Download - Journal Production Services - University of Toronto
67
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Download - Journal Production Services - University of Toronto


volume 83, number 1, December 2005 1
Cover Artist Lori WatersAfter earning a BFA from the University of Victoria, Lori was the commonwealth scholar to Ghana, where she completed her MFA at the University ofScience and Technology in Kumasi. Upon her return to Canada she worked in corporate communications while studying sciences part time. Looking for asocially-responsible way to combine art, life science, and computing, she found the Biomedical Communications program - the only accredited program ofits kind in Canada - which she entered in 2004. Lori's BMC masters research is on the visualization of dendritic enhancement of HIV infection. After grad-uation, Lori hopes to create medical and scientific educational materials, particularily HIV education materials.
5 Preface
6 News and ViewsChaoulli and Zeliotis vs. Quebec: A Primer on the Background, Decision and Impact on Health Care in CanadaMartin E. Betts, Peter Tanuseputro and Bobby Yanagawa
10 News at a GlanceJanice Kwan, Martin Betts, Sarah Perkins and Peter Tanuseputro
14 Ten Questions for Dr. Martin SchreiberMarieke Gardiner and Sam Silver
16 Medical MurmursSTAT3– A Promising Molecular Target for Cancer TherapyTomce Trajkovski
17 Back to BasicsMolecular Mechanisms of Aging: Telomerase and Cellular AgingMichael Sidiropoulos
19 In the LiteratureRisk-Treatment Mismatch in the Pharmacotherapy of Heart Failure - Another example of paradoxical lower levels of treatment in those at highest riskPeter Tanuseputro
20 Management of Non-ST elevation acute coronary syndromes: Insights from RITA 3 and ICTUSJohn D.D. Neary
22 Shaken Baby Syndrome: The Debate Rages OnJasrajbir Baath
Medical Education24 Professionalism for the Medical Student
Wayne C.V. Baici
Current Medical Perspectives26 June C. Carroll, MD, CCFP, FCFP
Evan Kwong and Rebecca Menzies
Morning Report29 SOB, Fevers, Murmurs...and CNS
Michael R. Humphreys
Clinicopathological Correlation32 Evaluating Hoarseness: How to Avoid Backing the
Wrong HorseGoran Jeremic, Mark Rafferty, Jonathan Irish, Dale Brown and David Goldstein
Quick Diagnosis 38 Case 1
Jennifer Singerman and Dr. Liesly Lee
39 Case 2Vicky Chan, Dr. Lyne Noël de Tilly and Dr. Yuna Lee
40 Case 3Daniel R. Ricciuto
Technology Review46 Handheld Computing in Medical Education
Ron Somogyi, Joy Abramson, John Kim and Joseph Koval
International Health50 The Indian Paradox: An Emerging Epidemic of
Cardiovascular DiseaseBehzad Hassani and Adnan Jalal
Complementary and Alternative Medicine53 Survey of First and Second Year Medical Students’
Familiarity and Comfort with Complementary and Alternative MedicineRebecca Brundin-Mather, Vishal Avinashi and Marja Verhoef
Philosophy and Medicine58 Trauma and Terrorism: How Do Humans Respond?
Behzad Hassani
Historical Review64 Gynaecological Surgery in the 19th Century: Diverging
Historical AccountsDelia Gavrus
Book Review68 The Making of a Surgeon in the 21st Century
Jasrajbir Baath
69 A Consumer’s Guide to Laboratory TestsAndrew J. Perrin
Table of Contents
University of Toronto Medical Journal2
EDITORS-IN-CHIEF
Diana Anderson, M.Arch. (0T8)Fiona Menzies, M.Sc. (0T8)
SENIOR ASSOCIATE EDITORS
Peter Ceponis, Ph.D. (0T8)Joanne Yu, Ph.D. (0T8)
JUNIOR ASSOCIATE EDITORS
Sagar Dugani, M.Sc. (0T9)Jonathan So, B.Sc. (0T9)
SENIOR MANAGING EDITORS
Mona Moosavian, B.Sc. (0T8)Lilly Teng, B.Sc. (0T8)
JUNIOR MANAGING EDITORS
Karen Jang, H.B.Sc. (0T9)Thomas O’Brien, B.Sc. (0T9)
SENIOR COPY EDITORS
Cynthia Chan, H.B.Sc. (0T8)Naomi Driman, M.Sc. (0T8)
JUNIOR COPY EDITORS
Danica Lam, B.A.Sc. (0T9)Nicolae Petrescu, B.Sc. (0T9)
SENIOR NEWS & VIEWS EDITORS
Martin Betts, B.Sc. (0T8)Peter Tanuseputro, M.H.Sc. (0T8)
JUNIOR NEWS & VIEWS EDITORS
Janice Kwan, B.Sc. (0T9)Adam Weathermon, M.A.Sc. (0T9)
SENIOR MORNING REPORT EDITORS
Praveena Sivananthan, B.Sc. (0T8)Amy Tung, B.Sc., B.Ed. (0T8)
Gwyneth Zai, M.Sc. (0T8)
JUNIOR MORNING REPORT EDITOR
Ashley Hawrylyshyn, B.Sc. (0T9)
SENIOR CLINICOPATHOLOGICAL CORRELATION EDITORS
Janice Wong, M.Sc. (0T8)
JUNIOR CLINICOPATHOLOGICAL CORRELATION EDITOR
Sivan Bega, M.Sc. (0T9)Adrian Sacher (0T9)
SENIOR ECONOMICS & HEALTH POLICY EDITOR
Jed Laughren, B.Sc. (0T8)
JUNIOR ECONOMICS & HEALTH POLICY EDITOR
Theresa Pazionis, M.A. (0T9)
SENIOR HISTORICAL REVIEW EDITORS
Bilal Ahmed, H.B.Sc. (0T8)Eric Morgen, H.B.Sc. (0T8)
JUNIOR HISTORICAL REVIEW EDITOR
Linda Sun (0T9)
SENIOR MEDICAL EDUCATION EDITORS
Behzad Hassani, H.BA. (0T8)Gevork Mnatzakanian, H.B.Sc. (0T8)
JUNIOR MEDICAL EDUCATION EDITOR
Ekta Khemani, M.Sc. (0T9)
SENIOR INTERNATIONAL HEALTH EDITORS
Brie Banks, H.B.Sc. (0T8)Deana Hathout, H.B.Sc. (0T8)Rishi Kapur, H.B.Sc. (0T8)
JUNIOR INTERNATIONAL HEALTH EDITORS
Alice Han, M.Sc. (0T9)Esther Li (0T9)
Melissa Vyvey, M.Phil. (0T9)
SENIOR QUICK DIAGNOSIS EDITORS
Kalam Karen Chan, M.Sc. (0T8)Andrew Lui, B.Sc. (0T8)
JUNIOR QUICK DIAGNOSIS EDITOR
Fereshte Samji (0T9)
SENIOR CURRENT MEDICAL PERSPECTIVES EDITOR
Evan Kwong, M.Sc. (0T8)
JUNIOR CURRENT MEDICAL PER.SPECTIVES EDITOR
Rebecca Menzies, H.B.Sc. (0T9)
SENIOR PHILOSOPHY AND MEDICINE EDITOR
Behzad Hassani, H.BA. (0T8)Jai Shah (0T8)
JUNIOR PHILOSOPHY AND MEDICINE EDITOR
Alex Mansfield (0T9)
SENIOR TECHNOLOGY REVIEW EDITORS
Joy Abramson, B.Sc. (0T8)Ron Somogyi, M.Sc. (0T8)
JUNIOR TECHNOLOGY REVIEW EDITORS
John Kim, M.Sc. (0T9)Joseph Koval, B.A, B.E.Sc. (0T9)
SENIOR ALTERNATIVE MEDICINE EDITOR
Kathryn Howe, Ph.D. (0T8)
SENIOR BOOK REVIEW EDITOR
Andrew Perrin, M.Res. (0T8)
JUNIOR BOOK REVIEW EDITOR
Brodie Ramin (0T9)
FINANCIAL OFFICER
Bilal Ahmed, H.B.Sc. (0T8)
GRAPHICS EDITORS
Diana Dai, M.D., M.Sc.BMC (c)Lori Waters, MFA, M.Sc.BMC (c)
WEBMASTER
Ben Bell, B.Sc. (0T8)
EDITORIAL BOARD
Hamideh Alasti, CCPMJudith Balogh, M.D.
Stephanie J. Brister, M.D.Janet Craik, M.Sc., OT Reg. (Ont.)
Ian Crandall, D.Phil.Marko Duic, M.D.
Kymm Feldman, M.D.Philip Hébert, M.D., Ph.D.
Maggie Lee Huckabee, Ph.D.Cheryl Jaigobin, M.D.
Richard J. Moulton, M.D.Richard Pittini, M.D.
Patrick Tang, M.D., Ph.D.James P. Waddell, M.D.V. Wee Yong, Ph.D.
FACULTY ADVISORY BOARD
Chair, Allan Detsky, M.D., Ph.D.Shabbir Alibhai, M.D.
Jane Aubin, Ph.D.Michael Baker, M.D.
John M. A. Bohnen, M.D.Wendy Levinson, M.D.
Irv Lipton, M.D.John F. MacDonald, Ph.D.David Naylor, M.D., D.Phil.Donald Redelmeier, M.D.Duncan Stewart, M.D.Sharon E. Straus, M.D.Donald Stuss, Ph.D.
Donald Wasylenki, M.D.
TYPESETTING
Type and Graphics Inc.
UTMJ Staff
E-mail: [email protected] • http://www.utmj.org • Phone: 416-946-3047 • Fax: 416-978-8730

volume 83, number 1, December 2005 3
UTMJ CorporateBenefactors Dr. Allan DetskyDr. John FlorasDr. David NaylorDr. John ParkerDr. Filoteo PasquiniThe FitzGerald Academy
UTMJ GrandBenefactors Dr. Michael A. BakerDr. David ByersEBSCO Canada Ltd. Dr. Barry J. GoldlistDr. Avrum GotliebDr. Michael L. GuinnessDr. R. HowardDr. Robert KyleDr. Ray D. MartinDr. Richard I. OgilviePeters-Boyd AcademyDr. K.P.H. PritzkerDr. Anita RachlisDr. Michael RobinetteDr. Fred SaibilDr. Ronald W. TaylorDr. Graham TropeDr. Robert WaldDr. Yeni Yucel
UTMJ Benefactors Dr. Sylvia L. AsaDr. Davy ChengDr. C. Mark CheungDr. Albert CheskesDr. H. Roslyn DevlinDr. Sheila DoyleDr. John EdmondsDr. Ronald S. FentonDr. Arnis FreibergDr. Kan Ying FungDrs. Joan S. &
Richard M. GladstoneDr. Alan L. Goldbloom
Dr. Jeffrey GollishDr. Larry GrossmanDr. Rajesh GuptaDr. Ian HarringtonHealthcare Materials,
Management and ServicesDr. Michael A. HutcheonDrs. Rita and Gabor KandelDr. Armand KeatingDr. John D. KempstonDr. Andrew W. MaykutDr. Hugh D. McGowanDr. David McNeelyDr. Howard OvensDr. G.L. RalphDr. James T. RutkaDr. Jerry ShimeDr. Morris ShustermanSunnybrook Hospital,
U of T ClinicDr. Ian TannockDr. Charles H. TatorDr. Gary WebbDr. Peter M. Webster
UTMJ PatronsDr. Joanne BargmanDr. Simon CaretteDr. Edward H. ColeDr. Donald H. CowanDr. David S. GoldbloomDr. Michael GordonDr. Bob HilliardDr. D. Linn HolnessDr. Robert H. HylandDr. Jay S. KeystoneDr. Stephen KraftDr. A.E. LangDr. Arlette Lefebvre-BedardDr. Lavina LickleyDr. Robert MaunderDr. Rosemary MeierDr. Ernest R. MichelDr. David MockDr. Fred R. PapsinDr. Robert L. PattenDr. Mel PetersielDr. Eliot A. Phillipson
Dr. Kenneth RobbDr. Irving B. RosenDr. Frank W. RosenbergDr. Donato A. RuggieroDr. Robert B. SalterDr. Steven ShadowitzDr. Katherine SiminovitchDr. James WaddellDr. Catharine WhitesideDr. Ronald M. Zuker
UTMJ FriendsAnderson Architects
Dr. A. Agur
Dr. Johanne Allard
Dr. Crawford Anglin
Dr. Mary Jane Ashley
Dr. Earl R.Bogoch
Dr. Iivi Campbell
Canada Institute for STI
Dr. Paul Dedumets
Dr. Helen P. Demshar
Dr. Tom L. Forbes
Dr. Steven Gallinger
Dr. Ian Graham
Dr. Jamie Graham
Dr. David Hedley
Dr. Sophie Hofstader
Dr. Marika Hohol
Hospital for Sick Children,
Library Hospital
Dr. Mark Iwanochko
Dr. Anna Jarvis
Dr. Moira Kapral
Dr. Colin D. Lambert
Dr. Bernard Langer
Dr. Peter Liu
Dr. J. T. Marotta
Dr. Martin McKneally
Dr. Donna McRitchie
Dr. Martin G. Myers
Dr. Daniel Panisko
Dr. Jacqui Pettersen
Dr. Kathleen L. Pritchard
Dr. Donald Redelmeier
Dr. W. John Reynolds
Dr. Robert N. Richards
Dr. Jay Rosenfield
UTMJ Subscribers
Dr. John R. Ross
Dr. Robert L. Ruderman
Dr. James Shaw
Dr. Kenneth Shulman
Dr. Ivan Silver
Dr. Melvin Silverman
Dr. Allan R. Slomovic
St Michael’s Hopsital,
Health Science Library
Dr. George Y. Takahashi
The Yao Trust c/o Dr. James Yao
Dr. Hugh Thomson
Dr. Jack Tu
Dr. Murray B. Urowitz
Dr. Richard D. Weisel
Woodward Library, University of
British Columbia
Dr. Anna Woo
Dr. John Wright
Dr. S. Zlotkin
The Editors apologize for any omis-sions to the above list; this list repre-sents our final version at press time.We will update the list in futureissues.
The University of Toronto Medical Journal is funded in part by its subscribers and the Medical Society. Patronage to the Journal issubdivided into five categories. Friend of the UTMJ - $50.00; UTMJ Patron - $75.00; UTMJ Benefactor - $100.00; UTMJ GrandBenefactor - > $100.00 and UTMJ Corporate Benefactor - >$200.00. To subscribe, please see the last page of the Journal. TheUTMJ wishes to thank the following patrons for their generous donations.

University of Toronto Medical Journal4
Dr. Dominick Amato
Dr. Eduardo Azevedo
Dr. Maria Bacchus
Dr. Jerald Bain
Dr. Meyer Balter
Dr. Alan Barolet
Dr. Martin Blackstein
Dr. Claire Bombardier
Dr. Louise Bordeleau
Dr. James Brunton
Dr. Ronald Burkes
Dr. Vivian Bykerk
Dr. Simon Carette
Dr. Charles Chan
Dr. Ed Cole
Dr. Jack Colman
Dr. Tim Cook
Dr. Allan Detsky
Dr. Shereen Ezzat
Dr. George Fantus
Dr. Denice Feig
Dr. S. Victor Feinman
Dr. John Floras
Dr. Shital Gandhi
Dr. Shiphra Ginsburg
Dr. Jewel Gold
Dr. Barry Goldlist
Dr. R. Goldstein
Dr. Pamela Goodwin
Dr. Allan Gordon
Dr. M. Gordon
Dr. Gordon Greenberg
Dr. Tony Hanley
Dr. Jacqueline James
Dr. Armand Keating
Dr. Ralph Kern
Dr. Ed Keystone
Dr. Stephen Lapinsky
Dr. Peter Lee
Dr. Gary Lewis
Dr. Ken Locke
Dr. Alexander Logan
Dr. Heather McDonald-Blumer
Dr. Susanna Mak
Dr. Sangeeta Mehta
Dr. Melita Mezody
Dr. Alvin Newman
Dr. Gary Newton
Dr. Mitra Niroumand
Dr. Mirek Otremba
Dr. John Parker
Dr. Yash Patel
Dr. Sue Quaggin
Dr. Cheryl Rosen
Dr. Douglas Ryan
Dr. Zion Sasson
Dr. James Shaw
Dr. Maureen Shandling
Dr. Mark Silverberg
Dr. Katherine Siminovitch
Dr. Hillary Steinhart
Dr. Thomas Stewart
Dr. Nicolas Szecket
Dr. Jerry Tenenbaum
Dr. Hillar Velland
Dr. Robert Wald
Dr. Randy Wax
Dr. Catherine Zahn
Dr. Noe Zamel
Dr. Bernard Zinman
Mount Sinai Hospital, Department of Medicine
The University of Toronto Medical Journal wishes to thank Dr. Allan Detsky and thefollowing patrons from the Department of Medicine at Mount Sinai Hospital for theirgenerous donations.

volume 83, number 1, December 2005 5
Supreme Court decision in Chaoulli and Zeliotis vs. Quebec: A
Primer on the Background, Decision and Impact on Health Care in
Canada. In the divided healthcare climate of today, this articleis especially relevant to our readers.
In Professionalism for the Medical Student: Past Lessons and Future
Challenges, Baici deals with a fundamental challenge facingmedical curriculums. Professional values and ethics of medi-cine are essential for the upcoming generation of physicians,in order for them to fulfill their important role in society.
All medical students strive to become good doctors. However,it is increasingly evident that this does not mean only an excel-lent knowledge and practice of clinical skills. In addition toprofessionalism, the ability to communicate knowledge andparticipate in debates surrounding healthcare issues is vital tofulfilling the obligations of a physician.
The University of Toronto Medical Journal is a tool withwhich medical students can refine these skills in collaborationwith qualified doctors and students in related university pro-grams. Therefore we would like to thank our patrons and sub-scribers for their continued support of this journal. It is great-ly appreciated.
Sincerely,
Diana Anderson and Fiona Menzies,Editors-in-chief
As the new Editors-in-Chief of the University of Toronto Medical
Journal for the academic year of 2005-2006, we are extremelyhonored to bring you the first issue.
This year we hope to lead the journal in some new directionswith the help of our dedicated editorial staff. We are in theprocess of establishing a review board for peer editing of arti-cles with the intention of making the reviewing process morevaluable to the authors. In an effort to reach as many poten-tial readers as possible, we have maintained an open accesswebsite which currently has an archive of the last seven vol-umes of the journal.
We are especially proud of the new design for the journal.This effort has allowed us to collaborate with the outstandingBiomedical Communications program. The Faculty ofMedicine at the University of Toronto encompasses manydiverse undergraduate and graduate programs, which we arebeginning to integrate into the UTMJ team. To this end, wehave expanded our consortium of authors to include studentsfrom other programs. An example of this collaboration is thearticle by Gavrus, Gynaecological Surgery in the 19th Century:
Diverging Historical Accounts, which is authored by a Ph.D. can-didate from the Institute for the History and Philosophy ofScience and Technology, University of Toronto.
Our readers will also appreciate the varied assortment of arti-cles we have from medical students. In The Indian Paradox: An
Emerging Epidemic of Cardiovascular Disease, Hassani and Jalaltackle the growing dilemma that a potentially greater geneticsusceptibility to cardiovascular disease may exist for the pop-ulation of India. This will have important implications for thetreatment of patients from this ethic group.
In our expanded News and Views section, Betts, Tanuseputroand Yanagawa provide an illuminating synopsis of the recent
Preface from the Editors

University of Toronto Medical Journal6
should be able to utilize private health insurance to reimbursethe cost of care obtained in the private sector.”2 Opposing thisposition, CAIR delegates were defeated in a conflicting motionearlier at the meeting to eliminate private insurance from thelist of possible solutions to the access to timely care problem.3
Underlying this debate is the near unanimous opinion ofCanadian physicians who believe that medical care be funda-mentally provisioned on need and not on ability to pay,2,3 a sen-timent continually expressed by the public in opinion polls.
Two significant groups have been conspicuously quiet amidstthis discourse. The first, the Canadian Federation of MedicalStudents (CFMS), is currently organizing a grassroots initiativeto study the issues further, galvanize its position and arrive ata policy position over the next few months. As such, the CFMSabstained its vote on the private insurance motion presented atthe CMA’s meeting. Perhaps more ominous has been theapparent reluctance of the federal and provincial governments,when faced with the Chaoulli decision, to publicly address orput forward effective and sustainable solutions to the challengesconfronting public healthcare.
Wait Lists: A Necessary Evil . . . But How Evil?In ruling that the healthcare system, as currently configured,violated the rights of Mr. Zeliotis the court is asserting that waitlists can be too long for certain procedures. In addition to thehip replacement surgery that was central to this case, kneereplacement, cataract surgery, diagnostic imaging, radiation ther-apy and cardiac care are all procedures that have been identi-fied by policy reports, professional associations, public opinionpolls and politicians as requiring more rigid criteria and bench-marks for maximum wait lengths. An important point to keepin mind is that the courts, in their ruling, considered the stateof health care in 1997, the period in which Mr. Zeliotis waswaiting for his hip replacement. The five-year period between1995 and 2000, using British Columbia (BC) as an example, sawa 42% growth rate in the number of surgical hip replacementprocedures and even higher growth rates for cataract surgeriesand knee replacements.4
Wait lists serve a necessary bureaucratic function within ourhealthcare system. They provide a mechanism for allocating
Chaoulli and Zeliotis vs. Quebec: A Primer on the Background, Decisionand Impact on Health Care in Canada
Martin E. Betts, B.Sc. (OT8)
Peter Tanuseputro, M.H.Sc. (OT8)
Bobby Yanagawa, Ph.D. (OT8)
This paper will provide an introduction to the background andimpact of the Supreme Court’s decision in Chaoulli and Zeliotisversus Quebec,1 reported in as balanced a manner as possible.The complexities of the issues cannot be fully addressed in sucha short review. Thus, we will focus on the reaction of majorstakeholder organizations, discuss dominant issues and addresspotential solutions. Our opportunities, as students, to influencehealth policy are modest, but significant, and it behooves us toremain vigilant on contemporary issues affecting access to carefor our future patients. It is our hope that this overview willstimulate thought, facilitate discussion and encourage engage-ment in rational policy debate leading to informed personalpositions.
Letting the Genie Out of the Bottle...On June 9, 2005, the Supreme Court of Canada ruled in astrategic 4-3 decision that the Quebec government cannot pre-vent Quebec residents from purchasing private insurance forprocedures covered under public healthcare.1 The complainant,George Zeliotis, had waited one year for hip replacementsurgery in 1996 and successfully argued that his wait was unrea-sonable, endangered his life and infringed on the guarantee ofthe right to life, liberty and security enshrined in the CanadianCharter of Rights and Freedoms. Similarly, Dr. JacquesChaoulli, Mr. Zeliotis’ physician, challenged the Quebec Hospital
Insurance Act and the Quebec Health Insurance Act. His request toset up a private hospital to offer services outside the umbrellaof public healthcare was previously denied by a Quebec court.Chaoulli fought to overturn the decision arguing that his ser-vices would improve the quality of health care. In their deci-sion the justices cited a public system that, in its current state,had failed to guarantee access to medical services in a timelymanner.
The impact of the court’s decision has reverberated withCanadians and throughout the media, triggering responses frommajor physician stakeholder organizations, namely the CanadianMedical Association (CMA) and the Canadian Association ofInternes and Residents (CAIR). At the CMA’s General CouncilMeeting in August a majority of delegates approved a motionsupporting “the principle that when timely access to care can-not be provided in the public health care system the patient
News and Views

volume 83, number 1, December 2005 7
resources, in the form of operating room time, essential tech-nologies and health personnel, according to clinical need andurgency. Wait lists are also valuable in maintaining the efficien-cy of the system, preventing resources that are costly and inhigh demand from sitting idle. What, then, determines whenwait times are too long?
The standard answer to this question has been that there isinsufficient evidence to know. However, the Wait TimeAlliance, a project involving physician specialty groups whosepractices are most affected by wait lists, has published waitingtime benchmarks and performance goals in its recently releasedfinal report.5 Similarly, the Western Canada Waiting List Projectis undertaking an ambitious project of incorporating symptoms,physical findings and other factors – including physician, patientand public consultation– to determine acceptable wait times forservices.6 Determining acceptable wait times for access to spe-cialist procedures is an important step in characterizing the cur-rent situation and will provide standards for ensuring no indi-vidual patient suffers longer than he or she should. Theseinitiatives and others are beginning to reduce the informationdeficit that has stalled action on reform.
Possible solution to the problem of excessive wait lists arenumerous and blame can be directed in many directions as towhy many feasible improvements to the system have not yetbeen put into practice. Systematic measures to better manageand coordinate waiting patients to available services have beenimplemented in a number of jurisdictions with positive results.Two successful and often cited examples are the Cardiac CareNetwork7 in Ontario and a comprehensive surgical wait listmanagement initiative by the province of Saskatchewan.8 Suchsystem-wide programs based on established evidence need to beconsidered for all jurisdictions.
Increasing capacity, by training more health professionals, isanother widely acknowledged requirement. However, the train-ing of nurses and doctors takes many years, a fact familiar tothis audience. During his tenure as the Premier of BC, the cur-rent federal Minister of Health did not recognize the impact ofreplacing the nearly 300 physicians lost annually to the provincewith only 120 medical school graduates. The consequences ofthis inaction are now clearly recognized in most jurisdictionsacross Canada as the number of citizens without a family physi-cian continues to rise. The addition of health professionals willimprove staffing levels to permit increased utilization of expen-sive capital infrastructure, including diagnostic equipment andoperating rooms. The increase in human resources and moreefficient management of waiting lists are two of the most obvi-ous and direct measures to curtail wait times.
There have been other suggestions, including more efficient useof health care personnel to free up more physician time for pro-cedures for which they alone are qualified. Family practicereform and electronic health records are other system-wideinterventions that all need stronger leadership from govern-ments and physicians to ensure the sustainability of our current
system. Of course, a more radical proposal, revitalized by theSupreme Court, includes removing the restrictions that preventprivate payment for services covered by public healthcare.
Is Private Insurance the Answer?Positions on the creation of a parallel private component to alargely publicly funded healthcare system have traditionally beenmarked by entrenched positions of ideologically focused organi-zations and opinions. In the past months grounds have shiftedwith traditional defenders of a public system, such as the CMA,considering private alternatives.
Underlying this newly invigorated debate is the fundamentalquestion of whether allowing private insurance will improveaccess to care for patients in Canada. It is presumed that thosewho can afford this luxury will receive preferential access tophysicians and procedures, leading to an overall increase in qual-ity of care. For those remaining within the public system, whatconsequences, if any, will second-tier status have on theirhealth? In a country proud of its traditions that ensure equali-ty for all, an ethos repeatedly reinforced by opinion polls andmore recently by delegates of the CMA,2 this unknown mustguide integration and regulation of any central changes to thestructure of healthcare in Canada.
It is argued that privately delivered, for-profit enterprises are dri-ven by market forces that compel them to increase efficiency inthe face of competition from similar businesses. The argumentfollows that privately funded care, in traditionally public sectors,would present more efficient enterprises that would lead to thereduction of public expenditures and ease the burden of astrained healthcare system. Additionally, overall health spendingwould likely increase as private citizens contribute funds aboveand beyond what they would have been responsible for in a sin-gle-payer system.
There continues to be opposition, however, to these arguments.First, healthcare in Canada is almost unanimously considered amerit good and not an ordinary market good which is requiredto drive traditional supply and demand dynamics. A merit goodhas a floor price that ensures it is not denied to anyone need-ing it, even those without adequate financial means.9 If one isanalyzing a privately funded, for-profit, private clinic system themarket forces model no longer applies since it does not makesense for private clinics to lower their prices to a level belowwhat the government is willing to pay for in the public system.The market model, in short, is questioned.
Data from the Organization for Economic Corporation andDevelopment (OECD) shows that countries seem to supportthe point that private systems do not lower the price of health-care. In these countries, a ten percent increase in private expen-diture was found to coincide, on average, with a one to threepercent decrease in public expenditures after controlling forother factors.10 If the two sectors are providing equal care thenit would seem that the private sector is less cost-efficient thanits public counterpart.

University of Toronto Medical Journal8
ed with a unique opportunity to make meaningful improve-ments to how healthcare is delivered in Canada. Our contribu-tion to this extraordinary and meaningful dialogue has neverbeen more important.
References1. Chaoulli v. Quebec (Attorney General). 2005 SCC 35.2. Canadian Medical Association [homepage on the Internet]. c1995-2005 [cited 2005
Oct 15]. Resolutions (unofficial) of the 138th General Meeting of the CanadianMedical Association. Available from: http://www.cma.ca/index.cfm/ci_id/45252/la_id/1.htm.
3. Hoyt B. Public versus private: the medical resident perspective. CMAJ. 2005 Oct 11;173(8):898-9.
4. McFarlane L. Supreme Court slaps for-sale sign on medicare. CMAJ. 2005 Aug2;173(3):269-70.
5. Wait Time Alliance for Timely Access to Health Care. It’s about time: achievingbenchmarks and best practices in wait time management. Ottawa: Canadian MedicalAssociation; 2005 [cited 2005 Oct 13]. Available from: http://www.cma.ca/multime-dia/CMA/Content_Images/Inside_cma/Media_Release/pdf/2005/wta-final.pdf.
6. WCWL - Western Canada Waiting List Project [homepage on the Internet]. Calgary:Western Canada Waiting List Project; c2003 [cited 2005 Oct 15]. Available from:www.wcwl.org.
7. Cardiac Care Network of Ontario [homepage on the Internet]. Toronto: Cardiac CareNetwork of Ontario; [cited 2005 Oct 15]. Available from: www.ccn.on.ca.
8. Saskatchewan Surgical Care Network [homepage on the Internet]. Regina:Saskatchewan Surgical Care Network; c2003 [cited 2005 Oct 15]. Available from:www.sasksurgery.ca.
9. Deber, RB. Getting What We Pay For: Myths and Realities about FinancingCanada’s Health Care System. Toronto: The Dialogue on Health Reform: SustainingConfidence in Canada’s Health Care System; 2000 [cited 2005 Oct 15]. Availablefrom: http://www.utoronto.ca/hpme/dhr/pdf/atrevised3.pdf.
10. Tuohy CH, Flood CM, Stabile M. How does private finance affect health care sys-tems: marshalling the evidence from OECD nations. J Health Polit Policy Law. 2004Jun;29(3):359-96.
11. Duckett SJ. Private care and public waiting. Aust Health Rev. 2005 Feb;29(1):87-93.12. Devereaux PJ, Choi PT, Lacchetti C, Weaver B, Schunemann HJ, Haines T, et al.
A systematic review and meta-analysis of studies comparing mortality rates of privatefor-profit and private not-for-profit hospitals. CMAJ. 2002 May 28;166(11):1399-406.
13. Himmelstein DU, Woolhandler S, Hellander I, Wolfe SM. Quality of care ininvestor-owned vs not-for-profit HMOs. JAMA. 1999 Jul 14;282(2):159-63.
14. Ipsos-Reid. In the wake of the Chaoulli decision by Supreme Court: Canada’s doc-tors and public reflect on implications for their health care system. Toronto: Ipsos-Reid; 2005 [cited 2005 Oct 15]. Available from: http://www.cma.ca/multimedia/CMA/Content_Images/Inside_cma/Media_Release/pdf/2005/Ipsos-Reid-Summary.pdf.
Results from the same study point out that private healthcaresystems tend to increase wait times and that parallel private sys-tems leave the sicker patients, who require more time- and cost-intensive procedures, to the care of the public system.10, 11 Thesingle-payer model in the publicly financed hospital and physi-cian system also seems to have greater purchasing power andhas a greater ability to hold down healthcare prices.9-10 Thehigher costs have been observed in some private, for-profitphysiotherapy clinics in Ontario and cataract eye surgery cen-tres in Alberta.9
The Chaoulli decision argued that an individual has the right topursue private healthcare for the betterment of his or her ownwell-being. In addition to the likely implications to the publichealthcare system there is, however, a lack of evidence sup-porting better care in a parallel private system. Patients in theprivate system have not been shown to experience improve-ments in life expectancy or quality of life and may even sufferworse health outcomes.12, 13 Beyond the evidence supporting agreater efficiency in the public healthcare system many arguethat a private system will preferentially benefit those who canpay for it and is contradictory to our Canadian value of equal-ity in healthcare.
The nature and extent of the ramifications of the ChaoulliSupreme Court decision remain uncertain. Recent polls havefound that 80% of physicians and 65% of Canadians believethat the decision will lead to shorter wait times for medical pro-cedures.14 Certainly, it has stimulated new debate. Whether thesolution for better health for citizens lies in a competitive, two-tiered landscape is debatable and evolving. The principle of ourcollective challenge is simple: to increase timely access to med-ical services without compromising equality or quality of care.Politicians, physicians and medical students have been present-

University of Toronto Medical Journal10
interactive decision theory, is a fundamental unifying frameworkfor the social sciences that explains why some groups succeed inpromoting cooperation while others suffer from conflict.
LiteratureHarold Pinter (United Kingdom)...“who in his plays uncovers the precipice under everyday prattleand forces entry into oppression’s closed rooms.” Pinter’s dramafocuses on the basic elements of the theatre creating “comedies ofmenace”. In addition, through his work he has long been an advo-cate of human rights.
http://nobelprize.org
U of T Initiative Facilitates Access to Medicines in GhanaSarah E. Perkins, Faculty of Law (UofT)
In May 2004 the Canadian Government passed the Jean Chretien
Pledge to Africa Act (Bill C-9). The passage of this legislation madeCanada the first nation in the world to take advantage of the flex-ibilities under the World Trade Organization Agreement on Trade-
Related Aspects of Intellectual Property Rights (TRIPS), permitting theexport of generic pharmaceuticals to developing nations for thetreatment of HIV/AIDS, tuberculosis and malaria. In May 2005C-9 officially came into force but unfortunately, since that time,not a single pill has been exported under the legislation.
This fall semester, the University of Toronto based Access toDrugs Initiative (ADI) will strive to bring the humanitarian objec-tives of C-9 to life. ADI, a collaboration between the Faculty ofLaw’s International Human Rights Program, Gilbert’s LLP, andMdlinx, has recently partnered with Ghana to assist Ghana inaccessing essential medicines, such as antiretrovirals, through C-9.
As a first step in this process, the group has received CIDA fund-ing to assist the Ghanaian government with draft amendments tothe Ghanaian patent law legislation. These amendments are nec-essary for Ghana to be able to legally import generic medicationsin compliance with the TRIPS Agreement. The draft amendmentsto Ghana’s legislation will also serve as model legislation for otherdeveloping nations interested in using C-9 to access generic phar-maceuticals.
And the winner is. . . An overview of the Nobel Prize Recipients for 2005Janice Kwan, B.Sc. (OT9)
Physiology or MedicineBarry J. Marshall (Australia) and J. Robin Warren (Australia)“...for their 1982 discovery of the bacterium Helicobacter pylori andits role in gastritis and peptic ulcer disease.” Prior to this finding,it was commonly thought that stress and lifestyle were the pre-vailing causes of gastric and duodenal ulcers.
PhysicsRoy J. Glauber (USA), John L. Hall (USA) and Theodor W. Hänsch (Germany)...for their “contribution to the quantum theory of optical coher-ence” and the “development of laser-based precision spec-troscopy.” Their work may lead to the development of extreme-ly accurate clocks and improved GPS technology.
ChemistryYves Chauvin (France), Robert H. Grubbs, and Richard R.Schrock“...for the development of the metathesis method of organic syn-thesis.” In metathesis reactions, double bonds are broken andmade between carbon atoms. These reactions result in the chang-ing of places between atom groups. The bond has been likenedto a pair of dancers that effectively exchange partners during thecourse of the reaction. The word metathesis means “changeplaces.”
PeaceInternational Atomic Energy Agency (IAEA) (Austria) andMohamed ElBaradei (Egypt)“...for their efforts to prevent nuclear energy from being used formilitary purposes and to ensure that nuclear energy for peacefulpurposes is used in the safest possible way.” The IAEA wasfounded in 1957 in Vienna, Austria. ElBaradei is its currentDirector General.
EconomicsRober J. Aumann (Israel and USA) and Thomas C. Schelling(USA)“...for having enhanced our understanding of conflict and cooper-ation through game-theory analysis.” Game theory, also known as
News at a Glance
News and Views

