
Cognitive-Behavioral Treatment of Personality Disorders
104
8 Cognitive-Behavioral Treatment of Personality Disorders ARTHUR FREEMAN and JAMES T. JACKSON Philadelphia College of Osteopathic Medicine, USA Introduction Personality-disordered patients encountered in many psychiatric settings often provide therapists with some of the most challenging patients in their clinical caseload. The diagnosis of personality disorder is evocative and frequently viewed as prognostically negative, indicative of potential treat- ment difficulty, predictive of storminess (both within and without the therapy work), with the patient having a potential for acting out, possibilities for displays of behavior that may lead to danger to self and others, or, at its worst, all of the above. Most often presenting (as do most patients) for treatment of their Axis I problems (i.e., for treatment of anxiety or depres- sion), Axis II patients frequently show poor response rates to standard treatment. Sometimes the Axis II behavior is obvious and evident early in treatment. At other times it only surfaces as the therapy progresses from simpler to more complex issues. The therapist may find that the therapy becomes more difficult and stormy, and the clinician finds the therapeutic issues becoming increasingly more complex, "messy," and crisis laden. At this point, the clinician may rightly, or wrongly, attribute these treatment dynamics to motivational deficits such as patient resistances rather than the more likely characterological problems inherent in the personality disorder. The frequent occurrence of such experiences in clinical practice points to the need for treatment approaches yielding more useful understanding and effective treatment of this common patient population. Given the long-term nature of the patients' characterological problems, their general avoidance of psychotherapy, their frequent referral through family pressure or legal remand, and their seeming reluctance or inability to
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Cognitive-Behavioral Treatment of Personality Disorders
8
Cognitive-Behavioral Treatment of Personality Disorders
ARTHUR FREEMAN and JAMES T. JACKSON
Philadelphia College of Osteopathic Medicine, USA
Introduction
Personality-disordered patients encountered in many psychiatric settings often provide therapists with some of the most challenging patients in their clinical caseload. The diagnosis of personality disorder is evocative and frequently viewed as prognostically negative, indicative of potential treat- ment difficulty, predictive of storminess (both within and without the therapy work), with the patient having a potential for acting out, possibilities for displays of behavior that may lead to danger to self and others, or, at its worst, all of the above. Most often presenting (as do most patients) for treatment of their Axis I problems (i.e., for treatment of anxiety or depres- sion), Axis II patients frequently show poor response rates to standard treatment. Sometimes the Axis II behavior is obvious and evident early in treatment. At other times it only surfaces as the therapy progresses from simpler to more complex issues. The therapist may find that the therapy becomes more difficult and stormy, and the clinician finds the therapeutic issues becoming increasingly more complex, "messy," and crisis laden.
At this point, the clinician may rightly, or wrongly, attribute these treatment dynamics to motivational deficits such as patient resistances rather than the more likely characterological problems inherent in the personality disorder. The frequent occurrence of such experiences in clinical practice points to the need for treatment approaches yielding more useful understanding and effective treatment of this common patient population.
Given the long-term nature of the patients' characterological problems, their general avoidance of psychotherapy, their frequent referral through family pressure or legal remand, and their seeming reluctance or inability to
104 Arthur Freeman and James T. Jackson
change, they are often the most difficult patients in a clinician's caseload. They generally require more work within the session, a longer time for therapy, and more therapist energy than do other patients. All of this expenditure occurs without the same rate of change and satisfaction as are gained with other patients.
Over the years, a number of theories have been developed that attempt to explain both the etiology and mechanisms involved in the developement and maintenance of the long-term, pervasive, and generally maladaptive patterns of thinking, feeling, and behaving diagnostic of Axis II disorders. Although a review of explanatory systems other than cognitive-behavioral lies beyond the scope of the present chapter, a brief discussion of neurobiological approaches to the understanding of personality disorders may help shed light on the refractory nature of such problems with concomitant implica- tions for treatment.
The idea that differences in the personalities of individuals may be rooted in differences in neurophysiological makeup is perhaps best represented by the work of Hans Eysenck (1952, 1967, 1970). Using the method of criterion analysis in his research, Eysenck became convinced that personality dimen- sions were dominated by a few types: introversion-extraversion, stability- instability, and later psychoticism. He took the position that differences in introversion versus extraversion were traceable, in part, to differences in the brain and central nervous system. Eysenck was able to demonstrate through electroencephalographic measures that introverts and extraverts differed in their baseline level of arousal. This difference was used to explain why introverts seem to avoid external stimulation while extraverts seem to continuously seek it. These apparent differences in overt behavior patterns were thought traceable to differences in the individual's genetically programmed capacity for cortical arousal.
Reflecting an increasing appreciation of the neurophysiological dimensions of personality, a number of theorists and researchers are following Eysenck's lead in challenging the dominance of psychosocial explanations of person- ality traits and disturbances. Recent work by Depue (1996), Raine (1993), for example, describes ongoing attempts to provide: (1) a clearer conceptual framework for understanding the neurobiological mechanisms underlying personality structure; and (2) a review of recent theoretical developments and research findings that attempt to illuminate the relationship between neuro- biological systems and personality traits (including those long-standing, pervasive, and generally maladaptive behavior patterns diagnostic of person- ality disorders.)
The implications of this body of literature for the treatment of personality disorders are consistent with the theoretical underpinnings of a cognitive- behavioral approach in the following ways.

Cognitive-Behavioral Treatment of Personality Disorders 105
(1) Both approaches recognize that so called resistance on the part of such patients may more accurately reflect a fear of making changes in their intrinsic nature or, who they "really are" and "have always been." Change, depending on the degree to which it is expected, may represent the threat of "a total loss of self."
(2) Implicit in both approaches is the notion that the patient is not to blame for his or her maladaptive personality style or faulty information processing. The neurophysiological approach offers the patient the opportu- nity of reframing these experiences as a natural outgrowth of certain neurobiological processes. Hope is offered that such inherent dispositions may be modifiable through pharmacotherapy and made less problematic through modifications of the individual's environmental context (see Fogel & Ratey, 1995, for more extensive discussion.) Similarly, the cognitive approach recognizes the intractable nature of certain "schemata" seen as the driving force underlying much of the patient's maladaptive personality style (Freeman, Pretzer, Fleming, & Simon, 1990; Beck, Freeman, & Associ- ates, 1990). Recommended interventions often involve helping the patient find an environmental context which represents a "good fit." In addition, the patient is helped to reframe their problem as a natural by-product of early experience in order to avoid self-blame or an inherent sense of "badness." In each conceptual system, the refractory nature of Axis II problem makes sense when viewed as intrinsic to the individual on both a psychological and a biological level.
Although the remainder of this chapter focuses primarily on cognitive- behavioral (CBT) approaches to the treatnment of personality disorders, it seems reasonable to suggest that an approach which considers both neuro- biological and cognitive factors will help provide a much more complete understanding of the powerful forces at work in maintaining these proble- matic personality styles.
Beck, Freeman and Associates (1990), Freeman (1988 a, b), Freeman and Leaf (1989), Layden, Newman, Freeman and Beyers-Morse (1993), Linehan (1988, 1993); and Young, (1990), Young and Swift (1988) have offered comprehensive cognitive behavioral treatment protocols for treating the Axis II behaviors. In so doing, these authors generally acknowledge the need to modify standard short-term cognitive behavioral approaches to better serve the patient with an Axis II disorder (cf. Fleming and Pretzer, 1990; Turner, 1987). Suggested modifications include placing an emphasis on individual case conceptualization when designing intervention strategies; collaborative development of clearly identified, shared goals; use of efficacy-enhancing and anxiety-reducing interventions; and a focus on identifying and modifying core beliefs or schema. To these goals we would add the following:

106 Arthur Freeman and James T. Jackson
(1) Stability of the framework for treatment (2) Increased activity of the therapist (2) The therapist's ability to tolerate negative transference (4) Establishing a connection between the patient's actions and feelings in the
present (5) Making self-destructive behaviors ungratifying (6) Blocking acting-out behaviors (7) Focusing clarifications and interpretations on the here-and-now (8) Paying careful attention to countertransference feelings (Waldinger &
Gunderson, 1987, pp. 8-9).
Cognitive theorists maintain that it is usually more productive to identify and modify "core problems" in treating personality disorders. This is in contrast with the treatment of more common Axis I problems wherein the problems may be dealt with without necessarily addressing and/or changing the personality. This Axis I focus, or "symptom therapy," approach is useful in working with many patients. For example, a patient may present for therapy as unassertive, socially anxious or "shy". The therapist might also diagnose the patient as having an avoidant personality disorder. With some patients with this symptom configuration, we might treat the social anxiety with assertiveness training, challenging of the anxiogenic thinking, relaxa- tion, imaginal and in vivo exposure, role playing and stress inoculation.
For another group of patients with the same configuration, the treatment will be confounded because the Axis II disorder fuels and exacerbates the Axis I anxiety. With this group it becomes essential to deal with the Axis II problems to reduce the manifest anxiety.
For yet another group, the Axis I anxiety problems excite and stimulate the Axis II avoidant personality disorder making it difficult to deal just with the anxiety.
For a final patient group that likely comprises the majority of those with a personality disorder, there is a bidirectional influence wherein the Axis I excites the Axis II and the Axis II fuels the Axis I. For the combination of Axis I and Axis II diagnoses, the course of treatment is far more complicated than for the typical non-Axis II patient with the same presenting complaints. The duration of treatment, frequency of treatment sessions, goals, and expecta- tions for both therapist and patient and the available techniques and strategies need to be altered in the CBT treatment of personality disorders.
A clinician may not be aware initially of the characterological nature, chronicity, and severity of the patient's problems when they first present for therapy (Koenigsberg, Kaplan, Gilmore, & Cooper, 1985; Fabrega, Mezzich, Mezzich & Coffman, 1985; Karno, Hough, Burnam, et al. 1986). Often, these are the very patients whose social functioning is poor (Casey, Tryer, & Platt, 1985). When Axis II problems are a focus at intake, the patient may not

Cognitive-Behavioral Treatment of Personality Disorders 107
be willing, at treatment onset, to work on the personality disorders, but rather may choose to work on the symptoms for which he or she was referred. It is important to remember that the patient's goals, and not those of others (including the therapist), are the initial focus of treatment. The patient's schemas are the agent, as well as target of therapeutic change. If an externally referred patient is not willing to work on "core" issues, the therapist may attempt to persuade the patient to be trusting, and to follow the therapist's agenda. This kind of agenda-setting can be set up as an experiment, and viewed as one of life's challenges.
The personality disorder is a prime example (and may appear to be a caricature) of personal, cultural, family, religious, gender, and age-related schema (Freeman, 1988a; Freeman & Leaf, 1989). In the case of the personality disorder, the schema, or basic rules of life, are so obvious that they are often unmistakable and will stand out in sharp relief. Generically, the schema serve to organize information, structure categorical judgment and assist in making classifications. Schema also provide the instructions to guide the directions and qualities of one's daily life. While the schema may not typically be in awareness, the products of this process are largely conscious and with special training can become more accessible to consciousness. Dysfunctional feelings and conduct are largely due to the function of certain schemas that tend to produce consistently biased judgments and a concomi- tant tendency to make cognitive errors in certain types of situations.
The personality-disordered patient will often see the difficulties that they encounter in dealing with other people or coping with life tasks as externally generated and independent of their behavior. Much of what they experience is, in their view, "done to them" or generally coming from the ill-will or negative actions of those around them. This "other-blaming" position often places them in conflict with peers, and often puts them in conflict with larger agencies and institutions. Such patients often have little idea about how they got to be the way they are, how they contribute to their life problems, or how to change. They are often referred by family members or friends who recognize a dysfunctional pattern, or who have reached their personal limit in attempting to cope with this individual. Their style of behaving and responding seems normal and reasonable to them and they generally see the problems they encounter as a product of other people's behavior or ill- will. Other personality disordered patients are very much aware of the self- defeating nature of their personality problems (for example, overdependence, inhibition, excessive avoidance) but are at a total loss as to how to change these patterns. Still other patients may have the motivation to change but lack the basic skills to modify their behavior or to alter their relationship and interactions with coworkers and significant others.

108 Arthur Freeman and James T. Jackson
Assessment and Diagnosis
In some cases, the behavior that is now part of the Axis II disorder has been functional in life. Witness the hard-driving executive who was up at 5:00 each morning and worked until 8:00 in the evening. He may have worked his way up in the company over the years, and may have been a harsh boss and task-master, demanding high levels of performance from himself and others. He may have been a "by-the-book" executive who followed policy and procedures to the letter. In his work life many appellations might have been appropr ia te~"workahol ic ," "type-A," or "dedicated."
Having worked so hard, been successful, become financially secure, and having been a good provider for his family, he is at a loss to explain his difficulty at the point of his retirement. He is depressed and feels himself to be a failure, based on his lack of productivity. The same schemas that have driven him to be successful now drive him to despair. At retirement, the life- long behavior is dysfunctional. He may now carry the diagnosis of obsessive- compulsive personality disorder. For many individuals appropriate (or fortuitous) life choices serve to structure their lives so that they are adaptive. When the structure offered by a job, a relationship, an organization, a behavioral regimen, or hobby are removed, what has always been in place becomes pathological. For example, dependent personalities may be a good fit for service in the military, government bureaucracies, or large corporations because they are compliant with orders and procedures. A 66-year-old man, diagnosed as obsessive-compulsive, dependent, and avoidant, stated, "The best time in my life was when I was in the army. I didn't have to worry about what to wear, what to do, or what to eat."
Axis II problems are not always diagnosed at intake, though early diagnosis and treatment planning are likely to be more effective (Morrison & Shapiro, 1987). Many Axis II patients are silent about their personality problems, or deny them, as a reflection of the disorders themselves. Whether or not they are diagnosed as having personality disorders, some patients believe that their personalities are an appropriate focus of treatment, while others fear such a focus. The collaborative nature of goal setting is one of the most important features of cognitive therapy. Power struggles over conflict- ing goals usually impede progress (Foon, 1985).
A summary of diagnostic signs that may point to the possibility of Axis II problems include the following scenarios: (1) A patient or significant other reports, "Oh, he/she has always done that, since he's a little boy/girl", or the patient may report, "I've always been this way". (2) The patient is not compliant with the therapeutic regimen. While noncompliance or resistance is common element in psychotherapy for many reasons, ongoing noncom- pliance should be used as a signal for further exploration of Axis II issues. (3)
Cognitive-Behavioral Treatment of Personality Disorders 109
Therapy seems to have come to a sudden, inexplicable stop. The clinician working with these patients can often help the patient to reduce the problems of anxiety or depression only to be blocked in further therapeutic work by the personality disorder. (4) The patient seems entirely unaware of the effect of their behavior on others. They report the responses of others, but fail to address any provocation or dysfunctional behavior that they might exhibit. (5) There is a question of the motivation of the patient to come for therapy and/or to change. This problem is especially true for those patients who have "been sent" to therapy by family members or the courts. (6) The patient's personality problems appear to be acceptable and natural for them. For example, a depressed patient without an Axis II diagnosis may say "I just want to get rid of this depression. I know what it is like to feel good and I want to feel that way again." The Axis II patient may see the problems as themselves: "This is how I am", "This is who I am".
The personality disorder is probably one of the most striking representa- tions of Beck's concept of schema (Beck, 1964, 1967; Beck, Freeman, & Associates, 1990; Freeman, 1988a, 1988b; Freeman, Pretzer, Fleming, & Simon, 1990). A therapist might begin to understand the personality disor- ders, for example, by focusing on clinically relevant schemas. The specific rules that govern information processing and behavior can be classified into a variety of useful categories such as personal, familial, cultural, religious, gender, or occupational schemas. Schemas can be inferred from behavior or assessed through interview and history taking. The degree to which particular schemas are on the continuum from active to inactive, as well as the degree to which they are on the continuum from unchangeable to changeable are essential dimensions in conceptualizing the patient's problems (Beck, 1964, 1967; Beck, Freeman, & Associates, 1990; Freeman, 1988a, 1988b; Free- man, Pretzen, Fleming, & Simon, 1990). The active schemas govern our usual integration of information and our everyday behavior. These schemas have to do with how we integrate other people's behavior, and how we generally relate to people and tasks. Inactive schemas are out of awareness and become active and serve to govern behavior. When the stimulus situation is no longer present, the inactive schemas recede to their previous state of dormancy. For example, a person may state "It's silly to be worried about what strangers think of you". However, if we were to put this person in the role of giving a speech to a room full of strangers, he may feel very anxious. In this instance the latent schema related to fear of disapproval or disgrace has been activated and becomes active. At this point it governs mood and behavior. When the stressor is removed and speech is over, the person may report that, "it really wasn't too bad." When a schema is activated across all situations, whether relevant to the specific schema or not, the schema is said to be active. This activity is particularly prominent in the neuroses (Axis I
110 Arthur Freeman and James T. Jackson
disorders) where every situation may be interpreted in terms of personal loss or defeat (depression) or danger (anxiety). In the personality disorders, the schemas are often highly charged and global.
Schemas may be classified and placed on a continuum from noncompelling to compelling. A noncompelling schema is one that the individual believes in but that can relatively easily be challenged and/or surrendered. Compelling beliefs are not easily challenged and are modified only with great difficulty, or not at all. Historical examples would be the religious or political martyrs who chose to die rather than surrender their compelling views of God, or unyielding allegiances to certain political beliefs. When faced with attack, the Zealots at Masada chose to die. At the beginning of the American revolution, the American patriot Patrick Henry spoke to the Virginia House of Burgesses and stated, "I know not what course others may take, but as for me give me liberty of give me death."
Since Axis II patients are generally governed by long-lasting habitual schemas, these deeply ingrained rules and beliefs are not easily changed, even when the patient is highly motivated to do so. The chronicity of the personality disorder results from the development of these dysfunctional schemas relatively early in life.
From birth through middle childhood, schemas are, ideally, in a constant stage of evolution. According to a Piagetian model, there is a continuous adaptation to the requirements of life. Through the interactive processes of assimilation and accommodation, these schemas facilitate the organization and understanding of the phenomenological world. For many reasons, some of the schemas do not mature and are maintained at an earlier level of development. This is the beginning of an Axis II problem. The schemas that are basically functional in this earlier part of life are being applied during later, more demanding times. While most of these early schemas were at one time functional, they have long since lost their functional value by dint of never having been modified by the individual to meet changing life/world experiences. For example, if a one-year-old child would like to be picked up, it conveys that message to a caretaker by lifting its arms and grunting or crying. The caretaker responds by picking the child up. We might infer that the child has a belief, "I am weak and helpless and need a large person to meet my needs." As the child matures, the schema, "I can do things for myself" develops, and the child no longer has the schematic world view that, "I need others to take care of me and meet my basic needs." When a child at age one is demanding of attention and help, it is often thought of as cute. When that same schema is manifested at age 31, it is not cute, but quite dysfunctional and given the diagnosis of 'dependent Personality Disorder." Given the chronic nature of the problems, one must question why these behaviors are maintained. They may cause difficulty at work, in school, or in one's personal life. In some cases they are reinforced by the society; what later
Cognitive-Behavioral Treatment of Personality Disorders 111
gets labeled as obsessive-compulsive may come when parents and teachers encourage a child who is "a real hard worker", "a kid that doesn't fool around", "a kid who hasn't messed around while other kids are messing around", "a kid who really works hard and gets all perfect grades". At later points, these compelling schema which a patient may often "know" are erroneous, are hard to change. They are rationalized by questioning: "What is wrong with wanting to do one's best?" These schema often become fixed when they are reinforced and/or modeled by parents.
One of the most important treatment considerations in working with personality-disordered individuals is to be aware that when the therapist approaches the active and compelling schema he or she will evoke anxiety. The individual is being asked to give up who they are and to step out of the safety zone. It may be uncomfortable, limiting, and lonely in there, but to go out means, "I may get hurt, and feel anxious". Before a patient will adopt an appropriate therapeutic strategy, the therapist will probably have to try to reshape the patient's initial expectations about the goals, time course, and procedures of therapy, help the patient achieve some relatively immediate and practical gains, and develop a trusting and supportive collaborative relation- ship, thus attempting to limit the anxiety.
Beck and Emery (1985) in discussing the treatment of agoraphobia, state: "It is crucial that the patient experience anxiety in order to ensure that the primitive cognitive levels have been activated (since these levels are directly connected to the affects). The repeated, direct, on-the-spot recognition that the danger signals do not lead to catastrophe ... enhance[s] the responsivity of the primitive level to more realistic inputs from above" (p. 129). In discussing plans for therapy with a patient diagnosed at intake as having depression and a borderline personality disorder the therapist discussed the possibility of the patient becoming increasingly anxious as the therapy progressed. In response, the patient asked "Why are you trying to control my anxiety? I'm depressed, I'm not anxious at all". At that point the therapist explained to her that as the therapy work challenged her strongly held beliefs, typically that anxiety would be increased. He also explained about the about the need therefore to master anxiety reduction skills. These skills, it was pointed out, would be an essential factor in successful therapy.
Unless the therapist starts to help the patient to cope with the increased anxiety, the therapy may grind to a halt or the patient may leave therapy prematurally. (Space limitations preclude a detailed discussion of anxiety treatment: cf. Beck & Emery (1985); Freeman & Simon (1989)).
Given the importance of the schematic changes, the therapist must recognize that schema are difficult to alter. The schema are held firmly in place by behavioral, cognitive, and affective elements. Changing only one factor will probably not be effective in changing the schema. The therapist must take a tripartite approach. The use of behavioral approaches alone will not lead to
112 Arthur Freeman and James T. Jackson
a successful outcome. Taking a cognitive approach and trying to argue the patient out of their distortions and schema will not work. Having the patient abreact within the session to fantasies or recollections will not be successful by itself. A therapeutic program that addresses all three areas is essential.
The patient's cognitive distortions serve as signposts that point to the schema. The goal of therapy is to help the patient to identify the different rules that they live by. The therapist has several options for what might be done to work with the schema. The first option is schematic restructuring. This may be likened to urban renewal. Having decided that a structure is unsound, the decision is made to tear down the old structure and build a new structure in its place. (This has been a goal of therapy for many years, particularly in psychoanalysis.) Whether this restructuring is reasonable is very questionable. An example of schematic restructuring is to have a paranoid personality become a fully trusting individual.
A second possibility is schematic modification. This involves smaller changes in the basic manner of responding to the world. An example would be to have the paranoid personality self-instruct not to respond as the response that they typically give is undesirable.
The third possibility is schematic reinterpretation. This involves helping the patient to understand and reinterpret their schema in more functional ways. They can also work on restructuring s c h e m a ~ i f that is possible. The most reasonable goal when working with an Axis II patient is to either modify or to reinterpret the schema. By focusing on schematic reinterpretation, the therapist can find ways for the patient to deal with their schema/rules in a more adaptive and functional manner. Given that the rules are not necessarily good or bad, it depends on how they are interpreted. For example, if someone had a great need to be loved or admired, they might choose to teach preschool children, who kiss and hug the teacher. If one wants to be looked up to and respected, earning or buying a title (e.g., Professor, Doctor, or Colonel) can meet the need for status. Many choices are made because the career or occupation offers an opportunity to meet the schematic press.
A final treatment focus is what we would term 'schematic camouflage'. This involves direct changes that are more cosmetic. For example, it was suggested that a schizoid individual try certain behaviors with a coworker. While the patient did not necessarily understand fully the meaning and subtleties of the behaviors, he was willing to do them, thereby making himself much more acceptable in the office.
Cognitive-Behavioral Treatment
The initial goal of therapy is an assessment of the problems and the development of a conceptualization of the patient's problems with appro- priate treatment plan. When therapists recognize that cases involve person- ality disorders, studies suggest that they will view the case as especially
Cognitive-Behavioral Treatment of Personality Disorders 113
difficult (Merbaum & Butcher, 1982; Rosenbaum, Horowitz, & Wilner, 1986). Anticipated patient "resistance" is probably the main source of such perceptions. In fact, these expectations are often accurate. When treating personality disorders, it may be difficult to agree about goals and to maintain good therapeutic collaboration. For example, a prominent wealthy business- man whose principal problem, in the view of the therapist, was a narcissistic personality disorder, entered therapy, in response to his wife's entreaties. His goal was to deal with problems of anger, anxiety, and guilt arising from marital conflict. Like most patients who were not self-referred, he was not interested in schema-therapy, but only in symptom-therapy (Chamberlain, Patterson, Reid, et al. 1984).
An excellent technique for assessment and structuring of the treatment is the use of the Diagnostic Profiling System (Freeman, 1997) using the diagnostic criteria of DSM-IV or ICD-10. This system provides the therapist with a tool to graph the severity of the DSM-IV criteria that comprise the patient's diagnosis. Since clients with the same diagnosis will usually differ in the severity and pattern of their symptoms, this assessment approach will enable the therapist and client to structure the therapy on the basis of objective assessment data reflecting the individual needs of each client.
Following the assessment, the therapist must make sure that the patient is socialized or educated to the CBT model. To make sure that there is appropriate informed consent for therapy, the therapist must explain what the therapy involves, the goals and plans of the therapy, the importance of therapeutic collaboration, the particular areas of difficulty that will be emphasized, and the likely techniques that will be used in therapy.
The initial therapeutic focus may be on relieving the presenting symptoms ~ anxiety or depression. In helping the patient to deal with their anxiety or depression, the therapist can teach the patient the basic cognitive therapy skills that are going to be necessary in working with the more difficult personality disorder. If the therapist can help the patient become less depressed or less anxious, the patient may accept that this therapy may have some value after all, and it may be worthwhile continuing to work in therapy.
The essential nature of the therapeutic collaboration and the building of a strong working alliance is nowhere more important than with the Axis II patient. The relationship will be one of the key ingredients in the therapy of the personality disorder. The therapeutic relationship will be a microcosm of the patient's responses to others in their environment. The sensitive nature of the relationship means that the therapist must exercise great care in working with this patient group. Being even two minutes late for a session with the dependent personality may evoke anxiety about abandonment. The same two minutes will raise the specter of being taken advantage of in the paranoid personality. Building and maintaining trust, essential to good therapy generally, is imperative. Given the imperative nature of trust in the relation- ship, few patients test the patience and mettle of a therapist more than

114 Arthur Freeman and James T. Jackson
the Axis II group. Issues of the therapist's countertransference must be acknowledged and addressed directly by the therapist.
The collaborative nature of the therapy must be constantly stressed. The therapy of the personality disorder must include a strong supportive/expres- sive component. Without the therapist's active support, the patient may quickly become frightened and disillusioned and leave therapy. The colla- borative set involves setting mutually acceptable, reasonable and proximal goals for therapy. By making small steps toward the desired goals, therapy can move ahead slowly but effectively.
The rate of treatment and flame of treatment must also be discussed. The patient who expects to be "cured" in 12-20 sessions must be apprised of the greater severity and chronicity of their problems and that these problems will take a longer time for treatment. The therapist must choose reasonable, goals for the time and duration of the available therapy. The "cure versus coping" issue suggests that the goal will be the psychoeducational building of coping skills.
The patient's significant others can be invaluable allies in the therapeutic endeavor by helping the patient to do homework and do reality testing, and offering support in making changes. The significant others can also be important sources of data about the patient's past behaviors. In a negative vein, meeting with the significant others may enable the therapist to piece together a family history of problems and understand the family system dynamics that keep the patient behaving in the same dysfunctional way. Finally, the significant others might be involved in marital or family therapy with the patient.
Summary
The nature of the Axis II problems makes treatment different from the Axis I therapy. One may skip steps when dealing with symptomatic problems (Axis I) where therapy may proceed rapidly, but in working with personality- disordered patients it is best to make sure they have a clear understanding of why schemata are the major focus of cognitive therapy, of the pace at which they can expect progress with their problems, and of the kind of support they can and cannot expect from their therapist.
References Beck, A. T. (1964). Thinking and depression: II. Theory and therapy. Archives of General
Psychiatry, 10, 561-571. Beck, A. T. (1967). Depression: Clinical, experimental, and theoretical aspects. New York:
Harper & Row. Beck, A. T., & Emery, G. (with Greenberg, R. L.) (1985). Anxiety disorders and phobias. A
cognitive perspective. New York: Basic Books.

