Does the Novel PET/CT Imaging Modality Impact on the Treatment of Patients With Metastatic...
10
ORIGINAL ARTICLES Does the Novel PET/CT Imaging Modality Impact on the Treatment of Patients With Metastatic Colorectal Cancer of the Liver? Markus Selzner, MD,* Thomas F. Hany, MD,† Peer Wildbrett, MD,* Lucas McCormack, MD,* Zakiyah Kadry, MD,†‡ and Pierre-Alain Clavien, MD, PhD* Objective: To compare the diagnostic value of contrast-enhanced CT (ceCT) and 2-18-F-fluoro-2-deoxyglucose-PET/CT in patients with metastatic colorectal cancer to the liver. Background: Despite preoperative evaluation with ceCT, the tumor load in patients with metastatic colorectal cancer to the liver is often underestimated. Positron emission tomography (PET) has been used in combination with the ceCT to improve identification of intra- and extrahepatic tumors in these patients. We compared ceCT and a novel fused PET/CT technique in patients evaluated for liver resec- tion for metastatic colorectal cancer. Methods: Patients evaluated for resection of liver metastases from colorectal cancer were entered into a prospective database. Each patient received a ceCT and a PET/CT, and both examinations were evaluated independently by a radiologist/nuclear medicine physician without the knowledge of the results of other diagnostic techniques. The sensitivity and the specificity of both tests regarding the detec- tion of intrahepatic tumor load, extra/hepatic metastases, and local recurrence at the colorectal site were determined. The main end point of the study was to assess the impact of the PET/CT findings on the therapeutic strategy. Results: Seventy-six patients with a median age of 63 years were included in the study. ceCT and PET/CT provided comparable findings for the detection of intrahepatic metastases with a sensitiv- ity of 95% and 91%, respectively. However, PET/CT was superior in establishing the diagnosis of intrahepatic recurrences in patients with prior hepatectomy (specificity 50% vs. 100%, P 0.04). Local recurrences at the primary colo-rectal resection site were detected by ceCT and PET/CT with a sensitivity of 53% and 93%, respectively (P 0.03). Extrahepatic disease was missed in the ceCT in one third of the cases (sensitivity 64%), whereas PET/CT failed to detect extrahepatic lesions in only 11% of the cases (sensitivity 89%) (P 0.02). New findings in the PET/CT resulted in a change in the therapeutic strategy in 21% of the patients. Conclusion: PET/CT and ceCT provide similar information regard- ing hepatic metastases of colorectal cancer, whereas PET/CT is superior to ceCT for the detection of recurrent intrahepatic tumors after hepatectomy, extrahepatic metastases, and local recurrence at the site of the initial colorectal surgery. We now routinely perform PET/CT on all patients being evaluated for liver resection for metastatic colorectal cancer. (Ann Surg 2004;240: 1027–1036) C olon cancer is the second most frequent malignancy in the Western hemisphere after breast cancer in women and lung cancer in men. In the United States, about 150,000 patients are diagnosed with colon cancer each year, and more than 50,000 of these patients will develop liver metastases. 1 Liver resection is the only therapeutic strategy that offers a chance of cure. This therapy has also gained increasing popularity over the past 2 decades due to improved surgical and peri-operative management with current mortality risks well below 5% in high-volume centers. 2–4 Many surgeons have developed strategies to improve resectability of large tumors such as the induction of hypertrophy of an estimated small remnant liver volume by selective portal vein emboli- zation 5 and the downstaging 6,7 of large liver tumors by chemotherapy. However, despite successful attempts at cur- ative resection in many situations, long-term survival has remained somewhat disappointing, ranging between 25% and 40%. 8 –10 Most patients after a curative resection develop recur- rent intra- or extrahepatic tumor manifestations. 11 The main reason for these tumor recurrences after putative complete tumor removal is the presence of undetected tumor at the time of surgery. Currently, patients undergo an extensive preop- erative work-up before liver resection to accurately define the hepatic lesions and to exclude the presence of extrahepatic From the *Department of Visceral and Transplantation Surgery, Zu ¨rich, Switzerland; the †Department of Nuclear Medicine, University Hospital, Zu ¨rich, Switzerland; and the ‡University of Pittsburgh Medical Center, Pittsburgh, PA. M.S. and T.F.H. contributed equally to this work. Reprints: Pierre-A. Clavien, MD, PhD, FACS Professor of Surgery Depart- ment of Surgery University Hospital Zu ¨ rich Ra ¨mistrasse 10, 8091 Zurich, Switzerland. E-mail: [email protected]. Copyright © 2004 by Lippincott Williams & Wilkins ISSN: 0003-4932/04/24006-1027 DOI: 10.1097/01.sla.0000146145.69835.c5 Annals of Surgery • Volume 240, Number 6, December 2004 1027
Transcript of Does the Novel PET/CT Imaging Modality Impact on the Treatment of Patients With Metastatic...
ORIGINAL ARTICLES
Does the Novel PET/CT Imaging Modality Impact on theTreatment of Patients With Metastatic Colorectal Cancer of
the Liver?
Markus Selzner, MD,* Thomas F. Hany, MD,† Peer Wildbrett, MD,* Lucas McCormack, MD,*Zakiyah Kadry, MD,†‡ and Pierre-Alain Clavien, MD, PhD*
Objective: To compare the diagnostic value of contrast-enhancedCT (ceCT) and 2-�18-F�-fluoro-2-deoxyglucose-PET/CT in patientswith metastatic colorectal cancer to the liver.Background: Despite preoperative evaluation with ceCT, the tumorload in patients with metastatic colorectal cancer to the liver is oftenunderestimated. Positron emission tomography (PET) has been usedin combination with the ceCT to improve identification of intra- andextrahepatic tumors in these patients. We compared ceCT and anovel fused PET/CT technique in patients evaluated for liver resec-tion for metastatic colorectal cancer.Methods: Patients evaluated for resection of liver metastases fromcolorectal cancer were entered into a prospective database. Eachpatient received a ceCT and a PET/CT, and both examinations wereevaluated independently by a radiologist/nuclear medicine physicianwithout the knowledge of the results of other diagnostic techniques.The sensitivity and the specificity of both tests regarding the detec-tion of intrahepatic tumor load, extra/hepatic metastases, and localrecurrence at the colorectal site were determined. The main endpoint of the study was to assess the impact of the PET/CT findingson the therapeutic strategy.Results: Seventy-six patients with a median age of 63 years wereincluded in the study. ceCT and PET/CT provided comparablefindings for the detection of intrahepatic metastases with a sensitiv-ity of 95% and 91%, respectively. However, PET/CT was superiorin establishing the diagnosis of intrahepatic recurrences in patientswith prior hepatectomy (specificity 50% vs. 100%, P � 0.04). Localrecurrences at the primary colo-rectal resection site were detected byceCT and PET/CT with a sensitivity of 53% and 93%, respectively(P � 0.03). Extrahepatic disease was missed in the ceCT in one thirdof the cases (sensitivity 64%), whereas PET/CT failed to detect
extrahepatic lesions in only 11% of the cases (sensitivity 89%) (P �0.02). New findings in the PET/CT resulted in a change in thetherapeutic strategy in 21% of the patients.Conclusion: PET/CT and ceCT provide similar information regard-ing hepatic metastases of colorectal cancer, whereas PET/CT issuperior to ceCT for the detection of recurrent intrahepatic tumorsafter hepatectomy, extrahepatic metastases, and local recurrence atthe site of the initial colorectal surgery. We now routinely performPET/CT on all patients being evaluated for liver resection formetastatic colorectal cancer.
