
Concerns About Serum Androgens Monitoring During Testosterone Replacement Treatments in Hypogonadal...
14
ORIGINAL RESEARCH—ENDOCRINOLOGY Concerns About Serum Androgens Monitoring During Testosterone Replacement Treatments in Hypogonadal Male Athletes: A Pilot StudyLuigi Di Luigi, MD,* Paolo Sgrò, MD,* Antonio Aversa, MD, † Silvia Migliaccio, MD,* Serena Bianchini, BLT,* Francesco Botrè, PhD ‡ , Francesco Romanelli, MD, † and Andrea Lenzi, MD † *Unit of Endocrinology, Department of Health Sciences, University of Rome “Foro Italico,” Rome, Italy; † Department of Experimental Medicine, University of Rome “Sapienza,” Rome, Italy; ‡ Department of Management, University of Rome “Sapienza”—Anti-Doping Laboratory of the Italian Federation of Sport Medicine (FMSI–CONI), Rome, Italy DOI: 10.1111/j.1743-6109.2011.02600.x ABSTRACT Introduction. A well-tailored testosterone replacement treatment (TRT) in male hypogonadal athletes plays a pivotal role to restore physiological performances, to reduce health risks, and to guarantee the ethic of competition. Few studies evaluated individual androgens profiles during TRT in trained individuals. Aim. The aim of this article was to verify the efficacy in restoring eugonadal serum and urinary androgens profiles after testosterone enanthate (TE) and gel (TG) administration. Methods. Ten male Caucasian-trained volunteers affected by severe hypotestosteronemia (<8 nmol/L) were included. Serum androgens and urinary testosterone metabolites were evaluated, in the same subjects, before and weekly for 5 weeks after both a single intramuscular TE injection (250 mg) and during a daily administration of TG (50 mg/die of testosterone), respectively. Main Outcome Measures. The main outcome measures of this article were serum total testosterone (TT), dihy- drotestosterone (DHT), calculated free and bioavailable testosterone (cFT, cBioT), 17-b-estradiol, and urinary glucuronide testosterone metabolites. Results. Supraphysiological TT concentrations were observed in 50% of our volunteers until 7 days after TE and in the 4% of total samples after TG. Serum DHT was high both after TE (all volunteers on day 7 and 50% on day 14) and during TG (32% of total samples). A relatively low number of samples showed normal cFT and cBioT both after TE and TG (20–44%, respectively). Urinary metabolites were related to the type of treatment and to serum androgens profile and resulted in the normal ranges from 15% to 60% of total samples. Conclusion. Besides well-known variations of mean serum TT, we showed a high percentage of serum and urinary samples with abnormal androgens, being TG safer than TE. We conclude that monitoring TRT with TT only may be inaccurate because of abnormal fluctuations of other circulating androgens. Further studies to identify the appropriate markers of eugonadism during TRT are highly warranted both in athletes and in non-athletes. Di Luigi L, Sgrò P, Aversa A, Migliaccio S, Bianchini S, Botrè F, Romanelli F, and Lenzi A. Concerns about serum androgens monitoring during testosterone replacement treatments in hypogonadal male athletes: a pilot study. J Sex Med 2012;9:873–886. Key Words. Testosterone; DHT; Free Testosterone; Bioavailable Testosterone; Doping; Sport Introduction I n the general population, males with low test- osterone concentrations are commonly submit- ted to a testosterone replacement treatment (TRT), if a clinical and biochemical diagnosis of hypogonadism (i.e., due to classical diseases affect- ing the hypothalamus-pituitary-gonadal axis) is established and if there are no contraindications [1]. In hypogonadal males engaged in competitive 873 © 2012 International Society for Sexual Medicine J Sex Med 2012;9:873–886
Transcript of Concerns About Serum Androgens Monitoring During Testosterone Replacement Treatments in Hypogonadal...
ORIGINAL RESEARCH—ENDOCRINOLOGY
Concerns About Serum Androgens Monitoring DuringTestosterone Replacement Treatments in Hypogonadal MaleAthletes: A Pilot Studyjsm_2600 873..886
Luigi Di Luigi, MD,* Paolo Sgrò, MD,* Antonio Aversa, MD,† Silvia Migliaccio, MD,*Serena Bianchini, BLT,* Francesco Botrè, PhD‡, Francesco Romanelli, MD,† and Andrea Lenzi, MD†
*Unit of Endocrinology, Department of Health Sciences, University of Rome “Foro Italico,” Rome, Italy; †Department ofExperimental Medicine, University of Rome “Sapienza,” Rome, Italy; ‡Department of Management, University of Rome“Sapienza”—Anti-Doping Laboratory of the Italian Federation of Sport Medicine (FMSI–CONI), Rome, Italy
DOI: 10.1111/j.1743-6109.2011.02600.x
A B S T R A C T
Introduction. A well-tailored testosterone replacement treatment (TRT) in male hypogonadal athletes plays apivotal role to restore physiological performances, to reduce health risks, and to guarantee the ethic of competition.Few studies evaluated individual androgens profiles during TRT in trained individuals.Aim. The aim of this article was to verify the efficacy in restoring eugonadal serum and urinary androgens profilesafter testosterone enanthate (TE) and gel (TG) administration.Methods. Ten male Caucasian-trained volunteers affected by severe hypotestosteronemia (<8 nmol/L) wereincluded. Serum androgens and urinary testosterone metabolites were evaluated, in the same subjects, before andweekly for 5 weeks after both a single intramuscular TE injection (250 mg) and during a daily administration of TG(50 mg/die of testosterone), respectively.Main Outcome Measures. The main outcome measures of this article were serum total testosterone (TT), dihy-drotestosterone (DHT), calculated free and bioavailable testosterone (cFT, cBioT), 17-b-estradiol, and urinaryglucuronide testosterone metabolites.Results. Supraphysiological TT concentrations were observed in 50% of our volunteers until 7 days after TE andin the 4% of total samples after TG. Serum DHT was high both after TE (all volunteers on day 7 and 50% on day14) and during TG (32% of total samples). A relatively low number of samples showed normal cFT and cBioT bothafter TE and TG (20–44%, respectively). Urinary metabolites were related to the type of treatment and to serumandrogens profile and resulted in the normal ranges from 15% to 60% of total samples.Conclusion. Besides well-known variations of mean serum TT, we showed a high percentage of serum and urinarysamples with abnormal androgens, being TG safer than TE. We conclude that monitoring TRT with TT only maybe inaccurate because of abnormal fluctuations of other circulating androgens. Further studies to identify theappropriate markers of eugonadism during TRT are highly warranted both in athletes and in non-athletes. Di LuigiL, Sgrò P, Aversa A, Migliaccio S, Bianchini S, Botrè F, Romanelli F, and Lenzi A. Concerns about serumandrogens monitoring during testosterone replacement treatments in hypogonadal male athletes: a pilotstudy. J Sex Med 2012;9:873–886.
Key Words. Testosterone; DHT; Free Testosterone; Bioavailable Testosterone; Doping; Sport
Introduction
I n the general population, males with low test-osterone concentrations are commonly submit-
ted to a testosterone replacement treatment
(TRT), if a clinical and biochemical diagnosis ofhypogonadism (i.e., due to classical diseases affect-ing the hypothalamus-pituitary-gonadal axis) isestablished and if there are no contraindications[1]. In hypogonadal males engaged in competitive
873
© 2012 International Society for Sexual Medicine J Sex Med 2012;9:873–886

sports or in heavy non-competitive physical activi-ties, an adequate TRT plays a pivotal role inrestoring physiological and functional conditionsand in reducing health risks during either physicalactivity or rest [2,3].
After puberty, endogenous testosterone largelymodifies body composition in males and influencesthe physiology of all the organs and tissuesinvolved in different motor behaviors (e.g.,walking, working, practicing physical exercise, andsports) and in the physiological short- and long-term mechanisms of adaptation to exercise-relatedstress [4–8]. Also, because of the observed linearrelationship between testosterone levels and legpress strength, thigh, and quadriceps musclevolume [6], a biologically normal serum total tes-tosterone (TT) concentration is fundamental inathletes to guarantee both a physiological exerciseperformance and a safe sport participation.
Because of the multiple genomic and nonge-nomic effects of testosterone, and even thoughevidence-based criteria does not exist, untreated ath-letes with hypotestosteronemia are theoreticallyexposed to further specific risks for health and fortheir biologically normal physical performances,when compared with sedentary hypogonadal indi-viduals [9,10]. For example, they are at increased riskof osteoporotic fractures in case of falling or trauma(e.g., cyclists, combat sports), of cardiovascular acci-dents related to high exercise strain, of worsenedsport-related anemia, and of reduced stress hor-mones balance (e.g., vs. cortisol). In addition, test-osterone deficiency alters the endocrine-metabolicand neuromuscular adaptations to exercise, reducesmuscles strength, aggressiveness in competition andproteins resynthesis during recovery, and increasesthe risk of overtraining. On these bases, and becausewe observed that the history of clinical symptoms ofhypogonadism may be inaccurate to diagnose test-osterone deficiency in trained individuals [3], webelieve that TRT should be considered in all athleteswith low serum testosterone due to true hypogo-nadism (e.g., not related to anabolic androgensabuse), independent of the presence of classicalsymptoms of hypogonadism.
True hypogonadal athletes should receive test-osterone at all ages, if there are no contraindica-tions [2,11,12], and after receiving a therapeuticuse exemption (TUE) by the respective anti-doping organization. In fact, since the early1970s, testosterone and other androgens are pro-hibited in athletes. Only recently has the com-plete ban of androgens makes an exception forathletes with androgen deficiency due to well-
established diagnostic entities, like pituitary ortesticular diseases [7,13–15].
Adequately tailoring and monitoring TRT inmale athletes is essential to reduce health risks, toguarantee physiological physical performances,and to respect the ethics of sport [2,12,16–18].This is of great importance because both lowandrogens concentrations are associated to specificconsequences for health and reduced performance,and long-term supraphysiological androgens con-centrations may increase the risk for side effectsand provide an unfair advantage for performancebecause of the dose-dependent effects of andro-gens on muscle mass, strength, and central nervoussystem (CNS) [2,6,12,19,20].
In the general population, it is recommended totailor TRT to maintain serum TT concentrationinto the midnormal range [11]. Furthermore, it issuggested to monitor injectable testosterone esters(such as enanthate or cypionate) or gel administra-tion by assessing serum TT midway between twoconsecutive testosterone esters injections or at anytime after patient has been on treatment with thegel for at least 1 week, respectively [11].
