
Demographic and socioeconomic links to cigarette smoking
23
This article was downloaded by: [Charles B Nam] On: 06 February 2014, At: 13:00 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Biodemography and Social Biology Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/hsbi20 Demographic and socioeconomic links to cigarette smoking Richard G. Rogers a , Charles B. Nam b & Robert A. Hummer c a Department of Sociology and Population Program , University of Colorado , Boulder, Colorado, 80309 b Department of Sociology and Center for the Study of Population , Florida State University , Tallahassee, Florida, 32306 c Department of Sociology , Louisiana State University , Baton Rouge, Louisiana, 70803 Published online: 23 Aug 2010. To cite this article: Richard G. Rogers , Charles B. Nam & Robert A. Hummer (1995) Demographic and socioeconomic links to cigarette smoking, Biodemography and Social Biology, 42:1-2, 1-21, DOI: 10.1080/19485565.1995.9988884 To link to this article: http://dx.doi.org/10.1080/19485565.1995.9988884 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be
Transcript of Demographic and socioeconomic links to cigarette smoking
This article was downloaded by: [Charles B Nam]On: 06 February 2014, At: 13:00Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number:1072954 Registered office: Mortimer House, 37-41 Mortimer Street,London W1T 3JH, UK
Biodemography and SocialBiologyPublication details, including instructions forauthors and subscription information:http://www.tandfonline.com/loi/hsbi20
Demographic andsocioeconomic links tocigarette smokingRichard G. Rogers a , Charles B. Nam b & RobertA. Hummer ca Department of Sociology and PopulationProgram , University of Colorado , Boulder,Colorado, 80309b Department of Sociology and Center for theStudy of Population , Florida State University ,Tallahassee, Florida, 32306c Department of Sociology , Louisiana StateUniversity , Baton Rouge, Louisiana, 70803Published online: 23 Aug 2010.
To cite this article: Richard G. Rogers , Charles B. Nam & Robert A. Hummer(1995) Demographic and socioeconomic links to cigarette smoking, Biodemographyand Social Biology, 42:1-2, 1-21, DOI: 10.1080/19485565.1995.9988884
To link to this article: http://dx.doi.org/10.1080/19485565.1995.9988884
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of allthe information (the “Content”) contained in the publications on ourplatform. However, Taylor & Francis, our agents, and our licensorsmake no representations or warranties whatsoever as to the accuracy,completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views ofthe authors, and are not the views of or endorsed by Taylor & Francis.The accuracy of the Content should not be relied upon and should be

independently verified with primary sources of information. Taylor andFrancis shall not be liable for any losses, actions, claims, proceedings,demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, inrelation to or arising out of the use of the Content.
This article may be used for research, teaching, and private studypurposes. Any substantial or systematic reproduction, redistribution,reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of accessand use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4

Demographic and Socioeconomic Linksto Cigarette Smoking
aRichard G. Rogers, bCharles B. Nam, and cRobert A. Hummer
aDepartment of Sociology and Population Program, University of Colorado, Boulder,Colorado 80309; bDepartment of Sociology and Center for the Study of Population, FloridaState University, Tallahassee, Florida 32306; and cDepartment of Sociology, Louisiana StateUniversity, Baton Rouge, Louisiana 70803
ABSTRACT: This paper illuminates the demographic and socioeconomic factors associated withsmoking statuses. It employs the 1990 National Health Interview Survey's Health Promotion andDisease Prevention Supplement and logistic regression to examine the covariates of smokingstatus among the U.S. adult population. Polychotomous logistic regression, which provides analternate way to examine smoking practices, simultaneously considers multiple variables andtheir interactions, controls for other important covariates, produces predicted values and pat-terns, and allows multiple comparisons. By examining interactions, we have found that agedisplays distinct, often curvilinear, patterns with smoking; that compared to females, males havehigher rates of cigarette consumption except at the youngest ages; that Anglos, especially Anglomales, exhibit high probabilities of cigarette consumption but also high probabilities of beingformer smokers; that Black males exhibit high probabilities of light smoking, but only at the olderages, and that they also exhibit high probabilities of being former light smokers; and thatMexican-American females are the least likely to currently smoke or to have ever smoked. Byclearly elucidating the demographic and socioeconomic variations in smoking, arguably the mostsalient marker of health behavior, we can better target programs and policies geared toward thereduction of smoking-related diseases and deaths.
There is a vast literature on the fac-tors that influence smoking. Much ofthis literature, however, examines onlyone or two smoking statuses, and muchof it is aimed at how to bring aboutsmoking cessation (cf. Giovinno et al.,1992). Our research focuses on multi-ple smoking statuses and aims to de-termine the underlying demographicand socioeconomic factors related tosmoking status.
Our research on tobacco smokingtakes into account several broad cate-gories of demographic and socio-economic factors. The central demo-graphic characteristics—age, sex, race/ethnicity—are those that are ascribedto the individual and are generally notsubject to change. The prevalence ofsmoking is low at the youngest ages,
peaks at ages 25-44, and then declinesat older ages (CDC, 1993a). Comparedto women, men are more likely tosmoke and to smoke more cigarettesper day, but they are also more likelyto quit. Furthermore, smoking preva-lence has declined since 1965 for menand since the late 1970's for women(CDC, 1993b).
Compared to whites, blacks exhibithigher rates of smoking, but initiatesmoking at later ages and smoke fewercigarettes per day (CDC, 1991). Al-though blacks try as often as whites,they are less successful at quitting. Lowblack cessation rates may be attributedto a high nicotine dependence, inducedby menthol cigarettes, and revealedthrough high black "wake-up" smok-
1
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4

Rogers et al. Social Biology
minutes of awakening (see Novotny etal., 1988; Orleans et al., 1989; Royce etal., 1993). Compared to other groups,Mexican-Americans are much morelikely to have never smoked; if they dosmoke, they smoke small quantities ofcigarettes (Rogers, 1991).
Socioeconomic status refers to thosefactors that describe an individual's rel-ative social position in society. In pastresearch, the variables under this ru-bric have included aspects of educa-tion, occupation, income, and wealth.In the context of this research, socio-economic status reflects the package ofsocial and economic resources thatgive persons the ability to acquire andmaintain good health. Compared tothe upper and middle classes, the lowerclasses take longer to adapt to newhealth practices, if they adapt at all.In England, men in the highest socialclass have largely stopped smoking,but men in the lowest social class haveyet to change their smoking beha-vior significantly (Fox and Goldblatt,1986). In the United States, those withless education and lower incomes aremore likely to smoke and less likely toquit (Novotny et al., 1988; Orleans etal., 1989; CDC, 1993a). Indeed, whilecigarette advertising seems to be en-couraging more lower-class women .and minorities to smoke, more upper-class men are beginning to quit, or tosmoke less (Susser et al., 1985; Coveyet al., 1992).
