Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics
11
Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics. Copyright © 2014. Constantine Kaniklidis. All rights reserved. 1 Research Perspective Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics Constantine Kaniklidis Director, Medical Research, No Surrender Breast Cancer Foundation (NSBCF) Member, European Association for Cancer Research (EACR) Editor, Evidence-based Medicine, Open Directory Project (ODP) Correspondence: Constantine Kaniklidis [email protected] ResearchGate: https://www.researchgate.net/profile/Constantine_Kaniklidis Date 6 November 2014 [publication pending] The author has no financial disclosures or potential conflicts of interest to declare. Abstract Ebola Virus Disease (EVD), formerly known as Ebola hemorrhagic fever (EHF), is caused by a genus of viruses called Ebolavirus first found in 1976 near the Ebola River in the Democratic Republic of Congo (then Zaire), and the current outbreak concentrated in West Africa is now the largest outbreak in history, exhibiting rapid human-to- human progression and high lethality requiring new and bolder international collaborative initiatives for management and treatment. Without any licensed therapy at this time, informed efforts must be directed towards a new understanding of its nature, transmission dynamics, and pathology, correcting much casual and misguided information in both the popular and even regulatory media. We therefore review the state-of-the-art in Ebola information, primarily towards the goal of founding and elucidating our review of new experimental treatments for prevention or therapeutics, including several using natural agents that have supporting data beyond the in vitro level. It will be only through an expansive view of both potential experimental and alternative treatment modalities that we may arrive at more effective interventions for achieving superior outcomes in the management of this Public Health Emergency of International concern (PHEIC). EBOLA VIRUS DISEASE (EVD), formerly known as Ebola hemorrhagic fever (renamed since some Ebola patients do not present hemorrhage), is caused by a genus of viruses called Ebolavirus, which was first found in 1976 near the Ebola River in the Democratic Republic of Congo (known at the time as Zaire) 1 , and is now the largest outbreak in history. Epidemiology/Ecology In March 2014, an outbreak of high case fatality viral febrile illness, Ebola Virus Disease (EVD), was identified in the Guéckédou region of the Republic of Guinea, more specifically within Guinea-Conakry (formerly French Guinea) in West Africa, with numbers increasing exponentially due to ongoing human-to-human transmission as the viral infection spread through Guinea– Conakry and into Liberia and Sierra Leone 34 , unfortunately bordering three countries on its south border (Sierra Leone, Liberia, and Côte d'Ivoire (Ivory Coast)). As of 31 October 2014, there were a total of 13,567 confirmed, probable, and suspected cases of Ebola virus disease (EVD) reported across eight affected countries (Guinea, Liberia, Mali, Sierra Leone, Spain, the United States of America (with to date isolated cases), Nigeria, Senegal), with 4951 reported deaths 3-8,32,33 , which is greater than in all previous Ebola outbreaks combined, and as a report from the Ebola Response Team of the World Health Organization 8 notes, the current EVD epidemic in
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics
Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics. Copyright © 2014. Constantine Kaniklidis. All rights reserved. 1
Research Perspective
Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics Constantine Kaniklidis
Director, Medical Research, No Surrender Breast Cancer Foundation (NSBCF) Member, European Association for Cancer Research (EACR) Editor, Evidence-based Medicine, Open Directory Project (ODP)
Correspondence: Constantine Kaniklidis [email protected] ResearchGate: https://www.researchgate.net/profile/Constantine_Kaniklidis Date 6 November 2014 [publication pending] The author has no financial disclosures or potential conflicts of interest to declare.
Abstract Ebola Virus Disease (EVD), formerly known as Ebola hemorrhagic fever (EHF), is caused by a genus of viruses called Ebolavirus first found in 1976 near the Ebola River in the Democratic Republic of Congo (then Zaire), and the current outbreak concentrated in West Africa is now the largest outbreak in history, exhibiting rapid human-to-human progression and high lethality requiring new and bolder international collaborative initiatives for management and treatment. Without any licensed therapy at this time, informed efforts must be directed towards a new understanding of its nature, transmission dynamics, and pathology, correcting much casual and misguided information in both the popular and even regulatory media. We therefore review the state-of-the-art in Ebola information, primarily towards the goal of founding and elucidating our review of new experimental treatments for prevention or therapeutics, including several using natural agents that have supporting data beyond the in vitro level. It will be only through an expansive view of both potential experimental and alternative treatment modalities that we may arrive at more effective interventions for achieving superior outcomes in the management of this Public Health Emergency of International concern (PHEIC).
EBOLA VIRUS DISEASE (EVD), formerly known as Ebola hemorrhagic fever (renamed since some Ebola patients do not present hemorrhage), is caused by a genus of viruses called Ebolavirus, which was first found in 1976 near the Ebola River in the Democratic Republic of Congo (known at the time as Zaire)1, and is now the largest outbreak in history. Epidemiology/Ecology In March 2014, an outbreak of high case fatality viral febrile illness, Ebola Virus Disease (EVD), was identified in the Guéckédou region of the Republic of Guinea, more specifically within Guinea-Conakry (formerly French Guinea) in West Africa, with numbers increasing
exponentially due to ongoing human-to-human transmission as the viral infection spread through Guinea–Conakry and into Liberia and Sierra Leone34, unfortunately bordering three countries on its south border (Sierra Leone, Liberia, and Côte d'Ivoire (Ivory Coast)). As of 31 October 2014, there were a total of 13,567 confirmed, probable, and suspected cases of Ebola virus disease (EVD) reported across eight affected countries (Guinea, Liberia, Mali, Sierra Leone, Spain, the United States of America (with to date isolated cases), Nigeria, Senegal), with 4951 reported deaths3-8,32,33, which is greater than in all previous Ebola outbreaks combined, and as a report from the Ebola Response Team of the World Health Organization8 notes, the current EVD epidemic in
Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics. Copyright © 2014. Constantine Kaniklidis. All rights reserved. 2
West Africa is both unprecedented in scale, and not principally due to the intrinsic biologic characteristics of the virus, but rather secondary to the state and characteristics of the affected populations, with control efforts insufficient to halt the spread of infection. In addition current statistical data collection methods understate the magnitude of the problem since these numbers are nonetheless themselves likely to be underestimates34,35. The case fatality rate among health care workers runs a spectrum from 56.1% in Guinea to 80.0% in Liberia34, largely confirmed by meta-analysis36 where it was concluded that the estimated case fatality rate was 65.4% but varied among the outbreaks, with a species effect identified, showing a higher case fatality rate for the Zaire species than for Sudan and Bundibugyo species. Thus, based on both exponential growth and high lethality, WHO declared on 8th August, 2014 the West Africa Ebola virus outbreak as a "Public Health Emergency of International Concern" (PHEIC), its highest level of alert. Ebola virus has five species - Zaire, Sudan, Tai Forest, Reston and Bundibugyo - and is a classical zoonotic disease, and data points to fruit bats (of the Pteropodidae family) as the most likely original reservoir for both Ebola and Marburg virus, with subsequent transmission through monkeys, gorillas, and chimpanzees, and ultimately, humans. Data finds that ZEBOV is the most severe species, with a case fatality rate approaching 90%, followed by Sudan EBOV (SEBOV) (53-66% mortality); Bundibugyo near 40%, with Tai Forest virus being described only in a single case now recovered from the disease2.
