Complete dissertation - Vrije Universiteit Amsterdam
155
VU Research Portal Maxillofacial fractures associated with accidents Ruslin, Muhammad 2019 document version Publisher's PDF, also known as Version of record Link to publication in VU Research Portal citation for published version (APA) Ruslin, M. (2019). Maxillofacial fractures associated with accidents: Epidemiology and consequences. General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal ? Take down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. E-mail address: [email protected] Download date: 05. Feb. 2022
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Complete dissertation - Vrije Universiteit Amsterdam
VU Research Portal
Maxillofacial fractures associated with accidents
Ruslin, Muhammad
2019
document versionPublisher's PDF, also known as Version of record
Link to publication in VU Research Portal
citation for published version (APA)Ruslin, M. (2019). Maxillofacial fractures associated with accidents: Epidemiology and consequences.
General rightsCopyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright ownersand it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights.
• Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal ?
Take down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
E-mail address:[email protected]
Download date: 05. Feb. 2022
Maxillofacial FracturesAssociated with Accidents:
Epidemiology and Consequences
Maxillofacial FracturesAssociated with Accidents:
Epidemiology and Consequences
MUHAMMAD RUSLIN
Maxillofacial Fractures Associated w
ith Accidents: Epidemiology and Consequences - M
uhamm
ad Ruslin

Maxillofacial fractures associated with accidents:
Epidemiology and consequences
Muhammad Ruslin
Maxillofacial fracturesassociated with accidents:
Epidemiology and consequences

The studies presented in this thesis were performed at the departement of Oral and Maxillofacial
Surgery, VU University Medical Center / Academic Centre for Dentistry Amsterdam (ACTA),
Amsterdam, the Netherlands.
Financial support for publication of this thesis was provided by :
Academic Centre for Dentistry Amsterdam
Cover design : M. Ruslin
Layout design : Asyraf Afif Alfian, M. Ruslin
Designer : van der Linden Grafische Dienstverlening
Printer by : van der Linden Grafische Dienstverlening
ISBN : 978-90-90313970-9
Copyright 2018, M. Ruslin, Amsterdam, the Netherlands
All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any
means, electronic or mechanical, including photocopy, recording, or any information storage and
retrieval system, without prior permission from the author.
The studies presented in this thesis were performed at the departement of Oral and Maxillofacial
Surgery, VU University Medical Center / Academic Centre for Dentistry Amsterdam (ACTA),
Amsterdam, the Netherlands.
Financial support for publication of this thesis was provided by :
Academic Centre for Dentistry Amsterdam
Cover design : M. Ruslin
Layout design : Asyraf Afif Alfian, M. Ruslin
Designer : van der Linden Grafische Dienstverlening
Printer by : van der Linden Grafische Dienstverlening
ISBN : 978-90-90313970-9
Copyright 2018, M. Ruslin, Amsterdam, the Netherlands
All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any
means, electronic or mechanical, including photocopy, recording, or any information storage and
retrieval system, without prior permission from the author.
door
Muhammad Ruslin
geboren te Pangkajene, Indonesië
Cover design : M. Ruslin
Layout design :AsyrafAfifAlfian,M.Ruslin
Designer : vanderLindenGrafischeDienstverlening
Printed by : vanderLindenGrafischeDienstverlening
ISBN : 978-90-9031397-9
Copyright 2018, M. Ruslin, Amsterdam, the Netherlands
Allrightsreserved.Nopartofthispublicationmaybereproducedortransmittedinanyformorbyany
means, electronic or mechanical, including photocopy, recording, or any information storage and
retrieval system, without prior permission from the author.

VRIJE UNIVERSITEIT
Maxillofacial fractures associated with accidents:
Epidemiology and consequences
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad Doctor aan
de Vrije Universiteit Amsterdam,
of gezag van de rector magnificus
prof.dr. V. Subramaniam,
in het openbaar te verdedigen
ten overstaan van de promotiecommissie
van de Faculteit der Tandheelkunde
op maandag 14 januari 2019 om 13.45 uur
in de aula van de universiteit
De Boelelaan 1105
door
Muhammad Ruslin
geboren te Pangkajene, Indonesië
door
Muhammad Ruslin
geboren te Pangkajene, Indonesië
,

promotor: prof.dr. T. Forouzanfar
copromotoren: prof.dr. D.B Tuinzing
dr. P. Boffano
promotor: prof.dr. T. Forouzanfar
copromotoren: prof.dr. D.B Tuinzing
dr. P. Boffano

promotiecommissie: prof.dr. D. Wismeijer
prof.dr. E.A.J.M. Schulten
prof.dr. B.J. van Royen
prof.dr. Y.Y. Harmas
dr. E.M. van Cann
paranimfen: Diandra Sabrina Natsir Kalla
Faqi Nurdiansyah Hendra

Contents
Chapter 1 : General introduction
1
Chapter 2 : Maxillofacial fractures associated with motor vehicle accidents: a review of the current literature
11
Chapter 3 : Motor-vehicle accidents related maxillofacial injuries: a multicenter and prospective study
21
Chapter 4 : Maxillofacial fractures associated with sport injuries: a review of the current literature
33
Chapter 5 : Chapter 6 :
Sport-related maxillofacial fractures Sport related maxillofacial fractures: a multicenter and prospective study
45
55
Chapter 7 : Dental trauma in association with maxillofacial fractures; an epidemiological study
69
Chapter 8 : The Maxillofacial Injury Severity Score (MFISS) and Facial Injury Severity Scale (FISS) as a predictor brain injury with maxillofacial fractures patients
82
Chapter 9 : The use of neuron-specific enolase to predict brain injury in motorcycle crash patients with maxillofacial fractures: a pilot study
91
Chapter 10 : The influence of helmet on the prevention of maxillofacial fractures sustained during motorcycle accidents
101
Chapter 11 : Summary, General discussion and Conclussion 111
Chapter 12 : Acknowledgements
Samenvatting
123
131
List of publications
137
Curriculum vitae
143
Allah will exalt those who believe among you, and those who have knowledge, to high ranks.
Al-Mujaadilah 11
Allah will exalt those who believe among you, and those who have knowledge, to high ranks.
Al-Mujaadilah 11

Contents
Chapter 1 : General introduction
1
Chapter 2 : Maxillofacial fractures associated with motor vehicle accidents: a review of the current literature
11
Chapter 3 : Motor-vehicle accidents related maxillofacial injuries: a multicenter and prospective study
21
Chapter 4 : Maxillofacial fractures associated with sport injuries: a review of the current literature
33
Chapter 5 : Chapter 6 :
Sport-related maxillofacial fractures Sport related maxillofacial fractures: a multicenter and prospective study
45
55
Chapter 7 : Dental trauma in association with maxillofacial fractures; an epidemiological study
69
Chapter 8 : The Maxillofacial Injury Severity Score (MFISS) and Facial Injury Severity Scale (FISS) as a predictor brain injury with maxillofacial fractures patients
82
Chapter 9 : The use of neuron-specific enolase to predict brain injury in motorcycle crash patients with maxillofacial fractures: a pilot study
91
Chapter 10 : The influence of helmet on the prevention of maxillofacial fractures sustained during motorcycle accidents
101
Chapter 11 : Summary, General discussion and Conclussion 111
Chapter 12 : Acknowledgements
Samenvatting
123
131
List of publications
137
Curriculum vitae
143
1
11
21
33
45
55
69
81
91
101
111
123
131
137
143

Chapter 1
General Introduction
General Introduction Maxillofacial fracture is defined as any physical insult caused to the face. It occurs quite commonly
after trauma and is often encountered in emergency medicine. If not properly managed, it can
negatively influence patients’ psychosocial and functional activities. Due to the specificity of this
anatomical region, maxillofacial injuries are serious clinical issues: it is in this region that the crucial
organs are placed and the digestive and respiratory systems begin. For this reason, injuries in this
part of the body are regarded as serious dysfunctions.
Maxillofacial injuries have various causes: traffic accidents, falls, assaults, and sports injuries. They
can be isolated or combined with other injuries. Thorough knowledge and understanding of the
epidemiology and consequences of these injuries is fundamental to the development of health
services and the adoption of new methods for preventing injuries.1-11
Epidemiology of Maxillofacial Fractures Globally, there have beed numerous epidemiological studies of maxillofacial fractures, especially in
the trauma, surgical, dental, and medical literature.11 Reports on developments in treatment
modalities in surgery and dental procedures vary according not only to the geographic area in
which the research is conducted and to the socioeconomic status of the patient group, but also to
the period of investigation.1-10 A range of studies have investigated the epidemiological features of
maxillofacial fractures in various population groups around the world1-12 Some have found that
maxillofacial fractures are more common among young adults, particularly males in the third and
fourth decades of life, often because they are involved in outdoor activities or reckless driving.13,14
One study found that the largest proportion of injuries occured in those whose ages ranged from 16
(48%) to 30 (68%).15 Another study also found that 68.6% of its study population lay in the 20-40
age range.13
With regard to the types of fractures, a systematic review published in 2013 found that mandibular
fracture was the most common fracture, accounting for 59.2% of the total.10,16 In contrast, other
studies in the western world found that nasal bone fractures and zygomatic complex fractures were
more common.5,17 Several studies found that the main fracture site in the mandible was the body,
which accounted for 40% of the total number of mandible fractures.5,10,17 In the middle third, the
zygoma was the most involved site.4 The relative predominance of the facial structure involved has
also been affected by a shift in the etiology of the injury, where an increase in the number of high-
speed motor vehicle accidents produced a shift from mandibular fractures to midface and
craniofacial fractures.18-23 While reports in low- and middle-income countries show that traffic
accidents are the main cause of maxillofacial fractures,9,19-22 data from high-income countries
indicates that the main cause lies in assaults.16,17,23-25
2
1Although assault is also becoming the most frequent cause in many low- and middle-income
countries, motor vehicle accidents (MVAs) are still among the world’s most frequent causes of
facial fractures.2,19,20 Traffic accidents account for 34.42–80.14% of all skeletal and soft tissue
injuries in the facial area.18 The recent literature shows clear differences between the incidence of
MVA-related facial fractures in high-income countries (20% in Japan, 35.2% in the Netherlands,
11% in Ireland) and low- and middle-incomes countries (72–85% in India, 46.7% in China).1
Sport are another important causes of maxillofacial injury. Approximately 5% of all mandible
fractures and 9% of fractures in the upper two-thirds of the face are caused by sport. Direct body
contact accounts for the majority of sports-related injuries, the most commonly associated soft
tissue injuries being found in the head and neck region.26 Sport-related accidents are also
responsible for approximately 10% of all midfacial trauma. In their study of sport-related injuries,
Elhammali et al.22 found a significant prevalence of the mid-facial complex (67%), followed by the
mandible (29%) and skull base (4%).16,17,22 In their review of sports-related maxillofacial trauma,
Kunamoto et al.16 suggested that a difference between the types of sports and the frequency and
type of fractures.16 While sports such as football, baseball, and hockey accounted for a high
percentage of facial injuries among young adults,16,17,22 horse riders most commonly incurred
fractures of the zygomatic bone (40%), and rugby players most commonly incurred mandible
fractures (65%).17 As no data are currently available on sport-related maxillofacial fractures in the
Netherlands, it is important to evaluate the possible relationships between the types of sport
practiced, the frequency, and nature of patients’ bone fractures.
Consequences of Maxillofacial Fractures Trauma to the facial region can cause injury to the dentition, facial soft tissues, and skeletal
components of the face such as the mandible, maxilla, zygoma, naso-orbitoethmoidal complex, and
supra-orbital structures.27 As facial traumas often underlie further aesthetic disturbances,11 cosmetic
deformities can be expected after nasal and naso-orbito-ethmoidal injuries.26 Victims of facial
injuries can sustain scars or disfigurements, with their resultant emotional and psychological
impact, such as posttraumatic stress syndrome and depression, which are common after facial
injuries have been sustained.28 Due to the centrality of the facial region as a key factor in human
identity, esthetics, and general well-being, the scarring caused even by minor facial injuries can be
costly and have a personal impact on the injured person.14 Before or after the reduction of a
fracture, vision-related complications can also be an issue, especially after a high Le Fort fracture.
Intraorbital or retrobulbar hemorrhage or damage to the optic nerve caused by bone fragments can
all lead to blindness, enophthalmos, and diplopia. While patients with zygomatic fractures may
suffer from trismus, other forms of maxillofacial injuries can also cause paranasal sinus fractures.26
1
3
1

Fracture of the alveolar process often causes damage to the soft tissues and teeth, increasing the
severity of craniofacial injuries.16 Various published article have reported on dental injury in
maxillofacial fracture, which occurs mainly in childhood and adolescence.29-36 Improper rigid fixation
of fracture segments will result in malocclusion, especially in patients with anterior open bites
and/or class III fracture patterns.26 A Study by Abbasi et al.27 found the presence of unerupted
mandibular third molars to be associated with an increased risk for mandibular angle fracture.27
Facial fractures can influence the treatment of dental injuries, as facial swelling may not always
allow dental treatment after fracture reduction. Premature tooth loss may result.30-36
Several studies on facial fractures found an association between traumatic brain injury (TBI) and
the trauma resulting from maxillofacial injuries.37 The presence of brain injuries in patients with a
maxillofacial fracture is a life-threatening condition. Over 50% of patients with these fractures have
multisystem trauma that requires special attention. Accurate diagnosis of TBI can be problematic: a
physician examining these injuries must assess the patient rapidly and according to a consistent
methodology. Diagnosis should be prompt, and the treatment should be appropriate.37
In recent years, the Glasgow Coma Scale (GCS) has been seen as the gold standard for assessing
the level of consciousness in patients who have sustained traumatic brain injury after trauma.38
However the GCS scale lacks the specificity necessary for determining the exact magnitude of any
brain injury sustained during such an event. Such injuries are also difficult to assess using clinical
techniques such as magnetic resonance imaging or by computer tomography.39 This explains the
development of Neuron Specific Enolase (NSE) to evaluate neuronal damage. A protein-based
enzyme found primarily within neurons, NSE is commonly used to assess the grade of neuronal
damage after trauma.40-43 As increased concentrations of NSE can be measured in the
cerebrospinal fluid and in the peripheral blood after neuronal damage, it provides a quick and
reliable laboratory indicator of the degree of brain-cell damage sustained after trauma.44
There are several severity for assessing the severity and probable outcome of injury,44-47 the most
commonly used classification scores being Facial Injury Severity Scale (FISS)15 and Maxillofacial
Injury Severity Score (MFISS).44,46 Based on the Abbreviated Injury Scale (AIS), these two scoring
systems combine the Injury Severity Score parameters of maxillofacial function and appearance
(e.g., limited opening of mouth, malocclusion, facial deformity).44-46 Although the FISS also
classifies the laceration of both facial soft tissue and bone, the classification of bones is not
sufficiently detailed, and cannot be used to distinguish between displaced and comminuted
fractures.45,46 As well as taking account of anatomic damage, subsequent scoring systems such as
the MFISS also take account of the impairment of maxillofacial function and facial appearance,
which can reflect the effect on quality of life (QoL) caused by maxillofacial injuries.
4

In some high-income countries, TBI was found to be a major cause of cyclists’ deaths and of
severe morbidity involving the head area as the impact zone.39-41 The exact pattern of such head
injuries depends on the magnitude and direction of the impact force and the trauma site.48
Althought previous studies assessing motorcycle accidents found that the risk of head and brain
injuries was significantly lower in riders who wore helmets than in those who did not, there is
currently very little information on the location and pattern of craniomaxillomandibular skull injuries
in cyclists (as distinct from motorcyclists) who wear helmets.
The prompt determination of brain injury in patients with maxillofacial fracture is crucial to improving
their survival and recovery. If a patient has multiple-system trauma or other pressing medical
concerns, facial frcatures may initially go unnoticed. In view of the consequences of untreated mild
brain injury, it is crucial to detect any brain injuries in maxillofacial trauma patients at an early
stage. It is also important to establish the incidence of maxillofacial fractures associated with
traumatic brain injuries.1-10
Prevention of Maxillofacial Fractures
Prevention modalities vary according to age and the cause of injury. The majority of injuries in
children occur during unstructured play and result in minor facial trauma. General provisions such
as safe play areas with soft surfaces will minimize falls and their impact. In older children, injuries in
organized sport will be minimized by the provision and wearing of appropriate safety gear..29
Some types of sport carry an increased risk of injury. In contact sports, custom-made molded
mouthguards have a proven efficacy in reducing both dental and oral trauma, and also in
minimizing concussion after lower-jaw impacts. Since mouthguards become compulsory in the
United States and New Zealand for high-school and college football and rugby players, the
proportion of face and mouth injuries is estimated to have fallen from 50% to < 0.5% of all football-
related injuries.29
Preventing maxillofacial injuries is important to improving the quality of life of the people involved,
and also to reducing the socioeconomic costs of traffic injuries. Traffic-related trauma continues to
decrease, due not only to the advent of better safety in automobiles (such as airbag and the use of
seat belts) but also to the enforcement of laws on alcohol and speed limits.48-54 With regard to
motorcycle accidents, we should acknowledge the crucial role of helmets. Recent studies have
shown that wearing a helmets can reduce the overall risk of head and brain injuries by 63%–88%
and can also reduce injuries to the upper and mid-facial area.41-51,53 It has also been reported that
wearing a standard, good-quality motorcycle helmet reduces the risk of mortality by 40% and the
risk of serious injury by over 70%.1-10
1
5
1
Aim of the Study Reports worldwide on the incidence and epidemiological causes of maxillofacial fractures1-10 show
that the greatest cause are traffic accidents and sport-related accidents. Maxillofacial trauma
especially in high-energy trauma is often associated with injuries to the cranium. While it remains a
challange to assess the exact extent of any brain damage caused by traffic accidents or other
traumatic injuries.48,54 It may now be possible to do so using NSE serum.40-43 The use of trauma
score and severity grade in trauma studies can also provide the basis for determining treatment
strategy, guiding anesthetization and surgery, predicting the survival probability of the injured
patients, and predicting the impact of maxillofacial fractures on future health status.44-47 This study
therefore evaluated the maxillofacial fractures related to various types of accidents. We also
investigated other factors, such as etiology, complication, assessment, and prevention of this type
of fracture.
Objectives:
• To understand the distribution and characteristics of MVA-related facial injuries and sport
accidents worldwide, a review of the literature was performed. The demographics and
patterns of MVA-related maxillofacial fractures and sport accidents were also studied in a
multicentre study.
• Retrospectively, we investigated the incidence and associated factors of dental trauma in all
patients presenting with facial trauma accompanied by dental injury.
• As well as investigating NSE serum levels in patients who had sustained maxillofacial
fractures during motor-vehicle accidents, we investigated the accuracy of neuron-specific
biomarkers in detecting mild brain injury.
• To our knowledge, the literature contains less information on the use of MFISS and FISS in
predicting TBI. We therefore assessed the value of MFISS and FISS in detecting brain
injury in patients with maxillofacial fractures.
• In motorcycle accidents, different helmet designs (i.e., full-coverage and half-coverage
helmets) can produce different effect on patients who sustain maxillofacial fractures. This
study therefore assessed the effects of half-coverage helmets worn in motorcycle accidents
by comparing helmeted and unhelmeted motorcyclists who had sustained maxillofacial
fractures during motorcycle accidents.
6

References 1. Yamamoto K, Matsusue Y, Horita S, Murakami K, Ueyama Y, Sugiura T, Kirita T. Maxillofacial fractures of pedestrians injured in a
motor vehicle accident. Craniomaxillofac Trauma Reconstr 2013;6(1):37–42.
2. Boffano P, Kommers SC, Karagozoglu KH, Forouzanfar T. Aetiology of maxillofacial fractures: a review of published studies during the last 30 years. Br J Oral Maxillofac Surg 2014;52(10):901–906.
3. Kommers SC, van den Bergh B, Boffano P, Verweij KP, Forouzanfar T. Dysocclusion after maxillofacial trauma: a 42 year analysis. J Craniomaxillofac Surg 2014;42(7):1083–1086.
4. Boffano P, Roccia F, Gallesio C, Karagozoglu KH, Forouzanfar T. Diplopia and orbital wall fractures. J Craniofac Surg 2014;25(2): e183–e185.
5. Boffano P, Roccia F, Gallesio C, Karagozoglu KH, Forouzanfar T. Bicycle-related maxillofacial injuries: a double-center study. Oral Surg Oral Med Oral Pathol Oral Radiol 2013;116(3):275–280.
6. Fasola AO, Lawoyin JO, Obiechina AE, Arotiba JT. Inner city maxillofacial fractures due to road traffic accidents. Dent Traumatol 2003;19(1):2–5.
7. Cini MA, Prado BG, Hinnig Pde F, Fukushima WY, Adami F. Influence of type of helmet on facial trauma in motorcycle accidents. Br J Oral Maxillofac Surg 2014;52(9):789–792.
8. Hitosugi M, Mizuno K, Nagai T, Tokudome S. Analysis of maxillofacial injuries of vehicle passengers involved in frontal collisions. J Oral Maxillofac Surg 2011;69(4):1146–1151.
9. Cox D, Vincent DG, McGwin G, MacLennan PA, Holmes JD, Rue 3rd LW. Effect of restraint systems on maxillofacial injury in frontal motor vehicle collisions. J Oral Maxillofac Surg 2004;62(5):571–575.
10. Ramli R, Abdul Rahman R, Abdul Rahman N, Abdul Karim F, Krsna Rajandram R, Mohamad MS, Mat Nor G, Sohadi RU. Pattern of maxillofacial injuries in motorcyclists in Malaysia. J Craniofac Surg 2008;19(2):316–321.
11. Pohchi A, Razak NHA, Rajion ZA, Alam MK. Maxillofacial fracture at hospital universiti sains malaysia (HUSM): a five year retrospective study. Int Med J 2013; 20(4):487–489.
12. Brasileiro BF, Passeri LA. Epidemiological analysis of maxillofacial fractures in Brazil: A 5-year prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;102(1):28–34.
13. Gerardo G, Germar, Cruz MAY. A Four-Year Study of the Demographic Distribution and Treatment of Maxillofacial Fractures Admitted at the Philippine General Hospital. Acta Med Philipp 2009;43(3):16–25.
14. Udeabor SE, Akinbami BO, Yarhere KS, Obiechina AE. Maxillofacial Fractures: Etiology, Pattern of Presentation, and Treatment in University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria. J Dent Surg 2014:1–5.
15. L ee KH, Snape L, Steenberg LJ, Worthington J. Comparison Between Interpersonal Violence and Motor Vehicle Accidents in the Aetiology of Maxillofacial Fractures. Anz J Surg 2007;77(8):695–698.
16. Kunamoto DP, Maeda Y. A literature review of sports-related orofacial trauma. Gen Dent 2004;52(3):270–280.
17. Tanaka N, Hayashi S, Amagasa T, Kohama G. Maxillofacial fractures sustained during sports. J Oral Maxillofac Surg 1996;54(6): 715–720
18. Gassner R, Tuli T, Hachl O, Rudisch A, Ulmer H. Cranio-maxillofacial trauma: a 10 year review of 9543 cases with 21067 injuries. J Craniomaxillofac Surg 2003;31(1):51–61.
19. Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, Kovačič Ž, Vesnaver A, Konstantinović VS, Petrović M, Stephens J, Kanzaria A, Bhatti N, Holmes S, Pechalova PF, Bakardjiev AG, Malanchuk VA, Kopchak AV, Galteland P, Mjøen E, Skjelbred P, Grimaud F, Fauvel F, Longis J, Corre P, Løes S, Lekven N, Laverick S, Gordon P, Tamme T, Akermann S, Karagozoglu KH, Kommers SC, Meijer B, Forouzanfar T. European Maxillofacial Trauma (EURMAT) in children: a multicenter and prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol 2015;119(5):499–504.
20. Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, Kovačič Ž, Vesnaver A, Konstantinović VS, Petrović M, Stephens J, Kanzaria A, Bhatti N, Holmes S, Pechalova PF, Bakardjiev AG, Malanchuk VA, Kopchak AV, Galteland P, Mjøen E, Skjelbred P, Koudougou C, Mouallem G, Corre P, Løes S, Lekven N, Laverick S, Gordon P, Tamme T, Akermann S, Karagozoglu KH, Kommers SC, Forouzanfar T. European Maxillofacial Trauma (EURMAT) project: a multicentre and prospective study. J Craniomaxillofac Surg 2015;43(1):62–70.
21. Allareddy V, Allareddy V, Nalliah RP. Epidemiology of facial fracture injuries. J Oral Maxillofac Surg 2011;69(1):2613–2618.
22. Elhammali N, Bremerich A, Rustemeyer J. Demographical and clinical aspects of sports-related maxillofacial and skull base fractures in hospitalised patients. Int J Oral Maxillofac Surg 2010;39(9):857–862
23. van den Bergh B, Karagozoglu KH, Heymans MW, Forouzanfar T. A etiology and incidence of maxillofacial trauma in Amsterdam: a retrospective analysis of 579 patients. J Craniomaxillofac Surg 2012;40(12):165–169.
24. Al Ahmed HE, Jaber MA, Abu Fanas SH, Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: a review of 230 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98(2):166–170.
25. Bali R, Sharma P, Garg A, Dhillon G. A comprehensive study on maxillofacial trauma conducted in Yamunanagar, India. J Inj Violence Res 2013;5(2):108–116.
26. Aktop S, Gonul O, Satilmis T, Garip H, Goker K. Management of Midfacial Fractures. A Textbook of Advanced Oral and Maxillofacial Surgery. Chapter 15:415–444.
27. Abbasi MM, Abbas I, Khan N, Shah SMH, Hameed H, Shad S, Zulfiqar K. Frequency of unerupted mandibular third molar in mandibular angle fractures. J Ayub Med Coll Abbottabad 2012;24(1):30–32.
28. Lee K. Global trends in maxillofacial fractures. Craniomaxillofac Trauma Reconstr 2012;5(4):213–222.
1
7
1

29. Barker R, Hockey R, Spinks D, Miles E. Facial Injury. Queensland Injury Surveillance Unit 2003;79:1–6.
30. Thoren H, Numminen L, Snall J, Korni E, Lindqvist C, Lizuka T. Tornwall J. Occurrence and types of dental injuries among patients with maxillofacial fractures. Int J Oral Maxillofac Surg 2010;39(8):774–778.
31. Lieger O, Zix J, Kruse A, Iizuka T. Dental injuries in association with facial fractures. J Oral Maxillofac Surg 2009;69(8):1680–1684.
32. Zhou HH, Ongodia D, Liu Q, Yang RT, Li ZB. Dental trauma in patients with maxillofacial fractures. Dental Traumatol 2013;29(4): 285–290.
33. da Silva AC, Passeri LA, Mazzonetto R, De Moraes M, Moreira RW. Incidence of dental trauma associated with facial trauma in Brazil: a 1-year evaluation. Dent Traumatol 2004;20(1):6–11.
34. Gassner R, Bosch R, Tuli R, Emshoff R. Prevalence of dental trauma in 6000 patients with facial injuries. Implication for prevention. Oral Surg Oral Med Oral Pathol Ral Radiol Endod 1999;87(1):27–33.
35. Roccia F, Boffano P, Bianchi FA, Ramieri G. An 11-year review of dental injuries associated with maxillofacial fractures in Turin, Italy. J Oral Maxillofac Surg 2013;17(4):269–274.
36. Iso-Kungas P, Tornwall J, Suominen AL, Lindqvist C, Thoren H. Dental injuries in pediatric patients with facial fractures are frequent and severe. J Oral Maxillofacial Surg 2012;70(2):396–400.
37. Salentijn EG, Peerdeman SM, Boffano P, van den Bergh B, Forouzanfar T. A ten-year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: incidence and aetiology. J Craniomaxillofac Surg 2014;42(6):705–710.
38. Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974;2(7872):81–84.
39. Kobeissy FH, Ottens AK, Zhang Z, Liu MC, Denslow ND, Dave JR, Tortella FC, Hayes RL, Wang KKW. Novel differential neuroproteomics analysis of traumatic brain injury in rats. Mol Cell Proteomics 2006;5(10):1887–1898.
40. Hayes RL. Biochemical markers of brain injury: applications to combat casualty care. Paper presented at: the RTO HFM Symposium on combat casualty care in ground based tactical situations: Trauma technology and emergency medical procedures; August 16-18, 2004;16–8; St. Pete Beach, USA
41. Pineda JA, Wang KKW, Hayes R. Biomarkers of proteolytic damage following traumatic brain injury. Brain Pathol 2004;14(2):202-209.
42. Wu YC, Zhao YB, Lu CZ, Qiao J, Tan YJ. Correlation between serum level of neuron-specific enolase and long-term functional outcome after acute cerebral infarction: prospective study. Hong Kong Med J 2004;10(4):251–254.
43. Wang KK, Ottens AK, Liu MC, Lewis SB, Meegan C, Oli MW, Tortella FC, Hayes RL. Proteomic identification of biomarkers of traumatic brain injury. Expert Rev Proteomics 2005;2(4):603–614.
44. Zhang J, Zhang Y, El-Maaytah M, Ma L, Liu L, Zhou LD. Maxillofacial Injury Severity Score: proposal of a new scoring system. Int J Oral Maxillofac Surg 2006;35(2):109–114.
45. Bagheri SC, Dierks EJ, Kademani D, Holmgren E, Bell RB, Hommer L, Potter BE. Application of a facial injury severity scale in craniomaxillofacial trauma. J Oral Maxillofac Surg 2006;64(3):408–414.
46. Chen C, Zhang Y, An JG, He Y, Gong X, Comparative study of four maxillofacial trauma scoring systems and expert score. J Oral Maxillofac Surg 2014;72(11):2212–2220.
47. Sahni V. Maxillofacial Trauma Scoring Systems: A Review. Injury 2016;47(7):1388–1392.
48. Leles JL, Santos EJ, Jorge FD, da Silva ET, Leles CR. Risk factors for maxillofacial injuries in a Brazilian emergency hospital sample. J Appl Oral Sci 2010;18(1):23–29.
49. Thompson DC, Rivara F, Thompson R. Helmets for preventing head and facial injuries in bicyclists. Cochrane Database Syst Rev. 10.1002/14651858. CD001855, October 25, 1999.
50. Attewel RG, Glase K, McFadden M. Bicycle helmet efficacy: a meta-analysis. Accid Anal Prev 2001;33(3):345–352.
51. Zibung E, Riddez L, Nordenvall C. Helmet use in bicycle trauma patients: a population-based study. Eur J Trauma Emerg Surg 2015;41(5):517–521.
52. Cripton PA, Dressler DM, Stuart CA, Dennison CR, Richards D. Bicycle helmets are highly effective at preventing head injury during head impact: head-form accelerations and injury criteria for helmeted and unhelmeted impacts. Accid Anal Prev 2014;70:1–7.
53. Ergun R, Bostanci U, Akdemir G, Beşkonakli E, Kaptanoğlu E, Gürsoy F, Taşkin Y. Prognostic value of serum neuron-specific enolase after head injury. Neural Res 1998;20(5):418–420.
54. Laterza OF, Modur VR, Crimmins DL, Olander JV, Landt Y, Lee JM, Ladenson JH. Identification of novel brain biomarkers. Clin Chem 2006;52(9):1713–1721.
8

9

10

Chapter 2
Maxillofacial fractures associated with
motor vehicle accidents:
A review of the current literature
This is an edited version of the manuscript:
Muhammad Ruslin, Jan Wolff, Tymour Forouzanfar, Paolo Boffano
Maxillofacial fractures associated with motor vehicle accidents: A review of the current literature
Journal of Oral and Maxillofacial Surgery, Medicine, and Pathology 2015 May;27(3):303–307.

Abstract
Introduction:
In many countries, traffic accidents are the most common cause of maxillofacial fractures.
Maxillofacial fractures can have various causes, such as traffic accidents, falls, assaults, sports
injuries, and others, in isolation or in combination with other injuries. The aim of this article was to
review and discuss papers that were published during the past 30 years regarding the distribution
and characteristics of motor vehicle accidents-related facial injuries throughout the world.
Methods:
We systematically reviewed all papers that were published in English between January 1980 and
December 2013 using MEDLINE and the MeSH term “facial fractures” together with the term
“motor vehicle”. Fourteen papers in other languages were excluded.
Results:
The percentage of motor vehicle accidents as etiological factors in epidemiological studies on
maxillofacial injuries ranged between 11% to 85%. On the whole, a progressively decreasing trend
was observed, particularly in North America, Brazil, and Europe. A further observed result was the
progressive decrease of incidence of facial injuries suffered by pedestrians in the last 30 years.
Facial fractures mainly involved the lower third or the middle third in all the considered studies.
Conclusion:
Motor vehicle accidents are still one of the most important etiological factors for maxillofacial
injuries. A great difference in the incidence of this kind of fractures between developed countries
and developing countries can be observed.
12

Introduction Maxillofacial fractures can have various causes, such as traffic accidents, falls, assaults, sports
injuries, and others, in isolation or in combination with other injuries.1-39 The epidemiology of these
fractures varies depending on the geographic area, socioeconomic status, and the period of
investigation.1-10 In many countries, traffic accidents are the most common cause of maxillofacial
fractures.1-10
Motor vehicle accidents (MVAs) are still among the most frequent causes of facial fractures all
over the world, although assault is becoming the most frequent cause in many developed
countries.2,40-42
Investigations of MVA-related maxillofacial injuries are crucial to clarify the mechanisms and
socioeconomic costs of MVA injuries, in particular because patients with oral and maxillofacial
injuries often acquire disabilities and require longterm treatment.1,2,6
In the last 30 years, the implementation of laws that require seat belts and/or airbags in cars and
helmets to be worn by motorcyclists has had an impact on the incidence of facial trauma in
developed countries.1,2,6,7
Furthermore, socioeconomic reasons such as poor roads and speed limits are a crucial factor that
influences the incidence of MVA.6,7
Preventing maxillofacial injuries is a valuable pursuit for improving the quality of life of the involved
subjects and decreasing the socioeconomic costs of motor vehicle collision injuries.6-8
Thorough knowledge and understanding of the etiology and epidemiology of MVA-related facial
injuries are fundamental for the development of health services, and the adoption of new methods
for preventing injuries.
The aim of this paper, therefore, was to review and discuss papers that were published during the
past 30 years regarding the distribution and characteristics of MVA-related facial injuries
throughout the world.
Material and Methods
We systematically reviewed all papers that were published in English between January 1980 and
December 2013 using MEDLINE and the MeSH term “facial fractures” together with the term
“motor vehicle”. Fourteen papers in other languages were excluded. Papers that presented
complete data about the etiology of motor vehicle accidents with appropriate information about car,
2
13
2

motorcycle and pedestrian accidents were identified and included. Data were collected on etiology
and characteristics of fractures and summarized in Table 2.1.
This article was exempt from IRB approval as it is a review of the literature. We followed Helsinki
Declaration guidelines.
Results
A total of 27 studies met the inclusion criteria and were included in this review (Tables 2.1 and 2.2). Table 2.1. Etiology of MVA-related maxillofacial fractures: review of epidemiologic studies
Country Number of patients
Percentage of MVA (%)
M:F ratio in MVA victims
Etiology of MVA Author Year Car (%) Motorcycle (%) Pedestrian struk by MV (%) Nigeria 1447 72.7 20.9:1 67.2 31.3 6.5 Adekeye Jordan [15] 1980
Jordan 131 61.1 - 50 20 30 Karyouti India [16] 1987 India 262 50 - 41.2 39.7 19.1 Sawhney and Ahuja [17] 1988
Nigeria 442 69.9 3.6:1 68.2 20.8 11.4 Ugboko et al. [18] 1998 The Netherlands 1324 36.6 - 60.2 33.4 6.4 van Beek and Merkx [19 1999
Japan 1502 38.8 - 33.6 59.4 7 Iida et al. [20] 2001 Nigeria 206 35 - 60 25.7 14.3 Olasoji Iran et al. [21] 2002
Iran 237 54 - 57 43 0 Motamedi [22] 2003 Brazil 1024 29.9 - 46.7 40.5 12.8 Brasileiro and Passeri [23] 2006
India 2748 85 4.5:1 73.3 26.7 0 Brasileiro and Passeri [23] 2007 Japan 674 20 - 23.7 65.9 10.4 Sasaki et al. [25] 2009
India 111 74.7 - 74.6 25.4 0 Kamath et al. [26] 2012 India 503 80.3 6.6:1 17 76 3 Kar and Mahavoi [27] 2012
The Netherlands 579 35.2 2.2:1 40 53.3 6.7 Van den Bergh et al. [28] 2012 Greece 727 50.8 5.8:1 36.6 56.1 7.3 Kostakis et al. [29] 2012
Ireland 82 11 2.6:1 94 3 3 Walker et al. [30] 2012 India 740 72 - 5.3 92.1 2.6 Bali et al. [31] 2013
China 1131 46.7 - 66.1 33.9 0 Zhou et al. [32] 2013
RTA: road traffic accidents. Bold character indicate the most frequent category for each author. Table 2.2. Characteristics of fractures in MVA-related trauma patients: review of epidemiological studies
Fractures Author Year Lower third (%) Middle third (%) Upper third (%) Combined (%) 54 32 - 14 Iida et al. [20] 2001
41 56 3 - Buchanan et al. [33 2005
22 70 8 - Erdmann et al. [34] 2008
50 15 4 31 Chalya et al. [35] 2011
41 59 - - Gandhi et al. [36] 2011
72 22 - 6 Mesgarzadeh et al. [37] 2011
50 47 3 - Kostakis et al .[29] 2012
38 48 - 24 Naveen Shankar et al. [38] 2012
69 31 - - Bali et al. [31] 2013
29 63 8 - Mijiti et al. [39] 2014
14
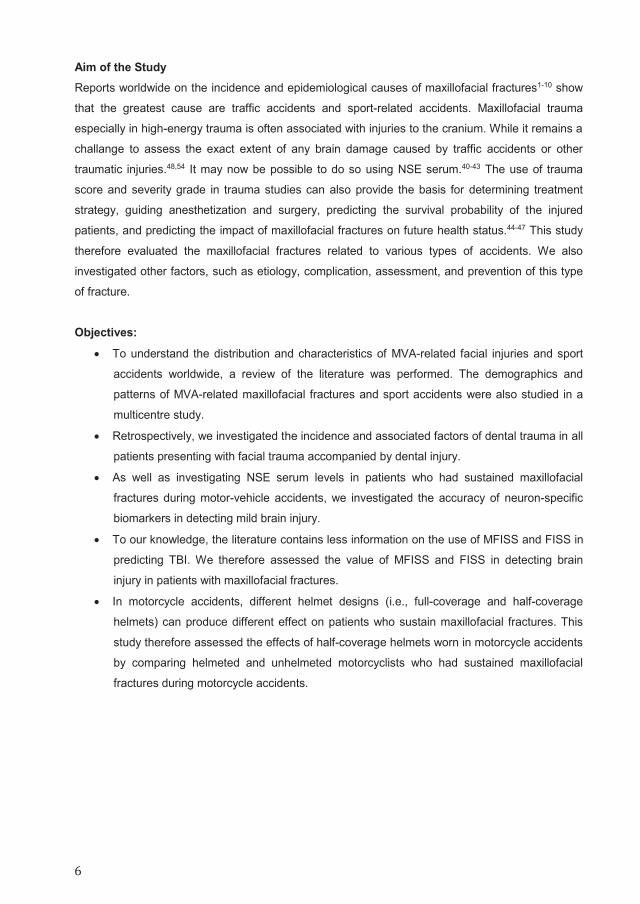
The percentage of MVA as etiological factors in epidemiological studies on maxillofacial injuries
ranged between 11%30 to 85%.24 On the whole, a progressively decreasing trend was observed,
particularly in North America, Brazil, and Europe. Data regarding male:female ratio were extremely
different too, with results between 2.2:1 and 20.9:1.
The percentages of the categories of MVAs (car, motorcycle and pedestrian) showed a
progressive trend all over the world: the incidence of maxillofacial injuries due to car accidents is
decreasing, whereas a continuous increase in motorcycle related facial injuries has been observed
in Asia (Japan, India) and Europe (The Netherlands, Greece). A further observed result was the
progressive decrease of incidence of facial injuries suffered by pedestrians in the last 30 years
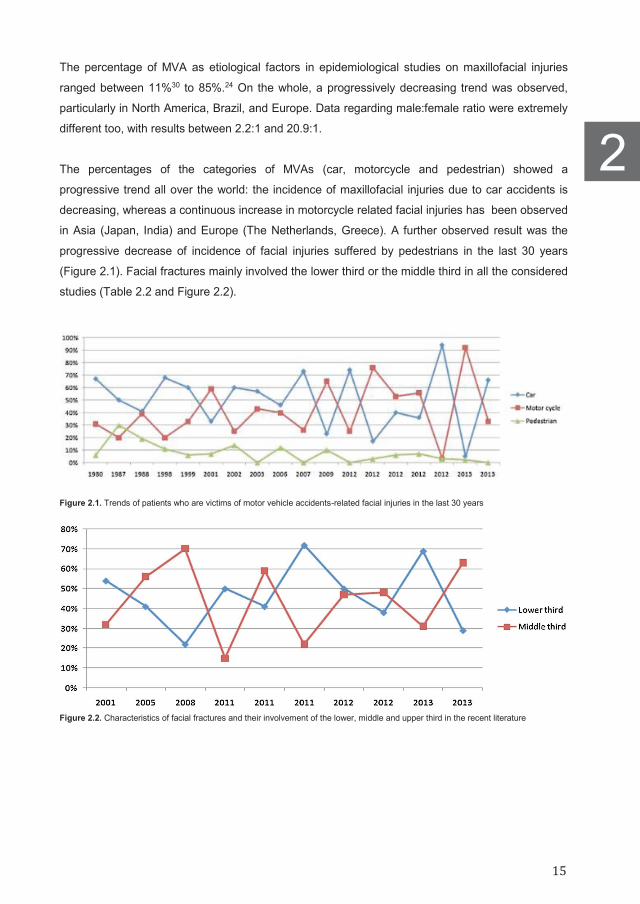
(Figure 2.1). Facial fractures mainly involved the lower third or the middle third in all the considered
studies (Table 2.2 and Figure 2.2).
Figure 2.1. Trends of patients who are victims of motor vehicle accidents-related facial injuries in the last 30 years
Figure 2.2. Characteristics of facial fractures and their involvement of the lower, middle and upper third in the recent literature
2
15
2
Discussion
Motor vehicle accidents are still one of the most important etiological factors for maxillofacial
injuries. Nowadays, their incidence widely varies, as various factors are involved in the prevention
of such accidents. In particular, not only road conditions, speed limits, and safety equipment, but
also the characteristics of used vehicles, socioeconomic conditions and regulations about alcohol
drinking before driving are fundamental for the prevalence of such injuries.
In the recent literature, a great difference in the incidence of MVA-related facial fractures between
developed countries (20% in Japan, 35.2% in the Netherlands, 11% in Ireland) and developing
countries (72–85% in India, 46.7% in China) can be easily observed. Of course, those data cannot
be really compared because of the aforementioned differences in regulations and their
implementations.
The etiology of MVA gives us important information, in particular regarding the progressive
decrease of pedestrians suffering from MVA-related injuries. This may be the first result of the
establishment and enforcement of more severe laws and regulations with regard to alcohol drinking
and speed limits. Unfortunately, there are too many variables to draw any conclusion about car and
motorcycle accidents.
However, for car accidents, detailed examinations for neck lesions are suggested for the patients
involved in MVAs. The decrease of the severity or incidence of head, chest, and abdominal injuries
of the vehicle occupants thanks to seat belt use is still controversial, whereas front seat
passengers are likely to suffer from less severe head or neck injuries than drivers because of the
absence of a steering wheel. Of course, it seems that although wearing a seat belt is effective for
preventing fatalities and generally decreasing the severity of injuries to the head or neck and to the
trunk, it cannot prevent all oral and maxillofacial injuries in motor vehicle occupants.1
Anyway, some authors confirmed that wearing a seat belt pre-vents the free flight of drivers within
the vehicle and contact with the interior of the vehicle (other than the steering wheel).8,9
Furthermore, airbags protect motor vehicle passengers by providing a cushioning barrier between
them and the vehicle’s interior hard surfaces, thus making the benefits of an airbag in decreasing
drivers’ fatality well recognized.8,9 Occupants of motor vehicles should heed the ubiquitous
message that proper seat belt use not only is a highly effective means to reduce the risk of injury in
general but also specifically reduces the risk of facial injury.8,9
As for motorcycle accidents, the crucial role of helmets has to be acknowledged. Three types of
helmets can be used: fixed full-face, articulated full-face, and open-face. Not only people who do
not wear helmets are 3–4 times more likely to sustain a head injury than those who do, but full-face
helmets in particular seem to bemostly effective in protecting the face.7,10 Studies on the wearing of
helmets by motorcyclists in urban areas have highlighted two main points: the effectiveness of laws
aimed at increasing their use and the protection provided against brain injuries and death.7,11
16

