
Does Alcohol Consumption Exacerbate the Mental Health Consequences of Interpersonal Violence
20
Violence Against Women 18(3) 289–308 © The Author(s) 2012 Reprints and permission: sagepub.com/journalsPermissions.nav DOI: 10.1177/1077801212442623 http://vaw.sagepub.com 442623VAW XX X 10.1177/107780121244 2623Kaplan et al.Violence Against Women © The Author(s) 2011 Reprints and permission: http://www. sagepub.com/journalsPermissions.nav 1 J. W. Goethe-Universitat Frankfurt, Frankfurt am Main, Germany 2 Florida State University, Tallahassee, FL, USA 3 Suffolk University, Boston, MA, USA Corresponding Author: Terrence D. Hill, Department of Sociology, Florida State University, 526 Bellamy Building, Tallahassee, FL 32306-2270, USA Email: [email protected] Does Alcohol Consumption Exacerbate the Mental Health Consequences of Interpersonal Violence? Lauren M. Kaplan 1 ,Terrence D. Hill 2 , and Gini R. Mann-Deibert 3 Abstract Although studies show that interpersonal violence is associated with poorer mental health, few studies specify the conditions under which victimization can be more or less detrimental to psychological well-being. Building on previous research, the authors test whether the association between interpersonal violence and psychological distress is moderated by alcohol consumption. Our analysis of longitudinal data from the Welfare, Children, and Families project suggests that interpersonal violence is more strongly associated with psychological distress in the context of more frequent intoxication. Programs designed to treat the combination of victimization and heavy alcohol consumption may make unique contributions to the well-being of women. Keywords alcohol consumption, interpersonal violence, mental health Introduction Studies consistently show that interpersonal violence—as indicated by child abuse and intimate partner violence—is associated with poorer mental health (Anderson, 2002; Banyard, 1999; Banyard & Williams, 1996; Caetano & Cunradi, 2003; Choi & Marks, 2008; Downs, Capshew, & Rindels, 2004; Draper et al., 2008; Hanson et al., 2001; Hill, Article at FLORIDA STATE UNIV LIBRARY on June 30, 2012 vaw.sagepub.com Downloaded from
Transcript of Does Alcohol Consumption Exacerbate the Mental Health Consequences of Interpersonal Violence
Violence Against Women18(3) 289 –308
© The Author(s) 2012Reprints and permission:
sagepub.com/journalsPermissions.nav DOI: 10.1177/1077801212442623
http://vaw.sagepub.com
442623 VAWXXX10.1177/1077801212442623Kaplan et al.Violence Against Women© The Author(s) 2011
Reprints and permission: http://www.sagepub.com/journalsPermissions.nav
1J. W. Goethe-Universitat Frankfurt, Frankfurt am Main, Germany2Florida State University, Tallahassee, FL, USA3Suffolk University, Boston, MA, USA
Corresponding Author:Terrence D. Hill, Department of Sociology, Florida State University, 526 Bellamy Building, Tallahassee, FL 32306-2270, USA Email: [email protected]
Does Alcohol Consumption Exacerbate the Mental Health Consequences of Interpersonal Violence?
Lauren M. Kaplan1, Terrence D. Hill2, and Gini R. Mann-Deibert3
Abstract
Although studies show that interpersonal violence is associated with poorer mental health, few studies specify the conditions under which victimization can be more or less detrimental to psychological well-being. Building on previous research, the authors test whether the association between interpersonal violence and psychological distress is moderated by alcohol consumption. Our analysis of longitudinal data from the Welfare, Children, and Families project suggests that interpersonal violence is more strongly associated with psychological distress in the context of more frequent intoxication. Programs designed to treat the combination of victimization and heavy alcohol consumption may make unique contributions to the well-being of women.
Keywords
alcohol consumption, interpersonal violence, mental health
Introduction
Studies consistently show that interpersonal violence—as indicated by child abuse and intimate partner violence—is associated with poorer mental health (Anderson, 2002; Banyard, 1999; Banyard & Williams, 1996; Caetano & Cunradi, 2003; Choi & Marks, 2008; Downs, Capshew, & Rindels, 2004; Draper et al., 2008; Hanson et al., 2001; Hill,
Article
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from

290 Violence Against Women 18(3)
Mossakowski, & Angel, 2007; Horwitz, Widom, McLaughlin, & White, 2001; Katz & Arias, 1999; Kaukinen & DeMaris, 2005; Miranda, Meyerson, Long, Marx, & Simpson, 2002; Resnick & Acierno, 1997; Springer, Sheridan, Kuo, & Carnes, 2007; Tolman & Rosen, 2001; Zlotnick, Johnson, & Kohn, 2006). This general pattern can be observed across a range of violence measures (e.g., nonspecific interpersonal violence, physical assault, psychological aggression, and sexual coercion) and mental health outcomes (e.g., depression, anxiety, posttraumatic stress disorder, and nonspecific psychological distress). The causal order of the association between violence and mental health is often difficult to establish (Kessler, Molnar, Feurer, & Appelbaum, 2001; Silver & Teasdale, 2005). However, available longitudinal evidence confirms that victimization can predict poorer mental health trajectories (Choi & Marks, 2008; Katz & Arias, 1999; Zlotnick et al., 2006).
Although previous research has made significant contributions to our understanding of the mental health consequences of interpersonal violence, few studies specify the conditions under which victimization can be more or less detrimental to psychological well-being. Studies have tested whether the effect of interpersonal violence varies according to respondents’ social position (e.g., sex, race, and socioeconomic status; Anderson, 2002; Buckner, Bassuk, & Beardslee, 2004; Carlson, McNutt, Choi, &, Rose, 2002; Williams & Mickelson, 2007) and level of psychosocial resources (e.g., self-esteem, sense of control, and social support; Arias, Lyons, & Street, 1997; Carlson et al., 2002; Coker et al., 2002; Holt & Espelage, 2005; Katz & Arias, 1999; Luster & Small, 1997; Skomorovsky, Matheson, & Anisman, 2006). To this point, however, surprisingly little attention has been devoted to relevant behavioral moderators such as substance use.
Building on previous research, we examine the moderating influence of alcohol con-sumption. Several studies show that interpersonal violence is associated with heavier drink-ing (Coker et al., 2002; Hill, Nielsen, & Angel, 2009; Kaukinen & DeMaris, 2005; Kilpatrick, Acierno, Resnick, Saunders, & Best, 1997; Martino, Collins, & Ellickson, 2005; Testa, Livingson, & Leonard, 2003; Tolman & Rosen, 2001; Wilsnack, Vogeltanz, Klassen, & Harris, 1997). If, as research suggests (Epstein, Saunders, Kilpatrick, & Resnick, 1998; Kaysen et al., 2007; Kilpatrick et al., 1997; Miranda et al., 2002; Ullman, Filipas, Townsend, & Starzynski, 2005; Wilsnack, Wilsnack, Kristjanson, & Harris, 1998), women often drink to cope with victimization, it is important to consider whether heavy alcohol consumption exacerbates the mental health consequences of interpersonal violence. To formally test this idea, we employ two waves of data collected from a large probability sample of low-income urban women with children. We focus on this population because studies consistently show that economically disadvantaged urban women exhibit high rates of child abuse and inti-mate partner violence (Baumrind, 1994; Benson, Wooldredge, Thistlethwaite, & Fox, 2004; Hill et al., 2007; Purvin, 2007; Tolman & Raphael, 2000).