Cognitive-Behavioral Treatment of Personality Disorders 115
Beck, A. T., Freeman, A., & Associates (1990). Cognitive therapy of personality disorders. New York: Guilford Press.
Casey, P. R., Tryer, P. J., & Platt, S. (1985). The relationship between social functioning and social functioning in primary care. Social Psychiatry, 20(1), 5-9.
Chamberlain, P., Patterson, G., Reid, J., Kavanaugh, K., & Forgatch, M. (1984). Observation of client resistance. Behavior Therapy, 15, 144-155.
Depue, R. A. (1996). A neurobiological framework for the structure of personality and emotion: implications for personality disorders. In J. F. Clarkin & M. L. Lenzenweger (Eds.), Major theories of personality disorder. New York: Guilford Press.
Eysenck, H. J. (1952). The scientific study of personality. London: Routledge and Kegan Paul. Eysenck, H. J. (1967). The biological basis of personality. Springfield, IL: Charles C. Thomas. Eysenck, H. J. (1970). The structure of human personality (3rd ed.). London: Methuen. Fabrega, H., Mezzich, J. E., Mezzich, A. C., & Coffman, G. A. (1985). Descriptive validity of
DSM~ depressions. Journal of Nervous and Mental Disease, 174(10), 573-584. Fogel, B. F., & Ratey, J. J. (1995). A neuropsychiatric approach to personality and behavior.
In J. J. Ratey (Ed.), Neuropsychiatry of personality disorders. Cambridge MA: Blackwell Science.
Fleming, B., & Pretzer, J. (1990). Cognitive-behavioral approaches to personality disorders. In M. Herson (Ed.), Advances in behavior therapy. Newbury Park, CA: Sage.
Foon, A. E. (1985). The effect of social class and cognitive orientation on clinical expectations. British Journal of Medical Psychology, 58(4) 357-364.
Freeman, A. (1988a). Cognitive therapy of personality disorders. In C. Perris, I. Blackburn, & H. Perris (Eds.), Cognitive psychotherapy: Theory and practice. New York: Springer Verlag.
Freeman, A. (1988b). Cognitive therapy of personality disorders. In C. Perris & M. Eismann (Eds.), Cognitive psychotherapy: An update. Umea, Sweden: DOPUU Press.
Freeman, A., & Leaf, R. C. (1989). Cognitive therapy applied to personality disorders. In A. Freeman, K. M. Simon, L. E. Beutler, & H. Arkowitz (Eds.), Comprehensive handbook of cognitive therapy. New York: Plenum Press.
Freeman, A., Pretzer, J., Fleming, B., & Simon, K. M. (1990). Clinical applications of cognitive therapy. New York: Plenum Press.
Freeman, A., & Simon, K. M. (1989). Cognitive therapy of anxiety. In A. Freeman, K. Simon, L. Beutler, & H. Arkowitz (Eds.), Comprehensive casebook of cognitive therapy. New York: Plenum Press.
Karno, M., Hough, R. L., Burnam, M. A., Escobar, J. I., Timbers, D. M., Santana, F., & Boyd, J. H. (1986). Lifetime prevelance of specific psychiatric disorders among Mexican Americans and non-Hispanic whites in Los Angeles. Archives of General Psychiatry, 44(8), 695-701.
Koeningsberg, H., Kaplan, R., Gilmore, M., & Cooper, A. (1985). The relationship between syndrome and personality disorder in DSM-III: Experience with 2,462 patients. American Journal of Psychiatry, 142, 207-212.
Layden, M. A., Newman, C. F., Freeman, A., & Byers-Morse, S. (1993). Cognitive therapy of borderline personality disorder. Needham Heights, MA : Allyn & Bacon.
Linehan, M. M. (1988). Perspectives on the interpersonal relationship in behavior therapy. Journal of Integrative and Eclectic Psychotherapy, 7, 278-290.
Linehan, M. M. (1993). Cognitive-behavioral treatment of borderline personality disorder. New York: Guilford Press.
Merbaum, M., & Butcher, J. N. (1982).Therapist's liking of their psychotherapy patients: Some issues related to severity of disorder and treatability. Psychotherapy: Theory, Research and Practice, 19(1), 6-76.
Morrison, L. A., & Shapiro, D. A. (1987). Expectancy and outcome in prescriptive vs. exploratory psychotherapy. British Journal of Clinical Psychology, 26(1), 59-60.

116 Arthur Freeman and James T. Jackson
Raine, A. (1993). The psychopathology of crime: Criminal behavior as a clinical disorder. San Diego CA: Academic Press.
Rosenbaum, R. L., Horowitz, M. J., & Wilner, N. (1986). Clinician assessments of patient difficulty. Psychotherapy, 23(3), 417-422.
Turner, S. M. (1987) The effects of personality disorder diagnosis on the outcome of social anxiety symptom reduction. Journal of Personality Disorders, 1,136-143.
Waldinger, R. J., & Gunderson, J. G. (1987). Effective psychotherapy with borderline patients: Case studies. New York: MacMillan.
Young, J. E. (1990). Cognitive therapy for personality disorders: A schema focused approach. Sarasota, FL: Professional Resource Exchange.
Young, J. E., & Swift, W. (1988). Schema focused cognitive therapy for personality disorders: Part I. International Cognitive Therapy Newsletter, 4(5), 13-14.

9
Applications of Cognitive Models of OCD in Clinical Practice
MARK H. FREESTON, ROBERT LADOUCEUR, JOSI~E RHEAUME, and ELIANE LINGER
Universit~ Laval, Quebec, Canada
Although cognitive-behavior therapy for obsessive-compulsive disorder (OCD) based on exposure and response prevention typically produces improvement in 80% of patients, it is also accepted that a significant number of patients do not benefit through refusal, dropout, or nonresponse. One subgroup has often been left out of treatment trials, namely, those with obsessive thoughts only (Ball, Baer, & Otto, 1996). However, breakthroughs in the conceptualization and treatment of this subgroup may help the efficacy of OCD treatment in general. In fact, the efficacy of cognitive-behavior therapy has only recently been established for obsessive thoughts when overt compulsions are absent (e.g., Freeston, Ladouceur, Gagnon, et al., 1997). The results of two clinical trials for patients without overt compulsions will be presented. The first was a controlled trial of cognitive-behavior therapy for obsessional thoughts only (Freeston et al., 1997). Treatment consisted of exposure to the obsessional thought using tape-loop exposure and response preven-tion of all effortful coping strategies (neutralization). Cognitive restructuring was also used as needed. Of 36 patients who were accepted for treatment, 29 patients were assigned to treatment or wait-list. The score on the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS; Goodman, Price, Rasmussen, et al., 1989) for the intention-to-treat sample is shown in Figure 9.1. The scores at posttest and follow-up are shown in Figure 9.1 for completers (n=22). For completers, 77% showed clinically significant
This paper was presented in (S. Taylor, chair) "Treatment of Obsessive-Compulsive Disorder: Current Status and Future Directions". Symposium presented at the XXVII Congress of the European Association for Behavioural and Cognitive Therapies, Venice, September, 1997.
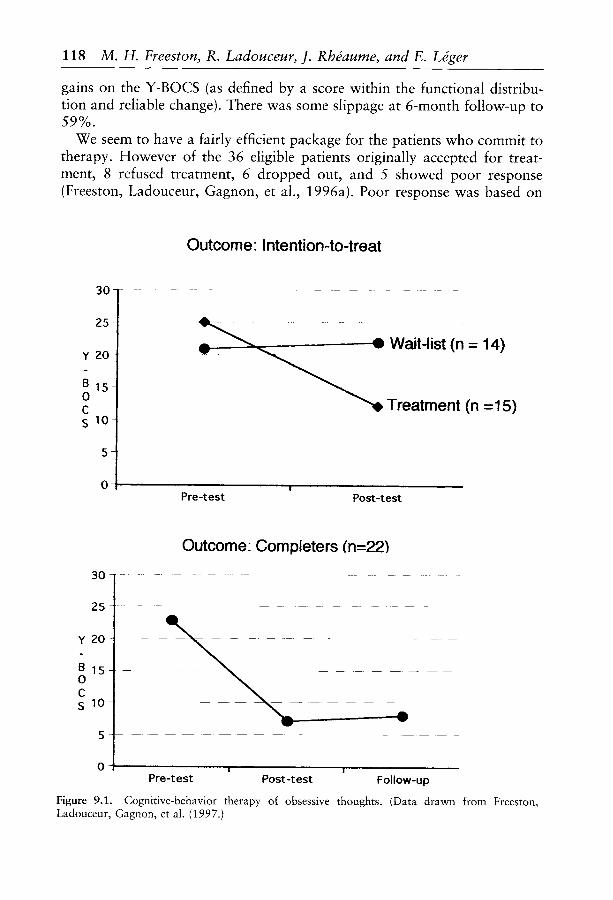
gains on the Y-BOCS (as defined by a score within the functional distribu- tion and reliable change). There was some slippage at 6-month follow-up to 59%.
We seem to have a fairly efficient package for the patients who commit to therapy. However of the 36 eligible patients originally accepted for treat- ment, 8 refused treatment, 6 dropped out, and 5 showed poor response (Freeston, Ladouceur, Gagnon, et al., 1996a). Poor response was based on
Outcome Intention-to-treat
30
25
Y 20-
B 1 5 - 0 C S 10-
_
0
3 0 -
.. ~ =- Wait-list (n = 14)
~ l ~ Treatment (n =15)
!
Pre-test Post-test
Outcome Completers (n=221
25-
Y 20-
BIS 0 C s l O -
. _
A
0
%
118 M. H. Freeston, R. Ladouceur, J. Rh#aume, and E. L@er
v V
A
. . . . . I I " ' ' I '
Pre-test Post-test Follow-up
Figure 9.1. Cognitive-behavior therapy of obsessive thoughts. (Data drawn from Freeston, Ladouceur, Gagnon, et al. (1997.)
Cognitive Models of OCD in Clinical Practice 119
end-state functioning across five measures (self and clinician ratings of OCD symptoms, interference in diverse life domains, anxiety, and depression). Those who refused treatment had received significantly less previous treat- ment and those who dropped out were older, more depressed, and reported more severe obsessions. Finally those who did poorly had relatively more checking behavior (not targeted during therapy), and used more reassurance- seeking and ruminative strategies. This last subgroup is especially interesting: poor response was associated with particular differences in the neutralizing strategies. We have made progress since this trial and are probably better equipped to address the neutralizing and the interpretations that are driving it. Despite good results, we still have a long way to go in reaching everyone.
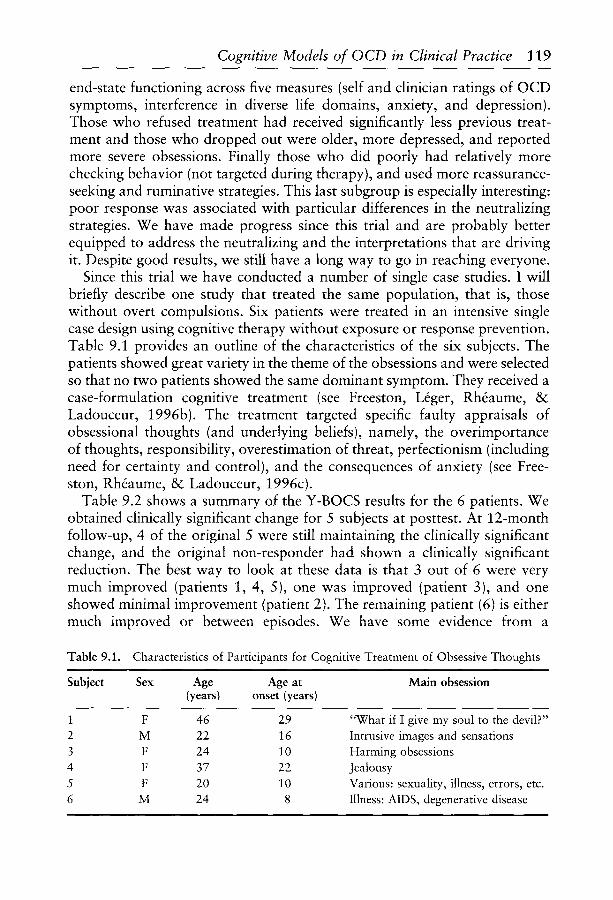
Since this trial we have conducted a number of single case studies. I will briefly describe one study that treated the same population, that is, those without overt compulsions. Six patients were treated in an intensive single case design using cognitive therapy without exposure or response prevention. Table 9.1 provides an outline of the characteristics of the six subjects. The patients showed great variety in the theme of the obsessions and were selected so that no two patients showed the same dominant symptom. They received a case-formulation cognitive treatment (see Freeston, L~ger, Rh~aume, & Ladouceur, 1996b). The treatment targeted specific faulty appraisals of obsessional thoughts (and underlying beliefs), namely, the overimportance of thoughts, responsibility, overestimation of threat, perfectionism (including need for certainty and control), and the consequences of anxiety (see Free- ston, Rh~aume, & Ladouceur, 1996c).
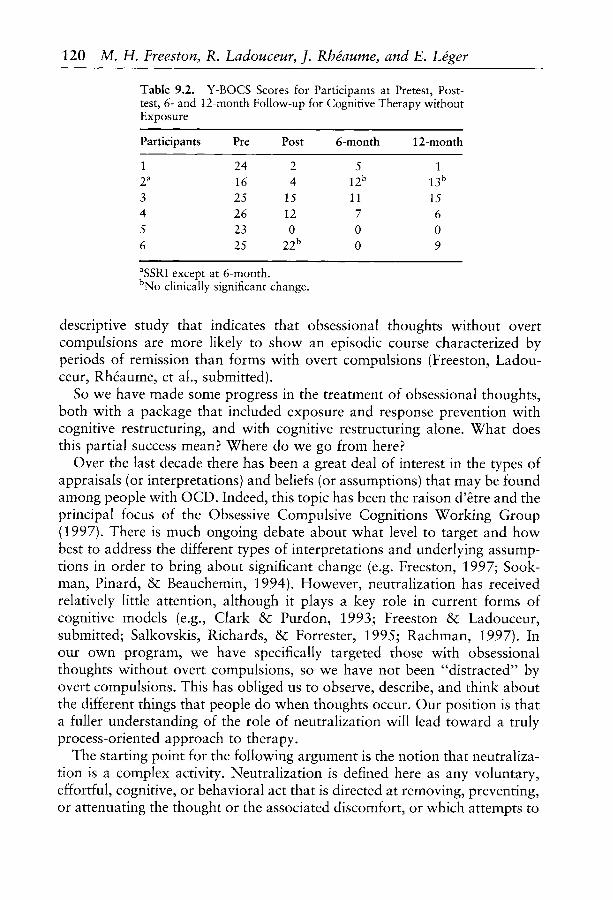
Table 9.2 shows a summary of the Y-BOCS results for the 6 patients. We obtained clinically significant change for 5 subjects at posttest. At 12-month follow-up, 4 of the original 5 were still maintaining the clinically significant change, and the original non-responder had shown a clinically significant reduction. The best way to look at these data is that 3 out of 6 were very much improved (patients 1, 4, 5), one was improved (patient 3), and one showed minimal improvement (patient 2). The remaining patient (6) is either much improved or between episodes. We have some evidence from a
Table 9.1. Characteristics of Participants for Cognitive Treatment of Obsessive Thoughts
Subject Sex Age Age at Main obsession (years) onset (years)
1 F 46 29 2 M 22 16 3 F 24 10 4 F 37 22 5 F 20 10 6 M 24 8
"What if I give my soul to the devil?" Intrusive images and sensations Harming obsessions Jealousy Various: sexuality, illness, errors, etc. Illness: AIDS, degenerative disease
120 M. H. Freeston, R. Ladouceur, J. RhOaume, and E. LSger
Table 9.2. Y-BOCS Scores for Participants at Pretest, Post- test, 6- and 12-month Follow-up for Cognitive Therapy without Exposure
Participants Pre Post 6-month 12-month
1 24 2 5 1 2 a 16 4 12 b 13 b
3 25 15 11 15 4 26 12 7 6 5 23 0 0 0 6 25 22 b 0 9
aSSRI except at 6-month. bNo clinically significant change.
descriptive study that indicates that obsessional thoughts without overt compulsions are more likely to show an episodic course characterized by periods of remission than forms with overt compulsions (Freeston, Ladou- ceur, Rh6aume, et al., submitted).
So we have made some progress in the treatment of obsessional thoughts, both with a package that included exposure and response prevention with cognitive restructuring, and with cognitive restructuring alone. What does this partial success mean? Where do we go from here?
Over the last decade there has been a great deal of interest in the types of appraisals (or interpretations) and beliefs (or assumptions) that may be found among people with OCD. Indeed, this topic has been the raison d'&re and the principal focus of the Obsessive Compulsive Cognitions Working Group (1997). There is much ongoing debate about what level to target and how best to address the different types of interpretations and underlying assump- tions in order to bring about significant change (e.g. Freeston, 1997; Sook- man, Pinard, & Beauchemin, 1994). However, neutralization has received relatively little attention, although it plays a key role in current forms of cognitive models (e.g., Clark & Purdon, 1993; Freeston & Ladouceur, submitted; Salkovskis, Richards, & Forrester, 1995; Rachman, 1997). In our own program, we have specifically targeted those with obsessional thoughts without overt compulsions, so we have not been "distracted" by overt compulsions. This has obliged us to observe, describe, and think about the different things that people do when thoughts occur. Our position is that a fuller understanding of the role of neutralization will lead toward a truly process-oriented approach to therapy.
The starting point for the following argument is the notion that neutraliza- tion is a complex activity. Neutralization is defined here as any voluntary, effortful, cognitive, or behavioral act that is directed at removing, preventing, or attenuating the thought or the associated discomfort, or which attempts to
Cognitive Models of OCD in Clinical Practice 121
change the meaning given to its presence or its content (see Freeston & Ladouceur, 1997, submitted). This is a functional definition of neutralization and covers all possible forms. The cognitive models referred to above all suggest that neutralizing is a response to the threat that results from the faulty appraisal of the intrusive thought, although they differ according to the type of threat that is believed to be primary.
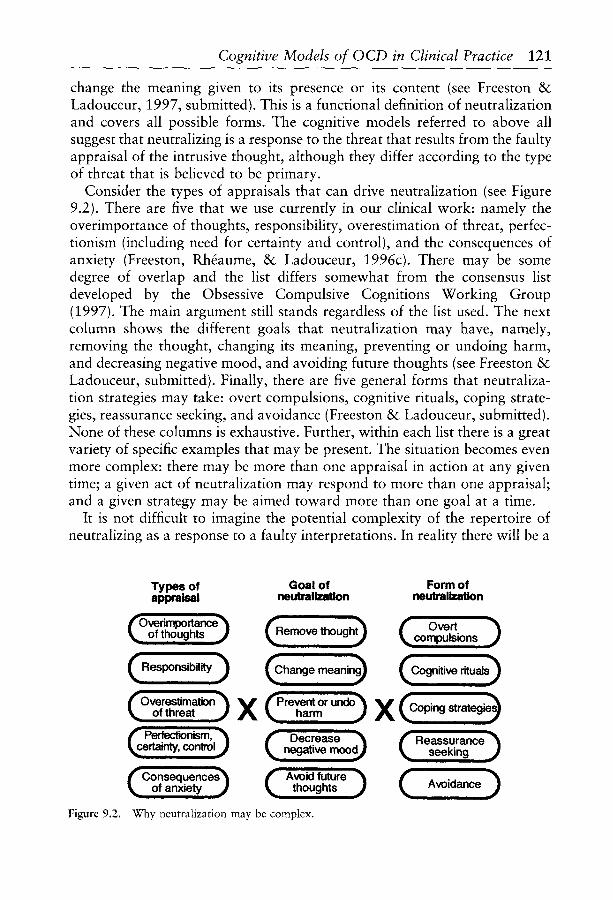
Consider the types of appraisals that can drive neutralization (see Figure 9.2). There are five that we use currently in our clinical work: namely the overimportance of thoughts, responsibility, overestimation of threat, perfec- tionism (including need for certainty and control), and the consequences of anxiety (Freeston, Rh~aume, & Ladouceur, 1996c). There may be some degree of overlap and the list differs somewhat from the consensus list developed by the Obsessive Compulsive Cognitions Working Group (1997). The main argument still stands regardless of the list used. The next column shows the different goals that neutralization may have, namely, removing the thought, changing its meaning, preventing or undoing harm, and decreasing negative mood, and avoiding future thoughts (see Freeston & Ladouceur, submitted). Finally, there are five general forms that neutraliza- tion strategies may take: overt compulsions, cognitive rituals, coping strate- gies, reassurance seeking, and avoidance (Freeston & Ladouceur, submitted). None of these columns is exhaustive. Further, within each list there is a great variety of specific examples that may be present. The situation becomes even more complex: there may be more than one appraisal in action at any given time; a given act of neutralization may respond to more than one appraisal; and a given strategy may be aimed toward more than one goal at a time.
It is not difficult to imagine the potential complexity of the repertoire of neutralizing as a response to a faulty interpretations. In reality there will be a
Types of Goal of Form of appraisal neutralization neutralizatk)n
fOverimportan~ (Remove thought-'~ r Overt ~_ ofthoughts ~ ~compulsions )
(Responsibility) (~hange mean;ng~ (Cognitive dtuals) i
~ ofthreat J X t~Ove'restimati~ ~ ~Prevent ~ and~ (C~ strateg~-~ harm X ~'"'Perfe~nism;' ~ ~ Decrease ~rtainty, contml~ ~ negative mood J ( ReassuranCeseeking )
i _
i ! i m m i I ~Consequences~ f~ Avoid future '~ ( ) of anxiety ~ ~ though!s ~ Avoidance i i i i
Figure 9.2. Why neutralization may be complex.

122 M. H. Freeston, R. Ladouceur, J. RhSaume, and E. LSger
fairly limited number of alternatives that are in play for a given patient in each column. There is often a clear hierarchy in terms of the relative importance of each appraisal-neutralization link. Now consider how neutra- lization may contribute to maintaining obsessional problems. Neutralization may act at several levels. It may influence (1) the occurrence of subsequent intrusions, (2) appraisals and underlying assumptions, (3) mood, and (4) subsequent neutralization. Only the first two will be addressed here, namely, the effects on intrusions and on appraisals (and underlying assumptions).
Figure 9.3 shows some ways in which neutralization may contribute to the occurrence of subsequent intrusions. Attempts to suppress may lead to enhancement and or r e b o u n d ~ b u t the jury is still out (see Purdon & Clark, in press, for a review). Any attempts to suppress or change meaning may also decrease the threshold for detection of subsequent thoughts. On the other hand, attempts to change meaning involve the recall and organization of thematically-related information: the person remains in the same content domain as the original intrusion, so it would not be surprising that other intrusions occur (this may be similar to a process in worry that has been described as tagging by Wells & Papageorgiou, 1995). Likewise, attempts to undo or prevent harm may also have same ef fec t~the actions performed remain connected by meaning to the original thought. (In addition, as the action often cannot objectively prevent or undo harm in a real-world way, and as people with OCD generally retain some degree of insight, it may also
Remove thought~~,,,,\\\,\,....,..,..\.~,,,\\~,. (l~nhancement, reboun~ l...a$,,,~,,n,,,,,,,, .IL ~both, or neither?
~Change meanin . (Decrease ~tetecfi0n Ill
m m m m m u m m m ~hreshold ,
(Recall, organization, ] h ~ " ~ ~ l ~ m ~ ~ ~ ! on thematically_ | P r e v e n t or undo i repetition, and acting |
lrelated information l i increases associations I
Avoid future ~ k~and leads to cuein J thoughts
~ fAssociating thoughts . . . . . . . . ]with evironmental or
emotional referents (Decrease negativ~ .................................. ~ ~ , ~ m o o d ....................................................
Figure 9.3. How neutralization may increase the frequency of subsequent intrusions.

Cognitive Models of O CD in Clinical Practice 123
be natural to doubt the efficacy of performing an objectively meaningless action and so a further intrusion may be triggered). If avoidance of future thoughts is the goal of the action, avoidance must be planned and so attention is actively allocated to intrusion-relevant material. At another level, attempts to prevent or undo harm and attempts to avoid future thoughts may both result in physical actions that occur in a particular context and so establish links to environmental referents. Similar effects may be observed when the goal is to decrease anxiety or negative mood. These linkages mean that the triggering can then occur when the referents or related cues are encountered. Once again, an associative network of intru- sion-related material remains accessible. Thus any of these potential mechan- isms may contribute to triggering and detecting subsequent intrusions.
Now consider the possible effects of neutralization on interpretations (and underlying assumptions). The thought-suppression literature indicates that attempts to suppress generally do not succeed, even if enhancement or rebound does not occur (Figure 9.4). Thus the continuing presence or the reoccurrence of the thought following attempted suppression or control may reinforce appraisals related to the overimportance of thoughts ("It won't go away, so it must be important"), the loss of mental control ("I'm losing control of my mind"), or contribute to a sense of agency through the omission bias ("If I keep on thinking about it, it means that I am still responsible"; see Salkovskis, Richards, & Forrester, 1995). Attempts to
I III
(Remove thought)..,.............,,.....,..~..,Nx~,.. ( Fails "> increases , , " I - importance
! - loss of control
( ' - - ' " ' " " ' " " ~ l ~ . _ qC sense of agency Change meaning
Prevent or undo harm
l i I i i
r o n l y the guilty need I t o proclaim their
innocence - QED
~ . . = ~ ~ ~ � 9 A v oi d future "
thoughts ~ (Generates confirmatory-'~ I evidence only |
A t - ]Prevents / [Decrease negative~_ ............................... .L ~ any ~ i s c o ~ r m a t i o n J kmood ,, J ............................................... . . . . .
Figure 9.4. How neutralization may strengthen appraisals and underlying beliefs.

124 M. H. Freeston, R. Ladouceur, J. Rh~aume, and E. L~ger
change meaning, or to prevent or undo harm, and avoidance of future intrusions will reinforce various appraisals according to the principle that only the guilty have to proclaim their innocence. That is, "I have to do this (change the meaning, undo, prevent, avoid, etc.) because it is important or might be true and the fact that I have to do this confirms that it is important or might be true, otherwise I wouldn't do it!" Finally, attempts to prevent or undo harm, avoid future intrusions, or decrease anxiety can only generate evidence relevant to confirming the original faulty conclusion. They also prevent new contradictory evidence from being generated.
What then are the implications of this speculative analysis? The analysis is based largely on observations with patients without overt compulsions. Structured interview data showed that patients with overt compulsions, in addition to their more familiar checking rituals, also showed a full range of other neutralizing activities such as those described among ruminators (Ladouceur, Freeston, Rh6aume, et al., submitted). Thus, it is logical to propose that the following points apply equally to OCD with and without overt com-pulsions. Response prevention (following exposure) can be a highly effective treatment strategy because 1) neutralizing will no longer contribute to trig-gering intrusions or keeping intrusion relevant material in mind, and 2) it will stop neutralizing from reinforcing the faulty appraisals and assumptions.
�9 Response prevention (following exposure) can be a highly effective treatment strategy because (1) neutralizing will no longer contribute to triggering intrusions or keeping intrusion relevant material in mind, and (2) it will stop neutralizing from reinforcing the faulty appraisals and assumptions.
�9 Response prevention will be less effective if key appraisal-neutralization links are not addressed. The patient may switch to less ritualized strategies or continue avoiding, which will maintain thoughts and continue to reinforce assumptions. Explicitly addressing the appraisal- neutralization link may help patients detect new or subtle forms of neutralization that, if ignored, could contribute to relapse.
�9 Cognitive strategies aimed at faulty appraisals, particularly strategies that use behavioral experiments where people act in different ways, may help people to stop neutralizing. A result equivalent to response prevention instructions should be obtained if faulty interpretations (and underlying assumptions) are corrected: people will stop neutralizing because there is no longer any need to respond to threat.
�9 Cognitive restructuring techniques will be ineffective if people continue to neutralize: intellectually accepting that an appraisal or interpretation is faulty will have little impact on symptoms if it is not followed up by action.

