
DEVELOPMENT AND EVALUATION OF A PERSONALIZED ...
151
DEVELOPMENT AND EVALUATION OF A PERSONALIZED MUSIC INTERVENTION FOR DEMENTIA EVAN G. SHELTON Master of Arts in Psychology of Adult Development and Aging Cleveland State University May 2014 submitted in partial fulfillment of requirements for the degree of DOCTOR OF PHILOSOPHY at the CLEVELAND STATE UNIVERSITY DECEMBER 2018
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of DEVELOPMENT AND EVALUATION OF A PERSONALIZED ...

DEVELOPMENT AND EVALUATION OF A PERSONALIZED MUSIC
INTERVENTION FOR DEMENTIA
EVAN G. SHELTON
Master of Arts in Psychology of Adult Development and Aging
Cleveland State University
May 2014
submitted in partial fulfillment of requirements for the degree of
DOCTOR OF PHILOSOPHY
at the
CLEVELAND STATE UNIVERSITY
DECEMBER 2018

We hereby approve this dissertation
For
Evan G. Shelton
Candidate for the Doctor of Philosophy degree.
for the Department of Psychology
And
CLEVELAND STATE UNIVERSITY
College of Graduate Studies by
_____________________________________ Katherine Judge, PhD, Dissertation Committee Chairperson
________________________________________________________
Department & Date
_____________________________________ Eric Allard, PhD, Dissertation Committee Member
________________________________________________________
Department & Date
_____________________________________ Toni Bisconti, PhD, Dissertation Committee Member
________________________________________________________
Department & Date
_____________________________________ Linda Francis, PhD, Dissertation Committee Member
________________________________________________________
Department & Date
_____________________________________ Harvey Sterns, PhD, Dissertation Committee Member
________________________________________________________
Department & Date
November 26, 2018
Student’s Date of Defense

ii
DEVELOPMENT AND EVALUATION OF A PERSONALIZED MUSIC
INTERVENTION FOR DEMENTIA
EVAN G. SHELTON
ABSTRACT
The use of personalized music as an intervention tool for dementia is garnering attention
in both research and practice. Personalized music aims to capitalize on the relatively
well-preserved pathways linking familiar music to memory. The use of personalized
music to engage persons with dementia (PWDs) represents a low-cost non-
pharmacological approach to improving well-being. Reductions in agitation and other
dementia-related behaviors often viewed as problematic have been reported in existing
personalized music interventions, and personalized music therapy poses little risk of side
effects in comparison to pharmacological interventions for dementia. There is currently a
scarcity of evidence in the academic literature detailing the dissemination of a music
therapy intervention to persons with dementia and family caregivers living in the
community. Moreover, few studies have examined the benefits of personalized music on
broad psychosocial constructs such as quality of life, mood, and relationship quality
between the CG and PWD.
This pilot study consisted of the development, implementation, and evaluation of
a personalized music intervention for PWDs living in the community. A randomized-
controlled trial with a two group (personalized music vs. unfamiliar music) pre-test and
post-test design was used to evaluate intervention efficacy. A one-month randomized-
controlled trial was conducted examining the effects of personalized music listening
relative to unfamiliar music listening on the PWD’s affect, anxiety, quality of life,

iii
behavioral expressions of dementia, and relationship strain between the PWD and an
informal CG. Results indicated that PWDs in the personalized music listening group
demonstrated significant reductions in anxiety (t(25) = -2.15, p = .04) and relationship
strain (t(25) = -2.61, p = .02) relative to PWDs in the unfamiliar music listening group.
Implications, acceptability/feasibility, limitations, and future directions are discussed.

iv
TABLE OF CONTENTS
ABSTRACT………………………………………………………………………. ii
CHAPTER
I. INTRODUCTION……………………………………………………... 1
1.1.Dementia Background................................................................ 2
1.2 The Illness Experience………………………………………... 5
1.2.1 Affect…………………………………………….. 7
1.2.2 Behavioral Expressions…………………………… 9
1.2.3 Anxiety…………………………………………….. 11
1.2.4 Quality of Life…………………………………….. 12
1.2.5 Relationship Strain………………………………… 14
1.3 Meeting the Demands of Dementia…………………………… 16
1.3.1 Pharmacological Approaches to Intervention for
PWDs………………………………………………. 16
1.3.2 Non-Pharmacological Approaches to Intervention for
PWDs………………………………………………. 18
1.4 Music and Memory…..……………………………………….. 20
1.4.1 The Neural Link Between Music and Memory……. 20
1.4.2 Familiar vs. Unfamiliar Music…………………….. 22
1.4.3 Music Intervention Impact on PWDs………...……. 23
1.4.4 Music Intervention and the Dyadic Relationship…...27
1.4.5 Cognitive Stimulation Therapy…………………….. 30

v
1.4.6 Personalized Music as a Humanistic Mode of
Intervention………………………………………… 32
1.5 Hypotheses…….……………………………………………… 35
II. METHODS……….………………….………………………………… 37
2.1 Study Design…………………………………………………. 37
2.2 Measures……………………………………………………… 37
2.2.1 Demographic Information…………………………. 38
2.2.2 Mini-Mental State Examination……………………. 38
2.2.3 Diary Based Fidelity Assessment………………….. 39
2.2.4 Outcome Measures………………………………… 39
2.3 Inclusion Criteria……………………………………………… 44
2.4 Participant Recruitment………………………………………. 45
2.4.1 Sample Size………………………………………… 46
2.5 Participant Characteristics….…………………………………. 47
2.6 Benjamin Rose Institute on Aging……………………………. 49
2.7 Procedure……………………………………………………… 50
2.7.1 Screening Phone Call………………………………. 50
2.7.2 In-Person Baseline Meeting……………………….. 51
2.7.3 In-Person 1-Month Follow-Up…………………….. 55
III. RESULTS…………………………………………………………….. 57
3.1 Statistical Analyses and Data Treatment…………………….. 57
3.2 Efficacy Testing………………………………………………. 60
3.2.1 Mood………………………………………………. 61

vi
3.2.2 Anxiety…………………………………………… 62
3.2.3 Behavioral Expressions of Dementia…………….. 63
3.2.4 Relationship Strain……………………………….. 64
3.2.5 Quality of Life……………………………………. 67
3.3 Acceptability and Feasibility………………………………… 67
IV. DISCUSSION………………………………………………………… 69
4.1 Efficacy………………………………………………………. 69
4.2 Acceptability and Feasibility…………………………………. 73
4.3 Clinical Implications…………………………………………. 77
4.4 Limitations……………………………………………………. 78
4.5 Future Directions for Research……………………………….. 81
REFERENCES…………………………………………………………………….. 86
APPENDICES…………………………………………………………………….. 116
A. Demographic information…………………………………………….. 117
B. Mini-Mental State Examination………………………………………. 118
C. The Assessment of Personalized Music Preference (patient version)… 122
D. The Assessment of Personalized Music Preference (family version)… 124
E. Diary-Based Fidelity Assessment Form (weeks 1-3)…………………. 126
F. Diary-Based Fidelity Assessment Form (week 4)........……………….. 127
G. Dementia Quality of Life Instrument – Positive Affect and Negative Affect
Subscales………………………………………………………………. 129
H. Quality of Life in Alzheimer’s Disease………………………………. 130
I. Zung Self-Rating Anxiety Scale………………………………………. 132

vii
J. Cohen-Mansfield Agitation Inventory – Short Form………………….. 133
K. Dyadic Relationship Strain ……………………………………………. 135
L. Telephone Screener…………………………………………………….. 136
M. Personalized Music Assessment……………………………………….. 140
N. Control Group Playlist…………………………………………………. 141
O. CONSORT Diagram…………………………………………………… 142
P. Commonly Selected Genres and Preferred Artists of Personalized Music
Group Participants…………………………………………………….. 143

1
CHAPTER I
INTRODUCTION
“Personalized music” refers to music that is meaningful and familiar to an
individual. The songs that a person learns over the course of his/her life are tied heavily
to the autobiographical memories associated with those songs, and the emotions that
accompany those memories (Baumgartner, 1992; Jäncke, 2008). If, for example, a
person hears the song they danced to at their wedding, or the rock and roll anthem of their
teen years, the memories of those events and the emotions that accompany them are often
recalled. Thus, familiar music can serve as a cue to the retrieval of the long-term
memories and positive emotions (Haj, Fasotti, & Allain, 2012). The ability to integrate
familiar musical stimuli with autobiographical memories and emotions is a well-
preserved aspect of cognition, even in individuals in the later stages of dementia
(Gerdner, 1997). Thus, the well-preserved connection between personalized music,
memory, and emotion has led to a surge in attention toward the use of personalized music
as a therapeutic tool for improving the lives of persons with dementia (PWDs). This
study aimed to accomplish the following: (1) to provide an in-depth overview of the
literature on the use of personalized music and dementia, (2) to identify important gaps in
the personalized music literature, and (3) to develop, implement, and assess the efficacy

2
of a personalized music intervention using a randomized-controlled trial in a community-
dwelling population of PWDs.
1.1. Dementia Background
Personalized music interventions for dementia attempt to circumvent the memory
deficits of PWDs in order to improve upon psychosocial well-being, or reduce psychical
and behavioral difficulties associated with the dementing illness. To begin this
discussion, it is important to have a general understanding of dementia and its impact on
the lives of those it affects.
Dementia is not a disease in itself. Rather, “dementia” is an umbrella term that
includes a group of conditions which lead to a global decline in memory and cognitive
ability. The most common form of dementia is Alzheimer’s disease, which accounts for
between 60% and 80% of dementia cases in the United States (Alzheimer’s Association,
2018). Other forms of dementia include vascular dementia, Frontotemporal dementia,
dementia with Lewy-bodies, dementia resulting from Parkinson’s disease, and prion
diseases such as Creutzfeldt-Jakob disease.
These varying etiologies lead to similar but distinct sets of symptoms, including
cognitive decline, memory loss, decline in physical ability and decline in the ability to
accomplish activities of daily living. Alzheimer’s disease and related dementias are often
associated with behavioral changes that are perceived by the caregiver (CG), friends, and
family to be inappropriate and out of character (Fauth & Gibbons, 2014, Finkel, 2000).
These behaviors might include wandering (Cipriani, Lucetti, Nuti, & Danti, 2014),
aggression/agitation (Cohen-Mansfield, 1997; Cohen-Mansfield, Marx, & Werner, 1992),

3
inappropriate sexual behaviors (Mendez & Shapira, 2013), and repetitive question asking
(Bourgoeis, 2002; Hwang, et al., 2000), for example. Among these types of behaviors,
apathy, depression, and agitation are among the most common, with behaviors such as
irritability, agitation, and delusions causing the greatest distress for CGs (Fauth &
Gibbons, 2014; Cohen-Mansfield, 2008). The Stress-Process Model posits that these
behaviors are primary stressors for CGs, which negatively impact the CG’s role strain,
intrapsychic strain, and psychosocial well-being outcomes (Pearlin, Mullan, Semple, &
Skaff, 1990). In line with this model, evidence from the literature suggests that CGs
providing care to PWDs who exhibit these types of behaviors are at a greater risk of
experiencing caregiver burden as well as depression (Ballard, Lowery, Powell, O’Brien,
& James, 2000). Further research applying the Stress-Process Model to PWDs suggests
that behavior problems may negatively impact PWDs in a similar way, including greater
role and intrapsychic strain, as well as increased depression and anxiety, and lower
physiological well-being and quality of life (Judge, Menne, & Whitlatch, 2010).
As dementia progresses, PWDs are more likely to have cognitive difficulties
related to executive function (Swanberg, Tractenberg, Mohs, Thal, & Cummings, 2004),
planning and problem solving (Allain et al., 2007; Piquard, Derouesné, Lacomblez, &
Siéroff, 2004), and orientation to time and place (Pai & Jacobs, 2004). The social well-
being of PWDs is often negatively impacted by increasing language difficulty and
embarrassment about memory problems (Ostwald, Duggleby, & Hepburn, 2002). This
often leads PWDs to withdraw from work and social activities (Ryan, Bannister, & Anas,
2009; Aminzadeh, Byszewski, Molnar, & Eisner, 2007). PWDs are also more likely to

4
experience changes in mood, increased depression, agitation, anxiety, and disturbances in
sleep (Alzheimer’s Association, 2018).
Although Alzheimer’s disease is not considered a part of normal aging, advancing
age is the greatest risk factor for Alzheimer’s (Thies & Bleiler, 2012). In 2018, the
number of individuals aged 65 and older with Alzheimer’s disease and other related
dementias in the United States is estimated at 5.7 million, and this number is projected to
grow to 8.4 million in 2030 and 13.8 million in 2050 (Alzheimer’s Association, 2018).
This drastic increase is projected to come as a result of a growing number of adults aged
65 and over as the baby boom generation enters later life. This “graying of the
population” has tremendous implications not only for those individuals who will develop
a dementing illness, but also for the healthcare systems and CGs who must meet the
challenge of providing quality care to PWDs. In the US, 83% of all older adults needing
care are cared for by an informal CG at home (Friedman, Shih, Langa, & Hurd, 2015).
Earlier estimates of PWD care place the proportion of PWDs cared for by a family or
friend at home between 65% and 75% (Aneshensel, Pearlin, Mullan, Zarit, & Whitlatch,
1995). In 2017, it was estimated that more than 16 million informal CGs provided
approximately 18.4 billion hours of unpaid care (Alzheimer’s Association, 2018). The
financial burden of caring for a PWD is not only represented in unpaid hours spent
providing care, but also in the cost of healthcare and, when it becomes necessary, long-
term care and hospice. The Alzheimer’s Association (2018) estimates that $277 billion
will be spent on these types of services for PWDs in 2018, with $60 billion of this cost
spent out-of-pocket.

5
1.2. The Illness Experience
Alzheimer’s disease remains a highly stigmatized condition due to its negative
impact on cognitive functioning and its association with loss of independence (Harman &
Clare, 2006). The negative impact of Alzheimer’s disease and related dementias on
social well-being has been linked to changes in self-identity (Clare, 2003). Moreover,
Clare (2003) suggested that the way PWDs perceive their illness (i.e., their “illness
representation”) has an impact on the PWD’s ability to cope with and adjust to the illness.
The subjective nature of the experiences of dementia translate into meaningful
information that cannot be obtained with confidence using observational measures or
proxy report data. Regarding the experience of dementia and quality of life, Testa and
Simonson (1996) state, "the patients' subjective perceptions and expectations translate
that objective assessment into the actual quality of life experienced."
Although CGs may have an accurate understanding of the feelings of the PWD,
the illness representations, coping, and the PWD’s illness experience in general are best
understood by the PWD. The use of self-report methodology to understand the illness
experience of PWDs, for example, indicates that embarrassment about memory loss is a
strong predictor of anxiety while depressive symptomology is better predicted by
physical health strain and role captivity (Dawson, Powers, Krestar, Yarry, & Judge,
2013). Although studies have long used CG proxy reports to obtain information about
the PWD, literature suggests that this proxy report data is often inaccurate. For example,
CG proxy reporters tend to have limited knowledge about the PWD’s care-related
preferences (Hawkins, Ditto, Danks, & Smucker, 2005), especially in the later stages of
the disease (Carpenter, Kissel, & Lee, 2007). Similarly, CG proxy reports often under-

6
estimate the importance of the PWD’s care values compared to self-report data from the
PWD (Reamy, Kim, Zarit, & Whitlatch, 2011; Reamy, Kim, Zarit, & Whitlatch, 2013).
In the development of the Dementia Quality of Life Assessment (DQoL; Brod, Stewart,
Sands, & Walton, 1999), the authors emphasize that self-report data from the perspective
of the PWD is the “gold standard” for assessing quality of life. Indeed, a recent study has
found that discrepancies do exist in proxy versus PWD reports of quality of life (Gomez-
Gallego, Gomez-Garcia, & Ato-Lozano, 2015). In a study of proxy and PWD reports of
anxiety, results showed that both self-report and proxy reports were accurate in predicting
clinically significant levels of anxiety, though proxy respondents tended to rate symptoms
as being more extreme that the PWDs (Bradford et al., 2013).
In general, the use of self-report data from PWDs is becoming more widely
advocated in the literature as a means of avoiding overestimation and underestimation
biases that exist in the use of proxy-report methodology for PWDs (Dawson et al., 2013;
Snow et al., 2005). Given that discrepancies are common between proxy report and self-
report data, the present study used PWD self-report methodology to assess the PWD’s
experience of anxiety, relationship strain, quality of life, and mood. Behavioral
expressions of dementia, in contrast, were measured using CG report. This study used
the Cohen-Mansfield Agitation Inventory-Short Form (Werner, Cohen-Mansfield,
Koroknay, & Braun, 1994), which has been used and validated for CGs. It is important
to note that the assessment of behavioral expressions of dementia from the CG’s
perspective does not require the CG to make judgments on behalf of the PWD. That is,
CGs are not asked to provide insights about the illness experience on behalf of the PWD.
Thus, the CG responses used in this study are not considered proxy-style responses.

7
Instead, this outcome, as it is used in this study, will represent the change in the CG’s
perception of behavioral expressions from baseline to post-test.
The use of self-report methodology for PWDs has been well-supported by the
literature as a valid and reliable means of obtaining data from persons with early to
moderate stage dementia (Moyle, Murfield, Griffiths, & Venturato, 2012; Brod, Stewart,
Sands, & Walton, 1999; Clark, Tucke, & Whitlatch, 2008; Whitlatch, Feinberg, & Tucke,
2005; Krestar, Looman, Powers, Dawson, & Judge, 2012). Moreover, the measures
chosen for this study have been developed and validated for use in populations with
dementia. Details about each measure are discussed fully in Chapter II.
This study sought to understand the impact of a personalized music intervention
on the above mentioned domains of psychosocial well-being: affect (overall mood),
anxiety, quality of life, and relationship strain, as well as behavioral expressions of
dementia. These domains were selected based on evidence from intervention research in
dementia as well as from our understanding of the psychosocial impact of dementia on
the PWD (discussed at length in the following sections of this Chapter). Each of the
following subsections details the psychosocial impact of dementia within the domains of
affect, behavioral expressions, anxiety, quality of life, and relationship strain. The
purpose of these sections is to call attention to the prevalence and importance of these
experiences from the perspective of the PWD, and to underscore the benefits of reducing
the negative psychosocial impact of dementia through targeted interventions such as the
personalized music intervention reported here.
1.2.1. Affect
8
Negative affect, mood, and mood disorders such as depression are common in
dementia (Zahodne, Ornstein, Cosentino, Devanand, & Stern, 2015). In the early stages,
and especially after receiving a dementia diagnosis, negative reactions such as fear,
anger, frustration, feelings of uncertainty, depression and embarrassment are common
(Cotrell & Schulz, 1993; Bamford & Bruce, 2000; Aminzadeh, et al., 2007). Worries
about the future and about memory function contribute to negative affect, as well
concerns including the loss of independence/autonomy, communication difficulty and
loss of control (De Boer et al., 2007). Harman and Clare (2006) found that individuals in
the early stages of dementia tended to have a concrete understanding of the fact that
dementia is a progressive illness with no medical cure. Anosognosia, or the lack of
awareness about one’s own condition, is more common in the middle and later stages of
dementia and has been negatively correlated with depressive symptomology (Mograbi &
Morris, 2013). In a study comparing affect across individuals with Alzheimer’s disease,
mild cognitive impairment, and healthy older adults, persons with Alzheimer’s disease
reported more negative emotions and confusion than the other groups (Ready, Carvalho,
Green, Gavett, & Stern, 2011).
In persons experiencing greater degrees of memory loss, positive and negative
mood resulting from emotional stimuli may persist well past the time that the stimulus is
forgotten (Feinstein, Duff, & Tranel, 2010). Two separate studies including participants
with amnesia (Feinstein et al., 2010) and individuals with probable Alzheimer’s disease
(Guzmán-Vélez, Feinstein, & Tranel, 2014) found that emotional responses to sad and
happy stimuli remained even after participants had forgotten the stimuli. These findings
have two important implications to consider if, in fact, personalized music listening does

9
have a positive impact on mood. First, experiences that are distressing for PWDs such as
confusion related to a situation or environment can have negative lasting effects on mood
even after the initial experience is forgotten. Second, the influence of positive emotional
experiences on mood, such as those associated with enjoyable music, may have lasting
effects, even after the actual stimulus is gone and forgotten. If sustained improvements in
mood can be achieved through personalized music listening, CGs may see further
benefits in ease of providing care with care tasks—even after the music has stopped. The
provision of help with personal activities of daily living such as bathing, toileting, and
eating, which may be uncomfortable for both the CG and the PWD, could benefit
substantially from improved mood of the PWD.
1.2.2. Behavioral Expressions
As dementia progresses, behaviors such as wandering, pacing, verbal agitation,
aggression, and repetitious mannerisms, become more likely (Lyketsos et al., 2002; Fauth
& Gibbons, 2014). These behaviors have been referred to as problem behaviors,
disruptive behaviors, disturbing behaviors, agitation (Cohen-Mansfield, 2001), and
behavioral expressions. For the purposes of this paper, the term “behavioral expressions”
will be used. This term has been most recently advocated in the literature as an
alternative to other terms which may imply that behaviors are a direct result of a
dementing illness (“symptoms”), or that the root problem leading to such behaviors lies
with the PWD rather than the environment or the provision of care, for example (Caspi,
2013).
The behavioral expressions associated with dementia often increase the suffering
of the PWD (Ballard, Day, Sharp, Wing, & Sorensen, 2008; Gilley, Whalen, Wilson, &

10
Bennett, 1991) and increase CG burden (van der Lee, Bakker, Duivenvoorden, & Dröes,
2014; Cohen-Mansfield, 2001). Moreover, PWDs who exhibit behaviors perceived to be
problematic by a CG are more likely to be institutionalized (Afram et al., 2014). While
not completely understood, research indicates that behavioral expressions of dementia
may stem from a combination of factors, including brain changes, pain, physical disease,
and an attempt to communicate unmet needs (Husebo, Ballard, & Aarsland, 2011;
Cohen-Mansfield & Werner, 1995). Several models exist to explain the nature of
problematic behaviors, but the perhaps the most supported model is the Unmet Needs
Model (Cohen-Mansfield, 2000; Cohen-Mansfield, Dakheel-Ali, Marx, Thein, & Regier,
2015; Cohen-Mansfield & Werner, 1995). This theory states that the needs of PWDs are
likely to go unmet as communication becomes more difficult and the ability to provide
for oneself diminishes. A variety of factors contribute to the development of behavioral
expressions, including personality (especially neuroticism and pre-morbid aggression;
Osborne, Simpson, & Stokes, 2010), environment, as well as physical and mental states
(Cohen-Mansfield et al., 2015). The Unmet Needs Hypothesis posits that behavioral
expressions are a way of attempting to fulfill needs, attempting to communicate, or an
outcome of frustration or negative affect combined with decreased inhibition (Cohen-
Mansfield, Dakheel-Ali, & Marx, 2009; Cohen-Mansfield et al., 2015). Personalized
music may facilitate improvement within several of these domains. Connecting with a
CG through music, for example, may improve communication between care partners.
Positive affect, as discussed in the previous section, may further translate into reduced
behavioral expressions, and frustration stemming from confusing and/or unfamiliar
stimuli might be circumvented by providing a stimulus that is familiar and enjoyable.

11
1.2.3. Anxiety
Anxiety is common across several different types of dementia, including
frontotemporal dementia, vascular dementia, and Alzheimer’s disease (Porter et al.,
2003). In Alzheimer’s disease, anxiety has been linked to individuals with greater levels
of cognitive impairment (Porter et al., 2003), with anxiety symptoms present in as many
as 70% of PWDs (Teri et al., 1998), though clinically significant anxiety is only prevalent
in about 7% of PWDs (Ferretti, McCurry, Logsdon, Gibbons, & Teri, 2001). Given the
high prevalence, anxiety symptomology is a major concern for research and practice in
dementia. Anxiety has been linked to reduced quality of life, reduced ADL ability,
increased behavioral expressions of dementia, and greater likelihood for nursing home
placement (Seignourel, Kunik, Snow, Wilson, & Stanley, 2008). The relationship
between anxiety and cognitive impairment is somewhat nuanced, with some studies
finding that higher levels of impairment are actually less likely to be associated with
anxiety (Kaiser et al., 2014). One explanation for these findings may be that anxiety is
greatest in the moderate stages of dementia when memory problems are present and
particularly troublesome compared to the early stages when symptoms are less noticeable
and the late stages when PWDs may be less aware of their memory deficits. Thus, it is
possible that PWDs in the middle stages of dementia may be able to derive the most
benefit from the use of personalized music in terms of anxiety reduction.
Findings from a small preliminary study suggest that the correlates of anxiety in
dementia may be different for those who develop early-onset Alzheimer’s disease
compared to late-onset Alzheimer’s disease. Those with early-onset Alzheimer’s disease
are more likely to present with anxiety symptomology if they are separated from their CG

12
and if they are male, while anxiety in late-onset Alzheimer’s disease is associated more
strongly with behavioral expressions of dementia (Kaiser et al., 2014). In both of these
demographics, however, the experience of anxiety in dementia is consistent with
Gerdner’s “Mid-Range Theory” of personalized music in dementia. This theory posits
that individuals with cognitive impairment may have more trouble and become more
confused when interpreting external stimuli from their environment, leading to anxiety
(Gerdner, 1997; more on this theory in the later sections of this Chapter). Indeed,
behavioral expressions of dementia and decreased ability to accomplish activities of daily
living have been identified as significant predictors of anxiety symptoms among PWDs
(Teri et al., 1998).
1.2.4. Quality of Life
Dementia poses a substantial obstacle to quality of life for PWDs. A long-
standing model in gerontology from Rowe & Kahn (1997) conceptualized successful
aging as (1) the avoidance of disability, (2) the maintenance of physical functioning, and
(3) engagement with life. Considering the life course of PWDs, the ominous trajectory of
dementia poses a substantial threat to each of these criteria. So, how can PWDs find
satisfaction and high quality of life in spite of these potential declines? Based on the
symptom profile of a PWD, it seems reasonable to turn to measures of cognitive
impairment and memory ability as indicators of quality of life. However, though
dementia is defined by general cognitive decline and memory impairment, objective
measures in such domains have provided little insight into the well-being of the PWD
(Logsdon, Gibbons, McCurry, & Teri, 2002; Banjeree et al., 2006).

