DISTRICT HEALTH ACTION PLAN 2012 – 2013
221
Page 1 of 221 DISTRICT HEALTH ACTION PLAN 2012 – 2013 Name of District: - Jehanabad District Patna District Patna Jehanabad Kako Modanganj Ratni Faridpur Ghosi Makhdumpur Hulasganj District Nalanda District Arwal District Gaya District Patna District Patna
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of DISTRICT HEALTH ACTION PLAN 2012 – 2013

Page 1 of 221
DISTRICT HEALTH ACTION PLAN 2012 –
2013
Name of District: - Jehanabad
District Patna
District Patna
Jehanabad
Kako Modanganj
Ratni Faridpur
Ghosi
Makhdumpur
Hulasganj
District Nalanda
District Arwal
District Gaya
District Patna District Patna

- 2 -
Acknowledgements This District Health Action plan prepared Under a Short & Hard Process of
about survey of one month and this was a good Opportunity to revisit the situation of health services status and national programmes in district as well as to have a positive dialogue with departments like Public Health Engineering, Women and Child Development, Maternal and Child Health care etc.
This document is an outcome of a collective effort by a number of individuals, related to our institutions and programmes:-
v Sri Balamurgan D ,Chairperson of District Health Society, Jehanabad was a source of inspiration towards this effort vide her inputs to this process during D.H.S review meetings.
v Dr.Arvind kumar (A.C.M.O) Nodal officer for this action plan who always supported this endeavor through his guiding words and language.
v Mr. Nimish Manan, District Programme Manager was incharge for the development of the DHAP(2012-13) .
v Mr Ravi Shankar Kumar, District Planning Coordinator has given full time effort in developing DHAP(2012-13).
v Mr. Kaushal Kumar Jha, District Account Manager has put huge effort in financial Planning.
v Mr. Arvind Kumar, M&E Officer is the technical advisor for the data introduced inside this DISTRICT HEALTH ACTION PLAN.
v Mr. Kushal Mukharji, District Programme Officer, DFID (SWASTH), Jehanabad has given Technical support in Plan Preparation.
v All district level Programme officer for various Health Programmes,DCHM, B.H.Ms, M.O.I.C, Hospital Manager, PHCs, Field Office Staff have supported with their full participations, cooperation and learning spirit through out this process.
we on behalf of the District Health Society, Jehanabad acknowledge the grateful contribution of all those mentioned above.
Dr. Smt. Shobha Sinha Sri Balamurgan D
Civil Surgeon-cum-member secretary, District Magistrate-cum-chairman
District Health Society, Jehanabad. District health society, Jehanabad

- 3 -
District Patna
District Patna
Jehanabad
Kako Modanganj
Ratni Faridpur
Ghosi
Makhdumpur
Hulasganj
District Nalanda
District Arwal
District Gaya
District Patna District Patna

- 4 -
Level 1,2,&3 facilities selected for 24*7 institutional delivery
N
Level2
District Patna
District Patna
Jehanabad Sadar
Kako Modanganj
Ratni Faridpur
Ghosi
Makhdumpurpur
Hulasganj
District Nalanda
District Arwal
District Gaya
District Patna District Patna
PHC
PHC
PHC
PHC PHC
Mandil
Dedsaiyaa
Bharthu
Dehuni
HSC Badheta
Level 1
Murgav
HSC Ikkil
Daraurt
Level 3
N
W
S
E
APHC Sikariya
APHC Shakurabad
Bandhuganj

- 5 -
STRUCTURE OF DISTRICT PLAN Chapter I: Introduction, profile of the district and process. PAGE NO § Introduction …………………………………………………………………………….. 8 § History of District………………………………………………………………………. 9 § District Profile…………………………………………………………………………… 11 § District Planning objective and priorities and planning Process… 19 Chapter II: *SWOT analysis……………… ……………………………………. 24 * HMIS DATA ANALYSIS…………………………………………………. 26 * Financial Progress up to NOV 2011…………………………….. 28 Chapter III: Part A
MATERNAL HEALTH 39
CHILD HEALTH 46
FAMILY PLANNING 53
Human Resource 55
ARSH 56
Human Resource 57
Training 61
NRHM Management Cost 62
Chapter IV: PART B
NRHM PART “ B”
ASHA 67
Untied Fund 71
Annual Maintance Grants 76
HOSPITAL STRENGTHENING 77
CORPUS GRANTS TO RKS 83
DE-CENTRALIZED PLANNING 84
PANCHAYTI RAJ INITIATIVE 85
IEC- BCC NRHM 86
MMU 87
REFERRAL TRANSPORT 88
PPP/NGO 89
MONITORING AND EVALUATION 91
PROCUREMENT 91

- 6 -
Chapter V:
Part C – Immunization 96
Routine Immunization/Polio
Chapter VI:
Part D – National Disease Control Programmes
IDSP 99
IDD 116
NVBDCP 117
RNTCP 126
SUMMARY OF BUDGET 154
Chapter VII (ANNEXURE)
SADAR HOSPITAL GAPS: …………………………………………………… 155
VILLAGE HEALTH ACTION PLAN……………………………………………… 158
HSC NAME WITH BUILDING STATUS………………………………………… 176
FINAL BUDGET SUMMARY……………………………………………………… 183

- 7 -
CHAPTER 1: INTRODUCTION, PROFILE OF THE DISTRICT & PROCESS

- 8 -
Introduction:
Jehanabad district was carved out of the old GAYA district on 1st
August 1986. Earlier it was a subdivision of Gaya since 1872. It is situated 56 km to
the south of the State Head Quarters, Patna and 47 km to the north of Gaya by
road and is well connected to both the stations via an electrified rail-route as well.
Again, in the year 2001, the district of Arwal was created out of the district of
Jehanabad.
Geography :
The district covers 941.4 sq. km. of geographical area in South Bihar.
The town of Jehanabad, which is the HQ of the district, is situated at the confluence
of rivers Dardha and Jamuna. Lying between 25-0’ to 25-15’ degree north latitude and
84-13’ to 85-15’ degree eastern longitude, the district is bounded by districts of Patna
in the north, Gaya in the south, Nalanda in the east and Arwal in the West.
Topography and Terrain :
Fertile alluvial soil locally called "Kewal" supports the District's
predominantly agricultural economy and is currently being tilled for production of
paddy, wheat, cane, potato, pulses, vegetables etc. The south-east area of the district
is hilly terrain bounding the district from this site and it offers favorable terrain for the
nexalites to operate and build their bases. Because of geographical constraints and
lack of Pucca road communication carrying out of anti naxal operations becomes a
tedious task. Naxalites take shelter in theses areas and they take advantage of the
porous inter district boarders. Naxals run trainings in these areas and commit crime
after which they easily sleep into the border of the neighboring district. The
geographical features become obstacles in the smooth movement of troops besides
being vulnerable to planting of land mines and becoming easy targets of ambush laid
by naxalites. Since, there several commoflause and concealment places the naxals
take shelter in these areas and convene secret meetings and out spread the
extremist ideology.

- 9 -
History :
Description of Jehanabad in the history is found in the famous book
"AINA-E-AKBARY" wrote by Abul Fazal. The book states that in the 17th century this
place was badly affected by famine and people were dying of hunger. Moghul
emperor Aurangzeb, in whose times the book was re-written established a "Mandi" for
relief of the people and named it 'JEHANARABAD'. The Mandi was under the direct
control of Jehanara and she spent a great deal of time here. In due course of time,
the place became 'JEHANARABAD' and later 'JEHANABAD'
Dialect :
The dialect spoken here is Magadhi (Magahi).
Socio-Economic :
The relatively small sized district is a cauldron of conflict as far as the
socio-economic situation is concerned. There were extreme caste tensions (with an
economic bearing) prevailing in the whole Magadh area (old Gaya district - now
broken into 5 districts of Gaya, Aurangabad, Nawada, Jehanabad and Arwal) and
they were manifested in their worst forms in this district. Thus this place has been
badly affected by Naxalism (PWG, MCC, ML(Lib) etc.) and has seen the emergence
of rival outfits such as Ranvir Sena.
In the result this district has witnessed horrifying spate of large scale
carnages in the past which has resulted in the killing of hundreds of innocents. Nonhi-
Nagwan, Parasbigha, Khagari-Damuha, Laxmanpur-Baathe, Rampur-Chauram,
Senari, Shankarbigha and Narainpur - there is a long list of villages where big
massacres have occurred.
Natural Resources
The rivers- Falgu, Dardha, Jamuna and Morhar flow by crossing the district's
plan topography. The river Falgu has got religious importance where 'PIND DAN' is

- 10 -
offered to their forefather's by the Hindus. All these rivers are mainly rainfed, have a
meagre discharge in the other parts of the year and go dry in the summers.
As far as minerals are concerned, the district has only minor ones. The sand
available with the river beds in the major part of the year is collected and transported
to other parts of the district besides to the adjoining districts and is useful in
construction work.
The soil is alluvial- textured brown gray which cracks open in the dry season
and gets very sticky in the rains and the mud tracks become unmotorable during that
period. The fertility is reasonably good.
The forest cover of the district is small- 1030 hectares, which is mainly
concentrated near the Barabar Hills. They belong to the category of reserve forests.
Human Resources
There are about 1.11 lakh cultivators including 92138 small and marginal
farmers, 1.78 lacs agricultural labourers, 7969 skilled labours, 5075 house hold
entrepreneurs and 95755 are engaged in allied agro business. The total population in
the working age group is 358723 out of which there are 236199 males and 122534
females.
Statistical Profile (based on 2011 census)
Sl. No.
Population Male Female Total
1. Bihar 54185347 49619290 103,804,637
2. Jehanabad 586202 537974 1124176
3. Rural Population 514724 475092 989816
4. Urban Population 71478 62882 134360
5. Literacy rate 79.30% 56.24% 68.27%
6. Rural 87.80% 88.31% 88.04%
7. Urban 12.20% 11.69% 11.96%
- 11 -
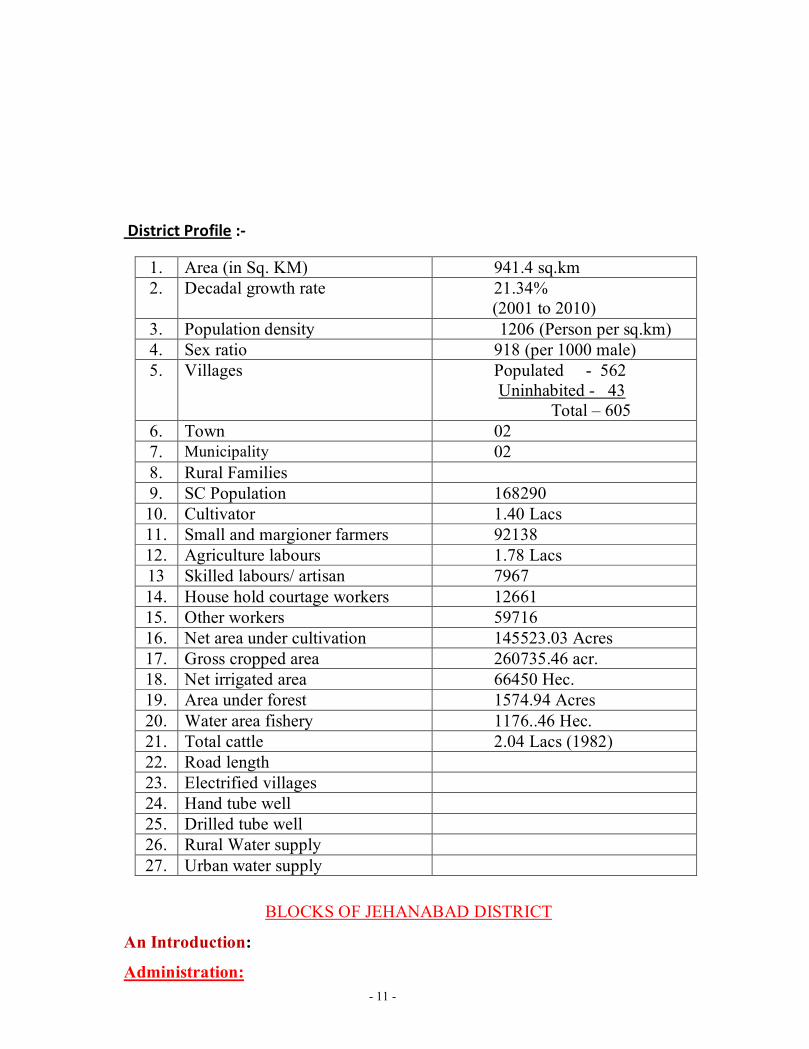
District Profile :-
1. Area (in Sq. KM) 941.4 sq.km 2. Decadal growth rate 21.34%
(2001 to 2010) 3. Population density 1206 (Person per sq.km) 4. Sex ratio 918 (per 1000 male) 5. Villages Populated - 562
Uninhabited - 43 Total – 605
6. Town 02 7. Municipality 02 8. Rural Families 9. SC Population 168290 10. Cultivator 1.40 Lacs 11. Small and margioner farmers 92138 12. Agriculture labours 1.78 Lacs 13 Skilled labours/ artisan 7967 14. House hold courtage workers 12661 15. Other workers 59716 16. Net area under cultivation 145523.03 Acres 17. Gross cropped area 260735.46 acr. 18. Net irrigated area 66450 Hec. 19. Area under forest 1574.94 Acres 20. Water area fishery 1176..46 Hec. 21. Total cattle 2.04 Lacs (1982) 22. Road length 23. Electrified villages 24. Hand tube well 25. Drilled tube well 26. Rural Water supply 27. Urban water supply
BLOCKS OF JEHANABAD DISTRICT
An Introduction:
Administration:

- 12 -
There is one subdivision - Jehanabad and seven blocks in the district
- Jehanabad, Kako, Makhdumpur, Ghosi, Ratni Faridpur, Hulasganj and
Modanganj. There are 93 Gram Panchayats, 7 Panchayat Samities and one Zila
Parishad in this district. One Nagar Panchayat is at Makhdumpur and one Nagar
Parishad at Jehanabad, M.P. constituency - 01, MLA constituency - 3
Infrastructure:
The district is linked to the bigger cities of Patna & Gaya both by
road and rail route. The recently electrified Patna-Gaya branch railway line (P.G.
line) traverses through the district and links the Grand Chord with Patna. There
are four railway stations- Jehanabad, Court, Tehta and Makhdumpur in the 31
km long stretch of the railways. National Highway No. 83 comes from Patna via
Masaurhi, goes directly to Gaya through Makhdumpur and runs almost parallel
to the railway line. There is a network of PWD roads and REO roads across the
district, albeit in a bad shape. The total length of surfaced roads is 541.65 kms
and mud tracks are 450.90 kms. The condition of the roads in the rural parts is
good.
The district has wide network of markets dealing mainly with grains
and vegetables. Major centers of trade and commerce are located in Jehanabad,
Ghosi, Kako and Makhdumpur. Besides in rural areas hats function usually once
in the week. The trade consists mainly of export of oil seeds, rice, gur, stone
chips and vegetables. The principal imports are coal, cement and other
construction materials, clothes, K. oil, tea, tobacco, fresh fruits and other
perishable/ non perishable consumer goods.
The telecommunication network in the district is good. The whole of the
district is either covered by basic or mobile phones.
The educational infrastructure available in the district can be summarized
as following-
Primary schools - 561

- 13 -
Middle schools - 198
High schools - 43
Sanskrit Schools - 07
Colleges - 02
Besides, the Sarva Shiksha Abhiyaan (SSA) has been started in the district
in a big way and there is a lot of improvement underway in the quality of the
buildings through additional classrooms, toilets, hand pumps, annual repair and
maintenance grants etc. Distribution of Teaching and learning materials, text
books etc. is being simultaneously carried out in a big way.
Credit facilities
Banks - 34 PACS - 62 Hospitals
District Hospital - 1 Sub-Divisional Hospital - 1 Referral Hospital - 2 Block P.H.C. - 7 Addl. PHCs - 32 Sub-centre - 96 T.B. Sanitarium - 1 Leprosy control unit - 1
The district has no big industrial unit but there is a network of
village and cottage industries comprising hand looms, local spinning units, shoe
making, carpenters, brick kiln, stone crushers etc.
As far as infrastructure for tourism is concerned, we have a few
places to mention. There are three historical places in the district. The foremost
one of Barabar or "Vanavar", situated 11 kms to the east of the NH - 31 from
Makhdumpur, has the temple of Lord Shiva in the name of Baba Sidheshwar
Nath, at the top of the hill, about 1100' above M.S.L. There are a few rock cut
caves namely Karna Chaupar and Sudama, relating to the times of Emperor
Ashoka. There is a Lomash Cave, named after a saint. A spring known as Patal
Ganga is said to be built by Ashoka. There is Nagarjuni caves located nearby.
The great Chinese traveler, Huen-Tsang, had visited this place and had described

- 14 -
it in his book. It has been described in E.M. Forster's "A Passage to India". In
recent times the district administration has renovated this place and constructed
two tourist bungalows, a restaurant, a cemented stair case to the top of the hill, a
children's park, boating facilities etc to promote tourism. Another Yatri Niwas is
coming up at the base camp under MPLADS. This place witnesses a huge fair in
the month of "Shravani" and it is estimated that about two to three lakhs of
devotees come to offer their prayers.
Situated 11 km south-east of Jehanabad railway station in Kako
block, Bhelawar is famous for an old temple of Lord Shiva. A big fair is
organised every year on the occasion of Maha Shivaratri. Specimens of art of the
Hindu and Muslim period have also been found here.
Also in Kako itself, which is equally important both for the Hindus
and the Muslims, there is a temple having old statue of Lord Sun in the North-
east of Kako village. It is said that Rani Kekai, wife of King Dasharatha and
step-mother of Lord Rama had domiciled here for sometime. On her name this
village got the name as 'Kako'. There is also a graveyard of a great Muslim Sufi
Lady-Hazrat Kamalo Bibi, aunt of Hazarat Makhdum Sahab of Bihar Sharif,
who is said to have been blessed with divine powers.

- 15 -
BLOCKS
Sl.No. Variable kako ratni ghoshi makdumpur okhari Jehanabad Hulasga
nj
Total area 33607.08 acres
142500 102463 100.63 SQ.Mile
23091
Total population
173770 147100 107649 259714 87262 254183 94498
Male population
90233 76740 55671 134612 45343 134116 49487
Female population
83536 70360 51978 125101 41918 120067 45014
Adolescent population (10-19yrs)
38340 15285
Sex Ratio
4380 2234
8760 7414
Child population: 0-6 months
:6mn-2yrs
:2-5yrs
13140 13925
7458 18410 21702 43701 16020 42720 21322 SC population :
0 00 00 ST population :
00 00 0 0
BPL population
17222 14826 13000 8847
No of Eligible couples
2499 21950 23138
Total no. of gram panchayat
16 14 10 22 08 14 09

- 16 -
Total no. of revenue villages
95 85 53 118 54 99 48
No of APHCs 04 07 06 05 03 05 02
No of HSCs 21 12 9 21 12 12 9
No. of Anganwadi centers
139/143 117/123
87/89 210/215 70/70 178/208 67/77
No of Doctors 9 9 8 13 7 7
No of ANMs 46 39 29 47 42 28
No of Grade A Nurse
4 8 7 8 7 4
No of Paramedicals
8 4 9 1
No. of Anganwadi workers
139 117 87 210 70 178 67
No of ASHA 145 128 90 180 75 136 87
Total No. of SHG/ Mahila mandals
136 120 76
No. of primary schools
154 122 53 59 108 15
No. of electrified villages
85 56
48
275
21412
No. of villages having source
of drinking water:
Well
Tube-well 5870

- 17 -
Pond- river
Piped water
Any other
No of villages having motorable roads
206 48

- 18 -
PLANNING GOAL,OBJECTIVE
AND
PRIORITIES

- 19 -
GOAL FOR YEAR 2012-13
Outcome indicator Bihar Jehanabad Goal for 2012-13
CBR 26.7 24.9 22
CDR 7.2 6.2 5
IMR 55 53 45
MMR 305 331 200
Neo Natal Mortality Rate
35 31 20
Source : Annual Health Survey 2010-11
Jehanabad District has targeted to reduce MMR from331 to 200 in year plan 2012-13, To reduce CBR 24.9 to 22 as CBR of Bihar State is 26.7, As IMR of District is 53 that has to bring at the point of 45. As District has Targeted to use more Contraceptive Pills according to DLHS 3 survey jehanabad has trend of use of contraceptive Pills 30%.
Planning Objective And Priorities
The Planning Objective for the District Health Action Plan 2012-13 has been decided on the basis of Goals of NRHM, Guidelines of State Health Society and DHAP of 2011-12. Followings are the Objective and priorities of planning of Jehanabad district:
1. Strengthening safe institutional Delivery by JBSY 2. Reducing Maternal and infant mortality rate by adopting tools of maternal
autopsy and increasing focus on neo natal child care by starting SNCU in the district headquarter. Strengthening VHSND.
3. Special focus on ARSH Programme by starting separate clinics for adolescents, and training frontline workers to create awareness regarding RTI/STI and UTI.
4. Vulnerable sections to be given priority in all health care facilities. 5. Increasing Immunization Coverage. 6. Family planning and unmet needs of contraceptives to be met with. 7. Increasing community participation in the health system by strengthening of
VHSC, effective functioning of Rogi Kalyan Samiti at PHC and Registration of RKS at APHC level and proper functioning of RKS at APHC level. Proper utilization of untied fund at PHC and HSC level and APHC level. To Functioning one APHC in each block as 24*7.
8. Training to all frontline facility providers to be given. 9. Awareness and BCC regarding all communicable and vector borne diseases. 10. To start one more NRC to Cover more SAM Children at Refral Hospital
Makhdumpur. 11. On PPP Mode Pathology Facility at APHC level. 12. To Insure at two HSC of District for Institutional Delivery. 13. To make sure use of Asha Drug Kit to better service quality at Village level. 14. Training to Asha on different Modules.

- 20 -
Specific and Non-Negotiable Steps to be taken by Jehanabad district in the year 2012-2013 with special focus on Blocks situation:
1. Initiating SNCU in the District hospital , Jehanabad 2. Radiology, Pathology and Ultrasound facilities in all PHCs and Referral
hospitals. 3. ISO certification for District Hospital, Makdumpur Referral and Kako PHC. 4. Generic Drug Storage at all seven PHC. Presently storage is only in District
Hospital. 5. To provide special health facility in Naxal affected areas of Jehanabad district. 6. Establishment of “ICU” in Sadar Hospital, Jehanabad.

- 21 -
Planning Process → Planning in the district began in October 2011 with Planning Team Formation. → The District Level planning team was formed and brifing was done by ACMO-
DPM-DPC. The District Level planning team consisted of the following members from Departments
· Civil Sirgeon · DPM · DPC · DAM · DIO · DPO-ICDS · Total Sanitation coordinator Phed · Development Partner DFID-Swasth- Unicef · MOIC of PHC The team after taking District level training organized a workshop in the District in which MOICs, BHMs and accountant of each block were trained for preparing Block level planning.
→ All officers of the district participated in the workshop along with District
accounts Manager/BHM/BAM/MEO/ASHA coordinator/DHM. → Civil Surgeon had delighted the workshop by giving her presence and
participation throughout the day. She clarified and explain the Efficacy of DHAP.ACMO, who is the nodal person facilitated the workshop and announced the district Programme officers as the nodal officers for different blocks. DPO-ICDS- Total Sanitation coordinator Phed- Development Partners- DFID-Swasth team - Unicef facilitated the process and components of planning. Further formats were discussed by DPM, DPC and queries were resolved.
→ Further at each block a workshop was done and all the members of Block PHC and ANMs were sensitized and given orientation regarding the planning with a Special focus on Village health planning and quality assurance of it The District Programme officers in charge for the block facilitated the workshop in their blocks.
→ All the blocks filled up the situation analysis format and took out the gaps present in their facilities.
→ Special focus was made for Village health action plan –the Facility survey-FGD-health services mapping and documentation process were explained and all the selected blocks Action Plan was prepared. The Dist Level Planning team members monitored the village level action Plan exercises at the block and villages
→ Thereby district compiled the data and added the information, goals, issues, strategies, activities and budget of the district and submitted it to the State by first week of January 2012.
The final Draft of District Health Action Plan of Jehanabad district for the year 2012-13. With Block as the basis of planning came in this final shape.

- 22 -
DISTRICT WORKSHOP: ----------------

- 23 -
CHAPTER 2 SWOT ANALYSIS

- 24 -
SWOT ANALYSIS
STRENGTH Every month DHS Meeting under the Leadership of District Magistrate and weekly meeting to review the progress and reduction of Gaps
*Experienced clinical and DHS staff.
* Experienced Doctors availibity.
Inter department coordination with ICDS-Phed-Education and development partner Unicef-WHO-DFID-MI-Nipi and NGOs
* Blood Bank at DH, and blood storage unit at RH Makhdumpur.
NRC is functional
* Better linkage facility to Gaya medical College and PMCH, Patna.
* Ambulance facility at all PHC to quick refers according to requirement.
* Good linkage facility and Pucca road village to PHC and higher level facility.
* Special Focus on Out reach area in RI Session.
All the blocks are having the New born corner
WEAKNESS · Lack of specialist Doctors. · Require More ANMS for quality service delivery
mechanism · Lack of all PHC Blood storage unit. · Lack of proper training to all clinical staff. · Lack of SNCU at district level. · Advanced Labor room required at PHC level & Delivery
Facility at HSC level. · Timely Availability of Drug. · Use the Fund of VHSC. · Demand of Doctor on HSC level. · OPD Daily Facility on HSC Level. · Drinking Water Facility should be made available in
Summer Season. · In cress in the APHC working Time. · Demand of 24*7 facility at APHC level.

- 25 -
OPPORTUNITY · Opportunity to Start one more Ne NRC. · Strengthen All clinical staff after giving training. · Opportunity to start SNCU. ASHA working at Grass root
level that is Good. · Availability of Drug through ASHA Kit at emergency
time has Good Impact on Villagers. · People are Satisfied with RI Facility. · Villagers are satisfied with counseling session during
there visit about sanitation, Family Planning. ·
THREAT · Threat of demotivation of clinical staff due to lack of HR Policies and NAXAL AFFECTED AREA which will initiate adverse affect.
· Threat of Drought.

- 26 -
ANC Registration against Expected Pregnancies 93%
TT1 given to Pregnant women against ANC Registraion 78%
3 ANC Check ups against ANC Reigtrations 58% 100 IFA Tablets given to Pregnant women against ANC Registraion 81%
Deliveries Unreported Deliveries against Estimated
Deliveries 24% HOME Deliveries( SBA& Non SBA)
against Estimated Deliveries 2%
Institutional Deliveries against Estimated Deliveries 64%
HOME Deliveries( SBA& Non SBA) against Reported Deliveries 49%
Institutional Deliveries against Reported Deliveries 49%
C Section Deliveries against Institutional Deliveries( Pvt & Pub) 6%
Births & Neonates Care Live Births Reported against Estimated Live
Births 44% New borns weighed against Reported
Live Births 55%
Still Births (Reported) 189 New borns weighed less than 2.5 kgs
against newborns weighed 10%
Sex Ratio at Birh 1,054 New borns breastfed within one hr of
Birth against Reported live Births 57%
Child Immunisation( 0 to 11 months)
BCG given against Expected Live Births 82% Measles given against Expected Live
Births 91%
OPV3 given against Expected Live Births 54% Fully Immunised Children against
Expected Live Births 54%
DPT3 given against Expected Live Births 80%
Family Planning Family Planning Methods Users (
Sterilisations(Male &Female)+IUD+ Condom pieces/72 + OCP Cycles/13)
7,779 IUD Insertions against reported FP
Methods 54%
Bihar- Jehanabad HMIS DATA ANALYSIS 2011-12
BIHAR-JEHANABAD- Data Month April to September 2011

- 27 -
Sterilisation against reported FP Methods 18% Condom Users against reported FP
Methods 18%
OCP Users against reported FP
Methods 10%
Other Services
OPD 4,91,846 Major Operations 870
IPD 13,766 Minor Operations 6,930

- 28 -
Financial Progress Up To NOV 2011
DISTRICT HEALTH SOCIETY JEHANABAD BUDGET WISE EXPENDITURE REPORT FOR FY 2011-12
NRHM PART "A"
S.N. Name of Scheme
OPENING BALANCE
AS ON 1.04.2011 (including Advance)
FUND RELASED
FROM SHSB
TOTAL FUND
APPROVED BUDGET
EXPENDITURE UPTO
November, 2011
CLOSING BALANCE as on 30-11-11
(DHS+Agency)
A Maternal Health
1 Monitoring Progress and quality of services delivery
50,000 5800
2 Operationalise 24x7 PHC
2,25,000 38720
3 Operationalise Sub Centre
1,00,000 0
4 RCH Outreach Camps 98,000 71310
5 Monthly Village Heatlh & Nutrition Day
5,01,500 36350
6 Home Delivery 1,02,000 1500
7 Institutonal Delivery Rural
3,32,49,430 18127580
8 Institutonal Delivery Urban
7,00,000 290000
9 Institutonal Delivery C-section
1,31,258 43500
10 Administrative Exp. 3,24,892 0
11 Maternal Death Review
53,025 4250
Sub Total 3,55,35,105 1,86,19,010
B Child Health
1 Implementation of IMNCI Activity
50,000 0
2 Facility Based New Born Care
7,75,000 0
3 Nutritional Rehabitation Centre
36,44,100 677688
Sub Total 44,69,100 6,77,688
C Family Planning
1 Quality Assurance of Sterlization Services
20,000 0
2 Female Sterlization Camps
10,80,000 18800

- 29 -
3 NSV Camps 20,000 29635
4 Compensatin for Female Sterlisation
42,70,000 1960437
5 Compensatin for Male Sterlisation
1,96,500 118115
6 Accredition of PP for Sterlisation
19,66,500 0
7 Pol for Family Planning
1,19,000 4856
8 IUD Camps 33,500 28500
9 Others (School Health)
723660
Sub Total 77,05,500 28,84,003
D ARSH
1 Arsh 0 0
Sub Total 0 0
E Tribal RCH
1 PNDT Sex Ratio 1,00,000 0
Sub Total 1,00,000 0
F
Infrastructure (Minor Civil
Work)Human Resource
(Except AYUSH)
1 ANM Staff Nurse 2,04,54,000 14050363
2 Laboratory Technican
3,60,000 0
3 Salary for MO in Blood Bank
4,20,000 0
4 FP Councellor 3,60,000 0
5 Muskan (Incentive to ASHA & ANM)
12,24,248 1557360
Sub Total 2,28,18,248 1,56,07,723
G Training
1 SBA 5,92,350 352440
2 Training of MO and Para Medical Staff
2,30,000 0
3 IMNCI Training 47,22,380 505036 4 NSSK Training 2,11,600 0 5 Minilap Training 70,237 0
6 Training of MO in IUD Insertion
55,289 0
7 Training of ANM in IUD Insertion
88,260 0

