Diabetes Attitudes, Wishes and Needs second study (DAWN2™): Cross-national benchmarking indicators...
10
Research: Educational and Psychological Issues Diabetes Attitudes, Wishes and Needs second study (DAWN2 TM ): Cross-national comparisons on barriers and resources for optimal care—healthcare professional perspective R. I. G. Holt 1 , A. Nicolucci 2 , K. Kovacs Burns 3 , M. Escalante 4 , A. Forbes 5 , N. Hermanns 6 , S. Kalra 7 , M. Massi-Benedetti 8 , A. Mayorov 9 , E. Men endez-Torre 10 , N. Munro 11 , S. E. Skovlund 12 , I. Tarkun 13 , J. Wens 14 and M. Peyrot 15 on behalf of the DAWN2 Study Group* 1 Faculty of Medicine, University of Southampton, Southampton, UK, 2 Consorzio Mario Negri Sud, Santa Maria Imbaro, Chienti, Italy, 3 Edmonton Clinic Health Academy, University of Alberta, Edmonton, AB, Canada, 4 University of Guadalajara, Instituto Mexicano del Seguro Social, Guadalajara, Jalisco, Mexico, 5 Kings College London, London, UK, 6 Research Institute Diabetes, Diabetes Zentrum Mergentheim, Bad Mergentheim, Germany, 7 Bharti Hospital and BRIDE, Karnal, India, 8 UBF for International Health Research, HIRS, Perugia, Italy, 9 National Research Centre for Endocrinology, Moscow, Russia, 10 Hospital Central de Asturias, Oviedo, Spain, 11 University of Surrey, Guildford, UK, 12 Novo Nordisk, Copenhagen, Denmark, 13 Kocaeli University, Kocaeli, Turkey, 14 University of Antwerp, Antwerp, Belgium and 15 Loyola University Maryland, Baltimore, MD, USA Accepted 22 May 2013 Abstract Aims The second Diabetes Attitudes, Wishes and Needs (DAWN2) study sought cross-national comparisons of perceptions on healthcare provision for benchmarking and sharing of clinical practices to improve diabetes care. Methods In total, 4785 healthcare professionals caring for people with diabetes across 17 countries participated in an online survey designed to assess diabetes healthcare provision, self-management and training. Results Between 61.4 and 92.9% of healthcare professionals felt that people with diabetes needed to improve various self-management activities; glucose monitoring (range, 29.3–92.1%) had the biggest country difference, with a between-country variance of 20%. The need for a major improvement in diabetes self-management education was reported by 60% (26.4–81.4%) of healthcare professionals, with a 12% between-country variance. Provision of diabetes services differed among countries, with many healthcare professionals indicating that major improvements were needed across a range of areas, including healthcare organization [30.6% (7.4–67.1%)], resources for diabetes prevention [78.8% (60.4–90.5%)], earlier diagnosis and treatment [67.9% (45.0–85.5%)], communication between team members and people with diabetes [56.1% (22.3–85.4%)], specialist nurse availability [63.8% (27.9–90.7%)] and psychological support [62.7% (40.6–79.6%)]. In some countries, up to one third of healthcare professionals reported not having received any formal diabetes training. Societal discrimination against people with diabetes was reported by 32.8% (11.4–79.6%) of participants. Conclusions This survey has highlighted concerns of healthcare professionals relating to diabetes healthcare provision, self-management and training. Identifying between-country differences in several areas will allow benchmarking and sharing of clinical practices. Diabet. Med. 30, 789–798 (2013) Introduction The rapidly increasing number of people with diabetes and disease burden may reach 552 million by 2030 [1]. This calls for a review of the current detection and management procedures and evaluation of additional measures necessary to support healthcare professionals, people with diabetes and their families. Correspondence to: Richard Holt. E-mail: [email protected] *Data access: the DAWN2 study is a global partnership initiative for the advancement of person-centred diabetes care and the results will be made available for public research purposes under the guidance of the DAWN2 International Publication Planning Committee (IPPC) once the primary publications are published. For more information contact [email protected] ª 2013 The Authors. Diabetic Medicine ª 2013 Diabetes UK 789 DIABETICMedicine DOI: 10.1111/dme.12242
Transcript of Diabetes Attitudes, Wishes and Needs second study (DAWN2™): Cross-national benchmarking indicators...

Research: Educational and Psychological Issues
Diabetes Attitudes, Wishes and Needs second study
(DAWN2TM): Cross-national comparisons on barriers and
resources for optimal care—healthcare professional
perspective
R. I. G. Holt1, A. Nicolucci2, K. Kovacs Burns3, M. Escalante4, A. Forbes5, N. Hermanns6,S. Kalra7, M. Massi-Benedetti8, A. Mayorov9, E. Men�endez-Torre10, N. Munro11,S. E. Skovlund12, I. Tarkun13, J. Wens14 and M. Peyrot15 on behalf of the DAWN2Study Group*
1Faculty of Medicine, University of Southampton, Southampton, UK, 2Consorzio Mario Negri Sud, Santa Maria Imbaro, Chienti, Italy, 3Edmonton Clinic Health
Academy, University of Alberta, Edmonton, AB, Canada, 4University of Guadalajara, Instituto Mexicano del Seguro Social, Guadalajara, Jalisco, Mexico, 5Kings
College London, London, UK, 6Research Institute Diabetes, Diabetes Zentrum Mergentheim, Bad Mergentheim, Germany, 7Bharti Hospital and BRIDE, Karnal,
India, 8UBF for International Health Research, HIRS, Perugia, Italy, 9National Research Centre for Endocrinology, Moscow, Russia, 10Hospital Central de Asturias,
Oviedo, Spain, 11University of Surrey, Guildford, UK, 12Novo Nordisk, Copenhagen, Denmark, 13Kocaeli University, Kocaeli, Turkey, 14University of Antwerp,
Antwerp, Belgium and 15Loyola University Maryland, Baltimore, MD, USA
Accepted 22 May 2013
Abstract
Aims The second Diabetes Attitudes, Wishes and Needs (DAWN2) study sought cross-national comparisons of
perceptions on healthcare provision for benchmarking and sharing of clinical practices to improve diabetes care.
Methods In total, 4785 healthcare professionals caring for people with diabetes across 17 countries participated in an
online survey designed to assess diabetes healthcare provision, self-management and training.
Results Between 61.4 and 92.9% of healthcare professionals felt that people with diabetes needed to improve various
self-management activities; glucose monitoring (range, 29.3–92.1%) had the biggest country difference, with a
between-country variance of 20%. The need for a major improvement in diabetes self-management education was
reported by 60% (26.4–81.4%) of healthcare professionals, with a 12% between-country variance. Provision of diabetes
services differed among countries, with many healthcare professionals indicating that major improvements were needed
across a range of areas, including healthcare organization [30.6% (7.4–67.1%)], resources for diabetes prevention
[78.8% (60.4–90.5%)], earlier diagnosis and treatment [67.9% (45.0–85.5%)], communication between team members
and people with diabetes [56.1% (22.3–85.4%)], specialist nurse availability [63.8% (27.9–90.7%)] and psychological
support [62.7% (40.6–79.6%)]. In some countries, up to one third of healthcare professionals reported not having
received any formal diabetes training. Societal discrimination against people with diabetes was reported by 32.8%
(11.4–79.6%) of participants.
Conclusions This survey has highlighted concerns of healthcare professionals relating to diabetes healthcare provision,
self-management and training. Identifying between-country differences in several areas will allow benchmarking and
sharing of clinical practices.
