Mucosa-associated microbiota drives pathogenic functions in ...
Upload
independentCategory
view
0download
0
PRELIMINARYCOMMUNICATION
Direct Detection of Bacterial Biofilmson the Middle-Ear Mucosa of ChildrenWith Chronic Otitis MediaLuanne Hall-Stoodley, PhDFen Ze Hu, PhDArmin Gieseke, PhDLaura Nistico, PhDDuc Nguyen, PhDJay Hayes, BSMichael Forbes, MDDavid P. Greenberg, MDBethany Dice, BSAmy Burrows, BSP. Ashley Wackym, MDPaul Stoodley, PhDJ. Christopher Post, MD, PhDGarth D. Ehrlich, PhDJoseph E. Kerschner, MD
OTITIS MEDIA (OM) IS THEmost common illness forwhich children visit a phy-sician, receive antibiotics,
or undergo surgery in the United States.Chronic OM includes both OM with ef-fusion (OME) and recurrent OM inwhich clinical evidence of OM and themiddle-ear effusion (MEE) resolves be-tween episodes. Otitis media with ef-fusion can result in conductive hear-ing loss, which has been linked to thedelayed development of speech and so-cialization skills.1 Streptococcus pneu-moniae, Haemophilus influenzae, andMoraxella catarrhalis are isolated fromapproximately 25% of children withOME, but polymerase chain reaction(PCR)-based methods have demon-
Author Affiliations: Center for Genomic Sciences, Al-legheny-Singer Research Institute, Pittsburgh, Pa (DrsHall-Stoodley, Hu, Gieseke, Nistico, Nguyen, Forbes,Stoodley, Post, and Ehrlich and Mr Hayes and Ms Dice);Department of Microbiology and Immunology, DrexelUniversity College of Medicine, Allegheny Campus,Pittsburgh (Drs Hall-Stoodley, Hu, Stoodley, Post, andEhrlich); Department of Molecular Ecology, Max PlanckInstitute for Marine Microbiology, Bremen, Germany
(Dr Gieseke); Children’s Hospital of Pittsburgh, Pitts-burgh (Dr Greenberg); and Children’s Hospital of Wis-consin, Medical College of Wisconsin, Department ofOtolaryngology, Milwaukee (Ms Burrows and DrsWackym and Kerschner).Corresponding Author: Garth D. Ehrlich, PhD, Cen-ter for Genomic Sciences, Allegheny-Singer ResearchInstitute, 320 E North Ave, Pittsburgh, PA 15212([email protected]).
Context Chronic otitis media (OM) is a common pediatric infectious disease. Previousstudies demonstrating that metabolically active bacteria exist in culture-negative pedi-atric middle-ear effusions and that experimental infection with Haemophilus influen-zae in the chinchilla model of otitis media results in the formation of adherent mucosalbiofilms suggest that chronic OM may result from a mucosal biofilm infection.
Objective To test the hypothesis that chronic OM in humans is biofilm-related.
Design, Setting, and Patients Middle-ear mucosa (MEM) biopsy specimens wereobtained from 26 children (mean age, 2.5 [range, 0.5-14] years) undergoing tympanos-tomy tube placement for treatment of otitis media with effusion (OME) and recurrentOM and were analyzed using microbiological culture, polymerase chain reaction (PCR)-based diagnostics, direct microscopic examination, fluorescence in situ hybridization, andimmunostaining. Uninfected (control) MEM specimens were obtained from 3 childrenand 5 adults undergoing cochlear implantation. Patients were enrolled between Febru-ary 2004 and April 2005 from a single US tertiary referral otolaryngology practice.
Main Outcome Measures Confocal laser scanning microscopic (CLSM) images wereobtained from MEM biopsy specimens and were evaluated for biofilm morphologyusing generic stains and species-specific probes for H influenzae, Streptococcus pneu-moniae, and Moraxella catarrhalis. Effusions, when present, were evaluated by PCRand culture for evidence of pathogen-specific nucleic acid sequences and bacterial growth,respectively.
Results Of the 26 children undergoing tympanostomy tube placement, 13 (50%)had OME, 20 (77%) had recurrent OM, and 7 (27%) had both diagnoses; 27 of 52(52%) of the ears had effusions, 24 of 24 effusions were PCR-positive for at least 1OM pathogen, and 6 (22%) of 27 effusions were culture-positive for any pathogen.Mucosal biofilms were visualized by CLSM on 46 (92%) of 50 MEM specimens fromchildren with OME and recurrent OM using generic and pathogen-specific probes.Biofilms were not observed on 8 control MEM specimens obtained from the patientsundergoing cochlear implantation.
Conclusion Direct detection of biofilms on MEM biopsy specimens from childrenwith OME and recurrent OM supports the hypothesis that these chronic middle-eardisorders are biofilm-related.JAMA. 2006;296:202-211 www.jama.com
202 JAMA, July 12, 2006—Vol 296, No. 2 (Reprinted) ©2006 American Medical Association. All rights reserved.

strated sequence-specific DNA andRNA for these pathogens in nearly 80%of cases.2-5
Evidence that OME is associated withpersistent bacterial infection in the ab-sence of culture, combined with its re-calcitrance to antibiotic treatment, ledto the development of the biofilm hy-pothesis.4,6 Biofilms consist of aggre-gated bacteria, usually adherent to a sur-face, surrounded by an extracellularmatrix, and have been implicated in sev-eral chronic bacterial infections.7-10
Previous laboratory studies with low-passage clinical isolates of H influen-zae have demonstrated that biofilmsform on the middle-ear mucosa (MEM)of the chinchilla6; however, no studieshave directly examined human MEMfor biofilms. Our objective in this studywas to perform imaging of MEM bi-opsy specimens from children withOME and recurrent OM to test the hy-potheses that these conditions are bio-film-related.
METHODSPatient Population
Institutional review board approval wasobtained from the Medical College ofWisconsin. Patients were invited to par-ticipate at the time of consultation foreither tympanostomy tube (TT) place-ment (study group) or cochlear im-plantation (control group). Written in-formed consent was obtained from theparents or guardians of the children inthe study and control groups, as wellas from adults in the control group.Consecutive patients fulfilling the studycriteria were invited to participate be-tween February 2004 and April 2005from a single tertiary referral pediatricotolaryngology practice (J.E.K.). Theparticipation rate was approximately50% in the TT group.
To be considered for inclusion, studypatients had to be between 6 monthsand 15 years of age and meet clinicalcriteria for TT insertion for either OMEor recurrent OM. Otitis media with ef-fusion was defined as the persistenceof an MEE for longer than 3 monthswith minimal constitutional symp-toms. Recurrent OM was defined as 3
or more acute OM presentations withina 6-month period in which clinical evi-dence of OM and MEE resolved be-tween episodes. Exclusion criteria in-cluded immunological abnormality,either intrinsic or pharmacological; ana-tomical or physiological defect of theear; syndrome associated with OM (eg,Down syndrome, cleft palate); senso-rineural hearing loss; and chronic mas-toiditis, cholesteatoma, or other OMcomplications except for conductivehearing loss.
