Early prosthetic joint infection after primary total joint arthroplasty
197
University of Groningen Early prosthetic joint infection after primary total joint arthroplasty Löwik, Claudia Aline Maria DOI: 10.33612/diss.97641504 IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2019 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Löwik, C. A. M. (2019). Early prosthetic joint infection after primary total joint arthroplasty: risk factors and treatment strategies. Rijksuniversiteit Groningen. https://doi.org/10.33612/diss.97641504 Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 15-03-2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Early prosthetic joint infection after primary total joint arthroplasty

University of Groningen
Early prosthetic joint infection after primary total joint arthroplastyLöwik, Claudia Aline Maria
DOI:10.33612/diss.97641504
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2019
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Löwik, C. A. M. (2019). Early prosthetic joint infection after primary total joint arthroplasty: risk factors andtreatment strategies. Rijksuniversiteit Groningen. https://doi.org/10.33612/diss.97641504
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 15-03-2022

Early prosthetic joint infection after primary total joint arthroplasty
Risk factors and treatment strategies
Claudia Aline Maria Löwik
51938_Claudia_Lowik.indd 1 19-08-19 11:12

The research published in this thesis was kindly supported by a grant from ZonMw and the Nederlandse Orthopaedische Vereniging (NOV). Publication of this thesis was �nancially supported by kind contributions from the University of Groningen (RUG), University Medical Center Groningen (UMCG), Research Institute SHARE and Anna Fonds | NOREF.
C.A.M. LöwikEarly prosthetic joint infection after primary total joint arthroplasty: risk factors and treatment strategies
ISBN: 978-94-034-1841-4 (printed version)ISBN: 978-94-034-1840-7 (electronic version)
Cover: Ferdinand van Nispen, my-thesis.nlLay-out: Ferdinand van Nispen, my-thesis.nlPrinting: GVO drukkers en vormgevers, Ede
© 2019, Claudia Löwik, Groningen, The Netherlands
All rights reserved. No part of this publication may be reproduced or transmitted in any form by any means, electronical, or mechanical, including photocopying, recording or otherwise, without the prior written permission of the copyright owner.
51938_Claudia_Lowik.indd 2 19-08-19 14:47

Early prosthetic joint infection after primary total joint arthroplasty
Risk factors and treatment strategies
Proefschrift
ter verkrijging van de graad van doctor aan de Rijksuniversiteit Groningen
op gezag van derector magni�cus prof. dr. C. Wijmenga
en volgens besluit van het College voor Promoties.
De openbare verdediging zal plaatsvinden op
maandag 25 november 2019 om 16.15 uur
door
Claudia Aline Maria Löwik
geboren op 5 augustus 1989te Zwolle
51938_Claudia_Lowik.indd 3 19-08-19 11:12
PromotoresProf. dr. S.K. BulstraDr. M. Stevens
CopromotorDr. P.C. Jutte
BeoordelingscommissieProf. dr. A.W. FriedrichProf. dr. R.G.H.H. NelissenProf. dr. ir. H.J. Busscher
51938_Claudia_Lowik.indd 4 19-08-19 11:12

ParanimfenMarco LöwikAnnet Wijnen
51938_Claudia_Lowik.indd 5 19-08-19 11:12
Contents
Chapter 1 General introduction and outline of this thesis 9
Chapter 2 Persistent wound drainage after total joint arthroplasty: a narrative review
21
Chapter 3 Periprosthetic joint infection in orthopaedic surgical oncology
39
Chapter 4 Obese patients have higher rates of polymicrobial and Gram-negative early periprosthetic joint infections of the hip than non-obese patients
53
Chapter 5 Predicting failure in early acute prosthetic joint infection treated with debridement, antibiotics, and implant retention: external validation of the KLIC score
71
Chapter 6 Use of gentamicin-impregnated beads or sponges in the treatment of early acute periprosthetic joint infection: a propensity score analysis
87
Chapter 7 Debridement, antibiotics and implant retention is a viable treatment option for early periprosthetic joint infection presenting more than four weeks after index arthroplasty
103
Chapter 8 Managing persistent wound leakage after total knee and hip arthroplasty. Results of a nationwide survey among Dutch orthopaedic surgeons
119
Chapter 9 LEAK study: design of a nationwide randomized controlled trial to �nd the best way to treat wound leakage after primary hip and knee arthroplasty
135
Chapter 10 General discussion and future perspectives 153
51938_Claudia_Lowik.indd 6 19-08-19 11:12
Summary 181Nederlandse samenvatting 185Dankwoord 190Curriculum vitae 194 SHARE: previous dissertations 195
51938_Claudia_Lowik.indd 7 19-08-19 11:12

51938_Claudia_Lowik.indd 8 19-08-19 11:12

Chapter 1
General introduction and outline of this thesis
51938_Claudia_Lowik.indd 9 19-08-19 11:12

51938_Claudia_Lowik.indd 10 19-08-19 11:12

General introduction
11
1Background
Osteoarthritis (OA) is the most common joint disorder worldwide.1 It can develop in any type of joint, although weight-bearing joints, such as the hip and knee, are most commonly a�ected. OA is recognized as a substantial source of disability, since it causes considerable pain and reduced mobility.2 Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are highly successful surgical treatment modalities for advanced OA of the hip and knee. In 2017, 29,937 primary THAs and 26,030 primary TKAs were performed in the Netherlands3 and over a million THAs and TKAs are performed annually in the USA.4 Due to general ageing of the population and increasing levels of obesity, the incidence of OA continues to rise. Because of this increasing incidence and changing thresholds for arthroplasty surgery, the demand for THA and TKA continues to rise too and is expected to keep rising in the coming decades.5
Although most patients experience good results after THA and TKA, some patients develop postoperative complications. One of the most serious complications after joint arthroplasty and an important cause for revision arthroplasty is prosthetic joint infection (PJI), developing in approximately 1-2% of primary arthroplasties and up to 10% of revision arthroplasties.6,7 Although this percentage is relatively low, the absolute number of patients with PJI is substantial, given the large and still-increasing number of patients who undergo total joint arthroplasty surgery. Prevention of PJI is therefore an important issue, especially given the signi�cant burden it poses on patients and society: PJI is associated with high morbidity and mortality, as well as high socioeconomic costs due to prolonged hospital stay, additional surgical procedures and antimicrobial treatment.8
Classi�cation of PJIPJI can develop at any time point after surgery. Several classi�cation systems for PJI have been composed over the years.9-14 Most systems divide PJI into early, late and hematogenous PJI, depending on the time from joint arthroplasty to development of PJI and duration of symptoms. A large proportion of PJIs occur within the �rst three months after implantation and are de�ned as early PJIs.15,16 Early PJIs are typically acquired at the time of surgery through intraoperative contamination and are caused by relatively virulent microorganisms, such as Staphylococcus aureus and Streptococcus species. Patients with early PJI typically
51938_Claudia_Lowik.indd 11 19-08-19 11:12

Chapter 1
12
have an acute presentation with a warm, swollen, painful, erythematous joint, often with features of sepsis. Late PJIs can also present acutely but usually have more subtle signs, such as chronic pain, a sinus tract with chronic drainage and sometimes prosthetic loosening at the bone-cement interface. Late PJIs present more than three months after index surgery. Just as early PJIs, they are also typically acquired at the time of index surgery but are caused by less virulent or indolent microorganisms, such as coagulase negative staphylococci. Some patients develop hematogenous PJI, in which the prosthetic joint gets infected after a longstanding infection-free period. These infections are typically secondary to an infection at a di�erent site in the body, such as dental infections. Patients with hematogenous PJI usually present with the same acute symptoms as patients with early PJI.
Risk factors for PJIMinimizing the risk of PJI after THA and TKA requires elimination of two types of risk factors: 1) factors that increase the risk of exposure of the hip or knee joint to microorganisms, and 2) factors that limit a patient’s ability to eliminate intra-articular microorganisms. One of the most important type-1 risk factors is prolonged wound leakage,17,18 a di�cult complication as it could be a symptom of an already existing PJI as well as a risk factor for developing PJI. Moreover, surgical wounds may show prolonged wound leakage for reasons other than infection (such as hematoma, seroma or fatty necrosis) and take longer to heal without development of an infection. As leaking wounds increase the risk of exposure to microorganisms by providing a porte d’entrée, prolonged wound leakage should be considered as potentially imminent PJI.19 Identi�ed type-2 risk factors include obesity, diabetes mellitus, immunode�ciency and rheumatoid arthritis.20,21 Literature indicates that the risk of PJI increases exponentially with body mass index.20,22 Patients with an oncological condition requiring tumor resection are often immunode�cient due to their need for chemotherapy or radiotherapy.23,24 Further, patients with rheumatoid arthritis are at increased risk due to their immunosuppressive therapy and susceptibility to infectious disorders of bone, joint and soft tissue.25 The number of comorbidities also limits a patient’s ability to eliminate intra-articular microorganisms, thus increasing the risk of PJI.26
51938_Claudia_Lowik.indd 12 19-08-19 11:12

General introduction
13
1Treatment strategies for PJIThere are several surgical and non-surgical treatment strategies for PJI, such as debridement, antibiotics and implant retention (DAIR), revision surgery and suppressive antibiotic therapy. The aim of performing a DAIR is to reduce the infective load of intra-articular microorganisms, provide extensive debridement and start antibiotic therapy in order to retain the prosthesis and avoid more invasive surgery (such as revision arthroplasty). During DAIR the pre-existing wound is opened and the joint cavity is debrided and thoroughly lavaged. If possible, modular components are exchanged. Multiple deep-tissue biopsies are subsequently obtained for culturing, broad-spectrum intravenous antibiotic treatment is started, and the wound is meticulously closed. DAIR is the recommended treatment for patients with early PJI, and is most successful for early acute PJI, in which symptoms exist for less than three weeks.27,28
The higher e�ectiveness of DAIR in early acute PJI compared with late PJI is due to bio�lm formation, a highly complex process in which microorganisms attach to a surface and proliferate into a mature bio�lm (Figure 1). Nearly all microorganisms are capable of forming a bio�lm, although some types of microorganisms are more potent than others. In vitro studies showed that a bio�lm already starts to form within hours of inoculation of bacteria,29 but these experiments are performed under optimal circumstances for bacterial growth and do not include the complexity of the host’s environment and the protective e�ect of its immune system.30 Recent in vivo models showed that a bio�lm is evident after two weeks, but extends and is covered by �brinous tissue and multiple host cells after six weeks.31 The process of bio�lm formation does vary widely between bacterial species, size of inoculum and hosts.32,33
Due to multiple phenotypic and genotypic changes in the process of bio�lm formation, embedded microorganisms become unresponsive to almost any antibiotic treatment once a mature bio�lm is formed.35,36 As a consequence, a PJI cannot be cured with DAIR without removal of the implant. In that case a di�erent surgical treatment option for PJI is revision arthroplasty, which involves replacing the primary prosthesis with a new prosthesis. The prosthesis, including the mature bio�lm, is removed, achieving infection control in approximately 90% of patients.37,38 However, bene�ts of DAIR over revision arthroplasty include retention of the prosthesis, preservation of bone stock, shorter duration of the surgical procedure, decreased risk of intraoperative fractures (caused by removal of components and implantation of cement spacers) and faster postoperative rehabilitation.39,40 And yet, rates of infection control after DAIR vary widely from
51938_Claudia_Lowik.indd 13 19-08-19 11:12

Chapter 1
14
37% to 88%.41-44 This variation in infection control after DAIR stresses the need for careful selection of eligible patients, especially since performing a DAIR procedure could reduce the e�ectiveness of subsequent revision surgery.45-48 Moreover, this indicates that surgical techniques of a DAIR procedure should be optimized to improve infection control after DAIR.
Aims and outline of this thesis
The studies described in this thesis aim to examine and evaluate the risk factors and treatment strategies for early PJI. The �rst part of the thesis focuses on patient groups at risk for PJI, such as obese patients, oncology patients and patients with prolonged wound leakage after THA and TKA. The second part of this thesis strives to provide insights on factors that can in�uence the treatment success of DAIR, such as patient selection, use of local antibiotics during DAIR and optimization of the timing of DAIR.
Part 1: Evaluation of patients at risk for early PJIChapter 2 presents a review of the available literature on the diagnosis and treatment of prolonged wound leakage after THA and TKA. As patients
Figure 1. Description of various stages involved in the development of a bio�lm. 1) Bacterial adhesion to the surface, 2) cell-to-cell adhesion, 3) attached cell monolayer, 4) maturation of a bio�lm and formation of exopolymeric substance, and 5) detachment. Image credit: D. Davis34
51938_Claudia_Lowik.indd 14 19-08-19 11:12

General introduction
15
1with prolonged wound leakage are at increased risk for developing PJI, it is important to optimally diagnose and treat these patients. Remarkably, there are no evidence-based guidelines on this topic that can guide orthopaedic surgeons in their decision-making process. The lack of scienti�c consensus motivated this review of the available literature.
Chapter 3 provides a review of the available literature on PJI in orthopaedic oncology patients. PJI rates among these patients are high due to local and systemic immunode�ciency caused by chemotherapy or radiotherapy. Moreover, these patients usually require large implants because of the need for extensive tumor resections. Even though this patient category is clearly di�erent than regular patients receiving THA or TKA, literature on oncologic PJI is scarce. Hence information on regular PJI is usually applied to oncology patients too. To outline the topics that need future research, conducted speci�cally on oncology patients, this review describes the current evidence on the de�nition, diagnosis and treatment of oncologic PJI.
Obese patients are another well-known patient category with an increased risk of PJI. Chapter 4 describes the clinical and microbiological characteristics of obese patients with early PJI, aiming to identify characteristics that contribute to this increased risk and to ultimately improve preventive measures for this speci�c patient category.
Part 2: Improving treatment strategies for early PJIChapter 5 shows the results of the external validation of a preoperative risk score for DAIR failure. As success rates of DAIR vary widely, it is important to select the right patients for this procedure: rates of infection control by DAIR could be optimized and the number of more extensive revision surgeries reduced. To estimate the risk of DAIR failure prior to surgery, thereby selecting the right patients for DAIR, Tornero et al. developed the KLIC score.49 This score preoperatively calculates the risk of DAIR failure by evaluating �ve patient-related factors: 1) chronic renal failure (Kidney), 2) Liver cirrhosis, 3) Index surgery, 4) Cemented prosthesis and 5) CRP >115 mg/L (KLIC). Before the KLIC score can be implemented as a standard tool in clinical practice, it has to be validated in an external cohort.
In addition to selecting the right patients for DAIR, infection control after DAIR can also be improved by optimizing surgical techniques and antibiotic treatment. Chapter 6 provides results on the e�cacy of gentamicin-
51938_Claudia_Lowik.indd 15 19-08-19 11:12

Chapter 1
16
impregnated beads and sponges in patients with early PJI treated with DAIR. In the Netherlands, gentamicin-impregnated beads and sponges are routinely applied to achieve higher rates of infection control. However, the bene�cial e�ects of applying these local antibiotic carriers have never been demonstrated.
Moreover, it is important to perform DAIR at the right time point. To this end, Chapter 7 describes the rate of infection control after DAIR according to the interval between index surgery and DAIR. As the success rate of DAIR is dependent on the time needed for bacteria to form a mature bio�lm at the surface of the prosthesis, PJI can no longer be cured by DAIR once embedded bacteria in the bio�lm become unresponsive to antibiotic treatment. So far, the time interval until formation of this mature bio�lm is unknown. Hence it cannot be estimated whether it is useful to perform a DAIR procedure at a certain time point after joint arthroplasty.
While Chapter 7 describes the optimal timing of DAIR in patients with early PJI in general, Chapters 8 and 9 focus on the optimal timing of DAIR in patients with prolonged wound leakage after THA and TKA. As there are no evidence-based guidelines on the best treatment for prolonged wound leakage, the Dutch orthopaedic community stated in 2015 that this topic constitutes an important knowledge gap. To address this gap, Consortium Orthopaedic Research (CORE) assembled the LEakage After primary Knee and hip arthroplasty (LEAK) study group. Chapter 8 provides the results of a survey the LEAK study group conducted among Dutch orthopaedic surgeons on the de�nition, diagnosis and treatment of prolonged wound leakage, to assess current clinical practice in the Netherlands.
Based on the results of this survey and the literature review in Chapter 2, the LEAK study group designed the LEAK study, which is described in Chapter 9. This nationwide multicenter randomized controlled trial compares the revision rates, clinical e�ectiveness and cost e�ectiveness of DAIR and non-surgical treatment. It is hypothesized that performing DAIR at an early time point is helpful in preventing and treating PJI and salvaging the implant in patients with prolonged wound leakage after THA and TKA.
Chapter 10 presents a general discussion on the main �ndings of the studies described in this thesis. It also provides future perspectives and implications for clinical practice.
51938_Claudia_Lowik.indd 16 19-08-19 11:12
General introduction
17
1References
1. Hiligsmann M, Cooper C, Arden N, Boers M, Branco JC, Luisa Brandi M, et al. Health economics in the �eld of osteoarthritis: an expert’s consensus paper from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Semin Arthritis Rheum 2013; 43(3): 303-13.
2. Moskowitz RW. The burden of osteoarthritis: clinical and quality-of-life issues. Am J Manag Care 2009; 15(8 Suppl): S223-9.
3. LROI. Online LROI annual report 2017: 10 years of registration, a wealth of information.4. Centers for Disease Control and Prevention. Number of all listed procedures for discharges from
short-stay hospitals, by procedure category and age: United States, 2010. www.cdc.gov.5. Kurtz SM, Lau E, Schmier J, Ong KL, Zhao K, Parvizi J. Infection burden for hip and knee arthroplasty
in the United States. J Arthroplasty 2008; 23(7): 984-91. 6. Kurtz SM, Ong KL, Lau E, Bozic KJ, Berry D, Parvizi J. Prosthetic joint infection risk after TKA in the
medicare population. Clin Orthop Relat Res 2010; 468(1): 52-6.7. Kunutsor SK, Whitehouse MR, Blom AW, Beswick AD, INFORM Team. Re-infection outcomes
following one- and two-stage surgical revision of infected hip prosthesis: a systematic review and meta-analysis. PLoS One 2015; 10(9): 1-15.
8. Kallala RF, Vanhegan IS, Ibrahim MS, Sarmah S, Haddad FS. Financial analysis of revision knee surgery based on NHS tari�s and hospital costs: does it pay to provide a revision service? Bone Joint J 2015; 97-B(2): 197-201.
9. Tsukayama DT, Estrada R, Gustilo RB. Infection after total hip arthroplasty: a study of the treatment of one hundred and six infections. J Bone Joint Surg Am 1996; 78(4): 512-23.
10. Fitzgerald RH Jr, Nolan DR, Ilstrup DM, van Scoy RE, Washington JA 2nd, Coventry MB. Deep wound sepsis following total hip arthroplasty. J Bone Joint Surg Am 1977; 59(7): 847-55.
11. McPherson EJ, Woodson C, Holtom P, Roidis N, Shufelt C, Patzakis M. Periprosthetic total hip infection: outcomes using a staging system. Clin Orthop Relat Res 2002; 403: 8-15.
12. Romanò CL, Romanò D, Logoluso N, Drago L. Bone and joint infections in adults: a comprehensive classi�cation proposal. Eur Orthop Traumatol 2011; 1(6): 207-17.
13. Zimmerli W, Trampuz A, Ochsner PE. Prosthetic-joint infections. N Engl J Med 2004; 351(16): 1645-54.
14. Giulieri SG, Graber P, Ochsner PE, Zimmerli W. Management of infection associated with total hip arthroplasty according to a treatment algorithm. Infection 2004; 32(4): 222-8.
15. Yokoe DS, Avery TR, Platt R, Huang SS. Reporting surgical site infections following total hip and knee arthroplasty: impact of limiting surveillance to the operative hospital. Clin Infect Dis 2013; 57(9): 1282-8.
16. Barrett L, Atkins B. The clinical presentation of prosthetic joint infection. J Antimicrob Chemother 2014; 69(Suppl 1): 25-8.
17. Surin VV, Sundholm K, Bäckman L. Infection after total hip replacement: with special reference to a discharge from the wound. J Bone Joint Surg Br 1983; 65(4): 412-8.
18. Saleh K, Olson M, Resig S, Bershadsky B, Kuskowski M, Gioe T, et al. Predictors of wound infection in hip and knee joint replacement: results from a 20 year surveillance program. J Orthop Res 2002; 20(3): 506-15.
19. Weiss AP, Krackow KA. Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993; 8(3): 285-9.
20. Chen J, Cui Y, Li X, Miao X, Wen Z, Xue Y, et al. Risk factors for deep infection after total knee arthroplasty: a meta-analysis. Arch Orthop Trauma Surg 2013; 133(5): 675-87.
21. Eka A, Chen AF. Patient-related medical risk factors for periprosthetic joint infection of the hip and knee. Ann Transl Med 2015; 3(16): 233.
22. Smith JO, Framptom CMA, Hooper GJ, Young SW. The impact of patient and surgical factors on the rate of postoperative infection after total hip arthroplasty – a New Zealand joint registry study. J Arthroplasty 2018; 33(6): 1884-90.
51938_Claudia_Lowik.indd 17 19-08-19 11:12

Chapter 1
18
23. Jeys LM, Luscombe JS, Grimer RJ, Abudu A, Tillman RM, Carter SR. The risks and bene�ts of radiotherapy with massive endoprosthetic replacement. J Bone Joint Surg Br 2007; 89-B(10): 1352-5.
24. Wafa H, Grimer RJ, Reddy K, Jeys LM, Abudu A, Carter SR, et al. Retrospective evaluation of the incidence of early periprosthetic infection with silver-treated endoprostheses in high-risk patients: case-control study. Bone Joint J 2015; 97-B(2): 252-7.
25. Doran MF, Crowson CS, Pond GR, O’Fallon WM, Gabriel SE. Frequency of infection in patients with rheumatoid arthritis compared with controls: a population-based study. Arthritis Rheum 2002; 46(9): 2287-93.
26. Lai K, Bohm ER, Burnell C, Hedden DR. Presence of medical comorbidities in patients with infected primary hip or knee arthroplasties. J Arthroplasty 2007; 22(5): 651-6.
27. Parvizi J, Gehrke T, Chen AF. Proceedings of the international consensus on periprosthetic joint infection. Bone Joint J 2013; 95-B(11): 1450-2.
28. Osmon DR, Berbari ER, Berendt AR, Lew D, Zimmerli W, Steckelberg JM, et al. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 2013; 56(1): 1-25.
29. Veerachamy S, Yarlagadda T, Manivasagam G, Yarlagadda PK. Bacterial adherence and bio�lm formation on medical implants: a review. Proc Inst Mech Eng H 2014; 228(10): 1083-99.
30. Bandyk DF, Kinney EV, Riefsnyder TI, Kelly H, Towne JB. Treatment of bacteria-bio�lm graft infection by in situ replacement in normal and immune-de�cient states. J Vasc Surg 1993; 18(3): 398-405.
31. Carli AV, Bhimani S, Yang X, Shirley MB, de Mesy Bentley KL, Ross FP, et al. Quanti�cation of peri-implant bacterial load and in vivo bio�lm formation in an innovative, clinically representative mouse model of periprosthetic joint infection. J Bone Joint Surg Am 2017; 99(6): e25.
32. Lovati AB, Bottagisio M, de Vecchi E, Gallazzi E, Drago L. Animal models of implant-related lowgrade infections: a twenty year review. Adv Exp Med Biol 2017; 971: 29-50.
33. Vidlak D, Kielian T. Infectious dose dictates the host response during Staphylococcus aureus orthopedic-implant bio�lm infection. Infect Immun 2016; 84(7): 1957-65.
34. Tshikantwa TS, Ullah MW, He F, Yang G. Current trends and potential applications of microbial interactions for human welfare. Front Microbiol 2018; 9: 1156. Available from: https://www.researchgate.net/figure/Description-of-various-stages-involved-in-the-development-of-a-bio�lm-1-Bacterial_�g2_325258657.
35. Lebeaux D, Ghigo JM, Beloin C. Bio�lm-related infections: bridging the gap between clinical management and fundamental aspects of recalcitrance toward antibiotics. Microbiol Mol Biol Rev 2014; 78(3): 510-43.
36. Davies D. Understanding bio�lm resistance to antibacterial agents. Nat Rev Drug Discov 2003; 2(2): 114-22.
37. Haleem AA, Berry DJ, Hanssen AD. Mid-term to long-term follow-up of two-stage reimplantation for infected total knee arthroplasty. Clin Orthop Relat Res 2004; 428: 35-9.
38. Hirakawa K, Stulberg BN, Wilde AH, Bauer TW, Secic M. Results of 2-stage reimplantation for infected total knee arthroplasty. J Arthroplasty 1998; 13(1): 22-8.
39. Choi HR, von Knoch F, Zurakowski D, Nelson SB, Malchau H. Can implant retention be recommended for treatment of infected TKA? Clin Orthop Relat Res 2011; 469(4): 961-9.
40. Fisman DN, Reilly DT, Karchmer AW, Goldie SJ. Clinical e�ectiveness and cost-e�ectiveness of 2 management strategies for infected total hip arthroplasty in the elderly. Clin Infect Dis 2001; 32(3): 419-30.
41. Sukeik M, Patel S, Haddad FS. Aggressive early débridement for treatment of acutely infected cemented total hip arthroplasty. Clin Orthop Relat Res 2012; 470(11): 3164-70.
42. Cobo J, Garcia San Miguel L, Euba G, Rodríguez D, García-Lechuz JM, Riera M, et al. Early prosthetic joint infection: outcomes with debridement and implant retention followed by antibiotic therapy. Clin Microbiol Infect 2011; 17(11): 1632-7.
43. Duque AF, Post ZD, Lutz RW, Orozco FR, Pulido SH, Ong AC. Is there still a role for irrigation and debridement with liner exchange in acute periprosthetic total knee infection? J Arthroplasty 2017; 32(4): 1280-4.
51938_Claudia_Lowik.indd 18 19-08-19 11:12

General introduction
19
144. Fehring TK, Odum SM, Berend KR, Jiranek WA, Parvizi J, Bozic KJ, et al. Failure of irrigation and
débridement for early postoperative periprosthetic infection. Clin Orthop Relat Res 2013; 471(1): 250-7.
45. Sherrell JC, Fehring TK, Odum S, Hansen E, Zmistowski B, Dennos A, et al. Fate of two-stage reimplantation after failed irrigation and débridement for periprosthetic knee infection. Clin Orthop Relat Res 2011; 469(1): 18-25.
46. Gardner J, Gioe TJ, Tatman P. Can this prosthesis be saved? Implant salvage attempts in infected primary TKA. Clin Orthop Relat Res 2011; 469(4): 970-6.
47. Brimmo O, Ramanathan D, Schiltz NK, Pillai AL, Klika AK, Barsoum WK. Irrigation and debridement before a 2-stage revision total knee arthroplasty does not increase risk of failure. J Arthroplasty 2016; 31(2): 461-4.
48. Nodzo SR, Boyle KK, Nocon AA, Henry MW, Mayman DJ, Westrich GH. The in�uence of a failed irrigation and debridement on the outcomes of a subsequent 2-stage revision knee arthroplasty. J Arthroplasty 2017; 32(8): 2508-12.
49. Tornero E, Morata L, Martínez-Pastor JC, Bori G, Climent C, García-Velez DM, et al. KLIC-score for predicting early failure in prosthetic joint infections treated with debridement, implant retention and antibiotics. Clin Microbiol Infect 2015; 21(8): 9-17.
51938_Claudia_Lowik.indd 19 19-08-19 11:12

51938_Claudia_Lowik.indd 20 19-08-19 11:12

Chapter 2
Persistent wound drainage after total joint arthroplasty: a
narrative review
Frank-Christiaan B.M. Wagenaar, Claudia A.M. Löwik, Akos Zahar, Paul C. Jutte, Thorsten Gehrke, Javad Parvizi
Published in: Journal of Arthroplasty 2019; 34(1): 175-182
51938_Claudia_Lowik.indd 21 19-08-19 11:12

Chapter 2
22
Abstract
BackgroundPersistent wound drainage after total joint arthroplasty (TJA) is an important complication with potential substantial adverse consequences, in particular periprosthetic joint infection.
MethodsThis review evaluated the available literature regarding several issues in the �eld of persistent wound drainage after TJA and o�ers a classi�cation of persistent wound drainage and an algorithmic approach to the decision-making process.
ResultsAvailable literature addressing the diagnosis and treatment of persistent wound drainage after TJA is scarce and an evidence-based clinical guideline is lacking. This is partially caused by the absence of a universally accepted de�nition of persistent wound drainage. In patients with persistent wound drainage, clinical signs and serological tests can be helpful in the diagnosis of a developing infection. Regarding the treatment of persistent wound drainage, non-surgical treatment consists of absorbent dressings, pressure bandages, and temporary joint immobilization. Surgical treatment is advised when wound drainage persists for more than �ve to seven days and consists of open debridement with irrigation and exchange of modular components and antimicrobial treatment.
ConclusionBased on this literature review, we proposed a classi�cation and algorithmic approach for the management of patients with persistent wound drainage after TJA. Hopefully, this o�ers the orthopaedic surgeon a practical clinical guideline by �nding the right balance between overtreatment and undertreatment, weighing the risks and bene�ts. However, this classi�cation and algorithmic approach should �rst be evaluated in a prospective trial.
51938_Claudia_Lowik.indd 22 19-08-19 11:12

Review on persistent wound drainage
23
2
Introduction
Persistent wound drainage (PWD) after total joint arthroplasty (TJA) is an important problem because of its potential adverse in�uence on the outcome following TJA, in particular development of a periprosthetic joint infection (PJI).1-8 PJI is associated with high morbidity and mortality, and a high socio-economic burden due to prolonged hospital stay, surgical procedure(s), antimicrobial treatment, and wound care.
Remarkably, PWD is rarely reported in literature and thereby literature fails to provide conclusive scienti�c evidence on many issues related to PWD after TJA, including the de�nition and treatment of PWD. This lack of evidence results in wide variation in diagnosis and treatment in daily practice, often only founded by the surgeon’s opinion. The absence of scienti�c consensus prompted this review of the available literature.
We performed a literature search and included all papers relevant to the subject of PWD (Table 1). Articles that were not written in English or did not have full text available were excluded. We included all relevant papers, regardless of the level of evidence.14 Although most articles were of low level of evidence, we included these articles because of the small number of available papers on the subject of PWD and due to the lack of articles with a higher level of evidence. Based on this literature review, we developed a classi�cation of PWD and an algorithmic approach to PWD after TJA that may guide clinicians in their decision-making process to select the appropriate treatment for PWD.
Incidence and relevance
The reported incidence of PWD after TJA varies between 0.2% and 21%,3-5,8,9,13 with higher incidences after revision TJA.8 This wide range in incidence is mainly caused by the variation in de�nitions of PWD (Table 1), illustrating the lack of consensus regarding the de�nition of PWD. Moreover, higher awareness results in higher incidences of PWD, as demonstrated by Maathuis et al. who found a 21% incidence of PWD when protocol-based surveillance was used to detect wound drainage after TJA.13
51938_Claudia_Lowik.indd 23 19-08-19 11:12

Chapter 2
24
Table 1. Overview of literature addressing wound drainage after total joint arthroplasty
Author Study type and sample size
Level of evidence
De�nition Incidence of wound drainage
ResultsDuration of drainage Amount of drainage
Adelani 9 Retrospective
N = 2221 TKAs
3 N/A N/A 0.2% 17 patients had non-infectious wound complications (including persistent wound drainage) and 12 patients had deep infection. Patients with complications had lower Knee Society function scores and a higher incidence of mild or greater pain.
Dennis 10 Opinion N/A >7 days after TJA N/A N/A Persistent wound drainage (not associated with erythema or purulence) can be managed with wound care and immobilization. If wound drainage persists beyond 5 to 7 days, spontaneous cessation of drainage is unlikely and surgical debridement is indicated.
Hansen 11 Prospective
N = 5627 THAs
4 >3-4 days after TJA Drainage that has soaked through the postoperative dressings
2.0% NPWT was started after 3-4 days of wound drainage in 109 patients and applied for 2 days. 76% did not need additional surgery, 10% needed super�cial debridement, 11% needed deep debridement, and 3% required component removal. Predictors for additional surgery were INR >2, previous hip surgery and NPWT >48 hours.
Jaberi 3 Retrospective
N = 11,785 TKAs / THAs
3 >2 days after TJA Drainage that has soaked through the postoperative dressings
2.9% 300 patients with wound drainage >48 hours were treated with local wound care and oral antibiotics. Wound drainage stopped between 2-4 days in 72%. The remaining patients underwent single debridement (76%) or additional treatment (repeat debridement, resection arthroplasty or long-term antibiotics). Timing of surgery and malnutrition predicted failure of the �rst debridement.
Lonner 12 Opinion N/A Several days after TJA N/A N/A Wound drainage beyond several days after surgery may increase the risk of infection. Drainage will usually stop after 24-48 hours of immobilization. If not, open debridement should be performed, including obtaining cultures, irrigation and meticulous wound closure. Exercises may be resumed once the wound is stable.
Maathuis 13 Retrospective
N = 558 TKAs / THAs
3 >5 days after TJA N/A 16.5% Comparison of an algorithmic approach to an ad hoc approach. In the algorithmic approach, registration of persistent wound drainage was two-fold (21% vs 11%), but the number of open debridements was lower (17% vs 30%) and the salvage rate higher (94% vs 85%)
Patel 4
Retrospective
N = 2437 TKAs / THAs
2 >5 days after TJA
≥2x2cm area of gauze covering the wound is wet or when �uid is noted to be originating from the surgical wound
20.1%
Persistent wound drainage results in longer hospital stay. Each day of wound drainage after day 5 increased the risk of wound infection by 42% following THA (p<.001) and by 29% following TKA (not signi�cant after correction for BMI).
Saleh 7 Prospective
N = 2305 TKAs / THAs
3 Wound drainage N/A N/A 33 patients developed a super�cial wound infection. Hematoma formation and days of wound drainage were signi�cant predictors of super�cial wound infection. 58% developed a prosthetic joint infection, patients with >5 days of wound drainage had 12.7 times more risk of developing a prosthetic joint infection.
Surin 5 Retrospective
N = 803 THAs
3 N/A N/A 12.6% 115 patients had super�cial wound drainage and cultures were positive in 70 wounds. 34 patients developed prosthetic joint infection. Patients with super�cial wound drainage had a 3.2 times higher risk of developing a prosthetic joint infection. The risk was further in�uenced by the character of the exudate and the use of prophylactic antibiotics.
Vince 1 Review / opinion N/A Limited amount of time
N/A N/A Persistent wound drainage should be treated by wound care and immobilization. If drainage does not stop after 3 to 7 days, open debridement should be performed. Aggressive surgery may prevent sepsis. Drainage that starts in the late postoperative phase is a great concern as it usually results from a prosthetic joint infection.
Weiss 8 Retrospective
N = 597 TKAs
4 ≥4 consecutive days beyond day 5 after TJA
≥2x2cm area of gauze covering the wound is wet or when �uid is noted to be originating from the surgical wound
1.3% 8 patients with persistent wound drainage. Open debridement was performed at an average of 12.5 days after index surgery. 25% of patients had positive tissue cultures. All patients were successfully treated with adjuvant antibiotics.
BMI: body mass index; INR: international normalized ratio; N/A: not applicable or not described; NPWT: negative pressure wound therapy; THA: total hip arthroplasty; TJA: total joint arthroplasty; TKA: total knee arthroplasty.
51938_Claudia_Lowik.indd 24 19-08-19 11:12

Review on persistent wound drainage
25
2
Table 1. Overview of literature addressing wound drainage after total joint arthroplasty
Author Study type and sample size
Level of evidence
De�nition Incidence of wound drainage
ResultsDuration of drainage Amount of drainage
Adelani 9 Retrospective
N = 2221 TKAs
3 N/A N/A 0.2% 17 patients had non-infectious wound complications (including persistent wound drainage) and 12 patients had deep infection. Patients with complications had lower Knee Society function scores and a higher incidence of mild or greater pain.
Dennis 10 Opinion N/A >7 days after TJA N/A N/A Persistent wound drainage (not associated with erythema or purulence) can be managed with wound care and immobilization. If wound drainage persists beyond 5 to 7 days, spontaneous cessation of drainage is unlikely and surgical debridement is indicated.
Hansen 11 Prospective
N = 5627 THAs
4 >3-4 days after TJA Drainage that has soaked through the postoperative dressings
2.0% NPWT was started after 3-4 days of wound drainage in 109 patients and applied for 2 days. 76% did not need additional surgery, 10% needed super�cial debridement, 11% needed deep debridement, and 3% required component removal. Predictors for additional surgery were INR >2, previous hip surgery and NPWT >48 hours.
Jaberi 3 Retrospective
N = 11,785 TKAs / THAs
3 >2 days after TJA Drainage that has soaked through the postoperative dressings
2.9% 300 patients with wound drainage >48 hours were treated with local wound care and oral antibiotics. Wound drainage stopped between 2-4 days in 72%. The remaining patients underwent single debridement (76%) or additional treatment (repeat debridement, resection arthroplasty or long-term antibiotics). Timing of surgery and malnutrition predicted failure of the �rst debridement.
Lonner 12 Opinion N/A Several days after TJA N/A N/A Wound drainage beyond several days after surgery may increase the risk of infection. Drainage will usually stop after 24-48 hours of immobilization. If not, open debridement should be performed, including obtaining cultures, irrigation and meticulous wound closure. Exercises may be resumed once the wound is stable.
Maathuis 13 Retrospective
N = 558 TKAs / THAs
3 >5 days after TJA N/A 16.5% Comparison of an algorithmic approach to an ad hoc approach. In the algorithmic approach, registration of persistent wound drainage was two-fold (21% vs 11%), but the number of open debridements was lower (17% vs 30%) and the salvage rate higher (94% vs 85%)
Patel 4
Retrospective
N = 2437 TKAs / THAs
2 >5 days after TJA
≥2x2cm area of gauze covering the wound is wet or when �uid is noted to be originating from the surgical wound
20.1%
Persistent wound drainage results in longer hospital stay. Each day of wound drainage after day 5 increased the risk of wound infection by 42% following THA (p<.001) and by 29% following TKA (not signi�cant after correction for BMI).
Saleh 7 Prospective
N = 2305 TKAs / THAs
3 Wound drainage N/A N/A 33 patients developed a super�cial wound infection. Hematoma formation and days of wound drainage were signi�cant predictors of super�cial wound infection. 58% developed a prosthetic joint infection, patients with >5 days of wound drainage had 12.7 times more risk of developing a prosthetic joint infection.
Surin 5 Retrospective
N = 803 THAs
3 N/A N/A 12.6% 115 patients had super�cial wound drainage and cultures were positive in 70 wounds. 34 patients developed prosthetic joint infection. Patients with super�cial wound drainage had a 3.2 times higher risk of developing a prosthetic joint infection. The risk was further in�uenced by the character of the exudate and the use of prophylactic antibiotics.
Vince 1 Review / opinion N/A Limited amount of time
N/A N/A Persistent wound drainage should be treated by wound care and immobilization. If drainage does not stop after 3 to 7 days, open debridement should be performed. Aggressive surgery may prevent sepsis. Drainage that starts in the late postoperative phase is a great concern as it usually results from a prosthetic joint infection.
Weiss 8 Retrospective
N = 597 TKAs
4 ≥4 consecutive days beyond day 5 after TJA
≥2x2cm area of gauze covering the wound is wet or when �uid is noted to be originating from the surgical wound
1.3% 8 patients with persistent wound drainage. Open debridement was performed at an average of 12.5 days after index surgery. 25% of patients had positive tissue cultures. All patients were successfully treated with adjuvant antibiotics.
BMI: body mass index; INR: international normalized ratio; N/A: not applicable or not described; NPWT: negative pressure wound therapy; THA: total hip arthroplasty; TJA: total joint arthroplasty; TKA: total knee arthroplasty.
51938_Claudia_Lowik.indd 25 19-08-19 11:12

Chapter 2
26
Wound drainage is usually a non-infectious disturbance in wound healing of short duration that occurs during the �rst days after TJA,2 but it may be an early symptom of a (developing) PJI. Research published between 1973 and 1983 described PWD as one of the main risk factors for developing a PJI,5,15-19 even though several researchers could not observe a correlation between PWD and PJI.20-23 Contemporary research underscored the adverse e�ects of wound complications, such as an increased risk of PJI, readmission, prolonged hospital stay, re-operations, and higher health care costs.1-4,6-8,12,24
Regarding the consequences of PWD after total knee arthroplasty (TKA), Galat et al. found a 6% increased cumulative risk of PJI in patients who required early surgical treatment for any early wound healing complication after TKA.2 Moreover, these patients had 5.3% risk of major additional surgical intervention (resection arthroplasty, muscle �aps or amputation) in the �rst two years following TKA.2 A di�erent study by Galat et al. showed an increased risk of 10.5% for PJI and 12.3% risk for major re-operation within two years after TKA in patients who required surgical intervention for post-operative hematoma.25
Regarding the consequences of PWD after both total hip arthroplasty (THA) and TKA, Parvizi et al. demonstrated that patients who developed a PJI were more likely to have experienced PWD and hematoma than patients without PJI (16.8 and 12.6 times more likely respectively).26 Similar results were reported by Saleh et al.7
Although most studies on wound-related complications after TJA have focused on the risk of developing PJI, wound-related complications also predispose patients to worse functional outcome.1-4,7-9,12,24,27-32 Mortazavi et al. found substantially worse patient satisfaction and lower Harris Hip Scores in patients requiring additional surgery for hematoma after THA.31 Adelani et al. observed similar worse functional outcome for patients with wound complications after TKA.9 Moreover, published data suggest that patients with PWD after TKA have an increased risk of residual pain and poor functional outcome, similar to patients who develop an infectious complication after TKA.9 Patient expectation after wound complications following TJA should therefore be tempered, even if wound complications do not result in PJI.
51938_Claudia_Lowik.indd 26 19-08-19 11:12

Review on persistent wound drainage
27
2
Theoretical and practical considerations
Wound drainage after TJA can be physiological in the �rst days after index surgery. However, it is unknown when wound drainage should be perceived as persistent or abnormal. Many other issues related to wound complications remain unanswered as well, such as the following: to what extent will wound drainage impair wound healing and/or o�er a retrograde gateway for entry of pathogens into the joint space?8 Where does wound drainage originate? If it originates from deeper layers of the joint, does it represent an early deep infection or merely normal drainage from defects in the soft tissues? If it originates from outside the joint, does it represent normal wound drainage or a draining hematoma or abscess?1 All these issues are important for the decision-making process but remain di�cult to clarify.
De�nition of PWDLiterature lacks a proven de�nition of PWD in terms of both duration and amount of drainage. Previous studies used a de�nition of duration of wound drainage varying from two to nine days after index surgery (Table 1).3,8 In 2013, the �rst International Consensus Meeting (ICM) on PJI de�ned PWD as >2x2cm of drainage in the wound dressing beyond 72 hours after index surgery.27,33 This consensus stated that limiting the de�nition of PWD to 72 hours postoperative allows for early intervention that may prevent the adverse consequences of PWD. However, the de�nition of PWD should be further speci�ed and evaluated.
Clinical and serological signs of a developing infectionClinical signs of wound infection (super�cial or deep) include systemic and local signs. Systemic signs involve fever, chills, and tachycardia. Local signs include induration, painful skin erythema (especially around the sutures), warmth, purulent drainage, and presence of a sinus tract.34 However, some of these clinical signs are frequently observed in the �rst days after uncomplicated TJA surgery as an early physiological response to surgical trauma.
Fever or pyrexia (generally de�ned as temperature >38.5ºC / >101ºF) is physiological in the �rst three to �ve days after index surgery.35-45 In this postoperative phase, additional tests for an underlying infectious cause of fever is unwarranted as it results in patient discomfort, has minor clinical yield, and is accompanied by considerable health care costs.35,36,39-46 However, temperatures
51938_Claudia_Lowik.indd 27 19-08-19 11:12

Chapter 2
28
>39ºC, particularly if present for multiple days and/or later than three to �ve days after surgery, require further diagnostic tests.46
Described blood serology parameters in the diagnosis of PJI are C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and white blood cell count (WBC). After uncomplicated TJA surgery the CRP level increases rapidly and reaches maximum level (up to 200-400 mg/L) within two to three days, followed by a quick decrease and normalization to preoperative level in two to eight weeks after uncomplicated TJA, even in patients with rheumatoid arthritis.47-61 An infectious complication in patients with PWD should be suspected if CRP levels increase later than 72 hours after TJA, or remain elevated beyond seven days after TJA.52,57-59,61,62
The WBC and ESR are less appropriate for the diagnosis of PJI in case of PWD, since the WBC increases only slightly after surgery and returns to normal within seven days after index surgery, while the ESR increases only gradually, with peak level between day �ve and 14 and normalization in 19 days up to nine months after index surgery.47,54,55,59-61,63
An algorithmic approach to the decision-making processIn clinical practice, assessment of the origin (intra- or extra-articular) and type of wound drainage (physiologic or infectious secretion) is often di�cult. Weiss and Krackow concluded that wound drainage can o�er a pathway where pathogens can enter the wound and joint, acting as a retrograde pathway for infection.8 This implies that PWD should be perceived as potential imminent PJI, hence justifying a low threshold for early surgical intervention.1,64 However, advocating early surgical intervention may result in unnecessary operations, while delaying early surgical intervention may result in development of PJI. An evidence-based algorithmic approach on PWD may ease the decision-making process in the diagnosis and timing of treatment. In literature, some authors merely provided general statements on the evaluation of wound complications.1,2,27 Only few studies speci�cally addressed PWD3-8,13 and only one of these studies described an algorithmic approach.13 In this study, the algorithmic approach was compared with an ad hoc approach in which the surgeon decided upon own discretion. Even though the reported percentage of PWD was two times higher in the algorithmic cohort (21% vs 11%), the number of surgical interventions was lower (17% vs 30%) and the salvage percentage was higher (94% vs 85%).13 This suggests that an algorithmic approach may
51938_Claudia_Lowik.indd 28 19-08-19 11:12

Review on persistent wound drainage
29
2
lead to increased awareness of PWD and an improved decision-making process with a lower frequency of surgical interventions and better outcome.
Timing of treatmentThe optimal timing of starting non-surgical or surgical treatment in patients with PWD remains to be established. Patel et al. stated that each day of PWD beyond day �ve after TJA surgery increased the risk of wound infection with 42% after THA and 29% after TKA.4 Saleh et al. found a 12.7 times higher risk of developing PJI when the wound drained for more than �ve days after THA/TKA compared with patients with shorter duration of wound drainage. Based on these �ndings, they advised on performing open debridement in case of hematoma or PWD for more than seven days postoperative.7
More recently, Jaberi et al. (de�ning wound drainage as persistent when drainage soaked postoperative dressings for more than two days) showed that draining wounds after THA and TKA healed uncomplicated within two to four days of non-surgical treatment (wound care and antimicrobial treatment) in 72% of patients.3 The remaining 28% underwent open debridement. This was successful in 76% of patients, while the remaining 24% underwent subsequent treatment including repeated debridement, resection arthroplasty, or suppressive antimicrobial treatment. These authors recommended early surgery within seven days after index surgery even though their successful DAIRs were performed at a mean of 14 days (range 4-32 days) after index surgery.3 Based on these studies, the ICM formulated the statement that surgical treatment should be performed if wound drainage persists for longer than �ve to seven days after index surgery.27
Non-surgical treatment strategiesNon-surgical treatment strategies are usually performed prior to surgical intervention.27 Since PWD is associated with an increased risk of PJI, observation only is highly discouraged.3,4,7,8 Acceptable non-surgical treatment is adequate wound care by using absorbent dressings and pressure bandages (hand-made spica for the hip), supplemented by several days of joint immobilization and interruption of physical therapy.3,65 Bed rest and braces may impair early rehabilitation, but this outweighs the potential risk of prolonging the duration of PWD and increasing the risk of PJI.1,12 Good results were reported on the use of silver-impregnated dressings66 and negative pressure wound therapy
51938_Claudia_Lowik.indd 29 19-08-19 11:12

Chapter 2
30
(NPWT).11,67-69 However, a Cochrane meta-analysis could not �nd de�nitive evidence for the e�ectiveness of NPWT.69
The ICM advised on early analysis and correction of anticoagulation, anemia, glucose regulation in diabetic patients, and malnutrition.27 One study retrospectively evaluated 11,785 THAs/TKAs and found malnutrition to predispose for failure of surgical debridement and an increased risk of PJI in patients with PWD. Therefore, they recommended consultation of a nutritional physician in case of wound drainage persisting longer than 48 hours.3 With regard to anticoagulation, Parvizi et al. showed that patients with a mean International Normalized Ratio higher than 1.5 had an increased risk of developing wound complications and PJI after THA/TKA. Hence, they stressed the importance of cautious anticoagulant treatment in order to prevent formation of a hematoma and subsequent wound drainage.26
Although antimicrobial treatment during PWD has been described,3 current consensus discourages antimicrobial treatment due to a lack of evidence on decreasing the risk of PJI.11,12 Furthermore, it may confound culture results thus impairing the diagnosis of an early PJI. And �nally, concerns about the increase of antimicrobial resistance cannot be ignored.34
Surgical treatment strategies Most publications advocate early surgical treatment in case wound drainage persists despite a period of adequate non-surgical treatment.1,3,10,27 Surgical treatment typically consists of open deep debridement and thorough irrigation, using six to nine liters of saline administered by low-pressure pulsatile jet lavage.70 Optionally, diluted povidone-iodine or chlorhexidine gluconate can be used to irrigate the joint cavity.71-73 However, it should be recognized that these recommendations on irrigation are derived from literature on primary TJA and trauma surgery, mostly from animal and basic science studies.
Whenever possible, modular components should be exchanged as it o�ers a better potential for thorough debridement and irrigation deep to these modular components. Moreover, modular component exchange is advised because the polyethylene component (acetabular liner or tibial inlay) may be colonized by pathogens.8 The soft tissue should be meticulously closed in a multilayer fashion.12,27 NPWT is a plausible alternative when wound closure is not possible.69 In these cases, consultation of a plastic surgeon is recommended.
51938_Claudia_Lowik.indd 30 19-08-19 11:12

