Distal Splenorenal Shunt for Management of Variceal Bleeding in Patients with Schistosomal Hepatic...
8
Distal Splenorenal Shunt for Management of Variceal Bleeding in Patients with Schistosomal Hepatic Fibrosis FAROUK A. EZZAT, F.R.C.S. MOHAMED A. ALY, M.D. OSAMA 0. BAHGAT, M.D. KAREEM M. ABU-ELMAGD, M.B.B.CH. OMAR M. FATHY, M.D. ATEF A. SALAM, M.D.* IBRAHIM Y. ALY, M.D. MOHSIN H. EL-BARBARY, M.D. MICHAEL H. KUTNER, PH.D.t The distal splenorenal shunt was performed in 60 patients with schistosomal hepatic fibrosis in whom no evidence of cirrhosis was documented by preoperative needle and operative wedge bi- opsy. No patients have been lost to follow-up with a median of 37 months (range: 17-86). The results showed low operative mortality (1.7%), high patency rate (92.5%), and low recurrent variceal hemorrhage (6.7%). Thrombosed shunts were treated either by refashioning the shunt (1 patient) or splenectomy and gastric devascularization (2 patients). Initial hyperbilirubinemia and reduction in serum albumin were found in the early post- operative period, with persistent hyperbilirubinemia in 32% of the patients. The 5-year survival was 88%, with liver disease related mortality in only three patients. Clinical encephalopathy was detected in three patients (5.1%); only one of them was in- capacitated. These data showed that: (1) selective shunt (distal splenorenal shunt, DSRS) is an effective surgical procedure in the treatment of schistosomal variceal bleeding, (2) shunt thrombosis is rare and can possible be corrected if detected early, (3) schistosomal patients have a better survival and a lower in- cidence of encephalopathy after DSRS than that reported in cir- rhotics, and (4) liver biopsy should be performed for proper as- sessment of the schistosomal population especially in the geo- graphic areas where the schistosoma parasite and viral hepatitis are endemic. B 5 LEEDING ESOPHAGEAL VARICES as a complication of portal hypertension is the most common cause of upper gastrointestinal hemorrhage in Egypt.' It is the leading cause of death in patients with schisto- somal hepatic fibrosis and portal hypertension. Although the initial bleeding episode may be fatal, patients usually have multiple episodes extending over many years.2 The economic impact of this disease is compounded by the fact that it affects individuals at the peak of their produc- tive life.3 From the Gastroenterology Unit, Department of Surgery, Mansoura University School of Medicine, Mansoura, Egypt Hepatic schistosomiasis represents the prototype of an intrahepatic presinusoidal block with normal architecture and cellular function.2'4 5 Therefore, any protection against recurrent variceal bleeding with maintained portal per- fusion, in such patients with good hepatic reserve could only improve long-term survival and quality of life. Considerable controversy still exists regarding the choice of a particular operative procedure for the treat- ment of portal hypertensive syndrome.6-" The present knowledge of the hemodynamics of schistosomal portal hypertension is at best incomplete. As a result, the rec- ommendation for a surgical approach in the treatment of these patients has been used on personal bias or the un- proven assumption that their response to a given proce- dure is similar to those with alcoholic or posthepatitic liver disease. The objective of this work is to evaluate specifically the clinical and hemodynamic responses of schistosomal por- tal hypertensive patients to the selective distal splenorenal shunt (DSRS). Although the clinical outcome of selective shunt has been carefully analyzed in the cirrhotic popu- lation,'2"13 only a few scattered publications have focused on this surgical procedure in the schistosomal patients.'4-'7 Because data emanating from the countries where schistosomiasis is endemic have suggested the co- existence of chronic active hepatitis and/or cirrhosis in patients with hepatosplenic schistosomiasis,'8"20 our study design was based on accurate histological and serological diagnosis of hepatic pathology. * Professor of Surgery, Emory University School of Medicine. t Department of Biometry, Emory University School of Medicine. Supported by Peace Fellowship Program for Egypt. Reprint requests: Farouk A. Ezzat, F.R.C.S., Gastroenterology Unit, Mansoura University Hospital, Mansoura, Egypt. Submitted for publication: March 18, 1986. Materials and Methods Patient Population The study population was a consecutive series of 60 patients with hepatosplenic schistosomiasis, portal hy- 566
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Distal Splenorenal Shunt for Management of Variceal Bleeding in Patients with Schistosomal Hepatic...

Distal Splenorenal Shunt for Management ofVariceal Bleeding in Patients with SchistosomalHepatic Fibrosis
FAROUK A. EZZAT, F.R.C.S. MOHAMED A. ALY, M.D. OSAMA 0. BAHGAT, M.D.KAREEM M. ABU-ELMAGD, M.B.B.CH. OMAR M. FATHY, M.D. ATEF A. SALAM, M.D.*IBRAHIM Y. ALY, M.D. MOHSIN H. EL-BARBARY, M.D. MICHAEL H. KUTNER, PH.D.t
The distal splenorenal shunt was performed in 60 patients withschistosomal hepatic fibrosis in whom no evidence of cirrhosiswas documented by preoperative needle and operative wedge bi-opsy. No patients have been lost to follow-up with a median of37 months (range: 17-86). The results showed low operativemortality (1.7%), high patency rate (92.5%), and low recurrentvariceal hemorrhage (6.7%). Thrombosed shunts were treatedeither by refashioning the shunt (1 patient) or splenectomy andgastric devascularization (2 patients). Initial hyperbilirubinemiaand reduction in serum albumin were found in the early post-operative period, with persistent hyperbilirubinemia in 32% ofthe patients. The 5-year survival was 88%, with liver diseaserelated mortality in only three patients. Clinical encephalopathywas detected in three patients (5.1%); only one of them was in-capacitated. These data showed that: (1) selective shunt (distalsplenorenal shunt, DSRS) is an effective surgical procedure inthe treatment of schistosomal variceal bleeding, (2) shuntthrombosis is rare and can possible be corrected if detected early,(3) schistosomal patients have a better survival and a lower in-cidence of encephalopathy after DSRS than that reported in cir-rhotics, and (4) liver biopsy should be performed for proper as-sessment of the schistosomal population especially in the geo-graphic areas where the schistosoma parasite and viral hepatitisare endemic.