Smoking habits represent the criti-cal broad category of our analysis andencompass a number of dimensions oftobacco smoking behavior. These be-haviors include whether persons haveever smoked, whether they stoppedsmoking if they once smoked, and,the amount of smoking for those whosmoked. Moreover, whereas most pre-
vious research has presented "aver-age" smoking characteristics, we illus-trate interactions by age, sex, and race,and mediated by socioeconomic char-acteristics. Thus, in this article, thecentral question we address is: Howare demographic and socioeconomicfactors related to smoking habits?
MATERIALS AND METHODS
We employ the 1990 NationalHealth Interview Survey, Health Pro-motion and Disease Prevention Sup-plement (HPDP), to examine the so-ciodemographic covariates of cigarettesmoking. NHIS data are derived froma household multistage sampling of thecivilian noninstitutional population ofthe United States through both clusterand stratified sampling techniques.The NHIS-HPDP is based on 41,104respondents aged 18 and over (NCHS,1993). In addition to smoking, theNHIS supplements asked respondentsabout other characteristics, includingdemographic factors and socioeco-nomic status.
Smoking categories follow the con-vention used by the Federal govern-ment: current smokers have smokedat least 100 cigarettes in their lifetimeand smoke at present; former smokershave smoked at least 100 cigarettesin the past but do not presentlysmoke; never smokers either havenever smoked at all or have smokedfewer than 100 cigarettes in their life-time. We have grouped current andformer smokers into light (fewer than20 cigarettes per day) and moderate-to-heavy smokers (20 or more).1
1Some studies have disaggregated current smok-ers into more categories, examining, say, light,moderate, and heavy smokers. Because of interac-tions with variables with low frequencies, particu-
2
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4
Vol. 42, No. 1-2 Cigarette Smoking
To measure ethnicity, we identi-fied three subpopulations: Mexican-Americans, Anglos, and Blacks. Re-spondents who identified themselvesas Mexican, Mexicano, Mexican-American, and Chicano were recordedas Mexican-American. Cubans, PuertoRicans, and the group "Other Hispan-ics" were excluded from the data setbecause they were too small to analyzeseparately and too diverse to combinewith Mexican-Americans. Anglos andBlacks were selected from amongthose who did not identify themselvesas Mexican-American.
We have included two measures ofsocioeconomic status: income and ed-ucation. Education was reported ascompleted years of schooling. A de-tailed question on family income wasasked, but 11 per cent of the respon-dents did not answer it. We insteaduse a broader question, which attaineda 98 per cent response rate, as towhether the person's family income is$20,000 or higher. Thus, our analysisis based on 37,282 Anglos, Blacks,and Mexican-Americans who providedincome, education, and smokinginformation.
To capture the smoking relation-ships within a multivariate framework,we perform polychotomous logistic re-gression analyses with the statisticalpackage BMDP (Dixon et al., 1988).2
larly with those involving ethnicity, we have re-tained the light and moderate-to-heavy smokingcategories. Few Mexican-American females smoke,especially at the higher levels of cigarette consump-tion.
2BMDP correctly calculates the coefficients forpolychotomous logistic regression, but does nottake into account NHIS-HPDP's complex samplingdesign in calculating the standard errors. On theother hand, SUDAAN correctly calculates the stan-dard errors from complex sample surveys for dichot-omous but not polychotomous logistic regression(see Shah et al., 1991). Therefore, to correctlyestimate the coefficients and the standard errors,
Polychotomous logistic regression,which provides an alternate way toexamine smoking practices, simulta-neously considers multiple variablesand their interactions, controls forother important covariates, producespredicted values and patterns, and al-lows multiple comparisons. In logisticregression, when the predictor variableX¡ changes by one unit, the corre-sponding B¡ coefficient indicates howmuch the log of the odds changes rel-ative to a baseline category (Knokeand Bohrnstedt, 1994).
In contrasting groups, we examinethe odds ratios. Odds ratios offer theadvantages of clear interpretation andvalues that do not vary even with shiftsin sample size or changes in the mar-ginal distributions (see Morgan andTeachman, 1988). To present the fig-ures, we examine the probabilities,which are calculated by:
Prob(event) = 1/(1 + e~z),
where
z = Bg + B^X^ + B2X2+ B3X3 + . . . + BnXn.
This procedure allows us to compare,say, the probabilities of never smokingand smoking low amounts of ciga-rettes, given certain characteristics,say, for young Mexican-American fe-males. In this way, we can demonstratehow smoking patterns vary by demo-graphic and socioeconomic factors.Note that the figures we present rep-resent predicted probabilities.
we used BMDP to calculate the coefficients, andSUDAAN for the standard errors. Because thestandard errors are calculated relative to specific co-efficients (Hosmer and Lemeshow, 1989), we havepresented the p-values but do not include standarderrors. GANSER LIBRARY
M!LLEÎÎÔV!LLE UNiVHtSITYM1LLERSVÍLLE.PA 17551
3
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4
Rogers et al. Social Biology
Interactions may take differentforms, so we define what we mean bythe presence and absence of interac-tions. If the association between oneindependent variable, say sex, and thedependent variable, smoking, is thesame within each level of another in-dependent variable, say age, thenthere is no interaction between age,sex, and smoking. If, however, the re-lationship between sex and smokingvaries by different ages, then an inter-action is present (see Hosmer andLemeshow, 1989).
RESULTS
COVARIATES OF SMOKING
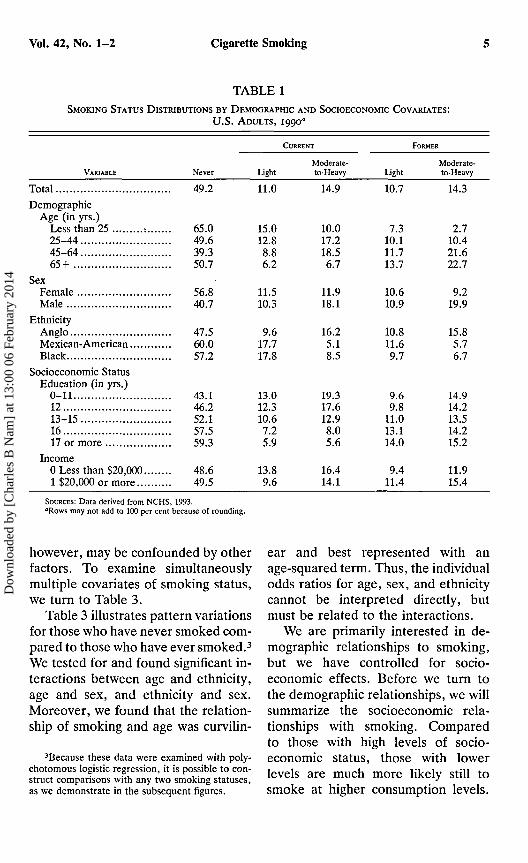
Table 1 shows the distribution ofsmoking habits by different factors.Each of the rows adds to 100 per cent.Thus, the first row shows that in1990 almost half of all adults havenever smoked, one-quarter continue tosmoke, and a similar proportion havequit. These results show curvilinear re-lations by age. For instance, there arehigh proportions of very young or oldnever smokers, but smaller propor-tions of never smokers in the middleyears. Among those young individualswho do smoke, most smoke few ciga-rettes. Few individuals younger than25 years of age are former smokersbecause there has been a limited timefor younger smokers to initiate andthen quit smoking. Compared to thoseyounger than 25, those 25-44 years ofage are less likely to have abstainedfrom smoking, are more likely to cur-rently smoke, and are substantiallymore likely to have quit. Those 65 andover are the most likely of all agegroups to have quit.
