
Correlation of Magnetic Resonance Imaging Findings and Reported Symptoms in Patients with Chronic...
9
The PDF of the article you requested follows this cover page. This is an enhanced PDF from The Journal of Bone and Joint Surgery 2010;92:353-360. doi:10.2106/JBJS.I.00031 J Bone Joint Surg Am. Seong and Tae Kyun Kim Jong Pil Yoon, Chong Bum Chang, Jae Ho Yoo, Sung Ju Kim, Ja Young Choi, Jung-Ah Choi, Sang Cheol Chronicity of an Anterior Cruciate Ligament Tear Correlation of Magnetic Resonance Imaging Findings with the This information is current as of March 1, 2010 Reprints and Permissions Permissions] link. and click on the [Reprints and jbjs.org article, or locate the article citation on to use material from this order reprints or request permission Click here to Publisher Information www.jbjs.org 20 Pickering Street, Needham, MA 02492-3157 The Journal of Bone and Joint Surgery
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Correlation of Magnetic Resonance Imaging Findings and Reported Symptoms in Patients with Chronic...

The PDF of the article you requested follows this cover page.
This is an enhanced PDF from The Journal of Bone and Joint Surgery
2010;92:353-360. doi:10.2106/JBJS.I.00031 J Bone Joint Surg Am.Seong and Tae Kyun Kim Jong Pil Yoon, Chong Bum Chang, Jae Ho Yoo, Sung Ju Kim, Ja Young Choi, Jung-Ah Choi, Sang Cheol
Chronicity of an Anterior Cruciate Ligament TearCorrelation of Magnetic Resonance Imaging Findings with the
This information is current as of March 1, 2010
Reprints and Permissions
Permissions] link. and click on the [Reprints andjbjs.orgarticle, or locate the article citation on
to use material from thisorder reprints or request permissionClick here to
Publisher Information
www.jbjs.org20 Pickering Street, Needham, MA 02492-3157The Journal of Bone and Joint Surgery
Correlation of Magnetic Resonance ImagingFindings with the Chronicity of anAnterior Cruciate Ligament Tear
By Jong Pil Yoon, MD, Chong Bum Chang, MD, PhD, Jae Ho Yoo, MD, PhD, Sung Ju Kim, MS, Ja Young Choi, MD,Jung-Ah Choi, MD, PhD, Sang Cheol Seong, MD, PhD, and Tae Kyun Kim, MD, PhD
Investigation performed at the Joint Reconstruction Center, Seoul National University Bundang Hospital, Seongnam, South Korea
Background: Although several findings on magnetic resonance imaging have been demonstrated after anterior cruciateligament injury, sequential changes on magnetic resonance imaging have not been comprehensively studied. We un-dertook to correlate four specific findings on magnetic resonance imaging of an anterior cruciate ligament injury over time.
Methods: One hundred and forty-five patients with a complete tear of the anterior cruciate ligament confirmed byarthroscopy were divided, according to the time from the injury to the acquisition of the magnetic resonance image, intofour groups: acute (within six weeks), subacute (more than six weeks to three months), intermediate (more than threemonths to one year), and chronic (more than one year). Four findings (anterior cruciate ligament morphology, jointeffusion, posterior cruciate ligament angle, and bone bruise) were evaluated for each study group.
Results: Strong correlations were found between the magnetic resonance imaging findings and the chronicity of theanterior cruciate ligament tear. Anterior cruciate morphology showed sequential changes with time (p < 0.001). Jointeffusion decreased with time, with a significant difference occurring between the acute and subacute groups at six weeks(p < 0.001). The posterior cruciate ligament angle decreased gradually over time (p < 0.001). Finally, the signal contrastof bone-bruising decreased with time, with a significant change occurring after three months (p = 0.049).
Conclusions: Our study confirmed that these four magnetic resonance imaging variables are closely correlated with thechronicity of an anterior cruciate ligament tear, and estimation of the chronicity of the tear can be facilitated by anintegrative interpretation of these findings.
Level of Evidence: Diagnostic Level II. See Instructions to Authors for a complete description of levels of evidence.
Estimates of the time elapsed from an anterior cruciateligament injury can be helpful in understanding thenatural history of the injury. To our knowledge, no
previous study has provided an integrated interpretation ofmagnetic resonance imaging findings following anterior cru-ciate ligament injury.
Direct findings on magnetic resonance imaging iden-tify changes in the substance of the anterior cruciate ligamentdue to injury, and indirect findings suggest an anterior cruci-ate ligament injury on the basis of an inferred injury mecha-nism or instability patterns, which develop following anteriorcruciate ligament insufficiency1-4. Of these magnetic reso-nance imaging findings, anterior cruciate ligament morphology,
joint effusion, posterior cruciate ligament buckling, and bone-bruising are magnetic resonance imaging signs with knownchronological importance. Previously, anterior cruciate liga-ment morphology had been reported to be useful in estimatingthe chronicity of anterior cruciate ligament tears, as acute tearsappear edematous and swollen, whereas chronic tears are hypo-intense and fragmented2,4. Joint effusion is a ubiquitous signof knee injury or pathology, but it is a nonspecific manifes-tation because it may be caused by many conditions, suchas trauma, overuse, synovitis, arthritis, or systemic disease5,6.Buckling of the posterior cruciate ligament results from an-terior subluxation of the tibia due to insufficiency of theanterior cruciate ligament, and chronic anterior cruciate
Disclosure: The authors did not receive any outside funding or grants in support of their research for or preparation of this work. Neither they nor amember of their immediate families received payments or other benefits or a commitment or agreement to provide such benefits from a commercialentity.
