Utilization of the Seniors Falls Investigation Methodology to Identify System-Wide Causes of Falls...
12
Vol. 49, No. 5, 2009 The Gerontologist © The Author 2009. Published by Oxford University Press on behalf of The Gerontological Society of America. Vol. 49, No. 5, 685–696 All rights reserved. For permissions, please e-mail: [email protected]. doi:10.1093/geront/gnp059 Advance Access Publication on June 12, 2009 685 Purpose: As a highly heterogeneous group, se- niors live in complex environments influenced by mul- tiple physical and social structures that affect their safety. Until now, the major approach to falls research has been person centered. However, in industrial set- tings, the individuals involved in an accident are seen as the inheritors of system defects. The objective of the present study was to investigate safety deficien- cies that contributed to falls in community-dwelling seniors using a systems approach. Design and Methods: The investigations were conducted us- ing the Seniors Falls Investigation Methodology (SFIM), an adapted version of a method used to ex- amine transportation accidents, such as airplane crashes. Fifteen seniors, who experienced a fall or near fall, participated in multiple case studies. A cross-case synthesis was used to summarize findings and identify common patterns of causes and safety deficiencies. Results: Falls and near falls are a result of latent unsafe conditions, and unsafe acts and decisions combined in a diverse set of circumstances. If not identified and removed, these unsafe conditions can cause falls for other se- niors. Implications: This study provided compel- ling evidence that causes of falling are systemic and develop over time. It demonstrated that the systems approach is needed to expand the focus from the in- dividual to multilayered organizational and supervi- sory causes. The SFIM demonstrated capability to identify causes of falls that will allow better preven- tion and management programs, hence advancing seniors’ safety. SFIM shows great potential for imple- mentation in organized settings, such as hospitals and long-term care homes. Key Words: Human factors, Systems approach, Accident investigations, Swiss cheese model, Safety deficiencies The fast growing body of knowledge in falls research produced great advances in understand- ing of the intrinsic and extrinsic risk factors of falling (Close, 2005). A number of randomized controlled trials demonstrated that modifying risk factors could reduce fall risk (Gillespie et al., 2002; Tinetti, McAvay, & Claus, 1996). However, dis- semination of research evidence into practice is lagging, which could explain why approximately one third of community-dwelling seniors are un- able to safely maneuver in their daily activities without falling at least once a year. Much is known about the risk factors (Ballinger & Payne, 2002; Fletcher & Hirdes, 2002; Salvà, Bolíbar, Pera, & Arias, 2004), but considerably less is known about the causes of falls and the circumstances surround- ing these adverse events (Campbell et al., 1990). In a review of literature on best practices in falls pre- vention for residents of long-term care (LTC) fa- cilities, Scott, Donaldson, and Gallagher (2003) indicated that comprehensive fall prevention plans Utilization of the Seniors Falls Investigation Methodology to Identify System-Wide Causes of Falls in Community-Dwelling Seniors Aleksandra A. Zecevic, PhD, 1,2 Alan W. Salmoni, PhD, 3 John H. Lewko, PhD, 4 Anthoney A. Vandervoort, PhD, 5 and Mark Speechley, PhD 6 1 Address correspondence to Aleksandra A. Zecevic, PhD, Faculty of Health Sciences, The University of Western Ontario, HSB 220, London, ON, Canada N6A 5B9. E-mail: [email protected] 2 School of Health Studies, Faculty of Health Sciences, The University of Western Ontario, London, Canada. 3 School of Kinesiology, Faculty of Health Sciences, The University of Western Ontario, London, Canada. 4 Centre for Research in Human Development, Laurentian University, Sudbury, Canada. 5 School of Physical Therapy, Faculty of Health Sciences, The Univer- sity of Western Ontario, London, Canada. 6 Department of Epidemiology and Biostatistics, The University of Western Ontario, London, Canada. by guest on July 6, 2016 http://gerontologist.oxfordjournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Utilization of the Seniors Falls Investigation Methodology to Identify System-Wide Causes of Falls...
Vol. 49, No. 5, 2009
The Gerontologist © The Author 2009. Published by Oxford University Press on behalf of The Gerontological Society of America. Vol. 49, No. 5, 685–696 All rights reserved. For permissions, please e-mail: [email protected]:10.1093/geront/gnp059 Advance Access Publication on June 12, 2009
685
Purpose: As a highly heterogeneous group, se-niors live in complex environments infl uenced by mul-tiple physical and social structures that affect their safety. Until now, the major approach to falls research has been person centered. However, in industrial set-tings, the individuals involved in an accident are seen as the inheritors of system defects. The objective of the present study was to investigate safety defi cien-cies that contributed to falls in community-dwelling seniors using a systems approach. Design and Methods: The investigations were conducted us-ing the Seniors Falls Investigation Methodology (SFIM), an adapted version of a method used to ex-amine transportation accidents, such as airplane crashes. Fifteen seniors, who experienced a fall or near fall, participated in multiple case studies. A cross-case synthesis was used to summarize fi ndings and identify common patterns of causes and safety defi ciencies. Results: Falls and near falls are a result of latent unsafe conditions, and unsafe acts and decisions combined in a diverse set of circumstances. If not identifi ed and removed, these unsafe conditions can cause falls for other se-niors. Implications: This study provided compel-ling evidence that causes of falling are systemic and
develop over time. It demonstrated that the systems approach is needed to expand the focus from the in-dividual to multilayered organizational and supervi-sory causes. The SFIM demonstrated capability to identify causes of falls that will allow better preven-tion and management programs, hence advancing seniors ’ safety. SFIM shows great potential for imple-mentation in organized settings, such as hospitals and long-term care homes.
Key Words: Human factors , Systems approach , Accident investigations , Swiss cheese model , Safety defi ciencies
The fast growing body of knowledge in falls research produced great advances in understand-ing of the intrinsic and extrinsic risk factors of falling ( Close, 2005 ). A number of randomized controlled trials demonstrated that modifying risk factors could reduce fall risk ( Gillespie et al., 2002 ; Tinetti, McAvay, & Claus, 1996 ). However, dis-semination of research evidence into practice is lagging, which could explain why approximately one third of community-dwelling seniors are un-able to safely maneuver in their daily activities without falling at least once a year. Much is known about the risk factors ( Ballinger & Payne, 2002 ; Fletcher & Hirdes, 2002 ; Salvà, Bolíbar, Pera, & Arias, 2004 ), but considerably less is known about the causes of falls and the circumstances surround-ing these adverse events ( Campbell et al., 1990 ). In a review of literature on best practices in falls pre-vention for residents of long-term care (LTC) fa-cilities, Scott, Donaldson, and Gallagher (2003) indicated that comprehensive fall prevention plans
Utilization of the Seniors Falls Investigation Methodology to Identify System-Wide Causes of Falls in Community-Dwelling Seniors
Aleksandra A. Zecevic , PhD , 1 , 2 Alan W. Salmoni , PhD , 3 John H. Lewko , PhD , 4 Anthoney A. Vandervoort , PhD , 5 and Mark Speechley , PhD 6
1 Address correspondence to Aleksandra A. Zecevic, PhD, Faculty of Health Sciences, The University of Western Ontario, HSB 220, London, ON, Canada N6A 5B9. E-mail: [email protected]
