Does lower extremity osteoarthritis exacerbate risk factors for falls in older adults?
14
685 CME ISSN 1745-5057 10.2217/WHE.12.53 © 2012 Future Medicine Ltd Women's Health (2012) 8 (6), 685–698 CME REVIEW Does lower extremity osteoarthritis exacerbate risk factors for falls in older adults? Mackenzie L Hoops* 1 , Noah J Rosenblatt 1 , Christopher P Hurt 2 , Jeremy Crenshaw 3 & Mark D Grabiner 1 The risk of falling reportedly increases almost 2.5-times in those with lower extremity osteoarthritis (OA LE ) compared with age-matched controls. However, the mechanisms underlying the increased risk are not clear. The risk factors for falls in people with OA LE found in the literature are mostly the same as the risk factors for people without OA LE . It is hypothesized that risk factors for falls are exacerbated by OA LE , such that these individuals are more likely to become dynamically unstable and, once this has occurred, are less able to perform an appropriate compensatory stepping response compared with people without OA LE . To the extent that this is true, task-specific training targeting the compensatory step, which decreases falls in middle-aged and older women, should be effective for people with OA LE . The purpose of the present review is to provide the rationale for the above hypothesis. Furthermore, the present authors present evidence that the fall risk of people with OA LE could be efficiently and effectively reduced using task-specific training previously shown to reduce falls in middle aged and older women. 1 Department of Kinesiology & Nutrition, University of Illinois at Chicago, 1919 W Taylor Street, Chicago, IL, USA 2 Department of Physical Therapy, University of Alabama Birmingham, 1530 3rd Avenue S, Birmingham, AL, USA 3 Department of Orthopedic Surgery, Mayo Clinic, 200 1st Street, Rochester, MN, USA *Author for correspondence: Tel.: +1 312 413 9432 [email protected] Keywords • aging • compensatory stepping • dynamic stability • falls • osteoarthritis • risk factor • task specificity Medscape: Continuing Medical Education Online This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Future Medicine Ltd. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians. Medscape, LLC designates this Journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test with a 70% minimum passing score and complete the evaluation at www.medscape.org/journal/wh; (4) view/print certificate. Release date: 26 November 2012; Expiration date: 26 November 2013 Learning objectives Upon completion of this activity, participants should be able to: • Analyze the risk of falls among older adults • Assess traditional risk factors for falls • Distinguish factors associated with osteoarthritis which increase the risk of falls • Evaluate means to reduce the risk of falls among patients with osteoarthritis of the lower extremities Financial & competing interests disclosure CME Author Charles P Vega, Health Sciences Clinical Professor; Residency Director, Department of Family Medicine, University of California, Irvine, CA, USA Disclosure: Charles P Vega has disclosed no relevant financial relationships. part of For reprint orders, please contact: [email protected]
Transcript of Does lower extremity osteoarthritis exacerbate risk factors for falls in older adults?

685
CME
ISSN 1745-505710.2217/WHE.12.53 © 2012 Future Medicine Ltd Women's Health (2012) 8(6), 685–698
CME REVIEW
Does lower extremity osteoarthritis exacerbate risk factors for falls in older adults?Mackenzie L Hoops*1, Noah J Rosenblatt1, Christopher P Hurt2, Jeremy Crenshaw3 & Mark D Grabiner1
The risk of falling reportedly increases almost 2.5-times in those with lower extremity osteoarthritis (OALE) compared with age-matched controls. However, the mechanisms underlying the increased risk are not clear. The risk factors for falls in people with OALE found in the literature are mostly the same as the risk factors for people without OALE. It is hypothesized that risk factors for falls are exacerbated by OALE, such that these individuals are more likely to become dynamically unstable and, once this has occurred, are less able to perform an appropriate compensatory stepping response compared with people without OALE. To the extent that this is true, task-specific training targeting the compensatory step, which decreases falls in middle-aged and older women, should be effective for people with OALE. The purpose of the present review is to provide the rationale for the above hypothesis. Furthermore, the present authors present evidence that the fall risk of people with OALE could be efficiently and effectively reduced using task-specific training previously shown to reduce falls in middle aged and older women.
1Department of Kinesiology & Nutrition, University of Illinois at Chicago, 1919 W Taylor Street, Chicago, IL, USA 2Department of Physical Therapy, University of Alabama Birmingham, 1530 3rd Avenue S, Birmingham, AL, USA 3Department of Orthopedic Surgery, Mayo Clinic, 200 1st Street, Rochester, MN, USA *Author for correspondence: Tel.: +1 312 413 9432 [email protected]
Keywords
• aging • compensatory stepping • dynamic stability • falls • osteoarthritis • risk factor • task specificity
Medscape: Continuing Medical Education Online
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Future Medicine Ltd. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Medscape, LLC designates this Journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test with a 70% minimum passing score and complete the evaluation at www.medscape.org/journal/wh; (4) view/print certificate.
Release date: 26 November 2012; Expiration date: 26 November 2013
Learning objectives
Upon completion of this activity, participants should be able to:
• Analyze the risk of falls among older adults
• Assess traditional risk factors for falls
• Distinguish factors associated with osteoarthritis which increase the risk of falls
• Evaluate means to reduce the risk of falls among patients with osteoarthritis of the lower extremities
Financial & competing interests disclosureCME AuthorCharles P Vega, Health Sciences Clinical Professor; Residency Director, Department of Family Medicine, University of California, Irvine, CA, USADisclosure: Charles P Vega has disclosed no relevant financial relationships. part of
For reprint orders, please contact: [email protected]

686 future science groupwww.futuremedicine.com
CMEREVIEW – Hoops, Rosenblatt, Hurt, Crenshaw & Grabiner
Conceptually, static postural stability is a condi-tion defined by the position of a person’s center of mass being within the boundaries of the base of support. The base of support is gener-ally defined by the perimeter established by the location of the feet or the perimeter established by the location of the feet and assistive devices such as a cane. Dynamic stability, however, is a condition defined by both the position of the person’s center of mass and the velocity of the center of mass relative to the base of support. Thus, a person may be dynamically unstable even when the condition of static stability is met. A fall occurs when a person becomes dynami-cally unstable and, subsequently, is unsuccessful at restoring dynamic stability. Consequently, a fall is the result of two sequential events: first, going from a state of dynamic or static stabil-ity to a state of dynamic instability followed by, the failure to compensate and restore a condi-tion of static or dynamic stability [1,2]. However, the risk of becoming dynamically unstable may not be an accurate determinant of the ability to restore static or dynamic stability and avoid a fall [3,4]. Each of the two events are associated with various risk factors that increase the likeli-hood of becoming dynamically unstable and/or decrease the likelihood of being able to restore static or dynamic stability. Furthermore, these risk factors may be modifiable or not modifi-able. For example, although a history of falling is one of the strongest risk factors for future falls [5], having had a previous fall is not modifiable. Muscle strength, on the other hand, is modi-fiable. In light of the increasing incidence of falls and fall-related injuries in older adults, as well as the economic burden that is placed on the healthcare system by these events, effective clinical interventions focusing on modifiable risk factors that are causally related to falls in older adults are highly warranted.
Falls in older adultsIn 2006, nearly 33% of older adults (age 65 years and older) in the USA reported at least one fall [6]. The number of older adults who fall annu-ally, which has increased from 28% since 1981 [7], suggests that efforts to reduce falls in older adults over the past 30 or more years have not been successful. The problem of falls is particu-larly relevant for women in light of their having higher incidence of falls than men (nearly twice as high), and because of postmenopausal loss of bone quality that increases the likelihood of fracture [7,8]. In the absence of effective fall pre-vention that can be delivered on a national scale, the absolute number of falls and fall-related inju-ries will increase with the population of older adults. The number of older adults in the USA is expected to reach 70 million by 2030 [9]. Consequently, the economic burden that falls contribute to healthcare costs will increase. In 2000, US$19 billion in direct medical costs were attributed to fall-related injuries to older adults [6]. The increases in fall-related injury, mortality and costs emphasize the need for fall-prevention methods that are time- and cost-effective, and scalable.