353
COPYRIGHT � 2010 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
J Bone Joint Surg Am. 2010;92:353-60 d doi:10.2106/JBJS.I.00031
ligament-deficient knees show greater degrees of buckling ofthe posterior cruciate ligament than do acute anterior cruciateligament-deficient knees because of the progressive laxity inthe secondary restraint that occurs after injury7,8. Bone-bruising has been described as a so-called footprint left at thetime of the injury 9, and has been detected on magnetic reso-nance images in >80% of acute ruptures of the anterior cru-ciate ligament10-12. Several studies have noted that bone bruisesgradually disappear from three weeks to several months afterthe injury13-17.
The aim of this study was to quantitatively correlate themagnetic resonance imaging findings with the chronicity ofanterior cruciate ligament injury over time in a large popula-tion. We hypothesized that these four findings on magneticresonance imaging change sequentially with time after the
injury and that the estimation of the chronicity of the anteriorcruciate ligament injury could be facilitated by their integratedinterpretation.
Materials and Methods
The study protocol was approved by our institutional reviewboard. We retrospectively reviewed the medical records of
474 patients with a complete tear of the anterior cruciate lig-ament that was confirmed by arthroscopy who were identifiedfrom a knee ligament reconstruction database at our institute.All operations were carried out by two of the authors (T.K.K.and C.B.C.) between February 2004 and September 2008, andall clinical information, including demographic data, medicalhistory, physical findings, arthroscopic findings, and details ofthe operative procedures, had been archived in the database.
Fig. 1-A Fig. 1-B
Fig. 1-C Fig. 1-D
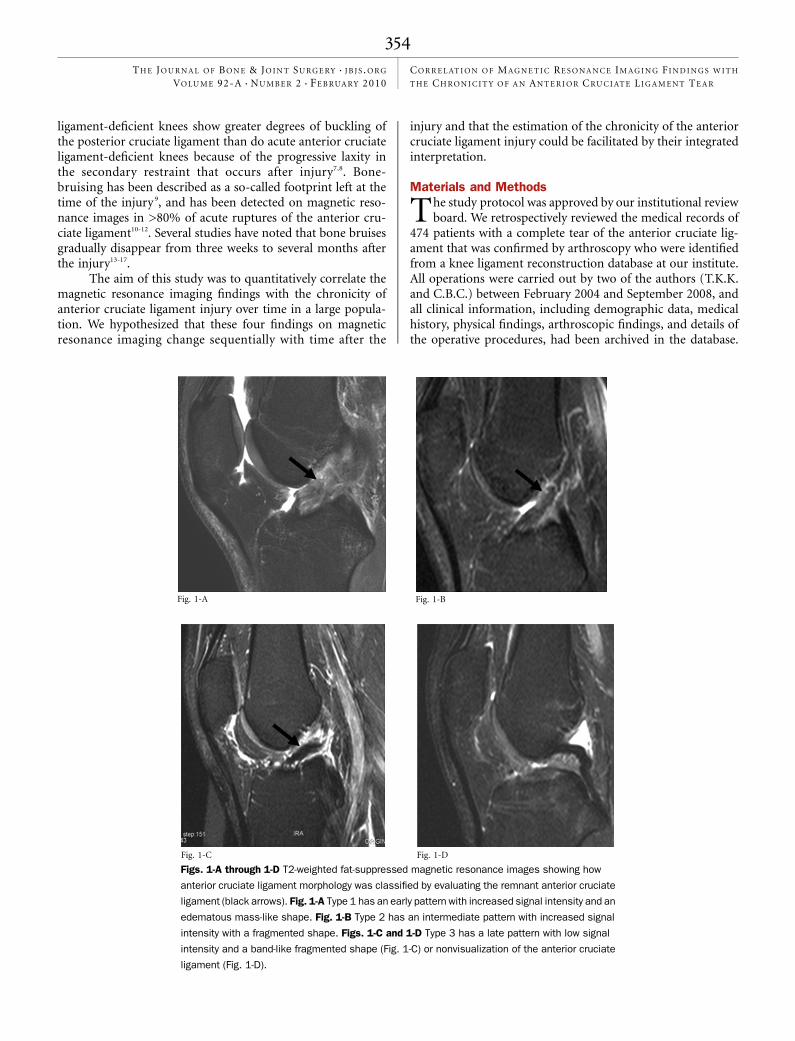
Figs. 1-A through 1-D T2-weighted fat-suppressed magnetic resonance images showing how
anterior cruciate ligament morphology was classified by evaluating the remnant anterior cruciate
ligament (black arrows). Fig. 1-A Type 1 has an early pattern with increased signal intensity and an
edematous mass-like shape. Fig. 1-B Type 2 has an intermediate pattern with increased signal
intensity with a fragmented shape. Figs. 1-C and 1-D Type 3 has a late pattern with low signal
intensity and a band-like fragmented shape (Fig. 1-C) or nonvisualization of the anterior cruciate
ligament (Fig. 1-D).