Cognitive Models of OCD in Clinical Practice 125
In other words, the ultimate goal of response prevention is to modify appraisals and the ultimate goal of correcting appraisals is response preven- tion. They may be seen as two sides of the same coin. Blanket response prevention may not always be very elegant, but it can be very effective. However, it may be difficult for some patients to accept exposure and response prevention, and so treatment is sometimes refused or response prevention is implemented partially. We normally use some degree of exposure and response prevention, in an explicitly cognitive framework. Initial cognitive restructuring prepares the way for exposure exercises which in many cases are presented as behavioral experiments. In this way we can ensure that people will act on the modified appraisals, and at the same time ensure that key faulty appraisals are not impeding response prevention. The approach outlined above is based on an understanding of the appraisal- neutralization link. It assumes a priori the presence of a complex repertoire of neutralizing behavior that is driven by appraisals. In turn, neutralizing contributes to maintaining and strengthening the assumptions and to the continuing occurrence of intrusive thoughts. Given that patients with overt compulsions also report a variety of other strategies (Ladouceur, Freeston, Rh~aume, et al., submitted), this broadened perspective on the use of cognitive and behavioral techniques within an understanding of the apprai- sal-neutralization link should extend the efficacy of treatment for OCD, regardless of whether overt compulsions are present or absent.
Acknowledgments The studies described in this chapter were supported by grants from le
Fonds de recherche en sant8 du Quebec and the Medical Research Council of Canada awarded to Robert Ladouceur. Mark Freeston received support from the Medical Research Council of Canada and the Social Sciences and Humanities Research Council of Canada.
Mark Freeston is now Chercheur adjoint at the D~partement de psychia- trie, Universit~ de Montreal.
References Ball, S. G., Baer, L., & Otto, M. W. (1996). Symptom subtypes of obsessive-compulsive
disorder in behavioral treatment studies: a quantitative review. Behaviour Research and Therapy, 34, 47-51.
Clark, D. A., & Purdon, C. (1993). New perspectives for a cognitive theory of obsessions. Australian Psychologist, 28, 161-167.
Freeston M. H. (1997, March). Levels of cognition in OCD: Conceptualization, assessment and change. In A. Pollard (Chair), Cognition in OCD. Symposium presented at the Annual Meeting of the Anxiety Disorders Association of America, New Orleans.
Freeston, M. H., & Ladouceur, R. (1997). What do patients do with their obsessive thoughts? Behaviour Research and Therapy, 35, 335-348.
126 M. H. Freeston, R. Ladouceur, J. Rh~aume, and E. LSger
Freeston, M. H., Ladouceur, R., Gagnon, F., Thibodeau, N., Rh~aume, J., Letarte, L., & Bujold, A. (1997). Cognitive-behavioral treatment of obsessional thoughts: A controlled study. Journal of Consulting and Clinical Psychology, 65, 405-413.
Freeston, M. H., Ladouceur, R., Gagnon, F., Thibodeau, N., Rhdaume, J., Letarte, H., & Bujold, A. (1996a, November). Classes of outcome in the treatment of obsessive thoughts. Communication presented at the Annual Meeting of the Association for the Advancement of Behavior Therapy, New York.
Freeston M. H., L~ger, E., Rhdaume, J., & Ladouceur, R. (1996b, November). The treatment utility of cognitive assessment in OCD. In G. Steketee (Chair), Cognitive aspects of OCD. Symposium presented at the Annual Meeting of the Association for the Advancement of Behavior Therapy, New York.
Freeston, M. H., Rh6aume, J., & Ladouceur, R. (1996c). Correcting faulty appraisals of obsessive thoughts. Behaviour Research and Therapy, 34, 433-446.
Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Fleischmann, R. L., Hill, C. L., Heniger, G. R., & Charney, D. S. (1989). The Yale-Brown Obsessive Compulsive Scale. I. Development, use and reliability. Archives of General Psychiatry, 46, 1006-1011.
Obsessive Compulsive Cognitions Working Group (1997). Cognitive assessment of obsessive- compulsive disorder. Behaviour Research and Therapy, 35, 667-681
Purdon, C., & Clark, D. A. (in press). White bears and other elusive cognitions: assessing the relevance of thought suppression for obsessional phenomena. Behaviour Modification.
Rachman, S. (1997). A cognitive theory of obsessions. Behaviour Research and Therapy, 35, 793-802.
Salkovskis, P. M., Richards, H. C., & Forrester, E. (1995). The relationship between obsessional problems and intrusive thoughts. Behavioural and Cognitive Psychotherapy, 23,281-299.
Sookman, D., Pinard, G., & Beauchemin, N. (1994). Multidimensional schematic restructur- ing treatment for obsessions: theory and practice. Journal of Cognitive Psychotherapy: An International Quarterly, 8, 175-194.
Wells, A., & Papageorgiou, C. (1995). Worry and the incubation of intrusive images following stress. Behaviour Research and Therapy, 33, 579-583.

10
Process of Change in Exposure Therapy of Phobias
K. GUNNAR GOTESTAM and BENGTA GOTESTAM
Norwegian University of Science and Technology, Trondheim, Norway
Introduction
Exposure has become the main principle for treating most of the phobias. For many specific phobias, a one-session treatment procedure has been developed (Ost, 1997). In our work with treatment and scientific investiga- tions of phobias, we have found the one-session procedure to be a useful tool for the investigation of the process of change. In a recent paper (G6testam & Berntzen, 1997), we pointed at the strong modeling effect in this situation. A natural development and use of this effect is to develop a group treatment procedure (G6testam, 1994; Ost, 1996).
In one study (Merluzzi, Taylor, Boltwood, & G6testam, 1991)we were able to show how blocking of the endorphin receptor system impedes the exposure effect, and later we also showed how blocking of the benzodiaze- pine receptor system reduces the exposure effect, while stimulation of the receptors improves it (G6testam, Taylor, & Trabert, 1995). However, the exposure procedure was incredibly potent, and overshadowed most of the other factors under study.
In the present study, we have taken the one-session exposure therapy paradigm further to study some other process phenomena. Our hypotheses are: (1) different treatment components, as observation versus exposure, have differential effects on the outcome; (2) personality changes do occur after exposure therapy of short duration; (3) "symptom substitution" will not be demonstrable, rather there is a generalization effect of exposure treatment.
128 K. Gunnar G6testam and Bengta G6testam
Methods
Setting
The setting is a university department, with a diverse research program, where some of the research efforts are directed toward anxiety disorders. We have studied fear of flying (Haug, Brenne, Johnsen, et al., 1987), dental phobia (G6testam, Berntzen, Grfiwe, et al., 1989), spider phobia (G6testam, Taylor, & Trabert, 1995), mouse and rat phobia (G6testam & Berntzen, 1997), tunnel phobia (G6testam & Svebak, 1996), and obsessive-compulsive disorder (OCD; G6testam & Vogel, 1997). On a clinical basis, we also treat other anxiety disorders, in connection with an outpatient unit (other animal phobias, blood/syringe phobia, social phobia, agoraphobia, claustrophobia, posttraumatic stress disorder (PTSD)).
Treatments
The treatments reported in this study are with small-animal phobias and with tunnel phobia.
One-session treatment. treatment.
The standard procedure is a 2-hour one-session
Pairs of phobias. Two patients are in the treatment room at the same time. One is treated with exposure for the phobia. The other patient "just wanted to observe", sits at a distance. When the treatment of the first patient is completed, the "observer" invariably wants to be exposed, and this treatment is completed wthin ten minutes (G6testam & Berntzen, 1997).
Group formats. Three different group conditions have been used (G6tes- tam, 1994): a live procedure (with 8 patients and 8 spiders); a model procedure (with 8 patients, and one model and spider); and a video procedure (with 8 patients in front of a video monitor, where the treatment of a patient is shown).
Tunnel phobia. A group was treated for tunnel phobia during a 2-day weekend (G6testam & Svebak, 1996). The same assessments were made, but in addition the claustrophobia scale was used.
Assessments
Cognitive anxiety. A questionnaire included 10 items with fearful thoughts if confronted to the animal, with responses between 0 (not at all) and 4 (all the time) (Ost & Hugdahl, 1981).

Process of Change in Exposure Therapy of Phobias 129
Somatic complaints. Another questionnaire included 17 somatic complaints related to confronting the animal, with responses between 0 (not at all) and 4 (very much) (C)st & Hugdahl, 1981).
Behavioral Approach Test (BAT). Patients were asked to approach the feared situation as far as they wanted without pressing themselves. The distance was about 10 meters, and 0-10 indicated the number of meters within which the patient approached the animal ( 0 - n o t moving, 10-approaching close to the animal). In addition, 11 indicated touching the animal, and 12 having the animal on/in ones's hands.
Basic Character Inventory (BCI). A questionnaire with 112 items (true/ false) was used to assess different personality traits (oral, compulsive, hysteric).
Stanford Acute Stress Reaction Questionnaire (SASRQ). A questionnaire with 20 items (0-5) was used to assess dissociative symptoms, as often seen in PTSD and in acute stress reactions.
Claustrophobia. Two questionnaires regarding claustrophobia, were used, one related to anxiety (20 items, 0 - n o anxiety, 4--extreme anxiety), and the other to avoidance of situations (20 items, 0 - n o avoidance, 2 - a l w a y s avoidant) (Ost, Johansson & Jerremalm, 1982). In the present study, the data are used as the weighed sum of the two scores.
Procedure
All assessments were made one week before treatment (mail), immediately before and after treatment (BAT only), and one week after treatment (mail). Follow-up assessments were made by mail after 3, 6, and 12 months.
Some patients with multiple phobias were treated for the most severe one, while the other phobias were assessed at the same time points. Patients with tunnel phobia (a special case of claustrophobia) were treated for their tunnel phobia, while more general symptoms of claustrophobia were assessed.
All general treatment efficacy data are reported elsewhere, as this presenta- tion is restricted to the study of the process of change.
Results
Observation versus Exposure
In the study with pairs of phobics, the patients undergoing direct exposure for about 2 hours showed the largest improvements in all measures. In their
130 K. Gunnar G6testam and Bengta G6testam
results, however, the improvement in approach behavior showed a higher proportion (91%), compared to the reduction of anxiety (9%). The "obser- ving" patient (who was at the same time exposed, although at greater distance and less intensity), showed a reversed pattern, with higher propor- tion of anxiety reduction (77%) and lower improvement in approach behavior (23 %).
If we look at the three group conditions, behavior avoidance test (BAT) showed greater improvement with more direct exposure (BAT change 20%, 40% and 45%, respectively, for video, model, and live exposure). On the other hand, the change in anxiety was greater in the model condition (43%) than in the live condition (34%). It thus seems that modeling works more on anxiety, while exposure works more on approach behavior.
We also have experience with patients (in clinical situations), who do not dare to approach more than one step toward the feared animal, but remains looking from that distance for the 2 hours. Afterwards they have reduced their anxiety and improved their approach behavior substantially, and at follow-up they have considered themselves as "greatly improved" or even in some cases "cured"!
It thus seems that it is important to include both the aspect of observation and real exposure in the treatment.
Personality Changes
If we look at the BCI (Basic Character Inventory) in a spider phobia study (G6testam, Hollup, & Grfiwe, 1996), from prior treatment to 3-month follow-up, there are decreases in the oral (28%), compulsive (19%), and hysteria trait (15%). The compulsive trait is then on the normal level, while the other two have approached normality.
The Stanford Acute Stress Inventory was applied to an ordinary spider phobia study, and the factors dissociation and anxiety were both substan- tially reduced (by 44% and 35%, respectively) from pre to post (1 week) assessments.
Generalization of Treatment Effects or "'Symptom Substitution"
The potential for generalization of treatment effects was assessed in two ways. Patients with dual phobias were treated for their most severe phobia, while the assessment of the other phobias was performed in parallel. The fear for the other phobia objects decreased on average to under 50%, which is roughly in the same range as the treatment results for the main phobia. Tunnel phobia patients were assessed in relation to their general claustro- phobia symptoms. After treatment, the claustrophobia symptoms (tunnel phobia not included) had been reduced by 15%, and after 6 months the total reduction was 44%.

Process of Change in Exposure Therapy of Phobias 131
Discussion
Our first hypothesis could be verified, in that exposure works more on behavioral avoidance, while observation seems to have better effect on anxiety.
Our second hypothesis was also verified, indicating that personality changes do occur during exposure therapy of short duration.
Our third hypothesis was also verified. There is a generalization effec of exposure treatment. This is an argument against the development of "symp- tom substitution" when a phobic symptom has been revealed. The "symptom substitution" hypothesis is built on the supposition that there is a back- ground, intraphysic reason for the phobic symptom, which, when it is erased, would be replaced by another symptom. Our results indicating personality changes after such short and effective therapy also support the result that no symptom substitution was shown
The result that anxiety is reduced, and avoidance behavior disappears, even after very distant exposure, evokes the question whether this is a matter of habituation or extinction. The original fear (the UCS; i.e., an animal) is neutralized by habituation, but conditioning is all the time going on in the phobic anxiety-provoking situation (the CS). Thus, there is also a certain amount of extinction involved in the anxiety reduction and approach behavior improvement.
It is difficult to know what the differential effect on anxiety reduction, without much approach improvement, really means. Probably the avoidance behavior cannot be relieved until the situation is behaviorally tested.
The importance of both observation and direct exposure calls for special procedures. We have developed a "rotation group procedure" in which a group of patients sit in a circle around a phobic object. Treatment starts with one of the patients (the "model") and after a while the next patient moves to his/her chair and becomes the model. In this way, all patients can observe the procedure all the time, but all patients will also be directly exposed (G6testam, 1995).
It is concluded that the one-session exposure treatment is a useful tool for the investigation of process of change in phobia, and that important aspects of the therapy process have been elucidated in the present study.
References
G6testam, K. G. (1994). Comparison of three group one-session treatments for spider phobia. Paper presented at 24th European Congress of Behaviour Therapy, Corfu, Greece, Sept 1994.
G6testam, K. G. (1995). A cost-effective group format for one-session treatment of specific animal phobias. Paper presented at 29th annual meeting of Association for the Advance- ment of Behavior Therapy, San Diego, USA, 1995.

132 K. Gunnar G6testam and Bengta G6testam
G6testam, K. G., & Berntzen, D. (1997). Use of the modeling effect in one-session exposure. Scandinavian Journal of Behavior Therapy, 26, 97-101.
G6testam, K. G., Berntzen, D., Grfiwe, R. W., Haug, T., & Lyngstad, G. (1989). Long term results after behavior therapy with dental phobia. In C. N. Stefanic, C. R. Soldatos, & A. D. Rabavilas (Eds.). Psychiatry today: Accomplishment and promises. Amsterdam: Excerpta Medica.
G6testam, K. G., Hol|up, S., & Grfiwe, R. W. (1996). Virtual reality in the treatment of spider phobia. An experimental controlled study. Paper presented at the 30tb Annual Meeting of Association for the Advancement of Behavior Therapy, New York, Nov 1996.
G6testam, K. G., & Svebak, S. (1996). Exposure treatment of tunnel phobia. Paper presented at 26th European Congress of Behavioural and Cognitive Therapies, Budapest, Hungary, Oct 1996.
G6testam, K. G., Taylor, C. B., & Trabert, W. (1995). Mechanisms of exposure treatment of phobia. In Y. Kasvikis (Ed.). 25 Years of scientific progress in behavioural and cognitive therapies (Vol. 1, pp. 13-25.) Athens: Ellinika Grammata.
G6testam, K. G., & Vogel, P. A. (1997). Treatment guidelines in obsessive-compulsive disorder. Paper presented at 25th Nordic Psychiatric Congress, Trondheim, Norway, May 1997.
Haug, T., Brenne, L., Johnsen, B. H., Berntzen, D., G6testam, K. G., & Hugdahl, K. (1987). A three-systems analysis of fear of flying: a comparison of a consonant versus a non- consonant treatment method. Behaviour Research and Therapy, 25, 187-194.
Merluzzi, T. V., Taylor, C. B., Boltwood, M., & G6testam, K. G. (1991). Opioid antagonist impedes exposure during exposure treatment of phobia. Journal of Clinical and Consult- ing Psychology, 59, 425-430.
(5st, L. G. (1996). One-session group treatment for spider phobics. Behaviour Research and Therapy, 34, 707-715.
Ost, L. G. (1997). Rapid treatment of specific phobias. In G. C. L. Davey (Ed.). Phobias. A handbook of theory, research and treatment (pp. 227-246). Chichester: Wiley.
(5st, L. G., & Hugdahl, K. (1981). Acquisition of phobias and anxiety response patterns in clinical patients. Behaviour Research and Therapy, 19, 439-447.
(5st, L. G., Johansson, J., & Jerremalm, A. (1982). Individual response patterns and the effects of different behavioral methods in the treatment of claustrophobia. Behaviour Research and Therapy, 20, 445-460.

11
The Clinical Implications of a Psychological Model of Paranoia
PETER KINDERMAN University of Manchester, UK
RICHARD P. BENTALL University of Liverpool, UK
Introduction
Psychotic phenomena in general, and delusions in particular, have recently become the focus for considerable academic study. The German psychiatrist Karl Jaspers considered the abnormal beliefs of psychiatric patients "unun- derstandable" (Jaspers, 1912/1963). This view appears influential, echoed by Berrios (1991) who asserted that delusions are "Empty speech acts, whose informational content refers to neither world nor self. They are not the symbolic expression of anything." Nevertheless, considerable evidence suggests not only that delusions are understandable but that they can be understood within conventional psychological models.
There appears to be a continuum from normal beliefs to delusions. Strauss (1969) identified abnormal beliefs that meet some, but not all, of the hallmarks of full-blown delusions. Subsequent investigators have shown that the beliefs of both normal individuals and psychiatric patients can be classified on independent dimensions such as conviction, extension, bizarre- ness, disorganization, preoccupation, and distressfulness (Garety & Hemsley, 1987; Harrow, Rattenbury, & Stoll, 1988; Kendler, Glazer, & Morgenstern, 1983). People with diagnosis of paranoid personality are described as "suspicious and cynical" and said to "bear grudges and take criticism extremely badly" (Chadwick & Trower, 1996; p. 9). Paranoid personality disorder appears to be common in the general population (Turkat & Banks, 1987) and has been placed on a continuum, where "paranoid schizophrenia
134 Peter Kinderman and Richard P. Bentall
should be regarded as a more severe form of paranoia, which is a more severe form of paranoid personality" (Romney, 1987; p. 651). It may also be claimed that paranoid personality disorder is a severe form of a schizotypal trait (Bentall, Claridge, & Slade, 1989; Claridge, 1989, 1993).
Delusions commonly observed in psychiatric patients (for example, beliefs of persecution or grandiosity) also reflect important existential issues (Musalek, Berner, & Katschnig, 1989) or concerns about the individual's position in the social universe (Bentall, 1994) that are common in "normal" psychology.
Delusions therefore are understandable in the sense that they are mean- ingful. More recent research, including a series of studies carried out at the University of Liverpool, UK, suggest that we can understand delusions of persecution in another way. Based on conventional psychological theories, a detailed model of paranoia has been developed that links persecutory delusions with the self-concept and attributional abnormalities.
Biases in Attent ion and Memory in Paranoia
Threat. It is well known that patients with a diagnosis of schizophrenia have relative deficits on measures of attention (Cutting, 1989; Green & Nuechterlein, 1994) and general information processing (see David and Cutting, 1994, for a review). In addition, abnormalities in the focus of attention have been discovered in paranoia.
Bentall and Kaney (1989) used the Stroop color-naming task to investigate attentional abnormalities in patients suffering from persecutory delusions and depressed and normal participants. When asked to color-name threat- related, depression-related, and neutral words, the paranoid patients showed abnormally slowed color-naming for the threat-related words. This finding has been replicated by Fear, Sharp and Healy (1996). Besides preferential attention for threat-related information, paranoid patients also display preferential recall of such information. Kaney, Wolfenden, Dewey, and Bentall (1992) asked paranoid, depressed, and normal participants to recall stories that either did nor did not contain propositions about threats. Although the patients with persecutory delusions recalled less information than the control participants, the recalled more information that was specifically threat-related. These findings suggest that threat-related material is particularly salient for paranoid patients.
Such selective information-processing is not restricted to threat-related material. Bentall, Kaney, and Bowen-Jones (1995) gave control participants and patients with delusions of persecution a flee-recall task in which they were presented with a mixed list of threat-related, depression-related, and neutral words. Whereas the depressed controls showed a specific recall bias

The Clinical Implications of a Psychological Model of Paranoia 135
for depression-related words, the paranoid patients showed a recall bias toward both threat-related and depression-related words.
Self-concept. Kinderman (1994) also used the Stroop paradigm, and asked depressed patients, patients with delusions of persecution, and nonpa- tient participants to color-name positive and negative trait words as well as neutral words. Both clinical groups but especially the patients with paranoid delusions, were slow to name the trait words, especially if the words were negative. Findings such as these have been interpreted (Bentall, Kinderman, & Kaney, 1994) as suggesting that paranoid patients have an implicit negative self-concept. It also appears that this implicit negative self-concept is explicitly denied. In the same study, Kinderman (1994) asked participants overtly to endorse negative and positive trait words according to whether they were felt to accurately describe the self before administering the emotional Stroop task. Paranoid patients, like nonpatients, endorsed many more positive than negative items. In contrast, however, the depressed patients and patients with paranoid delusions both displayed substantial interference when color-naming positive and especially negative trait words, indicating that such words were particularly salient for them.
Attributional Abnormalities in Paranoia
Considerable research has focused on the role of causal attributions (explanations) in paranoid delusions. Causal attributions are both common (Zullow, Oettingen, Peterson, & Seligman, 1988) and important elements of cognition. Psychologists such as Heider (1958) and Weiner (Weiner, 1986; Weiner, Russell, & Lerman, 1978) have regarded a person's conception of why significant events have occurred as important in determining their emotional and behavioral reactions to that event. In abnormal psychology, causal attributions have frequently been used to help explain depression.
In their "learned helplessness" model of depression, Abramson, Seligman, and Teasdale (1978) argued that depressed patients make abnormally inter- nal (self-blaming), stable and global explanations for negative events. Considerable empirical research has generally supported this hypothesis (Brewin, 1985; Sweeney, Anderson, & Bailey, 1986), although the exact nature of the attributional abnormalities in depression is still uncertain. Subsequent revisions of the learned helplessness model, such as Abramson, Metalsky, and Alloy's (1989) "hopelessness" model, have focused more on the stability and globalness of attributions than on internality judgments. Other researchers have suggested that the attributional style seen in depressed patients may be related to low self-esteem rather than depression (Tennen & Herzenberger, 1987; Tennen, Herzenberger, & Nelson, 1987). Generally, the

136 Peter Kinderman and Richard P. Bentall
causal status of attributions in depressive symptomatology has yet to be firmly established (Robbins & Hayes, 1995).
Kaney and Bentall (1989) used the Attributional Style Questionnaire (ASQ: Peterson, Semmel, Von Baeyer, et al., 1982) to investigate the causal attributions of paranoid patients. The ASQ requires participants to generate likely explanations for hypothetical positive and negative events affecting themselves. Participants then rate their own causal statements on three bipolar scales of internality (the degree to which the cause implicates the self as opposed to other people or circumstances), stability (the degree to which the cause will be present in the future), and globalness (the degree to which the cause influences a wide range of events in the individual's life, or 0nly the particular event described). Kaney and Bentall (1989) found that patients with persecutory delusions in comparison with nonpatient and depressed participants tended to make abnormally internal attributions for positive events and abnormally external attributions for negative events. This finding has been substantially replicated by Candido and Romney (1990) and by Fear and colleagues (1996). In a subsequent experimental investigation using computer games that were "rigged" so that participants either won or lost, Kaney and Bentall (1992) reported a similar result. While depressed participants reported little control in either condition, nonpatient participants displayed a robust "self-serving bias," reporting more control in the (contrived) win condition than the lose condition. As expected on the basis of the previous findings, patients with paranoid delusions reported a signifi- cantly greater self-serving bias.
Interestingly, this excessive self-serving attributional bias appears to be present in patients with paranoid delusions only on explicit measures. Winters and Neale (1985) developed a nonobvious measure of attributional style, the Pragmatic Inference Test (PIT). This is presented as a test of memory, such that participants are unaware that explanations are being requested. Lyon, Kaney, and Bentall (1994) found that both paranoid and depressed patients responded similarly on the PIT, making internal attribu- tions for negative events. On an explicit measure of attributional style, the patients with persecutory delusions made external attributions for negative events as outlined above. This pattern of results is interpreted as reflecting paranoid patients' explicit attempts to maintain a positive view of the self under the threat of implicit negative self-representations.
The suggestion that paranoid delusions have a defensive function has an impressive pedigree (see Winters & Neale, 1983, for a review). Freud, in particular, viewed paranoia as stemming from an individual's attempt to externalize unacceptable thoughts or impulses. More recently, Colby (1981; Colby, Faught, & Parkingson, 1979) suggested that paranoid delusions stem from a tendency to perceive or generate threats to self-esteem combined with a protective mechanism of projection and externalization of the threat to
The Clinical Implications of a Psychological Model of Paranoia 137
others. In the same vein, Zigler and Glick (1988) suggested that schizo- phrenia should be regarded as a form of camouflaged depression. This view has empirical support. Although psychotic patients, in general, show low- esteem (Ibelle, 1961; Kaplan, 1975; Rogers, 1958; Silverstone, 1991; Wylie, 1979), paranoid patients are an exception and tend to report high levels of self-esteem (Havner & Izard, 1962). More generally, psychotic patients have poorly elaborated (Robey, Cohen, & Gara, 1989) and contradictory (Gruba & Johnson, 1974) self-concepts.
A Detailed Model of Paranoia
Bentall, Kinderman, and Kaney (1994) proposed a detailed model of persecutory delusions incorporating certain features of self-discrepancy theory (Higgins, 1987). This is a condition of the long-held view that individuals' self-representations have multple aspects (Markus & Wurf, 1987). According to self-discrepancy theory, discrepancies may exist between different domains of the self (the actual-self, ideal-self, and ought-self, as perceived by me and as I believe other people see me). These discrepancies have important psychological consequences. Clinically depressed and dysthy- mic nonclinical participants report discrepancies between the actual-self and the ideal-self (self-actual:self-ideal discrepancies), whereas socially phobic or clinically anxious patients report discrepancies between the actual-self and the ought-self (Scott & O'Hara, 1994; Strauman, 1989; Strauman & Higgins, 1988). Moreover, manipulations of these self-discrepancies in normal individuals have been shown to lead to predictable changes in mood (Strauman & Higgins, 1987), autobiographical memory (Strauman, 1992), and even physiological functioning (Strauman, Lemieux & Coe, 1993).
In the Bentall, Kinderman, and Kaney (1994) model, persecutory delusions are seen as the consequence of an attributional process that reduces potential self-actual:self-ideal discrepancies. When external threats (i.e., negative social events) are encountered, these are rendered personally benign by explaining those events as caused by external factors. These external attributions apparently minimize self-actual:self-ideal discrepancies; however, they may also open discrepancies between self-representations and the views other people are believed to hold of the self. If other people are responsible for negative social interactions, it is likely that they will see one negatively. This model is represented graphically in Figure 11.1.
Self-Discrepancies in Paranoia
Specific prediction stemming from this model have been empirically tested. Kinderman and Bentall (1996b) elicited participants' actual-self, ideal-self,