Review on persistent wound drainage
31
2
Administration of prophylactic antimicrobial treatment is advised prior to incision.34,74 Various deep tissue samples for bacterial cultures are obtained, preferably �ve samples to increase pathogen detection. Each tissue sample is obtained using a clean instrument to avoid contamination. Tissue swabs are not advised.34 Tissue samples should be cultured up to 14 days and antimicrobial treatment is continued until culture results are de�nitive.34 In case of positive culture results, targeted antimicrobial treatment should be continued in consultation with an infectious diseases specialist, usually six to twelve weeks. Jaberi et al. found positive deep periprosthetic tissue cultures in 34% (28 of 83 cases) after surgical treatment for PWD after THA/TKA. Cultures were more often positive in the failure group (17 of 20, 85%) compared with the success group (11 of 63, 17%).3 Weiss and Krackow, reporting PWD in eight of 597 primary TKAs, showed that 25% (two of eight cases) had positive cultures after surgical debridement at a mean of 12.5 days after surgery (range 8-18 days).8 However, issues can be raised on the statistical power of this study cohort.
Summary
The reported incidence of PWD after TJA varies between 0.2% and 21%, with higher incidences after revision TJA. This wide range in incidence is mainly caused by the variation in de�nitions of PWD. The ICM formulated a de�nition that de�nes PWD as >2x2cm for longer than 72 hours, but this de�nition should be further speci�ed and validated.
Clinical signs of infection and blood serology can be helpful in diagnosing PJI in case of PWD, although some clinical signs can be a normal physiological response in the �rst days after TJA. An increase in CRP later than 72 hours after index surgery or persistent elevated levels of CRP beyond seven days can indicate development of an infectious complication.
Non-surgical treatment of PWD generally involves absorbent dressings, pressure bandages and temporary joint immobilization. Present consensus discourages the use of antimicrobial treatment. Nutritional consultation and correction of anticoagulation and metabolic imbalances should be considered.
Surgical treatment should be performed when wound drainage persists for more than �ve to seven days after index procedure despite adequate non-surgical treatment. Nonetheless, establishing this time frame needs validation in
51938_Claudia_Lowik.indd 31 19-08-19 11:12

Chapter 2
32
future research. Surgical treatment should include thorough open debridement and irrigation, obtaining tissue samples (cultured up to 14 days) and exchange of modular components. Empirical broad-spectrum antimicrobial treatment is administered in consultation with an infectious diseases specialist.
Proposed algorithm
Based on this literature review, the authors developed an algorithm to facilitate the decision-making process of PWD after TJA (Figure 1). Although we aimed to di�erentiate between PWD in THA and TKA in this algorithm, we did not �nd enough scienti�c evidence to make this distinction. In addition to the algorithm, we also propose a classi�cation of PWD that divides wound drainage into four categories based on the amount of drainage (Table 2). As this classi�cation is merged into the algorithm, the amount of drainage is combined with the duration of drainage (Figure 1), in which larger amounts of wound drainage are tolerated for a shorter period. Hopefully, this algorithm o�ers the orthopaedic surgeon a practical clinical guideline by �nding the right balance between overtreatment and undertreatment, weighing risks and bene�ts. Currently, a multicenter randomized controlled trial on the optimal treatment of PWD after TJA is being conducted to examine the validity and applicability of such a classi�cation and algorithm in daily clinical practice.75
Table 2. Proposed classi�cation of persistent wound drainage after total joint arthroplasty
Category Description1 (Limited) A stripe of blood in the wound dressing in the line of the wound or less than 2x2cm
in size a
2 (Moderate) More than 2x2cm drainage in absorbent gauze or dressing but without the need for changing the wound dressing (i.e. dressing is not soaked)
3 (Excessive) One dressing change per day due to soaked absorbent gauze or dressing4 (Massive) Two or more daily dressing changes due to soaked absorbent gauzes or dressings
a According to the 2013 international consensus meeting on periprosthetic joint infection.28,33
Conclusion
This review summarizes the available literature addressing several issues in the �eld of PWD after TJA. There are limited scienti�c data on PWD and absence of an
51938_Claudia_Lowik.indd 32 19-08-19 11:12

Review on persistent wound drainage
33
2
evidence-based guideline regarding diagnosis and treatment, partially caused by the lack of a universally accepted de�nition. We developed a classi�cation of PWD and an algorithmic approach for the management of PWD after TJA to o�er the orthopaedic surgeon a practical guideline for daily clinical practice.
2 4
POD 5
POD 7
POD 10
Persistent drainage
cally suspected?
cally suspected?
Increasing lab(ESR/CRP/Leuco)
ORCat. 3?
(immobilizer knee, bedrest), pressure bandage knee or hip spica, nu onal
n
If possible+ tel. consult POD 9
Baseline lab(ESR/CRP/Leuco),
24(immobilizer knee, bedrest) and
pressure bandageknee or hip spica
Surgical andt
24(immobilizer knee, bedrest) and
pressure bandage knee or hip spica
Persistent drainage
1Persistent drainage
(Cat. 1 4)
1
1
1Persistent drainage
ge
2
3+4
Cat. 4
Cat. 2 and 3 Cat. 1
Yes
No
No
No
Yes
Yes
Figure 1. Proposed algorithm for diagnosis and treatment of persistent wound drainage after total joint arthroplasty
51938_Claudia_Lowik.indd 33 19-08-19 11:12
Chapter 2
34
References
1. Vince K, Chivas D, Droll KP. Wound complications after total knee arthroplasty. J Arthroplasty 2007; 22(4 Suppl 1): 39-44.
2. Galat DD, McGovern SC, Larson DR, Harrington JR, Hanssen AD, Clarke HD. Surgical treatment of early wound complications following primary total knee arthroplasty. J Bone Joint Surg Am 2009; 91(1): 48-54.
3. Jaberi FM, Parvizi J, Haytmanek CT, Joshi A, Purtill J. Procrastination of wound drainage and malnutrition a�ect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008; 466(6): 1368-71.
4. Patel VP, Walsh M, Sehgal B, Preston C, DeWal H, Di Cesare PE. Factors associated with prolonged wound drainage after primary total hip and knee arthroplasty. J Bone Joint Surg Am 2007; 89(1): 33-8.
5. Surin VV, Sundholm K, Bäckman L. Infection after total hip replacement: with special reference to a discharge from the wound. J Bone Joint Surg Br 1983; 65(4): 412-8.
6. Butt U, Ahmad R, Aspros D, Bannister GC. Factors a�ecting wound ooze in total knee replacement. Ann R Coll Surg Engl 2011; 93(1): 54-6.
7. Saleh K, Olson M, Resig S, Bershadsky B, Kuskowski M, Gioe T, et al. Predictors of wound infection in hip and knee joint replacement: results from a 20 year surveillance program. J Orthop Res 2002; 20(3): 506-15.
8. Weiss AP, Krackow KA. Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993; 8(3): 285-9.
9. Adelani MA, Johnson SR, Keeney JA, Nunley RM, Barrack RL. Clinical outcomes following re-admission for non-infectious wound complications after primary total knee replacement. Bone Joint J 2014; 96-B(5): 619-21.
10. Dennis DA. Wound complications in total knee arthroplasty. In: Sculco TP, ed. Knee arthroplasty, 1st ed. New York, USA: Springer Vienna; 1997: p. 163-9.
11. Hansen E, Durinka JB, Costanzo JA, Austin MS, Deirmengian GK. Negative pressure wound therapy is associated with resolution of incisional drainage in most wounds after hip arthroplasty. Clin Orthop Relat Res 2013; 471(10): 3230-6.
12. Lonner JH, Lotke PA. Aseptic complications after total knee arthroplasty. J Am Acad Orthop Surg 1999; 7(5): 311-24.
13. Maathuis PGM, de Hartog B, Bulstra SK. Timing of open debridement for suspected infection of joint prosthesis: a report on 551 patients. Curr Orthop Pract 2009; 20(5): 541-5.
14. Howick J, Chalmers I, Glasziou P, Greenhalgh T, Heneghan C, Liberati A, et al. The Oxford 2011 levels of evidence. Oxford Center of Evidence-based Medicine.
15. McLaughlan J, Smylie HG, Logie JR, Smith G. A study of the wound environment during total hip arthroplasty. Postgrad Med J 1976; 52(611): 550-7.
16. Franco JA, Baer H, Enneking WF. Airborne contamination in orthopedic surgery: evaluation of laminar air �ow system and aspiration suit. Clin Orthop Relat Res 1977; 122: 231-43.
17. Fitzgerald RH Jr, Nolan DR, Ilstrup DM, van Scoy RE, Washington JA 2nd, Coventry MB. Deep wound sepsis following total hip arthroplasty. J Bone Joint Surg Am 1977; 59(7): 847-55.
18. Schwan A, Bengtsson S, Hambraeus A, Laurell G. Airborne contamination and postoperative infection after total hip replacement. Acta Orthop Scand 1977; 48(1): 86-94.
19. Andrews HJ, Arden GP, Hart GM, Owen JW. Deep infection after total hip replacement. J Bone Joint Surg Br 1981; 63-B(1): 53-7.
20. Aglietti P, Salvati EA, Wilson PD Jr. A study of the e�ectiveness of a surgical unidirectional �ltered air �ow unit during total prosthetic replacements of the hip. Arch Orthop Trauma Surg 1973; 77(4): 257-68.
21. Aglietti P, Salvati EA, Wilson PD Jr, Kutner LJ. E�ect of a surgical horizontal unidirectional �ltered air �ow unit on wound bacterial contamination and wound healing. Clin Orthop Relat Res 1974; 101: 99-104.
22. Wilson PD Jr. Joint replacement. South Med J 1977; 70(Suppl 1): 55-60.
51938_Claudia_Lowik.indd 34 19-08-19 11:12

Review on persistent wound drainage
35
2
23. Freeman MA, Challis JH, Zelezonski J, Jarvis ID. Sepsis rates in hip replacement surgery with special reference to the use of ultra clean air. Arch Orthop Trauma Surg 1977; 90(1): 1-14.
24. Berbari EF, Hanssen AD, Du�y MC, Steckelberg JM, Ilstrup DM, Harmsen WS, et al. Risk factors for prosthetic joint infection: case-control study. Clin Infect Dis 1998; 27(5): 1247-54.
25. Galat DD, McGovern SC, Hanssen AD, Larson DR, Harrington JR, Clarke HD. Early return to surgery for evacuation of a postoperative hematoma after primary total knee arthroplasty. J Bone Joint Surg Am 2008; 90(11): 2331-6.
26. Parvizi J, Ghanem E, Joshi A, Sharkey PF, Hozack WJ, Rothman RH. Does “excessive” anticoagulation predispose to periprosthetic infection? J Arthroplasty 2007; 22(6 Suppl 2): 24-8.
27. Ghanem E, Heppert V, Spangehl M, Abraham J, Azzam K, Barnes L, et al. Wound management. J Orthop Res 2014; 32(Suppl 1): S108-19.
28. Ng VY, Lusteberger D, Hoang K, Urchek R, Beal M, Calhoun JH, et al. Preoperative risk strati�cation and risk reduction for total joint reconstruction: AAOS exhibit selection. J Bone Joint Surg Am 2013; 95(4): 1-15.
29. Fernandez-Fairen M, Torres A, Menzie A, Hernandez-Vaquero D, Fernandez-Carreira JM, Murcia-Mazon A, et al. Economical analysis on prophylaxis, diagnosis, and treatment of periprosthetic infections. Open Orthop J 2013; 7: 227-42.
30. Kurtz SM, Lau E, Schmier J, Ong KL, Zhao K, Parvizi J. Infection burden for hip and knee arthroplasty in the United States. J Arthroplasty 2008; 23(7): 984-91.
31. Mortazavi SMJ, Hansen P, Zmistowski B, Kane PW, Restrepo C, Parvizi J. Hematoma following primary total hip arthroplasty: a grave complication. J Arthroplasty 2013; 28(3): 498-503.
32. Zmistowski B, Karam JA, Durinka JB, Casper DS, Parvizi J. Periprosthetic joint infection increases the risk of one-year mortality. J Bone Joint Surg Am 2013; 95(24): 2177-84.
33. Parvizi J, Gehrke T, Chen AF. Proceedings of the international consensus on periprosthetic joint infection. Bone Joint J 2013; 95-B(11): 1450-2.
34. Zmistowski B, Della Valle C, Bauer TW, Malizos KN, Alavi A, Bedair H, et al. Diagnosis of periprosthetic joint infection. J Arthroplasty 2014; 29(2 Suppl): 77-83.
35. Shaw JA, Chung R. Febrile response after knee and hip arthroplasty. Clin Orthop Relat Res 1999; 367: 181-9.
36. Kennedy JG, Rodgers WB, Zurakowski D, Sullivan R, Gri�n D, Beardsley W, et al. Pyrexia after total knee replacement: a cause for concern? Am J Orthop 1997; 26(8): 549-52.
37. Summersell PC, Turnbull A, Long G, Diwan A, Macdessi S, Cooke PJ, et al. Temperature trends in total hip arthroplasty: a retrospective study. J Arthroplasty 2003; 18(4): 426-9.
38. Athanassious C, Samad A, Avery A, Cohen J, Chalnick D. Evaluation of fever in the immediate postoperative period in patients who underwent total joint arthroplasty. J Arthroplasty 2011; 26(8): 1404-8.
39. Ghosh S, Charity RM, Haidar SG, Singh BK. Pyrexia following total knee replacement. Knee 2006; 13(4): 324-7.
40. Czaplicki AP, Borger JE, Politi JR, Chambers BT, Taylor BC. Evaluation of postoperative fever and leukocytosis in patients after total hip and knee arthroplasty. J Arthroplasty 2011; 26(8): 1387-9.
41. Ward DT, Hansen EN, Takemoto SK, Bozic KJ. Cost and e�ectiveness of postoperative fever diagnostic evaluation in total joint arthroplasty patients. J Arthroplasty 2010; 25(6 Suppl): 43-8.
42. Guinn S, Castro FP Jr, Garcia R, Barrack RL. Fever following total knee arthroplasty. Am J Knee Surg 1999; 12(3): 161-4.
43. Tai TW, Chang CW, Lin CJ, Lai KA, Yang CY. Elevated temperature trends after total knee arthroplasty. Orthopedics 2009; 32(12): 886.
44. Bindelglass DF, Pellegrino J. The role of blood cultures in the acute evaluation of postoperative fever in arthroplasty patients. J Arthroplasty 2007; 22(5): 701-2.
45. Anderson JT, Osland JD. Blood cultures for evaluation of fever after total joint arthroplasty. Am J Orthop 2009; 38(8): 134-6.
46. Chen AF, Haddad FS, Lachiewicz P, Bolognesi M, Cortes LE, Franceschini M, et al. Prevention of late PJI. J Arthroplasty 2014; 92(2 Suppl): 119-28.
51938_Claudia_Lowik.indd 35 19-08-19 11:12

Chapter 2
36
47. Bilgen O, Atici T, Durak K, Karaeminoğullari K, Bilgen MS. C-reactive protein values and erythrocyte sedimentation rates after total hip and total knee arthroplasty. J Int Med Res 2001; 29(1): 7-12.
48. Kolstad K, Levander H. In�ammatory laboratory tests after joint replacement surgery. Ups J Med Sci 1995; 100(3): 243-8.
49. Laiho K, Mäenpää H, Kautiainen H, Kauppi M, Kaarela K, Lehto M, et al. Rise in serum C reactive protein after hip and knee arthroplasties in patients with rheumatoid arthritis. Ann Rheum Dis 2001; 60(3): 275-7.
50. Moreschini O, Greggi G, Giordano MC, Nocente M, Margheritini F. Postoperative physiopathological analysis of in�ammatory parameters in patients undergoing hip or knee arthroplasty. Int J Tissue React 2001; 23(4): 151-4.
51. Neumaier M, Metak G, Scherer MA. C-reactive protein as a parameter of surgical trauma: CRP response after di�erent types of surgery in 349 hip fractures. Acta Orthop 2006; 77(5): 788-90.
52. Foglar C, Lindsey RW. C-reactive protein in orthopedics. Orthopedics 1998; 21(6): 687-91.53. Maury CPJ, Teppo AM, Raunio P. Control of the acute-phase serum amyloid A and C-reactive protein
response: comparison of total replacement of the hip and knee. Eur J Clin Invest 1984: 14(5): 323-8.54. Park KK, Kim TK, Chang CB, Yoon SW, Park KU. Normative temporal values of CRP and ESR in
unilateral and staged bilateral TKA. Clin Orthop Relat Res 2008: 466(1): 179-88.55. Honsawek S, Deepaisarnsakul B, Tanavalee A, Sakdinakiattikoon M, Ngarmukos S, Preativatanyou
K, et al. Relationship of serum IL-6, C-reactive protein, erythrocyte sedimentation rate, and knee skin temperature after total knee arthroplasty: a prospective study. Int Orthop 2011; 35(1): 31-5.
56. Choudry RR, Rice RP, Tri�t PD, Harper WM, Gregg PJ. Plasma viscosity and C-reactive protein after total hip and knee arthroplasty. J Bone Joint Surg Br 1992; 74(4): 523-4.
57. Niskanen RO, Korkala O, Pammo H. Serum C-reactive protein levels after total hip and knee arthroplasty. J Bone Joint Surg Br 1996; 78(3): 431-3.
58. White J, Kelly M, Dunsmuir R. C-reactive protein level after total hip and knee replacement. J Bone Joint Surg Br 1998; 80(5): 909-11.
59. Shih LY, Wu JJ, Yang DJ. Erythrocyte sedimentation rate and C-reactive protein values in patients with total hip arthroplasty. Clin Orthop Relat Res 1987; 225: 238-46.
60. Aalto K, Osterman K, Peltola H, Räsänen J. Changes in erythrocyte sedimentation rate and C-reactive protein after total hip arthroplasty. Clin Orthop Relat Res 1984; 184: 118-20.
61. Larsson S, Thelander U, Friburg S. C-reactive protein (CRP) levels after elective orthopedic surgery. Clin Orthop Relat Res 1992; 275: 237-42.
62. Yi PH, Cross MB, Moric M, Sporer SM, Berger RA, Della Valle CJ. Diagnosis of infection in the early postoperative period after total hip arthroplasty. Clin Orthop Relat Res 2014: 472(2): 424-9.
63. Covey DC, Albright JA. Clinical signi�cance of the erythrocyte sedimentation rate in orthopaedic surgery. J Bone Joint Surg Am 1987; 69(1): 148-51.
64. Wilson MG, Kelly K, Thornhill TS. Infection as a complication of total knee replacement arthroplasty: risk factors and treatment of sixty-seven cases. J Bone Joint Surg Am 1990; 72(6): 878-83.
65. Hahn GJ, Grant D, Bartke C, McCartin J, Carn RM. Wound complications after hip surgery using a tapeless compressive support. Orthop Nurs 1999; 18(3): 43-9.
66. Percival SL, Slone W, Linton S, Okel T, Corum L, Thomas JG. The antimicrobial e�cacy of a silver alginate dressing against a broad spectrum of clinically relevant wound isolates. Int Wound J 2011; 8(3): 237-43.
67. Pachowsky M, Gusinde J, Klein A, Lehrl S, Schulz-Drost S, Schlechtweg P, et al. Negative pressure wound therapy to prevent seromas and treat surgical incisions after total hip arthroplasty. Int Orthop 2012; 36(4): 719-22.
68. Masden D, Goldstein J, Endara M, Xu K, Steinberg J, Attinger C. Negative pressure wound therapy for at-risk surgical closures in patients with multiple comorbidities: a prospective randomized controlled study. Ann Surg 2012; 255(6): 1043-7.
69. Webster J, Scu�ham P, Stankiewicz M, Chaboyer WP. Negative pressure wound therapy for skin grafts and surgical wound healing by primary intention (review). Cochrane Database Syst Rev 2014; 10.
51938_Claudia_Lowik.indd 36 19-08-19 11:12

Review on persistent wound drainage
37
2
70. Crowley DJ, Kanakaris NK, Giannoudis PV. Irrigation of the wounds in open fractures. J Bone Joint Surg Br 2007; 89(5): 580-5.
71. Lineaweaver W, McMorris S, Soucy D, Howard R. Cellular and bacterial toxicities of topical antimicrobials. Plast Reconstr Surg 1985; 75(3): 394-6.
72. Brown NM, Cipriano CA, Moric M, Sporer SM, Della Valle CJ. Dilute betadine lavage before closure for the prevention of acute postoperative deep periprosthetic joint infection. J Arthroplasty 2012; 27(1): 27-30.
73. Ruder JA, Springer BD. Treatment of periprosthetic joint infection using antimicrobials: dilute povidone-iodine lavage. J Bone Joint Infect 2017; 2(1): 10-4.
74. Atkins BL, Athanasou N, Deeks JJ, Crook DW, Simpson H, Peto TEA, et al. Prospective evaluation of criteria for microbiological diagnosis of prosthetic-joint infection at revision arthroplasty. J Clin Microbiol 1998; 36(10): 2932-9.
75. Löwik CAM, Wagenaar FC, van der Weegen W, Poolman RW, Nelissen RGHH, Bulstra SK, et al. LEAK study: design of a nationwide randomised controlled trial to �nd the best way to treat wound leakage after primary hip and knee arthroplasty. BMJ Open 2017; 7(12): e018673.
51938_Claudia_Lowik.indd 37 19-08-19 11:12

51938_Claudia_Lowik.indd 38 19-08-19 11:12

Chapter 3
Periprosthetic joint infection in orthopaedic surgical oncology
Claudia A.M. Löwik, Roel-Jan W.J. Zuidhof, Joris J.W. Ploegmakers, Sander P.D. Dijkstra, Marjan Wouthuyzen-Bakker, Paul C. Jutte
Published in: Annals of Joint 2019; 4: 26
51938_Claudia_Lowik.indd 39 19-08-19 11:12

Chapter 3
40
Abstract
The use of tumor megaprostheses in patients with bone tumors has provided a successful limb salvaging treatment option in oncology patients. Unfortunately, the prevalence of periprosthetic infection is much higher after oncologic joint arthroplasty than after regular joint arthroplasty, ranging from 7% to 28%. This increased risk of infection is caused by local and systemic immunode�ciency due to chemotherapy and radiotherapy, long duration of surgery, large wound areas and the use of large implants. This review focused on speci�c issues regarding infected megaprostheses in oncology patients, aiming to give directions for the prevention, diagnosis and treatment of infected megaprostheses.
51938_Claudia_Lowik.indd 40 19-08-19 11:12

Periprosthetic joint infection in orthopaedic surgical oncology
41
3
Introduction
Total joint arthroplasties (TJAs) are highly successful orthopaedic surgical interventions and are most frequently applied in patients with degenerative joint disorders. The number of TJAs being implanted annually is still rising due to an ageing population. It is estimated that approximately four million TJAs will be performed in 2030 in the USA alone.1 Even though these procedures are usually successful with substantial improvement in the patient’s quality of life, 1-2% of patients with primary implants and 7% of patients with revised implants develop periprosthetic joint infection (PJI).2 Although the prevalence of PJI is relatively low, its clinical impact is evident. Due to formation of a bio�lm at the surface of the implant it is hard to treat PJI. This results in the need for extensive surgical re-interventions, which is accompanied by high morbidity.3
As with TJAs indicated for degenerative joint disorders, PJI is also reported in patients with oncologic TJAs (periprosthetic infection of a megaprosthesis (PMI)). The prevalence of PMI after oncologic TJA is much higher than after regular TJA and ranges from 7% to 28%.4-6 This higher prevalence is reasonably caused by local and systemic immunode�ciency, long duration of surgery, large wound areas and the use of large implants due to extensive tumor resection.7,8 Oncology patients are often immunode�cient because of the application of (neoadjuvant) chemotherapy or radiotherapy. Immunode�ciency leads to a decreased host defense, increased bleeding and compromised soft tissue healing. Moreover, due to prolonged duration of the procedure and a larger implant, the orthopaedic oncology patient has an even higher risk of compromised soft tissue healing. In addition, larger wound areas and resection could result in signi�cant dead space and subsequently massive hematoma formation which further increases the risk of infection.9
In order to assess the risk of infection after oncologic TJA this article focuses on speci�c issues regarding PJI in orthopaedic oncological implant surgery, aiming to give directions for the prevention, diagnosis and treatment of PMI.
51938_Claudia_Lowik.indd 41 19-08-19 11:12

Chapter 3
42
Prevention
Antibiotic prophylaxisPerioperative prophylactic antibiotic treatment has proven to be e�ective in reducing the risk of PJI after regular TJA from 5% to 1% when one preoperative dose and two postoperative doses of prophylactic antibiotics are administered within the �rst 24 hours after TJA.10 In oncologic TJA it is clinical practice in many hospitals to administer prophylactic antibiotics longer than 24 hours after TJA (up to 5 days). This is in line with the conclusions of a systematic review conducted by Racano et al. which showed that extended postoperative antibiotic prophylaxis can reduce the risk of PMI from 13% to 8%.8 Limitations of this review are the variety and inconsistency of antibiotics administered, lack of a clear de�nition of PMI, and low level of evidence of the included studies.8 These results emphasize the heterogeneity in the orthopaedic oncology patients compared with conventional orthopaedic patients, which indicates that various antibiotic prophylaxis strategies may be required. Thereby, it demonstrates the importance of composing evidence-based guidelines for antibiotic prophylaxis in oncologic orthopaedic surgery. Currently, an international multicentre study is performed to compare the e�ect of prophylactic antibiotic duration of 24 hours versus �ve days after oncologic TJA (PARITY study).11 The results of this study may provide su�cient evidence on the appropriate duration of antibiotic prophylaxis.
A di�erent method of administering antibiotic prophylaxis is soaking the endoprosthesis and/or allograft in antibiotic or antiseptic solutions before implantation. This soaking could result in a reduced infection rate by releasing local antimicrobials and thereby diminishing the bacterial load on the implant prior to implantation. However, only few studies have been conducted to evaluate the e�ectiveness of this type of prophylaxis. Therefore, implementation of soaking as standard antibiotic prophylaxis remains debatable.12
Endoprosthetic coatings The use of endoprosthetic coatings is an e�ective preventive measure for PMI. Endoprosthetic coatings provide a technique for the local delivery of antibiotics or antiseptics and show promising results in in vitro studies.13 These coatings can prevent bacterial colonization and promote ingrowth of the TJA, which is especially important in the application of cementless implants.
51938_Claudia_Lowik.indd 42 19-08-19 11:12

Periprosthetic joint infection in orthopaedic surgical oncology
43
3
Recent studies investigated the e�cacy of silver coatings.14 Silver coatings possess bactericidal properties operating by disrupting the cellular membrane of microorganisms and preventing DNA formation. Several studies reported a decrease of 50% in the prevalence of PMI when using a silver coating compared to uncoated TJAs.15,16 Hardes et al. showed that silver levels remained present in the serum up to 24 months after implantation of the silver coated TJA, but despite this �nding no adverse local tissue reactions or systemic toxicity were reported.17 Bosetti et al. determined the silver concentration in drains and seroma in patients with a silver coated megaprosthesis. Local argyria occurred in 23% of patients, independent of the silver concentration. No systemic toxic reactions to silver have been reported.18 Although results regarding silver coated prosthesis are promising, additional prospective studies are needed to con�rm the e�ectivity of silver coated TJAs in oncology patients.
De�nition and classi�cation
There are several guidelines that can be used for the de�nition and classi�cation of PMI. The most commonly used de�nitions for general PJI are based on the guidelines developed by the Infectious Diseases Society of America (IDSA) and Musculoskeletal Infection Society (MSIS).19,20 These general PJI de�nitions can also be applied to PMI. It is advised to use one of these two de�nitions, so that the results in literature are comparable and can be used for the estimation of the prognosis and success of treatment strategies.
Diagnosis
Regarding the diagnosis of PMI, similar principles apply as for general PJI. The suspicion of PMI can be raised based on symptoms, radiological signs, serological markers and synovial markers. Regarding the symptoms of PMI, pain at the site of implant is a consistent symptom of infection in over 90% of cases of PMI.21 As for radiological signs, the following signs indicate PMI: a periosteal reaction, scattered foci of osteolysis, or generalized bone resorption in the absence of implant wear.22
51938_Claudia_Lowik.indd 43 19-08-19 11:12

Chapter 3
44
Various serological markers are available for diagnostic screening. The most commonly used markers are C-reactive protein (CRP), erythrocyte sedimentation rate (ESR) and white blood cell count (WBC). The combined use of CRP and ESR can be helpful in the diagnosis of PMI, since their combined sensitivity and speci�city are 99% and 89%, respectively.23 After uncomplicated TJA the serum CRP level increases rapidly within two to three days, with normalization to the preoperative level in two to eight weeks.24,25 The ESR increases more gradually than the CRP, with peak level between day �ve and 14 and normalization in up to nine months after TJA.24,26 PMI should be suspected if CRP levels increase later than three days after TJA or remain elevated.25,27 Nevertheless, increased values of these serological markers may also be associated with oncologic conditions, which decreases their usefulness in oncology patients.28 Moreover, WBC may be reduced in oncology patients as a result of myelosuppressive chemotherapy.
If PMI is suspected based on clinical symptoms, radiological signs or serological markers, joint aspiration should be performed. There are several synovial markers that can be used, of which CRP, WBC and percentage of neutrophils are most frequently used. Synovial CRP shows sensitivity 70-97% and speci�city 79-100%,29,30 synovial WBC shows sensitivity 36-100% and speci�city 80-99%,31,32 and percentage of neutrophils shows sensitivity 84-100% and speci�city 80-99%.31,32 The sensitivity can be improved by serial aspirations. Currently, other synovial biomarkers are being tested with good results, such as leukocyte esterase,33 alpha-defensin,34 and calprotectin.35 When PMI is suspected but cannot be con�rmed by serological or synovial markers, bone scintigraphy, white blood cell scan or PET-scan can be performed.
The golden standard for diagnosing PMI is obtaining positive intra-articular cultures. Before obtaining these cultures, antibiotics should be withheld for a minimum of two weeks, to minimize the risk of false-negative results. Nevertheless, a single dose of prophylactic antibiotics does not alter intra-articular culture results and should therefore not be withheld.36 The incubation period of cultures should be at least seven days, although a minimum of two weeks is advised.37 The most common microorganisms causing PMI are Staphylococcus aureus and coagulase negative staphylococci. Together they account for over 50% of PMIs. A large proportion of PMIs are polymicrobial infections (21-45%).5,38
51938_Claudia_Lowik.indd 44 19-08-19 11:12

Periprosthetic joint infection in orthopaedic surgical oncology
45
3
Treatment
DAIR versus revision surgeryDebridement, antibiotics and implant retention (DAIR) is one of the treatment strategies frequently applied for PMI in orthopaedic oncology patients, especially in early PMI (within three months after index surgery).39,40 Nevertheless, infection control after DAIR varies widely with success rates varying from 39% to 70%.15,41,42 Several factors are associated with a higher rate of infection control after DAIR, including: early infection, short duration of symptoms, well-�xed implants and pre-operatively identi�ed microorganisms.43 Unfortunately, studies reporting DAIR results in oncology patients are scarce and have large variation in follow-up periods. In our opinion, DAIR should be used as the �rst treatment option in early PMI, especially considering the enormous consequences of removal of the large arthroplasty in oncology patients.
If DAIR fails to eradicate the infection, two-stage revision surgery is usually necessary. In literature, high rates of infection control are reported for two-stage revision surgery, with success rates varying from 63% to 100%.4,38,44 Other treatment strategies include one-stage revision, suppressive antibiotics and amputation, but all are considered less appropriate as initial treatment for PMI, most importantly since the rates of infection control after one-stage revision are worse than after two-stage revision.5,38,45 In addition, rates of infection control are higher when DAIR and two-stage revisions are performed in patients with a silver coated TJA.15
Use of a spacer in two-stage revision surgeryThe use of antibiotic-loaded cement spacers in two-stage revision surgery o�ers the advantages of delivering antibiotics locally at the site of infection while maintaining soft tissue tension to facilitate reimplantation of the TJA. In literature, no details are published on the design or composition of antibiotic-loaded cement spacers in case of two-stage revision surgery in PMI. Therefore, at this time point the current concepts of the use of spacers in two-stage revision in regular PJI should be applied to the oncology patients as well. According to these concepts, antibiotics added to the cement spacer should be heat-stable and should provide coverage for the identi�ed or suspected microorganisms causing the infection.46 Figure 1a illustrates the application of a customized spacer during the �rst stage of two-stage revision surgery. If the soft tissue is
51938_Claudia_Lowik.indd 45 19-08-19 11:12

Chapter 3
46
of acceptable quality at the time of surgery, a two-component spacer is a good option to prevent sti�ness of the joint. Figure 1b illustrates reimplantation of the implant during the second stage of revision surgery. Figure 1c shows that a gastrocnemius muscle �ap with free skin graft is used to cover the soft tissue defect. This indicates that it is valuable to collaborate with a plastic surgeon to provide good soft tissue coverage in two-stage revision surgery, especially in reconstructions in the proximal tibia and distal femur.
a
b
c
Figure 1. Two-stage revision surgery in a patient with PMI. a) Application of a customized two-component spacer after removal of a proximal tibia megaprosthesis. b) Reimplantation of a megaprosthesis. c) Use of a gastrocnemius muscle and free skin graft to cover the soft tissue defect.
51938_Claudia_Lowik.indd 46 19-08-19 11:12

Periprosthetic joint infection in orthopaedic surgical oncology
47
3
Use of antibiotics in the treatment of PMILiterature regarding the use of antibiotics in the surgical treatment of PMI is scarce. In the available literature on oncology patients, antibiotic regimens di�ered per patient according to the individual culture results and local protocol, about which no details were provided. Therefore, at this time point the current concepts for the use of antibiotics in regular PJI should be applied to oncology patients as well. In general, antibiotics are administered intravenously for at least two weeks, followed by oral antibiotics for at least ten weeks. The type of antibiotics is adjusted according to the culture results and resistance patterns, in consultation with an infectious diseases specialist.
In�uence of radiotherapy and chemotherapy on infection controlRadiotherapy increases the risk of PMI.45,47 Also, it increases the rate of failure after two-stage revision for PMI.4,44 Postoperative radiotherapy is of bigger in�uence on the infection rate than preoperative radiotherapy. This especially accounts for DAIR procedures, in which postoperative radiotherapy negatively in�uences the quality of the soft tissues and therefore hampers the local defence mechanisms and local availability of antibiotics.47
Several studies found an increased rate of PMI in patients receiving chemotherapy with incidences ranging from 18 to 32%,15,48,49 although other studies could not con�rm these results.5,43,50 In patients receiving two-stage revision surgery, it is advised to delay reimplantation of the TJA until completion of chemotherapy, because of the immunocompromised status of oncology patients receiving chemotherapy and the associated high risk regarding re-infection.43
Conclusion
While the diagnosis and treatment of regular PJI are already challenging, PMI poses additional challenges because of the immunocompromised status of oncology patients and extensive tumor resections. In general, regular PJI guidelines can be used for the prevention, diagnosis and treatment of PMI, although di�erences between regular patients and oncology patients should be kept in mind. Most importantly, wound healing after TJA should be monitored intensively, especially in patients receiving radiotherapy or
51938_Claudia_Lowik.indd 47 19-08-19 11:12

Chapter 3
48
chemotherapy, since these patients are immunocompromised and have a diminished quality of the soft tissues surrounding the joint. Perioperative antibiotic prophylaxis could be extended in these patients to reduce the risk of PMI. Current ongoing studies may provide clear recommendations for this in the future. Furthermore, silver coated TJAs could provide bene�cial e�ects in the prevention of PMI. In case PMI has developed, DAIR is the �rst choice of surgical treatment, especially in early infections. Two-stage revision surgery is a viable option in case DAIR is unsuccessful. Reimplantation of the TJA should be postponed until chemotherapy is completed.
51938_Claudia_Lowik.indd 48 19-08-19 11:12

Periprosthetic joint infection in orthopaedic surgical oncology
49
3
References
1. Darouiche RO. Treatment of infections associated with surgical implants. N Engl J Med 2004; 350(14): 1422-9.
2. Kurtz SM, Ong KL, Lau E, Bozic KJ, Berry D, Parvizi J. Prosthetic joint infection risk after TKA in the medicare population. Clin Orthop Relat Res 2010; 468(1): 52-6.
3. Abad CL, Haleem A. Prosthetic joint infections: an update. Curr Infect Dis Rep 2018; 20(7): 1–13. 4. Grimer RJ, Belthur M, Chandrasekar C, Carter SR, Tillman RM. Two-stage revision for infected
endoprostheses used in tumor surgery. Clin Orthop Relat Res 2002; 395: 193–203. 5. Hardes J, Gebert C, Schwappach A, Ahrens H, Streitburger A, Winkelmann W, et al. Characteristics
and outcome of infections associated with tumor endoprostheses. Arch Orthop Trauma Surg 2006; 126(5): 289–96.
6. Jeys LM, Grimer RJ, Carter SR, Tillman RM, Abudu A. Post operative infection and increased survival in osteosarcoma patients: are they associated? Ann Surg Oncol 2007; 14(10): 2887–95.
7. Nagano S, Yokouchi M, Setoguchi T, Sasaki H, Shimada H, Kawamura I, et al. Analysis of surgical site infection after musculoskeletal tumor surgery: risk assessment using a new scoring system. Sarcoma 2014; 1: 1-9.
8. Racano A, Pazionis T, Farrokhyar F, Deheshi B, Ghert M. High infection rate outcomes in long-bone tumor surgery with endoprosthetic reconstruction in adults: a systematic review. Clin Orthop Relat Res 2013; 471(6): 2017–27.
9. Kapoor SK, Thiyam R. Management of infection following reconstruction in bone tumors. J Clin Orthop Trauma 2015; 6(4): 244–51.
10. Yates AJ Jr. Postoperative prophylactic antibiotics in total joint arthroplasty. Arthroplast Today 2018; 4(1): 130–1.
11. Ghert M, Deheshi B, Holt G, Randall RL, Ferguson P, Wunder J, et al. Prophylactic antibiotic regimens in tumour surgery (PARITY): protocol for a multicentre randomised controlled study. BMJ Open 2012; 2(6).
12. Berriós-Torres SI, Umscheid CA, Bratzler DW, Leas B, Stone EC, Kelz RR, et al. Centers for disease control and prevention guideline for the prevention of surgical site infection. JAMA Surg 2017; 152(8): 784-91.
13. Neut D, Dijkstra RJB, Thompson JI, van der Mei HC, Busscher HJ. Antibacterial e�cacy of a new gentamicin-coating for cementless prostheses compared to gentamicin-loaded bone cement. J Orthop Res 2011; 29(11): 1654–61.
14. Romanò CL, Scarponi S, Gallazzi E, Romanò D, Drago L. Antibacterial coating of implants in orthopaedics and trauma: a classi�cation proposal in an evolving panorama. J Orthop Surg Res 2015; 10(1): 1–11.
15. Wafa H, Grimer RJ, Reddy K, Jeys LM, Abudu A, Carter SR, et al. Retrospective evaluation of the incidence of early periprosthetic infection with silver-treated endoprostheses in high-risk patients: case-control study. Bone Joint J 2015; 97-B(2): 252-7.
16. Donati F, Di Giacomo G, D’Adamio S, Ziranu A, Careri S, Rosa M, et al. Silver-coated hip megaprosthesis in oncological limb salvage surgery. Biomed Res Int 2016; 2016: 1–6.
17. Hardes J, Ahrens H, Gebert C, Streitbuerger A, Buerger H, Erren M, et al. Lack of toxicological side-e�ects in silver-coated megaprostheses in humans. Biomaterials 2007; 28(18): 2869–75.
18. Bosetti M, Massè A, Tobin E, Cannas M. Silver coated materials for external �xation devices: in vitro biocompatibility and genotoxicity. Biomaterials 2002; 23(3): 887-92.
19. Parvizi J, Zmistowski B, Berbari EF, Bauer TW, Springer BD, Della Valle CJ, et al. New de�nition for periprosthetic joint infection: from the workgroup of the musculoskeletal infection society. Clin Orthop Relat Res 2011; 469(11): 2992-4.
20. Osmon DR, Berbari ER, Berendt AR, Lew D, Zimmerli W, Steckelberg JM, et al. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 2013; 56(1): 1-25.
51938_Claudia_Lowik.indd 49 19-08-19 11:12

Chapter 3
50
21. Tsaras G, Osmon DR, Mabry T, Lahr B, St Sauveur J, Yawn B, et al. Incidence, secular trends, and outcomes of prosthetic joint infection: a population based study, Olmsted county, Minnesota, 1969-2007. Infect Control Hosp Epidemiol 2013; 33(12): 1207–12.
22. Ostlere S. How to image metal-on-metal prostheses and their complications. AJR Am J Roentgenol 2011; 197(3): 558–67.
23. Costa CR, Johnson AJ, Naziri Q, Maralunda GA, Delanois RE, Mont MA. E�cacy of erythrocyte sedimentation rate and C-reactive protein level in determining periprosthetic hip infections. Am J Orthop 2012; 41(4): 160–5.
24. Bilgen O, Atici T, Durak K, Karaeminoğullari K, Bilgen MS. C-reactive protein values and erythrocyte sedimentation rates after total hip and total knee arthroplasty. J Int Med Res 2001; 29(1): 7-12.
25. White J, Kelly M, Dunsmuir R. C-reactive protein level after total hip and knee replacement. J Bone Joint Surg Br 1998; 80(5): 909-11.
26. Honsawek S, Deepaisarnsakul B, Tanavalee A, Sakdinakiattikoon M, Ngarmukos S, Preativatanyou K, et al. Relationship of serum IL-6, C-reactive protein, erythrocyte sedimentation rate, and knee skin temperature after total knee arthroplasty: a prospective study. Int Orthop 2011; 35(1): 31-5.
27. Niskanen RO, Korkala O, Pammo H. Serum C-reactive protein levels after total hip and knee arthroplasty. J Bone Joint Surg Br 1996; 78(3): 431-3.
28. Van Hemelrijck M, Holmberg L, Garmo H, Hammar N, Walldius G, Binda E, et al. Association between levels of C-reactive protein and leukocytes and cancer: Three repeated measurements in the Swedish AMORIS study. Cancer Epidemiol Biomarkers Prev 2011; 20(3): 428–37.
29. Parvizi J, Jacovides C, Adeli B, Jung KA, Hozack WJ. Synovial C-reactive protein: a prospective evaluation of a molecular marker for periprosthetic knee joint infection. Clin Orthop Relat Res 2012; 470(1): 54–60.
30. Tetreault MW, Wetters NG, Moric M, Gross CE, Della Valle CJ. Is synovial C-reactive protein a useful marker for periprosthetic joint infection? Clin Orthop Relat Res 2014; 472(12): 3997–4003.
31. Dinneen A, Guyot A, Clements J, Bradley N. Synovial �uid white cell and di�erential count in the diagnosis or exclusion of prosthetic joint infection. Bone Joint J 2013; 95-B(4): 554–7.
32. Ghanem E, Parvizi J, Burnett RS, Sharkey PF, Keshavarzi N, Aggarwal A, et al. Cell count and di�erential of aspirated �uid in the diagnosis of infection at the site of total knee arthroplasty. J Bone Joint Surg Am 2008; 90(8): 1637–43.
33. Wetters NG, Berend KR, Lombardi AV, Morris MJ, Tucker TL, Della Valle CJ. Leukocyte esterase reagent strips for the rapid diagnosis of periprosthetic joint infection. J Arthroplasty 2012; 27(8 Suppl): 8–11.
34. Deirmengian C, Kardos K, Kilmartin P, Cameron A, Schiller K, Booth RE Jr, et al. The alpha-defensin test for periprosthetic joint infection outperforms the leukocyte esterase test strip. Clin Orthop Relat Res 2015; 473(1): 198–203.
35. Wouthuyzen-Bakker M, Ploegmakers JJW, Kampinga GA, Wagenmakers-Huizenga L, Jutte PC, Muller Kobold AC. Synovial calprotectin: a potential biomarker to exclude a prosthetic joint infection. Bone Joint J 2017; 99-B(5): 660-5.
36. Wouthuyzen-Bakker M, Benito N, Soriano A. The e�ect of preoperative antimicrobial prophylaxis on intraoperative culture results in patients with suspected or con�rmed prosthetic joint infection: a systematic review. J Clin Microbiol 2017; 55(9): 2765–74.
37. Fink B, Makowiak C, Fuerst M, Berger I, Schäfer P, Frommelt L. The value of synovial biopsy, joint aspiration and C-reactive protein in the diagnosis of late peri-prosthetic infection of total knee replacements. J Bone Joint Surg Br 2008; 90(7): 874-8.
38. Jeys LM, Grimer RJ, Carter SR, Tillman RM. Periprosthetic infection in patients treated for an orthopaedic oncological condition. J Bone Joint Surg Am 2005; 87(4): 842–9.
39. Yokoe DS, Avery TR, Platt R, Huang SS. Reporting surgical site infections following total hip and knee arthroplasty: impact of limiting surveillance to the operative hospital. Clin Infect Dis 2013; 57(9): 1282-8.
40. Barrett L, Atkins B. The clinical presentation of prosthetic joint infection. J Antimicrob Chemother 2014; 69(Suppl 1): 25-8.
41. Dhanoa A, Ajit Singh V, Elbahri H. Deep infections after endoprosthetic replacement operations in orthopedic oncology patients. Surg Infect (Larchmt) 2015; 16(3): 323–32.
51938_Claudia_Lowik.indd 50 19-08-19 11:12

Periprosthetic joint infection in orthopaedic surgical oncology
51
3
42. Peel TN, Cheng AC, Buising KL, Choong PFM. Microbiological aetiology, epidemiology, and clinical pro�le of prosthetic joint infections: are current antibiotic prophylaxis guidelines e�ective? Antimicrob Agents Chemother 2012; 56(5): 2386–91.
43. Mavrogenis AF, Papagelopoulos PJ, Coll-Mesa L, Pala E, Guerra G, Ruggieri P. Infected tumor prostheses. Orthopedics 2011; 34(12): 991–8.
44. Flint MN, Gri�n AM, Bell RS, Wunder JS, Ferguson PC. Two-stage revision of infected uncemented lower extremity tumor endoprostheses. J Arthroplasty 2007; 22(6): 859–65.
45. Funovics PT, Hip� C, Hofstaetter JG, Puchner S, Kotz RI, Dominkus M. Management of septic complications following modular endoprosthetic reconstruction of the proximal femur. Int Orthop 2011; 35(10): 1437–44.
46. Bloom�eld MR, Klika AK, Barsoum WK. Antibiotic-coated spacers for total hip arthroplasty infection. Orthopedics 2010; 33(9): 1–9.
47. Jeys LM, Luscombe JS, Grimer RJ, Abudu A, Tillman RM, Carter SR. The risks and bene�ts of radiotherapy with massive endoprosthetic replacement. J Bone Joint Surg Br 2007; 89-B(10): 1352-5.
48. Lee SH, Oh JH, Lee KS, Yoo KH, Kim HS. Infection after prosthetic reconstruction in limb salvage surgery. Int Orthop 2002; 26(3): 179–84.
49. McDonald DJ, Capanna R, Gherlinzoni F, Bacci G, Ferruzzi A, Casadei R, et al. In�uence of chemotherapy on perioperative complications in limb salvage surgery for bone tumors. Cancer 1990; 65(7): 1509–16.
50. Morii T, Yabe H, Morioka H, Beppu Y, Chuman H, Kawai A, et al. Postoperative deep infection in tumor endoprosthesis reconstruction around the knee. J Orthop Sci 2010; 15(3): 331–9.
51938_Claudia_Lowik.indd 51 19-08-19 11:12

51938_Claudia_Lowik.indd 52 19-08-19 11:12
Chapter 4
Obese patients have higher rates of polymicrobial and Gram-negative early
periprosthetic joint infections of the hip than non-obese
patients
Claudia A.M. Löwik, Wierd P. Zijlstra, Bas A.S. Knobben, Joris J.W. Ploegmakers, Baukje Dijkstra, Astrid J. de Vries, Greetje A. Kampinga, Glen Mithoe, Aziz Al
Moujahid, Paul C. Jutte, Marjan Wouthuyzen-Bakker, on behalf of the Northern Infection Network Joint Arthroplasty
Published in: PLoS One 2019; 14(4): e0215035
51938_Claudia_Lowik.indd 53 19-08-19 11:12
Chapter 4
54
Abstract
BackgroundObese patients are more likely to develop periprosthetic joint infection (PJI) after primary total joint arthroplasty. This study compared the clinical and microbiological characteristics of non-obese, obese and severely obese patients with early PJI, in order to ultimately optimize antibiotic prophylaxis and other prevention measures for this speci�c patient category.
MethodsWe retrospectively evaluated patients with early PJI of the hip and knee treated with debridement, antibiotics and implant retention (DAIR) between 2006 and 2016 in three Dutch hospitals. Only patients with primary arthroplasties indicated for osteoarthritis were included. Early PJI was de�ned as an infection that developed within 90 days after index surgery. Obesity was de�ned as a BMI ≥30kg/m2 and severe obesity as a BMI ≥35kg/m2.
ResultsA total of 237 patients were analyzed, including 64 obese patients (27.0%) and 62 severely obese patients (26.2%). Compared with non-obese patients, obese patients had higher rates of polymicrobial infections (60.3% vs 33.3%, p<0.001) with more often involvement of Enterococcus species (27.0% vs 11.7%, p=0.003). Moreover, severely obese patients had more Gram-negative infections, especially with Proteus species (12.9% vs 2.3%, p=0.001). These results were only found in periprosthetic hip infections, comprising Gram-negative PJIs in 34.2% of severely obese patients compared with 24.7% in obese patients and 12.7% in non-obese patients (p=0.018).
ConclusionOur results demonstrate that obese patients with early periprosthetic hip infections have higher rates of polymicrobial infections with enterococci and Gram-negative rods, which stresses the importance of improving preventive strategies in this speci�c patient category, by adjusting antibiotic prophylaxis regimens, improving disinfection strategies and optimizing postoperative wound care.
51938_Claudia_Lowik.indd 54 19-08-19 11:12

Periprosthetic joint infection in obese patients
55
4
Introduction
Obesity is a major health concern worldwide, as obesity has nearly tripled in the last decades. Currently, 39% of adults are overweight and 13% are obese.1 Obesity is not only associated with an increased risk of comorbidities, such as hypertension, diabetes mellitus and ischemic heart disease,2 but due to early development of osteoarthritis of weight-bearing joints, obese patients are also more likely to receive joint arthroplasty.3 Implantation of joint arthroplasties may lead to postoperative complications, particularly in obese patients.4 The most important complication is periprosthetic joint infection (PJI), occurring in approximately 1-2% of patients receiving joint arthroplasty.5 PJI has a large impact on patient’s quality of life and is accompanied by high health care costs. Literature indicates that the risk of PJI increases exponentially with the body mass index (BMI): i.e. severely obese patients have a four times increased risk of PJI compared with non-obese patients.6,7
There are many hypotheses for the increased risk of PJI in obese patients.8 First of all, obese patients are prone to diminished wound healing because of increased surface tension at the surgical site and prolonged wound leakage due to bulky subcutaneous tissue.9 Secondly, higher glucose levels in obese patients with diabetes mellitus increase the risk of infection.10 Thirdly, the applied cefazolin dosage as antibiotic prophylaxis may not be su�cient to achieve adequate tissue concentrations in obese patients, especially in patients weighing more than 120kg or with a BMI >40kg/m2.11-13 Finally, obese patients have increased bacterial colonization of the skin compared with non-obese patients, particularly in the groin.14,15 Currently applied antibiotic prophylaxis may not provide full coverage for these microorganisms.
To optimize prevention measures for obese patients receiving primary total joint arthroplasty, we aimed to describe the clinical and microbiological characteristics of early PJI in obese and severely obese patients.
Material and methods
Study designWe retrospectively reviewed patients with early PJI of the hip and knee who were treated with debridement, antibiotics and implant retention (DAIR) in
51938_Claudia_Lowik.indd 55 19-08-19 11:12