Legislations making helmet use compulsory for all motorcyclists are crucial to reduce the incidence
of facial injuries in this category.
As aforementioned in previous articles, it is demonstrated that motorcycle accidents in 100% of
the patients cause severe traumatic brain injury, followed by moped/scooter accidents (63.3%).
This may be due to the high velocity achieved by motorcycles in conjunction with the
inconvenience of wearing helmets, making them more vulnerable in traffic. Instead, car accidents
account for only 50% of the patients in the severe traumatic brain injury cases and furthermore for
only 16.7% of the patients in the mild cases. This is probably due to compulsory wearing of seat
belts and aggressive enforcement of “drinking and driving” laws.12,13
Finally, pedestrians are a peculiar category of patients involved in MVAs. Maxillofacial fractures are
not frequently seen in pedestrians injured in motor vehicle accidents. Injuries to the head,
shoulder/clavicle, and chest/ribs are observed frequently.1 Most pedestrians patients are children or
old persons. This epidemiology may be partly related to the fact that the ability of a pedestrian to
avoid a collision with a motor vehicle, or not to be injured seriously even if involved in an accident,
is quite different from age to age. The youngest patients may not pay attention to the dangers on
the street, whereas older pedestrians might not have high motor ability or reflexes due to the
physiological consequences of aging and the presence of systemic pathological conditions.1
In view of the overall cost of care to the society, emphasis should be placed on prevention of road
traffic accidents. The public should be adequately informed on the usage of seat belt and helmet,
and laws concerning speed limit and alcohol drinking.6
Alcohol initially leads to a reduction in attentiveness, a false perception of velocity, euphoria, and
difficulty in spatially discerning different light intensities. At higher concentrations, it determines
slow reaction times and sleepiness, a reduction in peripheral vision and poor performance in
routine activities, thus making alcohol drinking before driving a serious danger. Therefore, in
several countries the penalty for driving under the influence of alcohol has been increased, and
drivers who operate motor vehicles with high blood alcohol levels are criminalized.14
Conclusion Improving our understanding of the mechanisms of facial injuries in motor vehicle accidents can be
crucial for the adoption of new methods for preventing injuries, thus decreasing the associated
socioeconomic costs of these individuals. However, although fully restrained vehicle occupants are
less likely to sustain severe injuries, it may not be possible to entirely prevent maxillofacial injuries.
Further, multicentre studies with the assessment of the results of laws enforcement and
implementation are needed to clarify their efficacy for maxillofacial injury prevention.
2
17
2
References
1. Yamamoto K, Matsusue Y, Horita S, Murakami K, Ueyama Y, Sugiura T, Kirita T. Maxillofacial fractures of pedestrians injured in a
motor vehicle accident. Craniomaxillofac Trauma Reconstr 2013;6(1):37–42.
2. Boffano P, Kommers SC, Karagozoglu KH, Forouzanfar T. Aetiology of maxillo-facial fractures: a review of published studies during the last 30 years. Br J Oral Maxillofac Surg 2014;52(10):901–906.
3. Kommers SC, van den Bergh B, Boffano P, Verweij KP, Forouzanfar T. Dysocclusion after maxillofacial trauma: a 42 year analysis. J Craniomaxillofac Surg 2014;42(7):1083–1086.
4. Boffano P, Roccia F, Gallesio C, Karagozoglu KH, Forouzanfar T. Diplopia and orbital wall fractures. J Craniofac Surg 2014;25(2): e183–e185.
5. Boffano P, Roccia F, Gallesio C, Karagozoglu KH, Forouzanfar T. Bicycle-related maxillofacial injuries: a double-center study. Oral Surg Oral Med Oral Pathol Oral Radiol 2013;116(3):275–280.
6. Fasola AO, Lawoyin JO, Obiechina AE, Arotiba JT. Inner city maxillo-facial fractures due to road traffic accidents. Dent Traumatol 2003;19(1):2–5.
7. Cini MA, Prado BG, Hinnig Pde F, Fukushima WY, Adami F. Influence of type of helmet on facial trauma in motorcycle accidents. Br J Oral Maxillofac Surg 2014;52(9):789–792.
8. Hitosugi M, Mizuno K, Nagai T, Tokudome S. Analysis of maxillofacial injuries of vehicle passengers involved in frontal collisions. J Oral Maxillofac Surg 2011;69(4):1146–1151.
9. Cox D, Vincent DG, McGwin G, MacLennan PA, Holmes JD, Rue 3rd LW. Effect of restraint systems on maxillofacial injury in frontal motor vehicle collisions. J Oral Maxillofac Surg 2004;62(5):571–575.
10. Ramli R, Abdul Rahman R, Abdul Rahman N, Abdul Karim F, Krsna Rajandram R, Mohamad MS, Mat Nor G, Sohadi RU. Pattern of maxillofacial injuries in motorcyclists in Malaysia. J Craniofac Surg 2008;19(2):316–321.
11. Norvell DC, Cummings P. Association of helmet use with death in motor-cycle crashes: a matched-pair cohort study. Am J Epidemiol 2002;156(5):483–487.
12. Salentijn EG, Collin JD, Boffano P, Forouzanfar T. A ten year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: complications and treatment. J Craniomaxillofac Surg 2014;42(8):1717–1722.
13. Salentijn EG, Peerdeman SM, Boffano P, van den Bergh B, Forouzanfar T. A ten-year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: incidence and aetiology. J Craniomaxillofac Surg 2014;42(6):705–710.
14. Nóbrega LM, Cavalcante GM, Lima MM, Madruga RC, Ramos-Jorge ML, d’Avila S. Prevalence of facial trauma and associated factors in victims of road traffic accidents. Am J Emerg Med 2014;32(11):1382–1386.
15. Adekeye EO. The pattern of fractures of the facial skeleton in Kaduna, Nigeria. A survey of 1,447 cases. Oral Surg Oral Med Oral Pathol 1980;49(6):491–495.
16. Karyouti SM. Maxillofacial injuries at Jordan University Hospital. Int J Oral Maxillofac Surg 1987;16(3):262–265.
17. Sawhney CP, Ahuja RB. Faciomaxillary fractures in north India. A statistical analysis and review of management. Br J Oral Maxillofac Surg 1988;26(5):430–434.
18. Ugboko VI, Odusanya SA, Fagade OO. Maxillofacial fractures in a semi-urban Nigerian teaching hospital. A review of 442 cases. Int J Oral Maxillofac Surg 1998;27(4):286–289.
19. van Beek GJ, Merkx CA. Changes in the pattern of fractures of the maxillofacial skeleton. Int J Oral Maxillofac Surg 1999;28(6):424–428.
20. Iida S, Kogo M, Sugiura T, Mima T, Matsuya T. Retrospective analysis of 1502 patients with facial fractures. Int J Oral Maxillofac Surg 2001;30(4):286–290.
21. Olasoji HO, Tahir A, Arotiba GT. Changing picture of facial fractures in northern Nigeria. Br J Oral Maxillofac Surg 2002;40(2):140–143.
22. Motamedi MH. An assessment of maxillofacial fractures: a 5-year study of 237 patients. J Oral Maxillofac Surg 2003;61(1):61–64.
23. Brasileiro BF, Passeri LA. Epidemiological analysis of maxillofacial fractures in Brazil: a 5-year prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;102(1):28–34.
24. Subhashraj K, Nandakumar N, Ravindran C. Review of maxillofacial injuries in Chennai, India: a study of 2748 cases. Br J Oral Maxillofac Surg 2007;45(8):637–639.
25. Sasaki R, Ogiuchi H, Kumasaka A, Ando T, Nakamura K, Ueki T, Okada Y, Asanami S, Chigono Y, Ichinokawa Y, Satomi T, Matsuo A, Chiba H. Analysis of the pattern of maxillofacial fracture by five departments in Tokyo: a review of 674 cases. Oral Sci Int 2009;6(1):1–7.
26. Kamath RA, Bharani S, Hammannavar R, Ingle SP, Shah AG. Maxillofacial trauma in central Karnataka, India: an outcome of 95 cases in a regional trauma care centre. Craniomaxillofac Trauma Reconstr 2012;5(4):197–204.
27. Kar IB, Mahavoi BR. Retrospective analysis of 503 maxillo-facial trauma cases in Odisha during the period of Dec’04-Nov’09. J Maxillofac Oral Surg 2012;11(2):177–181.
28. van den Bergh B, Karagozoglu KH, Heymans MW, Forouzanfar T. Aetiology and incidence of maxillofacial trauma in Amsterdam: a retrospective analysis of 579 patients. J Craniomaxillofac Surg 2012;40(6):e165–e169.
18

29. Kostakis G, Stathopoulos P, Dais P, Gkinis G, Igoumenakis D, Mezitis M, Rallis G. An epidemiologic analysis of 1,142 maxillofacial fractures and concomitant injuries. Oral Surg Oral Med Oral Pathol Oral Radiol 2012;114(5 Suppl):S69–S73.
30. Walker TW, Donnellan J, Byrne S, McArdle N, Kerin MJ, McCann PJ. West of Ireland facial injury study. Part 2. Br J Oral Maxillofac Surg 2012;50(7):e99–e103.
31. Bali R, Sharma P, Garg A, Dhillon G.A comprehensive study on maxillofacial trauma conducted in Yamunanagar, India. J Inj Violence Res 2013;5(2):108–116.
32. Zhou HH, Ongodia D, Liu Q, Yang RT, Li ZB. Changing pattern in the characteristics of maxillofacial fractures. J Craniofac Surg 2013;24(3):929–933.
33. Buchanan J, Colquhoun A, Friedlander L, Evans S, Whitley B, Thomson M. Maxillofacial fractures at Waikato Hospital, New Zealand: 1989 to 2000. N Z Med J 2005;118(1217):U1529.
34. Erdmann D, Follmar KE, Debruijn M, Bruno AD, Jung SH, Edelman D, Mukundan S, Marcus JR. A retrospective analysis of facial fracture etiologies. Ann Plast Surg 2008;60(4):398–403.
35. Chalya PL, McHembe M, Mabula JB, Kanumba ES, Gilyoma JM. Etiological spectrum, injury characteristics and treatment outcome of maxillofacial injuries in a Tanzanian teaching hospital. J Trauma Manag Outcomes 2011;5(7):1–6.
36. Gandhi S, Ranganathan LK, Solanki M, Mathew GC, Singh I, Bither S. Pattern of maxillofacial fractures at a tertiary hospital in northern India: a 4-year retrospective study of 718 patients. Dent Traumatol 2011;27(4):257–262.
37. Mesgarzadeh AH, Shahamfar M, Azar SF, Shahamfar J. Analysis of the pattern of maxillofacial fractures in north western of Iran: a retrospective study. J Emerg Trauma Shock 2011;4(1):48–52.
38. Naveen Shankar A, Naveen Shankar V, Hegde N, Sharma, Prasad R. The pattern of the maxillofacial fractures - A multicentre retrospective study. J Craniomaxillofac Surg 2012;40(8):675–679.
39. Mijiti A, Ling W, Tuerdi M, Maimaiti A, Tuerxun J, Tao YZ, Saimaiti A, Morning A. Epidemiological analysis of maxillofacial fractures treated at a university hospital, Xinjiang, China: a 5-year retrospective study. J Craniomaxillofac Surg 2014;42(3):227–233.
40. Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, Kovačič Ž, Vesnaver A, Konstantinović VS, Petrović M, Stephens J, Kanzaria A, Bhatti N, Holmes S, Pechalova PF, Bakardjiev AG, Malanchuk VA, Kopchak AV, Galteland P, Mjøen E, Skjelbred P, Grimaud F, Fauvel F, Longis J, Corre P, Løes S, Lekven N, Laverick S, Gordon P, Tamme T, Akermann S, Karagozoglu KH, Kommers SC, Meijer B, Forouzanfar T. European Maxillofacial Trauma (EURMAT) in children: a multicenter and prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol 2015;119(5):499–504.
41. Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, Kovačič Ž, Vesnaver A, Konstantinović VS, Petrović M, Stephens J, Kanzaria A, Bhatti N, Holmes S, Pechalova PF, Bakardjiev AG, Malanchuk VA, Kopchak AV, Galteland P, Mjøen E, Skjelbred P, Bertin H, Marion F, Guiol J, Corre P, Løes S, Lekven N, Laverick S, Gordon P, Tamme T, Akermann S, Karagozoglu KH, Kommers SC, Forouzanfar T. Assault-related maxillofacial injuries: the results from the European Maxillofacial Trauma (EURMAT) multicenter and prospective collaboration. Oral Surg Oral Med Oral Pathol Oral Radiol 2015;119(4):385–391.
42. Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, Kovačič Ž, Vesnaver A, Konstantinović VS, Petrović M, Stephens J, Kanzaria A, Bhatti N, Holmes S, Pechalova PF, Bakardjiev AG, Malanchuk VA, Kopchak AV, Galteland P, Mjøen E, Skjelbred P, Koudougou C, Mouallem G, Corre P, Løes S, Lekven N, Laverick S, Gordon P, Tamme T, Akermann S, Karagozoglu KH, Kommers SC, Forouzanfar T. European Maxillofacial Trauma (EURMAT) project: a multicentre and prospective study. J Craniomaxillofac Surg 2015;43(1):62–70.
2
19
2

20

Chapter 3
Motor-vehicle accidents related
maxillofacial injuries: A multicenter and
prospective study
This is an edited version of the manuscript:
Muhammad Ruslin, Matteo Brucoli, Paolo Boffano, Arnaldo Benech, Jan Wolff, Emil Dediol, Vedran Uglešić, Žiga
Kovačič, Aleš Vesnaver, Vitomir S. Konstantinović, Milan Petrović, Jonny Stephens, Amar Kanzaria, Nabeel Bhatti,
Simon Holmes, Petia F. Pechalova, Angel G. Bakardjiev, Vladislav A. Malanchuk, Andrey V. Kopchak, Pål Galteland,
Even Mjøen, Per Skjelbred, Helios Bertin, F Marion, Julien Guiol, Pierre Corre, Sigbjørn Løes, Njål Lekven, Sean
Laverick, Peter Gordon, Tiia Tamme, Stephanie Akermann, K Hakki Karagozoglu, Sofie C. Kommers, Jan G. deVisscher,
Tymour Forouzanfar
Motor-vehicle accidents related maxillofacial injuries: A multicenter and prospective study.
Accepted for Publication

Abstract Introduction:
Facial injuries, including fractures, may have serious long-term implications for victims of motor
vehicle accidents (MVA) and important socio economic consequences. Preventing maxillofacial
injuries is a valuable pursuit for improving the quality of life of the involved subjects and decreasing
the socioeconomic costs of motor vehicle collision injuries. The purpose of this study is to present
and discuss the demographics and patterns of MVA-related maxillofacial fractures of a multicenter
study.
Methods:
This study is based on a systematic computer-assisted database that allowed to prospectively and
continuously record all patients hospitalized with maxillofacial fractures in the involved Maxillofacial
Surgery Units across Europe, since Monday 31st December 2012 to Sunday 29th December 2013.
Therefore, the following data were recorded for each patient: gender, age, etiology, etiology
mechanisms, site of facial fractures, Facial Injury Severity Score (FISS), date of injury. For this
study, only patients that were admitted to the hospital for MVA related maxillofacial injury were
considered.
Results:
Of the 3260 patients with maxillofacial fractures admitted within the study period, 326 traumas were
due to motor vehicle accidents with a male to female ratio of 2.2:1. The maximum incidence was
encountered in Zagreb (Croatia) (18%) and the minimum value was observed in Bergen (Norway)
(0%). The most frequent mechanisms were car accidents with 177 cases, followed by motorcycles.
The most frequently observed fracture involved the mandible with 199 fractures, followed by
maxilla-zygomatic-orbital (MZO) fractures. In all the three groups mandibular and MZO fractures
are the two most frequently observed fractures with some variations.
Conclusion:
The importance of the perseverance in analyzing MVA related facial injuries with their features and
characteristics should be stressed, as they may help to establish prevention strategies and
suggestions for all involved countries.
22
Introduction Injuries associated with traffic accidents are a problem faced in several countries, and their
prevention is often a priority for public health authorities.1-18 In fact, facial injuries, including
fractures, may have serious long term implications for victims of motor vehicle accidents (MVA) and
important socio economic consequences.1-8 Thus, the knowledge of the factors associated with
facial injuries stemming from MVAs is important for the prognosis, the identification of groups at
risk, and the establishment of measures to minimize the economic, emotional, psychological, and
social impacts of these events.1-8
Preventing maxillofacial injuries is a valuable pursuit for improving the quality of life of the involved
subjects and decreasing the socioeconomic costs of motor vehicle collision injuries.1-14 Several
studies in the literature have described the frequency and severity of facial injuries associated with
motor vehicle accidents. However, to our knowledge, no prospective multicentre study about MVA-
related maxillofacial injuries has been published. Therefore, several European centers, that had
already shown research experience in maxillofacial trauma.15-17 decided to collaborate to start a
prospective multicentre study about facial fracture epidemiology in Europe.
The purpose of this study is to present and discuss the demographics and patterns of MVA-related
maxillofacial fractures of a European multicenter prospective study about the epidemiology of facial
trauma during a year.
Material and Methods The present study was conducted at several European departments of oral and maxillofacial
surgery: the Department of Oral and Maxillofacial Surgery/Pathology at the VU Medical Center and
Academic Centre for Dentistry Amsterdam (Amsterdam, The Netherlands), the Department of
Maxillofacial Surgery at the University Hospital Dubrava (Zagreb, Croatia), the Maxilofacial
department at the UKC Ljubljana, (Ljubljana, Slovenia), the Clinic of Maxillofacial Surgery of the
School of Dentistry at the University of Belgrade (Belgrade, Serbia), the Department of Oral and
Maxillofacial Surgery of the Royal London Hospital at Barts Health NHS (London, UK), the
Department of maxilla-facial surgery at the Medical University (Plovdiv, Bulgaria), the Department
for Oral and Maxillofacial Surgery at the Bogomolets National Medical University (Kiev, Ukraine),
the Department of Maxillofacial Surgery at the Oslo University Hospital (Oslo, Norway), the Service
3
23
3

de Stomatologie et Chirurgie Maxillo-faciale at the Chu de Nantes (Nantes, France), the
Department of Maxillofacial Surgery at the University of Bergen (Bergen, Norway), the Department
of Oral and Maxillofacial Surgery at NHS Tayside and University of Dundee, (Dundee, UK), and the
Department of Maxillofacial surgery, Stomatology Clinic, Tartu University (Tartu, Estonia).
This study is based on a systematic computer-assisted database that allowed to prospectively and
continuously record all patients hospitalized with maxillofacial fractures in the involved Maxillofacial
Surgery Units across Europe, since Monday 31st December 2012 to Sunday 29th December 2013.
Therefore, the following data were recorded for each patient: gender, age, etiology, etiology
mechanisms, site of facial fractures, Facial Injury Severity Scale (FISS), date of injury. For this
study, only patients that were admitted to the hospital for MVA-related maxillofacial injury were
considered.
MVA-related injuries were analyzed and divided according to the type of injury: car accident,
motorcycle accidents, pedestrian hitten, unknown/other. Bicycle accidents were excluded.
Fractures were determined from a combination of physical examination and imaging (computed
tomography scans or conventional radiographs) at admission to hospital and classified in fractures
of the mandible, orbito-zygomatic-maxillary complex (OZM), orbit, nose, Le Fort, frontal sinus, and
naso-orbital-ethmoidal (NOE) fracture. Orbital fractures were subclassified according to the
involved walls and Le Fort fractures were divided according to Le Fort I, II, and III types. Frontal
sinus fractures were divided according to the involvement of the anterior and/or posterior tables.
Mandibular fractures included fractures of the symphysis, body, angle, ramus, coronoid, extra-
articular condyle, intra-articular condyle.
Associated injuries were classified as orthopedic, brain, abdominal, or thoracic. Patient
characteristics were analyzed using descriptive statistics. This study was exempt from institutional
review board approval as a chart review. We followed Helsinki Declaration guidelines.
Results
Of the 3260 patients with maxillofacial fractures admitted within the study period, 326 traumas were
due to motor vehicle accidents. Of course, in the different centers and countries the incidence of
MVA-related maxillofacial trauma varied, with the maximum value that was encountered in the
Zagreb (Croatia) center study population (39 patients, 18%) and the minimum value that was
observed in Bergen (Norway) (0 patients, 0%).
On the whole, 225 patients were male and 101 were female, with a male to female ratio of 2.2:1.
Mean age was 36.2 years.
Alcohol consumption was reported by 59 patients, whereas drugs use was noted in 4 cases.
24

The most frequent mechanisms of MVA related maxillofacial injury were car accidents with 177
cases, followed by motorcycles (91 patients), pedestrian hitten (33 cases), and other/unknown
mechanisms (25 patients). This result was quite uniformly observed in all centers, as showed in
Figure 3.1.
Figure 3.1. Percentages of mechanisms of MVA-related maxillofacial injury in the EURMAT centers. (BG, Bulgaria; EST, Estonia; F, France; HR, Croatia; N1, Oslo-Norway; N2, Bergen-Norway; NL, The Netherlands; SLO, Slovenia; SRB, Serbia; UA, Ukraine; UK1, London-England, United Kingdom; UK2, Dundee-Scotland, United Kingdom)
The most frequently observed fracture involved the mandible with 199 fractures, followed by
maxilla-zygomatic-orbital (MZO) fractures (136), orbital fractures (36), Le Fort fractures (32), nose
fractures (16 fractures), frontal sinus fractures (15), and NOE fractures (8).
FISS mean score in the whole study population was 2.39 (range, 1 – 12; median, 2; standard
deviation, 1.99). In the “car accident” group mean FISS was 2.54, in the “motorcycle” group the
observed mean FISS was 2.47, and in the “pedestrian” group, the mean value of FISS was 1.6.
Figure 3.2 shows the differences in fractures distribution according to the three etiological
categories.
3
25
3

Figure 3.2. Fractures distribution according to the three etiological categories
In all the three groups mandibular and MZO fractures are the two most frequently observed
fractures with some variations: in the car and motorcycle groups mandibular fractures are the main
site of injury, whereas in pedestrian MZO fractures are the most frequently observed fractures.
As for associated body injuries, brain and orthopedic lesions are the most frequently observed in all
the three groups, as shown by Figure 3.3.
Figure 3.3. Associated body injuries according to the three etiological categories
A peak of traumatic brain injuries has been observed in motorcycle accidents, whereas the peak of
orthopedic lesions was encountered in the car study population.
Finally, the analysis of the dates of injury showed that the summer months of July and August, as
well as November and December, present the highest incidence of MVA related maxillofacial
26
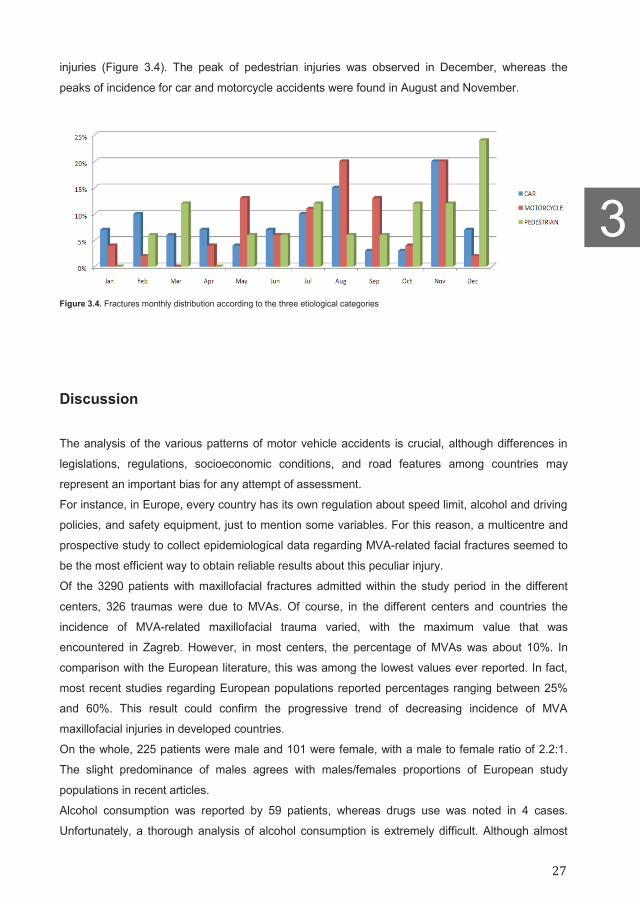
injuries (Figure 3.4). The peak of pedestrian injuries was observed in December, whereas the
peaks of incidence for car and motorcycle accidents were found in August and November.
Figure 3.4. Fractures monthly distribution according to the three etiological categories
Discussion
The analysis of the various patterns of motor vehicle accidents is crucial, although differences in
legislations, regulations, socioeconomic conditions, and road features among countries may
represent an important bias for any attempt of assessment.
For instance, in Europe, every country has its own regulation about speed limit, alcohol and driving
policies, and safety equipment, just to mention some variables. For this reason, a multicentre and
prospective study to collect epidemiological data regarding MVA-related facial fractures seemed to
be the most efficient way to obtain reliable results about this peculiar injury.
Of the 3290 patients with maxillofacial fractures admitted within the study period in the different
centers, 326 traumas were due to MVAs. Of course, in the different centers and countries the
incidence of MVA-related maxillofacial trauma varied, with the maximum value that was
encountered in Zagreb. However, in most centers, the percentage of MVAs was about 10%. In
comparison with the European literature, this was among the lowest values ever reported. In fact,
most recent studies regarding European populations reported percentages ranging between 25%
and 60%. This result could confirm the progressive trend of decreasing incidence of MVA
maxillofacial injuries in developed countries.
On the whole, 225 patients were male and 101 were female, with a male to female ratio of 2.2:1.
The slight predominance of males agrees with males/females proportions of European study
populations in recent articles.
Alcohol consumption was reported by 59 patients, whereas drugs use was noted in 4 cases.
Unfortunately, a thorough analysis of alcohol consumption is extremely difficult. Although almost
3
27
3

20% of patients’ victims of MVAs referred alcohol consumption, a strict and precise knowledge of
quantity, and type of alcohol beverages would be crucial. This kind of analysis would be extremely
difficult because several factors should be kept in mind, such as the little collaboration of some
patients in speaking about their usual alcohol consumption and the different laws about this topic.
The most frequent mechanisms of MVA-related maxillofacial injury were car accidents with 177
cases, followed by motorcycles (91 patients), pedestrian hitten (33 cases), and other/unknown
mechanisms (25 patients) (Figure 3.1). This result was quite uniformly observed in all centers, as
showed in Figure 3.2. In this article, bicycle accidents were excluded because they were
characterized by specific features and populations.
The most frequently observed fracture involved the mandible with 199 fractures, followed by MZO
fractures (136), orbital fractures (36), Le Fort fractures (32), nose fractures (16 fractures), frontal
sinus fractures (15), and NOE fractures (8) (Figure 3.2).
FISS mean score in the whole study population was 2.39. In the “car accident” group mean FISS
was 2.54, in the “motorcycle” group the observed mean FISS was 2.47, and in the “pedestrian”
group, the mean value of FISS was 1.6. Therefore, cars and motorcycles accidents seemed to
determine more severe injuries than “pedestrian accidents”. The reason could be the different
mechanism of this last type of injury: probably, the most severe impacts to pedestrian may easily
determine fatal outcomes, thus causing an underreporting of facial injuries in these patients.
Figure 3.2 shows the differences in fractures distribution according to the three etiological
categories. In all the three groups mandibular and MZO fractures are the two most frequently
observed fractures with just slight variations: in the car and motorcycle groups mandibular fractures
are the main site of injury, whereas in pedestrian MZO fractures are the most frequently observed
fractures.
Of course, further studies about safety equipment (seat belts, airbags, helmet) and their protective
effect against MVA-related facial injuries are needed, in spite of the challenge of such enquiry.10-14
As for associated body injuries, traumatic brain and orthopedic lesions are the most frequently
observed in all the three groups, as shown by Figure 3.3. A peak of traumatic brain injuries has
been observed in motorcycle accidents, whereas the peak of orthopedic lesions was encountered
in the car study population. The highest incidence of traumatic brain injuries associated with
motorcycle accidents was expected, due to the high velocity achieved by motorcycles in
conjunction with the lack of protection in comparison with cars. In spite of the inconvenience of
wearing helmets, the compulsory wearing of such protective equipment remains the only defense
for such severe injuries.10-14
Finally, the analysis of the dates of injury showed that the summer months of July and August, as
well as November and December, present the highest incidence of MVA-related maxillofacial
injuries (Figure 3.4). The peak of pedestrian injuries was observed in December, whereas the
peaks of incidence for car and motorcycle accidents were found in August and November. This
monthly distribution of MVA-related facial injuries confirms the acknowledged trend of maxillofacial
28

trauma that focuses in summer and winter seasons. In fact, in summer an increased use of
vehicles is frequently observed because of school holidays and better weather conditions, whereas
in winter months the more critical road conditions may facilitate MVAs because of precipitations.
Conclusion
This European multicenter study about MVA-related maxillofacial injury may represent another
important stand in our increasing understanding of vehicle accidents and their consequences. The
importance of the perseverance in analyzing MVA related facial injuries with their features and
characteristics should be stressed, as they may help to establish prevention strategies and
suggestions for all involved countries. Further prospective studies about alcohol consumption and
driving, as well as about safety equipment could be fundamental to appropriately assess this
socially important phenomenon.
3
29
3

References 1. Cini MA, Prado BG, Hinnig Pde F, Fukushima WY, Adami F. Influence of type of helmet on facial trauma in motorcycle accidents. Br
J Oral Maxillofac Surg 2014;52(9):789–792.
2. Cox D, Vincent DG, McGwin G, MacLennan PA, Holmes JD, Rue LW 3rd. Effect of restraint systems on maxillofacial injury in frontal motor vehicle collisions. J Oral Maxillofac Surg 2004;62(5):571–575.
3.
4. Fasola AO, Lawoyin JO, Obiechina AE, Arotiba JT. Inner city maxillofacial fractures due to road traffic accidents. Dent Traumatol 2003;19(1):2–5.
5. Hitosugi M, Mizuno K, Nagai T, Tokudome S. Analysis of maxillofacial injuries of vehicle passengers involved in frontal collisions. J Oral Maxillofac Surg 2011;69(4):114–651.
6. Iida S, Kogo M, Sugiura T, Mima T, Matsuya T. Retrospective analysis of 1502 patients with facial fractures. Int J Oral Maxillofac Surg 2001;30(4):286–290.
7. Lehto KS, Sulander PO, Tervo TM. Do motor vehicle airbags increase risk of ocular injuries in adults? Ophthalmology 2003;110(6): 1082–1088.
8. Nóbrega LM, Cavalcante GMS, Lima MMSM, Madruga RCR, Ramos-Jorge ML, d’Avila S. Prevalence of facial trauma and associated factors in victims of road traffic accidents. Am J Emerg Med 2014;32(11):1382–1386.
9. Oginni FO, Ugboko VI, Ogundipe O, Adegbehingbe BO. Motorcycle-related maxillofacial injuries among Nigerian intracity road users. J Oral Maxillofac Surg 2006;64(1):56–62.
10. Ramli R, Abdul Rahman R, Abdul Rahman N, Abdul Karim F. Krsna Rajandram R, Mohamad MS, Mat Nor G, Sohadi RU. Pattern of maxillofacial injuries in motorcyclists in Malaysia. J Craniofac Surg 2008;19(2):316–321.
11. Yamamoto K, Matsusue Y, Horita S, Murakami K, Ueyama Y, Sugiura T, Kirita T. Maxillofacial fractures of pedestrians injured in a motor vehicle accident. Craniomaxillofac Trauma Reconstr 2013;6(1):37–42.
12. Yokoyama T, Motozawa Y, Sasaki T, Hitosugi M. A retrospective analysis of oral and maxillofacial injuries in motor vehicle accidents. J Oral Maxillofac Surg 2006;64(12):1731–1735.
13. Salentijn EG, Peerdeman SM, Boffano P, van den Bergh B, Forouzanfar T. A ten-year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: incidence and aetiology. J Craniomaxillofac Surg 2014;42(6):705–710.
14. Salentijn EG, Collin JD, Boffano P, Forouzanfar T. A ten year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: Complications and treatment. J Craniomaxillofac Surg 2014;42(8):1717–1722.
15. Boffano P, Kommers SC, Karagozoglu KH, Forouzanfar T. Aetiology of maxillofacial fractures: a review of published studies during the last 30 years. Br J Oral Maxillofac Surg 2014;52(10):901–906.
16. Giarda M, Tavolaccini A, Arcuri F, Brucoli M, Benech A. Surgical approach to isolated bilateral orbital floor fractures. Acta Otorhinolaryngol Ital 2015;35(5):362–364.
17. Benech A, Nicolotti M, Brucoli M, Arcuri F. Intraoral extra-mucosal fixation of fractures in the atrophic edentulous mandible. Int J Oral Maxillofac Surg 2013;42(4):460–463.
18. Arcuri F, Brucoli M, Baragiotta N, Benech R, Ferrero S, Benech A. Analysis of complications following endoscopically assisted treatment of mandibular condylar fractures. J Craniofac Surg 2012;23(3):e196–e198.
19. Brucoli M, Arcuri F, Cavenaghi R, Benech A. Analysis of complications after surgical repair of orbital fractures. J Craniofac Surg 2011;22(4):1387–1390
References 1. Cini MA, Prado BG, Hinnig Pde F, Fukushima WY, Adami F. Influence of type of helmet on facial trauma in motorcycle accidents. Br
J Oral Maxillofac Surg 2014;52(9):789–792.
2. Cox D, Vincent DG, McGwin G, MacLennan PA, Holmes JD, Rue LW 3rd. Effect of restraint systems on maxillofacial injury in frontal motor vehicle collisions. J Oral Maxillofac Surg 2004;62(5):571–575.
3.
4. Fasola AO, Lawoyin JO, Obiechina AE, Arotiba JT. Inner city maxillofacial fractures due to road traffic accidents. Dent Traumatol 2003;19(1):2–5.
5. Hitosugi M, Mizuno K, Nagai T, Tokudome S. Analysis of maxillofacial injuries of vehicle passengers involved in frontal collisions. J Oral Maxillofac Surg 2011;69(4):114–651.
6. Iida S, Kogo M, Sugiura T, Mima T, Matsuya T. Retrospective analysis of 1502 patients with facial fractures. Int J Oral Maxillofac Surg 2001;30(4):286–290.
7. Lehto KS, Sulander PO, Tervo TM. Do motor vehicle airbags increase risk of ocular injuries in adults? Ophthalmology 2003;110(6): 1082–1088.
8. Nóbrega LM, Cavalcante GMS, Lima MMSM, Madruga RCR, Ramos-Jorge ML, d’Avila S. Prevalence of facial trauma and associated factors in victims of road traffic accidents. Am J Emerg Med 2014;32(11):1382–1386.
9. Oginni FO, Ugboko VI, Ogundipe O, Adegbehingbe BO. Motorcycle-related maxillofacial injuries among Nigerian intracity road users. J Oral Maxillofac Surg 2006;64(1):56–62.
10. Ramli R, Abdul Rahman R, Abdul Rahman N, Abdul Karim F. Krsna Rajandram R, Mohamad MS, Mat Nor G, Sohadi RU. Pattern of maxillofacial injuries in motorcyclists in Malaysia. J Craniofac Surg 2008;19(2):316–321.
11. Yamamoto K, Matsusue Y, Horita S, Murakami K, Ueyama Y, Sugiura T, Kirita T. Maxillofacial fractures of pedestrians injured in a motor vehicle accident. Craniomaxillofac Trauma Reconstr 2013;6(1):37–42.
12. Yokoyama T, Motozawa Y, Sasaki T, Hitosugi M. A retrospective analysis of oral and maxillofacial injuries in motor vehicle accidents. J Oral Maxillofac Surg 2006;64(12):1731–1735.
13. Salentijn EG, Peerdeman SM, Boffano P, van den Bergh B, Forouzanfar T. A ten-year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: incidence and aetiology. J Craniomaxillofac Surg 2014;42(6):705–710.
14. Salentijn EG, Collin JD, Boffano P, Forouzanfar T. A ten year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: Complications and treatment. J Craniomaxillofac Surg 2014;42(8):1717–1722.
15. Boffano P, Kommers SC, Karagozoglu KH, Forouzanfar T. Aetiology of maxillofacial fractures: a review of published studies during the last 30 years. Br J Oral Maxillofac Surg 2014;52(10):901–906.
16. Giarda M, Tavolaccini A, Arcuri F, Brucoli M, Benech A. Surgical approach to isolated bilateral orbital floor fractures. Acta Otorhinolaryngol Ital 2015;35(5):362–364.
17. Benech A, Nicolotti M, Brucoli M, Arcuri F. Intraoral extra-mucosal fixation of fractures in the atrophic edentulous mandible. Int J Oral Maxillofac Surg 2013;42(4):460–463.
18. Arcuri F, Brucoli M, Baragiotta N, Benech R, Ferrero S, Benech A. Analysis of complications following endoscopically assisted treatment of mandibular condylar fractures. J Craniofac Surg 2012;23(3):e196–e198.
19. Brucoli M, Arcuri F, Cavenaghi R, Benech A. Analysis of complications after surgical repair of orbital fractures. J Craniofac Surg 2011;22(4):1387–1390
References 1. Cini MA, Prado BG, Hinnig Pde F, Fukushima WY, Adami F. Influence of type of helmet on facial trauma in motorcycle accidents. Br
J Oral Maxillofac Surg 2014;52(9):789–792.
2. Cox D, Vincent DG, McGwin G, MacLennan PA, Holmes JD, Rue LW 3rd. Effect of restraint systems on maxillofacial injury in frontal motor vehicle collisions. J Oral Maxillofac Surg 2004;62(5):571–575.
3.
4. Fasola AO, Lawoyin JO, Obiechina AE, Arotiba JT. Inner city maxillofacial fractures due to road traffic accidents. Dent Traumatol 2003;19(1):2–5.
5. Hitosugi M, Mizuno K, Nagai T, Tokudome S. Analysis of maxillofacial injuries of vehicle passengers involved in frontal collisions. J Oral Maxillofac Surg 2011;69(4):114–651.
6. Iida S, Kogo M, Sugiura T, Mima T, Matsuya T. Retrospective analysis of 1502 patients with facial fractures. Int J Oral Maxillofac Surg 2001;30(4):286–290.
7. Lehto KS, Sulander PO, Tervo TM. Do motor vehicle airbags increase risk of ocular injuries in adults? Ophthalmology 2003;110(6): 1082–1088.
8. Nóbrega LM, Cavalcante GMS, Lima MMSM, Madruga RCR, Ramos-Jorge ML, d’Avila S. Prevalence of facial trauma and associated factors in victims of road traffic accidents. Am J Emerg Med 2014;32(11):1382–1386.
9. Oginni FO, Ugboko VI, Ogundipe O, Adegbehingbe BO. Motorcycle-related maxillofacial injuries among Nigerian intracity road users. J Oral Maxillofac Surg 2006;64(1):56–62.
10. Ramli R, Abdul Rahman R, Abdul Rahman N, Abdul Karim F. Krsna Rajandram R, Mohamad MS, Mat Nor G, Sohadi RU. Pattern of maxillofacial injuries in motorcyclists in Malaysia. J Craniofac Surg 2008;19(2):316–321.
11. Yamamoto K, Matsusue Y, Horita S, Murakami K, Ueyama Y, Sugiura T, Kirita T. Maxillofacial fractures of pedestrians injured in a motor vehicle accident. Craniomaxillofac Trauma Reconstr 2013;6(1):37–42.
12. Yokoyama T, Motozawa Y, Sasaki T, Hitosugi M. A retrospective analysis of oral and maxillofacial injuries in motor vehicle accidents. J Oral Maxillofac Surg 2006;64(12):1731–1735.
13. Salentijn EG, Peerdeman SM, Boffano P, van den Bergh B, Forouzanfar T. A ten-year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: incidence and aetiology. J Craniomaxillofac Surg 2014;42(6):705–710.
14. Salentijn EG, Collin JD, Boffano P, Forouzanfar T. A ten year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: Complications and treatment. J Craniomaxillofac Surg 2014;42(8):1717–1722.
15. Boffano P, Kommers SC, Karagozoglu KH, Forouzanfar T. Aetiology of maxillofacial fractures: a review of published studies during the last 30 years. Br J Oral Maxillofac Surg 2014;52(10):901–906.
16. Giarda M, Tavolaccini A, Arcuri F, Brucoli M, Benech A. Surgical approach to isolated bilateral orbital floor fractures. Acta Otorhinolaryngol Ital 2015;35(5):362–364.
17. Benech A, Nicolotti M, Brucoli M, Arcuri F. Intraoral extra-mucosal fixation of fractures in the atrophic edentulous mandible. Int J Oral Maxillofac Surg 2013;42(4):460–463.
18. Arcuri F, Brucoli M, Baragiotta N, Benech R, Ferrero S, Benech A. Analysis of complications following endoscopically assisted treatment of mandibular condylar fractures. J Craniofac Surg 2012;23(3):e196–e198.
19. Brucoli M, Arcuri F, Cavenaghi R, Benech A. Analysis of complications after surgical repair of orbital fractures. J Craniofac Surg 2011;22(4):1387–1390
30

31

32
Chapter 4
Maxillofacial fractures associated with
sport injuries: A review of the current
literature
This is an edited version of the manuscript:
Paolo Boffano, Muhammad Ruslin, Matteo Brucoli, Arnaldo Benech, Tymour Forouzanfar
Maxillofacial fractures associated with sport injuries: A review of the current literature.
Submitted