B5 LEEDING ESOPHAGEAL VARICES as a complicationofportal hypertension is the most common causeof upper gastrointestinal hemorrhage in Egypt.'
It is the leading cause of death in patients with schisto-somal hepatic fibrosis and portal hypertension. Althoughthe initial bleeding episode may be fatal, patients usuallyhave multiple episodes extending over many years.2 Theeconomic impact of this disease is compounded by thefact that it affects individuals at the peak of their produc-tive life.3
From the Gastroenterology Unit, Department of Surgery,Mansoura University School of Medicine, Mansoura, Egypt
Hepatic schistosomiasis represents the prototype ofanintrahepatic presinusoidal block with normal architectureand cellular function.2'4 5 Therefore, any protection againstrecurrent variceal bleeding with maintained portal per-fusion, in such patients with good hepatic reserve couldonly improve long-term survival and quality of life.
Considerable controversy still exists regarding thechoice of a particular operative procedure for the treat-ment of portal hypertensive syndrome.6-" The presentknowledge of the hemodynamics of schistosomal portalhypertension is at best incomplete. As a result, the rec-ommendation for a surgical approach in the treatment ofthese patients has been used on personal bias or the un-proven assumption that their response to a given proce-dure is similar to those with alcoholic or posthepatiticliver disease.The objective ofthis work is to evaluate specifically the
clinical and hemodynamic responses ofschistosomal por-tal hypertensive patients to the selective distal splenorenalshunt (DSRS). Although the clinical outcome of selectiveshunt has been carefully analyzed in the cirrhotic popu-lation,'2"13 only a few scattered publications have focusedon this surgical procedure in the schistosomalpatients.'4-'7 Because data emanating from the countrieswhere schistosomiasis is endemic have suggested the co-existence of chronic active hepatitis and/or cirrhosis inpatients with hepatosplenic schistosomiasis,'8"20 our studydesign was based on accurate histological and serologicaldiagnosis of hepatic pathology.
* Professor of Surgery, Emory University School of Medicine.t Department of Biometry, Emory University School of Medicine.Supported by Peace Fellowship Program for Egypt.Reprint requests: Farouk A. Ezzat, F.R.C.S., Gastroenterology Unit,
Mansoura University Hospital, Mansoura, Egypt.Submitted for publication: March 18, 1986.
Materials and Methods
Patient Population
The study population was a consecutive series of 60patients with hepatosplenic schistosomiasis, portal hy-
566

DSRS IN SCHISTOSOMAL PORTAL HYPERTENSION
pertension, and variceal bleeding, managed by distal sple-norenal shunt between February 1978 and July 1984.These patients were part of a larger total population of371 patients seen over the same time interval managed,as shown in Table 1. All patients included in this studyfulfilled the following criteria:
(1) History of at least one major episode of varicealbleeding. The minimal time interval between the last var-iceal hemorrhage and surgery was 4-6 weeks.
(2) Histological diagnosis of schistosomal hepatic fi-brosis by Tru-cutO needle and/or wedge biopsy with no
evidence of coexisting cirrhosis.(3) No symptoms or signs suggestive of encephalopa-
thy, schistosomal cor-pulmonale, and/or associatedchronic peptic ulcer.
There were 59 male and 1 female patients with a mean
(±SD) age of 36.5 ± 10 years (range: 19-62). Clinical andlaboratory assessment at presentation showed 49 Child'sclass A, 10 Child's B, and one Child's C.
Preoperative EvaluationAll patients included in the study were subjected to
stool and urine analysis, physical examination, hemato-logical studies, biochemical profile of liver and kidneyfunctions, endoscopy, intravenous pyelography, cardio-pulmonary assessment, neuropsychiatric examination,abdominal ultrasonography, and liver biopsy.
Stool and urine analyses were done for diagnosis andtreatment ofactive schistosomal infestation. Rectal biopsywas done in negative cases to exclude closed active lesions.The clinical, hematological, and biochemical exami-
nation focused on ascites, encephalopathy, platelet andwhite cell count, hematocrit, albumin, bilirubin, pro-
thrombin time, serum glutamic transaminases, and fastingplasma ammonia. In addition, renal function, fluid andelectrolyte status, and concomitant urinary or gastroin-testinal infection were assessed and managed before op-
eration.Endoscopic evaluation was done to document
esophagogastric varices and exclude any associated gastricor duodenal lesions such as chronic ulcer or malignancy.Endoscopy was done before and after DSRS under thesupervision of one endoscopist using a grading systemderived from the method of Conn and Brodoff2' as fol-lows: Grade 0-no or submucosal esophageal or gastricveins; Grade I-varices with a diameter less than 3 mm;Grade II-varices 3-5 mm in diameter; Grade III-var-ices with a diameter more than 5 mm.