(Ann Surg 2004;240: 1027–1036)
Colon cancer is the second most frequent malignancy inthe Western hemisphere after breast cancer in women
and lung cancer in men. In the United States, about 150,000patients are diagnosed with colon cancer each year, and morethan 50,000 of these patients will develop liver metastases.1
Liver resection is the only therapeutic strategy that offers achance of cure. This therapy has also gained increasingpopularity over the past 2 decades due to improved surgicaland peri-operative management with current mortality riskswell below 5% in high-volume centers.2–4 Many surgeonshave developed strategies to improve resectability of largetumors such as the induction of hypertrophy of an estimatedsmall remnant liver volume by selective portal vein emboli-zation5 and the downstaging6,7 of large liver tumors bychemotherapy. However, despite successful attempts at cur-ative resection in many situations, long-term survival hasremained somewhat disappointing, ranging between 25% and40%.8–10
Most patients after a curative resection develop recur-rent intra- or extrahepatic tumor manifestations.11 The mainreason for these tumor recurrences after putative completetumor removal is the presence of undetected tumor at the timeof surgery. Currently, patients undergo an extensive preop-erative work-up before liver resection to accurately define thehepatic lesions and to exclude the presence of extrahepatic
From the *Department of Visceral and Transplantation Surgery, Zurich,Switzerland; the †Department of Nuclear Medicine, University Hospital,Zurich, Switzerland; and the ‡University of Pittsburgh Medical Center,Pittsburgh, PA.
M.S. and T.F.H. contributed equally to this work.Reprints: Pierre-A. Clavien, MD, PhD, FACS Professor of Surgery Depart-
ment of Surgery University Hospital Zurich Ramistrasse 10, 8091 Zurich,Switzerland. E-mail: [email protected].
Copyright © 2004 by Lippincott Williams & WilkinsISSN: 0003-4932/04/24006-1027DOI: 10.1097/01.sla.0000146145.69835.c5
Annals of Surgery • Volume 240, Number 6, December 2004 1027

disease. This includes spiral contrast-enhanced computedtomography (ceCT), magnetic resonance imaging, andcolonoscopy. This strategy, however, is insufficient in viewof the poor long-term results and the fact that many patientsare still found to be unresectable at the time of surgery.
These shortcomings have prompted the development ofnew diagnostic tools. It has been shown for more than 50years that most tumors have a higher utilization and metab-olism rate of glucose.12,13 This has lead to the development ofan imaging modality using positron emission tomography(PET) of 18F-labeled glucose, 2-�18-F�-fluoro-2-deoxyglucose(FDG), to detect cancer cells. FDG is transported into tumorcells by hexose transporters and is then phosphorylated byhexokinase to FDG-6-phosphate. FDG-6-phosphate cannot befurther metabolized in most tumor cells, thereby it selectivelyaccumulates in the cancer tissue.14 FDG-PET offers new infor-mation on specific metabolic features of cancer cells rather thananatomic data on the localization of a lesion.
Several recent studies have demonstrated a high sensi-tivity and specificity of FDG-PET scanning for several typesof cancers,15–17 including colorectal cancer.18–20 Retrospec-tive studies have also suggested that the availability of PETallows improved selection of patients with metastatic colo-rectal cancer to the liver, resulting in better survival after liverresection.21 For example, in 1 study, PET imaging detectedextrahepatic tumor in 25% of patients found to have resect-able hepatic metastases by conventional preoperative work-up.21 However, PET is limited by a poor resolution and pooranatomic localization of positive PET lesions. As a result, thediagnosis ultimately relies on a correlation between findingsobtained on CT or magnetic resonance imaging and the PETscan. To overcome this limitation, a new technique combin-ing the same imaging session data of a full-ring PET-scannerwith a multi-detector row helical CT has been developed.22
With this novel technology, the PET-positive lesions areprojected directly into the CT scan to obtain simultaneousfunctional and anatomic information. These theoretical ad-vantages have recently been confirmed in lung cancer, wherePET/CT was significantly more accurate in predicting thetumor stage than PET or CT alone.16
PET/CT technology was introduced in our center inApril 2001, and patients with colorectal tumor referred for aliver resection underwent a PET/CT after conventional work-up. Data was prospectively collected to assess the ability ofPET/CT to detect new tumor lesions and to evaluate how theavailability of PET/CT imaging impacted on the selection ofpatients for surgery.
METHODS
Study DesignFrom January 2002 until July 2003, each patient being
considered for liver resection for metastases from colorectal
origin was included in the study. Cases with synchronousmetastases were not present in this series. Conventionalwork-up included ceCT of the chest and abdomen, and whenconventional imaging data from referring institutions wasinsufficient, that is, of poor quality or ceCT older than 15days, a new ceCT was performed in our center. A colonos-copy was also required within 6 months prior to surgery. APET/CT was obtained after completion of the conventionalwork-up. Any new lesion diagnosed on PET/CT was subse-quently confirmed by percutaneous or surgical biopsies. Thefinal decision to proceed with liver resection was based on allavailable data. In patients felt to have resectable lesions, astandard exploration of the abdominal cavity was performed,including routine intraoperative ultrasound by an independentinvestigator as well as biopsies of each lesion noted on ceCTor PET/CT. In patients who were considered nonoperable, theclinical course and serial ceCT (3 and 6 months) were used toconclusively establish the diagnosis of the initial ceCT andPET/CT findings. The PET/CT images were individuallyevaluated by a board-certified radiologist and nuclear medi-cine physician (T.F.H.) unaware of the other conventionalimaging findings. The main end point was to assess howPET/CT may change the indications for surgery comparedwith conventional radiology, that is, ceCT alone. Secondaryend points included the number of true- and false-positive and-negative PET/CT findings, the ability of ceCT and PET/CTto detect extrahepatic disease and recurrent liver tumor afterhepatectomy, and finally the influence of chemotherapy onthe detection of tumors by PET/CT. False-positive findingswere defined as benign lesion, which were diagnosed as livermetastases. Liver metastases, which were missed by an im-aging technique, were counted as false-negative findings.
ceCT Imaging ProtocolIn-house ceCT imaging was performed with a multi-
detector row scanner (Somatom Volume Zoom Siemens,Erlangen, Germany). For contrast-enhancement, 120 to 150mL of contrast media (Imagopaque, Amersham, AS, Oslo,Norway) was injected intravenously. An arterial as well as aporto-venous phase of the liver was acquired according to thefollowing parameters: 140 kV, 180mAs, collimation 4 � 1 to4 � 2.5 mm, pitch 1.5 to 1.25, reconstruction interval (mm) 1 to2, slice with 1.25 to 3 mm. Arterial phase imaging was per-formed with an automatic-bolus tracking system; the initiationof the porto-venous phase was set around 20 seconds after theend of the data acquisition of the arterial phase. Both scanscovered the thorax and abdomen to the level of the groins.
PET/CT Imaging ProtocolAll imaging and data acquisition was performed on a
combined PET/CT system (Discovery LS, GE Medical Sys-tems, Waukesha, WI) able to acquire CT images and PETdata on the same patient in 1 session. A GE Advance NXi
Selzner et al Annals of Surgery • Volume 240, Number 6, December 2004
© 2004 Lippincott Williams & Wilkins1028

PET scanner and a multidetector-row helical CT (LightSpeedPlus) are integrated in this dedicated system. The tableexcursion permitted scanning of 7 contiguous PET sectionscovering 1011 mm. This gave adequate coverage from headto pelvic floor in all patients examined. The PET and CT datasets were acquired on 2 independent computer consoles,which were connected by an interface to transfer CT data tothe PET scanner. For viewing of the images, the PET and CTdata sets were transferred to an independent, PC-based com-puter workstation by DICOM transfer. All viewing of coreg-istered images were performed with a dedicated softwaresystem (eNTEGRA, ELGEMS, Haifa, Israel). Whereas PETimages were acquired during free breathing and each imagewas obtained over multiple respiratory cycles, CT scans wereperformed during shallow breathing.