Diabet. Med. 30, 789–798 (2013)
Introduction
The rapidly increasing number of people with diabetes and
disease burden may reach 552 million by 2030 [1]. This calls
for a review of the current detection and management
procedures and evaluation of additional measures necessary
to support healthcare professionals, people with diabetes and
their families.
Correspondence to: Richard Holt. E-mail: [email protected]
*Data access: the DAWN2 study is a global partnership initiative for the
advancement of person-centred diabetes care and the results will be made
available for public research purposes under the guidance of the DAWN2
International Publication Planning Committee (IPPC) once the primary
publications are published. For more information contact
ª 2013 The Authors.Diabetic Medicine ª 2013 Diabetes UK 789
DIABETICMedicine
DOI: 10.1111/dme.12242

In 2001, the Diabetes, Attitudes, Wishes and Needs
(DAWN) study conducted in 13 countries evaluated the
non-medical factors that may prevent people with diabetes
from achieving optimal treatment outcomes [2]. DAWN
revealed that insufficient care and support was available to
meet the psychological and educational needs of people with
diabetes and their healthcare professionals in both developed
and developing countries. Improved collaboration within a
multidisciplinary team of healthcare professionals was iden-
tified as an important factor in improving outcomes for people
with diabetes [3]. A ‘patient-centred’ approach to diabetes
care, which emphasizes the individual’s role as part of the
treatment team, is essential for achieving optimal outcomes
and patient satisfaction [4,5], while a multidisciplinary
healthcare professional approach from the outset encourages
healthcare professionals to improve the delivery of care [6,7].
The DAWN study findings initiated a ‘DAWN Call to
Action’ programme that focused on new evidence-based
strategies for psychosocial and self-management education
for people with diabetes and support from healthcare
professionals [8,9]. Effective interaction and understanding
between people with diabetes and their healthcare profes-
sionals are paramount in diabetes self-management and
improving healthcare [10]. However, despite advances in
knowledge and improved collaboration, person-centred
diabetes care worldwide remains key to providing people
with diabetes with the care they deserve.
One decade after DAWN, the DAWN2 study was initiated
as a global partnership initiative between several established
national and international organizations, including the Inter-
national Diabetes Federation, the International Alliance of
Patients’ Organizations (IAPO) and the Steno Diabetes
Center, and Novo Nordisk [11] for the advancement of
person-centred diabetes care. This parallels the Global
DAWN Call to Action [8], World Health Organization
(WHO) frameworks for people-centred and innovative
chronic illness care and the IAPO declaration for patient-
centred health care [12]. The DAWN2 study aims to: (1)
improve our understanding of the unmet needs of people with
diabetes and those who care for them; (2) facilitate dialogue
and collaboration among all key stakeholders to strengthen
active patient involvement and self-management; and (3)
establish a cross-culturally validated multinational survey
system for assessing and benchmarking psychosocial and
educational aspects of diabetes care delivery. While a number
of different analyses and publications are expected from the
DAWN2 data, here we present the core descriptive data for
one of the DAWN2 surveys, which assessed the perceptions
and opinions of healthcare professionals on quality of life and
treatment burden, societal issues, involvement and empow-
erment of people with diabetes, self-management activities,
healthcare provision and education/training. This initial
report of cross-national benchmarking indicators with estab-
lished validity and reliability of source measures is intended to
serve the function of cross-national benchmarking in which
differences between countries can help identify country-spe-
cific needs and provide a baseline for future studies investi-
gating any changes in the needs and perceptions of healthcare
professionals treating people with diabetes. This report is one
of three linked papers within this edition of Diabetic
Medicine that describe the core data for the three stakeholder
groups surveyed in DAWN2 (people with diabetes, their
family members and healthcare professionals); each report
provides complementary data to the others.
Participants and methods
Study design and participants
Detailed methods for the international, interdisciplinary,
multi-stakeholder DAWN2 study (UTN no: U1111-1123-
7509; NCT01507116) have been described previously [11].
The study was conducted in 17 countries: Algeria, Canada,
China, Denmark, France, Germany, India, Italy, Japan,
Mexico, the Netherlands, Poland, Russian Federation, Spain,
Turkey, the UK and the USA.
A minimum of 280 healthcare professionals per country
was recruited with quotas for general practitioners/primary
care physicians, specialist physicians (endocrinologists and
diabetologists), diabetes nurses and dietitians. Sample quotas
were higher for physicians because worldwide they are the
main providers of diabetes care; quota for generalists were
higher than specialists for the same reason. All participating
healthcare professionals had been in practice for ≥ 1 year
and were treating ≥ 5 adults (aged ≥ 18 years) with diabetes
per month or ≥ 50 adults per month for diabetes specialists.
Recruitment methodology
Healthcare professionals were identified from online panels
and databases in each country, as well as telephone lists and
What’s new?
● The original DAWN study found that diabetes is often
associated with multiple psychosocial problems that are
barriers to self-management behaviours, and that cur-
rent healthcare resources in various countries are poorly
equipped or utilized to support people with diabetes.
● The current DAWN2 study has provided a new
in-depth understanding of the views and needs of
healthcare professionals, allowed for cross-national
comparisons and identified areas for improvement to
achieve optimal diabetes care.
● Healthcare professionals stress the importance of
improvinghealthcare organization, aswell as addressing
emotional problems and improving self-management
activities in people with diabetes.
790ª 2013 The Authors.
Diabetic Medicine ª 2013 Diabetes UK
DIABETICMedicine DAWN2: healthcare professional’s perspective � R. I. G. Holt et al.

physician directories. This hybrid approach ensured that the
study population is as representative as possible of the
healthcare professionals in each country and limits potential
bias if the entire sample is obtained through a single method.
Potential participants were then invited by email or
telephone and received a web link by email to a secure
server enabling them to complete the survey online.
Questionnaires
The healthcare professional survey comprised standardized
questions adapted from the original DAWN study and
modified versions of validated measures, including the
Healthcare Professional Patient Assessment of Chronic
Illness Care DAWN Short Form (HCP-PACIC-DSF) and
healthcare professional Health Care Climate DAWN Short
Form (HCP-HCC-DSF) questionnaires, as well as questions
developed for use with healthcare professionals specifically
for this survey. Finally, open-ended questions were included
to allow participants to share their experiences. The ques-
tionnaire was reviewed, approved and tested in English, then
translated into local languages before being back translated
to ensure harmonization [11]. The questionnaire was
reviewed and evaluated in each country by members of the
DAWN2 advisory board and the final questionnaire was
pilot-tested in detail with representatives of the respondent
group in each case prior to study execution. Measures
reported in this paper are described in the Supporting
Information (Table S1).
Ethical considerations
Surveys were conducted in accordance with the relevant
ethical requirements and followed local, national and
international guidelines relating to the conduct of non-
interventional studies [11].
Statistical analysis
Results from each country were subjected to descriptive
statistics for all variables and summarized as mean � stan-
dard deviation (SD) for continuous variables or percentages
for categorical variables. Questionnaire scores, calculated on
the entire study population (global score), are reported as
mean � SD. Results from single-item questions are shown as
the number and percentage of respondents. Data are reported
as median, minimum and maximum country scores. All the
scale scores range from 0 to 100, with higher values
indicating a higher level of the dimension measured.
Cronbach’s alpha coefficient was used to measure the
reliability (internal consistency) of multi-item questionnaires
(≥ 0.7 indicates an acceptable degree of internal consistency)
with median, minimum and maximum country coefficients.
Multi-level regression models [13,14] with an uncon-
structed correlation-type matrix [15] were used to account
for non-independent observations within countries and
estimate how much of the independent variation (residual
variance) is explained by differences between countries.