13
There are several conceptualizations of quality of life in dementia, with most
including factors related to affect, self-esteem, appraisal of physical function, social
functioning, the environment, and health (for an overview, see Ettema et al., 2005). More
recently, O’Rourke, Duggleby, Fraser, & Jerke (2015) further conceptualized quality of
life as including: relationships with others, agency in life today (i.e., purposefulness), the
PWD’s wellness perspective, and sense of place. Indeed, findings from the qualitative
literature indicate that the social aspects of dementia and an individual’s coping abilities
are better predictors of quality of life than cognitive impairment. Maintaining autonomy
over the disease course and contributing to others and the community in a positive and
meaningful way have been identified as some of the most important factors influencing a
positive quality of life for PWDs (Moyle et al., 2011; Everard, Lach, Fisher, & Baum,
2000).
At a functional level, declines in physical and cognitive ability threaten autonomy
by making activities of daily living (ADLs) more difficult. ADLs include a wide range of
personal (PADLs) and instrumental (IADLs) activities such as dressing, ambulating,
bathing, toileting, etc. for the former, and banking, shopping, cooking, doing laundry, etc.
for the latter. ADLs tend to decline differentially over the course of the illness, with
greater levels of ADL impairment present in populations with greater cognitive
impairment (Giebel, Sutcliffe, & Challis, 2015; Giebel et al., 2014). Giebel and
colleagues (2015) reported that difficulty with PADLs such as toileting, continence, and
feeding were significant predictors of quality of life for PWDs.
Among the various factors encompassing our understanding on quality of life in
dementia, personalized music may have a positive impact on quality of life through its

14
impact on affect, social functioning, and the environment. Cognitive and physical
impairment may interfere with the PWD’s ability to derive quality of life from the same
activities and experiences that they did before their illness. One possibility of using
personalized music for PWDs is that music listening will create new opportunities and
experiences from which the PWD can derive quality of life.
1.2.5. Relationship Strain
Improving the relationship between the PWD and the CG is an especially
important goal for non-pharmacological interventions in dementia given the tremendous
impact of social and relationship factors on the well-being of both the PWD and the CG.
Based on research linking high affective similarity in marital pairs (Bookwala & Schulz,
1996; Tower & Kasl, 1996), Schulz and Martire (2004) hypothesized that negative affect
experienced by either the CG or the PWD may have an adverse impact on the other care
partner. Thus, negative affect experienced by either care partner may adversely impact
the CG/PWD relationship as a whole.
The responsibility for providing care to a PWD typically falls on a family member
or friend who has not received formal training on how best to provide care (Schulz &
Martire, 2004; Brodaty & Donkin, 2009). Thus, CGs are at risk of experiencing strain
and stress from their increased workload and unfamiliar roles. PWDs also experience
role change, increased dependency, and the experience of the illness itself that threaten
the quality of the relationship with the CG. The progression of dementia and the role
acquisition of the CG and the PWD into a care-giver and care-receiver, respectively,
marks a drastic change in the familial or friend relationship. Informal CGs are typically
spouses, adult children, or children-in-law of the PWD (Pinquart & Sorensen, 2011)

15
whose role with respect to the PWD has traditionally been either a recipient of care
(parent-child) or a partner (spouse). Becoming a provider of care for the PWD requires
significant adjustment with respect to role change, with CGs often feeling trapped in their
new role (Brodaty & Donkin, 2009). Indeed, research suggests that CGs who are very
close to the PWD experience significantly higher levels of caregiver burden than CGs
who are not as close (Cantor, 1983). Spouses are typically the first to assume the CG role
if they are able to do so (Brody, 1981; Pinquart & Sorenson, 2011). Spousal CGs tend to
experience greater levels of caregiver burden than adult children or children–in-law,
including greater financial burden, physical burden, and relationship strain (Pinquart &
Sorensen, 2011), but are also less likely to place the PWD in a nursing home than an
adult child CG (Montgomery & Kosloski, 1994). Moreover, lower levels of marital
intimacy before and after the onset of dementia is predictive of higher levels of spousal
CG depression and strain (Morris, Morris, & Britton, 1988).
Family and friends—those individuals who are most likely to provide informal
care—typically represent a key source of social support and quality of life for PWDs
(Moyle et al, 2011). This further emphasizes the importance of a strong relationship
between the PWD and the CG. For PWDs, the maintenance of emotional social support
in late life has beneficial effects in a wide array of domains, including cardiovascular
function, endocrine function, immune function, and even mortality (Everard et al., 2000;
Uchino, Cacioppo, & Kiecolt-Glaser, 1996; Berkman & Syme, 1979). Social support
also serves as a strong predictor of life satisfaction, whereas social isolation and marital
status (being unmarried) is associated with lower life satisfaction (Eshkoor, Hamid,

16
Nudin, & Mun, 2014). Thus, improvement within the CG/PWD relationship may lead to
further improvement in broader domains of well-being.
1.3. Meeting the Demands of Dementia
Given the extraordinary prevalence and impact of dementia on those who will
develop a dementing illness, the individuals who will provide care for PWDs, and on the
health care system, efficacious treatments for dementia are in high demand. Approaches
to treating dementia typically fall within one of two categories: pharmacological
treatments and non-pharmacological treatments. While personalized music interventions
for dementia fall soundly within the non-pharmacological realm of treatment, it is
important to highlight the efficacy (or lack thereof) of pharmacology as a means of
addressing the problems associated with dementia in order to emphasize the important
role and therapeutic potential of non-pharmacology.
1.3.1 Pharmacological Approaches to Intervention for PWDs
Despite a tremendous medical effort over the past three decades to develop a cure
for Alzheimer’s disease and related dementias, no current pharmacological approaches to
treating dementia have been found to be curative. A meta-analysis of randomized,
controlled drug trials of several cholinesterase inhibitors (donepezil, galantamine,
rivastigmine, and tacrine) which were FDA-approved for treating dementia found
statistically significant but clinically marginal improvements in cognition and global
dementia assessment (Raina et al., 2008). Another recent meta-analysis (Matsunage,
Kishi, & Iwata, 2015) examining the efficacy of combination therapy using a
cholinesterase inhibitor and memantine, an NDMA receptor antagonist, resulted in

17
statistically significant improvements for individuals with moderate to advanced
dementia on some cognitive measures (Severe Impairment Battery [SIB; Panisset et al.,
1994]), but no improvements were found on other measures (Alzheimer’s Disease
Assessment Scale cognitive subscale [ADAS-cog; Rosen, Mohs, & Davis, 1984]; Mini-
Mental State Examination [MMSE; Folstein, Folstein, & McHugh, 1975]). While such
pharmacological treatments are arguably beneficially for PWDs, the currently available
medications only address the cognitive symptoms of dementia and do not alter the course
of the disease (Yiannopoulou & Papageorgiou, 2013). Recently developed medications
aimed at modifying the disease course have not been efficacious, though several
pharmacological treatments are currently undergoing clinical trials (Yiannopoulou &
Papageorgiou, 2013; Imbimbo & Giardina, 2011).
Pharmacological treatments aimed at addressing the behavioral expressions
associated with dementia are also common. The most frequently used medications for
PWDs include antipsychotics, antidepressants, and benzodiazepines (Seitz, et al., 2013),
though the most commonly used pharmacological treatments of problematic behavioral
expressions for PWDs are antipsychotics (Seitz, et al., 2013). The safety of using
antipsychotics for PWDs is a point of contention among many, with some studies
indicating that the most highly utilized antipsychotics increase risk of death (Huybrechts,
et al., 2012; Schneider, Dagerman, & Insel, 2005; Wang et al., 2005; Gill et al., 2007),
stroke (Herrmann, Mamdani, & Lanctot, 2004; Gill et al., 2005), and falls (Hien Le et al.,
2005), among other potentially dangerous adverse events (Seitz et al., 2012). Further, the
logistics of administering medications and maintaining medication adherence for PWDs
poses a challenge, particularly for PWDs living in the community (Arlt, Lindner, Rösler,

18
& von Renteln-Kruse, 2008). Researchers focusing on the use of antipsychotics for
treating the behavioral expressions associated with dementia consistently advocate the
use of non-pharmacological strategies for addressing behaviors before resorting to the use
of antipsychotics (Sink, Holden & Yaffe, 2005; Seitz et al., 2012). However, a major
barrier to the use of non-pharmacological approaches—and consequently the over-
administration of antipsychotic medications—is a relatively low understanding of and/or
unwillingness to implement non-pharmacological strategies of dementia care (Cohen-
Mansfield & Jensen, 2008). Since behavioral expressions may represent an underlying
problem (e.g., pain, interpersonal strain, environmental problems), it is important to rule
out such possibilities before resorting to the use of antipsychotics (Cohen-Mansfield &
Mintzer, 2005; Sink et al., 2005; Seitz et al., 2012). The widespread use of antipsychotics
in managing behavioral expressions of PWDs has garnered sharp criticism and opposition
from some, who maintain that behavioral expressions are attempts at communication
which can be addressed through rational non-pharmacological strategies. Perhaps the
most forward argument against the use of such medications comes from a humanistic
perspective of care:
“The medicalization of dementia has created a self-fulfilling prophecy, in which
persons with dementia are assigned a “sick person role,” are treated as children,
and then are medicated when they “act out” in rebellion to this treatment.” (Camp,
2017).
1.3.2. Non-Pharmacological Approaches to Intervention for PWDs

19
Non-pharmacological approaches to treating dementia are extremely varied in
scope and intention. The focus of these interventions and models ranges from policy-
level reforms of the healthcare system (Maslow, Fazio, Ortigara, Kuhn, & Zeisel, 2013;
Maslow, 2103) to support and skills training for CGs (Nichols, Martindale-Adams,
Burns, Graney, & Zuber, 2011; Judge, Yarry, & Orsulic-Jeras, 2010), cognitive
rehabilitation for PWDs (Bahar-Fuchs, Clare & Woods, 2013; Aguirre, Woods, Spector,
& Orrell, 2013; Clare & Woods, 2004), management of problematic behaviors (Solai,
Schultz, & Kunik, 2015; Livingston et al., 2014; Cohen-Mansfield, 2015; Ayalon, Gum,
Feliciano, & Areán, 2006), and training for staff in professional care settings (Spector,
Orrell, & Goyder, 2013; Noguchi, Kawano, & Yamanaka, 2013; Kuske et al., 2007).
Many different types of models and interventions now exist which aim to improve upon
the circumstances of the PWD and/or the CG. Within the domain of cognitive outcomes,
for example, non-pharmacological cognitive training techniques may lead to
improvements in cognitive outcomes. A systematic review by Sitzer and colleagues
(2006) revealed an overall effect size for cognitive training studies of Cohen’s d = .47,
with especially large improvements observed in domain specific outcomes of verbal and
visual learning (Cohen’s d = 2.16). Sitzer and colleagues (2006) argued that non-
pharmacological cognitive training and cognitive rehabilitation interventions may also
lead to improvements in depression, ADL ability, and general self-rated functioning,
though these non-cognitive outcomes of cognitive interventions were less well-supported
by a subsequent systematic review (Bahar-Fuchs, Clare, & Woods, 2013). Non-
pharmacological interventions aimed at improving upon the psychosocial well-being of
PWDs as well as behavioral expressions of dementia have demonstrated moderate

20
efficacy (for a review see: Livingston et al., 2014a; Livingston et al., 2014b; Cooper et
al., 2012), as will be discussed at length in the following sections.
Non-pharmacological interventions for dementia take multiple approaches,
including several different modes of intervention to improve upon the well-being of both
the PWD and the CG. While many non-pharmacological interventions have been
successful at improving key outcomes related to dementia, these types of interventions
are often expensive, require extensive training of staff or family members, and only target
one specific issue and one part of the illness continuum. In contrast, the use of
personalized music as a non-pharmacological tool for improving the lives of PWDs may
represent a low-cost yet efficacious approach to improving the lives of those with
dementia that can be implemented across the entire illness continuum. The subsequent
sections focus on the use of non-pharmacological interventions for dementia as a means
of improving psychosocial well-being (particular focus will be paid to quality of life,
affect, and anxiety), and behavioral expressions of dementia (including wandering,
agitation, etc.). In the following sections, discussion will begin with personalized music
interventions for dementia, and will draw on evidence from the broader non-
pharmacological intervention literature where the personalized music literature is lacking.
1.4. Music and Memory
1.4.1. The Neural Link between Music and Memory
Research indicates that memory for familiar music is well-preserved in
Alzheimer’s disease until the very late stages (Vanstone & Cuddy, 2009; Vanstone,
Cuddy, Duffin, & Alexander, 2009, Vanstone et al., 2012; Simmons-Stern, Budson, &
Ally, 2010). Several brain regions have been identified as important for musical
21
memory. The medial prefrontal cortex (mPFC) is a brain structure associated with
judgments regarding self-relevance and affect, as well as the integration of emotion,
autobiographical memory and music (Janata, 2009). Evidence from functional magnetic
resonance imaging (fMRI) suggests a “tonality structure” in the mPFC, such that changes
in tonal space are associated with a topographical activation patterns within the mPFC
(Janata, et al., 2002). Music that is familiar to the listener elicits a stronger response in the
mPFC than unfamiliar music (Plailly et al., 2007), and unfamiliar pleasant music elicits a
stronger mPFC response than unfamiliar unpleasant music (Blood et al., 1999). The
greater activation of the mPFC for familiar music relative to other forms of music may
indicate familiar music elicits a stronger (more positive) affective response than other
forms of music at an observable neural level. This underscores the importance of the
“personalized” aspect of music for dementia, which is discussed at greater length in the
following section.
In a comprehensive neuroimaging study, Jacobsen and colleagues (2015) used
fMRI to examine differences in brain activation regions while listening to familiar and
unfamiliar music. The regions identified by this study included the anterior cingulate
gyrus as well as the pre-supplementary motor area, which shares extensive connections
with the mPFC. While not traditionally thought to be associated with musical memory,
there is a growing body of evidence linking the pre-supplementary motor area and the
anterior cingulate gyrus to music familiarity (Pereira et al., 2011; Janata, 2009; Groussard
et al., 2010). Jacobsen and colleagues (2015) conducted a follow-up study in which they
examined grey matter atrophy, hypometabolism, and amyloid-β deposition in PWDs
using structural MRI and positron emission tomography (PET). Findings indicated that
22
the pre-supplementary motor area and the anterior cingulate gyrus are among the most
well-preserved brain regions in Alzheimer’s disease, with both regions demonstrating
significantly less grey matter atrophy and lower rates of hypometabolism than other brain
areas. While these areas contained levels of amyloid-β deposition similar to other
cortical areas, this accumulation of amyloid-β is representative of an earlier stage in the
disease process and a precursor to both hypometabolism and cortical atrophy. These
findings are supported by other neuroimaging studies of Alzheimer’s disease (Frisoni et
al., 2007; Benzinger et al., 2013; Jack & Holtzmann, 2013), and may help to explain the
preserved connection between music and memory for PWDs. These findings lend
support to the use of personalized music in dementia over the entire course of the
dementing illness—even into the later stages of the disease.
1.4.2. Familiar vs. Unfamiliar Music
The personalized aspect of musical interventions for dementia is underscored both
by theoretical models of music therapy (Gerdner, 1997) as well as the neuroscientific
evidence as discussed above. The articles discussed in the previous sectioned revealed a
difference in brain activation patterns when given familiar and unfamiliar music. From
the theoretical literature on music interventions for dementia, Gerdner hypothesized that
agitation was a result of a lowered stress threshold in dementia (1997). This lowered
stress threshold is thought to result from the increased difficulty of receiving and
processing sensory stimuli from the environment. As dementia progresses, external
stimuli may become confusing, and environmental cues may make it difficult for a PWD
to orient to time and place. Termed the “Mid-Range Theory,” it was hypothesized that
personalized music can serve as an attentional focus for PWDs, allowing them to focus
23
on something familiar and interpretable while filtering out more distressing external
stimuli (Gerdner, 1997). Thus, music that is familiar, interpretable, and tied to positive
memories and emotions should provide the best attentional focus for PWDs. Conversely,
novel, unfamiliar music which does not activate the well-preserved anterior cingulate
gyrus and pre-supplementary motor area is unlikely to capitalize on the link between
music, memory and emotion. Later biological support for the Mid-Range Theory came
from a randomized-controlled trial examining the impact of a personalized music
intervention on salivary chromogranin A, a biomarker of stress found in saliva, which
was significantly reduced among individuals in the personalized music condition relative
to a control condition (Suzuki, Kanamori, Nagasawa, Tokiko, & Takayuki, 2004;
Gerdner, 2010). A recent fMRI study provided further support for this theory, with
results suggesting increased functional connectivity immediately following the
presentation of personalized music (King et al., 2018).
The focus of the following sections will be on personalized music interventions
for dementia. While personalized music has garnered a substantial amount of evidence
for proximal outcomes such as agitation, behavioral expressions, and engagement, it is
important to note that the literature examining distal outcomes such as quality of life,
affect, and anxiety is sparse and methodologically inconsistent. Thus, where the
literature on personalized music is lacking, evidence will be drawn from literature on
music therapy (i.e., singing, dancing, live music, etc.), as well as the broader cognitive
stimulation literature.
1.4.3. Music Intervention Impact on PWDs

24
The preservation of musical memory in Alzheimer’s disease was recognized by
the scientific community as early as the mid-1980s (Crystal, Grober, and Masur, 1989
Norberg, Melin & Asplund, 1986). Some of the earliest studies of the effect of
personalized music on dementia focused on agitation in nursing home settings. Agitated
behaviors, or “behavioral expressions” as they are referred to in this paper, are
particularly relevant in this population. Behaviors that are verbally aggressive, repetitive,
or socially inappropriate are not only distressing for CGs, but are also associated with an
increased likelihood of the PWD being placed in a long-term care facility (Cohen-
Mansfield, Marx, & Rosenthal, 1989). Decreasing these types of behaviors may lead to
PWDs remaining in the home longer, reduce the cost of care, and reduce the burden
experienced by the CG.
Results from several studies demonstrated a reduction in agitation during a 30
minute music session and for 60 minutes immediately after listening (Gerdner, 1992;
Gerdner, 2005). A separate study found that participants with advanced dementia living
in a nursing home setting in a personalized music condition demonstrated significantly
reduced agitation compared to a classical music condition while listening and 30-minutes
after listening (Gerdner, 2000). The impact of music interventions of agitation for PWDs
has been well-supported in subsequent music intervention studies with few side effects
(Sung, Chang, & Abbey, 2006; Janata, 2012; Garland, Beer, Eppingstall, & O’Connor,
2007). The majority of studies assessing the impact of music on agitation in PWDs use
either the Cohen-Mansfield Agitation Inventory (Cohen-Mansfield, 1986) or the
Disruptive Behavior Scale (DBS; Beck et al., 1997) to assess agitation levels.

25
In several early studies, PWDs with late-stage dementia were found to benefit
from singing, as evidenced by behavioral observation of engagement and participation
(Norberg, Melin, & Asplund, 1986; Clair & Bernstein, 1990a; Clair & Bernstein, 1990b;
Clair, 1996). Engagement is also a consistent finding in music programming for nursing
home settings, demonstrating increased group singing participation, socializing, and
vocalizing (Olderog-Millard & Smith, 1989; Pollack & Namazi, 1992; Koger, Chaping,
& Brotons, 1999). Moreover, music has been identified in Validation Therapy as an
effective means of connecting with and engaging unresponsive late-stage PWDs (Feil,
2014), though little experimental evidence exists to support validation therapy as a whole
(Neal & Briggs, 2002).
Music intervention in dementia initially focused on proximal outcomes
(immediately after listening) rather than distal outcomes (sustained benefits over a period
of time). More recent studies have examined distal outcomes as a result of music
interventions for dementia. Unfortunately, there is very little consistency across these
interventions in terms of protocol and measurement, and very few studies of personalized
music have been conducted in the community. A recent meta-analysis of music use in
institutional settings concluded that the results of music interventions are promising, but
that further research is needed due to poor methodological quality of existing studies
(Blackburn & Bradshaw, 2014).
While the majority of studies examine music therapy in an institutional setting,
music interventions implemented in the community may pose similar benefits for the
PWD as well as benefits for the CG. Of the interventions that have been done in
community populations, one study found no impact on caregiver burden or behavioral

26
and psychological symptoms of dementia after 6, 12, and 24 months using a combined
music therapy and CG support group intervention (Berger et al., 2004). However, these
results may be due to insufficient dosage (1 hour long session per week), the lack of CG
involvement in the music portion of the intervention, minimal use of personalized music
during music therapy sessions, small sample size, and a large attrition rate. The use of
personalized music in community settings poses several benefits that are not applicable
(or less applicable) in institutional settings. For example, music’s ability to reconnect a
PWD and an informal family CG around shared musical memories from the course of
their lives is not possible in institutionalized populations. Any reductions seen in
behavioral expressions of dementia in the home may delay institutionalization and serve
as a major source of relief to a family caregiver who does not have formal training to care
for a person with dementia. Difficult behaviors that are more easily contained in long-
term care facilities such as wandering may be especially important outcomes for those
living in community settings.
Interventions in institutional settings may be more common due to the
convenience of recruiting participants and the ease of conducting music therapy sessions
in a group format. Two manuscripts from one larger study which used a 40 minute live
group music program administered three times a week for eight weeks found no positive
effects for agitation or anxiety for PWDs (Cooke, Moyle, Shum, Harrison, & Murfield,
2010a), but significant improvements in quality of life and depression for participants
with high baseline depression scores (Cooke, Moyle, Shum, Harrison, & Murfield,
2010b). A separate live music intervention conducted in Iceland using familiar songs
demonstrated a significant reduction in anxiety, aggressiveness, and activity disturbance

27
at a 6-week post-test, though results were not maintained four weeks post-intervention
(Svansdottir & Snaedal, 2006). In one nursing home study, PWDs were split into
personalized music and standard care conditions. After listening to personalized music
twice a week for six weeks, participants in the music condition demonstrated
significantly reduced levels of anxiety from baseline to week six relative to the control
condition (Sung, Chang, & Lee, 2010). One personalized music program examined the
impact of personalized music at different times of the day for residents in long-term care
(Janata, 2012). This study found that music intervention may reduce depressive
symptomology most in the late afternoon and evening.
1.4.4. Music Intervention and the Dyadic Relationship
Substantially less literature exists examining the impact of personalized music on
informal family CGs and their relationship with the PWD. To date, only one published
study has sought to examine the CG’s benefits of using mp3 players with personalized
music for PWDs living at home (Lewis, Bauer, Winbolt, Chenco, & Hanley, 2015). This
study was a pre-post design conducted in a community setting in Australia. CGs were
primarily spouses (71%), primarily female (69%), and nearly all CGs lived with the PWD
(94%). Significant quantitative outcomes for the informal family/friend CGs included
increased self-efficacy for managing dementia and reduced psychological distress,
evaluated using the Kessler-10 measure of Psychological Distress (anxiety and
depression; Kessler et al., 2002). Non-significant outcomes included general health and
life satisfaction, as well as caregiving stress. Significant reductions were observed from
Time 1 to Time 2 on a single item measure of relationship quality. It is likely that this
finding is due to the illness progression over the course of the study rather than mp3

28
usage, but the lack of control group makes it difficult to draw inferences about this
outcome. Qualitative items from the same study indicated that CGs felt that using mp3
players gave them a break from caregiving, helped to put the PWD in a better mood, and
CGs viewed the mp3 players as useful tools for providing care. A second study by Baker
and colleagues (2012) of spousal CGs and PWDs in the community setting included the
use of music as a therapeutic tool, but required the involvement of the CG in each music
session. For example, CGs were trained by a music therapist to utilize music techniques
such as singing familiar songs to the PWD, encouraging the PWD to move to music, and
having the PWD listen to quiet, relaxing music with closed eyes. Sessions were
approximately 20-30 minutes each, and CGs were instructed to ask the PWDs to recall
memories after listening to the music. Each CG kept track of sessions and responded to
qualitative questions using a diary during the 6-week program. Quantitative measures of
depression, anxiety, relationship quality, and satisfaction with the caregiving role did not
change significantly from Time 1 to Time 2, though this may be due to ceiling/floor
effects at Time 1, as well as a very small sample size (5 dyads). Qualitative interviews of
the participants indicated that CGs found the music activities to be relaxing for
themselves and the PWD, improved the quality of the time spent together, enabled the
CG and PWD to be more intimate, and increased satisfaction of the caregiving role. The
authors hypothesized that quantitative measures did not indicate any change from Time 1
to Time 2 because CGs were not presenting with depressive symptoms, anxiety, or
negative perceptions of their relationship with the PWD at Time 1. A third study
examining the effect of personalized music in the home measured CG reports of agitation
before, during and after a 30 minute listening session (Park & Pringle Specht, 2009).