Falls in people with lower extremity osteoarthritisArthritis has been recognized as increasing the likelihood of a fall for at least 25 years [10–28]. The risk of falling in people with arthritis is reportedly about 2.5-times that of older adults without arthritis [29]. However, many of the studies reporting a relationship between arthri-tis and falls have not reported which specific joints were affected, specified the type of arthri-tis being considered (i.e., osteoarthritis, rheu-matoid arthritis, lupus and so on), and have relied on self-report rather than a diagnosis by a physician. Indeed, in one review of risk factors
Financial & competing interests disclosure (cont.)Mackenzie L Hoops, Department of Kinesiology and Nutrition, University of Illinois at Chicago, IL, USADisclosure: Mackenzie L Hoops has disclosed no relevant financial relationships.Noah J Rosenblatt, Department of Kinesiology and Nutrition, University of Illinois at Chicago, IL, USADisclosure: Noah J Rosenblatt has disclosed no relevant financial relationships.Christopher P Hurt, Department of Physical Therapy, University of Alabama Birmingham, Birmingham, AL, USADisclosure: Christopher P Hurt has disclosed no relevant financial relationships.Jeremy Crenshaw, Department of Orthopedic Surgery, Mayo Clinic, Rochester, MN, USADisclosure: Jeremy Crenshaw has disclosed no relevant financial relationships.Mark D Grabiner, Department of Kinesiology and Nutrition, University of Illinois at Chicago, IL, USADisclosure: Mark D Grabiner has disclosed no relevant financial relationships.EditorElisa Manzotti, Publisher, Future Science GroupDisclosure: Elisa Manzotti has disclosed no relevant financial relationships.

687future science group Women's Health (2012) 8(6)
CME Risk factors for falls in people with lower extremity osteoarthritis – REVIEW
for falls, only one of the included studies was specific to osteoarthritis (OA) [30] and only one of the included studies was exclusive to lower extremity osteoarthritis (OA
LE) [31]. Given that
OA is the most prevalent form of arthritis [32] and that upper extremity arthritis would not be expected to directly increase fall risk, OA
LE is a
much more meaningful risk factor for falls when compared with general arthritis. Notably, two studies reported that more than 50% of people with knee OA reported a fall during the previous year [21,22]. This is higher than the 33% gener-ally attributed to older adults. One additional study reported that people with knee OA had a 30% increase in the incidence of falls compared with people without knee OA [25]. People with OA
LE also have an increased risk of hip frac-
ture compared with control subjects [17]. This is somewhat paradoxical considering individuals with OA generally have increased bone min-eral density compared with controls [33–35], and that increased bone mineral density is generally considered to confer protection from fracture. The increase in fracture risk may, in part, be due to the increased incidence of falls and/or an increase in the severity of falls [17].
The underlying mechanisms for the increased risk of falls in people with OA
LE are not clear.
The present authors propose that people with OA
LE may be at an increased risk of becoming
dynamically unstable and, once dynamically unstable, they are less able to perform an appro-priate compensatory stepping response. Either of these possibilities would increase fall risk. However, the factors that contribute to each possibility, as well as the clinical approaches to decrease the fall risk, are not necessarily the same. The present authors also propose that risk factors for falls in people with OA
LE found in
the literature are not different from the risk fac-tors for people without OA
LE. It is hypothesized
that the exacerbation of risk factors for falls in older adults with OA
LE increases the likeli-
hood of becoming dynamically unstable and decreases the ability to successfully perform a compensatory stepping response compared with people without OA
LE. Support for this hypoth-
esis would suggest the need for an intervention intended to address both dynamic stability and the ability to perform a successful compensatory stepping response.
Established risk factors for falls in older adultsIn addition to arthritis, the most commonly agreed modifiable risk factors for falls in older
adults include gait and balance impairments, and muscle weakness [29]. Fall risk scales linearly with the number of risk factors [36]. Indeed, absolute fall risk of older adults ranges from 11%, for those with no risk factors, to nearly 55%, for those who have multiple risk factors [37]. There are multiple functional outcomes associated with OA
LE, such as gait and balance impairments and
muscle weakness. These functional outcomes are not independent of other consequences associ-ated with OA
LE that have also been shown to be
related to falls (discussed later in this review). Whether considered as risk factors for falls in older adults or outcomes of OA
LE, the result is an
increased probability of becoming dynamically unstable and/or decreased ability to success-fully perform a compensatory stepping response (Table 1).
Gait impairmentsThe majority of falls in older adults occur dur-ing walking [38] and numerous studies have demonstrated associations between changes in gait and fall risk in older adults. Increased fall risk has been associated with slower walking velocity (although this appears to only be true for indoor falls [25,39]), shorter stride length, a wider step width and longer double-leg sup-port time [25,30,39–46]. Paradoxically, these char-acteristics tend to improve dynamic stability. Consequently, gait impairments associated with OA
LE are correlated with fall risk [29]. For exam-
ple, individuals with knee or hip OA have slower walking speeds, increased double support time and shorter stride lengths, and wider step width compared with healthy aging controls [47–52]. The extent to which these changes in gait are associated with, or more importantly cause, falls is not clear. Furthermore, the extent to which these spatial and temporal variables are modifi-able in people with OA
LE, as well as the effects
of modifying them, are unclear. For example, in isolation, faster walking velocity, which can be attained through lower extremity resistance training [53] may actually increase trip-related fall risk [54]. In general, gait impairments are organism-level changes that are secondary to, and reflective of, other functional changes at the system and tissue levels.
Balance impairments: static postural controlThe broad term ‘balance deficits’ was used to describe a category of risk factors that increased fall risk by threefold [29]. Effective postural control, whether static or dynamic, relies on
688 future science groupwww.futuremedicine.com
CMEREVIEW – Hoops, Rosenblatt, Hurt, Crenshaw & Grabiner
the integration of sensory input from multiple sensory systems with motor output that accu-rately matches the postural requirements. These sensorimotor systems degrade as a normal con-sequence of aging [55,56] and, as a result, there is an associated increase in static postural sway. People with OA
LE have larger postural sway
compared with age- and sex-matched control subjects [57–59]. The increase in static postural sway may increase the likelihood of a specific postural disturbance causing a person to become dynamically unstable. In fact, the ability to regain balance in response to small perturb-ations (where subjects are not allowed to take a step) is impaired in people with knee OA [60]. However, as indicated previously, the likelihood of becoming posturally unstable does not neces-sarily causally predict the inability to perform a compensatory stepping response and thereby prevent a fall.
Muscle weaknessLower extremity muscle weakness is frequently reported as a significant risk factor for falls [29,61]. This follows the notion that when a person becomes dynamically unstable, in addition to
the coordination required to perform a compen-satory stepping response, there can be substan-tial lower extremity joint muscle strength and power requirements to avoid a fall. The expected age-related decrease of muscle strength, as much as 3% per year beyond age 50 years [62–66], is accompanied by a reduction in the rate of force generation [67,68]. These important functional changes arise, in part, as a result of loss of muscle mass, which can be caused by the death of spi-nal motor neurons that lead to the loss of motor units (particularly large motor units that gener-ate high contraction force and power), disuse atrophy and muscle attenuation (i.e., infiltration of muscle by fat [69]). Collectively, these struc-tural and functional changes can contribute to the diminished ability to meet the biomechani-cal requirements of the compensatory stepping response. For example, the initial recovery step following a trip requires a knee extension moment that is sufficient to prevent the knee joint from buckling (i.e., flexing) [70]. Indeed, a potentially more important, but not widely studied aspect of this element of the compensa-tory stepping response is the power requirement at the knee joint, which can be quite large and
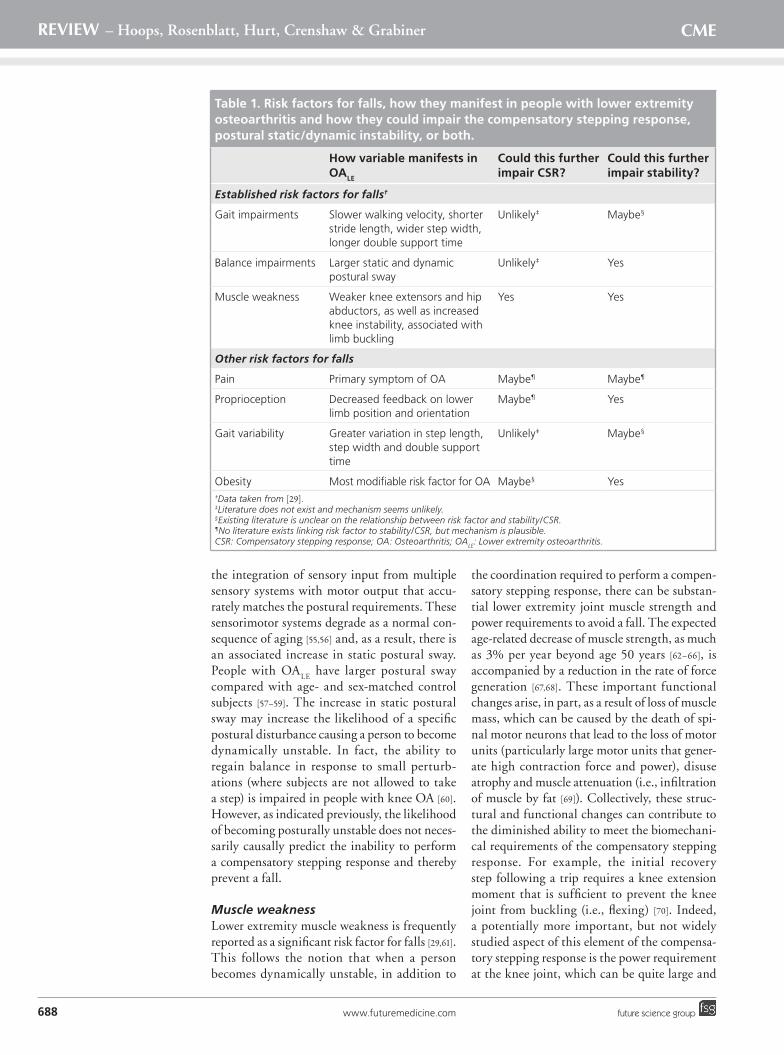
Table 1. Risk factors for falls, how they manifest in people with lower extremity osteoarthritis and how they could impair the compensatory stepping response, postural static/dynamic instability, or both.
