
Effect of asymmetric vocal fold stiffness on traveling wave velocity in the canine larynx.
12
Third Place .. Resident Basic Science Award 1992 Effect of asymmetric vocal fold stiffness on traveling wave velocity in the canine larynx STEVEN H. SLOAN, MD, GERALD S. BERKE, MD, and BRUCE R. GERRATT, PhD, Los Angeles. California The vocal fold (VF) traveling wave is essential to normal voice production. The present investigation describes a new method to determine traveling wave velocity (TWV) in the in vivo canine phonatory model. This method synchronizes photoglottographlc and electroglottographlc waveforms with videostroboscopic images to determine the du- ration of time the traveling wave moves between two tattoos placed a known distance apart between the upper and lower margins of each VF. Using this method, we com- pared the TWV of a paralyzed VF with the TWV of the contralateral, electrically stim- ulated VF during phonation in two canines. In addition, the presumed VFstiffness asym- metry in the simulated acute recurrent laryngeal nerve paralysis state was confirmed by measuring Young's modulus of each VF. The results indicated that the TWV of the paralyzed VF averaged 55% of the TWV of the normal, stiffer VFwhen the glottal gap was small and entrainment occurred. This study demonstrated the feasibility of quan- tifying traveling wave motion In asymmetric VF stiffness disorders. The potential use of TWV in human beings as a target to optimize the phonosurgical results in asymmetric VFstiffness disorders is discussed. (OTOlARYNGOL HEAD NECK SURG 1992;107:516.) The increasing interest in laryngostroboscopy as a clin- ical and research tool has recently focused attention on mucosal wave movement in the vocal fold during pho- nation. The vocal folds (VF) exhibit a wavelike motion that consists of vertical as well as horizontal compo- nents. The mucosal wave, propagated by the force of subglottic airflow, travels from the lower margin to the upper margin of the VF and then moves laterally, re- From UCLA Head and Neck Surgery. Supported by an NIH/NS grant (ROI DC00855-0l) and a VAMerit Review Grant. Presented at the Annual Meeting of the American Academy of Oto- laryngology-Head and Neck Surgery, Washington, D.C., Sept. 13-17, 1992. Received for publication May 29, 1992; accepted June 29, 1992. Reprint requests: Gerald S. Burke, MD, UCLA Head and Neck Surgery, CHS 62-132, 10833 Le Conte Ave., Los Angeles, CA 90024-1624. 23/1141107 516 sembling a wave breaking on the shoreline. The lower margins of the VF separate first and, before the upper margins separate, an elliptical volume of air is formed in the subglottic vault, confined by the upper margins superiorly and the lower margins laterally. As the upper margins move laterally, a puff of air is released (i.e., the glottal puff or pulse). 1 The lower margins then return to the midline to close the glottis, followed by the return to the midline of the upper margins as a new glottic vibratory cycle begins. The phase delay between the opening of the lower margins and the opening of the upper margins has been termed the mucosal traveling wave, because of its fluid-like movement when viewed on high-speed film or stroboscopy. The specific char- acteristics of this wave, such as its amplitude and ve- locity, modify the glottal air puffs. These puffs or pulses of air form the vocal source, influence the final acoustic signal emitted, and determine vocal quality. Conse- quently, the characteristics of the traveling wave are most important in determination of voice production. at UCLA on August 18, 2015 oto.sagepub.com Downloaded from at UCLA on August 18, 2015 oto.sagepub.com Downloaded from at UCLA on August 18, 2015 oto.sagepub.com Downloaded from
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Effect of asymmetric vocal fold stiffness on traveling wave velocity in the canine larynx.

Third Place .. Resident Basic Science Award 1992
Effect of asymmetric vocal fold stiffness ontraveling wave velocity in the canine larynxSTEVEN H. SLOAN, MD,GERALD S. BERKE, MD, and BRUCE R. GERRATT, PhD, Los Angeles. California
The vocal fold (VF) traveling wave is essential to normal voice production. The presentinvestigation describes a new method to determine traveling wave velocity (TWV) inthe in vivo canine phonatory model. This method synchronizes photoglottographlc andelectroglottographlc waveforms with videostroboscopic images to determine the duration of time the traveling wave moves between two tattoos placed a known distanceapart between the upper and lower margins of each VF. Using this method, we compared the TWV of a paralyzed VF with the TWV of the contralateral, electrically stimulated VFduring phonation in two canines. In addition, the presumed VFstiffness asymmetry in the simulated acute recurrent laryngeal nerve paralysis state was confirmedby measuring Young's modulus of each VF. The results indicated that the TWV of theparalyzed VF averaged 55% of the TWV of the normal, stiffer VF when the glottal gapwas small and entrainment occurred. This study demonstrated the feasibility of quantifying traveling wave motion In asymmetric VF stiffness disorders. The potential use ofTWV in human beings as a target to optimize the phonosurgical results in asymmetricVF stiffness disorders is discussed. (OTOlARYNGOL HEAD NECK SURG 1992;107:516.)
The increasing interest in laryngostroboscopy as a clinical and research tool has recently focused attention onmucosal wave movement in the vocal fold during phonation. The vocal folds (VF) exhibit a wavelike motionthat consists of vertical as well as horizontal components. The mucosal wave, propagated by the force ofsubglottic airflow, travels from the lower margin to theupper margin of the VF and then moves laterally, re-
From UCLA Head and Neck Surgery.Supported by an NIH/NS grant (ROI DC00855-0l) and a VA Merit
Review Grant.Presented at the Annual Meeting of the American Academy of Oto
laryngology-Head and Neck Surgery, Washington, D.C., Sept.13-17, 1992.
Received for publication May 29, 1992; accepted June 29, 1992.Reprint requests: Gerald S. Burke, MD, UCLA Head and Neck
Surgery, CHS 62-132, 10833 Le Conte Ave., Los Angeles, CA90024-1624.