Intravenous pyelography was done for every patientincluded in the study to verify the position of the leftkidney and to detect any obstructive lesions in the urinarytract. In those with obstruction, this was corrected priorto DSRS.The clinical examination of the cardiopulmonary sys-
tem included electrocardiography (ECG) and echocardi-
TABLE 1. Total Population Referred between February 1978and July 1984 with Variceal Bleeding by Disease Etiology
and Management Method
Schisto- Post-somal hepatitic* Mixed* Total
Selective shunt 60 54 36 150Splenectomy and
devascularization 15 20 15 50Total shunts 15 5 8 28Other surgical therapy
Splenectomy and coronaryvasoligation 105
Splenic artery and leftgastric ligation 15
Stappler esophageal trans-section 23
Total population 371
* Thirty per cent of these patients had chronic active hepatitis.
ography. These were mandatory in all patients to excludemoderate and severe degrees of schistosomal cor-pul-monale.The neuropsychiatric evaluation was done by the de-
partment of neurology and included neurological exam-ination and an electroencephalogram (EEG). ParsonSmith grading22 was used: grade C-mild; grade D-moderate; grade E-severe.Abdominal ultrasonography was done for the liver and
spleen to assess size and exclude any concomitant hepaticor splenic lesions such as lymphoma and malignancy.
Liver biopsy was done before operation by Tru-cutneedle in 90% of the patients.
Surgical Technique
The standard distal splenorenal shunt, as described byWarren et al.,7 was applied to all patients with interruptionof the collaterals connecting the gastrosplenic compart-ment to the portomesenteric axis. Operative time rangedfrom 4 to 5 hours. Blood loss was usually between 500-1000 ml. Temporary occlusion ofthe splenic artery duringsplenic vein dissection was helpful in minimizing bloodloss. Thickening of the splenic vein wall with degenerativeplaques was noticed in some patients but did not precludesatisfactory anastomosis. In most patients wedge biopsyfrom the liver was taken. Routine sump drainage for 12hours was done in the majority of the patients.
Longitudinal Follow-up
All patients had follow-up studies at 3, 6, and 12 monthsand every year thereafter. The median follow-up time was37 months (range: 17-86), with no patients being lost tofollow-up.
Postoperative studies included all the preoperativeclinical, biochemical, neurological, and medical assess-ments. Additionally, endoscopic evaluation was done at6 months, 1 year, and when clinically indicated. Liver
Vol. 204 * No. S 567
Ann. Surg. * November 1986EZZAT AND OTHERS
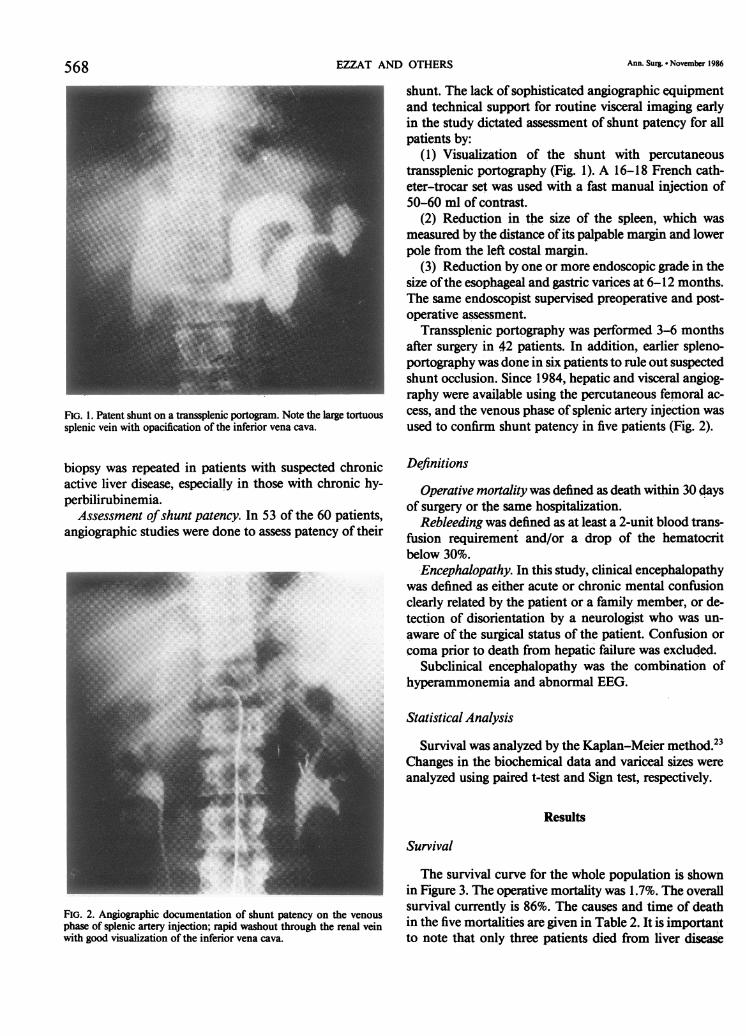
FIG. 1. Patent shunt on a transsplenic portogram. Note the large tortuoussplenic vein with opacification of the inferior vena cava.
biopsy was repeated in patients with suspected chronicactive liver disease, especially in those with chronic hy-perbilirubinemia.
Assessment ofshunt patency. In 53 of the 60 patients,angiographic studies were done to assess patency of their
FIG. 2. Angiographic documentation of shunt patency on the venous
phase of splenic artery injection; rapid washout through the renal veinwith good visualization of the inferior vena cava.
shunt. The lack of sophisticated angiographic equipmentand technical support for routine visceral imaging earlyin the study dictated assessment of shunt patency for allpatients by:
(1) Visualization of the shunt with percutaneoustranssplenic portography (Fig. 1). A 16-18 French cath-eter-trocar set was used with a fast manual injection of50-60 ml of contrast.
