Developing the evidence-base for Safe Communities: a multi-level, partly randomised, controlled...
12
This article was downloaded by: [Brought to you by Unisa Library], [Professor M. Seedat] On: 13 August 2012, At: 02:04 Publisher: Taylor & Francis Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK International Journal of Injury Control and Safety Promotion Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/nics20 Developing the evidence-base for Safe Communities: a multi-level, partly randomised, controlled trial M. Seedat a b , R. McClure a c , S. Suffla a b & A. van Niekerk a b a Institute for Social and Health Sciences, University of South Africa, Johannesburg, South Africa b Medical Research Council, University of South Africa Safety and Peace Promotion Research Unit, Cape Town, South Africa c Injury Research Institute, Monash University, Melbourne, Australia Version of record first published: 09 Aug 2012 To cite this article: M. Seedat, R. McClure, S. Suffla & A. van Niekerk (2012): Developing the evidence-base for Safe Communities: a multi-level, partly randomised, controlled trial, International Journal of Injury Control and Safety Promotion, DOI:10.1080/17457300.2012.705303 To link to this article: http://dx.doi.org/10.1080/17457300.2012.705303 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
-
Upload
southafricanmedicalresearchcouncil -
Category
Documents
-
view
1 -
download
0
Transcript of Developing the evidence-base for Safe Communities: a multi-level, partly randomised, controlled...
This article was downloaded by: [Brought to you by Unisa Library], [Professor M. Seedat]On: 13 August 2012, At: 02:04Publisher: Taylor & FrancisInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
International Journal of Injury Control and SafetyPromotionPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/nics20
Developing the evidence-base for Safe Communities: amulti-level, partly randomised, controlled trialM. Seedat a b , R. McClure a c , S. Suffla a b & A. van Niekerk a ba Institute for Social and Health Sciences, University of South Africa, Johannesburg, SouthAfricab Medical Research Council, University of South Africa Safety and Peace Promotion ResearchUnit, Cape Town, South Africac Injury Research Institute, Monash University, Melbourne, Australia
Version of record first published: 09 Aug 2012
To cite this article: M. Seedat, R. McClure, S. Suffla & A. van Niekerk (2012): Developing the evidence-base for SafeCommunities: a multi-level, partly randomised, controlled trial, International Journal of Injury Control and Safety Promotion,DOI:10.1080/17457300.2012.705303
To link to this article: http://dx.doi.org/10.1080/17457300.2012.705303
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form toanyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses shouldbe independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims,proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly inconnection with or arising out of the use of this material.

Developing the evidence-base for Safe Communities: a multi-level, partly randomised, controlled trial
M. Seedata,b*, R. McClurea,c, S. Sufflaa,b and A. van Niekerka,b
aInstitute for Social and Health Sciences, University of South Africa, Johannesburg, South Africa; bMedical Research Council,University of South Africa Safety and Peace Promotion Research Unit, Cape Town, South Africa; cInjury Research Institute,
Monash University, Melbourne, Australia
(Received 9 December 2011; final version received 19 June 2012)
Safe Communities, representing a global activation of the public health logic, may be strengthened through theoretical,methodological and empirical support. In the spirit of this Special Issue that aims to analyse the achievements andchallenges inherent to Safe Communities, we offer our contribution in the form of a methodology of a multi-countrychild safety, peace and health promotion study. The study, situated within an African-centred initiative calledUkuphepha – an isiZulu word meaning demonstrating African safety – is underpinned by four theoretical claims thatframe injury and violence prevention as a multi-disciplinary issue to be addressed through a suite of interventions tofamily and extended social systems. The interventions, sensitive to the priorities of each participating country, havebeen informed by the literature on effective interventions and the authors’ joint experiences of communitydevelopment. The study is designed as a population-based, multi-level, multi-intervention partly randomisedcontrolled trial, and there are potentially 24 participant communities representing South Africa, Mozambique, Egypt,Zambia, Uganda, Bangladesh, Malaysia and Australia – over three commencement phases. Whereas processevaluation will focus on community engagement, impact evaluation will consider risk and protective factors, andoutcome evaluation will examine the overall effectiveness of the interventions. Notwithstanding the many challenges,the study will provide insights into the methodology and mechanisms of ecologically-oriented interventions that locateinjury and violence prevention as an activity arising from safety, peace and health promotion.
Keywords: Safe Communities methodology; multi-level; multi-intervention; partly randomised controlled trial; Africa
Introduction
We use the principles entailed in the concepts of safety,peace and health to design and develop an Africa-centredchild injury and violence prevention study, with a view toillustrating how such an initiative may advance thetheoretical and scientific basis for the Safe Communitiesapproach. The Safe Communities approach represents aspecific global activation of the public health logic. Itrecognises the psychological, social, economic andcriminological dimensions of violence and injuries andinvolves the promotion of ecological actions to addressrisk and protective factors at multiple levels (individual,school, peers, family, community and society) usinginterventions aimed at universal, selected and indicatedgroups. The approach embodies a multi-disciplinary andmulti-sectorial engagement in the control of violence andinjuries and promotes interventions across the fullprimary, secondary and tertiary prevention continuum.The Safe Communities approach recognises the impor-tance of context, both in relation to the risk of injury andits prevention (Jansson, 2007; McClure, 2010).
The concept of Safe Communities that emerged inwestern Europe in the early 1980s and which resonateswith other earlier community development and commu-nity psychology perspectives originating in the 1960s and1970s in countries such as South Africa (see Seedat &Lazarus, 2011), gives substance to the public health logicby positioning multi-sectoriality, multi-disciplinarity,evidence, long-term investment, community participa-tion, registration of injuries, documentation, evaluationand dissemination as the guiding principles of commu-nity-based prevention actions. The global Safe Commu-nities network, which brings together more than 200demonstration programmes located in different regionsof the world, actualises these public health principles,ideals and overall approach.
Despite its inherent intentions, the Safe Commu-nities movement is fraught with challenges. Among thechallenges is the uneven operationalisation of SafeCommunities across different regions of the world.Most of the Safe Communities programmes arelocated in well-resourced contexts of Europe and
*Corresponding author. Email: [email protected]
International Journal of Injury Control and Safety Promotion
2012, 1–11, iFirst article
ISSN 1745-7300 print/ISSN 1745-7319 online
� 2012 Taylor & Francis
http://dx.doi.org/10.1080/17457300.2012.705303
http://www.tandfonline.com
Dow
nloa
ded
by [
Bro
ught
to y
ou b
y U
nisa
Lib
rary
], [
Prof
esso
r M
. See
dat]
at 0
2:04
13
Aug
ust 2
012

North America. In Africa and other resource chal-lenged environments however, the absence of a criticalmass of researchers, the lack of a community-basedinfrastructure, and competing public health priorities,hamper the uptake and translation of the vision andideals of the safe community model.