Criteria to evaluate indicators for benchmarking activities
included acceptable reliability in each country, as measured
with the Cronbach’s alpha coefficient, and statistically
significant between-country variation. The identical sampling
design for each country allowed us to make comparisons
without adjustment for differences in sample proportions.
Results
Between March and August 2012, 4785 healthcare profes-
sionals (2066 primary care physicians/general practitioners,
1350 diabetes specialists, 827 nurses and 542 dietitians) were
surveyed; participant characteristics are summarized in
Table 1.
Descriptive statistics for key indicators are presented in
Table 2. The country-level analysis showed that the Cron-
bach’s alpha coefficient was most reliable for recommenda-
tions relating to the ‘chronic illness care’ (HCP-PACIC-DSF)
questionnaire, but least reliable for assessment of perceived
‘helpfulness of active patient involvement’ (HAPI-DSF; Help-
fulness of Active Patient Involvement-DAWN short form),
with six countries falling below0.7. Four countries also had an
alpha score below 0.7 for the HCP-HCC-DSF questionnaire.
Cross-national comparison
There were significant between-country differences for all the
domains investigated, and the residual variancewas significant
for all the benchmarking indicators (P < 0.001), ranging
between 2% (‘need for more training on effective communi-
cation and motivation strategies to support long-term behav-
iour change’) and 23% [‘healthcare organization should
promote better communication within the team’ (Table 2)].
The estimated means or proportions (%) with 95%
confidence intervals that have been adjusted for clustering
for each indicator by country are presented in the figures and
in the Supporting Information (Table S2). All country-
specific references are based on these data. Individual data by
country were ranked according to the cluster-adjusted data
and, although some countries rank higher for certain
indicators, no country stands out as being consistently better
or worse than other countries.
Quality of life and treatment burden
Over half of healthcare professionals indicated that they had
discussed emotional issues with their patients; however,
approximately 13% reported a lack of resources to offer
support for people with diabetes who are emotionally
distressed or at risk of depression (Table 2; Fig. 1). In
addition, one third of healthcare professionals felt that people
with diabeteswere subjected to social discrimination, but there
ª 2013 The Authors.Diabetic Medicine ª 2013 Diabetes UK 791
Research article DIABETICMedicine
was a marked difference among the countries (11.4–79.6%;
Table 2); the lowest proportionwas inCanada and the highest
in Algeria (see also Supporting Information, Table S2).
Empowerment and self-care activities
A large proportion of respondents believe that it would be
helpful if people with diabetes could play a more active part
in the management of their condition (78.0 � 18.9; Table 2)
and take more responsibility for this (Table 2; see also
Supporting Information, Fig. S1). Sixty per cent of healthcare
professionals recommend a major improvement in self-man-
agement by people with diabetes, with physical activity
(92.9%), healthy eating (90.7%; Fig. 2) and maintaining a
healthy weight (89.8%) most commonly reported to require
greater attention. Improvements in self-monitoring of blood
glucose and dealing with emotion were recommended by
62.3 and 62.5% of healthcare professionals, respectively.
Opinions varied considerably across countries, with the
largest observed cross-national difference (29.3–92.1%)
being the need for glucose monitoring improvement; the
proportion of participants recommending improved glucose
monitoring was lowest in Denmark and highest in China (see
also Supporting Information, Table S2).
Healthcare provision
The provision of diabetes services differed among the 17
countries (Table 2). The majority of healthcare professionals
indicated the need for major improvements in the prevention
of Type 2 diabetes (78.8%), despite approximately 70%
reporting that resources such as interventions for weight loss
and physical exercise were available in their country. Early
diagnosis and treatment (67.9%) was another area requiring
improvement.
Several areas of healthcare provision requiring improve-
ment for chronic disease management were identified
(Table 2), including the availability of diabetes self-manage-
ment education [60.9% (see also Supporting Information,
Fig. S2)]. Only 30.6% believed that health care was well
organized for managing chronic conditions (Fig. 3). Respon-
dents agreed that diabetes should be a greater priority
(52.1%) and that better communication among healthcare
team members (56.1%) and greater availability of resources
to provide psychological support and care are needed
(62.7%; Fig. 4), including access to psychology or psychiatry
support (Table 2).
Nearly two thirds of respondents recognized the need for
more diabetes specialist nurses [63.8%; Table 2 (see also
Supporting Information, Fig. S3)] and the importance of
involving family members of people with diabetes (69.9%).
The need for formal training in effective communication for
all diabetes care specialists was also recognized (63.0%).
The provision of diabetes care by respondents during
regular clinic visits over the past 12 months was reported
according to the ‘chronic illness care’ (HCP-PACIC-DSF) and
‘healthcare climate’ (HCP-HCC-DSF) questionnaires. The
composite mean scores were 61.8 � 17.9 and 75.7 � 18.6,
respectively, indicating that many respondents felt that they
provided person-centred chronic illness care and high levels of
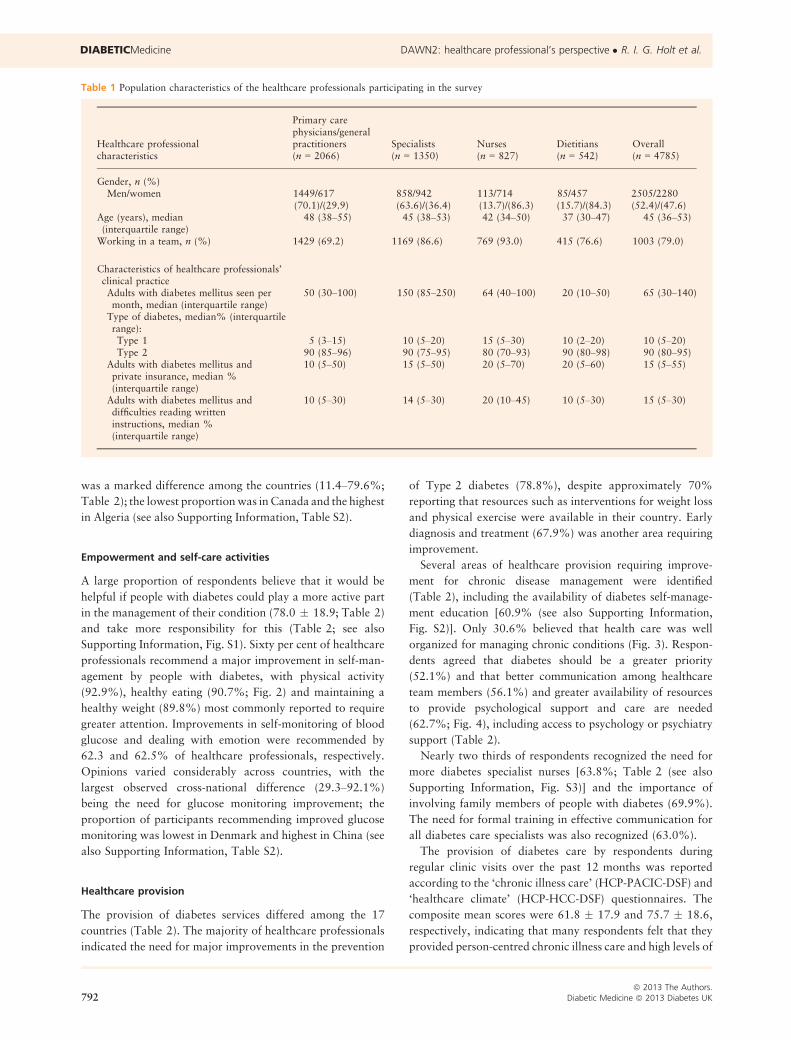
Table 1 Population characteristics of the healthcare professionals participating in the survey
Healthcare professionalcharacteristics
Primary carephysicians/generalpractitioners Specialists Nurses Dietitians Overall(n = 2066) (n = 1350) (n = 827) (n = 542) (n = 4785)
Gender, n (%)Men/women 1449/617
(70.1)/(29.9)858/942(63.6)/(36.4)
113/714(13.7)/(86.3)
85/457(15.7)/(84.3)
2505/2280(52.4)/(47.6)
Age (years), median(interquartile range)
48 (38–55) 45 (38–53) 42 (34–50) 37 (30–47) 45 (36–53)
Working in a team, n (%) 1429 (69.2) 1169 (86.6) 769 (93.0) 415 (76.6) 1003 (79.0)
Characteristics of healthcare professionals’clinical practiceAdults with diabetes mellitus seen permonth, median (interquartile range)
50 (30–100) 150 (85–250) 64 (40–100) 20 (10–50) 65 (30–140)
Type of diabetes, median% (interquartilerange):Type 1 5 (3–15) 10 (5–20) 15 (5–30) 10 (2–20) 10 (5–20)Type 2 90 (85–96) 90 (75–95) 80 (70–93) 90 (80–98) 90 (80–95)
Adults with diabetes mellitus andprivate insurance, median %(interquartile range)
10 (5–50) 15 (5–50) 20 (5–70) 20 (5–60) 15 (5–55)
Adults with diabetes mellitus anddifficulties reading writteninstructions, median %(interquartile range)
10 (5–30) 14 (5–30) 20 (10–45) 10 (5–30) 15 (5–30)
792ª 2013 The Authors.
