
Orders page 1 - ***** STAGING ***** - High Court of Australia
Upload
independentCategory
view
0download
0
Cost-effectiveness analysis of strategiesintroducing FDG-PET into the mediastinal staging ofnon-small-cell lung cancer from the Frenchhealthcare system perspective
K. Alzahouria, C. Lejeuneb, M.-C. Woronoff-Lemsic, P. Arveuxd,F. Guillemina,*
aCEC-Inserm, Service d’Epidemiologie et Evaluation Cliniques, C.H.U. de Nancy, bInserm EMI 01 06, Facultede Medecine, BP 87900, Dijon, cService Pharmacie, Unite Evaluation Medico-economique, Besancon, anddDepartement d’Information Medicale, Centre Georges-Francois Leclerc, Dijon, France
Received 4 June 2004; received in revised form 3 October 2004; accepted 8 October 2004
00do
SeNANa
KEYWORDSDecision trees; Cost-effectiveness;Economics; Non-small-cell lungcarcinoma;Fludeoxyglucose F18;Positron emissiontomography
09-9260/$ - see front matter q 200i:10.1016/j.crad.2004.10.010
* Guarantor and correspondent: F.rvice d’Epidemiologie et EvaluatNCY, 29 avenue du Marechal de Lncy, France. Tel.: C33 3 83 85 21 6E-mail address: f.guillemin@chu-na
AIM: To determine the most cost-effective strategy using PET for mediastinalstaging of potentially operable non-small-cell lung cancer (NSCLC).
METHODS: Four decision strategies based on French NSCLC work-up practices forthe selection of potential surgical candidates were compared, comprising CT only,PET for negative CT, PET for all with anatomical CT, and CT and PET for all cases. Themedical literature was surveyed to obtain values for all variables of interest. Costswere assessed with reimbursements from the French healthcare insurance for theyear 1999. Expected cost and life expectancy were calculated for all possibleoutcomes of each strategy. Sensitivity analysis was performed to determine theeffects of changing variables on the expected cost and life expectancy.
RESULTS: Compared with the CT only strategy, CT and PET for all resulted in arelative reduction of 70% of surgery for persons with mediastinal lymph nodemetastasis. PET for all with anatomical CT was shown to be a cost-effectivealternative to the CT only, with life expectancy increased by 0.10 years and expectedcost savings of 61 euros. This strategy was more favourable than PET for negative CT.Overall, sensitivity analyses showed the robustness of the results.
CONCLUSION: The introduction of thoracic PET for NSCLC staging is potentiallycost-effective in France. Further clinical investigation might help to validate thisresult.q 2005 The Royal College of Radiologists. Published by Elsevier Ltd. All rightsreserved.
Introduction
Prognosis of lung cancer remains poor and has notimproved appreciably over the last two decades. In
5 The Royal College of Radiolo
Guillemin, CEC-Inserm,ion Cliniques, C.H.U deattre de Tassigny, 540005; fax: C33 3 83 85 12 05.ncy.fr (F. Guillemin).
2000, lung cancers led to 27,164 deaths in Francewith a mortality rate standardized to Europe of 36.6per 100,000.1 There were 27,743 cases of newlydiagnosed lung cancers in France in 2000.2 Non-Small-Cell Lung Cancer (NSCLC) represents 80% ofall lung cancers. Its survival rate appears to bebetter if patient is medically operable and thetumor is resectable. Staging work-up of NSCLC aimsto identify patients who will potentially benefitfrom surgical treatment from those with
Clinical Radiology (2005) 60, 479–492
gists. Published by Elsevier Ltd. All rights reserved.

K. Alzahouri et al.480
mediastinal lymph nodes metastasis (stages N2 orN3). N2 status refers to metastasis to ipsilateralmediastinal and subcarinal lymph nodes. N3 statusrefers to metastasis to contralateral mediastinal,contralaterral hilar, ipsilateral or contralateralscalene, or to supraclavicular lymph nodes. N1refers to metastasis to lymph nodes in the peri-bronchial or the ipsilateral hilar region.3,4
Currently, Computed Tomography (CT) of thechest is an accepted tool for staging mediastinallymph nodes. Because of its low specificity, surgicalbiopsy by cervical mediastinoscopy or thoraco-scopy, or both, is necessary to achieve an accuratemediastinal stage. However theses surgical pro-cedures present inherent risks and significantcosts.5
2-[Fluorine-18] Flouro-2-Deoxy-D-Glocose (FDG)Positron Emission Tomography (PET) appears to beparticularly promising. PET can identify biopsy-proven metastasis that are not identified by othertests in 10% to 20% of potentially operable patientswith NSCLC.6 Recently, the PLUS study group (PETin LUng cancer Staging) conducted a randomisedclinical trial and concluded that addition of FDG-PET to conventional work-up staging of NSCLCprevented unnecessary surgery in one out of fivepatients with suspected NSCLC, therefore FDG-PETmay be included in the routine NSCLC stagingprotocol.7
Recent studies using decision-tree analysishave suggested the potential cost-effectivenessof using FDG-PET for the management ofNSCLC.8–13 This findings could not be valid inevery health care system without taking intoaccount specificity of costing of medical careand alternative clinical practices in health caresystem.14,15 Published decision tree modelsshould consider the specificity of medical costsdata or insurance reimbursement systems andshould reflect the practice of physician indifferent health care system.16 Consultation ofleader’s opinion in our academic universityhospital showed that the discrepancy betweenpublished decision tree analysis and reportedexperience in France health care system isparticularly high for staging NSCLC. Since costsstructures may differ in France from those inother countries and discrepancy exists betweenpublished models and actual practices, it wasfelt important that an incorporation of localcosts and practices should be made to adjust thepublished models.
The objective of this work was to develop adecision analysis model to compare the cost-effectiveness of various strategies of mediastinalstaging of potentially operable NSCLC combining
CT, PET and biopsy from the French health caresystem perspective.
Material and method
Base-case
The base-case was a 65-year-old patient, in whomNSCLC has been histologically established andassessed as operable. Distant metastases had notbeen detected and the tumour was assessed aslocally resectable by conventional staging. Esti-mates of the proportion of patients with a med-iastinal metastasis disease at presentation variedwith criteria for resectablity ranging from 28% to38%.17 So up to three-quarter of the patients withNSCLC were excluded from the base-case of ouranalysis.
General description of the model
We performed cost-effectiveness analysis from theFrench national public health system insuranceperspective using a decision tree model.18 Strat-egies comprised of sequences of particular clinicalevents with associated estimated transitional prob-abilities. At the end of each alternative arm of thetree (represented by a terminal node), payoffs wereassigned corresponding to the total cost of care andlife expectancy in years. Data 4.0 software (Tree-Age, Inc Williamston, MA) was used to construct thedecision tree and rolled back for analysis.
Structure of decision trees
Four strategies labelled CT only, PET for negativeCT, PET for all with anatomical CT, and CT and PETfor all were established (Fig. 1(a)–(d)).
The baseline strategy uses only thoracic CT fornon-invasive preoperative staging, whereas otherstrategies include the use of thoracic PET indifferent approaches. For all these strategies, weassumed that biopsy of mediastinal lymph nodes isperformed by cervical mediastinoscopy (CM), whichwas assumed to be equally sensitive to identifyipsilateral and contralateral mediastinal enlargedlymph node.