(2) Reduction in the size of the spleen, which wasmeasured by the distance of its palpable margin and lowerpole from the left costal margin.
(3) Reduction by one or more endoscopic grade in thesize ofthe esophageal and gastric varnces at 6-12 months.The same endoscopist supervised preoperative and post-operative assessment.
Transsplenic portography was performed 3-6 monthsafter surgery in 42 patients. In addition, earlier spleno-portography was done in six patients to rule out suspectedshunt occlusion. Since 1984, hepatic and visceral angiog-raphy were available using the percutaneous femoral ac-cess, and the venous phase of splenic artery injection wasused to confirm shunt patency in five patients (Fig. 2).
Definitions
Operative mortality was defined as death within 30 daysof surgery or the same hospitalization.
Rebleeding was defined as at least a 2-unit blood trans-fusion requirement and/or a drop of the hematocritbelow 30%.
Encephalopathy. In this study, clinical encephalopathywas defined as either acute or chronic mental confusionclearly related by the patient or a family member, or de-tection of disorientation by a neurologist who was un-aware of the surgical status of the patient. Confusion orcoma prior to death from hepatic failure was excluded.
Subclinical encephalopathy was the combination ofhyperammonemia and abnormal EEG.
Statistical Analysis
Survival was analyzed by the Kaplan-Meier method.23Changes in the biochemical data and variceal sizes wereanalyzed using paired t-test and Sign test, respectively.
Results
Survival
The survival curve for the whole population is shownin Figure 3. The operative mortality was 1.7%. The overallsurvival currently is 86%. The causes and time of deathin the five mortalities are given in Table 2. It is importantto note that only three patients died from liver disease
568

DSRS IN SCHISTOSOMAL PORTAL HYPERTENSION
1 2 3 4Years
5 6 7 8
FIG. 3. Kaplan-Meier survival plot for schistosomal patients after DSRSwith cumulative survival of 86% and standard error of 2.9%. The mean(±SD) follow-up period for these patients was 41 ± 24 months. Thepatient who died in an automobile accident is considered as censoredobservation.
related complications, two of hepatic cell failure and thethird of variceal hemorrhage.
Shunt Patency
Shunt patency was documented angiographically in 49of the 53 patients studied; giving a thrombosis rate of7.5%. Ofthe seven patients who did not have postoperativeangiography, six had a benign clinical course with reduc-tion of variceal and splenic sizes, providing indirect evi-dence of shunt patency. The time scale to thrombosis inthe four patients with angiographic evidence of shunt oc-clusion and the clinical course of these patients are givenin Table 3. It is interesting to note that one ofthese patientsdeveloped a large splenoportal collateral (Fig. 4). Follow-ing a conservative medical treatment in this patient, therewere no further bleeding episodes until he died from anautomobile accident.
Endoscopic evaluation of 55 patients before and at 6-12 months after DSRS showed a significant (p < 0.001)reduction in the size of varices. These changes are sum-marized in Table 4.
Rebleeding
Variceal rebleeding occurred in four patients for an in-cidence of6.7%. Two had documented shunt thrombosis,
TABLE 2. Deaths Following DSRS, with Time Intervaland Cause ofDeath
Time until Death(mo) Cause
I Hepatic cell failure4 Hepatic cell failure18 Complication of transsplenic portography30 Automobile accident78 Variceal hemorrhage
569TABLE 3. Patients with Documented Shunt Thrombosis
at Angiography, with Time and Clinical Course
Size ofTime Rebleeding Varices Management
5 days ++ 2++ Refashioned shuntSplenectomy and
7 days - 3+++ devascularizationSplenectomy and
10 days + 3+++ devascularization6 months - 3+++ Conservative
one had refashioning of the anastomosis, and the otherhad splenectomy and gastric devascularization (Table 3).The third died at 78 months and the status of his shuntwas never known, while the fourth had patent shunt(1.7%). The variceal bleeding in the patient with patentshunt occurred on the seventh postoperative day, re-
sponded to simple measures and did not require furthersurgery. Nonvariceal upper gastrointestinal hemorrhageoccurred in another patient 8 days after surgery becauseof postoperative pancreatitis and gastric erosions.
Ascites
Five patients developed moderate ascites in the earlypostoperative period, which was resolved with salt restric-tion and diuretics at 3 months in four patients and at 12months in one patient.
Encephalopathy
Absence of encephalopathy before surgery was a cri-terion for patient selection. Three patients (5.1%) devel-
FIG. 4. Thrombosed shunt with large splenoportal collateral on trans-splenic portogram 6 months after DSRS..
Vol. 204 * No. 5
IW. #
908070
3 60; 50OCDS 40
30*2010-
0
n=60
o MortalityA Alive

570 EZZAT AND OTHERS
TABLE 4. Endoscopic Changes in Variceal Size in 55 PatientsEvaluated prior to and 6-12 Months after DSRS
PreoperativePostoperative Grade
No. ofGrade* Patients 0 I II III
I 2 2II 16 11 5III 37 15 20 2 -
* Grades defined in the text.
oped clinical encephalopathy at some time during the fol-low-up period. The onset of encephalopathy was asso-
ciated with impairment of hepatocyte function, as shownby elevated serum bilirubin and fasting ammonia levels(Table 5).