Two groups of control biopsy speci-mens were obtained from patients inthe same otolaryngology practiceundergoing cochlear implantation: apediatric group (n=3), in which theage range was the same as for theexperimental group, and an adultgroup (n=5). For inclusion in eithercontrol group, patients had to have anegligible history of OM defined as 1or fewer episodes per year and nomiddle-ear pathology. Middle-earmucosa specimens were obtained atthe time of cochlear implantation andprepared in the same manner as thespecimens from the study group. Anti-biotic usage was not used as an exclu-sion criterion in any case.
Specimen Acquisitionand Tissue PreparationGeneral mask anesthesia was usedduring the surgical procedure. Usingan operating microscope (Carl ZeissInc, Thornwood, NY), a myringotomyincision was made in the anterior-inferior tympanic membrane. Middle-ear effusion was collected, if present,using a sterile tympanostomy trap forculture and PCR. A cup forceps wasinserted through the myringotomyincision using high-power magnifica-tion, and MEM specimens (!1 mm2)were obtained from the middle-earpromontory proximal to the eusta-chian tube.
The specimens were placed in Hankbalanced salt solution (HBSS) (Invit-rogen, Carlsbad, Calif ) and shippedovernight on ice to the Center for Ge-nomic Sciences. Because unfixed speci-mens were evaluated immediately af-
ter shipment it was not possible torandomize samples. Unfixed MEMspecimens were rinsed and incubatedwith either BacLight LIVE/DEADnucleic acid probes (Invitrogen) or withantipneumococcal antibody (PnAb) di-luted in HBSS, then rinsed to removeexcess probe and imaged in an en-closed coverslip chamber containingHBSS. Specimens for 16S rRNA fluo-rescence in situ hybridization (FISH)were fixed overnight and stored at!20°C prior to hybridization.
Aerobic Cultures. After collection,MEE specimens were immediatelytransported to the clinical microbiol-ogy laboratory for Gram staining andfor bacterial growth on blood agar,chocolate agar, MacConkey agar, andcolistin-naladixic acid, with incuba-tion in 5% CO2.
PCR-BasedBacterialDetection.DNAwas isolated from MEEs using TRIzol(Invitrogen). Twenty-microliter PCRswere performed containing 1.0 unit ofPlatinum Taq DNA polymerase (Invit-rogen); 5 mM each of the 4 deoxyribo-nucleotide triphosphates (Invitro-gen); 0.1 µM of each primer; 1.5 mMMgCl2; and 2 µL of DNA. A no-template negative control was used foreach reaction. The following primerswere used: H influenzae (forward)5"-GGAGTGGGTTGTACCAGAAG-TAGAT-3" [124–base pair [bp] ampli-con] and S pneumoniae (forward)5 " -AGTCGGTGAGGTAACCG-TAAG-3" [105-bp amplicon], both witha universal reverse 5"-AGGAGGT-GATCCAACCGCA-3" primer; and Mcatarrhalis (forward) 5"-TTGGCTTGT-GCTAAAATATC-3" [140-bp ampli-con] with an M catarrhalis (reverse)5"-GTCATCGCTATCATTCACCT-3"primer. The specificity of these prim-ers has been previously established.11
Thirty-six–cycle amplificationswere performed using a GeneAmpPCR System 2400 thermal cycler (Ap-plied Biosystems, Foster City, Calif )with 30 seconds of denaturation at95°C, 30 seconds of annealing at55°C, and 30 seconds of elongation at72°C. PCR products were restrictiondigested, electrophoretically sepa-
CHRONIC OTITIS MEDIA AS A BIOFILM DISEASE
©2006 American Medical Association. All rights reserved. (Reprinted) JAMA, July 12, 2006—Vol 296, No. 2 203

rated, and visualized using GelStarNucleic Acid Stain with a Kodakimage analysis system (EastmanKodak, Rochester, NY).
Microscopic ExaminationConfocal laser scanning microscopic(CLSM) imaging was performed usinga Leica DM RXE microscope attachedto a TCS SP2 AOBS confocal system us-ing high-resolution objectives (LeicaMicrosystems, Exton, Pa).
Evaluation of MEM SpecimensWith Pathogen-Specific Probes
Immunostaining. Specimens were in-cubated with 40 to 50 µg/mL of rabbitanti-S pneumoniae antibody (Biode-sign, Saco, Me) specific for S pneumo-niae serotypes 3, 4, 6, 7, 9, 14, 18, 19,and 23, washed to remove excess an-tibody, blocked with 10% fetal bovineserum (Hyclone, Logan, Utah) in HBSS,and incubated with 150 µg/mL of Af-f iniPure F(ab)2 fragment TexasRed!conjugated donkey antirabbit IgG(H#L chain) antibody (Jackson Immu-noResearch, West Grove, Pa). Speci-mens were rinsed with 10% fetal bo-vine serum/HBSS and evaluated usingthe CLSM transmission mode to de-fine the mucosal epithelium substra-tum and the fluorescent mode to de-tect the Texas Red–conjugated antibody.In vitro specificity studies demon-strated that this antibody reacted withall of the pneumococcal strains tested,and neither primary nor secondary an-tibodies cross-reacted with any of 31clinical isolates of H influenzae, M ca-tarrhalis, Pseudomonas aeruginosa, Sta-phylococcus aureus, or Klebsiella pneu-moniae (data not shown).
16S rRNA FISH. Middle-ear mu-cosa specimens were fixed with fresh4% paraformaldehyde in phosphate-buffered saline (PBS) followed bywashes with PBS and PBS-ethanol (1:1), with subsequent 3-minute incuba-tions in 80% and 100% ethanol. ForFISH, specimens were incubated with10 mg/mL of lysozyme (Sigma-Aldrich, St Louis, Mo) in 0.1-M Tris(hydroxymethyl) aminomethane hy-drochloride and 0.05-M Na2 EDTA at
37°C and washed with ultrapure wa-ter. The lysozyme step was omitted forsome specimens to optimize condi-tions for gram-negative bacteria.
To obtain bacterial species–specificinformation for the specimens fromchildren with recurrent OM, whichlacked effusions for PCR analyses, FISHprotocols were developed using 16SrRNA probes for H influenzae, S pneu-moniae, and M catarrhalis, as well as auniversal eubacterial 16S rRNA probe.These assays were also applied to OMEspecimens. A maximum of 3 FISHprobes could be performed on anysingle specimen due to limitations of thefluorescent dyes. Therefore, FISH pro-vides evidence that a specific patho-gen is present or absent when a spe-cific probe is used.