2 School of Health Studies, Faculty of Health Sciences, The University of Western Ontario, London, Canada.
3 School of Kinesiology, Faculty of Health Sciences, The University of Western Ontario, London, Canada.
4 Centre for Research in Human Development, Laurentian University, Sudbury, Canada.
5 School of Physical Therapy, Faculty of Health Sciences, The Univer-sity of Western Ontario, London, Canada.
6 Department of Epidemiology and Biostatistics, The University of Western Ontario, London, Canada.
by guest on July 6, 2016http://gerontologist.oxfordjournals.org/
Dow
nloaded from

The Gerontologist686
in LTC facilities should include “ a formal process for investigating individual falls and implementing tailored prevention plans ” (p. 144). The present study presents results from a unique approach to the study of falls in seniors, adapted from an acci-dent investigation methodology used in the trans-portation industry. Investigations of industrial accidents and falls have three things in common: the need to establish what happened, why it hap-pened, and how to prevent similar events from reoccurring. The present approach to falls investi-gation is based on retrospective identifi cation of the root causes and their contributors. Safety defi -ciencies are fi rst identifi ed through a structured and an in-depth investigative process and are then further considered for intervention on individual, supervisory, and organizational levels.
For the past 20 years, falls research benefi ted greatly from a person-centered approach, concen-trating on the characteristics of the faller and look-ing for counter measures affecting the person. A fall risk assessment is an example of this approach ( Cumming, 2002 ; Perell et al., 2002 ). Sometimes, these predisposing risk factors have been combined with person – environment interactions and situa-tional risk factors ( Feldman & Chaudhury, 2008 ; Lord, Menz, & Sherrington, 2006 ). However, in industrial settings, it has been shown that the indi-viduals involved at the “ sharp end ” of an accident are often “ the inheritors of system defects created by poor design, incorrect installation, faulty main-tenance and bad management decisions. ” The in-dividual ’ s part is usually that of “ adding the fi nal garnish to a lethal brew whose ingredients have already been long in the cooking ” ( Reason, 1990 , p. 173).
The objective of the present study was to iden-tify safety defi ciencies that contributed to falls in community-dwelling seniors using a systems ap-proach to human error and accident investigation. A secondary goal was to report on the application of the adapted accident investigation methodolo-gy, originally used to investigate accidents in the transportation industry, but used here to study falls in seniors.
For the purpose of this study, the “ system ” is defi ned in a very broad sense as a person interact-ing with the physical and social environment with-in which the person lives. In a systems approach, actions of humans are accepted as fallible and hu-man errors are expected ( Dekker, 2002 ). Falls are seen as the consequence of underlying causes or la-tent factors imbedded deep in the system that cre-
ate unsafe conditions ( Reason, 2000 ). The outcome of this approach is the identifi cation of safety defi -ciencies that lead to accidents. Active failures are errors committed by people at the end of a sequence of events that result in falls. Effects of active fail-ures are felt immediately, whereas latent failures, and their adverse consequences, may lie dormant within the system for a long period of time, only becoming evident when they combine with active failures and local triggers that create an opportu-nity for an accident ( Reason, 1990 , 2000 ). Where-as active failures are diffi cult to foresee and prevent, latent conditions can be identifi ed and corrected. Solutions in the systems approach accept that we cannot completely change the human condition but we can change the conditions in which humans operate. Interventions using a systems approach aim to eliminate circumstances that can provoke errors regardless of the people involved.
Methods
In this prospective case series study, a fall was defi ned as an event in which a person experienced an unexpected, unintentional, and uncontrollable loss of balance followed by landing on a lower level. In a near fall, a person recovered from the loss of balance before landing, on his or her own or with help of other people. A safety defi ciency was defi ned as an unsafe condition or underlying latent risk factor residing in the system, for which there were no adequate defenses. Persons aged 65 years or older were considered seniors.
The investigations of falls of community-dwell-ing seniors were conducted using the Seniors Falls Investigation Methodology (SFIM), an adapted version of an integrated safety investigation meth-od used in the transportation industry to investi-gate transportation accidents, such as airplane crashes ( Transportation Safety Board of Canada [TSB], 1998 ). Only a brief overview is presented subsequently as a detailed description of this meth-odology is available elsewhere ( Zecevic, Salmoni, Lewko, & Vandervoort, 2007 ).
Fifteen falls investigations of community-dwelling seniors were conducted in a naturally occurring re-tirement community in London, Ontario, Canada. The community consisted of 12 high-rise apartment buildings, where approximately 2,500 seniors resid-ed. According to a survey conducted in 1997, the average age of the tenants in the complex was 78 years. One third of the seniors had signifi cant mem-ory impairment, 21% had a caregiver, and 11% of
by guest on July 6, 2016http://gerontologist.oxfordjournals.org/
Dow
nloaded from

Vol. 49, No. 5, 2009 687
the seniors provided care for someone with whom they lived. Each year, an average of 700 – 800 falls and 8 – 10 hip fractures occurred in the community ( Kloseck, Crilly, & Misurak, 2002 ).
A total of 27 seniors who had experienced a fall or near fall were contacted and 15 were subse-quently interviewed. Twelve seniors were excluded due to one of the following reasons: the lengthy period of time since the fall, Mini-Mental Status Examination (MMSE; Folstein, Folstein, & McHugh, 1975 ) score below 26, loss of contact, refusal to sign a consent form or to be interviewed, and transfer to a LTC facility.
Participants were informed about the study us-ing fl yers mailed to all households, posters in all apartment buildings, personal recommendations by building superintendents, referrals by volun-teers in the Healthy Aging Program located in a nearby mall, short presentations to exercise classes, and referrals from local offi ces of the Victorian Order of Nurses (VON) and Community Care Ac-cess Centre (CCAC). Despite continuous efforts, recruitment for the in-depth investigations of falls was a diffi cult task because seniors were reluctant to discuss their experiences. For example, 11 (73%) senior fallers agreed to participate only after a rec-ommendation from a trusted third party or through a personal contact.
Recruitment was based on a maximum varia-tion sample strategy, with an intention to capture a variety of fall scenarios. Near falls and noninjuri-ous falls were included as they provide valuable op-portunities to identify and remove safety defi ciencies before they produce catastrophic consequences. To increase variation, we included in the study one se-nior with mild dementia, one acute case of a fre-quent faller, one senior who did not live in this particular community but fell while visiting a daughter who lived in the city, and one senior who had a low MMSE score due to illiteracy. All inves-tigations were conducted by the same investigator. The investigator was trained, mentored, and super-vised by two experienced human factors and work safety experts over the course of the study. The University of Western Ontario Research Ethics Board for health sciences research involving human subjects granted approval for this study and all participants provided written informed consent.
