Comparison of the osteoinductivity of bioimplants containing recombinant human bone morphogenetic...
10
Comparison of the osteoinductivity of bioimplants containing recombinant human bone morphogenetic proteins 2 (Infuse) and 7 (OP-1) Torin Barr, DDS, MSc, FRCDC, MSc, a Audrey J. A. McNamara, b George K. B. Sándor, MD, DDS, PhD, FRCDC, FRCSC, FACS, c Cameron M. L. Clokie, DDS, PhD, FRCDC, d and Sean A. F. Peel, PhD, e Toronto, Canada; Tampere and Oulu, Finland UNIVERSITY OF TORONTO; UNIVERSITY OF TAMPERE AND UNIVERSITY OF OULU Objectives. Recent research has focused on application of growth factors such as bone morphogenetic proteins (BMPs) as alternatives to autogenous bone grafting. Two bone graft substitute bioimplants containing recombinant human BMPs (rhBMPs), Infuse (rhBMP-2) and OP-1 (rhBMP-7), are approved for human application but have never been compared side by side. The aim of this study was to provide a direct comparison of the osteoinductive activity of the 2 commercially available and approved rhBMP-containing bioimplants in their clinically available forms. Study design. The activity of rhBMP-2 and -7 in solution were compared in vitro using the C2C12 cell-based assay. The activity of Infuse and OP-1 bioimplants containing 52.5 g of rhBMP-2 or rhBMP-7, respectively, were compared in vivo using a mouse muscle pouch assay and analyzed by microscopic CT (microCT) and histology. Results. The in vitro results showed that rhBMP-2 stimulated greater alkaline phosphatase production than rhBMP-7 over various time points and concentrations. The in vivo results showed that OP-1 induced greater bone volume than Infuse. Both implants induced bone of equivalent quality based on microCT and histologic evaluation. Conclusion. In their clinically available forms, the rhBMP-7– containing OP-1 induced greater bone volume than the rhBMP-2– containing Infuse in the mouse muscle pouch model. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109:531-540) Autogenous grafting is considered to be the gold stan- dard for repair and reconstruction of bony skeletal defects and stimulation of bone formation. Bone is the second most commonly transplanted tissue after blood, with over 2.2 million bone grafting procedures performed annually worldwide. 1 Autogenous grafts present no risk of disease transmission or graft rejection, and cancel- lous bone grafts include live osteocytes, osteoblasts, and all the requirements to begin formation of new bone. 2 However, autogenous bone is also associated with several disadvantages, including creation of a sec- ond surgical site and increased blood loss and time in surgery, which results in significantly increased patient morbidity. 2 The lack of an ideal grafting option has spurred extensive research into the potential of growth factors, including recombinant human bone morphogenetic proteins (rhBMPs). Several members of this group of endogenous growth factors have been shown to have the ability to stimulate the differentiation of mesenchy- mal stem cells (MSCs) into osteogenic cells (osteoin- duction), and 2, BMP-2 and BMP-7, have been ap- proved clinically for various indications related to bone repair. Comparisons of the activity of the various BMPs using in vitro and gene therapy models suggest that BMP-2 is more osteoinductive than BMP-7. 3,4 In commercially available bioimplants, the BMPs are combined with a scaffold to permit their retention at the wound site. The 2 commercially available BMP bioim- plants, Infuse, which contains rhBMP-2, and OP-1, which contains rhBMP-7, both use collagen. That being said, the bioimplants are prepared differently, with rh- Supported by the Oral and Maxillofacial Surgery Foundation of Canada and a grant from the Canadian Association of Oral and Maxillofacial Surgeons Foundation for Continuing Education and Research. A.M. was supported by a Network Oral Research Training summer student grant. a Chief Resident, Oral and Maxillofacial Surgery and Anesthesia. b Dental Student, Orthobiologics Group. c Professor and Head, Oral and Maxillofacial Surgery, University of Toronto; Coordinator, Pediatric Oral and Maxillofacial Surgical Ser- vices, Hospital for Sick Children and Bloorview Kids Rehab, To- ronto; Professor, Tissue Engineering, Regea Institute for Regenera- tive Medicine, University of Tampere, Tampere, Finland; Docent, Oral and Maxillofacial Surgery, University of Oulu, Oulu, Finland. d Professor, Oral and Maxillofacial Surgery, Director of Graduate Program, Oral and Maxillofacial Surgery and Anesthesia, University of Toronto. e Adjunct Professor, Orthobiologics Group, University of Toronto. Received for publication Jul 11, 2009; returned for revision Oct 5, 2009; accepted for publication Oct 21, 2009. 1079-2104/$ - see front matter © 2010 Mosby, Inc. All rights reserved. doi:10.1016/j.tripleo.2009.10.027 531
Transcript of Comparison of the osteoinductivity of bioimplants containing recombinant human bone morphogenetic...