Compared to males, females aremore likely to have never startedsmoking, are more likely to smokesmall quantities of cigarettes currentlybut less likely to smoke large quanti-ties, and are as likely to have quitsmoking small numbers of cigarettesbut more likely to have quit smokinglarge numbers of cigarettes. Blacks andMexican-Americans are more likelythan Anglos to smoke a pack or less ofcigarettes a day, but Anglos are morelikely than other ethnic groups tosmoke larger quantities of cigarettes.
Generally, higher levels of educa-tion are associated with an increase inthe propensity of individuals to havenever smoked and, if a smoker, to havequit (see CDC, 1993a; Pierce et al.,1989). For example, 43 per cent ofthose with 11 or fewer years of educa-tion have never smoked, compared to59 per cent of those with 17 or moreyears of schooling. Smoking differ-ences by income are slight, but suggestthat individuals with higher incomesare more likely to have never smokedand, if they ever smoked, to have quit(see also CDC, 1993a).
Table 2 shows the number of ciga-rettes consumed for current andformer smokers. Overall, current andformer smokers average a pack of cig-arettes a day, with former smokershaving smoked slightly more. Gener-ally, those 45-64 years of age, males,Anglos, and less-educated individualssmoke or smoked more cigarettes thantheir counterparts. For instance, thereis a large sex gap for current andformer smokers, but especially forformer smokers. Males who formerlysmoked average almost seven ciga-rettes more than similar females. Therelationships in this table and Table 1,
4
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4
Vol. 42, No. 1-2 Cigarette Smoking
TABLE 1
SMOKING STATUS DISTRIBUTIONS BY DEMOGRAPHIC AND SOCIOECONOMIC COVARIATES:
U.S. ADULTS, 1990a
CURRENT
VARIABLE Never
Total 49.2Demographic
Age (in yrs.)Less than 25 : 65.025-44 49.645-64 39.365+ 50.7
SexFemale 56.8Male 40.7
EthnicityAnglo 47.5Mexican-American 60.0Black 57.2
Socioeconomic StatusEducation (in yrs.)
0-11 43.112 46.213-15 52.116 57.517 or more 59.3
Income0 Less than $20,000 48.61 $20,000 or more 49.5
SOURCES: Data derived from NCHS, 1993."Rows may not add to 100 per cent because of rounding.
LightModerate-to-Heavy
FORMER
LightModerate-to-Heavy
11.0 14.9 10.7 14.3
15.012.88.86.2
11.510.3
9.617.717.8
13.012.310.67.25.9
13.89.6
10.017.218.56.7
11.918.1
16.25.18.5
19.317.612.98.05.6
16.414.1
7.310.111.713.7
10.610.9
10.811.69.7
9.69.8
11.013.114.0
9.411.4
2.710.421.622.7
9.219.9
15.85.76.7
14.914.213.514.215.2
11.915.4
however, may be confounded by otherfactors. To examine simultaneouslymultiple covariates of smoking status,we turn to Table 3.
Table 3 illustrates pattern variationsfor those who have never smoked com-pared to those who have ever smoked.3
We tested for and found significant in-teractions between age and ethnicity,age and sex, and ethnicity and sex.Moreover, we found that the relation-ship of smoking and age was curvilin-
3Because these data were examined with poly-chotomous logistic regression, it is possible to con-struct comparisons with any two smoking statuses,as we demonstrate in the subsequent figures.
ear and best represented with anage-squared term. Thus, the individualodds ratios for age, sex, and ethnicitycannot be interpreted directly, butmust be related to the interactions.
We are primarily interested in de-mographic relationships to smoking,but we have controlled for socio-economic effects. Before we turn tothe demographic relationships, we willsummarize the socioeconomic rela-tionships with smoking. Comparedto those with high levels of socio-economic status, those with lowerlevels are much more likely still tosmoke at higher consumption levels.
s
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4

Rogers et al. Social Biology
TABLE 2AVERAGE NUMBER OF CIGARETTES SMOKED FOR CURRENT AND FORMER SMOKERS BY DEMOGRAPHIC
AND SOCIOECONOMIC COVARIATES, U.S. ADULTS, 1990
Variable Current Former
Total 19.0 21.9Demographic
Age (in yrs).Less than 25 14.6 13.525-44 19.0 19.445-64 21.4 24.665+ 17.4 23.3
SexFemale 17.0 17.9Male 20.7 24.7
EthnicityAnglo 20.2 22.6Mexican-American 10.2 15.2Black 13.1 16.0
Socioeconomic StatusEducation (in yrs.)
0-11 19.2 23.112 19.2 22.613-15 18.5 21.016 18.2 20.617 or more 16.9 20.2
Income0 Less than $20,000 18.3 21.61 $20,000 or more 19.4 22.0
SOURCES: data derived from NCHS, 1993.
An additional year of education in-creases the odds of never smokingrather than current moderate smokingby one-quarter. Similar results occurfor income: compared to never smok-ers, individuals with low income areover 30 per cent more likely to smokecurrently than individuals with highincome. Generally, healthy practicesprogress from the higher to the lowersocioeconomic statuses (see Novotnyet al., 1988; Orleans et al., 1989).
DEMOGRAPHIC INTERACTIONS WITHCIGARETTE SMOKING
Table 3 also illustrates interactionsamong age, sex, ethnicity, and smok-ing, which suggests that the demo-
graphic relationships with smoking arecomplex. Because three two-way inter-actions are difficult to see and inter-pret, we display four figures. The firstfigure presents the probabilities of agearid sex interactions, controlling forother covariates; the second, age andethnicity interactions; the third, sexand ethnicity interactions; and thefourth figure, the predicted probabili-ties of smoking based on the three two-way interactions. The probabilities arecalculated for different age, sex, andethnic groups, holding the other cova-riates constant at their means. For ex-ample, in the first figure, we examinemales and females by age and smokingstatus, but (using the sample mean
6
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4

TABLE 3POLYCHOTOMOUS LOGISTIC REGRESSION COEFFICIENTS OF CIGARETTE SMOKING STATUS, DEMOGRAPHIC
AND SOCIOECONOMIC COVARIATES: U . S . ADULTS, I99O
£
2;oA. CURRENT
LIGHT
B. CURRENT
MODERA TE-TO-HEAVY
C. FORMER
LIGHT
VARIABLES
Age, sex, and ethnicityAgeAge2
SexAngloMexican-AmericanBlack
InteractionsAge by sexAge2 by sexAge by Mexican-AmericanAge2 by Mexican-AmericanAge by BlackAge2 by BlackSex by Mexican-AmericanSex by Black
SocioeconomicEducationHigh incomeIntercept
SOURCE: Data derived from NCHS, 1993.»PsO.OOl.