354
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010CO R R E L AT I O N O F MAG N E T I C RE S O N A N C E IM AG I N G F I N D I N G S W I T H
T H E CH R O N I C I T Y O F A N AN T E R I O R C RU C I AT E LI G A M E N T TE A R

The inclusion criteria were (1) a magnetic resonance imagingscan at our or another institute with use of a comparablemagnetic resonance imaging protocol and available in DICOM(Digital Imaging and Communications in Medicine) imageformat, and (2) a precise date for the anterior cruciate ligamentinjury with the history of an obvious single major injury con-firmed by a repeated history obtained in the emergency room,the outpatient clinic, and the first day of hospitalization. Theexclusion criteria were (1) a prior knee surgery, (2) an asso-ciated injury of the posterior cruciate ligament or partial ortotal disruption of one or both collateral ligaments, and (3) anobvious knee deformity or a history of fracture(s) in the kneeregion. After applying the above criteria, 329 subjects wereexcluded, and 145 knees in 145 patients (124 men and twenty-one women) were included. The mean age (and standard de-viation) was 31.3 ± 10.2 years (range, ten to fifty-six years).There were seventy-six right knees and sixty-nine left knees.
On the basis of previous studies4,14,18-21, study subjectswere allocated, according to the time elapsed between the in-jury of the anterior cruciate ligament and the acquisition ofmagnetic resonance imaging, into four groups: the acute group(within six weeks after the injury), the subacute group (morethan six weeks to three months after the injury), the inter-mediate group (more than three months to one year after theinjury), and the chronic group (more than one year after the
injury). There were sixty-seven acute injuries (in fifty-fourmale and thirteen female patients), nineteen subacute injuries(in seventeen male and two female patients), twenty-threeintermediate injuries (in twenty-one male and two femalepatients), and thirty-six chronic injuries (in thirty-two maleand four female patients). The mean time (and standard de-viation) between the anterior cruciate ligament injury andacquisition of the magnetic resonance imaging was 8.9 ± 10.7days for the acute group, 60.5 ± 10.7 days for the subacutegroup, 165.5 ± 68.1 days for the intermediate group, and2166.3 ± 1599.6 days for the chronic group.
All magnetic resonance images were acquired digitallywith use of a picture archiving and communication system(PACS) in DICOM format. Image assessments were subse-quently performed with use of PACS software (IMPAX; Agfa,Antwerp, Belgium) by a 1.5-T scanner (Intera; Philips, Best,The Netherlands). The imaging protocol consisted of T1-weighted sagittal sequences (repetition time, 450 ms; echotime, 20 ms); T2-weighted fat-suppressed sagittal images(repetition time, 2500 ms; echo time, 50 ms); proton density-weighted sagittal sequences (repetition time, 3300 ms; echotime, 12 ms); dual-echo proton-density and T2-weightedcoronal sequences (repetition time, 3300 ms; echo time, 12 msand 55 ms, respectively); proton density-weighted coronaloblique sequences (repetition time, 3300 ms; echo time, 12ms); and proton density-weighted fat-suppressed axial se-Fig. 2
Maximal anteroposterior dimension (black arrow) of the
suprapatellar fluid collection on the sagittal T2-weighted
fat-suppressed magnetic resonance images was used as
a surrogate for joint effusion.
Fig. 3
T2-weighted fat-suppressed magnetic resonance image showing the
posterior cruciate ligament angle, which was defined as the angle
between lines drawn through the central portions of the tibial and
femoral insertions of the posterior cruciate ligament.
355
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010CO R R E L AT I O N O F MAG N E T I C RE S O N A N C E IM AG I N G F I N D I N G S W I T H
T H E CH R O N I C I T Y O F A N AN T E R I O R C RU C I AT E LI G A M E N T TE A R

quences (repetition time, 2700 ms; echo time, 20 ms); a 16-cmfield of view; a 90� flip angle; a 3 to 4-mm thickness; and a512 · 512 matrix.
Four magnetic resonance imaging findings were inves-tigated. Anterior cruciate ligament morphology was evaluatedon sagittal images that best depicted the anterior cruciate lig-ament in its longest dimension and lowest signal intensity, andthree components were assessed: signal intensity, shape, and
nonvisualization, as described previously2,4,22. An abnormalsignal intensity was defined as an increased signal intensitywithin the anterior cruciate ligament on T2-weighted or pro-ton density-weighted images, whether it had a focal or diffusepattern or one that was continuous or interrupted. An ab-normal shape was defined as an edematous mass-like shapewith a large wavy contour, or a band-like fragmented shape.Nonvisualization was defined as a failure to visualize directlythe substance of the anterior cruciate ligament in any imageson T1-weighted, proton-density, and T2-weighted images atthe expected location. On the basis of previous reports2,4,19,anterior cruciate ligament morphology was categorized intothree types. Type 1 was defined as an early pattern with in-creased signal intensity and an edematous mass-like shape;Type 2, as an intermediate pattern with increased signal in-tensity and a band-like fragmented shape; and Type 3, as a latepattern with a low signal intensity and a band-like fragmentedshape, or as nonvisualized (Figs. 1-A through 1-D).
