How to Expertly Use Procalcitonin to Safely Reduce Antibiotic ...
Upload
khangminh22Category
view
1download
0
ii
COMPARING SERUM PROCALCITONIN AND SERIAL
C-REACTIVE PROTEIN AS SCREENING MARKERS FOR
NEONATAL BACTERIAL SEPSIS AT THE LAGOS UNIVERSITY
TEACHING HOSPITAL, IDI-ARABA LAGOS, NIGERIA
THIS DISSERTATION IS SUBMITTED IN PART FULFILLMENT
OF THE REQUIREMENTS FOR THE AWARD FOR THE
FELLOWSHIP OF THE NATIONAL POSTGRADUATE MEDICAL
COLLEGE OF NIGERIA IN THE FACULTY OF PAEDIATRICS.
BY
DR. MATTHEW-OKORE AMALACHUKWU NNENNA
MBBS (NIG) 2004
NOVEMBER 2016
iii
DECLARATION
It is hereby declared that this work is original unless otherwise acknowledged. The work has not been
presented to any other college in part fulfilment of the requirements for the award of a fellowship, nor
has it been submitted for publication in any academic journal.
……………………………………….
DR. MATTHEW- OKORE AMALACHUKWU
DATE: JANUARY 26TH 2017.
iv
ATTESTATION
We hereby certify that this work was done by Dr Matthew-Okore Amalachukwu in the department of
paediatrics Lagos University Teaching Hospital, Idi- Araba Lagos state under our supervision. we
also supervised the writing of the dissertation.
Names and addresses of the supervisors:
FIRST SUPERVISOR:
V.C EZEAKA, FWACP( PAED),
Professor/Consultant Paediatrician,
Department of Paediatrics,
College of medicine, university of Lagos and Lagos University Teaching Hospital,
Idi- Araba, Lagos.
………………………………
Signature/Date
Second Supervisor:
DR O.F ADENIYI, FMC(PAED),
Consultant Paediatrician,
Department of Paediatrics,
College of medicine, university of Lagos and Lagos university teaching hospital,
IDI- ARABA, LAGOS.
………………………………
Signature/Date
Third Supervisor
DR R OLADELE,
Consultant Microbiologist,
Department of Microbiology,
College of Medicine, University of Lagos and Lagos University Teaching Hospital,
IDI- ARABA, LAGOS.
………………………………
SIGNATURE/DATE

v
TABLE OF CONTENTS
TOPIC PAGE
Title i
Declaration ii
Attestation iii
Table of contents iv
Dedication vi
Acknowledgements vii
List of abbreviations viii
Definition of terms ix
List of tables xi
List of figures xii
Summary 1
Introduction 3
Literature review 7
Aim and specific objectives 23
Subjects and methods 24
Results 43
Discussion 60
Conclusion 68
Recommendations 69
Limitation 70
Areas of future research 71
References 72

vi
Appendix Ia (ethical approval) 86
Appendix Ib (extended ethical approval) 87
Appendix ii (consent form) 88
Appendix iii (Study Proforma) 93
Appendix iv (Researcher at Work) 97
Appendix v (Positive Procalcitonin Cassettes) 98
Appendix vi (Negative PCT cassettes) 99
Appendix vii (PCT interpretation card) 100
Appendix viii (Positive CRP Strips) 101
Appendix ix (positive blood culture samples) 102

vii
DEDICATION
This work is dedicated to:
The almighty god, without whom I am nothing.
My parents, Barr sir and Lady Goddy C Agbasi.
My husband, mr matthew okore and my wonderful children, Amarachi, Chidera,
Chukwuebuka and Onyinyechi.
To the Nigerian newborn- surviving against all odds!

viii
ACKNOWLEDGEMENTS
This work would not have been successful without the contributions from different persons in diverse
ways. Their kind contributions without which this work would not have been is eternally appreciated.
I express my deepest gratitude to my supervisors: Prof V.C Ezeaka, Dr (Mrs) O.F Adeniyi and dr.
(mrs) r. Oladele for their guidance. They painstakingly reviewed my work and guided me through the
rudiments of research. I deeply appreciate their efforts.
I also want to appreciate all the consultants in the department of Paediatrics who at different times
read through and added useful suggestions to my work. Their investment into my training is highly
appreciated.
I also appreciate the residents in the department of Paediatrics, especially the 2010 set.
I cannot forget Dr Bode- Sojobi, Dr Alli, Dr Igwe and Mrs Makinwa of the microbiology department
for taking me through the process of blood culture and analysis. Dr akpa, dr abiola and dr adeniran of
the community medicine department helped me through the confusing time of statistical analysis. I
deeply appreciate their kindness.
My appreciation also goes to Mr Sunday Isife and Mr Peter of the Paediatrics department laboratory.
They made the laboratory conducive for me to analyse my CRP and PCT samples, and shared my
excitement each time i got results. Dr. Moses, my research assistant, i am grateful.
My very sincere appreciation goes to all the parents and the subjects in this study.
Finally, I celebrate my parents, Barr. (Sir) and lady Goddy C. Agbasi who have never stopped
encouraging me to achieve my dreams. I cannot say how blessed i am to be your child. My siblings
Chizoba , Ijeoma, Uju and Obinna whose loss in the course of this work set me back, I appreciate
your support. To my aunty, Mrs Anthonia Ekeh, ‘Daa”, and my nanny, peace Ekawo, God bless you
richly.

ix
To my husband, Matthew and my wonderful children- Amarachi, Chidera, Chukwuebuka and
Onyinyechi, I will say, we did it!
To god who kept me alive and made all things possible be all the glory for ever more.
x
LIST OF ABBREVIATIONS
CBC COMPLETE BLOOD COUNT
CHER CHILDREN’S EMERGENCY ROOM
CRP C REACTIVE PROTEIN
ELBW EXTREMELY LOW BIRTH WEIGHT
EOS EARLY ONSET SEPSIS
IL INTERLEUKINS
LBW LOW BIRTH WEIGHT
LOS LATE ONSET SEPSIS
NBW NORMAL BIRTH WEIGHT
NICU NEONATAL INTENSIVE CARE UNIT
NPV NEGATIVE PREDICTIVE VALUE
PCT PROCALCITONIN
PPV POSITIVE PREDICTIVE VALUE
PROM PROLONGED RUPTURE OF MEMBRANES
SIRS SYSTEMIC INFLAMMATORY RESPONSE SYNDROME
TBA TRADITIONAL BIRTH ATTENDANTS
TNF TUMOR NECROSIS FACTOR.
VLBW VERY LOW BIRTH WEIGHT
WBC WHITE BLOOD CELL COUNT
WHO WORLD HEALTH ORGANISATION
xi
DEFINITION OF TERMS
1. Accuracy- The Degree To Which The Result Of A Measurement, Calculation Or
Specification Conforms To A Correct Value Or Standard.
2. Neonatal Sepsis- The Presence Of Infection (Probable Or Documented) With Systemic
Manifestations Of Infection In Babies Less Than 28 Days Of Life.
3. Early Onset Sepsis (Eos) - Sepsis Occurring Within The First 72 Hours Of Life.
4. Late Onset Sepsis (Los) – Sepsis Occurring From 4th To The 28th Day Of Life.
5. C- Reactive Protein (Crp) Level- Level Of C – Reactive Protein In A Patient Which Is
Measured In Mg/L Or Mg/Dl. (10mg/L= 1mg/Dl)
6. Procalcitonin (Pct) Level – Levels Of Procalcitonin In Patients Plasma Which Is Measured In
Ng/Ml. Normal Values Are <0.5ng/Ml.
7. Preterm Baby- Baby Delivered At Less Than 37 Completed Weeks Of Gestation.
8. Term Baby- A Baby Delivered At 37 To 41 Completed Weeks Estational Age.
9. Post Term Baby- A Baby Delivered At 42 Weeks Gestational Age And Above.
10. Extremely Low Birth Weight (Elbw) - Birth Weight Of Less Than 1000grams.
11. Very Low Birth Weight (Vlbw) - Birth Weight Of Less Than 1500grams.
12. Low Birth Weight (Lbw) - Birth Weight Of Less Than 2500grams.
13. Normal Birth Weight (Nbw) - Birth Weight Of 2500g To 4000grams.
14. Inborn Neonates- Babies Born At The Lagos University Teaching Hospital
15. Outborn Neonates- Babies Born Outside The Lagos University Teaching Hospital.
16. Definite Infection- Any Neonate With A Maternal Risk Factor For Sepsis Or At Least One
Clinical Sign Of Sepsis, Or Had A Positive Crp Or Pct And A Positive Blood Culture.

xii
17. Probable Infection- Any Baby With A Maternal Risk Factor For Sepsis Or At Least One
Clinical Sign Of Sepsis Who Had At Least A Positive Crp Or Pct And A Negative Blood
Culture.
18. No Infection- Any Baby With Any One Of The Risk Factors Of Sepsis Nor Any Of The
Clinical Features Of Sepsis, And Negative Crp, Pct And Blood Culture.
19. Sensitivity – The Ability Of A Test To Correctly Identify Subjects With A Disease. (True
Positives)
20. Specificity- The Ability Of A Test To Correctly Identify Subjects Without A Disease.(True
Negatives)
21. Positive Predictive Value (Ppv) - The Proportions Of The Positive Results In Diagnostic Tests
That Are True Positive Results.
22. Negative Predictive Value (Npv) - The Proportions Of The Negative Results In Diagnostic
Tests That Are All True Negative Results.
xiii
LIST OF TABLES
PAGE
TABLE I- ASSESSMENT OF VALIDITY 42
TABLE II- SOCIO-DEMOGRAPHIC CHARACTERISTICS OF STUDY
POPULATION 44
TABLE III- DESCRIPTIVE TABLE ON THE DISTRIBUTION OF SEPSIS BY SEX
AND PLACE OF BIRTH 45
TABLE IV- RELATIONSHIP BETWEEN SOCIAL CLASS AND CULTURE PROVEN
SEPSIS 46
TABLE V- SERIAL C-REACTIVE PROTEIN VALUES DURING THE COURSE OF
THE ADMISSION 49
TABLE VI- PROCALCITONIN VALUES AT PRESENTATION 50
TABLE VII- RELATIONSHIP BETWEEN MARKERS AND GESTATIONAL AGE 51
TABLE VIII- RELATIONSHIP BETWEEN MARKERS AND ONSET TIME OF SEPSIS 52
TABLE IX- BLOOD CULTURE RESULTS 53
TABLE X- RELATIONSHIP BETWEEN SERIAL CRP, PCT AND BLOOD CULTURE
OF SUBJECTS 56
TABLE XI- ASSESSMENT OF VALIDITY OF THE MARKERS 58
TABLE XII- RELATIONSHIP BETWEEN CRP AND PCT WITH OUTCOME OF
CARE 59
xiv
LIST OF FIGURES
PAGE
FIG 1A- SCHEMATIC REPRESENTATION OF CRP ASSAY PROCEDURE 34
FIG 1B- SCHEMATIC REPRESENTATION OF CRP ASSAY PROCEDURE 35
FIG 2- SCHEMATIC REPRESENTATION OF PCT ASSAY PROCEDURE 38
FIG 3- BAR CHART SHOWING RISK FACTORS FOR SEPSIS IN THE SUBJECTS 47
FIG 4- BAR CHART SHOWING CLINICAL FEATURES OF SEPSIS IN THE
SUBJECTS 48

1
SUMMARY
Neonatal sepsis (NNS) is a leading cause of morbidity and mortality in the developing countries
requiring early diagnosis and prompt treatment. The diagnosis of neonatal sepsis is very
challenging to the physician as the symptoms are non-specific and blood culture which is the
gold standard in the diagnosis requires a lot of blood, has a low sensitivity, is expensive and has
a long result turn out time. Screening markers like C –Reactive Protein (CRP) and Procalcitonin
(PCT) can help to make an early diagnosis thereby reducing the cost of care of the newborn with
sepsis.
The aim of the present study was to compare serial C- reactive protein and Procalcitonin as
screening markers for neonatal bacterial sepsis against blood culture which is the accepted gold
standard.
The study population was made up of neonates who were managed at the Lagos University
Teaching Hospital (LUTH) over a 6 month period. One hundred and five (105) neonates were
recruited into the study and samples for CRP, PCT and blood culture were taken from each
newborn. The CRP and PCT were analysed using point of care kits while the blood culture
samples were collected in the BACTEC culture bottles and incubated in the BACTEC 9050
machine. All samples were taken on presentation, prior to commencement of antibiotics, and
additional CRP samples were collected at 24 hours and at 72 hours. Levels of CRP and PCT
obtained were compared with blood culture results. The relationship between CRP, PCT and
specified variables: gestational age, onset time of sepsis and outcome of the treatment was
determined. Data was analysed using the Epi InfoTM 2008 version 3.4.1 software.

2
The sensitivity of CRP at presentation (0 hour) was 100% while at 24 hours it was 82% and
70% at 72 hours. The specificity of CRP at 0, 24 and 72 hours were 65%, 66% and 75%
respectively while the negative predictive values of CRP at 0, 24 and 72 hours were 100%, 97%
and 96% respectively.
On the other hand, PCT done on presentation had 100% sensitivity and negative predictive
values of 100%.
Blood culture was found to be positive in 11 neonates giving an overall infection rate of of
10.5%.
Both CRP and PCT were found to have significantly higher positivity rates in the term babies
compared to the preterm neonates. Both markers were also found to be more significant in late
onset sepsis.
In conclusion, PCT on the day of presentation has a high sensitivity and NPV and is useful in
early diagnosis of neonatal sepsis. However, serial CRP with high sensitivity and NPV can also
be used.
3
INTRODUCTION
Sepsis is defined as the presence of infection (probable or documented) with systemic
manifestations of infection.1,2 Systemic manifestations of infection, which is the systemic
inflammatory response syndrome (SIRS), is described as the presence of at least 2 of the
following criteria ( one of which must be abnormal temperature or leucocyte count):2
Core temperature of >38.30C or <36oC.
Tachycardia - Heart rate >180 beats/minute or bradycardia (heart rate <100 beats/minute.
Tachypnoea- respiratory rate >60 cycles/minute
Leucocytosis or leucopenia.
Neonatal sepsis is a major cause of neonatal morbidity and mortality throughout the world and
especially in the developing countries.3 The World Health Organisation (WHO) has estimated
that 4 million babies die in the first 28 days of life, and neonatal sepsis accounts for 26% of those
deaths.4 Ninety eight percent(98%) of neonatal deaths occur in developing countries.5 In Nigeria,
sepsis contributes significantly to under 5 mortality6,7 and hospital based studies suggest it
accounts for 20-25% of neonatal mortality.8
The diagnosis of neonatal sepsis is challenging to the physician because the features are non-
specific, and overlap with other non-infectious causes of systemic inflammation.9 Despite
research over the past decades, there is still no single ideal test for early diagnosis of neonatal
sepsis.10
The gold standard in the diagnosis of sepsis is blood culture .11,12 Blood culture is expensive, and
there is a delay of 48 hours before preliminary results are obtained.13,14 The yield of blood
culture is between 30 -70% and some cases of neonatal sepsis go undetected.15 This is because

4
of difficulty in obtaining enough blood samples16 and increasing use of intra-partum antibiotics
in women during labour and delivery.17
Therapeutic antibiotic use is recommended for infants with clinical features or risk factors for
sepsis.18 However, this results in overtreatment, unnecessary painful intravenous cannulations,
and mother- infant separations. 19 Antibiotic therapy greater than 72 hours has been found to
increase colonization by gram negative organisms and emergence of drug resistant strains.18
There is also associated altered gut colonization and increased risk of Candida colonization20 and
death. Also, prophylactic antibiotic treatment may result in the treatment of as many as 30
uninfected neonates for every infected one.19 The dilemma therefore is, ‘which babies need
antibiotics and for how long?’
Several newer markers of sepsis have been studied including C- reactive protein (CRP)3,14,21,
Procalcitonin (PCT),22-24 Tumor necrosis factor α (TNF),25-27 Fibronectin28 and Interleukins.27,29
In Port Harcourt, Nigeria, West et al30 observed that the qualitative method of CRP estimation
could correctly identify three quarters of neonates with sepsis. Ayazi et al 31 in Iran found serial
C- reactive protein levels useful in the evaluation of neonates with suspected sepsis.
Benitz et al19 found that when 3 serial CRP tests were done, their sensitivities increased
progressively, and negative predictive value of 3 serial CRP was 99.7% for proven sepsis.
Ibeh et al 22 in Benin reported that procalcitonin was superior to CRP as a predictor of neonatal
sepsis.
Considering these findings, this study aims to compare serial CRP and PCT as markers of
neonatal sepsis. This research hypothesized that serial CRP measurements is as effective as one
PCT measurement which other researchers have found to be very sensitive in making an early

5
diagnosis of neonatal sepsis, but quite expensive. The research was aimed at answering the
following research questions:
(a) Considering the fact that neonatal sepsis is common in our environment and is a leading
cause of prolonged, and sometimes unnecessary hospital admission, can serial CRP or PCT
be useful in early decision making?
(b) Can serial CRP be utilized as an effective marker for neonatal sepsis in our resource poor
country?
(c) Can these markers be used to monitor response to treatment in neonates being treated for
neonatal sepsis?
JUSTIFICATION
The practice of commencing every neonate with suspected sepsis on antibiotics has increased the
emergence of drug resistant organisms. 32 The cost of antibiotic therapy is also challenging in a
resource poor country especially if unnecessary.
The use of a reliable marker with high sensitivity and negative predictive value to select neonates
who do not require prolonged antibiotic therapy is desirable. The kits used for this study were
point of care kits which can give results in as fast as 30 minutes thereby identifying babies who
may not require antibiotics early. Most of the studies on these markers were done in developed
countries. Additionally, the sensitivity and specificity of CRP improves with serial
measurements. In Nigeria, to the best of the authors’ knowledge, no study has compared serial
CRP and PCT as markers of neonatal sepsis. Ibeh et al 22 in Benin compared PCT with a single
CRP reading.

