Determination of guidance levels of dose for diagnostic radiography in Taiwan
8
Determination of guidance levels of dose for diagnostic radiography in Taiwan C. J. Tung, H. Y. Tsai, and S. H. Lo Department of Nuclear Science, National Tsing Hua University, Hsinchu, Taiwan C. N. Guan and Y. B. Chen Department of Radiation Protection, Atomic Energy Council, Taipei, Taiwan ~Received 14 April 2000; accepted for publication 5 March 2001! The International Atomic Energy Agency has recommended guidance levels of dose for diagnostic radiography for a typical adult patient. These levels were intended to act as thresholds to trigger investigations or corrective actions in ensuring optimized protection of patients and maintaining appropriate levels of good practice. Since guidance levels should be derived from wide scale surveys of exposure factors performed in individual hospitals, a national survey was conducted recently in Taiwan to collect these factors for the most frequent radiographic procedures. A total of 276 completed questionnaires were received and analyzed. In the questionnaire, respondents were asked to check those projections that were routinely performed in their department and to report machine data, patient data, output measurements, and technical factors including kVp, mAs, focus- to-film distance, table-to-film distance, aluminum filtration, and focal spot size. Based on the survey data, entrance skin exposures in air, i.e., free air exposures at the point of intersection of the x-ray central beam with the entrance surface of the patient, were estimated using the RADCOMP program. Entrance surface doses to air and tissue with backscatter were then evaluated by the application of the exposure-dose conversion factor and the backscatter factor obtained from TLD measurements and Monte Carlo simulations. Guidance levels were determined from survey results on the entrance surface dose based on optimization considerations involving the cost-effectiveness analysis. Except for chest PA and LAT and skull LAT procedures, all guidance levels derived in this work are less than those recommended by the International Atomic Energy Agency. Survey data and guidance levels were provided to the national authorities to help them develop quality control and radiation protection programs for medical exposures. © 2001 American Association of Physicists in Medi- cine. @DOI: 10.1118/1.1368126# Key words: guidance level, reference level, investigation level, reference value, dose constraint I. INTRODUCTION Diagnostic imaging is the largest manmade source of radia- tion to the general public. It was estimated that diagnostic radiology and nuclear medicine contributed 88% to the col- lective effective dose from manmade sources in the US. 1 Similar estimates showed that this contribution was 96% in the U.K. 2 A national survey of patient doses in the U.K. demonstrated that there existed wide variations in the radia- tion dose received by patients for similar x-ray examinations. 3 The entrance surface dose ~ESD! per film for nominally the same type of radiograph typically ranged over factors of between 20 and 100 for individual patients. 4 A similar nationwide survey by the Food and Drug Adminis- tration of the US 5 revealed that the ratio of the maximum to minimum exposures ranged from 8.8 to 126.7. Clearly, these indicated that a good imaging technique was necessary to reduce patient doses to the lowest practicable levels consis- tent with the clinical purpose of the medical examination. The International Atomic Energy Agency ~IAEA! has rec- ommended guidance levels for the radiation dose to a typical adult patient. 6 These levels were intended to act as thresholds to trigger investigations or corrective actions in ensuring op- timized protection of patients and maintaining appropriate levels of good practices. Further guidance on what action to take was given by the Institute of Physics and Engineering in Medicine 7 ~IPEM! through the introduction of a remedial level and a suspension level at which remedial action was necessary and equipment should be removed from clinical use. Specific values of the ESD on the remedial level and the suspension level were suggested by the IPEM. The European experience with guidance levels has been encouraging. A follow-up study in the U.K. showed a 30% decrease in pa- tient doses for the common diagnostic x-ray procedures. 8 The draft of the ‘‘Ionizing Radiation Protection Act of the Republic of China’’ has adopted a mandatory quality control program for medical exposures. This draft is under review and expected to become law in 2001. To help the regulatory and health authorities to develop quality control standards and protocols, we recently conducted a national survey in Taiwan to collect exposure factors for all common radio- graphic procedures. A questionnaire survey form was sent to 665 hospitals; 276 of them completed and returned the form. Respondents were asked to provide exposure factors of stan- dard procedures on routine x-ray projections for all parts of the body. Free air exposure ~FAE! at the point of intersection of the x-ray central beam with the entrance surface of the 850 850 Med. Phys. 28 „5…, May 2001 0094-2405Õ2001Õ28„5…Õ850Õ8Õ$18.00 © 2001 Am. Assoc. Phys. Med.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Determination of guidance levels of dose for diagnostic radiography in Taiwan

Determination of guidance levels of dose for diagnostic radiographyin Taiwan
C. J. Tung, H. Y. Tsai, and S. H. LoDepartment of Nuclear Science, National Tsing Hua University, Hsinchu, Taiwan
C. N. Guan and Y. B. ChenDepartment of Radiation Protection, Atomic Energy Council, Taipei, Taiwan
~Received 14 April 2000; accepted for publication 5 March 2001!
The International Atomic Energy Agency has recommended guidance levels of dose for diagnosticradiography for a typical adult patient. These levels were intended to act as thresholds to triggerinvestigations or corrective actions in ensuring optimized protection of patients and maintainingappropriate levels of good practice. Since guidance levels should be derived from wide scalesurveys of exposure factors performed in individual hospitals, a national survey was conductedrecently in Taiwan to collect these factors for the most frequent radiographic procedures. A total of276 completed questionnaires were received and analyzed. In the questionnaire, respondents wereasked to check those projections that were routinely performed in their department and to reportmachine data, patient data, output measurements, and technical factors including kVp, mAs, focus-to-film distance, table-to-film distance, aluminum filtration, and focal spot size. Based on the surveydata, entrance skin exposures in air, i.e., free air exposures at the point of intersection of the x-raycentral beam with the entrance surface of the patient, were estimated using theRADCOMP program.Entrance surface doses to air and tissue with backscatter were then evaluated by the application ofthe exposure-dose conversion factor and the backscatter factor obtained from TLD measurementsand Monte Carlo simulations. Guidance levels were determined from survey results on the entrancesurface dose based on optimization considerations involving the cost-effectiveness analysis. Exceptfor chest PA and LAT and skull LAT procedures, all guidance levels derived in this work are lessthan those recommended by the International Atomic Energy Agency. Survey data and guidancelevels were provided to the national authorities to help them develop quality control and radiationprotection programs for medical exposures. ©2001 American Association of Physicists in Medi-cine. @DOI: 10.1118/1.1368126#
Key words: guidance level, reference level, investigation level, reference value, dose constraint
distoSi.