In addition to patent law amendments, a working group of lawstudents will be drafting a step-by-step guide to C-9 which willhelp other developing nations and pharmaceutical companies nav-igate the C-9 application procedure.
It is ADI’s hope that Ghana’s success will be a catalyst for theexport/import of generic pharmaceuticals to all nations in need,and for a sustained initiative that will ensure developing nationsaccess to essential medicines.
The Jean Chrétien Pledge to Africa, S.C. 2004, c.23.
http://www.wto.org/english/docs_e/legal_e/27-trips_01_e.htm.
Insight into the influenza virus of 1918Janice Kwan, B.Sc. (OT9)
In 1918, an unusually virulent strain of the human influenza virusswept around the planet, killing between 20 and 50 million peopleworldwide. Since then, virologists have been fascinated by this fluvirus strain and the reason for its immense virulency. This curios-ity has been heightened recently by the possibility of an H5N1avian influenza pandemic. In two breakthrough studies publishedrecently, researchers have made tremendous progress in our under-standing of the virus. Using sequence and phylogenetic analysesof frozen 1918 human lung tissue, Taubenberger et al. character-ized and described the full genome sequence of the 1918 virus.Employing the sequence provided by Taubenberger et al., Tumpeyet al. were able to recreate the virus and study its effects in mice.Predictably, this flu strain is more lethal to mice than are other flustrains.
Taubenberger et al. found that all eight of the genome segmentsfrom the 1918 virus differ from other human flu sequences, sug-gesting that the genome originates from a strain that did not infecthumans, and is likely bird in origin. By determining exactly whichmutations permitted the virus to jump from birds to humans, sci-entists may be able to recognize and predict other viruses likely tocause pandemics.
While some believe that these studies will provide essential infor-mation necessary to prevent a future influenza pandemic fromoccurring, others fear that the reconstruction of the lethal flustrain may prove to be a threat in its own right. Indeed, the eth-ical implications of producing a potential bioweapon have elicitedconcern in many in the scientific community.
Taubenberger JK, Reid AH, Lourens RM, Wang R, Jin G and Fanning TG.Characterization of the 1918 influenza virus polymerase genes. Nature 437: 889-93(2005).
Tumpey TM, Basler CF, Aguilar PV, Zeng H, Solorzano A, Swayne DE et al.Characterization of the reconstructed 1918 spanish influenza pandemic virus. Science 310:77-80 (2005).
Von Bubnoff A. The 1918 flu virus is resurrected. Nature 437: 794-795 (2005).
University of Toronto Researchers Win Lasker AwardMartin E. Betts. B.Sc. (OT8)
Ernest McCulloch and James Till, University of Toronto scientistsaffiliated with the Ontario Cancer Institute and the Institute ofMedical Science, were recently recognized with the 2005 AlbertLasker Award for Basic Medical Research. McCulloch and Till’spioneering work established the stem cell concept and has pro-vided an enduring framework through which stem cells are stud-ied today.
Beginning with a paper published in 1961 in the journal Radiation
Research, McCulloch and Till described the first quantitative methodto identify stem cells as self-replicating blood cell forming units inthe body. This led to a series of articles during the followingdecade contributing to knowledge on normal and abnormal bloodcell development.
The body of this work was initially recognized, shortly thereafterin 1969, by the Gairdner Foundation, through an award on simi-lar footing with the Lasker prize. The field of stem cell biologyhas grown exponentially in recent years, owing to much-hypedpotential in regenerative medicine and its involvement in cancersand cloning. The scientific, political, and ethical controversy sur-rounding the research and use of stem cells, both adult and embry-onic, has kept the field in the news and partially accounts for thisrenewed interest in the significant work of McCulloch and Till.
Priding itself on predicting future winners of the Nobel Prize, theLasker Foundation has presented annual awards for both basic andclinical medical research for 60 years, establishing its prize asamong the most coveted and prestigious in biomedical research.
http://www.laskerfoundation.org
Promising Vaccine for Cervical Cancer Peter Tanuseputro, M.H.Sc. (OT8)
Merck revealed in early October promising results from its phaseIII trial of Gardosil™, a genetically-engineered vaccine designed toblock infection from several strains of the Human Papilloma Virus(HPV). The HPV strains targeted are responsible for 70 percentof cervical cancer. 10,559 sexually active women between the ages16 to 26 years were enrolled, and of those who remained virus freeafter six months, none who received the 3 doses of the vaccineand 21 who received placebo shots developed cervical cancer orprecancerous lesions after an average of 2 years of follow up.Further analysis in a continuing study showed 97 percent vaccineeffectiveness in preventing cervical cancer after 1 dose of the vac-cine, with only 1 patient who received the vaccine, versus 36 whodid not, developing cervical cancer or precancerous lesions. It ishoped the vaccine will be ready for widespread clinical use in 2006.
volume 83, number 1, December 2005 11

University of Toronto Medical Journal12
During the period in question tuition for medical, dental, and lawprograms in Ontario increased 286%, 370%, and 173%, respec-tively. The proportion of the student population from the high-est socioeconomic background, those with a parent possessing agraduate or professional degree, increased and continued to beover-represented in professional programs in Ontario. Somewhatsurprisingly, given previous studies, the proportion of enrollmentof students from the lowest socioeconomic stratum, whose par-ents had no post-secondary education, also increased by a similarfactor of approximately 2. Students whose parents had post-sec-ondary qualifications below the graduate or professional levelshowed decreased enrollment. There were no significant changesin the class of students enrolling in professional programs in BCor Quebec, a control group with no change in tuition during theyears studied.
Prior to the substantial tuition increases in Ontario, student finan-cial aid was increased to prevent a decline in enrollment of stu-dents from disadvantaged backgrounds. This has been offered asan explanation in maintaining and even increasing enrollment ofstudents from these situations. However, this support may nothave qualified students of middle classes, resulting in a decreasedlikelihood of their being able to pay for tuition and a subsequentdecrease in their representation amongst professional programs inOntario.
http://www.statcan.ca/Daily/English/050927/d050927a.htm
Tuition and Diversity in Professional Programs in OntarioMartin E. Betts, B.Sc. (OT8)
A recent report from Statistics Canada has linked tuitionincreases for professional degree programs in Ontario with a shiftin the socioeconomic background of students enrolling in thoseprograms.
When tuition for medical, dental and law schools was deregulatedby the Ontario government in 1998, there was concern this actionwould further restrict access to students of low income families,minority groups, and rural areas, and that graduates would notreflect the diversity of the Canadian population. It is acknowl-edged that graduates from underrepresented groups are more like-ly to practice in underserviced communities, a requirement formaintaining the ideal of equity in Canadian services and society.
Using data collected from the 1995 and 2000 classes of theNational Graduates Survey, Marc Frenette of Statistics Canadaanalyzed the probabilities of graduates from Canadian post-sec-ondary institutions entering a program in medicine, dentistry orlaw within two years of their convocation date. These probabili-ties were stratified by an indirect measure of socioeconomic sta-tus, the highest education level achieved by a parent, and com-pared across provinces.

University of Toronto Medical Journal14
very serious student, I had this attitude that I needed to learneverything. Quoting my wife, “If I don’t learn this I might oneday hurt a patient for not knowing it.” This attitude wasreflected in my studies. I never sat in the front row but I’lladmit to being close, and I asked a fair number of questionsduring lectures. I spent my 2nd and 3rd years largely at TorontoWestern and I spent my second year there as a hospital rep. Iplayed volleyball and basketball; it was a terrific time. I hada lot of fun in medical school. Of course, I also met myfuture wife.
Any comments on intraclass relationships? Whatever works, right? I wouldn’t say it’s a great idea or a badidea anymore than a relationship with anyone else. Clearly, ithas the virtue of allowing for a partner who has a tremendousstore of empathy because he or she completely understands thechallenges and stresses that you’re facing. A downside is thatduring residency there are weeks when you’re on call frequent-ly and your call schedules don’t necessarily match. There weretimes when we hardly saw each other, and when we did seeeach other we were so exhausted. No exaggeration, there weremonths of one-in-three call where we both had different callschedules- and we would not go home at noon post-call. Wouldit be easier to be married to someone with normal hours? Sure,but my advice is to stick with whatever works.
Is it true that Ian Taylor introduced you to your wife?Absolutely true. Different cadaver, same lab. It was October of1983. Dr. Taylor walked over, tapped me on the shoulder andsaid, “There’s a young lady over there that is quite interested inyou.” I allegedly replied something like, “I’m sorry, I’m busydissecting.”
What has changed about medical school today as com-pared to when you were a student? It’s a very different landscape, actually. My class had about 33%women, now it’s up to 58% I understand. Many of my class-mates, myself included, had done only 2 years of undergradu-ate study. Today’s entrants have completed 3 or 4 years, if nota Masters or PhD. Students are more mature perhaps, at least
It’s 7:30 am on a drizzly Friday. Dr. Martin Schreiber has kindly agreed
to meet with us to answer some questions. What has dragged Sam Silver
and Marieke Gardner, second-year medical students and preclerkship rep-
resentatives for their class, to school at 7:30am you ask? Dr. Schreiber is
a busy man. As the newly appointed Preclerkship Director, Dr. Schreiber
sits on the Admissions Committee (and many others) and it is convening
at 8:00 am. There’s no time for an interview after the meeting, as he must
leave promptly in order to be on time for his children’s track meet. As a
nephrologist at St. Michael’s Hospital, Preclerkship Director, Foundations
of Medicine Course Coordinator, Associate Professor and dedicated fami-
ly man you start to wonder how he manages to do it all. Dr. Schreiber
will tell us it’s simply a matter of balance. (It probably doesn’t hurt to
have oodles of brains either. Dr. Schreiber was the Gold Medallist of the
University of Toronto Medicine Class of 8T7).
You’ve lived in Toronto most of your life …is there some-thing in the water? You’re right, I’ve been in Toronto for a while. I attended theUniversity of Toronto for my undergraduate (2 years, TrinityCollege), medical (4 years) and postgraduate (7 years) training.And finally as a teacher I’ve been here since 1994. I did take ayear during my postgraduate training (1992-3) to study at theUniversity of Dundee in Scotland. It was nice to get away forthat one year to experience something a little different andbring something different back.
Family connections have a lot to do with it. My parents werealways here. I met my wife as a classmate and she has strongfamily connections as well. Having two physicians in a familydoesn’t necessarily limit you to being in a large centre, but beingin a large centre makes it easier. Also, there haven’t really beenany compelling reasons to go elsewhere. The opportunities hereare excellent. I think it’s a great institution. There’s so muchvariety and diversity. The strengths are terrific. My own inter-est in education, which was the reason I went to Scotland, wasvery well fostered here. I’m not sure it’s something in the water,but there is definitely something very good about U of T.
What kind of medical student were you? I was quite young, only 19 when I started. I lived at home. A
Ten Questions for Dr. Martin Schreiber
Marieke Gardner, H.B.Sc. (OT8)
Sam Silver (OT8)
News and Views

older in years. The mentality of the class is also changing a lit-tle bit. Appropriately, students are more demanding as to whatthey will accept and are a little more empowered than we were.Undeniably, the fact that tuition has gone up 10-fold must besignificant. Technology. We did not have e-mail, the Internet,or the same electronic resources. We actually read textbooks.
As Preclerkship Director, what changes do you envisionover the next few years? Let me answer in a couple of different ways. I think that themost interesting change on the horizon is the potential expan-sion of the medical school into Mississauga and the communi-ty in general. I think that event is going to dominate any plansfor change in the near future. It’s hard to be specific becausewe don’t know by how much enrolment will increase or howthe larger program will be configured. Clearly, the expansion isgoing to have a feedback effect on the school as a whole. Withregards to other changes it’s hard to say we’re going to do A,B, and C because these may be negated or dominated by what’shappening with the expansion.
In a related sense, I gather a major force for change is thenotion of social accountability. It’s largely a force that comesfrom within all of us because we want to be accountable tosociety and to patients. We serve them, and in effect they’re theones who pay us and pay for our training. Government isdemanding we demonstrate that what we are doing in medicalschool is meeting the needs of society. For example, there is adesire to train an adequate number of family physicians. Thereis a crisis there. I feel it all the time as a specialist.
We need to make sure that, in the course of our curriculumplanning we make sufficient efforts to give students the oppor-tunity to make rational choices about their careers. I don’t thinkanybody would ever envisage a situation where people wereforced or coerced into any particular career path. One of thebest things about being a physician and going to medical schoolis that you don’t limit your options. However, I think we real-ly need to make sure that beginning right in preclerkship, thenotion of a career in primary care is not denigrated and that itis presented in a favourable light.
One major thing we need to continue to do is to make surethat our several excellent courses remain well integrated. Thereis a tendency for curricular drift and we need to avoid this.Each course has its own ideas, approaches, and topics anddelivers them very well. We need to ensure that they are deliv-ered as separate components of a cohesive unit. One mediumsized task I see is making sure that we as teachers workas coherently as possible so students get the best overallexperience.
If you could change one aspect of the preclerkship cur-riculum back to the way it was 20 years ago, what wouldit be? We used to have one day a week off for electives during eachof the first three years of school. It was a wonderful low stressway to spend time with physicians who were welcoming to stu-dents and interested in contributing to their education.
Are there any professors that are still here from whenyou were a student? Ian Taylor (Anatomy), Mike Wiley (Embryology and Histology),Valerie Watt (Metabolism and Nutrition) had just started teach-ing and Bob Richardson (Renal) to mention a few names thatyou would recognize from first year.
What do you do in your spare time? I like to read. I don’t read a lot of fiction though. I prefer non-fiction on topics like evolution and world history. Right now,I’m reading “Ideas: A History from Fire to Freud.” I like toplay with my kids. I like to travel. Our most recent family tripwas to the maritime provinces this past summer.
What advice can you offer the OT9 class on surviving thefirst year of medical school? The most important thing is balance. And I’m not talking aboutinput minus output (joke…please chuckle). Medical school is hard.That’s okay. If medical school were easy, why would we putyou through such a rigorous admissions process? I think if itwere easy, doctors wouldn’t be nearly as valuable. You really doneed to learn this stuff, it all matters. However, that’s not allthere is to life. If you don’t keep some balance, whether it behobbies, spending time with friends or family, things that makeyou complete, you’re much more likely to end up in trouble.
It is now 8:00 am and the interview closes. Dr. Schreiber, Marieke and
Sam have an Admissions Committee meeting to go to – part of our
balance.
volume 83, number 1, December 2005 15

Developing new and effective anticancer therapies has been verydifficult because of the vast number of genetic defects that canexist in a cancer cell. Research in the past has focused on cor-recting defective or deficient proteins, such as the tumor suppres-sor p53. Newer approaches have taken advantage of the conver-gence of many oncogenic signaling pathways on a limited set ofnuclear transcription factors, such as STAT3 (signal transducer andactivator of transcription 3).1 Targeting an overactive transcriptionfactor may negate the need to deal with the many upstream muta-tions that trigger the gene expression patterns that ultimately leadto malignancy.2 This new approach has led to exciting research thatfocuses on STAT3 as a promising target for the development ofa broad anticancer therapy.
STAT3 is one of seven transcription factors in the STAT familyof proteins that are activated in response to cytokines and growthfactors.1 STAT3 becomes activated by phosphorylation at a sin-gle tyrosine residue (Tyr-705), leading to dimerization through rec-iprocal SH2-phosphotyrosine interaction.3,6 Activated STAT3translocates to the nucleus where it binds consensus promotersequences that control fundamental biological processes includingcell proliferation, apoptosis, angiogenesis, and immune responses.2
In normal cells, STAT3 tyrosine phosphorylation is transient, last-ing from minutes to hours. However, in numerous cancer derivedcell lines or in primary tumours, STAT3 is persistently phospho-rylated, which appears to disrupt normal physiological control andleads to malignancy. Research has shown that blocking STAT3 sig-naling in tumour cells induces apoptosis, inhibits proliferation, sup-presses angiogenesis, and stimulates immune responses. Tumourcells that become dependent on persistent STAT3 signaling arealso more sensitive to STAT3 inhibitors than normal cells, pro-viding a therapeutic window based on transient or partial inhibi-tion of STAT3. Collectively, these findings point to STAT3 as apotential target for cancer therapy.2
STAT3 has been shown to be persistently active in a surprisingnumber of human cancer cell lines and tissues. The first evidenceof a link between STAT3 and human cancer came from findingsthat constitutive STAT3 activity was present in 95% of head andneck cancer cells and 50% of multiple myeloma cells.1 More recentstudies have linked persistent STAT3 activity with a variety ofleukemias and lymphomas as well as solid tumours such as breast,prostate, and lung.4,5
Work by Chiarle et al. has contributed to the mounting evidencethat targeting STAT3 may have beneficial anticancer effects.6 Usingmice, the researchers sought to determine if blocking the activa-tion of STAT3 with antisense oligonucleotides had a therapeuticeffect. Mice were challenged with a subcutaneous injection oftumour cells, and were treated one week later with antisenseoligonucleotides. In the treated mice, no tumour growth was seen,whereas after two weeks the control mice had large tumour mass-es. The researchers also showed that giving STAT3 antisenseoligonucleotides to mice with pre-existing tumours caused apop-tosis of cancer cells and substantially smaller tumours. It is impor-tant to note that the STAT3 antisense oligonucleotides killedtumour cells but had little effect on normal cells.
Further studies by Turkson et al.7 and Sun et al.8 showed thatSTAT3 was inhibited by platinum compounds and natural prod-ucts such as cucurbitacin (Cuc), which is produced by the cucum-ber plant. Song et al. recently discovered a new STAT3 inhibitorby virtual database screening. The researchers isolated a com-pound, STA-21, which was found to reduce the survival of breastcarcinoma cells that had constitutive STAT3 signaling, but hadminimal effect on the cells in which constitutive STAT3 signalingwas absent.3,6
Given these initial successes in therapies targeting STAT3, phar-macological blockage of constitutively active STAT3 seems to bea reasonable new approach for the treatment of many cancers.With more attention being paid to transcription factors as molec-ular targets, further success in developing a broadly applicable anti-STAT3 therapy may be on the horizon.
References1. Darnell JE. (2005) Validating Stat3 in cancer therapy. Nat Med. 2005 Jun;11(6):595-
96.2. Yu H, Jove R. (2004) The STATs of cancer – new molecular targets come of age.
Nat Rev Cancer. 2004;4: 97-105. 3. Song H, Wang R, Wang S, Lin J. A low-molecular-weight compound discovered
through virtual database screening inhibits Stat3 function in breast cancer cells. ProcNatl Acad Sci. 2005 Mar 29;102(13): 4700-5.
4. Bowman T, Garcia R, Turkson J, Jove R. (2000) STATs in oncogenesis. 2000May 25; Oncogene. 19(21): 2474-88.
5. Buettner R, Mora LB, Jove R. (2002) Activated STAT signaling in human tumorsprovides novel molecular targets for therapeutic intervention. Clin. Cancer Res. 2002Apr;8: 945–54.
6. Chiarle R, Simmons WJ, Cai H, et al. (2005) Dhall G, Zamo A, Raz R, et al. Stat3is required for ALK-mediated lymphomagenesis and provides a possible therapeu-tic target. Nat Med. 2005 May 15;11: 623-9.
7. Sun J, Blaskovich MA, Jove R, et al. (2005) C, Livingston SK, Coppola D, SebtiSM. Cucurbitacin Q: a selective STAT3 activation inhibitor with potent antitumoractivity. Oncogene. 2005 May 5;24(20): 3236-45.
8. Turkson J, Zhang S, Mora LB, Burns A, Sebti S, Jove R., et al. (2005) A novel plat-inum compound inhibits constitutive Stat3 signaling and induces cell cycle arrestand apoptosis of malignant cells. J Biol Chem. 2005 Sep 23;280(38): 32979-88.
University of Toronto Medical Journal16
Medical Murmurs
STAT3 – A Promising Molecular Target for Cancer Therapy
Tomce Trajkovski, B.Sc. (OT7)
News and Views

volume 83, number 1, December 2005 17
which is semi-conservative, DNA polymerase primers overlayand cover a portion of the terminal chromosome.Consequently, a portion of the telomere is not replicated andtherefore shortens with each cell division. Telomeres are knownto be shorter in senescent cells than in younger cells.10,11
Therefore, telomere shortening may be the “clock” that leadsto the shift toward senescent-associated gene expression andultimately cell senescence and the Hayflick limit.3
The Hayflick limit is a barrier to infinite replication, and hasvery few known exceptions.4 These exceptions include cancercells and the germ cell lineage.12,13 Certain stem cell lines, suchas gastrointestinal crypt cells, liver cells, and hematopoietic stemcells, also demonstrate replicative senescence, but do so with amuch extended cellular lifespan and a greater number of celldivisions in comparison with other somatic cell types.14
Surprisingly, this extension corresponds with a transient expres-sion of telomerase, which allows these cells to slow the rate atwhich their telomere bases disappear.15,16 Telomerase expressionalso occurs in the germ cell line and primordial stem cells. Sincethese cells are not limited by replicative senescence, they havea potential clinical application in the growth of tissues andorgans.3
The Cellular “Clock” The articles by Bodnar et al.1 and Vaziri and Benchimol,2 haveboth shed some light on what acts as the cellular “clock” thattimes replicative senescence. Bodnar et al. have shown that thetelomere is the clock of replicative senescence and that it canbe reset.1 Vaziri and Benchimol,2 as well as others,17 have inde-pendently confirmed the work. As previously mentioned,telomerases act by adding DNA bases to telomeres. This isdone through the use of a short RNA template that is presentin cells normally, and a catalytic protein component that is notfound in normal aging somatic cells. Bodnar et al. transfected agene for this catalytic component into cells and displayed thatthis resulted in extended telomeres.1 The extended telomeres inturn extended the replicative life span of the cells, giving thema pattern of gene expression identical to young cells, and show-ing 40% more population doublings.3
The study by Bodnar et al.1 effectively demonstrated that telom-
Numerous mechanisms have been proposed to explain theprocess of aging, including the prominent ‘telomerase theory’and the ‘mitochondrial theory’. Two recent papers, both pub-lished in 1998, highlight the significance of the telomerase the-ory in the everlasting debate over the aging cell.
The articles, by Bodnar et al.1 and Vaziri and Benchimol,2 bothdemonstrate that human cell senescence can be reversed bytransfection with a gene for the catalytic component of telom-erase. These startling articles suggest that the “Hayflick limit”can be extended, and propose numerous prospects for clinicalmedicine.3
A 1998 review article by Fossel3 provides a good review of thetelomerase theory of aging, and provides prospective expecta-tions and limitations of the theory in clinical applications. Thisarticle presents the relevant facts and findings from Fossel’spaper, and presents a simple description of the ‘telomerase the-ory’ of cellular aging and its potential clinical applications.
The Hayflick LimitNormal somatic cells have limited replicative potential, dubbedthe Hayflick limit, which has been demonstrated in young skinfibroblasts to be approximately 50 divisions.4 This replicativepotential is reached gradually, with progressive slowing of therate of divisions as well as manifestations of identifiable andpredictable morphological changes characteristic of “senescentcells.”5 These senescent cells also express definable patterns ofchanges in gene expression that accompany the replicativeblock, termed “senescence-associated gene expression.”3,6-8
Telomeres, Telomerases and DNA ShorteningEukaryotic chromosomes possess special structures, known astelomeres, at their ends. One strand of each telomere is com-posed of tandem repeats of short, guanine-rich regions. The G-rich telomere strand is made by an enzyme called telomerase.Telomerase is a reverse transcriptase comprised of a short RNAsequence that serves as the template for telomere synthesis andincludes a specific catalytic protein component. This mecha-nism ensures that chromosome ends can be rebuilt, and there-fore do not suffer shortening with each round of cell division.9
However, during the eukaryotic process of DNA replication,
Back to Basics
Molecular Mechanisms of Aging: Telomerase and Cellular Aging
Michael Sidiropoulos, M.Sc. (OT7)
News and Views

University of Toronto Medical Journal18
eres are the timepieces of replicative aging. It is now knownthat not only do telomeres shorten with cell aging, but also thatre-lengthening the telomere appears to reset gene expression,cell morphology, and the replicative life span. However, ques-tions remain about the role of cell senescence in the aging ofan entire organism, and whether our knowledge of cellularsenescence can be of potential therapeutic use in the treatmentof underlying age-related diseases. Possibilities for treatmentinclude alternatives to cancer therapy and effective preventionand treatment of immune senescence, atherosclerosis, dermato-logic aging, macular degeneration, and Alzheimer’s disease.3
References1. Bodnar AG, Ouellette M, Folkis M, Holt SE, Chiu CP, Morin GB, et al.
Extension of life-span by introduction of telomerase into normal human cells.Science. 1998 Jan 16;279(5349):334-5.
2. Vaziri H, Benchimol S. Reconstitution of telomerase activity in normal humancells leads to elongation of telomeres and extended replicattive life span. Curr
Biol. 1998 Feb 26;8(5):279-82.3. Fossel M. Telomerase and the aging cell: implications for human health. JAMA.
1998 Jun 3;279(21):1732-5.4. Hayflick L, Moorehead PS. The Limited in vitro lifetime of human diploid cell
strains. Exp Aging Res. 1961;25:585-621.5. Hayflick L. The cell biology of human aging. Sci Am. 1980;242:58-66.
6. Wright WE, Pereira-Smith OM, Shay JW. Reversible cellular senescence: impli-cations for immortalization of normal diploid fibroblasts. Mol Cell Biol. 1989July;9(7):3088-92.
7. Campisi J. The Biology of replicative senescence. Eur J Cancer. 1997Apr;33:703-9.
8. Faraghar RGA, Shall S. Gerontology and drug development: the challenge ofthe senescent cell. Drug Discovery Today. 1997 Feb;2(2):64-71.
9. Weaver RF. Molecular Biology. 1st ed. Boston: McGraw-Hill; 1999. p. 689-92.10. Harley CB, Futcher AB, Greider CW. Telomeres shorten during aging of
human fibroblasts. Nature. 1990 May 31;345:458-60.11. Hastie ND, Dempster M, Dunlop MG, Thompson AM, Green DK, Allshire
RC. Telomere reduction in human colorectal carcinoma and with aging. Nature.1990 Aug 30;346(6287):866-8.
12. Counter CM, Hirte HW, Bacchetti S, Harley CB. Telomerase activity in humanovarian carcinoma. Proc Natl Acad Sci. 1994;91:2900-4.
13. Kim NW, Piatyszek MA, Prowse KR, Harley CB, West MD, Ho PL. Specificassociation of human telomerase activity with immortal cells and cancer. Science.1994 Dec 23;266(5193):2011-5.
14. Chiu C-P, Dragowska W, Kim NW, Vaziri H, Yui J, Thomas TE, et al.Differential expression of telomerase activity in hematopoietic progenitors fromadult human bone marrow. Stem Cells. 1996 Mar;14(2):239-48.
15. Counter CM, Gupta J, Harley CB, Leber B, Bacchetti S. Telomerase activity innormal leukocytes and in hematologic malignancies. Blood. 1995 May1;85(9):2315-20.
16. Hiyama K, Hirai Y, Kyoizumi S, Akiyama M, Hiyama E, Piatyszek MA, et al.Activation of telomerase in human lymphocytes and hematopoietic progenitorcells. J Immunol. 1995 Oct 15;155(8):3711-5.
17. Counter CC, Meyerson M, Eaton EN, Ellisen LW, Caddle SD, Haber DA, etal. Telomerase activity is restored in human cells by ectopic expression ofhTERT (hEST2), the catalytic subunit of telomerase. Oncogene. 1998 Mar5;16(9):1217-22.

volume 83, number 1, December 2005 19
ImplicationsGiven the commonly observed constant relative risk reductionexperienced by all patients undergoing a particular therapy,patients who have the highest baseline risk of an outcome tobe treated by the therapy should receive the greatest absoluterisk reduction. This study has shown, however, that heart fail-ure patients who are at higher mortality risk, and thus poten-tially having more to gain from pharmacotherapy, have lowerprescription rates. This suggests that there exists a significantgap between the potential benefit of pharmacotherapy for heartfailure and what is currently achieved in the population. Theauthors refer to several other studies in areas such as the qual-ity of care received after an acute myocardial infarction and theprescribing of statins in elderly patients to demonstrate theirfinding of the paradox of people at higher risk receiving lowerlevels of care.2-8 Such patterns of care undoubtedly lead to anincrease in the avoidable burden of disease and contribute toinefficiencies in a health care system that is already strainedfrom the limited resources it possesses.
References1. Lee DS, Tu JV, Juurlink DN, Alter DA, Ko DT, Austin PC, et al. Risk-treat-
ment mismatch in the pharmacotherapy of heart failure. JAMA. 2005 Sep14;294(10):1240-7.
2. Alter DA, Manuel DG, Gunraj N, Anderson G, Naylor CD, Laupacis A. Age,risk-benefit trade-offs, and the projected effects of evidence-based therapies.Am J Med. 2004;116(8):540-5.
3. Bhatt DL, Roe MT, Peterson ED, Li Y, Chen AY, Harrington RA, et al.Utilization of early invasive management strategies for high-risk patients withnon-ST-segment elevation acute coronary syndromes: results from the CRU-SADE Quality Improvement Initiative. JAMA. 2004 Nov 3;292(17):2096-104.
4. Halon DA, Adawi S, Dobrecky-Mery I, Lewis BS. Importance of increasingage on the presentation and outcome of acute coronary syndromes in elderlypatients. J Am Coll Cardiol. 2004;43(3):346-52.
5. Rathore SS, Mehta RH, Wang Y, Radford MJ, Krumholz HM. Effects of ageon the quality of care provided to older patients with acute myocardial infarc-tion. Am J Med. 2003;114(4):307-15.
6. Barakat K, Wilkinson P, Deaner A, Fluck D, Ranjadayalan K, Timmis A. Howshould age affect management of acute myocardial infarction? A prospectivecohort study. Lancet. 1999;353(9157):955-9.
7. Stukel TA, Lucas FL, Wennberg DE. Long-term outcomes of regional varia-tions in intensity of invasive vs medical management of Medicare Patients withacute myocardial infarction. JAMA. 2005;293(11):1329-37.
8. Ko DT, Mamdani M, Alter DA Lipid-lowering therapy with statins in high-risk elderly patients: The treatment-risk paradox. JAMA. 2004;291(15):1864-70.
Risk-treatment Mismatch in the Pharmacotherapy ofHeart Failure1 – Another example of paradoxical lowerlevels of treatment in those at highest risk
BackgroundPharmacotherapy is a vital part of the management of heart fail-ure, a condition that is associated with a high burden of mor-tality and morbidity in individual patients and in the populationas a whole. Heart failure patients who are at higher risk ofmortality may benefit comparably to or to a greater extent frompharmacotherapy, and should then be expected to be treated atleast at the same rate as those at lower risk (after consideringfactors such as contraindications and life-limiting comorbidi-ties).
StudyLee et al. examined the rates of pharmacotherapy in heart fail-ure patients with different risks of death. The EnhancedFeedback for Effective Cardiac Treatment (EFFECT) studyexamined a population-based cohort of 9,942 patients whowere hospitalized in Ontario with heart failure from 1999-2001.One thousand four hundred and eighteen of these patients whowere younger than 79 years and had a left ventricular ejectionfraction equal to or less than 40% were included in the study.One-year mortality risk was predicted for each patient, and theprescription levels for angiotensin-converting enzyme (ACE)inhibitors, ACE inhibitors or angiotensin II receptor blockers(ARBs), and β-adrenoreceptor antagonists were observed.
ResultsPatients with a higher mortality risk were prescribed all threecategories of pharmacotherapy less often than those with lowerrisks. At time of hospital discharge, patients in the low, aver-age and high risk groups had prescription rates of 81%, 73%and 60%, respectively, for ACE inhibitors, 86%, 80% and65%, respectively, for ACE inhibitors or ARBs, and 40%, 33%and 24%, respectively, for β-adrenoreceptor antagonists (allp<0.001 for trends). Similar statistically significant trends exist-ed 90 days and 1 year following discharge. After adjusting forcontraindications and varying survival times, the hazard ratioscomparing the prescription rates in the low versus high mor-tality risk groups were 1.61 for ACE inhibitors or ARBs [95%confidence interval (CI): 1.49-1.74] and 1.80 for β-adrenore-ceptor antagonists [95% CI: 1.60-2.01].
In the Literature
Peter Tanuseputro, M.H.Sc. (OT8)
News and Views