Diabetic Medicine ª 2013 Diabetes UK
DIABETICMedicine DAWN2: healthcare professional’s perspective � R. I. G. Holt et al.
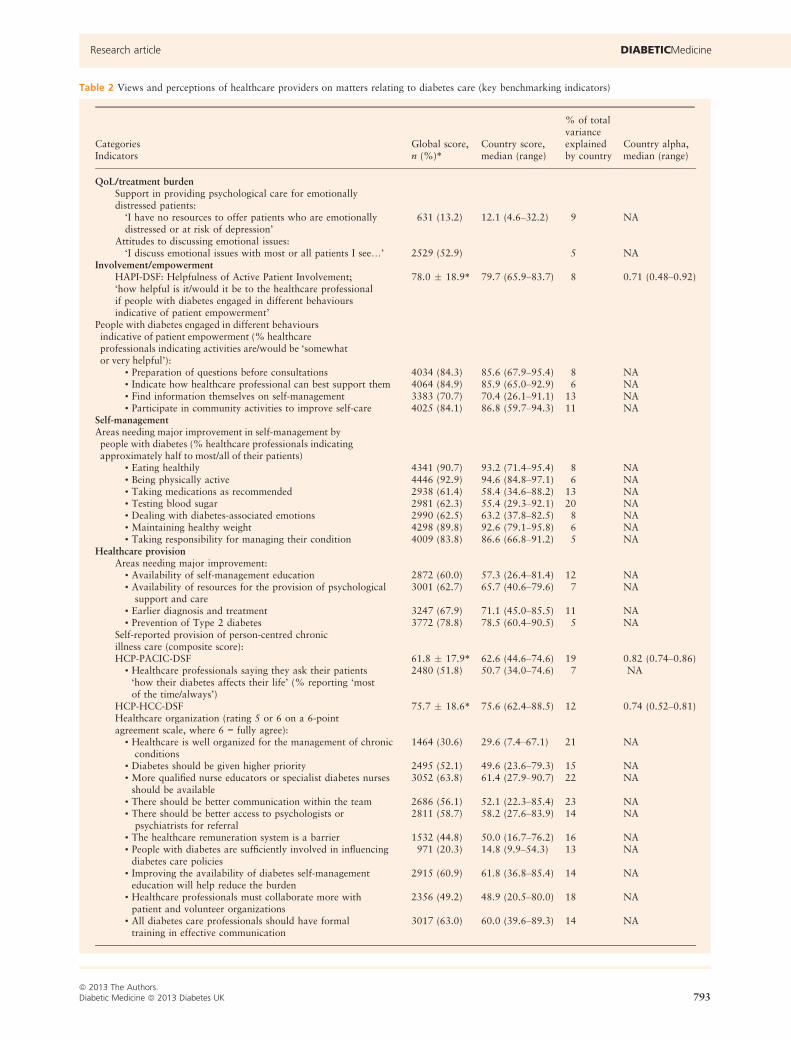
Table 2 Views and perceptions of healthcare providers on matters relating to diabetes care (key benchmarking indicators)
% of totalvarianceexplainedby country
Country alpha,median (range)
CategoriesIndicators
Global score,n (%)*
Country score,median (range)
QoL/treatment burdenSupport in providing psychological care for emotionallydistressed patients:
‘I have no resources to offer patients who are emotionallydistressed or at risk of depression’
631 (13.2) 12.1 (4.6–32.2) 9 NA
Attitudes to discussing emotional issues:‘I discuss emotional issues with most or all patients I see…’ 2529 (52.9) 5 NA
Involvement/empowermentHAPI-DSF: Helpfulness of Active Patient Involvement;‘how helpful is it/would it be to the healthcare professionalif people with diabetes engaged in different behavioursindicative of patient empowerment’
78.0 � 18.9* 79.7 (65.9–83.7) 8 0.71 (0.48–0.92)
People with diabetes engaged in different behavioursindicative of patient empowerment (% healthcareprofessionals indicating activities are/would be ‘somewhator very helpful’):
• Preparation of questions before consultations 4034 (84.3) 85.6 (67.9–95.4) 8 NA• Indicate how healthcare professional can best support them 4064 (84.9) 85.9 (65.0–92.9) 6 NA• Find information themselves on self-management 3383 (70.7) 70.4 (26.1–91.1) 13 NA• Participate in community activities to improve self-care 4025 (84.1) 86.8 (59.7–94.3) 11 NA
Self-managementAreas needing major improvement in self-management bypeople with diabetes (% healthcare professionals indicatingapproximately half to most/all of their patients)
• Eating healthily 4341 (90.7) 93.2 (71.4–95.4) 8 NA• Being physically active 4446 (92.9) 94.6 (84.8–97.1) 6 NA• Taking medications as recommended 2938 (61.4) 58.4 (34.6–88.2) 13 NA• Testing blood sugar 2981 (62.3) 55.4 (29.3–92.1) 20 NA• Dealing with diabetes-associated emotions 2990 (62.5) 63.2 (37.8–82.5) 8 NA• Maintaining healthy weight 4298 (89.8) 92.6 (79.1–95.8) 6 NA• Taking responsibility for managing their condition 4009 (83.8) 86.6 (66.8–91.2) 5 NA
Healthcare provisionAreas needing major improvement:
• Availability of self-management education 2872 (60.0) 57.3 (26.4–81.4) 12 NA• Availability of resources for the provision of psychologicalsupport and care
3001 (62.7) 65.7 (40.6–79.6) 7 NA
• Earlier diagnosis and treatment 3247 (67.9) 71.1 (45.0–85.5) 11 NA• Prevention of Type 2 diabetes 3772 (78.8) 78.5 (60.4–90.5) 5 NA
Self-reported provision of person-centred chronicillness care (composite score):HCP-PACIC-DSF 61.8 � 17.9* 62.6 (44.6–74.6) 19 0.82 (0.74–0.86)
• Healthcare professionals saying they ask their patients‘how their diabetes affects their life’ (% reporting ‘mostof the time/always’)
2480 (51.8) 50.7 (34.0–74.6) 7 NA
HCP-HCC-DSF 75.7 � 18.6* 75.6 (62.4–88.5) 12 0.74 (0.52–0.81)Healthcare organization (rating 5 or 6 on a 6-pointagreement scale, where 6 = fully agree):
• Healthcare is well organized for the management of chronicconditions
1464 (30.6) 29.6 (7.4–67.1) 21 NA
• Diabetes should be given higher priority 2495 (52.1) 49.6 (23.6–79.3) 15 NA• More qualified nurse educators or specialist diabetes nursesshould be available
3052 (63.8) 61.4 (27.9–90.7) 22 NA
• There should be better communication within the team 2686 (56.1) 52.1 (22.3–85.4) 23 NA• There should be better access to psychologists orpsychiatrists for referral
2811 (58.7) 58.2 (27.6–83.9) 14 NA
• The healthcare remuneration system is a barrier 1532 (44.8) 50.0 (16.7–76.2) 16 NA• People with diabetes are sufficiently involved in influencingdiabetes care policies