The patients were fasted for at least 4 hours before theintravenous administration of 10 mCi (370MBq) of FDG.Forty-five minutes postinjection, the combined examinationstarted. CT data were acquired first. The patients were posi-tioned on the table in a head-firs supine position. The arms ofthe patients were placed in an elevated position above thehead to reduce beam-hardening artifacts. However, in pa-tients unable to maintain this position, arms were positionedin front of the abdomen (n � 14). For the CT data acquisition,the following parameters were used: tube-rotation time 0.5seconds per evolution, 140kV, 80 mA, 22.5 mm per rotation,slice beam pitch 1.5 (high-speed mode), reconstructed slice-thickness 4.25 mm, scan length 867 mm, and acquisition time22.5 seconds per CT scan. No intravenous or oral contrastagents were used. After the CT data acquisition was com-pleted, the tabletop was automatically advanced into the PETgantry, and acquisition of PET data was started at the level ofthe pelvic floor. Six incremental table positions were acquiredwith minimal overlap, thereby covering 867 mm of tabletravel. For each position, 35 2-dimensional nonattenuation-corrected scans were obtained simultaneously over a5-minute period. No transmission scans were obtained be-cause CT data were used for transmission correction. Thetechnique for using CT data for attenuation correction hasbeen described in detail elsewhere.23 The images were recon-structed with iterative reconstruction with 2 iterations and 28subsets resulting in 35 2-dimensional sections over each axialfield-of-view increment of 14.6 cm, resulting in a slicethickness of 4.25 mm. Image reconstruction matrix was 128� 128 with a transaxial field of view of 49.7 � 49.7cm.
Data AnalysisThe attenuation-corrected PET images, the CT images,
and the coregistered PET/CT images were viewed simulta-neously by a board-certified radiologist using eNTEGRAsoftware. Image interpretation was based on the identificationof regions with increased FDG uptake on the PET images andthe anatomic delineation of all FDG-avid lesions on the coreg-
istered PET/CT images. Furthermore, all CT images wereviewed separately to identify additional lesions without FDGuptake using soft tissue, lung, and bone window leveling.
Statistical AnalysisDifferences in the ability to detect intrahepatic and
extrahepatic lesions between the CT scan and PET/CT werecalculated by the �2 test. A P value of less than 0.05 wasconsidered to be statistically significant. The statistical anal-ysis was performed with the Statistical Package and SoftwareSolution 9.0 (SPSS, Chicago, IL) software.
RESULTS
DemographicsSeventy-six patients (52 men, 24 women) with a me-
dian age of 63 years (range 35–78 years) were included in thestudy. Each patient was evaluated for resectability of meta-static colorectal cancer to the liver and received a ceCT anda PET/CT within a period of 2 weeks. The median timebetween colorectal resection and initial presentation was 14months (range 3–25 months). Sixty-two patients receivedchemotherapy after the colorectal cancer surgery with amedian interval between last chemotherapy and PET/CT of 3months (range 7 days to 15 months). The median follow-upof patients was 16 months (6 months to 3 years).
The data was analyzed in a step-by-step manner.1 First,a correlation of the ceCT and PET/CT findings was per-formed, including an analysis of all additional informationprovided by PET/CT. We then focused on2 identification ofeach positive and negative finding with ceCT and PET/CT,3
the ability of PET/CT to identify metastases at differentextrahepatic sites and at the site of local recurrence afterhepatectomy, and4 the potential effect of chemotherapy onfalse-negative PET/CT findings. Finally, as the main endpoint of the study, we assessed the impact of PET/CT on themanagement of patients with liver metastases.
How Does ceCT Compare to PET/CTRegarding the Detection of Intra- andExtrahepatic Metastases?
The presence of liver metastases was evaluated andallocated into the following groups: (A) unilobar disease upto 3 lesions; (B) unilobar disease with 4 or more lesions; and(C) bilobar disease. As shown in Table 1, liver lesions werediagnosed as benign in 8 patients by ceCT and in 14 patientsby PET/CT. About half of the remaining patients were ingroup A with either diagnostic modality, less than 5% were ingroup B, and about a third of patients were in group C.Therefore, no difference was noted between ceCT andPET/CT regarding the detection of intrahepatic metastasesaccording to the classification used. Local recurrence at thesite of the colorectal primary tumor was found in 9 patients(11%) in the ceCT and in 15 patients (20%) in the PET/CT
Annals of Surgery • Volume 240, Number 6, December 2004 PET/CT Imaging of Patients With Metastatic Colorectal Cancer
© 2004 Lippincott Williams & Wilkins 1029
(P � 0.27, Fisher’s exact test). The presence of extrahepaticdisease was identified by ceCT in 24 patients (31%), whereasPET/CT identified 34 patients (45%) with extrahepatic le-sions (P � 0.13). False-positive and -negative findings arepresented below.
What Was the Incidence of False-Negative andFalse-Positive Findings With ceCT and PET/CT?
An analysis of false-positive and -negative ceCT andPET/CT findings was performed. The final diagnosis wasbased on intraoperative findings including a comprehensiveultrasound evaluation, histology of the resected liver andother biopsies, and follow-up with serial ceCT in all patients,including those who did not undergo surgery.
Ten patients (13%) had only benign liver lesions with-out evidence of malignancy. ceCT correctly identified 7patients as cancer-free with false-positive results in 3 patients(2 adenomas and 1 hemangioma) (specificity 70%). PET/CTruled out cancer in 9 patients, with 1 patient being false-positive (liver abscess) (specificity 90%, P � 0.58). Amongthe 66 patients with documented liver metastases, ceCTmissed hepatic lesions in 3 patients (5%) and providedfalse-positive results in 1 case (sensitivity 95%). By contrast,PET/CT did not detect the liver metastasis in 6 patients (9%)(sensitivity 91%).
Local recurrence at the site of previously resectedcolorectal tumor was present in 15 patients. ceCT missed thediagnosis or provided inconclusive information in 7 patients
(53%; sensitivity 53%), whereas PET/CT allowed identifica-tion of 14 of the 15 patients, with 1 patient being false-negative (7%, sensitivity 93%, P � 0.03) (Table 2).
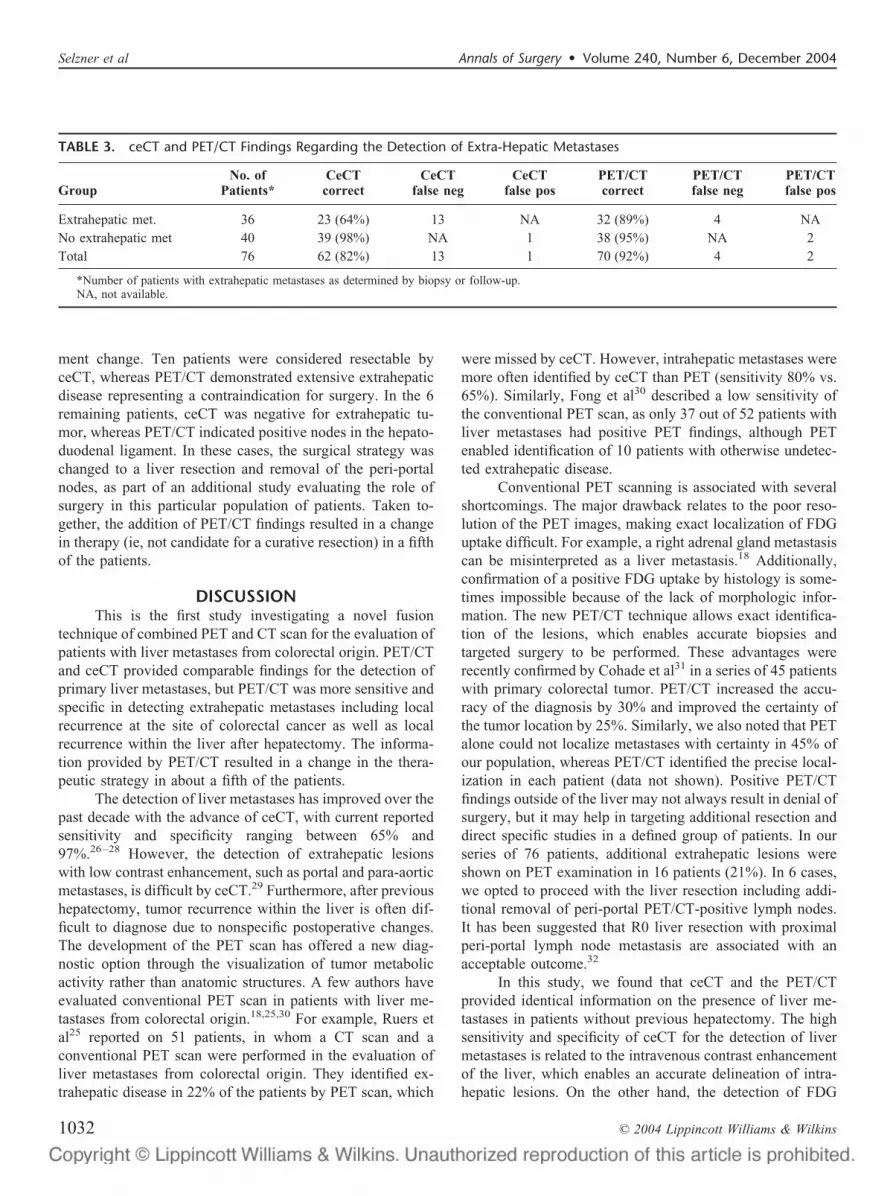
Extrahepatic metastases were present in 36 of the 66patients (55%) (Fig. 2). ceCT failed to diagnose extrahepaticmetastases in 13 of the 36 patients (36%) (sensitivity 64%),whereas PET/CT did not diagnose extrahepatic lesions inonly 4 (11%) of the 36 cases (sensitivity 89%; P � 0.02)(Table 3).