Reports that focused on the indications for CM inpatients with NSCLC are controversial. Someauthors recommend CM for all patients who arebeing considered for thoracotomies,5,19 whereasothers insist that CM is indicated only whenmediastinal involvement is suspected.20,21 Unfortu-nately, some lymph node levels are not accessible

Figure 1. (a) The strategy CT only. A square represents a decision node; circles are chance nodes; and diamonds denote terminal nodes (Biop., biopsy; CT, computedtomography; PET, positron emission tomography). (b) The strategy PET for negative CT. (Biop., biopsy; CT, computed tomography; PET, positron emission tomography).(c) The strategy PET for all with anatomical CT. (Biop., biopsy; CT, computed tomography; PET, positron emission tomography). (d) The strategy CT and PET for all.(Biop., biopsy; CT, computed tomography; PET, positron emission tomography).
Cost-e
ffective
ness
analysis
ofstra
tegie
sintro
ducin
gFD
G-PET
481

Figure
1(con
tinu
ed)
K. Alzahouri et al.482

Cost-effectiveness analysis of strategies introducing FDG-PET 483
by the standard CM, such as para-oesophageal (leveleight) nodes, pulmonary ligament (level nine)nodes, and in general hilar (level ten) nodes andall other intrapulmonary nodes. In addition, notaccessible to standard CM are the subaortic(aortopulmonary window, level five) and para-aortic (level six) nodes.22,23 French respiratoryphysicians and thoracic surgeons do not indicate aCM in all patients with CT positive for mediastinallymph node involvement (N1 or N2 lymph nodeswith more than 1 cm in the short-axis diameter).However, we have no evidence data about theproportion of patients with CT positive to whom CMwould be actually recommended. Based on theconsensus of multidisplinary experts, about half ofsuch patients would undergo surgical staging by CM.We integrated this parameter in staging work-up ofNSCLC for all strategies.
On the basis of the final diagnostic result of eachstaging strategy, patients are treated with chemo-radiation or surgical resection according to med-iastinal lymph nodes involvement or not.
CT onlyAccording to heterogeneity in practice, we assumedthat 50% of patients who are CT-positive formediastinal lymph node involvement (N2/N3) pro-ceed directly to chemo-radiation treatment andthat 50% of those patients have a biopsy to confirmthat the patient is not a surgical candidate. This 50%assumption reflects frequency of the practice ofmediastinoscopy for patients with CT positive assuggested by experts (see frequency of CM). If thebiopsy result is negative, patients proceed to lungresection. Patients who are CT negative formediastinal lymph node involvement (N0/N1) pro-ceed directly to thoracotomy.
PET for negative CT50% of patients who are CT positive proceed directlyto chemo-radiation and the other 50% of patientsundergo a confirming biopsy. If the biopsy result isnegative, they proceed to the necessary operation.TheCT-negativepatientsundergo thoracicPET. If thePET results are negative, patients proceed to thenecessary operation. Of patients with positive PET,50% had confirming biopsy and the remaining patientsproceed directly to chemo-radiation therapy.
PET for all with anatomical CTAll patients undergo thoracic CT and PET. Ofpatients with positive PET, 50% proceed to biopsyand the other 50% proceeded directly to chemo-radiation therapy. The PET-negative patients pro-ceed to thoracotomy. This strategy uses PETfunctional information for the staging decision and
CT information for anatomic location of mediastinalnodes whereas size is ignored. It simulates practicalscenario in which biopsy of mediastinal lymph nodecould be avoided in case of conflicting results of CTpositive and PET negative scanning.
CT and PET for allAll patients undergo systematically chest CT firstly,then thoracic PET. When both CT and PET demon-strate concordant results (negatives or positivesmediastinal lymph nodes), biopsy is not performed.In others cases, 50% of patients undergo lymphnodes biopsy, the others proceed directly tochemo-radiation therapy.
Data
The medical literature was surveyed to obtain abase-case value and range for all variables ofinterest, and we used short-term charges ratherthan cost.24 Since the precise values of probability,test parameters and cost varied in different studies,sensitivity analyses were performed. Values used inthe model, the ranges over which they were tested,and their sources are shown in Tables 1 and 2.
Stage of disease at presentation
The prevalence of contralateral and mediastinalnodal involvement, in patients with NSCLC beingconsidered for surgery was estimated at 30% on thebasis of review of a retrospective cohort of 217patients in our university hospital (unpublisheddata).
Sensitivity and specificity of tests
Estimates base-case values of the sensitivity andspecificity of thoracic CT to detect enlarged lymphnodes (N2/N3 disease) were provided by publishedstudies. We adopted sensitivity 0.57 (95% Confi-dence Interval CI, 0.49 to 0.66) and specificity 0.82(95% CI, 0.77 to 0.86) for thoracic CT obtained fromtwo meta-analyses of studies that used modern-generation scanner, CT criterion of O1 cm in theshort-axis diameter to represent mediastinal lymphnodes involvement, and pathologic confirmation bymediastinal lymph nodes sampling.25,26
The sensitivity and specificity for thoracic PEThas been reported in various subgroups according toCT results. We used these values for PET accordingto two meta-analyses recently published.13,27
The sensitivity and the specificity of CM wereobtained from meta-analysis of Toloza et al.28 Theoverall sensitivity was 0.81 (95% CI, 0.76 0.85). This
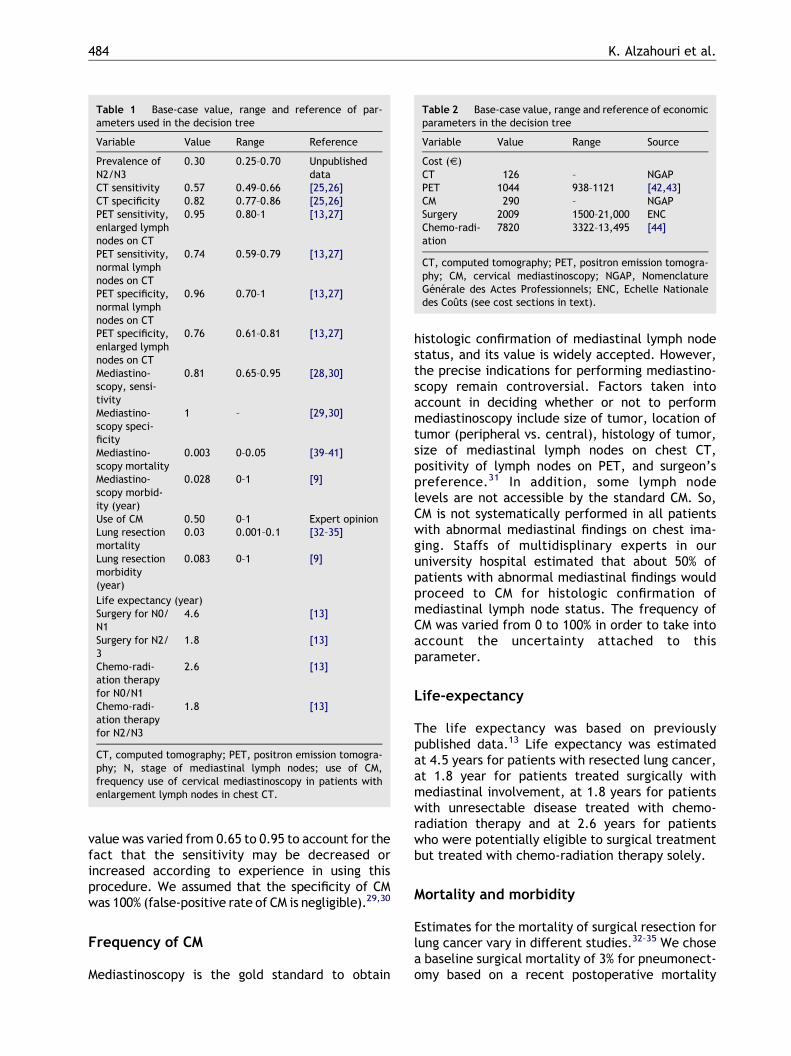
Table 1 Base-case value, range and reference of par-ameters used in the decision tree
Variable Value Range Reference