Theoretical BackgroundSubsequent analyses test whether the association between interpersonal violence and psychological distress is moderated by frequency of intoxication. We expect that interpersonal
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from
Kaplan et al. 291
violence will be more strongly associated with psychological distress in the context of more frequent intoxication. This expectation primarily flows from previous research on stressful life events and the physiological consequences of alcohol consumption. We also draw on evidence from prior work on victimization and substance abuse.
Studies show that heavy alcohol consumption can intensify the mental health conse-quences of stressful life events and chronic strains (Lipton, 1994; Marchand, Demers, Durand, & Simard, 2003; Neff, 1984, 1985; Neff & Husaini, 1982, 1985). Neff and Husaini report that stressful life events (e.g., total number of events and catastrophic events) are more strongly associated with depressive symptoms among heavy drinkers than moderate drinkers. Marchand and colleagues find that work-related physical risks (e.g., heavy lifting) and chemical exposures (e.g., pesticides) are more psychologically distressing for high-risk drinkers than low-risk drinkers.
These studies clearly demonstrate that heavy alcohol consumption can exacerbate the mental health consequences of stressful life events. Research also suggests that risky drinking practices can undermine the psychological benefits of positive life events. For example, Zabkiewicz and Schmidt (2009) show that mothers who enter welfare with drinking problems (regular consumption of five or more drinks per drink-ing occasion, at least one alcohol dependence symptom, and/or at least one alcohol-related social problem) are less likely to experience a decline in depressive symptoms following employment than mothers entering welfare without such problems. In this particular study, employment is actually unrelated to depressive symptoms among mothers with drinking problems.
Although research shows that risky drinking practices can make life conditions more distressing and less fulfilling, explanations for these patterns are not well established. There is also no direct evidence to suggest that this general process would apply to inter-personal violence.
Why might heavy alcohol consumption exacerbate the mental health consequences of interpersonal violence?
Child abuse and intimate partner violence are psychologically distressing because they are threatening and dangerous conditions. Victimization during the formative and devel-opmental years of childhood and adolescence can actually alter the structure of the brain to sensitize the physiological stress response to potential threats, real or imagined (McEwen, 2002; Watts-English, Fortson, Gibler, Hooper, & De Bellis, 2006). Kendall-Tackett (2002) explains that children with histories of abuse learn to see the world as a dangerous place and, as a consequence, tend to “. . . overestimate danger and adversity in their current environment” (p. 722). Lasting memories of abuse, chronic perceptions of threat, and more recent experiences with the insecurity and danger of intimate partner violence are taxing and fraught with classic symptoms of depression and anxiety, includ-ing feelings of sadness and hopelessness, fear and worry.
Interpersonal violence is stressful in itself, but risky drinking practices could, as in the case of stressful life events and chronic strains, make things worse. Research shows that alcohol use can be sufficient to stimulate the hypothalamic-pituitary-adrenal axis and trig-ger the release of cortisol into the bloodstream (McEwen, 2002; Sapolsky, 2004). By
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from

292 Violence Against Women 18(3)
extension, heavy alcohol consumption could result in chronic activation of the stress response and over-production of cortisol, thus contributing to allostatic load (McEwen, 2002). If the stress response to victimization (a stressor) can be prolonged by heavy drink-ing (yet another stressor), the combination of these conditions could heighten an individ-ual’s vulnerability to psychological distress.
In addition to direct physiological effects, heavy alcohol consumption could exacer-bate the mental health consequences of interpersonal violence in various indirect ways. Miethe and Deibert (2007) note that alcohol abuse can facilitate and escalate violent encounters. Heavy drinking can also trap women in cycles of self-destructive behavior that erode positive social ties with friends and family, diminish feelings of self-worth and control, and ultimately prevent the adoption of healthy and effective coping strategies (Kunz & Graham, 1998; Rodgers et al., 2000; Sayette, Wilson, & Elias, 1993; Seeman & Seeman, 1992).
MethodParticipants
The data for this investigation come from the Welfare, Children, and Families (WCF) project (see http://www.jhu.edu/~welfare/). The WCF project is a household-based, stratified random sample of 2,402 low-income women living in low-income neighbor-hoods in Boston, Chicago, and San Antonio. The WCF first sampled census blocks (or neighborhoods) with at least 20% of residents below the Federal poverty line based on the 1990 census. Within these neighborhoods, households under 200% of the poverty line were sampled, with an oversampling of households below 100% of the poverty line. Because one of the goals of the WCF project is to assess the impact of welfare policy and work on children, households were screened for the presence of children. Households with at least one infant or child (aged 0-4) or young adolescent (aged 10-14) were sam-pled. The children’s caregivers, all women, were interviewed face to face. The data were collected in 1999 with a follow-up in 2001. The baseline response rate was 75%, and 89% of the original sample participants were reinterviewed. The overall respondent-level response rate is 75%, with city-specific response rates of 74% (Boston), 71% (Chicago), and 79% (San Antonio). Subsequent analyses are weighted to account for variations in sample sizes across cities.
MeasuresPsychological distress is measured with the Brief Symptom Inventory (BSI-18), which contains subscales for depression, anxiety, and somatization (Derogatis, 2000). Psychological distress is measured as the mean response to 18 items (α = .92). For example, respondents were asked to indicate how much in the past 7 days they were distressed or bothered by “feeling no interest in things,” “feeling tense or keyed up,” and
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from

Kaplan et al. 293
“nausea or upset stomach.” Response categories for all psychological distress items were coded as (1) not at all, (2) a little bit, (3) moderately, (4) quite a bit, or (5) extremely.
Violence during childhood and adolescence is measured with two items. These items capture physical assault and sexual coercion before age 18. Respondents were asked to indicate whether they were ever hit, beaten up, burned, assaulted with a weapon, or whether their life had been threatened by an adult in their family or household before the age of 18. Respondents were also asked to indicate whether anyone—a stranger, friend, acquaintance, date, or relative—ever tried or succeeded in doing something sexual to them or made them do something sexual against their wishes. Original response catego-ries for these items were coded as (0) never, (1) once or twice, (2) several times, and (3) often. Due to limited incidence rates, these measures were coded into dummy variables. For each of the two measures, respondents were assigned a value of (1) if they reported being a victim of physical assault or sexual coercion before age 18, respectively, and (0) otherwise. These measures have been used in prior research to predict psychological dis-tress, frequency of intoxication, and self-rated health (Hill & Angel, 2005; Hill et al., 2007, Hill, Nielsen, & Angel, 2009; Hill, Schroeder, Bradley, Kaplan, & Angel, 2009).
Measures of violence in adulthood are drawn from the Revised Conflict Tactics Scales (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996). The CTS2 has established reliability and validity (Straus & Douglas, 2004; Straus et al., 1996). Drawing on the work of Straus and colleagues, we assess four major types of violence, including psycho-logical aggression, minor physical assault, severe physical assault, and sexual coercion. Psychological aggression captures nonphysical or verbal acts of violence. Respondents were asked to indicate how often in the past 12 months a romantic partner had threatened to (a) hit them, (b) use a weapon on them, and (c) hurt their child or take (him or her) away. Minor physical assault assesses nonsevere or “common couple” acts of physical violence. Respondents were asked to indicate how often in the past 12 months a romantic partner had (a) thrown something at them, and (b) pushed, grabbed, or shoved them. Severe physical assault measures some of the more brutal and vicious acts of physical violence. Respondents were asked to indicate how often in the past 12 months a romantic partner had (a) slapped, kicked, bit, or punched them, (b) beaten them, and (c) choked and burned them. Finally, sexual coercion is intended to capture forced sexual acts of violence. Respondents were asked to indicate how often in the past 12 months a romantic partner had forced them into any sexual activity against their will. Original response categories for all past-year violence items were coded as (0) never, (1) once or twice, (2) several times, and (3) often. Again, due to limited incidence rates, measures of adult violence were coded into dummy variables. Respondents were assigned a value of (1) if they reported a particular act of violence in the past 12 months and (0) otherwise. For example, the dummy variable for psychological aggression is coded as (1) for one or more acts of psychological aggression in the past year, and (0) for no acts of psychologi-cal aggression in the past year.
