
disease: 10-year results of a randomized trial extended field radiation therapy in early and...
32
doi:10.1182/blood-2003-05-1611 Prepublished online August 7, 2003; Catherine Traulle, Marc Bernard, Josette Briere, Pierre Colonna and Jean-Marie Andrieu Vigier, Christiane Ghandour, Said Atmani, Philippe Casassus, Herve Maisonneuve, Annick Le Mevel, Christine le Maignan, Bernard Desablens, Vincent Delwail, Mahmoud Dib, Christian Berthou, Magda disease: 10-year results of a randomized trial extended field radiation therapy in early and intermediate Hodgkin's (ABVD) or Epirubicin, Bleomycin, Velban, and Methotrexate (EBVM) plus Three cycles of Adriamycin, Bleomycin, Velban, and Dacarbazine (4212 articles) Neoplasia (3768 articles) Clinical Trials and Observations Articles on similar topics can be found in the following Blood collections http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requests Information about reproducing this article in parts or in its entirety may be found online at: http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprints Information about ordering reprints may be found online at: http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtml Information about subscriptions and ASH membership may be found online at: articles must include the digital object identifier (DOIs) and date of initial publication. priority; they are indexed by PubMed from initial publication. Citations to Advance online prior to final publication). Advance online articles are citable and establish publication yet appeared in the paper journal (edited, typeset versions may be posted when available Advance online articles have been peer reviewed and accepted for publication but have not Copyright 2011 by The American Society of Hematology; all rights reserved. Washington DC 20036. by the American Society of Hematology, 2021 L St, NW, Suite 900, Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.org From
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of disease: 10-year results of a randomized trial extended field radiation therapy in early and...

doi:10.1182/blood-2003-05-1611Prepublished online August 7, 2003;
Catherine Traulle, Marc Bernard, Josette Briere, Pierre Colonna and Jean-Marie AndrieuVigier, Christiane Ghandour, Said Atmani, Philippe Casassus, Herve Maisonneuve, Annick Le Mevel, Christine le Maignan, Bernard Desablens, Vincent Delwail, Mahmoud Dib, Christian Berthou, Magda disease: 10-year results of a randomized trialextended field radiation therapy in early and intermediate Hodgkin's(ABVD) or Epirubicin, Bleomycin, Velban, and Methotrexate (EBVM) plus Three cycles of Adriamycin, Bleomycin, Velban, and Dacarbazine
(4212 articles)Neoplasia � (3768 articles)Clinical Trials and Observations �
Articles on similar topics can be found in the following Blood collections
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
articles must include the digital object identifier (DOIs) and date of initial publication. priority; they are indexed by PubMed from initial publication. Citations to Advance online prior to final publication). Advance online articles are citable and establish publicationyet appeared in the paper journal (edited, typeset versions may be posted when available Advance online articles have been peer reviewed and accepted for publication but have not
Copyright 2011 by The American Society of Hematology; all rights reserved.Washington DC 20036.by the American Society of Hematology, 2021 L St, NW, Suite 900, Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly
For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 2, 2013. bloodjournal.hematologylibrary.orgFrom

1
TITLE
Three cycles of Adriamycin, Bleomycin, Velban and Dacarbazine (ABVD) or Epirubicin, Bleomycin, Velban and Methotrexate (EBVM) plus extended field radiation therapy in early and intermediate Hodgkin’s disease: 10-year results of a randomized trial.
SHORT TITLE
Combined modality therapy for Hodgkin’s disease
AUTHORS
Christine le Maignan (1), Bernard Desablens (2), Vincent Delwail (3), Mahmoud Dib (4), Christian Berthou (5), Magda Vigier (6), Christiane Ghandour (7), Saïd Atmani (8), Philippe Casassus (9), Hervé Maisonneuve (10), Annick Le Mevel (11), Catherine Traullé (12), Marc Bernard (13), Josette Brière (14), Pierre Colonna (1) and Jean-Marie Andrieu (1).
INSTITUTIONS
(1) Cancérologie Médicale, Hôpital Européen Georges Pompidou, Paris, France ; (2)Hématologie, Hôpital Sud, Amiens ; (3) Hématologie, Hôpital Jean Bernard, Poitiers ; (4) Maladies du Sang, CHU d’Angers ; (5) Hématologie, Hôpital Morvan, Brest ; (6) Hématologie, Hôtel Dieu, Nantes ; (7) 83 avenue Aristide Briand, Rennes ; (8) Hématologie, Hôpital Beaujon, Clichy ; (9) Hématologie, Hôpital Avicenne, Bobigny ; (10) Médecine A Centre Hospitalier Départemental, La Roche sur Yon ; (11) Centre René Gauducheau, Nantes ; (12) Centre Léon Bérard, Lyon ; (13) Hématologie, Hôpital Pontchaillou, Rennes ; (14) Anatomie Pathologique, Hôpital Saint-Louis, Paris.
RESEARCH GRANTS: Association de recherche sur les maladies tumorales et virales (AREMAS), Paris, France.
CORRESPONDING AUTHOR
Jean-Marie Andrieu, MDCancérologie médicale, Hôpital Européen Georges Pompidou, 20 rue Leblanc, 75908 Paris Cedex 15, FrancePhone: 33 1 56 09 34 71; Fax: 33 1 56 09 24 15 ; e-mail: Jean-Marie Andrieu <[email protected]>
WORDS COUNTS:
Text: 5432 wordsAbstract: 191 words
SCIENTIFIC HEADING:
Clinical observations, interventions and therapeutic trials
RUNNING HEAD
Hodgkin’s disease, tumor mortality, treatment mortality, randomized study, combined modality therapy, alkylating agents, radiation therapy
Copyright (c) 2003 American Society of Hematology
Blood First Edition Paper, prepublished online August 7, 2003; DOI 10.1182/blood-2003-05-1611
2
ABSTRACT
From 1990 to 1996, 386 adult patients with early/intermediate Hodgkin’s disease (HD) were
randomly assigned to receive three cycles of Adriamycin, Bleomycin, Vinblastin, Dacarbazine
(an alkylating agent) and Methylprednisolone (ABVDm, arm A) or Epirubicin, Bleomycin,
Vinblastin, Methotrexate and Methylprednisolone (EBVMm, arm E), a combination without
alkylating agent. Responding patients received extended field radiation therapy (RT). Post-
chemotherapy complete remission and 10-year freedom from progression rates were higher in
arm A (79.5% and 91.4%) than in arm E (70.4%, p=0.04 and 80%, p<.002).HD mortality
(HDM), treatment-related mortality (TRM) and overall survival (OS) were similar in both
arms (A 2.1%, 7.5% and 90.4%; B 3.9%, 5.5% and 90.3%). However TRM and OS rates were
lower in patients aged ≥40 years (p<0.005) reflecting the increasing incidence of background
fatal events with increasing age. Finally event-free survival (EFS) was higher in arm A
(84.6%) than in arm E (74.9%, p<0.02). In patients aged <40 years of arm A (74%), 10-year
EFS and OS rates were 88.9% and 95.4% with HDM and TRM rates as low as 0.7% and 3%.
Three courses of ABVDm plus RT are the best available option for treating early or
intermediate HD.

