
Drug development of MET inhibitors: targeting oncogene addiction and expedience
13
The MET tyrosine kinase is a cell surface receptor for hepatocyte growth factor (HGF , also known as scatter factor), a pleiotropic cytokine that conveys a unique combination of pro-migratory, anti-apoptotic and mitogenic signals 1,2 (FIG. 1). The MET signalling appara- tus includes several surface co-receptors and multiple downstream effectors (FIG. 2). MET activation by HGF can induce the disruption of intercellular contacts and the mobilization of cells from their primary location towards their adjacent surroundings. When cells leave their physiological niche, they are prone to rapid elimi- nation through an apoptotic process known as ‘anoikis’, which is induced by the detachment of cells. MET pathway activation has been shown to prevent anoikis by providing powerful survival cues 3,4 , thus favouring the colonization of inappropriate anatomical sites by these ‘nomadic’ cells. Finally, migration and survival are accompanied by rounds of cell division, which expand the number of migratory cells and allow population of the ‘settlements’ that have formed at distant sites. The spatial and temporal orchestration of these dis- tinct but complementary cellular activities — motility, protection from apoptosis and proliferation — is collect- ively defined as ‘invasive growth’ 1 . During embryonic development, invasive growth takes place during gas- trulation, when individual cells peel away from the ectoderm and migrate inwards to form the endoderm and the mesoderm. It also occurs when cells of the neural crest delaminate from the neural tube and disperse throughout the embryo, when myogenic precursors detach from the dermomyotome and undergo long- range migration to form the limb buds, and during angiogenesis. Consistently, all these morphogenetic processes are (or can be) mediated by the HGF/MET system 5–9 . In some cases, the signals for survival and proliferation dominate over those for migration: for example, HGF and MET also regulate the growth and development of the placenta and liver 5,10 . In the adult, invasive growth becomes quiescent, but it can be reactivated during wound healing and following organ damage, when the residual cells must expand and migrate to reconstitute the integrity of the injured tissues. In fact, the plasma levels of HGF rise after liver, heart or kidney injury 11–14 , suggesting that upregulation of HGF (and the ensuing activation of MET) might be part of a general, defensive physiological response to organ failure. The importance of the HGF/MET pathway in the control of tissue homeostasis is supported by the well-established protective activity of HGF in several degenerative diseases, including progressive nephropathies 15,16 , liver cirrhosis 17 and lung fibrosis 18 . It is now commonly accepted that the signalling pathways and the genetic programmes that orchestrate embryonic development and tissue morphogenesis are re-activated in cancer cells and can lead to the neo- plastic dissemination of tumours 10,19 . In line with this assumption, it has been shown that the propagation of MET-dependent invasive growth signals is a general and Division of Molecular Oncology, Institute for Cancer Research and Treatment (IRCC), University of Turin School of Medicine, Candiolo, Turin 10060, Italy. Correspondence to P.M.C. or L.T. e‑mails: [email protected]; [email protected] doi:10.1038/nrd2530 Drug development of MET inhibitors: targeting oncogene addiction and expedience Paolo M. Comoglio, Silvia Giordano and Livio Trusolino Abstract | The MET tyrosine kinase stimulates cell scattering, invasion, protection from apoptosis and angiogenesis, thereby acting as a powerful expedient for cancer dissemination. MET can also be genetically selected for the long-term maintenance of the primary transformed phenotype, and some tumours appear to be dependent on (or ‘addicted’ to) sustained MET activity for their growth and survival. Because of its dual role as an adjuvant, pro-metastatic gene for some tumour types and as a necessary oncogene for others, MET is a versatile candidate for targeted therapeutic intervention. Here we discuss recent progress in the development of molecules that inhibit MET function and consider their application in a subset of human tumours that are potentially responsive to MET-targeted therapies. REVIEWS 504 | JUNE 2008 | VOLUME 7 www.nature.com/reviews/drugdisc © 2008 Nature Publishing Group
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Drug development of MET inhibitors: targeting oncogene addiction and expedience

The MET tyrosine kinase is a cell surface receptor for hepatocyte growth factor (HGF, also known as scatter factor), a pleiotropic cytokine that conveys a unique combination of pro-migratory, anti-apoptotic and mitogenic signals1,2 (FIG. 1). The MET signalling appara-tus includes several surface co-receptors and multiple downstream effectors (FIG. 2). MET activation by HGF can induce the disruption of intercellular contacts and the mobilization of cells from their primary location towards their adjacent surroundings. When cells leave their physiological niche, they are prone to rapid elimi-nation through an apoptotic process known as ‘anoikis’, which is induced by the detachment of cells. MET pathway activation has been shown to prevent anoikis by providing powerful survival cues3,4, thus favouring the colonization of inappropriate anatomical sites by these ‘nomadic’ cells. Finally, migration and survival are accompanied by rounds of cell division, which expand the number of migratory cells and allow population of the ‘settlements’ that have formed at distant sites.
The spatial and temporal orchestration of these dis-tinct but complementary cellular activities — motility, protection from apoptosis and proliferation — is collect-ively defined as ‘invasive growth’1. During embryonic development, invasive growth takes place during gas-trulation, when individual cells peel away from the ectoderm and migrate inwards to form the endoderm and the mesoderm. It also occurs when cells of the neural crest delaminate from the neural tube and disperse
throughout the embryo, when myogenic precursors detach from the dermomyotome and undergo long-range migration to form the limb buds, and during angiogenesis. Consistently, all these morphogenetic processes are (or can be) mediated by the HGF/MET system5–9. In some cases, the signals for survival and proliferation dominate over those for migration: for example, HGF and MET also regulate the growth and development of the placenta and liver5,10.
In the adult, invasive growth becomes quiescent, but it can be reactivated during wound healing and following organ damage, when the residual cells must expand and migrate to reconstitute the integrity of the injured tissues. In fact, the plasma levels of HGF rise after liver, heart or kidney injury11–14, suggesting that upregulation of HGF (and the ensuing activation of MET) might be part of a general, defensive physiological response to organ failure. The importance of the HGF/MET pathway in the control of tissue homeostasis is supported by the well-established protective activity of HGF in several degenerative diseases, including progressive nephropathies15,16, liver cirrhosis17 and lung fibrosis18.
It is now commonly accepted that the signalling pathways and the genetic programmes that orchestrate embryonic development and tissue morphogenesis are re-activated in cancer cells and can lead to the neo-plastic dissemination of tumours10,19. In line with this assumption, it has been shown that the propagation of MET-dependent invasive growth signals is a general and
Division of Molecular Oncology, Institute for Cancer Research and Treatment (IRCC), University of Turin School of Medicine, Candiolo, Turin 10060, Italy. Correspondence to P.M.C. or L.T. e‑mails: [email protected]; [email protected]:10.1038/nrd2530
Drug development of MET inhibitors: targeting oncogene addiction and expediencePaolo M. Comoglio, Silvia Giordano and Livio Trusolino
Abstract | The MET tyrosine kinase stimulates cell scattering, invasion, protection from apoptosis and angiogenesis, thereby acting as a powerful expedient for cancer dissemination. MET can also be genetically selected for the long-term maintenance of the primary transformed phenotype, and some tumours appear to be dependent on (or ‘addicted’ to) sustained MET activity for their growth and survival. Because of its dual role as an adjuvant, pro-metastatic gene for some tumour types and as a necessary oncogene for others, MET is a versatile candidate for targeted therapeutic intervention. Here we discuss recent progress in the development of molecules that inhibit MET function and consider their application in a subset of human tumours that are potentially responsive to MET-targeted therapies.
R E V I E W S
504 | junE 2008 | voluME 7 www.nature.com/reviews/drugdisc
© 2008 Nature Publishing Group

Nature Reviews | Drug Discovery
P
P
P
P
P
P
P
MET
Ser975
Tyr1234Tyr1235
Tyr1349Tyr1356
Sema domain
Signal peptide (SP)Hairpin loop (HL)
Kringle (K) domain
Phospho-serine
Tyrosine kinasedomain
Phospho-tyrosine
Carboxy-terminal tail
PSI domain
IPT domain
SP HL K1 K2 K3 K4
HGF
R VS S
α-chain β-chaina
b
remarkable feature of highly aggressive tumours, which spawn ‘pioneer’ cells that move out, infiltrate adjacent tissues and establish metastatic lesions20,21. This, together with the observation that MET is expressed by endothe-lial cells and that HGF is a potent angiogenic factor9, implies that molecules that inhibit MET and HGF can potentially interfere with cancer onset and metastasis.
MET and cancerInappropriate activation of MET can be induced by specific genetic lesions, transcriptional upregulation or ligand-dependent autocrine or paracrine mechanisms1,21
(TABLE 1).Historically, MET was identified as the protein
product of a transforming oncogene: Translocated Promoter Region (TPR)–MET, which was derived from a chromosomal rearrangement in an osteosarcoma cell line treated with a chemical carcinogen22. The oncogenic TPR-MET fusion protein is constitutively active due to a leucine-zipper domain along the TPR moiety, which provides a structural dimerization motif that keeps the enzyme active. In animal models, transgenic expression of TPR-MET under a ubiquitous promoter leads to the development of mammary tumours and other malignan-cies23, whereas lentiviral-mediated somatic transduction of TPR-MET in the liver of adult mice generates hyper-plastic foci that invariably progress to overt malignan-cies24. In humans, the TPR-MET rearrangement has been detected in gastric cancers, in precursor lesions and in the adjacent normal mucosa, suggesting that this genetic translocation can predispose to the development of gastric carcinomas25. However, this finding should be viewed with caution due to the limited number of samples examined.
Amplification of the MET gene, with consequent protein overexpression and constitutive kinase activa-tion, has been reported in a number of human primary tumours, including gastric and oesophageal carcino-mas26–29, non-small-cell lung (nSCl) carcinomas with acquired resistance to epidermal growth factor receptor (EGFR) inhibitors30 and medulloblastomas31(TABLE 1). In agreement with these findings, conditional overex-pression of wild-type MET in hepatocytes of transgenic mice (an experimental condition that mimics the sponta-neous amplification of the MET gene observed in human tumours) is sufficient to cause hepatocellular carcino-mas that regress following transgene inactivation32. An increase in the MET gene copy number can be a genetic feature of the primary transformed phenotype, or a secondary occurrence that influences the subsequent phases of neoplastic progression. In some patients with colorectal carcinomas, for example, MET amplification was detected in a high percentage of liver metastases but not in the primary tumours33.
