Argonaute2 Mediates Compensatory Expansion of the Pancreatic β Cell

Compensatory Stepping: TheBiomechanics of a Preferred ResponseAmong Older Adults
Jody L. JensenDepartment of Kinesiology and Health Education,The University of Texas at Austin, Austin, Texas, USA
Lesley A. BrownDepartment of Kinesiology, University of Lethbridge,Lethbridge, Alberta, Canada
Marjorie H. WoollacottDepartment of Exercise and Movement Science,University of Oregon, Eugene, Oregon, USA
The purpose of this study was to evaluate age-related differences in themechanics of the compensatory stepping response to balance threats. Amoving platform was used to disturb the balance of 16 younger (21 to 35years) and 19 older (68 to 88 years) adults. Backward platformtranslations consisted of 15-cm displacements with peak accelerationsranging from 9.4 to 15.2 m=s2. Older adults were more likely to use a stepto recover balance and stepped at lower perturbation magnitudes thanyounger adults. Group differences were not found in time to step initiationor segmental momentum. The lack of group differences in momentumrevealed that lower perturbation accelerations created an equivalent orgreater magnitude of body motion in older adults compared to higher
Received 22 June 2000; accepted 15 March 2001.The authors gratefully acknowledge Mr. Dan Furgason (Department of Physics, University of
Lethbridge) for programming contributions and Mr. Ryan Sleik (Department of Kinesiology,University of Lethbridge) for manuscript formatting. This research was supported by a National
Institutes of Health Grant (AG05317) to M. Woollacott and a grant from the AmericanFederation for Aging Research to J. L. Jensen. L. A. Brown was also supported by grants from the
Alberta Heritage Foundation for Medical Research.Address correspondenc e to Jody L. Jensen, PhD, Department of Kinesiology and Health
Education, Bellmont Hall 222, The University of Texas at Austin, Austin, TX 78712, USA.E-mail: [email protected]
Experimental Aging Research, 27: 361±376, 2001
Copyright # 2001 Taylor & Francis
0361-073X /01 $12.00 + .00
361

accelerations experienced by younger adults. Older adults also showed areduced ability to attenuate the input acceleration and experiencedsignificantly greater linear acceleration of the head.
Loss of balance and falling is an unfortunate reality for many older adults. Whywe fall and what we can do about reducing the incidence of falling are centralthemes in prevention and rehabilitation research arenas. One approach tounderstanding the propensity for instability among the aged is to explore howthe strategies for balance recovery among older adults compare with those ofyounger adults who are not limited by balance dysfunction. For example, it hasbecome a common observation that older adults adopt a compensatory stepmore readily than younger adults (Brown, Shumway-Cook, & Woollacott,1999; McIlroy & Maki, 1996; Pai, Rogers, Patton, Cain, & Hanke, 1998;Luchies, Alexander, Schultz, & Ashton-Miller, 1994; Rogers, Hain, Hanke,& Janssen, 1996). It has also been noted that older adults adopt steps followingless severe balance disturbances than younger adults (Pai et al., 1998; Brownet al., 1999). Given the prevalence with which older adults utilize compensatorystepping to prevent imbalance, it is surprising that the basis for this apparentpreference remains largely undetermined. Here, we examine age-relateddifferences in the compensatory stepping response to examine the possibilit ythat the preference for stepping among older adults is mechanically based.
The occurrence of a step typically has been regarded as an inevitableconsequence of the horizontal movement of the center of mass (COM)beyond the limits of the base of support (BOS). Although steps of this typeare considered to be necessary outcomes of the laws of physics, recent workimplies that in both young and older adults, steps are also initiated when theCOM is located within the base of support (Brown et al., 1999; McIlroy &Maki, 1993; Pai et al., 1998). Thus the occurrence of a compensatory stepdoes not depend solely on the COM exceeding the base of support. Indeedrecent work by Pai and colleagues (1998, 1997) demonstrated that thevelocity of the COM is also a trigger for compensatory stepping. This workhas led to the conceptualization of the ``dynamic stability limits’’ for feasiblemovement termination, which predicted that the occurrence of a step dependson the interaction between the COM position and its velocity. Following thismodel, stepping may be necessary if there is a sufficiently high velocity ofCOM displacement, even if the COM is located within the BOS at stepinitiation . Thus, if older adults adopt steps following less severe disturbancesthan younger adults, and if these steps are initiated before the COM exceedsthe BOS, it would follow that a less intense balance disturbance would lead toan equivalent (or higher) COM velocity for older adults than for youngeradults. Thus, one issue that remains to be explored is how a less severeperturbation might create the momentum (Mass £ Velocity) in an older adultthat equates with that obtained following a larger perturbation experienced bya younger adult.
362 J. L. Jensen et al.