It is our opinion that the recommended strategies(i.e., evaluated hormones and timing of evaluation)for monitoring TRT with such testosterone prepa-rations during dose titration cannot permit per se theexact identification of the true serum androgensprofiles. In fact, besides a concomitant voluntaryabuse with testosterone (e.g., doping) during TRT,hypogonadal individuals might attain unwanted, andvery often unrevealed, abnormal TT serum concen-trations and/or fluctuations, depending upon thetype of testosterone preparations, doses, and timingof monitoring [19,21–24]. In addition, even if alsodihydrotestosterone (DHT)—a biologically activemetabolite of testosterone that is prohibited becauseof its anabolic and psychotropic effects—mayincrease after testosterone administration andinduce health concerns, it is not clear why it is notroutinely monitored during TRT. Furthermore,whereas in the future a possible doping control onrandom serum and urine samples may be used tosuspect both a not well-tailored TRT or an abusewith testosterone, few studies evaluated the risk todetect high serum androgens concentrations and theassociated urinary profile’s characteristics duringdifferent TRT [19].
The aim of this short-term exploratory open labelinvestigative study was to verify serum androgensand urinary testosterone metabolites profiles after asingle administration of a long half-life injectabletestosterone ester preparation, one of the most com-
874 Di Luigi et al.
J Sex Med 2012;9:873–886

monly used and abused testosterone preparation(e.g., mainly for their availability and low cost), andduring the administration of a newer TRT modality(e.g., testosterone gel [TG]) in trained males affectedby severe hypotestosteronemia. In particular, weaimed to evaluate both the probability of establish-ing drug-related abnormal androgens profiles andthe possible relationships between serum andurinary androgens profiles during such treatments.
Subjects and Methods
SubjectsTen male Caucasian hypogonadal volunteers prac-ticing noncompetitive physical activities wereincluded in the study; five were affected by primaryhypogonadism (e.g., three of them had bilateralanorchia and two a bilateral orchitis) and five bysecondary hypogonadism (e.g., congenital, idio-pathic), and their mean serum TT at diagnosis was2.91 � 2.32 nmol/L. All of them were alreadytreated with intramuscular (i.m.) testosteroneesters (250 mg every 3 weeks) and were consideredwell treated (inclusion criteria) because of normalserum TT (e.g., 14.1–24.5 nmol/L) as measuredmidway between two consecutive injections [11].At inclusion, the hypogonadal volunteers had thefollowing anthropometric characteristics asmean � standard deviation (SD): age 31.3 �7.5 years, height 176.8 � 7.4 cm, weight 73.4 �10.8 kg, and body mass index 27.4 � 4.8 kg/m2.The other inclusion criteria were: diagnosis ofsevere hypotestosteronemia (serum TT <8 nmol/L), diagnosed according to clinical, hormonal, andinstrumental criteria, and absence of positivehistory for diseases contraindicating testosteroneadministration, and of other factors influencingthe experimental evaluations (e.g., diseases,assumption of drugs or supplements, and so forth)[25–27]. University Ethical Committee’s approvaland written informed consent were obtained.
TreatmentsAfter 8 weeks of pharmacological washout, all vol-unteers first received a single i.m. injection con-taining testosterone enanthate (TE: 250 mg;Testo-Enant; Geymonat, Italy). Then, after5 weeks from TE administration, they started adaily application (e.g., at 08.00 am) of TG (50 mg/die of testosterone; Testogel; Bayer, ScheringHealthcare, Milan, Italy) for 5 weeks. Each volun-teer was his own control, receiving both TE andTG. The volunteers maintained their usual lif-estyle throughout all the study.
Blood Samples CollectionsImmediately before starting both TE and TGadministration, morning blood samples for serumhormones evaluations were collected from aforearm vein, under standardized conditionsafter an overnight fasting, between 07.30 and08.30 am and after 30 minutes in resting condi-tions (day 1). Then, morning blood samples werecollected on days 7, 14, 21, 28, and 35 after orduring TE and TG administration, respectively.Blood samples were immediately placed on iceuntil centrifugation (800 ¥ g) and serum separa-tion. Serum samples were frozen at -40°C untilanalyzed.
Urine Samples CollectionsImmediately before starting both TE and TGadministration, morning clean-catch urinesamples were collected (50 mL) after an overnightfast, from 06.00 to 07.00 am (day 1). Subsequently,morning urine samples were collected on days 7,14, 21, 28, and 35 after or during TE and TGadministration, respectively. Samples were frozenat -40°C until analyzed.
Blood and Urine Samples AnalysisSerum TT and sex hormone-binding globulin(SHBG) were measured by immunoradiometricassay using commercial kits (Spectria ORION,Espoo, Finland). Serum concentrations of DHTand 17-b-estradiol (E) were measured by radioim-munoassay (RIA) using commercial RIA kits(Diagnostic System Laboratory, Webster, TX,USA). All samples were analyzed in duplicate; theintra- and inter-assays coefficients of variationwere: 3.8% and 4.8% for TT, 3.7% and 6.9% forDHT, 5.3% and 8.1% for E, and 5.3% and 3.3%for SHBG, respectively. The sensitivity of themethods was: 0.1 nmol/L for TT, 0.014 nmol/Lfor DHT, 17.3 pmol/L for E, and 1.3 nmol/L forSHBG.
The serum concentrations of calculated freetestosterone (cFT) and calculated bioavailable tes-tosterone (cBioT), which includes free testoster-one plus testosterone weakly bound to albumin,were calculated from TT and SHBG concentra-tions, assuming an albumin concentration of 4.3 g/dL, by using published equations [28,29]. Thefree androgen index (FAI) was also calculated[FAI (nmol/nmol) = (TT/SHBG) ¥ 100]. SerumDHT/TT and TT/E ratios were calculated byserum DHT/TT (nmol/nmol) and TT/E (nmol/nmol).
Androgens Profile in Treated Male Hypogonadism 875
J Sex Med 2012;9:873–886

Urine samples were analyzed for free and glu-curonide androgen metabolites: testosterone (T),epitestosterone (EpiT), androsterone (A), etio-cholanolone (Et), 11b-hydroxyandrosterone (11-OH-A), 11b-hydroxyetiocholanolone (11-OH-E),5a-androstane-3a,17b-diol (5aAD3a17b), 5b-androstane-3a,17b-diol (5bAD3a17b), via gaschromatography–mass spectrometry (Agilent5890/5973, Agilent Technologies SpA, Cernuscosul Naviglio, Milan, Italy) as previously described[30]. The urinary metabolites concentration (C)per sample was corrected to a specific gravity of1.020 [C1020 = (1.020 - 1)/(specific gravitysample -1) · Csample]. Urinary T/EpiT, 5aAD3a17bl/5bAD3a17b, and A/Et ratios were calculated byrespective urinary metabolites ratios (ng/ng).
The serum hormones and proteins referenceranges reported by manufacturers for male indi-viduals (20–40 years) were as follows: TT, 8.2–34.6 nmol/L; DHT, 2.24–3.85 nmol/L; E,50–240 pmol/L; and SHBG, 16–61 nmol/L. Theintralaboratory reference ranges for absolute andcalculated testosterone fractions, evaluated on agematched healthy active male individuals, were: TT,12.9–27.7 nmol/L; SHBG, 14–50 nmol/L; cFT,0.30–0.58 nmol/L; cBioT, 6.9–14.1 nmol/L; andFAI, 33–101.
Statistical AnalysisResults are expressed as absolute values and asmean � SD. Serum and urine hormonal param-eters and calculated respective ratios (DHT/TT,TT/E, FAI, T/EpiT, 5aAD3a17bl/5bAD3a17b,A/Et), evaluated before and after treatments, wereanalyzed by anova for repeated measures to detectsignificant effects of two main factors: treatment(TE and TG) and time (before and after treat-ment). When a significant F-ratio (P < 0.05) wasobserved, the presence of significant differenceswas investigated using adequate post hoc tests. Alevel of 0.05 was selected for statistical signifi-cance. All other presented analyses were based ondescriptive statistics. At an individual level, toevaluate the number of samples within the normalranges (e.g., as percent of samples at each timepoints and as percent of total samples), we com-pared the serum hormones concentrations bothwith the manufacturer’s reference ranges (for TTand DHT) and with our laboratory referencesranges (for TT, cFT, cBioT, and FAI) and oururinary profiles with the existing reference rangesfor glucuronide metabolites of testosterone in aCaucasian athletic population, as reported by VanRenterghem et al. [31]. The concentrations of
urinary metabolites of testosterone has been alsoevaluated by grouping the urinary samples basedon the respective serum TT and DHT concentra-tions (normal, high, low) both after TE and duringTG administration. As reported in tables andfigures, because of the more common interval ofadministration of TE during TRT, for some sta-tistical evaluations, we considered the samples col-lected during the first 3 weeks after TEadministration and all the samples collected duringTG administration. The statistical software SPSS(version 18.0 for Windows; SPSS Inc., Chicago,IL, USA) was used.
Results
Clinical symptoms of hypogonadism (loss oflibido, erectile dysfunction, hot flushes, reducedvigor, weakness, etc.) have been observed at lowlevels of intensity in almost all volunteers duringthe last weeks of washout periods; none withdrewin the study because of severe symptoms ofhypogonadism and drug-related side effects.
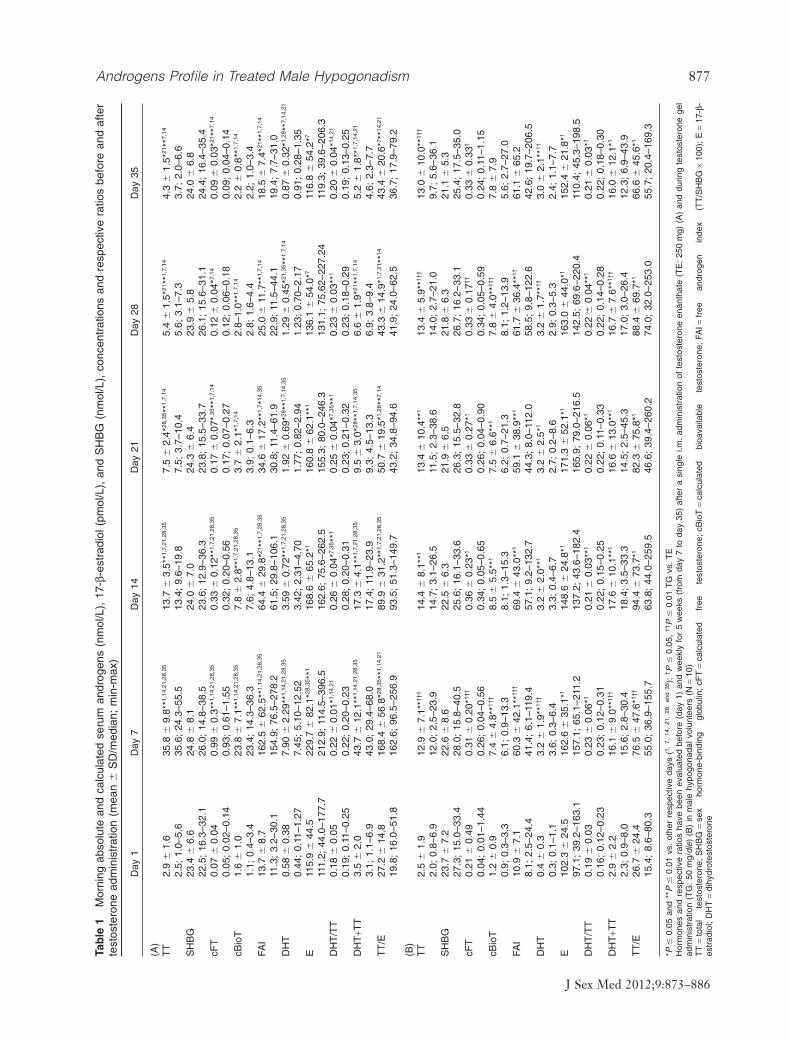
For all evaluated parameters, no differencesbetween pretreatments (day 1) mean serumsamples hormones concentrations were observed(Table 1). As expected, both TE and TG adminis-tration induced modifications in many of theevaluated or calculated serum and urinary param-eters. All results are reported in Tables 1–4 andFigures 1 and 2.
