
Normative data for two neuropsychological tests sensitive to frontal dysfunction
Deep brain stimulation of the centromedian thalamic
nucleus for the treatment of generalized and frontal
epilepsies*†Antonio Valent�ın, ‡EduardoGarc�ıa Navarrete, §¶RameshChelvarajah, ‡Cristina Torres,
‡MartaNavas, *#Lelia Vico, **Nerea Torres, ††Jesus Pastor, ¶Richard Selway, ‡Rafael G. Sola,
and *†‡‡Gonzalo Alarcon
Epilepsia, **(*):1–11, 2013doi: 10.1111/epi.12352
SUMMARY
Purpose: Deep brain stimulation (DBS) of the thalamus is an emerging surgical option for people withmedically refrac-
tory epilepsy that is not suitable for resective surgery, or in whom surgery has failed. Ourmain aim was to evaluate the
efficacy of bilateral centromedian thalamic nucleus (CMN) DBS for seizure control in generalized epilepsy and frontal
lobe epilepsy with a two-center, single-blind, controlled trial.
Methods: Participants were adults with refractory generalized or frontal lobe epilepsy. Seizure diaries were kept by
patients/carers prospectively from enrollment. The baseline preimplantation period was followed by a control period
consisting of a blind stimulation-OFF phase of at least 3 months, a 3-month blind stimulation-ON phase, and a 6-month
unblinded stimulation-ON phase. The control period was followed by an unblinded long-term extension phase with
stimulation-ON in those patients in whom stimulation was thought to be effective.
Key Findings: Eleven patients were recruited at King’s College Hospital (London, United Kingdom United King-
dom) and at University Hospital La Princesa (Madrid, Spain). Among the five patients with frontal lobe epilepsy,
only one patient had >50% improvement in seizure frequency during the blind period. In the long-term extension
phase, two patients with frontal lobe epilepsy had >50% improvement in seizure frequency. All six patients with
generalized epilepsy had >50% improvement in seizure frequency during the blind period. In the long-term exten-
sion phase, five of the six patients showed >50% improvement in the frequency of major seizures (one became sei-
zure free, one had >99% improvement, and three had 60–95% reduction in seizure frequency). Among patients
with generalized epilepsy, the DBS implantation itself appears to be effective, as two patients remained seizure
free during 12 and 50 months with DBS OFF, and the remaining four had 50–91% improvement in the initial
3 months with DBS OFF.
Significance: DBS implantation and stimulation of the CMN appears to be a safe and efficacious treatment, particularly
in patients with refractory generalized epilepsy. CMN stimulation was not as effective in frontal lobe epilepsy, which
requires further studies. DBS of the CMN should be considered as a treatment option, particularly in patients with
refractory generalized epilepsy syndromes.
KEYWORDS: Epilepsy, Seizure, Deep brain stimulation, Epilepsy surgery, Thalamus, Centromedian.
Accepted July 28, 2013.*Department of Clinical Neurophysiology, King’s College Hospital, London, United Kingdom; †Department of Clinical Neuroscience, Institute of
Psychiatry, King’s College London, London, United Kingdom; ‡Epilepsy Surgery Unit, University Hospital La Princesa, Madrid, Spain; §Department ofNeurosurgery, Queen Elizabeth Hospital Birmingham, Birmingham, United Kingdom; ¶Department of Neurosurgery, King’s College Hospital, London,United Kingdom; #Department of Clinical Neurophysiology, Royal Derby Hospital, Derby, United Kingdom; **Department of Neurophysiology, DoctorPeset Hospital, Valencia, Spain; ††Department of Neurophysiology, University Hospital La Princesa, Madrid, Spain; and ‡‡Department of Physiology,Faculty of Medicine, Complutense University, Madrid, Spain
Address correspondence to Antonio Valent�ın, Department of Clinical Neuroscience, Institute of Psychiatry, King’s College London, De CrespignyPark, London SE5 8AS, U.K. E-mail: [email protected]
Wiley Periodicals, Inc.© 2013 International League Against Epilepsy
1
FULL-LENGTHORIGINALRESEARCH

Approximately 25% of patients with epilepsy are notcontrolled by antiepileptic medication (Hart & Shorvon,1995; Lhatoo et al., 2003; Schuele & Luders, 2008; Kwanet al., 2011). Only around 20% of these patients have focalseizures not arising from eloquent cortex and can benefitfrom resective surgery. Furthermore, around 30–40% ofthe operated patients do not improve satisfactorily after re-sective surgical treatment (Tellez-Zenteno et al., 2005; deTisi et al., 2011). Consequently, approximately 20% ofpatients with epilepsy do not respond to medical or surgi-cal treatment, and consume substantial health resources,have significant social disadvantage, and are at risk ofaccidents during seizures and sudden death (Nashef &Ryvlin, 2009).
Electrical high frequency deep brain stimulation (DBS)of the thalamus is an emerging treatment for patients withmedically refractory epilepsy who are not suitable for resec-tive surgery. Several clinical studies have tested the efficacyof stimulation of different brain structures, including thecentromedian thalamic nucleus (Fisher et al., 1992; Velascoet al., 2007b), the anterior thalamic nucleus (SANTE trial;Fisher et al., 2010), the subthalamic nucleus (Loddenkem-per et al., 2001; Chabardes et al., 2002), medial temporalstructures (Vonck et al., 2005; Tellez-Zenteno et al., 2006;Velasco et al., 2007a), and other cortical structures (Sunet al., 2008; Morrell, 2011).
Stimulation of the centromedian thalamic nucleus(CMN) has been used by Velasco’s group for >20 years in>57 patients (Velasco et al., 1987, 1993, 1995, 2001,2007b). Their studies suggest that patients with generalizedepilepsy, in particular, appear to benefit from CMN stimula-tion, as demonstrated by reductions in the incidence of elec-troencephalography (EEG) spiking and in the frequency ofgeneralized tonic–clonic seizures and atypical absences.More specifically, patients with temporal lobe epilepsyappear not to improve with CMN stimulation.
Whereas Velasco’s studies benefit from a large numberof patients with specific syndromes stimulated over manyyears at a single target, these studies were neither controllednor blinded. A double-blind controlled crossover trial evalu-ated CMN stimulation on seven patients (Fisher et al.,1992). CMN stimulation was judged to induce little effect,with a seizure reduction of 30% during stimulation versus8% when stimulation was discontinued. However, threepatients that were recruited had temporal lobe epilepsy,which may explain the apparent lack of efficacy. Contradic-tory results have been reported by a few studies with smallpatient numbers (Chkhenkeli et al., 2004; Andrade et al.,2006; Cukiert et al., 2009).
In the present study, we carried out a controlled single-blind trial to revisit the efficacy of bilateral CMN stimula-tion on patients with generalized or frontal lobe epilepsies.We have evaluated the effect of CMN electrode implanta-tion and stimulation on seizure frequency and on patientreported outcome measures (PROs) in order to assess their
effects on the epilepsy and on broader aspects of thepatients’ lives.
MethodsPatients
Among a total of 11 patients (9 male, 2 female), 8patients were recruited at King’s College Hospital (London,United Kingdom) and 3 were recruited at University Hospi-tal La Princesa (Madrid, Spain). Six patients had removal ofthe vagus nerve stimulation (VNS) device before DBSimplantation. Age at surgery ranged from 18 to 51 years(mean 37). Average follow-up period was 2 years. Sixpatients had idiopathic or presumed symptomatic general-ized epilepsy and five had frontal epilepsy. Seizure diarieswere prospectively kept by patients/parents. Seven patientscompleted PROs, which included Quality of Life in Epi-lepsy-Patient-Weighted (QOLIE-31-P), Seizure SeverityScale and Hospital Anxiety Disorders before and after theprocedures.
Before implantation, patients had been evaluated withclinical history, examination, neuroimaging, and scalpEEG-video telemetry recorded with electrodes appliedaccording to the 10/20 or the Maudsley (Fern�andez Torreet al., 1999; Kissani et al., 2001) system. Patients wererecruited according to the following inclusion criteria: (1)age >18 years; (2) clear diagnosis of epilepsy (confirmedby scalp or intracranial telemetry); (3) patients were unsuit-able for resective surgery; (4) seizure frequency ≥10/month;(5) patients were able to give informed consent; (6) patientsor carers were able to keep seizure diaries; and (7) patientswere on stable dose of AEDs. Exclusion criteria were thefollowing: (1) major neurologic or psychiatric disorders; (2)history of poor compliance with medication; (3) temporallobe epilepsy; and (4) previous intracranial surgery. Allpatients and/or their carers were informed and signedwritten consent.