Insight into this issue may be gained by considering the momentumpossessed by the body prior to the initiation of the step. When weexperience a perturbation, the body is set in motion, and there is a changein momentum. In induced-momentum paradigms, momentum is ultimatelyconstrained by the generation of muscle torques to reduce segmentalmotion, and hence the linear momentum of the whole body. One hypothesisfor the increased incidence of stepping among older adults is that olderadults may be unable to generate the necessary counterbalancing muscletorques, either in magnitude or in rate of muscle torque development, tocontrol the body’s horizontal momentum. Evidence in support of thishypothesis comes from a number of studies showing an age-relatedreduction in voluntary muscle strength (Brown et al., 1999; McIlroy &Maki, 1993; Pai et al., 1998) and rate of muscle force production (Clarkson,Kroll, & Melchionda, 1981; Hakkinen & Hakkinen, 1991; Larsson, 1978).However, the results from voluntary muscle testing in the construction ofexplanations of function in reactive balance tasks should be viewed withsome caution. Two cautionary points can be made. First, the initial responseto a balance threat may not require a maximal muscle strength response(Gu, Schultz, Shepard, & Alexander, 1996). Secondly, there is evidence thatthe initial ankle muscle torque response to balance perturbations (e.g., up toapproximately 160 ms post perturbation) does not differ between youngerand older adults (Hall, Woollacott, & Jensen, 1999). These findings implythat the increased incidence of stepping among older adults may not be afunction of limitations in initial muscle torque production .
Although Hall et al. (1999) found the initial balance recovery response atthe ankle to be no different between younger and older adults, the possibilit yremains that the differences may be found in how the motion induced by theperturbation is propagated up the linked system. The purpose of this studywas to determine if there are age-related differences in the mechanics of thebalance response leading to step initiation . Our analyses were directed towardevaluating age-related differences in segmental momenta and accelerations atthe time of step initiation.
METHOD
Participants
The data from 35 females were analyzed in this study. There were 16younger adults and 19 older adults. The age of the younger participantsranged between 21 and 35 years (M ˆ 25.93, SD ˆ 4.62 years); the age of theolder participants ranged between 68 and 88 years (M ˆ 72.1, SD ˆ 3.78years). To qualify for participation in this study, all participants were screenedto ensure that they were free from any orthopedic, neurological, and=orcardiovascular disorders; the older adults were required to receive medical
Age Differences in Rapid Step Initiation 363

clearance to participate in the study. In addition, only those individuals whohad not experienced any fall episodes within the past year and did not have afear of falling (participant self-report) were invited to participate. Allparticipants were informed of the study protocol and indicated theirwillingness to participate through written consent. Study participation wasrestricted to females to control for potentially confounding gender-specificdifferences such as strength (Thelen, Schultz, & Alexander, 1996; Wolfson,Whipple, Derby, Amerman, & Nashner, 1994).
Protocol
Balance was disturbed using a translating force platform (mounted flushwith the surrounding surface). Each participant stood barefoot with armsfolded across the chest. They wore a lightweight climbing harness securedoverhead to ensure safety in the event of a stumble, misstep, or fall.Participants were asked to try to maintain their balance without moving theirfeet (i.e., stepping!the stepping area was unconstrained). A series of 18consecutive perturbations were delivered using both backward- and forward-directed platform displacements, ranging between 5 and 15 cm, withvelocities ranging between 10 and 80 cm=s. Perturbations were presentedin a pseudorandomized manner whereby less severe disturbances occurredwithin the early trials. This testing order served as a precautionary measure toensure that participants would not be exposed to the more severe disturbancesearly in the test session.
From these 18 trials, three backward-directed perturbation conditionswere selected for analysis: 15 cm at 40 cm=s; 15 cm at 60 cm=s; 15 cm at80 cm=s. In our previous work, these perturbation conditions were shown toelicit compensatory stepping in older and in younger adults (Brown et al.,1999). These perturbations represent a progressive increase in severity,presenting peak accelerations of 9.4, l2.5, and 15.2 m=s2 for the 40-, 60-,and 80-cm=s conditions, respectively. In all cases, the platform wastranslated using a ramp onset with parabolic offset displacement waveform.Figure 1 illustrates the displacement waveform and resulting accelera-tion=deceleration characteristics for the mid-severity condition (peakacceleration ˆ 12.5 m=s2).
Data were collected over a 5-s interval with platform translationsprogrammed to commence 1 s from the start of data collection. Datacollection was triggered after participants indicated that they were ready,though a variable wait period (approximately 1±3 s) was used so thatparticipants could not predict when the balance disturbance would occur. Inaddition, the three trials used in this analysis represented trials numbered 27(peak ˆ 9.4 m=s2), 21 (12.5 m=s2), and 18 (15.2 m=s2). Each trial waspreceded by a different perturbation condition, making anticipation of theprecise perturbation characteristics unlikely.
364 J. L. Jensen et al.