Serum TTAs expected, mean serum TT concentration sig-nificantly increased with respect to pretreatmentvalues both after TE and during TG administra-tion (Table 1). The mean TT concentrations werein the normal range only on day 14 after TEadministration and all time points during TGadministration.
The probability to find a sample containingserum TT within the normal manufacturer’s rangewas from 50% to 100% of samples at differenttime points (70% on total samples) during the first3 weeks after TE administration (Table 2). Par-ticularly, after TE administration serum, TT con-centrations were significantly above the upperlimit of the manufacturer’s reference range in the5/10 subjects on day 7, within the normal refer-ence range in 10/10 subjects on day 14, and clearlybelow the reference range (i.e., hypoandrogenism)in 5/10 subjects on day 21 and in all of subjects onday 28 and 35, respectively (Table 2, Figure 1).
876 Di Luigi et al.
J Sex Med 2012;9:873–886
Tab
le1
Mor
ning
abso
lute
and
calc
ulat
edse
rum
andr
ogen
s(n
mol
/L),
17-b
-est
radi
ol(p
mol
/L),
and
SH
BG
(nm
ol/L
),co
ncen
trat
ions
and
resp
ectiv
era
tios
befo
rean
daf
ter
test
oste
rone
adm
inis
trat
ion
(mea
n�
SD
/med
ian;
min
-max
)
Day
1D
ay7
Day
14D
ay21
Day
28D
ay35
(A)
TT
2.9
�1.
635
.8�
9.8*
*1,14
,21,
28,3
513
.7�
3.5*
*1,7,
21,2
8,35
7.5
�2.
4*28
,35 *
*1,7,
145.
4�
1.5*
21**
1,7,
144.
3�
1.5*
21**
7,14
2.5;
1.0–
5.6
35.6
;24
.3–5
5.5
13.4
;9.
6–19
.87.
5;3.
7–10
.45.
6;3.
1–7.
33.
7;2.
0–6.
6S
HB
G23
.4�
6.6
24.8
�8.
124
.0�
7.0
24.3
�6.
423
.9�
5.8
24.0
�6.
822
.5;
16.3
–32.
126
.0;
14.8
–38.
523
.6;
12.9
–36.
323
.8;
15.5
–33.
726
.1;
15.6
–31.
124
.4;
16.4
–35.
4cF
T0.
07�
0.04
0.99
�0.
3**1,
14,2
1,28
,35
0.33
�0.
12**
1,7,
21,2
8,35
0.17
�0.
07*,3
5 **1,
7,14
0.12
�0.
04*7,
140.
09�
0.03
*21**
7,14
0.05
;0.
02–0
.14
0.93
;0.
61–1
.55
0.32
;0.
20–0
.56
0.17
;0.
07–0
.27
0.12
;0.
06–0
.18
0.09
;0.
04–0
.14
cBio
T1.
6�
1.0
23.8
�7.
1**1,
14,2
1,28
,35
7.8
�2.
8**1,
7,21
,28,
353.
7�
2.1*
1,7,
142.
8–1.
0**1,
7,14
2.2
�0.
8**1,
7,14
1.1;
0.4–
3.4
23.4
;14
.3–3
6.3
7.6;
4.8–
13.1
3.9;
0.1–
6.3
2.8;
1.6–
4.4
2.2;
1.0–
3.4
FAI
13.7
�8.
716
2.5
�62
.5**
1,14
,21,
28,3
564
.4�
29.8
*21**
1,7,
28,3
534
.6�
17.2
**1,
7 *14
,35
25.0
�11
.7**
1,7,
1418
.5�
7.4*
21**
1,7,
14
11.3
;3.
2–30
.115
4.9;
76.5
–278
.261
.5;
29.8
–106
.130
.8;
11.4
–61.
922
.9;
11.5
–44.
119
.4;
7.7–
31.0
DH
T0.
58�
0.38
7.90
�2.
29**
1,14
,21,
28,3
53.
59�
0.72
**1,
7,21
,28,
351.
92�
0.69
*28**
1,7,
14,3
51.
29�
0.45
*21,3
5 **1,
7,14
0.87
�0.
32*1,
28**
7,14
,21
0.44
;0.
11–1
.27
7.45
;5.
10–1
2.52
3.42
;2.
31–4
.70
1.77
;0.
82–2
.94
1.23
;0.
70–2
.17
0.91
;0.
28–1
.35
E11
5.9
�44
.522
9.7
�82
.1*28
,35 *
*116
8.6
�65
.2*1
160.
8�
62.1
**1
136.
1�
54.0
*711
6.8
�54
.2*7
111.
2;44
.0–1
77.7
212.
9;11
4.5–
396.
516
2.6;
75.6
–262
.515
5.3;
80.0
–246
.313
1.1;
75.6
2–22
7.24
119.
3;39
.6–2
06.3
DH
T/T
T0.
18�
0.05
0.22
�0.
01*1,
14,2
10.
26�
0.04
*7,35
**1
0.25
�0.
04*7,
35**
10.
23�
0.03
**1
0.20
�0.
04*14
,21
0.19
;0.
11–0
.25
0.22
;0.
20–0
.23
0.28
;0.
20–0
.31
0.23
;0.
21–0
.32
0.23
;0.
18–0
.29
0.19
;0.
13–0
.25
DH
T+T
T3.
5�
2.0
43.7
�12
.1**
1,14
,21,
28,3
517
.3�
4.1*
*1,7,
21,2
8,35
9.5
�3.
0*28
**1,
7,14
,35
6.6
�1.
9*21
**1,
7,14
5.2
�1.
8**1,
7,14
,21
3.1;
1.1–
6.9
43.0
;29
.4–6
8.0
17.4
;11
.9–2
3.9
9.3;
4.5–
13.3
6.9;
3.8–
9.4
4.6;
2.3–
7.7
TT
/E27
.2�
14.8
168.
4�
56.8
*28,3
5 **1,
14,2
189
.9�
31.2
**1,
7,21
,28,
3550
.7�
19.5
*1,28
**7,
1443
.3�
14.9
*1,7,
21**
1443
.4�
20.6
*7 **14
,21
19.8
;16
.0–5
1.8
162.
6;96
.5–2
56.9
93.5
;51
.3–1
49.7
43.2
;34
.8–9
4.6
41.9
;24
.0–6
2.5
36.7
;17
.9–7
9.2
(B)
TT
2.5
�1.
912
.9�
7.1*
*1††
14.4
�8.
1**1
13.4
�10
.4**
113
.4�
5.9*
*1††
13.0
�10
.0**
1††
2.0;
0.8–
6.9
12.0
;2.
5–23
.914
.7;
3.1–
26.5
11.5
;2.
3–38
.614
.0;
2.7–
21.0
9.7;
5.6–
36.1
SH
BG
23.7
�7.
222
.6�
8.6
22.5
�6.
321
.9�
6.5
21.8
�6.
321
.1�
5.3
27.3
;15
.0–3
3.4
28.0
;15
.8–4
0.5
25.6
;16
.1–3
3.6
26.3
;15
.5–3
2.8
26.7
;16
.2–3
3.1
25.4
;17
.5–3
5.0
cFT
0.21
�0.
490.
31�
0.20
*1††
0.36
�0.
23*1
0.33
�0.
27*1
0.33
�0.
17††
0.33
�0.
33†
0.04
;0.
01–1
.44
0.26
;0.
04–0
.56
0.34
;0.
05–0
.65
0.26
;0.
04–0
.90
0.34
;0.
05–0
.59
0.24
;0.
11–1
.15
cBio
T1.
2�
0.9
7.4
�4.
8**1†
†8.
5�
5.5*
*17.
5�
6.6*
*17.
8�
4.0*
*1††
7.8
�7.
90.
9;0.
3–3.
36.
1;0.
9–13
.38.
1;1.
3–15
.36.
2;0.
7–21
.38.
1;1.
2–13
.95.
6;2.
7–27
.0FA
I10
.9�
7.1
60.3
�42
.1**
1††
69.4
�43
.0**
159
.1�
38.9
**1
61.7
�36
.4**
1†61
.1�
65.2
8.1;
2.5–
24.4
41.4
;6.
1–11
9.4
57.1
;9.
2–13
2.7
44.3
;8.
0–11
2.0
58.5
;9.
8–12
2.6
42.6
;19
.7–2
06.5
DH
T0.
4�
0.3
3.2
�1.
9**1†
†3.
2�
2.0*
*13.
2�
2.5*
13.
2�
1.7*
*1†3.
0�
2.1*
*1†
0.3;
0.1–
1.1
3.6;
0.3–
6.4
3.3;
0.4–
6.7
2.7;
0.2–
8.6
2.9;
0.3–
5.3
2.4;
1.1–
7.7
E10
2.3
�24
.516
2.6
�35
.1*1
148.
6�
24.8
*117
1.3
�52
.1*1
163.
0�
44.0
*115
2.4
�21
.8*1
97.1
;39
.2–1
63.1
157.
1;65
.1–2
11.2
137.
2;43
.6–1
82.4
165.
9;79
.0–2
16.5
142.
5;69
.6–2
20.4
110.
4;45
.3–1
98.5
DH
T/T
T0.
19�
0.03
0.23
�0.
06*1
0.21
�0.