Heavy alcohol consumption is indicated by frequency of intoxication. Frequency of intoxication is intended to measure the most fundamentally problematic aspect of alcohol consumption—getting drunk. Instead of asking respondents to recall specific alcohol
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from

294 Violence Against Women 18(3)
frequencies and quantities consumed, this measure requires respondents to estimate the number of occasions during which they were drunk. Respondents were asked, “In the past 12 months, how often have you gotten drunk?” Original response categories for this item were coded as (1) never, (2) once or twice, (3) several times, and (4) often. To isolate more frequent intoxication, respondents were assigned a value of (1) if they reported getting drunk several times or often and (0) otherwise. This measure of intoxication suffers from low reliability and imprecise response categories, but it has demonstrated construct valid-ity in previous research (Hill & Angel, 2005; Hill, Nielsen et al., 2009, Hill, Schroeder et al., 2009; Robbins, 1989). For example, using the 1985 National Survey on Drug Abuse, Robbins employed a similar measure of intoxication and found strong positive associa-tions with psychological distress, and social and behavioral problems.
In accordance with previous research on interpersonal violence and mental health among low-income women (e.g., Hill et al., 2007; Tolman & Rosen, 2001), our multi-variate analyses include controls for several relevant background factors, including age (in years), race/ethnicity (dummy variables for non-Hispanic White, Mexican, and other Hispanic compared with Black), education (in years), employment status (1 = worked for pay in the past week), family of origin welfare status (1 = respondent’s parents received public assistance), current welfare status (1 = currently receiving welfare), marital status (dummy variables for married-living with spouse and cohabiting-not married compared with singles and married-no spouse in house), and number of children (1 to 6 or more, top-coded continuous variable). Given the nature of the sample, it is important to capture the strain of financial hardship (i.e., the inability to provide for essential material needs). Hardship is measured as the mean response to 13 items (α = .83). For example, respon-dents were asked to indicate how often they had to “borrow money to pay bills.” Respondents were also asked to indicate whether they had enough money to “afford housing, food, and clothing,” and whether any adults or children in the household were “unable to eat for a whole day because there wasn’t enough money for food.” Because the original hardship items were measured with mixed question formats and response categories, each of these items has been standardized to account for metric differences.
Statistical ProceduresWe begin our analysis with the presentation of weighted descriptive statistics for the study sample, including minimum and maximum values, means, standard deviations, and alpha reliability estimates (Table 1). Next, we use ordinary least squares (OLS) regression to model baseline psychological distress and changes in distress (Table 2). Change score models, which are generally preferable to lagged endogenous dependent variable models (Johnson, 2005), assess 2-year distress trajectories. We first computed change scores by subtracting baseline (1999) distress scores from follow-up (2001) distress scores. These change scores are continuous variables that range from –2.50 to 2.50. Negative numbers indicate lower levels of psychological distress (i.e., fewer symptoms) in 2001 than in 1999. Positive numbers suggest higher levels of distress in 2001 than in 1999. Many respondents exhibit a change score of zero, which indicates no change across waves (i.e., same distress score in 1999 and in 2001).
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from
Kaplan et al. 295
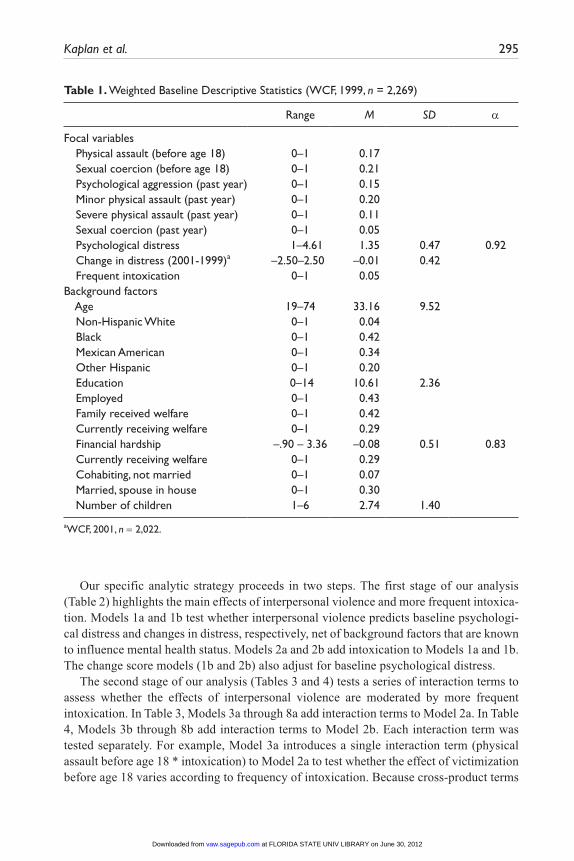
Table 1. Weighted Baseline Descriptive Statistics (WCF, 1999, n = 2,269)
Range M SD α
Focal variables Physical assault (before age 18) 0–1 0.17 Sexual coercion (before age 18) 0–1 0.21 Psychological aggression (past year) 0–1 0.15 Minor physical assault (past year) 0–1 0.20 Severe physical assault (past year) 0–1 0.11 Sexual coercion (past year) 0–1 0.05 Psychological distress 1–4.61 1.35 0.47 0.92 Change in distress (2001-1999)a –2.50–2.50 –0.01 0.42 Frequent intoxication 0–1 0.05 Background factors Age 19–74 33.16 9.52 Non-Hispanic White 0–1 0.04 Black 0–1 0.42 Mexican American 0–1 0.34 Other Hispanic 0–1 0.20 Education 0–14 10.61 2.36 Employed 0–1 0.43 Family received welfare 0–1 0.42 Currently receiving welfare 0–1 0.29 Financial hardship –.90 – 3.36 –0.08 0.51 0.83 Currently receiving welfare 0–1 0.29 Cohabiting, not married 0–1 0.07 Married, spouse in house 0–1 0.30 Number of children 1–6 2.74 1.40
aWCF, 2001, n = 2,022.
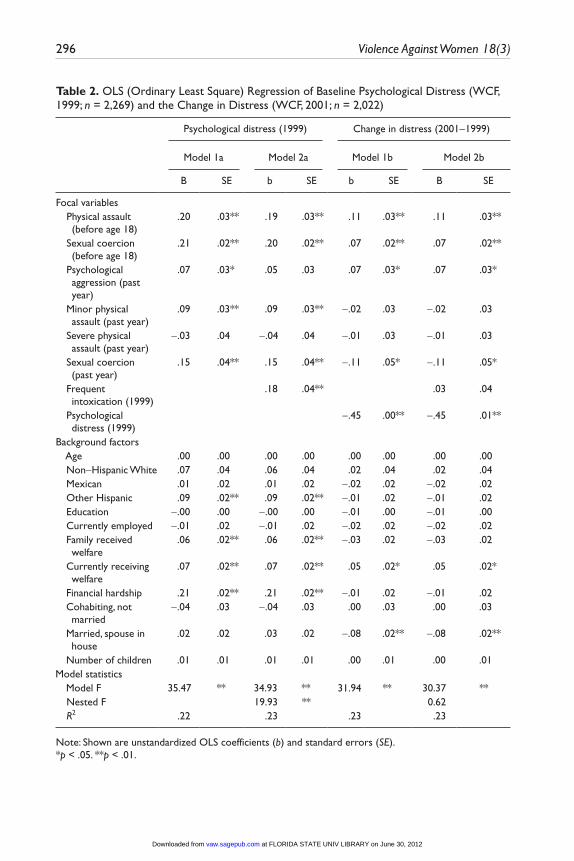
Our specific analytic strategy proceeds in two steps. The first stage of our analysis (Table 2) highlights the main effects of interpersonal violence and more frequent intoxica-tion. Models 1a and 1b test whether interpersonal violence predicts baseline psychologi-cal distress and changes in distress, respectively, net of background factors that are known to influence mental health status. Models 2a and 2b add intoxication to Models 1a and 1b. The change score models (1b and 2b) also adjust for baseline psychological distress.