- 30 -
8 DPMU Training 50,000 0 Sub Total 60,20,116 8,57,476
H NRHM
Management Cost
1 Mobility Support (DMO)
1,80,000 0
2 Contractual Staff for DPMU
11,86,284 894025
3
Equipment / Furniture and mobility support for DPMU Staff
9,86,000 167621
4 Block PMU 51,49,200 3476152
5 Uptration of Tally Erp 9
8,100 8100
6 ANC 22,500 0
7 Hospital Manager/Accountant Fru
9,00,000 357000
8 Annual Audit of Programme ( Stutory Audit)
36,000 0
9 Concurrent Audit 2,40,000 45000 Sub Total 87,08,084 49,47,898
Grand Total 23829506 46826270 706557
76 8,53,56,153 4,35,93,798 2,70,61,978
DISTRICT HEALTH SOCIETY JEHANABAD BUDGET WISE EXPENDITURE REPORT FOR FY 2011-12
NRHM PART "B"
S.N. Name of Scheme
OPENING BALANCE
AS ON 1.04.2011 (including Advance)
FUND RELASED
FROM SHSB
TOTAL FUND
APPROVED BUDGET
EXPENDITURE UPTO
NOVEMBER, 2011
CLOSING BALANCE as on 30-11-11
(DHS+Agency)
A ASHA
1 Selection & Training of ASHA
40,26,923 0
2 Procurement of ASHA drug Kit
2,17,750 0
3 TA /DA for ASHA Diwas
8,98,872 469296
4 Best Performance award to ASHA at District Level
14,000 1800

- 31 -
5 Identity Card for ASHA
360 0
6 ASHA Resource Center
18,10,750 607560
Sub Total 0 69,68,655 10,78,656
B Untied Fund
1 Untied Fund for SDH 50,000 6486 2 Untied Fund for PHC 2,25,000 104775
3 Untied Fund for APHC
8,00,000 39392
4 Untied Fund for HSC 9,20,000 644445
5 Untied Fund for VHSC
61,90,000 4350000
Sub Total 0 81,85,000 51,45,098
C Annual Maint.
Grant
1 Annual Maint. Grant for CHC
2,00,000
2 Annual Maint. Grant for PHC
2,00,000 27878
3 Annual Maint. Grant for APHC
7,50,000 210886
4 Annual Maint. Grant for HSC
5,10,000 33675
Sub Total 0 16,60,000 2,72,439
D Hospital
Strenthing
1 Installation of Solar Water System
3,20,500 8000
2 Sub-Centre Rent 3,06,000 13501
Sub Total 0 6,26,500 21,501
E New
Constraction & Renovation
1 Cons. Of HSC 0 3868000 2 Cons. Of APHC 0 0 3 Cons. Of PHC 0
4 Refurbishment of Existing Cold Chain Room
8,00,000 0
Sub Total 0 8,00,000 38,68,000
F Rogi Kalyan
Samiti
1 RKS SDH 5,00,000 407223 2 RKS Referral Hospital
3,00,000 18300
3 RKS PHC 7,00,000 1620029

- 32 -
4 RKS APHC 30,00,000 0
Sub Total 0 45,00,000 20,45,552
G Panchayati Raj
Initative
1 District Health Action Plan including Blocks & Village
4,51,000 192552
2
Orientation of Community leader of VHSC, PHS, PHC & CHC
1,39,500 10100
3
Orientation of Workshop, Training & Capacity building of PRI
61,800 0
Sub Total 0 6,52,300 2,02,652
H AYUSH
1 Salary for AYUSH MO 57,20,000 2848397
Sub Total 0 57,20,000 28,48,397
I BCC / IEC
1 Hording, Wall Painting & Others
4,05,000 218029
2 Health Mela (Leprocy)
4,000 0
Sub Total 0 4,09,000 2,18,029
J Referral
Transport
1 MMU 42,12,000 1497600 2 Dial 108 Ambulance
15,60,000 1064748
3 Dial 102 Ambulance 3,90,000 258675
Sub Total 0 61,62,000 28,21,023
K PPP/NGO
1 Outsourcing of Pathology & Radiology
40,00,000 1793382
2 Bio-Waste Management
11,04,000 0
Sub Total 0 51,04,000 17,93,382
L Innovations
1
Acceridition of Public and Private sector for safe abortion services
1,03,166 0
Sub Total 0 1,03,166 0
M Planning,
Implementation & Monitoring

- 33 -
1 Data Center (Dist. & Block)
8,10,000 673862
2 MCTS & HRIS 1,86,433 0 3 RI Monitoring 1,30,000 0 4 CPSMS 20,000 20000 5 HMIS 4,000 0
6 HMIS Supporting, Supervision & Data Validation
1,82,000 17500
Sub Total 0 13,32,433 7,11,362
N Procurement
1 Procurtement of Equipment (Labour Room)
18,42,104 458900
2 NBCC Equipment 4,02,328 272054 3 Minilap set 1,05,000 81180 4 NSV Kit 5,500 0 5 IUD Kit 15,000 0 6 Dental Chair 13,57,894 0 7 A.C 1.5 Ton Window
25,000 0
8 Parenteral Iron Sucrose
5,00,000 32425
9 IFA Tab. Pregnant Mother
6,57,456 0
10 IFA Small Tab/Syrup Children
8,18,438 0
11 IMNCI Drug Kit 6,00,000 0 12 General Drug Supply 48,78,900 1821842
Sub Total 0 1,12,07,620 26,66,401
O RNTCP
1 Supporting Strengthiing RNTCP
72,000 0
2 Payment of Monthly Bill to BSNL
27,240 0
Sub Total 0 99,240 0 Grand Total 17268995 30894015 48163010 5,35,29,914 2,36,92,492 2,44,70,518

- 34 -
DISTRICT HEALTH SOCIETY JEHANABAD
BUDGET WISE EXPENDITURE REPORT FOR FY 2011-12 NRHM PART "C"
A NAME OF SCHEME
OPENING BALANCE AS
ON 1.04.2011 (including Advance)
FUND RELEASED
FROM SHSB
TOTAL FUND
APPROVED BUDGET
EXPENDITURE
CLOSING BALANCE as on 30-11-11
(DHS+Agency)
1 C (RI) 2468357 28,03,461 1662947 2 C (PP) 1443961
75,47,851 3444300
3 Cold Chain Main.
25619
Sub Total 3912318 3910615 7822933 1,03,51,312 5132866 2690067
NRHM PART "D"
A NAME OF SCHEME
OPENING BALANCE AS
ON 1.04.2011 (including Advance)
FUND RELEASED
FROM SHSB
TOTAL FUND
APPROVED BUDGET
EXPENDITURE
CLOSING BALANCE as on 30-11-11
(DHS+Agency)
1 IDD 11,000 1200
Sub Total 34351 34351 11,000 1200 33151
NRHM PART "E"
A NAME OF SCHEME
OPENING BALANCE AS
ON 1.04.2011 (including Advance)
FUND RELEASED
FROM SHSB
TOTAL FUND
APPROVED BUDGET
EXPENDITURE
CLOSING BALANCE as on 30-11-11
(DHS+Agency)
1 IDSP 8,54,000 210945
Sub Total 112898 213500 326398 8,54,000 210945 115453
NRHM PART "F"
A NAME OF SCHEME
OPENING BALANCE AS
ON 1.04.2011 (including Advance)
FUND RELEASED
FROM SHSB
TOTAL FUND
APPROVED BUDGET
EXPENDITURE
CLOSING BALANCE as on 30-11-11
(DHS+Agency)
1 Maleria, Falaria & Kalazar
411896
Sub Total 1178402 10000 1188402 8,02,130 411896 776506
NRHM PART "G"

- 35 -
A NAME OF SCHEME
OPENING BALANCE AS
ON 1.04.2011 (including Advance)
FUND RELEASED
FROM SHSB
TOTAL FUND
APPROVED BUDGET
EXPENDITURE
CLOSING BALANCE as on 30-11-11
(DHS+Agency)
1 Leprocy 93663
Sub Total 146720 8378 155098 2,93,750 93663 61435 NRHM PART "H"
A NAME OF SCHEME
OPENING BALANCE AS
ON 1.04.2011
FUND RELEASED
FROM SHSB
TOTAL FUND
APPROVED BUDGET
EXPENDITURE
CLOSING BALANCE as on 30-11-11
(DHS+Agency)
1 Blindness 324799
Sub Total 2543770 0 2543770 31,07,015 324799 2218971
NRHM PART "I"
A NAME OF SCHEME
OPENING BALANCE AS
ON 1.04.2011 (including Advance)
FUND RELEASED
FROM SHSB
TOTAL FUND
APPROVED BUDGET
EXPENDITURE
CLOSING BALANCE as on 30-11-11
(DHS+Agency)
1 RNTCP 1057401
Sub Total 247647 1140550 1388197 24,08,475 1057401 330796

- 36 -
DISTRICT HEALTH SOCIETY, JEHANABAD SUMMRY REPORT
S.N. Name of Scheme
OPENING BALANCE AS
ON 1.04.2011 (including Advance)
FUND RELASED
FROM SHSB
TOTAL FUND
APPROVED ANNUAL BUDGET
EXPENDITURE UPTO
NOVEMBER, 2011
CLOSING BALANCE as on 30-
11-11 (DHS+Age
ncy)
NRHM PART "A" 23829506 46826270 70655776 85356153 43593798 27061978
NRHM PART "B" 17268995 30894015 48163010 53529914 23692492 24470518
NRHM PART "C" 3912318 3910615 7822933 10351312 5132866 2690067
NRHM PART "D" 34351 0 34351 11000 1200 33151
NRHM PART "E" 112898 213500 326398 854000 210945 115453
NRHM PART "F" 1178402 10000 1188402 802130 411896 776506
NRHM PART "G" 146720 8378 155098 293750 93663 61435
NRHM PART "H" 2543770 0 2543770 3107015 324799 2218971
NRHM PART "I" 247647 1140550 1388197 2408475 1057401 330796
Grand Total:- 49274607 83003328 132277935 156713749 74519060 57758875
Up to November, 2011 Total Annual Budget 156713749 Total Available Fund 132277935 Target Achived 74519060 Total Expenditure 74519060
Balance Target to be Achived 82194689 % Expenditure of Available Fund 56.34
% Of Achivment 47.55

- 37 -
The District Health Action Plan for the year 2012-13 has the following components and consists of following sections-: Part A: Reproductive and Child Health priority areas under RCH-II flexible pool (Sub-Components – Maternal Health, Child Health, Fmily Planning, ARSH, Urban RCH, Vulnerable Groups, Innovations/PPP/NGO, Infrastructure and Human Resources, Institutitonal Strengthening (HMIS, M&E), Training, Procurement, Programme Management). Part B: Additionalities under NRHM (ASHA, Infrastructure, Contractual Manpower, PPP-Referral & Emergency Transport, Diagnostics, Data Centres, Procurement, Planning) Part C: Routine Immunisation Part D – I : National Iodine Deficiency Disorders Control Programme (NIDDCP)
· Integrated Disease Surveillance project (IDSP)
· National Vector Borne Disease Control Programme (NVBDCP) (Malaria, Kalazar, Filaria)
· National Leprosy Elimination Programme (NLEP)
· National Programme for Control of Blindness (NPCB)
· Revised National Tuberculosis Control Programme (RNTCP)

- 38 -
CHAPTER 3
NRHM PART “A”

- 39 -
Part A- RCH FLEXIPOOL Current Status –
Indicator Bihar Jehanabad
CBR 26.7 24.9
CDR 7.2 6.2
IMR 55 53
MMR 305 331
TFR 2.1 2.9 ( SRS 2010-11)
Source: Annual Health Survey 2010-11
Important RCH indicators such as MMR, IMR, MMR are showing declining trends whereas institutional delivery in government facility, complete ANC, contraceptive use in the District has increased.
Indicator Bihar Jehanabad
Natural Growth Rate 19.5 18.7
Neo Natal Mortality Rate 35 31
Post Neo Natal Mortality Rate
19 21
Under Five Mortality Rate 77 67
Sex Ratio at Birth 919 935
Sex Ratio ( 0- 4 Years) 931 930
Sex Ratio (All Ages) 950 995
Source: Annual Health Survey 2010-11

- 40 -

- 41 -
Source: DLHS 3 ( 2007-08)

- 42 -
RCH II Programme Objectives and Strategies Vision Statement NRHM seeks to provide universal access to equitable, affordable and quality health care which is uncountable at the same time responsive to the needs of the people, reduction of child and maternal deaths as well as population stabilisation, gender and demographic balance in this process. The mission would help achieve goals set under the National Rural Health Policy and the Millennium Development Goals. To achieve these goals NRHM will: * Facilitate increased access and utilization of quality health services by all. * Forge a partnership between the Central, state and the local governments. * Set up a platform for involving the Panchayati Raj institutions and community in the management of primary health programmes and infrastructure. * Provide an opportunity for promoting equity and social justice. * Establish a mechanism to provide flexibility to the District and the community to promote local initiatives. * Develop a framework for promoting inter-sectoral convergence for promotive and preventive health care.

- 43 -
A.1 MATERNAL HEALTH
Maternal Health:
Introduction Maternal health indicator for Fifth Millennium Development Goal (MDG) is reduction of maternal mortality ratio to less than hundred. Safe maternal health through ensuring whole gamet of quality reproductive services from early registration of ANC, Intra-natal care and post natal care. Currently Jehanabad MMR is 335 which is higher than current MMR of State 305. In FY 2012-13 We have targeted, it bring at 200. Objective to Reduce MMR 335 to 200 Strategy that should be Adopted to Achieve Target 1. To increase Antenatal check up. 2. To increase the consumption of 100 IFA tablets. 3. To reduce anaemia among pregnant mothers. 4. To increase institutional delivery. 5. To increase birth assisted by trained health personnel. 6. To increase the coverage of Post Natal Care. 7. To reduce the no. of unsafe abortions Activities—
· Strengthen VHSND Day through supportive supervision. · Monitoring chart should be made to insure monitoring. · Involvement of PRI members or those member of community who have worth in
society. · Improved Access of ANC Care · At HSC level ANC Check up should be insure through fixed day ANC check up day
and that should be monitored through Doctors, Block and District official by visit of HSC.
· Organizing RCH camp in each Block PHC areas. · Refresher training of ANMs on ANC care. · Proper maintenance of ANC Register and Eligible Couple Register. · To insure 24*7 Facility in at least one APHC at each Block. · To make available of equipments like BP Apparatus, Weighing Machines,
Heamoglobinometer etc to sub Centers. · Counselling of Mothers about ANC check up, where to go at the time of Delivery and
about Post Natal Care and appropriate complementary feeding (ACF). · Timely Purchase of IFA tablet and Distribution. · To make sure of Keeping Buffer Stock. · Awarness among villagers use of IFA Tablets Through ANM,ASHA.
- 44 -
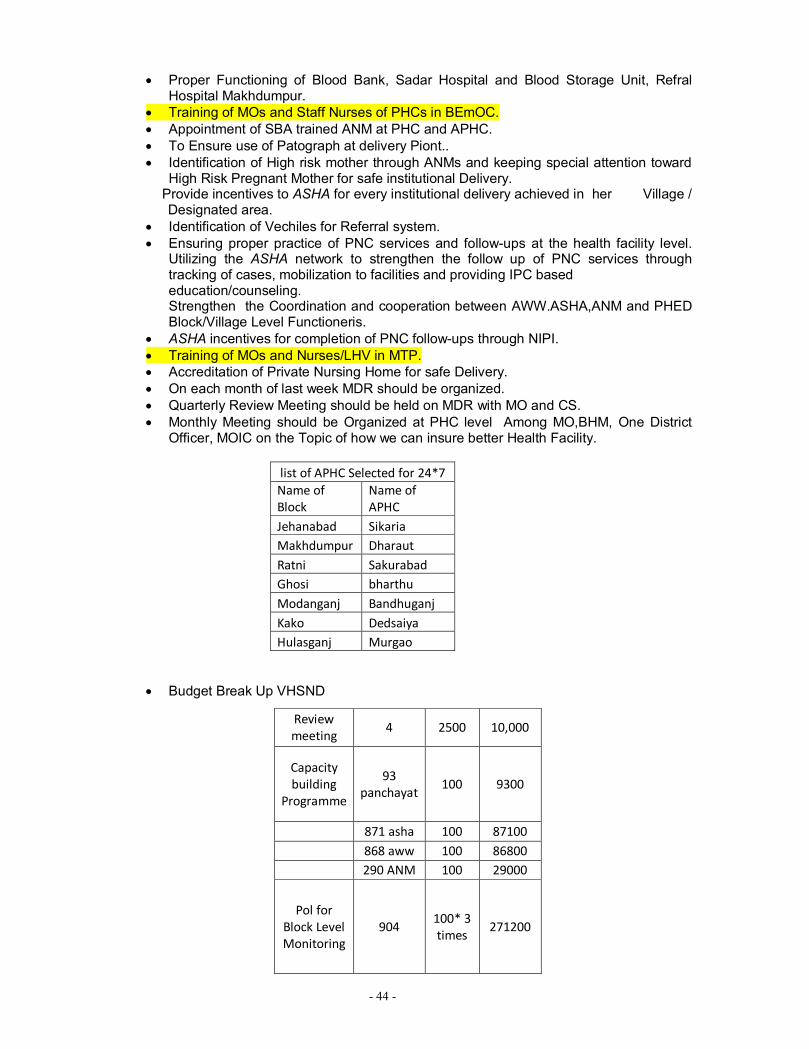
· Proper Functioning of Blood Bank, Sadar Hospital and Blood Storage Unit, Refral Hospital Makhdumpur.
· Training of MOs and Staff Nurses of PHCs in BEmOC. · Appointment of SBA trained ANM at PHC and APHC. · To Ensure use of Patograph at delivery Piont.. · Identification of High risk mother through ANMs and keeping special attention toward
High Risk Pregnant Mother for safe institutional Delivery. Provide incentives to ASHA for every institutional delivery achieved in her Village /
Designated area. · Identification of Vechiles for Referral system. · Ensuring proper practice of PNC services and follow-ups at the health facility level.
Utilizing the ASHA network to strengthen the follow up of PNC services through tracking of cases, mobilization to facilities and providing IPC based education/counseling. Strengthen the Coordination and cooperation between AWW.ASHA,ANM and PHED Block/Village Level Functioneris.
· ASHA incentives for completion of PNC follow-ups through NIPI. · Training of MOs and Nurses/LHV in MTP. · Accreditation of Private Nursing Home for safe Delivery. · On each month of last week MDR should be organized. · Quarterly Review Meeting should be held on MDR with MO and CS. · Monthly Meeting should be Organized at PHC level Among MO,BHM, One District
Officer, MOIC on the Topic of how we can insure better Health Facility.
list of APHC Selected for 24*7 Name of Block
Name of APHC
Jehanabad Sikaria Makhdumpur Dharaut Ratni Sakurabad Ghosi bharthu Modanganj Bandhuganj Kako Dedsaiya Hulasganj Murgao
· Budget Break Up VHSND
Review meeting
4 2500 10,000
Capacity building
Programme
93 panchayat
100 9300
871 asha 100 87100 868 aww 100 86800 290 ANM 100 29000
Pol for Block Level Monitoring
904 100* 3 times
271200

- 45 -
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost
Financial Requirement (in RS)
Committed Fund Required
A.1.1.1.2 Monitor Progress and Quality of Service Delivery
4 12500 50000
A.1.1.2 Operationalise 24*7 PHCs (MCH Centre- APHC)
7 25000 175000
A.1.1.5 Operationalise Sub Centres (MCH Centre- HSC)
2 50000 100000
A.1.3.1 RCH Outreach Camps/ Others
21 7000 147000
A.1.3.2 Monthly VHSND
904 4,93,400
A.1.4.1 Home Deliveries
300 500 150000
A.1.4.2.a Rural (Institutional Delivery)
23755 2000 4,75,10,000
A.1.4.2.b Urban (Institutional Delivery)
3224 1200 3,86,8800
A.1.4.2.C Institutional Deliveries C-section
260 1500 390,000
A.1.4.3 Administrative Expenses
324892
A.1.5 Maternal Death Review
200 750 150,000
Additional Budget
(A) Monitoring by MO Transportaion Expences to visit HSC on Fixed day in month three times at one HSC.
96 HSC* 3 Doctors*12 month
300 1,036,800
Total 54,395,892
Total 4,93,400

- 46 -
CHILD HEALTH
Introduction:---
The strategic approach for Child Health is reduction of neonatal and infant mortality, life cycle approach, improving service reach and coverage, inclusion of nutrition care in overall health care, skill building, public private partnership, inter-sectoral convergence, commoditization of services and effective IEC, BCC. Currently According to AHS 2010-11 IMR of Bihar is 55 while Jehanabad IMR is 53. In Financial year 2012-13 is has to bring upto 45. Neo Natal Mortality Rate of Bihar is 35 Jehanabad Neo Natal Mortality Rate is 31. In FY 2012-13 Target to Bring upto 20. Most deaths are caused by a few, preventable causes Three major causes contribute to 80% of deaths in the newborn period: Birth Asphyxia (inability to breathe well at birth), infections in the newborn and pre-maturity (being born before time). In addition, hypothermia (getting cold) contributes significantly. Most of these causes can be prevented or managed by a set of interventions delivered at household, community and health facility levels Inappropriate household practices increase the risk of newborn deaths. Besides the medical causes, certain practices at the household level increase the risk of deaths in the newborn period. Some of the key ones that are quiet prevalent in Jehanabad is : a) Delayed initiation of breastfeeding, breastfeeding is still delayed beyond the first hour, and in many cases beyond the first day. This increases the risk of dying by as much as 3 times. b) Delayed clothing and early bathing- babies are often not clothed adequately and bathed early: this increases the risk of baby getting cold (hypothermic) and subsequently dying. c) Not seeking care for newborns, babies are often not taken out of their households for first six weeks. This even applies for sick newborns, delaying seeking of appropriate care. d) Applying material on cord-stump-in many places, families put different material ranging from oil to cow-dung to the cord stump. This increases the risk of infection and sepsis among newborns. Strategy to Achieve the Target :--------
· Early initiation of breastfeeding: Initiation of breastfeeding within one hour of birth has been shown to improve newborn survival.
· Ensuring Warmth: Keeping babies warm at the time of birth improves newborn survival.
· Appropriate care of sick newborns at health facilities: When a newborn falls sick, she often requires specialized care at health facilities.
· Home visits to all newborns through IMNCI and through HBPNC Programme because of NIPI focus District.
· Strengthening PHCs for newborn care. · Special Care Newborn Units (SCNUs). · Reducing the load of Malnutritioned children through one more NRC.

- 47 -
· Micronutrient Management through initiation of ZINC Progamme.
Activities :-------
· To Ensure Early Breastfeeding through Mamta Health Worker. · Publication in News paper for generate awareness on Breastfeeding within one hour
of birth. · Vitamin A round to give micro nutrition. · Coordination with ICDS, PHED, local NGO, and Panchayti raj institution. · Joint meeting of MOIC,CDPO, Managers of Block for better implementation of
Programme. · Growth monitoring of Children and each quarter end Analysis of Data should be done
jointly with ICDS, Health Department. · Training to ASHA and AWW on Child growth measurement. · Insure to proper functioning and use of sick new born care in PHC. · To Start SNCU unit at District level. · To functioning of Newborn Stabilization Unit. · To make sure of Home visit by ASHA and AWW for Post Natal Care. · To conduct immunization session on fixed day for 100% coverage of Children. · Strengthen HMIS System to close monitoring and evaluation system on Child health
issue. · Increase strengthen ORS acceptance to stop Diarrhea. · New Building for NRC one for Sadar Hospital. · Organizing world breast feeding week and National Nutrition week as a part of theam
day at District,Block and HSC level with close coordination with ICDS and other Department.

- 48 -
A.2.7 Management of Childhood Diarrhea Through the Use of Zinc and ORS
District-Jehanabad
1. Introduction
India has a national policy for management of diarrhoea among children that recommends the use of Zinc tablets along with ORS in the treatment of diarrhoea as per the MOHFW, GoI directive dated 2nd Nov. 2006. A high-level meeting held under the chairmanship of Dr. M.K. Bhan, Secretary, Department of Biotechnology recommends for every case of diarrhoea, a dose of 20 mg/day for 14 days for children above age 6 months and 10mg/day for children aged 2-6 months.
The high-level committee recommendations emphasize that:
a) Zinc tablets should be available in all parts of the country including Anganwadicentres.. b) An effective communication strategy be put in place c) Health care providers including Anganwadi Workers and ASHAs are oriented and trained in the use of zinc along with ORS. 2. Situation Analysis:-
Indicator Jehanabad District
Bihar State
Source
Children suffered from Diarrhea in the last two weeks prior to survey (%)
7.0 12.1 DLHS-3
Children with Diarrhea in the last two weeks who were given treatment (%)
74.7 73.7 DLHS-3
Children with Diarrhea in the last two weeks who were received ORS (%)
13.6 22 DLHS-3
Women aware of ORS (%) 32.8 23.8 DLHS -3
IMR 53 55 Annual Health Survey,10-11
Under 5 Child Death 67 77 Annual Health Survey,10-11
3. Progress update and shortcomings during the current year (2011-12):
The HMIS data reveals that 3,323 cases of diarrhea and dehydration reported till the end of November 2011. However there is no data available with regard to the number of cases treated with ORS and Zinc.

- 49 -
The health and ICDS functionaries (MOs, CDPOs, LHVs, ANMs, Anganwadi Workers, ASHAs, BHMs, BCMs, Pharmacists, Staff Nurses) need to be trained on the childhood diarrhea management program using Zinc-ORS. Procurement of Zinc-ORS needs to happen at district-level and there is a need to ensure reporting of utilization of Zinc-ORS.
4. Plan of Action for 2012-2013:-
4.1 Specific Objectives (2012-13):
I) At least 1,19, 666 (50% of the total expected diarrheal cases in a year) childhood diarrheal episodes treated with ORS & Zinc through public health system (Sadar Hospital, PHCs, APHCs,HSCs, ASHAs and Anganwadi Workers)
II) At least 1, 19,666 numbers of Zinc syrup bottles and 2, 39,331 packets of ORS areprocured and distributed to AWWs, ASHAs, HSCs, APHCs, PHCs &Sadar Hospital. Population as per 2011 census
0-5 years Children (12.45% of the total population as per the CBR, Annual Health Survey, 10-11 for Jehanabad)
Expected yearly Childhood diarrheal cases (@1.71 per child/annual as per NCMH, 2005, GoI)
Target for 2012-13 (At least 50% cases will be reported and treated through public health system (At present 29% cases reported in public health system as per DLHS-3,India)
No. of bottles of Zinc Syrup to be procured for 12-13 (@ 1 bottle per episode)
No. of ORS packets to be procured for 12-13 (@ 2 packets per episode)
11,24,176 1,39,960 2,39,331 1,19,666 1,19,666 2,39,331
4.2 Implementation Strategies (2012-13):
· Procurement of Zinc Syrup & ORS packets at the district level. · Distribution of Zinc syrup & ORS packets to AWWs, ASHAs, HSCs, APHCs, PHCs &
District Hospital. · Ensure no stock-out of Zinc & ORS at all levels at all times · Training of all Medical Officers, CDPOs, ANMs, ICDS Supervisors, LHVs,
Pharmacists, Staff Nurses, BHMs, BCMs, AWWs, ASHAs on childhood Diarrhea management program and recording and reporting.
· Training of BCMs on supportive supervision and they will carry out supportive supervision visits to HSCs, AWCs, and ASHAs.
· Training of Data Entry Operators on recording and reporting. · Create awareness in the community about the importance of Zinc & ORS through
various BCC & Social Mobilization activities. · Celebrate important events like ORS-Zinc day/week · Quarterly review at district level under the chairmanship of DM/CS with key Health
and ICDS officials and quarterly review at block level under the chairmanship of MOIC with the presence of Health and ICDS officials.