Abstract Introduction:
Sport related maxillofacial injuries are progressively increasing, especially in the richest countries.
The aim of this paper, therefore, was to review and discuss articles that were published during the
past 20 years regarding the distribution and characteristics of sport-related facial injuries
throughout the world.
Methods:
We systematically reviewed all papers about sport related facial fractures that were published in
English between January 2000 and December 2017 using MEDLINE and the MeSH term “facial
fractures” together with the term “sport”. Sixteen papers in other languages were excluded.
Results:
The percentage of sport as an etiological factor for facial fractures was higher in Europe and
Oceania. In sport injuries, males outnumbered females. The most frequent sport was soccer, with
some peculiarities due to local diffusion of sports, such as rugby in New Zealand. In most studies
the two most frequent sites of injury were the mandible and the zygomatic maxillary complex.
Conclusion:
Further multicentre studies with the assessment of preventive measures and long-term observation
results are needed to clarify their efficacy for maxillofacial injury prevention.
34

Introduction
Maxillofacial fractures can have various causes, such as motor vehicle accidents, aggression, falls,
sports injuries, and others. The epidemiology of such fractures varies depending on the geographic
area, socioeconomic status, and the period of investigation. Sport related maxillofacial injuries are
progressively increasing, especially in the richest countries.
Injuries are due to player to- player contact, falls, or direct hits with equipment. Ball sports or sports
with projectiles also can be a cause of soft tissue injury. Overall, approximately 11% to 40% of all
sports injuries involve the face, and 8% of all facial soft tissue injuries are sports-related.
Regardless of sport or country, soft tissue injuries and fractures of the nose, zygoma, and mandible
represent the most frequent sites of injury.1
The great variety of sport related facial injuries and the complexity of facial structures makes
assessment and treatment of these problems highly important not only for the facial surgeon, but
also for the sideline physician. Team physicians should possess an understanding of the most
common facial injuries, the anatomy of the face, and the associated management of facial trauma
in athletics.1
Preventing maxillofacial injuries is a valuable pursuit for improving the quality of life of the involved
subjects. Thorough knowledge and understanding of the etiology and epidemiology of sport related
facial injuries are fundamental for the development of health services, and the adoption of new
methods for preventing injuries. The aim of this paper, therefore, was to review and discuss articles
that were published during the past 20 years regarding the distribution and characteristics of sport-
related facial injuries throughout the world.
Materials and Methods We systematically reviewed all papers that were published in English between January 2000 and
December 2017 using MEDLINE and the MeSH term “facial fractures” together with the term
“sport”. Sixteen papers in other languages were excluded. The percentage of sport injuries in any
epidemiological article about maxillofacial trauma since 2000 was recorded and grouped according
to continents. Then, only papers that were focused on sport related maxillofacial injuries and that
presented complete data about the etiology of different sport accidents with appropriate information
about type of injury and sites of fractures were included. Data were collected on etiology and
characteristics of fractures and summarized in tables. This article was exempt from IRB approval
as it is a review of the literature. We followed Helsinki Declaration guidelines.
4
35
4

Results
The percentages of sport related maxillofacial injuries in worldwide epidemiological studies were
recorded and are presented in Table 4.1.
Table 4.1. Percentages of sport related maxillofacial injuries in worldwide epidemiological studies
The percentage of sport as an etiological factor in epidemiological studies about maxillofacial
injuries ranged between 2.6% and 5% in Africa, between 7.4% and 11% in America, between 0.4%
and 14% in Asia, between 1.5% and 35% in Europe, and finally between 11.9% and 18% in
Continent First Author Year Country N of patients Sport injuries (%)
Africa Olasoji 2002 Nigeria 206 4 Adebayo 2003 Nigeria 443 5 Schaftenaar 2009 Tanzania 532 4.9 Chalya 2011 Tanzania 154 2.6
America Brasileiro 2006 Brazil 1024 8 Erdmann 2008 USA 437 11 De Lucena 2016 Brazil 718 7.4
Asia
Iida 2001 Japan 1502 9.7 Aksoy 2002 Turkey 553 0.4 Klenk 2003 United Arab Emirates 144 5 Motamedi 2003 Iran 237 6.3 Ansari 2004 Iran 2268 1 Al Ahmed 2004 United Arab Emirates 230 2.6 Erol 2004 Turkey 2901 1.1 Cheema 2006 Pakistan 702 0.5 Kadkhodaie 2006 Iran 7200 0.6 Al-Khateeb 2007 United Arab Emirates 288 3 Subhashraj 2007 India 2748 2 Sasaki 2009 Japan 674 14 Abbas 2009 Pakistan 952 10.9 Ozkaya 2009 Turkey 216 0.9 Lee 2010 Republic of Korea 318 11.9 Venugopal 2010 India 361 3 Gandhi 2011 India 718 0.8 Mesgarzadeh 2011 Iran 170 9.5 Zandi 2011 Iran 895 6.9 Naveen Shankar 2012 India 2027 1 Kapoor 2012 India 1000 1 Kar 2012 India 503 1 Abdullah 2013 Saudi Arabia 200 5.5 Almasri 2013 Saudi Arabia 101 3 Bali 2013 India 740 2 Jin 2013 China 627 1.3 Mijiti 2013 China 1350 3 Zhou 2013 China 1131 1.8 Motamedi 2014 Iran 7369 2.2 Kaul 2014 India 542 0.8 Pandey 2015 India 1108 3.29 Gaddipati 2015 India 1015 1 Kumar 2015 India 2731 1.9
Europe
Gassner 2003 Austria 9543 31 Bakardjiev 2007 Bulgaria 1706 1.5 Pombo 2010 Spain 643 11 Walker 2012 Ireland 82 35 Van den Bergh 2012 The Netherlands 579 8.3 Kostakis 2012 Greece 727 3 Kyrgidis 2013 Greece 1239 17.1 Rashid 2013 UK 1261 5 Van Hout 2013 The Netherlands 394 12 Ascani 2014 Italy 306 15.7 Boffano 2015 Europe 3396 11 Schneider 2015 Germany 409 7.1
Oceania Buchanan 2005 New Zealand 2527 18 Cabalag 2013 Australia 980 15 Moore 2015 New Zealand 1975 11.9
36
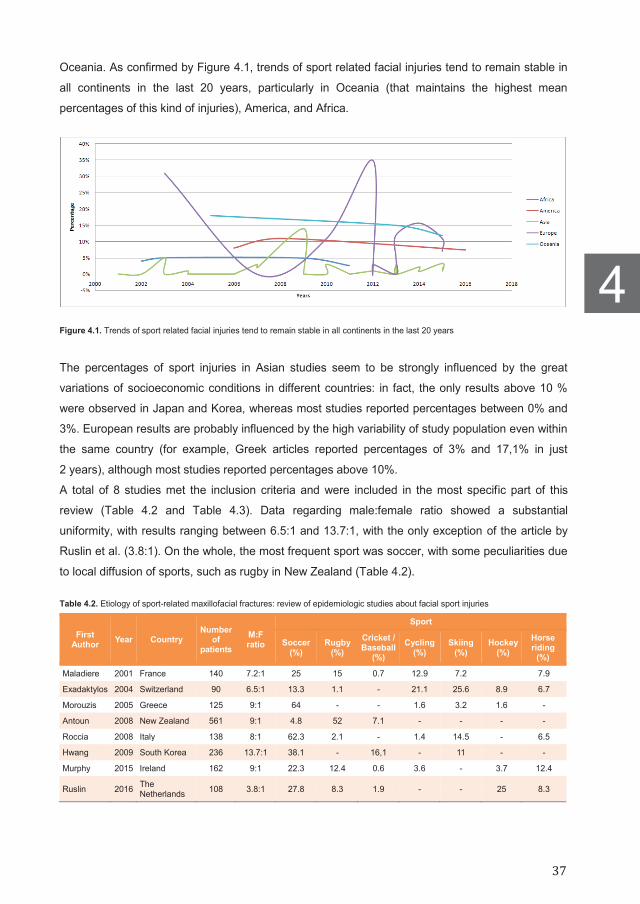
Oceania. As confirmed by Figure 4.1, trends of sport related facial injuries tend to remain stable in
all continents in the last 20 years, particularly in Oceania (that maintains the highest mean
percentages of this kind of injuries), America, and Africa.
Figure 4.1. Trends of sport related facial injuries tend to remain stable in all continents in the last 20 years
The percentages of sport injuries in Asian studies seem to be strongly influenced by the great
variations of socioeconomic conditions in different countries: in fact, the only results above 10 %
were observed in Japan and Korea, whereas most studies reported percentages between 0% and
3%. European results are probably influenced by the high variability of study population even within
the same country (for example, Greek articles reported percentages of 3% and 17,1% in just
2 years), although most studies reported percentages above 10%.
A total of 8 studies met the inclusion criteria and were included in the most specific part of this
review (Table 4.2 and Table 4.3). Data regarding male:female ratio showed a substantial
uniformity, with results ranging between 6.5:1 and 13.7:1, with the only exception of the article by
Ruslin et al. (3.8:1). On the whole, the most frequent sport was soccer, with some peculiarities due
to local diffusion of sports, such as rugby in New Zealand (Table 4.2).
Table 4.2. Etiology of sport-related maxillofacial fractures: review of epidemiologic studies about facial sport injuries
First Author Year Country
Number of
patients M:F ratio
Sport
Soccer (%)
Rugby (%)
Cricket / Baseball
(%) Cycling
(%) Skiing
(%) Hockey
(%) Horse riding
(%)
Maladiere 2001 France 140 7.2:1 25 15 0.7 12.9 7.2 7.9
Exadaktylos 2004 Switzerland 90 6.5:1 13.3 1.1 - 21.1 25.6 8.9 6.7
Morouzis 2005 Greece 125 9:1 64 - - 1.6 3.2 1.6 -
Antoun 2008 New Zealand 561 9:1 4.8 52 7.1 - - - -
Roccia 2008 Italy 138 8:1 62.3 2.1 - 1.4 14.5 - 6.5
Hwang 2009 South Korea 236 13.7:1 38.1 - 16,1 - 11 - -
Murphy 2015 Ireland 162 9:1 22.3 12.4 0.6 3.6 - 3.7 12.4
Ruslin 2016 The Netherlands 108 3.8:1 27.8 8.3 1.9 - - 25 8.3
4
37
4
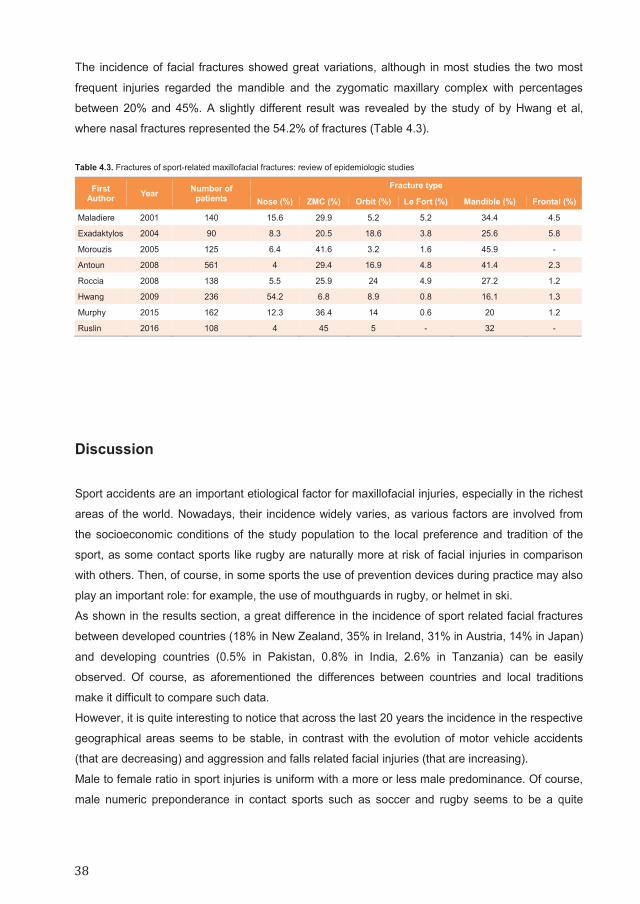
The incidence of facial fractures showed great variations, although in most studies the two most
frequent injuries regarded the mandible and the zygomatic maxillary complex with percentages
between 20% and 45%. A slightly different result was revealed by the study of by Hwang et al,
where nasal fractures represented the 54.2% of fractures (Table 4.3).
Table 4.3. Fractures of sport-related maxillofacial fractures: review of epidemiologic studies
First Author Year Number of
patients Fracture type
Nose (%) ZMC (%) Orbit (%) Le Fort (%) Mandible (%) Frontal (%)
Maladiere 2001 140 15.6 29.9 5.2 5.2 34.4 4.5
Exadaktylos 2004 90 8.3 20.5 18.6 3.8 25.6 5.8
Morouzis 2005 125 6.4 41.6 3.2 1.6 45.9 -
Antoun 2008 561 4 29.4 16.9 4.8 41.4 2.3
Roccia 2008 138 5.5 25.9 24 4.9 27.2 1.2
Hwang 2009 236 54.2 6.8 8.9 0.8 16.1 1.3
Murphy 2015 162 12.3 36.4 14 0.6 20 1.2
Ruslin 2016 108 4 45 5 - 32 -
Discussion
Sport accidents are an important etiological factor for maxillofacial injuries, especially in the richest
areas of the world. Nowadays, their incidence widely varies, as various factors are involved from
the socioeconomic conditions of the study population to the local preference and tradition of the
sport, as some contact sports like rugby are naturally more at risk of facial injuries in comparison
with others. Then, of course, in some sports the use of prevention devices during practice may also
play an important role: for example, the use of mouthguards in rugby, or helmet in ski.
As shown in the results section, a great difference in the incidence of sport related facial fractures
between developed countries (18% in New Zealand, 35% in Ireland, 31% in Austria, 14% in Japan)
and developing countries (0.5% in Pakistan, 0.8% in India, 2.6% in Tanzania) can be easily
observed. Of course, as aforementioned the differences between countries and local traditions
make it difficult to compare such data.
However, it is quite interesting to notice that across the last 20 years the incidence in the respective
geographical areas seems to be stable, in contrast with the evolution of motor vehicle accidents
(that are decreasing) and aggression and falls related facial injuries (that are increasing).
Male to female ratio in sport injuries is uniform with a more or less male predominance. Of course,
male numeric preponderance in contact sports such as soccer and rugby seems to be a quite
38

rational explanation for this result, in addition to the higher number of male athletes in comparison
to women.
The etiology of sport related maxillofacial injuries give us important information. Soccer is the most
frequently responsible sport for maxillofacial fractures. This result is naturally influenced by the
wide diffusion of soccer in the considered countries (France, Greece, Italy, South Korea, Ireland,
and The Netherlands). In fact, in New Zealand rugby related facial injuries were the most common,
whereas in Switzerland skiing and other winter sports were the most frequent causes of facial
injuries.
Finally, as for fractures type, from the analysis of the considered studies a predominance of
mandibular fractures in most articles was observed,57-61 followed by zygomatic fractures.63,64 The
only but important exception is represented by the article by Hwang et al. the authors reported an
incidence of 54.2% of nasal fractures that overwhelmed the other types of fractures.62 Of course,
this can be an important epidemiological issue, as a bias associated with the presence of
otolaryngology divisions and maxillofacial divisions within the same hospital is likely and it can be
due to the frequent referral of isolated nasal bone fractures to the otolaryngologist. The
consequence could be that in the study populations of maxillofacial centers an erroneously low
percentage of nasal bone fracture may be recorded.
Unfortunately, there are too many variables to draw any conclusion about sport related
maxillofacial injuries, as every single sport has different mechanism of injury, diffusion, and
preventive devices. However, educational courses for at risk sports players and coaches to
promote the use of preventive devices would be extremely important to increase their usage.
Sideline doctors, athletes and coaches should also be made aware and educated about most
important signs and symptoms of facial fractures to suspect this injury. Nevertheless, although the
use of simple preventive devices to prevent facial fractures, such as helmets, and mouth guards,
can be implemented, athletes still decide not to wear them, or do not know which is best, or choose
a poorly fitting device. Despite the availability of such items, the risk of injury can only be reduced,
and is dependent (in addition to the magnitude of force, source, and anatomical site) on the single
athlete.
Conclusion Improving our understanding of the mechanisms of facial injuries in sport accidents can be crucial
for the adoption of new methods for preventing injuries, thus decreasing the associated
socioeconomic costs of these individuals. Further multicentre studies with the assessment of
preventive measures and long-term observation results are needed to clarify their efficacy for
maxillofacial injury prevention.
4
39
4

References
1. Leinhart J, Toldi J, Tennison M. Facial Trauma in Sports. Curr Sports Med Rep 2017;16(1):23–29.
2. Olasoji HO, Tahir A, Arotiba GT. Changing picture of facial fractures in northern Nigeria. Br J Oral Maxillofac Surg 2002;40(2):140–143.
3. Adebayo ET, Ajike OS, Adekeye EO. Analysis of the pattern of maxillofacial fractures in Kaduna, Nigeria. Br J Oral Maxillofac Surg
2003;41(6):396–400. 4. Schaftenaar E, Bastiaens GJ, Simon EN, Merkx MA. Presentation and management of maxillofacial trauma in Dar es Salaam,
Tanzania. East Afr Med J 2009;86(6):254–825. 5. Chalya PL, McHembe M, Mabula JB, Kanumba ES, Gilyoma JM. Etiological spectrum, injury characteristics and treatment outcome
of maxillofacial injuries in a Tanzanian teaching hospital. J Trauma Manag Outcomes 2011;5:7. 6. Brasileiro BF, Passeri LA. Epidemiological analysis of maxillofacial fractures in Brazil: a 5-year prospective study. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod 2006;102(1):28–34. 7. Erdmann D, Follmar KE, Debruijn M, Bruno AD, Jung SH, Edelman D. Mukundan S, Marcus JR. A retrospective analysis of facial
fracture etiologies. Ann Plast Surg 2008;60(4):398–403. 8. de Lucena AL, da Silva Filho GF, de Almeida Pinto Sarmento TC, de Carvalho SH, Fonseca FR, de Santana Sarmento DJ.
Epidemiological profile of facial fractures and their relationship with clinical-epidemiological variables. J Craniofac Surg 2016; 27(2): 345–349.
9. Iida S, Kogo M, Sugiura T, Mima T, Matsuya T. Retrospective analysis of 1502 patients with facial fractures. Int J Oral Maxillofac
Surg 2001;30(4):286–290. 10. Aksoy E, Unlü E, Sensöz O. A retrospective study on epidemiology and treatment of maxillofacial fractures. J Craniofac Surg 2002;
13(6):772–775. 11. Klenk G, Kovacs A. Etiology and patterns of facial fractures in the United Arab Emirates. J Craniofac Surg 2003;14(1):78–84. 12. Motamedi MH. An assessment of maxillofacial fractures: a 5-year study of 237 patients. J Oral Maxillofac Surg 2003;61(1):61–64. 13. Ansari MH. Maxillofacial fractures in Hamedan province, Iran: a retrospective study (1987–2001). J Craniomaxillofac Surg 2004;
32(1):28–34. 14. Al Ahmed HE, Jaber MA, Abu Fanas SH, Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: a review
of 230 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98(2):166–170. 15. Erol B, Tanrikulu R, Görgün B. Maxillofacial fractures. Analysis of demographic distribution and treatment in 2901 patients (25-year
experience). J Craniomaxillofac Surg 2004;32(5):308–313. 16. Cheema SA, Amin F. Incidence and causes of maxillofacial skeletal injuries at the Mayo Hospital in Lahore, Pakistan. Br J Oral
Maxillofac Surg 2006;44(3):232–234. 17. Kadkhodaie MH. Three-year review of facial fractures at a teaching hospital in northern Iran. Br J Oral Maxillofac Surg 2006;44(3):
229–231. 18. Al-Khateeb T, Abdullah FM. Craniomaxillofacial injuries in the United Arab Emirates: a retrospective study. J Oral Maxillofac Surg
2007;65(6):1094–1101. 19. Subhashraj K, Nandakumar N, Ravindran C. Review of maxillofacial injuries in Chennai, India: a study of 2748 cases. Br J Oral
Maxillofac Surg 2007;45(8):637–639. 20. Sasaki R, Ogiuchi H, Kumasaka A, Ando T, Nakamura K, Ueki T, Okada Y, Asanami S, Chigono Y, Ichinokawa Y, Satomi T, Matsuo
A, Chiba H. Analysis of the pattern of maxillofacial fracture by five departments in Tokyo: A review of 674 cases. Oral Science International 2009;6(1):1–7.
21. Abbas I, Fayyaz M, Shah I, Khan MA, Qazi SH, Munir N, Bibi A, Abbasi M. Demographic distribution of maxillofacial fractures in
Ayub Teaching Hospital: 7-year review. J Ayub Med Coll Abbottabad 2009;21(2):110–112. 22. Ozkaya O, Turgut G, Kayali MU, Ugurlu K, Kuran I, Bas L. A retrospective study on the epidemiology and treatment of maxillofacial
fractures. Ulus Travma Acil Cerrahi Derg 2009;15(3):262–266. 23. Lee JH, Cho BK, Park WJ. A 4-year retrospective study of facial fractures on Jeju, Korea. J Craniomaxillofac Surg 2010;38(3):192–
196. 24. Venugopal MG, Sinha R, Menon PS, Chattopadhyay PK, Roy Chowdhury SK. Fractures in the maxillofacial region: A four year
retrospective study. Med J Armed Forces India 2010;66(1):14–17. 25. Gandhi S, Ranganathan LK, Solanki M, Mathew GC, Singh I, Bither S. Pattern of maxillofacial fractures at a tertiary hospital in
northern India: a 4-year retrospective study of 718 patients. Dent Traumatol 2011;27(4):257–262.
40

26. Mesgarzadeh AH, Shahamfar M, Azar SF, Shahamfar J. Analysis of the pattern of maxillofacial fractures in north western of Iran: A
retrospective study. J Emerg Trauma Shock 2011;4(1):48–52. 27. Zandi M, Khayati A, Lamei A, Zarei H. Maxillofacial injuries in western Iran: a prospective study. Oral Maxillofac Surg 2011;15(4):
201–209. 28. Naveen Shankar A, Naveen Shankar V, Hegde N, Sharma, Prasad R. The pattern of the maxillofacial fractures - A multicentre
retrospective study. J Craniomaxillofac Surg 2012;40(8):675–679. 29. Kapoor P, Kalra N. A retrospective analysis of maxillofacial injuries in patients reporting to a tertiary care hospital in East Delhi. Int J
Crit Illn Inj Sci 2012;2(1):6–10 30. Kar IB, Mahavoi BR. Retrospective analysis of 503 maxillo-facial trauma cases in odisha during the period of dec’04-nov’09. J
Maxillofac Oral Surg 2012;11(2):177–181. 31. Abdullah WA, Al-Mutairi K, Al-Ali Y, Al-Soghier A, Al-Shnwani A. Patterns and etiology of maxillofacial fractures in Riyadh City, Saudi
Arabia. Saudi Dent J 2013;25(1):33–38. 32. Almasri M. Severity and causality of maxillofacial trauma in the Southern region of Saudi Arabia. Saudi Dent J 2013;25(3):107–110. 33. Bali R, Sharma P, Garg A, Dhillon G. A comprehensive study on maxillofacial trauma conducted in Yamunanagar, India. J Inj
Violence Res 2013;5(2):108–116. 34. Jin Z, Jiang X, Shang L. Analysis of 627 hospitalized maxillofacial-oral injuries in Xi’an, China. Dent Traumatol 2014;30(2):147–153. 35. Mijiti A, Ling W, Tuerdi M, Maimaiti A, Tuerxun J, Tao YZ, Saimaiti A, Moming A. Epidemiological analysis of maxillofacial fractures
treated at a university hospital, Xinjiang, China: A 5-year retrospective study. J Craniomaxillofac Surg 2014;42(3):227–233. 36. Zhou HH, Ongodia D, Liu Q, Yang RT, Li ZB. Changing pattern in the characteristics of maxillofacial fractures. J Craniofac Surg
2013;24(3):929–933. 37. Motamedi MH, Dadgar E, Ebrahimi A, Shirani G, Haghighat A, Jamalpour MR. Pattern of maxillofacial fractures: a 5-year analysis of
8,818 patients. J Trauma Acute Care Surg 2014;77(4):630–634. 38. Kaul RP, Sagar S, Singhal M, Kumar A, Jaipuria J, Misra M. Burden of maxillofacial trauma at level 1 trauma center. J
Craniomaxillofac Trauma Reconstr. 2014;7(2):126–130. 39. Pandey S, Roychoudhury A, Bhutia O, Singhal M, Sagar S, Pandey RM. Study of the pattern of maxillofacial fractures seen at a
tertiary care hospital in north India. J Maxillofac Oral Surg 2015;14(1):32–39. 40. Gaddipati R, Ramisetti S, Vura N, Reddy KR, Nalamolu B. Analysis of 1,545 Fractures of Facial Region-A Retrospective Study.
Craniomaxillofac Trauma Reconstr 2015;8(4):307–314. 41. Kumar GB, Dhupar V, Akkara F, Kumar SP. Patterns of maxillofacial fractures in goa. J Maxillofac Oral Surg 2015;14(2):138–141 42. Gassner R, Tuli T, Hächl O, Rudisch A, Ulmer H. Cranio-maxillofacial trauma: a 10 year review of 9,543 cases with 21,067 injuries. J
Craniomaxillofac Surg 2003;31(1):51–61. 43. Bakardjiev A, Pechalova P. Maxillofacial fractures in Southern Bulgaria - a retrospective study of 1706 cases. J Craniomaxillofac
Surg 2007;35(3):147–150. 44. Pombo M, Luaces-Rey R, Pértega S, Arenaz J, Crespo JL, Garcia-Rozado A, Patino B, Lopez-Cedrun JL. Review of 793 facial
fractures treated from 2001 to 2008 in a coruna university hospital: types and etiology. Craniomaxillofac Trauma Reconstr 2010;3(1):49–54.
45. Walker TW, Donnellan J, Byrne S, McArdle N, Kerin MJ, McCann PJ. West of Ireland facial injury study. Part 2. Br J Oral Maxillofac
Surg 2012;50(7):e99–e103. 46. van den Bergh B, Karagozoglu KH, Heymans MW, Forouzanfar T. Aetiology and incidence of maxillofacial trauma in Amsterdam: a
retrospective analysis of 579 patients. J Craniomaxillofac Surg 2012;40(6):e165–e169. 47. Kostakis G, Stathopoulos P, Dais P, Gkinis G, Igoumenakis D, Mezitis M, Rallis G. An epidemiologic analysis of 1,142 maxillofacial
fractures and concomitant injuries. Oral Surg Oral Med Oral Pathol Oral Radiol 2012;114(5 suppl):S69–S73. 48. Kyrgidis A, Koloutsos G, Kommata A, Lazarides N, Antoniades K. Incidence, aetiology, treatment outcome and complications of
maxillofacial fractures. A retrospective study from Northern Greece. J Craniomaxillofac Surg 2013;41(7):637–643. 49. Rashid A, Eyeson J, Haider D, van Gijn D, Fan K. Incidence and patterns of mandibular fractures during a 5-year period in a London
teaching hospital. Br J Oral Maxillofac Surg 2013;51(8):794–798. 50. van Hout WM, Van Cann EM, Abbink JH, Koole R. An epidemiological study of maxillofacial fractures requiring surgical treatment at
a tertiary trauma centre between 2005 and 2010. Br J Oral Maxillofac Surg 2013;51(5):416–420 51. Ascani G, Di Cosimo F, Costa M, Mancini P, Caporale C. Maxillofacial fractures in the province of pescara, Italy: a retrospective
study. ISRN Otolaryngol. 2014 Jan 23;2014:101370. 52. Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, Kovačič Ž, Vesnaver A, Konstantinović VS, Petrović M, Stephens J, Kanzaria
A, Bhatti N, Holmes S, Pechalova PF, Bakardjiev AG, Malanchuk VA, Kopchak AV, Galteland P, Mjøen E, Skjelbred P, Koudougou
4
41
4
C, Mouallem G, Corre P, Løes S, Lekven N, Laverick S, Gordon P, Tamme T, Akermann S, Karagozoglu KH, Kommers SC, Forouzanfar T. European Maxillofacial Trauma (EURMAT) project: a multicentre and prospective study. J Craniomaxillofac Surg 2015 Jan;43(1):62–70.
53. Schneider D, Kämmerer PW, Schön G, Dinu C, Radloff S, Bschorer R. Etiology and injury patterns of maxillofacial fractures from the
years 2010 to 2013 in Mecklenburg-Western Pomerania, Germany: A retrospective study of 409 patients. J Craniomaxillofac Surg 2015 Dec;43(10):1948–1951.
54. Buchanan J, Colquhoun A, Friedlander L, Evans S, Whitley B, Thomson M. Maxillofacial fractures at Waikato Hospital, New
Zealand: 1989 to 2000. N Z Med J 2005;118(1217):U1529. 55. Cabalag MS, Wasiak J, Andrew NE, Tang J, Kirby JC, Morgan DJ. Epidemiology and management of maxillofacial fractures in an
Australian trauma centre. J Plast Reconstr Aesthet Surg 2014;67(2):183–189. 56. Moore BK, Smit R, Colquhoun A, Thompson WM. Maxillofacial fractures at Waikato Hospital, New Zealand: 2004 to 2013. N Z Med
J 2015;128(1426):96–102. 57. Maladière E, Bado F, Meningaud JP, Guilbert F, Bertrand JC. Aetiology and incidence of facial fractures sustained during sports: a
prospective study of 140 patients. Int J Oral Maxillofac Surg 2001;30(4):291–295. 58. Exadaktylos AK, Eggensperger NM, Eggli S, Smolka KM, Zimmermann H, Iizuka T. Sports related maxillofacial injuries: the first
maxillofacial trauma database in Switzerland. Br J Sports Med 2004;38(6):750–753. 59. Mourouzis C, Koumoura F. Sports-related maxillofacial fractures: a retrospective study of 125 patients. Int J Oral Maxillofac
Surg. 2005;34(6):635–638. 60. Antoun JS, Lee KH. Sports-related maxillofacial fractures over an 11-year period. J Oral Maxillofac Surg 2008;66(3):504–508. 61. Roccia F, Diaspro A, Nasi A, Berrone S. Management of sport-related maxillofacial injuries. J Craniofac Surg 2008;19(2):377–782. 62. Hwang K, You SH, Lee HS. Outcome analysis of sports-related multiple facial fractures. J Craniofac Surg 2009;20(3):825–829. 63. Murphy C, O'Connell JE, Kearns G, Stassen L. Sports-Related Maxillofacial Injuries. J Craniofac Surg 2015;26(7):2120–2123. 64. Ruslin M, Boffano P, ten Brincke YJ, Forouzanfar T, Brand HS. Sport-related maxillo-facial fractures. J Craniofac Surg 2016;27(1):
e91–e94. 65. Roccia F, Caldarelli C, Spada MC, Brucoli M, Beatrice F, Ruffino S, Benech A, Ramieri G, Berrone S. Development of a regional
database for studying epidemiology of maxillofacial trauma. J Craniofac Surg 2010;21(4):1045–1050.
42

43

44

Chapter 5
Sport-Related Maxillofacial Fractures
This is an edited version of the manuscript:
Muhammad Ruslin, Paolo Boffano, Y.J.D. ten Brincke, Tymour Forouzanfar, and Henk S. Brand
Journal of Craniofacial Surgery 2016 Jan;27(1):e91-e94

Abstract
Introduction:
Sports and exercise are important causes of maxillofacial injuries. Different types of sports might
differ in frequency and type of fractures. The aim of the present study was to explore the possible
relation between the types of sport practiced and the frequency and nature of the facial bone
fractures of patients presenting in an oral and maxillofacial surgery department of a Dutch
university center.
Methods:
This study is based on an analysis of patient records containing maxillofacial fractures sustained
between January 1, 2000 and April 1, 2014 at the Vrije Universiteit University Medical Center
(VUmc) in Amsterdam, The Netherlands.
Results:
The present study comprised data from 108 patients with 128 maxillofacial fractures. Seventy-nine
percent of the patients were male and 21% were female. The patients ranged in age from 10 to
64 years old with a mean age of 30.6 12.0. The highest incidence of sport-related maxillofacial
fractures occurred in individuals between the ages of 20 and 29. The most common sport-related
fractures were zygoma complex fractures, followed by mandible fractures. Soccer and hockey were
the most prominent causes of sport-related maxillofacial trauma in the present study. Coronoid
process fractures were only observed in soccer players and not in other sports groups. Mandible
angle fractures were relatively more frequent in rugby than in other sports.
Conclucion:
Based on the result of this study, we confirm a relation between type of sport and the nature and
frequency of the fractures causes and it causes. In addition, our findings are mostly in line with
other studies, which suggest that the data might be useful for the development of protocols to
prevent maxillofacial trauma in certain sports.
46

Introduction
Major causes of maxillofacial injuries are traffic accidents, falling, and (domestic) violence. Sports
and exercise are also important causes of maxillofacial injuries. Sport cause approximately 5% of
all mandible fractures and 9% of the fractures in the upper two-thirds of the face. Sport-related
accidents are also responsible for approximately 10% of all midfacial.1-4
Elhammali et al.5 found their study of sport-related injuries a significant prevalence of the mid-facial
complex (67%) followed by the mandible (29%) and skull base (4%).5 In their review study
concerning sports-related maxillofacial trauma, Kunamoto et al.6 suggested that different types of
sports differ in frequency and type of fractures. In Italy, soccer is the main cause of maxillofacial
trauma, with frequent fractures of the zygomatic bone (44%), the nasal bone (29%), and the
mandible (15%). A previous, larger study in Italy also found the same 3 types of fractures most
commonly in soccer players, but in different orders: nasal bone fractures (62%), zygomatic bone
fractures (15%), and mandible fractures (11%). In a study performed in Brazil, the investigators
found that the majority of soccer-related fractures consisted of nasal bone (35%) and orbito-
zygomatic complex (35%) followed by mandible (16%) orbital region (13%), frontal bone (2%), and
naso-orbito-ethmoid complex (2%).7 When soccer players suffer from mandible fractures, the
subcondylar site is most frequently affected (28,6%).8
Horse riders, on the other hand, suffer most frequently from fractures of the zygomatic bone
(40%),9 while rugby players suffer most frequently from mandible fractures (65%).10
Several authors stated that geographical differences might also play a role in the frequency and
type of sport-related maxillofacial fractures.6,8,11 In Austria, 55.3% of sport-related mandible
fractures were caused by skiing,8 and in Switzerland 27% of sport-related maxillofacial fractures
were sustained during skiing and snow-boarding.11 On the other hand, a study performed in the
United States reported no fractures due to skiing accidents.12 These geographical differences might
be affected by different numbers of individuals practicing specific sports.
Until now, no data are available on sport-related maxillofacial fractures in the Netherlands.
Therefore, the aim of the present study was to explore the possible relation between the types of
sport practiced, and the frequency and nature of the facial bone fractures of patients presenting in
the oral-maxillofacial department of a Dutch university center.
5
47
5

Material and Methods
This study is based on an analysis of a patient database from the Department of Oral and
Maxillofacial Surgery, Vrije Universiteit University Medical Center (VUmc), Amsterdam, The
Netherlands. The database consists of retrospectively collected data from January 1, 2000 until
January 1, 2010 and systematic computer-assisted databases that have continuously recorded
patients with maxillofacial fractures between January 1, 2010 and April 1, 2014.
Both surgically and nonsurgically treated patients were included. Only maxillofacial fractures
caused by sports were included in this study. The study was performed according to the guidelines
of the medical ethical committee of the Free University of Amsterdam.
Patients below the age of 4 and above the age of 80 were excluded, as these patients were not
expected to participate in community sports. From the medical records, the following data were
retrieved: sex, age, type of sports, and type of maxillofacial fracture. Maxillofacial fractures caused
by bicycle accidents were considered traffic accidents and were excluded from the study. Fractures
caused by skiing, snowboarding, and sled riding were combined into winter sports. Baseball and
softball fractures were also combined into softball.
The maxillofacial fractures were divided into mandible fractures (angle, body, condyle, guardsman
fractures, coronoid process, and symphysis), zygomatic complex fractures, mid-facial fractures (Le
Fort 1, 2, and 3, and alveolar process fractures of the maxilla), orbital walls fractures (orbital and
sphenoid sinus fractures), nasal bone and frontal sinus fractures, skull fractures (parietal and
temporal bone fractures), and multi-trauma (2 or more trauma from different complexes).
The IBM SPSS 21 package (IBM, Armonk, NY) was used to analyze associations among multiple
variables. Statistical significance was determined using x2, or Fisher exact test, if the sample sizes
were too small. P values <0.05 were considered statistically significant.
Results
The study population consisted of 108 patients with 128 maxillofacial fractures (79% male; 21%
female). A mean age of 30.6 years (SD, 12.0; range 10 – 64) was observed. The highest incidence
of maxillofacial fractures was observed in subjects between 20 and 29 years old (Table 5.1.).
48

Table 5.1. Age distribution of patients with maxillofacial fractures, stratified according to type of sport performed during the accident
Age Soccer Field Hockey
Horse Riding Rugby Martial Arts Ice Skating Winter
Sports Other Sports
Count (Percent
Within Age Intervals)
10–19 3 (10%) 2 (7%) 5 (56%) 0 (0%) 1 (17%) 0 (0%) 2 (40%) 5 (29%) 18 (17%)
20–29 9 (30%) 17 (63%) 2 (22%) 6 (67%) 1 (17%) 1 (20%) 0 (0%) 3 (18%) 39 (36%) 30–39 10 (33%) 6 (22%) 1 (11%) 1 (11%) 3 (50%) 1 (20%) 2 (40%) 3 (18%) 27 (25%)
40–49 7 (23%) 1 (4%) 0 (0%) 2 (22%) 1 (17%) 1 (20%) 1 (20%) 4 (24%) 17 (16%) 50–59 1 (3%) 1 (4%) 1 (11%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 2 (12%) 5 (5%)
60–69 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 2 (40%) 0 (0%) 0 (0%) 2 (2%) Total 30 (100%) 27 (100%) 9 (100%) 9 (100%) 6 (100%) 5 (100%) 5 (100%) 17 (100%) 108 (100%)
The patients had been engaged in 18 different sports as demonstrated in Table 5.2., where soccer
has been the major cause of maxillofacial trauma (28%) followed by field hockey (25%), horse
riding (8%), and rugby (8%).
Table 5.2. Frequency distribution of patients with orofacial fractures stratified according to type of sport performed during the accident
Type of Sport Number of Patients (Percentage) Soccer 30 (27.8) Field hockey 27 (25.0) Horse riding 9 (8.3) Rugby 9 (8.3) Martial arts 6 (5.6) Ice Skating 5 (4.6) Cricket 2 (1.9) Tennis 1 (0.9) Bicycle racing 1 (0.9) Winter sports, other than ice skating 5 (4.6) Sakeboarding 1 (0.9) Inline skating 3 (2.8) Ice hockey 1 (0.9) Skydiving 1 (0.9) Softball 3 (2.8) Gymnastics 1 (0.9) Go-karting 3 (2.8)
The most commonly sports observed related maxillofacial fractures were zygomatic complex
fractures (45%), followed by mandible fractures (32%) (Table 5.3.). Table 5.3. Maxillofacial fractures, stratified according to type of sport performed during the accident
Fracture Soccer Field Hockey
Horse Riding Rugby Martial
arts Ice
Skating
Winter Sports,
Other Than Ice Skating
Other Sports Total
Mandible 8 (27%) 10 (37%) 3 (33%) 2 (22%) 3 (50%) 0 (0%) 1 (20%) 7 (41%) 34 (32%) Zygoma complex 14 (47%) 13 (48%) 4 (44%) 5 (56%) 1 (17%) 4 (80%) 2 (40%) 6 (35%) 49 (45%)
Midface 0 (0%) 0 (0%) 1 (11%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (1%) Orbital wall 1 (3%) 0 (0%) 0 (0%) 0 (0%) 1 (17%) 0 (0%) 2 (40%) 1 (6%) 5 (5%)
Nasal bone / frontal sinus 1 (3%) 1 (4%) 0 (0%) 2 (22%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 4 (4%) Multiple 6 (20%) 3 (11%) 1 (11%) 0 (0%) 1 (17%) 1 (20%) 0 (0%) 3 (18%) 15 (14%)
Total 30 (100%) 27 (100%) 9 (100%) 9 (100%) 6 (100%) 5 (100%) 5 (100%) 17 (100%) 108 (100%)
5
49
5
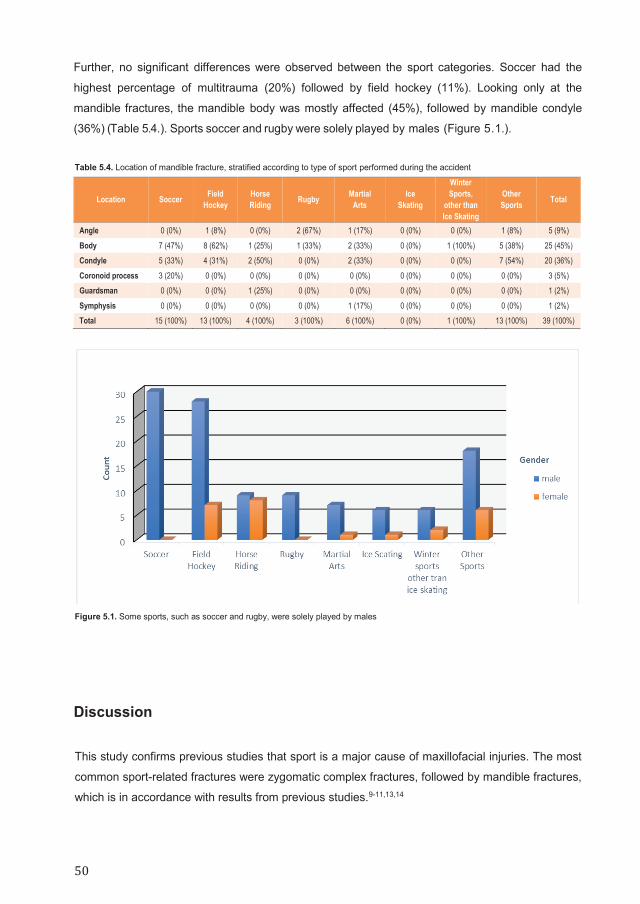
Further, no significant differences were observed between the sport categories. Soccer had the
highest percentage of multitrauma (20%) followed by field hockey (11%). Looking only at the
mandible fractures, the mandible body was mostly affected (45%), followed by mandible condyle
(36%) (Table 5.4.). Sports soccer and rugby were solely played by males (Figure 5.1.).
Table 5.4. Location of mandible fracture, stratified according to type of sport performed during the accident
Location Soccer Field Hockey
Horse Riding Rugby Martial
Arts Ice
Skating
Winter Sports,
other than Ice Skating
Other Sports Total
Angle 0 (0%) 1 (8%) 0 (0%) 2 (67%) 1 (17%) 0 (0%) 0 (0%) 1 (8%) 5 (9%)
Body 7 (47%) 8 (62%) 1 (25%) 1 (33%) 2 (33%) 0 (0%) 1 (100%) 5 (38%) 25 (45%) Condyle 5 (33%) 4 (31%) 2 (50%) 0 (0%) 2 (33%) 0 (0%) 0 (0%) 7 (54%) 20 (36%)
Coronoid process 3 (20%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 3 (5%) Guardsman 0 (0%) 0 (0%) 1 (25%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (2%)
Symphysis 0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (17%) 0 (0%) 0 (0%) 0 (0%) 1 (2%) Total 15 (100%) 13 (100%) 4 (100%) 3 (100%) 6 (100%) 0 (0%) 1 (100%) 13 (100%) 39 (100%)
Figure 5.1. Some sports, such as soccer and rugby, were solely played by males
Discussion
This study confirms previous studies that sport is a major cause of maxillofacial injuries. The most
common sport-related fractures were zygomatic complex fractures, followed by mandible fractures,
which is in accordance with results from previous studies.9-11,13,14
50