3
INTRODUCTION
Over the past 30 years, Hodgkin’s disease (HD) has been shown to be extremely sensitive to
both radiation therapy (RT) and multiagent chemotherapy (CT). As a result, a large array of
treatments ranging from RT alone to various CT, and to several combinations of CT and RT
has been offered to patients suffering from HD with increasing successes 1-3. However, these
treatments have been shown to have long term morbidity and mortality 4-12.
The objective of this study was to evaluate in the setting of a randomized trial comparing two
anthracycline-based CTs (one of which with a low toxicity anthracycline and without
alkylating agents) combined with the same RT, the two components of the 10-year mortality
rate: that resulting from HD itself and that occurring in complete remission (CR) from fatal
events attributable to the treatment.
In 1989, on the basis of the 5-year results of our previous trial (H81, 1981-1988, 407 patients
with clinical stages (CS) IA to IVB) combining 3 courses of ABVDm (Adriamycin,
Bleomycin, Vinblastin, Dacarbazine and Methylprednisolone) and high dose extended RT 13-
15, we identified a group of 264 patients with early/intermediate HD (i.e. with CS IA to IIIB
with a mediastinal mass ratio <0.45 and without involvement of both pelvic and lumboaortic
areas) which had 5-year freedom from progression and survival rates peaking at 95.1% and
95.9% respectively; these figures were very significantly different (p <0.0001) from those
observed in the group of the 143 remaining patients with advanced HD (65.7% and 75.1%,
respectively).
When we started preparing our H90-NM trial for early/intermediate HD, we were faced to the
fact that it would be difficult to further improve the remarkable above-mentioned results. We
thus decided to test in a randomized trial whether it would be possible to maintain these
4
excellent figures with an initial CT made of a combination of drugs potentially less toxic than
those of the ABVD association.
In ABVD, Adriamycin is known to cause severe or even fatal cardiac complications in some
patients, particularly when the drug is combined with mediastinal RT 10,16,17; moreover,
Dacarbazine which is an alkylating agent 18 may thus be potentially responsible for secondary
tumors. Based on previous reports where Epirubicin or Methotrexate were given in
association with Bleomycin and Velban in HD treatment 19,20, we designed the EBVMm
regimen, an association without any alkylating agent comprising Epirubicin, Bleomycin,
Vinblastin, Methotrexate and Methylprednisolone. In 1990, we thus initiated the H90-NM
randomized program (1990-1996), where patients with early/intermediate HD were randomly
assigned to 3 monthly courses of EBVMm (experimental arm) or ABVDm (reference arm);
patients of both arms enjoying complete or partial remission after CT received the same
tailored high dose extended RT as that given in our previous H81 trial. Besides recording
usual endpoints such as response to CT and to RT, relapses and deaths, we also prospectively
recorded all severe complications and their outcome.
Here we report the 10-year results of this randomized study including 386 patients. The
objective of the trial was to compare the freedom from progression and the HD mortality rates
as well as the incidence of life-threatening events occurring in CR and their resulting mortality
in both arms of the trial.

5
PATIENTS AND METHODS
Description of the H90-NM protocol, inclusion criteria
From January 1990 to December 1996, all consecutive patients aged 18 to 65 years with
untreated early/intermediate HD recruited in the 14 French centers affiliated to the “Groupe
Ouest-Est d’Etude des Leucémies et Autres Maladies du Sang” (GOELAMS) were enrolled in
the H90-NM trial. Patients with early/intermediate HD were defined as those having clinical
stage IA to IIIB with a mediastinal mass ratio <0.45 14,21-23 (or no mediastinal involvement)
and without involvement of both (uni or bilateral) pelvic and lumboaortic nodes.
Initial investigations included lymph node biopsy for diagnosis and histological classification,
physical examination, chest x-ray, bipedal lymphangiography (or abdominopelvic CT scan),
bone marrow biopsy, and biologic evaluation including blood count, sedimentation rate, and
kidney and liver chemistries. A liver biopsy was performed in case of liver enlargement and/or
a greater than twofold increase in serum alkaline phosphatase level. Clinical and radiological
examination of Waldeyer's ring, with a biopsy when necessary, was performed in patients with
upper cervical nodes. Patients were classified in CS IA to IIIB according to the Ann Arbor
criteria 24. The mediastinal mass ratio (MMR), i.e. the maximum mediastinal tumor width
divided by the thoracic width at vertebra T6, was measured in all patients with mediastinal
disease. The trial was conducted according to the guidelines of the Helsinki Declaration.
After verification of inclusion criteria (diagnosis of Hodgkin’s disease, age ≥ 18 and
≤ 65years, CS IA-IIIB with a mediastinal mass ratio < 0.45 or no mediastinal mass and
without involvement of both pelvic and lumboaortic nodes, no history of malignancy except
non melanoma skin tumors and carcinoma in situ of the cervix, no serious illness that would
limit survival or preclude CT or RT, absence of pregnancy, and informed signed consent),
patients were randomized (center by center) by a phone call to the central secretary of the

6
GOELAMS into one of the following arms: arm A, 3 cycles of ABVDm; arm E, 3 cycles of
EBVMm. Only one course of CT (ABVDm or EBVMm) was administered to patients with
cervical, axillary or inguinal CS IA with one pathological node not exceeding 2 cm diameter.
Schedules and dosages of the two CT regimens are listed in table 1. The dosage of each drug
was reduced to two thirds when the leukocyte count was between 2 and 2.5 G/l and/or the
platelet count between 60 and 80 G/l; chemotherapy infusion was postponed for 1 week when
leukocyte and/or platelet counts were less than 2 and/or 20 G/l, respectively.
Table 1. Chemotherapies of the randomized H90-NM trial.
Arm A (ABVDm)
1 cycle every 4 weeks
Arm E (EBVMm)
1 cycle every 4 weeks
Drugs i.v. Dose, mg/m2,
Days 1 and 14
Drugs i.v. Dose, mg/m2,
Days 1 and 14
Adriamycin 25 Epirubicin 30
Bleomycin 10 Bleomycin 10
Vinblastin 6 Vinblastin 6
Dacarbazine 375 Methotrexate 30
Methylprednisolone 120 Methylprednisolone 120
Two weeks after the last infusion of CT, patients’ status was assessed; complete remission
(CR) was defined as the complete disappearance of clinical or radiological disease, partial
remission (PR) as a ≥ 50% decrease of tumor burden, and failure as the persistence (<50%
decrease), progression, or reappearance of the disease. In case of failure to CT, patients
received salvage CT combinations, followed by RT whenever possible.
Patients in CR or PR after CT were irradiated. RT started 4 to 5 weeks after the last infusion
of CT. All patients were treated with megavoltage beam energy of 15 MV to 25 MV. RT of
initially involved nodes was given at a daily dose of 1.8 Gy per day (by equally weighted
7
parallel opposed AP-PA fields), 9 Gy per week up to 40 Gy. Non involved sites received
prophylactic RT (30 Gy).
In supradiaphragmatic CS I and II, the width of mediastinal radiation field was planned
according to the situation observed after CT; moreover when the upper cervical areas were not
initially involved, the upper limit of the RT field was the vertebra C3. When supraclavicular
nodes were involved, homolateral axillary area(s) received prophylactic RT (30 Gy); however,
the mediastinum was not irradiated when it was initially free of disease. On the other hand, all
patients with supradiaphragmatic CS I and II received prophylactic RT (30 Gy) to the spleen
and lumboaortic nodes (from vertebra T11/T12 to vertebra L3/L4).
In infradiaphragmatic CS I and II, unilateral or bilateral inguinal and pelvic areas (according
to initial involvement) were irradiated (40 Gy) while the non involved lumboaortic area (up to
T11/T12) and the spleen received prophylactic RT (30 Gy).
In CS III, supradiaphragmatic RT was the same as that given in CSI/II, except that the
mediastinum was prophylactically irradiated (30 Gy) when not initially involved. On the other
hand, infradiaphragmatic RT (40 Gy) encompassed the spleen and the lumboaortic area until
vertebra L5/S1.
Patient status was reassessed one month after completing RT. Patients without clinical and
radiological disease were considered in CR. Patients with a residual mediastinal mass after RT
were also considered in post-treatment CR provided their residual mass had not re-increased
within the six months after completion of RT. Other patients were considered as failures to
RT.
Remission status was checked every three months during the first year, then twice a year until
the fifth year, and once a year thereafter. At each follow-up consultation, the occurrence (or
absence of occurrence) of the following events was carefully recorded and dated: type and site

8
of second primary tumors (excluding non-melanoma skin cancers and carcinoma in situ of the
cervix), constrictive pericarditis, angina pectoris, myocardial infarction, cardiac dysrhythmia,
chronic dyspnea, severe lung or systemic infections; all other life-threatening or fatal events
were also recorded. Relapse was defined as the reappearance of the signs of the disease;
pathological material obtained at the time of relapse (biopsy or fine needle aspiration) was
examined in parallel with the initial material. Relapses were treated by salvage CT and RT
whenever possible. The pathological material of all secondary tumors was reviewed by a panel
of pathologists coordinated by one of us (J.B.).
Statistics
Probabilities of freedom from progression (FFP), event-free survival (EFS), and overall
survival (OS) as well as probabilities of HD mortality (HDM) and treatment-related mortality
(TRM) were calculated from the starting date of CT. Patients who were lost to follow-up were
censored at the date of their last examination. To calculate the probability of OS, all deaths
were taken into account; for FFP, events were failures (to CT or RT) and relapses. For EFS,
events were failures, relapses and deaths in first CR whatever their cause. For HDM, only
deaths from HD were considered as events while patients who died from other causes were
censored at the time of death; for TRM, events were restricted to deaths directly resulting
from the treatment or from all fatal events potentially attributable to the treatment (while
patients who died either from HD or from a cause clearly without any potential relation with
HD treatment were censored). Probabilities of development of second tumors and cardiac
events were calculated from the date of treatment completion. All the above-mentioned
probabilities were calculated by the Kaplan-Meier method, and the differences were assessed
by the log-rank test 25. The chi-square test or, when appropriate, the Fischer’s exact test (two-

9
tailed) was used to compare qualitative data. All computations were performed using the
SPSS 10.0 Package (SPSS Inc. France).