- 50 -
· Monthly review meeting with BCMs on the supportive supervision visit findings at the district level and monitoring visits by DCM to BCMs during supportive supervision visits.
· Strong coordination with the development partners
4.3 Supports by other Development Partners (2012-13):-
Micronutrient initiative will provide the following support in 2012-13 to the district Jehanabad:
1) Techno-managerial support through the placement of Divisional Coordinator 2) Training of all Medical Officers, ANMs, Staff Nurses, ICDS Supervisors,
CDPOs,BHMs, BCMs, LHVs, Pharmacists, Staff Nurses, ASHAs and Anganwadi Workers on childhood diarrhea management program using Zinc and ORS.
3) Training of BCMs on supportive supervision and mobility support for supportive supervision visits by the BCMs
4) Distribution of Inter personal communication (IPC) tool kit and compliance card for counseling by ANMs, Anganwadi Workers and ASHAs
5) Training of Data Entry Operators on recording and reporting 6) Support in organizing district and block level review meetings. 7) Provide prototype soft copy of poster, wall painting, and display board. 8) Supply of printed recording and reporting formats and supportive supervision
checklists. 4.4 Following activities proposed under NRHM budget (2012-13):
· Procurement of Zinc Syrup (1,19,666) and ORS packets (2,39,331) for 1,19,666 diarrheal episodes
· Print and distribute posters and display boards at Sadar Hospital, PHCs, APHCs, HSCs, AWCs
· Mobility support for hiring vehicle for the distribution of Zinc and ORS from the district to block PHCs
· Undertake wall paintings in villages · Mobility support for DCM to carry out monthly monitoring visits · Monthly Review meeting of BCMs at the district level. · Celebrate ORS –Zinc day and week at the district and block levels
4.5 Estimated budget under NRHM for 2012-13:
Sl.No. Name of Activity Unit Cost (Rs.)
Unit No. Total Cost (Rs.)
1 Procurement
1.1 Zinc Sulphate Suspension (20mg/5 ml-100 ml bottle) 5.58 1,19,666 6,67,736.00
1.2 ORS Packet 2.29 2,39,331 5,48,067.00
Sub Total 12,15,803.00

- 51 -
2 Mobility Support
2.1 Hiring Vehicle for transportation of Zinc syrup and ORS from the district to PHCs 3000 07 21,000.00
2.2
Hiring vehicle for visit by DCM/DDA(ASHA) to blocks and field for monitoring supportive supervision visits undertaken by BCM(@4 visits/month)
1000 48 48,000
Sub Total 69,000.00 3 Review Meeting
3.1 TA to BCMs to attend the monthly review meeting at the district level (@Rs.150/- per BCM per month)
150 84 12,600
3.2
Provision of refreshment (working lunch) for monthly review meeting of BCMs at district level including logistics arrangements like hiring chairs etc.(@ Rs.100/- per BCM)
100 84 8400
Sub Total 21,000
3 BCC and Social Mobilization activities
3.1 Design and print poster on zinc-ors for Sadar Hospital (1), PHC(7), APHC (32), HSCs (92) & AWCs (1024)
25 1156 28,900.00
3.2 Design and Print Display Board for Sadar Hospital (1) and PHCs(7), APHCs (32), HSCs ( 92)
300 132 39,600.00
3.3 Wall Painting (4*4)(@ 2 numbers in HSC catchment villages)(92 HSC*2=184)(@Rs 12 per sqft)
192 184 35,328.00
Sub Total 1,03,828.00
4 Celebration of ORS-Zinc Week/Day at District and Block levels
4.1
Rallies and other mobilization activities at block PHCs (07) and district (1) (Drawing, prize banners, refreshment for rally, poster competition)
10,000 8 8,000.00
Sub Total 8,000.00
Grand Total 14,17,631.00
Vitamin A Round:-------
· Two Times Round in year. One in June month second round in December 2012. · Jehanabad have around 160,000 target Children. · District Level Meeting before round and after round.
Vitamin A Round
Activity unit unit cost total Budget
DCC meeting 2 5000 10,000 Review
Meeting at District level after around
2 5000 10,000
BCC meeting 7*2 1000 14,000 Vtamin A syp 3520*2 40.32 2,83,853 Training for
Vaccinator at Block level
1100*2 25 55,000

- 52 -
Honorium for Additional site
Vaccinator 50*2 150 15,000
Total 3,87,853
Budget break up NRC NRC
running cost
3,61,000*12 month
43,32,000
Training of ANMs and
local Supervisor on NRC of
two focused
Block
70 participants*100
7000
Training of ASHA/AWW
of Two focused
block
300 participants*100
30000
Annual Maintance
Cost 1,03,535 1,03,535
Total 44,72,535
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
A.2.1.1 Implementation of IMNCI activities in districts
50000
A.2.2 New Born Stabilization Unit
1 7,75,000 7,75,000
A.2.6 Management of Diarrhoea, ARI and micronutrient malnutrition (NRC)
1 44,72,535 44,72,535
Innovation A.2.6 a Zinc ORS
programme 14,17,631
b. Promotion/ senitization programme on world breast
1* 2 event 7*2 event 96* 2 event
50000 10000 1000
100000 140000 192000
- 53 -
feeding week and National Nutrition week at District Block HSC level
A.2.7 Vitaming A round
2 Round 193926 387852
Total 6760018
‘

- 54 -
FAMILY PLANNING
Introduction:---
As we see the Data of District Health Society reported by PHCs. The total Data of Family Planning till November 2011 is 2076 while according to Population of Jehanabad census 2011 (1124176), We have to Achieve 1 % of total Population that is 11241. Its showing the only achievement of only 18.46% (till NOV.2011), which is poor condition. For better motherhood condition it is essential to be three years Gaps between children. So there is need to give more emphasis on family planning operation and using other method of Spacing. As total fertility rate of Bihar is 3.8 (source SRS 2008).
The Goal of Jehanabad is to Achieve the Target of Family Planning and more use of Spacing method.
Strategy:-------
· To achieve Target of Family Planning Operation at least 60% of Target. · More involvement of Male Participation in Family Planning Operation. · More focus on use of Contraceptive Pills, condoms, and IUD insetion. · Monitor of ensure to provide Quality services. · Focus on IEC display to generate awareness among communities. · Formation of Family Planning Cells at district and Block level comprises a team
member in the chairmanship of DM. Activities:---
· Organize RCH camp at HSC level. · In month at least two Family Planning Camp should be Organized. · Counselling session before Camp in concern area with high involvement of Doctors
and Block Team, after counseling session on the spot registration for Family Planning operation by help of ASHA, AWW,ANM.
· IEC display on family planning in surrounding. · Social Marketing on Contraceptive Pills, Condom through ASHA. · At Urban and Rural areas shop availability for Oral Pills and Condoms distribution. · Flex Banner on small family Benefit in villages. · Training on IUD insertion to ANMs. · Minilap training to MOs. · Incentive distribution to motivator and beneficiary.
INNOVATION-------------------
· Community debate competition one in month in Panchayat wise in presence of PRI member or the person who have worth among villagers.
· Counselling on family Planning Method to SHG and Mahila Mandal with the cooperation of ICDS and Women Development corporation (WDC).

- 55 -
· Micro plan preparation on Debate competition to each Block and involvement of Block and District officials and Doctors with Prize Distribution.
· Family Planning cell Member would be as: District Level— Chairman – District Magistrate. Members- Civil Surgeon, ACMO, DPM,DS, One Hospital Manager, M& E officer,DPO ICDS, Medical officer- 3 ( highly preferable Surgeon.) Block level Team--- Chairman— Pramukh of Block Members--- MOIC, Medical Officer- 3, CDPO, BHM, BCM,JCHM Health Educator, One ANM, one Block Based NGO. Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
A.3.1.1 Dissemination of Manuals on Sterilization Standers & QA of sterilization services
20000
A.3.1.2 Female Sterilization Camps
216 5000 10,80,000
A.3.1.3 NSV Camps 4 5000 20000
A.3.1.4 Compensation for Female Sterilization
6000 1000 60,00,000
A.3.1.5 Compensation for Male Sterilization
744 1500 1116000
A.3.1.6 Accreditation of Private Providers for sterilization services
1000 1500 1,500,000
A.3.3 POL for Family Planning
119000
A.3.5.4 Provide IUD services at
28 camps for Block.
1500 42000
- 56 -
Health Facility (IUD camps)
1 mega camp for District
2000
2000
Innovation
Prize for Debate competition
93 panchayat
500 46500
Total 9,945,500
ARSH
Adolescent Reproductive And Sexual Health programme is very important aspect of district. If we analyse the data of Adolescent, jehanabad has around 2 lakh school going children. On the basis of census 2011 Total women population of jehanabad is 537974 and Adolesecent Girls Population is around 16.75% of Total Women Population after calculation Around 90111 Adolescent Girls. For School going children there health check up is making them aware about there health condition. School Health programme name is now Nayi Pidi Sawasth Guarnatee Yojana. For Adoloscent Girls Weekly IFA Supplement Programme will Help in Preparing for future mother.
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
A.4.2 School Health Programme
15,00,000
Weekly IFA Supplementation Programme
90111 52 tabs/year per girls* RS 0.105
4,92,006
Training of ANM,ASHA,AWW
290 ANM
871 ASHA
868 AWW
Total 2029
70 1,42,030

- 57 -
Budget for Social Mobilization and IEC, BCC material
868 AWC
96 HSC
Total 964
50 48,200
A.7.2 PNDT Sex Ratio 1 1,00,000 1,00,000
Total 22,82,236
Infrastructure (Minor Civil Works) Human Resource (Except Ayush)
The Human Resource condition of the District is as:----
Human Resource (contract)
S.NO Name of post Total No
1 Surgeons 0
2 Obstetricians/ Gynecologist 0
3 No of Physicians 0 4 No of Pediatricians 0 5 Anaestheatist 0 6 Eye Surgeon 0 7 Pharmacist 0 8 Lab Technician 17 9 Radiographer 0
10 Female Docotor 0
11 Block Extension Educator 0
12 O.T. Assistant 0 13 Health Educator 0
14 Health Assistant (Male) 0
15 Medical Officer 30
16 Health Assistant (F)/ LHV 0

- 58 -
Human Resource (Regular)
S.NO Name of post Total No
1 Surgeons 2
2 Obstetricians/ Gynecologist 4
3 No of Physicians 2 4 No of Pediatricians 2
17 ANM 139 18 Staff Nurse 39
- 59 -
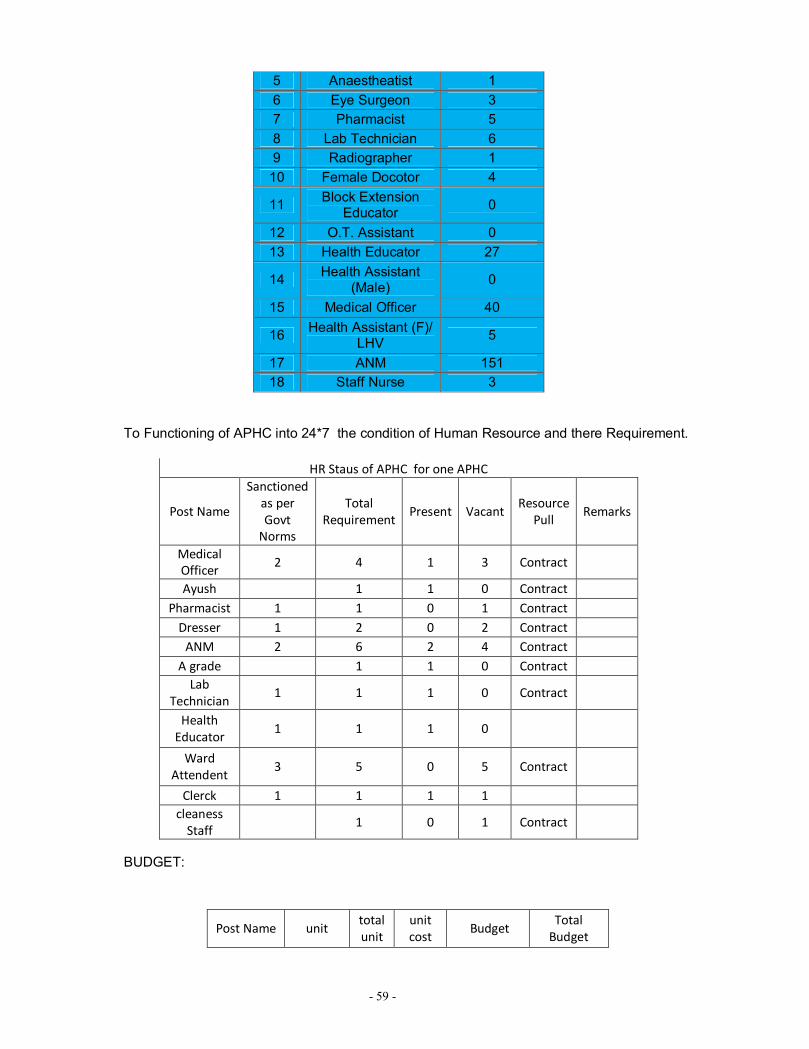
5 Anaestheatist 1 6 Eye Surgeon 3 7 Pharmacist 5 8 Lab Technician 6 9 Radiographer 1
10 Female Docotor 4
11 Block Extension Educator 0
12 O.T. Assistant 0 13 Health Educator 27
14 Health Assistant (Male) 0
15 Medical Officer 40
16 Health Assistant (F)/ LHV 5
17 ANM 151 18 Staff Nurse 3
To Functioning of APHC into 24*7 the condition of Human Resource and there Requirement.
HR Staus of APHC for one APHC
Post Name
Sanctioned as per Govt
Norms
Total Requirement
Present Vacant Resource
Pull Remarks
Medical Officer
2 4 1 3 Contract
Ayush 1 1 0 Contract Pharmacist 1 1 0 1 Contract
Dresser 1 2 0 2 Contract ANM 2 6 2 4 Contract
A grade 1 1 0 Contract Lab
Technician 1 1 1 0 Contract
Health Educator
1 1 1 0
Ward Attendent
3 5 0 5 Contract
Clerck 1 1 1 1 cleaness
Staff 1 0 1 Contract
BUDGET:
Post Name unit total unit
unit cost
Budget Total
Budget

- 60 -
BUDGET
FMR Code Budget Head
Physical Target (where
Applicable)
Unit Cost
Financial Requirement
(in RS)
Committed Fund
Required
A.8.1.1
ANMs, Staff Nurses,
Supervisory Nurses (salary
Contractual ANM/Contractual
SN)
A Grade 39 22000*12 10296000 858000
ANM 139 12650*12 21100200 1758350
A.8.1.2 Laboratory
Technicains in Blood Banks
3 11000*12 396000
A.8.1.5
Medical Officers at CHCs/ PHC
(Salary of Mo in Blood Banks)
1 35000*12 420000 35000
Medical Officer
3*7 APHC
21 30,000 6,30,000*12
month 75,60,000
Pharmacist 1*7APHC 7 12,000 84000*12
month 10,08,000
Dresser 2* 7
APHC 14 8,000
1,12,000*12 month
13,44,000
ANM 4*7
APHC 28 11,500
3,22,000*12 month
38,64,000
ward Attendent
5* 7 APHC
35 6,000 2,10,000*12
month 25,20,000
cleaness Staff
1* 7 APHC
7 5,000 35,000*12
month 4,20,000
Total 1,67,16,000

- 61 -
A.8.1.7
Others- Computer
Assistants/ BCC Co-ordination etc (FP Counsellors)
1 15000*12 180000
A.8.1.8
Incentive / Awardws etc. to
SN,ANMs etc.(Muskaan Programme- incentive to
ASHA and ANM
871 200*3 time 522600
Innovation
HR Requiremet
for 7 APHC Functioning
1,67,16,000
Total 49,630,800
2651350
Training
If we Analyze the Training Situation of District. We need more SBA trained ANM. To reduction of MMR and IMR relates with Training condition of Health Functioneries. Training Condition of District. Medical officers and Staff Nurses require BEmOC Training. They also Require MTP training. Budgetary Proposal:

- 62 -
FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost
Financial Requirement (in RS)
Committed Fund Required
A.9.3.1 Skilled Attendance at Birth
10 batch 88110 881100
A.9.3.7 Other MH training (any Integrated training,etc)
2 115000 230000
A.9.5.1 IMNCI 33 batches 2 TOT, 2 Follow up supervision
134760 159600 54860
4447080 319200 109720
A.9.5.5.3 NSSK Training 4 52900 211600
A.9.6.2 Minilap Training 1 70237 70237
A.9.6.4.1 Training of Medical Officers in IUD insertion
1 55300 55300
A.9.6.4.2 Training of ANMs/LHVs/SN in IUD Insertion
3 29425 88275
A.9.8.2 DPMU Training 1 50000 50000
Mamta Training 59 participants
48,785
Total 65,11,297
Programme /NRHM Management Costs
Programme Management is the one of important aspect of District Health Scoiety. The whole Programme implementation exist on DPMU and BPMU. At District level District Programme Manager, District Account Manager, District Planning Coordinator, M&E Officer, DCM (ASHA),DDA (ASHA), DCHM (NIPI), Epidemiologist, DDA (IDSP),DEO (IDSP),Assistant, Assistant (Account), Data operator is Present. While At Block level/ Sadar Hospital/ Refral Hospital has Hospital Manager, Block Health Manager, Block Account Manager, Block Community Mobilizer( ASHA), JCHM (NIPI)

- 63 -
is present. These personal require training and Skill Upgradation Session. We have experienced Managers.
· Beside these all things District Needed Physical and Financial Audit. · Quarterly Review meeting on How target can be Achieved. · Monthly Review meeting at District and Block Level in the Presence Civil surgeon. · Mobility Support for DPMU for supportive Supervision. · Provision of Ranking and according to Rank Reward provision. · Legal Advisor Provision on Call according to actual expense
Name of Post unit Cost Total
cost per month
Remarks
Assistant/Data Entry
Operator 2 12,000 24,000
Office Assistant
(Accounts) 1 12,000 12,000
Office Assistant
1 12,000 12,000
other expense (legal Advisor
Also) 57,000 57,000
There should be uniformity
in salary of
Assistant Grade and it should be similar to Block Account
Manager.
Total 1,05,000
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
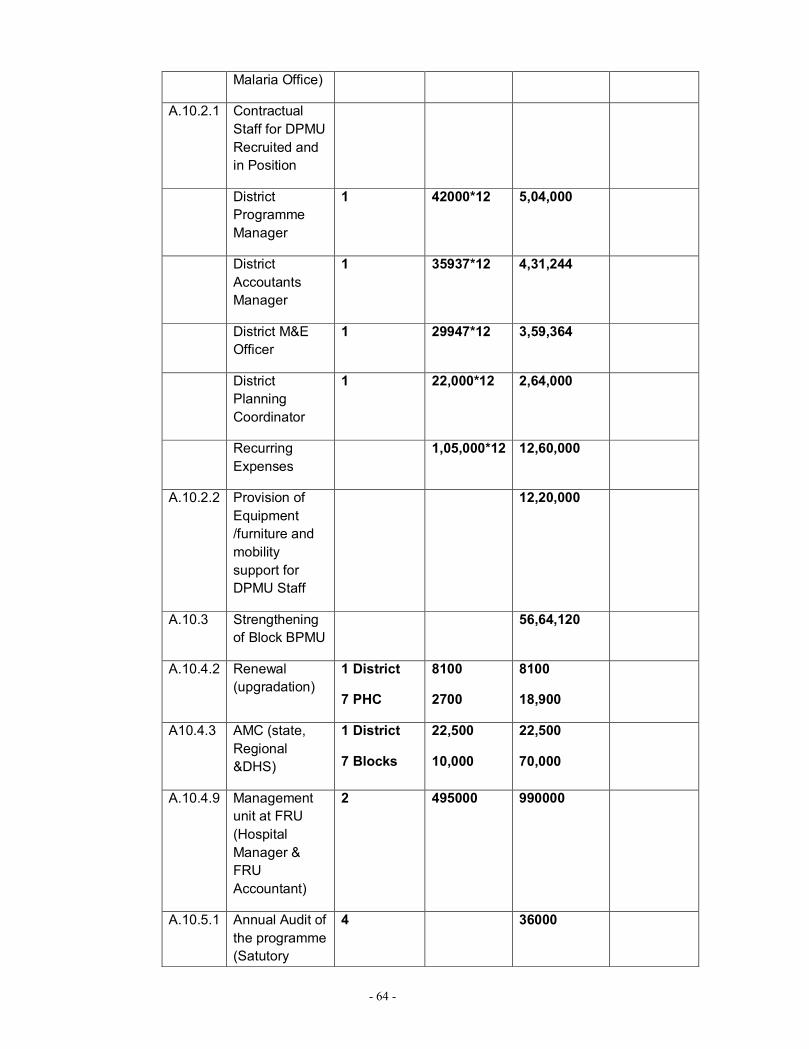
A.10.1.5 Mobility Support (District
180000
- 64 -
Malaria Office)
A.10.2.1 Contractual Staff for DPMU Recruited and in Position
District Programme Manager
1 42000*12 5,04,000
District Accoutants Manager
1 35937*12 4,31,244
District M&E Officer
1 29947*12 3,59,364
District Planning Coordinator
1 22,000*12 2,64,000
Recurring Expenses
1,05,000*12 12,60,000
A.10.2.2 Provision of Equipment /furniture and mobility support for DPMU Staff
12,20,000
A.10.3 Strengthening of Block BPMU
56,64,120
A.10.4.2 Renewal (upgradation)
1 District
7 PHC
8100
2700
8100
18,900
A10.4.3 AMC (state, Regional &DHS)
1 District
7 Blocks
22,500
10,000
22,500
70,000
A.10.4.9 Management unit at FRU (Hospital Manager & FRU Accountant)
2 495000 990000
A.10.5.1 Annual Audit of the programme (Satutory
4 36000
- 65 -
Audit)
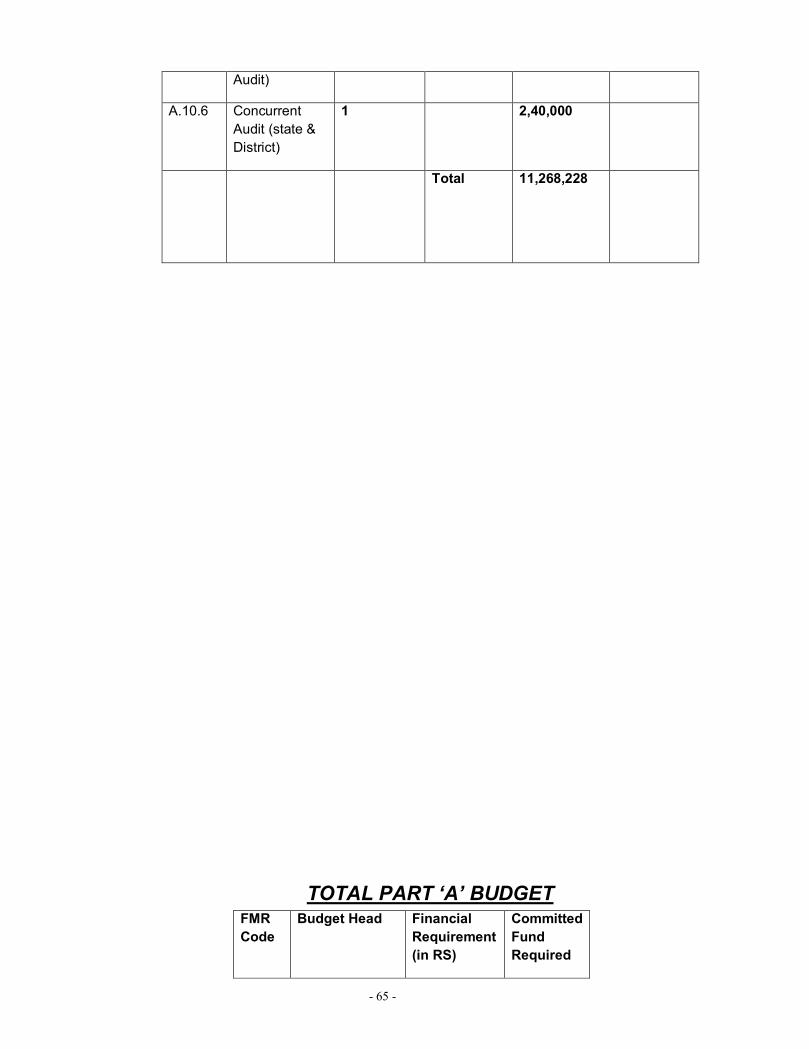
A.10.6 Concurrent Audit (state & District)
1 2,40,000
Total 11,268,228
TOTAL PART ‘A’ BUDGET FMR Code
Budget Head Financial Requirement (in RS)
Committed Fund Required

- 66 -
A.1 Maternal Health
54,395,892
A.2 Child Health 67,60,018
A.3 Family Planning
9,945,500
A.4 ARSH 22,82,236
A.8 Infrastructure (Minor civil Works) & Human Resources (Except Ayush)
49,630,800 26,51,350
A.9 Training 65,11,297
A.10 Programme/ NRHM Management Costs
11,268,228
Total 14,07,93,971
26,51,350

- 67 -
CHAPTER 4
NRHM PART”B”
About ASHA One of the key components of the National Rural Health Mission is to provide every village in the country with a trained female community health activist?? ASHA? or Accredited Social Health Activist. Selected from the village itself and accountable to it, the ASHA will be trained to work as an interface between the community and the public health system. Following are the key components of ASHA:

- 68 -
ASHA must primarily be a woman resident of the village? Married/ widowed/ divorced, preferably in the age group of 25 to 45 years.
She should be a literate woman with formal education up to class eight. This may be relaxed only if no suitable person with this qualification is available.
ASHA will be chosen through a rigorous process of selection involving various community groups, self-help groups, Anganwadi Institutions, the Block Nodal officer, District Nodal officer, the village Health Committee and the Gram Sabha.
Capacity building of ASHA is being seen as a continuous process. ASHA will have t undergo series of training episodes to acquire the necessary knowledge, skills and confidence for performing her spelled out roles.
The ASHAs will receive performance-based incentives for promoting universal immunization, referral and escort services for Reproductive & Child Health (RCH) and other healthcare programmes, and construction of household toilets.
Empowered with knowledge and a drug-kit to deliver first-contact healthcare, every ASHA is expected to be a fountainhead of community participation in public health programmes in her village.
ASHA will be the first port of call for any health related demands of deprived sections of the population, especially women and children, who find it difficult to access health services.
ASHA will be a health activist in the community who will create awareness on health and its social determinants and mobilise the community towards local health planning and increased utilisation and accountability of the existing health services. She would be a promoter of good health practices and will also provide a minimum package of curative care as appropriate and feasible for that level and make timely referrals.
ASHA will provide information to the community on determinants of health such as nutrition, basic sanitation & hygienic practices, healthy living and working conditions, information on existing health services and the need for timely utilisation of health & family welfare services.
She will counsel women on birth preparedness, importance of safe delivery, breast-feeding and complementary feeding, immunization, contraception and prevention of common infections including Reproductive Tract Infection/Sexually Transmitted Infections (RTIs/STIs) and care of the young child.
ASHA will mobilise the community and facilitate them in accessing health and health related services available at the Anganwadi/sub-centre/primary health centers, such as immunisation, Ante Natal Check-up (ANC), Post Natal Check-up supplementary nutrition, sanitation and other services being provided by the government.
She will act as a depot older for essential provisions being made available to all habitations like Oral Rehydration Therapy (ORS), Iron Folic Acid Tablet(IFA), chloroquine, Disposable Delivery Kits (DDK), Oral Pills & Condoms, etc.
At the village level it is recognised that ASHA cannot function without adequate institutional support. Women?s committees (like self-help groups or women?s health committees), village Health & Sanitation Committee of the Gram Panchayat, peripheral health workers especially ANMs and Anganwadi workers, and the trainers of ASHA and in-service periodic training would be a major source of support to ASHA.

- 69 -
ROLES & RESPONSIBILITIES ASHA will be a health activist in the community who will create awareness on health and its social determinants and mobilize the community towards local health planning and increased utilization and accountability of the existing health services. She would be a promoter of good health practices. She will also provide a minimum package of curative care as appropriate and feasible for that level and make timely referrals. Her roles and responsibilities would be as follows: Ø ASHA will take steps to create awareness and provide information to the community on determinants of health such as nutrition, basic sanitation & hygienic practices, healthy living and working conditions, information on existing health services and the need for timely utilization of health & family welfare services. She will counsel women on birth preparedness, importance of safe delivery, breastfeeding and complementary feeding, immunization, contraception and prevention of common infections including Reproductive Tract Infection/Sexually Transmitted Infection (RTIs/STIs) and care of the young child. Ø ASHA will mobilize the community and facilitate them in accessing health and health related services available at the village/sub-center/primary health centers, such as Immunization, Ante Natal Check-up (ANC), Post Natal Check-up (PNC), ICDS, sanitation and other services being provided by the government. Ø She will work with the Village Health & Sanitation Committee of the Gram Panchayat to develop a comprehensive village health plan.
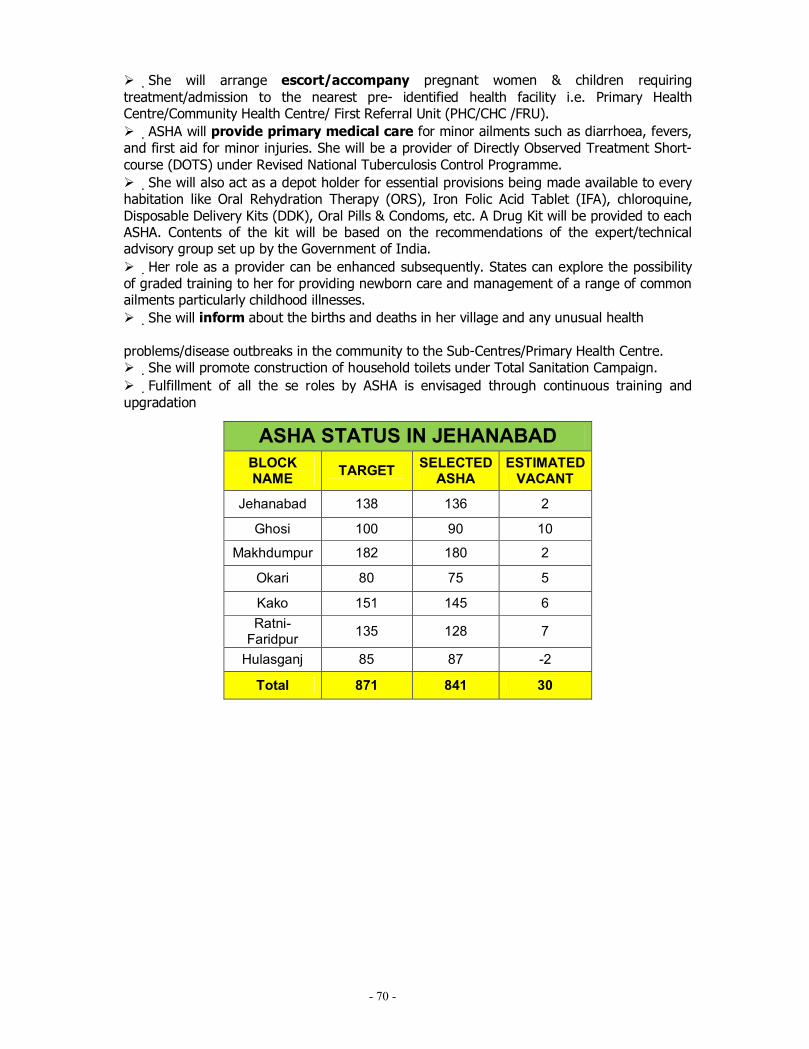
- 70 -
Ø She will arrange escort/accompany pregnant women & children requiring treatment/admission to the nearest pre- identified health facility i.e. Primary Health Centre/Community Health Centre/ First Referral Unit (PHC/CHC /FRU). Ø ASHA will provide primary medical care for minor ailments such as diarrhoea, fevers, and first aid for minor injuries. She will be a provider of Directly Observed Treatment Short-course (DOTS) under Revised National Tuberculosis Control Programme. Ø She will also act as a depot holder for essential provisions being made available to every habitation like Oral Rehydration Therapy (ORS), Iron Folic Acid Tablet (IFA), chloroquine, Disposable Delivery Kits (DDK), Oral Pills & Condoms, etc. A Drug Kit will be provided to each ASHA. Contents of the kit will be based on the recommendations of the expert/technical advisory group set up by the Government of India. Ø Her role as a provider can be enhanced subsequently. States can explore the possibility of graded training to her for providing newborn care and management of a range of common ailments particularly childhood illnesses. Ø She will inform about the births and deaths in her village and any unusual health problems/disease outbreaks in the community to the Sub-Centres/Primary Health Centre. Ø She will promote construction of household toilets under Total Sanitation Campaign. Ø Fulfillment of all the se roles by ASHA is envisaged through continuous training and upgradation
ASHA STATUS IN JEHANABAD BLOCK NAME TARGET SELECTED
ASHA ESTIMATED
VACANT
Jehanabad 138 136 2
Ghosi 100 90 10
Makhdumpur 182 180 2
Okari 80 75 5
Kako 151 145 6 Ratni-
Faridpur 135 128 7
Hulasganj 85 87 -2
Total 871 841 30

- 71 -
Budgetary Proposal
FMR Code
Budget Head
Physical Target (Where
Applicable)
Unit Cost
Fund Required
Committed Expenditure
B. 1.1.1 Asha Training 871 5100 44,42,100
B.1.1.2 Asha Drug kit
& Replenishment
871 250 2,17,750
B.1.1.3 Asha Divas 871 100 10,45,200
B.1.1.4.A Awards to Asha/ link 7 2000 14,000
2nd prize 7 1000 7,000 Worker 7 500 3,500
certificate Printing 21 250 5250
B.1.1.4.C Asha Identity Card 871 30 26,130
B.1.1.5 Asha Rsource centre DCM salry 1 22,000 2,64,000 DDA salary 1 18,150 2,17,800 BCM salary 7 13,200 11,08,800 Office expenditure T.A 7 1000 84000
mobile Recharge 2 300 7200
Internet Recharge 1 750 9000
BCM meeting Snacks 12 month 300 3600
Total 74,55,330