29
PWDs were over age 60, scored below 25 on the MMSE, and were exhibiting agitation.
CG demographics and inclusion criteria were not reported. As predicted, CGs reported
significantly reduced PWD agitation during and after listening as compared to before
listening. Though the authors mention that agitation is a direct contributor to caregiver
burden, there was no measure of caregiver burden to gauge the effect of reduced agitation
from music listening on CGs. The use of a more rigorous measure of relationship quality
in this study as well as the use of a control group to gauge the effects of the intervention
should provide much clearer insight into the impact of a personalized music intervention
on the CG/PWD relationship.
The benefits of general music therapy and music interventions for CGs have been
substantially more studied than personalized music, though the methodology used in
these studies varies widely. A recent systematic review of music therapy interventions
concluded that music therapy may reduce agitation and distressed behaviors in PWDs
while improving the quality of interactions between PWDs and CGs (Blackburn &
Bradshaw, 2014). The American Musical Therapy Association (2006) claims that music
therapy helps with the management of pain, stress, and anxiety for both the CG and the
PWD, provides opportunities for emotional intimacy, and opportunities for respite for the
CG. A musical therapy retreat study indicated that CGs felt less anxious and more than
half of CG participants reported improvements in the PWD’s social and emotional state
(Brotons & Marti, 2003). A 10-week group singing intervention found that quality of life
for the PWD and the CG remained stable over the course of the study despite steady
decline in cognitive status, behavioral and psychological symptoms of dementia, and
ADL ability (Camic, Williams, & Meeten, 2011). While not directly emblematic of a

30
“personalized” approach to music intervention in dementia, the results from the general
music therapy literature are encouraging. These results indicate that a musical approach
to intervention may be beneficial for both members of the dyad.
1.4.5. Cognitive Stimulation Therapy
The relatively sparse body of literature linking personalized music in dementia to
improvement within psychosocial domains warrants evidence from the broader cognitive
stimulation literature. Specifically, the personalized music intervention literature lacks
evidence that these types of interventions can result in sustained (as opposed to
immediately after the intervention is administered) well-being outcomes like quality of
life. Personalized music interventions are, arguably, cognitive stimulation interventions
at their core. The goal of personalized music is to engage the PWD cognitively while
providing an enjoyable and familiar attentional stimulus. The neuroscientific evidence
for personalized music captures a network of emotion and memory (discussed earlier in
this chapter) that may not be tapped in other cognitive stimulation approaches.
Nevertheless, there is evidence to be drawn from the cognitive stimulation literature
which may help to build the rationale and support the efficacy of personalized music
interventions for PWDs.
Cognitive stimulation approaches to intervention aim to engage the PWD in
activities that use cognitive resources, often in a social context (Aguirre, Woods, Spector,
& Orrell, 2013; Clare & Woods, 2004). Cognitive stimulation therapy relies on the
philosophy that cognitive stimulation can serve as a buffer against cognitive decline, and
that the lack of cognitive activity can, conversely, exacerbate this decline. Moreover,

31
cognitive stimulation therapy is based on the assumption that engagement in cognitively
stimulating activities is more enjoyable than disengagement.
Instead of targeting specific cognitive modalities, cognitive stimulation therapy
aims to benefit general cognitive functioning (Clare & Woods, 2004; Spector, Orrell, &
Woods, 2010). The types of activities commonly used in cognitive stimulation therapy
studies include discussion of past and recent events, engaging activities such as baking or
gardening, games and puzzles, as well as musical activities (Woods, Aguirre, Spector, &
Orrell, 2012). Intervention research on cognitive stimulation often utilizes several
different types of activities over the course of the study. For example, one RCT study
used a 14-session design in which participants engaged in physical games, sound,
childhood (reminiscence), food, current affairs, faces/scenes, word association, being
creative, categorizing objects, orientation, using money, number games, word games, and
team quizzes (Apóstolo, Cardoso, Rosa & Paúl, 2014). This study reported
improvements in cognition (using the Montreal Cognitive Assessment), but saw no
improvement in depression or independence related to ADLs. In addition to possible
cognitive benefits, some studies have found evidence for improvement of quality of life.
Spector and colleagues (2004) reported significantly improved quality of life for
participants in a cognitive stimulation therapy group compared to a treatment as usual
group. A study of the long-term effects of cognitive stimulation therapy found that
participants in a “maintenance” intervention group who participated in a weekly session
over the course of 6 months reported higher quality of life at month 3, and had higher
proxy ratings of quality of life, activities of daily living, and better mood at month 6
compared to a treatment as usual group (Orrell et al., 2014). Using a similar design,

32
Chapman and colleagues (2004) found that using a combination of donepezil and
cognitive stimulation therapy improved quality of life and slowed cognitive decline
relative to a donepezil only condition. In a Parkinson’s disease study, participants with
cognitive impairment in an individualized cognitive stimulation therapy intervention
showed some cognitive benefits, as measured by the Montreal Cognitive Assessment, as
well as improvements in quality of life, and ADL ability (Farzana et al., 2015). Based on
these findings, it stands to reason that the benefits of cognitive engagement observed
from this wider body of literature may be present also in a cognitively engaging
personalized music intervention. The link between cognitive engagement and quality of
life is especially relevant from this body of literature, as the personalized music
interventions which examine quality of life as an outcome are generally lacking in
methodological control.
1.4.6. Personalized Music as Humanistic Mode of Intervention
Personalized music interventions in dementia are built upon the philosophy that
PWDs are able to live well with dementia. Rather than taking a purely biomedical
approach that focuses on the illness at its detriments, personalized music aims to
circumvent the impairments of the PWD altogether and build instead upon the abilities of
the PWD. Bearing this in mind, the methodology desccribed in Chapter II is informed by
two approaches to care for persons with dementia: the “strength-based approach” and the
“person-centered approach.”
The philosophy behind the strength-based approach to intervention is to focus on
the strengths of the individuals rather than on weaknesses (Warchol, 2006; Judge, Yarry,
& Orsulic-Jeras, 2010; Yarry, Judge, & Orsulic-Jeras, 2010). A medicalized approach to

33
intervention for any chronic condition risks placing too heavy an emphasis on the disease
itself, its negative symptoms, and the limitations it places on the person with the disease.
The strength-based approach, conversely, places the emphasis entirely on the adaptive
and successful characteristics of each person individually. Though the efficacious
approaches to intervention discussed in this chapter are consistent with the strength-based
approach, the translation of the strength-based approach to intervention research was not
made until recently. The strength-based approach to intervention grew from the Solution-
focused approach to empowering clients within a counsellor-patient relationship (White
& Epston, 1990; Iveson, 2002). More recently, the strength-based approach has been
advocated as a humanistic framework for intervention for persons living with HIV/AIDs
(Orsulic-Jeras, Shepherd, & Britton, 2003) and for PWDs (Judge et al., 2010; Yarry et al.,
2010). The use of the strength-based model is particularly apropos for these populations
because it affords interventionists the ability to empower individuals who may feel
handicapped and stigmatized by their circumstances.
The “person-centered” approach to care is a term that has long been used and
advocated in research and in practice, though it lacks an agreed upon definition (Kogan,
Wilber, & Mosqueda, 2016; Lai, 2016). A recently published White Paper concerning
the quality of dementia care in the United States set out to provide a concrete outline for
what person-centered care is and is not, as well as to advocate for sweeping reforms
toward a person-centered model of healthcare (National Dementia Initiative, 2013). This
White Paper integrates the values espoused by various researchers on the topic of person-
centered care into a single framework. Thus, the person-centered approach, as defined by
the National Dementia Initiative (2013), is as follows:

34
(1) The core values and philosophy that we adopt must serve to foster a
meaningful relationship with the PWD, develop an understanding of the PWD’s
unique personhood, focus on strengths rather than weaknesses, and attempt to
enter the world of the PWD.
(2) We must build the structural elements of person-centered care within the long-
term care environment, including relationships within the community (a sense of
belonging), active and involved governance, reliable leadership (staff
empowerment and staff retention), care partners (staff training in core values of
person-centered care), services, meaningful engagement, a positive environment,
and accountability of person-centered care in practice.
(3) We must operationalize core and structural values in the development of broad
practices of person-centered care.
(4) Personalized practices must focus on specific ways of providing care and
embracing the personhood of each unique individual.
The National Dementia Initiative (2013) argues that health care in the United
States is fragmented and focuses too heavily on a biomedical approach. Instead, person-
centered healthcare aims to foster well-being in physical, psychological, social, and
spiritual domains.
The design and protocol of this intervention were made with careful consideration
given to the philosophies of both the person-centered approach as well as the strength-
based approach to dementia. In consideration of the strength-based approach, this
personalized music intervention relies on the remaining abilities of individuals with
dementia. As outlined in the previous sections, the ability to recognize familiar music

35
from throughout one’s life and draw on long-term memories and emotions is a remaining
strength of PWDs. The use of this type of music as a therapeutic tool may serve as a
means of circumventing the negative experiences associated with the dementing illness.
Thus, personalized music for dementia is strength-based insofar as it shifts focus away
from disease and disability and focuses instead on the abilities that remain over the
course of the disease. Consistent with the person-centered philosophy, the protocol of
this study includes the use of self-report methodology (discussed in Chapters I and II).
This approach aims to capture the perspective of the PWD from the perspective of the
PWD. Instead of using proxy report methodology or observational measures, the PWD is
treated as a valid and reliable respondent in the research process. Finally, the
personalized music aspect of this intervention capitalizes on the unique experiences,
preferences, and life circumstances of each participant.
1.5. Hypotheses
The development of the hypotheses presented in this section was informed by two
conceptual models. First, the Mid-Range Theory, as discussed earlier in this chapter,
links personalized music to positive affect (H1), reduced anxiety (H2), and reduced
behavioral expressions of dementia (H3) (Gerdner 1997; Gerdner, 2000). Second, the
Stress-Process Model, as discussed in Chapter I, posits that external resources or
“mediators” can alleviate the impact of dementia-related stressors (e.g., cognitive status,
functional problems, behavioral problems, perceived dependency, role captivity, and
perceived distress) on role strain and well-being (Judge et al., 2010). By treating
personalized music listening as an external resource for PWDs in the Stress-Process
Model, it was hypothesized that improvements would be seen in dyadic relationship

36
strain (H4, conceptualized as a secondary strain in the Stress-Process Model) as well as
quality of life (H5, a well-being outcome of the Stress-Process Model).
H1. Listening to personalized music over a four week period will improve the
overall mood of PWDs relative to participants in a control group.
H2. Listening to personalized music over a four week period will lead to reduced
anxiety for PWDs relative to participants in a control group.
H3. Listening to personalized music over a four week period will lead to fewer
behavioral expressions of dementia for PWDs relative to participants in a control group
H4. Listening to personalized music over a four week period will improve the
dyadic relationship between the PWD and the CG relative to dyads in the control group.
H5. Listening to personalized music over a four week period will improve the
quality of life of PWDs relative to participants in a control group.
An additional research question was to examine the acceptability and feasibility
of the intervention protocol. This was assessed using an acceptability questionnaire
(described in detail in the following sections), and by tracking dosage (amount of music
listening), adverse events, and attrition rates.

37
CHAPTER II
METHODS
2.1. Study Design
The current study was a one-month randomized, controlled trial with pre-test and
post-test assessments. Groups included one experimental (personalized music) condition
and one control (novel music) condition. After listening to novel music for one month,
the control condition participants were given the option of changing to a personalized
playlist following post-test assessments. The methodology described in this section was
approved by the Institutional Review Boards at Cleveland State University and at
Benjamin Rose Institute on Aging.
2.2. Measures
For the purposes of examining the impact of this personalized music intervention
on PWDs, self-report methodology was used to obtain the most valid insights into the
PWD’s perspective. All measures reported in the following sections were chosen based
on their reliability and validity for assessing populations with dementia. Affect, quality
of life, anxiety, and relationship strain measures were administered to the PWD in-person
by an interviewer. Response cards with visual response options were used to facilitate
responses to items for each measure. The following sections detail each of the measures

38
used in the study followed by a detailed account of the procedure for both the
experimental group and the control group.
2.2.1. Demographic Information
Initial eligibility information was collected via telephone. Information from this
call included details about the PWD’s memory loss (including when the memory
problems were first noticed, what the PWD’s memory-related symptoms are, whether or
not they have talked to a doctor about memory problems, and if the PWD is taking
medication for memory problems), how many days per week the CG provides care, when
the CG began providing assistance, the living arrangements of the CG and PWD, and
whether the CG has primary responsibility for the PWD. For a full account of these
questions, see Appendix I. If participants were eligible based on the information
provided via the initial telephone call, further demographic information was collected at
the first in-person meeting such as age, race/ethnicity, gender, marital status, relationship
between CG/PWD, employment status, income, and education level. Demographic
information was collected from both the PWD and the CG via a self-report questionnaire
(see Appendix A).
2.2.2. Mini-Mental State Examination
The Mini-Mental State Examination (MMSE) is a widely used assessment to
screen for cognitive impairment related to working memory, attention, orientation, and
language (see Appendix B; Folstein, Folstein, & McHugh, 1975). The MMSE is a brief
30-item assessment administered by an interviewer. Scores on the MMSE range from 0
to 30, with scores below 24 considered abnormal. In the present study, the MMSE will be
used to exclude participants scoring below 10. This cutoff point was chosen because of

39
the potentially diminished ability of individuals with severe dementia to self-report
reliably using a range of Likert response options on a variety of measures. While the
individuals were excluded from this RCT, individuals scoring below 10 on the MMSE
were referred for participation to the community rollout of Music & Memory offered
through the Benjamin Rose Institute on Aging.
2.2.3. Diary-Based Fidelity Assessment
All participants were given a goal “dosage” of 20 minutes of music listening at
least five days per week for four weeks. In order to account for dosage, a self-report
diary method was used to track time spent listening to music. These assessments were
provided to CGs at the in-person baseline meeting to be completed by CGs after each
listening session. This information was obtained via telephone on a weekly basis
throughout the duration of the study. This measure was administered to CGs because
CGs were typically the ones initiating music listening for the PWD. The diary-based
fidelity assessment was identical for the first three weeks of participation (see Appendix
E). The fourth and final diary-based fidelity assessment included all items from the first
three weeks in addition to a series of questions assessing the acceptability and feasibility
of the intervention (see Appendix F).
2.2.4. Outcome Measures
Affect
Overall affect of the PWD was measured using the positive affect subscale and
negative affect subscales of the Dementia Quality of Life Instrument (DQoL; see
Appendix G) (Brod, Stewart, Sands, & Walton, 1999). The positive and negative affect
subscales have indicated good reliability for use with PWDs, with Cronbach’s alpha for

40
the positive affect subscale of .83, and .89 for the negative affect subscale (Brod et al.,
1999). Taken as a whole, the five subscales of the DQoL (self-esteem, positive affect,
negative affect, feelings of belonging, and sense of aesthetics) measure the quality of life
of PWDs. While it is widely agreed upon in the literature that mood is an important
factor influencing quality of life (Logsdon, McCurry, & Teri, 2007; Thorgrimsen et al.,
2003; Banjeree et al., 2006), the DQoL Assessment places a substantially greater
emphasis on mood than other measures of quality of life (such as the QoL-AD, discussed
below; see Appendices G and H for a list of items). This has led researchers to use one or
both affect subscales from the DQoL independently from the remaining subscales of the
DQoL (Zarit, Femia, Kim & Whitlatch, 2010; Sabol et al, 2011; Shelton, Orsulic-Jeras,
Whitlatch, & Szabo, 2017). Indeed, a factor analysis of the DQoL indicated that at least
two separate factors of the DQoL exist: negative affect and the remaining items,
indicating that the affect items of the DQoL may be substantively unique from the
remaining subscales in their measurement (Edelman, Fulton, Kuhn, & Chang, 2005).
Thus, the two affect subscales from the DQoL served as an indicator of general mood and
are not thought to be redundant or indicative of global quality of life. Global quality of
life was assessed using a separate measure (discussed below). However, it may be
important to note that the quality of life measure discussed below includes a single item
related to overall mood in its conceptualization of quality of life.
Psychometric testing of PWDs’ responses to the DQoL in the present study
indicated excellent reliability at baseline and follow-up, with Chronbach’s alpha scores of
.86 and .88, respectively. As analyses were conducted with each of the mood subscales,
reliability analyses were conducted independently one the positive and negative affect

41
subscales as well as the full scale. Results for the positive DQoL subscale indicated a
Chronbach’s alpha of .84 and .86 at baseline and follow-up, respectively. The negative
DQoL subscale demonstrated Chronbach’s alpha reliability scores of .87 and .84 at
baseline and follow-up, respectively.
Quality of Life
Quality of Life of the PWD was assessed using the 13-item Quality of Life in
Alzheimer’s Disease questionnaire (QoL-AD; see Appendix H) (Logsdon, Gibbons,
McCurry, & Teri, 1999). The QoL-AD questionnaire is a brief self-report measure that
has demonstrated good acceptability, reliability, and validity for use with PWDs with
MMSE scores between 10 and 28 (Logsdon et al., 1999; Logsdon, McCurry, Gibbons, &
Teri, 2002). Thorgrimsen and colleagues (2003) have reported good reliability, with a
Cronbach’s alpha level of .83 for a sample of 261 respondents with a wide range of
dementia severity. The QoL-AD questionnaire includes items related to physical health,
energy, mood, social relationships, independence and ADL ability, and life as a whole
(for a full account of items, see Appendix H).
Psychometric testing of PWDs’ responses to the QOL-AD in the present study
indicated excellent reliability at baseline and follow-up, with Chronbach’s alpha scores of
.84 and .90, respectively.
Anxiety
Anxiety was measured using the Self-Rating Anxiety Scale (SAS; see Appendix
I) (Zung, 1971). The SAS is a widely used 20-item self-report questionnaire on which
participants rate how often they experience anxiety-related symptoms using a four point
Likert scale response format. Relatively fewer studies exist utilizing this scale as a self-

42
report questionnaire for PWDs. Studies from one sample reported good reliability
(Cronbach’s alpha of .73) using a 4-item version of the SAS (Dawson et al., 2013) and
acceptable reliability (Cronbach’s alpha of .68) using a 12-item version of the SAS
(Shelton, 2014). The SAS includes items about overall anxiety such as “I feel more
nervous and anxious than usual” and “I feel like I’m falling apart and going to pieces” as
well as items related to somatic concerns that are often indicative of anxiety such as “I
can feel my heart beating fast” and “My arms and legs shake and tremble.”
Psychometric testing of PWDs’ responses to the SAS in the present study
indicated good reliability at baseline and follow-up, with Chronbach’s alpha scores of .80
and .81, respectively.
Behavioral Expressions of Dementia
The frequency of behavioral expressions of dementia was assessed using the short
form of the Cohen-Mansfield Agitation Inventory (CMAI-SF; see Appendix J) (Werner,
Cohen-Mansfield, Koroknay, & Braun, 1994). This instrument was administered to CGs,
and asked about the frequency of 14 behaviors. CGs responded on a 5-point Likert scale
indicating how often the PWD has exhibited each behavior within the past two weeks.
Items on the CMAI-SF include behaviors such as verbal aggression, hitting/kicking,
pacing/wandering, repetitive question asking, hoarding, etc. The short form of the CMAI
was chosen over the long-form measure because the short form measure utilizes a 5-point
Likert-scale rather than a 7-point Likert scale. The simplicity of the 5-point Likert scale
makes remembering response options easier for CGs who may also have some degree of
memory difficulty. Fu, Moyle, & Cooke (2013) reported excellent reliability of the

43
CMAI-SF over five longitudinal measurements, with Cronbach’s alphas ranging from .87
to .91.
Psychometric testing of CGs’ responses to the CMAI-SF in the present study
indicated acceptable (albeit lower than previously reported) reliability at baseline and
follow-up, with Chronbach’s alpha scores of .71 and .79, respectively.
Relationship Strain
Relationship strain was measured using the Dyadic Relationship Scale (DRS; See
Appendix K) (Sebern & Whitlatch, 2007). The DRS includes 10 items with responses
recorded on a 4-point Likert scale. Two subscales are included in the DRS: a positive
dyadic interaction subscale and a dyadic strain subscale. The positive subscale includes
items such as “I felt that my relationship with my care partner has improved” and the
dyadic strain subscale includes items like “I felt angry toward him/her.” Sebern and
Whitlatch (2007) reported excellent reliability for CGs (Cronbach’s alphas of .85 for
positive interaction subscale and .89 for the dyadic strain subscale) as well as for
cognitively intact care recipients (Cronbach’s alphas of .86 for positive interaction
subscale and .84 for the dyadic strain subscale).
Chronbach’s alpha values for the PWDs’ scores on the DRS were .73 and .87 at
baseline and follow-up, respectively. Prior to the imputation of missing values in the
DRS, the reliability at baseline was .69—just below the widely accepted standard of .70
(Nunnally, 1978). There are two likely explanations for the low reliability prior to
imputation for the DRS. First, there were a higher number of missing values on items
comprising this scale relative to other measures. Two items in particular, I felt closer to
him/her than I have in a while, and I felt that communication between me and my care

44
partner improved were not answered at baseline by 7 and 6 participants, respectively.
Second, the DRS is composed of two distinct subscales, Positive Interaction and Role
Strain. When separated into its subscales, reliability for these domains was .81 (positive
interaction) and .83 (role strain) at baseline—a substantial improvement over the full-
scale reliability coefficient. These results indicate that the DRS is potentially more
informative when separated into its subscales. For the purposes of this study, analyses
were conducted both ways; with the full-scale DRS and with each individual subscale.
2.3. Inclusion Criteria
In order to be eligible for participation in the study, participants had to meet the
following criteria:
(1) The PWD must be 60 years of age or older. There was no age requirement for
the CG.
(2) Regarding memory impairment and dementia diagnosis, the goal of this study
was not to confirm or diagnose specific memory-related conditions, but to make
reasonable assumptions about inclusion. The inclusion criteria for the present study
mirrored closely the inclusion criteria of past research on personalized music
interventions for dementia (for an overview of samples used in personalized music
intervention studies, see Sung & Chang, 2005). In order to participate, PWDs had to
score 10 or above on the Mini-Mental State Examination (MMSE; Folstein, Folstein, &
McHugh, 1975). A score of 10 has been identified as a cutoff point for reliable self-
report responding on quality of life (Logsdon, Gibbons, McCury, & Teri, 2002; Mozley
et al., 1999) and was chosen to help to ensure that PWD self-report responses are reliable

45
(Feinberg & Whitlatch, 2001). Participants who scored above 27 on the MMSE must
have been diagnosed with dementia to be included in the study. This cutoff was chosen
based on literature suggesting that the conventional cutoff of 24 has a high degree of
specificity, but low sensitivity to detecting cognitive impairment (Kukull et al., 1994;
O’Bryant et al., 2008). These articles suggest an alternative score of 27 while noting that
differences in education levels may further impact performance.
(3) The PWD must live at home and receive care primarily from an informal
caregiver. There were no exclusions based on the relationship of the CG to the PWD
(e.g., spouse, son/daughter, friend, etc.). To be included, CGs must live with or visit the
PWD in-person at least five days out of the week. Since CGs were expected to help
initiate listening, this ensured that each CG will be able to provide the required music
listening dosage to the PWD.
2.4. Participant Recruitment
Several methods of recruitment were used to identify individuals to be screened
for participation. The predominant method of recruitment was through attendance at
caregiver support groups within the targeted geographical area. The principal researcher
attended 16 such support group meetings aimed at supporting caregivers of persons in the
early-to-moderate stages of dementia. Additionally, recruitment was conducted through
local adult day programs. Three adult day programs agreed to help identify and refer
appropriate participants for participation based on the eligibility requirements of the
study. Each of these organizations first contacted their clients to inform them of the
study and obtain a verbal agreement to share their contact information with the principal

46
researcher for a follow-up call. In addition to these recruitment methods, several other
recruitment efforts were made which yielded substantially fewer contacts. These
methods included outreach to local religious organizations, community talks about music
and memory, flyer postings at local establishments, outreach to senior apartment
buildings and home health care providers, and a description of the study in a local
homecare assistance newsletter.
2.4.1. Sample Size
Through the above recruitment efforts, 71 dyads expressed interest in
participating in the study. Of those 71 dyads, 46 were able to be contacted via telephone
and completed the telephone screener. Following the telephone screener, 8 participants
were excluded due to ineligibility (n = 1), declining to participate (n = 2), or other
reasons (n = 5). Thus, 38 dyads met with the principal investigator for the baseline
meeting. Of these, 4 did not meet MMSE eligibility requirements. The remaining 34
participants were randomly assigned to either the control group (N = 16) or the
experimental group (N = 18). Following assignment, 4 dyads withdrew from the study for
a total N-size of 30: 15 participants in the control group and 15 in the experimental
group. One of these dyads withdrew due to lack of interest. The other three dyads
withdrew due because they felt that the study required more time than their schedules
allowed. For a full CONSORT diagram detailing recruitment, see Appendix O.
An analysis was conducted to determine if there were any group differences in
baseline scores on outcome measures between completers and non-completers. Results
indicated no differences between completers and non-completers on mood, quality of life,

47
agitation, or relationship strain. However, participants who withdrew had lower baseline
anxiety scores on average (M = 1.25, SD = .04) than completers (M = 1.46, SD = .36).
2.5. Participant Characteristics
Potential participants were contacted by telephone and screened for inclusion and
exclusion criteria using the Telephone Screener (Appendix L). Informed consent was
obtained from both the CG and the PWD at the in-person baseline meeting.
For a full account of demographic information, see Table 1. Ten of the PWDs in
the control group were men, and 7 of the PWDs in the personalized music group were
men. Average age for participants in the control group was 73.5 (SD = 6.9) and 79.4 (SD
= 10.4) in the personalized music group. In the control group, 11 PWDs were white non-
Hispanic, 1 PWD was white Hispanic, and 3 PWDs were black. In the personalized
music group, 8 PWDs were white non-Hispanic and 7 PWDs were black. Three PWDs in
the control group and 4 PWDs in the personalized music group were veterans. In the
control group, 14 PWDs were married and 1 had never married. In the personalized
music group, 6 PWDs were married, 7 were widowed, 1 was divorced, and 1 had never
married.
Twelve PWDs in the control group received care from a spouse, 1 from an adult
child, and 2 from a non-relative. In the personalized music group, 6 PWDs received care
from a spouse, 7 from an adult child, 1 by another relative, and 1 by a non-relative.
Average MMSE score for PWDs in the control group was 22.7 (SD = 4.9), and 17.3 (SD
= 6.2) for PWDs in the personalized music group.