10
RESULTS
Characteristics of the patients and results of treatment
From January 1990 to December 1996, 393 patients with untreated early/intermediate HD
were enrolled onto the H90-NM multicenter trial in 14 French centers. Two patients older
than 65 years, 2 patients younger than 18 years and 2 patients with concurrent serious illness
(myocardial infarction and alcoholic liver cirrhosis) who were wrongly randomized were
excluded from the study, as well as one patient who decided not to be treated according to the
protocol after having been randomized. The remaining 386 patients included in the H90-NM
trial were assessable.
Initial characteristics of the patients are listed on Table 2. Median age was similar in both
arms at 30.5 years. Patients randomized in each of the two arms had well balanced
characteristics. Two hundred and seventy six (71.5%) patients were at CS IA-IIA; out of them,
211 were at supradiaphragmatic CS IA or IIA with a MMR <0.33. Fifty-nine patients with
peripheral CS IA with one node of less than 2 cm diameter received only one course of CT
(arm A 37, arm E 22). The median duration of the planned treatment was 6 months. CT was
administered at full dose to 379 patients (98.2%); the remaining 6 patients received ≥ 75% of
the planned doses. In January 2003, the median follow-up of living patients was 98 months
(72 to 140 months) and 5 patients, all in first CR, were lost to follow-up 91 to 116 months
after completion of treatment.
Treatment results are summarized on Table 3. After completion of CT, 290 patients entered in
CR, 159 in arm A (79.5%) and 131 is arm E (70.4%, p = 0.04). At completion of RT, which
was given to the 372 CT-responding patients, 96% of patients in arm A and 94.6% of patients
in arm E were in CR (p = NS). No severe toxicity occurred during CT or RT.

11
Table 2. Initial characteristics of the 386 adult patients with early/intermediate Hodgkin’s disease included in the H90-NM trial.
All Arm E(EBVMm-RT)
Arm A(ABVDm-RT)
Patients: 386 186 200
Sex: Male 206 90 116 Female 180 96 84
Age: < 40 years 279 132 147≥ 40 years 107 54 53
Histology: Nodular sclerosis 260 132 128 Other subtypes 126 54 72
Clinical stages: IA 81 33 48 IIA 195 95 100 IIIA 25 12 13 IB-IIB 65 36 29 IIIB 20 10 10
Clinical presentation: Supradiaphragmatic CS I/II: with MMR <0.33:
- no symptoms 211 96 115- symptoms 46 26 20
MMR ≥0.33 and <0.45 64 34 30 Infradiaphragmatic CS I/II 20 8 12 CS III 45 22 23
Contiguous extra nodal involvement : No 371 179 192 Yes 15 7 8
MMR: Mediastinal mass ratio (see methods section for definition)

12
Freedom from progression and HD mortality
The 14 patients who failed to respond to CT and the 4 patients who did not respond to RT
were given salvage therapies; 12 of them obtained a sustained CR among whom one died; the
six others achieved transient CR or even no CR and eventually died with HD (Table 3).
Table 3. Treatment results of the 386 patients with early/intermediate Hodgkin’s disease included in the H90-NM trial.
All patients Arm E
(EBVMm-RT)Arm A
(ABVDm-RT)
Patients submitted to CT 386 186 200
Complete remission after CT 290 (75.1%) 131 (70.4%) 159 (79.5%)
Partial remission after CT 82 48 34
Failure to CT 14 7 7
Patients submitted to RT 372 179 193after post CT CR / PR 290 / 82 131 / 48 159 / 34
Complete remission after RT 368 (95.3%) 176 (94.6%) 192 (96.0%)
Failure to RT 4 3 1
Patients submitted to salvage therapy 18 10 8
after failure to CT / RT 14 / 4 7 / 3 7 / 1
Alive with sustained CR 11 6 5
Deceased in CR 1 - 1
Deceased with active disease 6 4 2
Patients followed after post-RT CR 368 176 192
Alive with sustained first CR 317 144 173
Deceased in first CR 17 6 11
Relapsing after first CR 34 26 8
Alive with sustained second CR 27 22 5
Deceased in second CR 2 1 1
Deceased with active disease after relapse 5 3 2
CR, complete remission; CT, chemotherapy; RT, radiotherapy; PR, partial remission.

13
Out of the 368 patients who reached CR after the combined modality treatment, 34 relapsed (8
in arm A and 26 in arm E, p log rank = 0.01) after 8 to 110 months (median 26 months) of
CR.
After retreatment, 29 entered in permanent CR (among whom 2 deceased) while the 5 others
died from HD (Table 3). Out of the 92 patients of both arms whose mediastinum was not
irradiated, 2 suffered from a mediastinal relapse; both of them entered in sustained second CR
after salvage CT and mediastinal RT.
Overall, the FFP rate was 91.4 ± 2.1% in arm A and 80.0 ± 3.0% in arm E (p<0.002, figure
1A). In supradiaphragmatic CS IA or IIA with a MMR <0.33, FFP rates were 93.9 ± 2.2% in
arm A and 82.5 ± 4.1% in arm B (p = 0.016). On the other hand, patients of each arm with
post-CT CR had a significantly higher 10-year FFP rate than those who did not reach CR after
CT: 94.3 ± 2.1% vs. 80.5 ± 6.2% in arm A (p = 0.001), and 85.4 ± 3.3% vs. 67.2 ± 6.4% in
arm E
(p = 0.001).