Recruited patients were categorized as having either (1)“generalized epilepsies,” including patients with eithersymptomatic or idiopathic generalized epilepsy; or (2) “pre-sumed frontal epilepsy,” including patients with unilateralor bilateral frontal lobe epilepsy who were not suitable forresective surgery. Patients with presumed frontal lobe epi-lepsy had seizure semiology suggestive of frontal lobe sei-zures and had previously been assessed for resectivesurgery but no clear focus was identified on neuroimagingor on scalp EEG recordings. Noninvasive tests did not sug-gest a clear hypothesis for implantation of intracranial elec-trodes except in one patient, in whom intracranial videotelemetry failed to demonstrate a clear seizure focus. Tosimplify the wording throughout the paper, the patients withpresumed frontal lobe epilepsy will be simply referred to as“frontal lobe” patients.
The study has been approved by King’s College HospitalEthics Committee and the New Clinical Procedures
Epilepsia, **(*):1–11, 2013doi: 10.1111/epi.12352
2
A. Valent�ın et al.

Committee in 2005, and by the University Hospital La Prin-cesa Ethics Committee in 2009.
Study designThe study consists of a two-center, single-blind, non-ran-
domized, controlled trial. Essentially, in order to avoid theconfounding effects of implantation versus stimulation, thepatients were told that they were to be randomized, but theyall had an OFF period first, which acts as a “washout period”for the effects of implantation. Seizure outcome in allpatients was evaluated with daily seizure diaries filled in bythe patients and/or carers. The primary outcome measurewas the frequency of major seizures (the generalized tonic–clonic seizures, or the complex partial seizures with or with-out secondary generalization). The study was divided in fivestages: baseline, electrode implantation, parameter optimi-zation with system internalization, blind period, and open-label follow-up.
BaselineAll patients had a 3-month baseline period before implan-
tation during which the following tests were obtained andassessed: medical history, general and neurologic examina-tions, electrocardiography (ECG), electroencephalography(EEG) telemetry, magnetic resonance imaging (MRI), neu-ropsychological scores, and PRO questionnaires. Patientswere asked to keep a seizure diary 3 months prior to implan-tation and throughout the trial.
Electrode implantationOne four-contact electrode (K-3387 or K-3389, Medtron-
ic) was implanted stereotactically in the CMN of eachhemisphere under general anaesthesia. Target location foreach electrode was determined using frame (Leksell Coordi-nate Frame G, Elekta, Stockholm, Sweden)-based atlascoordinates and calculated with STEALTH FRAMELINK5 software (Medtronic, Inc., Minneapolis, MN, U.S.A.).Electrodes were implanted through bilateral frontal burrholes in a transparenchymal extraventricular trajectoryunder neurophysiologic monitoring (Fig. 1). The position ofimplanted electrodes was checked with intraoperative X-rayor computed tomography (CT) scan (Fig. 1).
Intraoperative scalp EEG was recorded in all patients. Inseven patients, additional intraoperative intracranial EEGwas also recorded with lateral frontal four- or eight-contactsubdural strip electrodes implanted bilaterally. In fourpatients, microelectrode recordings were performed at dif-ferent distances from the MRI target (Fig. 1). Scalp EEG inall patients, with additional subdural frontal electrodes inseven, were used to record cortical responses induced byelectrical stimulation at 0.2 and 6 Hz via the DBS electrodesat various distances from the target starting at 10 mm abovetarget. In all cases, electrical stimulation confirmed thatthere were cortical connections between deep structures andcortex. The final electrode position was decided on the basis
of atlas-derived coordinates, microelectrode intraoperativerecordings, and the thalamic location where stimulationinduced the largest cortical responses. General anesthesiawas induced with propofol and maintained with isoflurane.In seven patients the subdural frontal strips were notremoved after this procedure, and were used to record EEGresponses during postoperative telemetry recorded duringparameter optimization. The last four patients were not stud-ied with subdural electrodes, since it was observed that EEGresponses could be recorded on the scalp during parameteroptimization (see section below).
Parameter optimization and system internalizationAll 11 patients underwent 1-week scalp video telemetry
after DBS electrode implantation in order to identify theoptimal DBS stimulation parameters. In eight patients, DBSelectrodes were externalized during 1 week and were usedfor recording and stimulation. Among these eight patients,seven had subdural electrodes implanted bilaterally over thefrontal convexities. Recordings from subdural strips werenot used to estimate medium/long-term seizure outcome.The optimal stimulation parameters were identified by theevaluation of seizure frequency and cortical responses toCMN stimulation, including recruitment responses at 6 Hz(Fig. 2) and responses to single-pulse electrical stimulation(Lacruz et al., 2007; Flanagan et al., 2009;Alarcon&Valentin,2012; Alarcon et al., 2012; Kokkinos et al., 2013). Aftertelemetry, the subdural electrodes were removed, the systemwas internalized (Kinetra, Medtronic, Inc., Minneapolis,MN, U.S.A.), and the stimulator turned OFF.
Blind periodThe initial period after internalization was a single-blind
period during which patients did not know whether the stim-ulator was ON or OFF. Patients were told that during thisperiod that they would be randomized to 3 months of stimu-lation ON and 3 months of stimulation OFF, or vice versa.However, in all patients the first period consisted of stimula-tion OFF in order to washout the potential “micro-lesion-ing” effects of implantation and of the stimulation carriedout during parameter optimization.
Stimulation-OFF phase (at least 3 months). The initialstimulation-OFF period used for seizure frequencyevaluation was the first 3 months after implantation in allpatients. However, the stimulator was not turned on in thetwo patients who became seizure free after implantation/optimization, as it was considered unnecessary to turn ONthe stimulator in seizure-free patients on clinical grounds.Patient 1 has remained seizure free and stimulation OFF todate. In patient 2, the stimulator was turned on 13 monthsafter implantation, when seizures recurred.
Stimulation-ON phase (3 months). In the nine patients withseizures during the stimulation-OFF phase, stimulation was
Epilepsia, **(*):1–11, 2013doi: 10.1111/epi.12352
3
Centromedian DBS for Epilepsy
turned on 3 months after implantation. In patient 2, whoremained seizure free during the initial 3-month stimula-tion-OFF phase, stimulation was started 13 months afterimplantation. Patients remained blind for 3 months afterstarting stimulation. Patient 1 had remained seizure free andstimulation was never started (no stimulation-ON phaseavailable).
The initial stimulation protocol of the study was continu-ous stimulation, frequency of 130 Hz with pulse width of90 ls and up-to 5 V. Because the first two patients with thisprotocol did not show clear improvement in severity or fre-quency of seizures by comparing the stimulation-OFF andstimulation-ON phases, a new protocol was adopted: contin-uous stimulation, frequency at 60 Hz with pulse width of90 ls, and up to 5 V.
Open-label follow-up
Unblind stimulation-ON period (6 months). The single-blind period was followed by an open 6-month period withstimulation-ON.
Unblind long-term extension phase. The unblind stimula-tion-ON period was followed by an unlimited period withstimulation-ON in those patients who responded tostimulation.
Patient reported outcomesPatient reported outcome (PRO) questionnaires (Quality
of Life in Epilepsy-Patient-Weighted [QOLIE-31-P], Sei-zure Severity Scale, Hospital Anxiety Disorders) were
A
C E
B D
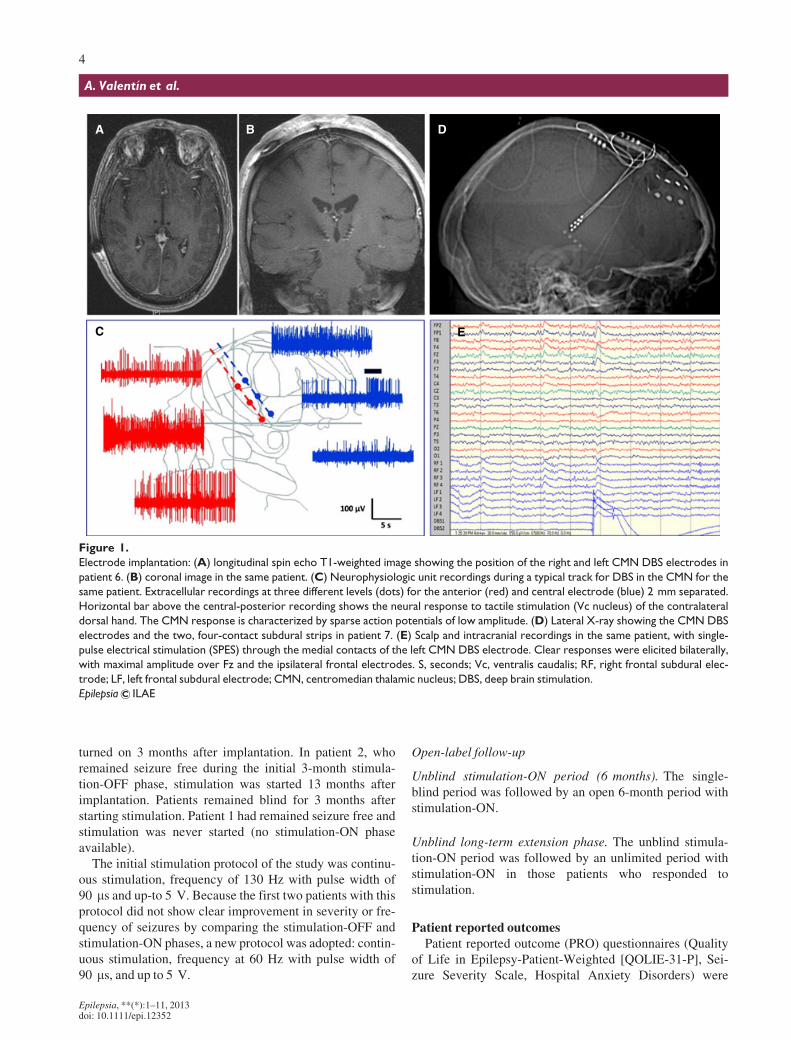
Figure 1.