Fluorescence in situ hybridizationwas performed as previously de-scribed12-14 using the following 16S ri-bosomal probe sequences: EUB338, 5"-GCTGCCTCCCGTAGGAGT-3" (16S[338-355]) Domain Bacteria12; Spn 5"-GTGATGCAAGTGCACCTT-3" (16S[195-212]) S pneumoniae13; Hinf 5"-CCGCACTTTCATCTCCG-3" (16S[185-202]) H influenzae14; and Mcat 5"-CCGCCACUAAGUAUCAGA-3" (16S[88-105]) M catarrhalis. Conditions forFISH were developed and rigorouslytested in vitro to ensure specificity foreach species probe, and the genericcharacter of the eubacterial probe (posi-tive and negative controls12,15) wastested using panels of bacterial strains.Probes were labeled with Cy3, Cy5, or6-FAM (Integrated DNA TechnologiesInc, Coralville, Iowa). Hybridizedsamples were evaluated using CLSM.
Specificity of 16S rRNA Probes.Clinical isolates of S pneumoniae, H in-fluenzae, M catarrhalis, P aeruginosa, Saureus, and K pneumoniae were ob-tained, cultured, and serotyped as de-scribed16,17 from the Children’s Hospi-tal of Pittsburgh and the MedicalCollege of Wisconsin for testing ofthe 16S probes. All H influenzae iso-lates hybridized with the H influenzaeprobe; no H influenzae isolates hybrid-ized with any probe for the other tar-get species. Streptococcus pneumoniae
and M catarrhalis probes were simi-larly specific (data not shown). Theeubacterial probe hybridized with allbacterial isolates, whereas a nonsense-sequence probe15 gave negative resultsfor all bacteria tested. Mixed pneumo-coccal/nontypeable H influenzae cul-tures examined with the S pneumo-niae, H influenzae, and eubacterial 16Sprobes demonstrated appropriate spe-cies-specific as well as eubacterial probehybridization (data not shown).
Image Analysis and InterpretationThe H influenzae6 and S pneumoniae(data not shown) chinchilla OM bio-film models were used as guides forassessing pediatric MEM specimens.Specimens were evaluated by 2 inde-pendent observers (L.H.-S., L.N.) (3observers for specimens evaluatedwith FISH [L.H.-S., L.N., P.S.]) forbacterial clusters showing morphol-ogy consistent with S pneumoniae andH influenzae based on in vivo andin vitro biofilms6,18; no instances ofdisagreement were recorded. Imagessuggestive of biofilm ultrastructurewere further evaluated using theCLSM electronic high-resolutionzoom function, and specimens werescored biofilm-positive when high-resolution images demonstrated bac-terial morphology. In specimens fromthe first 16 children in the studygroup (children 5-20), biofilms wereidentified solely by morphology usingstandard visual clues including size(approximately 1-2 µm), shape (coccior coccobacilli), and biofilm ultra-structure. When species-specificprobes (FISH and PnAb) were used,the same criteria were used in addi-tion to fluorescence with the appro-priate signal. The epithelial surface ofthe specimen was evident by stainingwith nonspecific dyes or by transmis-sion imaging. Control specimens wereexhaustively evaluated by 2 indepen-dent observers (L.H.-S., L.N.) for evi-dence of bacteria and biofilms usingidentical protocols and a comprehen-sive x-y raster scanning approach toensure that no minimal pockets ofbiofilm were missed.
CHRONIC OTITIS MEDIA AS A BIOFILM DISEASE
204 JAMA, July 12, 2006—Vol 296, No. 2 (Reprinted) ©2006 American Medical Association. All rights reserved.

Table 1. Results for Pediatric Middle-Ear Mucosa Biopsy Specimens Assayed With Multiple Molecular Methods for Otitis MediaPathogens—Study Group (Children Undergoing Tympanostomy Tube Placement)*
ChildNo.
Sex(Age, y) Ear Diagnosis Culture
PCR FISH 16S RNA Probe†BacLight
Probe PnAb BiofilmHI SP MC HI SP MC EUB5 F (13.8) L ROM NA NA NA NA # NA #
R OME NA ! # ! # NA #6 F (1.3) L ROM NA NA NA NA NA NA NA
R ROM NA NA NA NA # NA #7 F (4.5) L OME ! # ! ! NA NA NA
R ROM NA NA NA NA # NA !8 M (1.8) L OME ! # ! # NA #
R ROM NA NA NA NA # NA #9 F (0.8) L OME NA # ! ! # NA #
R ROM NA NA NA NA # NA #10 M (0.8) L OME #HI # ! ! # NA #
R OME ! # ! ! # NA #11 M (0.8) L OME NA NA NA NA # NA #
R ROM NA NA NA NA # NA #12 F (0.9) L ROM NA NA NA NA # NA #
R ROM NA NA NA NA # NA #13 M (2.0) L ROM NA NA NA NA # NA !
R OME ! # ! ! # NA #14 F (0.8) L OME #MC # ! ! # NA #
R OME ! # ! ! # NA #15 F (1.3) L ROM NA NA NA NA # NA #
R ROM NA NA NA NA # NA #16 M (0.8) L OME ! # ! ! # NA #
R ROM NA NA NA NA # NA #17 M (1.1) L ROM NA NA NA NA # NA #
R ROM NA NA NA NA # NA #18 M (2.8) L ROM NA NA NA NA # NA #
R OME NA # # # # NA #19 M (0.9) L OME NA ! # ! # NA #
R ROM NA NA NA NA # NA #20 F (4.5) L ROM NA NA NA NA # NA #
R ROM NA NA NA NA # NA #21 M (0.9) L OME ! # # ! NA # #
R OME ! # # ! NA # #22 F (2.5) L ROM NA NA NA NA NA # NA # NA # #
R ROM NA NA NA NA NA # NA # NA # #23 M (0.5) L OME #SP NA NA NA NA NA NA NA NA # #
R OME #SP NA NA NA NA NA NA NA NA # #24 F (0.8) L OME ! ! # ! NA # NA # NA # #
R OME #KP # # # # NA NA # NA # #25 M (1.2) L OME ! ! # ! NA NA NA NA NA # #
R OME ! # # # NA # NA # NA # #26 F (1.0) L ROM NA NA NA NA NA # NA # NA # #
R OME ! ! # ! NA # NA # NA # #27 F (7.8) L OME ! ! ! # NA NA # # NAD NA #
R OME ! ! ! # NA NA # # NA NA !‡28 M (7.8) L ROM NA NA NA NA # NA NA # NA ! !‡
R OME ! # ! ! # NA NA # NA NA #29 M (2.5) L OME ! # ! ! # # NA NA NA # #
R OME #HI # ! ! # # NA NA NA # #30 F (1.8) L ROM NA NA NA NA # # NA NA NA # #
R ROM NA NA NA NA # # NA NA NA # #
Abbreviations: EUB, eubacterial probe; FISH, fluorescence in situ hybridization; HI, Haemophilus influenzae (organism and probe); KP, Klebsiella pneumoniae; MC, Moraxella ca-tarrhalis (organism and probe); NA, not available (see below); OME, otitis media with effusion; PCR, polymerase chain reaction; PnAb, antipneumococcal antibody; ROM, recur-rent otitis media; SP, Streptococcus pneumoniae (organism and probe).