How variable manifests in OALE
Could this further impair CSR?
Could this further impair stability?
Established risk factors for falls†
Gait impairments Slower walking velocity, shorter stride length, wider step width, longer double support time
Unlikely‡ Maybe§
Balance impairments Larger static and dynamic postural sway
Unlikely‡ Yes
Muscle weakness Weaker knee extensors and hip abductors, as well as increased knee instability, associated with limb buckling
Yes Yes
Other risk factors for falls
Pain Primary symptom of OA Maybe¶ Maybe¶
Proprioception Decreased feedback on lower limb position and orientation
Maybe¶ Yes
Gait variability Greater variation in step length, step width and double support time
Unlikely‡ Maybe§
Obesity Most modifiable risk factor for OA Maybe§ Yes†Data taken from [29]. ‡Literature does not exist and mechanism seems unlikely. §Existing literature is unclear on the relationship between risk factor and stability/CSR.¶No literature exists linking risk factor to stability/CSR, but mechanism is plausible. CSR: Compensatory stepping response; OA: Osteoarthritis; OALE: Lower extremity osteoarthritis.

689future science group Women's Health (2012) 8(6)
CME Risk factors for falls in people with lower extremity osteoarthritis – REVIEW
involves eccentric contraction of the involved musculature. People with radiographic evidence OA
LE, particularly knee OA, tend to have knee
extensor strength that is approximately 20% lower than people without radiographic evi-dence of knee OA [50,59,71]. Notably, these losses are independent of pain, one of the most com-monly reported symptoms of OA [72], which may further alter the ability to perform a successful compensatory step.
Knee extensor weakness is associated with functional instability that manifests as knee buckling [73]. Knee buckling, or giving way, is characterized by an involuntary loss of postural support across the knee during weight bearing [73]. More than 60% of people with OA
LE report
sensations of knee buckling during activities of daily living [74]. Furthermore, 13% of those who report knee buckling also report falling as a result [73]. Thus, the associations between knee extensor weakness, knee buckling and falls reported for people with knee OA, even in the absence of pain, supports the hypothesis that the risk factors for falls in people with OA
LE found
in the literature are not different than those for people without OA
LE. However, the extent to
which the risk is increased is greater given the more frequent presence of risk factors in people with OA
LE.
Weakness of the hip joint musculature is also important with regards to fall risk. Specifically, strong hip abductors and adductors may be required to avoid laterally directed falls during gait, which increase the likelihood of hip frac-ture [75]. During the stance phase of walking, the hip musculature controls the frontal plane motion of the center of mass [76,77]. Weak hip abductors and adductors may diminish this control and increase the likelihood of a person becoming dynamically unstable. In general, compared with younger adults, older adults generate smaller maximum hip abduction and adduction isometric forces and do so at slower rates [78]. In people with OA
LE, hip abductor and
adductor strength may be 31 and 25% less than healthy controls, respectively [79].
Few studies have reported strength measures of the trunk or ankle musculature in people with OA
LE. Specifically, the ability to arrest and
reverse the trunk flexion following a trip, which, to a large extent, is a function of the trunk mus-culature, is a determinant of a fall following a laboratory-induced trip [54,80]. The ankle mus-culature contributes to static postural stability through control of postural sway and thus, can be linked to the initial loss of static postural
stability. During the compensatory stepping response, ankle plantar flexion is a key source of the propulsive ground reaction forces that are influential in avoiding a fall. Dorsiflexion weakness distinguished fallers from nonfallers in nursing home residents [81]. Plantar flexion and dorsiflexion strength of people with ankle OA is significantly lower than control subjects [82]. Collectively, however, given the limited data available on the ankle joint and trunk muscles of people with OA
LE, these are potentially impor-
tant areas of investigation for fall risk of people with OA
LE.
Other factors related to falls in older adults with & without OALE
PainPain, a hallmark symptom of OA, may partially explain the increased risk of falling [18,23,24,34]. In people with OA
LE, pain is the most com-
mon reason for seeking medical help [83] and is the most debilitating symptom of knee OA. Functionally, pain or even the perception of the potential for pain, may negatively influence coordination, postural sway, muscle strength and power, and the sensory components of muscle function (e.g., proprioception) [59]. These deficits provide potential mechanisms by which pain may influence fall risk by interfering with the requirements to preserve stability, as well as those needed to perform effective compensatory mechanisms. For example, women with wide-spread musculoskeletal pain had a 66% increase in fall risk compared with women with no pain or mild pain at one musculoskeletal site [12]. This appears to be the only published study of prospectively measured falls and lower extrem-ity pain. Further study of the contribution of pain to the increased risk of falling in people with OA
LE is warranted. For example, prospec-
tive analysis of individuals with radiographic evidence of OA, some of whom are in pain and others who are not, could help to establish if pain, as opposed to the structural and functional changes associated with OA, best explain the increase in falls in this population.
If pain partially explains the increased fall risk of people with OA
LE, then pain relief would be
expected to reduce this risk. However, while reductions in knee pain following intra-articular injections of local anesthetic increased maxi-mal voluntary knee extension force, this was not accompanied by concurrent improvement of proprioception or static postural sway. This suggests that factors other than pain account for these functional deficits [84]. Similarly, pain relief

690 future science groupwww.futuremedicine.com
CMEREVIEW – Hoops, Rosenblatt, Hurt, Crenshaw & Grabiner
was associated with increased walking velocity, although the walking velocity remained signifi-cantly slower than that of healthy controls [85]. It is important to note that pain relief may neg-atively alter gait. For example, patients taking a NSAID to reduce pain showed significantly greater peak external adduction knee joint moments and peak external knee joint exten-sion moments while walking compared with those with increased pain. This consequently increased knee joint forces, particularly in the medial knee joint compartment (the most fre-quently affected portion) [86]. These alterations in gait may reflect protective compensatory mechanisms that are secondary to pain, which act to reduce medial compartment forces by reducing the external adduction moment [86]. If so, medication use to reduce pain may have det-rimental consequences. Furthermore, relieving pain using medications influences gait, such as increased walking velocity, which could increase fall risk by making other risk factors for falls more pronounced.