diy
ve
is-toesys
.
icld
opat
toin
las
icaltheean. Aa-
erolewtoryrds
inio-t torm.tan-of
the
I. INTRODUCTION
Diagnostic imaging is the largest manmade source of ration to the general public. It was estimated that diagnoradiology and nuclear medicine contributed 88% to the clective effective dose from manmade sources in the U1
Similar estimates showed that this contribution was 96%the U.K.2 A national survey of patient doses in the U.Kdemonstrated that there existed wide variations in the ration dose received by patients for similar x-raexaminations.3 The entrance surface dose~ESD! per film fornominally the same type of radiograph typically ranged ofactors of between 20 and 100 for individual patients.4 Asimilar nationwide survey by the Food and Drug Admintration of the US5 revealed that the ratio of the maximumminimum exposures ranged from 8.8 to 126.7. Clearly, thindicated that a good imaging technique was necessarreduce patient doses to the lowest practicable levels content with the clinical purpose of the medical examination
The International Atomic Energy Agency~IAEA ! has rec-ommended guidance levels for the radiation dose to a typadult patient.6 These levels were intended to act as threshoto trigger investigations or corrective actions in ensuringtimized protection of patients and maintaining appropri
850 Med. Phys. 28 „5…, May 2001 0094-2405Õ2001Õ28„5
a-icl-.n
a-
r
etois-
als-e
levels of good practices. Further guidance on what actiontake was given by the Institute of Physics and EngineeringMedicine7 ~IPEM! through the introduction of a remedialevel and a suspension level at which remedial action wnecessary and equipment should be removed from clinuse. Specific values of the ESD on the remedial level andsuspension level were suggested by the IPEM. The Europexperience with guidance levels has been encouragingfollow-up study in the U.K. showed a 30% decrease in ptient doses for the common diagnostic x-ray procedures.8
The draft of the ‘‘Ionizing Radiation Protection Act of thRepublic of China’’ has adopted a mandatory quality contprogram for medical exposures. This draft is under reviand expected to become law in 2001. To help the regulaand health authorities to develop quality control standaand protocols, we recently conducted a national surveyTaiwan to collect exposure factors for all common radgraphic procedures. A questionnaire survey form was sen665 hospitals; 276 of them completed and returned the foRespondents were asked to provide exposure factors of sdard procedures on routine x-ray projections for all partsthe body. Free air exposure~FAE! at the point of intersectionof the x-ray central beam with the entrance surface of
850…Õ850Õ8Õ$18.00 © 2001 Am. Assoc. Phys. Med.

thckrseont
een
thedroe
fo
dordin
ay-mp,nae-tein
aia
aoruca
foth
toath
eri
-ti
et
ba
RPs,er-
cesorted
data-
s,ch
utair
thectoria-ize,sly
ayth
s ofall
see-
ins.ngits
orpa-
theal-
nd
aireleereerel-
851 Tung et al. : Determination of guidance levels 851
patient was determined using exposure factors andRADCOMP computer code. ESDs to air and tissue with bascatter were evaluated using the exposure-dose convefactor, the backscatter factor, and the ratio of the massergy absorption coefficients of tissue and air. Resultsevaluations were verified with experimental measuremefor a representative sample of x-ray machines to ensureaccuracy of these results. Analyses of ESDs were madderive the guidance levels of dose for the most frequentaminations in diagnostic radiography. These derivatiowere based on optimization considerations involvingcost-effectiveness analysis. Comparisons were made betwguidance levels of the present work and those recommenby the IAEA. Survey results and guidance levels were pvided to the national authorities in Taiwan to help them dvelop quality control and radiation protection programsmedical exposures.
II. MATERIALS AND METHODS
The determination of guidance levels should be mafrom wide scale surveys on ESD to an average patientreference phantom for the most frequent examinations inagnostic radiology.6 Such surveys have been conductedseveral countries. In the Nationwide Evaluation of X-rTrends~NEXT! survey program9,10 in the US, phantoms representing the standard patient were used for the measureof ESD. Data collected in the NEXT survey included kVHVL, type of film and screen, processing speed, etc. Ational protocol11 was developed in the U.K. for the measurment of patient dose using thermoluminescent dosime~TLDs!. Recording data recommended in the protocolcluded the focus-to-film distance~FFD!, kVp, mAs, filmsize, focal spot size, etc. A few other countries12 have alsoemployed TLDs for the measurement of ESD from their ntional surveys. Alternatively, the National Council on Radtion Protection and Measurements13 ~NCRP! has recom-mended the calculation of ESD based on the standexposure data and modified by the actual technical factComputing software was developed for such calculationsing either the NCRP standard exposure data or the userbrated output data. For instance, theRADCOMP X-ray En-trance Skin Exposure Software14 was applied to thedetermination of ESD and the genetically significant dosediagnostic radiology from a national survey in SouAfrica.15
For the dosimetry in x-ray radiography, it is convenientmeasure the FAE at the point where the x-ray central befirst strikes the body. Standard methods for measuringFAE for manual and automatic exposure control units wrecommended by the American Association of PhysicistsMedicine ~AAPM!.16 In the AAPM protocol, the ion chamber is placed approximately 23 cm above the table topminimize the backscattered radiation. Also, the x-ray fieldreduced so that it is slightly larger than the ion chambMeasured free-in-air exposure is then used to calculateFAE using the inverse square correction for the ion chamto the entrance surface position. Alternatively, the FAE c
Medical Physics, Vol. 28, No. 5, May 2001
e-ionn-ftshetox-seened--r
eai-
ent
-
rs-
--
rds.s-li-
r
meen
osr.heern
be estimated using exposure data from Table B 3 of NCReport No. 10213 and technical factors such as kVp, mAaluminum filtration, FFD, etc. In this work, we used thRADCOMP X-ray Entrance Skin Exposure Software to detemine the FAE from survey results. This software reproduthe NCRP-102 standard FAE using a scale factor of 1calculates the machine-specific FAE using user calibraoutput data. The principles ofRADCOMP involve some datastretching process that applies to the reference exposure~NCRP data or user data! by a statistical technique. Information required by theRADCOMP includes the phase~single orthree phase!, total filtration ~total equivalent aluminum orHVL !, scale factor or calibrated output data, kVp, mAFFD, table-to-film distance, and patient thickness. All suinformation was collected in the questionnaire survey.