Instrumentation
A hydraulically driven, strain-gauge force plate (30 £ 46 cm; Universityof Oregon, Institute of Neuroscience technical group) was used in this study.Analog outputs from a linear potentiometer, vertical and horizontal groundreaction forces, and the accompanying moment of force data were digitallysampled at 500 Hz.
Kinematic data were obtained from a two-camera WATSMART motionanalysis system (Northern Digital, Inc., Waterloo, Ontario). Light-emittingdiodes marked the following landmarks: (1) the head of the fifth metatarsal(`toe’), (2) the lateral calcaneus (`heel’), (3) the lateral malleolus (`ankle’),(4) the lateral femoral condyle (`knee’), (5) the greater trochanter (`hip’).(6) the acromion process (`shoulder’) , (7) the temporomandibula r joint(`ear’), (8) the temple (`head’), and (9) the platform. A calibrated volumemeasuring 1.7 £ 1.4 £ .55 m was defined. Average error (root meansquare) for the reconstruction of markers was less than 5 mm. Kinematicdata were sampled at 100 Hz.
Data Analyses
The presence of a step was determined from video data and confirmedusing center of pressure (COP) coordinates derived from the recorded vertical
FIGURE 1 Platform displacement and acceleration for the mid-severity condition of15 cm at 60 cm=s condition (12.5 m=s2), showing the ramp onset and parabolic offsetdisplacement waveform. NOTE: The perturbation conditions presented peakaccelerations of 9.4 m=s2, 12.5 m=s2, and 15.2 m=s2 for the 40, 60, and 80 cm=sconditions respectively.
Age Differences in Rapid Step Initiation 365

ground reaction force and moment of force data obtained from the forceplate. Step initiation was defined as the first deviation beyond the mean in thelateral COP signal. The criterion for deviation was a consistent change inslope over a 20-ms interval, leading to lift-off of the swing limb.
The body was modeled as a bilaterally symmetrical five-segment systemcomposed of feet, shanks, thighs, trunk (with arms), and head. Definitions ofsegment length proportion s and inertial characteristics were based onanthropometric data reported by Winter (1990). Kinematic data werereferenced to an inertial reference frame to compensate for plate motion.
The location of the body’s COM relative to the base of support in theanterior-posterior plane was used to describe the type of step response thatsubjects used to regain balance. In particular, we were interested inquantifying the prevalence of steps that do not occur as a consequence ofthe COM exceeding the base of support. We defined the functional base ofsupport as a distance equivalent to 80% of the length of the foot, measuredfrom the heel. If the horizontal location of the whole body COM was found tobe within this 80% boundary at the point of step initiation , then the step wasregarded to occur while the COM remained within the BOS.
Linear momentum (L) values at step initiation (for anterior-posterior planemotion) were determined for segmental and the whole body COM (L is theproduct of a body’s mass [m, segmental or whole body] and its linear velocity[v]; L ˆ mv). Angular momentum (H) was calculated for the trunk segmentonly (H is the product of a body’s inertia (I ) and its angular velocity (o);H ˆ Io). Trunk angular momentum (HTK) was used to categorize those stepsoccurring while the COM remained within the BOS to be either `delayed’ or`rapid.’ Steps initiated after HTK had reached its maximum were categorized as`delayed’ steps (Figure 2, Graphs A and C); steps initiated before maximumHTK were classified as `rapid’ steps (Figure 2, Graphs B and D).
Momentum represents the quantity of motion of a system at an instant intime. We were also interested in how the system was changing at the time ofstep initiation . Thus, we evaluated the horizontal linear acceleration (rate ofchange of velocity) of body segments relative to the acceleration of the toe todetermine how the velocity (thus the momentum) of the system was changingat the time of step initiation . We compared the motion of the body segmentsacross different perturbations by normalizing the magnitude of bodylandmark linear accelerations with respect to the peak acceleration associatedwith each perturbation.
Statistical Analyses
The frequency of stepping was compared between younger and olderadults using a chi-square test of association. Age differences in the measuresof interest were assessed using independent samples t tests with alpha set to0.05; a Bonferroni correction for multiple comparisons was used whenappropriate.
366 J. L. Jensen et al.