ProprioceptionProprioception, primarily in the lower extremi-ties, can contribute to static and dynamic pos-tural stability by providing feedback about limb position and joint orientation. Older adults have impaired proprioceptive feedback as a natural consequence of aging and are poorer at cor-recting errors in movement [87,88]. Diminished proprioception has been associated with falls in older adults [30,89–91]. In particular, lower extremity proprioceptive deficits, as measured using a joint angle matching task, prospectively discriminated older women who had multiple falls from nonfallers [26,27]. In people with knee OA, knee proprioception, measured using both knee (re)position sense and motion sensation tests, was significantly impaired compared with healthy controls [59,92–95].
Given the contributions of proprioception to static and dynamic stability, proprioceptive impairment exceeding that of ‘normal’ aging may cause a person to become dynamically unstable more frequently. To some extent, for people whose proprioception is impaired, moni-toring static and dynamic stability can still rely on other, redundant, sensory feedback systems (visual and vestibular/otolith) to signal dynamic instability [88]. However, these systems also tend to become impaired with age. Conceptually, proprioceptive impairment could contribute to signal processing delays that result in slower performance times, the result of which may be
insufficient time available for compensatory step-ping responses to occur. However, the effect of proprioceptive impairment associated with OA
LE
on the performance of a compensatory stepping response is not clear.
Gait variabilityThe topic of gait variability conceptually links increased movement variability with decreased neuromuscular control. As stated earlier, spatial and temporal step kinematics, such as increased step width, reduced stride length and slower walking speed, are associated with increased fall risk. However, for some populations, such as frail older adults, these changes may increase dynamic stability and decrease fall risk. Consequently, these variables may not necessar-ily represent meaningful clinical intervention targets. However, variability of step kinematics, particularly step width variability, has been pro-spectively associated with falling as variability may reflect errors in foot placement or ongoing attempts to compensate for an impaired abil-ity to control destabilizing motion of the body during gait [96,97]. Similarly, the variability of the height of the toe during swing (minimum toe clearance variability) has also been related to individuals with a history of trip-related falls [98]. However, the extent to which these variables are causally related to falls, the degree to which they are modifiable, and the methods through which they may be modified are not known.
Gait variability of people with OALE
may differ compared with people who do not have OA
LE. Individuals with knee OA have greater
coefficients of variation in step length, step width and double support time compared with healthy controls [99] suggesting a decreased pre-cision of the control of gait. The minimum toe clearance of people with symptomatic knee OA is not different than that of healthy asympto-matic control subjects; however, minimum toe clearance variability in people with OA
LE has not
been reported [100]. Overall, the topic of gait vari-ability as it relates to falls in people with OA
LE
represents a potentially important area of clinical research.
Obstacle crossing is a motor task that requires accurate interjoint coordination and swing foot control. Knee OA increases the tendency to trip during obstacle crossing [101]. In people with OA
LE, proprioceptive impairment may influ-
ence interlimb coordination patterns and may be associated with an increased variability in mini-mum toe clearance. This increase, in addition to the proprioceptive deficits, could increase the

691future science group Women's Health (2012) 8(6)
CME Risk factors for falls in people with lower extremity osteoarthritis – REVIEW
likelihood of the swing foot coming into contact with an obstacle. After receiving pain-relieving intra-articular knee injections, people with knee OA were 31% more successful in avoiding an obstacle, although the avoidance rate remained 20% smaller than that of healthy controls [102].
ObesityObesity is one of the most modifiable risk factors for OA [103,104] and a large majority of individ uals who are overweight/obese have OA
LE. Similar to
older adults and people with OA, obese adults have slower preferred walking speeds, shorter step lengths, increased double support time and larger step widths [105–107], all of which have been associated with fall risk, yet also associated with increased dynamic stability. In addition, similar to people with knee OA, obese people adapt their gait to reduce loading at the knee [106]. Obesity is linked to impaired static stability [108,109] and dynamic stability (as measured by the range and speed of the center of pressure motion during a maximum forward and backward lean task) [110] and impaired normalized knee extensor strength [111]. Furthermore, obesity is a risk fac-tor for falls [112], possibly linked to compromised compensatory stepping abilities [113]. Given the associations between obesity and gait/balance impairments, obese older adults with OA may be at high risk of falling compared with those with either OA or obesity alone.
Strategies for decreasing fall riskGiven the premise that a fall is the consequence of two sequential events, the loss of static or dynamic stability followed by an unsuccess-ful compensatory step, interventions targeting one or both of these events would likely reduce the occurrence of falls. In older adults, inter-ventions focusing on the ability to maintain static and dynamic stability by implementing balance training, in addition to an exercise pro-gram, reduces the occurrence of falls in approxi-mately 20% [114]. Given the imperative need for a compensatory mechanism following a loss of dynamic stability, novel concepts of training the compensatory step have been developed [115–117]. In particular, the present authors have developed an approach for reducing the occurrence of trip-related falls in focusing on training the compen-satory step following a disturbance simulating a trip, and have found reductions in trip-related falls of almost 80% [80].
Falls result from a wide variety of causes including trips, slips, stair ascent and descent, and missteps [Rosenblatt NJ, Unpublished Data] [29,118–119] .
For many trips and slips, which together account for approximately 50% of falls that occur dur-ing locomotion, it is possible to avoid falling by appropriately performing a compensatory step-ping response. However, the compensatory step-ping response associated with a trip and a slip involve considerably different environmental (and sensori motor) contexts. For example, when tripped, a person falls in the same direction of travel. When slipped, the person typically con-tinues to travel (i.e., slide) in the same direction, but actually falls backwards. Because the envi-ronmental contexts differ, the requirements of the compensatory stepping response also differ. The present authors’ approach to reducing fall risk has been to improve the ability of older women to successfully perform the compensatory stepping response in response to a simulated trip. This is a task that requires a high degree of motor skill. Given that a motor skill is being trained, the effec-tiveness of the protocol is significantly affected by the motor learning ‘principle of specificity’ [120]. Specificity is a quality underlying the proficiency with which a motor skill (e.g., muscle strength) learned under ‘practice’ conditions (resistance training) can be performed under a different set of ‘test’ conditions (sports). According to this principle, fall risk should decrease proportionally to the similarity between the practice conditions during which the motor skill of avoiding a fall after a trip are learned, and those conditions dur-ing an actual trip in the community.
Following laboratory-induced trips, trunk flexion and the length of initial recovery step distinguish fallers from nonfallers [54]. Moreover, similar mechanisms distinguished fallers from nonfallers in response to treadmill-delivered disturbances [4]. This suggests considerable between-protocol specificity. Indeed, a task-specific training protocol, employing treadmill-delivered disturbances, decreased the number of falls in middle-aged and older women after a laboratory-induced trip, during which the women who did not fall reduced trunk flexion and increased step length following the distur-bance [80]. A similar task-specific training pro-tocol decreased falls measured prospectively in the community [Rosenblatt NJ, Unpublished Data]
[Rosenblatt NJ, Marone J, Grabiner M. A novel step-
training paradigm to decrease prospective community-
based falls (2012), Manuscript in preparation] [121].
Compensatory step training to reduce falls in people with OALE
In the previous sections, the major risk factors for falls in older adults were presented in the

692 future science groupwww.futuremedicine.com
CMEREVIEW – Hoops, Rosenblatt, Hurt, Crenshaw & Grabiner
context of their overlapping with the risk factors for falls in people with OA
LE (Table 1). Even pain,
and particularly pain at the affected joint(s), cannot be considered to be a risk factor unique to OA because pain can arise from numerous joint-related conditions. Therefore, given that the risk factors are more similar than not, it seems reasonable to expect that the present authors’ task-specific training, found to be successful in reducing trip-related falls in older women, would also be effective in people with OA
LE.
The task-specific training targets performance of a compensatory stepping response following a posturally destabilizing disturbance deliv-ered by a computer-controlled treadmill. This type of training reduces the number of falls in both middle-age (55–65 years of age) and older (>65 years of age) community-dwelling women after laboratory-induced trips, and reduces all-cause falls in the community [Rosenblatt NJ,
Marone J, Grabiner M. A novel step-training paradigm
to decrease prospective community-based falls (2012),
Manuscript in preparation] [80,121]. The postural dis-turbances administered during the task-specific training simulated a trip [4,54,122], and were large enough to cause the subject to fall (safely into a harness) if they were not able to perform the required compensatory stepping response. The required compensatory stepping responses varied depending on the magnitude of the disturbance, where some may require one step, while others required several steps to restore dynamic stabil-ity. Biomechanically, the task-specific training significantly improved the ability of the women to restore control of the trunk following the disturbance and to coordinate this control with the recovery step(s). The risk of falling after a laboratory-induced trip decreased by 83% [80]
and prospectively measured trip-related fall risk decreased by approximately 60% [Rosenblatt NJ,
Marone J, Grabiner M. A novel step-training paradigm
to decrease prospective community-based falls (2012),
Manuscript in preparation] compared with control subjects. With regards to laterally directed dis-turbances where subjects are required to take a step in the mediolateral direction, compensatory stepping responses of young and older adults are quickly modified with practice [123,124]. This sug-gests that task-specific training may also decrease falls to the side, which significantly increases the risk of fall-related hip fracture.