Where safety promotion initiatives do exist in theseenvironments, they tend to be informed by models thatremain untested for their contextual and cultural fit, andrelevance for local conditions. A recent CochraneReview (Spinks, Turner, Nixon, & McClure, 2009)concluded that there was no consistent relationshipbetween status as a WHO designated Safe Communityand resultant changes in injury outcomes. Evaluationsfor 21 communities, collectively from Sweden, Austria,Norway, Australia and New Zealand, were included inthe review. Spinks et al. (2009) argue that the science ofcommunity-centred injury prevention is compromised bythe diversity and minimally demonstrated efficacy of safecommunity approaches and activities, the relative dearthof evaluations undertaken, methodological limitations incommunity-based evaluations, and the distinct variationin observed injury rates across identified communities.Similar findings were reported by Spinks and associatesin an earlier systematic review of community-basedchildhood injury prevention programmes undertaken in2004 (Spinks, Turner, McClure, & Nixon, 2004). Suchsystematic reviews, highlighting the under-developedtheoretical, methodological and empirical bases of SafeCommunities, offer a compelling case for robust studiesin the application of the safe community approach.
We argue that the Safe Communities approachdepends on the foundational concepts of safety, peaceand health. The aim of this paper is to articulate amethodology, based on these three foundationalconcepts that can be used to develop an evidencebase to support the intentions and achievements of theSafe Communities movement, within the multi-dis-ciplinary oriented, ecologically aligned public healthlogic. Within the context of this Special Issue thatintends to offer a critical reading of the successes,challenges and gaps in the Safe Communities move-ment, we describe the methodology in terms of a multi-country child violence and injury prevention studylocated within an initiative called Ukuphepha. Webegin with a brief description of Ukuphepha (an isiZuluword meaning demonstrating safety), and then outlinethe aims and scope of the child study itself.
Ukuphepha: demonstrating African safety, peace andhealth
Ukuphepha is an initiative that seeks to: implement,evaluate and maintain integrated safety, peace andhealth promotion programmes in resourced-challenged
communities in participating African countries; regu-larly convene scholarly fora dedicated to generatingcritical African-centred safety and peace promotiontheories and methodologies; and stimulate a network ofservice-based agencies. The initiative will establish sitesof study of innovative interventions, and combine injurydata collection with intervention applications andresearch-related community engagement. The initiativewill focus primarily on multi-site safety, peace andhealth promotion interventions that are responsive tothe emergent injury profiles of each participant com-munity. Emerging researchers and post-graduate stu-dents as well as community workers will be hosted at theinitiative’s sites for instruction and training on thetheory, methodology and implementation of injuryprevention and safety, peace and health promotion.The training and capacitation work is intended todevelop scarce skills and expertise across the region, aswell as create opportunities for longitudinal studies andongoing collaboration between partners. The Africa-centred group of scholars is expected to act as a resourcewithin the sector, contributing to the African and globalscience base and supporting safety, peace and healthpromotion initiatives in under-served communities inparticular. The network of service-based agencies,which is emerging rapidly, will both draw on, as wellas act as a resource to support the creation of safetypromotion and the development of skills linked totechnological improvement and innovation, and con-textual relevance.
The child injury and violence prevention study
Claims, organising logic and assumptions
This study is underpinned by four claims, whichprovide the organising and theoretical framework forthe study.
Injury and violence prevention is an activity arising fromthe integration of three streams: the promotion of safety,peace and health.
Safety, peace and health have historically beenconceptualised as distinct areas of focus, informed byinimitable epistemological, ontological and methodo-logical approaches, and accordingly observed to relateto injury and violence prevention in somewhat discreteand detached ways. However, conceptualisations ofsafety, peace and health have shared dominantassumptions about the drivers of individual, commu-nity and societal well-being in that each:
(1) is considered an essential individual, commu-nity and societal resource (e.g. World HealthOrganization, 1998);
2 M. Seedat et al.
Dow
nloa
ded
by [
Bro
ught
to y
ou b
y U
nisa
Lib
rary
], [
Prof
esso
r M
. See
dat]
at 0
2:04
13
Aug
ust 2
012

(2) is concerned with structural obstacles thatfunction to obstruct individual and collectivewelfare (e.g. Christie, Wagner, & Winter, 2001;Galtung, 1996);
(3) values the importance of catalysing change atthe levels of beliefs, attitudes, values, knowl-edge, behaviours and structures within thelocal, national and international milieu (e.g.Arya, 2004; Nastasi & Hitchcock, 2009); and
(4) recognises the capacity of individuals, collec-tives and broader systems to increase controlover the determinants of injury and violence(e.g. Stachtchenko & Jenicek, 1990).
The embedding of injury and violence preventionwithin such a multi-disciplinary and integrated frameresonates with critical perspectives on knowledge mak-ing and social praxis, which place the accent on: (1) thesocial determinants of violence and injury; (2) challengesto dominant discourses that support systemic exploita-tion, discrimination, oppression and inequity linked toinjury and violence; (3) honouring of multiple voices andknowledges in processes of social change; (4) adoptingan activist agenda in the pursuit of social justice; and (5)the sustainable satisfaction of basic human needs asessential for human development and well-being (e.g.Christie et al., 2001; Freire, 1970).
Effective promotion of safety, peace and health recog-nises and addresses multiple drivers at each of theecological levels: societal, community, household andindividual.
Safety, peace and health are the consequence ofinterconnected conditions and events (either risk orprotective factors) (Susser & Susser, 1996). Thepromotion of safety, peace and health, in resonancewith the large body of knowledge that demonstratesthe utility and complexities of multi-level interventions(e.g. Nastasi & Hitchcock, 2009), therefore relies on acomprehensive understanding of broad societal andcommunity factors (Rosen & Jansson, 2000), as well asmore localised factors at the household and individuallevel. Arguably, the targeting and application ofinterventions at each of these ecologic levels couldresult in a more sustained and successful population-based approach to injury prevention.
Communities are characterised by their distribution ofboth risk and protective characteristics
Protective factors, also referred to as assets, and whichmay include a focus on sense of community, communitycohesion, community resilience and other similar capa-cities directed towards transformation, may be mobilised
to mediate the deleterious consequences of risks andpromote safety, peace and health in the long-term. Withinthis context, social assets may be tangible (e.g. housingfacilities), behavioural (e.g. crossing roads at pedestriancrossings), social (e.g. development of a communitypatrol) or structural (e.g. good community leadershipand organisation). Research suggests that the fosteringand supporting of strong, protected, socially cohesivecommunities, which prioritise social capital, social con-nections and community life, is an important strategy forincreasing safety (e.g. Holdsworth & Hartman, 2009).
The promotion of safety, peace and health is partiallycontingent on democratic citizenship expressed throughactive community engagement in the design, implementa-tion, monitoring and evaluation of promotive initiatives.