6
Additionally, CRP is more readily available than PCT, so it would be useful to compare the
sensitivity and specificity, positive and negative predictive values of serial CRP and PCT to
determine if the use of serial CRP measurements can help to promptly identify newborns with
sepsis. This would significantly reduce duration of hospital stay, prevent emergence of antibiotic
resistance and ultimately reduce cost of healthcare. Early detection of infected neonates and early
discharge of the uninfected will help improve morbidity and mortality among these vulnerable
newborns.
It is hoped that the findings from this study will answer the research questions, add to the body
of knowledge, and contribute to policy formulation in the management of neonatal sepsis in
Nigeria.

7
LITERATURE REVIEW
Neonatal sepsis is a source of diagnostic challenge to the physician and a killer of newborns all
over the world. Among the major causes of death in the first month of life in Nigeria, severe
infections account for 26% and prematurity 28%.33 This is worrisome because preterm/low birth
weight is the risk factor most closely associated with early onset neonatal sepsis.34
Neonatal sepsis encompasses various systemic infections in the newborn such as septicemia,
meningitis and pneumonia, but does not include superficial infections like conjunctivitis and oral
thrush.35
CLASSIFICATION
Neonatal sepsis is classified into 2 major categories:36
Early onset sepsis (EOS): This usually occurs within the first 72hours. Neonates with (EOS)
typically present with respiratory distress.
Late onset sepsis (LOS): Usually occurs from 4 – 30days of delivery and is acquired in the
newborn unit or community.
Late, Late onset sepsis occurring after 30days has been reported, especially in the preterm very
low birth weight infants.36
Risk factors for early onset sepsis include: prematurity, chorioamnionitis, febrile illness in the
mother (within 2 weeks prior to delivery) and prolonged rupture of membranes (>18hours).

8
Preterms have a 3 -10 fold risk of acquiring infections more than term, normal weight infants.36
This is because of immaturity of the immune system, and maternal genital tract infection is an
important cause of preterm delivery.
Chorioamnionitis is characterized by intrapartum fever(>38oC), leucocytosis (WBC>15,000)
and uterine tenderness.37
THE BURDEN OF NEONATAL SEPSIS
Neonatal sepsis is accepted worldwide as a devastating complication for the newborn. This is
because of the high mortality associated with it, alongside long term complications such as
neurodevelopmental impairment. In the United States, the estimated annual incidence of severe
sepsis in the newborn is 0.3/ 1000 live births.10 The estimated mortality is 10.3%, with most
deaths occurring in the first 48 hours of infection.10 Neonatal sepsis contributes between 13- 15%
of neonatal deaths globally,38 and in developing countries, 30-50% of neonatal deaths.6,38,39
In 2012, West et al in Port Harcourt reported a prevalence of 33.1%.40 This is similar to 31.7%
reported by Antia- Obong et al in Calabar 7and 34.4% reported by Bode- Thomas et al in Jos.41
Lowest prevalence documented so far has been 10.7%42 reported by Njokanma et al in Ogun
state about two decades ago. The higher prevalences in Jos, Calabar and Port Harcourt may have
been because the studies were prospective and infants who had prior antibiotic therapy or whose
mothers were on antibiotics were excluded from the study.40 The use of antibiotics prior to blood
culture may suppress growth of bacteria in cultures.

9
At the Lagos University Teaching Hospital, Iroha et al 43 showed a prevalence of 35 per 1000
live births and accounted for 36% of neonatal deaths during the study period. Adejuyigbe et al 44
in Ile- Ife in 1995 had an incidence of 22.9 per 1000 live births and a mortality rate of 33.3%.
These studies from Nigeria are in sharp contrast to findings from the United Kingdom where an
incidence of 8/1000 live births was recorded,45 and the United States where an incidence of
0.76/1000 live births was recorded.46 In Saudi Arabia, 4.9/1000 live births was reported.47
The socio-economic burden of long term complications of neonatal sepsis has also been studied.
Mwaniki et al 48 in a review article documented that amongst 2442 neonates with sepsis, 40%
had sequelae which ranged from cognitive and learning difficulties, cerebral palsy, hearing loss,
loss of vision and co-ordination. These impairments may constitute huge financial, emotional
and social challenges for affected families.
PATHOGENESIS OF NEONATAL INFECTIONS
Before birth, the fetus is maintained in a sterile environment. The chorioamniotic membranes,
placenta and antibacterial factors in the amniotic fluid protect the fetus from infections.49 Sepsis
can begin in utero if the fetus swallows infected amniotic fluid. Organisms causing early onset
sepsis can also ascend from the birth canal either at rupture of amniotic membranes or during
labour, especially if the membranes ruptured for longer than 18 hours. The neonate can also
develop sepsis in the hours or days after birth when the mucosal surfaces are compromised ( e.g
in babies with omphalocele) 37
Sepsis results from the complex interaction between the invading organism and the host immune,
inflammatory and coagulation response.50 After invasion of the microorganisms, an acute
10
localized inflammatory reaction is initiated. The contact with bacterial endo or exotoxins initiates
the release of prostaglandin, leukotriene and histamine which activate further inflammatory cells.
Activated fibroblasts and leucocytes produce pro inflammatory cytokines including Interleukins
1 and 6, TNFα. IL-6 in synergy with IL-1 induce the hepatocytes to produce CRP.32
The high levels of cytokines and bacterial endotoxin in sepsis cause elevation of PCT by
inhibiting the final step in conversion of PCT to calcitonin.51 It is also postulated that the
elevation of PCT due to endotoxin release occurs mainly in parenchymal tissues. Parenchymal
cells unlike neuroendocrine cells lack the ability to cleave PCT into its mature form calcitonin
leading to a circulation of PCT in large amounts.52
Other factors predisposing to sepsis in the neonate include :diminished concentrations of
immunoglobulin, and reduced function of neutrophils and other cells involved in the response to
infection in both term and preterm infants.36 Despite these alterations in immunologic factors,
newborn infections are uncommon in the absence of predisposing obstetric factors.36
CAUSATIVE ORGANISMS AND CHANGING PATTERNS
Organisms causing neonatal sepsis vary according to locations, and even in the same location,
studies have shown that causative organisms vary periodically.
Iroha et al,43 at LUTH reported the common causative organisms to be more of gram negatives,
with Klebsiella pneumonia being dominant in both early and late onset sepsis. This was at
variance with a study done 20 years earlier in the same centre where E.coli was dominant.53
Other significant pathogens isolated in the LUTH study were Staphylococcus aureus and
Coagulase negative staphylococcus.43

11
Awoniyi et al,54 in Ife, Nigeria in 2009 found Staphylococcus aureus ( Staph aureus) to be the
dominant pathogen, followed by Pseudomonas(13%) , Klebsiella (13%) and Proteus (10%).
Adejuyigbe et al39 eight years earlier in the same center reported a similar pattern except for the
isolation of Listeria monocytogenes which is not a common cause of neonatal sepsis in the
tropics. These studies did not clearly state the pattern of infection amongst inborns and outborns,
however Adejuyigbe et al 39 noted that 56.6% of the neonates with risk factors and/or clinical
features of sepsis were delivered outside the hospital. Mokuolu et al 55 in 2002 in Ilorin in a
study that screened 198 neonates, isolated gram negative bacilli in early onset sepsis and Staph.
aureus was the commonest pathogen (29.5%) in late onset sepsis. 52% of the newborns with
sepsis were out born.
In 2007 at the University of Port Harcourt Teaching Hospital, West et al,56 in a study of 406
neonates with 169 positive cultures, isolated Klebsiella pneumonia and Staph aureus
predominantly in early onset sepsis(EOS) and late onset sepsis (LOS) respectively. Both
organisms were also predominant in the preterm and term newborns. In Bauchi, Yusuf et al 57 in
2008 isolated Escherichia coli as the predominant pathogen in EOS while Staph. aureus was the
predominant pathogen in LOS.57
These patterns are in contrast with studies from the United States where Group B streptococcus
(GBS) is the predominant pathogen in early onset sepsis followed by E. coli.34 GBS remains the
most significant pathogen in term infants, and E. Coli the most significant pathogen in preterm
infants with EOS.34 Similarly, a study from the United Kingdom has reported GBS to be the
most frequent pathogen, followed by coagulase negative staphylococcus.58 Though it appears
that GBS is uncommon in developing countries , a study done by Dawodu et al 59 in Ibadan
showed that there is a high vaginal carriage rate of GBS but low incidence of disease. Suara
12
et al 60 in Gambia postulated that the rarity of GBS disease in developing countries may be due
to the prevalence of maternally derived GBS antibodies, and lower prevalence of the virulent
GBS serotype III. From the studies above, it is notable that causative organisms of neonatal
sepsis vary from center to center, hence the need for continuous research and re-evaluation of
antibiotic sensitivity patterns.
DIAGNOSIS OF NEONATAL SEPSIS
Diagnosis of sepsis in the newborn is difficult because of non-specific clinical features which can
also be observed in non-infectious conditions. Available diagnostic testing is not useful in
deciding which neonate requires empirical antibiotics treatment, ( due to poor positive predictive
values e.g. full blood count ) but can help with the decision to discontinue treatment.61 The
diagnostic tests for neonatal sepsis may be specific or non-specific.
SPECIFIC TESTS:
BLOOD CULTURE
Blood culture is still recognized as the “gold standard” in the diagnosis of neonatal sepsis.14
However, it requires 48- 72 hours to get a preliminary result, and with maternal antibiotics, as
few as 2.7% of neonates with clinical sepsis may have positive cultures.62 The yield of blood
culture is 30-70%,15 and data shows that even in neonates who were critically ill and died, only
80% of autopsy proven sepsis was diagnosed by pre-mortem blood cultures.63 A positive blood
culture with a pathogenic organism confirms the diagnosis of neonatal sepsis, but a negative
blood culture does not rule out the disease.64 The use of antibiotics prior to collection of blood

13
culture samples can also affect the results. However, the BACTEC® blood culture systems
contain resins which neutralizes antimicrobial activity of antibiotics.65 Microbial culture using
BACTEC® has multiple advantages over conventional blood culture including rapidity, cost
effectiveness, recovery of fastidious organisms and lower risk of contamination due to the closed
system of blood collection.66 With the BACTEC® Peds Plus bottle, as low as 1ml of blood can
be used which makes it very useful for neonates.65
BACTEC® also improves the yield of clinically significant isolates with reduced time to
detection.67
Other specific tests include: Cerebrospinal fluid culture, urine culture and tracheal aspirate
cultures.
NON SPECIFIC TESTS:
I COMPLETE BLOOD COUNT.
The complete blood count (CBC) is one of the earlier markers evaluated. However, in the
interpretation of CBC, timing is important.68 The Manroes’s criteria, using the total white cell
count, immature neutrophil count and bands to neutrophil ratio is widely used.69 Makkar et al 70
in India showed immature to total neutrophil ratio as the most reliable indicator of sepsis in
neonates.
In Nigeria, micro ESR ( Erythrocyte Sedimentation Rate) has been studied by Boma West et al,71
and found to have a sensitivity of 75.7% which increased to 95.9% when combined with band
forms. This is also similar to 71% reported by Akpede and Abiodun.72
14
II INFLAMMATORY CYTOKINES
Inflammatory cytokines, (eg interleukins, tumor necrosis factor) are released in response to
inflammation. Interleukins 6 and 8 have been extensively studied. Cytokines are promising
diagnostic markers and their levels are increased early in the infective processes.27,73
Tumor necrosis factor has been studied by Ako-Nai in Ile- Ife,26 Nigeria and found to be a useful
marker of neonatal sepsis.
Some other biomarkers studied include serum amyloid,74 haptoglobulins75 and fibronectin.28,75
It has been postulated however, that a combination of markers often produces a screening test
with better sensitivity and specificity than a single marker.17,76,77
III C – REACTIVE PROTEIN
CRP is one of the most studied laboratory tests for neonatal sepsis. It was first described in 1930
by Tillet and Francis at Rockefeller University.78 A precipitation reaction was observed between
serum from patients suffering from acute pneumococcal pneumonia and the extracted
polysaccharide fraction C from the pneumococcal cell wall. This reaction was not observed when
using serum of healthy controls, or the patients after they had recovered.78
CRP is an acute phase reactant protein, produced in reaction to acute tissue injury or infection.
The production of CRP in the hepatocytes are induced by interleukin 6.79 CRP is normally
present as a trace component of the plasma.80 However, in the acute phase response, hepatic
synthesis can reach 1000 fold levels.81` Levels remain high as long as the inflammation persists
and then decreases rapidly.