The MET gene can also carry activating mutations, such as those found in a subset of patients with heredi-tary and sporadic papillary renal cancer34, childhood hepatocellular carcinoma35 and gastric carcinoma36. At least in hereditary cancers, single-allele mutations are usually accompanied by trisomy of the whole chromo-some 7 (where the MET locus resides), suggesting that
Figure 1 | Schematic structure of HGF and MET. a | Hepatocyte growth factor (HGF) is secreted as a single-chain, biologically inert precursor and is converted into its bioactive form by extracellular proteases, which cleave the bond between Arg494 and Val495. The mature form consists of an α- and a β-chain that are held together by a disulphide bond. The α-chain contains an N-terminal hairpin loop (HL) followed by four peculiar domains known as kringle (K) domains (80 amino acid double-looped structures formed by three internal disulphide bridges). The β-chain is homologous to serine proteases of the blood-clotting cascade, but lacks proteolytic activity owing to amino acid substitutions in the catalytic site. b | MET is a single-pass, disulphide-linked α/β heterodimer that is formed by proteolytic processing of a common precursor in the post-Golgi compartment. The extracellular portion of MET is composed of three domain types. The N-terminal 500 residues fold into a large Sema domain, which encompasses the whole α-subunit and part of the β-subunit, and shares sequence homology with domains found in the semaphorin and plexin families. The Sema domain is followed by a PSI domain – also found in the plexins, semaphorins and integrins, hence its name – that spans about 50 residues and contains four disulphide bonds. The PSI domain is connected to the transmembrane helix via four IPT domains, which are related to immunoglobulin-like domains and are named after their presence in plexins and transcription factors. The intracellular portion includes tyrosine kinase catalytic sites flanked by distinctive juxtamembrane and carboxy-terminal sequences. Phosphorylation of Tyr1234 and Tyr1235 within the catalytic site positively modulates enzyme activity, whereas phosphorylation of Ser975 in the juxtamembrane segment downregulates kinase activity. The carboxy-terminal tail includes two critical tyrosines (Tyr1349 and Tyr1356) that, once phosphorylated, act as a promiscuous docking site for the recruitment of several transducers and adaptors.
R E V I E W S
nATuRE REvIEWS | druG diScovEry voluME 7 | junE 2008 | 505
© 2008 Nature Publishing Group

Nature Reviews | Drug Discovery
MET MET
CD44v6
MET
Integrin α6β4
GRB2
GRB2
RAS
RASRAF
RAC1
ERK RAS
SRC
PI3K PI3K
HGF
PI3KGAB1PLCγ
STAT3
P PP
P
P
P
GRB2SHP2
SHC
SHP2P
P
Plexin B1
HGF
Enhancement ofRAS activation
Link to cytoskeleton
Docking platform
MET co-activator
Enhancement of PI3K, RAS and SRC activation
HGF-independent activation of MET signalsSOS
SOS
MEK
AKT
mutant heterozigosity must be complemented by dupli-cation of the mutated gene for full implementation of the transformed phenotype34. Also in this context, a genetically determined constitutive activation of MET can be a late event that potentiates a cell’s probability to incur secondary lesions: for instance, two different somatic mutations (Tyr1230Cys and Tyr1235Asp) appear to be selectively enriched during the metastatic spread of head and neck squamous-cell carcinomas, as cells positive for mutated (constitutively active) MET are found more frequently in the distal lymph node metastases than in the proximal lymph node stations or in the primary tumour of individual patients37. In animal models, the targeted introduction of different activating MET mutations in the murine met locus pre-disposes mice to diverse tumour types, some of which are metastatic and, similar to human cancers, display non-random duplication of the mutant met allele38.
The most frequent cause of constitutive MET activa-tion in human tumours is increased protein expression
as a consequence of transcriptional upregulation, in the absence of gene amplification. The list of neoplasms in which MET overexpression has been detected is constantly increasing and, at least for carcinomas, cases of excessive levels of MET expression have been found in virtually all types of this malignancy39. In cell-based assays, receptor overexpression can lead to local receptor oligomerization and reciprocal activa-tion, rendering cells responsive to sub-threshold ligand concentrations. This, together with the observations that HGF itself is able to activate the transcription of MET40 , that HGF is ubiquitously expressed through-out the body and that it is particularly active in the reactive stroma of tumours41,42, points to a role for this cytokine as a ‘landscaper factor’ (a widely distributed micro-environmental agent) that allows paracrine positive feedback loops to support the dissemination of cancer cells. Interestingly, this is in agreement with the observation that MET activating mutations require HGF to boost their catalytic efficiency43.
Figure 2 | MET-dependent signalling pathways. Using its promiscuous docking site at the carboxy-terminal tail, as well as association with the multi-adaptor GAB1, MET is able to recruit several SH2-domain-containing signal transducers that in turn activate a number of pathways, including the GRB2–SOS–RAS–RAF–MEK–ERK axis, the PI3K–AKT cascade, SRC, STAT3 and Rho-like GTPases such as RAC1. Compared with other purely mitogenic growth factors, hepatocyte growth factor (HGF) elicits a prolonged activation of downstream effectors that is likely to contribute to proper execution of invasive growth. Potency and endurance of MET-triggered pathways is secured by a network of upstream signalling co-receptors that physically associate with MET at the cell surface and that include the v6 splice variant of the hyaluronan receptor CD44, the laminin receptor α6β4 integrin and semaphorin receptors of the plexin B family. CD44 — specifically, the v6 splice variant — is necessary to link the MET cytoplasmic tail to the actin cytoskeleton and to optimise MET-triggered activation of the RAS–ERK cascade123,124; the α6β4 integrin acts as a supplementary docking platform for the additional recruitment of signalling molecules that amplify activation of PI3K, RAS and SRC-dependent pathways125–127; finally, plexins of the B family transactivate MET in the absence of HGF when stimulated by their semaphorin ligands, providing an alternative way to induce invasive growth and angiogenesis128–130. Together, these MET membrane partners amplify and/or diversify MET-dependent biochemical inputs and translate them into meaningful (and specific) biological outcomes. For details on MET domains see FIG. 1.
R E V I E W S
506 | junE 2008 | voluME 7 www.nature.com/reviews/drugdisc
© 2008 Nature Publishing Group

HGF can also aberrantly activate MET in an autocrine fashion, as described for gliobastomas44, breast carcino-mas45, rhabdomyosarcomas46 and osteosarcomas47. In experimental systems, exogenous co-expression of MET and HGF in several human and mouse cell lines leads to the formation of invasive tumours upon implantation in nude mice48–50, and mouse models that express HGF as a ubiquitous transgene develop different types of cancer and metastatic lesions51,52. Finally, ubiquitous expression of the HGF transgene in mice with a disruption of the genetic locus that contains the pRB regulator p16InK4a and the p53 regulator p14ARF (Ink4a–/–/Arf–/–) induces the development of malignant rhabdomyosarcomas with high penetrance and short latency53.
Strategies to target METSeveral different strategies have been pursued to inhibit MET, each focusing on one of the serial steps that regu-late MET activation (TABLES 2,3). The first event is the interaction between MET and its cognate ligand HGF. Such recognition can be blocked by HGF antagonists, which stoichiometrically compete with the ligand for receptor binding without leading to MET activation, and by HGF or MET neutralizing antibodies. Antibodies can also quantitatively downregulate MET by increasing its release (or ‘shedding’) from the cell surface.
upon ligand binding, the enzymatic activity of the kinase is unleashed by receptor dimerization and transphosphorylation of two catalytic tyrosine residues. Receptor oligomerization can be prevented by soluble fragments of the MET extracellular domain, which con-comitantly act as ‘decoy’ molecules that titre out ligand availability. MET catalytic activity can be blocked by small-molecule inhibitors that compete for ATP binding at the active site of the kinase.
Phosphorylation of the catalytic tyrosine residues is followed by phosphorylation of two additional tyrosines that act together as a multifunctional docking site for the concomitant recruitment of several SH2-containing transducers, including GRB2, PI3K, SRC and others1,2 (FIG. 2). Downstream propagation of MET-dependent signals can be obstructed by peptides competing with MET-associated signal transducers for access to the dock-ing site, or by combination therapies that block the activity of downstream signalling components.
HGF and MET biological antagonists. HGF is abundant in almost all tissues, where it is retained in the extracell-ular matrix — mainly in its precursor form — by low-affinity, high-avidity interactions with proteoglycans54,55. The stromal components of invasive tumours commonly overexpress proteases involved in pro-HGF activation, such as urokinase-type and tissue-type plasminogen activators56,57, thus utilizing the pro-HGF reservoir more efficiently than normal tissues and facilitating the paracrine activity of HGF on cancer cells41,42. Moreover, HGF/MET autocrine circuits have been described in some neoplasms44–47, suggesting that in addition to approaches that selectively target the receptor, strategies aimed at interfering with the recognition mechanisms between HGF and MET might have therapeutic value.
HGF contains two MET binding sites with different receptor affinities. The high-affinity binding site resides in the amino-terminal portion of the α-chain and can recognize a thus far uncharacterized region of MET independently of HGF processing and maturation58,59. The low-affinity site becomes accessible only upon pro-HGF conversion (that is, when HGF is fully active) and is essential for MET dimerization and activation through a specific association with the Sema domain of the MET extracellular portion60–63 (FIG. 3). These find-ings indicate that the inactive precursor of HGF, or HGF fragments that retain only the high-affinity site, interact with MET but do not induce MET signalling because they cannot induce MET dimerization, and thereby antagonise MET activation by mature HGF. They also suggest that the Sema domain of MET, either per se or in the context of the full-length, soluble MET extracellular portion, might competitively displace HGF and impair dimerization of the endogenous receptor.
Indeed, all these HGF and MET variants have been validated experimentally as powerful antagonists in vari-ous in vitro and in vivo models (TABLES 2,3). With regard to HGF competitive analogues, therapeutic activity of nK2, nK4 and uncleavable HGF has been demonstrated in preclinical models. nK2, a naturally occurring frag-ment of HGF that contains only the n-terminal hairpin loop (n domain) and the first two kringle domains (K2), has been shown to inhibit HGF-induced epithe-lial mitogenesis and morphogenesis in vitro64,65. nK4, a truncated form of HGF consisting of the entire α-chain (including the n-terminal domain and the four kringle domains) but devoid of the β-chain, is by far the most thoroughly studied HGF antagonist; its inhibitory activity has been demonstrated in various in vitro and in vivo models using different methods of compound delivery, ranging from administration of the purified protein to gene therapy approaches66,67. Interestingly, nK4 also acts as a generic angiogenesis inhibitor — regardless of MET blockade — because of its structural similarity with the anti-angiogenic molecule angiostatin68. uncleavable HGF, an unprocessable form of HGF that locks the mol-ecule in its inactive conformation, competes with active HGF for binding to MET and with pro-HGF convertases for HGF activation, thus it simultaneously blocks MET catalytic activation and HGF proteolytic maturation69.
As for MET competitive variants, decoy MET is a recombinant, enzymatically inactive molecule that corresponds to the whole MET extracellular domain; it interacts with both HGF and full-length MET, seques-tering the ligand and impairing dimerization of the native receptor, respectively70. Finally, the isolated Sema domain retains the ability to competitively inhibit ligand binding and receptor dimerization, impairs activation of MET-dependent transduction pathways and reduces HGF-triggered cell migration71.
Antibodies against HGF and MET. Recently, Amgen have reported the generation of some fully human monoclonal antibodies against HGF that exhibit thera-peutic potential in mice with subcutaneous xenografts of human glioma cell lines featuring an HGF-dependent
R E V I E W S
nATuRE REvIEWS | druG diScovEry voluME 7 | junE 2008 | 507
© 2008 Nature Publishing Group
autocrine loop72. Systemic administration of another anti-HGF antibody, l2G7 (Galaxy Biotech), proved to be particularly effective in inducing regression of both subcutaneous and intracranial glioma xenografts, sug-gesting that, unexpectedly, the blood–brain barrier does not impede l2G7 efficacy73. Amgen has also started clinical studies with AMG102, a fully human antibody (IgG2) recombinantly produced in mammalian cells74 that is being evaluated in Phase II clinical trials against advanced glioblastomas and kidney cancers75.