48
The type of music that was preferred by participants varied in genre. The most
commonly preferred genre of music was Gospel (n = 6), followed by Rock and Roll (n =
5). For a more detailed account of music preferences, see Appendix P.
Table 1
PWD Demographic Information
Characteristic Control (N = 15) Experimental (N = 15) Total (N = 30)
Gender
Female 5 (33%) 8 (53%) 13 (43%)
Age (Mean ± SD) 73.5 ± 6.9 79.4 ± 10.4 76.2 ± 9.2
Race
White Non-Hispanic 11 (73%) 8 (53%) 19 (63%)
Black/African American 3 (20%) 7 (47%) 10 (33%)
White Hispanic 1 (7%) 0 (0%) 1 (3%)
Marital Status
Married/Partnered 14 (93%) 6 (40%) 20 (67%)
Widowed 0 (0%) 7 (47%) 7 (23%)
Divorced 0 (0%) 1 (7%) 1 (3%)
Never Married 1 (7%) 1 (7%) 2 (7%)
Children
Yes 14 (93%) 11 (73%) 25 (83%)
No 1 (7%) 3 (20%) 4 (13%)
Relationship to Care Partner
Spouse 12 (80%) 6 (40%) 18 (60%)
Parent 1 (7%) 7 (47%) 8 (27%)
Other/Non-relative 2 (13%) 2 (13%) 4 (13%)
Level of Education
Some college or less 3 (20%) 11 (73%) 14 (47%)
College graduate or higher 12 (80%) 4 (27%) 16 (53%)
Household income
≤$40k per year 2 (15%) 11 (79%) 13 (48%)
>$40k per year 11 (85%) 3 (21%) 14 (52%)
MMSE Score (Mean ±SD) 22.67 ± 4.87 17.33 ± 6.20 20.00 ± 6.11
Efforts were made to schedule post-test meetings as close to the end of the one-
month intervention block as possible. The average number of days between baseline and
post-test for the control group participants was 34.9 days (SD = 7.7) and 47.9 days (SD =
49
23.2) for those in the experimental group. The average number of days between pre and
post-test for individuals in the experimental group was inflated due to three dyads. Two
PWDs in this group were hospitalized during the intervention. The time between pre and
post-test for these individuals was 106 days and 88 days. One additional post-test
meeting with a dyad was delayed due to health problems of a CG. The time between pre
and post-test for this dyad was 77 days. Between subjects differences were examined for
these individuals using the same approach as the final analyses (see Section 3.1 for
details). Rather than group assignment, a “delayed” variable was created and used as the
key predictor in each regression model. There were no significant differences between
these “delayed” participants and the rest of the experimental group in mood, quality of
life, anxiety, relationship strain, or behavioral expressions of dementia (all p’s > .05).
Thus, all participants were included in the final analyses.
2.6. Benjamin Rose Institute on Aging
This study was done with the support of an implementation study grant obtained
by Benjamin Rose Institute on Aging from the Ohio Department on Aging. This project
aimed to provide music equipment and music to PWDs living in the community in
Northeast Ohio. This dissertation study used a subset of the participants from the
implementation study to conduct a more rigorous examination of the benefits of
personalized music in dementia. In order to satisfy the terms of the grant, there are a few
methodological parameters that this dissertation study was required to meet. First, the
personalized music intervention was four weeks. This is the prescribed length of time
between pre-test and post-test deemed by the Ohio Department on Aging. This timeline

50
is consistent with previous personalized music interventions in dementia, which allow for
between 2 and 6 weeks between baseline and post-test measurements (Park & Pringle
Specht, 2009; Lewis et al., 2015; Gerdner, 2000). Second, Quality of Life was assessed
using the Quality of Life – Alzheimer’s Disease (QOL-AD) measure. Third, the
demographics assessment used in this study included all items required by the grant, and
was administered to both the PWD and the CG. Finally, this study used Apple® products
including iPod Shuffles® and iTunes® as the platform for obtaining and listening to
music.
2.7. Procedure
The following sections detail the study procedure for both the experimental and
control conditions throughout the study. To examine the acceptability and feasibility of
this protocol, pilot testing was conducted with the first three participants recruited, who
were automatically assigned to the experimental condition. This subsection of
participants allowed for the development and refinement of several key study
components, including questions used to assess personalized music (see Appendix M),
the procedure for training participants and setting up the music-related hardware and
software, and music tracking via the use of the diary-based fidelity assessments. The final
study protocol within each of these areas was finalized following interviews with the
initial three participants. Procedures and materials were adapted using insights gained
from these participants.
2.7.1. Screening Phone Call

51
Once a PWD or CG expressed interest in the program through community
recruitment efforts, they were contacted via telephone. A phone screener script and
questionnaire was utilized to facilitate the process of screening participants for eligibility
(for a full account of items and the script used in the screener, see Appendix L).
Caregivers contacted via telephone were asked about their care situation to determine
eligibility. The caller verified that the CG provides care for a person exhibiting memory
problems at least five days per week, that the PWD lives in the community, and is cared
for by a family CG. Additionally, participants were asked about their familiarity with
Apple® products, and if they have a computer with internet access that can store their
music. The goal of these questions was to identify how much assistance each dyad would
need to set up a personalized music database, create a playlist, and begin using a personal
music device. This helped determine what types of accommodations needed to be made
in terms of meeting location (for example, if participants plan to use a desktop computer
to house music located at the home, meetings should take place in this location).
All participants received an iPod Shuffle® with the accessories needed to begin
listening to personalized music (e.g., charger, charging cable, headphones, headphone
splitter, iTunes® gift card). Participants who did not have a home computer capable of
housing iTunes® and personalized music were given a pre-loaded iPod Shuffle® with
music identified as personally relevant through a personalized music assessment process
(discussed below). This method is used as an alternative to setting up an iTunes® account
for each participant because the ability to add, remove, or modify music in playlists is
easier if the device can be connected to a native desktop with iTunes®. Diary-based

52
fidelity questionnaires included an item to monitor whether technology complications
have prevented or deterred participants from engaging in music listening each week.
2.7.2. In-Person Baseline Meeting
If the participants met these inclusion criteria as determined in the screening call,
the researcher set up a time to meet with the CG and the PWD together in-person.
Options were provided to meet with the dyad in their home, at Benjamin Rose Institute
on Aging, or at another preferred location.
At the baseline meeting, a researcher obtained informed consent to participate in
the study from both the CG and the PWD. PWDs were administered the MMSE
(Appendix B) and demographic information was collected for both the PWD and the CG
(Appendix A). If participants met all eligibility requirements from the screening call and
the PWD scored 10 or above on the MMSE, the baseline assessment was administered.
Caregivers were asked to complete the following questionnaires independently: the
CMAI-SF (Appendix J), and the DRS (Appendix K). At the same time, an interviewer
administered the following questionnaires to the PWD in a separate room: DQoL affect
subscales (Appendix G), the QoL-AD (Appendix H), the SAS (Appendix I), and the DRS
(Appendix K). At this point, participants were randomly assigned to either the
experimental condition or the control condition. Blocked randomization was used to
ensure that each group contained approximately the same number of participants after
attrition.
Control Group – Baseline Meeting
If the participant is assigned to the control group of the intervention, the
researcher provided an iPod Shuffle® that had been preloaded with novel music.

53
Participants were given a goal music listening dosage of 20 minutes per day for at least
five days per week to match the dosage prescribed to the experimental condition. The
primary researcher provided 4 diary-based fidelity assessments (1 per week) to
participants in the control condition in order to capture actual amount of time spent
listening to music and to track any technology-related issues experienced by participants.
The primary researcher determined a weekly time to call participants to obtain diary-
based fidelity information via telephone. Participants in the control condition were asked
not to add any of their own music to the iPod® for the first month of listening. The
researcher explained that they will meet again in 4 weeks to follow up about the
questions they were asked at baseline. Finally, a researcher provided information and
resources related to the use of the iPod Shuffle® and participants were given study-
related information and contact information for a project researcher.
Experimental Group – Baseline Meeting
If the participant was assigned to the experimental condition, a personalized
music assessment was administered to determine the music preferences of the PWD. The
instrument used to assess personalized music preferences was based upon the Assessment
of Personal Music Preference questionnaire (APMP; Gerdner, Hartsock, & Buckwalter,
2000). Gerdner and colleagues developed two versions of the APMP; one version for
patients (see Appendix C), and one version for family members (see Appendix D). The
family version of the APMP used the CG as a proxy to respond on behalf of the PWD. A
single assessment was used in the present study (Appendix M), and was administered to
both the CG and the PWD jointly. This allowed the PWD to respond to questions about

54
favorite music themselves, and allowed CGs to weigh in with additional suggestions. A
summarized list of participants’ favorite music can be found in Appendix P.
Information obtained by the personalized music assessment helped the researcher
develop a playlist of 8-10 songs (or the amount of music that can be purchased using a
$10 iTunes® gift card). If the participants wished to add previously purchased music to
their playlist or add money to their iTunes account to purchase more music, the
researcher offered to help with this as well. Information was provided about how to add
music in the future if the participants so desire (more on this in the following paragraph).
If the participants owned a computer with internet access, the baseline meeting also
included setting up an iTunes account, purchasing music with the iTunes® gift card,
creating a playlist on the computer, transferring the music to an iPod Shuffle®, and
showing the participants how to use the device. If participants did not have a computer
that could store iTunes® and purchased music, the primary researcher had a laptop
available with internet access to download and transfer music to the participant’s iPod®.
As a final component of the baseline meeting, CGs in the experimental condition
were given a detailed information packet to serve as a resource for them after the
researcher left. This included the same information given to the participants in the control
group, additional information about the use and potential benefits of personalized music,
as well as information about how to use iTunes®. The researcher who met with the dyad
for the baseline session talked the CG through this information packet. In sum, this
information included:
The potential benefits of personalized music listening, including helping
with behavioral expressions that occur during certain times of the day or

55
during certain activities, decreasing anxiety and improving mood,
increasing quality of life, and providing an opportunity for the CG and the
PWD to reconnect around familiar music
How to use the iPod Shuffle®, iTunes®, and a list of resources available
to help with any technical or study-related questions.
A reminder about the amount of time PWDs and CGs should spend
listening to personalized music each week.
Finally, CGs were given the diary-based fidelity assessment forms (see
Appendices E and F) to track usage. As in the control group, a researcher set up a weekly
time to call participants to obtain diary-based fidelity information via telephone.
Participants were given the same goal “dosage” of 20 minutes per day of music listening,
at least five days per week over a period of 4 weeks. Actual dosage was tracked in the
diary-based fidelity assessment. The prescribed and actual dosage was captured and used
as a covariate in analyses.
2.7.3. In-Person 1-Month Follow-Up
Experimental Group – Follow-Up Meeting
At the end of the third week of the intervention, participants were contacted via
telephone to set up a final in-person meeting time. The meeting time was scheduled for
as close to one month from the baseline meeting as possible. At this follow-up meeting,
CGs were asked to complete the following questionnaires independently: the CMAI-SF
(Appendix J), and the DRS (Appendix K). At the same time, an interviewer administered
the following questionnaires to the PWD in a separate room: DQoL affect subscales
(Appendix G), the QoL-AD (Appendix H), the SAS (Appendix I), and the DRS

56
(Appendix K). This marked the termination of the study for participants in the
experimental group.
Control Group – Follow-Up Meeting
If the participant was assigned to the control group, they were given the option to
personalize the music on their iPod® to their taste. If they chose to fill the iPod® with
their favorite music, a researcher erased the unfamiliar music previously contained on the
iPod Shuffle® and helped the participants add their favorite music to the now blank
device in the exact same manner as the experimental group at Time 1. All participants
were allowed to keep the equipment (e.g., gift cards, mp3 players, headphones, chargers,
headphones splitters, etc.) that they were given for the intervention.

57
CHATPER III
RESULTS
3.1. Statistical Analyses and Data Treatment
SPSS Statistical Software (Version 24.0, IBM Statistics) was used to enter and
analyze data. Data were entered manually by the primary researcher. Reverse coded
items were reversed in the paper interview so as to avoid confusion during data entry.
Following data entry, descriptive statistics and frequency analyses were run for all items.
By examining range, any data points that exceeded the parameters of the scale were
identified, the hard copy of the interview was consulted, and the appropriate value was
filled in. All missing data were coded as ‘99’ and missing values were defined as ‘99’ for
all numerical variables in SPSS.
The “Analyze Patterns” function in SPSS was used to assess missing data for all
items composing outcome scales. In sum, 1.71% of all items were missing, with 98.29%
of values being present. Of the 30 cases, 16 had at least one missing value. Of the 144
variables, 33 (22.92%) had at least one missing value. For listening time, 3 participants
had missing data (i.e., participants failed to complete their weekly listening logbooks).
Each of these three dyads indicated to the primary researcher that they had listened to
music regularly over the month-long study, but failed to record their listening time.
58
Given the small percentage of missing data across cases, a single imputation
approach was used to handle missing data. Person-mean imputation was used to replace
missing values for all items within the outcome scales. Person-mean imputation is a
technique for substituting missing data using the mean of non-missing values within a
given Likert scale (Downey & King, 1998; Bono et al., 2007). If, for example, a
participant scores (4, 3, 4, 4, 99) on a 5-item Likert scale where 99 is missing, the value
would be replaced with the mean of (4, 3, 4, 4). The new data would be (4, 3, 4, 4, 3.75).
Regarding listening time, three participants had missing data. For this single
“dosage” variable, which was used as a covariate in the final analyses, item-mean
imputation was used to impute a value for the three missing data points. The item-mean
for this imputation was generated from the mean of the overall sample (as opposed to a
separate mean for the control/experimental group subsamples). Evidence suggests that
item-mean imputation for covariates produces unbiased estimates of the treatment effect
and maintains type 1 error rate accuracy in randomized-controlled trials (Kahan, 2014;
White & Thompson, 2005).
The dosage covariate was used in the final analyses was developed from the
PWD’s number of listening sessions as indicated in the weekly logbooks. Among three
dosage variables (total number of listening sessions, total listening time, and average time
per session), the number of listening sessions was the only dosage variable that was
significantly correlated with any of the DVs. Specifically, the number of listening
sessions was significantly correlated with Time 2 quality of life score (r = .37, p < .05),
and was trending toward a significant correlation with baseline quality of life score (r =
.31, p = .10). Regarding this dosage variable, it is possible that the total amount of time
59
spent listening was not as important as the number of listening sessions during the month-
long intervention. For example, suppose that PWD “A” listens for 45 minutes twice per
week and PWD “B” listens for 15 minutes six times per week. Both participants will
have listened for 1 hour and 30 minutes over the course of the week, but PWD “A” will
have gone 5 days of the week without listening compared to PWD “B’s” one day.
Typical approaches to analyzing intervention efficacy require a dosage of at least
80% of the prescribed intervention (Armijo-Olivo et al., 2009). However, given the
exploratory nature of this study, participants were not be excluded from analyses for
failing to meet 80% of their prescribed dosage. Rather, using ‘number of listening
sessions’ as a covariate in final analyses permitted insights about how dosage level
impacted the effectiveness of the intervention.
Multiple regression analyses were used to test each hypothesis. Each model was
structured using the following predictors: a centered baseline assessment of the DV being
tested, a dichotomized group assignment variable, MMSE score, and number of listening
sessions (dosage). The key variable in each model was the dichotomized group
assignment variable. The regression coefficient of this variable was assessed using a t-
test with n – k – 1 degrees of freedom, where n = sample size, and k = the number of
independent variables in the model. A significant regression coefficient for the group
assignment variable represented a significant difference in scores on the dependent
variable for PWDs in the personalized music listening group relative to the unfamiliar
music group (i.e., a significant regression coefficient for this variable indicates that group
assignment accounts for unique variance in the DV after accounting for the baseline score
on the outcome measure, MMSE score, and number of listening sessions).

60
The use of a regression framework for hypothesis testing in the current study was
chosen over an ANCOVA framework for its ability to maximize power in a small
sample. To illustrate, separate post-hoc power analyses were conducted using G*Power
(Faul et al., 2007). First, an analysis was conducted of a single regression coefficient
(two-tailed) in a linear fixed regression model, with a medium effect size of f2
= .25, 30
participants, 4 predictors, and an alpha level of .05. This yields an achieved power level
(1 – β error probability) of .75. The same analysis within an ANCOVA framework
(including main effects and interactions) yields an achieved power level of .16. The
multiple regression technique for assessing group differences has been used in similar
intervention studies in dementia (Judge et al., 2012; Bass et al., 2013).
3.2. Efficacy Testing
Results of each regression analysis are reported in the corresponding subsections
below. For each regression analysis, covariates included the number of listening sessions
(dosage), MMSE score of the PWD, and the centered baseline version of the dependent
variable. The unstandardized regression coefficient for group assignment (B) is reported
for each regression analysis.
Due to the existing differences at baseline from this small sample, analyses also
were conducted with the inclusion of the PWD’s age, income, relationship to care partner
(spouse/non-spouse), and the level of education. Across all analyses, none of these
demographic covariates added significant variance to the model. However, despite being
non-significant effects, the addition of these three variables led to reduced significance of
the key variable (group assignment) in the analyses for both relationship strain and

61
anxiety. It is likely that the drop in significance in this respect was due to high
multicollinearity between group assignment and income (r = -.59, p = .001), relationship
to the caregiver (r = -.41, p = .03), and age (r = .33, p = .08).
An additional concern regarding the inclusion of these non-significant predictors
in the final statistical model is over-fitting. It has been suggested that a minimum
number of subjects per variable in linear regression analysis be between 10 and 15
(Harrell, 2001; Green 1991). Thus, the required minimum sample size for a regression
model with the aforementioned demographic variables would be in the range of 70 to 105
dyads. For these reasons, demographic variables were not included in the final analyses
reported below. This issue is discussed in greater detail in the limitations section of this
study.
3.2.1. Mood
It was hypothesized (H1) that listening to personalized music over a four week
period would improve the overall mood of PWDs relative to participants in the control
group. Separate regression analyses were conducted for the positive and negative affect
subscales of the DQOL rather than a combined score. This decision was made due to
existing literature indicating that positive and negative affect are not opposite ends of a
single spectrum, but two separate constructs altogether (Russell & Carroll, 1999). That
is, a person can score high or low on both positive affect and negative affect.
In the regression model for negative mood, group assignment was non-significant,
B = .28, t(25) = 1.47, p = .16. Additionally, MMSE and session count were both non-
significant (p = .53 and p = .25, respectively). See Figure 1.
Figure 1:

62
In the regression model for positive mood, group assignment was a non-
significant predictor of positive mood at T2, B = .35, t(25) = 1.79, p = .09. MMSE score
was a significant covariate in the model for positive mood, B = .04, t(25) = -2.77, p = .01.
Session count remained non-significant, p = .38. See Figure 2.
Figure 2:
3.2.2. Anxiety
3
3.2
3.4
3.6
3.8
4
4.2
4.4
T1 T2
DQ
OL
(Ne
gati
ve M
oo
d S
ub
scal
e)
Unfamiliar Music Personalized Music
2.5
2.7
2.9
3.1
3.3
3.5
3.7
3.9
4.1
4.3
4.5
T1 T2
DQ
OL
(Po
siti
ve M
oo
d S
ub
scal
e)
Unfamiliar Music Personalized Music

63
It was hypothesized (H2) that listening to personalized music over a four week
period would lead to reduced anxiety for PWDs relative to participants in the control
group. In the regression model for anxiety (SAS score), group assignment was a
significant predictor of anxiety, B = -.17, t(25) = -2.15, p = .04. PWDs in the personalized
music group demonstrated greater reductions in anxiety relative to the unfamiliar music
group. MMSE and session count were both non-significant predictors of anxiety (p = .71
and p = .95, respectively). See Figure 3.
Figure 3:
3.2.3. Behavioral Expressions of Dementia
It was hypothesized (H3) that listening to personalized music over a four week
period would lead to fewer behavioral expressions of dementia for PWDs relative to
participants in the control group. In the regression model for behavioral expressions of
dementia (CMAI score), group assignment was non-significant, p > .05. PWDs in the
personalized music listening group did not demonstrate significantly fewer behavioral
expressions of dementia relative to the control group. MMSE and session count were
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
T1 T2
An
xie
ty
Unfamiliar Music Personalized Music

64
both non-significant predictors of behavioral expressions of dementia at T2 (p = .70 and p
= .19, respectively). See Figure 4.
Figure 4:
3.2.4. Relationship Strain
It was hypothesized (H4) that listening to personalized music over a four week
period would improve the dyadic relationship between the PWD and the CG relative to
dyads in the control group. In the regression model for relationship strain (DRS, full
scale), group assignment was a significant predictor of relationship strain at T2, B = -.33,
t(25) = -2.61, p = .02. PWDs in the personalized music group demonstrated greater
reductions in relationship strain relative to the unfamiliar music group. MMSE and
session count were both non-significant predictors of relationship strain (p = .15 and p =
.59, respectively). See Figure 5.
Figure 5:
1
1.1
1.2
1.3
1.4
1.5
1.6
1.7
1.8
1.9
2
T1 T2
Be
hav
iora
l Exp
ress
ion
s o
f D
em
en
tia
Unfamiliar Music Personalized Music

65
Separate identical regression analyses were conducted separately for the Positive
Interaction and Role Strain subscales of the DRS (see “Section 3.3: Psychometric
Testing” for a rationale). For the Positive Interaction subscale, group assignment
remained a significant predictor of positive interaction at T2, B = -.35, t(25) = -2.12, p =
.04. PWDs in the personalized music listening group showed greater improvement in
positive interaction at T2 relative to the unfamiliar music group (see Figure 5). MMSE
score and session count remained non-significant (p = .46 and p = .32, respectively). See
Figure 6.
Figure 6:
1
1.2
1.4
1.6
1.8
2
2.2
2.4
T1 T2
Re
lati
on
ship
Str
ain
(fu
ll sc
ale
)
Unfamiliar Music Personalized Music

66
*Note: Lower scores represent more positive interaction (less strain).
The Role Strain subscale of the DRS demonstrated similar results. Group assignment
remained a significant predictor of role strain at T2, B = -.42, t(25) = -2.21, p = .04. PWDs
in the personalized music listening group showed greater reductions in role strain at T2
relative to the unfamiliar music group (see Figure 6). MMSE score and session count
remained non-significant (p = .10 and p = .90, respectively). See Figure 7.
Figure 7:
1
1.2
1.4
1.6
1.8
2
2.2
2.4
T1 T2
Re
lati
on
ship
Str
ain
(p
osi
tive
in
tera
ctio
n)
Unfamiliar Music Personalized Music
1
1.2
1.4
1.6
1.8
2
2.2
2.4
T1 T2
Re
lati
on
ship
Str
ain
(ro
le s
trai
n)
Unfamiliar Music Personalized Music

67
3.2.5. Quality of Life
It was hypothesized (H5) that listening to personalized music over a four week
period would lead to improved quality of life for PWDs relative to participants in the
control group. In the regression model for quality of life (QOL score), group assignment
was non-significant, p = .15. MMSE score and session count were both non-significant
predictors of behavioral expressions of dementia at T2, although MMSE was nearing
significance (p = .06 and p = .12, respectively). See Figure 8.
Figure 8:
3.3. Acceptability and Feasibility
Questions designed to assess acceptability and feasibility were included in the
weekly logbooks. Given the potentially confusing nature of new technology, participants
were asked each week if they experienced any technology problems. At week one, one
participant reported a technology problem—the block charger in the kit wasn’t working.
2.5
2.6
2.7
2.8
2.9
3
3.1
3.2
3.3
3.4
3.5
T1 T2
Qu
alit
y o
f Li
fe
Unfamiliar Music Personalized Music

68
Another block charger was provided. At week two, two participants reported technology
problems—one participant couldn’t find the charging cable, but located it following a call
to the primary researcher. The second participant found that the iPod would not charge.
After contacting the primary researcher, it was discovered that the charging cable was not
plugged in all the way to the device. At week three, there were no technology problems
reported. At week four, one participant reported a technology problem—they were
having trouble adding additional music from iTunes.
Following the fourth week of recording listening times in the logbook, CGs were
asked to fill out a survey about their experience with the study. Items in this questionnaire
included “My loved one seemed to enjoy listening to personalized music,” and “I will
continue to play personalized music for my loved one in the future,” for example.
Overall, participants were very favorable toward the personalized music intervention.
For a full account of items and response means, see Table 2.
Table 2.
Acceptability and Feasibility Results for Participants in the Experimental Group (n = 12).
Item M SD
1. My loved one seemed to enjoy listening to personalized music 3.92 .29
2. I would recommend listening to personlized music to others in my situation 3.83 .39
3. I would recommend this study to others in my situation 3.83 .39
4. Playing personalized music for my loved one required too much effort on
my part 1.17 .58
5. The technology aspect of this study was too complicated to make it worth
my time. 1.33 .49
6. The researchers provided enough resources for me to be effective at
providing personalized music 3.75 .45
7. I will continue to play personalized music for my loved one in the future 3.92 .29
Note: Values are the mean of reported scores on a 4-point Likert scale (1 = strongly disagree, 4
= strongly agree).
M = mean, SD = standard deviation

69
CHAPTER IV
DISCUSSION
This study examined the efficacy of a personalized music listening intervention
on PWDs’ mood, behavioral expressions of dementia, anxiety, quality of life, and
relationship strain between the CG and PWD. Significant positive outcomes were found
for anxiety and relationship strain. Further, results indicated high levels of acceptability
and feasibility (discussed below).
4.2. Efficacy
Gerdner’s Mid-Range Theory was the conceptual model upon which the
hypotheses H1, H2, and H3 were based. Specifically, it was hypothesized that
personalized music listening would result in improved mood (H1), anxiety (H2), and
reduced behavioral expressions of dementia (H3). Following the Mid-Range Theory,
behavioral expressions of dementia should benefit most directly from personalized music
listening. The present study did not support this hypothesis. It is possible that behavioral
expressions of dementia are a proximal outcome of personalized music listening. That is,
behavioral symptoms of dementia may be reduced during listening and/or immediately
following listening (as articulated by the Mid-Range Theory), but when examined as a
distal outcome, as they were in this study, no effects were detected. Additionally, the

70
CG’s report of behavioral expressions of dementia was provided for the entire month in
retrospect during the follow-up interview. It is possible that if a different method of
tracking behavioral expression were utilized (such as a daily log or observational
approach, for example), a more precise measure of the number of behavioral expressions
of dementia could be determined. This may be a consideration for future studies.
Another possibility regarding the lack of change in behavioral expressions of dementia is
that the population of PWDs in the present study was in the mild-to-moderate stages of
dementia. In a population of PWDs in the moderate-to-late stages of dementia, when
behavioral expressions of dementia are more prevalent, perhaps a personalized music
intervention for PWDs in the community would be more effective in this regard.
This intervention demonstrated improvements in the domains of anxiety and
relationship strain, with a trend toward improvement in mood. This study attempted to
isolate the effects of personalized music listening on the PWD by utilizing a control
group that received an unfamiliar playlist of music. As such, this is one of the first
applied research studies designed to examine the benefits of the personalized music
listening relative to general music listening (as opposed to a care-as-usual comparison
group), in a population of PWDs (Gerdner, 2000). Moreover, this is the first study to
examine this research question in a population of community-dwelling PWDs. The
findings from this study provide support for the beneficial nature of personalized music
listening relative to unfamiliar music listening. These findings are consistent with the
existing literature indicating that personalized music listening for PWDs may be
especially engaging due to the well-preserved musical memory ability of PWDs
(Jacobsen, et al., 2015; Gerdner, 1997).