23/1141107
516
sembling a wave breaking on the shoreline. The lowermargins of the VF separate first and, before the uppermargins separate, an elliptical volume of air is formedin the subglottic vault, confined by the upper marginssuperiorly and the lower margins laterally. As the uppermargins move laterally, a puff of air is released (i.e.,the glottal puff or pulse). 1 The lower margins then returnto the midline to close the glottis, followed by the returnto the midline of the upper margins as a new glotticvibratory cycle begins. The phase delay between theopening of the lower margins and the opening of theupper margins has been termed the mucosal travelingwave, because of its fluid-like movement when viewedon high-speed film or stroboscopy. The specific characteristics of this wave, such as its amplitude and velocity, modify the glottal air puffs. These puffs or pulsesof air form the vocal source, influence the final acousticsignal emitted, and determine vocal quality. Consequently, the characteristics of the traveling wave aremost important in determination of voice production.
at UCLA on August 18, 2015oto.sagepub.comDownloaded from at UCLA on August 18, 2015oto.sagepub.comDownloaded from at UCLA on August 18, 2015oto.sagepub.comDownloaded from

Volume 107 Number 4October 1992 Effect of asymmetric vocal fold stiffness on traveling wave velocity 517
o DEGREETELESCOPE
..
MULTICHANNELSTORAGE
OSILLOSCOPE
t
t DIRECTCOMPUTERIZED
DIGITIZATION
FLOWMETER
tH••Wln.d...... al ..
V••tll.tor
Fig. 1. Schematic representation of experimental setup for determination of TVN.
Hirano'" has emphasized the importance of this mucosal traveling wave in his Body-Cover Theory of VFvibration. This theory divides the layers of the VF intotwo groups with different viscoelastic properties. Thecover, consisting of the epithelium and superficial lamina propria, is very pliable and can propagate a wavethat facilitates energy transfer from the glottal airstreamto the VF tissue. The body consists of the vocalis muscle. The passive stretch of the cover and the activecontraction of the body are the main contributors tooverall VF stiffness. 4 Changes in the stiffness of theVF affect the motion of the traveling wave.
Most theoretical models of VF function require thedetermination of stiffness or mechanical complianceparameters in order to define the motion of the massesconstituting the models.l" A number of authors"!' havemeasured the elastic modulus constants of the larynxin vitro in order to predict how laryngeal vibration may
work in vivo. These studies indicated the importanceof Young's elastic modulus in determination of the nature of laryngeal vibration.
Normal phonation is characterized by symmetric VFtraveling wave motion and presumably equal VF stiffness.":" Symmetric VF motion transforms aerodynamic energy to sound energy efficiently as a result offorceful, effective VF closure. In contrast, asymmetricVF stiffness-as in unilateral paresis/paralysisstates-produces asymmetric traveling wave motion.In this situation, the asymmetric motion and impairedVF closure results in less efficient transformation ofenergy and soft or breathy voice quality.
A number of techniques to study VF motion havebeen developed. Laryngeal stroboscopy allows VF vibration to be examined in detail during phonation. 14-16
Stroboscopy was first applied to the study of the larynxby Oertel in 1878. Modem laryngostroboscopes use a
at UCLA on August 18, 2015oto.sagepub.comDownloaded from

518 SLOAN et 01.
pulse light source to create a montage of the vibratingfolds. The pitch of phonation or a frequency generatoris used to control the strobe flash frequency in order tocreate the impression that the VFs are vibrating in slowmotion. The resultant videostroboscopic images provide a means for observing VF shape, movement, vibratory pattern, and timing relationships between opening and closure. Bless and Brandenburg 17 reported usingstroboscopy to differentiate functional and subtle structural abnormalities of the larynx. Von Leden" usedvideostroboscopy to evaluate the degree of infiltrationby cancerous lesions.
A less common application of laryngeal stroboscopyis in the diagnosis, treatment, and followup of laryngealparesis/paralysis states. IS Recurrent laryngeal nerve(RLN) paralysis causes a fixation of the VF in a nearmedian position. It also results in a loss of muscle tone,i.e. a reduction of stiffness in the "body" of the vocalfold. Equilibration of the stiffness of the mucosal coverand the muscular body then occurs, causing the VF tovibrate more as one margin. Stroboscopically, this isdemonstrated by the disappearance or diminution of themucosal traveling wave. Schoenharl'? studied laryngealparalysis with stroboscopy and found that in 55 of 62cases, the traveling wave was absent. The presence ofthe mucosal wave in patients with a paralyzed VF wasinterpreted as a sign of some degree of reinnervation,suggesting an improved prognosis. Isshiki et al. 20 published a detailed account of the effects of asymmetricVF tension. They concluded that the vibratory characteristics produced by asymmetric laryngeal stiffnessdepend on the degree of glottic closure. Moore et al. I
studied canine laryngeal paralysis with videostroboscopy and found that the mucosal wave was markedlydiminished, but not absent on the paralyzed side. Inaddition, it was found that RLN paralysis produced aloss of the normal two-mass laryngeal vibration. Similarfindings have been described in human beings." Manyother studies have qualitatively correlated laryngeal paralysis with stroboscopy, but quantification has beenlacking." An objective method to quantify vocal foldmotion in states of paralysis would be valuable.
Researchers have attempted to quantify the travelingwave velocity (TWV) in normal phonation. In excisedhuman larynges, Baer" found that each point along themucosal edge of the VF moved in a quasi-ellipticaltrajectory in the coronal plane. He calculated wave velocities of up to I meter/second, although velocity varied at different locations on the VF. More recently, theTWV has been determined in vivo. An accurate methodof calculating the TWV in the canine model has been
OlolaryngologyHeaa and Neck Surgery
developed by quantifying vocal fold motion stroboscopically." It was found that the TWV velocity variedfrom 800 to 1600 mm/second and was positively correlated with changes in VF stiffness. This correlationbetween VF stiffness and TWV has diagnostic and therapeutic implications. For example, if TWV could bemeasured and compared over time, the phonosurgicaltechniques used to treat lesions resulting in VF stiffnessasymmetries could be more objectively guided.