How Does PET/CT Compare to ceCT in theDetection of Local Recurrence in the LiverAfter Hepatectomy?
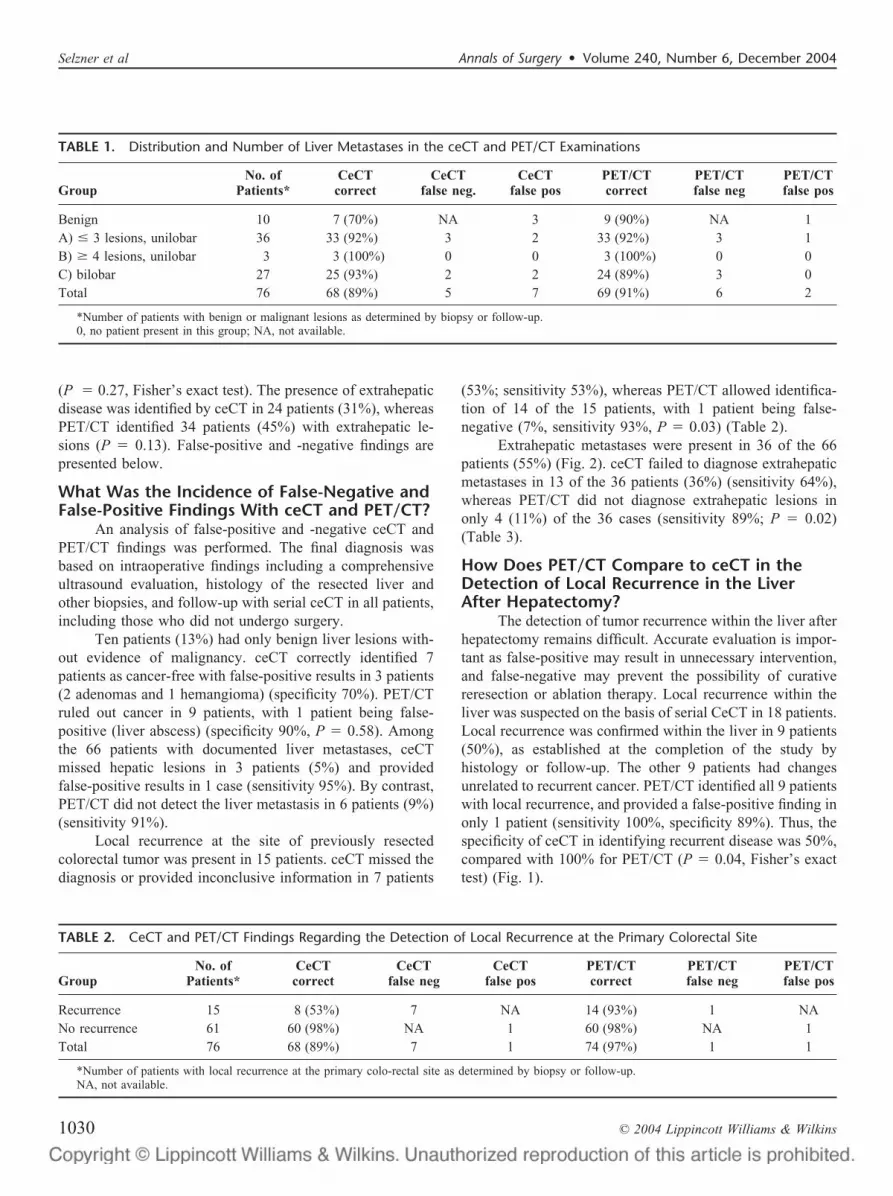
The detection of tumor recurrence within the liver afterhepatectomy remains difficult. Accurate evaluation is impor-tant as false-positive may result in unnecessary intervention,and false-negative may prevent the possibility of curativereresection or ablation therapy. Local recurrence within theliver was suspected on the basis of serial CeCT in 18 patients.Local recurrence was confirmed within the liver in 9 patients(50%), as established at the completion of the study byhistology or follow-up. The other 9 patients had changesunrelated to recurrent cancer. PET/CT identified all 9 patientswith local recurrence, and provided a false-positive finding inonly 1 patient (sensitivity 100%, specificity 89%). Thus, thespecificity of ceCT in identifying recurrent disease was 50%,compared with 100% for PET/CT (P � 0.04, Fisher’s exacttest) (Fig. 1).
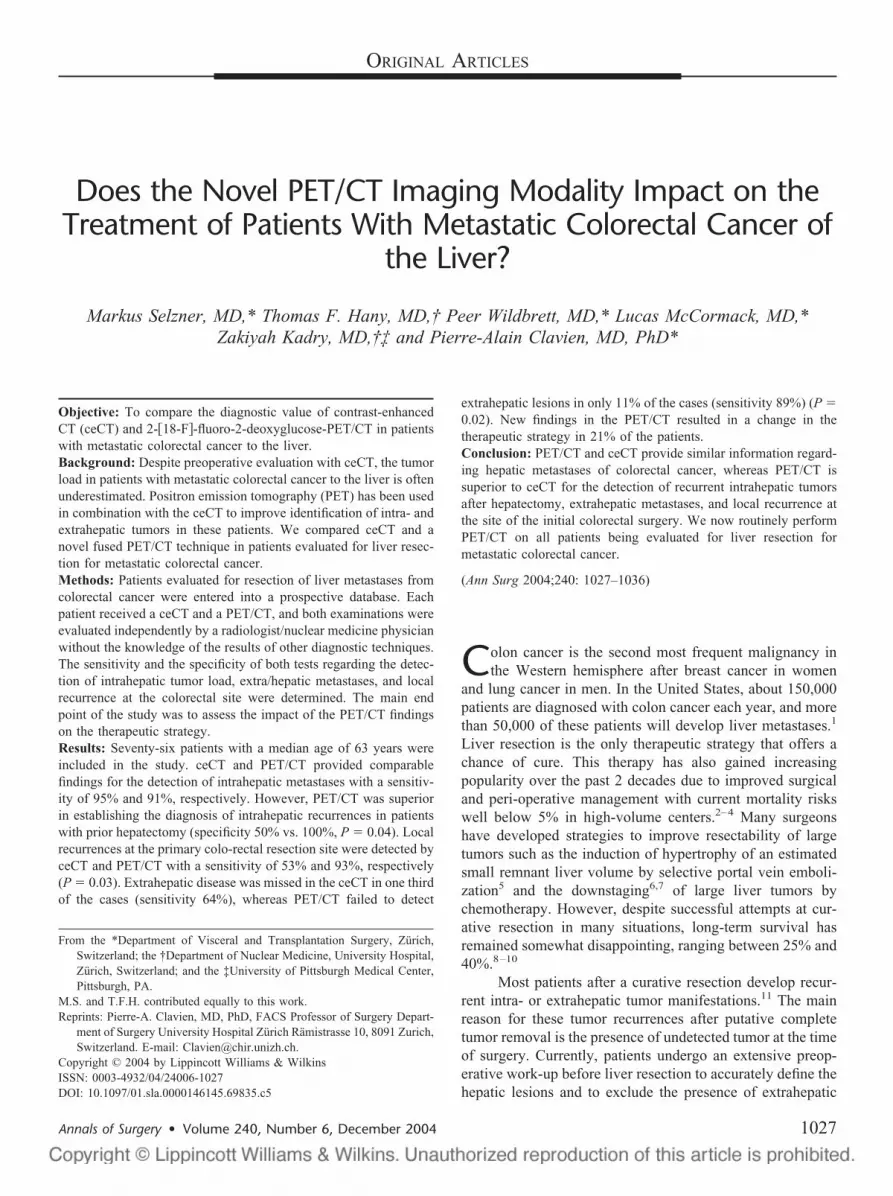
TABLE 1. Distribution and Number of Liver Metastases in the ceCT and PET/CT Examinations
GroupNo. of
Patients*CeCTcorrect
CeCTfalse neg.