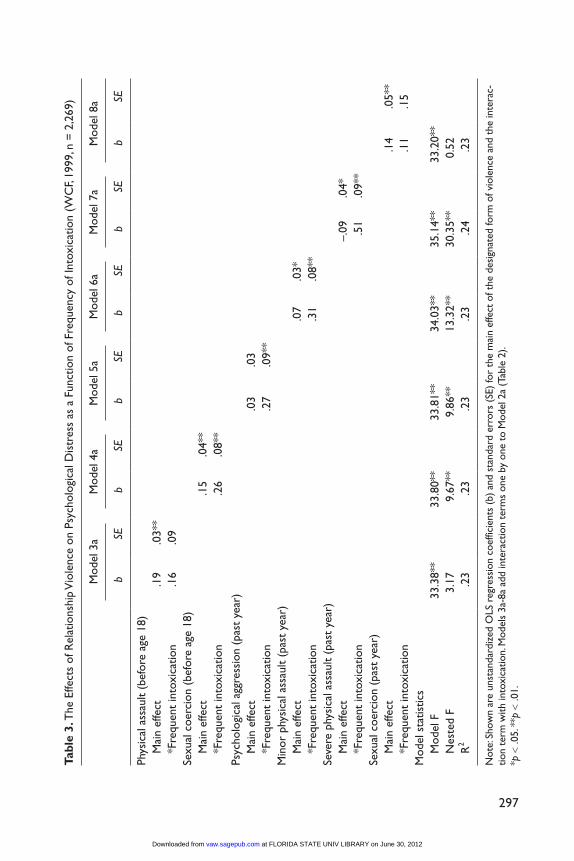
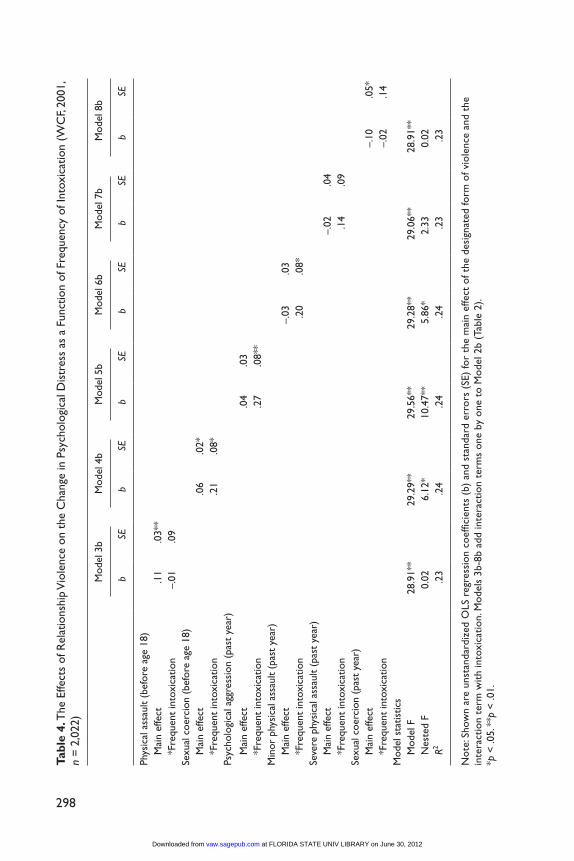
The second stage of our analysis (Tables 3 and 4) tests a series of interaction terms to assess whether the effects of interpersonal violence are moderated by more frequent intoxication. In Table 3, Models 3a through 8a add interaction terms to Model 2a. In Table 4, Models 3b through 8b add interaction terms to Model 2b. Each interaction term was tested separately. For example, Model 3a introduces a single interaction term (physical assault before age 18 * intoxication) to Model 2a to test whether the effect of victimization before age 18 varies according to frequency of intoxication. Because cross-product terms
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from
296 Violence Against Women 18(3)
Table 2. OLS (Ordinary Least Square) Regression of Baseline Psychological Distress (WCF, 1999; n = 2,269) and the Change in Distress (WCF, 2001; n = 2,022)
Psychological distress (1999) Change in distress (2001-1999)
Model 1a Model 2a Model 1b Model 2b
B SE b SE b SE B SE
Focal variables Physical assault
(before age 18).20 .03** .19 .03** .11 .03** .11 .03**
Sexual coercion (before age 18)
.21 .02** .20 .02** .07 .02** .07 .02**
Psychological aggression (past year)
.07 .03* .05 .03 .07 .03* .07 .03*
Minor physical assault (past year)
.09 .03** .09 .03** -.02 .03 -.02 .03
Severe physical assault (past year)
-.03 .04 -.04 .04 -.01 .03 -.01 .03
Sexual coercion (past year)
.15 .04** .15 .04** -.11 .05* -.11 .05*
Frequent intoxication (1999)
.18 .04** .03 .04
Psychological distress (1999)
-.45 .00** -.45 .01**
Background factors Age .00 .00 .00 .00 .00 .00 .00 .00 Non-Hispanic White .07 .04 .06 .04 .02 .04 .02 .04 Mexican .01 .02 .01 .02 -.02 .02 -.02 .02 Other Hispanic .09 .02** .09 .02** -.01 .02 -.01 .02 Education -.00 .00 -.00 .00 -.01 .00 -.01 .00 Currently employed -.01 .02 -.01 .02 -.02 .02 -.02 .02 Family received
welfare.06 .02** .06 .02** -.03 .02 -.03 .02
Currently receiving welfare
.07 .02** .07 .02** .05 .02* .05 .02*
Financial hardship .21 .02** .21 .02** -.01 .02 -.01 .02 Cohabiting, not
married-.04 .03 -.04 .03 .00 .03 .00 .03
Married, spouse in house
.02 .02 .03 .02 -.08 .02** -.08 .02**
Number of children .01 .01 .01 .01 .00 .01 .00 .01Model statistics Model F 35.47 ** 34.93 ** 31.94 ** 30.37 ** Nested F 19.93 ** 0.62 R2 .22 .23 .23 .23
Note: Shown are unstandardized OLS coefficients (b) and standard errors (SE).*p < .05. **p < .01.
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from
297
Tabl
e 3.
The
Effe
cts
of R
elat
ions
hip
Vio
lenc
e on
Psy
chol
ogic
al D
istr
ess
as a
Fun
ctio
n of
Fre
quen
cy o
f Int
oxic
atio
n (W
CF,
1999
, n =
2,2
69)
Mod
el 3
aM
odel
4a
Mod
el 5
aM
odel
6a
Mod
el 7
aM
odel
8a
b
SEb
SEb
SEb
SEb
SEb
SE
Phys
ical
ass
ault
(bef
ore
age
18)
M
ain
effe
ct.1
9.0
3**
*Fre
quen
t in
toxi
catio
n.1
6.0
9
Sexu
al c
oer c
ion
(bef
ore
age
18)
Mai
n ef
fect
.15
.04*
*
*F
r equ
ent
into
xica
tion
.26
.08*
*
Psyc
holo
gica
l agg
ress
ion
(pas
t ye
ar)
M
ain
effe
ct.0
3.0
3
*F
requ
ent
into
xica
tion
.27
.09*
*
Min
or p
hysi
cal a
ssau
lt (p
ast
year
)
Mai
n ef
fect
.07
.03*
*Fre
quen
t in
toxi
catio
n.3
1.0
8**
Se
vere
phy
sica
l ass
ault
(pas
t ye
ar)
M
ain
effe
ct–.