Restriction of dietary protein combined with lactuloseand neomycin therapy reduced the degree of clinical en-cephalopathy with improvement in the functional capac-ity. Only one patient was unable to return to his normaldaily productivity.
Subclinical encephalopathy was detected in three pa-tients with abnormal EEG and high fasting plasma am-
monia level. They had no limitation in their daily activity.
Biochemical Data
Serum albumin, bilirubin, and prothrombin time be-fore and 1 week after operation were analyzed in most ofthe patients. For long-term results, patients were dividedinto three subsets according to the length of their last fol-low-up.
Immediate postoperative changes showed significantreduction in albumin (p < 0.01) and increase in bilirubin(p < 0.001), with no significant change in prothrombintime (Table 6). At last evaluation time, the changes forpatients in each category are given in Table 7. While sta-tistical significance can be shown for increases in bilirubinand reduction in albumin at some time points, mainte-nance ofalbumin above the mean of 3.5 g/dl and bilirubinbelow 2.5 mg/dl suggests that these changes are not ofclinical significance.The most recent biochemical profile of all patients
showed chronic hyperbilirubinemia in 19 patients (32%),with a total serum bilirubin ranging from 2 to 5.3 mg/dl
TABLE 5. Patients with Clinical Encephalopathy
FastingClinical Onset Ammonia BilirubinDegree (mo) (,ug/dl) (mg/dl) EEG
Severe 6 140 4.3 CModerate 24 110 2.3Mild 6 130 3.2 B
Normal range of plasma ammonia in our laboratory is 5-83 ,g/dl.
Ann. Surg. * November 1986
TABLE 6. Seven to Ten Day Postoperative Changes in Serum Albumin,Bilirubin, and Prothrombin Time*
Preop Postop p Value
Albumin (N = 52) 4.0 ± 0.4 3.6 ± 0.6 <0.01Bilirubin (N = 50) 1.0 ± 0.4 1.3 ± 0.7 <0.001Prothrombin time(N =52) (+sec) 1.4 ± 1.0 1.3 ± 1.0 NS
* Normal values: albumin, 3-5.2 g/dl; bilirubin, 0.2-1.2 mg/dl.
and a mean of 3.0 ± 1 mg/dl. Their preoperative totalserum bilirubin was 1 ± 0.4 mg/dl. None ofthese patientsdeveloped viral hepatitis or cirrhosis after surgery, asshown by liver biopsies and/or serological studies for viralhepatitis.
Hemodynamic Studies
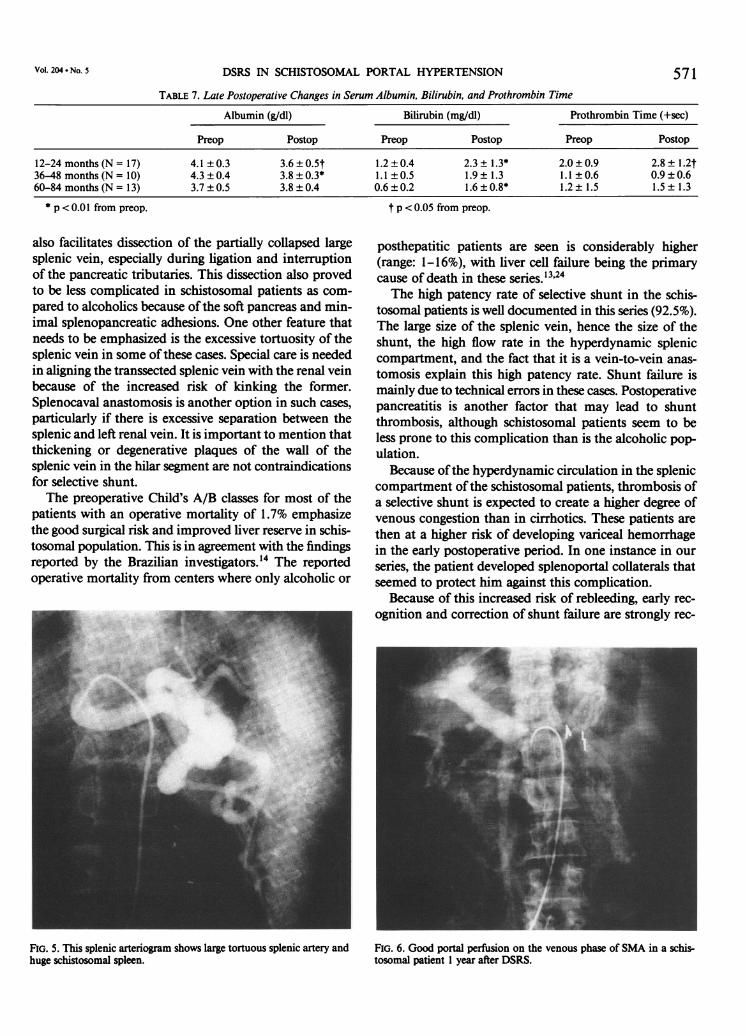
The preliminary results of the preoperative imagingstudies showed some of the angiographic features asso-ciated with hepatosplenic schistosomiasis. The hepaticwedge injection showed a homogenous parenchymogramwith nondistorted hepatic veins. The splenic artery injec-tion showed a large tortuous splenic artery and huge spleen(Fig. 5). Visualization of the portal system is variable,depending on contrast dilution. but the portal vein wasusually better seen on the venous phase of splenic arteryinjection than on the superior mesenteric artery injection.
In the five patients with angiographic studies 1 yearafter DSRS, portal perfusion was maintained in all pa-tients with minimal collateral formation (Fig. 6).