FIG
UR
E2
Gra
phs
Aan
dB
show
CO
Mtr
ajec
tori
esin
the
ante
rior=
pos
teri
or
(A=P
)dir
ecti
on
foll
owin
gpe
rturb
atio
nons
et(P
on
set,
mar
ked
bya
vert
ical
das
hed
line)
.H
ori
zont
allines
mar
kA
=Plo
cation
of
the
ankl
ejo
int
and
the
bas
e-of-
supp
ort
(BO
S)
lim
it.
Gra
phs
Can
dD
show
trun
kan
gul
arm
om
entu
m(H
)va
lues
.N
egat
ive
(posi
tive
)va
lues
are
asso
ciat
edw
ith
flex
ion
(exte
nsi
on)
ofth
etr
unk
on
the
thig
h.
Ste
pin
itia
tion
ism
arked
bya
soli
dve
rtic
alline.
367

RESULTS
Our results indicate that across the range of perturbations selected foranalysis older adults were more likely than younger adults to use a step torecover balance (w2 ˆ 6:85; p < :01). In particular, older adults (OA)stepped in 95% of the trials (n ˆ 54 out of 57 trials), whereas younger adults(YA) stepped in 62% of the trials (n ˆ 30 out of 48 trials). In addition, theseverity of the perturbation had a differential effect on OA compared to YA.As illustrated in Figure 3, 84% (16 of 19) of OA, but less than 15% (2 of 16)of YA, stepped following the low acceleration perturbation (9.4 m=s2)(w2 ˆ 10.89, p < :01). The medium acceleration condition (12.5 m=s2) elicitedsteps from 100% of OA and 75% of YA (w2 ˆ 1.58, p > :01). All participantsstepped following the most demanding condition (15.2 m=s2). These resultsshow the reliance of these older adults on the stepping response to regainequilibrium compared to these younger adults. Furthermore, these findingsdemonstrate the propensity among these older adults, compared to theseyounger adults, to use the stepping response following less demandingperturbations.
Of the step trials available for analysis (n ˆ 25=30 for YA; n ˆ 40=54 forOA), the COM was located within the base of support on 76% (19 of 25) ofthe step trials for YA and on 83% (33 of 40) of trials for OA. Of the stepstaken by YA with COM within BOS, 16% (3 of 19) were characterized asdelayed steps; that is, the steps were initiated after the angular momentum ofthe trunk had reached its maximum value (Figure 4, left). By definition,delayed steps are characterized by reduction in the motion of the trunk prior to
FIGURE 3 Prevalence (%) of stepping among young and older adults at eachperturbation condition.
368 J. L. Jensen et al.
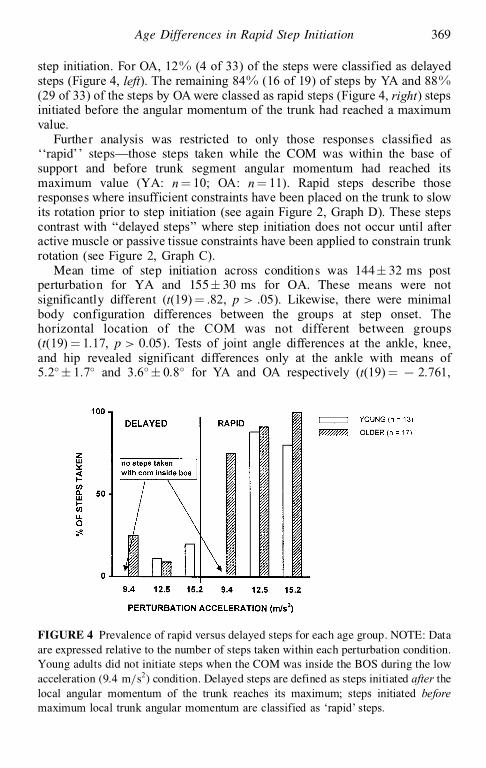
step initiation. For OA, 12% (4 of 33) of the steps were classified as delayedsteps (Figure 4, left). The remaining 84% (16 of 19) of steps by YA and 88%(29 of 33) of the steps by OA were classed as rapid steps (Figure 4, right) stepsinitiated before the angular momentum of the trunk had reached a maximumvalue.
Further analysis was restricted to only those responses classified as``rapid’’ steps!those steps taken while the COM was within the base ofsupport and before trunk segment angular momentum had reached itsmaximum value (YA: n ˆ 10; OA: n ˆ 11). Rapid steps describe thoseresponses where insufficient constraints have been placed on the trunk to slowits rotation prior to step initiation (see again Figure 2, Graph D). These stepscontrast with `̀ delayed steps’’ where step initiation does not occur until afteractive muscle or passive tissue constraints have been applied to constrain trunkrotation (see Figure 2, Graph C).
Mean time of step initiation across conditions was 144§ 32 ms postperturbation for YA and 155§ 30 ms for OA. These means were notsignificantly different (t(19) ˆ .82, p > :05). Likewise, there were minimalbody configuration differences between the groups at step onset. Thehorizontal location of the COM was not different between groups(t(19) ˆ 1.17, p > 0:05). Tests of joint angle differences at the ankle, knee,and hip revealed significant differences only at the ankle with means of5.2¯ § 1.7¯ and 3.6¯ § 0.8¯ for YA and OA respectively (t(19) ˆ 7 2.761,
FIGURE 4 Prevalence of rapid versus delayed steps for each age group. NOTE: Dataare expressed relative to the number of steps taken within each perturbation condition.Young adults did not initiate steps when the COM was inside the BOS during the lowacceleration (9.4 m=s2) condition. Delayed steps are defined as steps initiated after thelocal angular momentum of the trunk reaches its maximum; steps initiated beforemaximum local trunk angular momentum are classified as `rapid’ steps.
Age Differences in Rapid Step Initiation 369