138 Peter Kinderman and Richard P. Bentall
Self-Concept serf-actual:self-ideal discrepancies
Figure 11.1. A model of paranoid delusions.
Closure of self-actual:self-ideal Externalizing ~ discrepancies
attributional bias l =-~ Opening of
self-actual:other-actual discrepancies
I
and ought-self representations, and their beliefs about how their parents viewed them. In keeping with previous clinical research, nonpatient partici- pants showed high consistencies between all domains of the self-concept, while depressed patients showed marked self-discrepancies. Paranoid patients alone displayed small self-actual:self-ideal and self-actual :self-ought discre- pancies together with large discrepancies between self-perceptions and the believed perceptions of parents about the self. Paranoid patients also believed that their parents had more negative views of them than did other partici- pants. These findings are clearly consistent with Bentall, Kinderman, and Kaney's (1994) attributional model of paranoia outlined above.
Self-Representations and Causal Attributions
This attributional model of paranoia also makes explicit predictions about the dynamic relationship between self-representations and causal attribu- tions. Specifically, internal attributions for negative events should be asso- ciated with increases in self-actual:self-ideal and self-actual:self-ought discrepancies. Believing that you are responsible for the bad things that happen is likely to make you think worse about yourself. On the other hand, external attributions for negative events are likely to be associated with a closure or a minimization of such discrepancies. If you believe that you are free of blame, you are likely to feel no greater discrepancy from your self- guides.
This model also makes explicit predictions about discrepancies between self-representations and the perceived views of others. Kinderman and Bentall (1996b) reported low levels of agreement between self-perceptions and the believed view of others for both depressed and paranoid patients. In depressed individuals, these discrepancies reflected that fact th/lt self-percep- tions were more negative than the beliefs about the views of others. In paranoid patients this pattern was reversed, with self:other discrepancies reflecting positive self-representations and beliefs that other people held negative views. Within this pattern, therefore, internal attributions are
The Clinical Implications of a Psychological Model of Paranoia 139
likely to result in increased self:other discrepancies, as self-perceptions become increasingly negative. Paradoxically, extreme external attributions are also likely to result in increased self:other discrepancies. If you blame other people for the negative events that occur, it is reasonable to assume that those people will see you in a negative light. This will increase the gulf between a positive self-perception and these negative views.
These predictions were tested in an experimental study involving non- patient participants (Kinderman & Bentall, submitted). Participants completed a self-discrepancies questionnaire before and after completing a measure of causal attribution. Internal attributions for negative events were, as predicted, associated with increases in self-actual:self-ideal discrepancies. This suggests that external attributions have the consequence of protecting the self-concept from threat. In that study, however, the predicted conse- quences of excessively external attributions were not found. External attribu- tions were, instead, associated with reductions in self-actual:other-actual as well as self-actual:self-ideal discrepancies. Post hoc analyses revealed a significant difference between two types of external attribution. The nature of this analysis requires a little elaboration.
Internal, Personal and Situational Attributions
Studies of causal attribution following the tradition of learned helplessness have generally treated internality-externality as a bipolar dimension. This is reflected in the format and scoring of the ASQ (Peterson, Semmel, Von Baeyer, et al., 1982) on which the measure of causal attribution in the previous study was based. Other authors, however, have noted that partici- pants' responses on simple internality versus externality scales are incon- sistent and have proposed alternative ways of categorizing attributions for internality (Stratton, Munton, Hanks, et al., 1988; White, 1991). Three distinct attributional loci can be identified in the classification developed by Seligman and his colleagues: an internal locus (attributing the causes of events to self), a personal-external locus (attributing the causes of events to the actions or omission of identifiable others), and a situational-external locus (attributing the causes of events in terms of circumstance or chance). It is therefore unsurprising that the internality scale in Peterson and colleague's (1982) Attributional Style Questionnaire has frequently been criticized for its poor reliability (Rehm, 1988; Reivich, 1995; Tennen & Herzberger, 1985).
The post hoc analyses referred to above were based on this new taxonomy. These revealed that external attributions, if made to personal loci, were associated with decreased self-actual:self-ideal discrepancies and increased self-actual:other-actual discrepancies; situational-external attributions led to

140 Peter Kinderman and Richard P. Bentall
decreased self-actual:self-ideal and decreased self-actual: other-actual discre- pancies. These findings strongly suggest that previously conventional taxo- nomies of attributional locus may be inadequate for some investigations. For this reason Kinderman and Bentall (1996a) developed the Internal, Personal, and Situational Attributions Questionnaire (the IPSAQ), which indepen- dently measures attributions for positive and negative events made to internal, personal-external, and situational-external loci. It is interesting that this measure has significantly better internal consistency than the ASQ (Kinderman and Bentall, 1996a).
Following the development of the IPSAQ, the previous study investigating the psychological consequences of different types of causal attribution was replicated in the light of these three attributional loci (Kinderman & Bentall, submitted). This revealed an entirely predictable pattern of results. Attribu- tions made to internal (self-blaming) loci were associated with increased self- actual:self-ideal and increased self-actual:other-actual discrepancies. In other words, discrepancies between self-perceptions and the believed views of others. Attributions made to external personal (other-blaming) loci were associated with reduced self-actual:self-ideal discrepancies and increased self- actual: other-actual discrepancies. In contrast, attributions made to external situational loci were relatively benign, associated with reduced self- actual:self-ideal discrepancies and reduced self-actual:other-actual discre- pancies.
Extending these findings into the clinical population, Kinderman and Bentall (1997b) found that both paranoid and normal participants showed a robust self-serving bias; attributing more positive events than negative events to internal loci. Depressed patients lacked such a bias. In addition, the paranoid patients also showed a highly abnormal personalizing bias, with a majority of external attributions made to personal as opposed to situational loci. Paranoid patients made a few external-situational attributions for either positive or negative events.
These findings suggest that the separation of the two distinct loci of external attributions may be psychologically important. In addition, they provide valuable explanatory support for an attributional model of depres- sion and paranoia. The internal, self-blaming, attributions for negative events typically made by depressed individuals ("I'm late because I'm a poor driver") tend to lead to a more negative view of the self. The external- personal, other-blaming, attributions typically made by paranoid patients ("It's not my fault I'm late, this idiot on the motorway was deliberately driving at a snail's pace in the fast lane") are self-supporting, but tend to lead to the belief that other people think ill of one. Ordinary people, on the other hand, seem to be able to make situational attributions for negative events ("I'm late because there was fog on the motorway") which appear to preserve the self-concept without implicating others.
The Clinical Implications of a Psychological Model of Paranoia 141
Theory-of-Mind and Paranoia
Although the particular pattern of causal attributions of paranoid patients has only been reported recently, there have already been speculations as to its etiological pathway.
In the field of depression, there are considerable problems in attempting to find a pessimistic attributional style preceding the onset of depression (see Robbins & Hayes, 1995, for a review of this literature). Similar problems are certain to apply to paranoia. Nevertheless, there is evidence that suggests that an external locus of control (not dissimilar from an externalizing attribu- tional bias) in adolescents predicts later mental ill-health (Frenkel, Kugel- mass, Nathan, & Ingraham, 1995). More generally, an association has been observed between the attributional style (Hoffart & Torgesen, 1991; Selig- man, Peterson, Kaslow, et al., 1984) and the self-representations (Hammen, 1991; Hammen, Dyke, & Micklovitch, 1986) of parents and children. These findings together suggest that patterns of cognition can be learned, that these involve both self-representations and causal attributions, and that such cognitions may play an important role in the etiology of mental health problems.
In a slightly different slant on the possible etiology of the attributional biases and self-representations seen in paranoid individuals, high parental expressed emotion is known to precipitate psychiatric relapse (Brown, Birley, & Wing, 1972; Left & Vaughn, 1980; Rund, 1994) and has been associated with the onset of psychotic disorders in vulnerable individuals (Valone, Norton, Goldstein, & Doane, 1983). More precisely, it has been suggested that high levels of negative expressed emotions are associated with patient- blaming attributions (Brewin, MacCarthy, Duda, & Vaughn, 1991). This is particularly important as this would be precisely the kind of expressed parental cognition that would contribute to a bias towards external-personal attributions in children.
Although intriguing, these are not the only etiological speculations that can be drawn. A bias toward personal as opposed to situational external attributions can be seen as either a relative excess of personal attributions or a relative paucity of situational attributions. Detailed examination of the pattern of attributions made by paranoid individuals (Kinderman & Bentall, 1997b) suggests that the lack of situational external attributions reflects some form of deficit. That is, responses of this kind are at floor level for both positive and negative events.
It is well known that people with a diagnosis of schizophrenia experience general cognitive or information-processing impairments (Nuechterlein, Buchsbaum, & Dawson, 1994). It is possible that such information-proces- sing difficulties may be related to a difficulty in understanding and concep- tualizing the mental processes of other people. This ability--termed Theory

142 Peter Kinderman and Richard P. Bentall
of Mind (ToM)-- is believed to play an important role in ordinary social interactions (for a review, see Astington and Jenkins, 1995). ToM has been widely studied in the fields of autism and Asberger's syndrome (Baron- Cohen, Tager-Flusberg, & Cohen, 1993; Frith, 1989; Happ~ & Frith, 1994; Leslie, 1991) as well as psychosis, particularly paranoia (Corcoran, Mercer, & Frith, 1995; Frith, 1992, 1994; Frith & Corcoran, 1996).
A recent study in nonpatient participants has set out to examine this possibility. Kinderman, Dunbar, and Bentall, (1998) asked undergraduates to complete a highly complex ToM task and the IPSAQ. Participants were allocated to one of two groups on the basis of performence on the ToM task. Those individuals who were relatively poor at inferring the mental states of others attributed significantly more negative events to personal-external as opposed to situational-external causes. In addition, there was a tendency for people performing poorly on the ToM task to perform poorly on an assessment of memory. This is consistent with the hypothesis that ToM performance depends on more general cognitive resources, in particular executive function or working memory (Corcoran, Mercer, & Frith, 1995; Davis & Pratt, 1995).
Such a relationship between general cognitive information processing, ToM and causal attributions begins to form a coherent pattern. Situa- tional-external attributions are inherently complex, depending on the use of second-order explanations for events ("John did make an insulting remark, but that was because he was tired"). Any disruption or deficiency in such complex information processing is likely to affect ToM adversely and affect the choice of attributional locus. Such a disruption may be either temporary (as a result, for instance, of stress) or relatively permanent.
This is consistent with the observation that psychotic patients experience considerable dysfunctions of cognitive processes during acute phases of their illness (Nuechterlein & Dawson, 1984a; Neuchterlein, Dawson, Ventura, et al., 1991). These are likely to disrupt performance on complex tasks to a substantial extent. In such a state, the self-serving externalizing bias in causal attributions is likely to be expressed in a simplistic other-blaming manner. While nonpsychotic individuals can express these external attributions benignly, implicating situational causes, this elegance is beyond an acutely ill patient.
A Revised Model o f Paranoia
Clearly, a great deal of further research is required in this area. Never- theless, we propose an elaborated model of paranoid ideation. This model clearly forms an evolution of that proposed earlier. It has two important developments. First, the new tripartite taxonomy of attributional loci is explicitly incorporated. The psychological consequences of the three possi- bilities for causal explanations for negative events are described. Second, the

The Clinical Implications of a Psychological Model of Paranoia 143
Attenliono! ~ toward
se!f-referent material
im~i red in fo¢~l ion processing
Activation of implicit ~lf-ac t ual:self -ideal
discrepancies
Theory-of mind deficits
Extemalizlng a~ributional bias
Personal~ing bias in external attrilouflons
Closure of explicil ~tf.actual:~lf,ideol
discrepancies
Explanations for n @ t i v e so(:iol events imPlicatir~ the malign
actions of other oeoo~e
Opening of exPlicit self-actual:other-actual
discrepancies
Hgurc 11.2. A rc,,iwd modcl~)~pa~moid&!h>iolls.
possible role of cognitive disorganization in producing ToM deficits and therefore bias toward personal-external attributions is acknowledged. The revised model of paranoia is illustrated in Figure 11.2.
Clinical Implications The potential clinical implications of this model are great. There are
possible implications for clinical formulation of individual patients; for direct, face-to-face clinical work; and for indirect clinical work (for example, through consultation or ward-rounds).
Formulations are more than a simple enumeration of likely cognitive processes, but are instead intended to link, as well as list, personal difficulties (Persons, 1986). One of the challenges for clinicians is to construct a formulation that adequately explains how elements of cognition are asso- ciated. One of the strengths of the model of paranoid ideation outlined here may be felt to be the use of such cross linkages. This is particularly valuable in the field of schizophrenia, where there is such a plethora of research findings that one single cognitive process is highly unlikely to emerge as an

144 Peter Kinderman and Richard P. Bentall
explanation for the syndrome as a whole. Moreover, psychological formula- tions do not assume that behaviors and cognition are fixed in time. Etiological pathways and the iterative effects of a series of events and responses form important elements. Clinical interventions suitable for clin- icians in face-to-face contact with patients and for team-based consultation are briefly outlined below.
Attention and Memory Biases
It is to be expected that paranoid individuals would remember and attend to material related both to physical danger and threats to their self-concept. Clinical reports of paranoid individuals frequently refer to experiences that they interpret as related to personal threat. Patients would also be expected to be sensitive to experiences that the clinician can interpret as related to threats to the self-concept. At present the etiology of such attentional biases can only be speculative.
We can be clear about the possible clinical benefits of an understanding of these processes, however. Attention and memory are usually seen as relatively effortless processing, automatic in nature. While both attention and memory appear to be guided by higher information processing, biases in these areas are generally believed to provide direct evidence of characteristic schematic cognitive processing (Brewin, 1988). This information is clearly very useful in clinical formulation. If biases in memory and attention can be observed, this can help to identify the themes and nature of underlying cognitive schemata. Clinically, such schemata are thought to be related to the generation and maintenance of assumptions and beliefs that are believed to be responsible for the production of negative, automatic thoughts (Beck, 1967, 1976).
Central to the model of paranoid delusions outlined above is the idea that the self-concept is actively defended. In consequence, patients may possess attentional biases toward negative material, but they are also unlikely to acknowledge directly the presence of negative self-schemata. This will make direct therapeutic work very difficult. Moreover, biases in attention and memory may in themselves be very difficult to resolve. There is, however, the possibility that material useful for therapeutic work will be relatively easy to elicit. If patients tend to attend to and remember clinically important material, clinicians should not find themselves deprived of things to discuss.
Cognitive Disruption, Pharmacotherapy, and Neurocognitive Rehabilitation
It is well established that patients with schizophrenia exhibit dysfunctions of memory or attention (Nuechterlein, Buchsbaum, & Dawson, 1994;

The Clinical Implications of a Psychological Model of Paranoia 145
Nuechterlein & Dawson, 1984a, 1984b; Neuchterlein, Dawson, Ventura, et al., 1991). Such cognitive disruption may account for the observed patterns of attributions and theory-of-mind deficits. One can safely assume that it requires a considerable amount of intact cognitive processing ability to infer the mental states of others. Memory or attentional deficits may therefore make elegant and psychologically benign attributions difficult.
By far the most common treatment regime for people with a diagnosis of schizophrenia is the use of neuroleptic drugs. These are significantly effective in acute episodes of schizophrenia (Cole, Kleberman, & Goldberg, 1964). They are also effective in preventing relapse, reducing the relapse rate by between 70% and 40% (Hogarty, 1993). Nevertheless, neuroleptic medica- tion is a blunt tool and does not prove effective in all cases. While some two- thirds of patients will relapse on placebo medication, a third will relapse even if prescribed neuroleptics (see Day & Bentall, 1996, for a review). Neuro- leptics are also usually used to treat broad diagnostic entities such as schizophrenia rather than targeted at particular symptoms (Day & Bentall, 1996) or to address individual cognitive dysfunctions. It remains to be seen whether such targeted medical interventions may address neurocognitive deficits more precisely.
On a psychological level, psychosocial treatments of schizophrenia include neurocognitive rehabilitation aimed at ameliorating episode-linked cognitive and neuropsychological impairments (Corrigan, Hirschbeck, & Wolfe, 1995; Spaulding, Sullivan, Weiler, et al., 1994). This often includes intensive training and instruction in such cognitive tasks as vigilance, attention, memory, and decision-making. Such cognitive rehabilitation appears to be an effective intervention both in terms of specific measures of information processing (Penn, Mueser, Spaulding, et al., 1995) and impact on sympto- matology (Penn & Mueser, 1996).
Again, with particular relevance to the theoretical model outlined above, it is interesting to note that these neurocognitive psychological impairments are intimately related to social relationship difficulties (Corrigan, Green, & Toomey, 1994; Corrigan, Hirschbeck, & Wolfe, 1995; Lysaker, Bell, Zito, & Bioty, 1995; Penn, Mueser, Spaulding, et al., 1995; Wykes, 1994). This is believed by some researchers to have relevance for social-skills training and related therapies (Bellack, Sayers, Mueser, & Bennett, 1994; Bowen, Wallace, Glynn, et al., 1994; Wykes, 1994).
Theory-of-Mind
We described earlier how patterns of causal attribution apparently similar to those seen in paranoid individuals have been observed in people who perform relatively poorly on tests of theory-of-mind (Kinderman, Dunbar, &
146 Peter Kinderman and Richard P. Bentall
Bentall, 1998). More generally, deficits in the ability to understand the mental states of other people have been widely observed in individuals with (Frith, 1994; Frith & Corcoran, 1996; Frith & Done, 1988, 1989). Within the theoretical model outlined above, it is difficult to account for (negative) social interactions involving other individuals with reference to situational factors if you suffer from such deficits.
Clinically, therefore, difficulties in these related areas would be expected and may be conceptually interpretable. Theory-of-mind difficulties may be observed in terms of a lack of empathy and problems in social interactions. Higher-order theory-of-mind challenges, such as humour, irony, and decep- tion may reveal more subtle difficulties. Of course, we would predict consequent impairments of social attribution. Specifically, it is likely that paranoid individuals would find it difficult to account for the behavior of other individuals by making appropriate reference to the circumstances that might shape their view of the world. As in the earlier discussion of attribu- tions in social interactions, such an understanding may help to explain interpersonal difficulties and arguments.
More speculative therapeutic opportunities may be derived from our model. As mentioned above, theory-of-mind difficulties have been suggested as etiologically important in paranoia by other researchers (Frith, 1992, 1994). Our model makes quite explicit, if speculative, reference to ToM deficits. Some considerable effort has been expended in developing the theory-of-mind of people with autism or Asberger's syndrome (Baron- Cohen, Tager-Flusberg, & Cohen, 1993; Happ8 & Frith, 1994; Loveland & Tunali, 1991). It is not beyond the bounds of possibility to imagine therapeutic methods of developing empathy and social understanding in paranoid patients. Such interventions might involve the presentation of ambiguous or complex materials and the generation of appropriate alter- native accounts. The cognitive reconstructing of difficult or threatening social situations, events, and perceptions could also be incorporated into an opportunity to develop an individual's appropriate conceptualization of the mental state of others.
Causal Attributions
Attributional problems are, of course, central to the theoretical model outlined above. It is a simple empirical prediction that patients would show abnormalities in this area. More interestingly, these attributional abnormal- ities are likely to expose themselves in everyday settings as well as on standardized measures. In social interactions, paranoid individuals are unlikely to blame themselves and likely to blame others. This pattern should be visible in personal histories, during observed interactions between

The Clinical Implications of a Psychological Model of Paranoia 147
individuals (for instance, on wards) and, of course, on standardized psycho- logical measures. The consequences of these external-personal attributions (preserved self-actual:self-ideal consistency but more easily accessible self:other discrepancies) can also be predicted.
The problematic attributions central to the revised model of paranoia are predominantly social. That is, they involve social situations; people being rude to you, for instance. Moreover, paranoid attributions tend to implicate others. This may be a useful element in understanding difficult social interactions and interpersonal conflicts. Paranoid patients can be trouble- some, and people with paranoid personality disorders are notoriously querulant (Turkat & Banks, 1987). An understanding of the characteristic explanations deployed by such individuals may help carets and staff gain insight into such difficulties and hence intervene.
The most obvious clinical deviation of the research referred to above would be to tackle the attributional abnormalities directly. A number of cognitive-behavioral strategies have been developed for delusional phenom- ena. Watts, Powell, and Austin (1973) describe "belief modification," in which delusional beliefs are gently challenged and reframed. This approach has been developed by Chadwick and Lowe (1990), who have developed strategies by which patients are able to test their own delusional beliefs. Cognitive-behavioral techniques such as these are successful in small-scale studies (Garety, Kuipers, Fowler, et al., 1994; Kingdon, Turkington, & John, 1994; Tarrier, Beckett, Harwood, et al., 1993) and a number of large randomized control trials are underway.
Techniques such as these implicitly target causal attributions. Delusions are often exhibited as a set of attributions for real events, related to a delusional theme, and many statements related to delusional beliefs are essentially attributions ("I saw a man put his hand in his pocket [that's because], he is a special branch officer and he was radioing to headquarters"). The psychological model of paranoid ideation outlined above suggests that more explicit targeting of attributions may address core aspects of paranoid ideation. Moreover, the tripartite discrimination of attributional loci offers an opportunity for directly encouraging benign, nonparanoid, explanations for troubling events.
In a single-case study, Kinderman & Bentall (1997a) report an example of this kind of cognitive therapy. The patient' anxiety concerning the delusional presence of a plot to murder him was measured on a daily basis (on a simple scale labeled from "Not at all worried about any conspiracy" to "Extremely worried about a conspiracy") and frequent assessments of causal attributions were made. After a period of baseline measurement, the patient was encouraged to address his tendency to make personal (other-blaming) attributions. This encouragement was act ive-- the patient was asked to develop as many alternative explanations that involved situational or
148 Peter Kinderman and Richard P. Bentall
circumstantial factors as possible and to compare these with attributions involving blame to other people.
This structured cognitive behavioral intervention was conducted during approximately weekly sessions. Although the therapeutic target was specific paranoid ideation, therapy initially focused on less emotional topics. A cognitive approach to emotional disturbance was established by pointing out the links between feelings and the understanding of events. The impor- tance of causal explanation and the likely effects of the three types of attribution were emphasized. The patient was then asked to examine auto- matic assumptions about the causes of ordinary, everyday, events and encouraged to practice generating multiple explanations for everyday events, paying special attention to the consideration of situational attribu- tions.
As therapy developed, such situational attributions were encouraged for events that tended to elicit paranoid or delusional responses. Again, the patient was encouraged to develop alternative, situatl0nal, explanations for these. As an example, one event discussed in detail involved the patient seeing police officers on waste ground near his home and initially concluding that they intended to arrest or assault him. He then consciously generated the situational attribution that they were, in fact, exercising their dog (that is, that their presence was due to circumstantial, situational factors).
Such a therapeutic strategy employed is entirely compatible with conven- tional cognitive-behavior therapy based on engagement, elicitation of cogni- tive schemata, and reality testing. In this case, however, the specific intervention was directed at eliciting the client's explanations for negative or ambiguous events. The client was then helped to practice the generation of multiple possible alternatives. This developed a pattern of attributions for potentially threatening events that avoided the biases in attribution hypothe- sized to lie behind paranoid ideation.
In keeping with the model outlined above, the patient showed a tendency to make external-personal attributions for negative events while delusionally paranoid. As can be seen in Figure 11.3, at around the time that the active attributional therapy began, the patient's level of paranoid anxiety appeared to drop markedly. The patient's attributional style, as measured by the IPSAQ also changed, reverting to a more normal ratio of attributional loci.
These findings suggest that a relatively straightforward development of cognitive therapy, specifically designed around the new attributional model of paranoia, may be successful. Clearly a development such as this requires replication and elaboration, but it is also encouraging support for the model.
It is worth noting that the patient was urged to make situational external attributions. One opportunity provided by the novel tripartite taxonomy of causal attributions is that patients are offered a benign alternative to either self-blaming or other-blaming explanations. This is important. Logically, a

The Clinical Implications of a Psychological Model of Paranoia 149
Paranoia
10
8
6
4
2
I ! ! 1
0 10 20 30 40 Follow-up
Day
Figure 11.3. Daily recordings of paranoid ideation in a single-case study of attributional therapy for paranoid delusions (Kinderman & BentalI, 1997a). Recordings were made on a 10-cm visual analog scale labeled ranging from "Not at all worried about any conspiracy" to "Extremely worried about a conspiracy." Data are presented in two phases of treatment, with phase 1 being before and phase 2 after instructions to develop alternative situational explanations for ambiguous events. Follow-up records occurred on days 82 to 87 (the 12th week after commencement of treatment) and on day 147.
therapist working with paranoid individuals within the framework provided by the ASQ could only respond to the excessive externalizing biases exhibited by encouraging more self-blame. Such an alternative is no longer necessary. Goldwert (1993) commented on the teleological and religious quality of many delusions, and suggested that "a patient's recovery is heralded by the acceptance of the accidental in life" (p. 778). If the situational-external locus of causal attribution is meaningful, it is essentially an acceptance of the accidental.
Self-Discrepancies Disturbances in the self-concept are also key elements of the model
presented earlier. Despite the hypothesized centrality of disturbance of the self-concept in their problems, paranoid individuals are likely to report relatively small discrepancies between their self-perceptions and their ideals (Kinderman & Bentall, 1996b). In many senses they will have high self- esteem. At the same time, it is likely that they will report that they believe that other people hold critical views of them.

