
Dr. Chheang Sena - Partnership to Fight Chronic Disease
52
Prof. Chheang Sena, (DUR, Fr) 20-21/June/2011 Shangri-La in Jakarta, Indonesia
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Dr. Chheang Sena - Partnership to Fight Chronic Disease

Prof. Chheang Sena, (DUR, Fr)
20-21/June/2011 Shangri-La in Jakarta,
Indonesia

+ * *
+
General Overview
Non-communicable disease
prevention’s strategic plan
Discussion
Conclusion

More than 200 million people worldwide have diabetes !
Most of them do not receive the care they need !
STEPS Survey 2010

Demographic statusPopulation Pyramid of Kompong Cham province
Data Source Ministry of Planning & Ministry of Health 2005
F M

Goal: To estimate the prevalence of NCDs risk factors in order to establish the baseline information for the prevention and control of NCDs in Cambodia
Objectives: • To determine the prevalence of NCD risk factors including tobacco, alcohol, fruits and vegetables consumption, overweight and physical activity of the surveyed population; • To estimate the prevalence of raised blood pressure, diabetes and raised blood cholesterol among adult male and female population; • To compare NCDs prevalence and risk factors between urban and rural population, men and women, and across age groups.

STEP 1: Face-to-face
interview Information on: (1) tobacco use, (2) alcohol use, (3) intake of fruits and
vegetables (4) physical activities, (5) previously
diagnosed hypertension and diabetes.
STEP 2: Physical measurements of : (1) body weight and height, (2) waist and hip circumferences, (3) body fat, (4) blood pressure, and (5) physical fitness Using specific tests/ devices relevant to these measurements.
STEP 3: Biochemical measurements of capillary blood to determine (1) glucose (2) total cholesterol at sites Using dry chemical methods.
Three subsequent steps : Followed WHO Stepwise Approach to chronic disease risk factor surveillance methodology (closed supervision by HQ, WPRO and WHO-Cambodia

In accordance to the NCD multi-stage cluster survey method: 5,643 participants were selected; 5,433 responded (response rate of 96.3 %) Cover age group of 25-64 years old Stratified urban and rural (covered all geographical areas of Cambodia); Males and females
Selection of samples (WHO Kish Method): Primary sampling unit (PSU): commune level (Khum in rural areas/Khan in urban area; Secondary sampling unit (SSU): villages (Phum); Elementary unit (EU) a household and was selected at random.

Prior to survey: Total sample size calculated was 5,760
During the survey period of data collection: 5,643 were available 117 (2.0%) households were missing, being away for farming or other purposes
Of 5,643 households: Overall response rates ranged from 96.3% in STEPS 1, to 94.2% in STEPS 2, and to 92.7 % in STEPS 3.

Female Male
Percent


Percent
The two main tobacco indicators that are associated with an increased risk of developing chronic diseases are:

Percent

Percent

Net alcohol content of a standard drink is approximately 10g of Ethanol
1 STANDARD

Percent

The consumption of 5 or more standard drinks for males and 4 or more standard drinks for females on any day on the past 30 days


Percent
Eating less than five servings of fruit and/or vegetables per day is considered being a low fruit and vegetable intake and increases the risk to develop chronic diseases



A person not meeting any of the following criteria is considered being physically inactive and therefore at risk of chronic disease: 3 or more days of vigorous -intensity activity of at least 20 minutes per day; OR
5 or more days of moderate -intensity activity or walking of at least 30 minutes per day; OR
5 or more days of any combination of walking, moderate- or vigorous intensity activities achieving a minimum of at least 600 MET-minutes per week
Percent