Prevalence ofN2/N3
0.30 0.25–0.70 Unpublisheddata
CT sensitivity 0.57 0.49–0.66 [25,26]CT specificity 0.82 0.77–0.86 [25,26]PET sensitivity,enlarged lymphnodes on CT
0.95 0.80–1 [13,27]
PET sensitivity,normal lymphnodes on CT
0.74 0.59–0.79 [13,27]
PET specificity,normal lymphnodes on CT
0.96 0.70–1 [13,27]
PET specificity,enlarged lymphnodes on CT
0.76 0.61–0.81 [13,27]
Mediastino-scopy, sensi-tivity
0.81 0.65–0.95 [28,30]
Mediastino-scopy speci-ficity
1 – [29,30]
Mediastino-scopy mortality
0.003 0–0.05 [39–41]
Mediastino-scopy morbid-ity (year)
0.028 0–1 [9]
Use of CM 0.50 0–1 Expert opinionLung resectionmortality
0.03 0.001–0.1 [32–35]
Lung resectionmorbidity(year)
0.083 0–1 [9]
Life expectancy (year)Surgery for N0/N1
4.6 [13]
Surgery for N2/3
1.8 [13]
Chemo-radi-ation therapyfor N0/N1
2.6 [13]
Chemo-radi-ation therapyfor N2/N3
1.8 [13]
CT, computed tomography; PET, positron emission tomogra-phy; N, stage of mediastinal lymph nodes; use of CM,frequency use of cervical mediastinoscopy in patients withenlargement lymph nodes in chest CT.
Table 2 Base-case value, range and reference of economicparameters in the decision tree
Variable Value Range Source
Cost (V)CT 126 – NGAPPET 1044 938–1121 [42,43]CM 290 – NGAPSurgery 2009 1500–21,000 ENCChemo-radi-ation
7820 3322–13,495 [44]
CT, computed tomography; PET, positron emission tomogra-phy; CM, cervical mediastinoscopy; NGAP, NomenclatureGenerale des Actes Professionnels; ENC, Echelle Nationaledes Couts (see cost sections in text).
K. Alzahouri et al.484
value was varied from 0.65 to 0.95 to account for thefact that the sensitivity may be decreased orincreased according to experience in using thisprocedure. We assumed that the specificity of CMwas 100% (false-positive rate of CM is negligible).29,30
Frequency of CM
Mediastinoscopy is the gold standard to obtain
histologic confirmation of mediastinal lymph nodestatus, and its value is widely accepted. However,the precise indications for performing mediastino-scopy remain controversial. Factors taken intoaccount in deciding whether or not to performmediastinoscopy include size of tumor, location oftumor (peripheral vs. central), histology of tumor,size of mediastinal lymph nodes on chest CT,positivity of lymph nodes on PET, and surgeon’spreference.31 In addition, some lymph nodelevels are not accessible by the standard CM. So,CM is not systematically performed in all patientswith abnormal mediastinal findings on chest ima-ging. Staffs of multidisplinary experts in ouruniversity hospital estimated that about 50% ofpatients with abnormal mediastinal findings wouldproceed to CM for histologic confirmation ofmediastinal lymph node status. The frequency ofCM was varied from 0 to 100% in order to take intoaccount the uncertainty attached to thisparameter.
Life-expectancy
The life expectancy was based on previouslypublished data.13 Life expectancy was estimatedat 4.5 years for patients with resected lung cancer,at 1.8 year for patients treated surgically withmediastinal involvement, at 1.8 years for patientswith unresectable disease treated with chemo-radiation therapy and at 2.6 years for patientswho were potentially eligible to surgical treatmentbut treated with chemo-radiation therapy solely.
Mortality and morbidity
Estimates for the mortality of surgical resection forlung cancer vary in different studies.32–35 We chosea baseline surgical mortality of 3% for pneumonect-omy based on a recent postoperative mortality

Cost-effectiveness analysis of strategies introducing FDG-PET 485
reported by Wada et al.35 In addition, we sub-tracted 1 month (0.083 year, range from 0 to 1 year)for the morbidity associated with the recovery fromthoracotomy in decision analyses involving surgicalintervention for lung cancer.9,36–38 CM is usuallyassociated with minimal mortality (0% to 0.3%).39–41
We used the higher reported value of mortality asour base-case estimate (range from 0 to 5%). Weestimated the average morbidity for CM to be aboutone third of that for curative surgical resection(0.028 year) (10 days).9 The risk associated withchest CT is primarily attributable to administrationof intravenous contrast material. We assumed thatchest CT has neither morbidity nor mortality forpatients with NSCLC. The risk associated with PET isassumed to be negligible since there has been noreport to date of reaction or complications from theinjection of FDG.
Costs
The economic analysis was governed from thenational public health system insurance perspec-tive. Only medical direct costs were included in ourmodel. Because the sequence of events (diagnosisand hospital treatment) lasts maximum someweeks, costs were not discounted.
Cost of chest CT and CM were obtained from“Nomenclature Generale des Actes Professionnels”(NGAP) which is a fixed price scale of medicalinterventions. In France, available data concerningthe cost of a PET were reported by two Frenchsimulations including the cost of FDG, transportoperating costs, equipment operating, building,equipment, furniture and other miscellaneousitems.42,43 According to those findings, the cost ofPET was fixed at 1044 V. To estimate the costs ofsurgery treatment, a case-mix was derived from aregional database including various Diagnosis RelatedGroups (DRGs) for the year 1999 in the public healthcare sector. Cost was then measured using « EchelleNationale des Couts» (ENC), a national public costscale compiled by the Ministry of Health using datafrom a representative sample of French publichospitals for the year 1999. The ENC includes severalbudget headings, such as costs for labour, technicalprocedure, consumable products, maintenance, pro-vision for depreciation, laundering, and catering.Cost of chemo-radiation treatment for unresectableNSCLC was estimated from Schraub et al. study.44
Economic parameters are summarized in Table 2.
