Boosting in athletes with high-level spinal cord injury: Knowledge, incidence and attitudes of...
20
RESEARCH PAPER Boosting in athletes with high-level spinal cord injury: knowledge, incidence and attitudes of athletes in paralympic sport YAGESH BHAMBHANI 1 , JENNIFER MACTAVISH 2 , SHARON WARREN 1 , WALTER R. THOMPSON 3 , ANTHONY WEBBORN 4 , ELIZABETH BRESSAN 5 , MARCO TUILO DE MELLO 6 , SEAN TWEEDY 7 , LAURIE MALONE 8 , KENNET FROJD 9 , PETER VAN DE VLIET 10 & YVES VANLANDEWIJCK 11 1 Faculty of Rehabilitation Medicine, University of Alberta, Canada, 2 Faculty of Kinesiology and Recreation Management, University of Manitoba, Canada, 3 Department of Kinesiology and Health, Georgia State University, Atlanta, Georgia, USA, 4 Sussex Centre for Sport and Exercise Medicine, Chelsea School Research Centre, University of Brighton, UK, 5 Department of Sport Science, Stellenbosch University, South Africa, 6 Medicina e Biologia do Sono, Universidade Federal de Sao Paulo, Brazil, 7 School of Human Movement Studies, University of Queensland, Brisbane, Australia, 8 Lakeshore Foundation, Research and Education, Birmingham, Alabama, USA, 9 Swedish Development Centre for Disability and Sport and University of Gavle, Sweden, 10 Medical and Scientific Director, International Paralympic Committee, Bonn, Germany, and 11 Faculty of Kinesiology and Rehabilitation Sciences, Catholique University, Leuven, Belgium Accepted June 2010 Abstract Autonomic dysreflexia (AD) is unique to individuals with spinal injuries (SCI) at T6 or above and can be voluntarily induced. Although AD improves wheelchair racing performance in some athletes, it also elicits exaggerated blood pressure, which could be dangerous. The International Paralympic Committee considers AD doping and banned its use. Purpose. The purpose of this study is to evaluate AD knowledge, incidence and attitudes (KIA) of Paralympians with SCI. Methods. An existing questionnaire was modified to include questions of AD KIA, validated by three experts and piloted with a small sample. It was administered on-line, mailed to members of a scientific network and distributed during the Beijing Paralympic Games. Fisher Exact test was used to evaluate differences across gender, injury and education. Results. Of 99 participants, 54.5% had previously heard of AD while 39.4% were unaware; 16.7%, all males, had used AD to enhance performance. Participants reported that AD was (1) useful for middle (78.6%) and long distance (71.4%), marathon (64.3%) and wheelchair rugby (64.3%); (2) somewhat dangerous (48.9%), dangerous (21.3%) or very dangerous (25.5%) to health. Results were not influenced by age, injury level or injury duration. Conclusions. Findings indicate the need for educational programmes directed towards enhancing the AD knowledge of rehabilitation professionals, coaches and trainers working with SCI individuals. Keywords: Boosting survey, paralympic athletes Introduction There is no less contentious issue in elite sport than doping to enhance performance. Athletes are always looking to find the edge over opponents by fair means, or by foul in some cases. Potentially hazardous risks to health through doping are taken in the pursuit of sporting excellence. The increasing profile of sport for athletes with a disability and its potential rewards combined with the frailty of human nature has led some athletes with disabilities to seek improved performance through the administration of prohibited substances. However, there is a method unique to sport for athletes with a disability, which is termed ‘boosting’ for the intentional induction of autonomic dysreflexia (AD) to enhance performance [1–3]. This was deemed a prohibited method by the International Paralympic Committee (IPC) in 1994 [4], but this was later changed to being classed as a health risk and prohibits athletes from competing in a Correspondence: Yagesh Bhambhani, Faculty of Rehabilitation Medicine, University of Alberta, Edmonton, Alberta, Canada T6G 2G4. Tel: þ780-492-7248. E-mail: [email protected] Disability and Rehabilitation, 2010; 32(26): 2172–2190 ISSN 0963-8288 print/ISSN 1464-5165 online ª 2010 Informa UK, Ltd. DOI: 10.3109/09638288.2010.505678
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Boosting in athletes with high-level spinal cord injury: Knowledge, incidence and attitudes of...

RESEARCH PAPER
Boosting in athletes with high-level spinal cord injury: knowledge,incidence and attitudes of athletes in paralympic sport
YAGESH BHAMBHANI1, JENNIFER MACTAVISH2, SHARON WARREN1,
WALTER R. THOMPSON3, ANTHONY WEBBORN4, ELIZABETH BRESSAN5,
MARCO TUILO DE MELLO6, SEAN TWEEDY7, LAURIE MALONE8, KENNET FROJD9,
PETER VAN DE VLIET10 & YVES VANLANDEWIJCK11
1Faculty of Rehabilitation Medicine, University of Alberta, Canada, 2Faculty of Kinesiology and Recreation Management,
University of Manitoba, Canada, 3Department of Kinesiology and Health, Georgia State University, Atlanta, Georgia, USA,4Sussex Centre for Sport and Exercise Medicine, Chelsea School Research Centre, University of Brighton, UK, 5Department of
Sport Science, Stellenbosch University, South Africa, 6Medicina e Biologia do Sono, Universidade Federal de Sao Paulo,
Brazil, 7School of Human Movement Studies, University of Queensland, Brisbane, Australia, 8Lakeshore Foundation,
Research and Education, Birmingham, Alabama, USA, 9Swedish Development Centre for Disability and Sport and University
of Gavle, Sweden, 10Medical and Scientific Director, International Paralympic Committee, Bonn, Germany, and 11Faculty of
Kinesiology and Rehabilitation Sciences, Catholique University, Leuven, Belgium
Accepted June 2010
AbstractAutonomic dysreflexia (AD) is unique to individuals with spinal injuries (SCI) at T6 or above and can be voluntarily induced.Although AD improves wheelchair racing performance in some athletes, it also elicits exaggerated blood pressure, whichcould be dangerous. The International Paralympic Committee considers AD doping and banned its use. Purpose. The purposeof this study is to evaluate AD knowledge, incidence and attitudes (KIA) of Paralympians with SCI. Methods. An existingquestionnaire was modified to include questions of AD KIA, validated by three experts and piloted with a small sample. It wasadministered on-line, mailed to members of a scientific network and distributed during the Beijing Paralympic Games. FisherExact test was used to evaluate differences across gender, injury and education. Results. Of 99 participants, 54.5% hadpreviously heard of AD while 39.4% were unaware; 16.7%, all males, had used AD to enhance performance. Participantsreported that AD was (1) useful for middle (78.6%) and long distance (71.4%), marathon (64.3%) and wheelchair rugby(64.3%); (2) somewhat dangerous (48.9%), dangerous (21.3%) or very dangerous (25.5%) to health. Results were notinfluenced by age, injury level or injury duration. Conclusions. Findings indicate the need for educational programmes directedtowards enhancing the AD knowledge of rehabilitation professionals, coaches and trainers working with SCI individuals.
Keywords: Boosting survey, paralympic athletes
Introduction
There is no less contentious issue in elite sport than
doping to enhance performance. Athletes are always
looking to find the edge over opponents by fair
means, or by foul in some cases. Potentially
hazardous risks to health through doping are taken
in the pursuit of sporting excellence. The increasing
profile of sport for athletes with a disability and its
potential rewards combined with the frailty of human
nature has led some athletes with disabilities to seek
improved performance through the administration of
prohibited substances. However, there is a method
unique to sport for athletes with a disability, which is
termed ‘boosting’ for the intentional induction of
autonomic dysreflexia (AD) to enhance performance
[1–3]. This was deemed a prohibited method by the
International Paralympic Committee (IPC) in 1994
[4], but this was later changed to being classed as a
health risk and prohibits athletes from competing in a
Correspondence: Yagesh Bhambhani, Faculty of Rehabilitation Medicine, University of Alberta, Edmonton, Alberta, Canada T6G 2G4.
Tel: þ780-492-7248. E-mail: [email protected]
Disability and Rehabilitation, 2010; 32(26): 2172–2190
ISSN 0963-8288 print/ISSN 1464-5165 online ª 2010 Informa UK, Ltd.
DOI: 10.3109/09638288.2010.505678