Citizenship (Bulbulia, Seedat, & Lekoba, 2011), enactedthrough participatory processes that focus on a sharedownership of the injury challenge and associatedsolutions, recognition and mobilisation of communityassets, and collective responsibility for the identificationof priorities and appropriate interventions, is consideredas key for effective and sustainable injury preventionand safety, peace and health promotion (Klaasen,Morag MacKay, Moher, Walker, & Jones, 2000).
The interventions
The claims and assumptions described in the previoussection were used as the basis for developing theinterventions and evaluation design of the child study.The Ukuphepha child study seeks to deliver a suite ofinterventions to family and extended social and livingsystems through home visitations, as well as throughcommunity-wide interventions, including early child-hood development centres (ECDs) and outreach toplay parks. Priorities for the Ukuphepha interventionshave been determined by site-specific concerns andknown causes of childhood mortality and morbidity inthe selected communities. Both the characteristics ofthe study and the specific component interventionshave been selected from those that have previouslybeen demonstrated under research environments to beefficacious. The nature of the intervention deliverysystems (i.e. the nature of the study strategies andprocesses) has been developed from the literature oneffective interventions and informed by the authors’collective experiences of community development.
The basic organising structure of the study isillustrated by a three-dimensional matrix (see Figure1). One axis represents the risk/protective factor beingaddressed by the intervention and the second axisdepicts the nature of the factor being addressed by theprogramme (in terms of it being an economic, social or
International Journal of Injury Control and Safety Promotion 3
Dow
nloa
ded
by [
Bro
ught
to y
ou b
y U
nisa
Lib
rary
], [
Prof
esso
r M
. See
dat]
at 0
2:04
13
Aug
ust 2
012
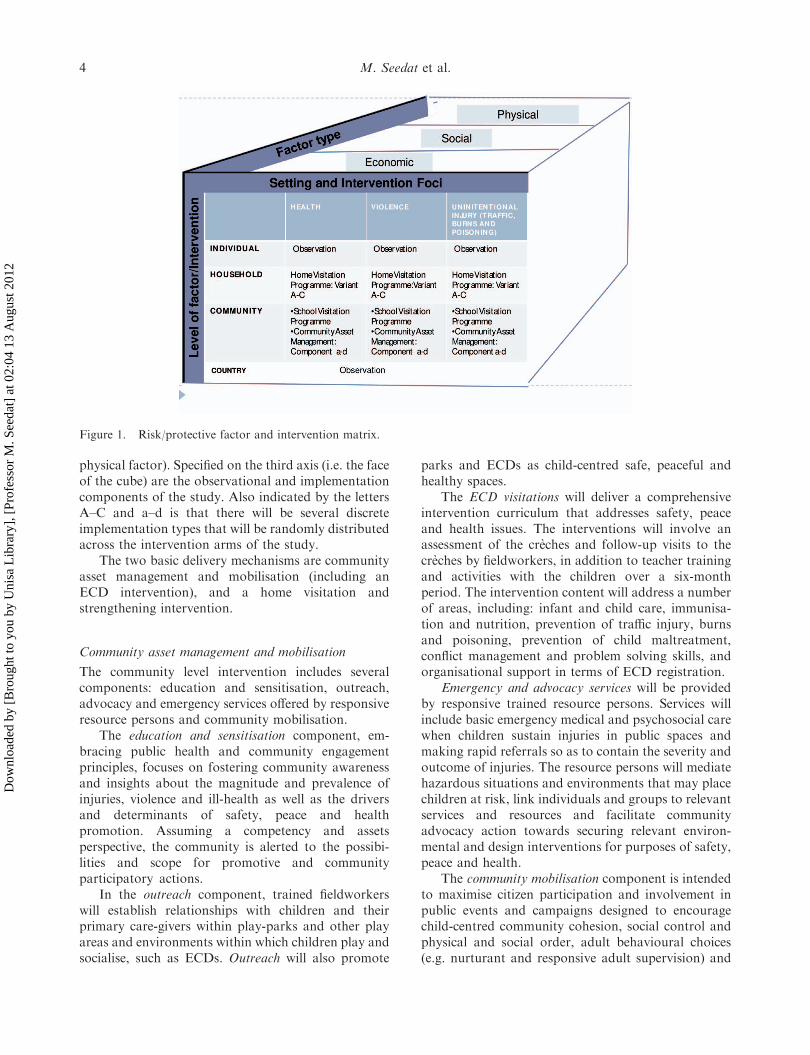
physical factor). Specified on the third axis (i.e. the faceof the cube) are the observational and implementationcomponents of the study. Also indicated by the lettersA–C and a–d is that there will be several discreteimplementation types that will be randomly distributedacross the intervention arms of the study.
The two basic delivery mechanisms are communityasset management and mobilisation (including anECD intervention), and a home visitation andstrengthening intervention.
Community asset management and mobilisation
The community level intervention includes severalcomponents: education and sensitisation, outreach,advocacy and emergency services offered by responsiveresource persons and community mobilisation.
The education and sensitisation component, em-bracing public health and community engagementprinciples, focuses on fostering community awarenessand insights about the magnitude and prevalence ofinjuries, violence and ill-health as well as the driversand determinants of safety, peace and healthpromotion. Assuming a competency and assetsperspective, the community is alerted to the possibi-lities and scope for promotive and communityparticipatory actions.
In the outreach component, trained fieldworkerswill establish relationships with children and theirprimary care-givers within play-parks and other playareas and environments within which children play andsocialise, such as ECDs. Outreach will also promote
parks and ECDs as child-centred safe, peaceful andhealthy spaces.
The ECD visitations will deliver a comprehensiveintervention curriculum that addresses safety, peaceand health issues. The interventions will involve anassessment of the creches and follow-up visits to thecreches by fieldworkers, in addition to teacher trainingand activities with the children over a six-monthperiod. The intervention content will address a numberof areas, including: infant and child care, immunisa-tion and nutrition, prevention of traffic injury, burnsand poisoning, prevention of child maltreatment,conflict management and problem solving skills, andorganisational support in terms of ECD registration.
Emergency and advocacy services will be providedby responsive trained resource persons. Services willinclude basic emergency medical and psychosocial carewhen children sustain injuries in public spaces andmaking rapid referrals so as to contain the severity andoutcome of injuries. The resource persons will mediatehazardous situations and environments that may placechildren at risk, link individuals and groups to relevantservices and resources and facilitate communityadvocacy action towards securing relevant environ-mental and design interventions for purposes of safety,peace and health.
The community mobilisation component is intendedto maximise citizen participation and involvement inpublic events and campaigns designed to encouragechild-centred community cohesion, social control andphysical and social order, adult behavioural choices(e.g. nurturant and responsive adult supervision) and
Figure 1. Risk/protective factor and intervention matrix.