71
The effect of personalized music listening on positive mood was approaching
significance in the present study. Similar to behavioral expressions of dementia, it may
be that mood is most improved proximally (during and immediately after listening).
Despite the lack of significance in this domain in the present study, it is recommended
that mood be considered as an outcome variable in future research. It may be that the
sample size in this pilot study was not sufficient to detect a significant effect of mood, or
that the one-month duration of the study was not long enough to promote a change in
overall mood.
Anxiety was significantly reduced in the personalized music group relative to the
unfamiliar music group over the one month intervention period. This is not the first study
to report anxiety-related benefits of personalized music listening for PWDs. Sung and
colleagues (2010) found similar outcomes for anxiety in an institutionalized population of
PWDs that were part of a personalized music listening group relative to a control (no
music) group after 6 weeks. Additionally, this finding is consistent with the Mid-Range
Theory supposition that personalized music provides an enjoyable and meaningful
stimulus for PWDs to focus their attention. This meaningful stimulus may occupy the
PWD’s attention in place of other potentially distressing and/or confusing stimuli that are
anxiety provoking. Moreover, in comparison to behavioral expressions of dementia and
mood, anxiety is relatively stable. Thus, it follows that anxiety may be a more
appropriate distal outcome measure of the effects of personalized music on well-being of
PWDs.
In the present study, the PWD’s quality of life did not demonstrate a significant
increase as a result of personalized music listening. There are several possibilities as to

72
why improvements were not seen in this domain. First, it is possible that there is a small
effect of personalized music listening on quality of life and this study did not have the
power to detect it. Indeed, the pattern of data for quality of life was similar to the pattern
of data for mood. Alternatively, it may be that the one-month duration of the present
intervention was not long enough to elicit an effect of quality of life. In contrast to mood,
quality of life is relatively stable over time (Atkinson, 1982). With an increased duration
of listening, it is possible that the slight trend visible from the present results would
continue over time and reach statistical significance. Another possibility is that
personalized music listening does not have a substantial impact on quality of life.
Questions from the quality of life measure used in the present study centered on highly
impactful domains of life such as finances, functional ability, marriage, hobbies, etc.
Personalized music, while enjoyable and engaging, may not be powerful enough to
impact many of these domains.
Findings from this study indicated that personalized music has a positive impact
on the relationship between the PWD and the CG—both in domains of role strain and
positive interaction. This finding may be unique to dyads living in the community relative
to PWDs living in long-term care receiving care from a professional CG. First,
personalized music may draw on shared memories between a PWD and an informal CG.
The use of personalized music by a CG to engage a PWD may be a source of positive
interaction between the two members of the dyad. Personalized music use in long-term
care facilities may provide more of an opportunity to engage residents while staff
members attend to other tasks. As such, interaction during listening sessions may be
more limited in this population.

73
During the in-person training with the CG on the iPod® and the general use of
personalized music, it was suggested that personalized music be used during the time of
the day when behavioral expressions of dementia are more common. For many PWDs,
sun-downing, or the prevalence of behavioral expressions of dementia later in the day, is
common. CGs were instructed to pre-empt these episodes if possible by engaging the
PWD in listening prior to these times of the day in order to increase mood and reduce the
likelihood of sun-downing. It is possible that this practice may have accounted for a
perceived improvement in relationship between the PWD and the CG. However, if this
were the case, it is unclear why improvements in behavioral expressions of dementia
were not detected in this study. Moreover, the instrument that was used for relationship
strain in this study demonstrated marginal reliability. Several of the items in this scale
had high rates of missing responses by participants. Despite this, the Dyadic
Relationship Scale is currently the only instrument aimed at assessing relationship strain
in this population. Future studies may consider modifying the items in this scale that had
high rates of missing data. Further, the reliability tests from the present study indicate
that the DRS may be most reliable when separated into its subscales.
4.2. Acceptability and Feasibility
Several factors were examined in the present study to assess the acceptability and
feasibility of this pilot intervention. Specifically, acceptability and feasibility were
assessed by examining attrition rates, adverse events, adherence to the study protocol,
and results from the acceptability questionnaire.
Of the 34 dyads that met all screening requirements and were randomly assigned
to the treatment or comparison group, 4 dyads ended up withdrawing from the study; an

74
11.8% attrition rate. Three of these participants were originally assigned to the
experimental group and one was assigned to the control group. In comparison to
previously published studies examining the benefits of personalized music for persons
with dementia, the present study demonstrated a slightly higher attrition rate. Sung and
colleagues (2006) reported a 10% attrition rate. In a subsequent study, Sung and
colleagues (2011) reported an attrition rate of 8.3%. The higher attrition rate in the
present study may be attributable to the fact that participants in this study were
community dwelling rather than institutionalized. In this particular intervention design,
the administration of the music listening was largely dependent on the initiative of an
informal CG in the home rather than a formal CG or a researcher in an institutional
setting. The added responsibility of an informal CG to engage the PWD in this study
may help to explain the higher attrition rate.
None of the non-completers in the present study reported withdrawing due to an
adverse event. One participant discontinued participation due to lack of interest, and
three participants withdrew because they felt that their schedules were too busy (or had
become too busy due to unforeseen circumstances) to continue participating. Among the
participants who completed the study, one adverse event was reported by a caregiver
during a weekly follow-up call. This PWD was in the personalized music group. The
CG reported that the PWD became upset by a song on the playlist that brought back
memories of the PWD’s father. During the follow-up call, the CG discussed the situation
with the primary researcher. It was decided that the best course of action was to remove
the song from the playlist. During the next week’s follow-up call, the CG reported that
the PWD experienced no adverse events during that week’s listening. Based on the

75
feedback of caregivers to the acceptability questionnaire, participants reported an
overwhelmingly positive experience participating in the study. Participants’ primary
recommendation for improving the study was to increase the number of songs on the
PWD’s playlist.
None of the participants in the control group reported familiarity with any of the
songs on the unfamiliar music playlist.
Regarding adherence to the treatment procedure, 27 participants of 30 completed
their weekly logbooks for the month. The three dyads that did not complete their
logbooks indicated that they did the listening, but failed to record their listening times.
All participants were given a goal listening dosage of 20 minutes per day for 5 days per
week for each week of the study. There were 20 participants during week 1 (66.7%) that
met this goal, 20 participants at week 2, 20 participants at week 3, and 14 participants at
week 4 (46.7%). There was quite a bit of variability in the number of sessions and the
duration of the listening sessions in which participants engaged. Some participants
preferred more frequent but shorter listening sessions while some participants preferred
fewer but longer listening sessions.
Given the lack of similar interventions for community-dwelling PWDs, it is
difficult to gauge whether this adherence rate is high or low. There are several factors
that may have influenced the adherence rate in this particular study. First, this
intervention protocol was extremely flexible in nature. Compared to other intervention
protocols wherein the number of sessions, the timing of sessions, and the content of each
session is rigidly controlled, this intervention relied on a much looser approach, allowing
CGs and PWDs to listen when they felt it was convenient, and for a duration that they

76
desired. While all participants were given a goal dosage, there was no penalty for failing
to meet this dosage. Another factor which may have contributed to the adherence rates of
participants was the equipment that participants were given to keep following their
completion of the program. Though there was no direct monetary incentive for
participating in the study, the ability to keep the iPod Shuffle® may have been an
incentive for some to participate, and to continue participating through the end of the
month-long participation window. Many CGs who were not previously familiar with
Apple® products were interested in learning how to use iTunes® in-depth so that they
could add, remove, and continue changing the PWD’s playlist after the study ended.
Finally, CGs may have been encouraged to use and continue using music as a means of
engaging PWDs after the baseline meeting with the primary researcher. During this
meeting, the primary researcher demonstrated how to use the iPod® and the CG had an
opportunity to witness the PWD using the iPod for the first time. Several CGs, especially
those in the personalized music group, indicated surprise during this meeting about how
positively the PWD responded to the use of the iPod® and to the music in general.
Overall, the uniqueness of the present protocol relative to other music-based
interventions designed for PWDs make firm conclusions about the treatment fidelity
difficult. The rate of completion, high acceptability as indicated by the acceptability
questionnaire, and the lack of adverse events support the feasibility of this intervention.
Regarding intervention dosage, a more rigid intervention protocol may increase the
number of PWDs who met the required dosage. However, a more structured approach to
either administering or monitoring the listening of the PWD comes with a potential

77
tradeoff of a time and resource-intensive experimental design and/or greater perceived
intrusion in the lives of the participants.
4.3. Clinical Implications
The present study supports the use of personalized music as a means of improving
several domains of psychosocial well-being for PWDs living in the community.
Personalized music interventions have predominantly been conducted in institutionalized
populations of PWDs such as those living in nursing homes or assisted living facilities.
This study takes a first step to extend these findings to individuals in the community.
Currently, it is estimated that 70% of persons with Alzheimer’s disease and related
dementias live in the community (Alzheimer’s Association, 2018). Among these
individuals, 74% live with an informal caregiver (Alzheimer’s Association, 2018). Thus,
community-dwelling individuals, as included in the current study, represent the largest
population of PWDs in the United States in terms of living arrangement. Although
accessibility to this population and implementation in the community are definite
challenges regarding the use of personalized music for these individuals, the present
study suggests that personalized music may nevertheless be a relatively low-cost means
of engaging these PWDs in a beneficial way.
The results from this study provide additional evidence to support the efficacy of
non-pharmacological approaches to intervention for PWDs. A primary benefit of this
type of intervention for PWDs is that engagement in personalized music, development of
a playlist, and implementation of the program does not require a high degree of
intervention expertise. Familiarity with the software and hardware used in the present

78
study is common, especially among the computer-savvy younger generations. In fact, the
Music and MemoryTM
organization relies heavily on high school age volunteers in
nursing homes and assisted living facilities to help PWDs setup and use their
personalized music devices.
The psychometric results from the PWD self-report data on the instruments used
in the present study adds further evidence to an existing body of literature suggesting that
PWDs are able to reliably self-report on subjective information (see Section 1.2). The
present sample included PWDs with an average MMSE score of 20 (SD = 6.1), indicating
a moderate level of impairment on average. This body of literature is important to ensure
that the true perspective of the PWD (as opposed to a potentially inaccurate proxy-report)
is obtained in dementia research.
4.4. Limitations
A primary limitation of the present study is the presence of group differences in
several key demographic areas. Participants assigned to the experimental group had, on
average, a lower level of education, lower income, lower MMSE score, were less likely
to have a spousal CG, and were older than those in the control group. In a study with a
larger sample size, the process of randomization likely would have been sufficient to
ensure that these variables matched across groups. While possible to control for these
demographic variables statistically in the regression analyses, the sample size and the
high multicollinearity between demographic factors and group assignment made the
inclusion of these variables statistically problematic (as discussed in the Efficacy Testing
subsection of the Results section). A “catch-22,” the increased N-size that would be
needed to include these predictors in the regression models would likely have been

79
sufficient to overcome the group differences merely through the process of random
assignment—hence eliminating the necessity for statistical control of these demographic
variables in the regression models altogether. Nevertheless, future studies should be sure
to consider these demographic factors when interpreting results.
A limitation is that the majority of participants in this study were recruited from
caregiver support groups via the Alzheimer’s Association. It is possible that this
recruitment method has some degree of inherent bias. Participants already engaged in
community-based resources aimed at helping PWDs and CGs may be more receptive and
engaged in the program and less likely to withdraw. With a sample of individuals
recruited via other means, it is possible that adherence would not have been as high as it
was in the present study. This potential source of bias presents a challenge for future
research in this area. Locating and recruiting PWDs and CGs from the community
without using existing community-based dementia services to access this population is
difficult. Potential sources of recruitment for future studies include hospitals, physicians’
offices, senior apartments, home healthcare organizations, and public advertisements.
An additional limitation to the present study was the restriction to an Apple®
framework and the limited resources (specifically, the number of songs) that could be
provided to each participant. Several alternative options exist which have the potential to
deliver a larger playlist to PWDs. An organization in Scotland called Playlist for Life®
has developed an app in recent years designed to engage PWDs with personalized music.
This app is installed on a smartphone or tablet, and requires a monthly fee to access
unlimited music via Spotify® streaming service. The app has a built in feature that helps
PWDs and CGs find their favorite music. This type of personalized music delivery has

80
the fantastic benefit of unlimited music, but requires a reliable internet connection, a
smartphone or tablet (rather than an iPod Shuffle®, which is very simplistic and easy to
use), and may be more costly in the long-term due to the monthly subscription. The
benefit of this app is that CGs would not have to learn to use iTunes® on a separate
computer in order to add or remove songs from a PWD’s playlist, nor would it be
necessary to learn to interface the iPod® and iTunes®. Moreover, a streaming service
does not require the storage of music files on a local computer or hard drive; music is
streamed in real time via the internet.
In the United States, internet access may be difficult to obtain or costly; especially
for low-SES families and families living in rural areas where there are few internet
service provider options. For these individuals, using an iPod® may be more cost
effective. Individuals can access iTunes® at a Wi-FiTM
hotspot such as a library or coffee
shop to add music to their playlist, and use the iPod® to engage PWDs at home in a
location without internet access. For institutions such as nursing homes, assisted living
facilities, and adult day care centers, the Apple® framework is cost effective.
Organizations can invest in a single computer with iTunes® to use as a hub for loading
multiple iPod Shuffles®, which are relatively inexpensive. As of yet, there is no one-
size-fits-all option for introducing personalized music to PWDs living in the community.
Future studies may consider a flexible approach to choosing a music service for this
population.
In the present study, participants in the control group were given a single playlist
of 24 songs (see Appendix N). Over the course of the one-month of listening, it is
possible that participants became familiar with the songs on the unfamiliar playlist. That

81
is, over time this music may have become familiar to participants, potentially posing a
similar benefit in the later weeks of the study as the personalized music provided to
PWDs in the personalized music group. In future studies, it may be beneficial to alter the
comparison group playlist during each listening session. This would be very challenging
and costly to accomplish with the iPod® and iTunes® approach, but would be reasonably
easy to implement if a streaming-based approach to music listening were used, such as
the Playlist for Life®, discussed above.
An additional limitation to the present study is that the primary researcher (who
conducted all interviews, training, and weekly follow-up calls), was not blinded to group
assignment, nor were the participants. Several efforts were made to minimize the impact
of experimenter bias in this regard. First, participants were randomly assigned to a group
after the completion of the baseline interview. Second, during the follow-up interview,
the experimenter was blinded to the baseline scores of the PWD. In future research, it
would be ideal to design a study in which the interviewer is blinded to group assignment
and a separate experimenter conducts the training and playlist development aspects of the
study. This would help to reduce potential sources of bias in the study design. As a final
limitation, participants in the personalized music listening group may have been primed
by the information packet they were given about the benefits of personalized music.
4.5. Future Directions for Research
It should be emphasized that the outcomes from this pilot study represent
preliminary results that should be used to guide future intervention development. The
most obvious future direction for this research is an increased sample size. Due to the
82
lack of existing data, the hypotheses presented and tested in this study require replication
and expansion to larger samples.
While this intervention was dyadic in nature, CG-derived benefits of personalized
music were not explored in the present study. Few studies have examined the impact of
personalized music on informal CGs. Given that personalized music may be a useful tool
for informal CGs regarding the engagement of persons with dementia, a potential
opportunity for CG respite, and (although not supported by the data from this study) a
potential means of reducing difficult behavioral expressions of dementia, CG outcomes
should be considered for inclusion in future research.
Due to the self-report nature of the PWD interviews at baseline and follow-up,
PWDs in the later stages of dementia were not included in the present study. Ultimately,
individuals in the later stages of dementia may stand to benefit the most from an
intervention of this nature. As cognitive and functional abilities decline later in the
course of the disease, the ability of personalized music to capitalize on a remaining
strength of PWDs may translate into a greater derived benefit for these individuals. A
notable difficulty of extending this type of protocol to PWDs in the later stages is
determining a way of measuring outcomes reliably from a population of individuals that
may have trouble communicating their own perspectives. In the present study, the
MMSE (particularly, a cutoff score of 10) was used to determine if the PWD would be
able to participate in the self-report process. While the MMSE is a widely used measure
of cognitive status for PWDs, it is an assessment of global cognitive functioning. Several
objective domains assessed by the MMSE such as orientation to time and place,
quantitative reasoning, and short-term memory for new information may not be relevant

83
to the PWD’s ability to participate in self-report research. An instrument aimed
specifically at assessing the subjective reporting capacity of PWDs (ability to
comprehend questions and communicate internal states, values and preferences, for
example) would be useful to extend this intervention to able PWDs who may have scored
below the MMSE cutoff used in the present study.
While several basic research studies in this field support the finding that musical
memory is well-preserved relatively late into the course of Alzheimer’s disease (Jacobsen
et al., 2015; King et al., 2018), no effort was made in the present study to confirm a
diagnosis of Alzheimer’s disease. All participants in the present study had a confirmed
or suspected diagnosis of dementia, and performed within a range on the MMSE which
indicated mild-to-moderate levels of impairment. If the preservation of musical memory
is a phenomenon that is unique to Alzheimer’s disease relative to other forms of
dementia, it is possible that the impact of a personalized music intervention would be
more robust in an Alzheimer’s-specific sample of PWDs. Alternatively, basic research in
neuroscience may benefit from examining preservation of the musical memory system in
PWDs with non-Alzheimer’s pathologies.
An increased intervention duration may be worthwhile to investigate the benefits
of personalized music listening over the long-term. This would allow for a better
understanding of how personalized music impacts relatively stable psychosocial
constructs such as quality of life or depression, for example. Additionally, a longer-term
intervention, or long-term follow-up after completion of the intervention would provide
insights into listening adherence over time. A replication of this research design with an
extended intervention period may pose some challenges, however. In this study, dyads

84
assigned to the control group were aware that the playlists they were given would be
personalized after the one-month intervention period. It may be less likely that dyads
would be receptive to listening to an unfamiliar playlist for an extended period of time
such as 3 months or 6 months. Furthermore, it is possible that PWDs in an unfamiliar
music listening group would come to learn and remember the music on a single playlist
after repeated exposure during an extended intervention period. This would seem to
necessitate a changing comparison group playlist, as discussed in the limitations sections
above.
One of the challenges associated with personalized music interventions is
determining which music is most personally meaningful to the PWD. For individuals in
the moderate-to-later stages of dementia, remembering specific songs, artists, and
composers poses a distinct challenge. Recommendations made by the CG and the use of
song sampling were used in the present study to overcome this challenge. While these
playlists appeared to be more beneficial than unfamiliar music in domains of anxiety and
relationship strain, it is difficult to know if there are personally meaningful songs missing
from the PWD’s playlist that would be even more effective. It would be particularly
interesting to see if playlists created prior to or immediately following a dementia
diagnosis (when the PWD is able to compile his or her ideal playlist) are more beneficial
in the moderate and later stages of the disease relative to playlists created by PWDs in
these stages with the help of a CG.
Additionally, most people have a preference for music that spans several genres
and moods. Future studies might examine the benefits of listening to a variety of such
genres and moods. For example, perhaps listening to a favorite relaxing orchestral piece

85
is best in the evening while listening to upbeat swing is best in the daytime. Future
assessments of personalized music should attempt to capture this detail of a PWD’s
preferred playlist. Questions such as “What type of music do you prefer to listen to when
you are sad/happy/angry?” might be a good starting point for creating separate favorite
playlists for different moods. While this study has highlighted some important overall
effects of personalized music, there is a great deal of specificity regarding the artists,
connections to the music, moods, genres, associated memories, etc. that have yet to be
explored in the personalized music literature.
In larger longitudinal studies, the benefits of a personalized music intervention
could be examined in several additional domains. For example, it would be particularly
interesting to know if the use of a personalized music intervention might delay the
progression of cognitive decline over time, if it would help to delay institutionalization of
PWDs living in the community, reduce caregiver burden over time, and/or to delay the
advancement of behavioral expressions of dementia. The Stress-Process Model, both for
individuals with dementia and for caregivers, may be a useful conceptual model to inform
the selection of outcome variables for PWDs and CGs in future studies.

86
REFERENCES
Afram, B., Stephan, A., Verbeek, H., Bleijlevens, M. H., Suhonen, R., Sutcliffe, C., ... &
Meyer, G. (2014). Reasons for institutionalization of people with dementia:
informal caregiver reports from 8 European countries. Journal of the American
Medical Directors Association, 15(2), 108-116.
Aguirre, E., Woods, R. T., Spector, A., & Orrell, M. (2013). Cognitive stimulation for
dementia: a systematic review of the evidence of effectiveness from randomised
controlled trials. Ageing research reviews,12(1), 253-262.
Allain, P., Chaudet, H., Nicoleau, S., Etcharry-Bouyx, F., Barré, J., Dubas, F., ... & Le
Gall, D. (2007). Étude de la planification de l’action au moyen du test du plan du
zoo dans la maladie d’Alzheimer. Revue Neurologique,163(2), 222-230.
Alzheimer's Association. (2018). 2018 Alzheimer's disease facts and figures. Alzheimer's
& Dementia, 12(4), 459-509.
American Music Therapy Association (AMTA) (2006) Music Therapy and Alzheimer’s
Disease. PDF Available at: http://www.musictherapy.org/
assets/1/7/MT_Alzheimers_2006.pdf.
Aminzadeh, F., Byszewski, A., Molnar, F. J., & Eisner, M. (2007). Emotional impact of
dementia diagnosis: exploring persons with dementia and caregivers’
perspectives. Aging and Mental Health, 11(3), 281-290.
Aneshensel, C. S., Pearlin, L. I., Mullan, J. T., Zarit, S. H., & Whitlatch, C. J. (1995).
Profiles in caregiving: The unexpected career. San Diego, CA US: Academic
Press.

87
Apóstolo, J. L. A., Cardoso, D. F. B., Rosa, A. I., & Paúl, C. (2014). The effect of
cognitive stimulation on nursing home elders: A randomized controlled
trial. Journal of Nursing Scholarship, 46(3), 157-166.
Arlt, S., Lindner, R., Rösler, A., & von Renteln-Kruse, W. (2008). Adherence to
medication in patients with dementia. Drugs & aging, 25(12), 1033-1047.
Armijo-Olivo, S., Warren, S., & Magee, D. (2009). Intention to treat analysis,
compliance, drop-outs and how to deal with missing data in clinical research: a
review. Physical therapy reviews, 14(1), 36-49.
Atkinson, T. (1982). The stability and validity of quality of life measures. Social
Indicators Research, 10(2), 113-132.
Ayalon, L., Gum, A. M., Feliciano, L., & Areán, P. A. (2006). Effectiveness of
nonpharmacological interventions for the management of neuropsychiatric
symptoms in patients with dementia: a systematic review. Archives of internal
medicine, 166(20), 2182-2188.
Bahar-Fuchs, A., Clare, L., & Woods, B. (2013). Cognitive training and cognitive
rehabilitation for mild to moderate Alzheimer’s disease and vascular
dementia. Cochrane Database Syst Rev, 6.
Baker, F. A., Grocke, D., & Pachana, N. A. (2012). Connecting through music: A study
of a spousal caregiver-directed music intervention designed to prolong fulfilling
relationships in couples where one person has dementia. Australian Journal of
Music Therapy, 23.

88
Ballard, C., Day, S., Sharp, S., Wing, G., & Sorensen, S. (2008). Neuropsychiatric
symptoms in dementia: importance and treatment considerations. International
Review of Psychiatry, 20(4), 396-404.
Ballard, C., Lowery, K., Powell, I., O'Brien, J., & James, I. (2000). Impact of behavioral
and psychological symptoms of dementia on caregivers. International
Psychogeriatrics, 12(S1), 93-105.
Bamford, C., & Bruce, E. (2000). Defining the outcomes of community care: the
perspectives of older people with dementia and their carers. Ageing and
Society, 20(05), 543-570.
Banerjee, S., Smith, S. C., Lamping, D. L., Harwood, R. H., Foley, B., Smith, P., …
Knapp, M. (2006). Quality of life in dementia: more than just cognition. An
analysis of associations with quality of life in dementia. Journal of Neurology,
Neurosurgery, and Psychiatry, 77(2), 146–148.
http://doi.org/10.1136/jnnp.2005.072983
Bass, D. M., Judge, K. S., Lynn Snow, A., Wilson, N. L., Morgan, R., Looman, W. J., ...
& Garcia‐Maldonado, M. (2013). Caregiver outcomes of partners in dementia
care: Effect of a care coordination program for veterans with dementia and their
family members and friends. Journal of the American Geriatrics Society, 61(8),
1377-1386.
Baumgartner, H. (1992). Remembrance of things past: Music, autobiographical memory,
and emotion. NA-Advances in Consumer Research Volume 19.

89
Beck, C., Heithoff, K., Baldwin, B., Cuffel, B., O'Sullivan, P., & Chumbler, N. (1997).
Assessing disruptive behavior in older adults: The Disruptive Behavior
Scale. Aging & Mental Health, 1(1), 71-80.
Benzinger, T. L., Blazey, T., Jack, C. R., Koeppe, R. A., Su, Y., Xiong, C., ... & Cairns,
N. J. (2013). Regional variability of imaging biomarkers in autosomal dominant
Alzheimer’s disease. Proceedings of the National Academy of Sciences, 110(47),
E4502-E4509.
Berger, G., Bernhardt, T., Schramm, U., Müller, R., Landsiedel‐Anders, S., Peters, J., ...
& Frolich, L. (2004). No effects of a combination of caregivers support group and
memory training/music therapy in dementia patients from a memory clinic
population. International Journal of Geriatric Psychiatry,19(3), 223-231.
Berkman, L. F., & Syme, S. L. (1979). Social networks, host resistance, and mortality: a
nine-year follow-up study of Alameda County residents. American journal of
Epidemiology, 109(2), 186-204.
Blackburn, R., & Bradshaw, T. (2014). Music therapy for service users with dementia: a
critical review of the literature. Journal of psychiatric and mental health
nursing, 21(10), 879-888.
Blood, A. J., Zatorre, R. J., Bermudez, P., & Evans, A. C. (1999). Emotional responses to
pleasant and unpleasant music correlate with activity in paralimbic brain
regions. Nature neuroscience, 2(4), 382-387.
Bookwala, J., & Schulz, R. (1996). Spousal similarity in subjective well-being: the
Cardiovascular Health Study. Psychology and aging, 11(4), 582.