03**
10.
22�
0.06
*10.
22�
0.04
**1
0.21
�0.
03*1
0.16
;0.
12–0
.23
0.23
;0.
12–0
.31
0.22
;0.
15–0
.25
0.22
;0.
11–0
.33
0.22
;0.
14–0
.28
0.22
;0.
18–0
.30
DH
T+T
T2.
9�
2.2
16.1
�9.
0**1†
†17
.6�
10.1
**1
16.6
�13
.0**
116
.7�
7.6*
*1††
16.0
�12
.1*1
2.3;
0.9–
8.0
15.6
;2.
8–30
.418
.4;
3.5–
33.3
14.5
;2.
5–45
.317
.0;
3.0–
26.4
12.3
;6.
9–43
.9T
T/E
26.7
�24
.476
.5�
47.6
*1††
94.4
�73
.7*1
82.3
�75
.8*1
88.4
�69
.7*1
66.6
�45
.6*1
15.4
;8.
6–80
.355
.0;
36.9
–155
.763
.8;
44.0
–259
.546
.6;
39.4
–260
.274
.0;
32.0
–253
.055
.7;
20.4
–169
.3
*P�
0.05
and
**P
�0.
01vs
.ot
her
resp
ectiv
eda
ys(1,
7,14
,21
,28
,an
d35
);† P
�0.
05,
††P
�0.
01T
Gvs
.T
EH
orm
ones
and
resp
ectiv
era
tios
have
been
eval
uate
dbe
fore
(day
1)an
dw
eekl
yfo
r5
wee
ks(f
rom
day
7to
day
35)
afte
ra
sing
lei.m
.ad
min
istr
atio
nof
test
oste
rone
enan
that
e(T
E:
250
mg)
(A)
and
durin
gte
stos
tero
nege
lad
min
istr
atio
n(T
G:
50m
g/di
e)(B
)in
mal
ehy
pogo
nada
lvol
unte
ers
(N=
10)
TT
=to
tal
test
oste
rone
;S
HB
G=
sex
horm
one-
bind
ing
glob
ulin
;cF
T=
calc
ulat
edfr
eete
stos
tero
ne;
cBio
T=
calc
ulat
edbi
oava
ilabl
ete
stos
tero
ne;
FAI=
free
andr
ogen
inde
x(T
T/S
HB
G¥
100)
;E
=17
-b-
estr
adio
l;D
HT
=di
hydr
otes
tost
eron
e
Androgens Profile in Treated Male Hypogonadism 877
J Sex Med 2012;9:873–886

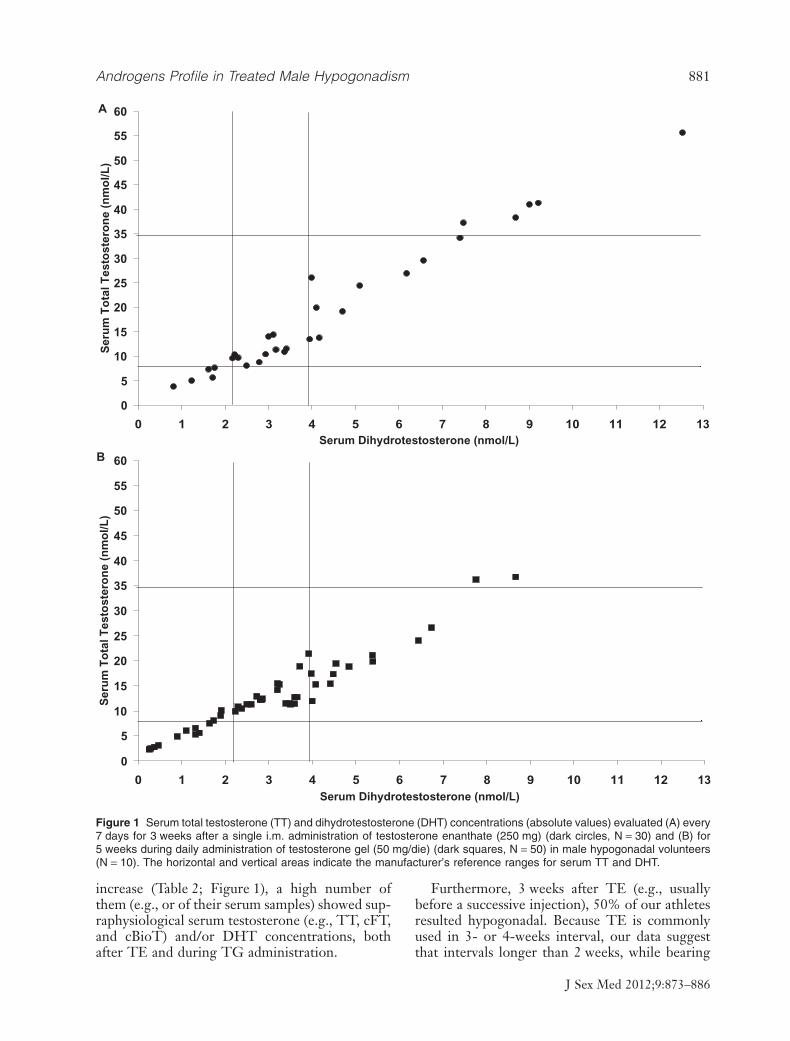
During TG administration, serum TT concen-trations were in the manufacturer’s referencerange from 60% to 90% of samples at differenttime points (78% on total samples) (Table 2),being the majority of abnormal samples because oflow TT concentrations in the same two subjects(i.e., probably because of reduced individual gelabsorption or for a relatively low TG dose), andonly two samples (e.g., 2/50) showed elevatedserum TT levels (Figure 1). Serum TT concentra-tion was significantly higher on day 7 after TEcompared with TG administration and, asexpected, was significantly higher on days 28 and35 during TG administration compared with TE.
The comparison with our laboratory referencerange for TT evidenced a lower number ofsamples in the normal range, with respect to themanufacturer’s range comparison, both after TEand during TG administration (Table 2).
Serum DHTMean serum DHT concentration significantlyincreased as compared with pretreatment valuesboth after TE and during TG administration(Table 1). The mean DHT concentrations werewithin the normal range at all time points after TEand during TG administration, respectively.
The probability to find a sample containingserum DHT within the normal range was from0% to 50% of samples at different time points(23% on total samples) during the first 3 weeksafter TE administration (Table 2). Particularly,after TE administration, serum DHT concentra-tions were above the upper limit in 10/10 subjectson day 7 and in 5/10 subjects on day 14, andnormal or below of the manufacturer’s referencerange from day 21 to day 35, respectively (Table 2,Figure 1).
During TG administration, serum DHT con-centrations were within the normal range from10% to 40% of samples at different time points(26% on total samples) during 5 weeks of TGadministration (Table 2); elevated serum DHTlevels were observed in 16/50 samples and lowDHT levels in 16/50 samples (Figure 1).
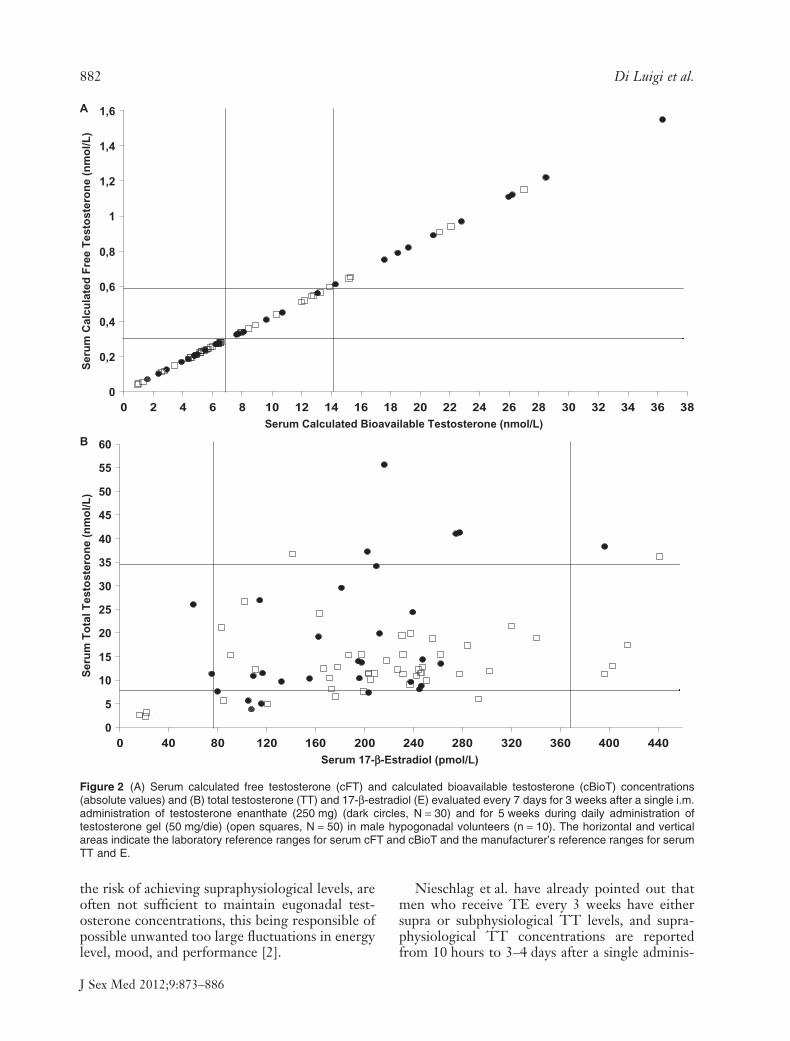
Serum Calculated HormonesAs expected, mean cFT, cBioT, and FAI increasedsignificantly both after TE and during TG admin-istration; serum cFT, cBioT, and FAI were signifi-cantly higher on day 7 after TE compared withTG administration (Table 1). It is of interest thatcompared with our laboratory reference ranges,cFT and cBioT were considered normal in60–70% of our volunteers only on day 7 after TE,particularly on day 7 after TE, all volunteersshowed high serum cFT and cBioT; on day 14,about 20% of them have low values and 20% havehigh values, and from day 21 to day 35, quite allvolunteers showed low cFT and cBioT values(Table 2, Figure 2). During 5 weeks of TG admin-istration, about 44% of total samples showednormal cFT and cBioT values; furthermore,whereas the majority of samples outside the refer-ence range values showed low cFT and cBioTlevels, in few samples (5/50), high values have beenalso observed (Table 2, Figure 2).