Data Collection and Analysis Using SFIM
The SFIM uses a systems approach to the inves-tigation of adverse events and employs a six-step
process: (a) planning and collection of occurrence data using a data collection tool F-SHEL — Faller, Software, Hardware, Environment, and Liveware ( Hawkins, 1993 ); (b) developing a sequence of events and identifying safety signifi cant events; (c) analyzing the error type and failure mode using the Generic Error Modeling System (GEMS; Rasmus-sen, 1987 ; Reason, 1990 ); (d) placing unsafe acts/decisions and unsafe conditions in context using an abbreviated version of the Swiss cheese accident causation model ( Reason, 2000 , 2003 ); (e) identi-fying safety defi ciencies and assessing risk; and (f) developing suggestions for safety action.
Data collection started as soon as possible after a fall and focused on content and interaction be-tween fi ve F-SHEL areas: the faller (F), documenta-tion and records (S), equipment (H), environmental (E), and other people involved (L). In the fi rst step, the investigator asked the faller to recount the fall in an attempt to reconstruct and understand the mindset of the faller at the time of the occurrence ( Dekker, 2002 ). Additional data collection inter-views were conducted with spouses, children, neighbors, friends, witnesses, CCAC case manag-ers, VON volunteers, pharmacists, building super-intendents, and property, casino, and grocery shop managers. For all but two falls, the faller and the investigator visited the site of the fall to reconstruct the event. A reenactment was videotaped while the faller instructed the investigator where to stand and look, what to do, what to hold in hands, and what to think. Frequently, only during the reenactment would the faller remember details of the occurrence and the full story would emerge. The investigator administered the MMSE to assess faller ’ s cognition and establish the credibility of the data collected from the faller. This determined the need for collec-tion of additional information from other sources. At times, data collected from the faller were unreli-able or unavailable. The SFIM accounts for this possibility in the same way the original TSB meth-odology accounts for the lack of survivors in air-plane accidents.
In the second step, the collected information was presented as a sequence of events ( Figure 1 ). This process linked the senior ’ s activities prior to and at the time of the event in a sequential and meaningful order and was updated as new infor-mation became available. After the initial inter-view, a draft of the event sequence was generated and then clarifi ed in consecutive interviews to en-sure accuracy. The completed sequence was re-viewed and discussed by the research team to
by guest on July 6, 2016http://gerontologist.oxfordjournals.org/
Dow
nloaded from

The Gerontologist688
identify safety-signifi cant events (bolded rectangles in Figure 1 ) by consensus.
In the third step, GEMS was used to link unsafe actions or decisions of the fallers with unsafe con-ditions present latently in the system. The GEMS analysis was performed for each safety-signifi cant event to determine intentionality of the action (intentional vs. unintentional) and determine the error type. Error types included failures of atten-tion (slips), failures of memory (lapses), errors of planning (mistakes), and deliberate decisions to act against a rule (adaptations, also called viola-tions). The human errors were then related to the unsafe conditions present at the time of the event. This analysis helps to understand the mindset of the faller in relation to latent unsafe conditions present at the time of the occurrence.
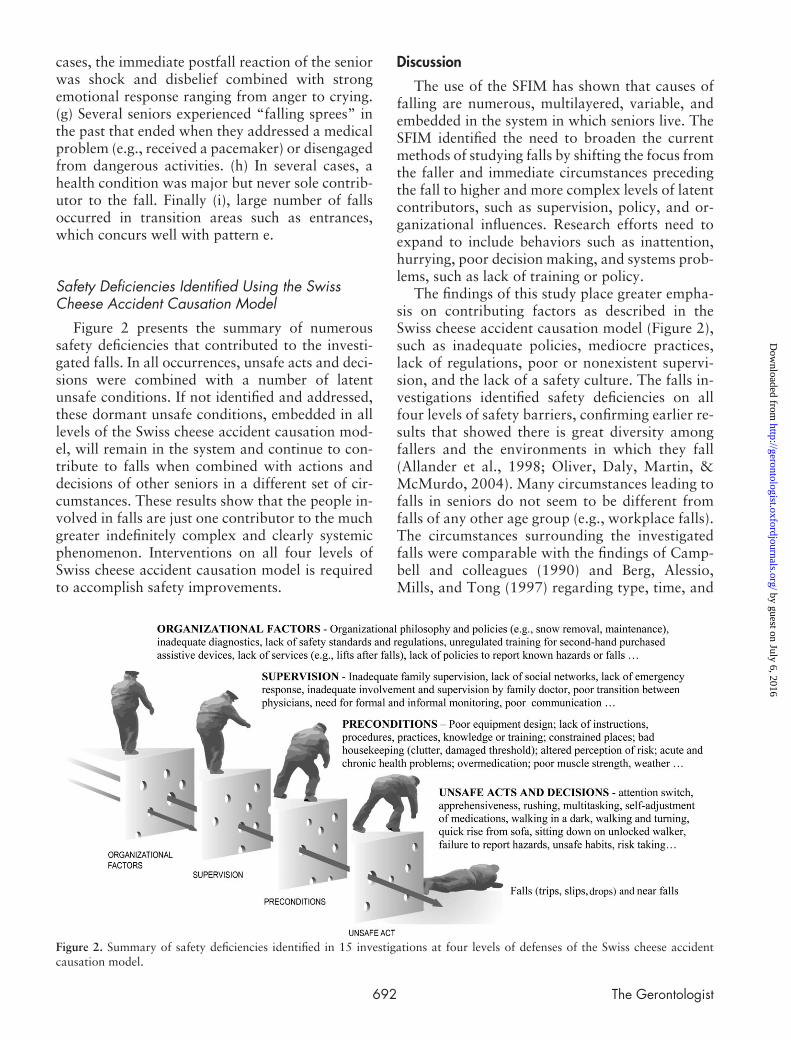
The fourth step in the analysis related the identifi ed errors and unsafe conditions with four predetermined categories of the Swiss cheese acci-dent causation model proposed by Reason (2000 ; Figure 2). In this model, “ slices of cheese ” represent safeguards, barriers, or defenses separating hazards and vulnerable persons. Optimally, the safeguards are intact, but in reality, the safeguards have many dynamic “ holes ” that constantly open, close, or shift locations. Accidents happen when holes on all levels align, allowing the accident trajectory arrow to pass through the barriers and connect the hazard
to the vulnerable person, in this case the faller. Our adapted version of the model consists of four de-fense levels: (a) the unsafe act describing the deci-sions and actions related to the fall; (b) preconditions for unsafe acts including internal (i.e., health, phys-ical abilities, habitual or atypical behavior) and ex-ternal (i.e., presence of hazards, equipment design, weather) risk factors; and (c) unsafe supervision , which includes informal supervisors (i.e., family, friends, neighbors, and other people not paid to care for seniors) and formal supervisors (i.e., physi-cian, nurse, physical therapist, occupational thera-pist, pharmacist, personal support worker, and others paid to provide services to seniors). Exam-ples of unsafe conditions identifi ed at this defense layer include inadequate training, management fail-ure, poor supervisory practice, lack of or inadequate communication, maintenance issues, and so forth; (d) organizational factors, including regulators and policymakers (e.g., senior advocacy groups, public health, researchers, municipal government, public transit, emergency medical services, property man-agement, etc.). Unsafe conditions at this level in-clude regulatory failures and inadequate policies.
The fi fth step in the investigation process assessed the level of risk and estimated the potential for ad-verse consequences. Based on this, priorities for safety actions were assigned. The sixth step involved proposing safety actions to prevent future falls.