Chapter 4
56
one university hospital (University Medical Center Groningen) and two general hospitals (Martini Hospital and Medical Center Leeuwarden) between January 2006 and December 2016. PJI was diagnosed according to the diagnostic criteria de�ned by the Musculoskeletal Infection Society (MSIS).16 In case of a single positive culture with a highly virulent microorganism, PJI was diagnosed in consultation with the infectious diseases specialist or medical microbiologist. Early PJI was de�ned as an infection developed within 90 days after index surgery.17 Only patients with primary arthroplasties indicated for osteoarthritis were included. Patients who underwent arthroscopic debridement or did not meet the MSIS criteria were excluded.
The following clinical variables were collected: sex, age, BMI, comorbidities, medication, in�ammatory markers and speci�cations of index surgery and the DAIR procedure. BMI was measured during the preoperative anesthetic screening prior to joint arthroplasty surgery. Patients were categorized according to BMI, with a cut-o� value of 30kg/m2 (i.e. class 1 obesity) and 35kg/m2 (i.e. class 2 obesity / severe obesity).1,18 Early failure was de�ned as the need for 1) a second DAIR procedure, 2) revision arthroplasty or de�nitive implant removal, 3) infection-related death or 4) suppressive antimicrobial treatment, all within 60 days after initial debridement. Overall failure was de�ned as infection-related death or the need for implant removal at any time point after initial debridement.
The following microbiological variables were collected: number of positive cultures, type of microorganism and resistance patterns of cultured microorganisms.
Index surgery and DAIR procedurePrior to joint arthroplasty patients performed a whole-body cleansing with chlorhexidine scrub. In case of abundant hair growth on the knee or groin region, hair was removed from the surgical site by use of a clipper. Prior to surgical incision, the skin was disinfected with a solution of povidone tincture in 75% alcohol. In case patients were allergic to povidone, the skin was disinfected by a chlorhexidine-alcohol solution. Cefazolin was administered as antibiotic prophylaxis 30 to 60 minutes prior to incision. According to local protocol, cefazolin dosage was one gram for patients <80kg and two grams for patients ≥80kg. In all patients receiving total hip arthroplasty the posterolateral approach was used. Total knee arthroplasties were inserted via the medial
51938_Claudia_Lowik.indd 56 19-08-19 11:12

Periprosthetic joint infection in obese patients
57
4
parapatellar approach. The incisions were closed with staples and dressed with absorbent bandages. In case of wound leakage in the postoperative period a pressure bandage was applied.
DAIR procedure consisted of opening the wound via the pre-existing incision, excising hematoma and avital tissue and irrigating the wound thoroughly with three to six liters of saline. Modular components were exchanged and optionally gentamicin-impregnated beads or sponges were inserted into the joint cavity according to local protocol and clinical judgement of the operating orthopaedic surgeon. Multiple cultures of deep tissue and synovial �uid were obtained during debridement. Cefuroxime was started as empirical intravenous antimicrobial treatment after obtaining cultures and was adjusted according to the culture results. Intravenous antimicrobial treatment was continued for at least two weeks before switching to an oral regimen, which was continued for an additional ten weeks. Rifampin was added to the antimicrobial treatment regimen in infections caused by rifampin-susceptible staphylococci.
Statistical analysisCategorical variables were presented in absolute frequencies and percentages. Continuous variables were expressed as mean and standard deviation (SD) or as median and interquartile range (IQR) when not normally distributed according to the Kolmogorov-Smirnov test of normality. The statistical comparison of categorical variables was performed using the Chi-square test. Parametric continuous variables were compared using the Student’s t-test and one-way ANOVA. Non-parametric continuous variables were compared with the Mann-Whitney U test. Statistical signi�cance was de�ned as a two-tailed p <0.05. Statistical assessment was carried out with IBM SPSS Statistics (version 24.0, Chicago, USA).
Ethical Review Committee statementThe Institutional Review Boards of the University Medical Center Groningen, Martini Hospital and Medical Center Leeuwarden approved this study. Each Institutional Review Board approved a waiver for obtaining written informed consent from the participants, since this was an observational study in which the data were analyzed anonymously. The study is conducted in accordance to the ethical standards in the 1964 Declaration of Helsinki, the Medical Research Involving Human Subjects Act (WMO) and the Good Clinical Practice standard (GCP).
51938_Claudia_Lowik.indd 57 19-08-19 11:12

Chapter 4
58
Results
Clinical characteristicsA total of 356 patients with early PJI of the knee or hip treated with DAIR were identi�ed. We excluded 52 patients with revision arthroplasties and 67 patients with primary arthroplasties placed for other indications than osteoarthritis (fracture (n=62), rheumatoid arthritis (n=2) and malignancy (n=3)). A total of 237 included patients had a mean age of 71.3 years (SD 10.5, range 27-91 years) and 63.7% of patients (n=151) were female. 160 patients (67.5%) had a periprosthetic hip infection and 77 patients (32.5%) had a periprosthetic knee infection. Patients experienced a mean duration of symptoms of infection of 6.8 days (SD 5.9, range 1-21 days) before DAIR procedure. DAIR procedure was performed at a mean of 20.7 days (SD 11.7, range 7-74 days) after index surgery. The median follow-up was 1.7 years (IQR 1.0-3.3) and was similar in obese and non-obese patients (1.8 years (IQR 1.0-3.1) vs 1.5 years (IQR 1.0-3.4), p=0.732).
From the included cohort (n=237) a total of 126 patients (53.2%) were obese. Of these obese patients 62 were severely obese (49.2%). Non-obese, obese and severely obese patients were of similar age (72.3 years vs 70.5 years vs 69.4 years, p=0.229), while severely obese patients were more often of female gender than non-severely obese patients (74.2% vs 60.0%, p=0.046). Regarding comorbidities, both obese and severely obese patients had a higher incidence of hypertension compared with non-obese patients and non-severely obese patients respectively (69.0% vs 56.8%, p=0.050 and 75.8% vs 58.9%, p=0.017), while diabetes mellitus only had a higher incidence in severely obese patients (35.5% vs 17.1%, p=0.003). Regarding symptoms at initial DAIR, severely obese patients had a higher incidence of redness of the wound compared with non-severely obese patients (39.4% vs 56.5%, p=0.020). There was a trend towards more wound leakage in obese patients, but this di�erence was not statistically signi�cant (82.0% vs 89.7%, p=0.088) (Table 1).
Comparing the variables of the joint replacement surgery and DAIR procedure we did not �nd any di�erences between non-obese, obese and severely obese patients (Table 1). Regarding the outcome after DAIR, rates of early failure and overall failure were comparable between non-obese, obese and severely obese patients (30.6% vs 33.3% vs 30.6%, p=0.740 and 9.0% vs 10.3% vs 9.7%, p=0.961 respectively). In the majority of patients (n=67, 88.2%) early failure was due to the need for a second DAIR, �ve patients (6.6%) needed
51938_Claudia_Lowik.indd 58 19-08-19 11:12
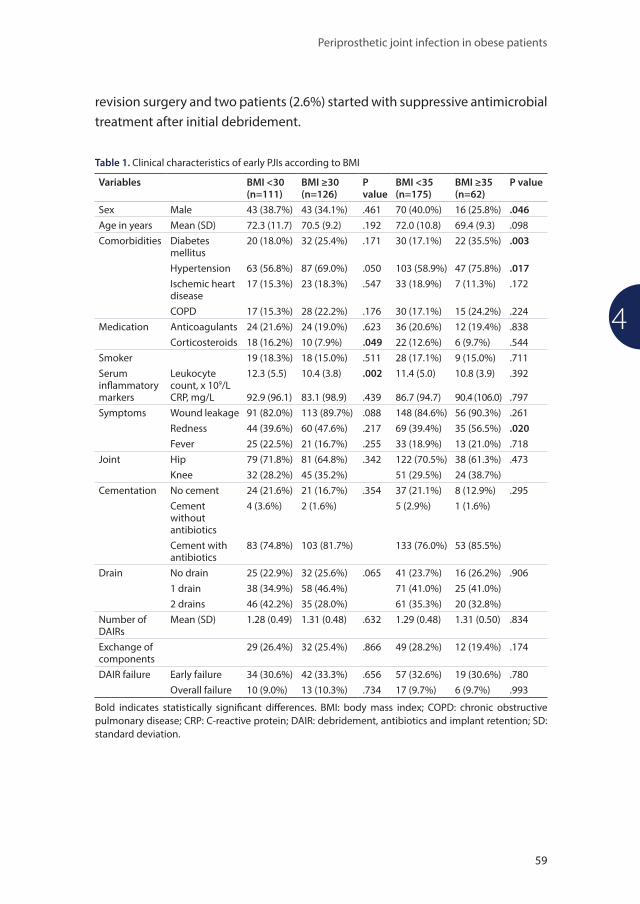
Periprosthetic joint infection in obese patients
59
4
revision surgery and two patients (2.6%) started with suppressive antimicrobial treatment after initial debridement.
Table 1. Clinical characteristics of early PJIs according to BMI
Variables BMI <30 (n=111)
BMI ≥30 (n=126)
P value
BMI <35 (n=175)
BMI ≥35 (n=62)
P value
Sex Male 43 (38.7%) 43 (34.1%) .461 70 (40.0%) 16 (25.8%) .046Age in years Mean (SD) 72.3 (11.7) 70.5 (9.2) .192 72.0 (10.8) 69.4 (9.3) .098Comorbidities Diabetes
mellitus20 (18.0%) 32 (25.4%) .171 30 (17.1%) 22 (35.5%) .003
Hypertension 63 (56.8%) 87 (69.0%) .050 103 (58.9%) 47 (75.8%) .017Ischemic heart disease
17 (15.3%) 23 (18.3%) .547 33 (18.9%) 7 (11.3%) .172
COPD 17 (15.3%) 28 (22.2%) .176 30 (17.1%) 15 (24.2%) .224Medication Anticoagulants 24 (21.6%) 24 (19.0%) .623 36 (20.6%) 12 (19.4%) .838
Corticosteroids 18 (16.2%) 10 (7.9%) .049 22 (12.6%) 6 (9.7%) .544Smoker 19 (18.3%) 18 (15.0%) .511 28 (17.1%) 9 (15.0%) .711Serum in�ammatory markers
Leukocyte count, x 109/LCRP, mg/L
12.3 (5.5)
92.9 (96.1)
10.4 (3.8)
83.1 (98.9)
.002
.439
11.4 (5.0)
86.7 (94.7)
10.8 (3.9)
90.4 (106.0)
.392
.797Symptoms Wound leakage 91 (82.0%) 113 (89.7%) .088 148 (84.6%) 56 (90.3%) .261
Redness 44 (39.6%) 60 (47.6%) .217 69 (39.4%) 35 (56.5%) .020Fever 25 (22.5%) 21 (16.7%) .255 33 (18.9%) 13 (21.0%) .718
Joint Hip 79 (71.8%) 81 (64.8%) .342 122 (70.5%) 38 (61.3%) .473Knee 32 (28.2%) 45 (35.2%) 51 (29.5%) 24 (38.7%)
Cementation No cement 24 (21.6%) 21 (16.7%) .354 37 (21.1%) 8 (12.9%) .295Cement without antibiotics
4 (3.6%) 2 (1.6%) 5 (2.9%) 1 (1.6%)
Cement with antibiotics
83 (74.8%) 103 (81.7%) 133 (76.0%) 53 (85.5%)
Drain No drain 25 (22.9%) 32 (25.6%) .065 41 (23.7%) 16 (26.2%) .9061 drain 38 (34.9%) 58 (46.4%) 71 (41.0%) 25 (41.0%)2 drains 46 (42.2%) 35 (28.0%) 61 (35.3%) 20 (32.8%)
Number of DAIRs
Mean (SD) 1.28 (0.49) 1.31 (0.48) .632 1.29 (0.48) 1.31 (0.50) .834
Exchange of components
29 (26.4%) 32 (25.4%) .866 49 (28.2%) 12 (19.4%) .174
DAIR failure Early failure 34 (30.6%) 42 (33.3%) .656 57 (32.6%) 19 (30.6%) .780Overall failure 10 (9.0%) 13 (10.3%) .734 17 (9.7%) 6 (9.7%) .993
Bold indicates statistically signi�cant di�erences. BMI: body mass index; COPD: chronic obstructive pulmonary disease; CRP: C-reactive protein; DAIR: debridement, antibiotics and implant retention; SD: standard deviation.
51938_Claudia_Lowik.indd 59 19-08-19 11:12

Chapter 4
60
Microbiological characteristics
Overall, early PJIs were polymicrobial in 113 patients (47.7%). Predominant microorganisms causing the infection were Staphylococcus aureus (44.3%), Staphylococcus epidermidis (34.6%), Streptococcus species (21.5%) and Enterococcus species (19.8%). Regarding polymicrobial infections, 66.4% solely involved Gram-positive microorganisms (n=75), 2.7% solely Gram-negative microorganisms (n=3), and 31.0% involved both Gram-positive and Gram-negative microorganisms (n=35). In patients with polymicrobial infections, each obtained culture was positive in 86.7% of cases (n=98). The mean number of species cultured in these polymicrobial infections was 2.64 (range 2-7), with 2 species being cultured in 56.6% (n=64), 3 species in 30.1% (n=34), 4 species in 8.0% (n=9), 5 species in 4.4% (n=5) and 7 species in 0.9% (n=1). In case of a polymicrobial infection, Staphylococcus epidermidis was involved in 46.0% of cases, Staphylococcus aureus in 41.6%, Enterococcus species in 38.1%, Streptococcus species in 29.2% and Proteus species in 10.6%. The most common combination of microorganisms was Staphylococcus aureus together with Streptococcus species (n=7) and Staphylococcus epidermidis together with Enterococcus species (n=6).
Obese patients had a higher rate of polymicrobial infections than non-obese patients (60.3% vs 33.3%, p<0.001), with higher prevalence of Enterococcus species (27.0% vs 11.7%, p=0.003). The same applies to severely obese patients compared with non-severely obese patients (polymicrobial infections in 59.7% vs 43.4%, p=0.028 and Enterococcus species in 32.2% vs 15.4%, p=0.004). Overall, there were no di�erences regarding Gram-negative microorganisms between obese and non-obese patients, but there were signi�cantly more infections caused by Proteus species in severely obese patients compared with non-severely obese patients (12.9% vs 2.3%, p=0.001).
Analyzing patients with PJI of the hip and knee separately, we found that the higher rate of polymicrobial infections in obese patients, including Enterococcus species and Gram-negative microorganisms, was only signi�cant in patients with periprosthetic hip infections (Table 2). Gram-negative rods were isolated in 34.2% of severely obese patients with hip PJI, compared with 24.7% in obese patients and 12.7% in non-obese patients (p=0.018). Proteus species were the main isolated Gram-negative microorganism, with a higher rate in severely obese patients compared with non-severely obese patients (18.4% vs 1.6%, p<0.001). Moreover, Morganella morganii was more often involved in
51938_Claudia_Lowik.indd 60 19-08-19 11:12

Periprosthetic joint infection in obese patients
61
4
severely obese patients (7.9% vs 0.0%, p=0.002). These di�erences were not signi�cant in obese patients compared with non-obese patients. Assessment of the microbiological characteristics in patients with periprosthetic knee infections only showed a signi�cant higher rate of involvement of Enterococcus faecium in severely obese compared with non-severely obese patients (8.3% vs 0.0%, p=0.037). There were no other signi�cant di�erences between non-obese, obese and severely obese patients (Table 3).
Regarding the susceptibility analyses of cefazolin and cefuroxime in Gram-negative microorganisms, results of these tests were only partially available. Microorganisms that are intrinsically resistant to cefazolin and cefuroxime (such as Enterococcus species, Enterobacter cloacae, Proteus vulgaris and Morganella morganii) are not indicated. E. coli was sensitive to cefazolin in all tested cases (n=3). Proteus mirabilis showed intermediate resistance to cefazolin in 33.3% (n=3). Regarding cefuroxime, E. coli (n=6), Klebsiella species (n=1) and Proteus mirabilis (n=11) all showed 100% sensitivity.
Discussion
This study describes the di�erences in clinical and microbiological characteristics of early PJI between non-obese, obese and severely obese patients. Our results demonstrated that obese and severely obese patients with periprosthetic hip infections had higher rates of polymicrobial infections with involvement of Enterococcus species. Moreover, severely obese patients with PJI of the hip had a higher rate of infections with Gram-negative microorganisms than non-severely obese patients. Interestingly, these results were not found in obese patients with periprosthetic knee infections, which indicates that infections of the hip and knee should be perceived as two separate entities and should therefore be approached di�erently. Even though the outcome after DAIR was comparable between non-obese, obese and severely obese patients, the di�erences in microbiological pro�le between obese and non-obese patients indicate that preventive measures should be adapted for hip arthroplasty surgery in obese patients.
51938_Claudia_Lowik.indd 61 19-08-19 11:12

Chapter 4
62
Tabl
e 2.
Isol
ated
mic
roor
gani
sms
durin
g D
AIR
in e
arly
PJI
s of
the
hip
acco
rdin
g to
BM
I
Vari
able
sBM
I <30
(n=7
9)BM
I ≥30
(n=8
1)P
valu
eBM
I <35
(n=1
22)
BMI ≥
35 (n
=38)
P va
lue
Perc
enta
ge o
f pos
itive
cul
ture
sM
ean
(SD
)91
.4 (2
0.1)
91.8
(18.
5).9
1790
.7 (2
0.9)
94.4
(12.
2).3
04Po
lym
icro
bial
infe
ctio
n27
(34.
2%)
55 (6
7.9%
)<.
001
56 (4
5.9%
)26
(68.
4%)
.015
Gra
m-p
ositi
ve m
icro
orga
nism
s76
(96.
2%)
78 (9
6.3%
).9
7511
7 (9
5.9%
)37
(97.
4%)
.678
Stap
hylo
cocc
us a
ureu
s33
(41.
8%)
32 (3
9.5%
).7
7051
(41.
8%)
14 (3
6.8%
).5
87St
aphy
loco
ccus
epi
derm
idis
25 (3
1.6%
)35
(43.
2%)
.131
43 (3
5.2%
)17
(44.
7%)
.291
Cory
neba
cter
ium
spe
cies
7 (8
.9%
)20
(24.
7%)
.008
22 (1
8.0%
)5
(13.
2%)
.484
Ente
roco
ccus
spe
cies
10 (1
2.7%
)24
(29.
6%)
.009
20 (1
6.4%
)14
(36.
8%)
.007
Ente
roco
ccus
faec
alis
7 (8
.9%
)20
(24.
7%)
.008
16 (1
3.1%
)11
(28.
9%)
.023
Ente
roco
ccus
faec
ium
1 (1
.3%
)0
(0.0
%)
.310
1 (0
.8%
)0
(0.0
%)
.576
Stre
ptoc
occu
s spe
cies
20 (2
5.3%
)16
(19.
8%)
.399
32 (2
6.2%
)4
(10.
5%)
.043
Oth
er g
ram
-pos
itive
s a
3 (3
.8%
)3
(3.7
%)
.975
4 (3
.3%
)2
(5.3
%)
.574
Gra
m-n
egat
ive
mic
roor
gani
sms
10 (1
2.7%
)20
(24.
7%)
.051
17 (1
3.9%
)13
(34.
2%)
.005
Ente
roba
cter
iace
aeEs
cher
ichi
a co
li2
(2.5
%)
3 (3
.7%
).6
703
(2.5
%)
2 (5
.3%
).3
86En
tero
bact
er c
loac
ae2
(2.5
%)
3 (3
.7%
).6
703
(2.5
%)
2 (5
.3%
).3
86Pr
oteu
s spe
cies
b2
(2.5
%)
7 (8
.6%
).0
942
(1.6
%)
7 (1
8.4%
)<.
001
Kleb
siel
la s
peci
es1
(1.3
%)
0 (0
.0%
).3
101
(0.8
%)
0 (0
.0%
).5
76M
orga
nella
mor
gani
i0
(0.0
%)
3 (3
.7%
).0
840
(0.0
%)
3 (7
.9%
).0
02N
on-fe
rmen
ters
Pseu
dom
onas
spe
cies
3 (3
.8%
)3
(3.7
%)
.975
5 (4
.1%
)1
(2.6
%)
.678
Acin
etob
acte
r spe
cies
1 (1
.3%
)2
(2.5
%)
.575
2 (1
.6%
)1
(2.6
%)
.694
Ana
erob
e m
icro
orga
nism
s3
(3.8
%)
4 (4
.9%
).7
244
(3.3
%)
3 (7
.9%
).2
24Ca
ndid
a sp
ecie
s0
(0.0
%)
1 (1
.2%
).3
220
(0.0
%)
1 (2
.6%
).0
72
Bold
indi
cate
s st
atis
tical
ly s
igni
�can
t di�
eren
ces.
BMI:
body
mas
s in
dex;
SD
: sta
ndar
d de
viat
ion.
a Mic
roco
ccus
lute
us (n
=2),
Mic
roba
cter
ium
�av
esce
ns (n
=1),
Dol
osig
ranu
losu
m p
igru
m (n
=1),
Kocu
ria s
peci
es (n
=1),
Roth
ia M
ucila
gino
sa (n
=1).
b 8/9
Pro
teus
spe
cies
that
wer
e is
olat
ed w
ere
Prot
eus m
irabi
lis, 1
/9 w
as P
rote
us v
ulga
ris.
51938_Claudia_Lowik.indd 62 19-08-19 11:12

Periprosthetic joint infection in obese patients
63
4
Tabl
e 3.
Isol
ated
mic
roor
gani
sms
durin
g D
AIR
in e
arly
PJI
s of
the
knee
acc
ordi
ng to
BM
I
Vari
able
sBM
I <30
(n=3
1)BM
I ≥30
(n=4
4)P
valu
eBM
I <35
(n=5
1)BM
I ≥35
(n=2
4)P
valu
ePe
rcen
tage
of p
ositi
ve c
ultu
res
Mea
n (S
D)
85.3
(30.
1)91
.3 (2
2.0)
.318
86.5
(28.
3)93
.8 (1
8.3)
.251
Poly
mic
robi
al in
fect
ion
9 (2
9.0%
)20
(45.
5%)
.150
18 (3
5.3%
)11
(45.
8%)
.382
Gra
m-p
ositi
ve m
icro
orga
nism
s27
(87.
1%)
42 (9
5.5%
).1
8946
(90.
2%)
23 (9
5.8%
).4
01St
aphy
loco
ccus
aur
eus
15 (4
8.4%
)24
(54.
5%)
.599
26 (5
1.0%
)13
(54.
2%)
.797
Stap
hylo
cocc
us e
pide
rmid
is8
(25.
8%)
14 (3
1.8%
).5
7315
(25.
5%)
9 (3
7.5%
).2
87Co
ryne
bact
eriu
m s
peci
es3
(9.7
%)
5 (1
1.4%
).8
165
(9.8
%)
3 (1
2.5%
).7
24En
tero
cocc
us s
peci
es3
(9.7
%)
10 (2
2.7%
).1
427
(13.
7%)
6 (2
5.0%
).2
29En
tero
cocc
us fa
ecal
is2
(6.5
%)
5 (1
1.4%
).4
715
(9.8
%)
2 (8
.3%
).8
38En
tero
cocc
us fa
eciu
m0
(0.0
%)
2 (4
.5%
).2
290
(0.0
%)
2 (8
.3%
).0
37St
rept
ococ
cus s
peci
es6
(19.
4%)
9 (2
0.5%
).9
0712
(23.
5%)
3 (1
2.5%
).2
65O
ther
gra
m-p
ositi
ves
a1
(3.2
%)
2 (4
.5%
).7
742
(3.9
%)
1 (4
.2%
).9
60G
ram
-neg
ativ
e m
icro
orga
nism
s4
(12.
9%)
7 (1
5.9%
).7
178
(15.
7%)
3 (1
2.5%
).7
16En
tero
bact
eria
ceae
Esch
eric
hia
coli
0 (0
.0%
)1
(2.3
%)
.398
1 (2
.0%
)0
(0.0
%)
.490
Ente
roba
cter
clo
acae
2 (6
.5%
)2
(4.5
%)
.718
3 (5
.9%
)1
(4.2
%)
.758
Prot
eus m
irabi
lis1
(3.2
%)
2 (4
.5%
).7
742
(3.9
%)
1 (4
.2%
).9
60Kl
ebsi
ella
spe
cies
0 (0
.0%
)0
(0.0
%)
1.00
00
(0.0
%)
0 (0
.0%
)1.
000
Mor
gane
lla m
orga
nii
0 (0
.0%
)0
(0.0
%)
1.00
00
(0.0
%)
0 (0
.0%
)1.
000
Non
-ferm
ente
rsPs
eudo
mon
as s
peci
es1
(3.2
%)
1 (2
.3%
).8
011
(2.0
%)
1 (4
.2%
).5
80Ac
inet
obac
ter s
peci
es0
(0.0
%)
1 (2
.3%
).3
981
(2.0
%)
0 (0
.0%
).4
90A
naer
obe
mic
roor
gani
sms
0 (0
.0%
)1
(2.3
%)
.398
1 (2
.0%
)0
(0.0
%)
.490
Cand
ida
spec
ies
0 (0
.0%
)0
(0.0
%)
1.00
00
(0.0
%)
0 (0
.0%
)1.
000
Bold
indi
cate
s st
atis
tical
ly s
igni
�can
t di�
eren
ces.
BMI:
body
mas
s in
dex;
SD
: sta
ndar
d de
viat
ion.
a Gra
nulic
atel
la a
diac
ens (
n=2)
, Sta
phyl
ococ
cus l
ugdu
nens
is (n
=1).
51938_Claudia_Lowik.indd 63 19-08-19 11:12

Chapter 4
64
The concept of abundant colonization with multiple microorganisms in the hip region14,15 is expected to mainly apply to direct anterior incisions, as previously described in literature.19,20 Interestingly, in our cohort obese patients showed abundant colonization with multiple microorganisms as well, even though posterolateral incisions were used for implantation of the hip arthroplasties. Contamination of the wound can occur primarily during surgery or secondarily in the postoperative period. Primary contamination may occur if inadequate antibiotic prophylaxis is applied (either by insu�cient dosage or inadequate type of antibiotics) or if the hip region is not thoroughly disinfected. The latter may be prevented by more thorough disinfection of the hip region, for example by using chlorhexidine-alcohol as a local disinfectant. Even though there are no large trials comparing chlorhexidine-alcohol with povidone tincture in 75% alcohol, it is proven that chlorhexidine-alcohol is more e�ective than povidone-iodine in reducing postoperative infections.21 This superior protection is mainly attributed to a reduction in Gram-positive skin �ora by rapid action and persistent activity despite exposure to bodily �uids.21 Nevertheless, there was a high number of polymicrobial infections in our cohort, caused by microorganisms susceptible to the local disinfectant as well as the antimicrobial prophylaxis. This may indicate that either the antibiotic dosage was too low or that a signi�cant proportion of PJIs developed due to secondary contamination in the postoperative period, maybe due to prolonged wound leakage, via the retrograde pathway.22 Although our data showed a trend towards a higher rate of wound leakage in obese patients, this di�erence was not statistically signi�cant. To prevent secondary contamination, it is important to provide adequate wound care with sterile absorbent dressings and pressure bandages.23 Therefore, obese patients should be evaluated more extensively after joint arthroplasty, to detect wound complications and provide adequate wound care at an early time point.
A di�erent option for improving preventive measures in obese patients receiving total hip arthroplasty is to increase the dosage of cefazolin, especially since previous studies showed that the currently applied cefazolin dosage as antibiotic prophylaxis may not be su�cient to achieve adequate tissue concentrations in obese patients.11-13 Another reason to increase the dosage of cefazolin is the higher rate of infections caused by Proteus species in obese patients in our cohort, since Proteus species have a higher minimum inhibitory concentration for cefazolin than other Enterobacteriaceae.24 Recently the Dutch
51938_Claudia_Lowik.indd 64 19-08-19 11:12

Periprosthetic joint infection in obese patients
65
4
guideline for antibiotic prophylaxis was adjusted, in which it is now advised to administer three grams of cefazolin in patients with a BMI >40 kg/m2,25 although our results suggest that this higher dosage may also be bene�cial for patients with a BMI >35 kg/m2.
Another option is to broaden the antibiotic prophylaxis during total hip arthroplasty surgery in obese patients, especially since cefazolin does not cover for Enterococcus species and most of the Gram-negative rods.26 Broadening the prophylaxis to cefuroxime combined with vancomycin or teicoplanin may be an option. Previous studies compared the e�cacy of various antibiotic prophylaxis regimens in reducing infection rates after joint arthroplasty, mostly by adding an antibiotic agent with a broader Gram-positive spectrum (such as a glycopeptide). Two studies compared the e�cacy of cefazolin with a combined regimen of cefazolin and vancomycin.27-28 Liu et al. found a reduction in infections in the combined regimen group,27 while Sewick et al. did not detect a di�erence between the regimens.28 Other studies compared the use of cefuroxime and a combined regimen of cefuroxime and teicoplanin and found a reduced infection rate in the combined treatment group.29,30 The higher e�cacy of the combined regimens in these studies was mainly based on a reduction in infections caused by methicillin-resistant Staphylococcus aureus.
Tornero et al. studied the e�cacy of dual prophylaxis (cefuroxime plus teicoplanin) and found a reduction in PJI rate solely in obese patients when adding teicoplanin to the antimicrobial regimen.30 This reduction was mainly observed for PJI due to methicillin-susceptible Staphylococcus aureus, which supports the hypothesis that the dosage of antimicrobial prophylaxis may be insu�cient in obese patients, since methicillin-susceptible Staphylococcus aureus should be fully covered by cefuroxime. A randomized controlled trial is needed to provide conclusive scienti�c evidence regarding the most e�ective antibiotic prophylaxis regimen for obese patients. This randomized trial should compare di�erent antibiotic regimens and should show whether the absolute percentage of PJIs indeed decreases when adapting the antibiotic prophylaxis regimen in obese patients receiving total hip arthroplasty.
There are several limitations to our study. First of all, we merely included patients with early PJI treated with DAIR. We did not include chronic infections, which could have provided additional insights, as these patients may have di�erent microbiological pro�les. We did not collect data on the total number of joint arthroplasties implanted in the participating hospitals during the
51938_Claudia_Lowik.indd 65 19-08-19 11:12

Chapter 4
66
study period. Therefore, we do not know the exact incidence of PJI in our cohort. However, previous studies clearly demonstrated a higher rate of PJI in obese patients,6,7 and therefore, it is likely that implementing the proposed prevention strategies will result in an absolute reduction of PJIs in the obese population. A second limitation is the retrospective design of this study. However, due to thorough recording of clinical and microbiological �ndings in the electronic patient �les of patients with PJI there were few missing variables, by which the results are representative for the included patients. Finally, we did not collect data on the exact disinfective agent that has been applied prior to surgery, because we could not reliably collect the allergies of included patients. However, in consultation with the orthopaedic surgeons in the participating hospitals we are con�dent that the disinfection procedure has been carried out correctly in each patient, whether with a povidone-alcohol solution or with a chlorhexidine-alcohol solution.
A strength of this study is that we were able to select a large homogenous group of patients with early PJI. Our initial statistical analyses showed that non-obese patients had a signi�cantly higher rate of arthroplasties indicated for fracture than obese patients (27.6% vs 10.6%, p<0.001, S1 File). Since literature indicates that fracture-related PJIs have a lower rate of Gram-negative infections and a higher failure rate compared with primary PJIs,31 we decided to only analyze patients with primary arthroplasties indicated for osteoarthritis.
In conclusion, obese and severely obese patients with early periprosthetic hip infections have higher rates of polymicrobial infections with involvement of enterococci and Gram-negative rods, which emphasizes the importance of improving preventive strategies in this speci�c patient category.
51938_Claudia_Lowik.indd 66 19-08-19 11:12

Periprosthetic joint infection in obese patients
67
4
References
1. World Health Organization. Obesity and overweight. Report 2018. www.who.int. 2. Pi-Sunyer X. The medical risks of obesity. Postgrad Med 2009; 121(6): 21-33.3. Bourne R, Mukhi S, Zhu N, Keresteci M, Marin M. Role of obesity on the risk for total hip or knee
arthroplasty. Clin Orthop Relat Res 2007; 465: 185-8.4. Arsoy D, Woodcock JA, Lewallen Dg, Trousdale RT. Outcomes and complications following total hip
arthroplasty in the super-obese patient, BMI >50. J Arthroplasty 2014; 29(10): 1899-905.5. Kurtz SM, Ong KL, Lau E, Bozic KJ, Berry D, Parvizi J. Prosthetic joint infection risk after TKA in the
medicare population. Clin Orthop Relat Res 2010; 468(1): 52-6.6. Chen J, Cui Y, Li X, Miao X, Wen Z, Xue Y, et al. Risk factors for deep infection after total knee
arthroplasty: a meta-analysis. Arch Orthop Trauma Surg 2013; 133(5): 675-87. 7. Smith JO, Framptom CMA, Hooper GJ, Young SW. The impact of patient and surgical factors on the
rate of postoperative infection after total hip arthroplasty – a New Zealand joint registry study. J Arthroplasty 2018; 33(6): 1884-90.
8. Eka A, Chen AF. Patient-related medical risk factors for periprosthetic joint infection of the hip and knee. Ann Transl Med 2015; 3(16): 233.
9. Patel VP, Walsh M, Sehgal B, Preston C, DeWal H, Di Cesare PE. Factors associated with prolonged wound drainage after primary total hip and knee arthroplasty. J Bone Joint Surg Am 2007; 89(1): 33-8.
10. Dowsey MM, Choong PF. Obese diabetic patients are at substantial risk for deep infection after primary TKA. Clin Orthop Relat Res 2009; 467(6): 1577-81.
11. Grupper M, Kuti JL, Swank ML, Maggio L, Hughes BL, Nicolau DP. Population pharmacokinetics of cefazolin in serum and adipose tissue from overweight and obese women undergoing cesarean delivery. J Clin Pharmacol 2017; 57(6): 712-9.
12. Kram JJF, Greer DM, Cabrera O, Bulage R, Forgie MM, Siddiqui DS. Does current cefazolin dosing achieve adequate tissue and blood concentrations in obese women undergoing cesarean section? Eur J Obstet Gynecol Biol 2017; 210: 334-41.
13. Rondon AJ, Kheir MM, Tan TL, Shohat N, Greenky MR, Parvizi J. Cefazolin prophylaxis for total joint arthroplasty: obese patients are frequently underdosed and at increased risk for periprosthetic joint infection. J Arthroplasty 2018; 33(11): 3551-4.
14. Boni L, Kuster SP, Bartik B, Zbinden R, Zingg PO, Achermann Y. Association of Cutibacterium avidum colonization in the groin with obesity: a potential risk factor for hip periprosthetic joint infection. Clin Infect Dis 2018: 67(12): 1878-82.
15. Font-Viczarra L, Tornero E, Bori G, Bosch J, Mensa J, Soriano A. Relationship between intraoperative cultures during hip arthroplasty, obesity and the risk of early prosthetic joint infection: a prospective study of 428 patients. Int J Artif Organs 2011; 34(9): 870-5.
16. Parvizi J, Zmistowski B, Berbari EF, Bauer TW, Springer BD, Della Valle CJ, et al. New de�nition for periprosthetic joint infection: from the workgroup of the musculoskeletal infection society. Clin Orthop Relat Res 2011; 469(11): 2992-4.
17. Barrett L, Atkins B. The clinical presentation of prosthetic joint infection. J Antimicrob Chemother 2014; 69(Suppl 1): 25-8.
18. Centers for Disease Control and Prevention. De�ning adult overweight and obesity. Report 2016. www.cdc.gov.
19. Hodgkiss-Harlow KD, Bandyk DF. Antibiotic therapy of aortic graft infection: treatment and prevention recommendations. Semin Vasc Surg 2011; 24(4): 191-8.
20. Ilchmann T, Zimmerli W, Bolliger L, Graber P, Clauss M. Risk of infection in primary, elective total hip arthroplasty with direct anterior approach or lateral transgluteal approach: a prospective cohort study of 1104 hips. BMC Muskuloskelet Disord 2016; 17(1): 471.
21. Darouiche RO, Wall MJ Jr, Itani KM, Otterson MF, Webb AL, Carrick MM, et al. Chlorhexidine-alcohol versus povidone-iodine for surgical-site antisepsis. N Engl J Med 2010; 362(1): 18-26.
51938_Claudia_Lowik.indd 67 19-08-19 11:12

Chapter 4
68
22. Weiss AP, Krackow KA. Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993; 8(3): 285-9.
23. Jaberi FM, Parvizi J, Haytmanek CT, Joshi A, Purtill J. Procrastination of wound drainage and malnutrition a�ect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008; 466(6): 1368-71.
24. European Committee on Antimicrobial Susceptibility Testing. Data from the EUCAST MIC distribution website. www.eucast.org.
25. Bauer M, van de Garde E, van Kasteren M, Prins J, Vos M. SWAB-richtlijn: perioperatieve profylaxe. www.swab.nl.
26. Turnidge JD. Cefazolin and enterobacteriaceae: rationale for revised susceptibility testing breakpoints. Clin Infect Dis 2011; 52(7): 917-24.
27. Liu C, Kakis A, Nicols A, Ries MD, Vail TP, Bozic KJ. Targeted use of vancomycin as perioperative prophylaxis reduces periprosthetic joint infection in revision TKA. Clin Orthop Relat Res 2014; 472(1): 227-31.
28. Sewick A, Makani A, Wu C, O’Donnell J, Baldwin KD, Lee GC. Does dual antibiotic prophylaxis better prevent surgical site infections in total joint arthroplasty? Clin Orthop Relat Res 2012; 470(10): 2702-7.
29. Soriano A, Popescu D, García-Ramiro S, Bori G, Martínez-Pastor JC, Balasso V, et al. Usefulness of teicoplanin for preventing methicillin-resistant Staphylococcus aureus infections in orthopedic surgery. Eur J Clin Microbiol Infect Dis 2006; 25(1): 35-8.
30. Tornero E, Garcí-Ramiro S, Martínez-Pastor JC, Bori G, Bosch J, Morata L, et al. Prophylaxis with teicoplanin and cefuroxime reduces the rate of prosthetic joint infection after primary arthroplasty. Antimicrob Agents Chemother 2015; 59(2): 831-7.
31. De Vries LMA, Neve WC, Steens J. Prosthesis retention after an infected hip prosthesis: hip fractures versus primary total hip prosthesis, data from 1998-2015. J Bone Joint Infect 2018; 3(3): 118-22.
51938_Claudia_Lowik.indd 68 19-08-19 11:12

51938_Claudia_Lowik.indd 69 19-08-19 11:12

51938_Claudia_Lowik.indd 70 19-08-19 11:12

Chapter 5
Predicting failure in early acute prosthetic joint infection treated
with debridement, antibiotics, and implant retention: external
validation of the KLIC score
Claudia A.M. Löwik, Paul C. Jutte, Eduard Tornero, Joris J.W. Ploegmakers, Bas A.S. Knobben, Astrid J. de Vries, Wierd P. Zijlstra, Baukje Dijkstra,
Alex Soriano, Marjan Wouthuyzen-Bakker, on behalf of the Northern Infection Network Joint Arthroplasty
Published in: Journal of Arthroplasty 2018; 33(8): 2582-2587
51938_Claudia_Lowik.indd 71 19-08-19 11:12

Chapter 5
72
Abstract
BackgroundDebridement, antibiotics and implant retention (DAIR) is a widely used treatment modality for early acute prosthetic joint infection (PJI). A preoperative risk score was previously designed for predicting DAIR failure, consisting of chronic renal failure (K), liver cirrhosis (L), index surgery (I), cemented prosthesis (C) and C-reactive protein >115mg/L (KLIC). The aim of this study was to validate the KLIC score in an external cohort.
MethodsWe retrospectively evaluated patients with early acute PJI treated with DAIR between 2006 and 2016 in three Dutch hospitals. Early acute PJI was de�ned as less than 21 days of symptoms and DAIR performed within 90 days after index surgery. Failure was de�ned as the need for 1) second DAIR, 2) implant removal, 3) suppressive antimicrobial treatment or 4) infection-related death within 60 days after debridement.
ResultsA total of 386 patients were included. Failure occurred in 148 patients (38.3%). Patients with KLIC scores of ≤2, 2.5-3.5, 4-5, 5.5-6.5 and ≥7 had failure rates of 27.9%, 37.1%, 49.3%, 54.5% and 85.7% respectively (p<0.001). The receiver operating characteristic curve showed an area under the curve of 0.64 (95% con�dence interval 0.59-0.69). A KLIC score higher than 6 points showed a speci�city of 97.9%.
ConclusionThe KLIC score is a relatively good preoperative risk score for DAIR failure in patients with early acute PJI and appears to be most useful in clinical practice for patients with low or high KLIC scores.
51938_Claudia_Lowik.indd 72 19-08-19 11:12

Predicting DAIR failure using the KLIC score
73
5
Introduction
Total joint arthroplasty is a widely used treatment modality for osteoarthritis of the hip and knee, with 310,800 total hip arthroplasties and 639,400 total knee arthroplasties performed in the United States in 2010.1,2 In general, joint arthroplasty is a successful procedure with large improvement in the patient’s quality of life. However, prosthetic joint infection (PJI) is a major complication after joint arthroplasty with high impact on the patient’s well-being, occurring in 1-2% of primary joint arthroplasties and up to 10% in revision arthroplasties.3,4 Most of these infections occur within the �rst three months after implantation and are de�ned as early infections.5,6
Surgical debridement, antibiotics and implant retention (DAIR) is the recommended treatment for patients with early PJI, being most successful in early acute PJI, in which symptoms exist for less than three weeks.7,8 Nevertheless, rates of infection control after DAIR vary widely from 37% to 88%.9-
16 Therefore, it is important to be able to predict DAIR failure to select eligible patients before surgery, especially because performing a DAIR procedure could negatively in�uence the outcome of subsequent revision arthroplasty. A couple of studies showed a higher failure rate of two-stage revisions after failed DAIR,17,18 although this has not been con�rmed by others.19,20
Previous studies identi�ed risk factors for DAIR failure, including high in�ammatory parameters, infection with Staphylococcus aureus, longer duration of symptoms, polyethylene retention, and arthroscopic debridement.21-30 In addition, Tornero et al. designed a preoperative risk score with a high accuracy for predicting failure (area under the curve (AUC) 0.84).31 This score consists of �ve preoperative factors, which were identi�ed as independent predictors of failure in 222 patients with early acute PJI: 1) chronic renal failure (Kidney), 2) Liver cirrhosis, 3) Index surgery (revision surgery or prosthesis indicated for a fracture), 4) Cemented prosthesis and 5) C-reactive protein (CRP) >115 mg/L.
To implement the KLIC score in other hospitals as a standard tool for predicting DAIR failure in early acute PJI, it is important to validate the risk score in an external cohort. Therefore, we assessed the predictive value of the KLIC score in a large cohort of patients with early acute PJI treated with DAIR in the Netherlands.
51938_Claudia_Lowik.indd 73 19-08-19 11:12

Chapter 5
74
Material and methods
Study designWe retrospectively analyzed patients with early acute PJI who were treated with DAIR between January 2006 and December 2016 in two general hospitals (Martini Hospital and Medical Center Leeuwarden) and one university hospital (University Medical Center Groningen) in the Netherlands. Patients who developed a PJI within three months after joint arthroplasty and had a duration of symptoms of less than 21 days were included. Diagnosis of PJI was determined according to the diagnostic criteria de�ned by the Musculoskeletal Infection Society (MSIS).32 Patients who did not meet the MSIS criteria were excluded from the analysis, as well as patients who underwent arthroscopic debridement instead of open surgical debridement.
Variables that were collected included demographics, body mass index (BMI), preoperative American Society of Anesthesiologists (ASA) classi�cation, co-morbidities, medication, clinical signs, serological markers, culture results and data of the index procedure and DAIR. The same de�nitions and cut-o�s values of these variables were used as described by Tornero et al.31 Sepsis was de�ned as presence of ≥2 systemic in�ammatory response syndrome criteria and a suspected source of infection. Consistent with Tornero et al.,31 we appointed scores to the preoperative variables of the KLIC score, adding up to a score ranging from 0 to 9.5 points (Table 1). The score was categorized into ≤2 points, 2.5-3.5 points, 4-5 points, 5.5-6.5 points and ≥7 points.
Table 1. Preoperative variables of the KLIC score with appointed scores
Variable ScoreK Chronic renal failure (kidney) 2L Liver cirrhosis 1.5I Index procedure (revision surgery or prosthesis indicated for a fracture) 1.5C Cemented prosthesis 2C C-reactive protein >115 mg/L 2.5
De�nition of outcomePrimary outcome was early failure, de�ned as one of the following events within 60 days after initial debridement: 1) second DAIR, 2) revision surgery or implant removal, 3) infection-related death, or 4) suppressive antimicrobial treatment. In case a second DAIR procedure was solely performed for removal
51938_Claudia_Lowik.indd 74 19-08-19 11:12

Predicting DAIR failure using the KLIC score
75
5
of gentamicin-impregnated beads, without clinical and biochemical signs of persistent infection, second debridement was not considered as failure.
Surgical and antimicrobial treatmentSurgical treatment consisted of DAIR, in which the wound was opened via the pre-existing incision and hematoma and avital tissue were extensively excised. Subsequently, the wound was thoroughly lavaged using three to six liters of saline. According to local protocols and the clinical judgement of the orthopaedic surgeon, modular components were optionally exchanged and gentamicin-impregnated beads or sponges were inserted into the joint cavity. After obtaining multiple deep tissue biopsies for culture, broad-spectrum intravenous antimicrobial treatment was started, if necessary adjusted according to the antibiogram, and maintained for two weeks. Subsequently, oral antimicrobial treatment was administered for ten weeks. Rifampin was added to the antimicrobial treatment regimen in infections caused by staphylococci.
Statistical analysisCategorical variables were expressed in absolute frequencies and percentages. Continuous variables were presented as mean and standard deviation (SD) or as median and interquartile range (IQR) when not normally distributed. Categorical variables were compared using the Chi-square test. Continuous variables were compared using the Student’s t-test or the Mann-Whitney U test according to the Kolmogorov-Smirnov test of normality.
Failure rates were reported for each risk group of the KLIC score and a receiver operating characteristic (ROC) curve was used to examine its accuracy for predicting DAIR failure. In addition, a binary logistic regression analysis was performed to evaluate whether additional important variables were associated with failure. Multicollinearity of variables was assessed. Multivariate logistic regression analysis was performed to identify independent predictors for failure. All preoperative variables with p<0.20 in the univariate analyses were assessed in the multivariate regression analysis. Statistical signi�cance was de�ned as a two-tailed p<0.05. Statistical analyses were performed using IBM SPSS Statistics (version 24.0, Chicago, USA).
51938_Claudia_Lowik.indd 75 19-08-19 11:12
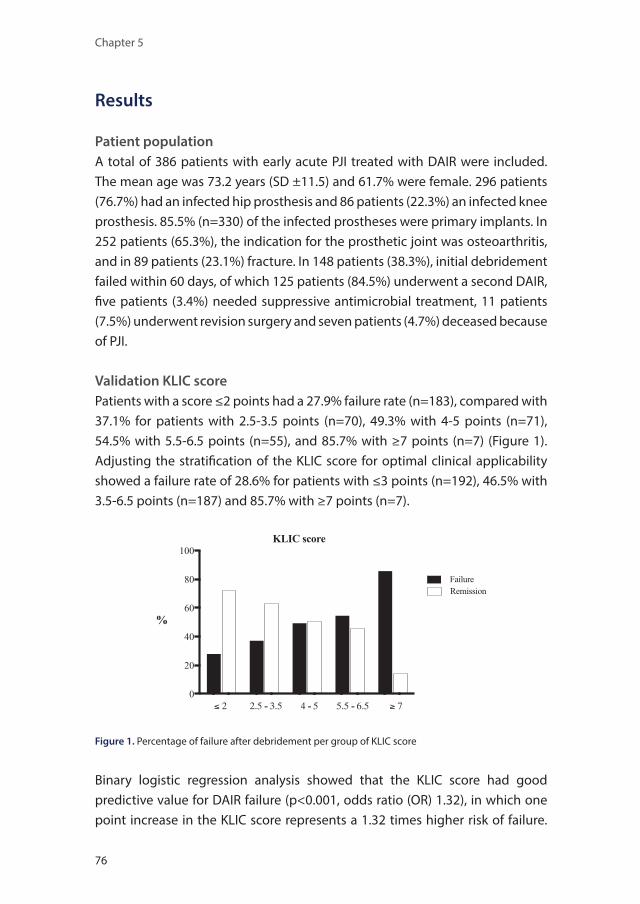
Chapter 5
76
Results
Patient populationA total of 386 patients with early acute PJI treated with DAIR were included. The mean age was 73.2 years (SD ±11.5) and 61.7% were female. 296 patients (76.7%) had an infected hip prosthesis and 86 patients (22.3%) an infected knee prosthesis. 85.5% (n=330) of the infected prostheses were primary implants. In 252 patients (65.3%), the indication for the prosthetic joint was osteoarthritis, and in 89 patients (23.1%) fracture. In 148 patients (38.3%), initial debridement failed within 60 days, of which 125 patients (84.5%) underwent a second DAIR, �ve patients (3.4%) needed suppressive antimicrobial treatment, 11 patients (7.5%) underwent revision surgery and seven patients (4.7%) deceased because of PJI.
Validation KLIC scorePatients with a score ≤2 points had a 27.9% failure rate (n=183), compared with 37.1% for patients with 2.5-3.5 points (n=70), 49.3% with 4-5 points (n=71), 54.5% with 5.5-6.5 points (n=55), and 85.7% with ≥7 points (n=7) (Figure 1). Adjusting the strati�cation of the KLIC score for optimal clinical applicability showed a failure rate of 28.6% for patients with ≤3 points (n=192), 46.5% with 3.5-6.5 points (n=187) and 85.7% with ≥7 points (n=7).
Figure 1. Percentage of failure after debridement per group of KLIC score
Binary logistic regression analysis showed that the KLIC score had good predictive value for DAIR failure (p<0.001, odds ratio (OR) 1.32), in which one point increase in the KLIC score represents a 1.32 times higher risk of failure.
51938_Claudia_Lowik.indd 76 19-08-19 11:12

Predicting DAIR failure using the KLIC score
77
5
The ROC curve showed an AUC of 0.64 (95% CI 0.59-0.69) (Figure 2). A score of 3.5 points showed the optimal cut-o� point value with a sensitivity and speci�city of 52.2% and 70.9% respectively. A score higher than 6 points showed a speci�city of 97.9%.
Figure 2. Receiver operating characteristic curve for the KLIC score
Di�erences between cohortsConsidering the lower accuracy of the KLIC score in our cohort (AUC 0.64) compared with Tornero et al. (AUC 0.84), we additionally evaluated the di�erences between both cohorts. The incidence of variables used in the KLIC score di�ered. The incidence of liver cirrhosis in our cohort was signi�cantly lower compared with Tornero et al. (1.0% vs 10.4%, p<0.001), and the incidence of cemented prostheses and CRP >115 mg/L was signi�cantly higher (83.9% vs 74.3%, p=0.004 and 32.4% vs 24.5%, p=0.046, respectively). There were no di�erences in incidence of chronic renal failure and index procedure.
Additional notable di�erences between cohorts were the number of PJIs of the hip (76.7% vs 38.3%, p<0.001) and the number of infections caused by Staphylococcus aureus (46.9% vs 36.5%, p=0.013). Polyethylene exchange was performed to a lesser extent in our cohort compared with that of Tornero et al. (21.0% vs 72.9%, p<0.001). Furthermore, in our cohort, gentamicin-impregnated beads and sponges were placed during a DAIR procedure in 184 patients (47.7%) and 109 patients (28.2%) respectively, while Tornero et al. did not use any local antimicrobials. The accuracy of the KLIC score did not change in the presence or absence of the above-mentioned variables (data not shown).
51938_Claudia_Lowik.indd 77 19-08-19 11:12