p ˆ .012). Knee joint angle excursions of 2.3¯ (§ 1.7¯) and 1.2¯ (§ 1.0¯) forYA and OA were nonsignificant (t(19) ˆ 7 2.18, p ˆ 0.04; Bonferronicorrection for multiple t tests), as were differences in hip joint excursions of2.6¯ (§ 2.1¯) and 3.0¯ (§ 1.3¯) for YA and OA, respectively (t(19)ˆ ¡0:38,p ˆ .71).
Analysis of the perturbation conditions that first led to the execution ofrapid steps revealed that 70% of OA produced a rapid step at the 9.4 m=s2
condition while the remaining 30% of OA first made rapid steps followingthe 12.5 m=s2 condition (Figure 5). No young adults produced a rapid step atthe 9.4 m=s2 condition (though 2 of 13 YA produced delayed steps atthis condition) . Younger adults did not begin to produce rapid steps until the12.5 m=s2 condition. Fifty percent of YA first produced rapid steps at the12.5 m=s2 condition. The remaining 50% first produced rapid steps atthe 15.2 m=s2 condition.
The interesting observation in Figure 5 is that OA adopted the rapid stepfollowing lower perturbation accelerations than YA. Figure 6A, shows thecomparison of group mean horizontal segmental momenta at the time of stepinitiation for the transition condition (the lowest perturbation acceleration thatelicited a rapid step). The data have been normalized to perturbation impulse(time integral of the horizontal force between the onset of the perturbation andthe initiation of the rapid step) to account for age group differences in the inputacceleration producing the rapid step. Thus the data in Figure 6 (A or B) maybe interpreted as the momentum achieved as a consequence of each unit of
FIGURE 5 Percent of each age group employing a rapid step in each accelerationcondition. NOTE: The bars represent the smallest acceleration to elicit the rapid stepin each group. Rapid steps were characterized by (1) the location of the COM beingwithin the BOS at step initiation and (2) that steps were initiated before the localangular momentum of the trunk reached its maximum value.
370 J. L. Jensen et al.