15
CRP is synthesized within 4-6 hours after exposure to an infective process or tissue damage,
peaks at 24-48 hours and then diminishes.82 In studies using CRP 1mg/dl as cut off value, the
range of reported statistical outcomes for culture proven sepsis is as follows: sensitivity 30-40%,
specificity 88-91% and negative predictive value of 97-99%.19,83 CRP elevations in non-infective
conditions such as meconium aspiration, recent vaccination, surgery, perinatal asphyxia and
intraventricular hemorrhage are also thought to affect the specificity of the test.84
The predictive value of CRP improves with time and is most predictive 24- 48 hours after a
newborn presents with suspected infection. Serial measurements (more than one) are therefore
recommended rather than a single value.19 Benitz et al 19 performed 3 CRP measurements- on
admission and next two mornings, while Nuntnarumit et al 85 performed 2 measurements at
initial assessment and 24-48hours later. In both studies, the predictive values of CRP increased
with serial testing.
Ayazi et al,31 in a study done in Iran determined CRP levels in neonates with suspected bacterial
infection. CRP levels were determined at initial evaluation and 24 hours later. Their results
showed that the sensitivity, specificity, positive and negative predictive values of CRP increased
with the second test. They concluded that normal CRP values obtained 24 hours after the initial
CRP indicate that infection is unlikely.
Lee et al,21 also applied a protocol of measuring CRP serially in the management of suspected
early neonatal sepsis. They measured CRP levels at initial evaluation, 8- 16 hours later and 24
hours later. Antibiotics were discontinued if two serial CRP were within normal range and blood
culture negative at the time of CRP report. They found that this protocol reduced the duration of
16
hospitalization and antibiotic use in the patients and none of the subjects required re-admission
within 1 week of discharge.
Benitz et al 19 in the study titled,’’ Serial serum C- reactive protein levels in the diagnosis of
neonatal infection”, evaluated 1002 newborns between 32weeks – 40 weeks gestational age.
CRP was done at initial evaluation and the next 2 mornings. The negative predictive values for 3
CRP tests were 99.7% and 98.7% for proven and probable sepsis. They concluded that two
normal CRP levels obtained 24 hours apart, show that a bacterial infection is unlikely. The
sensitivity of a normal CRP at the initial evaluation is not sufficient to justify withholding
antibiotic therapy.19 Furthermore Phillip et al 86 in their study guided the duration of antibiotic
therapy using serial monitoring of CRP. With this protocol, antibiotics were discontinued when
CRP levels became normal. The mean duration of treatment was thus reduced to 3.1 days and no
infant initially treated with antibiotics and discharged when the CRP returned to normal was re-
admitted.86
A normal repeat CRP 24-48 hours after the initiation of antibiotic therapy has been reported to
have a 99% negative predictive value in accurately identifying infants not infected in the
neonatal period.86
In summary, determination of serial CRP levels can be helpful in diagnosing neonatal sepsis,
monitoring the response to treatment in infected neonates and determining the duration of
antibiotic therapy .19,86

17
METHODS OF ASSAYING CRP
CRP can be assayed by several methods which may be qualitative, Semi quantitative or
quantitative. All methods are based on the ability of CRP to form antigen antibody complexes,
clump and precipitate, and then be visualized and measured. Examples of these methods are:
Latex agglutination method: This was the first laboratory method developed for CRP
assay. It is a qualitative method which measures the presence or absence of agglutination
or precipitation and indicates only whether CRP is present or absent in the sample.
Turbidimetric method: This quantitative method assesses agglutination of latex particles
coated with antibody against CRP by quantifying the absorbed light with a
spectrophotometer.87
Nephelometric method: This quantitative method measures the agglutination of particles
by quantifying the scattered light using a nephelometer.
Immunochromatography method: This method is based on the principle of flow through
immunochromatography and uses whole blood. It is a semi- quantitative method.
The quantitative methods are more widely used in developed countries. They provide highly
sensitive and specific results but require costly analysers.88 On the other hand, the qualitative and
semi quantitative methods are available for bedside testing and can provide results within 5-15
minutes. They also require less skill and may be more feasible in resource poor settings.
Furthermore, some researchers have found that the CRP values from semiquantitative methods
correlate well with the quantitative methods.88

18
IV PROCALCITONIN
Procalcitonin (PCT), an acute phase marker has been investigated for its diagnostic role in
neonatal sepsis since the mid 1990’s. Serum levels are reported to rise from 2 hours after
exposure to bacterial endotoxin, peak at 6-8 hours and reach a plateau after about 12 hours.89 It
reduces to its normal values after 2-3 days.82 It is the preliminary molecule of calcitonin. It is a
116 amino acid polypeptide with a molecular weight of 145kda.90
Procalcitonin is produced and secreted in the C cells of the thyroid gland in normal metabolic
conditions and levels are undetectable in the blood of healthy people.91 In cases of sepsis, PCT
has an extrathyroidal production in macrophages and monocytic cells of organs like the liver.89,92
In severe bacterial, fungal and parasitic infections with systemic manifestations, a significant rise
in procalcitonin levels are seen. Normal serum PCT level is <0.5ng/ml.93,94 Levels above this are
accepted as pathological. The unique feature that PCT levels increase in bacterial and fungal
infections , but remain unchanged even in severe viral infections makes it attractive as a potential
diagnostic variable for the diagnosis of bacterial infection.94
There are some challenges which have been noted with the use of PCT in the diagnosis of
neonatal infections. First is that infants with respiratory distress syndrome, perinatal asphyxia,
intracranial hemorrhage and pneumothorax may have raised serum PCT which may not differ
from those of septic neonates after onset of clinical signs of distress or infection.95 This raised
PCT is because the systemic response seen in severe infections could also occur in inflammatory
processes without infection such as ischaemia, multiple trauma and conditions listed above. 96
Available data also shows that PCT and CRP values are higher for neonates born to diabetic
mothers.97,98 Also, a physiological increase in PCT has been reported up to 36 hours
19
postpartum.99 Chiesa et al in Rome concluded that despite increase in PCT caused by these
perinatal events, PCT response to infection is much higher.97 They found that PCT levels in
infected neonates got as high as 500ng/ml depending on the severity of infection, while increases
caused by perinatal events such as respiratory distress rose to a mean of 2ng/ml.
METHODS OF PROCALCITONIN ASSAY.
Procalcitonin can be assayed quantitatively or semi- quantitatively. The semi- quantitative
method is an immunochromatographic assay. It utilizes the point of care kits which are faster to
use, inexpensive and do not require equipment or calibration. However, the colour intensity must
be evaluated by a technician and so is subject to individual observer variation.100
The quantitative assay is a luminometric immunoassay. Two antigen specific monoclonal
antibodies that bind PCT are added to serum or plasma. One of the antibodies is luminescence
labelled (the tracer). The antibodies react with the PCT and form “sandwich complexes”. The
luminescence labelled antibody then binds to the inner surface of the tube and excess tracer is
then removed. The amount of tracer on the test tube wall is then read with a luminometer. This
method is cumbersome, requires equipment and is more expensive.
The quantitative method is thought to be more reliable than the semi- quantitative method,
however, Manzano et al found the correlation between the two methods is moderate.100

20
COMPARING CRP AND PROCALCITONIN
CRP and PCT have been studied both independently and together. CRP is thought to be the most
extensively studied biomarker of sepsis and is the most frequent marker used in diagnosis and
monitoring of infections in the neonate.10
For a screening marker to be described as effective, ideally it should recognize all infected
neonates (highly sensitive) so that disease can be excluded with negative results (High negative
predictive value).101 Khashabi et al102 stated that the most important criteria of a reliable test are
its high sensitivity combined with a high negative predictive value. Kocabas et al27 also stated
that it is desirable for an ideal diagnostic marker to have about 100% sensitivity and NPV. It
should also have a reasonably high specificity and PPV of greater than 85%.
In Port Harcourt, Nigeria, West et al 30 studied 420 neonates and found that the qualitative
method of estimating CRP was cheap, had moderate sensitivity, specificity and negative
predictive value and could correctly identify close to three quarters of neonates with sepsis.
Similarly, Ibeh et al 22 in a study done among sixty neonates in University of Benin Teaching
Hospital, Nigeria found that PCT could be helpful for early detection of neonatal sepsis, and that
any increase in PCT in a critically ill neonate should warn of possible sepsis. Arowosegbe et al
103 in Abeokuta Ogun state studied 85 neonates with risk factors and/or clinical features of sepsis.
They found that at a cut off level 0.5ng/ml, the negative predictive value (NPV) of PCT was 80%
and the positive predictive value (PPV) was 39%. They also found that a higher percentage of
neonates who died (96%) had elevated PCT levels compared to those who survived (46%). They
concluded that any increase in PCT in an ill neonate should suggest the possibility of a

21
septicemic infection. They also stated that PCT is of great advantages where prediction of
severity and mortality is concerned.
Even though other critical illnesses in the newborn (Respiratory distress syndrome, severe
perinatal asphyxia) can elevate PCT, Chiesa et al97 found that PCT response in infection is much
higher, so a high index of suspicion of neonatal sepsis is required when PCT is elevated.
Naglaa et al 104in Egypt studied 60 neonates with suspected sepsis and found that PCT and CRP
are both reliable with the same diagnostic accuracy. In their study, both CRP an PCT had
positive predictive value (PPV) of 90%, while the negative predictive values ( NPV) were 87.5%
for PCT and 66.3% for CRP. The area under the curve (AUC) values were 0.92 and 0.88 for
PCT and CRP without any significant statistical difference. Their findings agree with
Franz et al 105 in Germany and Blommendahl et al106 in Finland.
However, some studies reported that PCT is a more reliable marker than CRP. This was found by
Sucilathangam et al in India93 who studied 50 neonates and found that PCT was superior to CRP
in diagnosing neonatal sepsis. In their study, an elevated PCT was detected in 22 of the 50
neonates, whereas an elevated CRP was detected in 18 cases. 14 of the 50 neonates were culture
positive, and PCT was elevated in 13 cases (92.85), while CRP was elevated in 7 cases (50%).
Based on their results, they recommended that commencement of antibiotics in newborn infants
should be based on the PCT results on the day of admission to the Neonatal Intensive Care Unit
(NICU).
Koksal et al107 in Turkey studied 67 neonates and found that PCT was superior to CRP in
diagnosing neonatal sepsis, detecting the severity of illness and evaluating response to
22
treatment. Furthermore, Mamdouh et al in Egypt108 and Adib et al109 also reported similar
findings.
Considering all the findings of previous researchers, this study seeks to compare serial CRP and
PCT as we seek to further improve newborn care. It is hoped that the results from this study will
significantly impact on policy formulations and management of neonatal sepsis in Nigeria.
23
AIM AND OBJECTIVES
AIM
1. This study aims to compare the efficacy of procalcitonin and serial C- reactive protein as
screening markers of neonatal bacterial sepsis at the Lagos University Teaching Hospital,
Idi Araba, Lagos.
SPECIFIC OBJECTIVES
1. To determine the levels of C-reactive protein and procalcitonin in the study subjects.
2. To compare C- reactive protein and Procalcitonin levels in neonatal sepsis by gestational
age, onset time of sepsis and socio-demographic factors.
3. To compare the sensitivity, specificity, positive and negative predictive values of serial
measurements of C- reactive protein with procalcitonin in neonatal sepsis using blood
culture as the gold standard.

24
SUBJECTS AND METHODS
STUDY LOCATION
The study was conducted at the inborn and out born wards of the neonatal unit at the Lagos
University Teaching Hospital (LUTH), Idi Araba, Lagos. Lagos is a metropolitan city in
Southwest Nigeria with an estimated population of 18 million, annual birth rate of 360,000 and
about 14,000 neonatal deaths annually, 20% of which are caused by infections.110
LUTH is a tertiary hospital with about 760 beds and provides healthcare services to the residents
of Lagos and its neighboring states. It is a training centre for undergraduates, post graduate
students and resident doctors.
The neonatal unit consists of 2 wards, the New Neonatal Unit (NNU) and Ward D1. The unit
averages 1400 admissions yearly and is run by 4 consultants, 8 resident doctors and 8 interns.
The NNU (in born ward) caters for inborn babies delivered in the labour ward of LUTH. It
shares the same complex with the delivery rooms and theatre. Babies are admitted here mainly
for prematurity, risks for sepsis, neonatal jaundice and congenital anomalies. This unit has the
capacity for 36 newborns.
Ward D1 (outborn unit) caters for referred babies admitted via the Children’s Emergency Room
(CHER). They are referred from other hospitals, maternity homes and traditional birth
attendants. Reasons for admission are similar to NNU except for neonatal tetanus, severe birth
asphyxia and severe hyperbilirubinaemia which are uncommon in inborn patients.

25
Babies born in LUTH without clinical features or risk factors for sepsis join their mothers in
postnatal wards C2 and C3. These babies are reviewed daily by the neonatal team. They are
discharged after 72hours except the baby develops jaundice or other problems.
For this study, subjects were recruited from NNU, D1 and Children Emergency Room after
obtaining parental consent. Both term and preterm neonates were recruited.
STUDY DESIGN
This was a cross sectional study carried out between September 2015 and February 2016.
STUDY POPULATION
The study population comprised of newborns, aged 0-28 days with risk factors and/ or clinical
features of sepsis. Neonates were recruited from the NNU for inborn babies, and CHER or ward
D1for outborn babies.
For the purpose of this study, the subjects were divided into 3 groups according to the criteria
suggested by White et al111:
Definite Infection: Any neonate with a maternal risk factor for sepsis or at least one clinical sign
of sepsis, or had a positive C-reactive protein or Procalcitonin, and a positive blood culture.
Probable Infection: Any baby with a maternal risk factor for sepsis or at least one clinical sign of
sepsis who had at least a positive C- reactive protein or Procalcitonin and a negative blood
culture.

26
No infection: Any baby with any one of the risk factors of sepsis or at least one of the clinical
features of sepsis, and negative CRP and PCT and blood culture.
INCLUSION CRITERIA.
Neonates who had risk factors for neonatal sepsis. These factors include
chorioamnionitis, maternal pyrexia > 38oC, foul smelling liquor, prematurity, prolonged
rupture of membranes > 18hours, history of maternal urinary tract infection.
Neonates who had clinical signs suggestive of sepsis. These factors include temperature
instability, feeding difficulties, abdominal distension, apnoea, abnormal glucose
homeostasis, non-physiologic jaundice, tachypnea, grunting respirations, irritability,
lethargy or seizures.
EXCLUSION CRITERIA
Babies who had already commenced antibiotics.
Infants of diabetic mothers.
Neonates with severe birth asphyxia.
No parental consent.

27
SAMPLE SIZE DETERMINATION.
Subjects were patients who met the inclusion criteria
The level of significance and power of the study was set at 5% and 80% respectively.
The formula for comparison of 2 proportions according to Varkevisser et al112 was used:
N= (u+ v)2{P1 (100- P 1) + P2 (100- P2) }
(P1 – P2)2
Where:
N = Sample size
u = One sided percentage point of the normal distribution, corresponding to 100% - the
power = 0.84.
v= Percentage point of the normal distribution, corresponding to the 2 sided 5%
significance level = 1.96
P1 = Proportion of proven septic neonates with positive CRP according to a previous
study93 = 50%
P2 = Proportion of non-septic neonates with positive CRP93 = 30.5%
N= (0.84 + 1.96)2 87
(50-30.5)2
7.84{2500 + 2119.75}
380.25
7.84 x 4619.75 = 36218.84
380.25 380.25
95.25.