*Cells marked NA indicate that assay was not performed due to sample limitations. PCR and culture were only possible if an effusion was present and therefore were never per-formed on ROM samples. For microscopic examination, the small size of the sample (!1 mm) did not allow subsectioning and, therefore, limited the examination to performanceof a subset of visualization techniques for any given sample.
†FISH assays began with patient 22.‡Denotes 16S signal in the absence of conclusive biofilm morphology.
CHRONIC OTITIS MEDIA AS A BIOFILM DISEASE
©2006 American Medical Association. All rights reserved. (Reprinted) JAMA, July 12, 2006—Vol 296, No. 2 205

RESULTSPatient CharacteristicsOf 52 MEM specimens obtained from26 children undergoing TT placement,50 were evaluated by CLSM for evi-dence of bacterial biofilms. Of these26 children, 13 (50%) had a diagnosisof OME, 20 (77%) had a diagnosis ofrecurrent OM, and 7 (27%) had bothdiagnoses. Of the 26 children withOM, 13 (50%) were girls, and themean age was 2.5 (range, 0.5-14)years. Uninfected control specimenswere obtained from 3 pediatricpatients (mean age, 5.8 [range, 0.9-14.8] years). All 3 pediatric controlpatients were boys. In addition, MEMspecimens from 5 adult patientsreceiving cochlear implantation (4women) were evaluated (mean age,49.9 [range, 22.9-69.9] years).
Among the 26 children undergoingTT placement, 27 (52%) of their 52 earshad effusions, and 24 of these 27 effu-sions were assayed by PCR for H influ-enzae, S pneumoniae, and M catarrha-lis; the 3 remaining effusions yieldedinsufficient effusion for both cultureand PCR or produced no testable DNA.Only 5 (19%) of the 27 effusions wereculture-positive for any of the 3 majorOM pathogens (H influenzae [2], Spneumoniae [2], M catarrhalis [1]), with1 additional effusion testing positive forKlebsiella species. However, all 24 ef-fusions assessed by PCR were positivefor at least 1 OM pathogen (H influen-zae [17], S pneumoniae [12], M ca-tarrhalis [6]). Of the 24 effusions, 4(17%) were PCR-positive for all 3 bac-teria, and 3 (13%) were PCR-positivefor both H influenzae and S pneumo-niae (TABLE 1).
Evidence of BiofilmsMiddle-ear mucosa specimens from allpatients were examined by CLSM forevidence of bacterial biofilms usingtechniques that included genericnucleic acid labeling of cells with theBacLight kit, FISH, and pneumococ-cal immunostaining. Because of thesmall specimen size (!1 mm2), only asubset of these analyses could be per-formed on each specimen. Of 30 OM
Figure 1. CLSM Imaging of MEM Biopsy Specimens From Children With Chronic OtitisMedia Stained With BacLight LIVE/DEAD Nucleic Acid Probes
Child 7, Right Ear, ROM; Culture NA, PCR NAA
Child 5, Right Ear, OME; Culture NA, PCR + (Streptococcus pneumoniae)B
10 µm
Child 13, Right Ear, OME; Culture !, PCR + (Haemophilus influenzae)C
10 µm
Biofilms (arrowheads) on an MEM specimen from an ear with an effusion that was PCR-positive for H influenzae.
Abbreviations: CLSM, confocal laser scanning microscopy; NA, not available (see Table 1 footnote); OME, otitis media with effusion; PCR, polymerase chain reaction; ROM, recurrent otitis media.
Above, illustration showing the location of the cochlear promontory in the middle ear where middle-ear mucosa (MEM) biopsy specimens where obtained. Left, MEM specimen showing only host-cell nuclei and no evidence of adherent bacterial clusters. Green fluorescence indicates live, healthy cells; red, dead cells; yellow and orange, cells with membrane damage.
Left, MEM specimen with matrix-encased bacterial clusters (biofilms; arrowheads) adherent to damaged MEM epithelial cells, which are readily distinguished from bacterial cells by morphology and larger size. The square panel is an x-y plan view showing matrix-encased bacterial clusters and cocci (green) localized on epithelial cells (nuclei stained red). Z-axes sections (below and right of plan view) demonstrate that the bacterial cell clusters are approximately 10-12 µm thick. Right, diagrams of how the rectangular (z-axes) sections are constructed (dotted lines in the confocal stack indicate plane of sections).
10 µm
B1
B2
Z-Y SectionB1
Z-X Section
Y Z
XB2
ReconstructedConfocal Stack
X-Y Plan Image(Merged X-Y
Sections)
ReconstructedConfocal Stack
Anatomy of Middle Ear (Lateral View,Tympanic Membrane Removed)
CochlearPromontory
Malleus
Incus
Stapes
RoundWindow
CHRONIC OTITIS MEDIA AS A BIOFILM DISEASE
206 JAMA, July 12, 2006—Vol 296, No. 2 (Reprinted) ©2006 American Medical Association. All rights reserved.

specimens examined using the BacLightkit, 28 were positive for bacterial bio-films based on morphological criteria.In these images, green fluorescence in-dicates live bacteria and healthy hostcells, and red stains the nuclei of deadcells (FIGURE 1). Yellow and orangefluorescence indicates the presence ofboth stains within a particular host cell,suggesting cell membrane damage. Aspecimen from a patient with an effu-sion that was PCR-positive for S pneu-moniae shows clusters of cocci that ap-pear to be adherent to the MEM (seez-axes images) that are surrounded by
an amorphous matrix that stains lightlywith the Syto 9 (green) nucleic acid–binding dye (Figure 1B). Similarly, aspecimen with an effusion that wasPCR-positive for H influenzae showsbacteria in matrix-enclosed bacterialclusters (Figure 1C). Overall, biofilmswere present on 46 (92%) of 50 OMspecimens and were not limited to thosecases in which an effusion was presentbut were also present on specimens ofchildren with recurrent OM (Table 1).
To obtain bacterial species!specificinformation for the specimens fromchildren with recurrent OM, which
lacked effusions, 16S RNA FISH was de-veloped for the major OM pathogens(FIGURE 2). Fluorescence in situ hy-bridization for H influenzae was posi-tive for 6 of 7 MEM specimens (86%),including 2 of 3 recurrent OM speci-mens. These specimens showed a rangeof biofilm morphologies, from micro-colonies to large clusters of bacteria. Of4 specimens from OME cases that wereFISH-positive for H influenzae, all 4 alsohad effusions that were PCR-positive forH influenzae.