MALE FEMALE
Percent
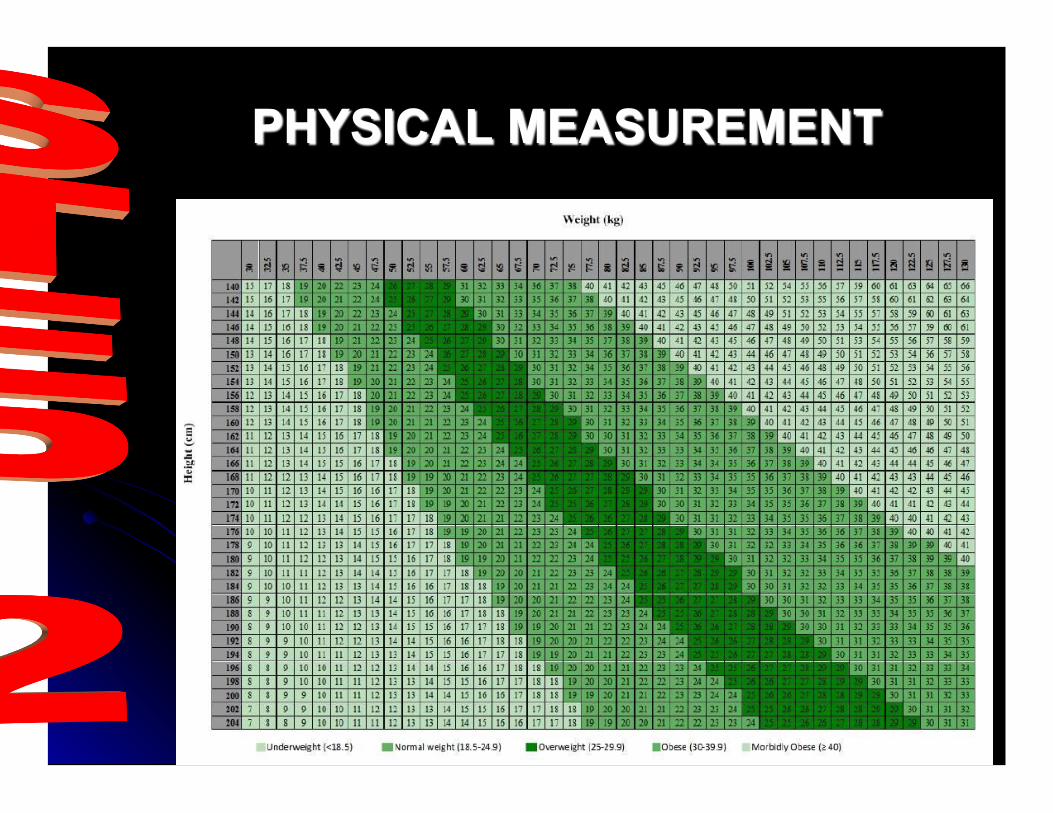
Overweight: having BMI ≥ to 25 kg/m2 and below 30 kg/m2 Obesity: BMI greater than or equal to 30 kg/m2
Percent

Percent

Percent

Percent

Percent

The current survey found that the prevalence of diabetes was 2.9% for the total respondents, not significantly different between men and women (2.5 vs. 3.3%); twice higher in the urban than in the rural area (5.6 vs. 2.3%), and increased with age, This prevalence of diabetes is by half lower than that found by a survey in 2004 in a semi-urban ( 5.6 vs 11.4%) and rural ( 2.3 vs 4.8% ) province of Cambodia. This difference might be mainly due to the fact that: The survey 2004 had the sample population from 25 to 65 years and above, the prevalence of diabetes based on non- fasting blood glucose, and only 4 villages were selected to present rural and semi-urban areas

In the present survey the sample population were limited to 25-64 years of age, blood samples were tested in the early morning by trained laboratory technicians using Accutrend Plus instruments and solutions purchased by the WHO Geneva, and 180 surveyed villages were stratified and randomly selected from the recent sampling frame to represent the urban and rural areas, and data were properly weighted and finalized by using the WHO STEPS EpiInfo program
In regards to blood pressure, the present survey found that 11.2% of the total population had raised blood pressure or hypertension (SBP≥140 and/or DBP≥90mmHg), and this prevalence was higher in men than in women (12.8 vs. 9.6%), was also higher in the urban
than in the rural area (16.9 vs 10.0 % ) and was increasing with age.

