �0.03 �0.77 0.71 0.08 �0.35 0.50
400 to 599 0.53 �0.05 1.12 0.07 �0.27 0.40
600 to 1199 0.11 �0.28 0.49 0.09 �0.13 0.31
�1200 0.41 �0.24 1.07 0.19 �0.19 0.56
Total vitamin D intake, IU/d¶ 0.15 0.65
�200 0.21 �0.23 0.65 0.05 �0.21 0.30
200 to �400 0.75 0.13 1.37 0.25 �0.11 0.60
�400 0.02 �0.39 0.43 0.08 �0.15 0.32
(Continued )
Margolis et al Calcium and Vitamin D Supplements and BP 851
by guest on December 19, 2015http://hyper.ahajournals.org/Downloaded from
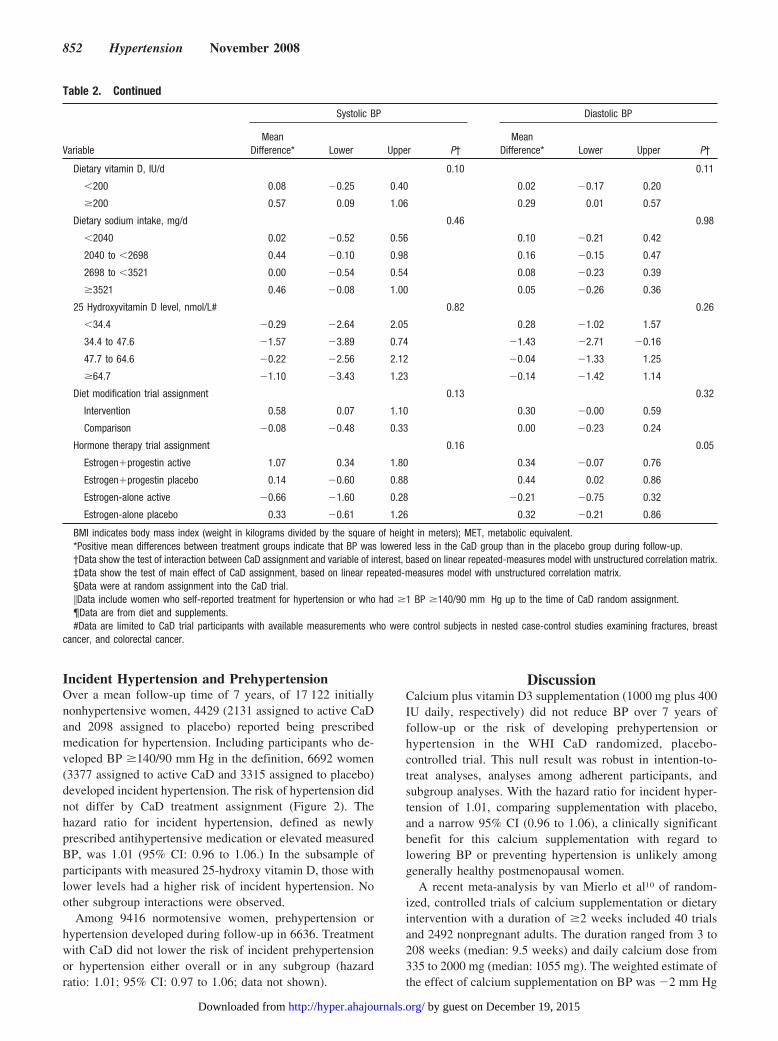
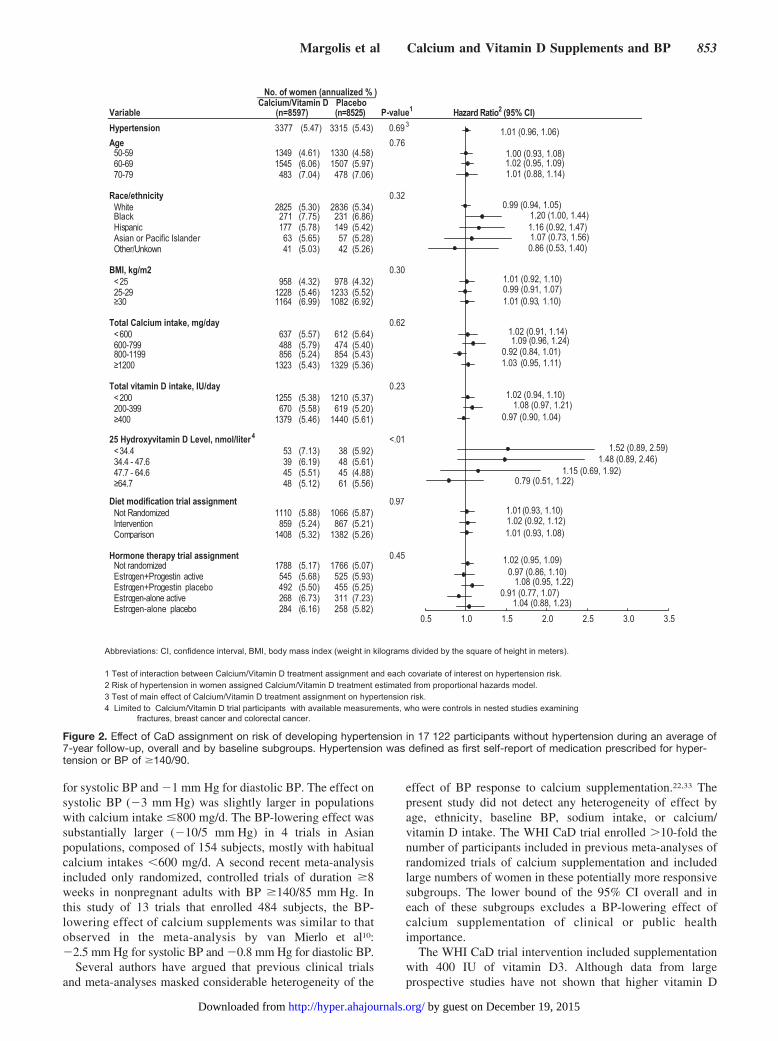
Incident Hypertension and PrehypertensionOver a mean follow-up time of 7 years, of 17 122 initiallynonhypertensive women, 4429 (2131 assigned to active CaDand 2098 assigned to placebo) reported being prescribedmedication for hypertension. Including participants who de-veloped BP �140/90 mm Hg in the definition, 6692 women(3377 assigned to active CaD and 3315 assigned to placebo)developed incident hypertension. The risk of hypertension didnot differ by CaD treatment assignment (Figure 2). Thehazard ratio for incident hypertension, defined as newlyprescribed antihypertensive medication or elevated measuredBP, was 1.01 (95% CI: 0.96 to 1.06.) In the subsample ofparticipants with measured 25-hydroxy vitamin D, those withlower levels had a higher risk of incident hypertension. Noother subgroup interactions were observed.
Among 9416 normotensive women, prehypertension orhypertension developed during follow-up in 6636. Treatmentwith CaD did not lower the risk of incident prehypertensionor hypertension either overall or in any subgroup (hazardratio: 1.01; 95% CI: 0.97 to 1.06; data not shown).
DiscussionCalcium plus vitamin D3 supplementation (1000 mg plus 400IU daily, respectively) did not reduce BP over 7 years offollow-up or the risk of developing prehypertension orhypertension in the WHI CaD randomized, placebo-controlled trial. This null result was robust in intention-to-treat analyses, analyses among adherent participants, andsubgroup analyses. With the hazard ratio for incident hyper-tension of 1.01, comparing supplementation with placebo,and a narrow 95% CI (0.96 to 1.06), a clinically significantbenefit for this calcium supplementation with regard tolowering BP or preventing hypertension is unlikely amonggenerally healthy postmenopausal women.