In the past, efforts to develop antibodies endowed with anti-tumour activity against MET were largely unsuccessful because the antibodies tended to have agonistic rather than antagonistic properties. This is due to the bivalent structure of the immunoglobulins, which act as natural dimerizing agents for the tyrosine kinase receptors. This limitation has been circumvented with a ‘one-armed’ antibody (oA-5D5), consisting of a monovalent Fab fragment with murine variable domains for the heavy and light chains fused to human IgG1 constant domains. In preclinical studies, oA-5D5 can almost completely inhibit intracerebral growth of HGF-expressing glioblastoma cells when delivered
locally76. The antibody is now reported to be in the early stages of clinical development143.
Another monoclonal antibody against the MET extracellular domain, Dn30, has been shown to reduce anchorage-independent growth and xenograft develop-ment of gastric carcinoma cells bearing amplification of the MET gene, as well as melanoma cell metastasis77. notably, the mechanism of action of this antibody relies on its ability to induce proteolytic cleavage of the MET extracellular portion, which on the one hand decreases the number of receptor molecules on the cell surface and, on the other hand, generates a ‘decoy effect’ that inhibits HGF binding and subsequent MET dimerization.
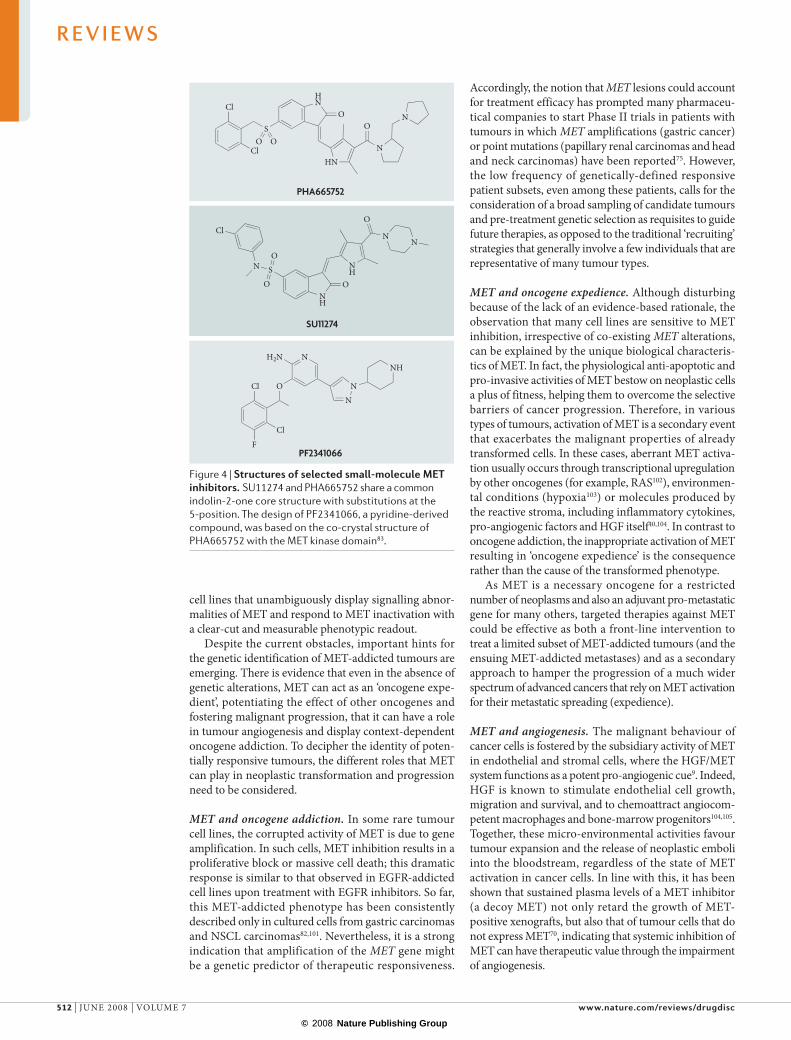
Small-molecule MET inhibitors. Initial attempts to identify ATP-competitive MET inhibitors led to the characterisation of K252a, a staurosporine analogue and broad-spectrum kinase inhibitor that blocks MET kinase activity at sub-micromolar concentrations78. Further chemical studies by Sugen (now Pfizer) resulted in the production of more selective MET inhibitors, all defined by the indolin-2-one core structure (FIG. 4). These com-pounds share the indolinone motif substituted at the 5-position of the indolinone core with 3-chlorobenzyl-sulphonamide groups (Su11274) or with 3,5-dimethyl pyrrole groups (PHA665752). Results from in vitro assays with various cancer cell lines show that both compounds inhibit MET-dependent biochemical and biological responses, with PHA665752 exhibiting at least 10-fold greater potency compared with Su11274 (REFS 79,80). Interestingly, Su11274 displays a selective inhibition pattern towards the different MET mutants identified in papillary renal carcinomas81, whereas PHA665752 is particularly effective in tumour cell lines and xenografts harbouring amplification of the MET gene82.
These small-molecule inhibitors have been limited to in vitro experiments or brief in vivo studies, and were not viable clinical agents due to poor pharmacokinetic proper-ties, resulting in low oral bioavailability. Based on the co-crystal structure of PHA665752 with the MET kinase domain, Pfizer designed PF2341066, an orally available 2-amino-3-benzyloxy-5-arylpyridine compound (FIG. 4) that selectively targets MET and anaplastic lymphoma kinase (AlK). PF2341066 shows efficacy at well-tolerated
doses, including marked cytoreductive anti-tumour activity and anti-angiogenic activity, in several neoplastic models featuring constitutively activated forms of MET. It is currently in Phase I/II clinical trials83.
Several other small molecules against MET have been produced by different companies and are now being tested in clinical trials. Xl880 (Exelixis) inhibits a fairly broad spectrum of kinases including MET, vascular endothelial growth factor receptor 2 (vEGFR2) and, to a lesser extent, platelet-derived growth factor receptor (PDGFR), Ron, KIT and TIE2 (REF. 84). It was the first orally bioavailable anti-MET small molecule to enter the clinic in 2005 and is presently undergoing Phase II trials in patients with poorly differentiated diffuse gastric cancer, head and neck squamous-cell carcinomas, and papillary renal cell carcinoma75. Interim results from the latter trial indicated that 14 out of 18 patients had a decrease in tumour size
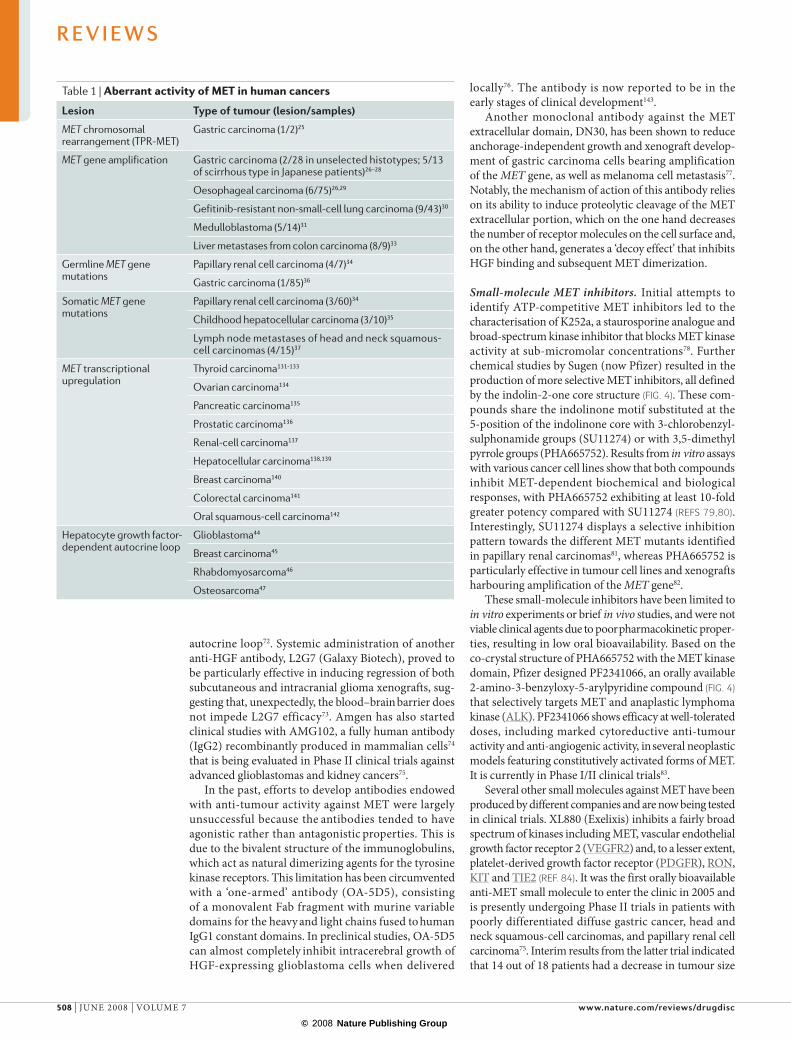
Table 1 | Aberrant activity of MET in human cancers
Lesion Type of tumour (lesion/samples)
MET chromosomal rearrangement (TPR-MET)
Gastric carcinoma (1/2)25
MET gene amplification Gastric carcinoma (2/28 in unselected histotypes; 5/13 of scirrhous type in Japanese patients)26–28
Oesophageal carcinoma (6/75)26,29
Gefitinib-resistant non-small-cell lung carcinoma (9/43)30
Medulloblastoma (5/14)31
Liver metastases from colon carcinoma (8/9)33
Germline MET gene mutations
Papillary renal cell carcinoma (4/7)34
Gastric carcinoma (1/85)36
Somatic MET gene mutations
Papillary renal cell carcinoma (3/60)34
Childhood hepatocellular carcinoma (3/10)35
Lymph node metastases of head and neck squamous- cell carcinomas (4/15)37
MET transcriptional upregulation
Thyroid carcinoma131-133
Ovarian carcinoma134
Pancreatic carcinoma135
Prostatic carcinoma136
Renal-cell carcinoma137
Hepatocellular carcinoma138,139
Breast carcinoma140
Colorectal carcinoma141
Oral squamous-cell carcinoma142
Hepatocyte growth factor-dependent autocrine loop
Glioblastoma44
Breast carcinoma45
Rhabdomyosarcoma46
Osteosarcoma47
R E V I E W S
508 | junE 2008 | voluME 7 www.nature.com/reviews/drugdisc
© 2008 Nature Publishing Group

Table 2 | Summary of biological antagonists and antibodies against HGF/MET
compound Stage of development comments
HGF/MET biological antagonists
NK2 (REFS 64,65) Preclinical • Inhibits HGF-induced proliferation in B5/589 mammary epithelial cells• Inhibits HGF-induced tubule formation in MCF-10A mammary epithelial
cells and in HUVECs
NK4 (REFS 66-68) Preclinical • The best-characterized HGF antagonist • Competitively inhibits HGF binding to MET• Inhibits HGF-dependent proliferation in hepatocytes• Inhibits invasion of different tumour cells in vitro and in xenografts• Inhibits angiogenesis in vitro and in xenografts
Uncleavable HGF69 Preclinical • Inhibits protease-mediated HGF conversion• Inhibits HGF-induced MET activation in A549 lung carcinoma cells• Suppresses tumour growth and metastasis in xenografts (A549,
MDA-MB-435 melanoma and HCT-116 colon carcinoma)• Impairs angiogenesis in xenografts• Systemic delivery does not perturb major physiological functions
Decoy MET70 Preclinical • Inhibits HGF binding and MET dimerization• Impairs MET constitutive activation in GTL16 gastric carcinoma cells• Impairs proliferation and migration in A549 cells• Impairs survival and invasion in MDA-MB-435 cells• Suppresses tumour growth and metastasis in xenografts (A549 and
MDA-MB-435)• Impairs angiogenesis in xenografts• Synergises with radiotherapy in inducing tumour regression• Systemic delivery does not perturb major physiological functions
Sema71 Preclinical • Inhibits HGF binding and MET dimerization• Inhibits activation of MET-dependent transduction pathways• Reduces HGF-driven migration of MDA-MB-435 cells
Antibodies against HGF
Various mAbs72 (1.29.1-1.74.1-1.75.1-2.4.4-2.12.1, Amgen)
Preclinical • Display sub-nanomolar affinities for HGF• Block binding of human HGF to MET• Inhibit HGF-mediated transduction pathways in PC3 prostate
carcinoma cells• Inhibit invasion of MDA-MB-435 cells in vitro• Cause regression of established U-87 MG (glioblastoma) subcutaneous
tumour xenografts
L2G7 (Galaxy Biotech)73 Preclinical • Blocks binding of HGF to MET• Inhibits HGF-induced scattering of MDCK cells• Inhibits HGF-induced proliferation of Mv-1-Lu cells in vitro• Inhibits HGF-induced proliferation and morphogenesis of HUVECs in vitro• Inhibits HGF-induced protection from apoptosis in U87-MG cells in vitro• Inhibits growth of established U-87 MG subcutaneous tumor xenografts• Systemic administration induces regression of intracranial U87-MG
xenografts
AMG102 (Amgen)74,75 Phase II trial: advanced glioblastoma; kidney carcinoma
• Enhances temozolomide- and docetaxel-induced anti-proliferative effects in U87-MG cells in vitro
• Increases docetaxel-induced apoptosis in U87-MG in vitro• Enhances temozolomide- and docetaxel-induced anti-growth effects in
U87-MG xenografts
Antibodies against MET
OA-5D5 (Genentech)76 Preclinical • ‘One-armed’ antibody• Inhibits HGF-induced MET phosphorylation in U87-MG cells• Inhibits proliferation and migration of U87-MG cells in vitro• Enhances staurosporin-induced apoptosis in U87-MG cells• Local treatment inhibits growth of intracranial U87-MG xenografts• Reduces angiogenesis in U87-MG xenografts
