Comparative study between breast tomosynthesis and classic digital mammography in the evaluation of...
9
ORIGINAL ARTICLE Comparative study between breast tomosynthesis and classic digital mammography in the evaluation of different breast lesions Sahar Mansour a,d, * , Lamia Adel a,d , Omina Mokhtar b,d , Omar Sherif Omar c,d a Radiology Department (Women’s Imaging Unit), Faculty of Medicine, Cairo University, Egypt b Radiology Department (Women’s Imaging Unit), National Cancer Institute of Cairo, Egypt c Surgery Department (Breast Specialist), Faculty of Medicine, Cairo University, Egypt d Wadi El-Neel Hospital, Radiology Department, Breast Imaging Unit Incorporation with Institute Gustave-Roussy (IGR), Dusseldorf Breast Cancer Center, Helsinki Breast Cancer Center and Institute Curie, Saint Cloud, France Received 19 February 2014; accepted 14 March 2014 Available online xxxx KEYWORDS Breast; Digital mammography; Biopsy; Computer applications-3D; Calcifications Abstract Objective: To evaluate the impact of adding 3D Tomosynthesis to Full Field Digital Mammography (FFDM) in the detection and diagnosis of breast lesions. Subjects and methods: The study included 166 mammograms with indeterminate findings selected from 1600 mammograms. They were classified into two groups: group 1 ‘Diagnostic mammograms’ of symptomatic women and group 2 ‘Screening mammograms’. Dense breasts assigned as ACR3 and ACR4 presented 69% (n = 114/166) of the studied cases. FFDM and 3D tomosynthesis examination was done and imaging findings were evaluated before and after the use of 3D tomosynthesis images. Results: Both modalities were compared regarding detection and diagnosis, each individually assessed, using the Pearson Chi Square tests. Detection (P value: 0.006) and diagnosis (P value: 0.048) of breast lesions dramatically improved when 3D tomosynthesis images were considered in the evaluation. The sensitivity, specificity, and accuracy of digital mammography was 60%, 20.7% and 48% have significantly enhanced on applying tomosynthesis to be 94.5%, 74% and 89.7%. Conclusion: Three-dimensional tomosynthesis significantly enhanced the detection and character- ization of breast lesions on digital mammography especially in the context of dense breast paren- chyma (ACR 3&4). Ó 2014 Production and hosting by Elsevier B.V. on behalf of Egyptian Society of Radiology and Nuclear Medicine. * Corresponding author at: Kasr ElAiny Hospital, Cairo University, Egypt. Tel.: +20 1006029047. E-mail address: [email protected] (S. Mansour). Peer review under responsibility of Egyptian Society of Radiology and Nuclear Medicine. Production and hosting by Elsevier The Egyptian Journal of Radiology and Nuclear Medicine (2014) xxx, xxx–xxx Egyptian Society of Radiology and Nuclear Medicine The Egyptian Journal of Radiology and Nuclear Medicine www.elsevier.com/locate/ejrnm www.sciencedirect.com 0378-603X Ó 2014 Production and hosting by Elsevier B.V. on behalf of Egyptian Society of Radiology and Nuclear Medicine. http://dx.doi.org/10.1016/j.ejrnm.2014.03.007 ARTICLE IN PRESS Please cite this article in press as: Mansour S. et al., Comparative study between breast tomosynthesis and classic digital mammography in the evaluation of different breast lesions, Egypt J Radiol Nucl Med (2014), http://dx.doi.org/10.1016/j.ejrnm.2014.03.007
Transcript of Comparative study between breast tomosynthesis and classic digital mammography in the evaluation of...

The Egyptian Journal of Radiology and Nuclear Medicine (2014) xxx, xxx–xxx
ARTICLE IN PRESS
Egyptian Society of Radiology and Nuclear Medicine
The Egyptian Journal of Radiology andNuclearMedicine
www.elsevier.com/locate/ejrnmwww.sciencedirect.com
ORIGINAL ARTICLE
Comparative study between breast tomosynthesis
and classic digital mammography in the evaluation
of different breast lesions
* Corresponding author at: Kasr ElAiny Hospital, Cairo University, Egypt. Tel.: +20 1006029047.
E-mail address: [email protected] (S. Mansour).
Peer review under responsibility of Egyptian Society of Radiology and Nuclear Medicine.
Production and hosting by Elsevier
0378-603X � 2014 Production and hosting by Elsevier B.V. on behalf of Egyptian Society of Radiology and Nuclear Medicine.
http://dx.doi.org/10.1016/j.ejrnm.2014.03.007
Please cite this article in press as: Mansour S. et al., Comparative study between breast tomosynthesis and classic digital mammographevaluation of different breast lesions, Egypt J Radiol Nucl Med (2014), http://dx.doi.org/10.1016/j.ejrnm.2014.03.007
Sahar Mansoura,d,*, Lamia Adel
a,d, Omina Mokhtar
b,d, Omar Sherif Omar
c,d
a Radiology Department (Women’s Imaging Unit), Faculty of Medicine, Cairo University, Egyptb Radiology Department (Women’s Imaging Unit), National Cancer Institute of Cairo, Egyptc Surgery Department (Breast Specialist), Faculty of Medicine, Cairo University, Egyptd Wadi El-Neel Hospital, Radiology Department, Breast Imaging Unit Incorporation with Institute Gustave-Roussy (IGR),Dusseldorf Breast Cancer Center, Helsinki Breast Cancer Center and Institute Curie, Saint Cloud, France
Received 19 February 2014; accepted 14 March 2014
Available online xxxx
KEYWORDS
Breast;
Digital mammography;
Biopsy;
Computer applications-3D;
Calcifications
Abstract Objective: To evaluate the impact of adding 3D Tomosynthesis to Full Field Digital
Mammography (FFDM) in the detection and diagnosis of breast lesions.