28
The same calculation was done for PCT using:
P1 = Proportion of proven septic neonates with positive PCT according to a previous study93 =
92.85%
P2 = Proportion of non-septic neonates with positive PCT93 = 25%.
(0.84+ 1.96)2 (92.85(100-92.85) + 25(100-25)
(92.85-18)2
7.84(663.88 +1875)
4603.62
= 4.32 (Not statistically significant)
The higher value was taken113: 95.25
However, in order to increase precision and possible attrition (from early neonatal deaths,
discharge against medical advice) 10% of the sample size was added.
95.25 + 9.525 = 104.775
105 subjects were recruited for this study.
29
CLINICAL AND LABORATORY DATA COLLECTION
STUDY PROCEDURE:
ETHICAL CONSIDERATION:
Ethical approval was obtained from the Lagos University Teaching Hospital’s Ethics and
Research committee before commencing the study. (Appendix I)
INFORMED CONSENT
Parents/ caregivers of newborns with risk factors and or clinical features of sepsis admitted into
the neonatal ward were approached for their consent for their wards to be enrolled in the study.
The details of the study were explained to them in simple language and they were given
opportunity to ask questions. An informed consent was obtained after this. (Appendix 1I)
PATIENT HANDLING PROCEDURE
Patients were recruited from NNU, ward D1 and Children’s Emergency Centre. At recruitment,
the parents / caregivers were interviewed. Informed consent was obtained for each subject.
Relevant history which included socio-demographic data, weight, gestational age, ante natal,
pregnancy and delivery history was obtained. Gestational age was determined from the last
menstrual period (LMP), but if unknown, antenatal ultrasound reports or Ballards score was
utilized if baby presented within 72 hours of life.
Particular attention was paid to obtaining information on the risk factors for sepsis for each
newborn. A questionnaire and consent form was given to the parent of each subject after which
a physical examination was done. The questionnaires were filled by the parents with the research
30
assistant providing support to the illiterate and semi-literate parents. This included a general
examination for pallor, fever, jaundice, respiratory distress and lethargy and systemic
examination which included a central nervous system examination, respiratory and abdominal
examination was also done. The babies were weighed free of any clothing, using the My weigh®
(Ultrascale MBSC-55) weighing scale. The scale was adjusted to zero before each measurement.
The researcher was assisted by a trained medical officer. Three residents in the neonatal unit
were also trained on sample collection for blood culture and assisted the researcher in taking
some samples.
SAMPLE COLLECTION
On recruitment, blood samples were taken (following strict universal precaution protocol for
asepsis) from the subjects before the commencement of antibiotics. Samples were taken for
CRP, PCT and blood culture. Sample bottles for the research were labelled and made available in
all the neonatal wards.
On presentation, 1ml of blood was collected in an EDTA bottle for serum procalcitonin and
CRP. Samples were collected with the babies kept under a radiant warmer or in other areas
designated for sample collection. The samples were analysed immediately, but if collected after
work hours, was refrigerated at 2-8oC and analysed not later 48 hours after collection.
The BACTEC Peds Plus® (Becton Dickinson, New Jersey, USA) blood culture broth media
were used. In the subjects, a peripheral vein was located and the area was cleaned with
methylated spirit, then povidone iodine. To reduce the risk of contamination, closed blood
sample collection system (butterfly needle attached to the BACTEC® bottle) was used to collect

31
the sample (about 2 mls). At least 2mls of blood was collected to increase the likelihood of
recovering an organism, especially for fastidious organisms like Haemophilus species. The flip
off caps of the vials were removed and the septum swabbed with alcohol pads before introducing
the sample. The samples were transported immediately to the Department of Medical
Microbiology laboratory; overnight samples collected were kept outside the refrigerator and sent
to the laboratory within 10 hours of collection.
Samples for repeat CRP (1 ml each) were collected at 24 and 72 hours (total of 3 samples) after
the initial CRP.
LABORATORY ANALYSIS
For PCT and CRP, samples were analysed immediately, but for babies whose samples were
collected after 4pm, the samples were stored at 2-8oC temperature and analysed within 48 hours.
The CRP and PCT samples were analysed by the researcher, supervised by the medical
laboratory scientist with experience in hematology and use of point of care kits in the Paediatrics
department side laboratory.
CRP ASSAY
For CRP, the actim® CRP by Medix Biochemica ,Finland114 was used. It was visually interpreted
based on immunochromatography method for semi- quantitative determination of CRP in whole
blood samples. This kit detected elevated serum CRP levels of >10mg/l (1mg/dl) to >80mg/l
(8mg/dl).
Each CRP test pack comprised of:
One dipstick in a sealed aluminium pouch with a dessicant.

32
One tube of specimen dilution buffer (0.5ml). The buffer solution contains buffer salts,
bovine serum albumin and preservatives.
10ul end to end capillary tubes.
The 10ul capillary tubes were used to take blood from the EDTA bottles and dropped into the
specimen dilution buffer tube. Sample was mixed into the buffer by inverting the tube upside
down repeatedly until the sample has completely transferred into the buffer and there is no
visible whole blood in the capillary.
The aluminum foil with the dipstick was opened carefully without touching the yellow dip area
at the lower part of the dipstick. The dipstick was used shortly after its removal from the pouch.
Specimen, if stored in the refrigerator was allowed to reach room temperature before testing. The
yellow dip area (lower end of the dipstick) was placed into the diluted sample and held there
until the liquid front entered the result area. The dipstick was removed from the solution and was
placed in a horizontal position.
The result was available in 5 minutes and lines appearing later than 5 minutes were ignored. A
red line (control line) appeared which confirmed correct performance of the test. If the control
line did not appear, the test is considered invalid and is repeated with another dipstick.
The results of the CRP are read off as follows114:
Control line with NO blue line- CRP<10mg/l
Control line with one blue line- CRP >10-40mg/l
Control line with 2 blue lines- CRP >40-80mg/l

33
Control line with 3 blue lines- CRP >80mg/l.
For ease of analysis, the results were categorised as follows:
A- Negative
B- >10 -40mg/l
C- >40-80mg/l
D- >80mg/l.
Babies who had values within the range of 10mg/l to >80mg/l fell into groups B- D and were
considered CRP positive.

34
SCHEMATIC REPRESENTATION OF CRP ASSAY PROCEDURE
FIGURE 1A: SCHEMATIC REPRESENTATION OF CRP ASSAY PROCEDURE

35
FIGURE 1B: SCHEMATIC REPRESENTATION OF CRP ASSAY PROCEDURE.

36
PROCALCITONIN ASSAY
For Procalcitonin a rapid diagnostic kit (one step procalcitonin test by Artron Laboratories
Canada)115 was used. It is a rapid and convenient immune chromatographic assay for the semi
quantitative detection of procalcitonin in human serum or plasma. Monoclonal antibodies
specifically against PCT are conjugated with colloidal gold and deposited on the conjugate pad
and immobilized in the test zone of the cassette. When an adequate volume of the test sample is
added, the gold antibody conjugate is rehydrated and the PCT, if any in the sample will interact
with the colloidal gold conjugated antibodies. The antigen- antibody colloidal gold complex
migrates towards the test window until the test zone where they are captured by immobilized
antibodies, forming a visible pink test line indicating a positive result. The colour intensity of the
band is directly proportional to the PCT concentration in the sample and is interpreted with a
reference card. This cassette can be used for serum or plasma. For PCT, values >0.5ng/ml was
taken as positive.
After the sample for CRP was taken, the remaining sample in the EDTA was centrifuged for
about 5mins to separate the plasma.
The testing device was removed from the sealed pouch and placed on a level surface. A sample
dropper (included in the pouch) was used to add three full drops (120ul) of the specimen into the
sample well marked with an arrow on the cassette.
The result was read in 30minutes and the colour blocks were compared with the interpretation
card included. If there was no visible band in the control region, the test was repeated with a
new device. Results were reported as:
<0.5ng/ml No T band – Negative. Systemic infections are unlikely.116

37
>0.5-<2ng/ml Intensity of the T band is stronger than colour block 0.5ng/ml, but weaker than
that of colour block 2. – Moderate risk for progression to severe infection.116
>2 -<10 intensity of the T band is stronger than colour block 2 but weaker than colour block 10.
High risk for progression to severe systemic infection.116
>10ng/ml the intensity of the T band is stronger than colour block 10ng/ml. High likelihood of
severe sepsis or septic shock.116 (See interpretation card in appendix VII)

38
SCHEMATIC REPRESENTATION OF PROCALCITONIN ASSAY PROCEDURE

39
CRP and PCT levels were analyzed by the researcher in the Paediatrics department laboratory.(
see appendix IV) At intervals, samples were also analysed by the laboratory scientist with a
different test kit to ensure accuracy and quality control.
The Blood culture samples were analysed by the microbiologist assisted by the researcher. The
researcher was trained on blood culture processing by the consultant microbiologist for 4 weeks
prior to commencement of the study.
The BACTEC Peds Plus™ / F culture vials were used. The vials are enriched with soybean-
casein digest broth and carbon dioxide and are for aerobic cultures. They are principally used
with the BACTEC(R) fluorescent series instruments for the qualitative culture and recovery of
aerobic microorganisms. These bottles require 1-3 mls of blood only which makes it a good
choice for neonates.
After the blood samples were collected, they were taken to the microbiology laboratory and
incubated in the BACTEC 9050 machine for a maximum period of 5 days. The BACTEC 9050
machine is a controlled environment where the vials are maintained at 370C. It is able to incubate
50 vials at the same time, and each vial is identified by its unique barcode. It continuously
agitates the vials, leading to an earlier detection of positives. Each culture vial has a sensor which
detects increase in carbon dioxide produced by the growth of microorganisms as they metabolise
the substrates present in the vial. The sensor is monitored by the instrument every 10 minutes for
an increase in its fluorescence, which is proportional to the amount of carbon dioxide present. A
positive reading indicates the presumptive presence of microorganisms in the vial. Bottles will be
checked for microbial activity evidenced by flagging of the machine. (This identifies the bottle
growing an organism). This usually occurs within 48-72 hours.

40
Bottles with growth were sub cultured on blood agar, chocolate agar and MacConkey agar and
organisms were further identified by the Microbact 24E oxoid identification system (This is a
semi-automated identification system). MacConkey agar is a differential medium and is useful
for enteric pathogens e.g Klebsiella, E.coli Blood agar is useful for Streptococcus species while
chocolate agar is useful for fastidious organisms e.g Haemophilus influenza and Neiserria
species.
A direct gram stain was done alongside the subcultures in the plate. This helps to rapidly identify
any organisms and rule out a contamination.
Positive isolates had antimicrobial susceptibility testing using disc diffusion method to determine
the antibiotic sensitivity pattern.
SOCIOECONOMIC CLASS (SEC)
Socio-economic class classification was done using the method described by Oyedeji117. Scores
from 1 to 5 were given for each criteria assessed. The criteria were maternal educational
attainment, maternal occupation, paternal educational attainment and paternal occupation. The
score from the 4 criteria were added and an average found by dividing by 4. The result
approximated to the nearest whole number gave the socio-economic class 1 to 5. For analysis,
SEC 1 and 2 were lumped together as the upper socioeconomic class; SEC 3 was regarded as
middle class while SEC 4 and 5 were put together as lower class.
41
DATA MANAGEMENT
Data was initially entered into a Microsoft excel spreadsheet (2010 version) then analysis was
done using the Epi InfoTM 2008 version 3.4.1 software.
Quantitative variables were presented as mean ± standard deviation in a normal distribution.
However, if the distribution was skewed, median and interquartile range were used to present the
data. Qualitative variables were presented as frequency tables and charts.
Association between two categorical variables were assessed using chi square statistics or
Fisher’s exact test when expected values in any of the cells is less than 5, while the difference in
mean was assessed using student t test statistics in two groups and Analysis of variance
(ANOVA/ F test) in > 2 groups.
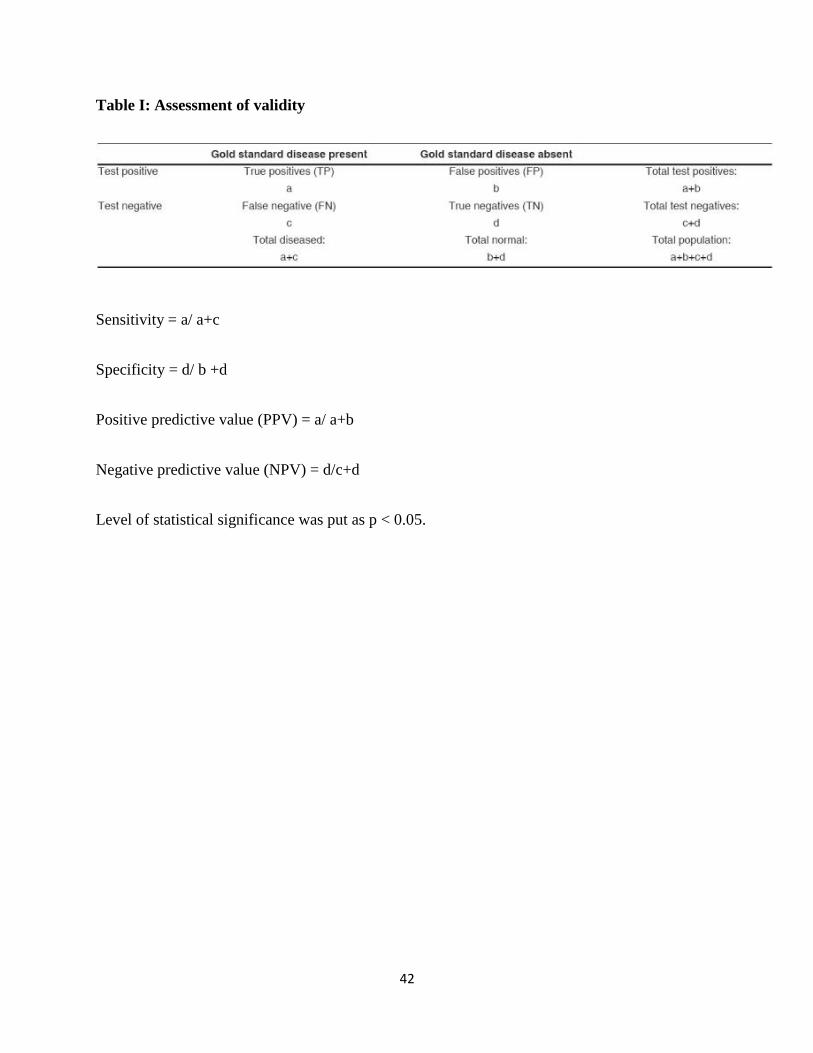
Assessment of validity was by calculating sensitivity, specificity, positive predictive value and
negative predictive value. Calculation of validity followed the 2x2 table shown in table 1.
42
Table I: Assessment of validity
Sensitivity = a/ a+c
Specificity = d/ b +d
Positive predictive value (PPV) = a/ a+b
Negative predictive value (NPV) = d/c+d
Level of statistical significance was put as p < 0.05.

43
RESULTS
DEMOGRAPHIC CHARACTERISTICS OF THE STUDY POPULATION
A total of 120 hospitalised neonates were screened for the study out of which 105 neonates were
recruited. They all had blood culture and procalcitonin tests assayed. All babies also had 3 CRP
tests except for the 9 mortalities who had at least 2 tests done. The study population consisted of
72 (68.6%) preterm and 33(31.4%) term neonates. 54 of the subjects were males (51.4%) while
51 (48.6%) were females with a male:female ratio of 1.1:1. The postnatal ages ranged from 1
hour to 624 hours with a mean age (SD) of 78.05(202.2) hours. The estimated gestational ages of
the babies ranged from 27 to 43 weeks with a mean (SD) of 33. 5(4.3) weeks. Majority of the
study participants were between 27-36 weeks (68.5%) while 1.9% were 43 weeks. (See Table II).
The weight of the subjects at the time of recruitment was between 500 grams and 4100 grams
with a mean weight (SD) of 1939 (842.6) grams. One third of the subjects (30.5%) were Low
birth weight (LBW) while 14.3% were extremely low birth weight (ELBW). (See table II)
Most of the study participants were recruited from the New Neonatal Unit (54.3%) which is for
inborn neonates. Sixty (57.1%) babies were delivered through caesarean section while 45
(42.9%) were spontaneous vaginal delivery.
Amongst the 11 babies with confirmed sepsis, 8(72.7%) were males and 8 (72.7%) of these
babies were outborn. (See table III)

44
Table 1I SOCIODEMOGRAPHIC CHARACTERISTICS OF STUDY POPULATION
Variable Number (%) of subjects
N=105(100%)
MEAN (SD)
SEX
Male
Female
54(51.43%)
51(58.57%)
M:F ratio= 1.1:1
GESTATIONAL AGE (WEEKS)
27-30
31-33
34-36
37-39
40-42
43
26(24.7%)
21(20%)
25(23.8%)
27(25.7%)
4 (3.8%)
2(1.9%)
33.5(4.3)
WEIGHT (GRAMS)
<1000g (ELBW)
>1000g - <1500g (VLBW)
>1500g -2499g ( LBW)
>2500-4000g (NBW)
15(14.3%)
28(26.7%)
32(30.5%)
30(28.6%)
1939.1g(842.6g)
ELBW-Extremely Low Birth Weight, VLBW- Very Low Birth Weight, LBW-Low Birth Weight, NBW- Normal
Birth Weight.