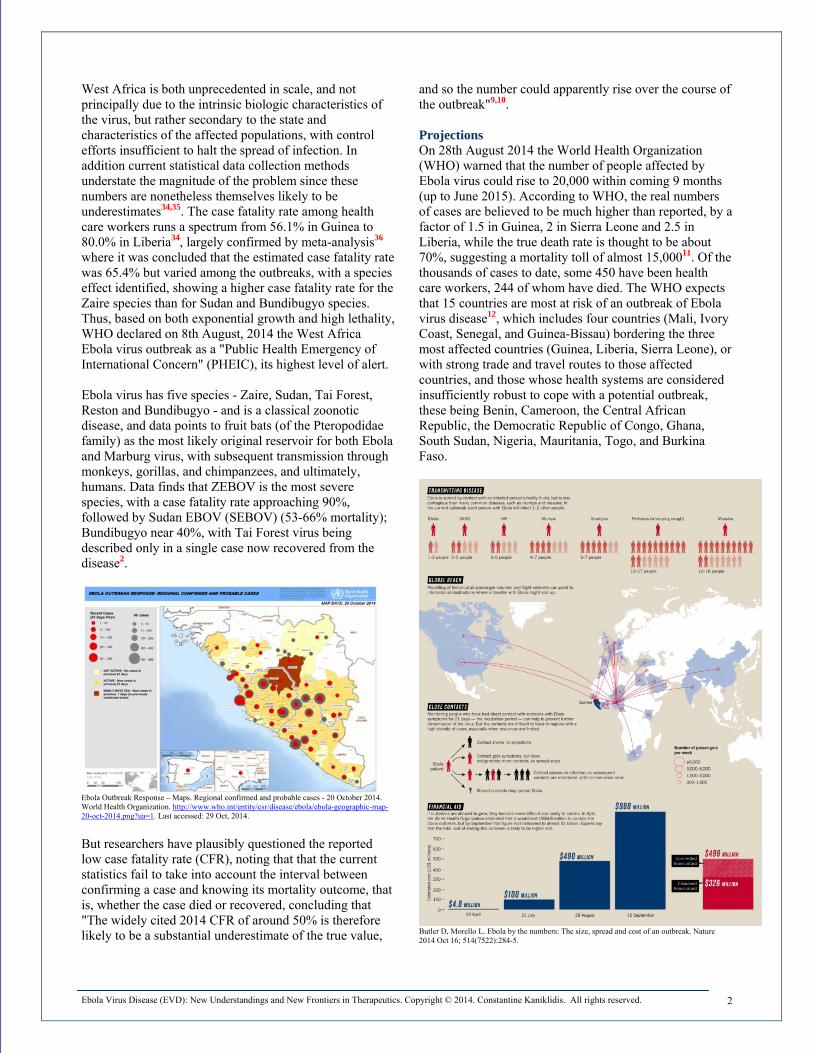
Ebola Outbreak Response – Maps. Regional confirmed and probable cases - 20 October 2014. World Health Organization. http://www.who.int/entity/csr/disease/ebola/ebola-geographic-map-20-oct-2014.png?ua=1. Last accessed: 29 Oct, 2014.
But researchers have plausibly questioned the reported low case fatality rate (CFR), noting that that the current statistics fail to take into account the interval between confirming a case and knowing its mortality outcome, that is, whether the case died or recovered, concluding that "The widely cited 2014 CFR of around 50% is therefore likely to be a substantial underestimate of the true value,
and so the number could apparently rise over the course of the outbreak"9,10. Projections On 28th August 2014 the World Health Organization (WHO) warned that the number of people affected by Ebola virus could rise to 20,000 within coming 9 months (up to June 2015). According to WHO, the real numbers of cases are believed to be much higher than reported, by a factor of 1.5 in Guinea, 2 in Sierra Leone and 2.5 in Liberia, while the true death rate is thought to be about 70%, suggesting a mortality toll of almost 15,00011. Of the thousands of cases to date, some 450 have been health care workers, 244 of whom have died. The WHO expects that 15 countries are most at risk of an outbreak of Ebola virus disease12, which includes four countries (Mali, Ivory Coast, Senegal, and Guinea-Bissau) bordering the three most affected countries (Guinea, Liberia, Sierra Leone), or with strong trade and travel routes to those affected countries, and those whose health systems are considered insufficiently robust to cope with a potential outbreak, these being Benin, Cameroon, the Central African Republic, the Democratic Republic of Congo, Ghana, South Sudan, Nigeria, Mauritania, Togo, and Burkina Faso.
Butler D, Morello L. Ebola by the numbers: The size, spread and cost of an outbreak. Nature 2014 Oct 16; 514(7522):284-5.
Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics. Copyright © 2014. Constantine Kaniklidis. All rights reserved. 3
t is clear therefore, that without more effective coordinated disease control37, prevention and treatment measures including:
An Ebola Action Checklist 1. Improvements in contact tracing 2. Stringent case isolation with more rigorous
implementation of safety protocols for both health care professionals (including as to more effective PPE (personal protective equipment) which too often appears despite rigorous compliance to have not disallowed transmission), and for innocent/secondary contacts
3. Heightened levels of and support for clinical management through improvements in dysfunctional and underresourced health systems
4. Safe burial practice that must include culturally sensitive disposal of infectious cadavers
5. Higher community engagement with informed and culturally respectful efforts to overcome distrust in local populations
6. Centralized event reporting with greater validation of disease and outcome statistics
7. A higher level of coordination across governments, public health agencies, research institutions, international partners, and other engaged international stakeholders, a coordination notably absent to date
8. More rapid and targeted development of a broader spectrum of treatment strategies, including: (1) conventional infectious disease control management, (2) experimental traditional interventions such as biological therapies and immunotherapies/vaccines, as well as (3) potential non-traditional CAM (complimentary and alternative medicine) modalities, for both prevention and treatment
9. The launching of methodologically robust controlled clinical trials for therapeutic interventions
10. Improved dissemination of safety, prevention and treatment information, both to the public and to health professionals, that has to date been of relatively low quality and reliability, with considerable unclarities and inconsistencies. [see commentary below]
the prognosis will remain grim, with the very high likelihood of further and wider epidemic level transmission and greater lethality, especially among and in poorly served and underserved populations and regions.
Commentary on Information Dissemination Two issues should be noted: (1) the recent highly successful Senegal experience using information outreach via harnessing a preexisting SMS/texting mobile platform65 mDiabetes suggest that mobile communication technology can play a vital and productive role in information dissemination, disease awareness and contact infinitives; (2) there is a disconcerting lack of inconsistency even in core definitions: thus, the fever threshold differs across countries being, for example either 38.0°C (100.4°F) or a history of fever for the UK, France and Australia, 38.3°C (100.94°F) for India, and 38.6°C (101.48°F) for Spain and USA, while some countries
(New Zealand) set no threshold and specify only sudden fever onset, as does also WHO. These divergent criteria could hamper and cloud reliable early detection. Given that 87% of patients with confirmed or probable Ebola have presented with sudden fever onset8, we advocate this criterion as more productive and relevant than that of fever in excess of a predetermined - and arbitrary - threshold, in agreement with researchers at the University of Lyon66.