09.0
4*
*F
requ
ent
into
xica
tion
.51
.09*
*
Sexu
al c
oerc
ion
(pas
t ye
ar)
M
ain
effe
ct.1
4.0
5**
*F
requ
ent
into
xica
tion
.11
.15
Mod
el s
tatis
tics
M
odel
F33
.38*
*33
.80*
*33
.81*
*34
.03*
*35
.14*
*33
.20*
*
N
este
d F
3.17
9.67
**9.
86**
13.3
2**
30.3
5**
0.52
R2
.23
.23
.23
.23
.24
.23
Not
e: S
how
n ar
e un
stan
dard
ized
OLS
reg
ress
ion
coef
ficie
nts
(b)
and
stan
dard
err
ors
(SE)
for
the
mai
n ef
fect
of t
he d
esig
nate
d fo
rm o
f vio
lenc
e an
d th
e in
tera
c-tio
n te
rm w
ith in
toxi
catio
n. M
odel
s 3a
-8a
add
inte
ract
ion
term
s on
e by
one
to
Mod
el 2
a (T
able
2).
*p <
.05.
**p
< .0
1.
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from
298
Tabl
e 4.
The
Effe
cts
of R
elat
ions
hip
Vio
lenc
e on
the
Cha
nge
in P
sych
olog
ical
Dis
tres
s as
a F
unct
ion
of F
requ
ency
of I
ntox
icat
ion
(WC
F, 20
01,
n =
2,0
22)
Mod
el 3
bM
odel
4b
Mod
el 5
bM
odel
6b
Mod
el 7
bM
odel
8b
b
SEb
SEb
SEb
SEb
SEb
SE
Phys
ical
ass
ault
(bef
ore
age
18)
M
ain
effe
ct.1
1.0
3**
*Fre
quen
t in
toxi
catio
n–.
01.0
9
Sexu
al c
oerc
ion
(bef
ore
age
18)
Mai
n ef
fect
.06
.02*
*Fre
quen
t in
toxi
catio
n.2
1.0
8*
Psyc
holo
gica
l agg
r ess
ion
(pas
t ye
ar)
M
ain
effe
ct.0
4.0
3
*F
requ
ent
into
xica
tion
.27
.08*
*
Min
or p
hysi
cal a
ssau
lt (p
ast
year
)
M
ain
effe
ct–.
03.0
3
*F
requ
ent
into
xica
tion
.20
.08*
Se
vere
phy
sica
l ass
ault
(pas
t ye
ar)
Mai
n ef
fect
–.02
.04
*Fre
quen
t in
toxi
catio
n.1
4.0
9
Sexu
al c
oerc
ion
(pas
t ye
ar)
Mai
n ef
fect
–.10
.05*
*F
requ
ent
into
xica
tion
–.02
.14
Mod
el s
tatis
tics
Mod
el F
28.9
1**
29.2
9**
29.5
6**
29.2
8**
29.0
6**
28.9
1**
Nes
ted
F0.
026.
12*
10.4
7**
5.86
*2.
330.
02
R2
.23
.24
.24
.24
.23
.23
Not
e: S
how
n ar
e un
stan
dard
ized
OLS
reg
ress
ion
coef
ficie
nts
(b)
and
stan
dard
err
ors
(SE)
for
the
mai
n ef
fect
of t
he d
esig
nate
d fo
rm o
f vio
lenc
e an
d th
e in
tera
ctio
n te
rm w
ith in
toxi
catio
n. M
odel
s 3b
-8b
add
inte
ract
ion
term
s on
e by
one
to
Mod
el 2
b (T
able
2).
*p <
.05.
**p
< .0
1.
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from

Kaplan et al. 299
were included in this stage of the analysis, all continuous variables have been centered to avoid problems due to multicollinearity (Aiken & West, 1991). The potential for multcol-linearity was formally diagnosed by examining variance inflation factors (VIF) for each regression coefficient. VIFs above 10.00 are generally considered to indicate problematic multicollinearity (Myers, 1986). All VIFs were below 2.00 throughout our analysis.
Supplemental Attrition AnalysisWhen considering changes in outcomes over time, it is customary to examine the issue of bias due to sample attrition. The primary concern is whether or not there are any sys-tematic changes in the sample across waves. To formally assess this issue, we estimated a series of binary logistic regression models predicting the log odds of sample attrition (results not shown). The dependent variable in this case is dummy-coded such that respondents who completed questionnaires for both waves were given a value of zero, and those who completed the Wave 1 questionnaire only were given a value of 1. The independent variables include all interpersonal violence measures, psychological distress, frequency of intoxication, and all background factors. Approximately 12% of the partici-pants (272) were lost to follow-up. The logistic regression results show very little evi-dence of bias due to sample attrition. Only education was statistically significant at conventional levels (OR = .94, p < .05). Sexual coercion before age 18 was marginally significant (OR = .72, p < .10). Since we adjust for these factors in our analysis, attrition is unlikely to bias regression coefficients (Winship & Radbill, 1994).
ResultsDescriptive Analysis
Table 1 provides weighted descriptive statistics for the study sample. Although reports of physical assault (17%) and sexual coercion (21%) before age 18 are similar to national lifetime prevalence rates, 12-month incidence rates for psychological aggression (15%), minor physical assault (20%), severe physical assault (11%), and sexual coercion (5%) are noticeably higher than expectations derived from national estimates (see Tjaden & Thoennes, 2000). Table 1 also shows that the average respondent exhibits low levels of psychological distress and intoxication. With respect to the change scores, we observe an average decline in psychological distress. This pattern suggests that mental health status improved over the study period.
Baseline AnalysisTable 2 shows the OLS regression of baseline psychological distress (1999). Model 1a includes interpersonal violence and all background factors. These results indicate that physical assault and sexual coercion before age 18 and psychological aggression, minor physical assault, and sexual coercion in the past year are associated with higher levels of
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from

300 Violence Against Women 18(3)
psychological distress. To our surprise, the coefficient for severe physical assault failed to reach statistical significance. Model 2a adds intoxication to the regression equation. According to these results, more frequent intoxication is also associated with higher levels of psychological distress. With the addition of intoxication in Model 2a, the association between psychological aggression in the past year and psychological distress is reduced (from Model 1a) by approximately 29% ([.07 – .05] / .07) and is no longer statistically significant at conventional levels. Taken together, these patterns suggest that frequency of intoxication may mediate the association between psychological aggression and psycho-logical distress.
Table 3 presents the results of our baseline moderation analysis. In this table, we test six interaction terms to formally assess whether the association between interpersonal violence and psychological distress varies according to frequency of intoxication. We observe statistically significant interaction terms for sexual coercion before age 18 and psychological aggression, minor physical assault, and severe physical assault in the past year. As expected, the nature of each interaction term is positive. This suggests that these forms of interpersonal violence are more psychologically distressing in the context of more frequent intoxication. To further illustrate these patterns, Table 5 presents adjusted psychological distress means for each statistically significant interaction from Table 3. For example, the adjusted distress mean associated with sexual coercion before age 18 is 1.47 for those who reported sporadic intoxication (never/once or twice) and 1.73 for those who reported more frequent intoxication (several times/often).