Joint effusion was defined as a fluid collection betweenthe quadriceps tendon and fat pad in the posterior suprapa-tellar pouch visualized as a low signal intensity on T1-weightedimages and as a high signal intensity on T2-weighted images.The amount of joint effusion was equated to the maximaldimension (in millimeters) in the anteroposterior direction ofthe suprapatellar fluid collection on the sagittal T2-weightedcuts5,6,23 (Fig. 2). The posterior cruciate ligament angle wasdefined as the angle between the lines drawn through thecentral portion of the tibial and femoral insertions of theposterior cruciate ligament1 (Fig. 3), and posterior cruciateligament buckling meant an increase in this angle. Bone-bruising was defined as an increased signal intensity in thebone marrow compared with muscle as described by the In-ternational Cartilage Repair Society classification24. This wasdetermined with use of fat-suppressed T2-weighted sagittalimages at the anterior side of the lateral femoral condyle andat the posterior portion of the lateral tibial plateau. Signalintensity values of bone bruises were measured with use ofa modified circular region of interest based upon previous
Fig. 4
A bone bruise was represented on a T2-weighted fat-suppressed
magnetic resonance image by signal contrast, which was defined as
the ratio of the mean signal intensity of a bone bruise (black circle)
to the mean signal intensity of a normal metaphyseal area (white
circle). Each circle is 1 cm2 in area.
TABLE I Comparison of the Magnetic Resonance Imaging Findings with Chronological Importance Among the Acute, Subacute,
Intermediate, and Chronic Groups
Group
Type of AnteriorCruciate Ligament Morphology*
Joint EffusionAmount† (mm) PCL Angle† (deg)
Bone Bruise
1 2 3 Prevalence* Signal Contrast†
Acute (n = 67) 55 (82) 5 (8) 7 (10) 11.5 ± 5.7‡ 125.1 ± 15.1 55 (82) 3.0 ± 1.2
Subacute (n = 19) 16 (84) 2 (11) 1 (5) 5.1 ± 4.3‡ 116.2 ± 14.1 16 (84) 2.7 ± 1.2§
Intermediate (n = 23) 7 (30) 7 (30) 9 (39) 4.9 ± 3.8 110.4 ± 15.4 13 (57) 1.8 ± 0.9§
Chronic (n = 36) 6 (17) 4 (11) 26 (72) 4.5 ± 4.0 98.7 ± 18.2 4 (11) 1.2 ± 0.6
*The values are given as the number of knees, with the percentage in parentheses. †The values are given as the mean and the standarddeviation. PCL = posterior cruciate ligament. ‡The difference between acute and subacute groups was significant (p < 0.001). §The differencebetween subacute and intermediate groups was significant (p = 0.049).
356
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010CO R R E L AT I O N O F MAG N E T I C RE S O N A N C E IM AG I N G F I N D I N G S W I T H
T H E CH R O N I C I T Y O F A N AN T E R I O R C RU C I AT E LI G A M E N T TE A R
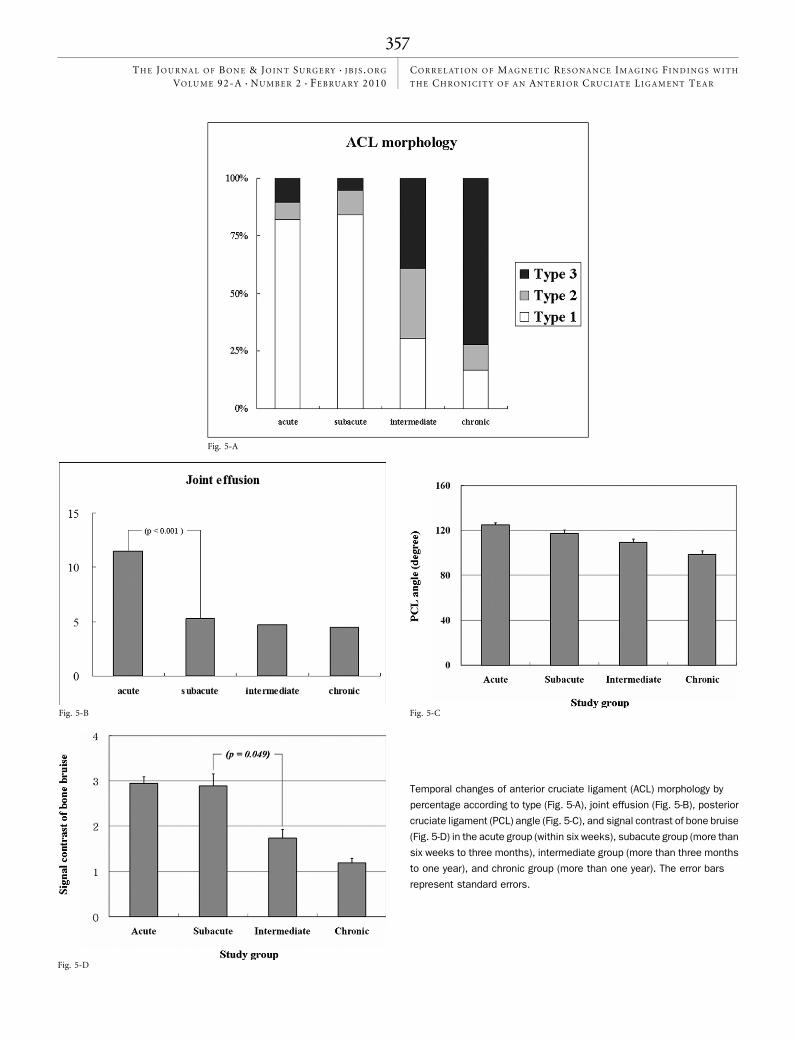
Fig. 5-A
Fig. 5-B Fig. 5-C
Fig. 5-D
Temporal changes of anterior cruciate ligament (ACL) morphology by
percentage according to type (Fig. 5-A), joint effusion (Fig. 5-B), posterior
cruciate ligament (PCL) angle (Fig. 5-C), and signal contrast of bone bruise
(Fig. 5-D) in the acute group (within six weeks), subacute group (more than
six weeks to three months), intermediate group (more than three months
to one year), and chronic group (more than one year). The error bars
represent standard errors.