For people with OALE
, foot placement of the initial recovery step may be a significant factor limiting their ability to avoid a trip-related fall. Following contact with the ground, the ini-tial weight-bearing phase of the recovery step involves eccentric contraction of the knee exten-sor muscles, which contributes to both reducing the angular momentum of the body and pre-venting the knee from buckling. Furthermore, the external knee adduction moment will likely increase as the width of the recovery step increases. A recovery step following a trip can thus result in relatively high compressive and shear loads at the knee joint [125]. For a person with OA
LE, such loads could elicit knee pain or
even the anticipation of pain, and could lead to buckling of the knee or reluctance to complete an appropriate compensatory step to avoid a fall. Thus, training the compensatory stepping response to minimize pain, or the anticipation of pain, may increase the likelihood of suc-cessfully executing the compensatory stepping response, if and when necessary, and avoiding a fall. This may be possible by training subjects with knee pain to take steps that do not elicit
Executive summary
• On average, one-third of older adults fall each year, and women fall more often than men.
• Falls in older adults are a leading cause of injury and death.
• People with lower extremity osteoarthritis have an unexplained higher incidence of falls than age-matched, healthy controls and women have a higher incidence of lower extremity osteoarthritis than men.
• Established risk factors for falls in older adults, which include gait impairments, balance deficits, muscle weakness, pain, increased gait variability and obesity, overlap with the risk factors associated with falls in people with lower extremity osteoarthritis.
• These risk factors are not necessarily easily improved/modifiable.
• From a biomechanical perspective, falls occur as a result of two sequential events:– Loss of static or dynamic stability;– Failed compensatory stepping response.
• A task-specific intervention focused only on improving the compensatory stepping response was shown to prospectively decrease falls in older women in the community.
• Given that the risk factors for falls in people with lower extremity osteoarthritis are mostly the same as those for people who do not have lower extremity osteoarthritis, this task-specific intervention will likely be an effective fall prevention approach in this large and growing clinical population.

693future science group Women's Health (2012) 8(6)
CME Risk factors for falls in people with lower extremity osteoarthritis – REVIEW
high loads on the joints of the lower extrem-ity. This too, could be addressed using a task-specific training protocol focused on reducing the external moments across the lower extremity joints.
Conclusion & future perspectiveOur study of falls and fall prevention in healthy older adults has led us to hypothesize that, rela-tive to healthy older adults, the symptoms asso-ciated with OA
LE negatively affect the ability to
maintain static/dynamic stability and/or the ability to successfully meet the biomechanical
requirements of the compensatory stepping response following dynamic instability. Task-specific training of the compensatory step-ping response induces changes in performance marked by improvement in biomechanical vari-ables, which have been shown to be causally related to falls in women. The next logical step of this work is to test the hypothesis, perhaps by determining the extent to which falls in people with OA
LE can be decreased by a task-specific
training protocol that improves the ability to perform compensatory stepping responses while minimizing the load on diseased joints.
ReferencesPapers of special note have been highlighted as:• of interest•• of considerable interest
1. Grabiner MD, Jahnigen DW. Modeling recovery from stumbles: preliminary data on variable selection and classification efficacy. J. Am. Geriatr. Soc. 40(9), 910–913 (1992).
2. Owings TM, Pavol MJ, Foley KT, Grabiner PC, Grabiner MD. Exercise: is it a solution to falls by older adults? J. Appl. Biomech. 15, 56–63 (1999).
3. Owings TM, Pavol MJ, Foley KT, Grabiner MD. Measures of postural stability are not predictors of recovery from large postural disturbances in healthy older adults. J. Am. Geriatr. Soc. 48(1), 42–50 (2000).
•• Recoveryfollowingposturaldisturbancescouldnotbepredictedfrommeasuresofposturalstability.
4. Owings TM, Pavol MJ, Grabiner MD. Mechanisms of failed recovery following postural perturbations on a motorized treadmill mimic those associated with an actual forward trip. Clin. Biomech. 16(9), 813–819 (2001).
• Olderwomencanimproveresponsestoatreadmill-inducedposturaldisturbanceinasfewasfivetrials.
5. Tinetti ME, Kumar C. The patient who falls: “It’s always a trade-off”. JAMA 303(3), 258–266 (2010).
6. Stevens JA, Corso PS, Finkelstein EA, Miller TR. The costs of fatal and non-fatal falls among older adults. Inj. Prev. 12(5), 290–295 (2006).
7. Prudham D, Evans JG. Factors associated with falls in the elderly: a community study. Age Ageing 10(3), 141–146 (1981).
8. Cummings SR, Nevitt MC, Browner WS et al. Risk factors for hip fracture in white women. Study of Osteoporotic Fractures Research Group. N. Engl. J. Med. 332(12), 767–773 (1995).
9. Gillespie LD, Robertson MC, Gillespie WJ et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2, CD007146 (2009).
10. Blake AJ, Morgan K, Bendall J et al. Falls by elderly people at home: prevalence and associated factors. Age Ageing 17(6), 365–372 (1988).
11. Lawlor DA, Patel R, Ebrahim S. Association between falls in elderly women and chronic diseases and drug use: cross sectional study. BMJ 327(7417), 712–717 (2003).
12. Leveille SG, Bean J, Bandeen-Roche K, Jones R, Hochberg M, Guralnik JM. Musculoskeletal pain and risk for falls in older disabled women living in the community. J. Am. Geriatr. Soc. 50(4), 671–678 (2002).
13. Leveille SG, Jones RN, Kiely DK et al. Chronic musculoskeletal pain and the occurrence of falls in an older population. JAMA 302(20), 2214–2221 (2009).
14. Schwartz AV, Villa ML, Prill M et al. Falls in older Mexican–American women. J. Am. Geriatr. Soc. 47(11), 1371–1378 (1999).
15. Stalenhoef PA, Crebolder HFJM, Knottnerus JA, Van der horst FGEM. Incidence, risk factors and consequences of falls among elderly subjects living in the community. Eur. J. Public Health 7(3), 328–334 (1997).
16. Sturnieks DL, Tiedemann A, Chapman K, Munro B, Murray SM, Lord SR. Physiological risk factors for falls in older people with lower limb arthritis. J. Rheumatol. 31(11), 2272–2279 (2004).
17. Arden NK, Crozier S, Smith H et al. Knee pain, knee osteoarthritis, and the risk of fracture. Arthritis Care Res. 55(4), 610–615 (2006).
18. Foley SJ, Lord SR, Srikanth V, Cooley H, Jones G. Falls risk is associated with pain and dysfunction but not radiographic osteoarthritis in older adults: Tasmanian Older Adult Cohort study. Osteoarthritis Cartilage 14(6), 533–539 (2006).
19. Granek E, Baker SP, Abbey H et al. Medications and diagnoses in relation to falls in a long-term care facility. J. Am. Geriatr. Soc. 35(6), 503–511 (1987).
20. Arnold CM, Faulkner RA. The history of falls and the association of the timed up and go test to falls and near-falls in older adults with hip osteoarthritis. BMC Geriatr. 7, 17 (2007).
21. Williams SB, Brand CA, Hill KD, Hunt SB, Moran H. Feasibility and outcomes of a home-based exercise program on improving balance and gait stability in women with lower-limb osteoarthritis or rheumatoid arthritis: a pilot study. Arch. Phys. Med. Rehabil. 91(1), 106–114 (2010).
22. Brand C, Aw J, Lowe A, Morton C. Prevalence, outcome and risk for falling in 155 ambulatory patients with rheumatic disease. APLAR J. Rheumatol. 8(2), 99–105 (2005).