Electrode implantation: (A) longitudinal spin echo T1-weighted image showing the position of the right and left CMN DBS electrodes in
patient 6. (B) coronal image in the same patient. (C) Neurophysiologic unit recordings during a typical track for DBS in the CMN for the
same patient. Extracellular recordings at three different levels (dots) for the anterior (red) and central electrode (blue) 2 mm separated.
Horizontal bar above the central-posterior recording shows the neural response to tactile stimulation (Vc nucleus) of the contralateral
dorsal hand. The CMN response is characterized by sparse action potentials of low amplitude. (D) Lateral X-ray showing the CMN DBS
electrodes and the two, four-contact subdural strips in patient 7. (E) Scalp and intracranial recordings in the same patient, with single-
pulse electrical stimulation (SPES) through the medial contacts of the left CMN DBS electrode. Clear responses were elicited bilaterally,
with maximal amplitude over Fz and the ipsilateral frontal electrodes. S, seconds; Vc, ventralis caudalis; RF, right frontal subdural elec-
trode; LF, left frontal subdural electrode; CMN, centromedian thalamic nucleus; DBS, deep brain stimulation.
Epilepsia ILAE
Epilepsia, **(*):1–11, 2013doi: 10.1111/epi.12352
4
A. Valent�ın et al.
completed before and 6 months after implantation in sevenpatients. Questionnaires were answered by patients and rel-atives within 30–45 min, allowing for the assessment ofquality of life, anxiety and depression levels, number andseverity of habitual seizures, and for the identification newseizure types that might have arisen in the course of thestudy.
StatisticsFisher exact test was used to assess significant differ-
ences between frontal and generalized epilepsy groupswith regard to the proportion of patients with good/pooroutcomes (>50% vs. <50% change in seizure frequencycompared to baseline) at 6 or 12 months after DBSimplantation. Wilcoxon matched-pairs signed-rank testwas used to compare PRO values before and afterimplantation.
ResultsPatients
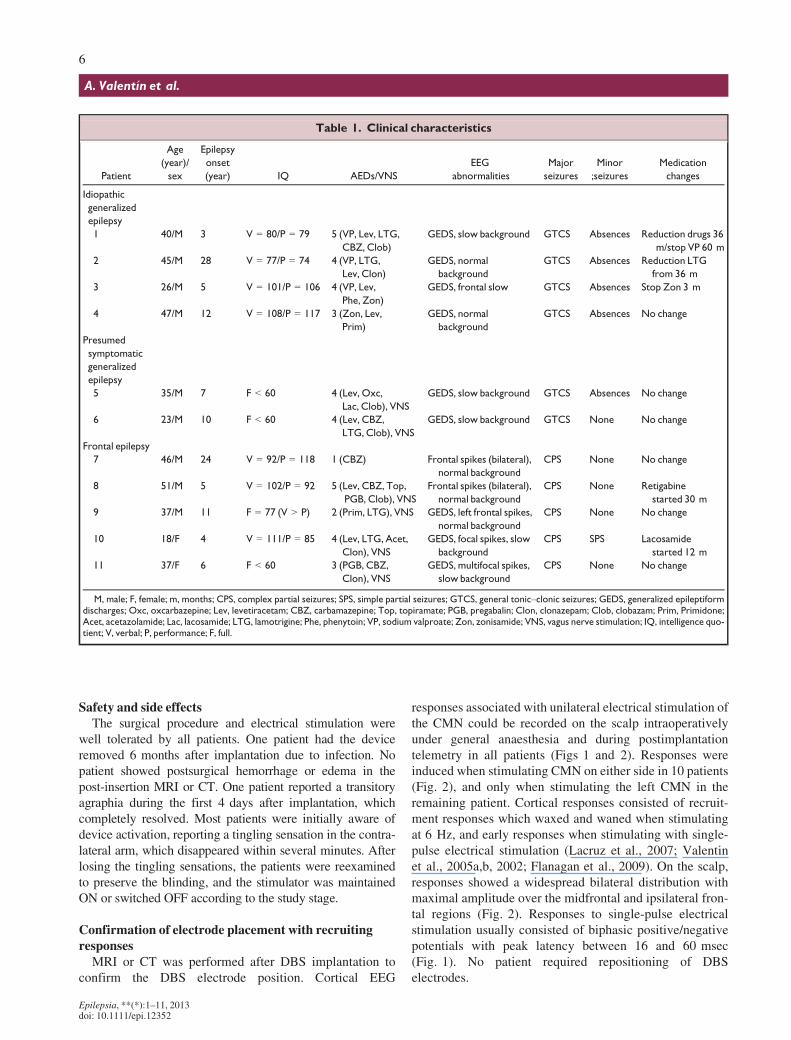
Table 1 shows the electroclinical characteristics ofpatients. The study included 11 patients, 2 female and 9male, aged between 18 and 65 years. Four patients had
idiopathic generalized epilepsy, two patients had pre-sumed symptomatic generalized epilepsy, and fivepatients had frontal lobe epilepsy. All patients with idio-pathic or presumed symptomatic generalized epilepsieshad normal imaging. Among the frontal patients, two hadnormal imaging and two showed mild cortical atrophy.All patients showed generalized or bilateral interictal epi-leptiform discharges. Among the six patients with general-ized epilepsy, all had convulsive generalized tonic–clonicseizures and five also had absence seizures. Among thefive frontal patients, all had complex partial seizures (withor without secondary generalization) and one also hadsimple partial seizures. The frequency of major seizures(the convulsive generalized tonic–clonic seizures or thecomplex partial seizures) was the main variable used toevaluate treatment efficacy as shown in Figs 3 and 4. Nolocalized seizure onset was demonstrated by ictal record-ings. All six patients with generalized epilepsy were onpolytherapy. Among the frontal patients, one was onmonotherapy, one on two antiepileptic drugs, and threewere on polytherapy. During the first 12 months afterimplantation, 10 patients had no medication changes, andzonisamide was stopped in the remaining patient after3 months.
A B
C D
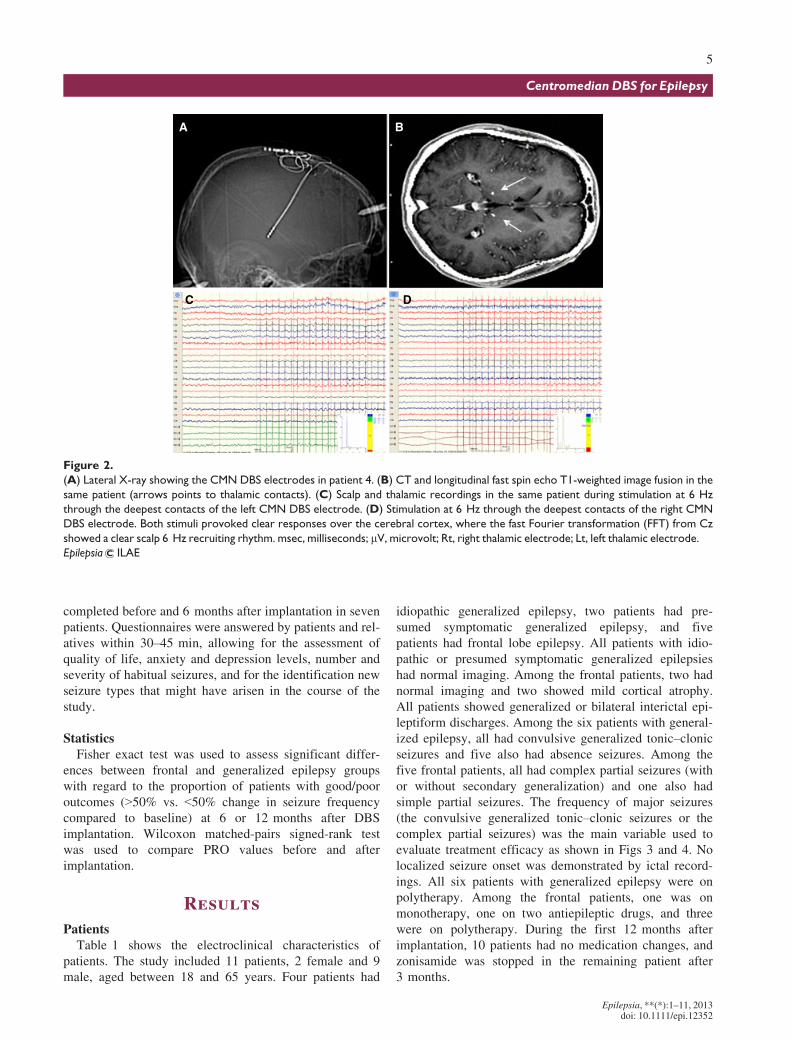
Figure 2.