input acceleration delivered by the perturbation. Independent samples t testsfailed to reveal age group differences for the lower extremity segments(t(19) ˆ 1.99, p ˆ .06; t(19) ˆ 1.9, p ˆ .07; t(19) ˆ 1.92, p ˆ .07 for the foot,shank, and thigh, respectively). Nor were age group differences found for thehead-arms-trunk (HAT) segment (t(19) ˆ 1.51, p ˆ .15) or for the whole bodyCOM (t(19) ˆ 1.10, p ˆ .28) (Figure 6B). This finding indicates that an
FIGURE 6 (A) Horizontal linear momenta for the foot, shank, thigh, and HATsegments. (B) Whole body COM horizontal linear momentum at the point of stepinitiation for young and older adults. NOTE: Data presented have been normalized tothe perturbation impulse (time integral of the horizontal force between the onset of theperturbation and the initiation of the rapid step) and are expressed in absolute valueterms.
Age Differences in Rapid Step Initiation 371

equivalent magnitude of body motion between younger and older adults isachieved following different input acceleration values. In particular, a lowerperturbation acceleration creates an equivalent magnitude of body motion inan older adult that a higher perturbation acceleration creates for a youngeradult.
At step initiation , the groups were not distinguishe d by any of thehorizontal segmental momentum terms. There was a consistent pattern,however, for the older adults to have larger momentum values. Given therapidity with which the steps were initiated, it is conceivable that theresimply was insufficient time for the motion differences to become apparentbetween the groups. Velocity terms (upon which momentum is based) revealthe instantaneous state of motion of a body or system. Acceleration termsreveal the rate at which velocity is changing. Thus, we evaluated thehorizontal linear acceleration of segments to determine how the system,specifically segment velocities, were changing. At the onset of the step,segmental velocities could be quite similar between the groups, but the rate atwhich the velocities were changing could be quite different.
Figure 7 presents the horizontal linear acceleration of segmental endpointsat step initiation. The data reveal how the input acceleration was reduced, oraugmented, across segments as the consequences of the perturbation werepropagated through the linked system. As illustrated, there was a noticeabledecrease in acceleration between the ankle and the head in YA. In contrast,this trend of attenuation was not seen among OA. For OA, there was a slightdecrease in the resultant acceleration from the ankle to the hip; however,acceleration magnitudes subsequently increased from hip to head. As the
FIGURE 7 The horizontal acceleration of each joint relative to the linear accelerationof the toe. NOTE: Data presented were obtained at the point of step initiation and havebeen normalized for the magnitude of perturbation acceleration.
372 J. L. Jensen et al.

head contains the apparatus for acceleration detection, we did an analysis ofthe differences in acceleration at the head. Indeed, the independent samplet test confirmed that there was a significant effect of age for horizontalacceleration at the head, with OA showing greater resultant accelerations thanYA (t(19) ˆ 2.41, p ˆ .02).
DISCUSSION
All participants were instructed to recover balance without moving theirfeet (i.e., stepping). Despite that instructiona l constraint, both young andolder adults employ a rapid step as a balance recovery response. Our resultsalso reveal that older adults employ a rapid stepping response more oftenwhen compared under similar conditions to younger adults. Older adults,compared to young adults, also resort to the step as a balance recoverystrategy under less threatening conditions . The propensity of older adults touse the rapid step was not due to these adults having a larger momentum atthe time of step initiation , though a trend for greater momenta in the olderadults was evident. What did distinguish the older adults from their youngeradult counterparts was their failure to attenuate the destabilizing accelerationsintroduced by the perturbation.
The difference between younger and older adults leading to rapid steppingunder less threatening conditions is not a matter of older adults adopting adifferent behavioral response compared to younger adults. For example, inboth groups, steps were initiated (on average) within the first 150 msfollowing onset of the perturbation. The older adults were neither quicker norslower in responding to the balance threat. Further, the older adults were notin a more tenuous position at the time of step initiation . The bodyconfiguration at the moment of the step showed minimal differences betweenyounger and older adults, with the older adults showing smaller jointexcursions at the ankle and knee and slightly larger excursions at the hip.
The issue here is also not one of older adults being unable to contain thecenter of mass trajectory to excursions within the limits of the base ofsupport. Our results clearly show that rapid steps, those initiated well beforethe whole body COM has exceeded the base of support and before trunkangular momentum has reached its maximum value, are a typical responseamong both younger and older adults. The interesting observation is thatolder adults employ these rapid step responses under less threateningcircumstances than younger adults!and not because they are thrown into amore precarious posture. Thus if the positional constraints of the COM didnot require establishing a new base of support, was there another mechanicaldemand requiring the step?
Such a mechanical demand could arise from a system that has gathered agreat deal of momentum. It has been suggested that controlling the horizontalmomentum of the COM is a strategy employed to maintain balance during
Age Differences in Rapid Step Initiation 373