45
Table III: Descriptive table on the distribution of sepsis by sex and place of birth.
VARIABLE Definite
SEPSIS
N= 11
PROBABLE
SEPSIS
N= 48
No
SEPSIS
N= 46
SEX
Male
Female
8 (72.7%)
3 (27.3%)
26 (54.1%)
22 (45.8%)
20 (43.5%)
26(56.5%)
Place of birth
Inborn
LUTH
Outborn
PRIVATE HOSP
GENERAL HOSP
TBA
HOME DELIVERY
3 (27.3%)
6(54.5%)
1(9.0%)
1 (9%)
0(0%)
25 (52.0%)
17 (35.4%)
3 (6.3%)
1 (2.0%)
2 (4.2%)
27 (58.6%)
11 (23.9%)
5 (10.4%)
2 (4.3%)
1 (2.0%)
TBA-Traditional Birth Attendant. LUTH-Lagos University Teaching Hospital

46
RELATIONSHIP BETWEEN SOCIAL CLASS AND CULTURE PROVEN SEPSIS
Social classification was done according to Oyedeji’s117 classification. Forty two (40%) of the
mothers were in social class III (see table IV). It was also found that culture proven sepsis was
highest in the lower social class 5(45.4%).
Table IV: Relationship between socioeconomic classification and culture proven sepsis
Social class culture proven sepsis
N 105(%) N 11(%)
Upper 35 (33.3%) 2(18.1%)
Middle 42 (40.0%) 4(36.3%)
Lower 28 (26.7%) 5(45.4%)

47
RISK FACTORS AND CLINICAL FEATURES OF SEPSIS
Among the risk factors for sepsis, prematurity was the highest with 72 babies (68.6%), while
maternal UTI was the lowest in 8 babies (3.8%) (See Fig 3). Respiratory distress was present in
72.4% of babies. (See fig 4)
Fig 3: Risk factors for sepsis in the subjects

48
Fig 4: Clinical features of sepsis in the subjects.

49
VALUES OF MARKERS FOR SEPSIS
Values of C- reactive protein
On presentation, 61(58.1%) babies had a negative CRP while 44(41.9%) had positive CRP.
At 24 hours, 63(60%) babies had negative CRP while 41(39%) had positive CRP.
At 72 hours, 67(63.8%) of the babies were CRP negative which was a 3.8% increase from the
number at 24 hours. However, 9(8.6%) of the subjects had died. (See table V)
Table V: Serial C-reactive protein values during the course of the admission
CRP(mg/l) Negative 10-40 40-80 >80
Presentation 58.1 25.7 7.6 8.6
24hrs 60 12.4 15.2 11.4
72hrs 63.8 14.3 5.7 6.7
Values are in percentage(%)
- -
50
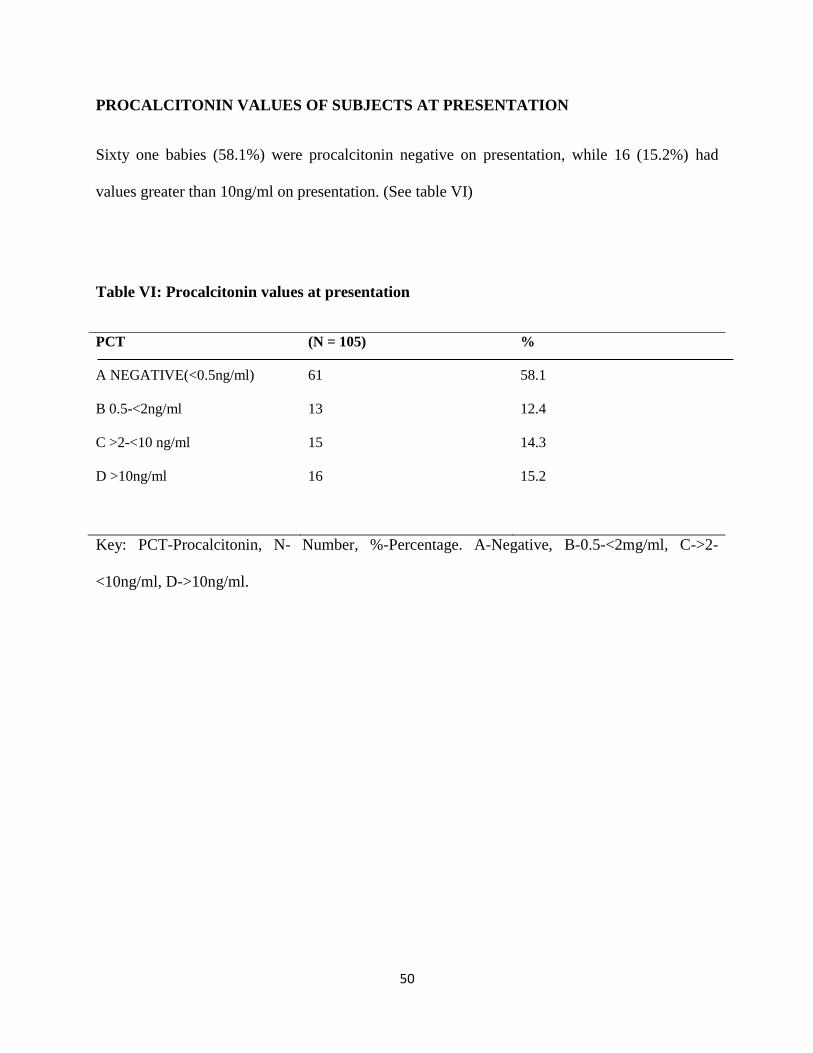
PROCALCITONIN VALUES OF SUBJECTS AT PRESENTATION
Sixty one babies (58.1%) were procalcitonin negative on presentation, while 16 (15.2%) had
values greater than 10ng/ml on presentation. (See table VI)
Table VI: Procalcitonin values at presentation
PCT (N = 105) %
A NEGATIVE(<0.5ng/ml) 61 58.1
B 0.5-<2ng/ml 13 12.4
C >2-<10 ng/ml 15 14.3
D >10ng/ml 16 15.2
Key: PCT-Procalcitonin, N- Number, %-Percentage. A-Negative, B-0.5-<2mg/ml, C->2-
<10ng/ml, D->10ng/ml.
51
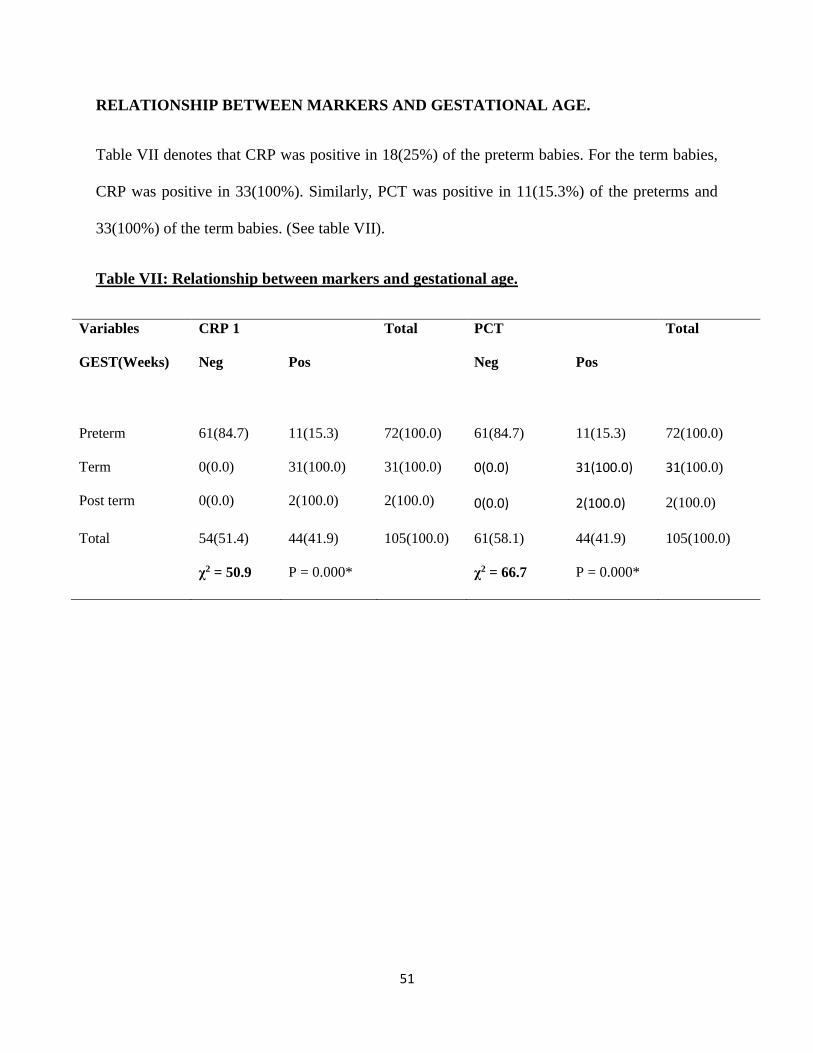
RELATIONSHIP BETWEEN MARKERS AND GESTATIONAL AGE.
Table VII denotes that CRP was positive in 18(25%) of the preterm babies. For the term babies,
CRP was positive in 33(100%). Similarly, PCT was positive in 11(15.3%) of the preterms and
33(100%) of the term babies. (See table VII).
Table VII: Relationship between markers and gestational age.
Variables CRP 1 Total PCT Total
GEST(Weeks) Neg Pos Neg Pos
Preterm 61(84.7) 11(15.3) 72(100.0) 61(84.7) 11(15.3) 72(100.0)
Term
Post term
0(0.0)
0(0.0)
31(100.0)
2(100.0)
31(100.0)
2(100.0)
0(0.0)
0(0.0)
31(100.0)
2(100.0)
31(100.0)
2(100.0)
Total 54(51.4) 44(41.9) 105(100.0) 61(58.1) 44(41.9) 105(100.0)
χ2 = 50.9 P = 0.000* χ2 = 66.7 P = 0.000*

52
RELATIONSHIP BETWEEN MARKERSAND ONSET TIME OF SEPSIS
The positivity rates were higher in late onset sepsis than early onset sepsis for both CRP and
PCT. (See table VIII)
Table VIII: Relationship between markers and onset time of sepsis
CRP PCT
SEPSIS ONSET Negative Positive Total Negative Positive Total
Early 50(63.3) 29(36.7) 79(100.0) 58(73.4) 21(26.6) 79(100.0)
Late 4(15.4) 22(84.6) 26(100.0) 3(11.5) 23(88.5) 26(100.0)
Total 54(51.4) 51(48.6) 105(100.0) 61(58.1) 44(41.9) 105(100.0)
χ2 = 17.9 P = 0.000* χ2 = 30.8 P = 0.000*
Key: CRP- C-reactive protein, PCT-Procalcitonin. *- Statistically significant

53
BLOOD CULTURE RESULTS AND MICROBIOLOGICAL PROFILE OF SUBJECTS
Blood culture results are as shown in figure 6. Eleven (10.5%) samples had positive growth on
blood culture while 89.5% of the neonates had a negative growth on blood culture.
Acinetobacter Baumanii, Eschericia coli, Klebsiella, Streptococci and Methycillin resistant
staphylococcus aureus (MRSA) were isolated from two neonatal samples each while Coagulase
negative Staphylococcus(CONS) was isolated from one sample.
Table IX: BLOOD CULTURE RESULTS
BLD CULTURE ORGANISM N = 105 % = 100.0
A.BAUMANII 2 1.9
CONS 1 1.0
E.COLI 2 1.9
KLEBSIELLA 2 1.9
STREPTOCOCCI 2 1.9
MRSA 2 1.9
NEGATIVE 94 89.5

54
Relationship between CRP, PCT and positive blood cultures.
CRP was positive in 11(100.0%) neonates with positive cultures, and in 40 (42.6%) neonates
with negative cultures. (See table X). PCT was positive in 11(100.0%) neonates with positive
growth on blood culture, and also positive in 33(35.1%) neonates with a negative blood culture.

55
Table X: Relationship between serial CRP, PCT and blood culture of subjects
Blood Culture
Test Positive Negative χ2 P value
CRP 1
Positive 11(100.0) 33(35.1) 17.0 <0.001
Negative 0(0.0) 61(64.9)
Total 11(100.0) 94(100.0)
CRP2
Positive 9(81.8) 32(34.4) 9.3 0.003*
Negative 2(18.2) 61(65.6)
Total 11(100.0) 93(100.0)
CRP3
Positive 7(70.0) 21(24.7) 8.8 0.006*
Negative 3(30.0) 64(75.3)
Total 10(10.5) 85(89.5)
PCT
Positive 11(100.0) 33(35.1) 17.0 <0.001
Negative 0(0.0) 61(64.9)
Total 11(100.0) 94(100.0)
CRP- C-Reactive protein. CRP1- on admission. CRP2- 24hours of admission CRP 3- at 72hours.
PCT-Procalcitonin on admission.* Statistically significant
56
The sensitivity of CRP 1 was 100%, Specificity was 65%, Positive and negative predictive
values were 25% and 100% respectively. (See table XI).
The sensitivity, specificity, positive and negative predictive values of PCT were 100%, 65%,
22% and 100% respectively. (See table XI)
Based on the results of the CRP, PCT and blood culture, babies could be said to fall into 3
groups as stated earlier based on the classification used by White et al.111 Eleven (10.5%)
neonates were found to have definite sepsis, 48(45.7%) had probable sepsis while 46(43.8%) had
no sepsis.

57
Table XI: Assessment of validity of the markers.
Sensitivity Specificity PPV NPV
CRP1 100% 65% 25% 100%
CRP2 82% 66% 22% 97%
CRP3 70% 75% 22% 96%
PCT 100% 65% 25% 100%
Key: CRP- C reactive protein. PCT- Procalcitonin, PPV- Positive Predictive Value, NPV-
Negative Predictive Value.

58
Relationship of CRP and PCT to outcome of study participants
Of the 105 subjects, 1(1.0%) discharged against medical advice (DAMA) due to financial
constraints. 15(14.3%) babies died during the admission out of which 10 babies died within 72
hours of admission. Of the 15 mortalities, 2(13.3%) had CRP >80mg/l at presentation. Also
amongst the mortalities were 9 (60%) babies who had PCT >10ng/ml on presentation (See table
X)

59
Table XI : Relationship between CRP and PCT with outcome of care
VARIABLE NUMBER(%AFFECTED
CRP 1 DAMA DEAD ALIVE P-VALUE
A. 0(0.0) 5(33.3) 56(62.9) χ2 = 14.0 0.1222
B. 1(100.0) 4(26.7) 22(24.7)
C. 0(0.0) 4(26.7) 4(4.5)
D. 0(0.0) 2(13.3) 7(7.9)
Total 1(100.0) 15(100) 89(100.0)
CRP 2
A. 0(0.0) 1(6.7) 62(69.7) χ2 = 35.3 0.0001
B. 0(0.0) 2(13.3) 11(12.4)
C. 0(0.0) 7(46.7) 9(10.1)
D. 1(7.7) 5(33.3) 7(7.9)
Total 1(100.0) 15(100.0) 89(100.0)
CRP 3
A. 0(0.0) 1(14.2) 66(74.1) X2 = 48.5 0.0000
B. 0(0.0) 0(0.0) 15(16.9)
C. 0(0.0) 1(14.2) 5(5.6)
D. 0(0.0) 5(71.4) 2(2.2)
Total 0(0.0) 7(100.0) 89(100.0)
PCT
A. 0(0.0) 1(6.7) 60(67.4) X2 = 41.8 0.0000
B. 0(0.0) 1(6.7) 12(13.5)
C. 1(100.0) 4(26.7) 10(11.2)
D. 0(0.0) 9(60.0) 7(7.86)
Total 1(100.0) 15(100.0) 89(100)
Key: CRP 1-C reactive protein on presentation, CRP 2- at 24hours, CRP 3- at 72 hours.
CRP A- Negative, B-10-40mg/l, C- 40-80mg/l, D- >80mg/l.
PCT- PROCALCITONIN PCT- A- Negative, B-0.5-<2mg/ml, C>2-<10ng/ml, D>10ng/ml.