Compared to Never Smoker
D. FORMER
MODERATE-TO-HEAVY
0.154»-0.022»-0.374*
ref-0.587-1.511e
0.0780.0020.368*
-0.025*0.533
-0.0371.0030.493
-0.162»-0.333
0.796
0.901"0.077»0.102ref
2.211»2.594»
0.102e
0.0022.2850.034d
0.338*0.023*0.886*0.670»
0.301»0.398»0.794»
0.197»-0.013»-0.288d
ref-1 .101 e
-2.123»
0.0520.0060.261d
-0.0170.602»
-0.041»0.5980.245
-0.0160.113*
-2.060»
0.752»0.050»0.291ref
2.289e
1.651*
0.199*0.0010.1880.0080.1470.0100.525d
0.382*
0.108»0.138»2.722»
n¡gai
1rexnaoE
03
'PsO.Ol.'PsO.lO.
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4

Rogers et al. Social Biology
values) hold constant ethnic and so-cioeconomic characteristics. In thesecond figure, we examine Mexican-Americans, Blacks, and Anglos by ageand smoking status, but hold constantsex and socioeconomic factors.4
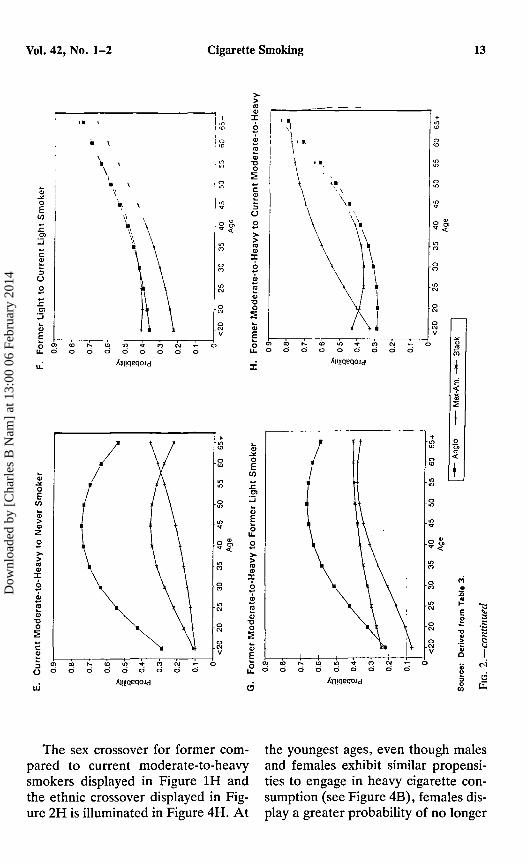
Age and Sex. —To understand howsmoking varies by age and sex, Figure1 presents the probabilities calculatedfrom Table 3.5 We present eight ofthe ten combinations.6 The first fourpanels contrast different ever smokersto never smokers. Figure IE comparestwo groups of current smokers whoconsume different amounts of tobacco.Figure IG provides a similar contrast,but for former smokers. And FiguresIF and 1H each contrast subgroupsthat currently smoke to others thathave quit. Therefore, unlike smokingprevalence rates or quit rates, whichcompare, say, former smokers to eversmokers, these figures provide moredetail, comparing the probabilities thatindividuals will be in one category oranother, say, former light or currentlight smokers. As Figure 1 demon-strates, such contrasts reveal patternsunexposed by prevalence or quit rates.
Smoking varies by age, with a dis-tinct curvilinear pattern for ever smok-ers. In Figures 1A, IB, and IE, the
4The sample means were 0.47 for sex, 0.05 forMexican-Americans, 0.11 for Blacks, 12.97 for ed-ucation, 0.67 for incomes of $20,000 or more, 6.17for age, 48.17 for age2, 2.86 for age by sex, 21.85 forage2 by sex, 0.22 for age by Mexican-American,0.64 for age by Black, 1.37 for age2 by Mexican-American, and 4.73 for age2 by Black. Age is codedin 5-year age intervals from age 1 (less than 20 yearsof age) to 11 (age 65 and above).
5Except for the age extremes, age is presented inthe figures as the initial age of the 5-year interval.
6We do not present current light to formermoderate-to-heavy smokers or current moderate-to-heavy to former light smokers because these twocombinations do not compare subpopulations thatare in similar categories.
probabilities of ever smoking beginlow in young years, peak in the middleyears, and taper to low levels at olderyears. For example, in Figure 1A, theprobability that males are current lightsmokers rather than never smokers islow at the youngest ages, peaks atages 40-44, and declines from ages 45on. Former smokers, especially formerlight smokers, display a more linearpattern. Figures 1C and IF indicatethat older individuals are more likelythan younger individuals to have quit,and that the probability of being aformer light smoker instead of a neversmoker or current light smoker is high-est for the oldest ages.
Several sex differences emerge fromthese figures. First, males generallyexhibit higher probabilities than fe-males of smoking and of smokinglarger quantities (see Figures 1A, IB,and IE). But these higher probabilitiesare partially offset by the greater prob-abilities males show for having quitsmoking, especially at higher levels ofcigarette consumption (see Figures 1C,ID, and IG).
Third, the peaks for smoking sta-tuses vary by sex, with females peakingat earlier ages than males (see Ernster1993). For example, the peak for cur-rent moderate smokers is at ages 45-49for males, but five years earlier for fe-males. A fourth and interrelated find-ing is that, between the sexes, thereare several age crossovers. Figure 1Ashows that, relative to never smokers,young females are more likely thanyoung males to smoke less than a packof cigarettes a day. These figures, then,help reveal the interrelations amongage, sex, and smoking statuses.