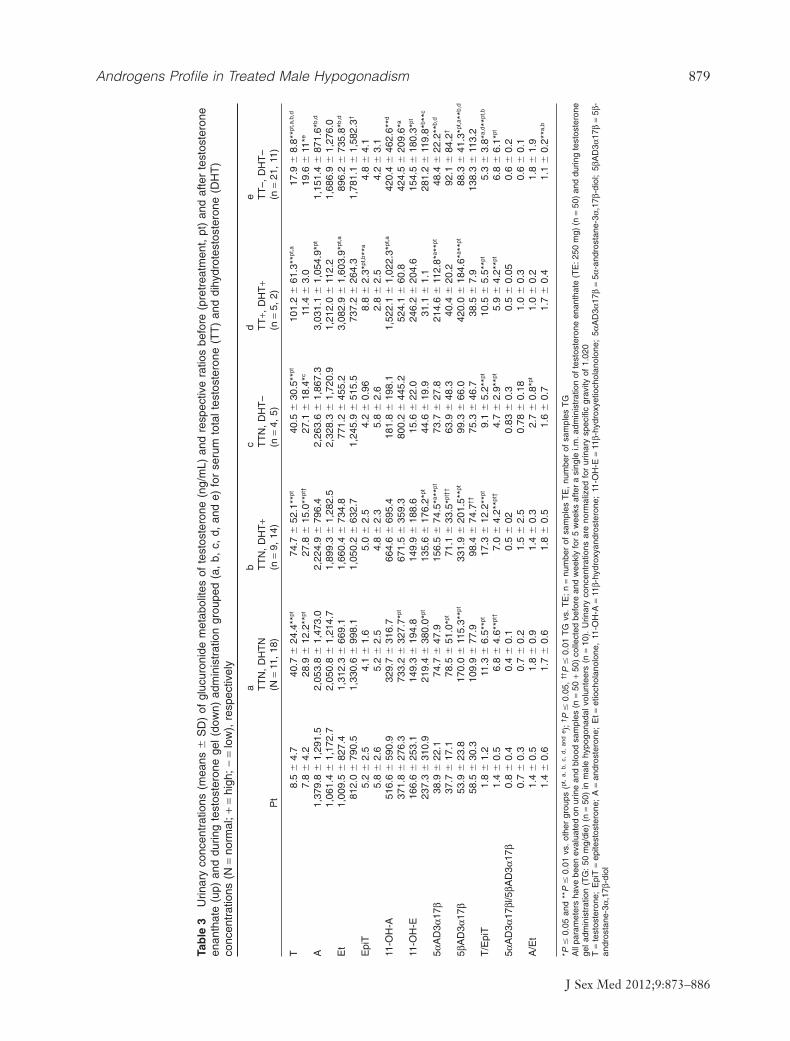
Urinary Testosterone Metabolites ProfilesThe evaluated glucuronide metabolites of test-osterone differently increased after TE and duringTG administration, also depending on serum TTand DHT profiles (Table 3). Particularly, theobserved differences in the evaluated urinary test-osterone metabolites concentrations were mainlyrelated to serum TT concentrations (normal, high,
Table 2 Percentage of serum samples with absolute and calculated androgens concentrations within the manufacturer’s(m) or laboratory (lab) reference ranges (% NR)
% NR after TE vs. % NR during TG
Day 7 Day 14 Day 21 Day 28 Day 35 Total§
TT (m) 50*14,28,35 vs. 80 100*7**21,28,35‡ vs. 80 50*28,35**14‡‡ vs. 60‡ 0*7,21**14 vs. 90†† 0*7,21**14 vs. 70†† 70‡‡ vs. 78‡‡
TT (lab) 40 vs. 50 60*28,35**21 vs. 50 0**14 vs. 30*28 0*14 vs. 70*21†† 0*14 vs. 40 33.3 vs. 48DHT (m) 0**14 vs. 40† 60*28**7 vs. 10 20 vs. 40 0*14 vs. 50† 0*14 vs. 20 23.3 vs. 46cFT (lab) 0**14 vs. 50† 60*21**7,28,35 vs. 20† 30*14 vs. 10 0**14 vs. 50† 0**14 vs. 10 20 vs. 44cBioT (lab) 0**14 vs. 40 70*21**7,28,35 vs. 20† 20*14 vs. 10*28 0**14 vs. 60*21,35†† 0**14 vs. 10*28 23.4 vs. 44FAI (lab) 0*21**14 vs. 40 70**7,35 vs. 60 40*7,35 vs. 60 20 vs. 70 0*21**14 vs. 70† 40 vs. 62
*P � 0.05 and **P � 0.01 vs. other respective days (1, 7, 14, 21, 28, and 35); †P � 0.05, ††P � 0.01 TG vs. TE; ‡P � 0.05, ‡‡P � 0.01 vs. lab§Evaluated during 3 weeks after TE administration (n = 30) and during 5 weeks of TG administration (N = 50)Measurements of % NR have been evaluated from serum samples collected weekly for 5 weeks after a single i.m. administration of testosterone enanthate (TE:250 mg) and during testosterone gel administration (TG: 50 mg/die) in male hypogonadal volunteers (N = 10)TT = total testosterone; DHT = dihydrotestosterone; cFT = calculated free testosterone; cBioT = calculated bioavailable testosterone; FAI = free androgen index(TT/SHBG ¥ 100)
878 Di Luigi et al.
J Sex Med 2012;9:873–886
Tab
le3
Urin
ary
conc
entr
atio
ns(m
eans
�S
D)
ofgl
ucur
onid
em
etab
olite
sof
test
oste
rone
(ng/
mL)
and
resp
ectiv
era
tios
befo
re(p
retr
eatm
ent,
pt)
and
afte
rte
stos
tero
neen
anth
ate
(up)
and
durin
gte
stos
tero
nege
l(do
wn)
adm
inis
trat
ion
grou
ped
(a,
b,c,
d,an
de)
for
seru
mto
talt
esto
ster
one
(TT
)an
ddi
hydr
otes
tost
eron
e(D
HT
)co
ncen
trat
ions
(N=
norm
al;
+=
high
;-
=lo
w),
resp
ectiv
ely
Pt
ab
cd
eT
TN
,D
HT
NT
TN
,D
HT
+T
TN
,D
HT
–T
T+,
DH
T+
TT
–,D
HT
–(N
=11
,18
)(n
=9,
14)
(n=
4,5)
(n=
5,2)
(n=
21,
11)
T8.
5�
4.7
40.7
�24
.4**
pt74
.7�
52.1
**pt
40.5
�30
.5**
pt10
1.2
�61
.3**
pt,a
17.9
�8.
8**pt
,a,b
,d
7.8
�4.
228
.9�
12.2
**pt
27.8
�15
.0**
pt†
27.1
�18
.4*c
11.4
�3.
019
.6�
11*e
A1,
379.
8�
1,29
1.5
2,05
3.8
�1,
473.
02,
224.
9�
796.
42,
263.
6�
1,86
7.3
3,03
1.1
�1,
054.
9*pt
1,15
1.4
�87
1.6*
b,d
1,06
1.4
�1,
172.
72,
050.
8�
1,21
4.7
1,89
9.3
�1,
282.
52,
328.
3�
1,72
0.9
1,21
2.0
�11
2.2
1,68
6.9
�1,
276.
0E
t1,
009.
5�
827.
41,
312.
3�
669.
11,
660.
4�
734.
877
1.2
�45
5.2
3,08
2.9
�1,
603.
9*pt
,a89
6.2
�73
5.8*
b,d
812.
0�
790.
51,
330.
6�
998.
11,
050.
2�
632.
71,
245.
9�
515.
573
7.2
�26
4.3
1,78
1.1
�1,
582.
3†
Epi
T5.
2�
2.5
4.1
�1.
65.
0�
2.5
4.2
�0.
968.
8�
2.3*
pt,b**
a4.
8�
4.1
5.8
�2.
65.
2�
2.5
4.8
�2.
35.
8�
2.6
2.8
�2.
54.
2�
3.1
11-O
H-A
516.
6�
590.
932
9.7
�31
6.7
664.
6�
695.
418
1.8
�19
8.1
1,52
2.1
�1,
022.
3*pt
,a42
0.4
�46
2.6*
*d
371.
8�
276.
373
3.2
�32
7.7*
pt67
1.5
�35
9.3
800.
2�
445.
252
4.1
�60
.842
4.5
�20
9.6*
a
11-O
H-E
166.
6�
253.
114
9.3
�19
4.8
149.
9�
188.
615
.6�
22.0
246.
2�
204.
615
4.5
�18
0.3*
pt
237.
3�
310.
921
9.4
�38
0.0*
pt13
5.6
�17
6.2*
pt44
.6�
19.9
31.1
�1.
128
1.2
�11
9.8*
b **c
5aA
D3a
17b
38.9
�22
.174
.7�
47.9
156.
5�
74.5
*a **pt
73.7
�27
.821
4.6
�11
2.8*
a **pt
48.4
�22
.2**
b,d
37.7
�17
.178
.5�
51.0
*pt71
.1�
33.5
*pt††
63.9
�48
.340
.4�
20.2
92.1
�84
.2†
5bA
D3a
17b
53.9
�23
.817
0.0
�11
5.3*
*pt33
1.9
�20
1.5*
*pt99
.3�
66.0
420.
0�
184.
6*a *
*pt88
.3�
41.3
*pt,a**
b,d
58.5
�30
.310
9.9
�77
.998
.4�
74.7
††75
.3�
46.7
38.5
�7.
913
8.3
�11
3.2
T/E
piT
1.8
�1.
211
.3�
6.5*
*pt17
.3�
12.2
**pt
9.1
�5.
2**pt
10.5
�5.
5**pt
5.3
�3.
8*a,
d **pt
,b
1.4
�0.
56.
8�
4.6*
*pt†
7.0
�4.
2**pt
†4.
7�
2.9*
*pt5.
9�
4.2*
*pt6.
8�
6.1*
pt
5aA
D3a
17bl
/5bA
D3a
17b
0.8
�0.
40.
4�
0.1
0.5
�02
0.83
�0.
30.
5�
0.05
0.6
�0.
20.
7�
0.3
0.7
�0.
21.
5�
2.5
0.78
�0.
181.
0�
0.3
0.6
�0.
1A
/Et
1.4
�0.
51.
8�
0.9
1.4
�0.
32.
7�
0.8*
pt1.
0�
0.2
1.8
�1.
91.
4�
0.6
1.7
�0.
61.
8�
0.5
1.6
�0.
71.
7�
0.4
1.1
�0.
2**a,
b
*P�
0.05
and
**P
�0.
01vs
.ot
her
grou
ps(pt
,a,
b,c,
d,an
de )
;† P
�0.
05,
††P
�0.