Streptococcus pneumoniae–specificFISH demonstrated bacterial morphol-
Figure 2. FISH of Bacterial Biofilms on MEM Biopsy Specimens From Children With Chronic Otitis Media
16S rRNA H influenzae Probe
Child 30, Right Ear, ROM; Culture NA, PCR NA, FISH + (Haemophilus influenzae, Streptococcus pneumoniae)A
Child 27, Left Ear, OME; Culture !, PCR + (Moraxella catarrhalis), FISH + (M catarrhalis, Eubacteria)B
16S rRNA S pneumoniae Probe Overlay
10 µm 10 µm10 µm
16S rRNA M catarrhalis Probe 16S rRNA Eubacterial Probe Overlay
CLSM images showing bacterial morphology in cell clusters of an MEM specimen visualized by FISH with, left, FAM-labeled M catarrhalis 16S rRNA probe (green); middle, Cy5-labeled eubacterial 16S probe (red); and right, overlay of both (yellow). This specimen was also PCR-positive for M catarrhalis.
Abbreviations: See Figure 1.
CLSM images showing coinfection by H influenzae and S pneumoniae on a middle-ear mucosa (MEM) biopsy specimen visualized by fluorescence in situ hybridization (FISH) with 16S rRNA probes specific for H influenzae (left) labeled with Cy5 (red), for S pneumoniae (middle) labeled with Cy3 (green), and overlay of both (right). Each species colonizes discrete regions not inhabited by the other.
10 µm 10 µm 10 µm
CHRONIC OTITIS MEDIA AS A BIOFILM DISEASE
©2006 American Medical Association. All rights reserved. (Reprinted) JAMA, July 12, 2006—Vol 296, No. 2 207

ogy in clusters from 10 of 10 speci-mens examined. Six of these 10 werealso hybridized with the eubacterialprobe, which colocalized with theS pneumoniae 16S in all cases. The4 remaining FISH-positive pneumo-coccal specimens were hybridizedwith the H influenzae 16S probe;al l demonstrated hybridization(Figure 2A). Of 5 children with MEMspecimens that were FISH-positive forS pneumoniae, 3 also had MEEs thatwere PCR-positive for S pneumoniae.Of 2 specimens examined using FISHfor M catarrhalis, 1 was positive.Overall, FISH and PCR gave compa-rable percentages of positive resultsfor H influenzae, S pneumoniae, andM catarrhalis.
Pneumococcal-specific immun-ostaining with PnAb was developed asa confirmatory assay for children withrecurrent OM and FISH-positive MEMspecimens that lacked a cognate effu-sion (ie, an effusion from the samechild, same ear). When the 2 pneumo-coccal-specific in situ visualizationmethods were used sequentially, 5 of5 specimens demonstrated S pneumo-niae by both methods (Table 1). A re-current OM specimen that lacked a cog-nate effusion was PnAb-positive andalso FISH-positive using pneumococcal-specific and eubacterial 16S probes(FIGURE 3B). Immunostaining alsoprovided confirmation of S pneumo-niae biofilms in patients with pneumo-coccal-specific PCR-positive effusions(Figure 3C).
Overall, biofilm structures wereidentified by at least 2 methods in 18(90%) of 20 specimens assayed usingin situ pathogen-specific probes. Thiscompares with 28 of 30 specimens(93%) that were biofilm-positive usingnonspecific probes. Of ears assayedwith 2 or more specific modalities, 12of 12 were PCR effusion–positive, 14of 15 (93%) were FISH-positive, and16 of 17 (94%) were PnAb-positive.Five of 6 (83%) of recurrent OMspecimens lacking effusions were posi-tive for OM pathogens using 1 ormore specific in situ methods (FISH orimmunostaining).
Figure 3. Biofilms on MEM Biopsy Specimens Visualized by FISH and Immunostaining With PnAb
10 µm 10 µm
Patient 4 (Control) Patient 4 (Control) Patient 4 (Control) A
Child 26, Right Ear, OME; Culture !, PCR + (S pneumoniae), FISH + (S pneumoniae, Eubacteria), PnAb +C
10 µm
10 µm
10 µm
10 µm
Overlay of 3 CLSM fluorescence in situ hybridization (FISH) images using Haemophilus influenzae, Streptococcus pneumoniae, and eubacterial 16S rRNA probes, and a transmission channel image (gray) of an uninfected middle-ear mucosa (MEM) specimen from a control patient undergoing cochlear implantation. Bacterial signals are completely absent.
Overlay of 2 CLSM FISH images of an MEM specimen from a child with recurrent OM using Cy3-labeled (green) S pneumoniae–specific and Cy5-labeled (red) eubacterial-specific 16S rRNA probes shows hybridization with bacteria on the MEM surface (transmission channel, gray). Yellow indicates hybridization with both the S pneumoniae and the conserved eubacterial 16S rRNA probes. Higher-magnification CLSM images (right, top) show pneumococcal morphology (arrowheads indicate diplococci) in cell clusters hybridizing with both the Cy3-labeled S pneumoniae 16S probe (green) and the Cy5-labeled eubacterial 16S probe (red). This specimen was also positive for pneumococcus by immunostaining with PnAb (right, bottom).
Left, Low-magnification CLSM image in fluorescent and transmission mode of a PnAb-positive MEM specimen. The pneumococci stain red (Texas Red–conjugated antibody, fluorescent channel) and the MEM surface appears gray (transmission channel). White box indicates the area of the specimen detail (right). Right, Detail of cell clusters with bacterial coccal morphology that stain with PnAb.
Child 22, Left Ear, ROM; Culture NA, PCR NA, FISH + (S pneumoniae, Eubacteria)B
16S rRNA EubacterialProbe
16S rRNA S pneumoniaeProbe
Overlay
PnAb Immunostain
Abbreviations: PnAb, antipneumococcal antibody. See Figure 1 for expansions of other terms.