Comparison of the osteoinductivity of bioimplants containingrecombinant human bone morphogenetic proteins 2(Infuse) and 7 (OP-1)Torin Barr, DDS, MSc, FRCDC, MSc,a Audrey J. A. McNamara,b
George K. B. Sándor, MD, DDS, PhD, FRCDC, FRCSC, FACS,c
Cameron M. L. Clokie, DDS, PhD, FRCDC,d and Sean A. F. Peel, PhD,e Toronto, Canada;Tampere and Oulu, FinlandUNIVERSITY OF TORONTO; UNIVERSITY OF TAMPERE AND UNIVERSITY OF OULU
Objectives. Recent research has focused on application of growth factors such as bone morphogenetic proteins(BMPs) as alternatives to autogenous bone grafting. Two bone graft substitute bioimplants containing recombinanthuman BMPs (rhBMPs), Infuse (rhBMP-2) and OP-1 (rhBMP-7), are approved for human application but have neverbeen compared side by side. The aim of this study was to provide a direct comparison of the osteoinductive activity ofthe 2 commercially available and approved rhBMP-containing bioimplants in their clinically available forms.Study design. The activity of rhBMP-2 and -7 in solution were compared in vitro using the C2C12 cell-based assay.The activity of Infuse and OP-1 bioimplants containing 52.5 �g of rhBMP-2 or rhBMP-7, respectively, were comparedin vivo using a mouse muscle pouch assay and analyzed by microscopic CT (microCT) and histology.Results. The in vitro results showed that rhBMP-2 stimulated greater alkaline phosphatase production than rhBMP-7over various time points and concentrations. The in vivo results showed that OP-1 induced greater bone volume thanInfuse. Both implants induced bone of equivalent quality based on microCT and histologic evaluation.Conclusion. In their clinically available forms, the rhBMP-7–containing OP-1 induced greater bone volume than therhBMP-2–containing Infuse in the mouse muscle pouch model. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod
2010;109:531-540)Autogenous grafting is considered to be the gold stan-dard for repair and reconstruction of bony skeletaldefects and stimulation of bone formation. Bone is thesecond most commonly transplanted tissue after blood,with over 2.2 million bone grafting procedures performedannually worldwide.1 Autogenous grafts present no risk
Supported by the Oral and Maxillofacial Surgery Foundation ofCanada and a grant from the Canadian Association of Oral andMaxillofacial Surgeons Foundation for Continuing Education andResearch. A.M. was supported by a Network Oral Research Trainingsummer student grant.aChief Resident, Oral and Maxillofacial Surgery and Anesthesia.bDental Student, Orthobiologics Group.cProfessor and Head, Oral and Maxillofacial Surgery, University ofToronto; Coordinator, Pediatric Oral and Maxillofacial Surgical Ser-vices, Hospital for Sick Children and Bloorview Kids Rehab, To-ronto; Professor, Tissue Engineering, Regea Institute for Regenera-tive Medicine, University of Tampere, Tampere, Finland; Docent,Oral and Maxillofacial Surgery, University of Oulu, Oulu, Finland.dProfessor, Oral and Maxillofacial Surgery, Director of GraduateProgram, Oral and Maxillofacial Surgery and Anesthesia, Universityof Toronto.eAdjunct Professor, Orthobiologics Group, University of Toronto.Received for publication Jul 11, 2009; returned for revision Oct 5,2009; accepted for publication Oct 21, 2009.1079-2104/$ - see front matter© 2010 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2009.10.027of disease transmission or graft rejection, and cancel-lous bone grafts include live osteocytes, osteoblasts,and all the requirements to begin formation of newbone.2 However, autogenous bone is also associatedwith several disadvantages, including creation of a sec-ond surgical site and increased blood loss and time insurgery, which results in significantly increased patientmorbidity.2
The lack of an ideal grafting option has spurredextensive research into the potential of growth factors,including recombinant human bone morphogeneticproteins (rhBMPs). Several members of this group ofendogenous growth factors have been shown to havethe ability to stimulate the differentiation of mesenchy-mal stem cells (MSCs) into osteogenic cells (osteoin-duction), and 2, BMP-2 and BMP-7, have been ap-proved clinically for various indications related to bonerepair. Comparisons of the activity of the various BMPsusing in vitro and gene therapy models suggest thatBMP-2 is more osteoinductive than BMP-7.3,4
In commercially available bioimplants, the BMPs arecombined with a scaffold to permit their retention at thewound site. The 2 commercially available BMP bioim-plants, Infuse, which contains rhBMP-2, and OP-1,which contains rhBMP-7, both use collagen. That being
said, the bioimplants are prepared differently, with rh-531
OOOOE532 Barr et al. April 2010
BMP-2 soaked onto a collagen sponge immediatelybefore use in the case of the Infuse bioimplant andrhBMP-7 lyophilized onto collagen granules before usein the case of OP-1. These differences could alter thebioactivity of the implant in vivo. At the time of writ-ing, there were no studies providing a direct compari-son of these commercially available bioimplant formsof rhBMP-2 and rhBMP-7. The aim of the presentstudy was to provide a direct comparison of the os-teoinductive activity of Infuse and OP-1.
MATERIALS AND METHODSTwo separate approaches were undertaken to address
the aim of this study. An in vitro series of experimentscompared the activity of the 2 different rhBMPs used inthe bioimplants in solution. The second approach di-rectly compared the BMPs combined with their scaf-folds as they are used clinically in an in vivo assay forosteoinductive activity.
In vitro experimentsThese experiments were based on the observation
that osteoinductive BMPs stimulate mouse muscle–derived C2C12 cells to change their differentiationpathway from a myogenic to an osteogenic one result-ing in an increase in alkaline phosphatase (ALP) ex-pression that is proportional to the amount of BMPadded.5,6 The stimulation of ALP can thus be used as anindex of the osteogenic potential of the test agents.
In vitro assay. The in vitro assay was performed aspreviously described.6 Briefly, C2C12 cells (ATCC,Manassas, VA) were seeded at 0.5 � 105 cells/mLalpha-MEM � 15% fetal bovine serum, 1 mL per wellof a 24-well plate, and allowed to attach overnight. Thefollowing day, the medium was removed and freshmedium with the test article added (day 0). Upon ter-mination, the medium was removed, the wells washed3 times with Tris-buffered saline (10 mmol/L Tris, 137mmol/L NaCl, pH 7.4), and the cell layer lysed withlysis buffer (M-Per; Fisher Scientific, Ottawa, Canada).The lysate was then assayed for ALP activity usingpara-nitrophenol phosphate (Sigma Aldrich, St. Louis,MO) and protein content using the Coomassie Plus kit(Fisher Scientific).
Comparison of rhBMPs in solution. Because the rh-BMPs from the commercially available bioimplantswere not both available separate from their carriers,rhBMP-2 and rhBMP-7 were purchased from R&DSystems (Minneapolis, MN). Both of these recombi-nant proteins were manufactured using Chinese ham-ster ovary cells and are similar to the rhBMPs used inboth of the commercially available BMP bioimplants.
In the first series of experiments, C2C12 cells were
cultured with 25 or 50 ng/mL rhBMP-2 or rhBMP-7 for24 hours and then terminated. In a second series ofexperiments, attachment cells were exposed to 20, 40,or 80 ng/mL rhBMP-2 or rhBMP-7 and cultured forvarious times up to 6 days. In these experiments thewells were refed on day 3 with fresh medium withoutthe rhBMP.
In all experiments, a control group was included thatwas exposed to medium without BMP.
OP-1 in vitro. In this experiment, on day 0 the me-dium was replaced with either fresh medium only (con-trol), medium containing a suspension of OP-1 granulesequivalent to 50 ng/mL rhBMP-7 (OP-1) or 50 ngrhBMP-2. When cultures were refed on day 3, care wastaken not to remove the collagen beads, and freshmedium without any additional rhBMP was added toeach well. Cultures were terminated on day 5 andassayed for ALP and protein as described above.
In vivo experimentsTo evaluate the osteoinductive activity of bioimplants
in an in vivo model, the Urist mouse muscle pouch assaywas used.7,8 The size of the induced bone formed in thisassay is proportional to the amount of BMP tested.
Preparation of bioimplants. OP-1 (Stryker, Cam-bridge, MA) and Infuse (Medtronic, Minneapolis, MN)were prepared according to the manufacturers’ specifi-cations. Briefly, 15 mg OP-1 powder, which contains52.5 �g of rhBMP-7 lyophilized onto bovine collagengranules, was weighed and placed into a #5 gelatincapsule (Torpac, Fairfield, NJ). For the Infuse implant,the collagen sponge was cut into 4 � 8 mm sections tofit into the #5 gelatin capsules. On the morning of thesurgery, the rhBMP-2 powder was reconstituted withthe sterile water provided in the Infuse package accord-ing to the package instructions to a final concentrationof 1.5 mg of rhBMP-2/mL. At the time of surgery, thegelatin capsule was placed in the muscle pouch andthen 35 �L of the solution, which contained 52.5 �g ofrhBMP-2, was applied to the collagen sponge.
