Deterioration of Quality of Life of High-Risk Breast Cancer Patients Treated with High-Dose...
10
Deterioration of Quality of Life of High-Risk Breast Cancer PatientsTreated with High-Dose Chemotherapy: The PEGASE 01 Quality of Life Study Patricia Marino, PhD, 1,10,11 Henri Roché, PhD, 2 Pierre Biron, MD, 3 Maud Janvier, MD, 4 Dominique Spaeth, MD, 5 Michel Fabbro, MD, 6 Claude Linassier, MD, 7 Thierry Delozier, MD, 8 Anne-Laure Martin, MS, 9 Gaelle Santin, MS, 1 Jean-Paul Moatti, PhD, 1,10 on behalf of the PEGASE Group 1 Inserm, Unit Research 912, Marseilles, France; 2 Institut Claudius Regaud,Toulouse, France; 3 Centre Léon Bérard, Lyon, France; 4 Centre René Huguenin, Saint Cloud, France; 5 Centre Alexis Vautrin, Nancy, France; 6 Centre Paul Lamarque, Montpellier, France; 7 CHU,Tours, France; 8 Centre François Baclesse, Caen, France; 9 FNCLCC, Paris, France; 10 Aix Marseille Université, Marseille, France; 11 Institat Paoli-Calmettes, Marseilles, France ABSTRACT Objective: The aim of this study was to compare the quality of life (QOL) of high-risk breast cancer patients included in a randomized clinical trial (PEGASE 01) comparing conven- tional chemotherapy versus adding an additional high-dose chemotherapy (HDC) cycle with blood stem cell support. Methods: A total of 314 patients were included in the clini- cal trial. QOL evaluations were available for 199 patients. QOL was assessed over a 1-year follow-up period, using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C-30. The results were analyzed using a linear mixed-effects model. Results: Toxicity of HDC has a strong negative impact on patients’ QOL during the treatment phase. This negative impact tended to last longer in the HDC group, as for most of the QLQ-C30 scales, the QOL scores of HDC patients tend to improve at a slower rate than that of patients receiving stan- dard chemotherapy. In particular, physical functioning remains deteriorated 1 year after inclusion for HDC patients comparatively to conventional chemotherapy patients (85.99 vs. 76.65, P = 0.021), and the pain score was still higher in the HDC group at that time (28.32 vs. 15.97, P = 0.004). Conclusion: HDC has a negative impact on QOL even after treatment phase. In the absence of an overall survival benefit of using HDC for high-risk breast cancer patients, QOL studies with a longer follow-up play an important role in informing the complex trade-off implied by HDC between higher toxicity, reduced risk of relapse, and QOL decrease after the active phase of treatment. Keywords: breast cancer, high-dose chemotherapy, quality of life. Introduction The prognosis of breast cancer patients with major axillary invasion remains poor, despite the progress related to adjunction of chemotherapy to treatment combining surgery and radiotherapy. Since the early diffusion of adjuvant chemotherapy using anthracycline-containing regimen administered at con- ventional doses, there has been much debate about the complex trade-off between the potential, however limited, gains in terms of survival and the negative impact on patients’ quality of life (QOL) because of the toxic side effects involved. These recurrent debates have increased since high-dose chemotherapy (HDC) supported by hematopoietic growth factors and peripheral stem cell transplantation was introduced in the early 1990s. These “dose-intensive” chemotherapy regimens have been tested on both advanced and high- risk breast cancer patients with the hope of increasing long-term disease-free survival (DFS) [1]. Nevertheless, to date, only one randomized trial has shown the exist- ence of any benefits of HDC in terms of overall sur- vival (OS) [2], while no benefits of this treatment were observed in other studies [3–8], and a few studies have suggested that HDC may decrease the risk of relapse and thus improve DFS [2,9,10]. In addition, HDC is known to be associated with greater toxicity than standard-dose chemotherapy regimens. Previous studies have shown that increasing dose intensity has distinctly detrimental effect on patients’ QOL [11,12]. These studies suggested that this negative impact tends to be transient and to dis- appear soon after the active treatment phase [13,14]. Some of these studies have dealt, however, with HDC in the context of metastatic breast cancer, and there is little evidence available so far about the impact on QOL of adjuvant HDC regimens. The impact of this treatment may in fact be rather complex: the decrease in QOL due to the toxic effects of HDC may Address correspondence to: Patricia Marino, INSERM U379, 232, Bd de Sainte Marguerite, 13273 Marseilles Cedex 9, France. E-mail: [email protected] 10.1111/j.1524-4733.2007.00306.x Volume 11 • Number 4 • 2008 VALUE IN HEALTH © 2008, International Society for Pharmacoeconomics and Outcomes Research (ISPOR) 1098-3015/08/709 709–718 709
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Deterioration of Quality of Life of High-Risk Breast Cancer Patients Treated with High-Dose...

Deterioration of Quality of Life of High-Risk Breast CancerPatients Treated with High-Dose Chemotherapy:The PEGASE 01 Quality of Life Study
Patricia Marino, PhD,1,10,11 Henri Roché, PhD,2 Pierre Biron, MD,3 Maud Janvier, MD,4 Dominique Spaeth, MD,5
Michel Fabbro, MD,6 Claude Linassier, MD,7 Thierry Delozier, MD,8 Anne-Laure Martin, MS,9 Gaelle Santin, MS,1
Jean-Paul Moatti, PhD,1,10 on behalf of the PEGASE Group1Inserm, Unit Research 912, Marseilles, France; 2Institut Claudius Regaud,Toulouse, France; 3Centre Léon Bérard, Lyon, France; 4Centre RenéHuguenin, Saint Cloud, France; 5Centre Alexis Vautrin, Nancy, France; 6Centre Paul Lamarque, Montpellier, France; 7CHU,Tours, France;8Centre François Baclesse, Caen, France; 9FNCLCC, Paris, France; 10Aix Marseille Université, Marseille, France; 11Institat Paoli-Calmettes,Marseilles, France
ABSTRACT
Objective: The aim of this study was to compare the qualityof life (QOL) of high-risk breast cancer patients included in arandomized clinical trial (PEGASE 01) comparing conven-tional chemotherapy versus adding an additional high-dosechemotherapy (HDC) cycle with blood stem cell support.Methods: A total of 314 patients were included in the clini-cal trial. QOL evaluations were available for 199 patients.QOL was assessed over a 1-year follow-up period, usingthe European Organization for Research and Treatment ofCancer Quality of Life Questionnaire C-30. The results wereanalyzed using a linear mixed-effects model.Results: Toxicity of HDC has a strong negative impact onpatients’ QOL during the treatment phase. This negativeimpact tended to last longer in the HDC group, as for most ofthe QLQ-C30 scales, the QOL scores of HDC patients tend to
improve at a slower rate than that of patients receiving stan-dard chemotherapy. In particular, physical functioningremains deteriorated 1 year after inclusion for HDC patientscomparatively to conventional chemotherapy patients (85.99vs. 76.65, P = 0.021), and the pain score was still higher in theHDC group at that time (28.32 vs. 15.97, P = 0.004).Conclusion: HDC has a negative impact on QOL even aftertreatment phase. In the absence of an overall survival benefitof using HDC for high-risk breast cancer patients, QOLstudies with a longer follow-up play an important role ininforming the complex trade-off implied by HDC betweenhigher toxicity, reduced risk of relapse, and QOL decreaseafter the active phase of treatment.Keywords: breast cancer, high-dose chemotherapy, quality oflife.