DN30 (Metheresis)77 Preclinical • Reduces MET activation in GTL16 cells• Stimulates shedding of the MET ectodomain in GTL16 and MDA-MB-435 cells• Inhibits anchorage-independent growth of GTL16 cells• Inhibits growth of GTL16 xenografts• Inhibits growth and metastasis of MDA-MB-435 xenografts
HGF, hepatocyte growth factor; HUVECs, human umbilical vein endothelial cells; MDCK, Madin–Darby canine kidney cells; Mv-1-Lu, mink lung epithelial cells; NK, HGF fragment consisting of N domain and Kringle domains.
R E V I E W S
nATuRE REvIEWS | druG diScovEry voluME 7 | junE 2008 | 509
© 2008 Nature Publishing Group

Table 3 | Summary of small-molecule MET inhibitors
compound Stage of development comments
K252 (REF. 78) Preclinical • Broad-spectrum kinase inhibitor• Phospho-MET IC50: 500 nM in HGF-stimulated MLP29 fetal mouse liver cells• HGF-dependent motility IC50: 30 nM in MLP29 cells• Viability IC50: 100 nM in GTL16 gastric carcinoma cells• Partial reversion of TPR-MET transformed phenotype: 75 nM in NIH3T3 mouse
fibroblasts• More effective at inhibiting MET active mutant (M1268T) than wild-type MET
SU11274 (Pfizer)79,81 Preclinical • MET-specific inhibitor (10–100 times more selective than 7 other kinases tested)• Enzyme IC50: 20 nM• Phospho-MET IC50: 1 µM in HGF-stimulated A549 lung carcinoma cells• Phospho-MET IC50 in M1268T and H1112Y MET mutants: 500 nM in NIH-3T3 cells• Viability IC50: 320 nM in GTL16 cells; 0.8–4.4 µM in various NSCLC cells; 2.5 µM in
various mesothelioma cell lines; 1–2.5 µM in various melanoma cell lines• Induces apoptosis in TPR-MET transformed BaF3 mouse pre-B cells
PHA665752 (Pfizer)80,82
Preclinical • MET-specific inhibitor (over 50 times more selective than 12 other kinases tested)• Enzyme IC50: 9 nM• Phospho-MET IC50: 25 nM in HGF-stimulated A549 cells• Viability IC50: 25 nM in GTL16 and other gastric carcinoma cells; 1–2 µM in
HGF-expressing mesothelioma cells• HGF-dependent motility IC50: 40 nM in MDCK cells• Induces regression of GTL16 xenografts• Inhibits growth and angiogenesis in xenografts from various lung carcinoma
cell lines
PF2341066 (Pfizer)83 Phase I/II trials started in August 2006: advanced carcinomas (various types)
• MET- and ALK-specific inhibitor ( more than 100 times more selective than 120 other kinases tested)
• Orally available• Enzyme IC50: 4 nM• Phospho-MET IC50: 10 nM in various tumour cell lines and HUVECs• Viability IC50: 10 nM in GTL16 cells• HGF-dependent motility IC50: 15 nM in MDCK cells• HGF-dependent invasion IC50: 6 nM in NCI-H441 lung carcinoma; 35 nM in HUVECs• HGF-dependent survival IC50: 14 nM in HUVECs
XL880 (Exelixis)75,84,85 • Phase I trial started in July 2005• Phase II trial started in June 2006:
papillary renal; gastric, head and neck carcinoma
• Broad spectrum kinase inhibitor (mainly MET and VEGFR2)• Enzyme IC50: 0.4 nM
ARQ197 (ArQule)75,86-
91• Phase I trial started in February
2006• Phase II trial started in November
2007: pancreatic carcinoma
• Non ATP competitive, MET-specific inhibitor (10–100 times more selective than 230 other kinases tested)
• Enzyme IC50: 50 nM• Phospho-MET IC50: 100 nM in NCI-H441 cells• Viability IC50: 100 nM in NCI-H441 cells• Invasion IC50: 80 nM in NCI-H441 cells• Inhibits growth in MDA-MB-231 (breast carcinoma), PC3 (prostate carcinoma),
HT29 (colon carcinoma) and PaCa2 (pancreatic carcinoma) xenografts• Inhibits metastasis formation in experimental metastatic models of orthotopic
colon cancer xenografts
MK2461 (Merck)75 • Phase I trial started in August 2007 in the United States
• Phase I/II trial started in July 2007 in Japan and Korea
• No information available
MP470 (SuperGen)92 Phase I trial started in July 2007 • Broad spectrum kinase inhibitor (MET, RET, mutant forms of KIT, PDGFR and FLT3)
SGX523 (SGX Pharmaceuticals)75,93,
Phase I trial started in January 2008 • Highly specific MET inhibitor (over 1,000 times more selective than 211 other kinases tested)
• Enzyme IC50: 35 nM• Phospho-MET IC50: 24 nM in GTL16 cells• Viability IC50: 93 nM in GTL16 cells• Inhibits migration in MDCK and A549 cells• Inhibits growth of GTL16 xenografts
JNJ38877605 (Johnson & Johnson)94
Preclinical • Highly specific MET inhibitor (selective over other 229 kinases tested)• Enzyme IC50: 4 nM• Phospho-MET IC50: 50 nM• Induces regression of U87-MG xenografts
FLT3, FMS-like tyrosine kinase 3; HGF, hepatocyte growth factor; HUVECs, human umbilical vein endothelial cells; MDCK, Madin–Darby canine kidney cells; NSCLC, non-small cell lung cancer; PDGFR, platelet derived growth factor receptor; VEGFR2, vascular endothelial growth factor receptor 2.
R E V I E W S
510 | junE 2008 | voluME 7 www.nature.com/reviews/drugdisc
© 2008 Nature Publishing Group

a bHGF
Sema
414400382
377
311
301
C
PSI
N
56 7 1
2ABCD
3
Top
Bottom
Nature Reviews | Drug Discovery
(ranging between 1 and 25%) after the first 8 weeks and at follow-up evaluations, after several months of treatment, 12 patients had stable disease and one patient exhibited a partial response (prolonged tumour shrinkage)85.
ARQ197 (ArQule) is a non ATP competitive drug that was identified as a selective MET inhibitor in a screen that assessed the biochemical profile of 230 kinases86-89. According to early data from Phase I trials, out of 37 patients with a broad range of solid tumours, 3 achieved a partial response and 20 had stable disease90. notably, 11 out of 19 patients treated for 6 weeks or less devel-oped novel metastatic lesions in the following 6 months, whereas 18 out of 19 patients treated for 12 weeks or longer did not, suggesting a potential anti-invasive activity for this compound91. A randomized Phase II study of ARQ197 versus gemcitabine in treatment-naive patients with unresectable, locally advanced or metastatic pancreatic adenocarcinoma is ongoing75.
Based on unpublished information available on the internet, several other small-molecule compounds are entering the clinic for initial studies. Merck is recruit-ing patients for Phase I/II studies on MK2461, a small-molecule inhibitor of MET for which no details are provided75. SuperGen has just started a Phase I trial with MP470, an oral, multi-targeted tyrosine kinase inhibitor of MET, RET and mutant forms of KIT, PDGFR and FlT3 (REF. 92). SGX523 (SGX Pharmaceuticals) and jnj38877605 (johnson & johnson) are reported to be highly specific MET inhibitors, with selective anti-MET activity over more than 200 other human kinases profiled in vitro93,94. Phase I clinical trials with SGX523 started in january 2008 (REF. 75) and trials with jnj38877605 are imminent.
Further approaches to inhibit MET signalling. Additional strategies to target MET signalling are aimed at MET co-receptors, such as CD44, the α6β4 integrin and B plexins, as well as ubiquitous downstream effectors that channel MET-dependent transduction pathways95 (see also FIG. 2). The inactivation of co-receptors could be achieved, for example, by designing antibodies or peptides that disrupt the MET-based heterocomplexes. Indeed, it has been demonstrated that a peptide frag-ment of CD44 prevents activation of MET-triggered signals and MET-induced migration in vitro96.
For targeting downstream effectors, combination therapies targeting multiple pathways could be envis-aged. This roughly involves three categories of signal-ling molecules: pro-survival effectors, comprising the PI3K–Akt cascade and STAT3; mitogenic effectors, consisting of the Grb2–SoS–RAS–RAF–MEK–ERK pathway; and pro-migratory effectors, including small GTPases of the Rho family and SRC. Ideally, inhibi-tors directed against different key components of this network (in combination with anti-MET inhibitors) might provide greater therapeutic efficacy, especially in those cases in which MET monotherapy becomes ineffective. Propagation of MET-dependent signals can be also blocked by peptides competing with MET-associated signal transducers for access to the dock-ing site. Specifically, attempts have been made with artificial tripeptide-based inhibitors of the Grb2 SH2 domain97 and with phospho-peptides that obstruct binding of STAT3 to MET and STAT3 dimerization98.