This prevalence of hypertension was lower than that reported 5 years ago by a survey in a semi-urban and rural province of Cambodia where up to 25% and 11.7% of the surveyed population
had raised blood pressure respectively. The prevalence of tobacco smoking in the current survey was 54.1% men and 5.9% women; it was higher than country-wide survey in 2005-2006 where only 48% of men and 3.6% of women smoked cigarettes The high prevalence of alcohol consumption ( 1 in every 2 respondents were current drinkers; with men drink more often and much more than women The high prevalence of alcohol drinking found by the current survey might be partly resulted from aggressive advertisements of beer and other alcohol products throughout the country in recent decades

The high prevalence of raised total blood cholesterol ( 1in every 5 respondents)
The low prevalence of fruit and vegetable consumption ( 8 in every 10 respondents ate less than five servings of fruit and/or vegetables on average per day).
The proportion of overweight and/or obese population ( BMI ≥ 25kg/m² ) was twice in the urban area as compared to the rural area (26.7 vs. 13.0%) and was 1.6 times higher in women than in men ( 19.0 vs. 11.6% ).
The prevalence of respondents with 3 or more risk factors for NCDs was twice higher in men than in women ( 14.1 vs. 6.5% ), also twice higher for ages 45-64 than for ages 25-44 ( 15.7 vs. 7.3% ), and significantly higher in the urban than rural areas ( 15.9 vs. 9.1% )

The Cambodian STEPs survey results provided valuable baseline information for the prevalence of major NCDs and their associated risk factors at the national level as well as at urban and rural levels of Cambodia. The survey revealed that the prevalence of diabetes and hypertension in Cambodia were lower than that reported in previous surveys in Cambodia and in some neighboring countries Even though, major risk factors for NCDs were alarmingly prevalent, including alcohol consumption and tobacco use, especially among urban and male population, and overweight among women and aging population

+ * *
+


Objective of the survey: Diabetes prevalence determination
Date of activity: started from 2004 to 2005
Survey site: Kompong Cham, Battam Bong, Siem Reap
Criteria adopted: WHO, 1999
Results: in Kg Cham, Battambang and Phnom Penh:10 % adults have diabetes, ¼ adult: high blood pressure, poor rural community surveyed in Siem Reap: 5% of adults had diabetes and 12% were hypertensive patients.
Non-communicable diseases is become the top problem of developing country !

It is not so early to act from now !
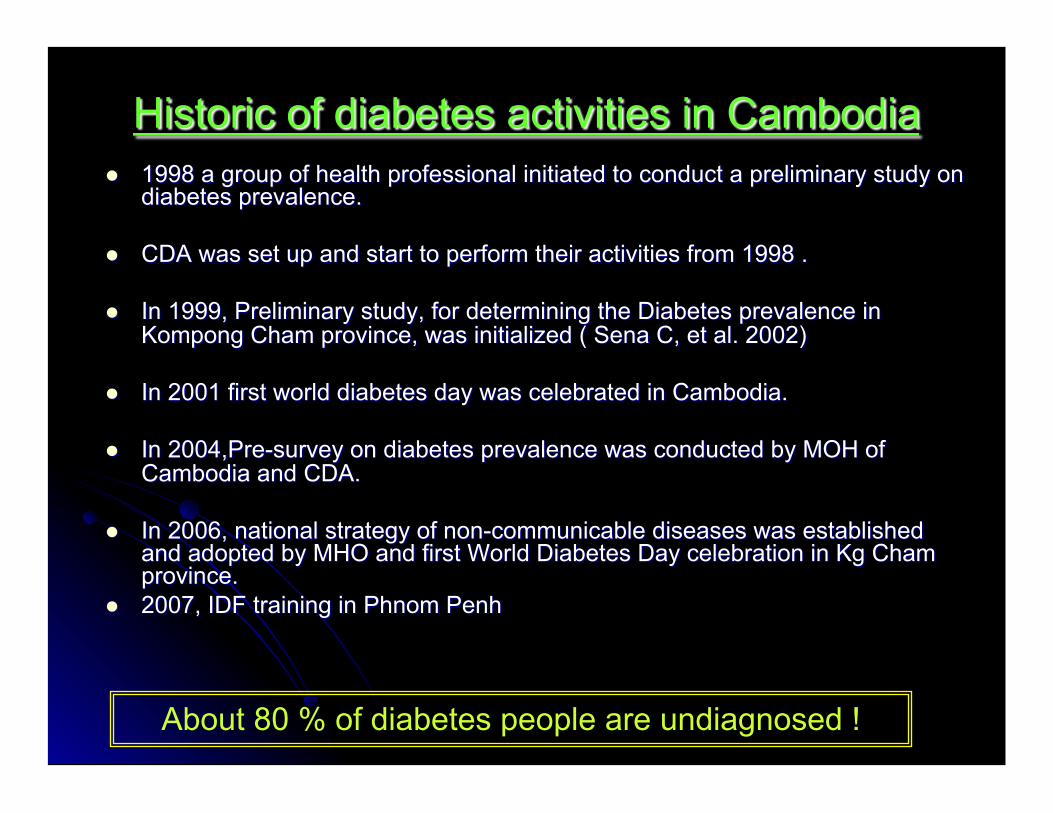
About 80 % of diabetes people are undiagnosed !