Introduction
The prognosis of breast cancer patients with majoraxillary invasion remains poor, despite the progressrelated to adjunction of chemotherapy to treatmentcombining surgery and radiotherapy. Since theearly diffusion of adjuvant chemotherapy usinganthracycline-containing regimen administered at con-ventional doses, there has been much debate about thecomplex trade-off between the potential, howeverlimited, gains in terms of survival and the negativeimpact on patients’ quality of life (QOL) because ofthe toxic side effects involved. These recurrent debateshave increased since high-dose chemotherapy (HDC)supported by hematopoietic growth factors andperipheral stem cell transplantation was introduced inthe early 1990s. These “dose-intensive” chemotherapy
regimens have been tested on both advanced and high-risk breast cancer patients with the hope of increasinglong-term disease-free survival (DFS) [1]. Nevertheless,to date, only one randomized trial has shown the exist-ence of any benefits of HDC in terms of overall sur-vival (OS) [2], while no benefits of this treatment wereobserved in other studies [3–8], and a few studies havesuggested that HDC may decrease the risk of relapseand thus improve DFS [2,9,10].
In addition, HDC is known to be associated withgreater toxicity than standard-dose chemotherapyregimens. Previous studies have shown that increasingdose intensity has distinctly detrimental effect onpatients’ QOL [11,12]. These studies suggested thatthis negative impact tends to be transient and to dis-appear soon after the active treatment phase [13,14].Some of these studies have dealt, however, with HDCin the context of metastatic breast cancer, and thereis little evidence available so far about the impacton QOL of adjuvant HDC regimens. The impact ofthis treatment may in fact be rather complex: thedecrease in QOL due to the toxic effects of HDC may
Address correspondence to: Patricia Marino, INSERM U379,232, Bd de Sainte Marguerite, 13273 Marseilles Cedex 9, France.E-mail: [email protected]
10.1111/j.1524-4733.2007.00306.x
Volume 11 • Number 4 • 2008V A L U E I N H E A L T H
© 2008, International Society for Pharmacoeconomics and Outcomes Research (ISPOR) 1098-3015/08/709 709–718 709

be balanced by future QOL improvements because ofthe lower risk of relapse.
In the absence of any evidence of benefits in terms ofOS, the effects of HDC on breast cancer patients havegenerally been assumed by the clinical community tobe negative, and HDC has not been adopted as stan-dard clinical practice. In this context, a better knowl-edge about the impact of these regimens on QOLbecomes a key parameter for both clinical decision-making and public health authorities’ decisions aboutthe diffusion of these innovative treatments.
A QOL study was therefore carried out in thecontext of a prospective randomized trial (PEGASE01) evaluating the clinical impact of adding one HDCcourse following standard chemotherapy for high-riskbreast cancer patients. The aim of this study was tocompare the effects on QOL of the two treatmentregimens, during a 1-year follow-up period.
Methods
The PEGASE 01 Clinical TrialWomen eligible for inclusion in the PEGASE 01 trialhad a nonmetastatic breast cancer with more thanseven axillary lymph nodes involved. They had to beless than 60 years of age with a World Health Orga-nization performance status �2. Between December1994 and December 1998, 314 patients at 29 medicalcenters were included in the trial. The protocol wasapproved by the ethical committee (Consultative Com-mittee for Protection of Persons Participating in Bio-medical Research) and all the patients gave theirwritten informed consent before being included in thestudy. All the patients included in the PEGASE 01protocol were eligible for the QOL study.
After surgery, patients were randomized to receivefour cycles of FEC100 (Epirubicin 100 mg/m2; Cyclo-phosphamide 500 mg/m2; 5-Fluorouracil 500 mg/m2)and then, either no further chemotherapy (standardarm, n = 155) or one additional cycle of HDC (Mitox-antrone 45 mg/m2 day -6; Cyclophosphamide60 mg/kg days -5 and -4; and Melphalan 140 mg/m2
day -2; HDC arm, n = 159). In the HDC treatmentarm, peripheral blood stem cells were harvested afterthe second and/or third FEC100 cycles under 5 mg/kgfilgrastim stimulation and reinfused on day 0. Granu-locyte colony-stimulating factor (G-CSF) (5 mg/kg/day)began on day 1 after stem cell transplantation and wasgiven until the absolute neutrophil count > 1 ¥ 109/Lfor three consecutive days.
After chemotherapy, radiotherapy was undergoneby the women in both treatment groups and positivehormonal receptor menopausal women were giventamoxifen for 3 years.
The primary end point defined in the clinical pro-tocol was DFS. QOL and economic outcomes [15]were secondary end points.
Assessment of QOLQuality of life was assessed using the self-administeredEuropean Organization for Research and Treatment ofCancer Quality of Life Questionnaire C-30 (EORTCQLQ-C30). This questionnaire, which was specificallydesigned for cancer patients [16], has been validatedfor international use and its psychometric propertiesfor breast cancer patients have been reported [17]. Itcontains 30 items subdivided into five functioningscales (physical, role, emotional, cognitive and socialfunctioning), three symptom scales (fatigue, nausea/vomiting, pain), and six single items (dyspnea, sleepdisturbance, loss of appetite, constipation, diarrhea,and financial difficulties).
Patients’ answers to the EORTC QLQ-C30 werescored using the algorithms supplied by the EORTC[18]. All scores range from 0 to 100, where a higherscore corresponds to a higher functional level or ahigher level of symptoms.
Timing of the AssessmentThe number of questionnaires administered duringfollow-up period was chosen to minimize the burdenon the patients. Consequently, the EORTC QLQ-C30was administered five times: 1) on the first day of thelast cycle of FEC100; 2) at the end of radiotherapy forstandard arm patients and after blood stem cell trans-plantation for HDC patients; 3) 1 month after radio-therapy for standard arm patients and at the end ofradiotherapy for HDC patients; 4) 3 months afterradiotherapy for both arms; and 5) 1 year after inclu-sion for both arms. FEC-related side effects wereassessed at the last FEC cycle for both arms. HDC-related side effects were measured at discharge fromtransplantation unit for HDC patients. In addition,patients’ sociodemographic characteristics were re-corded at inclusion.
Patient’s compliance in completion of question-naires was defined as the ratio between the number ofcompleted questionnaires returned and those expected.The expected number of questionnaires was the totalnumber which should have been completed by eachpatient according to the protocol, depending on howlong they survived.
Statistical AnalysisParticularly close attention was devoted to the prob-lems that may be related to missing data in the QOLstudy. Standard statistical analysis of repeated mea-sures usually considers that the probability that somedata are missing is independent of the value of thesedata. According to the classification developed byRubin [19], such data should be considered as MissingCompletely At Random (MCAR) and classical analysisof variance remains appropriate for statistical analysisin this case. MCAR data should, however, be distin-
710 Marino et al.

guished from missing-at-random (MAR) data. In thelatter case, which is more likely to happen in thecontext of longitudinal assessment of QOL embeddedin a clinical trial, the probability some data are missingmay depend on the previous (observed) values of thedata, but does not depend on the specific value of themissing data.