Rational identification of responsive tumoursExperience with EGFR tyrosine kinase inhibitors has demonstrated that they are only efficacious in a small subset of tumours, those that exhibit genetic alterations of the receptor itself99. Intriguingly, cultured cell lines bearing the same EGFR genetic lesions that are present in human tumours in vivo undergo cell-cycle arrest or apoptosis in response to EGFR inhibition, even under otherwise optimal conditions. This phenomenon, called ‘oncogene addiction’, applies to all those settings in which cancer cells appear to be dependent on a single over-active oncogene for their proliferation and survival99,100 (BOX 1).
In the case of MET, the lesson that genetic alterations of the kinase might induce oncogene addiction and there-fore predict therapeutic responsiveness, has not been fully appreciated. The biochemical and biological char-acterization of each of the inhibitors mentioned above and in TABLES 2,3 has been carried out using a bewilder-ing amount of different cell lines, most of which have not been characterized in genetic terms. Data appear to be even more confusing because some results have been obtained in cells in which MET is basally inactive, others in the presence of exogenous HGF, and others in cells displaying variable levels of MET overexpression. The rational selection of consistently responsive cell lines will be mandatory to build a preclinical foundation for the oriented recruitment of potentially responsive patients. Furthermore, reliable in vitro models in which to test MET inhibition should be based on genetically defined
Figure 3 | complex between the MET Sema domain and the HGF β-chain. Ribbon representation of the complex between MET and hepatocyte growth factor (HGF); the HGF β-chain is shown in grey and MET in various colours. The N-terminus of MET is coloured dark blue and the C-terminus is coloured red. Disordered regions are indicated with dotted lines and the numbers refer to the last and first residues of the ordered regions. a | Sema domain of MET forms a seven-bladed β propeller (subunits labelled 1-7) and its overall shape resembles a funnel with an inner diameter of about 25 Å at the wide portion and 10 Å in the narrowest part. The β strands in blade 1 are labelled A–D. Each of the blades consists of four anti-parallel β strands with strand A in the centre of the propeller, followed by strands B and C, and with strand D forming the outermost strand of the blade. b | Side view of the same complex. Figure modified with permission from REF. 61 (2004) Macmillan Publishing Ltd.
R E V I E W S
nATuRE REvIEWS | druG diScovEry voluME 7 | junE 2008 | 511
© 2008 Nature Publishing Group
Nature Reviews | Drug Discovery
Cl
S
ClO O
HN
O
HN
N
ON
Cl
F
Cl
O
NH2N
N
N
NH
PHA665752
PF2341066
SU11274
NH
O
SNO
O
NH
N
O
NCl
cell lines that unambiguously display signalling abnor-malities of MET and respond to MET inactivation with a clear-cut and measurable phenotypic readout.
Despite the current obstacles, important hints for the genetic identification of MET-addicted tumours are emerging. There is evidence that even in the absence of genetic alterations, MET can act as an ‘oncogene expe-dient’, potentiating the effect of other oncogenes and fostering malignant progression, that it can have a role in tumour angiogenesis and display context-dependent oncogene addiction. To decipher the identity of poten-tially responsive tumours, the different roles that MET can play in neoplastic transformation and progression need to be considered.
MET and oncogene addiction. In some rare tumour cell lines, the corrupted activity of MET is due to gene amplification. In such cells, MET inhibition results in a proliferative block or massive cell death; this dramatic response is similar to that observed in EGFR-addicted cell lines upon treatment with EGFR inhibitors. So far, this MET-addicted phenotype has been consistently described only in cultured cells from gastric carcinomas and nSCl carcinomas82,101. nevertheless, it is a strong indication that amplification of the MET gene might be a genetic predictor of therapeutic responsiveness.
Accordingly, the notion that MET lesions could account for treatment efficacy has prompted many pharmaceu-tical companies to start Phase II trials in patients with tumours in which MET amplifications (gastric cancer) or point mutations (papillary renal carcinomas and head and neck carcinomas) have been reported75. However, the low frequency of genetically-defined responsive patient subsets, even among these patients, calls for the consideration of a broad sampling of candidate tumours and pre-treatment genetic selection as requisites to guide future therapies, as opposed to the traditional ‘recruiting’ strategies that generally involve a few individuals that are representative of many tumour types.
MET and oncogene expedience. Although disturbing because of the lack of an evidence-based rationale, the observation that many cell lines are sensitive to MET inhibition, irrespective of co-existing MET alterations, can be explained by the unique biological characteris-tics of MET. In fact, the physiological anti-apoptotic and pro-invasive activities of MET bestow on neoplastic cells a plus of fitness, helping them to overcome the selective barriers of cancer progression. Therefore, in various types of tumours, activation of MET is a secondary event that exacerbates the malignant properties of already transformed cells. In these cases, aberrant MET activa-tion usually occurs through transcriptional upregulation by other oncogenes (for example, RAS102), environmen-tal conditions (hypoxia103) or molecules produced by the reactive stroma, including inflammatory cytokines, pro-angiogenic factors and HGF itself40,104. In contrast to oncogene addiction, the inappropriate activation of MET resulting in ‘oncogene expedience’ is the consequence rather than the cause of the transformed phenotype.
As MET is a necessary oncogene for a restricted number of neoplasms and also an adjuvant pro-metastatic gene for many others, targeted therapies against MET could be effective as both a front-line intervention to treat a limited subset of MET-addicted tumours (and the ensuing MET-addicted metastases) and as a secondary approach to hamper the progression of a much wider spectrum of advanced cancers that rely on MET activation for their metastatic spreading (expedience).
MET and angiogenesis. The malignant behaviour of cancer cells is fostered by the subsidiary activity of MET in endothelial and stromal cells, where the HGF/MET system functions as a potent pro-angiogenic cue9. Indeed, HGF is known to stimulate endothelial cell growth, migration and survival, and to chemoattract angiocom-petent macrophages and bone-marrow progenitors104,105. Together, these micro-environmental activities favour tumour expansion and the release of neoplastic emboli into the bloodstream, regardless of the state of MET activation in cancer cells. In line with this, it has been shown that sustained plasma levels of a MET inhibitor (a decoy MET) not only retard the growth of MET-positive xenografts, but also that of tumour cells that do not express MET70, indicating that systemic inhibition of MET can have therapeutic value through the impairment of angiogenesis.
Figure 4 | Structures of selected small-molecule MET inhibitors. SU11274 and PHA665752 share a common indolin-2-one core structure with substitutions at the 5-position. The design of PF2341066, a pyridine-derived compound, was based on the co-crystal structure of PHA665752 with the MET kinase domain83.
R E V I E W S
512 | junE 2008 | voluME 7 www.nature.com/reviews/drugdisc
© 2008 Nature Publishing Group

Intriguingly, MET is transcriptionally upregulated by hypoxia103, an obvious consequence of anti-angiogenic treatments aimed to cut off the tumour’s blood supply. In turn, increased MET expression stimulates cell invasive-ness as an escape route towards more oxygenated tissues. This points to the therapeutic necessity of suppressing MET activity when targeting angiogenesis to prevent the potential dissemination of cancer cells, which would be promoted as a result of intratumoural oxygen deprivation. The fact that inactivation of MET has both anti-invasive effects in the tumour and anti-angiogenic effects in the microenvironment invigorates the use of MET inhibitors as a ‘two-for-one’ combination therapy that concomitantly impairs metastatic spreading and tumour neo-vascularization106,107.
Context-dependent oncogene addiction. Besides direct oncogene addiction, tumours might also display a con-text-dependent addiction on certain signalling compo-nents. As tyrosine kinase receptors are able to activate signalling pathways that are part of complex molecular circuitries shared with other receptors, their signalling cascades can be negatively or positively controlled at multiple levels108. Accordingly, activation of a specific receptor can lead to different outcomes depending on the additional genes that, in a defined tumour context, are functionally gained or lost.
This concept has important implications for the design of molecularly targeted combination therapies. A notable example is the role of the tumour suppres-sor PTEn in the modulation of MET-dependent gene expression. Dysregulated activation of MET together
with loss of PTEn is a relatively common occurrence in tumours such as malignant gliomas44. In this situation, loss of PTEn leads to transcriptional upregulation of the EGFR agonist TGF-α, which induces constitutive activa-tion of EGFR in an autocrine manner109. This indicates that EGFR signalling can contribute to the malignant phenotype in cells displaying a constitutively active form of MET, setting the stage for combined therapies against MET and EGFR whenever a concomitant deficiency of PTEn is observed. Intriguingly, inactivation of PTEn, which results in continual anti-apoptotic signalling, is usually associated with resistance to tyrosine kinase inhibitors, but combined inhibition of MET and EGFR in a glioblastoma model in which both receptors are con-stitutively hyperactive can circumvent PTEn deficiency and restore therapeutic responsiveness110.
Another example of molecular cross-talk between members of the EGFR family and MET has recently been highlighted in lung tumours with acquired resistance to the EGFR small-molecule inhibitors gefitinib and erlo-tinib30,111. In such tumours, resistance to EGFR inhibitors might be achieved through amplification of the MET gene, which leads to MET hyperactivation and MET-dependent phosphorylation of HER3. Phosphorylated HER3 can, in turn, recruit PI3K and stimulate PI3K-based survival pathways that confer resistance. In agree-ment with these findings, obstruction of MET signalling in these resistant cells restores their sensitivity to EGFR inhibitors, so that only the simultaneous blockade of both MET and EGFR impairs tumour growth.
OutlookIn the early days of anti-cancer therapy, the observation that tumours are hyperproliferative lesions prompted the development of anti-mitotic and cytostatic compounds with the hope that they would function indiscriminately as magic bullets. As it became clear that cancers have multiple aetiologies, and that neoplastic progression is associated with a combination of genetic and epigenetic alterations, the task of developing therapies suitable for treatment of the full spectrum of cancers was depicted as Herculean and almost impossible.
Things have now changed: it is well established that inactivation of individual oncogenes can block tumour growth and even lead to tumour regression, despite the multitude of genetic alterations harboured by trans-formed cells. This has given an unprecedented clinical value to the concept that cancer is a disease of genes, allowing a novel classification of tumours based on the presence of defined genetic lesions. Classical histopatho-logical diagnosis is still important to evaluate the extent of phenotypic aggressiveness, but personalized molecular diagnosis is needed to understand whether a tumour in one specific patient carries a particular genetic alteration that could be targeted by therapy.
In the case of MET, the challenge is to identify the genetically-defined responsive patient subsets that could benefit from MET inhibition. This calls for a vast preclin-ical strategy of tumour categorization based on genetic makeup, responsiveness to MET inhibition and follow-up validation of surrogate indicators of MET activity.