Incremental cost-effectiveness ratio
The subsequent cost effectiveness analysis was
performed according to the recommendations forreference-case analysis on the Panel by Cost-Effectiveness in Health and Medicine45 and thoseof Drummond et al.46 Calculations of expected costand life expectancy of competing strategies wereperformed by summing the products of probabilitiesand values of each outcome.
Conventional staging with CT only is the mostwidely used strategy and was chosen as baselinestrategy to which each PET-based strategy wascompared by calculating the Incremental Cost-Effectiveness Ratio (ICER).
ICER ¼ðCOSTstrategy�COSTbaselineÞ
ðLEstrategy � LEbaselineÞ
where COSTbaseline and LEbaseline represented thecost and the life expectancy for CT only strategyand COSTstrategy and LEstrategy represented the costand life expectancy for each PET-based strategy.The results of ICER were presented in term of Eurosper Life Year Saved (V/LYS).
A negative numerator and positive denominatormean that the strategy under evaluation has lowercost and higher life expectancy being beneficial in allmeans. A positive numerator and negative denomi-nator also yield a negative ICER. In that case the newstrategy is dominated, because it has higher cost andlower life expectancy and should be rejected.
Positive numerator and denominator mean thatthe new strategy saves life years at an increasedcost. In this case, cost per life year saved might becalculated and the acceptability of this valuethreshold of ICER could be discussed. Negativenumerator and denominator (cost savings and areduction in life expectancy) yield a positive ICERbut a conflicting ethical consideration of costsavings per life year lost.
Sensitivity analyses
Sensitivity analyses were performed to evaluate therobustness of our results when we varied theprobabilities and assumptions used in the model.The range of values over which probability and costswere tested was obtained from the medicalliterature and expert opinion.
Results
Base-case values
Table 3 showed the proportion of therapeuticmanagement of patients according to the strategies
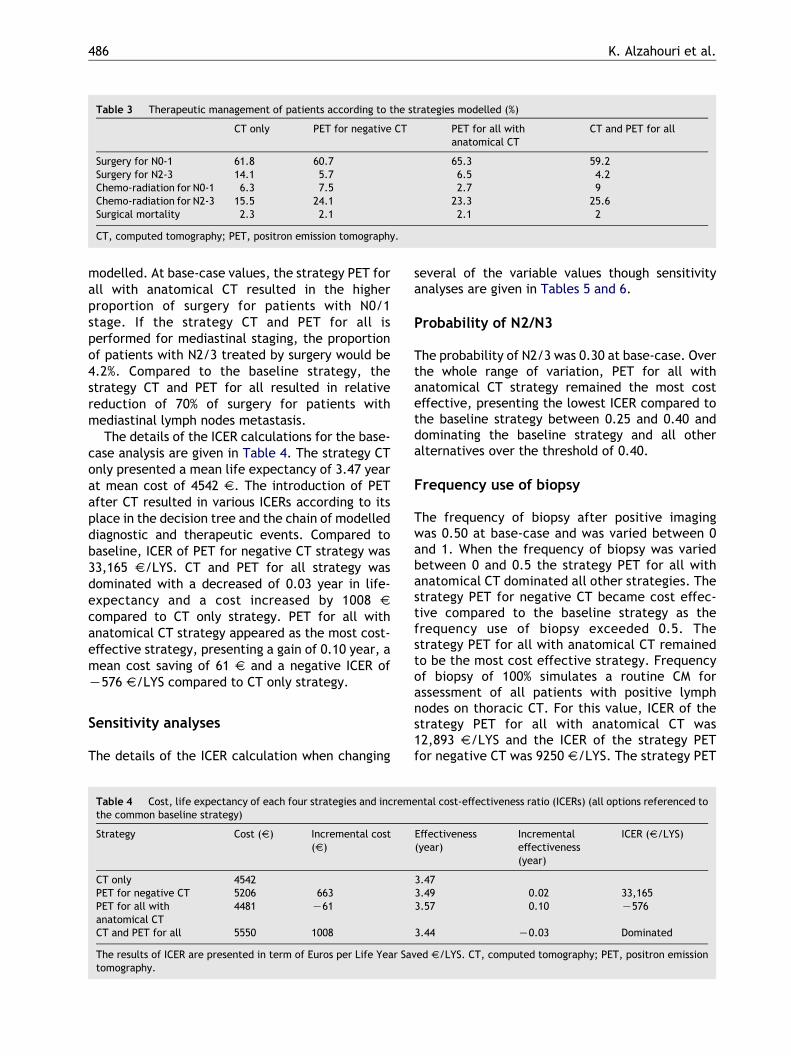
Table 3 Therapeutic management of patients according to the strategies modelled (%)
CT only PET for negative CT PET for all withanatomical CT
CT and PET for all
Surgery for N0-1 61.8 60.7 65.3 59.2Surgery for N2-3 14.1 5.7 6.5 4.2Chemo-radiation for N0-1 6.3 7.5 2.7 9Chemo-radiation for N2-3 15.5 24.1 23.3 25.6Surgical mortality 2.3 2.1 2.1 2
CT, computed tomography; PET, positron emission tomography.
K. Alzahouri et al.486
modelled. At base-case values, the strategy PET forall with anatomical CT resulted in the higherproportion of surgery for patients with N0/1stage. If the strategy CT and PET for all isperformed for mediastinal staging, the proportionof patients with N2/3 treated by surgery would be4.2%. Compared to the baseline strategy, thestrategy CT and PET for all resulted in relativereduction of 70% of surgery for patients withmediastinal lymph nodes metastasis.
The details of the ICER calculations for the base-case analysis are given in Table 4. The strategy CTonly presented a mean life expectancy of 3.47 yearat mean cost of 4542 V. The introduction of PETafter CT resulted in various ICERs according to itsplace in the decision tree and the chain of modelleddiagnostic and therapeutic events. Compared tobaseline, ICER of PET for negative CT strategy was33,165 V/LYS. CT and PET for all strategy wasdominated with a decreased of 0.03 year in life-expectancy and a cost increased by 1008 Vcompared to CT only strategy. PET for all withanatomical CT strategy appeared as the most cost-effective strategy, presenting a gain of 0.10 year, amean cost saving of 61 V and a negative ICER ofK576 V/LYS compared to CT only strategy.
Sensitivity analyses
The details of the ICER calculation when changing
Table 4 Cost, life expectancy of each four strategies and incremthe common baseline strategy)
Strategy Cost (V) Incremental cost(V)
CT only 4542PET for negative CT 5206 663PET for all withanatomical CT
4481 K61
CT and PET for all 5550 1008
The results of ICER are presented in term of Euros per Life Year Satomography.
several of the variable values though sensitivityanalyses are given in Tables 5 and 6.
Probability of N2/N3
The probability of N2/3 was 0.30 at base-case. Overthe whole range of variation, PET for all withanatomical CT strategy remained the most costeffective, presenting the lowest ICER compared tothe baseline strategy between 0.25 and 0.40 anddominating the baseline strategy and all otheralternatives over the threshold of 0.40.