14
A total of 11 patients died with HD, 6 after failing to initial CT or RT and 5 after a relapse
(Table 3). HDM rate was thus 2.1 ± 1.0% and 3.9 ± 1.5% in arms A and E, respectively
(p = NS; figure 1B). In supradiaphragmatic CS IA or IIA with a MMR <0.33, HDM rates were
0% in arm A and 1.0 ± 1.0% in arm B (p = NS). In arm A, the post-CT status did not
influence HDM rate (CR vs. no CR 1.3 ± 1% vs. 4.9% ± 2.9%, p = 0.14) while it was a
significant prognosis marker in arm E (CR vs. no CR 0.8 ± 0.8% vs. 11.2 ± 4%, p<0.001) . In
arm A, HDM was lower in patients aged less than 40 years (0.7 ± 0.7%) than in patients over
this age (5.9 ± 3.2%, p=0.02) while HDM of patients of arm E was identical in both age
groups (3.8 ± 1.7% vs.4.1 ± 2.8%, respectively).
Life-threatening events and treatment mortality rates
Second cancers: A total of 23 patients (arm A 16; arm E 7) developed a second cancer: 22 of
them were in first CR when their second malignancy developed (Table 4). On the other hand,
two second tumors (one breast cancer and one non Hodgkin’s lymphoma (NHL)) occurred 2
and 3 months after completion of HD treatment and were thus not associated with HD
treatment. Nine patients (all in first CR) suffered from an hematological malignancy; after
having excluded the above-mentioned NHL, this corresponds to a 10-year probability of 2.6
± .9% for the whole group, higher in arm A (7 events, 4.5 ± 1.7%) than in arm E (1 event, 0.6
± 0.6%, p = 0.04; figure 2A). Gender of the patients was also predictive of the development of
an hematological malignancy (M, 8 events: 4.8 ± 1.7%, vs. F, no event, p=0.007).
On the other hand, a solid tumor developed in 14 patients (9 deaths); once having excluded
the above-mentioned breast cancer, this corresponds to a 10-year incidence of 4.9 ± 1.4%,
without any difference between arms A and E (4.2 ± 1.6% and 5.8 ± 2.4%, respectively,
p=0.92; figure 2B). Gender was not predictive of a solid tumor (p=0.5) while age at treatment
(< 40 years vs. ≥ 40 years) was a significant prognostic factor of the incidence of a second
15
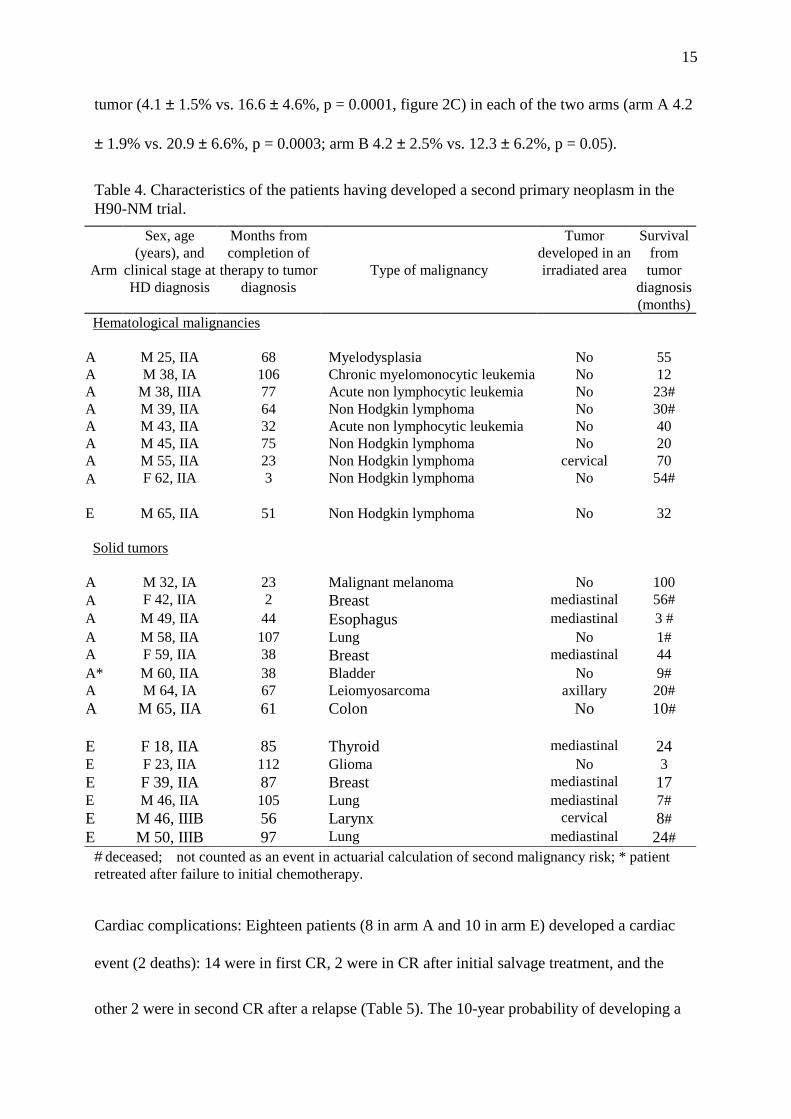
tumor (4.1 ± 1.5% vs. 16.6 ± 4.6%, p = 0.0001, figure 2C) in each of the two arms (arm A 4.2
± 1.9% vs. 20.9 ± 6.6%, p = 0.0003; arm B 4.2 ± 2.5% vs. 12.3 ± 6.2%, p = 0.05).
Table 4. Characteristics of the patients having developed a second primary neoplasm in the H90-NM trial.
Arm
Sex, age (years), and
clinical stage at HD diagnosis
Months from completion of
therapy to tumor diagnosis
Type of malignancy
Tumor developed in an irradiated area
Survival from tumor
diagnosis (months)
Hematological malignancies
A M 25, IIA 68 Myelodysplasia No 55A M 38, IA 106 Chronic myelomonocytic leukemia No 12A M 38, IIIA 77 Acute non lymphocytic leukemia No 23#A M 39, IIA 64 Non Hodgkin lymphoma No 30#A M 43, IIA 32 Acute non lymphocytic leukemia No 40A M 45, IIA 75 Non Hodgkin lymphoma No 20A M 55, IIA 23 Non Hodgkin lymphoma cervical 70A • F 62, IIA 3 Non Hodgkin lymphoma No 54#
E M 65, IIA 51 Non Hodgkin lymphoma No 32
Solid tumors
A M 32, IA 23 Malignant melanoma No 100A • F 42, IIA 2 Breast mediastinal 56#A M 49, IIA 44 Esophagus mediastinal 3 #A M 58, IIA 107 Lung No 1#A F 59, IIA 38 Breast mediastinal 44A* M 60, IIA 38 Bladder No 9#A M 64, IA 67 Leiomyosarcoma axillary 20#A M 65, IIA 61 Colon No 10#
E F 18, IIA 85 Thyroid mediastinal 24E F 23, IIA 112 Glioma No 3E F 39, IIA 87 Breast mediastinal 17E M 46, IIA 105 Lung mediastinal 7#E M 46, IIIB 56 Larynx cervical 8#E M 50, IIIB 97 Lung mediastinal 24#
# deceased; • not counted as an event in actuarial calculation of second malignancy risk; * patient retreated after failure to initial chemotherapy.
Cardiac complications: Eighteen patients (8 in arm A and 10 in arm E) developed a cardiac
event (2 deaths): 14 were in first CR, 2 were in CR after initial salvage treatment, and the
other 2 were in second CR after a relapse (Table 5). The 10-year probability of developing a

16
cardiac event was 5.6 ± 1.3% without any difference between both arms (A 4.5 ± 1.6%, E 7.0
± 2.2%; p = 0.51).
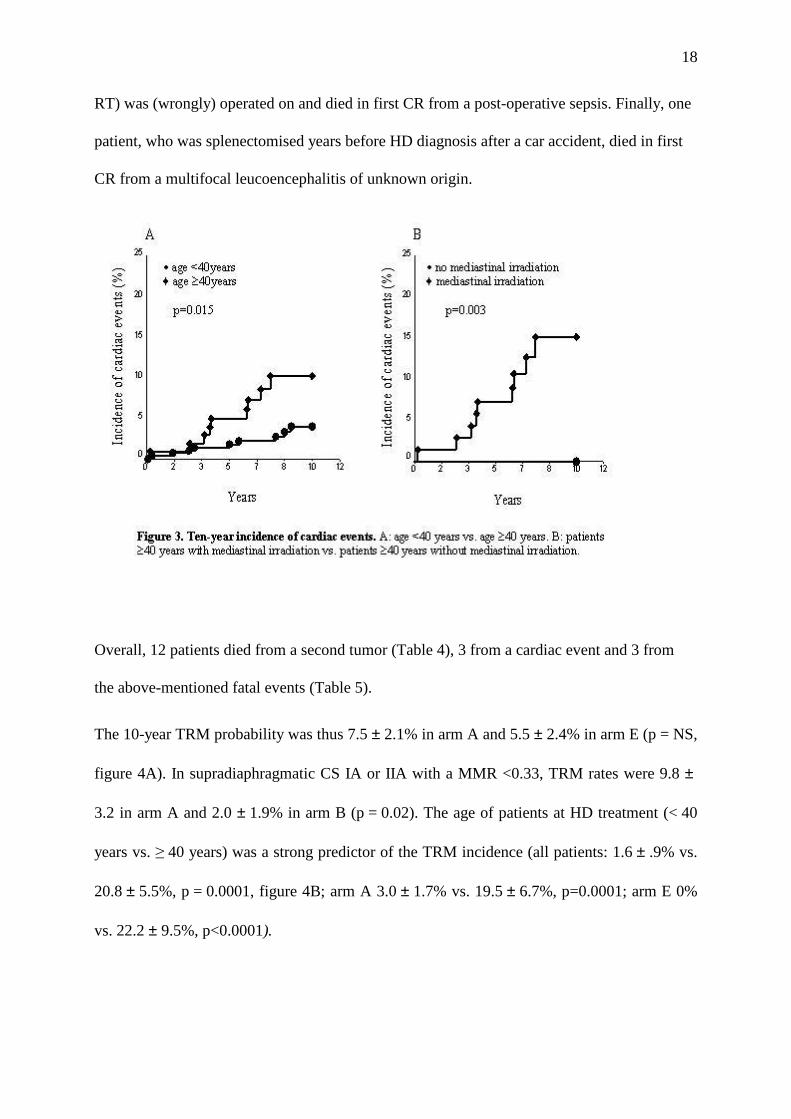
However, the cardiac events incidence was significantly associated with the age of patients at
HD treatment (< 40 years 4.0 ± 1.3% vs. ≥ 40 years 10.2 ± 3.3%, p = 0.015, figure 3A), and
marginally with their gender (male 7.9 ± 2.2% vs. female 2.9 ± 1.3%, p = 0.10). Out of the 52
patients who received a second treatment (which included Adriamycine in most of the cases) 4
developed a cardiac event vs. 14 among the 334 patients who had only one treatment
(p logrank = 0.93). On the other hand, the probability of a cardiac event was higher (without
reaching statistical significance) in the group of patients whose mediastinum was irradiated
(6.7 ± 1.6%) than in the group whose mediastinum was not irradiated (2.3 ± 1.6%; p = 0.2);
however, this difference became statistically significant in the group of patients aged ≥ 40
years at treatment : those who had their mediastinum irradiated had a 10-year risk of cardiac
events as high as 15.0 ± 4.8%, while those whose mediastinum was not irradiated did not