Chapter 5
78
Preoperative and perioperative variables according to outcomeTable 2 shows the results of preoperative variables in relation to the outcome of debridement in our cohort. Various preoperative variables showed signi�cant di�erences between patients with remission and failure after debridement, including: CRP (78.8 vs 132.4 mg/L, p<0.001), age (72.0 vs 75.1 years, p=0.009), days from arthroplasty to debridement (21.0 vs 18.2 days, p=0.018), ASA classi�cation (2.29 vs 2.44, p=0.021), and leukocyte count (11.0 vs 12.2 x109/L, p=0.027).
Moreover, failure rates were signi�cantly higher for the following preoperative variables: CRP >115mg/L (55.2% vs 30.3%, p<0.001), left-sided prosthesis (46.7% vs 31.1%, p=0.002), presence of sepsis (52.1% vs 35.1%, p=0.007), ischemic heart disease (50.6% vs 35.3%, p=0.013), and prosthesis indicated for a fracture (52.8% vs 33.3%, p=0.047). Multicollinearity analyses revealed that a left-sided prosthesis was associated with a higher percentage of positive cultures (93.6% vs 89.3%, p=0.028), sepsis (25.0% vs 13.6%, p=0.004), and Staphylococcus aureus infection (57.8% vs 37.4%, p<0.001). Presence of a �stula was associated with a signi�cant lower failure rate after debridement (22.0% vs 40.3%, p=0.022) and was associated with younger age (67.5 vs 73.9, p=0.001) and a lower percentage of positive cultures (85.0% vs 92.1%, p=0.032). Multivariate regression analysis showed that the following preoperative variables were signi�cant independent predictors for DAIR failure in our cohort: gender (OR 2.03), ischemic heart disease (OR 1.84), laterality of the arthroplasty (OR 1.80), age (OR 1.03), CRP (OR 1.01), and days from arthroplasty to debridement (OR 0.97).
Table 2. Preoperative patient characteristics according to outcomeCharacteristics Remission (n=238) Failure (n=148) P valueAge in years Mean (SD) 72.0 (11.5) 75.1 (11.2) .009
≥70 years 152 (63.9%) 105 (70.9%) .152Gender Male 79 (33.2%) 69 (46.6%) .080BMI in kg/m2 Mean (SD) 30.2 (SD 6.5) 29.1 (SD 5.6) .117
≥35 kg/m2 50 (22.3%) 23 (17.4%) .269Preoperative ASA score Mean (SD) 2.29 (SD 0.65) 2.44 (SD 0.60) .021
3-4 90 (37.8%) 65 (43.9%) .234Comorbidities Hypertension 147 (61.8%) 92 (62.2%) .938
Ischemic heart disease 38 (16.0%) 39 (26.4%) .013Heart failure 22 (9.2%) 19 (12.8%) .265Diabetes mellitus 46 (19.3%) 36 (24.3%) .243Malignancy 57 (23.9%) 30 (20.3%) .400COPD 43 (18.1%) 38 (25.7%) .074Chronic renal failure 15 (6.3%) 11 (7.4%) .667
51938_Claudia_Lowik.indd 78 19-08-19 11:12

Predicting DAIR failure using the KLIC score
79
5
Table 2. continuedCharacteristics Remission (n=238) Failure (n=148) P value
Liver cirrhosis 1 (0.4%) 3 (2.0%) .130Dementia 8 (3.4%) 8 (5.4%) .327Rheumatoid arthritis 17 (7.1%) 11 (7.4%) .915
Medication Anticoagulants 51 (21.4%) 44 (29.7%) .066Steroid therapy 23 (9.7%) 21 (14.2%) .174
Site of arthroplasty Knee 54 (22.7%) 32 (21.6%) .697Hip 181 (76.1%) 115 (77.7%)
Laterality Left 96 (40.3%) 83 (56.8%) .002Indication for arthroplasty Osteoarthritis 168 (70.6%) 84 (56.8%) .047
Fracture 42 (17.6%) 47 (31.8%)Type of surgery Primary 207 (87.0%) 123 (83.1%) .294
Revision 31 (13.0%) 25 (16.9%)Type of cementation Not cemented 43 (18.1%) 19 (12.8%) .274
Cemented (without antibiotics)
8 (3.4%) 8 (5.4%)
Cemented (with antibiotics)
187 (78.6%) 121 (81.8%)
Days from prosthesis to debridement
Mean (SD) 21.0 (13.0) 18.2 (9.9) .018
>28 days 33 (13,9%) 13 (8,8%) .134Days of symptoms Mean (SD) 6.7 (6.0) 7.2 (6.0) .425Clinical signs Fever 42 (17.6%) 31 (20.9%) .421
Pain 77 (32.4% 39 (26.4%) .211Redness 97 (40.8%) 64 (43.2%) .630Wound drainage 207 (87.0%) 127 (85.8%) .745Skin necrosis 6 (2.5%) 7 (4.7%) .242Presence of �stula 32 (13.4%) 9 (6.1%) .022Sepsis 35 (14.7%) 38 (25.7%) .007
Antimicrobial treatment before debridement
42 (17.6%) 24 (16.2%) .717
Leukocyte count in x109/L Mean (SD) 11.0 (4.4) 12.2 (5.8) .027≥10 x109/L 121 (50.8%) 85 (57.4%) .207
CRP in mg/L Mean (SD) 78.8 (86.2) 132.4 (108.0) <.001>115 mg/L 56 (23.5%) 69 (46.6%) <.001
Creatinin in mg/L Mean (SD) 79.9 (30.4) 79.2 (33.9) .831>110 mg/L 30 (12.6%) 15 (10.1%) .454
Glycaemia Mean (SD) 7.2 (1.9) 7.6 (2.7) .277
Bold indicates statistically signi�cant di�erences. ASA: American Society of Anesthesiologist; BMI: body mass index; COPD: chronic obstructive pulmonary disease, CRP: C-reactive protein; SD: standard deviation.
Table 3 shows the results of perioperative variables in relation to the outcome of debridement. Positive cultures in all of the obtained intraoperative tissues and bacteremia were associated with a signi�cant higher failure rate (41.7% vs 26.2%, p=0.010 and 57.7% vs 34.4%, p=0.008 respectively), just as the use
51938_Claudia_Lowik.indd 79 19-08-19 11:12

Chapter 5
80
of gentamicin-impregnated beads or sponges (43.0% vs 23.7%, p=0.001). Multicollinearity analyses showed that use of local antimicrobials was associated with a higher CRP value (105.9 vs 78.6 mg/L, p=0.020) and a higher number of Staphylococcus aureus infections (50.2% vs 36.6%, p=0.022).
Infection with Staphylococcus aureus showed a higher failure rate (47.5% vs 30.2%, p<0.001), as well as infection with anaerobe microorganisms (i.e. Cutibacterium acnes (n=4), Bacteroides fragilis (n=4) and Finegoldia magna (n=4)) (66.7% vs 37.2%, p=0.021), although anaerobe microorganisms were isolated in only a limited number of cases (n=15). Although gram-negative microorganisms in general were not associated with DAIR failure (42.5% vs 37.3%, p=0.390), infection with Proteus species did show a signi�cant higher failure rate (61.1% vs 37.2%, p=0.042). However, Proteus species were also isolated in only a limited number of cases (n=18). Infection with Corynebacterium species and other gram-positive microorganisms showed a signi�cant lower failure rate (23.5% vs 40.6%, p=0.020 and 8.3% vs 39.3%, p=0.030 respectively).
Discussion
We evaluated the preoperative predictive value of the KLIC score for DAIR failure in a large external cohort of 386 patients. Our study showed that the KLIC score is a relatively good preoperative risk score for predicting failure, but its predictive value was lower than previously described, with an AUC of 0.64 in our cohort compared with 0.84 in the study by Tornero et al.31 This lower predictive accuracy is probably due to the retrospective design of this study and di�erences in local epidemiology, clinical characteristics, and surgical techniques. Although performing an additional prospective study could be useful, our results demonstrated that the KLIC score is applicable in clinical practice in patients with a low (<3.5 points) or high (>6 points) KLIC score for predicting DAIR failure.
Di�erences between cohorts are the most important reason that a predictive model should be validated externally before it can be implemented in clinical practice in other countries and hospitals. Therefore, validating the KLIC score in a large external cohort of patients in the Netherlands is one of the strengths of our study. In addition, by using the exact same variables, inclusion criteria, de�nition of failure, and cut-o� values as Tornero et al., the process of
51938_Claudia_Lowik.indd 80 19-08-19 11:12

Predicting DAIR failure using the KLIC score
81
5
validation of the KLIC score was executed legitimately. Although our study demonstrated that the KLIC score does predict failure,
the sensitivity, speci�city and accuracy were lower than previously described. A cause for this could be that we performed a retrospective database research while Tornero et al. carried out a prospective study.31 In addition, di�erences in incidence of variables in the KLIC score, a higher number of PJIs of the hip, more infections caused by Staphylococcus aureus and the use of local antimicrobials could be the cause of the lower accuracy of the KLIC score. Furthermore, there was a lower percentage of polyethylene exchange in our cohort, partially because of the use of certain types of arthroplasties in which polyethylene exchange was not possible (i.e. AGC prostheses). Moreover, we observed an evident increase in the percentage of polyethylene exchange from 0% in 2006
Table 3. Perioperative patient characteristics according to outcome
Characteristics Remission (n=238)
Failure (n=148)
P value
Polyethylene exchange 47 (19.8%) 34 (23.0%) .462Local antimicrobials No antimicrobials 71 (29.8%) 22 (14.9%) .001
Gentamicin beads 12 (5.0%) 16 (10.8%)Gentamicin sponges 113 (47.5%) 71 (48.0%)Gentamicin beads + sponges 42 (17.6%) 39 (26.4%)
Need for muscle �ap 3 (1.3%) 5 (3.4%) .156Bacteremia 11 (4.6%) 15 (10.1%) .008Percentage of positive cultures Mean (SD) 89.4 (21.6) 94.5 (16.3) .009All cultures positive 176 (73.9%) 126 (85.1%) .010Polymicrobial infection 109 (45.8%) 67 (45.3%) .919Microorganism Staphylococcus aureus 95 (39.9%) 86 (58.1%) <.001
MRSA 0 (0%) 0 (0%) 1.000Staphylococcus epidermidis 85 (35.7%) 41 (27.7%) .103Corynebacterium species 39 (16.4%) 12 (8.1%) .020Enterococcus species 44 (18.5%) 26 (17.6%) .820Streptococcus species 44 (18.5%) 22 (14.9%) .358Other gram-positives 11 (4.6%) 1 (0.7%) .030Escherichia coli 11 (4.6%) 8 (5.4%) .729Pseudomonas species 15 (6.3%) 4 (2.7%) .112Enterobacter cloacae 10 (4.2%) 5 (3.4%) .684Proteus species 7 (2.9%) 11 (7.4%) .042Other gram-negatives 11 (4.6%) 12 (8.1%) .159Anaerobes 5 (2.1%) 10 (6.8%) .021Candida species 1 (0.4%) 2 (1.4%) .311
Bold indicates statistically signi�cant di�erences. MRSA: methicillin-resistant Staphylococcus aureus; SD: standard deviation.
51938_Claudia_Lowik.indd 81 19-08-19 11:12

Chapter 5
82
to 46.3% in 2016 in our cohort, as the importance of exchanging modular components became more evident in recent years.7,22
Most of the preoperative and perioperative risk factors for DAIR failure were in concordance with previous studies, including the preoperative variables: in�ammatory parameters,22,25,27,28 ASA classi�cation,29,30 and duration of symptoms,21,23,26,27,30 and perioperative variables: bacteremia, a higher percentage of positive cultures, and infection with Staphylococcus aureus.11,29,33
In our cohort, multivariate regression analysis revealed that additional preoperative variables other than the variables included in the KLIC score were predictive of failure, indicating the dynamics in risk scores because of di�erences in studied populations, thereby stressing the need for validation of risk scores in external cohorts.
A remarkable di�erence between the cohorts is the failure rate of debridement (38.3% vs 23.4%), which could be explained by the higher percentage of Staphylococcus aureus infections and higher CRP values in our cohort. Over the years, the failure rate decreased gradually from 45.5% in 2006 to 31.7% in 2016 in our cohort, possibly because of the increase in polyethylene exchange. Nonetheless, our failure rate is comparable with previous studies.9,11,12,14,15
Preoperative risk factors for DAIR failure can be used in the decision-making process to select eligible patients for debridement. The KLIC score is an easy and clinical applicable risk score which can help the clinician in discussing the risk of DAIR failure with the patient. Although a DAIR procedure is in general a good treatment modality for patients with early acute PJI, in patients with a high estimated preoperative failure risk, the physician may consider a di�erent treatment approach with a higher chance of infection control. For example, performing revision surgery instead of debridement or starting suppressive antimicrobial treatment after debridement in patients who are not eligible for revision surgery due to severe comorbidity.
In conclusion, we demonstrated in an external cohort that the KLIC score is a relatively good preoperative risk score for DAIR failure in patients with early acute PJI. Its predictive value seems most prominent and therefore clinical applicable in patients with low or high KLIC scores. Ideally, additional validation in a prospective study should con�rm these �ndings.
51938_Claudia_Lowik.indd 82 19-08-19 11:12

Predicting DAIR failure using the KLIC score
83
5
References
1. Williams SN, Wolford ML, Bercovitz A. Hospitalization for total knee replacement among inpatients aged 45 and over: United States, 2000-2010. NCHS Data Brief 2015; 210: 1-8.
2. Wolford ML, Palso K, Bercovitz A. Hospitalization for total hip replacement among inpatients aged 45 and over: United States, 2000-2010. NCHS Data Brief 2015; 186: 1-8.
3. Kurtz SM, Ong KL, Lau E, Bozic KJ, Berry D, Parvizi J. Prosthetic joint infection risk after TKA in the medicare population. Clin Orthop Relat Res 2010; 468(1): 52-6.
4. Kunutsor SK, Whitehouse MR, Blom AW, Beswick AD, INFORM Team. Re-infection outcomes following one- and two-stage surgical revision of infected hip prosthesis: a systematic review and meta-analysis. PLoS One 2015; 10(9): 1-15.
5. Yokoe DS, Avery TR, Platt R, Huang SS. Reporting surgical site infections following total hip and knee arthroplasty: impact of limiting surveillance to the operative hospital. Clin Infect Dis 2013; 57(9): 1282-8.
6. Barrett L, Atkins B. The clinical presentation of prosthetic joint infection. J Antimicrob Chemother 2014; 69(Suppl 1): 25-8.
7. Parvizi J, Gehrke T, Chen AF. Proceedings of the international consensus on periprosthetic joint infection. Bone Joint J 2013; 95-B(11): 1450-2.
8. Osmon DR, Berbari ER, Berendt AR, Lew D, Zimmerli W, Steckelberg JM, et al. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 2013; 56(1): 1-25.
9. Faschingbauer M, Kappe T, Trubrich A, Bieger R, Reichel H. Retention of the prosthesis in early periprosthetic infection after total hip arthroplasty. Z Orthop Unfall 2015; 153(2): 192-7.
10. Sukeik M, Patel S, Haddad FS. Aggressive early débridement for treatment of acutely infected cemented total hip arthroplasty. Clin Orthop Relat Res 2012; 470(11): 3164-70.
11. Cobo J, Garcia San Miguel L, Euba G, Rodríguez D, García-Lechuz JM, Riera M, et al. Early prosthetic joint infection: outcomes with debridement and implant retention followed by antibiotic therapy. Clin Microbiol Infect 2011; 17(11): 1632-7.
12. Duque AF, Post ZD, Lutz RW, Orozco FR, Pulido SH, Ong AC. Is there still a role for irrigation and debridement with liner exchange in acute periprosthetic total knee infection? J Arthroplasty 2017; 32(4): 1280-4.
13. Fehring TK, Odum SM, Berend KR, Jiranek WA, Parvizi J, Bozic KJ, et al. Failure of irrigation and débridement for early postoperative periprosthetic infection. Clin Orthop Relat Res 2013; 471(1): 250-7.
14. Bergkvist M, Mukka SS, Johansson L, Ahl TE, Sayed-Noor AS, Sköldenberg OG, et al. Debridement, antibiotics and implant retention in early periprosthetic joint infection. Hip Int 2016; 26(2): 138-43.
15. Westberg M, Grøgaard B, Snorrason F. Early prosthetic joint infections treated with debridement and implant retention: 38 primary hip arthroplasties prospectively recorded and followed for median 4 years. Acta Orthop 2012; 83(3): 227-32.
16. Aboltins CA, Dowsey MM, Peel T, Lim WK, Parikh S, Stanley PA, et al. Early prosthetic hip joint infection treated with debridement, prosthesis retention and bio�lm-active antibiotics: functional outcomes, quality of life and complications. Intern Med J 2013; 43(7): 810-5.
17. Sherrell JC, Fehring TK, Odum S, Hansen E, Zmistowski B, Dennos A, et al. Fate of two-stage reimplantation after failed irrigation and débridement for periprosthetic knee infection. Clin Orthop Relat Res 2011; 469(1): 18-25.
18. Gardner J, Gioe TJ, Tatman P. Can this prosthesis be saved? Implant salvage attempts in infected primary TKA. Clin Orthop Relat Res 2011; 469(4): 970-6.
19. Brimmo O, Ramanathan D, Schiltz NK, Pillai AL, Klika AK, Barsoum WK. Irrigation and debridement before a 2-stage revision total knee arthroplasty does not increase risk of failure. J Arthroplasty 2016; 31(2): 461-4.
20. Nodzo SR, Boyle KK, Nocon AA, Henry MW, Mayman DJ, Westrich GH. The in�uence of a failed irrigation and debridement on the outcomes of a subsequent 2-stage revision knee arthroplasty. J Arthroplasty 2017; 32(8): 2508-12.
51938_Claudia_Lowik.indd 83 19-08-19 11:12

Chapter 5
84
21. Triantafyllopoulos GK, Poultsides LA, Sakellariou VI, Zhang W, Sculco PK, Ma Y, et al. Irrigation and debridement for periprosthetic infections of the hip and factors determining outcome. Int Orthop 2015; 39(6): 1203–9.
22. Kim JG, Bae JH, Lee SY, Cho WT, Lim HC. The parameters a�ecting the success of irrigation and debridement with component retention in the treatment of acutely infected total knee arthroplasty. Clin Orthop Surg 2015; 7(1): 69-76.
23. Triantafyllopoulos GK, Poulsides LA, Zhang W, Sculco PK, Ma Y, Sculco TP. Periprosthetic knee infections treated with irrigation and debridement: outcomes and preoperative predictive factors. J Arthroplasty 2015; 30(4): 649-57.
24. Kuiper JWP, van den Bekerom MPJ, van der Stappen J, Nolte PA, Colen S. 2-stage revision recommended for treatment of fungal hip and knee prosthetic joint infections. Acta Orthop 2013; 84(6): 517-23.
25. Vilchez F, Martínez-Pastor JC, García-Ramiro S, Bori G, Maculé F, Sierra J, et al. Outcome and predictors of treatment failure in early post-surgical prosthetic joint infections due to Staphylococcus aureus treated with debridement. Clin Microbiol Infect 2011; 17(3): 439-44.
26. Buller LT, Sabry FY, Easton RW, Klika AK, Barsoum WK. The preoperative prediction of success following irrigation and debridement with polyethylene exchange for hip and knee prosthetic joint infections. J Arthroplasty 2012; 27(6): 857-64.
27. Kuiper JW, Vos CJ, Saouti R, Vergroesen DA, Graat HC, Debets-Ossenkopp YJ, et al. Prosthetic joint-associated infections treated with DAIR (debridement, antibiotics, irrigation, and retention): analysis of risk factors and local antibiotic carriers in 91 patients. Acta Orthop 2013; 84(4): 380-6.
28. Martínez-Pastor JC, Muñoz-Mahamud E, Vilchez F, García-Ramiro S, Bori G, Sierra J, et al. Outcome of acute prosthetic joint infections due to gram-negative bacilli treated with open debridement and retention of the prosthesis. Antimicrob Agents Chemother 2009; 53(11): 4772-7.
29. Azzam KA, Seeley M, Ghanem E, Austin MS, Purtill JJ, Parvizi J. Irrigation and debridement in the management of prosthetic joint infection: traditional indications revisited. J Arthroplasty 2010; 25(7): 1022-7.
30. Fink B, Schuster P, Schwenninger C, Frommelt L, Oremek D. A standardized regimen for the treatment of acute postoperative infections and acute hematogenous infections associated with hip and knee arthroplasties. J Arthroplasty 2017; 32(4): 1255-61.
31. Tornero E, Morata L, Martínez-Pastor JC, Bori G, Climent C, García-Velez DM, et al. KLIC-score for predicting early failure in prosthetic joint infections treated with debridement, implant retention and antibiotics. Clin Microbiol Infect 2015; 21(8): 9-17.
32. Parvizi J, Zmistowski B, Berbari EF, Bauer TW, Springer BD, Della Valle CJ, et al. New de�nition for periprosthetic joint infection: from the workgroup of the musculoskeletal infection society. Clin Orthop Relat Res 2011; 469(11): 2992-4.
33. Byren I, Bejon P, Atkins BL, Angus B, Masters S, McLardy-Smith P, et al. One hundred and twelve infected arthroplasties treated with ‘DAIR’ (debridement, antibiotics and implant retention): antibiotic duration and outcome. J Antimicrob Chemother 2009; 63(6): 1264-71.
51938_Claudia_Lowik.indd 84 19-08-19 11:12

51938_Claudia_Lowik.indd 85 19-08-19 11:12

51938_Claudia_Lowik.indd 86 19-08-19 11:12

Chapter 6
Use of gentamicin-impregnated beads or sponges in the treatment of early acute
periprosthetic joint infection: a propensity score analysis
Marjan Wouthuyzen-Bakker, Claudia A.M. Löwik, Bas A.S. Knobben, Wierd P. Zijlstra, Joris J.W. Ploegmakers, Glen Mithoe, Aziz Al Moujahid, Greetje A. Kampinga, Paul C. Jutte, on behalf of the Northern Infection
Network Joint Arthroplasty
Published in: Journal of Antimicrobial Chemotherapy 2018; 73(12): 3454-3459
51938_Claudia_Lowik.indd 87 19-08-19 11:12

Chapter 6
88
Abstract
BackgroundEarly acute periprosthetic joint infections (PJIs) treated with debridement, antibiotics and implant retention (DAIR) have failure rates ranging from 10% to 60%. We determined the e�cacy of applying local gentamicin-impregnated beads and/or sponges during debridement in early PJI.
MethodsPatients with early acute PJI, de�ned as less than 21 days of symptoms and treated with DAIR within 90 days after index surgery, were retrospectively evaluated. Early failure was de�ned as PJI-related death, the need for implant removal or a second DAIR or antibiotic suppressive therapy owing to persistent signs of infection, all within 60 days after initial debridement. Overall failure was de�ned as implant removal at any time point during follow-up. A 1:1 propensity score matching was performed to correct for confounding factors.
ResultsA total of 386 patients were included. Local gentamicin was applied in 293 patients (75.9%) and was withheld in 93 patients (24.1%). Multivariate analysis demonstrated that the use of local gentamicin was independently associated with early failure (OR 1.97, 95% CI 1.12 - 3.48). After propensity matching, early failure was 40.3% in the gentamicin group versus 26.0% in the control group (p=0.06) and overall failure was 5.2% in the gentamicin group versus 2.6% in the control group (p=0.40). These numbers remained when solely analyzing the application of gentamicin-impregnated sponges.
ConclusionEven after propensity score matching, failure rates remained higher if local gentamicin-impregnated beads and/or sponges were administered in early acute PJI. Based on these results, their use should be discouraged.
51938_Claudia_Lowik.indd 88 19-08-19 11:12

Gentamicin-impregnated beads and sponges
89
6
Introduction
Periprosthetic joint infection (PJI) is a major complication after total joint arthroplasty, occurring in approximate 1-2% of primary arthroplasties and in up to 10% of revision arthroplasties.1-2 The majority of these infections occur in the early post-surgical period and are treated with debridement, antibiotics and implant retention (DAIR). Successful treatment of early PJI by DAIR depends on multiple host- and implant-related factors, such as the causative microorganism(s) and their susceptibility to antibiotics.3-18
As treatment success ranges from 40 to 90%, it is crucial to improve surgical techniques and optimize antibiotic treatment to achieve infection control without the need for additional surgeries.19-25 Indeed, many studies report the importance of exchanging the modular components during debridement and emphasize the need for prescribing antibiotics with high e�cacy against bio�lms.3-8,13-15 In addition, applying local antibiotics during surgical debridement may be another option to achieve higher cure rates, by rapidly obtaining su�cient levels of antibiotics at the site of the infection. For this reason, gentamicin-impregnated beads and sponges were introduced many years ago. Gentamicin is eluted from beads over a course of 2-6 weeks and sponges provide a burst release in the �rst 24 hours and are ‘empty’ after three days.26-28 Both are able to obtain levels of local gentamicin far above the MIC values but, until now, retrospective analyses did not show any bene�t in clinical outcome.29-30
It is well known that retrospective studies are prone to selection bias, particularly in evaluating treatment strategies as a more aggressive treatment approach is often applied in severe infections compared with milder clinical courses. By means of a propensity score analysis, this particular type of bias can be addressed. Therefore, we determined the e�cacy of gentamicin-impregnated beads and/or sponges in a large cohort of early acute PJI patients by using a propensity score analysis to control for confounding factors.
51938_Claudia_Lowik.indd 89 19-08-19 11:12

Chapter 6
90
Material and methods
Study designPatients with early acute PJI of the hip, knee, shoulder or elbow and treated with DAIR between January 2006 and December 2016 were retrospectively analyzed. Early acute PJI was de�ned as a PJI that developed within three months after the index surgery with less than 21 days of symptoms. Diagnosis of PJI was determined according to the diagnostic criteria de�ned by the Musculoskeletal Infection Society (MSIS).31 Patients who did not meet the MSIS criteria were excluded from the analysis, as well as patients who underwent arthroscopic debridement instead of open surgical debridement. Patients were recruited in two general hospitals (Martini Hospital and Medical Center Leeuwarden) and one university hospital (University Medical Center Groningen) in the Netherlands. Informed consent was retrieved when required by the ethics committee of the participating center.
Surgical and antimicrobial treatmentAs previously described in this cohort of patients, surgical treatment consisted of a DAIR procedure, in which the wound was opened via the pre-existing incision.17 Hematoma and avital tissue were extensively excised and the wound was thoroughly irrigated using three to six liters of saline. According to the clinical judgement of the orthopaedic surgeon, mobile components were exchanged and gentamicin-impregnated beads or sponges were inserted into the joint cavity. After obtaining multiple deep tissue biopsies for culture, empirical broad-spectrum intravenous antimicrobial treatment was started and, if necessary, adjusted according to results of the antibiogram. Intravenous treatment was maintained for at least two weeks before switching to an oral regimen that was continued for an additional ten weeks. Rifampicin was added to the antimicrobial treatment regimen in infections caused by rifampin-susceptible staphylococci.
De�nition of failureThe primary outcome was early treatment failure, de�ned as one of the following events within 60 days after initial debridement: 1) a second DAIR procedure, 2) implant removal, 3) PJI-related death, or 4) long-term suppressive antimicrobial treatment in the case of persistent clinical signs of infection.
51938_Claudia_Lowik.indd 90 19-08-19 11:12

Gentamicin-impregnated beads and sponges
91
6
In case of a second DAIR procedure being solely performed for removal of gentamicin-impregnated beads that were placed during initial debridement, without clinical and biochemical signs of persistent infection, the second debridement was not considered to be a failure. The secondary outcome was overall failure and was de�ned as the need for implant removal at any time point during follow-up.
Statistical analysisA Chi-square test was used to analyze di�erences between groups for categorical variables. To correct for bias between the gentamicin group and the control group, a propensity score matching was performed. A propensity score was calculated using a logistic regression model in which the use of local gentamicin was used as the dependent variable, and several (pre)operative variables that were statistically di�erent between both groups as covariates. Matching was performed using a caliper of two decimals and identical propensity scores were randomized to perform the matching. In addition, a logistic regression analysis was performed to identify risk factors for early and overall failure. Variables with a di�erence between both groups, de�ned as a P value <0.10 in the univariate analysis, were subsequently included in the multivariate analysis. All analyses were two-tailed and P values <0.05 were considered statistically signi�cant. A Kaplan-Meier survival curve with a cox regression analysis was performed to evaluate failure rate in time. Statistical analysis was performed using SPSS, version 23.0 (SPSS Inc., Chicago, IL, USA).
Results
Patient characteristics A total of 386 patients were included in the �nal analysis, including 86 knees and 296 hips (comprising 99% of the total cohort). Local gentamicin was applied in 293 patients (75.9%) and was withheld in 93 patients (24.1%). In the gentamicin group, gentamicin-impregnated beads were administered in 28 patients (9.6%), gentamicin-impregnated sponges were administered in 184 patients (62.8%) and both were administered in 81 patients (27.6%). The mean number of inserted gentamicin-impregnated beads was 66.4 (SD 22.0) and the mean number of inserted gentamicin-impregnated sponges was 2.6 (SD 1.0).
51938_Claudia_Lowik.indd 91 19-08-19 11:12

Chapter 6
92
Table 1 shows the baseline characteristics of analyzed patients, separated according to insertion of local gentamicin. The gentamicin group had a signi�cantly higher rate of hypertension and chronic renal insu�ciency, longer duration of symptoms, a higher rate of fractures as an indication for arthroplasty, higher in�ammatory parameters at clinical presentation, a higher rate of pus during debridement and infection that was more often polymicrobial in origin and/or caused by Staphylococcus aureus. Additional variables that are known in literature to be associated with worse outcome, like rheumatoid arthritis, revised or cemented prostheses, not exchanging the modular components and the use of antibiotics with low e�cacy against bio�lms were similar in both groups (Table 1). 3-8,13-16
Clinical outcome: gentamicin group versus control groupTable 1 shows the outcome of both groups before and after propensity matching. Before propensity matching, early failure within 60 days after initial debridement was observed in 43.0% of patients who were treated with local gentamicin versus 23.7% in whom local gentamicin was withheld (p=0.001). For both groups, the majority of failure (>80%) was due to the need for a second debridement because of persistent clinical signs of infection. Implant removal was necessary in 9.2% of the gentamicin group versus 2.2% of the control group (p=0.02). After 1:1 propensity score matching for variables that were signi�cantly di�erent between the gentamicin group and the control group, a total of 77 patients in each group remained eligible for analysis (n=154). Although not statistically signi�cant (p=0.06), early failure within 60 days after initial debridement remained higher in the gentamicin group (40.3% versus 26.0%). Implant removal was necessary in 5.2% of patients in whom local gentamicin was applied compared with 2.6% in whom it was withheld (p=0.40). Figure 1 shows the failure rate in time after propensity score matching. Additional multivariate analysis demonstrated that the use of local gentamicin was independently associated with early failure (OR 1.97, 95% CI 1.12-3.48), as well as overall failure (OR 4.46, 95% CI 0.99-20.07).
51938_Claudia_Lowik.indd 92 19-08-19 11:12

Gentamicin-impregnated beads and sponges
93
6
Table 1. Clinical characteristics and outcome in patients receiving or not receiving local gentamicin during debridement
Total patient group Propensity matching 1:1Local gentamicin a (n=293)
Control (n=93) P value
Local gentamicin a (n=77)
Control (n=77)
P value
Baseline characteristicsMale 60.4% 177/293 65.6% 61/93 0.37 42.9% 33/77 37.7% 29/77 0.51Age >80 years 33.1% 97/293 32.3% 30/93 0.88 23.4% 18/77 37.7% 29/77 0.05BMI >30 kg/m2 47.4% 127/268 37.5% 33/88 0.10 52.1% 37/71 37.5% 27/72 0.08ASA classi�cation ≥3
41.3% 121/293 36.6% 34/93 0.42 28.6% 22/77 41.6% 32/77 0.09
Medical historyHypertension 66.2% 194/293 48.4% 45/93 0.002 48.1% 37/77 54.5% 42/77 0.42Ischemic heart disease
22.2% 65/293 12.9% 12/93 0.05 23.4% 18/77 15.6% 12/77 0.22
Heart failure 11.3% 33/293 8.6% 8/93 0.47 9.1% 7/77 10.4% 8/77 0.79Diabetes mellitus
22.2% 65/293 18.3% 17/93 0.42 14.3% 11/77 18.2% 14/77 0.51
COPD 22.5% 66/293 16.1% 15/93 0.19 22.1% 17/77 18.2% 14/77 0.55Chronic renal insu�ciency
8.2% 24/293 2.2% 2/93 0.04 2.6% 2/77 2.6% 2/77 1.00
Liver cirrhosis 1.4% 4/293 0.0% 0/93 0.26 0.0% 0/77 0.0% 0/77 1.00Rheumatoid arthritis
7.8% 23/293 5.4% 5/93 0.45 7.8% 6/77 6.5% 5/77 0.75
MedicationOral anticoagulant
25.3% 74/293 22.6% 21/93 0.60 19.5% 15/77 26.0% 20/77 0.34
Immune-suppressive drugs
11.3% 33/293 11.8% 11/93 0.88 7.8% 6/77 11.7% 9/77 0.42
Characteristics of infected implantHip 78.2% 229/293 72.0% 67/93 0.22 80.5% 62/77 72.7% 56/77 0.25Knee 20.8% 61/293 26.9% 25/93 0.22 19.5% 15/77 27.3% 21/77 0.25Indication prosthesis: fracture
37.9% 111/293 25.8% 24/93 0.03 23.4% 18/77 26.0% 20/77 0.71
Revision prosthesis
14.3% 42/293 15.1% 14/93 0.86 6.5% 5/77 14.3% 11/77 0.11
Cemented stem 84.6% 248/293 81.7% 76/93 0.50 79.2% 61/77 85.7% 66/77 0.29Clinical presentation
Duration of symptoms ≥10 days
30.3% 88/293 44.1% 41/93 0.01 36.4% 28/77 37.7% 29/77 0.87
Temperature >38.3 °C
19.8% 58/293 16.1% 15/93 0.43 19.5% 15/77 16.9% 13/77 0.68
Redness 44.4% 130/293 33.3% 31/93 0.06 46.8% 36/77 33.8% 26/77 0.10Wound leakage 87.4% 256/293 83.9% 78/93 0.39 85.7% 66/77 85.7% 66/77 1.00Pus 22.9% 67/293 8.6% 8/93 0.002 15.6% 12/77 10.4% 8/77 0.34
51938_Claudia_Lowik.indd 93 19-08-19 11:12

Chapter 6
94
Table 1. continued
Total patient group Propensity matching 1:1Local gentamicin a
(n=293)
Control (n=93) P value
Local gentamicin a
(n=77)
Control (n=77)
P value
Sepsis 19.5% 57/293 17.2% 16/93 0.63 19.5% 15/77 18.2% 14/77 0.84CRP >115 mg/L 35.8% 105/293 21.5% 20/93 0.01 23.4% 18/77 22.1% 17/77 0.85Leucocytes >12 cells/µL
35.8% 105/293 34.4% 32/93 0.80 33.8% 26/77 33.8% 26/77 1.00
Identi� ed microorganismsPolymicrobial 48.8% 143/293 35.5% 33/93 0.03 39.0% 30/77 39.0% 30/77 1.00Staphylococcus aureus
50.2% 147/293 36.6% 34/93 0.02 33.8% 26/77 36.4% 28/77 0.74
Enterococcusspecies
18.1% 52/293 18.3% 17/93 0.97 16.9% 13/77 19.5% 15/77 0.68
Gram-negative bacilli
21.2% 62/293 19.4% 18/93 0.71 11.7% 9/77 19.5% 15/77 0.18
Gentamicin resistance of (one of ) the infecting micro-organisms
19.5% 57/293 25.8% 24/93 0.19 13.0% 10/77 28.6% 22/77 0.02
Surgical and antibiotic treatmentExchange modular components
21.8% 64/293 18.5% 17/92 0.49 18.2% 14/77 19.5% 15/77 0.84
Debridement ≥21 days after index arthroplasty
31.4% 92/293 28.0% 26/93 0.53 14.3% 11/77 9.1% 7/77 0.32
Use of rifampicin for staphylococci
83.0% 122/147 84.8% 28/33 0.79 73.6% 39/53 73.7% 42/57 0.99
Use of � uoro-quinolones for Gram-negatives
56.5% 35/62 61.1% 11/18 0.73 55.6% 5/9 53.3% 8/15 0.92
OutcomeEarly failure (<60 days)
43.0% 126/293 23.7% 22/93 0.001 40.3% 31/77 26.0% 20/77 0.06
Second DAIR owing to uncontrolled infection
84.9% 107/126 81.8% 18/22 93.5% 29/31 80.0% 16/20
Overall failure (implant removal)
9.2% 27/293 2.2% 2/93 0.02 5.2% 4/77 2.6% 2/77 0.40
Values in bold are statistically signi� cant. ASA: American society of anesthesiologists; CRP: C-reactive protein.a Local gentamicin consisted of gentamicin-impregnated beads, sponges or both.
51938_Claudia_Lowik.indd 94 19-08-19 11:12

Gentamicin-impregnated beads and sponges
95
6
Figure 1. Failure rate early acute PJI according to the application of local gentamicin impregnated bead and/or sponges in the
propensity matched cohort. Early failure (A) is defined a second debridement because of persistent clinical signs of infection, implant
removal, PJI related death or the need for suppressive antibiotic therapy. Overall failure (B) is defined as implant removal at any time
point during follow-up.
A
0 10 20 30 40 50 600
5050
60
70
80
90
100
%early failure Local gentamicin (n=77)
Control (n=77)
days
logrank test p = 0.09, HR 1.64 (CI 95% 0.94-2.86)
0 250 500 750 10000
5050
60
70
80
90
100
%overall failure
Local gentamicin (n=77)Control (n=77)
days
logrank test p = 0.37, HR 2.22 (CI 95% 0.44-11.0)
B
Figure 1. Failure rate early acute PJI according to the application of local gentamicin impregnated bead and/or sponges in the
propensity matched cohort. Early failure (A) is defined a second debridement because of persistent clinical signs of infection, implant
removal, PJI related death or the need for suppressive antibiotic therapy. Overall failure (B) is defined as implant removal at any time
point during follow-up.
A
0 10 20 30 40 50 600
5050
60
70
80
90
100
%early failure Local gentamicin (n=77)
Control (n=77)
days
logrank test p = 0.09, HR 1.64 (CI 95% 0.94-2.86)
0 250 500 750 10000
5050
60
70
80
90
100
%overall failure
Local gentamicin (n=77)Control (n=77)
days
logrank test p = 0.37, HR 2.22 (CI 95% 0.44-11.0)
B
Figure 1. Failure rate or early acute PJI according to the application of local gentamicin-impregnated beads and/or sponges in the propensity matched cohort. Early failure (A) is de� ned as second debridement because of persistent clinical signs of infection, implant removal, PJI-related death or the need for suppressive antibiotic therapy. Overall failure (B) is de� ned as implant removal at any time point during follow-up.
Subgroup analysisTo determine whether certain subgroups may bene� t from local gentamicin, we performed several subanalyses. Compared with the control group, the administration of local gentamicin did not show any bene� cial e� ect on early failure in the following groups: old age (>80 years) (23.3% (7/30) versus 52.6% (51/97), p=0.005); DAIR performed more than 21 days after index surgery (30.8% (8/26) versus 29.3% (27/92), p=0.89); DAIR performed in patients with more than ten days of symptoms (24.4% (10/41) versus 50.0% (44/88), p=0.006); presence of wound leakage (23.1% (18/78) versus 42.6% (109/256), p=0.002); Staphylococcus aureus infections (41.2% (14/34) versus 49.0% (72/147), p=0.41);
51938_Claudia_Lowik.indd 95 19-08-19 11:12

Chapter 6
96
enterococcal infections (29.4% (5/17) versus 39.6% (21/53), p=0.45); and polymicrobial infections (33.3% (11/33) versus 39.2% (56/143), p=0.53).
Mechanisms for higher failure rate in the gentamicin groupTo assess whether the second procedure for the removal of gentamicin-impregnated beads exposed patients to a higher risk of recurrent infection, we compared the outcome in patients who underwent one DAIR (n=204) with patients who underwent one DAIR and an additional lavage for the removal of gentamicin-impregnated beads without signs of persistent infection (n=57). In this analysis, in which failure was de�ned as the need for implant removal, PJI-related death or the need for suppressive therapy, failure rates were 9.7% and 10.5%, respectively (p=0.9).
In addition, since sponges do not need extra surgery for removal, but can remain in situ, we performed a subanalysis on solely gentamicin-impregnated sponges. Early failure within 60 days after initial debridement was 38.6% (71/184) in the sponge group versus 23.7% (22/93) in patients without local gentamicin (p=0.013). Removal of the implant was necessary in 2.2% (2/93) in the control group versus 7.1% (13/184) in the sponge group (p=0.09). After performing 1:1 propensity analysis, early failure was 40.4% (21/52) in the sponge group versus 26.0% (20/77) in the control group (p=0.09), and implant removal was necessary in 5.8% (3/52) and 2.6% (2/77) (p=0.36), respectively. We additionally performed a subanalysis in PJI cases with solely gentamicin-intermediate or -susceptible strains (n=305): early failure was 41.5% in the gentamicin group and 26.1% in the control group (p=0.02) and overall failure was 8.1% in the gentamicin group and 1.4% in the control group (p=0.05).
Discussion
By applying a propensity score matching analysis to correct for confounding factors, our study demonstrates an approximate two-fold higher failure rate with the use of gentamicin-impregnated beads and/or sponges in the treatment of early acute PJI. This failure rate included not only the need for a second surgical debridement owing to persistent clinical signs of infection in the early post-surgical course, but also included the necessity for implant removal during the whole follow-up period. Despite its retrospective design,
51938_Claudia_Lowik.indd 96 19-08-19 11:12

Gentamicin-impregnated beads and sponges
97
6
our data clearly indicate that the application of gentamicin-impregnated beads and/or sponges in a DAIR procedure has no advantage and, therefore, their use should be discouraged.
By providing both dead-space management and by achieving high concentrations of antibiotics at the site of infection, application of gentamicin beads and/or sponges should theoretically lead to higher cure rates in severe orthopaedic infections, like PJIs. However, their application so far does not seem to be bene�cial in actual clinical outcome. Few studies have been published on the additional value of gentamicin beads/sponges to systemic antibiotic therapy in PJI. One retrospective study performed by Kuiper et al. demonstrated a higher cure rate when using gentamicin-impregnated sponges and a higher failure rate when using gentamicin-impregnated beads, but this association was not found in the multivariate analysis.29 Only one small randomized controlled trial has been performed (with approximate 14 patients in each arm), demonstrating no bene�cial e�ect of gentamicin beads.32-34 However, in this study the application of local antibiotics was compared with systemic antibiotics, instead of complementary use. Other studies only described the outcome of their routine usage, without the inclusion of a control group.34-37
In some studies, including ours, applying gentamicin carriers in orthopaedic infections even appear to do more harm than good. To illustrate, Blaha et al. performed a randomized study in a large cohort of chronic osteomyelitis patients and demonstrated a higher recurrence rate when gentamicin-containing polymethyl-methacrylate (PMMA) beads were implanted at the site of infection compared with systemic antibiotic treatment alone.33 In addition, a high recurrence rate (17%) has also been observed in a large observational study performed by Walenkamp et al. in patients with chronic osteomyelitis treated with the sole use of gentamicin-impregnated PMMA beads.34 It has been postulated that the lack of e�cacy may be due to reduced activity of gentamicin in an environment with a low pH and low oxygen level, which is the case in the presence of a bio�lm.30 Indeed, Neut et al. demonstrated bacterial growth on the majority of removed gentamicin-impregnated beads, suggesting that the beads maintain rather than treat the infection.35 Although this may partially be explained by the presence of gentamicin-resistant strains, a previous study observed no di�erence in cure rate between strains with high and low MICs of gentamicin.36 Our results also showed no di�erence in outcome when solely analyzing PJIs with gentamicin-susceptible strains. We
51938_Claudia_Lowik.indd 97 19-08-19 11:12

Chapter 6
98
did not �nd any other potential explanation for the worse outcome in the gentamicin group; according to subanalyses, the additional surgery to remove the gentamicin beads did not seem to expose patients to a higher risk for reinfection and the higher failure rate was also observed in the sole use of gentamicin-impregnated sponges that can remain in situ. These sponges form a kind of sludge and may well act as a foreign body just like beads after they have emptied their load.
Future studies should address whether other types of local antibiotic application may be useful in the treatment of acute PJI in patients with a high risk of failure. A promising type appears to be the administration of vancomycin powder, which has been applied as prevention measure in hip and knee revision arthroplasty and does not necessitate additional surgery for its removal.38,39 Riesgo et al. retrospectively evaluated the infection-free survivorship in acute PJI after implementing a vancomycin povidone-iodine protocol and demonstrated a reduction in failure rate from 37% to 17% in a cohort of 74 cases.39 Its use and potential bene�t should be con�rmed and further explored in future studies.
Despite the fact that propensity matching is an important strength of our study, it has limitations as well. Although propensity matching corrects for confounding factors, remaining selection bias cannot be ruled out, since one can only correct for objective variables and not for the clinical judgement of the orthopaedic surgeon who decided to apply local gentamicin. In addition, the matched cohort only included a subselection of patients of the total cohort (40%). However, despite this subselection, the high failure rates remained the same in the matched cohort, which makes it unlikely that the matched analysis was performed in cases with less severe infections. Moreover, subgroup analysis in high-risk groups for failure did not show any bene�t from local gentamicin either and the use of local gentamicin was an independent predictor for failure in the multivariate analysis as well.
In conclusion, the use of gentamicin-impregnated beads and/or sponges is associated with higher failure rates in early PJI and, therefore, their use should be discouraged. Future studies should conclude whether other types of local antibiotics can improve treatment outcome.
51938_Claudia_Lowik.indd 98 19-08-19 11:12
Gentamicin-impregnated beads and sponges
99
6
References
1. Kurtz SM, Ong KL, Lau E, Bozic KJ, Berry D, Parvizi J. Prosthetic joint infection risk after TKA in the medicare population. Clin Orthop Relat Res 2010; 468(1): 52-6.
2. Kunutsor SK, Whitehouse MR, Blom AW, Beswick AD, INFORM Team. Re-infection outcomes following one- and two-stage surgical revision of infected hip prosthesis: a systematic review and meta-analysis. PLoS One 2015; 10(9): 1-15.
3. Tsang SJ, Ting J, Simpson AHRW, Gaston P. Outcomes following debridement, antibiotics and implant retention in the management of periprosthetic infections of the hip: a review of cohort studies. Bone Joint J 2017; 99–B(11): 1458–66.
4. Zhang C, Yan CH, Chan PK, Ng FY, Chiu KY. Polyethylene insert exchange is crucial in debridement for acute periprosthetic infections following total knee arthroplasty. J Knee Surg 2017; 30(1): 36-41.
5. Choi HR, von Knoch F, Zurakowski D, Nelson SB, Malchau H. Can implant retention be recommended for treatment of infected TKA? Clin Orthop Relat Res 2011; 469(4): 961-9.
6. Lora-Tamayo J, Murillo O, Iribarren JA, Soriano A, Sánchez-Somolinos M, Baraia-Etxaburu JM, et al. A large multicenter study of methicillin-susceptible and methicillin-resistant Staphylococcus aureus prosthetic joint infections managed with implant retention. Clin Infect Dis 2013; 56(2): 182-94.
7. Lora-Tamayo J, Senneville É, Ribera A, Bernard L, Dupon M, Zeller V, et al. The not-so-good prognosis of streptococcal periprosthetic joint infection managed by implant retention: the results of a large multicenter study. Clin Infect Dis 2017; 64(12): 1742-52.
8. Rodríguez-Pardo D, Pigrau C, Lora-Tamayo J, Soriano A, del Toro MD, Cobo J. Gram-negative prosthetic joint infection: outcome of a debridement, antibiotics and implant retention approach. A large multicentre study. Clin Microbiol Infect 2014; 20(11): O911-9.
9. Urish KL, Bullock AG, Kreger AM, Shah NB, Jeong K, Rothenberger SD. A multicenter study of irrigation and debridement in total knee arthroplasty periprosthetic joint infection: treatment failure is high. J Arthroplasty 2018; 33(4): 1154-9.
10. Triantafyllopoulos GK, Poultsides LA, Sakellariou VI, Zhang W, Sculco PK, Ma Y, et al. Irrigation and debridement for periprosthetic infections of the hip and factors determining outcome. Int Orthop 2015; 39(6): 1203–9.
11. Marculescu CE, Berbari EF, Hanssen AD, Steckelberg JM, Harmsen SW, Mandrekar JN, et al. Outcome of prosthetic joint infections treated with debridement and retention of components. Clin Infect Dis 2006; 42(4): 471-8.
12. Buller LT, Sabry FY, Easton RW, Klika AK, Barsoum WK. The preoperative prediction of success following irrigation and debridement with polyethylene exchange for hip and knee prosthetic joint infections. J Arthroplasty 2012; 27(6): 857-64.
13. Tornero E, Morata L, Martínez-Pastor JC, Angulo S, Combalia A, Bori G, et al. Importance of selection and duration of antibiotic regimen in prosthetic joint infections treated with debridement and implant retention. J Antimicrob Chemother 2016; 71(5): 1395-401.
14. El Helou OC, Berbari EF, Lahr BD, Eckel-Passow JE, Razonable RR, Sia IG, et al. E�cacy and safety of rifampin containing regimen for staphylococcal prosthetic joint infections treated with debridement and retention. Eur J Clin Microbiol Infect Dis 2010; 29(8): 961-7.
15. Martínez-Pastor JC, Muñoz-Mahamud E, Vilchez F, García-Ramiro S, Bori G, Sierra J, et al. Outcome of acute prosthetic joint infections due to gram-negative bacilli treated with open debridement and retention of the prosthesis. Antimicrob Agents Chemother 2009; 53(11): 4772-7.
16. Tornero E, Morata L, Martínez-Pastor JC, Bori G, Climent C, García-Velez DM, et al. KLIC-score for predicting early failure in prosthetic joint infections treated with debridement, implant retention and antibiotics. Clin Microbiol Infect 2015; 21(8): 9-17.
17. Löwik CAM, Jutte PC, Tornero E, Ploegmakers JJW, Knobben BAS, de Vries AJ, et al. Predicting failure in early acute prosthetic joint infection treated with debridement, antibiotics and implant retention: external validation of the KLIC score. J Arthroplasty 2018; 33(8): 2582-7.
18. Vilchez F, Martínez-Pastor JC, García-Ramiro S, Bori G, Maculé F, Sierra J, et al. Outcome and predictors of treatment failure in early post-surgical prosthetic joint infections due to Staphylococcus aureus treated with debridement. Clin Microbiol Infect 2011; 17(3): 439-44.
51938_Claudia_Lowik.indd 99 19-08-19 11:12