Implantation. All animal work was conducted fol-lowing approval by the University of Toronto animalcare committee. Twenty male CD-1 mice aged 37-42days were divided into 2 groups of 10 animals each.Under anesthesia bilateral pouches were made in thethigh muscles of the hind limbs of each animal by bluntdissection. Within each group, half of the animals re-ceived the bioimplant on the left and the other half onthe right. The other side in both groups received agelatin capsule containing collagen sponge alone.
Microscopic CT analysis. The animals were killedon post-operative day 28. The hind limbs were re-moved and fixed with 10% buffered formalin. Afterfixation, the specimens were imaged using a General
Electric Healthcare eXplore Locus SP microscopic CT
in yel
OOOOEVolume 109, Number 4 Barr et al. 533
(microCT) scanner. Samples were scanned and recon-structed using the manufacturer’s software with a result-ant resolution of 59 �m. After image reconstruction, aregion of interest (ROI) was determined. This area wasset to encompass all areas containing the bioimplant-induced bone. These could be easily distinguished fromthe skeletal bones based on location and density (Fig. 1).
To analyze the quantity and quality of bone withinthe ROI, the voxels of the microCT images were seg-mented into bone and nonbone phases. Segmentationwas achieved by determining a threshold value for thevoxel gray level at which the voxel was counted asbone.9 The total volume (TV), bone volume (BV),mineral density of the total volume (TV-MD), mineraldensity of the bone volume (BV-MD), mineral contentof the total volume (TV-MC), mineral content of thebone volume (BV-MC), and bone volume fraction(BVF) of the ROI were determined for each sample.
Because more than half (12 out of 20) of the speci-mens demonstrated �1 distinct ossicle, the ossicleswere categorized into 2 groups: primary and secondary.Primary ossicles were defined as the largest contiguousinduced ossicle. Secondary ossicles were all other in-duced bony ossicles in the ROI (Fig. 1).
The bone analysis parameters were applied individ-ually to the primary and secondary ossicles as well as tothe total induced bone which included primary andsecondary ossicles.
Histologic analysis. After completion of themicroCT analysis, the specimens were decalcified in
A
Fig. 1. Screen shot of a single slice through the hind limbsprotein–induced bony ossicle can be easily distinguished fromdensity of the bone. Every 10 slices, the ossicle is manually ousoftware to generate the region of interest (ROI). Once the3-dimensional reconstructed image with the ROI highlighted
formic acid and embedded in wax. Sections from each
specimen were stained with hematoxylin and eosin(H&E) and examined by light microscopy.
StatisticsAll results were analyzed using Sigma Stat v3.5 statis-
tical software (Systat, Richmond CA). All data was eval-uated for normality and equal variance. The in vitro assayresults were compared by ANOVA. In the in vivo studiesresults that were normally distributed were compared us-ing the Student T test. If the distribution was found to benonparametric, the T test was aborted and the Mann-Whitney Rank Sum Test was used. A p value � 0.05 wasconsidered to be significant.
RESULTS
In vitro studiesComparison of rhBMPs in solution in vitro. Expo-
sure of the C2C12 cells to both experimental agentsresulted in an increase in ALP production. Productionof ALP was markedly higher in the rhBMP-2 group atall time points and doses studied (P � .001). The meanALP concentrations for rhBMP-2 were �6 timesgreater than for rhBMP-7 at 3 days and 3 times greaterat 6 days (Fig. 2).
OP-1 in vitro. OP-1 samples in vitro demonstratedincreased ALP activity at both 3 and 5 days. At bothtime points the rhBMP-2 group had significantlyhigher ALP activity than the OP-1 group (P � .001)
which the ossicle is outlined (A). The bone morphogeneticnes of the skeleton, which are much brighter due to the higherand intervening splices interpolated using the manufacturer’sas generated, it was checked for accuracy by viewing the
low (B).
B
fromthe botlinedROI w
(Fig. 3).
OOOOE534 Barr et al. April 2010
In vivo studyDuring the process of harvesting it was noted that the
induced bony ossicle was not limited to the side of theimplant but that in many specimens, the ossicle spannedthe vertebral column (Fig. 1).
MicroCT analysis. MicroCT analysis revealed that theBMP bioimplants induced irregularly shaped ossicles
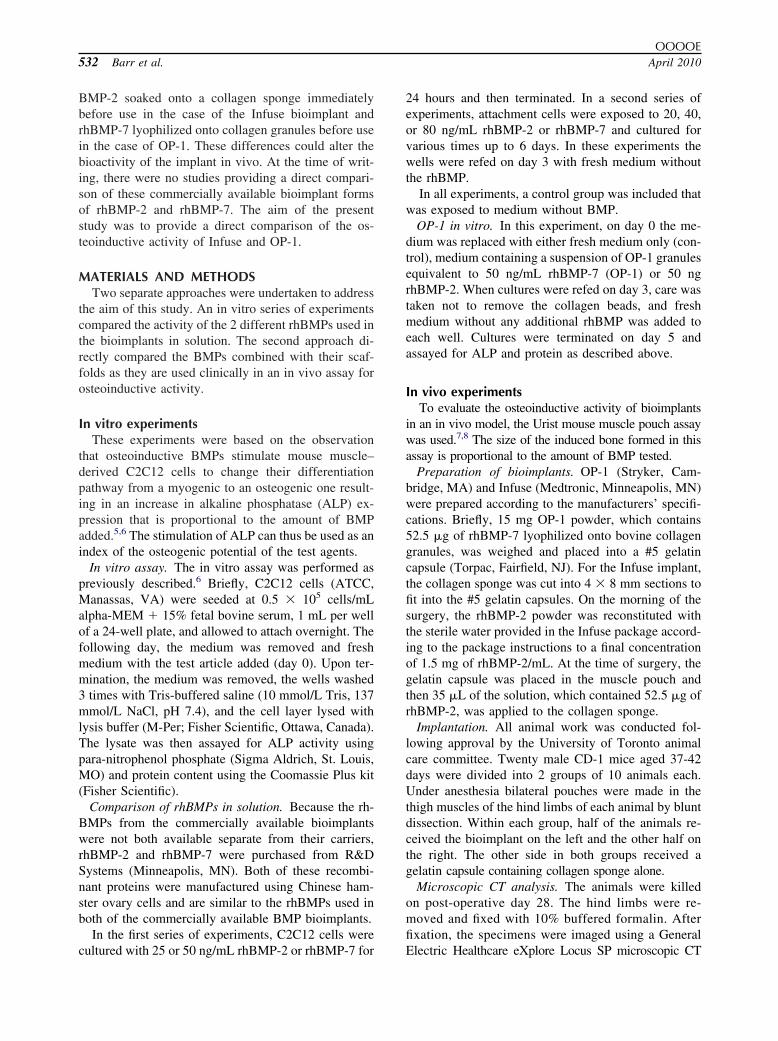
Fig. 2. A, C2C12 cells were exposed to 25 or 50 ng/mL ofrhBMP-2 or rhBMP-7 for 24 hours. After termination, thecultures were assayed for alkaline phosphatase (ALP) activ-ity. Results were normalized to protein content. Both rh-BMP-2 and rhBMP-7 stimulated ALP activity compared withcontrol (medium alone); however, the increase was signifi-cantly greater in the rhBMP-2–treated cultures (P � .001). B,C2C12 cells were exposed to 20 ng/mL of rhBMP-2 orrhBMP-7 or medium alone (Ctrl) for up to 6 days. Cultureswere terminated on day 1, 3, and 6 and assayed for ALP andprotein. ALP activity was greatest in rhBMP-2–treated cul-tures at all time points (P � .001).