Current American and European guidelines recommend an earlyinvasive strategy for the management of high-risk patients withnon-ST elevation acute coronary syndromes (NSTEACS).1,2 Theserecommendations are largely based on the findings of seven ran-domized trials (enrolling 9208 patients) published between 1994and 2002 that compared early invasive against selectively invasivestrategies in NSTEACS.3-9 The first three of these studies (TIMIIIIB, MATE, and VANQWISH) showed no compelling benefit toan early invasive strategy.3-5 However, subsequent advances ininterventional cardiology (including coronary stenting and peripro-cedural use of thienopyridines and GP IIb/IIIa blockade) prompt-ed a second wave of trials (FRISC II, TACTICS-TIMI 18, VINO,and RITA 3) which demonstrated improvements in a variety ofclinical outcomes in the early invasive group.6-9
Two more recent publications provide very different insights intothe appropriate management of NSTEACS. The five-year follow-up of the RITA 3 trial suggests that the benefits of an early inva-sive strategy may only become fully apparent over long-term fol-low-up.10 By contrast, the ICTUS trial argues that advances inmedical therapy may have eliminated the advantage of an earlyinvasive strategy in unselected patients.11
Before the two-year RITA 3 data were published in 2002, threetrials6-8 had already argued for an advantage to early invasive strate-gies in NSTEACS. However, skeptics criticized these studies onseveral grounds. FRISC II and TACTICS employed more strin-gent diagnostic criteria (i.e. higher serum levels of cardiac enzymes)for periprocedural myocardial infarction (MI) than for spontaneousMI, tending to decrease the number of events in the early invasivegroup relative to the selectively invasive group. FRISC II showeda mortality benefit but employed unusually stringent criteria forcardiac catheterization in the conservatively managed group.VINO showed a benefit in the composite endpoint of death ornonfatal MI but was by far the smallest of the trials (131 patients,as compared to 2457 in FRISC II and 2220 in TACTICS).
RITA 3 enrolled 1810 British patients with NSTEACS between1997 and 2001. Patients randomized to early invasive managementhad coronary angiography performed within 72 hours after ran-domization. Patients in the conservative management arm under-went angiography if medical management failed to control anginal
symptoms or noninvasive tests demonstrated evidence of ischemia.Primary endpoints were the combined rate of death, nonfatal MI,or refractory angina at four months and the combined rate ofdeath or nonfatal MI at one year. The 2002 publication reporteda lower rate of the first endpoint (ARR 4.9%, RRR 34%, p=0.001)but not the second (ARR 0.7%, RRR 9%, p=0.58) in the earlyinvasive group.9 These data confirmed TACTICS’ observation ofa decreased incidence of recurrent angina in the early invasivegroup. However, whereas TACTICS also showed a benefit inrecurrent MI and the composite endpoint of death or nonfatal MI,RITA 3 showed no significant differences in these endpoints. TheRITA 3 investigators suggested that this difference might beexplained by TACTICS’ use of more stringent diagnostic criteriafor periprocedural MI than for spontaneous MI. Moreover, theyargued that this use of differential thresholds for the diagnosis ofMI was not justified on prognostic grounds.12
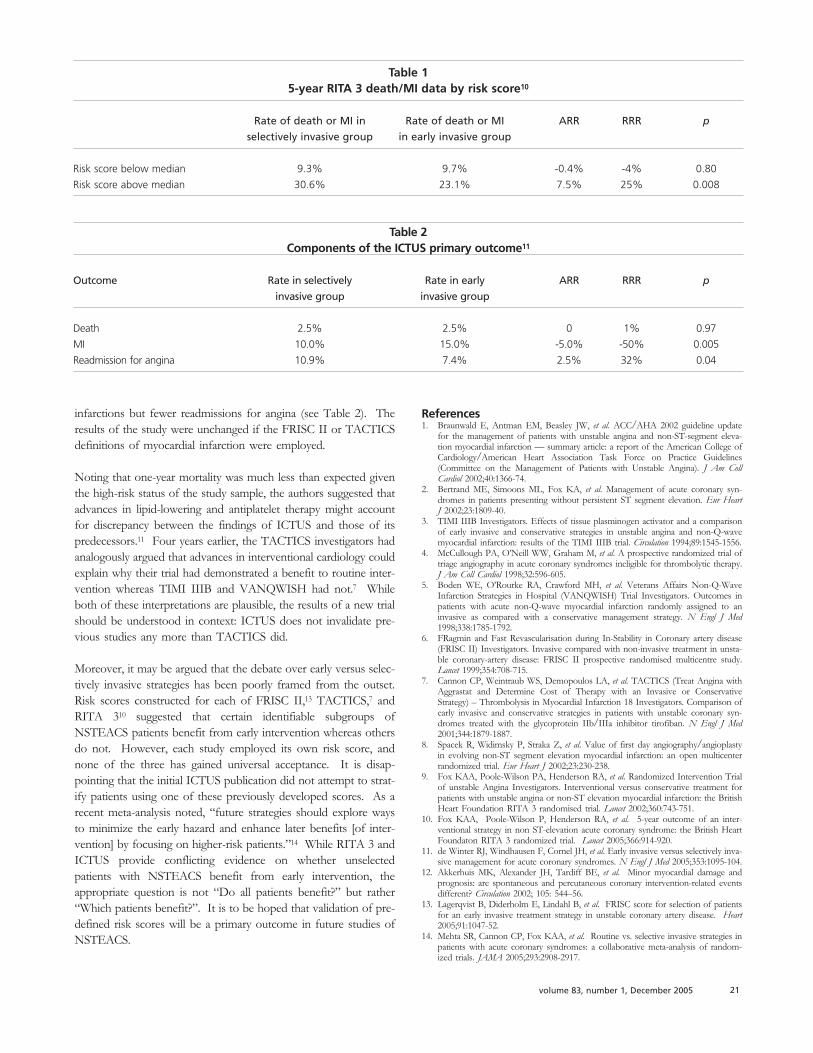
Therefore, after the publication of the two-year data from RITA3, the only major single outcome for which an early invasive strat-egy had clearly demonstrated a benefit was recurrent angina. Therecently published five-year data10 provide evidence for a benefitin death or nonfatal MI (ARR 3.4%, RRR 17%, p=0.044); thereduction in all-cause mortality alone was barely insignificant (ARR3.0%, RRR 20%, p=0.054). When a risk score was developedusing a predefined exploratory analysis, the benefit of an early inva-sive strategy was found to be limited to patients in the top half ofrisk (see Table 1). This comparison, however, was not stated tobe prespecified.
Published in the same week as the five-year RITA 3 follow-up,ICTUS11 was the fourth large trial of early versus selectively inva-sive management of NSTEACS in the era of coronary stentingand multi-agent platelet inhibition. It was also the first such trialto recommend early use of clopidogrel and a high-dose statin(atorvastatin 80 mg). ICTUS enrolled 1200 troponin-positiveDutch patients between 2001 and 2003; the primary endpoint wasthe combined rate of death, recurrent MI, or rehospitalization forangina within one year. Surprisingly (given the results of previousstudies), the rate of this endpoint was nonsignificantly higher in theearly invasive group (22.7% vs. 21.2%, ARR -1.5%, RRR -7%,p=0.33). Breaking the primary endpoint down into its compo-nents, the early invasive group experienced more myocardial
University of Toronto Medical Journal20
Management of Non-ST Elevation Acute Coronary Syndromes: Insights from RITA 3 and ICTUS
John D.D. Neary, H.B.Sc. (OT6)
News and Views
volume 83, number 1, December 2005 21
References1. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA 2002 guideline update
for the management of patients with unstable angina and non-ST-segment eleva-tion myocardial infarction — summary article: a report of the American College ofCardiology/American Heart Association Task Force on Practice Guidelines(Committee on the Management of Patients with Unstable Angina). J Am Coll
Cardiol 2002;40:1366-74.2. Bertrand ME, Simoons ML, Fox KA, et al. Management of acute coronary syn-
dromes in patients presenting without persistent ST segment elevation. Eur Heart
J 2002;23:1809-40.3. TIMI IIIB Investigators. Effects of tissue plasminogen activator and a comparison
of early invasive and conservative strategies in unstable angina and non-Q-wavemyocardial infarction: results of the TIMI IIIB trial. Circulation 1994;89:1545-1556.
4. McCullough PA, O’Neill WW, Graham M, et al. A prospective randomized trial oftriage angiography in acute coronary syndromes ineligible for thrombolytic therapy.J Am Coll Cardiol 1998;32:596-605.
5. Boden WE, O’Rourke RA, Crawford MH, et al. Veterans Affairs Non-Q-WaveInfarction Strategies in Hospital (VANQWISH) Trial Investigators. Outcomes inpatients with acute non-Q-wave myocardial infarction randomly assigned to aninvasive as compared with a conservative management strategy. N Engl J Med
1998;338:1785-1792.6. FRagmin and Fast Revascularisation during In-Stability in Coronary artery disease
(FRISC II) Investigators. Invasive compared with non-invasive treatment in unsta-ble coronary-artery disease: FRISC II prospective randomised multicentre study.Lancet 1999;354:708-715.
7. Cannon CP, Weintraub WS, Demopoulos LA, et al. TACTICS (Treat Angina withAggrastat and Determine Cost of Therapy with an Invasive or ConservativeStrategy) – Thrombolysis in Myocardial Infarction 18 Investigators. Comparison ofearly invasive and conservative strategies in patients with unstable coronary syn-dromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med
2001;344:1879-1887.8. Spacek R, Widimsky P, Straka Z, et al. Value of first day angiography/angioplasty
in evolving non-ST segment elevation myocardial infarction: an open multicenterrandomized trial. Eur Heart J 2002;23:230-238.
9. Fox KAA, Poole-Wilson PA, Henderson RA, et al. Randomized Intervention Trialof unstable Angina Investigators. Interventional versus conservative treatment forpatients with unstable angina or non-ST elevation myocardial infarction: the BritishHeart Foundation RITA 3 randomised trial. Lancet 2002;360:743-751.
10. Fox KAA, Poole-Wilson P, Henderson RA, et al. 5-year outcome of an inter-ventional strategy in non ST-elevation acute coronary syndrome: the British HeartFoundaton RITA 3 randomized trial. Lancet 2005;366:914-920.
11. de Winter RJ, Windhausen F, Cornel JH, et al. Early invasive versus selectively inva-sive management for acute coronary syndromes. N Engl J Med 2005;353:1095-104.
12. Akkerhuis MK, Alexander JH, Tardiff BE, et al. Minor myocardial damage andprognosis: are spontaneous and percutaneous coronary intervention-related eventsdifferent? Circulation 2002; 105: 544–56.
13. Lagerqvist B, Diderholm E, Lindahl B, et al. FRISC score for selection of patientsfor an early invasive treatment strategy in unstable coronary artery disease. Heart
2005;91:1047-52.14. Mehta SR, Cannon CP, Fox KAA, et al. Routine vs. selective invasive strategies in
patients with acute coronary syndromes: a collaborative meta-analysis of random-ized trials. JAMA 2005;293:2908-2917.
infarctions but fewer readmissions for angina (see Table 2). Theresults of the study were unchanged if the FRISC II or TACTICSdefinitions of myocardial infarction were employed.
Noting that one-year mortality was much less than expected giventhe high-risk status of the study sample, the authors suggested thatadvances in lipid-lowering and antiplatelet therapy might accountfor discrepancy between the findings of ICTUS and those of itspredecessors.11 Four years earlier, the TACTICS investigators hadanalogously argued that advances in interventional cardiology couldexplain why their trial had demonstrated a benefit to routine inter-vention whereas TIMI IIIB and VANQWISH had not.7 Whileboth of these interpretations are plausible, the results of a new trialshould be understood in context: ICTUS does not invalidate pre-vious studies any more than TACTICS did.
Moreover, it may be argued that the debate over early versus selec-tively invasive strategies has been poorly framed from the outset.Risk scores constructed for each of FRISC II,13 TACTICS,7 andRITA 310 suggested that certain identifiable subgroups ofNSTEACS patients benefit from early intervention whereas othersdo not. However, each study employed its own risk score, andnone of the three has gained universal acceptance. It is disap-pointing that the initial ICTUS publication did not attempt to strat-ify patients using one of these previously developed scores. As arecent meta-analysis noted, “future strategies should explore waysto minimize the early hazard and enhance later benefits [of inter-vention] by focusing on higher-risk patients.”14 While RITA 3 andICTUS provide conflicting evidence on whether unselectedpatients with NSTEACS benefit from early intervention, theappropriate question is not “Do all patients benefit?” but rather“Which patients benefit?”. It is to be hoped that validation of pre-defined risk scores will be a primary outcome in future studies ofNSTEACS.
Table 15-year RITA 3 death/MI data by risk score10
Rate of death or MI in Rate of death or MI ARR RRR p
selectively invasive group in early invasive group
Risk score below median 9.3% 9.7% -0.4% -4% 0.80
Risk score above median 30.6% 23.1% 7.5% 25% 0.008
Table 2Components of the ICTUS primary outcome11
Outcome Rate in selectively Rate in early ARR RRR p
invasive group invasive group
Death 2.5% 2.5% 0 1% 0.97
MI 10.0% 15.0% -5.0% -50% 0.005
Readmission for angina 10.9% 7.4% 2.5% 32% 0.04

University of Toronto Medical Journal22
victims of SBS.9 Duhaime et al. also advocated, based on availablebiomechanical data from subhuman primates, that shaking alonewas not enough to cause the SBS findings. Duhaime’s findingswere, however, disputed by other studies, and the concept of SBSas a purely shaking based phenomenon remained.10,11 A more seri-ous challenge to the prevailing beliefs about SBS was provided bynumerous studies in the early 1990’s that disputed the diagnosticnature of many of the syndrome’s findings. Principal amongthese were ophthalmologic findings such as extensive subretinal,intraretinal, and preretinal hemorrhages. Even more specific find-ings such as folding of the retina around the macular region (per-imacular retinal folds) and the separation of any of the retinal lay-ers in the region of the macula (traumatic macular retinoschisis)were challenged. Although the differential diagnosis of retinal hem-orrhages in infancy is quite broad, including hemorrhages from thebirthing process as well as hemorrhages due to coagulopathies,retinal hemorrhages were not considered likely in short distanceaccidental falls.12 This was important because the most commonhistory for SBS victims as given by the parent or guardian was oneof an accidental household fall. The finding of retinal hemor-rhages in these supposed accidental cases would point to shakingas the true cause of the injury.13 However, studies finding thatretinal hemorrhages could be found after Cardio PulmonaryResuscitation (CPR) raised concerns that children unconscious dueto reasons other than abuse could be wrongly deemed to havebeen abused.14,15 Although retinal hemorrhages were no longerpathognomonic for SBS, numerous studies reconfirmed the highprevalence of SBS in infants with retinal hemorrhage.12,13,16,17
Other studies questioned the finding that CPR can cause retinalhemorrhages or indicated that CPR retinal hemorrhages, which aretypically small punctate hemorrhages, were easily distinguishablefrom the characteristic pattern of SBS retinal hemorrhages whichconsisted of extensive, often confluent, hemorrhages found in sub-retinal and preretinal regions as well as extensively throughout thelayers of the retina.18,19 Thus, despite many challenges, by the turnof the century, a somewhat uniform picture of SBS had emerged.Infants, usually below the age of two but sometimes up to the ageof five, presenting with histories of accidental trauma who had lit-tle evidence of external head injury but who suffered form sub-dural and retinal hemorrhages were quickly scrutinized for the pos-sibility of SBS if no other obvious causes, such as a severecoagulopathy, were found.20
Since 2001, many of the traditionally held beliefs about SBS havebeen called into question. Prior to 2001, the prevailing view was
AbstractThere is an ongoing debate in the scientific literature about thebiomechanics, histopathology, prevalence, and pathophysiology ofthe constellation of cranial and ocular findings referred to as theShaken Baby Syndrome (SBS). This paper presents a briefoverview of the literature on SBS and details the debate that is rag-ing. The results of this debate are already having a significantimpact on child abuse litigation around the world.
In July of 2005, the London Court of Appeals overturned theconvictions of three cases of a particular form of child abuse andaccepted up to 90 more such cases for review.1 This decisioncalls attention to the rigorous debate raging in the scientific com-munity about the constellation of child abuse findings labeled“The Shaken Baby Syndrome.” The fear of the consequences ofshaking babies is etched into the back of many young parents’minds and, due to public education by various experts and agen-cies, the Shaken Baby Syndrome (SBS) has become a common-place term in both scientific and layman circles. However, with-in the past few years, many of the supposedly typical SBS findingshave been questioned, and the quality of the evidence for the syn-drome criticized. This has divided the scientific community intoexperts that continue to espouse the traditional or slightly modi-fied views of this syndrome versus those that have begun ques-tioning its foundations.
Child abuse has long been a part of human life, but SBS is a rel-atively new concept. It can be traced back to two publications inthe early 1970’s by Caffey who described the constellation of find-ings in infants that had been shaken while held by the extremi-ties.2,3 These findings included the presence of subduralhematomas and ocular hemorrhages due to a whiplash force andthe absence of signs of external head trauma. Caffey referred thisas “The Whiplash Shaken Infant Syndrome.” Many studies there-after supported Caffey’s diagnosis and also added many new find-ings, including the presence of perimacular retinal folds and trau-matic macular retinoschisis as ocular lesions highly specific for thesyndrome.4-8 By the 1980’s, these findings were being referred toas the now familiar “Shaken Baby Syndrome.”5
Although by the end of the last century questions were still beingposed about the pathophysiology, mechanism, and true prevalenceof SBS, the literature seemed to espouse a unified view of mostof the critical aspects of the syndrome. A study by Duhaime et al.in 1986 found that blunt trauma was present in most supposed
Shaken Baby Syndrome: The Debate Rages On
Jasrajbir Baath, B.Sc.(0T8)
News and Views

volume 83, number 1, December 2005 23
Experts in the field have an opportunity to make a significant con-tribution by continuing to conduct objective and more advancedbiomechanical and pathological research in the attempt to comecloser to the truth on SBS. Allowing child abusers to escape jus-tice or innocent parents and guardians to be falsely accused ofabusing children are both serious miscarriages of justice.
References1. Gray L. (2005). Appeals put new doubts on cases of shaken baby syndrome.
Retrieved September 05th, 2005 from the World Wide Web: http://thescots-man.scotsman.com/index.cfm?id=1664122005.
2. Caffey J. (1972). On the theory and practice of shaking infants. Its potential resid-ual effects of permanent brain damage and mental retardation. Am J Dis Child.124:161-169.
3. Caffey J. (1974). The whiplash shaken infant syndrome: manual shaking by theextremities with whiplash-induced intracranial and intraocular bleedings, linked withresidual permanent brain damage and mental retardation. Pediatrics. 54: 396-403.
4. Greenwald MJ, Weiss A, Oesterle CS and Friendly DS. (1986). Traumaticretinoschisis in battered babies. Ophthalmology. 93: 618-625.
5. Gaynon MW, Koh K, Marmor MF and Frankel LR. (1988). Retinal folds in theshaken baby syndrome. Am J Ophthalmol. 106: 423-425.
6. Han DP and Wilkinson WS. (1990). Late ophthalmic manifestations of the shakenbaby syndrome. J Pediatr Ophthalmol Strabismus. 27: 299-303.
7. Elner SG, Elner VM, Arnall M and Albert DM. (1990). Ocular and associated sys-temic findings in suspected child abuse. A necropsy study. Arch Ophthalmol.108:1094-1101.
8. Massicotte SJ, Folberg R, Torczynski E et al. (1991). Vitreoretinal traction and per-imacular retinal folds in the eyes of deliberately traumatized children. Ophthalmology.98: 1124-1127.
9. Duhaime AC, Gennarelli TA, Thibault LE et al. (1987). The shaken baby syndrome.A clinical, pathological, and biomechanical study. J Neurosurg. 66: 409-415.
10. Hadley MN, Sonntag VK, Rekate HL and Murphy A. (1989). The infant whiplash-shake injury syndrome: a clinical and pathological study. Neurosurgery. 24: 536-540.
11. Alexander R, Sato Y, Smith W and Bennett T. (1990). Incidence of impact traumawith cranial injuries ascribed to shaking. Am J Dis Child. 144: 724-726.
12. Duhaime AC, Alario AJ, Lewander WJ et al. (1992). Head injury in very young chil-dren: mechanisms, injury types, and ophthalmologic findings in 100 hospitalizedpatients younger than 2 years of age. Pediatrics. 90: 179-185.
13. Buys YM, Levin AV, Enzenauer RW et al. (1992). Retinal findings after head trau-ma in infants and young children. Ophthalmology. 99:1718-1723.
14. Weedn VW, Mansour AM and Nichols MM. (1990). Retinal hemorrhage in aninfant after cardiopulmonary resuscitation. Am J Forensic Med Pathol. 11: 79-82.
15. Goetting MG and Sowa B. (1990). Retinal hemorrhage after cardiopulmonaryresuscitation in children: an etiologic reevaluation. Pediatrics. 85: 585-588.
16. Johnson DL, Braun D and Friendly D. (1993). Accidental head trauma and retinalhemorrhage. Neurosurgery. 33: 231-234.
17. Gilliland MG, Luckenbach MW and Chenier TC. (1994). Systemic and ocular find-ings in 169 prospectively studied child deaths: retinal hemorrhages usually meanchild abuse. Forensic Sci Int. 68: 117-132.
18. Gilliland MG and Luckenbach MW. (1993). Are retinal hemorrhages found afterresuscitation attempts? A study of the eyes of 169 children. Am J Forensic Med Pathol.14: 187-192.
19. Odom A, Christ E, Kerr N et al. (1997). Prevalence of retinal hemorrhages in pedi-atric patients after in-hospital cardiopulmonary resuscitation: a prospective study.Pediatrics.99: E3.
20. Levin AV. (2002). Ophthalmology of shaken baby syndrome. Neurosurg Clin N Am.13: 201-211.
21. Case ME, Graham MA, Handy TC et al. (2001). Position paper on fatal abusivehead injuries in infants and young children. Am J Forensic Med Pathol. 22: 112-122.
22. Geddes JF, Hackshaw AK, Vowles GH et al. (2001). Neuropathology of inflictedhead injury in children. I. Patterns of brain damage. Brain.124:1290-1298.
23. Geddes JF, Vowles GH, Hackshaw AK et al. (2001). Neuropathology of inflictedhead injury in children. II. Microscopic brain injury in infants. Brain. 124:1299-1306.
24. Geddes JF, Tasker RC, Hackshaw AK et al. (2003). Dural haemorrhage in non-traumatic infant deaths: does it explain the bleeding in ‘shaken baby syndrome’?Neuropathol Appl Neurobiol. 29:14-22.
25. Donohoe, M. (2003). Evidence-based medicine and shaken baby syndrome: part I:literature review, 1966-1998. Am J Forensic Med Pathol. 24: 239-242.
26. Lantz PE, Sinal SH, Stanton CA and Weaver RG Jr. (2004). Perimacular retinalfolds from childhood head trauma. BMJ. 328: 754-756.
27. Geddes JF and Plunkett J. (2004). The evidence base for shaken baby syndrome.BMJ. 328: 719-720.
28. Plunkett J. (2001). Fatal pediatric head injuries caused by short-distance falls. Am JForensic Med Pathol. 22: 1-12.
29. Reece RM. (2004). The evidence base for shaken baby syndrome: response to edi-torial from 106 doctors. BMJ. 328: 1316-1317.
30. Geddes JF and Plunkett J. (2004). The evidence base for shaken baby syndrome:Authors’ reply. BMJ. 328:1317.
31. Lantz PE. (2004). The evidence base for shaken baby syndrome: response to Reeceet al from 41 physicians and scientists. BMJ. 329: 741-742.
that whiplash forces caused subdural hemorrhages through therupture of bridging veins and retinal hemorrhages through theeffect of these shearing forces on the well-adherent vitreoretinaljunction in infants.17,21 A series of neuropathological studiesbrought into question this traumatic rupture mechanism. Autopsyfindings indicated that the most common mechanism of cranialinjury in supposed SBS cases was global hypoxic damage andeventual brain swelling leading to the bleed.22-24 Another study in2003 by Donohoe presented a review of the SBS literature up to1998 and found that there existed numerous errors in methodol-ogy and logic as well as misinterpretation of data.25 The studiesexamined were mostly retrospective in nature and Donohoebelieved that the authors stretched their interpretations to fit pre-conceived notions about SBS. He concluded that the literatureand thus the prevailing viewpoints on SBS did not appropriatelyfit the criteria for evidence-based medicine.
The neuropathology studies and the study by Donohoe laid thefoundation for other researchers wanting to dispute the prevalentthinking about SBS. An article by Lantz et al. accompanied by aseries of editorials in a 2004 British Medical Journal (BMJ) issuewere particularly critical.26 Lantz et al. described a 14-month-oldchild with all of the supposed findings of SBS, including thosedeemed to be highly specific for the syndrome such as extensiveretinal hemorrhages and perimacular retinal folds.26 All the otherpieces of evidence in the case, including the corroborated acci-dental history, however, pointed to accidental causes for the child’sinjury. An accompanying editorial by Geddes and Plunkett builton the Lantz article to question not just the diagnostic findings ofSBS, but also whether enough evidence existed to even support areasonable belief in the syndrome’s existence.27 Plunkett had pre-viously published a study in 2001 that found subdural and retinalhemorrhages in children with short distance falls from playgroundequipment.28 In their BMJ article, Plunkett and Geddes combinedthese results with those of Lantz and Donohoe to assert that adiagnosis of SBS is much less reliable than generally thought. Theresponse to these BMJ articles was very strong. A letter was sub-mitted to the BMJ signed by numerous experts on child abuse thatrefuted the articles of Donohoe, Lantz, Geddes, and Plunkett forvarious reasons but failed to provide any new data to support theirclaims.29 The response to Reece from Geddes, Plunkett, andLantz followed in subsequent BMJ issues but once again reiterat-ed old findings and failed to address the fundamental issues of thedebate with any new data.30-31
The mere fact that this debate exists, however, has had a monu-mental impact on child abuse litigation. Ophthalmologists can nolonger claim in the court that a child has been abused because ofthe presence of retinal findings he/she believes is specific for SBS.Defense lawyers for those suspected of causing SBS assert thatthere is disagreement between the experts and, therefore, the courtshould not use ocular findings as proof of abuse.1 Influencedlargely by the published BMJ articles, the diagnosis of SBS hasbeen called into serious question in Britain and elsewhere. TheJudge in the three SBS cases overturned in July 2005 felt that thecourt should take more notice of a changing scientific theory.1

IntroductionMedicine is changing at an unprecedented rate in this generation.Advances in technology, higher patient expectations, health carereform and a focus on cost containment have put new pressureson physicians, including tests to their devotion to medicine and totheir professional behaviour. During the 1960s and 1970s, criticsaccused the medical profession for putting its own welfare abovethat of society.1 There was a perception that medicine was placingemphasis on income and power and on protecting incompetent orunethical physicians. In the past decade, there has been a renewedsense of the importance of professionalism in medicine, especiallyduring medical training. In January 1996, the Association ofAmerican Medical Colleges established the Medical SchoolObjectives Project (MSOP) to create a report that addressed theseconcerns.2 In response, the medical literature has refined its defi-nition of medical professionalism, the role professionalism playsbetween medicine and society and the current status of profes-sional behaviour in medical students. An educational curriculumhas been designed to teach the professional values and ethics ofmedicine to the upcoming generation of doctors.
Discourse SynopsisIn order for medical students to understand their obligations dur-ing study, a clear definition of the concept of professionalism mustbe achieved. The Oxford English Dictionary defines a professionas “the occupation which one professes to be skilled in and to fol-low; a vocation in which a professed knowledge of some depart-ment of learning or science is used in its application to the affairsof others, or in the practice of an art founded upon it”.3 Centralto this definition is that a profession possesses a body of knowl-edge and skills over which it has exclusive control, as well as a com-mitment to service. This definition however is too simplistic anddoes not fully address the complexity of modern medicine or itshistory.
According to medical literature, there are two roles that a doctormust fulfill: that of the healer and that of the professional.4
Although there is much overlap between these roles, they arisefrom separate historical backgrounds and entail different sets ofobligations – the resolution of which is at the heart of professionalbehaviour. The tradition of the physician healer in Western Societydates back to Hippocrates. The Hippocratic Oath is at the centreof medicine’s identity and defines its morality. Furthermore, med-icine is to keep those whom it serves from harm and injustice. Theorigin of the professional is more recent; it was a result of an
industrial society that afforded its citizens the ability to purchasemedical care at a time when science gave physicians a serviceworth purchasing. The professional was thus a concept that arosewhich provided an organisational framework to manage the ser-vices of physicians.1
The resolution of the two roles, that of the healer and that of theprofessional, underlies the modern definition of medical profes-sionalism. Medical professionalism is defined as a set of funda-mental behaviours.5 First and foremost, physicians both in train-ing and in practice must subordinate their interests to the interestsof others. Conflicts of interests will undoubtedly arise between thephysician, the health care system and the individual patient, but itis imperative that the physician foremost meets the needs of thepatient. Second, physicians must adhere to high ethical and moralstandards. These standards have their roots in the principles ofbeneficence and non-maleficence; they require physicians to alwaysdo right and to do no wrong. Moreover, physicians must also dis-play core humanitarian values including honesty and integrity, car-ing and compassion, altruism and empathy and a respect for oth-ers. These values stem from the fact that the practice of medicineis a human endeavour requiring humanistic ideals. Finally, physi-cians must be accountable to themselves and also to their col-leagues. Such accountability reinforces and supports professionalbehaviours.
The integrity of medical professionalism must be maintained dueto the role it plays in society and the medical organization. Medicalprofessionalism is a contract between medicine and society.Professional status is not a right, but a privilege that society affordsmedicine as a return for its services. Thus, physicians have anobligation to maintain the integrity of the profession and meet theexpectations of society.4 A breach in this contract on the part ofphysicians permits society to re-evaluate the privileges it grants,including physicians’ autonomy and self-regulation.
As an example, the world was shocked in the spring of 1965 whenthe anaesthetist Henry K. Beecher revealed documented unethicalmedical research funded by the U.S. government at a conferenceheld by the Upjohn Pharmaceutical Company. He presented 22examples of unethical studies published in major medical journals,including three studies that withheld effective treatment fromexperimental subjects.6 This was especially unpalatable by theAmerican audience who had believed that the horrors of theNuremberg Trials in Germany could never happen in America.
University of Toronto Medical Journal24
Professionalism for the Medical Student
Wayne C.V. Baici, B.Sc. (McMaster 2006)
Medical Education

volume 83, number 1, December 2005 25
Future DirectionsIf a formal curriculum in professional behaviour is required, whatshould be its form? To assist medical schools in this endeavour, theAssociation of American Medical Colleges established the MedicalSchool Objective Project (MSOP).2 Their report identified fourattributes that a medical student should possess at the time of grad-uation. Two of the four attributes identified were domains thatmedical schools traditionally excelled at teaching. First, physiciansmust be knowledgeable; that is, they must understand the normalstructure of the body’s organ systems and related pathology.Second, physicians must also be skilful; they must be able to per-form a complete medical history and physical examination. Theremaining two attributes have its focus in professional behaviour.Physicians must be dutiful; they must possess knowledge of thesocial, economic, psychological and cultural determinants of diseaseand a commitment to advocate health care access to underservedmembers of society. Moreover, physicians must be altruistic. Thereare seven learning objectives required to meet this attribute; some ofthe more salient ones include knowledge of theories and principlesof ethical decision-making, honesty and integrity in interpersonalinteractions, a placement of the patient’s welfare above one’s ownand an understanding of the conflicts of interests inherent in thefinancial and organizational arrangements of medicine that places athreat on medical professionalism. The MSOP report is confidentthat attainment of these four attributes will allow physicians-in-train-ing to completely address the evolving needs of modern society.
ConclusionMedical professionalism is an ideal to be aspired. Through its pur-suit, ever-higher standards will be set leading to higher levels of eth-ical behaviour. While the medical curriculum can help studentsachieve these ideals, it is implicit in the very nature of medical workthat students will aspire to a high ethical code. Through a vigor-ous selection process, medical schools select a body of medical stu-dents who already exhibit many of the qualities deemed essential forphysicians, including integrity, trustworthiness and compassion. Itis essential for the individual student to further develop these attrib-utes, as well as recognize and correct their personal deficits. Sucha dedication towards medical professionalism will not only serve thestudent well during their medical training, but it will also preparethem for their future calling as a physician.
References1. Cruess RL, Cruess SR. Teaching medicine as a profession in the service of healing.
Acad Med. 1997;72:941-952.2. Medical School Objective Writing Group. Learning objectives for medical student edu-
cation – Guidelines for medical school: Report 1 of the medical school objectives pro-ject. Acad Med. 1999;74:13-18.
3. Oxford English Dictionary. Oxford: Clarendon Press; 2001.4. Cruess SR, Cruess RL. Professionalism must be taught. BMJ. 1997;315:1674-1677.5. Swick HM. Toward a normative definition of medical professionalism. Acad Med.
2000;75:612-6166. Kopp VJ. Henry Knowles Beecher and the development of informed consent in anes-
thesia research. Anesthesiology. 1999;90:1756-1765.7. Hensel WA, Dickey NW. Teaching professionalism: Passing the torch. Acad Med.
1999;74:878-884.8. Rennie SC, Crosby JR. Are “tomorrow’s doctors” honest? Questionnaire study explor-
ing medical students’ attitudes and reported behaviour on academic misconduct. BMJ.2001;332:274-5.
9. Green MJ, Farber NJ, et al. Lying to each other. Arch Intern Med. 2000;160:2317-2323.10. Sierles F, Hendricks I, Circle S. Cheating in medical school. J Med Educ. 1980;55:124-
5.11. Fehser J. Teaching professionalism: a student’s perspective. Mount Sinai J Med.
2002;69:412-14.12. Rezler AG. Attitude changes during medical school: A review of the literature. J Med
Educ. 1974;49:1023-30.13. Roche WP, Scheetz, AP, et al. Medical students’ attitudes in a PBL curriculum: Trust,
altruism, and cynicism. Acad Med. 2003;78: 398-402.
His seminal article “Ethics and Clinical Research” in the 1966 issueof the New England Journal of Medicine influenced subsequent med-ical ethics and the modern day notion of informed consent.
Medical professionalism also underlies the foundation upon whichmedical society organizes itself. The medical profession is orga-nized on what is called the ‘community structure’.7 This is a net-work of equal interrelationships between its members who areunited together by a common goal. Such an organizational networkdiffers considerably from the corporate or hierarchical structurethat underlies the organization of trades. A community structurerequires an ethical code even more stringent than set by society’slegal codes. This creates a system of trust among its members withthe requirement that each is self-accountable. Without such self-regulation, the community network would collapse.
Lessons LearnedProfessional development begins during training. It is thus impor-tant for the medical community to take a proactive approach anddirect its efforts toward teaching professionalism to the next cohortof doctors. Does the current generation of students require a cur-riculum in professionalism? A study by Rennie and Crosby evalu-ated medical students’ attitudes towards academic misconduct.8 Ofthose who replied, one third of students admitted that they woulddiscuss an Objective Structured Clinical Examination (OSCE) tostudents who had not taken the exam, write in a patient’s chart thata nervous system examination was normal when in fact it hadn’tbeen performed and resubmit work from another part of thecourse. Failures in medical professionalism were also observed dur-ing residency. A report by Green and Farber evaluated the use ofdeception between internal medicine residents.9 Their resultsshowed 36% of the residents would use deception to avoidexchanging call, 14% would fabricate a laboratory value to anattending physician and 5% would lie to cover up a medical mis-take. Professional misbehaviour is not a new phenomenon. In1980, fifty-eight percent of the 428 American students surveyedreported cheating at one time during their medical school training.10Such misconduct by medical students is concerning and potential-ly forecasts a future career of professional breeches, if not correct-ed during their formative years in education.
It has been suggested that misconduct by medical students may beattributed to the unusual degree of stress encountered in medicalschool. Medical training places students under tremendous stressdue to the volume of information to be learned, increasing levelsof responsibility and fierce competition that may lead to non-coop-eration.11 In fact, due to these pressures, studies have shown thatmedical students become more cynical and less altruistic as theyadvance in training.12 It appears that medical education underminesidealism that medical students may have had before entering. Areport by Roche and Schertz suggests that such a process of ‘de-idealization’ may be curriculum-specific.13 In their study of a prob-lem-based learning (PBL) curriculum at Mercer University Schoolof Medicine, they showed that students during their second year ina PBL curriculum actually show an increase in their altruistic idealsand a decrease in their level of cynicism. Moreover, these positivequalities remained throughout their medical school training. Afocus on formative rather than summative evaluations, and a colle-gial rather than a competitive environment, seems to foster desir-able qualities in physicians-in-training.