Missing data are indeed very rarely MCAR incancer clinical trials, and statistical methods based onthe assumption that data are rather MAR are prefer-able for analysis [20]. The approach we used thereforeassumed that the missing data mechanism was MAR,and analysis was performed using a linear mixed-effects model, unbiased under the MAR assumption[21,22]. The general form of the model is Yi = Xib+ Zigi + ei where Yi is the QOL vector for ith individual,Xi the matrix of fixed effects (i.e., the covariates), andZi the matrix of random effects. The intrasubject cor-relations (repeated measures) are modeled with inclu-sion of random effects in the model.
Our model included an intercept and a slope asrandom effects. This means that the baseline value ofthe scores, as well as their evolution in time, may differbetween patients. Time was fitted in the model as acontinuous variable, because the timing of the assess-ments varied across patients.
In order to account for the decrease in QOLobserved at the second assessment (Q2) for HDC
patients (due to the intensification phase), we includedin the model an indicator variable for the secondassessment (EvalQ2 = 1 if it was the second assess-ment, and 0 otherwise) as in the study by Jacqmin-Gadda et al. [23]. This additional variable allowed usto model the change in the slope after the second QOLassessment.
Our model can therefore be written as follows:
Y Arm Time Arm TimeEvalQ EvalQ A
ij i ij i ij= + + + ×( ) ++ ×
β β β βγ γ
0 1 2 3
1 22 2 rrmTime
i i
i ij ij
( ) + ++
νν ε
0
1
It was estimated using the SAS Proc Mixed procedure[24].
Results
Clinical ResultsThe baseline data on the 314 patients included in theclinical protocol, such as age, stage, number of positivelymph nodes, hormonal status, estrogen and progest-erone receptor, and histological types, were well bal-anced between the two treatment arms.
Patients’ main clinical characteristics and survivaltime are summarized in Table 1. After a medianfollow-up period of 61.2 months, a significant differ-ence in DFS was observed, with mean DFS durations
Table 1 Clinical characteristics and outcomes for patients included in the PEGASE 01 trial
All PEGASE 01 patients Patients in the QOL study
Standard group(n = 155)
HDC group(n = 159)
Standard group(n = 99)
HDC group(n = 100)
Age (year), median (range) 47 (29–60) 48 (25–59) 47 (27–49) 47 (25–59)Breast conserving surgery (%) 60 (39) 75 (47) 38 (38) 50 (50)Tumor classification (%)
T0 5 (3) 2 (1) 2 (2) 2 (2)T1 42 (27) 43 (27) 24 (24) 29 (29)T2 70 (45) 91 (57) 49 (49) 53 (53)T3–4 28 (18) 20 (13) 20 (20) 16 (16)Undetermined 10 (6) 3 (2) 4 (4) 0 (0)
Histological grade SBRI 8 (5) 15 (9) 7 (7) 11 (11)II 70 (45) 50 (31) 41 (41) 29 (29)III 64 (41) 82 (52) 45 (45) 53 (53)Unknown 13 (8) 12 (8) 6 (6) 7 (7)
Positive nodesMedian (range) 13 (8–36) 11 (8–36) 13 (8–34) 12 (8–26)
Receptor statusER positive 91 (59) 105 (66) 57 (57) 70 (70)PR positive 87 (56) 86 (54) 60 (60) 54 (54)
Hormonal status (%)Premenopausal 108 (70) 109 (69) 70 (71) 68 (68)Postmenauposal 47 (30) 50 (31) 29 (29) 32 (32)
Toxicity duration (month)*Mean (SD) 5.24 (0.07) 6.88 (0.09) 5.21 (0.74) 7.03 (0.81)
Overall survivalMean duration 70.27 71.78 69.30 72.155-year rate (%) 67.8 73.7 68.0 75.0
Disease-free survivalMean duration 49.5 61.1 48.9 64.15-year rate (%) 40.7 60.0 41.0 61.9
*Toxicity was calculated as the total duration of treatment, until the end of radiotherapy.ER,estrogen receptor; HDC, high-dose chemotherapy; PR, progesterone receptor; QOL, quality of life; SBR, Scarff Bloom Richardson; SD, standard deviation.
QOL of High-Risk Breast Cancer Patients 711
(95% confidence interval [CI]) of 49.5 months (CI44.1–54.8) and 61.1 months (CI 56.1–65.8) instandard treatment arm and HDC arm, respectively(P < 0.001). The 5-year DFS rates were 40.7% and60% (65 relapses occurred in the standard treatmentarm vs. 44 in the HDC arm), respectively.
Nevertheless, OS was the same in both treatmentgroups with mean durations of 70.3 months (CI 65.5–75.1) in standard arm and 71.8 months (CI 67.8–75.7)in HDC arm. The 5-year OS rates were 67.8% and73.7% in the standard and HDC arms, respectively.
Recruitment and Participation in the QOL StudyAmong the 314 patients included in the PEGASE 01trial, 50 patients could not be included in the QOLstudy for the following reasons: three centers refusedto participate in the QOL study (41 patients); ques-tionnaires could not be administered to seven patientswho were treated outside the participating center; twopatients were illiterate and could not complete ques-tionnaires. In addition, 65 patients expressly refused toparticipate in the QOL study.
We present the QOL results on the 199 patientswho completed at least one QOL questionnaire (99 inthe standard group and 100 in the HDC group). Char-acteristics of these patients are given in Table 1. Therewere no statistically significant differences in termsof the main clinical characteristics between the 199patients included in the QOL study and the 115patients not included in the study.
The response rate of the 199 participating patientsto QOL questionnaires was good: it amounted to 90%during the active phase of treatment and 76% duringthe first year of follow-up. There was no statisticallysignificant difference in the compliance rates betweenthe two treatment arms (88% and 73% in the standardtreatment arm vs. 91% and 79% in the HDC arm).Nevertheless, it is worth noting that 48% of therespondents answered all five questionnaires, whereas52% did not answer at least one of the questionnairesduring the study period.
Sociodemographic CharacteristicsThe 199 patients included in our analysis had thefollowing sociodemographic characteristics (HDC armvs. standard arm): 1) the great majority of the patientswere married (77% vs. 66%) and had at least one child(81% in both arms); 2) more than half of these patientswere not secondary school or university graduates(55% vs. 62%), but the great majority had a profes-sional activity before incurring the disease (68% vs.61%). No statistically significant differences wereobserved between the sociodemographic characteris-tics of the two groups of patients.