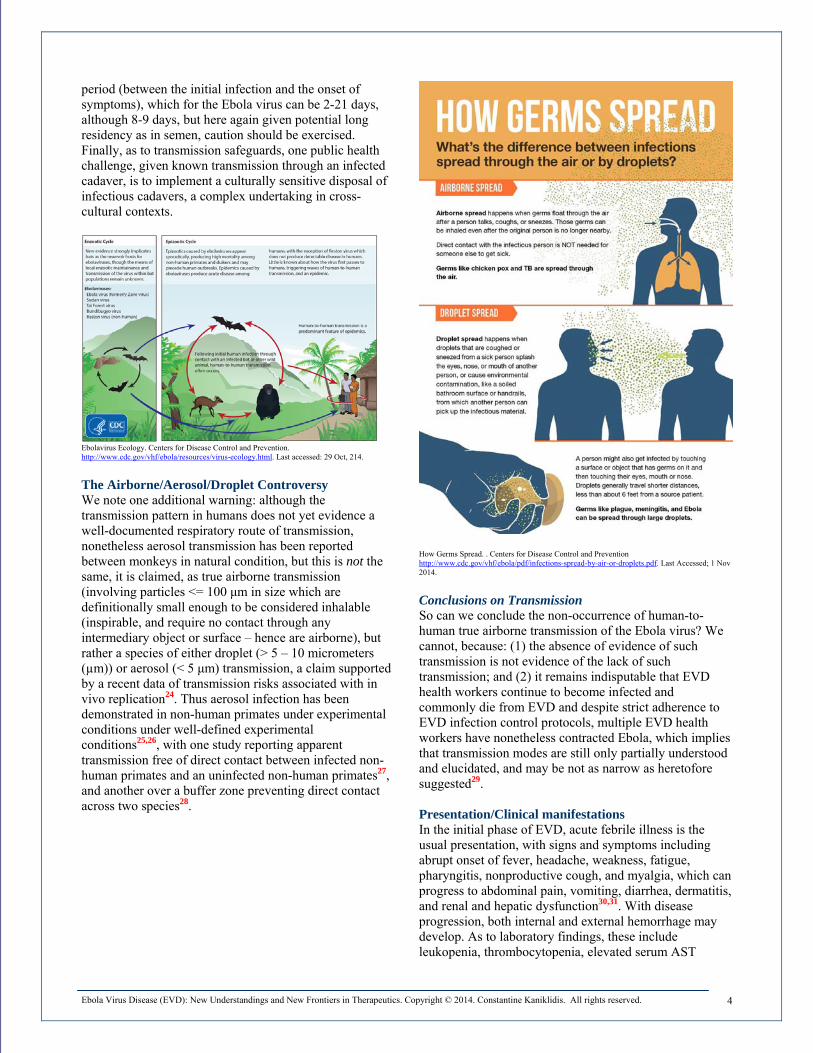
Pathology/Presentation Incubation ranges from 3 to 21 days13, with the Zaire species having an incubation period of 12.7 ± 4.3 days14. EVD appears to exhibit a typical duration of 5 to 15 days15. Symptom onset is sudden and resembles those of influenza syndrome, with fever, headache, abdominal pain, arthralgia and myalgia, with approximately half of patients complaining of cough, sore throat, and dysphagia. These are variably followed by the digestive adverse events of diarrhea, nausea, and vomiting. Hemorrhage, apparently associated with the severity of infection, may occur in 30-80% of patients clustered towards end of illness, presenting with symptoms of purpura, epistaxis, gingival bleeding, gastrointestinal or other bleeding16. It has been demonstrated that immune response inhibition, including reduction in interferon production, favors the rapid spread of the virus in the body17. Transmission Human to human transmission is responsible for spreading the outbreak, mainly through direct contact with patient's or a patient's cadaver's blood, or various body, including urine and bowel excretions/ bloody stool, semen or genital secretion, sweat, vomitus and indirect or secondary contact with any environment contaminated with infected body fluids, the virus gaining entry into the body through mucosa, skin abrasion or directly through blood16,18. The Ebola virus persists in breast milk and genital secretions and semen, in the later for up to 7 weeks after recovery from the illness suggesting the possibility of sexual mode of transmission19 during convalescence and even up to 13 weeks after recovery, as also reported in other supporting data on the sexual transmission as a route of Ebola infection20,21, confirmed also for the transmission of Crimean-Congo Hemorrhagic Fever Infection (CCHFI) via transmission through sexual intercourse with a convalescing patient22. Finally, the risk of transmission from fomites (inanimate objects that can carry a transmittable infectious agent, including towels, clothes, bedding/sheets, skin cells, hair) especially during convalescence appears to be low and protectable through basic measures23, although we warn that given the number of infections that have occurred for which we lack a verifiable “chain of causation”, this suggests caution in interpreting the potential for transmission from fomites which may be significant but not yet wholly documented. Furthermore, it is thought that the Ebola virus is not human-to-human transmittable during the incubation
Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics. Copyright © 2014. Constantine Kaniklidis. All rights reserved. 4
period (between the initial infection and the onset of symptoms), which for the Ebola virus can be 2-21 days, although 8-9 days, but here again given potential long residency as in semen, caution should be exercised. Finally, as to transmission safeguards, one public health challenge, given known transmission through an infected cadaver, is to implement a culturally sensitive disposal of infectious cadavers, a complex undertaking in cross-cultural contexts.
Ebolavirus Ecology. Centers for Disease Control and Prevention. http://www.cdc.gov/vhf/ebola/resources/virus-ecology.html. Last accessed: 29 Oct, 214.
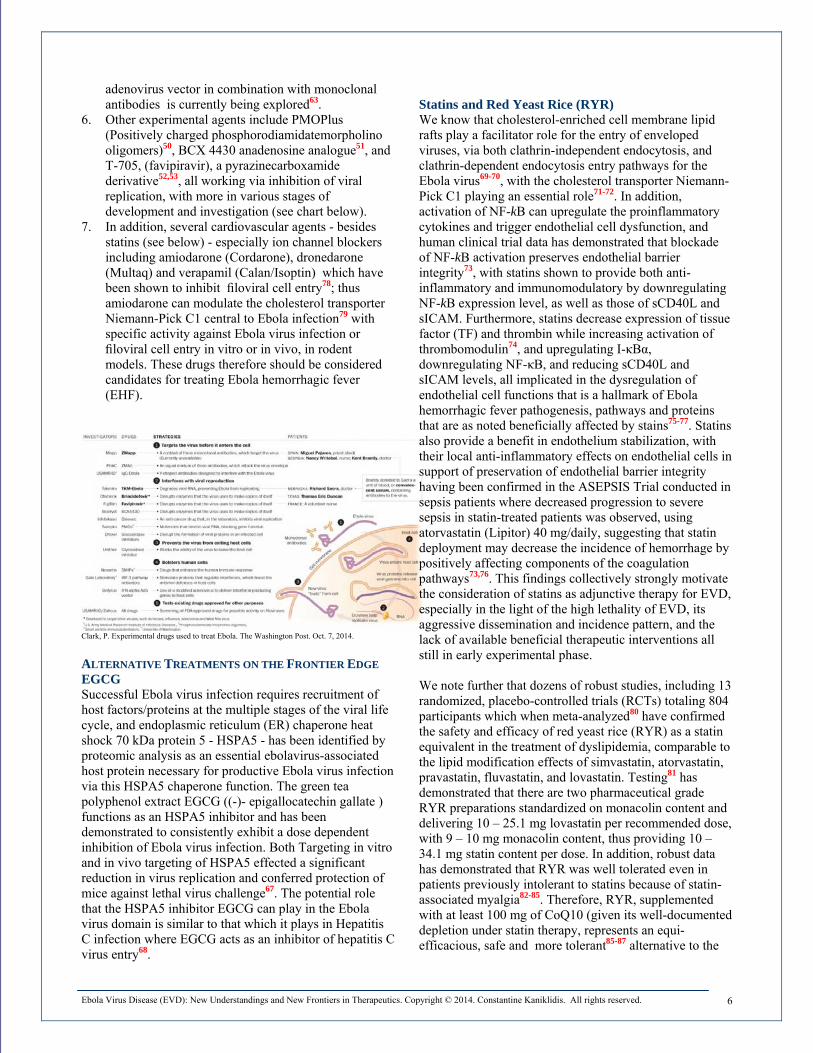
The Airborne/Aerosol/Droplet Controversy We note one additional warning: although the transmission pattern in humans does not yet evidence a well-documented respiratory route of transmission, nonetheless aerosol transmission has been reported between monkeys in natural condition, but this is not the same, it is claimed, as true airborne transmission (involving particles <= 100 μm in size which are definitionally small enough to be considered inhalable (inspirable, and require no contact through any intermediary object or surface – hence are airborne), but rather a species of either droplet (> 5 – 10 micrometers (µm)) or aerosol (< 5 μm) transmission, a claim supported by a recent data of transmission risks associated with in vivo replication24. Thus aerosol infection has been demonstrated in non-human primates under experimental conditions under well-defined experimental conditions25,26, with one study reporting apparent transmission free of direct contact between infected non-human primates and an uninfected non-human primates27, and another over a buffer zone preventing direct contact across two species28.