dysreflexia state whether intentional or not. This is
akin to the use of placing limits on haematocrit levels
in competitive skiing.
The athlete with a high-level spinal injury has
limited physiological potential for improvements in
cardiac output and maximal oxygen uptake, which
are known to improve racing performance. The loss
of sympathetic cardiac innervation results in a
maximum heart rate between 110 and 130 beats
per minute determined by intrinsic sino-atrial activity
[5–7]. The restricted heart rate reserve and reduced
stroke volume are further compounded by a loss of
catecholamine response to exercise and by the
absence of the muscular venous pump in the lower
limbs. These physiological limitations lead some
athletes with high-level spinal cord injuries to partly
compensate for the loss by the induction of the
dysreflexic state. During training and competition,
some athletes had noticed that the dysreflexic state
actually reduced the rating of perceived exertion and
faster top velocities were attained. Although initially
the phenomenon was occurring spontaneously, it
was found that the condition could be voluntarily
induced by practices including clamping of the
urinary catheter to produce bladder distension,
excessive tightening of the leg straps, twisting and/
or sitting on the scrotum. Athletes felt that in this
way they could induce the boosted state on
command [3].
A boosting study [1] conducted on eight wheel-
chair athletes during simulated racing confirmed
significant performance enhancement with the most
striking change being a 9.7% improvement in 7.5 K
race performance time. This would be approximately
equivalent to reducing the able-bodied marathon
record by 12 min! In the boosted state at rest, there
was a lower heart rate; and during exercise, subjects
were able to achieve levels in excess of the normal
maximum. Significant rises in noradrenaline levels
were seen, but no change in adrenaline levels
occurred. However, blood pressure increased to a
significantly higher level in the boosted compared to
the unboosted state and in some cases rose to
dangerously high levels.
The IPC, having determined boosting to be a
prohibited method, have a practical problem with
enforcement. Although the concern is for the safety
of athletes, there are comparisons with growth
hormone abuse – unless you catch the athlete in
the act, how do you detect it? AD occurs sponta-
neously in athletes with high-level spinal cord
injuries, and so to prohibit its use it is necessary that
there be a method of not only detecting an athlete in
a dysreflexic state, but also proving that the state was
intentionally induced. Blood pressure measurements
were made in the call-up room at the 1996 Atlanta
Paralympics and other major sanctioned events, and
the potential threat was to withdraw athletes with
abnormally high readings. The ‘normal value’ of
blood pressure in a call-up room before a Paralympic
final event is difficult to predict. For the sports
physician, coaches and trainers working with athletes
with this disability it is important to be aware of this
condition, whether intentionally induced or not [8].
The immediate management is to remove the
nociceptive stimulus where possible and to admin-
ister sublingual nifedipine to reduce the blood
pressure. The IPC has a fiduciary responsibility to
ensure that athletes compete in a safe manner at the
events that are sanctioned by the organisation [9].
Therefore, it was imperative that a study which
addresses these issues be conducted, so that the IPC
can implement policies that are conducive to their
mission and to protect the athletes.
The World Anti Doping Agency (WADA) Social
Sciences Research Grant Programme has identified
‘increasing knowledge of causes and of risk and
protective factors in doping behaviour’ as one of its
research priorities. To date, there is no published
information pertaining to the knowledge, incidence
and attitudes of paralympic athletes regarding
boosting (i.e. voluntary induction of AD). Therefore,
the current research project was designed to (1)
develop and validate a comprehensive boosting
questionnaire to provide such information, and (2)
evaluate these aspects of boosting in male and female
paralympic wheelchair athletes with spinal cord
injuries at or above the T6 level. This study tested
the following hypotheses: (1) a significant proportion
of the wheelchair athletes with spinal cord lesion
levels above T6 will indicate that they used boosting
to enhance their physical performance during train-
ing and/or competition, (2) there would be no
significant difference between males and females in
the prior knowledge and incidence of boosting, (3)
boosting knowledge would not be influenced by the
education level and injury duration of the athletes,
(4) athletes of both genders would demonstrate
awareness of the signs and symptoms regarding
boosting and (5) a majority of the athletes would find
boosting to be unacceptable for improving perfor-
mance during training and/or competition.
Methods
This study was implemented over a 2-year (yr)
period from March 2007 to February 2009. In
accordance with the Declaration of Helsinki, ethics
approval was obtained from the Health Research
Ethics Board at the University of Alberta prior to
initiating the study. The research design used to
complete this study is illustrated in Figure 1.
Boosting in paralympic athletes 2173

Phase I – validation
During this 9-month phase (March to December
2007), the boosting questionnaire originally published
by Burnham et al. [1] was used as a starting point for
developing a comprehensive questionnaire to evaluate
the knowledge, incidence and attitudes of athletes
towards boosting. Several questions related to these
three themes were added to the questionnaire and
subsequently validated by experts in the area of
questionnaire design. Initially, the questionnaire was
reviewed by two experts in survey research from the
University of Alberta, Edmonton, Canada. Their
recommendations were incorporated into the ques-
tionnaire, which was then reviewed by an expert from
the University of Manitoba, Winnipeg, Canada.
Following these revisions, the modified questionnaire
was sent to the IPC Sports Science Committee (IPC
SSC) for a final review before its implementation. The
validated questionnaire is included in the Appendix.
Phase II – pilot study
A pilot study, which was designed to test the content
and readability of the validated questionnaire, was
conducted from January to March 2008. Fifteen
competitive athletes were contacted through the
International Network for the Advancement of
Paralympic Sport through Science (INAPSS). Ath-
letes from Australia (3), Belgium (2), Brazil (4),
Sweden (2), South Africa (2) and the United States
(2) received the questionnaire from their sports
administrators. These questionnaires were com-
pleted by the athletes and forwarded to the IPC
head office in Bonn, Germany or directly to the
principal investigator at the University of Alberta.
The athletes were asked to comment on the content
and readability of the questionnaire. Their feedback
was used to make final changes to the questionnaire
before its actual implementation.
Phase III - data collection
Data collection was initiated in three ways: (1) an on-
line version of the questionnaire, which was developed
at the end of the validation phase, was posted on the
IPC web site so that athletes could complete it at their
convenience. The on-line questionnaire was available
from August through October 2008. (2) The validated
questionnaire was sent to members of INAPSS for
distribution, and upon completion returned to the
IPC headquarters. (3) Data were collected during the
Paralympic Games in Beijing from 7 to 17 September
2008. This latter process included a number of steps.
First, managers and team physicians of the National
Paralympic Committees (NPCs) who attended the
Paralympic Games were informed of the study at an
orientation meeting one day before the Games
commenced. A covering letter from the Chairperson
of the IPC SSC and the study principal investigator,
along with sufficient copies of the questionnaire, were
subsequently placed in their individual mail boxes for
distribution to the spinal cord injured athletes who met
the inclusion criteria of the study. This letter clearly
specified that only athletes with spinal cord injuries at
or above the T6 level were eligible to participate in the
study. A written reminder was sent to the NPC
managers during the Paralympic Games to encourage
their athletes to complete the questionnaire. As well, a
final reminder was sent to the NPC managers after the
conclusion of the Games, requesting them to remind
the athletes to complete the on-line version of the
questionnaire if they did not have the opportunity of
completing it during the Games in Beijing. Second,
appropriate signage was placed at strategic locations in
the Paralympic Village to inform athletes about the
Figure 1. Experimental design of the study.
2174 Y. Bhambhani et al.