(A) Lateral X-ray showing the CMN DBS electrodes in patient 4. (B) CT and longitudinal fast spin echo T1-weighted image fusion in the
same patient (arrows points to thalamic contacts). (C) Scalp and thalamic recordings in the same patient during stimulation at 6 Hz
through the deepest contacts of the left CMN DBS electrode. (D) Stimulation at 6 Hz through the deepest contacts of the right CMN
DBS electrode. Both stimuli provoked clear responses over the cerebral cortex, where the fast Fourier transformation (FFT) from Cz
showed a clear scalp 6 Hz recruiting rhythm. msec, milliseconds; lV, microvolt; Rt, right thalamic electrode; Lt, left thalamic electrode.
Epilepsia ILAE
Epilepsia, **(*):1–11, 2013doi: 10.1111/epi.12352
5
Centromedian DBS for Epilepsy
Safety and side effectsThe surgical procedure and electrical stimulation were
well tolerated by all patients. One patient had the deviceremoved 6 months after implantation due to infection. Nopatient showed postsurgical hemorrhage or edema in thepost-insertion MRI or CT. One patient reported a transitoryagraphia during the first 4 days after implantation, whichcompletely resolved. Most patients were initially aware ofdevice activation, reporting a tingling sensation in the contra-lateral arm, which disappeared within several minutes. Afterlosing the tingling sensations, the patients were reexaminedto preserve the blinding, and the stimulator was maintainedON or switched OFF according to the study stage.
Confirmation of electrode placement with recruitingresponses
MRI or CT was performed after DBS implantation toconfirm the DBS electrode position. Cortical EEG
responses associated with unilateral electrical stimulation ofthe CMN could be recorded on the scalp intraoperativelyunder general anaesthesia and during postimplantationtelemetry in all patients (Figs 1 and 2). Responses wereinduced when stimulating CMN on either side in 10 patients(Fig. 2), and only when stimulating the left CMN in theremaining patient. Cortical responses consisted of recruit-ment responses which waxed and waned when stimulatingat 6 Hz, and early responses when stimulating with single-pulse electrical stimulation (Lacruz et al., 2007; Valentinet al., 2005a,b, 2002; Flanagan et al., 2009). On the scalp,responses showed a widespread bilateral distribution withmaximal amplitude over the midfrontal and ipsilateral fron-tal regions (Fig. 2). Responses to single-pulse electricalstimulation usually consisted of biphasic positive/negativepotentials with peak latency between 16 and 60 msec(Fig. 1). No patient required repositioning of DBSelectrodes.
Table 1. Clinical characteristics
Patient
Age
(year)/
sex
Epilepsy
onset
(year) IQ AEDs/VNS
EEG
abnormalities
Major
seizures
Minor
;seizures
Medication
changes
Idiopathic
generalized
epilepsy
1 40/M 3 V = 80/P = 79 5 (VP, Lev, LTG,
CBZ, Clob)
GEDS, slow background GTCS Absences Reduction drugs 36
m/stop VP 60 m
2 45/M 28 V = 77/P = 74 4 (VP, LTG,
Lev, Clon)
GEDS, normal
background
GTCS Absences Reduction LTG
from 36 m
3 26/M 5 V = 101/P = 106 4 (VP, Lev,
Phe, Zon)
GEDS, frontal slow GTCS Absences Stop Zon 3 m
4 47/M 12 V = 108/P = 117 3 (Zon, Lev,
Prim)
GEDS, normal
background
GTCS Absences No change
Presumed
symptomatic
generalized
epilepsy
5 35/M 7 F < 60 4 (Lev, Oxc,
Lac, Clob), VNS
GEDS, slow background GTCS Absences No change
6 23/M 10 F < 60 4 (Lev, CBZ,
LTG, Clob), VNS
GEDS, slow background GTCS None No change
Frontal epilepsy
7 46/M 24 V = 92/P = 118 1 (CBZ) Frontal spikes (bilateral),
normal background
CPS None No change
8 51/M 5 V = 102/P = 92 5 (Lev, CBZ, Top,
PGB, Clob), VNS
Frontal spikes (bilateral),
normal background
CPS None Retigabine
started 30 m
9 37/M 11 F = 77 (V > P) 2 (Prim, LTG), VNS GEDS, left frontal spikes,
normal background
CPS None No change
10 18/F 4 V = 111/P = 85 4 (Lev, LTG, Acet,
Clon), VNS
GEDS, focal spikes, slow
background
CPS SPS Lacosamide
started 12 m
11 37/F 6 F < 60 3 (PGB, CBZ,
Clon), VNS
GEDS, multifocal spikes,
slow background
CPS None No change
M, male; F, female; m, months; CPS, complex partial seizures; SPS, simple partial seizures; GTCS, general tonic–clonic seizures; GEDS, generalized epileptiformdischarges; Oxc, oxcarbazepine; Lev, levetiracetam; CBZ, carbamazepine; Top, topiramate; PGB, pregabalin; Clon, clonazepam; Clob, clobazam; Prim, Primidone;Acet, acetazolamide; Lac, lacosamide; LTG, lamotrigine; Phe, phenytoin; VP, sodium valproate; Zon, zonisamide; VNS, vagus nerve stimulation; IQ, intelligence quo-tient; V, verbal; P, performance; F, full.
Epilepsia, **(*):1–11, 2013doi: 10.1111/epi.12352
6
A. Valent�ın et al.
Seizure outcome
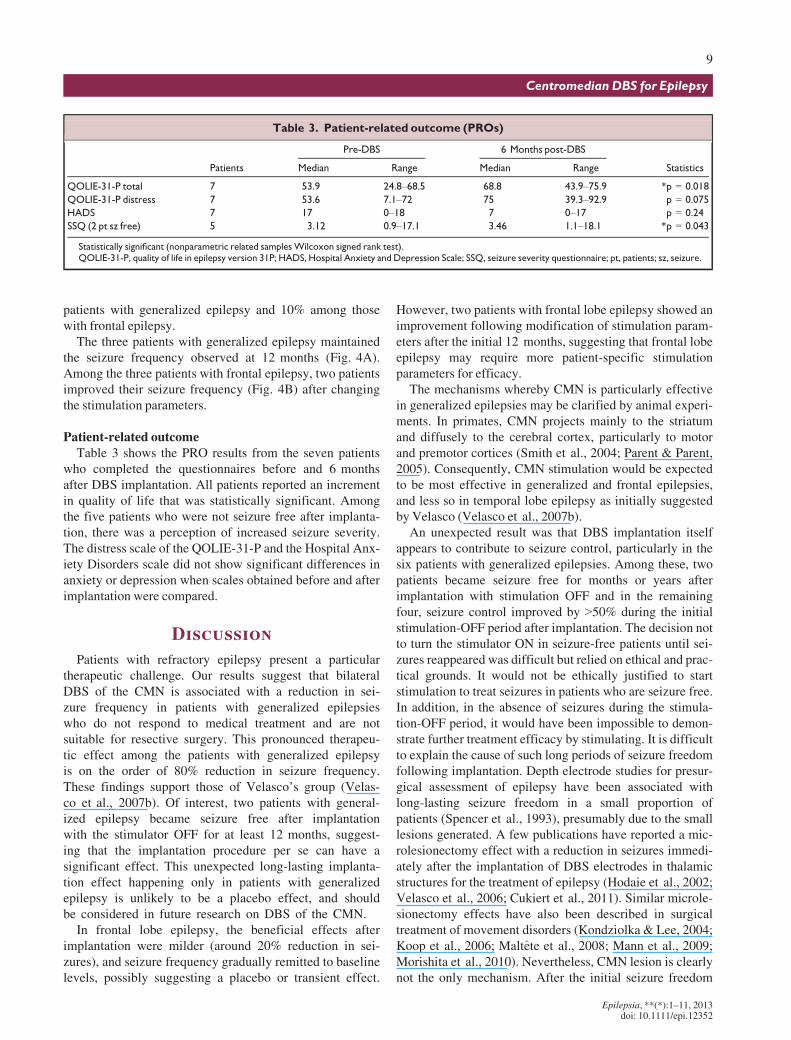
Symptomatic or idiopathic generalized epilepsyThe follow-up period in six patients with symptomatic or
idiopathic generalized epilepsy ranged between 12 and66 months (Table 2). During the blind period, all patientshad >50% improvement in seizure frequency. In the long-term extension phase, five of the six patients showed >50%improvement in the frequency of major seizure. Amongthese five patients, three became seizure free and two had67–80% reduction in seizure frequency. All patients had≥50% improvement in the frequency of minor seizures.