Many students may wonder whether family physicians can con-duct medical research. Dr. June Carroll is a prime example of afamily physician who is actively involved in research.
Academic and Professional HistoryDr. Carroll was one of the first in herfamily to go to university. Initially,she did not plan to go into medicine:she was interested in genetics.However, she soon discovered thatone of her strengths was workingwith people. After taking two years ofundergraduate science in biology, Dr.Carroll began studying medicine atthe University of Toronto. She ispresently a clinician, a teacher, and ascientist involved in genetics research.
During medical school, Dr. Carroll had always debated whetherto work overseas or in underdeveloped areas in Canada. Shechose family medicine because she loved working with peopleand having long-term relationships with them throughout theirlives. During her residency in family medicine at North YorkGeneral and Women’s College, she participated in an elective atthe Sioux Lookout Program, which is a program that enablesfamily medicine residents (among others) to work and train atclinics in First Nations reserves in northwestern Ontario.
After completing her residency, she was invited back to theSioux Lookout Program as a staff member. She spent two yearsworking at this program with her newlywed husband, who is
also a family physician. From a base hospital in Sioux Lookout,a total of four family physicians would fly out for a week ortwo each month to First Nations reserves. There, they workedin clinics alongside nurses and community health workers.
After taking an eight-month trip to Europe with her husband,Dr. Carroll started her family practice at Mount Sinai in 1980.Over the years, her role at Mount Sinai has changed. At first,she started out with a full spectrum practice as a clinician-teacher. Approximately ten years later, she became very inter-ested in research.
ResearchDr. Carroll became interested in research partly because of themany questions that came out of her practice as a family physi-cian. She also ran into many mentors in family medicine whoconducted studies to answer research questions; they led her tobelieve that she could also do the same. Initially, she joinedsome of their projects, and later on, she started to develop pro-jects on her own. Thus, she gradually received more trainingand changed her focus of work to research and health policy.
Dr. Carroll’s main focus of research is in studying and facili-
tating the integration of genetics research into primary care. Herresearch projects include educational and knowledge translationprojects. In order to integrate genetics research into primarycare, Dr. Carroll develops educational tools for patients andphysicians to teach them how to critically assess genetic tests.
University of Toronto Medical Journal26
June C. Carroll, MD, CCFP, FCFP
Associate Professor, Department of Family & Community Medicine, University of TorontoRay D. Wolfe Department of Family Medicine, Mount Sinai Hospital
Evan Kwong, B.Sc., M.Sc. (0T8)
Rebecca Menzies, B.Sc. (0T9)
“I loved it, because it just threw meinto doing everything.”
– Dr. Carroll speaking about the Sioux Lookout Program
“As you practice you start to wonderabout things; you start to have lots ofquestions, and I realized that I couldanswer some of them.”
– Dr. Carroll speaking about howshe gained interest in research
Current Medical Perspectives

volume 83, number 1, December 2005 27
members of the patient’s family. Thus, confidentiality is animportant issue to consider when conducting genetic tests.
In addition to developing educational tools, part of Dr.Carroll’s research includes evaluating them in the community.However, due to pressure to see patients in the community,some family physicians may not have the time to participate inthe evaluation studies. Nevertheless, once a good educationaltool has been developed and introduced, many physicians areenthusiastic and welcoming. It is also important to cater toeveryone by offering both pencil-and-paper tools as well aselectronic tools (e.g. PDAs and integration into electronic med-ical records).
Because of her vision for her genetics research, Dr. Carroll hasrecently been awarded the Sydney G. Frankfort Chair in FamilyMedicine, which gives her more time to devote to research andacademic pursuits. She has also received the 2004-2006 DonaldRice Award from The College of Family Physicians of Canada.This award is a travelling lectureship that allows her to travelacross Canada to present talks about her genetics research.
As she has become more successful in research, Dr. Carroll haswondered whether or not she should give up practice and onlydo research. However, Dr. Carroll feels that she has a fantasticpractice full of patients whom she has known for over 20 years.In addition, having a family practice allows her to understandhow her research may impact other practicing physicians in thecommunity.
Personal HistoryHometown: Toronto, Ontario
Family: Dr. Carroll’s husband, Dr. David White, is also a fami-ly doctor. They have three children who are all studying in dif-ferent fields at various universities across Canada.
Pets: Unfortunately, Dr. Carroll’s lovely black labrador retrieverpassed away in May at the age of 13. They will wait for a whilebefore getting another dog.
Hobbies: Dr. Carroll enjoys swimming and kayaking at her cot-tage in Muskoka. Her favourite place to be is sitting on thedock at the cottage reading a novel. Dr. Carroll also enjoysmusic and travelling. Her family went to Italy this past summer.
Questions
What advice would you give to a medical student who isinterested in research? If you have an interest in research or an academic type of prac-tice, I would encourage you to get the training early on—eithera Master’s or PhD. I would certainly encourage anyone who isthinking about research to do some sort of formal training.There are lots of resources for this now. To conduct the genet-
With the advent of the Human Genome Project, her hypothe-sis is that there will be more genetics tests available in medi-cine. Some of these genetic tests will be tests for adult-onsetdiseases, such as the current ones for hereditary breast, ovari-an, and colorectal cancer. Perhaps one day there will be genet-ic tests to determine a predisposition for certain common dis-orders that are seen in family medicine, such as diabetes orasthma. There is no doubt that the technology will be there.However, the more important questions are, “What significancewill these genetic tests have? What do their results really meanin practice? Is there added value? Will the results change theway of decision-making?” Some of the genetic tests may nothave added value. For example, one would probably not con-duct a genetic test for a predisposition for cardiovascular dis-ease in someone who smokes, is obese, and has hypertension.In other cases, a genetic test may be of benefit, such as a testfor hereditary breast cancer. If a woman has a family historythat is suggestive of being at a high risk for the BRCA muta-tion, then having a genetic test may change the way the physi-cian does surveillance or screening, and may also affect thepatient’s decision-making about prevention or treatment. Somegenetic tests may even be potentially worrisome. For example,if a patient is tested for a predisposition for Alzheimer’s dis-ease, there may not be any information about when the diseasewill begin, and even whether or not it is certain that the patientwill get Alzheimer’s. Currently, there is also no preventativetreatment available. Therefore, having this genetic test donemay only cause a lot of anxiety for the patient, without muchbenefit.
There are many other issues with integrating genetic tests intopractice. For example, one of the unique things about genetictests is that having one done may give information about other
“I would like to see more support forresearch in knowledge translation and in primary care, because they havethe opportunity to impact on patientsdirectly.”
– Dr. Carroll speaking about thesupport for primary care research
“New discoveries in medicine are con-stantly being made, but these discoverieswill not have any meaning unless theyare translated from bench to office tocommunity.”
– Dr. Carroll speaking about translation of research into practice

ics research that I do now, if I were younger and starting in thesame situation today, I would probably do a Master’s degree ineducation or public health or epidemiology work. It is alsoimportant to note that, in research, you don’t have to do every-thing. It is essential to build a good team that includes otherswho are experts in their field, e.g. biostatisticians, methodolo-gists, etc.
What was the best advice you received from a mentor? I received some of the best advice when I was transitioningfrom a full-time clinical practice to research. A career in medi-cine can change over time; you don’t have to be in the samecareer. There are two important points to note. Firstly, you donot need to feel that you have to do it all at once. You can goback to school and do further training if you wish; go whereyour interests take you. Secondly, you also need to pay atten-tion to your life outside of medicine. When you have a familyand kids, things may slow down a bit; yet, when the childrengrow up things may begin to gear up again. Opportunities willkeep coming.
What career would you have chosen if not medicine orresearch?If I weren’t in anything to do with medicine or research, Iprobably would have become a teacher.
What is your favourite book?I read lots of novels, but it is hard for me to think of afavourite. I do quite like Margaret Atwood’s novels, and alsobooks by Barbara Kingsolver. The last book I read wasAmsterdam, by Ian McEwan.
What is your favourite quote?”Nothing changes if nothing changes.”
- Alcoholics Anonymous truism
This is the one I am using the most with my patients. It is aninteresting quote to think about if you are trying to makechanges to your life. If you keep going on the same way, doingthe same things, nothing will change. It has application in alco-holism and drug addiction, but it certainly applies to manyother situations. If you don’t do something different or don’topen yourself up to do something different, you won’t be dif-ferent.
Do you have anything else you would like to add?In Canada, patients are likely to turn to their family physiciansto help them make informed choices. It is a privilege to be afamily physician; I am honoured to have long-term doctor-patient-family relationships. It is vital for people to have a fam-ily physician – to have a first contact into the health care sys-tem. However, it is disturbing to all of us that there are somany people who don’t have someone like that now. Familymedicine needs to be valued in society, valued in medicalschool, and valued by specialists.
University of Toronto Medical Journal28
“Balance is most important; ensure thatyou do not forget your non-medicalinterests, as well as your family andfriends.”
– Dr. Carroll speaking about acareer in medicine
“It’s the joy of family medicine, It isreally quite lovely.”
– Dr. Carroll speaking about the doctor-patient-relationship

volume 83, number 1, December 2005 29
sweating at night three months ago and had since beenexperiencing intermittent episodes of fever with chills.His family physician tried a course of clarythromycin with-out success.
Given the additional history, which diagnosis is critical torule out first?Infectious Endocarditis (IE). With patients who present with newonset of heart failure in the face of unexplained fevers andchills, IE must be ruled out, especially considering the patient’sknown history of valvular disease.
IE is an infection of the endocardium of the heart by amicrobe. Traditionally, it has been classified as acute or suba-cute based on the rapidity and severity of clinical symptoms;generally, acute IE involves healthy valves while subacute IEinvolves prosthetic or diseased valves.2 More recently, IE isfrequently classified as native valve-, prosthetic valve- or pace-maker-associated IE. The pathological vegetation that charac-terizes IE is an amalgamation of fibrin, platelets, and inflam-matory cells intermeshed with the microorganism responsiblefor the vegetation. Although predominantly a disease of valves,IE can infect any component of the endocardium.3
Describe the epidemiology for native valve IE, and therisk factors that should be elicited in the history.The epidemiology of native valve IE in developed countries ischanging due to the increased incidence of nosocomial IE, aspatients with significant risk factors live longer on an increas-ing amount of interventions. The incidence of native valve IEin these countries varies between 1.7 to 6.2 cases per 100,000person-years.3 Rheumatic heart disease is the most importantcardiac risk factor. Other risk factors for native valve IEinclude intravenous drug use (IVDU), recent gastrointestinal orgenitourinary surgery, human immunodeficiency virus (HIV),poor dentition, diabetes, renal replacement therapy, congenitalheart disease, mitral valve prolapse (MVP) with associatedregurgitation, degenerative valve lesions, and indwellingcatheters.3,4 In particular, IVDU often predisposes patients toright-sided IE.5
Two weeks prior, the patient underwent a dental extrac-tion with antibiotic prophylaxis. He denied a history ofIV drug use and had no indwelling lines. Additional past
Case PresentationA 68-year-old male presented for a scheduled trans-oesophageal echocardiogram (TEE) at an outpatient car-diovascular surgery clinic for consideration of a mitralvalve replacement (MVR)/repair. He reported orthopnea,requiring three pillows to sleep at night for the past fourmonths. He also complained of progressing shortness ofbreath (SOB) on exertion, which would worsen after hewalked up just one flight of stairs. According to his wife,he had been waking up at night with increasing SOB andcough, which was relieved temporarily upon arising froma supine position and going to the bathroom. Before thispresentation, he was admitted to hospital three weeksprior and investigated thoroughly for acute coronary syn-drome; cardiac angioplasty showed no evidence of disease.
What are the differential diagnoses for this patient’sshortness of breath (SOB) with the limited history pre-sented thus far?The differential diagnoses of shortness of breath (SOB) are bestclassified according to system.1 Cardiac: cardiac heart failure,coronary artery disease, myocardial infarction, pericarditis,arrhythmia, valvular disease, infectious endocarditis, myocardi-tis, anaemia. Pulmonary: asthma, pneumonia, pneumothorax,pulmonary edema, pleural effusion, metastatic disease, chronicobstructive pulmonary disease, restrictive lung diseases. Upperairway: epiglottitis, croup, mononucleosis, foreign body.Psychogenic: anxiety, panic disorder, pain. Endocrine: meta-bolic acidosis. Central: neuromuscular disorders, pain, overdose(aspirin).1
The patient was found to be in florid pulmonary oedemaand was sent to the emergency department. On furtherreview, he was determined to have a long history of mitralvalve (MV) disease. As a teenager, his sister had previ-ously been diagnosed with rheumatic fever and subse-quently developed a heart murmur. He had displayedsymptoms at the time, but was never formally diagnosedwith rheumatic fever. Twenty years ago, he developed aheart murmur and had subsequently been followed by acardiologist. His cardiologist counselled him on the pos-sible benefits of an MVR/repair several months ago andconsequently an assessment was arranged. The patientreported an onset of fever, myalgias, cough, and some
SOB, Fevers, Murmurs . . . and CNS
Michael R. Humphreys, B.Sc. (OT6)
Morning Report

111µmol/l, and BUN 7.6mmol/l. Liver enzymes and liverfunction tests were within normal limits. Urinalysis wasnormal. Chest X-ray revealed cardiomegaly with enlargedleft ventricle (LV), perihilar infiltrates, and the presence ofKerley B lines bilaterally. ECG was normal. The TEE(Figure 1) reported mildly dilated ventricles and severelydilated left atria with normal LV function. Severe mitralregurgitation was noted. The posterior mitral valve leafletwas flail and thickened, and a 1.5cm mobile mass wasseen. Likewise, the anterior mitral valve leaflet had anattached spherical 1.4cm x 11.1cm mass with mobile fin-ger-like projections. Both the tricuspid valve and aorticvalve, which was tri-leaflet, displayed mild regurgitation.
Why was a TEE performed, as opposed to a transthoracicechocardiogram (TTE)?While the TTE is a specific diagnostic test for IE, it is not verysensitive; conversely, TEE has a high sensitivity in the diagno-sis of IE because of the proximity of the valves to the esoph-agus.2
What are some additional investigations that could beperformed to rule out embolic phenomenon?A CT head or MRI is useful to rule out microabscesses,mycotic aneurysms, and intracranial hemorrhage. CT or MRIof the abdomen and pelvis, and CT of the thorax are useful inidentifying splenic abscesses or emboli to the renal, hepatic,iliac, or mesenteric arteries.3
Do we have enough evidence to diagnose IE? What are the diagnostic criteria?The currently accepted diagnostic criteria for IE are the modi-fied Dukes criteria. Diagnosis is confirmed with fulfillment oftwo major criteria or one major and three of five minor crite-ria. Diagnosis is also confirmed with pathologic or bacterio-logic evaluation of vegetations, intracardiac abscess, or majoremboli.4
Major criteria include positive blood cultures in at least twoconsecutive specimens of microbes typical for IE (or threespecimens if not separated by 12 hours; however, they must beseparated by one hour), or a single positive culture or serolog-ic evidence of C. burnetti.4 Also included as a major criterion isa TEE or TTE showing evidence of IE (oscillating intracardiacmass, abscess, or prosthetic valve dehiscence) or demonstratingnew valvular regurgitation.
Minor criteria include: 1) predisposing cardiac condition orIVDU; 2) temperature greater than 38ºC; 3) embolic-relatedphenomenon: septic pulmonary infarct, mycotic aneurysms,intracranial hemorrhage, arterial emboli, conjunctival hemor-rhage, or Janeway’s lesions; 4) immunologic-related phenome-non: Osler nodes, Roth spots, rheumatoid factor, glomeru-lonephritis; 5) positive blood cultures or echocardiogramsuggestive of IE but failing criterion as a major criteria.4
In the case presented here, we have fulfillment of one major
medical history included hypertension and hypothy-roidism. The patient was taking ramipril, hydrochloroth-iazide, ECASA, L-thyroxine and furosemide, the latter ofwhich had recently been increased from 40mg PO OD to60mg PO OD. The patient also revealed that he had nottaken his diuretics for the past couple of days because ofconcerns over increased urinary frequency while he wastravelling.
What are the physical findings associated with IE?Low-grade fevers are often present with subacute IE; high-grade fevers are associated with acute IE. With the exceptionof right-sided IE, the vast majority of patients with subacute IEhave detectable heart murmurs.2 Many patients with IE have apredisposing murmur; however, only a small fraction of thispopulation exhibits a change in the quality of the murmur.2
About one third of acute IE patients do not have murmurs.Examination of patients’ vitals may indicate sepsis.
Peripheral signs of IE are rarely observed due to detection andtreatment with antibiotics; they are either the result of septicemboli or immune complex deposition. Petechiae may beobserved on the soft palate, oral mucosa, and conjunctivae, aswell as on the anterior trunk or dorsa of extremities.2,3 Splinterhemorrhages can be seen under the nail beds. Osler nodes arepainful nodules located in the distal pulp spaces of digits andare immune complex-related.3 Conversely, Janeway lesions arepainless, emboli-related, and present as macules often on themore proximal thenar and hypothenar eminences.2 Clubbingmay be noted. Roth spots on fundoscopy represent hemor-rhage of the retina, an immunologic phenomenon.Splenomegaly, meningitis, neural deficits (including hemiplegiaand unilateral blindness), and hematuria can occur secondary toseptic emboli.2,3 Right-sided IE emboli can present like multi-focal pneumonia.5 Lumbosacral back pain mediated by immunecomplex deposition occurs frequently.2 Patients with acute IEoften present with signs of congestive heart failure. Patientsshould also be evaluated for uremic symptoms, synovitis, andarthralgias secondary to immune complex deposition.
On physical exam, the patient’s temperature was 38.3ºC,BP 129/85, HR 72bpm with an oxygen saturation of 91%on room air. His JVP was elevated at 7cm above the ster-nal angle. Precordial auscultation revealed a soft S1, wide-ly split S2, presence of an S3, and a pan-systolic ejectionmurmur prominent at the mitral area and radiating to theaxilla. Marked crackles were present bilaterally; there wasno evidence of peripheral edema. Exam was negative forJaneway lesions, Osler’s nodes, and splinter hemorrhages.Fundoscopy was positive for a single white area of pallorsurrounded by hemorrhage on the inferior aspect of theleft superotemporal arcade. Dental consult suggestedpoor dentition and need for additional dental surgery.
Initial laboratory investigations showed normocytic ane-mia (hemoglobin 109g/dl), WBC 9.0x103/µl, platelets267x103/µl, electrolytes within normal range, creatinine
University of Toronto Medical Journal30

volume 83, number 1, December 2005 31
mitral valve was replaced with preservation and relocationof chordae, and his left ventricle outflow tract and tricus-pid valve were repaired. Pathology of the mitral valveanterior leaflet revealed gram positive cocci (1+) and poly-morphs (3+) on gram stain with no culture growth. Hewas discharged from hospital two weeks later with com-plete resolution of symptoms and received a peripherallyinserted central catheter (PICC) line for completion of IVantibiotic therapy as an outpatient.
References1. Zoorob RJ, Campbell JS. Acute dyspnea in the office. Am Fam Phys. 2003 Nov
1;68(9):1803-10.2. Brusch JL. Infectious Endocarditis. eMedicine.com. 2005 Aug 15 [cited 2005
Oct 7]. Available from: http://www.emedicine.com/MED/topic671.htm. 3. Mylonakis E, Calderwood S. Infective endocarditis in Adults. N Engl J Med.
2001 Nov 1;345(18):1318-30.4. Moreillon P, Que YA. Infective endocarditis. Lancet. 2004 Jan 10;363(9403):139-
49.5. Eykyn SJ. Endocarditis: basics. Heart. 2001 Oct;86(4):476-80.6. Anguera I, Del Rio A, Miro JM, Matinez-Lacasa X, Marco F, Guma JR, et al.
Staphylococcus lugdunensis infective endocarditis: description of 10 cases andanalysis of native valve, prosthetic valve and pacemaker lead endocarditis clin-ical profiles. Heart. 2005 Feb;91(2):e10.
7. Delahaye F, Celard M, Roth O, de Gevigney G. Indications and optimal tim-ing for surgery in infective endocarditis. Heart. 2004 Jun;90(6):618-20.
criterion, based on the results of the TEE, and three minor cri-teria, with the presence of a Roth spot, temperature of 38.3ºC,and previous history of mitral valve insufficiency likely sec-ondary to rheumatic fever.
Blood cultures in two consecutive vials grew coagulase-negative staphylococcus (CNS), and following administra-tion of antibiotics, no growth was observed. Susceptibilityresults indicated sensitivity to cefazolin, cloxicillin, andvancomycin.
What are the common microbes causing native valve IE?The microbiology of native valve IE is age-dependent. In theadult population (ages 16-60), the most common pathogen isstreptococcus species (45-65%), followed by Staphylococcus aureus(30-40%). The remaining pathogens include gram-negativebacilli (5-10%), enterococcus species (5-8%), CNS (4-8%),fungi, culture negative and HACEK organisms (haemophilus,actinobacillus, cardiobacterium, eikenella and kingella), anddiptheroids.3,5
Does CNS mean infection of IE with Staphylococcus epidermidis?No: while the most common CNS causing IE is S. epidermidis,which has an affinity for prosthetic valves, S. lugdunensis and S.hominis are among several other CNS associated with IE.6 S.
lugdunensis often follows a more ominous course, with increasedvalvular destruction, increased incidence of septic embolicevents, antibiotic resistance, and increased mortality; hence, thedistinction is important.6 Unlike S. epidermidis, S. lugdunensis
shows no affinity for prosthetic valves and is just as likely tobe found on native valves.5 Unfortunately, labs will often notspeciate CNS further, as with the case presented here.
Does this patient need surgery?The mortality rate of native valve IE presenting with heart fail-ure is 55-85% with conservative medical management, versusonly 10-35% with surgical treatment.7 Heart failure is the mostcommon indication for IE cardiac surgery. Mitral regurgitation-associated heart failure is more readily tolerated than aorticregurgitation, due to the inability of the ventricle to adapt tothe extra volume. As the waiting time for surgery increases, therisk of perivalvular infection also increases.7 Other indicationsfor urgent surgery include valvular obstruction, perivalvularinfection, and vegetations with documented embolic events. Inthe case of large mobile vegetations with documented embolicevents, urgent surgery is indicated; however, without evidenceof embolic events, the indication for surgery is less clear.7
EpilogueThe patient was stabilized in the ICU and improved withmedical management of his heart failure. When antibiot-ic sensitivities of the bacteria were known, he wasswitched from empiric antibiotics to vancomycin 1mg IVq12h for a six-week course. Following stabilization of hisheart failure and one week of antibiotic treatment, thepatient received a dental extraction and cleaning. His

Case Presentation A 63-year-old male presented to his family physician with atwo month history of hoarseness. 3 weeks prior to presenta-tion, he was diagnosed with laryngitis at a walk-in clinic andprescribed antibiotics. There was no improvement in hissymptoms with the medication. The hoarseness wasdescribed by the patient as a ‘huskiness’ that developed grad-ually with no precipitating event. The patient denied anyincidents of laryngeal trauma, upper respiratory tract viralinfection or foreign body ingestion. His voice had notreturned to normal at any point and there was no fluctuationin severity. No associated symptoms of hemoptysis, dys-phagia, odynophagia or otalgia were reported. The mandenied any history of vocal abuse or misuse and works in anenvironment without loud noise or noxious fumes. Hesmoked 1 pack of cigarettes per day for the past 40 years andconsumed 3 to 4 alcoholic drinks per week.
His past medical history was unremarkable. There was nohistory of heart, lung or liver disease. The only medicationhe used was Prevacid for gastro-esophageal reflux disease.
On examination he was noted to have a hoarse voice. Therewas no evidence of stridor or respiratory distress. A head andneck examination performed by the family physician wasnormal. A mirror examination was attempted but the ante-rior vocal cords could not be visualized. No cervical lym-phadenopathy was present.
Based on a prolonged history of non-resolving hoarseness in apatient with a smoking history and difficulty with visualization ofthe larynx, the patient was referred to an otolaryngologist.Endoscopic examination was performed at the referral visit, whichshowed an exophytic lesion on the right vocal cord that was sus-picious for an early stage squamous cell carcinoma. The patientunderwent diagnostic endoscopy under a general anesthetic and abiopsy was performed that confirmed squamous cell carcinoma.He was staged as a T1b glottic carcinoma (involving the vocal cordonly with no extension to the anterior commissure or oppositecord).
Table 1Differential Diagnosis of Hoarseness
Organic
Infectious Inflammatory
acute viral laryngitis
bacterial tracheitis / laryngitis
Non-infectious Inflammatory
vocal cord nodules
vocal cord polyps / Reinke’s edema
contact ulcer / granuloma
Laryngeal Trauma
blunt or sharp external trauma
intubation injury
Laryngeal Cysts
ductal cyst
saccular cyst
laryngocele
Neoplasms
benign: papilloma, chondroma, lipoma, neurofibroma
malignant: squamous cell carcinoma
Systemic
endocrine (hypothyroidism, high estrogen state)
rheumatoid arthritis, SLE, amyloidosis
Neurologic
central lesions (CVA, Guillaume Barre, head injury, neural tumours)
peripheral lesions from tumours, surgery, cardiac disease
myasthenia gravis, spastic dysphonia, presbylaryngeus
Inorganic (Functional)
Psychogenic Aphonia
Habitual Aphonia
Ventricular Dysphonia
University of Toronto Medical Journal32
Evaluating Hoarseness: How to Avoid Backing the Wrong Horse
Goran Jeremic, B.Sc. (0T7)Mark Rafferty, MB, FRCSIJonathan Irish, MB, BCh, FRCSCDale Brown, MB, BCh, FRCSC David Goldstein, B.A., MD
Clinicopathological Correlation

Clinical DiagnosisT1b glottic carcinoma.
Vocal Cord Dysphonia
Anatomy, Etiology, and Clinical FeaturesThe laryngeal skeleton is comprised of cartilaginous structures con-nected by membranes and ligaments that form a structural systemthat forces air from the trachea through the true vocal cords toproduce sound.
The larynx can be divided anatomically into three distinct regions:the supraglottis, glottis and subglottis. The glottis consists of thetrue vocal cords and the space between them through which airpasses. The supraglottis, commonly called the vestibule, is the areaabove the true vocal cords and inferior to and including theepiglottis.1 It consists of the epiglottis, vestibular folds (the falsevocal cords), the area between the vestibular and vocal foldsreferred to as the ventricle, the arytenoids and the aryepiglottic
folds. The saccule is a recess within the ventricle that containsmucous secreting glands which function to keep the true vocalcords moist and well lubricated. The subglottis is the area belowthe vocal cords and superior to the inferior border of the cricoidcartilage.
The muscles that control the size and shape of the glottis, as wellas the amount of tension on the vocal ligaments, are referred toas the intrinsic muscles of the larynx. With the exception of thecricothyroid muscle, these muscles are supplied by a branch of thevagus nerve, the recurrent laryngeal nerve.
The vocal cords are covered by a stratified squamous epitheliumdevoid of glands and follicles. The lack of underlying submucosagives the vocal cords their pearly white appearance on gross exam-ination. The area between the epithelium and elastic tissue is calledReinke’s space. The remainder of the larynx is lined by respirato-ry epithelium with submucosal connective tissue containingmucous glands. Lymphatics are abundant throughout the larynxexcept in the glottic area, which contains only a sparse network oflymphatics.2
Speech production is a complex process that involves the lungs,larynx, pharynx, tongue and lips. The role of the larynx is to pro-vide the sound source for speech. During phonation, a columnof air forces the adducted vocal cords to open producing a vibra-tory wave across the mucosal cover of the vocal cords. It is thisvibratory wave that produces sound. Since the epithelium of thetrue vocal cords is only loosely adherent to the underlying tissue,vibration occurs.2 The sound produced by mucosal vibration isenhanced in volume and resonance as it passes through the oraland nasal cavity. As the sound passes through the oral cavity it isshaped into speech by the tongue, palate, cheeks and lips. Volumeis varied by the amount of air passing through the vocal cords.The tension of the vocal cords determines the frequency at whichthe cords will vibrate, and therefore the pitch of the sound pro-duced. Interference with either adduction of the cords or the pro-duction or propagation of the mucosal wave secondary to edema,dehydration or lesions of the vocal cords can produce hoarseness.3
volume 83, number 1, December 2005 33
Figure 1. Endoscopic view of vocal cords
Figure 2. Laryngeal squamous cell carcinoma
Figure 3. Appearance of normal vocal cords using Direct Laryngoscopy

University of Toronto Medical Journal34
by the otolaryngologist.8 The mirror examination is an inexpensiveand easy means for one to view the larynx. The entire laryngealstructure should be examined (Table 2), with special attention tothe color and character of the mucosa overlying the true vocalcords and arytenoids.
The resting abducted position of the vocal cords during quietbreathing should be noted, with demonstration of normal andsymmetrical adduction while the patient says ‘e’. The appearanceof the normal larynx as appears on direct laryngoscopy can be seenin Figure 3.
Indirect laryngoscopy should be performed on any patients pre-senting with hoarseness and is mandatory for hoarseness of greaterthan two weeks duration in order to rule out laryngeal carcinoma.Chronic hoarseness is an indication for referral to an otolaryngol-ogist (other indications for referral are listed in Table 3), asadvanced diagnostic and therapeutic techniques may be requiredsuch as videostroboscopy or direct laryngoscopy.
Table 3Indications for Referral to an Otolaryngologist
in a Patient with Hoarseness
1) present for greater than 2 weeks
2) unable to adequately visualize the larynx on indirect laryngoscopy
3) history with risk factors for malignancy
4) fails to respond with conservative therapy
5) needs further investigations to obtain a diagnosis
6) pathology seen requires biopsy or surgical management
Videostroboscopy demonstrates the vocal cord mucosal wave bysynchronizing a light flash with the patients voice frequency. It isan excellent means of detecting subtle abnormalities of the mucos-al wave or early lesions that cannot be seen by layngoscopy.4
Direct laryngoscopy involves using a rigid laryngoscope to providea direct view of the larynx while the patient is under a generalanesthesia for biopsy of laryngeal lesions or surgical treatment.
Differential Diagnosis and Management of Hoarseness
Inflammatory
Infectious InflammatoryThe most common cause of hoarseness seen by the family practi-tioner is acute viral laryngitis.9 In viral laryngitis hoarseness is oftenassociated with concurrent or prior symptoms of an upper respi-ratory tract infection (URTI).10 Laryngoscopy reveals bilateral edemaand erythema of the vocal cords and surrounding mucosal mem-branes. It is a self-limiting disease where the hoarseness improveswith resolution of the infection. Treatment involves analgesia, voicerest and adequate hydration.4 Mucolytics may be employed in thepresence of thick mucous production irritating the vocal cords.Decongestants should be avoided since they tend to further dehy-drate the mucosal membranes.4 Bacterial laryngitis, is less common,and occurs as a secondary super-infection typically with S. pneumo-
A thorough history and physical examination can determine theetiology in most patients. It is important to differentiate acute (lessthan two weeks) from chronic hoarseness, since the latter is morecommonly associated with laryngeal malignancy.4 A history of pre-cipitating factors such as vocal abuse, neck trauma, upper respira-tory tract infection (URTI), or chronic throat clearing should beelicited. A history of fluctuating hoarseness with periods of thepatient’s voice returning to normal would make a fixed lesion aless likely etiology.4
A thorough functional inquiry may reveal associated symptomssuch as post-nasal drip, sinusitis, allergies, chronic cough, hypothy-roid symptoms, or gastro-esophageal reflux, which may provideinsight to the etiology. A history of otalgia, sore throat, dyspha-gia, odynophagia, hemoptysis or stridor may accompany hoarse-ness in patients with laryngeal or thyroid carcinoma.5
The past medical history should include a search for diseases orsurgical procedures, listed in Table 1 that may account for thepatient’s hoarseness. Medications that dry mucous membranes,such as diuretics and anti-histamines can cause hoarseness.6 It isimportant to identify and quantify the amount of alcohol con-sumption and smoking, as both are significant risk factors forlaryngeal malignancy. Occupations that involve excessive vocal usehave work environments with irritating fumes, places people at riskfor laryngeal irritation and inflammation.
The physical examination should begin with listening to thepatient’s speech. The nature of the dysphonia often provides cluesas to the fundamental problem. For example, hoarseness with abreathy voice indicates air escape suggestive of a unilateral vocalcord paralysis, while a rough sound to the voice may indicate alesion on the vocal cord.
A thorough head and neck examination should be performed onany patient presenting with hoarseness. The nasal cavity, oral cav-ity and oropharynx should be examined for signs of a URTI, acuteor chronic rhinitis, sinusitis or post-nasal discharge. Otoscopyshould be performed in the hoarse patient with associated otalgiaas a normal appearing external and middle ear often indicatesreferred pain from other sources such as a laryngeal malignancy.7
The neck should be evaluated for lymphadenopathy or thyroidmasses.
Table 2Areas to be Examined on Laryngoscopy
1) vallecula 4) false vocal cords
2) epiglottis 5) true vocal cords
3) pyriform sinuses 6) subglottic area
The most important aspect of the physical examination is visual-ization of the larynx by indirect laryngoscopy. Indirect laryn-goscopy can be performed by mirror examination, flexible laryn-goscope or by rigid Hopkin’s scope. The latter two provide amore enhanced and comprehensive view and are usually employed

nia, H. Flu, M. Cattaralas, or Mycoplasma.4 It should be suspectedif there is a marked increase in temperature, severe pharyngitis, oran associated bronchitis in those with a preceding viral laryngitis.Antibiotics are used if a bacterial super-infection is suspected or con-firmed by culture. Laryngeal tuberculosis is a rare cause of hoarse-ness that should be considered in patients with a history of pul-monary tuberculosis or risk factors for tuberculosis.11
Non-Infectious InflammatoryChronic inflammation of the vocal cords can result from a chron-ic cough, smoking, vocal abuse and less frequently from post-nasaldrip and environmental toxin exposure.9 Associated symptomsinclude dry throat, cough, and constant need to clear the throat.Chronic irritation of any cause may produce edema and erythemaof the vocal cords in the early stages and mucosal hypertrophy andkeratinization in later stages. The latter may appear as white patch,commonly known as leukoplakia. Leukoplakia is a descriptiveterm for the gross appearance of any number of histologic find-ings including hyperkeratosis, dysplasia, carcinoma in situ (CIS), orcarcinoma.12 The presence of leukoplakia should prompt a referralfor biopsy to rule out either a pre-malignant or malignant lesion.
Vocal cord nodules, also called singer’s or screamer’s nodules,result from submucosal inflammation with eventual callus forma-tion. They most commonly arise in singers, women and childrenand present with hoarseness, which is often aggravated by URTIs,sinusitis, tobacco and alcohol.13 The nodules tend to arise bilater-ally at the junction of the anterior and middle one-third of thevocal cords, and appear soft and red in their early stages and hardand white in their chronic stages.14 Conservative treatment withvoice rest and speech therapy usually leads to improvement or res-olution.14 If an adequate trial of conservative therapy fails micro-laryngoscopic excision may be indicated.
Vocal cord polyps are benign inflammatory masses that aresmooth and soft appearing and appear to be either sessile orpedunculated.9 They most commonly result from vocal abuse orsmoking.14 Polyps may be single or multiple but are most oftenunilateral. Depending on polyp size, hoarseness may be associat-ed with dyspnea, cough, dysphagia, or a sensation of a mass in thethroat. The most effective management is microscopic excision.8
Reinke’s edema or polypoid degeneration of the vocal cords is aunilateral or bilateral collection of fluid in Reinke’s space. The eti-ology is the same as for polyps. Initial management involvessmoking cessation and speech therapy, however, conservativemanagement often fails because of the poor vocal cord lymphaticsupply.14 Therefore, surgical removal is often employed with post-operative speech therapy to help prevent recurrence.14
Gastro-esophageal reflux disease (GERD) is a common cause ofhoarseness. It is often worse in the morning after lying supineduring the night.4 Chronic acid reflux results in mucosal thicken-ing and inflammation overlying the vocal process of the arytenoidswith occasional progression to contact ulcer or granuloma forma-tion.4 The hoarseness usually responds well to aggressive anti-reflux therapy.15 Granulomas or contact ulcers that do notrespond to conservative management are usually excised.14 Post-operative intralesional steroid injection and treatment of the under-lying causes have been shown to decrease recurrence rates.13 Other
causes of granuloma formation or contact ulcers includes chroniccoughing or voice clearing, and forceful adduction of the vocalcords at the onset of speaking. The latter is seen in males whospeak in a low pitch and with great emphasis.13
Laryngeal CystsThe main cystic lesions of the larynx that can present with hoarse-ness include ductal cysts, saccular cysts and laryngoceles. Ductalcysts are mucous retention cysts caused by obstruction of mucos-al glands. On laryngoscopy, they appear as a swelling of the lat-eral aspect of the true vocal cord with sparing of the free edge,where mucous glands are absent.14 A saccular cyst, which occursless frequently than ductal cysts, is a sub-mucosal mucus-filleddilatation of the saccule.14 They may be seen as either anterior orlateral swellings of the ventricle or false cords. Laryngoceles areair filled cyst-like dilatations of the saccule and are acquired lesionsthat predominantly occur among caucasian males over the age of60.5 They may appear as a swelling of the false cords, which canoften be accentuated by a valsalva maneuver. Large laryngocelesmay also appear as a lateral compressible neck mass. Patients withany of these cystic lesions may have associated symptoms such ascough, dyspnea, dysphagia, stridor, neck mass, or foreign bodysensation. A CT scan often aids in the diagnosis of the latter twocysts, and in determining the extent of the lesions. It is importantto note that laryngeal malignancies may obstruct the saccule pro-ducing a laryngocele, and therefore carcinoma must be ruled outin any adult presenting with a laryngocele.16
TraumaLaryngeal injury should be suspected in any patient with blunt orsharp trauma to the anterior neck. Common causes of laryngealtrauma include contact sports, motor vehicle accidents and endo-tracheal intubation. Post-traumatic hoarseness can occur sec-ondary to vocal cord edema, hematoma, rupture, scarring, ary-tenoid dislocation, cartilaginous or bony laryngeal fractures orvagus/recurrent laryngeal nerve damage. Following any trauma tothe anterior neck, a full laryngeal examination and CT scan is indi-cated. Mild hoarseness secondary to vocal cord edema is commonafter short periods of intubation, but should not persist for longerthan 3 days.17 Management involves repairing mucosal lacerationsand ensuring adequate stability of the skeletal framework of thelarynx. Post-traumatic vocal rehabilitation is needed to preventhabitual dysphonia, which is a chronic post-traumatic dysphoniathat results from attempts to compensate for the initial traumaticdisability.14
Neoplasms of the Larynx
Benign NeoplasmsSquamous papillomas, believed to be caused by the human papil-loma virus,18 account for approximately 80% of benign laryngealtumors.14 Although they are seen most frequently in children, theycan occur in patients of all ages. In the adult population single ormultiple papillomas may be found throughout the larynx, with thetrue vocal cords being the most frequent site of occurrence.19 Theyappear as white to reddish shiny verrucous masses, located at thejunction of the anterior commissure and true vocal cord. Themainstay of treatment is microlaryngoscopic excision. The CO2
volume 83, number 1, December 2005 35