Figure 1. An example of the sequence of events for a near fall. Bolded rectangles present safety-signifi cant events that are further analyzed through Generic Error Modeling System.
by guest on July 6, 2016http://gerontologist.oxfordjournals.org/
Dow
nloaded from

Vol. 49, No. 5, 2009 689
On average, investigations took 10 – 20 hrs to complete and prepare an investigation summary. Each fall investigation was reported as a single case in a multiple case study design ( Yin, 1989 ). By summarizing multiple cases, categories and pat-terns of safety defi ciencies were identifi ed. The in-formation about causes of falling is essential for design of both individual and community-based falls prevention programs that focus on improve-ments in safety.
Results
The Study Population A total of 15 seniors participated in the study.
Eleven (73%) were women. The average age was 79 years ( SD ± 7, range 65 – 93) and the majority (80%) lived alone in an apartment. Prior to the fall, two thirds (67%) had an acute medical con-dition and were using, on average, seven prescrip-tion medications ( SD ± 4, range 1 – 14). Most participants (87%) did not exercise and two se-niors (13%) were smokers. Six seniors (40%) used a cane or a walker and the majority (74%) required some help with activities of daily living and instrumental activities of daily living. The average MMSE score was 28/30 ( SD ± 2, range 22 – 30).
Maximum variability sampling resulted in the inclusion of a variety of fall occurrences: two near falls where one senior recovered from loss of bal-ance and a second senior was caught by their daughter before landing; a fall of a senior with mild dementia; three falls of seniors who suffered from diseases that increase the propensity for fall-ing, such as Parkinson ’ s or chronic pain; a fall of a younger senior (65 years of age); and a fall of a very old senior (93 years of age), all of whom lived independently in community.
Characteristics of the Investigated Falls
Most falls (80%) occurred during a routine dai-ly activity, such as going to the bathroom, walking through the apartment, walking the dog, returning from the mall, taking off shoes, opening or locking the entrance door, picking up mail, or going out to the balcony to check the weather. Only 20% of falls occurred during nonroutine activities, such as painting a spot on the wall, rushing to check a fl ood in the laundry room, stopping the bus on the opposite side of the street, or entering a casino. Alcohol consumption was not reported in any of
the investigated falls. Four fallers (27%) grabbed something after losing their balance and before landing on the ground. Three fallers (20%) were using an assistive device at the time of the fall. Most seniors (73%) were unaccompanied when they fell. Six falls (40%) were witnessed. Four se-niors (27%) were accompanied by a family mem-ber (daughters, sons-in-law, a friend, or husband). Three fallers (20%) were engaged in conversation immediately prior to the fall.
Immediate causes of the fall included trips, a slip, a loss of consciousness due to hypotension, “ frozen leg ” , loss of support, overreach, misstep, pain, and syncope. Noteworthy, 40% of fallers re-quired immediate help as they were not able to get up on their own after the fall. A summary of the most common characteristics of the investigated falls is provided in Table 1 .
After all 15 investigations were completed and summarized, we applied a cross-case synthesis technique to identify common patterns and themes. This helped uncover the origins, causes, and contributors to falling. To aid to understand-ing of the depth of SFIM investigation and sys-tem-wide nature of its outcomes, the following examples are summaries of three investigated falls. The following case summary explains how actions and decisions of humans combine with latent contributing factors that result in safety de-fi ciencies on all four levels of Swiss cheese acci-dent causation model. Summaries for all 15 cases are available in Zecevic (2006) . Please note that each case was unique and none could be declared typical.
Table 1 . Summary of the Most Common Characteristics of the Falls Experienced by Community-Dwelling Seniors
Investigated
Falls characteristics %
Walking just before the fall 81 Indoor falls 80 Routine activity 80 Injurious falls (mild, moderate, and serious) a 73 Laying on the fl oor or ground after landing 73 Wore shoes 60 Entrance area 54 Time of the fall between 12 and 5 p.m. 54 Forward fall 53 Medical help sought after the fall 47 Trip 47 Required help of another person to get up 47
Note: a A high percentage of injurious falls is in part the consequence of recruitment due to head and facial injuries.
by guest on July 6, 2016http://gerontologist.oxfordjournals.org/
Dow
nloaded from

The Gerontologist690
Three Example Case Summaries
Case 10: Sitting Down on an Unlocked Walker. — The senior fell in the seniors ’ activity club in her apartment building when attempting to sit on her unlocked walker. The faller was a 71-year-old wom-en who suffered from severe osteoarthritis, increased blood pressure, high cholesterol, and chronic back pain caused by herniated discs and spinal stenosis. She used seven prescription medications daily. She experienced three mini-strokes in the past 3 years that resulted in partial loss of control of the right leg and slurred speech but did not have memory prob-lems. The faller lived alone and had no family in town but had well-developed network of friends in the building. Her 83-year-old neighbor was helping with laundry, shopping, and dog walking. The se-nior was well aware of available community services but did not think that she needs their help.
In the fall 2004, the senior bought a walker from a neighbor. She never asked for or got any training or written instructions on how to use the walker. She adjusted the height of the handles on her own but did not know how to put the brakes on. She planned to use the walker in a few years time but soon after the purchase she started using it daily for the afternoon walk with her dog. She did not know that this particular model of walker was recommended for indoor use. Companies sell-ing walkers have a system in place where a physi-cal or occupational therapist visits seniors who purchase new assistive devices to provide initial adjustment and training. This system does not ex-ist for assistive devices purchased second hand. Hence, the faller did not know how to lock the walker ’ s brakes, walk through the door, or prop-erly sit on the walker seat.
On the day of the fall, she just returned from a 15-min afternoon walk with her friend and the dog. They were standing and talking in the activity club when she felt increasing discomfort and pain in her lower back. For the fi rst time, she decided to sit on the walker seat and not one of many chairs available in the room. She perceived chairs in the club to be too low and uncomfortable. While talk-ing to a friend, she held the walker with one hand and fl exed hips to sit on it. The walker slowly moved backward and the senior very slowly slid down to the fl oor. A thick winter coat she wore made a soft landing. The senior was unable to get up on her own and her 83-year-old friend was un-able to help. The building superintendent was in the next room and came to assist her get up.
The identifi ed safety defi ciencies in this case in-clude the following:
Unsafe acts/decisions: not locking the brakes on •the walker before sitting on it, not knowing cor-rect way to sit on the walker, multitasking (talk-ing with friend), and deciding to change routine and sit on the walker seat for the fi rst time Preconditions: chronic back pain with unsatis- •factory pain management, purchase of second-hand assistive device without instructions on how to safely use it, and using assistive devices without being properly trained Supervision: lack of community services to pro- •vide safety training for seniors who purchase as-sistive devices secondhand and lack of adequate formal (community services, family doctor) and informal (family) supervision Organizational factors: lack of policies requir- •ing appropriate training programs for users of secondhand assistive devices and lack of in-formation and awareness about prevalence of secondhand assistive devices purchases and implications to seniors ’ safety.