study and seek their participation. Third, members of
the investigative team also personally contacted team
managers and coaches at the various practice venues to
increase athlete participation. Finally, members of the
investigative team telephoned the Operations Man-
agers of the NPCs periodically asking them to remind
the athletes to complete the questionnaires. The
completed questionnaires were returned by the
athletes to the IPC SSC office at the Paralympic
Village either directly or via their NPC managers to
ensure anonymity.
Phase IV – data analysis
A total of 99 participants completed the survey that
was used for data analysis. Following is the break-
down of the completed questionnaires that were used
for analysis: 15 from the pilot study, 34 from the
INAPSS network, 46 completed at the Beijing
Paralympic Games and four completed online. Some
of the participants did not respond to all the questions
in the survey, and therefore, the analysis to the
pertinent questions is based on varying number of
responses. The information from these 99 partici-
pants who completed the questionnaire (hereafter
referred to as respondents) was entered into Survey
Monkey (www.surveymonkey.com), which is a soft-
ware programme used for processing questionnaire
data. The data were then exported into SPSS to
perform the Fisher Exact test to compare the
frequencies of the responses with respect to the
following variables: (1) gender, (2) level of education,
(3) duration of injury and (4) sport participation. This
statistical technique has been designed specifically for
the analysis of contingency tables of categorical data
where the sample sizes are small and/or when there
are fewer than five subjects per cell (Fisher 1970).
The test produces an exact probability but a was set at
0.05. Caution needs to be applied in interpretation of
the results even though this test was used because in
many instances cell sizes were small and often zero.
Consequently trends in the descriptive characteristics
have been reported where pertinent.
Results
Characteristics of participants
Personal characteristics (Questions 19–21). A descrip-
tive overview of the 99 participants who completed
Table I. Characteristics of male and female participants.
Group* Variable Number of participants in each category
Males Age group 16–21 22–27 28–33 34–39 40–45 46þN¼85 4 17 21 26 12 5
Status S-PT S-FT A-PT A-FT A-SF A-SG/OF
N¼72 6 3 9 9 21 17/7
Employment PE-PT PE-FT SE-PT SE-FT UE-LW UE-NLW
N¼60 15 13 8 10 4 10
Education SHS HSG SPS SU UD GD
N¼83 15 25 10 10 10 13
Females Age group 16–21 22–27 28–33 34–39 40–45 46þN¼11 1 2 1 4 0 3
Status S-PT S-FT A-PT A-FT A-SF A-SG/OF
N¼15 0 2 0 2 3 2/6
Employment PE-PT PE-FT SE-PT SE-FT UE-LW UE-NLW
N¼5 2 1 1 1 0 0
Education SHS HSG SPS SU UD GD
N¼10 1 2 1 0 3 3
Combined Age group 16–21 22–27 28–33 34–39 40–45 46þN¼99 5 20 23 31 12 8
Status S-PT S-FT A-PT A-FT A-SF A-SG/OF
N¼90 6 5 9 13 24 20/13
N¼65 Employment PE-PT PE-FT SE-PT SE-FT UE-LW UE-NLW
17 14 9 11 4 10
N¼96 Education SHS HSG SPS SU UD GD
17 28 11 10 13 17
N, number of participants who responded to that question; S-PT, student part time; S-FT, student full time; A-PT, athlete part time; A-FT,
athlete full time; A-SF, athlete self funded; A-SGOF, athlete state/government/other funding; PE-PT, paid employee, part time; PE-FT,
paid employee, full time; A-PT, athlete, part time; A-FT, athlete, full time; A-SF, athlete, self funded; A-SG/OF, athlete, state funded/other
source; SHS, some high school; HSG, high school graduation; SPS, some post secondary education; SU, some university (no degree); ED,
undergraduate degree; GD, graduate degree.
*Three participants did not indicate their gender on the questionnaire (Question #25).
Boosting in paralympic athletes 2175
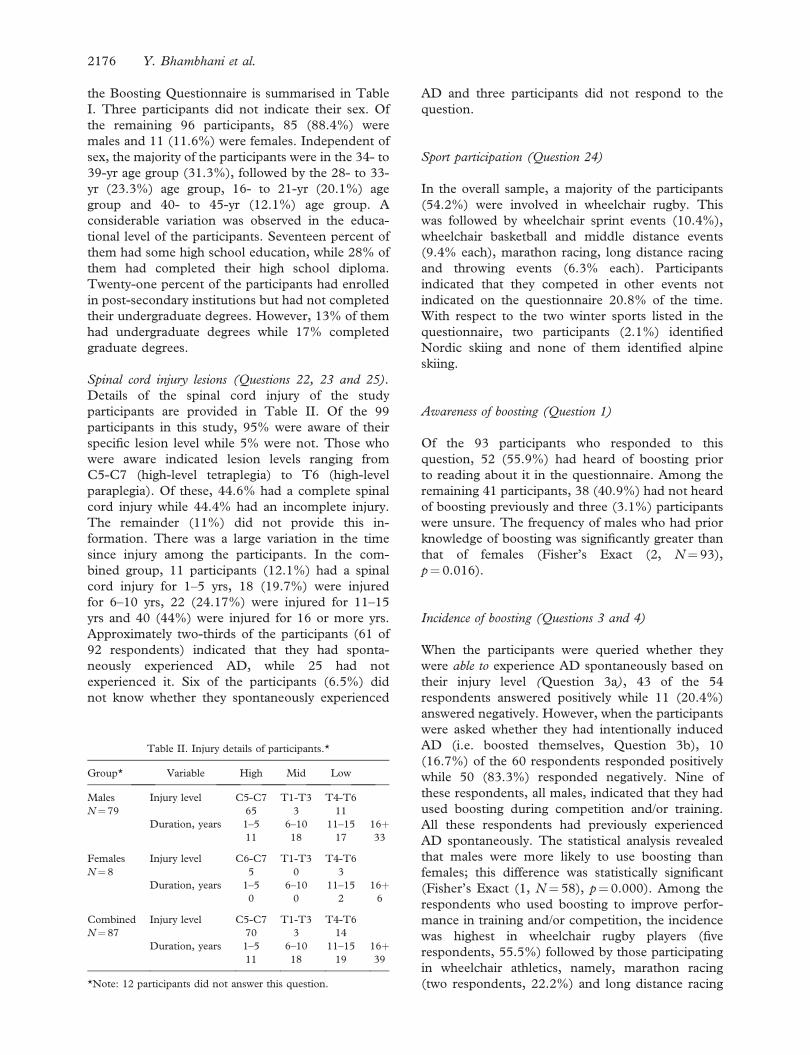
the Boosting Questionnaire is summarised in Table
I. Three participants did not indicate their sex. Of
the remaining 96 participants, 85 (88.4%) were
males and 11 (11.6%) were females. Independent of
sex, the majority of the participants were in the 34- to
39-yr age group (31.3%), followed by the 28- to 33-
yr (23.3%) age group, 16- to 21-yr (20.1%) age
group and 40- to 45-yr (12.1%) age group. A
considerable variation was observed in the educa-
tional level of the participants. Seventeen percent of
them had some high school education, while 28% of
them had completed their high school diploma.
Twenty-one percent of the participants had enrolled
in post-secondary institutions but had not completed
their undergraduate degrees. However, 13% of them
had undergraduate degrees while 17% completed
graduate degrees.
Spinal cord injury lesions (Questions 22, 23 and 25).
Details of the spinal cord injury of the study
participants are provided in Table II. Of the 99
participants in this study, 95% were aware of their
specific lesion level while 5% were not. Those who
were aware indicated lesion levels ranging from
C5-C7 (high-level tetraplegia) to T6 (high-level
paraplegia). Of these, 44.6% had a complete spinal
cord injury while 44.4% had an incomplete injury.
The remainder (11%) did not provide this in-
formation. There was a large variation in the time
since injury among the participants. In the com-
bined group, 11 participants (12.1%) had a spinal
cord injury for 1–5 yrs, 18 (19.7%) were injured
for 6–10 yrs, 22 (24.17%) were injured for 11–15
yrs and 40 (44%) were injured for 16 or more yrs.
Approximately two-thirds of the participants (61 of
92 respondents) indicated that they had sponta-
neously experienced AD, while 25 had not
experienced it. Six of the participants (6.5%) did
not know whether they spontaneously experienced
AD and three participants did not respond to the
question.
Sport participation (Question 24)
In the overall sample, a majority of the participants
(54.2%) were involved in wheelchair rugby. This
was followed by wheelchair sprint events (10.4%),
wheelchair basketball and middle distance events
(9.4% each), marathon racing, long distance racing
and throwing events (6.3% each). Participants
indicated that they competed in other events not
indicated on the questionnaire 20.8% of the time.
With respect to the two winter sports listed in the
questionnaire, two participants (2.1%) identified
Nordic skiing and none of them identified alpine
skiing.
Awareness of boosting (Question 1)
Of the 93 participants who responded to this
question, 52 (55.9%) had heard of boosting prior
to reading about it in the questionnaire. Among the
remaining 41 participants, 38 (40.9%) had not heard
of boosting previously and three (3.1%) participants
were unsure. The frequency of males who had prior
knowledge of boosting was significantly greater than
that of females (Fisher’s Exact (2, N¼ 93),
p¼ 0.016).
Incidence of boosting (Questions 3 and 4)
When the participants were queried whether they
were able to experience AD spontaneously based on
their injury level (Question 3a), 43 of the 54
respondents answered positively while 11 (20.4%)
answered negatively. However, when the participants
were asked whether they had intentionally induced
AD (i.e. boosted themselves, Question 3b), 10
(16.7%) of the 60 respondents responded positively
while 50 (83.3%) responded negatively. Nine of
these respondents, all males, indicated that they had
used boosting during competition and/or training.
All these respondents had previously experienced
AD spontaneously. The statistical analysis revealed
that males were more likely to use boosting than
females; this difference was statistically significant
(Fisher’s Exact (1, N¼ 58), p¼ 0.000). Among the
respondents who used boosting to improve perfor-
mance in training and/or competition, the incidence
was highest in wheelchair rugby players (five
respondents, 55.5%) followed by those participating
in wheelchair athletics, namely, marathon racing
(two respondents, 22.2%) and long distance racing
Table II. Injury details of participants.*
Group* Variable High Mid Low
Males Injury level C5-C7 T1-T3 T4-T6
N¼79 65 3 11
Duration, years 1–5 6–10 11–15 16þ11 18 17 33
Females Injury level C6-C7 T1-T3 T4-T6
N¼8 5 0 3
Duration, years 1–5 6–10 11–15 16þ0 0 2 6
Combined Injury level C5-C7 T1-T3 T4-T6
N¼87 70 3 14
Duration, years 1–5 6–10 11–15 16þ11 18 19 39
*Note: 12 participants did not answer this question.
2176 Y. Bhambhani et al.