Frequency use of biopsy
The frequency of biopsy after positive imagingwas 0.50 at base-case and was varied between 0and 1. When the frequency of biopsy was variedbetween 0 and 0.5 the strategy PET for all withanatomical CT dominated all other strategies. Thestrategy PET for negative CT became cost effec-tive compared to the baseline strategy as thefrequency use of biopsy exceeded 0.5. Thestrategy PET for all with anatomical CT remainedto be the most cost effective strategy. Frequencyof biopsy of 100% simulates a routine CM forassessment of all patients with positive lymphnodes on thoracic CT. For this value, ICER of thestrategy PET for all with anatomical CT was12,893 V/LYS and the ICER of the strategy PETfor negative CT was 9250 V/LYS. The strategy PET
ental cost-effectiveness ratio (ICERs) (all options referenced to
Effectiveness(year)
Incrementaleffectiveness(year)
ICER (V/LYS)
3.473.49 0.02 33,1653.57 0.10 K576
3.44 K0.03 Dominated
ved V/LYS. CT, computed tomography; PET, positron emission

Table 5 Sensitivity analysis for epidemiologic parameters (all options referenced to the common baseline strategy)
CT only PET for negative CT PET for all with anatomical CT CT and PET for all
Cost LE Cost LE ICER Cost LE ICER Cost LE ICER
Base-case
4542 3.47 5206 3.49 33,165 4481 3.57 K576 5550 3.44 Dominated
Probability of N2/N30.25 4233 3.59 4945 3.61 60,855 4275 3.70 402 5283 3.56 Dominated0.43 5348 3.15 5885 3.19 12,909 5019 3.26 K2956 6246 3.13 Dominated0.61 6464 2.70 6825 2.77 5056 5764 2.82 K5922 7208 2.71 79,1490.7 7022 2.47 7295 2.56 3160 6136 2.59 K7280 7689 2.49 32,222
Use of CMa
0.00 4839 3.37 5537 3.34 Dominated 3799 3.51 K7355 5847 3.34 Dominated0.20 4721 3.41 5405 3.40 Dominated 4072 3.53 K5098 5729 3.38 Dominated0.30 3661 343 5339 3.42 Dominated 4209 3.55 K3754 5669 3.40 Dominated0.80 4365 3.53 5007 3.58 13,156 4891 3.62 6166 5373 3.50 Dominated1 4246 3.57 4875 3.64 9250 5164 3.65 12,893 5254 3.54 Dominated
(PET Sp/CTK)0.70 4543 3.47 5661 3.35 Dominated 4936 3.44 Dominated 6005 3.30 Dominated0.73 4543 3.47 5608 3.37 Dominated 4884 3.46 Dominated 5953 3.32 Dominated0.81 4543 3.47 5451 3.42 Dominated 4726 3.50 5529 5796 3.37 Dominated
(PET Sn/CTK)0.59 4543 3.47 5234 3.48 59,060 4510 3.57 K337 5579 3.44 Dominated0.67 4543 3.47 5219 3.49 41,988 4495 3.57 K469 5564 3.44 Dominated0.79 4543 3.47 5196 3.49 28,767 4472 3.58 K651 5541 3.44 Dominated
(PET Sn/CTC)0.61 4543 3.47 5206 3.49 33,150 4465 3.56 K875 5603 3.42 Dominated0.73 4543 3.47 5206 3.49 33,150 4478 3.57 K632 5561 3.44 Dominated0.81 4543 3.47 5206 3.49 33,150 4487 3.58 K500 5533 3.45 Dominated
The results of ICER are presented in term of Euros by Life Year Saved V/LYS. LE, life expectancy; ICER, incremental cost-effectiveness ratio; CM, cervical mediastinoscopy; CT, computed tomography; PET, positron emission tomography; (PET Sn/CTK).PET sensitivity for normal lymph nodes on CT PET; (PET Sp/CTC). PET specificity for enlarged lymph nodes on CT.a The probability of performing cervical mediastinoscopy after abnormal mediastinal findings on chest imaging.
Cost-effectiveness analysis of strategies introducing FDG-PET 487
for all with anatomical CT increased cost and lifeexpectancy with ICER of 9312 V/LYS comparedwith the strategy PET for negative CT (data notshown).
Sensitivity and specificity of PET
The one-way sensitivity analysis of parameters ofPET showed that only the specificity of PET afternegative CT (PET Sp/CTK), had threshold valuesbeyond which PET for all with anatomical CTstrategy was the strategy of choice. Base-casevalue for this parameter was 0.96 and it wasvaried between 0.70 and 1. For a (PET Sp/CTK)lower than 0.73, the CT only strategy dominatedall other strategies. Above this value the strategyPET for all with anatomical CT was the most cost-effective strategy. Through the ranges of otherparameters of PET (sensitivity of PET afternegative CT, sensitivity of PET after positive CTand specificity of PET after positive CT) thesensitivity analysis showed that the strategy PETfor all with anatomical CT remained the cost-effective strategy (Table 5).
Cost of FDG-PET
The cost of PET was 1044 V for base-case. Varyingthe costs of PET (including cost of FDG) for valueabove 1044 V the results remain the same. When itwas raised at 1121 V, the strategy PET for all withanatomical CT increased cost and life expectancywith ICER of 170 V/LYS compared with the strategyCT only.
Cost of surgery
The cost of surgery was 2009 V for base-case. Whenthe cost of surgery was raised above 10,000 V thestrategy PET for negative CT produced negativeratios of K9200 V/LYS in comparison with thestrategy CT only. The strategy PET for all withanatomical CT also saved cost and increased lifeexpectancy with ICER of K4083 V/LYS. If savingcost was the sole consideration, the strategy PETfor negative CT would be the best strategy. TheICER of PET for all with anatomical CT strategy wasK2897 V/LYS in comparison with the PET fornegative CT strategy which means that the strategy

Table 6 Sensitivity analysis for economic parameters (all options referenced to a common baseline strategy)
CT only PET for negative CT PET for all with anatomical CT CT and PET for all
Cost LE Cost LE ICER Cost LE ICER Cost LE ICER
Base-case 4542 3.47 5206 3.49 33,165 4481 3.57 K576 5550 3.44 Dominated
Cost of PET938 4542 3.470 5131 3.49 29,450 4376 3.57 K1658 5481 3.44 Dominated975 4542 3.470 5157 3.49 30,750 4412 3.57 K1299 5536 3.44 Dominated1030 4542 3.470 5196 3.49 32,700 4467 3.57 K749 5628 3.44 Dominated1084 4542 3.470 5234 3.49 34,550 4522 3.57 K210 5481 3.44 Dominated1121 4542 3.470 5260 3.49 35,900 4559 3.57 170 5591 3.44 Dominated
Cost of surgery3954 6064 3.47 6537 3.49 23,650 5919 3.58 K1364 6822 3.44 Dominated7308 8687 3.47 8831 3.49 7200 8397 3.58 K2728 9014 3.44 Dominated10,662 11,309 3.47 11,125 3.49 K9200 10,875 3.58 K4083 11,206 3.44 346814,016 13,932 3.47 13,420 3.49 K25,600 13,354 3.58 K5437 13,399 3.44 17,94617,370 16,555 3.47 15,714 3.49 K42,050 15,832 3.58 K6802 15,591 3.44 32,45820,724 19,178 3.47 18,008 3.49 K58,500 18,311 3.58 K8156 17,783 3.44 46,970
Cost of chemo-radiation7391 4389 3.47 5046 3.49 32,850 4384 3.58 K47 5384 3.44 Dominated10,443 5483 3.47 6183 3.49 35,000 5079 3.58 K3801 6569 3.44 Dominated13,495 6577 3.47 7319 3.49 37,100 5775 3.58 K7545 7753 3.44 Dominated
The results of ICER are presented in term of Euros by Life Year Saved V/LYS. CT, computed tomography; PET, positron emission tomography; ICER, incremental cost-effectiveness ratio.