23. Scott D, Blizzard L, Fell J, Jones G. Prospective study of self-reported pain, radiographic osteoarthritis, sarcopenia progression, and falls risk in community-dwelling older adults. Arthritis Care. Res. (Hoboken) 64(1), 30–37 (2012).
24. Nahit ES, Silman AJ, Macfarlane GJ. The occurrence of falls among patients with a new episode of hip pain. Ann. Rheumatic Dis. 57(3), 166–168 (1998).
25. Kelsey JL, Berry SD, Procter-Gray E et al. Indoor and outdoor falls in older adults are different: the maintenance of balance, independent living, intellect, and zest in the elderly of Boston study. J. Am. Geriatr. Soc. 58(11), 2135–2141 (2010).
26. Lord SR, Clark RD, Webster IW. Physiological factors associated with falls in an elderly population. J. Am. Geriatr. Soc. 39(12), 1194–1200 (1991).
27. Lord SR, Ward JA, Williams P, Anstey KJ. Physiological factors associated with falls in older community-dwelling women. J. Am. Geriatr. Soc. 42(10), 1110–1117 (1994).
694 future science groupwww.futuremedicine.com
CMEREVIEW – Hoops, Rosenblatt, Hurt, Crenshaw & Grabiner
28. Fallah Yakhdani HR, Bafghi HA, Meijer OG et al. Stability and variability of knee kinematics during gait in knee osteoarthritis before and after replacement surgery. Clin. Biomech. 25(3), 230–236 (2010).
29. Rubenstein LZ, Josephson KR. The epidemiology of falls and syncope. Clin. Geriatr. Med. 18(2), 141–158 (2002).
• Comprehensivereviewofthemostcommoncausesandriskfactorsforfalls.
30. Lipsitz LA, Jonsson PV, Kelley MM, Koestner JS. Causes and correlates of recurrent falls in ambulatory frail elderly. J. Gerontol. 46(4), M114–M122 (1991).
31. Campbell AJ, Borrie MJ, Spears GF. Risk factors for falls in a community-based prospective study of people 70 years and older. J. Gerontol. 44(5), M112–M117 (1989).
32. Lawrence CR, David TF, Charles GH et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: part II. Arthritis Rheum. 58, 26–35 (2008).
33. Jones G, Nguyen T, Sambrook PN, Lord SR, Kelly PJ, Eisman JA. Osteoarthritis, bone density, postural stability, and osteoporotic fractures: a population based study. J. Rheumatol. 22(5), 921–925 (1995).
34. Arden NK, Nevitt MC, Lane NE et al. Osteoarthritis and risk of falls, rates of bone loss, and osteoporotic fractures. Arthritis Rheum. 42(7), 1378–1385 (1999).
35. Nevitt MC, Lane NE, Scott JC et al. Radiographic osteoarthritis of the hip and bone mineral density. Arthritis Rheum. 38(7), 907–916 (1995).
36. Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. N. Engl. J. Med. 319(26), 1701–1707 (1988).
37. Delbaere K, Close JC, Heim J et al. A multifactorial approach to understanding fall risk in older people. J. Am. Geriatr. Soc. 58(9), 1679–1685 (2010).
38. Overstall PW, Exton-Smith AN, Imms FJ, Johnson AL. Falls in the elderly related to postural imbalance. Br. Med. J. 1(6056), 261–264 (1977).
39. Quach L, Galica AM, Jones RN et al. The nonlinear relationship between gait speed and falls: the Maintenance of Balance, Independent Living, Intellect, and Zest in the Elderly of Boston Study. J. Am. Geriatr. Soc. 59(6), 1069–1073 (2011).
40. Guimaraes RM, Isaacs B. Characteristics of the gait in old people who fall. Int. Rehabil. Med. 2(4), 177–180 (1980).
41. Imms FJ, Edholm OG. Studies of gait and mobility in the elderly. Age Ageing 10(3), 147–156 (1981).
42. Tinetti ME, Franklin Williams T, Mayewski R. Fall risk index for elderly patients based on number of chronic disabilities. Am. J. Med. 80(3), 429–434 (1986).
43. Wolfson L, Whipple R, Amerman P, Tobin JN. Gait assessment in the elderly: a gait abnormality rating scale and its relation to falls. J. Gerontol. 45(1), M12–M19 (1990).
44. Woo J, Ho SC, Lau J, Chan SG, Yuen YK. Age-associated gait changes in the elderly: pathological or physiological? Neuroepidemiology 14(2), 65–71 (1995).
45. Luukinen H, Koski K, Laippala P, Kivelä S. Predictors for recurrent falls among the home-dwelling elderly. Scand. J. Prim. Health Care 13(4), 294–299 (1995).
46. Gehlsen GM, Whaley MH. Falls in the elderly: part I, gait. Arch. Phys. Med. Rehabil. 71(10), 735–738 (1990).
47. Al-Zahrani K, Bakheit AMO. A study of the gait characteristics of patients with chronic osteoarthritis of the knee. Disabil. Rehabil. 24(5), 275–280 (2002).
48. Gyory AN, Chao EY, Stauffer RN. Functional evaluation of normal and pathologic knees during gait. Arch. Phys. Med. Rehabil. 57, 571–577 (1976).
49. Messier SP, Loeser RF, Hoover JL, Semble EL, Wise CM. Osteoarthritis of the knee: effects on gait, strength, and flexibility. Arch. Phys. Med. Rehabil. 73, 29–36 (1992).
50. Stauffer RN, Chao EY, Gyory AN. Biomechanical gait analysis of the diseased knee joint. Clin. Orthop. Relat. Res. (126), 246–255 (1977).
51. Andriacchi TP, Ogle JA, Galante JO. Walking speed as a basis for normal and abnormal gait measurements. J. Biomech. 10(4), 261–268 (1977).
52. Brinkmann JR, Perry J. Rate and range of knee motion during ambulation in healthy and arthritic subjects. Phys. Ther. 65(7), 1055–1060 (1985).
53. Fiatarone MA, Marks EC, Ryan ND, Meredith CN, Lipsitz LA, Evans WJ. High-intensity strength training in nonagenarians. Effects on skeletal muscle. JAMA 263(22), 3029–3034 (1990).
54. Pavol MJ, Owings TM, Foley KT, Grabiner MD. Mechanisms leading to a fall from an induced trip in healthy older adults. J. Gerontol. A Biol Sci. Med. Sci. 56(7), M428–M437 (2001).
• Identifiesbiomechanicalmechanismsrequiredforsuccessfulrecoveryfollowingalaboratory-inducedtrip.
55. Horak FB, Shupert CL, Mirka A. Components of postural dyscontrol in the elderly: a review. Neurobiol. Aging 10(6), 727–738 (1989).
56. Lord SR, Menz HB. Visual contributions to postural stability in older adults. Gerontology 46(6), 306–310 (2000).
57. Wegener L, Kisner C, Nichols D. Static and dynamic balance responses in persons with bilateral knee osteoarthritis. J. Orthop. Sports Phys. Ther. 25(1), 13–18 (1997).
58. Hinman RS, Bennell KL, Metcalf BR, Crossley KM. Balance impairments in individuals with symptomatic knee osteoarthritis: a comparison with matched controls using clinical tests. Rheumatology 41(12), 1388–1394 (2002).
59. Hassan BS, Mockett S, Doherty M. Static postural sway, proprioception, and maximal voluntary quadriceps contraction in patients with knee osteoarthritis and normal control subjects. Ann. Rheumatic Dis. 60(6), 612–618 (2001).
60. Kiss RM. Effect of degree of knee osteoarthritis on balancing capacity after sudden perturbation. J. Electromyogr. Kinesiol. 22(4), 575–581 (2012).
61. Moreland JD, Richardson JA, Goldsmith CH, Clase CM. Muscle weakness and falls in older adults: a systematic review and meta-analysis. J. Am. Geriatr. Soc. 52(7), 1121–1129 (2004).
62. Aniansson A, Hedberg M, Henning G, Grimby G. Muscle morphology, enzymatic activity, and muscle strength in elderly men: a follow-up study. Muscle Nerve 9(7), 585–591 (1986).
63. Cahalan TD, Johnson ME, Liu S, Chao EY. Quantitative measurements of hip strength in different age groups. Clin. Orthop. Relat. Res. (246), 136–145 (1989).