- 72 -
Untied Funds
Untied funds of Sadar Hospital, Refrral Hospital, Primary Health Centre, APHC, HSC, Village Health Sanitation Committee is used but problem occure in HSC and VHSC untied fund.
Activities proposed:----
· Calling PRI member for meeting on making awareness on Untied fund expenditure. · At block level training of ANM on Cash Book Management. · Monthly meeting between VHSC member on HSC.
Detail of Village Health Sanitation Committee Block Wise Name of Block – Okari
SNO Name of VHSC No of
Revenuue Village
Name of Mukhiya (President)
Mobile No Name of ANM
(Secretary) Mobile no
1 Okari 8 Shyamnandan Sharma 9431617368 Sarsawati Kumari 7654398629 2 Jaitipur Kurua 6 Naresh Bind 9801746472 Manju Devi 9576270601
3 Saristabad 6 Tulshi Kumar Albela 8809036672 Kumari Premlata
sinha 9955279500
4 Niama 8 Raj kishor Prasad 7739113917 Chinta Kumari 9955004106 5 Bandanduganj 7 Pritima Devi 9801510979 Kamla Kumari 8873074048
6 Gandhar 8 Shailesh Kumar
Ambedkar 9973163880 Kumari Manju Sinha 9430606079
7 Dewra 5 Kamlesh Devi 9973715992 Saroj Kumari 9525352384 8 Modanganj 6 Neha Sharma 9934235933 Durgawati Devi 9006238971 54

- 73 -
NAME OF BLOCK-- Jehanabad
SNO Name of VHSC No of
Revenuue Village
Name of Mukhiya (President)
Mobile No Name of ANM
(Secretary) Mobile no
1 Sewnan 6 Manju Kumari Sinha 8797299575 SANTOSH KUMARI 9507208874
2 Pandui 5 Pratima Devi 9955627630 GITA PRASAD SINGH 8434601606
3 Kalpa 4 Binay Kumar 9572228555 ANJU KUMARI 9279770173
4 Jamuk 7 Madan Kumar 9631624500 LILA SINHA 9430009521
5 Sikariya 9 Prabha Devi 8809252202 MANORMA KUAMRI 8434364157
6 Muther 6 Sanjay Singh 9263453500 SUSHILA KUMARI 9576149502
7 Nauroo 5 Sumantri Devi 9431830163 SNJOG KUMARI 9973592479
8 Gonwan 8 Belmanti Devi 9546516788 SUSHILA KUMARI 9386278983
9 Larsa 8 Dhannajay Kumar 9906376865 SRI KUMARI 9931935011
10 Amain 11 Sumitra Devi 9661241280 USHA KUMARI 9431618167
11 Mandil 6 Savitri Devi 9771879313 SHAIL KUMARI 9801398127
12 Bhawanichak 8 Rama Yadav 9955500784 SILA KUMARI 9931182972
13 Mandebigha 9 Tej Pratap Singh 9934634797 KRI. KIRAN SINGH 9931226417
14 Kinari 7 Arun Singh 8809256824 SUNAINA KUMARI 9934835807
Total 99
NAME OF BLOCK-- Makhdumpur
SNO Name of VHSC No of
Revenuue Village
Name of Mukhiya (President)
Mobile No Name of ANM
(Secretary) Mobile no
1 Bela Bira 6 Abhiram Paswan 9771854848 Bimala Sinha 9708984870 2 Solhanda 6 Saroj Devi 9771994104 Dayamanti Kumari 3 Rampur 4 Awadesh Sharma 9470851905 Meena Devi 9430841306 4 Bhaikh 3 Siyaram Prasad 9934621731 Shashikala Kumari 5 Darnai 5 Ajay Yadav 9934414377 Indu Kumari 8083385654 6 Kachnama 7 Ashok Kumar 9263675431 Anita Kumari 7677274664 7 Chariyari 6 Omprakash Singh 9431830378 Kalayani Kumari 9934485447 8 Pundha 11 Nirmala Devi 9801707913 Sarshawati Devi 9905487227
9 Kumardih 6 Asha Devi 9931878131 Binita Kumari
10 Manjhosh 5 Sunita Devi 9934103908 Pramila Devi 11 Kohara 4 Usha Devi 9934811871 Manju Devi 12 Paschim Saren 1 Sunita Devi 7739664914 Rina Kumari 13 Purvi Saren 6 Nirmala Devi 8298704877 Sita Devi 9708829804 14 Sugao 2 Lakhichand Yadav 9939988804 Madhuri Pandey 15 Kalanaur 6 Dukhanram 7250085634 Shakuntala Devi 9835343753 16 Makarpur 6 Abhiyanta Kumari 9162854521 Rina Kumari 8002670214 17 Dakara 7 Sushma Kumari 9006836931 Chinta Devi 9234665515 18 Dharaut 3 Mahendra Manjhi 9525887515 Shashikala Kumari 19 Malathi 8 Ramanand Manjhi 9576009517 Shakuntala Devi 9835343753 20 Sumera 4 Dayanand Prasad 9934907245 Lalti Kumari 9525426458 21 Jagpura 8 Israt Khan 9308002599 Sanju Kumari 9135092477 22 Jamanganj 4 Shivpujan Yadav 8521868191 Rita Kumari 9097932421
118
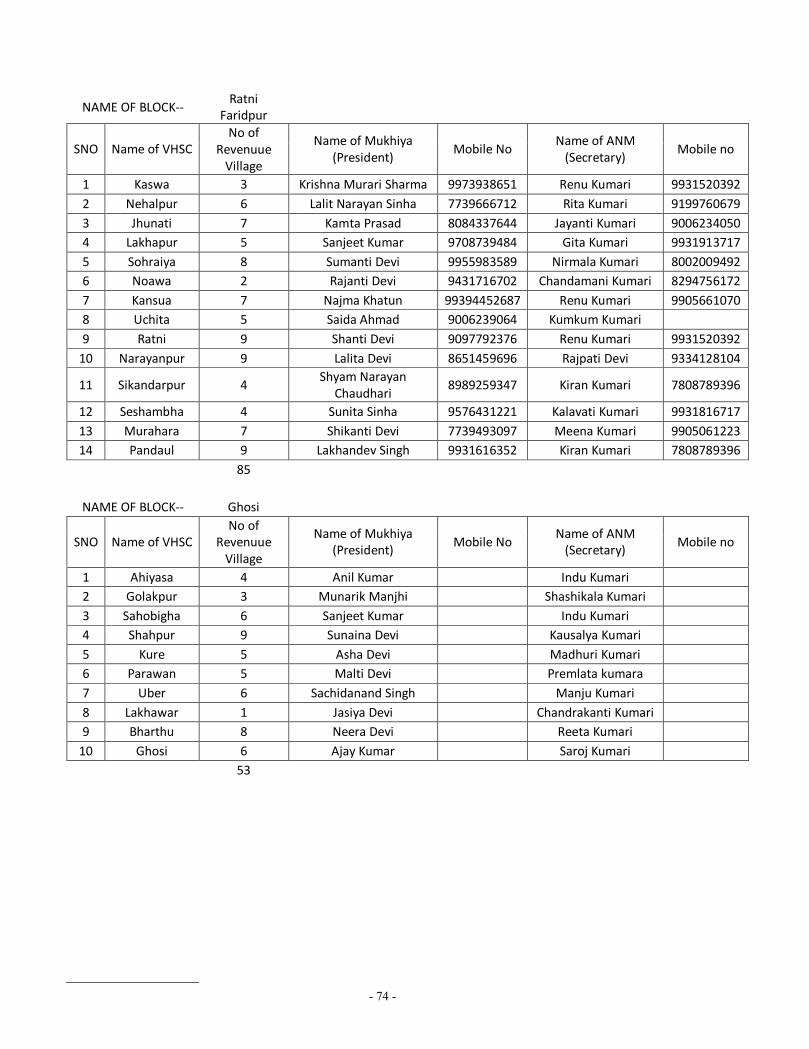
- 74 -
NAME OF BLOCK-- Ratni
Faridpur
SNO Name of VHSC No of
Revenuue Village
Name of Mukhiya (President)
Mobile No Name of ANM
(Secretary) Mobile no
1 Kaswa 3 Krishna Murari Sharma 9973938651 Renu Kumari 9931520392 2 Nehalpur 6 Lalit Narayan Sinha 7739666712 Rita Kumari 9199760679 3 Jhunati 7 Kamta Prasad 8084337644 Jayanti Kumari 9006234050 4 Lakhapur 5 Sanjeet Kumar 9708739484 Gita Kumari 9931913717 5 Sohraiya 8 Sumanti Devi 9955983589 Nirmala Kumari 8002009492 6 Noawa 2 Rajanti Devi 9431716702 Chandamani Kumari 8294756172 7 Kansua 7 Najma Khatun 99394452687 Renu Kumari 9905661070 8 Uchita 5 Saida Ahmad 9006239064 Kumkum Kumari 9 Ratni 9 Shanti Devi 9097792376 Renu Kumari 9931520392
10 Narayanpur 9 Lalita Devi 8651459696 Rajpati Devi 9334128104
11 Sikandarpur 4 Shyam Narayan
Chaudhari 8989259347 Kiran Kumari 7808789396
12 Seshambha 4 Sunita Sinha 9576431221 Kalavati Kumari 9931816717 13 Murahara 7 Shikanti Devi 7739493097 Meena Kumari 9905061223 14 Pandaul 9 Lakhandev Singh 9931616352 Kiran Kumari 7808789396
85
NAME OF BLOCK-- Ghosi
SNO Name of VHSC No of
Revenuue Village
Name of Mukhiya (President)
Mobile No Name of ANM
(Secretary) Mobile no
1 Ahiyasa 4 Anil Kumar Indu Kumari 2 Golakpur 3 Munarik Manjhi Shashikala Kumari 3 Sahobigha 6 Sanjeet Kumar Indu Kumari 4 Shahpur 9 Sunaina Devi Kausalya Kumari 5 Kure 5 Asha Devi Madhuri Kumari 6 Parawan 5 Malti Devi Premlata kumara 7 Uber 6 Sachidanand Singh Manju Kumari 8 Lakhawar 1 Jasiya Devi Chandrakanti Kumari 9 Bharthu 8 Neera Devi Reeta Kumari
10 Ghosi 6 Ajay Kumar Saroj Kumari 53

- 75 -
Name of Block- Kako
SNO Name of VHSC No of
Revenuue Village
Name of Mukhiya (President)
Mobile No Name of ANM
(Secretary) Mobile no
1 Paschimi Kako 1 Renu Kumari Manju Kumari Sinha 2 Maniyawa 6 Aditya Kumar Vaijanti Kumari 3 Purvi Kako 1 Survila Kumari Pratima Kumari 4 Nonhi 5 Sikandra Prasad Kiran kumara 5 Khalispur 4 MD. Idris Radha Kumari 6 Sulemanpur 11 Yogendra Paswan Sadhana Kumari 7 Bhadauna 10 Anita Devi Dharmashila Kumari 8 Barawa 8 Usha Devi Rashmi Ranjan 9 Uttarserthu 5 Ranjay Kumar Singh Manisha Kumari
10 Saidabad 4 Rekha Devi Meena Kumari 11 Damuha 7 Shashi Bhushan Prasad Renu Kumari 12 Nerthua 5 Tilak Chauhan Renu Bharti 13 Pinjoura 8 Surjmani Devi Usha Kumari 14 Dedsaiya 7 Rakesh Kumar Meera Kumari Bharti 15 Bara 5 Ganga Sagar Urmila Devi 16 Amthua 8 Pramila Devi Pravila Kumari
95
NAME OF BLOCK-- Hulasganj
SNO Name of VHSC No of
Revenuue Village
Name of Mukhiya (President)
Mobile No Name of ANM
(Secretary) Mobile no
1 Murgao 4 Sumintra Devi 8809221323 Rita Sinha 9955052328 2 Kokarasa 5 Vijay Bind 9162144700 Kanti Devi 9608285046 3 Keur 5 Kamlesh Prasad 9572010409 Manju Kumari 9608771040 4 Tira 6 Puja Devi 9006934792 Reeta Devi 9955052230 5 Dawathu 5 Umashankar Sharma 9934240667 Unil Kumari 9955131972 6 Bauri 6 Ravikant Sharma 88098544875 Savitri Devi 9631288474 7 Surajpur 4 Kapil Paswan 9507099210 Sunita Sinha 8873710467 8 Chiri 7 Madhuri Devi 9006029448 Malti Devi 9570696125 9 Khudauri 6 Bhibha Devi 9931215804 Malti Kumari 9934513156 48

- 76 -
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B.2.1 Untied Fund for SDH/CHC
2 50000 1000000
B.2.2.a Untied Fund for PHCs
9 25000 225000
B.2.2 b Untied fund for APHCs
32 25000 800000
B.2.3 Untied fund for sub centre
96 10000 960000
B.2.4 Untied fund for VHSC
552 10000 5520000
Total 8505000

- 77 -
Annual Maintenance Grants
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B.3.1 CHC (Referral Hospital)
2 3,00,000 6,00,000
B.3.2 Annual Maintenance Grant for PHCs
7 2,00,000 14,00,000
B.3.2.a Annual Maintenance Grant for APHCs
32 1,00,000 32,00,000
B.3.3 Annual Maintenance Grant for Sub Centre
96 25,000 24,00,000
Annual Maintance Grants For DH
1 5,00,000 5,00,000
Total 81,00,000

- 78 -
Hospital Strengthening
In financial year 2012-13 proposal of construction of HSC, APHC, NRC building Sadar Hospital Up gradation as are:
NAME OF BLOCK JEHANABAD
NAME OF SCHEME PARTICULARS NO OF UNITS
UNIT COST
TOTAL Assumed FUND Reqrired (lakh)
Cosntruction of PHC one more building
required on the above of build building
1 20
Renovation of PHC Renovation of Shabha
Ghar 1 9
Cosntruction of HSC 0 0 Renovation of HsC 0 0
Construction of APHC Kalpa ( Land Available) 1 75.99 75.99
Chainpura (Land
Available) 1 75.99 75.99
Mandil (Land Available) 1 75.99 75.99 Bistaul 1 75.99 75.99 land Reqrired 1acre 20 20
Renovation of APHC 0 0 Total 352.96
Construction of the
Building of Sadar Hospital Central Registration Hall 1 5
NRC Building 1 30
MO Quarter Multistorage
18 100
Staff Quarter Multi
Storage 30 200
DS Quarter 1 50 CS Quarter 1 60 New Building For Indoor 1 100
Renovation of the Building of Sadar Hospital
Renovation of Main Building
1 50
Total 595

- 79 -
Name of Block Kako
NAME OF SCHEME PARTICULARS NO OF UNITS
UNIT COST
TOTAL FUND REQURED (lakh)
Cosntruction of PHC Asha Rest Room 1 5 Male ward Room 1 10 Office 1 5
Quarter mo Multi
Storage 4 5 20
Quarter Staff Multi
Storage 6 5 30
Renovation of PHC 0 0 Cosntruction of HSC Barawa 1 9.5 9.5
Pinjaura 1 9.5 9.5 Asiyawa 1 9.5 9.5 Purvi Kako 1 9.5 9.5 Pashchami Kako 1 9.5 9.5 Bibipur 1 9.5 9.5 Land for ALL 6 6 3 18
Renovation of HSC Uttar Serthu Major
repairing 3
Safepur ( Baundary
wall) 2
Ainwa (Major Repairing) 3
Hatee ( Major
Repairing) 3
Emaliya (Baundary) 2 Bembhai (Baundary) 2 Nonhi (Baundary wall) 2
Choti Murari (Baundary
Wall) 2
Construction of APHC Ali Nagar Pali 1 75.99 75.99
Renovation of APHC Bhelawar (Major
Repairing) 1 6 6
Kajisariya (major
Repairing) 1 6 6
Dedsaiya ( Major
Repairing) 1 6 6
Total 257.99

- 80 -
Name of Block Ghosi
NAME OF SCHEME PARTICULARS NO OF UNITS
UNIT COST
TOTAL FUND REQURED (lakh)
Cosntruction of PHC Women ward 1 10 baundary Wall 1 15 Indoor Building 1 15
Quarter mo ( Multi
Storage) 2 10
Quarter Staff ( Multi
Storage) 8 18
Rogi Sade 1 5 meeting Hall 1 5
Renovation of PHC 0 0 0 0 Cosntruction of HSC Dhuriyari 1 9.5 9.5
Lakhawar 1 9.5 9.5 Ahiyasa 1 9.5 9.5 Saho Bigha 1 9.5 9.5 Uber 1 9.5 9.5 Land for All 5 Hsc 5 2 10
Renovation of HSC 0 0 Construction of APHC Nandana 1 75.99 75.99
Kora 1 75.99 75.99 Sonwa 1 75.99 75.99 Lakhawar 1 75.99 75.99 Land For all 4 APHC 4 5 20
Construction of Incomple referral Hospital
0 0
Total 459.46
Name of Block Hulasganj
NAME OF SCHEME PARTICULARS NO OF UNITS
UNIT COST
TOTAL FUND REQURED (lakh)
Cosntruction of PHC 0 0 Renovation of PHC 0 0
Cosntruction of HSC Khudauri (land Available but controversial)
1 9.5 9.5
Adrakhi bigha 1 9.5 9.5 land for one Hsc 1 2 2
Renovation of HSC Murgao 1 3 Construction of APHC Murgao (land Available) 1 75.99 75.99
Keur 1 75.99 75.99 Land for 1 APHC 1 5 5 Total 180.98

- 81 -
Name of Block Okari
NAME OF SCHEME PARTICULARS NO OF UNITS
UNIT COST
TOTAL FUND REQURED (lakh)
Cosntruction of PHC MO Quarter Multistorage
7 30
Quarter Staff (Multi
Storage) 10 50
Renovation of PHC Repairing of Old
Building 1 8
Cosntruction of HSC Naima 1 9.5 9.5 Modanganj 1 9.5 9.5 Land for 2 Hsc 2 2 4
Renovation of HSC Dewara Minor 1 1 Aarhit Major 1 3 Saistabad Minor 1 1 Muriya Bigha Major 1 3 Baina Minor 1 1 Sakrautha minor 1
Construction of APHC Bandhuganj Land
Available 1 75.99 75.99
Jalalpur Land Available 1 75.99 75.99 Total 272.98
Name of Block Ratni Faridpur
NAME OF SCHEME PARTICULARS NO OF UNITS
UNIT COST
TOTAL FUND REQURED (lakh)
Cosntruction of PHC Quarter MO (Multi
Storage) 2 15
Quarter Staff ( Multi
Storage) 6 30
Sakurabad Meeting Hall 1 5 Renovation of PHC Old building Sakurabad 1 6
Cosntruction of HSC Dhanadihri 1 9.5 9.5 sarta 1 9.5 9.5 Pokhawa 1 9.5 9.5 Ratni-bazar 1 9.5 9.5 Kundila 1 9.5 9.5 Sohriya 1 9.5 9.5 Murhara land Available 1 9.5 9.5 land for all 6 6 2 12
Construction of APHC Nehalpur 1 75.99 75.99 Lakhapur 1 75.99 75.99 Uttarapati 1 75.99 75.99 Pandual 1 75.99 75.99 Kaswa 1 75.99 75.99

- 82 -
Noawa 1 75.99 75.99 land for all 6 6 5 30 Total 620.44
Name of Block Makhdumpur
NAME OF SCHEME PARTICULARS NO OF UNITS
UNIT COST
TOTAL FUND REQURED (lakh)
Cosntruction of PHC 0 0
Renovation of PHC Renovation of PHC
Building 1 5
Cosntruction of HSC Newari 1 9.5 9.5 suppi 1 9.5 9.5 shekhpura 1 9.5 9.5 tilkai 1 9.5 9.5 Makarpur 1 9.5 9.5 Sugao 1 9.5 9.5 Nawabganj 1 9.5 9.5 Mahamatpur 2 1 9.5 9.5 Machil 1 9.5 9.5 Land for all 9 9 2 18
Renovation of HSC Ikil (Baundary Wall) 1 3 Sumera (Major) 1 3 Dhoda (minor) 1 1 Umta (Minor) 1 1 Vishunganj (Minor) 1 1
Construction of APHC Sagarpur land avialble 1 75.99 75.99 Chatiyana land available 1 75.99 75.99 Tehta 1 75.99 75.99 Saren 1 75.99 75.99 land for 2 aphc 2 5 10 Total 431.46
Grand Total 6322.54
Quarters for Medical officers and Staffs.

- 83 -
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B.4.3 Sub Centre Rent and Contingencies
36 500 2,16,000
B.5.2 b
Construction of Residential quarters for Doctors and Staff nurses
15 45,000,00
B.5.2 c Strengthening of Cold Chain
800000
Construction, Renovation of PHC,APHC,HSC,SD (fund Demanded through District PIP- through DM Office)
6322.54 (Lakh) proposed Budget
Bihar Govt.
B.5.2.a
Construction of APHC
2 75.99lakh
88,20,000
Construction of HSC
6 9.50 lakh 22,80,000
Total 5,516,000
1,11,00,000

- 84 -
CORPUS GRANTS TO RKS
Rogi Kalyan Samiti is operational in District Hospital, All Referral Hospital, All PHCs. In APHC RKS Registration done account opening is in process. In FY 2012-13 Special attention toward Strengthening of APHC RKS Functioning, so that we could make possible to provide 24*7 Services at APHCs.
Activities:---
· Timely Meeting of RKS.
· Change of Membership after completion of time period of 3 year.
· Insure presence of Member in RKS meeting.
· RKS members Joint Meeting with District Official in the Chairmanship of District Magistrate.
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B.6.1 District Hospitals
1 500000 500000
B.6.2 CHCs (RH) 2 100000 200000
B.6.3 PHCs 7 100000 700000
B.6.4 Others (APHCs) 32 100000 3200000
Total 4,600,000

- 85 -
District Action Plans (including Block, Village)
To Keeping the view of Decentralization Plan preparation of District is directed throw bottom down to top up. Now plan is prepared first on village then at HSC, that is compiled in Block Plan finally District Plan Prepared and send to state for further process. Now District has Strategic Planning Expert District Planning Coordinator. District need strengthen Planning Process. FY 2012 -13 has target of 25 villages Plan, 92 HSC plan, 7 Block Health action Plan.
Activities:--
· Capacity Building workshop to all ASHA, AWW, ANM, Block and District officer on Planning with the Help of State, so that it could be strengthen.
· One full time vehicle hiring for DPC for supportive supervision.
· One Data operator to strengthen Planning Cell.
· Orientation to all PRI members for important role in Planning Process at HSC and at Village level Planning.
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B.7 District Action Plans (including Block, Village)
96 HSC
25 village
7 PHC
1 DHAP
1 Data Operator
1500
1000
5000
50,000
6000
1,44,000
25000
35000
50,000
72,000
Total 3,26,000

- 86 -
Panchayati Raj Initiative
Panchayati Raj Initiative is one the important aspect of Strengthening of NRHM Goal. We could access Complete Health Package for Villagers. A common efforts of All department including Panchayati Raj reduce MMR,IMR others Health target. Prosperity of Villagers would be Better after involvement of PRI Members.
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost
Financial Requirement (in RS)
Committed Fund Required
B8.1 Constitution and orientation of Community leader & of VHSC, CHC,PHC,SHC etc.
93 1500 139500
B.8.2 Orientation workshops, trainings and capacity Building of PRI at State/ District Health Societies,CHC,PHC
102 606 61812
Total 201,312
Mainstreaming of AYUSH
Jehanabad has 27 AYUSH Doctors. They all are Posted at APHC. There is Challangeous Task of Mainstreaming of AUSH Doctors.
Activities:---
· Orientation of AYUSH Doctors.
· Fixed Day Counselling session at APHC to Villagers twice in Week for use of Home made Treatment/ Natural Therapy.
· At school level visit Of AYUSH Doctors to Teach Children on use of local/ Natural Resources for better Health condition.
· Regular Drug Supply for AYUSH.

- 87 -
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B.9.1 a AYUSH Specialists
27 20,000 64,80,000
Total 64,80,000
IEC-BCC NRHM
IEC-BCC Activities has deep impression on Community and Villagers. The condition of IEC Activity in District is not good as it should be. So In FY there is Need on Focus on IEC activities as:--
Activities:--
· Miking at Block and Village level.
· Wall writing and Flex ,VHDND,FP, other Health Programme.
· One Big Hording at Block PHC,and at all APHC.
· Quarterly BCC Campaign with Help of other Partner Agencies.
· Organizing Health Mela.
· Publication in Newspaper during Breast feeding week about benefit of Breastfeeding to children.
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B10.1 Development and operationalize of State BCC/IEC Strategy
1400000
B 10.3 Health Mela 2 5000 10000

- 88 -
(Leprosy)
Total 1410000
Mobile Medical Units (including Recurring expenditure)
MMU fit for Jehanabad Naxal Affected area. The Out reach area where People have Problem to Communicate nearest Health Facilities. There MMU is helpful. The Monitoring Aspect of MMU is week. There is Need of special Focus on Monitoring Aspect so we could reach Quality service of MMU to Villagers.
Activities:--
· Microplan Preparation of MMU Visit.
· Monitoring chart preparation at Block and District level.
· Identification of One Nodal Officer at District and at Block Level.
· Assurance of Quality Service Delivery through MMU.
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B.11 MMU 1 4212000
Micro plan Preparation at District and at Block Level with Monitoring Chart
7 1500 10,500
Total 42,22,500

- 89 -
Referral Transport
Ambulance status of Jehanabad
Sno Name of Facility Ambulance
1 Sadar Hospital,Jehanabad
Tata Winger- 2, Red Cross - 1, 108
ambulance
2 PHC, Jehanabad Red Cross- 1
3 PHC, Ratni Faridpur Maruti Eco-1
4 Referral Hospital, Makhdumpur Maruti Eco-1
5 PHC, Hulasganj Red Cross- 1
6 PHC, Okari Maruti Eco-1
7 PHC, Ghosi Maruti Eco-1 8 PHC, kako Red Cross- 1
9 Referral Hospital, Ghosi Nil
· To convert 24*7, Seven APHC require one Ambulance at each centre.
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B.12.2.d 102 Ambulance Service
7 (APHC) 15000*12 1,260,000
B.12.2.c 108 ambulance
1 1,716,000
B.12.2.c BLS Ambulance
8 1,16,700*12 11,203,200
Total 1,41,79,200

- 90 -
PPP/NGOs
The above Data reveals that in PHC Ghosi, Ratni faridpur have not Radiology facility.
And in 7 APHC In FY 2012-13 have to start Pathology Service.
7 silent Gensate for APHC & Dietry Provision at APHC.
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B.13.3.b Outsourcing of Pathology and Radiology Services from PHCs to DH
14 4,500,000
B.13.3.d IMEP (Bio Waste Management)
13 1,104,000
District Health Society,Jehanbad Pathology and Radiology Status
Pathology unit/ Collection
Centre Radiology Unit
Sl.No Facility Name
Govt. Private Govt. X-ray
Private X-ray
Private Ultra
sound
Remarks
1 Sadar
Hospital Yes Yes Yes Yes Yes
2 Kako No Yes No Yes No 3 Ghosi Yes Yes No No No 4 Ghosi Refral Yes NO Yes No No
5 Makhdumpur Yes Yes No Yes No
6 Ratni
Faridpur No Yes No No No
7 Hulasganj No Yes No Yes No
8 Okari/
Modanganj No Yes No Yes No
9 Sadar Block Jehanabad
No Yes No No No

- 91 -
Pathological Services for APHC
7 300,000
Outsourcing of Silent Gensate of 5 KV
7 RS 150 *24 hrs *30 days*12 month
9,072,000
Outsourcing of dietry Provision at APHC
7 RS 50*5 patient* 30 days *12 month
6,30,000
Total 1,56,06,000
INNOVATIONS Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B.14.b Yukti Yojana Accreditation of Public and Private Sector For Providing Safe Abortion Services
304 103166
Total 103166

- 92 -
Monitoring and Evaluation Programme implementation then Monitoring and Evaluation of the Programme is one of important aspect of the District. Expected Outcome will come after Supportive Supervision and taking remedial Action.
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B.15.3.1.a State, District , Divisional, Block Data Centre
9 10,000*12 1,080,000
B.15.3.2.a MCTS and HRIS
6 186433
B.15.3.2.b RI Monitoring 7 130000
B.15.3.3.b Plan for HMIS supportive Supervision and Data Validation
182000
Total 15,78,433
Procurement
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B.16.1.1 Procurement of Equipment : (MH Labour Room)
11 167,464 1842104

- 93 -
B.16.1.2 Procurement of equipment : CH (SCNU &NBCC ,icu
For ICu Equipment
49,00,000
B.16.1.3.a Procurement of Minilap Set :FP
35 3000 105000
B.16.1.3.b Procurement of NSV Kit (FP)
5 1100 5500
B.16.1.3.c Procurement of IUD Kit (FP)
1 15,000 15,000
B.16.2.1.A Parental Iron sucrose (IV/IM) as therapeutic measure to pregnant women with severe Anemia
1 7,00,000 7,000,00
B.16.2.1.B IFA Tablets for Pregnant & Lactating Mothers
800000
B.16.2.2.a IFA small Tablets and syrup for children 6-59 months
1,000,000
B.16.2.2.b IMNCI Drug kit 2400 250 6,00,000
B.16.2.5 General Drugs & Supplies for Health Facilities
12400000
Total 22,367,604
- 94 -
Support Services
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
B.22.4 Support Strengthening RNTCP
79,200
B.23.A Payment of Monthly Bill to be BSNL
29,964
Total 1,09,164
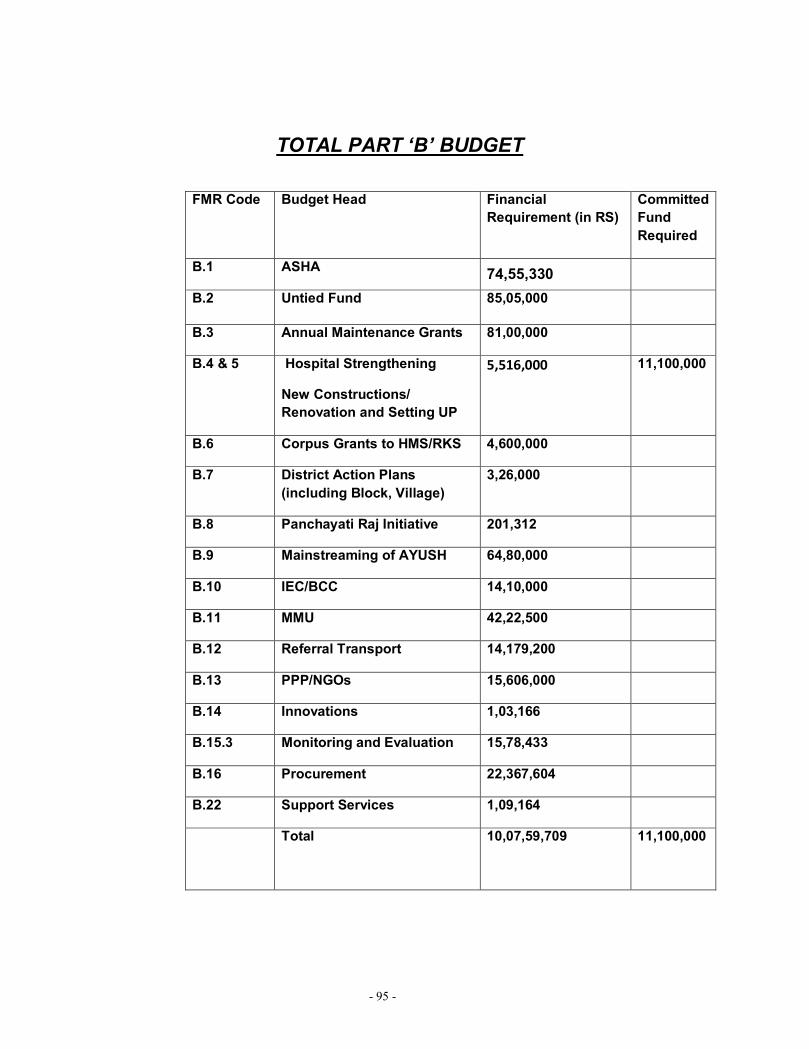
- 95 -
TOTAL PART ‘B’ BUDGET
FMR Code Budget Head Financial Requirement (in RS)
Committed Fund Required
B.1 ASHA 74,55,330
B.2 Untied Fund 85,05,000
B.3 Annual Maintenance Grants 81,00,000
B.4 & 5 Hospital Strengthening
New Constructions/ Renovation and Setting UP
5,516,000 11,100,000
B.6 Corpus Grants to HMS/RKS 4,600,000
B.7 District Action Plans (including Block, Village)
3,26,000
B.8 Panchayati Raj Initiative 201,312
B.9 Mainstreaming of AYUSH 64,80,000
B.10 IEC/BCC 14,10,000
B.11 MMU 42,22,500
B.12 Referral Transport 14,179,200
B.13 PPP/NGOs 15,606,000
B.14 Innovations 1,03,166
B.15.3 Monitoring and Evaluation 15,78,433
B.16 Procurement 22,367,604
B.22 Support Services 1,09,164
Total 10,07,59,709
11,100,000

- 96 -
CHAPTER 5
NRHM PART “C”

- 97 -
Routine Immunization & PP
Objective:- To Achieve 100% Coverage.
Gaps: --
· Lack of Drug of Trivalent for OPV.
· Require New Cold Chain Room At District level for better Management of Logistic.
· Specail Genset Require 10 kv for Cold Chain.
· Require Automatic ILR- 1 * 7 PHC = 7
4 ILR for District
Activities:--
· Refreshment Training to all MOIC, BHM, MO on RI.
· RI Micro plan Preparation.
· Regular incentive Payment to all ASHA, ANM.
· Additional session plan and manpower for 100% coverage.
· Supportive supervision and RI Monitoring.
· Additional Manpower required for Additional Session Plan.
· Specail attention toward low coverge Blocks.
·

- 98 -
Budgetary Proposal: FMR Code
Budget Head Physical Target (where Applicable)
Unit Cost Financial Requirement (in RS)
Committed Fund Required
C. RI 3,364,153
Pulse Polio
9,45,914
Total 3,364,153 9,45,914
- 99 -
CHAPTER 6
NRHM PART “D - I”

- 100 -
Integrated Disease Surveillance Project (IDSP)
(Use of revised guidelines subject to approval of restructuring and extension of IDSP project)
DSU IDSP JEHANABAD

- 101 -
INTEGRATED DISEASE SURVEILLANCE PROJECT (IDSP)
BACKGROUND:
The Government of India has initiated a decentralized, state based Integrated Disease
Surveillance Project (IDSP) in the country in response to a long felt need expressed by
various expert committees. The project would be able to detect early warning signals
of impending outbreaks and help us to initiate effective response in a timely manner. It
is also expected to provide essential data to monitor progress of ongoing disease
control programs and help to allocate health resources more optimally.
The project is assisting the State to:
¨ Surveillance of limited number of health conditions / diseases and risk factors;
¨ strengthen data quality, analysis and links to action;
¨ Improve laboratory support;
¨ Train stakeholders in disease surveillance and action;
¨ Coordinate and decentralize surveillance activities;
¨ Integrate disease surveillance at the state and district levels, and involve communities
and other stakeholders, particularly the private sector.