University of Toronto Medical Journal36
surgery have equal success rates in preventing recurrence.24
Radiation is the preferred method of treatment since it preservesthe best quality of voice, with surgery reserved for salvage. Latestage glottic carcinomas at diagnosis (T3 or T4) are treated pri-marily with either concomitant chemoradiation or a total laryngec-tomy. The majority of glottic carcinomas at diagnosis are eitherT1 or T2, since these lesions tend to present early.21 The five-yearcure rate for T1 and T2 lesions of the glottic larynx are 80-95%,and 70-80% respectively.16,21 Voice and speech rehabilitation arean integral aspect in helping the patient maintain communicativeabilities post-treatment.
Table 5Risk Factors for Hoarseness Related to Carcinoma
Laryngeal Carcinoma Advanced Glottic Carcinoma
1) Smoking 1) Dysphagia
2) Alcohol 2) Referred Otalgia
3) Nickel exposure 3) Foreign body sensation
4) Radiation exposure 4) Dyspnea or stridor
5) Human Papilloma Virus 5) Cough/Hemoptysis
6) Herpes Virus 6) Regional Lymphadenopathy
7) Syphilis
Table 6Staging for Glottic Cancers
Tis: Carcinoma in situ
T1: Tumor confined to vocal folds or folds with normal mobility
(includes involvement of anterior and posterior commissures)
T2: Supraglottic or subglottic extension with normal or impaired vocal
fold mobility
T3: Tumor confined to larynx with vocal cord fixation
T4: Massive tumor with thyroid cartilage destruction and/or extension
beyond the confines of the larynx
Systemic Causes of DysphoniaPatients with hypothyroidism may present with hoarseness andvocal fatigue secondary to myxedema of the vocal cords.14
Pregnancy may cause hoarseness secondary to vocal cord edema.25
Connective tissue diseases such as systemic lupus erythematosis,rheumatoid arthritis and amyloidosis14,16,26 can involve the vocalcords. Diagnosis is based on either supportive evidence of thesediseases from history and physical examination, and fromhistopathology of any laryngeal lesions. Management most ofteninvolves treating the underlying systemic conditions.
Neurological Causes of Dysphonia
Vocal Cord ParalysisVocal cord paralysis often occurs secondary to recurrent laryngealnerve damage, and less frequently to vagal nerve damage. Paralysismay be either unilateral or bilateral, the former presenting withhoarseness, and the latter presenting with dyspnea or stridor. Inaddition to hoarseness, patients with unilateral vocal cord paralysisoften have a breathy voice due to air escape from incomplete glot-tic closure on phonation. Occasionally, symptoms of aspiration
laser is often used to remove the lesions. Recurrence is notuncommon in respiratory papillomatosis, particularly in the pedi-atric population. There are a number of local and systemic treat-ments being studied to reduce recurrence on these lesions.
Other less common benign tumors that should be included inthe differential diagnosis include chondromas, neurofibromas,lipomas, and hemangiomas. Diagnosis is based on the patho-logic examination.
Malignant NeoplasmsExcluding skin cancer, laryngeal carcinoma is the second mostcommon malignancy of the head and neck (Table 4).20 It occursmost commonly in males aged 45 to 75. Over 90% of laryngealcarcinomas are of the squamous cell type.21
Table 4Relative Frequencies of Primary Head and Neck Tumors
at the Anatomic Sites
Oral Cavity 40%
Larynx 25%
Oro/hypopharynx 7%
Major Salivary Glands 7%
Remaining Sites 13%
The major risk factors include cigarette smoking and excessivealcohol consumption, other suggested predisposing risk factors arehighlighted in Table 5. Laryngeal carcinoma is subdivided anatom-ically into glottic, supraglottic and subglottic categories, with theformer accounting for 65-75% of all laryngeal malignancies.21
Glottic carcinoma tend to be well differentiated and slow growingwith lymph node metastases occurring in less than 10% of casesdue to the sparse lymphatic network of the vocal cords.22 Fourpercent of dysplastic laryngeal lesions and 10-15% of CIS lesionsof the larynx progress to invasive carcinoma.5
Glottic carcinoma, dysplasia and CIS tend to present early withhoarseness. Advanced glottic carcinoma at presentation is lesscommon, presenting with symptoms other than hoarseness (Table5). Supraglottic and subglottic carcinomas present late, the formerwith either difficulty swallowing (dysphagia) or pain on swallowing(odynophagia) and the latter with stridor and dyspnea. On laryn-goscopy, dysplasia and CIS often appear as areas of leukoplakia,while carcinomas tend to appear as either exophytic or ulcerativelesions and may cause cord paralysis. A biopsy of the lesion forhistologic examination needs to be obtained to make a diagnosisof glottic carcinoma. The tumor is staged based on the results ofthe physical examination and CT/MRI (Table 6).23 Endoscopy(laryngoscopy, esophagoscopy and tracheobronchoscopy) undergeneral anesthetic is performed to rule out a possible synchronousprimary, as well as to determine the extent of the tumor.
Dysplasia and CIS are usually treated with microsurgical excisionor vocal cord mucosal striping and close follow-up.21 Preservationof the larynx and voice are the goals of treatment for laryngealmalignancies. For early glottic carcinoma radiation therapy and

may be present. The severity of symptoms depends upon theamount of abduction of the paralyzed cord and the degree towhich the contralateral cord can compensate. The most commoncause of unilateral vocal cord paralysis is iatrogenic injury of therecurrent laryngeal nerve from surgery, such as from thyroid orthoracic surgery, or from endotracheal intubation.14 Other com-mon causes of unilateral vocal cord paralysis are listed in Table 7.The etiology can usually be identified on history and physicalexamination; however, in approximately 20% of cases no cause canbe identified.14
Table 7Causes of Unilateral Vocal Cord Paralysis
1) Iatrogenic- thyroid surgery- thoracic or cardiac surgery- endotracheal intubation
2) Compression by neoplasms of the:- jugular foramen- esophagus- trachea/bronchi- thyroid- upper mediastinum
3) Mediastinal Sclerosing/ Inflammatory Disorders- Tuberculosis- Sarcoidosis
4) Cardiac Disease causing:- aortic arch abnormalities- left atrial enlargement
5) Idiopathic
On examination, these patients demonstrate a weak cough.Laryngoscopy reveals abduction of the paralyzed cord at rest, withlimited or no adduction on phonation. When there is no causeapparent on history and physical examination, a chest x-ray andCT of the head and neck is warranted.4 Electromyography (EMG)can be employed to aid in differentiating neuropathies, myopathiesand neuromuscular transmission abnormalities.16
Expectant management is initially indicated for patients with uni-lateral vocal cord paralysis and an intact nerve, as function will usu-ally recover in 6 to 12 months.16 Surgery is indicated in patientswho are either aspirating, severely distressed about their dyspho-nia, or who remain hoarse for greater than one year. Surgery aimsto medialize the paralyzed vocal cord, with either Teflon, fat orcollagen injection, or by a medialization laryngeal frameworksurgery (thyroplasty), allowing for the apposition of the vocal cordson adduction to decrease air escape and the breathiness quality ofvoice and prevent aspiration.
Neuromuscular DisordersSpasmodic dysphonia is a condition characterized by a strained orbroken voice that is caused by excessive involuntary adduction ofvocal cords during phonation. Initial management involves speechtherapy. For patients that fail conservative management botulinumtoxin A injections into the thyroarytenoid muscles is being usedwith good results.27
Presbylaryngeus, the natural ageing changes of the larynx, is themost common cause of hoarseness in the elderly, with females
being more frequently affected.4 With increasing age the tone ofthe muscles decreases and the vocal folds take on a bowed appear-ance when adducted, preventing adequate apposition of the vocalcords on phonation.
ConclusionTreatment options of transoral laser surgery and radiation wereoffered to the patient after the risks and benefits of each wereexplained. The patient opted for transoral laser surgery with com-plete resection on pathology.
Hoarseness is a distressing symptom, which usually causes peopleto seek medical attention. Fortunately, the majority of cases seenby the family physician are benign, with viral laryngitis being themost common. However, hoarseness may be a symptom of moreserious disease. It is an early symptom of laryngeal cancer, whichallows it to be detected early in its course. Early detection candecrease patient morbidity and mortality. Therefore, it is impor-tant for the family physician to be able to recognize patients withrisk factors for malignancy, and feel comfortable using indirectlaryngoscopy to determine which patients need to be referred toan otolaryngologist.
References1. Pillsbury III HC, Rose AS. Biology of the Ears, Nose, and Throat. Dorland’s
Illustrated Medical Dictionary. 29th ed. Philadelphia: WB Saunders; 2002. p. 1244-7.2. Akesson EJ, Loeb JA, Wulson-Pauwels L. Thompson’s Core Textbook of Anatomy.
2nd ed. Philadelphia: J.B. Lippincott Co; 1990.3. Ruben RJ.Throat Disorders. In: Beers, MH, editor. The Merck Manual of Medical
Information. New York: Merck & Co.; 2003. p. 1267-70.4. Garret GC, Ossoff RH. Hoarseness: Contemporary Diagnosis and Management.
Comprehensive therapy. 1995;21(12):705-710.5. Meyerhoff WL, Rice DH. Otolaryngology- Head and Neck Surgery. Philidalphia:
W.B. Saunders; 1992.6. Rosen CA, Anderson D, Murry T. Evaluating hoarseness: keeping your patient’s
voice healthy. Am Fam Physician. 1998;57(11):2775–82. 7. Bailey BJ, Calhoun KH. Head and Neck Surgery-Otolaryngology. 3rd ed.
Philadelphia: Lippincott-Raven; 2002. 8. Koufman JA, Isaacson G. Approach to the patient with a voice disorder.
Otolaryngologic Clinics of North America, W.B. Saunders: 1991. p. 989-998.9. Berke GS, Kevorkian KF. The Diagnosis and Management of Hoarseness.
Comprehensive Therapy; 1996;22(4):251-255.10. Dettelbach M, Eibling DE, Johnson JT. Hoarseness: From Viral Laryngitis to Glottic
Cancer. Post-Graduate Medicine; 1994;95(5):143-163.11. Yencha MW, Linfesty R, Blackmon A. Laryngeal tuberculosis. Am J Otolaryngol. 2000
Mar-Apr;21(2):122-6.12. Wenig B. Atlas of Head and Neck Pathology. Philadelphia: WB Saunders; 1993.13. Lucente FE, Sobol SM. Essentials of Otolaryngology. 3rd ed. New York: Raven
Press; 1993.14. Savoury LW, Glckman JL: Cervical metastasis. In: Paparella MM, Shumrick DA,
Myeroff WL, eds. Otolaryngology. 3rd ed. Philadelphia: WB Saunders Co;1991:2565-2568.
15. Waring J, Lacayo L Katz E, Suwak B. Chronic cough and hoarseness in patientswith severe gastroesophageal reflux disease: Diagnosis and response to therapy.Digestive Diseases and Sciences. 1995;40(5):1093-1097.
16. Cummings CW, Fredrickson JM, Harker LA, Krause CJ, Schuller DE.Otolaryngology Head and Neck Surgery. 3rd ed. St. Louis: Mosby; 1998.
17. English G. Otolaryngology. Philadelphia: Lippincott Rowen Publishers; 1996.18. Aaltonen LM, Rihkanen H, Vaheri A. Human papillomavirus in larynx. Laryngoscope.
2002 Apr;112(4):700-7.19. Wiatrak BJ. Overview of recurrent respiratory papillomatosis. Curr Opin Otolaryngol
Head Neck Surg. 2003 Dec;11(6):433-41.20. Rice DH, Spiro R. Current concepts in head and neck cancer. American Cancer Society.
1989 Nov;19(4):637-45.21. Rhys Evans PH, Montgomery PQ, Gullane PJ. Principles and Practice of Head and
Neck Oncology. London: Martin Dunitz; 2003. 22. Shah JP, Patel SG. Head and Neck Surgery and Oncology. 3rd ed. London: Mosby;
2003. 23. Greene FL, Page DL, Fleming ID, Fritz AG, Balch CM, Haller DG, et al. AJCC
Cancer Staging Manual. 6th ed. New York: Springer; 2002.24. Smith JC, Johnson JT, Cognetti DM, Landsittel DP, Gooding WE, Cano ER et al.
Quality of life, functional outcome, and costs of early glottic cancer. Laryngoscope.2003 Jan 113(1):68-76.
25. Lyons B. Doctor my Voice seems Husky. Austrialian Family Physician. 1994;23(11):2111-2119.
26. Tsunoda K, Soda Y. Hoarseness as the initial manifestation of systemic lupus ery-thematosus. Journal of Laryngology and Otology; 1996;110(5):478-479.
27. Blitzer A, Sulica L. Botulinum toxin: basic science and clinical uses in otolaryngolo-gy. Laryngoscope. 2001 Feb 111(2):218-26.
volume 83, number 1, December 2005 37

Case 1Jennifer Singerman, B.Sc. (OT7)Dr. Liesly Lee, MD, Neurology, Sunnybrook and Women’s CollegeHospital
A previously healthy 59-year-old woman is brought by ambulance tothe emergency department. She presents with a 3-week history ofblurred vision and progressive gait ataxia. On admission, her childrennote that she seems to startle easily and has become increasingly con-fused. She is not responding appropriately to questions or instructions,seems unfamiliar with her normal surroundings, and is “not makingsense” when talking. The family suggests the possibility that theirmother has also been suffering from hallucinations.
The patient’s past medical history is unremarkable. She immigrated toCanada from Sri Lanka three and a half years earlier, and speaks onlyTamil. Her regular medications include ASA and a calcium supplement.She had been prescribed betahistine dihydrochloride three weeks earli-er for dizziness, and nitrazepam one week earlier for insomnia. Shedenies any drug or food allergies.
On exam, the patient appears frightened and confused. She is not ori-ented to time or place. Her heart rate is 98 and regular; respiratory rateis 18; blood pressure is 141/84; temperature is 36ºC. Head and neckexams are unremarkable except for arcus senilis. Her respiratory andcardiac exams are normal.
On neurologic examination, a full mini-mental status examination can-not be completed due to presence of a language barrier and her cog-nitive status. She is unable to count backwards from 20, nor is she ableto name the days of the week or the months of the year backwards.She is able to name a pen and a shoe.
On cranial nerve assessment, the patient cannot identify the number offingers held up one foot in front of her eyes. She is able to track facesand reach for items in her visual field. On fundoscopy there is no evi-dence of haemorrhage or papilloedema. Pupils are equal and reactiveto light. She has full extra-ocular movements with saccadic intrusions.The rest of the cranial nerves are normal.
On motor examination, she has an abnormal dystonic posturing of herupper limbs. There is a mild right hemiparesis with a right pronatordrift. The patient has cogwheel rigidity in her wrists and elbows, moremarked on the right side. There is “waxy flexibility” in her upper limbs,in which her arms remain in any position put into place by the examin-er. The patient also exhibits stimulus-sensitive myoclonus (i.e.myoclonus in response to a loud noise like clapping). All deep-tendonreflexes are normal. The Babinski reflexes are equivocal. She has nopalmo-mental nor grasp reflexes. On sensory examination, the patientis grossly responsive to pain in all 4 limbs. She does not appear to haveneglect. The patient’s stance is unsteady, with a wavering gait.
A number of investigations are carried out. Toxin screen is negative.She has a normal lumbar puncture. Her ESR is slightly elevated, but C3,C4, RF, vitamin B12, vitamin B6, and TSH levels are all normal. There isno evidence for a fungal infection. Head CT shows basilar artery tipcalcification. MRI shows bilateral cortical ribbon enhancement posteri-orly, and cortical atrophy in excess of what would be expected for thepatient’s age (Figure 1). An EEG shows 1 Hz periodic complexes.
The patient becomes more confused and unresponsive followingadmission. She stops responding to questions, and then becomes fullymute. She begins to have jerky movements in her limbs, and her bodybecomes very rigid. Soon after, she begins having stimulus-sensitiveseizures. She is then transferred to the Palliative Care unit, 3 weeks fol-lowing hospital admission.
What is the Diagnosis?
University of Toronto Medical Journal38
Case Reports from the University of Toronto Faculty of Medicine
Figure 1.1.
Quick Diagnosis

volume 83, number 1, December 2005 39
Case 2Vicky Chan, B.Sc. (OT6)Lyne Noël de Tilly, MD, FRCPCYuna Lee, MD, FRCPC
A 33-year old, right-handed, Caucasian man presented to theEmergency Department (ED) in late spring with worsening headacheand left-sided weakness. One month prior to his presentation, he wasadmitted to the hospital with left-sided weakness. MagneticResonance Imaging (MRI) at the time revealed abnormal increased sig-nal on the T2- weighted images and FLAIR sequence along the rightaspect of the pons and midbrain, with further cephalic extension alongthe right thalamus and adjacent deep brain structures (Figure 2.1).Patchy enhancement was also present along the right midbrain. Alumbar puncture (LP) showed an elevated protein level of 0.55 g/L, butculture and cytology of the cerebrospinal fluid (CSF) were negative.Other than physiotherapy, he did not receive any medical treatmentwhile in hospital. His symptoms gradually improved and he was dis-charged after 2 weeks to follow-up with neurology.
On this presentation, his gradual onset of left-sided weakness was sim-ilar to the prior incident and he needed a cane for walking. In addi-tion, he also experienced nausea and vomiting with headache.
His past medical history included an episode of infectious colitis 2 yearsago. On review of systems, it was discovered that he had been suffer-
ing from intermittent fever that was associated with skin nodules in thecalves and triceps for the past 5 years. These episodes lasted for 3-4days and were relieved with NSAIDs. On one occasion, he had 2painful ulcers in the genital area, but all tests for sexually transmittedinfections were negative. He has also had a history of recurring painfuloral ulcers since childhood.
On physical examination, the patient appeared well. His blood pressurewas 115/80 mmHg, heart rate was 80 beats/min and regular, respira-tory rate was 16 beats/min, and his temperature was 37.2ºC. His car-diovascular, respiratory and abdominal examinations were all normal.Cranial nerve examination revealed a mild left facial droop and saccadiceye movements. The remainder of the cranial examination was normal.Tone on his left side was increased. Power was 5+ on the right and 4+on the left. His deep tendon reflexes were 2+ on the right, 3+ in theleft upper extremity and 4+ (clonus >4 beats) in the left lower extrem-ity. The Babinski reflex was present on the left. Sensation was intactother than a mild decrease in vibration sensation in the left lowerextremity. He also had an antalgic, wide-based gait.
Investigations in the hospital included a repeat lumbar puncture thatshowed elevated protein (0.81 g/L) and increased leukocyte count (403with 79% of lymphocyte). An oligoclonal band was absent. Culturesand serology tests of blood and CSF were negative including those fortuberculosis, fungal infection, Listeria, herpes simplex virus, toxoplas-mosis, syphilis and Lymes disease. HIV testing was also negative.Serology of West Nile virus was not done since his symptoms developed
in the spring when the incidence of West Nileinfection is low. A vasculitic work-up was nega-tive. His serum angiotensin-converting enzyme(ACE) level was also normal. A repeat MRI of thehead showed new involvement of the left-sidedmidbrain. There were persistent abnormal signalsin the right midbrain and cerebral peduncle, butthe involvement in the right thalamus and basalganglia were improved (Figure 2.2). An MRI ofthe C-spine was normal, along with a ComputedTomogram (CT) of his chest and pelvis. A galliumscan of the whole body and an ophthalmologicexam were both unremarkable.
Figure 2.1. Axial FLAIR brain MRI on presentation.
Patchy increased signal in the right midbrain extending
in the right thalamus and adjacent deep brain.
Figure 2.2. Axial FLAIR brain MRI on second admis-
sion. Interval extension of the increased signal along the
left midbrain, with improvement of the right thalamic
lesion.
What is the diagnosis?

Case 3Daniel R. Ricciuto, H.BMSc (OT6)
A 32-year-old male with end stage renal disease (ESRD) is referred to therheumatology service for polyarthralgia. He presented to the EmergencyDepartment five days earlier with a three week history of worsening hipand back pain, as well as swollen, painful fingertips in his right hand. Thepain was continuous, associated with impaired mobility, and was refracto-ry to treatment with acetaminophen or ibuprofen. He did not experiencemorning stiffness. He did not have a rash, oral lesions or eye symptoms,nor did he experience fevers, weight loss or night sweats. There was nohistory of trauma.
The patient’s past history is significant for familial thrombocytopenic pur-pura (TTP) and subsequent end stage renal disease (ESRD); treatment withhemodialysis (HD) began three years earlier. He also suffers from hyper-tension. He is an intravenous drug user and has had recurrent presenta-tions for Gram-negative bacteremia in the previous eight months. He doesnot have a history of arthritis or connective tissue disease, nor does he havea family history of any such disease. However, he states that he has hadmild pain in his back and hips for several months. He does not have a his-tory of inflammatory bowel disease and has not suffered from a recentdiarrheal illness. He is sexually active, but does not have a known sexuallytransmitted disease, dysuria or urethral discharge.
His medications at the time of admission were: methadone, atenolol,amlodipine, ramipril, sevelamer, calcium carbonate, aspirin, folic acid anddarbepoetin alfa.
On examination, the patient was alert and in no distress. His heart rate was96 beats/min and regular, respiratory rate 14, blood pressure 175/90, andoral temperature 36.9°C. Examination of the musculoskeletal systemrevealed tender clubbing with a drumstick appearance in all digits on theright hand and the second digit of the left hand. Percussion tendernesswas present over the thoracic, lumbar and sacral spine; range of motion ofthe back was limited by pain. There was stress tenderness over the sacroil-iac (SI) joints bilaterally. Flexion and extension of the hips were normal, butthere was a decrease in the range of internal and external rotation bilater-ally. There were no rashes, skin lesions, conjunctival injection or orallesions. The cardiovascular exam revealed normal heart sounds withoutmurmurs. Peripheral stigmata of endocarditis were absent. The neurolog-ical, respiratory and abdominal examinations were within normal limits.
Laboratory investigations revealed a haemoglobin level of 96 g/L (normalrange, 140-180 g/L) with a MCV of 74.1 fL (normal range, 80-96 fL), leuko-cyte count of 9.8 x 109/L (normal range, 4.0-11.0 x 109/L) and a plateletcount of 210 x 109/L (normal range, 150-450 x 109/L). Creatinine was ele-vated at 518 umol/L (normal range, 50-130 umol/L). Total serum calciumwas normal at 2.34 mmol/L (normal range, 2.1-2.6 mmol/L) and serumphosphate was elevated at 1.68 mmol/L (normal range, 0.84-1.45mmol/L). All other serum electrolytes were within normal limits. Alkalinephosphatase (ALP) was elevated at 298 U/L (normal range, 45-115 U/L) andalbumin was 30 g/L (normal range, 31-43 g/L). The results of all other liverenzymes and function tests were within normal limits. Two sets of bloodcultures did not yield any organisms after four days incubation.
Radiography of the patient’s hands revealed phalangeal tuft resorption andacro-osteolysis of the second to fifth digits of the right hand and the sec-ond digit of the left hand. Subperiosteal resorption along the radial aspectsof the middle phalanges with a lace-like appearance of the bone was alsopresent. As well, several of the interdigital arteries were calcified (see Figure3.1). Computed tomography (CT) of the pelvis revealed several erosions ofthe lower lumbar and sacral spine, with intervening calcification along theanterior superior endplate of L5 (see Figure 3.2). Widening, erosions, scle-rosis and numerous calcifications were present within the SI joints bilater-ally (see Figure 3.3). A bone scan revealed increased activity in the acromio-clavicular, sternoclavicular, sternal, vertebral, costochondral and SI joints, inaddition to the skull, symphysis pubis and patellae (see Figure 3.4).
What is the diagnosis?
University of Toronto Medical Journal40
Figure 3.1. Plain x-rays of the left and right hands showing distal tuft resorp-tion, subperiosteal bone resorption and calcification of the interdigital arteries.
Figure 3.2. Reconstruction ofa CT pelvis in the sagittal planeshowing erosions of the lumbarand sacral spine and calcificationof the anterior superior aspect ofL5.
Figure 3.3. AxialCT image showingwidening, erosionsand sclerosis of thesacroiliac joints.
Figure 3.4. Bone scan show-ing increased activity through-out axial skeleton.

3M™ Littmann® Stethoscopes
You want the best for your patients.
The best care begins with careful listening and the right tools.
That’s why doctors have counted on the reliability and superior acoustics of 3M™ Littmann® Stethoscopes more than any
other brand. From the popular 3M™ Littmann® Cardiology III Stethoscope to the most advanced
3M™ Littmann® Electronic Stethoscope Model 4000WS that allows you to see what you hear, 3M listens to what
you need and delivers. When second best isn’t good enough, count on 3M™ Littmann® Stethoscopes -
the Tools of the Trade.
To learn more, call 3M Canada at 1-800-3M HELPS (1-800-364-3577) or visit www.3M.com/Littmann.
3M is a trademark of 3M and Littmann is a registered trademark of 3M. Used under license in Canada. © 3M 2005. 0508-CP-23050-a-E 3 Innovation
isten to life.

University of Toronto Medical Journal42
thalamus on T2-weighted images, plus cerebral atrophy) andEEG (1 Hz periodic complexes) patterns make the diagnosishighly probable.5 The only way to definitively diagnose CJD iswith a brain biopsy, however, this is not usually done. Prionscannot be killed by autoclaving,8 hence the biopsy equipmentwould need to be destroyed. If one were to complete a biop-sy, it would show spongiform degeneration. In addition, acti-vated astrocytes and microglia would be seen.2
Unfortunately, there is no treatment for CJD. Purely palliativemeasures should be taken, such as opiates for pain manage-ment, and benzodiazepines or sodium valproate for myoclonus.
References1. Aguzzi A, Polymenidou M. Mammalian prion biology: One century of evolv-
ing concepts. Cell. 2004; 116:313-27.2. Glatzel M, Soeck K, Seeger H. Human prion diseases: Molecular and clinical
aspects. Arch Neur. 2005; 62(4):545-52.3. Aguzzi A, Montrasio F, Kaeser PS. Prions: Health scare and biological chal-
lenge. Nat Rev Mol Cell Biol. 2001; 2:118-26.4. Gambetti P, Kong Q, Zou W. Sporadic and familial CJD: Classification and
characterisation. Br Med Bull. 2003; 66:213-39.5. Wisniewski T. Prion-related diseases [monograph on the Internet]. Omaha:
eMedicine.com ; 2004 [cited 2005 Oct 19]. Available from: http://www.emed-icine.com/neuro/topic662.htm.
6. Brown P, Preece M, Brandel JP. Iatrogenic Creutzfeld-Jakob disease at the mil-lennium. Neurology. 2000; 55:1075-81.
7. Harder A, Jendroska K, Kreuz F. Novel twelve-generation kindred of fatalfamilial insomnia from Germany representing the entire spectrum of diseaseexpression. Am J Med Genet. 1999; 87:311-6.
8. Alper T. The Scrapie enigma: Insights from radiation experiments. Radiat Res.1993; 135:283-92.
Case 2 Diagnosis: Neuro-Behçet’s Syndrome
Behçet’s Syndrome (BS) was named in 1937 by Hulusi Behçet,a Turkish dermatologist who described the triad of recurrentoral apthous ulcers, genital ulcers and uveitis.1 It is anautoimmune disorder of recurring vasculitis involving vesselsof any type and any size.2 Up to 85% of patients may alsopresent with skin lesions in the form of papulopustularlesions, erythema nodosum or pathergy reaction (see belowunder clinical diagnosis).3 Other organ systems may be affect-ed as a result of vasculitis and involvement of the intestines,lungs, vessels and central nervous system are often associatedwith poor prognosis.4
Neurological involvement in BS occurs in about 5-10% ofpatients and tends to occur several years after the initial onsetof Behçet disease.4 Neuro-Behçet syndrome (NBS) can besubdivided into two major forms: intra-axial NBS and extra-axial NBS.3 Intra-axial NBS is the result of vascular inflamma-tion in the CNS with focal or multifocal parenchymal involve-ment, whereas extra-axial NBS is the consequence of cerebralvenous sinus thrombosis and often presents with limited symp-toms. In addition to the two most common forms, neuro-psy-cho-BS and peripheral nervous system involvement may alsooccur.
And the diagnosis is . . .
Case 1Diagnosis: Sporadic Creutzfeld-Jakob Disease (sCJD)
Creutzfeld-Jakob Disease (CJD) is a neurodegenerative infec-tious prion disease that is invariably fatal.1 The disease iscaused by a misfolding of a single protein, PrPc, a ubiquitouscell surface protein found particularly on neuronal cells. InCJD, the PrPc protein is misfolded into an aberrant version,PrPsc (the “sc” refers to scrapie, the corresponding prion dis-ease found in sheep). The PrPsc proteins aggregate and inducefurther PrPc proteins to mutate into the PrPsc form. The exactfunction of the normal PrPc proteins is unclear, but researchsuggests that they may function as signal-transducing molecules,superoxide dismutase, or proteases.2 The mutated PrPsc can-not perform these vital functions, and disease ensues.
There are four types of CJD: sporadic (sCJD), iatrogenic(iCJD), familial (fCJD), and variant (vCJD). Sporadic CJD is arare disease occurring all over the world, showing no particulargeographic predilection. Most countries report an incidence of0.6-1.2 x106, although higher numbers have been reported.3
Males and females are affected in equal numbers, and the meanage of onset is between 55 and 65 years of age.2 The etiologyof sCJD is unclear. Early symptoms include diminished cogni-tive function, sleep disturbances, and behaviour abnormalities.As the disease progresses, patients experience pyramidal andextrapyramidal symptoms, visual disturbances, ataxia, cerebellardysfunction, and myoclonus. Finally, as the disease enters itslate stages, patients exhibit akinetic mutism, and finally death.4
The median time of survival is 5 months, and 90% of patientswill die within one year of diagnosis.2,5
The iatrogenic type of CJD is exceedingly rare, and usuallyresults from contaminated neurosurgery instruments. Theother causes of iCJD include dura mater grafts or pituitarygrowth hormone injections from infected donors.6
Familial CJD is an autosomal dominant disease, resulting froma mutation in the PRNP gene on chromosome 20, the geneencoding for PrPc.7 This form has the best prognosis of alltypes of CJD, with a mean prognosis of 26 months.5
The ingestion of infected animal products causes the variantform of CJD; this typically involves beef from cows withBovine Spongiform Encephalopathy (BSE), otherwise known asMad Cow Disease. The patient profile is somewhat differentfrom those with sCJD, as the mean age of patients with vCJDis 29 years, and the median survival rate is 14 months. As well,more than half of patients present with psychiatric symptoms,a characteristic not known to sCJD.2
The diagnosis of CJD is usually made on clinical grounds.Typical MRI (hyperintense signals in the basal ganglia and the

EpidemiologyBehçet’s Syndrome is most prevalent along the ancient SilkRoad from eastern Asia to the Mediterranean area. The inci-dence in this area is roughly 1/10,000, compared to1/1,000,000 in Europe and North America.5 Men are affectedmore often (world average of 1.4:1) and with more severe dis-ease. Behçet’s Syndrome can occur at any age, but frequentlyin the third decade of life.
Neurological involvement also occurs more commonly in men,with a male to female ratio of up to 4:1.3 Of the two majorforms of NBS, intra-axial NBS has a poorer prognosis and ismuch more common than extra-axial NBS.
PathophysiologyBehçet’s Syndrome is characterized by infiltration of lympho-cytes and neutrophils into the affected organs.6 The causativeagent is unknown although over the years, genetic, immuno-logical, infectious and vascular causes have been examined.
GeneticA strong genetic association has been shown between BS andthe human leukocyte antigen (HLA)-B 51 gene. It was foundthat about 20% of healthy individuals carry the HLA-B51locus, compared with 50-80% of BS patients.5 The directinvolvement of the gene remains unproven, although studiesdone on mice have shown that the presence of HLA-B51results in excessive function of neutrophils, which is a char-acteristic of BS.
Immunological Like most other autoimmune disorders, the cytokine profile ofBS is skewed towards the Th1-type immune responses. Somestudies have shown that the Th1 pro-inflammatory cytokinesinterleukin-2 (IL-2) and interferon-g are increased in peripher-al blood and positively correlate with disease activity in BS.7
Infectious AgentsBefore the 1980s, it was thought that the disease process wasa result of an aseptic inflammatory response. Recently, viraland bacterial infections such as Streptococcus sanguis, herpes sim-plex virus and heat shock protein are thought to play some rolein the pathogenesis of the disease.5
Vascular AbnormalitiesAnti-endothelial cell antibodies are more prevalent in BS andmay contribute to the vasculitic process commonly present inthe histopathological specimens of oral ulcers, genital ulcersand central nervous system lesions. There are also rare casesof venous thrombi in patients with BS, and they are often asso-ciated with factor V Leiden and prothrombin gene G20210Amutations.7
Craniotomic biopsies in NBS typically demonstrate multifocalnecrotizing lesions with inflammatory cell reactions mainlyaround small veins. These CNS lesions are most commonlyseen in the brain stem, followed by the cerebral basal ganglia.4
Clinical DiagnosisThe diagnosis of BS is based on clinical signs and symptomsbecause there are no pathognomonic laboratory findings. In1990, an international group of physicians established the crite-ria for the diagnosis of BS.8 According to this guideline, apatient must have recurring oral ulcerations (at least 3 occasionsin a year) plus two of the following four: recurrent genital ulcer-ations, uveitis or retinal vasculitis, skin lesions or positivepathergy test (appearance of red bump or pustule after forearmis pricked with a small, sterile needle). Several tools have beendesigned to improve the accuracy of diagnosing BS. The mostrecent one is the arithmetic method, which is reported to havea sensitivity of 97.2%, a specificity of 96.7% and an accuracyof 97.1%.9 In this method, ocular lesions are given five points,oral aphthosis four points, genital ulcer three points, pathergyphenomenon two points and skin manifestations one point; atotal of seven points or higher is the cutoff for the diagnosisof BS. However, further studies are required to verify the sen-sitivity and specificity of the test.
Intra-axial NBS may present as a spectrum with symptomsvarying from headache, confusion, and seizures to stroke-likemanifestations. The most common region affected in intra-axial NBS is the brainstem and results in cranial nerve defects,dysarthria, corticospinal tract lesions and ataxia. However,hemiparesis, cognitive-behavioral changes or extrapyramidalsigns may also be seen. Extra-axial NBS, on the other hand, isthe result of venous thrombosis and often presents with severeheadache, mental changes, and motor ocular palsies as a resultof increased intracranial pressure.3
The differential diagnosis for brain stem lesions in a youngadult include multiple sclerosis (MS), infections such as tuber-culosis, Listeria and West Nile virus, neurosarcoidosis, braintumour including lymphoma, and vasculitic diseases (systemiclupus erythematosus, Behçet disease). Results from MRI andCSF analysis can help differentiate NBS from MS. In patientswith NBS, MRI often reveals large, diffuse brainstem lesionswith an upward extension to diencephalic structures or a down-ward extension to the pontobulbar region. In contrast to MS,periventricular and subcortical lesions are rare in NBS.Cerebrospinal fluid content may show inflammatory changes inNBS, but such abnormalities occur less frequently in MS.3
Infections can be ruled out by serology and cultures of CSF andblood. Meningeal involvement is common in neurosarcoidosis;however, other organ systems are often involved in thesepatients and they may have an elevated serum ACE level.Finally, the clinical course as well as the presence of associatedsystemic findings may help distinguish neoplastic and vasculiticdiseases.
ManagementSimilar to other autoimmune inflammatory diseases, BS is oftentreated with anti-inflammatory drugs as well as immunosup-pressants. The choice of treatment depends on the clinicalmanifestations. For example, those that are confined to themucocutaneous region (oral, genital, skin) usually respond well
volume 83, number 1, December 2005 43

University of Toronto Medical Journal44
Case 3Diagnosis: Renal osteodystrophy (osteitis fibrosa)
Renal osteodystrophy is the umbrella term given to the changes inmineral metabolism and bone structure that occur secondary toESRD. Several subdivisions of renal osteodystrophy exist, includ-ing osteomalacia, adynamic bone disease and osteitis fibrosa.Patients with more than one component are said to have mixeddisease. Osteomalacia is characterized by a low rate of boneturnover, defective mineralization and accumulation of unmineral-ized bone matrix (osteoid).1 Adynamic bone disease is differenti-ated from osteomalacia by a low rate of bone turnover without anincrease in osteoid formation.1 Osteitis fibrosa results fromincreased bone turnover due to secondary hyperparathyroidism.
Hyperphosphatemia is the main culprit in the development ofhyperparathyroidism in patients with renal failure.1,2 As theglomerular filtration rate (GFR) decreases early in renal failure, thefiltered phosphate load is decreased leading to phosphate retention.Hyperphosphatemia is thought to cause hyperparathyroidism byseveral mechanisms, such as the generation of hypocalcemia,decreased formation of calcitriol (1,25α-hydroxyvitamin D) and adirect effect on the stimulation of parathyroid hormone (PTH)secretion.2 In some patients, oversecretion of PTH can lead tohypercalcemia. This phenomenon, termed tertiary hyperparathy-roidism, results from severe hyperplasia of the parathyroid glandunresponsive to serum calcium levels.2,3
Patients with secondary hyperparathyroidism may experience bonepain, ectopic calcification and pruritis; however, the diagnosis ofrenal osteodystrophy is made based on laboratory, imaging andhistological investigations.3 Bone biopsy is the gold standard andcan differentiate between the subtypes of renal osteodystrophy, butit is invasive, costly and impractical for routine diagnosis.4Biochemical investigations may reveal hyperphosphatemia,hypocalcemia or an elevated ALP, although levels depend on theacuity of renal failure, the degree of active bone resorption and theeffects of any concurrent treatments. Parathyroid hormone canalso be measured and, by definition, is elevated in osteitis fibrosa.
Imaging is essential in the diagnosis of renal osteodystrophy andcan help to differentiate between the different subtypes of the dis-ease. Hyperparathyroidism causes several distinct radiologicalchanges. Hand radiography may reveal subperiosteal bone resorp-tion at the tufts of the terminal phalanges and/or the radial aspectsof the middle phalanges with a typical lace-like appearance.Trabecular bone resorption can lead to loss of definition of thecranial vault, termed “salt and pepper skull”. Subchondral boneresorption commonly affects the sternoclavicular, acromioclavicu-lar and sacroiliac joints, as well as the symphysis pubis and inter-vertebral discs. The changes seen in the sacroiliac joints can mimicankylosing spondilitis. Brown tumours (osteoclastomas), whichappear as cavitary lesions most commonly in the pelvis, ribs, femo-ra and facial bones can also be seen in hyperparathyroidism. Softtissue calcification, which can occur in tendons or vasculature,adjacent to joints or within organs, is another feature of renalosteodystrophy.5
to topical steroids and non-immunosuppressive agents such ascolchicine. Those with moderate systemic disease may require oralcorticosteroids.1
For patients who have involvement of the CNS, high-dose steroidsare often used along with other immunosuppressants. Such agentsmay include methotrexate, interferon-g, azathioprine, cyclosporineand thalidomide.1,6
OutcomeCentral nervous system involvement in BS usually takes a relaps-ing remitting course, although a single episode or a secondary pro-gression is also seen. Intra-axial NBS has a high morbidity andmortality rate, with 50% of patients reaching moderate to severedisability after 10 years.3 Like patients with other chronic diseases,people with BS should be educated about the disease process,prognosis and the sequelae of long-term treatment.
Back to the CaseIn this case, the patient presented with his second episode of pre-sumed NBS. The criteria for diagnosis of BS were met by histo-ry; however, a definitive diagnosis was not possible since a biopsyof his CNS lesions could not be obtained. Over the course of hishospitalization, his neurological symptoms improved only mini-mally. After he was identified to have other systemic symptomson history consistent with Behçet’s disease, he was given high-dosesteroids before discharge. His strength improved significantly twoweeks post-treatment. A repeat MRI of the brain 20 days afterinitiation of steroid treatment showed a significant reduction in thenumber of brainstem lesions.
Given the rapid improvement of the brainstem lesions after steroidtreatment, MS as well as neoplasms are less likely. Particularly,lymphoma is unlikely since his neurological symptoms improvedwithout any treatment in the initial presentation. The diagnosis ofneurosarcoidosis could not be ruled out completely, although givenhis improved clinical course without treatment in the initial pre-sentation, the normal serum level of ACE, and the lack of involve-ment of other organ systems, this is less probable. With his his-tory of recurrent rash, oral and genital lesions and the rapidresponse to steroid treatment, NBS seemed to be the most likelydiagnosis. Neuro-Behçet syndrome should be considered as partof the differential diagnosis in young patients presenting withbrainstem lesions.
References1. Lee S, Bang D, Lee ES. (2004). Behçet Disease. [cited 2005 Jun 11]. Available
from: http://www.emedicine.com/ derm/topic49.htm.2. Johns Hopkins Vasculitis Center. [homepage on the Internet]. c2004. Behçet’s
Disease. [cited 2005 Jun 11]. Available from.3. Siva A, Altintas A, Saip S. Behçet’s syndrome and the nervous system. Curr Opin
Neurol. 2004;17(3):347-57. 4. Matsuo K, Yamada K, Nakajima K, Nakagawa M. Neuro-Behçet Diease
Mimicking Brain Tumor. AJNR Am J Neuroradiol. 2005;26(3):650-3.5. Suzuki Kurokawa M, Suzuki N. Behçet’s Disease. Clin Exp Med. 2004;4(1):10-20.6. Arayssi R, Hamdan A. New insights into the pathogenesis and therapy of Behçet’s
disease. Curr Opin Pharmacol. 2004;4(2):183-8.7. Direskeneli H. Behçet’s disease:infectious aetiology, new autoantigens, and HLA-
B51. Ann Rheum Dis. 2001;60(11):996-1002.8. Wechsler, B, Davatchi, F, Hamza, M, Dilsen, N, et al. Criteria for diagnosis of
Behçet’s disease. Lancet. 1990; 335(8697): 1078-1080.9. Davatchi F, Chitsaz S, Jamshidi AR, Nadji AH, Chams-Davatchi C, Shams H, et
al. New simple way to use the classification tree for the diagnosis of Behçet’s dis-ease. APLAR Journal of Rheum. 2005;8(1):43-44.