Change Score AnalysisTable 2 also presents the OLS regression of psychological distress change scores (2001-1999). These results indicate that physical assault and sexual coercion before age 18 and psychological aggression in the past year predict increases in psychological distress over the study period. Unexpectedly, sexual coercion in the past year is associated with fewer symp-toms of psychological distress from baseline to follow-up. Model 2b adds frequency of intoxication to Model 1b. Because baseline frequency of intoxication is unrelated to changes in psychological distress, the patterns for interpersonal violence are identical across models.
Table 4 presents the results of our change score moderation analysis. Similar to the patterns revealed in Table 3, we observe statistically significant interaction terms for sexual coercion before age 18 and psychological aggression and minor physical assault in the past year. Once again, the nature of each interaction term is positive. This suggests that women who reported experiences with these forms of violence and more frequent intoxication at baseline were especially vulnerable to increases in psychological distress over the study period. Table 5 presents adjusted change score means for each statistically significant interaction from Table 4. For instance, the adjusted mean change score asso-ciated with psychological aggression in the past year is 0.02 for those who reported sporadic intoxication (never/once or twice) and 0.29 for those who reported more frequent intoxication (several times/often).
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from

Kaplan et al. 301
DiscussionAlthough numerous studies show that interpersonal violence is associated with poorer mental health, few studies specify the conditions under which this association is more or less pronounced. Using data collected from a large probability sample of low-income women with children living in Boston, Chicago, and San Antonio, we predicted psycho-logical distress over 2 years with multiple measures of interpersonal violence and a host of relevant background factors. Building on previous research, we examined the moderat-ing influence of frequency of intoxication.
The results of our baseline analysis indicate that physical assault and sexual coercion before age 18 and minor physical assault and sexual coercion in the past year are associ-ated with higher levels of psychological distress. Psychological aggression in the past year was initially associated with higher levels of distress, but this association was apparently mediated by frequency of intoxication. These patterns are generally consis-tent with previous research (e.g., Downs et al., 2004; Hanson et al., 2001; Hill et al., 2007; Katz & Arias, 1999; Miranda et al., 2002; Resnick & Acierno, 1997). It is unclear why severe physical assault is unrelated to psychological distress when multiple studies report otherwise (e.g., Cascardi & O’Leary, 1992; Romito, Turan, & De Marchi, 2005;
Table 5. Adjusted Psychological Distress Means for Statistically Significant Interactions (from Tables 3 and 4) Between Relationship Violence and Frequency of Intoxication
Mean psychological distress (1999)
Mean change in distress (2001-1999)
Sexual Coercion (before age 18) × Frequency of Intoxication
Intoxicated never/once or twice 1.47 0.04 Intoxicated several times/often 1.73 0.25Psychological Aggression (Past Year)
× Frequency of Intoxication
Intoxicated never/once or twice 1.35 0.02 Intoxicated several times/often 1.62 0.29Minor Physical Assault (Past Year) ×
Frequency of Intoxication
Intoxicated never/once or twice 1.38 –0.03 Intoxicated several times/often 1.69 0.16Severe Physical Assault (Past Year) ×
Frequency of Intoxication
Intoxicated never/once or twice 1.24 Intoxicated several times/often 1.75
Note: All means are adjusted for baseline relationship violence, frequency of intoxication, and background factors. Change means also adjust for baseline psychological distress.
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from
302 Violence Against Women 18(3)
Tolman & Rosen, 2001). One possibility is that low incidence rates for severe physical assault may limit our ability to detect statistically significant differences.
Our change score analysis demonstrates that physical assault and sexual coercion before age 18 and psychological aggression in the past year predict increases in psycho-logical distress over the study period. Although these patterns support previous research (e.g., Banyard & Williams, 1996; Katz & Arias, 1999), our results for minor and severe physical assault are inconsistent with other longitudinal studies (e.g., Choi & Marks, 2008; Zlotnick et al., 2006). It is conceivable that minor physical assault may only con-tribute to distress in the immediate future. The nonsignificant pattern for severe physical assault confirms our baseline analysis. It is unclear why sexual coercion in the past year is associated with fewer symptoms of distress over time. Our baseline analysis suggests that sexual coercion is psychologically distressing in the short term. Perhaps the experi-ence of sexual violence can be followed by traumatic growth over time (see Tedeschi & Calhoun, 1996).
The results of our baseline moderation analysis show that sexual coercion before age 18 and psychological aggression, minor physical assault, and severe physical assault in the past year are more psychologically distressing in the context of more frequent intoxi-cation. Our change score moderation analysis is generally consistent with our baseline analysis. Specifically, women who report more frequent intoxication along with sexual coercion before age 18 and psychological aggression and minor physical assault in the past year are especially vulnerable to increases in psychological distress over the study period. These results are generally consistent with previous studies showing that heavy drinking can exacerbate the mental health consequences of stressful life conditions (e.g., Marchand et al., 2003; Neff & Husaini, 1982). However, to the best of our knowledge, we are first to consider whether heavy alcohol consumption moderates the association between interpersonal violence and psychological distress.
Overall, our results clearly emphasize the need for additional research, prevention policies, and treatment programs focused directly on the problem of interpersonal vio-lence among low-income urban women. In addition to highlighting the basic need for violence prevention initiatives, the results of our moderation analysis provide some guid-ance concerning the design of future polices and treatment programs. We observe that more frequent intoxication consistently exacerbates the mental health consequences of interpersonal violence over the 2-year study period and across several forms of interper-sonal violence. In our view, these results suggest that interventions designed to screen for and treat the combination of interpersonal violence and heavy alcohol consumption may make unique contributions to the psychological well-being of women. We would like to emphasize, however, that the viability of this approach is contingent upon replication and further testing of the moderating influences of risky drinking behaviors.
The present study makes several contributions to previous work on interpersonal violence and mental health. As stated, very little research has sought to specify the con-ditions under which violent experiences can be more or less detrimental to mental health. Our work suggests that risky drinking practices can exacerbate the psychological consequences of victimization. Previous studies are also often based on data collected
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from

Kaplan et al. 303
from small nonprobability samples that are characterized by limited variation in victim-ization experiences and mental health status. However, our analysis employs data col-lected from a large probability sample of low-income urban women. Although studies are usually limited to one or two measures of interpersonal violence, we examine the effects of multiple types of child abuse and intimate partner violence. Because most studies of interpersonal violence and mental health are based on cross-sectional designs, causal order is often unclear. The combination of our baseline and change score analy-ses helps to clarify this issue.
Our study also has several limitations. We would first like to acknowledge the limita-tions of our measurement of heavy alcohol consumption. Although it is customary to measure multiple aspects of drinking behavior with precise frequencies and quantities, our measure of intoxication is based on a single item with a narrow range of imprecise response categories. Although this measure has been used in previous research and has demonstrated construct validity (e.g., Hill & Angel, 2005; Robbins, 1989), the reliability of this single item is a cause for concern. However, because this measure exhibits low reliability, the associations presented in this article likely reflect conservative estimates.
Although the WCF survey is a valuable data source for examining the effects of interpersonal violence, it does have certain restrictions. Although it is preferable to specify the age of victimization, our measures of violence in early life are limited to experiences before age 18. Our measure of physical assault before age 18 also includes psychological aggression. A more precise measure would yield a more accurate assess-ment of the effect of physical assault in early life. Data limitations also prevent us from considering the effects of verbal abuse, witnessing violence, and general neglect. We were also unable to assess the effects of important aspects of intimate terrorism, including dominance, control, and isolation.