Subjects and methods: The study included 166 mammograms with indeterminate findings selected
from 1600 mammograms. They were classified into two groups: group 1 ‘Diagnostic mammograms’
of symptomatic women and group 2 ‘Screening mammograms’. Dense breasts assigned as ACR3 and
ACR4 presented 69% (n= 114/166) of the studied cases. FFDMand 3D tomosynthesis examination
was done and imaging findings were evaluated before and after the use of 3D tomosynthesis
images.
Results: Both modalities were compared regarding detection and diagnosis, each individually
assessed, using the Pearson Chi Square tests. Detection (P value: 0.006) and diagnosis (P value:
0.048) of breast lesions dramatically improved when 3D tomosynthesis images were considered in
the evaluation. The sensitivity, specificity, and accuracy of digital mammography was 60%,
20.7% and 48% have significantly enhanced on applying tomosynthesis to be 94.5%, 74% and
89.7%.
Conclusion: Three-dimensional tomosynthesis significantly enhanced the detection and character-
ization of breast lesions on digital mammography especially in the context of dense breast paren-
chyma (ACR 3&4).� 2014 Production and hosting by Elsevier B.V. on behalf of Egyptian Society of Radiology and Nuclear
Medicine.
y in the

2 S. Mansour et al.
ARTICLE IN PRESS
1. Introduction
Mammography is an effective imaging tool for the detection ofearly-stage breast cancer, and it is the only screening modality
proved to reduce mortality from breast cancer (1–3). However,the appearance of overlapping tissue on mammograms poses asignificant obstacle to interpretation (4–7).
Breast tomosynthesis is anew tool that canbe expected toame-liorate this problem by reducing or eliminating tissue overlap (8).
The purpose of this study is to evaluate the potential impactof adding 3D Tomosynthesis to Full Field Digital Mammogra-
phy on the detection and diagnosis of breast lesions.
2. Material and methods
This study is a prospective analysis approved by the EthicsCommittee inWadi El-Neel Hospital, where radiological exam-ination of the study cases had been performed in a well
equipped and organized breast imaging unit incorporation withInstitute Gustave-Roussy (IGR), the leading European anti-cancer center. Included cases have given informed consents.
2.1. Material
The study included 166 consecutive mammograms with posi-
tive findings on the standard mammography examination.Studies were performed during the period of 13 months.Included cases were classified into two groups according to
the objective of their referral: Group 1: ‘Diagnostic mammo-grams’ of symptomatic women. Group 2: ‘Screening mammo-grams’ of non symptomatic women referred for their regularannual check up.
2.2. Methods
2.2.1. Mammography examination
A combined FFDM and 3D tomosynthesis examination wasdone by Hologic Selenia Dimensions Digital Tomosynthesis
System using the following steps:
� Position views: Images are taken both in the cranio-caudal(CC) and medio-lateral oblique (MLO) views.
� Acquisition: The system attains a ‘‘Combo-mode’’ imagingtechnique (2D + 3D imaging) that acquires a traditionaldigital mammogram and a tomosynthesis scan in the same
compression. During a tomosynthesis scan, multiple (11–15), low-dose images of the breast are acquired at differentangles while the X-ray tube moves in an arc across the
breast. These images are then used to produce a series ofone-millimeter thick images (from 60 to 90 slices) that canbe reconstructed to a three dimensional image of the breast.
� Displaymethodology: Images are displayed on dedicated highresolution workstations with special capabilities that are tai-lored for breast imaging. The re-constructed tomosynthesisimages can be viewed as one slice at a time or in a cine loop.
2.2.2. Ultrasound examination
A complementary ultrasound examination was performed forall cases using both B-mode and elastography ultrasound on
Please cite this article in press as: Mansour S. et al., Comparative study bevaluation of different breast lesions, Egypt J Radiol Nucl Med (2014), ht
Aplio XG device (Toshiba, Japan) to confirm or exclude mam-mography identified abnormalities. Examination was done by6–9 MHz high frequency probes.
2.3. Image analysis
According to the ‘‘Breast Imaging Data and Reporting
System’’ (9) mammograms of all patients were assigned an ini-tial BIRADS category in view of their Full Field Digital mam-mography (FFDM) findings by two independent readers (A.L.
and M.S. of 18 and 15 years experience) into: (i) BIRADS 3 orBIRADS 4 mammograms: with indeterminate benign ormalignant mammography findings, (ii) BIRADS 1 and BIR-
ADS 2 mammograms: if the tomosynthesis images addednew undetected lesions in BIRADS 1 or changed the categoryof detected ones in BIRADS 2 and (iii) BIRADS 5 cases: whenadditional findings were reported on reviewing the tomosyn-
thesis images (e.g. additional undetected lesions or widertumor extent).
A second look of the mammograms established by another
individual reader (M.O. of 20 years experience) and anotherBIRADS category assigned after a combined review of boththe tomosynthesis and the regular digital mammography
images.The authors were blinded regarding the image analysis per-
formed by each of them and both the initial mammogram(only regular mammogram) and re-evaluation (combined
tomosynthesis and regular mammography images) were per-formed without knowledge of the pathology results. At thestage of final evaluation, there was multidisciplinary discussion
of findings with the authors and the breast surgery consultant(O.O.).
On reporting the mammogram, we answered the following
questions before and after evaluating the 3D tomosynthesisimages:
1. Can we detect any abnormality? (mass lesions, parenchymaldistortion, focal asymmetries, micro calcifications or diffusebreast edema pattern).
2. Can we characterize/ diagnose this abnormality? (i.e. classify
as benign, indeterminate or malignant).3. Which BIRADS category could we assign?
4. Should we recommend or deter further biopsy?
5. Does the FFDM findings whether or not combined with 3D
tomosynthesis concomitant with the pathology results?
6. Do we need a follow up study for confirming the current
mammography findings?
Ultrasound guided core biopsy using a 14G biopsy needlewas performed in 63% (n= 104) for malignant looking (BI-
RADS 5), suspicious (BI-RADS 4) and indeterminate lesions(BI-RADS 3). The remaining BI-RADS 3 category (n= 26)and BI-RADS 2 category (n = 35) lesions were managed
according to the ACR guideline which is determined duringthe follow up: a one year stable lesion was considered ofbenign nature.