How Germs Spread. . Centers for Disease Control and Prevention http://www.cdc.gov/vhf/ebola/pdf/infections-spread-by-air-or-droplets.pdf. Last Accessed; 1 Nov 2014. Conclusions on Transmission So can we conclude the non-occurrence of human-to-human true airborne transmission of the Ebola virus? We cannot, because: (1) the absence of evidence of such transmission is not evidence of the lack of such transmission; and (2) it remains indisputable that EVD health workers continue to become infected and commonly die from EVD and despite strict adherence to EVD infection control protocols, multiple EVD health workers have nonetheless contracted Ebola, which implies that transmission modes are still only partially understood and elucidated, and may be not as narrow as heretofore suggested29. Presentation/Clinical manifestations In the initial phase of EVD, acute febrile illness is the usual presentation, with signs and symptoms including abrupt onset of fever, headache, weakness, fatigue, pharyngitis, nonproductive cough, and myalgia, which can progress to abdominal pain, vomiting, diarrhea, dermatitis, and renal and hepatic dysfunction30,31. With disease progression, both internal and external hemorrhage may develop. As to laboratory findings, these include leukopenia, thrombocytopenia, elevated serum AST

Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics. Copyright © 2014. Constantine Kaniklidis. All rights reserved. 5
(aspartate aminotransferase) and ALT (alanine aminotransferase), and proteinuria.
When Caring for Suspect or Confirmed Patients with Ebola. . Centers for Disease Control and Prevention. http://www.cdc.gov/vhf/ebola/hcp/caring-for-ebola-suspects.html. Last accessed: 29 Oct, 2014.
TREATMENT AND MANAGEMENT Given the absence of any licensed prophylaxis or treatment, then other than experimental therapies and vaccines, conventional care for patients with EVD is largely empiric and supportive: remedying any intravascular volume depletion, blood pressure maintenance, fluids and electrolyte balancing to avoid hyponatremia, hypokalemia, and hypocalcemia, maintenance of oxygen levels, use of anticoagulant therapy, blood transfusion if necessary, the avoidance of the complications of shock, maintenance of good nutrition, and comfort care, while waiting for the immune system to mobilize an immune response), addressing the known and presenting symptoms and their management in a EVD-specialized facility with proper containment and barrier isolation procedures and following the latest protocols for protection of health professionals and staff caring for or coming into contact with EVD patients and the patient environment, and with careful hemodynamic monitoring, and empiric antimicrobial therapy if vomiting, diarrhea, and/or other signs of severe gastrointestinal dysfunction and/or signs of sepsis warrant38,39,40.
Given the urgency of the EVD situation globally and the unavailability of any licensed prophylaxis or treatment, the World Health Organization (WHO) at an expert panel convened on August 11, 201443 examined the ethical considerations44 of experimental deployment and “concluded unanimously that it would be acceptable on both ethical and evidential grounds to use as potential treatments or for prevention unregistered interventions that have shown promising results in the laboratory and in animal models but have not yet been evaluated for safety and efficacy in humans, provided that certain conditions are met”43. EXPERIMENTAL THERAPIES Experimental therapies41,42;45-64 include: 1. Vaccine therapies, the two major EVD vaccine
candidates42,64 being cAd3-EBOV (cAd3), from GlaxoSmithKline (GSK) NIAID (the U.S. National Institute of Allergy and Infectious Diseases), and rVSVΔG-EBOV-GP (rVSV), from NewLink Genetics and the Public Health Agency of Canada (PHAC), with studies in nonhuman primates indicating 100% efficacy for both these vaccine candidates. One live virus vaccine, VSV-Ebola, derived via recombinant vesicular stomatitis virus (VSV) encoding the Ebola or Marburg surface glycoproteins is showing promise in humans and non-human primates at about a 50% death prevention rate56-60.
2. Biological therapies (including monoclonal antibodies), most notably Zmapp (Mapp Biopharmaceutical), a cocktail of three humanized" monoclonal antibodies (MB-003) derived from tobacco plant Nicotiana, which targets different epitopes (portions of a molecule to which an antibody binds of the Ebola virus glycoprotein, with an apparent 67% survival rate in humans (2 of 3 patients) but, we caution, this may have been secondary to the high quality of care received rather than to Zmapp itself, and a time-of-administration-dependent 43 – 100% survival rate in non-human primates (67 – 100% when within 48 hours post-infection after onset of viremia and fever)45-47.
3. RNA-based therapies like siRNAs (small interfering RNA molecules), notably Tekmira's TKM-Ebola48,49, a siRNA targets the L gene of Ebola's RNA polymerase, approved by FDA for use in infected patients, and when three siRNAs encapsulated in stable nucleic acid lipid particles (SNALPs) are combined, there is apparent 100% protection against Ebola virus if given 30 minutes post-infection.
4. Antibody therapy derived from the whole blood or serum of convalescent EVD survivors54,55.
5. Although some preclinical data on interferon-alpha appeared promising, in nonhuman primates the licensed product human interferon-alpha-2b, had only a marginal effect on delay of the disease onset and death61,62; however interferon delivery via an
Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics. Copyright © 2014. Constantine Kaniklidis. All rights reserved. 6
adenovirus vector in combination with monoclonal antibodies is currently being explored63.
6. Other experimental agents include PMOPlus (Positively charged phosphorodiamidatemorpholino oligomers)50, BCX 4430 anadenosine analogue51, and T-705, (favipiravir), a pyrazinecarboxamide derivative52,53, all working via inhibition of viral replication, with more in various stages of development and investigation (see chart below).
7. In addition, several cardiovascular agents - besides statins (see below) - especially ion channel blockers including amiodarone (Cordarone), dronedarone (Multaq) and verapamil (Calan/Isoptin) which have been shown to inhibit filoviral cell entry78; thus amiodarone can modulate the cholesterol transporter Niemann-Pick C1 central to Ebola infection79 with specific activity against Ebola virus infection or filoviral cell entry in vitro or in vivo, in rodent models. These drugs therefore should be considered candidates for treating Ebola hemorrhagic fever (EHF).