17
developed any cardiac event thus far (p = 0.03, figure 3B).
Table 5. Characteristics of the patients having developed a cardiac event or an other life-threatening or fatal event in the H90-NM trial.
Arm
Sex, age(years), and clinical
stage at HD diagnosis
Months from completionof therapyto event
Event developed in an irradiated area Type of event
Survival from event
(months)
Cardiac eventsA F 26, IIIA 66 Yes Myocardial infarction 63A M 34, IIB 31 No Myocardial infarction 107A F 35, IIA 19 Yes Myocardial infarction 76A M 36, IIA 35 Yes Myocardial infarction 81A M 36, IIA 60 No Myocardial infarction 28A M 37, IA 94 Yes Myocardial infarction 0 #A F 40, IIA 73 Yes Myocardial infarction 2
+A M 57, IIA 42 Yes Myocardial infarction 55
E M19, IIIA 104 Yes Myocardial infarction 39E F 23, IIB § 4 Yes Congestive heart failure 96E M 36, IIB § 99 Yes Myocardial infarction 14E M 42, IIA 75 Yes Angina pectoris 37E M 45, IIA § 47 Yes Angina pectoris 59E M 46, IIIB 46 Yes Myocardial infarction 19 *E M 60,IIB 74 Yes Dysrhythmia 62E M 65, IIIB § 31 Yes Myocardial infarction 0 #E M 65, IIA 90 Yes Angina pectoris 15 #E F 65, IA 2 Yes Myocardial infarction 88
Other eventsA M 45, IA § 15 No Stroke 0 #A M 49, IIIB 36 Yes Post-operative sepsis 1 #
E F 58, IIIB 8 NoMultifocal leucoencephalitis
1 #
# deceased; § patient having received a second line anthracycline-based chemotherapy;* patient deceased from larynx cancer (see Table 4).
Other complications (Table 5): no patient developed constrictive pericarditis, chronic dyspnea,
severe lung or systemic infection so far. On the other hand, one patient died from a stroke
with normal blood counts after having completed the treatment of his relapse. Another patient
who had a limited pachypleuritis of the left costo-diaphragmatic pleura (resulting from splenic
18
RT) was (wrongly) operated on and died in first CR from a post-operative sepsis. Finally, one
patient, who was splenectomised years before HD diagnosis after a car accident, died in first
CR from a multifocal leucoencephalitis of unknown origin.
Overall, 12 patients died from a second tumor (Table 4), 3 from a cardiac event and 3 from
the above-mentioned fatal events (Table 5).
The 10-year TRM probability was thus 7.5 ± 2.1% in arm A and 5.5 ± 2.4% in arm E (p = NS,
figure 4A). In supradiaphragmatic CS IA or IIA with a MMR <0.33, TRM rates were 9.8 ±
3.2 in arm A and 2.0 ± 1.9% in arm B (p = 0.02). The age of patients at HD treatment (< 40
years vs. ≥ 40 years) was a strong predictor of the TRM incidence (all patients: 1.6 ± .9% vs.
20.8 ± 5.5%, p = 0.0001, figure 4B; arm A 3.0 ± 1.7% vs. 19.5 ± 6.7%, p=0.0001; arm E 0%
vs. 22.2 ± 9.5%, p<0.0001).

19
Overall survival
A total of 31 patients died: 11 with HD, 18 (15 in first CR) from a second tumor, a cardiac
event or an other treatment-related or potentially treatment-related event, and the last 2 (both
in first CR) from an unrelated cause (murder, car accident). Of note the fact that in January
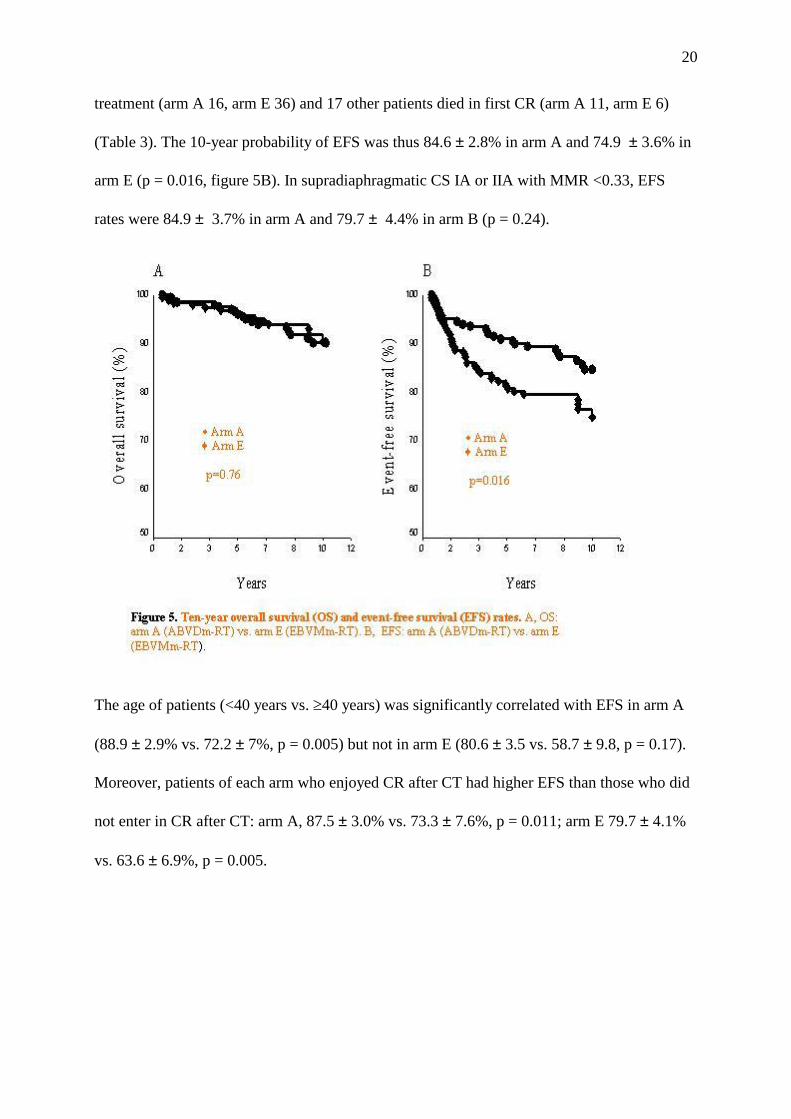
2003 all living patients were in CR. Ten-year survival rate was thus 90.4 ± 2.3% in arm A and
90.3 ± 2.7% in arm E (p = NS, figure 5A). In supradiaphragmatic CS IA or IIA with a MMR
<0.33, corresponding figures were 89.4 ± 3.3% in arm A and 96.0 ± 2.4% in arm B (p =0.10).
Survival rate was strongly associated with the age of patients at treatment, higher in patients
< 40 years than in patients ≥ 40 years (arm A 95.7 ± 1.9% vs. 74.3 ± 6.8%, p< 0.0001; arm E
95.4 ± 1.8% vs. 74.7 ± 9.6%, p=0.01). However the post-CT status (CR vs. no CR) was a
significant predictor of survival in arm E (p=0.01) but not in arm A (p=0.3).
Event-free survival
A total of 52 patients either failed to respond to CT or RT or relapsed after completion of
20
treatment (arm A 16, arm E 36) and 17 other patients died in first CR (arm A 11, arm E 6)
(Table 3). The 10-year probability of EFS was thus 84.6 ± 2.8% in arm A and 74.9 ± 3.6% in
arm E (p = 0.016, figure 5B). In supradiaphragmatic CS IA or IIA with MMR <0.33, EFS
rates were 84.9 ± 3.7% in arm A and 79.7 ± 4.4% in arm B (p = 0.24).
The age of patients (<40 years vs. ≥40 years) was significantly correlated with EFS in arm A
(88.9 ± 2.9% vs. 72.2 ± 7%, p = 0.005) but not in arm E (80.6 ± 3.5 vs. 58.7 ± 9.8, p = 0.17).
Moreover, patients of each arm who enjoyed CR after CT had higher EFS than those who did
not enter in CR after CT: arm A, 87.5 ± 3.0% vs. 73.3 ± 7.6%, p = 0.011; arm E 79.7 ± 4.1%
vs. 63.6 ± 6.9%, p = 0.005.