64. Larsson L, Grimby G, Karlsson J. Muscle strength and speed of movement in relation to age and muscle morphology. J. Appl. Physiol. 46(3), 451–456 (1979).
65. Vandervoort AA, McComas AJ. Contractile changes in opposing muscles of the human ankle joint with aging. J. Appl. Physiol. 61(1), 361–367 (1986).
66. Winegard KJ, Hicks AL, Sale DG, Vandervoort AA. A 12-year follow-up study of ankle muscle function in older adults. J. Gerontol. Series A Biol Sci. Med. Sci. 51A(3), B202–B207 (1996).
67. Hakkinen K, Hakkinen A. Muscle cross-sectional area, force production and relaxation characteristics in women at different ages. Eur. J. Appl. Physiol. Occup. Physiol. 62(6), 410–414 (1991).
68. Thelen DG, Schultz AB, Alexander NB, Ashton-Miller JA. Effects of age on rapid
695future science group Women's Health (2012) 8(6)
CME Risk factors for falls in people with lower extremity osteoarthritis – REVIEW
ankle torque development. J. Gerontol. Series A Biol Sci. Med. Sci. 51A(5), M226–M232 (1996).
69. Taaffe DR, Henwood TR, Nalls MA, Walker DG, Lang TF, Harris TB. Alterations in muscle attenuation following detraining and retraining in resistance-trained older adults. Gerontology 55(2), 217–223 (2009).
70. Pavol MJ, Owings TM, Foley KT, Grabiner MD. Influence of lower extremity strength of healthy older adults on the outcome of an induced trip. J. Am. Geriatr. Soc. 50(2), 256–262 (2002).
71. Slemenda C, Brandt KD, Heilman DK et al. Quadriceps weakness and osteoarthritis of the knee. Ann. Intern. Med. 127(2), 97–104 (1997).
72. Davis MA, Ettinger WH, Neuhaus JM, Mallon KP. Knee osteoarthritis and physical functioning: evidence from the NHANES I epidemiologic follow up Study. J. Rheumatol. 18(4), 591–598 (1991).
73. Felson DT, Niu J, McClennan C et al. Knee buckling: prevalence, risk factors, and associated limitations in function. Ann. Intern. Med. 147(8), 534–540 (2007).
74. Fitzgerald GK, Piva SR, Irrgang JJ. Reports of joint instability in knee osteoarthritis: its prevalence and relationship to physical function. Arthritis Care Res. 51(6), 941–946 (2004).
75. Greenspan SL, Myers ER, Maitland LA, Resnick NM, Hayes WC. Fall severity and bone mineral density as risk factors for hip fracture in ambulatory elderly. JAMA 271(2), 128–133 (1994).
76. MacKinnon CD, Winter DA. Control of whole body balance in the frontal plane during human walking. J. Biomech. 26(6), 633–644 (1993).
77. Pandy MG, Lin Y, Kim HJ. Muscle coordination of mediolateral balance in normal walking. J. Biomech. 43(11), 2055–2064 (2010).
78. Johnson ME, Mille M, Martinez KM, Crombie G, Rogers MW. Age-related changes in hip abductor and adductor joint torques. Arch. Phys. Med. Rehabil. 85(4), 593–597 (2004).
79. Arokoski MH, Arokoski JPA, Haara M et al. Hip muscle strength and muscle cross sectional area in men with and without hip osteoarthritis. J. Rheumatol. 29(10), 2185–2195 (2002).
80. Grabiner M, Bareither M, Gatts S, Marone J, Troy KL. Task-specific training reduces trip-related fall risk in women. Med. Sci. Sports Exerc. doi:10.1249/MSS.0b013e318268 c89f (2012) (Epub ahead of print).
•• Short-termtask-specificsteptrainingimprovesthemechanismsrequiredfortriprecovery.
81. Fukagawa NK, Wolfson L, Judge J, Whipple R, King M. Strength is a major factor in balance, gait, and the occurrence of falls. J. Gerontol. Series A Biol Sci. Med. Sci. 50, Spec No 64–67 (1995).
82. Valderrabano V, von Tscharner V, Nigg BM et al. Lower leg muscle atrophy in ankle osteoarthritis. J. Orthop. Res. 24(12), 2159–2169 (2006).
83. O’Reilly SC, Muir KR, Doherty M. Effectiveness of home exercise on pain and disability from osteoarthritis of the knee: a randomised controlled trial. Ann. Rheumatic Dis. 58(1), 15–19 (1999).
84. Hassan BS, Doherty SA, Mockett S, Doherty M. Effect of pain reduction on postural sway, proprioception, and quadriceps strength in subjects with knee osteoarthritis. Ann. Rheumatic Dis. 61(5), 422–428 (2002).
85. Shrader MW, Draganich LF, Pottenger LA, Piotrowski GA. Effects of knee pain relief in osteoarthritis on gait and stair-stepping. Clin. Orthop. Relat. Res. (421), 188–193 (2004).
86. Hurwitz DE, Ryals AR, Block JA, Sharma L, Schnitzer TJ, Andriacchi TP. Knee pain and joint loading in subjects with osteoarthritis of the knee. J. Orthop. Res. 18, 572–579 (2000).
87. Kaplan FS, Nixon JE, Reitz M, Rindfleish L, Tucker J. Age-related changes in proprioception and sensation of joint position. Acta Orthop. 56(1), 72–74 (1985).
88. Robbins S, Waked E, Mcclaran J. Proprioception and stability: foot position awareness as a function of age and footware. Age Ageing 24(1), 67–72 (1995).
89. Mion LC, Gregor S, Buettner M, Chwirchak D, Lee O, Paras W. Falls in the rehabilitation setting: incidence and characteristics. Rehabil. Nurs. 14(1), 17–22 (1989).
90. Rossat A, Fantino B, Nitenberg C et al. Risk factors for falling in community-dwelling older adults: which of them are associated with the recurrence of falls? J. Nutr. Health Aging 14(9), 787–791 (2010).
91. Tinetti ME. Preventing falls in elderly persons. N. Engl. J. Med. 348(1), 42–49 (2003).
92. Knoop J, Steultjens MPM, van der Leeden M et al. Proprioception in knee osteoarthritis: a narrative review. Osteoarthritis Cartilage 19(4), 381–388 (2011).
93. Barrett D, Cobb A, Bentley G. Joint proprioception in normal, osteoarthritic and replaced knees. J. Bone Joint Surg. Br. 73(1), 53–56 (1991).
94. Marks R, Quinney HA, Wessel J. Proprioceptive sensibility in women with normal and osteoarthritic knee joints. Clin. Rheumatol. 12(2), 170–175 (1993).
95. Sharma L, Pai Y, Holtkamp K, Rymer WZ. Is knee joint proprioception worse in the arthritic knee versus the unaffected knee in unilateral knee osteoarthritis? Arthritis Rheum. 40(8), 1518–1525 (1997).
96. Maki BE. Gait changes in older adults: predictors of falls or indicators of fear. J. Am. Geriatr. Soc. 45(3), 313–320 (1997).
97. Hausdorff JM, Rios DA, Edelberg HK. Gait variability and fall risk in community-living older adults: a 1-year prospective study. Arch. Phys. Med. Rehabil. 82(8), 1050–1056 (2001).
98. Khandoker AH, Taylor SB, Karmakar CK, Begg RK, Palaniswami M. Investigating scale invariant dynamics in minimum toe clearance variability of the young and elderly during treadmill walking. IEEE Trans. Neural Syst. Rehabil. Eng. 16(4), 380–389 (2008).
99. Kiss RM. Effect of severity of knee osteoarthritis on the variability of gait parameters. J. Electromyogr. Kinesiol. 21(5), 695–703 (2011).
100. Levinger P, Lai DTH, Menz HB et al. Swing limb mechanics and minimum toe clearance in people with knee osteoarthritis. Gait Posture 35(2), 277–281 (2012).
101. Pandya NK, Draganich LF, Mauer A, Piotrowski GA, Pottenger L. Osteoarthritis of the knees increases he propensity to trip on an obstacle. Clin. Orthop. Relat. Res. (431), 150–156 (2005).
102. Pandya NK, Piotrowski GA, Pottenger L, Draganich LF. Pain relief in knee osteoarthritis reduces the propensity to trip on an obstacle. Gait Posture 25(1), 106–111 (2007).