CHRONIC OTITIS MEDIA AS A BIOFILM DISEASE
208 JAMA, July 12, 2006—Vol 296, No. 2 (Reprinted) ©2006 American Medical Association. All rights reserved.
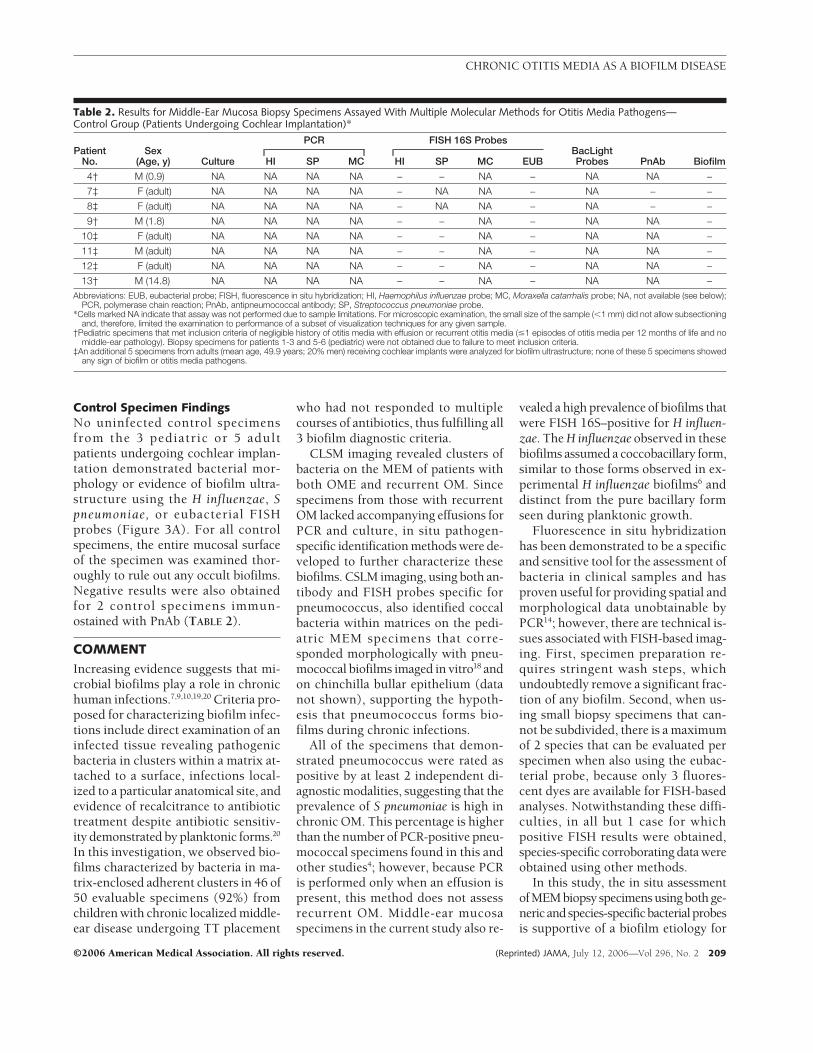
Control Specimen FindingsNo uninfected control specimensfrom the 3 pediatric or 5 adultpatients undergoing cochlear implan-tation demonstrated bacterial mor-phology or evidence of biofilm ultra-structure using the H influenzae, Spneumoniae, or eubacterial FISHprobes (Figure 3A). For all controlspecimens, the entire mucosal surfaceof the specimen was examined thor-oughly to rule out any occult biofilms.Negative results were also obtainedfor 2 control specimens immun-ostained with PnAb (TABLE 2).
COMMENTIncreasing evidence suggests that mi-crobial biofilms play a role in chronichuman infections.7,9,10,19,20 Criteria pro-posed for characterizing biofilm infec-tions include direct examination of aninfected tissue revealing pathogenicbacteria in clusters within a matrix at-tached to a surface, infections local-ized to a particular anatomical site, andevidence of recalcitrance to antibiotictreatment despite antibiotic sensitiv-ity demonstrated by planktonic forms.20
In this investigation, we observed bio-films characterized by bacteria in ma-trix-enclosed adherent clusters in 46 of50 evaluable specimens (92%) fromchildren with chronic localized middle-ear disease undergoing TT placement
who had not responded to multiplecourses of antibiotics, thus fulfilling all3 biofilm diagnostic criteria.
CLSM imaging revealed clusters ofbacteria on the MEM of patients withboth OME and recurrent OM. Sincespecimens from those with recurrentOM lacked accompanying effusions forPCR and culture, in situ pathogen-specific identification methods were de-veloped to further characterize thesebiofilms. CSLM imaging, using both an-tibody and FISH probes specific forpneumococcus, also identified coccalbacteria within matrices on the pedi-atric MEM specimens that corre-sponded morphologically with pneu-mococcal biofilms imaged in vitro18 andon chinchilla bullar epithelium (datanot shown), supporting the hypoth-esis that pneumococcus forms bio-films during chronic infections.
All of the specimens that demon-strated pneumococcus were rated aspositive by at least 2 independent di-agnostic modalities, suggesting that theprevalence of S pneumoniae is high inchronic OM. This percentage is higherthan the number of PCR-positive pneu-mococcal specimens found in this andother studies4; however, because PCRis performed only when an effusion ispresent, this method does not assessrecurrent OM. Middle-ear mucosaspecimens in the current study also re-
vealed a high prevalence of biofilms thatwere FISH 16S–positive for H influen-zae. The H influenzae observed in thesebiofilms assumed a coccobacillary form,similar to those forms observed in ex-perimental H influenzae biofilms6 anddistinct from the pure bacillary formseen during planktonic growth.
Fluorescence in situ hybridizationhas been demonstrated to be a specificand sensitive tool for the assessment ofbacteria in clinical samples and hasproven useful for providing spatial andmorphological data unobtainable byPCR14; however, there are technical is-sues associated with FISH-based imag-ing. First, specimen preparation re-quires stringent wash steps, whichundoubtedly remove a significant frac-tion of any biofilm. Second, when us-ing small biopsy specimens that can-not be subdivided, there is a maximumof 2 species that can be evaluated perspecimen when also using the eubac-terial probe, because only 3 fluores-cent dyes are available for FISH-basedanalyses. Notwithstanding these diffi-culties, in all but 1 case for whichpositive FISH results were obtained,species-specific corroborating data wereobtained using other methods.
In this study, the in situ assessmentof MEM biopsy specimens using both ge-neric andspecies-specificbacterialprobesis supportive of a biofilm etiology for
Table 2. Results for Middle-Ear Mucosa Biopsy Specimens Assayed With Multiple Molecular Methods for Otitis Media Pathogens—Control Group (Patients Undergoing Cochlear Implantation)*
PatientNo.
Sex(Age, y) Culture
PCR FISH 16S ProbesBacLightProbes PnAb BiofilmHI SP MC HI SP MC EUB
4† M (0.9) NA NA NA NA ! ! NA ! NA NA !7‡ F (adult) NA NA NA NA ! NA NA ! NA ! !8‡ F (adult) NA NA NA NA ! NA NA ! NA ! !9† M (1.8) NA NA NA NA ! ! NA ! NA NA !
10‡ F (adult) NA NA NA NA ! ! NA ! NA NA !11‡ M (adult) NA NA NA NA ! ! NA ! NA NA !12‡ F (adult) NA NA NA NA ! ! NA ! NA NA !13† M (14.8) NA NA NA NA ! ! NA ! NA NA !
Abbreviations: EUB, eubacterial probe; FISH, fluorescence in situ hybridization; HI, Haemophilus influenzae probe; MC, Moraxella catarrhalis probe; NA, not available (see below);PCR, polymerase chain reaction; PnAb, antipneumococcal antibody; SP, Streptococcus pneumoniae probe.
*Cells marked NA indicate that assay was not performed due to sample limitations. For microscopic examination, the small size of the sample (!1 mm) did not allow subsectioningand, therefore, limited the examination to performance of a subset of visualization techniques for any given sample.
†Pediatric specimens that met inclusion criteria of negligible history of otitis media with effusion or recurrent otitis media ($1 episodes of otitis media per 12 months of life and nomiddle-ear pathology). Biopsy specimens for patients 1-3 and 5-6 (pediatric) were not obtained due to failure to meet inclusion criteria.
‡An additional 5 specimens from adults (mean age, 49.9 years; 20% men) receiving cochlear implants were analyzed for biofilm ultrastructure; none of these 5 specimens showedany sign of biofilm or otitis media pathogens.