2.4. Statistical analysis
Imaging findings were tabulated and categorical results of Full
Field Digital Mammography and 3D Digital Tomosynthesis
etween breast tomosynthesis and classic digital mammography in thetp://dx.doi.org/10.1016/j.ejrnm.2014.03.007
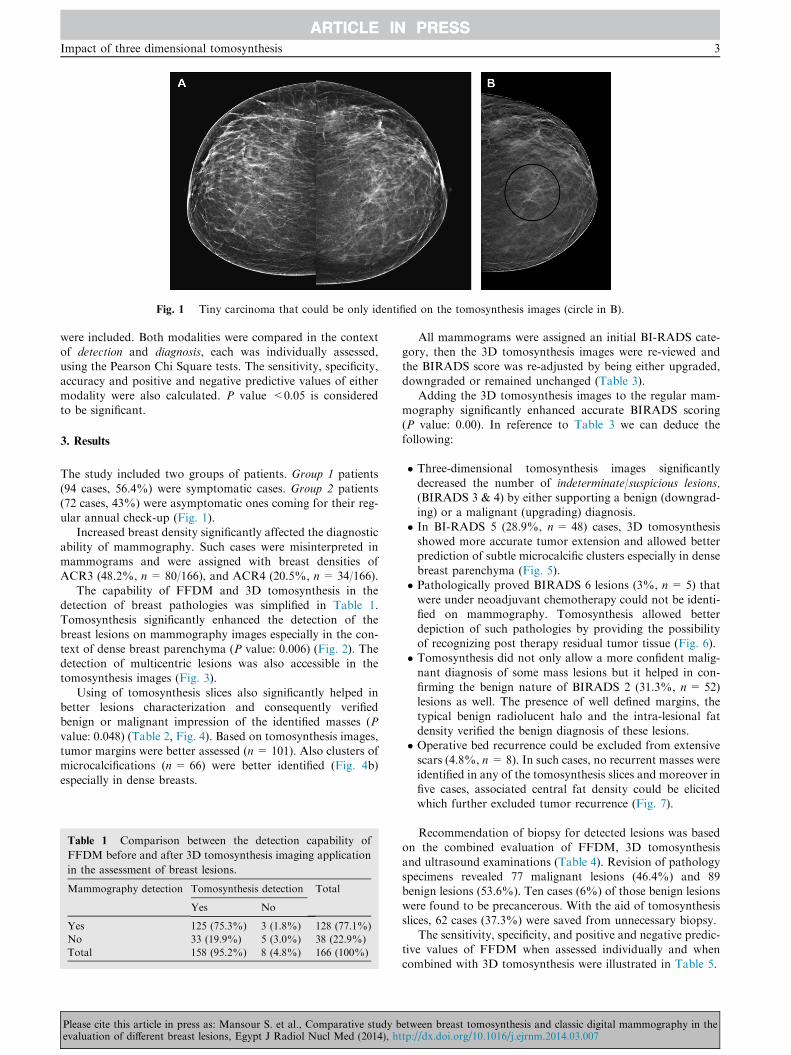
Fig. 1 Tiny carcinoma that could be only identified on the tomosynthesis images (circle in B).
Impact of three dimensional tomosynthesis 3
ARTICLE IN PRESS
were included. Both modalities were compared in the contextof detection and diagnosis, each was individually assessed,using the Pearson Chi Square tests. The sensitivity, specificity,
accuracy and positive and negative predictive values of eithermodality were also calculated. P value <0.05 is consideredto be significant.
3. Results
The study included two groups of patients. Group 1 patients
(94 cases, 56.4%) were symptomatic cases. Group 2 patients(72 cases, 43%) were asymptomatic ones coming for their reg-ular annual check-up (Fig. 1).
Increased breast density significantly affected the diagnostic
ability of mammography. Such cases were misinterpreted inmammograms and were assigned with breast densities ofACR3 (48.2%, n = 80/166), and ACR4 (20.5%, n= 34/166).
The capability of FFDM and 3D tomosynthesis in thedetection of breast pathologies was simplified in Table 1.Tomosynthesis significantly enhanced the detection of the
breast lesions on mammography images especially in the con-text of dense breast parenchyma (P value: 0.006) (Fig. 2). Thedetection of multicentric lesions was also accessible in thetomosynthesis images (Fig. 3).
Using of tomosynthesis slices also significantly helped inbetter lesions characterization and consequently verifiedbenign or malignant impression of the identified masses (P
value: 0.048) (Table 2, Fig. 4). Based on tomosynthesis images,tumor margins were better assessed (n= 101). Also clusters ofmicrocalcifications (n = 66) were better identified (Fig. 4b)
especially in dense breasts.
Table 1 Comparison between the detection capability of
FFDM before and after 3D tomosynthesis imaging application
in the assessment of breast lesions.
Mammography detection Tomosynthesis detection Total
Yes No
Yes 125 (75.3%) 3 (1.8%) 128 (77.1%)
No 33 (19.9%) 5 (3.0%) 38 (22.9%)
Total 158 (95.2%) 8 (4.8%) 166 (100%)
Please cite this article in press as: Mansour S. et al., Comparative study bevaluation of different breast lesions, Egypt J Radiol Nucl Med (2014), ht
All mammograms were assigned an initial BI-RADS cate-gory, then the 3D tomosynthesis images were re-viewed andthe BIRADS score was re-adjusted by being either upgraded,
downgraded or remained unchanged (Table 3).Adding the 3D tomosynthesis images to the regular mam-
mography significantly enhanced accurate BIRADS scoring(P value: 0.00). In reference to Table 3 we can deduce the
following:
� Three-dimensional tomosynthesis images significantly
decreased the number of indeterminate/suspicious lesions,(BIRADS 3 & 4) by either supporting a benign (downgrad-ing) or a malignant (upgrading) diagnosis.