Nasal bone fractures were nearly absent in the present data, since these fractures are usually
treated by the ear nose throat (ENT) department and therefore not included in the database used.
The highest incidence of sport-related maxillofacial fractures occurred in individuals between the
ages of 20 and 29 (Table 5.1.). Other studies found similar results, although the 36% in the present
study is slightly lower than the 41.4% to 52.9% in previous studies.4,5,8,10,13,14 Most sport-related
fractures occurred in males, which is also in accordance with previous studies.7-10,13,14
Soccer and hockey were the most prominent causes of sport-related maxillofacial trauma in the
present study. This is in line with the large number of people playing soccer in the Netherlands.
Hockey, on the other hand, is only the ninth most popular sport in the Netherlands (Centraal
Bureau Statistiek; CBS).15,16 However, field hockey participation in the Amsterdam and the
adjacent Amstelveen suburb is high, with 6.5% of all Dutch hockey players playing in this area
(CBS). We suspect that this may contribute to the prominence of hockey-related trauma in our
data. However, this high number could also be a result of hockey being a high-risk sport for
maxillofacial trauma. In Ireland,17 gaelic football was the sport responsible for most fractures
followed by cricket and soccer, respectively, while in Japan10 and Great Britain18 rugby proved to
be the main cause. In Switzerland11 most fractures were sustained during skiing and snow-
boarding during team sports such as soccer or ice hockey and cycling. In Brazil, nasal fractures
were the most common soccer-related facial fractures. In a retrospectively performed review about
451 Germans soccer players who had suffered injuries during soccer games, the head was
affected in 23.9% of cases. The areas most frequently involved were the facial and occipital
regions.19
An interesting observation of the present study is that coronoid process fractures were only
observed in soccer players and not in other sports groups. This might be due to the fact that the
most common cause of accident in soccer is impact against another player.10 However, in the
study of Emshoff et al.8 no fractures in the coronoid region were observed among 28 fractures
related to soccer. Mandible angle fractures were more seen in rugby than in other sports. Other
studies also demonstrated that the mandible is often a site of injury in rugby,9,10 but these previous
studies did not specify the frequency of mandible angle fractures in rugby players. Other authors
reported the most frequent fracture site of the mandible was the angle followed by the symphysis in
maxillofacial fractures sustained during sports played with ball.20
The present study has several potential limitations. In the first place, it is a single-center study.
Amsterdam has 3 other hospitals where patients with maxillofacial injuries are treated. As the
patients are not equally divided into the 4 hospitals in Amsterdam, some hospitals may see more
and different kinds of patients than the other hospitals. Therefore, the results in the present study
might not be fully representative for the Netherlands. As the data were partly collected
retrospectively, this may also have introduced information bias.
5
51
5

Conclusion In conclusion, the results of this study suggest a relation between type of sport and the nature and
frequency of the fractures it causes. Furthermore, we confirm a relation between type of sport and
the nature and frequency of the fractures causes and it causes. Our findings are mostly in line with
other studies, which suggest that the data might be useful for the development of protocols to
prevent maxillofacial trauma in certain sports.
52

References
1. Van den Bergh B, van Es C, Forouzanfar T. Analysis of mandibular fractures. J Craniofac Surg 2011;22(5):1631–1634.
2. Van den Bergh B, Karagozoglu KH, Heymans MW, Forouzanfar T. Aetiology and incidence of maxillofacial trauma in Amsterdam: a retrospective analysis of 579 patients. J Craniomaxillofac Surg 2012;40(6):e165–e169.
3. Salentijn EG, Van den Bergh B, Forouzanfar T. A ten-year analysis of midfacial fractures. J Craniomaxillofac Surg 2013;41(7):630–636.
4. Gassner R, Bosh R, Tuli T, Emshoff R. Prevalence of dental trauma in 6000 patients with facial injuries: implication for prevention. Oral Surg Oral Med Oral Pathol Radiol Endod 1999;87(1):27–33.
5. Elhammali N, Bremerich A, Rustemeyer J. Demographical and clinical aspects of sports-related maxillofacial and skull base fractures in hospitalised patients. Int J Oral Maxillofac Surg 2010;39(9):857–862.
6. Kunamoto DP, Maeda Y. A literature review of sports-related maxillofacial trauma. Gen Dent 2004;52(3):270–280.
7. Goldenberg DC, Dini GM, Pereira MD, Gurgel A, Bastos EO, Nagarkar P, Gemperli R, Ferreira LM. Soccer-related facial trauma: multicenter experience in 2 Brazilian University Hospitals. Plast Reconstr Surg Glob Open 2014;2(6):e168.
8. Emshoff R, Scho ning H, Ro thler G, Waldhart E. Trends in the incidence and cause of sport-related mandibular fractures: a retrospective analysis. J Oral Maxillofac Surg 1997;55(6):585–592.
9. Frenguelli A, Ruscito P, Bicciolo G, Rizzo S, Massarelli M. Head and neck trauma in sporting activities. Review of 208 cases. J Craniomaxillofac Surg 1991;19(4):178–181.
10. Tanaka N, Hayashi S, Amagasa T, Kohama G. Maxillofacial fractures sustained during sports. J Oral Maxillofac Surg 1996;54(6): 715–719.
11. Exadaktylos AK, Eggensperger NM, Eggali S, Smolka KM, Zimmermann H, Lizuka T. Sports related maxillofacial injuries: the first maxillofacial trauma database in Switzerland. Br J Sports Med 2004;38:750–753.
12. Soporowski NJ, Tesini DA, Weiss AI. Survey of ofacial sports-related injuries. J Mass Dent Soc 1994;43(4):16–20.
13. Cerulli G, Carboni A, Mercurio A, Perugini M, Becelli R. Soccer-related craniomaxillofacial injuries. J Craniofac Surg 2002;13(5): 627–630.
14. Mourouzis C, Koumoura F. Sports-related maxillofacial fractures: a retrospective study of 125 patients. Int J Oral Maxillofac Surg 2005;34(6):635–638.
15. Centraal Bureau Statistiek. Available at: http://www.cbs.nl. Accessed June 25, 2014
16. Koninklijke Nederlandse Hockey Bond. Available at: http://www.knhb.nl. Accessed June 25, 2014
17. Fasola AO, Obiechina AE, Arotiba JT. Sports related maxillofacial fractures in 77 Nigerian patients. Afr J Med Med Sci 2000;29(3-4):215–217.
18. Hill CM, Burford K, Martin A, Thomas DW. A one-year review of maxillofacial sports injuries treated at an accident and emergency department. Br J Oral Maxillofac Surg 1998;36(1):44–47.
19. Kolodziej MA, Koblitz S, Nimsky C, Hellwig D. Mechanisms and consequences of head injuries in soccer: a study of 451 patients. Neurosurg Focus 2011;31(5):E1
20. Delilbasi C, Yamazawa M, Nomura K, Lida S, Kogo M. Maxillofacial fractures sustained during sports played with a ball. Oral Surg Oral Med Oral Pathol Radiol Endod 2004;97(1):23–27.
5
53
5

54
Chapter 6
Sport related maxillofacial fractures:
A multicenter and prospective study
This is an edited version of the manuscript:
Muhammad Ruslin, Matteo Brucoli, Paolo Boffano, Arnaldo Benech, Emil Dediol, Vedran Uglešić, Žiga Kovačič, Aleš
Vesnaver, Vitomir S. Konstantinović, Milan Petrović, Jonny Stephens, Amar Kanzaria, Nabeel Bhatti, Simon Holmes,
Petia F. Pechalova, Angel G. Bakardjiev, Vladislav A. Malanchuk, Andrey V. Kopchak, Pål Galteland, Even Mjøen, Per
Skjelbred, Helios Bertin, Pierre Corre, Sigbjørn Løes, Njål Lekven, Sean Laverick, Peter Gordon, Tiia Tamme, Stephanie
Akermann, K Hakki Karagozoglu, Sofie C. Kommers, Jan G. de Visscher, Tymour Forouzanfar
Sport related maxillofacial fractures: A multicenter and prospective study
Submitted

Abstract
Introduction:
The purpose of this study is to present and discuss the demographics and patterns of sport–related
maxillofacial fractures of a multicenter study.
Methods:
This study is based on a systematic computer-assisted database that allowed to prospectively and
continuously record all patients hospitalized with maxillofacial fractures in the involved Maxillofacial
Surgery Units across Europe, since Monday 31st December 2012 to Sunday 29th December 2013.
Results:
The 3260 patients with maxillofacial fractures admitted within the study period, 275 traumas were
due to sport accidents with a male to female ratio of 4.1:1. Soccer was most frequently responsible
for maxillofacial injuries (33%), followed by rugby (18%) and skiing (12%). The most frequently
observed fracture involved the mandible with 116 fractures, followed by maxilla-zygomatic-orbital
(MZO) fractures.
Conclusion:
There are still too many variables to draw any conclusion about sport-related maxillofacial injuries,
as every single sport has different mechanism of injury, diffusion, and preventive devices.
56

Introduction
Injuries associated with sport accidents are a problem faced in several countries, and their
prevention is often a priority for public health authorities. Sport related maxillofacial injuries are
progressively increasing, especially in the richest countries.1-52 Injuries are due to player to-player
contact, falls, or direct hits with equipment.
In fact, facial injuries, including fractures, may have serious long-term implications for victims of
sport accidents and important socio economic consequences.1-8 The great variety of sport related
facial injuries and the complexity of facial structures makes assessment and treatment of these
problems highly important not only for the facial surgeon, but also for the sideline physician.
Thus, the knowledge of the factors associated with facial injuries stemming from sport accidents is
important for the prognosis, the identification of groups at risk, and the establishment of measures
to minimize the economic, emotional, psychological, and social impacts of these events.1-8
Preventing maxillofacial injuries is a valuable pursuit for improving the quality of life of the involved
subjects.1-14 Several studies in the literature have described the frequency and severity of facial
injuries associated with sport accidents. However, to our knowledge, no prospective multicentre
study about sport-related maxillofacial injuries has been published. Therefore, several European
centers, that had already shown research experience in maxillofacial trauma,1-16 decided to
collaborate to start a prospective multicentre study about facial fracture epidemiology in Europe.
The purpose of this study is to present and discuss the demographics and patterns of sport related
maxillofacial fractures of a European multicenter prospective study about the epidemiology of facial
trauma during a year.
Material and Methods
The present study was conducted at several European departments of oral and maxillofacial
surgery: the Department of Oral and Maxillofacial Surgery/Pathology at the VU Medical Center and
Academic Center for Dentistry Amsterdam (Amsterdam, The Netherlands), the Department of
Maxillofacial Surgery at the University Hospital Dubrava (Zagreb, Croatia), the Maxilofacial
department at the UKC Ljubljana, (Ljubljana, Slovenia), the Clinic of Maxillofacial Surgery of the
School of Dentistry at the University of Belgrade (Belgrade, Serbia), the Department of Oral and
Maxillofacial Surgery of the Royal London Hospital at Barts Health NHS (London, UK), the
Department of maxilla-facial surgery at the Medical University (Plovdiv, Bulgaria), the Department
for Oral and Maxillo-facial Surgery at the Bogomolets National Medical University (Kiev, Ukraine),
the Department of Maxillofacial Surgery at the Oslo University Hospital (Oslo, Norway), the Service
6
57
6

de Stomatologie et Chirurgie Maxillo-faciale at the Chu de Nantes (Nantes, France), the
Department of Maxillofacial Surgery at the University of Bergen (Bergen, Norway), the Department
of Oral and Maxillofacial Surgery at NHS Tayside and University of Dundee, (Dundee, UK), and the
Department of Maxillofacial surgery, Stomatology Clinic, Tartu University (Tartu, Estonia).
This study is based on a systematic computer-assisted database that allowed to prospectively and
continuously record all patients hospitalized with maxillofacial fractures in the involved Maxillofacial
Surgery Units across Europe, since Monday 31st December 2012 to Sunday 29th December 2013.
Therefore, the following data were recorded for each patient: gender, age, etiology (type of sport),
site of facial fractures, Facial Injury Severity Scale (FISS), date of injury. For this study, only
patients that were admitted to the hospital for sport related maxillofacial injury were considered.
Sport-related injuries were analyzed and divided according to the type of sport. Fractures were
determined from a combination of physical examination and imaging (computed tomography scans
or conventional radiographs) at admission to hospital and classified in fractures of the mandible,
orbito-zygomatic-maxillary complex (OZM), orbit, nose, Le Fort, frontal sinus, and naso-orbital-
ethmoidal (NOE) fracture. Orbital fractures were subclassified according to the involved walls and
Le Fort fractures were divided according to Le Fort I, II, and III types. Frontal sinus fractures were
divided according to the involvement of the anterior and/or posterior tables. Mandibular fractures
included fractures of the symphysis, body, angle, ramus, coronoid, extra-articular condyle, intra-
articular condyle.
Associated injuries were classified as orthopedic, brain, abdominal, or thoracic. Patient
characteristics were analyzed using descriptive statistics.
This study obtained institutional review board approval from the leading center. We followed
Helsinki Declaration guidelines.
Results
Of the 3260 patients with maxillofacial fractures admitted within the study period, 275 traumas
(8.4%) were due to sport accidents.
On the whole, 222 patients were male and 53 were female, with a male to female ratio of 4.1:1.
Mean age was 27.6 years (median, 24; range, 3 – 66; standard deviation, 14.1). The most
numerous decade of age was the first (10 – 19 years) with 87 patients (31.6%), followed by the
second decade (20 – 29 years) that included 76 patients (27.6%), and the third (51 patients,
18.5%) (Figure 6.1).
58

Figure 6.1. Decades of age of patients affected by sport-related maxillofacial injury in the study population
As for the male to female ratio according to decades of age, Figure 6.2 shows that percentages of
men and women were similar at all ages with a remarkable predominance of males, ranging
between 5.9:1 (2nd decade) and 2.5:1 (4th decade).
Figure 6.2. Male and female distribution according to decades of age in the study population
As for etiology, soccer was most frequently responsible for maxillofacial injuries (33%), followed by
rugby (18%), skiing (12%), basketball (5%), hockey (4.5%), and combat sports (2.5%); the
remaining cases were from unspecified or other sports (Figure 6.3).
6
59
6
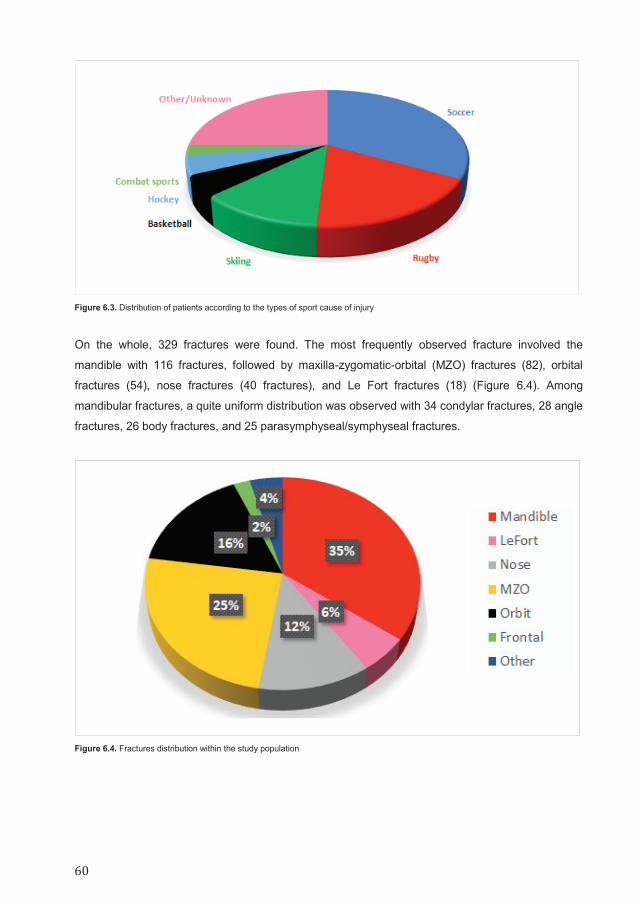
Figure 6.3. Distribution of patients according to the types of sport cause of injury
On the whole, 329 fractures were found. The most frequently observed fracture involved the
mandible with 116 fractures, followed by maxilla-zygomatic-orbital (MZO) fractures (82), orbital
fractures (54), nose fractures (40 fractures), and Le Fort fractures (18) (Figure 6.4). Among
mandibular fractures, a quite uniform distribution was observed with 34 condylar fractures, 28 angle
fractures, 26 body fractures, and 25 parasymphyseal/symphyseal fractures.
Figure 6.4. Fractures distribution within the study population
60

FISS mean score in the whole study population was 1.8 (range, 1 – 6; median, 1; standard
deviation, 1.22).
Associated body injuries were observed in few patients (18 patients) that mainly suffered from brain
(14 patients) and orthopedic lesions (6 patients). A peak of traumatic brain injuries and orthopedic
injuries was observed in rugby and skiing accidents.
Finally, the analysis of the dates of injury showed a quite uniform distribution, with the final months
of the year from September to December presenting the highest incidence of sport related
maxillofacial injuries (Figure 6.5).
Figure 6.5. Fractures monthly distribution
Discussion The analysis of the various patterns of sport related accidents is crucial, although differences in
socioeconomic conditions and traditions among countries may represent an important bias for any
attempt of assessment.
The incidence of sport related facial fractures widely varies, also because some contact sports like
rugby are naturally more at risk of facial injuries in comparison with others. Then, of course, in
some sports the use of prevention devices during practice may also play an important role: for
example, the use of mouthguards in rugby, or helmet in ski. In our study population, an incidence of
6
61
6

about 8.4% was found, that appeared to be quite low in comparison with recent articles from
developed countries (18% in New Zealand, 35% in Ireland, 31% in Austria), but higher than
developing countries (0.5% in Pakistan, 0.8% in India, 2.6% in Tanzania).
The male to female ratio observed in our study population of 4.1:1 confirmed the expected male
predominance, due to the male numeric preponderance in contact sports such as soccer and rugby
and to the higher number of male athletes in comparison to women. Furthermore, no surprise
derived from the age of the considered patients, as about 59% of the study population age was
between 10 and 29 years.
The etiology of sport related maxillofacial injuries give us important information. In our study,
soccer was the most frequently responsible sport for maxillofacial fractures, although this result is
naturally influenced by the wide diffusion of soccer in the some of the considered countries
(France, The Netherlands, United Kingdom). As expected, rugby and skiing were important
etiological factors too.
The most frequently observed fracture involved the mandible with 116 fractures, followed by
maxilla-zygomatic-orbital (MZO) fractures (82), orbital fractures (54), nose fractures (40 fractures),
and Le Fort fractures (18) (Figure 6.4). Among mandibular fractures, a curiously quite uniform
distribution was observed between condylar, angle fractures, body fractures, and parasymphyseal/
symphyseal fractures.
An important epidemiological issue can be represented by nose fractures, as the presence of
otolaryngology divisions and maxillofacial divisions within the same hospital may determine the
frequent referral of isolated nasal bone fractures to the otolaryngologist, and thus the exclusion
from the present study. The consequence could be that in the study populations of maxillofacial
centers an erroneously low percentage of nasal bone fracture may be recorded.
The low FISS mean score in the whole study population of 1.8 and the rarity of associated body
injuries (18 patients) seem to suggest that the habitual character of sport related facial injury is a
“puntiform” trauma, with the involvement of a single bone in most cases. Skiing may represent the
most frequent exception, which more often causes polytrauma because of the high speed and
energy trauma.
Finally, the analysis of the dates of injury curiously showed a highest incidence of sport related
maxillofacial injuries during the final months of the year, with no apparent explanation.
Unfortunately, there are still too many variables to draw any conclusion about sport related
maxillofacial injuries, as every single sport has different mechanism of injury, diffusion, and
preventive devices. However, educational courses for at risk sports players and coaches to
promote the use of preventive devices would be extremely important to increase their usage.
Despite the availability of such items, the risk of injury can only be reduced, and is dependent (in
addition to the magnitude of force, source, and anatomical site) on the single athlete.
62
Conclusion
This European multicenter study about sport related maxillofacial injury might represent another
important stand in our increasing understanding of the epidemiology of sport accidents and their
consequences. The importance of the perseverance in analyzing sport related facial injuries with
their features and characteristics should be stressed, as they may help to establish prevention
strategies and suggestions for all involved countries.
6
63
6

References 1. Olasoji HO, Tahir A, Arotiba GT. Changing picture of facial fractures in northern Nigeria. Br J Oral Maxillofac Surg 2002;40(2):140–
143.
2. Adebayo ET, Ajike OS, Adekeye EO. Analysis of the pattern of maxillofacial fractures in Kaduna. Nigeria Br J Oral Maxillofac Surg 2003;41(6):396–400.
3. Schaftenaar E, Bastiaens GJ, Simon EN, Merkx MA. Presentation and management of maxillofacial trauma in Dar es Salaam, Tanzania. East Afr Med J 2009;86(6):254–258.
4. Chalya PL, McHembe M, Mabula JB, Kanumba ES, Gilyoma JM. Etiological spectrum, injury characteristics and treatment outcome of maxillofacial injuries in a Tanzanian teaching hospital. J Trauma Manag Outcomes 2011;5:7.
5. Brasileiro BF, Passeri LA. Epidemiological analysis of maxillofacial fractures in Brazil: a 5-year prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;102(1):28–34.
6. Erdmann D, Follmar KE, Debruijn M, Bruno AD, Jung SH, Edelman D, Mukundan S, Marcus JR. A retrospective analysis of facial fracture etiologies. Ann Plast Surg 2008;60(4):398–403.
7. de Lucena AL, da Silva Filho GF, de Almeida Pinto Sarmento TC, de Carvalho SH, Fonseca FR, de Santana Sarmento DJ. Epidemiological profile of facial fractures and their relationship with clinical-epidemiological variables. J Craniofac Surg 2016;27(2):345–349.
8. Iida S, Kogo M, Sugiura T, Mima T, Matsuya T. Retrospective analysis of 1502 patients with facial fractures. Int J Oral Maxillofac Surg 2001;30(4):286–90.
9. Aksoy E, Unlü E, Sensöz O. A retrospective study on epidemiology and treatment of maxillofacial fractures. J Craniofac Surg 2002;13(6):772–775.
10. Klenk G, Kovacs A. Etiology and patterns of facial fractures in the United Arab Emirates. J Craniofac Surg 2003;14(1):78–84.
11. Motamedi MH. An assessment of maxillofacial fractures: a 5-year study of 237 patients. J Oral Maxillofac Surg 2003;61(1):61–64.
12. Ansari MH. Maxillofacial fractures in Hamedan province, Iran: a retrospective study (1987-2001). J Craniomaxillofac Surg 2004;32(1):28–34
13. Al Ahmed HE, Jaber MA, Abu Fanas SH, Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: a review of 230 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98(2):166–170.
14. Erol B, Tanrikulu R, Görgün B. Maxillofacial fractures. Analysis of demographic distribution and treatment in 2901 patients (25–year experience). J Craniomaxillofac Surg 2004;32(5):308–313.
15. Cheema SA, Amin F. Incidence and causes of maxillofacial skeletal injuries at the Mayo Hospital in Lahore, Pakistan. Br J Oral Maxillofac Surg 2006;44(3):232–234.
16. Kadkhodaie MH. Three-year review of facial fractures at a teaching hospital in northern Iran. Br J Oral Maxillofac Surg 2006;44(3): 229–231.
17. Al-Khateeb T, Abdullah FM. Craniomaxillofacial injuries in the United Arab Emirates: a retrospective study. J Oral Maxillofac Surg 2007;65:1094–101.
18. Subhashraj K, Nandakumar N, Ravindran C. Review of maxillofacial injuries in Chennai, India: a study of 2748 cases. Br J Oral Maxillofac Surg 2007;45:637–9.
19. Sasaki R, Ogiuchi H, Kumasaka A, Ando T, Nakamura K, Ueki T, Okada Y, Asanami S, Chigono Y, Ichinokawa Y, Satomi T, Matsuo A, Chiba H. Analysis of the pattern of maxillofacial fracture by five departments in Tokyo: A review of 674 cases. Oral Science International 2009;6(1):1–7.
20. Abbas I, Fayyaz M, Shah I, Khan MA, Qazi SH, Munir N, Bibi A, Abbasi M. Demographic distribution of maxillofacial fractures in Ayub Teaching Hospital: 7-year review. J Ayub Med Coll Abbottabad 2009;21(2):110–112.
21. Ozkaya O, Turgut G, Kayali MU, Ugurlu K, Kuran I, Bas L. A retrospective study on the epidemiology and treatment of maxillofacial fractures. Ulus Travma Acil Cerrahi Derg 2009;15(3):262–266.
22. Lee JH, Cho BK, Park WJ. A 4-year retrospective study of facial fractures on Jeju, Korea. J Craniomaxillofac Surg 2010;38(3): 192–196.
23. Venugopal MG, Sinha R, Menon PS, Chattopadhyay PK, Roy Chowdhury SK. Fractures in the maxillofacial region: A four-year retrospective study. Med J Armed Forces of India 2010;66:14–17.
24. Gandhi S, Ranganathan LK, Solanki M, Mathew GC, Singh I, Bither S. Pattern of maxillofacial fractures at a tertiary hospital in northern India: a 4-year retrospective study of 718 patients. Dent Traumatol 2011;27:257–262.
25. Mesgarzadeh AH, Shahamfar M, Azar SF, Shahamfar J. Analysis of the pattern of maxillofacial fractures in north western of Iran: A retrospective study. J Emerg Trauma Shock 2011;4(1):48–52.
26. Zandi M, Khayati A, Lamei A, Zarei H. Maxillofacial injuries in western Iran: a prospective study. Oral Maxillofac Surg 2011;15(4): 201–209.
27. Naveen Shankar A, Naveen Shankar V, Hegde N, Hegde N, Sharma, Prasad R. The pattern of the maxillofacial fractures–A multicentre retrospective study. J Craniomaxillofac Surg 2012;40(8):675–679.
28. Kapoor P, Kalra N. A retrospective analysis of maxillofacial injuries in patients reporting to a tertiary care hospital in East Delhi. Int J Crit Illn Inj Sci 2012;2(1):6–10
64
29. Kar IB, Mahavoi BR. Retrospective analysis of 503 maxillo-facial trauma cases in odisha during the period of Dec ‘04–Nov ‘09. J Maxillofac Oral Surg 2012;11(2):177–181.
30. Abdullah WA, Al-Mutairi K, Al-Ali Y, Al-Soghier A, Al-Shnwani A. Patterns and etiology of maxillofacial fractures in Riyadh City, Saudi Arabia. Saudi Dent J 2013;25(1):33–38.
31. Almasri M. Severity and causality of maxillofacial trauma in the Southern region of Saudi Arabia. Saudi Dent J 2013;25(3):107–110.
32. Bali R, Sharma P, Garg A, Dhillon G. A comprehensive study on maxillofacial trauma conducted in Yamunanagar, India. J Inj Violence Res 2013;5(2):108–116.
33. Jin Z, Jiang X, Shang L. Analysis of 627 hospitalized maxillofacial-oral injuries in Xi’an, China. Dent Traumatol 2014;30(2):147–153.
34. Mijiti A, Ling W, Tuerdi M,Maimaiti A, Tuerxun J, Tao YZ, Saimaiti A, Moming A. Epidemiological analysis of maxillofacial fractures treated at a university hospital, Xinjiang, China: A 5-year retrospective study. J Craniomaxillofac Surg 2014;42(3):227–233.
35. Zhou HH, Ongodia D, Liu Q, Yang RT, Li ZB. Changing pattern in the characteristics of maxillofacial fractures. J Craniofac Surg 2013;24(3):929–933.
36. Motamedi MH, Dadgar E, Ebrahimi A, Shirani G, Haghighat A, Jamalpour MR. Pattern of maxillofacial fractures: a 5-year analysis of 8,818 patients. J Trauma Acute Care Surg 2014;77(4):630–634.
37. Kaul RP, Sagar S, Singhal M, Kumar A, Jaipuria J, Misra M. Burden of maxillofacial trauma at level 1 trauma center. J Craniomaxillofac Trauma Reconstr 2014;7(2):126–130.
38. Pandey S, Roychoudhury A, Bhutia O, Singhal M, Sagar S, Pandey RM. Study of the pattern of maxillofacial fractures seen at a tertiary care hospital in north India. J Maxillofac Oral Surg 2015;14(1):32–39.
39. Gaddipati R, Ramisetti S, Vura N, Reddy KR, Nalamolu B. Analysis of 1,545 Fractures of Facial Region-A Retrospective Study. Craniomaxillofac Trauma Reconstr 2015;8(4):307–314.
40. Kumar GB, Dhupar V, Akkara F, Kumar SP. Patterns of maxillofacial fractures in goa. J Maxillofac Oral Surg 2015;14(2):138–141.
41. Gassner R, Tuli T, Hächl O, Rudisch A, Ulmer H. Cranio-maxillofacial trauma: a 10 year review of 9,543 cases with 21,067 injuries. J Craniomaxillofac Surg 2003;31(1):51–61.
42. Bakardjiev A, Pechalova P. Maxillofacial fractures in Southern Bulgaria - a retrospective study of 1706 cases. J Craniomaxillofac Surg 2007;35(3):147–150.
43. Pombo M, Luaces-Rey R, Pértega S, Arenaz J, Crespo JL, Garcia-Rozado A, Patino B, Lopez-Cedrun JL. Review of 793 facial fractures treated from 2001 to 2008 in a coruna university hospital: types and etiology. Craniomaxillofac Trauma Reconstr 2010;3(1):49–54.
44. Walker TW, Donnellan J, Byrne S, McArdle N, Kerin MJ, McCann PJ. West of Ireland facial injury study. Part 2. Br J Oral Maxillofac Surg 2012;50(7):e99–e103.
45. van den Bergh B, Karagozoglu KH, Heymans MW, Forouzanfar T. Aetiology and incidence of maxillofacial trauma in Amsterdam: a retrospective analysis of 579 patients. J Craniomaxillofac Surg 2012;40(6):e165–e169.
46. Kostakis G, Stathopoulos P, Dais P, Gkinis G, Igoumenakis D, Mezitis M, Rallis G. An epidemiologic analysis of 1,142 maxillofacial fractures and concomitant injuries. Oral Surg Oral Med Oral Pathol Oral Radiol 2012;114(5 suppl):S69–S73.
47. Kyrgidis A, Koloutsos G, Kommata A, Lazarides N, Antoniades K. Incidence, aetiology, treatment outcome and complications of maxillofacial fractures. A retrospective study from Northern Greece. J Craniomaxillofac Surg 2013;41(7):637–643.
48. Rashid A, Eyeson J, Haider D, van Gijn D, Fan K. Incidence and patterns of mandibular fractures during a 5-year period in a London teaching hospital. Br J Oral Maxillofac Surg 2013;51(8):794–798.
49. van Hout WM, Van Cann EM, Abbink JH, Koole R. An epidemiological study of maxillofacial fractures requiring surgical treatment at a tertiary trauma centre between 2005 and 2010. Br J Oral Maxillofac Surg 2013;51(5):416–420.
50. Ascani G, Di Cosimo F, Costa M, Mancini P, Caporale C. Maxillofacial fractures in the province of pescara, Italy: a retrospective study. ISRN Otolaryngol 2014;23:101370.
51. Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, Kovačič Ž, Vesnaver A, Konstantinović VS, Petrović M, Stephens J, Kanzaria A, Bhatti N, Holmes S, Pechalova PF, Bakardjiev AG, Malanchuk VA, Kopchak AV, Galteland P, Mjøen E, Skjelbred P, Koudougou C, Mouallem G, Corre P, Løes S, Lekven N, Laverick S, Gordon P, Tamme T, Akermann S, Karagozoglu KH, Kommers SC, Forouzanfar T. European Maxillofacial Trauma (EURMAT) project: a multicentre and prospective study. J Craniomaxillofac Surg 2015;43(1):62–70.
52. Schneider D, Kämmerer PW, Schön G, Dinu C, Radloff S, Bschorer R. Etiology and injury patterns of maxillofacial fractures from the years 2010 to 2013 in Mecklenburg-Western Pomerania, Germany: A retrospective study of 409 patients. J Craniomaxillofac Surg 2015;43(10):1948–51.
53. Buchanan J, Colquhoun A, Friedlander L, Evans S, Whitley B, Thomson M. Maxillofacial fractures at Waikato Hospital, New Zealand: 1989 to 2000. N Z Med J 2005;118(1217):U1529.
54. Cabalag MS, Wasiak J, Andrew NE, Tang J, Kirby JC, Morgan DJ. Epidemiology and management of maxillofacial fractures in an Australian trauma centre. J Plast Reconstr Aesthet Surg 2014;67(2):183–189.
55. Moore BK, Smit R, Colquhoun A, Thompson WM. Maxillofacial fractures at Waikato Hospital, New Zealand: 2004 to 2013. N Z Med J 2015;128(1426):96–102.
56. Maladière E, Bado F, Meningaud JP, Guilbert F, Bertrand JC. Aetiology and incidence of facial fractures sustained during sports: a prospective study of 140 patients. Int J Oral Maxillofac Surg 2001;30(4):291–295.
6
65
6
57. Exadaktylos AK, Eggensperger NM, Eggli S, Smolka KM, Zimmermann H, Iizuka T. Sports related maxillofacial injuries: the first maxillofacial trauma database in Switzerland. Br J Sports Med 2004;38(6):750–753.
58. Mourouzis C, Koumoura F. Sports-related maxillofacial fractures: a retrospective study of 125 patients. Int J Oral Maxillofac Surg 2005;34(6):635–638.
59. Antoun JS, Lee KH. Sports-related maxillofacial fractures over an 11-year period. J Oral Maxillofac Surg 2008;66(3):504–508.
60. Roccia F, Diaspro A, Nasi A, Berrone S. Management of sport-related maxillofacial injuries. J Craniofac Surg 2008;19(2):377–382.
61. Hwang K, You SH, Lee HS. Outcome analysis of sports-related multiple facial fractures. J Craniofac Surg 2009;20(3):825–829.
62. Murphy C, O'Connell JE, Kearns G, Stassen L. Sports-Related Maxillofacial Injuries. J Craniofac Surg 2015;26(7):2120–2123.
63. Ruslin M, Boffano P, ten Brincke YJ, Forouzanfar T, Brand HS. Sport-Related Maxillo-Facial Fractures. J Craniofac Surg 2016; 27(1):e91–e94.
64. Roccia F, Caldarelli C, Spada MC, Brucoli M, Beatrice F, Ruffino S, Benech A, Ramieri G, Berrone S. Development of a regional database for studying epidemiology of maxillofacial trauma. J Craniofac Surg 2010;21(4):1045–1050.
65. Leinhart J, Toldi J, Tennison M. Facial Trauma in Sports. Curr Sports Med Rep 2017;16(1):23–29.
66. Salentijn EG, Peerdeman SM, Boffano P, van den Berg B, Forouzanfar T. A ten-year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: incidence and aetiology. J Craniomaxillofac Surg 2014;42(6):705–170.
67. Salentijn EG, Collin JD, Boffano P, Forouzanfar T. A ten-year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: Complications and treatment. J Craniomaxillofac Surg 2014;42(8):1717–1722.
68. Boffano P, Kommers SC, Karagozoglu KH, Forouzanfar T. Aetiology of maxillofacial fractures: a review of published studies during the last 30 years. Br J Oral Maxillofac Surg 2014;52(10):901–906.
69. Giarda M, Tavolaccini A, Arcuri F, Brucoli M, Benech A. Surgical approach to isolated bilateral orbital floor fractures. Acta Otorhinolaryngol Ital 2015;35(5):362–364.
70. Benech A, Nicolotti M, Brucoli M, Arcuri F. Intraoral extra-mucosal fixation of fractures in the atrophic edentulous mandible. Int J Oral Maxillofac Surg 2013;42(4):460–463.
71. Arcuri F, Brucoli M, Baragiotta N, Benech R, Ferrero S, Benech A. Analysis of complications following endoscopically assisted treatment of mandibular condylar fractures. J Craniofac Surg 2012;23(3):e196–e198.
72. Brucoli M, Arcuri F, Cavenaghi R, Benech A. Analysis of complications after surgical repair of orbital fractures. J Craniofac Surg 2011;22(4):1387–1390
66