971 (20.3) 14.8 (9.9–54.3) 13 NA
• Improving the availability of diabetes self-managementeducation will help reduce the burden
2915 (60.9) 61.8 (36.8–85.4) 14 NA
• Healthcare professionals must collaborate more withpatient and volunteer organizations
2356 (49.2) 48.9 (20.5–80.0) 18 NA
• All diabetes care professionals should have formaltraining in effective communication
3017 (63.0) 60.0 (39.6–89.3) 14 NA
ª 2013 The Authors.Diabetic Medicine ª 2013 Diabetes UK 793
Research article DIABETICMedicine
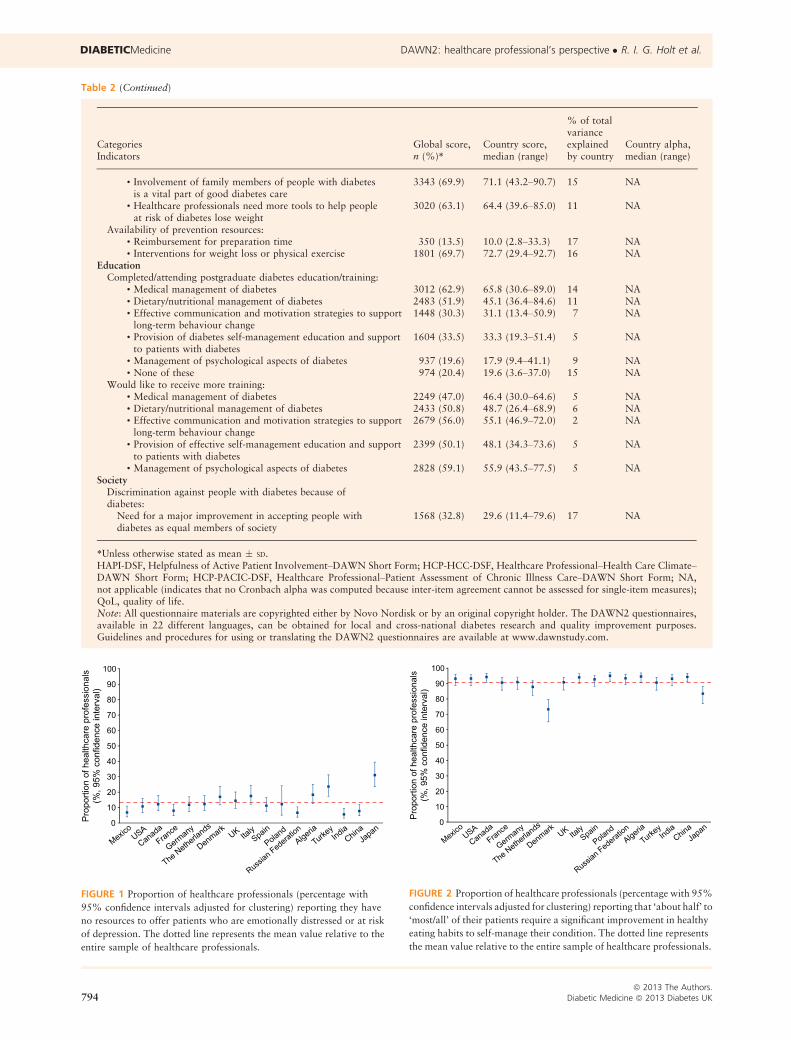
Table 2 (Continued)
% of totalvarianceexplainedby country
Country alpha,median (range)
CategoriesIndicators
Global score,n (%)*
Country score,median (range)
• Involvement of family members of people with diabetesis a vital part of good diabetes care
3343 (69.9) 71.1 (43.2–90.7) 15 NA
• Healthcare professionals need more tools to help peopleat risk of diabetes lose weight
3020 (63.1) 64.4 (39.6–85.0) 11 NA
Availability of prevention resources:• Reimbursement for preparation time 350 (13.5) 10.0 (2.8–33.3) 17 NA• Interventions for weight loss or physical exercise 1801 (69.7) 72.7 (29.4–92.7) 16 NA
EducationCompleted/attending postgraduate diabetes education/training:
• Medical management of diabetes 3012 (62.9) 65.8 (30.6–89.0) 14 NA• Dietary/nutritional management of diabetes 2483 (51.9) 45.1 (36.4–84.6) 11 NA• Effective communication and motivation strategies to supportlong-term behaviour change
1448 (30.3) 31.1 (13.4–50.9) 7 NA
• Provision of diabetes self-management education and supportto patients with diabetes
1604 (33.5) 33.3 (19.3–51.4) 5 NA
• Management of psychological aspects of diabetes 937 (19.6) 17.9 (9.4–41.1) 9 NA• None of these 974 (20.4) 19.6 (3.6–37.0) 15 NA
Would like to receive more training:• Medical management of diabetes 2249 (47.0) 46.4 (30.0–64.6) 5 NA• Dietary/nutritional management of diabetes 2433 (50.8) 48.7 (26.4–68.9) 6 NA• Effective communication and motivation strategies to supportlong-term behaviour change
2679 (56.0) 55.1 (46.9–72.0) 2 NA
• Provision of effective self-management education and supportto patients with diabetes
2399 (50.1) 48.1 (34.3–73.6) 5 NA
• Management of psychological aspects of diabetes 2828 (59.1) 55.9 (43.5–77.5) 5 NASociety
Discrimination against people with diabetes because ofdiabetes:
Need for a major improvement in accepting people withdiabetes as equal members of society
1568 (32.8) 29.6 (11.4–79.6) 17 NA
*Unless otherwise stated as mean � SD.HAPI-DSF, Helpfulness of Active Patient Involvement–DAWN Short Form; HCP-HCC-DSF, Healthcare Professional–Health Care Climate–DAWN Short Form; HCP-PACIC-DSF, Healthcare Professional–Patient Assessment of Chronic Illness Care–DAWN Short Form; NA,not applicable (indicates that no Cronbach alpha was computed because inter-item agreement cannot be assessed for single-item measures);QoL, quality of life.Note: All questionnaire materials are copyrighted either by Novo Nordisk or by an original copyright holder. The DAWN2 questionnaires,available in 22 different languages, can be obtained for local and cross-national diabetes research and quality improvement purposes.Guidelines and procedures for using or translating the DAWN2 questionnaires are available at www.dawnstudy.com.
FIGURE 2 Proportion of healthcare professionals (percentage with 95%
confidence intervals adjusted for clustering) reporting that ‘about half’ to
‘most/all’ of their patients require a significant improvement in healthy
eating habits to self-manage their condition. The dotted line represents
the mean value relative to the entire sample of healthcare professionals.