The FAE determined above is defined free in air withoany backscatter. To obtain the entrance surface dose towith backscatter (ESDair), the following formula may beused. It is given by
ESDair~mGy!5FAE~mR!30.008 773BSF, ~1!
where 0.008 77 converts the exposure, in units mR, intoabsorbed dose to air, in units mGy, and the backscatter fa~BSF! accounts for the contribution from backscatter radtion. The BSF depends on factors such as kVp, field sFFD, body tissue, etc. This quantity was studied previouby TLD measurements17 and Monte Carlo simulations18 fordifferent x-ray radiographic procedures. Further, one mconvert the ESDair into the entrance skin dose to tissue wibackscatter (ESDtissue) by the relation
ESDtissue~mGy!5ESDair~mGy!3~men /r! tissue
~men /r!air, ~2!
where the ratio of the mass energy absorption coefficienttissue and air depends on the x-ray energy. For practicallydiagnostic x-ray spectra, this ratio is 1.0661%.18
The ESDair was recommended by the IAEA as the dodescriptor for guidance levels in diagnostic radiography. Bcause of its simplicity and indication of the maximum skdose, it was used for the periodic checking of patient dose19
However, the ESD has little biological significance regardithe health risks.20 As the x-ray passes through the body,flux drops significantly. The absorbed doses to tissuesorgans should be used for estimating the likelihood oftients to develop stochastic effects.21 In addition, the effec-tive dose should be used to estimate the total detriment ofwhole body.22 These radiation protection doses may be cculated from ESDair or ESDtissue by the application of con-version factors obtained using Monte Carlo simulations amathematical phantoms.23–25
III. RESULTS
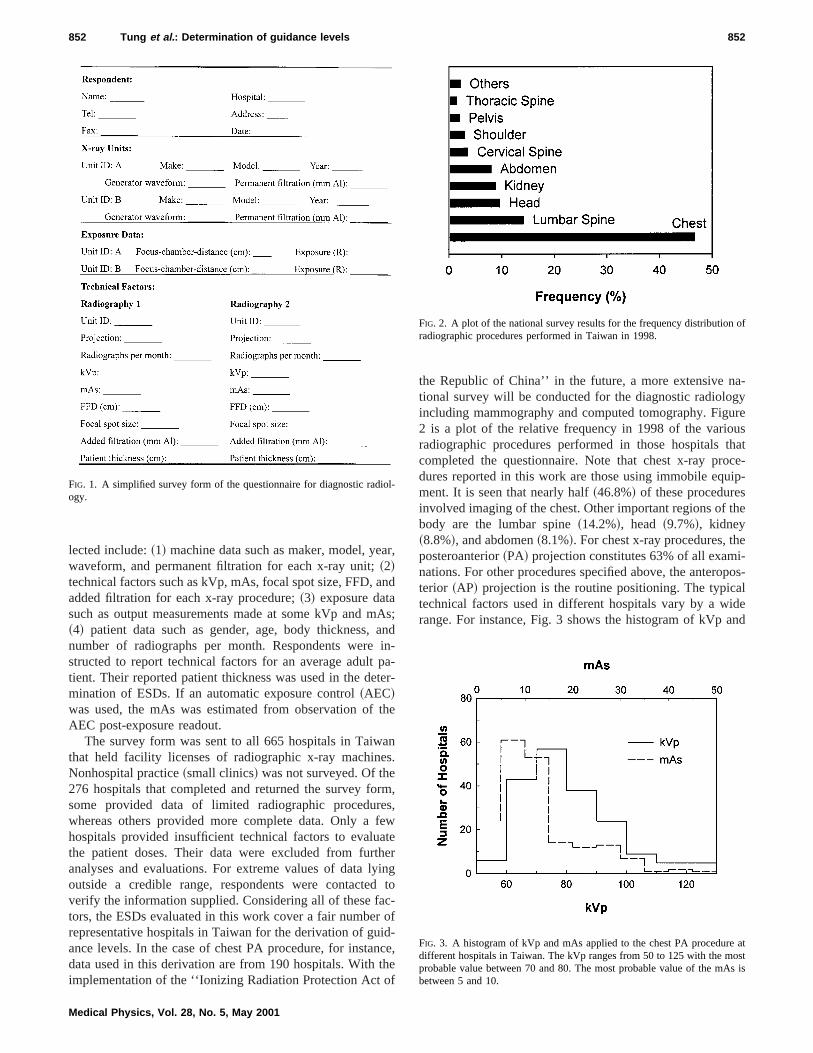
Figure 1 shows some essential part of the questionnform. The original survey form contains a listing of possibprojections for each part of the body. Respondents wasked to provide information on those projections that wroutinely performed in their department. Information co
a
an
Aai
pte
th
ans
rmesfeatheyidc
r oidncthf
a-gyureusthatce-ip-
he
ei-pos-l
idend
ol-
of
atosts is
852 Tung et al. : Determination of guidance levels 852
lected include:~1! machine data such as maker, model, yewaveform, and permanent filtration for each x-ray unit;~2!technical factors such as kVp, mAs, focal spot size, FFD,added filtration for each x-ray procedure;~3! exposure datasuch as output measurements made at some kVp and m~4! patient data such as gender, age, body thickness,number of radiographs per month. Respondents werestructed to report technical factors for an average adulttient. Their reported patient thickness was used in the demination of ESDs. If an automatic exposure control~AEC!was used, the mAs was estimated from observation ofAEC post-exposure readout.
The survey form was sent to all 665 hospitals in Taiwthat held facility licenses of radiographic x-ray machineNonhospital practice~small clinics! was not surveyed. Of the276 hospitals that completed and returned the survey fosome provided data of limited radiographic procedurwhereas others provided more complete data. Only ahospitals provided insufficient technical factors to evaluthe patient doses. Their data were excluded from furtanalyses and evaluations. For extreme values of data loutside a credible range, respondents were contacteverify the information supplied. Considering all of these fators, the ESDs evaluated in this work cover a fair numberepresentative hospitals in Taiwan for the derivation of guance levels. In the case of chest PA procedure, for instadata used in this derivation are from 190 hospitals. Withimplementation of the ‘‘Ionizing Radiation Protection Act o
FIG. 1. A simplified survey form of the questionnaire for diagnostic radiogy.