Box 1 | Oncogene addiction and oncogene overdose
The mechanisms underlying oncogene addiction are still elusive. One hypothesis relies on the observation that many oncogenes paradoxically convey both pro-survival and pro-apoptotic signals115,116. Acute inactivation of the addicting oncoprotein could result in a quantitative and/or temporal signalling imbalance in which the pro-apoptotic outputs prevail over survival pathways, leading to cell death99,100.
Because of the genomic instability inherent in cancer, neoplastic cells accrue genetic alterations and undergo genetic drift over time. This heavy mutational baggage renders tumour cells much more vulnerable than normal cells, so that they undergo apoptosis whenever novel oncogenic insults overload their stressed biochemical circuits with additional signals (‘oncogene overdose’). The first intimation that deregulated oncogenic cues trigger expeditious cell death came from the unexpected discovery that oncoproteins like MYC, E1A and c-JUN can function as potent pro-apoptotic molecules115. Similarly, mammary carcinoma cells co-expressing high levels of epidermal growth factor receptor (EGFR) and human epidermal growth factor receptor 2 (HER2) undergo apoptosis in response to epidermal growth factor117.
Intriguingly, something similar has been described for the hepatocyte growth factor (HGF)/MET system. It is notable that HGF was initially named ‘tumour cytotoxic factor’ for its ability to elicit apoptotic responses in sarcoma118 and hepatoma119 cells. More recently, HGF has been shown to enhance apoptosis in ovarian cancer cells treated with conventional chemotherapeutics through a p38 MAPK-dependent pathway120,121. Together, these findings suggest that, in some cellular settings and upon activation of specific signalling cascades, HGF can act as a death-inducing cytokine. Obviously, HGF cannot be used as an anti-cancer pro-apoptotic molecule because of its intrinsic pro-invasive activity. However, mutant forms of HGF that retain some beneficial properties while lacking adverse pro-metastatic effects have already been produced and therapeutically validated122. Possibly, HGF analogues with selective pro-apoptotic function on some tumour types will be developed in the future.
R E V I E W S
nATuRE REvIEWS | druG diScovEry voluME 7 | junE 2008 | 513
© 2008 Nature Publishing Group

The current availability of high-throughput DnA sequencing, genome-wide transcriptional profiling and proteomics provides a unique opportunity to organize a joint effort to achieve these objectives. Pilot cellular models of sensitivity to MET inhibition have been characterized and preliminary information on the signalling and transcriptional consequences of MET overactivation and inhibition in vitro is now avail-able24,82,101,112–114. Changes in protein phosphorylation, indicative of changes in protein activity, and gene
expression signatures could be exploited to derive a list of molecules that might be used as biomarkers of MET activation in vivo. This knowledge should be comple-mented by the analysis of how the abnormal activity of other oncogenes or oncosuppressors can affect cellular responsiveness to MET inhibition, which can be clini-cally relevant for the use of combined therapies. only when this information is verified and validated, will it be possible to translate all these preclinical observations into a promising therapeutic approach.
1. Trusolino, L. & Comoglio, P. M. Scatter-factor and semaphorin receptors: cell signalling for invasive growth. Nature Rev. Cancer 2, 289–300 (2002).
2. Birchmeier, C., Birchmeier, W., Gherardi, E. & Vande Woude, G. F. Met, metastasis, motility and more. Nature Rev. Mol. Cell. Biol. 4, 915–925 (2003).
3. Xiao, G. H. et al. Anti-apoptotic signaling by hepatocyte growth factor/Met via the phosphatidylinositol 3-kinase/Akt and mitogen-activated protein kinase pathways. Proc. Natl Acad. Sci. USA 98, 247–252 (2001).
4. Zeng, Q. et al. Hepatocyte growth factor inhibits anoikis in head and neck squamous cell carcinoma cells by activation of ERK and Akt signaling independent of NF-κB. J. Biol. Chem. 277, 25203–25208 (2002).
5. Bladt, F., Riethmacher, D., Isenmann, S., Aguzzi, A. & Birchmeier, C. Essential role for the c-met receptor in the migration of myogenic precursor cells into the limb bud. Nature 376, 768–771 (1995).
6. Streit, A. et al. A role for HGF/SF in neural induction and its expression in Hensen’s node during gastrulation. Development 121, 813–824 (1995).
7. Andermacher, E., Surani, M. A. & Gherardi, E. Co-expression of the HGF/SF and c-met genes during early mouse embryogenesis precedes reciprocal expression in adjacent tissues during organogenesis. Dev. Genet. 18, 254–266 (1996).
8. Takayama, H., La Rochelle, W. J., Anver, M., Bockman, D. E. & Merlino, G. Scatter factor/hepatocyte growth factor as a regulator of skeletal muscle and neural crest development. Proc. Natl Acad. Sci. USA 93, 5866–5871 (1996).
9. Bussolino, F. et al. Hepatocyte growth factor is a potent angiogenic factor which stimulates endothelial cell motility and growth. J. Cell Biol. 119, 629–641 (1992).
10. Schmidt, C. et al. Scatter factor/hepatocyte growth factor is essential for liver development. Nature 373, 699–702 (1995).
11. Michalopoulos, G. K. & DeFrances, M. C. Liver regeneration. Science 276, 60–66 (1997).
12. Nakamura, T., Mizuno, S., Matsumoto, K., Sawa, Y. & Matsuda, H. Myocardial protection from ischemia/reperfusion injury by endogenous and exogenous HGF. J. Clin. Invest. 106, 1511–1519 (2000).
13. Matsumoto, K. & Nakamura, T. Hepatocyte growth factor: renotropic role and potential therapeutics for renal diseases. Kidney Int. 59, 2023–2038 (2001).
14. Rabkin, R. et al. Hepatocyte growth factor receptor in acute tubular necrosis. J. Am. Soc. Nephrol. 12, 531–540 (2001).
15. Okada, H. & Kalluri, R. Cellular and molecular pathways that lead to progression and regression of renal fibrogenesis. Curr. Mol. Med. 5, 467–474 (2005).
16. Liu, Y. & Yang, J. Hepatocyte growth factor: new arsenal in the fights against renal fibrosis? Kidney Int. 70, 238–240 (2006).
17. Ueki, T. et al. Hepatocyte growth factor gene therapy of liver cirrhosis in rats. Nature Med. 5, 226–230 (1999).
18. Watanabe, M. et al. Hepatocyte growth factor gene transfer to alveolar septa for effective suppression of lung fibrosis. Mol. Ther. 12, 58–67 (2005).
19. Boccaccio, C. & Comoglio, P. M. Invasive growth: a MET-driven genetic programme for cancer and stem cells. Nature Rev. Cancer 6, 637–645 (2006).
20. Comoglio, P. M. & Trusolino, L. Invasive growth: from development to metastasis. J. Clin. Invest. 109, 857–862 (2002).
21. Danilkovitch-Miagkova, A. & Zbar, B. Dysregulation of Met receptor tyrosine kinase activity in invasive tumors. J. Clin. Invest. 109, 863–867 (2002).
22. Cooper, C. S. et al. Molecular cloning of a new transforming gene from a chemically transformed human cell line. Nature 311, 29–33 (1984).
23. Liang, T. J., Reid, A. E., Xavier, R., Cardiff, R. D. & Wang, T. C. Transgenic expression of tpr-met oncogene leads to development of mammary hyperplasia and tumors. J. Clin. Invest. 97, 2872–2877 (1996).
24. Boccaccio, C. et al. The MET oncogene drives a genetic programme linking cancer to haemostasis. Nature 434, 396–400 (2005).First in vivo demonstration that lentiviral-mediated somatic transduction of oncogenic MET in hepatocytes of adult mice leads to the development of hepatocellular carcinomas.
25. Soman, N. R., Correa, P., Ruiz, B. A. & Wogan, G. N. The TPR-MET oncogenic rearrangement is present and expressed in human gastric carcinoma and precursor lesions. Proc. Natl Acad. Sci. USA 88, 4892–4896 (1991).
26. Houldsworth, J., Cordon-Cardo, C., Ladanyi, M., Kelsen, D. P. & Chaganti, R. S. Gene amplification in gastric and esophageal adenocarcinomas. Cancer Res. 50, 6417–6422 (1990).
27. Kuniyasu, H. et al. Frequent amplification of the c-met gene in scirrhous type stomach cancer. Biochem. Biophys. Res. Commun. 189, 227–232 (1992).
28. Hara, T. et al. Amplification of c-myc, K-sam, and c-met in gastric cancers: detection by fluorescence in situ hybridization. Lab. Invest. 78, 1143–1153 (1998).
29. Miller, C. T. et al. Genomic amplification of MET with boundaries within fragile site FRA7G and upregulation of MET pathways in esophageal adenocarcinoma. Oncogene 25, 409–418 (2006).
30. Bean, J. et al. MET amplification occurs with or without T790M mutations in EGFR mutant lung tumors with acquired resistance to gefitinib or erlotinib. Proc. Natl Acad. Sci. USA 104, 20932–20937 (2007).
31. Tong, C. Y. et al. Detection of oncogene amplifications in medulloblastomas by comparative genomic hybridization and array-based comparative genomic hybridization. J. Neurosurg. 100, 187–193 (2004).
32. Wang, R., Ferrell, L. D., Faouzi, S., Maher, J. J. & Bishop, J. M. Activation of the Met receptor by cell attachment induces and sustains hepatocellular carcinomas in transgenic mice. J. Cell Biol. 153, 1023–1034 (2001).First in vivo demonstration that transgenic overexpression of wild-type MET in mouse hepatocytes leads to the development of hepatocellular carcinomas.
33. Di Renzo, M. F. et al. Overexpression and amplification of the MET/HGF receptor gene during the progression of colorectal cancer. Clin. Cancer Res. 1, 147–154 (1995).
34. Schmidt, L. et al. Germline and somatic mutations in the tyrosine kinase domain of the MET proto-oncogene in papillary renal carcinomas. Nature Genet. 16, 68–73 (1997).First identification of naturally-occurring oncogenic mutations of MET in humans.
35. Park, W. S. et al. Somatic mutations in the kinase domain of the MET/hepatocyte growth factor receptor gene in childhood hepatocellular carcinomas. Cancer Res. 59, 307–310 (1999).
36. Lee, J. H. et al. A novel germ line juxtamembrane MET mutation in human gastric cancer. Oncogene 19, 4947–4953 (2000).
37. Di Renzo, M. F. et al. Somatic mutations of the MET oncogene are selected during metastatic spread of human HNSC carcinomas. Oncogene 19, 1547–1555 (2000).
First report of a direct involvement of MET in tumour metastasis in humans. Neoplastic cells harbouring activating mutations of the MET gene undergo clonal expansion during the metastatic spreading of head and neck squamous-cell carcinomas.
38. Graveel, C. et al. Activating Met mutations produce unique tumor profiles in mice with selective duplication of the mutant allele. Proc. Natl Acad. Sci. USA 101, 17198–17203 (2004).
39. Danilkovitch-Miagkova, A. & Zbar, B. Dysregulation of Met receptor tyrosine kinase activity in invasive tumors. J. Clin. Invest. 109, 863–867 (2002).
40. Boccaccio, C., Gaudino, G., Gambarotta, G., Galimi, F. & Comoglio, P. M. Hepatocyte growth factor (HGF) receptor expression is inducible and is part of the delayed-early response to HGF. J. Biol. Chem. 269, 12846–12851 (1994).