Diabetes care is for every one in the worldwide !

Tranche d’âge (année)
Nombre total de sujets
Nombre de sujet ayant une glycémie (mg/dl)
<100 100-109 >110
Homme + Femme Homme + Femme Homme + Femme
N % N % N %
<34 23 22 95,6 0 0 1 4,3
34-64 440 365 83,0 16 3,6 59 13,4
>64 57 41 71,9 5 8 ,8 11 19,3
N : nombre des personnes % : pourcentages déterminés en fonction du nombre de sujets de la tranche d’âge


To develop and strengthen the institutional management and implementation structure for non communicable diseases.
To develop a surveillance system for NCD risk factors and selected diseases.
To stall the epidemic of NCDs through the population reduction in the main risk factors of poor diet, physical inactivity, smoking, harmful alcohol use and the aggressive management of high risk individuals.
To strengthen and equip health delivery systems to provide affordable, equitable and quality management of non communicable diseases through the public health system.

1-Lack of net work and diabetes institutional management: Provincial structure Infrastructure National guideline… Provincial strategy
2-Lack of human resources : Health professional, Experiences, diabetes care and control knowledge 3-Traditional myth behavior: Life style, traditional drug using…
4-Diabetes is not well known in the country: National prevalence,
Diabetes selves care and prevention…
5-Disadvantaged and vulnerable community: Concerning to equitable health services
and diabetes care people at risk…