A recent meta-analysis by van Mierlo et al10 of random-ized, controlled trials of calcium supplementation or dietaryintervention with a duration of �2 weeks included 40 trialsand 2492 nonpregnant adults. The duration ranged from 3 to208 weeks (median: 9.5 weeks) and daily calcium dose from335 to 2000 mg (median: 1055 mg). The weighted estimate ofthe effect of calcium supplementation on BP was �2 mm Hg
Table 2. Continued
Variable
Systolic BP Diastolic BP
MeanDifference* Lower Upper P†
MeanDifference* Lower Upper P†
Dietary vitamin D, IU/d 0.10 0.11
�200 0.08 �0.25 0.40 0.02 �0.17 0.20
�200 0.57 0.09 1.06 0.29 0.01 0.57
Dietary sodium intake, mg/d 0.46 0.98
�2040 0.02 �0.52 0.56 0.10 �0.21 0.42
2040 to �2698 0.44 �0.10 0.98 0.16 �0.15 0.47
2698 to �3521 0.00 �0.54 0.54 0.08 �0.23 0.39
�3521 0.46 �0.08 1.00 0.05 �0.26 0.36
25 Hydroxyvitamin D level, nmol/L# 0.82 0.26
�34.4 �0.29 �2.64 2.05 0.28 �1.02 1.57
34.4 to 47.6 �1.57 �3.89 0.74 �1.43 �2.71 �0.16
47.7 to 64.6 �0.22 �2.56 2.12 �0.04 �1.33 1.25
�64.7 �1.10 �3.43 1.23 �0.14 �1.42 1.14
Diet modification trial assignment 0.13 0.32
Intervention 0.58 0.07 1.10 0.30 �0.00 0.59
Comparison �0.08 �0.48 0.33 0.00 �0.23 0.24
Hormone therapy trial assignment 0.16 0.05
Estrogen�progestin active 1.07 0.34 1.80 0.34 �0.07 0.76
Estrogen�progestin placebo 0.14 �0.60 0.88 0.44 0.02 0.86
Estrogen-alone active �0.66 �1.60 0.28 �0.21 �0.75 0.32
Estrogen-alone placebo 0.33 �0.61 1.26 0.32 �0.21 0.86
BMI indicates body mass index (weight in kilograms divided by the square of height in meters); MET, metabolic equivalent.*Positive mean differences between treatment groups indicate that BP was lowered less in the CaD group than in the placebo group during follow-up.†Data show the test of interaction between CaD assignment and variable of interest, based on linear repeated-measures model with unstructured correlation matrix.‡Data show the test of main effect of CaD assignment, based on linear repeated-measures model with unstructured correlation matrix.§Data were at random assignment into the CaD trial.�Data include women who self-reported treatment for hypertension or who had �1 BP �140/90 mm Hg up to the time of CaD random assignment.¶Data are from diet and supplements.#Data are limited to CaD trial participants with available measurements who were control subjects in nested case-control studies examining fractures, breast
cancer, and colorectal cancer.
852 Hypertension November 2008
by guest on December 19, 2015http://hyper.ahajournals.org/Downloaded from
for systolic BP and �1 mm Hg for diastolic BP. The effect onsystolic BP (�3 mm Hg) was slightly larger in populationswith calcium intake �800 mg/d. The BP-lowering effect wassubstantially larger (�10/5 mm Hg) in 4 trials in Asianpopulations, composed of 154 subjects, mostly with habitualcalcium intakes �600 mg/d. A second recent meta-analysisincluded only randomized, controlled trials of duration �8weeks in nonpregnant adults with BP �140/85 mm Hg. Inthis study of 13 trials that enrolled 484 subjects, the BP-lowering effect of calcium supplements was similar to thatobserved in the meta-analysis by van Mierlo et al10:�2.5 mm Hg for systolic BP and �0.8 mm Hg for diastolic BP.
Several authors have argued that previous clinical trialsand meta-analyses masked considerable heterogeneity of the
effect of BP response to calcium supplementation.22,33 Thepresent study did not detect any heterogeneity of effect byage, ethnicity, baseline BP, sodium intake, or calcium/vitamin D intake. The WHI CaD trial enrolled �10-fold thenumber of participants included in previous meta-analyses ofrandomized trials of calcium supplementation and includedlarge numbers of women in these potentially more responsivesubgroups. The lower bound of the 95% CI overall and ineach of these subgroups excludes a BP-lowering effect ofcalcium supplementation of clinical or public healthimportance.