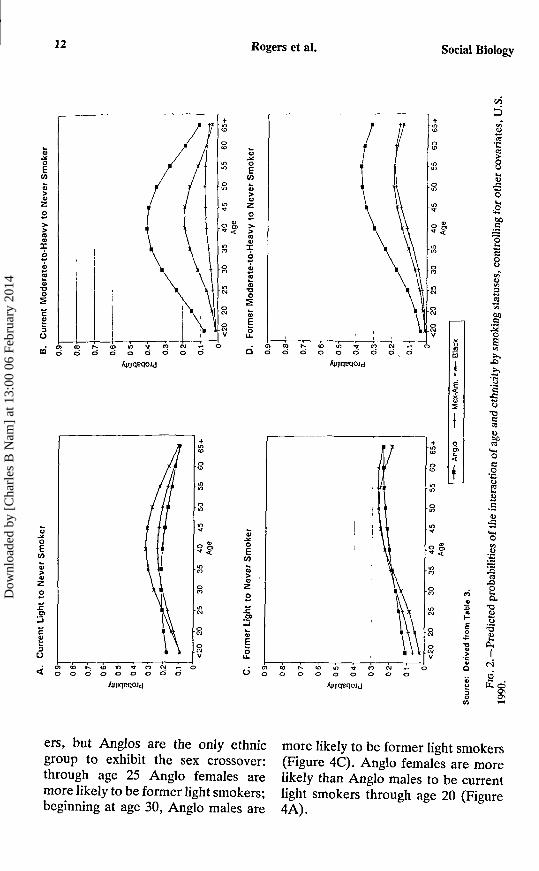
Age and Ethnicity.—Figure 2 pre-sents age and ethnicity interactions by
8
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4

Vol. 42, No. 1-2 Cigarette Smoking
smoking status. Again, observe thegeneral curvilinear relations with age.In most figures, Mexican-Americansand Blacks display similar patterns,but with a few unique deviations byMexican-Americans. For example,while Anglos and Blacks displaycurvilinear relations between currentmoderate-to-heavy and light smoking,Mexican-Americans exhibit a lineargradation. The probability of being acurrent moderate-to-heavy relativeto current light smoker peaks at age45 and then declines for Anglos andBlacks, but continues to increasethrough the oldest ages for Mexican-Americans. And whereas the proba-bility of being a former smoker, ra-ther than current moderate-to-heavysmoker, is low at the youngest agesand increases slowly until the oldestages, the probabilities for Mexican-Americans are more progressive.Compared to never smokers, Blackswho smoke are more likely than othergroups to smoke less than a pack ofcigarettes a day (see Rogers andCrank, 1988). Anglos continue to ex-hibit the highest levels of moderate-to-heavy smoking, but also exhibit thegreatest chances of quitting atmoderate-to-heavy levels (see Figures2B, 2D, 2E, and 2G).
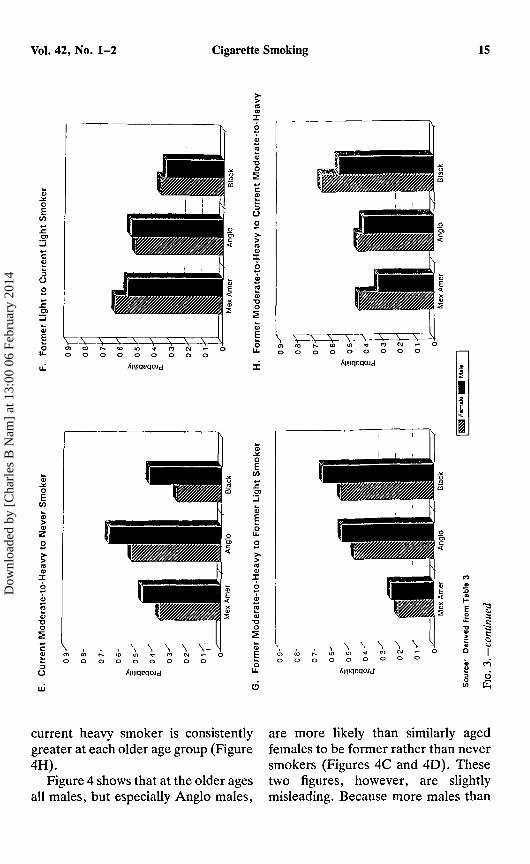
Sex and Ethnicity. —Figure 3 revealsinteractions between sex, ethnicity,and smoking. Males are generallymore likely than females to have eversmoked, especially at higher levels ofconsumption. But compared to neversmokers, the probability of being alight smoker is greater for Anglo fe-males than males. Usually, Anglofemales are more likely than Blackfemales, who are more likely thanMexican-American females, to have
ever smoked. The exception is Blackfemale current light smokers. Anglomales are more likely than othermales to be current moderate-to-heavysmokers or to have quit moderatesmoking.
SMOKING PREDICTIONS BASED ONTHREE TWO-WAY INTERACTIONS
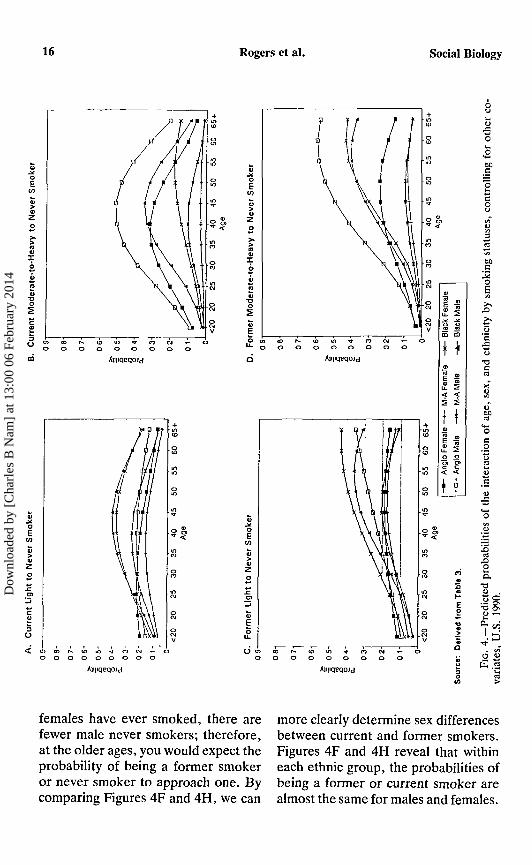
Figure 4 portrays the predictedprobabilities of smoking based on thethree two-way interactions of age, sex,and ethnicity on cigarette smokingas calculated from Table 3. Buildingon the previous figures, we can discernseveral patterns. Figure 2 showedhigher rates of current light smokingfor Blacks than other ethnic groups.Figure 4A shows an interaction amongethnicity, sex, age, and smoking. Blackmales and females exhibit higher ratesof light smoking than their Anglo maleand female counterparts, but only inthe middle years. For example, com-pared to Anglo females, Black femalesare less likely to be current light thannever smokers below age 25 and atages 65 and above (Figure 4A). Butyoung Anglo females are twice aslikely as Black females to be currentlight than never smokers (see alsoGeronimus et al., 1993). Nevertheless,Black middle-aged males are by farthe most likely groups to smoke lessthan a pack of cigarettes a day. Thechances of a 45-49 year old Black malebeing a current light rather than neversmoker is 1 in 2.5; the similar proba-bility for Mexican-American females isjust 1 in 7.