60
DISCUSSION
This study aimed to compare the efficacy of serial CRP and PCT as screening markers of
neonatal bacterial sepsis.
CRP and PCT were compared with blood culture which is widely reported as the gold standard
in the diagnosis of NNS. In the present study, the incidence of culture proven sepsis was low
(10.5%). This is similar to the findings of Iroha et al43 also at LUTH. The reason for this low
yield may be because 93% of the subjects in this study were born in a hospital environment with
better hygiene practices than the non- hospital environment. However, Boma West et al71 in
2012 in Port- Harcourt Nigeria had an incidence of 41.6% which may have been because of a
much larger neonatal sample size in addition to a high number of outborn subjects. Naher et al118
in Dhaka, Bangladesh reported a low incidence of 6% which they attributed to sample collection
after commencing antibiotics and faulty sample collection procedure. It has been generally
reported that the yield of blood culture is generally poor, and serial blood culture sampling
which can be used to improve yield is not practicable in the newborn due to low blood volumes
and difficulty in collecting adequate samples.119
In this study, CRP correctly identified 100% of the babies with culture proven infection and
42.6% of babies with probable infection. This is higher than the results of West et al30 in Port
Harcourt, Nigeria who found that CRP correctly identified 74% babies with culture proven
(definite) infection. This difference may be because the kits used in this study were semi-
quantitative and may be more sensitive than the qualitative assay used by West et al30. West et
al30 opined that that this finding would mean that one out of every four neonates with sepsis will
be missed which is unacceptably high considering the devastating effects of untreated neonatal

61
sepsis. This finding by West et al30 is one of the reasons why serial CRP sampling is preferred.
Ibeh et al22 in Benin found CRP levels in proven and probable sepsis to be as high as 130.1mg/l
and 96.7mg/l respectively. Sucilathangam et al93 in India also found high levels of CRP in
proven and probable sepsis. Similarly, Benitz et al19 found that proven or probable sepsis was
strongly correlated with elevated CRP levels.
PCT levels in this study were also found to be elevated in neonates with definite infection and
probable infection. This finding is similar to findings from studies done by Arowosegbe et al103
and Ibeh et al22 in Nigeria. Sucilathangam et al93 also found that PCT levels were remarkably
high in neonates with definite and suspected sepsis. In their study, in some cases of culture
positive sepsis, other sepsis screening tests (e.g White cell count) were negative but PCT was
elevated. Furthermore, this present study found that 45.7% of the subjects had probable sepsis
and their CRP and /or PCT were elevated, alongside risk factors and clinical features of sepsis,
however they had negative blood cultures. Arowosegbe et al also described a similar pattern
whereby 21.2% of babies with clinical features and positive PCT had negative blood cultures.
Other than sepsis, this pattern may also be seen in babies with clinical findings like respiratory
distress and intracranial haemorrhage which can also trigger off the inflammatory response.
These findings re –emphasize previous postulations that blood culture can remain negative
despite bacterial sepsis.27,107,118
CRP was found to be significantly positive in the term and post term babies, compared to the
preterm babies. The explanation for this may be the same as adduced by Hofer et al32 who also
reported lower CRP response to infection in preterms and suggested that reasons for this may
include the use of more frequent prophylactic antibiotics in the mothers of the preterm babies
and timing of blood sampling which is usually earlier in the preterm newborns.32 They also

62
stated that CRP is thought to play a role in innate immunity, as an early defense system against
infections and as far as the endogenous immune response depends on the gestational age, CRP
responses may be lower due to the preterms less mature immunological system.32
Similarly, Kawamura et al120 also reported a lower sensitivity of CRP in preterms compared to
term newborns.
For PCT, 100% of the term babies had positive PCT compared to 15.3% of the preterms. This
finding may be due to the fact that PCT is thought to rise slower in the preterm, possibly because
of their immature immune system. Liu et al in China studied physiological changes in
procalcitonin concentration in neonates and found that serum PCT of premature infants will
remain at relatively low levels within 36 hours after birth while term babies peak within 24
hours.121
Nevertheless, Arowosegbe et al103 in Nigeria found that PCT seemed equally accurate for the
diagnosis of neonatal sepsis in both preterm and term neonates. This is similar to the findings of
Savagner et al10 and Kocabas et al27 in Turkey. The conclusion from this study is that there is a
significant difference in the reaction of procalcitonin in term and pre term babies.
The relationship between CRP, PCT and onset time of sepsis denotes that CRP was found to be
significantly positive in 84.6% of newborns with late onset sepsis (LOS). This may be because
the babies have started building up some innate immunity which is important in CRP response.
In Ife, Nigeria Ako- Nai et al26 found no difference in the rate of CRP elevation in early and late
onset sepsis. However, they studied only 30 subjects and so their findings may not be very
representative of the general populace. Naglaa et al104 using categorization of EOS to be < 7
days and term babies only found CRP to be significantly higher in early onset sepsis. The
63
importance of stating their criteria for onset time of sepsis is that after 72 hours, other researchers
would have classified the babies as having late onset sepsis. Benitz et al19 however found CRP to
be more sensitive in late onset sepsis (<72 hours) and suggested that this may be because their
infections had been present for a longer time.
PCT in this study was also significantly more sensitive in late onset sepsis. PCT was positive in
26.6% of early onset sepsis and 88.5% of late onset sepsis. The reason for this is not immediately
known. However, Arowosegbe et al103 in their study found no difference in PCT performance in
early and late onset sepsis. In contrast, Naglaa et al104 found PCT to be more sensitive in early
onset sepsis, but as has been stated above , their definition of early onset sepsis differs from the
generally accepted 72 hours, and some of the babies may actually have late onset sepsis.36 The
conclusion from this study however, is that procalcitonin is more sensitive in late onset sepsis.
The relationship of social class with sepsis has also been well documented. In our study, 73.3%
of the neonates were in the upper and middle class while 26.7% were from the lower social class.
This may be attributed to the fact that in Lagos state, free healthcare for children under age 5 is
provided in state owned facilities so more people of lower socioeconomic status will likely
patronize those centres more than a fee paying centre like LUTH. However, amongst the
neonates with culture proven sepsis, 45.4% were from the low socio economic status. Other
workers in Nigeria found a significant relationship between culture proven sepsis and social
class.39,122 This is in consonance with the results of Javed et al123 in Pakistan who also found that
mothers belonging to lower social income groups and significantly, mothers with primary
education had more neonates with sepsis than mothers with secondary education. This
association of social class with proven sepsis may be because mothers of lower social income

64
groups are more likely to deliver in unsterile environments, and have poorer health seeking
behaviours than those of the upper class.
In terms of place of delivery and the incidence of culture proven sepsis, a high proportion of the
outborn babies (72.5%) had confirmed sepsis. Adejuyigbe et al103 documented a similar finding
with 72.7% of the subjects with culture proven sepsis being outborn. Mukuolu et al in their study
in Ilorin and West et al56 in Port Harcourt had similar findings. This pattern is not surprising as
most deliveries outside government owned hospitals, or well-equipped private hospitals are
usually done in very unsterile environments.
The overall sensitivity of CRP in this present study was found to be 100%, and NPV was 100%.
However, West et al30 in Port Harcourt, Nigeria got sensitivity of 74% in their study. The
difference in results may be due to the methods of assay used. In our study, a semi quantitative
assay method was used which may have a higher sensitivity than the qualitative assay used by
West et al. However, Nuntnarumit85 in Bangkok, using a quantitative assay got an overall
sensitivity, specificity, PPV and NPV of 100%,94%, 91.6% and 100% respectively. These values
were similar to the results of the present study.
C reactive protein levels are elevated in only 35% to 65% of neonates at the onset of the
illness.19 Recognising that there is a delay of at least several hours due to the cascade of events
which leads to the elevation of CRP (activation of neutrophils, production of interleukin-6 and
induction of hepatic synthesis of CRP) led to an initial criticism of this test as having insufficient
sensitivity to guide therapy.19 However, with further research, Phillip et al124 noted that CRP
levels are consistently elevated 24 to 48 hours after the onset of infection and suggested that
serial normal levels may indicative of absent bacterial infection.124 In this study the sensitivity of

65
CRP 1 was higher than CRP 2 and 3. This is in contrast to the findings of Benitz et al19 who
demonstrated increasing sensitivity (35%,78.9% and 88.9%) over 3 days in both preterm and
term babies. This pattern was also found by other researchers.31,85,120 The reason for this
difference in pattern may be that with response to antibiotic therapy, CRP levels which were
initially elevated will start returning to normal range. Hindocha et al125 in their study also
observed this. However, the negative predictive values (NPV) were 67%, 88% and 83%
respectively which is similar to the pattern observed by other researchers.19 Similar results were
also obtained by Lee et al21. Khashabi et al102 in Iran studied 110 patients out of which 91 had
negative CRP and blood culture. The overall NPV of serial CRP was used as a guide to
discontinue antibiotic treatment. They reported that only one patient of this cohort was re-
admitted after 21 days of discharge with symptoms unrelated to the initial admission. Mathai et
al 126 in India concluded that serial testing of CRP may not be of much use in diagnosis but may
help in identifying uninfected babies. Based on the findings from this study, it may also be
concluded that serial negative testing of CRP will be more useful in identifying uninfected
babies.
In this study, at a cut off value of 0.5ng/ml, the sensitivity and NPV of PCT were both 100%. In
their studies, Arowosegbe et al103 in Abeokuta and Ibeh et al22 in Benin, Nigeria also got high
values in these validity tests. Arowosegbe used a semi quantitative point of care test, similar to
what was used in this study while Ibeh et al used the quantitative Kryptor® immunoassay random
assess analyser. The PPV and NPV from Arowosegbe et al were 84% and 83%, while Ibeh et al
reported 91.6% and 80%. The moderate difference between both methods of assay further
buttresses the fact that in centres with minimal resources who cannot afford quantitative
analysers, point of care kits could be used. Similarly, Suciathangam et al93 in India using a

66
quantitative immune- luminometry method got 92.8%,75%,59% and 96% for sensitivity,
specificity, NPV and PPV respectively. They studied a similar cohort of subjects with this study
and concluded that PCT done on the day of admission can help in early diagnosis of neonatal
sepsis.93 Furthermore, Kocabas et al27 in Turkey using a quantitative assay got sensitivity and
NPV of PCT to be 100% . \
The results from the present study showed that 93.3% of the 15 mortalities showed progressively
rising CRP values (See table XI). Among the mortalities in this study, CRP levels progressively
rose to >80mg/l over 72 hours getting to such high levels in 71.4% of the mortalities at 72hours.
This is similar to Lai et al127 in their study at Taiwan who found that high CRP levels were
significantly associated with more severe clinical symptoms and worse outcomes. They also
found that more mortalities (13.6%) occurred in the groups with CRP >100mg/l compared to
4.9% in the low CRP group.127 Oberhoffer et al128 also postulated that high levels of CRP on
admission may predispose to a fatal outcome in patients with sepsis.
Similarly, PCT values in neonatal sepsis may be a good predictor of mortality. This study shows
that 93% of the mortalities had PCT levels of >2mg/ml to >10 ng/ml. Of this number, 60% had
PCT levels of >10ng/ml which is indicative of a high likelihood of severe sepsis or septic shock.
This is in agreement with Arowosegbe et al103 in Abeokuta, Nigeria as 96.3% of the mortalities
in their study had elevated PCT. Adib et al109 and Suciathangam et al93 also found that PCT
correlated well with the progression and severity of infection and is useful for prognostication.
The results from this study have shown that PCT on the day of presentation has a high
sensitivity and NPV and is useful in early diagnosis of neonatal sepsis and prognostication.

67
Similarly, CRP which also has equal sensitivity with PCT and a good NPV can also be used in
making early diagnosis of neonatal sepsis.

68
CONCLUSION
1. The levels of CRP and PCT rise in the presence of neonatal bacterial sepsis.
2. Both CRP and PCT perform better as markers in the term babies and in late onset sepsis.
3. Serial negative CRP in a neonate may confidently rule out the possibility of a septicaemic
illness.
4. PCT has a high sensitivity and NPV for sepsis if done within 24hours.

69
RECOMMENDATIONS
The present recommendations are made based on the results and conclusions from the present
study:
1. CRP and PCT should be routinely used in our newborn nurseries as an adjunct to blood
culture for the screening of newborns with risk factors and / or clinical features of sepsis.
2. Serial CRP measurements done over 72 hours in conjunction with clinical and other
laboratory parameters can be used to facilitate early decision on discharge for babies with
suspected sepsis.

70
LIMITATION
1. A quantitative assay using nephelometry method would have been a more objective
assessor of the values of CRP and PCT. However, the cost of doing this was out of the
researchers reach.

71
AREAS FOR FUTURE RESEARCH
1. A multi-center study on these markers should be carried out. This will help to obtain a
larger sample size which would be more reflective of the general population, and
subsequently nationally accepted protocols for the management of this group of newborns
can be formulated.
2. Research comparing the use of point of care kits in comparison with quantitative methods
of assay can be conducted.
3. A research can also be conducted on using serial CRP testing to discontinue antibiotic
therapy in the newborn unit. It would be interesting to find out how it impacts on cost of
care, service delivery and patient satisfaction.
72
REFERENCES
1. Dellinger PR, Levy M, Rhodes A, Annane D, Gerlach H, Opal S et al. Surviving sepsis
campaign:International guidelines for the management of severe sepsis and septic shock.
Crit Care Med 2013;41(2):580-637.
2. Goldstein B, Giror B, Randolph A. International pediatric sepsis consensus conference:
definitions for sepsis and organ dysfunction in Pediatrics. Pediat Crit Care 2005;6:2-8.
3. Osrin D, Vergano S, Costello A. Serious bacterial infections in newborn infants in
developing countries. Curr Opin Infect Dis 2004;17:217-24.
4. World Health Organisation. Neonatal and perinatal mortality. Country, regional and global
estimates. 2006;2-5.
5. World Health Organization. Perinatal mortality: a listing of available information. Geneva
1996;1-10.
6. Dawodu AH, Alausa OK. Neonatal Septicemia in the Tropics. Afri J Med Sci 1980; 2:1-6.
7. Antia-Obong OE, Utsalo SJ, Udo JJ, Udo KT. Neonatal Septicemia in Calabar, Nigeria.
Central Afr J Med 1992;36:161-5.
8. Omokhodion S, Adeyemo A, Akindele J. Neonatal sepsis in Ibadan: Implications for
neonatal care in developing countries. Early Child Development and Care 1993;91(1):77-85.
9. Barruti- Gaffuri Z, Pacarazi H, Zhubi B, Begolli L, Topciu V . The importance of
determining procalcitonin and C- reactive protein in different stages of sepsis. Bosn J Basic
Med Sciences 2010; 10:60-4.
10. Savagner C, Leboucher B, Gascoin- Lachambre G, Gras-Leguen C. Relevance of
procalcitonin for the diagnosis of early and late onset sepsis in newborns. In: Azevedo

73
L,editor. Sepsis -an ongoing and significant challenge. Croatia:Intech publishers; 2012.249-
58.
11. Panero A, Paificco L, Rossi N, Mancuso G, Stegagno M, Chiesa C. Interleukin 6 in
neonates with early and late onset infections. Paediatr Infect Dis J 1997;16:370-75.
12. Santosh K, Dipanwita R, Ranjana B, Debdutta C, Swapan K. Neonatal sepsis: Role of a
battery of immunohematological tests in early diagnosis. Int J App Basic Med Res
2012;2:43-7.
13. Bomela H, Ballot D, Cory B, Cooper P. Use of C- reactive protein to guide duration of
empiric antibiotic therapy in suspected early neonatal sepsis. Pediatr Infect Dis J
2000;19:531-5.
14. Mustafa S, Farooqui S, Waheed S, Mahmook K. Evaluation of C- reactive protein as early
indicator of blood culture positivity in neonates. Pak J Med Sci 2005:69-73.
15. Chandna A, Rao M, Srinivas M, Shayamala S. Rapid diagnostic tests in neonatal septicemia.
Indian J Pediatr 1988;55(6):947-53.
16. Escobar G. What have we learned from observational studies in neonatal sepsis? Pediatr
Crit Care Med 2005;6:138-45.
17. Resch B, Hofer N, Muller W. Challenges in the diagnosis of sepsis in the neonate. In:
Azevedo L,editor. Sepsis - an ongoing and significant challenge. Croatia. Intech publishers;
2012:233-47.
18. Centers for Disease Control and Prevention. Prevention of perinatal Group B streptococcal
disease: a public health perspecive. MMWR 1996;45:1-24.
19. Benitz E, Han M, Madan A, Ramachandra P. Serial Serum C- reactive proteinin the
diagnosis of neonatal infection. Pediatrics 1998;102:41-51.