Case 17: Trip Over the Box. — At approximately 11:00 p.m., an 84-year-old women fell in her apart-ment kitchen. She tripped over a heavy box that, earlier that evening, she fi lled up with sweets and jars of jam. Earlier that week, she was instructed to remove all sweet foods from home, after being diag-nosed with Type 2 diabetes. She left the box on the fl oor near the kitchen entrance. She planned to move the box out of the way in the morning and to give it to her daughter the following weekend. Habitually, the senior leaves items on the fl oor when she plans to take them out of the apartment. This creates clut-ter that was present at several places in her bedroom during the investigation. The senior had cleaned out her closet and prepared multiple bags of items for her daughter to take away. On the day of the fall, it was the fi rst time the senior left an obstacle (box) in the middle of the walking path to the kitchen.
After fi nishing her before-bed routine in the bathroom, she turned off all the lights in the apart-ment (to conserve energy) and quickly walked from the bathroom to the kitchen to throw a piece of wrapping paper into the garbage bin. Her right foot hit the heavy box, both feet blocked behind the box; she lost balance and fell forward hitting the carpeted fl oor with her face. The impact broke her nose; her glasses made deep indentations around her eyes that later caused severe facial bruising. Both her knees were also bruised. She
by guest on July 6, 2016http://gerontologist.oxfordjournals.org/
Dow
nloaded from

Vol. 49, No. 5, 2009 691
called an ambulance concerned about heavy bleed-ing from her nose. The ambulance took her to the emergency room, from where she was released the same night. At the time of the fall, the senior lived alone, did not have acute medical illness, and was regularly taking three prescription medications. Her daughters lived in nearby townships and came to visit on holidays.
The identifi ed safety defi ciencies in this case in-clude the following:
Unsafe acts/decisions: leaving heavy box on •kitchen fl oor, turning off all lights in the apart-ment, walking through the apartment in com-plete darkness, and hurry Preconditions: habit of creating obstacles by •leaving things on the fl oor and habitual walking around apartment in darkness Supervision: lack of family involvement in mon- •itoring seniors ’ unsafe behaviors (i.e., creating hazardous obstacles) Organizational factors: need for public health •agency to address the issue of energy conser-vation and how it infl uences seniors ’ safety at home.
Case 18: Trip Over a Loaded Shopping Buggy. — The senior fell over a loaded shopping buggy on the sidewalk between a nearby mall and her apart-ment building. The faller, a 65-year-old petite women, was returning from a grocery store push-ing a heavier than usual shopping buggy in front of her. Unexpectedly, the buggy ’ s small front wheels got trapped in a crack between two sidewalk slabs and halted the buggy. In an attempt to initiate for-ward movement, the senior strongly pushed the buggy handle, which caused the buggy to quickly collapse forward pulling the senior over it. As she fell, the senior struck her chin on the handle of the buggy, causing severe pain, swelling, and bruising of her lower jaw, chin, and neck.
At the time of the fall, the senior did not have acute health issues and she lived alone in the com-munity. The shopping buggy was imported and sold in a local grocery store. The target customers were people who do not drive a car or are not able to carry groceries. Approximately 1,000 buggies were sold monthly across the country and on aver-age four to fi ve were returned to the distributor ev-ery month due to damage caused by problems such as overloading and striking an uneven surface.
Government safety regulations require that only electrical products imported to Canada be inspect-ed. The buggy was designed to fold so it can be
stored vertically. It did not have a safety feature that would lock the buggy in an “ open ” position, such as is available on strollers designed for chil-dren, that would prevent collapsing if front wheels were trapped and the handle was pushed forward. According to the confusing loading instructions, which the senior discarded at the time of purchase, several months prior to the incident, the buggy ’ s maximal loading was not exceeded, but this was the fi rst time senior loaded it so heavily.
The identifi ed safety defi ciencies in this case in-clude the following:
Unsafe acts/decisions: pushing on the buggy •handle when front wheels were trapped and decision to load the buggy more than ever before Preconditions: uneven concrete slabs on the •sidewalk, poor design of the shopping buggy (small front wheels, lack of safety device to pre-vent collapse during use), confusing loading in-structions, and limited experience in using the buggy for shopping (the senior usually utilized it to transport laundry to and from the laundry room within the apartment building) Supervision: lack of apt practice for reporting •and removing known hazards in public places, the uneven concrete slabs on the sidewalk and gaps between them were well known to walker, wheelchair, and scooter users in the community. Two years earlier, an attempt to deal with this problem resulted in rejection by municipal gov-ernment as gaps were narrower than required by the policy that warrants intervention Organizational factors: lack of safety standards •for import of poorly designed devices, and inad-equate regulations to prevent sales of poorly de-signed products to vulnerable populations, such as seniors.
Nine patterns emerged from 15 investigations (Table 2): (a) In every fall, there were several dis-tinct latent unsafe conditions that combined with unsafe acts and decisions performed by the fallers. (b) This always occurred in a sequence of undesir-able events where multiple opportunities for safety improvements were over looked. This introduced a new dimension of time into etiology of falls. (c) Seniors have over time developed successful safety strategies to cope with limitations in their func-tional abilities. (d) At the time of the fall, their usual strategies failed due to urgency or (e) novelty of the situation (doing some thing for the fi rst time or doing it in a different way). (f) In almost all
by guest on July 6, 2016http://gerontologist.oxfordjournals.org/
Dow
nloaded from
The Gerontologist692
cases, the immediate postfall reaction of the senior was shock and disbelief com bined with strong emotional response ranging from anger to crying. (g) Several seniors experi enced “falling sprees” in the past that ended when they addressed a medical problem (e.g., received a pacemaker) or disengaged from dangerous activi ties. (h) In several cases, a health condition was major but never sole contrib-utor to the fall. Finally (i), large number of falls occurred in transition areas such as entrances, which concurs well with pattern e.
Safety Defi ciencies Identifi ed Using the Swiss Cheese Accident Causation Model
Figure 2 presents the summary of numerous safety defi ciencies that contributed to the investi-gated falls. In all occurrences, unsafe acts and deci-sions were combined with a number of latent unsafe conditions. If not identifi ed and addressed, these dormant unsafe conditions, embedded in all levels of the Swiss cheese accident causation mod-el, will remain in the system and continue to con-tribute to falls when combined with actions and decisions of other seniors in a different set of cir-cumstances. These results show that the people in-volved in falls are just one contributor to the much greater indefi nitely complex and clearly systemic phenomenon. Interventions on all four levels of Swiss cheese accident causation model is required to accomplish safety improvements.
Discussion
The use of the SFIM has shown that causes of falling are numerous, multilayered, variable, and embedded in the system in which seniors live. The SFIM identifi ed the need to broaden the current methods of studying falls by shifting the focus from the faller and immediate circumstances preceding the fall to higher and more complex levels of latent contributors, such as supervision, policy, and or-ganizational infl uences. Research efforts need to expand to include behaviors such as inattention, hurrying, poor decision making, and systems prob-lems, such as lack of training or policy.