Of interest, two patients became seizure free immediatelyafter implantation. Patient 1 has remained seizure free todate with stimulator OFF (follow-up of 60 months). Patient2 remained seizure free for 12 months and then had five sei-zures in 1 month. Stimulation was then turned on (60 Hz)and the patient was almost seizure free for 45 months (onlyone seizure in this period). The stimulator then stoppedworking for technical reasons and the patient had three sei-zures in a month. After stimulation was resumed, he becameseizure free to date (3 months).
Frontal epilepsyThe five patients with frontal lobe epilepsy had follow-up
periods between 6 and 36 months (Table 2). During theblind period, only one patient had ≥50% improvement inseizure frequency. In the long-term extension phase, onepatient had 90% improvement in seizure frequency, onepatient had a 60% improvement, one had a 50% improve-ment, and two patients did not show any clear improvementin frequency or severity.
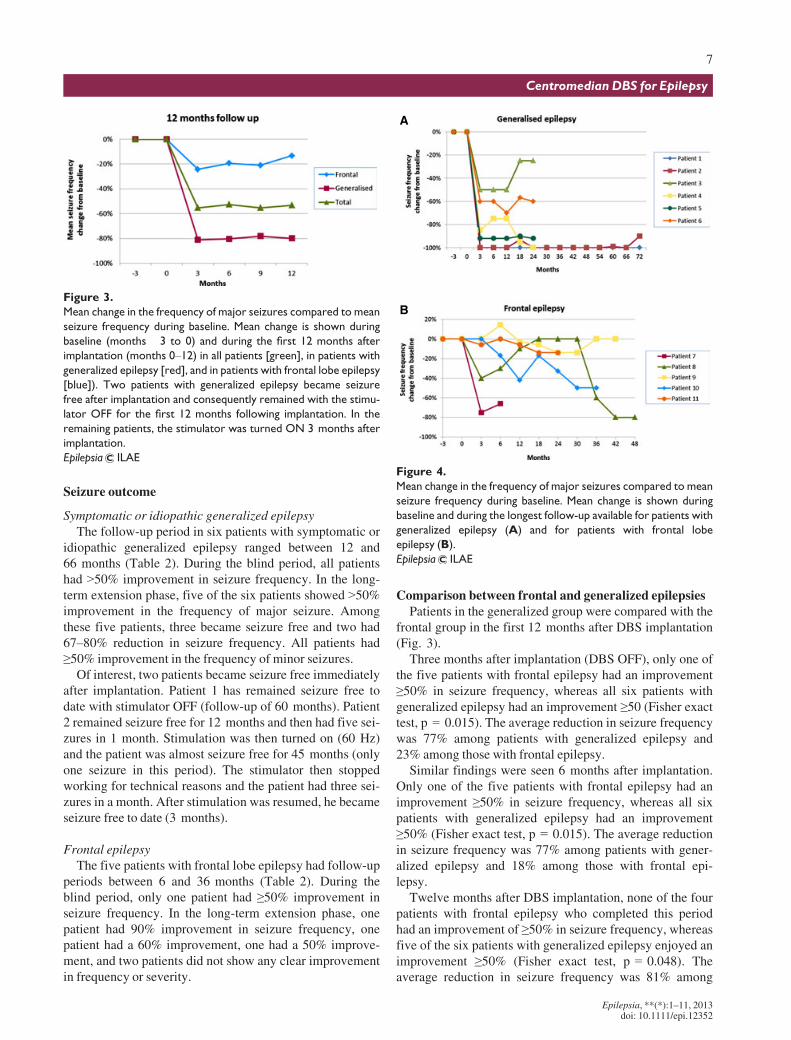
Comparison between frontal and generalized epilepsiesPatients in the generalized group were compared with the
frontal group in the first 12 months after DBS implantation(Fig. 3).
Three months after implantation (DBS OFF), only one ofthe five patients with frontal epilepsy had an improvement≥50% in seizure frequency, whereas all six patients withgeneralized epilepsy had an improvement ≥50 (Fisher exacttest, p = 0.015). The average reduction in seizure frequencywas 77% among patients with generalized epilepsy and23% among those with frontal epilepsy.
Similar findings were seen 6 months after implantation.Only one of the five patients with frontal epilepsy had animprovement ≥50% in seizure frequency, whereas all sixpatients with generalized epilepsy had an improvement≥50% (Fisher exact test, p = 0.015). The average reductionin seizure frequency was 77% among patients with gener-alized epilepsy and 18% among those with frontal epi-lepsy.
Twelve months after DBS implantation, none of the fourpatients with frontal epilepsy who completed this periodhad an improvement of ≥50% in seizure frequency, whereasfive of the six patients with generalized epilepsy enjoyed animprovement ≥50% (Fisher exact test, p = 0.048). Theaverage reduction in seizure frequency was 81% among
Figure 3.
Mean change in the frequency of major seizures compared to mean
seizure frequency during baseline. Mean change is shown during
baseline (months �3 to 0) and during the first 12 months after
implantation (months 0–12) in all patients [green], in patients with
generalized epilepsy [red], and in patients with frontal lobe epilepsy
[blue]). Two patients with generalized epilepsy became seizure
free after implantation and consequently remained with the stimu-
lator OFF for the first 12 months following implantation. In the
remaining patients, the stimulator was turned ON 3 months after
implantation.
Epilepsia ILAE
A
B
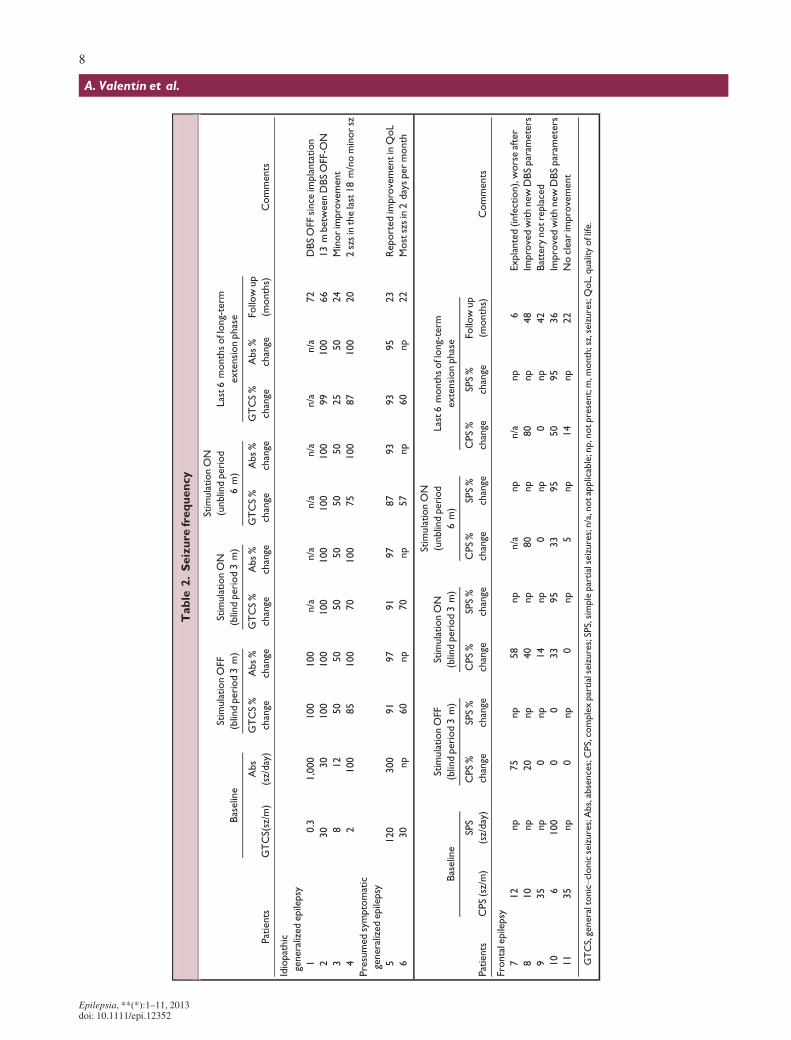
Figure 4.