There has been a recent proliferation of surgical techniques to correct dysphonias associated with travelingwave abnormalities. These include methods that medialize the VF, augment the tissues using alloplasticmaterial, or reinnervate the paralyzed VF.23-27 Despitethese new surgical methods, no objective means arepresently used by surgeons to evaluate and optimize theresults of their interventions. Instead, the surgeon usually gauges the changes made to the VF by visual inspection or by listening to the voice and making someperceptual judgment. A method to measure VF motionhas the potential to objectively determine the bestphonosurgical result. For example, Trapp et al. 28 optimized vocal function with Teflon injection of the paralyzed canine VF to the point where mechanical compliance or stiffness between the two vocal folds wasgrossly equivalent. At this point, symmetric travelingwave motion and a subsequent increase in the amplitudeof the upper harmonics of the acoustic signal were observed.
The purpose of this study was two-fold. First, wewanted to investigate and describe a new method todetermine TWV in the in vivo canine phonatory model.This method synchronizes photoglottographic (PGG)and electroglottographic (EGG) waveforms with videostroboscopic images in order to determine the quantity of time the traveling wave moves between twotattoos placed a known distance apart on each VF. Second, using this new method, we wanted to compare theTWV of a paralyzed VF (acute RLN paralysis) withthe contralateral, normally innervated VF during phonation. In addition, the presumed VF stiffness asymmetry in the acute RLN paralysis state was confirmedby determining Young's elastic modulus of each VF.
METHODS
Experimental preparation. The experimentalpreparation was similar to that previously reported instudies of the in vivo canine model." Figure I providesa diagrammatic representation of the experimentalsetup. Four healthy adult male mongrel dogs (25 kgeach) were studied. Two dogs had aperiodic phonation
at UCLA on August 18, 2015oto.sagepub.comDownloaded from

Volume 107 Number 4October 1992 Effect of asymmetric vocal fold stiffness on traveling wave velocity 519
Fig.2. Videostroboscopic image of dots piaced at upper and lower margin of left VFduring closedphased. u denotes upper dot. L denotes lower dot. The arrow indicates the midline.
with a unilateral RLN paralysis and, as a result, theirTWV could not be determined. Aperiodic phonationwas defined as an inability of the stroboscope to triggerperiodic light flashes. In this case, images of VF vibration were not interpretable. The other two dogsphonated periodically, so TWV could be analyzed.
The animals were premedicated with acepromazinemaleate intramuscularly. Intravenous pentobarbital wasthen administered to a level of corneal sensation lossand additional amounts were used to maintain this levelof anesthesia throughout the experiment. The animalswere placed in supine position and direct laryngoscopywas performed to confirm normal laryngeal anatomy.A 7 mm orotracheal tube was inserted and the animalswere given assisted ventilation with 95% oxygen.
A midline neck incision was made to expose thetrachea and larynx. The strap and sternocleidomastoidmuscles were retracted laterally. A low tracheotomywas performed at the level of the suprasternal notch,through which an endotracheal tube was passed to allowventilator-assisted respiration. A second tracheotomywas performed in a more superior location, throughwhich a cuffed endotracheal tube was passed in a rostraldirection and positioned with the tip resting 10 em below the glottis. The cuff of this tube was inflated tojust seal the trachea. Room air from a compressed airtank was bubbled through 5 cm of water at 37° C forwarming and humidification and passed through thisrostral tube. Flow was controlled with a needle valve
(Whitey, Highland Heights, Ohio) and measured witha flowmeter (Gilmont No. 1500, Great Neck, N.Y.).A 1 em button was used to suspend the epiglottis froma fixed point to provide direct visualization of the larynxthrough the oral cavity.
Tattooing procedure. To determine traveling wavevelocity, tattooing of the vocal folds was performed byplacing Higgins waterproof black india ink in the submucosal plane. A custom-made stainless steel ink dotapplicator with two sharp prongs placed 1.5 mm apartfrom each other was used. This applicator was gentlyadvanced deep to the glottic mucosa, forming two indelible distinct dots. One pair of dots was placed oneach VF, halfway between the anterior commissure andthe vocal process of the arytenoid on the medial surfacecorresponding to the upper and lower margins of eachvocal fold. Each dot was 0.5 mm in diameter. Figure2 shows the appearance of the upper and lower dotapplied to the left canine VF.
Electrical stimulation. A 1 em segment of the external branch of each superior laryngeal nerve (SLN)was isolated and Harvard subminiature electrodes (Harvard Apparatus, Inc., South Natick, Mass.) were applied to each nerve. Only one recurrent laryngeal nerve(RLN) was isolated 5 em inferior to the larynx and aHarvard electrode was applied. A Grass model 54Hstimulator (Grass Instrument Co., Quincy, Mass.) provided voltage stimulation to both SLNs. A constantcurrent stimulator (RLN Stimulator, Model S2LH, WR
at UCLA on August 18, 2015oto.sagepub.comDownloaded from

520 SLOAN et 01.
Medical Electronics, St. Paul, Minn.) was used to provide varying amounts of current to the RLN. The frequency of stimulation was 80 Hz, with a pulse durationof 1.5 milliseconds for both nerve stimulators. Voltagewas kept constant at 1.9 volts for the Grass stimulatorand currents ranged from 0.09 to 0.15 rnA for the RLNstimulator. Electrical isolation between the RLN andSLN was verified by direct observation. Maximal stimulation of the unilateral RLN to the point at which thestrap muscles contracted (approximately 9 volts) wasnot observed to produce contraction of the cricothyroidmuscle. In addition, no lengthening or thinning of thevocal folds occurred during maximal RLN stimulation.Isolated maximal stimulation of the SLNs to the pointof strap muscle contraction did not demonstrate tensingor bulging of the vocalis muscle on direct laryngoscopicexamination. No arytenoid adduction nor phonationcould be elicited by maximal SLN stimulation.