357
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010CO R R E L AT I O N O F MAG N E T I C RE S O N A N C E IM AG I N G F I N D I N G S W I T H
T H E CH R O N I C I T Y O F A N AN T E R I O R C RU C I AT E LI G A M E N T TE A R

studies14,25,26. A circle with an area of 1 cm2 was created over anarea of bone bruise with use of the circular region-of-interesttool in the PACS software package, and the maximum signalintensity of the lesion was read. Signal intensity values ofcontrol bone marrow were then measured with use of the samemethod in normal metaphyseal bone marrow on the sameimage (Fig. 4). The degree of bone contusion was equated tosignal contrast, which was calculated by determining the ratioof the signal intensity values of the bone-bruise area to the areaof control bone marrow.
All measurements were performed by two fellowship-trained musculoskeletal radiologists (J.Y.C. and J.-A.C.) whowere blinded to patient data. When there was disagreement onthe radiographic findings, a consensus opinion was obtained. Asubset sample of twenty magnetic resonance images wererandomly selected and repeatedly measured for the four find-ings by the two radiologists for an interobserver reliabilityanalysis. Intraclass correlation coefficients showed a good levelof reliability for anterior cruciate ligament morphology type(0.79; p < 0.001) and excellent levels for joint effusion (0.85;p < 0.001) and the posterior cruciate ligament angle (0.82;p < 0.001), similar to previous studies2,8,27-29. The intraclasscorrelation coefficient for the signal intensity of bone-bruisingwith use of the circular region-of-interest method was also atthe excellent level (0.95; p < 0.001).
The four temporal groups were compared with regardto the four magnetic resonance imaging findings of anteriorcruciate ligament morphology, joint effusion, posterior cru-ciate ligament angle, and bone bruise. The anterior cruciateligament morphology and the prevalence of bone-bruise find-ings were compared with use of the Mantel-Haenszel chi-square test. The other continuous variables (joint effusion,posterior cruciate ligament angle, and signal contrast of thebone bruise) were analyzed by one-way analysis of varianceand the Scheffe multiple comparison test as a post hoc analysis.In addition, correlation analyses were performed to evaluatethe relationships between the chronicity of the anterior cru-ciate ligament tear and the three continuous magnetic reso-nance imaging variables, namely, joint effusion, posteriorcruciate ligament angle, and bone-bruise signal contrast, andtheir results were represented by the Spearman coefficient. TheSpearman correlation coefficients were interpreted as follows:>0.5 indicated a large association; 0.3 to 0.5, a moderate as-sociation; and 0.1 to 0.3, a small association30. A p value of<0.05 was considered significant.
Source of FundingNo external source of funding was received for this study.
Results
Demographic variables, namely, age, sex, and injury side,were not significantly different for the four study groups
(p > 0.05). Obvious correlations were observed between thechronicity of the anterior cruciate ligament tear and the fourmagnetic resonance imaging findings (Table I, Figs. 5-A through5-D). The anterior cruciate ligament morphology showed se-
quential changes with the passage of time that were significant(p < 0.001). Type-1 morphology was dominant (83%; seventy-one of eighty-six knees) until three months, whereas Type 3dominated (59%; thirty-five of fifty-nine knees) at more thanthree months after the injury. A joint effusion was observed inall four study groups, but the amount was larger in the acutegroup than in the other groups. Although the mean amount ofjoint effusion decreased with time, a significant difference wasobserved between the acute and the subacute groups (p <0.001). A close correlation (Spearman coefficient = –0.543)was found between the chronicity of injury and joint effusion(p < 0.001). The posterior cruciate ligament angle decreasedwith the chronicity of injury. Although no significant differ-ence was found between the mean values of adjacent groups, astrong correlation (Spearman coefficient = –0.563) was foundbetween the chronicity of injury and posterior cruciate liga-ment angle (p < 0.001). Bone-bruise prevalence reduced withthe chronicity of the injury. The acute and subacute groupshad bone-bruise rates of >80%, while the intermediate andchronic groups had bone-bruise rates of 57% and 11%, re-spectively. The bone-bruise signal contrast also decreased withthe chronicity of the injury. The signal contrast of a bonebruise in the acute and subacute groups (less than threemonths after the injury) was greater than the contrast in theintermediate and chronic groups (more than three monthsafter the injury) by post hoc analysis (p = 0.049). Further-more, a strong correlation (Spearman coefficients = –0.595)was found between the chronicity of the injury and the meansignal contrast of the bone bruise (p < 0.001).