67

68

Chapter 7
Dental trauma in association with
maxillofacial fractures:
An epidemiological study
This is an edited version of the manuscript:
Muhammad Ruslin, Jan Wolff, Henk S. Brand, Paolo Boffano, Tymour Forouzanfar
Dental trauma in association with maxillofacial fractures: An epidemiological study
Dental Traumatology 2015; August;31(4):318-323
Abstract Introduction:
Dental injury and facial soft tissue are one of the most commonly seen injuries in patients with
maxillofacial trauma. The prevalence of dental injury is highly worldwide and mostly occurs in
childhood and adolescence. The aim of this study was to retrospectively investigate the incidence
and associated factors of dental trauma in patients with maxillofacial fractures at the VU Medical
Center in Amsterdam.
Methods:
Data from 707 patients who were treated surgically for maxillofacial fractures were evaluated. The
data were collected retrospectively from patient files and other available databases. The data
collected included date of fracture, age, gender, type of fracture, and injured teeth.
Results:
Of the total 707 patients, 164 patients (23.2%) presented dental injuries associated with facial
fractures. Mandibular condylar fractures, mandibular parasymphyseal fractures, Le Fort fractures,
and mandibular body fractures were found to be significantly more associated with dental injury.
Zygomatic arch or zygomatic complex fractures were significantly less associated with dental
injury. Women had a significant higher risk of facial fractures with dental injuries than men. The
maxilla demonstrated the highest incidence of injured teeth. The most affected teeth were the
maxillary incisors (33.1%), followed by mandible incisors (13.6%), mandible molars (12.8%), and
maxillary premolars (12.6%).
Conclusion:
Our findings show a higher risk of dental injury among patients with a mandibular condylar fracture
and mandibular parasymphyseal fracture but a lower risk of dental injury among patients with a
zygomatic arch or zygomatic complex fracture. On average, patients had more than three injured
teeth, with most of the injured teeth being in the upper jaw. The maxillary incisors, followed by the
mandible incisors, were the most injured teeth.
70
Introduction
When a maxillofacial trauma occurs, the most common types of injuries are facial soft tissue injury
and dental injury. The prevalence of dental injury is highly worldwide and mostly occurs in
childhood and adolescence.1-6 Andreasen et al.1,7 found injuries to permanent anterior teeth in one
in four adults and in one in five children. The prevalence of dental injury varies considerably
between countries,2-6 and it is determined by many factors such as behavioral and cultural diversity,
social and economic status, the age of the population that is investigated, and the lack of
standardization in dental trauma research.
Depending on the severity of the accident, fractures to facial bones may also occur. Trauma
resulting in only maxillofacial fractures has been frequently studied.8-15 Findings show the age
group most susceptible to only facial fractures is 19–30 years,9,10,12,14,15 although some researchers
have reported that the 20–40 years age group is the most susceptible.11-13
Dental injury that is associated with other maxillofacial trauma is also commonly seen. At the time
of writing, seven articles have been published in several countries that describe the frequency and
type of dental injury associated with maxillofacial fractures.2,12-17 These studies have shown that the
prevalence of dental injuries in patients with facial bone fractures ranges from 13% up to
23%.2,12,13,16,17 Exceptions to these findings are the research of Zhou et al.14 and da Silva et al.15
These researchers found the prevalence of patients with dental injuries in combination with facial
fractures to be 41.8% and 2.1%, respectively. Many of the patients studied were aged between 20
and 30 years.14,16
Dental trauma may influence the treatment of facial fractures and usually requires postoperative
dental treatment, which in turn requires good communication with the treating dentist. Furthermore,
facial fractures can also have an influence on the treatment of dental injuries. In some cases,
dental treatment is not possible after fracture reduction due to facial swelling and can lead to
subsequent premature tooth loss in some cases.
In the Netherlands, maxillofacial surgeons commonly perform first aid dental treatment. This makes
it important to understand the prevalence of dental trauma in relation to facial fractures. A previous
study performed in the Netherlands by van den Bergh et al.9 investigated the incidence and
etiology of maxillofacial trauma. They found zygomatic and mandibular bone fractures to be the
most common bone fracture in both men and women. Together, these fractures account for
approximately 80% of all facial fractures. A study that investigates the relationship between dental
injuries and facial fractures in the Netherlands has yet to be performed. The aim of this present
study was therefore to retrospectively investigate the incidence and associated factors of dental
trauma in patients with maxillofacial fractures at the VU University Medical Center, Amsterdam,
from January 2000 until March 2013.
7
71
7
Material and methods
This study is based on an analysis of a patient database from the Department of Oral and
Maxillofacial Surgery, Vrije Universiteit University Medical Center (VUmc), Amsterdam, the
Netherlands. The patient database comprised retrospectively collected data from January 1, 2000,
until January 1, 2010, and a systematic computerassisted database that has continuously recorded
patients with maxillofacial fractures between January 1, 2010, and March 1, 2013. The study was
performed according to the guidelines of the Medical Ethics Committee of the Free University of
Amsterdam.
Only surgically treated patients were included in the study. Totally edentulous patients, patients
with a nose fracture or fractures in the dentoalveolar complex, and patients who received no
surgical treatment were excluded from the study. The patient data included date of fracture, age,
gender, type of fracture, and site of injured teeth. In the study, patients were divided into three
groups based on their age at the time of trauma: children (0–12 years), teenagers (13–19 years),
and adults (20 years and older). Adult patients were further categorized into the age groups: 20-29,
30-39, 40-49, 50-59, 60-69, 70-79, and 80 years and older.
The facial fractures were subdivided into fractures of the frontal sinus, orbital fractures, fractures of
the zygoma complex, zygomatic arch fractures, Le Fort I/II/III fractures, mandibular coronoid
fractures, condylar fractures, mandibular ramus fractures, mandibular angulus fractures,
mandibular body fractures, and parasymphyseal fractures. All of these fractures were registered on
the left side, the right side, or on both sides. The site of the injured teeth was classified as maxillary
or mandibular and then further subdivided in incisors, canines, premolars, and molars. The type of
dental injury was not further specified.
Statistical analysis was performed using SPSS (version 18.0) to assess the relationship between
dental injury and other relevant variables. The data were analyzed using the chi-squared test, the
independent-sample t-test, and the one-sample t-test, and P-values of 0.005 or less were
considered to be statistically significant.
Results
In total, 707 patients with facial fractures were included in the study. Table 7.1. shows the
descriptive statistics. The study population comprised 525 males and 182 females, giving a male-
to-female ratio of 2.9:1. The mean age of the patients was 33.6 years, with a range from 2 to 88
years. The majority of patients (233 patients, 33.0%) with facial fractures were aged 20 to 29 years.
No significant difference between males and females was found (chi-squared test). Of these
72

patients, 164 patients (23.2%) presented dental injuries associated with facial fractures. Of these,
106 were male and 58 female, giving a male-to-female ratio of 1.8:1. Their mean age was 31.4
years, ranging from 5 to 69 years. Most of the patients (55 patients, 33.5%) with associated dental
injury were aged 20–29 years (Table 7.1). Furthermore, results showed women had a significant
higher risk of facial fractures with dental injuries than men (chi-squared, P = 0.001), and men had a
significant higher risk of only facial fractures than women (P = 0.001).
Table 7.1. Descriptive statistic
Age (years) Total patient group Patients with only dental injuries
Gender Gender Male (%) Female (%) Total (%) Male (%) Female (%) Total (%)
0-9 3 (0.6) 3 (1.6) 6 (0.8) 0 - 1 (1.7) 1 (0.6) 10-19 73 (13.9) 22 (12.1) 95 (13.4) 22 (20.8) 10 (17.2) 32 (19.5) 20-29 182 (34.7) 51 (28) 233 (33) 37 (35) 18 (31) 55 (33.5) 30-39 118 (22.5) 37 (20.3) 155 (21.9) 24 (22.6) 14 (24.1) 38 (23.2) 40-49 88 (16.8) 33 (18.1) 121 (17.1) 11 (10.4) 9 (15.5) 20 (12.2) 50-59 38 (7.2) 17 (9.3) 55 (7.8) 8 (7.5) 3 (5.2) 11 (6.7) 60-69 17 (3.2) 12 (6.6) 29 (4.1) 4 (3.8) 3 (5.2) 7 (4.3) 70-79 4 (0.8) 6 (3.3) 10 (1.4) 0 - 0 - 0 - 80-89 2 (0.4) 1 (0.5) 3 (0.4) 0 - 0 - 0 - Total 525 (100) 182 (100) 707 (100) 106 (100) 58 (100) 164 (100)
Among the total group, 1231 maxillofacial bone fractures were recorded, which accounts for a
mean of 1.74 fractures per patient. The mean for patients with dental injury associated with
fractures proved to be higher (mean 2.48; P < 0.05). Table 7.2. shows that the zygomatic complex
is the most fractured bone (25.35%), followed by the mandibular condyle (22.7%). In contrast to
this finding, the lower third of the face was more susceptible to fractures than the upper two-thirds.
Looking at the group with facial fractures and dental injuries, the mandibular condylus proved to be
most fractured bone (38.7%), followed by fractures of the mandibular parasymphyseal region
(22.4%). No dental injury was found with the zygomatic arch fractures. In this group, the lower third
of the face was also more susceptible to fractures than the upper two-thirds of the face. Statistical
analysis showed that dental injury occurred significantly more frequently in association with
mandibular condylar fracture (P < 0.001), mandibular parasymphyseal fracture (P < 0.001), Le Fort
fracture (P < 0.001), and mandibular body fracture (P = 0.049) (Table 7.2). There is a significantly
lower risk for dental injury in association with injury in the zygomatic region (P < 0.001).
7
73
7
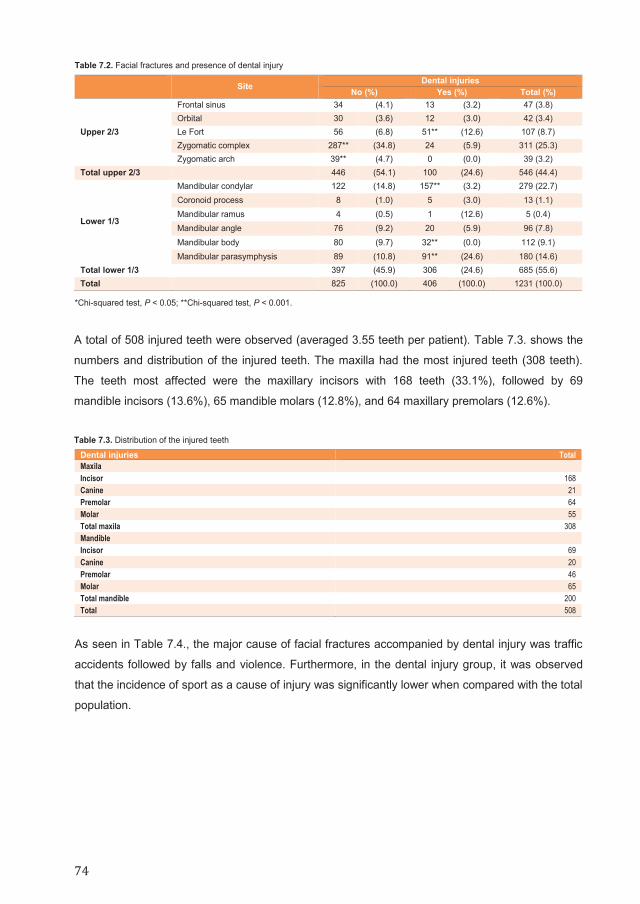
Table 7.2. Facial fractures and presence of dental injury
Site Dental injuries No (%) Yes (%) Total (%)
Upper 2/3
Frontal sinus 34 (4.1) 13 (3.2) 47 (3.8) Orbital 30 (3.6) 12 (3.0) 42 (3.4) Le Fort 56 (6.8) 51** (12.6) 107 (8.7) Zygomatic complex 287** (34.8) 24 (5.9) 311 (25.3) Zygomatic arch 39** (4.7) 0 (0.0) 39 (3.2)
Total upper 2/3 446 (54.1) 100 (24.6) 546 (44.4)
Lower 1/3
Mandibular condylar 122 (14.8) 157** (3.2) 279 (22.7) Coronoid process 8 (1.0) 5 (3.0) 13 (1.1) Mandibular ramus 4 (0.5) 1 (12.6) 5 (0.4) Mandibular angle 76 (9.2) 20 (5.9) 96 (7.8) Mandibular body 80 (9.7) 32** (0.0) 112 (9.1) Mandibular parasymphysis 89 (10.8) 91** (24.6) 180 (14.6)
Total lower 1/3 397 (45.9) 306 (24.6) 685 (55.6) Total 825 (100.0) 406 (100.0) 1231 (100.0)
*Chi-squared test, P < 0.05; **Chi-squared test, P < 0.001.
A total of 508 injured teeth were observed (averaged 3.55 teeth per patient). Table 7.3. shows the
numbers and distribution of the injured teeth. The maxilla had the most injured teeth (308 teeth).
The teeth most affected were the maxillary incisors with 168 teeth (33.1%), followed by 69
mandible incisors (13.6%), 65 mandible molars (12.8%), and 64 maxillary premolars (12.6%).
Table 7.3. Distribution of the injured teeth
Dental injuries Total Maxila Incisor 168 Canine 21 Premolar 64 Molar 55 Total maxila 308 Mandible Incisor 69 Canine 20 Premolar 46 Molar 65 Total mandible 200 Total 508
As seen in Table 7.4., the major cause of facial fractures accompanied by dental injury was traffic
accidents followed by falls and violence. Furthermore, in the dental injury group, it was observed
that the incidence of sport as a cause of injury was significantly lower when compared with the total
population.
74

Table 7.4. Etiologi of maxillofacial fractures
Patients with maxillofacial fractures (%) Patients with maxillofacial fractures and dental injuries (%) Fail 128 (18.1) 43* (26.2) Traffic accident pedestrian 16 (2.3) 2 (1.2) Traffic accident bicycle 159 (22.5) 64* (39.0) Traffic accident TMMW 90 (12.7) 20 (12.2) Traffic accident CAR 34 (4.8) 7 (4.3) Sport 83 (11.7) 5* (3.0) Violence 173 (24.5) 20* (12.2) Work 7 (1.0) 1 (0.6) Other 17 (2.4) 2 (1.2) Total 707 (100) 164 (100)
*Significance, P < 0.001
Dicussion Our study evaluated all patients presenting with facial trauma accompanied with dental injury at the
VU University Medical Center (VUmc) in Amsterdam, the Netherlands, over a period of 13 years.
VU University Medical Center is a University Hospital and one of the main hospitals that treats
facial injuries in the greater Amsterdam area. Patients who did not receive surgical treatment were
excluded from the study. In this study, we found a prevalence of dental injury in association with
facial fractures of 23.2%. Iso-Kungas et al.17 found a similar prevalence of 22.5%, although their
population comprised only pediatric patients. Our prevalence of dental injury in association with
facial fractures was higher than the prevalence found by Lieger et al.13 with 19.5%, Thoren et al.12
with 16%, Gassner et al.18 with 18.9%, Roccia et al.16 with 13.1%, but lower than the prevalence
found by Zhou et al.14 (41.8%). The relatively high prevalence of dental injury in our study can
partly be explained by our inclusion criteria. We were mainly interested in patients who had
received surgical treatment for their maxillofacial injury. Therefore, patients treated nonsurgically
had probably suffered less severe trauma without any associated dental injury.
In our total study population, most of the patients were aged between 20 and 29 years. This is in
agreement with the majority of the recent studies that have investigated facial fractures.8-12,14,15
Lieger et al.13 found that most patients were between 31 and 40 years old. However, their study
group also contained totally edentulous patients. Of the 164 patients with facial fractures and dental
injury, most were between 20 and 29 years old. This finding is in line with other recent studies on
maxillofacial fractures.14,16,18 The prevalence of isolated dental injury varies considerably,1 but tends
to occur most frequently in children and adolescents.1,2,4,5,18 Iso-Kungas et al.17 investigated a
group of pediatric patients and found higher figures than were found in other studies that focused
on adults. They concluded that dental injury together with facial fractures was generally more
complicated in children than in adults.17
7
75
7

As in other studies, we found a male predominance in both the total group and the group with
dental injury with facial fractures.8,12-18 This is a similar finding to studies that investigated dental
injury only. Many of these studies found a male-to-female ratio of 2:1.4,9,21 However, in our study we
found that women had a statistically higher association for dental injuries with facial fractures
compared with their male counterparts. Roccia et al.16 found the same association. However,
Thoren et al.12 worked in the same field and found no significant association between gender and
incidence of dental injury.
In this present study, the bone most susceptible to fracture was the zygomatic complex, followed
by the mandibular condylar. Thoren et al.12 reported slightly different results, with mandibular
fractures being the most prevalent, followed by zygomatico-orbital fractures. In the group with facial
fractures and dental injury, the mandibular condyle was the most fractured bone, followed by the
mandibular parasymphyseal region. This corresponds to the findings of Roccia et al.16 who
reported the same results. Furthermore, we found that the lower third of the face was more
susceptible to fractures than the upper two-thirds of the face in both the group with dental injury
and the group without dental injury. This contrasts with the findings of other researchers who found
that most fractures occurred in the upper two-thirds of the face in the group without dental
injury.12,15,16 However, in accordance with the findings of our survey, most studies have reported
the lower third of the face to be more susceptible to fractures in the group with facial fractures and
dental injury.12,15-17 One explanation for the higher incidence of facial fractures in the lower third of
the face found in our study could be that most patients in the Amsterdam area are treated for
bicycle accidents and not for interpersonal violence. As a result, those patients treated for bicycle
accidents at the VUMC have a higher susceptibility to fractures in the lower third of the face.
Our results showed that the mandibular condylar fracture, mandibular parasymphyseal fracture,
Le Fort fracture, and mandibular body fracture were significantly more associated with dental injury.
Lieger et al.13 found that patients with dental injury had a higher risk of symphysis fractures,
followed by condylar fractures. Zhou et al.14 also found significantly more dental injury with only
symphysis fractures. Other authors reported that dental injury was significantly more associated
with mandibular fractures.12,16,17 However, da Silva et al.15 observed more maxillary fractures than
mandibular fractures with dental injury, although this conclusion was based on only seven patients
with facial fractures combined with dental injury.
The results of the present study show a mean of 3.55 injured teeth per patient. This is higher than
the findings of Thoren et al.12 who found a mean of 2.5 injured teeth, Iso-Kungas et al.17 who found
a mean of 3.2 injured teeth, and Roccia et al.16 who found a mean of 2.8 injured teeth per patient.
Zhou et al.14 found a higher mean number of injured teeth per patient (4.68 teeth), but they also
reported a higher number of patients with dental injuries than in our study. The maxilla contained
the most injured teeth in our patient group. Other studies have reported similar results:12-14,16 one
study found a similar number of injured teeth in the upper and lower jaw.17 Similar to other
studies,2-14,16,17 our study found maxillary incisors to be the teeth most effected, followed by the
76

mandibular incisors. This corresponds with the findings of studies that investigated isolated dental
injuries, where most of the injured teeth were in the anterior segment.4,7,19-22
Several studies22-26 have reported a temporal shift in the importance of different causes of facial
bone fractures. In particular, the role of traffic accidents as a cause of facial bone fracture has
decreased, whereas the number of facial bone fractures caused by violence and sport injuries has
increased. However, in our study, we found injuries caused by two-wheeled motor vehicle (TWMV)
accidents have increased significantly and sport-related accidents have significantly decreased.
Although we did not find a significant difference, we also observed a slight and slow increase in the
number of fractures caused by violence over the study period. When we examined the causes of
maxillofacial fractures with associated dental injuries, we found a similar trend for violence as an
increasing cause.
The present study had several potential limitations. In the first place, it was a single-center study.
There are three other hospitals in Amsterdam where patients with maxillofacial injuries are treated.
As the patients are not divided equally among the four hospitals in Amsterdam, some hospitals
may see more and different kinds of patients than other hospitals. Therefore, the results in the
present study might not be fully representative for the Netherlands. As the data were partly
collected retrospectively, this may also introduce information bias. Nevertheless, the results found
in this study are mostly in line with other studies and suggest that the data might be useful for the
development of protocols to prevent maxillofacial trauma accompanied with or without dental injury.
Because oral and maxillofacial injuries are associated with functional, socioeconomic, and
psychological factors, it is important to take appropriate preventative measures. Prevention can be
accomplished with various safety measures such as seatbelts, airbags, stricter speed limits, road
safety training, using different lanes for different types of vehicles, tougher drunk driving laws, and
the use of protective sport equipment such as helmets, mouth guards, and face shields.23,25,27–29 In
the Netherlands, very few people wear helmets while cycling. Although helmets provide significant
protection against brain injury,28,30 they are less useful against facial fractures of the mandible
because the chin area is not protected.
Conclusion The results of this study showed that men had the most fractured bones, but women had a
significantly higher risk of facial fractures with dental injury. We found a higher risk of dental injury
among patients with a mandibular condylar fracture, mandibular parasymphyseal fracture, Le Fort
fracture, or mandibular body fracture and a lower risk among patients with zygomatic arch or
zygomatic complex fractures. On average, patients had more than three injured teeth, with most of
7
mandibular incisors. This corresponds with the findings of studies that investigated isolated dental
injuries, where most of the injured teeth were in the anterior segment.4,7,19-22
Several studies22-26 have reported a temporal shift in the importance of different causes of facial
bone fractures. In particular, the role of traffic accidents as a cause of facial bone fracture has
decreased, whereas the number of facial bone fractures caused by violence and sport injuries has
increased. However, in our study, we found injuries caused by two-wheeled motor vehicle (TWMV)
accidents have increased significantly and sport-related accidents have significantly decreased.
Although we did not find a significant difference, we also observed a slight and slow increase in the
number of fractures caused by violence over the study period. When we examined the causes of
maxillofacial fractures with associated dental injuries, we found a similar trend for violence as an
increasing cause.
The present study had several potential limitations. In the first place, it was a single-center study.
There are three other hospitals in Amsterdam where patients with maxillofacial injuries are treated.
As the patients are not divided equally among the four hospitals in Amsterdam, some hospitals
may see more and different kinds of patients than other hospitals. Therefore, the results in the
present study might not be fully representative for the Netherlands. As the data were partly
collected retrospectively, this may also introduce information bias. Nevertheless, the results found
in this study are mostly in line with other studies and suggest that the data might be useful for the
development of protocols to prevent maxillofacial trauma accompanied with or without dental injury.
Because oral and maxillofacial injuries are associated with functional, socioeconomic, and
psychological factors, it is important to take appropriate preventative measures. Prevention can be
accomplished with various safety measures such as seatbelts, airbags, stricter speed limits, road
safety training, using different lanes for different types of vehicles, tougher drunk driving laws, and
the use of protective sport equipment such as helmets, mouth guards, and face shields.23,25,27–29 In
the Netherlands, very few people wear helmets while cycling. Although helmets provide significant
protection against brain injury,28,30 they are less useful against facial fractures of the mandible
because the chin area is not protected.
Conclusion The results of this study showed that men had the most fractured bones, but women had a
significantly higher risk of facial fractures with dental injury. We found a higher risk of dental injury
among patients with a mandibular condylar fracture, mandibular parasymphyseal fracture, Le Fort
fracture, or mandibular body fracture and a lower risk among patients with zygomatic arch or
zygomatic complex fractures. On average, patients had more than three injured teeth, with most of
7
77
7

the injured teeth being in the upper jaw. The maxillary incisors, followed by the mandibular incisors,
were the most injured teeth. Traffic accidents were found to be the major cause of dental injuries.
Further, research on various safety measures and on the treatment and survival of injured teeth to
improve patient treatment strategy is recommended.
78

References 1. Glendor U, Marcenes W, Andreasen JO. Classification, epidemiology and etiology. In: Andreasen JO, Andreasen FM, Andersson L,
editors. Textbook and color atlas of traumatic injuries to the teeth. Oxford, UK: Bleckwell Publishing; 2007. p. 217–54.
2. Gassner R, Bosch R, Tuli R, Emshoff R. Prevalence of dental trauma in 6000 patients with facial injuries. Implication for prevention. Oral Surg Oral Med Oral Pathol Ral Radiol Endod 1999;87(1):27–33.
3. Andreasen JO. Etiology and pathogenesis of traumatic dentalinjuries. A clinical studie of 1,298 cases. Scand J Dent Res 1970;78(4): 329–342.
4. Glendor U, halling A, Andersson L, Elier-Petersson E. Incidence of traumatic tooth injuries in children and adolescents in the country of Vastmanland, Sweden. Swed Dent J 1996;20(1-2):15–28.
5. Glendor U. Epidemiology of traumatic dental injuries-a12 year review of the literature. Dent Traumatol 2008;24(6):603–611. 6. Bastone EB, Freer TJ, McNamara JR. Epidemiology of dental trauma: a review of the literature. Aust Dent J 2000;45(1):2–9. 7. Kastle LM, Gift HC, Bhat M, Swango PA. Prevalence of incisor trauma in persons 6-50 years of age: United States, 1988–1991. J
Dent Res 1996;75:696–705. 8. Naveen Shankar A, Naveen Shankar V, Hedge N, Sharma, Prasad R. The pattern of the maxillofacial fractures - A multicenter
retrospective study. J Craniomaxillofac Surg 2012;40(8):675–679. 9. van den Bergh B, Karagozoglu KH, Heymans MW, Forouzanfar T. Aetiology and incidence of maxillofacial trauma in Amsterdam: a
retrospective analysis of 579 patients. J Craniomaxillofac Surg 2012;40(6):e165–e169. 10. Al Ahmed HE, Jaber MA, Abu Fanas SH, Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: a review
of 230 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98(2):166–170. 11. Bali R, Sharma P, Garg A, Dhillon G. A comprehensive study on maxillofacial trauma conducted in Yamunanagar, India. J Inj
Violence Res 2013;5(2):108–116. 12. Thoren H, Numminen L, Snall J, Kormi E, Lindqvist C, Lizuka T, Tornwall J. Occurrence and types of dental injuries among patients
with maxillofacial fractures. Int J Oral Maxillofac Surg 2010;39(8):774–778. 13. Lieger O, Zix J, Kruse A, Iizuka T. Dental injuries in association with facial fractures. J Oral Maxillofac Surg 2009;67(8):1680–1684. 14. Zhou HH, Ongodia D, Liu Q, Yang RT, Li ZB. Dental trauma in patients with maxillofacial fractures. Dental Traumatol 2013;29(4):
285–290. 15. da Silva AC, Passeri LA, Mazzonetto R, De Moraes M, Moreira RW. Incidence of dental trauma associated with facial trauma in
Brazil: a 1-year evaluation. Dent Traumatol 2004;20(1):6–11. 16. Roccia F, Boffano P, Bianchi FA, Ramieri G. An 11-year review of dental injuries associated with maxillofacial fractures in Turin,
Italy. J Oral Maxillofac Surg 2013;17(4):269–274. 17. Iso-Kungas P, Tornwall J, Suominen AL, Lindqvist C, Thoren H. Dental injuries in pediatric patients with facial fractures are frequent
and severe. J Oral Maxillofacial Surg 2012;70(2):396–400. 18. Gassner R, Tuli T, Hachl O, Rudisch A, Ulmer H. Craniomaxillofacial trauma: a 10 year review of 9,543 cases with 21,067 injuries. J
Craniomaxillofac Surg 2003;31(1):51–61. 19. Lauridsen E, Hermann NV, Gerds TA, Kreiborg S, Andreasen JO. Pattern of traumatic dental injuries in the permanent dentition
among children, adolescents, and adults. Dent Traumatol 2012;28(5):358–363. 20. Caldas AD, Burgos MEA. A retrospective study of traumatic dental injuries in Brazilian dental trauma clinic. Dent Traumatol
2001;17(6):250–253. 21. Rajab LD. Trumatic dental injuries in children presenting for treatment at the Department of Pediatric Dentistry, Faculty of Dentistry,
University of Jordan, 1997–2000. Dent Traumatol 2003;19(1):6–11. 22. Borssen E, Holm AK. Traumatic dental injuries in a cohort of 16-years-olds in Northern Sweden. Endod Dent Traumatol 1997;13(6):
276–280. 23. Fasola AO, Nyako EA, Obiechina AE, Arotiba JT. Trends inthe characteristics of maxillofacial fractures in Nigeria. J Oral Maxillofac
Surg 2003;61(10):1140–1143. 24. Kyrgidis A, Koloutsos G, Kommata A, Lazarides N, Antoniades K. Incidence, aetiology, treatment outcome and complications of
maxillofacial fractures. A retrospective study from Northern Greece. J Craniomaxillofac Surg 2013;41(7):637–643. 25. van Beck GJ, Merkx CA. Changes in the pattern of fractures of the maxillofacial skeleton. Int J Oral Maxillofac Surg 1999;28(6):424–
428. 26. Kostakis G, Stathopoulus P, Dais P, Gkinis G, Igoumenakis D, Mezitis M, Rallis G. An epidemiologic analysis of 1142 maxillofacial
fractures and concomitant injuries. Oral Surg Oral Med Oral Pathol Oral Radiol 2012;114(5 Suppl):S69–S73. 27. Exadaktylos AK, Eggensperger NM, Eggli S, Smolka KM, Zimmermann H, Iizuka T. Sports related maxillofacial injuries: the first
maxillofacial trauma database in Switzerland. Br J Sports Med 2004;38(6):750–753. 28. Thompson DC, Nunn ME, Thompson RS, Rivara FP. Effectiveness of bicycle safety helmets in preventing serious facial injury.
JAMA 1996;276(24):1974–1975. 29. McMullin BT, Rhee JS, Pintar FA, Szabo A, Yoganandan N. Facial fractures in motor vehicle collisions. Arch Facial Plast Surg
2009;11(3):165–170. 30. Lee JH, Cho BK, Park WJ. A 4-year retrospective study of facial fractures on Jeju, Korea. J Craniomaxillofac Surg 2010;38(3):192–
196.
7
79
7

80

Chapter 8
The Maxillofacial Injury Severity Score (MFISS) and
Facial Injury Severity Scale (FISS) as a predictor brain
injury with maxillofacial fractures patients
This is an edited version of the manuscript:
Muhammad Ruslin, Paolo Boffano, HCW de Vet, M Brucoli, KH Karagozoglu, Tymour Forouzanfar
The Maxillofacial Injury Severity Score (MFISS) and Facial Injury Severity Scale (FISS)
as a predictor brain injury with maxillofacial fractures patients
Submitted
Abstract Introduction:
The aims of this study were to assess prognostic value of Maxillofacial Injury Severity Score
(MFISS) and Facial Injury Severity Scale (FISS) in detecting brain injury and maxillofacial fractures
patients at the VU Medical Center in Amsterdam.
Methods:
The data were collected retrospectively from patient files and other available databases. The data
collected included age, gender, cause of trauma, and diagnosis of moderate to severe traumatic
brain injury (TBI). Two commonly used systems were selected: MFISS and FISS, each patient was
graded according to these two systems. Results of the two scoring systems score were compared,
and statistical analysis was performed to assess association between brain injury and age, etiology
and trauma score values.
Results:
Of the total 1326 patients, 52 patients were diagnosed with TBI. Both FISS and MFISS proved to
be associated significantly with TBI. Higher FISS and MFISS were associated with a higher TBI
cases. The sensitivity and specificity analyses demonstrated that the best values were for the FISS
3 and 5, and for the MFISS 7. Other parameters such as age, gender, location of the facture ets,
did not improve the results.
Conclusion:
FISS and MFISS proven to be useful and valuable assessment tools for diagnosing TBI. However,
the clinician can choose the cut-off point with the best sensitivity and specificity fitting in the
depending on the hospital policy. Combinations with other patient specific parameters did not
improve the results.
82

Introduction
The most common types of injuries after maxillofacial injuries are facial soft tissue injury, and
depending on the severity of the accident, fractures to facial bones may also occur. Trauma
resulting in only maxillofacial fractures has been frequently studied.1-4 The facial skeleton
comprises the bone of the maxilla, zygoma, and the bony walls of the nasal cavity, paranasal
sinuses, and orbit and the mandible. It is one of the most complex arrangements of curving bony
structures in the body and it is commonly involved in brain injury.5
Maxillofacial trauma with associated traumatic brain injury (TBI) carries significant potential for
mortality and neurological morbidity.6,7 TBI is defined as loss of consciousness and/or post-
traumatic amnesia in a patient with a non-penetrating head injury.8 The association between
maxillofacial trauma and brain injury is still a matter of current debate. Numerous studies on
maxillofacial trauma accompanies with traumatic brain injury have been carried out.9-14 According
to Davidoff et al.8 facial fractures proven to be strongly associated with traumatic brain injury.8 On
the other hand, Haug et al.15 found a 76% incidence of neurologic injury associated with facial
fractures. Furthermore, Haug et al.15 stressed that, in case of a trauma to the midface, energy will
be directly transmitted to the cranium, causing damage to the brain.15 In contrast to these studies,
many authors have the opinion that no association exists between maxillofacial trauma and brain
injury. In their study Lee et al.16 demonstrated that facial fractures are not associated with an
increased risk of traumatic brain injury, theorizing that facial bones act as a protective cushion for
the brain.16 This is in line with the study performed by Chang et al.17 who stated that the maxilla
and the surrounding midfacial bones act as an absorption barrier against high impact energy
caused by trauma, thus protecting the brain from damage. Due to these mechanisms fewer brain
injuries are expected to occur. Knowing the consequences of untreated brain injury, it is very
important to detect in early stage the brain injuries accompanied the maxillofacial fractures.
In the literature several severity indices for maxillofacial trauma are noted.18-21 Two most used
classification scores are and Facial Injury Severity Scale (FISS)19 and the Maxillofacial Injury
Severity Score (MFISS).18,20 Both systems combine the Injury Severity Score parameters of
maxillofacial function and appearance (e.g., limited opening of mouth, malocclusion, facial
deformity). Furthermore, they are based on the Abbreviated Injury Scale (AIS).18-20 The FISS
includes the classification of laceration of facial soft tissue as well as that of bone. However, the
classification of bones is not very detailed. Therefore, it cannot be used to distinguish displaced
and comminuted fractures.19,20 Scoring systems such as the MFISS are useful to classify not only
anatomic damages, but also the impairment of maxillofacial function and facial appearance,
subsequently reflecting the effect of maxillofacial injury on quality of life.
The use of trauma score and severity grade in trauma studies can provide the basis to decide the
most appropriate treatment strategy, and to predict the survival probability of injured patients and
8
83
8
the impact on health status in the future.18 To our knowledge there is lack of information in the
literature concerning the association of FISS and MFISS with TBI.
The aim of the present study was twofold. First, to investigate the correlation between FISS, and
MFISS with TBI. Second, to study the sensitivity and specificity of these classifications in detecting
brain injury in patients with maxillofacial fractures. In doing so the authors wanted to investigate the
clinical use of these tests.
Materials and Methods This study is based on an analysis of a patient database from the Department of Oral and
Maxillofacial Surgery, Vrije Universiteit University Medical Center (VUmc), Amsterdam, the
Netherlands. The patient database comprised retrospectively collected data from January 1, 2002,
until January 1, 2010, and a systematic computer-assisted database that has continuously
recorded patients with maxillofacial fractures between January 1, 2010, and April 1, 2013. The
study was performed according to the guidelines of the Medical Ethics Committee of the Free
University of Amsterdam.
Surgically and non-surgically treated maxillofacial trauma patients with and without TBI were
included in the study. Totally edentulous patients, patients with a nose fracture or dentoalveolar
fractures were excluded. The patient data included date of fracture, age, gender, type of fracture,
and diagnosis of moderate/severe traumatic brain injury.
The facial fractures were subdivided into fractures of the frontal sinus, orbital fractures, fractures of
the zygoma complex, zygomatic arch fractures, Le Fort I/II/III fractures, mandibular coronoid
fractures, condylar fractures, mandibular ramus fractures, mandibular angulus fractures,
mandibular body fractures, and parasymphyseal fractures. All of these fractures were registered on
the left side, the right side, or on both sides. The FISS and MFISS were calculated for each patient.
Statistical analysis was performed using SPSS (version 18.0) to assess the relationship between
brain injury and FISS and MFISS. We used 2 X 2 tables to calculate the sensitivity and specificity
values for different cut-off points of FISS and MFISS in showing brain injury (Table 8.1). The best
cut-off point was selected by 2 authors (T.F. and R.d.V) and was defined as one with best balance
of sensitivity and specificity.
Further, data were analyzed using logistic regression analysis, chi-squared test, the independent-
sample t-test, and the one-sample t-test, and p-values of 0.05 or less were considered to be
statistically significant.
84
Table 8.1. Calculation of sensitivity and specificity
Cut-off MFISS of FISS NO brain injury Brain injury
≥ Cut-off A B
< Cut-off C D
Sensitivity, a/(a+c); Specificity, d/(b+d)
Results On the whole, between 2002 and 2013, 1326 patients affected by maxillofacial fractures were
referred and treated at the Department of Oral and Maxillofacial Surgery at the VUmc.
The mean age of patients whom suffered from maxillofacial injuries was 39.2 years (range 5 – 98,
SD 19.64). Most patients were grouped in the 2nd decade (20–29 years) with 351 cases, followed
by the 3rd (30 – 39 years) and the 4th (40 – 49 years).
Most patients were males (68.25%). The etiology of the maxillofacial injuries was mostly from fall
(24.5%), followed by traffic bicycle accidents (20.14%) and assaults (18.29 %).
Out of 1326 patients of the study population, 52 subjects (4%) were diagnosed with a moderate to
severe TBI. A motor vehicle accident was the main etiological factor in patients who presented with
traumatic brain injury, with 22 patients with TBI out of 52 (42,3%). A statistically significant
association was observed between motor vehicle accidents (MVA) related maxillofacial injuries and
the diagnosis of TBI (p < 0.05). In fact, among the various mechanisms of injury, patients who had
MVAs were most likely to have moderate to severe traumatic brain injuries, whereas age did not
seem to represent a particular risk factor for TBI.
According to decades of age, a quite uniform distribution of traumatic brain injury was observed
with no statistically significant differences.
FISS mean value was found to be 2.25 (range, 1 – 21; SD, 1.93), with the most frequent observed
values being 1 (55%), followed by 4 (15%), and 3 (11%). MFISS mean calculated value was 5.70
(range, 1 – 48; SD, 3.90), with the most frequent observed values of 6 (57%), 3 (20%), and
2 (10%).
FISS seemed to statistically associated with TBI (p < 0.00005, IC95% 9.7 – 31.9, OR 17.6), but risk
of neurotrauma only increased with FISS > or = 5. The value of MFISS was statistically associated
with the diagnosis of TBI too (p < 0.00005, IC95% 3.9 – 12.6, OR 7). With this score system, risk of
neurotrauma only increased with MFISS > or = 7.
In Table 8.2a., and 8.2b., the calculated sensitivity and specificity of FISS and MFISS according to
different cut-off points are demonstrated. The best results were seen in the FISS with the cut-off
point of 3 and 5. For MFISS the best cut-off point proved to be 7. The cross-tabs for the two best
points of the FISS are shown in Table 8.3a and 8.3b as an example.
8
85
8
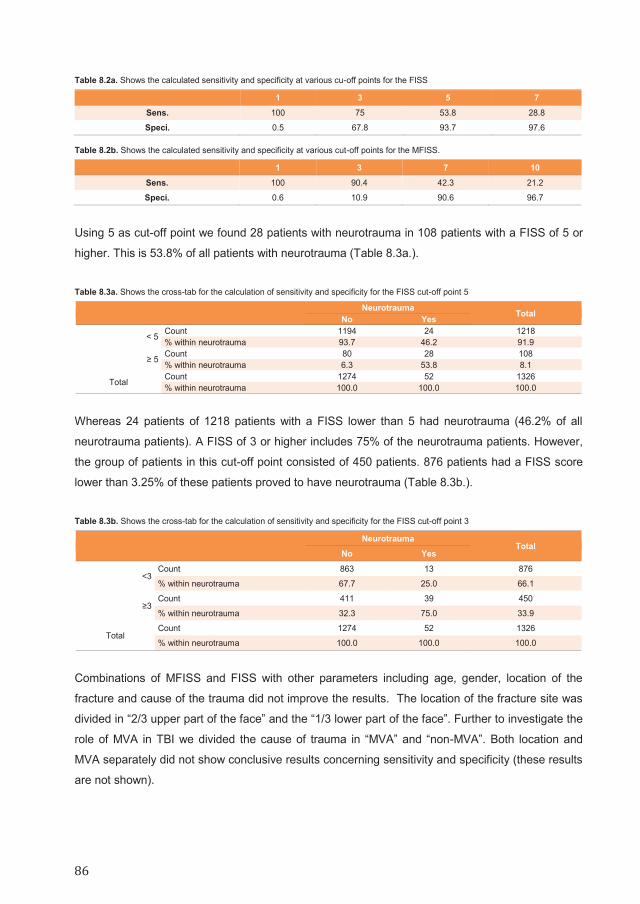
Table 8.2a. Shows the calculated sensitivity and specificity at various cu-off points for the FISS
1 3 5 7
Sens. 100 75 53.8 28.8
Speci. 0.5 67.8 93.7 97.6
Table 8.2b. Shows the calculated sensitivity and specificity at various cut-off points for the MFISS.
1 3 7 10
Sens. 100 90.4 42.3 21.2
Speci. 0.6 10.9 90.6 96.7
Using 5 as cut-off point we found 28 patients with neurotrauma in 108 patients with a FISS of 5 or
higher. This is 53.8% of all patients with neurotrauma (Table 8.3a.).
Table 8.3a. Shows the cross-tab for the calculation of sensitivity and specificity for the FISS cut-off point 5
Neurotrauma Total
No Yes
< 5 Count 1194 24 1218
% within neurotrauma 93.7 46.2 91.9
≥ 5 Count 80 28 108 % within neurotrauma 6.3 53.8 8.1
Total Count 1274 52 1326 % within neurotrauma 100.0 100.0 100.0
Whereas 24 patients of 1218 patients with a FISS lower than 5 had neurotrauma (46.2% of all
neurotrauma patients). A FISS of 3 or higher includes 75% of the neurotrauma patients. However,
the group of patients in this cut-off point consisted of 450 patients. 876 patients had a FISS score
lower than 3.25% of these patients proved to have neurotrauma (Table 8.3b.).
Table 8.3b. Shows the cross-tab for the calculation of sensitivity and specificity for the FISS cut-off point 3
Neurotrauma
Total
No Yes
<3 Count 863 13 876
% within neurotrauma 67.7 25.0 66.1
≥3 Count 411 39 450
% within neurotrauma 32.3 75.0 33.9
Total Count 1274 52 1326
% within neurotrauma 100.0 100.0 100.0
Combinations of MFISS and FISS with other parameters including age, gender, location of the
fracture and cause of the trauma did not improve the results. The location of the fracture site was
divided in “2/3 upper part of the face” and the “1/3 lower part of the face”. Further to investigate the
role of MVA in TBI we divided the cause of trauma in “MVA” and “non-MVA”. Both location and
MVA separately did not show conclusive results concerning sensitivity and specificity (these results
are not shown).
86
Discussion Early recognition of associated TBIs is a fundamental part of initial assessment and treatment
planning in facial trauma patients and could significantly reduce morbidity and mortality associated
with these life threatening injuries.22
There may be important risks to the patient if the diagnosis of minor head injury is missed. In fact,
symptoms such as impaired memory and concentration and persistent headaches can become
chronic and limit function and safe return to work. Finally, if the severity of concussion is not
diagnosed, then patients may be given inadequate advice regarding follow-up and return to sports
or work.23
According to a recent study based on finite element analysis of maxillofacial trauma associated
with TBIs, site and direction of facial impact played a key role in determining the severity and
location of the facial bone fracture, which in turns influenced those of the traumatic brain injury.22
This study confirmed that severity of brain injury is highly associated with the proximity of location
of impact to the brain: in particular, owing to its close proximity to the brain, the anterior-inferior
frontal lobe experiences injuries with higher severity.22
Previous studies demonstrated that the presence of facial bone fractures is actually a marker for
increased risk of brain injury, observing that patients with facial fracture had a greater chance of
presenting with TBI compared with non-facial fracture patients.13
Therefore, it seems that facial fracture might act as a sentinel for TBI as hypothesized by some
authors that suggested that facial fracture might be a predictable marker for TBI.24 In our
investigation, FISS and MFISS proved to be useful and valuable assessment tools. Higher values
of both FISS and MFISS revealed to be statistically associated with the diagnosis of TBI.
In addition to this crucial finding from the literature, we managed to add further important
information to the current literature. In fact, in our study, more severe facial damage (higher FISS
and MFISS values) was associated with traumatic brain injury, thanks to a positive correlation
between the severity of maxillofacial injuries and the occurrence of traumatic brain injury.
This is of clinical importance as it indicates that in severely injured patients with severe and
complex facial fractures, early neurosurgical/neurological assessment is most probably needed and
emergency computed tomography should be performed without delay to prevent the morbidity
associated with TBI.
Quick neurological diagnosis and early intervention is fundamental to prevent or at least decrease
the occurrence of avoidable complications as well as mortality and to give the most appropriate
multidisciplinary treatment, as even a short duration of hypoxia and edema might lead to significant
neurological deficits.
It is important to consider that the incidence of head injury in patients with maxillofacial trauma
might be attributed to the transfer of force from the facial skeleton to the cranium. The mechanism
of force transmission that occurs through the head and the neck during facial trauma is not well
8
87
8

understood.23 Traditionally, the face has been thought to have an impact absorbing property,
thereby protecting the neurocranium from severe injury. Nevertheless, some authors have
suggested that the facial skeleton may actually transmit the significant forces required to induce
fractures of the facial skeleton directly to the neurocranium, resulting in serious brain injury.22
In the results we noted the sensitivity and specificity of different cut-off points for the FISS and
MFISS. It is difficult to point one specific cut-off point as the best. The cut off point 3 and 5 for the
FISS showed the best sensitivity and specificity. Using 3 as cut-off point the reliability to diagnose
neurotrauma is higher than the other point. However, the patient number in our population having a
FISS of 3 or higher is very high. It is questionable if we had to admitt all these patients to the
department of neurology for an early neurosurgical/neurological assessment to identify 75% of all
patients with a TBI. However, as we showed the results of different cut-off points for FISS and
MFISS a clinician can choose which cut-off point suits better to their hospital protocols.
The main limitations of the present study are due to the local and not fully national
representativeness, as well as to the retrospective nature of the investigation. Nevertheless, the
results found in this study are mostly in line with other studies, and suggest that the data might be
useful for the development of protocols to prevent maxillofacial trauma accompanied with or
without brain injury.
Conclusion
The results of our study seem to confirm that severe facial fractures are associated with traumatic
brain injury. In fact, severe facial fractures mean more mechanical force insult and affect more
severe injury to brain. Our data showed that despite the association between severity of the trauma
and traumatic brain injury it is very difficult to identify a parameter or a set of parameters with a high
sensitivity and specificity for diagnosing traumatic brain injuries.
88
References
1. Naveen Shankar A, Naveen Shankar V, Hedge N, Sharma, Prasad R. The pattern of the maxillofacial fractures - a multicenter
retrospective study. J Craniomaxillofac Surg 2011;40(8):675–679.
2. van den Bergh B, Karagozoglu KH, Heymans MW, Forouzanfar T. An etiology and incidence of maxillofacial trauma in Amsterdam: a retrospective analysis of 579 patients. J Craniomaxillofac Surg 2012;40(6):e165–e169.
3. Al Ahmed HE, Jaber MA, Abu Fanas SH, Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: a review
of 230 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98(2):166–170. 4. Bali R, Sharma P, Garg A, Dhillon G. A comprehensive study on maxillofacial trauma conducted in Yamunanagar, India. J Inj
Violence Res 2013;5(2):108–116. 5. Hussain K, Wijetunge DB, Grubnic S, Jackson IT. A comprehensive analysis of craniofacial trauma. J Trauma 1994;36(1):34–47. 6. Bogusiak K, Arkuszewski P. Characteristics and epidemiology of zygomaticomaxillary complex fractures. J Craniofac Surg
2010;21(4):1018–1023. 7. Stiver SI. Complications of decompressive craniectomy for traumatic brain injury. Neurosurg Focus 2009;26(6):E7. 8. Davidoff G, Jakubowski M, Thomas D, Alpert M. The spectrum of closed-head injuries in facial trauma victims: incidence and
impact. Ann Emerg Med 1988;17(1):6–9. 9. Salentijn EG, Peerdeman S, Boffano P, van den Bergh B, Forouzanfar T. A ten-year analysis of the traumatic maxillofacial and brain
injury patient in Amsterdam: incidence and aetiology. J Craniomaxillofac Surg 2014;42(6):705–710. 10. Salentijn EG, Collin JD, Boffano P, Forouzanfar T. A ten-year analysis of the traumatic maxillofacial and brain injury patient in
Amsterdam: Complications and treatment. J Craniomaxillofac Surg 2014;(42(8):1717–1722. 11. Gassner R, Tuli T, Hachl O, Rudisch A, Ulmer H. Cranio-maxillofacial trauma: a 10 year review of 9543 cases with 21067 injuries. J
Craniomaxillofac Surg 2003;31(1):51–61. 12. Thoren H, Snall J, Salo J, Suominen-Taipale L, Kormi E, Lindqvist C, Törnwall J. Occurrence and types of associated injuries in
patients with fractures of the facial bones. J Oral Maxillofac Surg 2010;68(4):805–810. 13. Rajandram RK, Syed OSN, Rashdi MF, Abdul JMN. Maxillofacial injuries and traumatic brain injury - a pilot study. Dent Traumatol
2014;30(2):128–132. 14. Rajendra PB, Mathew TP, Agrawal A, Sabharawal G. Characteristics of associated craniofacial trauma in patients with head injuries:
An experience with 100 cases. J Emerg Trauma Shock. 2009;2(2):89–94. 15. Haug RH, Savage JD, Likavec MJ, Conforti PJ. A review of 100 closed head injuries associated with facial fractures. J Oral
Maxillofac Surg 1992;50(3):218–222. 16. Lee KF, Wagner LK, Lee YE, Suh JH, Lee SR. The impact-absorbing effects of facial fractures in closed-head injuries. An analysis
of 210 patients. J Neurosurg 1987;66(4):542–547. 17. Chang CJ, Chen YR, Noordhoff MS, Chang CN. Maxillary involvement in central craniofacial fractures with associated head injuries.
J Trauma 1994;37(5):807–811. 18. Zhang J, Zhang Y, El-Maaytah M, Ma L, Liu L, Zhou LD. Maxillofacial Injury Severity Score: proposal of a new scoring system. Int J
Oral Maxillofac Surg 2006;35(2):109–114. 19. Bagheri SC, Dierks EJ, Kademani D, Holmgren E, Bell RB, Hommer L, Potter BE. Application of a facial injury severity scale in
craniomaxillofacial trauma. J Oral Maxillofac Surg 2006;64(3):408–414. 20. Chen C, Zhang Y, An J-G, He Y, Gong X, Comparative study of four maxillofacial trauma scoring systems and expert score. J Oral
Maxillofac Surg 2014;72(11):2212–2220. 21. Sahni V, Maxillofacial Trauma Scoring Systems: A Review. Injury 2016;47(7):1388–1392. 22. Tse KM, Tan LB, Lee SJ, Lim SP, Lee HP. Investigation of the relationship between facial injuries and traumatic brain injuries using
a realistic subject-specific finite element head model. Accid Anal Prev 2015;79:13–32. 23. Grant AL, Ranger A, Young GB, Yazdani A. Incidence of major and minor brain injuries in facial fractures. J Craniofac Surg
2012;23(5):1324–1328. 24. You N, Choi MS, Roh TH, Jeong D, Kim SH. Severe facial fracture is related to severe traumatic brain injury. World Neurosurg
2018;111;e47–e52. 25. Aladelusi T, Akinmoladun V, Olusanya A, Akadiri O, Fasola A. Analysis of road traffic crashes-related maxillofacial injuries severity
and concomitant injuries in 201 patients seen at the UCH, Ibadan. Craniomaxillofac Trauma Reconstr 2014;7(4):284–289.
8
89
8

90

Chapter 9
The use of neuron-specific enolase to
predict mild brain injury in motorcycle
crash patients with maxillofacial
fractures: A pilot study
This is an edited version of the manuscript: Muhammad Ruslin, Jan Wolff, Harmas Y. Yusuf, Muhammad Z. Arifin, Paolo Boffano, Tymour Forouzanfar
The use of neuron-specific enolase to predict mild brain injury in motorcycle crash patients with maxillofacial fractures:
A pilot study
Accepted for Publication

Abstract
Introduction:
Mild traumatic brain injury (TBI) is common but accurate diagnosis and its clinical consequences
have been a problematic, maxillofacial trauma does have an association with traumatic brain injury.
Neuron-specific enolase (NSE) have been developed to evaluate neuronal damage. The aim of this
study was to investigate the accuracy of neuron-specific enolase (NSE) serum levels to detect mild
brain injury of patients with sustained maxillofacial fractures during motor vehicle accidents.
Methods:
Blood samples were drawn from 40 healthy (control group) and 48 trauma patients who had
sustained isolated maxillofacial fractures and mild brain injury assessed employing Glasgow Coma
Scale. In the trauma group, correlations between the NSE serum values and different facial fracture
sites were assessed.
Results:
The mean NSE serum level in the group of 48 patients who had sustained maxillofacial fracture
was 13.12 ng/ml with SD (standard deviation) of 9.68 ranging from 3.19 to 54.51 ng/ml. These
values were significantly higher than those measured in the healthy control group (p <0.001). The
mean NSE serum levels in the lower part of the facial skeleton (15.44 ng/ml with SD of 15.34) were
higher than those in the upper facial part (12.42 ng/ml with SD 7.68); and the mean NSE level in
middle-and lower part 11.97 ng/ml with SD 5.63, was higher than in the middle part (7.88 with SD
2.64).
Conclusion:
NSE serum levels can be observed in patients who have sustained maxillofacial fractures and mild
brain injury.
92
IncreasedNSEserumlevelscanbeobservedinpatientswhohavesustainedmaxillofacialfractures
and mild brain Injury.