(2 respondents, 22.2%). None of the respondents
involved in wheelchair basketball and throwing
events used boosting to enhance performance in
training or competition. The statistical analysis
revealed that there was no significant difference in
the incidence of boosting across sports (Fisher’s
Exact (4, N¼ 48), p¼ 0.506). Seven of the 10
athletes who used boosting indicated that they did
not use it during regular training, while training to
peak for competition, and in both national and
international competitions. Two of these athletes
used boosting during the training phases and
competitions identified earlier, while on athlete
reported using boosting all the time to improve
performance during national and international com-
petitions.
A comparison of the incidence of boosting across
age, education level and injury level of the respon-
dents is provided in Table III. The younger subjects
aged between 16 and 27 yrs and the oldest subjects
aged above 46 yrs had never voluntarily used
boosting to enhance their performance in training
and/or competition. However, 12.5, 15.8 and 33.3%
of the respondents aged between 28 and 33, 34–39
and 40–45 yrs, respectively, used boosting to
improve their performance in training and/or com-
petition. The statistical analysis indicated that there
was no significant difference in the incidence of
boosting among age categories (Fisher’s Exact (4,
N¼ 59), p¼ 0.339).
Most of the subjects surveyed, regardless of the
level of education, had not voluntarily used boosting
to enhance their performance in training and/or
competition. Of these 48 respondents, eight indi-
cated that they had used boosting to enhance training
and/or competition. Three respondents (37.5%) had
some postsecondary education, one (12.5%) had
some university education and four (50%) had
graduate degrees. The statistical analysis revealed
that as the educational level increased the frequency
of boosting increased (Fisher’s Exact (4, N¼ 48),
p¼ 0.033). Although the incidence of boosting
appeared to be higher in respondents with cervical
injuries (C5 to C7), when compared to respondents
with injuries at the thoracic level (T1 to T3 and T4 to
T6 collapsed), the statistical analysis revealed that
there was no significant difference in the incidence of
boosting by level of injury (Fisher’s Exact (2,
N¼ 55), p¼ 0.370).
Knowledge and use of boosting
A comparison of knowledge of boosting across
education level and injury duration of the respon-
dents is provided in Table IV. The descriptive
statistics showed that respondents who had gradu-
ated from high school were less likely (44%) to have
previously heard of boosting compared to those who
had some post-secondary education (54.5%), some
university education (60%), an undergraduate de-
gree (61.5%) and a graduate university degree
(64.7%). However, the statistical analysis revealed
that there was no significant difference in their
previous knowledge about boosting by level of
education (Fisher’s Exact (8, N¼ 76), p¼ 0.717).
The percentages of respondents who had previous
knowledge of boosting as a performance enhancing
strategy were 27.3, 55.6, 63.2 and 65% in the 1–5, 6–
10, 11–15 and 416 yrs post-injury duration,
respectively. There was no significant difference in
previous knowledge about boosting by duration of
injury (Fisher’s Exact (6, N¼ 88), p¼ 0.12), but
there was a trend towards greater knowledge of
boosting 6 yrs post injury.
With respect to the use of boosting in their sport,
approximately 27.1% of the respondents reported
that boosting was commonly used in their sport while
35.4% were not sure about its use. The results in
Table V indicated that there was no significant
Table III. Incidence of boosting in athletes with high level spinal injury: influence of age, education and injury levels (responses to Question
3b, Appendix A).
Variable
Question 3b: Have you ever intentionally induced autonomic dysreflexia during training or competition to improve your
performance?
Age 22–27 years 28–33 years 34–39 years 40–45 years 46þ years Total Per cent Fisher Exact
Yes 0 2 3 4 0 9 15.3 p¼0.339
No 8 14 16 8 5 51 84.7
Education level HSG SPS SU UD GD Total Per cent Fisher Exact
Yes 0 3 1 0 4 8 16.7 p¼0.033
No 15 5 4 7 9 40 83.3
Injury level High: C5-C7 Mid: T1-T3 Low: T4-T6 Total Per cent Fisher Exact
Yes 8 1 1 10 18.2 p¼0.370
No 33 1 11 45 81.8
SHS, some high school; HSG, high school graduation; SPS, some post-secondary education; SU, some university (no degree); ED,
undergraduate degree; GD, graduate degree.
Boosting in paralympic athletes 2177

difference on knowledge about boosting in their
sport by educational level (Fisher’s Exact (16,
N¼ 48), p¼ 0.584) although there was a trend for
those with some post-secondary education to believe
that it was commonly used in their sport. When these
responses were analysed with respect to injury
duration, 29.1% of the respondents indicated that
it was commonly used in their sport while 32.7%
were not sure of the frequency of its use. Once again,
there was no significant difference (Table V) on
knowledge about boosting and injury duration of the
respondents (Fisher’s Exact (12, N¼ 55), p¼ 0.217),
although there was a trend for those with 16þ yrs
injury duration to believe that it was more commonly
used.
Twenty-nine (28 males and 1 female) of the 99
participants who responded to this question reported
that boosting was most useful (Figure 2, panel A) in
middle distance events (78.6%), long distance events
(71.4%), marathon racing (64.3%) and wheelchair
rugby (64.3%). This was followed by sprint events
(57.1%), wheelchair basketball (32.1%), Nordic
skiing (21.4%), alpine skiing (10.7%), throwing
events (10.7%) and other events (3.6%). When
queried about the sport in which boosting would be
the least useful (Figure 2, panel B), a majority of the
respondents identified throwing events (55.6%) and
alpine skiing (51.9%). Smaller percentages of the
respondents identified middle distance (3.7%), long
distance (11.1%) and marathon racing (25.9%) as
the events that were least benefited by boosting.
Corresponding values for sprinting events, wheel-
chair basketball and wheelchair rugby were 25.9,
25.9 and 11.1%, respectively.
A majority of the respondents indicated that
boosting was most useful during competition (80.5%)
when compared to the other phases such as during
training (9.8%) or immediately prior to competition
(7.3%). The frequencies of the variables that they felt
benefited the most from boosting during competition
are illustrated in Figure 3. The four most frequently
reported benefits of boosting during competition
were increased circulation, less fatigue and increased arm
endurance along with increased aggression and increased
Table IV. Knowledge of boosting in athletes with high level spinal injury: influence of education level and injury duration (responses to
Question 3b, Appendix A).
Variable
Question 3a: Before reading about it on this questionnaire, have you every heard of boosting as a performance
enhancing strategy?
Education level HSG SPS SU UD GD Total Per cent Fisher Exact
Yes 11 6 6 8 11 42 55.3 p¼0.717
No 12 5 4 5 6 32 42.1
Not sure 2 0 0 0 0 2 2.6
Injury duration 1–5 years 6–10 years 11–15 years 16þ years Total Per cent Fisher Exact
Yes 3 10 12 26 51 58.0 p¼0.120
No 7 7 7 13 34 38.6
Not sure 1 1 0 1 3 3.4
SHS, some high school; HSG, high school graduation; SPS, some post-secondary education; SU, some university (no degree); ED,
undergraduate degree; GD, graduate degree.
Table V. Use of boosting in athletes with high level spinal injury: influence of education level and injury duration.
Variable Question 6: To your knowledge, would you boosting is:
Education level HSG SPS SU UD GD Total Per cent Fisher Exact
Commonly used 2 2 3 2 4 13 27.1 p¼0.584
Infrequently used 4 1 0 2 3 10 20.8
Rarely used 4 0 0 0 1 5 10.4
Not used 2 0 0 0 1 3 6.3
Not sure of its use 4 3 1 6 3 17 35.4
Injury duration 1–5 years 6–10 years 11–15 years 16þ years Total Per cent Fisher Exact
Commonly used 0 2 2 12 16 29.1 p¼0.217
Infrequently used 2 3 3 4 11 20.0
Rarely used 1 2 1 4 8 14.5
Not used 0 1 0 1 2 3.6
Not sure of its use 0 2 8 8 18 32.7
SHS, some high school; HSG, high school graduation; SPS, some post-secondary education; SU, some university (no degree); ED,
undergraduate degree; GD, graduate degree.
2178 Y. Bhambhani et al.

alertness. However, some athletes also reported
increased anxiety and greater frustration as possible
effects of boosting during competition. The respon-
dents reported that the main source of knowledge
was their personal experience (62.5%) and reports
from other athletes (46.4%).
Knowledge pertaining to health effects of boosting
(Question 11)
A summary of the respondents’ knowledge pertain-
ing to the dangers of boosting is provided in Table
VI. Forty-nine percent of the male and female
respondents agreed that boosting was somewhat
dangerous to health. However, 21.1 and 24.6% of
the respondents also felt that boosting was dangerous
or very dangerous to health, respectively. Only a
small proportion (5.3%) felt that boosting was not at
all dangerous to health. In general, both males and
females had a similar opinion regarding the dangers
of boosting. Statistically, there were no significant
differences in the frequency of responses regarding
the dangers of boosting by gender when the category
not dangerous at all was compared to any level of
danger, although males were more spread over the
various categories (Fisher’s Exact (3, N¼ 57),
p¼ 0.615). Similarly, there were no significant
differences in the frequency of responses with respect
to dangers of boosting when they were examined by
education level (Fisher’s Exact (12, N¼ 47),
p¼ 0.106) or the injury duration (Fisher’s Exact (9,
N¼ 54), p¼ 0.421) of the respondents.
With respect to the symptoms of boosting, most of
the respondents identified headache (70.9%), ex-
cessive sweating (80.6%) and high blood pressure
(83.3%) as the most frequent ones. Shivering
(36.8%) and blurred vision (26%) were less fre-
quently reported by them. The frequencies of these
symptoms are illustrated in Figure 4. The main
source of knowledge regarding the symptoms of
boosting was their personal experience (61.7%) and
reports from other athletes (50%). The respondents
gained some information by reading about boosting
(22.9%) and received only minimal information
(2.1%) from their coaches. When queried about
the consequences of boosting, most of the subjects
identified high blood pressure (86%), stroke/cerebral
hemorrhage (59.6%) and death (44%) as possible
outcomes. Only a small proportion (16.1%) identi-
fied seizures as a possible consequence of boosting.
Attitude towards boosting
A majority of the males and females indicated that
using boosting to improve training capacity, max-
imise performance during competition, and because
their competitors were using it was unacceptable.
There was no significant gender difference in the
frequency of the responses to this question (Fisher’s
Figure 2. Events that will most (panel A) and least (Panel B) likely
benefit from boosting in high-level spinal injured athletes (N¼29
responses). MR, marathon racing; LDE, long distance events;
MDE, middle distance events; SPR, sprint races; THR, throwing
events; WCB, wheelchair basketball; WCR, wheelchair rugby; NS,
Nordic skiing; AS, Alpine skiing; OTH, other events. Note: only
one female participant responded to this question. Her response is
illustrated in wheelchair rugby. Many athletes participated in more
than one sport, and therefore, the total of all the frequencies
exceeds 100%.
Figure 3. Variables that would benefit the most from boosting
during competition (N¼50 responses). IAST, increased arm
strength; IAE,¼ increased arm endurance; LAS, less arm stiffness;
LDB, less difficulty breathing; IC, increased circulation; LF, less
fatigue; IAG, increased aggression; IAL, increased alertness; IAN,
increased anxiety; IF, increased frustration.
Boosting in paralympic athletes 2179