21
DISCUSSION
In this large group of patients with early or intermediate HD, we first explored in the setting of
a randomized trial whether 3 courses of EBVMm or ABVDm, followed by the same RT,
resulted in similar rates of CR and FFP. Our results showed that this was not the case.
EBVMm induced a significantly lower rate of CR than ABVDm; moreover, despite enjoying
similar rates of CR after RT in both arms, patients of the EBVMm arm had higher relapse
rate, and lower FFP and EFS rates than patients of the ABVDm arm. EBVMm is thus clearly
a less potent multiagent CT than ABVDm. A randomized trial comparing Methotrexate
Cyclophosphamide, Bleomycin and prednisolone plus Adriamycin (50 mg/m2) or Epirubicin
(75 mg/m2, i.e. + 50%) in a large group of intermediate and high grade non Hodgkin’s
lymphomas showed that both association had the same incidence of adverse effects as well as
the same CR rates (58.1% vs. 58.5%) 26. In our H90-NM trial, the dose of Epirubicin (30
mg/m2) was only 20% higher than that of Adriamycin (25 mg/m2). The lower efficacy of
EBVMm vs. ABVDm was thus likely resulting partly from an insufficient dose of Epirubicin
and possibly from the lower efficacy of Methotrexate compared with Dacarbazine.
In both arms of our trial, entering in CR after initial CT had also a favorable impact on FFP
and EFS rates. The prognostic value of the result of the first 3 courses of CT has been shown
twenty years ago in patients treated by MOPP followed by RT 27 and was confirmed more
recently by our group in patients treated by ABVD combined with RT 14,21. This information
underlines the importance of taking into account this intermediate endpoint to direct the
second part of the treatment whether it is RT or CT. It remains fortunately that most of the
patients treated with EBVMm who did not enter in CR after CT or relapsed after completion
of RT enjoyed a second sustained CR after salvage therapies; as a result, patients of both arms
had finally the same HDM and OS rates.
22
The other important objective of this trial was to observe the long-term complications and the
resulting mortality rates associated with this combined modality program. Concerning second
tumors, recent studies gathering large numbers of HD patients with follow-up reaching
sometimes more than 20 years have brought very robust information 6,7,11,28-32. However, the
results of this trial are of particular interest because, besides that all severe complications were
prospectively recorded, it is to our knowledge the first study comparing a CT (EBVMm)
which did not contain any alkylating agent with the reference ABVDm combination which
comprised Dacarbazine, which is an alkylating agent 18.
Importantly, we showed that second hematological malignancies, all of which occurred in
male patients and in first CR, had a significantly lower incidence in the EBVMm arm than in
the ABVDm arm (p = 0.04). No secondary leukemia occurred in the EBVMm-RT arm (no
alkylating agent) which is in keeping with the very low rate (≤0.5%) observed after RT alone
29,30,33; in contrast, 4 secondary leukemias (2 acute non lymphoblastic leukemias (ANLL), 1
myelodysplastic syndrome, 1 chronic myelomonocytic leukemia) developed after ABVDm-
RT which corresponds to an incidence of 2.7 ± 1.4% (p = 0.05). Thus far, it was known that
the combination of ABVDm plus RT was less leukemogenic than that of MOPP (an
association including two alkylating agents, Mechlorethamine and Procarbazine) plus RT 34.
This randomized study demonstrated that the leukemogenic impact of ABVDm plus RT was
however significantly higher than that of EBVMm plus RT. ABVD alone is almost not
leukemogenic 35, but when alkylating agent(s) is (are) associated with RT, the rate of second
leukemia has been shown to be dependant of the extent of RT 34.
On the other hand, EBVMm combined with high dose extended RT was associated with a
very low 10-year rate of non-Hodgkin’s lymphomas (1 case, i.e. 0.6% ± 0.6%) which is not in
favor of the idea that NHLs could be part of the natural history of HD or of an underlying

23
immunodeficiency as suggested by others 36,37. A recent review on the occurrence of NHLs
after HD is in keeping with our observation; combined modality therapy such as MOPP-RT
was shown to result in an increased risk of NHLs compared to RT alone; moreover it was also
suggested that CTs comprising one alkylating agent resulted in lower risk of NHLs than CTs
comprising two alkylating agents 30. Interestingly, no case of NHL has so far occurred after
the 70th month following completion of treatment (344 patients still at risk). This suggests
that the pattern of secondary NHL development would possibly resemble that of secondary
ANLL. Longer follow-up of this randomized cohort of patients is needed to have a clearer
answer to this question.
On the other hand, the incidence of solid tumors was similar in both arms of the trial ; this
most likely reflects that the additional carcinogenic role of Dacarbazine is very weak in
comparison to the role of high dose extended RT 38-42. The 10-year rate of solid tumors
observed in this prospective trial is indeed in the range of what has been reported in a much
larger cohort of patients with longer follow-up 32. As others, we observed the significant
impact of the age of patients (< 40 years vs. ≥ 40 years) at HD treatment on the development
of solid tumors; this is, to a large extent, the result of the increasing incidence of background
tumors with increasing age 31.
Life threatening or fatal cardiac events were suspected to be associated with mediastinal
irradiation for decades 43. This was confirmed by our study where all severe complications
have been prospectively recorded. Overall, the cumulative rate of cardiac events approached
6% by 10 years. The age of the patients at HD treatment was predictive of a cardiac event with
a lower risk when the treatment was applied before 40 years (4.0 ± 1.4%) and a significantly
higher risk after this age (10.2 ± 3.3%, p=0.015) confirming previous findings 44. The increase
of risk with age at treatment has been demonstrated to result at least partly from background