Mean change in the frequency of major seizures compared to mean
seizure frequency during baseline. Mean change is shown during
baseline and during the longest follow-up available for patients with
generalized epilepsy (A) and for patients with frontal lobe
epilepsy (B).
Epilepsia ILAE
Epilepsia, **(*):1–11, 2013doi: 10.1111/epi.12352
7
Centromedian DBS for Epilepsy
Table
2.Seizure
frequency
Patients
Baseline
StimulationOFF
(blindperiod3m)
StimulationON
(blindperiod3m)
StimulationON
(unblindperiod
6m)
Last6monthsoflong-term
extensionphase
Comments
GTCS(sz/m
)
Abs
(sz/day)
GTCS%
change
Abs%
change
GTCS%
change
Abs%
change
GTCS%
change
Abs%
change
GTCS%
change
Abs%
change
Followup
(months)
Idiopathic
generalizedepilepsy
10.3
1,000
�100
�100
n/a
n/a
n/a
n/a
n/a
n/a
72
DBSOFF
since
implantation
230
30
�100
�100
�100
�100
�100
�100
�99
�100
66
13mbetw
een
DBSOFF-O
N
38
12
�50
�50
�50
�50
�50
�50
�25
�50
24
Minorimprovement
42
100
�85
�100
�70
�100
�75
�100
�87
�100
20
2szsinthelast18m/nominorsz
Presumedsymptomatic
generalizedepilepsy
5120
300
�91
�97
�91
� 97
�87
�93
�93
�95
23
Reported
improvementinQoL
630
np
�60
np
�70
np
�57
np
�60
np
22
Mostszsin2dayspermonth
Patients
Baseline
StimulationOFF
(blindperiod3m)
StimulationON
(blindperiod3m)
StimulationON
(unblindperiod
6m)
Last6monthsoflong-term
extensionphase
Comments
CPS(sz/m)
SPS
(sz/day)
CPS%
change
SPS%
change
CPS%
change
SPS%
change
CPS%
change
SPS%
change
CPS%
change
SPS%
change
Followup
(months)
Frontalepilepsy
712
np
�75
np
�58
np
n/a
np
n/a
np
6Explanted(infection),worseafter
810
np
�20
np
�40
np
�80
np
�80
np
48
ImprovedwithnewDBSparam
eters
935
np
0np
14
np
0np
0np
42
Battery
notreplaced
10
6100
00
�33
�95
�33
�95
�50
�95
36
ImprovedwithnewDBSparam
eters
11
35
np
0np
0np
�5np
�14
np
22
Noclear
improvement
GTCS,generaltonic–clonicseizures;Abs,absences;CPS,complexpartialseizures;SPS,simplepartialseizures;n/a,notapplicable;np,notpresent;m,m
onth;sz,seizures;QoL,qualityoflife.
Epilepsia, **(*):1–11, 2013doi: 10.1111/epi.12352
8
A. Valent�ın et al.
patients with generalized epilepsy and 10% among thosewith frontal epilepsy.
The three patients with generalized epilepsy maintainedthe seizure frequency observed at 12 months (Fig. 4A).Among the three patients with frontal epilepsy, two patientsimproved their seizure frequency (Fig. 4B) after changingthe stimulation parameters.
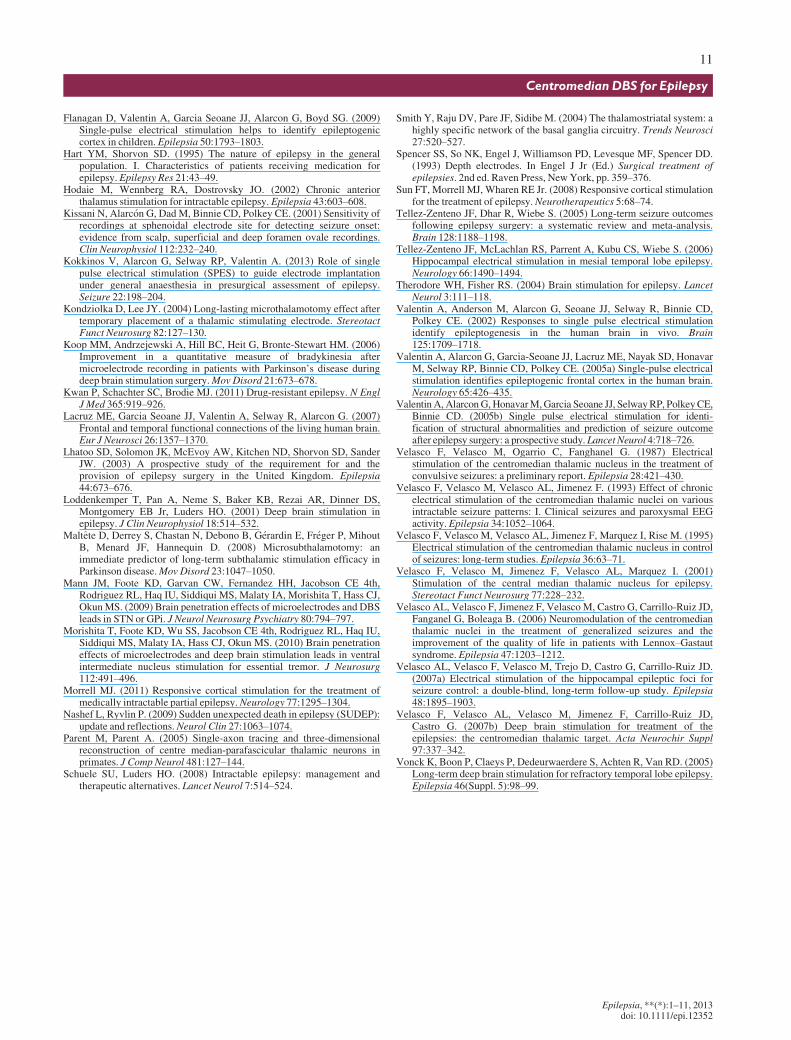
Patient-related outcomeTable 3 shows the PRO results from the seven patients
who completed the questionnaires before and 6 monthsafter DBS implantation. All patients reported an incrementin quality of life that was statistically significant. Amongthe five patients who were not seizure free after implanta-tion, there was a perception of increased seizure severity.The distress scale of the QOLIE-31-P and the Hospital Anx-iety Disorders scale did not show significant differences inanxiety or depression when scales obtained before and afterimplantation were compared.
DiscussionPatients with refractory epilepsy present a particular
therapeutic challenge. Our results suggest that bilateralDBS of the CMN is associated with a reduction in sei-zure frequency in patients with generalized epilepsieswho do not respond to medical treatment and are notsuitable for resective surgery. This pronounced therapeu-tic effect among the patients with generalized epilepsyis on the order of 80% reduction in seizure frequency.These findings support those of Velasco’s group (Velas-co et al., 2007b). Of interest, two patients with general-ized epilepsy became seizure free after implantationwith the stimulator OFF for at least 12 months, suggest-ing that the implantation procedure per se can have asignificant effect. This unexpected long-lasting implanta-tion effect happening only in patients with generalizedepilepsy is unlikely to be a placebo effect, and shouldbe considered in future research on DBS of the CMN.
In frontal lobe epilepsy, the beneficial effects afterimplantation were milder (around 20% reduction in sei-zures), and seizure frequency gradually remitted to baselinelevels, possibly suggesting a placebo or transient effect.
However, two patients with frontal lobe epilepsy showed animprovement following modification of stimulation param-eters after the initial 12 months, suggesting that frontal lobeepilepsy may require more patient-specific stimulationparameters for efficacy.
The mechanisms whereby CMN is particularly effectivein generalized epilepsies may be clarified by animal experi-ments. In primates, CMN projects mainly to the striatumand diffusely to the cerebral cortex, particularly to motorand premotor cortices (Smith et al., 2004; Parent & Parent,2005). Consequently, CMN stimulation would be expectedto be most effective in generalized and frontal epilepsies,and less so in temporal lobe epilepsy as initially suggestedby Velasco (Velasco et al., 2007b).