The fi ndings of this study place greater empha-sis on contributing factors as described in the Swiss cheese accident causation model ( Figure 2 ), such as inadequate policies, mediocre practices, lack of regulations, poor or nonexistent supervi-sion, and the lack of a safety culture. The falls in-vestigations identifi ed safety defi ciencies on all four levels of safety barriers, confi rming earlier re-sults that showed there is great diversity among fallers and the environments in which they fall ( Allander et al., 1998 ; Oliver, Daly, Martin, & McMurdo, 2004 ). Many circumstances leading to falls in seniors do not seem to be different from falls of any other age group (e.g., workplace falls). The circumstances surrounding the investigated falls were comparable with the fi ndings of Camp-bell and colleagues (1990) and Berg, Alessio, Mills, and Tong (1997) regarding type, time, and
Figure 2 . Summary of safety defi ciencies identifi ed in 15 investigations at four levels of defenses of the Swiss cheese accident causation model.
by guest on July 6, 2016http://gerontologist.oxfordjournals.org/
Dow
nloaded from

Vol. 49, No. 5, 2009 693
Table 2 . Patterns and Emerging Themes Summarized From 15 Investigations of Falls Experienced by Community-Dwelling Seniors
Patterns Examples from investigated cases
Every fall was the result of multiple, combined, and cumulative unsafe acts decisions and latent unsafe conditions
Poorly designed shopping buggy was combined with uneven sidewalks and a senior ’ s strong push on the handle Heavily loaded box, senior left on the kitchen fl oor, was combined with darkness in the apartment and unplanned walk back to the kitchen Not knowing how to lock the walker, purchased from a neighbor, was combined with acute back pain and a decision to sit on the walker ’ s seat for the fi rst time Senior ’ s decision to go out in extreme cold weather was combined with slippery snow-covered sidewalks, rushing to stop the approaching bus, and an omission of a visual check of the intended walking path
A fall was the outcome of a sequence of undesirable events: The initiating event was followed by a sequence of adverse acts or decisions that occur in the presence of unsafe conditions
The faller placed a box on the fl oor → she fi lled up the box with unwanted food → the box was too heavy to move → she left the box in a narrow kitchen entrance → 3 hrs later the faller turned off all lights in the apartment → she walked in darkness to kitchen → she tripped over the box → she broke her nose The senior walked over several scattered rugs at the casino entrance → her daughter asked if the paper on the fl oor was her mother ’ s → the senior turned around → senior saw a paper → senior realized it is not hers → senior turned around while stepping forward → her foot caught the edge of the carpet → carpet folded → senior lost balance → she dropped on her knees A shopping buggy was imported from China → the senior purchased shopping buggy in a local mall → she loaded the buggy with heavy cans of juice that were on sale → the small front wheels of the buggy got caught between two concrete slabs on the sidewalk → she pushed the buggy handle forward → the buggy collapsed pulled by heavy load → she fell over the buggy → her chin hit the pavement
Seniors develop safety strategies to cope with diminishing functional abilities (e.g., they are more careful, walk slower, do not climb on chairs, go out only when supervised, and use assistive devices)
The senior usually takes time to get up from laying down position to allow her fl uctuating blood pressure to stabilize The senior successfully adapted her gait speed to accommodate severe arthritis in right knee by walking slower and paying attention to where she was stepping The senior was careful to visually check his walking path to compensate for blindness in his left eye
Rushing, urgency, and startle caused failures of the senior ’ s usually successful coping strategies (the same cases as aforementioned were used to illustrate the detrimental infl uence of rushing)
The senior was startled by a loud knock; she got up quickly from laying on a sofa to answer the door; she collapsed in the hallway due to hypotension Surprised by a commotion in the laundry room and loud shouts for help from her daughter, the senior rushed down the hallway, turned the corner to the laundry room, and slipped on soapy washing machine – released water on the fl oor The senior spotted the bus coming from the opposite direction; in a rush to attract the driver ’ s attention, he stepped forward to cross the street; he did not see and tripped over a pile of frozen snow on his path
Change of routine or novelty of the situation contributed to falling
Senior loaded the shopping buggy heavier than ever before Senior decided to sit on the seat of her walker for the fi rst time Senior left Lifeline ® bracelet on the kitchen shelf for the fi rst time
Immediate postfall reactions of the seniors were surprisingly similar
Senior was alone and in distress, initially experiencing strong emotional response such as disbelief, crying, or anger. The faller was uncertain of what to do, was unable to get up on his/her own, and struggled to get help (i.e., crawling to the telephone, shouting for help, creating noise)
Occasionally, seniors experience “ falling sprees ” or multiple fall events in a short period of time
Detailed falling histories revealed that seniors periodically experienced multiple falls, usually related to an acute medical condition of unsafe behaviors. When the problem was addressed (i.e., syncope) and resolved (i.e., pacemaker), or a behavioral change was implemented (i.e., stop climbing on chairs to water fl owers), the falling stopped
Some health conditions were major, but not sole, contributors to the fall
Syncope, Parkinson ’ s disease, “ frozen leg, ” hypotension, and foot/knee problems were signifi cant contributors to falls but were always coupled with other latent unsafe conditions
Falls often occurred in transition areas (i.e., entrances)
Falls occurred in entrances to buildings, apartments, rooms, or balconies.
by guest on July 6, 2016http://gerontologist.oxfordjournals.org/
Dow
nloaded from
The Gerontologist694
location of the fall, activities preceding the event or injury type. Most investigated falls occurred in-doors and in the afternoon, which is comparable with results of the studies of Norton, Campbell, Lee-Joe, Robinson, and Butler (1997) and Gallagher and Brunt (1996) respectively. Gill, Williams, and Tinetti (2000) found that living rooms, bedrooms, and kitchens were the most fre-quent places of nonsyncopal falls but that hall-ways had the highest relative risk for hazard exposure. This study found that 54% of the falls occurred in entrance areas to buildings, apartments, or rooms. The investigations also confi rmed that most falls occur while walking ( Gallagher & Brunt ), with seniors tripping over an object ( Luukinen et al., 2000 ) and falling forward (Nevitt et al., 1993 ).
The Swiss cheese accident causation model pro-vided an effi cient and logical framework to orga-nize the identifi ed safety defi ciencies causing falls and to present them symbolically as dynamic ever-changing “ holes ” in safeguards, barriers, or de-fenses that separate hazards and vulnerable persons. This framework is the fi rst to introduce an additional component of time into the causa-tion of falls, demonstrating that causes of falls are sequential and evolve over time. The sequence of events illustrated that the origin of each fall is an initiating event, which can occur years, days, or minutes before the fall, followed by a sequence of undesirable acts or decisions that interact with la-tent unsafe conditions.
In terms of the Swiss cheese accident causation model, most of the knowledge accumulated in the past two decades has focused on two defense levels, namely, unsafe acts (biomechanics and tribology) and preconditions for unsafe acts (epi-demiology, occupational therapy, nursing, geron-tology, geriatrics, rehabilitation, and psychology). The levels of supervision and organizational infl u-ences have received much less attention. This study identifi ed a need for increased formal supervision of family physicians, personal support workers, nurses, occupational and physical therapists, and other people who provide services to seniors. The safety defi ciencies included but were not limited to inadequate diagnosis of illnesses (e.g., syncope), overmedication, lack of community-based services for safety education, and the need to improve strategies for seniors needing to subscribe to a Lifeline ® (e.g., direct contact with emergency ser-vices). The present fi ndings also indicated a lack of safety awareness among informal supervisors such as family members, friends, neighbors, or commu-
nity volunteers. The safety defi ciencies included complete or partial lack of family involvement and monitoring, poor communication, and lack of lo-cal social networks. Six participants (40%) lived alone and either completely lacked family involve-ment or their family members lived more than 1 hr away.