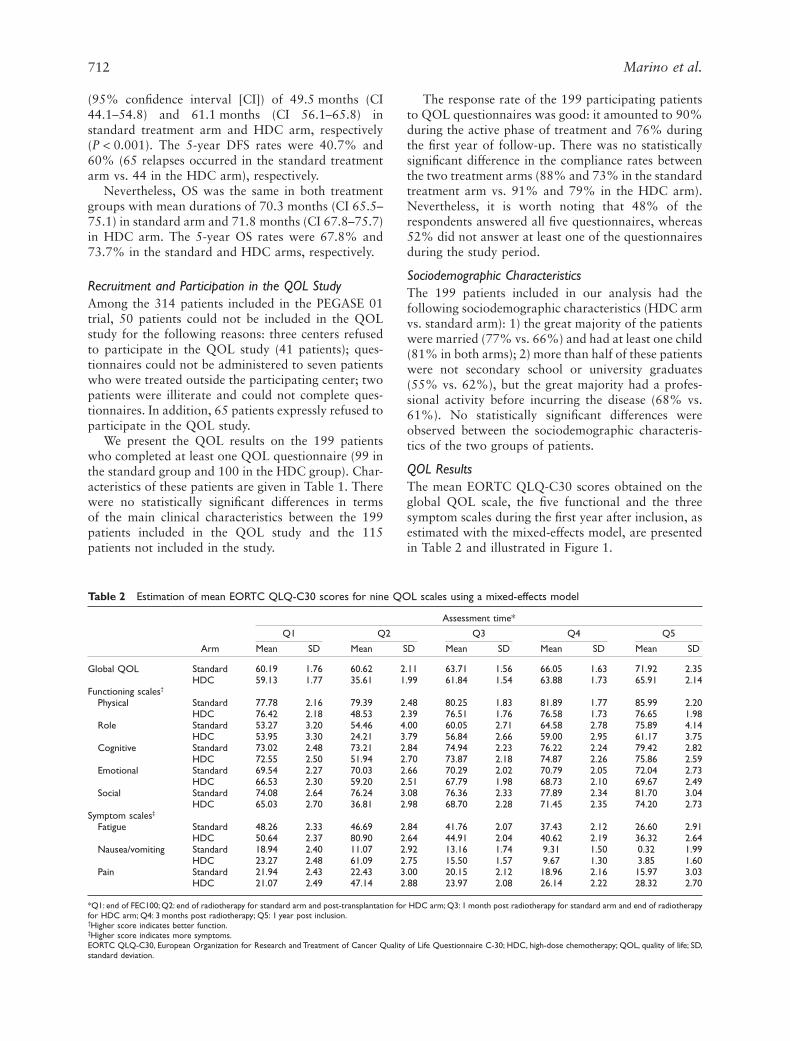
QOL ResultsThe mean EORTC QLQ-C30 scores obtained on theglobal QOL scale, the five functional and the threesymptom scales during the first year after inclusion, asestimated with the mixed-effects model, are presentedin Table 2 and illustrated in Figure 1.
Table 2 Estimation of mean EORTC QLQ-C30 scores for nine QOL scales using a mixed-effects model
Arm
Assessment time*
Q1 Q2 Q3 Q4 Q5
Mean SD Mean SD Mean SD Mean SD Mean SD
Global QOL Standard 60.19 1.76 60.62 2.11 63.71 1.56 66.05 1.63 71.92 2.35HDC 59.13 1.77 35.61 1.99 61.84 1.54 63.88 1.73 65.91 2.14
Functioning scales†
Physical Standard 77.78 2.16 79.39 2.48 80.25 1.83 81.89 1.77 85.99 2.20HDC 76.42 2.18 48.53 2.39 76.51 1.76 76.58 1.73 76.65 1.98
Role Standard 53.27 3.20 54.46 4.00 60.05 2.71 64.58 2.78 75.89 4.14HDC 53.95 3.30 24.21 3.79 56.84 2.66 59.00 2.95 61.17 3.75
Cognitive Standard 73.02 2.48 73.21 2.84 74.94 2.23 76.22 2.24 79.42 2.82HDC 72.55 2.50 51.94 2.70 73.87 2.18 74.87 2.26 75.86 2.59
Emotional Standard 69.54 2.27 70.03 2.66 70.29 2.02 70.79 2.05 72.04 2.73HDC 66.53 2.30 59.20 2.51 67.79 1.98 68.73 2.10 69.67 2.49
Social Standard 74.08 2.64 76.24 3.08 76.36 2.33 77.89 2.34 81.70 3.04HDC 65.03 2.70 36.81 2.98 68.70 2.28 71.45 2.35 74.20 2.73
Symptom scales‡
Fatigue Standard 48.26 2.33 46.69 2.84 41.76 2.07 37.43 2.12 26.60 2.91HDC 50.64 2.37 80.90 2.64 44.91 2.04 40.62 2.19 36.32 2.64
Nausea/vomiting Standard 18.94 2.40 11.07 2.92 13.16 1.74 9.31 1.50 0.32 1.99HDC 23.27 2.48 61.09 2.75 15.50 1.57 9.67 1.30 3.85 1.60
Pain Standard 21.94 2.43 22.43 3.00 20.15 2.12 18.96 2.16 15.97 3.03HDC 21.07 2.49 47.14 2.88 23.97 2.08 26.14 2.22 28.32 2.70
*Q1: end of FEC100; Q2: end of radiotherapy for standard arm and post-transplantation for HDC arm; Q3: 1 month post radiotherapy for standard arm and end of radiotherapyfor HDC arm; Q4: 3 months post radiotherapy; Q5: 1 year post inclusion.†Higher score indicates better function.‡Higher score indicates more symptoms.EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C-30; HDC, high-dose chemotherapy; QOL, quality of life; SD,standard deviation.
712 Marino et al.
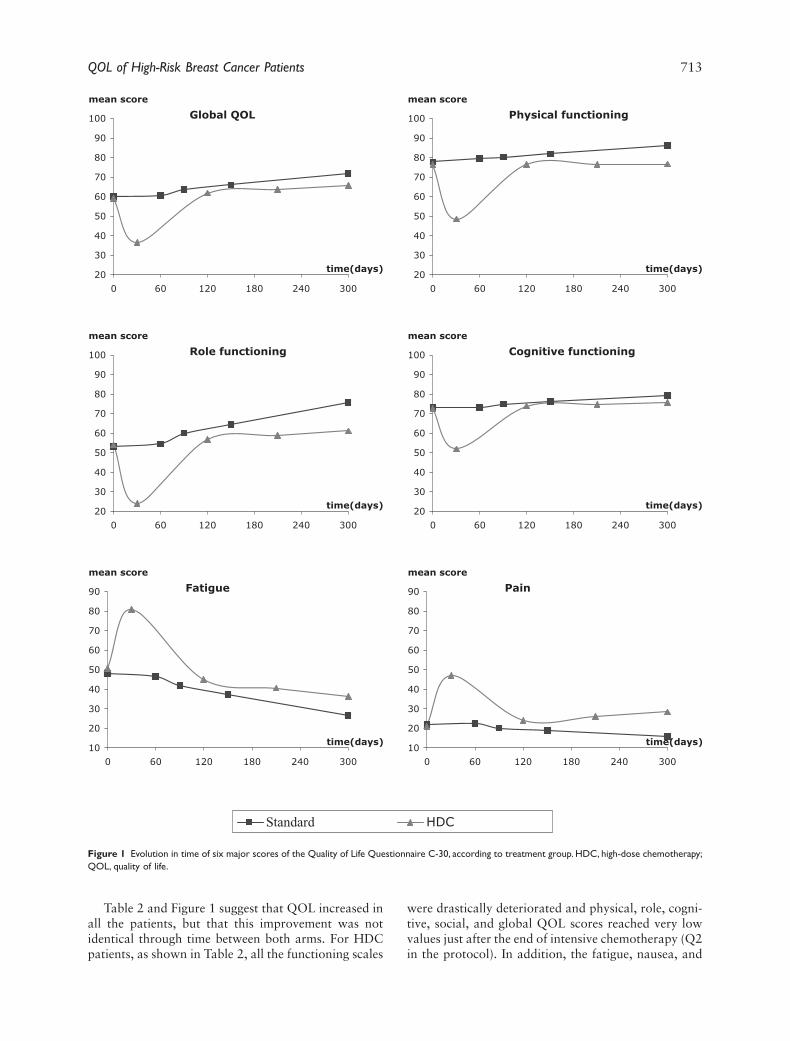
Table 2 and Figure 1 suggest that QOL increased inall the patients, but that this improvement was notidentical through time between both arms. For HDCpatients, as shown in Table 2, all the functioning scales
were drastically deteriorated and physical, role, cogni-tive, social, and global QOL scores reached very lowvalues just after the end of intensive chemotherapy (Q2in the protocol). In addition, the fatigue, nausea, and
Standard HDC
mean score
20
30
40
50
60
70
80
90
100
0 60 120 180 240 300
time(days)
Global QOL
mean score
20
30
40
50
60
70
80
90
100
0 60 120 180 240 300
time(days)
Physical functioning
mean score
20
30
40
50
60
70
80
90
100
0 60 120 180 240 300
time(days)
Role functioning
mean score
20
30
40
50
60
70
80
90
100
0 60 120 180 240 300
time(days)
Cognitive functioning
mean score
10
20
30
40
50
60
70
80
90
0 60 120 180 240 300
time(days)
Fatigue
mean score
10
20
30
40
50
60
70
80
90
0 60 120 180 240 300
time(days)
Pain
Figure 1 Evolution in time of six major scores of the Quality of Life Questionnaire C-30, according to treatment group. HDC, high-dose chemotherapy;QOL, quality of life.