4 M. Seedat et al.
Dow
nloa
ded
by [
Bro
ught
to y
ou b
y U
nisa
Lib
rary
], [
Prof
esso
r M
. See
dat]
at 0
2:04
13
Aug
ust 2
012

environmental arrangements. The public campaignsand events will focus on priority safety, peace andhealth issues. International and nationally recognisedevents, such as the World Health Day, World Day forthe Prevention of Child Abuse and World Day ofRemembrance for Road Traffic Victims, may be usedas vehicles to mobilise community action around, keysafety, peace and health priorities.
Home visitation and strengthening interventions
The three variants comprise: a core home visitationcurriculum and microfinancing and economic solidar-ity; core curriculum and hazard reduction; and a corecurriculum and both the microfinancing and hazardreduction packages.
The home visitation and strengthening interventionwill offer a core health and safety curriculum deliveredto primary caregivers that integrates child health(focussed on nutrition and immunisation) and familyfunctioning, child abuse and unintentional injury(traffic, burns and poisoning) prevention components.The intervention will involve visitors calling 8–10 timeson the intervention households over a six-monthperiod. The content of visits focuses on two basicissues: (i) reducing the stressors that mediate injury andmaltreatment, and (ii) strengthening the protectivefactors that will prevent this from happening (Butch-art, Harvey, Mian, & Furness, 2006; Swart, VanNiekerk, Seedat, & Jordaan, 2008).
During each of these visits, trained home visitorswill provide the primary caregivers with informationon safety practices, complete a related injury hazardchecklist, and discuss possible changes to reduce risksfor specific child injury types. Each visit will lastapproximately 30–40 min. This curriculum will com-prise the core home visitation programme; the coreprogramme will, for some households, be supplemen-ted by additional home visitation components thatinclude either specific safety equipment or micro-financing based on the principles of economicsolidarity.
The microfinancing and economic solidarity varia-tion of the home visitation intervention will combinethe core health and safety curriculum (Odendaal, VanNiekerk, Jordaan, & Seedat, 2009; Swart et al., 2008),with social empowerment and economic solidarity thatresonates with the IMAGE (Intervention with Micro-finance for AIDS and Gender Equity) (Pronyk et al.,2005) and Stepping Stones interventions (Jewkes et al.,2008). This integration will comprise two components:a poverty-focussed microfinance and economic soli-darity scheme, and a health and gender equitycomponent. The primary caregivers will comprise thetarget group for the intervention; only caregivers who
had not received microfinance training before theintervention will be included in the study.
This hazard reduction aspect of the intervention willcombine the core health and safety curriculum withinformation on the safe use of a domestic stove and theprovision of a designated safe stove. This aspect of theintervention provides specific instructions and demon-strations of the utilisation of one of the paraffin stovesthat meet current country-specific South Africanlegislation. Paraffin stoves, despite the hazardousnature of the fuel that they use, are in widespreaduse in impoverished settings. However, some of thenewer such stoves host a number of safety features.These stoves are reported to self-extinguish whenmoved, do not explode (because of the physicalseparation of paraffin and air, except in the burneritself), have reportedly no harmful emissions, have noheated loose parts which may fall on to flammableliquids or materials when knocked over (such as thecooking oil in the pan), and cannot be refuelled whenalight (e.g. Promethea Corporation, 2009).
Feasibility and Sustainability
The Ukuphepha interventions have been developed toenable the eventual integration of its implementationprocedures, intervention materials and curricula intoexisting primary health care, educational and socialsupport systems, in participating sites and countries.An implementation manual has collated these inter-vention processes and materials to facilitate a cost-effective replication of the component interventions asrequired by participating sites (Abrahams & Suffla,2011). This replication would initially be from the pilotsites in South Africa, across partner sites, for eventualconsideration, implementation and maintenance byexisting country health and care systems. The im-plementation manual would, for example, provide abasis for government health care workers to integratethe home visitation curriculum into their routinehealth care training and activities, and for teachers tointegrate the ECD safety, peace and health pro-grammes into daily classroom activities (Abrahams &Suffla, 2011).
Evaluation design
The study is an international, population-based, multi-level, multi-intervention, partly randomised controlledtrial. The key design levels are: (i) country, (ii)community, and (iii) household primary caregiver/child. Interventions will be undertaken at each level asdescribed below. While the ultimate focus of this trial,and consequently the study sample, are children 0–7,the multi-level design implies a target group for each of
International Journal of Injury Control and Safety Promotion 5
Dow
nloa
ded
by [
Bro
ught
to y
ou b
y U
nisa
Lib
rary
], [
Prof
esso
r M
. See
dat]
at 0
2:04
13
Aug
ust 2
012
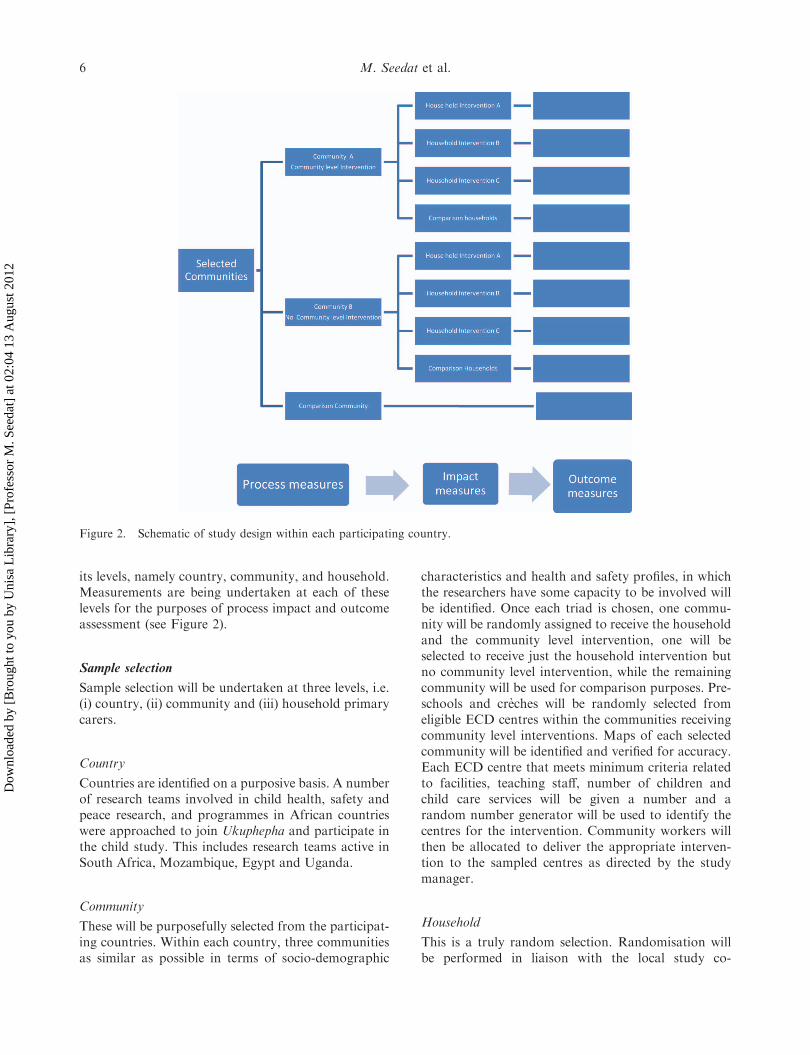
its levels, namely country, community, and household.Measurements are being undertaken at each of theselevels for the purposes of process impact and outcomeassessment (see Figure 2).