150 Peter Kinder,nan and Richard P. Bentall
These self-concept abnormalities relate to the individuals' causal attribu- tions. We suggest that an advance of self-blaming explanations for negative events serves a self-protective function, minimizing self-actual:self-ideal discrepancies. At the same time, other-blaming attributions open discrepan- cies between self-perceptions and beliefs concerning how one is seen by other people. This relationship between the self-concept and causal attributions also illustrates a second broad benefit of a theoretical model such as that outlined above.
The benefits of understanding the nature and themes of a patient's cognitive schemata were briefly mentioned when discussing abnormalities of attention and memory. Clearly an understanding of an individual's self- concept is an extremely important element of a clinical formulation and a common focus for clinical intervention. In the revised model of paranoia, it is suggested that these cognitive schemata center on the self-concept. This has two important clinical consequences.
First, the centrality of the self-concept in paranoid ideation suggests that material related to the self is particularly salient, and that it is from this perspective that the world is viewed. Paranoid individuals are likely, there- fore, to be narcissistic and to see frequent references to them in circumstantial events. This is entirely consistent with the clinical observations that, in paranoid schizophrenia and paranoid personality disorder, narcissism and ideas of reference are common (Gelder, Gath, & Mayou, 1993; Hamilton, 1985). Aspects of self-referent schematic processing identified in other areas of psychopathology are also likely to be important. Thus, issues related to both achievement and affiliation (Gotlib & Hammen, 1996) should be carefully examined.
Second, an understanding of the centrality of the self-concept in the cognitive schemata of paranoid individuals may provide other useful clues for clinical information. When the self-concept is seen as central, aspects of its self-regulatory nature (Markus & Wurf, 1978) may be seen as important. There appear to be a number of self-regulatory processes in normal psychol- ogy (Taylor, 1988). These involve self-reinforcing biases in attention and memory (Higgins & Bargh, 1987; Markus & Wurf, 1987) whereby positive self-representations are more likely to be processed efficiently and easily recalled (Greenberg & Pyszczynski, 1985).
Although researchers and clinicians from different perspectives are likely to concentrate on different aspects of the model, it could be argued that self- concept abnormalities are central. It is interesting, therefore, to observe that self-discrepancy theorists have begun to develop specific therapeutic strate- gies aimed at reconfiguring self-representations in disorders such as depres- sion and anxiety. These strategies may have value in paranoia.
Tim Strauman and his colleagues (Strauman, 1994, 1996a, 1996b; Strau- man & Kolden, 1996) describe a set of strategies based on conventional

The Clinical Implications of a Psychological Model of Paranoia 151
cognitive restructuring techniques that are designed to address problematic self-representations and distressing discrepancies. Patients reporting a large number of negative self-descriptive words in their self-actual representations might be encouraged to reappraise the degree to which they feel that these words are characteristic, or techniques might be employed to reduce the accessibility of this material. At the same time, patients may be encouraged to reflect on positive aspects of the self that they would acknowlege but that may not be easily accessible. Patients may also be helped to develop more positive self-concepts by including new material in their actual-self represen- tations. Thus social interactions, cognitive therapy, nursing care and, perhaps most usefully, occupational therapy may be used to develop an individual's positive sense of self.
As an example of these techniques in depression, one might imagine a patient using words such as "bad mother, .... inadequate," and "stupid" in the self-actual domain. Therapeutic strategies might involve cognitive techniques aimed at challenging the evidential basis of these self-descriptions. The patient might be asked to review the evidence that she is a bad mother-- or rather consider evidence suggesting that she is a good mother. Similarly, the evidence against inadequacy and stupidity could be weighed against evidence in favor of adequacy and intelligence. Other techniques may address the accessibility of such negative self-referent material, perhaps via the development of metacognitive strategies, and increase the accessibility of more positive self-descriptions. In the latter context, the patient may be reminded of (and asked to encourage herself to remember) less well-remem- bered positive components. In addition, cognitive and (probably more successfully) occupational therapeutic techniques could be used to introduce new, positive, material into the self-actual representation. Creative or artistic projects might help introduce new material, as might social skills training, assertiveness, and therapeutic workshops aimed at clinical elements such as anxiety or anger management.
Material in the self-ideal and self-ought domains can be addressed in similar ways: reducing the degree to which excessive guides are felt appro- priate, increasing the degree to which the patients believe they have met their guides, and reappraising evidence suggesting that guides are met. Self- actual:self-ideal discrepancies (and other discrepancies) can also be addressed directly, encouraging the patients to examine evidence regarding the degree to which they fall short of their ideals.
Again as an illustration of such approaches with depressed individuals, self-guides such as "strong" might emerge as important. A depressed individual might display a tendency toward self-criticism if emotional fortitude were seen as both vital and inflexible. Such views could clearly be targets for modification via cognitive therapy. More directly, the patient might be asked to consider evidence of their appropriate emotional strength.
152 Peter Kinderman and Richard P. Bentall
A woman coping with the pressures of a career and a young child might be asked to reflect on the emotional coping necessary. It is possible that evidence would be uncovered that suggests that such strength is indeed present. It may be tess than complete, and it might not be seen when stresses are severe, but wide self-actual:self-ideal discrepancies may be reduced.
Other therapeutic strategies may be useful here, especially at later, more insightful stages of therapy. Unrealistic, excessive, or contradictory self- guides may be explicable in terms of early upbringing, family dynamics, or abusive childhood experiences. It is possible that therapeutic work in this regard may be beneficial.
Of course, depressive cognitions are not the same as paranoid delusions. There are likely to be a number of problems translating these techniques to paranoid individuals. In particular, the fact that a paranoid individual is likely to report highly positive self-representations despite an implicit nega- tive self-concept may present difficulties. Attempting to initiate self-discre- pancy therapy with individuals who are already actively using processes addressing the same processes could lead to any number of difficulties.
Nevertheless, a therapeutic approach focusing directly on self-representa- tions may have value. Abnormalities in self-discrepancies occupy a central role in the model of paranoid delusions outlined above. As such they appear an obvious therapeutic target. Moreover, such self-discrepancy therapy may be acceptable even to paranoid patients. Even with high apparent self-esteem, it is likely to prove acceptable to boost self-esteem. A skilled therapist may be able to work with an individual expressing delusionally positive self-repre- sentations and still develop a healthy self-concept. In contrast to the hypothetical depressed individual imagined above, an individual with para- noid delusions may well describe himself as "charismatic, ... . intelligent," and "crafty." Despite the positive nature of these apparent self-representations, our modelof paranoid ideation would predict a negative implicit self-concept. Although one would not choose to challenge these descriptors, as in the previous example, a therapist may decide to help the patient include other positive material in his self-representations. Other, perhaps more reasonable, material not initially included might be made more accessible. Such material could well be less paranoid in flavor than initial self-descriptors. Again as above, social or occupational strategies might help the patient incorporate new, positive, material into his self-actual representation. As with depression, creative or artistic projects could generate new self-descriptive material, and social skills training, assertiveness classes, anxiety management, and anger management have clear benefits.
In addition, within a framework like this, targeting of the self-concept is powerful but less than totally explicit. If a patient is successfully engaged, a skilled therapist can address the self-representations through behavioral interventions, occupational therapy, and more general practical advice
The Clinical Implications of a Psychological Model of Paranoia 153
concerning lifestyle and activities in addition to using cognitive techniques. Assuming a good therapeutic relationship has been developed, such inter- ventions are unlikely to be resisted. If resistance is encountered, this is unlikely to lead to the psychological reactance that can occur wit h cognitive techniques.
Perhaps most importantly, such benign interventions with patients with paranoid beliefs often lead to more general discussions concerning the self- concept. Although paranoid ideation is associated with defensive attributions and a delusionally-enhanced self-concept, patients are also assumed to possess negative implicit self-representations. Once an empathic and suppor- tive discussion concerning self-esteem is initiated, and if that discussion is seen to develop the self-concept as opposed to threatening it, these more negative self-representations may emerge. Direct therapeutic work can then begin, focused on these issues.
Family Therapy
It is now well established that close contact with relatives showing high levels of expressed emotion is a major risk factor for relapse in schizophrenia (the seminal work in this area being Vaughn and Left, 1976). The causes and nature of high expressed emotion remain unclear. The level of observed expressed emotion is not necessarily stable (Tarrier, Barrowclough, Vaughn, et al., 1988), and probably reflects a response by carets to a family member with a diagnosis of schizophrenia (Birchwood & Smith, 1987; Macmillan, Gold, Crow, et al., 1986).
Interventions (family therapy) have been developed in an attempt to reduced expressed emotion and thus reduce relapse rates (see Leff, 1994, for an overview). Such programs generally include education about schizo- phrenia as well as family therapeutic sessions. These are aimed at improving communication, teaching problem-solving skills, lowering criticism and over- involvement, reducing face-to-face contact between patient and relatives, and expanding social networks. In addition, individual therapy is often imple- mented, including social-skills training, anxiety management, and cognitive therapy for residual psychotic symptoms.
Such programs have been highly successful (Dixon & Lehman, 1995; Falloon, Boyd, McGill, et al., 1982; Left, Kuipers, Berkowitz, et al., 1982; Penn & Mueser, 1996; Tarrier, Barrowclough, Porceddu, & Fitzpatrick, 1994). Family interventions are generally reported as being highly effective in reducing expressed emotion, in improving relapse rates and outcomes, and in reducing the burden on carers (Penn & Mueser, 1996).

154 Peter Kinderman and Richard P. Bentall
Clearly, further research is needed to identify which patients will benefit from family therapy and isolate the "active" ingredients of family interven- tions (Penn & Mueser, 1996). There are again some interesting links to the revised model of paranoia outlined above. Of particular interest is the observation that expressed emotion reflects the causal attributions of family members. Brewin, MacCarthy, Duda, and Vaughn (1991) found that high, negative, expressed emotion was correlated with a tendency by family members to attribute the blame for symptomatic problems within the patient. Thus, if abnormal behavior is attributed to characteristics of the patient, and seen as potentially controllable, blame and negative emotions will follow. There are clear and direct links with the pattern of causal attributions seen in paranoid individuals.
More usefully, it may be the case that addressing this issue may be one of the "active ingredients" sought by Penn and Mueser (1996). Our work summarized in the model above also highlights direct problems that may further focus interventions with families. Direct evidence of discrepancies between the self-representations of paranoid people and the believed views of their parents has emerged (Kinderman & Bentall, 1996b). Clearly, this is relevant to family therapy, as is the secondary observation that the percep- tions of paranoid individuals concerning what they believe their parents think of them are markedly negative (Kinderman & Bentall, 1996b).
It is worth noting that an obvious consequence of the revised model of paranoia outlined above is increased self-other discrepancies. It is clear that these will involve discrepancies between self-representations and the believed views of parents or carets, as found by Kinderman and Bentall (1996b). Even in the absence of the etiological significance of expressed emotion, therapy aimed at ameliorating these (and consequent) conflicts is likely to be valuable.
Educational and behavioral family therapy for the relatives of people with a diagnosis of schizophrenia tends to have a more specific focus than traditional systemic family therapy. Nevertheless, perceptions by and of family members remain central. The model of paranoid ideation outlined above makes explicit reference to such perceptions. In attempting to amelio- rate potentially dysfunctional relationships within the family, understanding of such discrepancies may prove useful. Although it is clear from the discussion above that any discussion of the etiology of discrepancies between self-actual representations and beliefs about what one's parents think must remain speculative, placing these ideas within a formulation of paranoid thought may be important. It may be relevant, for example, to consider whether relationship difficulties are driven by such self-actual :parent-actual discrepancies, whether the perceptions are mutual between parent and child, and whether these discrepancies should be seen as elements of paranoia or reflections of other familial tension.

The Clinical Implications of a Psychological Model of Paranoia 155
On a more practical level, discrepancies between a patient's self-represen- tations and his beliefs about how his parents seen him may explain and contextualize antagonism and conflict. We discussed earlier how self-discre- pancies may become a focus of therapy. In addition to an examination of self- representations and beliefs with an individual, beliefs about how one is perceived by others could be addressed directly. Therapy directly involving the discrepant views of family members could have the disadvantage of potentially triggering unpleasant emotions. It might have the benefit, however, of attempting to address fundamental issues.
Summary Recent research into psychological processes in paranoia has led to the
development of a detailed defensive model of paranoia. This model focuses on abnormalities in causal attributions and self-representations. Patients with persecutory delusions have been shown to attend preferentially to negative self-referent stimuli while endorsing primarily positive self-descriptive words. Negative social events are attributed by paranoid patients to external factors; specifically paranoid individuals blame other people for their misfortunes. These attributional abnormalities appear to be responsible for a pattern of high consistency between self-actual and self-ideal representations as well as large discrepancies between self-actual representations and the believed perceptions of others in paranoid individuals. Finally, recent research suggests that theory-of-mind deficits (a relative inability to comprehend the mental states of other people) may play a role in the etiology of these attributional abnormalities.
Each aspect of this model has clinical implications for both formulation and therapy. The proposed model may help explain disturbances of attention and memory. These, in turn, can offer pointers to the themes and natures of cognitive schemata in paranoia. Attributional abnormalities may explain both individual and interpersonal difficulties, and attributional therapies may be developed. Disturbances of the self-concepts are central to the revised model of paranoia. These may be of great value in explaining a number of features of the clinical presentation, from delusional explanations for commonplace events, through cognitive schemata, to narcissm and ideas of reference. As in other areas, direct therapeutic strategies may be developed.
Etiological aspects of the model include cognitive disruption, theory-of- mind dysfunction, and family difficulties. Once again, each aspect of the model can help explain paranoia and could be amenable to therapeutic interventions. Patterns of information-processing difficulties can be linked

156 Peter Kinderman and Richard P. Bentall
with other aspects of a paranoid presentation, and can be amenable to psychological, pharmacological, and rehabilitative interventions. Theory-of- mind difficulties have the potential to explain a range of interpersonal and intrapersonal problems. Although theory-of-mind therapy is presently nonexistent, it may be possible to develop some form of intervention. Finally, family problems are implicated both as consequences of the pattern of cognition in the new model of paranoia and as etiological factors. Family therapy is already known to be successful. Developments in this area, specifically related to this model of paranoia, may be useful.
Clearly, further research is necessary. Nevertheless, it appears not only that academic research can develop theoretical models but that these models can directly influence clinical practice.
References
Abramson, L. Y., Metalsky, G. I., & Alloy, L. B. (1989). Hopelessness depression: A theory- based subtype of depression. Psychological Review, 96, 358-372.
Abramson, L. Y., Seligman, M. E. P., & Teasdale, J. D. (1978). Learned helplessness in humans: Critique and reformulation. Journal of Abnormal Psychology, 78, 40-74.
Astington, J. W., & Jenkins, J. M. (1995). Theory of mind development and social under- standing. Cognition and Emotion, 9, 151-165.
Baron-Cohen, S., Tager-Flusberg, H., & Cohen, D. J. (1993). Understanding other minds: Perspectives from autism. Oxford: Oxford University Press.
Beck, A. T. (1967). Depression: Clinical, experimental and theoretical aspects. New York: Harper and Row.
Beck, A. T. (1976). Cognitive therapy and the emotional disorders. New York: International Universities Press.
Bellack, A. S., Sayers, M., Mueser, K. T., & Bennett, M. (1994). Evaluation of social problem solving in schizophrenia. Journal of Abnormal Psychology, 103, 371-378.
Bentall, R. P. (1994). Cognitive biases and abnormal beliefs: towards a model of persecutory delusions. In: A. S. David & J. Cutting (Eds.), The neuropsychology of schizophrenia. London: Lawrence Erlbaum.
Bentall, R. P., Claridge, G. S., & Slade, P. D. (1989). The multidimensional nature of schizotypal traits: a factor-analytic study with normal subjects. British Journal of Clinical Psychology, 28, 363-375.
Bentall, R. P., Kaney, S. & (1989). Content-specific information processing and persecutory delusions: an investigation using the emotional Stroop test. British Journal of Medical Psychology, 62, 355-364.
Bentall, R. P., Kaney, S., & Bowen-Jones, K. (1995). Persecutory delusions and recall of threat- related, depression-related and neutral words. Cognitive Therapy and Research, 19, 331-343.
Bentall, R. P., Kinderman, P., & Kaney, S. (1994). The self, attributional processes and abnormal beliefs: towards a model of persecutory delusions. Behaviour Research and Therapy, 32, 331-341.
Berrios, G. (1991). Delusions as "wrong beliefs": A conceptual history. British Journal of Psychiatry, 159, 6-13.
Birchwood, M., & Smith, J. (1987). Schizophrenia in the family. In J. Orford (Ed.), Coping with disorder in the family. London: Croom Helm.
The Clinical Implications o f a Psychological Model o f Paranoia 157
Bowen, L., Wallace, C. J., Glynn, S. M., Nuechterlein, K. H., Lutzker, J. R., & Kuehnel, T. G. (1994). Schizophrenic individuals' cognitive functioning and performance in interperso- nal interactions and skills training procedures. Journal of Psychiatric Research, 28, 289-301.
Brewin, C. (1988). Cognitive foundations of clinical psychology. London: Lawrence Erlbaum. Brewin, C. R. (1985). Depression and causal attributions: What is their relation? Psychological
Bulletin, 98, 297-309. Brewin, C. R., MacCarthy, B., Duda, K., & Vaughn, C. (1991). Attribution and expressed
emotion in the relatives of patients with schizophrenia. Journal of Abnormal Psychology, 100, 546-554.
Brown, G. W., Birley, J. L. T., & Wing, J. K. (1972). Influence of family life on the course of schizophrenia disorders: replication. British Journal of Psychiatry, 121,241-258.
Candido, C. L., & Romney, D. M. (1990). Attributional style in paranoid vs depressed patients. British Journal of Medical Psychology, 63, 355-363.
Chadwick, P., & Lowe, C. F. (1990). The measurement and modification of delusional beliefs. Journal of Consulting and Clinical Psychology, 58, 225-232.
Chadwick, P., & Trower, P. (1996). Cognitive therapy for punishment paranoia: A single-case experiment. Behaviour Research and Therapy, 34, 351-356.
Claridge, G. S. (1987). The schizophrenias as nervous types revisited. British Journal of Psychiatry, 151,735-743.
Claridge, G. (1993). What is schizophrenia? Common theories and divergent views. Journal of Mental Health, 2, 251-252.
Colby, K. M. (1981). Modelling a paranoid mind. Behavioral and Brain Sciences, 4, 515-560. Colby, K. M., Faught, W. S., & Parkinson, R. C. (1979). Cognitive therapy of paranoid
conditions: heuristic suggestions based on a computer simulation. Cognitive Therapy and Reasearch, 3, 55-60.
Cole, J., Kleberman, G. L., & Goldberg, S. C. (1964). Phenothiazine treatment of acute schizophrenia. Archives of General Psychiatry, 10, 246-261.
Corcoran, R., Mercer, G., & Frith, C. D. (1995). Schizophrenia, symptomatology and social inference: investigating "theory of mind" in people with schizophrenia. Schizophrenia Research, 17, 5-13.
Corrigan, P. W., Green, M. F., & Toomey, R. (1994). Cognitive correlates to social cue perception in schizophrenia. Psychiatry Research, 53, 141-151.
Corrigan, P. W., Hirschbeck, J. N., & Wolfe, M. (1995). Memory and vigilance training to improve social perception in schizophrenia. Schizophrenia Research, 17, 257-265.
Cutting, J. (1989). Gestalt theory and psychiatry: discussion paper. Journal of the Royal Society of Medicine, 82,429-431.
David, A. S., & Cutting, J. C. (Eds.). (1994). The neuropsychology of schizophrenia Hove: Erlbaum.
Davis, H. L., & Pratt, C. (1995). The development of children's theory of mind: the working memory explanation. Austrialian Journal of Psychology, 47, 25-31.
Day, J. C., & Bentall, R. P. (1996). Neuroleptic medication and the psychosocial treatment of psychotic symptoms: Some neglected issues. In G. Haddock & P. Slade (Eds.), Cognitive- behavioural interventions with psychotic disorders. London; Routledge.
Dixon, L. B., & Lehman, A. F. (1995). Family interventions for schizophrenia. Schizophrenia Bulletin, 21,631-643.
Falloon, I., Boyd, J., McGill, C., Razoni, J., Moss, H., & Gilderman, A. (1982). Family management in the prevention of exacerbation of schizophrenia: a controlled study. New England Journal of Medicine, 306, 1437-1440.
Fear, C. F., Sharpe, H., & Healy, D. (1996). Cognitive processes in delusional disorders. British Journal of Psychiatry, 168, 61-67.
Frenkel, E., Kugelmass, S., Nathan, M., & Ingraham, L. J. (1995). Locus of control and mental health in adolescence and adulthood. Schizophrenia Bulletin, 21,219-226.
158 Peter Kinderman and Richard P. Bentall
Frith, C. (1994). Theory of mind in schizphrenia. In A. S. David & J. C. Cutting (Eds.), The neuropsychology of schizophrenia. Hove: Erlbaum.
Frith, C. D. (1992). The cognitive neuropsychology of schizophrenia. Hillsdale, NJ: Lawrence Erlbaum.
Frith, C. D., & Corcoran, R. (1996). Exploring "theory of mind" in people with schizo- phrenia. Psychological Medicine, 26, 521-530.
Frith, C. D., & Done, C. J. (1988). Towards a neuropsychology of schizophrenia. British Journal of Psychiatry, 153, 437-443.
Frith, C. D., & Done, C. J. (1989). Experiences of alien control in schizophrenia reflect a disorder in the central monitoring of action. Psychological Medicine, 19, 359-363.
Frith, U. (1989). Autism: Explaining the enigma. Oxford: Blackwell. Garety, P. A., & Hemsley, D. R. (1987). The characteristics of delusional experience.
European Archives of Psychiatry and Neurological Sciences, 236, 294-298. Garety, P. A., Kuipers, L., Fowler, D., Chamberlain, F., & Dunn, G. (1994). Cognitive
behavioral therapy for drug-resistant psychosis. British Journal of Medical Psychology, 67, 259-271.
Gelder, M., Gath, D., & Mayou, R. (1983). Oxford textbook of psychiatry. Oxford: Oxford University Press.
Goldwert, M. (1993). Paranoia and the accidental. Psychological Reports, 72, 778. Gotlib, I. H., & Hammen, C. L. (1996). Psychological aspects of depression: Towards a
cognitive-interpersonal integration. London: Wiley. Green, M. F., & Nuechterlein, K. H. (1994). Mechanism of backward masking in schizo-
phrenia. In A. S. David & J. C. Cutting (Eds.), The neuropsychology of schizophrenia. Hove: Erlbaum.
Greenberg, J., & Pyszczynski, T. (1985). Compensatory self-inflation: a response to the threat of self-regard of public failure. Journal of Personality and Social Psychology, 49, 273-280.
Gruba, F. P., & Johnson, J. E. (1974). Contradictions within the self-concepts of schizo- phrenics. Journal of Clinical Psychology, 30, 253-254.
Hamilton, M. (Ed.). (1985). Fish's psychopathology: Signs and symptoms in psychiatry. Bristol: Wright.
Hammen, C.(1991). Depression runs in families: The social context of risk and resilience in children of depressed mothers. London: Springer-Verlag.
Hammen, C. L., Dyke, D. G., & Micklovitch, D. J. (1986). Stability and severity parameters of depressive self-schema responding. Journal of Social and Clinical Psychology, 4, 23-45.
Happd, F., & Frith, U. (1994). Theory of mind in autism. In E. Schopler & G. B. Mesibov (Eds.), Learning and cognition in autism. New York: Plenum Press.
Harrow, M., Rattenbury, F., & Stoll, F. (1988). Schizophrenic delusions: and analysis of their persistence, of related premorbid ideas and three major dimensions. In T. F. Oltmanns & B. A. Maher (Eds.), Delusional beliefs. New York: Wiley.
Havner, P. H., & Izard, C. E. (1962). Unrealistic self-enhancement in paranoid schizophrenics. Journal of Consulting Psychology, 26, 65-68.
Heider, F.(1958). The psychology of interpersonal relations. New York: Wiley. Higgins, E. T. (1987). Self-discrepancy: a theory relating self and affect. Psychological Reveiw,
94, 319-340. Higgins, E. T., & Bargh, J. A. (1987). Social cognition and social perception. Annual review of
Psychology, 38, 369-425. Hoffart, A., & Torgesen, S. (1991). Causal attributions in first degree relatives of depressed
and agoraphobic inpatients. Comprehensive Psychiatry, 32, 458-464. Hogarty, G. E. (1993). Prevention of relapse in chronic schizophrenia patients. Journal of
Clinical Psychiatry, 54, 18-23. Ibelle, B. P. (1961). Discrepancies between self-concepts and ideal self-concepts in paranoid
schizophrenics and normals. Dissertation Abstracts, 21, 2004-2005.

The Clinical Implications o f a Psychological Model o f Paranoia 159
Jaspers, K. (1912/1963). General psychopathology (Hoenig, J & Hamilton, M. W., Trans.). Manchester: Manchester University Press.
Kaney, S., & Bentall, R. P. (1989). Persecutory delusions and attributional style. British Journal of Medical Psychology, 62, 191-198.
Kaney, S., & Bentall, R. P. (1992). Persecutory delusions and the self-serving bias. Journal of Nervous and Mental Disease, 180, 773-780.
Kaney, S., Wolfenden, M., Dewey, M. E., & Bentalt, R. P. (1992). Persecutory delusions and the recall of threatening and non-threatening propositions. British Journal of Clinical Psychology, 31, 85-87.
Kaplan, H. B. (1975). Self-attitudes and deviant behaviour. Pacific Pallisades: Goodyear. Kendler, K. S., Glazer, W., & Morgenstern, H. (1983). Dimensions of delusional experience.
American Journal of Psychiatry, 140, 466-469. Kinderman, P. (1994). Attentional bias, persecutory delusions and the self concept. British
Journal of Medical Psychology, 67, 53-66. Kinderman, P., & Bentall, R. P. (1996a). A new measure of causal locus: The internal,
Personal and Situational Attributions Questionnaire. Personality and Individual Differ- ences, 20, 261-264.
Kinderman, P., & Bentall, R. P. (1996b). Self-discrepancies and persecutory delusions: Evidence for a defensive model of paranoid ideation. Journal of Abnormal Psychology, 106, 106-114.
Kinderman, P., & Bentall, R. P. (1997a). Attributional therapy for paranoid delusions: A case study. Behavioural and Cognitive Psychotherapy, 25, 269-280.
Kinderman, P., & Bentall, R. P. (1997b). Causal attributions in paranoia and depression: Internal, personal and situational attributions for negative events. Journal of Abnormal Psychology, 106, 341-345.
Kinderman, P., Dunbar, R., & Bentall, R. P. (1998). Theory-of-mind, attributional style and paranoia. British Journal of Psychology, 89, 191-204.
Kingdon, D., Turkington, D., & John, C. (1994). Cognitive behaviour therapy for schizo- phrenia: The amenability of delusions and hallucinations to reasoning. British Journal of Psychiatry, 164, 581-587.
Left, J. (1994). Working with the families of schizophrenic patients. British Journal of Psychiatry, 164 (Supplement 23), 71-76.
Left, J. P., Kuipers, L., Berkowitz, R., Ebstein-Vries, R., & Sturgeon, D. (1982). A controlled trial of social intervention in the families of schizophrenic patients. British Journal of Psychiatry, 141,121-134.
Left, J. P., & Vaughn, C. (1980). The interaction of life-events and relatives' expressed emotion in schizophrenia and depressive neurosis. British Journal of Psychiatry, 136, 146-153.
Leslie, A. M. (1991). The theory of mind impairment in autism: evidence for a modular mechanism of development? In A. Whiten (Ed.), Natural theories of mind. Oxford: Blackwell.
Loveland, K. A., & Tunali, B. (1991). Social scripts for conversational interactions in autism and Down's syndrome. Journal of Autism and Developmental Disorders, 21, 177-186.
Lyon, H. M., Kaney, S., & Bentatt, R. P. (1994). The defensive function of persecutory delusions: evidence from attribution tasks. British Journal of Psychiatry, 164, 637-646.
Lysaker, P. H., Bell, M. D., Zito, W. S., & Bioty, S. M. (1995). Social skills at work. Deficits and predictors of improvement in schizophrenia. Journal of Nervous and Mental Diseases, 183, 688-692.
Macmillan, J. F., Gold, A., Crow, T. J., Johnson, A. L., & Johnstone, E. C. (1986). The Northwick Park study of first episodes of schizophrenia. IV. Expressed emotion and relapse. British Journal of Psychiatry, 148, 133-143.
Markus, H., & Wurf, E. (1987). The dynamic self-concept: A social psychological perspective. Annual Review of Psychology, 38, 299-337.