The present investigation is also limited by the self-report nature of the data. Specifically, we would like to recognize the potential for bias due to social desirability. In an effort to protect individual values, self-concepts, and identities, it is possible that some individuals might falsely respond to questions by underreporting violent experiences, symptoms of dis-tress, and episodes of intoxication. Since we are unable to control for social desirability in our models, our results may misrepresent the strength of many observed associations.
Finally, we would like to emphasize some of the more basic limitations of the data. The sample is restricted to predominantly Black and Hispanic low-income women with chil-dren from Boston, Chicago, and San Antonio. Although women with these characteristics tend to exhibit high violence-risk profiles (Baumrind, 1994; Benson et al., 2004; Hill et al., 2007; Purvin, 2007; Tolman & Raphael, 2000), it is unclear whether our results can be generalized beyond these specific population parameters.
Despite the limitations of our study, our results clearly demonstrate that more frequent intoxication can exacerbate the mental health consequences of interpersonal violence over two years. In light of this evidence, it is important for future research to replicate our work with more reliable assessments of alcohol consumption and across other indicators of mental health (e.g., posttraumatic stress disorder) and substance abuse (e.g., illicit drug use). Clearly, additional attention must be devoted to precise explanations for why substance
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from

304 Violence Against Women 18(3)
abuse might intensify the psychological costs of victimization. Continued research will eventually lead to a more detailed understanding of the association between interpersonal violence and mental health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Aiken, L., & West, S. (1991). Multiple regression: Testing and interpreting interactions. Thousand Oaks, CA: Pine Forge Press.
Anderson, K. (2002). Perpetrator or victim? Relationships between intimate partner violence and well-being. Journal of Marriage and Family, 64, 851-863.
Arias, I., Lyons, C., & Street, A. (1997). Individual and marital consequences of relationship violence: Moderating effects of relationship efficacy and spouse support. Journal of Family Violence, 12, 193-210.
Banyard, V. (1999). Childhood maltreatment and the mental health of low-income women. American Journal of Orthopsychiatry, 69, 161-171.
Banyard, V., & Williams, L. (1996). Characteristics of child sexual abuse as correlates of women’s adjustment: A prospective study. Journal of Marriage and Family, 58, 853-865.
Baumrind, D. (1994). The social context of child maltreatment. Family Relations, 43, 360-368.Benson, M., Wooldredge, J., Thistlethwaite, A., & Fox, G. L. (2004). The correlation between
race and domestic violence is confounded with community context. Social Problems, 51, 326-342.
Buckner, J., Bassuk, E., & Beardslee, W. (2004). Exposure to violence and low-income chil-dren’s mental health: Direct, moderated, and mediated relations. American Journal of Orthopsychiatry, 74, 413-423.
Caetano, R., & Cunradi, C. (2003). Intimate partner violence and depression among whites, blacks, and Hispanics. Annals of Epidemiology, 13, 661-665.
Carlson, B., McNutt, L., Choi, D., & Rose, I. (2002). Intimate partner abuse and mental health: The role of social support and other protective factors. Violence Against Women, 8, 720-745.
Cascardi, M., & O’Leary, D. (1992). Depressive symptomatology, self-esteem, and self-blame in battered women. Journal of Family Violence, 7, 249-259.
Choi, H., & Marks, N. (2008). Marital conflict, depressive symptoms, and functional impair-ment. Journal of Marriage and Family, 70, 377-390.
Coker, A., Smith, P., Thompson, M., McKeown, R., Betheas, L., & Davis, K. (2002). Social support protects against the negative effects of partner violence on mental health. Journal of Women’s Health & Gender-Based Medicine, 11, 465-476.
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from
Kaplan et al. 305
Derogatis, L. (2000). Brief Symptom Inventory 18, administration, scoring, and procedures manual. Minneapolis, MN: National Computer System.
Downs, W., Capshew, T., & Rindels, B. (2004). Relationships between adult women’s alcohol problems and their childhood experiences of parental violence and psychological aggres-sion. Violence Against Women, 8, 785-815.
Draper, B., Pfaff, J., Pirkis, J., Snowdon, J., Lautenschlager, N., Wilson, I., et al. (2008). Long-term effects of childhood abuse on the quality of life and health of older people: results from the depression and early prevention of suicide in general practice project. Journal of the American Geriatrics Society, 56, 262-271.
Epstein, J., Saunders, B., Kilpatrick, D., & Resnick, H. (1998). PTSD as a mediator between childhood rape and alcohol use in adult women. Child Abuse & Neglect, 22, 223-234.
Hanson, R., Saunders, B., Kilpatrick, D., Resnick, H., Crouch, J., & Duncan, R. (2001). Impact of childhood rape and aggravated assault on adult mental health. American Journal of Orthopsychiatry, 71, 108-119.
Hill, T., & Angel, R. (2005). Neighborhood disorder, psychological distress, and heavy drinking. Social Science & Medicine, 61, 965-975.
Hill, T., Mossakowski, K., & Angel, R. (2007). Relationship violence and psychological distress among low-income urban women. Journal of Urban Health, 84, 537-551.
Hill, T., Nielsen, A., & Angel, R. (2009). Relationship violence and frequency of intoxication among low-income urban women. Substance Use & Misuse, 44, 684-701.
Hill, T., Schroeder, R., Bradley, C., Kaplan, L., & Angel, R. (2009). The long-term health con-sequences of relationship violence: An examination of low-income women from Boston, Chicago, and San Antonio. American Journal of Public Health, 99, 1645-1650.
Holt, M., & Espelage, D. (2005). Social support as a moderator between dating violence rela-tionship violence and depression/anxiety among African American and Caucasian adoles-cents. School Psychology Review, 34, 309-328.
Horwitz, A., Widom, C., McLaughlin, J., & White, H. (2001). The impact of childhood abuse and neglect on adult mental health: A prospective study. Journal of Health and Social Behavior, 42, 184-201.
Johnson, D. (2005). Two-wave panel analysis: Comparing statistical methods for studying the effects of transitions. Journal of Marriage and Family, 67, 1061-1075.
Katz, J., & Arias, I. (1999). Psychological abuse and depressive symptoms in dating women: Do different types of abuse have differential effects. Journal of Family Violence, 14, 281-295.
Kaukinen, C., & DeMaris, A. (2005). Age at first sexual assault and current substance use and depression. Journal of Interpersonal Violence, 20, 1244-1270.
Kaysen, D., Dillworth, T., Simpson, T., Waldrop, A., Larimer, M., & Resick, P. (2007). Domestic violence and alcohol use: Trauma-related symptoms and motives for drinking. Addictive Behaviors, 32, 1272-1283.
Kendall-Tackett, K. (2002). The health effects of child abuse: Four pathways by which abuse can influence health. Child Abuse & Neglect, 26, 715-729.
Kessler, R., Molnar, B., Feurer, I., & Appelbaum, M. (2001). Patterns of mental health predic-tors of domestic violence in the United States: Results from the national comorbidity survey. Law and Psychiatry, 24, 487-508.
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from
306 Violence Against Women 18(3)
Kilpatrick, D., Acierno, R., Resnick, H., Saunders, B., & Best, C. (1997). A 2-year longitudinal analysis of the relationships between violent assault and substance use in women. Journal of Consulting and Clinical Psychology, 65, 834-847.
Kunz, J., & Graham, K. (1998). Drinking patterns, psychosocial characteristics and alcohol consequences. Addiction, 93, 1079-1090.