Airflow. The rate of air flow was 520 em/sec. Thisrate of flow was required to provide sustained oscillation in a canine hemiparalyzed larynx. Flow was controlled by a valve at the laboratory wall outlet andpassed through the air warming chamber before entryinto the larynx.
Vldeostroboscopy. Videostroboscopy was performed using a model 8000 Storz laryngostroboscope(Karl Storz Endoscopy-America Inc., Culver City,CA) connected with a fiberoptic cable to a 0° Storztelescope for observation of vocal fold vibratory excursion and traveling wave speed. Images were recorded using a CCD camera (Toshiba IK C30A, BuffaloGrove, Ill.) and %-inch videotape recorder (SONY VO9850, Park Ridge, N.J.). Recorded video images wereviewed on a SONY video monitor (PVM 1341) andanalyzed frame-by-frame.
Glottographic techniques. Events in the glottalcycle were monitored by PGG and EGG. The larynxwas illuminated from above by a fiberoptic xenon lightsource secured in the oral cavity and directed towardthe glottis. Light transmission through the vocal cordswas transduced with a photosensor (Centronics OSD50-2, Mountainside, N.J.) placed on the animal's trachea approximately 3 em below the larynx. EGG electrodes (Synchrovoice, Harrison, N.J.) were sutured indirect contact on either side of the thyroid cartilage,with the reference electrode sutured to the skin. PGGand EGG tracings were observed on a storage oscilloscope (Tektronix 5116, Beaverton, Ore.), low-passfiltered at 3000 Hz and digitized at 20,000 Hz. Thewaveforms were analyzed using a commercially available software package for the PC system (C-Speech,Paul Milenkovic, Madison, Wis.).
OfolaryngologyHead and Neck Surgery
Synchronization and TWV calculation. Videostroboscopic images were synchronized with glottographic signals to provide information about the timingof events in acute RLN paralysis. This allowed us todetermine the amount of time it took the traveling waveto move from the lower dot to the upper dot placed oneach VF. From determining this quantity of time andknowing the distance between dots, TWV could becalculated. Further details about the synchronizationmethod is being published in a separate report from thislaboratory." Briefly, a 5 millisecond (msec) squarewave pulse (SWP) was digitized and simultaneouslyrecorded on the audio channel of the videotape recorder. By correlating the 5 msec SWP with the vertical synchronization trace of the video signal, the position of the strobe flash on the glottographic waveformcould be precisely correlated with individual videoimages.
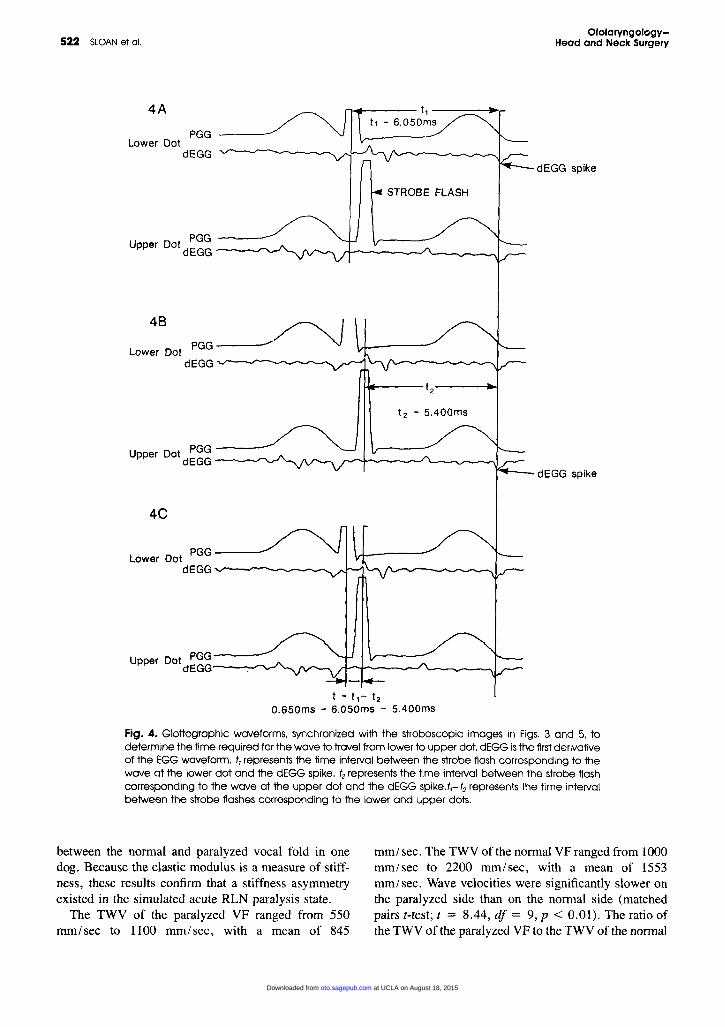
The videostroboscopic image in Fig. 3 shows thetraveling wave at the center of the lower dot (labeledL) at the beginning of the open phase. Figure 4, A showsthe synchronous waveforms of PGG, and the first derivative of EGG (dEGG). t l , Is defined as a time intervalfrom the center of the strobe flash to the point on theglottographic wave that is consistently found at the samelocation within the vibratory cycle. The dEGG downgoing spike at the moment of closure of the vibratorycycle has been shown to have this characteristic." Asa result, t l is the time interval between the middle ofthe strobe flash (when the traveling wave reached thelower dot) and the dEGG spike. This time, 6.05 msec,is represented by the distance between the cursors.
The image in Fig. 5 shows the traveling wave at thecenter of the upper dot (labeled u) later in the openphase of the glottal cycle. Figure 4, B depicts the corresponding PGG and dEGG waveforms. Similarly, t2
is the time interval between the middle of the strobeflash spike (when the traveling wave reached the upperdot) and the dEGG spike (moment of closure). Thistime, 5.400 msec, is represented by the distance between the cursors.