which were composed of bone and soft tissue. The OP-1
bioimplants induced significantly larger ossicles (TV: P �.001) with significantly more bone (BV: P � .031) andmore mineral content (TV-MC: P � .05; BV-MC: P �.05) than the Infuse group (Table I).
However, there was no significant difference in themineral density of the total volume or bone volume orin the bone volume fractions of the induced ossiclesbetween the OP-1 and Infuse groups (Table I).
Primary ossicle and secondary ossicles. The resultswhen comparing only the primary ossicles were similar
Fig. 3. C2C12 cells were cultured in the presence of 50ng/mL rhBMP-2 in solution or OP-1 containing 50 �g ofrhBMP-7 lyophilized onto collagen granules. Even whenrhBMP-7 was combined with its collagen scaffold it was lessactive than rhBMP-2 in solution (P � 0.01).
Table I. Microscopic computerized tomography(microCT) results for total induced bone (primary �secondary ossicles)
MicroCT parameter OP-1 Infuse P value
Quantity measuresTotal volume (mm3) 526 � 209 226 � 93 �.001Bone volume (mm3) 118 � 66 61 � 41 .031*Bone mineral content
(mg Ca)66.2 � 33.8 34.0 � 22.8 .023
Tissue mineral content(mg Ca)
42.4 � 24.0 23.9 � 18.2 .045*
Quality measuresBone mineral density 131 � 21 141 � 43.2 .600Tissue mineral density 361 � 21 376 � 29 .186*Bone volume fraction 0.23 � 0.08 0.25 � 0.08 .500
For both the total induced bone and the primary ossicles only (TableII), significant differences were seen with all the quantity measuresbetween the 2 groups, with OP-1 producing larger ossicles with morebone and calcium. However, no significant differences were seen inthe quality of the tissue produced as assessed by bone mineraldensity, tissue mineral density, or bone volume fraction.*P values were generated using the Mann-Whitney U test, becausethe values for these parameters were not normally distributed.
to those for the total induced bone, with the OP-1 group

OOOOEVolume 109, Number 4 Barr et al. 535
having significantly higher TV, BV, TV-MC, andBV-MC and equivalent TV-MD, BV-MD, and BVFcompared with the Infuse group (Table II).
Analysis of the secondary ossicles demonstrated thatthey represented approximately 1% of the total volumeof the ossicles and that there were no significant dif-ferences between the OP-1 and Infuse groups for any ofthe parameters.
Histologic analysis. Inspection of the histologicspecimens revealed bone formation in both the Infuseand the OP-1 groups. No bone formation was noted inthe control samples.
Specimens from the Infuse group demonstrated bothwoven bone formation and a significant cartilaginouscomponent. The immature woven bone contained nor-mal-appearing osteocytes within lacunae and osteoblas-tic rimming (Fig. 4). Several specimens showed signif-icant areas of hypertrophic cartilage undergoing vascularinvasion from the marrow space (Fig. 5).
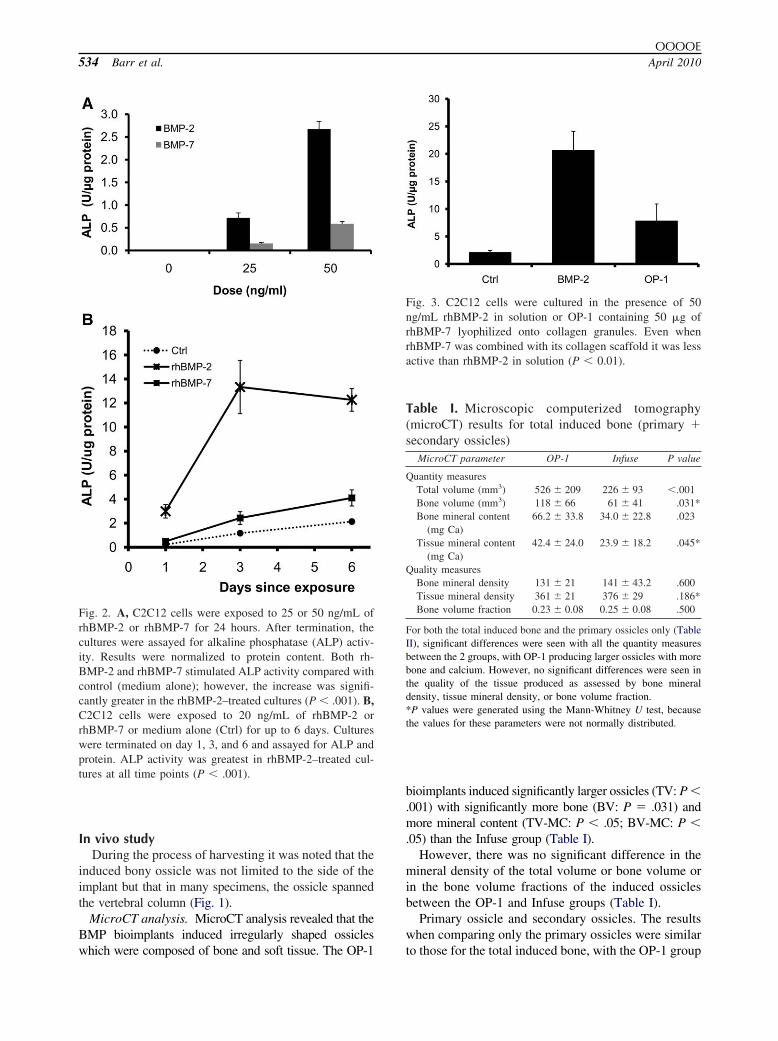
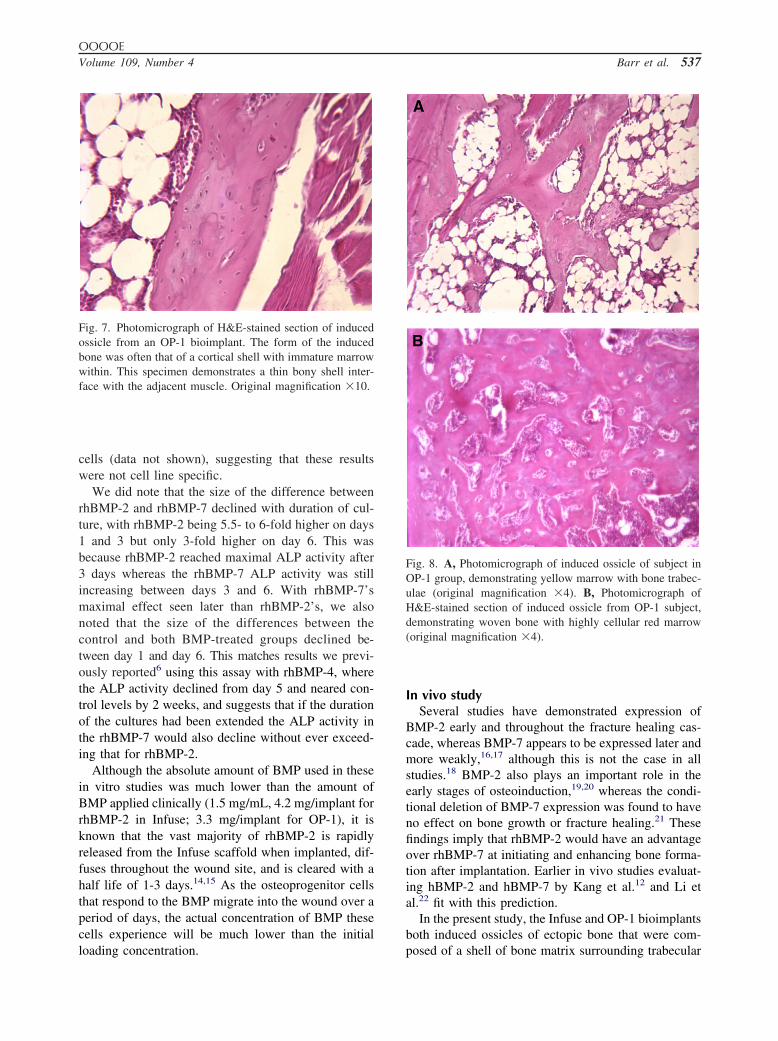
Histology of the OP-1 specimens also demonstratedwoven bone with embedded osteocytes in lacunae.However, the cartilage in the OP-1 specimens was lessobvious, had a more chondro-osteoid appearance, andwas surrounded by bone (Fig. 6). Bone formation wasoften found in the form of a thin peripheral shell(Fig. 7). OP-1 specimens overall demonstrated greaterorganization of the bony trabeculae and marrow space,with examples of both red and yellow marrow (Fig. 8).
DISCUSSIONSurgeons around the world are presented with a daily
Table II. Microscopic computerized tomography(microCT) results for primary ossicle analysis
MicroCT parameter OP-1 Infuse P value