CHRONIC OTITIS MEDIA AS A BIOFILM DISEASE
©2006 American Medical Association. All rights reserved. (Reprinted) JAMA, July 12, 2006—Vol 296, No. 2 209

chronic OM. The vast majority of MEMspecimens obtained from children un-dergoing TT placement evidenced ma-trix-enclosed adherent bacteria, whereascontrol specimens from patients under-going cochlear implantation had no evi-dence of bacteria. Moreover, these datasuggest that the bacterial species in-volved in these mucosal biofilms are thesame pathogens commonly associatedwith OM. However, because of the smallamount of tissue and the inability to si-multaneously perform positive and nega-tive 16S controls on each specimen, wecannot entirely exclude the possibility ofnonspecific interactions with the probesused in these analyses. We attempted toaddress this limitation by using a largernumber of tests in the aggregate thancould be performed on each specimen.Moreover, in vitro evaluations of allof the 16S and antibody probes used inthis investigation identified no cross-reactivity when tested against a batteryof clinical strains representing the com-mon human mucosal pathogens. A sec-ond limitation of this investigation wasthe small number of age-matched con-trols who were available for participa-tion in the study; to partially compen-sate for this difficulty, we expandedthe age range for obtaining control speci-mens.
Collectively, the data presented in thisstudy support the hypothesis that bio-films may play a role in the pathogen-esis and chronicity of OME and also pro-vide evidence that at least some mucosalspecimens from patients with recur-rent OM harbor bacterial biofilms. Thisfinding is surprising in light of the bodyof literature that suggests that consecu-tive episodes of acute OM are associ-ated with unique bacterial strains.21 Ourfindings are more consistent with re-current OM as a chronic disease withepisodic acute exacerbations. Leibo-vitz et al22 have demonstrated that ap-proximately 30% of cases of recurrentOM result from relapses attributable tothe original organism. The true relation-ship between bacterial persistence dem-onstrated on biopsy and the clinical ob-servation of a disease-free period clearlyrequires further investigation.
Importantly, the findings from ourstudy do not exclude other potentialpathogenic factors associated with OME,such as an antecedent viral upper respi-ratory infection, eustachian tube dys-function with impaired gas exchange, agenetically predisposed host, persistentinflammatory mediators, or exacerba-tion by gastroesophageal reflux. How-ever, these findings do argue against thenotion that OME is the result of a non-bacterial inflammatory process and alsoindicate that equating culture negativ-ity and absence of bacteria is incorrect.
The finding that biofilms are presentin almost all cases of OME in this studymay help to explain the lack of antibi-otic efficacy for this disorder, given thatbiofilm bacteria are more antibiotic re-sistant than single cells in suspen-sion.23-28 This resistance may stem fromthe fact that oxygen and nutrient limi-tation within biofilms induces meta-bolic quiescence, which in turn re-duces antibiotic effectiveness.2,23 Otherevidence suggests that biofilm bacte-ria may have genetic mechanisms, se-lected for in the biofilm, that provideantimicrobial protection.29-31 In addi-tion, the biofilm provides a physicalbarrier that enhances pathogen resis-tance to host defenses such as opsoniza-tion, lysis by complement, and phago-cytosis.7
CONCLUSIONSDirect detection of biofilms on MEM bi-opsy specimens from children withOME and recurrent OM supports thehypothesis that these chronic middle-ear disorders may be biofilm-related andmay help to explain multiple patho-physiological aspects of chronic OM.Much remains to be learned about themechanisms by which bacteria in thesebiofilms persist and resist both the hostimmune response and antibiotic treat-ment.
Author Contributions: Dr Ehrlich had full access to allof the data in the study and takes responsibility forthe integrity of the data and the accuracy of the dataanalysis.Study concept and design: Hall-Stoodley, Hu, Forbes,Burrows, Stoodley, Post, Ehrlich, Kerschner.Acquisition of data: Hall-Stoodley, Hu, Gieseke, Nistico,Nguyen, Hayes, Forbes, Greenberg, Dice, Burrows,Wackym, Stoodley, Ehrlich, Kerschner.
Analysis and interpretation of data: Hall-Stoodley, Hu,Gieseke, Nguyen, Hayes, Stoodley, Ehrlich, Kerschner.Drafting of the manuscript: Hall-Stoodley, Hu, Gieseke,Nistico, Nguyen, Hayes, Forbes, Dice, Burrows,Stoodley, Ehrlich, Kerschner.Critical revision of the manuscript for important in-tellectual content: Hall-Stoodley, Hu, Nguyen,Greenberg, Burrows, Wackym, Stoodley, Post, Ehrlich,Kerschner.Statistical analysis: Hall-Stoodley, Hu, Nistico, Nguyen,Hayes, Forbes, Stoodley, Ehrlich, Kerschner.Obtained funding: Post, Ehrlich, Kerschner.Administrative, technical, or material support: Hall-Stoodley, Hu, Gieseke, Nistico, Nguyen, Hayes, Forbes,Greenberg, Dice, Burrows, Stoodley, Ehrlich, Kerschner.Study supervision: Hu, Ehrlich, Kerschner.Financial Disclosures: Dr Post reports having servedas a speaker for Pfizer and Alcon and as scientific ad-visor to Medtronic/Xomed. Dr Ehrlich reports havingreceived a research grant from Merck to study the ef-ficacy of using montelukast as a prophylactic agentfor OM in an animal model. Dr Kerschner reports hav-ing served as a member of the speakers’ bureaus forDaiichi and Alcon. No other authors reported finan-cial disclosures.Funding/Support: This work was supported by Al-legheny General Hospital, the Allegheny-Singer Re-search Institute, the Medical College of Wisconsin, Na-tional Institute on Deafness and Other CommunicationDisorders grants DC 05659 ( J.C.P.), DC 02148(G.D.E.), DC 04173 (G.D.E.), and DC 00192 and DC007903 ( J.E.K.), and the Health Resources and Ser-vices Administration of the Department of Health andHuman Services.Role of the Sponsors: None of the funding organiza-tions or institutional sponsors had any role in the de-sign and conduct of the study; the collection, analy-sis, and interpretation of the data; or the preparation,review, or approval of the manuscript.Acknowledgment: We thank Mary O’Toole, Centerfor Genomic Sciences, Allegheny-Singer Research In-stitute, for help in the preparation of the manuscriptand R. M. Wadowsky, ScD, University of PittsburghMedical Center Graduate School of Public Health,for bacterial clinical isolates. Ms O’Toole and DrWadowsky received no compensation for their assis-tance.