voluntary movements (e.g., gait: Kaya, Krebs, & Riley, 1998; sit-to-stand:Kaya et al., 1998; Pai & Lee, 1994; Pai & Rogers, l990; 1991). The strategywould be to limit the segmental or whole body momenta to those levels thatcan be managed by the application of an opposing impulse (the application ofmuscle force over time). The data presented did not strictly support thishypothesis in that we found no significant group differences in horizontalCOM momentum at the time of step initiation . We did, however, observe atendency for older adults to be described by larger segmental and whole bodymomenta. It was this observation that led to the consideration of not just theinstantaneous state of the system as represented by the velocity-basedmomentum variable, but how the system was changing as revealed in theacceleration analysis.
Based on the acceleration analysis, the production of rapid steps by olderadults under relatively less threatening conditions is related to the rate atwhich the body is gaining momentum. Although the groups were notdistinguishe d by differences in the momentum of the body possessed at steponset, the older adults were experiencing larger accelerations. Older adultsdemonstrated only a very modest reduction in the horizontal accelerationacross the lower extremity segments. The trunk and head, in fact, experiencedaugmented accelerations!thus increasing gains in momentum. This findingis consistent with previous reports of age-related differences in theattenuation of horizontal segmental accelerations during gait. Winter(1991) found that younger adults were able to reduce head acceleration to23% of the pelvic acceleration magnitude. Older adults attenuated theacceleration to only 42% of pelvic magnitudes. Our results reveal the sametendency. Both younger and older adults reduced the horizontal accelerationof segments up to the level of the hip joint. It is at the hip joint, however,where age-related differences in the pattern of attenuation emerge (see Figure7). Although the acceleration at the shoulder is greater than that at the hip forboth age groups, the magnitude of acceleration increases substantially amongolder adults, with the cumulative effect that older adults experience largerhorizontal accelerations of the head than younger adults per unit ofperturbation acceleration. Thus it is possible that older adults perceivesmaller challenges to balance (relative to threats experienced by youngeradults) as more threatening because the undamped accelerations experiencedat the head imply a larger threat to balance than actually exists.
Allum and Pfaltz (1985) have shown that acceleration of the headfollowing a platform perturbation activates the vestibular system and leads toearly (within 150 ms) postural adjustments serving to stabilize the body(activation of ankle musculature) and head (activation of head musculature).Given the timing of this vestibular-based response, one may infer that thevestibular system also underlies the origin of the rapid step response. Furtherwork investigating the postural compensations used by vestibular-deficien tpatients following rapid platform accelerations is needed to elucidate thispossibility.
374 J. L. Jensen et al.