Clark, P. Experimental drugs used to treat Ebola. The Washington Post. Oct. 7, 2014. ALTERNATIVE TREATMENTS ON THE FRONTIER EDGE EGCG Successful Ebola virus infection requires recruitment of host factors/proteins at the multiple stages of the viral life cycle, and endoplasmic reticulum (ER) chaperone heat shock 70 kDa protein 5 - HSPA5 - has been identified by proteomic analysis as an essential ebolavirus-associated host protein necessary for productive Ebola virus infection via this HSPA5 chaperone function. The green tea polyphenol extract EGCG ((-)- epigallocatechin gallate ) functions as an HSPA5 inhibitor and has been demonstrated to consistently exhibit a dose dependent inhibition of Ebola virus infection. Both Targeting in vitro and in vivo targeting of HSPA5 effected a significant reduction in virus replication and conferred protection of mice against lethal virus challenge67. The potential role that the HSPA5 inhibitor EGCG can play in the Ebola virus domain is similar to that which it plays in Hepatitis C infection where EGCG acts as an inhibitor of hepatitis C virus entry68.
Statins and Red Yeast Rice (RYR) We know that cholesterol-enriched cell membrane lipid rafts play a facilitator role for the entry of enveloped viruses, via both clathrin-independent endocytosis, and clathrin-dependent endocytosis entry pathways for the Ebola virus69-70, with the cholesterol transporter Niemann-Pick C1 playing an essential role71-72. In addition, activation of NF-kB can upregulate the proinflammatory cytokines and trigger endothelial cell dysfunction, and human clinical trial data has demonstrated that blockade of NF-kB activation preserves endothelial barrier integrity73, with statins shown to provide both anti-inflammatory and immunomodulatory by downregulating NF-kB expression level, as well as those of sCD40L and sICAM. Furthermore, statins decrease expression of tissue factor (TF) and thrombin while increasing activation of thrombomodulin74, and upregulating I-κBα, downregulating NF-κB, and reducing sCD40L and sICAM levels, all implicated in the dysregulation of endothelial cell functions that is a hallmark of Ebola hemorrhagic fever pathogenesis, pathways and proteins that are as noted beneficially affected by stains75-77. Statins also provide a benefit in endothelium stabilization, with their local anti-inflammatory effects on endothelial cells in support of preservation of endothelial barrier integrity having been confirmed in the ASEPSIS Trial conducted in sepsis patients where decreased progression to severe sepsis in statin-treated patients was observed, using atorvastatin (Lipitor) 40 mg/daily, suggesting that statin deployment may decrease the incidence of hemorrhage by positively affecting components of the coagulation pathways73,76. This findings collectively strongly motivate the consideration of statins as adjunctive therapy for EVD, especially in the light of the high lethality of EVD, its aggressive dissemination and incidence pattern, and the lack of available beneficial therapeutic interventions all still in early experimental phase. We note further that dozens of robust studies, including 13 randomized, placebo-controlled trials (RCTs) totaling 804 participants which when meta-analyzed80 have confirmed the safety and efficacy of red yeast rice (RYR) as a statin equivalent in the treatment of dyslipidemia, comparable to the lipid modification effects of simvastatin, atorvastatin, pravastatin, fluvastatin, and lovastatin. Testing81 has demonstrated that there are two pharmaceutical grade RYR preparations standardized on monacolin content and delivering 10 – 25.1 mg lovastatin per recommended dose, with 9 – 10 mg monacolin content, thus providing 10 – 34.1 mg statin content per dose. In addition, robust data has demonstrated that RYR was well tolerated even in patients previously intolerant to statins because of statin-associated myalgia82-85. Therefore, RYR, supplemented with at least 100 mg of CoQ10 (given its well-documented depletion under statin therapy, represents an equi-efficacious, safe and more tolerant85-87 alternative to the
Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics. Copyright © 2014. Constantine Kaniklidis. All rights reserved. 7
experimental use of statins in the potential treatment of Ebola virus disease. Rutin/Vitamin P and Vitamin C It is known that cell adhesion molecules (CAMs), including selectin, intercellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1), play critical roles in cell adhesion to the vascular endothelium cell extravasation and vascular inflammation. Rutin, or vitamin P, is a major flavonoid which appears of benefit in Crimean-Congo Hemorrhagic Fever Infection (CCHF) and epidemic hemorrhagic fever to protect vascular barrier integrity, via its ability to inhibit the expression of cell adhesion molecules (CAMs), thus inhibiting the adhesion and migration of leukocytes and modulating vascular barrier integrity88,89. Vitamin C, or ascorbic acid, can also be used in CCHF and epidemic hemorrhagic fever89, potentially preventing endothelial dysfunction via stimulation of endothelial proliferation, modulating blood flow by sparing endothelial cell-derived nitric oxide and increasing the level of type IV collagen in the basement membrane90. Melatonin The hallmarks of EVD-induced infection and mortality are: (1) disruption or destruction of the vascular endothelium (cells lining the entire circulatory system and regulating vascular wall function); (2) disseminated intravascular coagulation (DIC), a condition of systemic intravascular activation of blood coagulation resulting in the generation and deposition of fibrin, leading to microvascular thrombi in various organs and contributing, finally to multiple organ dysfunction syndrome (MODS), with the consumption and subsequent depletion or exhaustion of coagulation proteins/factors and platelets secondary to the ongoing activation of coagulation ultimately inducing severe bleeding, (3) fibrinolysis (the process by which fibrin is removed (fibrin dissolution, by means of plasmin, a proteolytic enzyme) from damaged blood vessels, thus breakdown clots), and followed by (4) multi-organ hemorrhage / multiple organ dysfunction syndrome (MODS), a systemic, dysfunctional inflammatory response characterized by incremental degrees of physiologic derangements in individual organs. In this process a cascade of reactions of immune- and inflammatory responses involving monocytes, macrophages, and dendritic cells play the central role in endothelial injury, triggering an excessive immuno-inflammatory cascade of reactions producing certain immune system cell proteins known as cytokines, including chemotactic cytokines called chemokines (a family of chemoattractant molecules, attracting leukocytes to areas of inflammation), these cytokines regulating
responses to infection or injury such as inflammation, the most notable EVD-induced cytokines being TNF- α (tumor necrosis factor alpha), IFN- α (Interferon alfa), IL6 (interleukin 6), IL8 (interleukin 8), TF (tissue factors), and MCP-1 (monocyte chemoattractant protein-1). Melatonin directly targets all these major components of cascade of immuno-inflammatory responsive events associated with and triggered by the Ebola virus infection91, suppressing the levels of key cytokines TNF- α, IFN- α, IL6, IL8, TF, MCP-1, as well as VEGF, JNK phosphorylation, and tight junctional protein degradation while reducing endothelial apoptosis92-94, and - as with statins - can also decrease expression of tissue factor (TF)95, collectively providing the kind of protection against endothelial cell injury and preservation of vascular structure and function to assist in avoiding late stage EVD hemorrhage. In addition, melatonin may assist against the dysregulation of blood coagulation and fibrinolysis associated with disseminated intravascular coagulation (DIC), providing dual-mode anti-coagulant activity in both the reduction of TF, platelet activation and coagulation factor VIII levels and the stimulation of vascular endothelial cells to secrete tissue factor pathway inhibitor (TPPI)95, activity confirmed in preclinical in vivo96 as well as human clinical, including RCT, data97,98. This is consonant with a vast body of data demonstrating melatonin's benefits in the treatment and management of a wide spectrum of viral infections, via positive regulation of immune function, and of programmed cell death (PCD) in viral disease, its activity as an inflammation inhibitor, a free radical scavenger, and a potent antioxidant enzyme inducer99. Methodology for this Review A search of the PUBMED, Cochrane Library / Cochrane Register of Controlled Trials, MEDLINE, EMBASE, AMED (Allied and Complimentary Medicine Database), CINAHL (Cumulative Index to Nursing and Allied Health Literature), PsycINFO, ISI Web of Science (WoS), BIOSIS, LILACS (Latin American and Caribbean Health Sciences Literature), ASSIA (Applied Social Sciences Index and Abstracts), and SCEH (NHS Evidence Specialist Collection for Ethnicity and Health) was conducted without language or date restrictions, and updated again current as of date of publication, with systematic reviews and meta-analyses extracted separately. Search was expanded in parallel to include just-in-time (JIT) medical feed sources as returned from Terkko (provided by the National Library of Health Sciences - Terkko at the University of Helsinki). Unpublished studies were located via contextual search, and relevant dissertations were located via NTLTD (Networked Digital Library of Theses and Dissertations) and OpenThesis. Sources in languages foreign to this reviewer were translated by language translation software.
Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics. Copyright © 2014. Constantine Kaniklidis. All rights reserved. 8
References 1. Breman JG, Johnson KM. Ebola Then and Now. N Engl J Med 2014 Sep 10. 2. Mishra B. The threat of Ebola: An update. Indian J Med Microbiol 2014 Oct-Dec; 32(4):364-70. 3. Ebola Response Roadmap Situation Report Update. 25 October 2014.
http://apps.who.int/iris/bitstream/10665/137185/1/roadmapupdate25Oct14_eng.pdf?ua=1. Last accessed: 29 Oct 2014.
4. Rapid Risk Assessment: Outbreak of Ebola virus disease in West Africa - Seventh update, 17 October 2014. European Centre for Disease Prevention and Control (ECDC). http://www.ecdc.europa.eu/en/publications/_layouts/forms/Publication_DispForm.aspx?List=4f55ad51-4aed-4d32-b960-af70113dbb90&ID=1187. Last accessed: 29 Oct 2014.
5. Epidemiological update: outbreak of Ebola virus disease in West Africa. European Centre for Disease Prevention and Control (ECDC). http://www.ecdc.europa.eu/en/press/news/_layouts/forms/News_DispForm.aspx?List=8db7286c-fe2d-476c-9133-18ff4cb1b568&ID=1097. Last accessed: 29 Oct 2014.
6. 2014 Ebola Outbreaks - Timeline October 29. http://healthmap.org/ebola/#timeline. Last accessed: 29 Oct 2014. 7. Update: Ebola Virus Disease Outbreak — West Africa, October 2014. Morbidity and Mortality Weekly Report
(MMWR). Centers for Disease Control and Prevention. Early Release. October 28, 2014 / 63(Early Release);1-4. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm63e1028a1.htm?s_cid=mm63e1028a1_w. Last accessed: 29 Oct 2014.
8. WHO Ebola Response Team. Ebola virus disease in West Africa--the first 9 months of the epidemic and forward projections. N Engl J Med 2014 Oct 16; 371(16):1481-95.
9. Kucharski AJ, Edmunds WJ. Case fatality rate for Ebola virus disease in west Africa. Lancet 2014 Oct 4; 384(9950):1260.
10. Gomes MFC, Pastore y Piontti A, Rossi L, Chao D, Longini I, Halloran ME, Vespignani A. Assessing the International Spreading Risk Associated with the 2014 West African Ebola Outbreak. PLOS Currents Outbreaks. 2014 Sep 2.
11. Butler D, Morello L. Ebola by the numbers: The size, spread and cost of an outbreak. Nature 2014 Oct 16; 514(7522):284-5.
12. Gulland A. Fifteen countries are at risk of Ebola outbreak, says WHO. BMJ 2014; 349:g6305. 13. Okware SI, Omaswa FG, Zaramba S, et al. An outbreak of Ebola in Uganda. Trop Med Int Health 2002,
7(12):1068-1075. 14. Eichner M, Dowell SF, Firese N. Incubation period of Ebola hemorrhagic virus subtype Zaire. Osong Public Health
Res Perspect 2011, 2(1):3-7. 15. Baron RC, McCormick JB, Zubeir OA. Ebola virus disease in southern Sudan: hospital dissemination and
intrafamilial spread. Bull World Health Organ 1983, 61(6):997-1003. 16. Chippaux JP. Outbreaks of Ebola virus disease in Africa: the beginnings of a tragic saga. J Venom Anim Toxins
Incl Trop Dis 2014; 20(1):44. 17. Kühl A, Pöhlmann S. How Ebola virus counters the interferon system. Zoonoses Public Health 2012, 59(Suppl
2):116-131. 18. Review of Human-to-Human Transmission of Ebola Virus. Centers for Disease Control and Prevention.
http://www.cdc.gov/vhf/ebola/transmission/human-transmission.html. Page last updated: October 29, 2014. Last accessed: 29 Oct 2014.
19. Ebola virus disease. Available from: http://www.who.int/mediacentre/factsheets/fs103/en. Last accessed: 29 Oct 2014.
20. Rodriguez LL, De Roo A, Guimard Y, et al. Persistence and genetic stability of Ebola virus during the outbreak in Kikwit, Democratic Republic of the Congo, 1995. J. Infect. Dis 1999; 179 (Suppl 1), S170–176.
21. Rowe AK, Bertolli J, Khan AS., et al. Clinical, virologic, and immunologic follow-up of convalescent Ebola hemorrhagic fever patients and their household contacts, Kikwit, Democratic Republic of the Congo. Commission de Lutte contre les Epidemies a Kikwit. J. Infect. Dis 1999; 179 (Suppl 1), S28–35.
22. Ergonul O, Battal I. Potential sexual transmission of Crimean-Congo hemorrhagic fever infection. Jpn J Infect Dis 2014; 67(2):137-8.
23. Bausch DG, Towner JS, Dowell SF, et al. Assessment of the risk of Ebola virus transmission from bodily fluids and fomites. J Infect Dis 2007; 196(Suppl 2):S142-S147.
24. Alimonti J, Leung A, Jones S, et al. Evaluation of transmission risks associated with in vivo replication of several high containment pathogens in a biosafety level 4 laboratory. Sci Rep 2014; 4: 5824.
Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics. Copyright © 2014. Constantine Kaniklidis. All rights reserved. 9
25. Geisbert TW, Daddario-Dicaprio KM, Geisbert JB, et al. Feldmann H. Vesicular stomatitis virus-based vaccines protect nonhuman primates against aerosol challenge with Ebola and Marburg viruses. Vaccine 2008 Dec 9; 26(52):6894-900.
26. Johnson E, Jaax N, White J, Jahrling P. Lethal experimental infections of rhesus monkeys by aerosolized Ebola virus. Int J Exp Pathol 1995; 76(4):227-36.
27. Jaax NK, Davis KJ, Geisbert TJ, et al. Lethal experimental infection of rhesus monkeys with Ebola-Zaire (Mayinga) virus by the oral and conjunctival route of exposure. Arch Pathol Lab Med 1996; 120(2):140-55.
28. Weingartl HM, Embury-Hyatt C, Nfon C, Leung A, Smith G, Kobinger G. Transmission of Ebola virus from pigs to non-human primates. Sci Rep 2012; 2:811.