QOL of High-Risk Breast Cancer Patients 713
pain scores increased considerably during this activephase of treatment, which suggest that these sideeffects of the treatment greatly affected the patients’QOL. Although HDC patients’ scores remainedunchanged during the first year, QOL graduallyincreased in the standard treatment group. In particu-lar, the physical score remained practically the sameat Q3, Q4, and Q5 assessments in HDC patients,but increased from 80.3 to 86.0 in standard grouppatients. One year after inclusion, large differencesexisted between the two arms for some major scores,such as physical functioning, role functioning, fatigue,and pain. In addition, during the last few months offollow-up, QOL continued to improve in the case ofstandard treatment patients, but remained stable inthat of HDC patients.
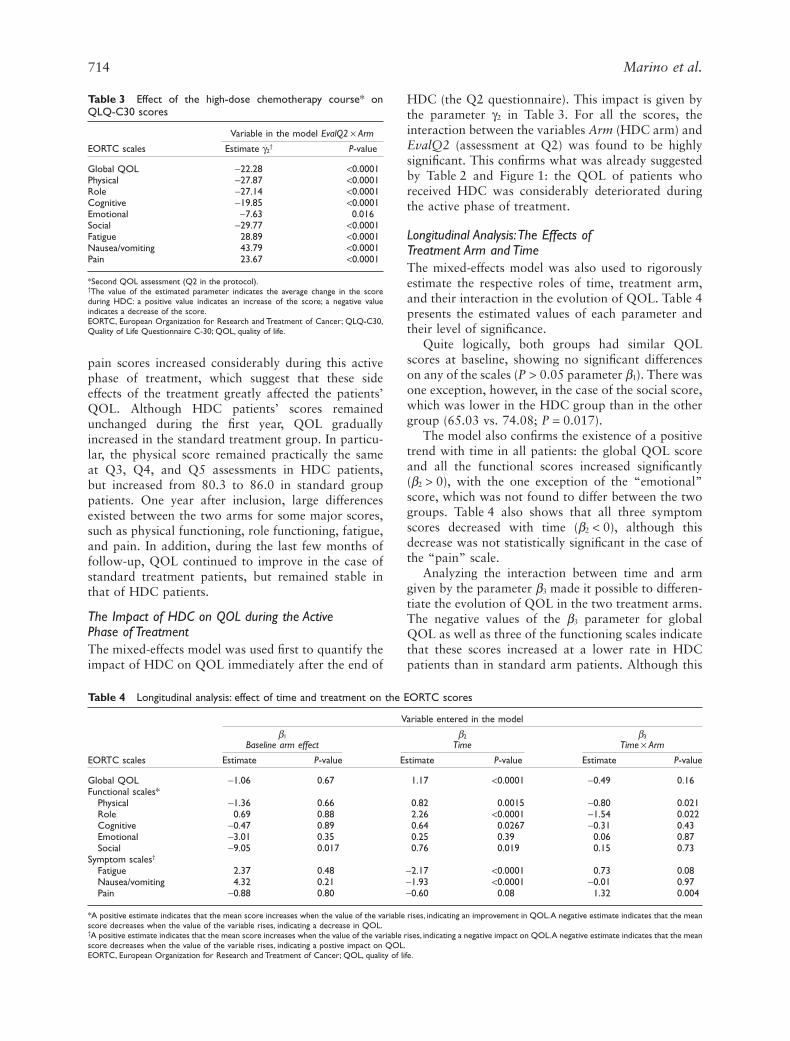
The Impact of HDC on QOL during the ActivePhase of TreatmentThe mixed-effects model was used first to quantify theimpact of HDC on QOL immediately after the end of
HDC (the Q2 questionnaire). This impact is given bythe parameter g2 in Table 3. For all the scores, theinteraction between the variables Arm (HDC arm) andEvalQ2 (assessment at Q2) was found to be highlysignificant. This confirms what was already suggestedby Table 2 and Figure 1: the QOL of patients whoreceived HDC was considerably deteriorated duringthe active phase of treatment.
Longitudinal Analysis:The Effects ofTreatment Arm and TimeThe mixed-effects model was also used to rigorouslyestimate the respective roles of time, treatment arm,and their interaction in the evolution of QOL. Table 4presents the estimated values of each parameter andtheir level of significance.
Quite logically, both groups had similar QOLscores at baseline, showing no significant differenceson any of the scales (P > 0.05 parameter b1). There wasone exception, however, in the case of the social score,which was lower in the HDC group than in the othergroup (65.03 vs. 74.08; P = 0.017).
The model also confirms the existence of a positivetrend with time in all patients: the global QOL scoreand all the functional scores increased significantly(b2 > 0), with the one exception of the “emotional”score, which was not found to differ between the twogroups. Table 4 also shows that all three symptomscores decreased with time (b2 < 0), although thisdecrease was not statistically significant in the case ofthe “pain” scale.
Analyzing the interaction between time and armgiven by the parameter b3 made it possible to differen-tiate the evolution of QOL in the two treatment arms.The negative values of the b3 parameter for globalQOL as well as three of the functioning scales indicatethat these scores increased at a lower rate in HDCpatients than in standard arm patients. Although this
Table 3 Effect of the high-dose chemotherapy course* onQLQ-C30 scores
EORTC scales
Variable in the model EvalQ2 ¥ Arm
Estimate g2† P-value
Global QOL -22.28 <0.0001Physical -27.87 <0.0001Role -27.14 <0.0001Cognitive -19.85 <0.0001Emotional -7.63 0.016Social -29.77 <0.0001Fatigue 28.89 <0.0001Nausea/vomiting 43.79 <0.0001Pain 23.67 <0.0001
*Second QOL assessment (Q2 in the protocol).†The value of the estimated parameter indicates the average change in the scoreduring HDC: a positive value indicates an increase of the score; a negative valueindicates a decrease of the score.EORTC, European Organization for Research and Treatment of Cancer; QLQ-C30,Quality of Life Questionnaire C-30; QOL, quality of life.