- 102 -
Original Project Development objectives (PDOs) and scope
The original project development objective was to improve the information available to the government health services and private health care providers on a set of high priority diseases and risk factors, with a view to improving the on the ground responses to such diseases and risk factors.
The five year project (launched in 2004) was to support the longer-run program to consolidate and integrate disease surveillance in the country. The new integrated disease surveillance system was to put greater emphasis on building the links between the collection and analysis of information and the actual on the ground interventions (medical or otherwise) by the public and private sectors. The long run goal was to effect a complete shift from the present centrally driven, fragmented disease surveillance system, to an integrated disease surveillance and control program coordinated by the center but fully implemented by the States, districts and communities.
The project was to assist the Government of India and the States and Union Territories to:
· Surveil a limited number of health conditions and risk factors; · Strengthen data quality, analysis and links to action; · Improve laboratory support; · Train stakeholders in disease surveillance and action; · Coordinate and decentralized surveillance activities; · Integrate disease surveillance at the State and district levels, and involve
communities and other stakeholders, particularly the private sector.
3. Proposed changes in the restructured project
3.1 Modified Project Development Objectives (PDO) for 2010-2012:
To support the first phase of India's long run vision to improve and integrate disease surveillance compliant with the IHR 2005 requirement by:
I. Supporting a nation-wide effort for surveillance preparedness for immediate reporting of outbreaks, regular surveillance and weekly reporting with emphasis on provisional diagnosis by medically trained staff from public and private sectors to generate early warning signals for appropriate and timely public health actions.
II. Demonstrating establishment and operation of decentralized surveillance
systems meeting performance standards (timeliness, improved quality of outbreak investigation including mobilizing the human and other appropriate samples for confirming the diagnosis by laboratory network, Strengthening analysis and use of surveillance data and response) in at least 9 Indian States, viz. Tamil-Nadu,Karnataka, Gujarat, Punjab, West Bengal, Andhra Pradesh, Rajasthan, Maharashtra and Uttarakhand.
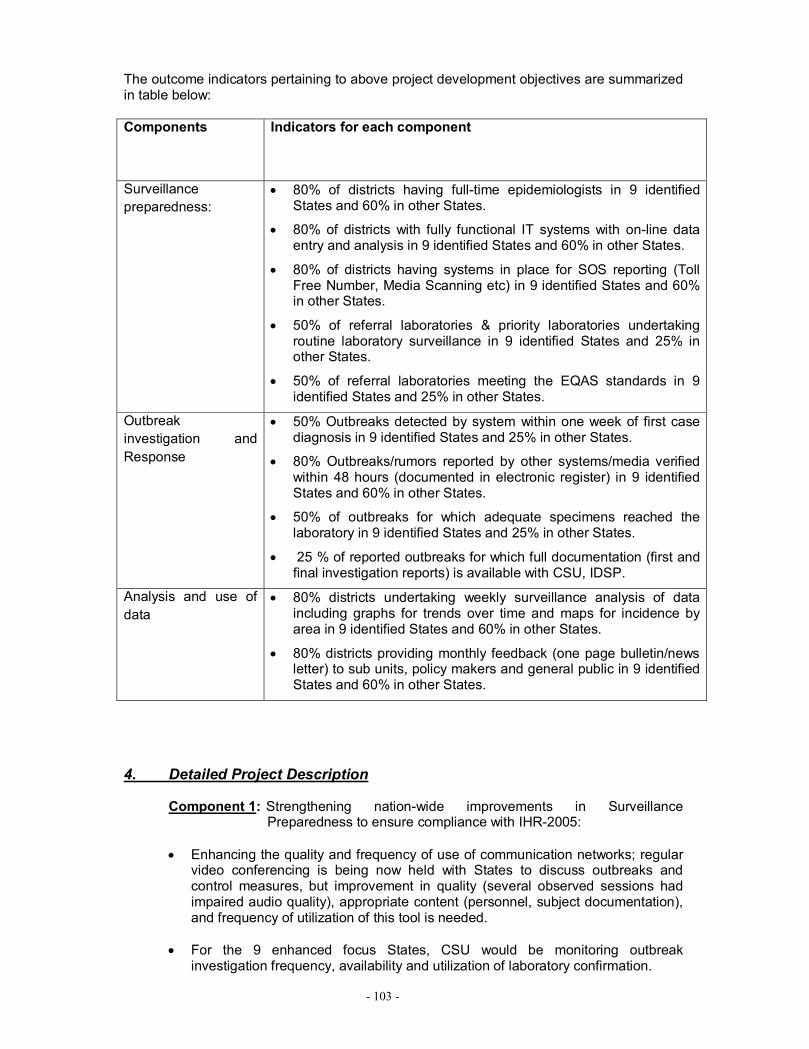
- 103 -
The outcome indicators pertaining to above project development objectives are summarized in table below:
Components Indicators for each component
Surveillance preparedness:
· 80% of districts having full-time epidemiologists in 9 identified States and 60% in other States.
· 80% of districts with fully functional IT systems with on-line data entry and analysis in 9 identified States and 60% in other States.
· 80% of districts having systems in place for SOS reporting (Toll Free Number, Media Scanning etc) in 9 identified States and 60% in other States.
· 50% of referral laboratories & priority laboratories undertaking routine laboratory surveillance in 9 identified States and 25% in other States.
· 50% of referral laboratories meeting the EQAS standards in 9 identified States and 25% in other States.
Outbreak investigation and Response
· 50% Outbreaks detected by system within one week of first case diagnosis in 9 identified States and 25% in other States.
· 80% Outbreaks/rumors reported by other systems/media verified within 48 hours (documented in electronic register) in 9 identified States and 60% in other States.
· 50% of outbreaks for which adequate specimens reached the laboratory in 9 identified States and 25% in other States.
· 25 % of reported outbreaks for which full documentation (first and final investigation reports) is available with CSU, IDSP.
Analysis and use of data
· 80% districts undertaking weekly surveillance analysis of data including graphs for trends over time and maps for incidence by area in 9 identified States and 60% in other States.
· 80% districts providing monthly feedback (one page bulletin/news letter) to sub units, policy makers and general public in 9 identified States and 60% in other States.
4. Detailed Project Description
Component 1: Strengthening nation-wide improvements in Surveillance Preparedness to ensure compliance with IHR-2005:
· Enhancing the quality and frequency of use of communication networks; regular
video conferencing is being now held with States to discuss outbreaks and control measures, but improvement in quality (several observed sessions had impaired audio quality), appropriate content (personnel, subject documentation), and frequency of utilization of this tool is needed.
· For the 9 enhanced focus States, CSU would be monitoring outbreak
investigation frequency, availability and utilization of laboratory confirmation.

- 104 -
· Further training for district epidemiologists and data managers on use of the
portal (and confirming and enhancing portal functioning) will provide needed analytic capacity at the district level.
· With the approval of modified P and L forms for IDSP, there would be definite
improvement in quality and timeliness of reporting. New P and L forms were uploaded in portal. The rollout of the new forms to the States and districts were done.
Component 2: Demonstrating timeliness and improved quality of outbreak
investigation and response in all States: · The CSU would expand the variables collected systematically in the Outbreak
Reporting System. CSU would also continuously monitor the data collected by this system, and work with States and districts if the CSU identify evident problems with timeliness of reporting, laboratory confirmation, and appropriate interventions will be ensured.
· The 1075 call centre will be publicized to health professionals, and would
particularly serve as an important supplement source of information and outbreaks in areas where surveillance infrastructure is yet to develop.
· Similarly, the media scanning service would be useful for all these States, but
may be particularly important as a supplement in areas where surveillance infra-structure is still under-development.
· The CSU would establish real time collaboration modalities between the newly
recruited epidemiologists and National/ State Microbiologists/ State laboratory coordinators.
· Outbreaks reported and responded by IDSP system would be subjected to competency assessment tool developed for this purpose.
· Medical colleges would be involved in disease surveillance and reponse Component 3: Strengthening analysis and use of surveillance data in 9
States that achieved surveillance preparedness demonstrating quality data analysis and assessing analytic quality of outbreak investigations:
· Epidemiologists in CSU would formally review a sample of outbreaks reported
using the suitably adapted assessment tool created for the outbreak investigation module.
· CSU epidemiologists would undertake analyses of IDSP data to better
understand data contained in the system. · Effective communication of key findings and issues to IDSP sub-units, State and
national policy leaders, and as appropriate, to the public. To facilitate this, the NCDC requires support from experts in disciplines like communications, economics and public policy.
· Interesting and well conducted outbreak investigations would be actively used as
models—e.g. through write-ups in IDSP bulletins, presentations on teaching and video-conferences.

- 105 -
Component 4: Supporting human health related activities under India’s avian
influenza pandemic control program: · The health sub-component of IDSP Avian Influenza (AI) component aided to
strengthen and network reference laboratories for prompt confirmation of AI human cases & H1N1 and re-establish Seasonal Influenza surveillance system for India building on the network established by the Department of Health Research (DHR).
· In the proposed AI lab network CSU, NCDC Delhi would take care of some
critical operational issues such as (a) strict compliance with the definition of Influenza Like Illness; (b) adequate training of epidemiologists and lab personnel to ensure quality in sample collection, transport and testing; (c) use of standardized testing strategy developed in consultation with National Institute of Virology, Pune and WHO.
5. Activities Agreed under different Components
(a) Surveillance Preparedness:
· Training of epidemiologists (district and State), microbiologists (State and priority labs) and entomologists by NHSRC, the recruiting agency has the responsibility of capacity building of the newly recruited additional dedicated IDSP staff. They have completed the Master Trainers training through faculty development programme. Subsequent training of actual staff will be done regionally by drawing the faculty from the resource group. The entomologists and microbiologists group training will be facilitated by respective units of NCDC.
· Training of District Surveillance Teams: the regular training under IDSP is due in some of the States specially Phase III states.
· Additional Training for improved reporting and decentralized analysis will be done for health supervisors, block health management teams, pharmacists etc. This is a key activity to be taken up fresh in the nine priority States. The pharmacists, Medical Record Technicians, Nurses attached to sub-district, district and Medical college hospitals @ 5 to 6 per facility will be trained in simple tasks of collating the data from multiple OPDs, in patients and laboratory and preparing weekly report to be shared with DSU.
· Ensuring fully functional IT systems in Place :
Ø A mechanism will be developed to enhance data integration and flow from Telephone (mobile, voice and text, and landlines), Email, and Fax.
Ø Decentralization of the recruitment and management of the IT Human Resource (DMs and DEOs) directly to the SSUs/ DSUs, to enhance accountability.

- 106 -
Ø Revision of remuneration to bring these at par with other national health projects will reduce attrition.
Ø SSUs/ DSUs will now be authorized to have broadband connectivity thru BSNL and disburse their broadband bills.
Ø Training of DMs and DEOs has been initiated – training modules have been developed and a detailed training schedule has been prepared.
Ø Bandwidth capacity of EDUSAT will be upgraded from the present 512 Kbps to 1 Mbps.
Ø The causes of the Toll free number issues are being analyzed and investigated. This analysis will form the basis of corrective actions that could include resolving technical issues, changing of the 1075 service provider and/or the Call Centre service provider.
Ø To promote the use of the toll- free services, the number will be publicized amongst health providers in conferences of IMA, IAP, private hospitals and amongst the general public by tagging to other information and dissemination opportunities such as advertisements, bulletins on public health etc.
Ø The CSU/ SSU- Andhra Pradesh is conducting an independent assessment of the SMS syndromic-reporting model, incorporate any necessary revisions / refinements and scale up the model in A.P. and the other priority States.
Ø The existing infrastructure at SSU/DSU will be used to implement a Media Scanning and Verification System in the 9 priority States. Karnataka has initiated such efforts and it appears that existing equipment and Human Resource are adequate to establish and implement the system. The Media Surveillance System functional at the CSU will serve as the model for the State Media Scanning Cells. The CSU will develop guidelines; provide training, hand holding and monitoring support.
· For 50 Priority district labs:
Ø Procurement of equipments by the States to be expedited through rigorous monitoring- Ensure maintenance of equipment.
Ø Develop a specimen collection system within the district.
Ø To expedite placements of new medical and non medical microbiologists at district labs and at State level under IDSP

- 107 -
Ø To organize training for new microbiologists by identifying 3 additional training institutes. An informal dialogue with representatives from CMC Vellore, BJ Medical College, Pune was initiated through NHSRC on course content and methodology of training. This activity dependent on joining of the selected candidates.
Ø To prepare and distribute SOP manuals for the district priority labs inclusive of bio waste management guidelines and mechanisms for internal quality controls.
Ø Regular monitoring of the functioning of district priority labs
Ø Providing guidelines for procurement of quality kits and supervise the implementation of these guidelines.
Ø To identify one or two External Quality Assessment Scheme (EQAS) organizers and organize EQAS once the district priority labs become functional, by early 2010 (depends upon the units to be functional for at least 3 months).
· For Referral laboratory Network in 9 priority States:
Ø Enabling the States to establish a system of collection and transport of samples from linked districts to the referral labs.
Ø Providing guidelines for procurement of quality kits and supervise the implementation of these guidelines.
Ø To hold meeting with the SSU & all other stake holders in the Referral Plan & enabling them to establish a Referral Network for the identified state.
Ø Regular (yearly, quarterly?) supervising and evaluating of the functioning of the lab network and adapt according to the local and national needs
Ø Identifying specialized laboratories for testing of rare but contagious diseases. Establishing a system of EQAS for the referral labs, by early 2010.
Ø Identifying good examples of networking among these States and sharing with the other States (yearly)
· For entomological surveillance:
Ø Training of newly recruited entomologist will be completed.

- 108 -
Ø Mapping, monitoring entomological density and bionomics and sensitivity to insecticides will be done by these entomologists in consultation of programme officer of NVBDCP & DMO
Ø Undertake entomological investigations whenever there are vector borne disease outbreaks.
(b) Outbreak investigation and Response:
· 50% Outbreaks detected by system within one week of first case diagnosis in 9 identified States and 25% in other States.
· 80% Outbreaks/rumors reported by other systems/media verified within 48 hours (documented in electronic register) in 9 identified States and 60% in other States.
· 50% of outbreaks for which adequate specimens reached the laboratory in 9 identified States and 25% in other States.
· Full documentation (first and final investigation reports) of 25 % of reported outbreaks in 9 priority States will be available on the IDSP portal.
(c) Analysis and use of data:
· 80% districts undertaking weekly surveillance analysis of data including graphs for trends over time and maps for incidence by area in 9 identified States and 50% in other States.
· 80% districts providing monthly feedback (one page bulletin/news letter) to sub units, policy makers and general public in 9 identified States and 60% in other States.
Major Components of IDSP
• Integration and Decentralization of Surveillance activities
• Strengthening of Public Health Laboratories
• Human Resource Development - Training of SSO, DSO, RRT, other medical
and paramedical staff

- 109 -
• Use of Information Technology for collection, compilation, analysis &
dissemination of data
Organizational structure
National Surveillance Committee
(Central Surveillance Unit)
State Surveillance Committee
(State Surveillance Unit)
District Surveillance Committee
(District Surveillance Unit)
Reporting Unit
(PRU)
Data source
S, P & L forms (Weekly Reporting)
- Form S
(Syndromic Reporting) - Health Workers (Sub Centres)
– Form P
(Probable Cases which are clinically diagnosed by a medical doctor) - PHC, CHC,
Hospitals
– Form L - Lab Confirmed Cases
A probable case that is Laboratory confirmed
Data source
Weekly & SOS reporting on EWS format and monitoring of outbreaks

- 110 -
• Supplemental Information:
– IDSP 24x7 Call Centre
Information about outbreaks received on a toll free number – 1075 &
information shared with SSO/DSO
– Media Scanning & Verification Cell
Provides information about outbreaks by scanning media; shared with stakeholders
Data transmission methods
• e-mail: S,P,L forms & EWS
• IDSP Portal (www.idsp.nic.in)
• SMS reporting thru mobiles.

- 111 -
•

- 112 -
L For
Format for instantaneous reporting of Early Warning Signal / outbreaks
as soon as it is detected
State : District: Date of reporting:
Is there any unusual increase in Cases/Deaths or unusual event in any area? Yes/No
If yes, provide the following information
Response Mechanism
§ Multidisciplinary Rapid Response Team (RRT) constituted/ trained at all State and
district headquarters; comprises of:
1.Public Health Expert – Epidemiologist/(District Surveillance Officer/ Faculty of Community
Medicine)
2. Clinician
3. Microbiologist/ Lab personnel
4. Entomologist (for Vector Borne Diseases)
§ Video Conferencing for interaction on outbreak investigations.
Important Purposes of data analysis
� Identifying outbreaks / Potential outbreaks (alert the health services system) e.g. a
case of measles should alert services system
� Identifying ‘High-risk population groups’ (person/place) so that targeted intervention
can be provided
� Identifying regional differences for improving services (e.g. measles: low vaccination
in a area)
� Predicting changes in disease trends over time (prevention/IEC)
- 113 -
Identifying problems in health systems so that gaps can be effectively plugged (e.g. possibility
of increased vector density/poor mosquito control/migration of infected people to the region)
Reports to be generated
1. Timeliness/completeness
2. Description by time, place and person
3. Trends over time
4. Compare with Threshold levels
5. Compare reporting units
6. Compare private / public
7. Compare health providers and laboratory
2. SITUATION ANALYSIS:
The project is being implemented at the State, District and Peripheral level by
· Formation of District Surveillance Units at Revenue Districts.
· Strengthening the existing laboratory facilities at Peripheral, District and State
levels (L1, L2 and L3)
· Provision of Satellite Interactive Terminal (EDUSAT) and modern
communication facilities (Computers / Fax) by statewide networking for the
rapid flow of information for immediate action
· Improvement of management and technical skills to the health and laboratory
personnel by training.
ACTION PLAN FOR THE YEAR 2012-13
Manpower
Ø To ensure 100 % Appointment by 2013
Civil work & Furniture/Fixtures:
Furniture and fixtures have been procured and installed in DSUs for the videoconferencing facility (EDUSAT) at the District Surveillance Office. Similarly, lab.furnitures and fixtures have been supplied to 20 district level laboratories

- 114 -
Training Ø Initiate Training for RRT – Members (will be done by CSU)
Ø Conduct Orientation Training for Data Entry Operators
Ø Re – Orientation training for Data Managers
Ø Training the District Accountants in Booking Keeping and Double Entry System of
Accounting etc.,
Ø Reorientation training for Lab personals at all levels.
Information Technology Ø To ensure, effective functioning of EDUSAT in all places.
Ø Interact with all the DSUs and Govt. Medical Colleges from the State Surveillance Units
Ø Online reporting through EDUSAT
Reporting Ø To improve reporting of clinically confirmed cases by promoting coordination between
different players within public sector such as major hospitals, medical colleges and local
self NGOs.
Ø To improve the timeliness of reporting.
Ø To improve the reports collected from private sector and to involve private lab.
Ø To achieve 100% reporting from District Head Quarters Lab.-L2
Ø To achieve 100% quality report from all L1, L2 and L3 laboratories.
Ø Analysis of the data based on time, place, person.
Ø To involve all major private hospital and private medical colleges in surveillance.
Review Ø To conduct regular and in-depth district performance evaluation and review
Ø Monitor the Training conducted by the Districts.
Ø Surprise visit to Public / Private Reporting units

- 115 -
*SUB –ACTIVITY TASKS –JEHANABAD UNIT COST.2012-13
- To conduct regular and in-depth District performance evaluation and review.
- Monitor the training conducted by the Districts.
- Surprise visit to public/private Reporting units 1. Budgeting
Draft - Annexure
Budget Sheet for DSU JEHANABAD(BIHAR)
Sub-activity
Tasks Unit Cost
No. of Units
2012 - 13 Remarks
1.1 Epidemiologists 33,000 1
33,000 *12=
396,000
Epidemiologists salary per month
1.2 District Data Manager
14,850 1
14,850 * 12 =
178,200
DDM Salary per month
1. Staff Salary
1.3
1.4
Data Entry Operator
Administrative Assistant
9350
7000
1
1
9350 * 12 =
112,200
7000x12
=84000
per month for future which is mention in IDSP PIP (Tentative cost)
Sub Total 770,400
2.1 Mobility Support 20000 1 20000 * 12 =240000
20000 Per month for Each District
2.2 Office Expenses 10000 1 10000 * 12 =120000
10000 Per month for Each District
2. Operational Cost
2.3 ASHA incentives for Outbreak reporting
100 10 1000*12=
12000
Estimated to get 10 information’s per month from volunteers a total of 120 such information in a year per district. Each informant to be given an incentive of

- 116 -
Rs.100/-
2.4 Consumables for District Labs
150000 1 150000
2.5 Collection & transportation of samples
75000 1 75000
2.6 IDSP reports including alerts 20 52 * 1 1040
2.7 Printing of Reporting Forms 20 52 *15 15600
2.8 Broadband Expenses 2000 1 1000 * 12 =
24000
Sub Total 6,37,640
3. New Innovations 3.1 IEC at District
Level 50000 1 50000*1
=50000 1 Districts
3.2 Advertisement Media and local media
30000 1 30000*1=
30000 I Districts
3.3
Laptop for presentation and mobile work of office
40000 2 40000*2
=80000
DSU for Epidemiologists and Data Manager
3.4 Mobility support for DSU &RRT Team
50000 1 50000*1=
50000 1 Districts
3.5 Mobile expenses for DSUl 500 2
500*2*12=
12000
Each DSU two mobile for Epidemiologists and Data Manager
Sub Total 222000
TOTAL 1630040

- 117 -
PRONE DESIASE LIST OF JEHANABAD DISTRICT
1. MALARIA
2. LEPROSY
3. FALIRIA
4. ACUTE DIARRHOEAL DISEASE DYSENTERY
LIST OF PATHOLOGICAL LABORATORY REGISTERED AND UNREGISTERED IN JEHANABAD
THESE LAB WORKING UNDER DHS CONTRACT
1. CENTAL DIAGNOSTIC RATNI PHC 2. CENTRAL DIAGNOSTIC KAKO PHC 3. CENTRAL DIAGNOSTIC HULASGANG PHC 4. CENTRAL DIAGNOSTIC SADAR PHC 5. CENTRAL DIAGNOSTIC OKARI PHC 6. CENTRAL DIAGNOSTIC GHOSI PHC 7. CENTRAL DIAGNOSTIC MAKDUMPUR PHC 8. CENTRAL DIAGNOSTIC SADAR HOSPITAL JEHANABAD .
IDD · Before Round District Level Coordinatiion Meeting in the Presence of District
Magistrate and Civil Surgeon.
· Block level Meeting.
· Training Before round to ASHA,ANM, AWW.
Budgetary Proposal
FMR Code
Budget Head
Physical Target (where
Applicable
Unit Cost
Financial Requirement
(inRS) Committed Fund
Required
D IDD 11000
Total 11000

- 118 -
NVBDCP
Kalaazar
Gaps Objective Strategy Activities
To increase the coverage of DDT spray in the endemic zone , there should be proper monitoring by the supervisors, capacity building of the sprayer, supervisors and other healthcare professionals
1. Ensure planning for timely spray of DDT in Feb-March and May-June for 40 days in each block
2. Identification of Houses with Kala-azar patients by ANM & ASHA @ 50/ per village.
3. Two round of spraying scheduled in Feb-March and May-June should be strictly observed
1
Poor coverage of DDT spray
Vector control through
insecticide spray in
the attack area
Monitoring of the
spraying squad by
MOIC
4. DDT spray should be at the rate of 1gm/sq. meter upto the height of 6 feet.