Lipton, R. (1994). The effect of moderate alcohol use on the relationship between stress and depression. American Journal of Public Health, 84, 1913-1917.
Luster, T., & Small, S. (1997). Sexual abuse history and problems in adolescence: Exploring the effects of moderating variables. Journal of Marriage and the Family, 59, 131-142.
Marchand, A., Demers, A., Durand, P., & Simard, M. (2003). The moderating effect of alcohol intake on the relationship between work strains and psychological distress. Journal of Stud-ies on Alcohol, 64, 419-427.
Martino, S., Collins, R., & Ellickson, P. (2005). Cross-lagged relationships between substance use and intimate partner violence among a sample of young adult women. Journal of Studies on Alcohol, 66, 139-148.
McEwen, B. (2002). The end of stress as we know it. Washington, DC: Joseph Henry Press.Miethe, T., & Deibert, G. (2007). Fight time: the normative rules and routines of interpersonal
violence. Long Grove, IL: Waveland Press.Miranda, R., Meyerson, L., Long, P., Marx, B., & Simpson, S. (2002). Sexual assault and alco-
hol use: Exploring the self-medication hypothesis. Violence and Victims, 17, 205-217.Myers, R. (1986). Classical and modern regression with applications. Boston, MA: Duxbury
Press.Neff, J. (1984). The stress-buffering role of alcohol consumption: The importance of symptom
dimension. Journal of Human Stress, 19, 35-42.Neff, J. (1985). Evaluating the stress-buffering role of alcohol consumption: Variation by type
of event and type of symptom. Alcohol & Alcoholism, 20, 391-401.Neff, J., & Husaini, B. (1982). Life events, drinking patterns and depressive symptomatol-
ogy: The stress-buffering role of alcohol consumption. Journal of Studies on Alcohol, 43, 301-318.
Neff, J., & Husaini, B. (1985). Stress-buffer properties of alcohol consumption: The role of urbanicity and religious identification. Journal of Health and Social Behavior, 26, 207-222.
Purvin, D. (2007). At the crossroads and in the crosshairs: Social welfare policy and low-income women’s vulnerability to domestic violence. Social Problems, 54, 188-210.
Resnick, H., & Acierno, R. (1997). Health impact of interpersonal violence 2: Medical and mental health outcomes. Behavioral Medicine, 23, 65-79.
Robbins, C. (1989). Sex differences in psychosocial consequences of alcohol and drug abuse. Journal of Health and Social Behavior, 30, 117-130.
Rodgers, B., Korten, A., Jorm, A., Christensen, H., Henderson, S., & Jacomb, P. (2000). Risk factors for depression and anxiety in abstainers, moderate drinkers and heavy drinkers. Addiction, 95, 1833-1845.
Romito, P., Turan, J., & De Marchi, M. (2005). The impact of current and past interpersonal violence on women’s mental health. Social Science & Medicine, 60, 1717-1727.
Sapolsky, R. (2004). Why zebras don’t get ulcers. New York: Owl Books.
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from
Kaplan et al. 307
Sayette, M., Wilson, T., & Elias, M. (1993). Alcohol and aggression: A social information pro-cessing analysis. Journal of Studies on Alcohol, 54, 399-407.
Seeman, M., & Seeman, A. (1992). Life strains, alienation, and drinking behavior. Alcoholism: Clinical and Experimental Research, 16, 199-205.
Silver, E., & Teasdale, B. (2005). Mental disorder and violence: Stressful life events and impaired social support. Social Problems, 52, 67-78.
Skomorovsky, A., Matheson, K., & Anisman, H. (2006). The buffering role of social support perceptions in relation to eating disturbances among women in abusive dating relationships. Sex Roles, 54, 627-638.
Springer, K., Sheridan, J., Kuo, D., & Carnes, M. (2007). Long-term physical and mental health consequences of childhood physical abuse: Results from a large population-based sample of men and women. Child Abuse and Neglect, 31, 517-530.
Straus, M., & Douglas, E. (2004). A short form of the revised conflict tactics scales, and typolo-gies for severity and mutuality. Violence and Victims, 19, 507-520.
Straus, M., Hamby, S., Boney-McCoy, S., & Sugarman, D. (1996). The Revised Conflict Tactics Scales (CTS2): Development and preliminary psychometric data. Journal of Family Issues, 17, 283-316.
Tedeschi, R., & Calhoun, L. (1996). The Posttraumatic Growth Inventory: Measuring the posi-tive legacy of trauma. Journal of Traumatic Stress, 9, 455-471.
Testa, M., Livingson, J., & Leonard, K. (2003). Women’s substance use and experiences of intimate partner violence. Addictive Behaviors, 28, 1649-1664.
Tjaden, P., & Thoennes, N. (2000). Full report of the prevalence, incidence, and consequences of violence against women: Findings from the National Violence against Women Survey. Washington, DC: U.S. Department of Justice, National Institute of Justice.
Tolman, R., & Raphael, J. (2000). A review of research on welfare and domestic violence. Jour-nal of Social Issues, 56, 655-682.
Tolman, R., & Rosen, D. (2001). Domestic violence in the lives of women receiving wel-fare: Mental health, substance dependence, and well-being. Violence Against Women, 7, 141-158.
Ullman, S., Filipas, H., Townsend, S., & Starzynski, L. (2005). Trauma exposure, posttraumatic stress disorder and problem drinking in sexual assault survivors. Journal of Studies on Alco-hol, 66, 610-619.
Watts-English, T., Fortson, B., Gibler, N., Hooper, S., & De Bellis, M. (2006). The psychobiol-ogy of maltreatment in childhood. Journal of Social Issues, 62, 717-736.
Williams, S., & Mickelson, K. (2007). A psychosocial resource impairment model explaining partner violence and distress: Moderating role of income. American Journal of Community Psychology, 40, 13-25.
Wilsnack, S., Vogeltanz, N., Klassen, A., & Harris, T. (1997). Childhood sexual abuse and women’s substance abuse: national survey findings. Journal of Studies on Alcohol, 58, 264-271.
Wilsnack, R., Wilsnack, S., Kristjanson, A., & Harris, T. (1998). Ten-year prediction of wom-en’s drinking behavior in a national representative sample. Women’s Health, 4, 199-230.
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from
308 Violence Against Women 18(3)
Winship, C., & Radbill, L. (1994). Sampling weights and regression analysis. Sociological Methods and Research, 22, 230-257.
Zabkiewicz, D., & Schmidt, L. (2009). The mental health benefits of work: Do they apply to welfare mothers with a drinking problem? Journal of Behavioral Health Services & Research, 36, 96-110.
Zlotnick, C., Johnson, D., & Kohn, R. (2006). Intimate partner violence and long-term psy-chosocial functioning in a national sample of American women. Journal Interpersonal Violence, 21, 262-275.
Bios
Lauren M. Kaplan is a doctoral student in the Department of Sociology at Goethe-Universität, Frankfurt am Main, Germany. Her research focuses on the social distribution of health and health-relevant behaviors. She is especially interested in the areas of stress, violence, neighbor-hood conditions, and HIV.
Terrence D. Hill is an assistant professor of sociology at Florida State University, with a secondary appointment in the Department of Public Health. His research focuses on the social distribution of health and health-relevant behaviors. He is especially interested in the effects of social relationships, religious involvement, neighborhood conditions, and socioeconomic status.
Gini R. Mann-Deibert is an assistant professor of sociology at Suffolk University. Her research centers on crime and delinquency, with a particular focus on the intersection of crime and sexuality.
at FLORIDA STATE UNIV LIBRARY on June 30, 2012vaw.sagepub.comDownloaded from




