It is in the performance of voluntary tasks that we acquire a sense of forceproduction limits and set thresholds that define our strategic choices. In theface of an unexpected perturbation, it is these limits, defined under voluntaryconditions and past experience, that provide the first approximations for howto perform the `novel’ task. What we observed was the possibility of areduced acceleration attenuation response in the older adults. Whether this isa physical limitation or a learned response is not clear from these results.Changing the consequences of taking a step (e.g., Brown & Frank, 1997)would allow us to probe limitations in physical capacity versus learned limitsand examine in greater detail the age-related behavioral response differencesnow typically observed during balance-control tasks.
REFERENCES
Allum, J. H. J., & Pfaltz, C. R. (1985). Visual and vestibular contributions to pitch sway sta-bilization in the ankle muscles of normals and patients with bilateral peripheral vestibular
de®cits. Experimental Brain Research, 58, 82±94.Brown, L. A., & Frank, J. S. (1997). Postural compensations to the potential consequence s of
instability: Kinematics. Gait and Posture, 6, 89±97.Brown, L. A., Shumway-Cook , A., & Woollacott, M. H. (1999). Attentional demands and
postural recovery: The effects of aging. Journal of Gerontology : Medical Sciences, 54A,M165±M171.
Clarkson, P. M., Kroll, W., & Melchionda, A. M. (1981). Age, isometric strength, rate of tensiondevelopment and ®ber type composition. Journal of Gerontology: Medical Sciences, 36,
M648±M653.Gu, M. J., Schultz, A. B., Shepard, N. T., & Alexander, N. B. (1996) . Postural control in young and
elderly adults when stance is perturbed: Dynamics. Journal of Biomechanics, 29, 319±329.Hakkinen, K., & Hakkinen, A. (1991). Muscle cross-sectional area, force production and
relaxation characteristics in women at different ages. European Journal of Applied Physiol-
ogy, 62, 410±414.
Hall, C. D., Woollacott, M. H., & Jensen, J. L. (1999). Rate and magnitude of force development :Implications for balance control. Journal of Gerontology: Medical Sciences, 54A, M507±
M513.Kaya, B. K., Krebs, D. E., & Riley, P. O. (1998). Dynamic stability in elders: Momentum control
in locomotor ADL. Journal of Gerontology: Medical Sciences, 53A, M126±M134.Larsson, L. (1978). Morphological and functional characteristics of the aging skeletal muscle in
man: A cross-sectional study. Acta Physiologica Scandinavica, 45(Suppl.), 5±36.Luchies, C. W., Alexander. N. B., Schultz, A. B., & Ashton-Miller, J. A. (1994). Stepping
responses of young and old adults to postural disturbances: Kinematics. Journal of the
American Geriatrics Society, 42, 506±512.
McIlroy, W. E., & Maki, B. E. (1993). Task constraints on foot movement and the incidence of
compensatory stepping following perturbation of upright stance. Brain Research, 616, 30±38.McIlroy, W. E., & Maki, B. E. (1996). Age-related changes in compensatory stepping in response
to unpredictable perturbations. Journal of Gerontology : Medical Sciences, 51A, M289±M296.
Pai, Y., Rogers, M. W., Patton, J., Cain, T. D., & Hanke, T. A. (1998). Static versus dynamic
predictions of protective stepping following waist-pull perturbations in young and olderadults. Journal of Biomechanics, 31, 1111±1118.
Age Differences in Rapid Step Initiation 375

Pai, Y. C., & Lee, W. A. (1994). Effect of a terminal constraint on control of balance during sit-to-stand. Journal of Motor Behavior, 26, 247±256.
Pai, Y. C., & Patton, J. L. (1997). Center of mass velocity-displacemen t predictions for balancecontrol. Journal of Biomechanics, 30, 347±354.
Pai, Y. C., & Rogers, M. W. (1990). Control of body mass transfer as a function of speed ofascent in sit-to-stand. Medicine and Science in Sports and Exercise, 22, 378±384.
Pai, Y. C., & Rogers, M. W. (1991). Segmental contributions to total body momentum in sit-to-stand. Medicine and Science in Sports and Exercise, 23, 225±230.
Rogers, M. W., Hain, T. C., Hanke, T. A., & Janssen, I. (1996). Stimulus parameters and inertialload: Effects on the incidence of protective stepping responses in healthy human subjects.
Archives of Physical Medicine and Rehabilitation, 77, 363±368.Thelen, D. G., Schultz, A. B., & Alexander, N. B. (1996). Effects of age on rapid ankle torque
development. Journals of Gerontology: Medical Sciences, 51, 5, M226±M232.Winter, D. A. (1990) . Biomechanics and motor control of human movement (2nd ed.). Toronto :
John Wiley & Sons.Winter, D. A. (1991). The biomechanics and motor control human gait: Normal, elderly, and
pathological (2nd ed.). Waterloo, Ontario: University of Waterloo Press.
Wolfson, L., Whipple, R., Derby, C. A., Amerman, P., & Nashner, L. (1994). Gender differencesin the balance of healthy elderly as demonstrated by dynamic posturography . Journal of
Gerontology : Medical Sciences, 49, M160±M167.
376 J. L. Jensen et al.
Copyright © 2022 FDOKUMEN