01T
Gvs
.T
E;
n=
num
ber
ofsa
mpl
esT
E,
num
ber
ofsa
mpl
esT
GA
llpa
ram
eter
sha
vebe
enev
alua
ted
onur
ine
and
bloo
dsa
mpl
es(n
=50
+50
)co
llect
edbe
fore
and
wee
kly
for
5w
eeks
afte
ra
sing
lei.m
.adm
inis
trat
ion
ofte
stos
tero
neen
anth
ate
(TE
:250
mg)
(n=
50)
and
durin
gte
stos
tero
nege
ladm
inis
trat
ion
(TG
:50
mg/
die)
(n=
50)
inm
ale
hypo
gona
dalv
olun
teer
s(n
=10
).U
rinar
yco
ncen
trat
ions
are
norm
aliz
edfo
rur
inar
ysp
ecifi
cgr
avity
of1.
020
T=
test
oste
rone
;E
piT
=ep
itest
oste
rone
;A
=an
dros
tero
ne;
Et=
etio
chol
anol
one,
11-O
H-A
=11
b-hy
drox
yand
rost
eron
e;11
-OH
-E=
11b-
hydr
oxye
tioch
olan
olon
e;5a
AD
3a17
b=
5a-a
ndro
stan
e-3a
,17b
-dio
l;5b
AD
3a17
b=
5b-
andr
osta
ne-3
a,17
b-di
ol
Androgens Profile in Treated Male Hypogonadism 879
J Sex Med 2012;9:873–886

or low) and as observed in the group TT-normal/DHT-high, probably also to the serum DHT (e.g.,vs. TT-normal/DHT-normal for 5aAD3a17b)and to the type of treatment (e.g., mainly forurinary T, 5aAD3a17b, and 5bAD3a17b)(Table 3).
The concentrations of evaluated urinary param-eters resulted within the normal reference ranges[31] in about 30–60% of total urinary samples, andfor some parameters, the great relative percentageurine samples with normal concentrations wereobserved only when serum was TT-high/DHT-high. Depending on respective serum androgensprofile, differences were between TE and TGadministration for some urinary metabolites con-centrations (e.g., for A, 11-OH-A, 5aAD3a17b,5bAD3a17b, T/EpiT, 5aAD3a17b/5bAD3a17b,and A/Et) were observed (Table 4). Only forurinary EpiT ratio, quite all samples showed lowconcentrations, independently from serum andro-gens concentrations (Table 4).
Discussion
Few investigations evaluated the prevalence of truehypogonadism or the effects of TRT in male ath-letes, and no cross-sectional or longitudinal trialsevaluated the consequences of untreated testoster-one deficiency or of a not well-tailored TRT onathletes’ health and/or performance [3,32]. Themajority of clinical studies on TRT have been per-formed in sedentary males and focused on moni-
toring specific clinical target and/or mean serumhormones variations (e.g., TT, LH, etc.) after tes-tosterone administration [13,24,33–37]. Very fewclinical data on individual absolute androgensprofiles during TRT exist, because of the greatinterest for individual androgens profile uponpharmacological loading, with different testoster-one preparations, coming from sport-linked orga-nizations faced with detecting testosterone abusein healthy and in hypogonadal athletes [19,38–40].
TRT Monitoring in Male Hypogonadal AthletesIn the present study, we partially confirmed somealready known variations of mean serum andro-gens concentrations upon the administrations ofTE and TG in hypogonadal males. At individuallevel, we showed that it is really difficult to mimicphysiological androgens rhythm by using thesepreparations. Furthermore, we also confirmedthat, at individual level, it is inaccurate to identifythe presence of a normal and stable androgensprofile during TRT only by evaluating serum TT,as actually recommended. This is of great impor-tance for male athletes, where it is highlyrecommended to reproduce a true and stablephysiological androgenization.
Even if, according to the common strategy formonitoring TRT, all of our volunteers resultedsubstantially well treated (e.g., for past history andbecause of normal serum TT in all volunteers onday 14 after TE and in the 60–80% of totalsamples during TG) or needing a TG dose’s
Table 4 Percentage of urinary samples with glucuronide metabolites of testosterone within the reported referenceranges (% NR) for athletes (from Van Renterghem et al. [31]) total and grouped (a, b, c, d, and e) for serum totaltestosterone (TT) and dihydrotestosterone (DHT) concentrations (N = normal; + = high; - = low), respectively
% NR after TE vs. % NR during TG
a b c d e
Total§TTN, DHTN TTN, DHT+ TTN, DHT– TT+, DHT+ TT–, DHT–(n = 11, 18) (n = 9, 14) (n = 4, 5) (n = 5, 2) (n = 21, 11)
T 86*b,c,e**d vs. 69*e 25 vs. 50 0 vs. 50 0 vs. 0 43 vs. 22 43.3 vs. 56A 43 vs. 38 88*c**e vs. 25†† 0 vs. 50 75*e vs. 0 24 vs. 22 53.3 vs. 46Et 57 vs. 38 75*e vs. 33 50 vs. 75*e 25 vs. 0 33 vs. 11 50 vs. 46EpiT 0 vs. 0 0 vs. 0 0 vs. 0 0 vs. 0 10 vs. 0 0 vs. 011-OH-A 43 vs. 62 25 vs. 58 0 vs. 50 50 vs. 100 33 vs. 33 26.6 vs. 62†
11-OH-E 14 vs. 15*e 25 vs. 8*e 0 vs. 0 50 vs. 0 24 vs. 56 16.6 vs. 365aAD3a17b 71*b,d vs. 38 13*e vs. 42 50 vs. 25 0*e vs. 100*e† 62 vs. 22†† 33.3 vs. 505bAD3a17b 71*b,d vs. 62 13*e vs. 42 50 vs. 50 0**e vs. 0 76 vs. 22†† 40 vs. 46T/EpiT 43*b vs. 0† 0 vs. 0 0 vs. 50 0 vs. 0 24 vs. 11 0 vs. 25aAD3a17bl/5bAD3a17b 86 vs. 23*e†† 63 vs. 42 50 vs. 25 100 vs. 0† 52 vs. 67 63.3 vs. 50†
A/Et 29 vs. 85† 38 vs. 67 0 vs. 50 50 vs. 100 48 vs. 67 56.7 vs. 74††
*P � 0.05 and **P � 0.01 vs. other groups (a, b, c, d, and e); †P � 0.05, ††P � 0.01 TG vs. TE§Evaluated during 3 weeks after TE administration (n = 30) and during 5 weeks of TG administration (n = 50)Measurements of % NR have been evaluated from urine samples collected weekly for five weeks after a single i.m. administration of testosterone enanthate (TE:250 mg) (n = 50) and during testosterone gel administration (TG: 50 mg/die) (n = 50) in male hypogonadal volunteers (n = 10)T = testosterone; EpiT = epitestosterone; A = androsterone; Et = etiocholanolone, 11-OH-A = 11b-hydroxyandrosterone; 11-OH-E = 11b-hydroxyetiocholanolone;5aAD3a17b = 5a-androstane-3a,17b-diol; 5bAD3a17b = 5b-androstane-3a,17b-diol
880 Di Luigi et al.
J Sex Med 2012;9:873–886
increase (Table 2; Figure 1), a high number ofthem (e.g., or of their serum samples) showed sup-raphysiological serum testosterone (e.g., TT, cFT,and cBioT) and/or DHT concentrations, bothafter TE and during TG administration.
Furthermore, 3 weeks after TE (e.g., usuallybefore a successive injection), 50% of our athletesresulted hypogonadal. Because TE is commonlyused in 3- or 4-weeks interval, our data suggestthat intervals longer than 2 weeks, while bearing
0
5
10
15
20
25
30
35
40
45
50
55
60
0 1 2 3 4 5 6 7 8 9 10 11 12Serum Dihydrotestosterone (nmol/L)
Ser
um
To
tal T
esto
ster
on
e (n
mo
l/L)
13
A
0
5
10
15
20
25
30
35
40
45
50
55
60
0 1 2 3 4 5 6 7 8 9 10 11 12Serum Dihydrotestosterone (nmol/L)
Ser
um
To
tal T
esto
ster
on
e (n
mo
l/L)
13
B
Figure 1 Serum total testosterone (TT) and dihydrotestosterone (DHT) concentrations (absolute values) evaluated (A) every7 days for 3 weeks after a single i.m. administration of testosterone enanthate (250 mg) (dark circles, N = 30) and (B) for5 weeks during daily administration of testosterone gel (50 mg/die) (dark squares, N = 50) in male hypogonadal volunteers(N = 10). The horizontal and vertical areas indicate the manufacturer’s reference ranges for serum TT and DHT.
Androgens Profile in Treated Male Hypogonadism 881
J Sex Med 2012;9:873–886
the risk of achieving supraphysiological levels, areoften not sufficient to maintain eugonadal test-osterone concentrations, this being responsible ofpossible unwanted too large fluctuations in energylevel, mood, and performance [2].
Nieschlag et al. have already pointed out thatmen who receive TE every 3 weeks have eithersupra or subphysiological TT levels, and supra-physiological TT concentrations are reportedfrom 10 hours to 3–4 days after a single adminis-
0
0,2
0,4
0,6
0,8
1
1,2
1,4
1,6
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38
Serum Calculated Bioavailable Testosterone (nmol/L)
Ser
um
Cal
cula
ted
Fre
e T
esto
ster
on
e (n
mo
l/L)
A
0
5
10
15
20
25
30
35
40
45
50
55
60
0 40 80 120 160 200 240 280 320 360 400 440
Serum 17-β-Estradiol (pmol/L)
Ser
um
To
tal T
esto
ster
on
e (n
mo
l/L)
B
Figure 2 (A) Serum calculated free testosterone (cFT) and calculated bioavailable testosterone (cBioT) concentrations(absolute values) and (B) total testosterone (TT) and 17-b-estradiol (E) evaluated every 7 days for 3 weeks after a single i.m.administration of testosterone enanthate (250 mg) (dark circles, N = 30) and for 5 weeks during daily administration oftestosterone gel (50 mg/die) (open squares, N = 50) in male hypogonadal volunteers (n = 10). The horizontal and verticalareas indicate the laboratory reference ranges for serum cFT and cBioT and the manufacturer’s reference ranges for serumTT and E.