CeCTfalse pos
PET/CTcorrect
PET/CTfalse neg
PET/CTfalse pos
Benign 10 7 (70%) NA 3 9 (90%) NA 1A) � 3 lesions, unilobar 36 33 (92%) 3 2 33 (92%) 3 1B) � 4 lesions, unilobar 3 3 (100%) 0 0 3 (100%) 0 0C) bilobar 27 25 (93%) 2 2 24 (89%) 3 0Total 76 68 (89%) 5 7 69 (91%) 6 2
*Number of patients with benign or malignant lesions as determined by biopsy or follow-up.0, no patient present in this group; NA, not available.
TABLE 2. CeCT and PET/CT Findings Regarding the Detection of Local Recurrence at the Primary Colorectal Site
GroupNo. of
Patients*CeCTcorrect
CeCTfalse neg
CeCTfalse pos
PET/CTcorrect
PET/CTfalse neg
PET/CTfalse pos
Recurrence 15 8 (53%) 7 NA 14 (93%) 1 NANo recurrence 61 60 (98%) NA 1 60 (98%) NA 1Total 76 68 (89%) 7 1 74 (97%) 1 1
*Number of patients with local recurrence at the primary colo-rectal site as determined by biopsy or follow-up.NA, not available.
Selzner et al Annals of Surgery • Volume 240, Number 6, December 2004
© 2004 Lippincott Williams & Wilkins1030
What Is the Ability of PET/CT to IdentifyTumors at Specific Extrahepatic Locations?
Because the ability to detect extrahepatic metastases byceCT or PET/CT could be dependent on the location, weseparately evaluated metastases in the lung, portal, or para-aortic lymph nodes, as well as in bone.
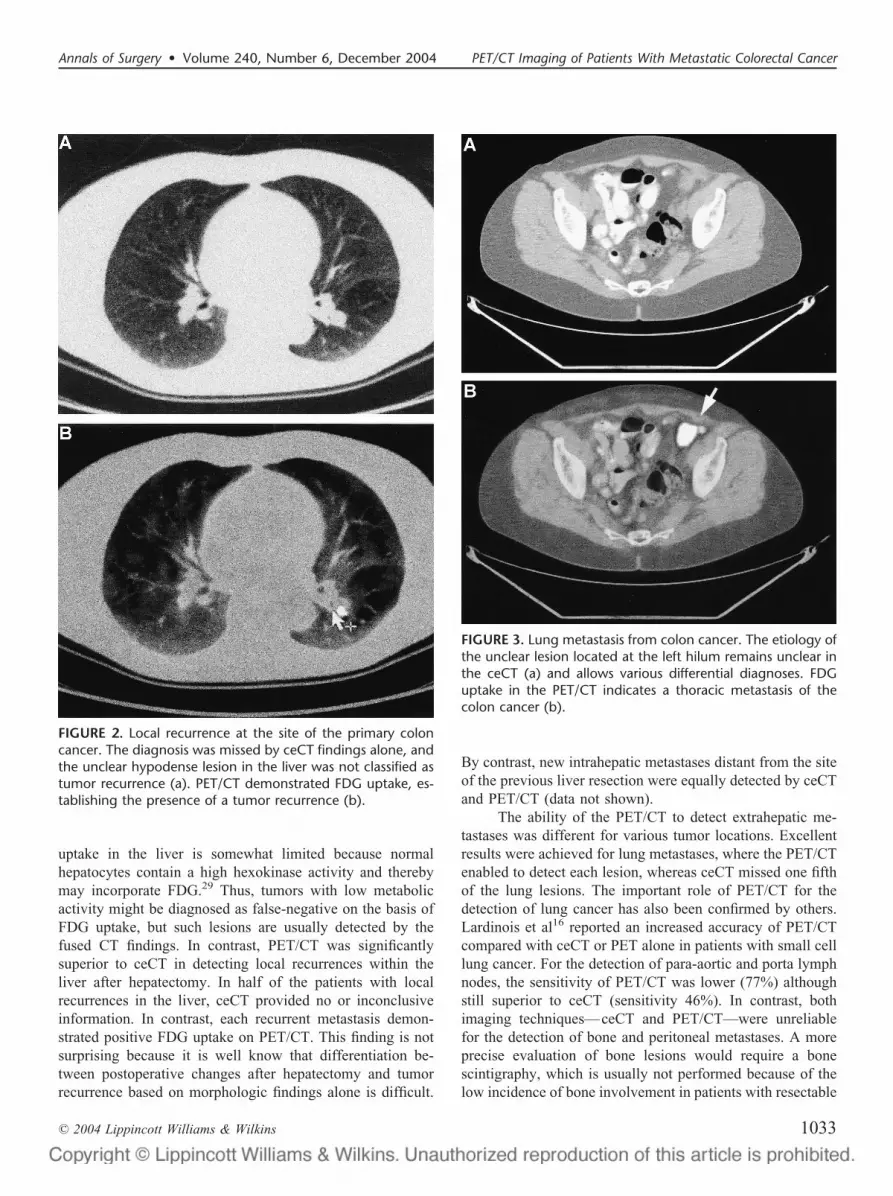
Lung metastases were present in 18 patients and werecorrectly diagnosed in each patient by PET/CT (sensitivity
100%). By contrast, ceCT failed to detect lung metastases in4 (22%) of the 18 patients (sensitivity 78%, P � 0.1) (Fig. 3).Portal and para-aortic lymph node metastases were present in13 patients. ceCT failed to identify these lesions in 7 patients(54%, sensitivity 46%), whereas PET/CT missed this diag-nosis in 3 patients (23%) (sensitivity 77%, P � 0.4). Bonemetastases were noted in 4 patients at the time of the initialpresentation. These bone lesions were missed by ceCT in 2patients and by PET/CT in 1.
Does the Use of Chemotherapy Before PET/CTInfluence FDG Uptake of ColorectalMetastases?
It has been suggested that the use of chemotherapywithin a month of a PET examination may decrease thesensitivity of PET scan in detecting tumors24, although othershave challenged this shortcoming.25 To address this issue, wedetermined the number of false-negative FDG-uptake in pa-tients with previous chemotherapy versus those without pre-vious chemotherapy administration. Eighteen received che-motherapy within 1 month prior to PET/CT. FDG uptake wasabsent in the liver metastases in 5 patients (28%) in the groupwith recent chemotherapy (sensitivity 72%) and in 1 of 58patients (5%) in the group without recent chemotherapy(sensitivity 98%, P � 0.14, Fisher’s exact test).
Extrahepatic metastases were present in 9 of the 18patients with recent chemotherapy. No FDG uptake wasnoted in 3 of these 9 patients (sensitivity 66%). By contrast,among the 58 patients without recent chemotherapy, 27 hadextrahepatic metastases. FDG uptake was negative in 1patient(sensitivity 96%; P � 0.05, Fisher’s exact test).