Discussion
In this study, we aimed to investigate the correlation betweenthe magnetic resonance imaging findings and the chronicity
of an anterior cruciate ligament injury. We used one directfinding (anterior cruciate ligament morphology) and threeindirect findings (joint effusion, posterior cruciate ligamentangle, and bone bruise) on magnetic resonance imaging of alarge number of subjects with varying chronicity of injuryof the anterior cruciate ligament. The four magnetic reso-nance imaging findings correlated well with the chronicity ofthe anterior cruciate ligament injury. Although several previ-ous studies have investigated the natural course and the as-sociated magnetic resonance imaging changes of anteriorcruciate ligament injury13-17, we believe this is the first com-prehensive interpretation of the temporal changes of magneticresonance imaging findings after an anterior cruciate ligamentinjury.
The principal finding of this study is that there is adistinct correlation between the four magnetic resonanceimaging findings and the chronicity of the anterior cruciateligament tear. Anterior cruciate ligament morphology duringthe acute and chronic stages after injury has been well docu-mented4,22. A previous study has described cloud-like edemaduring the acute stage and a small fragmented anterior cruciateligament shape in chronic injury4. Nonvisualization of the sub-stance of the anterior cruciate ligament is another common
358
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010CO R R E L AT I O N O F MAG N E T I C RE S O N A N C E IM AG I N G F I N D I N G S W I T H
T H E CH R O N I C I T Y O F A N AN T E R I O R C RU C I AT E LI G A M E N T TE A R

and specific finding of chronic injury 22. In the present study, weoften observed a mixed pattern of anterior cruciate ligamentmorphology during the subacute and intermediate stages, asshown in Figure 1-B. We classified anterior cruciate ligamentmorphology into three types to ensure reliability. Joint effusionwas 125% greater in the acute group than in the subacutegroup. It then diminished and remained at a low level after sixweeks, which indicates that joint effusion is a sensitive sign ofintra-articular pathology in the acute setting, with a rapiddecrease in volume being seen over time. The posterior cru-ciate ligament angle is known to be a secondary sign of anteriorcruciate ligament insufficiency, which is attributed to anteriortranslation of the tibial plateau that increases with time7,8. Ingeneral, in this study, the posterior cruciate ligament angle wasfound to be well-correlated with the chronicity of the anteriorcruciate ligament injury, but no significant difference wasobserved between adjacent groups, which means that thechanges in the posterior cruciate ligament angle were dis-tributed over a long period of time, not occurring in just onephase. The prevalence and degree of bone-bruising had dif-ferent characteristics before and after three months, althoughon occasion it persisted for as long as one year after the injury.The prevalence of bone-bruising during the acute and sub-acute phases was >80%, but this rate fell to 57% in the inter-mediate phase and to 11% in the chronic phase. Signalcontrasts were significantly greater in the acute and subacutephases as well. A previous study found that bone-bruisingdiminishes after six weeks15, and another previous study foundthat it persisted for twelve to fourteen weeks14. We speculatethat these different interpretations may be due to the use ofmagnetic resonance acquisition sequences with differentsensitivities.
Bone-bruising is an indirect magnetic resonance imag-ing finding, which changes with time after injury. Brittbergand Winalski24 proposed the International Cartilage RepairSociety classification, which compared the signal intensityvalues of bone bruises with those of muscle to evaluate bonemarrow changes after cartilage repair. Viskontas et al.21 used aclassification system to evaluate the amount of bone-bruisingfollowing rupture of the anterior cruciate ligament. Wemodified this system and compared the signal intensity val-ues of bone bruises with neighboring, normal metaphysealbone marrow. We also utilized a modified circular region-of-interest method to quantify the intensities of the bruises.Previous studies with use of a region of interest have dependedon manual drawing guided by the naked eye25 or computer-assisted analysis31, but both methods can be unreliable orimpractical. In contrast, we utilized the PACS software tocalculate the region of interest, which we believe to be a morereliable and practical method. Our results showed that thistechnique fairly represented the chronicity of anterior cruciateligament injury and that it could contribute to estimating thetime after injury.
The temporal changes of the four individual findings onmagnetic resonance imaging can be integrated to constitute thecharacteristics of each group. The acute group (less than six
weeks) features a typical edematous mass-shaped anteriorcruciate ligament with high signal intensity, a large joint ef-fusion, a small posterior cruciate ligament angle, and bonebruise(s) with high signal contrast, all of which typify the in-tense posttraumatic tissue reaction. In the subacute group(more than six weeks to three months), the edematous ante-rior cruciate ligament morphology and bone-bruising persist,but the joint effusion decreases. Therefore, the most notabledifference between the acute and subacute periods is theamount of joint effusion. The intermediate group (more thanthree months to one year) is characterized by the resolutionof the edematous anterior cruciate ligament morphology andbone-bruising. By this time, the amount of joint effusion hasalready decreased considerably; hence, no further discerniblereduction is seen. Since the posterior cruciate ligament angledecreases gradually without a steep change, there is no note-worthy difference between the subacute and intermediategroups with regard to this angle. In the chronic group (morethan one year), most of the acute injury stigmata have dis-appeared so that the anterior cruciate ligament morphology iscommonly Type 3 (fragmented or nonvisualized), and there islittle joint effusion, and rarely bone-bruising. The decrease inthe posterior cruciate ligament angle progressed in the chronicgroup because of the long-term insufficiency of the anteriorcruciate ligament. We believe that integrating the interpreta-tions of these four magnetic resonance imaging findings canhelp to estimate the chronicity of an anterior cruciate ligamentinjury. However, it should be noted that highly precise deter-mination of the injury chronicity can still be elusive becausesome of the changes in the magnetic resonance imaging find-ings are subtle, with substantial overlap occurring between thevarious time frames.