REFERENCES
1. Bennett KE, Haggard MP, Silva PA, Stewart IA. Be-haviour and developmental effects of otitis media witheffusion into the teens. Arch Dis Child. 2001;85:91-95.2. Post JC, Preston RA, Aul JJ, et al. Molecular analy-sis of bacterial pathogens in otitis media with effusion.JAMA. 1995;273:1598-1604.3. Aul JJ, Anderson KW, Wadowsky RM, et al. Acomparative evaluation of culture and PCR for the de-tection and determination of persistence of bacterialstrains and DNAs in the Chinchilla laniger model ofotitis media. Ann Otol Rhinol Laryngol. 1998;107:508-513.4. Rayner MG, Zhang Y, Gorry MC, Chen Y, Post JC,Ehrlich GD. Evidence of bacterial metabolic activity inculture-negative otitis media with effusion. JAMA.1998;279:296-299.5. Dingman JR, Rayner MG, Mishra S, et al. Corre-lation between presence of viable bacteria and pres-ence of endotoxin in middle-ear effusions. J ClinMicrobiol. 1998;36:3417-3419.6. Ehrlich GD, Veeh R, Wang X, et al. Mucosalbiofilm formation in middle-ear mucosa in the chin-chilla model of otitis media. JAMA. 2002;287:1710-1715.7. Costerton JW, Stewart PS, Greenberg EP. Bacte-rial biofilms: a common cause of persistent infections.Science. 1999;284:1318-1322.8. Stoodley P, Sauer K, Davies DG, Costerton JW. Bio-
CHRONIC OTITIS MEDIA AS A BIOFILM DISEASE
210 JAMA, July 12, 2006—Vol 296, No. 2 (Reprinted) ©2006 American Medical Association. All rights reserved.

films as complex differentiated communities. Annu RevMicrobiol. 2002;56:187-209.9. Costerton W, Veeh R, Shirtliff M, Pasmore M, PostC, Ehrlich G. The application of biofilm science to thestudy and control of chronic bacterial infections. J ClinInvest. 2003;112:1466-1477.10. Hall-Stoodley L, Costerton JW, Stoodley P. Bac-terial biofilms: from the natural environmentto infectious diseases. Nat Rev Microbiol. 2004;2:95-108.11. Gok U, Bulut Y, Keles E, Yalcin S, Doymaz MZ.Bacteriological and PCR analysis of clinical material as-pirated from otitis media with effusions. Int J PediatrOtorhinolaryngol. 2001;60:49-54.12. Amann RI, Binder BJ, Olson RJ, Chisholm SW, De-vereux R, Stahl DA. Combination of 16S rRNA-targeted oligonucleotide probes with flow cytometryfor analyzing mixed microbial populations. Appl En-viron Microbiol. 1990;56:1919-1925.13. Kempf VA, Trebesius K, Autenrieth IB. Fluores-cent in situ hybridization allows rapid identification ofmicroorganisms in blood cultures. J Clin Microbiol.2000;38:830-838.14. Hogardt M, Trebesius K, Geiger AM, Hornef M,Rosenecker J, Heesemann J. Specific and rapid detec-tion by fluorescent in situ hybridization of bacteria inclinical samples obtained from cystic fibrosis patients.J Clin Microbiol. 2000;38:818-825.15. Manz W, Amann R, Ludwig W, Wagner M, Schlei-fer K-H. Phylogenetic oligodeoxynucleotide probesfor the major subclasses of proteobacteria: problems
and solutions. Syst Appl Microbiol. 1992;15:593-600.16. Shen K, Antalis P, Gladitz J, et al. Identification,distribution, and expression of novel genes in 10 clini-cal isolates of nontypeable Haemophilus influenzae.Infect Immun. 2005;73:3479-3491.17. Shen K, Gladitz J, Antalis P, et al. Characteriza-tion, distribution and expression of novel genes amongeight clinical isolates of Streptococcus pneumoniae.Infect Immun. 2006;74:321-330.18. Allegrucci M, Hu FZ, Shen K, et al. Phenotypic char-acterization of Streptococcus pneumoniae biofilmdevelopment. J Bacteriol. 2006;188:2325-2335.19. Donlan RM, Costerton JW. Biofilms: survivalmechanisms of clinically relevant microorganisms. ClinMicrobiol Rev. 2002;15:167-193.20. Parsek MR, Singh PK. Bacterial biofilms: an emerg-ing link to disease pathogenesis. Annu Rev Microbiol.2003;57:677-701.21. Harabuchi Y, Faden H, Yamanaka N, Duffy L, WolfJ, Krystofik D. Nasopharyngeal colonization with non-typeable Haemophilus influenzae and recurrent oti-tis media. J Infect Dis. 1994;170:862-866.22. Leibovitz E, Greenberg D, Piglansky L, et al. Re-current acute otitis media occurring within one monthfrom completion of antibiotic therapy: relationship tothe original pathogen. Pediatr Infect Dis J. 2003;22:209-216.23. Borriello G, Werner E, Roe F, Kim AM, Ehrlich GD,Stewart PS. Oxygen limitation contributes to anti-biotic tolerance of Pseudomonas aeruginosa in bio-
films. Antimicrob Agents Chemother. 2004;48:2659-2664.24. Roberts ME, Stewart PS. Modelling protection fromantimicrobial agents in biofilms through the forma-tion of persister cells. Microbiology. 2005;151:75-80.25. Anderl JN, Zahller J, Roe F, Stewart PS. Role ofnutrient limitation and stationary-phase existence inKlebsiella pneumoniae biofilm resistance to ampicil-lin and ciprofloxacin. Antimicrob Agents Chemother.2003;47:1251-1256.26. Fux CA, Wilson S, Stoodley P. Detachment char-acteristics and oxacillin resistance of Staphyloccocusaureus biofilm emboli in an in vitro catheter infectionmodel. J Bacteriol. 2004;186:4486-4491.27. Stewart PS, Costerton JW. Antibiotic resistanceof bacteria in biofilms. Lancet. 2001;358:135-138.28. Fux CA, Stoodley P, Hall-Stoodley L, CostertonJW. Bacterial biofilms: a diagnostic and therapeuticchallenge. Expert Rev Anti Infect Ther. 2003;1:667-683.29. Mah TF, Pitts B, Pellock B, Walker GC, StewartPS, O’Toole GA. A genetic basis for Pseudomonasaeruginosa biofilm antibiotic resistance. Nature. 2003;426:306-310.30. Drenkard E, Ausubel FM. Pseudomonas biofilmformation and antibiotic resistance are linked to phe-notypic variation. Nature. 2002;416:740-743.31. Christensen BB, Sternberg C, Andersen JB, et al.Establishment of new genetic traits in a microbialbiofilm community. Appl Environ Microbiol. 1998;64:2247-2255.
I am not yet so lost in lexicography as to forget thatwords are the daughters of earth, and that things arethe sons of heaven. Language is only the instrumentof science, and words are but the signs of ideas: I wish,however, that the instrument might be less apt to de-cay, and that signs might be permanent, like the thingswhich they denote.
—Samuel Johnson (1709-1784)
CHRONIC OTITIS MEDIA AS A BIOFILM DISEASE
©2006 American Medical Association. All rights reserved. (Reprinted) JAMA, July 12, 2006—Vol 296, No. 2 211
Copyright © 2022 FDOKUMEN