882 Di Luigi et al.
J Sex Med 2012;9:873–886

tration of 200–250 mg of TE [21,22,41]. Even ifour results were partially predictable [41], they areof great interest for doping concerns in hypogo-nadal athletes. In fact, we highlight the observedhigh probability (e.g., at least 50%) to find out atan individual level a random serum sample withsupraphysiological TT level until 7 days after TEadministration compared with the 4% of totalsamples during fixed dose TG administration atthe doses we used. Consequently, based on ourdata, a great percentage of hypogonadal athletesassuming 250 mg of TE every 3 weeks may behyperandrogenic for serum TT for one-third ofthe period between two consecutive TE adminis-tration (i.e., at the common, 3-weeks interval ofadministration) and for about 120 days per year,and even more if also DHT is considered. In fact,the probability to find out an hyperandrogenicserum sample for DHT resulted higher both afterTE (e.g., in all volunteers on day 7 and in 50% ofthem on day 14) and during TG (e.g., in 32%of total samples); we also highlight that for some ofour volunteers the of TG dose and/or absorptionwere low, based on the observed low serum TTconcentration (Figure 1).
On this basis, we believe that it is not easy totitrate TRT to obtain stable and eugonadal serumTT without major fluctuations and/or elevationsin DHT concentrations in all hypogonadal ath-letes treated with TE or TG. We might alsohypothesize the possible use of low doses of5a-reductase inhibitors, to reduce both the con-version of testosterone to DHT and, indirectly,also the doses of administered exogenous test-osterone. However, this is only a very speculativehypothesis, because we do not know if thisco-treatment could be really useful, safe, andethical.
Finally, we also highlight that even if aromati-zation of testosterone to E during TRT is tradi-tionally related to the extent of adipose tissue,which in trained athletes is often low (e.g., unfor-tunately we did not evaluate body composition),our data showed both the presence of active aro-matization of both TE and TG that it is likely tooccur also at muscle site or at testicular level [42]and a large fluctuation of serum E and TT/Eratio only after TE administration (Table 1).In addition, no differences for TT/E ratiobetween subjects affected by primary and second-ary hypogonadism were observed (unpublishedresults).
As already reported [2], when necessary (e.g.,difficulty in dose tailoring with testosterone esters
or gel) and/or possible (e.g., drugs and/or moneyavailability, and so forth), the best way to generatea more physiological and long-life stable andro-gens profile (e.g., normal serum TT and DHT)may be to start TRT with newer testosteronepreparations (e.g., parenteral testosterone unde-canoate, subdermal testosterone implants) [43–45]or delivery systems (e.g., devices releasing variableamounts of testosterone), particularly when indi-vidualized dose titration are necessary.
Based on our results, the concepts of testoster-one dose tailoring and monitoring during TRT inhypogonadal individuals should be probablyreevaluated, particularly for athletes. In fact, wehave both clinical and ethical concerns about thepresence of often unrevealed abnormal circulatingandrogens concentrations during TRT. Because ofthe possible short-term effects of supraphysiologi-cal doses of testosterone and DHT, and also to thefact that serum TT fluctuations are necessary toinduce some physiological effects of testosterone,we cannot exclude that also a transitory hyperan-drogenism may influence health and/or exerciseperformance [8]. Unfortunately, we actually do notknow whether the commonly observed side effectsof TRT (e.g., increased hematocrit and prostategrowth) could be also related to the presence oftoo often unrevealed and prolonged transitoryabnormally high circulating TT and DHT con-centrations (also for high cFT and cBioT?) duringdifferent TRT. Furthermore, it is not knownwhether the observed fluctuation and/or abnormal(e.g., low or high) levels of circulating androgensafter TE and TG could negatively or positivelyaffect athlete’s physical adaptations (e.g., neuro-logical, muscular, metabolic) and performance[46].
Unwanted Hyperandrogenism and Anti-DopingDuring TRT in Hypogonadal AthletesTestosterone is voluntary abused by healthy ath-letes not only for its proteo-anabolic properties(e.g., long-term effects) but also for its acuteeffects on CNS, neuromuscular system, andmetabolisms [6,8]. Consequently, besides the well-known long-term effects on muscles (e.g., hyper-trophy, increased strength), also an unwantedtransitory hyperandrogenism (e.g., hyper-TTand/or hyper-DHT) during TRT may furtherimprove athlete’s performance. The onset ofaction and time course of testosterone action ondifferent target organs are poorly investigated [47].For example, when an athlete’s behavior and cog-nition are concerned, a transitory increase of
Androgens Profile in Treated Male Hypogonadism 883
J Sex Med 2012;9:873–886

androgenization degree may reduce the sense offatigue, increase aggressiveness, and amelioratecognitive processes during competition. Conse-quently, during authorized TRT with TE, as actu-ally tailored, hypogonadal athletes are expected tobenefit from transitory hyperandrogenism. This ismainly based on anecdotal reports, because it isnot demonstrated that soon reaching supraphysi-ological androgen levels during competition mayyield in the short-term to favorable muscular per-formances [47].
When anti-doping is concerned, exogenoustestosterone abuse in healthy athletes may be sus-pected for urinary T/EpiT ratio higher than aproper cutoff value, and it is confirmed by evalu-ating the 13C/12C ratio with gas chromatography-combustion-isotope ratio mass spectrometryand/or by specific laboratory reports on longitudi-nal urinary steroids profiles and expert’s dataanalyses [48]. However, actually, no data are avail-able on possible strategies for suspecting and con-firming testosterone misuse or abuse during TRTin male hypogonadal athletes. A specific monitor-ing strategy and the institution of a specific bio-logical passport for treated hypogonadal athletescould be very useful in anti-doping activity intreated hypogonadal athletes [49].
Even if, theoretically, hypogonadal active indi-viduals, competitive, and not competitive athletes,at all ages are probably numerous in the world,there are few competitive true hypogonadal ath-letes treated with testosterone who are exposed todoping controls [3]. However, based on ourresults, we can hypothesize that a relatively highpercentage of worldwide hypogonadic athletes(e.g., and also non-athletes) may involuntary “liveand work” for many days with inappropriate serumTT and /or DHT concentrations during a lifelongTRT with the testosterone ester or gel used in thepresent study. Consequently, if in the future theevaluation of serum TT and DHT during arandom serum doping control is introduced byanti-doping organizations, the risk of suspecting atestosterone misuse or abuse in this populationcould be really high. In addition, the use of moresophisticated delivery systems that would alloweasier dose-titration controls for testosterone arenecessary.
Our study was not designed to study metabolicpathways or to identify a procedure to confirmdoping with testosterone during TRT with TEand TG. Based on the observed relationshipsbetween serum and urinary androgens profiles(Tables 3 and 4), we suggest that the future
methods to detect testosterone abuse during TRTshould be based on the parallel evaluation of bothserum androgens and specific urinary metabolitesof testosterone, whose respective cutoffs should beidentified for each type of testosterone prepara-tion, timing of doping control, and serum andro-gens profile. In fact, besides the relatively lownumber of samples, we observed significant differ-ences in the urinary concentrations of some test-osterone metabolites, both between TE and TGadministration and between urinary samplesgrouped for serum TT and DHT concentrations(Table 3). Being our urinary metabolites of test-osterone within the reported reference ranges forhealthy athletes only from the 15% to 60%, dif-ferent TRT related reference ranges for eachurinary testosterone metabolite should be identi-fied, only when TRT is tailored to obtain normalserum TT and DHT concentrations.
Conclusion
Considering the results of this study, we believethat in hypogonadal male athletes it is incorrect tomonitor a TRT only by evaluating serum TT. Inaddition, it is necessary to identify and standardizethe optimal target for serum androgens profile(e.g., in terms of TT, cFT, cBioT, and DHT con-centrations) both to guarantee health status andphysiological performances and to adequatelymanage doping controls to suspect and confirm apossible testosterone abuse during TRT.
Waiting for further clinical investigations, theoptimal target for a correct TRT in athletes shouldbe to induce a long-life stable eugonadal andro-gens profile throughout an individualized well-tailored treatment; this means to avoid as much aspossible also transitory hypo or hyperandro-genisms. Because few studies are available ongenetic differences in individual testosteronemetabolism and androgen receptors sensitivityduring TRT in athletes [50], the optimal testoster-one formulation would allow each athlete to titratethe dose, in order to guarantee at least both physi-ological and stable serum TT and DHT concen-trations. Furthermore, from a practical point ofview, it is advisable to document this target beforea TUE request, by evaluating serum TT andDHT at different time points during the first dosestitration, depending by different available specifictestosterone formulations, doses, and frequency ofadministration [2,13].
Because of some limitations of our study (e.g.,reduced number of volunteers, lack of evaluations
884 Di Luigi et al.
J Sex Med 2012;9:873–886

of long-term effects on health and performance,lack of comparison with other TRT, and so forth),related to the difficulty in finding and evaluatingfor a long period hypogonadal competitive ath-letes, further and larger experimental and clinicalevaluations are highly warranted on this issues, bystudying also newer TRT modalities, both in ath-letes and in non-athletes.
Acknowledgment
This study was supported by a grant of Italian Ministryof Health—Commission for Vigilance on Doping andAthletes’ Health.
Corresponding Author: Luigi Di Luigi, MD, Unit ofEndocrinology, Department of Health Sciences, Uni-versity of Rome “Foro Italico,” Rome 00135, Italy. Tel:+390636733563; Fax: +390636733231; E-mail:[email protected]
Conflict of Interest: None.
Statement of Authorship
Category 1(a) Conception and Design
Luigi Di Luigi(b) Acquisition of Data
Antonio Aversa; Serena Bianchini; Francesco Botrè;Silvia Migliaccio; Francesco Romanelli; Paolo Sgrò
(c) Analysis and Interpretation of DataAntonio Aversa; Luigi Di Luigi; FrancescoRomanelli; Paolo Sgrò
Category 2(a) Drafting the Article
Luigi Di Luigi(b) Revising It for Intellectual Content
Luigi Di Luigi; Andrea Lenzi
Category 3(a) Final Approval of the Completed Article
Luigi Di Luigi; Paolo Sgrò; Antonio Aversa; SilviaMigliaccio; Serena Bianchini; Francesco Botrè;Francesco Romanelli; Andrea Lenzi
References
1 Cunningham GR, Toma SM. Clinical review: Why is andro-gen replacement in males controversial? J Clin EndocrinolMetab 2011;96:38–52.
2 Gooren LJ, Behre HM. Testosterone treatment of hypogo-nadal men participating in competitive sports. Andrologia2008;40:195–9.
3 Di Luigi L, Sgrò P, Fierro V, Bianchini S, Battistini G, MaginiV, Jannini EA, Lenzi A. Prevalence of undiagnosed testoster-
one deficiency in aging athletes: Does exercise training influ-ence the symptoms of male hypogonadism? J Sex Med2010;7:2591–601.
4 Zitzmann M, Nieschlag E. Effects of androgen replacement onmetabolism and physical performances in male hypogonadism.J Endocrinol Invest 2003;26:886–92.
5 Isidori AM, Giannetta E, Greco EA, Gianfrilli D, Bonifacio V,Isidori A, Lenzi A, Fabbri A. Effects of testosterone on bodycomposition, bone metabolism and serum lipid profile inmiddle-aged men: A meta-analysis. Clin Endocrinol2005;63:280–93.