90
Bourgeois, M. S. (2002). “Where is my wife and when am I going home?” The challenge
of communicating with persons with dementia. Alzheimer's Care Today, 3(2),
132-144.
Bradford, A., Brenes, G. A., Robinson, R. A., Wilson, N., Snow, A. L., Kunik, M. E., ...
& Amspoker, A. B. (2013). Concordance of self-and proxy-rated worry and
anxiety symptoms in older adults with dementia. Journal of anxiety
disorders, 27(1), 125-130.
Brod, M., Stewart, A. L., Sands, L., & Walton, P. (1999). Conceptualization and
measurement of quality of life in dementia: The dementia quality of life
instrument (DQoL). The Gerontologist, 39(1), 25-36.
Brodaty, H., & Donkin, M. (2009). Family caregivers of people with dementia.
Dialogues Clin Neurosci, 11(2), 217-228.
Brody, E. M. (1981). “Women in the middle” and family help to older people. The
Gerontologist, 21(5), 471-480.
Brotons, M., & Marti, P. (2003). Music therapy with Alzheimer's patients and their
family caregivers: a pilot project. Journal of Music Therapy, 40(2), 138-150.
Camic, P. M., Williams, C. M., & Meeten, F. (2013). Does a ‘Singing Together Group’
improve the quality of life of people with a dementia and their carers? A pilot
evaluation study. Dementia, 12(2), 157-176.
Camp, C. J. (2017). Flexibility in persons with dementia In J. D. Sinnott (Ed.), Identity
flexibility during adulthood. (pp. 99-114). Cham, Switzerland: Springer
International Publishing AG.

91
Cantor, M. H. (1983). Strain among caregivers: A study of experience in the United
States. The Gerontologist.
Carpenter, B. D., Kissel, E. C., & Lee, M. M. (2007). Preferences and life evaluations of
older adults with and without dementia: reliability, stability, and proxy
knowledge. Psychology and aging, 22(3), 650.
Caspi, E. (2013). Time for change: Persons with dementia and “behavioral expressions,”
not “behavior symptoms.” Journal of the American Medical Directors
Association, 14(10), 768–769. http://doi.org/10.1016/j.jamda.2013.05.019
Chapman, S. B., Weiner, M. F., Rackley, A., Hynan, L. S., & Zientz, J. (2004). Effects of
cognitive-communication stimulation for Alzheimer's disease patients treated with
donepezil. Journal of Speech, Language, and Hearing Research, 47(5), 1149-
1163.
Cipriani, G., Lucetti, C., Nuti, A., & Danti, S. (2014). Wandering and dementia.
Psychogeriatrics, 14(2), 135-142.
Clair, A. A. (1996). The effect of singing on alert responses in persons with late stage
dementia. Journal of Music Therapy, 33(4), 234-247.
Clair, A. A., & Bernstein, B. (1990a). A comparison of singing, vibrotactile and
nonvibrotactile instrumental playing responses in severely regressed persons with
dementia of the Alzheimer's type. Journal of Music Therapy, 27(3), 119-125.
Clair, A. A., & Bernstein, B. (1990b). A preliminary study of music therapy
programming for severely regressed persons with Alzheimer's-type dementia.
Journal of Applied Gerontology, 9(3), 299-311.

92
Clare, L. (2003). Managing threats to self: awareness in early stage Alzheimer's
disease. Social science & medicine, 57(6), 1017-1029.
Clare, L., & Woods, R. T. (2004). Cognitive training and cognitive rehabilitation for
people with early-stage Alzheimer's disease: A review.Neuropsychological
rehabilitation, 14(4), 385-401.
Cohen‐Mansfield, J. (1986). Agitated behaviors in the elderly: II. Preliminary results in
the cognitively deteriorated. Journal of the American Geriatrics Society, 34(10),
722-727.
Cohen-Mansfield, J. (1997). Conceptualization of agitation: results based on the Cohen-
Mansfield agitation inventory and the agitation behavior mapping
instrument. International Psychogeriatrics, 8(S3), 309-315.
Cohen-Mansfield, J. (2000). Theoretical Frameworks for Behavioral Problems in
Dementia. Alzheimer's Care Today, 1(4), 8-21.
Cohen-Mansfield, J. (2001). Nonpharmacologic interventions for inappropriate behaviors
in dementia: a review, summary, and critique. The American Journal of Geriatric
Psychiatry: Official Journal of the American Association for Geriatric Psychiatry,
9(4), 361–381. http://doi.org/10.1176/appi.ajgp.9.4.361
Cohen-Mansfield, J. (2008). Agitated behavior in persons with dementia: the relationship
between type of behavior, its frequency, and its disruptiveness. Journal of
psychiatric research, 43(1), 64-69.
Cohen-Mansfield, J. (2015). Non-pharmacological interventions for agitation in
dementia: various strategies demonstrate effectiveness for care home residents;
further research in home settings is needed. Evidence Based Nursing.

93
Cohen-Mansfield, J., Dakheel-Ali, M., & Marx, M. S. (2009). Engagement in persons
with dementia: the concept and its measurement. The American journal of
geriatric psychiatry, 17(4), 299-307.
Cohen-Mansfield, J., Dakheel-Ali, M., Marx, M. S., Thein, K., & Regier, N. G. (2015).
Which unmet needs contribute to behavior problems in persons with advanced
dementia? Psychiatry research, 228(1), 59-64.
Cohen-Mansfield, J., & Jensen, B. (2008). Assessment and treatment approaches for
behavioral disturbances associated with dementia in the nursing home: Self-
reports of physicians' practices. Journal of the American Medical Directors
Association, 9(6), 406-413.
Cohen-Mansfield, J., Marx, M. S., & Rosenthal, A. S. (1989). A description of agitation
in a nursing home. Journal of Gerontology, 44(3), M77-M84.
Cohen-Mansfield, J., Marx, M. S., & Werner, P. (1992). Agitation in elderly persons: an
integrative report of findings in a nursing home. International
Psychogeriatrics, 4(04), 221-240.
Cohen-Mansfield, J., & Mintzer, J. E. (2005). Time for change: the role of
nonpharmacological interventions in treating behavior problems in nursing home
residents with dementia. Alzheimer Disease & Associated Disorders,19(1), 37-40.
Cohen-Mansfield, J., & Werner, P. (1995). Environmental influences on agitation: An
integrative summary of an observational study. American Journal of Alzheimer's
Disease and Other Dementias, 10(1), 32-39.
Cooke, M. L., Moyle, W., Shum, D. H., Harrison, S. D., & Murfield, J. E. (2010a). A
randomized controlled trial exploring the effect of music on agitated behaviours

94
and anxiety in older people with dementia. Aging and Mental Health, 14(8), 905-
916.
Cooke, M., Moyle, W., Shum, D., Harrison, S., & Murfield, J. (2010b). A randomized
controlled trial exploring the effect of music on quality of life and depression in
older people with dementia. Journal of Health Psychology,15(5), 765-776.
Cooper, C., Mukadam, N., Katona, C., Lyketsos, C. G., Ames, D., Rabins, P., ... &
Brodaty, H. (2012). Systematic review of the effectiveness of non-
pharmacological interventions to improve quality of life of people with
dementia. International Psychogeriatrics, 24(06), 856-870.
Cotrell, V., & Schulz, R. (1993). The perspective of the patient with Alzheimer’s disease:
a neglected dimension of dementia research. The Gerontologist, 33(2), 205–211.
http://doi.org/10.1093/geront/33.2.205
Clark, P. A., Tucke, S. S., & Whitlatch, C. J. (2008). Consistency of information from
persons with dementia An analysis of differences by question
type. Dementia, 7(3), 341-358.
Crystal, H. A., Grober, E., & Masur, D. A. V. I. D. (1989). Preservation of musical
memory in Alzheimer's disease. Journal of Neurology, Neurosurgery &
Psychiatry, 52(12), 1415-1416.
Dawson, N. T., Powers, S. M., Krestar, M., Yarry, S. J., & Judge, K. S. (2013). Predictors
of self-reported psychosocial outcomes in individuals with dementia. The
Gerontologist, 53(5), 748-759.

95
De Boer, M. E., Hertogh, C. M., Dröes, R. M., Riphagen, I. I., Jonker, C., & Eefsting, J.
A. (2007). Suffering from dementia–the patient's perspective: A review of the
literature. International Psychogeriatrics, 19(06), 1021-1039.
Dileo, C. & Bradt, J. (2005). Medical music therapy: A Meta-analysis of the literature
and an agenda for future research. Cherry Hill, NJ: Jeffrey Books.
Eshkoor, S. A., Hamid, T. A., Nudin, S. S. H., & Mun, C. Y. (2014). Does substance
abuse contribute to further risk of falls in dementia. Aging, Neuropsychology, and
Cognition, 21(3), 317-324.
Everard, K. M., Lach, H. W., Fisher, E. B., & Baum, M. C. (2000). Relationship of
activity and social support to the functional health of older adults. The Journals of
Gerontology. Series B, Psychological Sciences and Social Sciences, 55(4), S208–
S212. http://doi.org/10.1093/geronb/55.4.S208
Ettema, T. P., Dröes, R. M., de Lange, J., Ooms, M. E., Mellenbergh, G. J., & Ribbe, M.
W. (2005). The concept of quality of life in dementia in the different stages of the
disease. International Psychogeriatrics, 17(03), 353-370.
Farzana, F., Sreekanth, V., Mohiuddin, M. K., Mohan, V., Balakrishna, N., & Ahuja, Y.
R. (2015). Can individual home‐based cognitive stimulation therapy benefit
Parkinson's patients with mild to moderate cognitive impairment? International
journal of geriatric psychiatry, 30(4), 433-435.
Faul, F., Erdfelder, E., Buchner, A., & Lang, A. G. (2009). Statistical power analyses
using G* Power 3.1: Tests for correlation and regression analyses. Behavior
research methods, 41(4), 1149-1160.

96
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G* Power 3: A flexible
statistical power analysis program for the social, behavioral, and biomedical
sciences. Behavior research methods, 39(2), 175-191.
Fauth, E. B., & Gibbons, A. (2014). Which behavioral and psychological symptoms of
dementia are the most problematic? Variability by prevalence, intensity, distress
ratings, and associations with caregiver depressive symptoms. International
journal of geriatric psychiatry, 29(3), 263-271.
Feil, N. (2014). Validation therapy with late-onset dementia populations. Caregiving in
dementia: Research and applications, 199-218.
Feinberg, L. F., & Whitlatch, J. (2002). Decision-making for persons with cognitive
impairment and their family caregivers. American journal of Alzheimer's disease
and other dementias, 17(4), 237-244.
Feinstein, J. S., Duff, M. C., & Tranel, D. (2010). Sustained experience of emotion after
loss of memory in patients with amnesia. Proceedings of the National Academy of
Sciences, 107(17), 7674-7679.
Ferretti, L., McCurry, S. M., Logsdon, R., Gibbons, L., & Teri, L. (2001). Anxiety and
Alzheimer's disease. Journal of Geriatric Psychiatry and Neurology, 14(1), 52-
58.
Finkel, S. (2000). Introduction to behavioural and psychological symptoms of dementia
(BPSD). International journal of geriatric psychiatry.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). “Mini-mental state”: a practical
method for grading the cognitive state of patients for the clinician.Journal of
psychiatric research, 12(3), 189-198.

97
Friedman, E. M., Shih, R. A., Langa, K. M., & Hurd, M. D. (2015). US prevalence and
predictors of informal caregiving for dementia. Health Affairs,34(10), 1637-1641.
Frisoni, G. B., Pievani, M., Testa, C., Sabattoli, F., Bresciani, L., Bonetti, M., ... &
Thompson, P. M. (2007). The topography of grey matter involvement in early and
late onset Alzheimer's disease. Brain, 130(3), 720-730.
Garland, K., Beer, E., Eppingstall, B., & O'Connor, D. W. (2007). A comparison of two
treatments of agitated behavior in nursing home residents with dementia:
simulated family presence and preferred music. The American journal of geriatric
psychiatry, 15(6), 514-521.
Gerdner, L. A. (1992). The effects of individualized music on elderly clients who are
confused and agitated. Unpublished Masters thesis, University of Iowa.
Gerdner, L. A. (1997). An individualized music intervention for agitation. Journal of the
American Psychiatric Nurses Association, 3(6), 177-184.
Gerdner, L. A. (2000). Effects of individualized versus classical “relaxation” music on
the frequency of agitation in elderly persons with Alzheimer's disease and related
disorders. International Psychogeriatrics, 12(01), 49-65.
Gerdner, L. A. (2005). Use of individualized music by trained staff and family:
translating research into practice. Journal of gerontological nursing, 31(6), 22-30.
Gerdner, L. A. (2010). Individualized Music for Elders with Dementia. Journal of
Gerontological Nursing, 36(6), 7–15. http://doi.org/10.3928/00989134-20100504-
01
Gerdner, L. A., Hartsock, J., & Buckwalter, K. C. (2000). Assessment of Personal Music
Preference (family version). The University of Iowa Gerontological Nursing

98
Interventions Research Center: Research Development and Dissemination Core,
Iowa City, Iowa.
Giebel, C. M., Sutcliffe, C., Stolt, M., Karlsson, S., Renom-Guiteras, A., Soto, M., …
Challis, D. (2014). Deterioration of basic activities of daily living and their impact
on quality of life across different cognitive stages of dementia: a European study.
International Psychogeriatrics, 26(08), 1283–1293.
http://doi.org/10.1017/S1041610214000775
Giebel, C. M., Sutcliffe, C., & Challis, D. (2015). Activities of daily living and quality of
life across different stages of dementia: a UK study. Aging & mental health,
19(1), 63-71.
Gill, S. S., Bronskill, S. E., Normand, S. L. T., Anderson, G. M., Sykora, K., Lam, K., ...
& Gurwitz, J. H. (2007). Antipsychotic drug use and mortality in older adults with
dementia. Annals of internal medicine, 146(11), 775-786.
Gill, S. S., Rochon, P. A., Herrmann, N., Lee, P. E., Sykora, K., Gunraj, N., ... &
Mamdani, M. (2005). Atypical antipsychotic drugs and risk of ischaemic stroke:
population based retrospective cohort study. Bmj, 330(7489), 445.
Gilley, D. W., Whalen, M. E., Wilson, R. S., & Bennett, D. A. (1991). Hallucinations and
associated factors in Alzheimer's disease. The Journal of neuropsychiatry and
clinical neurosciences.
Gómez-Gallego, M., Gomez-García, J., & Ato-García, M. (2014). Confirmatory factor
analysis of the quality of life in Alzheimer’s disease scale in patients with
Alzheimer’s disease. Experimental aging research,40(3), 266-279.

99
Green, S. B. (1991). How many subjects does it take to do a regression analysis.
Multivariate behavioral research, 26(3), 499-510.
Groussard, M., Viader, F., Hubert, V., Landeau, B., Abbas, A., Desgranges, B., ... &
Platel, H. (2010). Musical and verbal semantic memory: two distinct neural
networks?. Neuroimage, 49(3), 2764-2773.
Guetin, S., Portet, F., Picot, M. C., Pommié, C., Messaoudi, M., Djabelkir, L., ... &
Touchon, J. (2009). Effect of music therapy on anxiety and depression in patients
with Alzheimer’s type dementia: randomised, controlled study. Dementia and
geriatric cognitive disorders, 28(1), 36-46.
Guzmán-Vélez, E., Feinstein, J. S., & Tranel, D. (2014). Feelings without memory in
Alzheimer disease. Cognitive and Behavioral Neurology, 27(3), 117-129.
El Haj, M., Fasotti, L., & Allain, P. (2012). The involuntary nature of music-evoked
autobiographical memories in Alzheimer’s disease. Consciousness and
Cognition, 21(1), 238-246.
Harman, G., & Clare, L. (2006). Illness representations and lived experience in early-
stage dementia. Qualitative health research, 16(4), 484-502.
Harrell, F. E. (2001) Regression Modeling Strategies, with Applications to Linear
Models, Survival Analysis and Logistic Regression. New York, NY: Springer.
Hawkins, N. A., Ditto, P. H., Danks, J. H., & Smucker, W. D. (2005). Micromanaging
death: process preferences, values, and goals in end-of-life medical decision
making. The Gerontologist, 45(1), 107-117.
Herrmann, N., Mamdani, M., & Lanctot, K. L. (2004). Atypical antipsychotics and risk
of cerebrovascular accidents. American Journal of Psychiatry,161(6), 1113-1115.

100
Hien Le, T., Cumming, R. G., Cameron, I. D., Chen, J. S., Lord, S. R., March, L. M., ...
& Sambrook, P. N. (2005). Atypical antipsychotic medications and risk of falls in
residents of aged care facilities. Journal of the American Geriatrics
Society, 53(8), 1290-1295.
Hsu, M. H., Flowerdew, R., Parker, M., Fachner, J., & Odell-Miller, H. (2015).
Individual music therapy for managing neuropsychiatric symptoms for people
with dementia and their carers: a cluster randomised controlled feasibility
study. BMC geriatrics, 15(1), 1.
Hwang, J. P., Tsai, S. J., Yang, C. H., Liu, K. M., & Lirng, J. F. (2000). Repetitive
phenomena in dementia. The International Journal of Psychiatry in
Medicine, 30(2), 165-171.
Husebo, B. S., Ballard, C., & Aarsland, D. (2011). Pain treatment of agitation in patients
with dementia: a systematic review. International journal of geriatric
psychiatry, 26(10), 1012-1018.
Huybrechts, K. F., Gerhard, T., Crystal, S., Olfson, M., Avorn, J., Levin, R., ... &
Schneeweiss, S. (2012). Differential risk of death in older residents in nursing
homes prescribed specific antipsychotic drugs: population based cohort
study. Bmj, 344, e977.
Imbimbo, B. P., & Giardina, G. A. M. (2011). γ-secretase inhibitors and modulators for
the treatment of Alzheimer's disease: disappointments and hopes. Current topics
in medicinal chemistry, 11(12), 1555-1570.
Iveson, C. (2002). Solution-focused brief therapy. Advances in Psychiatric
Treatment, 8(2), 149-156.

101
Jacobsen, J. H., Stelzer, J., Fritz, T. H., Chételat, G., La Joie, R., & Turner, R. (2015).
Why musical memory can be preserved in advanced Alzheimer’s
disease. Brain, 138(8), 2438-2450.
Jack, C. R., & Holtzman, D. M. (2013). Biomarker modeling of Alzheimer’s disease.
Neuron, 80(6), 1347-1358.
Janata, P. (2009). The neural architecture of music-evoked autobiographical
memories. Cerebral Cortex, bhp008.
Janata, P. (2012). Effects of widespread and frequent personalized music programming
on agitation and depression in assisted living facility residents with Alzheimer-
type dementia. Music and Medicine, 4(1), 8-15.
Janata, P., Birk, J. L., Van Horn, J. D., Leman, M., Tillmann, B., & Bharucha, J. J.
(2002). The cortical topography of tonal structures underlying Western
music. science, 298(5601), 2167-2170.
Jäncke, L. (2008). Music, memory and emotion. Journal of biology, 7(6), 1.
Johanson, G. A., & Brooks, G. P. (2009). Initial scale development: sample size for pilot
studies. Educational and Psychological Measurement.
Judge, K. S., Menne, H. L., & Whitlatch, C. J. (2010). Stress process model for
individuals with dementia. The Gerontologist, 50(3), 294–302.
http://doi.org/10.1093/geront/gnp162
Judge, K. S., Yarry, S. J., & Orsulic-Jeras, S. (2010). Acceptability and feasibility results
of a strength-based skills training program for dementia caregiving dyads. The
Gerontologist, 50(3), 408-417.

102
Julious, S. A. (2005). Sample size of 12 per group rule of thumb for a pilot study. Pharm
Stat, 4(4), 287-291.
Kaiser, N. C., Liang, L. J., Melrose, R. J., Wilkins, S. S., Sultzer, D. L., & Mendez, M. F.
(2014). Differences in anxiety among patients with early-versus late-onset
Alzheimer’s disease. The Journal of neuropsychiatry and clinical
neurosciences, 26(1), 73-80.
Kessler, R. C., Andrews, G., Colpe, L. J., Hiripi, E., Mroczek, D. K., Normand, S. L., ...
& Zaslavsky, A. M. (2002). Short screening scales to monitor population
prevalences and trends in non-specific psychological distress. Psychological
medicine, 32(06), 959-976.
King, J. B., Jones, K. G., Goldberg, E., Rollins, M., MacNamee, K., Moffit, C., ... &
Breitenbach, K. R. (2018). Increased Functional Connectivity After Listening to
Favored Music in Adults With Alzheimer Dementia. The Journal of Prevention of
Alzheimer's Disease, 1-7.
Koger, S. M., Chapin, K., & Brotons, M. (1999). Is music therapy an effective
intervention for dementia? A meta-analytic review of literature.Journal of Music
Therapy, 36(1), 2-15.
Kogan, A. C., Wilber, K., & Mosqueda, L. (2016). Person‐Centered Care for Older
Adults with Chronic Conditions and Functional Impairment: A Systematic
Literature Review. Journal of the American Geriatrics Society, 64(1), e1-e7.
Krestar, M. L., Looman, W., Powers, S., Dawson, N., & Judge, K. S. (2012). Including
individuals with memory impairment in the research process: the importance of

103
scales and response categories used in surveys. Journal of Empirical Research on
Human Research Ethics, 7(2), 70-79.
Kuske, B., Hanns, S., Luck, T., Angermeyer, M. C., Behrens, J., & Riedel-Heller, S. G.
(2007). Nursing home staff training in dementia care: a systematic review of
evaluated programs. International Psychogeriatrics,19(05), 818-841.
Lai, C. (2016). Person‐Centered Dementia Care. The Encyclopedia of Adulthood and
Aging.
Lewis, V., Bauer, M., Winbolt, M., Chenco, C., & Hanley, F. (2015). A study of the
effectiveness of MP3 players to support family carers of people living with
dementia at home. International Psychogeriatrics, 27(03), 471-479.
Livingston, G., Kelly, L., Lewis-Holmes, E., Baio, G., Morris, S., Patel, N., ... & Cooper,
C. (2014a). A systematic review of the clinical effectiveness and cost-
effectiveness of sensory, psychological and behavioural interventions for
managing agitation in older adults with dementia.
Livingston, G., Kelly, L., Lewis-Holmes, E., Baio, G., Morris, S., Patel, N., ... & Cooper,
C. (2014b). Non-pharmacological interventions for agitation in dementia:
systematic review of randomised controlled trials. The British Journal of
Psychiatry, 205(6), 436-442.
Logsdon, R. G., Gibbons, L. E., McCurry, S. M., & Teri, L. (1999). Quality of life in
Alzheimer's disease: Patient and reports. Journal of Mental Health and Aging, 5,
21–32.

104
Logsdon, R. G., Gibbons, L. E., McCurry, S. M., & Teri, L. (2002). Assessing quality of
life in older adults with cognitive impairment. Psychosomatic medicine, 64(3),
510-519.
Logsdon, R. G., McCurry, S. M., & Teri, L. (2007). Evidence-based psychological
treatments for disruptive behaviors in individuals with dementia. Psychology and
aging, 22(1), 28.
Lyketsos, C. G., Lopez, O., Jones, B., Fitzpatrick, A. L., Breitner, J., & DeKosky, S.
(2002). Prevalence of neuropsychiatric symptoms in dementia and mild cognitive
impairment: results from the cardiovascular health study. Jama, 288(12), 1475-
1483.
Maslow, K. (2013). Person centered care for people with dementia: Opportunities and
challenges. Generations, 37(3), 8-15.
Maslow, K., Fazio, S., Ortigara, A., Kuhn, D., & Zeisel, J. (2013). From Concept to
Practice: Training in Person-Centered Care for People with
Dementia. Generations, 37(3), 100-107.
Matsunaga, S., Kishi, T., & Iwata, N. (2015). Memantine monotherapy for Alzheimer’s
disease: a systematic review and meta-analysis. PloS one, 10(4), e0123289.
Mendez, M. F., & Shapira, J. S. (2013). Hypersexual behavior in frontotemporal
dementia: a comparison with early-onset Alzheimer’s disease. Archives of sexual
behavior, 42(3), 501-509.
Montgomery, R. J., & Kosloski, K. (1994). A longitudinal analysis of nursing home
placement for dependent elders cared for by spouses vs adult children. Journal of
Gerontology, 49(2), S62-S74.

105
Morris, L. W., Morris, R. G., & Britton, P. G. (1988). The relationship between marital
intimacy, perceived strain and depression in spouse caregivers of dementia
sufferers. British Journal of Medical Psychology, 61(3), 231-236.
Moyle, W., Venturto, L., Griffiths, S., Grimbeek, P., McAllister, M., Oxlade, D., &
Murfield, J. (2011). Factors influencing quality of life for people with dementia:
A qualitative perspective. Aging & Mental Health, 15(8), 970–977.
http://doi.org/10.1080/13607863.2011.583620
Moyle, W., Murfield, J. E., Griffiths, S. G., & Venturato, L. (2012). Assessing quality of
life of older people with dementia: A comparison of quantitative self‐report and
proxy accounts. Journal of Advanced Nursing, 68(10), 2237-2246.
Mozley, C. G., Huxley, P., Sutcliffe, C., Bagley, H., Burns, A., Challis, D., &
Cordingley, L. (1999). ‘Not knowing where I am doesn't mean I don't know what
I like’: cognitive impairment and quality of life responses in elderly people.
International journal of geriatric psychiatry, 14(9), 776-783.
National Dementia Initiative (2013) Dementia care: The quality chasm. Retrieved from:
https://www.leadingage.org/uploadedFiles/Content/Members/Nursing_Homes/Qu
ality/DementiaCareTheQualityChasm.pdf
Neal, M., & Briggs, M. (2003). Validation therapy for dementia. Cochrane Database Syst
Rev, 3.
Nichols, L. O., Martindale-Adams, J., Burns, R., Graney, M. J., & Zuber, J. (2011).
Translation of a dementia caregiver support program in a health care system—
REACH VA. Archives of Internal Medicine, 171(4), 353-359.