Several limitations should be noted when interpretingour findings. First, the magnetic resonance images we usedwere not acquired as a sequential series in the same subject,which is neither practical nor cost-effective. Instead, we eval-uated the findings of a relatively large number of patients overa wide range of time and used a statistical approach to evaluatethem. Second, the time of injury was determined from thepatients’ history, and the anterior cruciate ligament injury wasconfirmed by arthroscopy. Although we tried to confine sub-jects to those with an obvious single traumatic event, thereremains a possibility that some repeat traumatic events wereincluded. Third, not all magnetic resonance imaging findingshaving chronological importance, such as cartilage lesions,were included in this study because we found it difficult tomeasure cartilage lesions reproducibly on magnetic resonanceimaging.
In conclusion, our study demonstrates that the fourmagnetic resonance imaging findings of anterior cruciate lig-ament morphology, joint effusion, posterior cruciate ligamentangle, and bone-bruising correlate well with the chronicity ofanterior cruciate ligament injury. Estimating the chronicity ofanterior cruciate ligament injury can be facilitated by an in-tegrated interpretation of these four magnetic resonance imagingfindings. n
359
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010CO R R E L AT I O N O F MAG N E T I C RE S O N A N C E IM AG I N G F I N D I N G S W I T H
T H E CH R O N I C I T Y O F A N AN T E R I O R C RU C I AT E LI G A M E N T TE A R
Jong Pil Yoon, MDChong Bum Chang, MD, PhDJung-Ah Choi, MD, PhDTae Kyun Kim, MD, PhDJoint Reconstruction Center (J.P.Y., C.B.C., and T.K.K.) and theDepartment of Radiology (J.-A.C.), Seoul National University BundangHospital, 300 Gumidong, Bundangu,Seongnam-si, Gyunggido 463-707, South Korea.E-mail address for T.K. Kim: [email protected]
Jae Ho Yoo, MD, PhDDepartment of Orthopaedic Surgery,Soonchunhyang University Hospital, Bucheon,
1174 Jung-dong, Wonmi-gu,Bucheon-si, Gyeonggi-do 420-767, South Korea
Sung Ju Kim, MSDepartment of Statistics, Korea University,Anam-dong, Seongbuk-gu,Seoul 136-701, South Korea
Ja Young Choi, MDSang Cheol Seong, MD, PhDDepartments of Radiology (J.Y.C.) and Orthopaedic Surgery (S.C.S.),Seoul National University Hospital,28 Yongondong Chongnogu, Seoul 110-774, South Korea
References
1. McCauley TR, Moses M, Kier R, Lynch JK, Barton JW, Jokl P. MR diagnosis oftears of anterior cruciate ligament of the knee: importance of ancillary findings. AJRAm J Roentgenol. 1994;162:115-9.
2. Robertson PL, Schweitzer ME, Bartolozzi AR, Ugoni A. Anterior cruciate ligamenttears: evaluation of multiple signs with MR imaging. Radiology. 1994;193:829-34.
3. Tung GA, Davis LM, Wiggins ME, Fadale PD. Tears of the anterior cruciate liga-ment: primary and secondary signs at MR imaging. Radiology. 1993;188:661-7.
4. Vahey TN, Broome DR, Kayes KJ, Shelbourne KD. Acute and chronic tears of theanterior cruciate ligament: differential features at MR imaging. Radiology. 1991;181:251-3.
5. Johnson MW. Acute knee effusions: a systematic approach to diagnosis. AmFam Physician. 2000;61:2391-400.
6. Kolman BH, Daffner RH, Sciulli RL, Soehnlen MW. Correlation of joint fluid andinternal derangement on knee MRI. Skeletal Radiol. 2004;33:91-5.
7. Dimond PM, Fadale PD, Hulstyn MJ, Tung GA, Greisberg J. A comparison of MRIfindings in patients with acute and chronic ACL tears. Am J Knee Surg. 1998;11:153-9.
8. Gentili A, Seeger LL, Yao L, Do HM. Anterior cruciate ligament tear: indirect signsat MR imaging. Radiology. 1994;193:835-40.
9. Sanders TG, Medynski MA, Feller JF, Lawhorn KW. Bone contusion patterns ofthe knee at MR imaging: footprint of the mechanism of injury. Radiographics.2000;20 Spec No:S135-51.
10. Rosen MA, Jackson DW, Berger PE. Occult osseous lesions documented bymagnetic resonance imaging associated with anterior cruciate ligament ruptures.Arthroscopy. 1991;7:45-51.