Medical Physics, Vol. 28, No. 5, May 2001
r,
d
s;ndn-a-r-
e
.
,,wer
ngto
-f-e,e
the Republic of China’’ in the future, a more extensive ntional survey will be conducted for the diagnostic radioloincluding mammography and computed tomography. Fig2 is a plot of the relative frequency in 1998 of the varioradiographic procedures performed in those hospitalscompleted the questionnaire. Note that chest x-ray produres reported in this work are those using immobile equment. It is seen that nearly half~46.8%! of these proceduresinvolved imaging of the chest. Other important regions of tbody are the lumbar spine~14.2%!, head ~9.7%!, kidney~8.8%!, and abdomen~8.1%!. For chest x-ray procedures, thposteroanterior~PA! projection constitutes 63% of all examnations. For other procedures specified above, the anteroterior ~AP! projection is the routine positioning. The typicatechnical factors used in different hospitals vary by a wrange. For instance, Fig. 3 shows the histogram of kVp a
FIG. 2. A plot of the national survey results for the frequency distributionradiographic procedures performed in Taiwan in 1998.
FIG. 3. A histogram of kVp and mAs applied to the chest PA proceduredifferent hospitals in Taiwan. The kVp ranges from 50 to 125 with the mprobable value between 70 and 80. The most probable value of the mAbetween 5 and 10.
al12p
fortiopn
mhe
io-eenl
thein
ch-uip-nol-nt.ich
therned
A
ntht a
asla-
re 5
air
Dout
ical
air
a-
in
do
ren
853 Tung et al. : Determination of guidance levels 853
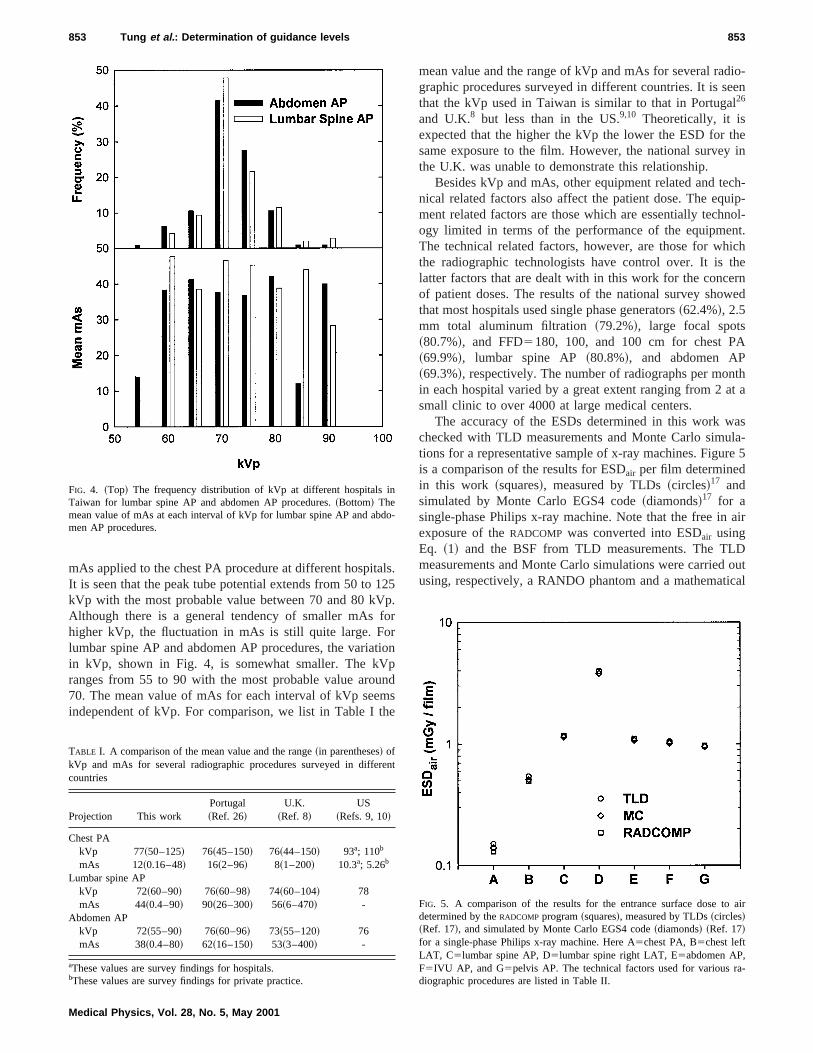
mAs applied to the chest PA procedure at different hospitIt is seen that the peak tube potential extends from 50 tokVp with the most probable value between 70 and 80 kVAlthough there is a general tendency of smaller mAshigher kVp, the fluctuation in mAs is still quite large. Folumbar spine AP and abdomen AP procedures, the variain kVp, shown in Fig. 4, is somewhat smaller. The kVranges from 55 to 90 with the most probable value arou70. The mean value of mAs for each interval of kVp seeindependent of kVp. For comparison, we list in Table I t
FIG. 4. ~Top! The frequency distribution of kVp at different hospitalsTaiwan for lumbar spine AP and abdomen AP procedures.~Bottom! Themean value of mAs at each interval of kVp for lumbar spine AP and abmen AP procedures.
TABLE I. A comparison of the mean value and the range~in parentheses! ofkVp and mAs for several radiographic procedures surveyed in diffecountries
Projection This workPortugal~Ref. 26!
U.K.~Ref. 8!
US~Refs. 9, 10!
Chest PAkVp 77~50–125! 76~45–150! 76~44–150! 93a; 110b
mAs 12~0.16–48! 16~2–96! 8~1–200! 10.3a; 5.26b
Lumbar spine APkVp 72~60–90! 76~60–98! 74~60–104! 78mAs 44~0.4–90! 90~26–300! 56~6–470! -
Abdomen APkVp 72~55–90! 76~60–96! 73~55–120! 76mAs 38~0.4–80! 62~16–150! 53~3–400! -
aThese values are survey findings for hospitals.bThese values are survey findings for private practice.