Quantity measuresTotal volume (mm3) 521 � 216 224 � 100 .002*Bone volume (mm3) 117 � 66 61 � 41 .038*Bone mineral content
(mg Ca)65.3 � 34.1 33.8 � 23.0 .026
Tissue mineral content(mg Ca)
42.0 � 24.1 23.6 � 18.2 .045*
Quality measuresBone mineral density 132 � 45 141 � 43 .628Tissue mineral density 361 � 20 375 � 30 .212*Bone volume fraction 0.23 � 0.09 0.25 � 0.08 .605
For both the total induced bone (Table I) and the primary ossiclesonly, significant differences were seen with all the quantity measuresbetween the 2 groups, with OP-1 producing larger ossicles with morebone and calcium. However, no significant differences were seen inthe quality of the tissue produced as assessed by bone mineraldensity, tissue mineral density, or bone volume fraction.*P values were generated using the Mann-Whitney U test, becausethe values for these parameters were not normally distributed.
dilemma of finding the best methodology of recon-
structing bony defects, solving fracture nonunions, andaugmenting existing bone volumes. Autogenous bonegrafts have long been considered to be the gold stan-dard for the surgical reconstruction of bone defects.Harvesting of autogenous bone necessitates a secondsurgical site, with its own set of associated morbiditiesand complications, including pain, neurovascular in-jury, and infection.10 Alternatives to autogenous graft-ing have been used with mixed results. To date, noalternative has been able to replicate the success andrelative predictability of autogenous grafting.
The recent introduction of bone morphogenetic pro-teins (BMP) bioimplants to clinical practice has pro-vided a new alternative. For these BMPs to be effective,they are combined with a carrier or delivery system to
Fig. 4. A, Photomicrograph of H&E-stained induced ossiclefrom an Infuse implant, showing irregularly spaced osteo-cytes within large lacunae and osteoblasts along immaturebony trabeculae. (original magnification �10). B, Higher-power photomicrograph of immature bony trabecula withosteocytes within lacunae (original magnification �40).
form a bioimplant.11 At the time of writing, there were

OOOOE536 Barr et al. April 2010
2 rhBMP-based bioimplants in clinical use: Infuse,containing rhBMP-2, and OP-1, using rhBMP-7.
Studies directly comparing the activity of differentBMPs are not common in the literature, and there areno reports comparing the osteoinductive ability of the 2commercially available rhBMPs when combined withtheir carriers in the bioimplants which are used clini-cally. Therefore, the aim of the present investigationwas to compare the activity of the component BMPsalone and as bioimplants in their clinical form.
In vitro studiesThe in vitro assay evaluated rhBMP-2 and rhBMP-7
alone. Both rhBMP-2 and rhBMP-7 were able to sig-nificantly increase ALP activity in mouse myoblastC2C12 cells severalfold. At all doses and time points,rhBMP-2 generated a significantly greater responsethan rhBMP-7. Studies from different investigators di-rectly comparing the osteogenic activity of BMPs invitro have repeatedly shown that BMP-2 consistentlystimulates a greater response than BMP-7.4,12,13 Thosestudies used baculoviral or adenoviral vectors to trans-fect cell lines with the cDNA for the various hBMPsand then measured ALP in the transfected cells as ameasure of osteoinductivity. However, in those studiesno efforts were made to standardize results to theamount of BMP produced by the cells after transfec-tion, and therefore the results could reflect differencesin the expression levels of the recombinant proteinsrather than the activity of the proteins themselves.