FIGURE 1 Proportion of healthcare professionals (percentage with
95% confidence intervals adjusted for clustering) reporting they have
no resources to offer patients who are emotionally distressed or at risk
of depression. The dotted line represents the mean value relative to the
entire sample of healthcare professionals.
794ª 2013 The Authors.
Diabetic Medicine ª 2013 Diabetes UK
DIABETICMedicine DAWN2: healthcare professional’s perspective � R. I. G. Holt et al.
practical or communicative support for people with diabetes,
such as actively listening, encouraging and involving patients
in their own care management. Notably, over half (51.8%) of
healthcare providers indicated that they had asked their
patients how diabetes impacted their life (Table 2).
Education and information
Access to diabetes education or training programmes is
limited, with one in five healthcare professionals (median
19.6%, but up to one third in some countries) not receiving
any postgraduate training. Over 50% of respondents showed
an interest in attending training programmes that would
equip them with the knowledge and tools to provide better
care for people with diabetes (Table 2).
Discussion
A review of the perceptions of healthcare professionals
treating adult patients with diabetes regarding their diabetes
practice, management and procedures is an important step to
ensure that people with diabetes and all those involved in their
care receive the best possible support. The original DAWN
studyprovided insights fromamultinational perspectiveon the
needs of both people with diabetes and healthcare profession-
als to help improve diabetes care locally and internationally
[2,3]. DAWN also highlighted a good relationship between
healthcare professionals and people with diabetes, and that
better collaboration between these groupswas associatedwith
favourable outcomes [16]. This allowed healthcare profes-
sionals to assess the needs of people with diabetes more
effectively and implement appropriate changes to current care.
The DAWN2 study provides a multinational insight into
current health care for the management of people with
diabetes from the perspectives of healthcare professionals,
people with diabetes and their family members. This report
has highlighted the concerns of healthcare professionals
regarding diabetes healthcare provision, self-management
and training. The DAWN2 results show substantial variation
in the perceptions of healthcare professionals in different
countries. Despite these differences, healthcare professionals
across all countries considered the current healthcare provi-
sion for people with diabetes to be inadequate. Consistent
with DAWN [17], the majority of healthcare professionals
who participated in DAWN2 believe that, despite techno-
logical advances and the availability of improved treatments,
current national healthcare systems remain poorly equipped
to manage and treat people with diabetes effectively; and
although self-management education was considered to be
important, its provision was seen as lacking.
DAWN2 highlighted that psychosocial support is consid-
ered a key aspect of diabetes care, but that healthcare
professionals lack adequate resources, training and reim-
bursement to provide it. Some healthcare professionals
reported having no resources to address emotional problems
in people with diabetes, and only approximately half
reported that they discuss emotional problems with their
patients or ask about the impact of diabetes on their patients’
lives, but the latter may differ from the perception of people
with diabetes being asked about this. Dealing with the
emotional difficulties faced by people with diabetes and their
lack of adherence to treatment can leave healthcare profes-
sionals feeling overwhelmed and frustrated [18,19]. There is
often a lack of clarity for healthcare professionals regarding
who should manage the psychosocial aspects of diabetes and
many avoid addressing these issues, concerned that they are
ill-equipped or have insufficient education and training
[2,18,20]. A number of countries have introduced national
postgraduate education programmes for professionals to
improve their knowledge and understanding of diabetes and
the requirements of people with diabetes to ensure that they
FIGURE 3 Proportion of healthcare professionals (percentage with
95% confidence intervals adjusted for clustering) reporting that
healthcare in their country is well organized for the management of
chronic conditions, including diabetes (rating 5 or 6 on a 6-point scale).
The dotted line represents the mean value relative to the entire sample
of healthcare professionals.
FIGURE 4 Proportion of healthcare professionals (percentage with
95% confidence intervals adjusted for clustering) reporting that a
major improvement is needed in making resources available for the
provision of psychological support and care. The dotted line represents
the mean value relative to the entire sample of healthcare professionals.
ª 2013 The Authors.Diabetic Medicine ª 2013 Diabetes UK 795
Research article DIABETICMedicine

are offering comprehensive, effective diabetes self-manage-
ment education. Although the type of specialist training
offered differs between countries, the benefits of such
programmes have been demonstrated [21,22].
Healthcare professionals agreed that diabetes self-manage-
ment is suboptimal and needs improving; however, there may
be differences between healthcare professionals and people
with diabetes in their perceptions of how to encourage
self-management. Peoplewith diabetes often face psychosocial
issues when accepting and making and maintaining lifestyle
changes to improve the management of their diabetes. To help
support people with diabetes, healthcare professionals should
be able to identify and consider societal issues such as
discrimination, intolerance, lack of community support and
religious practices (e.g. fasting during themonth ofRamadan).
Ultimately, healthcare professionals also need to engage
people with diabetes better to develop a plan that allows the
individual to lead a full and active life, to encourage hope, and
to console them and help them understand the consequences
when treatment goals are not met [4,5,23].
Healthcare professionals agreed that involving family
members of people with diabetes is a vital part of diabetes
care. However, family members also need education on
diabetes to help support their relative with diabetes, and may
also require psychological and emotional support; both of
these factors can contribute to a positive outcome [24,25].
Successful management of diabetes is facilitated by good
relationships between people with diabetes, their family
members and a multidisciplinary team of professionals,
including doctors trained in diabetes, dietitians, nurses and
psychologists [26]. Close collaboration within the multidis-
ciplinary team is key to ensuring that people with diabetes
receive the correct level of support at the correct time.
Communication should be extended not only to people with
diabetes, but also to individuals considered to be at high risk
of this condition [26,27].
Over two thirds of healthcare professionals indicated the
need for major improvements in diabetes prevention, early
diagnosis and treatment. The development and implementa-
tion of diabetes prevention programmes worldwide has been
a challenge, but advances in scientific research and clinical
trials have led to pragmatic improvements in the primary
healthcare setting [27,28]. Many healthcare professionals in
this survey indicated that, while resources to help prevent the
onset of diabetes were available in their country, there is a
need to improve the delivery of such resources to those at risk.
The ability to monitor the quality of diabetes care across
the globe has been limited by the lack of standard definitions
of indicators of the disease and lack of standard systems for
providing these indicators in representative population sam-
ples [29]. The DAWN2 questionnaires contain a series of
reliable tools suitable for measuring desired outcomes, as
well as their barriers and drivers, in healthcare professionals
across countries. This allows us to understand the differences
in several aspects of diabetes care between countries, and
therefore permits benchmarking and sharing of better clinical
policies and practices. However, several study limitations can
be noted, such as the challenges of ensuring a representative
population of the country and areas sampled [11]. The
proportion of healthcare professionals in the various disci-
plines differed across countries and participants included
only those healthcare professionals who treat adults, result-
ing in a lack of input from paediatric diabetes services.
Furthermore, as participation was voluntary, this sample of
healthcare professionals may be more motivated than
non-participants and therefore, results from DAWN2 may
not wholly reflect the entire population of diabetes health-
care professionals. In addition, caution is required when
drawing conclusions from healthcare professionals describ-
ing their own behaviour and practices. Finally, although
every effort was made to ensure appropriate translations into
native languages, this process is fraught with difficulty and
may result in misinterpretation or misunderstanding.
The outcomes examined here may be partially explained by
differences in the organization of chronic illness care between
the countries, including national diabetes and chronic illness
policies.Many other factors may have influenced the DAWN2
findings, such as socio-economic and cultural factors and
disciplinary differences. For outcomes in the healthcare
professional survey, disciplinary differences may vary by
and interact with country, rather than being consistent across
countries. While analysis and discussion of these issues are
beyond the scope of this manuscript, further analyses are
ongoing to identify and investigate differences between
countries, professions and stakeholder groups. For healthcare
professionals, further analyses are required to elucidate and
understand fully the specific needs of the individual disciplines
within diabetes teams. Subsequent DAWN2 publications will
combine data for people with diabetes, family members and
the different healthcare disciplines, as well as health policy
perspectives, to generate multi-perspective analyses of barri-
ers and drivers for the provision of optimal person-centred
diabetes care in participating countries.