An unexpected result was that DBS implantation itselfappears to contribute to seizure control, particularly in thesix patients with generalized epilepsies. Among these, twopatients became seizure free for months or years afterimplantation with stimulation OFF and in the remainingfour, seizure control improved by >50% during the initialstimulation-OFF period after implantation. The decision notto turn the stimulator ON in seizure-free patients until sei-zures reappeared was difficult but relied on ethical and prac-tical grounds. It would not be ethically justified to startstimulation to treat seizures in patients who are seizure free.In addition, in the absence of seizures during the stimula-tion-OFF period, it would have been impossible to demon-strate further treatment efficacy by stimulating. It is difficultto explain the cause of such long periods of seizure freedomfollowing implantation. Depth electrode studies for presur-gical assessment of epilepsy have been associated withlong-lasting seizure freedom in a small proportion ofpatients (Spencer et al., 1993), presumably due to the smalllesions generated. A few publications have reported a mic-rolesionectomy effect with a reduction in seizures immedi-ately after the implantation of DBS electrodes in thalamicstructures for the treatment of epilepsy (Hodaie et al., 2002;Velasco et al., 2006; Cukiert et al., 2011). Similar microle-sionectomy effects have also been described in surgicaltreatment of movement disorders (Kondziolka & Lee, 2004;Koop et al., 2006; Maltete et al., 2008; Mann et al., 2009;Morishita et al., 2010). Nevertheless, CMN lesion is clearlynot the only mechanism. After the initial seizure freedom
Table 3. Patient-related outcome (PROs)
Patients
Pre-DBS 6 Months post-DBS
StatisticsMedian Range Median Range
QOLIE-31-P total 7 53.9 24.8–68.5 68.8 43.9–75.9 *p = 0.018
QOLIE-31-P distress 7 53.6 7.1–72 75 39.3–92.9 p = 0.075
HADS 7 17 0–18 7 0–17 p = 0.24
SSQ (2 pt sz free) 5 3.12 0.9–17.1 3.46 1.1–18.1 *p = 0.043
Statistically significant (nonparametric related samplesWilcoxon signed rank test).QOLIE-31-P, quality of life in epilepsy version 31P; HADS, Hospital Anxiety and Depression Scale; SSQ, seizure severity questionnaire; pt, patients; sz, seizure.
Epilepsia, **(*):1–11, 2013doi: 10.1111/epi.12352
9
Centromedian DBS for Epilepsy

after implantation with stimulation OFF, seizures recurredin patient 2 approximately 12 months after implantation.Stimulation was then started and he recovered seizure free-dom for 40 months. The stimulator then went OFF forunclear technical reasons and in a month he had three sei-zures, which stopped when the stimulator was switched ONagain. The findings imply that CMN lesion and stimulationmay have additive effects, and suggest that the effects ofelectrical stimulation may derive from inactivating theCMN.
Our study incorporates a number of modifications overprevious reports on CMN stimulation that may have contrib-uted to showing efficacy. Our study design was equippedwith sufficient flexibility to avoid removing from the trialprecisely those patients in whom the procedure was mosteffective, due to either implantation or stimulation. Follow-ing Velasco’s findings (Velasco et al., 2007b), recruitmentwas restricted to patients with generalized or frontal epilep-sies. Patients with temporal lobe epilepsy were excluded incontrast to the study by Fisher et al. (1992), where effectsmight have been diluted by the inclusion of temporal epi-lepsy. To accommodate the effects of the implantation pro-cedure, our design is a single-blind study with no time limitbetween the stimulation-OFF and stimulation-ON phases(i.e., DBS was maintained OFF if patients remained seizurefree during the first 3 months after implantation). We haveused EEG responses to optimize implantation and the con-tacts chosen for stimulation. The initial parameters (130 Hzand 90 ls) were chosen following typical stimulation set-tings for DBS for epilepsy (Therodore & Fisher, 2004).After unclear effects with stimulation frequency at 130 Hz,we decided to follow Velasco’s and Fisher’s protocols at60 Hz for the CMN (Fisher et al., 1992; Velasco et al.,2001), which indeed appeared to be more effective in ourpatients. Based on our experience in >80 children withmovement disorders, we chose continuous stimulation.Finally, we have excluded patients with focal resections,hemispherectomy, or callosotomy in order to avoidpotential confounding factors.
It is interesting to note that although all seven patientswho completed the PRO questionnaires showed animprovement in quality of life, the five patients who werenot seizure free reported a mild increase in the severity ofseizures. Consequently, it appears that the reductionobserved in seizure frequency is associated with an incre-ment in quality of life, despite a mild increment in seizureseverity. More importantly, the procedure was notassociated with anxiety or depression.
ConclusionDBS implantation and stimulation of CMN appears to be
a safe and efficacious treatment, particularly in patients withgeneralized epilepsy for which medical treatment has failed.CMN stimulation was less effective in frontal lobe epilepsy,
which requires further studies. DBS of CMN should beconsidered as a treatment option in patients with refractorygeneralized epilepsy syndromes.
AcknowledgmentsThis work has been partially funded by a grant from Fund for Epilepsy,
and the Plan Nacional de Investigaci�on Cient�ıfica, Desarrollo e Innovaci�onTecnol�ogica (I + D + I), Instituto de Salud Carlos III, PI12/02839.
DisclosureWe confirm that we have read the Journal’s position on issues involved
in ethical publication and affirm that this report is consistent with thoseguidelines. A Valentin has received funding for travel, expert advice, andspeaker honoraria from Medtronic. R Selway and R Chelvarajah havereceived speaker honoraria from Cyberonics. The remaining authors reportno disclosures or potential conflict of interest.
ReferencesAlarcon G, Valentin A. (2012) Cortical stimulation with single electrical
pulses in human epilepsy.Clin Neurophysiol 123:223–224.Alarcon G, Martinez J, Kerai SV, Lacruz ME, Quiroga RQ, Selway RP,
Richardson MP, Garcia Seoane JJ, Valentin A. (2012) In vivo neuronalfiring patterns during human epileptiform discharges replicated byelectrical stimulation. Clin Neurophysiol 123:1736–1744.
Andrade DM, Zumsteg D, Hamani C, Hodaie M, Sarkissian S, Lozano AM,Wennberg RA. (2006) Long-term follow-up of patients with thalamicdeep brain stimulation for epilepsy. Neurology 66:1571–1573.
Chabardes S, Kahane P, Minotti L, Koudsie A, Hirsch E, Benabid AL.(2002) Deep brain stimulation in epilepsy with particular reference tothe subthalamic nucleus. Epileptic Disord 4(Suppl. 3):S83–S93.
Chkhenkeli SA, Sramka M, Lortkipanidze GS, Rakviashvili TN, BregvadzeES, Magalashvili GE, Gagoshidze TS, Chkhenkeli IS. (2004) Electro-physiological effects and clinical results of direct brain stimu-lationfor intractable epilepsy. Clin Neurol Neurosurg 106:318–329.
Cukiert A, Burattini JA, Cukiert CM, Argentoni-Baldochi M, Baise-ZungC, Forster CR, Mello VA. (2009) Centro-median stimulation yieldsadditional seizure frequency and attention improvement in patientspreviously submitted to callosotomy. Seizure 18:588–592.
Cukiert A, Burattini JA, Lima AM, Cukiert CM, Forster CR, Baise-Zung C,Argentoni-Baldochi M, Mello VA. (2011) Microlesional, attentional,anticonvulsant and proconvulsant effects of thalamic and hippocampaldeep brain stimulation (DBS). Abstract No 1.310, 2011 AmericanEpilepsy Society Annual Meeting, www.aesnet.org.
de Tisi J, Bell GS, Peacock JL, McEvoy AW, Harkness WF, Sander JW,Duncan JS. (2011) The long-term outcome of adult epilepsy surgery,patterns of seizure remission, and relapse: a cohort study. Lancet378:1388–1395.
Fern�andez Torre JL, Alarc�on G, Binnie CD, Polkey CE. (1999)Comparison of sphenoidal, foramen ovale and anterior temporalplacements for detecting interictal epileptiform discharges inpresurgical assessment for temporal lobe epilepsy. Clin Neurophysiol110:895–904.
Fisher RS, Uematsu S, Krauss GL, Cysyk BJ, McPherson R, Lesser RP,Gordon B, Schwerdt P, Rise M. (1992) Placebo-controlled pilot studyof centromedian thalamic stimulation in treatment of intractableseizures. Epilepsia 33:841–851.
Fisher R, Salanova V, Witt T, Worth R, Henry T, Gross R, Oommen K,Osorio I, Nazzaro J, Labar D, Kaplitt M, Sperling M, Sandok E, Neal J,Handforth A, Stern J, DeSalles A, Chung S, Shetter A, Bergen D,Bakay R, Henderson J, French J, Baltuch G, Rosenfeld W, Youkilis A,Marks W, Garcia P, Barbaro N, Fountain N, Bazil C, Goodman R,McKhann G, Babu Krishnamurthy K, Papavassiliou S, Epstein C,Pollard J, Tonder L, Grebin J, Coffey R, Graves N. (2010) Electricalstimulation of the anterior nucleus of thalamus for treatment ofrefractory epilepsy. Epilepsia 51:899–908.