The significant and growing burden of diabetes must be prevented and controlled in the country.
NCDs care is for everyone
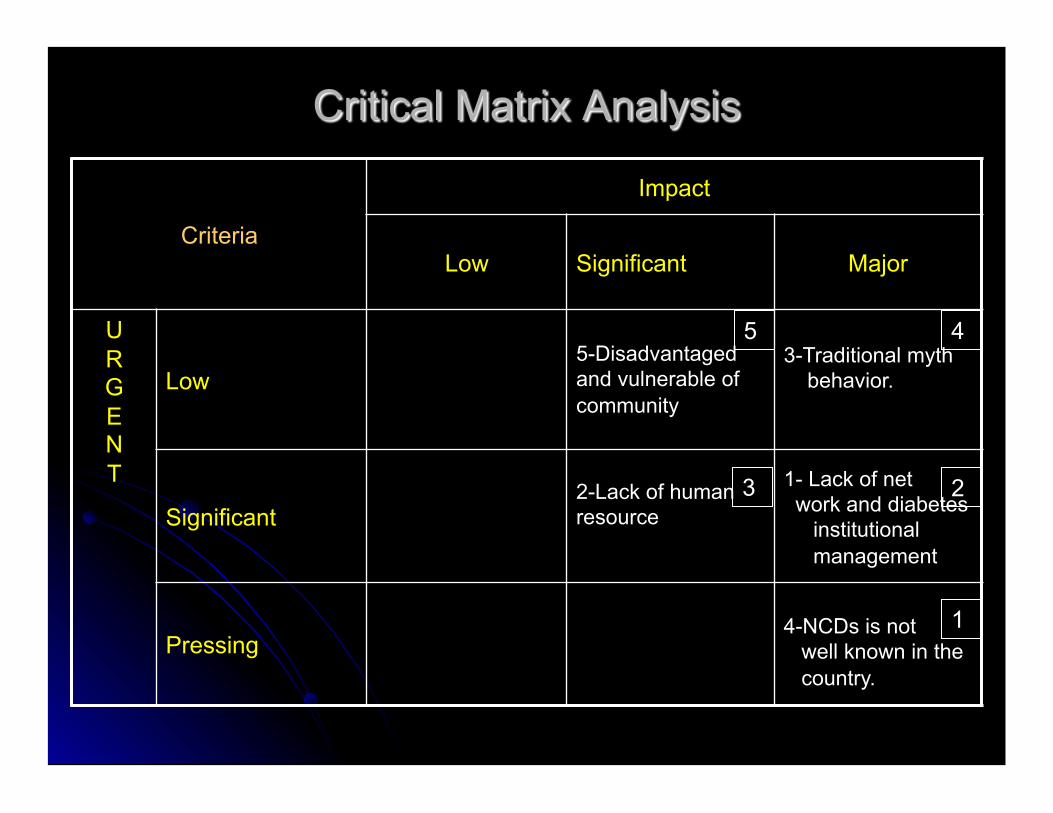
Criteria
Impact
Low Significant Major
U R G E N T
Low 5-Disadvantaged and vulnerable of community
3-Traditional myth behavior.
Significant 2-Lack of human resource
1- Lack of net work and diabetes institutional management
Pressing 4-NCDs is not well known in the country.
5 4
2 3
1