29. Cohen J. Infectious diseases. When Ebola protection fails. Science 2014 Oct 3; 346(6205):17-8. 30. Feldmann H, Geisbert TW. Ebola haemorrhagic fever. Lancet. 2011; 377:(9768):849–862. 31. Turner C. Ebola virus disease: An emerging threat. Nursing 2014; 44(9):68-9. 32. 2014 Ebola Outbreak in West Africa - Case Counts. Centers for Disease Control and Prevention. Update: 31 Oct
2014. http://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/case-counts.html. Last accessed: 1 Nov 2014. 33. Zhang L, Wang H. Forty years of the war against Ebola. J Zhejiang Univ Sci B 2014 Sept.; 15(9):761-765. 34. Baden LR, Kanapathipillai R, Campion EW, Morrissey S, Rubin EJ, Drazen JM. Ebola--an ongoing crisis. N Engl J
Med 2014 Oct 9; 371(15):1458-9. 35. Kupferschmidt K. Infectious Disease. Estimating the Ebola epidemic. Science 2014 Sep 5; 345(6201):1108. 36. Lefebvre A, Fiet C, Belpois-Duchamp C, Tiv M, Astruc K, Aho Glélé LS. Case fatality rates of Ebola virus
diseases: A meta-analysis of World Health Organization data. Med Mal Infect 2014; 44(9):412-6. 37. Farrar JJ, Piot P. The Ebola emergency--immediate action, ongoing strategy. N Engl J Med 2014 Oct 16;
371(16):1545-6. 38. Fowler RA, Fletcher T, Fischer WA 2nd, et al. Caring for critically ill patients with ebola virus disease.
Perspectives from west Africa. Am J Respir Crit Care Med 2014; 190:733. 39. Lamontagne F, Clément C, Fletcher T, et al. Doing Today's Work Superbly Well - Treating Ebola with Current
Tools. N Engl J Med 2014; 371:1565. 40. Checklist for patients being evaluated for Ebola virus disease (EVD) in the United States. Centers for Disease
Control and Prevention. http://www.cdc.gov/vhf/ebola/pdf/checklist-patients-evaluated-us-evd.pdf. Last accessed: 1 Nov 2014.
41. Joffe S. Evaluating novel therapies during the Ebola epidemic. JAMA 2014 Oct 1; 312(13):1299-300. 42. Kanapathipillai R, Restrepo AM, Fast P, et al. Ebola Vaccine - An Urgent International Priority. N Engl J Med
2014 Oct 7. 43. Krech R, Kieny M-P. Advisory Panel to the World Health Organization. Ethical considerations for use of
unregistered interventions for Ebola viral disease. Bulletin of the World Health Organization 2014;92:622. http://www.who.int/bulletin/volumes/92/9/14-145789/en/. Last accessed: 1 Nov 2014.
44. Yakubu A, Folayan MO, Sani-Gwarzo N, Nguku P, Peterson K, Brown B. The Ebola outbreak in Western Africa: ethical obligations for care. J Med Ethics 2014 Sep 9.
45. Goodman JL. Studying "Secret Serums"-Toward Safe, Effective Ebola Treatments. N Engl J Med 2014. 46. Z Mapp Information Sheet. www.mappbio.com/zmapinfo.pdf. Last accessed on 7 Sept 2014. 47. Qiu X, Wong G, Audet J, et al. Reversion of advanced Ebola virus disease in nonhuman primates with ZMapp.
Nature 2014; 514:47. 48. Geisbert TW, Lee AC, Robbins M, Geisbert JB, Honko AN, Sood V, et al. Postexposure protection of non-human
primates against a lethal Ebola virus challenge with RNA interference: A proof-of-concept study. Lancet 2010;375:1896-905.
49. Mullard A. Experimental Ebola drugs enter the limelight. Lancet 2014;384:649. 50. Warren TK, Warfield KL, Wells J, Swenson DL, Donner KS, Van Tongeren SA, et al. Advanced antisense
therapies for postexposure protection against lethal filovirus infections. Nat Med 2010;16:991-4. 51. Falzarano D, Feldmann H. Possible leap ahead in filovirus therapeutics. Cell Res 2014;24:647-8. 52. Oestereich L, Lüdtke A, Wurr S, Rieger T, Muñoz-Fontela C, Günther S. Successful treatment of advanced Ebola
virus infection with T-705 (favipiravir) in a small animal model. Antiviral Res. 2014 May;105:17-21. Epub 2014 Feb 26.
53. Smither SJ, Eastaugh LS, Steward JA, Nelson M, Lenk RP, Lever MS. Post-exposure efficacy of oral T-705 (Favipiravir) against inhalational Ebola virus infection in a mouse model. Antiviral Res. 2014 Apr;104:153-5. Epub 2014 Jan 24.
54. Burnouf T, Seghatchian J. Ebola virus convalescent blood products: Where we are now and where we may need to go. Transfus Apher Sci 2014.
Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics. Copyright © 2014. Constantine Kaniklidis. All rights reserved. 10
55. Use of convalescent whole blood or plasma collected from patients recovered from Ebola virus disease for transfusion, as an empirical treatment during outbreaks: interim guidance for national health authorities and blood transfusion services. World Health Organization. Version 1.0 September 2014. http://apps.who.int/iris/bitstream/10665/135591/1/WHO_HIS_SDS_2014.8_eng.pdf?ua=1. Last accessed: 1 Nov 2014.
56. Geisbert TW, Feldmann H. Recombinant vesicular stomatitis virus-based vaccines against Ebola and Marburg virus infections. J Infect Dis 2011; 204 Suppl 3:S1075.
57. Geisbert TW, Daddario-DiCaprio KM, Williams KJ, et al. Recombinant vesicular stomatitis virus vector mediates postexposure protection against Sudan Ebola hemorrhagic fever in nonhuman primates. J Virol 2008; 82:5664.
58. Feldmann H, Jones SM, Daddario-DiCaprio KM, et al. Effective post-exposure treatment of Ebola infection. PLoS Pathog 2007; 3:e2.
59. Daddario-DiCaprio KM, Geisbert TW, Ströher U, et al. Postexposure protection against Marburg haemorrhagic fever with recombinant vesicular stomatitis virus vectors in non-human primates: an efficacy assessment. Lancet 2006; 367:1399.
60. Jones SM, Feldmann H, Ströher U, et al. Live attenuated recombinant vaccine protects nonhuman primates against Ebola and Marburg viruses. Nat Med 2005; 11:786.
61. Bray M. The role of the Type I interferon response in the resistance of mice to filovirus infection. J Gen Virol 2001; 82:1365.
62. Jahrling PB, Geisbert TW, Geisbert JB, et al. Evaluation of immune globulin and recombinant interferon-alpha2b for treatment of experimental Ebola virus infections. J Infect Dis 1999; 179 Suppl 1:S224.
63. Qiu X, Wong G, Fernando L, et al. mAbs and Ad-vectored IFN-α therapy rescue Ebola-infected nonhuman primates when administered after the detection of viremia and symptoms. Sci Transl Med 2013; 5:207ra143.
64. Stanley DA, Honko AN, Asiedu C, et al. Chimpanzee adenovirus vaccine generates acute and durable protective immunity against ebolavirus challenge. Nat Med 2014; 20:1126.
65. Government of Senegal boosts Ebola awareness through SMS campaign. World Health Organization. Nov 2014. http://www.who.int/features/2014/senegal-ebola-sms/en/. Last accessed: 4 Nov 2014.