24
cardiac events, the incidence of which increases with increasing age 12. However the impact of
RT, when given at ≥ 40 years, was clearly demonstrated in this trial where the incidence of
cardiac events was significantly higher in the patients whose mediastinum was irradiated (9
events, 5.0 ± 4.8%) than in those whose mediastinum was not irradiated (no event, p = 0.032)
which is also in keeping with previous observations 4-12. Overall, our results confirm the
predominant role of high dose RT and the weak impact of anthracyclines (at the doses they
were given in our trial) on the genesis of cardiac complications.
Importantly, most solid tumors as well as most cardiac events developed in the mediastinal
irradiated area (40 Gy) and none in prophylactically irradiated areas (30 Gy). Limiting RT to
involved fields without modifying its dose (40 Gy) would thus probably not decrease the rate
of second solid tumors or cardiac events; in contrast it would certainly increase the rate of
lumboaortic/splenic relapses, which were prevented to occur in this trial by prophylactic
lumboaortic and splenic RT which sterilize occult infradiaphragmatic disease in
supradiaphragmatic CS I/II HD 45.
The preservation of the low rate of HDM observed in this trial and, at the same time, the
decrease of the incidence of second tumors and/or cardiac events could only be achieved by
increasing the efficacy of CT, either by increasing its number of cycles 46 or by increasing its
dose 47. In patients enjoying CR, this would allow to sterilize occult disease and at the same
time to decrease the dose of RT (limited to initially involved areas), or even to completely
eliminate RT 48,49. These strategies should be adequately tested in the setting of large
randomized trials.
Overall, it is of great concern to observe the high incidence of mortality resulting from second
tumors, cardiac and other life-threatening events. Such an incidence reached 4.4% by 10 years
and the slope of the curve strongly suggests that this incidence should continue to increase
25
with increasing lengths of follow-up as recently shown in cohorts of patients followed 20 or
more years 12,32. Importantly, TRM was significantly associated with age of patients at
treatment in both arms of the trial. In the group of patients treated at the age of 40 or beyond,
the 10-year risk of dying from an event potentially attributable to the treatment reached 20%
(19.5% in arm A and 22.2% in arm E), which reflects the increasing incidence of mortality
from background events (which would have occurred in the absence of treatment) with
increasing age as it has been repetitively demonstrated 11,12,32. Thus, in this age group (28% of
our patients), although HDM was low (5.9% in arm A and 4.1% in arm E), OS was only
74.3% in arm A and 74.7% in arm E. In contrast, in the group of patients treated before the
age of 40 years (72% of our cohort), HDM rates were similarly low (0.7% in arm A and 3.8%
in arm E) but TRM rates were very low 3% in arm A, 0% in arm E) because of the absence of
background fatal events in this age group. On the basis of HDM and TRM, there was thus no
final advantage of one arm over the other, which was also shown by 10-year survival rates of
arms A and E which were the same (95.7% and 95.4%, respectively). However, EFS (i.e. no
failure to CT or RT, no relapse and no death in first CR), which is the most frequently used
index of the success or failure of a treatment, is significantly higher in arm A (84.6% than in
arm E (74.9%, p = 0.016). Three courses of ABVDm plus RT remains thus the best available
option to treat early/intermediate HD.
We have now reach a point in the history of CS I and II HD treatment where it has become
clear that combining CT and RT is a better option than RT alone, as shown by several groups
50-52 and most recently by the 3-year FFS results of a large randomized trial comparing in early
HD (supradiaphragmatic CS IA or IIA with a MMR <0.33) 3 courses of Adriamycin plus
Velban combined with subtotal RT (EFS: 94%) vs. subtotal RT alone (EFS: 81%, p = 0.001)
53. Three-year EFS rates of our H90-NM for patients with similar characteristics were: arm A
95%, arm E 90% (p = NS). Improving these results will be a difficult task with currently

26
available methods of treatment. For the present time, it remains that the only way to reduce
the worrying rate of mortality resulting from cardiac events or second cancers is to
disseminate specific guidelines to concerned people (patients, general practionners,
hematologists, oncologists, radiation therapists) indicating the necessity of a life-time follow-
up for all HD patients and particularly for those treated at the age of 40 or beyond. It should
include systematic and iterative programs of early detection of cancers and heart diseases by
appropriate means as well as the fight against smoking (which is known to increase
background tumors and cardiac events).

27
ACKNOWLEDGMENT
We would like to thank Dr Malika Djeridane for excellent assistance in data collection and
technical help in several computer techniques.

28
REFERENCES
1. Connors JM, Noordijk EM, Horning SJ. Hodgkin's lymphoma: basing the treatment on the evidence. Hematology (Am Soc Hematol Educ Program). 2001:178-193
2. Tirelli U, Vaccher E, Spina M, Carbone A. Hodgkin's disease: clinical presentation and treatment. Cancer Treat Res. 2001;104:247-265
3. Yung L, Linch D. Hodgkin's lymphoma. Lancet. 2003;361:943-951
4. Cosset JM, Henry-Amar M, Pellae-Cosset B, et al. Pericarditis and myocardial infarctions after Hodgkin's disease therapy. Int J Radiat Oncol Biol Phys. 1991;21:447-449
5. Boivin JF, Hutchison GB, Lubin JH, Mauch P. Coronary artery disease mortality in patients treated for Hodgkin's disease. Cancer. 1992;69:1241-1247
6. Vaughan Hudson B, Vaughan Hudson G, Linch DC, Anderson L. Late mortality in young BNLI patients cured of Hodgkin's disease. Ann Oncol. 1994;5 Suppl 2:65-66
7. Boivin JF, Hutchison GB, Zauber AG, et al. Incidence of second cancers in patients treated for Hodgkin's disease. J Natl Cancer Inst. 1995;87:732-741
8. Henry-Amar M, Joly F. Late complications after Hodgkin's disease. Ann Oncol. 1996;7 Suppl 4:115-126
9. Hoppe RT. Hodgkin's disease: complications of therapy and excess mortality. Ann Oncol. 1997;8:115-118.
10. Hancock SL. Cardiovascular late effects after treatment of Hodgkin's disease. In: Mauch PM, Armitage JD, Diehl V, Hoppe RT, Weiss LM, eds. Hodgkin's disease. Philadelphia: Lippincott Williams & Wilkins; 1999:647-659
11. Dores GM, Metayer C, Curtis RE, et al. Second malignant neoplasms among long-term survivors of Hodgkin's disease: a population-based evaluation over 25 years. J Clin Oncol. 2002;20:3484-3494.
12. Ng AK, Bernardo MP, Weller E, et al. Long-term survival and competing causes of death in patients with early-stage Hodgkin's disease treated at age 50 or younger. J Clin Oncol. 2002;20:2101-2108.
13. Ifrah N, Hunault M, Jais JP, et al. Infradiaphragmatic Hodgkin's disease: long term results of combined modality therapy. Leuk Lymphoma. 1996;21:79-84
14. Colonna P, Jais JP, Desablens B, et al. Mediastinal tumor size and response to chemotherapy are the only prognostic factors in supradiaphragmatic Hodgkin's disease treated by ABVD plus radiotherapy: ten-year results of the Paris-Ouest-France 81/12 trial, including 262 patients. J Clin Oncol. 1996;14:1928-1935.