Generally, current moderate-to-heavy smokers are more likely to bemale than female (see Figure 1) andAnglo rather than Mexican-American
9
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4

10 Rogers et al. Social Biology
d
/imqeqoJd
aZO
i ]
• Í
1\
C/5
3
O
T3Cta
!CL
•a
I
or Black (see Figure 2). Indeed, Anglomales consistently exhibit the highestrates of current moderate-to-heavysmoking (see Figures 4B and 4E). An-glo females are more likely than all
sex and ethnic groups, save Anglomales, to be current moderate-to-heavy smokers through age 35 (Figure4B); beginning at age 40, the probabil-ities that Anglo females will be current
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4

Vol. 42, No. 1-2 Cigarette Smoking 11
3O
E05
•ao
cQ> V "
t odui
Xó
O
3O
Ió
•oo
E
I¿
AllüqeqoJd00
moderate-to-heavy smokers quickly and than Mexican-American males un-diminishes. Anglo females are more til age 55.likely to be current moderate-to-heavy Figure 1 identified sex crossovers bysmokers than Black males until age 40 age for current and former light smok-
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4
12 Rogers et al. Social
+to
oCD
mm
o
m*r
o g»* <mCO
Biology
c/SD»,te
sar
i
>8U
0
t260
Olli
ntr
8
oEco
zo
60
co
mCO
oCM
O
V
ri
S
o
rive
d i
O
ities
*J3
prob
•edi
cted
1
ers, but Anglos are the only ethnie more likely to be former light smokersgroup to exhibit the sex crossover: (Figure 4C). Anglo females are morethrough age 25 Anglo females are likely than Anglo males to be currentmore likely to be former light smokers; light smokers through age 20 (Figurebeginning at age 30, Anglo males are 4A).
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4
Vol. 42, No. 1-2 Cigarette Smoking 13
AllliqeqoJd
The sex crossover for former com-pared to current moderate-to-heavysmokers displayed in Figure 1H andthe ethnic crossover displayed in Fig-ure 2H is illuminated in Figure 4H. At
the youngest ages, even though malesand females exhibit similar propensi-ties to engage in heavy cigarette con-sumption (see Figure 4B), females dis-play a greater probability of no longer
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4

14 Rogers et al. Social Biology
i6
• o
m
E10
zo
AllliqeqoJd
zo
0)J £O
E
>ZO
O)
•mer
£
i'i | UHR
i
11n_\—\_A—^—-N—-
•a
caJDOex-a%'•5&,I
smoking rather than smoking at highconsumption levels (Figure 4H). Atthe older ages, however, males aremore likely than their ethnic counter-parts to be former rather than current
moderate-to-heavy smokers (Figure4H). Mexican-American males andfemales distinguish themselves as theonly two groups in which the proba-bilities of being a former rather than
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4
Vol. 42, No. 1-2 Cigarette Smoking 15
0)j e
: Sm
o
c
do
.cJ
rmer
s. \ \ \en co r
EH
fmmXwtMxk
\ \ \S fS í-i r
:
BÊJÊHHHÊÊÊÊÊ
M M •JaiH|HH|
ÍÜÜ! Lj I
\ \ \ \r o-i ei
CJ i- C
V
j eO
m
o
5
-£
IX2
IÓ
)te
-
o5
csco
>
nav
X
óa
nai•o
oS
Fo
rmer
oZo
•
•oo
3ü
o> to i*.
i«
\ •. s \ \ N N
H
AltliqeqoJd
1
o
current heavy smoker is consistently are more likely than similarly agedgreater at each older age group (Figure females to be former rather than never4H). smokers (Figures 4C and 4D). These
Figure 4 shows that at the older ages two figures, however, are slightlyall males, but especially Anglo males, misleading. Because more males than
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4
16 Rogers et al. Social Biology
A|i|iqcqoJd
to r-~ w o oj . -
:k F
em
ale
~1
*«-
Bla
c
i
CD
CO
A F
ern
t(D
3o F
en-
î:k
Male
1
*-
Bla
c
i
w
to
Ï
ID
C'Sio
i-a
. CA
ü o
tC 2
females have ever smoked, there arefewer male never smokers; therefore,at the older ages, you would expect theprobability of being a former smokeror never smoker to approach one. Bycomparing Figures 4F and 4H, we can
more clearly determine sex differencesbetween current and former smokers.Figures 4F and 4H reveal that withineach ethnic group, the probabilities ofbeing a former or current smoker arealmost the same for males and females.
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4

Vol. 42, No. 1-2 Cigarette Smoking 17
to
Oo
AlüiqeqoJd
o
1/5
có ÔJ ^ o ó c\j ~̂
AlüiqeqOJd
8
03
U.
Ü
roCÛ
<l
«3
EQ)
U_
«Í
S
t<D
E<D
U .
OCTc<
île
o
CD
+
<t
s!,
1o0)<
3ü
O Ö
Anglo and Black males have greater greater probability than males of beingprobabilities than comparable females a former rather than current lightof being a former light smoker. But smoker at every age. And Mexican-Mexican-American females exhibit a American females exhibit a greater
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4
18 Rogers et al. Social Biology
probability than males of being aformer rather than current moderate-to-heavy smoker at all but the oldestages.
Royce et al. (1993) reported thatBlacks were motivated but often un-successful at quitting smoking. Figures1C and ID illustrate that Blacks, espe-cially older males, succeed in quitting.Because Blacks begin smoking at olderages, relatively few young Black malesare at risk of quitting. At older ages,however, more Blacks smoke and aretherefore at risk of quitting; many doquit. Thus, detailed smoking distribu-tions by age and race clarify otherwiseparadoxical findings.
One pervasive finding is thatMexican-American females are themost likely among sex-ethnic combina-tions to be never smokers. Therefore,we find pronounced differences inthe odds ratios between Mexican-American females and groups who ex-hibit a high propensity to smoke. Forexample, compared to similarly agedMexican-American females, Blackmales aged 45-49 are about 4 timesmore likely to be current light smokersrather than never smokers; Anglo fe-males aged 40-44 are 15 times morelikely to be current moderate-to-heavyrather than never smokers; Mexican-American males aged 65 and over are5 times more likely to be former lightthan never smokers; and Anglo malesaged 55-59 are 17 times more likely tobe former moderate-to-heavy thannever smokers.
CONCLUSION
Demographic and socioeconomicvariables influence the odds of a personbeing a never smoker, current smoker,or former smoker. Past research has
established the consequences of smok-ing tobacco for the deterioration of aperson's health and increased chancesof dying prematurely (see Elo andPreston, 1992; Rogers and Powell-Griner, 1991). Because the deleteriouslong latency influences of smoking usu-ally affect individuals most when theyare at adult ages, smoking is a criticalbehavior for the maintenance of healthand long life for adults. Indeed, smok-ing may contribute to leukemia, pepticulcer disease, diabetes, and declines inbone density, and is clearly implicatedin its association with respiratory dis-eases, circulatory diseases, and can-cer, especially lung cancer (see CDC,19936; Nam et al., 1994; Rimm et al.,1993; Rowe and Kahn, 1987). There-fore, better understanding of the socialand demographic factors that influencesmoking behavior could result in im-proved ways to encourage individualsto abstain from smoking, to reducetheir smoking, or to quit, and there-by reduce morbid conditions, chronicdiseases, and disability.