Treatment should initially be aimed at preventing phosphate accu-mulation and secondary hyperparathyroidism. Early in the courseof renal failure, dietary phosphate restriction through limited pro-tein intake may reduce the level of serum phosphate. Howeverthis dietary measure must be balanced with the risk of malnutri-tion.6 In patients with worsening renal function or patients whorequire dialysis, oral phosphate binders are needed. Calcium salts,such as calcium carbonate or acetate, taken with meals are first-line therapies and should be considered when serum phosphatelevels are greater than 1.80 mmol/L.6 Serum calcium levels shouldbe maintained at low-normal range to help prevent the formationof insoluble calcium-phosphate products and their subsequentdeposition in arteries and soft tissues. Sevelamer is a cationic poly-mer that does not contain calcium and therefore theoreticallydecreases the risk of hypercalcemia and heterotopic calcification.However, sevelamer is expensive and has not been shown to besafer or more efficacious than calcium acetate.6
In patients with continued hypocalcemia and/or hyperparathy-roidism despite correction of serum phosphate, vitamin D sup-plementation should be considered. Serum calcium levels shouldbe monitored periodically because of the risk of hypercalcemia.7
Refractory hyperparathyroidism in ESRD can lead to severehypercalcemia, extraskeletal calcification and renal osteodystrophy.
In these patients, parathyroidectomy may be indicated if PTH lev-els are markedly elevated.8
In this particular case, the main differential diagnoses consideredwere septic arthritis, chronic osteomyelitis and seronegativespondyloarthropathy. A diagnosis of secondary hyperparathy-roidism (osteitis fibrosa) was made primarily through the classicradiographic findings described above and an elevated PTH levelof 86 pmol/L. The patient was already being treated with phos-phate binding agents and was not a candidate for vitamin D sup-plementation due to serum calcium levels in the high-normalrange. The patient was assessed by general surgery for parathy-roidectomy.
References1. Hruska KA, Teitelbaum SL. Renal Osteodystrophy. N Engl J Med.
1995;333:166-174.2. Rose BD, Henrich WL. Pathogenesis of renal osteodystrophy. [cited 2005 Oct
11]. Available from: http://www.utdol.com.3. Potts JT. Hypercalcemia associated with renal failure. In: Braunwald E et al.,
editors. Harrison’s Principles of Internal Medicine, 15th ed. New York:McGraw-Hill; 2001. p. 2216-2217.
4. Martin KJ, Olgaard K. Diagnosis, assessment, and treatment of bone turnoverabnormalities in renal osteodystrophy. Am J Kidney Dis. 2004;43:558-565.
5. Jevtic V. Imaging of renal osteodystrophy. Eur J Radiol. 2003;46:85-95.6. Cronin RE. Treatment of hyperphosphatemia in chronic renal failure. [cited
2005 Oct 11]. Available from: http://www.utdol.com.
volume 83, number 1, December 2005 45

University of Toronto Medical Journal46
Two recent studies have examined the effectiveness of PDA-basedpatient encounter logs. In the first, at the Indiana UniversitySchool of Medicine, a pilot study was conducted to assess the basicclinical skills encounters for third-year medical students. UsingPalm PDAs, the students logged each clinical skill encounter,recording detailed information including the site, date, procedure,whether they observed, performed, or assisted in the skill and thementor’s name. In addition, for each procedure logged, the stu-dent’s supervisor would sign directly on the screen of the PDA todocument the student’s involvement.
The results after nine months of tracking were surprising. Of the52 core basic clinical skills identified by the Indiana UniversitySchool of Medicine, there was not a single skill or procedure thatall students performed as a group. In fact, only 10 skill encoun-ters occurred commonly among the group as a whole, and fewerthan half of students had any exposure to common clinical skillencounters such as intravenous catheter placements, splinting,injections or venipuncture.6 Preceptors reviewing paper logswould receive this information only once the student had alreadycompleted a rotation, thus preventing feedback from being usedto improve the student’s experience. In contrast, a log collectedon a PDA and uploaded daily or weekly would allow the precep-tor and student alike to continually evaluate the experience and toadjust schedules to ensure that the student receives optimalinstruction and opportunities.
A second study conducted at the College of Physicians andSurgeons at Columbia University offered students the option ofusing their PDA instead of scanned cards to track clinical encoun-ters. A simple patient-tracking program was installed on the PDAsof participating students. Information tracked on the PDA mir-rored the information tracked with the optically scanned cards.The major difference between the cards and the PDA was in thediagnosis category; the cards included a selected list of 116 diag-noses commonly encountered in outpatient settings and organizedby organ system, whereas the PDAs were linked to an abbreviat-ed, searchable International Classification of Diseases (ICD-9)database of 1882 commonly encountered outpatient diagnosesorganized by diagnosis number.
In the Columbia study, too, PDA tracking had advantages over
Introduction Undergraduate medical education is changing in the new millenni-um. Students spend a majority of their time in school learning howto access up-to-date, accurate information. In the past, resourceswere limited to and consisted predominantly of library texts andprinted journals. Today, this information is available electronically tobe accessed by computer and, more recently, on handheld portabledigital assistants (PDAs). A decade ago, PDAs were bulky and slowand had limited use. Today, they are small, have impressive amountsof memory, a wide array of software applications and some high techbells and whistles, such as wireless Web, e-mail, colour andaudio/video features. Portable digital assistants support an extensivecollection of medical applications that will help health care providersand physicians-in-training whether they are in the classroom, officeor making rounds. Most of these applications can be updated imme-diately as new information becomes available. Data can be enteredinto a PDA at any site and information transferred by infrared, ordownloaded by linking to a desktop computer.
Many articles have examined the utility of the PDA in medicineand reviewed the availability of medical software for use withPDAs. The focus of this article, however, is the application ofPDA technology and software to the field of UndergraduateMedical Education from both the institutions’ perspective and thatof the student.
Patient Encounter LogsAt many medical schools, a “patient encounter log” is used to mon-itor student experiences in diverse clinical settings. These logs aregenerally used to track the nature of students’ clinical exposure withrespect to case mix and disease severity, as well as to record students’opportunities to perform certain identified procedures.1,2 Logs areuseful for determining whether appropriate supervision and feedbackis occurring, particularly in ambulatory and community-based sites.3
Others have used student logs to study the impact of differencesamong ambulatory experiences in terms of patient characteristics andpractice settings on student learning outcomes.4 In the UnitedStates, documentation of student clinical experience via these logs isconsidered essential both for accreditation processes and internalprogram evaluations.5 While traditionally, these logs have taken theform of notebooks or optically scanned cards, many schools are nowmoving to a PDA-based system for logging.
Handheld Computing in Medical Education
Ron Somogyi, B.Sc., M.Sc. (0T8)Joy Abramson, B.Sc.(MD/PhD)John Kim B.Sc., M.Sc. (0T9)Joseph Koval, BESc., B.A. (0T9)
Technology Review

paper tracking. In particular, the percentage of missing data washigher for scanned card users than PDA users. Anecdotally, stu-dents reported that they found the PDAs easy to use, and thatrecording basic encounter information took less than 30 seconds.7
Thus, initial studies indicate significant advantages to using PDAsfor tracking patient encounters over traditional paper-based meth-ods. The immediate feedback to students and instructors allowsfor direct improvement of educational experiences, more completerecords, and easier and more convenient systems for student use.The disadvantages of a PDA-based logging system were not dis-cussed in depth, but included such issues as cost, privacy and databackup.
Clinical Reference Software for Medical EducationIn addition to patient tracking, the second major use of PDAs inmedical education is for access to reference sources in a formatconvenient for the clinical setting. There is a huge and rapidlygrowing selection of medical software available encompassingthousands of titles. This includes PDA versions of popular text-books and various medical utilities, particularly drug reference listsand medical calculators. Several of the most popular softwarepackages for students are listed in Table 1.8 All are available forboth Palm and Pocket PC platforms.
Many studies have examined data on medical student PDA usage,evaluating its effectiveness for both patient encounter logging andinformation access. While most of the data comes through self-reporting by the students, one study used analysis software pre-installed on the PDA that automatically collected data on students’use of both medical and nonmedical software. In this study, theDepartment of Family Medicine at the Northeastern Ohio
Universities College of Medicine provided PDAs to third-year stu-dents during a six-week family medicine rotation. The PDAs wereinitially provided with both general usage software (address book,calculator, date book, expense account, memo pad, graffiti teach-ing program and to-do list) as well as medical software: Griffith’s5 Minute Clinical Consult®, ePocrates qRx®, ePocrates qID®,iSilo® (a document reader), HanDBase® (logbook program),MedCalc® and Application Usage® (tracking software). TheHanDBase® logbook, in which students entered all patients seenand procedures performed during the family medicine rotation,was the only required use of the PDA. After HanDBase®, themost often used programs were ePocrates qRx and Griffith’s 5Minute Clinical Consult®.9
This study also looked at the students’ subjective ratings of theusefulness of each of the programs in enhancing learning and doc-umenting clinical exposure during the clerkship experience. Onboth pre-rotation and post-rotation questionnaires, an over-whelm-ing majority of students believed the PDA would enhance theirclerkship experience, increase their confidence with patients andincrease their confidence in interactions with residents and attend-ing physicians. On the post-rotation evaluation, thirty-three of the85 students included reported that the PDA altered the way theyaccessed clinical information. Changes in accessing clinical infor-mation was significantly related to self-reported enhancement ofthe clerkship due to PDA use.
However, whether PDA use can improve objective assessments ofstudents’ educational achievements such as exam scores is stillunknown. Subjectively, on self-reported measures, students reportthat they like the PDA format and that the PDA improved theirexperience.
volume 83, number 1, December 2005 47
Table 1Popular PDA Software for Medical Students
Title DescriptionHarrison’sManual of Medicine An electronic version of the popular internal medicine textbook. It covers topics in therapeutics, signs and($60 USD) symptoms, differential diagnosis, clinically relevant pathophysiology, clinical manifestations, lab findings and
practice guidelines. (www.unboundmedicine.com)
Griffith’s 5 Minute Clinical Consult This is another PDA version of a popular textbook. It contains facts on more than 1,000 medical and surgical($65 USD) conditions and is indexed with more than 7,500 terms and medications. (www.skyscape.com)
DrDrugs ($50 USD) DrDrugs includes over 4500 trade and generic drugs, nearly 130 drug classifications, over 1000 drug monographs, including the dosage amount of the active generic ingredient as well as information on drugaction and interactions. Each drug file is divided into 15 different sections of information.(www.skyscape.com)
LexiDrugs ($75 USD) Viewed as the most comprehensive drug database covering 1600 drug monographs covering over 7000 U.S.and Canadian brand names. The information for each drug is under 24 categories. More comprehensive thanDrDrugs, but higher-priced. (www.lexi.com)
Stedman’s Concise Medical Dictionary This technical dictionary includes 51,000 terms, has clearly written definitions, features common prefixes, ($35 USD) suffixes and combining forms
Sanford Guide to Antimicrobial Therapy This infections disease reference software has the same content as the reference text and includes ($30 USD) ambulatory, inpatient, adult and pediatric information. It is evidence-based and has extensive reference
citations. (http://handheld.medicine.dal.ca)
Netter’s Anatomy Flashcards A useful study aid for students, this program contains over 350 high resolution anatomy images, covering all($50 USD) body areas

University of Toronto Medical Journal48
Table 2Canadian Medical School Handheld Websites
McMaster University: http://hsl.mcmaster.ca/resources/pda/
McGill University: http://www.health.library.mcgill.ca/research/pda/
UBC:
http://www.cme.med.ubc.ca/scripts/index_.asp?action=31&U_ID=0&P_ID=5635
University of Alberta: http://www.library.ualberta.ca/pdazone/health/
University of Calgary (Rural Medicine):
http://www.ruralnet.ab.ca/medinfo/handheld/
University of Ottawa:
http://www.medicine.uottawa.ca/medtech/laptop/eng/palm.html
University of Toronto: http://www.library.utoronto.ca/gerstein/pda/
Dalhousie University: http://handheld.medicine.dal.ca/
At the University of Toronto, the PDA program began in 2003.The Gerstein Science Library first attempted to identify whichsoftware they should license to be of most use to medical students.Because there were numerous software options available, and agreat deal of overlap between the options, this was a difficult task.In contrast to the past, where science libraries were able to focustheir efforts on acquiring high quality and peer-reviewed researchmaterials, the PDA market consists predominantly of republishedinformation, distilled from many sources and reformatted for thepurpose of making information faster and easier for the user toaccess. For the first time, the library had to consider ‘ease of use’,software memory usage and PDA platform.
With so many software options, the library chose to target theundergraduate medical student – focusing on software designed toaid the student on the ward. In addition, they were cognizant of thefact that the student’s pocket book is not as large as the profes-sional’s or the clinician’s. Specifically, the library decided to focuson two kinds of content: drug information and basic disease &condition information. When considering the obvious overlapbetween the various software publishers, the library put its empha-sis on the software that was most frequently updated and moststrongly supported evidence-based approaches.10
Costs and Implementation IssuesEducational institutions are constantly struggling with the signifi-cant costs associated with new technologies. For PDAs, the infra-structure set-up costs, including technical support and data analy-sis (in the case of student logging), represent the largest burden.The per-use cost of PDA technology is relatively small. A studyat Columbia University on procedure logging estimated the aver-age cost per student over four years to be approximately $9 USDfor the PDAs, compared to US$15 for an optical scanning cardsystem.8 These cost estimates were based on purchase costs ofPDAs, design and printing of scan cards and software; they do notreflect the purchase or maintenance of the optical scanner, whichwould further magnify the price difference. At many schools,medical students are required to purchase their own PDAs, furtherreducing the financial burden for the university.
PDA Use in Canadian Medical SchoolsWith recent advances in PDA technology, more physicians andmedical students are using PDAs. As a result, medical schoolsare establishing networks that support PDA use by their students.Dalhousie University and the University of Calgary are two exam-ples of Canadian medical schools that have established programsfor handheld computing in medical education.
Dalhousie University recognized the increasing popularity of PDAsin the medical field and established a committee in 2001 to reviewand provide up-to-date recommendations of handhelds and theirsoftware in relation to medicine. The most recent review tookplace in 2005 and the review recommendations have recently beenmade public on their website.8 In addition to forming a reviewcommittee, Dalhousie University developed a website called“mobileMedix” that is better suited for PDAs that are capable ofwireless connection to the internet. Commonly, websites seen ondesktop computers are too large for the small screen of a hand-held. In contrast, mobileMedix is a text-only site, designed specif-ically for small screens. Through mobileMedix, medical studentscan find information regarding curriculum, evaluations, telephonedirectories and pertinent news related to their education.
The University of Calgary began their PDA initiative by providingall first-year medical students with a Palm handheld (PalmTungsten C). The PDA initiative began with the class of 2006.To complement the PDA initiative, the University of Calgarydeveloped the Curriculum Information System (CIS). The CIS issimilar to Dalhousie’s mobileMedix in that it is a website consist-ing of class schedules, telephone directories and updates. The CIS,however, is more extensive and provides access to course notes,discussion forums and other web-based medical references such asdigital libraries. The PDA initiative has been running for the pastthree years and has received positive feedback from the studentbody.
In addition to taking advantage of the capability of handhelds toconnect with the internet and their large storing capacity for ref-erence materials, handhelds are also being used in Canadian med-ical education to monitor the student’s clinical experiences. TheUniversity of British Columbia introduced this monitoring pro-gram to third-year medical students during their PaediatricClerkship. One objective of this program was to allow the clerksupervisors to monitor their clerks and ensure that all the requiredskills were learned in a timely manner.
Handhelds are becoming more common in the medical field.Although not all schools have provided support for PDAs likeDalhousie University and the University of Calgary, many schoolsdo recognize the more prominent roles of PDAs with the num-ber of schools providing a website indexing useful PDA resources(Table 2). In order to encourage the medical students’ use of PDAtechnology and help to alleviate the financial burden of buyingexpensive medical software, many Canadian universities have alsobegun to buy general licenses for the more popular programs.

The Future of PDA’s in Medical EducationToday, PDAs continue to command a significant portion of thetechnology market: sales of PDAs worldwide increased by 25% inthe first three months of 2005, compared to the same period ayear earlier, to 3.4 million units.11 Similarly, handheld computingwithin the medical profession is becoming ubiquitous: in 2003, theCMAJ reported that 53% of physicians under the age of 35 usedPDAs as part of their medical practice.12 That number has almostcertainly increased in the past two years.
For medical students in particular, PDAs have become an essen-tial tool independent of required curricular uses. It is simply con-venient to carry several thick textbooks in a device that weights acouple hundred grams and fits into a small pocket and the orga-nizational tools are useful for medical students, just as they are forany busy person. But PDAs can provide much more for medicaleducation than simply a high tech agenda book and miniaturebook reader. As discussed earlier, logging medical procedures elec-tronically improves accuracy and allows for timely feedback.Electronic drug guides can be updated much more frequently thanpaper ones, and interactive tools can help students to learn.
Portable digital assistants, like all technology, are quickly evolving.We are currently seeing three notable improvements that have sig-nificant potential to change how medical students interact withhandheld computing. First, the quantity of storage space availablein a typical PDA is increasing tremendously. With the continuingdrop in prices for external memory such as Secure Digital cards,and the introduction of PDAs with a larger built-in memory capac-ity such as palmOne’s LifeDrive™, this limitation is quickly dis-appearing. Students will no longer have to choose which textbookor programs are most essential – they will have room for all ofthem.
Secondly, the ability of handhelds to connect to the internet, otherexternal sites or to each other has been gradually improving.While many new handhelds feature WiFi or Bluetooth wirelessaccess, it is still typical to transfer most information to the PDAthrough hardwired synchronization with a desktop computer, andaccess to the internet is limited. With widespread wireless accessbecoming more common in clinical settings, fully up-to-date med-ical information will be constantly available.
Lastly, the introduction of “convergence” devices has given fargreater utility to the PDA. It is now possible to purchase a PDAwith the additional features of a cellular phone, a music player anda camera within the price range of the typical medical student. Asmore functions become combined into the same small package, itbecomes difficult to even guess what capabilities these devices mayprovide in the future. What remains certain is that the availabili-ty of handheld computers and ready access to information in anysetting has changed medical education and will continue to do so.
References1. Parkerson GR Jr, Baker C. Clinical experience of medical students in North
Carolina family medicine preceptorships. J Med Educ. 1980;55(1): 42-7.2. Rattner SL, Louis DZ, Rabinowitz C, Gottlieb JE, Nasca TJ, Markham FW, et al.
Documenting and comparing medical students’ clinical experiences. J Am Med
Assoc. 2001;286(9): 1035–1040.3. Kowlowitz V, Slatt LM, Kollisch DO, Strayhorn G. Monitoring students’ clinical
experiences during a third-year family medicine clerkship. Acad Med. 1996;71(4):387-9.
4. Kurth RJ, Irigoyen MM, Schmidt HJ, Li S. The effects of patient characteristicsand practice settings on students’ participation in a primary care clerkship. Acad
Med. 2000;75(6): 634-8. 5. McVeigh S, Williams R, Pangaro L. An Internet home page to log students’ patient
contacts. Acad Med. 1997;72(5): 417-8.6. Engum SA. Do you know your students’ basic clinical skills exposure? Am J Surg.
2003;186(2): 175-81.7. Kurth RJ, Silenzio V, Irigoyen MM. Use of personal digital assistants to enhance
educational evaluation in a primary care clerkship. Med Teach. 2002;24(5): 488-90.8. Dalhousie University Faculty of Medicine [homepage on the Internet]. Halifax:
c2003-2005 [updated 2005 April 18; cited 2005 October 12]. Recommendations forHandheld Hardware and Software; [about 35 screens]. Available from: http://hand-held.medicine.dal.ca/.
9. Sutton J, Stockton L, McCord G, Gilchrist VJ, Fedyna D. Handheld computer usein a family medicine clerkship. Academic Medicine. 2004;79(11): 1114-9.
10. Rita Vine. E-Health Specialist, Gerstein Science Information Centre, University ofToronto. October 12, 2005. Personal Communication.
11. Lemon S. PDA sales increase sharply: Driven by demand for wireless devices, ship-ments hit a new high, researcher says. PC World [serial on the internet]. 2005 May[cited 2005 October 12]; [about 1 p.]. Available from:http://www.pcworld.com/news/article/0,aid,120698,00.asp.
12. Martin S. More than half of MDs under age 35 now using PDAs. CMAJ.2003;169(9): 952.
volume 83, number 1, December 2005 49
University of Toronto Medical Journal50
the structure of the health care system. In this section, we willpresent an analysis of the aforementioned culprits by focusingon the Indian experience.
In the second half of the twentieth century, the life expectan-cy in India rose from 41.2 years in 1951-1961 to 61.4 years in1991-1996 – a major surge indeed.8 This was of course a suc-cess story: significant decline in mortality rates in infancy, child-hood, and adolescence were realized due to more effective pub-lic health responses to perinatal, infectious and nutritionaldeficiency disorders. Improvement in social and economicindicators (per capita income, female literacy) further augment-ed the effect. Ironically, such increased longevity, hard earnedthough it may have been, elevated the ranks of middle-aged andolder adults. This in turn made possible longer periods ofexposure to the risk factors of CVD and increased the proba-bility of clinically manifest CVD events.9 Thus, the modernepidemiological transition from infectious and nutritional dis-eases to CVD and chronic illnesses occurred in India as it didelsewhere in the developed world. It is speculated that half ofdeaths in India by the year 2015 will likely be caused by coro-nary artery disease alone, a figure of disastrous epidemic pro-portion.
The impacts of epidemiological transition are likely augmentedby the lifestyle changes in the Third World. Industrialization,urbanization, globalization ... the seemingly progressive devel-opments of the modern world have often been unkind to lessprivileged countries. India, often acknowledged as an “eco-nomic power”, has not been immune to these trends.Substantially higher levels of CVD risk factors (higher levels ofbody mass index, hypertension, physical inactivity, higher pro-portion of cholesterol and triglycerides and diabetes) and coro-nary heart disease have been observed among the urban Delhiresidents when compared to their rural counterparts.10 Theever-increasing use of tobacco in India will further augment themortality rates of CVD,11 which will rise beyond the rates pre-dicted from demographic changes alone.
A further side effect of urbanization and globalization of foodproduction and marketing is the dietary/nutritional transitionobserved in the Third World. India, in fact, embodies this dis-
Contemplation…Although cardiovascular disease (CVD) is often thought of asa disease of affluence, its brunt is increasingly being borne bydeveloping countries. India, the world’s second most populouscountry, has been particularly hard hit by the CVD epidemic.There were 2.3 million CVD-related deaths in India in 1990. By2002, CVD accounted for 2.8 million deaths per year and isexpected to cause nearly 5 million deaths by 2020.12 Studies sug-gest that Indians may have greater genetic susceptibility to CVDthan other ethnic groups.3 In addition, increased life expectan-cy has led to a progressive aging of the population.Consequently, chronic degenerative diseases such as CVDaccount for a growing proportion of total morbidity and mor-tality.4 Furthermore, like many developing countries, India isundergoing rapid urbanization. The accompanying changes indietary patterns, occupation and lifestyle are thought to beimportant contributors to the rapidly rising prevalence ofCVD.5 This article provides a brief overview of the epidemiol-ogy and risk factors of CVD in Indians, and it assesses the pre-ventive efforts of India’s health care system.
Researchers have been investigating the epidemiology of CVDin Indians since the 1960s, with much of their research focus-ing on coronary artery disease – a subset of CVD. Studies inIndia have established the prevalence of coronary artery diseaseas 7.6%-12.6% in urban areas, and 3.1%-7.4% in rural areas. Aplausible explanation for the urban-rural gradient is the lowerrisk factors in rural areas.6 In addition, the proportion of CVD-related mortality at an earlier age is considerably higher inIndians (52.2% of deaths at <70 years) than in established mar-ket economies (22.8%).7 Despite considerable research in thisarea, analysis and comparison across studies remain limited bydifferences in methodology and criteria for the diagnosis ofCVD, paucity of large prospective cohort studies and theunder- representation of women.
Enigma Unravelled...The Third World contributes more than two thirds of theworld CVD mortality. To understand this unexpected shift inthe global patterns of CVD, one must consider several para-meters such as epidemiological transition, lifestyle changes,nutritional transition, tobacco trends, role of genetics as well as
The Indian Paradox: An Emerging Epidemic of Cardiovascular Disease
Behzad Hassani, H.B.A. (OT8)
Adnan Jalal, B.Sc. (OT8)
International Health

ruptive development. Although the increased use of cheap veg-etable oils and fats can be seen among all developing nations,the Indian diet has been hit hardest. The traditional SouthAsian diet is high in complex carbohydrates and proteins andlow in fat. Modern Indian diet shows an overall decline in theproportion of calories derived from complex carbohydrates tothe advantage of the proportion derived from saturated fats.12
Frying in saturated fats and heavy seasoning in salt are com-mon and excessive themes in Indian cooking.13 The result isan energy-dense diet poor in dietary fiber and micronutrients.
Among the vices of civilization, tobacco is by far the deadliest.Although developed nations have managed to reduce tobaccoconsumption in the past decades, a sharp rise is seen in thedeveloping world. It is postulated that in India alone, thetobacco-attributable death toll will rise from 1.4% in 1990 to13.3% in 2020, a significant component of which will manifestas CVD.14 At this point, a word must be said about the mar-keting efforts of the trans-national tobacco corporations in theThird World.15 The tobacco industry has been trying to makeup for stagnating sales in the USA by creating markets in theThird World countries that provide a much more favourablepolitical and social climate for business.16 In addition, the lackof awareness of the health risks of tobacco and the scarcity ofanti-smoking campaigns further the cause of the industry. Theoutcome is a fertile market for this prestigious product import-ed from the West. The US government has been involved inthis problem: millions of dollars of Commodity CreditCorporation loans and price supports have gone to tobaccogrowers of the Third World; surplus tobacco has been pur-chased by the government from the US distributors and sup-plied to the developing countries; and US trade policy hasexerted sanctions against Asian countries who have refused toimport tobacco from the American corporations.17 This cam-paign may very well be called “a new opium war”18 on Asia.To further add salt to a devastating wound, the tar and nico-tine, removed from the American cigarettes, have been ‘recy-cled’ into the products bound for the Third World.19
Furthermore, a role for genetic predisposition to CVD amongIndians may be proposed. Several studies have focused on thedisturbingly high incidence of CVD in Asian Indians livingabroad.20,21 In a recent London study, much higher numbers ofmetabolic derangements were seen among South Asians com-pared to the Europeans. The signs included hypertension,higher waist-hip ratio, and higher fasting blood levels of triglyc-erides, glucose and insulin. A recent US study reported preva-lence rates of CVD and associated risk factors that were threetimes more frequent in Asian Indian men compared to theFramingham Study population. Higher levels of lipoprotein (a)and elevated incidence of postprandial hyperlipidemia andmetabolic syndrome were also observed among South Asians.However, note that these findings, although suggestive ofgenetic involvement, do not preclude a role for dietary orlifestyle factors.
Who is My Brother’s Keeper?In the midst of this inevitable epidemic, it is critical for us toassess the status and capability of the health care system inIndia. The deaths of 15 children in a public hospital in the EastIndian state of West Bengal in 2002 flamed a debate on thecompetence of the Indian health care system.22 Dr. Amit SenGupta, the spokesman of India’s Public Health Campaign, com-mented on the event in an interview with the BBC, “The inci-dent has taken place in a metropolitan city therefore there is somuch of media attention. The main point is that basic healthcare is almost non-existent in rural areas.” Gross overcrowd-ing is a common theme in the country’s public sector hospitalsthat serve the less privileged classes of the Indian society. Thecentral government, that pours billions into India’s nuclearweapons programs, spends less than 0.09% of the GDP onhealth care. Sixteen percent of the health care expenditure isthe contribution of the state, and the remaining 84% comesfrom the private sector.23 The Indian constitution envisions awelfare state that embodies the ideals of equality and social jus-tice. Those lofty ideals are for now just that – ideals!
In brief, India is not prepared to cope with this booming epi-demic. Health care facilities that would be capable of provid-ing appropriate acute and long-term management programs arefew. The concept of prevention is lacking. The two-tier sys-tem of health care delivery discriminates against the vast pop-ulation who live far below the poverty line. Intuitively, pooreducational and economic status is associated with higher riskof CVD in the Indian population.24 As is often the case, theworst off are the most vulnerable and the least protected.
IlluminationDespite all, hope strives in the midst of despair. The low lev-els of traditional CVD risk factors among the rural populationof India may offer a window of opportunity for the control ofthe CVD epidemic. Comprehensive population based policiesshould, therefore, be formulated that emphasize primordial andprimary prevention. This strategy, which is more cost-effectivethan a pharmacological approach, may benefit from the exist-ing primary health care and social welfare channels that haveoutreached at the grass-roots level. In addition, health profes-sionals at primary and secondary care settings should haveaccess to inexpensive, effective interventions such as aspirin.They should also be encouraged to adopt suitable clinical algo-rithms for diagnosis. Finally, it should be ensured that tertiarycare practices optimize resources, avoiding heavy investment inexpensive but low-yield technologies.25,26 The prevention ofCVD is a daunting task that will require the sustained involve-ment of individuals, communities, health policy makers andother key stakeholders.
References1. Murray CJ, Lopez AD. The global burden of disease: A comprehensive assess-
ment of mortality and disability from diseases, injuries and risk factors in 1990and projected to 2020. Boston: Harvard School of Public Health; 1996.
2. World Health Organization. Global Burden of Disease Estimate 2002. Availablefrom: http://www3.who.int/whosis/menu.cfm?path=evidence,burden.
volume 83, number 1, December 2005 51

University of Toronto Medical Journal52
14. World Health Organization. Tobacco or Health? First Global Status Report.World Health Organization. Geneva, Switzerland; 1996.
15. Baer HA, Singer M, Susser I. Legal Addictions, Up in Smoke. In MedicalAnthropology and the World System: A Critical Perspective. Westport,Connecticut: Bergin & Garvey; 1997. p.102-125.
16. Chapman S, Leng WW. Tobacco control in the third world: a resource atlas.Penang, Malaysia: International Organisation of Consumers Unions; 1990.
17. Baer HA, Singer M, Susser I. Legal Addictions, Up in Smoke. In MedicalAnthropology and the World System: A Critical Perspective. Westport,Connecticut: Bergin & Garvey; 1997. p.102-125.
18. Ibid.19. Ibid.20. Enas EA, Yusuf S, Mehta JL. Prevalence of coronary artery disease in Asian
Indians. American Journal of Cardiology. 1992;70: 945-949.21. Enas EA, Garg A, Davidson MA, et al. Coronary heart disease and its risk
factors in first-generation immigrant Asian Indians to the United States ofAmerica. Indian Heart Journal. 1996;48(4):343-53.
22. Singh J. India’s deteriorating health care system. BBC News Online September3rd. [c2002]. [cited 2005 Sept 11]. Available from: http://news.bbc.co.uk/.
23. Ibid.24. Gupta R, Gupta VP, Ahluwalia NS. Educational status, coronary heart disease
and coronary risk factor prevalence in a rural population in India. British Medical
Journal. 1994;307:1332-1336.25. Reddy KS, Yusuf S. Emerging epidemic of cardiovascular disease in develop-
ing countries. Circulation. 1998;97(6): 596-601.26. Nishtar S. Prevention of coronary heart diseases in south Asia. Lancet.
2002;360(9338):1015-8.
3. Gopalan C. Rising incidence of obesity, coronary heart disease and diabetes inthe Indian urban middle class. Possible role of genetic and environmental fac-tors. World Rev Nutr Diet. 2001;90:127-43.
4. Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular dis-eases: Part II: variations in cardiovascular disease by specific ethnic groups andgeographic regions and prevention strategies. Circulation. 2001;104(23):2855-64.
5. Gopalan C. Rising incidence of obesity, coronary heart disease and diabetes inthe Indian urban middle class. Possible role of genetic and environmental fac-tors. World Rev Nutr Diet. 2001;90:127-43.
6. Bahl VK, Prabhakaran D, Karthikeyan G. Coronary artery disease in Indians.Indian Heart J. 2001;53(6): 707-13.
7. Murray CJ, Lopez AD. Global comparative assessments in the health sector. Geneva:World Health Organization, 1994.
8. World Bank. World Development Report: Investing in Health. New York, NY:Oxford University Press; 1993.
9. Reddy KS. Cardiovascular disease in India. World Health Stat Q. 1993;46:101-107.
10. Bahl VK, Prabhakaran D, Karthikeyan G. Coronary artery disease in Indians.Indian Heart J. 2001;53(6): 707-13.
11. Chapman S, Leng WW. Tobacco control in the third world: a resource atlas.Penang, Malaysia: International Organisation of Consumers Unions; 1990.
12. Lang T. The public health impact of globalization of food trade. In: ShettyPS, McPherson K, eds. Diet, Nutrition and Chronic Disease: Lessons FromContrasting Worlds. Chichester, UK: Wiley; 1997. p. 173-187.
13. Ahmed S. Coronary heart disease: the Indian Asian diet. Nursing Standard.1999;13(27), 45-47.