Mayer et al.3 monitored DNA synthesis activity in
Fig. 5. Photomicrograph of H&E-stained induced ossicle inan Infuse subject, demonstrating histologic pattern consistentwith endochondral bone formation, including hypertrophicchondrocytes and vascular invasion from the marrow (origi-nal magnification �10).
periosteal cells and epiphyseal and sternal chondrocytes
in embryonic chicks after exposure to rhBMP-2, -4, -5,-6, and -7. They noted the greatest response fromBMP-2 and -4 and the lowest specific activity withBMP-7. However, this was not a model that reflectedthe osteogenic differentiation of the cells, but rathertheir proliferation.
In the present study, the osteoinductive activity ofthe BMPs was assessed based on stimulating the dif-ferentiation of mouse muscle–derived C2C12 cellsalong an osteogenic lineage, and therefore it can beconsidered to be a more direct evaluation of the os-teoinductive potential of the BMPs. The pattern ofrhBMP-2 being more active than rhBMP-7 was seen atall doses and times tested. We obtained similar results
Fig. 6. A, Photomicrograph of H&E-stained section of in-duced bony ossicle from an OP-1 bioimplant; basophilicstaining areas represent tissue of cartilaginous origin sur-rounded by woven bone (original magnification �10). B,Photomicrograph of H&E-stained section of induced ossiclefrom an OP-1 bioimplant, demonstrating osteocytes in lacu-nae (original magnification �40).
using mouse W20-17 stromal cells and rat L6 myogenic
OOOOEVolume 109, Number 4 Barr et al. 537
cells (data not shown), suggesting that these resultswere not cell line specific.
We did note that the size of the difference betweenrhBMP-2 and rhBMP-7 declined with duration of cul-ture, with rhBMP-2 being 5.5- to 6-fold higher on days1 and 3 but only 3-fold higher on day 6. This wasbecause rhBMP-2 reached maximal ALP activity after3 days whereas the rhBMP-7 ALP activity was stillincreasing between days 3 and 6. With rhBMP-7’smaximal effect seen later than rhBMP-2’s, we alsonoted that the size of the differences between thecontrol and both BMP-treated groups declined be-tween day 1 and day 6. This matches results we previ-ously reported6 using this assay with rhBMP-4, wherethe ALP activity declined from day 5 and neared con-trol levels by 2 weeks, and suggests that if the durationof the cultures had been extended the ALP activity inthe rhBMP-7 would also decline without ever exceed-ing that for rhBMP-2.
Although the absolute amount of BMP used in thesein vitro studies was much lower than the amount ofBMP applied clinically (1.5 mg/mL, 4.2 mg/implant forrhBMP-2 in Infuse; 3.3 mg/implant for OP-1), it isknown that the vast majority of rhBMP-2 is rapidlyreleased from the Infuse scaffold when implanted, dif-fuses throughout the wound site, and is cleared with ahalf life of 1-3 days.14,15 As the osteoprogenitor cellsthat respond to the BMP migrate into the wound over aperiod of days, the actual concentration of BMP thesecells experience will be much lower than the initial
Fig. 7. Photomicrograph of H&E-stained section of inducedossicle from an OP-1 bioimplant. The form of the inducedbone was often that of a cortical shell with immature marrowwithin. This specimen demonstrates a thin bony shell inter-face with the adjacent muscle. Original magnification �10.
loading concentration.
In vivo studySeveral studies have demonstrated expression of
BMP-2 early and throughout the fracture healing cas-cade, whereas BMP-7 appears to be expressed later andmore weakly,16,17 although this is not the case in allstudies.18 BMP-2 also plays an important role in theearly stages of osteoinduction,19,20 whereas the condi-tional deletion of BMP-7 expression was found to haveno effect on bone growth or fracture healing.21 Thesefindings imply that rhBMP-2 would have an advantageover rhBMP-7 at initiating and enhancing bone forma-tion after implantation. Earlier in vivo studies evaluat-ing hBMP-2 and hBMP-7 by Kang et al.12 and Li etal.22 fit with this prediction.
In the present study, the Infuse and OP-1 bioimplantsboth induced ossicles of ectopic bone that were com-
Fig. 8. A, Photomicrograph of induced ossicle of subject inOP-1 group, demonstrating yellow marrow with bone trabec-ulae (original magnification �4). B, Photomicrograph ofH&E-stained section of induced ossicle from OP-1 subject,demonstrating woven bone with highly cellular red marrow(original magnification �4).
posed of a shell of bone matrix surrounding trabecular

OOOOE538 Barr et al. April 2010
bone and marrow. However, contrary to our expecta-tions, the rhBMP-7–containing OP-1 bioimplants pro-duced larger ossicles containing greater amounts ofbone than the rhBMP-2–containing Infuse bioimplants.
Kang et al.12 evaluated the osteogenic ability of 14BMPs using both in vitro and in vivo assays. The invivo portion of that study included 2 methods of testingthe BMPs. In the first, C2C12 cells transfected with theadenoviral vector for each of the 14 BMPs were in-jected into the quadriceps muscle of mice. The secondapproach involved the injection of the adenoviral vec-tors directly into the muscle. In a similar model com-paring bone formed using cells transfected with 5 dif-ferent BMPs Li et al.22 also reported rhBMP-2 wasmore osteoinductive than rhBMP-7, although the hier-archy of activity between the other BMPs differed fromthat determined by Kang et al.
One explanation for the differences between our invivo results and those in the literature relates to differ-ences in experimental design. The earlier studies in-volved implantation of either cells transfected withadenovirus expressing BMPs or direct injection of theadenovirus itself. It has been previously reported thatthe amount of rhBMP-2 and rhBMP-7 secreted by trans-fected cells is much lower than for other cells transfectedwith other proteins of similar size23,24 and that there arevariations in amounts secreted between the differentBMPs.25 Therefore, it is possible that rhBMP-7 yieldsafter transfection were consistently lower than rh-BMP-2, leading to the dose of rhBMP-7 in vivo beinglower. In contrast, in the present study we have com-pared the 2 rhBMPs at the same dose prepared withtheir collagen carriers in their approved clinical form.
This does not explain the differences between our invitro and in vivo results. One difference between theimplants is that OP-1 uses bovine type 1 collagenobtained from bony sources and Infuse uses bovinetype 1 collagen from the Achilles tendon. However, thisis unlikely to be the cause of the difference in activity,because the type 1 collagen in bone and tendon isbiochemically similar.26 Further, when we comparedALP activity from cells cultured with OP-1 granules tothose exposed to a similar concentration of rhBMP-2 insolution, the ALP activity of the cultures exposed torhBMP-2 was 2.5-fold higher, indicating that the in-creased activity of OP-1 in vivo was not due to asynergistic effect of the collagen scaffold.