Introduction Mild traumatic brain injury (TBI) is common but accurate diagnosis and its clinical consequences
have been a problematic. Mild TBI causes transient neurophysiologic brain dysfunction, sometimes
with structural axonal and neuronal damage. Clinically mild TBI includes acute early phase post-
traumatic symptoms such as headache, dizziness, imbalance, fatigue, sleep disruption, and
impaired cognition. These symptoms resolve for several days even weeks and they are largely
related to brain trauma and concomitant injuries. The late phase post-traumatic symptoms exist in
minority of patients consist of somatic, emotional, and cognitive symptoms. Effective early phase
management may prevent or limit the later phase symptoms and should include education about
symptoms and expectations for recovery, as well as recommendations for activity modifications.1
In a recent retrospective study, Salentijn et al.2 found that maxillofacial trauma does have an
association with traumatic brain injury. In comparison to the overall maxillofacial trauma population,
their results demonstrate that frontal sinus fractures are more commonly diagnosed in brain injury
and the location of impact in these kinds of traumas is potentially considered to be the cause.
Despite substantial progress in post-traumatic neuro-monitoring it still remains difficult to quantify
the exact extent of brain injury sustained during such fractures. To date the Glasgow Coma Scale
(GCS) is still considered to be the gold standard in assessing the consciousness level of patients
having sustained traumatic brain injury after trauma.3 However the GCS scale lacks of specificity to
assess the exact magnitude of brain injury sustained during the traumatic brain. Even with the
current used scale like the Marshall CT classification, such injuries still remain difficult to assess.4
Despite numerous studies on maxillofacial trauma accompanies with traumatic brain injury have
been carried out,5-9 there is still a lack of information on undetected mild brain injury to patients with
maxillofacial trauma after vehicle accidents. Knowing the consequences of untreated mild brain
injury, it is very important to detect in early stage the brain injuries exist in maxillofacial trauma
patients. Therefore, this study is especially carried out to detect mild degree of brain injury in
patients with maxillofacial trauma after vehicle accidents.
In recent years, several new biomarkers have been developed to evaluate neuronal injuries and
have ever since also become increasingly important supplements to the GCS. Neuron-specific
enolase (NSE) is one of such protein-based enzyme found primarily within neurons and it is
commonly used to assess the grade of neuronal damage after trauma.10-14 Increased concentration
of NSE can be measured in the cerebrospinal fluid and in the peripheral blood after neuronal
damage in which it provides a quick and reliable laboratory indicator of the degree of brain cell
damage sustained after trauma.15
The present pilot study was aimed at investigating the neuron-specific enolase serum levels in
patients that had sustained maxillofacial fractures during motor vehicle accidents. Furthermore, we
9
93
9

also assessed the differences of NSE serum values at different maxillofacial fracture sites. The
eventual future aim would be to investigate prospectively the accuracy neuron-specific biomarkers
in detecting mild brain injury in patients with maxillofacial trauma.
Material and Methods
Ethical approval was granted by the Health Research Ethics Committee at the Faculty of Medicine
University of Padjadjaran / Dr. Hasan Sadikin General Hospital Bandung, Indonesia. The first group
consisted of 48 adult patients who had sustained isolated maxillofacial fractures during motor
vehicle accidents in the Bandung area. The fracture locations were divided into three parts: upper,
middle and lower part. The upper part of facial skeleton comprising the frontal bone, the middle part
comprising the midfacial bone: the maxilla, the nasoethmoid, and lateral midfacial bone-zygoma,
and the lower part comprising the mandible. The second group of 40 control patients were healthy
adult subjects with no history of facial trauma that were undergoing routine medical checkup at the
Dr. Hasan Sadikin Hospital in Bandung.
A detail analysis was carried out on all patients who satisfied the inclusion and exclusion criteria.
The inclusion criteria for the first group are all patients whom presented with isolated maxillofacial
injuries during motor vehicle accidents, structural imaging normal, loss of consciousness 0–30 min,
alteration of consciousness/mental state up to 24 h, and post-traumatic amnesia 0–1 day. Only
patients with a mild brain injury (GCS score 13 – 15) were included in this study. Patients with
multiple traumas with Abbreviated Injury Score (AIS) ≥ 3 in other body region were excluded from
the study. Prognosis of all patients was good.
The brain injury was measured using the GCS. The GCS was introduced in 1974 as a method for
determining objectively the severity of brain dysfunction and coma six hours after the occurrence of
the head trauma. The GCS scale is composed of three different tests namely: eye, verbal, and
motor response. Mild available score is 13 – 15, moderate score is 9 – 12 and severe if its score
range is < 9.3
All blood samples were withdrawn from both patient groups by peripheral vein puncture. All NSE
measurements were performed with an electrochemiluminescence immunoassay (ECLIA), using a
sandwich technique in duplicate, with NSE kits (Roche, Mannheim, Germany) and the Elecsys
2010 analyzer (Roche Diagnostics, Mannheim, Germany). Since the half-life of NSE in the serum is
approximately 48 hours,16 all trauma and healthy patients in this study underwent NSE screening
within 24 hours.
The time from injury to blood drawn in one trauma patient in our study was in 30 hours, one trauma
patient was in 28 hours and the rest of them drawn in < 24 hours. Furthermore it must be noted
94
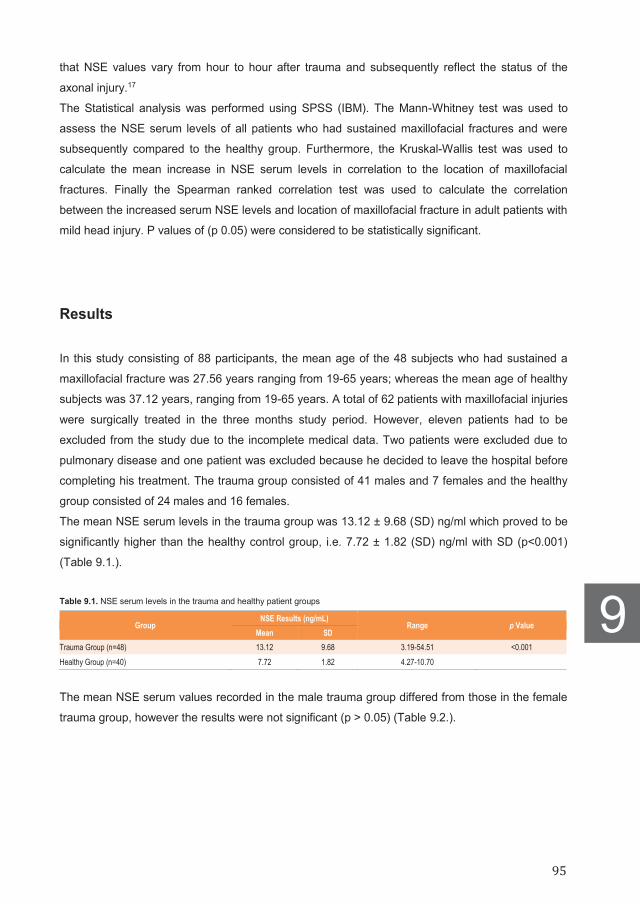
that NSE values vary from hour to hour after trauma and subsequently reflect the status of the
axonal injury.17
The Statistical analysis was performed using SPSS (IBM). The Mann-Whitney test was used to
assess the NSE serum levels of all patients who had sustained maxillofacial fractures and were
subsequently compared to the healthy group. Furthermore, the Kruskal-Wallis test was used to
calculate the mean increase in NSE serum levels in correlation to the location of maxillofacial
fractures. Finally the Spearman ranked correlation test was used to calculate the correlation
between the increased serum NSE levels and location of maxillofacial fracture in adult patients with
mild head injury. P values of (p 0.05) were considered to be statistically significant.
Results
In this study consisting of 88 participants, the mean age of the 48 subjects who had sustained a
maxillofacial fracture was 27.56 years ranging from 19-65 years; whereas the mean age of healthy
subjects was 37.12 years, ranging from 19-65 years. A total of 62 patients with maxillofacial injuries
were surgically treated in the three months study period. However, eleven patients had to be
excluded from the study due to the incomplete medical data. Two patients were excluded due to
pulmonary disease and one patient was excluded because he decided to leave the hospital before
completing his treatment. The trauma group consisted of 41 males and 7 females and the healthy
group consisted of 24 males and 16 females.
The mean NSE serum levels in the trauma group was 13.12 ± 9.68 (SD) ng/ml which proved to be
significantly higher than the healthy control group, i.e. 7.72 ± 1.82 (SD) ng/ml with SD (p<0.001)
(Table 9.1.).
Table 9.1. NSE serum levels in the trauma and healthy patient groups
Group NSE Results (ng/mL)
Range p Value Mean SD
Trauma Group (n=48) 13.12 9.68 3.19-54.51 <0.001 Healthy Group (n=40) 7.72 1.82 4.27-10.70
The mean NSE serum values recorded in the male trauma group differed from those in the female
trauma group, however the results were not significant (p > 0.05) (Table 9.2.).
9
95
9
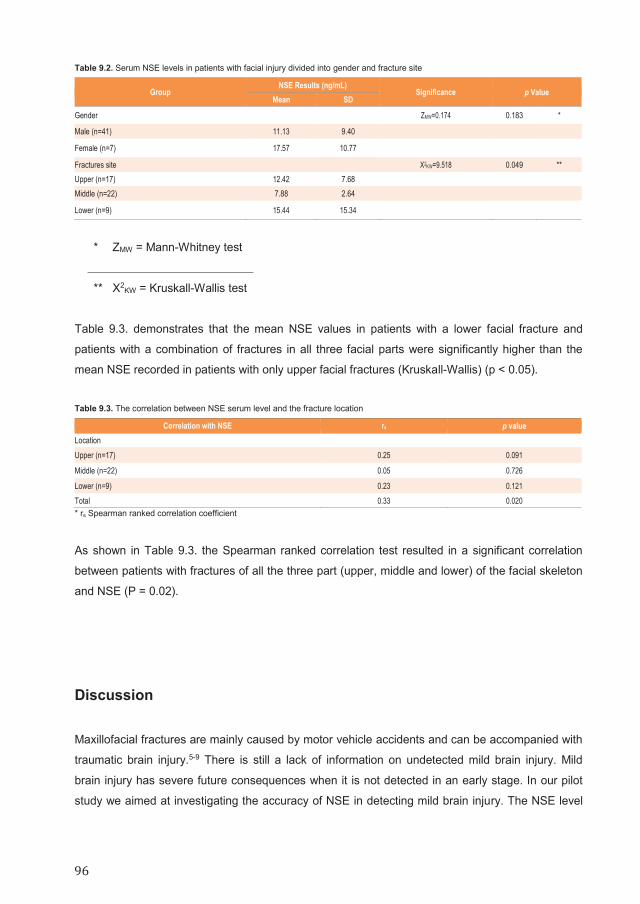
Table 9.2. Serum NSE levels in patients with facial injury divided into gender and fracture site
Group NSE Results (ng/mL)
Significance p Value Mean SD
Gender ZMW=0.174 0.183 *
Male (n=41) 11.13 9.40
Female (n=7) 17.57 10.77
Fractures site X2KW=9.518 0.049 ** Upper (n=17) 12.42 7.68 Middle (n=22) 7.88 2.64
Lower (n=9) 15.44 15.34
* ZMW = Mann-Whitney test
** X2KW = Kruskall-Wallis test
Table 9.3. demonstrates that the mean NSE values in patients with a lower facial fracture and
patients with a combination of fractures in all three facial parts were significantly higher than the
mean NSE recorded in patients with only upper facial fractures (Kruskall-Wallis) (p < 0.05).
Table 9.3. The correlation between NSE serum level and the fracture location
Correlation with NSE rs p value Location Upper (n=17) 0.25 0.091
Middle (n=22) 0.05 0.726
Lower (n=9) 0.23 0.121 Total 0.33 0.020 * rs Spearman ranked correlation coefficient
As shown in Table 9.3. the Spearman ranked correlation test resulted in a significant correlation
between patients with fractures of all the three part (upper, middle and lower) of the facial skeleton
and NSE (P = 0.02).
Discussion
Maxillofacial fractures are mainly caused by motor vehicle accidents and can be accompanied with
traumatic brain injury.5-9 There is still a lack of information on undetected mild brain injury. Mild
brain injury has severe future consequences when it is not detected in an early stage. In our pilot
study we aimed at investigating the accuracy of NSE in detecting mild brain injury. The NSE level
96

of patients with maxillofacial fractures accompanied with mild brain injury were compared to the
levels of normal persons. The findings indicate that patients having sustained facial fractures have
higher NSE values than healthy controls. Furthermore, the results of this study showed no gender
differences in serum NSE levels in adult patients that had sustained facial fractures. These results
are comparable to those reported by Hayes10 and Wu et al.12 suggest that serum NSE levels are
not gender bases. Furthermore, the NSE levels in patients with facial fractures differed significantly
depending on the location of the facial fractures. The lowest NSE levels were recorded in the
midfacial part implying that the midfacial bony structures absorb traumatic forces better than other
bony structures and subsequently protect the neurocranium from heavy trauma.18 The midface
anatomy is unique in its scaffold-like structure and offers vertical supporting structures, i.e.,
nasomaxillar, zigomaticomaxillar, and pterigomaxillar buttresses; and horizontal supporting
structures, i.e., lateral anthrum, medial nasal wall, and zygomatic arc.19
The aforementioned differences in sight specific NSE values can be due to biomechanical
differences in the bony structures of the upper facial area when compared to the mid face region.
The upper facial bones often lack of sufficient amount of cancellous bone, therefore the scaffold
like structure of the mid face respond with a minimum deformation to a load increase induced by a
trauma. This lack of deformation subsequently leads to higher forces induced on the skull and
increases the risk of head injury as previously reported by Lee et al.18 and by Salentijn et al.2
Interestingly all patients who had sustained blows to their lower jaws in our study had higher NSE
values. These results agree with a study held by Keenan et al.20 indicating that facial fractures are
markers to a high risk of brain injury. However, these results are contradictive to the same study
mentioned earlier by Lee et al.18 who reported that patients who had sustained injuries in the lower
facial part (mandible) had less risk for sustaining a head injury.
One explanation for the higher NSE values in the patients who sustained fractures in the lower jaw
could be due to the direct energy transmission into the skull base and brain. Upon impact to the
lower jaw forces are transmitted through the condyles into the disks and directly into the temporal
bone, hence skull base causing a possible increase in the NSE serum values. Interestingly in
clinical settings, mandible fractures are often classified as being less problematic than midface
traumas. A recent study by Salentijn et al.2 reported that fractures of the midface and upper third
part of the skull are more prone to cause brain injury than mandibular fractures. The results of the
present study are not in good agreement with the aforementioned clinical studies by Salentijn et al.2
In several recent articles, authors state that NSE is released into the blood by hemolysis, which
may be a serious source of error in some cases.21 Furthermore, increases in NSE levels have been
observed in multiple types of trauma with and without traumatic brain injury, limiting its ability to
properly discriminate the magnitude of brain injury.21 As our pilot study is limited in NSE
investigation level in patients with maxillofacial injury without mild brain injury, further research
using a more comparable control group should conduct to decisively sum up a conclusion on this
9
97
9

issue. In addition, the number of the case involved in this study is limited, thus should be enhanced
in subsequent research.
Conclusion
Despite the shortcomings of the present pilot study, it can carefully be concluded that an increase
in NSE serum levels can be observed in patients who have sustained maxillofacial fractures and
mild brain injury. Further, our findings suggest that patients with maxillofacial fractures can sustain
mild brain injuries which can remain undiagnosed in clinical settings. However, to draw firm
conclusion on the accuracy of NSE measurement in discriminating between patients with
maxillofacial trauma accompanied with mild brain injury and patients with maxillofacial injury
without brain injury, a prospective study consisting of these two group of patients is mandatory.
98

References 1. Katz DI, Cohen SI, Alexander MP. Mild traumatic brain injury. Handb Clin Neurol. 2015;127:131–56.
2. Salentijn EG, Peerdeman SM, Boffano P, van den Bergh B. A ten-year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: incidence and aetiology. J Craniomaxillofac Surg 2014;42(6):705–710.
3. Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974;2(7872):81–84.
4. Kobeissy FH, Ottens AK, Zhang Z, Liu MC, Denslow ND, Dave JR, Tortella FC, Hayes RL, Wang KKW. Novel differential neuroproteomics analysis of traumatic brain injury in rats. Mol Cell Proteomics 2006;5(10):1887–1898.
5. Gassner R, Tuli T, Hachl O, Rudisch A, Ulmer H. Cranio-maxillofacial trauma: a 10 year review of 9,543 cases with 21,067 injuries. J Craniomaxillofac Surg 2003;31(1):51–61.
6. Thoren H, Snall J, Salo J, Suominen-Taipale L, Kormi E, Lindqvist C, Tornwall J. Occurrence and types of associated injuries in patients with fractures of the facial bones. J Oral Maxillofac Surg 2010;68(4):805–810.
7. Naveen Shankar A, Naveen Shankar V, Hegde N, Sharma, Prasad R. The Pattern of the maxillofacial fractures – A multicenter retrospective study. J Craniomaxillofac Surg 2012;40(8):675–679.
8. Allareddy V, Allareddy V, Nalliah RP. Epidemiology of facial fracture injuries. J Oral Maxillofac Surg 2011;69(10):2613–2618.
9. Rajandram RK, Syed OSN, Rashdi MF, Abdul Jabar MN. Maxillofacial injuries and traumatic brain injury – a pilot study. Dent Traumatol 2014;30(2):128–132.
10. Hayes RL. Biochemical markers of brain injury: applications to combat casualty care. Paper presented at: the RTO HFM Symposium on combat casualty care in ground based tactical situations: Trauma technology and emergency medical procedures; August 16–18, 2004;16–8; St. Pete Beach, USA
11. Pineda JA, Wang KK, Hayes RL. Biomarkers of proteolytic damage following traumatic brain injury. Brain Pathol 2004;14(2):202–209.
12. Wu YC, Zhao YB, Lu CZ, Qiao J, Tan YJ. Correlation between serum level of neuron-specific enolase and long-term functional outcome after acute cerebral infarction: prospective study. Hong Kong Med J. 2004;10:251–254.
13. Wang KK, Ottens AK, Liu MC, Lewis SB, Meegan C, Oli MW, Tortella FC, Hayes RL. Proteomic identification of biomarkers of traumatic brain injury. Expert Rev Proteomics 2005;2(4):603–614.
14. Laterza OF, Modur VR, Crimmins DL, Olander JV, Landt Y, Lee JM, Ladenson JH. Identification of novel brain biomarkers. Clin Chem. 2006;52(9):1713–1721.
15. Ergün R, Bostanci U, Akdemir G, Beşkonakli E, Kaptanoğlu E, Gürsoy F, Taşkin Y. Prognostic value of serum neuron-specific enolase after head injury. Neural Res 1998;20(5):418–420.
16. Wunderlich MT, Ebert AD, Kratz T, Goertler M, Jost S, Herrmann M. Early neurobehavioral outcome after stroke is related to release of neurobiochemical markers of brain damage. Stroke 1999;30(6):1190–1195.
17. Bazarian JJ, Merchant-Borna K. Tau, s-100 calcium-binding protein B, and neuron-specific enolase as biomarkers of concussion. JAMA Neurol 2014;71(7):925–926.
18. Lee KF, Wagner LK, Lee YE, Suh JH, Lee SR. The impact-absorbing effect of facial fractures in closed-head injuries. J Neurosurg 1987;66(4):542–547.
19. Plaisier BR, Punjabi AP, Super DM, Haug RH. The relationship between facial fractures and death from neurologic injury. J Oral Maxillofac Surg 2000;58(7):708–712.
20. Keenan HT, Brundage SI, Thompson DC, Maier RV, Rivara FP. Does the face protect the brain? A case-control study of traumatic brain injury and facial fractures. Arch Surg 1999;134(1):14–17.
21. Yokobori S, Hosein K, Burks S, Sharma I, Gajavelli S, Bullock R. Biomarkers for the clinical differential diagnosis in traumatic brain injury; a systematic review. CNS Neurosci Ther 2013;19(8):556–565.
9
99
9

100
Chapter 10
The influence of helmet on the
prevention of maxillofacial fractures
sustained during motorcycle accidents
This is an edited version of the manuscript:
Muhammad Ruslin, Harmas Y. Yusuf, Muhammad Z. Arifin, Jan Wolff, Paolo Boffano, Tymour Forouzanfar
The influence of helmet design on the prevention of maxillofacial fractures sustained
during motorcycle accidents
Accepted for Publication

Abstract Introduction:
Traffic accidents are among the main etiologic factors of maxillofacial injuries. Of all the different
types of motor vehicles used worldwide, motorcycle riders sustain the most serious injuries in the
head and neck area. Therefore, this study aimed to assess the effect of half-coverage helmet use
in motorcycle accidents and to investigate the difference in neuron-specific enolase serum levels in
helmeted and unhelmeted person who had sustained maxillofacial fractures during motorcycle
accidents.
Methods:
The study comprised of half-coverage helmeted and unhelmeted patients who had sustained
maxillofacial fractures during motorcycle accidents. Only hospitalized patients with maxillofacial
fractures and a mild head injury that had been surgically treated within 48 hours were included in
this study. The riders whose helmet flied out before their head hit the ground were included as
unhelmetted patients. All patients who had sustained moderate or severe head injuries were
excluded from the study.
Results:
A total of 48 subjects (22 helmeted and 26 unhelmeted) sustained maxillofacial fractures were
divided into three parts: upper, middle, and lower facial. All patients were scored using the
Glasgow Coma Scale upon arrival at the hospital. The most prevalent maxillofacial fracture site in
helmeted group was the mid-face (40.9%) and the upper-middle-lower face (26.9%) in unhelmeted
group. There was no statistical significant difference between neuron-specific enolase serum levels
in helmeted group (11.5 mg/ml) compared to unhelmeted group (14.49 ng/ml) (p > 0.05).
Conclusion:
Half-coverage helmets provided motorcyclists with only limited protection in the head and facial
area. Unhelmeted motorcycle riders sustained comparable injuries compared to half-coverage
helmeted users. It should be noted that the same clinicians carried out this investigation, and the
same protocol was used throughout the present study.
102

Introduction
Due to the increase of motor vehicle ownership and rapid economic development, the number of
road traffic injuries is unexpectedly increasing; significantly in the next decade.1 Traffic accidents
are among the main etiologic factors of maxillofacial injuries and account for 34.42 – 80.14% of all
skeletal and soft tissue injuries in the facial area.2 Of all the different types of motor vehicles used
worldwide, motorcycle riders sustain the most serious injuries in the head and neck area which
often lead to a disability or in some cases lead to mortality.3
Previous studies focused on the assessment of motorcycle accidents and have found a significant
reduction in the risk of head and brain injuries in helmeted motorcycle riders compared to
unhelmeted persons.4-6 Another group reported that wearing a standard good quality motorcycle
helmet reduces the risk of mortality by 40% and the risk of serious injury by over 70%.7 Conrad et
al.8 conclude that although motorcycle riders appear to comply with the motorcycle helmet law, it is
a "token compliance," less than 50% of riders were maximally protected by helmets and very little
safety consciousness was found among riders.8
Assessing the exact extent of brain damage caused after motorcycle accidents remains a
challenge. In recent years several new biomarkers have been developed to assess the degree of
neuronal injury sustained during a trauma. These biomarkers are becoming increasingly important
as supplements for the Glasgow Coma Scale (GCS). Another existing biomarker is neuron-specific
enolase (NSE), a protein-based enzyme found within neurons that can be used to quantify the
degree of neuronal damage sustained after a head trauma.9-12 Increased concentration of NSE can
be measured in the cerebrospinal fluid and in peripheral blood after trauma; hence, neuronal
damage offers a quick and reliable method of assessing the degree of brain cell damage sustained
after motorcycle accidents.13
The aims of this study were to assess the effects of different helmet designs (full and half-coverage
helmets) in motorcycle accidents and to carry out further investigation on the difference NSE
serum levels in half-coverage helmeted and unhelmeted persons that had sustained maxillofacial
fractures during motorcycle accidents. Furthermore, correlations between NSE serum values and
different maxillofacial fracture sites were also assessed.
10
103
10

Material and Methods
This study was approved by the Health Research Ethics Committee of Medical faculty, the
University of Padjadjaran/Dr. Hasan Sadikin General Hospital Bandung, Indonesia. The study
comprised of half-coverage helmeted and unhelmeted patients who had sustained maxillofacial
fractures during motorcycle accidents at the urban Bandung area in Indonesia. Only hospitalized
patients with maxillofacial fractures and a mild head injury that had been surgically treated within
48 hours were included in this study. The riders whose helmet flied out before their head hit the
ground were included as unhelmetted patients. All patients who had sustained moderate or severe
head injuries were excluded from the study. Furthermore, multiple trauma and alcoholized patients
were excluded from the study. The maxillofacial fractures were divided into three parts upper,
middle, and lower facial. The upper part of facial skeleton comprising the frontal bone, the middle
part comprising the midfacial bone: the maxilla, the nasoethmoid, and lateral midfacial bone-
zygoma, and the lower part comprising the mandible. All patients in this study were scored using
the GCS upon arrival at the hospital. Furthermore, computed tomography scans of all patients
were also performed. Blood samples were taken from all studied patients and centrifuged for 10
minutes at 2.500 rotations per minute. Neuron-specific enolase measurements were performed
with an electrochemiluminescence immunoassay (ECLIA) using a sandwich technique in duplicate
with NSE kits (Roche, Mannheim, Germany) and the Elecsys 2010 analyzer (Roche Diagnostics,
Mannheim, Germany). This study underwent NSE screening within 24 hours since the half-life of
NSE in the serum is approximately 48 hours.14 The NSE cut-off value is 10 ng/ml.15 Statistical analyses were performed using statistical package for social science (SPSS) version
22.0. The Chi-Square test was used to assess the gender, age, and site of fracture of helmeted
motorcyclist. Furthermore, the independent t-test was used to calculate the mean admission of
GCS, life-time NSE, and NSE results in correlation with the helmeted motorcyclist, and finally the
two-way ANOVA test was used to calculate the NSE serum value related to half-coverage
helmeted (Figure 10.1A.) and unhelmeted motorcyclist that had sustained maxillofacial fractures.
Figure 10.1. Types of helmet: A. Half-coverage helmet. B. Full-coverage helmet
104

Results A total of 62 patients with mild head injuries were surgically treated in the three months study
period. However, fourteen patients should be excluded from the study since eleven patients had
incomplete medical data, two patients have pulmonary disease and one patient decided to leave
the hospital before completing his treatment. From all subjects (48 patients) included in this study,
it has been found that 45% (22 patients) were half-coverage helmeted and 54% (26 patients)
unhelmeted. The group consisted of 41 males patients (85%) and seven females (14%) with a
mean age was 27.57 years old ranging from 19 to 65 years old. The most prevalent group was
between 16–25 years old with 45% (22 subjects) were half-coverage helmeted and 54% (26
subjects) were unhelmeted. The most prevalent maxillofacial fracture site was the mid-face 40.9% in the half-coverage
helmeted group and 26.9% in upper-middle-lower in the unhelmeted group (Figure 10.2.).
Figure 10.2. Half-coverage helmeted and unhelmeted distribution stratified according to maxillofacial fractures site
All patients sustained a mild head injury during the traffic accident with the mean GCS 13.95
values upon admission were 13.95 in the half-coverage helmeted group and 13.73 in the
unhelmeted group. The mean life-time NSE values were 10.89 hours in the half-coverage
helmeted and 13.24 hours in the unhelmeted group. Furthermore, the mean NSE serum levels of
the patients who had sustained a maxillofacial fracture was 11.52 ng/ml in the half-coverage
Half-coverage helmeted
Unhelmeted
10
105
10

helmeted group and 14.49 ng/ml in the unhelmeted group; however, there was no statistically
significant difference between the two groups (p > 0.05) (Table 10.2.).
Table 10.1. Patients’ demographic and maxillofacial fractures, GCS, and NSE characteristics of half-coverage helmeted motorcyclist compared with unhelmeted motorcyclist involved
Characteristic Half-coverage helmeted (n = 22)
Unhelmeted (n = 26) p-value
Gender Male 18 (81.8%) 23 (88.5%) 0.516a
Female 4 (18.2%) 3 (11.5%) - Age Group (years) 16–25 9 (41%) 17 (65.4%) 0.342a 26–35 8 (36.4%) 4 (15.4%) - 36–45 3 (13.6%) 4 (15.4%) - 46–55 1 (4.5%) 1 (3.8%) - 56–65 1 (4.5%) - - Fractures site Upper 5 (22.7%) 4 (15.4%) 0.118a
Upper-middle - - - Upper-lower - - - Upper-middle-lower 1 (4.5%) 7 (26.9%) - Middle 9 (40.9%) 4 (15.4%) - Middle-lower 3 (13.6%) 6 (23.1%) - Lower 4 (18.2%) 5 (19.2%) - Mean admission GCS 13.95 (0.58) 13.73 (0.72) 0.239b
Mean life-time NSE 10.98 (5.26) 13.24 (4.88) 0.133b
Mean NSE results 11.52 (6.83) 14.49 (11.52) 0.294b
a) Chi-Square test; b) independent t-test, p < 0.05
The two-way ANOVA analyses showed that the NSE serum values in the half-coverage helmeted
subjects who had sustained maxillofacial fractures in the upper-middle-lower sites were 33.01
ng/ml. These values were slightly higher than those recorded in the unhelmeted group 19.45 ng/ml;
however, there was no statistical significant difference between the groups (p > 0.05) (Table 10.2.).
Table 10.2. Half-coverage helmeted and unhelmeted motorcyclist related NSE serum level and maxillofacial fracture site
Fracture site NSE p-value Half-coverage helmeted Unhelmeted Upper 12.91 11.82
0.480
Upper-middle - - Upper-lower - - Upper-middle-lower 33.01 19.45 Middle 8.82 5.79 Middle-lower 8.17 13.87 Lower 13.01 17.40
*) p-value two-way ANOVA, p < 0.05
The NSE serum values in the unhelmeted subjects who had sustained maxillofacial fractures in the
lower sites were 17.40 ng/ml. These values were slightly higher than those recorded in the half-
coverage helmeted group 13.01 ng/ml; however, there was no statistical significant difference
between the groups (p > 0.05) (Table 10.2.).
106

Discussion
Motorcycles are the fastest growing sector of motor vehicles worldwide and comprise the majority
of all motor vehicles in low- and middle- income countries.16 This study revealed that males (half-coverage helmeted 81.8% and unhelmeted 88.5%) are more
frequently subjected to maxillofacial fractures than females (half-coverage helmeted 18.2% and
unhelmeted 11.5%). Furthermore, maxillofacial fractures resulting from motorcycle accidents are
most common amongst patients aged in the range of 16–25. These results, however, differed from
those reported by Cavalcante et al.17 who studied the influence of helmets on facial trauma in
motorcycle accidents and reported that most victims were between 21 and 40 years old (62.9%). A
recent study by Cavalcante et al.17 reported that (94.5%) of the patients were male and the majority
of patients were using a helmet (80.1%) during the accident. Furthermore, Conrad et al.8 reported
that motorcycle riders in the urban Yogyakarta area in Indonesia did not always wear helmets
especially at night when no police were around. The main reasons for not wearing helmets were
discomfort and absence of police surveillance.
One of the findings in our study shows that half-coverage helmets provide limited protection
against head and brain injuries. Interestingly there is no significant difference between the half-
coverage helmeted and unhelmeted group (mean GCS is 13.95 for half-coverage helmeted and
13.73 for unhelmeted). Nevertheless, intracranial cerebral injury; intracranial hemorrhage; and
face, skull vault, and cervical spine injuries are more likely to be found in fatally injured to
unhelmeted motorcyclist compared to helmeted motorcyclist.18 However, a helmet is only effective
when it remains on the head during the accident. Based on the findings of this study, continued
efforts should be warranted to encourage the use of full coverage (Figure 10.1B.) motorcycle
helmet in Bandung. One possible method of increasing the comfort of full coverage helmets is by
developing lighter helmets with better ventilation especially in hot countries.
One explanation for the higher incidence of facial fractures in the upper and the middle third of the
face in the half-coverage helmeted group could be due to the fact that most patients probably did
not strap their helmets properly and subsequently exposed their chin area unprotected.
Nevertheless, the half-coverage helmeted subjects had lower NSE values when compared to
unhelmeted subjects in this study. These finding demonstrated that half-coverage helmeted offers
more brain protection than unhelmeted. Interestingly, the NSE serum values in the half-coverage
helmeted group who had sustained maxillofacial fractures in the upper-middle-lower sites were
slightly higher than in the unhelmeted group of patients. It indicates that half-coverage helmeted
does not protect the upper-middle-lower regions of the face and, half-coverage helmeted only
protects the posterior parts of the head. Furthermore, the NSE serum values in the unhelmeted
group that had sustained maxillofacial fractures in lower facial region were slightly higher than in
the half-coverage helmeted group indicating that the helmet strap may have a positive damping
10
107
10

effect. The results of this study demonstrated that more concern should be given to helmet design
(fracture driven design).
This study has several limitations since some information was not gathered directly from the
motorcycle riders experienced the accidents; hence, there are some measurement bias associated
with observations of the speed, crash area of helmet, incorrect helmet uses, and rider
characteristics. Many helmets may appear to be standard helmets on visual inspection but in fact
they may lack those energy absorption layer that may protect the rider from injury in the event of
an accident, nonetheless the prevalence of non-standard helmets may be underestimated. In
addition, the number of the case involved in this study is limited. Futher, to drow firm conclusion on
the protection of helmeted and unhelmeted motorcycle riders associated with maxillofacial trauma,
more quantitative data is a mandatory.
Conclusion
In conclusion, the findings of this study revealed that half-coverage helmets provided motorcyclists
with only limited protection in the head and facial area. Unhelmeted motorcycle riders sustained
comparable injuries compared to half-coverage helmeted users. It should be noted that the same
clinicians carried out this investigation, and the same protocol was used throughout the present
study.
108

References 1. Ameratunga S, Hijar M, Norton R. Road-traffic injuries: confronting disparities to address a global-health problem. Lancet 2006;
367(9521):1533–1540.
2. Wood EB, Freer TJ. Incidence and aetiology of facial injuries resulting from motor vehicle accidents in Queensland for three-year period. Aust Dent J 2001;46(4):248–288.
3. World Health Organization. (2013a). Global status report on road safety 2013: Supporting a decade of action. Geneva, Switzerland: World Health Organization.
4. Rowland J, Rivara F, Salzberg P, Soderberg R, Maier R, Koepsell. Motorcycle helmet use and injury outcome and hospitalization costs from crashes in Washington State. Am J Public Health 1996;86(1):41–45.
5. Houston DJ, Richardson LE. Motorcyclist fatality rates and mandatory helmet-use laws. Accid Anal and Prev 2008;40(1):200–208.
6. Crompton JG, Bone C, Oyetunji T, Pollack KM, Bolorunduro O, Villegas C, Stevens K, Cornwell EE 3rd, Efron DT, Haut ER, Haider AH. Motorcycle helmets associated with lower risk of cervical spine injury: debunking the myth. J Am Coll Surg 2011;212(3):295–300.
7. World Health Organization. (2103b, Janury 2). Road traffic injuries. Retrieved from http://www.who.int/mediacentre/factsheets/fs358/
8. Conrad P, Bradshaw YS, Lamsudin R, Kasniyah N, Costello C. Helmets, injuries and cultural definitions: motorcycle injury in urban Indonesia. Accid Anal Prev 1996;28(2):193–200.
9. Hayes RL, Wang KKW, Tortella FC, Dave JR, Lu XCM. Biochemical markers of brain injury: applications to combat casualty care. Presented at the RTO HFM Symposium on combat casualty care in ground based tactical situations: Trauma technology and emergency medical procedures. USA, (2004).16–18.
10. Pineda JA, Wang KKW, Hayes RL. Biomarkers of proteolytic damage following traumatic brain injury. Brain Pathol 2004;14:202–209.
11. Wu YC, Zhao YB, Lu CZ, Qiao J, Tan YJ. Correlation between serum level of neuron-specific enolase and long-term functional outcome after acute cerebral infarction: prospective study. Hong Kong Med J 2004;10:251–254.
12. Wang KK, Ottens AK, Liu MC, Lewis SB, Meegan C, Oli MW, Tortella FC, Hayes R. Proteomic identification of biomarkers of traumatic brain injury. Expert Rev Proteomics 2005;2(4):603–614.
13. Ergun R, Bostanci U, Akdemir G, Beşkonakli E, Kaptanoğlu E, Gursoy F, Taşkin Y. Prognostic value of serum neuron-specific enolase after head injury. Neurol Res 1998;20(5):418–420.
14. Wunderlich MT, Ebert AD, Kratz T, Goertler M, Jost S, Herrman M. Early neurobehavioral outcome after stroke is related to release of neurobiochemical markers of brain damage. Stroke 1999;30:1190–1195.
15. Bazarian JJ, Merchant-Borna K. Tau, s-100 calcium-binding protein B, and neuron-specific enolase as biomarkers of concussion-reply. JAMA Neurol 2014;71(7):926–927.
16. De Rome L, Ivers R, Fitzharris M, Du W, Haworth N, Heritier S, Richardson D. Motorcycle protective clothing: protection from injury or just the weather? Accid Anal Prev 2011;43(6):1893–1900.
17. Cavalcante JR, Oka SC, de Santana Santos T, Dourado E, de Oliveira E Silva ED, Gomes AC. Influence of helmet use in facial trauma and moderate traumatic brain injury victims of motorcycle accidents. J Craniofac Surg 2012;23(4):982–985.
18. Richter M, Otte D, Lehmann U, Chinn B, Schuller E, Doyle D, Sturrock K, Krettek C. Head injury mechanisms in helmet-protected motorcyclists: prospective multicenter study. J Trauma 2001;51(5):949–958.
10
109
10