Epilepsia, **(*):1–11, 2013doi: 10.1111/epi.12352
10
A. Valent�ın et al.
Flanagan D, Valentin A, Garcia Seoane JJ, Alarcon G, Boyd SG. (2009)Single-pulse electrical stimulation helps to identify epileptogeniccortex in children. Epilepsia 50:1793–1803.
Hart YM, Shorvon SD. (1995) The nature of epilepsy in the generalpopulation. I. Characteristics of patients receiving medication forepilepsy. Epilepsy Res 21:43–49.
Hodaie M, Wennberg RA, Dostrovsky JO. (2002) Chronic anteriorthalamus stimulation for intractable epilepsy. Epilepsia 43:603–608.
Kissani N, Alarc�on G, Dad M, Binnie CD, Polkey CE. (2001) Sensitivity ofrecordings at sphenoidal electrode site for detecting seizure onset:evidence from scalp, superficial and deep foramen ovale recordings.Clin Neurophysiol 112:232–240.
Kokkinos V, Alarcon G, Selway RP, Valentin A. (2013) Role of singlepulse electrical stimulation (SPES) to guide electrode implantationunder general anaesthesia in presurgical assessment of epilepsy.Seizure 22:198–204.
Kondziolka D, Lee JY. (2004) Long-lasting microthalamotomy effect aftertemporary placement of a thalamic stimulating electrode. StereotactFunct Neurosurg 82:127–130.
Koop MM, Andrzejewski A, Hill BC, Heit G, Bronte-Stewart HM. (2006)Improvement in a quantitative measure of bradykinesia aftermicroelectrode recording in patients with Parkinson’s disease duringdeep brain stimulation surgery.MovDisord 21:673–678.
Kwan P, Schachter SC, Brodie MJ. (2011) Drug-resistant epilepsy. N EnglJ Med 365:919–926.
Lacruz ME, Garcia Seoane JJ, Valentin A, Selway R, Alarcon G. (2007)Frontal and temporal functional connections of the living human brain.Eur J Neurosci 26:1357–1370.
Lhatoo SD, Solomon JK, McEvoy AW, Kitchen ND, Shorvon SD, SanderJW. (2003) A prospective study of the requirement for and theprovision of epilepsy surgery in the United Kingdom. Epilepsia44:673–676.
Loddenkemper T, Pan A, Neme S, Baker KB, Rezai AR, Dinner DS,Montgomery EB Jr, Luders HO. (2001) Deep brain stimulation inepilepsy. J Clin Neurophysiol 18:514–532.
Maltete D, Derrey S, Chastan N, Debono B, G�erardin E, Fr�eger P, MihoutB, Menard JF, Hannequin D. (2008) Microsubthalamotomy: animmediate predictor of long-term subthalamic stimulation efficacy inParkinson disease.Mov Disord 23:1047–1050.
Mann JM, Foote KD, Garvan CW, Fernandez HH, Jacobson CE 4th,Rodriguez RL, Haq IU, Siddiqui MS, Malaty IA, Morishita T, Hass CJ,OkunMS. (2009) Brain penetration effects of microelectrodes and DBSleads in STN or GPi. J Neurol Neurosurg Psychiatry 80:794–797.
Morishita T, Foote KD, Wu SS, Jacobson CE 4th, Rodriguez RL, Haq IU,Siddiqui MS, Malaty IA, Hass CJ, Okun MS. (2010) Brain penetrationeffects of microelectrodes and deep brain stimulation leads in ventralintermediate nucleus stimulation for essential tremor. J Neurosurg112:491–496.
Morrell MJ. (2011) Responsive cortical stimulation for the treatment ofmedically intractable partial epilepsy.Neurology 77:1295–1304.
Nashef L, Ryvlin P. (2009) Sudden unexpected death in epilepsy (SUDEP):update and reflections.Neurol Clin 27:1063–1074.
Parent M, Parent A. (2005) Single-axon tracing and three-dimensionalreconstruction of centre median-parafascicular thalamic neurons inprimates. J Comp Neurol 481:127–144.
Schuele SU, Luders HO. (2008) Intractable epilepsy: management andtherapeutic alternatives. Lancet Neurol 7:514–524.
Smith Y, Raju DV, Pare JF, Sidibe M. (2004) The thalamostriatal system: ahighly specific network of the basal ganglia circuitry. Trends Neurosci27:520–527.
Spencer SS, So NK, Engel J, Williamson PD, Levesque MF, Spencer DD.(1993) Depth electrodes. In Engel J Jr (Ed.) Surgical treatment ofepilepsies. 2nd ed. Raven Press, NewYork, pp. 359–376.
Sun FT, Morrell MJ, Wharen RE Jr. (2008) Responsive cortical stimulationfor the treatment of epilepsy.Neurotherapeutics 5:68–74.
Tellez-Zenteno JF, Dhar R, Wiebe S. (2005) Long-term seizure outcomesfollowing epilepsy surgery: a systematic review and meta-analysis.Brain 128:1188–1198.
Tellez-Zenteno JF, McLachlan RS, Parrent A, Kubu CS, Wiebe S. (2006)Hippocampal electrical stimulation in mesial temporal lobe epilepsy.Neurology 66:1490–1494.
Therodore WH, Fisher RS. (2004) Brain stimulation for epilepsy. LancetNeurol 3:111–118.
Valentin A, Anderson M, Alarcon G, Seoane JJ, Selway R, Binnie CD,Polkey CE. (2002) Responses to single pulse electrical stimulationidentify epileptogenesis in the human brain in vivo. Brain125:1709–1718.
Valentin A, Alarcon G, Garcia-Seoane JJ, Lacruz ME, Nayak SD, HonavarM, Selway RP, Binnie CD, Polkey CE. (2005a) Single-pulse electricalstimulation identifies epileptogenic frontal cortex in the human brain.Neurology 65:426–435.
ValentinA, AlarconG,HonavarM,Garcia Seoane JJ, SelwayRP, PolkeyCE,Binnie CD. (2005b) Single pulse electrical stimulation for identi-fication of structural abnormalities and prediction of seizure outcomeafter epilepsy surgery: a prospective study. LancetNeurol 4:718–726.
Velasco F, Velasco M, Ogarrio C, Fanghanel G. (1987) Electricalstimulation of the centromedian thalamic nucleus in the treatment ofconvulsive seizures: a preliminary report. Epilepsia 28:421–430.
Velasco F, Velasco M, Velasco AL, Jimenez F. (1993) Effect of chronicelectrical stimulation of the centromedian thalamic nuclei on variousintractable seizure patterns: I. Clinical seizures and paroxysmal EEGactivity. Epilepsia 34:1052–1064.
Velasco F, Velasco M, Velasco AL, Jimenez F, Marquez I, Rise M. (1995)Electrical stimulation of the centromedian thalamic nucleus in controlof seizures: long-term studies. Epilepsia 36:63–71.
Velasco F, Velasco M, Jimenez F, Velasco AL, Marquez I. (2001)Stimulation of the central median thalamic nucleus for epilepsy.Stereotact Funct Neurosurg 77:228–232.
Velasco AL, Velasco F, Jimenez F, Velasco M, Castro G, Carrillo-Ruiz JD,Fanganel G, Boleaga B. (2006) Neuromodulation of the centromedianthalamic nuclei in the treatment of generalized seizures and theimprovement of the quality of life in patients with Lennox–Gastautsyndrome. Epilepsia 47:1203–1212.
Velasco AL, Velasco F, Velasco M, Trejo D, Castro G, Carrillo-Ruiz JD.(2007a) Electrical stimulation of the hippocampal epileptic foci forseizure control: a double-blind, long-term follow-up study. Epilepsia48:1895–1903.
Velasco F, Velasco AL, Velasco M, Jimenez F, Carrillo-Ruiz JD,Castro G. (2007b) Deep brain stimulation for treatment of theepilepsies: the centromedian thalamic target. Acta Neurochir Suppl97:337–342.
Vonck K, Boon P, Claeys P, Dedeurwaerdere S, Achten R, Van RD. (2005)Long-term deep brain stimulation for refractory temporal lobe epilepsy.Epilepsia 46(Suppl. 5):98–99.
Epilepsia, **(*):1–11, 2013doi: 10.1111/epi.12352
11
Centromedian DBS for Epilepsy
Copyright © 2022 FDOKUMEN




