Table 4 Longitudinal analysis: effect of time and treatment on the EORTC scores
EORTC scales
Variable entered in the model
b1
Baseline arm effectb2
Timeb3
Time ¥ Arm
Estimate P-value Estimate P-value Estimate P-value
Global QOL -1.06 0.67 1.17 <0.0001 -0.49 0.16Functional scales*
Physical -1.36 0.66 0.82 0.0015 -0.80 0.021Role 0.69 0.88 2.26 <0.0001 -1.54 0.022Cognitive -0.47 0.89 0.64 0.0267 -0.31 0.43Emotional -3.01 0.35 0.25 0.39 0.06 0.87Social -9.05 0.017 0.76 0.019 0.15 0.73
Symptom scales†
Fatigue 2.37 0.48 -2.17 <0.0001 0.73 0.08Nausea/vomiting 4.32 0.21 -1.93 <0.0001 -0.01 0.97Pain -0.88 0.80 -0.60 0.08 1.32 0.004
*A positive estimate indicates that the mean score increases when the value of the variable rises, indicating an improvement in QOL.A negative estimate indicates that the meanscore decreases when the value of the variable rises, indicating a decrease in QOL.†A positive estimate indicates that the mean score increases when the value of the variable rises, indicating a negative impact on QOL.A negative estimate indicates that the meanscore decreases when the value of the variable rises, indicating a postive impact on QOL.EORTC, European Organization for Research and Treatment of Cancer; QOL, quality of life.
714 Marino et al.

difference was not significant for global QOL, itreached significance level in the case of two importantfunctional scales: physical (P = 0.021) and role (P =0.022). The positive values of the pain and fatiguescores show that these two symptoms decreased at alower rate in the HDC arm: this difference was clearlysignificant in the case of pain (P = 0.004), but notfatigue (P = 0.08).
Conclusion
High-dose chemotherapy is known to decrease QOLduring a relatively short period of time because of theside effects commonly associated with cytotoxicdrugs. As to date only one randomized trial has beenable to demonstrate that HDC offers a benefit interms of OS [2], and even if we can hope it willreduce the risk of relapse, toxicity may jeopardize theuse of these innovative treatments. In this context,the impact of HDC on QOL becomes a centralparameter on which to base medical decision-making,but very little is known about this impact as very fewstudies of adjuvant HDC with autologous blood stemcell transplantation have included QOL assessment[25–28].
The aim of this study was to assess the impact ofHDC on the QOL of breast cancer patients withaxillary lymph node invasion during a 12-monthperiod. Using a mixed effects model, the QOL ofpatients receiving HDC was compared to that ofpatients who received standard-dose chemotherapy.The results of our study showed that the toxicity ofHDC has a strong negative impact on patients’ QOLduring the active phase of treatment. In addition, thisnegative impact on patients’ QOL tends to last longerthan for patients treated with standard chemo-therapy. The parameter reflecting the interactionsbetween time and treatment group (b3) was signifi-cant or at borderline significance level for somemajor QOL scales, showing that the pattern of QOLin time differed between treatment groups. In particu-lar, physical functioning was obviously still deterio-rated 1 year after inclusion in HDC patients, andthe negative impact of pain (and possibly fatigue)remains more important for them. Our results showthat the QOL of HDC patients tends to improve at aslower rate than that of patients treated with stan-dard chemotherapy, at least during the first year afterthe start of treatment. Therefore, gains in QOL dueto the decreased risk of relapse may indeed be lowerthan they were previously thought to be. Interest-ingly, the emotional score did not increase signifi-cantly during the 1-year follow-up period, and didnot differ between treatment groups. The most deci-sive factor here therefore seems to be the diseasestatus, and not the type of treatment undergone.
The results of this study are interesting as thoseof previous QOL studies suggested that the negativeimpact of adjuvant chemotherapy does not affect theacceptability of this treatment [11,13,29–31]. In thespecific context of adjuvant HDC, the authors of pre-vious studies concluded that more intensive therapieswere associated with a decrease in QOL because of theside effects occurring during the treatment period, butthat this decrease was transient and tended to disap-pear quite soon after treatment was completed[14,27,28]. In a study by Peters et al., however, breastcancer patients treated with HDC with autologoustransplantation reported having a number of problemssuch as sleep disturbance, anxiety, and fatigue 1 yearafter the end of treatment, but did not suffer from anymajor decrease in their QOL [32].
One possible reason for the differences betweenthe results of this study and previous ones may haveto do with the methods used. Standard statisticalmethods for repeated measures require completedata, and the statistical analysis is therefore restrictedto those patients who answered all the QOL ques-tionnaires during the study period. In situationswhere data were missing because of the disease or itstreatment, this approach may introduce significantbiases into the statistical analysis. This is particularlytrue in the case of patients in the advanced stages ofthe disease: if their disease prevents patients fromanswering QOL questionnaires, including only thosepatients who completed all the QOL questionnairesmight lead to overestimating QOL [33]. The mixed-effects model used here was based on the assumptionthat missing data are MAR, which is highly plausiblein the case of our data. This approach has been usedin previous research on cancer patients to analyzelongitudinal QOL data [34–37], but to our knowl-edge, this is the first study in which this approach hasbeen used to assess how HDC affects QOL in breastcancer patients. It is always difficult to choose themost appropriate method for dealing with missingQOL data in longitudinal follow-up studies, and thistopic has recently been studied by several authors[38–41]. In particular, analyzing QOL during alonger follow-up period may require the use of othertypes of models.
The clinical significance of differences in QOL is animportant point which has to be discussed in QOLstudies. It was recently concluded that all the methodsdesigned to assess what might be called a meaningfuldifference in QOL scores lead to the same conclusion[42]. A difference of 5 to 10 points in patients’ scoreson a 0–100-point scale is generally considered to bemeaningful [43], and that was the criterion adoptedhere. The large statistical difference in the QOL scoresobserved in this study between groups therefore seemsto reflect a clinically significant difference which wasperceivable by the patients.
QOL of High-Risk Breast Cancer Patients 715

Study LimitationsOne of the main limitations of this study, as in otherstudies carried out alongside clinical trials, is that wecannot completely exclude the possibility that somebias may have occurred in our QOL assessments,because a proportion of the patients participating inthe clinical trial could not be included in the QOLstudy itself. Nevertheless, no differences were found toexist between the socioeconomic and clinical charac-teristics of the PEGASE 01 patients who were includedin the QOL study and those who were not. In addition,the use of a mixed-effects model allowed us to takeinto account in the statistical analysis all the informa-tion available on each of the 199 patients who partici-pated in the QOL study.