Medical Physics, Vol. 28, No. 5, May 2001
s.5.r
n
ds
mean value and the range of kVp and mAs for several radgraphic procedures surveyed in different countries. It is sthat the kVp used in Taiwan is similar to that in Portuga26
and U.K.8 but less than in the US.9,10 Theoretically, it isexpected that the higher the kVp the lower the ESD forsame exposure to the film. However, the national surveythe U.K. was unable to demonstrate this relationship.
Besides kVp and mAs, other equipment related and tenical related factors also affect the patient dose. The eqment related factors are those which are essentially techogy limited in terms of the performance of the equipmeThe technical related factors, however, are those for whthe radiographic technologists have control over. It islatter factors that are dealt with in this work for the conceof patient doses. The results of the national survey showthat most hospitals used single phase generators~62.4%!, 2.5mm total aluminum filtration~79.2%!, large focal spots~80.7%!, and FFD5180, 100, and 100 cm for chest P~69.9%!, lumbar spine AP ~80.8%!, and abdomen AP~69.3%!, respectively. The number of radiographs per moin each hospital varied by a great extent ranging from 2 asmall clinic to over 4000 at large medical centers.
The accuracy of the ESDs determined in this work wchecked with TLD measurements and Monte Carlo simutions for a representative sample of x-ray machines. Figuis a comparison of the results for ESDair per film determinedin this work ~squares!, measured by TLDs~circles!17 andsimulated by Monte Carlo EGS4 code~diamonds!17 for asingle-phase Philips x-ray machine. Note that the free inexposure of theRADCOMP was converted into ESDair usingEq. ~1! and the BSF from TLD measurements. The TLmeasurements and Monte Carlo simulations were carriedusing, respectively, a RANDO phantom and a mathemat
FIG. 5. A comparison of the results for the entrance surface dose todetermined by theRADCOMP program~squares!, measured by TLDs~circles!~Ref. 17!, and simulated by Monte Carlo EGS4 code~diamonds! ~Ref. 17!for a single-phase Philips x-ray machine. Here A5chest PA, B5chest leftLAT, C5lumbar spine AP, D5lumbar spine right LAT, E5abdomen AP,F5IVU AP, and G5pelvis AP. The technical factors used for various rdiographic procedures are listed in Table II.
-
t
tou
tht
ire.4eshaeliza
thant
-
vel.ncefis
e-
tiveforc-to
levelined
r-
e
nce
arl
foth
854 Tung et al. : Determination of guidance levels 854
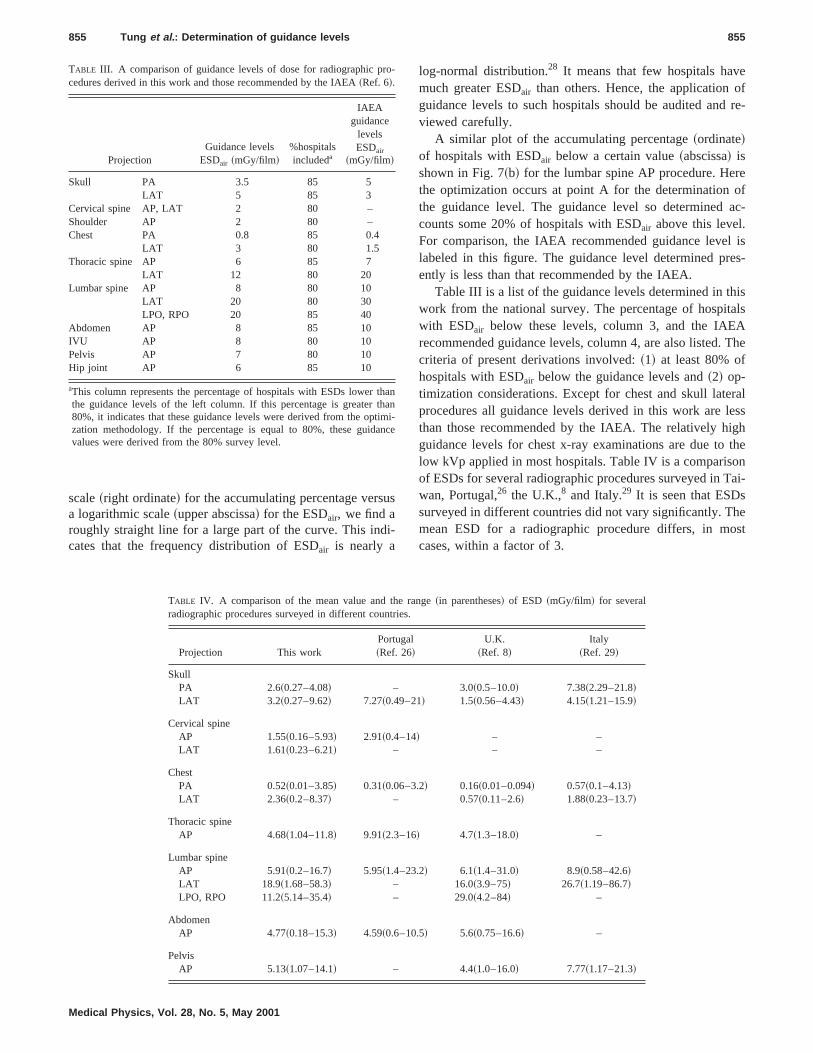
phantom. The radiographic procedures and technical facused are listed in Table II. The agreement among all resis quite good. The percent differences between data ofRAD-
COMP calculations and TLD measurements are213%,29.3%, 1.7%,20.76%, 0.91%,21.9%, and 2.1% for chesPA, chest left LAT, lumbar spine AP, lumbar spine rigLAT, abdomen AP, IVU AP, and pelvis AP, respectively.