11. Speer KP, Spritzer CE, Bassett FH 3rd, Feagin JA Jr, Garrett WE Jr. Osseousinjury associated with acute tears of the anterior cruciate ligament. Am J SportsMed. 1992;20:382-9.
12. Spindler KP, Schils JP, Bergfeld JA, Andrish JT, Weiker GG, Anderson TE,Piraino DW, Richmond BJ, Medendorp SV. Prospective study of osseous, articular,and meniscal lesions in recent anterior cruciate ligament tears by magneticresonance imaging and arthroscopy. Am J Sports Med. 1993;21:551-7.
13. Costa-Paz M, Muscolo DL, Ayerza M, Makino A, Aponte-Tinao L. Magneticresonance imaging follow-up study of bone bruises associated with anterior cruciateligament ruptures. Arthroscopy. 2001;17:445-9.
14. Davies NH, Niall D, King LJ, Lavelle J, Healy JC. Magnetic resonance imagingof bone bruising in the acutely injured knee—short-term outcome. Clin Radiol.2004;59:439-45.
15. Graf BK, Cook DA, De Smet AA, Keene JS. "Bone bruises" on magnetic reso-nance imaging evaluation of anterior cruciate ligament injuries. Am J Sports Med.1993;21:220-3.
16. Roemer FW, Bohndorf K. Long-term osseous sequelae after acute trauma of theknee joint evaluated by MRI. Skeletal Radiol. 2002;31:615-23.
17. Vellet AD, Marks PH, Fowler PJ, Munro TG. Occult posttraumatic osteochondrallesions of the knee: prevalence, classification, and short-term sequelae evaluatedwith MR imaging. Radiology. 1991;178:271-6.
18. Bretlau T, Tuxoe J, Larsen L, Jorgensen U, Thomsen HS, Lausten GS. Bonebruise in the acutely injured knee. Knee Surg Sports Traumatol Arthrosc.2002;10:96-101.
19. Chen WT, Shih TT, Tu HY, Chen RC, Shau WY. Partial and complete tear of theanterior cruciate ligament. Acta Radiol. 2002;43:511-6.
20. Klass D, Toms AP, Greenwood R, Hopgood P. MR imaging of acute anteriorcruciate ligament injuries. Knee. 2007;14:339-47.
21. Viskontas DG, Giuffre BM, Duggal N, Graham D, Parker D, Coolican M. Bonebruises associated with ACL rupture: correlation with injury mechanism. Am J SportsMed. 2008;36:927-33.
22. Mink JH, Deutsch AL. Magnetic resonance imaging of the knee. Clin OrthopRelat Res. 1989;244:29-47.
23. Schweitzer ME, Falk A, Berthoty D, Mitchell M, Resnick D. Knee effusion: nor-mal distribution of fluid. AJR Am J Roentgenol. 1992;159:361-3.
24. Brittberg M, Winalski CS. Evaluation of cartilage injuries and repair. J Bone JointSurg Am. 2003;85 Suppl 2:58-69.
25. Schmid MR, Hodler J, Vienne P, Binkert CA, Zanetti M. Bone marrow abnor-malities of foot and ankle: STIR versus T1-weighted contrast-enhanced fat-suppressed spin-echo MR imaging. Radiology. 2002;224:463-9.
26. Vogl TJ, Schmitt J, Lubrich J, Hochmuth K, Diebold T, Del Tredici K, Sudkamp N.Reconstructed anterior cruciate ligaments using patellar tendon ligament grafts:diagnostic value of contrast-enhanced MRI in a 2-year follow-up regimen. Eur Radiol.2001;11:1450-6.
27. Boks SS, Vroegindeweij D, Koes BW, Hunink MM, Bierma-Zeinstra SM. Mag-netic resonance imaging abnormalities in symptomatic and contralateral knees:prevalence and associations with traumatic history in general practice. Am J SportsMed. 2006;34:1984-91.
28. Lee K, Siegel MJ, Lau DM, Hildebolt CF, Matava MJ. Anterior cruciate ligamenttears: MR imaging-based diagnosis in a pediatric population. Radiology. 1999;213:697-704.
29. Mellado JM, Calmet J, Olona M, Gine J, Sauri A. Magnetic resonance imaging ofanterior cruciate ligament tears: reevaluation of quantitative parameters andimaging findings including a simplified method for measuring the anterior cruciateligament angle. Knee Surg Sports Traumatol Arthrosc. 2004;12:217-24.
30. Fleiss JL. Statistical methods for rates and proportions. 2nd ed. New York: JohnWiley; 1981.
31. Mayerhoefer ME, Breitenseher M, Hofmann S, Aigner N, Meizer R, Siedentop H,Kramer J. Computer-assisted quantitative analysis of bone marrow edema of theknee: initial experience with a new method. AJR Am J Roentgenol. 2004;182:1399-403.
360
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010CO R R E L AT I O N O F MAG N E T I C RE S O N A N C E IM AG I N G F I N D I N G S W I T H
T H E CH R O N I C I T Y O F A N AN T E R I O R C RU C I AT E LI G A M E N T TE A R




