Another limitation of this study is the short durationof the follow-up period (1 year), as side effects mayoccur in the long term and not be limited to the first fewmonths after the treatment phase. It has in fact beenreported in studies on bone marrow transplantation[44] that some side effects may not be properly assessedwithin a single year of follow-up. In particular, somedebate is focusing today on questions about cognitivefunction [45,46]. Long-term QOL is of considerableimportance, as it contributes decisively to the overallvalue of intensified regimens. As the ultimate goal ofadjuvant treatment is to improve long-term survival,short-term toxicity should be readily accepted in situa-tions where a therapeutic benefit is observed in terms ofOS. Of course, in cases where the OS benefits are notvery clear, it can be argued that DFS should be used asa surrogate criterion because a relapse of cancer is atraumatic event which can have serious psychologicalconsequences [47–49]. This implies, however, thatdelaying relapses translates into a better QOL forpatients as long as they remain disease-free. The resultsof the PEGASE 01 protocol suggest that in the case ofHDC for high-risk breast cancer patients, such assump-tion should be handled with caution: HDC patientsundergo a longer active phase of treatment, which isassociated with significantly higher toxicity, whereasthe mean time elapsing before a relapse occurs is longerthan for standard arm patients. The extent to whichdelays in relapses actually compensate for the highertoxicity to which patients are exposed during theirtreatment depends strongly on the level of patients’QOL during the remission period.
No comorbidity data were available in this study, asour study population consisted of fairly young women(<60 years of age). Nevertheless, changes in comorbid-ity may have a significant effect on QOL in the longterm, and this point should therefore be included infuture studies evaluating HDC for breast cancerpatients.
In conclusion, the gains in QOL obtained by delay-ing relapse with HDC should be balanced with thelosses incurred by HDC patients not only during the
active phase of treatment but afterward. Future QOLstudies should be carried out during longer follow-upperiod to clarify the difficult trade-off which ariseswith HDC between greater toxicity, the lower risk ofrelapse and the persistent decrease in QOL even afterthe active phase of treatment.
The authors are extremely grateful to the patients for theiractive cooperation in this study. We also thank all those whoadministered quality-of-life questionnaires at each center andthe Fédération Nationale des Centres de Lutte Contre leCancer (FNCLCC) who promoted the PEGASE program. Wewould also like to thank all the participating institutions:Institut C. Regaud, Toulouse; Institut Curie, Paris; Center L.Berard, Lyon; Institut G. Roussy, Villejuif; Center R. Hugue-nin, St Cloud; Center A. Vautrin, Nancy; Center Vald’Aurelle, Montpellier; Hôpital Bretonneau, Tours; Center F.Baclesse, Caen; Center J. Perrin, Clermont-Ferrand; InstitutBergonié, Bordeaux; Center O. Lambret, Lille; Center P.Papin, Angers; Center A. Lacassagne, Nice; Hôpital R.Dubos, Pontoise; Hospices Civils, Lyon; Hospidale Card-arelli, Napoli; Institut Paoli-Calmettes, Marseille; Institut J.Godinot, Reims; Hôpital Metz; CHU La Tronche, Grenoble;Hôpital Bourg-en-Bresse; Hôpital H. Mondor; CHUDupuytren, Limoges; Hôpital J. Bernard, Poitiers; HôpitalPasteur, Colmar; Hôpital St Etienne; Hôpital P. Brousse,Villejuif; Hôpital Brive.
Source of financial support: The work of Patricia Marino wassupported by Association pour la Recherche sur le Cancer.The PEGASE program was supported by the Ligue NationaleContre le Cancer. The QOL study was partly supported bythe Fondation de France.
References
1 Peters WP, Dansey RD, Klein JL, Baynes RD. High-dose chemotherapy and peripheral blood progenitorcell transplantation in the treatment of breast cancer.Oncologist 2000;5:1–13.
2 Nitz UA, Mohrmann S, Fischer J, et al. Comparisonof rapidly cycled tandem high-dose chemotherapyplus peripheral-blood stem-cell support versus dose-dense conventional chemotherapy for adjuvanttreatment of high-risk breast cancer: results of a mul-ticentre phase III trial. Lancet 2005;366:1935–44.
3 Rodenhuis S, Richel DJ, van der Wall E, et al. Ran-domised trial of high-dose chemotherapy and hae-mopoietic progenitor-cell support in operable breastcancer with extensive axillary lymph-node involve-ment. Lancet 1998;352:515–21.
4 Hortobagyi GN, Buzdar AU, Theriault RL, et al. Ran-domized trial of high-dose chemotherapy and bloodcell autografts for high-risk primary breast carcinoma.J Natl Cancer Inst 2000;92:225–33.
5 Bergh J, Wiklund T, Erikstein B, et al. Tailored fluo-rouracil, epirubicin, and cyclophosphamide comparedwith marrow-supported high-dose chemotherapy asadjuvant treatment for high-risk breast cancer: a ran-domised trial. Scandinavian Breast Group 9401 study.Lancet 2000;356:1384–91.
716 Marino et al.
6 Schrama JG, Faneyte IF, Schornagel JH, et al. Ran-domized trial of high-dose chemotherapy and hemato-poietic progenitor-cell support in operable breastcancer with extensive lymph node involvement: finalanalysis with 7 years of follow-up. Ann Oncol2002;13:689–98.
7 Peters WP, Rosner GL, Vredenburgh JJ, et al. Pro-spective, randomized comparison of high-dosechemotherapy with stem-cell support versus inter-mediate-dose chemotherapy after surgery and adju-vant chemotherapy in women with high-risk primarybreast cancer: a report of CALGB 9082, SWOG 9114,and NCIC MA-13. J Clin Oncol 2005;23:2191–200.
8 Coombes RC, Howell A, Emson M, et al. High dosechemotherapy and autologous stem cell transplanta-tion as adjuvant therapy for primary breast cancerpatients with four or more lymph nodes involved:long-term results of an international randomised trial.Ann Oncol 2005;16:726–34.
9 Rodenhuis S, Bontenbal M, Beex LV, et al. High-dosechemotherapy with hematopoietic stem-cell rescue forhigh-risk breast cancer. N Engl J Med 2003;349:7–16.
10 Farquhar C, Basser R, Marjoribanks J, Lethaby A.High dose chemotherapy and autologous bonemarrow or stem cell transplantation versus conven-tional chemotherapy for women with early poor prog-nosis breast cancer. Cochrane Database Syst Rev2003:CD003139.
11 Macquart-Moulin G, Viens P, Palangie T, et al. High-dose sequential chemotherapy with recombinantgranulocyte colony-stimulating factor and repeatedstem-cell support for inflammatory breast cancerpatients: does impact on quality of life jeopardizefeasibility and acceptability of treatment? J ClinOncol 2000;18:754–64.
12 Partridge AH, Bunnell CA, Winer EP. Quality of lifeissues among women undergoing high-dose chemo-therapy for breast cancer. Breast Dis 2001;14:41–50.
13 Hürny C, Bernhard J, Coates AS, et al. Impact ofadjuvant therapy on quality of life in women withnode-positive operable breast cancer. Lancet 1996;347:1279–84.
14 Fairclough DL, Fetting JH, Cella D, et al. Quality oflife and quality adjusted survival for breast cancerpatients receiving adjuvant therapy. Eastern Coopera-tive Oncology Group (ECOG). Qual Life Res 1999;8:723–31.