At the organizational level, the investigations recognized that philosophies, policies, and prac-tices of organizations directly or indirectly pro-viding services to seniors also contributed to the fall occurrences. For example, the policy of a mu-nicipal government contributed to excessive snow on the sidewalks and bus stops, the federal gov-ernment lacks regulations related to import of poorly designed devices targeting seniors, an ex-port/import company imports poorly designed shopping buggy, there are no training require-ments for the fi rst-time users of walkers bought “ secondhand, ” and so forth. Better safety stan-dards, regulations, training, policies, and services are integral parts of creating safer communities. An example of a successful intervention at the or-ganizational level is a recent report on The evolu-tion of seniors ’ falls prevention in British Columbia ( Herman, Gallagher, & Scott, 2006 ). By coordinated action and collaboration between the Federal Public Health Agency, the Provincial Ministry of Health, and academics from three universities, the annual hospital cost of fall-related injuries among seniors has been reduced by an estimated 13.7% ($24 million) between 2000 and 2005.
The present investigations also identifi ed favor-able safety mechanisms already functioning well in this community. For example, building superinten-dents working in the apartment complex were well trained and acutely aware of senior ’ s capabilities and needs. The superintendents were often the fi rst responders and quickly helped resolve emergency situations. The investigation of the near fall of a senior who tripped over a damaged threshold ( Fig-ure 1 ) identifi ed several safety defi ciencies related to property maintenance. The investigative report was provided to the property management and within weeks the company changed the policy re-garding replacement of thresholds in the apart-ments of seniors who use assistive devices. Now, all walker users in this senior ’ s complex have safer thresholds installed. These good practices could act as models for other communities.
Research on highly reliable systems (e.g., air traf-fi c control centers) illustrates that the best accident
by guest on July 6, 2016http://gerontologist.oxfordjournals.org/
Dow
nloaded from

Vol. 49, No. 5, 2009 695
safeguards are a collective preoccupation with safe-ty and timely adjustments to match local circum-stances ( Reason, 2000 ). This approach is different from current practices that govern prevention and management of falls in seniors, where falls are fre-quently kept undisclosed. Although an earlier study found that approximately 700 – 800 falls occurred yearly in this apartment complex ( Kloseck et al., 2002 ), only 27 seniors contacted the study inter-viewer over the period of 1 year. Seniors reported that they assumed that the letter they had received and posters in their buildings were for “ someone else, ” whereas others thought their falls were not “ bad enough. ” A concerted effort is needed to con-vince seniors that falls should be discussed in the same way as other medical problems. Involvement of seniors in creating their own culture of safety is essential.
This study supports the need for prevention programs that will address systemic causes of fall-ing. Although multifactorial strategies have been implemented with some success in the past ( Chang et al., 2004 ; Feder, Cryer, Donovan, & Carter, 2000 ; Gillespie et al., 2002 ; Hill-Westmoreland, Soeken, & Spellbring, 2002 ), none was as compre-hensive as the SFIM identifi ed they should be. This study illustrated how an entire community needs to act together to address causes of falls and their negative consequences. It seems that working si-multaneously on population-based risk factor re-duction and localized investigation of systemic causes of falling could be the best approach to falls management and prevention.
Currently, two pilot studies are under way to ex-plore potential of the SFIM to improve patient safety in hospitals, nursing, and LTC homes. A Web-based Falls Database© was created to systematically gather evidence from falls investigations and, over time, allow exchange of recommendations between falls prevention programs. The present study will inform the design of a survey to investigate the prevalence of identifi ed safety defi ciencies and establish a team of stakeholders that will continue to work on improvement of safety in this community.
Limitations
Although 15 investigated cases are inadequate to generalize the fi ndings, the identifi ed associations clearly illustrate the potency of this method. It may only take one fall to identify a defi ciency in the sys-tem that, if corrected, could prevent many future falls. The presented case study approach requires
substantial resources and time to complete each in-vestigation. Investigators have to be trained in hu-man factors and mentored over several months before conducting independent investigations. Nev-ertheless, every case is an analogue to an experi-ment with strength to provide evidence about causes of falls. Reluctance of seniors to discuss their falls in depth resulted in recruitment of six seniors who sustained visible face and head injuries. This might have resulted in better understanding of serious in-jurious falls. In spite of this recruitment bias, we achieved the goal of maximum variation sampling as each investigation captured distinctly different fall scenarios.
Conclusions
This multiple case study presented an innova-tive and promising systems approach to identify safety defi ciencies that contribute to falls in com-munity-dwelling seniors. The study demonstrated the potential of the SFIM to expand the focus from the faller and his or her immediate environment to multilayered organizational and supervisory con-tributors to falling. Falls are a result of latent un-safe conditions, combined with unsafe acts and decisions in a diverse set of circumstances. The fu-ture application of SFIM has the potential to ad-vance seniors ’ safety in the community, hospitals, and LTC homes by identifying causes and contrib-uting factors to falls. Implementation of recom-mendations, designed to address safety defi ciencies, will allow creation of safety culture that will self-initiate safety action.
Funding
The Ontario Neurotrauma Foundation is acknowledged for funding this project.
Acknowledgments
The authors thank the seniors who took part in the study, their fami-lies, friends, family doctors, support workers, and neighbors; ESAM group; and partners in the Cherryhill Healthy Aging Program (VON, CCAC, specialized geriatric services), who collectively contributed to im-proving the safety of seniors in this community. Tricia Armstrong is ac-knowledged for editing the fi nal version of the text .
References Allander , E. , Gullberg , B. , Johnell , O. , Kanis , J. A. , Ranstam , J. , & Elffors ,
L. ( 1998 ). the MEDOS Study Group . Circumstances around the fall in a multinational hip fracture risk study: A diverse pattern for preven-tion . Accident Analysis and Prevention , 30 , 607 – 616 .
Ballinger , C. , & Payne , S. ( 2002 ). The construction of the risk of falling among and by older people . Ageing and Society , 22 , 305 – 324 .
Berg , W. P. , Alessio , H. M. , Mills , E. M. , & Tong , C. ( 1997 ). Circum-stances and consequences of falls in independent community-dwelling older adults . Age and Ageing , 26 , 261 – 268 .
by guest on July 6, 2016http://gerontologist.oxfordjournals.org/
Dow
nloaded from

The Gerontologist696
Campbell , J. A. , Borrie , M. J. , Spears , G. F. , Jackson , S. L. , Brown , J. S. , & Fitzgerald , J. L. ( 1990 ). Circumstances and consequences of falls experienced by a community population 70 years and over during a prospective study . Age and Ageing , 19 , 136 – 141 .
Chang , J. T. , Morton , S. C. , Rubenstein , L. Z. , Mojca , W. A. , Maglione , M. , Suttorp , M. J. , et al. ( 2004 ). Interventions for the prevention of falls in older adults: Systematic review and meta-analysis of ran-domised clinical trials . British Medical Journal , 328 , 680 – 686 .