106
Noguchi, D., Kawano, Y., & Yamanaka, K. (2013). Care staff training in residential
homes for managing behavioural and psychological symptoms of dementia based
on differential reinforcement procedures of applied behaviour analysis: A process
research. Psychogeriatrics, 13(2), 108-117.
Norberg, A., Melin, E., & Asplund, K. (1986). Reactions to music, touch and object
presentation in the final stage of dementia. An exploratory study.International
Journal of Nursing Studies, 23(4), 315-323.
Nunnally, J. C. (1978). Psychometric theory (2nd ed.). New York: McGraw-Hill.
O’Bryant, S. E., Humphreys, J. D., Smith, G. E., Ivnik, R. J., Graff-Radford, N. R.,
Petersen, R. C., & Lucas, J. A. (2008). Detecting dementia with the mini-mental
state examination in highly educated individuals. Archives of neurology, 65(7),
963-967.
Olderog-Millard, K. A., & Smith, J. M. (1989). The influence of group singing therapy
on the behavior of Alzheimer's disease patients. Journal of Music Therapy, 26(2),
58-70.
Orrell, M., Aguirre, E., Spector, A., Hoare, Z., Woods, R. T., Streater, A., ... & Russell, I.
(2014). Maintenance cognitive stimulation therapy for dementia: single-blind,
multicentre, pragmatic randomised controlled trial. The British Journal of
Psychiatry, 204(6), 454-461.
O'Rourke, H. M., Duggleby, W., Fraser, K. D., & Jerke, L. (2015). Factors that affect
quality of life from the perspective of people with dementia: a
metasynthesis. Journal of the American Geriatrics Society, 63(1), 24-38.

107
Orsulic-Jeras, S., Shepherd, J. B., & Britton, P. J. (2003). Counseling older adults with
HIV/AIDS: A strength-based model of treatment. Journal of Mental Health
Counseling, 25(3), 233.
Osborne, H., Simpson, J., & Stokes, G. (2010). The relationship between pre-morbid
personality and challenging behaviour in people with dementia: A systematic
review. Aging & mental health, 14(5), 503-515.
Ostwald, S. K., Duggleby, W., & Hepburn, K. W. (2002). The stress of dementia: view
from the inside. American journal of Alzheimer's disease and other
dementias, 17(5), 303-312.
Pai, M. C., & Jacobs, W. J. (2004). Topographical disorientation in community‐residing
patients with Alzheimer's disease. International journal of geriatric
psychiatry, 19(3), 250-255.
Panisset, M., Roudier, M., Saxton, J., & Boiler, F. (1994). Severe impairment battery: a
neuropsychological test for severely demented patients. Archives of
neurology, 51(1), 41-45.
Park, H., & Pringle Specht, J. K. (2009). Effect of individualized music on agitation in
individuals with dementia who live at home. Journal of gerontological
nursing, 35(8), 47-55.
Pearlin, L. I., Mullan, J. T., Semple, S. J., & Skaff, M. M. (1990). Caregiving and the
stress process: An overview of concepts and their measures. The
gerontologist, 30(5), 583-594.
Pereira, C. S., Teixeira, J., Figueiredo, P., Xavier, J., Castro, S. L., & Brattico, E. (2011).
Music and emotions in the brain: familiarity matters.PloS one, 6(11), e27241.

108
Pinquart, M., & Sörensen, S. (2011). Spouses, adult children, and children-in-law as
caregivers of older adults: a meta-analytic comparison. Psychology and
aging, 26(1), 1.
Piquard, A., Derouesné, C., Lacomblez, L., & Siéroff, É. (2004). Planification et activités
de la vie quotidienne dans la maladie d’Alzheimer et les dégénérescences
frontotemporales. Psychologie & NeuroPsychiatrie du vieillissement, 2(2), 147-
156.
Plailly, J., Tillmann, B., & Royet, J. P. (2007). The feeling of familiarity of music and
odors: the same neural signature?. Cerebral cortex, 17(11), 2650-2658.
Pollack, N. J., & Namazi, K. H. (1992). The effect of music participation on the social
behavior of Alzheimer's disease patients. Journal of Music Therapy, 29(1), 54-67.
Porter, V. R., Buxton, W. G., Fairbanks, L. A., Strickland, T., O'Connor, S. M.,
Rosenberg-Thompson, S., & Cummings, J. L. (2003). Frequency and
characteristics of anxiety among patients with Alzheimer's disease and related
dementias. The Journal of neuropsychiatry and clinical neurosciences, 15(2),
180-186.
Raglio, A., Bellandi, D., Baiardi, P., Gianotti, M., Ubezio, M. C., & Granieri, E. (2013).
Listening to music and active music therapy in behavioral disturbances in
dementia: a crossover study. Journal of the American Geriatrics Society, 61(4),
645-647.
Raina, P., Santaguida, P., Ismaila, A., Patterson, C., Cowan, D., Levine, M., ... &
Oremus, M. (2008). Effectiveness of cholinesterase inhibitors and memantine for

109
treating dementia: evidence review for a clinical practice guideline. Annals of
internal medicine, 148(5), 379-397.
Ready, R. E., Carvalho, J. O., Green, R. C., Gavett, B. E., & Stern, R. A. (2011). The
structure and validity of self-reported affect in mild cognitive impairment and
mild Alzheimer's disease. International Psychogeriatrics,23(06), 887-898.
Reamy, A. M., Kim, K., Zarit, S. H., & Whitlatch, C. J. (2011). Understanding
discrepancy in perceptions of values: individuals with mild to moderate dementia
and their family caregivers. The Gerontologist, 51(4), 473-483.
Reamy, A. M., Kim, K., Zarit, S. H., & Whitlatch, C. J. (2013). Values and preferences
of individuals with dementia: perceptions of family caregivers over time. The
Gerontologist, 53(2), 293-302.
Rosen, W. G., Mohs, R. C., & Davis, K. L. (1984). A new rating scale for Alzheimer's
disease. The American journal of psychiatry.
Rowe, J. W., & Kahn, R. L. (1997). Successful aging. The gerontologist,37(4), 433-440.
Russell, J. A., & Carroll, J. M. (1999). On the bipolarity of positive and negative affect.
Psychological bulletin, 125(1), 3.
Ryan, E. B., Bannister, K. A., & Anas, A. P. (2009). The dementia narrative: Writing to
reclaim social identity. Journal of Aging Studies, 23(3), 145-157.
Sabol, V. K., Resnick, B., Galik, E., Gruber-Baldini, A. L., Morton, P. G., & Hicks, G. E.
(2011). Exploring the factors that influence functional performance among
nursing home residents. Journal of aging and health,23(1), 112-134.
110
Schneider, L. S., Dagerman, K. S., & Insel, P. (2005). Risk of death with atypical
antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-
controlled trials. Jama, 294(15), 1934-1943.
Schulz, R., & Martire, L. M. (2004). Family caregiving of persons with dementia:
prevalence, health effects, and support strategies. The American journal of
geriatric psychiatry, 12(3), 240-249.
Sebern, M. D., & Whitlatch, C. J. (2007). Dyadic relationship scale: A measure of the
impact of the provision and receipt of family care. The Gerontologist, 47(6), 741-
751.
Seignourel, P. J., Kunik, M. E., Snow, L., Wilson, N., & Stanley, M. (2008). Anxiety in
dementia: A critical review. Clinical Psychology Review, 28, 1071–1082.
doi:10.1016/j.cpr.2008.02.008
Seitz, D. P., Brisbin, S., Herrmann, N., Rapoport, M. J., Wilson, K., Gill, S. S., ... &
Conn, D. (2012). Efficacy and feasibility of nonpharmacological interventions for
neuropsychiatric symptoms of dementia in long term care: a systematic
review. Journal of the American Medical Directors Association,13(6), 503-506.
Seitz, D. P., Gill, S. S., Herrmann, N., Brisbin, S., Rapoport, M. J., Rines, J., ... & Conn,
D. K. (2013). Pharmacological treatments for neuropsychiatric symptoms of
dementia in long-term care: a systematic review. International
Psychogeriatrics, 25(02), 185-203.
Shelton, E. G. (2014). Stage of change discrepancies among individuals with dementia
and caregivers. Master’s Thesis. Cleveland State University.

111
Shelton, E. G., Orsulic-Jeras, S., Whitlatch, C. J., & Szabo, S. M. (2017). Does it Matter
if We Disagree? The Impact of Incongruent Care Preferences on Persons with
Dementia and Their Care Partners. The Gerontologist, 58(3), 556-566.
Simmons-Stern, N. R., Budson, A. E., & Ally, B. A. (2010). Music as a memory
enhancer in patients with Alzheimer's disease. Neuropsychologia, 48(10), 3164-
3167.
Sink, K. M., Holden, K. F., & Yaffe, K. (2005). Pharmacological treatment of
neuropsychiatric symptoms of dementia: a review of the evidence. Jama, 293(5),
596-608.
Sitzer, D. I., Twamley, E. W., & Jeste, D. (2006). Cognitive training in Alzheimer's
disease: a meta‐analysis of the literature. Acta Psychiatrica Scandinavica, 114(2),
75-90.
Snow, A. L., Kunik, M. E., Molinari, V. A., Orengo, C. A., Doody, R., Graham, D. P., &
Norris, M. P. (2005). Accuracy of self-reported depression in persons with
dementia. Journal of the American Geriatrics Society, 53, 389–396.
doi:10.1111/j.1532-5415.2005.53154.x
Solai, L., Schultz, S. K., & Kunik, M. E. (2015). Non-Pharmacological Management of
Behavioral Disturbance in Dementia. The American Journal of Geriatric
Psychiatry, 23(3), S22-S23.
Spector, A., Orrell, M., & Goyder, J. (2013). A systematic review of staff training
interventions to reduce the behavioural and psychological symptoms of dementia.
Ageing research reviews, 12(1), 354-364.

112
Spector, A., Orrell, M., & Woods, B. (2010). Cognitive Stimulation Therapy (CST):
effects on different areas of cognitive function for people with
dementia. International journal of geriatric psychiatry, 25(12), 1253-1258.
Spector, A., Throgrimsen, L., Woods, B., Orrell, M., & Hirsch, C. H. (2004). Cognitive
stimulation therapy improved cognition and quality of life in dementia. Evidence-
based medicine, 9(2), 49.
Sung, H. C., Chang, A. M., & Abbey, J. (2006). The effects of preferred music on
agitation of older people with dementia in Taiwan. International journal of
geriatric psychiatry, 21(10), 999.
Sung, H. C., Chang, A. M., & Lee, W. L. (2010). A preferred music listening intervention
to reduce anxiety in older adults with dementia in nursing homes. Journal of
clinical nursing, 19(7‐8), 1056-1064.
Suzuki, M., Kanamori, M., Nagasawa, S., Tokiko, I., & Takayuki, S. (2007). Music
therapy‐induced changes in behavioral evaluations, and saliva chromogranin A
and immunoglobulin A concentrations in elderly patients with senile
dementia. Geriatrics & gerontology international, 7(1), 61-71.
Svansdottir, H. B., & Snaedal, J. (2006). Music therapy in moderate and severe dementia
of Alzheimer's type: a case–control study. International psychogeriatrics, 18(04),
613-621.
Swanberg, M. M., Tractenberg, R. E., Mohs, R., Thal, L. J., & Cummings, J. L. (2004).
Executive dysfunction in Alzheimer disease. Archives of Neurology, 61(4), 556-
560.

113
Testa, M. A., & Simonson, D. C. (1996). Assessment of quality-of-life outcomes. New
England journal of medicine, 334(13), 835-840.
Teri, L., Ferretti, L. E., Gibbons, L. E., Logsdon, R. G., McCurry, S. M., Kukull, W. A.,
... & Larson, E. B. (1999). Anxiety in Alzheimer's disease: Prevalence and
comorbidity. The Journals of Gerontology Series A: Biological Sciences and
Medical Sciences, 54(7), M348-M352.
Thorgrimsen, L., Selwood, A., Spector, A., Royan, L., de Madariaga Lopez, M., Woods,
R. T., & Orrell, M. (2003). Whose quality of life is it anyway?: The validity and
reliability of the Quality of Life-Alzheimer's Disease (QoL-AD) scale. Alzheimer
Disease & Associated Disorders, 17(4), 201-208.
Tower, R. B., & Kasl, S. V. (1996). Depressive symptoms across older spouses:
longitudinal influences. Psychology and aging, 11(4), 683.
Uchino, B. N., Cacioppo, J. T., & Kiecolt-Glaser, J. K. (1996). The relationship between
social support and physiological processes: a review with emphasis on underlying
mechanisms and implications for health.Psychological bulletin, 119(3), 488.
Van Breukelen, G. J. (2006). ANCOVA versus change from baseline had more power in
randomized studies and more bias in nonrandomized studies. Journal of clinical
epidemiology, 59(9), 920-925.
van der Lee, J., Bakker, T. J., Duivenvoorden, H. J., & Dröes, R. M. (2014). Multivariate
models of subjective caregiver burden in dementia: a systematic review. Ageing
research reviews, 15, 76-93.
Vanstone, A. D., & Cuddy, L. L. (2009). Musical memory in Alzheimer disease. Aging,
Neuropsychology, and Cognition, 17(1), 108-128.

114
Vanstone, A. D., Cuddy, L. L., Duffin, J. M., & Alexander, E. (2009). Exceptional
preservation of memory for tunes and lyrics. Annals of the New York Academy of
Sciences, 1169(1), 291-294.
Vanstone, A. D., Sikka, R., Tangness, L., Sham, R., Garcia, A., & Cuddy, L. L. (2012).
Episodic and semantic memory for melodies in Alzheimer's disease. Music
Perception: An Interdisciplinary Journal, 29(5), 501-507.
Wang, P. S., Schneeweiss, S., Avorn, J., Fischer, M. A., Mogun, H., Solomon, D. H., &
Brookhart, M. A. (2005). Risk of death in elderly users of conventional vs.
atypical antipsychotic medications. New England Journal of Medicine, 353(22),
2335-2341.
Warchol, K. (2006). Facilitating Functional and Quality‐of‐Life Potential: Strength‐based
Assessment and Treatment for All Stages of Dementia. Topics in Geriatric
Rehabilitation, 22(3), 213-227.
Werner, P., Koroknay, V., Braun, J., & Cohen‐Mansfield, J. (1994). Individualized care
alternatives used in the process of removing physical restraints in the nursing
home. Journal of the American Geriatrics Society,42(3), 321-325.
White, M., & Epston, D. (1990). Narrative means to therapeutic ends. WW Norton &
Company.
Whitlatch, C. J., Feinberg, L. F., & Tucke, S. (2005). Accuracy and consistency of
responses from persons with cognitive impairment.Dementia, 4(2), 171-183.
Woods, B., Aguirre, E., Spector, A. E., & Orrell, M. (2012). Cognitive stimulation to
improve cognitive functioning in people with dementia.Cochrane Database Syst
Rev, 2.

115
Yarry, S. J., Judge, K. S., & Orsulic-Jeras, S. (2010). Applying a strength-based
intervention for dyads with mild to moderate memory loss: Two case
examples. Dementia, 1471301210384315.
Yiannopoulou, K. G., & Papageorgiou, S. G. (2013). Current and future treatments for
Alzheimer’s disease. Therapeutic advances in neurological disorders, 6(1), 19-
33.
Zahodne, L. B., Ornstein, K., Cosentino, S., Devanand, D. P., & Stern, Y. (2015).
Longitudinal relationships between Alzheimer disease progression and psychosis,
depressed mood, and agitation/aggression. The American Journal of Geriatric
Psychiatry, 23(2), 130-140.
Zarit, S. H., Femia, E. E., Kim, K., & Whitlatch, C. J. (2010). The structure of risk factors
and outcomes for family caregivers: implications for assessment and
treatment. Aging & mental health, 14(2), 220-231.
Zung, W. W. (1971). A rating instrument for anxiety disorders.Psychosomatics, 12(6),
371-379.

116
APPENDIX

117
Appendix A: Demographic Information
Demographic Item CR Response CG Response
Can you please tell me your first and last name?
How would you identify your gender?
Male Female Male Female
What is your marital status? Married Single Divorced Widowed
Married Single Divorced Widowed
What is your relationship to your family member with memory and thinking challenges/ your loved one/ your family member with dementia?
Spouse Child Other relative Non-relative Parent
Spouse Child Other relative Non-relative Parent
Are you Hispanic or Latino? yes no yes no
How would you identify your race?
White non-hispanic White hispanic American Indian/Alaska
Native Asian Black or African-American Native Hawaiian/other
Pacific Islander Other race not specified Persons reporting 2 or more
races
White non-hispanic White hispanic American Indian/Alaska
Native Asian Black or African-American Native Hawaiian/other
Pacific Islander Other race not specified Persons reporting 2 or more
races
Are you a Veteran? yes no yes no
What is your education level? Less than a high school diploma
High school diploma or GED diploma
Some College Bachelor’s degree Master’s degree
Less than a high school diploma
High school diploma or GED diploma
Some College Bachelor’s degree Master’s degree

118
Appendix B: Mini-Mental State Examination (Folstein, Folstein, & McHugh, 1975)
Now I’d like to ask you a few questions and give you some problems to solve. Please try to answer as best as you can. 1. What
WRITE DOWN RESPONSE Incorrect Correct
year is this? 0 1
season is this? 0 1
month of the year is this? 0 1
is today’s date? 0 1
day of the week is this? 0 1
2. What
WRITE DOWN RESPONSE Incorrect Correct
county are we in? 0 1
state are we in? 0 1
city/town are we in? 0 1
is the name of this place/room? 0 1
floor of this place are we on? 0 1
3. I am going to name three objects. After I have said all three objects, I want you to repeat
them. Remember what they are because I am going to ask you to name them again in a few minutes.
“ball” “car” “man” Please repeat the three items for me.
RECORD EXACT RESONSE
0 1 2 3
NUMBER OF TRIALS
SCORE ONE POINT FOR EACH CORRECT ANSWER. IF RESP DOES NOT REPEAT ALL THREE, REPEAT UNTIL THEY HAVE LEARNED ALL THREE, OR UP TO A MAXIMUM OF 5 TIMES. ALLOW 20 SECONDS FOR REPLY. SCORE FIRST RESPONSE ONLY.
4. Spell the word WORLD. Now would you please spell WORLD backwards? (ALLOW 30
SECONDS)
D L R O W RECORD EXACT RESPONSE
0 1 2 3 4 5

119
SCORE ONE POINT FOR EACH LETTER IN THE CORRECT ORDER.
5. Now what were the names of the three objects that I asked you to remember?
RECORD EXACT RESONSE
0 1 2 3
ONE POINT FOR EACH CORRECT ANSWER: BALL CAR MAN. ALLOW 10 SECONDS
6. Could you please tell me what this is (POINT TO PENCIL) and what this is (POINT TO
WATCH).
RECORD EXACT RESPONSE 0 1 2
HAVE THE IWD NAME THEM AS YOU POINT. ONE POINT FOR EACH CORRECT ANSWER. ALLOW 10 SECONDS EACH.
7. I’d like you to repeat the following phrase after me: “No ifs, ands, or buts.” (ALLOW 10
SECONDS)
RECORD EXACT RESPONSE 0 1
8. Please read this and do what it tells you to do: [USE CHOICE CARD A]
CLOSE YOUR EYES 0 1
IF IWD JUST READS AND DOES NOT THEN CLOSE EYES, THEN PROBE: “PLEASE READ THE WORDS ON THIS PAGE AND DO WHAT IT TELLS YOU TO DO”. ALLOW 10 SECONDS.
REMINDER: TRY TO HAVE RESP. FINISH QUESTIONS 9-11. IF RESP. IS PHYSICALLY UNABLE TO USE HAND(S), NOTE THIS AND SCORE MMSE ACCORDINGLY (I.E., _____/25). SKIP TO NEXT SECTION.
9. Could you please tell me if you are left or right handed? (Alternate left/right in statement,
e.g., if RESP is right handed, ask them to take paper in left hand.) Now I’d like you to
take this paper in your right/left hand

120
fold the paper in half 0 1 2 3
and put the paper on the table
SCORE ONE POINT FOR EACH CORRECTLY PERFORMED COMMAND. ALLOW 30 SECONDS.
10. Would you please write any complete sentence on this piece of paper.
SENTENCE CORRECT? 0
NO 1
YES
SENTENCE MUST CONTAIN A SUBJECT, VERB, AND MAKE SENSE. IGNORE SPELLING ERRORS. IF RESPONDENT CANNOT WRITE, ASK HIM OR HER TO SAY A SENTENCE. ALLOW 30 SECONDS.
11. Now I’d like you to copy this design please. [USE CHOICE CARD B]
DESIGN CORRECT? 0
NO 1
YES
ALL 10 ANGLES MUST BE PRESERVED, AND THE 2 MUST INTERSECT TO FORM A 4-SIDED FIGURE. ALLOW 60 SECONDS.
WHILE IWD IS COPYING DESIGN, USE THE TIME TO GO BACK AND CALCULATE TOTAL MMSE SCORE.
Total number correct out of 30 ___ ___ 88
Total number correct out of 25 ___ ___ 88

121
Choice Card A [remove text before administering]
CLOSE YOUR EYES.
______________________________________________________________________________
Choice Card B [remove text before administering]

122
Appendix C: The Assessment of Personal Music Preference (Patient Version) (Gerdner,
Hartsock, & Buckwalter, 2000)
Music is often a very important part of people’s lives. Please complete the following
based on your personal music preference.
Before illness, how important a role did music play in your life?
_____ 1. Very Important
_____ 2. Moderately Important
_____ 3. Slightly Important
_____ 4. Not Important
Do/did you play a musical instrument?
If yes, please specify (examples: piano, guitar).
Do/did you enjoy singing?
If yes, please specify (examples: around-the house, church choir).
Do/did you enjoy dancing?
If yes, please specify (examples: attended dance lessons, participated in dance contests)
The following is a list of different types of music. Please indicate your three (3) most
favorite types with 1 being the most favorite, 2 the next, and 3 the third favorite.
_____ 1. Country and Western
_____ 2. Classical
_____ 3. Spiritual/Religious
_____ 4. Big Band/Swing
_____ 5. Folk
_____ 6. Blues
_____ 7. Jazz
_____ 8. Rock and Roll
_____ 9. Easy Listening
_____ 10. Cultural or Ethnic Specific (examples: Czech polkas, Ravi Shankar Indian
sitar)
_____ 11. Other: _____________________________________________
What form does your favorite music take?
_____ 1. Vocal
_____ 2. Instrumental
_____ 3. Both
Please identify specific songs/selections which make you feel happy.
Please identify specific artist(s)/performers(s) that you enjoy listening to the most.

123
Please identify specific albums, audio-cassette tapes, or compact discs contained in your
personal music library.
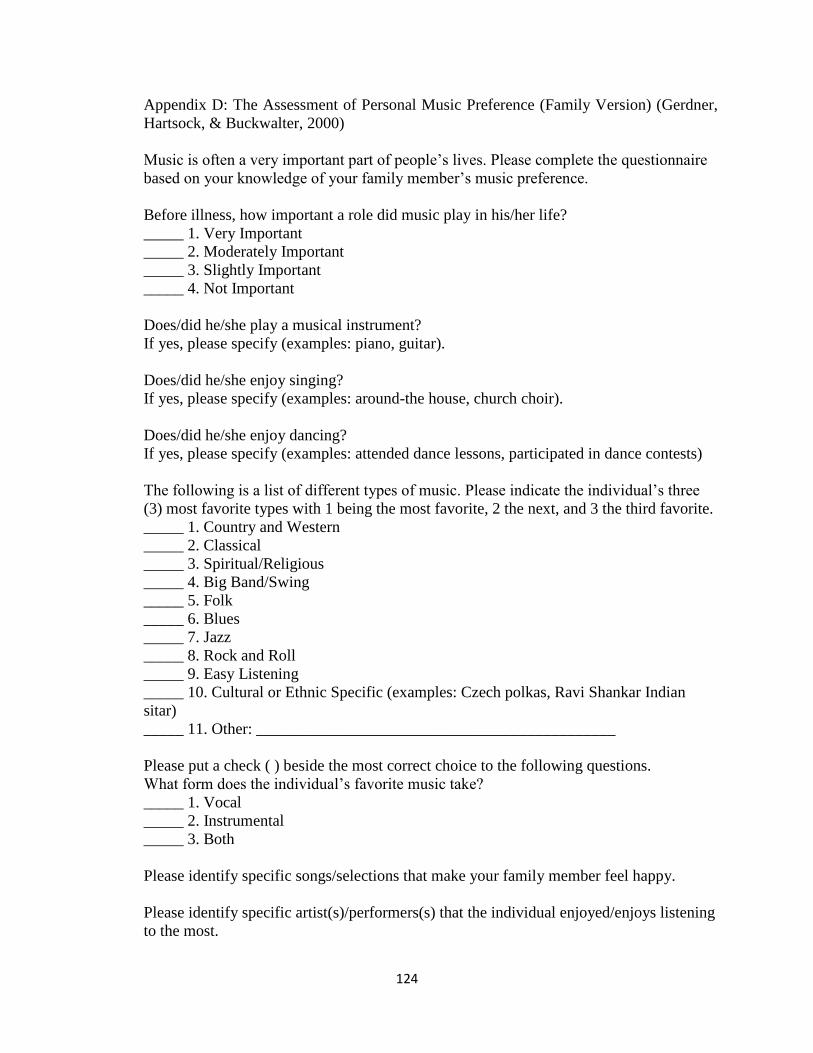
124
Appendix D: The Assessment of Personal Music Preference (Family Version) (Gerdner,
Hartsock, & Buckwalter, 2000)
Music is often a very important part of people’s lives. Please complete the questionnaire
based on your knowledge of your family member’s music preference.
Before illness, how important a role did music play in his/her life?
_____ 1. Very Important
_____ 2. Moderately Important
_____ 3. Slightly Important
_____ 4. Not Important
Does/did he/she play a musical instrument?
If yes, please specify (examples: piano, guitar).
Does/did he/she enjoy singing?
If yes, please specify (examples: around-the house, church choir).
Does/did he/she enjoy dancing?
If yes, please specify (examples: attended dance lessons, participated in dance contests)
The following is a list of different types of music. Please indicate the individual’s three
(3) most favorite types with 1 being the most favorite, 2 the next, and 3 the third favorite.
_____ 1. Country and Western
_____ 2. Classical
_____ 3. Spiritual/Religious
_____ 4. Big Band/Swing
_____ 5. Folk
_____ 6. Blues
_____ 7. Jazz
_____ 8. Rock and Roll
_____ 9. Easy Listening
_____ 10. Cultural or Ethnic Specific (examples: Czech polkas, Ravi Shankar Indian
sitar)
_____ 11. Other: _____________________________________________
Please put a check ( ) beside the most correct choice to the following questions.
What form does the individual’s favorite music take?
_____ 1. Vocal
_____ 2. Instrumental
_____ 3. Both
Please identify specific songs/selections that make your family member feel happy.
Please identify specific artist(s)/performers(s) that the individual enjoyed/enjoys listening
to the most.