In summary, despite improvements in healthcare provision
and healthcare organization, feedback from healthcare pro-
fessionals indicates the need for better resources, education,
training and collaboration among an interdisciplinary team of
healthcare professionals caring for people with diabetes.
Healthcare professionals remain concerned about the gap in
healthcare provision to meet the needs of people with diabetes
and family members. The increasing prevalence of diabetes
and the lack of resources for effective care calls for a new,
proactive and preventive approach, in which psychosocial
issues are managed within collaborative teams, including
people with diabetes and their family members. DAWN2
provides benchmarks for further study to determine the
progress made and to identify the barriers that remain in
diabetes care. As a collaborative study that has involved global
organizations, it is anticipated that the DAWN2 findings will
help drive multinational changes in patient-centred care.
796ª 2013 The Authors.
Diabetic Medicine ª 2013 Diabetes UK
DIABETICMedicine DAWN2: healthcare professional’s perspective � R. I. G. Holt et al.

Funding sources
The DAWN2 study is funded by Novo Nordisk A/S. Medical
writing and editorial support in the preparation of this
manuscript, which was funded by Novo Nordisk A/S, was
provided by Bioscript Medical Ltd. In collaboration with
national, regional and global partners, including the Inter-
national Diabetes Federation, International Alliance of
Patient Organizations and the international Steno Diabetes
Center, the DAWN2 survey working group, the DAWN2
International Publication Planning Committee (IPPC) and
Harris Interactive, Novo Nordisk has assisted with the
planning and designing of the DAWN2 study. Data collec-
tion was independently performed by Harris Interactive, who
were funded by Novo Nordisk. Data analysis and publica-
tion preparation were performed by members of the
DAWN2 IPPC and authors.
Competing interests
RIGH has received funding for travel and accommodation to
attend DAWN2 IPPC meetings, but has not received any fee
for this work from Novo Nordisk. He has acted as an
advisory board member and speaker for Novo Nordisk, and
as a speaker for Sanofi-Aventis, Eli Lilly, Otsuka and
Bristol-Myers Squibb. He has received grants in support of
investigator trials from Novo Nordisk. AN has received
research grants in the last year from Novo Nordisk, Eli Lilly,
Sanofi-Aventis, Merck Sharp and Dohme, Bristol-Myers
Squibb/Astra Zeneca and Bayer. KKB and AF have been
reimbursed for travel and accommodation expenses from
Novo Nordisk to attend the DAWN2 IPPC meetings, but
have not received any fee for this work from Novo Nordisk.
ME has acted as an advisory board member for Novo
Nordisk, Eli Lilly, Sanofi and Boehringer. He also received
speaking honoraria from Novo Nordisk, Eli Lilly, Bris-
tol-Myers Squibb and BoehringerMexico. NH is a member of
the IPPC of the DAWN2 study and member of the national
German DAWN2 Advisory Board supported by Novo Nor-
disk. He is further a member of the global Diabetes Educator
Advisory Board of Eli Lilly. Research support was obtained
from Eli Lilly, Sanofi-Aventis, Berlin Chemie and DEXCOM.
SK is a member of the IPPC and has been reimbursed for
travel and accommodation expenses from Novo Nordisk to
attend the DAWN2 IPPC meetings, but has not received any
fee for this work from Novo Nordisk. MMB is a non-paid
member of the Board of the NN Italian Barometer Initiative
and of the Steering Committee of the International Diabetes
Federation (IDF) Good Metabolic Control campaign sup-
ported by Sanofi Italy. He has received speaking honoraria
from Sanofi. AM has received funding from Novo Nordisk,
Eli Lilly, Life Scan and Roche Diagnostic for attending
scientific meetings and congresses and received honoraria for
lectures. EM-T is a member of the International DAWN2
Advisory Board. He has received speaking honoraria from
Novo Nordisk, Novartis, Eli Lilly and Sanofi. NM has acted
in an advisory board (Advisory Panel) or teaching capacity
(Speakers Bureau) for Abbott, AstraZeneca/Bristol-Myers
Squibb, Boehringer Ingelheim, Eli Lilly, Novo Nordisk,
Merck Sharp and Dohme and Sanofi in the last 12 months.
SES is an employee of Novo Nordisk A/S, Copenhagen,
Denmark. _IT has received speaking honoraria in the last year
from Novo Nordisk, Bristol-Myers Squibb, Astra Zeneca and
Eli Lilly. JW has acted as an advisory board member for Eli
Lilly, AstraZeneca/Bristol-Myers Squibb and Novo Nordisk.
MP has recently received research grants and/or consulting
fees from Amylin, Genentech, Eli Lilly, MannKind, Med-
tronic, and Novo Nordisk. He has received speaking hono-
raria from Novo Nordisk and has participated in advisory
panels for Novo Nordisk and Roche. He has received
financial support from Novo Nordisk for his participation
as Principal Investigator for the DAWN2 study.
Acknowledgements
The DAWN2 Study Group consists of a national lead
investigator from each country and members of the DAWN2
IPPC: Rachid Malek, Algeria; Johan Wens, Belgium; Jo~ao
Eduardo Salles, Brazil; Katharina Kovacs Burns and Michael
Vallis, Canada; Xiaohui Guo, China; Ingrid Willaing and
Søren Eik Skovlund, Denmark; G�erard Reach, France;
Norbert Hermanns and Bernd Kulzer, Germany; Sanjay
Kalra, India; Antonio Nicolucci and Marco Comaschi, Italy;
Hitoshi Ishii, Japan; Miguel Escalante, Mexico; Frans
Pouwer, the Netherlands; Andrzej Kokoszka, Poland; Alex-
ander Mayorov, Russia; Edelmiro Men�endez Torre, Spain;
Ilhan Tarkun, Turkey; Melanie Davies, Richard Holt, Angus
Forbes and Neil Munro, the UK; Mark Peyrot, the USA.
The authors wish to acknowledge the contribution of the
International Diabetes Federation and the numerous other
international and national experts and patient advocates who
have contributed directly to the design of the DAWN2 study
during 2010–2011. The complete list of study experts and
people with diabetes advisers is available at www.dawn
study.com. Fabio Pellegrini, Giuseppe Lucisano and Basilio
Pintaudi from Consorzio Mario Negri Sud performed the
statistical analyses for this study and prepared the figures
presented in this publication, and Christine Mullan-Jensen
assisted with the design and execution of the study and
provided input to this publication.
All DAWN2 surveys were conducted by Harris Interactive
Inc., an independent research organization. The authors wish
to acknowledge Anna Ginovker of Harris Interactive for
directing the global fieldwork and Bioscript Medical Ltd for
providing assistance with obtaining ethical approvals in
several countries, as well as Tawhid Ahmad and Helen
Swainston of Bioscript Medical Ltd for medical writing and
editorial support. Harris Interactive conducted the surveys,
and provided expertise in designing the questionnaires and
planning survey implementation, including sampling frames
ª 2013 The Authors.Diabetic Medicine ª 2013 Diabetes UK 797
Research article DIABETICMedicine

and strategies, questionnaire administration strategies,
weighting criteria, etc.
References
1 International Diabetes Federation. Diabetes Atlas, 5th Edition.
2012. Available at http://www.idf.org/diabetesatlas/(2012). Last
accessed 22 January 2013.