The bioimplants tested differ greatly in the way theBMP is applied to the collagen carrier. OP-1 is suppliedas a dry powder, with the BMP-7 already lyophilizedonto the collagen granules. The Infuse implant is de-signed to be prepared by soaking the absorbable colla-gen sponge (ACS) with the reconstituted BMP-2 solu-
tion for 15 minutes and then implanting the sponge.Thus, differences in the way that BMP is applied to thecollagen may have contributed to differences in theactivity of the bioimplants.
Another explanation for the differences between thein vitro and in vivo results relates the fact that boneformation is affected by more than differentiation ofosteoblasts. Considerable evidence exists demonstrat-ing that osteogenesis and bone healing are linked toangiogenesis27 and that vascularization occurs just be-fore osteogenesis.28 Several members of the transform-ing growth factor family have been shown to possessangiogenic properties, including BMP-2 and -7.29,30
The mechanism of BMP-induced angiogenesis is mostlikely via stimulation of secretion of the proangiogenicgrowth factor vascular endothelial growth factor byBMPs.31,32 Thus, the greater bone formed by OP-1implants may be due to a greater potential to stimulateangiogenesis which indirectly increases osteogenesis,rather than a direct stimulation of osteogenesis.
In evaluating the applicability of these results to theclinical situation, it should be noted that the musclepouch assay has been used previously to demonstratethe potential of rhBMPs, including rhBMP-2 and -7, toinduce bone formation33,34 and to compare the activityof BMPs in different carriers7,35 and the effect of tem-perature on rhBMP activity.36 The use of an intramus-cular implantation site rather than an intraskeletal oneallowed us to measure the amount of newly inducedbone without the confounding presence of the hostbone. In rats, it has been reported that there is a greaterosteogenic response when BMPs are implanted in anintraskeletal site compared with an intramuscular one,37
possibly due to the recruitment of preosteoblasts andstromal cells not present in muscle, although it is un-known whether intraskeletal implantation would alterthe conclusion that OP-1 forms more bone than Infuse.Furthermore, some clinical situations, such as the repairof large defects where the implant is surrounded bymuscle along its length and only in contact with bone ateither end,38 may be better modeled by intramuscularimplantation.
The time course of BMP-induced osteoinduction inthe present model is: proliferation of mesenchymalcells (day 3), formation of new cartilage (day 7), in-duction of woven bone (days 10 and 14), and remod-eling of woven bone into lamellar bone and develop-ment of bone marrow (days 21 and 28).7,39 The inducedbone ossicle of rhBMP-2 collagen implants is com-pletely resorbed by 8 weeks.40 Thus, by 28 days theentire sequence of events after BMP implantation hasoccurred.
The dose used in the present study was much lessthan that used clinically (50 �g compared with 3-4 mg),
because studies have demonstrated that the amount of
OOOOEVolume 109, Number 4 Barr et al. 539
BMP required for osteoinduction in rodents is 30 to 50times less than is required in patients,41 although it isunclear why.
In summary, the results of the present investigationsuggest that although rhBMP-7 is less active than rh-BMP-2 in vitro, the rhBMP-7–containing OP-1 bioim-plant induces greater amounts of bone in vivo thanInfuse. Although our in vitro results agree with those ofearlier studies, the results of the muscle pouch assay donot match earlier in vivo data. The potential of thesebioimplants to form bone are likely related to more thanthe osteoinductive activity of their component BMPsalone. The delivery system, release profile, host bed,and effect on other elements of the biologic healingcascade, including angiogenesis, likely play an impor-tant role in determining the amount of bone formed.Despite our expectation from the available in vitro andin vivo data that rhBMP-2 would form more bone invivo, when formulated in the form of the clinical bio-implant it was the rhBMP-7–containing OP-1 implantthat formed more bone in this model.
The authors thank Ms. Susan Carter and Ms. Aileen Zhoufor their assistance with the surgery and microCT and Ms.Alice Varghese and Ms. Katherine Lee for assistance with thein vitro work.
REFERENCES1. Giannoudis PV, Dinopoulos H, Tsiridis E. Bone substitutes: an
update. Injury 2005;36(Suppl 3):S20-7.2. Hubble MJ. Bone grafts. Surg Technol Int 2002;10:261-5.3. Mayer H, Scutt AM, Ankenbauer T. Subtle differences in the
mitogenic effects of recombinant human bone morphogeneticproteins -2 to -7 on DNA synthesis on primary bone-formingcells and identification of BMP-2/4 receptor. Calcif Tissue Int1996;58:249-55.
4. Cheng H, Jiang W, Phillips FM, Haydon RC, Peng Y, Zhou L, etal. Osteogenic activity of the fourteen types of human bonemorphogenetic proteins (BMPs). J Bone Joint Surg Am 2003;85-A:1544-52.
5. Katagiri T, Yamaguchi A, Komaki M, Abe E, Takahashi N,Ikeda T, et al. Bone morphogenetic protein-2 converts the dif-ferentiation pathway of C2C12 myoblasts into the osteoblastlineage. J Cell Biol 1994;127:1755-66.
6. Peel SA, Hu ZM, Clokie CM. In search of the ideal bonemorphogenetic protein delivery system: in vitro studies on de-mineralized bone matrix, purified, and recombinant bone mor-phogenetic protein. J Craniofac Surg 2003;14:284-91.
7. Clokie CM, Urist MR. Bone morphogenetic protein excipients:comparative observations on poloxamer. Plast Reconstr Surg2000;105:628-37.
8. Kawai T, Urist MR. Quantitative computation of induced hete-rotopic bone formation by an image analysis system. Clin Orthop1988;233:262-7.
9. Fajardo RJ, Ryan TM, Kappelman J. Assessing the accuracy ofhigh-resolution X-ray computed tomography of primate trabec-ular bone by comparisons with histological sections. Am J Phys
Anthropol 2002;118:1-10.10. Dinopoulos H, Giannoudis PV. The use of bone morphogeneticproteins (BMPs) in long-bone nonunions. Curr Orthop 2007;21:268-79.
11. Winn SR, Uludag H, Hollinger JO. Sustained release emphasiz-ing recombinant human bone morphogenetic protein-2. AdvDrug Deliv Rev 1998;31:303-18.
12. Kang Q, Sun MH, Cheng H, Peng Y, Montag AG, Deyrup AT,et al. Characterization of the distinct orthotopic bone-formingactivity of 14 BMPs using recombinant adenovirus-mediatedgene delivery. Gene Ther 2004;11:1312-20.
13. Luu HH, Song WX, Luo X, Manning D, Luo J, Deng ZL, et al.Distinct roles of bone morphogenetic proteins in osteogenicdifferentiation of mesenchymal stem cells. J Orthop Res 2007;25:665-77.
14. Winn SR, Uludag H, Hollinger JO. Carrier systems for bonemorphogenetic proteins. Clinical orthopaedics and related re-search 1999;367(Suppl):S95-106.