125
Please identify specific albums, audio-cassette tapes, or compact discs contained in your
family member’s personal music library.

126
Appendix E: Diary-Based Fidelity Assessment Form (Weeks 1-3)
Music Tracking Logbook
Please complete this assessment once per week over the course of the study.
Name _______________________ Date_________________________
1. Please use this form to keep track of music listening for the week:
Sunday Monday Tuesday Wednesday Thursday Friday Saturday
How many minutes did your loved one spend listening to music?
2. Have you had any technology problems that have prevented or deterred you or your
loved one from listening to personalized music?
____Yes
____No
Please describe:
________________________________________________________________________
________________________________________________________________________
3. Have you listened to music with your loved one during the past week?
____Yes
____No
4. Has listening to music helped to resolve any behavioral problems associated with
your loved one’s memory loss in the past week? (e.g., agitation, unwillingness to eat,
repetitive question asking, etc.)
____Yes
____No
Please describe:
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________

127
Appendix F: Diary-Based Fidelity Assessment Form (Week 4)
Music Tracking Logbook
Please complete this assessment once per week over the course of the study.
Name _______________________ Date_________________________
1. Please use this form to keep track of music listening for the week:
Sunday Monday Tuesday Wednesday Thursday Friday Saturday
How many minutes did your loved one spend listening to music?
2. Have you had any technology problems that have prevented or deterred you or your
loved one from listening to personalized music?
____Yes
____No
Please specify:
________________________________________________________________________
________________________________________________________________________
3. Have you listened to music with your loved one during the past week?
____Yes
____No
4. Has listening to music helped to resolve any behavioral problems associated with
your loved one’s memory loss in the past week? (e.g., agitation, unwillingness to eat,
repetitive question asking, etc.)
____Yes
____No
If yes, please specify:
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________

128
Please respond to the following questions on a scale of 1. STRONGLY DISAGREE, 2.
DISAGREE, 3. AGREE, and 4. STRONGLY AGREE (circle that which applies)
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
1. My loved one seemed
to enjoy listening to
personalized music
Strongly Disagree Disagree Agree Strongly Agree
2. I would recommend
listening to personalized
music to others in my
situation
Strongly Disagree Disagree Agree Strongly Agree
3. I would recommend
this study to others in my
situation
Strongly Disagree Disagree Agree Strongly Agree
4. Playing personalized
music for my loved one
required too much effort
on my part
Strongly Disagree Disagree Agree Strongly Agree
5. The technology aspect
of this study was too
complicated to make it
worth my time.
Strongly Disagree Disagree Agree Strongly Agree
6. The researchers
provided enough
resources for me to be
effective at providing
personalized music
Strongly Disagree Disagree Agree Strongly Agree
7. I will continue to play
personalized music for
my loved one in the
future
Strongly Disagree Disagree Agree Strongly Agree
8. Any other comments
about this study that you
would like to share?
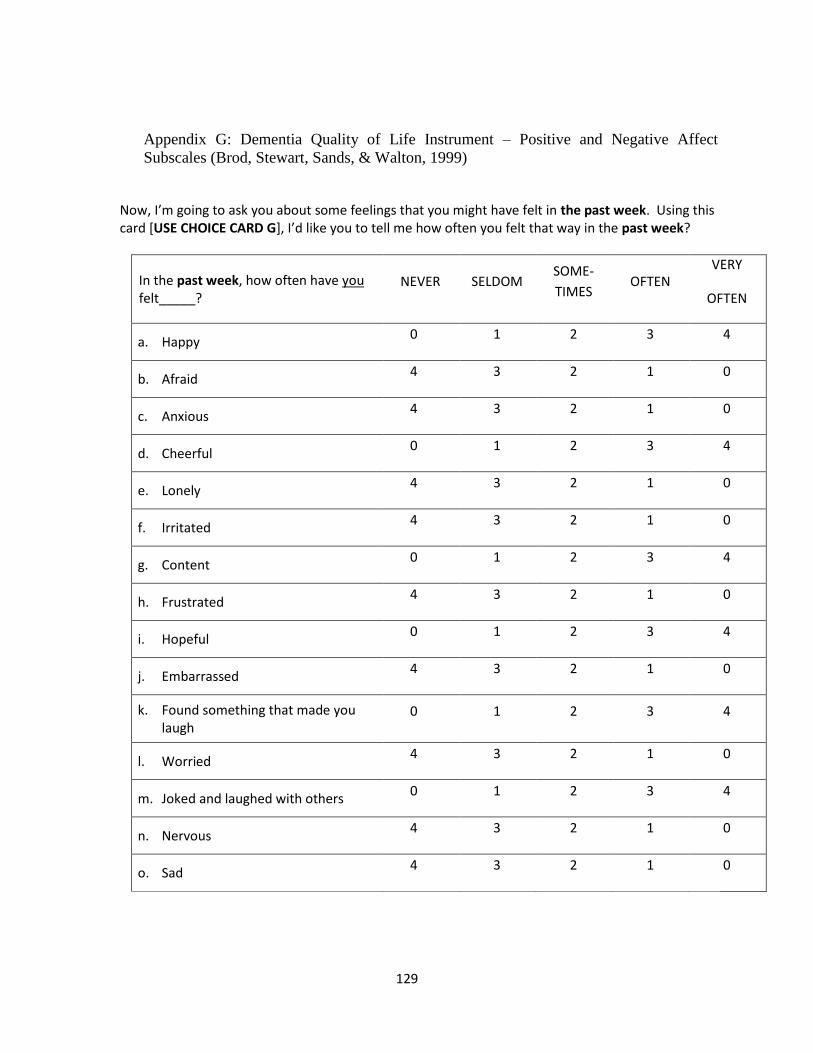
129
Appendix G: Dementia Quality of Life Instrument – Positive and Negative Affect
Subscales (Brod, Stewart, Sands, & Walton, 1999)
Now, I’m going to ask you about some feelings that you might have felt in the past week. Using this card [USE CHOICE CARD G], I’d like you to tell me how often you felt that way in the past week?
In the past week, how often have you felt_____?
NEVER SELDOM SOME-
TIMES OFTEN
VERY
OFTEN
a. Happy 0 1 2 3 4
b. Afraid 4 3 2 1 0
c. Anxious 4 3 2 1 0
d. Cheerful 0 1 2 3 4
e. Lonely 4 3 2 1 0
f. Irritated 4 3 2 1 0
g. Content 0 1 2 3 4
h. Frustrated 4 3 2 1 0
i. Hopeful 0 1 2 3 4
j. Embarrassed 4 3 2 1 0
k. Found something that made you laugh
0 1 2 3 4
l. Worried 4 3 2 1 0
m. Joked and laughed with others 0 1 2 3 4
n. Nervous 4 3 2 1 0
o. Sad 4 3 2 1 0

130
Appendix H: Quality of Life in Alzheimer’s Disease (QoL-AD) (Logsdon, Gibbons,
McCurry, & Teri, 1999)
Quality of Life-AD
Instructions for Interviewers
The QOL-AD is administered in interview format to individuals with dementia, following the
instructions below. Hand the form to the participant, so that he or she may look at it as you give
the following instructions (instructions should closely follow the wording given in bold type):
I want to ask you some questions about your quality of life and have you rate different
aspects of your life using one of four words: poor, fair, good, or excellent.
Point to each word (poor, fair, good, and excellent) on the form as you say it.
When you think about your life, there are different aspects, like your physical health,
energy, family, money, and others. I’m going to ask you to rate each of these areas. We
want to find out how you feel about your current situation in each area.
If you’re not sure about what a question means, you can ask me about it. If you have
difficulty rating any item, just give it your best guess.
It is usually apparent whether an individual understands the questions, and most individuals who
are able to communicate and respond to simple questions can understand the measure. If the
participant answers all questions the same, or says something that indicates a lack of
understanding, the interviewer is encouraged to clarify the question. However, under no
circumstances should the interviewer suggest a specific response. Each of the four possible
responses should be presented, and the participant should pick one of the four.
If a participant is unable to choose a response to a particular item or items, this should be noted in
the comments. If the participant is unable to comprehend and/or respond to two or more items,
the testing may be discontinued, and this should be noted in the comments.
As you read the items listed below, ask the participant to circle her/his response. If the participant
has difficulty circling the word, you may ask her/him to point to the word or say the word, and
you may circle it for him or her. You should let the participant hold his or her own copy of the
measure, and follow along as you read each item.
1. First of all, how do you feel about your physical health? Would you say it’s poor, fair,
good, or excellent? Circle whichever word you think best describes your physical health
right now.
2. How do you feel about your energy level? Do you think it is poor, fair, good, or excellent?
If the participant says that some days are better than others, ask him or her to rate how she/he has
been feeling most of the time lately.
3. How has your mood been lately? Have your spirits been good, or have you been feeling
down? Would you rate your mood as poor, fair, good, or excellent?
4. How about your living situation? How do you feel about the place you live now?
Would you say it’s poor, fair, good, or excellent?

131
5. How about your memory? Would you say it is poor, fair, good, or excellent?
6. How about your family and your relationship with family members? Would you describe
it as poor, fair, good, or excellent? If the respondent says they have no family, ask about
brothers, sisters, children, nieces, nephews.
7. How do you feel about your marriage? How is your relationship with (spouse’s name). Do
you feel it’s poor, fair, good, or excellent? Some participants will be single, widowed, or
divorced. When this is the case, ask how they feel about the person with whom they have the
closest relationship, whether it’s a family member or friend. If there is a family caregiver, ask
about their relationship with this person. It there is no one appropriate, or the participant is
unsure, score the item as missing. If the participant's rating is of their relationship with someone
other than their spouse, note this and record the relationship in the comments section.
8. How would you describe your current relationship with your friends? Would you say it’s
poor, fair, good, or excellent? If the respondent answers that they have no friends, or all their
friends have died, probe further. Do you have anyone you enjoy being with besides your
family? Would you call that person a friend? If the respondent still says they have no friends,
ask how do you feel about having no friends—poor, fair, good, or excellent?
9. How do you feel about yourself—when you think of your whole self, and all the different
things about you, would you say it’s poor, fair, good, or excellent?
10. How do you feel about your ability to do things like chores around the house or other
things you need to do? Would you say it’s poor, fair, good, or excellent?
11. How about your ability to do things for fun, that you enjoy? Would you say it’s poor,
fair, good, or excellent?
12. How do you feel about your current situation with money, your financial situation? Do
you feel it’s poor, fair, good, or excellent? If the respondent hesitates, explain that you don’t
want to know what their situation is (as in amount of money), just how they feel about it.
13. How would you describe your life as a whole. When you think about your life as a whole,
everything together, how do you feel about your life? Would you say it’s poor, fair, good, or
excellent?
SCORING INSTRUCTIONS FOR THE QOL:
Points are assigned to each item as follows: poor=1, fair=2, good=3, excellent=4.
The total score is the sum of all 13 items.

132
Appendix I: Zung Self-Rating Anxiety Scale (SAS) (Zung, 1974)
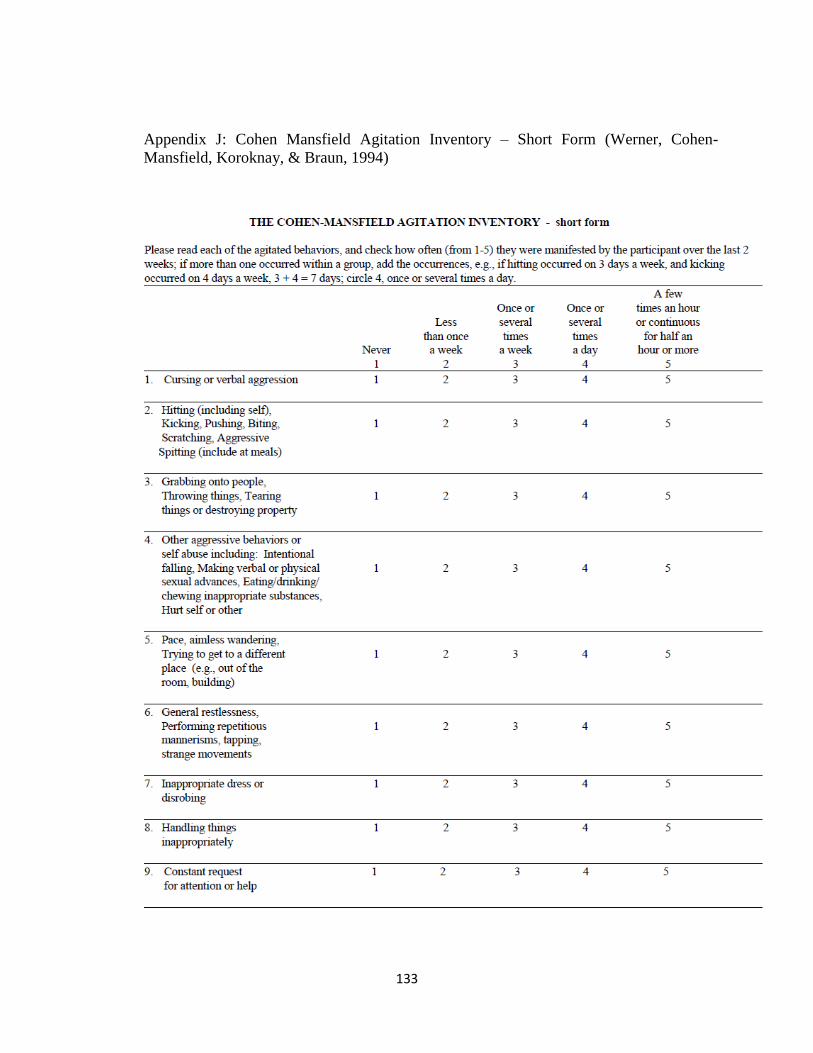
133
Appendix J: Cohen Mansfield Agitation Inventory – Short Form (Werner, Cohen-
Mansfield, Koroknay, & Braun, 1994)

134
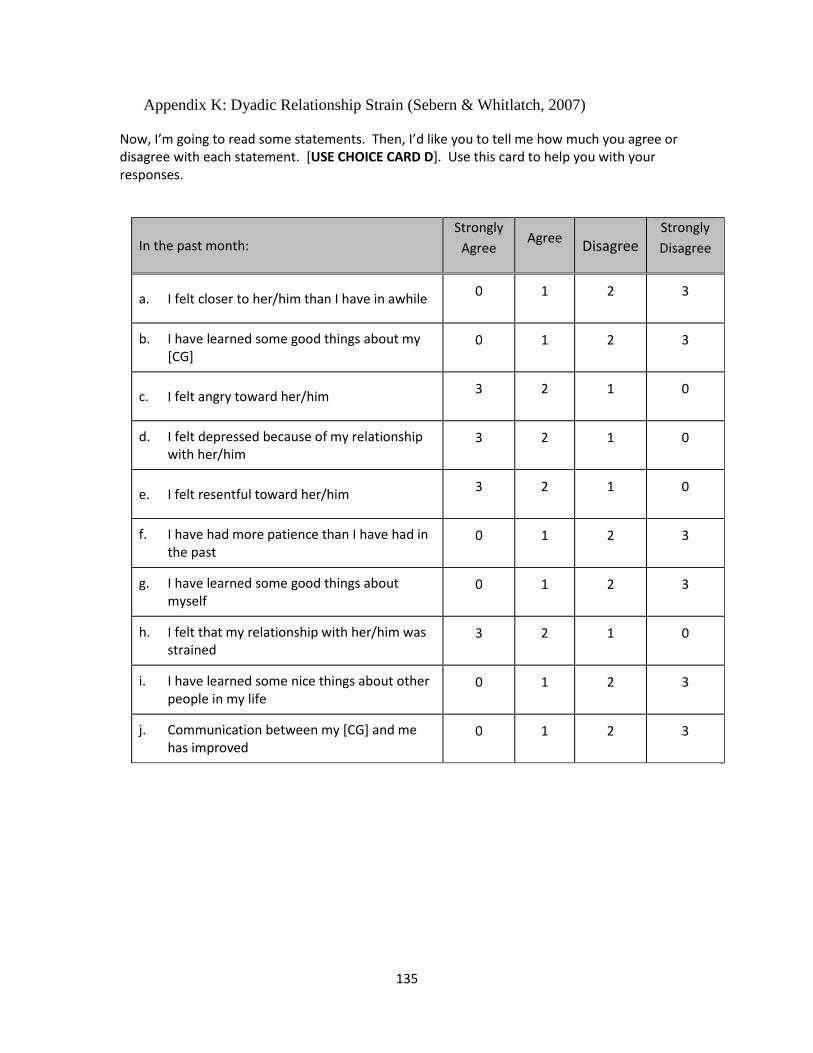
135
Appendix K: Dyadic Relationship Strain (Sebern & Whitlatch, 2007)
Now, I’m going to read some statements. Then, I’d like you to tell me how much you agree or disagree with each statement. [USE CHOICE CARD D]. Use this card to help you with your responses.
In the past month: Strongly
Agree Agree
Disagree Strongly
Disagree
a. I felt closer to her/him than I have in awhile 0 1 2 3
b. I have learned some good things about my [CG]
0 1 2 3
c. I felt angry toward her/him 3 2 1 0
d. I felt depressed because of my relationship with her/him
3 2 1 0
e. I felt resentful toward her/him 3 2 1 0
f. I have had more patience than I have had in the past
0 1 2 3
g. I have learned some good things about myself
0 1 2 3
h. I felt that my relationship with her/him was strained
3 2 1 0
i. I have learned some nice things about other people in my life
0 1 2 3
j. Communication between my [CG] and me has improved
0 1 2 3

136
Appendix L: Telephone Screener
Music and MemorySM
Telephone Recruitment Script
Hello, may I speak with __________?
Hello! My name is ________________ [Insert Name] from __________________ [Insert
organization]. I am calling to talk with you about the Music and Memory program that we are
offering in conjunction with Benjamin Rose and the Ohio Department on Aging. If you have
about 15 minutes to talk, I’d like to tell you about the program. If you’re interested in you and
your loved one participating, I’d also like to ask you some questions. Is now an okay time to
talk?
Great! Before we begin, I would like to make sure you are in a safe place and can talk freely
with me.
Thank you!
Benjamin Rose Institute on Aging is working with the Ohio Department on Aging to implement a
program called Music and Memory. The goal of this program is to help you connect with the
music you know and love. Research shows that listening to music can help people with a wide
range of challenges. Many people find renewed joy in life through music, especially when the
music is personally meaningful. The family members of people who participate in Music and
Memory also frequently benefit from the program. The program itself is being offered to you at
no cost, with the exception of any equipment and/or music you wish to purchase in the future.
As part of your participation in the Music and Memory program, a student from Cleveland State
University will set up a time to meet with you in person to gather some basic information about
you and your loved one. With the information you provide, we will share with you with the
equipment and information you’ll need to get started with Music and Memory. This may include
sending you equipment, such as an iPod Shuffle and headphones for listening to personalized
music at home, as well as helping to start a music library on your home computer. We will
provide some forms for you to fill out and send back to us over the course of one month which
will tell us about how things are going with the music. After one month of using the Music and
Memory program, a student from Cleveland State University will contact you for a final time to

137
ask you similar questions again in order to monitor how the program is going. The information
you provide will be very useful in helping us learn whether the program is working and also how
to make the program available to others who could benefit.
Does this sound like something you’d be interested in?
IF NO: That’s okay. If you change your mind or if you have any further questions, please call the
Music and Memory staff at Benjamin Rose at (216) 373-1615 -or- email at
[email protected]. Thank you for your time.
IF YES, THEN CONTINUE: Great! I’d like to ask you a few questions to make sure that you are
eligible for the program, before I go on. The reason is that the program is designed for people in
a particular situation.
I. Eligibility *Required questions
Screener Item CG Response
1) *Does the person you provide care for
have trouble with his/her memory? yes no (If no, STOP)
2) What year was CR’s memory
problem first noticed?
3) What are the CR’s memory-related
symptoms?
4) Has CR talked to a doctor about memory
concerns? yes no
5) Does CR have a diagnosis for memory
problems? yes no (If no, go to #7)
6) If diagnosed, what is diagnosis? Alzheimer’s Disease
Other Dementia
Vascular Dementia
Other Diagnosis:
7) What year was CR diagnosed?
8) Is CR taking medications for memory
problems? yes no (If no, go to #10)
9) What medications is CR taking for memory
problems?
Aricept (Donepezil)
Reminyl (Galantimine)
Excelon (Rivastigmine)
Namenda (Memantine)
Other:
10) *Does CR receive assistance from a CG as
a result of having memory challenges? yes no
11) When did CG begin assisting CR due to
memory?
12) How many days out of the week does the

138
Not Eligible Script: I’m very sorry, but unfortunately, you are not eligible for this program. This program requires that you (STATE THE REASON THAT THE PERSON IS NOT ELIGIBLE). I thank you for your time and wish you the best of luck. Please feel free to contact Benjamin Rose for other programs that you may be qualifies for. END CALL Eligible Script: Thank you. Based on your responses, you are eligible to participate in Music and Memory. Would it be all right to set up a meeting with you and your loved-one in-person to get started with the program? We are able to meet at the Benjamin Rose Institute on Aging in Cleveland (11890 Fairhill Rd, Cleveland, OH 44120), at your own home, or at another location if you prefer.
If YES, “Great, where would you prefer to meet?” ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
“When would be a good day and time to meet with you?
_____________________________________________________________________________________________________________________________________________________________________________________________________________
CG help the CR with care tasks? (If less than 5, STOP)
13) Does the CR still drive? yes (If yes, go to #13) no
14) If CR does not drive, why?
15) Does person have primary responsibility
for CR? yes no
16) Where does the CR reside? Alone in community
With CG
With another family member
Non-community
Other:
(If in Nursing Home, STOP)
17) *Do you have a computer with internet
access?
18) *If yes, is this computer a portable laptop,
or a desktop workstation?
yes no
19) *Are you familiar with iPods, iTunes, or
other Apple products?
yes no
(If YES, go to #19)
20) *Do you own an iPhone or iPod? yes no

139
“Excellent. I will plan on seeing you and your loved one at _______(PLACE) on the_______(DAY) at ________(TIME). In the meantime, in case I need to contact you, is this phone number the best place to reach you?
If NO, “For this project, it would be a requirement to meet in person to set up the Music and Memory program. I can give you a phone number to call and set up a meeting if you change your mind. Does this sound okay?

140
Appendix M: Personalized Music Assessment
Personalized Music Assessment (Experimental group T1, Control group T2)
Participant ID: ____________
1. Did CG/PWD/family create a playlist before interview? YES NO
2. What style(s) of music does the PWD prefer?
3. What specific artists does the PWD prefer?
4. What specific songs does the PWD prefer?
If possible, the interviewer should sample identified songs for the PWD before purchasing them
(in the iTunes store, play song preview). Respond to the following questions regarding this
sampling process.
5. Was the interviewer able to sample songs for the PWD to listen to? YES NO
i. If not, why? _____________________________________________________
6. Did the PWD exhibit a physical response to hearing the music samples? (e.g., foot tapping,
swaying, head bobbing, smiling). YES NO
While sampling each song, ask the PWD: “Do you like this song?”
7. Was PWD able to respond yes/no? YES NO
While sampling each song, ask the PWD: “Would you like me to add this song to your playlist?”
8. Was PWD able to respond yes/no? YES NO

141
Appendix N. Control Group Playlist

142
Appendix O: CONSORT Diagram
Excluded (n= 8)
Not meeting inclusion criteria (n= 1)
Declined to participate (n= 2)
Other reasons (n= 5)
Non-completers (n= 1)
Completers (n= 15)
Allocated to control (n= 16)
Non-completers (n= 3)
Completers (n= 15)
Allocated to intervention (n= 18)
Allocation
Follow-Up
PWD given MMSE (n= 38)
Expressed interest (n= 71)
Completed phone screener
(n= 46)
Excluded
Did not meet MMSE requirements
(n= 4)

143
Appendix P: Commonly Selected Genres and Preferred Artists of Personalized Music
Group Participants
Genre Number of Participants Favorite Artists
Gospel 6
Luther Vandross, Mahalia Jackson, Sam Cooke, Mississippi Mass Choir, Shirley Caesar, Chicago Mass Choir, Marvin Sapp, Yolanda Adams, Heziah Walker, James Cleveland
Rock/Classic Rock 5
Billy Joel, P!nk, Supertramp, Journey, The Rolling Stones, The Who, Jethro Tull, John Fogerty, The Eagles, Pete Seger, Bruce Springsteen, Fats Domino, J Giles Band, Chuck Berry, Elvis Presley
Golden Oldies 4 Nat King Cole, Dean Martin, Frank Sinatra, The Temptations, The Beatles, The Beach Boys
Big Band/Swing/Jazz 4 Billie Holiday, Nat King Cole, The Rat Pack, Sinatra, Ella Fitzgerald, Louis Armstrong, Glenn Miller
Blues 3 B.B. King, Muddy Waters, John Lee Hooker
RnB 3 Mariah Carey, Aretha Franklin, Diana Ross
Classical 3 Beethoven, flute music, piano concertos, misc artists
Pop/Soft Rock 3 Barry Manilow, Josh Groban, Perry Como, Beach Boys
Country/Folk 3 Alan Jackson, Garth Brooks, Jimmy Rodgers, Hank Williams, Johnny Cash
Bluegrass 2 Bill Monroe, Jimmy Martin
Musicals 2 Irving Berlin, Rogers and Hammerstein, Jerome Kern
Polka/Waltz/Accordion 1 Frankie Yankovic, misc artists




