41. Aguirre Ghiso, J. A., Alonso, D. F., Farias, E. F., Gomez, D. E. & de Kier Joffe, E. B. Deregulation of the signaling pathways controlling urokinase production. Its relationship with the invasive phenotype. Eur. J. Biochem. 263, 295–304 (1999).
42. Parr, C., Watkins, G., Mansel, R. E. & Jiang, W. G. The hepatocyte growth factor regulatory factors in human breast cancer. Clin. Cancer Res. 10, 202–211 (2004).
43. Michieli, P. et al. Mutant Met-mediated transformation is ligand-dependent and can be inhibited by HGF antagonists. Oncogene 18, 5221–5231 (1999).
44. Koochekpour, S. et al. Met and hepatocyte growth factor/scatter factor expression in human gliomas. Cancer Res. 57, 5391–5398 (1997).
45. Tuck, A. B., Park, M., Sterns, E. E., Boag, A. & Elliott, B. E. Coexpression of hepatocyte growth factor and receptor (Met) in human breast carcinoma. Am. J. Pathol. 148, 225–232 (1996).
46. Ferracini, R. et al. Retrogenic expression of the MET proto-oncogene correlates with the invasive phenotype of human rhabdomyosarcomas. Oncogene 12, 1697–1705 (1996).
47. Ferracini, R. et al. The Met/HGF receptor is over-expressed in human osteosarcomas and is activated by either a paracrine or an autocrine circuit. Oncogene 10, 739–749 (1995).
48. Rong, S., Segal, S., Anver, M., Resau, J. H. & Vande Woude, G. F. Invasiveness and metastasis of NIH 3T3 cells induced by Met-hepatocyte growth factor/scatter factor autocrine stimulation. Proc. Natl Acad. Sci. USA 91, 4731–4735 (1994).
49. Bellusci, S. et al. Creation of an hepatocyte growth factor/scatter factor autocrine loop in carcinoma cells induces invasive properties associated with increased tumorigenicity. Oncogene 9, 1091–1099 (1994).
50. Jeffers, M., Rong, S., Anver, M. & Vande Woude, G. F. Autocrine hepatocyte growth factor/scatter factor signalling induces transformation and the invasive/metastatic phenotype in C127 cells. Oncogene 13, 853–861 (1996).
51. Takayama, H. et al. Diverse tumorigenesis associated with aberrant development in mice overexpressing hepatocyte growth factor/scatter factor. Proc. Natl Acad. Sci. USA 94, 701–706 (1997).
52. Otsuka, T. et al. c-Met autocrine activation induces development of malignant melanoma and acquisition of the metastatic phenotype. Cancer Res. 58, 5157–5167 (1998).
53. Sharp, R. et al. Synergism between INK4a/ARF inactivation and aberrant HGF/SF signaling in rhabdomyosarcomagenesis. Nature Med. 8, 1276–1280 (2002).
54. Kobayashi, T. et al. Hepatocyte growth factor specifically binds to sulfoglycolipids. J. Biol. Chem. 269, 9817–9821 (1994).
R E V I E W S
514 | junE 2008 | voluME 7 www.nature.com/reviews/drugdisc
© 2008 Nature Publishing Group

55. Lyon, M., Deakin, J. A., Mizuno, K., Nakamura, T. & Gallagher, J. T. Interaction of hepatocyte growth factor with heparan-sulfate. Elucidation of the major heparan sulfate structural determinants. J. Biol. Chem. 269, 11216–11223 (1994).
56. Naldini, L. et al. Extracellular proteolytic cleavage by urokinase is required for activation of hepatocyte growth factor/scatter factor. EMBO J. 11, 4825–4833 (1992).
57. Mars, W. M., Zarnegar, R. & Michalopoulos, G. K. Activation of hepatocyte growth factor by the plasminogen activators uPA and tPA. Am. J. Pathol. 143, 949–958 (1993).
58. Lokker, N. A. et al. Structure–function analysis of hepatocyte growth factor: identification of variants that lack mitogenic activity yet retain high affinity receptor binding. EMBO J. 11, 2503–2510 (1992).
59. Lietha, D., Chirgadze, D. Y., Mulloy, B., Blundell, T. L. & Gherardi, E. Crystal structures of NK1-heparin complexes reveal the basis for NK1 activity and enable engineering of potent agonists of the MET receptor. EMBO J. 20, 5543–5555 (2001).
60. Matsumoto, K., Kataoka, H., Date, K. & Nakamura, T. Cooperative interaction between α- and β-chains of hepatocyte growth factor on c-Met receptor confers ligand-induced receptor tyrosine phosphorylation and multiple biological responses. J. Biol. Chem. 273, 22913–22920 (1998).
61. Stamos, J., Lazarus, R. A., Yao, X., Kirchhofer, D. & Wiesmann, C. Crystal structure of the HGF β-chain in complex with the Sema domain of the Met receptor. EMBO J. 23, 2325–2335 (2004).
62. Kirchhofer, D. et al. Structural and functional basis of the serine protease-like HGF beta-chain in Met binding and signaling. J. Biol. Chem. 279, 39915–39924 (2004).
63. Trusolino L, Pugliese L, Comoglio PM. Interactions between scatter factors and their receptors: hints for therapeutic applications. FASEB J. 12, 1267–1280 (1998).
64. Chan, A. M. et al. Identification of a competitive HGF antagonist encoded by an alternative transcript. Science 254, 1382–1385 (1991).
65. Montesano, R. et al. Differential effects of hepatocyte growth factor isoforms on epithelial and endothelial tubulogenesis. Cell Growth Differ. 9, 355–365 (1998).
66. Matsumoto, K. & Nakamura, T. NK4 (HGF-antagonist/angiogenesis inhibitor) in cancer biology and therapeutics, Cancer Sci. 94, 321–327 (2003).
67. Matsumoto, K. & Nakamura, T. NK4 gene therapy targeting HGF-Met and angiogenesis. Front. Biosci. 13, 1943–1951 (2008).
68. Kuba, K. et al. HGF/NK4, a four-kringle antagonist of hepatocyte growth factor, is an angiogenesis inhibitor that suppresses tumor growth and metastasis in mice. Cancer Res. 60, 6737–6743 (2000).
69. Mazzone, M. et al. An uncleavable form of pro-scatter factor suppresses tumor growth and dissemination in mice. J. Clin. Invest. 114, 1418–1432 (2004).
70. Michieli, P. et al. Targeting the tumor and its microenvironment by a dual-function decoy Met receptor. Cancer Cell 6, 61–73 (2004).
71. Kong-Beltran, M., Stamos, J. & Wickramasinghe, D. The Sema domain of Met is necessary for receptor dimerization and activation. Cancer Cell 6, 75–84 (2004).
72. Burgess, T. et al. Fully human monoclonal antibodies to hepatocyte growth factor with therapeutic potential against hepatocyte growth factor/c-Met-dependent human tumors. Cancer Res. 66, 1721–1729 (2006).
73. Kim, K. J. et al. Systemic anti-hepatocyte growth factor monoclonal antibody therapy induces the regression of intracranial glioma xenografts. Clin. Cancer Res. 12, 1292–1298 (2006).
74. Jun, H. T. et al. AMG 102, a fully human anti-hepatocyte growth factor/scatter factor neutralizing antibody, enhances the efficacy of temozolomide or docetaxel in U-87 MG cells and xenografts. Clin. Cancer Res. 13, 6735–6742 (2007).
75. Registry of federally and privately supported clinical trials conducted in the United States [online] <www.clinicaltrials.gov>
76. Martens, T. et al. A novel one-armed anti-c-Met antibody inhibits glioblastoma growth in vivo. Clin. Cancer Res. 12, 6144–6152 (2006).
77. Petrelli, A. et al. Ab-induced ectodomain shedding mediates hepatocyte growth factor receptor down-regulation and hampers biological activity. Proc. Natl Acad. Sci. USA 103, 5090–5095 (2006).
78. Morotti, A., Mila, S., Accornero, P., Tagliabue, E. & Ponzetto, C. K252a inhibits the oncogenic properties of Met, the HGF receptor. Oncogene 21, 4885–4893 (2002).
79. Sattler, M. et al. A novel small molecule met inhibitor induces apoptosis in cells transformed by the oncogenic TPR-MET tyrosine kinase. Cancer Res. 63, 5462–5469 (2003).
80. Christensen, J. G. et al. A selective small molecule inhibitor of c-Met kinase inhibits c-Met-dependent phenotypes in vitro and exhibits cytoreductive antitumor activity in vivo. Cancer Res. 63, 7345–7355 (2003).
81. Berthou, S. et al. The Met kinase inhibitor SU11274 exhibits a selective inhibition pattern toward different receptor mutated variants. Oncogene 23, 5387–5393 (2004).
82. Smolen, G. A et al. Amplification of MET may identify a subset of cancers with extreme sensitivity to the selective tyrosine kinase inhibitor PHA-665752. Proc. Natl Acad. Sci. USA 103, 2316–2321 (2006).
83. Zou, H. Y. et al. An orally available small-molecule inhibitor of c-Met, PF-2341066, exhibits cytoreductive antitumor efficacy through antiproliferative and antiangiogenic mechanisms. Cancer Res. 67, 4408–4417 (2007).
84. Eder, J. P. et al. Phase I experience with c-MET inhibitor XL880 administered orally to patients (pts) with solid tumors. J. Clin. Oncol. 25, 3526 (2007).
85. Ross, R. W. et al. A phase 2 study of the dual MET/VEGFR2 inhibitor XL880 in patients with papillary renal carcinoma. Abstract B249. AACR-NCI-EORTC: Molecular Targets and Cancer Therapeutics, San Francisco, California, USA (2007).
86. Jeay, S. et al. ARQ197, a highly selective small molecule inhibitor of c-Met, with selective antitumor properties in a broad spectrum of human cancer cells. Abstract 2369. AACR Annual Meeting, Los Angeles, California, USA (2007).
87. Munshi, N. et al. ARQ197, a highly selective inhibitor of c-Met, inhibits invasive and metastatic growth of cancer cells. Abstract 2367. AACR Annual Meeting, Los Angeles, California, USA (2007).
88. Youzhi, L. I. et al. Anti-metastatic activity of ARQ197, a highly selective oral small molecule inhibitor of c-Met, in experimental metastatic models of colon cancer. Abstract 2191. AACR Annual Meeting, Los Angeles, California, USA (2007).
89. Youzhi, L. I. et al. Broad spectrum anti-cancer activity of ARQ197, a highly selective oral c-Met inhibitor, in multiple xenograft models. Abstract 2216. AACR Annual Meeting, Los Angeles, California, USA (2007).
90. Garcia, A. et al. Phase 1 study of ARQ 197, a selective inhibitor of the c-Met RTK in patients with metastatic solid tumors reaches recommended phase 2 dose. Abstract 3525. ASCO Annual Meeting, Chicago, Illinois, USA (2007).
91. Conquering cancer with novel therapeutics. ArQule website [online] <http://phx.corporate-ir.net/phoenix.zhtml?c=82991&p=irol-presentations>
92. SuperGen reports dosing of first patient in Phase I trial of novel tyrosine kinase inhibitor. SuperGen website [online] <http://ir.supergen.com/phoenix.zhtml?c= 105560&p=irol-newsArticle&ID=1022920& highlight>
93. Froning, K. J. et al. SGX523: a potent and highly selective small molecule inhibitor of the MET receptor tyrosine kinase. Abstract 2366. AACR Annual Meeting, Los Angeles, California, USA (2007).