Discussion
A few reports are available in the English literaturedealing with selective shunt in the schistosomal popula-tion.'4-'7 Most of these studies consist of a small serieswith incomplete and short term follow-up. Also none ofthese reports has emphasized the importance of histolog-ical diagnosis of hepatic schistosomiasis. Therefore, thepossibility of coexistence of other entities of liver diseasesuch as cirrhosis and chronic active hepatitis cannot beexcluded in such studies.
This current study represents the largest consecutiveseries of patients, with histologically proven schistosomalhepatic fibrosis, treated with selective splenorenal shunt.It is also the first clinical trial to address long-term survivalafter DSRS in this patient population.Some technical aspects of the DSRS procedure in
schistosomal patients need to be addressed. The large sizeof the spleen and the congestion in the gastrosplenopan-creatic compartment, particularly during clamping ofthesplenic vein, carry the potential for significant blood loss.Routine temporary clamping of the splenic artery priorto dissection of the splenic vein has proved to be veryhelpful in minimizing blood loss. Splenic arterial clamping
DSRS IN SCHISTOSOMAL PORTAL HYPERTENSION 571TABLE 7. Late Postoperative Changes in Serum Albumin, Bilirubin, and Prothrombin Time
Albumin (g/dl) Bilirubin (mg/dl) Prothrombin Time (+sec)
Preop Postop Preop Postop Preop Postop
12-24 months(N= 17) 4.1±0.3 3.6±0.5t 1.2±0.4 2.3±1.3* 2.0±0.9 2.8± 1.2t36-48 months (N = 10) 4.3 ± 0.4 3.8 ± 0.3* 1.1 ±0.5 1.9 ± 1.3 1.1 ± 0.6 0.9 ± 0.660-84 months (N = 13) 3.7 ± 0.5 3.8 ± 0.4 0.6 ± 0.2 1.6 ± 0.8* 1.2 ± 1.5 1.5 ± 1.3
* p < 0.01 from preop. t p < 0.05 from preop.
also facilitates dissection of the partially collapsed largesplenic vein, especially during ligation and interruptionof the pancreatic tributaries. This dissection also provedto be less complicated in schistosomal patients as com-pared to alcoholics because of the soft pancreas and min-imal splenopancreatic adhesions. One other feature thatneeds to be emphasized is the excessive tortuosity of thesplenic vein in some ofthese cases. Special care is neededin aligning the transsected splenic vein with the renal veinbecause of the increased risk of kinking the former.Splenocaval anastomosis is another option in such cases,particularly if there is excessive separation between thesplenic and left renal vein. It is important to mention thatthickening or degenerative plaques of the wall of thesplenic vein in the hilar segnent are not contraindicationsfor selective shunt.The preoperative Child's A/B classes for most of the
patients with an operative mortality of 1.7% emphasizethe good surgical risk and improved liver reserve in schis-tosomal population. This is in agreement with the findingsreported by the Brazilian investigators.'4 The reportedoperative mortality from centers where only alcoholic or
posthepatitic patients are seen is considerably higher(range: 1-16%), with liver cell failure being the primarycause of death in these series.'3'24The high patency rate of selective shunt in the schis-
tosomal patients is well documented in this series (92.5%).The large size of the splenic vein, hence the size of theshunt, the high flow rate in the hyperdynamic spleniccompartment, and the fact that it is a vein-to-vein anas-tomosis explain this high patency rate. Shunt failure ismainly due to technical errors in these cases. Postoperativepancreatitis is another factor that may lead to shuntthrombosis, although schistosomal patients seem to beless prone to this complication than is the alcoholic pop-ulation.
Because ofthe hyperdynamic circulation in the spleniccompartment ofthe schistosomal patients, thrombosis ofa selective shunt is expected to create a higher degree ofvenous congestion than in cirrhotics. These patients arethen at a higher risk of developing variceal hemorrhagein the early postoperative period. In one instance in ourseries, the patient developed splenoportal collaterals thatseemed to protect him against this complication.
Because of this increased risk of rebleeding, early rec-ognition and correction of shunt failure are strongly rec-
FIG. 5. This splenic arteriogram shows large tortuous splenic artery andhuge schistosomal spleen.
Vol. 204 - No. S
FIG. 6. Good portal perfusion on the venous phase of SMA in a schis-tosomal patient I year after DSRS.

Ann. Surg. November 1986EZZAT AND OTHERS572
A-
A
100
80 .
60 .co
=C-, 40 .
20 .
0 2 4 6 8 10Years
Warren et alAnn Surg 1982
B0'L0
ommended to prevent death from exsanguination. If theshunt cannot be salvaged, the surgeon has a choice be-tween a total shunt or splenectomy with gastric devas-cularization. However, total shunt has two major disad-vantages in this situation. First, it might fail to immedi-ately decompress the splenic compartment; second, itexposes the patient to the risk of developing disablingencephalopathy. Our preference in these cases is to dosplenectomy and gastric devascularization. It is question-able whether sclerotherapy would give lasting protectionagainst variceal bleeding in these occluded patients. How-ever, in patients with a patent shunt, sclerotherapy is avaluable technique in the control ofvariceal bleeding untilthe shunt attains its maximal decompressive effect.Our results indicate that DSRS is highly effective in
protecting against a recurrence of variceal bleeding. Onlyfour patients had variceal rebleeding (6.7%), and one ofthese four had a patent shunt (1.7%). For reasons that arenot clear to us, the Brazilian investigators reported a higherincidence ofrebleeding after selective shunt in their schis-tosomal patients.'4 They cited an incidence of 16.6% butdid not elaborate on the causes of bleeding, nor did theyspecify the functional status ofthe shunt in those patients.