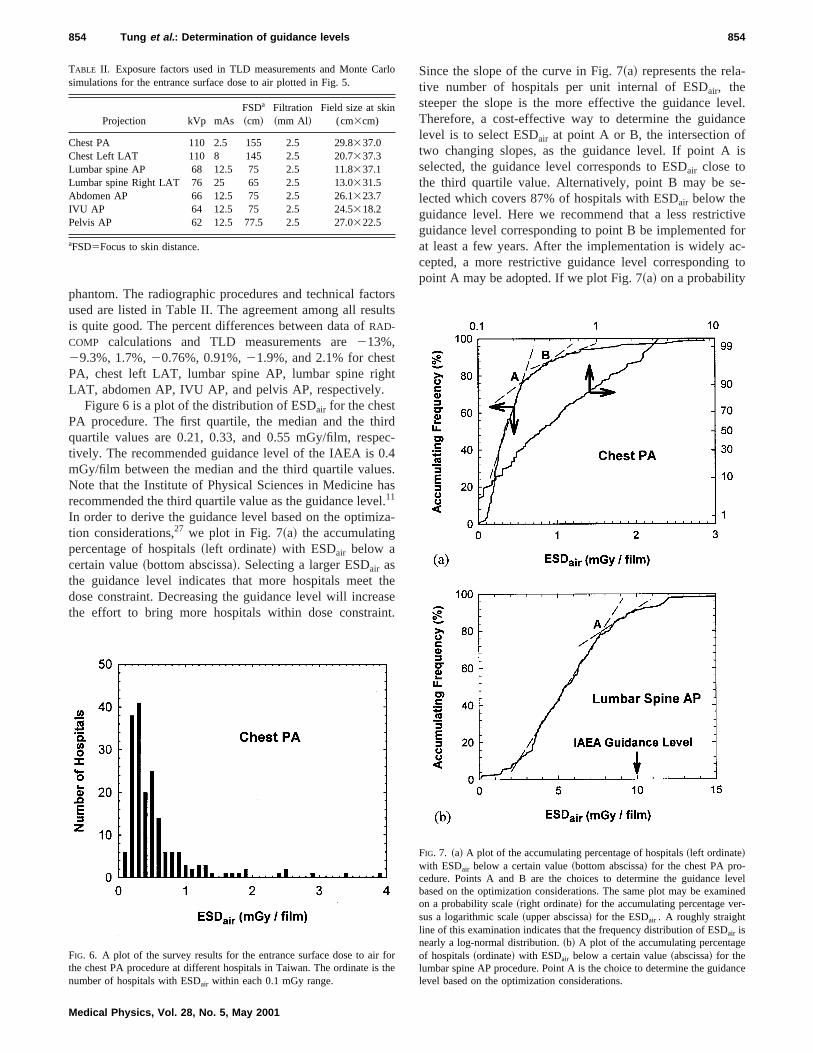
Figure 6 is a plot of the distribution of ESDair for the chestPA procedure. The first quartile, the median and the thquartile values are 0.21, 0.33, and 0.55 mGy/film, resptively. The recommended guidance level of the IAEA is 0mGy/film between the median and the third quartile valuNote that the Institute of Physical Sciences in Medicinerecommended the third quartile value as the guidance lev11
In order to derive the guidance level based on the optimtion considerations,27 we plot in Fig. 7~a! the accumulatingpercentage of hospitals~left ordinate! with ESDair below acertain value~bottom abscissa!. Selecting a larger ESDair asthe guidance level indicates that more hospitals meetdose constraint. Decreasing the guidance level will increthe effort to bring more hospitals within dose constrai
TABLE II. Exposure factors used in TLD measurements and Monte Csimulations for the entrance surface dose to air plotted in Fig. 5.
Projection kVp mAsFSDa
~cm!Filtration~mm Al!
Field size at skin(cm3cm)
Chest PA 110 2.5 155 2.5 29.8337.0Chest Left LAT 110 8 145 2.5 20.7337.3Lumbar spine AP 68 12.5 75 2.5 11.8337.1Lumbar spine Right LAT 76 25 65 2.5 13.0331.5Abdomen AP 66 12.5 75 2.5 26.1323.7IVU AP 64 12.5 75 2.5 24.5318.2Pelvis AP 62 12.5 77.5 2.5 27.0322.5
aFSD5Focus to skin distance.
FIG. 6. A plot of the survey results for the entrance surface dose to airthe chest PA procedure at different hospitals in Taiwan. The ordinate isnumber of hospitals with ESDair within each 0.1 mGy range.
Medical Physics, Vol. 28, No. 5, May 2001
rslts
dc-
.s.-
ese.
Since the slope of the curve in Fig. 7~a! represents the relative number of hospitals per unit internal of ESDair, thesteeper the slope is the more effective the guidance leTherefore, a cost-effective way to determine the guidalevel is to select ESDair at point A or B, the intersection otwo changing slopes, as the guidance level. If point Aselected, the guidance level corresponds to ESDair close tothe third quartile value. Alternatively, point B may be slected which covers 87% of hospitals with ESDair below theguidance level. Here we recommend that a less restricguidance level corresponding to point B be implementedat least a few years. After the implementation is widely acepted, a more restrictive guidance level correspondingpoint A may be adopted. If we plot Fig. 7~a! on a probability
FIG. 7. ~a! A plot of the accumulating percentage of hospitals~left ordinate!with ESDair below a certain value~bottom abscissa! for the chest PA pro-cedure. Points A and B are the choices to determine the guidancebased on the optimization considerations. The same plot may be examon a probability scale~right ordinate! for the accumulating percentage vesus a logarithmic scale~upper abscissa! for the ESDair . A roughly straightline of this examination indicates that the frequency distribution of ESDair isnearly a log-normal distribution.~b! A plot of the accumulating percentagof hospitals~ordinate! with ESDair below a certain value~abscissa! for thelumbar spine AP procedure. Point A is the choice to determine the guidalevel based on the optimization considerations.
o
re
us
i-
eof
re-
reofac-
l ises-
isalsAThe
ralessghthe
onai-
heost
ro-
ththatiman
855 Tung et al. : Determination of guidance levels 855
scale~right ordinate! for the accumulating percentage versa logarithmic scale~upper abscissa! for the ESDair, we find aroughly straight line for a large part of the curve. This indcates that the frequency distribution of ESDair is nearly a
TABLE III. A comparison of guidance levels of dose for radiographic pcedures derived in this work and those recommended by the IAEA~Ref. 6!.
ProjectionGuidance levels
ESDair ~mGy/film!%hospitalsincludeda
IAEAguidance
levelsESDair
~mGy/film!