110
Chapter 11
Summary, General discussion and
Conclusion

Summary Chapter 2 systematically reviews all papers published worldwide in the last 30 years on the
distribution and characteristics of facial injuries related to motor-vehicle accidents (MVA). The
percentage of MVA as etiological factors in epidemiological studies on maxillofacial injuries ranged
between 11% to 85%. Overall, a progressively decreasing trend was observed, particularly in
North America, Brazil, and Europe. The recent literature clearly shows a wide difference in the
incidence of MVA-related facial fractures between developed countries (20% in Japan, 35.2% in
the Netherlands, 11% in Ireland) and developing countries (72%–85% in India and 46.7% in
China). Naturally, differences in regulations and their implementation make it difficult to fully
compare these data.
Studies on the wearing of helmets by motorcyclists in urban areas have highlighted two main
points: the effectiveness of laws intended to increase their use, and the protection helmets have
provided against brain injuries and death.1,2 Legislation making helmet use compulsory for all
motorcyclists is crucial to reducing the incidence of facial injuries in this category: previous articles
have demonstrated that motorcycle accidents involving unhelmeted riders cause severe traumatic
brain injury in 100% of the patients, followed by 63.3% of moped/scooter accidents. This may be
due to the high velocity achieved by motorcycles in conjunction with their riders unwilling to
wearing helmets, making them doubly vulnerable in traffic.3,4
Injuries associated with traffic accidents are a problem in many countries, and their prevention is
often a priority for the public health authorities.1,2,5-16 As Chapter 3 shows, MVAs caused the
maxillofacial fractures of 326 of the 3260 patients admitted to the various different European
centers during the study period. Naturally, the incidence of MVA-related maxillofacial trauma
varied, with the maximum value that was encountered in Zagreb (18%), In most centers, however,
the percentage of MVAs was approximately 10%. In comparison with the European literature, this
was among the lowest values ever reported - a result that may confirm the decreasing incidence of
MVA-related maxillofacial injuries in high-income countries. The most common causes of MVA-
related maxillofacial injury mechanisms in high-income countries were car accidents (177 patients),
followed by motorcycle accidents (91 patients), pedestrians (33 patients), and other/unknown (25
patients).
Chapter 4 and 5 highlight a second cause of maxillofacial injuries, maxillofacial fractures
associated with sport-related injuries, and chapter 6 present the demographics and patterns of
sport-related maxillofacial fractures in a multicenter study. The percentage of sport as a cause of
facial fractures was higher in Europe and Oceania. The number of sport injuries involving males
112
also outnumbered that involving females. Comprising data on 108 patients with 128 maxillofacial
fractures, our study in chapter 5 confirmed previous findings that sport is a major cause of
maxillofacial injuries, in which the most common sport-related fractures were zygomatic complex
fractures, followed by mandible fractures. Our finding that soccer and hockey were the most
prominent causes of sport-related maxillofacial trauma is consistent with the large number of
people playing soccer in the Netherlands.17,18 In chapter 6, we found soccer (33%) to be the sport
most responsible for maxillofacial injuries, followed by rugby (18%) and skiing (12%). A noteworthy
finding is that coronoid process fractures were observed only in soccer players, and not in other
sports groups-possibly a consequense of the fact that impact against another player is the most
common cause of accident in soccer.17 Our findings in this study are largely consistent with those
of other studies, suggesting that the data may be useful for the development of protocols to
prevent maxillofacial trauma in certain sports.
Chapter 7 evaluated all patients presenting with facial trauma accompanied by dental injury at the
VU University Medical Center (VUmc) in Amsterdam, where 164 (23.2%) patients of the total 707
patients presented with dental injuries associated with facial fractures. We found that the
prevalence of dental injury associated with facial fractures was higher than that found in numbers
of previous studies (18.9% and 22.5%)19,20 except fort hat of Zhou et al.21 where the prevalence we
found was lower (41.8%). We found mandibular condylar fractures, mandibular parasymphyseal
fractures, Le Fort fractures, and mandibular body fractures to have a significantly higher
association with dental injury, and zygomatic arch or zygomatic complex fractures to have a
significantly lower association. In both groups-i.e., that with dental injury and that without- we also
found that the lower third of the face was more susceptible to fractures than the upper two-thirds. A
possible explanation for the higher incidence of facial fractures we found in the lower third of the
face is that most patients in the Amsterdam area are treated for bicycle accidents and not for
interpersonal violence. The highest incidence of injured teeth was in the maxilla. The teeth most
affected were the maxillary incisors (33.1%), followed by the mandible incisors (13.6%), mandible
molars (12.8%), and maxillary premolars (12.6%). Our results are largely in line with those in other
published studies.19-23
In fractures of the alveolar process, the soft tissues and teeth are often damaged, thereby
increasing the severity of craniofacial injuries. In our study, traffic accidents were the major cause
of dental injuries. While the overall role of traffic accidents as a cause of facial bone fracture is
known to have decreased and the overall number of facial bone fractures caused by violence and
sport injuries to have increased, we found that injuries caused by two-wheeled motor vehicles
(TWMV) accidents had significantly increased and that sport-related accidents had significantly
decreased. Although we did not find a significant difference between TWMV and sport-related
11
113
11
markers of a high risk of brain injury. One explanation for the higher NSE values in the patients
who sustained fractures in the lower jaw may concern direct energy transmission into the skull
base and brain. Upon impact to the lower jaw, forces are transmitted through the condyles into the
disks and directly into the temporal bone, and thust the skull base. This may increase NSE serum
values.
Chapter 10 of this study explores the effect of helmet use in bicycle and motorcycle accidents in
preventing head injuries by reducing the impact of forces to the head.27 It also investigates the
difference in NSE serum levels in helmeted and unhelmeted people who had sustained
maxillofacial fractures during motorcycle accidents. According to injury site, a total of 48 subjects
(22 helmeted and 26 unhelmeted) who had sustained such fractures were divided into three parts:
upper, middle, and lower facial. Upon arrival in hospital, all were scored using the Glasgow Coma
Scale (GCS). The most prevalent maxillofacial fracture site in the helmeted group was the mid-face
(40.9%); in the unhelmeted grup it was upper-middle-lower face (26.9%) in. Although NSE serum
levels in helmeted group (11.5 mg/ml) did not differ significantly from those in the unhelmeted
group (14.49 ng/ml) (p > 0.05), patients who had been wearing half-coverage helmets had lower
NSE values than those who had worn no helmet. This demonstrates that half-coverage helmets
offered more brain protection than no helmet.
11
accidents, we also observed a slight and gradual increase over the study period in the number of
fractures caused by violence. Examination of the causes of maxillofacial fractures with associated
dental injuries showed a similar trend: that violence was an increasing cause of such injuries.19-23
Chapter 8 assesses the prognostic values of two commonly used scoring systems-the
Maxillofacial Injury Severity Score (MFISS) and Facial Injury Severity Scale (FISS)-in detecting
brain injury and maxillofacial fractures patients at the VU Medical Center in Amsterdam. Between
2002 and 2013, a total of 1326 patients affected by maxillofacial fractures were treated, 52 of
whom had been diagnosed with TBI. Each patient had been graded according to the MFISS and
FISS. The mean value of MFISS 5.70 and that of FISS was 2.25. Motor vehicle accidents were the
most frequent cause of TBI (22 patients; p < 0.05). Both values of MFISS and FISS were
statistically associated with the presence of TBI, we found both systems to be valuable
assessment tools for the predicting TBI. High-energy trauma, such as MVA, which causes multiple
and complex facial fractures (higher MFISS and FISS values), represents a higher risk of being
associated with brain injuries. A recent study based on finite element analysis of the maxillofacial
trauma associated with TBIs showed that the site and direction of facial impact played a key role in
determining the severity and location of the facial bone fracture, which in turns influenced the
severity and location of the traumatic brain injury.24
As there is still little information on undetected mild brain injury in patients with maxillofacial
trauma, chapter 9 investigates the accuracy of neuron-specific enolase (NSE) serum levels in
detecting mild brain injury in patients with sustained maxillofacial fractures after motor vehicle
accidents. Blood samples were drawn from 40 healthy patients (control group) and 48 trauma
patients who had sustained isolated maxillofacial fractures and mild brain injury assessed with the
Glasgow Coma Scale. In the trauma group, correlations between the NSE serum values and
different facial fracture sites were assessed. The mean NSE serum level in the group of 48 patients
who had sustained maxillofacial fracture was 13.12 ng/ml. These values were significantly higher
than those measured in the healthy control group. The mean NSE serum levels in the lower part of
the facial skeleton (15.44 ng/ml) were higher than those in the upper facial part; and the mean NSE
level in the middle-lower parts (11.97 ng/ml) was higher than that in the middle part. The NSE
levels in patients with facial fractures also differed significantly according to the location of the
facial fractures. The lowest NSE levels were recorded in the midfacial part, implying that the
midfacial bony structures absorb traumatic forces better than other bony structures, and
subsequently protect the neurocranium from heavy trauma.25
Interestingly, all the patients in our study who had sustained blows to their lower jaws had higher
NSE values. These results agree with a study by Keenan et al.26 indicating that facial fractures are
114

markers of a high risk of brain injury. One explanation for the higher NSE values in the patients
who sustained fractures in the lower jaw may concern direct energy transmission into the skull
base and brain. Upon impact to the lower jaw, forces are transmitted through the condyles into the
disks and directly into the temporal bone, and thust the skull base. This may increase NSE serum
values.
Chapter 10 of this study explores the effect of helmet use in bicycle and motorcycle accidents in
preventing head injuries by reducing the impact of forces to the head.27 It also investigates the
difference in NSE serum levels in helmeted and unhelmeted people who had sustained
maxillofacial fractures during motorcycle accidents. According to injury site, a total of 48 subjects
(22 helmeted and 26 unhelmeted) who had sustained such fractures were divided into three parts:
upper, middle, and lower facial. Upon arrival in hospital, all were scored using the Glasgow Coma
Scale (GCS). The most prevalent maxillofacial fracture site in the helmeted group was the mid-face
(40.9%); in the unhelmeted grup it was upper-middle-lower face (26.9%) in. Although NSE serum
levels in helmeted group (11.5 mg/ml) did not differ significantly from those in the unhelmeted
group (14.49 ng/ml) (p > 0.05), patients who had been wearing half-coverage helmets had lower
NSE values than those who had worn no helmet. This demonstrates that half-coverage helmets
offered more brain protection than no helmet.
11
115
11
General Discussion In short the aims of this theses were threefold. First, we investigated the incidence, epidemiology
and concequences of facial trauma caused by traffic and sport related accidents. Second, the use
of trauma severity measurements in detecting mild brain injury were assessed and third, the
protective value of different helmets in motorcyclists was studied.
MVA Motor Vehicle and Sport accident related injury The etiology of MVA gives us important information. The available data demonstrates that motor
vehicle accidents are still one of the most important etiological factors for maxillofacial injuries.
Nowadays, their incidence widely varies, as various factors are involved in the prevention of such
accidents. In particular, not only road conditions, speed limits, and safety equipment, but also the
characteristics of used vehicles, socioeconomic conditions and regulations about alcohol drinking
before driving are fundamental for the prevalence of such injuries.7 A great difference in the
incidence of MVA-related facial fractures between developed countries (20% in Japan, 35.2% in
the Netherlands, 11% in Ireland) and developing countries (72–85% in India, 46.7% in China) can
be easily observed.31 In past studies regarding European populations reported percentages
ranging between 25% and 60%. The results of the presented multicenter study in this thesis
however showed an incidence of 10 % in most centers. This result could confirm the progressive
trend of increased use of protective measures like seat belts and helmets. Wearing a seat belt
proved to be effective for preventing fatalities and generally decreasing the severity of injuries to
the head or neck and to the trunk.1 Further, it reduces the risk of facial injury, however it should be
noted that even proper seat belt use cannot prevent all oral and maxillofacial injuries in motor
vehicle occupants. Concerning motorcycle accidents, the crucial role of helmets has to be
acknowledged. On the market there are several types of helmets available, with their own
advantages and disadvantages. All of them have in common that they can prevent head injuries,
but in particular full-face helmets seem to be mostly effective in protecting the face.9,32
Sport accidents are an important etiological factor for maxillofacial injuries, especially in the richest
areas of the world.5,21,30 Nowadays, their incidence widely varies, as various factors are involved
from the socioeconomic conditions of the study population to the local preference and tradition of
the sport, as some contact sports like rugby are naturally more at risk of facial injuries in
comparison with others.33 A great difference in the incidence of sport related facial fractures
between developed countries (18% in New Zealand, 35% in Ireland, 31% in Austria, 14% in Japan)
and developing countries (0.5% in Pakistan, 0.8% in India, 2.6% in Tanzania) can be easily
observed. However, it is quite interesting to notice that across the last 20 years the incidence in the
116
MVA and Sport accident related injury

respective geographical areas seems to be stable, in contrast with the evolution of MVA, that are
decreasing.
Soccer is the most frequently responsible sport for maxillofacial fractures. This result is naturally
influenced by the wide diffusion of soccer in the considered countries (France, Greece, Italy, South
Korea, Ireland, and The Netherlands).33-40 Further, although the use of simple preventive devices
such as helmets, and mouth guards have proven to prevent facial fractures, athletes still decide not
to wear them, or do not know which is best, or choose a poorly fitting device
Finally, concerning the fractures type, from the analysis of the considered studies on MVA and
sport related injuries a predominance of mandibular fractures33-37 followed by midfacial fractures
was observed.39-40
Trauma severity measurement Trauma severity scores and NSE blood level could be of use as an indicators for brain injury.42-46
However to implement these measurement as standard assessments in patients with facial trauma
more prospective studies are required. Our assessment of the prognostic value of MFISS47-49 and
FISS48 during the detection of brain injury and maxillofacial fractures showed that MFISS and FISS
were valuable assessment tools for diagnosing TBI, and that higher MFISS and FISS were
associated with a higher TBI cases. This is of clinical importance. In severely injured patients with
severe and complex facial fractures, it indicates that early neurosurgical/neurological assessment
is almost certainly needed, and that emergency computed tomography should be performed
without delay to prevent the morbidity associated with TBI. However, for further use, the clinician
should choose the cut-off point with the best sensitivity and specificity fitting in the hospital policy.
With regard to protection of the brain, we found that a half-coverage helmet offers more brain
protection than no helmet.49 Interestingly the NSE serum values in those who had sustained
maxillofacial fractures to the upper-middle-lower sites when wearing half-coverage helmets were
slightly higher than in those who had not been wearing a helmet. The NSE serum values in the
unhelmeted group whose maxillofacial fractures that had been sustained in the lower facial region
were also slightly higher than in the half-coverage helmeted group, indicating that the helmet strap
may have a positive damping effect. These results stress the need for greater attention to be paid
to helmet design (i.e., fracture-driven design).
Concerning the association between maxillofacial fracture and TBI, our findings suggest that
patients with maxillofacial fractures can sustain mild brain injuries that remain undiagnosed in a
clinical settings. While an increase in NSE serum levels can be observed in patients who have
sustained maxillofacial fractures and mild brain injury, firm conclusions on the accuracy of NSE
11
117
11

measurement in discriminating between patients with maxillofacial trauma accompanied by mild
brain injury and in those with maxillofacial injury without brain injury can be drawn only in a
prospective study consisting of these two groups of patients. In our opinion, such a study is
mandatory.
Protective value of helmet in MVA. In view of the overall cost of care to the society, emphasis should be placed on the prevention of
road traffic accidents. Although helmets provide significant protection against brain injury, they are
less useful against fractures of the mandible, as the chin area is not protected.50,51 Further, many
helmets appear on visual inspection to be standard helmets, they often lack the energy-absorption
layer that can protect a rider from injury in the event of an accident. The prevalence of bicycle
helmet use remains low despite research indicating the high level of head injury risk when bicycling
without a helmet and the significant protection afforded by bicycle helmets. Several studies
investigated the reasons of riders not wearing helmets. They demonstrated that the most common
reason for not wearing a helmet were "uncomfortable," "annoying," "it's hot," "don't need it," and
"don't own one."52 In several countries wearing of a bicycle helmet is mandatory. On the other hand
other countries in which it is not mandatory to wear a helmet hide behind the fact that probably
legal obligation will result in reduced cycling, concequently leading to reduced physical activity.
Several authors however, demonstrated that there is limited evidence of reduced cycling if wearing
of helmets is mandatory. They propose obligations should be coupled with physical activity
promotion.
118

Conclusion Since oral and maxillofacial injuries are associated with functional, socioeconomic, and
psychological factors, it is important to take appropriate preventative measures. Despite the
retrospective nature of the present thesis the data may represent another important contribution in
our increasing understanding of different accident related facial injuries and their consequences.
This can be crucial for the adoption of new methods for preventing injuries, thus decreasing the
associated socioeconomic costs of these individuals. Injury severity assessment tests could be
helpful as prognostic modalities in predicting short term and long term consequences of the injury
as both MVA and sport related accidents can result in brain injury. Studies about safety equipment
and their protective effect against MVA and sport related facial injuries are needed. Further,
legislations making the use of these safety equipment’s mandatory could be crucial to reduce the
incidence of facial injuries in these categories.
11
119
11
References
1. Yamamoto K, Matsusue Y, Horita S, Murakami K, Ueyama Y, Sugiura T, Kirita T. Maxillofacial fractures of pedestrians injured in a motor vehicle accident. Craniomaxillofac Trauma Reconstr 2013;6(1):37–42.
2. Boffano P, Kommers SC, Karagozoglu KH, Forouzanfar T. Aetiology of maxillofacial fractures: a review of published studies during the last 30 years. Br J Oral Maxillofac Surg 2014;52(10):901–906.
3. Kommers SC, van den Bergh B, Boffano P, Verweij KP, Forouzanfar T. Dysocclusion after maxillofacial trauma: a 42 year analysis. J Craniomaxillofac Surg 2014;42(7):1083–1086.
4. Boffano P, Roccia F, Gallesio C, Karagozoglu KH, Forouzanfar T. Diplopia and orbital wall fractures. J Craniofac Surg 2014;25(2):e183–e185.
5. Lida S, Kogo M, Sugiura T, Mima T, Matsuya T. Retrospective analysis of 1502 patients with facial fractures. Int J Oral Maxillofac Surg 2001;30(4):286–290.
6. Lehto KS, Sulander PO, Tervo TM. Do motor vehicle airbags increase risk of ocular injuries in adults? Ophthalmol 2003;110(6):1082–1088.
7. Nóbrega LM, Cavalcante GMS, Lima MMSM, Madruga RCR, Ramos-Jorge ML, d’Avila S. Prevalence of facial trauma and associated factors in victims of road traffic accidents. Am J Emerg Med 2014;32(11):1382–1386.
8. Oginni FO, Ugboko VI, Ogundipe O, Adegbehingbe BO. Motorcycle-related maxillofacial injuries among Nigerian intracity road users. J Oral Maxillofac Surg 2006;64(1):56–62.
9. Ramli R, Abdul Rahman R, Abdul Rahman N, Abdul Karim F. Krsna Rajandram R, Mohamad MS, Mat Nor G, Sohadi RU. Pattern of maxillofacial injuries in motorcyclists in Malaysia. J Craniofac Surg 2008;19(2):316–321.
10. Yokoyama T, Motozawa Y, Sasaki T, Hitosugi M. A retrospective analysis of oral and maxillofacial injuries in motor vehicle accidents. J Oral Maxillofac Surg 2006;64(12):1731–1735.
11. Salentijn EG, Peerdeman SM, Boffano P, van den Bergh B, Forouzanfar T. A ten-year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: incidence and aetiology. J Craniomaxillofac Surg 2014;42(6):705–710.
12. Salentijn EG, Collin JD, Boffano P, Forouzanfar T. A ten year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: Complications and treatment. J Craniomaxillofac Surg 2014;42(8):1717–1722.
13. Giarda M, Tavolaccini A, Arcuri F, Brucoli M, Benech A. Surgical approach to isolated bilateral orbital floor fractures. Acta Otorhinolaryngol Ital 2015;35(5):362–364.
14. Benech A, Nicolotti M, Brucoli M, Arcuri F. Intraoral extra-mucosal fixation of fractures in the atrophic edentulous mandible. Int J Oral Maxillofac Surg 2013;42(4):460–463.
15. Arcuri F, Brucoli M, Baragiotta N, Benech R, Ferrero S, Benech A. Analysis of complications following endoscopically assisted treatment of mandibular condylar fractures. J Craniofac Surg 2012;23(3):e196–e198.
16. Brucoli M, Arcuri F, Cavenaghi R, Benech A. Analysis of complications after surgical repair of orbital fractures. J Craniofac Surg 2011;22(4): 1387–1390
17. Centraal Bureau Statistiek. Available at: http://www.cbs.nl. Accessed June 25, 2014
18. Koninklijke Nederlandse Hockey Bond. Available at: http://www.knhb.nl. Accessed June 25, 2014
19. Gassner R, Tuli T, Hachl O, Rudisch A, Ulmer H. Craniomaxillofacial trauma: a 10 year review of 9543 cases with 21067 injuries. J Craniomaxillofac Surg 2003;31(1):51–61.
20. Iso-Kungas P, Tornwall J, Suominen AL, Lindqvist C, Thoren H. Dental injuries in pediatric patients with facial fractures are frequent and severe. J Oral Maxillofacial Surg 2012;70(2):396–400.
21. Zhou HH, Ongodia D, Liu Q, Yang RT, Li ZB. Dental trauma in patients with maxillofacial fractures. Dental Traumatol 2013;29(4):285–290.
22. Lauridsen E, Hermann NV, Gerds TA, Kreiborg S, Andreasen JO. Pattern of traumatic dental injuries in the permanent dentition among children, adolescents, and adults. Dent Traumatol 2012;28(5):358–363.
23. Caldas AD, Burgos MEA. A retrospective study of traumatic dental injuries in Brazilian dental trauma clinic. Dent Traumatol 2001;17(6):250–253.
24. Tse KM, Tan LB, Lee SJ, Lim SP, Lee HP. Investigation of the relationship between facial injuries and traumatic brain injuries using a realistic subject-specific finite element head model. Accid Anal Prev 2015;79:13–32.
25. Lee KF, Wagner LK, Lee YE, Suh JH, Lee SR. The impact-absorbing effect of facial fractures in closed-head injuries. J Neurosurg 1987;66(4):542–547.
26. Keenan HT, Brundage SI, Thompson DC, Maier RV, Rivara FP. Does the face protect the brain? A case-control study of traumatic brain injury and facial fractures. Arch Surg 1999;134(1):14–17.
27. Persaud N, Coleman E, Zwolakowski BA, Lauwers B, Cass D. Nonuse of bicycle helmets and risk of fatal head injury: a proportional mortality, case-control study. CMAJ 2012;184(17):921–923.
28. Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, Kovačič Ž, Vesnaver A, Konstantinović VS, Petrović M, Stephens J, Kanzaria A, Bhatti N, Holmes S, Pechalova PF, Bakardjiev AG, Malanchuk VA, Kopchak AV, Galteland P, Mjøen E, Skjelbred P, Grimaud F, Fauvel F, Longis J, Corre P, Løes S, Lekven N, Laverick S, Gordon P, Tamme T, Akermann S, Karagozoglu KH, Kommers
SC, Meijer B, Forouzanfar T. European Maxillofacial Trauma (EURMAT) in children: a multicenter and prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol 2015;119(5):499–504.
29. Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, Kovačič Ž, Vesnaver A, Konstantinović VS, Petrović M, Stephens J, Kanzaria A, Bhatti N, Holmes S, Pechalova PF, Bakardjiev AG, Malanchuk VA, Kopchak AV, Galteland P, Mjøen E, Skjelbred P, Bertin H, Marion F, Guiol J, Corre P, Løes S, Lekven N, Laverick S, Gordon P, Tamme T, Akermann S, Karagozoglu KH, Kommers SC, Forouzanfar T. Assault-related maxillofacial injuries: the results from the European Maxillofacial Trauma (EURMAT) multicenter and prospective collaboration. Oral Surg Oral Med Oral Pathol Oral Radiol 2015;119(4):385–391.
30. Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, Kovačič Ž, Vesnaver A, Konstantinović VS, Petrović M, Stephens J, Kanzaria A, Bhatti N, Holmes S, Pechalova PF, Bakardjiev AG, Malanchuk VA, Kopchak AV, Galteland P, Mjøen E, Skjelbred P, Koudougou C, Mouallem G, Corre P, Løes S, Lekven N, Laverick S, Gordon P, Tamme T, Akermann S, Karagozoglu KH, Kommers SC, Forouzanfar T. European Maxillofacial Trauma (EURMAT) project: a multicentre and prospective study. J Craniomaxillofac Surg 2015;43(1):62–70.
31. Subhashraj K, Nandakumar N, Ravindran C. Review of maxillofacial injuries in Chennai, India: a study of 2748 cases. Br J Oral Maxillofac Surg 2007;45(8):637–639.
32. Cini MA, Prado BG, Hinnig Pde F, Fukushima WY, Adami F. Influence of type of helmet on facial trauma in motorcycle accidents. Br J Oral Maxillofac Surg 2014;52(9):789–792.
33. Exadaktylos AK, Eggensperger NM, Eggli S, Smolka KM, Zimmermann H, Iizuka T. Sports related maxillofacial injuries: the first maxillofacial trauma database in Switzerland. Br J Sports Med 2004;38(6):750–753.
34. Maladière E, Bado F, Meningaud JP, Guilbert F, Bertrand JC. Aetiology and incidence of facial fractures sustained during sports: a
prospective study of 140 patients. Int J Oral Maxillofac Surg 2001;30(4):291–295. 35. Mourouzis C, Koumoura F. Sports-related maxillofacial fractures: a retrospective study of 125 patients. Int J Oral Maxillofac
Surg. 2005;34(6):635–638. 36. Antoun JS, Lee KH. Sports-related maxillofacial fractures over an 11-year period. J Oral Maxillofac Surg 2008;66(3):504–508. 37. Roccia F, Diaspro A, Nasi A, Berrone S. Management of sport-related maxillofacial injuries. J Craniofac Surg 2008;19(2):377–782.
38. Murphy C, O'Connell JE, Kearns G, Stassen L. Sports-Related Maxillofacial Injuries. J Craniofac Surg 2015;26(7):2120–2123.
39. Hwang K, You SH, Lee HS. Outcome analysis of sports-related multiple facial fractures. J Craniofac Surg 2009;20(3):825–829.
40. Ruslin M, Boffano P, ten Brincke YJ, Forouzanfar T, Brand HS. Sport-related maxillo-facial fractures. J Craniofac Surg 2016;27(1): e91–e94.
41. Hayes RL. Biochemical markers of brain injury: applications to combat casualty care. Paper presented at: the RTO HFM
Symposium on combat casualty care in ground based tactical situations: Trauma technology and emergency medical procedures; August 16–18, 2004;16–8; St. Pete Beach, USA
42. Pineda JA, Wang KK, Hayes RL. Biomarkers of proteolytic damage following traumatic brain injury. Brain Pathol 2004;14(2):202–
209. 43. Wu YC, Zhao YB, Lu CZ, Qiao J, Tan YJ. Correlation between serum level of neuron-specific enolase and long-term functional
outcome after acute cerebral infarction: prospective study. Hong Kong Med J. 2004;10:251–254. 44. Wang KK, Ottens AK, Liu MC, Lewis SB, Meegan C, Oli MW, Tortella FC, Hayes RL. Proteomic identification of biomarkers of
traumatic brain injury. Expert Rev Proteomics 2005;2(4):603–614. 45. Laterza OF, Modur VR, Crimmins DL, Olander JV, Landt Y, Lee JM, Ladenson JH. Identification of novel brain biomarkers. Clin
Chem. 2006;52(9):1713–1721. 46. Zhang J, Zhang Y, El-Maaytah M, Ma L, Liu L, Zhou LD. Maxillofacial Injury Severity Score: proposal of a new scoring system. Int J
Oral Maxillofac Surg 2006;35(2):109–114. 47. Bagheri SC, Dierks EJ, Kademani D, Holmgren E, Bell RB, Hommer L, Potter BE. Application of a facial injury severity scale in
craniomaxillofacial trauma. J Oral Maxillofac Surg 2006;64(3):408–414. 48. Chen C, Zhang Y, An J-G, He Y, Gong X, Comparative study of four maxillofacial trauma scoring systems and expert score. J Oral
Maxillofac Surg 2014;72(11):2212–2220. 49. Richter M, Otte D, Lehmann U, Chinn B, Schuller E, Doyle D, Sturrock K, Krettek C. Head injury mechanisms in helmet-protected
motorcyclists: prospective multicenter study. J Trauma 2001;51(5):949–958.
50. Thompson DC, Nunn ME, Thompson RS, Rivara FP. Effectiveness of bicycle safety helmets in preventing serious facial injury. JAMA 1996;276(24):1974–1975.
51. Lee JH, Cho BK, Park WJ. A 4-year retrospective study of facial fractures on Jeju, Korea. J Craniomaxillofac Surg 2010;38(3):192–196.
52. Conrad P, Bradshaw YS, Lamsudin R, Kasniyah N, Costello C. Helmets, injuries and cultural definitions: motorcycle injury in urban Indonesia. Accid Anal Prev 1996;28(2):193–200.
11
120

SC, Meijer B, Forouzanfar T. European Maxillofacial Trauma (EURMAT) in children: a multicenter and prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol 2015;119(5):499–504.
29. Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, Kovačič Ž, Vesnaver A, Konstantinović VS, Petrović M, Stephens J, Kanzaria A, Bhatti N, Holmes S, Pechalova PF, Bakardjiev AG, Malanchuk VA, Kopchak AV, Galteland P, Mjøen E, Skjelbred P, Bertin H, Marion F, Guiol J, Corre P, Løes S, Lekven N, Laverick S, Gordon P, Tamme T, Akermann S, Karagozoglu KH, Kommers SC, Forouzanfar T. Assault-related maxillofacial injuries: the results from the European Maxillofacial Trauma (EURMAT) multicenter and prospective collaboration. Oral Surg Oral Med Oral Pathol Oral Radiol 2015;119(4):385–391.
30. Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, Kovačič Ž, Vesnaver A, Konstantinović VS, Petrović M, Stephens J, Kanzaria A, Bhatti N, Holmes S, Pechalova PF, Bakardjiev AG, Malanchuk VA, Kopchak AV, Galteland P, Mjøen E, Skjelbred P, Koudougou C, Mouallem G, Corre P, Løes S, Lekven N, Laverick S, Gordon P, Tamme T, Akermann S, Karagozoglu KH, Kommers SC, Forouzanfar T. European Maxillofacial Trauma (EURMAT) project: a multicentre and prospective study. J Craniomaxillofac Surg 2015;43(1):62–70.
31. Subhashraj K, Nandakumar N, Ravindran C. Review of maxillofacial injuries in Chennai, India: a study of 2748 cases. Br J Oral Maxillofac Surg 2007;45(8):637–639.
32. Cini MA, Prado BG, Hinnig Pde F, Fukushima WY, Adami F. Influence of type of helmet on facial trauma in motorcycle accidents. Br J Oral Maxillofac Surg 2014;52(9):789–792.
33. Exadaktylos AK, Eggensperger NM, Eggli S, Smolka KM, Zimmermann H, Iizuka T. Sports related maxillofacial injuries: the first maxillofacial trauma database in Switzerland. Br J Sports Med 2004;38(6):750–753.
34. Maladière E, Bado F, Meningaud JP, Guilbert F, Bertrand JC. Aetiology and incidence of facial fractures sustained during sports: a
prospective study of 140 patients. Int J Oral Maxillofac Surg 2001;30(4):291–295. 35. Mourouzis C, Koumoura F. Sports-related maxillofacial fractures: a retrospective study of 125 patients. Int J Oral Maxillofac
Surg. 2005;34(6):635–638. 36. Antoun JS, Lee KH. Sports-related maxillofacial fractures over an 11-year period. J Oral Maxillofac Surg 2008;66(3):504–508. 37. Roccia F, Diaspro A, Nasi A, Berrone S. Management of sport-related maxillofacial injuries. J Craniofac Surg 2008;19(2):377–782.
38. Murphy C, O'Connell JE, Kearns G, Stassen L. Sports-Related Maxillofacial Injuries. J Craniofac Surg 2015;26(7):2120–2123.
39. Hwang K, You SH, Lee HS. Outcome analysis of sports-related multiple facial fractures. J Craniofac Surg 2009;20(3):825–829.
40. Ruslin M, Boffano P, ten Brincke YJ, Forouzanfar T, Brand HS. Sport-related maxillo-facial fractures. J Craniofac Surg 2016;27(1): e91–e94.
41. Hayes RL. Biochemical markers of brain injury: applications to combat casualty care. Paper presented at: the RTO HFM
Symposium on combat casualty care in ground based tactical situations: Trauma technology and emergency medical procedures; August 16–18, 2004;16–8; St. Pete Beach, USA
42. Pineda JA, Wang KK, Hayes RL. Biomarkers of proteolytic damage following traumatic brain injury. Brain Pathol 2004;14(2):202–
209. 43. Wu YC, Zhao YB, Lu CZ, Qiao J, Tan YJ. Correlation between serum level of neuron-specific enolase and long-term functional
outcome after acute cerebral infarction: prospective study. Hong Kong Med J. 2004;10:251–254. 44. Wang KK, Ottens AK, Liu MC, Lewis SB, Meegan C, Oli MW, Tortella FC, Hayes RL. Proteomic identification of biomarkers of
traumatic brain injury. Expert Rev Proteomics 2005;2(4):603–614. 45. Laterza OF, Modur VR, Crimmins DL, Olander JV, Landt Y, Lee JM, Ladenson JH. Identification of novel brain biomarkers. Clin
Chem. 2006;52(9):1713–1721. 46. Zhang J, Zhang Y, El-Maaytah M, Ma L, Liu L, Zhou LD. Maxillofacial Injury Severity Score: proposal of a new scoring system. Int J
Oral Maxillofac Surg 2006;35(2):109–114. 47. Bagheri SC, Dierks EJ, Kademani D, Holmgren E, Bell RB, Hommer L, Potter BE. Application of a facial injury severity scale in
craniomaxillofacial trauma. J Oral Maxillofac Surg 2006;64(3):408–414. 48. Chen C, Zhang Y, An J-G, He Y, Gong X, Comparative study of four maxillofacial trauma scoring systems and expert score. J Oral
Maxillofac Surg 2014;72(11):2212–2220. 49. Richter M, Otte D, Lehmann U, Chinn B, Schuller E, Doyle D, Sturrock K, Krettek C. Head injury mechanisms in helmet-protected
motorcyclists: prospective multicenter study. J Trauma 2001;51(5):949–958.
50. Thompson DC, Nunn ME, Thompson RS, Rivara FP. Effectiveness of bicycle safety helmets in preventing serious facial injury. JAMA 1996;276(24):1974–1975.
51. Lee JH, Cho BK, Park WJ. A 4-year retrospective study of facial fractures on Jeju, Korea. J Craniomaxillofac Surg 2010;38(3):192–196.
52. Conrad P, Bradshaw YS, Lamsudin R, Kasniyah N, Costello C. Helmets, injuries and cultural definitions: motorcycle injury in urban Indonesia. Accid Anal Prev 1996;28(2):193–200.
11
121

122

Chapter 12
Samenvatting

Hoofdstuk 2: Maxillofaciale fracturen geassocieerd met auto-ongelukken: een overzicht van de recente literatuur.
De afgelopen dertig jaar zijn alle onderzoeken die zijn gepubliceerd over de verspreiding en
karakteristieken van aan auto-ongeluk-gerelateerd letsel aan het gelaat systematisch beoordeeld.
Het percentage auto-ongelukken als etiologische factor in epidemiologische onderzoeken over
maxillofaciaal letsel varieert tussen de 11% en 85%. Over het geheel genomen werd een
progressieve afname geconstateerd, met name in Noord-Amerika, Brazilië en Europa. In recente
publicaties is eenvoudig een groot verschil op te merken in de incidentie van aan auto-ongelukken
gerelateerde gelaatsfracturen in ontwikkelde landen (20% in Japan, 35,2 % in Nederland, 11% in
Ierland) en ontwikkelingslanden (72-85% in India, 46,6 % in China). Natuurlijk kunnen deze data
niet echt vergeleken worden vanwege de verschillen in wet- en regelgeving en implementatie
daarvan.
Uit onderzoeken over het dragen van een helm door motorrijders in stedelijke gebieden kwamen
als twee belangrijkste punten naar voren: de effectiviteit van wetten gericht op het gebruik van de
helm en de bescherming die deze biedt tegen hersenbeschadiging en overlijden. Wetgeving die
het gebruik van een helm verplicht voor alle motorrijders, is cruciaal om de incidentie van faciaal
letsel te verminderen. In eerdere artikelen hierover is aangetoond dat motorongelukken bij 100%
van de patiënten ernstig traumatisch hersenletsel veroorzaakt, gevolgd door bromfiets/scooter
ongelukken (63,3%). Dit kan een gevolg zijn van de hoge snelheid die motoren kunnen bereiken in
samenhang met het ongemak van het dragen van een helm, hetgeen ze kwetsbaarder maakt in
het verkeer.
Hoofdstuk 3: Auto-ongelukken gerelateerd aan maxillofaciaal letsel: een Europees multicenter en prospectief onderzoek.
In dit onderzoek worden de demografische ontwikkeling en patronen van door auto-ongelukken
gerelateerde maxillofaciale fracturen beoordeeld en besproken. Van de 3260 patiënten die binnen
de onderzoeksperiode zijn opgenomen met maxillofaciale fracturen waren 326 trauma’s aan auto-
ongelukken toe te schrijven, met een man-vrouw verhouding van 2,2:1. De hoogste incidentie
(18%) werd in Zagreb (Kroatië) gemeten en het laagste aantal (0%) in Bergen (Noorwegen).
Ongelukken met auto’s kwamen met 177 gevallen het meest voor, gevolgd door motorrijders. De
124

mandibulaire fractuur werd met 199 gevallen het meest waargenomen, gevolgd door de orbitaal-
zygoma-fracturen (MZO). In alle drie de groepen waren mandibulaire- en MZO fracturen, met een
paar variaties, de twee meest geziene fracturen. Het grote belang van volharding in het analyseren
van alle facetten en bijzonderheden van auto-ongeluk gerelateerde faciale verwondingen moet
worden benadrukt.
Hoofdstuk 4: Maxillofaciale fracturen geassocieerd met sportblessures: een overzicht van de hedendaagse literatuur.
Publicaties van de afgelopen twintig jaar over de wereldwijde verspreiding en karakteristieken van
aan sport gerelateerde faciale verwondingen zijn bestudeerd en besproken. Uit deze evaluatie
kwam naar voren dat het percentage van sport als etiologische factor voor faciale fracturen hoger
lag in Europa en Oceanië. Er kwamen meer sportblessures voor bij mannen dan bij vrouwen.
Verreweg de meeste ongevallen deden zich voor bij voetbal, met sommige uitzonderingen,
veroorzaakt door lokale verschillen in sport, zoals rugby in Nieuw-Zeeland. In de meeste
onderzoeken bleken het mandibulaire en het zygomatic-maxillaire complex de meest voorkomende
verwonding. Verdere multicenter onderzoeken met de nadruk op preventieve maatregelen en
lange-termijn observaties zijn noodzakelijk om hun doeltreffendheid aan te tonen in zake de
preventie van maxillofaciale verwondingen.
Hoofdstuk 5: Sportgerelateerde maxillofaciale fracturen.
Het huidige onderzoek bevat data van 108 patiënten met 128 maxillofaciale fracturen. Het
bevestigt de uitkomst van eerdere onderzoeken dat sport een majeure oorzaak is van
maxillofaciale verwondingen. De meest voorkomende sport gerelateerde fracturen waren zygoma
fracturen, gevolgd door mandibulaire fracturen. Dit komt overeen met uitkomsten van eerder
gedane studies. Het is ook in lijn met het grote aantal mensen dat voetbalt in Nederland. Een
interessante observatie in het onderhavige onderzoek is dat fracturen van de processus
coronoideus alleen werden gezien bij voetballers en niet bij andere sporters. Mandibulaire
fracturen werden relatief vaker gezien bij rugby dan bij andere sporten. De resultaten van dit
onderzoek zijn overwegend vergelijkbaar met andere onderzoeken, waarmee deze data nuttig
kunnen zijn voor de ontwikkeling van protocollen teneinde maxillofaciale fracturen te voorkomen bij
bepaalde sporten.
12 125
12
Hoofdstuk 6: Aan sport gerelateerde maxillofaciale fracturen: een multicenter en prospectief onderzoek.
In een multicenter onderzoek werd de demografische ontwikkeling en patronen van aan sport
gerelateerde maxillo-faciale fracturen onderzocht. Van de 3260 patienten die werden opgenomen
met maxillofaciale verwondingen gedurende de onderzoeksperiode waren 275 traumata toe te
schrijven aan sportongelukken met een man-vrouw verhouding van 4,1:1. Voetbal was meestal de
oorzaak voor maxillofaciale fracturen (33%), gevolgd door rugby (18%) en skiën (12%). De meest
voorkomende fractuur wet gezien in onderkaak met 116 fracturen, gevolgd door maxillo zygomatic
orbital fracturen. Er blijken echter nog steeds teveel variabelen te zijn om conclusies te trekken
voor wat betreft aan sport gerelateerd letsel, omdat bij iedere sport afzonderlijk verschillende
mechanismen voor wat betreft letsel, diffusie, en preventieve middelen worden gehanteerd.
Hoofdstuk 7: Gebitstrauma in combinatie met maxillofaciale fracturen; een epidemiologisch onderzoek.
Alle patiënten met faciaal trauma gepaard aan letsel aan het gebit werden gezien aan het VU
Medisch Centrum (VUmc) in Amsterdam. Van in totaal 707 patiënten hadden 164 patiënten
(23,2%) letsel aan het gebit gepaard aan faciale fracturen. In dit onderzoek bleek dat een
prevalentie van gebitsletsel samen met faciale fracturen hoger uitviel dan in vorige onderzoeken
werd gevonden (41,8%). Le Fort fracturen en condylaire, parasymphysis fracturen van de
onderkaak kwamen significant vaker voor in combinatie met gebitsletsel. De combinatie van
gebitsletsel met zygoma fracturen was significant minder. Voorts bleek uit ons onderzoek dat het
onderste deel van het gezicht vatbaarder is voor fracturen dan de bovenste delen in zowel de
groep met gebitsletsel als de groep zonder gebitsletsel. Een oorzaak van de hogere incidentie van
faciale fracturen kan zijn dat de meeste patiënten in de regio Amsterdam behandeld worden als
gevolg van fietsongelukken en niet door interpersoonlijk geweld. De maxilla toonde de hoogste
incidentie van tandletsel. De gebits elementen, die het meest aangetast werden waren de boven
tanden (maxillaire snijtanden) (33,1%), gevolgd door ondertanden (mandibulaire snijtanden)
(13,6%), kiezen in onderkaak (molaren) (12,8%) en kiezen in de bovenkaak (premolaren) (12,6%).
De resultaten uit dit onderzoek zijn grotendeels in lijn met andere onderzoeken in de literatuur.
126