TWV was calculated as d / t, in which d = distancebetween the dots and t = t, - (2, the time required forthe wave to travel from the lower to the upper dot(6.050 - 5.400 = 0.650 msec). Figure 4,C depictsthis time interval as the distance between the cursors.The distance between the lower and upper dots on eachVF was measured using a vernier caliper and an operating microscope after the larynx was excised.
Measurement of elastic modulus. In order to confirm a stiffness asymmetry in the simulated acute RLNparalysis condition, direct measurement of the elastic
at UCLA on August 18, 2015oto.sagepub.comDownloaded from

Volume 107 Number 4October 1992 Effect of asymmetric vocal fold stiffness on traveling wave velocity 521
Fig. 3. Videostroboscopic image of traveling wave at the lower dot at beginning of open phase.
modulus was made from both vocal folds of each canine. Other researchers have emphasized the importance of the elastic modulus in determining travelingwave motion.5.22.32.33 Young's elastic modulus is a measure of VF stiffness and is calculated from the followingequation:
. (Stress) (F /A)Young's modulus'" = Y = =--
(Strain) (x)
in which F = force required for lateral movement;A = area over which force was applied; x =displacement or change in length in x from the initiallength.
Elastic modulus values were compared between theparalyzed and normally innervated VF using a "tensionometer" device. Normal innervation was producedat the same RLN and SLN stimulation values usedduring TWV testing. The details of the constructionand operation of this stiffness-measuring device are reviewed in another publication. 12.13 In brief, this devicemeasures the transverse or horizontal elastic modulusof the VF. It is sensitive to small changes in the modulusand can be maneuvered into position easily and rapidly.Two modulus testing trials were performed on each dogfor each amount of displacement from the resting position. The amount of displacement studied for eachtrial was 0.5, 1.0, 1.5, and 2.0 mm.
Experimental design. The effect of acute RLN paralysis on. TWV was studied by simultaneously stimulating both SLN and one RLN to produce phonation
at constant air flow rate of 520 cc/sec. While the SLNwas stimulated bilaterally at 1.9 V, the animals werephonated at unilateral RLN intensities between 0.09 and0.15 mAo The amount of RLN stimulation was randomly varied to produce periodic phonation. Flow ratesless than 520 cc / sec and RLN intensities less than 0.09rnA resulted in breathy, aperiodic phonation in all fourdogs.
The elastic modulus of both the paralyzed and normally innervated vocal folds in the two dogs with periodic phonation was determined, as just described, after the phonatory trials were completed.
Data Analysis
Separate TWV calculations were made for each rightand left VF for all the trials with periodic vibration andinterpretable stroboscopic images. TWV could not becalculated for trials with aperiodic vibration. This prevented the determination of TWV in all trials in two ofthe four dogs. Consequently, a total of 10 trials wereanalyzed (six from one dog, four from the other). Because results were similar in the two dogs, they werecombined for analysis. Similarly, Young's elastic modulus values were calculated for each paralyzed and normally innervated VF as a function of displacement inthe two dogs with periodic phonation.
RESULTS
Figure 6 compares the Young's elastic modulus indynes/em? as a function of displacement in millimeters
at UCLA on August 18, 2015oto.sagepub.comDownloaded from
522 SLOAN et 01.Ofolaryngology
Head and Neck Surgery
STROBE FLASH
dEGG spike
~f---- 11 ------.,~....
t1 ~ 6.050ms4A
PGG
PGG ---Upper Dol dEGG --_r-.....-'
Lower DotdEGG
dEGG spike
12 ~ 5.400ms
4C
Upper Dot PGGdEGG--""""""""''-
Lower Dot PGG---dEGG '-/'"'-....--------~.................
48 ~Lower Dot PGG
dEGG -...r--..",.... ~......... .....
Upper Dot PGGdEGG---r-\"..r'
t = 11 - 12
O.650ms = 6.050ms - 5.400ms
Fig. 4. Glottographic waveforms, synchronized with the stroboscopic images in Figs. 3 and 5. todetermine the time required for the wave to travel from lower to upper dot. dEGG isthe firstderivativeof the EGG waveform. t, represents the time interval between the strobe flash corresponding to thewave at the lower dot and the dEGG spike. t2 represents the time interval between the strobe flashcorresponding to the wave at the upper dot and the dEGG spike,t,-t2 represents the time intervalbetween the strobe flashes corresponding to the lower and upper dots.
between the normal and paralyzed vocal fold in onedog. Because the elastic modulus is a measure of stiffness, these results confirm that a stiffness asymmetryexisted in the simulated acute RLN paralysis state.
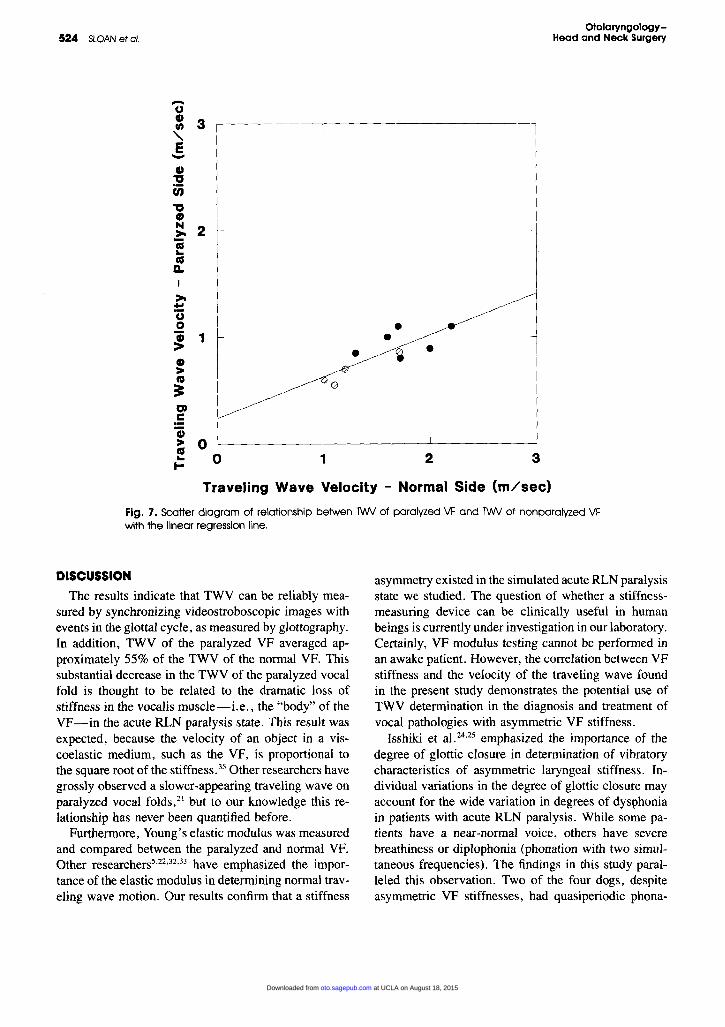
The TWV of the paralyzed VF ranged from 550mm/sec to 1100 mm/sec, with a mean of 845
mm /sec. The TWV of the normal VF ranged from 1000mm/sec to 2200 rum/sec, with a mean of l553mm/sec. Wave velocities were significantly slower onthe paralyzed side than on the normal side (matchedpairs z-test; t = 8.44, df = 9, p < 0.0l). The ratio ofthe TWV of the paralyzed VF to the TWV of the normal
at UCLA on August 18, 2015oto.sagepub.comDownloaded from

Volume 107 Number 4October 1992 Effect of asymmetric vocal fold stiffness on traveling wave velocily 523
Fig. 5. Videostroboscopic image of traveling wave at the upper dot later In the open phase.