We have uncovered several smokingpatterns by age and sex. Generally, ageis curvilinearly related to smoking,such that the probability of being anever smoker is highest at the age ex-tremes. At the youngest ages, beforeindividuals are initiated into smoking,there are a large number of neversmokers. Thus, to maintain a high pro-portion of never smokers requires thatsocial and public health programs pre-vent youths from ever becoming fullinitiates. At the older ages, three sep-arate phenomena may produce a largeproportion of never smokers. First,since smoking practices have changedover time, older individuals may rep-resent a cohort who never startedsmoking. Individuals aged 50 and over
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4

Vol. 42, No. 1-2 Cigarette Smoking 19
would have been adolescents, the agegroup at highest risk of smoking initi-ation, before cigarette consumptionreached its peak, in 1963 (Ravenholt1990). Second, older individuals whosmoked briefly or in the distant pastmay consider themselves never smok-ers even though they do have a pastsmoking history. Third, since eversmokers have higher mortality thannever smokers, this higher mortalitymay selectively kill smokers leavingnever smokers at the older ages. Mostlikely the three explanations combineto account for the high proportion ofnever smokers, with the first explana-tion the most salient.
At younger ages, females are aslikely as males to consume high num-bers of cigarettes and more likely toconsume low to moderate numbers ofcigarettes. Thus, at the younger ages,females are not only paralleling butare exceeding male smoking habits.Fortunately, young females exhibithigh probabilities of quitting. If fe-males exhibited low rates of smokingand high rates of quitting, we would ex-pect that subsequent lung cancer diag-nosis and mortality attributed to ciga-rettes would be substantially lowerthan, rather than close to, male rates.
There are interactions by sex andethnicity. Generally, never smokersare more likely to be female andMexican-American; current moderate-to-heavy smokers are more likely tobe male and Anglo (see also Fiore etal., 1989). Thus, we can expect thelargest differences between Mexican-American females and Anglo males. Infact, compared to Mexican-Americanfemales aged 45-49, Anglo males atsimilar ages are 33 times more likely tobe moderate-to-heavy smokers ratherthan never smokers. This suggests that
there are substantial differences insmoking by age, sex, and ethnicity thatmust be recognized in any publichealth or policy decisions.
Several studies reported high Blackmotivation but low success in smokingcessation (see Orleans et al., 1989;Royce et al., 1993). Others have notedthat education moderates the race ef-fects in smoking: "Education is nega-tively related to age of smoking onset,amount smoked, and perceived diffi-culties quitting; it is positively relatedto plans to quit, beliefs that smokingis related to lung cancer and thatlung cancer would have serious con-sequences" (Manfredi et al., 1992, p.268). We have shown that many Blackssuccessfully quit smoking, especially atolder ages. Thus, age and educationadjustments clarify Black smoking pat-terns. Nevertheless, continued anti-smoking programs are warranted, par-ticularly for the poor. For example,Lacey et al. (1993) recommend thatprograms deal with the root causes ofsmoking, including, for example, theunique stress, isolation, and limited so-cial and economic resources apparentin public housing.
Like most previous studies, we haveexamined smokers at one point in timeto compare one smoking status to an-other. These relations illustrate howsmoking is affected by demographicvariables and other covariâtes, but wehave not been able to compare smok-ing transitions. Such comparisons,which require longitudinal data, arewarranted for future research andcould show, for instance, the quit ratesfor people at different consumptionlevels.
These results can inform healthplanners and policy makers. Policy de-cisions and health care strategies can
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4

20 Rogers et al. Social Biology
be effective at the individual or struc-tural levels.
For examples, policies can influenceindividual health behaviors, but aremediated by demographic characteris-tics—age, sex, race, and ethnicity—and also by major social institutions-family, school, and work. Individualsmoking choices are often based onpeer norms, whether family memberssmoke, and larger social norms andvalues.
Structural forces can promote posi-tive individual health behavior: theAmerican Cancer Society and theAmerican Heart Association can spon-sor such programs as the Great Amer-ican Smokeout; federal, state, and lo-cal governments can legislate smokingpractices; schools can teach smokingprevention curricula; businesses canenact policies to prevent smoking; themedia can promote anti-smoking cam-paigns; and health care providers canadvise smokers to quit (see CDC,1993c; DHHS, 1991; Shopland, 1993).Such programs help, but are dwarfed
by the advertising and influence of thetobacco industry (Davis, 1987; Barry,1991).
Ultimately, then, individuals them-selves must opt for healthy lifestylesfree of cigarettes. This article hasfurther elucidated both the complexnature and patterned responses tosmoking. By clearly elucidating thedemographic and socioeconomic vari-ations in smoking, arguably the mostsalient marker of health behavior,we can better target programs and pol-icies geared toward the reduction ofsmoking-related diseases and deaths.
ACKNOWLEDGMENTS
This research was supported in part byNational Institute on Aging grant No. 1R01AG10113-01A2. An earlier version of thispaper was presented at the annual meetingsof the Southern Demographic Associationheld October 21-23,1993, in New Orleans,LA. The authors are grateful for statisticaladvice from Jay Teachman, research assis-tance from Jacqueline Carrigan, and wordprocessing from Susan Spika.
REFERENCES
BARRY, MICHELLE. 1991. The influence of theU.S. tobacco industry on the health, econ-omy, and environment of developing coun-tries. New Eng. J. Med. 324(13):917-919.
CENTERS FOR DISEASE CONTROL. 1993a. Cigarettesmoking among adults—United States, 1991.Morbid. Mortal. Wkly. Rep. 42(12):230-233.
_____. 1993b. Cigarette smoking—Attributablemortality and years of potential life lost-United States, 1990. Morbid. Mortal. Wkly.Rep. 42(33):645-649.
_____. 1993c. The Great American Smokeout,November 18, 1993. Morbid. Mortal. Wkly.Rep. 42(44):853.
_____. 1991. Differences in the age of smokinginitiation between blacks and whites—United States. Morbid. Mortal. Wkly. Rep.40:754-757.
COVEY, LIRIO S., EDITH A. ZANG, and ERNST L.WYNDER. 1992. Cigarette smoking and occu-
pational status: 1977 to 1990. Amer. J. Publ.Hlth. 82(9):1230-1234.
DAVIS, RONALD M. 1987. Current trends in cig-arette advertising and marketing. New Eng.J. Med. 316(12):725-732.