The WHI CaD trial intervention included supplementationwith 400 IU of vitamin D3. Although data from largeprospective studies have not shown that higher vitamin D
Abbreviations: CI, confidence interval, BMI, body mass index (weight in kilograms divided by the square of height in meters).
1 Test of interaction between Calcium/Vitamin D treatment assignment and each covariate of interest on hypertension risk.2 Risk of hypertension in women assigned Calcium/Vitamin D treatment estimated from proportional hazards model.3 Test of main effect of Calcium/Vitamin D treatment assignment on hypertension risk.4 Limited to Calcium/Vitamin D trial participants with available measurements, who were controls in nested studies examining
fractures, breast cancer and colorectal cancer.
Variable P-value 1
Hypertension 3377 (5.47) 3315 (5.43) 0.69 3
Age 0.76943195-05 (4.61) 1330 (4.58)545196-06 (6.06) 1507 (5.97)38497-07 (7.04) 478 (7.06)
Race/ethnicity 0.325282etihW (5.30) 2836 (5.34)
Black 271 (7.75) 231 (6.86)Hisp 771cina (5.78) 149 (5.42)Asian or Pacific Islander 63 (5.65) 57 (5.28)
14nwoknU/rehtO (5.03) 42 (5.26)
BMI, kg/m2 0.3085952< (4.32) 978 (4.32)822192-52 (5.46) 1233 (5.52)
≥ 461103 (6.99) 1082 (6.92)
Total Calcium intake, mg/day 0.62736006< (5.57) 612 (5.64)884997-006 (5.79) 474 (5.40)6589911-008 (5.24) 854 (5.43)
≥ 32310021 (5.43) 1329 (5.36)
Total vitamin D intake, IU/day 0.235521002< (5.38) 1210 (5.37)076993-002 (5.58) 619 (5.20)
≥ 9731004 (5.46) 1440 (5.61)
25 Hydroxyvitamin D Level, nmol/liter 4 <.01354.43< (7.13) 38 (5.92)936.74 - 4.43 (6.19) 48 (5.61)546.46 - 7.74 (5.51) 45 (4.88)
≥ 847.46 (5.12) 61 (5.56)
Diet modification trial assignment 0.970111dezimodnaR toN (5.88) 1066 (5.87)958noitnevretnI (5.24) 867 (5.21)
Comp 8041nosira (5.32) 1382 (5.26)
Hormone therapy trial assignment 0.458871dezimodnar toN (5.17) 1766 (5.07)
Estrogen+Prog 545evitca nitse (5.68) 525 (5.93)Estrogen+Progestin placebo 492 (5.50) 455 (5.25)Estrog 862evitca enola-ne (6.73) 311 (7.23)Estrogen-alone p 482obecal (6.16) 258 (5.82)
No. of women (annualized % )Calcium/Vitamin D
(n=8597)Placebo
oitaR drazaH)5258=n( 2 (95% CI)
0.5 1.0 1.5 2.0 2.5 3.0 3.5
1.01 (0.96, 1.06)
1.00 (0.93, 1.08)1.02 (0.95, 1.09)1.01 (0.88, 1.14)
0.99 (0.94, 1.05)1.20 (1.00, 1.44)1.16 (0.92, 1.47)1.07 (0.73, 1.56)0.86 (0.53, 1.40)
1.01 (0.92, 1.10)0.99 (0.91, 1.07)1.01 (0.93, 1.10)
1.02 (0.91, 1.14)1.09 (0.96, 1.24)
0.92 (0.84, 1.01)1.03 (0.95, 1.11)
1.02 (0.94, 1.10)1.08 (0.97, 1.21)
0.97 (0.90, 1.04)
1.52 (0.89, 2.59)1.48 (0.89, 2.46)
1.15 (0.69, 1.92)0.79 (0.51, 1.22)
1.01 (0.93, 1.10)1.02 (0.92, 1.12)1.01 (0.93, 1.08)
1.02 (0.95, 1.09)0.97 (0.86, 1.10)
1.08 (0.95, 1.22)0.91 (0.77, 1.07)
1.04 (0.88, 1.23)
Figure 2. Effect of CaD assignment on risk of developing hypertension in 17 122 participants without hypertension during an average of7-year follow-up, overall and by baseline subgroups. Hypertension was defined as first self-report of medication prescribed for hyper-tension or BP of �140/90.