� In BI-RADS 5 (28.9%, n = 48) cases, 3D tomosynthesisshowed more accurate tumor extension and allowed betterprediction of subtle microcalcific clusters especially in dense
breast parenchyma (Fig. 5).� Pathologically proved BIRADS 6 lesions (3%, n= 5) thatwere under neoadjuvant chemotherapy could not be identi-fied on mammography. Tomosynthesis allowed better
depiction of such pathologies by providing the possibilityof recognizing post therapy residual tumor tissue (Fig. 6).� Tomosynthesis did not only allow a more confident malig-
nant diagnosis of some mass lesions but it helped in con-firming the benign nature of BIRADS 2 (31.3%, n = 52)lesions as well. The presence of well defined margins, the
typical benign radiolucent halo and the intra-lesional fatdensity verified the benign diagnosis of these lesions.� Operative bed recurrence could be excluded from extensivescars (4.8%, n = 8). In such cases, no recurrent masses were
identified in any of the tomosynthesis slices and moreover infive cases, associated central fat density could be elicitedwhich further excluded tumor recurrence (Fig. 7).
Recommendation of biopsy for detected lesions was basedon the combined evaluation of FFDM, 3D tomosynthesis
and ultrasound examinations (Table 4). Revision of pathologyspecimens revealed 77 malignant lesions (46.4%) and 89benign lesions (53.6%). Ten cases (6%) of those benign lesions
were found to be precancerous. With the aid of tomosynthesisslices, 62 cases (37.3%) were saved from unnecessary biopsy.
The sensitivity, specificity, and positive and negative predic-tive values of FFDM when assessed individually and when
combined with 3D tomosynthesis were illustrated in Table 5.
etween breast tomosynthesis and classic digital mammography in thetp://dx.doi.org/10.1016/j.ejrnm.2014.03.007
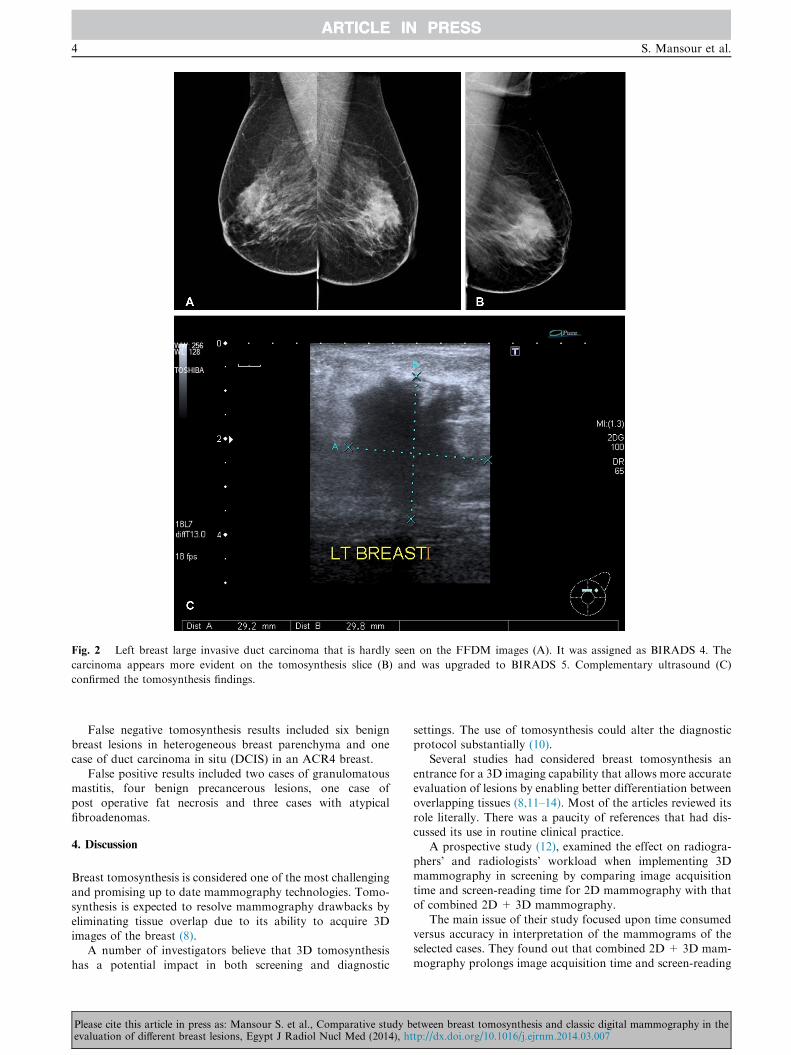
Fig. 2 Left breast large invasive duct carcinoma that is hardly seen on the FFDM images (A). It was assigned as BIRADS 4. The
carcinoma appears more evident on the tomosynthesis slice (B) and was upgraded to BIRADS 5. Complementary ultrasound (C)
confirmed the tomosynthesis findings.
4 S. Mansour et al.
ARTICLE IN PRESS
False negative tomosynthesis results included six benignbreast lesions in heterogeneous breast parenchyma and onecase of duct carcinoma in situ (DCIS) in an ACR4 breast.
False positive results included two cases of granulomatousmastitis, four benign precancerous lesions, one case ofpost operative fat necrosis and three cases with atypical
fibroadenomas.
4. Discussion
Breast tomosynthesis is considered one of the most challengingand promising up to date mammography technologies. Tomo-synthesis is expected to resolve mammography drawbacks by
eliminating tissue overlap due to its ability to acquire 3Dimages of the breast (8).
A number of investigators believe that 3D tomosynthesis
has a potential impact in both screening and diagnostic
Please cite this article in press as: Mansour S. et al., Comparative study bevaluation of different breast lesions, Egypt J Radiol Nucl Med (2014), ht
settings. The use of tomosynthesis could alter the diagnosticprotocol substantially (10).