Similar results were found regarding local recurrence atthe site of previous colorectal surgery. Such recurrence waspresent in 3 patients (17%) in the recent chemotherapy group.FDG uptake was negative in 1 of these 3 patients (sensitivity66%), whereas documented local recurrence remained FDG-negative in only 1 of 12 patients in the group withoutchemotherapy (sensitivity 92%; P � 0.08). This patient wasdiagnosed as a local recurrence by ceCT and PET/CT, despitea negative FDG-uptake, because of an obvious large tumormass infiltrating the sacrum.
How Does the Availability of PET/CT Impacton the Management of Patients With LiverMetastases?
The main end point of the study was to determinewhether the availability of PET/CT may influence the thera-peutic strategy in patients with suspected liver metastases. Inall 76 patients, a treatment plan was defined after the ceCTexamination and re-evaluated after obtaining the PET/CTdata. In 60 patients (79%), PET/CT did not change thetherapeutic strategy based on the ceCT findings alone. In 16patients (21%), the findings on PET/CT resulted in a treat-
FIGURE 1. Recurrence of a colon cancer metastasis in the liverafter previous liver resection. The ceCT (a) shows a hypodenselesion of unclear etiology. The PET/CT (b) demonstrates FDGuptake highly suggestive for tumor recurrence. The patientwas reoperated and the tumor recurrence was confirmed bypathology (c).
Annals of Surgery • Volume 240, Number 6, December 2004 PET/CT Imaging of Patients With Metastatic Colorectal Cancer
© 2004 Lippincott Williams & Wilkins 1031
ment change. Ten patients were considered resectable byceCT, whereas PET/CT demonstrated extensive extrahepaticdisease representing a contraindication for surgery. In the 6remaining patients, ceCT was negative for extrahepatic tu-mor, whereas PET/CT indicated positive nodes in the hepato-duodenal ligament. In these cases, the surgical strategy waschanged to a liver resection and removal of the peri-portalnodes, as part of an additional study evaluating the role ofsurgery in this particular population of patients. Taken to-gether, the addition of PET/CT findings resulted in a changein therapy (ie, not candidate for a curative resection) in a fifthof the patients.
DISCUSSIONThis is the first study investigating a novel fusion
technique of combined PET and CT scan for the evaluation ofpatients with liver metastases from colorectal origin. PET/CTand ceCT provided comparable findings for the detection ofprimary liver metastases, but PET/CT was more sensitive andspecific in detecting extrahepatic metastases including localrecurrence at the site of colorectal cancer as well as localrecurrence within the liver after hepatectomy. The informa-tion provided by PET/CT resulted in a change in the thera-peutic strategy in about a fifth of the patients.
The detection of liver metastases has improved over thepast decade with the advance of ceCT, with current reportedsensitivity and specificity ranging between 65% and97%.26–28 However, the detection of extrahepatic lesionswith low contrast enhancement, such as portal and para-aorticmetastases, is difficult by ceCT.29 Furthermore, after previoushepatectomy, tumor recurrence within the liver is often dif-ficult to diagnose due to nonspecific postoperative changes.The development of the PET scan has offered a new diag-nostic option through the visualization of tumor metabolicactivity rather than anatomic structures. A few authors haveevaluated conventional PET scan in patients with liver me-tastases from colorectal origin.18,25,30 For example, Ruers etal25 reported on 51 patients, in whom a CT scan and aconventional PET scan were performed in the evaluation ofliver metastases from colorectal origin. They identified ex-trahepatic disease in 22% of the patients by PET scan, which
were missed by ceCT. However, intrahepatic metastases weremore often identified by ceCT than PET (sensitivity 80% vs.65%). Similarly, Fong et al30 described a low sensitivity ofthe conventional PET scan, as only 37 out of 52 patients withliver metastases had positive PET findings, although PETenabled identification of 10 patients with otherwise undetec-ted extrahepatic disease.
Conventional PET scanning is associated with severalshortcomings. The major drawback relates to the poor reso-lution of the PET images, making exact localization of FDGuptake difficult. For example, a right adrenal gland metastasiscan be misinterpreted as a liver metastasis.18 Additionally,confirmation of a positive FDG uptake by histology is some-times impossible because of the lack of morphologic infor-mation. The new PET/CT technique allows exact identifica-tion of the lesions, which enables accurate biopsies andtargeted surgery to be performed. These advantages wererecently confirmed by Cohade et al31 in a series of 45 patientswith primary colorectal tumor. PET/CT increased the accu-racy of the diagnosis by 30% and improved the certainty ofthe tumor location by 25%. Similarly, we also noted that PETalone could not localize metastases with certainty in 45% ofour population, whereas PET/CT identified the precise local-ization in each patient (data not shown). Positive PET/CTfindings outside of the liver may not always result in denial ofsurgery, but it may help in targeting additional resection anddirect specific studies in a defined group of patients. In ourseries of 76 patients, additional extrahepatic lesions wereshown on PET examination in 16 patients (21%). In 6 cases,we opted to proceed with the liver resection including addi-tional removal of peri-portal PET/CT-positive lymph nodes.It has been suggested that R0 liver resection with proximalperi-portal lymph node metastasis are associated with anacceptable outcome.32
In this study, we found that ceCT and the PET/CTprovided identical information on the presence of liver me-tastases in patients without previous hepatectomy. The highsensitivity and specificity of ceCT for the detection of livermetastases is related to the intravenous contrast enhancementof the liver, which enables an accurate delineation of intra-hepatic lesions. On the other hand, the detection of FDG
TABLE 3. ceCT and PET/CT Findings Regarding the Detection of Extra-Hepatic Metastases
GroupNo. of
Patients*CeCTcorrect
CeCTfalse neg
CeCTfalse pos
PET/CTcorrect
PET/CTfalse neg
PET/CTfalse pos
Extrahepatic met. 36 23 (64%) 13 NA 32 (89%) 4 NANo extrahepatic met 40 39 (98%) NA 1 38 (95%) NA 2Total 76 62 (82%) 13 1 70 (92%) 4 2
*Number of patients with extrahepatic metastases as determined by biopsy or follow-up.NA, not available.
Selzner et al Annals of Surgery • Volume 240, Number 6, December 2004
© 2004 Lippincott Williams & Wilkins1032
uptake in the liver is somewhat limited because normalhepatocytes contain a high hexokinase activity and therebymay incorporate FDG.29 Thus, tumors with low metabolicactivity might be diagnosed as false-negative on the basis ofFDG uptake, but such lesions are usually detected by thefused CT findings. In contrast, PET/CT was significantlysuperior to ceCT in detecting local recurrences within theliver after hepatectomy. In half of the patients with localrecurrences in the liver, ceCT provided no or inconclusiveinformation. In contrast, each recurrent metastasis demon-strated positive FDG uptake on PET/CT. This finding is notsurprising because it is well know that differentiation be-tween postoperative changes after hepatectomy and tumorrecurrence based on morphologic findings alone is difficult.
By contrast, new intrahepatic metastases distant from the siteof the previous liver resection were equally detected by ceCTand PET/CT (data not shown).
The ability of the PET/CT to detect extrahepatic me-tastases was different for various tumor locations. Excellentresults were achieved for lung metastases, where the PET/CTenabled to detect each lesion, whereas ceCT missed one fifthof the lung lesions. The important role of PET/CT for thedetection of lung cancer has also been confirmed by others.Lardinois et al16 reported an increased accuracy of PET/CTcompared with ceCT or PET alone in patients with small celllung cancer. For the detection of para-aortic and porta lymphnodes, the sensitivity of PET/CT was lower (77%) althoughstill superior to ceCT (sensitivity 46%). In contrast, bothimaging techniques—ceCT and PET/CT—were unreliablefor the detection of bone and peritoneal metastases. A moreprecise evaluation of bone lesions would require a bonescintigraphy, which is usually not performed because of thelow incidence of bone involvement in patients with resectable
FIGURE 2. Local recurrence at the site of the primary coloncancer. The diagnosis was missed by ceCT findings alone, andthe unclear hypodense lesion in the liver was not classified astumor recurrence (a). PET/CT demonstrated FDG uptake, es-tablishing the presence of a tumor recurrence (b).
FIGURE 3. Lung metastasis from colon cancer. The etiology ofthe unclear lesion located at the left hilum remains unclear inthe ceCT (a) and allows various differential diagnoses. FDGuptake in the PET/CT indicates a thoracic metastasis of thecolon cancer (b).