Margolis et al Calcium and Vitamin D Supplements and BP 853
by guest on December 19, 2015http://hyper.ahajournals.org/Downloaded from

intake lowered the incidence of hypertension, participants inthese studies with plasma levels of 25-hydroxy vitamin D inthe deficient range had an increase in the risk of incidenthypertension (6-fold in men and 3-fold in women).16 In thepresent study, we did not find evidence of lower BP inwomen who received the active vitamin D3–containingsupplement in the lowest quartile of measured 25-hydroxyvitamin D, which fell into the range generally considereddeficient. In fact, there was a trend toward an increased riskof hypertension with supplementation in women with lowervitamin D levels. This was not statistically significant forhypertension defined only by antihypertensive treatment pre-scription. Because of the number of subgroup interactionsthat we examined, this finding may be attributable to chance.
There are a number of potential limitations to this study.First, only postmenopausal women were included, so ourresults may not apply to men or younger women, althoughthere is little basis to believe that these populations wouldrespond differently to calcium supplementation.10 Second,nonadherence may have biased results toward the null;however, sensitivity analyses accounting for this suggestedthat the study result was robust. Third, the baseline level ofdietary calcium intake was higher in the WHI CaD trial thanaverage for older women in the United States (825 versus 660mg/d), and many women took supplemental calcium andvitamin D at baseline and as open-label supplements duringthe trial. However, because of the large size of the study,subgroup analyses included substantial numbers of partici-pants with low intake of these nutrients, and a clinicallyimportant BP effect was also excluded in these subgroups.Fourth, different results might have been observed with adifferent formulation or dose of calcium or a higher dose ofvitamin D3. The dose of 400 IU of vitamin D in particular hasbeen questioned as being inadequate to reduce the incidenceof hip fracture and colorectal cancer, the main end points ofthe trial.27,28 The lack of any degree of BP lowering even insubgroups with low intakes of calcium or vitamin D or inwomen with low vitamin D levels argues against this possi-bility, however. In addition, meta-analyses have not showndifferences in BP lowering with higher (�1000 to 1200mg/d) versus lower doses of calcium supplements.34,35 Fi-nally, it is possible that combining calcium with othernutrients or other minerals or simultaneous dietary interven-tion focused on calcium and vitamin D rich foods might haveled to different results. However, a meta-analysis of 3 trials ofcombinations of calcium, magnesium, and potassium supple-mentation in 277 participants did not find a significant effecton BP.36 Although 1 meta-analysis suggested the possibilityof a trend toward a greater BP-lowering effect of dietaryversus nondietary provision of calcium,9 unequivocally effec-tive dietary interventions to lower BP have generally includedsodium restriction and manipulation of multiple foods groups,macronutrients, and minerals.11
This study also has important strengths. The large size ofthe study allowed us to examine subgroups that had beenhypothesized to have potential for greater benefit: blacks,Asians, hypertensive subjects, women with low habitualintake of calcium, and women with low serum levels ofvitamin D. The study methodology was double blind and
included adequate concealment of treatment assignment. Thestudy was longer than any trial reported previously, and therewas little loss to follow-up.
In conclusion, in postmenopausal women over 7 years offollow-up, calcium plus vitamin D3 supplementation did notreduce either BP or the risk of developing hypertension.There was no subgroup that appeared to benefit from CaDsupplementation, and the precision of this study excludes aBP-lowering effect of calcium supplementation of clinical orpublic health importance.