Exact (4, N¼ 61), p¼ 0.875) although there was a
trend according to the descriptive statistics for males
to see it as being more acceptable. When these
responses were analyzed with respect to level of
education, there were no significant differences in
the frequency of these responses in either gender
(Fisher’s Exact (16, N¼ 51), p¼ 0.773). Evaluation
of these responses with respect to injury duration
revealed that there was no significant influence in
either gender (Fisher’s Exact (12, N¼ 58),
p¼ 0.793). When queried whether boosting should
not be banned because it can happen unintentionally their
opinion was split. Approximately 25% of the
respondents found this unacceptable while 37% were
in agreement with the statement. Similarly, the
respondents expressed a range of views about the
statement: boosting should not be banned because any
athlete with T6 or higher spinal cord injury can decide to
induce AD. Statements that the majority of the
respondents did not agree with included: (1) only
practices that are not available to all athletes in the
same class should be banned and (2) showcasing the
talents of athletes, and by extension the capabilities
of people with disabilities, is far more important than
whether or not someone is boosting.
Discussion
A total of 99 athletes participated in this study, with
the majority (89%) of them being males. It is not
surprising, therefore, that the males demonstrated
considerable variability with respect to their age, level
of education, employment status and source of
funding compared to the females (Table I). The
male participants also had greater variability with
respect to the level of injury (C5 to T6) and duration
of injury (1–18 yrs) compared to the females (C5 to
T4 and 3–16 yrs, respectively) (Table II). It is
noteworthy that only 25% of the combined sample
was within the 16–27 year age group, while 20% was
above 40 yrs old. Approximately 55% of the overall
sample was within the 28- to 40-yr age range, which
was likely an artifact of many having sustained their
spinal cord injuries later in life and, consequently,
launched their paralympic sport careers later as well.
Also, many of these athletes devoted several yrs to
training post-injury before becoming elite athletes,
which further contributes to the advanced age. The
participants in this study represented three main
summer sports, namely, athletics (track and field),
wheelchair basketball and wheelchair rugby. A
majority of them competed in wheelchair rugby
(54.2%), followed by wheelchair track events (mara-
thon, long distance, middle distance and sprints;
32%), wheelchair basketball (9.4%) and field events
(6.3%).
Table VI. Knowledge of dangers of boosting in athletes with high-level spinal injury: influence of education level and injury duration.
Variable Question 6: To your knowledge, would you boosting is:
Gender Male Female Total Per cent Fisher Exact
Not at all dangerous 3 0 3 5.3 p¼0.615
Somewhat dangerous 24 4 28 49.1
Dangerous 12 0 12 21.1
Very dangerous 13 1 14 24.6
Education level HSG SPS SU** UD GD Total Per cent Fisher Exact
Not at all dangerous 1 0 0 1 0 2 p¼0.106
Somewhat dangerous 5 2 1 8 7 23
Dangerous 2 3 2 0 3 10
Very dangerous 5 0 3 1 3 12
Injury duration 1–5 years 6–10 years 11–15 years 16þ years Total Per cent Fisher Exact
Not at all dangerous 0 1 1 1 3 p¼0.421
Somewhat dangerous 1 5 10 11 27
Dangerous 0 3 2 5 10
Very dangerous 2 2 1 9 14
SHS, some high school; HSG, high school graduation; SPS, some post-secondary education; SU, some university (no degree); ED,
undergraduate degree; GD, graduate degree.
Figure 4. Symptoms of boosting reported by respondents with
high-level spinal injuries (N¼58 responses). HEAD, headache;
SHIV, shivering; SWEAT, excessive sweating; HBP, high blood
pressure; BV, blurred vision.
2180 Y. Bhambhani et al.

The current results indicated that 52 of the 96
participants whose gender was known (54.1%) had
previously heard of boosting to enhance perfor-
mance, while 40.1% of them were unaware of this
practice and the remainder was unsure. Contrary to
our hypothesis, awareness was significantly greater in
males compared to female participants and did not
differ by the age and the injury duration (Table III)
of the participants in either gender. Although male
participants who had university undergraduate or
postgraduate degrees were more aware of this
practice, this finding should be interpreted with
caution due to the relatively small number of
participants. A similar finding was observed with
respect to the duration of injury; i.e. those who had
longer injury histories tended to have greater
awareness of boosting than their counterparts with
less history. For athletes with spinal cord injuries
above T6 in particular, knowledge of boosting was
limited and makes them, along with women athletes
prime audiences to target educational initiatives.
Only 60 of the 99 participants responded to the
question: Have you every intentionally induced AD to
boost your performance in training or competition. The
reason for the low response rate to this question is
not known, but it could be due to their apprehension
for disclosing information that could possibly in-
criminate them in a technique that is deemed illegal
by the IPC (www.paralympic.org). This was despite
the questionnaire being designed to ensure anonym-
ity; the participants were not required to provide
their name or country of origin on the questionnaire.
Furthermore, the participants deposited the com-
pleted questionnaire into a mailbox and not to any of
the investigators involved in the study Consistent
with our hypothesis, 15.5% (9 of 58) indicated that
they had previously used boosting to enhance
performance in training or competition, while the
remaining 84.5% had not used this method. It is
particularly noteworthy that all the respondents who
used this method were males (Note: one respondent
did not identify their gender), with a majority of
them competing in wheelchair rugby (five of nine or
55.5% of the respondents). The other four positive
responses were received from athletes who competed
in long- and middle-distance wheelchair racing
events. Our finding that a majority of the ‘boosters’
were wheelchair rugby players was most likely
because they comprised the largest proportion
(54.2%) of the respondents in this study. With
respect to the frequency of boosting, approximately
two-thirds of the athletes indicated that they had not
used it during training or during national and
international competitions. A small percentage of
the participants (6–14%) reported using this techni-
que to enhance performance during training and
competition, while only one participant indicated
that he used it all the time in national and
international competitions to enhance performance.
The observation that several participants used
boosting during training is of serious concern
because most athletes, particularly those competing
in individual sports, tend to train on their own with
minimal amount of supervision. The possibility of an
adverse event due to an exaggerated blood pressure
response resulting from boosting during training has
important implications for developing educational
programmes pertaining to this practice.
The results of this preliminary investigation
indicated that the incidence of boosting did not
differ by the age of the respondents (Table III).
This is most likely because a spinal cord injury can
occur at any stage in life, and therefore, may not
have any bearing on the athlete’s decision to boost
or not to boost. Theoretically, it is likely that
respondents with the higher lesion levels would
most likely benefit the most from boosting.
However, the current findings revealed that there
was no significant difference in the incidence of
boosting by the level of spinal injury of the
respondents. To further explore this question, the
difference in the incidence of boosting between
respondents who spontaneously experienced AD
(Question 22) and those who decided to boost
themselves to enhance performance during training
and/or competition was examined (Question 3b).
Once again, the results indicated that there was no
significant difference (Fisher Exact (2, N¼ 48),
p¼ 0.312) by these two variables, suggesting that
prior experience of AD did not influence the
respondents’ decision to boost for performance
enhancement. However, contrary to our hypoth-
esis, the incidence of boosting was significantly
associated with the level of education of the
respondents (Table III). Those who had graduate
university degrees (N¼ 4) boosted more frequently
when compared to respondents who had some high
school (N¼ 0) and some post-secondary (N¼ 3)
education. The theoretical reason(s) for these
findings are unclear at present and need to be
further investigated. However, this finding should
be interpreted with caution because of the small
number of subjects that boosted in each of the
educational categories.
Knowledge pertaining to the effects of boosting on
athletic performance was quite varied. Approxi-
mately 40% of the athletes believed that boosting
definitely had a beneficial effect on some sports,
while an equal proportion was unsure of such
benefits. Wheelchair racing events such as the
marathon, long distance and middle distance races
(Figure 3) were identified by the majority of the
respondents as the sports that would most benefit
from boosting. From a physiological standpoint,
Boosting in paralympic athletes 2181