- 119 -
Less time spent on spraying DDT
Training and capacity building for proper spraying
Regular capacity building training on prescribed module for the sprayer to ensure that very corner of the house is properly spray up to height of six feet from ground level.
Poor condition of Sprayer, pump and nozzles etc No of Pumps available-0, No of pumps required-30, No of bucket savailable-70, No of buckets required-70, No of gallon available-21, No of gallon required-49, No of pond measure available-21, No of pond measure required-49, .
Regular checking of the spraying pumps for better functioning and timely replacement of the faulty pieces.
Fund allocation and timely release for : maintanceof old sprayer pumps, Purchase of new pumps and other articles needed- buckets, mugs etc.
Inadequate stock of DDT, DDT available-9.5mt. (Not required)
Making available DDT during spraying round
Ensure adequate Stock of DDT through proper & timely indenting to improve the quality of spray

- 120 -
Faulty payment plan
Appropriate fund allocation for the payment of the spraying of DDT
Fund would be allocated for regular payment of wages (147 SFW to be used and 735 FW to be used for monitoring and spraying work)
Early diagnosis and treatment through PHC system
Case detection rate should be increased with appropriate diagnostic test
Increase efficiency of case detection through training of Community workers on signs and symptoms of Kala-azar: 1) three weeks persisten fever not responding to antibitics, malaria being excluded, with palpable spleen.2) Ensure availability of aldehyde test at PHC level 3) Purchase of RK 39 kit for detection of Kalazar
1. Ensuring availability of Amphotoricin at all level
Loss of wages for KZ patients(case detection in year 2007-3275)
2. Replacing of medicines on priority based
2
Poor rate of case
detection of Kalazar
Reduction of kala-
azar mortality
and morbidity
Early diagnosis
and treatment
through PHC system
3. Training of ANMs and ASHA for IM injection
3
Lack of monitoring
and supervision mechanism,
Monitoring and supervision mechanism
Preparation of Monthly visit plan for supervision :
- Checking spraying schedule - For supervision & treatment follow
up
Office expenses
4 Lack of Increasing Community 1. Fund allocation for training activities

- 121 -
2. Identification of NGO/Private partner as trainer
3. Knowledge sharing with the community on signs and symptoms of Kala-azar through VHSC
4. Training of VHSC/PRI and community health worker on sign & symptom of Kala-azar
5. Regular monitoring of IEC activities
6. IEC activities through nukkad natak, kalajatha mass media like radio
7.Activity for survilence like polio survilence
8.Wall painting of Tretment protocole and provisions for pateints in PHC in Hindi.
appropriate BCC &
Community Mobilization.
awareness for
prevention of Kala-
azar
participation in reducing
mortality and morbidity
due to Kala-azar
IEC van for each PHC
Blindness Issues Strategy Activities
Staff shortage Recruitment Recruitment of Eye Specialists and surgeons on contractual basis.
Recruitment of Opthalmic Assistants on contractual basis.
Untrained staffs Capacity building Training of Doctors on IOL technique
Training of Opthalmic Assistant

- 122 -
Low achievement Increasing noof camps Organising Operations at District level
PPP
Accreditation of Nursing Homes capable of doing Cataract surgeries
Establishing another Cataract Operation Center at PHC Kako.
Purchase of equipments and medicines
Lackof awareness Awareness building Assigning LHV/Supervisor counseling work
Organising eye screening camps in villages/ schools
IEC on cataract and its facilities
InvolvingNGOs Meeting with Local NGOs onthis issue
Lackof adequate referal services
Strengthening referal system
Arrangement of carrying patients to the Operation Centers and then taking them back homes
Monitoring and follow up
Monitoring and follow up Mobility support for Visiting homes of the patients tomanage any post treatment complication.
Developing records of cataract cases from OPD registers at PHC level

- 123 -
Leprosy
Gaps issues Strategy
Activities
· Existing PR of the district is 1.1 and the target is only 1, so the existing program performance is good.
· Lack of awareness is still a problem with the Leprosy Program as most of the cases are detected accidentally.
Lack of Awareness
Awareness generation
IEC on Leprosy
· Inadequate staff, Only 6 supervisors and 11 Non Medical Assistants are working while the requirement of Supervisor is 17 and that of NMA is 33( One NMAeach in each APHC)
Lack of Human Resource
Staff Recruitment in contract basis
Recruitment of 11 supervisors
· There is no active involvement of the Medical officers at sector and Block levels.
Orientation of Mos and staffs on Leprosy
Case validation, to have check on wrong diagnosis and re registration
Prompt and early detection of the cases to avoid deformity and disability,
· Lack of PHC staff involvement. No manpower support,
Strengthen
Health Care
Services
Ulcer care foot ware reorientation training of medical & para medical staff.
No lab testing facility in the district Infrastructure
Establishing Lab
Establishing Lab at district level

- 124 -
Gap Recurring expenditure like reagents
Updation of master register
Mobility support for DLO
Lack of monitoring at all level Monitoring Gap
Increasing
mobility
Office expenses
Fileria
Gaps issues
Strategy Activities
Line listing of the cases
Purchse of equipments for the management of Filaria cases like towel, Bucket, soap, mug etc
DEC distribution through AWCs and paying hon to AWWs for this.
It affects mainly the economically weaker sections of
communities
1. Single dose DEC mass therapy once a year in identified blocks and selected DEC treatment in filariasis endemic areas.
Purchse of DEC

- 125 -
Training to AWWs/ASHA on DEC distribution and filaria case management
Result in low priority being accorded by governments for the control of lymphatic filariasis.
2. Continuous use of vector control measures.
Meeting with VHSC members
Low effectiveness of the tools used by the control programme
Detection and treatment of micro-Filaria carriers, treatment of acute and chronic filariasis.
The chronic nature of the disease
4. IEC for ensuring community awareness and participation in vector control as well as personal protection measures.
Wall paintings
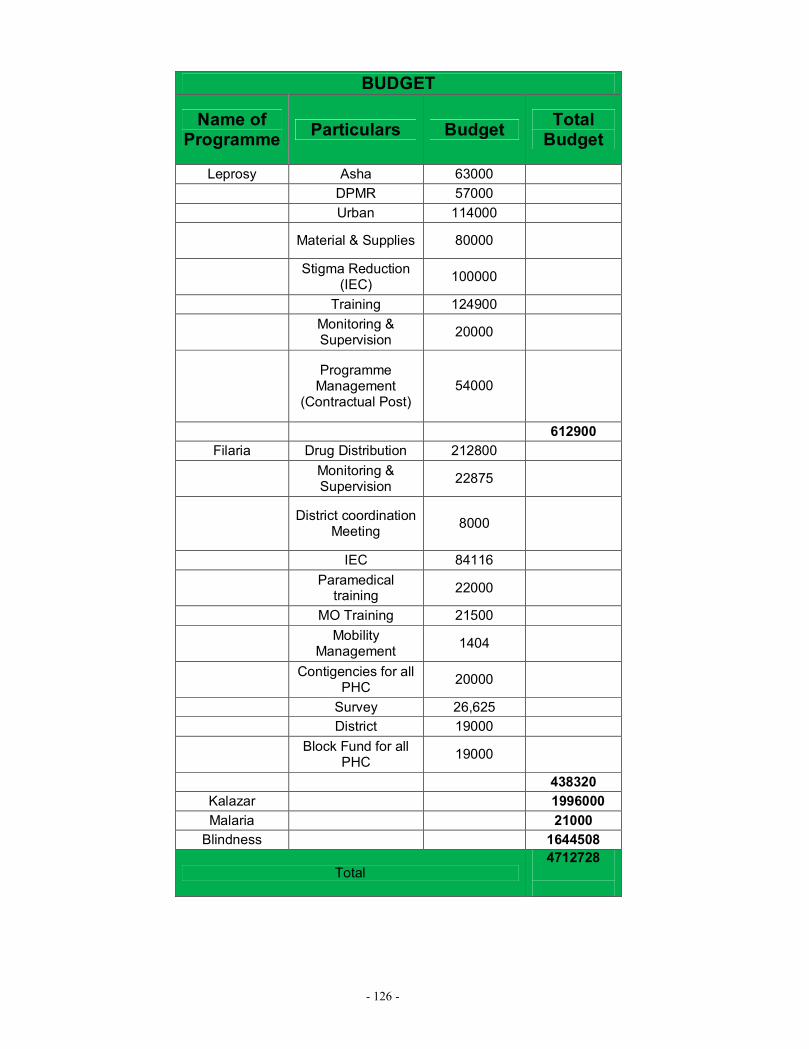
- 126 -
BUDGET
Name of Programme Particulars Budget Total
Budget
Leprosy Asha 63000 DPMR 57000 Urban 114000
Material & Supplies 80000
Stigma Reduction (IEC) 100000
Training 124900
Monitoring & Supervision 20000
Programme
Management (Contractual Post)
54000
612900 Filaria Drug Distribution 212800
Monitoring & Supervision 22875
District coordination Meeting 8000
IEC 84116
Paramedical training 22000
MO Training 21500
Mobility Management 1404
Contigencies for all PHC 20000
Survey 26,625 District 19000
Block Fund for all PHC 19000
438320 Kalazar 1996000 Malaria 21000
Blindness 1644508
Total 4712728

- 127 -
TUBERCULOSIS----------------------------
ANNUAL PLAN FOR PROGRAMME PERFORMANCE & BUDGET FOR THE YEAR
1ST APRIL 2012 TO 31ST MARCH 2013 District:- JEHANABAD. State :- BIHAR.
Name_Dr. Vijay Kumar Singh, Designation_DTO_ _____
Section-A – General Information about the District
1 Population (in lakh) please give projected population 2009 1154545*
2 Urban population 102061
3 Tribal population -
4 Hilly population -
5 Any other known groups of special population for specific interventions
(e.g. nomadic, migrant, industrial workers, urban slums)
-
(These population statistics may be obtained from Census data /District Statistical Office)
Does the district have a DTC Yes
ORGANIZATION OF SERVICES IN THE DISTRICT:
Please indicate if the TU is-
No. of MCs S. No.
Name of the TU Population (in Lakhs)
Govt NGO Govt NGO Private
1 DTC, Jehanabad. 681323 1 0 4 0 0
2 Ghosi 473222 1 0 4 0 0
DISTRICT 1154545 02 0 08 0 0

- 128 -
RNTCP performance indicators:
Important: Please give the performance for the last 4 quarters i.e. July 2010 to June 2011
Plan for the next year
TB Unit
Total number
of patients put on
treatment
Annualized total case detection rate (per lakh pop)
No of new
smear positive
cases put on
treatment
Annualized New
smear positive
case detection rate (per lakh p op)
Cure rate for cases
detected in the last 4
corresponding quarters
Annualized NSP CDR
Cure rate
(85%)
Proportion of TB
patients tested for
HIV
DTC 682 56% 264 234 65% 85%
Ghosi 360 39% 118 150 65% 85%
District 1042 382
Section B – List Priority areas for achieving the objectives planned:
S.No. Priority areas Activity planned under each priority area
1 Training Training of MO's
Training of ASHA, ANM worked in all PHC by STS
2 IEC / Publicity Wall Writing, Hording, Banners, Print Publicity, Mice.
3 Supervision Vehicle Hiring for DTO & MO-TC
4 Human Resource To Fill up all Contractual vacancies and to make a Panel of reserved Candidates
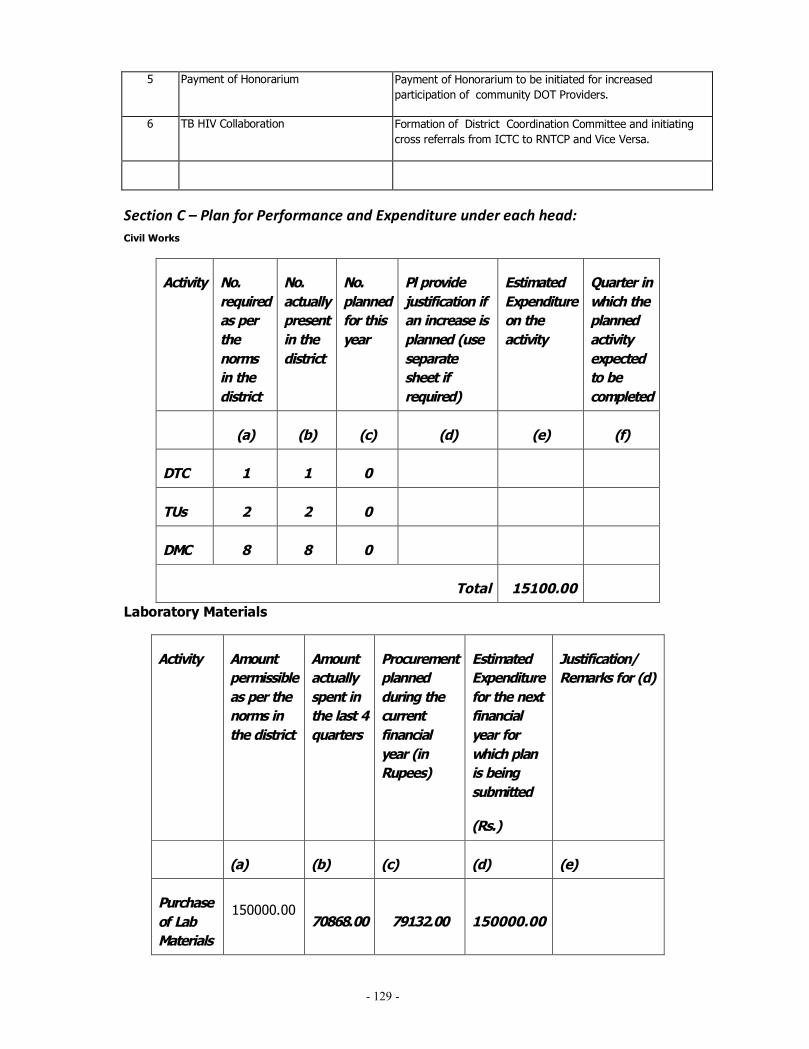
- 129 -
5 Payment of Honorarium Payment of Honorarium to be initiated for increased participation of community DOT Providers.
6 TB HIV Collaboration Formation of District Coordination Committee and initiating cross referrals from ICTC to RNTCP and Vice Versa.
Section C – Plan for Performance and Expenditure under each head: Civil Works
Activity No. required as per the norms in the district
No. actually present in the district
No. planned for this year
Pl provide justification if an increase is planned (use separate sheet if required)
Estimated Expenditure on the activity
Quarter in which the planned activity expected to be completed
(a) (b) (c) (d) (e) (f)
DTC 1 1 0
TUs 2 2 0
DMC 8 8 0
Total 15100.00
Laboratory Materials
Activity Amount permissible as per the norms in the district
Amount actually spent in the last 4 quarters
Procurement planned during the current financial year (in Rupees)
Estimated Expenditure for the next financial year for which plan is being submitted
(Rs.)
Justification/ Remarks for (d)
(a) (b) (c) (d) (e)
Purchase of Lab Materials
150000.00 70868.00 79132.00 150000.00

- 130 -
Honorarium
Activity
Amount permissible as per the norms in
the district
Amount actually spent in the last 4 quarters
Expenditure (in Rs)
planned for current financial
year
Estimated Expenditure for the next
financial year for
which plan is being
submitted
(Rs.)
Justification/ Remarks for (d)
(a) (b) (c) (d) (e)
Honorarium for DOT providers (both tribal and non tribal districts)
200000.00 35000.00 165000.00
200000.00 We have planed to
distribute the recommended
insentive to DOT
Providers for cured /
completed TB Patients.
Honorarium for DOT providers of Cat IV patients
12500.00
Equipment Maintenance:
Item
No. actually present in the district
Amount actually spent in the last
4 quarters
Amount Proposed
for Maintenance
during current
financial yr.
Estimated Expenditure for the next
financial year for
which plan is being
submitted
Justification/ Remarks for
(d)

- 131 -
(Rs.)
(a) (b) (c) (d) (e)
Office Equipment
(Maintenance includes computer software and hardware upgrades, repairs of photocopier, fax, OHP etc)
1 3500.00 26500.00
30000.00
Binocular Microscopes ( RNTCP)
8 0.00 13500.00
43500.00
Training:
No. planned to be trained in RNTCP during each quarter of next FY
(c)
Activity No. in the district
No. already trained in RNTCP
Q1 Q2 Q3 Q4
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being submitted
(Rs.)
Justification/ remarks
(a) (b) (d) (e) (f)
Training of MOs
Training of LTs of DMCs-
Govt + Non Govt
15000.00
Training of MPWs
Training of

- 132 -
MPHS, pharmacists,
nursing staff, BEO etc
Training of Comm Volunteers
Training of Pvt Practitioners
Other trainings #
Re- training of MOs
84 66 20 20 20 20 32000
Re- Training of LTs of DMCs
10 10 10 10 5000 20000.00
Re- Training of MPWs
20000.00
Re- Training of MPHS
10000.00
Re- Training of Pharmacists
Re- Training of nursing staff, BEO
Re- Training of CVs
Re-training of Pvt Practitioners
700 700 200 200 150 150 38000.00

- 133 -
TB/HIV Training of MOs
10000.00
TB/HIV Training of STLS, LTs , MPWs, MPHS, Nursing Staff, Community Volunteers etc
TB/HIV Training of STS
Training of MOs and Para medicals in DOTS Plus for management of MDR TB
Provision for Update Training at Various Levels(key staff & MO-PHIs)
10000.00
Any Other Training Activity( Key staff & MO-PHIs)
75000.00 75000.00
# Please specify
Vehicle Maintenance:

- 134 -
Type of Vehicle
Number permissible as per the norms in the district
Number actually present
Amount spent on POL and Maintenance in the previous 4 quarters
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being submitted
(Rs.)
Justification/ remarks
(a) (b) (c) (d) (e) (f)
Four Wheelers
- - - -
Two Wheelers
02 02 7958.00 42042.00 50000.00
Vehicle Hiring:
Hiring of Four Wheeler
Number permissible as per the norms in the district
Number actually present
Amount spent in the previous 4 quarters
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being submitted (Rs.)
Justification/ remarks
(a) (b) (c) (d) (e) (f)
For DTO 01 01 71750.00 42042.00 268800
For MO-TC
02 02 0.00 58800.00
197050 268800
NGO/ PP Support: (New schemes w.e.f. 01-10-2008)

- 135 -
Activity No. of currently involved in RNTCP in the district
Additional enrolment planned for this year
Amount spent in the previous 4 quarters
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being submitted
(Rs.)
Justification/ remarks
(a) (b) (c) (d) (e) (f)
ACSM Scheme: TB advocacy, communication, and social mobilization
1 150000.00
It is planned to give ACSM
scheme to one NGO to cover
both the TUs in the district
SC Scheme: Sputum Collection Centre/s
Transport Scheme: Sputum Pick-Up and Transport Service
DMC Scheme: Designated Microscopy Cum Treatment Centre (A & B)
LT Scheme: Strengthening RNTCP diagnostic services
Culture and DST Scheme: Providing Quality Assured

- 136 -
Culture and Drug Susceptibility Testing Services
Adherence scheme: Promoting treatment adherence
Slum Scheme: Improving TB control in Urban Slums
Tuberculosis Unit Model
TB-HIV Scheme: Delivering TB-HIV interventions to high HIV Risk groups (HRGs)
TOTAL 150000.00

- 137 -
Miscellaneous:
Activity* Amount permissible as per the norms in the district
Amount spent in the previous 4 quarters
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being submitted
(Rs.)
Justification/ remarks
(a) (b) (c) (d) (e)
150000.00 28018.00
121982.00 150000.00 For payment of telephone and internet bills and for office furniture for DTC and TU.
150000.00
* Please mention the main activities proposed to be met out through this h
Contractual Services:
Activity No. required as per the norms in the district
No. actually present in the district
No. planned to be additionally hired during this year
Amount spent in the previous 4 quarters
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being submitted
(Rs.)
Justification/ remarks
(a) (b) (c) (d) (e)
Medical Officer-DTC
1 - 1 - 120000.00 336000.00
STS 02 02 00 190426.00 151200.00 302400.00
STLS 02 02 00 216031.00 151200.00 302400.00
TBHV 00 00 01 0.00 32000.00 96000.00
MO will be recruited in the coming financial year

- 138 -
DEO 01 01 00 79739.00 56100.00 112200.00
Accountant – part time
00 00 01 0.00 12000.00 36000.00
Contractual LT
04 00 289520.00 252000.00 504000.00
DOTS Plus cum TB HIV supervisor 0 01 90000.00 180000.00 1869000
Printing:
Activity Amount permissible as per the norms in the district
Amount spent in the previous 4 quarters
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being submitted
(Rs.)
Justification/ remarks
(a) (b) (c) (d) (e)
Printing*
100000.00 26936.00
73064.00 100000.00
* Please specify items to be printed

- 139 -
Research and Studies:
Any Operational Research project planned (Yes)
(Post Graduate grant for one research paper from each Medical College)
Estimated Budget (to be approved by STCS).___________________________________
Medical Colleges
Activity Amount permissible as per norms
Estimated Expenditure for the next financial year(Rs.)
Justification/ remarks
(a) (b) (c)
Contractual Staff:
§ MO (In place: Yes/No)
§ STLS (In place: Yes/No)
§ LT (In place: Yes/No)
§ TBHV (In place: Yes/No)
Research and Studies:
§ Thesis of PG Student
§ Operations Research*
Travel Expenses for attending STF/ZTF meetings
IEC: Meetings and CME planned

- 140 -
Procurement of Vehicles:
Equipment No. actually present in the district
No. planned for this year
Estimated Expenditure for the next financial year for which plan is being submitted (Rs.)
Justification/ remarks
(a) (b) (c) (d)
4-wheeler **
2-wheeler
** Only if authorized in writing by the Central TB Division
Procurement of Equipment:
Equipment No. actually present in the district
No. planned for this year
Estimated Expenditure for the next financial year for which plan is being submitted (Rs.)
Justification/ remarks
(a) (b) (c) (d)
Office Equipment (computer, modem, scanner, printer, UPS etc)
Any Other

- 141 -
Section D: Summary of proposed budget for the district –
Budget estimate for the coming FY 2012- 13
S.No. Category of Expenditure (To be based on the planned activities and expenditure in Section
C)
1 Civil works 15100.00
2 Laboratory materials 150000.00
3 Honorarium 212500.00
4 IEC/ Publicity 75000.00
5 Equipment maintenance 43500.00
6 Training 75000.00
7 Vehicle maintenance 50000.00
8 Vehicle hiring 268800.00
9 NGO/PP support 150000.00
10 Miscellaneous 150000.00
11 Contractual services 1869000.00
12 Printing 100000.00
13 Research and studies 0.00
14 Medical Colleges 0.00
15 Procurement –vehicles 0.00
16 Procurement – equipment 0.00
TOTAL 3158900.00
** Only if authorized in writing by the Central TB Divisio
Annual Action Plan Format Advocacy, Communication and Social Mobilization (ACSM) for RNTCP

- 142 -
1) Information on previous year’s Annual Action Plan- a) Budget proposed in last Annual Action Plan: b) Amount released by the state: c) Amount Spent by the district-
2) Permissible budget as per norm : 3) Budget for next financial year for the district as per action plan detailed
below:
Program Challenges to be tackled by ACSM during the Year 2009 - 10
WHY
ACSM Objective
For WHOM
Target Audience
WHAT
ACSM Activities
When
Time Frame
By WHO
M
Monitoring and Evaluation
Budget
Based on existing TB indicators and analysis of communication challenges
(Maximum 3 Challenges )
Desired behavior or action (make SMART: specific, measurable, achievable, realistic & time bound objectives)
Activities
Media/
Material Required
Q1
Q2
Q3
Q4
Key implementer and RNTCP officer responsible for supervision
Outputs;
Evidence that the activities have been done
Outcomes:
Evidence that it has been effective
Total expenditure for the activity during the financial year
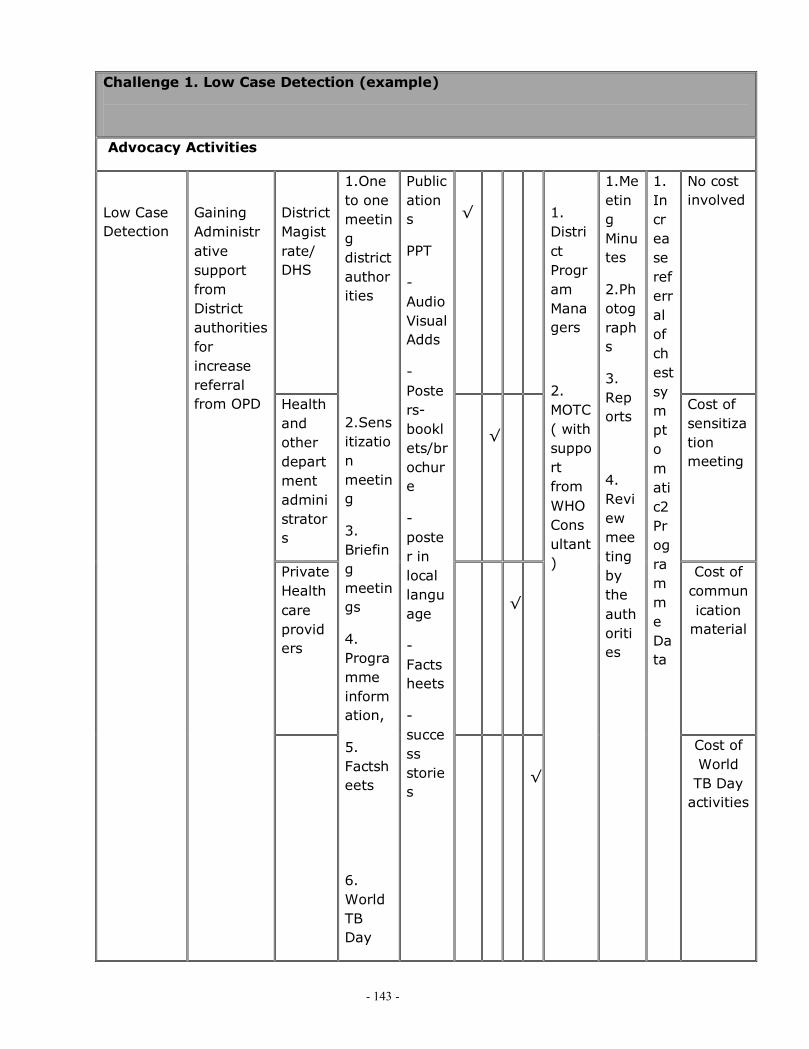
- 143 -
Challenge 1. Low Case Detection (example)
Advocacy Activities
District Magistrate/ DHS
√
No cost involved
Health and other department administrators
√
Cost of sensitization meeting
Private Health care providers
√
Cost of communication
material
Low Case Detection
Gaining Administrative support from District authorities for increase referral from OPD
1.One to one meeting district authorities
2.Sensitization meeting
3. Briefing meetings
4. Programme information,
5. Factsheets
6. World TB Day
Publications
PPT
-Audio Visual Adds
-Posters-booklets/brochure
-poster in local language
-Factsheets
-success stories
√
1. District Program Managers
2. MOTC ( with support from WHO Consultant)
1.Meeting Minutes
2.Photographs
3. Reports
4. Review meeting by the authorities
1. Increase referral of chest symptomatic2 Programme Data
Cost of World TB Day
activities
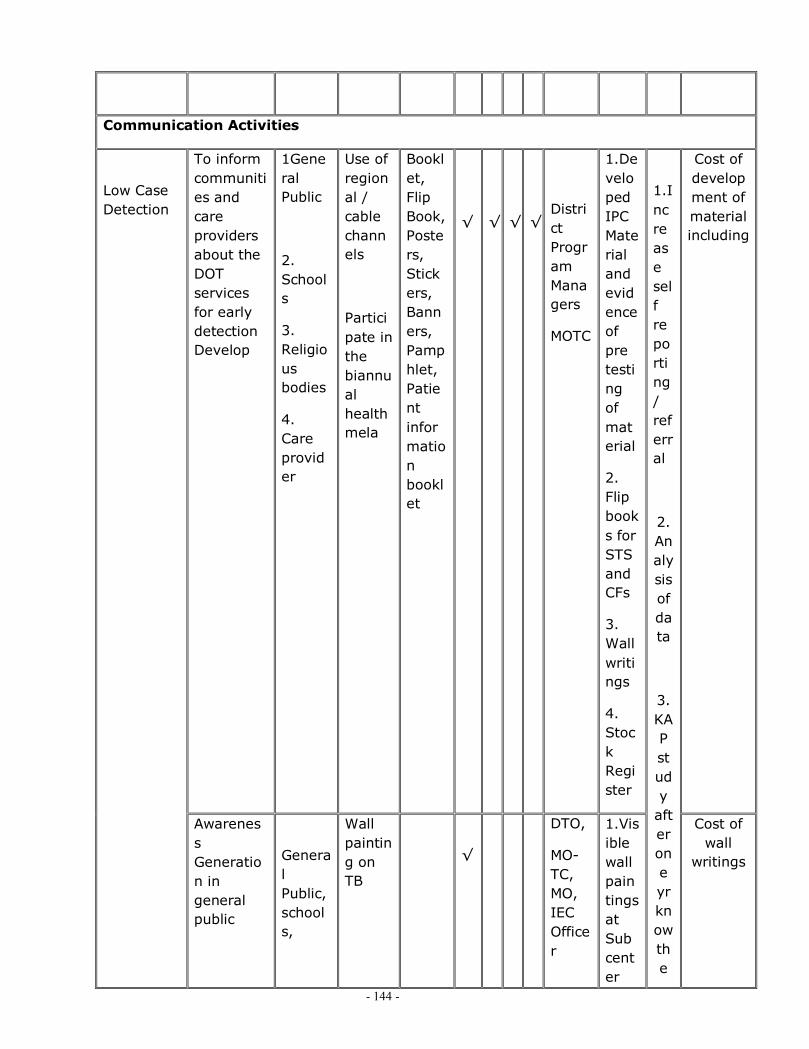
- 144 -
Communication Activities
To inform communities and care providers about the DOT services for early detection Develop
1General Public
2. Schools
3. Religious bodies
4. Care provider
Use of regional / cable channels
Participate in the biannual health mela
Booklet, Flip Book, Posters, Stickers, Banners, Pamphlet, Patient information booklet
√
√
√
√
1. DTO
District Program Managers
MOTC
1.Developed IPC Material and evidence of pre testing of material
2. Flip books for STS and CFs
3. Wall writings
4. Stock Register
Cost of development of material including
Low Case Detection
Awareness Generation in general public
General Public, schools,
Wall painting on TB
√
DTO,
MO-TC, MO, IEC Officer
1.Visible wall paintings at Sub center
1.Increase self reporting/ referral
2.Analysis of data
3. KAP study
after one yr know the
Cost of wall
writings
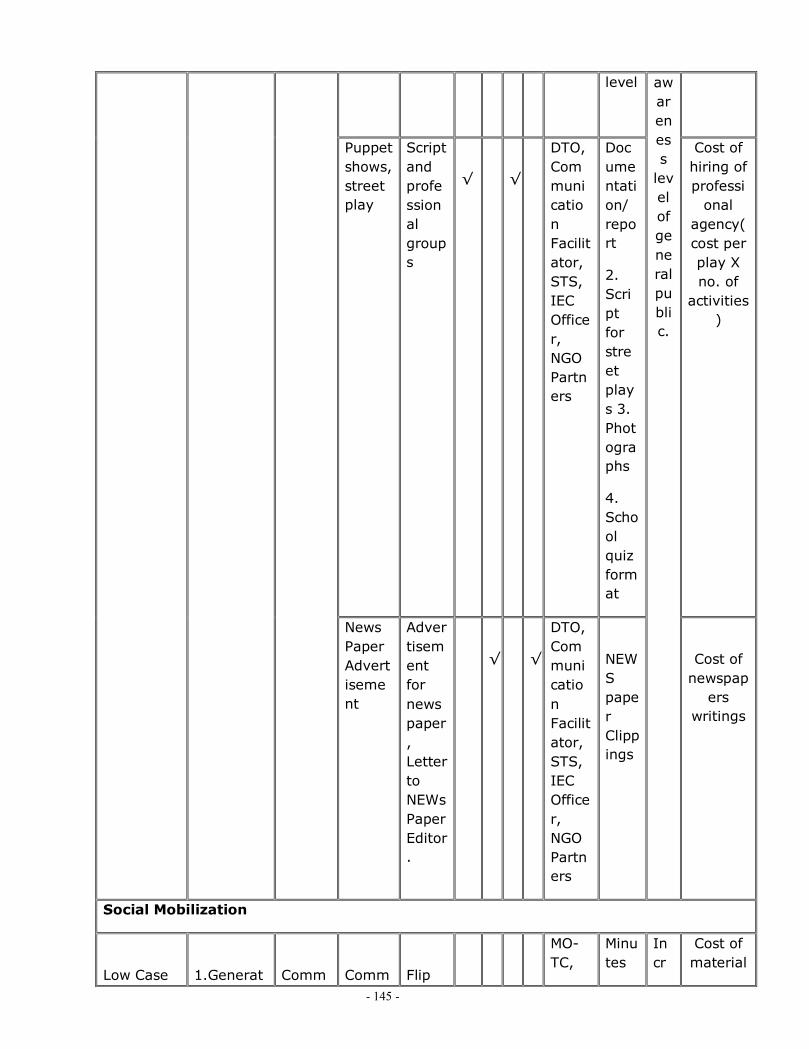
- 145 -
level
Puppet shows, street play
Script and professional groups
√
√
DTO, Communication Facilitator, STS, IEC Officer, NGO Partners
Documentation/ report
2. Script for street plays 3. Photographs
4. School quiz format
Cost of hiring of professi
onal agency( cost per play X no. of
activities)
News Paper Advertisement
Advertisement for news paper, Letter to NEWs Paper Editor.
√
√
DTO, Communication Facilitator, STS, IEC Officer, NGO Partners
NEWS paper Clippings
awareness
level of general public.
Cost of newspap
ers writings
Social Mobilization
Low Case
1.Generat
Comm
Comm
Flip
MO-TC,
Minutes
Incr
Cost of material

- 146 -
unity Meeting
Chart and Posters, Talks
√
√
√
√
IEC Officer, Communication Facilitator, STS
of Meetings
Display of Posters
Flip Chart
ease Self reporting in chest symptomatic
+ cost of
community
meetings total
number of
meetings
planned
Celebration of World TB day
Display Material for World TB Day
DTO, MO-TC, MO, Communication Facilitator, STS
Documentation of l world TB Day activities
Pre- post evaluation of WTB Day activities with specific objectives
Budgeted above
Detection e Awareness in general public
2. Encourage early self reporting
3. Community Groups. PRI
unity
General Public, Patients, DOTs Providers
Exhibitions
display
DTO, MO-
Docume
Incr
Cost of Hiring of