15 Marino P, Siani C, Roche H, Moatti JP. Impact ofuncertainty on cost-effectiveness analysis of medicalstrategies: the case of high-dose chemotherapy forbreast cancer patients. Int J Technol Assess HealthCare 2005;21:342–50.
16 Aaronson NK, Ahmedzai S, Bergman B, et al. TheEuropean Organization for Research and Treatmentof Cancer QLQ-C30: a quality-of-life instrument foruse in international clinical trials in oncology. J NatlCancer Inst 1993;85:365–76.
17 Osoba D, Zee B, Pater J, et al. Psychometric propertiesand responsiveness of the EORTC Quality of LifeQuestionnaire (QLQ-C30) in patients with breast,ovarian and lung cancer. Qual Life Res 1994;3:353–64.
18 Fayers P, Aaronson NK, Bjordal K, et al. EORTCQLQ-C30 scoring manual. EORTC Quality of LifeDocumentation 1995.
19 Rubin D. Inference and missing data. Biometrika1976;63:581–92.
20 Fairclough DL, Peterson HF, Chang V. Why aremissing quality of life data a problem in clinicaltrials of cancer therapy? Stat Med 1998;17:667–77.
21 Laird NM, Ware JH. Random-effects models for lon-gitudinal data. Biometrics 1982;38:963–74.
22 Diggle P, Kenward M. Informative drop-out in longi-tudinal data analysis. Appl Stat 1994;43:49–93.
23 Jacqmin-Gadda H, Fabrigoule C, Commenges D, Dar-tigues JF. A 5-year longitudinal study of the Mini-Mental State Examination in normal aging. Am JEpidemiol 1997;145:498–506.
24 Littell R, Milliken G, Stroup W, Wolfinger R. SASSystem for Mixed Models. Cary, NC: SAS Institute,1996.
25 Goodwin PJ, Black JT, Bordeleau LJ, Ganz PA.Health-related quality-of-life measurement in ran-domized clinical trials in breast cancer-taking stock. JNat Cancer Inst 2003;95:263–81.
26 van Dam FS, Schagen SB, Muller MJ, et al. Impair-ment of cognitive function in women receiving adju-vant treatment for high-risk breast cancer: high-doseversus standard-dose chemotherapy. J Natl CancerInst 1998;90:210–18.
27 Peppercorn J, Herndon J, 2nd, Kornblith AB, et al.Quality of life among patients with Stage II and IIIbreast carcinoma randomized to receive high-dosechemotherapy with autologous bone marrow supportor intermediate-dose chemotherapy: results fromCancer and Leukemia Group B 9066. Cancer2005;104:1580–9.
28 Brandberg Y, Michelson H, Nilsson B, et al. Qualityof life in women with breast cancer during the firstyear after random assignment to adjuvant treatmentwith marrow-supported high-dose chemotherapywith cyclophosphamide, thiotepa, and carboplatin ortailored therapy with fluorouracil, epirubicin, andcyclophosphamide: Scandinavian Breast Group Study9401. J Clin Oncol 2003;21:3659–64.
29 Jansen Hjermstad M, Kaasa S. Quality of life inadult cancer patients treated with bone marrowtransplantation––a review of the literature. Eur JCancer 1995;31A:163–73.
30 Swain SM, Rowland J, Weinfurt K, et al. Intensiveoutpatient adjuvant therapy for breast cancer: resultsof dose escalation and quality of life. J Clin Oncol1996;14:1565–72.
31 Hjermstad MJ, Evensen SA, Kvaloy SO, et al. Health-related quality of life 1 year after allogeneic or autolo-gous stem-cell transplantation: a prospective study. JClin Oncol 1999;17:706–18.
32 Peters WP, Ross M, Vredenburgh JJ, et al. High-dosechemotherapy and autologous bone marrow supportas consolidation after standard-dose adjuvant therapyfor high-risk primary breast cancer. J Clin Oncol1993;11:1132–43.
33 Wang-Clow F, Lange M, Laird NM, Ware JH. Asimulation study of estimators for rates of change in
QOL of High-Risk Breast Cancer Patients 717
longitudinal studies with attrition. Stat Med 1995;14:283–97.
34 Bottomley A, Biganzoli L, Cufer T, et al. Randomized,controlled trial investigating short-term health-relatedquality of life with doxorubicin and paclitaxel versusdoxorubicin and cyclophosphamide as first-line che-motherapy in patients with metastatic breast cancer:European Organization for Research and Treatmentof Cancer Breast Cancer Group, Investigational DrugBranch for Breast Cancer and the New Drug Devel-opment Group Study. J Clin Oncol 2004;22:2576–86.
35 Moinpour CM, Lyons B, Grevstad PK, et al. Qualityof life in advanced non-small-cell lung cancer: resultsof a Southwest Oncology Group randomized trial.Qual Life Res 2002;11:115–26.
36 Bordeleau L, Szalai JP, Ennis M, et al. Quality of lifein a randomized trial of group psychosocial support inmetastatic breast cancer: overall effects of the inter-vention and an exploration of missing data. J ClinOncol 2003;21:1944–51.
37 Ganz PA, Guadagnoli E, Landrum MB, et al. Breastcancer in older women: quality of life and psychoso-cial adjustment in the 15 months after diagnosis. JClin Oncol 2003;21:4027–33.
38 Bernhard J, Cella DF, Coates AS, et al. Missingquality of life data in cancer clinical trials: seriousproblems and challenges. Stat Med 1998;17:517–32.
39 Fayers P, Machin D. Quality of Life: Assessment,Analysis and Interpretation. Chichester: Wiley, 2000.
40 Fairclough D. Design and Analysis of Quality of Lifein Clinical Trials. New York: Chapman & Hall/CRC,2002.
41 Fairclough D, Gagnon D, Zagari M. Evaluation ofquality of life in a clinical trial with nonrandomdropout: the effect of epoetin in anemic cancerpatients. Qual Life Res 2003;12:1013–27.
42 Norman GR, Sloan JA, Wyrwich KW. Interpretationof changes in health-related quality of life: the remark-able universality of half a standard deviation. MedCare 2003;41:582–92.
43 Osoba D, Bezjak A, Brundage M, et al. Analysis andinterpretation of health-related quality-of-life datafrom clinical trials: basic approach of The NationalCancer Institute of Canada Clinical Trials Group. EurJ Cancer 2005;41:280–7.
44 Andrykowski MA, Greiner CB, Altmaier EM, et al.Quality of life following bone marrow transplanta-tion: findings from a multicentre study. Bri J Cancer1995;71:1322–9.
45 Rugo HS, Ahles T. The impact of adjuvant therapy forbreast cancer on cognitive function: current evidenceand directions for research. Semin Oncol 2003;30:749–62.
46 O’Shaughnessy J. Chemotherapy-related cognitivedysfunction in breast cancer. Semin Oncol Nurs 2003;19(Suppl. 2):S17–24.
47 Cella DF, Mahon SM, Donovan MI. Cancer recur-rence as a traumatic event. Behav Med 1990;16:15–22.
48 Jenkins PL, May VE, Hughes LE. Psychological mor-bidity associated with local recurrence of breastcancer. Int J Psychiatry Med 1991;21:149–55.
49 Bull AA, Meyerowitz BE, Hart S, et al. Quality of lifein women with recurrent breast cancer. Breast CancerRes Treat 1999;54:47–57.
718 Marino et al.