these races are primarily dependent upon aerobic
metabolism and would therefore benefit the most
when the athletes are in a boosted state [10,11].
What is surprising, however, is that 64.3% of the
respondents also indicated that boosting would
benefit wheelchair rugby performance which is a
high intensity, intermittent sport that is not depen-
dent primarily upon aerobic metabolism. It is
possible that factors such as increased aggression
and alertness [12] that were reported by some
athletes (Figure 3), which could be attributed to
the enhanced catecholamine response in the boosted
state during exercise [11,13], could explain this
response. A recent study [14] on professional able-
bodied rugby players suggested that players with high
levels of self-reported aggression were more likely to
use excessive force to injure an opponent and obtain
an advantage during the game. As well, it has been
documented [15] that hormonal changes (testoster-
one and cortisol) during competition in able-bodied
karate athletes could interact with their personality
traits to enhance competitive performance. Research
along these lines should be conducted on athletes
with disabilities to validate these findings.
The current findings support the hypothesis that
athletes of both genders would demonstrate awareness
of the signs and symptoms pertaining to boosting.
Approximately 50% of the respondents felt that
boosting was somewhat dangerous, while 46% of
them reported that it was dangerous or very dangerous
to health. Further analysis revealed that 7 of 9
respondents who had used boosting indicated that it
was somewhat dangerous to health, while one respon-
dent indicated that it was very dangerous and the
remaining one felt that it was not at all dangerous to
health. Excessive sweating, high blood pressure and
headache were identified as the most frequent
symptoms of boosting, while shivering and blurred
vision were reported less frequently. Two of these
symptoms, namely excessive sweating and shivering,
are easily visible and are frequently used to identify
whether spinal cord injured athletes are in the boosted
state during competitions [6]. When queried about the
consequences of boosting, approximately 60% of the
respondents identified stroke/cerebral haemorrhage
and 44% identified death as possible outcomes. The
awareness of the signs/symptoms and consequences of
boosting was not associated with their education level
or injury duration. Respondents indicated that they
gained most of this knowledge through their personal
experiences or from discussions with other athletes.
Only 22.9% of them indicated that they learned about
boosting from reading, while 2.1% leaned about it
from their coaches. These findings are not surprising
because of the following reasons. First, although much
has been written about the clinical effects of AD which
occurs spontaneously [16–18], there is minimal
published scientific information pertaining to its
voluntary induction (i.e. boosting) that is available
to athletes. The available boosting studies have
focused strictly on the physiological responses of
the athletes during exercise [1,11,13]. Second, the
findings of two surveys [10,19] indicated that a
majority of the elite athletes with disabilities do not
have professionally trained coaches, and therefore,
rely on themselves for acquiring relevant informa-
tion. One former paralympic athlete [20] clearly
stated that education should be given to athletes about all
the aspects of boosting. To permit participation of
‘unboosted’ athletes, new standards should be fixed to
ensure rights for those who do not use boosting. These
findings reiterate the need for developing suitable
educational programs not only for the athletes, but
also for the coaches, trainers and rehabilitation
professionals responsible for their overall health and
safety. The male and female respondents in this
study were strongly opposed to the use of boosting to
improve training capacity, enhance performance
during competition and cause their competitors were
using it. This opinion was independent of their
education level, employment status and duration of
injury. Despite their knowledge pertaining to the
dangers and adverse health effects of boosting
(Figure 4), 16.7% of the respondents indicated that
they had used it to enhance performance during
training and/or competition. This finding should be
of concern to the athletes, coaches and trainers and
the governing bodies of the paralympic sport
organisations.
Random monitoring of athletes suspected of
boosting was first implemented at the Sydney
Paralympic Games in 2000. During the 2008 Beijing
Paralympic Games, a total of 20 athletes, 16 wheel-
chair racers and four-hand cyclists were tested for
boosting shortly before competition. This is a
relatively small number compared to the total
number of athletes with high-level spinal cord
injuries that participated in the Games and the
overall number of events in which they competed.
None of these athletes demonstrated a positive
response on the basis of their blood pressure
measurements. However, it is possible that some
athletes could have induced boosting during the
competition and circumvented the initial screening
process. This is difficult to monitor and poses a real
challenge to the procedures for monitoring boosting
in these athletes. The results of this study indicated
that only one participant used boosting all the time
during national and international competitions. It is
recommended that the frequency of boosting tests at
the Paralympic games and other IPC sanctioned
events be increased considerably so that the trends
in this method of coping can be systematically
evaluated.
2182 Y. Bhambhani et al.