400000
Cf)
::J --a-- Nonparalyzed RVe-::J 300000"'D • Paralyzed Lve0~_Cf)
2000000)C::J0>- 100000<J
O+--.,...--......----,r----,..---..,..-----r-----r----'to 2 3 4
Displacement (mm)Fig. 6. Plot of Young's elastic modulus in dvnes/crrr' vs. displacement In millimeters for paralyzedand nonparalyzed VF.
VF ranged was from 0.44 to 0.65, with a mean ratioof 0.55. (SD ± 0.078).
Simple linear regression was used to analyze the relationship between TWV on the normal and paralyzedVF. TWV on the paralyzed side increased significantly
as a function of TWV on the normal side(F[I,8] = 14.83, P < 0.05). Figure 7 represents themoderately high correlation between the two variables.The linear function fits the data well, despite the smallnumber of trials (r2 = 0.65).
at UCLA on August 18, 2015oto.sagepub.comDownloaded from
524 SLOAN et al.
-CJ
: 3-,E-CD
"(i;"0CD
~ 2'i..asa.J
>..'uo~ 1
CD>'"~OJC.-'i> 0~ 0I- 1
••• •
2 3
OlolaryngologyHead and Neck Surgery
Traveling Wave Velocity - Normal Side (m/sec)
Fig. 7. SCatterdiagram of relationship be1wen NI/Vof paralyzed VF and NI/V of nonparalyzed VFwith the linear regression line.
DISCUSSION
The results indicate that TWV can be reliably measured by synchronizing videostroboscopic images withevents in the glottal cycle, as measured by glottography.In addition, TWV of the paralyzed VF averaged approximately 55% of the TWV of the normal VF. Thissubstantial decrease in the TWV of the paralyzed vocalfold is thought to be related to the dramatic loss ofstiffness in the vocalis muscle-i.e., the "body" of theVF-in the acute RLN paralysis state. This result wasexpected, because the velocity of an object in a viscoelastic medium, such as the VF, is proportional tothe square root of the stiffness." Other researchers havegrossly observed a slower-appearing traveling wave onparalyzed vocal folds," but to our knowledge this relationship has never been quantified before.
Furthermore, Young's elastic modulus was measuredand compared between the paralyzed and normal VF.Other researchers5 ,22,32,33 have emphasized the importance of the elastic modulus in determining normal traveling wave motion. Our results confirm that a stiffness
asymmetry existed in the simulated acute RLN paralysisstate we studied. The question of whether a stiffnessmeasuring device can be clinically useful in humanbeings is currently under investigation in our laboratory.Certainly, VF modulus testing cannot be performed inan awake patient. However, the correlation between VFstiffness and the velocity of the traveling wave foundin the present study demonstrates the potential use ofTWV determination in the diagnosis and treatment ofvocal pathologies with asymmetric VF stiffness.
Isshiki et al. 24,25 emphasized the importance of thedegree of glottic closure in determination of vibratorycharacteristics of asymmetric laryngeal stiffness. Individual variations in the degree of glottic closure mayaccount for the wide variation in degrees of dysphoniain patients with acute RLN paralysis. While some patients have a near-normal voice, others have severebreathiness or diplophonia (phonation with two simultaneous frequencies). The findings in this study paralleled this observation. Two of the four dogs, despiteasymmetric VF stiffnesses, had quasiperiodic phona-
at UCLA on August 18, 2015oto.sagepub.comDownloaded from

Volume 107 Number 4October 1992 Effect of asymmetric vocal fold stiffness on traveling wave velocity 525
tion and, as a result, TWV could be compared betweenvocal folds. The phenomenon of entrainment-the simultaneous opening and closing of both vocal foldswas observed in these two dogs. Entrainment, althoughpoorly understood, is thought to occur through tissueproximity and airflow. When it occurs, only modestreductions in vocal efficiency and mild abnormalitiesin acoustic measures occur. In contrast, when asymmetric stiffness conditions are associated with decoupling of the vocal folds or a lack of entrainment as aresult of large glottal gaps, severe aberrations in vibration and acoustic signals can occur. Entrainment doesnot occur in this condition, and results in the perceptionof diplophonia (phonation with two simultaneous fundamental frequencies). 36-38 Because stroboscopy represents a composite or average over many vibratorycycles, the cycle-to-cycle variation of motion or aperiodicity associated with wide glottal gaps and the lackof entrainment prevent meaningful stroboscopic analysis. We assume this occurred in two of the dogs inthis study, because they were observed to have largeglottal gaps and aperiodic phonation.