2 Peyrot M, Rubin RR, Lauritzen T, Snoek FJ, Matthews DR,
Skovlund SE. Psychosocial problems and barriers to improved
diabetes management: results of the Cross-National Diabetes
Attitudes, Wishes and Needs (DAWN) Study. Diabet Med 2005;
22: 1379–1385.
3 Skovlund SE, Peyrot M. The Diabetes Attitudes, Wishes, and Needs
(DAWN) program: a new approach to improving outcomes in
diabetes care. Diabetes Spectr 2005; 18: 136–142.
4 Murphy K, Casey D, Dinneen S, Lawton J, Brown F. Participants’
perceptions of the factors that influence diabetes self-management
following a structured education (DAFNE) programme. J Clin Nurs
2011; 20: 1282–1290.
5 Serrano-Gil M, Jacob S. Engaging and empowering patients to
manage their type 2 diabetes, Part I: a knowledge, attitudes, and
practice gap? Adv Ther 2010; 27: 321–333.
6 Rasekaba TM, Graco M, Risteski C, Jasper A, Berlowitz DJ,
Hawthorne G et al. Impact of a diabetes disease management
program on diabetes control and patient quality of life. Popul
Health Manag 2012; 15: 12–19.
7 American Association of Clinical Endocrinologists (AACE).
Diabetes care plan guidelines. Endocr Pract 2011; 17: 1–53.
8 Conference Report: 2nd International DAWN Summit: a call--
to-action to improve psychosocial care for people with diabetes.
Pract Diabetes Int 2004; 21: 201–208.
9 International Diabetes Federation. Putting people at the centre of
care: DAWN in action. Diabetes Voice 2004; 49: 1–49.
10 Morrison F, Shubina M, Goldberg SI, Turchin A. Performance of
primary care physicians and other providers on key process
measures in the treatment of diabetes. Diabetes Care 2013; 36:
1147–1152.
11 Peyrot M, Kovacs Burns K, Davies M, Forbes A, Hermanns N, Holt
R et al. Diabetes Attitudes Wishes and Needs 2 (DAWN2): a
multinational, multi-stakeholder study of psychosocial issues in
diabetes and person-centred diabetes care. Diabetes Res Clin Pract
2013; 99: 174–184.
12 International Alliance of Patients’ Organizations (IAPO).
Patient-Centred Healthcare Indicators Review. 2012. Available at
http://www.patientsorganizations.org/attach.pl/1438/1332/PCH
Indicators Review.pdf. Last accessed 13 May 2013.
13 Snijders TAB, Bosker RJ. Multi-Level Analysis: An Introduction to
Basic and Advanced Multi-Level Modelling. London: SAGE, 1999.
14 De Berardis G, Pellegrini F, Franciosi M, Belfiglio M, Di Nardo B,
Greenfield S et al. Quality of care and outcomes in type 2 diabetic
patients: a comparison between general practice and diabetes
clinics. Diabetes Care 2004; 27: 398–406.
15 Singer JD, Willett JB. Applied Longitudinal Data Analysis: Mod-
eling Change and Event Occurrence. New York: Oxford University
Press, 2003.
16 Rubin RR, Peyrot M, Siminerio L, on behalf of the International
DAWN Advisory Panel. Health care and patient-reported out-
comes: results of the cross-national Diabetes Attitudes, Wishes, and
Needs study. Diabetes Care 2006; 29: 1249–1255.
17 Peyrot M, Rubin RR, Lauritzen T, Skovlund SE, Snoek FJ,
Matthews DR et al. International DAWN Advisory Panel. Patient
and provider perceptions of care for diabetes: results of the
cross-national DAWN study. Diabetologia 2006; 49: 279–288.
18 Beverly EA, Hultgren BA, Brooks KM, Ritholz MD, Abrahamson
MJ, Weinger K. Understanding physicians’ challenges when treat-
ing type 2 diabetic patients’ social and emotional difficulties: a
qualitative study. Diabetes Care 2011; 34: 1086–1088.
19 Wens J, Vermeire E, Van Royen P, Sabbe B, Denekens J. GPs’
perspectives of type 2 diabetes patients’ adherence to treatment: a
qualitative analysis of barriers and solutions. BMC Fam Pract
2005; 6: 20.
20 RoyT,LloydCE,PouwerF,HoltRI,SartoriusN.Screening toolsused
for measuring depression among people with Type 1 and Type 2
diabetes: a systematic review.DiabetMed 2012; 29: 164–175.
21 Doni�cov�a V, Bro�z J, Sorin I. Health care provision for people with
diabetes and postgraduate training of diabetes specialists in
Eastern European countries. J Diabetes Sci Technol 2011; 5:
1124–1136.
22 MurugesanN,ShobanaR,SnehalathaC,KapurA,RamachandranA.
Immediate impact of a diabetes training programme for primary
care physicians – an endeavour for national capacity building for
diabetes management in India. Diabetes Res Clin Pract 2009; 83:
140–144.
23 Stenner KL, Courtenay M, Carey N. Consultations between nurse
prescribers and patients with diabetes in primary care: a qualitative
study of patient views. Int J Nurs Stud 2011; 48: 37–46.
24 White P, Smith SM, Hevey D, O’Dowd T. Understanding type 2
diabetes: including the family member’s perspective. Diabetes Educ
2009; 5: 810–817.
25 Keogh KM, Smith SM, White P, McGilloway S, Kelly A, Gibney J
et al. Psychological family intervention for poorly controlled type 2
diabetes. Am J Manag Care 2011; 2: 105–113.
26 Graffy J, Grant J, Williams K, Cohn S, Macbay S, Griffin S et al.
More than measurement: practice team experiences of screening for
type 2 diabetes. Fam Pract 2010; 27: 386–394.
27 National Institute for Health and Clinical Excellence (NICE). Public
Health Guidance on Diabetes. 2012. Available at http://www.nice.
org.uk/nicemedia/live/13791/59951/59951.pdf. Last accessed 22 Jan-
uary 2013.
28 Lindstr€om J, Neumann A, Sheppard KE, Gilis-Januszewska A,
Greaves CJ, Handke U et al. Take action to prevent diabetes – the
IMAGE toolkit for the prevention of type 2 diabetes in Europe.
Horm Metab Res 2010; 42 (Suppl 1): S37–55.
29 International Diabetes Federation. Diabetes Atlas, 4th Edition.
2009. Available at http://archive.diabetesatlas.org/content/
monitoring-global-quality-care. Last accessed 19 April 2013.
Supporting Information
Additional Supporting Information may be found in the
online version of this article:
Figure S1. Proportion of healthcare professionals reporting
that ‘about half’ to ‘most/all’ of their patients require a
significant improvement in taking responsibility for manag-
ing their own condition.
Figure S2. Proportion of healthcare professionals reporting
that a major improvement is needed in making self-manage-
ment education available to people with diabetes.
Figure S3. Proportion of healthcare professionals indicating
that more qualified nurse-educators or specialist diabetes
nurses should be available.
Table S1. DAWN2 HCP Questionnaire Measures.
Table S2. The views and perceptions of healthcare profes-
sionals on matters relating to diabetes care.
798ª 2013 The Authors.
Diabetic Medicine ª 2013 Diabetes UK
DIABETICMedicine DAWN2: healthcare professional’s perspective � R. I. G. Holt et al.





![[Innovative]Teacher Day Wishes, Message, SMS, Quotes, Whats App Status {Hindi, English}](https://static.fdokumen.com/doc/165x107/6342895a3130fea02d0c04ad/innovativeteacher-day-wishes-message-sms-quotes-whats-app-status-hindi-english.jpg)