Several studies had considered breast tomosynthesis an
entrance for a 3D imaging capability that allows more accurateevaluation of lesions by enabling better differentiation betweenoverlapping tissues (8,11–14). Most of the articles reviewed its
role literally. There was a paucity of references that had dis-cussed its use in routine clinical practice.
A prospective study (12), examined the effect on radiogra-
phers’ and radiologists’ workload when implementing 3Dmammography in screening by comparing image acquisitiontime and screen-reading time for 2D mammography with thatof combined 2D+ 3D mammography.
The main issue of their study focused upon time consumedversus accuracy in interpretation of the mammograms of theselected cases. They found out that combined 2D + 3D mam-
mography prolongs image acquisition time and screen-reading
etween breast tomosynthesis and classic digital mammography in thetp://dx.doi.org/10.1016/j.ejrnm.2014.03.007

Fig. 3 Screening mammogram showed a subtle mid upper breast area of parenchymal distortion that became more apparent on one of
the tomosynthesis slices in addition to another lesion (arrows). Complementary ultrasound proved the presence of an underlying two tiny
spiculated mass lesions.
Table 2 Comparison between the diagnostic ability of FFDM
before and after combining the 3D tomosynthesis imaging in
the assessment of breast lesions.
Mammography diagnosis Tomosynthesis diagnosis Total
Yes No
Yes 51 (30.7%) 4 (2.4%) 55 (33.1%)
No 90 (54.2%) 21 (12.7%) 111 (66.9%)
Total 141 (84.9%) 25 (15.1%) 166 (100%)
Impact of three dimensional tomosynthesis 5
ARTICLE IN PRESS
time (at initial implementation), yet appears to be associatedwith improved screening accuracy, which consequently help
in detection of more cancers (12).Skaane et al. compared digital mammography and digital
breast tomosynthesis (DBT) in a side-by-side feature analysis
for cancer conspicuity, and assessed whether there is a poten-tial additional value of DBT to standard conventional imagingregarding the detection of additional malignancies. The study
included 129 women and actually biopsied 45 breasts (theremaining 84 cases were dismissed with a normal/definitelybenign finding that presented no need for biopsy). Accordingto their work; the side-by-side feature analysis showed higher
conspicuity scores for tomosynthesis compared to conven-tional 2D for cancers presenting as spiculated masses and dis-tortions (15).
Hakim et al. (10) subjectively compared additional mam-mographic views to DBT when characterizing known masses,architectural distortions, or asymmetries. The study considered
mammography of 25 women with known masses. After reviewof the examinations, radiologists rated their relative preferencein terms of classifying the finding in question twice; one timewhen aided by the additional views and another when aided
by DBT. The diagnostic BI-RADS rating of both examina-tions was correlated. They found that FFDM and DBT(combined) were perceived to be better for diagnosis in 50%
of cases. Finally they concluded that DBT may be an alterna-tive to obtaining additional mammographic views in most
Please cite this article in press as: Mansour S. et al., Comparative study bevaluation of different breast lesions, Egypt J Radiol Nucl Med (2014), ht
cases especially if the presentation of the concerned lesion isnot by calcification.
During our experience; the 3D tomosynthesis images hadincreased the sensitivity and accuracy of mammography and
significantly enhanced accurate BIRADS scoring (P value:0.00). The proved malignant lesions (n= 77) were correctlydiagnosed by mammography in 14 cases (18.1%), such estima-
tion became more accurate when 3D tomosynthesis included inthe evaluation to be 48 cases (62.3%). Even when malignantmass lesions were identified on mammograms, 3D tomosyn-
thesis still has a role in defining actual tumor size and exten-sion (Fig. 5). We have to admit that the diagnostic accuracypercentage for FFDM was very low to be accepted on a stan-
dard basis; yet it is a unique situation in this study as most ofthe malignant cases were of dense breast categories.
Tomosynthesis significantly enhanced the cancer detectionrate of mammography as it showed a sensitivity of 94.5% com-
pared to only 60% in solo mammography evaluation. This wascoupled with its impact on the diagnostic accuracy of mam-mography that had upgraded from 48% to 89.7%. Improved
depiction of clustered microcalcifications, together with bettermargin delineation and superior resolution has paved way formaking an accurate diagnosis (Fig. 4b).
In a study done in 2012, DBT was compared with mammo-graphic spot views (MSVs) in characterizing 67 breast massesas benign (n = 37) or malignant (n = 30). In this small-samplestudy, mass characterization in terms of visibility ratings,
reader performance, and BI-RADS assessment with DBTwas similar to that with MSVs. Preliminary findings suggestthat MSV might not be necessary for mass characterization
when performing DBT (16).From our point of view, tomosynthesis being a ‘‘slice fold-
ing’’ technique has only the capability to locate the site of cal-
cific clusters but not to accurately suggest the possiblepathology of clusters. Regarding this issue spot magnificationview is a better method of evaluation.