PerspectivesCalcium supplementation, and, to a lesser extent, vitamin Dsupplementation have long been hypothesized to lower BPand delay the onset of hypertension. The results of previouscalcium supplementation trials have been mixed but ingeneral have shown a small BP–lowering benefit. The WHICaD supplementation trial provides the most definitive an-swer to the question: no benefit was seen overall or in anysubgroup of postmenopausal women. Although the dose ofboth supplements was modest, particularly the vitamin D, thelack of benefit in women with low intake of these nutrients orlow levels of vitamin D argues against a different result haddosages been higher. Because the WHI trial did not includeyounger women or men, no firm conclusions can be drawnabout the effect of calcium or vitamin D on BP in thesegroups. This study also did not address the question of BPlowering by dietary calcium intake or dairy foods, but itsuggests that short cuts with dietary supplements cannot besubstituted for encouraging people to adopt dietary patternsthat have been shown to lower BP and decrease the risk ofhypertension.
Sources of FundingThe Women’s Health Initiative program is funded by the NationalHeart, Lung, and Blood Institute, National Institutes of Health, USDepartment of Health and Human Services, through contractsN01WH22110, 24152, 32100-32102, 32105-32106, 32108-32109,32111-32113, 32115, 32118-32119, 32122, 42107-42126, 42129-42132, and 44221.
DisclosuresNone.
References1. Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Sacks FM,
Bray GA, Vogt TM, Cutlet JA, Windhauser MM, Lin PH, Karania N. Aclinical trial of the effects of dietary patterns on blood pressure. DASHCollaborative Research Group [see comment]. N Engl J Med. 1997;336:1117–1124.
2. Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA, Harsha D,Obarzanek E, Conlin PR, Miller ER, Simons-Morton DG, Karania N, LinPH. Effects on blood pressure of reduced dietary sodium and the DietaryApproaches to Stop Hypertension (DASH) diet. DASH-Sodium Collab-orative Research Group. N Engl J Med. 2001;344:3–10.
3. Dauchet L, Kesse-Guyot E, Czernichow S, Bertrais S, Estaquio C, PeneauS, Vergnaud AC, Chat-Yung S, Castetbon K, Deschamps V, Brindel P,Hercberg S. Dietary patterns and blood pressure change over 5-yfollow-up in the SU.VI.MAX cohort. Am J Clin Nutr. 2007;85:1650–1656.
4. Wang L, Manson JE, Buring JE, Lee IM, Sesso HD. Dietary intake ofdairy products, calcium, and vitamin D and the risk of hypertension inmiddle-aged and older women. Hypertension. 2008;51:1073–1079.
854 Hypertension November 2008
by guest on December 19, 2015http://hyper.ahajournals.org/Downloaded from
5. Cappuccio FP, Elliott P, Allender PS, Pryer J, Follman DA, Cutler JA.Epidemiologic association between dietary calcium intake and bloodpressure: a meta-analysis of published data. Am J Epidemiol. 1995;142:935–945.
6. Allender PS, Cutler JA, Follmann D, Cappuccio FP, Pryer J, Elliott P.Dietary calcium and blood pressure: a meta-analysis of randomizedclinical trials. Ann Intern Med. 1996;124:825–831.
7. Birkett NJ. Comments on a meta-analysis of the relation between dietarycalcium intake and blood pressure. Am J Epidemiol. 1998;148:223–228,discussion 32–33.
8. Bucher HC, Cook RJ, Guyatt GH, Lang JD, Cook DJ, Hatala R, Hunt DL.Effects of dietary calcium supplementation on blood pressure. A meta-analysis of randomized controlled trials. JAMA. 1996;275:1016–1022.
9. Griffith LE, Guyatt GH, Cook RJ, Bucher HC, Cook DJ. The influence ofdietary and nondietary calcium supplementation on blood pressure: anupdated metaanalysis of randomized controlled trials. Am J Hypertens.1999;12:84–92.
10. van Mierlo LA, Arends LR, Streppel MT, Zeegers MP, Kok FJ, GrobbeeDE, Geleijnse JM. Blood pressure response to calcium supplementation:a meta-analysis of randomized controlled trials. J Hum Hypertens. 2006;20:571–580.
11. Dickinson HO, Mason JM, Nicolson DJ, Campbell F, Beyer FR, CookJV, Williams B, Ford GA. Lifestyle interventions to reduce raised bloodpressure: a systematic review of randomized controlled trials.J Hypertens. 2006;24:215–233.