Ascites was a minimal problem during the postoperativeperiod and nonexistent at the end of the first year. TheBrazilian group has reported a 10% incidence of ascitesafter DSRS in their patient population.'4 This overall in-cidence of early postoperative ascites in the schistosomalpatients compared to the cirrhotic population (10-56%)'3may be related to good liver reserve and lower sinusoidalpressure in schistosomal hepatic fibrosis.4The significant drop in albumin and increase in bili-
rubin, in both the immediate postoperative period andalso at late follow-up, reflects some degree ofparenchymalinvolvement in schistosomal hepatic fibrosis26 that be-come accentuated after DSRS. This encroachment on thehepatic reserve may be explained by impairment in theperfusion ofhepatocytes due to sinusoidal obstruction byextensive hepatic fibrosis,27-30 and deposition of collagen
FIGS. 7A and B. Kaplan-Meier survival plot for pres-ent study (schistosomal)compared to Emory series(cirrhotics). Five-year sur-
n = 60 vival is 88% in schistosomalSchistosomal Hepatic Fibrosis patients (B), 70% in nonal-
coholics, and 40) in alco-a . a a a a ~~~~~~~~holicpatients (A).
1 2 3 4 5 6 7 8Years
in the perisinusoidal (Disse) spaces.3" In addition, thepiecemeal necrosis in the periportal areas and the periph-eral nodules formed in the hepatic parenchyma under-neath the liver capsule2 may also indicate some degree ofparenchymal damage in these patients.One ofthe important findings ofthis study is the initial
and chronic rise in total serum bilirubin (32%). The initialrise can be reduced by temporary clamping ofthe splenicartery, especially during interruption ofthe splenic outflowand shunt performance (unpublished data from our cen-ter).25 Chronic hyperbilirubinemia in these patients isusally associated with reasonable serum albumin andnormal prothrombin time. Similar observations have beenmade by other investigators.'4'25 Theoretically, this hy-perbilirubinemia may be attributed to a hemolytic mech-anism as well as reduced clearance by the liver. The in-creased hemolysis can be explained by the increased tur-bulent splenic blood flow in the splenic sinusoidal bedand across the splenorenal anastomosis. Also, impairedclearance possibly may be due to hepatocellular dysfunc-tion and/or diversion of the hemolytic pigments awayfrom the liver.'4 These assumptions need further hema-tological and hemodynamic investigations.The quality of life after shunt therapy is largely deter-
mined by the presence or absence ofencephalopathy. Withthe hemodynamic and metabolic advantages of selectiveshunt, clinical encephalopathy was detected in only 5.1%of our series. The reported higher incidence (13.3%) inthe same population by the Brazilian group'4 may reflectthe broad spectrum of this syndrome with the lack ofclear-cut criteria for its diagnosis and evaluation. The on-set ofencephalopathy in our patients was associated withevidence ofimpairment in the hepatocyte functions. Thelower incidence of postselective shunt encephalopathy inthe schistosomal patients as compared to that in cirrhotics,12% in the first 5 years and up to 27% at 10 years,'3'24emphasizes the importance of underlying liver disease asa factor in the development of this complication.The interrelationship between liver pathology and sur-

Vol. 204 * No.5 DSRS IN SCHISTOSOMAL PORTAL HYPERTENSION 573vival after selective shunt has been addressed by other in-vestigators.'2'32 Our study of schistosomal patients showeda 5-year survival rate of 88% as compared to 40% in al-coholic and 70% in nonalcoholic patients'2"3 (Fig. 7).Our results substantiate the superiority ofDSRS in the
management of variceal bleeding in the schistosomalpopulation. Postshunt encephalopathy is sharply reducedas compared to total shunt operations. 433 Also, the fa-vorable 5-year survival rate after the selective shunt ascompared to the total shunts underscores the importanceofpreservation ofportal perfusion. Compared to nonshuntoperations, DSRS is a far more effective procedure in pro-tecting the patients against recurrence of variceal hem-orrhage.
In view of these findings, removal ofthe spleen shouldbe avoided in the schistosomal patients. Variceal hem-orrhage in splenectomized patients can be managed bysclerotherapy, which may not be effective in many ofthesepatients.
ConclusionThis clinical trial proves that DSRS is effective in the
management of variceal hemorrhage in schistosomal pa-tients. The operative mortality ofthe procedure was 1.7%.Recurrent variceal hemorrhage occurred in only 6.7%.Five-year survival was 88%. Ofparticular importance wasthe reduced incidence ofclinical encephalopathy of 5. 1%.This low incidence ofpostshunt encephalopathy is ofgreatvalue in allowing these patients to maintain gainful em-ployment. Until the role of sclerotherapy as a definitivemethod oftreatment is fully investigated, we consider theselective shunt as the method of choice for the treatmentof variceal hemorrhage in the schistosomal patients.
AcknowledgmentsThe authors would like to thank the Emory liver team for their guidance
in formulating this worlk The appreciation is extended to the departmentof medical illustration for their technical assistance.
References1. Bessa SM, Helmy I. Injection sclerotherapy for esophageal varices
caused by schistosomal hepatic fibrosis. Surgery 1985; 97:164-168.
2. Dunn MA, Kamel R. Hepatic schistosomiasis. Hepatology 1981; 1:653-661.
3. Abdel-Wahab MF. Schistosomiasis in Egypt. Florida: CRS PressInc., 1982.
4. Continho A. Hemodynamic studies of portal hypertension in schis-tosomiasis. Am J Med 1968; 44:547-556.
5: Warren KS. The kinetics of hepatosplenic schistosomiasis. SeminLiver Dis 1984; 4:293-300.