6 Bhasin S, Woodhouse L, Casaburi R, Singh AB, Bhasin D,Berman N, Chen X, Yarasheski KE, Magliano L, Dzekov C,Dzekov J, Bross R, Phillips J, Sinha-Hikim I, Shen R, StorerTW. Testosterone dose-response relationships in healthyyoung men. Am J Physiol Endocrinol Metab 2001;281:E1172–81.
7 Nieschlag E, Behre HM, Bouchard P, Corrales JJ, Jones TH,Stalla GK, Webb SM, Wu FC. Testosterone replacementtherapy: Current trends and future directions. Hum ReprodUpdate 2004;10:409–19.
8 Crewther BT, Cook C, Cardinale M, Weatherby RP, Lowe T.Two emerging concepts for elite athletes: The short-termeffects of testosterone and cortisol on the neuromuscularsystem and the dose-response training role of these endog-enous hormones. Sports Med 2011;41:103–23.
9 Darby E, Anawalt BD. Male hypogonadism: An update ondiagnosis and treatment. Treat Endocrinol 2005;4:293–309.
10 Seftel AD. Male hypogonadism. Part I: Epidemiology ofhypogonadism. Int J Impot Res 2006;18:115–20.
11 Bhasin S, Cunningham GR, Hayes FJ, Matsumoto AM,Snyder PJ, Swerdloff RS, Montori VM. Testosterone therapyin men with androgen deficiency syndromes: An EndocrineSociety clinical practice guideline. J Clin Endocrinol Metab2010;95:2536–59.
12 Gooren LJ. Advances in testosterone replacement therapy.Front Horm Res 2009;37:32–51.
13 Gooren LJ, Bunck MC. Androgen replacement therapy:Present and future. Drugs 2004;64:1861–91.
14 Nieschlag E. Testosterone treatment comes of age: Newoptions for hypogonadal men. Clin Endocrinol 2006;65:275–81.
15 Isidori AM, Lenzi A. Testosterone replacement therapy: Whatwe know is not yet enough. Mayo Clin Proc 2007;82:11–3.
16 Di Luigi L, Romanelli F, Lenzi A. Androgenic-anabolic ste-roids abuse in males. J Endocrinol Invest 2005;28(3 suppl):81–4.
17 Modlinski R, Fields KB. The effect of anabolic steroids on thegastrointestinal system, kidneys, and adrenal glands. CurrSports Med Rep 2006;5:104–9.
18 Rhoden EL, Morgentaler A. Risks of testosterone-replacement therapy and recommendations for monitoring. NEngl J Med 2004;350:482–92.
19 Di Luigi L, Sgrò P, Romanelli F, Mazzarino M, Donati F,Braganò MC, Bianchini S, Fierro V, Casasco M, Botrè F,Lenzi A. Urinary and serum hormones profiles after test-osterone enanthate administration in male hypogonadism:Concerns on the detection of doping with testosterone intreated hypogonadal athletes. J Endocrinol Invest 2009;32:445–53.
20 Hartgens F, Kuipers H. Effects of androgenic-anabolic ste-roids in athletes. Sports Med 2004;34:513–54.
21 Dobs AS, Meikle AW, Arver S, Sanders SW, Caramelli KE,Mazer NA. Pharmacokinetics, efficacy, and safety of apermeation-enhanced testosterone transdermal system incomparison with bi-weekly injections of testosterone enan-thate for the treatment of hypogonadal men. J Clin EndocrinolMetab 1999;84:3469–78.
Androgens Profile in Treated Male Hypogonadism 885
J Sex Med 2012;9:873–886

22 Nieschlag E, Cüppers HJ, Wiegelmann W, Wickings EJ. Bio-availability and LH-suppressing effect of different testosteronepreparations in normal and hypogonadal men. Horm Res1976;7:138–45.
23 Behre HM, Nieschlag E. Comparative pharmacokinetic ofandrogen preparations: Applications of computer analysis andsimulation. In: Nieschlag E, Behre HM, eds. Testosteroneaction, deficiency, substitution. Berlin: Springer-Verlag; 1990:115–35.
24 Wang C, Berman N, Longstreth JA, Chuapoco B, Hull L,Steiner B, Faulkner S, Dudley RE, Swerdloff RS. Pharmaco-kinetics of transdermal testosterone gel in hypogonadal men:Application of gel at one site versus four sites: A general clinicalresearch center study. J Clin Endocrinol Metab 2000;85:964–9.
25 Seftel A. Male hypogonadism. Part II: Etiology, pathophysiol-ogy, and diagnosis. Int J Impot Res 2006;18:223–8.
26 Di Luigi L, Guidetti L, Pigozzi F, Baldari C, Casini A, NordioM, Romanelli F. Acute amino acids supplementation enhancespituitary responsiveness in athletes. Med Sci Sports Exerc1999;31:1748–54.
27 Di Luigi L, Rossi C, Sgrò P, Fierro V, Romanelli F, Baldari C,Guidetti L. Do non-steroidal anti-inflammatory drugs influ-ence the steroid hormone milieu in male athletes? Int J SportsMed 2007;28:809–14.
28 Sodergard R, Backstrom T, Shanbhag V, Carstensen H. Cal-culation of free and bound fractions of testosterone andestradiol-17b to human plasma proteins at body temperature. JSteroid Biochem 1982;16:801–10.
29 Vermeulen A, Verdonck L, Kaufman JM. A critical evaluationof simple methods for the estimation of free testosterone inserum. J Clin Endocrinol Metab 1999;84:3666–72.
30 Mazzarino M, Botrè F. A fast liquid chromatographic/massspectrometric screening method for the simultaneous detec-tion of synthetic glucocorticoids, some stimulants, anti-oestrogen drugs and synthetic anabolic steroids. RapidCommun Mass Spectrom 2006;20:3465–76.
31 Van Renterghem P, Van Eenoo P, Geyer H, Schänzer W,Delbeke FT. Reference ranges for urinary concentrations andratios of endogenous steroids, which can be used as markers forsteroid misuse, in a Caucasian population of athletes. Steroids2010;75:154–63.
32 Hackney AC. Effects of endurance exercise on the reproduc-tive system of men: The “exercise-hypogonadal male condi-tion”. J Endocrinol Invest 2008;31:932–8.
33 Morelli A, Corona G, Filippi S, Ambrosini S, Forti G,Vignozzi L, Maggi M. Which patients with sexual dysfunctionare suitable for testosterone replacement therapy? J Endo-crinol Invest 2007;30:880–8.
34 Swerdloff RS, Wang C, Cunningham G, Dobs A, IranmaneshA, Matsumoto AM, Snyder PJ, Weber T, Longstreth J,Berman N. Long-term pharmacokinetics of transdermal test-osterone gel in hypogonadal men. J Clin Endocrinol Metab2000;85:4500–10.
35 Rolf C, Kemper S, Lemmnitz G, Eickenberg U, Nieschlag E.Pharmacokinetics of a new transdermal testosterone gel ingonadotrophin-suppressed normal men. Eur J Endocrinol2002;146:673–9.
36 Chik Z, Johnston A, Tucker AT, Chew SL, Michaels L, AlamCA. Pharmacokinetics of a new testosterone transdermal deliv-ery system, TDS-testosterone in healthy males. Br J Clin Phar-macol 2006;61:275–9.
37 Snyder PJ, Lawrence DA. Treatment of male hypogonadismwith testosterone enanthate. J Clin Endocrinol Metab 1980;51:1335–9.
38 Palonek E, Gottlieb C, Garle M, Björkhem I, Carlström K.Serum and urinary markers of exogenous testosterone admin-istration. J Steroid Biochem Mol Biol 1995;55:121–7.
39 Kicman AT, Brooks RV, Collyer SC, Cowan DA, Nanjee MN,Southan GJ, Wheeler MJ. Criteria to indicate testosteroneadministration. Br J Sports Med 1990;24:253–64.
40 Dehennin L, Matsumoto AM. Long-term administration oftestosterone enanthate to normal men: Alterations of theurinary profile of androgen metabolites potentially useful fordetection of testosterone misuse in sport. J Steroid BiochemMol Biol 1993;44:179–89.
41 Behre HM, Wang C, Handelsman DJ, Nieschlag E.Pharmacology of testosterone preparations. In: NieschlagE, Behre HM, eds. Testosterone action, deficiency, substitu-tion. Cambridge: Cambridge University Press; 2004:405–44.
42 Isidori AM, Caprio M, Strollo F, Moretti C, Frajese G, IsidoriA, Fabbri A. Leptin and androgens in male obesity: Evidencefor leptin contribution to reduced androgen levels. J ClinEndocrinol Metab 1999;84:3673–80.
43 von Eckardstein S, Nieschlag E. Treatment of male hypogo-nadism with testosterone undecanoate injected at extendedintervals of 12 weeks: A phase II study. J Androl 2002;23:419–25.
44 Fennell C, Sartorius G, Ly LP, Turner L, Liu PY, Conway AJ,Handelsman DJ. Randomized cross-over clinical trial of inject-able vs. implantable depot testosterone for maintenance oftestosterone replacement therapy in androgen deficient men.Clin Endocrinol (Oxf) 2010;73:102–9.
45 Yassin AA, Saad F. Plasma levels of dihydrotestosterone remainin the normal range in men treated with long-acting parenteraltestosterone undecanoate. Andrologia 2007;39:181–4.
46 Vingren JL, Kraemer WJ, Ratamess NA, Anderson JM, VolekJS, Maresh CM. Testosterone physiology in resistance exerciseand training: The up-stream regulatory elements. Sports Med2010;40:1037–53.
47 Saad F, Aversa A, Isidori AM, Zafalon L, Zitzmann M, GoorenLJ. Onset of effects of testosterone treatment and time spanuntil maximum effects are achieved. Eur J Endocrinol 2011;165:675–85.
48 Van Renterghem P, Van Eenoo P, Sottas PE, SaugyM, Delbeke F. A pilot study on subject-based comprehen-sive steroid profiling: Novel biomarkers to detect testoster-one misuse in sports. Clin Endocrinol (Oxf) 2011;75:134–40.
49 Sottas PE, Saugy M, Saudan C. Endogenous steroid profilingin the athlete biological passport. Endocrinol Metab ClinNorth Am 2010;39:59–73.
50 Bowers LD. Testosterone doping: Dealing with genetic differ-ences in metabolism and excretion. J Clin Endocrinol Metab2008;93:2469–71.
886 Di Luigi et al.
J Sex Med 2012;9:873–886




