74
20. Saiman L, Ludington E, Dawson JD, Patterson JE,Rangel- Frausto S, Wiblin RT et al. Risk
factors for Candida species colonization of neonatal intensive care unit patients. Pediatr
Infect Dis J 2001;20(12):1119-24.
21. Lee W, Chan M, Young B. Reducing hospitalization and antibiotic use in suspected early
neonatal sepsis through serial measurements of C- reactive proteins. HK J Pediatr (new
series) 2005;10:3-9.
22. Ibeh N, Osifo J, Iyere I, Ibeh G, Olowe A. Serum procalcitonin, early detection of neonatal
bacteremia and septicemia in a tertiary healthcare facility. North Am J Med Sci 2011;3:157-
60.
23. Stocker M, Fontana M, El Helou S,Wegscheider K, Berger TM. Use of Procalcitonin-
guided decision making to shorten antibiotic therapy in suspected neonatal early onset
sepsis: prospective randomised control trial. Neonatology. 2010;97(2):165-74.
24. Boo N, Nor A, Rohana J. Usefulness of semi-quantitative procalcitonin test kit for early
diagnosis of neonatal sepsis. Singapore Med J 2008;49(3):204-7.
25. Smith K, Bigham M. Biomarkers in pediatric sepsis. The Open Inflammation Journal
2011;4:24-30.
26. Ako- Nai A, Lawal O, Adejuyigbe E, Kassim O, Onipede A. The determination of C-
reactive protein and tumor necrosis factor alpha in sera of neonates with sepsis. Int. J Trop
Med 2011;6(2):30-4.
27. Kocabas E, Sankcioglu A, Aksaray N, Seydaoglu G, Seyhun Y, Yaman A. Role of
Procalcitonin, C- reactive protein, interleukin 6,interleukin 8 and tumor necrosiis factor
alpha in the diagnosis of neonatal sepsis. Turk J Pediatr 2007;49(1):7-20.

75
28. Mojgan M, Seyyed H, Mehrdad H, Farnaz S, Amin N, Mohammad F. Evaluation of
Fibronectin and C- reactive protein levels in patients with sepsis: A case-control study. Acta
Med Iranica 2012;50:404-10.
29. Boskabadi H, Maamouri G, Afshari T, Ghayour- Mobarhan M, Shakeri M. Serum
interleukin as a diagnostic marker in neonatal sepsis. Iran J Ped 2010;20:41-7.
30. West B, Peterside O, Ugwu R, Eneh A. Prospective evaluation of the usefulness of C-
reactive protein in the diagnosis of neonatal sepsis in sub Saharan African region.
Antimicrob Resist Infect Control 2012;1:22-26.
31. Ayazi P, Daneshi M, Hashemi H. The role of serial serum C- reactive protein in the
diagnosis of neonatal infection. Iran J Ped 2007;1:47-51.
32. Hofer N, Zacharias E, Muller W, Resch B. An update on the use of C- Reactive Protein in
early onset neonatal sepsis :Current insights and new tasks. Neonatology 2012:102(1)25-36.
33. Federal Ministry of Health . Saving Newborns lives in Nigeria: Newborn health in the
context of the integrated maternal, newborn and child health strategy. 2nd edition. 2011:24-
32.
34. Stoll B, Hansen N, Sanchez P, Faix R, Poindexter B, Krisa P et al. Early onset neonatal
sepsis: The burden of group B Streptococcal and E.coli disease continues. Pediatrics
2011;127(5):817-26.
35. Sankar M, Agarwal R, Deorari A, Paul V. Sepsis in the newborn. Indian J Pediatr
2008;75:261-66.
36. Stoll BJ. Infections of the newborn infant.In: Kliegman R, Behrman RE, Jenson HB,
Stanton BF editors. Nelson textbook of pediatrics.19th edition. Philadelphia: Saunders
Elsevier: 2011.p. 623-628.

76
37. Polin R. Management of neonates with suspected or proven early onset bacterial sepsis.
Pediatrics 2012;129:1006-115.
38. Omene J. Neonatal septicemia in Benin city, Nigeria. a review of 74 cases. Trop Geogr Med
1979;31:35-9.
39. Adejuyigbe E, Adeodu O, Ako- Nai A, Taiwo O, Owa J. Septicemia in high risk neonates at
a hospital in Ile-Ife, Nigeria. East Afr Med J 2001;78:540-3.
40. West B, Peterside O. Sensitivity pattern among bacterial isolates in neonatal septicaemia in
Port Harcourt. Ann Clin Microbiol Antimicrob 2012;11:7.
41. Bode-Thomas F, Ikeh E, Ejeliogu E. Current aetiology of neonatal sepsis in Jos University
Teaching Hospital. Niger J Med 2004;13:130-5.
42. Njokanma C, Olanrewaju D, Akesode F. Antibiotic resistance among bacterial isolates in
neonatal septicaemia. Niger J Paediatr 1994;21:47-51.
43. Iroha E, Egri-Okwaji M, Kesah C, Odugbemi T. Changing patterns of causative organisms
of neonatal septicemia at the Lagos University Teaching Hospital. Niger J Pediatr
1998;25:1-5.
44. Adejuyigbe E, Adeodu O, Ako-Nai A, Taiwo O, Owa J. Septicaemia in high risk neonates
at a teaching hospital in Ile-Ife, Nigeria. East Afr Med J 2001:78: 540-3
45. Vergano S, Menson E, Kennea N, Embleton N, Russel AB, Watts T et al. Neonatal
infections in England: the NeonIN surveillance network. Arch Dis Child Fetal Neonatal Ed
2011 Jan;96(1):F9-F14.
46. Weston EJ, Pondo T, Lewis MM,Martell-Cleary P, Morin C,Jewell B et al. The burden of
invasive early- onset neonatal sepsis in the United States, 2005-2008. Pediatr Infect Dis J
2011;30(11):937-41.

77
47. Dawodu A, Al-Umram K, Twum-danso K. A case control study of neonatal sepsis:
experience from Saudi Arabia. J Trop Pediatr 1997;43:84-8.
48. Mwaniki MK, Atieno M, Lawn JE, Newton CR. Long term neurodevelopmental outcomes
after intrauterine and neonatal insults: a systematic review. Lancet 2012;379:445-52.
49. Klein JO, Nizet V. Bacterial sepsis and meningitis.In: Infectious diseases of the fetus and
newborn infant, 7th ed, Remington JS, Klein JO, Wilson CB,et al (Eds), Elsevier Saunders,
Philadelphia 2011.p.222.
50. Hotchkiss RS. The pathophysiology and treatment of sepsis. N Engl J Med 2003;348:138-
50.
51. Jones AE, Fiechtl JF, Brown MD,Ballew JJ, Kline JA . Procalcitonin test in the diagnosis of
bacteremia: a meta analysis. Ann Emerg Med 2007 Jul;50(1):34-41.
52. Ali AM, Elkhatib WF, Abdelaziz SS. Procalcitonin versus C- Reactive Protein in neonatal
sepsis. J Immunol Infect Dis 2014:1: 103
53. Ahmed I, Fadahunsi H, Ogunbi O. Bacterial spectrum in sepsis at the neonatal unit, Lagos
University Teaching Hospital. Nig J Med 1974;4:22-4.
54. Awoniyi D, Udo S, Oguntibeju O. An epidemiological survey of neonatal sepsis in a
hospital in Western Nigeria. Afr J Microbiol Res. 2009;3(6):385-9.
55. Mokuolu A, Jiya N, Adesiyun O. Neonatal septicaemia in Ilorin; bacterial pathogens and
antibiotic sensitivity pattern. Afri J Med Sci 2002;31:127-30.
56. West BA, Tabansi PN. The prevalence of Neonatal sepsis in the University of Port Harcourt
Teaching Hospital,Nigeria. Niger J Pead 2014;41(1):33-37.

78
57. Yusuf M, Abdul- Hamid T. Isolation and identification of bacteria associated with neonatal
septicaemia at the specialist hospital, Bauchi.Journal of pharmacy and biological sciences
2012;2(6):47-50.
58. Muller-Pebody B, Johnson A, Heath P, Gilbert R, Henderson K, Sharland M. Empirical
treatment of neonatal sepsis: are the current guidelines adequate? Arch Dis Child Fetal
Neonatal Ed. 2011 Jan;96(1):F4- 8.
59. Dawodu A, Danmole I, Onile B. Epidemiology of group B streptococcal carriage among
pregnant women and their neonates: an African experience. Trop Geogr Med 1983;35:145-
50.
60. Suara R, Adegbola R, Mulholland. Seroprevalence of antibodies to Group B Streptococcal
polysaccharides in Gambian mothers and their newborns. J Natl Med Assoc 1998;90:109-
14.
61. Gerdes J. Clinicopathologic approach to the diagnosis of neonatal sepsis. Clin perinatol
1991;18:361-81.
62. Ottolini M, Lundgreen K, Mirkinson L, Cason S. Utility of Complete blood count and blood
culture screening to diagnose neonatal sepsis in the asymptomatic at risk newborn. Pediatr
Infect Dis J 2003;22:430-4.
63. Squire E, Favara B, Todd J. Diagnosis of neonatal bacterial infection: hematologic and
pathologic findings in fatal and non fatal cases. Paediatrics 1979 Jul;64(1):60-4.
64. Gerdes J. Diagnosis and management of bacterial infection in the neonate. Pediatr Clin
North Am 2004;51:939-59.b
65. .BACTECTM PEDS PLUS/F Culture (package insert). Sparks,USA: Becton, Dickinson and
Company,2012.

79
66. Bagyalakshmi R TK, Malathi J, Mahalaksmi B, Prasanna S, Madhavan H. Comparative
evaluation of BACTEC culture using Peds plus F broth with standard microbiological
methods in detection of microbial aetiologies in vitreous aspirates in infectious
endophthalmitis. Internet journal of ophthalmology and visual science 2009;8:1
67. Cetin E, Kaya, S. Demirci, M Aridogan, BC. Comparison of the BACTEC blood culture
system versus conventional methods for culture of normally sterile body fluids. Adv Ther
2007;24:1271-7.
68. Rozycki H, Stahl G, Baumgart S. Impaired sensitivity of a single early leucocyte count in
screening for neonatal sepsis. Pediatr Infect Dis J 1987;6:440-2.
69. Manroe B, Weinberg A, Rosenfeld C, Browne R. The neonatal blood count in health and
disease. Reference values for neutrophillic cells. . J Paediatr 1979;95(1):89-98.
70. Makkar M, Gupta C, Pathak R, Garg S, Mahajan N. Performance evaluation of hematologic
scoring system in early diagnosis of neonatal sepsis. J Clin Neonatol 2013;2(1):25-9.
71. West BA, Tabansi PN, Ugwu RO, Eneh AU. The predictive value of Micro- Erythrocyte
sedimentation rate in neonatal sepsis in a low resource country. Pediatr Therapeut
2012;S2:002:1-4.
72. Akpede GO, Abiodun PO. The micro erythrocyte sedimentation rate as a screening test for
bacteraemia in young children with non- focal infections. West Afr J Med 1995;14:147-51.
73. Khassawneh M, Hayajneh W, Kofahi H, Khader Y, Amarin Z, Daoud A. Diagnostic
markers for neonatal sepsis: Comparing C-reactive protein,Interleukin 6 and Immunoglobin
M. Scand J Immunol 2007;65(2):171 -5.

80
74. Yuan H, Huang J, Bokun LV, Wenying Y, Guang H, Wang J et al. Diagnosis value of
serum amyloid A test in neonatal sepsis: A meta analysis. Biomed Res Int 2013;ID 520291-
9.
75. Kalayci A, Yilmazer F, Adam B, Sancak R, Kucukoduk S. The importance of fibronectin,
haptoglobulin, ceruloplasmin and transferrin in the early diagnosis of neonatal sepsis. Turk J
Med Sci 2000;30(2): 151-5.
76. Mondal K, Nag D, Bandyopadhyay R, Chakraborty D, Sinha S. neonatal sepsis: Role of a
battery of immunohaematological tests in early diagnosis. Int J of App Basic Med Res
2012;2: 43-7.
77. Carcillo J, Planquois J, Goldstein B. Early markers of infection and sepsis in newborns and
children. Adv Sepsis 2006;5: 118-25.
78. Tillet W, Francis T. Serological reactions in pneumonia with a non-protein somatic
fractionof pneumococcus. J Exp Med 1930;52:561-71.
79. Weinhold B, Ruther U. Interleukin 6 dependent and independent regulation of the human C
-reactive protein gene. Biochem J 1997; 327(pt 2):425-9.
80. Ajay H, Agarwal R, Sharma S, Agarwal S. Predictive signifiance of C reactive protein in
spontaneous preterm delivery: a prospective cohort study. Int J Reprod Contracept Obstet
Gynaecol 2013; 2:47-51.
81. Volanakis JE. Human C- reactive protein: expression, structure and function.Mol Immunol
2001; 38(2-3):189-97.
82. Gabay C, Kushner I. Acute phase proteins and other systemic responses to inflammation. N
Engl J Med 1999; 340:448-54.