Sample selection
Sample selection will be undertaken at three levels, i.e.(i) country, (ii) community and (iii) household primarycarers.
Country
Countries are identified on a purposive basis. A numberof research teams involved in child health, safety andpeace research, and programmes in African countrieswere approached to join Ukuphepha and participate inthe child study. This includes research teams active inSouth Africa, Mozambique, Egypt and Uganda.
Community
These will be purposefully selected from the participat-ing countries. Within each country, three communitiesas similar as possible in terms of socio-demographic
characteristics and health and safety profiles, in whichthe researchers have some capacity to be involved willbe identified. Once each triad is chosen, one commu-nity will be randomly assigned to receive the householdand the community level intervention, one will beselected to receive just the household intervention butno community level intervention, while the remainingcommunity will be used for comparison purposes. Pre-schools and creches will be randomly selected fromeligible ECD centres within the communities receivingcommunity level interventions. Maps of each selectedcommunity will be identified and verified for accuracy.Each ECD centre that meets minimum criteria relatedto facilities, teaching staff, number of children andchild care services will be given a number and arandom number generator will be used to identify thecentres for the intervention. Community workers willthen be allocated to deliver the appropriate interven-tion to the sampled centres as directed by the studymanager.
Household
This is a truly random selection. Randomisation willbe performed in liaison with the local study co-
Figure 2. Schematic of study design within each participating country.
6 M. Seedat et al.
Dow
nloa
ded
by [
Bro
ught
to y
ou b
y U
nisa
Lib
rary
], [
Prof
esso
r M
. See
dat]
at 0
2:04
13
Aug
ust 2
012
Table
1.
Ukuphephachildstudy:phase
twosite
inform
ation*.
Studysite
MachavaSede
Port
said
Ismaliagovernorate
Bwaise,
MakerereII
community
Opit
Vlakfontein
Nomzamo
Studylocation
Matola,Maputo
Province,
Mozambique
North-easterncity
inEgypt
Alongthewestbankof
theSuez
Canal,Egypt
Four-km
northof
Kawem
pedivision,
Uganda
NorthernUganda
South
ofJohannesburg,
Gauteng,South
Africa
South
East
ofCape
Town,Western
Cape,
South
Africa
Urbanorruralcontext
Industrialarea(urban
andperi-urbanareas)
Urban
Urban
Peri-urban
Rural(post-w
arperiod)
Urban(low-income,
inform
alsettlement)
Peri-urban(low-income)
Communitysize
No.ofresidents,
No.of
adults,
Children
aged
0–12
34,880,16,853men
and
18,027women,11,755
children
600,000,N/A
,N/A
882,500,23.4%
are
less
than10years
old,
N/A
8000,5000adults,3000
childrenaged
0–12
years
16,800,N/A
,N/A
32,000,N/A
,N/A
+2500,16,250(65%
of
population),7500
children
Community
infrastructure
Schools,Clinics,
Churches,
NGOs,CBOs
Threeelem
entary,three
secondary,three
technical,tw
ohospitals,tw
ohealth
centres,oneprivate
clinic,125churches,
twoMuslim
mosques
University,Schools,N/A
,N/A
,Approxim
ately
220activeNGO’s
713schools,Suez
Canal
University
Hospital,
N/A
,N/A
,N/A
Threeprimary
schools,
twosecondary
schools,onesm
all
highinstitutionof
learning,threeclinics,
twopharm
acies,three
churches,onehome-
basedMosque,
one
smallpolice
post,one
CBO
women’s
organisation,one
police
post
Primary
school,
secondary
school,
vocationschool,
Healthunitmission
hospital,N/A
,Police
post,soldiers’
barracks
Creches,20pre-schools,
twoprimary,one
secondary,skills
developmentcentre,
oneclinic,N/A
,N/A
25–30creches,three
primary,one
secondary,oneclinic,
3–4churches,tw
oNPO’s
Housingtypes
Mostly
madeofreed,
woodandzinc,
There
are
someconventional
houses
Urbanhousing,withslum
areas
Urbanandruralareas
andslum
housing
New
lyconstructed
homes
are
ofpermanent
materials.Old
structuresare
semi-
permanentmaterials
Sem
i-permanenthousing,
mudandgrass
structuresi.e.
temporary
housing
6100form
alhousing
Mixed
housing:+3500
form
alRDPhousing,
and+
1500inform
al
dwellings
Socio-economic
profile
Unem
ployment
rate,income
rate
N/A
,low
sources
of
income
N/A
,N/A
N/A
,middle
class
citizens
N/A
,mainly
low
income
earners
N/A
,N/A
N/A
,N/A
+35–40%
more
women
employed,N/A
Child(0–12
years)injury
patternsand
priorities
–including
availability
ofexisting
data,detail
ofavailable
data
Injury
priorities
andpatterns,
available
data
N/A
,N/A
Roadtrafficinjury,82%
ofchildinjuries
occur
inthestreet;male
childrenhavegreater
risk
forinjury
Roadtrafficinjury,child
abuse
and
maltreatm
ent,0–11
agegroup,551
childrenwereinjured:
falls(60%),road
trafficinjuries
(15%),
burns(7%),poisoning
(3%)andnear
drowning/drowning
(2%)(G
lobal
Childhood
UnintentionalInjury
Surveillance
(GCUIS),2007)
Roadtraffic,
burnsand
falls.N/A
Violence,N/A
Pedestrianinjuries,burns,
falls,childabuse
and
neglect,N/A
Roadtrafficinjuries,
Burns,Falls,
Incidentsfor:Traffic–
17,Burns–6,Falls–
40,+
25%
of
unintentionalinjuries
forchildreninclude
poisoning (continued)
International Journal of Injury Control and Safety Promotion 7
Dow
nloa
ded
by [
Bro
ught
to y
ou b
y U
nisa
Lib
rary
], [
Prof
esso
r M
. See
dat]
at 0
2:04
13
Aug
ust 2
012
Table
1.