Chapter 6
100
19. Sukeik M, Patel S, Haddad FS. Aggressive early débridement for treatment of acutely infected cemented total hip arthroplasty. Clin Orthop Relat Res 2012; 470(11): 3164-70.
20. Cobo J, Garcia San Miguel L, Euba G, Rodríguez D, García-Lechuz JM, Riera M, et al. Early prosthetic joint infection: outcomes with debridement and implant retention followed by antibiotic therapy. Clin Microbiol Infect 2011; 17(11): 1632-7.
21. Duque AF, Post ZD, Lutz RW, Orozco FR, Pulido SH, Ong AC. Is there still a role for irrigation and debridement with liner exchange in acute periprosthetic total knee infection? J Arthroplasty 2017; 32(4): 1280-4.
22. Fehring TK, Odum SM, Berend KR, Jiranek WA, Parvizi J, Bozic KJ, et al. Failure of irrigation and débridement for early postoperative periprosthetic infection. Clin Orthop Relat Res 2013; 471(1): 250-7.
23. Bergkvist M, Mukka SS, Johansson L, Ahl TE, Sayed-Noor AS, Sköldenberg OG, et al. Debridement, antibiotics and implant retention in early periprosthetic joint infection. Hip Int 2016; 26(2): 138-43.
24. Westberg M, Grøgaard B, Snorrason F. Early prosthetic joint infections treated with debridement and implant retention: 38 primary hip arthroplasties prospectively recorded and followed for median 4 years. Acta Orthop 2012; 83(3): 227-32.
25. Aboltins CA, Dowsey MM, Peel T, Lim WK, Parikh S, Stanley PA, et al. Early prosthetic hip joint infection treated with debridement, prosthesis retention and bio�lm-active antibiotics: functional outcomes, quality of life and complications. Intern Med J 2013; 43(7): 810-5.
26. Kelm J, Anagnostakos K, Regitz T, Schmitt E, Schneider G, Ahlhelm F. MRSA-infections-treatment with intraoperatively produced gentamycin-vancomycin PMMA beads. Chirurg 2004; 75(10): 988-95.
27. Swieringa AJ, Goosen JH, Jansman FG, Tulp NJ. In vivo pharmacokinetics of a gentamicin-loaded collagen sponge in acute periprosthetic infection: serum values in 19 patients. Acta Orthop 2008; 79(5): 637-42.
28. Moojen DJ, Hentenaar B, Vogely CH, Verbout AJ, Castelein RM, Dhert WJ. In vitro release of antibiotics from commercial PMMA beads and articulating hip spacers. J Arthroplasty 2008; 23(8): 1152-6.
29. Kuiper JW, Vos CJ, Saouti R, Vergroesen DA, Graat HC, Debets-Ossenkopp YJ, et al. Prosthetic joint-associated infections treated with DAIR (debridement, antibiotics, irrigation, and retention): analysis of risk factors and local antibiotic carriers in 91 patients. Acta Orthop 2013; 84(4): 380-6.
30. Barth RE, Vogely HC, Hoepelman AIM, Peters EJ. ‘To bead or not to bead?’ Treatment of osteomyelitis and prosthetic joint-associated infections with gentamicin bead chains. Int J Antimicrob Agents 2011; 38(5): 371-5.
31. Parvizi J, Zmistowski B, Berbari EF, Bauer TW, Springer BD, Della Valle CJ, et al. New de�nition for periprosthetic joint infection: from the workgroup of the musculoskeletal infection society. Clin Orthop Relat Res 2011; 469(11): 2992-4.
32. Nelson CL, Evans RP, Blaha JD, Calhoun JH, Henry SL, Patzakis MJ. A comparison of gentamicin-impregnated polymethylmethacrylate bead implantation to coventional parenteral antibiotic therapy in infected total hip and knee arthoplasty. Clin Orthop Relat Res 1993: 295: 96-101.
33. Blaha JD, Calhoun JH, Nelson CL, Henry SL, Seligson D, Esterhai JL Jr, et al. Comparison of the clinical e�cacy and tolerance of gentamicin PMMA beads on surgical wire versus combined and systemic therapy for osteomyelitis. Clin Orthop Relat Res 1993; 295: 8-12.
34. Walenkamp GH, Kleijn LL, de Leeuw M. Osteomyelitis treated with gentamicin-PMMA beads: 100 patients followed for 1-12 years. Acta Orthop Scand 1998; 69(5): 518-22.
35. Neut D, van de Belt H, Stokroos I, van Horn JR, van der Mei HC, Busscher HJ. Biomaterial-associated infection of gentamicin-loaded PMMA beads in orthopaedic revision surgery. J Antimicrob Chemother 2001; 47(6): 885-91.
36. Janssen DMC, Geurts JAP, Jütten LMC, Walenkamp GH. 2-stage revision of 120 deep infected hip and knee prostheses using gentamicin-PMMA beads. Acta Orthop 2016; 87(4): 324-32.
37. Geurts JAP, Janssen DMC, Kessels AG, Walenkamp GH. Good results in postoperative and hematogenous deep infections of 89 stable total hip and knee replacements with retention of prosthesis and local antibiotics. Acta Orthop 2013; 84(6): 509-16.
51938_Claudia_Lowik.indd 100 19-08-19 11:12

Gentamicin-impregnated beads and sponges
101
6
38. Otte JE, Politi JR, Chambers B, Smith CA. Intrawound vancomycin powder reduces early prosthetic joint infections in revision hip and knee arthroplasty. Surg Technol Int 2017; 30: 284-9.
39. Riesgo AM, Park BK, Herrero CP, Yu S, Schwarzkopf R, Iorio R. Vancomycin povidone-iodine protocol improves survivorship of periprosthetic joint infection treated with irrigation and debridement. J Arthroplasty 2018; 33(3): 847-50.
51938_Claudia_Lowik.indd 101 19-08-19 11:12

51938_Claudia_Lowik.indd 102 19-08-19 11:12

Chapter 7
Debridement, antibiotics and implant retention is a viable
treatment option for early periprosthetic joint infection
presenting more than four weeks after index arthroplasty
Claudia A.M. Löwik, Javad Parvizi, Paul C. Jutte, Wierd P. Zijlstra, Bas A.S. Knobben, Chi Xu, Karan Goswami, Katherine A. Belden, Ricardo Sousa, André
Carvalho, Juan Carlos Martínez-Pastor, Alex Soriano, Marjan Wouthuyzen-Bakker, on behalf of the Northern Infection Network Joint Arthroplasty and
ESCMID study group for implant-associated infections
Submitted
51938_Claudia_Lowik.indd 103 19-08-19 11:12

Chapter 7
104
Abstract
BackgroundSuccess of debridement, antibiotics and implant retention (DAIR) in early periprosthetic joint infection (PJI) largely depends on the presence of a mature bio�lm. At what time point DAIR should be disrecommended is unknown. This multicenter study evaluated the outcome of DAIR in relation to time after index arthroplasty.
MethodsWe retrospectively evaluated PJIs occurring within 90 days after surgery and treated with DAIR. Patients with bacteremia, arthroscopic debridements and a follow-up <1 year were excluded. Treatment failure was de�ned as 1) any further surgical procedure related to infection 2) PJI-related death, 3) long-term suppressive antibiotics.
Results769 patients were included. Treatment failure occurred in 294 patients (38%) and was similar between time intervals: week 1-2: 42% (95/226); week 3-4: 38% (143/378); week 5-6: 29% (29/100), week 7-12: 42% (27/65). Exchange of modular components was performed to a lesser extent in the early compared with the late post-surgical course (41% vs 63%, p<0.001). The causative microorganisms, comorbidities and duration of symptoms were comparable between time intervals.
ConclusionDAIR is a viable option in patients with early PJI presenting more than four weeks after index surgery, as long as DAIR is performed as soon as PJI is diagnosed and modular components are exchanged.
51938_Claudia_Lowik.indd 104 19-08-19 11:12

E�cacy of DAIR according to the time interval
105
7
Introduction
Total joint arthroplasty (TJA) is a widely used treatment modality for advanced osteoarthritis of the hip and knee.1 Although this procedure is highly successful, in 1-2% of TJAs a periprosthetic joint infection (PJI) develops, which is a major complication with large impact on a patient’s well-being.2 When PJI develops within three months after index arthroplasty, these infections are classi�ed as early PJI.3-8
The preferred surgical treatment for early PJI is debridement, antibiotics and implant retention (DAIR). DAIR is considered as a less invasive surgical treatment option than revision surgery since the prosthesis can be retained, allowing preservation of bone stock, shorter duration of the surgical procedure, decreased risk of intraoperative fractures and faster postoperative rehabilitation.9,10 The success rate for DAIR varies widely from 30% to 80%.11-
15 Although there are no absolute contraindications for performing a DAIR procedure in patients with PJI, it is accepted that DAIR should be performed in patients with acute PJI.16
Multiple factors in�uence the outcome of DAIR, that includes host- and implant-related factors, clinical presentation, intraoperative variables, causative microorganisms and the applied antimicrobial regimen.15,17-20 Moreover, several studies have demonstrated that DAIR failure increases when the infection exists for a longer time period.17,18,21-24 This �nding can be explained by the fact that once a mature bio�lm developed, the infection cannot be cured without removing the implant.25,26 For this reason, the Infectious Disease Society of America (IDSA) guideline published in 2013 recommends to remove the implant when a PJI develops more than 30 days after the index arthroplasty.27 An important limitation of this approach is that it does not take into account the fact that the process of bio�lm formation varies substantially based on the type of causative microorganism, the inoculum size that contaminates the wound during surgery and host-related factors.28,29 Therefore, performing a DAIR merely based on a short time interval from the index arthroplasty may lead to unnecessary removal of the implant in a large subset of patients.
This multicenter study was designed to evaluate the in�uence of important variables on the outcome of DAIR, in particular the time interval from index surgery to DAIR. The study sought to determine if DAIR is still a viable option for patients with PJI occurring more than 30 days after index arthroplasty.
51938_Claudia_Lowik.indd 105 19-08-19 11:12

Chapter 7
106
Material and methods
Study designAll patients with early PJI of the hip or knee treated with DAIR from 1999 to 2016 in six hospitals in four di�erent countries (the United States, Spain, Portugal and the Netherlands) were included and retrospectively analyzed. Early PJI was de�ned as an infection occurring within 90 days of index arthroplasty.30 The diagnosis of PJI was determined according to the criteria of the International Consensus Meeting, published in 2013.31 Patients who underwent arthroscopic debridement, those with positive blood cultures and patients with a follow-up of less than one year were excluded.
Surgical treatmentThe details of how DAIR was performed were retrieved from the clinical records. The DAIR procedure involved an arthrotomy, extensive synovectomy, and irrigation of the joint with three to six liters of irrigation �uid. The modular components were exchanged in some cases and retained in others. Empirical broad-spectrum intravenous antibiotic treatment was started after obtaining multiple deep tissue biopsies for culture and, if necessary, adjusted according to the culture results. Intravenous antibiotics were continued for at least two weeks before switching to an oral regimen that was continued for an additional ten weeks. Rifampin was added to the antibiotic treatment regimen in infections caused by rifampin-susceptible staphylococci. DAIR was performed as soon as the orthopaedic surgeon detected a clinical suspicion of infection, consisting of infective symptoms such as fever, redness of the wound, persisting or recurrent wound leakage and/or elevated in�ammatory serum parameters.
De�nition of outcomeThe main outcomes were treatment failure and implant failure. Treatment failure was de�ned as one of the following events within one year after DAIR: 1) the need for any further surgical procedure related to infection (i.e.: a second DAIR, implant removal or amputation); 2) PJI-related death; or 3) the need for administration of long-term suppressive antimicrobial treatment. Implant failure was de�ned as the need for implant removal at any time point after DAIR.
51938_Claudia_Lowik.indd 106 19-08-19 11:12

E�cacy of DAIR according to the time interval
107
7
Statistical analysisCategorical variables were expressed in absolute frequencies and percentages. Continuous variables were presented as mean and standard deviation (SD) or as median and interquartile range (IQR) when not normally distributed according to the Kolmogorov-Smirnov test of normality. The chi-square test was used to compare categorical variables. Parametric continuous variables were compared using the Student’s t-test or one-way ANOVA. Non-parametric continuous variables were compared with the Mann-Whitney U test. Failure rates were calculated for each two-week time interval from index surgery to DAIR. Subsequently, logistic regression analysis was performed to identify independent risk factors for treatment failure. Variables with a di�erence between groups, de�ned as a P value <0.15 in the univariate analysis were included in the multivariate analysis. Statistical signi�cance was de�ned as a two-tailed P value <0.05. Statistical analyses were performed using IBM SPSS Statistics (version 24.0; Chicago, IL, USA).
Results
Patient characteristicsThe study cohort consisted of 769 patients with early PJI treated with DAIR. Data were collected from 981 patients, but 212 patients were excluded due to a time interval more than 90 days from index arthroplasty to DAIR (n=122), positive blood cultures (n=42) or a follow-up of less than one year (n=48). 463 patients (60%) had a PJI of the hip and 306 patients (40%) of the knee. The mean age was 70 years (SD ± 12, range 24-97 years) and 57% (n=431) were female. PJI occurred after primary TJA in 622 patients (82%) and after revision TJA in 140 patients (18%) The median follow-up was 3.2 years (range 1-15 years), with a signi�cant di�erence in follow-up between intervals: week 1-2: 3.2 years (range 1-14); week 3-4: 3.0 years (range 1-14); week 5-6: 4.0 (range 1-14); week 7-12: 4.0 (range 1-15) (p=0.008).
Failure rates according to time interval after index surgeryOverall, 294 patients (38%) had treatment failure within one year after DAIR. More than half of the patients (161 patients, 55%) required a second DAIR, 82 patients (28%) required revision surgery for infection, 42 patients (14%) were
51938_Claudia_Lowik.indd 107 19-08-19 11:12

Chapter 7
108
placed on long-term suppressive antimicrobial treatment, 8 patients (3%) deceased due to PJI and one patient (0.3%) required an amputation. There were no statistically signi�cant di�erences in type of failure between time intervals (p=0.414). The treatment failure rates per time interval from index arthroplasty to DAIR were as follows: week 1: 39% (11/28); week 2: 42% (84/198); week 3: 41% (104/255); week 4: 32% (39/123); week 5: 30% (21/71); week 6: 28% (8/29); week 7-12: 42% (27/65) (Figure 1a and 2). Analyzing additional intervals from week 7 to 12, no di�erences in treatment failure rates were observed between week 7-8 and week 9-12 (40% (12/30) vs 43% (15/35), p=0.816). The implant failure rates per time interval from index arthroplasty to DAIR were as follows: week 1: 21% (6/28); week 2: 15% (30/198); week 3: 17% (42/255); week 4: 20% (25/123); week 5: 17% (12/71); week 6: 10% (3/29); week 7-12: 23% (15/65) (Figure 1b). Analyzing additional intervals from week 7 to 12, there were no di�erences in implant failure rates between week 7-8 and week 9-12 (30% (9/30) vs 17% (6/35), p=0.220).
Using univariate binary logistic regression analysis, time interval from index arthroplasty to DAIR was not a statistically signi�cant factor for predicting treatment failure using time interval both as a continuous variable (OR 0.99, 95% CI 0.98–1.00, p=0.266) and categorical variable (with four time-interval categories) (OR 0.58, 95% CI 0.30–1.10, p=0.154). These results were in agreement with the outcome of the univariate binary regression on implant failure in relation to time interval (OR 1.00, 95% CI 0.99–1.01, p=0.899 and OR 0.54, 95% CI 0.25–1.19, p=0.499, respectively). The multivariate binary logistics regression analysis showed that several preoperative variables were independent predictors for treatment failure: the C-reactive protein (CRP) (OR 1.01, 95% CI 1.00–1.01, p<0.001), revision arthroplasty (OR 4.34, 95% CI 1.62-11.64, p=0.004), arthroplasty indicated for fracture (OR 2.36, 95% CI 1.25-4.48, p=0.008) and female gender (OR 1.89, 95% CI 1.14-3.13, p=0.013). Not exchanging the modular components (OR 1.70, 95% CI 0.96–3.00, p=0.067) and cemented arthroplasties (OR 1.84, 95% CI 0.96–3.52, p=0.074) showed a trend towards worse outcome.
51938_Claudia_Lowik.indd 108 19-08-19 11:12

E�cacy of DAIR according to the time interval
109
7
1a
1b
Figure 1. Failure rates according to time interval from index arthroplasty to DAIR (n=769). The de�nitions of treatment failure and implant failure are described in the material and methods section of the paper. 1a) Treatment failure. 1b) Implant failure.
0 50 100 150 200 250 300 3500
102030405060708090
100
%treatment success
week 1-2
week 3-4
follow-up (days)
logrank test p = 0.11
week 5-6
week 7-12
Figure 2. Treatment success of DAIR during follow-up according to time interval from index arthroplasty to DAIR (n=769).
51938_Claudia_Lowik.indd 109 19-08-19 11:12

Chapter 7
110
Preoperative variables according to time interval after index surgeryThe general patient characteristics were comparable among patients in di�erent time intervals for DAIR (Table 1). The mean CRP value and the duration of symptoms of PJI were also the same in patient groups divided based on interval from index arthroplasty to DAIR. The leukocyte count was higher in patients undergoing DAIR within two weeks or later than six weeks after index arthroplasty (p<0.001). When the time interval from index arthroplasty to DAIR increased, the number of patients experiencing pain increased (p=0.004), as well as the number of patients with red wounds (p=0.002). Patients who were treated in the late post-surgical course (week 7-12) had a lower rate of wound leakage than patients who were treated earlier (p=0.003). DAIR was performed at an earlier time point in patients with PJI of the hip compared with patients with PJI of the knee (p<0.001) and patients with PJI of the hip experienced wound leakage more often than patients with PJI of the knee (84% vs 67%, p<0.001). Subanalyses comparing PJI of the hip and knee showed no statistically signi�cant di�erences in treatment failure and implant failure (39% vs 38%, p=0.737 and 16% vs 19%, p=0.237, respectively).
Intraoperative variables according to time interval after index surgeryExchange of modular components was performed to a lesser extent in the early (week 1-2) compared to the late (week 7-12) post-surgical course (41% vs 63%, p<0.001) (Table 2). Predominant microorganisms causing PJI were Staphylococcus aureus (44%), Staphylococcus epidermidis (34%), Enterococcus species (15%) and Streptococcus species (11%). PJI was polymicrobial in 286 patients (37%). There were no major di�erences in causative microorganisms per time interval. Only methicillin-resistant Staphylococcus aureus (MRSA) was cultured more often when DAIR was performed more than six weeks after index arthroplasty (p=0.032). The number of positive cultures gradually decreased when DAIR was performed at a later time point (p<0.001). The failure rates per causative microorganism were comparable for di�erent time intervals (Table 3). There were no statistical di�erences in the use of correct ‘antibio�lm’ antibiotic treatment between time intervals, for both rifampicin in case of infections caused by staphylococci (p=0.676) and cipro�oxacin in case of infections caused by Gram-negative microorganisms (p=0.543).
51938_Claudia_Lowik.indd 110 19-08-19 11:12

E�cacy of DAIR according to the time interval
111
7
Table 1. Patient characteristics according to time interval from index arthroplasty to DAIR (n=769)
Variables Week 1-2 (n=226)
Week 3-4 (n=378)
Week 5-6 (n=100)
Week 7-12 (n=65)
P value
Age in years Mean (SD) 69.5 (11.8) 70.5 (11.8) 67.3 (13.3) 69.6 (13.2) .149Gender Male 108 (48.0%) 153 (40.7%) 39 (39.8%) 31 (48.4%) .220BMI in kg/m2 Mean (SD) 31.0 (7.1) 31.2 (6.2) 31.3 (5.8) 30.7 (6.5) .920Comorbidities Diabetes mellitus 41 (18.1%) 77 (20.4%) 16 (16.0%) 13 (20.0%) .757
COPD 46 (20.4%) 62 (16.4%) 10 (10.0%) 8 (12.3%) .095Malignancy 30 (13.3%) 57 (15.1%) 17 (17.0%) 12 (18.5%) .695Renal failure 16 (7.1%) 20 (5.3%) 7 (7.0%) 10 (15.4%) .032Liver cirrhosis 8 (3.5%) 9 (2.4%) 7 (7.0%) 3 (4.6%) .154Rheumatoid arthritis 11 (4.9%) 23 (6.1%) 10 (10.0%) 3 (4.6%) .321
Type of arthroplasty Primary 179 (80.6%) 315 (83.8%) 79 (79.0%) 49 (76.6%) .414Revision 43 (19.4%) 61 (16.2%) 21 (21.0%) 15 (23.4%)
Site of arthroplasty Hip 164 (72.6%) 228 (60.3%) 38 (38.0%) 33 (50.8%) <.001Knee 62 (27.4%) 150 (39.7%) 62 (62.0%) 32 (49.2%)
Indication for arthroplasty
Osteoarthritis 151 (68.6%) 281 (74.7%) 84 (84.8%) 47 (73.4%) .108Fracture 42 (19.1%) 54 (14.4%) 7 (7.1%) 10 (15.6%)
Days of symptoms Mean (SD) 6.0 (4.7) 7.3 (6.6) 6.7 (5.2) 6.1 (6.6) .135Type of symptoms Fever 29 (17.2%) 43 (14.2%) 11 (14.7%) 11 (26.2%) .235
Pain 48 (32.2%) 98 (37.0%) 25 (44.6%) 25 (62.5%) .004Redness 65 (43.6%) 138 (52.1%) 30 (53.6%) 31 (77.5%) .002Wound leakage 115 (77.2%) 220 (82.7%) 42 (75.0%) 23 (57.5%) .003
Leukocyte count in x109/L
Mean (SD) 11.4 (6.3) 9.7 (3.9) 9.0 (3.4) 9.8 (4.0) <.001
CRP value in mg/L Mean (SD) 101.6 (98.4) 93.6 (95.5) 88.7 (92.7) 86.2 (93.4) .567KLIC score Mean (SD) 2.9 (1.9) 2.9 (1.7) 2.8 (1.6) 2.8 (2.0) .947
Bold indicates statistically signi�cant di�erences. BMI: body mass index; COPD: chronic obstructive pulmonary disease; CRP: C-reactive protein; SD: standard deviation.
51938_Claudia_Lowik.indd 111 19-08-19 11:12

Chapter 7
112
Table 2. Intraoperative variables according to time interval from index arthroplasty to DAIR (n=769)
Variables Week 1-2 (n=226)
Week 3-4 (n=378)
Week 5-6 (n=100)
Week 7-12 (n=65)
P value
Exchange of modular components
85 (40.7%) 158 (44.4%) 56 (59.6%) 36 (63.2%) <.001
Percentage of positive cultures
Mean (SD) 88.6% (22.4) 86.5% (24.5) 75.1% (33.8)
63.2% (39.3) <.001
All of the obtained cultures positive
141 (74.2%) 228 (69.5%) 46 (52.9%) 22 (43.1%) <.001
Polymicrobial 79 (35.0%) 157 (41.5%) 32 (32.0%) 18 (27.7%) .066Gram-positive microorganisms
196 (86.7%) 334 (88.4%) 82 (82.0%) 50 (76.9%) .054
Staphylococcus aureus
94 (41.6%) 174 (46.0%) 50 (50.0%) 21 (32.3%) .101
MRSA 15 (6.6%) 17 (4.5%) 8 (8.0%) 9 (13.8%) .032Staphylococcus epidermidis
80 (35.4%) 134 (35.4%) 26 (26.0%) 19 (29.2%) .257
Enterococcus species
36 (15.9%) 52 (13.8%) 15 (15.0%) 11 (16.9%) .852
Streptococcus species
28 (12.4%) 44 (11.6%) 5 (5.0%) 8 (12.3%) .224
Other Gram-positives
26 (15.4%) 64 (21.1%) 12 (16.0%) 7 (16.7%) .412
Gram-negative microorganisms
57 (25.2%) 99 (26.2%) 26 (26.0%) 13 (20.0%) .765
Escherichia coli 16 (7.1%) 26 (6.9%) 9 (9.0%) 2 (3.1%) .536Pseudomonas species
14 (8.3%) 20 (6.6%) 7 (9.3%) 3 (7.1%) .831
Enterobacter cloacae
11 (4.9%) 15 (4.0%) 4 (4.0%) 3 (4.6%) .957
Proteus species 7 (3.1%) 24 (6.3%) 4 (4.0%) 3 (4.6%) .329Other Gram-negatives
18 (8.0%) 33 (8.7%) 9 (9.0%) 5 (7.7%) .978
Anaerobe microorganisms
2 (0.9%) 9 (2.4%) 1 (1.0%) 2 (3.1%) .437
Candida species 2 (0.9%) 1 (0.3%) 0 (0.0%) 2 (3.1%) .054
Bold indicates statistically signi�cant di�erences. MRSA: methicillin-resistant Staphylococcus aureus; SD: standard deviation.
51938_Claudia_Lowik.indd 112 19-08-19 11:12

E�cacy of DAIR according to the time interval
113
7
Table 3. Failure rates according to causative microorganism and time interval from index arthroplasty to DAIR (n=769)
Variables Week 1-2 Week 3-4 Week 5-6 Week 7-12 P value
Polymicrobi-al infections
38/79 (48.1%) 57/157 (36.3%) 8/32 (25.0%) 9/18 (50.0%) .080
Gram-posi-tive micro- organisms
88/196 (44.9%) 126/334 (37.7%) 24/82 (29.3%) 19/50 (38.0%) .094
Staphylococcus aureus
51/94 (54.3%) 77/174 (44.3%) 18/50 (36.0%) 10/21 (47.6%) .185
MRSA 9/15 (60.0%) 4/17 (23.5%) 4/8 (50.0%) 6/9 (66.7%) .102Staphylococcus epidermidis
32/80 (40.0%) 37/134 (27.6%) 5/26 (19.2%) 8/19 (42.1%) .094
Enterococcus species
16/36 (44.4%) 20/52 (38.5%) 5/15 (33.3%) 5/11 (45.5%) .861
Streptococcus species
11/28 (39.3%) 16/44 (36.4%) 1/5 (20.0%) 3/8 (37.5%) .877
Other Gram-positives
11/26 (42.3%) 15/64 (23.4%) 4/12 (33.3%) 3/7 (42.9%) .286
Gram-neg-ative micro- organisms
25/57 (43.9%) 38/99 (38.4%) 7/26 (26.9%) 4/13 (30.8%) .479
Escherichia coli 8/16 (50.0%) 11/26 (42.3%) 4/9 (44.4%) 0/2 (0.0%) .608Pseudomonas species
4/14 (28.6%) 6/20 (30.0%) 1/7 (14.3%) 1/3 (33.3%) .864
Enterobacter cloacae
5/11 (45.5%) 4/15 (26.7%) 1/4 (25.0%) 1/3 (33.3%) .764
Proteus species 5/7 (71.4%) 9/24 (37.5%) 2/4 (50.0%) 2/3 (66.7%) .388Other Gram-negatives
7/18 (38.9%) 17/33 (51.5%) 1/9 (11.1%) 2/5 (40.0%) .184
Anaerobe micro- organisms
1/2 (50.0%) 6/9 (66.7%) 1/1 (100.0%) 2/2 (100.0%) .626
Candida species
2/2 (100.0%) 1/1 (100.0%) 0/0 (0.0%) 1/2 (50.0%) .392
MRSA: methicillin-resistant Staphylococcus aureus
Discussion
This multicenter, multinational study consisting of a large group of patients with early PJI of the hip and knee is one of the �rst studies to refute the importance of time interval from index arthroplasty to DAIR on the outcome of DAIR. The results demonstrated that, although failure rates were highest when DAIR was performed 7-12 weeks after index arthroplasty, DAIR was still successful in approximately 60% and the implant could be retained in 75% of
51938_Claudia_Lowik.indd 113 19-08-19 11:12

Chapter 7
114
patients. Moreover, within the �rst six weeks after index arthroplasty, failure rates tended to gradually decrease, instead of increase, which may be due to a lower bacterial inoculum observed in these cases. Our results do not only question current guidelines stating that DAIR is not recommended when PJI develops more than 30 days after index arthroplasty,27 but clearly demonstrate that DAIR is still a viable surgical treatment option in a large proportion of these patients. Our results do not imply or justify postponing DAIR though. In fact, based on the recommendation of the second International Consensus Meeting, DAIR should be performed as soon as symptoms of infection arise.16 These �ndings are in agreement with existing literature, demonstrating that each day of delaying DAIR decreases the chance of treatment success with approximately 10%, depending on the a�ected joint.17 Indeed, in our study, symptom duration was comparable between time intervals which con�rms the fact that a DAIR procedure was performed as soon as the suspicion of a PJI arose.
Although we expected di�erences in the type of microorganism causing the infection per time interval, i.e. virulent microorganisms in the early post-surgical course (e.g. Staphylococcus aureus and Gram-negatives) and low-virulent microorganisms in the late post-surgical course (e.g. Coagulase negative staphylococci and enterococci), no di�erences were observed. Our observation that treatment failure and implant failure increased when DAIR was performed more than six weeks after index arthroplasty is supported by in vivo studies evaluating the time to develop a mature bio�lm.33-35 Carli et al. demonstrated in a mouse model with a proximal tibial implant that although a bio�lm is evident two weeks after injection with Staphylococcus aureus, it matures and is covered by �brinous tissue and multiple host cells after six weeks.35 However, the fact that treatment was still successful in approximately 60% of patients when DAIR was performed in the late post-surgical course (week 7-12) and remained equally successful between six and twelve weeks after index arthroplasty, illustrates that the development of a bio�lm is a variable process which does not only depend on time, but also on the causative microorganism, the inoculum size and the host.28,29
What could be perceived as a limitation of this study is the exclusion of patients with bacteremia. Nevertheless, since we could not be certain that the PJI was the cause of the bacteremia and not secondary to the bacteremia itself, we considered it more accurate to exclude this patient category. If a PJI occurs
51938_Claudia_Lowik.indd 114 19-08-19 11:12

E�cacy of DAIR according to the time interval
115
7
due to bacteremia by another focus (for example via a central venous catheter), the joint will be contaminated / infected by bacteria at that particular time point which precludes the possibility to solely evaluate time intervals after index surgery in relation to outcome. Nevertheless, the outcome of our analysis was not di�erent when we included patients with bacteremia (data not shown). Another limitation is the statistically signi�cant di�erence in follow-up per time interval, although this di�erence is clinically irrelevant since all patients had a follow-up more than one year with comparable ranges, by which the treatment failure rates are unbiased by this di�erence.
In conclusion, we believe the outcome of DAIR is a�ected by a number of factors that are in complex interplay. Basing a surgical decision solely on the time interval from index arthroplasty to DAIR is neither logical nor evidence-based. Further studies are needed to examine the in�uence of all factors on the outcome of DAIR in isolation and in combination. Machine learning and/or arti�cial intelligence may need to be used to develop an algorithm that will better help surgeons deciding on when to perform DAIR in patients with early PJI. Until such an algorithm is developed, DAIR can be perceived as a viable treatment option in patients presenting more than four weeks after index surgery in case DAIR is performed as soon as symptoms of infection arise and modular components are exchanged.
51938_Claudia_Lowik.indd 115 19-08-19 11:12

Chapter 7
116
References
1. Hiligsmann M, Cooper C, Arden N, Boers M, Branco JC, Brandi ML, et al. Health economics in the �eld of osteoarthritis: an expert’s consensus paper from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Semin Arthritis Rheum 2013; 43(3): 303–13.
2. Kurtz SM, Ong KL, Lau E, Bozic KJ, Berry D, Parvizi J. Prosthetic joint infection risk after TKA in the medicare population. Clin Orthop Relat Res 2010; 468(1): 52–6.
3. Tsukayama DT, Estrada R, Gustilo RB. Infection after total hip arthroplasty: a study of the treatment of one hundred and six infections. J Bone Joint Surg Am 1996; 78(4): 512–23.
4. Fitzgerald Jr RH, Nolan DR, Ilstrup DM, van Scoy RE, Washington 2nd JA, Coventry MB. Deep wound sepsis following total hip arthroplasty. J Bone Joint Surg Am 1977; 59(7): 847–55.
5. McPherson EJ, Woodson C, Holtom P, Roidis N, Shufelt C, Patzakis M. Periprosthetic total hip infection: outcomes using a staging system. Clin Orthop Relat Res 2002; 403: 8–15.
6. Romanò CL, Romanò D, Logoluso N, Drago L. Bone and joint infections in adults: a comprehensive classi�cation proposal. Eur Orthop Traumatol 2011; 1(6): 207–17.
7. Zimmerli W, Trampuz A, Ochsner PE. Prosthetic-joint infections. N Engl J Med 2004; 351(16): 1645–54.
8. Giulieri SG, Graber P, Ochsner PE, Zimmerli W. Management of infection associated with total hip arthroplasty according to a treatment algorithm. Infection 2004; 32(4): 222–8.
9. Choi HR, von Knoch F, Zurakowski D, Nelson SB, Malchau H. Can implant retention be recommended for treatment of infected TKA? Clin Orthop Relat Res 2011; 469(4): 961–9.
10. Fisman DN, Reilly DT, Karchmer AW, Goldie SJ. Clinical e�ectiveness and cost-e�ectiveness of 2 management strategies for infected total hip arthroplasty in the elderly. Clin Infect Dis 2001; 32(3): 419–30.
11. Faschingbauer M, Kappe T, Trubrich A, Bieger R, Reichel H. Retention of the prosthesis in early periprosthetic infection after total hip arthroplasty. Z Orthop Unfall 2015; 153(2): 192–7.
12. Duque AF, Post ZD, Lutz RW, Orozco FR, Pulido SH, Ong AC. Is there still a role for irrigation and debridement with liner exchange in acute periprosthetic total knee infection? J Arthroplasty 2017; 32(4): 1280–4.
13. Fehring TK, Odum SM, Berend KR, Jiranek WA, Parvizi J, Bozic KJ, et al. Failure of irrigation and débridement for early postoperative periprosthetic infection. Clin Orthop Relat Res 2013; 471(1): 250–7.
14. Westberg M, Grøgaard B, Snorrason F. Early prosthetic joint infections treated with debridement and implant retention. Acta Orthop 2012; 83(3): 227–32.
15. Tsang SJ, Ting J, Simpson AHRW, Gaston P. Outcomes following debridement, antibiotics and implant retention in the management of periprosthetic infections of the hip: a review of cohort studies. Bone Joint J 2017; 99-B(11): 1458–66.
16. Argenson JN, Arndt M, Babis G, Battenberg A, Budhiparama N, Catani F, et al. Hip and knee section. Treatment: debridement and retention of implant: proceedings of international consensus on orthopedic infections. J Arthroplasty 2019; 34: S399-419.
17. Triantafyllopoulos GK, Poultsides LA, Sakellariou VI, Zhang W, Sculco PK, Ma Y, et al. Irrigation and debridement for periprosthetic infections of the hip and factors determining outcome. Int Orthop 2015; 39(6): 1203–9.
18. Triantafyllopoulos GK, Poultsides LA, Zhang W, Sculco PK, Ma Y, Sculco TP. Periprosthetic knee infections treated with irrigation and debridement: outcomes and preoperative predictive factors. J Arthroplasty 2015; 30(4): 649–57.
19. Kim JG, Bae JH, Lee SY, Cho WT, Lim HC. The parameters a�ecting the success of irrigation and debridement with component retention in the treatment of acutely infected total knee arthroplasty. Clin Orthop Surg 2015; 7(1): 69–76.
20. Vilchez F, Martínez-Pastor JC, García-Ramiro S, Bori G, Maculé F, Sierra J, et al. Outcome and predictors of treatment failure in early post-surgical prosthetic joint infections due to Staphylococcus aureus treated with debridement. Clin Microbiol Infect 2011; 17(3): 439–44.
51938_Claudia_Lowik.indd 116 19-08-19 11:12

E�cacy of DAIR according to the time interval
117
7
21. Buller LT, Sabry FY, Easton RW, Klika AK, Barsoum WK. The preoperative prediction of success following irrigation and debridement with polyethylene exchange for hip and knee prosthetic joint infections. J Arthroplasty 2012; 27(6): 857–64.
22. Kuiper JWP, Vos CJ, Saouti R, Vergroesen DA, Graat HCA, Debets-Ossenkopp YJ, et al. Prosthetic joint-associated infections treated with DAIR (debridement, antibiotics, irrigation, and retention): analysis of risk factors and local antibiotic carriers in 91 patients. Acta Orthop 2013; 84(4): 380–6.
23. Fink B, Schuster P, Schwenninger C, Frommelt L, Oremek D. A standardized regimen for the treatment of acute postoperative infections and acute hematogenous infections associated with hip and knee arthroplasties. J Arthroplasty 2017; 32(4): 1255–61.
24. Brandt CM, Sistrunk WW, Du�y MC, Hanssen AD, Steckelberg JM, Ilstrup DM, et al. Staphylococcus aureus prosthetic joint infection treated with debridement and prosthesis retention. Clin Infect Dis 1997; 24(5): 914–9.
25. Lebeaux D, Ghigo JM, Beloin C. Bio�lm-related infections: bridging the gap between clinical management and fundamental aspects of recalcitrance toward antibiotics. Microbiol Mol Biol Rev 2014; 78(3): 510–43.
26. Davies D. Understanding bio�lm resistance to antibacterial agents. Nat Rev Drug Discov 2003; 2(2): 114–22.
27. Osmon DR, Berbari EF, Berendt AR, Lew D Zimmerli W, Steckelberg JM, et al. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 2013; 56(1): 1–25.
28. Lovati AB, Bottagisio M, de Vecchi E, Gallazzi E, Drago L. Animal models of implant-related lowgrade infections. A twenty year review. Adv Exp Med Biol 2017; 971: 29–50.
29. Vidlak D, Kielian T. Infectious dose dictates the host response during Staphylococcus aureus orthopedic-implant bio�lm infection. Infect Immun 2016; 84(7): 1957–65.
30. Barrett L, Atkins B. The clinical presentation of prosthetic joint infection. J Antimicrob Chemother 2014; 69(Suppl 1): 25–8.
31. Parvizi J, Gehrke T, Chen AF. Proceedings of the international consensus on periprosthetic joint infection. Bone Joint J 2013; 95-B(11): 1450–2.
32. Vilchez F, Martínez-Pastor JC, García-Ramiro S, Bori G, Tornero E, García E, et al. E�cacy of debridement in hematogenous and early post-surgical prosthetic joint infections. Int J Artif Organs 2011; 34(9): 863–9.
33. Veerachamy S, Yarlagadda T, Manivasagam G, Yarlagadda PK. Bacterial adherence and bio�lm formation on medical implants: a review. Proc Inst Mech Eng H 2014; 228(10): 1083–99.
34. Bandyk DF, Kinney EV, Riefsnyder TI, Kelly H, Towne JB. Treatment of bacteria-bio�lm graft infection by in situ replacement in normal and immune-de�cient states. J Vasc Surg 1993; 18(3): 398–405.
35. Carli AV, Bhimani S, Yang X, Shirley MB, de Mesy Bentley KL, Ross FP, et al. Quanti�cation of peri-implant bacterial load and in vivo bio�lm formation in an innovative, clinically representative mouse model of periprosthetic joint infection. J Bone Joint Surg Am 2017; 99(6): e25.
51938_Claudia_Lowik.indd 117 19-08-19 11:12

51938_Claudia_Lowik.indd 118 19-08-19 11:12

Chapter 8
Managing persistent wound leakage after total knee and hip arthroplasty. Results of a
nationwide survey among Dutch orthopaedic surgeons
Claudia A.M. Löwik, Frank-Christiaan B.M. Wagenaar, Martin Stevens, Sjoerd K. Bulstra, Yvette Pronk, Inge van den Akker-Scheek,
Marjan Wouthuyzen-Bakker, Rob G.H.H. Nelissen, Rudolf W. Poolman, Walter van der Weegen, Paul C. Jutte, on behalf of the LEAK study group
Published in: Journal of Bone and Joint Infection 2017; 2(4): 202-207
51938_Claudia_Lowik.indd 119 19-08-19 11:12

Chapter 8
120
Abstract
BackgroundPersistent wound leakage after joint arthroplasty is a scantily investigated topic, despite the claimed relation with a higher risk of periprosthetic joint infection. This results in a lack of evidence-based clinical guidelines for the diagnosis and treatment of persistent wound leakage after joint arthroplasty. Without such guideline, clinical practice in orthopaedic hospitals varies widely. In preparation of a nationwide multicenter randomized controlled trial on the optimal treatment of persistent wound leakage, we evaluated current Dutch orthopaedic care for persistent wound leakage after joint arthroplasty.
MethodsWe conducted a questionnaire-based online survey among all 700 members of the Netherlands Orthopaedic Association, consisting of 23 questions on the de�nition, classi�cation, diagnosis and treatment of persistent wound leakage after joint arthroplasty.
Results The questionnaire was completed by 127 respondents, representing 68% of the Dutch hospitals that perform orthopaedic surgery. The results showed wide variation in the classi�cation, de�nition, diagnosis and treatment of persistent wound leakage among Dutch orthopaedic surgeons. 56.7% of the respondents used a protocol for diagnosis and treatment of persistent wound leakage, but only 26.8% utilized the protocol in every patient. Most respondents (59.1%) reported a maximum period of persistent wound leakage before starting non-surgical treatment of three to seven days after index surgery and 44.1% of respondents reported a maximum period of wound leakage of ten days before converting to surgical treatment.
ConclusionThe wide variety in clinical practice underscores the importance of developing an evidence-based clinical guideline for the diagnosis and treatment of persistent wound leakage after joint arthroplasty. To this end, a nationwide multicenter randomized controlled trial will be conducted in the Netherlands, which may provide evidence on this important and poorly understood topic.
51938_Claudia_Lowik.indd 120 19-08-19 11:12

Survey on persistent wound leakage
121
8
Introduction
The diagnosis and treatment of persistent wound leakage is an important and poorly understood topic in the �eld of joint arthroplasty. Persistent wound leakage after total knee and hip arthroplasty is associated with a higher risk of developing periprosthetic joint infection (PJI).1-5 PJI is a serious complication with great impact on a patient’s physical functioning and quality of life. Moreover, PJI is a high �nancial burden for society. Additional medical costs of PJI are approximately €30,000 per patient,6,7 with even higher societal costs because of productivity loss, home care and informal care provided by relatives. Unfortunately, there are no evidence-based guidelines for the diagnosis and treatment of persistent wound leakage after joint arthroplasty.
Numerous issues hamper the development of sound guidelines. First of all, research on wound leakage is hard, as PJI is the major endpoint of wound leakage treatment, which has a low incidence.8 Secondly, there is no uniformly accepted de�nition of wound leakage or when to call it persistent. This lack of clear de�nitions hampers comparison of clinical reports to such an extent that there is no clear evidence for any treatment modality for persistent wound leakage. Finally, in clinical practice the amount of drainage may also play a role in the decision-making process, e.g. agreement on the optimal treatment of severe persistent wound leakage is usually easier than agreement on the treatment of less severe wound leakage.
As a result of this lack of clarity, there is still insu�cient evidence for the development of a clinical guideline. In 2013 consensus statements on current practices for prevention, diagnosis and management of PJI were developed during the �rst International Consensus Meeting (ICM) on PJI.9 One of these statements suggested that wound leakage is considered to be persistent when it continues for more than three days after index surgery. Moreover, they stated that surgical management of persistent wound leakage should be performed without delay if wound leakage persists for �ve to seven days after index surgery.10 However, there is no de�nitive evidence for these statements, as there have been no randomized controlled trials on persistent wound leakage.
Without a guideline, clinical practice in orthopaedic hospitals varies widely. Moreover, there is no insight into the modalities used for diagnosis and treatment of persistent wound leakage after joint arthroplasty. This paper reports the results of a questionnaire-based online survey among Dutch
51938_Claudia_Lowik.indd 121 19-08-19 11:12

Chapter 8
122
orthopaedic surgeons on current care for persistent wound leakage after joint arthroplasty. The survey is part of the preparation for a nationwide multicenter randomized controlled trial in the Netherlands on the optimal treatment of persistent wound leakage after total knee and hip arthroplasty.
Material and methods
ProcedureTo evaluate current clinical practice of Dutch orthopaedic surgeons on persistent wound leakage after knee and hip arthroplasty, a questionnaire-based online survey was sent to all 700 members of the Netherlands Orthopaedic Association (NOV), working as orthopaedic surgeons in Dutch hospitals. Surveys completed by residents and members working outside the Netherlands were excluded. The web-based survey tool used for this questionnaire was google.forms. In January 2016 the questionnaire was disseminated by the NOV via e-mail invitation with a link to the survey. Reminder e-mails were sent after two and four weeks to increase the response rate. Data collection was closed six weeks after sending the �rst e-mail.
QuestionnaireThe questionnaire consisted of 23 questions regarding the de�nition, classi�cation, diagnosis and treatment of persistent wound leakage after arthroplasty (Appendix). The questionnaire was developed by the LEAK study group (LEakage After Knee and hip arthroplasty). This group was appointed by the NOV and its Consortium Orthopaedic Research (CORE), as part of the preparation for a nationwide multicenter randomized controlled trial on the treatment of persistent wound leakage after total knee and hip arthroplasty. The LEAK study group involved 25 members who are experts in the �eld of prosthetic joint infections (orthopaedic surgeons, epidemiologists, researchers and an infectious diseases specialist). Three consensus rounds were used to form the �nal questionnaire (Appendix).
Statistical analysesStatistical analyses were performed using IBM SPSS Statistics (version 23.0, Chicago, USA). Results were analyzed using descriptive statistics.
51938_Claudia_Lowik.indd 122 19-08-19 11:12

Survey on persistent wound leakage
123
8
Results
RespondentsA total of 127 respondents �lled in the questionnaire (18.1% of NOV members), representing 70 of all 103 institutions where knee and hip arthroplasty surgeries are performed (68.0%). Most respondents work in general non-training hospitals (61.4%) and 48.8% of the respondents had more than ten years of working experience (Table 1).
Table 1. Descriptives of respondents (n=127)
Variable Value Respondents (%)Clinic type General hospital 78 (61.4%)
Orthopaedic training hospital 39 (30.7%)University hospital 10 (7.9%)
Experience in years 0-10 65 (51.2%)10-20 38 (29.9%)>20 24 (18.9%)
Classi�cation and de�nition of wound leakageMost respondents did not use a classi�cation system for wound leakage (81.2%) (Table 2). Of the 24 respondents who reported using a classi�cation system, 12 referred to their de�nition of wound leakage in days (9.4%) and the other 12 all used di�erent classi�cation systems (9.4%).
Just over half of the respondents (51.2%) used a de�nition of persistent wound leakage, based on duration of wound leakage after index surgery (Table 2). The used cut-o� points showed a large range of 1 to 14 days. Of the 65 respondents who used a de�nition of persistent wound leakage, 24 de�ned wound leakage as persistent when present for more than �ve days (36.9%), 11 as present for more than seven days (16.9%) and 19 for more than ten days (29.2%) (Figure 1a).
Protocol for persistent wound leakageMore than half of the respondents used a protocol for diagnosis and treatment of persistent wound leakage (56.7%), but only 26.8% utilized the protocol in every patient. Patients were regularly discharged by 48.8% of the respondents regardless of wound leakage. A similar percentage of respondents almost never discharged patients with wound leakage (43.3%). The majority of respondents
51938_Claudia_Lowik.indd 123 19-08-19 11:12

Chapter 8
124
reported monitoring patients after discharge (90.2%), e.g. via telephone consultation (Table 2).
Table 2. De�nition, classi�cation and protocol for wound leakage (n=127)
Variable Value Respondents (%)Classi�cation for wound leakage Yes 24 (18.8%)
No 103 (81.2%)Uniform de�nition of wound leakage Yes 65 (51.2%)
No 62 (48.8%)Uniform protocol in case of wound leakage Yes, used in all cases 34 (26.8%)
Yes, not always used 38 (29.9%)No 55 (43.3%)
Discharge patients with wound leakage Yes, always 4 (3.2%)Yes, regularly 62 (48.8%)No, almost never 55 (43.3%)No, never 6 (4.7%)
Monitoring wound leakage after discharge* Yes 111 (90.2%)No 12 (9.8%)
* 4 missing values
Diagnostic modalitiesMost clinical parameters used to evaluate persistent wound leakage were redness (92.9%), fever (92.9%), pain (69.3%), course of recovery (67.7%) and/or swelling (52.7%). Warmth was evaluated by fewer respondents (38.6%). Nearly all respondents used a combination of at least three clinical parameters (86.6%) (Figure 2a). The most popular combination was redness, fever, course of recovery and pain (used by 42.5% of the respondents), with another 27.5% of the respondents evaluating these parameters in combination with warmth and swelling.
For in�ammatory parameters, plasma C-reactive protein (CRP) was used as a diagnostic modality by 92.1% of respondents. Similarly, most (82.7%) perceived CRP as the most important in�ammatory parameter in persistent wound leakage. Moreover, 70.9% of the respondents felt that the trend or dynamics of CRP are important.
Non-surgical treatment modalitiesThe maximum period of persistent wound leakage before starting non-surgical treatment was three to seven days according to most respondents (59.1%) (Figure 1b). 20.5% of respondents stated no maximum period before
51938_Claudia_Lowik.indd 124 19-08-19 11:12

Survey on persistent wound leakage
125
8
starting non-surgical treatment, as they only use surgical treatment modalities. The miscellaneous group used clinical presentation instead of the above-mentioned time-based parameter (10.2%).
Regarding non-surgical treatment modalities for persistent wound leakage most respondents used wound care (60.6%), bed rest (49.6%), pressure bandages (36.2%), admittance (23.6%) and antibiotics (23.6%). A wide variety of combinations was reported (in total 36), all comprising small groups (ranging from one to eight respondents): 54.4% of the respondents used 1-2 non-surgical treatment modalities, 40.9% used 3-4 modalities and 4.7% reported using 5-7 modalities (Figure 2b). The most popular combination was admittance and wound care (5.5%).
Surgical treatment modalitiesMost respondents reported a maximum period of wound leakage before converting to surgical treatment of ten days after index surgery (44.1%) (Figure 1c), yet with a wide range from 5 to 21 days. From the miscellaneous group (31.5%), 14 respondents favored a 14-day cut-o�, while another 14 respondents stated basing their decision on aspects other than duration of wound leakage (e.g. type and/or amount of wound leakage, clinical parameters and/or in�ammatory parameters).
The most-used surgical treatment modalities were lavage (96.1%), obtaining cultures (94.4%), surgical debridement (79.5%), antibiotics (77.2%) and exchange of mobile components (67.7%). The majority of the respondents (52.0%) favored a combined use of all these �ve treatment modalities as a surgical treatment regime; 34.6% of respondents used 3-4 surgical treatment modalities and 13.4% used 1-2 modalities (Figure 2c). The miscellaneous group (3.1%) comprised of two respondents using local gentamicin carriers, one removing the prosthesis and one other respondent performing only super�cial debridement in case of an intact joint capsule and iliotibial tract.
51938_Claudia_Lowik.indd 125 19-08-19 11:12