29
15. Andrieu JM, Jais JP, Colonna P, et al. Ten-year results of a strategy combining three cycles of ABVD and high- dose extended irradiation for treating Hodgkin's disease at advanced stages. Ann Oncol. 1998;9:195-203
16. Merrill J, Greco FA, Zimbler H, Brereton HD, Lamberg JD, Pomeroy TC. Adriamycin and radiation: synegistic cardiotoxicity. Ann Intern Med. 1975;82:122-123
17. Billingham ME, Bristow MR, Glatstein E, Mason JW, Masek MA, Daniels JR. Adriamycin cardiotoxicity: endomyocardial biopsy evidence of enhancement by irradiation. Am J Surg Pathol. 1977;1:17-23
18. Colvin OM. Antitumor alkylating agents. In: DeVita VT, Jr, Hellman S, Rosenberg SA, eds. Cancer Principles and practice of oncology (ed 6th). Philadelphia: Lippincott Williams & wilkins; 2001:363-376
19. Zittoun R, Eghbali H, Audebert A, et al. Association d'épirubicine, bléomycine, vinblastine, et prednisone (EBVP) avant radiothérapie dans les stades localisés de la maladie de Hodgkin. Essai de phase II. Bull Cancer. 1987;74:151-157.
20. Horning SJ, Hoppe RT, Hancock SL, Rosenberg SA. Vinblastine, bleomycin, and methotrexate: an effective adjuvant in favorable Hodgkin's disease. J Clin Oncol. 1988;6:1822-1831
21. Desablens B, Tourani JM, Casassus P, et al. Traitement des formes localisées de la maladie de hodgkin par 3 cures de chimiothérapie (ABVD-MP) associées à une radiothérapie focale élargie et lombo-splénique prophylactique. Presse Med. 1989;18:1917-1921.
22. Straus DJ, Gaynor JJ, Myers J, et al. Prognostic factors among 185 adults with newly diagnosed advanced Hodgkin's disease treated with alternating potentially noncross-resistant chemotherapy and intermediate-dose radiation therapy. J Clin Oncol. 1990;8:1173-1186
23. Gisselbrecht C, Ferme C. Prognostic factors in advanced Hodgkin's disease: problems and pitfalls. Towards an international prognostic index. Leuk Lymphoma. 1995;15 Suppl 1:23-24
24. Carbone PP, Kaplan HS, Musshoff K, Smithers DW, Tubiana M. Report of the Committee on Hodgkin's Disease Staging Classification. Cancer Res. 1971;31:1860-1861
25. Peto R, Pike MC, Armitage P, et al. Design and analysis of randomized clinical trials requiring prolonged observation of each patient. II. analysis and examples. Br J Cancer. 1977;35:1-39.
26. Nair R, Ramakrishnan G, Nair NN, et al. A randomized comparison of the efficacy and toxicity of epirubicin and doxorubicin in the treatment of patients with non-Hodgkin's lymphoma. Cancer. 1998;82:2282-2288
27. Kuentz M, Reyes F, Brun B, et al. Early response to chemotherapy as a prognostic factor in Hodgkin's disease. Cancer. 1983;52:780-785
28. Henry-Amar M. Second cancer after the treatment for Hodgkin's disease: a report from the International Database on Hodgkin's Disease. Ann Oncol. 1992;3 Suppl 4:117-128
30
29. Swerdlow AJ, Douglas AJ, Hudson GV, Hudson BV, Bennett MH, MacLennan KA. Risk of second primary cancers after Hodgkin's disease by type of treatment: analysis of 2846 patients in the British National Lymphoma Investigation. Bmj. 1992;304:1137-1143
30. van Leeuwen FE, Swerdlow AJ, Valagussa P, Tucker MA. Second cancers after treatment of Hodgkin's disease. In: Mauch PM, Armitage JD, Diehl V, Hoppe RT, Weiss LM, eds. Hodgkin's disease. Philadelphia: Lippincott Williams & Wilkins; 1999:607-632
31. Swerdlow AJ, Barber JA, Hudson GV, et al. Risk of second malignancy after Hodgkin's disease in a collaborative British cohort: the relation to age at treatment. J Clin Oncol. 2000;18:498-509
32. Ng AK, Bernardo MV, Weller E, et al. Second malignancy after Hodgkin disease treated with radiation therapy with or without chemotherapy: long-term risks and risk factors. Blood. 2002;100:1989-1996.
33. Tucker MA, Coleman CN, Cox RS, Varghese A, Rosenberg SA. Risk of second cancers after treatment for Hodgkin's disease. N Engl J Med. 1988;318:76-81
34. Delwail V, Jais JP, Colonna P, Andrieu JM. Fifteen-year secondary leukaemia risk observed in 761 patients with Hodgkin's disease prospectively treated by MOPP or ABVD chemotherapy plus high-dose irradiation. Br J Haematol. 2002;118:189-194.
35. Valagussa P, Santoro A, Fossati Bellani F, Franchi F, Banfi A, Bonadonna G. Absence of treatment-induced second neoplasms after ABVD in Hodgkin's disease. Blood. 1982;59:488-494
36. van Rijswijk RE, Verbeek J, Haanen C, Dekker AW, van Daal WA, van Peperzeel HA. Major complications and causes of death in patients treated for Hodgkin's disease. J Clin Oncol. 1987;5:1624-1633
37. Zarate-Osorno A, Medeiros LJ, Longo DL, Jaffe ES. Non-Hodgkin's lymphomas arising in patients successfully treated for Hodgkin's disease. A clinical, histologic, and immunophenotypic study of 14 cases. Am J Surg Pathol. 1992;16:885-895
38. Hancock SL, Tucker MA, Hoppe RT. Factors affecting late mortality from heart disease after treatment of Hodgkin's disease. Jama. 1993;270:1949-1955
39. Henry-Amar M. Quantitative risk of second cancer in patients in first complete remission from early stages of Hodgkin's disease. NCI Monogr. 1988:65-72
40. Jenkin D, Doyle J, Berry M, et al. Hodgkin's disease in children: treatment with MOPP and low-dose, extended field irradiation without laparotomy. Late results and toxicity. Med Pediatr Oncol. 1990;18:265-272
41. Zanini M, Viviani S, Santoro A, et al. Extended-field radiotherapy in favorable stage IA-IIA Hodgkin's disease (prognostic role of stage). Int J Radiat Oncol Biol Phys. 1994;30:813-819
31
42. Chronowski GM, Wilder RB, Tucker SL, et al. Analysis of in-field control and late toxicity for adults with early-stage Hodgkin's disease treated with chemotherapy followed by radiotherapy. Int J Radiat Oncol Biol Phys. 2003;55:36-43.
43. Hancock SL, Donaldson SS, Hoppe RT. Cardiac disease following treatment of Hodgkin's disease in children and adolescents. J Clin Oncol. 1993;11:1208-1215
44. Tarbell NJ, Thompson L, Mauch P. Thoracic irradiation in Hodgkin's disease: disease control and long-term complications. Int J Radiat Oncol Biol Phys. 1990;18:275-281.
45. Andrieu JM, Dana M, Desprez-Curely JP, Jacquillat C, Weil M. MOPP chemotherapy plus irradiation for Hodgkin's disease, stages IA to IIIB. Long-term results of the prospective trial H72 (1972-1976, 334 patients). Hematol Oncol. 1985;3:219-231.
46. Duggan DB, Petroni GR, Johnson JL, et al. Randomized comparison of ABVD and MOPP/ABV hybrid for the treatment of advanced Hodgkin's disease: report of an intergroup trial. J Clin Oncol. 2003;21:607-614
47. Diehl V, Franklin J, Pfreundschuh M, et al. Standard and increased-dose BEACOPP chemotherapy compared with COPP-ABVD for advanced Hodgkin's disease. N Engl J Med. 2003;348:2386-2395
48. Ferme C, Sebban C, Hennequin C, et al. Comparison of chemotherapy to radiotherapy as consolidation of complete or good partial response after six cycles of chemotherapy for patients with advanced Hodgkin's disease: results of the groupe d'etudes des lymphomes de l'Adulte H89 trial. Blood. 2000;95:2246-2252
49. DeVita VT, Jr. Hodgkin's disease--clinical trials and travails. N Engl J Med. 2003;348:2375-2376
50. Noordijk EM, Carde P, Mandard AM, et al. Preliminary results of the EORTC-GPMC controlled clinical trial H7 in early-stage Hodgkin's disease. EORTC Lymphoma Cooperative Group. Groupe Pierre-et-Marie-Curie. Ann Oncol. 1994;5 Suppl 2:107-112
51. Pavlovsky S, Schvartzman E, Lastiri F, et al. Randomized trial of CVPP for three versus six cycles in favorable-prognosis and CVPP versus AOPE plus radiotherapy in intermediate-prognosis untreated Hodgkin's disease. J Clin Oncol. 1997;15:2652-2658
52. Moody AM, Pratt J, Hudson GV, Smith P, Lamont A, Williams MV. British National Lymphoma Investigation: pilot studies of neoadjuvant chemotherapy in clinical stage Ia and IIa Hodgkin's disease. Clin Oncol (R Coll Radiol). 2001;13:262-268
53. Press OW, LeBlanc M, Lichter AS, et al. Phase III randomized intergroup trial of subtotal lymphoid irradiation versus doxorubicin, vinblastine, and subtotal lymphoid irradiation for stage IA to IIA Hodgkin's disease. J Clin Oncol. 2001;19:4238-4244




