(Continued)
Studysite
MachavaSede
Port
said
Ismaliagovernorate
Bwaise,
MakerereII
community
Opit
Vlakfontein
Nomzamo
Existingrelationshipswith
communityleadersandother
stakeholders(e.g.schools,
municipality)
NGO’s}
SAUDECO,
CA-PAZ,
AMORTREVO,
ADIC
AE,REMAR;
NGO’scollaborate
withProvincial
Department(H
IV);
Health;CityCouncil;
Administrativepost;
LocalCourt;local
authorities;civil
society/church
Haverelationshipswith
communityleaders
anddifferent
stakeholders(e.g.
schools,
municipality).
Partnershipsand
collaborationbetween
thedifferentsectors
such
asthehealth,
socialandcivil
sectors.Collaboration
withUNISA
(2005).
Havegoodrelationships
withcommunity
leadersanddifferent
stakeholders(e.g.
schools,
municipality).
Partnershipsand
collaborationbetween
thedifferentsectors
such
asthehealth,
socialandcivil
sectors.Partnerships
withvariousNGO’s,
MinistryofHealth
(MOH).
Localcommunity,
women’sgroups,
possible
coordinator
(seven
years
experience
with
safety).
Localcommunity,health
workers,possible
coordinator(10years
experience
onschool
violence).
Partnershipsand
collaborationswith
thelocalcivic;local
municipality;creches;
localschools;NGOs
&government
departments
(e.g.
CommunitySafety,
Human
Development).
Partnershipsand
collaborationswith
thelocalcivic;local
municipality;creches;
localschools;NGOs
andgovernment
departments
(e.g.
CommunitySafety,
Human
Development).
Currentchildsafety
promotion
interventionstakingplace
at
either
household,schoolor
communitylevel
Hostingorphans(H
IV);
recoveryofproperties;
acquisitionofschools
supplies,uniform
s,schoolfees;support
thegenerationof
incomevia
subsistence
agriculture
inorder
topromote
self-
sustainability
1998schoolpedestrian
safety
initiative(12–13
years).Safe
CommunityGroup
2005spreadthe
importance
ofinjury
andviolence
preventionatdifferent
levels;served
the
communityand
assistedin
solving
problemsrelatedto
childrenandsafety.
Port
Said
InternationalSchools
Initiative(2005)–
promotedawareness
andpreventionof
accidentaltransport
injuries.2007UN
InternationalWeek
forRoadSafety.
TheUniversity
isinvolved
inmany
injury
control
programmes
such
as
RS10(W
HO/M
OH
jointroadtraffic
injury
control).In
2004,theSchool-
BasedProgram
for
Injury
Preventionand
Safety
Promotionwas
implementedin
Ismailia
city.
Aschoolinjury
clubis
locatedin
oneofthe
primary
schools).
Injury
Control
Centre–Uganda
(ICCU)currentlyhas
Injury
Prevention
Intervention
programmes
atoneof
thecommunity
schools(focus:burns,
trafficinjuries).
Planningforinjury
preventionactivitiesis
takingplace;
Currently,noinjury
programme.
Childsafety
campaign:
addressingpedestrian
safety;burns;child
abuse
andneglect-
implementedat
primary
schoolsand
creches
Childsafety
campaign:
addressingpedestrian
safety;burns;child
abuse
andneglect
–im
plementedat
primary
schoolsand
creches
Note:*Zambia
sitesin
theprocess
ofbeingidentified.
8 M. Seedat et al.
Dow
nloa
ded
by [
Bro
ught
to y
ou b
y U
nisa
Lib
rary
], [
Prof
esso
r M
. See
dat]
at 0
2:04
13
Aug
ust 2
012

ordinating centre using the following process. Maps ofeach community will be identified and verified foraccuracy. Based on earlier studies, eligible householdscould be ‘families with children 7 years or younger wholived in that house, visited there more than once amonth, or stayed there during school holidays’ (Swartet al., 2008, p. 184). The same randomisation processwill be used for the selection of households for each ofthe communities involved in interventions at thehousehold level.
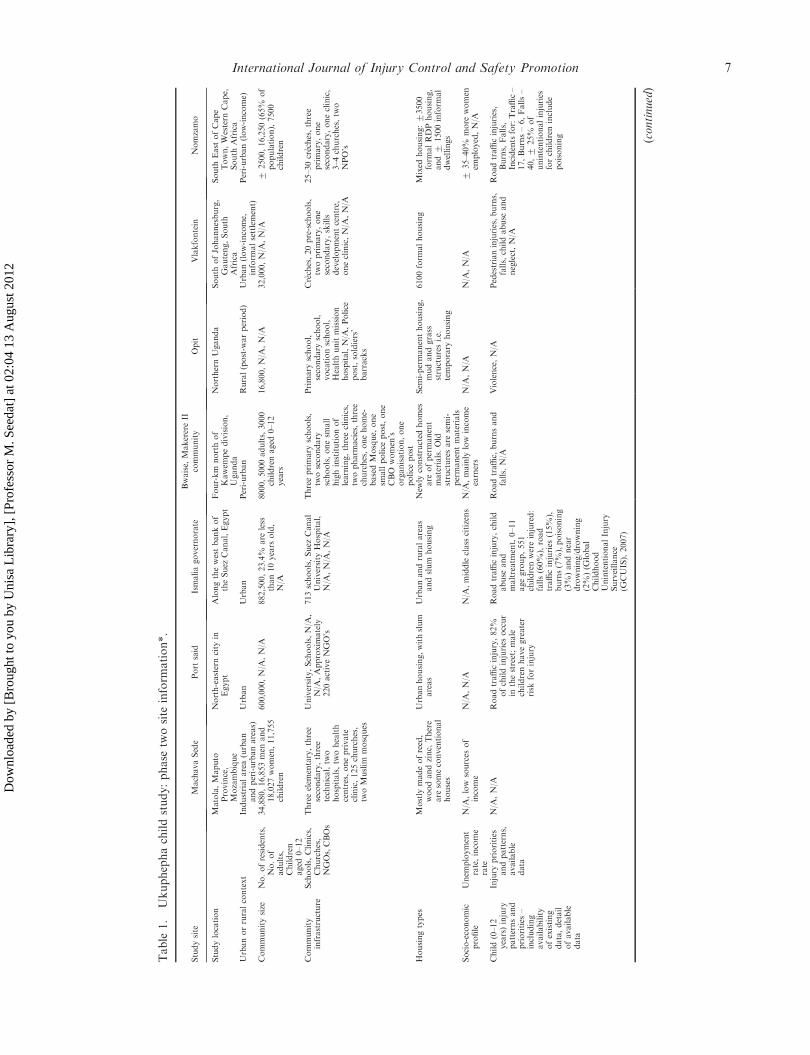
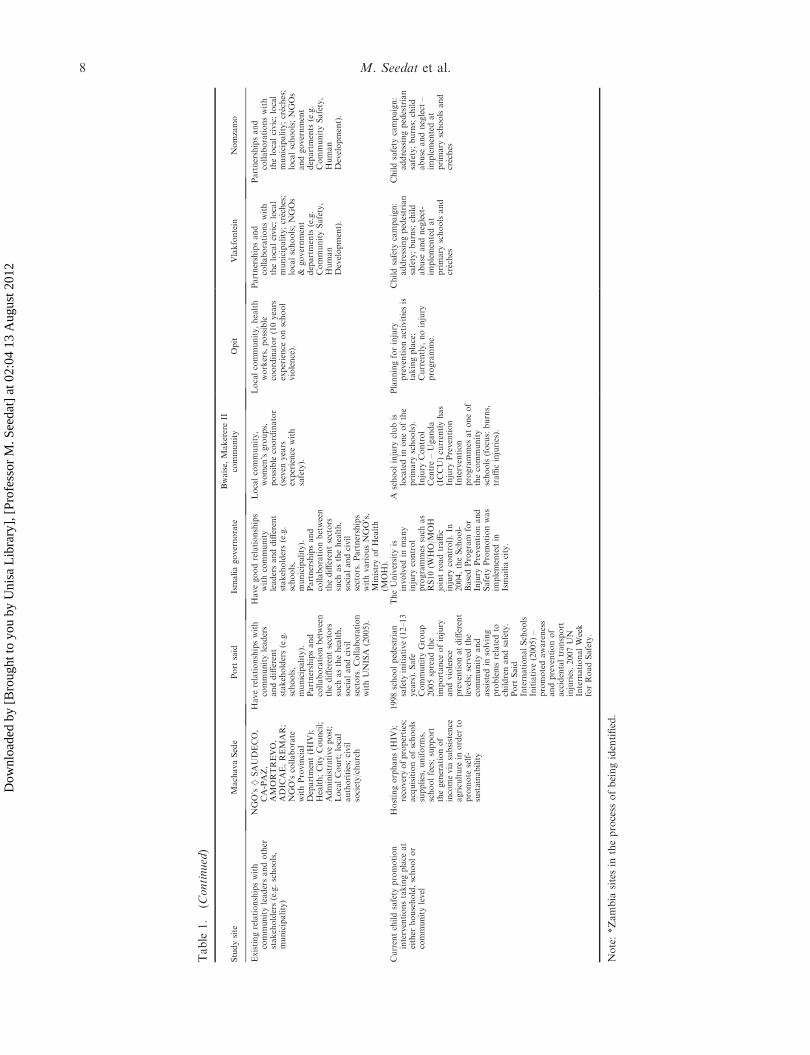
Study sites
There will potentially be 24 communities involved inthis stage over three commencement phases. Studysites will include three communities per countryinvolved in the study. Phase one study sites are inSouth Africa, where the full intervention basket isbeing prepared for piloting and implementation. Phasetwo study sites will potentially involve communitiesfrom South Africa, Egypt, Uganda, Zambia andMozambique (see Table 1). In phase three, indigenouscommunities in Australia, and communities fromBangladesh and Malaysia will be added. Phase twoand phase three study sites may involve the imple-mentation of the full intervention basket or interven-tions at selected levels only. Each site will have its ownlocal study centre and there will also be a co-ordinatingcentre. A description of the phase one and phase twosites is included in the table below.
Evaluation
Process evaluation