66. Dananché C, Bénet T,Vanhems P. Ebola: fever definitions might delay detection in non-epidemic areas. The Lancet, Early Online Publication, 3 November 2014.
67. Reid SP, Shurtleff AC, Costantino JA, et al. HSPA5 is an essential host factor for Ebola virus infection. Antiviral Res 2014 Jul 10.
68. Ciesek S von Hahn T Colpitts CC et a. The green tea polyphenol, epigallocatechin-3-gallate, inhibits hepatitis C virus entry. Hepatology 2011;54:1947-55.
69. Aleksandrowicz, P., Marzi, A., Biedenkopf, N. et al. Ebola virus enters host cells by macropinocytosis and clathrin-mediated endocytosis. J Infect Dis. Nov 2011; 204: S957–S967.
70. Bhattacharyya, S., Warfield, K.L., Ruthel, G., Bavari, S., Aman, M.J., and Hope, T.J. Ebolavirus uses clathrin-mediated endocytosis as an entry pathway. Virology. May 25 2010; 401: 18–28.
71. Carette JE Raaben M Wong AC et a. Ebola virus entry requires the cholesterol transporter Niemann-Pick C1. Nature 2011;477:340-3.
72. Cote M Misasi J Ren T et a. Small molecule inhibitors reveal Niemann-Pick C1 is essential for Ebola virus infection. Nature 2011;477:344-8.
73. Patel JM, Snaith C, Thickett DR, et al. Randomized double-blind placebo-controlled trial of 40 mg/day of atorvastatin in reducing the severity of sepsis in ward patients (asepsis trial). Crit Care, 2012, 16: R231.
74. Undas A, Brummel-Ziedins KE, Mann KG. Anticoagulant effects of statins and their clinical implications. Thromb Haemost, 2014, 111: 392–400.
75. Hensley LE, Geisbert TW. The contribution of the endothelium to the development of coagulation disorders that characterize Ebola hemorrhagic fever in primates. Thromb Haemost 2005; 94(2):254-61.
76. Fedson DS. Treating influenza with statins and other immunomodulatory agents. Antiviral Res 2014;99:417-35. 77. McElroy AK, Erickson BR, Flietstra TD, et al. Biomarker Correlates of Survival in Pediatric Patients with Ebola
Virus Disease. Emerg Infect Dis 2014; 20(10). 78. Gehring G, Rohrmann K, Atenchong N, Mittler E, Becker S, Dahlmann F, Pohlmann S, Vondran FW, David S,
Manns MP, Ciesek S, von Hahn T. The clinically approved drugs amiodarone, dronedarone and verapamil inhibit filovirus cell entry. J Antimicrob Chemother, 2014, 69: 2123–2131.
79. Piccoli E Nadai M Caretta CM et al. Amiodarone impairs trafficking through late endosomes inducing a Niemann-Pick C-like phenotype. Biochem Pharmacol 2011;82:1234-49.
80. Li Y, Jiang L, Jia Z, et al. A Meta-Analysis of Red Yeast Rice: An Effective and Relatively Safe Alternative Approach for Dyslipidemia. PLoS One 2014; 9(6):e98611.
Ebola Virus Disease (EVD): New Understandings and New Frontiers in Therapeutics. Copyright © 2014. Constantine Kaniklidis. All rights reserved. 11
81. Red Yeast Rice Supplements Review. ConsumerLab. 15 Aug 2014. https://www.consumerlab.com/reviews/Red-Yeast-Rice-Supplements-Review/Red_Yeast_Rice/. Last accessed: 1 Nov 2014.
82. Marazzi G, Cacciotti L, Pelliccia F, Iaia L, Volterrani M, et al. Long-term effects of nutraceuticals (berberine, red yeast rice, policosanol) in elderly hypercholesterolemicpatients. Adv Ther 2011; 28: 1105–1113.
83. Affuso F, Ruvolo A, Micillo F, Saccà L, Fazio S. Effects of a nutraceutical combination (berberine, red yeast rice and policosanols) on lipid levels and endothelialfunction randomized, double-blind, placebo-controlled study. Nutr Metab Cardiovasc Dis 2010; 20: 656–661.
84. Becker DJ, Gordon RY, Halbert SC, French B, Morris PB, et al. Red yeast rice for dyslipidemia in statin-intolerant patients: a randomized trial.Ann Intern Med 2009; 150: : 830–839, W147–149.
85. Halbert SC, French B, Gordon RY, Farrar JT, Schmitz K, et al. Tolerability of red yeast rice (2,400 mg twice daily) versus pravastatin (20 mg twice daily) in patients with previousstatin intolerance. Am J Cardiol 2010; 105: 198–204.
86. Becker DJ, Gordon RY, Morris PB, Yorko J, Gordon YJ, et al. Simvastatin vs therapeutic lifestyle changes and supplements: randomized primary prevention trial. Mayo Clin Proc 2008; 83: 758–764.
87. Cicero AF, Brancaleoni M, Laghi L, Donati F, Mino M. Antihyperlipidaemic effect of a Monascus purpureus brand dietary supplement on a large sample of subjects at low risk for cardiovascular disease: a pilot study. Complement Ther Med 2005; 13: 273–278.
88. Lee W, Ku SK, Bae JS. Barrier protective effects of rutin in LPS-induced inflammation in vitro and in vivo. Food Chem Toxicol, 2012, 50: 3048–3055.
89. Whitehouse CA. Crimean-Congo hemorrhagic fever. Antiviral Res, 2004, 64: 145–160. 90. May JM, Harrison FE. Role of vitamin C in the function of the vascular endothelium. Antioxid Redox Signal, 2013,
19: 2068–2083. 91. Tan DX, Reiter RJ, Manchester LC. Ebola virus disease: Potential use of melatonin as a treatment. J Pineal Res
2014 Sep 27. 92. Song J, Kang SM, Lee WT et al. The beneficial effect of melatonin in brain endothelial cells against oxygen-
glucose deprivation followed by reperfusion-induced injury. Oxid Med Cell Longev 2014; 2014:639531. 93. Alamili M, Bendtzen K, Lykkesfeldt J et al. Melatonin suppresses markers of inflammation and oxidative damage
in a human daytime endotoxemia model. J Crit Care 2014; 29:184.e9–184.e13. 94. Ozdemir G, Ergün Y, Bakariş S et al. Melatonin prevents retinal oxidative stress and vascular changes in diabetic
rats. Eye (Lond) 2014; 28:1020–1027. 95. Kostovski E, Dahm AE, Iversen N et al. Melatonin stimulates release of tissue factor pathway inhibitor from the
vascular endothelium. Blood Coagul Fibrinolysis 2011; 22:254–259. 96. Tunali T, Sener G, Yarat A et al. Melatonin reduces oxidative damage to skin and normalizes blood coagulation in
a rat model of thermal injury. Life Sci 2005; 76:1259–1265. 97. Wirtz PH, Spillmann M, Bärtschi C et al. Oral melatonin reduces blood coagulation activity: a placebo-controlled
study in healthy young men. J Pineal Res 2008; 44:127–133. 98. Wirtz PH, Bärtschi C, Spillmann M et al. Effect of oral melatonin on the procoagulant response to acute
psychosocial stress in healthy men: a randomized placebo-controlled study. J Pineal Res 2008; 44:358–365. 99. Boga JA, Coto-Montes A, Rosales-Corral SA, Tan DX, Reiter RJ. Beneficial actions of melatonin in the
management of viral infections: a new use for this "molecular handyman"? Rev Med Virol 2012; 22(5):323-38.