PLANNING WORKSHEET-1
CAMBODIA Plan Period: Jan/2009-Dec/2011
Issue 4-Diabetes is not well known in the country and province
With assumption The detail is in appendix-1,2,3
Objective-1: Promote the public awareness on NCDS burden and healthy lifestyle in the Community.
Strategies Action steps Responsible Organization
Time Targets Resource / Bud-get
1-Raise public awareness of NCDs burden and healthy lifestyles
1-Celebrate the yearly World Diabetes Day
2-Running monthly outreach education in community and public health facilities.
3-Develop and print IEC materials regarding to diabetes and its risk factors : - poster, self-management, leaflet, palm let, brochure, Gazette…etc
- CDA
-CDA & PHD-MOH
14 Nov
Every month
- Feb-09
- 400 participants had attended
- Report of activity at two HC every month
- Diet pyramid poster Leaflet, Brochure, T-Shirt, and Newsletters was print out.
-NGOs -CDA -MOH
-NGOs -CDA -MOH
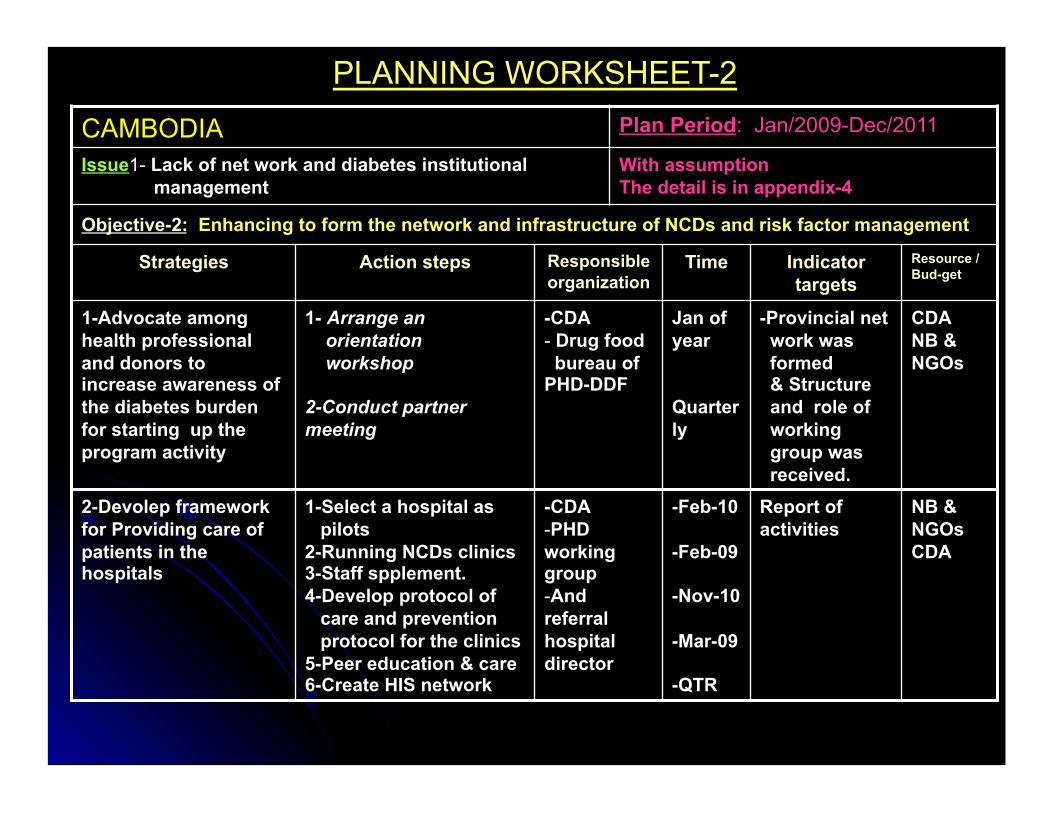
PLANNING WORKSHEET-2
CAMBODIA Plan Period: Jan/2009-Dec/2011
Issue1- Lack of net work and diabetes institutional management
With assumption The detail is in appendix-4
Objective-2: Enhancing to form the network and infrastructure of NCDs and risk factor management
Strategies Action steps Responsible organization
Time Indicator targets
Resource / Bud-get
1-Advocate among health professional and donors to increase awareness of the diabetes burden for starting up the program activity
1- Arrange an orientation workshop
2-Conduct partner meeting
-CDA - Drug food bureau of PHD-DDF
Jan of year
Quarterly
-Provincial net work was formed & Structure and role of working group was received.
CDA NB & NGOs
2-Devolep framework for Providing care of patients in the hospitals
1-Select a hospital as pilots 2-Running NCDs clinics 3-Staff spplement. 4-Develop protocol of care and prevention protocol for the clinics 5-Peer education & care 6-Create HIS network
-CDA - PHD working group - And referral hospital director
-Feb-10
-Feb-09
-Nov-10
-Mar-09
-QTR
Report of activities
NB & NGOs CDA