Annals of Surgery • Volume 240, Number 6, December 2004 PET/CT Imaging of Patients With Metastatic Colorectal Cancer
© 2004 Lippincott Williams & Wilkins 1033

liver metastases from colorectal cancer. Peritoneal lesionscan be detected by laparoscopy prior to laparotomy, and ourresults indicate that PET/CT cannot replace staging laparos-copy for the diagnosis of peritoneal lesions.
Local recurrence at the site of the primary colorectalcancer is often missed by conventional ceCT, and positivefindings are difficult to interpret due to the inherent changesrelated to previous colectomy and sometimes to postoperativeinfection. In this study, 15 patients (20%) had a local colo-rectal recurrence at the time of evaluation for liver resection.ceCT enabled the detection of only half of these patients,whereas all but 1 (93%) were correctly diagnosed by PET/CT. Of note, the patient with a false-negative lesion receivedchemotherapy within a week of the CT/PET scan. A potentialpitfall of PET/CT is the inability to differentiate betweentumor and chronic infection, because both situations areassociated with an increased FDG uptake. Although no false-positive findings regarding local recurrence were present inthe current series, this shortcoming needs to be considered.Whether PET/CT can obviate the need for colonoscopyremains to be demonstrated, but it is likely that PET/CT issuperior because local recurrence is often extraluminal,which may remain undetected by endoscopy.
Although our study demonstrates that PET/CT providesvaluable new information, several shortcomings need to behighlighted. FDG uptake is often not detected in small tumors(eg, �5 mm), which are also often missed on ceCT. There arecurrently no tests that can prevent such false-negative find-ings. As mentioned above, there are also false-positive find-ings, particularly in the setting of infection because FDGuptake will occur in infected lymph nodes.19,30 Furthermore,the clinical history should be well known because high bloodglucose levels or recent chemotherapy may prevent FDGuptake by cancer cells. In this study, we found that the use ofchemotherapy within 1 month of PET/CT resulted in a highincidence of false-negative results. Therefore, FDG uptakeseems to be unreliable in patients with recent chemotherapy.However, whereas FDG uptake was negative, most of theselesions were seen by the fused CT findings. Thus, if theclinician is aware of this limitation, findings on PET/CT canstill be of value.
In this study, we performed PET/CT without the use ofintravenous contrast; therefore intrahepatic vascular struc-tures were poorly delineated. This information is crucial inthe planning of the surgical strategy. In addition, infiltrationand thrombosis of portal vein branches are important piecesof information with prognostic significance. As a result, wenow evaluate PET/CT with intravenous contrast, because thismay obviate the need for additional ceCT or magnetic reso-nance imaging, or perhaps colonoscopy. Such a strategywould be attractive, enabling a one-step diagnostic procedurewith a potential reduction in cost.
In conclusion, we demonstrate that PET/CT providesimportant additional information in patients with presumedresectable colorectal metastases to the liver, resulting in achange of therapy in a fifth of patients. The most significantadditional information relates to the accurate detection ofextrahepatic spread of tumor. Also, PET/CT was particularlyvaluable in detecting local recurrence at the margin of aprevious liver resection and at the site of the primary colo-rectal surgery. Future studies should evaluate whetherPET/CT with the simultaneous use of intravenous contrastwould enable an accurate anatomic staging of patients withliver metastases without the need for additional tests.
REFERENCES1. Parker S, Tong T, Bolden S, et al. Cancer statistics. Cancer J Clin.
1997;47:5–27.2. Selzner M, Clavien PA. Resection of liver tumors: Special emphasis on
neoadjuvant and adjuvant therapy. In: Clavien PA, editor. MalignantLiver Tumors: Current and Emerging Therapies. Malden: BlackwellScience; 1999:137–149.
3. Belghiti J, Hiramatsu K, Benoist S, et al. Seven hundred forty-sevenhepatectomies in the 1990s: an update to evaluate the actual risk of liverresection. J Am Coll Surg. 2000;191:38–46.
4. Clavien PA, Selzner M, Rudiger H, et al. A prospective randomizedstudy in 100 consecutive patients undergoing major liver resection withvs. without ischemic preconditioning. Ann Surg. 2003;238:843–852.
5. Azoulay D, Castaing D, Smail A, et al. Resection of nonresectable livermetastases from colorectal cancer after percutaneous portal vein embo-lization. Ann Surg. 2000;231:480–486.
6. Clavien PA, Selzner N, Morse M, et al. Downstaging of hepatocellularcarcinoma and metastasis from colorectal cancer by selective intraarterial chemotherapy. Surgery. 2002;131:433–442.
7. Bismuth H, Adam R, Levi F, et al. Resection of nonresectable livermetastases from colorectal cancer after neoadjuvant chemotherapy. AnnSurg. 1996;224:509–522.
8. Figueras J, Farran L, Benasco C, et al. Vascular occlusion in hepaticresections in cirrhotic rat livers: an experimental study in rats. LiverTransplant Surg. 1997;3:617–623.
9. Fong Y, Fortner J, Sun RL, et al. Clinical score for predicting recurrenceafter hepatic resection for metastatic colorectal cancer: analysis of 1001consecutive cases. Ann Surg 1999;230:309–321.
10. Millikan KW, Staren ED, Doolas A. Invasive therapy of metastaticcolorectal cancer to the liver. Surg Clin North Am. 1997;77:27–48.
11. Scheele J, Stangl R, Altendorf-Hoffmann A. Indicators of prognosis afterhepatic resection for colorectal secondaries. Surgery. 1991;110:13–15.
12. Warburg O, Wind F, Neglers E. On the Metabolism of Tumors in theBody. London: Constable; 1930.
13. Som P, Atkins H, Bandopadhyay D, et al. A fluorinated glucose analoge,2-fluoro-2-deoxy-D-glucose (F18): nontoxic tracer for rapid tumor de-tection. J Nucl Med 1980;21:670–675.
14. Lewis P, Griffin S, Marsden P, et al. Whole-body 18F-fluorodeoxyglu-cose positron emission tomography in preoperative evaluation of lungcancer. Lancet. 1994;344:1265–1266.
15. Lowe V. Positron emission tomography scanning in lung cancer. RespCare Clin North Am. 2003;9:119–136.
16. Lardinois D, Weder W, Hany T, et al. Staging of non-small-cell lungcancer with integrated positron-emission tomography and computedtomography. N Engl J Med. 2003;348:2500–2507.
17. Prichard R, Hill A, Skehan S, O’Higgins N. Positron emission tomog-raphy for staging and management of malignant melanoma. Br J Surg.2002;89:389–396.
18. Lai D, Fulham M, Stephen M, et al. The role of whole-body positronemission tomography with �18�fluorodeoxyglucose in identifying oper-able colorectal cancer metastases to the liver. Arch Surg. 1996;131:703–707.
Selzner et al Annals of Surgery • Volume 240, Number 6, December 2004
© 2004 Lippincott Williams & Wilkins1034

19. Desai C, Zervos E, Arnold M, et al. Positron emission tomographyaffects surgical management in recurrent colorectal cancer patients. AnnSurg Oncol. 2003;10:59–64.
20. Topal B, Flamen P, Aert R, et al. Clinical value of whole-body positronemission tomography in potentially curable colorectal liver metastases.EJSO. 2001;27:175–179.
21. Fernandez FG, Drebin JA, Linehan DC, Dehdashti F, Siegel BA,Strasberg SM. Five-year survival after resection of hepatic metastasesfrom colorectal cancer in patients screened by positron emission tomog-raphy with F-18 fluorodeoxyglucose. Ann Surg. 2004;240:438–447.
22. Hany T, Steinert H, Goerres G, et al. PET diagnostic accuracy: improve-ment with in-line PET-CT system: Initial results. Radiology. 2002;225:575–581.
23. Kamel E, Hany TF, Burger C, et al. CT vs 68Ge attenuation correctionin a combined PET/CT system: evaluation of the effect of lowering theCT tube current. Eur J Nucl Med Mol Imaging. 2002;29:346–350.