Kontos et al. in 2011 presented a correlation between theparenchymal texture features at DBT and digital mammogra-phy with breast percent density (PD) in a screening population
etween breast tomosynthesis and classic digital mammography in thetp://dx.doi.org/10.1016/j.ejrnm.2014.03.007
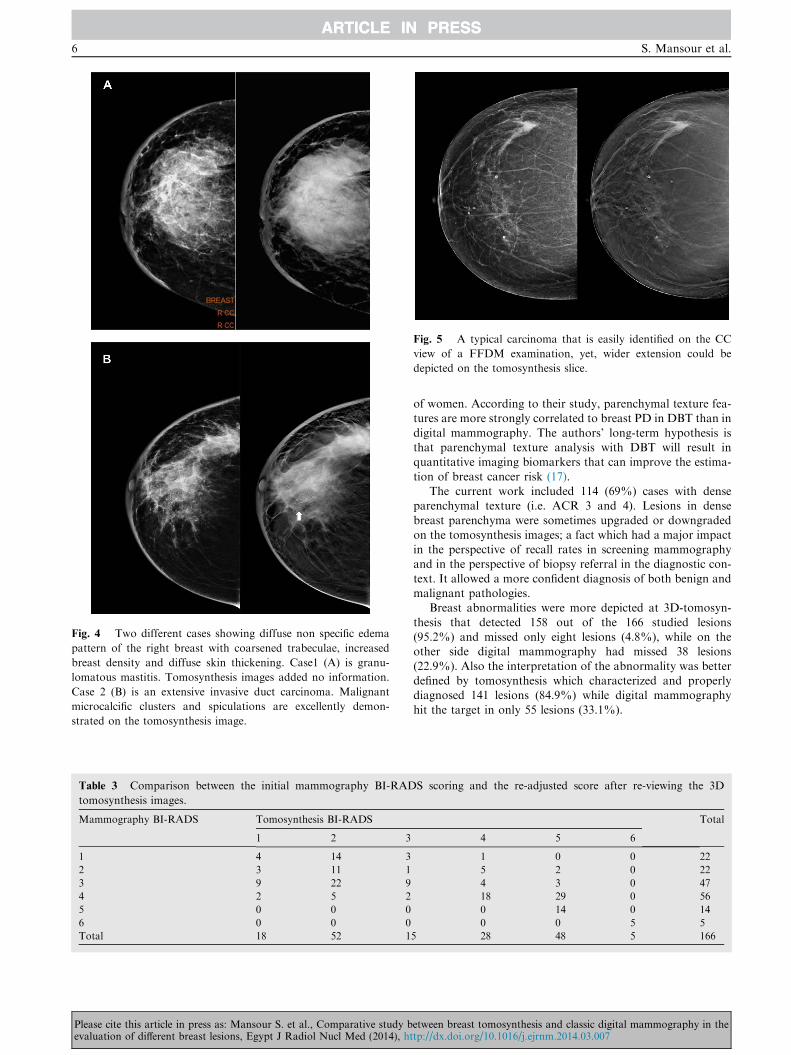
Fig. 4 Two different cases showing diffuse non specific edema
pattern of the right breast with coarsened trabeculae, increased
breast density and diffuse skin thickening. Case1 (A) is granu-
lomatous mastitis. Tomosynthesis images added no information.
Case 2 (B) is an extensive invasive duct carcinoma. Malignant
microcalcific clusters and spiculations are excellently demon-
strated on the tomosynthesis image.
Table 3 Comparison between the initial mammography BI-RAD
tomosynthesis images.
Mammography BI-RADS Tomosynthesis BI-RADS
1 2 3
1 4 14 3
2 3 11 1
3 9 22 9
4 2 5 2
5 0 0 0
6 0 0 0
Total 18 52 1
Fig. 5 A typical carcinoma that is easily identified on the CC
view of a FFDM examination, yet, wider extension could be
depicted on the tomosynthesis slice.
6 S. Mansour et al.
ARTICLE IN PRESS
Please cite this article in press as: Mansour S. et al., Comparative study bevaluation of different breast lesions, Egypt J Radiol Nucl Med (2014), ht
of women. According to their study, parenchymal texture fea-tures are more strongly correlated to breast PD in DBT than in
digital mammography. The authors’ long-term hypothesis isthat parenchymal texture analysis with DBT will result inquantitative imaging biomarkers that can improve the estima-
tion of breast cancer risk (17).The current work included 114 (69%) cases with dense
parenchymal texture (i.e. ACR 3 and 4). Lesions in dense
breast parenchyma were sometimes upgraded or downgradedon the tomosynthesis images; a fact which had a major impactin the perspective of recall rates in screening mammographyand in the perspective of biopsy referral in the diagnostic con-
text. It allowed a more confident diagnosis of both benign andmalignant pathologies.
Breast abnormalities were more depicted at 3D-tomosyn-
thesis that detected 158 out of the 166 studied lesions(95.2%) and missed only eight lesions (4.8%), while on theother side digital mammography had missed 38 lesions
(22.9%). Also the interpretation of the abnormality was betterdefined by tomosynthesis which characterized and properlydiagnosed 141 lesions (84.9%) while digital mammography
hit the target in only 55 lesions (33.1%).
S scoring and the re-adjusted score after re-viewing the 3D
Total
4 5 6
1 0 0 22
5 2 0 22
4 3 0 47
18 29 0 56
0 14 0 14
0 0 5 5
5 28 48 5 166
etween breast tomosynthesis and classic digital mammography in thetp://dx.doi.org/10.1016/j.ejrnm.2014.03.007

Fig. 6 Proved carcinoma under neo-adjuvant chemotherapy. Tumor is in-apparent on FFDM image (A). It becomes clearly illustrated
on the tomosynthesis images (arrow in B).
Fig. 7 A 37-year-old female with history of right conservative
breast surgery. She recently noticed a palpable operative bed
lump. Her mammogram showed operative bed microcalcifications
and spiculations. She was assigned BI-RADS 4 score with
suspicious recurrence. Tomosynthesis images showed a central
radio-lucency with fine egg shell calcifications; a picture that is
typical for operative bed fat necrosis. She was downgraded to BI-
RADS 2 score.
Table 4 Number of performed breast biopsies and results of
revision of pathology specimens.
Pathology Total No.
of cases
Biopsy
performed
Biopsy
deterred
Benign 79 (47.6%) 17 62
Fibroadenomas 5 1
Mammary dysplasia 2 –
Fibrocystic changes 2 25
Mastitis 6 1
Normal 2 9
Scar 8
Duct ectasia 2
Precancerous 10 (6%) 10 –
Malignant 77 (46.4%) 77 –
DCIS 6
Lobular carcinoma 3
Malignant phylloids 1
Invasive duct carcinoma 67
Total 166 104 62
Table 5 Calculated sensitivity, specificity, accuracy, and
positive and negative predictive values of FFDM before and
after combining the 3D tomosynthesis in the assessment of
breast lesions.