AbstractComplementary and alternative medicine (CAM) is widelyused throughout Canada, yet most physicians know littleabout these therapies and may find it difficult to talk to theirpatients about their use. As part of a national initiative todevelop curricula on CAM for undergraduate medical edu-cation programs, an anonymous questionnaire was distrib-uted to all first and second year medical students in Canadain order to assess their comfort with, beliefs about, and expo-sure to CAM. The average response rate was 44%, rangingfrom 4% to 79% across schools. Although 89% of all stu-dents reported that they would ask their future patients aboutCAM, only 45% indicated that they currently felt prepared todiscuss CAM with patients or colleagues. Eighty-four pere-cent agreed that CAM research must meet the same stan-dards as conventional research to be valid and acceptable,but only half agreed that a therapy that has not been provenby western science should not be recommended to patients.Across schools, students agreed that there is a need forincreased CAM curricula in UME, yet only 25% of respon-dents reported receiving CAM education (range from 1% to84%). Results of this questionnaire highlighted the interestand expectation of pre-clerkship medical students in Canadato learn about CAM and to apply this knowledge in theirfuture practice.
IntroductionComplementary and alternative medicine (CAM) is a group ofdiverse medical and health care systems, practices, and productsthat are not presently considered to be part of conventional med-icine.1 Examples of CAM are acupuncture, ayurveda, chiropractic,natural health products, and homeopathy. Although individualscommonly report wanting to talk to their physicians about the useof CAM, they tend not to do so.2-5 Reasons for this lack of com-munication include physicians not asking patients about their CAMuse as well as patient perceptions that (a) their physician will notapprove of their CAM use, (b) their CAM use is not relevant infor-mation for their physician, and (c) their physician lacks knowledgeabout CAM.
Although studies do show that knowledge about CAM is lackingamongst practicing physicians, there is ample research that shows
that physicians are interested in learning more about CAM, includ-ing wanting more attention paid in undergraduate, graduate, andcontinuing education courses.6-9 Moreover, the public’s demandfor CAM has spurred some physicians to make referrals to com-plementary and alternative practitioners, to provide these services,and to take the initiative to become educated regarding the safety,efficacy and assumptions of CAM approaches.3,10,11
Medical student surveys also indicate that students (1) lack knowl-edge about CAM, (2) want to become more familiar with CAM intheir undergraduate medical education, but (3) become less inter-ested in knowing about CAM as they progress through medicalschool.12,13
In 1999, Ruedy et al., reported that 81% (13/16) of Canadian med-ical schools included CAM in their curriculum.14 However, theyprovided few details in their study about the depth and breadth ofCAM inclusion in undergraduate medical education (UME) pro-grams. We know from our own research, conducted as part of alarge-scale effort to generate and collate CAM curriculum forUME programs, that there is tremendous variability acrossCanadian medical schools in CAM content.15,16 For those schoolsthat offer some CAM teaching, integration into the existing cur-riculum is limited with most teaching being “add on” and elective.At the same time, there is an identified need and a strong desirefor CAM education that focuses on definitions, evidence, safety,doctor-patient communication, and attitudes/respect.
Many stakeholders are involved in the process of changing med-ical school curriculum including deans, curriculum committees,administrators, teaching faculty, and medical students. While theremay have been brief local surveys of medical students, to datethere has not yet been a national survey of medical students inCanada about CAM. Consequently, we surveyed pre-clerkshipmedical students in the 16 Canadian schools about CAM in orderto document student interest and involvement with CAM, and toidentify specific CAM curricular needs in this area. To this end, we asked medical students about their:1 comfort in discussing CAM, 2 general beliefs about CAM research and evidence, and3 exposure to, and opinions about, CAM education in UME.
volume 83, number 1, December 2005 53
Survey of First and Second Year Medical Students’ Familiarity and
Comfort with Complementary and Alternative Medicine
Rebecca Brundin-Mather, MAScVishal Avinashi, MDMarja Verhoef, Ph.D.
Complementary and Alternative Medicine

University of Toronto Medical Journal54
Don’t Know) to a four category format. In addition, one questionon licensing was modified to reflect the Canadian context, anditems added that asked more detailed feedback about CAM edu-cation in UME. The questionnaire was translated from English toFrench in order to survey students attending Université deSherbrooke, Université Laval, and Université de Montréal. Thequestionnaire was reviewed by several members of the CAM inUME project advisory group prior to being distributed.
Descriptive analyses were conducted on all the questions. Chisquare analyses and t-tests were conducted to compare first andsecond year responses to each question. Although between-schooldifferences were not statistically analyzed due to the extreme vari-ability in response rate across schools and the lack of homogene-ity of variance within some schools, some school differences willbe reported where relevant.
This study was approved by the University of Calgary ConjointHealth Research Ethics Board and the Saskatchewan BehaviouralResearch Ethics.*
ResultsAll 16 medical schools agreed to participate in the survey. Themean response rate was 44%, though the response rate varied
Materials and Methods
ParticipantsThere were approximately 3500 first and second year medical stu-dents attending Canada’s 16 medical schools at the time of the sur-vey. To facilitate distribution of the questionnaire, school repre-sentatives were recruited from the Canadian Federation of MedicalStudents (CFMS) and the Fédération des étudiants medicines duQuébec (FEMQ). Given that medical students are typically over-surveyed and less likely to respond to questionnaires left in theirmail box, each school representative was asked to hand out thequestionnaire to first and second year students at the end of amandatory class. As this was not possible for all third and fourthyear classes, they were excluded from the sample population.Participation in the study was voluntary. The questionnaire wasanonymous and took approximately 5 minutes to complete. Asan incentive, a cash prize of $200 was offered to the school withthe highest percentage of completed questionnaires.
QuestionnaireQuestions on the two page survey were predominantly drawnfrom an unvalidated 10-item questionnaire developed at theUniversity of Maryland Complementary Medicine Program.17 TheComplementary Therapies Questionnaire was designed for medical stu-dents, and serves as a course evaluation tool as well as a generalsurvey of knowledge and attitudes. The Maryland questionnairewas modified by changing the three-category format (Yes, No, and
•As Dr. Avinashi was a medical student at the University of Saskatchewan at the time ofour ethics submission. Thus, as a co-investigator on this project, we required ethicsapproval from his home institution.
Figure 1. Survey response rate of first and second year medical students.

across schools from 4% at the University of British Columbia to79% at Memorial University of Newfoundland (Figure 1). In addi-tion to low response rates, not all schools returned surveys fromboth 1st and 2nd year students. Of the 1641 students whoresponded, 716 were first year students and 925 were second yearstudents. There were no statistically significant differencesbetween first and second year student responses to surveyquestions.
General KnowledgeFirst and second year medical students estimated on average that44% of the Canadian population uses CAM, and that 52% ofpatients do not tell their physician that they use CAM. Moststudents reported that between 2 and 4 of the 13 provincial andterritorial licensing authorities in Canada have policies addressingphysician practice of CAM and/or physician referral to CAMpractitioners.
Comfort with CAM and General Beliefs about CAM EvidenceSeventy-five percent of all first and second year medical students
agreed or strongly agreed that patients should first see a medicaldoctor before undergoing CAM treatment(s), and 92% felt thatmedical licensing boards should have written policies addressingphysician practice of CAM and/or physician referral to CAM prac-titioners. Table 1 presents the total student response rate on ques-tions assessing their comfort with CAM and their beliefs aboutCAM evidence. There was generally greater dispersion of scoresacross the four response categories on questions ‘current scientif-ic evidence supporting CAM is scanty and poor,’ ‘should not rec-ommend a therapy that is not proven effective by western science,’and on ratings of ‘feeling prepared to discuss CAM with patientsor colleagues.’ Across schools, the aggregate agreement score var-ied between 30% and 66% on these questions, with the greatestrange on feeling prepared to discuss CAM (from 23% at McMasterUniversity to 89% at Université de Laval).
Table 2 presents the results of student ratings of the safety andeffectiveness of nine CAM areas. The question format permittedstudents to check each therapy as (a) safe, (b) unsafe, (c) effective,(d) ineffective, and/or (e) one that they personally had used. With
volume 83, number 1, December 2005 55
Table 1Medical students’ ratings of their comfort with CAM and beliefs about CAM research.
Survey Question Strongly Disagree Disagree Agree Strongly Agree
When I am in practice, I will always ask my patients 1% 9% 52% 37%about their use of CAM
When I am in practice, I think I will feel comfortable 1% 4% 49% 45%asking patients about their use of CAM
I feel prepared to discuss one or more forms of CAM 14% 31% 36% 17%with patients or colleagues
CAM research must meet the same standards as 2% 13% 46% 38%conventional research to be valid and acceptable
Current scientific evidence support CAM is scanty and poor 3% 31% 51% 12%
Should not recommend a therapy that is not proven 5% 39% 42% 13%effective by western science
Table 2Medical students’ ratings of the safety, effectiveness, and personal use of CAM
Complementary Therapy Safe Unsafe Effective Ineffective Personally Use
Massage 82% 2% 69% 7% 33%
Prayer/Spiritual Healing 76% 2% 44% 22% 14%
Acupuncture 72% 10% 56% 12% 11%
Mind-Body Therapies 66% 4% 35% 22% 5%
Vitamins 65% 15% 57% 13% 34%
Hypnosis 53% 12% 26% 33% 2%
Homeopathy 48% 16% 20% 40% 9%
Chiropractic 42% 37% 47% 18% 19%
Herbs 35% 38% 36% 24% 14%

University of Toronto Medical Journal56
these two groups in their ratings of feeling prepared to discussCAM.
Table 4 presents medical student ratings of the usefulness ofseven teaching methods in helping prepare them to advisepatients about CAM. The top two teaching methods that stu-dents rated as ‘useful’ or ‘very useful’ were lectures and text-book readings, while using CAM to promote one’s own healthwas most frequently reported as ‘somewhat useful’ or ‘not at alluseful.’
Discussion and ConclusionThe push for increased curriculum about complementary andalternative medicine in undergraduate medical education is notnew. In many medical schools, medical students have, in fact,been the dominant driving force of curriculum.15 This ques-tionnaire was the first national survey of Canadian medical stu-dent’s attitudes and beliefs about CAM as well as opinions ofCAM education in UME. Although our response rate was lowin some medical schools, the results mirror similar surveys inthe published literature. There is clearly a willingness on thepart of first and second year medical students to discuss CAMwith their patients. However, whether this positive attituderemains throughout medical school and even residency cannotbe answered in this study. There is some evidence in the lit-erature to suggest that as medical students progress throughtheir training, they become more skeptical towards CAM.13 Amore inclusive cross-sectional design or a longitudinal designthat surveys students at multiple time periods throughout theirtraining would provide important information in this area.
Although the students in this survey know the prevalence ofCAM use in Canada and the average rate of non-disclosure ofCAM use to physicians, they appear to lack knowledge aboutthe growing evidence base on CAM therapies. There is per-haps greater caution on questions requiring more specificknowledge of CAM research with 84% of all medical studentsagreeing or strongly agreeing that CAM research must meet thesame standards as conventional research to be valid, and only55% agreed or strongly agreed that a therapy that is not provenby conventional standards should not be recommended. Fivepercent of all participants (7% of first year and 4% of secondyear) did not attempt to assess the safety and effectiveness ofthe nine complementary therapies, quite possibly because theydid not feel that they had the knowledge to rate the therapies.Certainly, there were many students, particularly in some med-ical schools, who reported that they did not currently feel pre-pared to discuss CAM with patients or with colleagues.
A lack of preparation and/or knowledge about CAM is notsurprising given that only a quarter of students reported receiv-ing formal CAM education. At the same time, a comparisonof students who reported receiving formal CAM and those whodid not shed little light on whether CAM education impacts onstudents comfort with CAM or perceptions and knowledge ofCAM. Given that there may also be a social desirability biason the part of some participants, future research should exam-
this approach, the percentages in “safe” and “unsafe” and “effec-tive” and “ineffective” may not add up to 100. Although not aone-to-one correspondence, the therapies most frequently rated assafe and effective were also least likely to be rated as unsafe andineffective. Massage was most frequently rated by students as safeand as effective, herbs as unsafe, and homeopathy as ineffective.Fifty-nine percent of students reported having used some CAMpersonally, most frequently citing vitamins and massage.
Exposure to, and opinions about, CAM in UMEEighty-seven percent of all students agreed or strongly agreed thatthere is a need for increased CAM curricula in undergraduate med-ical education. Across schools, the combined percentages rangedfrom 71% at UBC to 96% at Dalhousie. Overall, 25% of partic-ipants, 18% of first year and 30% of second year, reported receiv-ing some formal CAM education. Yet the variability betweenschools was extreme with reports ranging from 1% at Universitéde Sherbrooke to 84% at University of Western Ontario (see Table3). Of the 430 students who reported receiving CAM education,73% agreed that this education was useful in making them feelmore comfortable with discussing the topic with patients, but only46% were satisfied with the content and delivery of theinstruction.
Table 3Medical students’ reports of having
received CAM education
School Yes No Don’t Know
Western Ontario 84% 15% 2%
Saskatchewan 54% 44% 3%
Memorial 49% 47% 4%
Manitoba 46% 49% 5%
McGill 36% 60% 4%
Queen’s 21% 74% 6%
Dalhousie 19% 80% 1%
Montreal 16% 81% 3%
Laval 10% 88% 2%
McMaster 9% 90% 1%
Alberta 9% 91% 0
Toronto 8% 92% 0
Ottawa 7% 91% 2%
Sherbrooke 1% 99% 0
Explorative analyses on the sub samples of students who hadreceived CAM education and those who did not producedsome interesting results. In some schools, such as theUniversité de Sherbrooke where essentially no students report-ed receiving formal CAM education, 85% of students agreed orstrongly agreed that they felt prepared to discuss CAM withpatients and colleagues. Ninety-four percent of students whohad not received any education in CAM agreed that they wouldalways ask their patients about CAM and would feel comfort-able doing so. There were no significant differences between

volume 83, number 1, December 2005 57
ine the nature and duration of CAM education in order to drawmore solid conclusions.
CAM in UMEIt is encouraging that 87% of students who responded to this ques-tionnaire see a need for increased CAM in UME. Furthermore,this study provides insight into teaching methods that may bestimpact student learning about CAM. Although lectures are ratedas useful by most students, other more experiential approaches thatmay make a more lasting impact in acquired knowledge, skills, andattitudes also appear to be desirable. In responding to suggestionsfor CAM-related topics to include in UME, many students com-mented that education about CAM should be evidence-based.Forjuoh et al. reported initial success with teaching medical studentsabout CAM using evidence-based medicine principles as a vehicle.18
This approach served two important UME learning objectivesincluding (1) how to read, understand, and appraise the medical lit-erature, and (2) knowing about CAM. Folding CAM into a moremainstream concept such as evidence-based medicine may also easeits integration into undergraduate medical education programs.
While the response rate was too low in some schools to generalizeto all first and second year medical students, it is apparent that themajority of students who responded to this survey are interested inknowing about CAM and expect to receive this education duringtheir undergraduate training in order to discuss it with patients.Within the past five years there has been an increase in CAM cur-riculum development in medical schools across Great Britain,19,20
the European Union,21 the United States,22,23 and Canada.16 Suchcurriculum changes are partially based on the belief that doctorsmust have an understanding of all the health services their patientsmay be accessing, particularly in order to appropriately assess andrespond to potential interactions between various health treatments.The results of this survey provide further support from an impor-tant stakeholder group that medical schools in Canada must con-tinue to work to integrate CAM into UME.
AcknowledgmentsWe wish to acknowledge the assistance of the school representa-tives to the Canadian Federation of Medical Students and theFédération des étudiants medicines du Québec who distributed and
collected the questionnaires on our behalf. This study was madepossible through a grant from the Canadian InterdisciplinaryNetwork for Complementary & Alternative Medicine Research.
References1. National Center for Complementary and Alternative Medicine. Bethesda: National
Institutes of Health. Get the facts: What is complementary and alternative medi-cine (CAM)? [updated 2005 Jul 12; cited 2002 Oct 6]. Available from:http://nccam.nih.gov/health/whatiscam/.
2. Ramsay C, Walker W, Alexander J. Alternative medicine in Canada: Use and pub-lic attitudes. Public Policy Sources. 1999; 21: 3-31.
3. Astin JA, Marie A, Pelletier KR, Hansen E, Haskell WL. A Review of the incor-poration of complementary and alternative medicine by mainstream physicians.Arch Intern Med. 1998; 158: 2303-10.
4. Sibinga EM, Ottolini MC, Duggan AK, Wilson MH. Parent-pediatrician commu-nication about complementary and alternative medicine use for children. Clin Pediatr(Phila). 2004; 43: 367-73.
5. Robinson A, McGrail MR. Disclosure of CAM use to medical practitioners: AReview of qualitative and quantitative studies. Comp Ther in Med. 2004; 12: 90-8.
6. Winslow LC, Shapiro H. Physicians want education about complementary andalternative medicine to enhance communication with their patients. Arch Intern Med.2002;162:1176-81.
7. Rampes H, Sharples F, Maragh S, Fisher P. Introducing complementary medicineinto the medical curriculum. J R Soc Med. 1997; 90: 19-22.
8. Verhoef M, Best A, Boon H. Role of complementary medicine in medical educa-tion: opinions of medical educators. Annals RCPSC. 2002; 35: 166-70.
9. Kreitzer MJ, Mitten D, Harris I, Shandeling J. Attitudes toward CAM among med-ical, nursing and pharmacy faculty and students. Alt Ther Health Med. 2002; 8: 44-54.
10. Goldszmidt M, Levitt C, Duarte-Franco E, Kaczorowski J. Complementary health-care services: A Survey of general practitioners’ views. Can Med Assoc J. 1995; 153:29-35.
11. Verhoef MJ, Sutherland L. Alternative medicine and general practitioners. Can FamPhys 1995; 41: 1005-11.
12. Duggan K, Verhoef MJ, Hilsden RJ. First-year medical students and complemen-tary and alternative medicine: Attitudes, knowledge, and experiences. Ann R CollPhysicians Surg Can. 1999; 32: 157-60.
13. Furnham A, McGill C. Medical students’ attitudes about complementary and alter-native medicine. J Altern Complement Med. 2003; 9: 275-84.
14. Ruedy J, Kaufman DM, MacLeod H. Alternative and complementary medicine inCanadian medical schools: A Survey. CMAJ. 1999; 160:816-7.
15. Verhoef MJ, Brundin-Mather R, Jones A, Boon H, Epstein M. Complementaryand Alternative Medicine in Undergraduate Medical Education: Associate Deans’Perspective. (Editorial) Can Fam Phys. 2004; 50: 847-9.
16. The CAM in UME Project. Calgary: National Working Group [updated 2005 Feb28, cited 2005 Oct 6]. Available from: http://www.fp.ucalgary.ca/CAMinUME.
17. Covington M. (2002). Complementary therapies questionnaire. In: Proceedingsfrom the Evaluation Conference for CAM CurriculumProceedings of a workingconference on evaluation of CAM curricula. 2002 June 17-18, Ann Arbor, US.Michigan: University of Michigan; 2002., Ann Arbor
18. Forjuoh SN, Rascoe TG, Symm B, Edwards JC. Teaching medical students com-plementary and alternative medicine using evidence-based principles. J AlternComplement Med. 2003; 9:429-39.
19. Morgan D, Glanville H, Mars S, Nathanson V. Education and training in comple-mentary and alternative medicine: A Postal survey of UK universities, medicalschools and faculties of nurse education. Complement Ther Med. 1998; 6:64-70.
20. Owen DK, Lewith G, Stephens CR. Can doctors respond to patients’ increasinginterest in complementary and alternative medicine? BMJ. 2001; 322:154-7.
21. Barberis L, De Toni E, Schiavone M, Zicca A, Ghio R. Unconventional medicineteaching at the Universities of the European Union. J Altern Complement Med.2001; 7:337-343.
22. Wetzel MS, Eisenberg DM, Kaptchuk TJ. Courses involving complementary andalternative medicine at U.S. medical schools. JAMA. 1998; 280:784-7.
23. Maizes V, Schneider C, Bell I, Weil A. Integrative medical education: Developmentand implementation of a comprehensive curriculum at the University of Arizona.Acad Med. 2002; 77:851-60.
Table 4Medical students’ ratings of the usefulness of different teaching methods in helping prepare them
to advise patients about CAM
Not at all Useful Somewhat Useful Useful Very Useful
Lectures 3% 14% 54% 27%
Hands on experience with CAM and patients in clinical settings 5% 17% 41% 32%
Observations of CAM practitioners 7% 20% 40% 28%
Articles on clinical trials of CAM 4% 25% 43% 24%
Case-base learning 7% 24% 45% 21%
Textbook readings 9% 45% 35% 6%
Using CAM to promote my own health 23% 36% 26% 9%

University of Toronto Medical Journal58
The SpectrumTerrorism is a prototypic traumatic event for those whose lifeand physical integrity are directly threatened and for those whoexperience sudden loss of a loved one.2 However, one mustalso consider that the ultimate goal of terrorism is to instill fearin society at large, in addition to threatening the integrity of sin-gle individuals and small groups. Thus, collateral effects devel-op among individuals and communities who are not directlyaffected by the event, particularly since such occurrencesreceive extensive coverage by the mass media. The burden maypersist with individuals as chronic disorders for years to come,and could very well change the fabric of the society drastically.Therefore, terrorism defies the boundaries of space and time.This unique quality complicates any effort undertaken for thepurpose of assessment and organization of the psychosocialimpacts of this phenomenon – but we shall try.
Human ReactionsIt is said that up to 90% of victims of a terrorist attack mayexhibit some adverse psychological reaction in the hours imme-diately following the event.2 In most instances, symptoms sub-side over the weeks to come, although by 12 weeks, approxi-mately 30% of the victims may still bear significant distress.The numbers continue to drop afterwards, even though delayedresponses or responses to later consequences of the incidentcontinue to appear. In brief, most who are distressed in thefirst weeks will recover. This process can best be observed inthe New York City experience following the 9/11 attacks.3,4
Surveys conducted by the New York Academy of Medicine fiveto eight weeks following the attacks reported a Post-TraumaticStress Disorder (PTSD) prevalence rate of 7.5%, with thosehaving the most severe exposure or personal loss at higher riskthan others. Six months following the attacks, this figuredropped to a mere 0.6% for PTSD and an additional 4.7% forsub-syndromal PTSD.
Notice, however, that the above study does not present thecomplete picture. First, it points to the flaws of the earlyassessment and estimation of PTSD prevalence based on earlysymptoms. In other words, early symptoms did not constitutea real clinical syndrome requiring treatment in all cases; manyof the early indicators were simply a reflection of transient dis-tress. Furthermore, the short period of time covered by thestudy protocol could not include the delayed-onset cases ofPTSD, nor could the design distinguish between acute versuschronic distress. It remains clear, however, that strong physio-
The Sick Rose
O Rose thou art sick.
The invisible worm,
That flies in the night
In the howling storm:
Has found out thy bed
Of crimson joy:
And his dark secret love
Does thy life destroy.
William Blake
The BeginningTerrorism is a reality of our time. The US State Departmentdefines terrorism as “premeditated, politically motivated vio-lence perpetrated against non-combatant targets by sub-nation-al groups or clandestine agents, usually intended to influence anaudience.”1 Although the statement above is a worthy attemptat defining this age-old phenomenon, it fails to encompass thegrand spectrum of societal implications that terrorism creates.
Terrorism erodes, at both the individual and the communitylevel, the sense of security and safety of daily life. It defies ournatural need to conceptualize life on earth as predictable, order-ly, logical, and controllable. Terrorism destroys lives, shattersfamilies, and destabilizes societies. As such, it compromises themental and the spiritual well-being of humans, in addition to itsobvious physical and material consequences. Recent attacks –September 11, 2001, on the Twin Towers and Washington; theLondon and Madrid bombings; and the extensive yet chronicIsraeli experience with terror, intensified following the Intifada– have focused the world’s attention on the psychologicalimpacts of terrorism.
This brief account strives to address the human response to ter-rorism from the perspective of the individual as well as thecommunity. Needless to say, treatises can be written on suchprofound a topic and the present endeavour aims merely topresent a brief survey outlining the far-reaching psychologicalimplications of this bitter reality.
Trauma and Terrorism: How Do Humans Respond?
Behzad Hassani, H.B.A. (OT8)
Philosophy and Medicine

logical, cognitive and emotional responses to trauma exist thatare simply normal reactions to extreme situations and not a signof mental disorder or moral weakness. Nevertheless, even suchbenign reactions can interfere with the ability of individuals toregain control of their lives, and hence must be addressed bymental health professionals.
Now that we have confronted a few of the methodologicalobstacles, we can make an effort to categorize the disorderlycontinuum of psychosocial responses to terrorism. We can doso by conceptualizing the aftermath of a terrorist attack interms of a series of stages or phases, each with its own uniquecharacteristics and psychiatric profile on the individual andcommunity level:5
Phase 1: Immediate Response and the “Rescue Stage”During the first hours to days after the terrorist event, the focuslies on rescuing victims and seeking to stabilize the situation.In this stage, various types of acute emotional response areobserved: heightened autonomic arousal, diffuse anxiety, fear,confusion, survivor guilt, and ambivalence about learning thetruth. Furthermore, the release of stress hormones and periph-eral cathecolamines following the traumatic event result inimproved cognitive performance. However, as stress persists,behavioural and cognitive performance may become narrowlyfocused, leading to a loss of flexibility. This may give rise todisorganized thinking, which in turn results in either a fight orflight response or a freeze response (psychic numbing).Internal conflicts over acceptance/rejection of nurturance maydevelop, and affective instability or brief reactive psychosis andhysteria may be observed.
Contrary to popular belief, victims show little panic and oftenengage in heroic or altruistic acts. Many of the above behav-iours are adaptive and ensure short-term survival. Suchresponse to trauma was perhaps best observed following the9/11 attacks, when tens of thousands of people peacefully evac-uated Manhattan and thousands volunteered to care for theemergency workers and donated blood and food. Most unchar-acteristically, New Yorkers stopped going to work and spoke tostrangers on the streets!6 A further instance of surprisinghuman kindness was replicated in London following the sub-way bombings of July 7: one London shop owner posted a signinviting passers-by to “come in and stay as long as you like.Join us for tea, soft drinks, coffee, and soup on the house.”7
As noted, most of the acute reactions dissipate over time, andeven though they are normal responses to extreme conditions,the symptoms may be perceived by the victims as socially inap-propriate, shameful, and as evidence of inadequacy. This inturn will lead to further distress. On a community level, therisk of mass panic and acute outbreaks of medically unexplainedsymptoms (OMUS) is at its peak. These topics will beaddressed in a later section.
volume 83, number 1, December 2005 59
Phase 2: Intermediate Response – Adaptation, Arousal,and Avoidance: the “Inventory stage”From one week to several months after the event, the attentionturns to longer-term solutions with bureaucratic forms of helpreplacing the heroic rescue missions. Victims may initially expe-rience a transient “honeymoon” phase: a feeling of relief atbeing safe and optimism about the roads that lie ahead. Soonafter, a more realistic appraisal of the lasting consequences willbe performed and disillusionment may set in. Intrusive recol-lections of the event, heightened and persistent autonomicarousal, avoidance of stimuli linked with the trauma, and somat-ic symptoms (dizziness, headache, fatigue, nausea) are com-monly found. Stress may even precipitate early labour and maycause fetal distress. Several psychiatric disorders develop in thisstage. Anger, irritability, apathy, disordered grief, abnormalbereavement, and social withdrawal are common manifesta-tions. Major depression, panic disorder, generalized anxiety dis-order, substance/alcohol abuse (as was demonstrated in aManhattan study),8 and somatoform disorders are further con-sequences of trauma in this period.2 Although the emphasis ofthe present account will be on PTSD and some culture-specif-ic manifestations, one must note that the other syndromes mayalso prove terribly debilitating and cause significant pathologyamong the survivors.
Post Traumatic Stress Disorder (PTSD)As mentioned earlier, the mechanisms of natural recovery fromtraumatic events are strong in humans and will bring aboutgradual dissipation of acute post-traumatic symptoms, many ofwhich are recognized PTSD symptoms. However, some maydevelop psychiatric disorders in the long term; most common-ly, PTSD, which occurs in as many as 30% of individualsexposed to a terrorist attack.6 Thus, the pathologic processinvolved in PTSD is a reflection of a failure of recovery fromearly symptoms. Studies of the Israeli experience have shownthat the rate of PTSD following terrorist attacks is twice as highas that observed in other traumatic events.9 Interestingly, therecovery course of PTSD during an era of chronic terror is sim-ilar to that of other traumatic events. Studies of 9/11 victimssuggest that severity of the experience and the degree of expo-sure are the best predictors of PTSD.4 Those whose lives aredirectly affected, who are physically injured, and who witnessgrotesque events are at higher risk. It is notable, however, thateven indirect exposure could render individuals vulnerable toPTSD: family members and friends of survivors, rescue work-ers, and health care workers have been among the reportedcases. The domain of influence is such that even those whowatch more media coverage are also at higher risk for PTSD.10
Furthermore, a multi-generational component to post-traumat-ic reactions has been observed: adult children of Holocaust sur-vivors with PTSD show a greater prevalence of PTSD to theirown traumatic experiences compared to adult children ofHolocaust survivors without PTSD.11 The rate is also higheramong monozygotic compared with dizygotic twins.12 Furtherrisk factors for PTSD are: family history of psychopathology,prior exposure to trauma, lower IQ, lower educational attain-

University of Toronto Medical Journal60
tations of the human experience in the post-modern multicul-tural world of today. Psychiatry must transcend its Eurocentricroots and its rigid definitions and strive to ponder the univer-sal human condition. The courage to embrace Nature’s chaosand uncertainty is at the heart of this process.
Phase 3: Long-term Response – Recovery, Reconstruction,Impairment, and Change13
A year or more after the traumatic event, relative stability mayhave been restored to the victims’ lives. However, many mayexperience feelings of resentment and disappointment if initialhopes for assistance or restoration are not met. Symptoms ofthe “Inventory Stage” may persist, and a significant late onsetincidence of PTSD, depression and anxiety may manifest.Rates of suicide may increase, and late-appearing somatoformsymptoms may disrupt daily life. More complex syndromesmay appear among survivors of prolonged, repeated, andintense trauma (chronic experience with terrorism), an exampleof which is survivor syndrome. The survivor journeys through life“without a spark.”13 The joy of life is gone and the will to liveis overshadowed by despair. The spectrum of behaviour rangesfrom depression and guilt to chronic aggression and an “addic-tion to hate.”13 Family dynamics are disrupted, and on a grandscale the sense of community is weakened. The collectiveresponse of a community is most peculiar in this stage andabounds with paradox and subtleties.
Communities in DistressThe disruptive force of terrorism transcends the individual.The very aim of terrorism is to create tears in the fabric ofsocial life by instilling fear and instituting chaos. The acute col-lective community response to terrorism includes symptoms ofemotional distress, misattribution of somatic symptoms, andsocial symptoms such as loss of confidence in the administra-tion, resentment of authority figures, social isolation, demoral-ization, marginalization, and scapegoating using traditional divi-sions in the society (e.g. along religious or ethnic lines).14,15 Inthis section, we will survey the general group responses to ter-rorism and take a closer look at the Israeli society, the onlynation-state to have had decades of experience with this dis-ruptive phenomenon.
Three specific collective reactions to trauma have been docu-mented in the literature: mass panic,14 acute outbreaks of med-ically unexplained symptoms (OMUS),16 and chronic cases ofmedically unexplained physical symptoms (MUPS).17
Furthermore, it is worthwhile to consider the communityresponse to biological and chemical attacks separately as sever-al unique features of the agents make them particularly terrify-ing to the public.
Mass panic, simply phrased, is an intense and contagious fearwhereby the individual’s only reference of conduct becomes the“self”.18 Extremes of behaviour are expected: desire to escapeor, alternatively, behavioural paralysis. Chaos ensues in thecommunity, and social organization and cultural roles are com-promised. In spite of the popular myth, mass panics are rela-
ment, history of heavy alcohol use, female gender, and poorposttraumatic social support.2
It must be emphasized that a small proportion of people whoexperience more persistent stressors after the initial trauma (e.g.chronic experience with terror, subsequent threat of attacks,biological agents) can apparently develop PTSD after a delayedperiod of time (six months to years) following the initial trau-matic event.2 This quality further complicates the aetiology,detection, and treatment of PTSD in the affected population.Cardinal features of PTSD are as follows:13
Persistent and intrusive re-experiencing of the traumatic eventvia nightmares or flashbacks is a critical manifestation of PTSD.The patient may experience intense psychological distress andphysiological reactivity on exposure to internal or external cuesthat symbolize the event. Re-enactments of the events throughsubtle and repetitive play may occur among children.
Persistent avoidance of reminders and cues associated with thetrauma as well as persistent emotional numbing are furthersigns of PTSD. Patients may evade activities, places, or peoplethat remind them of the experience, and may develop a fatalistsense of a foreshortened future without expectations of a nor-mal lifespan or life.
Persistent symptoms of autonomic hyper-arousal, such asinsomnia, anger, and hypervigilance are further manifestationsof PTSD.
It is noteworthy that even though the above cluster of PTSDsymptoms has been reported in every part of the world, signif-icant cultural variations in manifestation exist. In less industri-alized nations, avoidance and numbing are less common andinstead dissociative and trance-like states, in which fragments ofthe event are relived, are more common.
Culture-Specific Disorders13
A comprehensive analysis of culture-specific syndromes cannotbe undertaken in the present account. However, a brief syn-opsis is included in order to draw attention to this much-neglected, yet vital topic. The boundaries between disorders ofthe “mind” and the “body” are often porous and at best arbi-trary. In other words, the Cartesian dichotomy of “mind vs.body” is nothing but an illusion and a futile attempt at simpli-fying life’s chaotic reality. The interpenetration of the twospheres is most visible in the study of culture-specific manifes-tations of psychiatric disorders. In many cultures, depression isoften experienced largely in somatic terms: complaints of“nerves”, headaches, chronic diffuse pain, fatigue, trance disor-ders, problems of the “heart”, feelings of “heat”, and fears ofsomatic illness are merely a few examples. Some culture-spe-cific post-traumatic syndromes with irregular somatoform pre-sentations include: Susto (Latin America), Amok (Malaysia,Philippines), Dhat (India), Latah (South Pacific, southeast Asia),and Khoucheraug (Cambodia). It is axiomatic that much empha-sis need be placed on the analysis of these “irregular” manifes-

tively uncommon. The trials of the Tokyo sarin attack, theIsraeli SCUD missile attacks, the Oklahoma City bombing, andeven the Hiroshima and Nagasaki nuclear attacks bear witnessto this claim. As mentioned earlier, altruistic and heroic acts(adaptive behaviours) are the norm after the trauma of a ter-rorist attack.14 It is understandable, however, that factors suchas feelings of utter hopelessness or lack of confidence in theauthorities could increase the likelihood of a mass panic. Onceagain, extensive mass media coverage of such events could con-tribute to the propagation of fear and the inducement of emo-tional trauma, and subsequently heighten the risk for chaos.
The human stress response is comprised of arousal, anxiety,and vigilance: evolution’s solution to trauma. However, thephysiological reactions of the survival response may be mistak-enly attributed to the effect of biological/chemical agents ormedical illness. The symptoms may manifest on a large scaleand present as mass outbreaks of medically unexplained symp-toms (OMUS). Although no identifiable medical cause can beascertained, the condition appears contagious, spreads by sightand sound, and presents in public places or among socialgroupings. Rapid onset and remission of symptoms – such ashyperventilation, shortness of breath, dizziness, nausea, syn-cope, and abdominal distress – characterize this esoteric phe-nomenon. Often, these symptoms mimic the reported or per-ceived effects of an infectious or chemical agent.19 Remarkableepidemics of such somatization have been observed in the USAand the West Bank following false reports of poisonous gasleaks.20 OMUS may lead to significant chaos and social dis-ruption following chemical and biological attacks, and mayimpose a tremendous burden on an already stressed healthcaresystem.
As mentioned earlier, rapid onset and remission characterize theOMUS. However, acute to chronic transition of the afore-mentioned enigmatic symptoms is a possibility. Althoughresearch has not yet identified terrorism-induced clusters ofmedically unexplained physical symptoms (MUPS), evidencefrom World War I and the Vietnam War is abundant.17 It islikely that biological and chemical attacks could bring about theformation of MUPS in the affected societies. The above symp-toms have often been categorized as “somatoform”. Thisvague convention casts more shadow upon the doctor-patientrelationship than light. The manifestations of MUPS are debil-itating in the long run. Naturally, the patient may become con-vinced of the medical nature of their condition and in frustra-tion demand a treatment. On the other hand, the physician issceptical of any medical diagnosis for the problem and mayimplicitly convey to the patient that the symptoms are not“real”. The tension will inevitably lead to alienation andamount to a doctor-patient standoff. Once again, the vitalityof mediators such as trust, respect, understanding, empathy,and validation for patients’ concerns is highlighted in practice.
In recent years, the presentation and management of chemi-cal/biological attacks have become the topics of intense debateamong healthcare professionals and the focus of dramatic cov-
erage in mass media as well as Hollywood. Chemical/biologi-cal agents are often invisible and odourless. The symptomsmay often mimic those of common illnesses and thereforeevade early detection. Some agents cause gross deformities(small pox, mustard gas) and thus terrify the public and height-en the fear of contagious spread. To complicate the situationfurther, the agents and their symptomatology are often unfa-miliar to physicians. Even our preventive response to theseagents is problematic: the protective gear worn during theattacks increases social isolation, and limits intra-group interac-tion. Indeed, it increases the incidence of psychiatric ailments.21
In brief, the likelihood of mass panic and occurrence of MUPSis increased following biochemical terrorist campaigns. Forexample, twice as many gas hysteria cases were observed dur-ing World War I as there were actual gas exposure cases.18 Onthe other hand, many biological and chemical agents directlyaffect the central nervous system and cause symptoms such aslethargy, depression, disorientation, and psychosis.19
Furthermore, it is likely that different behavioural responseswould present for biological versus chemical agents. Each hasits own peculiar onset, presentation, and aetiology and is tend-ed to by different groups of professionals and first responders.It is due to these complicating parameters that social prepared-ness and structured response are even more critical during andfollowing biological/chemical attacks.
In keeping with its peripatetic scientific roots, medicine oftenstrives to categorize, routinize, and organize symptoms andconditions. In essence, it aims to render the unpredictable, pre-dictable. Similar reaction is expected when exploring thehuman response to terrorism. However, in the realm of psy-chiatry, the chaos and disorderliness of life presents a genuineand insurmountable challenge to our preconceived and simpli-fied constructs. One example of such contention is seen in thelandmark study by Israeli scientists, who found that terrorattacks in Israel produced a transient quiescence in light auto-mobile accidents one day after the event, followed by a 35%spike in fatal accidents precisely three days subsequent to theattack.22 Furthermore, public reports of decline in New YorkCity murder rates following 9/11 attacks highlighted the broad-based, short-term societal responses to terror that cannot beeasily explained.23 Understanding such paradoxical population-wide reactions to traumatic events is critical if the medical com-munity is to devise measures to detect and address the subtleand indirect human responses to terrorism.
Towards New HorizonsTerrorism is a blight on humanity’s record. It targets innocentcivilians and instills horror in populations. Terrorism carriesthe element of uncertainty in human life to devastating heights.It destroys lives, property and material culture. The psychiatricimplications of such traumatic events have only recentlybecome the focus of academic attention. What can be done toalleviate the pain? The best approach would be to abolish thetrauma. The next best remedy would be to foster resilience andbolster support so that individuals can develop the necessarycoping capacity prior to the event. In the future, academic
volume 83, number 1, December 2005 61