160 Peter Kinderman and Richard P. Bentall
Musalek, M., Berner, P., & Katschnig, H. (1989). Delusional theme, sex and age. Psycho- pathology, 22, 260-267.
Nuechterlein, K. H., Buchsbaum, M. S., & Dawson, M. E. (1994). Neuropsychological vulnerability to schizophrenia. In A. S. David & J. C. Cutting (Eds.), The neuropsychol- ogy of schizophrenia. Hove: Erlbaum.
Nuechterlein, K. H., & Dawson, M. E. (1984a). A heuristic vulnerability-stress model of schizophrenic episodes. Schizophrenia Bulletin, 10, 300-312.
Nuechterlein, K. H., & Dawson, M. E. (1984b). Information processing and attentional functioning in the developmental course of schizophrenic disorders. Schizophrenia Bulletin, 10, 160-203.
Nuechterlein, K. H., Dawson, M. E., Ventura, J., Fogelson, D., Gitlin, M., & Mintz, J. (1991). Testing vulnerability models: stability of potential vulnerability indicators across clinical state. In H. Hafner & W. W. Gattaz (Eds.), Search for the causes of schizophrenia. Heidelberg: Springer.
Penn, D. L., & Mueser, K. T. (1996). Research update on the psychosocial treatment of schizophrenia. American Journal of Psychiatry, 153, 607-617.
Penn, D. L., Mueser, K. T., Spaulding,W., Hope, D. A. & Reed, D. (1995). Information processing and social competence in chronic schizophrenia. Schizophrenia Bulletin, 21, 269-281.
Persons, J. B. (1986). The advantages of studying psychological phenomena rather than psychiatric diagnoses. American Psychologist, 41, 1252-1260.
Peterson, C., Semmel, A., Von Baeyer, C., Abramson, L., Metalsky, G. I., & Seligman, M. E. P. (1982). The Attributional Style Questionnaire. Cognitive Therapy and Research, 3, 287-300.
Rehm, L. P. (1988). Assessment of depression. In A. S. Bellack & M. Hersen (Eds.), Behavioural assessment: A practical handbook (3rd edn.). Oxford: Pergamon.
Reivich, K. (1995). The measurement of explanatory style. In G. M. Buchanan & M. E. P. Seligman (Eds.), Explanatory style. Hillsdale, NJ: Lawrence Erlbaum.
Robbins, C. J., & Hayes, A. M. (1995). The role of causal attributions in the prediction of depression. In G. M. Buchanan & M. E. P. Seligman (Eds.), Explanatory style. Hillsdale, NJ: Erlbaum.
Robey, K. L., Cohen, B. D., & Gara, M. A. (1989). Self-structure in schizophrenia. Journal of Abnormal Psychology, 98, 436-442.
Rogers, A. H. (1958). The self-concept in paranoid schizophrenia. Journal of Clinical Psychology, 14, 365-366.
Romney, D. M. (1987). A simplex model of the paranoid process: Implications for diagnosis and prognosis. Acta Psychiatrica Scandinavica, 75, 651-655.
Rund, B. R. (1994). The relationship between psychosocial and cognitive functioning in schizophrenic patients and expressed emotion and communication deviance in their parents. Acta Psychiatrica Scandinavica, 90, 133-140.
Scott, L., & O'Hara, M. W. (1993). Self-discrepancies in clinically anxious and depressed university students. Journal of Abnormal Psychology, 102, 282-287.
Seligman, M. E., Peterson, C., Kaslow, N. J. Tanenbaum, R. L., Alloy, L. B. & Abramson, L. B. (1984). Attributional style and depressive symptoms among children. Journal of Abnormal Psychology, 93, 235-238.
Silverstone, P. H., (1991). Low self-esteem in different psychiatric conditions. British Journal of Clinical Psychology, 30, 185-188.
Spaulding, W. D., Sullivan, M., Weiler, M., Reed, D., Richardson, C. & Storzback, D. (1994). Changing cognitive functioning in rehabilitation of schizophrenia. Acta Psychiatrica Scandinavica, 384, 116-124.
Stratton, P., Munton, A. G., Hanks, H. G. I., Heard, D., Brewin, C. R., & Davidson, C. (1988). The Leeds Attributional Coding System Manual. Leeds: Leeds Family Therapy Research Centre.
The Clinical Implications o f a Psychological Model o f Paranoia 161
Strauman, T. J. (1989). Self-discrepancies in clinical depression and social phobia: cognitive structures that underlie emotional disorders? Journal of Abnormal Psychology, 98, 14-22.
Strauman, T. J. (1992). Self-guides, autobiographical memory, and anxiety and dysphoria: toward a cognitive model of vulnerability to emotional distress. Journal of Abnormal Psychology, 101(1), 87-95.
Strauman, T. J. (1994). Self-representations and the nature of cognitive change in psychother- apy. Journal of Psychotherapy Integration, 4, 291-316.
Strauman, T. J. (1996a). Psychopathology from a self-regulation perspective. Journal of Psychotherapy Integration, 5, 313-321.
Strauman, T. J. (1996b). Self-discrepancy theory: validity and clinical implications. Interna- tional Journal of Psychology, 31, 2050.
Strauman, T. J., & Higgins, E. T. (1987). Automatic activation of self-discrepancies and emotional syndromes: when cognitive structures influence affect. Journal of Abnormal Psychology, 98, 14-22.
Strauman, T. J., & Higgins, E. T. (1988). Self-discrepancies as predictors of vulnerability to distinct syndromes of chronic emotional distress. Journal of Personality, 56, 685-707.
Strauman, T. J., & Kolden, G. G. (1996). Self-discrepancy and psychotherapy for depression. International Journal of Psychology, 31, 2054.
Strauman, T. J., Lemieux, A. M., & Coe,C. L. (1993). Self-discrepancy and natural killer cell activity: immunological consequences of negative self-evaluation. Journal of Personality and Social Psychology, 64, 1042-1052.
Strauss, J. S. (1969). Hallucinations and delusions as points on continua function: rating scale evidence. Archives of General Psychiatry, 21,581-586.
Sweeney, P., Anderson, K., & Bailey, S. (1986). Attributional style and depression: a meta- analytic review. Journal of Personality and Social Psychology, 50, 774-791.
Tarrier, N., Barrowclough, C., Porceddu, K., & Fitzpatrick, E. (1994). The Salford Family Intervention Project: relapse rates of schizophrenia at five and eight years. British Journal of Psychiatry, 165, 829-832.
Tarrier, N., Barrowclough, C., Vaughn, C. E., Bamrah, J. S., Porceddu, K., Watts, S., & Freeman, H. (1988). The community management of schizophrenia. British Journal of Psychiatry, 153, 532-542.
Tarrier, N., Beckett, R., Harwood, S., Baker, A., Yusupoff, L., & Ugarteburu, I. (1993). A trial of two cognitive-bebavioural methods of treating drug-resistant residual psychotic symptoms in schizophrenic patients. I. Outcome. British Journal of Psychiatry, 162, 524-532.
Taylor, S. E. (1988). Positive illusions. New York: Basic Books. Tennen, H., & Herzeberger, S. (1985). Attributional Style Questionnaire. In S. J. Keyser & R.
C. Sweetland (Eds.), Test critiques. Westport: Test Corporation of America. Tennen, H., & Herzeberger, S. (1987). Depression, self-esteem and the absence of self-
protective attributional biases. Journal of Personality and Social Psychology, 52, 72-80. Tennen, H., Herzenberger, S., & Nelson, H. F. (1987). Depressive attributional style: the role
of self-esteem. Journal of Personality, 55, 631-660. Turkat, I. D. & Banks, D. S. (1987). Paranoid personality and its disorder. Journal of
Psychopathology and Behavioural Assessment, 9, 295-304. Valone, K., Norton, J. P., Goldstein, M. J., & Doane, J. A. (1983). Parental expressed emotion
and affective style in an adolescent sample at risk of schizophrenia spectrum disorders. Journal of Abnormal Psychology, 92, 279-285.
Vaughn, C. E., & Left, J. (1976). The influence of family and social factors on the course of psychiatric illness: A comparison of schizophrenic and depressed neurotic patients. British Journal of Psychiatry, 129, 125-137.
Watts, F. N., Powell, E. G., & Austin, S. V. (1973). The modification of abnormal beliefs. British Journal of Medical Psychology, 46, 359-363.
162 Peter Kinderman and Richard P. Bentall
Weiner, B. (1986). Cognition, emotion and action. In R. M. Sorrentino & E. T. Higgins (Eds.), Handbook of motivation and cognition: Foundations of social behaviour. New York: Guildford Press.
Weiner, B., Russell, D., & Lerman, D. (1978). Affective consequences of causal attributions. In J. H. Harvey, W. Ickes, & R. F. Kidd (Eds.), New directions in attribution research. Hillsdale: Erlbaum.
White, P. A. (1991). Ambiguity in the internal/external distinction in causal attribution. Journal of Experimental Social Psychology, 27, 259-270.
Winters, K. C., & Neale, J. M. (1983). Delusions and delusional thinking: a review of the literature. Clinical Psychology Review, 3, 227-253.
Winters, K. C., & Neale, J. M. (1985). Mania and low self-esteem. Journal of Abnormal Psychology, 94, 282-290.
Wykes, T. (1994). Predicting symptomatic and behavioural outcomes of community care. British Journal of Psychiatry, 165, 486-492.
Wylie, R. C. (1979). The self-concept (revised edition). Lincoln: University of Nebraska Press. Zigler, E., & Glick, M. (1988). Is paranoid schizophrenia really camouflaged depression?
American Psychologist, 43,284-290. Zullow, H. M., Oettingen, G., Peterson, C., & Seligman, M. E. P. (1988). Pessimistic
explanatory style in the historical record: CAVing LBJ, Presidential candidates, and East versus West Berlin. American Psychologist, 43, 673-682.

12
Self-Directed Experience and Personal Therapy: The Situation in the German-Speaking Countries and the "State of the Art" of Empirical Research
ANTON-RUPERT LAIREITER University of Salzburg, Austria
Terminology A few introductory words on terminology are necessary. The title of this
chapter contains two terms, "self-directed experience" and "personal ther- apy." This duality results from two things: first from terminological difficul- ties and pluralities of the phenomena this paper deal with, and second from problems in translating the relevant terms from German into English. The classic method, which at the same time is also the model for most of the subsequent conceptions and methods in other psychotherapeutic schools, is the so called Lehranalyse, most often translated as "training analysis" in psychoanalysis that goes back to Freud, Ferenczi, and other psychoanalysts of the first generation.
Primarily trained in psychodynamic psychotherapy, but later having dissociated themselves from it, many founders of subsequent psychothera- peutic schools took over this training element and integrated it into their own models of training and educating psychotherapists. This was the case in most of the psychodynamic (Adlerian, Jungian, neo-analytic, interpersonal) but also in the humanistic and experiential psychotherapies, such as Gestalt therapy, client-centered therapy, or transactional analysis. In most of the humanistic therapies this element is no longer called "training analysis";

164 Anton-Rupert Laireiter
according to the terminology of these schools, different terms are used here, such as Gestalt-Lehranalyse ("Gestalt training analysis") in Gestalt-therapy, Lehrtherapie ("teaching therapy/training therapy") in client-centered ther- apy, or most often just pers6nliche Therapie or Eigentherapie (personal therapy) in most other psychotherapeutic schools.
In some contexts, especially in group dynamics and the encounter move- ment, this phenomenon was also called Selbsterfahrung, a term which is difficult to translate into English, because the English language does not have a term comparable to this German word. "Self-experience," which would be the literal translation, does not sound well for English ears. So, at best it may translated as "self-centering," "self-related," "self-directed," or "self-focus- ing experience," o r ~ t o use a term more usual in Engl ish~"personal therapy." However, training in cognitive-behavioral psychotherapy in the German-speaking countries does not favor personal therapy for psychothera- pists (Lange, 1994; Schmelzer, 1996). Thus, this term is not be used to describe the phenomenon that will be discussed here. As a compromise, therefore, both terms are used to make clear to English-speaking readers the subject of the present paper.
What does "self-directed experience" as a translation of the German word Selbsterfahrung mean? In its narrowest sense, it describes the application of the strategies and methods of a certain psychotherapeutic m e t h o d ~ i n our case cognitive-behavioral therapy (CBT)~ to a psychotherapist's own person: his or her self, personal life, and problems. Because the therapist and his/her self are of primary concern in this training element, we may also speak of a self-directed (self-centering, self-related, self-focusing, or personal) psychotherapeutic experience of the therapist. This is the meaning of the German term Selbsterfahrung in the context of CBT.
As one may easily imagine, this kind of experience has not so far had great importance for the development and tradition of CBT, as well as for other psychotherapeutic schools that focus on external conditions in the regulation of human behavior, such as systemic and family therapies. The question that follows then is: Why has it received so much attention in cognitive-behavioral psychotherapy in the German-speaking countries for the last a few years? In the author's view three major factors are responsible for this development:
(1) reasons related to the development of CBT itself; (2) reasons related to self-centered experience in particular; and (3) reasons related to the specific professional and political situation in the
German-speaking countries.
In relation to (1), three aspects are important. First, during recent years, cognitive behavioral psychotherapy learned a lot about the importance of personal and interpersonal factors in therapy, as well as about the im- portance of the therapist-patient relationship as a major contributor to

Self-Directed Experience and Personal Therapy 165
therapeutic effectiveness (Kanfer, Reinecker, & Schmelzer, 1996; Laireiter, 1995; Margraf & Brengelmann, 1992; Raue & Goldfried, 1994; Schindler, 1991). Therefore, developing personal features and interpersonal behaviors that are favorable for psychotherapy and that improve the psychotherapeutic outcome became important goals in training cognitive-behavioral psychotherapists. Methods of personal therapy and self-directed experience seemed to be most suitable to many authors and trainers for training these competencies and behaviors (cf. Kanfer, Reinecker, & Schmelzer, 1996; Laireiter & Elke, 1994). Second, many studies demonstrated negative effects of unfavorable interpersonal styles and behaviors on the outcome of psychotherapy. Consequently, reducing noxious personal and interpersonal effects of therapists became a major goal in the training of future cognitive behavioral psychotherapists. Again, self-directed personal experience, and in some cases personal therapy, were proposed as very important methods for reaching this goal (Kanfer, Reinecker, & Schmelzer, 1996; Zimmer, 1983). Third, many results of research on therapeutic training made it evident that the application of the methods and strategies a therapist is trained in to his own person and behavior, for example, by role-playing, "peer-therapy" micro-teaching and so on, improves the effects of training (Matarazzo & Garner, 1992), which gave self-directed experiences additional importance.
Concerning (2), many results show that a great number of psychotherapists attend personal therapy during their training period as well as in later professional life, with no difference between obligatory and voluntary attendance (see, for example, Mahoney & Craine, 1991; Norcross, Straus- ser-Kirtland & Missar, 1988; Pope & Tabachnik, 1994; Prochaska & Norcross, 1983). One may conclude, therefore, that attending one or even more personal therapies seems to be a very important feature of the psychotherapeutic community in general. Consequently, it may be hypothe- sized that this promoted discussion of the importance of and necessity of a personal therapy for cognitive-behavioral psychotherapists also, especially in the German-speaking countries where psychodynamic reasoning is still very powerful in the psychotherapeutic field.
The Professional and Political Situation in the German-speaking Countries
There are two specific professional and political reasons why this subject is so intensively discussed in the German-speaking countries. First, as mentioned above, psychodynamic reasoning is still very powerful within psychotherapy in these countries. Second, legal and professional regulations of the therapeutic practice and training, which are strongly influenced by psychodynamic reasoning, make self-directed experience obligatory for each trainee in CBT in these countries.

166 Anton-Rupert Laireiter
Although the legal and state regulations situations are very different in Austria, Germany, and Switzerland, the amount of self-directed experience in therapeutic training is comparable, especially between Switzerland and Austria. Behavior therapists in training have to attend at least 100 hours of self-directed experience in Germany, and between 200 and 300 hours in Austria and about the same amount in Switzerland. In Austria this amount is laid down in the Psychotherapiegesetz", a law on the practice and training in psychotherapy; in Germany and Switzerland other legal regulations are in force (regulations related to the medical profession or resulting from insur- ance law).
The legal orders do not regulate the contents and the theoretical models of self-directed experience in psychotherapy. However, it is laid down that every psychotherapeutic school has to develop its own theoretical models and methods for this training element, which must correspond to the general theoretical models of each school and, more importantly, must be integrated into the general conceptions and goals of training in that particular school. Accordingly, CBT also was forced to develop its own models and methods of self-related experience and personal therapy in the late 1980s and early 1990s in the German-speaking countries. During this time, many authors and scholars developed their own methods, which resulted in a very heterogenous and difficult situation, because the conceptions and methods were very different and attendants from different training institutions received very different forms of training and self-directed modes of experience (see Laireiter, 1994). In the meantime, this diversity has been reduced a little and more general developments have become generally adopted. However, the situation is still far from any general and broadly accepted conception of self-related experience in CBT (Bruch & Hoffmann, 1996; Laireiter & Elke, 1994; Lieb, 1997-98a).
Despite the heterogeneity of the models and methods, some general rules guide their development. The following three are most important.
(1)
(2)
(3)
Models of self-directed experience have to correspond to the general theoretical and methodological principles of CBT and should originate from its theoretical and methodological background. Consequently, these models should be based on CBT and should not be imported from any other psychotherapeutic school. Related to (1), methods and strategies of cognitive-behaviorally orientied self-directed experience should originate primarily from the fund of methods and strategies of CBT. Models and methods of self-directed experience should not only corre- spond to the general goals of training in CBT, they should cover important subgoals that are not represented by any other method or element of training. Consequently, the models must refer to the general

Self-Directed Experience and Personal Therapy 167
goals of training and must also represent specific parts of them. In any case it may not be a pointless addition to the conventional methods of training of cognitive-behavior therapists devoid of any meaningful func- tion.
Goals of Self-Directed Experience in Training Therapists
Although the discussion of the functions and goals of this training element brought forth many different and sometimes very heterogenous views in German CBT, they can be combined into a system of five general goals: didactic, educational, preventive, therapeutic and resource-improving goals (see Table 12.1). It is interesting to note also that authors from English- speaking countries have made similar suggestions (see Laireiter & Fiedler, 1996; Norcross, in Dryden, 1991).
In relation to the didactic goals, it will be expected that ongoing therapists should become more acquainted with the general strategies and methods of cognitive-behavioral psychotherapy, which should improve the general effects of training in the therapeutic strategies and methods. Additionally, this personal acquaintanceship should also result in a more personal identi- fication of the ongoing psychotherapist with the methods he is trained in (Laireiter & Elke, 1994).
Regarding the educational goals, it is proposed that future therapists will encounter intensive experience with the client- or patient-role and should therefore develop intensive empathy for this role as well as for the personal needs of clients. Additionally, other therapeutically relevant behaviors may also be learned in this setting, such as favorable interpersonal skills, self- awareness, self-reflectivity, interpersonal sensitivity, social assertiveness, self- monitoring-skills and so on (Kanfer, Reinecker, & Schmelzer, 1996).
Some authors emphasize preventive effects of self-directed experiences (see Kanfer, Reinecker, & Schmelzer, 1996). In their opinion, attending courses of self-directed experience should lead to a greater sensitivity of future therapists to the problematic parts of their own personalities and behaviors. Addition- ally, intensive self-confrontation in such a setting should reduce so called "blind spots" of poor self-knowledge and intensify self-monitoring of their interpersonal behaviors, especially problematic ones. These (problematic and noxious interpersonal) behaviors and personal features may also be reduced by actively applying therapeutic methods.
In relation to point (4), several authors stress the necessity of treating the personal problems of the future therapist (e.g., Pope & Tabachnik, 1994; Prochaska & Norcross, 1983). Different studies demonstrate that trainees as well as practicing therapists do have personal problems that must be treated in order to reduce impaired effectivity and to prevent early burn-out and the

168 Anton-Rupert Laireiter
Table 12.1. Goals of Personal Therapy and Self-Directed Personal Experience in Psychotherapy
1. Didactic goals �9 Learning to practice cognitive-behavioral psychotherapy:
by observing a model by conducting client-behaviors
�9 Getting acquainted with the therapeutic process �9 Learning cognitive-behavioral strategies and methods by encounting them �9 Getting identified with the principles and methods of cognitive-behavioral psychotherapy
2. Educational goals �9 Learning therapeutically relevant behaviors:
empathy by taking over the client's role self-awarenes and self-monitoring skills interpersonal skills and interpersonal sensitivity social assertiveness
3. Preventive goals �9 Reduction of negative, noxious effects of the therapist �9 Enhancing the sensitivity for problematic behavior of the therapist �9 Reduction of "blind spots" and improving self-knowledge
4. Therapeutic goals �9 Treatment of personal problems �9 Management of negative problematic personal areas
5. Resource-improving goals: �9 Developing personal and interpersonal resources
well-being self-esteem positive self-view
�9 Prevention of actual and potential burn-out
intensification of these personal problems. Because "s tandard" self-directed experience methods most often do not achieve these ends adequately, most training institutions prescribe personal therapy for therapists with personal problems additionally to their "normal" self-directed experience courses. In other authors ' view (see Frank, 1998; Norcross, in Dryden, 1991; Schmelzer, 1996), self-directed experience should also focus on the personal and interpersonal resources of the therapist and might therefore actively prevent actual and potential burn-out, irrespective of whether personal problems exist or not. Burn-out is a major problem in the helping professions, especially in psychotherapy, and its prevention therefore appears an impor- tant goal of training in psychotherapy.

Self-Directed Experience and Personal Therapy 169
Models and Methods of Self-Directed Experience in the German-speaking Countries
As pointed out above, many different models have been developed, which may, however, be classified into five groups (Laireiter, 1996b; see also Table 12.2): models focusing on the person of the therapist (person-related models); models focusing on personal and interpersonal aspects of the therapist in practicing psychotherapy (practice-focusing models); models stressing the application of cognitive-behavioral methods and strategies by the future therapist (methods-centered models); models that emphasize the importance of some kind of personal therapy in the dyadic and group-setting (personal therapy-models); and models that combine elements of models (1) to (4) (combined models).
Person-related models concentrate primarily on the person of the psychotherapist in training without focusing on his professional activities. Most of these experiences are completed in two different forms: modified cognitive behavioral groups, and structured thematic groups dealing with "themes of life" (Schmelzer, 1996), such as one's own learning history, family background, interactional and interpersonal behaviors, problematic aspects of one's own personality, and so on. The primary goal of these methods is to become acquainted with the methods and strategies of cognitive behavioral psychotherapy and to become sensitized for one's own behavior and person- ality, especially on the interpersonal level.
Practice-focussing models also deal with the person of the ongoing psychotherapist; however, they concentrate on the therapist's behavior and interpersonal performance in the therapeutic situation. Three different conceptions may be added to this group: (i) self-reflection on these aspects in goal-directed working groups, most comparable to thematic supervision or intervision groups; in these groups the reflection on one's own behavior and interactive strategies of the therapist is the subject of the work; (ii) the attendance at specific goal-directed groups dealing with specific "themes of professional life" (Schmelzer, 1996); (iii) the focusing on personal and interpersonal aspects of the therapist in psychotherapy supervision.
Methods-centered models concentrate on the direct and personal experi- ence of the future therapist with the most important methods, strategies and treatment manuals of cognitive behavior therapy. During this kind of self- directed experience, each trainee applies different singular and combined methods as well a s ~ i n some cases~total treatment manuals to his or her own person. This application most often takes place in groups guided by a teaching therapist; however, in some cases it also is done alone or in unguided groups. One of the most important forms of this self-application of methods and strategies of CBT, which is also very often used within person-centered models, is the completion of self-modification and self-
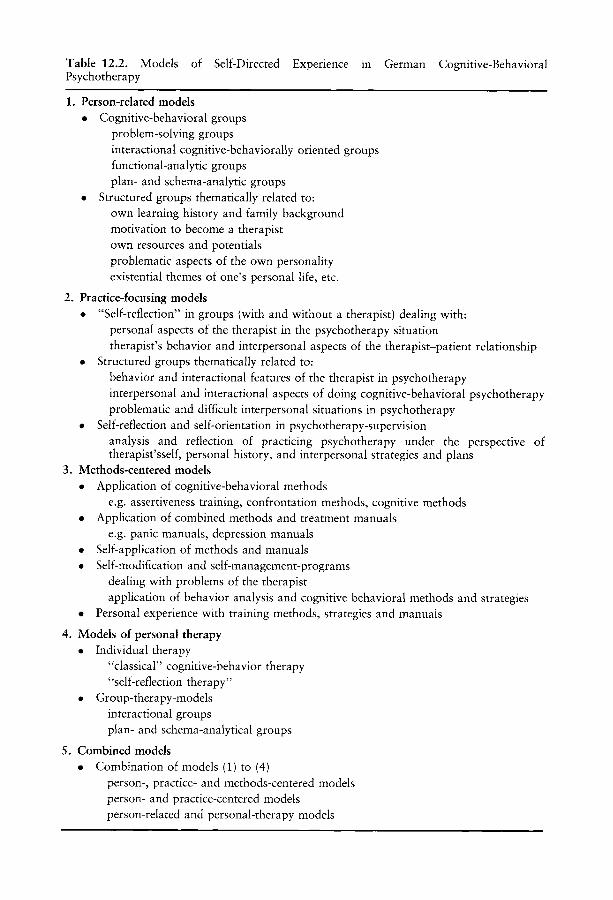
Table 12.2. Models of Self-Directed Experience in German Cognitive-Behavioral Psychotherapy
1. Person-related models �9 Cognitive-behavioral groups
problem-solving groups interactional cognitive-behaviorally oriented groups functional-analytic groups plan- and schema-analytic groups
�9 Structured groups thematically related to: own learning history and family background motivation to become a therapist own resources and potentials problematic aspects of the own personality existential themes of one's personal life, etc.
2. Practice-focusing models �9 "Self-reflection" in groups (with and without a therapist) dealing with:
personal aspects of the therapist in the psychotherapy situation therapist's behavior and interpersonal aspects of the therapist-patient relationship
�9 Structured groups thematically related to: behavior and interactional features of the therapist in psychotherapy interpersonal and interactional aspects of doing cognitive-behavioral psychotherapy problematic and difficult interpersonal situations in psychotherapy
�9 Self-reflection and self-orientation in psychotherapy-supervision analysis and reflection of practicing psychotherapy under the perspective of therapist'sself, personal history, and interpersonal strategies and plans
3. Methods-centered models �9 Application of cognitive-behavioral methods
e.g. assertiveness training, confrontation methods, cognitive methods �9 Application of combined methods and treatment manuals
e.g. panic manuals, depression manuals �9 Self-application of methods and manuals �9 Self-modification and self-management-programs
dealing with problems of the therapist application of behavior analysis and cognitive behavioral methods and strategies
�9 Personal experience with training methods, strategies and manuals
4. Models of personal therapy �9 Individual therapy
"classical" cognitive-behavior therapy "self-reflection therapy"
�9 Group-therapy-models interactional groups plan- and schema-analytical groups
5. Combined models �9 Combination of models (1) to (4)
person-, practice- and methods-centered models person- and practice-centered models person-related and personal-therapy models

Self-Directed Experience and Personal Therapy 171
management programs to change one's own problematic behaviors (e.g., smoking, working behaviors, cognitions, problematic coping with stress). In almost every training course in behavior therapy in the German-speaking countries, trainees have to complete at least one of these programs during their training period (Laireiter, 1994; Ziesing & Pfingsten, 1994).
Models of personal therapy are rather complex. One finds classic cognitive- behavior therapy in individual as well as in group settings but also more complex models such as the so-called "self-reflection therapy" (Laireiter & Fiedler, 1996), which combines functional analysis and cognitive-behavioral methods based on the general treatment model of CBT with intensive self- reflection and self-encounter by analyzing and working through personal life experiences, actual and past conflicts, interpersonal behaviors and plans of the therapist and the motives and meanings lying behind them (see also Grawe, 1997, for related methods).
Most training programs for cognitive behavior therapy in the German- speaking countries do not use singular models; they are usually combined. However, very different combinations can be observed. D6ring-Seipel, Schiiler, and Seipel (1995), for instance, combined person-, practice-, and methods-centered elements to develop their program. G6rlitz and Hippler (1992) only integrated person-related and practice-centered elements; and Zimmer, Zimmer, and Wagner (1994) developed a purely person-centered model by integrating a short personal therapy in a dyadic setting into a person-related group conception.
It becomes evident that the development of models of self-directed experi- ence in training cognitive-behavioral psychotherapists in the German-speak- ing countries is not yet finished and is still far from any broadly accepted general structure.
Empirical Studies and Results andSelf-Directed Experience
o n Personal Therapy
Studies in the German-speaking Countries
So much for the conceptual situation of personal therapy and self-centered experience in the German-speaking countries. The most important question that follows now is: What is known about the effects of the different models? Since they were introduced only a short time ago, they have not yet been fully evaluated empirically. Therefore, only very few data are available on their effects and their acceptibility to the participants of the training courses at present. These results are primarily related to combined models; no study has been conducted to evaluate the effects of the individual models (see models (1) to (4) in Table 12.2).