15. Uludag H, Gao T, Porter TJ, Friess W, Wozney JM. Deliverysystems for BMPs: factors contributing to protein retention at anapplication site. J Bone Joint Surg Am 2001;83-A(Suppl 1 Pt2):S128-35.
16. Onishi T, Ishidou Y, Nagamine T, Yone K, Imamura T, Kato M,et al. Distinct and overlapping patterns of localization of bonemorphogenetic protein (BMP) family members and a BMP typeII receptor during fracture healing in rats. Bone 1998;22:605-12.
17. Cho TJ, Gerstenfeld LC, Einhorn TA. Differential temporalexpression of members of the transforming growth factor betasuperfamily during murine fracture healing. J Bone Miner Res2002;17:513-20.
18. Spector JA, Luchs JS, Mehrara BJ, Greenwald JA, Smith LP,Longaker MT. Expression of bone morphogenetic proteins dur-ing membranous bone healing. Plast Reconstr Surg 2001;107:124-34.
19. Okubo Y, Bessho K, Fujimura K, Konishi Y, Kusumoto K,Ogawa Y, et al. Osteoinduction by recombinant human bonemorphogenetic protein-2 at intramuscular, intermuscular, subcu-taneous and intrafatty sites. Int J Oral Maxillofac Surg 2000;29:62-6.
20. Ngo TQ, Scherer MA, Zhou FH, Foster BK, Xian CJ. Expressionof bone morphogenic proteins and receptors at the injured growthplate cartilage in young rats. J Histochem Cytochem 2006;54:945-54.
21. Tsuji K, Cox K, Gamer L, Graf D, Economides A, Rosen V.Conditional deletion of BMP7 from the limb skeleton does notaffect bone formation or fracture repair. J Orthop Res 2009[Epub ahead of print].
22. Li JZ, Li H, Sasaki T, Holman D, Beres B, Dumont RJ, et al.Osteogenic potential of five different recombinant human bonemorphogenetic protein adenoviral vectors in the rat. Gene Ther2003;10:1735-43.
23. Israel DI, Nove J, Kerns KM, Moutsatsos IK, Kaufman RJ.Expression and characterization of bone morphogenetic pro-tein-2 in Chinese hamster ovary cells. Growth Factors 1992;7:139-50.
24. Swencki-Underwood B, Mills JK, Vennarini J, Boakye K, Luo J,Pomerantz S, et al. Expression and characterization of a humanBMP-7 variant with improved biochemical properties. ProteinExpr Purif 2008;57:312-9.
25. Hammonds RG, Jr., Schwall R, Dudley A, Berkemeier L, Lai C,Lee J, et al. Bone-inducing activity of mature BMP-2b producedfrom a hybrid BMP-2a/2b precursor. Mol Endocrinol 1991;5:149-55.
26. Friess W. Collagen—biomaterial for drug delivery. Eur J Pharm
Biopharm 1998;45:113-36.
OOOOE540 Barr et al. April 2010
27. Hausman MR, Schaffler MB, Majeska RJ. Prevention of fracturehealing in rats by an inhibitor of angiogenesis. Bone 2001;29:560-4.
28. Winet H, Bao JY, Moffat R. A control model for tibial cortexneovascularization in the bone chamber. J Bone Miner Res1990;5:19-30.
29. Smadja DM, Bieche I, Silvestre JS, Germain S, Cornet A, Lau-rendeau I, et al. Bone morphogenetic proteins 2 and 4 areselectively expressed by late outgrowth endothelial progenitorcells and promote neoangiogenesis. Arterioscler Thromb VascBiol 2008;28:2137-43.
30. Ramoshebi LN, Ripamonti U. Osteogenic protein-1, a bonemorphogenetic protein, induces angiogenesis in the chick cho-rioallantoic membrane and synergizes with basic fibroblastgrowth factor and transforming growth factor-beta1. Anat Rec2000;259:97-107.
31. Deckers MM, van Bezooijen RL, van der Horst G, HoogendamJ, van Der Bent C, Papapoulos SE, et al. Bone morphogeneticproteins stimulate angiogenesis through osteoblast-derived vas-cular endothelial growth factor A. Endocrinology 2002;143:1545-53.
32. Yeh LC, Lee JC. Osteogenic protein-1 increases gene expressionof vascular endothelial growth factor in primary cultures of fetalrat calvaria cells. Mol Cell Endocrinol 1999;153:113-24.
33. Wang EA, Rosen V, D’Alessandro JS, Bauduy M, Cordes P,Harada T, et al. Recombinant human bone morphogenetic pro-tein induces bone formation. Proc Natl Acad Sci U S A1990;87:2220-4.
34. Sampath TK, Maliakal JC, Hauschka PV, Jones WK, Sasak H,Tucker RF, et al. Recombinant human osteogenic protein-1(hOP-1) induces new bone formation in vivo with a specificactivity comparable with natural bovine osteogenic protein andstimulates osteoblast proliferation and differentiation in vitro.J Biol Chem 1992;267:20352-62.
35. Saito N, Okada T, Toba S, Miyamoto S, Takaoka K. New
synthetic absorbable polymers as BMP carriers: plastic propertiesof poly-D,L-lactic acid-polyethylene glycol block copolymers.J Biomed Mater Res 1999;47:104-10.
36. Ohta H, Wakitani S, Tensho K, Horiuchi H, Wakabayashi S,Saito N, et al. The effects of heat on the biological activity ofrecombinant human bone morphogenetic protein-2. J BoneMiner Metab 2005;23:420-5.
37. Okubo Y, Bessho K, Fujimura K, Kusumoto K, Ogawa Y, TaniY, et al. Comparative study of intramuscular and intraskeletalosteogenesis by recombinant human bone morphogenetic pro-tein-2. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1999;87:34-8.
38. Clokie CM, Sándor GK. Reconstruction of 10 major mandibulardefects using bioimplants containing BMP-7. J Can Dent Assoc2008;74:67-72.
39. Okubo Y, Bessho K, Fujimura K, Kusumoto K, Ogawa Y, IizukaT. Expression of bone morphogenetic protein in the course ofosteoinduction by recombinant human bone morphogenetic pro-tein-2. Clin Oral Implants Res 2002;13:80-5.
40. Kim CS, Kim JI, Kim J, Choi SH, Chai JK, Kim CK, et al.Ectopic bone formation associated with recombinant human bonemorphogenetic proteins-2 using absorbable collagen sponge andbeta tricalcium phosphate as carriers. Biomaterials 2005;26:2501-7.
41. Valentin-Opran A, Wozney J, Csimma C, Lilly L, Riedel GE.Clinical evaluation of recombinant human bone morphogeneticprotein-2. Clin Orthop 2002;395:110-20.
Reprint requests:
Professor George K. B. SándorFaculty of DentistryUniversity of TorontoHospital for Sick Children S-525555 University AvenueToronto, OntarioCanada M5G 1X8
[email protected]