K.Alzah
ourietal.
488

Cost-effectiveness analysis of strategies introducing FDG-PET 489
PET for all with anatomical CT increased lifeexpectancy and saved cost when it was comparedwith strategy PET for negative CT. When the cost ofsurgery was raised above 17,000V, the strategy PETfor all with anatomical CT increased cost and lifeexpectancy with ICER of 1367V/LYS compared withthe strategy PET for negative CT (Table 6).
Cost of chemoradiation
Doubling or even tripling estimated cost of chemo-radiation therapy did not change the order of ICERamong four strategies tested.
Discussion
The results of this decision analysis clearly supportthe use of thoracic PET as preoperative mediastinalstaging procedure for patients with NSCLC. Thestrategy PET for all with anatomical CT has shownto be the most cost-effective alternative comparedwith the CT only management strategy. It savedcost and increased life expectancy resulting in K576 V/LYS. Even under a wide range of assump-tions, the results of sensitivity analyses showed therobustness of this conclusion. Varying model par-ameters simulates the possibility of seeing indi-cation for this new test to be transferred fromspecialised centres to the routine practice in non-specialized centres. It provides a degree of confi-dence on results of this cost-effectiveness analysesin France even if variations in practice exist.
Assuming a widespread diffusion of PET FDG, thediscrepancies between the results of PET and CTabout the involvement of mediastinal lymph nodeswould be the cornerstone to avoid invasive med-iastinal staging. The strategy PET for all withanatomical CT simulates this practical scenario.However, we believe that when FDG-PET results arenegative, decision to perform CM or surgery withcurative intent should be guided by the pre-testprobability of mediastinal metastasis, the risk forsurgical complications, and the patient prefer-ences. While our results can help to inform clinicaldecision making, more investigations are needed todetermine when surgery without previous mediast-inal biopsy can be performed.
Uncertainty exists in regards to the results ofcost effectiveness analysis because the level ofuncertainty in each calculated ICER is unknown. Inthe absence of data at the patient level we usedsensitivity analyses. Recently, a number of alterna-tive complex methods based on simulation haveappeared in the literature for computing
confidence intervals around calculated ICER.47,48
However, a number of practical problems areassociated with such methods for quantifyinguncertainty of ICER.49
The optimal overall strategy for staging patientswith NSCLC remains controversial. Although chestCT can be used to assess patients’ T and M status,the ability of CT to accurately assess mediastinalinvolvement is suboptimal. CM provides a moreaccurate way to stage the mediastinum, but it isassociated with additional risks and costs. In thepresent study strategy CT and PET for all resulted inrelative reduction of 70% of surgery for patientswith mediastinal lymph nodes metastasis. Thisdiffers from results of a recent randomized clinicaltrial concluding that PET does not lead to a majorreduction of surgery for in patients with NSCLC.50
Since there is a difference in selection of patientsentering the workup processes, our results do notcontradict this, in so far as less than 8% of patientsrecruited into the Viney study had medisatinalmetastasis to N2 or N3 lymph nodes, while ourmodel was based on observational practices with aproportion of patients with a mediastinal metas-tasis disease of 30% as base-case.
Several studies have attempted to identify thebest strategy for staging the mediastinum ofpatients with NSCLC. Scott et al. used decisionanalysis to compare various staging strategiescombining PET, CT, and biopsy.9 In their model,patients without mediastinal disease underwentresection, whereas patients with evidence ofmediastinal involvement (metastases to N2/N3lymph nodes) were candidate for thoracotomy andlung resection as only therapy. The analysis wasperformed from the United States health caresystem perspective and Medicare reimbursementscosts were used. The authors concluded thatstrategy that used CT PET after negative CT tostage the mediastinum generates an ICER of$ 25,286 per life-year saved.
More recently, Dietlein et al.13 performed a cost-effectiveness analysis comparing CT and PET tostage mediastinal lymph nodes. Patients withproven NSCLC were enrolled into the model.Patients without evidence of mediastinal diseaseunderwent resection, whereas patients with med-iastinal involvement were considered to haveunresectable disease and were not considered formultimodal therapy. The economic analysis waslimited to hospital costs and professional fees. Theauthors demonstrated that use CT and PET tostaging patients with NSCLC is cost-effective forthe German health system. The authors concludedthat the implantation of PET in Germany wouldresult in an additional cost of only 32,000 V.

K. Alzahouri et al.490
In Japan, Kosuda et al. have proposed anotherdecision tree that might be adapted for practices inJapan health care system.11 The results of themodels showed that whole body PET in the place ofCT for staging NSCLC patients avoided unnecessarybronchoscopies and thoracotomies for incurableand benign diseases. The authors concluded thatthe strategy that uses whole-body PET for managingNSCLC would be potentially cost-effective in Japan.
Critical appraisal of theses literatures showedthat several assumptions were made to facilitateprocedural modelling in terms of the architectureof the decision tree model. These assumptions wererelated to different approaches for the manage-ment of NSCLC given the results of FDG-PETscanning. In addition not all possible costs wereincluded in these studies. Neither the cost ofpalliative care nor the cost of chemotherapy wasincluded in the decision tree of Scott et al. Thecosts of palliative care and chemotherapy would beincurred in the specific population with non-resectable cancer, and so it influences the com-parison between strategies. Moreover, at the timeour analysis was designed, evidence suggests thatpractice and costs may differ in France from thosein other countries. CM is not routinely used incurrent management of patients with CT positive toconfirm that they are not surgical candidates. Animportant cause for such a discrepancy in Francemedical practice from other countries might be dueto the fact that France health care system is publicsystem and financed by national budget.51–54
Our study has some limitations. Firstly, it doesnot consider all plausible options for the use of PET.Recently, the ability of PET-CT fusion imaging toimprove on the sensitivity and specificity of PETalone has been reported.55 Moreover, studies haveshown an additional value of PET in determiningextra-thoracic spread of disease for patients withNSCLC.56,57 At this time, adequate data are avail-able for evaluating the role of the PET in theassessment of mediastinal lymph nodes includingthese from two rigorous meta-analyses. There aremuch fewer data available regarding the sensitivityand specificity of PET for the detection of liver orbone metastases. However, several small serieshave suggested that the high accuracy of PET mayobviate the need for a bone scan.58,59 Assessment ofthe role of these new approaches awaits furtherstudies. Secondly, the simple approach taken bycombining expert opinion based on their practicesand original data from the literature on thesensitivity and specificity of tests independentlymight be inappropriate. It is likely that discrepancymight arise between the published data and thetest performance as a routine procedure. The
usefulness of PET in the mediastinal staging oflung cancer is evolving. So, the initial enthusiasmfor PET as the staging tool for mediastinal diseasemight be tempered by the results of recentstudies.60,61 But sensitivity analyses showed thateven with lower sensitivity of PET, the strategy PETfor all patients with anatomical CT is still cost-effective. On the other hand, we have no evidencedata about the proportion of patients with med-iastinal abnormality for whom CM would be per-formed. Therefore, we adapted expert opinionestablished in multidisplinary staffs in our univer-sity hospital to set up the base-case for this study.Nevertheless, the frequency of use of biopsy wasvaried between 0 and 100% to consider thevariability in practice of biopsy after positivesresults of thoracic imaging. Thirdly, the costs inthis study are taken from France’s national per-spective, and hence cannot be extended to othercountries. Although, an optimal approach wouldhave estimated the true costs of each subgroup ofpatient, we lacked data about adjustment cost ofsurgery and chimoradiotherapy for target subgrouppatient. Finally, our work did not account for costsassociated with bronchoscopy, bone scan, abdomi-nal CT or others procedures that could be per-formed to identify underlying diseases such asChronic Obstructive Pulmonary Diseases (COPD) orother co-morbidity. Since all the strategiesassumed that patients were potential candidatesfor surgery and they could be operated, such co-morbidity cost consideration in the analysis isbeyond the scope of the present study.