12. Dickinson HO, Nicolson DJ, Cook JV, Campbell F, Beyer FR, Ford GA,Mason J. Calcium supplementation for the management of primary hyper-tension in adults. Cochrane Database Syst Rev. 2006:CD004639.
13. Trumbo PR, Ellwood KC. Supplemental calcium and risk reduction ofhypertension, pregnancy-induced hypertension, and preeclampsia: anevidence-based review by the US Food and Drug Administration. NutrRev. 2007;65:78–87.
14. Krause R, Buhring M, Hopfenmuller W, Holick MF, Sharma AM. Ultra-violet B and blood pressure. Lancet. 1998;352:709–710.
15. Pfeifer M, Begerow B, Minne HW, Nachtigall D, Hansen C. Effects of ashort-term vitamin D(3) and calcium supplementation on blood pressureand parathyroid hormone levels in elderly women. J Clin EndocrinolMetab. 2001;86:1633–1637.
16. Forman JP, Giovannucci E, Holmes MD, Bischoff-Ferrari HA, TworogerSS, Willett WC, Curhan GC. Plasma 25-hydroxyvitamin D levels and riskof incident hypertension. Hypertension. 2007;49:1063–1069.
17. Li YC, Kong J, Wei M, Chen ZF, Liu SQ, Cao LP. 1,25-Dihydroxyvitamin D(3) is a negative endocrine regulator of the renin-an-giotensin system. J Clin Invest. 2002;110:229–238.
18. Carthy EP, Yamashita W, Hsu A, Ooi BS. 1,25-Dihydroxyvitamin D3and rat vascular smooth muscle cell growth. Hypertension. 1989;13:954–959.
19. Borges AC, Feres T, Vianna LM, Paiva TB. Cholecalciferol treatmentrestores the relaxant responses of spontaneously hypertensive rat arteriesto bradykinin. Pathophysiology. 2002;8:263–268.
20. Feres T, Vianna LM, Paiva AC, Paiva TB. Effect of treatment withvitamin D3 on the responses of the duodenum of spontaneously hyper-tensive rats to bradykinin and to potassium. Br J Pharmacol. 1992;105:881–884.
21. McCarron DA. Role of adequate dietary calcium intake in the preventionand management of salt-sensitive hypertension. Am J Clin Nutr. 1997;65:712S–716S.
22. Resnick LM. The role of dietary calcium in hypertension: a hierarchicaloverview. Am J Hypertens. 1999;12:99–112.
23. Geleijnse JM, Grobbee DE. Calcium intake and blood pressure: anupdate. J Cardiovasc Risk. 2000;7:23–29.
24. Suter PM, Sierro C, Vetter W. Nutritional factors in the control of bloodpressure and hypertension. Nutr Clin Care. 2002;5:9–19.
25. Hays J, Hunt J, Hubbell F, Anderson GL, Limacher M, Allen C, RossouwJE. The Women’s Health Initiative recruitment methods and results. AnnEpidemiol. 2003;13:S18–S77.
26. Jackson RD, Lacroix AZ, Cauley JA, Mcgowan J. The Women’s HealthInitiative Calcium-Vitamin D trial: overview and baseline characteristicsof participants. Ann Epidemiol. 2003;13:S98–S106.
27. Jackson RD, LaCroix AZ, Gass M, Wallace B, Robbins J, Lewis CE,Bassford T, Beresford SA, Black HR, Blanchette P, Bonds DE, BrunnerRL, Brzyski RG, Caan B, Cauley JA, Chlebowski RT, Cummings SR,Granek I, Hays J, Heiss G, Hendrix SL, Howard BV, Hsia J, Hubbell FA,Johnson KC, Judd H, Kotchen JM, Kuller LH, Langer RD, Lasser NL,Limacher MC, Ludlam S, Manson JE, Margolis KL, McGowan J, OckeneJK, O’Sullivan MJ, Phillips L, Prentice RL, Sarto GE, Stefanick ML, VanHorn L, Wactawski-Wende J, Whitlock E, Anderson GL, Assaf AR,Barad D. Calcium plus vitamin D supplementation and the risk offractures. N Engl J Med. 2006;354:669–683.