The process evaluation will focus on the level ofcommunity engagement in delivery and the achieve-ment of implementation targets. Qualitative processinformation will be recorded on an ongoing basis bythe study officers and includes descriptive data regard-ing staffing, costs of delivery, exposure in the commu-nity, participants, growth over time, changes tointervention based on feedback, decision-making andgovernance issues. Data collection instruments anddata collection training manuals are being developedto support community workers record thisinformation.
Impact evaluation
The impact evaluation will include the administrationof a household demographic and risk/protective factorquestionnaire to identify injury and selected healthrisks at household level. A community asset and riskaudit to identify assets and risks at community level
will be administered. Data collection is to be under-taken by trained assessors in each participatingcommunity. Data collectors responsible for the admin-istration of the household risk assessment question-naire – pre- and post-study intervention – will beblinded to group allocation. Data collection instru-ments and data collection training manuals are beingdeveloped to support trained assessors record thisinformation.
Outcome evaluation
The outcome evaluation will focus on the effectivenessof interventions. The injury definition used for theintervention specific outcome includes all conditionsthat can be coded by the external cause codes of theICD-10; V01-Y36 (inclusive of all causes and allcategories of intent but excluding adverse medicalevents). The measured outcomes include frequency ofinjury resulting in more than 24 h abstaining fromplay, frequency of medically treated injury, frequencyof hospital admissions for treatment of injury andmortality from injury. Injury will be defined by intent(both intentional and unintentional injury are includedin the study), nature of injury, body part injured,severity of injury (coded using AIS) and by location,activity at time of injury and mechanism of injury(coded using ICECI). Data collection is via medicalrecord review which is to be undertaken by trainedassessors in each participating community. Datacollectors responsible for obtaining injury outcomedata – pre- and post-study intervention – will beblinded to group allocation. Data collection instru-ments and data collection training manuals are beingdeveloped to support trained assessors record thisinformation.
Ethical and cultural issues
Each of the participating countries would seek ethicsapproval from a designated national human researchethics authority. Study participants will be informedabout the risks involved and the voluntary nature oftheir and their children’s participation. All fieldworkersare to have a list of appropriate child care services towhich the child and their caregiver may be referred toand will take the responsibility of arranging referrals andappointments. In cases, where the research indicates thatthe child’s safety and health are compromised in anyway, we will be obligated and ethically bound to reportthis to the necessary authorities such as a social worker.Confidentiality will be maintained unless there is evidentrisk of harm to the child. Assent will be taken from allchildren participating in the study, while their caregiverswill provide written consent. All households except for
International Journal of Injury Control and Safety Promotion 9
Dow
nloa
ded
by [
Bro
ught
to y
ou b
y U
nisa
Lib
rary
], [
Prof
esso
r M
. See
dat]
at 0
2:04
13
Aug
ust 2
012

those belonging to the comparison group for thecombined community, ECD and home visitation inter-ventions will benefit by receiving the health, educationaland safety packages. These households will be invited tojoin an intervention that is supported by the findings ofthe current Ukuphepha implementation.
Conclusion
Despite the self-evident appropriateness of the safecommunity approach and the tremendous support forthe movement, the literature indicates that the evidencebase in support of such programmes is under devel-oped (Spinks et al., 2004, 2009). In this article, we haveshown that formal evaluations using high-qualitystudy designs are achievable within the safe communitycontext and describe an Africa-centred, multi-national,multi-intervention, partially randomised controlledtrail that is currently underway. We have used theprinciples entailed in the concepts of safety, peace andhealth to design and develop an Africa-centred childviolence and injury prevention study with a view toillustrating how such an initiative may advance thetheoretical and scientific basis for the Safe Commu-nities approach.