The determination of TWV in the in vivo caninemodel required tattooing of the VF. This process createdeasily visible, distinct marks on the VF. The exactplacement of dots on the VF was crucial. For example,the level at which the dots were placed on each VF hadto be the same, because TWV could be different atdifferent locations on the vocal fold." It also becameapparent that the dots had to be made closer together.This was especially true on the paralyzed VF, becausethe amplitude of traveling wave appeared less and onlya small amount of the vertical dimension of the VF wasinvolved in the mucosal wave motion. Furthermore, theink needed to be placed deep to the mucosa. Any markplaced topically on the VF mucosa washed off or became distorted during phonation. Although this tattooing method is invasive, no VF bleeding occurred andwave motion appeared unchanged after the marks weremade. This method for determining TWV proved effective in the canine model, but is too traumatic forapplication to human beings.
Future studies should seek to quantify VF wave motion in other types of voice disorders. VF edema, scarring, and mass lesions all affect traveling wave motionand thus may have unique stroboscopic appearances.Quantification of these VF traveling wave abnormalitieshas not been clinically applicable previously. If TWVcould be reliably and noninvasively determined in human beings, it could serve as a reliable marker to targetintraoperative phonosurgical results and optimize the
treatment of these lesions. In addition, further researchis needed to determine the relationship of this asymmetric TWV, the glottal flow pulse, and the resultingacoustic signal.
CONCLUSION
This study describes a method to determine the velocity of the traveling wave in the in vivo canine model.Videostroboscopic images were synchronized withglottographic waveforms to determine the time requiredfor the traveling wave to move between two tattoosplaced a known distance apart on each VF. The TWVof a paralyzed VF was compared with the TWV of thecontralateral, electrically stimulated VF. The results indicated that when the glottal gap was relatively small,entrainment occurred and the TWV of the paralyzedVF averaged 55% of the TWV of the innervated, stifferVF. The quantification of traveling wave motion mayimprove our understanding of laryngeal function andour ability to effectively diagnose and treat patients withvocal pathologies.
REFERENCES
I. Moore OM, Berke GS, Hanson DG, Ward PH. Videostroboscopy of the canine larynx: the effects of asymmetric laryngealtension. Laryngoscope 1987;97:543-53.
2. Hirano M. Structure of the vocal fold in normal and diseasestates anatomical and physical studies. ASHA Rep 1981;II :1127.
3. Hirano M. Morphological structure of the vocal cord as a vibratorand its variations. Folia Phoniatr (Basel) 1976;26:89-94.
4. Sloan S, Berke GS, Gerratt BR, Ye M. Determination of vocalfold mucosal wave velocity in an in vivo canine model. Acceptedfor publication. Laryngoscope.
5. Titze IR. The physics of small amplitude oscillations of the vocalfolds. J Acous Soc Am 1988;80:1526-32.
6. Ishizaka K, Flanagan JL. Synthesis of voiced sounds from a twomass model of the vocal cords. Bell System Tech J 1972;51:123368.
7. Ishizaka K, Matsudaira M. Fluid mechanical considerations ofvocal cord distribution. SCRL Monograph No.8, Santa Barbara,Calif., 1972.
8. Stevens KN. Physics of laryngeal behavior and larynx nodes.Phonetica 1977;34:264-79.
9. Ishizaka K, Kaneko T. On equivalent mechanical constants ofthe vocal cords. J Acoust Soc Jpn 1968;24:312-3.
10. Kakita Y, Hirano M. Ohmaru K. Physical properties of the vocalfold tissue: Measurement on excised larynx. In: Stevens KN andHirano M, eds. Vocal fold physiology. Tokyo: University ofTokyo Press, 1981.
II. Stevens KS. Acoustic phonetics. Chapters 2 and 3. (In preparation), 1992.
12. Berke GS. Intraoperative measurement of the elastic modulus ofthe vocal fold: Part I. Device development. Laryngoscope1992;102:760-9.
at UCLA on August 18, 2015oto.sagepub.comDownloaded from

526 SLOAN et 01.
13. Berke GS, Smith ME. Intraoperative measurement of the elasticmodulus of the vocal fold: Part 2 Preliminary results. Laryngoscope 1992;102:770-8.
14. Bless DM, Hirano M, Feder RJ. Videostroboscopic evaluationof the larynx. Ear Nose Throat J 1987;66:48-58.
15. Kitzing P. Stroboscopy-a pertinent laryngological examination. J Otolaryngol 1985:14:151-7.
16. Koike Y, Imaizumi S. Objective evaluation of Iaryngostroboscopic findings. In: Fujimura 0, ed. Vocal physiology: voiceproduction, mechanisms and functions. New York: Raven Press,Ltd., 1988:433-41.
17. Bless DM, Brandenburg JH. Stroboscopic evaluation of "functional" voice disorders. Presented at the Middle Section of theTriological Society. Madison, Wisconsin: January 1983.
18. Von Leden H. The electric synchron-stroboscope: its value forthe practicing laryngologist. Ann Otol Rhinol Laryngol1961;70:881-93.
19. Schoenharl E. Die stroboskopie in der praktischen laryngologie.Stuttgart, Germany: Georg Thieme Verlag, 1960.
20. Isshiki N, Tanabe M, Ishizada K, Broad D. Clinical significanceof asymmetrical vocal cord tension. Ann Otol Rhinol Laryngol1977;86:58-66.
21. Sercarz JA, Berke GS, Ming Y, Gerratt BR, Natividad M. Videostroboscopy of human vocal fold paralysis. Ann Otol RhinolLaryngoI1992;101:567-77.
22. Baer T. Investigation of the phonatory mechanism. In: LudlowCI, O'Connell M, eds. Proceedings of the Conference on theAssessment of Vocal Pathology. Rockville, Md.: ASHA Reports1981;11:38-47.
23. Arnold GE. Vocal rehabilitation of paralytic dysphonia. VIII.Phoniatric methods of vocal compensation. Arch Otolaryngol1962;76:76-83.