DIXON, W. J., M. B. BROWN, L. ENGELMAN,M. A. HILL, and R. I. JENNRICH. 1988.BMDP statistical software manual. Volume2. Univ. of California Press, Los Angeles,CA.
ELO, IRMA T., and SAMUEL H. PRESTON. 1992.Effects of early-life conditions on adult mor-tality: A review. Pop. Index 58(2):186-212.
ERNSTER, VIRGINIA L. 1993. Women and smok-ing. Amer. J. Pub. Hlth. 83(9):1202-1204.
FIORE, M. C., T. E. NOVOTNY, J. P. PIERCE, E. J.HATZIANDREU, K. M. PATEL, and R. M.DAVIS. 1989. Trends in cigarette smokingin the United States: The changing influenceof gender and race. J. Amer. Med. Assoc.261:49-55.
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4
Vol. 42, No. 1-2 Cigarette Smoking 21
Fox, JOHN, and PETER GOLDBLATT. 1986. Haveinequalities in health widened? A prelimi-nary study of recent changes in social classdifferences in male mortality. In Spcioeco-nomic differential mortality. InternationalSeminar on the Socio-Economic Aspects ofDifferential Mortality. Statistical PublishingHouse, Hungary.
GERONIMUS, ARLINE T., LISA J. NEIDERT, andJOHN BOUND. 1993. Age patterns of smokingin U.S. black and white women of child-bearing age. Amer. J. Pub. Hlth. 83(9):1258-1264.
GIOVINNO, GARY A., MICHAEL P. ERIKSEN, andJEFFREY W. MCKENNA. 1992. The vital diver-sity of tobacco control research. Amer. J.Publ. Hlth. 82(9):1203-1205.
HOSMER, DAVID W., and STANLEY LEMESHOW.1989. Applied logistic regression. John Wileyand Sons, NY.
KNOKE, DAVID, and GEORGE W. BOHRNSTEDT.1994. Statistics for social data analysis. 3rded. F. E. Peacock Publishers, Itasca, IL.
LACEY, LORETTA P., CLARA MANFREDI, GEORGEBALCH, RICHARD B. WARNECKE, KARENALLEN, and CONSTANCE EDWARDS. 1993. So-cial support in smoking cessation amongblack women in Chicago public housing. Pub.Hlth. Rep. 108(3):387-394.
MANFREDI, CLARA, LORETTA LACEY, RICHARDWARNECKE, and MARIANNE BUIS. 1992.Smoking-related behavior, beliefs, and socialenvironment of young black women in sub-sidized public housing in Chicago. Amer. J.Publ. Hlth. 82(2):267-272.
MORGAN, S. PHILIP, and JAY D. TEACHMAN.1988. Logistic regression: Descriptions, ex-amples, and comparisons. J. Marr. Fam.50(4):929-936.
NAM, CHARLES B., ROBERT A. HUMMER, andRICHARD G. ROGERS. 1993. Underlying andmultiple cases of death related to smoking.Pop. Res. Pol. Rev. 13(3):305-326.
NATIONAL CENTER FOR HEALTH STATISTICS. 1993.National Health Interview Survey, 1990:Health promotion and disease preventionsupplement. Public Use Sample, documenta-tion, and codebook. NCHS, Hyattsville,MD.
NOVOTNY, THOMAS E., KENNETH E. WARNER,JULIETTE S. KENDRICK, and PATRICK L. REM-INGTON. 1988. Smoking by blacks and whites:Socioeconomic and demographic differ-ences. Amer. J. Pub. Hlth. 78(9):1187-1189.
ORLEANS, CAROLE TRACY, VICTOR J. SCHOEN-
BACH, MARY ANNE SALMON, VICTOR J.STRECHER, WILLIAM KALSBEEK, DANAQUADE, EDWARD F. BROOKS, ROBERT KON-RAD, CHARLES BLACKMON, and CHARLES D.WATTS. 1989. A survey of smoking and quit-ting patterns among black Americans. Amer.J. Pub. Hlth. 79(2):176-181.
PIERCE, J. P., M. C. FIORE, T. E. NOVOTNY, E. J.HATZIANDREU, and R. M. DAVIS. 1989.Trends in cigarette smoking in the UnitedStates: Educational differences are increas-ing. J. Amer. Med. Assoc. 261:56-60.
RAVENHOLT, R. T. 1990. Tobacco's global deathmarch. Pop. Develop. Rev. 16(2):213-240.
RIMM, ERIC B., JOANN E. MANSON, MEIR J.STAMPFER, GRAHAM A. COLDITZ, WALTER C.WILLETT, BERNARD ROSNER, CHARLES H.HENNEKENS, and FRANK E. SPEIZER. 1993.Cigarette smoking and the risk of diabetes inwomen. Amer. J. Pub. Hlth. 83(2):211-219.
ROGERS, RICHARD G. 1991. Demographic char-acteristics of cigarette smokers in the UnitedStates. Soc. Biol. 38(1-2):1-12.
ROGERS, RICHARD G., and JOHN P. CRANK. 1988.Ethnic differences in smoking patterns:Findings from NHIS. Pub. Hlth. Rep.103(4):387-393.
ROGERS, RICHARD G., and EVE POWELL-GRINER.1991. Life expectancies of cigarette smokersand non-smokers in the United States. Soc.Sci. Med. 32(10):1151-1159.
ROWE, JOHN W., and ROBERT L. KAHN. 1987.Human aging: Usual and successful. Science237:143-149.
ROYCE, JACQUELINE M., NORMAN HYMOWITZ,KITTY COBETT, TYLER D. HARTWELL, andMARIO A. ORLANDI. 1993. Smoking cessationfactors among African Americans andwhites. Amer. J. Publ. Hlth. 82(2):220-226.
SHAH, BABUBHAI V., BETH G. BARNWELL, P. Ni-LEEN HUNT, and LISA M. LAVANGE. 1991.SUDAAN user's manual. Research TriangleInstitute, Research Triangle Park, NC.
SHOPLAND, DONALD R. 1993. Smoking controlin the 1990's: A National Cancer InstituteModel for Change. Amer. J. Publ. Hlth.83(9):1208-1210.
SUSSER, MERVYN W., WILLIAM WATSON, and KIMHOPPER. 1985. Sociology in medicine. OxfordUniv. Press, New York.
U.S. DEPARTMENT OF HEALTH AND HUMAN SER-VICES. 1991. Healthy people: National healthpromotion and disease prevention objec-tives. USGPO, Washington, DC.
Dow
nloa
ded
by [
Cha
rles
B N
am]
at 1
3:00
06
Febr
uary
201
4








![[Demographic and socioeconomic differences in consumption of sugar-sweetened beverages among Colombian children and adolescents]](https://static.fdokumen.com/doc/165x107/63415b16189652a6680a7eb3/demographic-and-socioeconomic-differences-in-consumption-of-sugar-sweetened-beverages.jpg)