6. Hassab MA. Gastophageal decongestion and splenectomy in thetreatment of esophageal varices in bilharzial cirrhosis: furtherstudies with a report on 355 operations. Surgery 1967; 61:169-176.
7. Warren WD, Zeppa R, Fomon JJ. Selective trans-splenic de-compression of gastroesophageal varices by distal splenorenalshunt. Ann Surg 1967; 166:437-455.
8. Westaby D, Macdougall BRD, Williams R. Improved survival fol-lowing injection sclerotherapy for esophageal varices: final analysisof a controlled trial. Hepatology 1985; 5:827-830.
9. Kern AK, Bower RH, Fischer JE. Surgery for portal hypertension.Semin Liver Dis 1982; 2:242-252.
10. Westaby D, Williams R. Variceal bleeding. In Williams R, MaddreyWC, eds. Liver (Butterworths International Medical Reviews,Gastroenterology 4). Butterworths: London-Boston, 1984; 12:284-307.
11. Donovan AJ. Surgical treatment ofportal hypertension: a historicalperspective. World J Surg 1984; 8:626-645.
12. Warren WD, Milikan WJ, Henderson JM, et al. Ten years portalhypertensive surgery at Emory: results and new perspectives. AnnSurg 1982; 195:530-542.
13. Henderson JM, Warren WD. Current status ofthe distal splenorenalshunt. Semin Liver Dis 1983; 3:251-263.
14. Raia S, Meis S, Macedo AL. Surgical treatment ofportal hypertensionin schistosomiasis. World J Surg 1984; 8:738-752.
15. Cruz NI, Marquez E. Distal splenorenal shunts: the experience atthe Puerto Rico University Hospital. Bol Asoc Med PR 1981,73:335-340.
16. Machado AL, Felho JEB, Campos AB, et al. Selective distal sple-norenal shunts: technique and results. Am J Surg 1981; 142:281-284.
17. Habashi AHF. Trans-splenic decompression of esophageal varicesby selective distal splenorenal shunt. J Egypt Med Assoc 1977;60:23-28.
18. Nooman ZM, Khaiil M, Nafehy M, et al. Hepatitis B antigen inbilharzial HB, positive subjects infected with viral hepatitis. InAbdlallah A, ed. Proceedings of the International Conference onSchistosomiasis. Cairo: Egyptian Ministry of Health 1975; 1:149-155.
19. Bassily S, Farid Z, Higashi GI, et al. Chronic hepatitis B-antigenemiain patients with hepatosplenic schistosomiasis. J Trop Med Hyg1979; 82:248-251.
20. Lyra LG, Reboucas G, Andrade ZA. Hepatitis B surface antigencarrier state in hepatosplenic schistosomiasis. Gastroenterology1976; 71:641-645.
21. Conn HD, Brodoff M. Emergency esophagoscopy in the diagnosisof upper gastrointestinal hemorrhage: a critical evaluation of itsdiagnostic accuracy. Gastroenterology 1964; 47:505-512.
22. Parsons-Smith BG, Summerskill WHJ, Dawson AM, Sherlock S.The electroencephalograph in liver disease. Lancet 1957; 2:867-871.
23. Kaplan EL, Meier P. Nonparametric estimation from incompleteobservations. J Am Stat Assoc 1958; 53:457-481.
24. Millikan WJ, Warren WD, Henderson JM, et al. The Emory pro-spective randomized trial: selective versus nonselective shunt tocontrol variceal bleeding. Ann Surg 1985; 201:712-722.
25. Raia S. Portal hypertension in schistosomiasis. In Orloff MJ, StipaS, Ziparo V, eds. Medical and Surgical Problems of Portal Hy-pertension. London: Academic, 1980; 301-312.
26. Beker GS, Valencia-Parparcen J. Portal hypertension syndrome.Am J Dig Dis 1968; 13:1047-1054.
27. Andrade ZA. Hepatic schistosomiasis: morphological aspects. InPopper H, Schaffner F, eds. Progress in Liver Diseases. New York:Grune and Stratton, 1965; 11:228-241.
28. Hidayat MA, Wahid HA. A study ofthe vascular changes in bilharialhepatic fibrosis and their significance. Surg Gynecol Obstet 1971;132:997-1004.
29. Alves CAP, Alves AR, Abreu WN, Andrade ZA. Hepatic arteryhypertrophy and sinusoidal hypertension in advanced schisto-somiasis. Gastroenterology 1977; 72:126-128.
30. Mies S, Mori T, Larsson E, et al. Hepatic vein in mansonic schis-tosomiasis: angiographic and hemodynamic pattern. Gastroen-terology 1980; 78:1314.
31. Grimaud JA, Borjevic R. Chronic human schistosomiasis: pathologyof Disse's space. Lab Invest 1977; 36:268-273.
32. Zeppa R, Hutson DG, Levi JU, Livingstone AS. Factors influencingsurvival after distal splenorenal shunt. World J Surg 1984; 5:733-738.
33. Aly IY. Interposition, H-graft, mesocaval shunt for treatment ofvariceal bleeding in schistosomal portal hypertension. M.S. Thesis,Mansoura University, Egypt, 1979.
34. Barsoum MS, Bohous Fl, El-Rooby AA, et al. Tamponade andinjection sclerotherapy in the management ofbleeding esophagealvarices. Br J Surg 1982; 69:76-78.