Skull PA 3.5 85 5LAT 5 85 3
Cervical spine AP, LAT 2 80 –Shoulder AP 2 80 –Chest PA 0.8 85 0.4
LAT 3 80 1.5Thoracic spine AP 6 85 7
LAT 12 80 20Lumbar spine AP 8 80 10
LAT 20 80 30LPO, RPO 20 85 40
Abdomen AP 8 85 10IVU AP 8 80 10Pelvis AP 7 80 10Hip joint AP 6 85 10
aThis column represents the percentage of hospitals with ESDs lowerthe guidance levels of the left column. If this percentage is greater80%, it indicates that these guidance levels were derived from the opzation methodology. If the percentage is equal to 80%, these guidvalues were derived from the 80% survey level.
Medical Physics, Vol. 28, No. 5, May 2001
log-normal distribution.28 It means that few hospitals havmuch greater ESDair than others. Hence, the applicationguidance levels to such hospitals should be audited andviewed carefully.
A similar plot of the accumulating percentage~ordinate!of hospitals with ESDair below a certain value~abscissa! isshown in Fig. 7~b! for the lumbar spine AP procedure. Hethe optimization occurs at point A for the determinationthe guidance level. The guidance level so determinedcounts some 20% of hospitals with ESDair above this level.For comparison, the IAEA recommended guidance levelabeled in this figure. The guidance level determined prently is less than that recommended by the IAEA.
Table III is a list of the guidance levels determined in thwork from the national survey. The percentage of hospitwith ESDair below these levels, column 3, and the IAErecommended guidance levels, column 4, are also listed.criteria of present derivations involved:~1! at least 80% ofhospitals with ESDair below the guidance levels and~2! op-timization considerations. Except for chest and skull lateprocedures all guidance levels derived in this work are lthan those recommended by the IAEA. The relatively higuidance levels for chest x-ray examinations are due tolow kVp applied in most hospitals. Table IV is a comparisof ESDs for several radiographic procedures surveyed in Twan, Portugal,26 the U.K.,8 and Italy.29 It is seen that ESDssurveyed in different countries did not vary significantly. Tmean ESD for a radiographic procedure differs, in mcases, within a factor of 3.
anni-ce
TABLE IV. A comparison of the mean value and the range~in parentheses! of ESD ~mGy/film! for severalradiographic procedures surveyed in different countries.
Projection This workPortugal~Ref. 26!
U.K.~Ref. 8!
Italy~Ref. 29!
SkullPA 2.6~0.27–4.08! – 3.0~0.5–10.0! 7.38~2.29–21.8!LAT 3.2~0.27–9.62! 7.27~0.49–21! 1.5~0.56–4.43! 4.15~1.21–15.9!
Cervical spineAP 1.55~0.16–5.93! 2.91~0.4–14! – –LAT 1.61~0.23–6.21! – – –
ChestPA 0.52~0.01–3.85! 0.31~0.06–3.2! 0.16~0.01–0.094! 0.57~0.1–4.13!LAT 2.36~0.2–8.37! – 0.57~0.11–2.6! 1.88~0.23–13.7!
Thoracic spineAP 4.68~1.04–11.8! 9.91~2.3–16! 4.7~1.3–18.0! –
Lumbar spineAP 5.91~0.2–16.7! 5.95~1.4–23.2! 6.1~1.4–31.0! 8.9~0.58–42.6!LAT 18.9~1.68–58.3! – 16.0~3.9–75! 26.7~1.19–86.7!LPO, RPO 11.2~5.14–35.4! – 29.0~4.2–84! –
AbdomenAP 4.77~0.18–15.3! 4.59~0.6–10.5! 5.6~0.75–16.6! –
PelvisAP 5.13~1.07–14.1! – 4.4~1.0–16.0! 7.77~1.17–21.3!

atl ozehoenVo
thcla
ves
ncdxlsin
t is.rore-aie
eftffoannchlithll
gyo.th3
Rhe
ion
a-tin
. 1
n-dia-
77,iag-
to’’
of
of’’
nt
K., andon
Re-ion
’’
hef-
1,s’’
ofns,’’
anrlo
di-f
iondio-
ree’’
a-ce
venal
onof
ose
ion’’
856 Tung et al. : Determination of guidance levels 856
IV. DISCUSSION
A national survey was conducted recently to investigpatient doses for diagnostic radiographs in Taiwan. A tota276 completed questionnaires were received and analyIn the questionnaire, respondents were asked to check tprojections that were routinely performed in their departmand to report exposures and technical factors including kmAs, FFD, aluminum filtration, focal spot size, etc. Basedsurvey data, FAEs were estimated using theRADCOMP pro-gram. ESDs were evaluated by the application ofexposure-dose conversion factor and the backscatter faobtained from TLD measurements and Monte Carlo simutions. Guidance levels of dose were derived using surresults on ESDair based on the optimization considerationExcept for chest and skull lateral procedures all guidalevels derived in this work are less than those recommenby the IAEA. The large guidance levels for chest x-ray eaminations are due to the low kVp applied in most hospitaLow tube potentials are also found from national surveysfor instance, Portugal and U.K. despite suggestions thacreasing the applied voltage should reduce patient dose30
Guidance levels of dose for diagnostic radiography pvide the benchmark for the comparison of x-ray exposufrom different facilities. It is important to implement guidance levels for the reduction of patient doses and the mtenance of good image quality. Diagnostic guidance levshould not be regarded as state-of-the art data, as theyappropriated only in state-of-the practice. Guidance levchange over time due to changes in technology. The drathe ‘‘Ionizing Radiation Protection Act of the Republic oChina’’ has adopted a mandatory quality control programmedical exposures. This program requires that registrand licensees of radiographic facilities to report the entrasurface dose for a typical adult patient for each radiograpprocedure. To help the national authorities to develop quacontrol standards and protocols, we provided them withsurvey results on ESDair and guidance levels of dose for acommon radiographic procedures.
ACKNOWLEDGMENTS
This work was supported in part by the Atomic EnerCouncil of the Republic of China under Contract N892001DRP014 and by the National Science Council ofRepublic of China under Contract No. 87-2312-B-007-00NU.
1National Council on Radiation Protection and Measurements, NCRPport No. 93, ‘‘Ionizing Radiation Exposure of the Population of tUnited States’’~NCRP, Bethesda, Maryland, 1987!.
2National Radiological Protection Board, NRPB Report R263, ‘‘RadiatExposure of the U.K. Population—1993 Review’’~NRPB, Chilton, Did-cot, U.K., 1993!.