Hoofdstuk 8: De Maxillofacial Injury Severity Score (MFISS) en Facial Injury Severity Scale (FISS) als een voorspelling voor hersenletsel bij patiënten met een maxillofaciale fractuur
Dit onderzoek is gebaseerd op een analyse van een patiënten database van de afdeling Orale en
Maxillofaciale Chirurgie van VUmc in Amsterdam. Tussen 2002 en 2013 werden 1326 patiënten
behandeld in verband met maxillofaciale fracturen. Op het totaal aantal patiënten werden 52
patiënten met traumatisch hersenletsel (TBI) gediagnosticeerd. Twee algemeen gebruikte
systemen werden geselecteerd: MFISS en FISS. Iedere patiënt kreeg aan de hand van deze
systemen een score. De gemiddelde waarde van MFISS was 5,70, de gemiddelde waarde van
FISS kwam op 2,25. Een auto ongeluk was de meest voorkomende oorzaak van TBI; dit kwam bij
22 patiënten voor (p < 0,05). De waarden van zowel FISS als MFISS werden statistisch
geassocieerd met de aanwezigheid van TBI. Op basis van onze resultaten was de uitkomst dat
FISS en MFISS nuttige en waardevolle onderzoeksmiddelen zijn voor het voorspellen van TBI.
High-energy-trauma, zoals bij MVA (auto-ongeluk) dat gedetermineerd wordt door meervoudige en
complexe faciale fracturen (hogere FISS en MFISS waarden) laat een hoger risico zien op
associatie met hersenletsel. Volgens een recent onderzoek dat is gebaseerd op de Finite Element
Analysis van maxillofaciaal trauma geassocieerd met TBI’s, speelt de locatie en de richting van het
geweld een grote rol bij het vaststellen van de ernst van het hersenletsel. Dit onderzoek bevestigt
dat er een hoge associatie tussen de afstand en de locatie van de botsing tot het brein bestaat.
Met name de anterior-interior frontale kwab, vanwege de directe nabijheid tot de hersenen, levert
aanzienlijk ernstiger letsel op.
Hoofdstuk 9: Het gebruik van neuron specifiek enolase (NSE)
om licht hersenletsel te voorspellen bij patiënten die als gevolg van een motorongeluk maxilla-faciale fracturen hebben opgelopen: een pilot onderzoek.
Er werd bij 40 gezonde mensen (controle groep) bloed afgenomen en bij 48 trauma patiënten die
geïsoleerde maxillofaciale fracturen hadden opgelopen waarbij door toepassing van de Glasgow
Coma Scale lichte hersenschade was vastgesteld. In de traumagroep werden correlaties
vastgesteld tussen de NSE serum waarden en verschillende faciale fracturen. De gemiddelde NSE 12 127
12

serum waarde binnen de groep van 48 patiënten die een maxillofaciale fractuur hadden
doorgemaakt was 13,12 ng/ml. Deze waarden waren significant hoger dan de gemeten waarden
binnen de gezonde controle groep. De gemiddelde NSE serum waarden in het lage gedeelte van
het faciale skelet waren hoger dan de waarden in het bovenste faciale gedeelte. En de gemiddelde
NSE waarden in het middelste en lagere gedeelte was met 11,97 ng/ml hoger dan van het
middelste gedeelte. Voorts verschilden de NSE waarden van patiënten met faciale fracturen
significant, afhankelijk van de locatie van de faciale fracturen. De laagste NSE waarden werden
aangetroffen bij patiënten met fracturen in het middenfaciale gedeelte, wat impliceert dat de
middenfaciale botstructuur beter in staat is om traumatische klappen op te vangen dan andere
botstructuren waardoor het neurocranium beschermd wordt tegen ernstig trauma. Interessant is
dat alle patiënten in ons onderzoek die klappen hadden doorgemaakt tegen hun onderkaak hogere
NSE waarden hadden. De resultaten van dit onderzoek zijn overwegend vergelijkbaar met andere
onderzoeken aangegeven dat faciale fracturen een hoger risico van hersenletsel markeren. Een
verklaring voor de hogere NSE waarden bij patiënten die fracturen in de onderkaak hebben
doorstaan, zou kunnen zijn door de directe energie transmissie naar de schedelbasis en de
hersenen. Door de botsing met de onderkaak worden krachten overgedragen door de condylus
naar het slaapbeen, vandaar naar de schedelbasis, mogelijk leidend tot een toename van de NSE
serumwaarden.
Hoofdstuk 10: De invloed van helm op de preventie van maxillofaciale fracturen bij motorongelukken
Het doel van dit onderzoek was om uit te vinden of helmgebruik bij motorongelukken leidt tot een
vermindering van letsel bij botsingen met het hoofd. Het verschil in NSE serumwaarden bij
patiënten met helm en zonder helm met maxillofaciale fracturen na een motorongeluk werd ook
onderzocht. In totaal 48 personen (22 met helm en 26 zonder helm) met maxillofaciale fracturen
werden onderverdeeld in drie gebieden: boven-, midden- en onder gezicht. Alle patiënten werden
na aankomst in het ziekenhuis kregen een score door toepassing van de Glasgow Coma Scale.
Het meest prevalente gebied van de maxillofaciale fractuur bij de gehelmde groep was het midden
gezicht (40,9%) en bij de ongehelmde groep was het boven-midden-onder gezicht (26,9%). Er was
geen significant verschil tussen de NSE serumwaarden van de gehelmde groep (11,5 mg.nl) en
die van de groep zonder helm (14,49 ng/ml) (p>0,05). Desalniettemin hadden de half gehelmden in
dit onderzoek lagere NSE waarden dan de groep zonder helm. Deze uitkomst laat zien dat half
gehelmden beter beschermd zijn tegen hersenletsel dan mensen zonder helm.
128

129

130

Acknowledgements

Al-ḥamdu li-llāhi rabbi l-ʿālamīn, all the praises and thanks to Allah Subḥānahu wa ta'alā, the Lord
of the universes. Today is the day of finishing my thesis after an intensive learning. Writing this
thesis has given a big impact on me. I would never have been able to finish my thesis without the
guidance of colleagues, help from friends, and support from my family. Here, I would like to reflect
on the people who have generously contributed to the work presented in this thesis.
Foremost, I would like to express my sincere gratitude to my promotor, Prof. dr. Tymour
Forouzanfar for the continuous support of my Ph.D study. I am particularly indebted to have you as
my promotor. Thank you so much for encouraging my research and for allowing me to grow as a
research scientist. Your enthusiasm, trust, enormous support, and motivation on finishing my study
are infinite. I have been extremely lucky to have a supervisor who cared so much about my work.
Special mention goes to my enthusiastic co-promotor Prof. dr. D.B. (Bram) Tuinzing, thank you
very much for your brilliant comments and critical suggestions. You really gave me the strength to
keep on going and finishing my study. My Ph.D has been an amazing experience, not only
because your tremendous academic support, but also for giving me lots of wonderful opportunities
on scientific matters which improve my thesis so much, also for giving me lots of wonderful
opportunities on clinical matters which improved my proficiency. You have been there to support
me not only as my mentor, but really as my family here in the Netherlands.
Similar, profound gratitude to my co-promotor dr. Paolo Boffano, thank you very much for your
whole heartedly for an enormous contribution to my study. You have always welcomed me to
discuss my research, helped me to develope new ideas, and responded to my questions and
queries so promptly. Hard times became so much easier with you always being around. You are all
such God’s blessing. The three of you guided me with unconditional supports to strive toward my
goals. It has been a great honor for me to do this Ph.D under your supervision.
Besides my advisor, I would like to thank the members of my doctoral committee, Prof. dr.
D. Wismeijer, Prof. dr. E.A.J.M. Schulten, Prof. dr. B.J. van Royen, Prof. Dr. drg. Y.Y. Harmas, dr.
E.M. van Cann, for reviewing this thesis, for their insightful comments, and for the willingness to
join the committee.
I would like to thank people from the Department of Oral and Maxillofacial Surgery/Oral Pathology
VUmc, Prof. dr. I. van der Waal, Prof. dr. E.A.J.M. Schulten, K.H. Karaqozoglu, dr. M.N. Helder,
M.S Maningky, B.A. Meijer, Prof. dr. J.G.A.M. de Visscher, M.Gilijamse, dr. A. Ridwan Pramana,
who made me feel welcome, and also special thank to dr. Martijn van Steenbergen, this study
would have not finished without the enormous help from all of you. I would also like to thank
Annelies van de Geest and all the members of staff administration and to all the other committed
people at the Department of Oral and Maxillofacial Surgery/Oral Pathology VUmc in Amsterdam.
My VUmc Ph.D colleagues, Dessy Rachmawati, Diandra Sabrina N. Kalla & Family, Faqi
Nurdiansyah Hendra & Family, Rifaat Nurrahma, Hasanuddin, Aisha A. Hussein, Salem Al Kaabi,
thanks for the collaboration. You were not only my colleagues, but also a good friends during my
time here. My thoughts are also going to all other Indonesian best friends in The Netherlands,
Abbas Makkassau & Oktiva Dwi Prihatin, Dijo Amin & Fatimah Dijo, Daniel & Family, Ronny
Anthonijz & Family, L.C. Tse, M. Wijono & Family, Sunarti Heersink Tutu & Family, thank you for
the lovely friendship and also for joining together, to keep us close to our roots. Also to the
Indonesian students group in the Netherlands, Firdaus Hamid, Andi Rofian Sultan, Andi Ahmad
Yani & Family, Andriany Qanitha & Family, Aldian Irma Amaruddin & Family, Amalia Mulia Utami &
Family, Nurul Qalby & Family, Nur Isdah Idris & Family, thank you for all your support and
friendship. Thanks to all of you, for your loving companionship in the Netherlands. Thank you prof.
Jan Passchier, you always gathered Indonesian students together, and also always listened to us
and were there when we needed any help.
To all my colleagues, Charlotte R.A. Verlinden, Manon Weijers, Wilhelmus J.J.M. Martin, it was my
pleasure to work with you on cleft charity journey together in Makassar, Indonesia, Dear Rtn.
Manon thanks for your support with your Rotary Club Alkmaar together with Rotary Club
Ujangpandang for supported the schisis Project at South Celebes. I am as Rotarian now with new
Rotary Club Makassar City Center, always be the inspiration.
Also two colleagues, Jill Knips (Germany), Laura Gabriela Gonzalez Valdez (Mexico), it was my
pleasure to work with you on cleft charity journey together to advancement of skills and science of
oral and maxillofacial surgery, during your fellowship of the International Association of Oral and
Maxillofacial Surgeons (IAOMS) in cleft lip, and palate craniofacial surgery in Makassar, Indonesia.
To all my Dutch students research-internship in my Department of Oral and Maxillofacial Surgery,
Faculty of Dentistry, Hasanuddin University, Makassar, Indonesia, Lawrence S. Dom, Amanda M.
Scholtes, David Hardjosantoso, Arian Vojdani, Eveline Konijnendijk, K. Joanna Li, Shanice van
Stenus, Kiara N. van Trikt, (all from VUmc-ACTA, Amsterdam), and also to Dagmar E. Wortmann
A
132
I would like to thank people from the Department of Oral and Maxillofacial Surgery/Oral Pathology
VUmc, Prof. dr. I. van der Waal, Prof. dr. E.A.J.M. Schulten, K.H. Karaqozoglu, dr. M.N. Helder,
M.S Maningky, B.A. Meijer, Prof. dr. J.G.A.M. de Visscher, M.Gilijamse, dr. A. Ridwan Pramana,
who made me feel welcome, and also special thank to dr. Martijn van Steenbergen, this study
would have not finished without the enormous help from all of you. I would also like to thank
Annelies van de Geest and all the members of staff administration and to all the other committed
people at the Department of Oral and Maxillofacial Surgery/Oral Pathology VUmc in Amsterdam.
My VUmc Ph.D colleagues, Dessy Rachmawati, Diandra Sabrina N. Kalla & Family, Faqi
Nurdiansyah Hendra & Family, Rifaat Nurrahma, Hasanuddin, Aisha A. Hussein, Salem Al Kaabi,
thanks for the collaboration. You were not only my colleagues, but also a good friends during my
time here. My thoughts are also going to all other Indonesian best friends in The Netherlands,
Abbas Makkassau & Oktiva Dwi Prihatin, Dijo Amin & Fatimah Dijo, Daniel & Family, Ronny
Anthonijz & Family, L.C. Tse, M. Wijono & Family, Sunarti Heersink Tutu & Family, thank you for
the lovely friendship and also for joining together, to keep us close to our roots. Also to the
Indonesian students group in the Netherlands, Firdaus Hamid, Andi Rofian Sultan, Andi Ahmad
Yani & Family, Andriany Qanitha & Family, Aldian Irma Amaruddin & Family, Amalia Mulia Utami &
Family, Nurul Qalby & Family, Nur Isdah Idris & Family, thank you for all your support and
friendship. Thanks to all of you, for your loving companionship in the Netherlands. Thank you prof.
Jan Passchier, you always gathered Indonesian students together, and also always listened to us
and were there when we needed any help.
To all my colleagues, Charlotte R.A. Verlinden, Manon Weijers, Wilhelmus J.J.M. Martin, it was my
pleasure to work with you on cleft charity journey together in Makassar, Indonesia, Dear Rtn.
Manon thanks for your support with your Rotary Club Alkmaar together with Rotary Club
Ujangpandang for supported the schisis Project at South Celebes. I am as Rotarian now with new
Rotary Club Makassar City Center, always be the inspiration.
Also two colleagues, Jill Knips (Germany), Laura Gabriela Gonzalez Valdez (Mexico), it was my
pleasure to work with you on cleft charity journey together to advancement of skills and science of
oral and maxillofacial surgery, during your fellowship of the International Association of Oral and
Maxillofacial Surgeons (IAOMS) in cleft lip, and palate craniofacial surgery in Makassar, Indonesia.
To all my Dutch students research-internship in my Department of Oral and Maxillofacial Surgery,
Faculty of Dentistry, Hasanuddin University, Makassar, Indonesia, Lawrence S. Dom, Amanda M.
Scholtes, David Hardjosantoso, Arian Vojdani, Eveline Konijnendijk, K. Joanna Li, Shanice van
Stenus, Kiara N. van Trikt, (all from VUmc-ACTA, Amsterdam), and also to Dagmar E. Wortmann
A
(University of Groningen), Lara S. van de Lande (Erasmus University Rotterdam), Munifa Amira
Anthonijz (The Hague University of Applied Sciences), it was my pleasure to work with you.
Frida Tjiook-Tan & Yang Tjiook, thank you for all your support and also with your Soroptimist
International Club Amsterdam Amstel for supporting the Schisis Project Celebes Ceft Center at
Makassar.
Here also I would like to express the deepest appreciation to the Prof. Dr. Dwia Aries Tina
Pulubuhu, MA., Rector of Hasanuddin University, and also to Prof. Dr. Ir. Muh. Restu, MP., Prof.
Dr. Ir. Sumbangan Baja, M.Sc., Prof. Dr. drg. A. Arsunan, M.Kes, vice Rector of Hasanuddin
University, and also thanks to Prof. Dr. dr. Idrus A. Paturusi, SpB., Sp.OT.(K), Prof. Dr. Eng.
Dadang Ahmad Suriamihardja, M.Eng., and, Prof. Dr. dr. A. Wardihan Sinrang, MS., former Rector
and former vice Rector of Hasanuddin University, who have been giving me a great support for my
study. Thanks to the Ministry of Research, Technology and Higher Education of the Republic of
Indonesia, for their scholarship for overseas.
Thanks to Prof. Makoto Noguchi, DDS., Ph.D., Prof. Keng-Liang Ou, Ph.D., Prof. Lun Jou Lo, MD.,
thanks to you all, for giving me lots of wonderful opportunities on clinical and scientific matters
which can improved my proficiency and special thank to Prof. dr. Chairuddin Rasyad, Ph.D., Sp.B.,
Sp.OT.(K)., drg. Hj. Halimah Dg. Sikati, Prof. drg. Tet Soeparwadi, Sp.BM.(K) (late), Prof. dr. A.
Husni Tanra, Ph.D., Sp.An.(K)., and Prof. Dr. drg. Eky Soeria Soemantri, Sp.Ort.(K)., Dr. dr.
Warsinggih, Sp.B-KBD., who always supported me from the very beginning. You helped and
inspired me to find a way to achieve my passion to study abroad. I am very grateful to have you in
my life.
Then, for the Faculty of Dentistry, Hasanuddin University, I would like to thank to Prof. drg. H.M.
Hatta Hasan S., Ph.D., Sp.BM., Prof. drg. Mansjur Nasir, Ph.D., Prof. Dr. drg. Burhanuddin Dg.
Pasiga, M.Kes., Prof. Dr. drg. Sumintarti, MS., Prof. Dr. drg. Hasanuddin, MS., Prof. Dr. drg.
Rasmidar Samad, MS., Prof. Dr. drg. Harlina, M.Kes., Prof. Dr. drg. M. Hendra Chandha, MS.,
Prof. drg. M. Dharmautama, Ph.D., Sp.Pros.(K)., Prof. Dr. drg. Sri Oktawati, Sp.Perio.(K)., Prof. Dr.
drg. Sherly Horax, MS., Prof. Dr. drg. Barunawaty Yunus, M.Kes., Sp.RKG.(K)., Prof. Dr. drg.
Bahruddin Thalib, M.Kes., Sp.Pros., Prof. Dr. drg. Edy Machmud, Sp.Pros.(K)., Prof. Dr. drg.
Fajriani, M.Si., and also to all my seniors, best friends thanks to you all, for your enormous support
when I needed a hand, even though I was so far away. Thanks to all my colleagues in the
Department of Oral and Maxillofacial Surgery, Prof. drg. H.M. Hatta Hasan S., Ph.D., Sp.BM., Prof.
Dr. drg. M. Hendra Chandha, MS., drg. Netty N. Kawulusan, M.Kes., drg. Surijana Mappangara,
M.Kes., Sp.Perio., drg. Nasman Nuralim, Ph.D., (late), drg. Hasmawati Hasan, M.Kes., drg. Andi
Tajrin, M.Kes., Sp.BM.(K)., drg. Abul Fauzi, Sp.BM., drg. M. Irfan Rasul, Sp.BM, and also I would
like to express the deepest appreciation to the Dean of Faculty of Dentistry, Hasanuddin
A
133

(University of Groningen), Lara S. van de Lande (Erasmus University Rotterdam), Munifa Amira
Anthonijz (The Hague University of Applied Sciences), it was my pleasure to work with you.
Frida Tjiook-Tan & Yang Tjiook, thank you for all your support and also with your Soroptimist
International Club Amsterdam Amstel for supporting the Schisis Project Celebes Ceft Center at
Makassar.
Here also I would like to express the deepest appreciation to the Prof. Dr. Dwia Aries Tina
Pulubuhu, MA., Rector of Hasanuddin University, and also to Prof. Dr. Ir. Muh. Restu, MP., Prof.
Dr. Ir. Sumbangan Baja, M.Sc., Prof. Dr. drg. A. Arsunan, M.Kes, vice Rector of Hasanuddin
University, and also thanks to Prof. Dr. dr. Idrus A. Paturusi, SpB., Sp.OT.(K), Prof. Dr. Eng.
Dadang Ahmad Suriamihardja, M.Eng., and, Prof. Dr. dr. A. Wardihan Sinrang, MS., former Rector
and former vice Rector of Hasanuddin University, who have been giving me a great support for my
study. Thanks to the Ministry of Research, Technology and Higher Education of the Republic of
Indonesia, for their scholarship for overseas.
Thanks to Prof. Makoto Noguchi, DDS., Ph.D., Prof. Keng-Liang Ou, Ph.D., Prof. Lun Jou Lo, MD.,
thanks to you all, for giving me lots of wonderful opportunities on clinical and scientific matters
which can improved my proficiency and special thank to Prof. dr. Chairuddin Rasyad, Ph.D., Sp.B.,
Sp.OT.(K)., drg. Hj. Halimah Dg. Sikati, Prof. drg. Tet Soeparwadi, Sp.BM.(K) (late), Prof. dr. A.
Husni Tanra, Ph.D., Sp.An.(K)., and Prof. Dr. drg. Eky Soeria Soemantri, Sp.Ort.(K)., Dr. dr.
Warsinggih, Sp.B-KBD., who always supported me from the very beginning. You helped and
inspired me to find a way to achieve my passion to study abroad. I am very grateful to have you in
my life.
Then, for the Faculty of Dentistry, Hasanuddin University, I would like to thank to Prof. drg. H.M.
Hatta Hasan S., Ph.D., Sp.BM., Prof. drg. Mansjur Nasir, Ph.D., Prof. Dr. drg. Burhanuddin Dg.
Pasiga, M.Kes., Prof. Dr. drg. Sumintarti, MS., Prof. Dr. drg. Hasanuddin, MS., Prof. Dr. drg.
Rasmidar Samad, MS., Prof. Dr. drg. Harlina, M.Kes., Prof. Dr. drg. M. Hendra Chandha, MS.,
Prof. drg. M. Dharmautama, Ph.D., Sp.Pros.(K)., Prof. Dr. drg. Sri Oktawati, Sp.Perio.(K)., Prof. Dr.
drg. Sherly Horax, MS., Prof. Dr. drg. Barunawaty Yunus, M.Kes., Sp.RKG.(K)., Prof. Dr. drg.
Bahruddin Thalib, M.Kes., Sp.Pros., Prof. Dr. drg. Edy Machmud, Sp.Pros.(K)., Prof. Dr. drg.
Fajriani, M.Si., and also to all my seniors, best friends thanks to you all, for your enormous support
when I needed a hand, even though I was so far away. Thanks to all my colleagues in the
Department of Oral and Maxillofacial Surgery, Prof. drg. H.M. Hatta Hasan S., Ph.D., Sp.BM., Prof.
Dr. drg. M. Hendra Chandha, MS., drg. Netty N. Kawulusan, M.Kes., drg. Surijana Mappangara,
M.Kes., Sp.Perio., drg. Nasman Nuralim, Ph.D., (late), drg. Hasmawati Hasan, M.Kes., drg. Andi
Tajrin, M.Kes., Sp.BM.(K)., drg. Abul Fauzi, Sp.BM., drg. M. Irfan Rasul, Sp.BM, and also I would
like to express the deepest appreciation to the Dean of Faculty of Dentistry, Hasanuddin
University, Prof. Dr. drg. Bahruddin Thalib, M.Kes., Sp.Pros, and also all former Dean of Faculty of
Dentistry, Hasanuddin University, drg. Hj. Halimah Dg. Sikati, Prof. drg. H.M. Hatta Hasan S.,
Ph.D., Sp.BM., drg. M. Amin Kansi, MS., Ph.D., Prof. drg. Moh. Dharmautama, Ph.D., Sp.Pros.(K),
and Prof. drg. Mansjur Nasir, Ph.D., for always support and encourage me to obtain this Ph.D.
I would like to extend my sincere thanks to the colleagues vice directors of the Dental Hospital
Hasanuddin University, drg. Andi Tajrin, M.Kes., SpBM.(K)., drg. Adam Malik Hamudeng,
M.MedEd., drg. Surijana Mappangara, M.Kes., SpPerio., and Dr. drg. Aries Chandra Trilaksana,
Sp.KG.(K), for keeping in touch and sharing the ups and downs in life, and all staf members of the
Dental Hospital Hasanuddin University.
My special thank also to my mentors in Indonesia, Prof. drg. Sunardi Mangundjaja, Sp.BM.(K)
(Padjadjaran University, Bandung), Prof. Dr. drg. Benny Sjariefsyah Latief, Sp.BM.(K) (University
of Indonesia, Jakarta), Prof. drg. R.M. Coen Pramono Danudiningrat, SU., Sp.BM.(K) (Airlangga
University, Surabaya), Prof. drg. Iwan Tofani, Ph.D., Sp.BM (University of Indonesia, Jakarta),
Prof. Dr. drg. Harmas Yazid Yusuf, Sp.BM.(K) (Padjadjaran University, Bandung), and drg. M.
Masykur Rahmat, Sp.BM.(K) (late) (Gadjah Mada University, Yogyakarta), for always support and
encourage me to improved my proficiency. Also to my paranymphs, Diandra Sabrina Natsir Kalla
and Faqi Nurdiansyah Hendra, thanks for helping me on the thesis defense preparation. Best of
luck for you Ph.D.
Last, but most importantly, my deepest gratitude and regards to my mother for her continued
support and encouragement. She continually amazed me for supporting me spiritually throughout
my life. I can see myself completing this highest educational qualification because of your teaching
in my life and your blessings, and very much treasure the loves of my life. My special thanks to my
dear wife Nilla Mayasari, I thank you for your unconditional love, patience, understanding, and
support, it was sometimes really hard to be on such a distance, where would I be without you,
giving me spirit and unconditional love. My daughter Naila Nursyifa Ruslin and my son Nabil Syafi
Ruslin, thank to you for being part of this journey and for embracing the joys, excitements, and
desperations of this venture. I dedicate this thesis to all of you.
Many thanks to my mother in law, and to my brothers and sister, also to my brothers in law, for
your encouragement and support.
It is not possible to mention all the names here but there any many more colleagues, friends, and
family whom I wish to offer my gratitude for their help, encouragement, and nice memories during
to finish this thesis.
A
134

University, Prof. Dr. drg. Bahruddin Thalib, M.Kes., Sp.Pros, and also all former Dean of Faculty of
Dentistry, Hasanuddin University, drg. Hj. Halimah Dg. Sikati, Prof. drg. H.M. Hatta Hasan S.,
Ph.D., Sp.BM., drg. M. Amin Kansi, MS., Ph.D., Prof. drg. Moh. Dharmautama, Ph.D., Sp.Pros.(K),
and Prof. drg. Mansjur Nasir, Ph.D., for always support and encourage me to obtain this Ph.D.
I would like to extend my sincere thanks to the colleagues vice directors of the Dental Hospital
Hasanuddin University, drg. Andi Tajrin, M.Kes., SpBM.(K)., drg. Adam Malik Hamudeng,
M.MedEd., drg. Surijana Mappangara, M.Kes., SpPerio., and Dr. drg. Aries Chandra Trilaksana,
Sp.KG.(K), for keeping in touch and sharing the ups and downs in life, and all staf members of the
Dental Hospital Hasanuddin University.
My special thank also to my mentors in Indonesia, Prof. drg. Sunardi Mangundjaja, Sp.BM.(K)
(Padjadjaran University, Bandung), Prof. Dr. drg. Benny Sjariefsyah Latief, Sp.BM.(K) (University
of Indonesia, Jakarta), Prof. drg. R.M. Coen Pramono Danudiningrat, SU., Sp.BM.(K) (Airlangga
University, Surabaya), Prof. drg. Iwan Tofani, Ph.D., Sp.BM (University of Indonesia, Jakarta),
Prof. Dr. drg. Harmas Yazid Yusuf, Sp.BM.(K) (Padjadjaran University, Bandung), and drg. M.
Masykur Rahmat, Sp.BM.(K) (late) (Gadjah Mada University, Yogyakarta), for always support and
encourage me to improved my proficiency. Also to my paranymphs, Diandra Sabrina Natsir Kalla
and Faqi Nurdiansyah Hendra, thanks for helping me on the thesis defense preparation. Best of
luck for you Ph.D.
Last, but most importantly, my deepest gratitude and regards to my mother for her continued
support and encouragement. She continually amazed me for supporting me spiritually throughout
my life. I can see myself completing this highest educational qualification because of your teaching
in my life and your blessings, and very much treasure the loves of my life. My special thanks to my
dear wife Nilla Mayasari, I thank you for your unconditional love, patience, understanding, and
support, it was sometimes really hard to be on such a distance, where would I be without you,
giving me spirit and unconditional love. My daughter Naila Nursyifa Ruslin and my son Nabil Syafi
Ruslin, thank to you for being part of this journey and for embracing the joys, excitements, and
desperations of this venture. I dedicate this thesis to all of you.
Many thanks to my mother in law, and to my brothers and sister, also to my brothers in law, for
your encouragement and support.
It is not possible to mention all the names here but there any many more colleagues, friends, and
family whom I wish to offer my gratitude for their help, encouragement, and nice memories during
to finish this thesis.
A
A
135

136

List of publications
Published 1. The anthropological aspects of dentofacial deformities: A comparison between Indonesian and
Dutch cohorts. Muhammad Ruslin, Tymour Forouzanfar, Ida A. Astuti, Eky S. Soemantri, Dirk B. Tuinzing Journal of Dentomaxillofacial Science 2014 Feb;13(1):48–54.
2. Dental trauma in association with maxillofacial fractures; An epidemiological study.
Muhammad Ruslin, Jan Wolff, Henk S. Brand, Paolo Boffano, Tymour Forouzanfar Dental Traumatology 2015 April;31(4):318–323.
3. Maxillofacial fractures associated with motor vehicle accidents: A review of the current literature. Muhammad Ruslin, Jan Wolff, Tymour Forouzanfar, Paolo Boffano Journal Oral and Maxillofacial Surgery, Medicine, and Pathology 2015 May;27(3):303–307.
4. The epidemiology, treatment, and complication of dentofacial deformities in an Indonesian
population: A 21-year analysis. Muhammad Ruslin, Tymour Forouzanfar, Ida A. Astuti, Eky S. Soemantri, Dirk B. Tuinzing Journal Oral and Maxillofacial Surgery, Medicine, and Pathology 2015 Sep;27(5):601–607.
5. Effect of nanostructured thin film on minimally invasive surgery devices applications:
Characterization, cell cytotoxicity evaluation and an animal study in rat. Keng-Liang Ou, Chao-Chia Weng, Erwan Sugiatno, Muhammad Ruslin, Yun-Ho Lin, Han-Yi Cheng Surgical Endoscopy 2015 Nov:30(7);3035–3049.
6. Sport related maxillo-facial fractures. Muhammad Ruslin, Paolo Boffano, Y.J.D. ten Brincke, Tymour Forouzanfar, Henk S. Brand Journal of Craniofacial Surgery 2016 Jan;27(1):e91–e94.
7. Assessing the need for a protocol in monitoring weight loss and nutritional status in
orthognathic surgery based on patients experiences. Muhammad Ruslin, Hannah Dekker, Dirk B. Tuinzing, Tymour Forouzanfar Journal of Clinical and Experimental Dentistry 2017 Feb;9(2):e272–e275.
8. Micro/nanostructured surface modification using femtosecond laser pulses on minimally invasive electrosurgical devices. Chia-Cheng Lin, Hao-Jan Lin, Yun-Ho Lin, Erwan Sugiatno, Muhammad Ruslin, Chen-Yao Su, Keng-Liang Ou, Han-Yi Cheng
Journal of Biomedical Materials Researc Part B Applied Biomaterials 2017 May;105(4):865–873.
9. An innovative a–calcium sulfate hemihydrate bioceramic as a potential bone graft substitute.
Heng-Jui Hsu, Rahmat Abd Waris, Muhammad Ruslin, Yun-Ho Lin, Chin-Sung Chen, Keng-Liang Ou Journal of the American Ceramic Society 2017 August;101(1):419–427.
10. The difference uses of panoramic photo and CBCT evaluation of the gnathoplasty surgery
outcome. Ayu Wahyuni, Muliaty Yunus, Muhammad Ruslin Journal of Dentomaxillofacial Science 2017 August;2(2):110–113.
138
11. The application of silver nano-particles on developing potential treatment for chronic rhinosinusitis: Antibacterial action and cytotoxivity effect on human nasal epithelial cell model. Hsin-Hua Chou, Min-Tsan Huang, Sylvia L.F. Pender, Muhammad Ruslin, Yun-Ho Lin, Keng-Liang Ou Materials Science & Engineering C Materials for Biological Applications 2017 Nov;80:624–630.
12. 3D assessment of damaged bicycle helmets and corresponding craniomaxillo mandibular skull
injuries: A feasibility study. Gustaaf J.C. van Baar, Muhammad Ruslin, Maureen van Eijnatten, George K. Sandor, Tymour Forouzanfar, Jan Wolff Injury, 2017 Des:48(12):2872–2878.
13. The epidemiology, treatment, and complication of ameloblastoma in East-Indonesia : 6 Years
Retrospective Study. Muhammad Ruslin, Faqi N. Hendra, Arian Vojdani, David Hardjosantoso, Mohammad Gazali, Andi Tajrin, Jan Wolff, Tymour Forouzanfar Medicina Oral Patologia Oral y Cirugia Bucal 2018 Jan;23(1):e58–e58.
14. Hybrid micro/nanostructural surface offering improved stress distribution and enhanced
osseointegration properties of the biomedical titanium implant. Ping-Jen Hou, Keng-Liang Ou, Chin-Chieh Wang, Chiung-Fang Huang, Muhammad Ruslin, Erwan Sugiatno, Tzu-Sen Yang, Hsin-Hua Chou Journal of the Mechanical Behavior of Biomedical Materials 2018 Mar;79:173–180.
15. The potential of the stem cells composite hydrogel wound dressings for promoting wound
healing and skin regeneration: In vitro and in vivo evaluation. Ling-Chuan Hsu, Bou-Yue Peng, May-Show Chen, Bahruddin Thalib, Muhammad Ruslin, Tran Dang Xuan Tung, Hsin-Hua Chou, Keng-Liang Ou Journal of Biomedical Materials Researc Part B Applied Biomaterials Mar 2018. Epub ahead of print.
16. Long exposure of argon plasma coagulation induces more thermal damage accompanied by a
higher expression of NF-kB and caspase-3. Rahmat A. Waris, Keng-Liang Ou, Muhammad Ruslin, Bahruddin Thalib, Chung-Ming Liu, Hsin-Hua Chou Journal of Dentomaxillofacial Science 2018 April;3(1):62–69.
17. Total tannin levels analysis of brown algae (sargassum sp. and padina sp.) to prevent blood
loss in surgery. Abul Fauzi, Satriani Lamma, Muhammad Ruslin Journal of Dentomaxillofacial Science 2018 April;3(1):37–40.
18. Utilization of pedicled buccal fat pads for coverage of the lateral relaxing wound: A review of
literature and a case series of 15 patients. Muhammad Ruslin, Andi S. Hajrah Yusuf, Andi Tajrin, Lun-Jou Lo, Tymour Forouzanfar Journal of Clinical and Experimental Dentistry 2018 May;10(5):e502–506.
19. Evaluation of surface characteristics and hemocompatibility on the of the oxygen plasma-
modified biomedical titanium. Hsi-Jen Chiang, Hsin-Hua Chou, Keng-Liang Ou, Erwan Sugiatno, Muhammad Ruslin, Rahmat Abd Waris, Chiung-Fang Huang, Chung-Ming Liu, Pei-Wen Peng Metals 2018 July;8(7):513.
P P
139

20. Analysis of total flavonoid levels in brown algae (Sargassum sp. and Padina sp.) as analgesic drug therapy. Muhammad Ruslin, Akbar Fuad Husain, Hajrah Yusuf AS, Subehan Asian Journal of Pharmaceutical and Clinical Research 2018 July;11(7):81–83.
Accepted for publication 21. Motor-vehicle accidents related maxillofacial injuries: A multicenter and prospective study.
Muhammad Ruslin, Matteo Brucoli, Paolo Boffano, Arnaldo Benech, Jan Wolff, Emil Dediol, Vedran Uglešić, Žiga Kovačič, Aleš Vesnaver, Vitomir S. Konstantinović, Milan Petrović, Jonny Stephens, Amar Kanzaria, Nabeel Bhatti, Simon Holmes, Petia F. Pechalova, Angel G. Bakardjiev, Vladislav A. Malanchuk, Andrey V. Kopchak, Pål Galteland, Even Mjøen, Per Skjelbred, Helios Bertin, F Marion, Julien Guiol, Pierre Corre, Sigbjørn Løes, Njål Lekven, Sean Laverick, Peter Gordon, Tiia Tamme, Stephanie Akermann, K Hakki Karagozoglu, Sofie C. Kommers, Jan G. de Visscher, Tymour Forouzanfar. Oral Surg Oral Med Oral Pathol Oral Radiol
22. The influence of helmet on the prevention of maxillofacial fractures sustained during motorcycle accidents. Muhammad Ruslin, Jan Wolff, Harmas Y. Yusuf, Muhammad Z. Arifin, Jan Wolff, Paolo Boffano, Tymour Forouzanfar Cogent Engineering
23. The use of neuron-specific enolase to predict brain injury in maxillofacial fractures after vehicle accidents: A pilot study. Muhammad Ruslin, Harmas Yazid Yusuf, Muhammad Zaifullah Arifin, Jan Wolff, Paolo Boffano, Tymour Forouzanfar Chinese Journal of Traumatology
24. Establishing cleft services in developing countries: complications of cleft lip and palate surgery in rural areas of Indonesia. Muhammad Ruslin, Lawrence Dom, Andi Tajrin, A.S. Hajrah Yusuf, Syafri K. Arif, Andi H. Tanra, Keng Liang Ou, Tymour Forouzanfar Archives of Plastic Surgery
Submitted 25. Rapid and efficient fabrication of the biocompatible bioceramic for bone graft substitute
applications: Phase transformation, in vitro cytocompatibility and an in vivo study in the chick chorioallantoic membrane model. Keng-Liang Ou, Heng-Jui Hsu, Yun-Ho Lin, Muhammad Ruslin, Ching-Zong Wu, Rahmat A. Waris
26. Intraoperative and early postoperative complications using the buccal fat pad during cleft
palate surgery in East Indonesia. Muhammad Ruslin, Diandra Sabrina N. Kalla, Andi S. Hajrah Yusuf, Andi Tajrin, Paolo Boffano, Tymour Forouzanfar
27. Maxillofacial fractures associated with sport injuries: A review of the current literature.
Paolo Boffano, Muhammad Ruslin, Matteo Brucoli, Arnaldo Benech, Tymour Forouzanfar
140

28. High-energy plasma modification induced phase transformation and variation of the surface properties on the nanostructured oxide layer of biomedical titanium implant. Hsi-Jen Chiang, Chung-Ming Liu, Keng-Liang Ou, Bahruddin Thalib, Rahmat Waris, Muhammad Ruslin, Chiung-Fang Huang
29. The Maxillofacial Injury Severity Score (MFISS) and Facial Injury Severity Scale (FISS) as a
predictor brain injury with maxillofacial fractures patients. Muhammad Ruslin, Paolo Boffano, HCW de Vet, M Brucoli, KH Karagozoglu, Tymour Forouzanfar
30. A promising of nanostructured-gold surface offering improved thermomechanical and anti-
adhesive properties of the electrosurgical electrode for biomedical applications. Hsi-Jen Chiang, Chung-Ming Liu, Bahruddin Thalib, Muhammad Ruslin, Keng-Liang Ou, Pei-Wen Peng, Chiung-Fang Huang
31. Surface characterization and thermomechanical behavior of nanostructured-gold layer for
biomedical applications. Keng-Liang Ou, Chi-Ming Wu, Rahmat A Waris, Erwan Sugiatno, Muhammad Ruslin, Chung-Ming Liu, Hsin-Hua Chou
32. Sport related maxillofacial fractures: A multicenter and prospective study.
Muhammad Ruslin, Matteo Brucoli, Paolo Boffano, Arnaldo Benech, Emil Dediol, Vedran Uglešić, Žiga Kovačič, Aleš Vesnaver, Vitomir S. Konstantinović, Milan Petrović, Jonny Stephens, Amar Kanzaria, Nabeel Bhatti, Simon Holmes, Petia F. Pechalova, Angel G. Bakardjiev, Vladislav A. Malanchuk, Andrey V. Kopchak, Pål Galteland, Even Mjøen, Per Skjelbred, Helios Bertin, Pierre Corre, Sigbjørn Løes, Njål Lekven, Sean Laverick, Peter Gordon, Tiia Tamme, Stephanie Akermann, K Hakki Karagozoglu, Sofie C. Kommers, Jan G. de Visscher, Tymour Forouzanfar
33. Global incidence and profile of ameloblastoma: A systematic review and meta-analysis. Faqi Nurdiansyah Hendra, Ellen Van Cann, Muhammad Ruslin, Jan de Visscher, Tymour Forouzanfar, Henrica de Vet
34. Towards tissue engineering application of cleft palate defects: A review.
Diandra Sabrina N. Kalla, Faqi Nurdiansyah Hendra, Muhammad Ruslin, Melvin Maningky, Tymour Forouzanfar, Marco N. Helder
35. Long-term stability counterclockwise surgical advancement mandibular deficiency in patients
with high mandibular plane angle. Part I – Dental and skeletal aspect. Muhammad Ruslin, Tymour Forouzanfar, R.B. Greebe, Dirk B. Tuinzing
36. Long-term stability counterclockwise surgical advancement mandibular deficiency in patients
with high mandibular plane angle. Part II – Double and single surgery aspect. Muhammad Ruslin, Tymour Forouzanfar, R.B. Greebe, Dirk B. Tuinzing
37. The role of endodontics after tooth injuries to prevent root resorption: A review and case
presentation. Syamsiah Syam, Andi Sumidarti, A. S. Hajrah-Yusuf, Aries Chandra Trilaksana, M. Hendra Chanda, Muhammad Ruslin
38. Global perspective on facial deformity: Cultural and religious perspective.
Hasanuddin, Muhammad Ruslin, Tymour Forouzanfar
P P
141
SyamsiahSyam,AndiSumidarti,A.S.Hajrah-Yusuf,AriesChandraTrilaksana,M.HendraChanda, Muhammad Ruslin

142

Curriculum vitae

Muhammad Ruslin, was born in Pangkajene, Indonesia on the 2nd of
July 1973. He is currently an Associate Professor in Oral and
Maxillofacial Surgery, at Department of Oral and Maxillofacial Surgery,
Faculty of Dentistry, Hasanuddin University. He is also a Consultant of
Oral and Maxillofacial Surgeon at Hasanuddin University Hospital and
Dental Hospital Hasanuddin University. He graduated his Bachelor and
Doctor of Dental Surgery from Faculty of Dentistry, Hasanuddin
University, Makassar, Indonesia in 2000 and obtained a Master Degree
in Oral and Maxillofacial Surgery from Faculty of Medical, University of Padjadjaran, Bandung,
Indonesia in 2009. He had his residency training at Department of Oral and Maxillofacial Surgery
Faculty of Dentistry, University of Padjadjaran, Bandung, Indonesia (2003-2009), he registered as
Oral and Maxillofacial Surgeon by Indonesian College of Oral and Maxillofacial Surgeons in 2009,
and he registered as Consultant of Oral and Maxillofacial Surgery by Indonesian College of Oral
and Maxillofacial Surgeons in 2017. He did a visiting research fellow in Department of Oral and Maxillofacial Surgery, Graduate School
of Medicine and Pharmaceutical Sciences for Research, University of Toyama (Prof. Makoto
Noguchi, DDS., PhD) (2014. Jan-Mar). He did a Clinical Fellow in Department of Plastic and
Reconstruction Surgery, Chang Gung Memorial Hospital, Taouyuan, Taiwan (Prof. Lun Jou Lo.)
(2015). Since 2012, he has been a PhD researcher at Department of Oral and Maxillofacial
Surgery/Oral Pathology, VU University Medical Center/Academic Centre for Dentistry Amsterdam
(ACTA), Amsterdam, The Netherlands (Promotor Prof. Tymour Forouzanfar, MD., DDS., PhD., and
copromotors Prof. D. Bram Tuinzing, DMD and Paolo Boffano, MD., PhD). His research and
clinical interests include oromaxillofacial trauma, congenital anomalies, dentofacial deformities,
temporomandibular joint disorders, stem cells/tissue engineering and surgical implants. He has
established Celebes Cleft Center Foundation in 2011 as non-profit organization.
He has been the councilor at International Association of Oral and Maxillofacial Surgeons, the vice
chairman of the Indonesian College of Oral and Maxillofacial Surgeons and Director of Dental
Hospital Hasanuddin University.
C
144

Maxillofacial FracturesAssociated with Accidents:
Epidemiology and Consequences
Maxillofacial FracturesAssociated with Accidents:
Epidemiology and Consequences
MUHAMMAD RUSLIN
Maxillofacial Fractures Associated w
ith Accidents: Epidemiology and Consequences - M
uhamm
ad Ruslin