103. Felson DT, Joyce G, Jingbo N, Yuqing Z, David JH. The effect of body weight on progression of knee osteoarthritis is dependent on alignment. Arthritis Rheum. 50, 3904–3909 (2004).
104. Reijman M, Pols HAP, Bergink AP et al. Body mass index associated with onset and progression of osteoarthritis of the knee but not of the hip: The Rotterdam Study. Ann. Rheum. Dis. 66, 158–162 2007).
105. Browning RC, Kram R. Effects of obesity on the biomechanics of walking at different speeds. Med. Sci. Sports Exercise 39, 1632–1641 (2007).
106. DeVita P, Hortobagyi T. Obesity is not associated with increased knee joint torque and power during level walking. J. Biomech. 36, 1355–1362 (2003).
107. Spyropoulos P, Pisciotta JC, Pavlou KN, Cairns MA, Simon SR. Biomechanical gait
696 future science groupwww.futuremedicine.com
CMEREVIEW – Hoops, Rosenblatt, Hurt, Crenshaw & Grabiner
analysis in obese men. Arch. Phys. Med. Rehabil. 72, 1065–1070 (1991).
108. Maffiuletti NA, Agosti F, Proietti M et al. Postural instability of extremely obese individuals improves after a body weight reduction program entailing specific balance training. J. Endocrinol. Invest. 28(1), 2–7 (2005).
109. Handrigan G, Hue O, Simoneau M et al. Weight loss and muscular strength affect static balance control. Int. J. Obes. (Lond.) 34(5), 936–942 (2010).
110. Jadelis K, Miller ME, Ettinger WH, Messier SP. Strength, balance, and the modifying effects of obesity and knee pain: results from the Observational Arthritis Study in Seniors (OASIS). J. Am. Geriatr. Soc. 49(7), 884–891 (2001).
111. Hulens M, Vansant G, Lysens R, Claessens AL, Muls E, Brumagne S. Study of differences in peripheral muscle strength of lean versus obese women: an allometric approach. Int. J. Obes. Relat. Metab. Disord. 25(5), 676–681 (2001).
112. Fjeldstad C, Fjeldstad A, Acree L, Nickel K, Gardner A. The influence of obesity on falls and quality of life. Dyn. Med. 7(1), 4 (2008).
113. Rosenblatt NJ, Grabiner MD. Relationship between obesity and falls by middle-aged and
older women. Arch. Phys. Med. Rehabil. 93(4), 718–722 (2012).
114. Gillespie LD, Gillespie WJ, Robertson MC, Lamb SE, Cumming RG, Rowe BH. Interventions for preventing falls in elderly people. Cochrane Database Syst. Rev. 4, CD000340 (2003).
115. Mansfield A, Peters AL, Liu BA, Maki BE. A perturbation-based balance training program for older adults: study protocol for a randomised controlled trial. BMC Geriatr. 7, 12 (2007).
116. Protas EJ, Mitchell K, Williams A, Qureshy H, Caroline K, Lai EC. Gait and step training to reduce falls in Parkinson’s disease. NeuroRehabilitation 20(3), 183–190 (2005).
117. Shimada H, Obuchi S, Furuna T, Suzuki T. New intervention program for preventing falls among frail elderly people: the effects of perturbed walking exercise using a bilateral separated treadmill. Am. J. Phys. Med. Rehabil. 83(7), 493–499 (2004).
118. Li W, Keegan TH, Sternfeld B, Sidney S, Quesenberry CP Jr, Kelsey JL. Outdoor falls among middle-aged and older adults: a neglected public health problem. Am. J. Public Health 96(7), 1192–1200 (2006).
119. Berg WP, Alessio HM, Mills EM, Tong C. Circumstances and consequences of falls in
independent community-dwelling older adults. Age Ageing 26(4), 261–268 (1997).
120. Henry FM. Specificity versus generality in learning motor skill. In: Classical Studies on Physical Activity. Brown RC, Kenon GS (Eds). Prentice Hall, Englewood Cliffs, NJ, USA, 331–340 (1968).
121. Rosenblatt NJ, Marone J, Grabiner M. Task-specific training decreases falls by older women in the community: 6 month prospective data. Gerontologist 50, 550 (2010).
122. Troy KL, Grabiner MD. The presence of an obstacle influences the stepping response during induced trips and surrogate tasks. Exp. Brain Res. 161(3), 343–350 (2005).
123. Hurt CP, Rosenblatt NJ, Grabiner MD. Form of the compensatory stepping response to repeated laterally directed postural disturbances. Exp. Brain Res. 214(4), 557–566 (2011).
124. Yungher DA, Morgia J, Bair W et al. Short-term changes in protective stepping for lateral balance recovery in older adults. Clin. Biomech. 27(2), 151–157 (2012).
125. Cyr M, Smeesters C. Instructions limiting the number of steps do not affect the kinetics of the threshold of balance recovery in younger adults. J. Biomech. 40(13), 2857–2864 (2007).
697future science group Women's Health (2012) 8(6)
CME Risk factors for falls in people with lower extremity osteoarthritis – REVIEW
To obtain credit, you should first read the journal article. After reading the article, you should be able to answer the following, related, multiple-choice questions. To complete the questions (with a minimum 70% passing score) and earn continuing medical education (CME) credit, please go to www.medscape.org/journal/wh. Credit cannot be obtained for tests completed on paper, although you may use the worksheet below to keep a record of your answers. You must be a registered user on Medscape.org. If you are not registered on Medscape.org, please click on the New Users: Free Registration link on the left hand side of the website to register. Only one answer is correct for each question. Once you successfully answer all post-test ques-tions you will be able to view and/or print your certificate. For questions regarding the content of this activity, contact the accredited provider,
[email protected]. For technical assistance, contact [email protected]. American Medical Association’s Physician’s Recognition Award (AMA PRA) credits are accepted in the US as evidence of participation in CME activi-ties. For further information on this award, please refer to http://www.ama-assn.org/ama/pub/category/2922.html. The AMA has deter-mined that physicians not licensed in the US who participate in this CME activity are eligi-ble for AMA PRA Category 1 Credit(s)™. Through agreements that the AMA has made with agencies in some countries, AMA PRA credit may be acceptable as evidence of partici-pation in CME activities. If you are not licensed in the US, please complete the questions online, print the AMA PRA CME credit certificate and present it to your national medical association for review.
Activity evaluation: where 1 is strongly disagree and 5 is strongly agree.
1 2 3 4 5
The activity supported the learning objectives.
The material was organized clearly for learning to occur.
The content learned from this activity will impact my practice.
The activity was presented objectively and free of commercial bias.
1. You are seeing a 70-year-old woman with a history of bilateral knee osteoarthritis (OA). The patient’s daughter is with her and expresses concern regarding her mother’s risk of falling. What can you tell her regarding the background of falls, especially in cases of OA?
£ A Nearly one third of all older adults experienced a fall in 2006
£ B OA of the knee joint specifically increases the risk of falling more than tenfold
£ C Arthritis itself does not significantly affect the risk of falling
£ D The principal mechanism promoting a higher risk of falling among patients with OA is muscle weakness
Does lower extremity osteoarthritis exacerbate risk factors for falls in older adults?
2. What should you consider regarding traditional risk factors for falls among older adults?
£ A Longer stride length promotes a higher risk of falls
£ B A wider step width reduces dynamic stability
£ C Longer double-leg support time can increase the risk of falls
£ D Knee extensor weakness is the principal reason for knee buckling
698 future science groupwww.futuremedicine.com
CMEREVIEW – Hoops, Rosenblatt, Hurt, Crenshaw & Grabiner
3. What can you tell this patient and her daughter regarding changes associated with OA and her risk of falls?
£ A Pain relief with corticosteroid injections will reduce static postural sway and the risk of falls
£ B The main disability associated with higher fall risk among patients with OALE is reduced proprioception
£ C Toe clearance during ambulation is reduced by OALE
£ D Obesity is common among patients with OALE and is associated with multiple gait abnormalities, which promote falls
4. What should you recommend regarding a rehabilitation program to reduce this patient’s risk of fall?
£ A Training should focus on increasing flexibility in the joint affected by OALE
£ B Training should focus on improving the compensatory step following a disturbance
£ C Training cannot improve the fall risk among adults at age 65 years or older
£ D It is particularly difficult to protect patients against laterally-directed disturbances