The authors recognise that as such the study is anambitious yet considered contribution towards sup-porting the development of the Safe Communities’empirical and theoretical base and examining itsrelevance feasibility, sustainability, and appropriate-ness for resourced-challenged situations. Notwith-standing the risks and challenges, the study will yieldmany lessons for data management in large-scaleinternational studies, research partnerships and colla-borations, and implementing ecologically orientedinterventions that locate injuries and violence ascross-disciplinary issues key to the promotion ofchildhood safety, peace and health.
Acknowledgements
The authors would like to thank the members of theUkuphepha child study group for their inputs to thecollective knowledge production process from which thisarticle draws. They would also like to thank Najuwa Arendsefor assisting in the editing of this article.
References
Abrahams, T., & Suffla, S. (2011). Child safety, peace andhealth: A trainer’s manual. Cape Town: Medical Re-search Council-University of South Africa’s Safety andPeace Promotion Research Unit.
Arya, N. (2004). Peace through health I: Development anduse of a working model. Medicine, Conflict and Survival,20, 242–257. doi: 10.1080/1362369042000248893. Re-trieved from www.fes.uwaterloo.ca/. . ./narya/peace/. . ./AryaPeacethroughHealthModelMCS.pdf.
Bulbulia, S., Seedat, M., & Lekoba, R. (2011). Community-based pedestrian safety promotion initiatives: Lessons fromSouth Africa. Unpublished manuscript, Institute forSocial & Health Sciences, University of South Africa,Johannesburg.
Butchart, A., Harvey, A.P., Mian, M., & Furness, T. (2006).Preventing child maltreatment: A guide to taking actionand generating evidence. Geneva: World Health Organi-zation. Retrieved from http://whqlibdoc.who.int/publi-cations/2006/9241594365_eng.pdf).
Christie, D.J., Wagner, R.V., & Winter, D.D. (2001).Introduction to peace psychology. In D.J. Christie,R.V. Wagner, & D.D. Winter (Eds.), Peace, conflict,and violence: Peace psychology for the 21st century (pp. 1–14). Englewood Cliffs, NJ: Prentice-Hall.
Freire, P. (1970). Pedagogy of the oppressed. New York:Herder & Herder.
Galtung, J. (1996). Peace by peaceful means: Peace andconflict, development and civilization. London: Sage.
Holdsworth, L., & Hartman, Y. (2009). Indicators ofcommunity cohesion in an Australian country town.Commonwealth Journal of Local Governance, 2, 76–97.
Jansson, B. (2007). Research on the prevention of fall injuriesmakes prediction for practice difficult. Age and Ageing,35, 351–352.
Jansson, B., Ponce De Leon, A., Ahmed, N., & Jansson, V.(2006). Why does Sweden have the lowest childhoodinjury mortality in the world? The roles of architectureand public pre-school services. Journal of Public HealthPolicy, 27, 146–165.
Jewkes, R., Nduna, M., Levin, J., Jama, N., Dunkle, K.,Puren, A., & Duvvury, N. (2008). Impact of steppingstones on incidence of HIV and HSV-2 and sexualbehaviour in rural South Africa: Cluster randomisedcontrolled trial. British Medical Journal, 337, a506.
Klaasen, T.P., Morag MacKay, J., Moher, D., Walker, A., &Jones, A.L. (2000). Community-based injury preventioninterventions; the future of children. UnintentionalInjuries in Childhood, 10(1), 83–110.
McClure, R.J. (2010). Injury risk and prevention in context.Injury Prevention, 16, 361–362.
Nastasi, B.K., & Hitchcock, J. (2009). Challenges ofevaluating multi-level interventions. American Journalof Community Psychology, 43, 360–376.
Odendaal, W., Van Niekerk, A., Jordaan, E., & Seedat, M.(2009). The impact of a home visitation programme onhousehold hazards associated with unintentional child-hood injuries: a randomised controlled trial. AccidentAnalysis and Prevention, 41(1), 183–190.
Promethea Corporation. (2009). Parasafe stoves: Uniquesafety features. Retrieved from http://www.promothea.-biz/parasafe_safety.html.
Pronyk, P.M., Kim, J.C., Hargreaves, J.R., Makhubele,M.B., Morison, L., Watts, C., & Porter, J.D.H. (2005).Integrating microfinance and HIV prevention – Perspec-tives and emerging lessons from rural South Africa.Small Enterprise Development, 16, 26–38.
Rosen, M., & Jansson, B. (2000). How to act - implementinghealth and safety promotion in organizations. HealthPolicy and Planning, 15(3), 247–254.
Seedat, M., & Lazarus, S. (2011). Community psychology inSouth Africa: Origins, developments, and manifestations.Journal of Community Psychology, 39, 241–257.
Spinks, A., Turner, C., McClure, R., & Nixon, J. (2004).Community based prevention programs targeting allinjuries for children. Injury Prevention, 10, 180–185.
10 M. Seedat et al.
Dow
nloa
ded
by [
Bro
ught
to y
ou b
y U
nisa
Lib
rary
], [
Prof
esso
r M
. See
dat]
at 0
2:04
13
Aug
ust 2
012

Spinks, A., Turner, C., Nixon, J., & McClure, R.J. (2009).The ‘WHO Safe Communities’ model for the preventionof injury in whole populations. Cochrane Database ofSystematic Reviews, 3, Article No.: CD004445. doi:10.1002/14651858.CD004445.pub3.
Stachtchenko, S., & Jenicek, M. (1990). Conceptual differ-ences between prevention and health promotion: Re-search implications for community health programs.Canadian Journal of Public Health, 8, 53–59.
Susser, M., & Susser, E. (1996). Choosing a future forepidemiology: II. From black box to Chinese boxes andeco-epidemiology. American Journal of Epidemiology, 86,674–677.
Swart, L., Van Niekerk, A., Seedat, M., & Jordaan, E.(2008). Paraprofessional home visitation programme toprevent childhood injuries in low-income communities: Acluster randomised controlled trial. Injury Prevention, 14,194–169.
World Health Organization. (1998). WHO CollaboratingCentres on Safety Promotion and Injury Prevention,Quebec, and Community Safety Promotion. Safetyand safety promotion: Conceptual and operationalaspects. Stockholm: Karolinska Institute. Retrievedfrom http://www.phs.ki.se/csp/pdf/Publications/safety_promotion1998%20.pdf.
International Journal of Injury Control and Safety Promotion 11
Dow
nloa
ded
by [
Bro
ught
to y
ou b
y U
nisa
Lib
rary
], [
Prof
esso
r M
. See
dat]
at 0
2:04
13
Aug
ust 2
012