Chapter 8
126
1a
>5 days36,9%
>7 days16,9%
>10 days29,2%
0 days
>1 day
>3 days
>4 days
>5 days
>7 days
>8 days
>10 days
>14 days
1b
3 days14,2%
5 days26,0%
7 days18,9%
10 days10,2%
No treatment20,5%
Other10,2% 3 days
5 days
7 days
10 days
No treatment
Other
1c
7 days14,2%
10 days44,1%
Other31,5%
3 days
5 days
7 days
10 days
No treatment
Other
Figure 1. De�nition of persistent wound leakage and maximum period of wound leakage before start of (non-)surgical treatment (n=127).
1a. De�nition of wound leakage (in days). 1b. Number of days before starting non-surgical treatment. 1c. Number of days before starting surgical treatment
51938_Claudia_Lowik.indd 126 19-08-19 11:12

Survey on persistent wound leakage
127
8
2a
0%
20%
40%
60%
80%
100%
2b
0%
10%
20%
30%
40%
50%
60%
70%
2c
0%
20%
40%
60%
80%
100%
Figure 2. Clinical parameters, non-surgical treatment modalities and surgical treatment (n=127)
2a. Clinical parameters2b. Non-surgical treatment modalities2c. Surgical treatment modalities
51938_Claudia_Lowik.indd 127 19-08-19 11:12

Chapter 8
128
Discussion
In this online survey we evaluated current Dutch orthopaedic care for persistent wound leakage after joint arthroplasty. This survey revealed considerable variation in clinical practice among Dutch orthopaedic surgeons in terms of classi�cation, de�nition, diagnosis and treatment of persistent wound leakage after joint arthroplasty. This variety in clinical practice is likely the result of a lack of evidence-based guidelines, caused by the scarce evidence on this topic.1-5,10-12
Regarding the de�nition of persistent wound leakage after joint arthroplasty most respondents based the de�nition on the duration of wound leakage after index surgery. Preferred cut-o� points were more than �ve days and more than ten days, yet with a large range (1 to 14 days). This lack of agreement is in accordance with reports in the literature, reporting using time (with a range of two to seven days), presence of microbial content or type of secretion (purulent, hematogenous or clear) as de�nition.1-5,11-16 The ICM statements de�ne persistent wound leakage as a wound leaking >2 x 2cm for more than three days, arguing that this time frame would allow for earlier intervention and may limit the claimed adverse consequences (e.g. PJI).10 Still, there is no scienti�c data con�rming this statement.
In the Netherlands there is dearth of a uniform approach to the classi�cation, de�nition, diagnosis and treatment of persistent wound leakage. Only 18.7% of respondents used a classi�cation and all used a di�erent classi�cation. In the literature there is a complete lack of data regarding amount of wound leakage, while this amount and its dynamics play a large role in the decision-making process. This missing classi�cation of type and amount of wound leakage impairs comparison and interpretation of the scarce literature on the topic.
This survey showed that there is no consensus on a protocol. Only 26.5% used a protocol consistently, and 30.5% did not use the protocol in all cases. In the literature only Maathuis et al. have described a standardized method to approach persistent wound leakage after arthroplasty.1 Compared with an ad hoc approach, their algorithm resulted in fewer open debridements (17% versus 30%) and a higher salvage percentage (95% versus 85%).
The clinical parameters most respondents used when evaluating persistent wound leakage were redness, fever, pain, swelling and a course of recovery. A combination of at least two clinical parameters was used by nearly all
51938_Claudia_Lowik.indd 128 19-08-19 11:12

Survey on persistent wound leakage
129
8
respondents (96.9%). However, 24 di�erent combinations were reported, underscoring an apparent lack of evidence and consensus for an optimal combination of clinical parameters.
Our results showed that orthopaedic surgeons used several clinical and in�ammatory parameters to provide the necessary information to guide clinical decision-making. For in�ammatory parameters, 92.1% of respondents used CRP at some point in their decision-making process. Moreover, most respondents reported CRP to be the primary parameter and 70.9% reported that the trend or dynamics of CRP are important - e.g. a rise in CRP is considered a worrisome sign, whereas a decrease is generally interpreted as a sign of absence of infection. Nevertheless, responses to the exact use of CRP were wide and diverse, probably in relation to the fact that an elevated CRP, as well as some other clinical infectious symptoms (such as fever and tachycardia), may be a physiological response in the early postoperative period.17-23
In this survey the maximum period of wound leakage before starting non-surgical treatment was three to seven days after index surgery. The most popular treatment modalities included wound care, bed rest, pressure bandages and/or antibiotics. Still, more than 30 combinations of treatment modalities were used, stressing the lack of consensus on optimal non-surgical treatment. Literature on this topic is limited, suggesting several days of immobilization,15,16 sterile dressings,3 and/or antibiotics.3 The use of antibiotics among 23.4% of respondents was a surprising and disturbing �nding, as the e�cacy of antibiotic treatment in persistent wound leakage after arthroplasty has not been studied. Antibiotics can also have substantial negative e�ects, such as increased risk of resistance, poor penetration into the bio�lm, and complicated early diagnosis and treatment of infection, given that they can mask infection and confound culture �ndings.10,15 For these reasons, the ICM advises against the use of antibiotics in persistent wound leakage after joint arthroplasty.9,10
Most respondents (43.8%) convert to surgical treatment if wound leakage is present for ten days after index surgery, implying a non-surgical treatment period of three to seven days. The literature o�ers little guidance on this topic, but suggests that wound leakage more than �ve to nine days after arthroplasty should be managed by surgical treatment to give a higher chance of preventing PJI.2-4,14,16 Based on these �ndings, the ICM states that surgical treatment should be performed if wound leakage persists for more than �ve to seven days.10
51938_Claudia_Lowik.indd 129 19-08-19 11:12

Chapter 8
130
However, it seems reasonable to use parameters other than merely duration of wound leakage in the clinical decision-making process. In this survey a minority of respondents used other aspects, such as type or amount of wound leakage, clinical parameters and/or infectious parameters.
A total of 16 combinations were reported as surgical treatment protocol. The majority (52.3%) favored a combined protocol consisting of �ve modalities (surgical debridement, lavage, cultures, exchange of mobile components, and start of antibiotic treatment). These modalities are comparable to the ICM’s, stating a moderate agreement on deep open debridement, cultures (>3) and modular component exchange.10,24
This survey can be viewed as a fair representation of the practices of the Dutch orthopaedic community. The main weakness of this study is that it is by design a questionnaire-based survey. Although this study design led to a relatively low response rate of 18.1% among all NOV members, the respondents represented the majority (68.0%) of orthopaedic clinics, which leads to a reasonable assumption that respondents provided a correct representation of clinical practice in the Netherlands. Respondents were not obliged to �ll in the name of the hospital they worked in, since it was anticipated that orthopaedic surgeons could consider this a barrier for �lling in the survey. Because of this, 15 respondents did not provide data on the hospital they worked in. Taking this into account, the actual representation of orthopaedic clinics may be even higher than 68.0%.
In conclusion, the data from this nationwide survey among Dutch orthopaedic surgeons on persistent wound leakage after joint arthroplasty demonstrated a wide variation in clinical practice of classi�cation, de�nition, diagnosis and treatment of persistent wound leakage. This underscores the lack of consensus, which is mainly due to a dearth of clear evidence on the correct diagnosis and treatment of wound leakage. This survey may be representative for current daily clinical practice of the global orthopaedic community and stresses the need for further research on this important topic.
51938_Claudia_Lowik.indd 130 19-08-19 11:12

Survey on persistent wound leakage
131
8
Appendix
Table 3. QuestionnaireQuestion Answer options
1 Years of experience 0-10 years10-20 years>20 years
2 Clinic type General hospitalOrthopaedic training hospitalUniversity hospital
3 Do you have/use a uniform de�nition of Yespersistent wound leakage after arthroplasty? No
4 If so, please specify your uniform de�nition of persistent wound leakage after arthroplasty.
Speci�cation
5 Do you use some classi�cation of (persistent) Yeswound leakage after arthroplasty? No
6 If so, specify your classi�cation of (persistent) wound leakage after arthroplasty.
Speci�cation
7 Do you use a uniform protocol in case of Yes, and this is used in all cases(persistent) wound leakage after arthroplasty? Yes, but this is not always
followedNo
8 Do you discharge patients with wound leakage Yes, alwaysafter arthroplasty? Yes, regularly
No, almost neverNo, never
9 If so, do you have a monitoring system for wound Yesleakage after discharge from your clinic? No
10 Do you have a maximum period of wound 3 daysleakage after arthroplasty after which you start 5 daysnon-surgical treatment? 7 days
10 daysNo, there is no surgical treatmentOther
11 If your answer is other, what is the maximum number of days you follow?
Speci�cation
12 What non-surgical treatment modalities do you (Re-)admittance to clinicuse? Multiple answers are possible. Antibiotic treatment
Bed restPressure bandages / hip spicaWound careNo shower policyOther
13 If your answer is other, what non-surgical modalities do you use?
Speci�cation
51938_Claudia_Lowik.indd 131 19-08-19 11:12

Chapter 8
132
Table 3. continuedQuestion Answer options
14 Do you have a maximum period of wound 3 daysleakage after arthroplasty at which you decide to 5 daysdo surgical treatment? 7 days
10 daysNo, there is no surgical treatmentOther
15 If your answer is other, what is the maximum number of days you follow?
Speci�cation
16 What components comprise your surgical Debridementtreatment protocol? Multiple answers are Lavagepossible. Antibiotics
CulturesExchange of mobile componentsProsthesis removalOther
17 If your answer is other, which modalities do you use as your surgical treatment?
Speci�cation
18 Do you use C-reactive protein (CRP) in your Yestreatment decision process in case of persistent Nowound leakage after arthroplasty?
19 If so, what are your considerations in using CRP in your decision-making process?
Speci�cation
20 Which serological parameter do you think is the BSEmost important in persistent wound leakage after CRParthroplasty? Leucocyte count
Other21 If your answer is other, describe your parameter. Speci�cation22 What clinical parameter(s) do you use in your Redness
decision-making process in case of persistent Feverwound leakage after arthroplasty? Multiple. Course of recoveryanswers are possible Pain
WarmthSwellingOther
23 If your answer is other, describe your parameter. Speci�cation
51938_Claudia_Lowik.indd 132 19-08-19 11:12

Survey on persistent wound leakage
133
8
References
1. Maathuis PGM, de Hartog B, Bulstra SK. Timing of open debridement for suspected infection of joint prosthesis: a report on 551 patients. Curr Orthop Pract 2009; 20(5): 541-5.
2. Weiss AP, Krackow KA. Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993; 8(3): 285-9.
3. Jaberi FM, Parvizi J, Haytmanek CT, Joshi A, Purtill J. Procrastination of wound drainage and malnutrition a�ect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008; 466(6): 1368-71.
4. Saleh K, Olson M, Resig S, Bershadsky B, Kuskowski M, Gioe T, et al. Predictors of wound infection in hip and knee joint replacement: results from a 20 year surveillance program. J Orthop Res 2002; 20(3): 506-15.
5. Patel VP, Walsh M, Sehgal B, Preston C, DeWal H, Di Cesare PE. Factors associated with prolonged wound drainage after primary total hip and knee arthroplasty. J Bone Joint Surg Am 2007; 89(1): 33-8.
6. Kurtz SM, Lau E, Schmier J, Ong KL, Zhao K, Parvizi J. Infection burden for hip and knee arthroplasty in the United States. J Arthroplasty 2008; 23(7): 984-91.
7. Kallala RF, Vanhegan IS, Ibrahim MS, Sarmah S, Haddad FS. Financial analysis of revision knee surgery based on NHS tari�s and hospital costs: does it pay to provide a revision service? Bone Joint J 2015; 97-B(2): 197-201.
8. Kurtz SM, Ong KL, Lau E, Bozic KJ, Berry D, Parvizi J. Prosthetic joint infection risk after TKA in the medicare population. Clin Orthop Relat Res 2010; 468(1): 52-6.
9. Parvizi J, Gehrke T, Chen AF. Proceedings of the international consensus on periprosthetic joint infection. Bone Joint J 2013; 95-B(11): 1450-2.
10. Ghanem E, Heppert V, Spangehl M, Abraham J, Azzam K, Barnes L, et al. Wound management. J Orthop Res 2014; 32(Suppl 1): S108-19.
11. Butt U, Ahmad R, Aspros D, Bannister GC. Factors a�ecting wound ooze in total knee replacement. Ann R Coll Surg Engl 2011; 93(1): 54-6.
12. Surin VV, Sundholm K, Bäckman L. Infection after total hip replacement. With special reference to a discharge from the wound. J Bone Joint Surg Br 1983; 65(4): 412-8.
13. Hansen E, Durinka JB, Costanzo JA, Austin MS, Deirmengian GK. Negative pressure wound therapy is associated with resolution of incisional drainage in most wounds after hip arthroplasty. Clin Orthop Relat Res 2013; 471(10): 3230-6.
14. Dennis DA. Wound complications in total knee arthroplasty. In: Sculco TP, ed. Knee Arthroplasty, 1st ed. New York, USA: Springer Vienna 1997: 163-9.
15. Vince K, Chivas D, Droll KP. Wound complications after total knee arthroplasty. J Arthroplasty 2007; 22(4 Suppl 1): 39-44.
16. Lonner JH, Lotke PA. Aseptic complications after total knee arthroplasty. J Am Acad Orthop Surg 1999; 7(5): 311-24.
17. Aalto K, Osterman K, Peltola H, Räsänen J. Changes in erythrocyte sedimentation rate and C-reactive protein after total hip arthroplasty. Clin Orthop Relat Res 1984; 184: 118-20.
18. Bilgen O, Atici T, Durak K, Karaeminoğullari K, Bilgen MS. C-reactive protein values and erythrocyte sedimentation rates after total hip and total knee arthroplasty. J Int Med Res 2001; 29(1): 7-12.
19. Moreschini O, Greggi G, Giordano MC, Nocente M, Margheritini F. Postoperative physiopathological analysis of in�ammatory parameters in patients undergoing hip or knee arthroplasty. Int J Tissue React 2001; 23(4): 151-4.
20. Niskanen RO, Korkala O, Pammo H. Serum C-reactive protein levels after total hip and knee arthroplasty. J Bone Joint Surg Br 1996; 78(3): 431-3.
21. Shih LY, Wu JJ, Yang DJ. Erythrocyte sedimentation rate and C-reactive protein values in patients with total hip arthroplasty. Clin Orthop Relat Res 1987; 225: 238-46.
22. White J, Kelly M, Dunsmuir R. C-reactive protein level after total hip and knee replacement. J Bone Joint Surg Br 1998; 80(5): 909-11.
23. Honsawek S, Deepaisarnsakul B, Tanavalee A, Sakdinakiattikoon M, Ngarmukos S, Preativatanyou K, et al. Relationship of serum IL-6, C-reactive protein, erythrocyte sedimentation rate, and knee skin temperature after total knee arthroplasty: a prospective study. Int Orthop 2011; 35(1): 31-5.
24. Zmistowski B, Parvizi J. Identi�cation and treatment of infected total hip arthroplasty. Expert Rev Anti Infect Ther 2012; 10(4): 509-18.
51938_Claudia_Lowik.indd 133 19-08-19 11:12

51938_Claudia_Lowik.indd 134 19-08-19 11:12

Chapter 9
LEAK study: design of a nationwide randomized
controlled trial to �nd the best way to treat wound leakage
after primary hip and knee arthroplasty
Claudia A.M. Löwik, Frank-Christiaan B.M. Wagenaar, Walter van der Weegen, Rudolf W. Poolman, Rob G.H.H. Nelissen, Sjoerd K. Bulstra, Yvette Pronk,
Karin M. Vermeulen, Marjan Wouthuyzen-Bakker, Inge van den Akker-Scheek, Martin Stevens, Paul C. Jutte, on behalf of the LEAK study group
Published in: BMJ Open 2017: 7; e018673
51938_Claudia_Lowik.indd 135 19-08-19 11:12

Chapter 9
136
Abstract
BackgroundTotal hip and knee arthroplasty are highly successful treatment modalities for advanced osteoarthritis. However, prolonged wound leakage after arthroplasty is linked to prosthetic joint infection (PJI), which is a potentially devastating complication. On the one hand, wound leakage is reported as a risk factor for PJI with a leaking wound acting as a porte d’entrée for microorganisms. On the other hand, prolonged wound leakage can be a symptom of PJI. Literature addressing prolonged wound leakage is scarce, contradictory and of poor methodological quality. Hence, treatment of prolonged wound leakage varies considerably with both non-surgical and surgical treatment modalities. There is a de�nite need for evidence concerning the best way to treat prolonged wound leakage after joint arthroplasty.
MethodsA prospective nationwide randomized controlled trial will be conducted in 35 hospitals in the Netherlands. The goal is to include 388 patients with persistent wound leakage 9-10 days after total hip or knee arthroplasty. These patients will be randomly allocated to non-surgical treatment (pressure bandages, (bed) rest and wound care) or surgical treatment (debridement, antibiotics and implant retention (DAIR)). DAIR will also be performed on all non-surgically treated patients with persistent wound leakage at day 16-17 after index surgery, regardless of amount of wound leakage, other clinical parameters or C-reactive protein. Clinical data are entered into a web-based database. Patients are asked to �ll in questionnaires about disease-speci�c outcomes, quality of life and cost e�ectiveness at 3, 6 and 12 months after surgery. Primary outcome is the number of revision surgeries due to infection within a year of arthroplasty.
Ethics and disseminationThe Review Board of each participating hospital has approved the local feasibility. The results will be published in peer-reviewed scienti�c journals.
Trial registration numberNTR 5960.
51938_Claudia_Lowik.indd 136 19-08-19 11:12

Design of the LEAK study
137
9
Strengths and limitations of this study- This nationwide study is the �rst randomized controlled trial to compare
outcomes of non-surgical treatment and surgical treatment in patients with prolonged wound leakage after total hip and knee arthroplasty.
- This study is an initiative of the Netherlands Orthopaedic Association. The optimal treatment for persistent wound leakage is unknown and is considered an important knowledge gap. This is why numerous Dutch hospitals participate, allowing for inclusion of a large number of patients.
- Since literature addressing wound leakage is scarce, there is no evidence for the optimal timing of DAIR. Therefore, timing of the early intervention (DAIR at day 9-10) is based on consensus instead of evidence.
- Orthopaedic surgeons may be reluctant to randomize patients in case of minimal wound leakage (LEAK class 1). This may induce biased results.
51938_Claudia_Lowik.indd 137 19-08-19 11:12

Chapter 9
138
Introduction
Osteoarthritis (OA) is the most common joint disorder worldwide and is recognized as a substantial source of disability.1 Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are highly successful and widely accepted surgical treatment modalities for advanced OA of the hip and knee. In 2015, 28,798 THAs and 27,082 TKAs were performed in the Netherlands2 and 310,800 THAs and 693,400 TKAs were performed in the United States in 2010.3,4 The demand for joint arthroplasty continues to rise due to an ageing population and changing thresholds for surgery and is expected to keep increasing in the coming decades.5 Unfortunately, this results in higher absolute numbers of complications after joint arthroplasty. One of the most serious and potentially devastating complications is prosthetic joint infection (PJI).
Persistent wound leakage after primary THA or TKA is associated with PJI. Wound leakage is induced in the postoperative phase by an in�ammatory response.6 Conversely, surgical wounds may also show prolonged leakage for other reasons (hematoma, seroma or fatty necrosis) and take longer to heal without development of a PJI. Prolonged wound leakage is a risk factor for PJI as a leaking wound can be a porte d’entrée for microorganisms (retrograde infection pathway).7 Bacteria can rapidly form a bio�lm on the metal surface of the prosthesis, thereby decreasing the e�ectiveness of the host defense and antimicrobial therapy. It is estimated that in the Netherlands about 2200 patients annually (4% of ±55,000 THA/TKA) have wound leakage at day nine after index surgery.2,6 As PJI is a serious and potentially devastating complication, prolonged wound leakage should be considered as potentially imminent PJI, with �uid production as a symptom or a risk factor for infection.
PJI has an enormous impact on patients as well as society, as it often results in septic revision surgery, requiring removal of the infected implant to eradicate the infection and hopefully allowing subsequent re-implantation. This septic revision surgery is accompanied by a large negative impact on the quality of life of patients and high health care costs (± € 30,000 per patient with PJI in the United Kingdom),8 due to extended hospital stays, costly surgical procedures, prolonged use of antibiotics and impaired function of the hip or knee. The Dutch Arthroplasty Register reports a total of 3809 THA and 2667 TKA revision surgeries performed in 2015.2 Revision surgery within one year of index surgery was necessary in more than 600 patients, and at least 30% of these were PJI-related.2
51938_Claudia_Lowik.indd 138 19-08-19 11:12

Design of the LEAK study
139
9
Persistent wound leakage can be treated by non-surgical and surgical treatment modalities. Non-surgical treatment can consist of relative rest (no exercise and bed rest), pressure bandages (hip spica or knee pressure bandage) and wound care with sterile bandages. Hospital admission can be required. Surgical treatment typically consists of debridement, antibiotics and implant retention (DAIR).9,10 A DAIR procedure is meant to clean the prosthesis and wound, including breaking down the bio�lm, in order to treat the infection and render further infection treatment unnecessary. Treatment of persistent wound leakage varies considerably amongst Dutch hospitals, as con�rmed recently by a nationwide questionnaire-based survey regarding both non-surgical and surgical treatment modalities.11 However, these modalities have never been studied comparatively.
Several authors have investigated the e�ect of DAIR for treatment of persistent wound leakage and reported various results and/or made (opinion-based) statements, generally in favor of early DAIR.6,10-15 The most recent PJI consensus meeting suggests �ve to seven days of wound leakage as the threshold to perform DAIR, but there is no solid evidence for this statement.16 Therefore, the optimal timing of DAIR is yet to be established, which could imply that either overtreatment or undertreatment may occur. As the treatment decision-making process is generally relatively easy in patients with severe wound leakage and a high suspicion of infection, this study particularly aims to provide evidence for the best treatment of patients with a low suspicion of infection.
As early DAIR is hypothesized to be helpful in treating or preventing infection and salvaging the implant, the objective of this study is to determine the clinical outcome and cost e�ectiveness of early surgical intervention (DAIR at day 9-10 after index procedure) versus non-surgical treatment in patients with prolonged wound leakage after primary THA/TKA. In addition, the impact on disease-speci�c and general health-related quality of life will be determined. Our hypothesis, based on the scarce literature mentioned above, is that performing a DAIR at day 9-10 will result in a 50% reduction rate of revision surgery for PJI up to one year after primary THA/TKA compared with non-surgical treatment.
51938_Claudia_Lowik.indd 139 19-08-19 11:12

Chapter 9
140
Methods and design
Study design and procedureA prospective nationwide multicenter randomized controlled trial (RCT) will be conducted. The study will be carried out in 35 hospitals throughout the Netherlands. All patients aged 18 or older and scheduled to undergo primary THA/TKA in the participating hospitals will receive written and oral information about the LEakage After primary Knee and hip arthroplasty (LEAK) study. Patients with persistent wound leakage at day 5-7 after index surgery will be monitored carefully and receive non-surgical treatment. Clinical examination, wound classi�cation and C-reactive protein (CRP) will be carried out at day 5-7 and day 9-10. In case of persistent leakage at day 9-10 after index surgery, the patient will be included in the study (after signing the informed consent form) and randomized to either surgical treatment (DAIR at 9-10) or continued non-surgical treatment. Patients allocated to the non-surgical treatment group with persistent wound leakage at day 16-17 after index surgery will also be subjected to a DAIR, regardless of amount of wound leakage, other clinical parameters or CRP. Patients in the non-surgical treatment group with clear signs of infection (de�ned as temperature >38.5°C, increasing wound leakage, redness, pain, and increasing CRP (>25% compared with day 9-10)) earlier than day 16-17 will receive surgical treatment at that time point. Patients with clear signs of infection earlier than or at day nine after index surgery will receive surgical treatment without randomization (Figure 1). The extended version of the study protocol �owchart is enclosed in Figure 2 in the Appendix.
Randomization will be performed by a web-based system (developed by Interactive Studios, Rosmalen, The Netherlands), based on the software Apache and MySQL. Each participating hospital receives an individual login in order to register and randomize patients. A two-day time window for randomization (day 9-10) is chosen to facilitate implementation of the protocol, as some patients undergo surgery on days of the week that result in follow-up moments in the weekend, which may hamper inclusion. Since there is no uniform classi�cation for wound leakage, experts in the �eld of PJI (the LEAK study group) developed a wound leakage classi�cation system based on amount of wound leakage, called the LEAK classi�cation, consisting of four classes: LEAK class 0: dry wound; LEAK class 1: mild wound leakage (<2x2cm in gauze per 24 hour); LEAK class 2: moderate wound leakage (>2x2cm in gauze
51938_Claudia_Lowik.indd 140 19-08-19 11:12
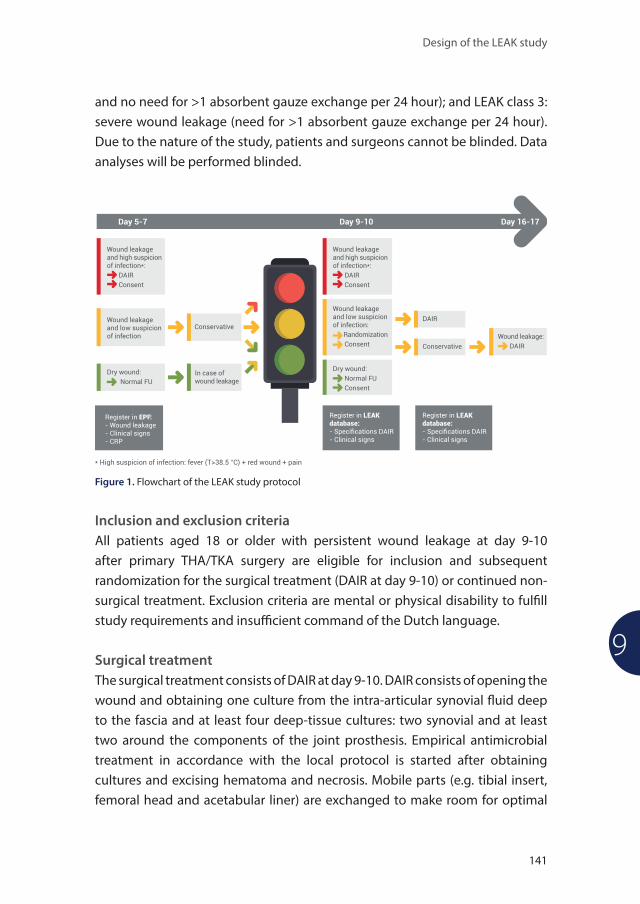
Design of the LEAK study
141
9
and no need for >1 absorbent gauze exchange per 24 hour); and LEAK class 3: severe wound leakage (need for >1 absorbent gauze exchange per 24 hour). Due to the nature of the study, patients and surgeons cannot be blinded. Data analyses will be performed blinded.
Figure 1. Flowchart of the LEAK study protocol
Inclusion and exclusion criteriaAll patients aged 18 or older with persistent wound leakage at day 9-10 after primary THA/TKA surgery are eligible for inclusion and subsequent randomization for the surgical treatment (DAIR at day 9-10) or continued non-surgical treatment. Exclusion criteria are mental or physical disability to ful� ll study requirements and insu� cient command of the Dutch language.
Surgical treatmentThe surgical treatment consists of DAIR at day 9-10. DAIR consists of opening the wound and obtaining one culture from the intra-articular synovial � uid deep to the fascia and at least four deep-tissue cultures: two synovial and at least two around the components of the joint prosthesis. Empirical antimicrobial treatment in accordance with the local protocol is started after obtaining cultures and excising hematoma and necrosis. Mobile parts (e.g. tibial insert, femoral head and acetabular liner) are exchanged to make room for optimal
51938_Claudia_Lowik.indd 141 19-08-19 11:12

Chapter 9
142
debridement. The wound is extensively debrided and lavaged using 3-6 liters of saline (alternative is a povidone iodine solution or chlorhexidine solution). Mechanical scrubbing of the visible prosthetic parts is advised.
Non-surgical treatmentThe non-surgical treatment consists of relative rest (stop exercise and start bed rest), pressure bandages (hip spica or knee pressure bandage) and wound care with sterile bandages. The non-surgical treatment is optionally carried out in a hospital admission setting. Patients in the non-surgical treatment group do not receive antimicrobial treatment. In non-surgically treated patients clinical examination, wound classi�cation and CRP are performed at day 16-17 after index surgery. A DAIR will also be performed on all patients with persistent wound leakage at day 16-17 after index surgery, regardless of amount of wound leakage, other clinical parameters or CRP.
Outcome measuresPrimary outcome is the percentage of reoperations for PJI within one year of index surgery. Reoperation refers to any kind of septic revision surgery (one or two stage revision, Girdlestone, arthrodesis or amputation). In addition, any other PJI treatment modalities are recorded (repeated DAIR, start of suppressive antimicrobial treatment or watchful neglect).
Secondary outcomes are the impact of surgical treatment compared with non-surgical treatment on disease-speci�c outcome and general health-related quality of life and the economic evaluation (cost e�ectiveness and cost utility) of the surgical and non-surgical treatment. Self-reported questionnaires will be used to measure these outcome parameters. All questionnaires used are recommended by the Netherlands Orthopaedic Association (NOV) as a quality assessment tool of orthopaedic care and are included in the standard Patient Reported Outcome Measure (PROM) list for both THA and TKA patients. Randomized patients will �ll in these questionnaires 3, 6 and 12 months after index surgery.
Clinical dataClinical data will be recorded from randomized patients, patients who undergo surgical treatment earlier or at day nine because of clear signs of infection and patients with persistent wound leakage at day 5-7 but a dry wound at day 9-10
51938_Claudia_Lowik.indd 142 19-08-19 11:12

Design of the LEAK study
143
9
after index surgery. Data are recorded in the web-based database. Demographic characteristics, body mass index, American Society of Anesthesiologists score, immunosuppressant medication, diabetes and anticoagulants will be recorded. Further data include information about the index surgery, reoperation for PJI, postoperative complications, clinical signs of infection, use of antibiotics and measurement of CRP. For those patients who are allocated to surgical treatment, details of the DAIR procedure and culture results will be recorded. In case of repeated DAIR procedures, the information will also be speci�ed in the database. The clinical data are �lled in by a physician of the participating hospital, to preserve doctor-patient con�dentiality.
Disease speci�c outcome and general health-related quality of lifeQuestionnaires that will be used to measure disease-speci�c outcome are the Hip and Knee disability and Osteoarthritis Outcome Score – physical function short form (HOOS-PS/KOOS-PS)17,18 and the Oxford Hip and Knee Score (OHS/OKS).19,20 General health-related quality of life will be measured by the EuroQol-5D-5L (EQ-5D-5L).21,22
The HOOS-PS and KOOS-PS are disease-speci�c PROMs derived from the original HOOS and KOOS questionnaires. These questionnaires inform after hip or knee disability in patients with osteoarthritis. The HOOS-PS consists of �ve items assessing physical function with interval-level properties. Questions are answered using a Likert scale, in which a higher score re�ects more symptoms and limitations. The KOOS-PS contains seven items. Questions are answered using a Likert scale, with higher scores indicating more limitations in physical functioning. The raw scores are converted to a 0-to-100 scale with 100 as the best outcome. The Dutch language versions of the HOOS-PS and KOOS-PS are considered reliable and valid.17,18
The OHS and OKS are disease-speci�c PROMs. These questionnaires consist of twelve questions covering function and pain associated with the hip or knee. Questions are answered using a Likert scale. Scoring involves summating the total for each item to produce a �nal score between 0 and 48, with a higher score indicating greater disability. The questionnaires are considered reliable, valid and sensitive to clinically important changes over time and are available in the Dutch language.19,20
The EQ-5D-5L is a widely used and valid generic instrument to measure general health-related quality of life, and is validated in the Dutch language.21,22
51938_Claudia_Lowik.indd 143 19-08-19 11:12

Chapter 9
144
The EQ-5D-5L consists of two parts. The �rst part consists of �ve dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each dimension is scored using a Likert scale. The combined scores of these �ve dimensions are converted to the EQ-5D index score.22 The second part consists of a 20 cm visual analog scale (EQ-VAS) that has endpoints labeled “best imaginable health state” and “worst imaginable health state” anchored at 100 and 0, respectively. Respondents are asked to indicate how they rate their own health by writing down the number representing the point on the EQ-VAS which best represents their own health on that day.21,22 The EQ-5D-5L is embedded in this study protocol, as it is especially useful in combination with the economic evaluation that will be conducted in order to calculate utilities.
Economic evaluationThe primary aim of the economic evaluation will be to estimate the societal costs of the strategy to perform a DAIR at day 9-10 and compare this with the costs of a continued non-surgical treatment strategy. Secondary aim will be to estimate the cost e�ectiveness of the surgical treatment compared with non-surgical treatment (from a societal perspective), based on the primary measure of e�ectiveness (number of infections prevented).
Cost e�ectiveness analyses (CEA) and cost utility analyses (CUA) based on EQ-5D-5L-de�ned utilities will be performed to describe the �nancial consequences of both surgical and non-surgical treatment. All items of resource use will be collected at the patient level, using case report forms and the patient questionnaires Medical Consumption Questionnaire (iMCQ) and Productivity Cost Questionnaire (iPCQ). The iMCQ is a generic instrument for measuring medical costs. The questionnaire includes 31 questions related to frequently occurring contacts with health care providers.23 The iPCQ is a standardized generic instrument for measuring and valuing productivity losses. The questionnaire includes 12 questions divided into three modules measuring productivity losses of paid work due to absenteeism, presenteeism and productivity losses related to unpaid work.24,25
The CEA and CUA integrate two quantities: the additional costs (or savings) of surgical treatment compared with non-surgical treatment and the additional health bene�ts. Based on these two quantities the incremental cost e�ectiveness ratio is calculated, which is the di�erence in costs divided by the di�erence in e�ects. Results of the CEA will display the additional costs or
51938_Claudia_Lowik.indd 144 19-08-19 11:12

Design of the LEAK study
145
9
savings with surgical treatment in order to prevent one additional patient with an infection compared with non-surgical treatment. In the CUA, the impact on quality adjusted life year (QALY) will rely on the results based on the EQ-5D-5L. Results of the CUA will display the additional costs or savings with surgical treatment in order to gain one QALY compared with non-surgical treatment.
Health care will be valued using standard prices,26 with time and travel costs included in the CEA and CUA. Productivity losses will be valued using both the friction-cost method (primary analysis) and the human-capital method (sensitivity analysis). The time horizon will be 12 months; therefore, the analysis will not include discounting of costs and e�ects. Bootstrap resampling will be performed on the cost as well as on the cost and e�ect pairs in order to calculate con�dence intervals. Cost e�ectiveness acceptability curves will be plotted to estimate the probability of surgical treatment being more cost-e�ective than non-surgical treatment, for di�erent amounts of money that a decision-maker may be willing to pay for one additional unit of e�ect (infection avoided or QALY).
Sample sizeThe power analysis is based on the assumption that 20% of patients with persistent wound leakage at day 9-10 will necessitate revision surgery. It is hypothesized that surgical treatment (DAIR at day 9-10) will prevent 50% of PJIs and consequently revision surgery compared with non-surgical treatment. In order to detect this 50% reduction with 80% power at a signi�cance level of 0.05, 155 patients are required in the surgical treatment group and 155 in the non-surgical treatment group. With an expected dropout rate of approximately 20%, a sample size of 194 patients per group is needed, making up a total required patient group of 388 patients.
Statistical analysisDescriptive statistics will be used to analyze patient characteristics. The primary outcome of the study is revision surgery for PJI within one year of index surgery (a binary variable). At least two measurements will be collected, namely at the time of randomization (at day 9-10) and one year after index surgery. The dependency of the measurements within the patient is our focal interest. To take into account other dependencies (e.g. the hospital in which the patient is treated), a multilevel logistic regression model with three levels will be used
51938_Claudia_Lowik.indd 145 19-08-19 11:12

Chapter 9
146
to analyze the data. The three levels are hospitals, patients and measurements. As this study is designed as an RCT, every patient can be classi�ed as a case (surgical treatment) or control (non-surgical treatment). The e�ect of the intervention will be controlled for relevant covariates such as age and gender. Intention-to-treat analyses will be conducted. Subanalyses will be performed for patients with wound leakage after THA and TKA separately, to gain insight into the e�ectiveness of the intervention. Moreover, subanalyses will be performed within both treatment groups to distinguish between patients who initially received non-surgical treatment but were treated with a DAIR at day 16-17 versus patients who only received non-surgical treatment (non-surgical treatment group) and between patients who received one DAIR versus two DAIRs (surgical treatment group).
For all analyses, a one–tailed signi�cant level of p <0.05 is considered to be statistically signi�cant. All statistical analyses will be performed using SPSS Version 24.0 for Windows (IBM, Armonk, New York, USA).
Ethics and dissemination
The Review Board of each participating hospital has examined and approved the local feasibility. The study will be conducted according to the principles of the Medical Research Involving Human Subjects Act (WMO), the Good Clinical Practice standard (GCP) and the Declaration of Helsinki. Eligible patients will be informed about the study and will sign an informed consent form in order to participate. Serious adverse events will be recorded and reported to an independent data and safety monitoring board. Auditing and monitoring will be carried out throughout the duration of the study. We began recruitment in February 2017 and expect to have completed recruitment by August 2018 and completed data collection by August 2019. The results of this study will be published in international peer-reviewed scienti�c journals.
Discussion
Wound leakage is associated with PJI, with �uid production as a symptom or a risk factor for infection. With increasing numbers of joint arthroplasties
51938_Claudia_Lowik.indd 146 19-08-19 11:12

Design of the LEAK study
147
9
worldwide, the number of PJIs is rising as well. Without an evidence-based guideline, there is huge variation in clinical practice regarding the treatment of persistent wound leakage in the Netherlands and abroad, with both non-surgical and surgical treatment modalities being used.11 The most recent PJI consensus meeting suggests �ve to seven days of wound leakage as the threshold to perform a DAIR-procedure.16 However, this statement remains unproven and comparative studies on early surgical intervention (DAIR) versus non-surgical treatment are lacking. There is a need for an unambiguous clinical guideline to treat persistent wound leakage.
Objective of the LEAK study is to determine the outcome of surgical treatment (DAIR at day 9-10) versus non-surgical treatment. Performing surgical treatment at day 9-10 is a compromise between the recommendation of the most recent PJI meeting and usual clinical practice in the Netherlands.16 In preparation of designing this RCT, we performed a survey among Dutch orthopaedic surgeons to evaluate current Dutch orthopaedic care for persistent wound leakage after joint arthroplasty. As only 17.2% of Dutch orthopaedic surgeons started surgical treatment after 5-7 days of wound leakage and 44.1% after 10 days of wound leakage,11 we decided to perform surgical treatment at day 9-10 after joint arthroplasty.
Based on the scarce literature available, the conservative assumption is that wound leakage is associated with revision for PJI in 20% of cases, and it is hypothesized that surgical treatment (DAIR on day 9-10) will reduce this to a 10% revision rate for PJI, that is, a 50% reduction within one year of primary THA/TKA compared with continued non-surgical treatment. It is hypothesized that in the long run (more than one year) even a larger reduction can be achieved, as many cases of PJI are caused by lower-virulence pathogens, and PJI within 2-5 years is generally considered as related to the index surgery. In this study, participating patients will be followed-up for one year. This follow-up length is chosen because of restrictions from the subsidiary agency. Additional follow-up will be done through the Dutch National Registry for Orthopaedic Implants (LROI).
If the hypothesis as formulated in the LEAK study is con�rmed, this will o�er a �rm body of evidence for the development of a guideline for treatment of prolonged wound leakage, eventually resulting in a lower percentage of PJIs and therefore a signi�cant improvement of physical functioning and health-related quality of life for patients with prolonged wound leakage. Moreover,
51938_Claudia_Lowik.indd 147 19-08-19 11:12

Chapter 9
148
from an economic perspective, it will lead to signi�cant cost savings in orthopaedic health care. It is estimated that in the Netherlands about 2200 patients annually (4% of ± 55,000 THA/TKA) have wound leakage at day 9-10.2,6 It is hypothesized that the number of patients needing revision surgery for PJI with non-surgical treatment will be 200-400 compared with 100-200 with surgical treatment at day 9-10 after index surgery. Costs of standard treatment are di�cult to estimate due to large variations in current clinical practices. Costs of the study intervention (DAIR) are about €3,000. Additional savings include the avoided re-interventions, which amount to approximately €30,000 per procedure. The hypothesized reduction in orthopaedic health care costs by implementing the LEAK study protocol is €300,000 per year nationwide. This reduction in health care costs will be even greater considering the fact that PJI may develop later than one year after index surgery. Furthermore, it is hypothesized that performing surgical treatment (DAIR at day 9-10) can reduce the productivity loss associated with reoperations and can reduce the costs associated with prolonged home care and informal care provided by relatives, which come in addition to the health care costs.
During the design of the LEAK study, the project team discussed using a non-inferiority design. This was discarded, as it is estimated that the e�ect of surgical treatment is su�ciently large to provide evidence for the superiority of performing an early DAIR procedure.
In conclusion, clinical practice for the treatment of persistent wound leakage varies considerably. The dilemma is that not all postoperative prolonged wound leakages are a proxy for PJI, but delaying surgical treatment for too long may result in undertreatment and development of a PJI. At the present time, the literature shows no evidence for superiority of surgical over non-surgical treatment. The results of the current study will contribute to development of evidence-based guidelines on the optimal treatment and treatment timing of persistent wound leakage after THA and TKA.
51938_Claudia_Lowik.indd 148 19-08-19 11:12

Design of the LEAK study
149
9
Appendix
Figur e 2. Extended version of the � owchart of the LEAK study protocol
Note
A:
- Pati
ent r
ecei
ves ‘
Basic
info
rmati
on fl
yer L
EAK
stud
y’ a
t tim
e of
indi
catio
n fo
r prim
ary
THA
/ TKA
.
Note
B:
- Reg
ister
par
amet
ers i
n lo
cal e
lect
roni
c pati
ent fi
le in
a st
anda
rdize
d m
anne
r.
- Det
erm
ine
CRP.
- D
eter
min
e LE
AK cl
ass =
- LEA
K Cl
ass 0
, dry
- LEA
K Cl
ass 1
, mild
: str
ipe
of b
lood
in w
ound
dre
ssin
g or
≤2x
2 cm
in g
auze
per
24
hr
- L
EAK
Clas
s 2, m
oder
ate:
>2x
2 cm
in g
auze
and
no
need
for >
1 ab
sorb
ent g
auze
exc
hang
e pe
r 24
hr
- L
EAK
Clas
s 3, s
ever
e: n
eed
for >
1 ab
sorb
ent g
auze
exc
hang
e pe
r 24
hr
- Des
crib
e cli
nica
l par
amet
ers =
redn
ess,
feve
r (T
≥ 38
.5 d
egre
es C
elciu
s), p
ain,
swel
ling.
- N
on-s
urgi
cal t
reat
men
t = re
lativ
e re
st (s
top
exer
cise,
bed
rest
), w
ound
care
with
ster
ile b
anda
ges,
pres
sure
ban
dage
,
hosp
ital a
dmiss
ion
can
be co
nsid
ered
(not
app
licab
le a
t day
16)
. - H
igh
susp
icion
of i
nfec
tion
= fe
ver (
T ≥
38.5
deg
rees
Cel
sius)
+ re
d in
dura
ted
wou
nd +
pai
n.
Note
C:
- DAI
R (d
ebrid
emen
t, an
tibio
tics a
nd im
plan
t ret
entio
n) is
don
e to
clea
n th
e pr
osth
esis
and
the
wou
nd.
- The
com
pone
nts o
f DAI
R ar
e:
- W
ound
ope
ning
- 1 cu
lture
of fl
uid
deep
to th
e fa
scia
- Art
hrot
omy
and
than
≥4
deep
tiss
ue cu
lture
s (2
syno
vial
, and
≥1
arou
nd b
oth
com
pone
nts o
f the
join
t pro
sthe
sis)
- A
ntibi
otics
as s
tart
ed o
nly
after
taki
ng th
e cu
lture
s
- Mob
ile p
arts
(e.g
. tibi
al in
sert
, fem
oral
hea
d) a
re e
xcha
nged
to m
ake
room
for o
ptim
al d
ebrid
emen
t
- Ext
ensiv
e de
brid
emen
t is d
one,
i.e.
rese
ction
of h
emat
oma
and
necr
osis
and
syno
vect
omy
- T
horo
ugh
wou
nd la
vage
with
3-6
litr
es o
f sal
ine
- I
t is a
dvise
d to
use
scru
b sp
onge
s to
mec
hani
cally
clea
n al
l visi
ble
pros
thes
is pa
rts
- P
ovid
one
iodi
ne so
lutio
n of
chlo
rhex
idin
solu
tion
may
be
used
- F
ollo
w-u
p pr
oced
ure
after
DAI
R: w
ound
leak
clas
s reg
istra
tion
2-3
times
a w
eek
and
CRP
cont
rol 2
tim
es a
wee
k. C
ultu
re
re
sults
are
regi
ster
ed a
nd ti
me
to co
mpl
etel
y dr
y w
ound
. In
case
of p
ersis
tent
wou
nd le
akag
e a
seco
nd D
AIR
may
be
cons
ider
ed a
ccor
ding
to ju
dgm
ent o
f tre
ating
surg
eon.
Note
D:
- Pati
ent r
ecei
ves ‘
Patie
nt in
form
ation
LEAK
stud
y’ o
n da
y 5-
7 aft
er su
rger
y.
Note
E:
- If n
ew w
ound
leak
age
star
ts b
etw
een
day
5-7
and
9-10
afte
r sur
gery
, the
pati
ent i
s stil
l elig
ible
for r
ando
miza
tion
(at d
ay 9
-10)
. Per
form
DAI
R in
case
of h
igh
susp
icion
of i
nfec
tion
(see
Not
e B)
.
Note
F:
- If w
ound
leak
age
is ob
serv
ed o
nly
at d
ay 9
-10
after
surg
ery,
the
patie
nt is
still
elig
ible
for r
ando
miza
tion
(at d
ay 9
-10)
. - I
ncre
ase
in w
ound
leak
age
= in
crea
se o
f one
clas
s or m
ore
(see
Not
e B
for L
EAK
class
ifica
tion)
- I
ncre
ase
in C
RP =
≥ 2
5% in
crea
se co
mpa
red
with
pre
viou
s CRP
. - H
igh
susp
icion
of i
nfec
tion
= fe
ver (
T ≥
38.5
deg
rees
Cel
sius)
+ re
d in
dura
ted
wou
nd +
pai
n.
Ask
patie
nt p
erm
issio
n to
use
ano
nym
ized
data
for s
tudy
pur
pose
s and
reco
rd in
pati
ent fi
le.
- Ask
pati
ent p
erm
issio
n to
use
ano
nym
ized
data
for s
tudy
pur
pose
s and
reco
rd in
pati
ent fi
le.
- The
pati
ent i
s ran
dom
ized
at th
is m
omen
t bet
wee
n DA
IR (d
ay 9
-11
after
surg
ery)
and
conti
nued
non-
surg
ical t
reat
men
t.
ASK
PATI
ENT
PERM
ISSI
ON
ASK
PATI
ENT
PERM
ISSI
ON +
RA
NDOM
IZAT
ION
LEAK
stud
y flo
wch
art
Day
5-7
after
surg
ery,
ac
tive
patie
nt m
onito
ring
if w
ound
leak
age
is pr
esen
t
Day
9-10
afte
r sur
gery
Day
16-1
7 aft
er su
rger
y
Wou
nd le
akag
e?
Wou
nd le
akag
e?
Wou
nd le
akag
e?
Loca
l fol
low
-up
prot
ocol
+ LR
OI
1. D
AIR
(day
9-1
1 aft
er su
rger
y)
2. R
egist
er in
LEAK
stud
y da
taba
se
1. D
AIR
(day
9-1
1 aft
er su
rger
y 2.
Reg
ister
in LE
AK st
udy
data
base
1. C
ontin
ue n
on-s
urgi
cal t
reat
men
t 2.
Reg
ister
in LE
AK st
udy
data
base
1. Lo
cal f
ollo
w-u
p pr
otoc
ol +
LROI
2.
Reg
ister
in LE
AK st
udy
data
base
1. D
AIR
(day
16-
19 a
fter s
urge
ry)
2. R
egist
er in
LEAK
stud
y da
taba
se
No
Yes,
all o
ther
case
s
No
No
Yes
Yes
No
Yes a
nd h
igh
susp
icion
for
infe
ction
Yes a
nd lo
w
susp
icion
for
infe
ction
Star
t non
-sur
gica
l tre
atm
ent
ASK
PATI
ENT
PERM
ISSI
ON
ASK
PATI
ENT
PERM
ISSI
ON
ASK
PATI
ENT
PERM
ISSI
ON +
RA
NDOM
IZAT
ION
Prim
ary
TKA/
THA
Incr
ease
in
wou
nd le
akag
e AN
D In
crea
se C
RP
(com
pare
d to
day
5-7
)?
OR
High
susp
icion
of i
nfec
tion
A B B
B
B
C DA
IR
(day
5-8
afte
r sur
gery
)
C C C D
E
F
1. Lo
cal f
ollo
w-u
p pr
otoc
ol +
LROI
2.
Reg
ister
in LE
AK st
udy
data
base
51938_Claudia_Lowik.indd 149 19-08-19 11:12
Chapter 9
150
References
1. Hiligsmann M, Cooper C, Arden N, Boers M, Branco JC, Luisa Brandi M, et al. Health economics in the �eld of osteoarthritis: an expert’s consensus paper from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Semin Arthritis Rheum 2013; 43(3): 303-13.
2. LROI-rapportage. Blik op uitkomsten. Jaarrapportage uit de landelijke registratie orthopedische implantaten 2015.
3. Wolford ML, Palso K, Bercovitz A. Hospitalization for total hip replacement among inpatients aged 45 and over: United States, 2000-2010. NCHS Data Brief 2015; 186: 1-8.
4. Williams SN, Wolford ML, Bercovitz A. Hospitalization for total knee replacement among inpatients aged 45 and over: United States, 2000-2010. NCHS Data Brief 2015; 210: 1-8.
5. Kurtz SM, Lau E, Schmier J, Ong KL, Zhao K, Parvizi J. Infection burden for hip and knee arthroplasty in the United States. J Arthroplasty 2008; 23(7): 984-91.
6. Maathuis PGM, de Hartog B, Bulstra SK. Timing of open debridement for suspected infection of joint prosthesis: a report on 551 patients. Curr Orthop Pract 2009; 20(5): 541-5.
7. Weiss AP, Krackow KA. Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993; 8(3): 285-9.
8. Vanhegan IS, Malik AK, Jayakumar P, Ul Islam S, Haddad FS. A �nancial analysis of revision hip arthroplasty: the economic burden in relation to the national tari�. J Bone Joint Surg Br 2012; 94(5): 619-23.
9. Vince K, Chivas D, Droll KP. Wound complications after total knee arthroplasty. J Arthroplasty 2007; 22(4 Suppl 1): 39-44.
10. Ghanem E, Heppert V, Spangehl M, Abraham J, Azzam K, Barnes L, et al. Wound management. J Orthop Res 2014; 32(Suppl 1): S108-19.
11. Wagenaar FC, Löwik CAM, Stevens M, Bulstra SK, Pronk Y, van den Akker-Scheek I, et al. Managing persistent wound leakage after total knee and hip arthroplasty: results of a nationwide survey among Dutch orthopaedic surgeons. J Bone Joint Infect 2017; 2(4): 202-7.
12. Azzam KA, Seeley M, Ghanem E, Austin MS, Purtill JJ, Parvizi J. Irrigation and debridement in the management of prosthetic joint infection: traditional indications revisited. J Arthroplasty 2010; 25(7): 1022-7.
13. Geurts JAP, Janssen DMC, Kessels AG, Walenkamp GH. Good results in postoperative and hematogenous deep infections of 89 stable total hip and knee replacements with retention of prosthesis and local antibiotics. Acta Orthop 2013; 84(6): 509-16.
14. Kuiper JW, Vos CJ, Saouti R, Vergroesen DA, Graat HC, Debets-Ossenkopp YJ, et al. Prosthetic joint-associated infections treated with DAIR (debridement, antibiotics, irrigation, and retention): analysis of risk factors and local antibiotic carriers in 91 patients. Acta Orthop 2013; 84(4): 380-6.
15. Triantafyllopoulos GK, Poulsides LA, Zhang W, Sculco PK, Ma Y, Sculco TP. Periprosthetic knee infections treated with irrigation and debridement: outcomes and preoperative predictive factors. J Arthroplasty 2015; 30(4): 649-57.
16. Parvizi J, Gehrke T, Chen AF. Proceedings of the international consensus on periprosthetic joint infection. Bone Joint J 2013; 95-B(11): 1450-2.
17. De Groot IB, Reijman M, Terwee CB, Bierma-Zeinstra SMA, Favejee M, Roos EM, et al. Validation of the Dutch version of the hip disability and osteoarthritis outcome score. Osteoarthritis Cartilage 2007; 15(1): 104-9.
18. De Groot IB, Favejee MM, Reijman M, Verhaar JAN, Terwee CB. The Dutch version of the knee injury and osteoarthritis outcome score: a validation study. Health Qual Life Outcomes 2008; 6: 16.
19. Haverkamp D, Breugem SJ, Sierevelt IN, Blankevoort L, van Dijk CN. Translation and validation of the Dutch version of the Oxford 12-item knee questionnaire for knee arthroplasty. Acta Orthop 2005; 76(3): 347-52.
20. Gosens T, Hoefnagels NH, de Vet RC, Dhert WJ, van Langelaan EJ, Bulstra SK, et al. The “Oxford heup score”: the translation and validation of a questionnaire into Dutch to evaluate the results of total hip arthroplasty. Acta Orthop 2005; 76(2): 204-11.
51938_Claudia_Lowik.indd 150 19-08-19 11:12