94. Perera, T. Selective inhibition of Met kinase: JNJ38877605. Spring CTEP Early Drug Development Meeting, Rockville, Maryland, USA (2007).
95. Bertotti, A. & Comoglio, P. M. Tyrosine kinase signal specificity: lessons from the HGF receptor. Trends Biochem. Sci. 28, 527–533 (2003).
96. Matzke, A., Herrlich, P., Ponta, H. & Orian-Rousseau, V. A five-amino-acid peptide blocks Met- and Ron-dependent cell migration. Cancer Res. 65, 6105–6110 (2005).
97. Atabey, N. et al. Potent blockade of hepatocyte growth factor-stimulated cell motility, matrix invasion and branching morphogenesis by antagonists of Grb2 Src homology 2 domain interactions. J. Biol. Chem. 276, 14308–14314 (2001).
98. Boccaccio, C. et al. Induction of epithelial tubules by growth factor HGF depends on the STAT pathway. Nature 391, 285–288 (1998).
99. Sharma, S. V., Bell, D. W., Settleman, J. & Haber, D. A. Epidermal growth factor receptor mutations in lung cancer. Nature Rev. Cancer 7, 169–181 (2007).
100. Sharma, S. V. & Settleman, J. Oncogene addiction: setting the stage for molecularly targeted cancer therapy. Genes Dev. 21, 3214–3231 (2007).
101. Lutterbach, B. et al. Lung cancer cell lines harboring MET gene amplification are dependent on Met for growth and survival. Cancer Res. 67, 2081–2088 (2007).
102. Ivan, M., Bond, J. A., Prat, M., Comoglio, P. M. & Winford-Thomas, D. Activated ras and ret oncogenes induce over-expression of c-met (hepatocyte growth factor receptor) in human thyroid epithelial cells. Oncogene 14, 2417–2423 (1997).
103. Pennacchietti, S. et al. Hypoxia promotes invasive growth by transcriptional activation of the met protooncogene. Cancer Cell. 3, 347–361 (2003).
104. Bhowmick, N. A., Neilson, E. G. & Moses, H. L. Stromal fibroblasts in cancer initiation and progression. Nature 432, 332–337 (2004).
105. Kmiecik, T. E., Keller, J. R., Rosen, E. & Vande Woude, G. F. Hepatocyte growth factor is a synergistic factor for the growth of hematopoietic progenitor cells. Blood 80, 2454–2457 (1992).
106. Steeg, P. S. Angiogenesis inhibitors: motivators of metastasis? Nature Med. 9, 822–823 (2003).
107. Bottaro, D. P. & Liotta, L. A. Cancer: Out of air is not out of action. Nature 423, 593–595 (2003).
108. Amit, I., Wides, R. & Yarden, Y. Evolvable signaling networks of receptor tyrosine kinases: relevance of robustness to malignancy and to cancer therapy. Mol. Syst. Biol. 3, 151 (2007).
109. Abounader, R. et al. Regulation of c-Met-dependent gene expression by PTEN. Oncogene 23, 9173–9182 (2004).
110. Stommel, J. M. et al. Coactivation of receptor tyrosine kinases affects the response of tumor cells to targeted therapies. Science 318, 287–290 (2007).
111. Engelman, J. A. et al. MET amplification leads to gefitinib resistance in lung cancer by activating ERBB3 signaling. Science 316, 1039–1043 (2007).First description of MET gene amplification as a mechanism of acquired resistance to epidermal growth factor receptor inhibitors.
112. Kaposi-Novak, P. et al. Met-regulated expression signature defines a subset of human hepatocellular carcinomas with poor prognosis and aggressive phenotype. J. Clin. Invest. 116, 1582–1595 (2006).
113. Rikova, K. et al. Global survey of phosphotyrosine signaling identifies oncogenic kinases in lung cancer. Cell 131, 1190–1203 (2007).
114. Guo, A. et al. Signaling networks assembled by oncogenic EGFR and c-Met. Proc. Natl Acad. Sci. USA 105, 692–697 (2008).
115. Green, D. R. Even, G. I. A matter of life and death. Cancer Cell 1, 19–30 (2002).
116. Harrington, E. A., Fanidi, A. & Evan G. I. Oncogenes and cell death. Curr. Opin. Genet. Dev. 4, 120–129 (1994).
117. Tikhomirov, O. & Carpenter, G. Ligand-induced, p38-dependent apoptosis in cells expressing high levels of epidermal growth factor receptor and ErbB-2. J. Biol. Chem. 279, 12988–12996 (2004).
118. Shima, N. et al. Tumor cytotoxic factor/hepatocyte growth factor from human fibroblasts: cloning of its cDNA, purification and characterization of recombinant protein. Biochem. Biophys. Res. Commun. 180, 1151–1158 (1991).
119. Matteucci, E., Castoldi, R. & Desiderio, M. A. Hepatocyte growth factor induces pro-apoptotic genes in HepG2 hepatoma but not in B16-F1 melanoma cells. J. Cell. Physiol. 186, 387–396 (2001).
120. Rasola, A. et al. Hepatocyte growth factor sensitizes human ovarian carcinoma cell lines to paclitaxel and cisplatin. Cancer Res. 64, 1744–1750 (2004).
121. Coltella, N. et al. p38 MAPK turns hepatocyte growth factor to a death signal that commits ovarian cancer cells to chemotherapy-induced apoptosis. Int. J. Cancer 118, 2981–2990 (2006).
122. Michieli, P. et al. An HGF-MSP chimera disassociates the trophic properties of scatter factors from their pro-invasive activity. Nature Biotechnol. 20, 488–495 (2002).
123. Orian-Rousseau, V., Chen, L., Sleeman, J. P., Herrlich, P. & Ponta, H. CD44 is required for two consecutive steps in HGF/c-Met signaling. Genes Dev. 16, 3074–3086 (2002).
124. Orian-Rousseau, V. et al. Hepatocyte growth factor-induced Ras activation requires ERM proteins linked to both CD44v6 and F-actin. Mol. Biol. Cell 18, 76–83 (2007).
R E V I E W S
nATuRE REvIEWS | druG diScovEry voluME 7 | junE 2008 | 515
© 2008 Nature Publishing Group

125. Trusolino, L., Bertotti, A. & Comoglio, P. M. A signaling adapter function for α6β4 integrin in the control of HGF-dependent invasive growth. Cell 107, 643–654 (2001).
126. Bertotti, A., Comoglio, P. M. & Trusolino, L. β4 integrin is a transforming molecule that unleashes Met tyrosine kinase tumorigenesis. Cancer Res. 65, 10674–10679 (2005).
127. Bertotti, A., Comoglio, P. M. & Trusolino, L. β4 integrin activates a Shp2-Src signaling pathway that sustains HGF-induced anchorage-independent growth. J Cell Biol. 175, 993–1003 (2006).
128. Giordano, S. et al. The semaphorin 4D receptor controls invasive growth by coupling with Met. Nature Cell Biol. 4, 720–724 (2002).
129. Conrotto, P., Corso, S., Gamberini, S., Comoglio, P. M. & Giordano, S. Interplay between scatter factor receptors and B plexins controls invasive growth. Oncogene 23, 5131–5137 (2004).
130. Conrotto, P. et al. Sema4D induces angiogenesis through Met recruitment by Plexin B1. Blood 105, 4321–4329 (2005).References 123–130 provide information on how MET-dependent signals can be amplified and/or diversified by MET association with surface transmembrane partners, including CD44, β4 integrin and plexin B.
131. Di Renzo, M. F., et al. Overexpression of the c-MET/HGF receptor gene in human thyroid carcinomas. Oncogene 7, 2549–2553 (1992).
132. Ruco, L., et al. D. Expression of Met protein in thyroid tumours. J. Pathol. 180, 266–270 (1996).
133. Chen, B. K., et al. Overexpression of c-Met protein in human thyroid tumors correlated with lymph node metastasis and clinicopathologic state. Pathol. Res. Pract. 195, 427–433 (1999).
134. Di Renzo, M. F., et al. Overexpression of the Met/HGF receptor in ovarian cancer. Int. J. Cancer 58, 658–662 (1994).
135. Di Renzo, M. F., Poulsom, R., Olivero, M., Comoglio, P. M. & Lemoine, N. R. Expression of the Met/hepatocyte growth factor receptor in human pancreatic cancer. Cancer Res. 55, 1129–1138 (1995).
136. Humphrey, P. A., et al. Hepatocyte growth factor and its receptor (c-MET) in prostatic carcinoma. Am. J. Pathol. 147, 386–396 (1995).
137. Natali, P. G., et al. Overexpression of the met/HGF receptor in renal cell carcinomas. Int. J. Cancer 69, 212–217 (1996).
138. Ueki, T., Fujimoto, J., Suzuki, T., Yamamoto, H & Okamoto, E. Expression of hepatocyte growth factor and its receptor, the c-met proto-oncogene, in hepatocellular carcinoma. Hepatology 25, 619–623 (1997).
139. Tavian, D., et al. U-PA and c-MET mRNA expression is co-ordinately enhanced while hepatocyte growth factor mRNA is down-regulated in human hepatocellular carcinoma. Int. J. Cancer 87, 644–649 (2000).
140. Camp, R. L., Rimm, E. B. & Rimm, D. L. Met expression is associated with poor outcome in patients with axillary lymph node negative breast carcinoma. Cancer 86, 2259–2265 (1999).
141. Wielenga, V. J., et al. Expression of c-Met and heparan-sulfate proteoglycan forms of CD44 in colorectal cancer. Am. J. Pathol. 157, 1563–1573 (2000).
142. Morello, S., et al. MET receptor is overexpressed but not mutated in oral squamous cell carcinomas. J. Cell. Physiol. 189, 285–290 (2001).
143. Big biotechs take antibody approach to blocking Met receptor. Chemical & Engineering news [online] < http://pubs.acs.org/cen/coverstory/85/8534cover3.html >
AcknowledgementsWe thank A. Bertotti and C. Boccaccio for discussion and critical reading of the manuscript; J. Hickman, M. Burbridge, T. Perera and S. Buchanan for providing informative material; and A. Cignetto for excellent secretarial assistance. Work from the authors’ laboratory is supported by Associazione Italiana per la Ricerca sul Cancro, European Union Framework Programmes, Ministero dell’Università e della Ricerca, Compagnia di San Paolo and Fondazione CRT.
Competing interests statementThe authors declare competing financial interests: see web version for details.
DATABASESUniProtKB: http://ca.expasy.org/sprotALK | CD44 | EGFR | FLT3 | GRB2 | HER3 | HGF | KIT | p14ARF | p16INK4a | PDGFR | PTEN | RON | SRC | TGFα | TIE2 | VEGFR2
FURTHER INFORMATIONInstitute for Cancer Research and Treatment (IRCC): http://www.ircc.it
ALL LinkS ArE AcTivE in THE onLinE pdF
R E V I E W S
516 | junE 2008 | voluME 7 www.nature.com/reviews/drugdisc
© 2008 Nature Publishing Group




