- 147 -
/Mela’s / Popular Events in District.
Material ( Posters, Stickers, Banners, Pamphlet)
Interactive game s
√
√
TC, MO, Communication Facilitator, STS
ntation of activity
Write ups / brief used in plays
ease Self reporting of TB patients ( KAP study after one yr)
place and
display material & cost
interactive
games, prizes etc.
School Children
Drawing & Quiz Competitions
Games – Snake and ladder, Chakraview Game etc.
Pamphlets] IEC Material
√
√
√
DTO, Communication Facilitator, STS, IEC Officer, NGO Partners
Documentation of Activities/ Photographs
Pre- post intervention evaluation
Cost of one
school activity X no. of activities planned in the
distict=
College & School NSS Studen
TB Sessions during NSS caps
Games – Snake and ladder,
DTO, Communication Facilit
Documentation of Activ
Data Analysis
4000

- 148 -
ts in school and college, Drawing & Quiz Competitions
Help Mohan etc.
Pamphlets] IEC Material
ator, STS, IEC Officer, NGO Partners
ities/ Photographs
Challenge 2: High Default Rate (example 2)
Advocacy Activities
High Default Rate
Sensitizing district authorities about the importance of reducing default cases & for their support for necessary instructions to the Programme staff
1.Health care providers
Public & Private
2. STS
1.Interaction Meetings
2.One to One Interaction Meetings
3. Use of Information Booklet
Audio Visual Adds
-Posters-booklets/brochure
-poster in local language
-Factsheets
-success stories
District Program Managers
MOTC
Review of default case TU wise
Record of meetings
Reduction in default rate by 2% - Data analysis
Study to docu

- 149 -
ment default within one yr
Communication Activities
Patients, Their Family Members, DOTs Providers
Sharing of experience of cured patients / Patients during Treatment.
√
√
√
√
MO,
STS & Communication facilitators
High Default Rate
To motivate patients & their families for completion of treatment
Community TB Groups / NGOs
Patient interaction meetings & involvement of cured persons
Flip Chart Development
Development of material for Community DOT Provi
√
√
√
√
MO-TC, STS, ANMs
Records of meeting
Evidence of material development – pre testing
Increase in no. community base
Reduction in default rate by 2%- Analysis of programme data
Reducti

- 150 -
ders d NGOs involvement
on in time for retrieval of defaults
One to one meeting with the patient
Interpersonal communication with patients
Patient information booklet
√
√
√
√
MO, STS, DOT Provider
Evidence of such meeting
Patient information booklet
Reduction in defaults
Cost of patient informat
ion booklet (if not
budgeted above)
(no cost for one-to one IPC)
Social Mobilization
High Default Rate
To link poor patients to the welfare schemes
Sensitization of Departments Social welfare schemes
Posters, programme fact sheet,
Presentation
Annual
√
√
DTO, MO TC
Documentation, Records , Photographs
Data of
Reduction in defaults
Do
Cost of one
meeting no of
meetings

- 151 -
reports
referral of TB patients t symptomatic will increase
cumentation of effectiveness of such linkages through a study after one year
For mobilizing support from Community groups
Community support groups
Cured patients
Interaction meetings
Information material,
√
√
MO-TC, STS, Communication Facilitators
Formation of TB support groups in X no. of villages
Decrease in the no. of defaults
Cost of such
meetings

- 152 -
in such villages
Challenge 3:-
Advocacy activities
Communication activities
1.
Social Mobilization Activities
TOTAL
BUDGET PART D-I

- 153 -
FMR Code
Budget Head Financial Requirement (in RS)
Committed Fund Required
D IDD 11,000
E IDSP 1,630,040
F.1.1 Malaria 21,000
F.1.4 Filaria 438,220
F.2 Kalazar 19,96,000
G Leprosy 6,12,900
H Blindness 16,44,508
I RNTCP 31,58,900
Total 95,12,568
Total Budget

- 154 -
TOTAL BUDGET NRHM
PART NAME TOTAL
NRHM PART 'A' 14,07,93,971
NRHM PART 'B' 10,07,59,709
NRHM PART 'C' 33,64,153
NRHM PART 'D'-'I' 95,12,568
TOTAL 25,44,30,401

- 155 -
CHAPTER 7
ANNEXURE
ANNEXTURE
DISTRIC HOSPITAL GAPS:

- 156 -
Gaps of District Hospitals:---
# Safety and security and Dignity----1. there is need of patient privacy and during general OPD. 2. Free movement of patient attended in labor room and Gyne OT as needed guard for that to not inter in that area.
3. lack of proper documentation. 4. lack of the safety and security to patient personal property.
# Regulatory complains-------
1. X-ray machine are used without AERB clearness as State have to interven in this regard to IGMS System.
2. No fire safety.
# Administrative problem---------
1. lack of written communication 2. Negligence to medical services. 3. Lack of ABC inventory system so needed one operator and one desktop with all accessories. 4. Lack of Drug . 5. Lack of HR department at District level. 6. Lack of Feed back system so need of one feedback department. 7. Lack of intercom phone connectivity so that one department and other staff could
communicate with them so medical services should be insure properly. 8. Lack of central sterilization services department. 9. Lack of Regular Audit According to IPHS norms. Need quarterly audit after formation of Audit
team. 10. Lack of tries area. 11. Lack of cafeteria. 12. Need of insect cacher . 13. Lack of management in Dietary services Delivery. 14. Lack of Laundry department. 15. Lack of hot water arrangement.
HR Requirement in Disrict Hospital and some common Department for District.
Department Required Personal and Expected output.

- 157 -
name
Filling and Record maintains Department at district Hospital.
Need 10 personal ( in that 4 should be diploma in medical record + 4 clerks and 2 fourth grade staff with 24*7).
HR department for district
Need 2 Data operator 4 Clerks 2 Managers. Total of 8 personal team which will work for entire district and proper use of human resource could be used as DPC could work as HR Head of Department as it is immense part of Planning.
Data Operator and Accountant to Department
TB, NLEP need one Data operator and one Accountant.
Central Sterilization service Department for District Hospital.
4 personal for this department, they all will be master in sertization
OT assistant for district
30 OT assistant for all district so that C-Section could be Strengthen.
Sanctioned Current working Vacant position
ANM 307 290 17
MO
144 70 74
SPECIALIST 51 14 37
Training required for MO.
Facility Name Lsas Emoc Mtp Nssk f-imnci
Imnci Mini-lap
Laproscopy Nsv Iucd Others

- 158 -
Sadar Hp 4 4 4 4 4 4 2 2 4 4
RH Makhdumpur
4 4 4 4 4 4 4 4 4 4
PHC Ratni 4 4 4 4 4 4 4 4 4 4
PHC Hulasganj
2 2 2 2 2 2 2 2 2 2
PHC kako 2 2 2 2 2 2 2 2 2 2
PHC Sadar 2 2 2 2 2 2 2 2 2 2
PHC Okari 3 3 3 3 3 3 3 3 3 3
Total 21 21 21 21 21 21 19 19 21 21
Training Required to ANM.
Facility Name NSSK SBA IMCI IUCD OTHERS
PHC okari 9 6 9 9
PHC Sadar 9 6 9 9
PHC Kako 4 4 4 5
PHC Hulasganj 4 4 4 4
PHC Ratni 3 1 3 3
RH Makhdumpur 8 8 8 8
District Hospital 9 9 9 9
HSC OF all District 100 39 100 100
Total 146 77 146 147

- 159 -
VILLAGE HEALTH ACTION PLAN 2012 – 2013
MAKHPA, PHC MAKHDUMPUR
District Patna
District Patna
Jehanabad
Kako Modanganj
Ratni Faridpur
Ghosi
Makhdumpur
Hulasganj
District Nalanda
District Arwal
District Gaya
District Patna District Patna

- 160 -
Acknowledgements This Village Health Action plan prepared Under a Short & Hard Process of
about survey of concerned village and this was a good Opportunity to revisit the situation of health services status and national programmes in Village as well as to have a positive dialogue with departments like Public Health Engineering, Women and Child Development, Maternal and Child Health care etc.
This document is an outcome of a collective effort by a number of individuals, related to our institutions and programmes:-
v Mr Balamurgan D ,Chairperson of District Health Society, Jehanabad was a source of inspiration towards this effort vide her inputs to this process.
v Dr.Shobha Sinha (C.S) always supported throw her guiding words and language.
v Mr. Nimish Manan, District Programme Manager was in incharge for the development of the VHAP(2012-13) .
v Mr Ravi Shankar Kumar , Distirct Planning Coordinator has given full time effort in developing VHAP(2012-13).
v Dr B.N.Sharma (MOIC) Block level Nodal Officer PHC cum Referral Hospital, Makhdumpur has put huge effort in this Planning.
v Mr. Md. Shamshad Alam (Block Health Manager) PHC cum Referral Hospital, Makhdumpur has given full time efforts.
v Mr. Kunal Bharti (Hospital Manager) Referral Hospital, Makhdumpur has given huge support.
v All Village Level Staffs, ASHA, AWW, PRI member have supported with their full participations, cooperation and learning spirit through out this process. I on behalf of the Health Sub Centre, Dakara, PHC Makhdumpur
acknowledge the grateful contribution of all those mentioned above.
ANM (Nodal)
HSC Dakara,

- 161 -
PHC cum Referral Hospital, Makhdumpur
NAME OF BLOCK- Makhdumpur
Name of HSC - Dakra
Village Name- Makhapa
Introduction , Profile of the Block & Village:------
Introduction (Objective):------------
· To Analyze the Health Facility at the level of end User.
· Decentralization of Planning Process.
· To Full fill the Gaps of Health Services for Villagers.
Block & HSC Profile:---------
Introduction:-------
Makhdumpur PRIMARY HEALTH CENTER (P.H.C) cum Referral Hospital
Makhdumpur is situated at 18 km from the district head quarters. It is on the NH-83, which
connects Patna to Gaya..
Topography and Terrain :
Fertile alluvial soil locally called "Kewal" supports the district's predominantly
agricultural economy and is currently being tilled for production of paddy, wheat, cane, potato, pulses,
vegetables etc. graphical constraints and lack of metalled road communication carrying out of anti
naxal operations becomes a tedious task. Since, there several commoflause and concealment places the
naxals take shelter in these areas and convene secret meetings and out spread the extremist ideology.
Dialect :
The dialect spoken here is Magadhi (Magahi).
Administration:
There are 22 Gram Panchyats.
HSC Dakra is far away around 6 km from PHC Cum Referral Hospital Makhumpur.
ANM Name ----- Chinta Kumari ®, MO- 9234665515
Surekha Kumari © MO- NA
Village Profile:---------
Makhpa village is around 1400 populated Village. There are 1 Urdu Primary School, 1 AWC. This
Village Connectivity with Road (Gramin Sadak). Purley Muslim family Based Village. There incomes

- 162 -
Sources based on Agriculture and service. Educated peoples are living here. One of Famous leader of
JD (U) Md. Shakil Ahamad khan belongs to this village.
Team and Respondent Details:---------
Team Member-
A) BHM
B) ANM
C) ASHA
D) AWC
Respondent- Villagers

- 163 -
Process:------
District Level Meetingà Block Level meeting -à Selection of village--àSelection Of Team Member à Gram Shabha along With Villagers -à Collection of Feed back of Villagers -à Sharing with Block and District Officials-à Preparation of Village Health Action Planà Final approval through ANM.
General Information
Name of ANM ® Chinta Kumari SBA trinned
Name of ANM © Surekha Kumari
Name of HSC Dakara
Name of Panchayat Makhpa
Name of APHC tagged Dharaut
Distance of village from HSC 1 km
Distance of Village from PHC 6 km
Population of Village ( 2011 census) 1400
Number of AWC in Village 1
Total Population Covered SC
Male
Female
Total No of SHG in Village
Name of Asha Sita Devi
Total Population Adolescent the age
group of 10-19 Female population in the age of
Child population
M F Total M F Total 15-49 Above 49 years
0-6 months
6mn –
2yrs
2-6 years
Total
765 635 1400 88 82 170 366 187 25 73 63 161
CHILD HEALTH

- 164 -
Nutritional Status (weight for age) Name of AWC
No of Children in AWC
Grade I Grade II
Grade III
Grade IV
Total
0-3 years 20 28 15 5 68 Makhpa
3-6 years 28 40 10 0 78
Name of Village
Name of hamlet Source for Drinking water
Distance from the hamlets
Is it available round the year
Alternate source of
water
HAND PUMP Yes well
Makhpa
Village Health and Sanitation Committee:
VHSC
formed
Name of the
members
Designation Number of
meetings of the VHSC
Name of the VHSC member of monitoring committee
Designation Funds with the VHSC
No. of meetings
of the monitoring committee
Yes Shushma kumari
Chairman Shushma Kumari
Mukhiya 147460
Chinta Kumari
Secretary Sita Devi ASHA
Kiran Kumari
AWW
Village Details:

- 165 -
Distance from health centres in km
HSC APHC PHC
Motorable road
AWC
School
Electricity
A meeting
hall
1 km 7 km 6 km Yes Yes Yes Yes Yes
Diseases in summer season
Sun Stroke
Diarrea
Diseases in rainy season
Diarrea
Diseases in Winter season
Ashthma
Epidemiology pattern (Season wise major
illnesses)
Village Health & Nutrition Day (Till 0-4-2011 to 30-9-2011)
Name of the Village
VHND Day Participants in VHND Day
Major activities carried out on the day
Any suggestions for improvement
Makhpa 5 Villagers, ANM, ASHA,AWC
RI, Condom Distribution, FP
Counselling,ANC,PNC
Within 30 minutes Availability of Referral Transport:
SNO Name of Village
Name of ASHA
Vehicle Type
Vehicle No Name & Mobile No
Remarks
1 Makhpa Sita Devi

- 166 -
What are health services have Positive impact (villager’s findings)
· ASHA working at Grass root level that is Good. · Availability of Drug through ASHA Kit at emergency time has Good Impact on Villagers. · People are Satisfied with RI Facility. · Villagers are satisfied with counseling session during there visit about sanitation, Family
Planning.
What are the suggestions of community/ASHA/ANM/AWW
· Delivery Facility at HSC level. · Insure the Availability of Drug. · Use the Fund of VHSC. · Demand of Doctor on HSC level. · OPD Daily Facility on HSC Level. · Drinking Water Facility should be made available in Summer Season. · Need DDT spray in Village.

- 167 -
Conclusion
Makhpa Villagers are Satisfied with Govt. Facility but they have demand to open HSC daily, so that they find easy to avail services of health facility in easy way. They demanded more drugs available to ASHA / ANM so that they could find Drugs at emergency time. Demand of Doctor at HSC level was most Prerotisable. At HSC level demand of 24*7 Facility. Drinking Water Facility should be Available in Drought condition because of Drought Prone Area. Sanitation Problem should be Strengthen.

- 168 -
VILLAGE HEALTH ACTION PLAN 2012 – 2013
LODIPUR , PHC JEHANABAD
District Patna
District Patna
Jehanabad
Kako Modanganj
Ratni Faridpur
Ghosi
Makhdumpur
Hulasganj
District Nalanda
District Arwal
District Gaya
District Patna District Patna

- 169 -
Acknowledgements This Village Health Action plan prepared Under a Short & Hard Process of
about survey of concerned village and this was a good Opportunity to revisit the situation of health services status and national programmes in Village as well as to have a positive dialogue with departments like Public Health Engineering, Women and Child Development, Maternal and Child Health care etc.
This document is an outcome of a collective effort by a number of individuals, related to our institutions and programmes:-
v Mr Balamurgan D ,Chairperson of District Health Society, Jehanabad was a source of inspiration towards this effort vide her inputs to this process.
v Dr.Shobha Sinha (C.S) always supported throw her guiding words and language.
v Mr. Nimish Manan, District Programme Manager was in incharge for the development of the VHAP(2012-13) .
v Mr Ravi Shankar Kumar , Distirct Planning Coordinator has given full time effort in developing VHAP(2012-13).
v Dr Dilip Kumar Sinha (MOIC) Block level Nodal Officer PHC Jehanabad has put huge effort in this Planning.
v Mr. Anup Sinha Block Health Manager PHC Jehanabad has given full time efforts.
v Mr. Rajeev Ranjan has given huge support. v All Village Level Staffs, ASHA, AWW, PRI member have
supported with their full participations, cooperation and learning spirit through out this process.
I on behalf of the Health Sub Centre, Karuna, PHC Jehanabad acknowledge the grateful contribution of all those mentioned above.
ANM (Nodal)
HSC KARUNA,
PHC, JEHANABAD

- 170 -
NAME OF BLOCK- Jehanabad
Name of HSC - Karuna
Village Name- karuna
Introduction , Profile of the Block & Village:------
Introduction (Objective):------------
· To Analyze the Health Facility at the level of end User. · Decentralization of Planning Process. · To Full fill the Gaps of Health Services for Villagers.
Block & HSC Profile:-----------
Jehanabad PRIMARY HEALTH CENTER is situated at 1 km from the district
head quarters. It is on the NH-83, which connects Patna to Gaya.
Topography and Terrain : Fertile alluvial soil locally called "Kewal" supports the district's predominantly
agricultural economy and is currently being tilled for production of paddy, wheat, cane, potato,
pulses, vegetables etc. graphical constraints and lack of metalled road communication
carrying out of anti naxal operations becomes a tedious task. Since, there several
commoflause and concealment places the naxals take shelter in these areas and convene
secret meetings and out spread the extremist ideology.
Dialect : The dialect spoken here is Magadhi (Magahi).
Administration: There are 14 Gram Panchayats.
HSC Karuan is far away around 4km from Sadar Hospital.
ANM Name ----- Nitu Kumari,© MO- 8804243041
Maya Kumari © MO-
Village Profile:---------
Lodipur village is around 975 populated Village. There are 1 Middle School, 1 AWC. This
Village Connectivity with Train root and Road (Gramin Sadak). Peoples are well educated,
well cultered, Purley Hindu family Based Village. There incomes Sources based on
Agriculture.

- 171 -
Team and Respondent Details:---------
Team Member-
E) BHM
F) ANM
G) ASHA
H) AWC
Respondent- Villagers
Process:------
District Level Meetingà Block Level meeting -à Selection of village--àSelection Of Team Member à Gram Shabha along With Villagers -à Collection of Feed back of Villagers -à Sharing with Block and District Officials-à Preparation of Village Health Action Planà Final approval through ANM.
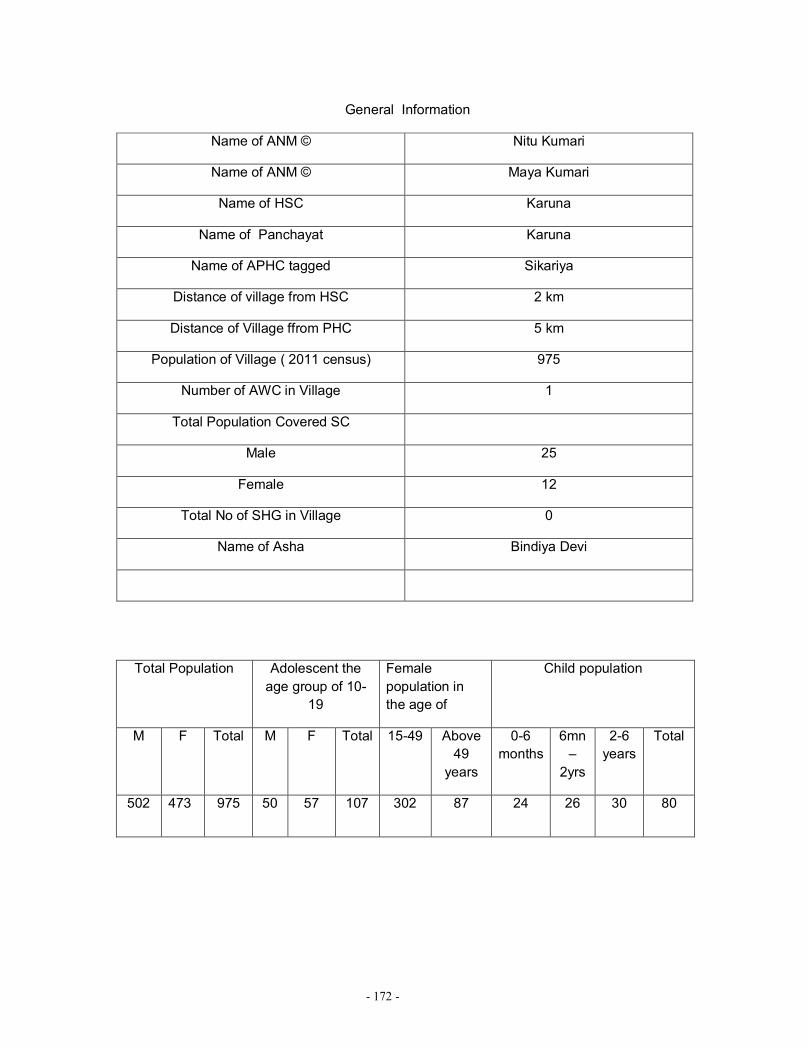
- 172 -
General Information
Name of ANM © Nitu Kumari
Name of ANM © Maya Kumari
Name of HSC Karuna
Name of Panchayat Karuna
Name of APHC tagged Sikariya
Distance of village from HSC 2 km
Distance of Village ffrom PHC 5 km
Population of Village ( 2011 census) 975
Number of AWC in Village 1
Total Population Covered SC
Male 25
Female 12
Total No of SHG in Village 0
Name of Asha Bindiya Devi
Total Population Adolescent the
age group of 10-19
Female population in the age of
Child population
M F Total M F Total 15-49 Above 49
years
0-6 months
6mn –
2yrs
2-6 years
Total
502 473 975 50 57 107 302 87 24 26 30 80

- 173 -
CHILD HEALTH
Nutritional Status (weight for age) Name of AWC
No of Children in AWC
Grade I Grade II
Grade III
Grade IV
Total
0-3 years 30 20 8 1 59 Lodipur
3-6 years 22 10 2 0 34
Name of Village
Name of hamlet Source for Drinking
water
Distance from the hamlets
Is it available round the year
Alternate source of
water
Hand pump Yes Well
Lodipur
Village Health and Sanitation Committee:
VHSC
formed
Name of the
members
Designation Number of
meetings of the VHSC
Name of the VHSC member
of monitoring committee
Designation Funds with the
VHSC
No. of meetings
of the monitoring committee
Yes Sanjay Kumar
Chairman 1 Manju Sinha
Mukhiya 10000
Sushila kumara
Secretary Bindiya Devi
ASHA
Village Details:

- 174 -
Distance from health centres in km
HSC APHC PHC
Motorable road
AWC
School
Electricity
A meeting
hall
2 km 6km 4 km Yes Yes Yes Yes Yes
Diseases in summer season
Sun Stroke
Diarrea
Diseases in rainy season
Diarrea
Diseases in Winter season
Ashthma Pneumonia
Epidemiology pattern (Season wise major
illnesses)
Village Health & Nutrition Day (Till 0-4-2011 to 30-9-2011)
Name of the Village
VHND Day Participants in VHND Day
Major activities carried out on the day
Any suggestions for improvement
Lodipur 5 Villagers, ANM, ASHA,AWC
RI, Condom Distribution, FP
Counselling,ANC,PNC
Done in Broad Manner

- 175 -
Within 30 minutes Availability of Referral Transport:
SNO Name of Village
Name of ASHA
Vehicle Type
Vehicle No Name & Mobile No
Remarks
1 Lodipur Bindiya Devi
Referral system is vey poor.
What are health services have Positive impact (villager’s findings)
· ASHA working at Grass root level that is Good. · Availability of Drug through ASHA Kit at emergency time has Good Impact on
Villagers. · People are Satisfied with RI Facility.
What are the suggestions of community/ASHA/ANM/AWW

- 176 -
· Delivery Facility at HSC level. · Insure the Availability of Drug. · Use the Fund of VHSC. · Demand of Doctor on HSC level. · OPD Daily Facility on HSC Level. · Regular Visit of ANM not only in RI Day.
Conclusion
Lodipur Villagers are Satisfied with Govt. Facility but they have demand to open new HSC in there village. Reffral system is very Poor. They Want Ambulance Facility over there. There attention toward AWC to more strengthen. They demanded more drugs available to ASHA so that they could find Drugs at emergency time.

- 177 -
NAME OF HEALTH SUB-CENTER
S.NO NAME OF PHC
Functional/ Sanc.
NAME OF HSC
Running in
Building
Land Availability
Remarks 1 Remarks 2
1 Jehanabad 12/13 1. kasai Own Govt. Building
2. Amain Own Govt. Building
3. Pinjaura Own Govt. Building
4. Gonma Rent Yes
khata no- 274, plot no- 2442
Iap, water lodging
5.Sewanan Own Govt. Building
6. Mustichak Panchayat Bhawan Yes
khata no- 32, plot no-
360
Iap, Started foundation
work
7. Paras Bhigha Rent Yes
khata no-
50,khasra- 94
Iap, Till linter work.
8. Kinari Own Govt. Building
9. Ramdev Chak Rent Yes
khata no-133, khasra no- 441
Iap, Foundation
work

- 178 -
10. Bhewad Own Govt. Building
11. Bhawani Chak Rent Yes
khata no-
76,khasra-2452
Iap, Plinth level
12. Karuna Hault
Own Govt. Building
13. Kamdev Bhigha ( Non Functional)
Yes
Building underconstruction floor not completed, window glasses not fixed, not
hand over
2 Modanganj 12/12 1. Dewara Own Govt Building Need minor
repair
2. Jalapur Rent Yes Iap,
Foundation work
3. Naima Rent No
4. Aarhit Own Govt Building Need minor
repair
5. Pitambarpur
In pustkalaya Yes Iap, Plinth
level
6. Saistabad Own Govt Building Need minor
repair
7. Masad Rent Yes Iap,
Foundation work
8. Muriya Bigha
Own Govt Building Need minor
repair 9. Modanganj Rent No
10. Baina Own Govt Building Need minor
repair
11.Sakrautha Own Govt Building Need minor
repair
12. Charui Own Govt Building
3 Makhdumpur 21/22 1. Newari Rent No
2. Ikkil Own Govt. Building Need
baundary
3. Supi Panchayat Bhawan No

- 179 -
4. Mahamat pur 1
Own Govt. Building
5. Shekhpura Rent No 6.Tilkai Rent No 7. Makarpura Rent No
8. Serthua Own Govt. Building
9. Sumera Own Govt. Building
Need Major
Repairing
10. Sugao Panchayat Bhawan No
11. Nawabganj Rent No
12. Bhimpura Own Govt. Building
13.
Mahamatpura 2
Rent No
14. Machil Rent No
15. Dhoda Own Govt. Building
Need Minor
Repairing
16. Umata Own Govt. Building Need minor
repairing
17. Dakara Own Govt. Building
18. Bishunganj
Own Govt. Building Need minor
repairing
19. Saidpur Own Govt. Building
20. Kohara Own Govt. Building Complete handed over
on 2-9-11
21. Indarpur
(Non Functional)
Yes Under consturction
22. kohra Own Govt. Building
4 Kako 21/21 1. Uttar Serthu
Own Govt. Building

- 180 -
2. Barwa Rent No
3. Sfepur Own Govt. Building
4. Chandaura Rent Yes Iap
5.Dewghara Rent Yes Iap, water logging
6.Ainwa Own Govt. Building
7. Saidabad Rent Yes Iap,fondation work
8. Firoji Running in AWC Yes
Govt. Building is ready, not hand over
yet
9. Hatee Own Govt. Building
10. Pinjaura Rent No
11. Nawada Own Govt. Building
12.
Paigamwar Pur
Own Govt. Building
13. Asiyawa Rent No
14. Emaliya Own Govt. Building
15. Bemabhai Own Govt. Building
16. Nonahi Own Govt. Building
17. Purbi
Kako ( Functional)
No
18. Pashchami
Kako ( Functional)
No
19. Maniyawa Running in AWC Yes
Building Undercons
truction
Building complete but not
functional

- 181 -
20. Bibipur Running in AWC No
Govt. Building is ready, not hand over
yet
21. Choti Murhari
Own Govt. Building
5 Ratni- Faridpur 12/12 1. Badetha Own Govt
Building
2. Jhunathi Panchayat Bhawan Yes
Building unconstructi
on during long time
3. Dhanadihari Rent No
4. Sarta Rent No
5. Sariya Bazar
Own Govt Building
6. Pokhawa Rent No
7. Ratni Bazar Rent No
8. Kundila Rent No 9. Sohraiya Rent No
10. Murhara
Own Govt old
Building ( working on rent)
Fully Damaged
that cannot be
repaired
11. Kansua Panchayat Bhawan No
12. Seshambha
Own Govt Building
New Building complete & hand
over
6 Hulasganj 9/11 1. Murgao Own Govt Building
2. Davathu Own Govt Building
3. Khudauri Rent Yes controversail Land
4. Adrakhi Bigha
In Indra Awas No
5. Ginji Own Govt Building
6. Kokarsa Own Govt Building