University of Toronto Medical Journal62
References1. US Department of State [homepage on the Internet]. Washington D.C.: Bureau
of Public Affairs, U.S. Department of State; c2005 [cited 2005 Sept 5]. Availablefrom: http://www.state.gov/.
2. Yehuda R, Bryant R, Marmar C, Zohar J. Pathological Response to Terrorism.Neuropsychopharmacology. 2005 Oct;30(10):1793-805. Epub 2005 Jul 13.
3. Galea S, Ahern J, Resnick H, Kilpratric D, Bucuvalas M, Gold J, et al.Psychological sequelae of the September 11 terrorist attacks. N Engl J Med.2002 Mar 23;346:982-7.
4. Galea S, Vlahov D, Resnick H, Ahern J, Susser E, Gold J, et al. Trends of prob-able post-traumatic stress disorder in New York City after the September 11terrorist attacks. Am J Epidemiol. 2003;158:514-24.
5. Ursano RJ, Fullerton CS, Norwood AE. Psychiatric dimensions of disaster:Patient care, community consultation, and preventive medicine. Harv Rev
Psychiatry. 1995 Nov-Dec;3(4):196-209. 6. Solnit R. The Uses of Disaster: Notes on Bad Weather and Good Government.
Harper’s Magazine. 2005 Oct;311(1865):33.7. Solnit R. The Uses of Disaster: Notes on Bad Weather and Good Government.
Harper’s Magazine. 2005 Oct;311(1865):33.8. Vlahov D, Galea S, Resnick H, Ahern J, Boscarino JA, Bucuvalas M, et al.
Increased use of cigarettes, alcohol, and marijuana among Manhattan, NewYork, residents after the September 11th terrorist attacks. Am J Epidemiol.2002;155(11):988-96.
9. Shalev AY, Freedman S. PTSD Following Terrorist Attacks: A ProspectiveEvaluation. Am J Psychiatry. 2005 Jun;162:1188-91.
10. Schuster MA, Stein BD, Jaycox L, Collins RL, Marshall GN, Elliot MN, et al.A national survey of stress reactions after the September 11, 2001, terroristattacks. N Engl J Med. 2001 Nov 15;345(20):1507-12.
11. Yehuda R, McFarlane AC, Shalev AY. Predicting the development of post-traumatic stress disorder from the acute response to a traumatic event. Biol
Psychiatry. 1998 Dec 15;44(12):1305-13.12. Stein MB, Jang KL, Taylor S, Vernon PA, Livesley WJ. Genetic and environ-
mental influences on trauma exposure and posttraumatic stress disorder symp-toms: a twin study. Am J Psychiatry. 2002 Oct;159:1675-81.
13. Fullerton CS, Ursano RJ. Psychological and Psychopathological Consequencesof Disasters. In: Lopez-Ibor JJ, Christodoulou G, Maj M, Sartorius N, OkashaA, editors. Disasters and Mental Health. Chichester, West Sussex; Hoboken,NJ: John Wiley & Sons; 2005. p. 13-37.
14. Glass TA, Schoch-Spana M . Bioterrorism and the people: How to vaccinatea city against panic. Clin Infect Dis. 2002;34:217-23.
15. Holloway HC, Norwood AE, Fullerton CS, Engel CC, Ursano RJ. The threatof biological weapons: prophylaxis and mitigation of psychological and socialconsequences. JAMA. 1997 Aug 6;278(5):425-7.
16. Pastel R. Outbreaks of medically unexplained physical symptoms after militaryaction, terrorist threat, or technological disaster. Mil Med. 2001;166(Suppl 2):44-6.
17. McLeod WR. Merphos poisoning or mass panic? Aust N Z J Psychiatry. 1975Dec;9(4):225-9.
18. Lacy TJ, Benedek DM. Terrorism and weapons of mass destruction: Managingthe behavioral reaction in primary care. South Med J. 2003 Apr;96(4):394-9.
19. Gamino LA, Elkins GR, Hackney KU. Emergency management of mass psy-chogenic illness. Psychosomatics. 1989 Fall;30(4):446-9.
20. DiGiovanni C Jr. Domestic terrorism with chemical or biological agents:Psychiatric aspects. Am J Psychiatry. 1999 Oct;156:1500-5.
21. Ritchie EC. Psychological problems associated with mission oriented protec-tive gear. Mil Med. 2001 Dec;166(12 Suppl):83-4.
22. Stecklov G, Goldstein JR. Terror attacks influence driving behavior in Israel.PNAS. 2004 Oct 5;101(40):14551-6.
23. Marks A. US crime rate up, ending decade of decline: Violent crime spikerenews debate over strategy: better technology or more police? Christian Science
Monitor. 2002 Jun 25;Sect. USA:2.24. Danieli Y, Brom D, Sills J, editors. The Trauma of Terrorism: Sharing
Knowledge and Shared Care – An International Handbook. Binghamton, NY:Haworth Maltreatment & Trauma Press; 2005.
emphasis must be placed on the refinement of risk factors, pre-dictors, and aetiological indicators of post-traumatic disorders.Early detection and treatment of traumatized individuals wouldfurther prevent a prolonged and debilitating stress response.
Furthermore, one must not neglect to acknowledge, reclaim,and harness the grand vitality of human resilience, a hard-earned virtue and a precious gift from our evolutionary past.Perhaps the most touching embodiment of this virtue is seenin a poem written by a 16-year-old Israeli girl following a dead-ly suicide bombing campaign:24
While you were showering
A mortar fell
And three people died.
While you were sleeping
Shots were fired
And eight soldiers were wounded.
While you were eating
Terrorists infiltrated
A house where children were sleeping.
And while you were saying the grace after meals
All that remained of the children
Were pieces.
While you were playing
A terrorist entered
A hall full of people.
And while you were losing
Their souls left their bodies
The guests, the bride and the groom.
So let’s hurry, let’s run, let’s get organized,
Let’s finish, let’s do as much as we can
For who knows what will happen,
The next time someone sits down to eat.
Martin Luther King, Jr. once wrote:
“Cowardice asks… ”Is it safe?”
Expedience asks… “Is it politic?”
Vanity asks… “Is it popular?”
Then comes a time
When one must take a position
That is neither safe, politic, nor popular,
But one must take it because it is right.”
With the hope that we ask the right question and take the rightposition...

University of Toronto Medical Journal64
Marr sketches the life and accomplishments of four surgeonswho practised in New York City. He devotes particular atten-tion and lavishes many exceptional compliments on MarionSims, whose “contributions to medical literature are many.”1
Sims is credited with devising a successful surgery for vesico-vaginal fistula. He was the first to build an instrument – thevaginal speculum – that allowed him to see the vaginal tearsthat caused urine to dribble uncontrollably and incessantly fromthe bladder and through the vagina. This terrible conditionaffected women who had experienced a difficult birth, andalthough it was not fatal, it caused a lot of physical discomfortand psychological pain to the sufferers. After operating unsuc-cessfully as many as thirty times on one black slave, Sims wasable to refine his technique and permanently close the fistula byusing silver-wire sutures.
The picture of Sims that emerges from Marr’s book is that ofa kind man who “persisted in treating charity patients even onSunday,”1 and who put his genius in the service of humanity:“He was motivated by the desire to benefit the human race byrelieving its suffering and advancing medical science.”1
Although Marr admits that Sims displayed his southern sympa-thies rather tactlessly during the Civil War, and that he couldbe “highly excitable and extremely jealous of his [priority]rights,”1 Marr squarely blames the dislike Sims evoked in manyof his contemporaries on their lack of vision. He accuses Sims’detractors of hating him “with the vindictiveness of the dull fora genius beyond their comprehension.”1 In Marr’s book, Sims’patients make only fleeting appearances as grateful recipients ofSims’ ministrations, and even surgeries where the patient diedare viewed as successes either because Sims was scientifically onthe right track or because these attempts were daring andcreative.
Marr also presents Edmund Randolph Peaslee, the New Yorkovariotomist and Sims’ colleague at the Women’s Hospital, in aflattering light. Peaslee started to practise ovariotomy liberallyin the mid 1800s, a time when doctors were still cautious aboutthis type of surgery since it was often fatal. More controver-sial still were hysterectomies, which had an even higher mor-tality rate: in the U.S. between 1853 and 1866, 42 hysterec-tomies were performed and only 9 women survived.1 Despite
AbstractDifferent historians have interpreted the beginnings ofgynaecological surgery in the 19th century as a legitimatemedical field in diverging ways. The early scholars extolthe advances in 19th century gynaecological interventions,and portray surgeons as heroes and visionaries. Somefeminist historians vilify the surgeons, attacking both theircharacter and their medical practice by pointing to thepower imbalance between the women patients and theirauthoritarian male physicians. A third group of historiansviews gynaecological surgery as an enterprise that hasboth negative and positive consequences, emphasizingdoctor-patient interaction and the social context in whichit occurs. An exploration of these three views shows theimportance of a more balanced interpretation and pointsto some ethical issues relevant to the present day.
Gynaecological Surgery in the 19th Century: Diverging Historical AccountsGynaecological surgery became a legitimate and widespreadenterprise during the 19th century with the success of inter-ventions such as the removal of diseased ovaries and the repair-ing of vesico-vaginal fistulas. However, these advances, alongwith the development of the field in general, are not withoutcontroversy, and scholars have expressed widely diverging viewsabout the history of gynaecology. Some historians write a glo-rifying account of heroic discoveries. Others – mainly feministhistorians – vilify the surgeons, attacking both their characterand medical practices, as well as pointing to the power imbal-ance between the women patients and their authoritarian malephysicians. Finally, since the late 1970s a number of scholarsoffer perhaps the most accurate view, situating themselvesbetween these two extremes to create a more nuanced pictureof 19th century gynaecological surgery, and acknowledging bothits positive and negative consequences.
Gynaecological Surgeons as HeroesIn the first six decades of the twentieth century, historians whowrote about gynaecological surgery produced laudatory biogra-phies of a few prominent surgeons, such as J. Marion Sims, andextolled these surgeons’ contributions to women’s health. Inhis book “Pioneering Surgeons of the Women’s Hospital,” James Pratt
Gynaecological Surgery in the 19th Century: Diverging Historical Accounts
Delia Gavrus, M.A., Ph.D. candidateInstitute for the History and Philosophy of Science and Technology, University of Toronto
Historical Review

these grim numbers, Marr sees Peaslee as a trail-blazing doctorwho stuck to his guns despite the fact that other doctors failedto share his insights regarding the importance of ovariotomyand hysterectomy. For instance, when Peaslee presented hisovariotomy monograph at the New York Academy of Medicine,“not a single surgeon in the audience defended the operation.”1
Some doctors thought the operation was too dangerous; othersconsidered it a fad that would quickly fade. Eventually, how-ever, following the introduction of anaesthesia and asepsis, ovar-iotomy became a widespread practice. Marr lauds Peaslee forputting “this operation on a secure footing [since] in New YorkCity in those early years Peaslee was the lone champion andfinal arbiter of this type of abdominal surgery.”1 Thus Peaslee,like Sims, is portrayed as a great visionary, a man ahead of histime.
Not only biographies, but also early histories of surgery praisethe resourcefulness of these 19th century gynaecological sur-geons. In “Eternal Eve,” Harvey Graham contends “the devel-opment of the major gynaecological operations began inAmerica and depended entirely upon the resource and courageof a handful of backwoods obstetricians.”2 In a heroic tone, hetells the story of the successful ovariotomies performed byEphraim McDowell as early as 1809, and then proceeds to namea dozen doctors who attempted with varied success to operateon women’s reproductive organs. Graham is sensitive to thepain that this type of surgery inflicted on women, often prais-ing women for their endurance, but generally, the patients donot command much of his attention. His admiration for thesurgical feats of the doctors is, on the other hand, very clear.Thus, ignoring the contribution of many men and women out-side the medical profession,1 Graham credits the founding ofthe Women’s Hospital in New York to “the genius, courage,and pertinacity of Marion Sims.”2
Gynaecological Surgeons as VillainsMany feminists in the 1970s mounted scathing attacks on pastand contemporary gynaecology. Mary Daly, for instance, wrotethat “sexual surgery became The Man’s means of restrainingwomen” and that Sims, “known for his hatred and abhorrenceof female organs, remedied his problems [...] by cutting upwomen’s bodies.”3 Barbara Ehrenreich and Deirdre Englishcautioned that “it should not be imagined that poor womenwere spared the gynaecologist’s exotic catalogue of tortures sim-ply because they couldn’t pay.”4 These feminists saw women asvictims of sadistic doctors who sought to control them bypathologizing their proto-feminist behaviour.
In his famous feminist book, “The Horrors of the Half-Known Life,”G. J. Barker-Benfield explores male attitudes regarding femalesexuality in 19th century America and comes to the conclusionthat “hostility toward women and competition among men werethe conditions for the rise of modern gynaecology.”5 Men weredisgusted with women’s genitals, Barker-Benfield affirms, whilealso fearing women’s sexual appetite. Moreover, men viewedwomen as being at the mercy of their physiology. They wereweak, emotional, and irrational as a result of their feminine
organs (ovaries, uterus, vagina, etc.), and thus were seen tohover “on the verge of hysteria, insanity, and crime.”5 This phi-losophy, which emphasized the somatic substrates of feminini-ty, led men to the natural conclusion that one effective way tocontrol women’s sexuality was to submit them to “bodyexperts”5 – that is, to doctors.
Barker-Benfield’s assessment of gynaecological surgeons isunequivocally negative. He emphasizes that Sims perfected hissurgical procedures on poor patients – first on black slaves, andlater on poor Irish immigrants at the Women’s Hospital. Heaccuses Sims of establishing the Women’s Hospital entirely for“provid[ing] guinea pigs for his self-education,” so that he couldlater charge “stupendous fees” in private practice.5 Thus Barker-Benfield attacks both Sims’ practice as a doctor and his charac-ter. Unlike the early historians, Barker-Benfield does not thinkthat Sims practiced medicine in order to save women from painand disease. His purpose, rather, was either to controlintractable behaviour or to restore women to their rightful posi-tion: that of baby-bearers. His preoccupation with this latterpurpose can be seen in Sims’ great interest in curing femaleinfertility. But even in instances when fertility was not desired,Sims could not justify helping a woman feel less discomfortduring intercourse if the intercourse did not lead to procreation.Barker-Benfield gives the example of one of Sims’ patients, awoman in her mid-thirties, who suffered from general pain inher vagina and who was a candidate for a surgical procedurethat consisted in an incision of the os and the cervix. Uponlearning that the woman did not plan to ever have childrenagain, Sims declined to help her unless she agreed to becomepregnant. She did, and Sims operated on her. This is a clearexample, Barker-Benfield concludes, that “Sims could not con-strue therapeutic action apart from preparing a woman for preg-nancy.”5
In some situations, Barker-Benfield writes, Sims and other sur-geons were all too happy to curtail women’s ability to repro-duce. They performed numerous ovariotomies and hysterec-tomies on women deemed inferior and not worthy ofreproducing (such as immigrants, blacks, and the mentally ill).Barker-Benfield always refers to ovariotomy as “female castra-tion” and contends that it was practiced in order to “normal-ize” a disorderly woman’s behaviour and to make her, in thewords of one doctor, “tractable, orderly, industrious, and clean-ly.”5 Doctors such as Robert Battey advocated the removal ofhealthy ovaries for a variety of non-ovary related symptoms,and many gynaecologists, including Sims, performed manyunnecessary castrations and clitoridectomies.5
Deborah Kuhn McGregor, a feminist historian writing closer tothe present, provides a slightly more tempered view of gynae-cological surgery than Barker-Benfield. She concedes that thecure for vesico-vaginal fistula was a success, but for McGregorthis success came at a very high price because it “deflectedattention from an accompanying increase in the practice ofovariotomy, with its attendant high rate of mortality.”6
McGregor asserts that Sims’ early success encouraged doctors
volume 83, number 1, December 2005 65

University of Toronto Medical Journal66
cians themselves were reluctant to operate. This held true forboth somatic and psychosomatic illness. Shorter documentsthat women who suffered from nervous symptoms did improveafter an ovariotomy or a clitoriodectomy as a result of theplacebo effect, but he also criticizes “this aberrant chapter inthe history of medicine”7 as resting on unscientific theories suchas reflex irritation. Moreover, reflex theory had a negativeimpact on men as well: they too were castrated, though not asoften as women. This evidence disproves claims by some fem-inist historians who have argued that “no doctor ever consid-ered perpetrating similar medical insults to the male organs.”8
Shorter asserts that medicine had an overall positive effect onwomen’s lives in the 19th century. He thinks it not a coinci-dence that the first wave of feminism arose at the beginning ofthe twentieth century, and he argues that the women’s move-ment “was made possible by the securing of good health forwomen.”9 Shorter notes the physical suffering and ill healththat women endured for centuries, an ill health that was respon-sible for women’s lower life expectancy. Gynaecological prob-lems were clearly at the forefront of women’s medical problems.Notwithstanding misguided surgical intervention for nervousdisorders, gynaecological surgery benefited many women. In astudy of admissions to the gynaecological ward of Mt. SinaiHospital in New York between 1883 and 1894, Shorter showsthat the vast majority of women suffered from pelvic infections,tumours, cysts, and other organic complaints, rather than fromhysteria or “ovarian madness.”9 Gynaecology thus providedrelief for these women and often gave them a new lease on life.However, Shorter’s account of medicine is not unfailingly pos-itive or uncritical. He accuses one doctor who refuses mor-phine to women suffering from “ill-defined pelvic pains” of aninability to empathize with his patients and of a “failure to makeany insightful, imaginative leap into the lives of his patients.”9
Furthermore, Shorter does not dispute that women were morelikely to submit to castration, for instance, since they more read-ily internalized doctors’ medical theories and submitted moreeasily to authority than men. Women were viewed as “poiso-nous, diseased, and inferior,” and they themselves concurredwith this judgment.9
Ann Dally takes a similarly balanced approach to gynaecologi-cal intervention. She too reacts to feminist histories: “Somefeminists write as if unpleasant, even sadistic, treatments weregiven only to women and always with sinister motives. This isnot the case.”10 Dally criticizes 19th-century doctors for exper-imenting on poor female patients and for not showing muchinterest in learning about female physiology, but she also pointsto the benefits of this surgery for women who suffered fromtumours. She admits that the death rate for ovariotomies wasvery high, but attributes some of it to the fact that doctorsoperated only on serious cases precisely because they wereaware of the high death rate.11 On the topic of gynaecologicalsurgery for psychosomatic complaints, Dally decries the poorscientific basis for this practice but feels that “it is important torealize that most doctors at the time genuinely believed that theovaries were the source of virtually all female sickness.”11
to experiment liberally with surgical interventions, and very soonmajor operations became common. Many doctors routinelyperformed Battey’s Operation (the removal of healthy ovaries)for nervous symptoms, insanity, and epilepsy, even though thedeath rate was extremely high. Furthermore, McGregor argues,by the time Sims died in 1883 the prevalence of vesico-vaginalfistula was rapidly decreasing for a number of reasons: medicalpractitioners had become more adept at delivering babies andhad better facilities and instruments at their disposal; slaveryended and thus the standard of living for black Americansincreased; the diet of most Americans improved and the inci-dence of rickets decreased, allowing women easier births.Ironically then, at the beginning of the twentieth century, mostwomen incurred vesico-vaginal fistulas from accidents duringgynaecological surgery. This line of reasoning seems to suggest,though McGregor never fully articulates it, that women wouldhave been better off without Sims’ vesico-vaginal fistula cure,given its negative consequences on further gynaecological inter-vention and the fact that the condition eventually disappeared.
McGregor believes that in the 19th century, “male dominanceof medical practice rested on the subordination of women andthe objectification of their bodies.”6 But even if all women wereobjectified, they were not all treated equally. McGregor showshow race and class affected the prescribed therapy. She givesthe example of a rich society lady who consulted Sims in 1857for a condition he called vaginismus. The lady could not standany physical contact of her genitalia, and thus could not engagein intercourse. Sims theorized that a cure for vaginismus wouldconsist of a Y-shaped incision in the vaginal wall, but he couldnot be sure because he had never attempted this procedure.Consequently, Sims refused to perform surgery on this ladybecause “an untried process was not justifiable on one in herposition in social life.”6 Clearly, he never expressed any suchsentiment for the black slaves and poor Irish women he exper-imented on. While McGregor’s approach is a little less extremethan Barker-Benfield’s, McGregor still writes from a positionthat ultimately indicts 19th century surgery for its treatment ofwomen and argues that little good, if any, came from surgicalinterventions.
A More Nuanced Look at Gynaecological SurgeonsA third and final group of historians, writing since the late1970s, offers a more nuanced view of gynaecological surgery inthe 19th century. Without ever going to the two extremes pre-sented above, some historians tend to emphasize the positiveaspects of gynaecological surgery, while others spend more timedwelling on the negative aspects. Regardless of these differ-ences, the historians in this third group agree that 19th centurygynaecological surgery had both good and bad consequences.
Edward Shorter argues that characterizing the relationshipbetween doctors and female patients as one of control and sub-mission is not accurate. Women were not completely passive,and not all of them were easily intimidated by medical authori-ty. Having heard of the wonders it could accomplish, theyoften insisted on gynaecological surgery even when the physi-

Battey’s operation unfortunately became a “fashionable” phe-nomenon, but Dally emphasizes that Battey was a “skilled andhighly moral American surgeon”11 whose motives were hon-ourable: he genuinely wanted to help sick women. In fact,Dally argues, he saw this intervention as a last resort, to be per-formed only for “any grave disease which is either dangerousto life or destructive to health and happiness, which is incur-able by other and less radical means.”11
Another historian who takes a balanced approach, ReginaMorantz-Sanchez, documents the career of Mary AmandaDixon Jones, a gynaecological surgeon in 19th centuryBrooklyn, and shows that she was just as eager as her male col-leagues to subject women patients to gynaecological surgery.Even though Dixon Jones always expressed a great desire tohelp women, and even though she considered herself morecapable of caring for women patients by virtue of being awoman herself, her therapeutics did not differ from those ofmale doctors. In fact, in a previous study, Regina MarkellMorantz and Sue Zschoche showed that women doctors in the19th century clung longer to traditional values than their malecolleagues.12 Thus, Morantz-Sanchez suggests a simplistic viewof sadistic male doctors and victimized female patients is notan accurate description of gynaecological surgery in the 19th
century. Although Morantz-Sanchez’s account is framed asintellectual history and differs somewhat from the social histo-ries of Shorter and Dally, it certainly shares a desire to moveaway from the oversimplifications of past scholarship. Thesehistorians may be of different theoretical persuasions, have dif-ferent writing styles, and may use different historical data (epi-demiological data in Shorter’s situation versus a case study ofmedical practice in Morantz-Sanchez’s situation), but they allshare a balanced approach to the history of gynaecologicalsurgery, in contrast with the early historians and with some ofthe feminist historians.
ConclusionAlthough the events comprising the story of 19th centurygynaecological surgery are of little debate, different groups ofscholars have subscribed to conflicting interpretations of thoseevents. The early historians extol the advances in gynaecolog-ical interventions and portray surgeons as heroes and visionar-ies. Some feminist historians swing to the other extreme, vili-
fying doctors and imputing them a desire to control and tor-ture women. A final group of historians favour a more tem-perate approach and consider the interaction between doctorsand patients, as well as the social context in which thisoccurred. These historians view gynaecological surgery as anenterprise that had both negative and positive consequences.When it was used to “treat” nervous disorders, surgery was anunnecessary and unfortunate intervention, but when it was usedlegitimately to remove dangerous tumours and to cure vesico-vaginal fistulas, gynaecological surgery benefited womenimmensely.
History is more than an exercise in enumerating the names ofpioneers and the dates of medical discoveries. Every genera-tion rewrites history, to some extent, by reinterpreting thesocial, political, and scientific context in which medical discov-eries were made. A balanced interpretation of the history ofmedicine suggests that even when medical innovation results inimproved health for patients, it can also lead at times to objec-tification, mistreatment, and occasional abuse. The formaliza-tion and systematization of ethics in common practice today isa welcome advance in light of some 19th century practices.
References1. Marr JP. Pioneer surgeons of the Women’s Hospital. Philadelphia: F.A. Davis;
1957.2. Graham H. Eternal Eve. London: Heinemann; 1950.3. Daly M. Gynecology: The Metaethics of radical feminism. Boston: Beacon
Press; 1978.4. Ehrenreich B, English D. For her own good: 150 of the Experts’ advice to
women. New York: Doubleday; 1979.5. Barker-Benfield GJ. The Horrors of the half-known life: Male attitudes toward
women in nineteenth-century America. New York: Routledge; 2000.6. McGregor DK. From midwives to medicine: The Birth of American gynecol-
ogy. New Jersey: Rutgers University Press; 1998.7. Shorter E. From paralysis to fatigue: A History of psychosomatic illness in the
modern era. New York: Free Press; 1992.8. Ehrenreich B, English D. Complaints and Disorders: The Sexual Politics of
Sickness. In: Seizing our bodies: The Politics of women’s health. Dreifus C,editor. New York: Vintage; 1977.
9. Shorter E. A History of women’s bodies. New York: Basic Books; 1982.10. Dally A. Women under the knife: A History of surgery. London: Hutchinson
Radius; 1991.11. Dally A. The Trouble with doctors: Fashions, motives and mistakes. London:
Robson Books; 2003.12. Morantz RM, Zschoche S. Professionalism, feminism, and gender roles: A
Comparative study of nineteenth-century medical therapies. JAH. 1980; 67(3):568-88.
volume 83, number 1, December 2005 67

University of Toronto Medical Journal68
The Making of a Surgeon in the 21st Century
Jasrajbir Baath, B.Sc. (OT8)
In this harrowing descriptionof life as a general surgeryresident, Dr. Craig A. Millerdescribes his five years at theOhio State UniversityMedical Center in Columbus,Ohio. This book, a self-pro-fessed modern day version ofthe1968 memoir “The Making
of a Surgeon” by Dr. WilliamA. Nolen, is a must read for all students. Even those not con-sidering surgery as a future career will find the detaileddescription of life in residency, from both personal and pro-fessional perspectives, to be highly valuable.
The book is a relatively quick read but provides extensive cov-erage on various aspects of residency. The twenty-two chap-ters provide insight into both each year of training and thelongitudinal aspects of postgraduate medical education. Mostinteresting amongst the longitudinal narratives is a chapterentitled “Publish or Perish” which provides an interesting lookat the pressure put on residents to publish significant researchwhile maintaining their already hectic clinical schedule.Although the book can become depressing at times, this isovercome with numerous episodes of comic relief, as well asstories of personal and clinical triumph.
It is not often that one finds a surgeon able to write anythingother than a scientific treatise. Dr. Miller, an avid musicianprior to entering medical school, has an artistic flair absent inmost members of the medical community. He is able to paintvivid images of the circumstances surrounding the complexcases, surgeries, and characters encountered throughout theretrospective. These characters include the oddly memorablepatients and physicians, for whom the author’s affectionsranged from loathing to admiration. The personal idiosyn-crasies of these characters, such as the chief resident with thehabit of falling asleep during awkward circumstances, or theintern who would sleep through all pages during an on-callnight, are brought to light with a descriptive touch usuallyreserved for full-time novelists.
The true core of the book lies, however, in the difficulties thatMiller faced during his five-year training period. He describesthe “scut” work assigned during first year, consisting of mun-dane tasks such as ordering tests and phoning in consults, that
did not allow him to gain surgical experience. He also detailsa number of instances in which he was publicly derided by hissuperiors for minor errors in knowledge – a victim of intel-lectual hazing.
The greatest difficulty was, of course, the schedule. Callschedules of 1 in 3 and being forced to work longer than thescheduled time took a great toll on Miller’s emotional and per-sonal life. He describes the dazed state one is in on a post-call day and the resultant propensity for error. Even Miller’smarriage, which began during the first year of residency, didnot survive the barbaric residency schedule.
There are, however, stories of triumph and excellence as well.Miller illustrates the system of graded responsibility used inresidency, whereby the resident is given more and moreresponsibility as their experience grows. This culminates in hisability to perform major operations independently, justifyingthe trust that his superiors now place in him. Not surprising-ly, Miller culminates his account with an ambivalent analysisof the process. Indeed the system is efficient in creating excel-lent surgeons, he says, but there must be an alternative to thedestruction of families.
Besides providing an eye-opening look into life as a surgeryresident, this book is also a valuable read for other reasons.First off, those who enjoy reading in their spare time will sim-ply find this entertaining. It is not an epic novel by any means,but well-written nonetheless. Secondly, those interested insurgery will learn a lot from this book as it provides briefoverviews of many surgical procedures, concepts, and prac-tices. Certainly one who reads this book will have a much bet-ter understanding of the role of a general surgeon in the over-all health care picture. Lastly, the book provides a look intothose aspects of residency that are common to all programsand not just specific to surgery. Knowing how to deal withissues such as fire-breathing faculty, difficult staff, and per-sonal problems is an important skill for all medical studentsand residents, thereby significantly increasing the book’s tar-get readership.
Overall, the book is a highly recommended read. It suffersfrom some minor problems such as surprisingly numerousspelling mistakes and the occasional awkwardly written sen-tence or paragraph. In general, however, Dr. Miller presents apleasing writing style that makes the description of his expe-riences that much more interesting. This book would be avaluable read to many, but is practically indispensable tosomeone considering a career in surgery.
The Making of a Surgeon in the 21st Century
Dr. Craig A. Miller
Blue Dolphin PublishingNevada City
2004
Book Reviews – Non-Fiction

volume 83, number 1, December 2005 69
A Consumer’s Guide to Laboratory Tests
Andrew J. Perrin, MRes (MD/PhD)
There is no shortage of self-help manuals, medical ency-clopediae or reference booksvying for the dollars oftoday’s patient. Indeed, ourinformation age has createdan insatiable urge to possessall knowledge relevant to adiagnosis, sometimes even
before it has been made. With patient demand for knowledgedriving them, medical publishers have sought to fill shelveswith volumes concerning every disease process imaginable,even to the point of redundancy. But, this redundancy is notcomprehensive; sorely lacking has been a reference discussingthe myriad of testing procedures encountered by patients – areference that would allow patients to decode the test requi-sitions written on their behalf. Into this gap Mary C. Ricottahas offered her Consumer’s Guide to Laboratory Tests.
Set like a road map to the modern clinical laboratory, Ricottabegins with a comprehensive overview of Haematology. Shesmartly outlines the classification of anemia and walks thereader through the complete blood count (CBC), relating CBCfindings to clinical disease. This is followed by a briefdescription of the major hematological pathologies and a dis-cussion of coagulation and its associated tests. Each of thefollowing sections, outlining respectively, ClinicalBiochemistry, Microbiology, Immunology, Serology,Cytotechnology, Histology and Molecular Diagnosis are con-structed in a similar fashion, which makes for a very cohesiveread. A fully cross-referenced appendix, linking diseaseprocess to the test used to detect or characterize it, furtherenhances this unity.
Despite this elegant organization, diagrams are used sparingly,often leaving the reader to formulate their own visuals. As aresult, the author fails to capitalize on the most effective ofteaching tools – a picture. Ricotta’s passages are also repletewith medical jargon. Her explanations, while direct and suc-cinct to the medically trained, are often difficult for untrainedreaders. Considering the target audience, these missteps sig-nificantly detract from the book.
Although the text presents a comprehensive tour of the clin-ical laboratory, I am surprised by the failure to mention themany other non-laboratory based tests that patients are likelyto encounter. For instance, no allusions are made to cardio-graphic studies or pulmonary function tests. Blending thiswith the already extensive discussion of laboratory tests couldonly benefit the reader, as it would allow patients to correlateelectrocardiographic findings with serum enzyme profiles inunderstanding acute myocardial infarction.
A Consumer’s Guide to Laboratory Tests represents an excellentideal. Mary Ricotta has attempted to fill a gap in patient edu-cation that is both needed and relevant. While her difficultyin communicating with patients undermines this goal, heroverview of the clinical laboratory represents a valuableresource for clinicians seeking a brief description of the majortesting methodologies.
A Consumer’s Guide toLaboratory Tests
Mary C. Ricotta
Prometheus Books2005
ISBN: 1-59102-247-9
301 pp
Non-Fiction – Book Reviews