Limitations of the study
Because of the relatively small sample size in this
study, the number of responses in the categorical
variables for many of the questions was very low.
Although the Fisher Exact test is specifically de-
signed for small sample sizes (below five per cell), the
current findings were limited by low statistical power
and distortion between categories because of the
small number of respondents in many cells. There-
fore, visual analysis of the descriptive statistics should
be given some weight despite any lack of statistical
significance.
The ratio of male (N¼ 84) to female (N¼ 11)
participants in this study was approximately 8:1. The
gender distribution of the 241 athletes with spinal
injuries above T6 who participated at the Beijing
Paralympic Games is not available, and therefore, it
is not clear whether the present distribution is
representative of their participation in the Games.
It is likely, however, that the males who met the
inclusion criteria outnumbered the females, because
all but one of the participants in wheelchair rugby,
the sport that comprised 96 of the 241 athletes
(40%), were males. Generalising the results of this
study to the female Paralympic population should be
viewed with caution.
The current questionnaire was administered only
in English, and therefore, was completed by indivi-
duals who were familiar with this language. There-
fore, the findings from this study could be
generalized mainly to athletes who could commu-
nicate in English. However, in some instances, non-
English speaking athletes (e.g., Brazil and Italy) were
assisted by their coaches and team managers in
completing the questionnaire during the Games and
are included in the total sample.
In the interest of ensuring anonymity of the
participants, the Health Research Ethics Board at
the University of Alberta stipulated that they not be
required to identify their country of residence on the
questionnaire. Therefore, it was not possible to
conduct an analysis of the results with respect to
the country of origin in this study. It is possible that
regional differences pertaining to boosting may exist,
and further research should be conducted to examine
this question.
The use of a self-report questionnaire to obtain
information on a sensitive issue such as doping runs
the risk of under-reporting by the athletes, and
therefore, could be misleading [21]. As well, the
reproducibility of the responses to these sensitive
issues may be questionable [22]. From a research
perspective, it is crucial that the perspectives of the
athletes’ be accurately documented, so that appro-
priate intervention strategies can be implemented by
the sport governing bodies.
Recommendations
This is the first study that has systematically
examined the incidence, knowledge and attitudes
towards boosting in paralympic athletes with high-
level spinal cord injuries. The lack of previous
research pertaining to this topic makes it difficult to
place the current results in perspective. However,
based on these findings, the following recommenda-
tions are made:
1. Educational materials pertaining to AD are
developed in simple language that can be
understood by individuals with SCI and
rehabilitation professionals responsible for
their regular care.
2. Specific educational materials pertaining to
the effects of boosting during exercise are
developed so that paralympic athletes can
increase their awareness and knowledge
about this method of doping which can be
dangerous to their health.
3. A concerted effort should be made to
increase boosting awareness in females as
they demonstrated considerable lack of
knowledge in this area.
4. Educational materials are developed in an
interactive manner in different languages so
as to enhance knowledge and learning by the
athletes, coaches and trainers internationally.
5. Coaches and trainers should be educated
about this practice and convey this informa-
tion to their athletes so that the overall
incidence of boosting can be reduced.
6. Boosting educational programmes be tar-
geted in geographical regions where the
awareness is most likely to be low.
7. Boosting programmes be initiated at the
junior level so that these individuals are fully
aware of its dangers when they become
competitive athletes.
8. Boosting workshops during the paralympic
games and other sanctioned competitions
should be considered so as to further educate
the athletes, coaches and trainers regarding
this practice.
9. Educational programmes be targeted to
specific sports (e.g. wheelchair rugby, wheel-
chair distance racing) in which the incidence
of boosting is likely to be high.
10. Increase the frequency of boosting tests at
sanctioned competitions so that the trends in
this practice can be systematically evaluated.
11. Further research should be conducted on a
larger sample size of competitive spinal cord
injured athletes of both genders with lesion
levels above T6 so that the findings can be
Boosting in paralympic athletes 2183
generalised to a larger segment of this
population.
Acknowledgements
We thank the following organisations and individuals
for facilitating this research study:
. World Anti-Doping Agency (WADA) for their
financial support.
. International Paralympic Committee (IPC) for
their administrative assistance in implementing
this study through their head office in Bonn
and at the Paralympic Games in Beijing.
. The IPC Sports Science Committee for its
approval of the study to be conducted at the
Beijing 2008 Paralympic Games.
. Dr. Wendy Rodgers, Professor, Faculty of
Physical Education and Recreation, University
of Alberta for reviewing the first draft of the
questionnaire.
. Dr. Kelly MacKay, Associate Dean (Aca-
demic) Faculty of Kinesiology and Recreation
Management, University of Manitoba for
reviewing the second draft of the questionnaire.
. Managers of the National Paralympic Com-
mittees for encouraging their athletes to
participate in this study.
. Team coaches who took the responsibility of
distributing the questionnaires to the athletes
and returning them in a timely fashion.
. Susan Armijo Olivo and Patricia Edney from
the Rehabilitation Research Center, University
of Alberta, for their assistance in conducting
the statistical analyses.
. All the participants who took the time to
complete this questionnaire during the Paral-
ympic Games in Beijing and via the on-line
submission process. Without your cooperation,
this research study would not have been
possible!
References
1. Burnham R. Wheeler G, Bhambhani Y, Belanger M, Eriksson
P, Steadward R. Intentional induction of autonomic dysre-
flexia among quadriplegic athletes for performance enhance-
ment: efficacy, safety, and mechanism of action. Clin J Sports
Med 1994;4:1–10.
2. Riding M. Boosting in Paralympic sport – some ethical
considerations. New horizons in sport for athletes with
disabilities; In Proceedings of the International Vista ‘99
Conference. Meyer & Meyer Sport; 2001. pp 267–272.
3. Webborn AD. ‘‘Boosting’’ performance in disability sport.
Brit J Sports Med 1999;33:74–75.
4. International Paralympic Committee. IPC handbook Part I.
2nd ed. Bonn: International Paralympic Committee; 2000.
5. Bhambhani Y. Principles of fitness assessment and training for
wheelchair athletes. In: Steadward R, Wheeler G, Watkinson
E, editors. Adapted physical activity. Edmonton, Canada:
University of Alberta Press; 2003. pp 511–540.
6. Bhambhani Y. Physiology of wheelchair racing in athletes with
spinal cord injury. Sports Med 2002;32:23–51.
7. Hoffman MD. Cardiorespiratory fitness and training in
quadriplegics and paraplegics. Sports Med 1986;3:312–330.
8. Smith J, Wilder RP. Musculoskeletal rehabilitation and sports
medicine. IV. Miscellaneous sports medicine topics. Arch
Phys Med Rehabil 1999;80(5 Suppl 1):S68–S89.
9. Riding M. Doping – a paralympic perspective. New horizons
in sport for athletes with disabilities. In: Proceedings of the
International Vista ‘99 Conference. Meyer & Meyer Sport;
2001. pp 273–280.
10. Bradbury T. Athletes doing it for themselves: self coaching
guidelines for elite athletes. New horizons in sport for athletes
with disabilities. In: Proceedings of the International Vista ‘99
Conference. Meyer & Meyer Sports; 2001. pp 81–96.
11. Schmid A, Schmidt-Trucksass A, Huonker M, Konig D,
Eisenbarth I, Sauerwein H, Brunner C, Storch MJ, Lehmann
M, Keul J. Catecholamines response of high performance
wheelchair athletes at rest and during exercise with autonomic
dysreflexia. Int J Sports Med 2001;22:2–7.
12. Avois L, Robinson N, Saudan C, Baume N, Mangin P, Saugy
M. Central nervous system stimulants and sport practice. Br J
Sports Med 2006;40 (Suppl 1):i16–i20.
13. Wheeler G, Cumming D, Burnham R, Maclean I, Sloley BD,
Bhambhani Y, Steadward R. Testosterone, cortisol and
catecholamine responses to exercise stress and autonomic
dysreflexia in elite quadriplegic athletes. Paraplegia
1994;32:292–299.
14. Maxwell JP, Visek AJ. Unsanctioned aggression in rugby union:
relationships among aggressiveness, anger, athletic identity, and
professionalization. Aggress Behav 2009;35:237–243.
15. Parmigiani S, Dadomo H, Bartolomucci A, Brain PF,
Carbucicchio A, Costantino C, Ferrari PF, Kalanza P, Volpi
R. Personality traits and endocrine response as possible
asymmetry factors of agonistic outcome in karate athletes.
Aggress Behav 2009;35:324–333.
16. Bloch RF. Autonomic dysfunction. In: Bloch RF, editor.
Management of spinal cord injuries. Baltimore: Williams &
Wilkins; 1986. pp 149–163.
17. Karlsson AK. Autonomic dysreflexia. Spinal Cord 1999;37:
383–391.
18. Lee BY, Karmakar MG, Herz BL, Sturgill RA. Autonomic
dysreflexia revisited. J Spinal Cord Med 1995;18:75–87.
19. Chow JW, Mindock LA. Discus throwing performances and
medical classification of wheelchair athletes. Med Sci Sports
Exerc 1999;31:1272–1279.
20. Raymond S. Boosting. In: Steadward R, Nelson E, Wheeler
G, editors. Vista ‘93 – the Outlook. Edmonton, Alberta,
Canada: Rick Hansen Center; 1994. pp 242–247.
21. Adams A, Soumerai S, Lomas J, Ross-Degnan, D. Evidence
of self-report in assessing adherence to guidelines. Int J Qual
Health Care 1999;11:187–192.
22. Dollinger SJ, Malmquist D. Reliability and validity of single-
item self-reports: with special relevance to college students’
alcohol use, religiosity, study, and social life. J Gen Psychol
2009;136:231–241.
2184 Y. Bhambhani et al.

Appendix. Validated boosting questionnaire
What is Boosting?
Some individuals with a high level spinal cord injury (SCI), usually above the T6 level, experience a reflex
condition known as autonomic dyreflexia in their daily lives. Some athletes with spinal cord injury may voluntarily
induce autonomic dysreflexia, which is commonly called boosting, to improve their performance.
The purpose of this questionnaire is to learn more about the perspectives of elite athletes on sport and
performance enhancing practices, particularly boosting, in the Paralympic movement. All the information on the
questionnaire is anonymous and completely confidential, and will not be used to identify you individually or to
compromise your eligibility to compete in IPC sanctioned competitions. Please feel free to skip any questions
you are not comfortable answering and to add any additional comments about the research that you deem
appropriate. If you need more space for your answers, please use the back of the pages or attach additional ones.
Thank you very much for your valued time and contribution! Please return your completed questionnaire to
the person who invited you to participate or directly to the IPC (see address below).
1. Before reading about it on this questionnaire, have you ever heard of boosting as a performance enhancing
strategy? Please check [�] one.
¤ Yes (go to question 2)
¤ No (go to question 16)
¤ Not sure (go to question 16)
2. If you answered yes to the previous question, would you define boosting in any way other than described in
the introduction to this questionnaire? If so, how.
3a. Based on your injury/lesion level is it possible for you to experience autonomic dysreflexia?
¤ Yes
¤ No (go to question 6)
3b. If you answered yes to question 3a, have you ever intentionally induced autonomic dysreflexia to boost
your performance in training or competition?
¤ Yes
¤ No
4. With 1 being never and 5 being all the time, please circle (�) the number that best reflects how often you use
boosting in: If you answered NO to question 3a please circle 6.
5. Who monitors your use of boosting during: Please check [�] all that apply.
Never Sometimes All the time Not applicable
Your regular training program: � � � � � �Your peaking for competition training program: � � � � � �National competitions: � � � � � �International competitions: � � � � � �
You Coach Doctor Other No one Not applicable
Regular training program: ¤ ¤ ¤ ¤ ¤ ¤Peaking for competition training ¤ ¤ ¤ ¤ ¤ ¤National competitions: ¤ ¤ ¤ ¤ ¤ ¤International competitions: ¤ ¤ ¤ ¤ ¤ ¤
Boosting in paralympic athletes 2185

6. To your knowledge, would you say boosting is:
¤ Commonly used in your sport ¤ Not used in your sport
¤ Infrequently used in your sport ¤ I am not sure of its use
¤ Rarely used in your sport
7. When do you think boosting is most useful? Please check [�] all that apply.
¤ In training ¤ During competition
¤ Immediately before competition ¤ Other: please explain
8. Do you think boosting is more useful in some sports than others?
¤ Yes, please answer question 9a and 9b
¤ No, please go to question #10a
¤ Do not know, please go to question #10a
9a. Which sports/events do you think boosting is most useful? Please check [�] all that apply.
¤ Wheelchair Athletics ¤ Wheelchair Basketball
¤ Marathon racing ¤ Quad Rugby
¤ Long distance events ¤ Nordic Skiing
¤ Middle distance events ¤ Alpine Skiing
¤ Sprints ¤ Other, please specify
¤ Throwing events
9b. Which sports/events do you think boosting is least useful? Please check [�] all that apply.
¤ Wheelchair Athletics ¤ Wheelchair Basketball
¤ Marathon racing ¤ Quad Rugby
¤ Long distance events ¤ Nordic Skiing
¤ Middle distance events ¤ Alpine Skiing
¤ Sprints ¤ Other, please specify
¤ Throwing events
10a. Of the listed items, which do you believe boosting affects and at what point in time (e.g., before, during or
after the event). Please check [�] that apply.
In Training
Immediately Before
Competition During Competition After Competition
Yes No Not Sure Yes No Not Sure Yes No Not Sure Yes No Not Sure
Increased arm strength
Increased arm endurance
Less arm stiffness
Less difficulty breathing
Improved circulation
Less fatigue
Increased aggression
Increased alertness
Increased anxiety
Increased frustration
Other (specify)
2186 Y. Bhambhani et al.