172 Anton-Rupert Laireiter
Studies evaluating these combined models conclude that the participants accept them as important training elements in cognitive behavioral psychotherapy (D6ring-Seipel, Schiiler, & Seipel, 1995; G6rlitz & Hippler, 1992; Lieb, 1998b); most of them are also highly valued by their participants (D6ring-Seipel, Schiiler, & Seipel, 1995; Lieb, 1998b). The major effect of having self-directed experience is related to its didactic and educational goals. Thus, in the aforementioned studies most trainees stated that they learned a lot about behavior therapy, its application, and its methods and strategies by applying its principles and methods to their own persons and behaviors (D6ring-Seipel, Schiiler, & Seipel, 1995; Lieb, 1998b). Additionally, most participants reported higher self-awareness and self-reflection (G6rlitz & Hippler, 1992) as well as an improvement of their interpersonal skills and a higher empathy for and a better understanding of their clients (D6ring- Seipel, Schiiler, & Seipel, 1995). In one study (Hoyer & Stangier, 1998) it was observed that the attendance at a weekend of (practice-focusing) self- directed experience resulted in a higher interpersonal sensitivity and a better client-therapist relationship in the following therapy sessions. This was also perceived and stated by the clients (assessed by questionnaires on the therapeutic process and the therapist-patient relationship). This study is the only one that demonstrated direct effects of this training element on practicing psychotherapy and therapeutic interpersonal behavior. Many more of these studies are needed in future.
In summary, the studies cited above report encouraging results of combined models of self-related experience according to their acceptance and some of their postulated goals (didactic and educational). However, most of these studies are based on subjective data (self-reports, subjective evalua- tions) from the therapists; only one used data from the patients. Future studies should more often use observational methods and data from patients. They should also explore the effects of self-directed experience on the effectiveness as well as the therapeutic and interpersonal behaviors of the therapists in their everyday work as well as the differential effects of the different models of self-directed experiece.
International Studies
If German research has not yet studied self-directed experience and its effects within CBT very intensively, has international research done so? Unfortunately, the answer is a clear "No"! Not one study on the effects of personal therapy and self-directed experience in cognitive-behavioral psychotherapy has been published in international journals. Most studies published deal with modes and effects of the psychoanalytic training analysis as well as with personal therapies in general, without differentiating their theoretical orientation (see Laireiter, 1996a; Schmelzer, 1996, for overviews).
Self-Directed Experience and Personal Therapy 173
Additionally, only very few studies deal with personal therapy and self- directed experience as a training element; many of them result from other contexts, such as the development of psychotherapists and their personal lives as well as the treatment of psychotherapists with mental disorders and professional impairment. This leads to the conclusion that research on training in psychotherapy is still in his infancy (see also Binder, 1993, for a related view). Only research on psychotherapy supervision (see Frank, 1997) and on teaching psychotherapeutic skills (e.g., Matarazzo & Garner, 1992) has received more scientific attention.
The major results of the studies on personal therapy and self-directed experience may be summarized under the following four heads:
(1) Prevalence of personal therapy in psychotherapy-trainees and practicing therapists
(2) Subjectively evaluated effects of personal therapy (3) Effects of personal therapy on the personal problems and impairments of
therapists (4) The direct effects of personal therapy on the therapeutic effectiveness
Because of limited space, the results on these topics are presented only in summary (for more details see Beutler, Machado, & Allstetter Neufeldt, 1994; Clark, 1986; Laireiter, 1996a; Macaskill, 1988; Schmelzer, 1996).
Concerning point (1), most studies found that about 80% of all psychotherapists attend a personal therapy at least once in their professional life; men do it less often (75%) than women (90%) and psychodynamically and humanistically oriented psychotherapists (85-90%) more often than cognitive-behaviorally and systemically oriented ones (40-50%) (Norcross, in Dryden, 1991; Pope & Tabachnik, 1994). Most therapies needed about 50 hours to be completed; however, in psychodynamic and humanistic psychotherapies longer personal therapies are usual (250 and more hours) (Pope & Tabachnik, 1994). The most often attended forms of therapy are psychodynamic, humanistic, eclectic, systemic, and cognitive-behavioral (in that order). It is interesting and important to note that cognitive-behavioral therapists most often complete psychodynamic and humanistic therapies, but very rarely cognitive or behavioral ones (Norcross, Strausser, & Faltus, 1988).
On point (2), most therapists report intensive and very positive effects of their personal therapies on their personal and professional lives. Additionally, they value it as a very helpful and necessary experience during their training period as well as in their later career (Greenberg & Staller, 1981; Macaskill, 1988; Norcross, 1990). About 60-70% of therapists regard it as an essential element in psychotherapeutic training. The following effects of personal therapy are reported most often (see Greenberg & Staller, 1981; Pope & Tabachik, 1994; Macaskill, 1988):

174 Anton-Rupert Laireiter
�9 Improvement of basic interpersonal skills such as empathy, warmth, genuiness, openess, etc.
�9 Improvement of self-esteem and personal and interpersonal assertiveness �9 Increase of self-awareness and the ability to reflect on one's own
behaviors, goals, and plans �9 Improved learning of therapeutic strategies and methods �9 Learning of basic interpersonal skills for conducting the therapist-
patient relationship �9 Improved interpersonal sensitivity and emotional expressivity
Under the perspective of the didactic and educational goals discussed above, the following effects of personal therapy, reported by the attendants, can be seen as very important:
�9 Getting acquainted with the therapeutic process �9 Being a client and experiencing the client role �9 Encountering the interpersonal processes of the therapeutic relationship
immediately and directly �9 Encountering processes of change of one's own behavior �9 Learning basic therapeutic and interpersonal behaviors by observing the
therapist as a model.
Most personal therapies result in positive effects on the personal problems and impairments of the therapists (Greenberg & Staller, 1981; Norcross, 1990; Sherman, 1996); however, lack of positive effects or even negative ones have been reported in about 10-20% of therapists (Macaskill, 1988). Not all studies found such negative effects.
In contrast to the very positive effects a personal therapy has on the problems and disorders of the therapist, the results concerning the direct effects of this experience on therapeutic effectiveness are very diverse and do not allow any firm conclusions. Most studies did not find any direct effect; very few found a positive one; and some also found negative effects of personal therapy on therapeutic effectiveness (see Beutler, Machado, & Allstetler Neufeld, 1994; Clark, 1986; Greenberg & Staller, 1981; Wheeler, 1991). Unfortunately, those studies that report positive effects show meth- odological problems. Most often they did not control the factor "length of professional activity," thus, confounding the results. Clark (1986) reports that controlling this factor in one study changed the positive effect of personal therapy into a negative one, that leads to the conclusion that the professional experience of a therapist is much more important for his therapeutic effectiveness than is his personal therapy (for a related conclu- sion, see Willutzki & Ambtihl, 1998). Although direct evidence of improved effectiveness of therapists having personal therapy is lacking, most of these therapists see their personal therapy as very helpful and effective for their
Self-Directed Experience and Personal Therapy 175
own psychotherapeutic practice. However, as Norcross (in Dryden, 1991) pointed out, this contradiction must not be a real contradiction for two reasons: First, the relationship has not yet been adequately explored; second, therapists could be referring to other aspects than therapeutic effectiveness, when speaking about the helpfulness and effectiveness of their own therapies. However, this contradiction could also be regarded as a real one and, thus, must be seen as a phenomenon of dissonance reduction (Festinger, 1957) and the justification of the efforts of the therapists (Cooper & Axsom, 1982).
In summary, the results presented can be interpreted as follows. A large number of psychotherapists, also with cognitive-behavioral orientation, attend personal therapy, even though it is not obligatory. If voluntary attendance is focused, most therapists prefer psychodynamic and humanistic schools for dealing with their problems and making their self-focusing experiences. Cognitive-behavioral psychotherapy does not seem to be in favor, which may have to do with its focus on problem-solving and changing behaviors (Norcross, in Dryden, 1991). Most therapists obviously like to improve their self-reflection and self-awareness and do not want to change specific problems.
In relation to the effects, the studies presented make evident that a personal therapy most successfully achieves the didactic, educational, and therapeutic goals and only to some extent the preventive ones mentioned above. It apparently has only scant effect on the therapeutic effectiveness of the attending therapist. But Norcross (in Dryden, 1991) has pointed out that it may be asked whether this is the primary and most important goal of this training element. Theoretical considerations as well as empirical results put other, more central goals and functions into the foreground, such as the development of important personal and interpersonal therapeutic skills, the improvement of the effects in psychotherapeutic training, the reduction of personal problems and mental disorders, and thus the prevention of noxious and problematic personal and interpersonal effects of the therapist. Are these effects not enough?
What conclusions can be drawn from these results for personal therapy and self-directed experience in CBT? Because most studies reported above deal with psychodynamically and humanistically orientied therapies, the conclusions cannot be fully and uncritically transfered to CBT. The effects of personal therapy and self-directed experience in this approach must be explored by specific studies. However, some of the results of the aforemen- tioned German studies support the notion that cognitive-behaviorally oriented self-centered experiences may also have similar effects and conse- quences, such as a better performance in the therapeutic situation, learning of more empathic and self-reflective behaviors, development of interpersonal skills and competencies, reduction of personal problems and conflicts, and consequent prevention of noxious effects of the therapist in his therapeutic

176 Anton-Rupert Laireiter
work with his patients. It will be the aim of further studies using a better methodology to test these hypotheses more extensively and directly.
Conclusions
The present paper has dealt with personal therapy and self-related experi- ence as a newly established element in training of cognitive-behavioral psychotherapists, with special reference to the German-speaking countries. However, we have also explored the international literature and could find no reference to a theoretical or practical model in the English-language literature, which leads to the question whether this element is or is not important in CBT in general. Looking at the literature and the international congresses, one must conclude that it evidently is not very significant in most training courses in the European and American associations and institutions of CBT. Theoretical considerations as well as the aforementioned empirical results lead to a different conclusion: Personal and self-directed experience in psychotherapeutic training has some very important practical functions and purposes. It should therefore receive more attention in the international community of cognitive-behavioral psychotherapists.
The importance of this training element in the German-speaking countries results from the historically founded strength of psychodynamic reasoning in psychotherapy in these countries. Owing to this specificity, CBT has a very specific situation in relation to personal therapy and self-directed experience in these countries. Again because of to this specificity, German CBT has done a lot of work in developing and evaluating theoretical and practical models of this training element. Although much has been done, further developments are still needed. As a first step, it will be necessary to evaluate the different models and conceptions more intensively and, as a second, more general and broadly accepted models of self-directed experience and personal therapy should be developed.
References Beutler, L. E., Machado, P. P. P. & Allstetter Neufeld, S. (1994). Therapist variables. In S. L.
Garfield & A. E. Bergin (Eds.), Handbook of psychotherapy and behavior change (4th ed., pp. 229-271). New York: Wiley.
Binder, J. L. (1993). Is it time to improve psychotherapy training? Clincial Psychology Review, 13, 301-318.
Bruch, M., & Hoffmann, N. (Eds.). Selbsterfahrung in der Verhaltenstherapie? [Self-directed experience in cognitive-behavioral psychotherapy?]. Berlin: Springer.
Clark, M. M. (1986). Personal therapy: A review of empirical research. Professional Psychotherapy: Research and Practice, 17, 541-543.
Cooper, J., & Axsom, D. (1982). Effort justification in psychotherapy. In G. Weary & H. L. Mirels (Eds.), Integrations of clinical and social psychology. New York: Oxford Univer- sity Press.

Self-Directed Experience and Personal Therapy 177
D6ring-Seipel, E., Sch~iler, P., & Seipel, K. H. (1995). Selbsterfahrung for Verhaltensthe- rapeuten: Konzept eines Trainings zielorientierter Selbstreflexion: Erste Erfahrungen [Self- directed experience in behavior therapy training: The conception of a training in goal- directed self-reflection: primary results]. Verhaltenstherapie, 5, 138-148.
Dryden, W. (1991). A dialogue with John Norcross. Toward Integration (chapter 5: Personal Therapy). Milton Keynes: Open University Press.
Festinger, L. (1957). A theory of cognitive dissonance. Evaston, IL: Stanford University Press. Frank, R. (1997). Die Relevanz der Supervisionsforschung fiir die Praxis der Psychotherapie
[The relevance of research on psychotherapy-supervision on practicing psychotherapy]. In H. Petzold & M. M~irtens (Eds.), Psychotherapieforschung und die Praxis der Psychotherapie. [Psychotherapy research and the practice of psychotherapy]. Paderborn: Junfermann.
Frank, R. (1998). Wohlbefinden von Psychotherapeutinnen und Psychotherapeuten: Evalua- tion von Selbsterfahrung w~ihrend der Fort- und Weiterbildung [Well-being of psychotherapists: evaluation of self-directed experience during therapeutic training]. In A.-R. Laireiter (Ed.), Selbsterfahrung in der Verhaltenstherapie~Empirische Befunde [Self-directed experience in cognitive-behavioral psychotherapy~empirical results]. Tiibingen: DGVT.
Grawe, K. (1997). Research-informed psychotherapy. Psychotherapy Research, 7, 1-20. Greenberg. R. P. & Staller, J. (1981). Personal therapy for therapists. American Journal of
Psychiatry, 138, 1457-1471. G6rlitz, G., & Hippler, B. (1992). Selbsterfahrung in der Ausbildung zum
Verhaltenstherapeuten~Erfahrungsbericht [Self-encounter in training of behavior therapists ~ experiential report]. Verhaltenstherapie, 2, 151-158.
Hoyer, J., & Stangier, U. (1998). Wirkt sich "Selbsterfahrung in der Ausbildung" auf die Qualit~it der Therapiestunden aus? Pilotstudie und Forschungsvorschl~ige [Does "self- directed experience in training of psychotherapists" influence the quality of psycho- therapeutic work? A pilot-study and proposals for future studies]. In A.-R. Laireiter (Ed.), Selbsterfahrung in der Verhaltenstherapie~Empirische Befunde. [Self-directed experi- ence in cognitive-behavioral psychotherapy~empirical results]. Tiibingen: DGVT.
Kanfer, F. H., Reinecker, H., & Schmelzer, D. (1996). Selbstmanagement-Therapie" Ein Lehrbuch fiir die klinische Praxis [Self-management Therapy: A teaching guide for clinical practice] (2d ed.). Berlin: Springer.
Laireiter, A.-R. (1994). Zum gegenw~irtigen Stand der Implementierung von Selbsterfahrung in deutschsprachige Ausbildungscurricula in Verhaltenstherapie [The implementation of self-directed experience into training courses of German-language cognitive-behavioral psychotherapy: present situation]. In A.-R. Laireiter & G. Elke (Eds.), Selbsterfahrung in der Verhaltenstherapie~ Konzepte und praktische Erfahrungen [Self-directed experience in cognitive-behavioral psychotherapy~conceptions and practical experiences] (pp. 201-229). Tiibingen: DGVT.
Laireiter, A.-R. (1995). Die Therapeut-Klient-Beziehung in der Verhaltenstherapie [The therapist-patient relationship in cognitive-behavioral psychotherapy]. Psychotherapie Forum, 3, 128-146.
Laireiter, A.-R. (1996a). Selbsterfahrung in der Ausbildung in Psychotherapie~ Schwerpunkt Verhaltenstherapie [Psychotherapist's personal therapy: outcome and consequences for training psychotherapists ~ special emphasis on cognitive-behavioral psychotherapy]. Psychologie in der Medizin, 7, 3-14.
Laireiter, A.-R. (1996b). Selbsterfahrung in der Verhaltenstherapie~Konzepte und Metho- den [Self-directed experience in cognitive-behavioral psychotherapy~conceptions and methods]. Psychotherapie Forum, 4, 210-216.
Laireiter, A.-R., & Elke, G. (Eds.) (1994). Selbsterfahrung in der Verhaltenstherapie~ Konzepte und praktische Erfahrungen [Self-directed experience in cognitive-behavioral psychotherapy~conceptions and practical experiences]. Tiibingen: DGVT.
178 Anton-Ruper t Laireiter
Laireiter, A.-R., & Fiedler, P. (1996). Selbsterfahrung und Eigentherapie [Self-directed experience and personal therapy]. In M.Bruch & N. Hoffmann (Eds.), Selbsterfahrung in der Verhaltenstherapie? [Self-directed experience in cognitive-behavioral psychother- apy?] (pp. 82-123). Berlin: Springer.
Lange, A. (1994). Nicht-schulspezifische Faktoren und die Pflicht zur Lehrtherapie: Eine kritische Auseinandersetzung [Nonspecific factors in psychotherapy and the obliga- tion for a personal therapy: a critical examination]. Psychologische Rundschau, 45, 148-156.
Lieb, H. (1998a). Selbsterfahrung fiir Psychotherapeuten [Self-directed experience for psychotherapists]. G6ttingen: Verlag fiir Angewandte Psychologie.
Lieb, H. (1998b). Evaluationsstudie IFKV Bad Diirkheim: Ver~inderung durch Selbsterfahrung~Wirkvariablen in der Selbsterfahrung [Evaluation study IFKV Bad Dtirkheim: Change through self-directed experience ~ working factors of self-directed experience]. In A.-R. Laireiter (Ed.), Selbsterfahrung in der Verhaltenstherapie~ Empirische Befunde. [Self-directed experience in cognitive-behavioral therapy~ empirical results]. Tiibingen: DGVT.
Macaskill, N. D. (1988). Personal therapy in the training of psychotherapist: Is it effective? British Journal of Psychology, 4, 219-226.
Mahoney, M. J., & Craine, M. H. (1991). The changing beliefs of psychotherapy experts. Journal of Psychotherapy Integration, 1,207-221.
Margraf, J., & Brengelmann, J. C. (Eds.) (1992). Die Therapeut-Patient-Beziehung in der Verhaltenstherapie [The therapist-patient relationship in cognitive-behavioral psychother- apy]. Miinchen: Gerhard R6ttger Verlag.
Matarazzo, R. G., & Garner, A. M. (1992). Research on training in psychotherapy. In K. D. Freedheim (Ed.), History of psychotherapy. A century of change (pp. 850-877). Washington DC.: American Psychological Association.
Norcross, J. C. (1990). Personal therapy for therapists: One solution. Psychotherapy in Private Practice, 8, 45-59.
Norcross, J. C., Strausser, D. J., & Faltus, F. J. (1988). The therapist's therapist. American Journal of Psychotherapy, 62, 53-66.
Norcross, J. C., Strausser-Kirtland, D. J., & Missar, C. D. (1988). The processes and outcomes of psychotherapists' personal treatment experiences. Psychotherapy, 25, 36-43.
Pope, K. S., & Tabachnik, B. G. (1994). Therapists as patients: A national survey of psychologists' experiences, problems and beliefs. Professional Psychology: Research and Practice, 25, 247-258.
Prochaska, J. O., & Norcross, J. C. (1983). Contemporary psychotherapists: A national survey of characteristics, practices, orientations, and attitudes. Psychotherapy: Theory, Research and Practice, 20, 161-173.
Raue, P. J., & Goldfried, M. R. (1994). The therapeutic alliance in cognitive-behavior therapy. In A.O. Horvath & L.S. Greenberg (Eds.), The working alliance. Theory, research and practice (pp. 131-152). New York: Wiley.
Schindler, L. (1991). Die empirische Analyse der therapeutischen Beziehung. Beitrdge zur Prozeflforschung in der Verhaltenstherapie [The empirical analysis of the therapeutic relationship. A contribution to process research in cognitive-behavioral psychotherapy]. Berlin: Springer.
Schmelzer, D. (1996). Selbsterfahrung in der Verhaltenstherapie~Grunderfordernis, Luxus oder notwendiges Ubel? [Self-directed experience in cognitive behavioral psychotherapy ~basic need, luxury or necessary evil?]. In M. Bruch & N. Hoffmann (Eds.), Selb- sterfahrung in der Verhaltenstherapie? [Self-directed experience in cognitive behavioral psychotherapy?] (pp. 125-194). Berlin: Springer.
Sherman, M. D. (1996). Distress and professional impairment due to mental health problems among psychotherapists. Clinical Psychology Review, 16, 299-315.

Self-Directed Experience and Personal Therapy 179
Wheeler, S. (1991). Personal therapy: An essential aspect of counsellor training or a distraction from focussing on the client. International Journal of the Advancement of Counselling, 14, 193-202.
Willutzki, U., & Ambiihl, H. (1998). Selbsterfahrung und professionelle Eutwichlung von Verhaltens-therapeuten. Eine empirische Perspektive [Self-directed experience and profes- sional development of cognitive-behavioral psychotherapists: An empirical perspective]. In A.-R. Cairciter (Ed.), Selbslerfahrung in der Verhaltenstherapie--Empirische Befunde [Self-directed experience in cognitive-behavioral psychotherapy-empirical results]. Tiibin- gen, DGVT.
Ziesing, F., & Pfingsten, U. (1994). Ausbildungsmanual 3: Selbstveriinderung--Verhal- tenstherapie selbst erfahren [Training manual No. 3: Self-change: Applying cognitive- behavioral psychotherapy on the self]. Tiibingen: DGVT.
Zimmer, D. (Ed.) (1983). Die therapeutische Beziehung [The therapist-patient relationship]. Weinheim: Edition Psychologie.
Zimmer, F. T., Zimmer, D., & Wagner, W. (1994). Selbsterfahrung in der verhaltensther- apeutischen Weiterbildung [Self-directed experience in training of cognitive-behavioral psychotherapy]. In A.-R. Laireiter & G. Elke (Eds.), Selbsterfahrung in der Verhal- tenstherapie: Konzepte und praktische Erfahrungen [Self-directed experience in cognitive- behavioral psychotherapy--conceptions and practical experiences] (pp. 17-31). Tiibingen: DGVT.

13
Cognitive Aspects of Posttraumatic Stress Disorder
RICHARD J. MCNALLY Harvard University
Introduction
The main goal of cognitive research on posttraumatic stress disorder (PTSD) is to elucidate the information-processing abnormalities constitutive of the syndrome. Cognitive researchers endeavor to describe how the brain, characterized at an information-processing level of analysis, gives rise to the signs and symptoms of the disorder.
Our research group has conducted cognitive studies on PTSD that fall under three broad categories (McNally, 1996). First, we have done studies documenting content-dependent information-processing abnormalities that emerge only when patients process information having certain meaning (e.g., related to traumatic memories). For example, studies have revealed that Vietnam combat veterans with PTSD exhibit selective Stroop interference when naming the colors of combat-related words, whereas healthy combat veterans do not (e.g., McNally, Kaspi, Riemann & Zeitlin, 1990).
Content-independent abnormalities emerge when patients display cogni- tive problems irrespective of the meaning of the information processed. For example, Vietnam veterans with PTSD not only exhibit selective Stroop interference for trauma words consistent with symptoms of intrusive cogni- tion, they often exhibit overall slowed color-naming suggestive of general concentration impairment (e.g., Kaspi, McNally, & Amir, 1995). Combat veterans with PTSD also exhibit impairments in recalling specific autobio- graphical memories that are not necessarily related to valence or to trauma (e.g., McNally, Lasko, Macklin, & Pitman, 1995).
Finally, we have conducted studies to test whether lower cognitive ability (intelligence) is a risk factor for developing PTSD (e.g., McNally & Shin, 1995).
182 Richard J. McNally
The purpose of this chapter is to provide a brief overview of some our recent research on the cognitive aspects of PTSD. Space limitations perforce confine the coverage to the first and third categories of cognitive research.
Content-dependent Abnormalities Many studies have shown that Vietnam veterans with PTSD exhibit greater
interference for trauma cues than do healthy combat veterans on the emotional Stroop task (e.g., McNally, Kaspi, Riemann, & Zeitlin, 1990). Given that patients seemingly cannot help but attend to the meaning of threat cues, at the expense of naming their colors, one might conclude that such processing is automatic. If so, is it the case that selective processing of threat cues in PTSD qualifies as automatic in other ways (McNally, 1995)? Psychologists have traditionally characterized as "automatic" those cognitive processes that occur involuntarily, that consume few cognitive resources, and that are capable of occurring outside awareness.
Using masked ("subliminal") and unmasked ("supraliminal") presenta- tions, we tested whether Vietnam combat veterans with PTSD, relative to healthy combat veterans, exhibit selective interference for subliminal as well as supraliminal trauma cues (McNally, Amir, & Lipke, 1996). Subjects color- named four types of stimulus: trauma-relevant, positive, categorized neutral (household items), and color-inconsistent words. Words appeared one at a time on a computer screen, and the subject's vocal color-naming latency was measured.
If the intrusive cognitive processes tapped by the Stroop paradigm are "automatic" in the sense of being initiated outside of awareness, we ought to detect enhanced interference for trauma words in the PTSD group in the subliminal condition as well as the supraliminal one. This is not, however, what we found. Indeed, we found no persuasive evidence that patients selectively processed masked trauma cues, although we did obtain evidence of delayed color-naming of trauma cues in the PTSD group when these cues appeared supraliminally.
These data imply a dissociation between two putative attributes of auto- maticity. PTSD patients automatically process trauma cues in the sense that they cannot help but do so (i.e., automaticity as involuntary processing), but they do not appear to detect these cues when masked (i.e., automaticity as occurring outside awareness).
Another topic we have studied recently is the reported ability of psychia- trically impaired adult survivors of childhood sexual abuse to employ an avoidant or dissociative encoding style (McNally, Metzger, Lasko, et al., in press). Some clinical experts hold that sexually abused children acquire an ability to disengage attention from threat cues during abuse episodes and to redirect it elsewhere. Dissociation at the time of traumatic events, however,

Cognitive Aspects of Posttraumatic Stress Disorder 183
seems to predict later PTSD, so this avoidant encoding style may be adaptive in childhood but presage problems later in adulthood.
To investigate this issue, we tested the hypothesis that psychiatrically impaired adult survivors of childhood sexual abuse are characterized by an enhanced ability to disengage attention, and therefore not encode, and remember, trauma-related cues. We accomplished this aim by testing three groups of subjects in an item-cueing directed forgetting paradigm. One group comprised women who had histories of childhood sexual abuse and PTSD; the second group had histories of childhood sexual abuse, but no PTSD; and the third group had never been exposed to traumatic events, like sexual abuse, and, of course, had no PTSD.
The subject sat in front of a computer screen and a series of words appeared one at a time. There were three word types: trauma words (e.g., incest), positive words (e.g., cheerful), and neutral words (e.g., table). Each word appeared for 2 seconds and was followed by either an RRRR or an FFFF instruction, notifying the subject either to remember or to forget the word. After the encoding task, subjects were asked to write down all words they remembered seeing during the encoding task, regardless of whether the word had been followed by a remember or a forget instruction.
A standard directed forgetting effect occurs when subjects exhibit better recall for remember-words than forget-words; and if this effect is preserved on recognition testing, then one can conclude that effects on recall are attributable to differential encoding of remember words relative to forget words (rather than to retrieval inhibition of forget items). Therefore, the avoidant encoding hypothesis implies that subjects in the two healthy groups ought to exhibit standard directed forgetting effects for all word types, whereas the impaired group ought to exhibit memory deficits for trauma words.
The results were dramatically at variance with the avoidant encoding hypothesis. Although both the healthy groups exhibited typical directed forgetting effects, the PTSD group did not. Indeed, they exhibited deficits for positive and neutral material they were instructed to remember, and tended to remember all too well trauma words they were supposed to forget as well as those they were supposed to remember.
Item-cueing directed forgetting protocols measure memory, but do so as a basis of making inferences about encoding processes. In other recent studies, our group has conducted experiments to test for implicit memory biases favoring the processing of trauma-cues in PTSD. Implicit memory tests are those that reveal the effects of previous experiences without directly requiring explicit recall of these experiences. Interest in implicit memory processes in the anxiety disorders is, in part, due to their putatively automatic character, and the ego-dystonic phenomenology of these syndromes implies that auto- matic, involuntary processes figure prominently in the maintenance, and perhaps the etiology, of these conditions.