Our study showed that the additional PET cost ismore than compensated for by the savings realizedfrom avoided surgeries. It allowed drawing atten-tion on consequences of sequence of NSCLC stagingprocedures. This theoretical decision model mightbe backed up by experience after implementationof this new technology for NSCLC work-up in Francehealth care system.
Acknowledgements
The authors would like to thank A. Bernard, P. Bey,A. Bizieux-Thaminy, S. Briancon, A. Depierre, P.Foucher, D. Jolly, Y. Martinet, O. Menard, E. Quoixand M. Velten for their fruitful contribution to thiswork. We are also grateful to E. Lebihan formethodological assistance. This work was sup-ported by grants from the French Ministry of Health,the Urban Community of Nancy area and theLorraine Region.
Cost-effectiveness analysis of strategies introducing FDG-PET 491
References
1. Menegoz F, Black RJ, Arveux P, et al. Cancer incidence andmortality in France in 1975–95. Eur J Cancer Prev 1997;6:442–66.
2. Institut de veille sanitaire. Evolution de l’incidence et dela mortalite par cancer en France de 1978 a 2000.(Accessed September 30, 2004 at http://www.invs.sante.fr/publications/).
3. Grondin SC, Liptay MJ. Current concepts in the staging ofnon-small cell lung cancer. Surg Oncol 2002;11:181–90.
4. Naruke T, Suemasu K, Ishikawa S. Lymph node mapping andcurability at various levels of metastasis in resected lungcancer. J Thorac Cardiovasc Surg 1978;76:832–9.
5. Luke WP, Pearson FG, Todd TR, et al. Prospective evaluationof mediastinoscopy for assessment of carcinoma of the lung.J Thorac Cardiovasc Surg 1986;91:53–6.
6. Pieterman RM, van Putten JW, Meuzelaar JJ, et al. Pre-operative staging of non-small-cell lung cancer with posi-tron-emission tomography. N Engl J Med 2000;343:254–61.
7. van Tinteren H, Hoekstra OS, Smit EF, et al. Effectiveness ofpositron emission tomography in the preoperative assess-ment of patients with suspected non-small-cell lung cancer:the PLUS multicentre randomised trial. Lancet 2002;359:1388–93.
8. Sloka JS, Hollett PD, Mathews M. Cost-effectiveness ofpositron emission tomography for non-small cell lungcarcinoma in Canada. Med Sci Monit 2004;10:MT73–MT80.
9. Scott WJ, Shepherd J, Gambhir SS. Cost-effectiveness ofFDG-PET for staging non-small cell lung cancer: a decisionanalysis. Ann Thorac Surg 1998;66:1876–83.
10. Miles KA. An approach to demonstrating cost-effectivenessof diagnostic imaging modalities in Australia illustrated bypositron emission tomography. Australas Radiol 2001;45:9–18.
11. Kosuda S, Ichihara K, Watanabe M, et al. Decision-treesensitivity analysis for cost-effectiveness of whole-body FDGPET in the management of patients with non-small-cell lungcarcinoma in Japan. Ann Nucl Med 2002;16:263–71.
12. Gugiatti A, Grimaldi A, Rossetti C, et al. Economic analyseson the use of positron emission tomography for the work-upof solitary pulmonary nodules and for staging patients withnon-small-cell-lung-cancer in Italy. Q J Nucl Med 2004;48:49–61.
13. Dietlein M, Weber K, Gandjour A, et al. Cost-effectiveness ofFDG-PET for the management of potentially operable non-small cell lung cancer: priority for a PET-based strategy afternodal-negative CT results. Eur J Nucl Med 2000;27:1598–609.
14. Dietlein M, Knapp WH, Lauterbach KW, et al. Economicevaluation studies in nuclear medicine: the need forstandardization. Eur J Nucl Med 1999;26:663–80.
15. Halliday RG, Darba J. Cost data assessment in multinationaleconomic evaluations: some theory and review of publishedstudies. Appl Health Econ Health Policy 2003;2:149–55.
16. Dolan JG. A survey of clinicians’ opinions regarding the valueof published decision analyses as sources of clinically usefulinformation. Med Decis Making 1997;17:427–30.
17. Dwamena BA, Sonnad SS, Angobaldo JO, et al. Metastasesfrom non-small cell lung cancer: mediastinal staging in the1990s—meta-analytic comparison of PET and CT. Radiology1999;213:530–6.
18. Singer ME, Applegate KE. Cost-effectiveness analysis inradiology. Radiology 2001;219:611–20.
19. Funatsu T, Matsubara Y, Ikeda S, et al. Preoperative
mediastinoscopic assessment of N factors and the need formediastinal lymph node dissection in T1 lung cancer.J Thorac Cardiovasc Surg 1994;108:321–8.
20. Daly BD, Mueller JD, Faling LJ, et al. N2 lung cancer:outcome in patients with false-negative computed tomo-graphic scans of the chest. J Thorac Cardiovasc Surg 1993;105:904–10.
21. Takamochi K, Nagai K, Yoshida J, et al. The role of computedtomographic scanning in diagnosing mediastinal node invol-vement in non-small cell lung cancer. J Thorac CardiovascSurg 2000;119:1135–40.
22. Hoffmann H. Invasive staging of lung cancer by mediastino-scopy and video-assisted thoracoscopy. Lung Cancer 2001;34(Suppl 3):S3–S5.
23. Passlick B, Kubuschock B, Sienel W, et al. Mediastinallymphadenectomy in non-small cell lung cancer: effective-ness in patients with or without nodal micrometastases—results of a preliminary study. Eur J Cardiothorac Surg 2002;21:520–6.
24. Finkler SA. The distinction between cost and charges. AnnIntern Med 1982;96:102–9.
25. Halter G, Buck AK, Schirrmeister H, et al. Lymph nodestaging in lung cancer using [18F]FDG-PET. Thorac Cardio-vasc Surg 2004;52:96–101.