24. Findlay M, Young H, Cunningham D, et al. Noninvasive monitoring oftumor metabolism using fluorodeoxyglucose and positron emission to-mography in colorectal cancer liver metastases: correlation with tumorresponse to fluorouracil. J Clin Oncol. 1996;14:700–708.
25. Ruers T, Neeleman N, Jager G, et al. Value of positron emissiontomography with �F-18�fluorodeoxyglucose in patients with colorectalliver metastases: a prospective study. J Clin Oncol. 2002;20:388–395.
26. Schiepers C, Penninckx F, Vadder N, et al. Contribution of PET in thediagnosis of recurrent colorectal cancer: comparison with conventionalimaging. Eur J Surg Oncol. 1995;21:517–522.
27. Vitola J, Delbeke D, Sandler M, et al. Positron emission tomography tostage suspected metastatic colorectal carcinoma to the liver. Am J Surg.1996;171:21–26.
28. Johnson K, Bakhsh A, Young D, et al. Correlating computed tomogra-phy and positron emission tomography scan with operative findings inmetastatic colorectal cancer. Dis Colon Rectum. 2001;44:354–357.
29. Beets G, Penninckx F, Schiepers C, et al. Clinical value of whole-bodypositron emission tomography with �18F�fluorodeoxyglucose in recur-rent colorectal cancer. Br J Surg 1994;81:1666–1670.
30. Fong Y, Saldinger P, Akhurst T, et al. Utility of �18�F-FDG positronemission tomography scanning on selection of patients for resection ofhepatic colorectal metastases. Am J Surg. 1999;178:282–287.
31. Cohade C, Osman M, Leal J, et al. Direct comparison of (18)F-FDGPET and PET/CT in patients with colorectal carcinoma. J Nucl Med.2003;44:1797–1803.
32. Jaeck D, Nakano H, Bachellier P, et al. Significance of hepatic lymphenode involvement in patients with colorectal liver metastases: a prospec-tive study. Ann Surg Oncol. 2002;9:430–438.
DiscussionsDR. JAECK: Thank you for the opportunity to discuss
this very nice paper. I think that you have to be congratulatedfor this very interesting study. It is the first prospective studycomparing contrast CT and PET-CT in the preoperativeevaluation of colorectal liver metastases. There was a realneed to perform such a study. The main end point of the studywas to evaluate how the PET-CT could change the surgicalindications. You showed that in 79% of the patients, it didnot. For the remaining 16 patients, the findings resulted in achange of treatment; however, 6 were still considered resect-able, but with extrahepatic disease resection, and finally only10 were not operated.
My first question concerns the cost-effectiveness ofPET-CT. My second question concerns the 6 patients that youdecided to operate on despite the presence of extrahepaticdisease. Were you able to differentiate the PET-CT-positive
nodes in the hepato-duodenal ligament from positive nodesaround the celiac axis, as we could show previously that onlyproximal periportal lymph node metastases are associatedwith acceptable outcome? My main concern is about the 10patients you decided not to operate. Indeed, if the extrahe-patic disease could have been resected, it would suppresswrongly for these patients any hope for cure. My question is,did you use additional exploration such as biopsy to confirmthe results of PET-CT and to avoid any false-positive? Sec-ondly, what is your policy concerning resectable extra-he-patic disease, as you did not mention this aspect in yourselection criteria?
Finally, it would be very interesting to compare CT toPET-CT with simultaneous use of intravenous contrast,which will probably add more information.
DR. SELZNER: Dr. Jaeck, thank you for your thoughtfulcomments. Cost-effectiveness was not an end point in ourstudy, and therefore we cannot give you detailed informationon this issue. However, since surgery was avoided in 10 outof 66 patients, substantial cost savings might be expected.Second, because of the high anatomic resolution of thePET/CT, we could convincingly differentiate PET positivelymph nodes in the hepato-duodenal ligament from thosearound the celiac axis. Third, in our series a biopsy wasperformed in each PET/CT positive finding, which was notseen by conventional ceCT. Fourth, we consider extrahepaticdisease as a contraindication for liver resection, except forresectable lung lesions and proximal periportal lymph nodemetastases.
DR. SENNINGER: Thank you very much for your presen-tation. You are well ahead of us with an instrument like this;we have a PET/CT in Munster since January this year.
I have 1 comment and 2 short questions. The commentwould be that in our experience we do not trust pelvic CTguided biopsies if they are negative. Whatever they show,during the exploration you can have a safe look at the liverand at the same time you can investigate if there is a leakageof the anastomosis that could result in a false-positive PETfinding. Can you describe the effects of a previous thermo-ablation in the liver on PET results, because the surroundinginflammation could give a false-positive PET enhancement?Second, could you please highlight the value of the PET/CTfor the differentiation of benign and malignant lesions? Everyliver center has 1 or 2 patients per year where benign lesionsare thought to be benign but turn out to be a malignant tumor.
DR. SELZNER: No patient received thermo-ablation priorto the PET/CT in our series. However, this is an importantquestion to address in future studies. Concerning your secondquestion, our study focused on patients with suspected livermetastases, and in this population PET/CT was superior to
Annals of Surgery • Volume 240, Number 6, December 2004 PET/CT Imaging of Patients With Metastatic Colorectal Cancer
© 2004 Lippincott Williams & Wilkins 1035

ceCT in identifying the nature of the liver lesion. A series ofpatients with suspected benign liver lesions would be neces-sary to properly address the role PET/CT in securing thebenignity of such lesions.
DR. NEUHAUS: Part of my questions has already beenanswered. I would, however, like to ask you what you woulddecide and how you would proceed if 6 or 9 months afterrectal excision or low anterior resection you have a singleresectable liver metastasis and a positive PET finding in thepelvis? Would you deny a possibly life-saving operationbecause of a positive PET result?
DR. SELZNER: Dr. Neuhaus, thank you for this question.At this point, curative liver resection should not be denied onthe basis of FDG-positive lesions alone in the pelvis orelsewhere. A histologic confirmation has to be obtained bypercutaneous or open biopsy, and the treatment adjustedaccordingly.
DR. LERUT: I would like to challenge a little bit yourresults on detecting the lung metastasis. I was surprised thatyou had 4 patients in which the lung metastasis were “missedon CT scan,” and I wonder whether they really were missedor whether it was just a confirmation by PET of an already onCT scan suspicious lesion. Indeed, if the PET shows ametastasis, you would expect that the diameter would be likeat least 1 cm or more, and those are lesions that with modernspiral CT scan no radiologist would miss today. Secondly,along the same lines, would you agree that multislice spiralCT for the subcentimetric lesions is still more accurate than
PET or PET-CT, because these lesions do not have sufficientcritical mass to show up on the PET scan?
DR. SELZNER: Thank you for this important question. Ireported here the data as evaluated by our nuclear medicine/radiologist author (T.F.H.) in a blind manner. I would like tolet Professor Clavien address this issue and conclude thediscussion.
DR. CLAVIEN: Dr. Lerut, this is an important point,which we have discussed in length with our “imaging”colleagues. PET/CT is a fusion of PET plus CT images, andthe FDG-uptake has to be evaluated in combination with theCT finding. The fusion of both techniques was better than theadditive information of each picture. CT missed these lesionsbecause they were not enough suspicious regarding shape,size, and location. Your next question is whether ceCT isbetter than CT plus PET/CT for small lesions. This might betrue today, although not apparent in our study. However, theforthcoming availability of PET/ceCT (ie, CT with intrave-nous contrast) will obviously be better than ceCT alone, andPET/ceCT may become the only test needed to assess thesepatients preoperatively. I would like to conclude that we(surgeons) should not see PET/CT as a tool which only leads todenial of surgery to many patients. PET/CT offers new oppor-tunities to better target our therapy, and we may well find thatpatients with extrahepatic lesions other than in the lung andperiportal nodes may also benefit from surgery. I believe thatPET/CT should now be included in each trial to better securehomogeneity of the studied populations.
Selzner et al Annals of Surgery • Volume 240, Number 6, December 2004
© 2004 Lippincott Williams & Wilkins1036