24. Isshiki N, Okamura H, Ishikawa T. Thyroplasty type 1 (lateralcompression) for dysphonia due to vocal cord paralysis or atrophy. Acta Otolaryngol (Stockh) 1975;80:465-73.
25. Isshiki N, Tanabe M, Sawada M. Arytenoid adduction for unilateral vocal cord paralysis. Arch Otolaryngol 1978;104:555-8.
OtolaryngologyHead and Neck Surgery
26. Crumley RL, Izdebski K, McMicken B. Nerve transfer versusTeflon injection for vocal cord paralysis: a comparison. Laryngoscope 1988;98:1200-4.
27. Tucker H. Laryngeal reinnervation for unilateral vocal cord paralysis. Ann Otol Rhinol Laryngol 1981;90:457-9.
28. Trapp T, Berke GS, Bell T, Hanson DG, Ward PH. The effectof vocal fold augmentation on laryngeal vibration in simulatedrecurrent laryngeal nerve paralysis: a study of Teflon and phonagel. Ann Otol Rhinol Laryngol 1988;98(3):220-7.
29. Berke GS, Moore DM, Hanson DG, Gerratt BR, et al. Laryngealmodeling: theoretical, in vitro, in vivo. Laryngoscope1987;97:871-81.
30. Sercarz JA, Berke GS, Ming Y, Gerratt BR, Kreiman J, Natividad M. Synchronizing videostroboscopic images of human laryngeal vibration with physiological signals. Am J Otolaryngol1992;13:40-4.
31. Childers DG, Hicks DM, Moore GP, Eskenazi L, Lalwani AL.Electroglottography and vocal fold physiology. J Speech HearRes 1990;33:245-54.
32. Titze IR. Biomechanics and distributed mass models of vocalfold vibration. In: Stevens KN, Hirano M, eds. Vocal fold physiology. Tokyo: University of Tokyo Press, 1981:245-70.
33. Titze IR. On the relation between subglottal pressure and fundamental frequency in phonation. J Acous Soc Am 1989;85:901-6.
34. Vennard JK. Elementary fluid mechanics. 2nd ed. New York:John Wiley & Sons, Inc.:1947.
35. Achenbach JD. Wave propagation in elastic solids. l sr ed. Amsterdam: Elsevier Science Publishers, 1987.
36. Ward PH, Sanders JW, Goldman R, Moore GP. Diplophonia.Ann Otol Rhinol Laryngol 1969;78:771-7.
37. Gerratt BR, Precoda K, Hanson DG, Berke GS. Source characteristics of diplophonia. J Acoust Soc Am 1988;83(SI):S66.
38. Smith ME, Berke GS, Gerratt BG, Kreiman J. Laryngealparalyses: theoretical considerations and effects on laryngeal vibration. J Speech Hear Res 1992;35:545-54.
at UCLA on August 18, 2015oto.sagepub.comDownloaded from

310 News and Announcements
held July 26-30, 1993,at the Tamarron Resort in Durango,Colorado.
This 28 hour review and update will encompass all theclinically important areas of MR imaging. Important newconcepts and pathological/imaging correlations in thebody, musculoskeletal system, ENT, head and neck, brain,and spine will be explored. Daily case presentations willsupplement these lectures and will serve to test the registrants' diagnostic abilities in MR imaging.
This complete review of MR imaging will be presentedby nationally recognized leaders in magnetic resonanceimaging. As a result of this comprehensive review, registrants will become familiar with current applications ofMR imaging and will be able to integrate many of theseapplications directly into their practice.
Program chairmen for this presentation will be RobertQuencer, MD (University of Miami), Victor Haughton,MD (Medical College of Wisconsin). Twenty-eight creditsof Category I will be available.
For further information, please contact Marti Carter,CME, Inc., 11011 West Nort Ave., Milwaukee, Wisconsin53226, or call (414) 771-9520.
Ear, Nose, and Throat Diseases: 1993 Update
Children's Hospital of Pittsburgh will hold its 18thAnnual Symposium, "Ear, Nose, and Throat Diseases inChildren: A 1993 Update." This symposium will be heldJuly 30-31, 1993. CME credits will be awarded.
CORRECTION
Otolaryngology Head and Neck Surgery
March 1993
For further information, please contact the Department of Pediatric Otolaryngology, Children's Hospital ofPittsburgh, 3705 Fifth Avenue at DeSoto St., Pittsburgh,Pennsylvania 15213, or call (412) 692-8577.
Twenty-fifth Annual Meeting - Head andNeck Oncologists
The Association of Head and Neck Oncologists ofGreat Britain will sponsor the Twenty-fifth Annual Meeting of Head and Neck Oncology, to be held in Edinburgh,Scotland, United Kingdom, on August 23-26, 1993.
International and local faculty will present extensivesocial and family programs.
For further information, please contact Mr. P. J. Bradley, Honorary Secretary, Department of Otorhinolaryngology-Head and Neck Surgery, University Hospital,Queens Medical Centre, Nottingham, NG7 2UH, England, or phone 0602421421.
Sixth International Congress onInterventlonal Ultrasound
The Sixth International Congress on InterventionalUltrasound will be held in Copenhagen, Denmark, onSeptember 7-10, 1993.
For further information, please contact Christian Nolsoe, Congress Secretary, Department of Ultrasound, Herlev Hospital, University of Copenhagen, DK-2730 HerlevDenmark, or call +45/ 44 53 53 00 ext. 3240.
The Supplement to the December 1992 issue of the JOURNAL (Volume 107, Number 6,Part 2), incorrectly listed Dr. Bruce R. Gordon as Chief of Otolaryngology at the Massachusetts Eye and Ear Institute. Dr. Joseph Nadol is Chief of Otolaryngology at the Massachusetts Eye and Ear Infirmary. Dr. Gordon is Chief of Otolaryngology at Cape Cod Hospital.




