Design of the LEAK study
151
9
21. Janssen MF, Pickard AS, Golicki D, Gudex C, Niewada M, Scalone L, et al. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: a multi-country study. Qual Life Res 2013; 22(7): 1717-27.
22. Versteegh MM, Vermeulen KM, Evers SMAA, de Wit GA, Prenger R, Stolk EA. Dutch tari� for the �ve-level version of EQ-5D. Value Health 2016; 19(4): 343-52.
23. Bouwmans C, Hakkaart-van Roijen M, Koopmanschap M, Krol M, Severens H, Brouwer W. Handleiding iMTA medical consumption questionnaire (iMCQ). Rotterdam: iMTA, Erasmus Universiteit, 2013. www.imta.nl.
24. Bouwmans C, Hakkaart-van Roijen M, Koopmanschap M, Krol M, Severens H, Brouwer W. Handleiding iMTA productivity cost questionnaire (iPCQ). Rotterdam: iMTA, Erasmus Universiteit, 2013. www.imta.nl.
25. Bouwmans C, Krol M, Severens H, Koopmanschap M, Brouwer W, Hakkaart-van Roijen L. The iMTA productivity cost questionnaire: a standardized instrument for measuring and valuing health-related productivity losses. Value Health 2015; 18(6): 753-8.
26. Zorginstituut Nederland. Kostenhandleiding: methodologie van kostenonderzoek en referentieprijzen voor economische evaluaties in de gezondheidszorg: geactualiseerde versie 2015.
51938_Claudia_Lowik.indd 151 19-08-19 11:12

51938_Claudia_Lowik.indd 152 19-08-19 11:12

Chapter 10
General discussion and future perspectives
51938_Claudia_Lowik.indd 153 19-08-19 11:12

51938_Claudia_Lowik.indd 154 19-08-19 11:12

General discussion and future perspectives
155
10
The studies in this thesis aimed to examine and evaluate the risk factors and treatment strategies for early prosthetic joint infection (PJI). PJI is one of the most serious complications after joint arthroplasty and can develop at any time point after surgery.1,2 Although it is important to prevent all types of PJI (early PJI, late PJI and hematogenous PJI), the studies in this thesis focused solely on patients with early PJI, as a large proportion of PJIs occur in the early post-surgical course. The �rst part of this thesis evaluated patient groups at risk for PJI, including obese patients, oncology patients and patients with prolonged wound leakage after total hip arthroplasty (THA) and total knee arthroplasty (TKA), while the second part of the thesis examined factors that can in�uence the treatment success of DAIR, including patient selection, use of local antibiotics during DAIR and the timing of DAIR. The present chapter presents a general discussion on the main �ndings of the studies in this thesis and o�ers future perspectives and implications for clinical practice.
Part 1: Evaluation of patients at risk for early PJIEven though we cannot see them, microorganisms are everywhere. They are present in the air, in water, on the surface of the skin and in about each object in an operating room. Even though many preventive measures are put in place to prevent microorganisms from in�ltrating the joint during total joint arthroplasty surgery, complete protection is an impossibility. Fortunately, the immune system provides additional protection by eradicating microorganisms that in�ltrate the joint. Prevention of PJI is therefore aimed at identifying and eliminating two types of risk factors: 1) factors that increase the risk of exposure of the joint to microorganisms, and 2) factors that limit the host’s ability to eradicate contamination of the joint with microorganisms. Literature identi�ed that an important type-1 risk factor is prolonged wound leakage with or without development of a sinus,3,4 as a leaking wound increases the risk of exposing the joint to microorganisms by providing a porte d’entrée. Hence patients at risk for prolonged wound leakage should be carefully evaluated postoperatively, to identify and treat postoperative complications at an early time point and thereby minimize the risk of PJI. Type-2 risk factors identi�ed in previous studies include obesity, diabetes mellitus, oncological conditions and rheumatoid arthritis.5,6 Knowledge about these risk factors can be used to estimate the risk of PJI before implantation of the joint arthroplasty. This risk estimation can support the decision-making process of both patient and health
51938_Claudia_Lowik.indd 155 19-08-19 11:12

Chapter 10
156
care professional on: 1) whether or not to perform joint arthroplasty surgery, and 2) whether or not to deploy additional strategies before, during and after joint arthroplasty surgery to prevent PJI. Moreover, e�orts towards optimizing these risk factors can minimize the risk of PJI, for example by performing the joint surgery when the immune system is the least compromised, by reducing weight or by improving antibiotic prophylaxis regimens. The studies in this thesis focused on three patient categories at increased risk for PJI: obese patients, oncology patients and patients with prolonged wound leakage.
Obese patientsObesity is a major health concern worldwide, with a tripled number of obese patients in recent decades.7 Although many papers have shown that obesity is a risk factor for PJI, the causes for this increased risk remain unclear. There are several factors that contribute to impaired wound healing and thus prolonged wound leakage in obese patients: 1) Obese patients have abundant subcutaneous tissue, which is relatively avascular.8,9 2) Obese patients are at increased risk of formation of pooled blood or serous �uids due to large dead space. The formation of these hematomas or seromas increase the internal pressure on the wound and sutures, which further impairs wound healing.10 3) In order to achieve proper cellular response in the wound healing process the body needs su�cient proteins, vitamins and minerals. Since obese patients su�er from a paradoxical malnutrition, resulting from a calorie-dense diet high in carbohydrates and fats and low in vitamins and minerals, they have nutritional de�ciencies that impede such cellular response.11
In addition, the results of chapter 4 showed that periprosthetic hip infections in obese patients are caused by di�erent microorganisms than in non-obese patients. Obese patients had higher rates of polymicrobial infections and more infections with Enterococcus species. Moreover, severely obese patients with hip PJI had more infections with Gram-negative rods, mainly Proteus species and Morganella morganii. These results support the hypothesis of abundant colonization with multiple microorganisms in the groin, which may be due to the large surface of skin with favorable moist conditions for microorganisms in the skin folds of obese patients. This implies that preventive measures should be adapted for obese patients receiving THA.
In future research the orthopaedic infection community should explore feasible adaptations of these preventive measures. There are several options to
51938_Claudia_Lowik.indd 156 19-08-19 11:12

General discussion and future perspectives
157
10
this end. First of all, obese patients could receive a higher dosage of cefazolin, considering the higher minimum inhibitory concentration (MIC) of cefazolin for Proteus species and the fact that currently applied cefazolin dosage may not be su�cient to achieve adequate tissue concentrations in obese patients.12-15 The newest SWAB guideline (Stichting Werkgroep Antibiotica Beleid) already advises administering 3000mg cefazolin to patients with a BMI >40kg/m2 (instead of the previous 2000mg).16-17 Our results nonetheless indicate that the higher dosage of cefazolin may also be bene�cial for patients with a BMI >35kg/m2 receiving THA, since the rate of Proteus species was signi�cantly higher in severely obese patients. It will be interesting to compare incidences of PJI before and after implementation of this new guideline, especially with regard to the number of infections caused by Proteus species.
Secondly, the type of antibiotic prophylaxis in obese patients during primary hip arthroplasty could be modi�ed to cover a broader spectrum of microorganisms - for example, by adding a glycopeptide such as vancomycin or teicoplanin to the standard antibiotic prophylaxis regimen, as these types of antibiotics cover Enterococcus species. Gram-negative microorganisms, commonly found in obese patients with hip PJI, are inherently resistant to both vancomycin and teicoplanin. Substituting cefazolin with cefuroxime would be more e�ective in providing full coverage for Gram-negative microorganisms, but unfortunately cefuroxime does not cover Enterococcus species. Combining a glycopeptide with cefazolin would be the preferred option, especially when the cefazolin dosage is adjusted to the BMI. Although this raises the concern of developing antibiotic resistance, it may be a minor concern since antibiotic prophylaxis is only administered for a limited, maximum period of 24 hours. While some studies already compared the e�cacy of various antibiotic prophylaxis regimens in reducing infection rates after joint arthroplasty,18-20 only one considered BMI in their results. Tornero et al. showed a reduction of PJI rates in obese patients receiving cefuroxime plus teicoplanin compared with cefuroxime only.21 This reduction was mainly observed for PJI due to Staphylococcus aureus, which supports the hypothesis that the dosage of antimicrobial prophylaxis may be insu�cient for obese patients, as Staphylococcus aureus should be fully covered by cefuroxime.
Thirdly, disinfection of the hip region could be performed more thoroughly in patients who will receive THA. Chlorhexidine-alcohol 2% should be applied as disinfectant, as it is proven to be more e�ective than povidone-iodine in
51938_Claudia_Lowik.indd 157 19-08-19 11:12

Chapter 10
158
reducing postoperative infections.22 Currently there are no studies comparing the e�cacy of chlorhexidine-alcohol with povidone tincture in 75% alcohol though. Moreover, obese patients could be treated with mupirocin nasal cream preoperatively and be required to take chlorhexidine gluconate showers for �ve days before index surgery in order to decolonize the skin.23 Although this is only proven to e�ectively reduce infections caused by Staphylococcus aureus (which is not the main cause of the higher number of PJIs in obese patients), a substantial number of infections could be prevented by standard application of this regimen in obese patients.
Lastly, since surgical wounds in obese patients are prone to prolonged wound leakage, it is essential that obese patients be evaluated more extensively after joint arthroplasty, especially after THA. Although follow-up after joint arthroplasty di�ers per hospital, as shown by the survey on wound leakage among Dutch orthopaedic surgeons, obese patients (especially with BMI >35kg/m2) should be re-evaluated at the outpatient clinic one week after index surgery. In this way wound complications can be detected at an early time point and treated adequately.
Oncology patientsPatients with bone tumors requiring joint arthroplasty after resection of tumor tissue are at increased risk for developing PJI. The prevalence of oncologic PJI is 7% to 28%24-26 compared with approximately 1% for regular PJI.27 Multiple factors cause this increased risk, such as immunode�ciency due to radiotherapy or chemotherapy, longer duration of surgery, larger wounds and use of larger implants due to extensive tumor resection.28 Unfortunately, little is known speci�cally about oncologic PJI, which is shown in the literature review presented in this thesis. Most guidelines for oncologic PJI are therefore derived from research on patients with regular PJI. Although this may work for some aspects of PJI, such as diagnostic criteria, several topics need research speci�cally conducted on patients with oncologic PJI.
First of all, administration of adequate antibiotic prophylaxis is important to reduce the risk of PJI in oncology patients. In regular total joint arthroplasty, there is consensus that antibiotic prophylaxis should not be administered for longer than 24 hours after index arthroplasty.29 There is no consensus on antibiotic prophylaxis in oncology patients though. Since oncology patients represent a heterogenous population, it is di�cult to compare studies on
51938_Claudia_Lowik.indd 158 19-08-19 11:12

General discussion and future perspectives
159
10
this topic. A systematic review by Racano et al. suggests that administering antibiotic prophylaxis longer than 24 hours is bene�cial for oncology patients.30 A multicenter randomized controlled trial called the PARITY trial (Prophylactic Antibiotic Regimens In Tumor surgerY) is currently being conducted to compare the e�cacy of 24 hours with 5 days of antibiotic prophylaxis.31 These results may lead to the composition of an evidence-based guideline for antibiotic prophylaxis in oncology patients.
Secondly, the application of coated arthroplasties can have positive e�ects on the reduction of oncologic PJI. One of the most reported types of coated arthroplasties is silver-coated arthroplasty. Because of its e�ective local antimicrobial activity and relatively low toxicity, the silver coating seems a viable option for oncology patients.32,33 Only few patients reported local side e�ects of the silver, such as dermal argyria.34 Other coating options include the use of iodine-coated arthroplasty, which showed potential in a study by Tsuchiya et al.35 This type of coating should be examined more thoroughly before it is standardly applied in clinical practice.
Thirdly, the timing of chemotherapy and radiotherapy can in�uence the risk of PJI. Although radiotherapy is not routinely applied in the treatment of bone tumors, it may be used preoperatively for radiosensitive tumors (such as Ewing’s sarcoma)36 or postoperatively in case of inadequate surgical margins, poor response to chemotherapy or local recurrence.37 Infection rates are 23% in patients who received radiotherapy before index arthroplasty and 35% when radiotherapy was started after index arthroplasty.26 This is because radiotherapy impairs wound healing by damaging �broblasts, which leads to necrosis, slow growth of skin cells and thereby reduced strength of the wound.38,39 Neo-adjuvant chemotherapy is often applied in bone tumors. A review on the e�ects of neo-adjuvant chemotherapy showed that immunode�ciency after chemotherapy is associated with an increased risk of PJI,28 although others did not �nd any e�ect of chemotherapy on infection rate.40 While radiotherapy and chemotherapy likely in�uence the risk of PJI in oncology patients, there is no established optimal timing for oncologic tumor resection. This should be examined in future studies.
Patients with prolonged wound leakageProlonged wound leakage is a di�cult problem since wound leakage can be a symptom of an already existing PJI or a risk factor for developing PJI (by
51938_Claudia_Lowik.indd 159 19-08-19 11:12

Chapter 10
160
providing a porte d’entrée for microorganisms4). Surgical wounds may also show prolonged leakage for reasons other than infection (such as hematoma, seroma or fatty necrosis) and take longer to heal without developing an infection, especially in certain patient categories such as obese patients or patients on anticoagulant medication. If prolonged wound leakage is caused by an infection, surgical treatment is preferred and typically consists of DAIR.41-
43 If prolonged wound leakage is caused by factors other than infection, non-surgical treatment is preferred, aiming to prevent the development of a PJI. Non-surgical treatment consists of relative rest (bed rest and no exercise), pressure bandages and wound care with sterile bandages.42,44 Unfortunately, distinguishing between these types of wound leakage is often challenging, which hinders adequate treatment and optimal timing of treatment of prolonged wound leakage.
Remarkably, literature on this topic is scarce; this is clearly shown by the literature review in this thesis. Because of this lack of scienti�c evidence, there are no national or international evidence-based guidelines. Most current guidelines are based on consensus, in particular the international consensus meetings on prosthetic joint infections in 2013 and recently in July 2018 in Philadelphia.29,42,45 Moreover, many orthopaedic surgeons base their decision on the treatment of prolonged wound leakage solely on their own past experiences. This is clearly demonstrated in the results of the survey among Dutch orthopaedic surgeons on current clinical practice for prolonged wound leakage, indicating wide variation in all aspects of its diagnosis and treatment.
Interestingly, only half of the hospitals had a protocol for prolonged wound leakage and only 26% used this protocol regularly. This reveals the di�culty of composing a protocol due to the lack of scienti�c evidence. It also indicates that prolonged wound leakage is a complex problem for which orthopaedic surgeons feel it is necessary to evaluate each patient individually to decide on the best treatment. Although an individual approach can be bene�cial for patients, it also has disadvantages. If a patient has prolonged wound leakage, the timing of surgical treatment is usually considered for several days; in other words, it may take several days before the medical practitioner decides whether it is necessary to perform a DAIR. This results in uncertainty and concern for the patient, who may be fearful of a second surgical procedure and worry about potentially more extensive surgeries such as revisions. Standardized use of a protocol in hospitals reduces uncertainties for patients, since they know that
51938_Claudia_Lowik.indd 160 19-08-19 11:12

General discussion and future perspectives
161
10
surgical treatment will be performed when wound leakage persists beyond a certain time point.
Composing a protocol for prolonged wound leakage not only bene�ts patients, it also provides advantages for medical practitioners. The current lack of evidence-based guidelines and the large variety in current clinical practice stresses the need for high-quality evidence on this topic. The results of the LEAK study can provide such high-quality evidence, which will help medical practitioners in the clinical decision-making process. Besides the main aim of the LEAK study to evaluate the timing of DAIR in patients with prolonged wound leakage, there are several other topics of interest. By collecting data on C-reactive protein (CRP) values at several time points after index arthroplasty, the LEAK study can assess the possibility of estimating risk of infection in patients with prolonged wound leakage based on the postoperative trend of the CRP values. Moreover, data on the clinical aspect of the surgical wound at various time points after index arthroplasty are collected, which may indicate that, for example, patients with hematoma experience prolonged wound leakage more often without developing an infection. Patient-related factors such as BMI, comorbidities and medication are also collected, with the ultimate goal to estimate risk of infection for various clinical pro�les according to number of days and classi�cation of wound leakage. To illustrate: a patient with obesity and steroid therapy with wound leakage class 2 at day 9 has a 43% estimated risk of infection. Drafting such a prediction model will greatly support the clinical decision-making process.
As there is still no optimal tool to diagnose PJI without performing surgery, and certainly not for patients with prolonged wound leakage, it would be interesting to test the accuracy of various synovial biomarkers for diagnosing PJI in these patients. Two promising biomarkers are alpha-defensin and leukocyte esterase, with sensitivity and speci�city reaching nearly 100% for alpha-defensin, and 81% sensitivity and 97% speci�city for leukocyte esterase.46 Advantage of leukocyte esterase is that it is a point-of-care test that can be used as a bedside marker, while alpha defensin is tested by immunoassay, whose results take longer to obtain. Moreover, the alpha-defensin test is very expensive. A cheaper biomarker would be calprotectin, which showed high accuracy in a recent study by Wouthuyzen-Bakker et al.47 It is already used routinely as a fecal marker in patients with in�ammatory bowel disease and is currently available as a point-of-care test. However, neither biomarker has
51938_Claudia_Lowik.indd 161 19-08-19 11:12

Chapter 10
162
yet been tested to diagnose PJI in patients with prolonged wound leakage. Another option would be to culture synovial �uid. Its main bene�t is that the causative microorganisms can be identi�ed before DAIR, so that adequate antibiotic treatment can be started immediately after obtaining intraoperative cultures. A downside is that there is little time to wait for positive cultures in patients with prolonged wound leakage. Medical practitioners will only wait a few days before proceeding to DAIR, at which point it will only culture virulent microorganisms. Hence synovial �uid culture cannot be used to rule out PJI in patients with wound leakage, as it would be necessary to wait two weeks before culture results are de�nitively negative. Synovial �uid culture can however still be used to rule in PJI, as the speci�city of 95% is indicative of a few false-positive cultures.48 It would be an option to test samples of wound exudate, since these are available at any time in patients with wound leakage and can be obtained non-invasively. Cultures of super�cial exudate samples have proven to be inadequate though.49 This is why new biomarkers should be developed and examined for this new method of diagnosing PJI in patients with prolonged wound leakage. Currently, bacterial toxins seem a viable option, although the accuracy of these toxins should be studied more extensively.50
Part 2: Improving treatment strategies for early PJIAlthough the main objective should be to prevent PJI, once PJI develops it should be e�ectively treated. The ideal treatment consists of selecting the right treatment modality for the speci�c patient and optimally administering it. There are several options to treat early PJI. While two-stage revision arthroplasty provides the highest cure rates (ranging from 85% to 100%),51,52 it is accompanied with high morbidity and mortality as well as high health care costs. DAIR can treat PJI without the need for removal of the prosthesis, but has an evidently lower cure rate than two-stage revision (ranging from 40% to 90%).53-56 Although it is useful to try to cure PJI with less invasive surgery (DAIR) before proceeding to revision surgery, there are some downsides. First of all, it is not yet clear whether performing a DAIR prior to revision surgery decreases the cure rate of revision surgery.57-60 Moreover, if the infection is not cured by DAIR patients are subjected to additional surgical procedures before the implant is removed and infection is treated. Still, there are many bene�ts of DAIR over revision surgery, such as faster postoperative rehabilitation, preservation of bone stock, decreased risk of intraoperative fractures and shorter duration of
51938_Claudia_Lowik.indd 162 19-08-19 11:12

General discussion and future perspectives
163
10
the surgical procedure.61,62 These bene�ts outweigh the downsides of DAIR, but do stress the importance of proper patient selection and excellent performance in order to optimize DAIR cure rates.
Selecting patients for DAIRTo explain the large variation in success rates of DAIR, previous studies identi�ed several patient-related, surgical and microbiological risk factors for DAIR failure. For patient-related risk factors, they found that a high ASA score,63,64 arthroplasty indicated for fracture,65 longer duration of symptoms,64,66-73 and high serological in�ammatory markers are related to an increased risk of DAIR failure.67,69,74-76 Moreover, surgical risk factors such as arthroscopic debridements,77-79 purulent discharge at the site of the implant,63 and DAIRs without exchange of modular components also increase the risk of DAIR failure,61,74 just as culturing Staphylococcus aureus as causative microorganism.63,66,77,80,81
Although all these factors are known to contribute to an increased risk of DAIR failure, so far there is no practical tool available that can estimate this risk for each speci�c patient, which could help orthopaedic surgeons in their decision-making process. A tool for predicting DAIR failure should meet two conditions: it should be available preoperatively and be easy to use, to facilitate its implementation in daily clinical practice. Tornero et al. designed a predictive tool that meets both conditions: the KLIC score, which consists of �ve preoperative patient-related risk factors: 1) chronic renal failure (Kidney), 2) Liver cirrhosis, 3) Index surgery, 4) Cemented prosthesis and 5) CRP >115 mg/L (KLIC).82 Our results showed that the KLIC score can signi�cantly predict DAIR failure, where a higher KLIC score corresponds with a higher failure rate. Despite the signi�cant predictive value of this risk score, our study showed a much lower accuracy than Tornero et al.; this could be ascribed to di�erences in local epidemiology, patient characteristics and surgical techniques. For example, orthopaedic surgeons in our cohort performed exchange of modular components in only 21% of patients, while Tornero et al. did in 72.9%. Remarkably, the exchange of modular components was not associated with DAIR failure in this study, while previous literature clearly identi�es it as a risk factor.61,74 It is nonetheless advisable to exchange all modular components during a DAIR procedure for three reasons: �rstly, it is important to create free space for optimal debridement (without removal of modular components the deeper compartments of the joint cannot be irrigated and debrided
51938_Claudia_Lowik.indd 163 19-08-19 11:12

Chapter 10
164
thoroughly); secondly, any microorganisms and bio�lm present on the modular components should be removed and clean components reinserted; �nally, removed modular components can be used to diagnose PJI when sent for sonication.
The lower accuracy in our cohort indicates that medical practitioners should be cautious when implementing this risk score routinely in daily clinical practice. Nevertheless, our study did show that the score is useful in patients with low (<3.5 points) or high (>6 points) KLIC scores. In patients with low KLIC scores medical practitioners should always perform a DAIR procedure before turning to other, more invasive surgical treatment modalities. However, in patients with high KLIC scores and therefore a high estimated risk of DAIR failure of 60% to 90% an orthopaedic surgeon may consider a di�erent treatment approach with a higher chance of infection control. The downside of choosing a di�erent treatment approach in patients with a high KLIC score is withholding a less invasive surgical treatment from patients while there is a chance that they may bene�t from this milder treatment. Moreover, medical practitioners should consider the great impact of revision surgery on patients’ quality of life when choosing to perform extensive revision surgery without trying to cure the infection with DAIR. Due to the relatively low accuracy of the KLIC score in our cohort, medical practitioners should not base this decision solely on the KLIC score but should consider the treatment options per individual patient. Currently the preferred strategy is that all patients can undergo the DAIR procedure to try and cure the infection, but in patients with high KLIC scores other treatment options or postoperative suppressive antibiotic treatment should be considered to optimize the chances of infection control.
Future research should aim to develop a preoperative risk score for DAIR failure with a higher accuracy than the KLIC score. In our cohort we found it important for the CRP value and arthroplasty indicated for fracture to be included in the risk score. Other variables such as age, exchange of modular components and number of days from arthroplasty to DAIR could also be included. The CRIME80 score is currently used to predict DAIR failure in patients with hematogenous PJI.83 It consists of seven variables, each with appointed scores, where a higher CRIME80 score is associated with a higher risk of DAIR failure: COPD (2 points), CRP >150mg/l (1 point), rheumatoid arthritis (3 points), arthroplasty indicated for fracture (3 points), male (1 point), exchange of modular components (-1 point), age >80 years (2 points).83 Although it is
51938_Claudia_Lowik.indd 164 19-08-19 11:12

General discussion and future perspectives
165
10
preferable to use the same risk score for DAIR failure in both early PJI and late acute PJI, the score remains to be validated for patients with early PJI.
Use of gentamicin beads and spongesImproving outcome after DAIR by administering local antibiotics is a longstanding strategy in Dutch hospitals, yet the bene�cial e�ect of these antibiotics has never been demonstrated and its use remained con�ned to the Netherlands. In theory, achieving high concentrations of antibiotics at the site of infection and providing dead space management should help cure PJI. Because of the local e�ect of the gentamicin-impregnated beads and sponges in the joint cavity, systemic toxic side e�ects are uncommon,84,85 although Swieringa et al. have reported a decrease in renal function after application of gentamicin-impregnated sponges.86
The application of gentamicin-impregnated beads and sponges does not seem to in�uence clinical outcome though. One study by Kuiper et al. demonstrated that applying gentamicin-impregnated sponges is associated with a lower failure rate of DAIR while using gentamicin beads showed higher failure rates, although these di�erences were not observed in the multivariate analysis.69 Two di�erent studies did not show any bene�cial e�ect of gentamicin beads,87,88 while other studies only described the outcome of routinely using gentamicin beads, without comparing with controls.89-92 Chapter 6 of this thesis showed higher failure rates after DAIR in the gentamicin group, even after propensity score matching for confounding factors. Moreover, patients on whom gentamicin-impregnated beads or sponges were used needed implant removal twice as often than control patients (5.2% vs 2.6%). Although these results were not statistically signi�cant, they clearly demonstrate that applying gentamicin-impregnated beads or sponges does not improve the outcome after DAIR and may even have adverse e�ects. Accordingly, its use for this indication should be discontinued.
A reason for the lack of e�cacy of local gentamicin may be its reduced activity in the joint cavity in patients with PJI, due to a low pH and low oxygen level caused by the presence of a bio�lm.93 Moreover, local gentamicin levels may be below the MIC levels, reducing their e�cacy. Even though both gentamicin beads and sponges can get gentamicin levels far above the MIC levels in the joint cavity, the release of gentamicin is maximal in the �rst few days after insertion and decreases afterwards.94-96 For instance: gentamicin sponges
51938_Claudia_Lowik.indd 165 19-08-19 11:12

Chapter 10
166
release up to 95% of their antibiotics in the �rst two hours after insertion.97 After releasing gentamicin, the beads and sponges lose their purpose and can be perceived as a foreign body. Indeed, Neut et al. demonstrated bacterial growth on the majority of removed gentamicin-impregnated beads, which suggests that these beads may preserve the infection rather than cure it.90
Future studies should assess whether applying local antibiotics can be useful when using other types of antibiotics and antibiotic carriers. Vancomycin could be an alternative to gentamicin, as the e�cacy of vancomycin does not decrease when used in an environment with low pH and low oxygen levels, which is usually the case in PJI. Vancomycin can be administered as a powder, so it does not necessitate a second DAIR procedure to remove an antibiotic carrier and does not become a foreign body. Recent studies showed good results with use of vancomycin powder during DAIR procedures.98,99 A large systematic review on vancomycin powder in 6701 cases of spinal surgery showed nephrotoxicity in one case and ototoxicity in one case.101 A di�erent study showed a higher rate of wound complications when vancomycin powder was administered during total hip arthroplasty.102 Future studies are warranted before vancomycin powder is applied standardly, but its application is encouraged for patients at a high risk of DAIR failure, estimated by calculating the KLIC score or CRIME80 score.83
Optimal timing of DAIRAlthough there are no absolute contraindications to perform a DAIR procedure in patients with early PJI, DAIR is only advised when the risk of failure is acceptable. The risk of failure depends on multiple host- and implant-related factors, as described above. Most of the guidelines applied to decide whether it is viable to perform a DAIR procedure are based on duration of symptoms and time interval from index arthroplasty to DAIR. Most authors suggest that DAIR should be performed within a few days of the onset of symptoms in order to achieve infection control.64,67,73 Moreover, current guidelines suggest that DAIR should not be performed when PJI develops more than 30 days after index arthroplasty.100
Using a guideline solely based on number of days from index arthroplasty to DAIR has advantages. Whereas the duration of symptoms is usually subjective, the number of days from index arthroplasty is objective. Besides, the precise onset of symptoms can be di�cult to establish, as it is confounded
51938_Claudia_Lowik.indd 166 19-08-19 11:12

General discussion and future perspectives
167
10
by the physiological healing process, for example in case of pain or wound leakage in the early post-surgical course. The study in this thesis showed that the time interval from index arthroplasty to DAIR is not a reliable predictor for treatment success of DAIR in early PJI. Although treatment failure was highest when performing DAIR in the late post-surgical course (7-12 weeks), DAIR was successful in approximately 60% of these patients. This still makes it a viable treatment option when performed more than 30 days after index arthroplasty, in contrast to previously published guidelines.100
The increase in failure rates when DAIR was performed more than six weeks after index arthroplasty is supported by previous studies evaluating the time to develop a mature bio�lm. These studies showed that a bio�lm is already evident within two weeks of inoculation with microorganisms.103-105 In the complex process of bio�lm formation, embedded microorganisms become unresponsive to almost any antibiotic treatment because of multiple phenotypic and genotypic changes.106,107 Within six weeks a mature bio�lm has developed, at which time point PJI can no longer be cured with antibiotics only, without removal of the implant. The results in this thesis illustrate that the development of a bio�lm is a variable process that depends not only on time but also on the causative microorganism, the size of inoculum that contaminated the wound during surgery, and the host.108,109
Future studies should aim to compose a predictive model for the time needed to form a mature bio�lm. Since this depends on multiple variables, in vitro studies are probably needed �rst, adding variables one at a time. For example, time until formation of a mature bio�lm should be evaluated for di�erent microorganisms. Next, time until formation of a mature bio�lm should be examined for di�erent inoculum sizes in each individual type of microorganism. This should be followed by in vivo studies, where time until formation of a mature bio�lm should be examined per site of infection, as this may vary per type of joint. Complementarily, di�erences in host-related factors should be tested, such as various concentrations of white blood cells at the site of infection. Unfortunately, even if such a prediction model could be composed, not all these variables can be determined in patients with PJI, like the inoculum size that contaminated the wound during surgery. Another useful option when evaluating time from index arthroplasty to formation of a mature bio�lm is the use of �uorescent biomarkers which can visualize the progress of bio�lm formation in the joint. Current studies have used genetically encoded
51938_Claudia_Lowik.indd 167 19-08-19 11:12

Chapter 10
168
�uorescent proteins to identify the stage of bio�lm formation.110 So far these techniques have only been studies in vitro, so there is no solution yet that can be applied in the clinical situation of PJI. Future studies should aim to investigate the applicability of the real-time administration of �uorescent proteins, so that the presence and stage of a bio�lm can be observed intraoperatively using a �uorescence scope. Until more is known about time to formation of a mature bio�lm, DAIR should be considered a viable treatment option in patients with PJI presenting within 90 days of index arthroplasty.
Barriers and facilitators in the LEAK studyUnfortunately, the results of the LEAK study cannot be presented in this thesis, as inclusion is behind schedule. Although a large group of 38 Dutch hospitals are participating in this multicenter randomized controlled trial, it was not yet possible to include the necessary number of 388 patients. There are several reasons for this. Firstly, due to lengthy procedures for assessing local feasibility in the participating hospitals (which take on average 150 days), a large number of hospitals started at a later time point than the initially estimated date of 1 February 2017. For future multicenter clinical trials, national authorities should ensure prevention of unnecessary additional procedures, especially since conducting a second medical ethical examination is against national regulations. For that reason, ethical approval of the coordinating center should be considered su�cient to approve local feasibility, which is not yet the case at the moment. This issue unnecessarily hampers clinical studies and should be given high priority on the national research agenda.
Secondly, it appears that orthopaedic surgeons are hesitant to randomize patients, as they are used to their own treatment methods and believe that either surgical or non-surgical treatment is better for a particular patient, even though there is no evidence to support that statement. This viewpoint is especially interesting, since the orthopaedic community itself has stated that the topic of prolonged wound leakage constitutes an important knowledge gap. Surgeons are hesitant to perform a DAIR procedure in patients with a low risk of PJI, given the uncertainty as to whether the joint is infected. If there is no current infection, the DAIR would be performed too soon and unnecessarily, and this second intervention would be adding a risk of introducing infection. Still, ongoing wound leakage is a risk factor for developing an infection by providing a porte d’entrée for microorganisms,4 so postponing DAIR may also
51938_Claudia_Lowik.indd 168 19-08-19 11:12

General discussion and future perspectives
169
10
lead to an increased risk of PJI. Unfortunately, the optimal timing of DAIR remains to be established, although the LEAK study can improve insights on this important topic. A solution o�ered for the hesitance toward randomization is assessment of the patient by an independent surgeon (i.e. a colleague). Moreover, in each regional training group of orthopaedics (ROGO) an ambassador is available for consultation about patient eligibility. And yet the optimal solution is actually quite simple: each patient with prolonged wound leakage should be randomized, so that the type of treatment is automatically chosen by randomization.
Thirdly, identi�cation of eligible patients for randomization is di�cult in hospitals where patients are discharged one to three days after index surgery. These patients are usually checked at the outpatient clinic at 14 days, 6 weeks or 3 months, which is too late for randomization. Even though the participating hospitals give these patients clear instructions to contact the hospital if wound leakage persists for longer than 5 to 7 days, most patients fail to do so, or do it too late (e.g. after 14 days). An innovative app will be introduced soon that can improve identi�cation of these patients: the Wound care app is an application on mobile phone or tablet in which patients state the amount of wound leakage and signs of infection daily for the �rst 30 days after total joint arthroplasty. Based on an algorithm, patients receive a pop-up message to contact the hospital in case of an increased risk of infection or wound leakage lasting longer than 5 to 7 days. This will hopefully help identify patients earlier. In a pilot study recently conducted at Leiden University Medical Center and Alrijne Hospital by H. Schepers, the Wound care app showed good feasibility and patients reported that the app was easy to use. The Wound care app is currently being used in several hospitals participating in the LEAK study.
Finally, orthopaedic surgeons are worried about receiving negative reviews on inspection by insurance companies, because of having performed more DAIR procedures in the context of the LEAK study. All orthopaedic arthroplasties are registered in the Dutch Arthroplasty Register (LROI). When revision surgery is needed, this is also registered in the LROI, including the reason for revision (such as infection or aseptic loosening). When exchange of modular components is performed during a DAIR procedure, this is registered as revision surgery due to infection. Hence performing a high number of DAIRs with exchange of modular components can be incorrectly interpreted by insurance companies as performing a high number of revisions because of
51938_Claudia_Lowik.indd 169 19-08-19 11:12
Chapter 10
170
infection. The Netherlands Orthopaedic Association (NOV) sent a letter to the major insurance companies to clarify these concerns, so participating hospitals do not need to worry about this issue anymore. It may nonetheless be a good thing to modify the registration in the LROI so that DAIRs can be registered as such, especially since performing a higher number of DAIRs could be perceived as bene�cial as they can prevent the need for more extensive revision surgery in case of infection.
Future perspectives
Unfortunately, there are only a limited number of topics that can be explored in the scope of a thesis. Many other interesting topics remain unsolved and should be examined in the future. Additional questions and hypotheses arose while investigating the topics described in this thesis. Some of the most interesting subjects to investigate in the future are described below.
Is it useful to perform a second DAIR if infectious signs persist after the �rst DAIR?The topic of performing multiple DAIRs has not been studied extensively, as most studies regard the need for further surgical procedures as DAIR failure. Studies that did assess this topic displayed di�erent results. While Moojen et al. report similar results for single and multiple DAIRs,111,112 and Mont et al. describe good results for second and third DAIRs,113 others describe higher failure rates for second DAIR.76,81 Analyses of our cohort of 386 patients showed comparable failure rates for the �rst and second DAIR (unpublished data). Failure rates of a third DAIR were also assessed, but this group was too small to draw reliable conclusions. It would be interesting to compare the results of a protocol in which patients with failed DAIRs are treated with revision surgery to a protocol in which patients with failed DAIRs are treated with a second and, if necessary, a third DAIR.
Is it useful to irrigate the joint with povidone-iodine or chlorhexidine-alcohol during DAIR? Currently, most medical practitioners irrigate the joint with saline pulse lavage during DAIR. It is postulated that povidone-iodine and chlorhexidine-alcohol
51938_Claudia_Lowik.indd 170 19-08-19 11:12

General discussion and future perspectives
171
10
are more e�ective in treating the infection. Both agents are frequently used to prevent PJI,22,114 but not yet very often in its treatment. A recent study showed good results of using povidone-iodine lavage during DAIR.115 Also, chlorhexidine-alcohol lavage showed promising results in an in vitro study,116 but future studies are warranted before these solutions can be implemented in daily clinical practice - especially since local e�ects on soft tissue and systemic e�ects from intra-articular appliance are unknown. It would be interesting to compare the e�cacy of povidone-iodine, chlorhexidine-alcohol and saline in a randomized controlled trial.
How many dosages of prophylactic antibiotics should be administered to adequately prevent PJI?In the prevention of PJI it may be equally e�ective to give one dosage of antibiotic prophylaxis instead of three dosages. A systematic review including four randomized controlled trials could not �nd any evidence that three dosages are more e�ective than one.117 Unfortunately, the quality of evidence of these trials was very low according to the GRADE criteria. Additional trials are therefore warranted.
Which method of wound closure best prevents wound leakage and PJI? For deep closure, a biomechanical study showed that microorganisms adhere less to barbed sutures than to conventional braided sutures (such as Vicryl).118 Moreover, barbed sutures allow for faster closure.119 For super�cial closure, several studies found no di�erences in number of patients with wound leakage and super�cial wound infections between staples, sutures and adhesives.120-122 A recent study by Roerdink et al. shows that adding a subcuticular layer of continuous sutures reduces the incidence of prolonged wound leakage from 11.7% to 1.9%. The incidence of PJI decreased from 1.5% to 0.4%.123 However, super�cial and deep closure techniques combined have not been studied yet, nor have the e�ect of using vacuum dressings in the early post-surgical course and the technique of wound closure to prevent PJI.
Should tranexamic acid be standardly applied to patients who receive joint arthroplasty in order to prevent prolonged wound leakage and PJI? Tranexamic acid is an anti�brinolytic agent that reduces blood loss during and after joint arthroplasty. It is proven to be safe and can e�ectively reduce
51938_Claudia_Lowik.indd 171 19-08-19 11:12

Chapter 10
172
the need for blood transfusions.124 Reducing blood loss should hypothetically result in less hematoma formation, which reduces the risk of PJI,125 but the e�ect of tranexamic acid on wound leakage and PJI has not yet been studied.
Conclusion
Although some research questions regarding risk factors and treatment strategies in early PJI were answered in this thesis, an important one remains unsolved: the optimal treatment of prolonged wound leakage after TKA/THA. Even though the results of the LEAK study are not available yet, we believe that these can provide important insights toward future treatment protocols for prolonged wound leakage. Coordinating the LEAK study has evidenced the challenge of performing large-scale randomized controlled trials. With the development of collaboration in CORE this may become easier in the future.
In terms of the risk factors for PJI, the studies in this thesis described that obese patients, oncology patients and patients with wound leakage are at an increased risk of developing PJI, drawing the following conclusions: 1) Antibiotic prophylaxis regimens should be adapted to reduce this risk of periprosthetic hip infections in obese patients. 2) Many aspects of the topic of oncologic PJI require additional research. Regarding the treatment of PJI, the following conclusions can be drawn based on this thesis: 1) The KLIC score can be used to estimate the risk of treatment failure after DAIR, although a risk score with a higher accuracy should be developed. 2) Application of gentamicin-impregnated beads and sponges should be discontinued in patients with early PJI undergoing a DAIR procedure. 3) DAIR is still a viable treatment option when patients with PJI present more than four weeks after index arthroplasty.
51938_Claudia_Lowik.indd 172 19-08-19 11:12

General discussion and future perspectives
173
10
References
1. Tsukayama DT, Estrada R, Gustilo RB. Infection after total hip arthroplasty: a study of the treatment of one hundred and six infections. J Bone Joint Surg Am 1996; 78(4): 512-23.
2. McPherson EJ, Woodson C, Holtom P, Roidis N, Shufelt C, Patzakis M. Periprosthetic total hip infection: outcomes using a staging system. Clin Orthop Relat Res 2002; 403: 8-15.
3. Surin VV, Sundholm K, Bäckman L. Infection after total hip replacement: with special reference to a discharge from the wound. J Bone Joint Surg Br 1983; 65(4): 412-8.
4. Weiss AP, Krackow KA. Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993; 8(3): 285-9.
5. Chen J, Cui Y, Li X, Miao X, Wen Z, Xue Y, et al. Risk factors for deep infection after total knee arthroplasty: a meta-analysis. Arch Orthop Trauma Surg 2013; 133(5): 675-87.
6. Eka A, Chen AF. Patient-related medical risk factors for periprosthetic joint infection of the hip and knee. Ann Transl Med 2015; 3(16): 233.
7. World Health Organization. Obesity and overweight. Report 2018. www.who.int.8. Patel VP, Walsh M, Sehgal B, Preston C, DeWal H, Di Cesare PE. Factors associated with prolonged
wound drainage after primary total hip and knee arthroplasty. J Bone Joint Surg Am 2007; 89(1): 33-8.9. Wilson JA, Clark JJ. Obesity: impediment to postsurgical wound healing. Adv Skin Wound Care
2004; 17(8): 426-35.10. Armstrong M. Obesity as an intrinsic factor a�ecting wound healing. J Wound Care 1998; 7(5): 220-1.11. Xanthakos SA. Nutritional de�ciencies in obesity and after bariatric surgery. Pediatr Clin North Am
2009; 56(5): 1105-21.12. European committee on antimicrobial susceptibility testing. Data from the EUCAST MIC distribution
website. www.eucast.org.13. Grupper M, Kuti JL, Swank ML, Maggio L, Hughes BL, Nicolau DP. Population pharmacokinetics of
cefazolin in serum and adipose tissue from overweight and obese women undergoing cesarean delivery. J Clin Pharmacol 2017; 57(6): 712-9.
14. Rondon AJ, Kheir MM, Tan TL, Shohat N, Greenky MR, Parvizi J. Cefazolin prophylaxis for total joint arthroplasty: obese patients are frequently underdosed and at increased risk for periprosthetic joint infection. J Arthroplasty 2018; 33(11): 3551-4.
15. Kram JJF, Greer DM, Cabrera O, Bulage R, Forgie MM, Siddiqui DS. Does current cefazolin dosing achieve adequate tissue and blood concentrations in obese women undergoing cesarean section? Eur J Obstet Gynecol Biol 2017; 210: 334-41.
16. Bauer M, van de Garde E, van Kasteren M, Prins J, Vos M. SWAB richtlijn: perioperatieve profylaxe. www.swab.nl.
17. Brill MJ, Houwink AP, Schmidt S, van Dongen EP, Hazebroek EJ, van Ramshorst B, et al. Reduced subcutaneous tissue distribution of cefazolin in morbidly obese versus non-obese patients determined using clinical microdialysis. J Antimicrob Chemother 2014; 69(3): 715-23.
18. Liu C, Kakis A, Nicols A, Ries MD, Vail TP, Bozic KJ. Targeted use of vancomycin as perioperative prophylaxis reduces periprosthetic joint infection in revision TKA. Clin Orthop Relat Res 2014; 472(1): 227-31.
19. Sewick A, Makani A, Wu C, O’Donnell J, Baldwin KD, Lee GC. Does dual antibiotic prophylaxis better prevent surgical site infections in total joint arthroplasty? Clin Orthop Relat Res 2012; 470(10): 2702-7.
20. Soriano A, Popescu D, García-Ramiro S, Bori G, Martínez-Pastor JA, Balasso V, et al. Usefulness of teicoplanin for preventing methicillin-resistant Staphylococcus aureus infections in orthopedic surgery. Eur J Clin Microbiol Infect Dis 2006; 25(1): 35-8.
21. Tornero E, Garcí-Ramiro S, Martínez-Pastor JC, Bori G, Bosch J, Morata L, et al. Prophylaxis with teicoplanin and cefuroxime reduces the rate of prosthetic joint infection after primary arthroplasty. Antimicrob Agents Chemother 2015; 59(2): 831-7.
22. Darouiche RO, Wall MJ Jr, Itani KM, Otterson MF, Webb AL, Carrick MM, et al. Chlorhexidine-alcohol versus povidone-iodine for surgical-site antisepsis. N Engl J Med 2010; 362(1): 18-26.
51938_Claudia_Lowik.indd 173 19-08-19 11:12

Chapter 10
174
23. Sporer SM, Rogers T, Abella L. Methicillin-resistant and methicillin-sensitive Staphylococcus aureus screening and decolonization to reduce surgical site infection in elective total joint arthroplasty. J Arthroplasty 2016; 31(9 Suppl): 144-7.
24. Grimer RJ, Belthur M, Chandrasekar C, Carter SR, Tillman RM. Two-stage revision for infected endoprostheses used in tumor surgery. Clin Orthop Relat Res 2002; 395: 193–203.
25. Hardes J, Gebert C, Schwappach A, Ahrens H, Streitburger A, Winkelmann W, et al. Characteristics and outcome of infections associated with tumor endoprostheses. Arch Orthop Trauma Surg 2006; 126(5): 289–96.
26. Jeys LM, Grimer RJ, Carter SR, Tillman RM. Periprosthetic infection in patients treated for an orthopaedic oncological condition. J Bone Joint Surg Am 2005; 87(4): 842–9.
27. Kurtz S, Ong K, Lau E, Bozic K, Berry D, Parvizi J. Prosthetic joint infection risk after TKA in the medicare population. Clin Orthop Relat Res 2010; 468(1): 52–6.
28. Kapoor SK, Thiyam R. Management of infection following reconstruction in bone tumors. J Clin Orthop Trauma 2015; 6(4): 244–51.
29. Parvizi J, Gehrke T, Chen AF. Proceedings of the international consensus on periprosthetic joint infection. Bone Joint J 2013; 95-B(11): 1450-2.
30. Racano A, Pazionis T, Farrokhyar F, Deheshi B, Ghert M. High infection rate outcomes in long-bone tumor surgery with endoprosthetic reconstruction in adults: a systematic review. Clin Orthop Relat Res 2013; 471(6): 2017–27.
31. Ghert M, Deheshi B, Holt G, Randall RL, Ferguson P, Wunder J, et al. Prophylactic antibiotic regimens in tumour surgery (PARITY): protocol for a multicentre randomised controlled study. BMJ Open 2012; 2(6).
32. Donati F, Di Giacomo G, D’Adamio S, Ziranu A, Careri S, Rosa M, et al. Silver-coated hip megaprosthesis in oncological limb salvage surgery. Biomed Res Int 2016; 2016: 1–6.
33. Hardes J, von Ei� C, Streitbuerger A, Balke M, Budny T, Henrichs MP, et al. Reduction of periprosthetic infection with silver-coated megaprostheses in patients with bone sarcoma. J Surg Oncol 2010; 101(5): 389–95.
34. Hardes J, Ahrens H, Gebert C, Streitbuerger A, Buerger H, Erren M, et al. Lack of toxicological side-e�ects in silver-coated megaprostheses in humans. Biomaterials 2007; 28(18): 2869–75.
35. Tsuchiya H, Shirai T, Nishida H, Murakami H, Kabata T, Yamamoto N, et al. Innovative antimicrobial coating of titanium implants with iodine. J Orthop Sci 2012; 17(5): 595–604.
36. Choi Y, Lim DH, Lee SH, Lyu CJ, Im JH, Lee YH, et al. Role of radiotherapy in the multimodal treatment of Ewing sarcoma family tumors. Cancer Res Treat 2015; 47(4): 904–12.
37. Ciernik IF, Niemierko A, Harmon DC, Kobayashi W, Chen YL, Yock T, et al. Proton-based radiotherapy for unresectable or incompletely resected osteosarcoma. Cancer 2011; 117(19): 4522–30.
38. Hill RP, Kaspler P, Gri�n AM, O’Sullivan B, Catton C, Alasti H, et al. Studies of the in vivo radiosensitivity of human skin �broblasts. Radiother Oncol 2007; 84(1): 75–83.
39. Rudolph R, Vande Berg J, Schneider JA, Fisher JC, Poolman WL. Slowed growth of cultured �broblasts from human radiation wounds. Plast Reconstr Surg 1988; 82(4): 669–77.
40. Morii T, Yabe H, Morioka H, Beppu Y, Chuman H, Kawai A, et al. Postoperative deep infection in tumor endoprosthesis reconstruction around the knee. J Orthop Sci 2010; 15(3): 331–9.
41. Vince K, Chivas D, Droll KP. Wound complications after total knee arthroplasty. J Arthroplasty 2007; 22(4 Suppl 1): 39-44.
42. Ghanem E, Heppert V, Spangehl M, Abraham J, Azzam K, Barnes L, et al. Wound management. J Orthop Res 2014; 32(Suppl 1): S108-19.
43. Maathuis PGM, de Hartog B, Bulstra SK. Timing of open debridement for suspected infection of joint prosthesis: a report on 551 patients. Curr Orthop Pract 2009; 20(5): 541-5.
44. Jaberi FM, Parvizi J, Haytmanek CT, Joshi A, Purtill J. Procrastination of wound drainage and malnutrition a�ect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008; 466(6): 1368-71.
45. Argenson JN, Arndt M, Babis G, Battenberg A, Budhiparama N, Catani F, et al. Hip and knee section. Treatment: debridement and retention of implant: proceedings of international consensus on orthopedic infections. J Arthroplasty 2019; 34(2 Suppl: S399-419.
51938_Claudia_Lowik.indd 174 19-08-19 11:12