28. Wactawski-Wende J, Kotchen JM, Anderson GL, Assaf AR, Brunner RL,O’Sullivan MJ, Margolis KL, Ockene JK, Phillips L, Pottern L, PrenticeRL, Robbins J, Rohan TE, Sarto GE, Sharma S, Stefanick ML, Van HornL, Wallace RB, Whitlock E, Bassford T, Beresford SA, Black HR, BondsDE, Brzyski RG, Caan B, Chlebowski RT, Cochrane B, Garland C, GassM, Hays J, Heiss G, Hendrix SL, Howard BV, Hsia J, Hubbell FA,Jackson RD, Johnson KC, Judd H, Kooperberg CL, Kuller LH, LaCroixAZ, Lane DS, Langer RD, Lasser NL, Lewis CE, Limacher MC, MansonJE. Calcium plus vitamin D supplementation and the risk of colorectalcancer. N Engl J Med. 2006;354:684–696.
29. Institute of Medicine Standing Committee on the Scientific Evaluation ofDietary Reference Intakes. Dietary Reference Intakes for Calcium, Phos-phorous, Magnesium, Vitamin D, and Fluoride. Washington, DC:National Academy Press; 1997.
30. Anderson GL, Manson J, Wallace R, Lund B, Hall D, Davis S, ShumakerS, Wang CY, Stein E, Prentice RL. Implementation of the Women’sHealth Initiative study design. Ann Epidemiol. 2003;13:S5–S17.
31. Patterson R, Kristal A, Tinker L, Carter R, Bolton M, Agurs-Collins T.Measurement characteristics of the Women’s Health Initiative food fre-quency questionnaire. Ann Epidemiol. 1999;9:178–187.
32. Ainsworth B, Haskell W, Leon A, Ainsworth BE, Haskell WL, Leon AS,Jacobs DR Jr, Montoye HJ, Sallis JF Jr, Paffenbarger RS Jr. Compendiumof physical activities: Classification of energy costs of human physicalactivities. Med Sci Sports Exerc. 1993;25:71–80.
33. Zemel MB. Calcium modulation of hypertension and obesity: mech-anisms and implications. J Am Coll Nutr. 2001;20:428S–435S, dis-cussion 40S–42S.
34. Dickinson HO, Nicolson DJ, Cook JV, Campbell F, Beyer FR, Ford GA,Mason J. Calcium supplementation for the management of primary hyper-tension in adults. Cochrane Database Syst Rev. 2006;(2):CD004639.
35. van Mierol LA, Arends LR, Streppel MT, Zeegers MP, Kok FJ, GrobbeeDE, Geleijnse JM. Blood pressure response to calcium supplementation:a meta-analysis of randomized controlled trials. J Hum Hypertens. 2006;20:571–580.
36. Beyer FR, Dickinson HO, Nicolson DJ, Ford GA, Mason J. Combinedcalcium, magnesium and potassium supplementation for the managementof primary hypertension in adults. Cochrane Database Syst Rev. 2006;(3):CD004805.
Margolis et al Calcium and Vitamin D Supplements and BP 855
by guest on December 19, 2015http://hyper.ahajournals.org/Downloaded from
for the Women�s Health Initiative InvestigatorsThomson and James C. Torner
Grimm, Jr, Theodore A. Kotchen, Lewis H. Kuller, Sylvia Wassertheil-Smoller, Cynthia A.Henry R. Black, Shirley A.A. Beresford, Stephanie A. Connelly, J. David Curb, Richard H.
Karen L. Margolis, Roberta M. Ray, Linda Van Horn, JoAnn E. Manson, Matthew A. Allison,Health Initiative Randomized Trial
Effect of Calcium and Vitamin D Supplementation on Blood Pressure: The Women's
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 2008 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/HYPERTENSIONAHA.108.114991
2008;52:847-855; originally published online September 29, 2008;Hypertension.
http://hyper.ahajournals.org/content/52/5/847World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org/content/suppl/2008/09/29/HYPERTENSIONAHA.108.114991.DC1.htmlData Supplement (unedited) at:
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertensionin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on December 19, 2015http://hyper.ahajournals.org/Downloaded from




