- 182 -
7. Keur Own Govt Building
8. Tira Own Govt Building
9. Narma Own Govt Building
10. Kandaul (
Non Functional)
Own Govt Building
11. Bhagwan
pur (Non functional)
Yes
New Building Under
construction
7 Ghosi 9/12 1. Dhuriyari Rent No
2. Bajitpur Own Govt Building
3. Lakhawar Rent No 4. Ahiyasa Rent No
5. Bharthu Own Govt Building
6. Dehuni Rent Yes
Building complete
but Plaster of Floor, windows,
work septic tank
and bathroom work not
complete.
7. Sahobigha Rent No
8. Uber Panchayat Bhawan No
9. Kure Own Govt Building
10. Birpur (
Non Functional)
Yes Building
Underconstruction
11. Daharpur
( Non Functional)
Yes Building
Underconstruction
12 Parawan
(Non functional)
Yes Building
Underconstruction
Total 96/103
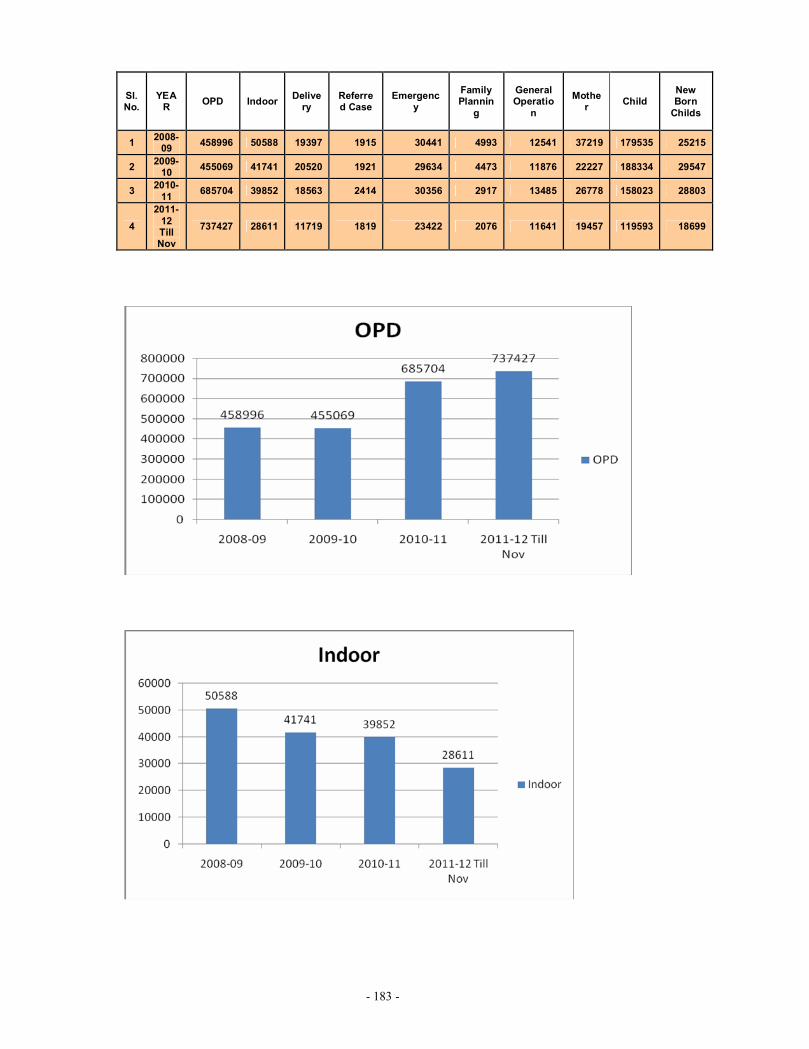
- 183 -
Sl. No.
YEAR OPD Indoor Delive
ry Referred Case
Emergency
Family Plannin
g
General Operatio
n
Mother Child
New Born
Childs
1 2008-09 458996 50588 19397 1915 30441 4993 12541 37219 179535 25215
2 2009-10 455069 41741 20520 1921 29634 4473 11876 22227 188334 29547
3 2010-11 685704 39852 18563 2414 30356 2917 13485 26778 158023 28803
4 2011-
12 Till Nov
737427 28611 11719 1819 23422 2076 11641 19457 119593 18699
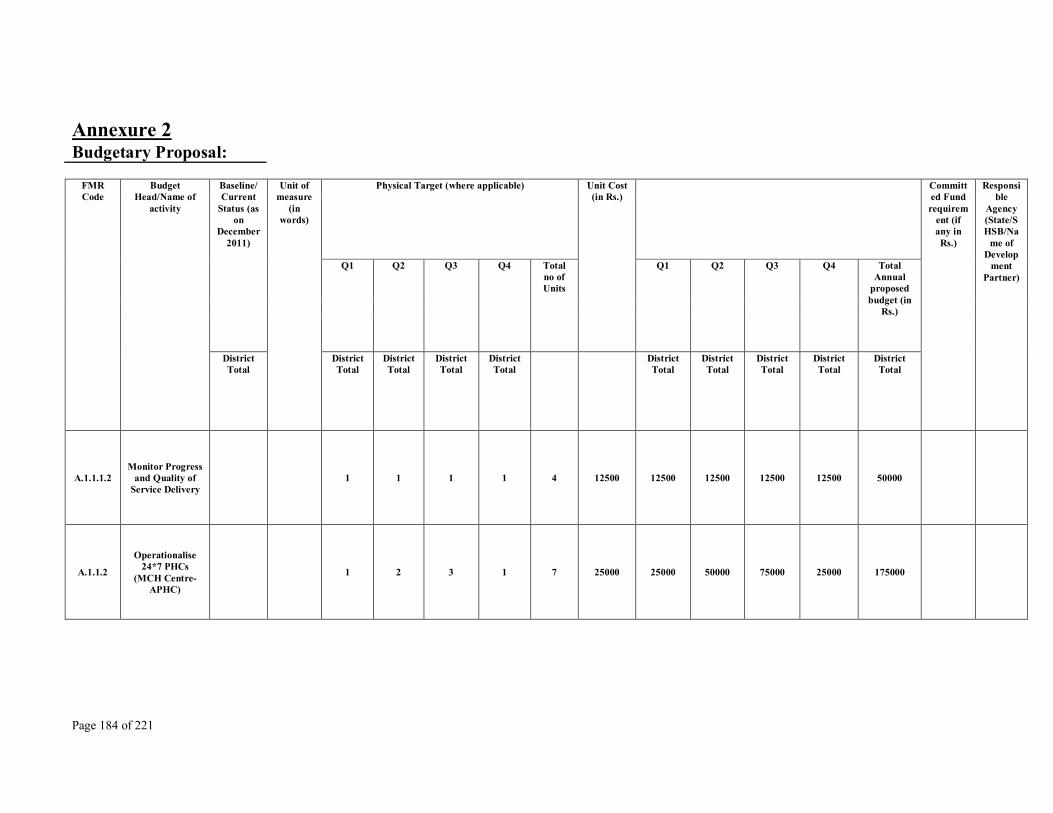
Page 184 of 221
Annexure 2 Budgetary Proposal:
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A.1.1.1.2 Monitor Progress
and Quality of Service Delivery
1 1 1 1 4 12500 12500 12500 12500 12500 50000
A.1.1.2
Operationalise 24*7 PHCs
(MCH Centre- APHC)
1 2 3 1 7 25000 25000 50000 75000 25000 175000
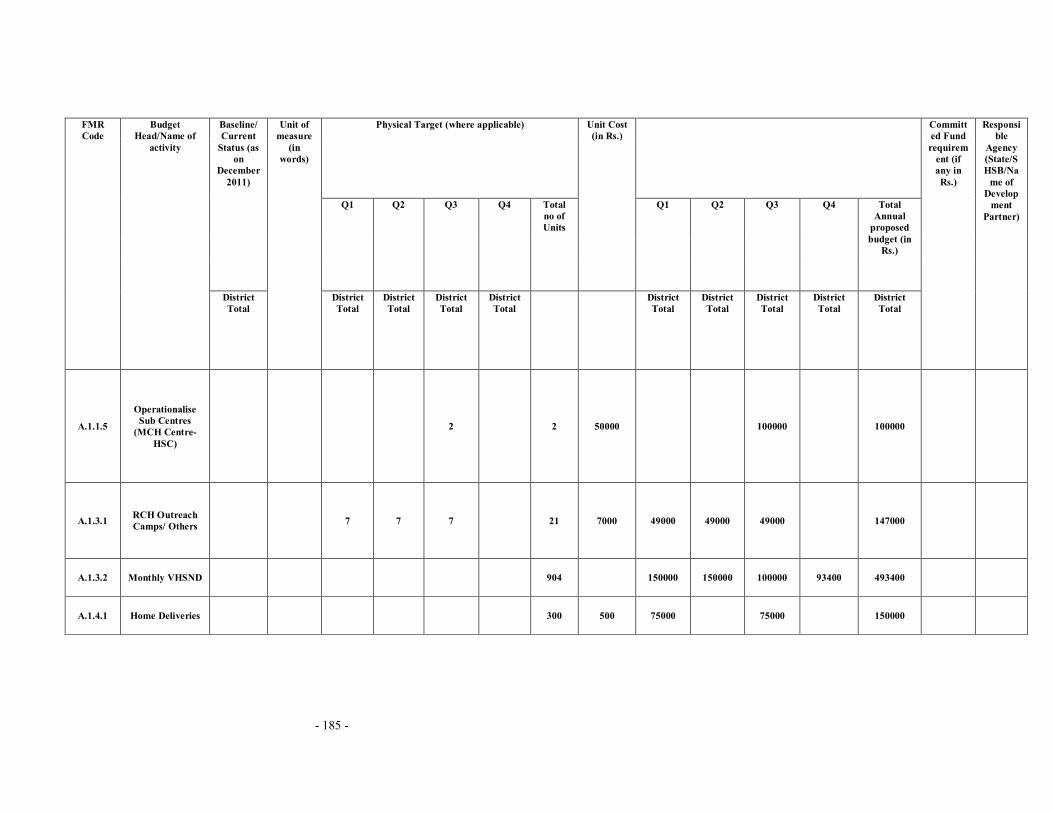
- 185 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A.1.1.5
Operationalise Sub Centres
(MCH Centre- HSC)
2 2 50000 100000 100000
A.1.3.1 RCH Outreach Camps/ Others 7 7 7 21 7000 49000 49000 49000 147000
A.1.3.2 Monthly VHSND 904 150000 150000 100000 93400 493400
A.1.4.1 Home Deliveries 300 500 75000 75000 150000

- 186 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A.1.4.2.a Rural
(Institutional Delivery)
8000 6000 5000 4755 23755 2000 16000000 12000000 10000000 9510000 47510000
A.1.4.2.b Urban
(Institutional Delivery)
1000 800 800 624 3224 1200 1200000 960000 960000 748800 3868800
A.1.4.2.C Institutional Deliveries C-
section 70 70 60 60 260 1500 105000 105000 90000 90000 390000
A.1.4.3 Administrative Expenses 81223 81223 81223 81223 324892
A.1.5 Maternal Death Review 50 50 50 50 200 750 37500 37500 37500 37500 150000
innovation 0

- 187 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
(A)
Monitoring by MO
Transportaion Expences to visit
HSC on Fixed day in month
three times at one HSC.
864 864 864 864
96 HSC* 3 times*1
2 month
300 259200 259200 259200 259200 1036800
A.2.1.1
Implementation of IMNCI
activities in districts
50000 50000
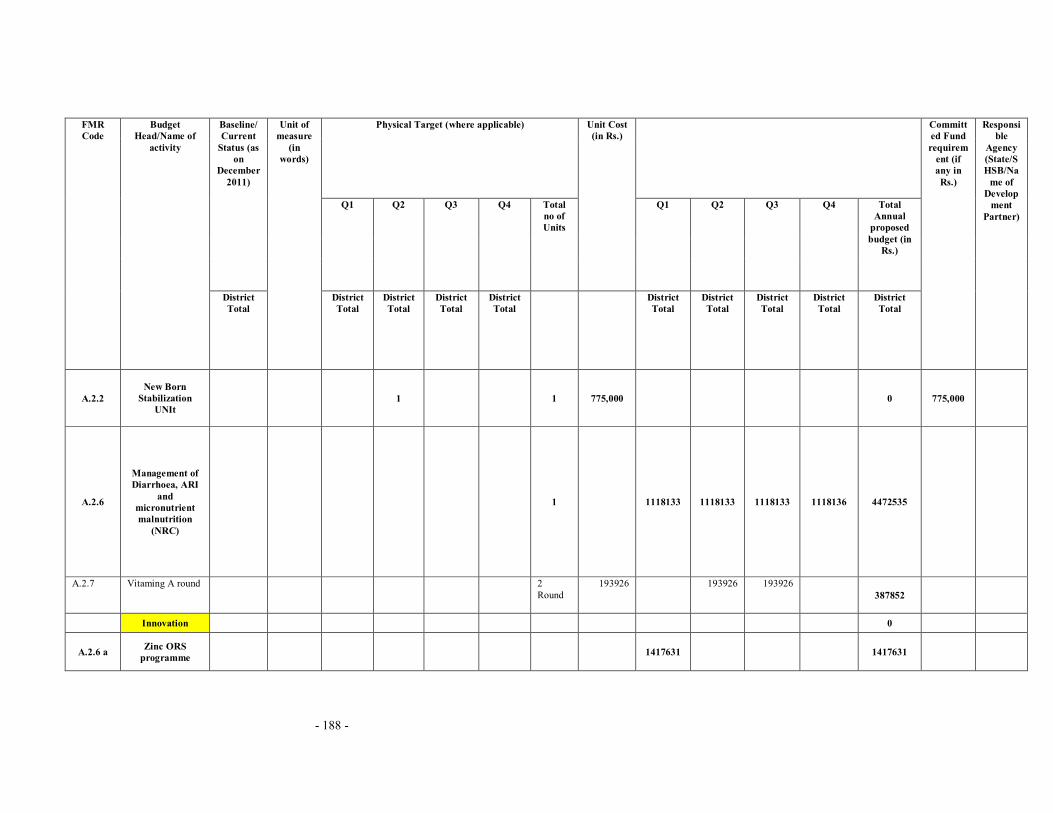
- 188 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A.2.2 New Born
Stabilization UNIt
1 1 775,000 0 775,000
A.2.6
Management of Diarrhoea, ARI
and micronutrient malnutrition
(NRC)
1 1118133 1118133 1118133 1118136 4472535
A.2.7 Vitaming A round
2 Round
193926
193926 193926 387852
Innovation 0
A.2.6 a Zinc ORS programme 1417631
1417631

- 189 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
Promotion/ senitization
programme on world breast
feeding week and National
Nutrition week at District
1* 2 event 50000 100000 100000
Block 7*2 event 10000 140000 140000
b.
HSC level 96* 2 event 1000 192000 192000

- 190 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A.3.1.1
Dissemination of Manuals on Sterilization
Standers & QA of sterilization
services
20000 20000
A.3.1.2 Female
Sterilization Camps
54 54 54 54 216 5000 270000 270000 270000 270000 1080000
A.3.1.3 NSV Camps 1 1 1 1 4 5000 5000 5000 5000 5000 20000
A.3.1.4 Compensation
for Female Sterilization
1800 1000 2000 1200 6000 1000 1800000 1000000 2000000 1200000 6000000

- 191 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A.3.1.5 Compensation
for Male Sterilization
186 186 186 186 744 1500 279000 279000 279000 279000 1116000
A.3.1.6
Accreditation of Private Providers for sterilization
services
200 300 200 300 1000 1500 300000 450000 300000 450000 1500000
A.3.3 POL for Family Planning 29750 29750 29750 29750 119000
A.3.5.4
Provide IUD services at Health
Facility (IUD camps)
7 7 7 7
28 camps
for Block.
1500 10500 10500 10500 10500 42000

- 192 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
1
1 mega camp
for District
2000 2000 2000
Innovation 0
Prize for Debate competition 22 24 23 24
93 pancha
yat 500 11000 12000 11500 12000 46500
A.4.2 School Health Programme 1500000 1500000
Weekly IFA
Supplementation Programme
90111
52 tabs/year per girls* RS 0.105
123000 123000 123000 123006 492006

- 193 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
Training of
ANM,ASHA,AWW
2029 2029 70 142030 142030
Budget for Social Mobilization and
IEC, BCC material
964 50 12050 12050 12050 12050 48200
A.7.2 PNDT Sex Ratio 1 100,000 25000 25000 25000 25000 100000

- 194 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A.8.1.1
ANMs, Staff Nurses,
Supervisory Nurses (salary Contractual
ANM/Contractual SN)
0
A Grade 39 22000*12 2574000 2574000 2574000 2574000 10296000 858000
ANM 139 12650*12 5275050 5275050 5275050 5275050 21100200 1758350
A.8.1.2 Laboratory
Technicains in Blood Banks
3 11000*12 99000 99000 99000 99000 396000

- 195 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A.8.1.5
Medical Officers at CHCs/ PHC
(Salary of Mo in Blood Banks)
1 35000*12 105000 105000 105000 105000 420000 35000
A.8.1.7
Others- Computer
Assistants/ BCC Co-ordination etc (FP Counsellors)
1 15000*12 45000 45000 45000 45000 180000
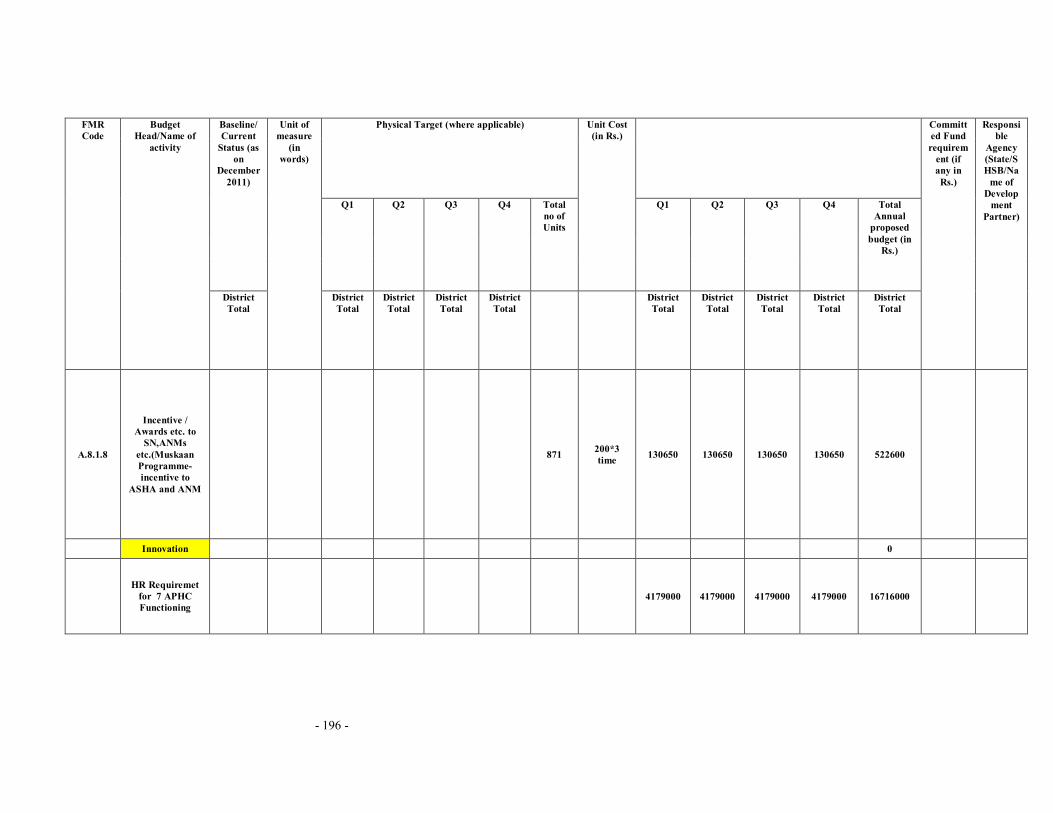
- 196 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A.8.1.8
Incentive / Awards etc. to
SN,ANMs etc.(Muskaan Programme- incentive to
ASHA and ANM
871 200*3 time 130650 130650 130650 130650 522600
Innovation 0
HR Requiremet
for 7 APHC Functioning
4179000 4179000 4179000 4179000 16716000

- 197 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A.9.3.1 Skilled
Attendance at Birth
3 3 2 2 10 batch 88110 264330 264330 176220 176220 881100
A.9.3.7
Other MH training (any
Integrated training,etc)
1 1 2 115000 115000 115000 230000
A.9.5.1 IMNCI 8 9 8 8 33 batches 134760 1078080 1212840 1078080 1078080 4447080
2 TOT, 159600 159600 159600 319200
2 Follow
up supervi
sion
54860 54860 54860 109720

- 198 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A.9.5.5.3 NSSK Training 1 1 1 1 4 52900 52900 52900 52900 52900 211600
A.9.6.2 Minilap Training 1 1 70237 70237 70237
A.9.6.4.1 Training of
Medical Officers in IUD insertion
1 1 55300 55300 55300
A.9.6.4.2 Training of
ANMs/LHVs/SN in IUD Insertion
1 1 1 3 29425 29425 29425 29425 88275
A.9.8.2 DPMU Training 1 50000 50000 50000

- 199 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
Mamta Training 59
participants
48785 48785
A.10.1.5 Mobility Support (District Malaria
Office) 45000 45000 45000 45000 180000
A.10.2.1
Contractual Staff for DPMU
Recruited and in Position
0

- 200 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
District
Programme Manager
1 42000*12 126000 126000 126000 126000 504000
District
Accoutants Manager
1 35937*12 107811 107811 107811 107811 431244
District M&E Officer 1 29947*12 89841 89841 89841 89841 359364
District Planning Coordinator 1 22,000*12 66000 66000 66000 66000 264000
Recurring Expenses 1,05,000*
12 315000 315000 315000 315000 1260000

- 201 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A.10.2.2
Provision of Equipment
/furniture and mobility support for DPMU Staff
305000 305000 305000 305000 1220000
A.10.3 Strengthening of Block BPMU 1416030 1416030 1416030 1416030 5664120
A.10.4.2 Renewal (upgradation)
1 district,
7 blocks
8100 2700 27000 27000

- 202 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A10.4.3 AMC (state, Regional &DHS)
1 district,
7 blocks
22,500 10,000 92500 92500
A.10.4.9
Management unit at FRU (Hospital Manager & FRU
Accountant)
2 495000 247500 247500 247500 247500 990000
A.10.5.1 Annual Audit of the programme (Satutory Audit)
4 36000 36000

- 203 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
A.10.6 Concurrent
Audit (state & District)
1 60000 60000 60000 60000 240000
B. 1.1.1 Asha Training 871 5100 2221050 2221050 4442100
B.1.1.2 Asha Drug kit & Replenishment 871 250 217750 217750
B.1.1.3 Asha Divas 871 100 261300 261300 261300 261300 1045200
B.1.1.4.A Awards to Asha/ link 7 2000 14000 14000
2nd prize 7 1000 7000 7000
Worker 7 500 3500 3500
certificate Printing 21 250 5250 5250

- 204 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
B.1.1.4.C Asha Identity Card 871 30 26130 26130
B.1.1.5 Asha Rsource centre 0
DCM salry 1 22,000 66000 66000 66000 66000 264000
DDA salary 1 18,150 54450 54450 54450 54450 217800
BCM salary 7 13,200 277200 277200 277200 277200 1108800
office Expence 0
T.A 7 1000 21000 21000 21000 21000 84000
mobile Recharge 2 300 1800 1800 1800 1800 7200
Internet Recharge 1 750 2250 2250 2250 2250 9000

- 205 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
BCM meeting Snacks 12
month 300 900 900 900 900 3600
B.2.1 Untied Fund for SDH/CHC 2 50000 1,000,000 1000000
B.2.2.a Untied Fund for PHCs 9 25000 225000 225000
B.2.2 b Untied fund for APHCs 32 25000 800000 800000
B.2.3 Untied fund for sub centre 96 10000 960000 960000
B.2.4 Untied fund for VHSC 552 10000 5520000 5520000
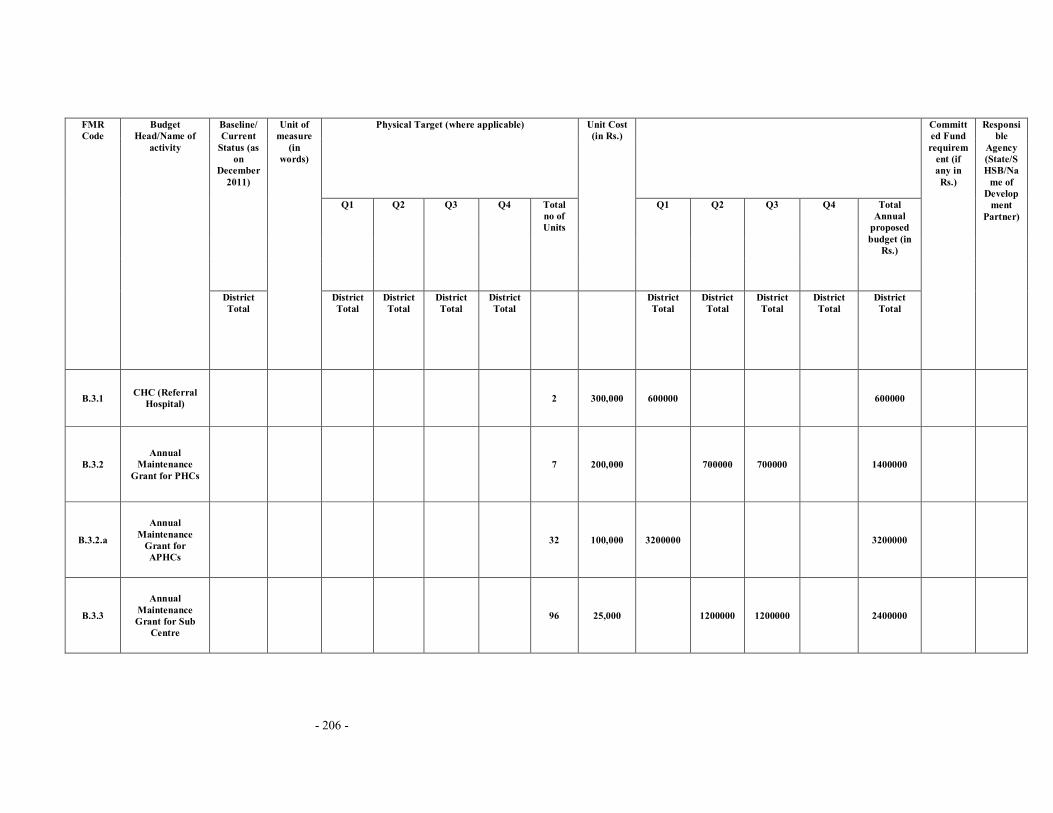
- 206 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
B.3.1 CHC (Referral Hospital) 2 300,000 600000 600000
B.3.2 Annual
Maintenance Grant for PHCs
7 200,000 700000 700000 1400000
B.3.2.a
Annual Maintenance
Grant for APHCs
32 100,000 3200000 3200000
B.3.3
Annual Maintenance Grant for Sub
Centre
96 25,000 1200000 1200000 2400000

- 207 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
Annual
Maintance Grants For DH
1 500,000 250000 250000 500000
B.4.3 Sub Centre Rent
and Contingencies
36 500 54000 54000 54000 54000 216000
B.5.2 b
Construction of Residential quarters for
Doctors and Staff nurses
15 2250000 2250000 4500000

- 208 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
B.5.2 c Strengthening of Cold Chain 800000 800000
Construction, Renovation of
PHC,APHC,HSC,SD (fund Demanded
through District PIP- through DM
Office)
0
632254000
Demanded
through Bihar Govt

- 209 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
B.5.2.a Construction of APHC 2 75.99lakh 0 8,820,000
Construction of HSC 6 9.50 lakh 0 2,280,000
B.6.1 District Hospitals 1 500000 500000 500000
B.6.2 CHCs (RH) 2 100000 200000 200000
B.6.3 PHCs 7 100000 700000 700000
B.6.4 Others (APHCs) 8 8 8 8 32 100000 800000 800000 800000 800000 3200000
B.7 District Action
Plans (including Block, Village)
96 HSC 1500 144000 144000

- 210 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
25 village 1000 25000 25000
7 PHC 5000 35000 35000
1 DHAP 50,000 50000 50000
1 Data Operat
or 6000 18000 18000 18000 18000 72000
B8.1
Constitution and orientation of Community leader & of
VHSC, CHC,PHC,SHC
etc.
93 1500 69750 69750 139500

- 211 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
B.8.2
Orientation workshops,
trainings and capacity Building of PRI at State/ District Health
Societies,CHC,PHC
102 606 61812 61812
B.9.1 a AYUSH Specialists 27 20,000 1620000 1620000 1620000 1620000 6480000

- 212 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
B10.1
Development and operationalize of State BCC/IEC
Strategy
500000 400000 300000 200000 1400000
B 10.3 Health Mela (Leprosy) 1 1 2 5000 5000 5000 10000
B.11 MMU 1 1053000 1053000 1053000 1053000 4212000
Micro plan Preparation at District and at
Block Level with Monitoring
Chart
7 1500 10500 10500

- 213 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
B.12.2.d 102 Ambulance Service
7 (APHC
) 15000*12 315000 315000 315000 315000 1260000
B.12.2.c 108 ambulance 1 429000 429000 429000 429000 1716000
B.12.2.c BLS Ambulance
8 1,16,700*12 2,800,800 2,800,800 2,800,800 2,800,800 11203200
B.13.3.b
Outsourcing of Pathology and
Radiology Services from PHCs to DH
14 1125000 1125000 1125000 1125000 4500000

- 214 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
B.13.3.d IMEP (Bio Waste Management) 13 276000 276000 276000 276000 1104000
Pathological Services for
APHC 7 75000 75000 75000 75000 300000
Outsourcing of
Silent Gensate of 5 KV at aphc
7
RS 150 *24 hrs
*30 days*12 month
2268000 2268000 2268000 2268000 9072000

- 215 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
Outsourcing of dietry Provision
at APHC 7
RS 50*5 patient* 30 days
*12 month
157500 157500 157500 157500 630000
B.14.b
Yukti Yojana Accreditation of
Public and Private Sector For Providing Safe Abortion
Services
304 25791 25791 25791 25793 103166

- 216 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
B.15.3.1.a
State, District , Divisional, Block
Data Centre 9 10,000 270000 270000 270000 270000 1080000
B.15.3.2.a MCTS and HRIS 6 46608 46608 46608 46609 186433
B.15.3.2.b RI Monitoring 7 32500 32500 32500 32500 130000
B.15.3.3.b
Plan for HMIS supportive
Supervision and Data Validation
45500 45500 45500 45500 182000

- 217 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
B.16.1.1
Procurement of Equipment : (MH Labour
Room)
11 167,464 1842104 1842104
B.16.1.2
Procurement of equipment : CH (SCNU &NBCC, ICU equipment)
4,900,000
4900000
B.16.1.3.a
Procurement of Minilap Set :FP 35 3000 52500 52500 105000

- 218 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
B.16.1.3.b
Procurement of NSV Kit (FP) 5 1100 5500 5500
B.16.1.3.c Procurement of IUD Kit (FP) 1 15,000 15000 15000
B.16.2.1.A
Parental Iron sucrose (IV/IM) as therapeutic
measure to pregnant women
with severe Anemia
1 700,000 350000 350000 700000

- 219 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
B.16.2.1.B
IFA Tablets for Pregnant & Lactating Mothers
200000 200000 200000 200000 800000
B.16.2.2.a
IFA small Tablets and
syrup for children 6-59
months
250000 250000 250000 250000 1000000
B.16.2.2.b IMNCI Drug kit 2400 250 300000 300000 600000

- 220 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
B.16.2.5 General Drugs &
Supplies for Health Facilities
3100000 3100000 3100000 3100000 12400000
B.22.4 Support
Strengthening RNTCP
19800 19800 19800 19800 79200
B.23.A Payment of
Monthly Bill to be BSNL
7491 7491 7491 7491 29964
C. pulse Polio 0 945914
C. RI 841038 841038 841038 841039 3364153
D.3 IDD 11000 11000
E IDSP 407510 407510 407510 407510 1630040
F.1.1 Malaria 21000 21000

- 221 -
Physical Target (where applicable) Baseline/Current
Status (as on
December 2011)
Q1 Q2 Q3 Q4 Total no of Units
Unit Cost (in Rs.)
Q1 Q2 Q3 Q4 Total Annual
proposed budget (in
Rs.)
FMR Code
Budget Head/Name of
activity
District Total
Unit of measure
(in words)
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
District Total
Committed Fund requirem
ent (if any in Rs.)
Responsible
Agency (State/SHSB/Na
me of Develop
ment Partner)
F.1.4. Filaria 109555 109555 109555 109555 438220
F.1.5 Kalazar 499000 499000 499000 499000 1996000
G Leprosy 153225 153225 153225 153225 612900
H Blindness 600000 600000 444508 1644508
I RNTCP 789725 789725 789725 789725 3158900
Total 84383579 64538866 55415069 50092887 254430401 15472264