Statistics Mammography (%) Tomosynthesis (%)
Sensitivity 60 94.5
Specificity 20.7 74
Accuracy 48 89.7
Positive predictive value 62 92
Negative predictive value 20 80
Impact of three dimensional tomosynthesis 7
ARTICLE IN PRESS
Nevertheless we have to admit that breast tomosynthesissometimes does not save the case, it holds the challenge of‘‘absence of mass effect’’. Lesions with no associate architec-
tural compression and/or distortion may be indiscernible fromthe related parenchyma in breast with ACR 3&4 categories(Fig. 8). Such condition may present with a number of consid-
ered pathologies such as: Intraductal epithelial hyperplasia,lobular carcinoma in situ and ductal carcinoma in situ (DCIS).Presence of an area of abnormal echo pattern on complemen-tary breast US could draw attention to biopsy and conse-
quently solve such problem.
Please cite this article in press as: Mansour S. et al., Comparative study bevaluation of different breast lesions, Egypt J Radiol Nucl Med (2014), ht
Bernardi et al. (12), in 2012 stated that there is limited evi-dence on the role of 3D mammography with tomosynthesis in
breast screening, although early studies suggest that it mayimprove specificity. They evaluated the effect of integrating3D mammography on 158 consecutive recalls to assessment
in asymptomatic subjects and finally found out that their study
etween breast tomosynthesis and classic digital mammography in thetp://dx.doi.org/10.1016/j.ejrnm.2014.03.007
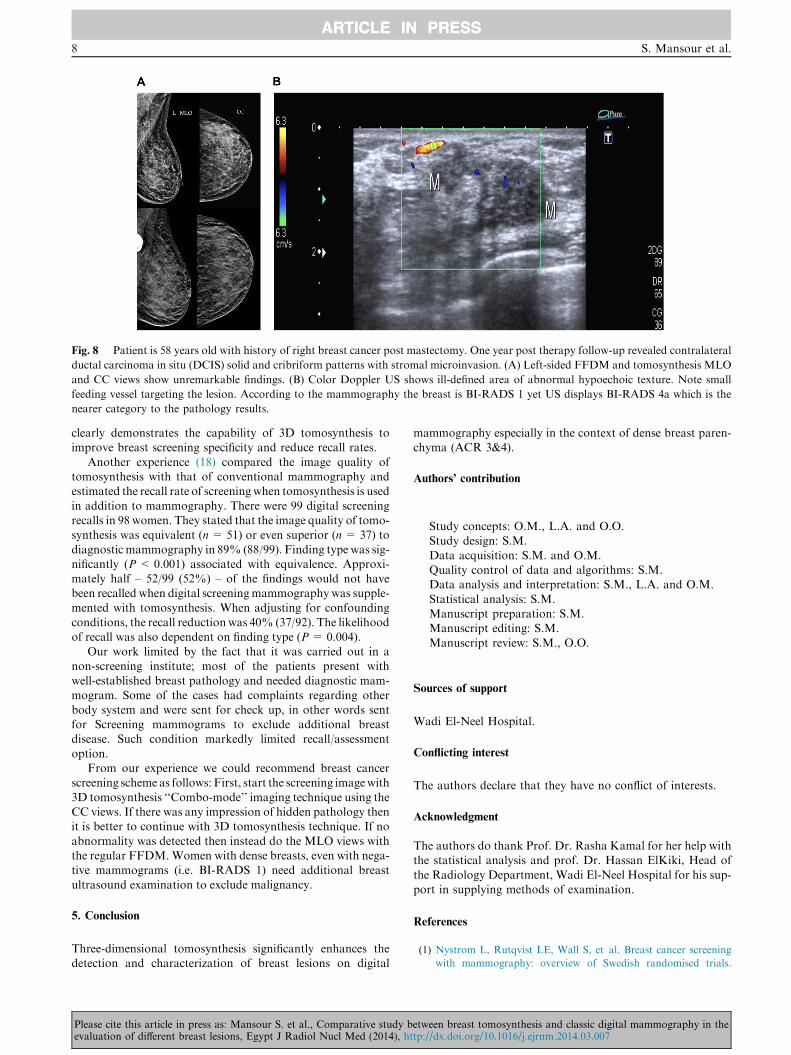
Fig. 8 Patient is 58 years old with history of right breast cancer post mastectomy. One year post therapy follow-up revealed contralateral
ductal carcinoma in situ (DCIS) solid and cribriform patterns with stromal microinvasion. (A) Left-sided FFDM and tomosynthesis MLO
and CC views show unremarkable findings. (B) Color Doppler US shows ill-defined area of abnormal hypoechoic texture. Note small
feeding vessel targeting the lesion. According to the mammography the breast is BI-RADS 1 yet US displays BI-RADS 4a which is the
nearer category to the pathology results.
8 S. Mansour et al.
ARTICLE IN PRESS
clearly demonstrates the capability of 3D tomosynthesis toimprove breast screening specificity and reduce recall rates.
Another experience (18) compared the image quality oftomosynthesis with that of conventional mammography andestimated the recall rate of screeningwhen tomosynthesis is used
in addition to mammography. There were 99 digital screeningrecalls in 98 women. They stated that the image quality of tomo-synthesis was equivalent (n= 51) or even superior (n = 37) to
diagnostic mammography in 89% (88/99). Finding type was sig-nificantly (P < 0.001) associated with equivalence. Approxi-mately half – 52/99 (52%) – of the findings would not havebeen recalled when digital screeningmammography was supple-
mented with tomosynthesis. When adjusting for confoundingconditions, the recall reductionwas 40% (37/92). The likelihoodof recall was also dependent on finding type (P = 0.004).
Our work limited by the fact that it was carried out in anon-screening institute; most of the patients present withwell-established breast pathology and needed diagnostic mam-
mogram. Some of the cases had complaints regarding otherbody system and were sent for check up, in other words sentfor Screening mammograms to exclude additional breastdisease. Such condition markedly limited recall/assessment
option.From our experience we could recommend breast cancer
screening scheme as follows: First, start the screening imagewith
3D tomosynthesis ‘‘Combo-mode’’ imaging technique using theCC views. If there was any impression of hidden pathology thenit is better to continue with 3D tomosynthesis technique. If no
abnormality was detected then instead do the MLO views withthe regular FFDM.Women with dense breasts, even with nega-tive mammograms (i.e. BI-RADS 1) need additional breast
ultrasound examination to exclude malignancy.