PLANNING WORKSHEET-3
CAMBODIA Plan Period: Jan/2009-Dec/2011
Issue-2:Lack of human resource With assumption The detail is in appendix-5,6
Objective-3: Develop and strengthening the quality of equip health delivery system among RH and PHD staffs to provide affordable care and equitable diseases management
Strategies Action steps Responsible persons
Time Targets Resource / Bud-get
1-Enforce to run NCDs program in the province
Establish a PHD working group for running NCD program
PHD Director
Sep-11 A working group that has a secretariat from nutrition unit
NB
1-Providing the quality of NCDs education and care skill to medical practitioners, clinic staffs.
1-Develop curriculum of the training 2-select the trainers 3-select the trainees 4-Financial support request 5-Monitoring and evaluation program
-NCDs working group
Oct-11 -25 trainees from RH & HC were trained
WDF NGOs NB
2-Strengthening the quality of diabetes educator and medical practitioner skill.
1-Provide the regular update and refreshment training in diabetes
-NCD working group
-Dec of every year
-25 trainees from RH & HC were attended In the training
WDF NGOs NB CDA
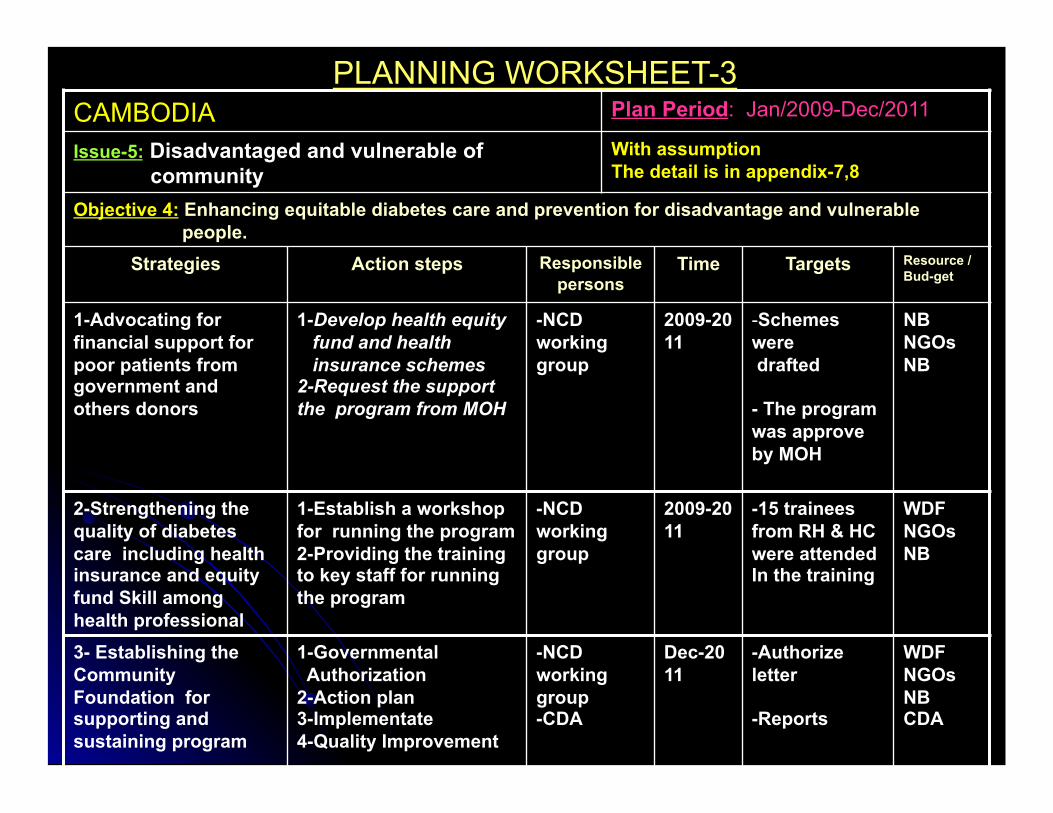
PLANNING WORKSHEET-3 CAMBODIA Plan Period: Jan/2009-Dec/2011
Issue-5: Disadvantaged and vulnerable of community
With assumption The detail is in appendix-7,8
Objective 4: Enhancing equitable diabetes care and prevention for disadvantage and vulnerable people.
Strategies Action steps Responsible persons
Time Targets Resource / Bud-get
1-Advocating for financial support for poor patients from government and others donors
1-Develop health equity fund and health insurance schemes 2-Request the support the program from MOH
-NCD working group
2009-2011
- Schemes were drafted
- The program was approve by MOH
NB NGOs NB
2-Strengthening the quality of diabetes care including health insurance and equity fund Skill among health professional
1-Establish a workshop for running the program 2-Providing the training to key staff for running the program
-NCD working group
2009-2011
-15 trainees from RH & HC were attended In the training
WDF NGOs NB
3- Establishing the Community Foundation for supporting and sustaining program
1-Governmental Authorization 2-Action plan 3-Implementate 4-Quality Improvement
-NCD working group -CDA
Dec-2011
-Authorize letter
-Reports
WDF NGOs NB CDA





