10b. In answering the previous question (10a), what are your responses based on? Please check [�] all that
apply.
¤ Personal experience
¤ Reports form other athletes you know personally
¤ Coaches
¤ Reading
¤ Other (Specify):
11. Based on what you know about boosting, would you say it is:
¤ Not at all dangerous
¤ Somewhat dangerous
¤ Dangerous
¤ Very dangerous
12a. Which of the following, if any, do you believe are symptoms of boosting. Please check [�] all that apply.
12b. In answering the previous question (12a), what is your main source of information? Please check [�] all
that apply.
¤ Personal experience
¤ Reports form other athletes you know personally
¤ Coaches
¤ Reading
¤ Other (Specify):
13. Which, if any, of the listed health risks do you think are possible consequences of boosting and how do you
know this? Please check [�] all that apply.
Symptom Yes No Not Sure
Headache
Shivering
Excessive Sweating
High blood pressure
Blurred vision
Other (specify)
Information Sources
Possible consequence Yes No Not Sure Personal Experience Other Athletes Coaches Reading Other (specify)
High blood pressure
Seizures
Stroke/cerebral haemorrhage
Death
Other (specify)
Boosting in paralympic athletes 2187

14. With 1 being totally not acceptable and 5 being totally acceptable, please circle (�) the number that best
reflects your opinion about boosting.
15. Please circle (�) the number that best reflects the extent to which you agree (1¼ strongly disagree and
5¼ strongly agree) with the following statements.
16. In the column provided please list any other methods you currently use for improving performance (e.g.,
nutritional supplements, carbohydrate replacement) in training/competition that have not been addressed
in this questionnaire and indicate (�) whether you believe the method/practice to be effective, legal, and
whether it has associated health risks.
17. Recent sport news includes numerous examples of ‘‘doping’’ scandals in sport generally. From your
perspective, which of the following statements best captures your opinion about this issue? With 1 being
totally not acceptable and 5 being totally acceptable, please circle (�) the number that best reflects your
view about each statement.
TotallyNot Acceptable
SometimesAcceptable
TotallyAcceptable
Boosting to improve training capacity is: � � � � �Boosting to maximize performance in competition is: � � � � �Boosting because you know your competitors are is: � � � � �Boostino is: � � � � �
StronglyDisagree
SomewhatAgree
TotallyAgree
Boosting should not be banned becauseit can happen unintentionally.
� � � � �Boosting should not be banned because any athlete with T6
or higher spinal cord injury can decide to induceautonomic dysreflexia.
� � � � �Only practices that are not available to all athletes in
the same class should be banned.� � � � �
The message—show casing the talents of athletes and by extensionthe capabilities of people with disabilities—is far more importantthan whether or not someone is boosting.
� � � � �
Effective Legal Health Risks
Method/Practice Yes No Not Sure Yes No Not Sure Yes No Not Sure
TotallyNot Acceptable
SometimesAcceptable
TotallyAcceptable
Using banned drugs to improve training capacity is: � � � � �Using banned drugs to maximize
performance in competition is:� � � � �
Using banned drugs because youknow your competitors are is:
� � � � �Using banned drugs is: � � � � �
2188 Y. Bhambhani et al.
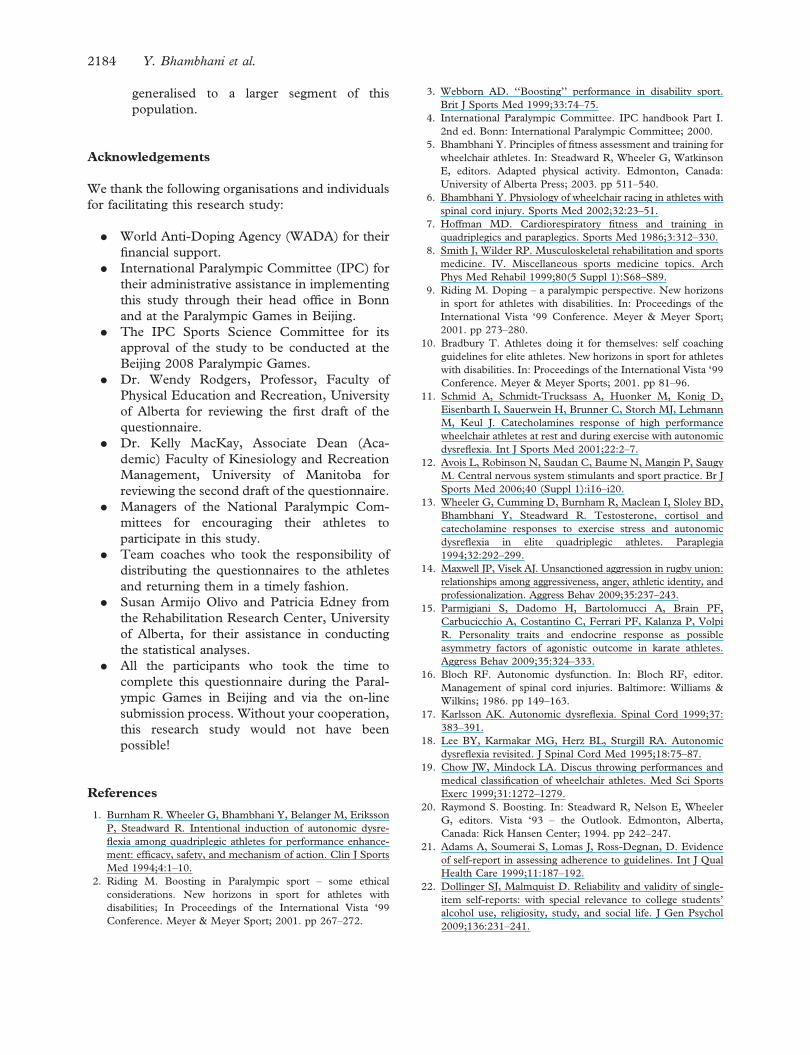
18. To what extent, if any, do you think doping is a concern in Paralympic Sports? Please check [�] one.
¤ Not a concern at all
¤ Sometimes a concern
¤ A major concern
Please add additional comments to explain your answer to question 18.
Background Information
Questions in this section of the questionnaire are designed to provide background information. Once again, this
information will not be used to identify you but to provide information about the sample group involved in the
research. Please feel free to skip any questions you are not comfortable answering.
19. What is the highest level of education you have completed? Please check [�] one.
¤ Some high school ¤ Undergraduate university degree(s)
¤ High school graduation Specify area:
¤ Some post-secondary (not university) ¤ Graduate university degree Specify area:
¤ Some university (no degree)
20. Which of the following best describes your status? Please check [�] all that apply.
¤ Paid employee � ¤ part-time ¤ full-time
¤ Self employed � ¤ part-time ¤ full-time
Please describe the kind of work you do:
¤ Unemployed � ¤ looking for work ¤ not looking for work
¤ Student � ¤ part-time ¤ full-time
¤ Athlete � ¤ part-time ¤ full-time
As an athlete are you: ¤ self-funded
¤ state/government funded
¤ funded by other source: please specify:
21. Please check [�] the appropriate box for each of the following items
Sex: ¤ Female ¤ Male
Age: ¤ 16 to 21 ¤ 34 to 39
¤ 22 to 27 ¤ 40 to 45
¤ 28 to 33 ¤ 46 and over
22. Have you ever spontaneously (not intentionally induced) experienced autonomic dysreflexia?
¤ Yes (go to question 23)
¤ No (go to question 24)
¤ I don’t know (go to question 24)
23. If you answered yes to question 22, how often does this happen? Please specify:
24. Which sport(s) do you participate in? Please check [�] all that apply.
¤ Wheelchair Athletics ¤ Wheelchair Basketball
¤ Marathon racing ¤ Quad Rugby
¤ Long distance events ¤ Nordic Skiing
¤ Middle distance events ¤ Alpine Skiing
¤ Sprints ¤ Other, please specify
¤ Throwing events
Boosting in paralympic athletes 2189

25a. Please specify the date of your initial spinal cord injury: ______/______/______
Day Month Year
25b. Please specify the lesion level of your injury:
Level of Lesion:
¤ I do not know the lesion level of my injury
25c. Please indicate whether your spinal cord injury: Please check [�] one box only
¤ Complete
¤ Incomplete
¤ I do not know the answers to this question
26. Is there anything else you would like to convey to the IPC about doping, boosting, or any other legal or
banned performance enhancing strategy? If yes, please explain.
2190 Y. Bhambhani et al.

Copyright of Disability & Rehabilitation is the property of Taylor & Francis Ltd and its content may not be
copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written
permission. However, users may print, download, or email articles for individual use.