26. Toloza EM, Harpole L, McCrory DC. Noninvasive staging ofnon-small cell lung cancer: a review of the current evidence.Chest 2003;123:137S–146.
27. Gould MK, Kuschner WG, Rydzak CE, et al. Test performanceof positron emission tomography and computed tomographyfor mediastinal staging in patients with non-small-cell lungcancer: a meta-analysis. Ann Intern Med 2003;139:879–92.
28. Toloza EM, Harpole L, Detterbeck F, et al. Invasive staging ofnon-small cell lung cancer: a review of the current evidence.Chest 2003;123:157S–166.
29. Esnaola NF, Lazarides SN, Mentzer SJ, et al. Outcomes andcost-effectiveness of alternative staging strategies for non-small-cell lung cancer. J Clin Oncol 2002;20:263–73.
30. Kelly RF, Tran T, Holmstrom A, et al. Accuracy and cost-effectiveness of [18F]-2-fluoro-deoxy-D-glucose-positronemission tomography scan in potentially resectable non-small cell lung cancer. Chest 2004;125:1413–23.
31. Chang MY, Sugarbaker DJ. Surgery for early stage non-smallcell lung cancer. Semin Surg Oncol 2003;21:74–84.
32. Ginsberg RJ, Hill LD, Eagan RT, et al. Modern thirty-dayoperative mortality for surgical resections in lung cancer.J Thorac Cardiovasc Surg 1983;86:654–8.
33. Roeslin N, Morand G. Complications and mortality of surgeryfor bronchogenic cancers. Rev Pneumol Clin 1992;48:231–6.
34. Vogt-Moykopf I, Fritz T, Meyer G, et al. Bronchoplastic andangioplastic operation in bronchial carcinoma: long-termresults of a retrospective analysis from 1973 to 1983. Int Surg1986;71:211–20.
35. Wada H, Nakamura T, Nakamoto K, et al. Thirty-dayoperative mortality for thoracotomy in lung cancer.J Thorac Cardiovasc Surg 1998;115:70–3.
36. Beck JR, Kassirer JP, Pauker SG. A convenient approximationof life expectancy (the “DEALE”). I. Validation of themethod. Am J Med 1982;73:883–8.
37. Beck JR, Pauker SG, Gottlieb JE, et al. A convenientapproximation of life expectancy (the “DEALE”). II. Use inmedical decision-making. Am J Med 1982;73:889–97.
38. Moroff SV, Pauker SG. What to do when the patient outlivesthe literature, or DEALE-ing with a full deck. Med DecisMaking 1983;3:313–38.
39. Cybulsky IJ, Bennett WF. Mediastinoscopy as a routineoutpatient procedure. Ann Thorac Surg 1994;58:176–8.

K. Alzahouri et al.492
40. Hammoud ZT, Anderson RC, Meyers BF, et al. The currentrole of mediastinoscopy in the evaluation of thoracicdisease. J Thorac Cardiovasc Surg 1999;118:894–9.
41. Puhakka HJ. Complications of mediastinoscopy. J LaryngolOtol 1989;103:312–5.
42. Bergeal E. Evalutaion medico-economique de la Tomogra-phie a Emission de Positons: le projet Champardennais,these de Doctorat en medecine. Universite de Reims2000;40–58.
43. Fauchet MVJ. Tomographie par emission de positons etoncologie : technique, clinique, offre industrielle, mise enœuvre. RBM 1998;20:113–82.
44. Schraub S, Arveux P, Mercier M, et al. Surgical health carepatterns and cancer cost: two studies using populationregistry data. Rev Epidemiol Sante Publique 1996;44(Suppl1):S33–S9.
45. Siegel JE, Weinstein MC, Russell LB, et al. Recommendationsfor reporting cost-effectiveness analyses. Panel on Cost-Effectiveness in Health and Medicine. JAMA 1996;276:1339–41.
46. Drummond MF, Jefferson TO. Guidelines for authors andpeer reviewers of economic submissions to the BMJ. The BMJEconomic Evaluation Working Party. BMJ 1996;313:275–83.
47. O’Brien BJ, Drummond MF, Labelle RJ, et al. In search ofpower and significance: issues in the design and analysis ofstochastic cost-effectiveness studies in health care. MedCare 1994;32:150–63.
48. Siani C, Moatti JP. The handling of uncertainty in economicevaluations of health care strategies. Rev Epidemiol SantePublique 2003;51:255–76.
49. Briggs A, Fenn P. Confidence intervals or surfaces? Uncer-tainty on the cost-effectiveness plane Health Econ 1998;7:723–40.
50. Viney RC, Boyer MJ, King MT, et al. Randomized controlledtrial of the role of positron emission tomography in themanagement of stage I and II non-small-cell lung cancer.J Clin Oncol 2004;22:2357–62.
51. McPherson K, Wennberg JE, Hovind OB, et al. Small-areavariations in the use of common surgical procedures: aninternational comparison of New England, England, andNorway. N Engl J Med 1982;307:1310–4.
52. Rosenau PV. Managing medical technology: lessons for theUnited States from Quebec and France. Int J Health Serv2000;30:617–39.
53. Cherkin DC, Deyo RA, Loeser JD, et al. An internationalcomparison of back surgery rates. Spine 1994;19:1201–6.
54. Volinn E, Diehr P, Ciol MA, et al. Why does geographicvariation in health care practices matter? (And sevenquestions to ask in evaluating studies on geographicvariation) Spine 1994;19:2092S–2100.
55. Lardinois D, Weder W, Hany TF, et al. Staging of non-small-cell lung cancer with integrated positron-emission tomogra-phy and computed tomography. N Engl J Med 2003;348:2500–7.
56. MacManus MP, Hicks RJ, Matthews JP, et al. High rate ofdetection of unsuspected distant metastases by pet inapparent stage III non-small-cell lung cancer: implicationsfor radical radiation therapy. Int J Radiat Oncol Biol Phys2001;50:287–93.
57. Stroobants SG, D’Hoore I, Dooms C, et al. Additional value ofwhole-body fluorodeoxyglucose positron emission tomogra-phy in the detection of distant metastases of non-small-celllung cancer. Clin Lung Cancer 2003;4:242–7.
58. Cheran SK, Herndon JE, Patz Jr EF. Comparison of whole-body FDG-PET to bone scan for detection of bone metastasesin patients with a new diagnosis of lung cancer. Lung Cancer2004;44:317–25.
59. Gayed I, Vu T, Johnson M, et al. Comparison of bone and 2-deoxy-2-[18F]fluoro-D-glucose positron emission tomographyin the evaluation of bony metastases in lung cancer. MolImaging Biol 2003;5:26–31.
60. Gonzalez-Stawinski GV, Lemaire A, Merchant F, et al. Acomparative analysis of positron emission tomography andmediastinoscopy in staging non-small cell lung cancer.J Thorac Cardiovasc Surg 2003;126:1900–5.
61. Reed CE, Harpole DH, Posther KE, et al. Results of theAmerican College of Surgeons Oncology Group Z0050 trial:the utility of positron emission tomography in stagingpotentially operable non-small cell lung cancer. J ThoracCardiovasc Surg 2003;126:1943–51.
Copyright © 2022 FDOKUMEN




