81
83. Chiesa C, Pellegrini G, Panero A, Osborn J, Signore F, Assumma M,et al. C- reactive
protein, Interleukin-6 and procalcitonin in the immediate postnatal period: Influence of
illness severity,risk status, antenatal and perinatal complications and infection. Clin Chem
2003;49:60-68.
84. Forest J, lariviere F, Dolsc P, Masson M, Nadeau L. C- reactive protein as a biochemical
indicator of bacterial infection in neonates. Clin Biochem 1986; 19:192-4.
85. Nuntnarumit PO, Kitiwanwanich S. Predictive values of serial C- reactive protein in
neonatal sepsis. J Med Assoc Thai 2002; 85:1151-8
86. Phillip AG, Mills PC. Use of C- reactive protein in minimising antibiotic exposure:
experience with infants initially admitted to a well baby nursery. Pediatrics 2000
Jul;106(1):E4.
87. Luis C, Jose C, Gerstenblith G, Luis P, Dumet J Luis CL et al. Correlation between
turbidimetric and nephelometric methods of measuring C- reactive protein in patients with
unstable angina or non ST elevation acute myocardial infarction. Arq Bras Cardio(internet)
2003;81:133-6.
88. Naik PR, Bharadwaj SB, Desai PB. Comparison of rapid semi- quantitative card test against
immunoturbidimetric quantitative test for determination of C-reactive protein levels in
neonatal sepsis. Int. J. Pharm.Life.Sci. 2013;4(11):38-42.
89. Dandona P, Nix D, Wilson MF, Aljada A, Love J, Assicot M, Bohuon C. Procalcitonin
increase after endotoxin injection in normal subjects. J Clin Endocrinol Metab 1994;
79(6):1605-8.
90. Whicher J, Bienvenu J, Monneret G. Procalcitonin as an acute phase marker. Ann Clin
Biochem 2001; 38(Pt 5):483-93.
82
91. Athan F, Akagunduz B, Genel F, Bak M, Can D. Procalcitonin: A marker of neonatal sepsis.
J Trop Pediatr. 2002; 48(1):10-4.
92. Assicot M,Gendrel D, Carsin H, Bohoun C, Raymond J, Guilbaud J. High serum
procalcitonin concentrations in patients with sepsis and infection. Lancet 1993;341:515-518.
93. Sucilathangam G, Amuthavalli K, Velvizhi G, Ashihabegum M, Jeymurugan T,
Palaniappan N. Early diagnostic markers for neonatal sepsis: comparing Procalcitonin and
C- reactive protein. J Clin Diagn Res 2012; 6(4):627-31.
94. Van Rossum A, Wulkan R, Oudesluys-Murphy A. Procalcitonin as an early marker of
infection in neonates and children. Lancet Infectious diseases 2004; 4:620-30.
95. Bonac B, Derganc M, Wraber B, Hojker S. Interleukin 8 and procalcitonin in early
diagnosis of severe bacterial infection in critically ill neonates. Pfulgers Arch. 2000;440(5
Suppl): R72-4.
96. Vincent J. Definition of sepsis and non infectious Systemic Inflammatory Response (SIRS).
In Cavaillon JM, Adrie C (eds) Sepsis and non infectious systemic inflammation: From
Biology to critical care. Wiley Blackwell 2009:p 4.
97. Chiesa C, Panero A, Rossi N,Stegagno M, De Giusti M, Osborn J, et al. Reliability of
Procalcitonin Concentrations for the diagnosis of sepsis in critically ill neonates. Clin Infect
Dis 1998; 26:664-72.
98. Lindegaard M, Svarrer E, Damm P, Mathiesen E, Nielsen L. Increased LDL cholesterol and
CRP in infants of mothers with type 1 diabetes. Diabetes Metab Res Rev 2008; 24:465-71.
99. Monneret G, Labaune J, Issac C, Bienvenu F, Putet G, Bienvenu J. Procalcitonin and C-
reactive protein levels in neonatal infections. Acta Paediatr 1997;86(2):209-12.

83
100. Manzano S, Girodias JB, Cousineau J, Delvin E,Gervale A. Comparison of procalcitonin of
procalcitonin measurement by a semi- quantitative method and an ultra sensitive method in
a paediatric emergency department. Clin. Biochem.2009;42:1557-60.
101. Younis S, Sheikh M, Raza A. Diagnostic accuracy of C- Reactive protein in neonatal sepsis.
JBM 2014;1:33-42.
102. Khashabi J, Karamiyar M, Taghinejad H, Shirazi M. Use of serial C-Reactive Protein
measurements for determination of length of empiric antibiotic therapy in suspected
neonatal sepsis. Iran J Med Sci 2004;29:31-5.
103. Arowosegbe AO, Ojo DA, Dedeke IOF, Shittu OB, Akinloye OA. Diagnostic value of
procalcitonin in neonatal sepsis. Niger J Paed; 43 (1): 15 - 19.
104. Naglaa F, Abeer S, Mohammad M, Yousef L. Procalcitonin and C- reactive protein as
diagnostic markers of neonatal sepsis. Aust J Basic Appl Sci 2012;6(4):108-14.
105. Franz A, Kron M, Pohlandt F, Steinbach G. Comparison of procalcitonin with interleukin
8,C-reactive protein and differential white blood cell count for the early diagnosis of
bacterial infections in newborn infants. Pediatr Infect Dis J 1999; 18(8):666-71.
106. Blommendahl J, Janas M, Laine S, Miettinen P, Ashorn P. Comparison of procalcitonin
with CRP and differential white blood cell count for the diagnosis of culture proven
neonatal sepsis. Scand J Infect Dis 2002; 34:620-2.
107. Koksal N, Harmanci R, Cetinkaya M, Hacimustafaoglu M. Role of procalcitonin and CRP
in diagnosis and follow up of neonatal sepsis. Turk J Pediatr 2007; 49:20-9.
108. Mamdouh M, Hassan A, Moghazy H, Sadek A. Procalcitonin or C- reactive protein or both
for diagnosis of neonatal sepsis. J Appl Sci Res 2012; 8:4615-23.

84
109. Adib M, Bakhshiani Z, Navaei F, Fosoul F, Fouladi S, Kazemzadeh H. Procalcitonin: A
reliable marker for the diagnosis ofneonatal sepsis. Iran J Basic Med Sci 2012; 15:777-82.
110. Ezeaka C, Shittu O, Olufunlayo F, Ekekwe G, Onuekwusi N, Odeku M et al. Saving
newborn lives in Nigeria:Newborn health in context of the integrated maternal, newborn and
child health strategy. Abuja:Federal Ministry of Health, Save the children,ACCESS
2009:82.
111. White D, Ballot D, Cooper P, Perovic O, Galpin J. Can a negative procacitonin level guide
antibiotic therapy in early onset neonatal sepsis? SAJCH 2007; 1: 146-50.
112. Varkevisser C, Pathmanathan I, Brownlee A. Designing and conducting health systems
research projects. Ottawa canada International development research centre 1991:213-6.
113. Daly L, Bourke G. Interpretation and uses of Medical Statistics. Saunders Elsevier 2000;5th
edition:271.
114. Artron® Procalcitonin rapid test (package insert). Burnaby Canada: Artron laboratories Inc,
Ltd;2014.
115. Actim® CRP test (package insert). Kauniainen, Finland: Medix Biochemica.,2010.
116. Bone RC,Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA et al. American College
of Chest Physicians/ Society/Society of Critical Care Medicine Consensus
Conference:definitions for sepsis and organ failure and guidelines for the use of innovative
therapies in sepsis. Crit Care Med 1992 Jun;20(6):864-74
117. Oyedeji G. Socioeconomic and cultural background of hospitalised children in Ilesha. Nig J
Paediatr 1985;12:111-17.
118. Naher B, Mannan M, Noor K. Role of serum procalcitonin and C- Reactive Protein in the
diagnosis of neonatal sepsis. Bangladesh Med Res Counc Bull 2011;37:40-6.

85
119. Buttery J. Blood cultures in newborns and children: optimising an everyday test. Arch Dis
Child Fetal Neonatal.2002;87(1):F25-F28.
120. Kawamura M, Nishida H. The usefulness of serial c-reactive protein measurement in
managing neonatal infection. Acta Medica Paediatrica.1995;10:3-7.
121. Liu YF, Tong XM, Zheng FY, Piao MH, Ning YZ. Physiological changes in serum
procalcitonin in premature infants early after birth. Chin J Contemp Pediatr.2013;15:81-4
122. Onyedibe K, Utoh O.Nedosa A, Okolo M, Ita O, Udoh U, Bode-Thomas F. The impact of
socio-economic factors on neonatal sepsis in Jos,Nigeria.Jos J Med 2011;6:54-8.
123. Javed M, Memon A. Maternal risk factors in early neonatal sepsisat a tertiary care teaching
hospital. Saudi Med J. 2009;30:1301-4.
124. Phillip AGS. Commentary. In:Oski FA, Stockman JA,eds. Year Book of Pediatrics.
Chicago,IL:Year Book Medical Publishers;1981:17.
125. Hindocha P,Gould JD, Wojeciechowski A, Wood CBS. Serial study of C- reactive protein
in neonatal septicaemia.Arch Dis Child 1984;59:435-438.
126. Mathai E, Christopher U, Mathai M, Jana A,Rose D, Bergstrom S. Is C- Reactive protein
useful in differentiating infected from uninfected neonates among those at risk of infection?
Indian Pediatr 2004;41:895-900.
127. Mei-Yin L, Ming-Hong T, Chang-Wen L, Ming-Chou C, Reyin L, Ren-Huei F et al.
Characteristics of neonates with culture proven blood stream infection who have low levels
of c-reactive protein. BMC Infect Dis. 2015;15:321-9.
128. Oberhoffer M, Russwurm S. Outcome prediction by traditional and new markers of
inflammation in patients with sepsis. Clin Chem Lab Med 1999;37:363-8.
86
APPENDIX I
ETHICAL APPROVAL 1a

87
APPENDIX I
EXTENDED ETHICAL APPROVAL 1B

88
APPENDIX I1
INFORMED CONSENT AND CONSENT FORM (Subjects)
“To evaluate serum procalcitonin and serial C-reactive protein as screening markers for
neonatal bacterial sepsis at the Lagos University Teaching hospital.”
Name and affiliation of researcher.
This research is being conducted by Dr Matthew-Okore Amalachukwu, a senior registrar in the
Department of Paediatrics, Lagos University Teaching Hospital, Idi-Araba, Lagos State.
Sponsor of Research
This research is sponsored by Dr Matthew-Okore A
Purpose of Research
The purpose of this research is to find out if serial C reactive protein is comparable to serum
procalcitonin as markers of neonatal sepsis in LUTH.
Procedure of the Research “To compare serum procalcitonin and serial C-reactive protein
as screening markers for neonatal bacterial sepsis at the Lagos University Teaching
hospital Idi - Araba.”
On admission, blood samples will be taken under strict asepsis using sterile gloves and injection
packs. 1ml will be collected in an EDTA bottle for serum procalcitonin and CRP in subjects. A
repeat sample for CRP will be collected at 24 hours and 72 hours in the subjects.
The BACTEC blood culture systems will be used for blood culture. 2mls of blood will be
collected.
89
Expected duration of research and of participant(s)’ involvement
The research is expected to last four (4) months. You will be interviewed on admission and small
quantity of blood sample will be collected thrice.
Risks
The study will not cause any physical harm to your child. There will be slight pain when taking
the blood sample from the vein but this will resolve with pain reliever.
Cost Implication to the participants
Participation in this research will be free of any financial cost to the parents/guardian.
Benefits
Studies have shown that use of early markers for diagnosis of neonatal sepsis can reduce hospital
stay and reduce costs in management of neonatal sepsis. This study seeks to evaluate serial CRP
and procalcitonin to determine which of the markers that could be adapted to our environment.
Confidentiality
Any information you provide will be treated with utmost confidentiality.
Your child’s name or any identifier will not be used in any publication or report from this study.
Voluntariness
Your participation in this study is entirely voluntary.
Alternatives to Participation

90
Your refusal to participate in the study will not in any way affect the healthcare services you
would receive in this hospital.
Due Inducement
If you are requested to come after clinic hours, you will be compensated for cost of
transportation to and from research site but you will not be paid any dues for participating in this
research.
Consequences of participants’ decision to withdraw from research and procedure for
orderly termination of participation.
You are free to withdraw your participation at any time in the study even if you had earlier
agreed but changed your mind.
Your decision will not affect your ability to receive medical care or lose any benefit to which
you would, otherwise, be entitled.
Modality for providing treatment and action(s) to be taken in case of injury or adverse
event(s):
If you suffer any injury as a result of your participation in the research, you will be treated in the
Lagos University Teaching Hospital and the research will bear the cost of treatment.
What happens to the research participants when the research is over?
During the research, you will be given any information that may affect your continued
participation or your health. There is no expected negative effect on participant at the end of

91
research. If your child is identified with neonatal sepsis, he or she would be treated by the
neonatal unit.
Statement about sharing of benefits of this research:
The results of the tests will be communicated to you. And may be helpful in your treatment by
your doctors.
Statement of person obtaining informed consent:
I have fully explained this research to ………………………………………………………. and
have given sufficient information, including risks and benefits, to make an informed decision.
DATE:__________________ Signature_____________________
Name_________________________________
Statement of the person giving consent:
I have read the description of this research or have had it translated into language I understand
and I have also talked it over with the doctor to my satisfaction. I understand that my
participation is voluntary. I know enough about the purpose, methods, risks and benefits of the
research to judge that I want to take part in it. I understand that I may freely stop being part of
this study at any time. I have received a copy of this consent form and additional information
sheet to keep for myself.
Date_______________ Signature __________________
Name____________________________Name of parent/guardian _____________________

92
Signature_____________ Date_______________________
Researcher’s Contact:
Dr Matthew-Okore Amalachukwu;
Department of Paediatrics, Lagos University Teaching Hospital, Idi-Araba, Lagos.
Telephone mobile: 08033941972
Email: [email protected]
Institutional Health Research Ethics Committee’s Contact:
LUTH Health Research Ethics Committee;
Room 107, Administrative Building, LUTH, Idi-Araba, Lagos.

93
APPENDIX III
STUDY PROFORMA
Neonatal data
Identification/ Personal data
Serial No …………………………… Interview date …………………………
Date of birth …………………….
Sex Male Female
Age ……………………………………..
Gestational age……………… APGAR Score ………………Birth weight ……………
Ballards score ………………………..Address ……………………………
Tribe Hausa Yoruba Igbo
Religion Christianity Islam Traditional Others.
Educational level of parents: Father Mother
Post graduate
University graduate/equivalent
SSCE/GCE+ Professional training

94
SSCE/GCE+ Grade teacher training
SSCE/GCE
JSS completed
Primary school
No formal education
Occupation of parents/ care giver
Senior public servant/Professional/manager
Large scale trader/Contractor
Intermediate public servant
JSS teachers/clerk/typist/artisan
Petty trader/laborer/messenger
Unemployed /full time house wife/student
MATERNAL DATA
Age
LUTH Patient Yes No
Mode of delivery SVD Caesarean section Others (Specify).........
Place of delivery Govt hosp Private hosp TBA Home delivery

95
RISK FACTORS FOR SEPSIS
Maternal factors
Chorioamnionitis Prolonged labour Maternal UTI
PROM > 18hours
Maternal pyrexia (>380C) Meconium stained liquor
NEWBORN FACTORS
Prematurity
Very Low birth weight
Sustained Fetal tachycardia (>180beats/min)
Multiple gestation
CLINICAL EVALUATION
Fever
Poor suck
Seizures
Hypothermia / Hyperthermia
Respiratory distress
Abdominal distension
Skin mottling/ sclerema

96
Lethargy
Others (please indicate)………………………………………..
Samples taken CRP PCT Blood culture Time of collection

97
APPENDIX IV
RESEARCHER AT WORK

98
APPENDIX V-
POSITIVE PROCALCITONIN CASSETTES.

99
APPENDIX VI
NEGATIVE PROCALCITONIN CASSETTES.

100
APPENDIX VII
Artron PCT Interpretation card

101
APPENDIX VIII
POSITIVE CRP STRIPS

102
APPENDIX IX
POSITIVE (CLOUDY) BLOOD CULTURE BOTTLES
Copyright © 2022 FDOKUMEN



![The Chanticleer [serial]](https://static.fdokumen.com/doc/165x107/632863a3051fac18490eb46f/the-chanticleer-serial.jpg)