5. Conclusion
Three-dimensional tomosynthesis significantly enhances thedetection and characterization of breast lesions on digital
Please cite this article in press as: Mansour S. et al., Comparative study bevaluation of different breast lesions, Egypt J Radiol Nucl Med (2014), ht
mammography especially in the context of dense breast paren-chyma (ACR 3&4).
Authors’ contribution
Study concepts: O.M., L.A. and O.O.Study design: S.M.
Data acquisition: S.M. and O.M.Quality control of data and algorithms: S.M.Data analysis and interpretation: S.M., L.A. and O.M.
Statistical analysis: S.M.Manuscript preparation: S.M.Manuscript editing: S.M.
Manuscript review: S.M., O.O.
Sources of support
Wadi El-Neel Hospital.
Conflicting interest
The authors declare that they have no conflict of interests.
Acknowledgment
The authors do thank Prof. Dr. Rasha Kamal for her help withthe statistical analysis and prof. Dr. Hassan ElKiki, Head of
the Radiology Department, Wadi El-Neel Hospital for his sup-port in supplying methods of examination.
References
(1) Nystrom L, Rutqvist LE, Wall S, et al. Breast cancer screening
with mammography: overview of Swedish randomised trials.
etween breast tomosynthesis and classic digital mammography in thetp://dx.doi.org/10.1016/j.ejrnm.2014.03.007

Impact of three dimensional tomosynthesis 9
ARTICLE IN PRESS
Lancet 1993;341(8851):973–8 [Published correction appears in,
Lancet 1993; 342(8883):1372.].
(2) Tabar L, Fagerberg CJ, Gad A, et al. Reduction in mortality
from breast cancer after mass screening with mammography:
randomised trial from the Breast Cancer Screening Working
Group of the Swedish National Board of Health and Welfare.
Lancet 1985;1(8433):829–32.
(3) Lewin JM, D’Orsi CJ, Hendrick RE. Digital mammography.
Radiol Clin North Am 2004;42(5):871–84.
(4) Holland R, Mravunac M, Hendriks JH, Bekker BV. So-called
interval cancers of the breast: pathologic and radiologic analysis
of sixty-four cases. Cancer 1982;49(12):2527–33.
(5) Martin JE, Moskowitz M, Milbrath JR. Breast cancer missed by
mammography. AJR 1979;132(5):737–9.
(6) Feig SA, Shaber GS, Patchefsky A, et al. Analysis of clinically
occult and mammographically occult breast tumors. AJR
1977;128(3):403–8.
(7) Bird RE, Wallace TW, Yankaskas BC. Analysis of cancers missed
at screening mammography. Radiology 1992;184(3):613–7.
(8) Park JM, Franken Jr EA, Garg M, Fajardo LL, Niklason LT.
Breast tomosynthesis: present considerations and future applica-
tions. Radiographics 2007;27(Suppl. 1):S231–40.
(9) Lazarus E, Mainiero MB, Schepps B, et al. BIRADS Lexicon for
US and mammography: interobserver variability and positive
predictive value. Radiology 2006;239(2):385–91.
(10) Hakim CM, Chough DM, Ganott MA, Sumkin JH, Zuley ML,
Gur D. Digital breast tomosynthesis in the diagnostic environ-
ment. A subjective side-by-side review. AJR 2010;195(2):172–6.
Please cite this article in press as: Mansour S. et al., Comparative study bevaluation of different breast lesions, Egypt J Radiol Nucl Med (2014), ht
(11) Helvie MA. Digital mammography imaging: breast tomosynthesis
and advanced applications. Radiol Clin North Am 2010;48(5):
917–29.
(12) Bernardi D, Ciatto S, Pellegrini M, et al. Prospective study of
breast tomosynthesis as a triage to assessment in screening. Breast
Cancer Res Treat 2012;133(1):267–71.
(13) Sahiner B, Chan HP, Hadjiiski LM, et al. Computer-aided
detection of clustered microcalcifications in digital breast tomo-
synthesis: a 3D approach. Med Phys 2012;39(1):28–39.
(14) Yang G, Qian X, Phan T, et al. Design and feasibility studies of a
stationary digital breast tomosynthesis system. Nucl Instrum
Methods Phys Res, Sect A 2011;648(Suppl 1):S220–3.
(15) Skaane P, Gullien R, Bjørndal H, et al. Digital breast tomosyn-
thesis (DBT): initial experience in a clinical setting. Acta Radiol
2012;53(5):524–9.
(16) Noroozian M, Hadjiiski L, Rahnama-Moghadam S, et al. Digital
breast tomosynthesis is comparable to mammographic spot views
for mass characterization. Radiology 2012;262(1):61–8.
(17) Kontos D, Ikejimba LC, Bakic PR, Troxel AB, Conant EF,
Maidment AD. Analysis of parenchymal texture with digital
breast tomosynthesis: comparison with digital mammography
and implications for cancer risk assessment. Radiology 2011;
261(1):80–91.
(18) Poplack SP, Tosteson TD, Kogel CA, Nagy HM. Digital
breast tomosynthesis: initial experience in 98 women with
abnormal digital screening mammography. AJR 2007;189(3):
616–23.
etween breast tomosynthesis and classic digital mammography in thetp://dx.doi.org/10.1016/j.ejrnm.2014.03.007

![Breast percent density estimation from 3D reconstructed digital breast tomosynthesis images [6913-43]](https://static.fdokumen.com/doc/165x107/6336264964d291d2a302c4a3/breast-percent-density-estimation-from-3d-reconstructed-digital-breast-tomosynthesis.jpg)