Close , J. C. ( 2005 ). Prevention of falls — A time to translate evidence into practice . Age and Ageing , 34 , 98 – 100 .
Cumming , R. G. ( 2002 ). Intervention strategies and risk-factor modifi ca-tion for falls prevention. A review of recent intervention studies . Clin-ics in Geriatric Medicine , 18 , 175 – 189 .
Dekker , S. W. A. ( 2002 ). The fi eld guide to human error investigations . Aldershot, England : Ashgate .
Feder , G. , Cryer , C. , Donovan , S. , & Carter , Y., ( 2000 ). Guidelines Devel-opment Group . on behalf of the Guidelines for the prevention of falls in people over 65 . British Medical Journal , 321 , 1007 – 1011 .
Feldman , F. , & Chaudhury , H. ( 2008 ). Falls and the physical environ-ment: A review and a new multifactorial falls-risk conceptual frame-work . Canadian Journal of Occupational Therapy , 75 , 82 – 95 .
Fletcher , P. C. , & Hirdes , J. P. ( 2002 ). Risk factors for falling among community-based seniors using home care services . Journal of Geron-tology: Medical Sciences , 57 , M504 – M510 .
Folstein , M. F. , Folstein , S. E. , & McHugh , P. R. ( 1975 ). “ Mini-mental state. ” A practical method for grading the cognitive state of patients for the clinician . Journal of Psychiatric Research , 12 , 189 – 198 .
Gallagher , E. M. , & Brunt , H. ( 1996 ). Head over heels: Impact of health promotion program to reduce falls in the elderly . Canadian Journal on Aging , 15 , 84 – 96 .
Gill , T. M. , Williams , C. S. , & Tinetti , M. E. ( 2000 ). Environmental haz-ards and the risk of nonsyncopal falls in the homes of community-living older persons . Medical Care , 38 , 1174 – 1183 .
Gillespie , L. D. , Gillespie , W. J. , Robertson , M. C. , Lamb , S. E. , Cumming , R. G. , & Rowe , B. H. ( 2002 ). Interventions for preventing falls in elderly people (Cochrane Review) . In The Cochrane Library, Issue 1 . Oxford, England : Update Software .
Hawkins , F. H. ( 1993 ). Human factors in fl ight . Aldershot, England : Ash-gate .
Herman , M. , Gallagher , E. , & Scott , V. ( 2006 ). The evolution of seniors ’ falls prevention in British Columbia. British Columbia Ministry of Health, Healthy Children, Women and Seniors Branch, Population Health and Wellness Division . Retrieved May 14, 2006, from http://www.healthservices.gov.bc.ca/cpa/publications/falls_report.pdf
Hill-Westmoreland , E. , Soeken , K. , & Spellbring , A. M. ( 2002 ). A meta-analysis of fall prevention programs for the elderly . Nursing Research , 51 , 1 – 8 .
Kloseck , M. , Crilly , R. G. , & Misurak , L. ( 2002 ). A health care model for community seniors: A community-systems approach. The Cherryhill Healthy Ageing Program: Six-year outcomes. Invited report . London, Ontario, Canada : Geriatric Medicine, Parkwood Hospital .
Lord , S. R. , Menz , H. B. , & Sherrington , C. ( 2006 ). Home environment risk factors for falls in older people and the effi cacy of home modifi ca-tions . Age and Ageing , 35 (Suppl). 2, ii55 – ii59 .
Luukinen , H. , Herala , M. , Koski , K. , Honkanen , R. , Laippala , P. , & Kivela , S.L. ( 2000 ). Fracture risk associated with a fall according to type of fall among the elderly . Osteoporosis International , 11 , 631 – 634 .
Nevitt , M. C. , Cummings , S. R. , & the Study of Osteoporotic Fractures Research Group ( 1993 ). Type of fall and risk of hip and wrist frac-tures: The study of osteoporotic fractures . Journal of the American Geriatrics Society , 41 , 1226 – 1234 .
Norton , R. , Campbell , J. A. , Lee-Joe , T. , Robinson , E. , & Butler , M. ( 1997 ). Circumstances of falls resulting in hip fractures among old people . Journal of the American Geriatrics Society , 45 , 1108 – 1112 .
Oliver , D. , Daly , F. , Martin , F. C. , & McMurdo , M. E. T. ( 2004 ). Risk factors and risk assessment tools for falls in hospital in-patients: A systematic review . Age and Ageing , 33 , 122 – 130 .
Perell , K. L. , Nelson , A. , Goldman , R. L. , Luther , S. L. , Prieto-Lewis , N. , & Rubenstein , L. Z. ( 2002 ). Fall risk assessment measures: An ana-lytic review . Journal of Gerontology: Medical Sciences , 56 , M761 – M766 .
Rasmussen , J. ( 1987 ). Reasons, causes and human error . In J. Rasmussen , K. Duncan , & J. Leplat (Eds.), New technology and human error (pp. 293 – 301 ). Toronto, Ontario, Canada : John Wiley .
Reason , J. ( 1990 ). Human error . New York : Cambridge University Press . Reason , J. ( 2000 ). Human error: Models and management . British Medi-
cal Journal , 320 , 768 – 770 . Reason , J. ( 2003 ). Beyond the organisational accident: The need for “ error
wisdom ” on the frontline . Quality & Safety in Health Care , 13 (Suppl. 2) , ii28 – ii33 .
Salvà , A. , Bolíbar , I. , Pera , G. , & Arias , C. ( 2004 ). Incidence and conse-quences of falls among elderly people living in the community . Medicina Clinica (Barcelona) , 122 , 172 – 176 .
Scott , V. , Donaldson , M. , & Gallagher , E. ( 2003 ). A review of the litera-ture on best practices in falls prevention for residents of long-tem care facilities. Monograph . Vancouver, British Columbia, Canada : BC In-jury Research and Prevention Unit .
Tinetti , M. E. , McAvay , G. , & Claus , E. ( 1996 ). Does multiple risk factor reduction explain the reduction in fall rate in the Yale FICSIT Trial? Frailty and Injuries Cooperative Studies of Intervention Techniques . American Journal of Epidemiology , 144 , 389 – 399 .
Transportation Safety Board of Canada . ( 1998 ). An integrated process for investigating human factors . Hull, Quebec, Canada : Author .
Yin , R. L. ( 1989 ). Case study research: Design and methods . Newbury Park, CA : Sage .
Zecevic , A. A. ( 2006 ). A human factors perspective of falls in older adults (Doctoral dissertation, University of Western Ontario, 2006) . Disser-tation Abstracts International , 68 , 171 .
Zecevic , A. A. , Salmoni , A. W. , Lewko , J. H. , & Vandervoort , A. A. ( 2007 ). Seniors Falls Investigation Methodology (SFIM) — A systems approach to the study of falls in seniors . Canadian Journal on Aging , 26 , 277 – 286 .
Received August 20 , 2008 Accepted October 24 , 2008 Decision Editor: Nancy Schoenberg, PhD
by guest on July 6, 2016http://gerontologist.oxfordjournals.org/
Dow
nloaded from