3National Radiological Protection Board, NRPB Report R200, ‘‘A Ntional Survey of Doses to Patients Undergoing a Selection of RouX-ray Examinations in English Hospitals’’~NRPB, Chilton, Didcot,U.K., 1986!.
4National Radiological Protection Board, Documents of the NRPB, VolNo. 3, ‘‘Patient Dose Reduction in Diagnostic Radiology’’~NRPB, Chil-ton, Didcot, U.K., 1990!.
Medical Physics, Vol. 28, No. 5, May 2001
efd.set
p,n
etor-y
.e
ed-.,
n-
-s
n-lsarelsof
rtseictye
e-
e-
e
,
5J. Gray, ‘‘Reference values-what are they?’’ AAPM Newsletter24, 9–10~1999!.
6International Atomic Energy Agency, IAEA Safety Series No. 115, ‘‘Iternational Basic Safety Standards for Protection Against Ionizing Ration and for the Safety of Radiation Sources’’~IAEA, Vienna, Austria,1996!.
7The Institute of Physics and Engineering in Medicine, Report No.‘‘Recommended Standards for the Routine Performance Testing of Dnostic X-ray Imaging Systems’’~IPEM, York, U.K., 1997!.
8National Radiological Protection Board, NRPB Report R289, ‘‘DosesPatients from Medical X-ray Examinations in the U.K.—1995 Review~NRPB, Chilton, Didcot, U.K., 1996!.
9Center for Devices and Radiological Health, ‘‘Nationwide EvaluationX-ray Trends~NEXT!: 1994 P/A Chest X-ray Data’’~CDRH, Food andDrug Administration!.
10Center for Devices and Radiological Health, ‘‘Nationwide EvaluationX-ray Trends ~NEXT!: 1995 Abdomen and LS Spine X-ray Data~CDRH, Food and Drug Administration!.
11Institute of Physical Sciences in Medicine, ‘‘National Protocol for PatieDose Measurements in Diagnostic Radiology’’~IPSM, York, U.K.,1992!.
12K. Schneider, H. Fendel, C. Bakowski, E. Stein, M. Kohn, M. Kellner,Schweighofer, G. Cartagena, R. Padovani, W. Panzer, C. ScheurerB. Wall, ‘‘Results of a dosimetry study in the European Communityfrequent x-ray examinations in infants,’’ Radiat. Prot. Dosim.43, 31–36~1992!.
13National Council on Radiation Protection and Measurements, NCRPport No. 102, ‘‘Medical X-ray Electron Beam and Gamma-ray Protectfor Energies up to 50-MeV’’~NCRP, Bethesda, MD, 1989!.
14R. G. Zamenhof, ‘‘RADCOMP X-ray Entrance Skin Exposure Software~Nuclear Associates, Victoreen, Inc., New York, 1990!.
15E. R. Hering, T. J. van W. Kotze, and G. J. Maree, ‘‘An estimation of tgenetically significant dose from diagnostic radiology for the South Arican population, 1990–1991,’’ Health Phys.74, 419–428~1998!.
16American Association of Physicists in Medicine, AAPM Report No. 3‘‘Standardized Methods for Measuring Diagnostic X-ray Exposure~Medical Physics Publishing, Madison, WI, 1991!.
17C. J. Tung, C. Y. Cheng, T. C. Chao, and H. Y. Tsai, ‘‘Determinationentrance skin doses and organ doses for medical x-ray examinatioRadiat. Prot. Dosim.85, 417–420~1999!.
18National Radiological Protection Board, NRPB Report R186, ‘‘OrgDoses from Medical X-ray Examinations Calculated Using Monte CaTechniques’’~NRPB, Chilton, Didcot, U.K., 1985!.
19A. Robinson, ‘‘Radiation protection and patient doses in diagnostic raology,’’ in Grainger & Allison’s Diagnostic Radiology: A Textbook oMedical Imaging, edited by R. G. Grainger and D. Allison~ChurchillLivingstone, New York, 1990!, pp. 169–189.
20K. Faulkner, A. P. Jones, and A. Walker,Safety in Diagnostic Radiology~IPSM, York, U.K., 1995!.
21International Commission on Radiological Protection, ICRP Publicat60, ‘‘1990 Recommendations of the International Commission on Ralogical Protection’’~Pergamon, Oxford, 1991!.
22National Radiological Protection Board, NRPB Report R261, ‘‘Softwafor Evaluating the Detriment Associated with Radiation Exposur~NRPB, Chilton, Didcot, U.K., 1993!.
23National Radiological Protection Board, NRPB Report R262, ‘‘Estimtion of Effective Dose in Diagnostic Radiology from Entrance SurfaDose and Dose-Area Product Measurements’’~NRPB, Chilton, Didcot,U.K., 1994!.
24M. Zonkl, N. Petoussi, and G. Drexler, ‘‘Effective dose and effectidose equivalent—the impact of the new ICRP definition for exterphoton irradiation,’’ Health Phys.62, 395–399~1992!.
25S. H. Stern, M. J. Dennis, G. Williams, and M. Rosenstein, ‘‘Simulatiof the upper gastrointestinal fluoroscopic examination for calculationabsorbed dose in tissue,’’ Health Phys.69, 391–395~1995!.
26R. Serro, J. V. Carreiro, J. P. Galvao, and R. Peis, ‘‘Population dassessment from radiodiagnosis in Portugal,’’ Radiat. Prot. Dosim.43,65–68~1992!.
27International Commission on Radiological Protection, ICRP Publicat55, ‘‘Optimization and Decision-Making in Radiological Protection~Pergamon, Oxford, 1989!.

io-Ch
857 Tung et al. : Determination of guidance levels 857
28C. C. Yu, C. J. Tung, I. F. Hung, and C. L. Tseng, ‘‘Analyses of radactive aerosols to support accurate internal dose assessments atShan nuclear power plant,’’ Health Phys.65, 147–155~1993!.
29R. E. Gallini, S. Belletti, V. Berna, and U. Giugni, ‘‘Adult and child
Medical Physics, Vol. 28, No. 5, May 2001
in–doses in standardized x-ray examinations,’’ Radiat. Prot. Dosim.43,41–47~1992!.
30K. L. Bontrager,Radiographic Positioning and Related Anatomy, 4th ed.~Mosby, St. Louis, MO, 1997!.