General discussion and future perspectives
175
10
46. Wyatt MC, Beswick AD, Kunutsor SK, Wilson MJ, Whitehouse MR, Blom AW. The alpha-defensin immunoassay and leukocyte esterase colorimetric strip test for the diagnosis of periprosthetic infection: a systematic review and meta-analysis. J Bone Joint Surg Am 2016; 98(12): 992-1000.
47. Wouthuyzen-Bakker M, Ploegmakers JJW, Kampinga GA, Wagenmakers-Huizenga L, Jutte PC, Muller Kobold AC. Synovial calprotectin: a potential biomarker to exclude a prosthetic joint infection. Bone Joint J 2017; 99-B(5): 660-5.
48. Fink B, Makowiak C, Fuerst M, Berger I, Schäfer P, Frommelt L, et al. The value of synovial biopsy, joint aspiration and C-reactive protein in the diagnosis of late periprosthetic infection of total knee replacement. J Bone Joint Surg Br 2008; 90(7): 874-8.
49. Elamurugan TP, Jagdish S, Kate V, Chandra Parija S. Role of bone biopsy specimen culture in the management of diabetic foot osteomyelitis. Int J Surg 2011; 9(3): 214-6.
50. Ovington L. Bacterial toxins and wound healing. Ostomy Wound Manage 2003; 49(7A Suppl); 8-12.51. Hirakawa K, Stulberg BN, Wilde AH, Bauer TW, Secic M. Results of 2-stage reimplantation for
infected total knee arthroplasty. J Arthroplasty 1998; 13(1): 22-8. 52. Haleem AA, Berry DJ, Hanssen AD. Mid-term to long-term follow-up of two-stage reimplantation
for infected total knee arthroplasty. Clin Orthop Relat Res 2004; 428: 35-9. 53. Sukeik M, Patel S, Haddad FS. Aggressive early débridement for treatment of acutely infected
cemented total hip arthroplasty. Clin Orthop Relat Res 2012; 470(11): 3164-70. 54. Cobo J, Garcia San Miguel L, Euba G, Rodríguez D, García-Lechuz JM, Riera M, et al. Early prosthetic
joint infection: outcomes with debridement and implant retention followed by antibiotic therapy. Clin Microbiol Infect 2011; 17(11): 1632-7.
55. Duque AF, Post ZD, Lutz RW, Orozco FR, Pulido SH, Ong AC. Is there still a role for irrigation and debridement with liner exchange in acute periprosthetic total knee infection? J Arthroplasty 2017; 32(4): 1280-4.
56. Fehring TK, Odum SM, Berend KR, Jiranek WA, Parvizi J, Bozic KJ, et al. Failure of irrigation and débridement for early postoperative periprosthetic infection. Clin Orthop Relat Res 2013; 471(1): 250-7.
57. Sherrell JC, Fehring TK, Odum S, Hansen E, Zmistowski B, Dennos A, et al. Fate of two-stage reimplantation after failed irrigation and débridement for periprosthetic knee infection. Clin Orthop Relat Res 2011; 469(1): 18-25.
58. Gardner J, Gioe TJ, Tatman P. Can this prosthesis be saved? Implant salvage attempts in infected primary TKA. Clin Orthop Relat Res 2011; 469(4): 970-6.
59. Nodzo SR, Boyle KK, Nocon AA, Henry MW, Mayman DJ, Westrich GH. The in�uence of a failed irrigation and debridement on the outcomes of a subsequent 2-stage revision knee arthroplasty. J Arthroplasty 2017; 32(8): 2508-12.
60. Brimmo O, Ramanathan D, Schiltz NK, Pillai AL, Klika AK, Barsoum WK. Irrigation and debridement before a 2-stage revision total knee arthroplasty does not increase risk of failure. J Arthroplasty 2016; 31(2): 461-4.
61. Choi HR, von Knoch F, Zurakowski D, Nelson SB, Malchau H. Can implant retention be recommended for treatment of infected TKA? Clin Orthop Relat Res 2011; 469(4): 961-9.
62. Fisman DN, Reilly DT, Karchmer AW, Goldie SJ. Clinical e�ectiveness and cost-e�ectiveness of 2 management strategies for infected total hip arthroplasty in the elderly. Clin Infect Dis 2001; 32(3): 419-30.
63. Azzam KA, Seeley M, Ghanem E, Austin MS, Purtill JJ, Parvizi J. Irrigation and debridement in the management of prosthetic joint infection: traditional indications revisited. J Arthroplasty 2010; 25(7): 1022-7.
64. Fink B, Schuster P, Schwenninger C, Frommelt L, Oremek D. A standardized regimen for the treatment of acute postoperative infections and acute hematogenous infections associated with hip and knee arthroplasties. J Arthroplasty 2017; 32(4): 1255-61.
65. Bergkvist M, Mukka SS, Johansson L, Ahl TE, Sayed-Noor AS, Sköldenberg OG, et al. Debridement, antibiotics and implant retention in early periprosthetic joint infection. Hip Int 2016; 26(2): 138-43.
66. Brandt CM, Sistrunk WW, Du�y MC, Hanssen AD, Steckelberg JM, Ilstrup DM, et al. Staphylococcus aureus prosthetic joint infection treated with debridement and prosthesis retention. Clin Infect Dis 1997; 24(5): 914–9.
51938_Claudia_Lowik.indd 175 19-08-19 11:12

Chapter 10
176
67. Buller LT, Sabry FY, Easton RW, Klika AK, Barsoum WK. The preoperative prediction of success following irrigation and debridement with polyethylene exchange for hip and knee prosthetic joint infections. J Arthroplasty 2012; 27(6): 857-64.
68. Hartman MB, Fehring TK, Jordan L, Norton HJ. Periprosthetic knee sepsis: the role of irrigation and debridement. Clin Orthop Relat Res 1991; 273: 113-8.
69. Kuiper JW, Vos CJ, Saouti R, Vergroesen DA, Graat HC, Debets-Ossenkopp YJ, et al. Prosthetic joint-associated infections treated with DAIR (debridement, antibiotics, irrigation, and retention): analysis of risk factors and local antibiotic carriers in 91 patients. Acta Orthop 2013; 84(4): 380-6.
70. Marculescu CE, Berbari EF, Hanssen AD, Steckelberg JM, Harmsen SW, Mandrekar JN, et al. Outcome of prosthetic joint infections treated with debridement and retention of components. Clin Infect Dis 2006; 42(4): 471-8.
71. Schoifet SD, Morrey BF. Treatment of infection after total knee arthroplasty by débridement with retention of the components. J Bone Joint Surg Am 1990; 72(9): 1383-90.
72. Tattevin P, Crémieux Ac, Pottier P, Huten D, Carbon C. Prosthetic joint infection: when can prosthesis salvage be considered? Clin Infect Dis 1999; 29(2): 292-5.
73. Triantafyllopoulos GK, Poultsides LA, Sakellariou VI, Zhang W, Sculco PK, Ma Y, et al. Irrigation and debridement for periprosthetic infections of the hip and factors determining outcome. Int Orthop 2015; 39(6): 1203–9.
74. Kim JG, Bae JH, Lee SY, Cho WT, Lim HC. The parameters a�ecting the success of irrigation and debridement with component retention in the treatment of acutely infected total knee arthroplasty. Clin Orthop Surg 2015; 7(1): 69-76.
75. Martínez-Pastor JC, Muñoz-Mahamud E, Vilchez F, García-Ramiro S, Bori G, Sierra J, et al. Outcome of acute prosthetic joint infections due to gram-negative bacilli treated with open debridement and retention of the prosthesis. Antimicrob Agents Chemother 2009; 53(11): 4772-7.
76. Vilchez F, Martínez-Pastor JC, García-Ramiro S, Bori G, Maculé F, Sierra J, et al. Outcome and predictors of treatment failure in early post-surgical prosthetic joint infections due to Staphylococcus aureus treated with debridement. Clin Microbiol Infect 2011; 17(3): 439-44.
77. Byren I, Bejon P, Atkins BL, Angus B, Masters S, McLardy-Smith P, et al. One hundred and twelve infected arthroplasties treated with ‘DAIR’ (debridement, antibiotics and implant retention): antibiotic duration and outcome. J Antimicrob Chemother 2009; 63(6): 1264-71.
78. Waldman BJ, Hostin E, Mont MA, Hungerford DS. Infected total knee arthroplasty treated by arthroscopic irrigation and débridement. J Arthroplasty 2000; 15(4): 430-6.
79. Chung JY, Ha CW, Park YB, Song YJ, Yu KS. Arthroscopic debridement for acutely infected prosthetic knee: any role for infection control and prosthesis salvage? Arthroscopy 2014; 30(5): 599-606.
80. Betz M, Abrassart S, Vaudaux P, Gjika E, Schindler M, Billières J, et al. Increased risk of joint failure in hip prostheses infected with Staphylococcus aureus treated with debridement, antibiotics and implant retention compared to Streptococcus. Int Orthop 2015; 39(3): 397-401.
81. Deirmengian C, Greenbaum J, Lotke PA, Booth RE Jr, Lonner JH. Limited success with open debridement and retention of components in the treatment of acute Staphylococcus aureus infections after total knee arthroplasty. J Arthroplasty 2003; 18(7 Suppl 1): 22-6.
82. Tornero E, Morata L, Martínez-Pastor JC, Bori G, Climent C, García-Velez DM, et al. KLIC-score for predicting early failure in prosthetic joint infections treated with debridement, implant retention and antibiotics. Clin Microbiol Infect 2015; 21(8): 9-17.
83. Wouthuyzen-Bakker M, Sebillote M, Lomas J, Taylor A, Palomares EB, Murillo O, et al. Clinical outcome and risk factors for failure in late acute prosthetic joint infections treated with debridement and implant retention. J Infect 2019; 78(1): 40-7.
84. Walenkamp GH, Vree TB, van Rens TJ. Gentamicin-PMMA beads. Pharmacokinetic and nephrotoxicological study. Clin Orthop Relat Res 1986; 205: 171-83.
85. Wahlig H, Dingeldein E, Bergmann R, Reuss K. The release of gentamicin from polymethylmethacrylate beads: an experimental and pharmacokinetic study. J Bone Joint Surg Br 1978; 60-B(2): 270-5.
86. Swieringa AJ, Tulp NJ. Toxic serum gentamicin levels after the use of gentamicin-loaded sponges in infected total hip arthroplasty. Acta Orthop 2005; 76(1): 75-7.
51938_Claudia_Lowik.indd 176 19-08-19 11:12

General discussion and future perspectives
177
10
87. Nelson CL, Evans RP, Blaha JD, Calhoun J, Henry SL, Patzakis MJ. A comparison of gentamicin-impregnated polymethylmethacrylate bead implantation to conventional parenteral antibiotic therapy in infected total hip and knee arthroplasty. Clin Orthop Relat Res 1993; 295: 96-101.
88. Blaha JD, Calhoun JH, Nelson CL, Henry SL, Seligson D, Esterhai JL Jr, et al. Comparison of the clinical e�cacy and tolerance of gentamicin PMMA beads on surgical wire versus combined and systemic therapy for osteomyelitis. Clin Orthop Relat Res 1993; 295: 8-12.
89. Walenkamp GH, Kleijn LL, de Leeuw M. Osteomyelitis treated with gentamicin-PMMA beads: 100 patients followed for 1-12 years. Acta Orthop Scand 1998; 69(5): 518-22.
90. Neut D, van de Belt H, Stokroos I, van Horn JR, van der Mei HC, Busscher HJ. Biomaterial-associated infection of gentamicin-loaded PMMA beads in orthopaedic revision surgery. J Antimicrob Chemother 2001; 47(6): 885-91.
91. Janssen DM, Geurts JAP, Jütten LM, Walenkamp GH. 2-stage revision of 120 deep infected hip and knee prostheses using gentamicin-PMMA beads. Acta Orthop 2016; 87(4): 324-32.
92. Geurts JAP, Janssen DMC, Kessels AG, Walenkamp GH. Good results in postoperative and hematogenous deep infections of 89 stable total hip and knee replacements with retention of prosthesis and local antibiotics. Acta Orthop 2013; 84(6): 509-16.
93. Barth RE, Vogely HC, Hoepelman AIM, Peters EJ. ‘To bead or not to bead?’ Treatment of osteomyelitis and prosthetic joint-associated infections with gentamicin bead chains. Int J Antimicrob Agents 2011; 38(5): 371-5.
94. Kelm J, Anagnostakos K, Regitz T, Schmitt E, Schneider G, Ahlhelm F. MRSA-infections-treatment with intraoperatively produced gentamycin-vancomycin PMMA beads. Chirurg 2004; 75(10): 988-95.
95. Swieringa AJ, Goosen JH, Jansman FG, Tulp NJ. In vivo pharmacokinetics of a gentamicin-loaded collagen sponge in acute periprosthetic infection: serum values in 19 patients. Acta Orthop 2008; 79(5): 637-42.
96. Moojen DJ, Hentenaar B, Vogely CH, Verbout AJ, Castelein RM, Dhert WJ. In vitro release of antibiotics from commercial PMMA beads and articulating hip spacers. J Arthroplasty 2008; 23(8): 1152-6.
97. Sørensen TS, Sørensen AI, Merser S. Rapid release of gentamicin from collagen sponge. In vitro comparison with plastic beads. Acta Orthop Scand 1990; 61(4): 353-6.
98. Otte JE, Politi JR, Chambers B, Smith CA. Intrawound vancomycin powder reduces early prosthetic joint infections in revision hip and knee arthroplasty. Surg Technol Int 2017; 30: 284-9.
99. Riesgo AM, Park BK, Herrero CP, Yu S, Schwarzkopf R, Iorio R. Vancomycin povidone-iodine protocol improves survivorship of periprosthetic joint infection treated with irrigation and debridement. J Arthroplasty 2018; 33(3): 847-50.
100. Osmon DR, Berbari ER, Berendt AR, Lew D, Zimmerli W, Steckelberg JM, et al. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 2013; 56(1): 1-25.
101. Dial BL, Lampley AJ, Green CL, Hallows R. Intrawound vancomycin powder in primary total hip arthroplasty increases rate of sterile wound complications. Hip Pelvis 2018; 30(1): 37-44.
102. Ghobrial GM, Cadotte DW, Williams K Jr, Fehlings MG, Harrop JS. Complications from the use of intrawound vancomycin in lumbar spinal surgery: a systematic review. Neurosurg Focus 2015; 39(4): E11.
103. Veerachamy S, Yarlagadda T, Manivasagam G, Yarlagadda PK. Bacterial adherence and bio�lm formation on medical implants: a review. Proc Inst Mech Eng H 2014; 228(10): 1083-99.
104. Bandyk DF, Kinney EV, Riefsnyder TI, Kelly H, Towne JB. Treatment of bacteria-bio�lm graft infection by in situ replacement in normal and immune-de�cient states. J Vasc Surg 1993; 18(3): 398-405.
105. Carli AV, Bhimani S, Yang X, Shirley MB, de Mesy Bentley KL, Ross FP, et al. Quanti�cation of peri-implant bacterial load and in vivo bio�lm formation in an innovative, clinically representative mouse model of periprosthetic joint infection. J Bone Joint Surg Am 2017; 99(6): e25.
106. Lebeaux D, Ghigo JM, Beloin C. Bio�lm-related infections: bridging the gap between clinical management and fundamental aspects of recalcitrance towards antibiotics. Microbiol Mol Biol Rev 2014; 78(3): 510-43.
51938_Claudia_Lowik.indd 177 19-08-19 11:12

Chapter 10
178
107. Davies D. Understanding bio�lm resistance to antibacterial agents. Nat Rev Drug Discov 2003; 2(2): 114-22.
108. Lovati AB, Bottagisio M, de Vecchi E, Gallazzi E, Drago L. Animal models of implant-related lowgrade infections: a twenty year review. Adv Exp Med Biol 2017; 971: 29-50.
109. Vidlak D, Kielian T. Infectious dose dictates the host response during Staphylococcus aureus orthopedic-implant bio�lm infection. Infect Immun 2016; 84(7): 1957-65.
110. Monmeyran A, Thomen P, Jonquière H, Sureau F, Li C, Plamont MA, et al. The inducible chemical-genetic �uorescent marker FAST outperforms classical �uorescent proteins in the quantitative reporting of bacterial bio�lm dynamics. Sci Rep 2018; 8(1): 10336.
111. Moojen DJ, Zwiers JH, Scholtes VA, Verheyen CC, Poolman RW. Similar success rates for single and multiple debridement surgery for acute hip arthroplasty infection. Acta Orthop 2014: 85(4): 383-8.
112. Romanò CL, Manzi G, Logoluso N, Romanò D. Value of debridement and irrigation for the treatment of peri-prosthetic infections: a systematic review. Hip Int 2012; 22(Suppl 8): S19-24.
113. Mont MA, Waldman B, Banerjee C, Pacheco IH, Hungerford DS. Multiple irrigation, debridement, and retention of components in infected total knee arthroplasty. J Arthroplasty 1997; 12(4): 426-33.
114. Brown NM, Cipriano CA, Moric M, Sporer SM, Della Valle CJ. Dilute betadine lavage before closure for the prevention of acute postoperative deep periprosthetic joint infection. J Arthroplasty 2012; 27(1): 27-30.
115. Ruder JA, Springer BD. Treatment of periprosthetic joint infection using antimicrobials: dilute povidone-iodine lavage. J Bone Joint Infect 2017; 2(1): 10-4.
116. Schwechter EM, Folk D, Varshney AK, Fries BC, Kim SJ, Hirsh DM. Optimal irrigation and debridement of infected joint implants: an in vitro methicillin-resistant Staphylococcus aureus bio�lm model. J Arthroplasty 2011; 26(6 Suppl): 109-13.
117. Thornely P, Evaniew N, Riediger M, Winemaker M, Bhandari M, Ghert M. Postoperative antibiotic prophylaxis in total hip and knee arthroplasty: a systematic review and meta-analysis of randomized controlled trials. CMAJ Open 2015; 3(3): E338-43.
118. Fowler JR, Perkins TA, Buttaro BA, Truant AL. Bacteria adhere less to barbed mono�lament than braided sutures in a contaminated wound model infection. Clin Orthop Relat Res 2013; 471(2): 665-71.
119. Sah AP. Is there an advantage to knotless barbed suture in TKA wound closure? A randomized trial in simultaneous bilateral TKAs. Clin Orthop Relat Res 2015; 473(6): 2019-27.
120. Khan RJ, Fick D, Yao F, Tang K, Hurworth M, Nivbrant B, et al. A comparison of three methods of wound closure following arthroplasty: a prospective, randomised, controlled trial. J Bone Joint Surg Br 2006; 88-B(2): 238-42.
121. Miller AG, Swank ML. Dermabond e�cacy in total joint arthroplasty wounds. Am J Orthop 2010; 39(10): 476-8.
122. Krebs VE, Elmallah RK, Khlopas A, Chughtai M, Bonutti PM, Roche M, et al. Wound closure techniques for total knee arthroplasty: an evidence-based review of the literature. J Arthroplasty 2018; 33(2): 633-8.
123. Roerdink RL, Plat AW, van Hove RP, Leenders ACAP, van der Zwaard BC. Reduced wound leakage in arthroplasty with modi�ed wound closure: a retrospective cohort study. Arch Orthop Trauma Surg 2019; Epub ahead of print.
124. Poeran J, Rasul R, Suzuki S, Danninger T, Mazumdar M, Opperer M, et al. Tranexamic acid use and postoperative outcomes in patients undergoing total hip and knee arthroplasty in the United States: retrospective analysis of e�ectiveness and safety. BMJ 2014; 349: 1-10.
125. Galat DD, McGovern SC, Hanssen AD, Larson DR, Harrington JR, Clarke HD. Early return to surgery for evacuation of a postoperative hematoma after primary total knee arthroplasty. J Bone Joint Surg Am 2008; 90(11): 2331-6.
51938_Claudia_Lowik.indd 178 19-08-19 11:12

Summary
Nederlandse samenvatting
51938_Claudia_Lowik.indd 179 19-08-19 11:12

51938_Claudia_Lowik.indd 180 19-08-19 11:12

181
S
Summary
Summary
Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are highly successful surgical treatment modalities for advanced osteoarthritis of the hip and knee. One of the most serious complications after joint arthroplasty is prosthetic joint infection (PJI). PJI develops in approximately 1-2% of primary arthroplasties and is associated with high morbidity and mortality as well as high socioeconomic costs. Prevention of PJI is therefore important to reduce the number of patients that experience its devastating e�ects. Furthermore, PJIs should be treated as e�ectively as possible once a PJI has developed. This thesis therefore focused on risk factors and treatment strategies for early PJI.
Part 1: Evaluation of patients at risk for early PJIChapter 2 provided a review of the available literature on the diagnosis and treatment of prolonged wound leakage after THA and TKA. As patients with prolonged wound leakage are at increased risk for developing PJI, it is important to optimally diagnose and treat these patients. Remarkably, there are no evidence-based guidelines on this topic that can guide orthopaedic surgeons in their decision-making process. As a �rst step toward such a guideline, we reviewed the available literature. This review revealed the availability of only a small number of papers on the diagnosis and treatment of prolonged wound leakage, most with a low level of evidence. Based on this literature review, we developed a classi�cation of prolonged wound leakage and an algorithmic approach to its diagnosis and treatment, which may guide orthopaedic surgeons in their decision-making process when selecting the proper treatment.
Chapter 3 provided a review of the available literature on PJI in orthopaedic oncology patients. PJI rates among these patients are high due to local and systemic immunode�ciency caused by chemotherapy or radiotherapy. Moreover, these patients usually require large implants because of the need for extensive tumor resections. Even though this patient category is clearly di�erent than regular patients receiving THA or TKA, the literature review showed that few papers speci�cally address PJI in oncology patients. There is evidence that the administration of chemotherapy or radiotherapy increases the risk of PJI. The use of silver-coated joint arthroplasties can reduce the risk of PJI. Additional research is needed on the de�nition of oncologic PJI, use of prophylactic antibiotics and optimal treatment of PJI in oncology patients.
51938_Claudia_Lowik.indd 181 19-08-19 11:12

182
Summary
Obese patients are another well-known patient category with an increased risk of PJI. This may be due to diminished wound healing, insu�cient dosage of antibiotic prophylaxis during joint arthroplasty or increased bacterial colonization of the skin. Chapter 4 examined the di�erences in clinical and microbiological characteristics between non-obese, obese and severely obese patients with early PJI. This study showed that obese patients with hip PJI had higher rates of polymicrobial infections than non-obese patients, and there was more involvement of Enterococcus species and Gram-negative microorganisms. These results stress the importance of improving preventive measures in obese patients and suggest that antibiotic prophylaxis during hip arthroplasty surgery should be broadened for this speci�c patient category.
Part 2: Improving treatment strategies for early PJIChapter 5 described the results of the external validation of a preoperative risk score for DAIR failure. As success rates of DAIR vary widely, it is important to select the right patients for this procedure. Rates of infection control by DAIR could be optimized and the number of more extensive revision surgeries reduced. To estimate the risk of DAIR failure prior to surgery, thereby selecting the right patients for DAIR, Tornero et al. developed the KLIC score. This score calculates the risk of DAIR failure preoperatively by evaluating �ve patient-related factors: 1) chronic renal failure (Kidney), 2 Liver cirrhosis, 3) Index surgery, 4) Cemented prosthesis and 5) CRP >115 mg/L (KLIC). A high KLIC score is associated with a high risk of DAIR failure. The study in this thesis showed that the KLIC score is a relatively good preoperative risk score, especially in patients with low or high KLIC scores. In patients with a low KLIC score (<3.5 points), orthopaedic surgeons should always perform a DAIR before turning to more invasive surgical treatment modalities. In patients with a high KLIC score (>6 points), they may consider other treatment options or postoperative suppressive antibiotic treatment to optimize the chances of infection control. In addition to selecting the right patients for DAIR, infection control after DAIR can also be improved by optimizing surgical techniques and antibiotic treatment. Chapter 6 provided results on the e�cacy of gentamicin-impregnated beads and sponges in patients with early PJI treated with DAIR. In the Netherlands, gentamicin-impregnated beads and sponges are routinely inserted in the joint cavity during DAIR to achieve higher rates of infection control. The bene�cial e�ects of applying these local antibiotic carriers have
51938_Claudia_Lowik.indd 182 19-08-19 11:12

183
S
Summary
never been demonstrated though. Interestingly, the study in this thesis showed that gentamicin-impregnated beads and sponges do not improve the outcome after DAIR and may even be associated with higher failure rates after DAIR. These results remained unchanged when a propensity score analysis was conducted to control for confounding factors. Use of gentamicin-impregnated beads and sponges should therefore be discontinued for this indication.
Infection control after DAIR can be improved by performing DAIR at the right time point. Chapter 7 thus focused on the rates of infection control after DAIR according to the interval between index surgery and DAIR procedure. As the success rate of DAIR is dependent on the time needed for bacteria to form a mature bio�lm at the surface of the prosthesis, PJI can no longer be cured by DAIR once embedded bacteria in the bio�lm become unresponsive to antibiotic treatment. Up to now, the time interval until formation of this mature bio�lm was unknown, therefore the time frame to successfully perform a DAIR procedure had not been established. Current guidelines suggest that DAIR should not be performed when PJI develops more than 30 days after index arthroplasty. However, the study in this thesis showed that the time interval from index arthroplasty to DAIR is not a reliable predictor for treatment success of DAIR in early PJI. Although treatment failure was highest when DAIR was performed in the late post-surgical course (7-12 weeks), DAIR was still successful in approximately 60% of these patients. This indicates that DAIR is still a viable treatment option when performed more than 30 days after index arthroplasty.
While Chapter 7 described the optimal timing of DAIR in patients with early PJI in general, Chapters 8 and 9 focused on the optimal timing of DAIR in patients with prolonged wound leakage after THA and TKA. Currently there are no evidence-based guidelines on the optimal treatment of prolonged wound leakage. A survey was conducted among Dutch orthopaedic surgeons to assess current clinical practice in the Netherlands. Chapter 8 provided the results of this survey, which showed a wide variation in the classi�cation, de�nition, diagnosis and treatment of prolonged wound leakage.
Based on the results of this survey and the literature review in Chapter 2, Consortium Orthopaedic REsearch (CORE) designed the LEAK study, which is described in Chapter 9. This nationwide multicenter randomized controlled trial compares the revision rates, clinical e�ectiveness and cost e�ectiveness of DAIR and non-surgical treatment. It is hypothesized that performing DAIR at an early time point is helpful in preventing and treating PJI and salvaging
51938_Claudia_Lowik.indd 183 19-08-19 11:12

184
Summary
the implant in patients with prolonged wound leakage after THA and TKA. The results of this trial will be presented in a separate publication.
Chapter 10 presented a general discussion on the main �ndings of the studies described in this thesis. It also provided future perspectives and implications for clinical practice.
51938_Claudia_Lowik.indd 184 19-08-19 11:12
185
S
Nederlandse samenvatting
Nederlandse samenvatting
Knie- en heupprothesen zijn zeer succesvolle chirurgische behandelmethoden voor gevorderde artrose van de knie en heup. Echter ontwikkelt ongeveer 1-2% van alle patiënten met een knie- of heupprothese een prothese-infectie. Het is belangrijk om deze infecties te voorkomen, omdat prothese-infecties een negatieve invloed hebben op de kwaliteit van leven van een patiënt en gepaard gaan met hoge medische kosten. Daarom zijn de studies in dit proefschrift gericht op de risicofactoren voor het ontwikkelen van een prothese-infectie en de optimale behandeling van een prothese-infectie.
Deel 1: Patiënten met een verhoogd risico op een prothese-infectieHoofdstuk 2 geeft een overzicht van studies die zijn uitgevoerd op het gebied van de diagnose en behandeling van verlengde wondlekkage na het plaatsen van een knie- of heupprothese. Aangezien patiënten met verlengde wondlekkage een verhoogd risico hebben op het ontwikkelen van een prothese-infectie, is het belangrijk om verlengde wondlekkage zo goed mogelijk te diagnosticeren en behandelen. Opmerkelijk genoeg zijn er geen evidence-based richtlijnen die orthopedisch chirurgen kunnen ondersteunen in hun besluitvoering rondom dit probleem. Als een eerste stap richting de ontwikkeling van een dergelijke richtlijn hebben we de beschikbare literatuur op het gebied van verlengde wondlekkage verzameld en beoordeeld. Dit literatuuroverzicht laat zien dat er slechts een klein aantal studies is uitgevoerd naar de diagnose en behandeling van verlengde wondlekkage, waarvan bij de meeste studies een de�nitie voor verlengde wondlekkage ontbreekt en de kwaliteit matig is. Om orthopedisch chirurgen een leidraad te kunnen bieden voor het kiezen van een geschikte behandeling in het geval van verlengde wondlekkage hebben we een classi�catie voor verlengde wondlekkage ontwikkeld en een algoritme opgesteld voor de diagnose en behandeling van verlengde wondlekkage.
Hoofdstuk 3 geeft een overzicht van studies die zijn uitgevoerd op het gebied van prothese-infecties bij orthopedische oncologische patiënten. Het percentage prothese-infecties is hoog bij oncologische patiënten door lokale en systemische immunode�ciëntie veroorzaakt door chemotherapie of radiotherapie. Bovendien wordt bij deze patiënten vaak een grotere prothese geplaatst vanwege uitgebreide tumorresectie. Ook al verschilt de
51938_Claudia_Lowik.indd 185 19-08-19 11:12

186
Nederlandse samenvatting
oncologische patiënt duidelijk van de doorsnee patiënt die een totale knie- of heupprothese krijgt, toch zijn er maar enkele studies uitgevoerd die speci�ek gericht zijn op prothese-infecties in oncologische patiënten. In deze studies is aangetoond dat de toediening van chemotherapie of radiotherapie het risico op een prothese-infectie verhoogt, terwijl het gebruik van zilver gecoate prothesen het infectierisico kan verlagen. Aanvullend onderzoek is nodig om meer duidelijkheid te krijgen over de de�nitie van een prothese-infectie in oncologische patiënten, het gebruik van profylactische antibiotica en de optimale behandeling van een prothese-infectie in oncologische patiënten.
Een andere bekende patiëntengroep met een verhoogd risico op het ontwikkelen van een prothese-infectie zijn obese patiënten. Dit verhoogde risico wordt veroorzaakt doordat obese patiënten matige wondgenezing hebben, een relatief te lage dosering antibioticaprofylaxe krijgen tijdens het plaatsen van de knie- of heupprothese en uitgebreidere kolonisatie van de huid met bacteriën hebben. In hoofdstuk 4 is onderzocht welke verschillen in klinische en microbiologische kenmerken er bestaan tussen niet-obese, obese en morbide obese patiënten met een prothese-infectie. De resultaten van deze studie laten zien dat obese patiënten met een geïnfecteerde heupprothese vaker een polymicrobiële infectie hebben dan niet-obese patiënten. Daarnaast worden meer infecties veroorzaakt door Enterococcus species en Gram-negatieve micro-organismen. Deze resultaten onderstrepen het belang van het verbeteren van preventieve maatregelen bij obese patiënten en suggereren dat de antibioticaprofylaxe tijdens het plaatsen van een heupprothese moet worden uitgebreid in deze patiëntengroep.
Deel 2: Optimale behandeling van prothese-infectiesIn hoofdstuk 5 worden de resultaten beschreven van de externe validatie van een preoperatieve risicoscore voor de succeskans van DAIR. Het feit dat de succespercentages van DAIR sterk variëren in de literatuur geeft aan dat het belangrijk is om geschikte patiënten te selecteren voor deze procedure. Daardoor kunnen de succespercentages van DAIR verbeterd worden en het aantal benodigde aanvullende operaties gereduceerd. Om vooraf aan een DAIR de succeskans te kunnen inschatten (om daarmee de geschikte patiënten te kunnen identi�ceren) hebben Tornero et al. de KLIC-score ontwikkeld. Deze score berekent preoperatief de succeskans van DAIR door vijf patiënt-gerelateerde factoren te beoordelen: 1) chronisch nierfalen (Kidney), 2) Levercirrose, 3) Index
51938_Claudia_Lowik.indd 186 19-08-19 11:12

187
S
Nederlandse samenvatting
operatie, 4) geCementeerde prothese en 5) CRP >115 mg/L (KLIC). Een hoge KLIC-score is geassocieerd met een lage succeskans van DAIR. De resultaten laten zien dat de KLIC-score een relatief goede preoperatieve risicoscore is, met name bij patiënten met hoge of juist lage KLIC-scores. Bij patiënten met een lage KLIC-score (<3.5 punten) zouden orthopedisch chirurgen altijd een DAIR moeten uitvoeren voordat wordt overgegaan tot uitgebreidere operaties. Bij patiënten met een hoge KLIC-score (>6 punten) kunnen orthopedisch chirurgen overwegen om een andere behandeloptie te kiezen of postoperatief suppressieve antibiotica te starten om de kans op controle van de infectie te vergroten.
Aanvullend aan het selecteren van geschikte patiënten voor DAIR is het belangrijk om de operatietechniek en antibiotische behandeling van DAIR te verbeteren. In hoofdstuk 6 worden de resultaten beschreven van de e�ectiviteit van gentamicinekralen en -matjes in patiënten met vroege prothese-infecties die behandeld zijn middels DAIR. In Nederland worden tijdens een DAIR vaak gentamicinekralen en -matjes achtergelaten in de gewrichtsholte om de succeskans van DAIR te vergroten. Echter is het e�ect van deze lokale antibiotica nooit aangetoond. De resultaten tonen aan dat gentamicinekralen en -matjes geen gunstig e�ect hebben op het succespercentage van DAIR en zelfs geassocieerd zijn met een lager succespercentage. Deze resultaten bleven onveranderd na het toepassen van een propensity score analyse waarbij gecorrigeerd is voor verstorende variabelen. Naar aanleiding van deze resultaten wordt geadviseerd gentamicinekralen en -matjes niet meer toe te passen voor deze indicatie.
Het succespercentage van DAIR kan vergroot worden door de DAIR op het juiste moment uit te voeren. Daarom heeft hoofdstuk 7 de succespercentages van DAIR uitgezet tegen het tijdsinterval van het plaatsen van de prothese tot de DAIR-procedure. Doordat de succeskans van DAIR met name afhangt van de tijd die micro-organismen nodig hebben om een volledige bio�lm te vormen, kan een prothese-infectie niet meer genezen worden door middel van DAIR indien een volledige bio�lm gevormd is waarbij micro-organismen niet meer gevoelig zijn voor antibiotica. Tot op heden is niet vastgesteld hoe lang het duurt voordat deze volledige bio�lm gevormd is. Daardoor is niet duidelijk binnen welke periode een DAIR nog succesvol kan worden uitgevoerd. De huidige literatuur geeft aan dat DAIR niet moet worden verricht als de prothese-infectie zich meer dan 30 dagen na het plaatsen van de prothese
51938_Claudia_Lowik.indd 187 19-08-19 11:12

188
Nederlandse samenvatting
ontwikkelt. De studie in dit proefschrift laat zien dat het tijdsinterval tussen het plaatsen van de prothese en de DAIR-procedure geen betrouwbare voorspeller is voor het succes van DAIR bij een vroege prothese-infectie. Ook al was het succespercentage het laagst als de DAIR zeven tot twaalf weken na het plaatsen van de prothese werd uitgevoerd, DAIR was alsnog succesvol bij 60% van deze patiënten. Dit geeft aan dat DAIR ook een goede behandeloptie is voor een vroege prothese-infectie als de DAIR meer dan 30 dagen na het plaatsen van de prothese wordt uitgevoerd.
Terwijl hoofdstuk 7 de optimale timing van DAIR beschrijft bij patiënten met een vroege prothese-infectie in het algemeen, richten hoofdstuk 8 en 9 zich op de optimale timing van DAIR bij patiënten met verlengde wondlekkage na een knie- of heupprothese. Op dit moment zijn er geen evidence-based richtlijnen voor de optimale behandeling van verlengde wondlekkage. Om de huidige gang van zaken in de klinische praktijk in Nederland te onderzoeken werd een enquête afgenomen onder Nederlandse orthopedisch chirurgen. Hoofdstuk 8 geeft de resultaten van deze enquête weer, waaruit blijkt dat er tussen Nederlandse orthopedisch chirurgen grote variatie bestaat in de classi�catie, de�nitie, diagnose en behandeling van verlengde wondlekkage.
Op basis van de resultaten van de enquête en het literatuuroverzicht in hoofdstuk 2 is vanuit Consortium Orthopaedic REsearch (CORE) de LEAK-studie opgezet, welke beschreven staat in hoofdstuk 9. Deze nationale multicenter gerandomiseerde studie vergelijkt de kostene�ectiviteit, de klinische e�ectiviteit en het aantal revisie-operaties tussen DAIR en conservatieve behandeling. Hierbij wordt verondersteld dat het tijdig uitvoeren van een DAIR-procedure een prothese-infectie kan voorkomen of vroegtijdig kan behandelen, waardoor de prothese behouden kan blijven in patiënten met verlengde wondlekkage na een knie- of heupprothese. De resultaten van dit onderzoek zullen op een later moment gepubliceerd worden.
Hoofdstuk 10 geeft een algemene discussie van de belangrijkste bevindingen van de studies die zijn beschreven in dit proefschrift. Daarnaast worden toekomstperspectieven beschreven en worden de implicaties voor de klinische praktijk benoemd.
51938_Claudia_Lowik.indd 188 19-08-19 11:12

Dankwoord
Curriculum vitae
SHARE: previous dissertations
51938_Claudia_Lowik.indd 189 19-08-19 11:12

190
Dankwoord
Dankwoord
Dit proefschrift is mede tot stand gekomen dankzij het werk en de steun van velen. Ik wil iedereen hiervoor hartelijk bedanken, maar een aantal mensen wil ik in het bijzonder noemen.
Dr. M. Wouthuyzen-Bakker, beste Marjan. Al ben je niet o�cieel mijn co-promotor, samen met de andere (co)promotoren sta je bovenaan mijn dankwoord. Jouw enthousiasme voor het bedenken en uitvoeren van nieuwe onderzoeken is erg aanstekelijk. Op een mooie manier heb je mij bij je internationale projecten betrokken, waardoor ik veel nieuwe en interessante personen heb ontmoet. Ook breng je veel gezelligheid met je mee, onder andere tijdens onze tripjes naar Nantes en Helsinki. Je bent altijd beschikbaar voor overleg en onze artikelen worden in rap tempo geschreven. Hopelijk blijft deze samenwerking ook na het afronden van dit proefschrift bestaan. Bedankt voor je fantastische inzet.
Dr. P.C. Jutte, beste Paul. Bedankt voor de kansen die je mij hebt geboden in het orthopedische onderzoek. Al voor de PhD begon werkten we goed samen aan de diagnostische richtlijn voor prothese-infecties. Je vertelde me enthousiast over het komende PhD-traject over de LEAK-studie en had het vertrouwen in mij om dit grote project te gaan coördineren, wat een prachtige ervaring is geworden. Ook wil ik je graag bedanken voor alle hulp die je me verder hebt geboden. Ondanks alle drukte van het klinische werk in combinatie met de vele (inter)nationale reizen nam je toch altijd de tijd om te overleggen en adviezen te geven. Bedankt voor de kansen die je me hebt gegeven en nog steeds geeft.
Dr. M. Stevens, beste Martin. Jouw deur staat altijd open. Als ik ergens over twijfelde of even een luisterend oor nodig had, was jij altijd beschikbaar. De kritische wetenschappelijke blik van jou en Inge heeft mijn schrijven naar een hoger niveau getild, en is perfect in combinatie met de klinische blik van Paul en Marjan. Jij bent degene die me tijdens mijn wetenschappelijke stage van de opleiding Geneeskunde al hebt geholpen en ook degene die me aan Paul heeft gekoppeld toen ik verder wilde in het wetenschappelijk onderzoek in de orthopedie. Hartelijk bedankt voor het vertrouwen in mij en je bereidheid om te helpen.
51938_Claudia_Lowik.indd 190 19-08-19 11:12

191
S
Dankwoord
Prof. dr. S.K. Bulstra, beste Sjoerd. Je enthousiasme straalt op iedereen af, waardoor er een goede sfeer op de werkvloer ontstaat. Iedereen staat ervoor open om hulp te bieden en vragen te beantwoorden, waardoor ik met veel plezier in het UMCG heb gewerkt. Graag wil ik je bedanken voor de moeite die je hebt genomen om me te helpen om in opleiding te komen tot orthopedisch chirurg. Bedankt dat je mijn promotor wilde zijn.
Dr. I. van den Akker-Scheek, beste Inge. Je hebt een scherpe blik en doordat je kritisch naar methodieken, abstracts en andere voorstellen kijkt, zorg je ervoor dat onduidelijkheden en onzuiverheden in de epidemiologie vroegtijdig uitgeroeid worden. Jouw inbreng in het wekelijkse overleg van de LEAK-studie was dan ook onmisbaar, bedankt daarvoor.
Geachte leden van de beoordelingscommissie, prof. dr. A.W. Friedrich, prof. dr. R.G.H.H. Nelissen en prof. dr. ir. H.J. Busscher. Hartelijk bedankt voor jullie bereidwilligheid om de wetenschappelijke waarde van dit proefschrift te beoordelen.
Beste deelnemende ziekenhuizen van de LEAK-studie. Hartelijk bedankt voor jullie inzet. Het is prachtig om met zo’n groot aantal ziekenhuizen samen te werken aan een project. De samenwerkingsverbanden opgebouwd tijdens de LEAK-studie zijn een mooie opmaat naar het in de toekomst uitvoeren van meer studies over lastig te onderzoeken vraagstukken. Immers, vele handen maken licht werk!
Projectgroep LEAK-studie, beste Frank-Christiaan Wagenaar, Walter van der Weegen, Yvette Pronk, Rob Nelissen, Rudolf Poolman, Karin Vermeulen en Gera Welker. Met deze mooi diverse en gemotiveerde studiegroep hebben we in een korte tijdsperiode de LEAK-studie opgezet. Bedankt voor jullie inzet voor deze prachtige studie.
Nederlandse Orthopaedische Vereniging, beste Marloes Schmitz, Edith Rijnsburger. Met de LEAK-studie als groot CORE-project hebben we veel mogen samenwerken, wat ik als erg prettig heb ervaren. Door goed overleg en praktisch denkwerk hebben we mooie stappen gemaakt in het leggen van de basis voor verdere CORE-projecten. Bedankt voor deze prachtige mogelijkheid en veel succes met toekomstige projecten!
51938_Claudia_Lowik.indd 191 19-08-19 11:12

192
Dankwoord
Drs. H. Scheper, beste Henk. Fijn dat we onze krachten hebben kunnen bundelen om samen het mooie project van de Wondzorg app te kunnen opstarten. Proost op een goede verdere samenwerking!
Dr. A. Soriano, dear Alex. Thank you so much for your enthousiasm in the �eld of prosthetic joint infections. It is very nice to collaborate with you and I am delighted that you will come to Groningen for the defense of my thesis.
Mede-auteurs van de Northern Infection Network Joint Arthroplasty (NINJA), beste Aziz al Moujahid, Baukje Dijkstra, Greetje Kampinga, Bas Knobben, Glen Mithoe, Joris Ploegmakers, Astrid de Vries en Wierd Zijlstra. Bedankt voor jullie hulp bij het samenstellen van de grote database van patiënten met prothese-infecties en jullie kritische blik bij het trekken van conclusies hieruit. De NINJA is een prachtig netwerk voor de diagnostiek en behandeling van prothese-infecties en zal zeker bijdragen aan het optimaliseren van de patiëntenzorg bij prothese-infecties. Ga zo door!
Co-authors, dear Katherine Belden, André Carvalho, Sander Dijkstra, Thorsten Gehrke, Karan Goswami, Juan Carlos Martínez-Pastor, Javad Parvizi, Ricardo Sousa, Eduard Tornero, Chi Xu, Akos Zahar and Roel-Jan Zuidhof. It has been an honor to work together with you to assemble a large international database on patients with prosthetic joint infection treated with DAIR. Hopefully we will continue this nice collaboration in the future. Thank you so much for all your e�orts.
Beste Siebe Kuipers, bedankt voor het maken van het online magazine voor de LEAK-studie, een mooi innovatief project. Ook zou ik graag Rudolf Poolman, Rob Nelissen en Wierd Zijlstra willen bedanken voor de interviews die ze hebben gegeven.
Beste mede PhD-ers, Annet, Eric, Louren, Olivier, Rinne, Sjoukje, Tim en Tjerk. Als collega-promovendi hebben we elkaar altijd kunnen helpen waar het nodig was en hebben we het heel gezellig gehad op onze onderzoekskamer. Bedankt voor jullie luisterend oor en de leuke tijd die ik heb gehad.
51938_Claudia_Lowik.indd 192 19-08-19 11:12

193
S
Dankwoord
Beste Els en Yvonne, wat is het toch �jn om altijd bij jullie te kunnen binnenlopen voor vragen of gewoon een gezellig praatje. Jullie hebben me altijd heel goed geholpen en daar ben ik jullie erg dankbaar voor.
Paranimfen, Annet Wijnen en Marco Löwik, bedankt voor jullie ondersteuning bij de afronding van mijn PhD. Het is erg prettig om samen naar de lay-out van het proefschrift te kijken en natuurlijk is samen een feest plannen veel gezelliger dan alleen.
Lieve Robert, bedankt dat je me altijd aan het lachen maakt en �jn dat je altijd klaarstaat om problemen te relativeren en oplossingen te bedenken.
Lieve familie, bedankt voor jullie onvoorwaardelijke steun. Door problemen met jullie te bespreken worden ze overzichtelijker en kan ik ze oplossen. Jullie zijn fantastisch.
Lieve vrienden, jullie geven me de ontspanning waardoor ik elke dag weer hard aan het werk kan. Met name het spelen van spelletjes en de uren op de tennisbaan zijn om van te genieten. Bedankt dat jullie er voor mij zijn.
51938_Claudia_Lowik.indd 193 19-08-19 11:12

194
Curriculum vitae
Curriculum vitae
Claudia Aline Maria Löwik was born on the 5th of August 1989 in Zwolle, the Netherlands. She attended secondary school at the Thomas à Kempis college in Zwolle and graduated in 2007. That same year she started the study Medicine at the University of Groningen, which she �nished in 2014.
After graduation, she worked as a clinical resident at the emergency room at the Bethesda Hospital in Hoogeveen. One year later, she started working as a
clinical resident at the department of general surgery at the Scheper Ziekenhuis in Emmen. During this time period she performed a literature review on the diagnostic modalities for prosthetic joint infections under supervision of dr. P.C. Jutte. This was the start of this thesis on the risk factors and treatment strategies for early prosthetic joint infections. Until the start of her PhD, she worked as a clinical resident at the department of general surgery at the University Medical Center Groningen. From December 2016 to November 2018 she did full-time research at the department of orthopaedic surgery at the University Medical Center Groningen.
After �nishing her thesis, she started to work as a clinical resident at the department of orthopaedic surgery at the Medical Center Leeuwarden. It is her ambition to become an orthopaedic surgeon.
51938_Claudia_Lowik.indd 194 19-08-19 11:12

195
S
SHARE: previous dissertations
Research Institute SHARE
This thesis is published within the Research Institute SHARE (Science in Healthy Ageing and healthcaRE) of the University Medical Center Groningen / University of Groningen. Further information regarding the institute and its research can be obtained from our internet site: http://www.share.umcg.nl/
More recent theses can be found in the list below. ((co-) supervisors are between brackets)
2019
Dierselhuis EF. Advances of treatment in atypical cartilaginous tumours (prof SK Bulstra, prof AJH Suurmeijer, dr PC Jutte, dr M Stevens)
Gils A van. Developing e-health applications to promote a patient-centered approach to medically unexplained symptoms (prof JGM Rosmalen, prof RA Schoevers)
Notenbomer A. Frequent sickness absence; a signal to take action (prof U Bultmann, prof W van Rhenen, dr CAM Roelen)
Bishanga DR. Improving access to quality maternal and newborn care in low-resource settings: the case of Tanzania (prof J Stekelenburg, dr YM Kim)
Tura AK. Safe motherhood: severe maternal morbidity and mortality in Eastern Ethiopia (prof SA Scherjon, prof J Stekelenburg, dr TH van den Akker)
Vermeiden CJ. Safe motherhood: maternity waiting homes in Ethiopia to improve women’s access to maternity care (prof J Stekelenburg, dr TH van den Akker)
Schrier E. Psychological aspects in rehabilitation (prof PU Dijkstra, prof JHB Geertzen)
51938_Claudia_Lowik.indd 195 19-08-19 11:12

196
SHARE: previous dissertations
Malinakova K. Spirituality and health: their associations and measurement problems (prof SA Reijneveld, prof P Tavel, dr JP van Dijk)
Dijkhuizen A. Physical �tness and performance of daily activities in persons with intellectual disabilities and visual impairment; towards improving conditions for participation (prof CP van der Schans, dr A Waninge, dr WP Krijnen)
Graaf MW de. The measurement and prediction of physical functioning after trauma (prof E Heineman, dr IHF Reininga, dr KW Wendt)
Vrijen C. Happy faces and other rewards; di�erent perspectives on a bias away from positive and toward negative information as an underlying mechanism of depression (prof AJ Oldehinkel, prof CA Hartman, prof P de Jonge)
Moye Holz DD. Access to innovative medicines in a middle-income country; the case of Mexico and cancer medicines (prof HV Hogerzeil, prof SA Reijneveld, dr JP van Dijk)
Woldendorp KH. Musculoskeletal pain & dysfunction in musicians (prof MF Reneman, prof JH Arendzen, dr AM Boonstra)
Mooyaart JE. Linkages between family background, family formation and disadvantage in young adulthood (prof AC Liefbroer, prof F Billari)
Maciel Rabello L. The in�uence of load on tendons and tendinopathy; studying Achilles and patellar tendons using UTC (prof J Zwerver, prof RL Diercks, dr I van den Akker-Scheek, dr MS Brink)
Holvast F. Depression in older age (prof PFM Verhaak, prof FG Schellevis, prof RC Oude Voshaar, dr H Burger)
For earlier theses visit our website
51938_Claudia_Lowik.indd 196 19-08-19 11:12