184 Richard J. McNally
We did two experiments that involved procedures adapted from those developed by Jacoby and his colleagues (Jacoby, Allan, Collins, & Larwill, 1988; Jacoby & Dallas, 1981). In the first one, we used a perceptual identification paradigm (McNally & Amir, 1996). Our subjects were Viet- nam combat veterans with and without PTSD. The words were drawn from three categories: trauma words (e.g., claymore, [rag), positive words (e.g., rejoice, optimism), and neutral words drawn from the category of "house- hold items" (e.g., doorknob, porch).
The procedure was straightforward. Subjects saw each word on a compu- ter screen for 3 seconds, and read it out loud. They were later presented with these 60 "old" words intermixed with 60 "new" distractor words drawn from the same category. This time, however, each word appeared for only 100 milliseconds, and was followed by a random character mask for 2700 milliseconds. The subject's task was to identify (name out loud) each word, and to guess if uncertain.
In a perceptual identification paradigm, implicit memory is revealed by subjects' correctly identifying more old words than new words. If a trauma- relevant implicit memory bias were operative in PTSD, this priming advan- tage for old words ought to be enhanced for trauma-relevant material. More fluent processing of trauma cues ought therefore be present in PTSD.
The results revealed strong overall priming effects. Subjects identified old words more readily than new ones, but there was no evidence of enhanced priming for trauma words in the PTSD group.
This paradigm, however, is strongly influenced by the perceptual ~ in this case, orthographic ~ features of input. Accordingly, upon reflection, perhaps it is not entirely surprising that a strongly perceptually driven paradigm would be insensitive to emotional variables such as trauma-relevance and psychiatric diagnosis. Therefore, in our next experiment, we used an implicit memory procedure that involves processing of more conceptually complex materials: entire sentences (Amir, McNally, & Wiegartz, 1996).
This procedure, dubbed the "white noise" paradigm, works as follows. During the encoding phase, subjec ts~ in this case Vietnam veterans with and without P T S D ~ h e a r d a series of sentences one at a time that were prerecorded on a Macintosh computer. Half were trauma sentences like, "The chopper landed in hot LZ," and half were neutral like "The shiny red apple sat on the table."
After encoding, subjects were given practice with the white noise rating task. They heard a series of unrelated neutral sentences against a background of varying levels of white noise. Their task was to rate the loudness of the background noise in which the sentences were embedded.
Following this phase, they were given the implicit memory task. In this task, they heard four kinds of sentences: old trauma sentences, new trauma sentences, old neutral sentences, and new neutral sentences. All were

Cognitive Aspects of Posttraumatic Stress Disorder 185
embedded in white noise of varying volumes. Subjects repeated each sentence as best as they could, and rated the volume of the noise accompanying each sentence.
Implicit memory for old sentences is revealed by subjects perceiving the noise accompanying old sentences as being less loud than the noise accom- panying new sentences. We computed an implicit memory index to indicate the magnitude of priming by subtracting the perceived volume ratings for the noise accompanying old sentences from the perceived volume ratings for the noise accompanying new sentences. The greater the priming index, the greater the implicit memory effect. Now, if PTSD is associated with a cognitive system biased toward fluent processing of trauma information, the priming index ought to be greater for trauma sentences than for neutral sentences in PTSD patients, but not in combat veterans without the disorder.
Although the effects were not always significant at each noise level, the pattern of results was the same: greater priming for trauma sentences in PTSD and the opposite pattern in the control group.
Cognitive Ability and Risk for PTSD
As a first-pass, rough approximation of the meaning of "intelligence" we might conceptualize it as "problem-solving ability." Coping with the emotional consequences of exposure to traumatic events is surely a "problem to be solved," and a person's ability to do so, to put their experiences into words, to process them emotionally, to recruit social support, and so forth, may be relatedto their general ability to solve problems. That is, relatively higher intelligence may be a protective factor against PTSD among those exposed to trauma. Stated differently, lower intelligence may be a risk factor for PTSD. Not everyone exposed to traumatic events develops PTSD, and therefore researchers need to identify what variables predict severity of PTSD.
In our first study on 105 Vietnam veterans (McNally & Shin, 1995), we obtained a zero-order correlation of r = 0.41 between PTSD symptoms and combat exposure, thereby confirming the dose-response effect. The correla- tion between PTSD symptoms and IQ was r = - 0.33, and it was not diminished when we partialed out the effects of combat exposure: r = - 0.35. Therefore, lower IQ predicted variance in PTSD symptoms beyond that predicted by extent of combat exposure.
Regression analyses revealed that combat exposure accounted for 17% of the variance in PTSD symptoms, and IQ accounted for an additional 10%, boosting the R-squared to 0.27.
Although these data are consistent with the possibility that lower cognitive ability is a risk factor for PTSD, they are also consistent with the possibility that chronic PTSD lowers estimated current IQ, perhaps by impairing concentration.
186 Richard J. McNally
Therefore, in our next study, we obtained premilitary IQ scores as well as current IQ scores, measures of combat exposure, and measures of PTSD symptoms (Macklin, Metzger, Litz, et al., 1998). We replicated our previous zero-order correlation between IQ and PTSD symptoms: r = - 0 . 3 7 . Strik- ingly, preservice IQ was just as strongly related to PTSD symptoms as was current IQ: r = - 0.45. Combat exposure was also strongly related to PTSD symptoms: r = 0.59. Importantly, the relation between PTSD symptoms and decline in IQ from premilitary to current was nonsignificant: r = 0.08. This implies that PTSD symptoms do not cause a drop in IQ.
Correlations with combat exposure partialed out showed that premilitary IQ remained significantly related to current PTSD: r = - 0 . 3 3 ; and current IQ had a similar relation: r = - 0 . 2 7 .
Taken together, these studies suggest several conclusions. First, lower intelligence is a risk factor for the development of chronic PTSD symptoms. Second, chronic PTSD does not appear related to change (or decrease) in estimated IQ. Third, estimated IQ may be a proxy measure for generalized problem-solving capability, including coping with the problem of recovering from exposure to horrific events. I suspect our results would have been even stronger had we a valid measure of "emotional intelligence" (Goleman, 1995).
R e f e r e n c e s
Amir, N., McNally, R. J., & Wiegartz, P. S. (1996). Implicit memory bias for threat in posttraumatic stress disorder. Cognitive Therapy and Research, 20, 625-635.
Goleman, D. (1995). Emotional intelligence. New York: Bantam Books. Jacoby, L. L., Allan, L. G., Collins, J. C., & Larwill, L. K. (1988). Memory influences
subjective experience: Noise judgments. Journal of Experimental Psychology: Learning, Memory, and Cognition, 14, 240-247.
Jacoby, L. L., & Dallas, M. (1981). On the relationship between autobiographical memory and perceptual learning. Journal of Experimental Psychology: General, 110, 306-340.
Kaspi, S. P., McNally, R. J., & Amir, N. (1995). Cognitive processing of emotional information in post-traumatic stress disorder. Cognitive Therapy and Research, 19, 433-444.
Macklin, M. L., Metzger, L. J., Litz, B. T., McNally, R. J., Lasko, N. B., Orr, S. P., & Pitman, R. K. (1998). Lower pre-combat intelligence is a risk factor for posttraumatic stress disorder. Journal of Consulting and Clinical Psychology, 66, 323-326.
McNally, R. J. (1995). Automaticity and the anxiety disorders. Behaviour Research and Therapy, 33, 747-754.
McNally, R. J. (1996). Cognitive bias in the anxiety disorders. Nebraska Symposium on Motivation, 43, 211-250.
McNally, R. J., & Amir, N. (1996). Perceptual implicit memory for trauma-related informa- tion in post-traumatic stress disorder. Cognition and Emotion, 10, 551-556.
McNally, R. J., Amir, N., & Lipke, H. J. (1996). Subliminal processing of threat cues in posttraumatic stress disorder? Journal of Anxiety Disorders, 10, 115-128.

Cognitive Aspects of Posttraumatic Stress Disorder 187
McNally, R. J., Kaspi, S. P., Riemann, B. C., & Zeitlin, S. B. (1990). Selective processing of threat cues in posttraumatic stress disorder. Journal of Abnormal Psychology, 99, 398-402.
McNally, R. J., Lasko, N. B., Macklin, M. L., & Pitman, R. K. (1995). Autobiographical memory disturbance in combat-related posttraumatic stress disorder. Behaviour Research and Therapy, 33, 619-630.
McNally, R. J., Metzger, L. J., Lasko, N. B., Clancy, S. A., & Pitman, R. K. (in press). Directed forgetting of trauma cues in women with histories of childhood sexual abuse with and without posttraumatic stress disorder. Journal of Abnormal Psychology.
McNaUy, R. J., & Shin, L. M. (1995). Association of intelligence with severity of posttrau- matic stress disorder symptoms in Vietnam combat veterans. American Journal of Psychiatry, 152, 936-938.

14
A Behavior Analyst in the Land of Behavior Therapy, or the Evolution of Behavior Science
PAOLO M O D E R A T O University of Parma, Italy
I shall try to analyze the development of behavior therapy from its first systematic applications in the early 1960s to the present day. To do so we need to answer two questions. First, has there been an evolution in behavior therapy? And if so, of what nature has this evolution been? Second, does the social representation of behavior therapy among those psychologists and psychotherapists not belonging to a behaviouristic framework corre- spond to the reality of facts; that is, the present scientific statute (as laid down by the scientific community) and the regular procedures for therapy practice.
To try to answer these questions I would like to introduce a page of historical psychology taken from the book by Eysenck and Rachman The causes and cures o f neurosis, published in 1965 and translated into Italian in 1971. This is also an explicit acknowledgment to Hans Jurgen Eysenck, who has been for many Italian behaviorists the most prominent figure in the field.
This book can be considered in many respects the Manifesto of Behavior therapy, as the paper by Watson "The psychology as a behaviorist views it" is considered the Manifesto of Behaviorism. In many respects both the authors have had a common fate: the criticism of their ideas has often shifted into personal aggression. The same thing happened to other people who challenged the establishment in different fields: Galileo, Darwin, Skinner, and also painters, musicians, and so on. Only many years later have their ideas, in their respective fields, have been accepted; and this has happened only to some of them, not yet to others.

190 Paolo Moderato
The term BT seems to have been introduced essentially independently by three separated research groups: by Skinner, Solomon, and Lindsley in 1953 in the United States; by Lazarus (1958) in South Africa to refer to Wolpe's application of his "reciprocal inhibition" technique to neurotic patients; and by Eysenck's Maudsley group in the United Kingdom to define a new look of clinical work.
What follows is an e-mail I received from one of researchers I mentioned above:
18 June 1996
Thank you for coming to the "source" while the source still lives.
I first coined the term "Behavior Therapy" on 8 June 1953 when searching for a name and address for our new project in applying free operant investigations to the behavior of chronic psychotics in Metropolitan State Hospital. I still have the laboratory notebook listing the other alternative names: Behavior Therapy Research, Behavior Reclamation, Reinforcement Therapy, and Behavior Reconditioning.
The notes page also lists suggestions of my reasons for choosing that name at the time.
"Behavior Therapy~(cure of behavior by behaving)
Behavior Therapy~(The reconditioning of diseased behavior)
I select 'Behavior T h e r a p y ~ it is novel, clear-cut, short, easy to say and spell, catchy with a pun in it, descriptive ~ philosophical orientation, subject + method of treatment, and ties in with traditional methods' names: i.e. occupational therapy, fever therapy, electro-shock therapy, hydro-therapy, etc."
When I called Fred Skinner on the phone a week later on 15 June 1953 to get approval for the name, he said "Good, it also gives the notion we are not trying to do too much we are not tampering with the ego, or id, but are merely trying to change the behavior a little . . . . "
We used the name "Studies in Behavior Therapy" in our Boston telephone listing, on our letterhead and envelopes, and on our proposals and Status Reports I, II, and II for the Office of Naval Research Contract N5ori-07662 from 1 June 1953 through 31 December 1954. I have copies of these items which I can send you by airmail if you need them.
On 1 January 1955, I felt secure enough in our hospital setting and with the clinical psychiatrists at Harvard to change our name to Behavior Research Labora to ry~ which was what we were doing all along. This well may be the first use of that term. At that time I considered Behavior Research a higher calling than Behavior Therapy and still do to this day.
Thanks for your interest,
Ogden Lindsley
But let us go back to Eysenck and Rachman's The causes and cures o f neurosis. In a table at page 32 the authors propose a comparison between what they refer to as "Psychotherapy," which has an underlying psycho-

A Behavior Analyst in the Land of Behavior Therapy 191
analytic base, and "behaviour therapy." I had in two previous papers faced this topic (Moderato, Di Benedetto, & Orlando, 1993; Moderato & Smith, 1993) in two symposia where the major psychotherapeutic approaches challenged each other in terms of their implicit and explicit theoretical and metatheoretical basis. Here attention will be focused only on the latter column (Tab. 14.1), which concerns behaviour therapy, to see which if any of the various arguments used by Eysenck and Rachman are still valid and conversely to discover those that are now changed.
Table 14.1. Important Differences between Psychotherapy and Behavior Therapy
Psychotherapy Behavior therapy
1. Based on inconsistent theory, never properly formulated in postulate form.
2. Derived from clinical observation and made without necessary control obser- vations or experiments.
3. Considers symptoms the visible upshot of unconscious caused ("complexes").
4. Regards symptoms as evidence of repression.
5. Believes that symptomatology is deter- mined by defense mechanisms.
6. All treatment of neurotic disorders must be historically based.
7. Cures are achieved by handling the underlying (unconscious) dynamics, not by treating the symptom itself.
8. Interpretation of symptoms, dreams, acts, etc., is an important element of treatment.
9. Symptomatic treatment leads to the elaboration of new symptoms.
10. Transference relations are essential for cures of neurotic disorders.
1. Based on consistent, properly formu- lated theory leading to testable deduc- tions.
2. Derived from experimental study specifically designed to test basic theory and deductions made there- from.
3. Considers symptoms as unadaptive conditioned responses.
4. Regards symptoms as evidence of faulty learning.
5. Believes that symptomatology is deter- mined by individual differences in conditionability and autonomic labi- lity, as well as accidental environmen- tal circumstances.
6. All treatment of neurotic disorders is concerned with habits existing at present; the historical development is largely irrelevant.
7. Cures are achieved by treating the symptom itself, i.e., by extinguishing unadaptive C.Rs and establishing desirable C.Rs.
8. Interpretation, even if not completely subjective and erroneous, is irrelevant.
9. Symptomatic treatment leads to permanent recovery, provided auto- nomic as well as skeletal CRs are extinguished.
10. Personal relations are not essential for cures of neurotic disorders, although they may be useful in certain circum- stances.

192 Paolo Moderato
The first point states that behavior therapy is based on a consistent theory, well formulated, from which we can obtain testable deductions. The form of the statement is obviously tied to the Zeitgeist of the 1940s and 1950s, which in epistemological terms means Logical Positivism and Operationism, and in theoretical terms means "The Grand Theories" of learning, mainly those of Hull and Spence, and the attempt to explain the whole of human behavior using the principles of learning.
There is no doubt that compared to the theoretical and epistemological weakness of psychoanalytic theory the learning principles are still strong and consistent. Despite some cognitive revolutionary proclamations, if you review a handbook of psychology, whichever you choose, even those who define themselves as purely or mainly cognitivist, in the chapter on "Learning" you will find more or less the sequence: respondent learning, operant learning, social learning, that is, basically data and principles coming from the research of Pavlov, Skinner, and Bandura. The same old story, with one main difference: There is no mention of any theory of learning. The apparent paradox is that the illusion of the big learning theory fell down just when all researchers agreed on the fact that learning influences almost all human phenomena, be they biological, psychological, or social.
Thus the first statement, with slight changes, retains its scientific value.
Point (2) states that behavior therapy stems from experimental research, designed to prove the basis of the theory and its corresponding deductions. Therefore, considering what has been said as regards the theory and the formulation of its basic assumption, there can be no doubt that behavior therapy is firmly aligned to the experimental procedures typical of the natural sciences. This fortunately is still true today. All behavior therapy procedures are experimentally validated, unlike "psychiatric treatments which are usually established ad hoc and are not derived by scientifically established principles" (Eysenck, 1978, p. 10). Davidson & Goldfried (1973) assert that behavior therapy originates from the general guidelines used in clinical work, to which was later added an experimental approach with the practical aim of studying human behavior. Moreover, the experimental influence of beha- viour therapy extended out of its field: In several countries there are projects of research that analyse and evaluate the real effects and the costs and benefits of different psychotherapeutic approaches. This is certainly due in part to financial considerations, but would not have happened without the methodological contribution of behavioral psychology.
In the third point, the symptoms are considered as maladjusted condi- tioned responses. Here we see the classic Pavlovian-type framework that made up the early life-force of behavior therapy both in the early studies of Watson, Rayner, and Cover Jones and in the more systematic studies made by Wolpe. If we think of the range of techniques available today in the
A Behavior Analyst in the Land of Behavior Therapy 193
behavioral field, we can easily see how these studies are only partially referable to reconditioning techniques, derived from the Pavlovian paradigm. Nevertheless, in a wider sense, symptoms are the maladjusted result of learning. The intrinsic mechanism of learning is evolutionary adaptive, not its contents: The same principle is responsible of the "loss" of fear of soldiers in a battle and of phobia for butterflies.
In point (4) the symptoms are believed to be evidence of faulty learning. From this point we may infer an implicit correspondence between learning and behavior; this recalls point 1 and the "Big Learning Theories" of the 1950s, which proposed that any animal and human behavior was explain- able in terms of learning. We could update this argument by saying that the symptoms are made up of interactions which are either problematic, insuffi- cient, or exaggerated in some way, or out of specific or contextual control. Actually, learning~either learning how or learning w h a t ~ i s in any case involved.
The fifth point states that the symptomatology is determined as much from the individual differences in susceptibility to conditioning and weakness of the sympathetic nervous system as to the fortuitous circumstances of the environment. This formulation is somewhat vague in that it takes into account only certain factors such as the individual physiological differences or fortuitous/causal environmental circumstances, but neglects others such as the context in which the interaction takes place, or how these individual differences have developed. Moreover, not enough relevant emphasis is placed on each group of factors.
According to point (6), all treatments of nervous disorders refer to the habits that exist in the "present": their historical development is largely irrelevant. This is a typical associationist view in which the individual's history is (at least in theory) completely underrated. The role of the individual's history is then subsequently reassessed by Contextualism, which root metaphor is the ongoing act. It is difficult for behavior therapy today to identify itself with this point, even though this statement, in my opinion, was a ballon d'essai to polemically dispute against the historic sexual determinism of psychoanalysis, more than a suggestion for practice. We will come back to this point later.
The seventh point says that recovery is achieved by dealing directly with the symptoms themselves, that is, extinguishing the maladjusted conditioned responses and establishing the desired conditioned responses. This formula- tion, which is true as regards the direct treatment of the symptoms, is nevertheless misleading in that it is too restricting to match behaviour therapy to the extinction of the undesired conditioned responses and the establish- ment of the desired conditioned responses (see later)
In point (8) Eysenck and Rachman state that, even if interpretation is not completely subjective and erroneous, it is nevertheless totally irrelevant. This

194 Paolo Moderato
belief is still widely held. It is necessary however, to understand what one means by the term Interpretation, and what kind of therapeutic practices one includes in the concept. In any case there is no doubt that BT cannot be put in a hermeneutic paradigm.
According to the ninth point, treating the symptom leads to a permanent recovery, provided that the autonomous, skeletal conditioned responses become extinct. This is to contrast what is stated by psychotherapists from a psychoanalytic f f a m e w o r k ~ t h a t treatment of the symptoms in itself leads either to a reappearance of the symptom or to relapse. This point is still interesting because it has also been made by many "cognitive constructionist scientists." My personal opinion (Anchisi, Dessy, & Moderato, 1997) is that a dangerous tendency can be discerned to abandon or underemphasise a most important field of BT, behavioral assessment and functional analysis. An inaccurate, routinely run or, what is worst, interpretative assessment causes false hypotheses for treatment. It is not the rationale of behavior therapy but the method of therapy that can be wrong, in that it does not operate on the cause of the problem. Some years later Eysenck (1978) clearly explains that behavior therapy is not a collection of techniques to apply to any disease like cookery recipes. Without an appropriate analysis of the variables working in each case, and without correct choice of the right treatment, behavior therapy does not work any better than any other psychotherapy. According to Eysenck, each case is to be considered as a research, formulating hypotheses about the causes of symptoms, predicting the possible reactions to one treatment or to another and evaluating the role of client setting events, those out of therapist's control.
I would stress that behaviour therapists should not fear using words such as "cause" in their studies. This stands clearly for a scientific theory of human behavior and not for insidious homunculus theories that should be consid- ered a step back to prescientific animistic psychology.
The tenth and final point looks at the relation with the therapist: A personal relationship is not essential to the cure of nervous disorders, although it may turn out to be useful in certain circumstances. The idea, widely held in the predominant years of behavior therapy was that relational variables had little influence or in any event were secondary to the real mechanisms of change. For example, Costello (1963), referring to the differences between conventional types of psychotherapy and behavior therapy, states that "many psychotherapists encourage the patients to estab- lish a close emotional relationship with them, a relationship of dependence. However, in behavior therapy this type of emotional tie is discouraged because it could interfere with the relearning procedures. Obviously the behavior therapist asks for collaboration from his patient and must avoid anything that may give rise to feeling of mistrust or rejection by the patient."

A Behavior Analyst in the Land of Behavior Therapy 195
In recent times even behavior therapists have begun to consider the role that the relationship between therapist and client plays (even if only as a mediator) in clinical recovery. According to Sibilia (1994) a relationship is defined by a pattern of interdependent (and often not always congruent) attitudes, actions, and emotions that shape the interactional sequences of the participants. So far, however, little has been done to systematically study on an experimental basis the relational variables that influence therapeutic change. An area that could show interesting developments is that regarding the relationship as the context (context in the Kantorian sense of the word) in which therapeutic interactions take place. Therapeutic relations are no longer seen as "anathema" to behavior therapists. From a contextualistic point of view it is such a context (in Kantor's words the "setting events") that confers greater or lesser meaning and value to any specific stimulus configuration (the technical procedures). Even the choice of the term "setting" shows on the one hand the evolution of behavior therapy, and on the other the possibility of opening a debate within the constellation of psychotherapies (obviously I refer to those that are scientifically accredited). This means being able to use terms such as cause, in common with others, that are, at least in part if not totally, reciprocally comprehensible.
At this point a critical question can be posed "What relationship applies today between behaviorism and behavior therapy?" However, this defers to another question: "What do we mean by behaviorism today?" From a brief analysis of the literature, it emerges that the following attributes have been ascribed to behaviorism: standard, social, paradigmatic, purposive, cognitive, methodological, operant, classical, radical; related concepts are interbeha- viorism, behavior analysis, behaviorology.
Behaviorism, intended as a guiding framework for behavior and cognitive therapy, is rather far from the Behaviorism outlined in Watson's paper in 1913 (Moderato & Ziino, 1994; Moderato & Chase, 1995). This does not mean, as someone says, that we have to reject that behaviorism, or worse behaviorism in total. Then, for a science as young as psychology was, it was a natural and almost forced choice of undertaking the walk already run, through the 19th and the 20th centuries, by the other natural organic and inorganic sciences. As for the other sciences, the laboratory was the place where the researcher could achieve better control, a place where reality could be simplified by treating simple stimuli. Actually, Watson started this difficult and sometimes unrewarding trip.
Watson's behaviorism represented a revolutionary step for the advance- ment of modern science. First of all it allowed the psychology to be definitely detached from the animistic conception ~ the hardest obstacles to the progress of any science ~ favoring the abandonment of myths and super- stitions and supporting the removal of all entities that are the transcendent or without spatial-temporal dimension.
196 Paolo Moderato
In the second place it has contributed in substantial way to the constitution of the epistemological status of scientific psychology speeding the separation from philosophical speculation and bringing it instead to scientific compar- ison with things and events of the real world. The things that define the scientific approach, as opposed to the philosophical approach, are direct observation, experimentation, and unbiased analysis and interpretation of the events as they are observed, as they happen, and as they are altered by specific circumstances.
Watson's behaviorism was a form of behaviorism that gave rise to behavior therapy, following on from Pavlov's research on conditioned responses. Reading the original passages by Wat son~no t the quotation of the quotation of the quotation e t c . ~ I am sure that everyone would find them much more modern than they would ever expect. But this is not the point n o w .
Eysenck interpreted and handed down the spirit of Watson in the therapeutic field. His therapeutic revolution, his criticism against psycho- analytic psychotherapy, charges of ineffectiveness, his polemics again the establishment, have been of great intensity and, in many respects, upsetting like those of Watson.
Thus, let us go back to the initial question: Has there been an evolution in behavior therapy and, if so, of what nature has this evolution been? Even if behavior therapy was born within an S-R behavioristic framework, surely the greater part of Behaviorism in the late 1990s is not an S-R psychology but a holistic and contextualistic psychology that traces its roots in the work of many psychologists, among whom I mention Kantor, the scholar who from 1925 onward (until 1984 when he died) elaborated a nondualistic psycho- logical system (an interactional system known as Interbehaviorism). Accord- ing to Kantor, stimulus and response do not exist one without the other and cannot be defined independently of the context. Moreover, Kantor places great emphasis on the individual history, which he refers to in terms of reactional biography. Reactional biography is the biopsychological history of each individual that is fundamental in giving meaning to the interactions that take place hic et nunc.
If classical behaviorism can be described as a mechanical theory, physica- listic, reductionist, and environmentalist, modern behaviorism, by contrast, is functionalist, nonreductionist, interactional, and situation-specific. Human behavior is described in terms of interactions.
The overall global view of this behaviorism is both contextualistic and pragmatic. Its root metaphor is the concept of becoming; the concept of change is thus a basic category for it. A holistic view characterizes this behaviorism, the organism being conceived in an active sense; its relations with the social environment are explained in terms of functional analysis as opposed to causal. The explanation of behavior involves not a deterministic

A Behavior Analyst in the Land of Behavior Therapy 197
but a probabilistic relation, since complete control over human relationships is quite impossible. However, probabilistic control is still a control in accordance with the experimental methods of the natural sciences. The science to refer to is no longer physics, as in logical positivism, but biology, a science that mixes up chaotic and casual principles and causal ones.
Other sciences have followed the same path I have outlined here: the "simple" mechanistic physics of Newton and Laplace, have become a science of "fields," much more complex but still anchored to scientific and experi- mental methodology.
From this perspective emerges the figure of a human being who is no longer described in naive mechanical terms and is immersed in his becoming. Behavioral techniques, for the most part nonaversive and progressively more ecological, may be applied in diverse settings and for diverse goals, but mainly to allow him to interact with his or her external environment in a more comfortable and less problematic way.
References
Anchisi, R., Dessy, M. G., & Moderato, P. (1997). Analisi e terapia del comportamento nell'infanzia e nell'adolescenza. Torino: Cortina.
Borgo, S., & Sibilia, L. (1994). The patient therapist relationship. Its many dimensions. Roma: Consiglio Nazionale delle Ricerche.
Eysenck, H. J. (1978). Prefazione. In E. Sanavio (Ed.) Le nevrosi apprese. Milano: F. Angeli. Eysenck, H. J., & Rachman S. (1965). The causes and cures of neurosis. London: Routledge. Costello, C. G. (1963). Behaviour therapy: criticisms and confusions. Davidson, G. C., & Goldfried, M. R. (1973). Postdoctoral training in clinical behavior
therapy. In: I. B. Weiner (Ed.) Postdoctral education in clinical psychology. Topeka KA: Menningen Foundation.
Goldfried, M. R., & Davidson, G. C. (1976). Clinical behavior therapy. New York: Holt, Rinehart and Winston.
Kantor, J. R. (1959). Interbehavioral psychology. Chicago: Principia Press. Krasner, L. (1971). The operant approach in behavior therapy. In A. E. Bergin & S. L.
Gaefield (Eds.), Handbook of psychotherapy and behavior change (pp. 612-652). New York: Wiley.
Lazarus, A. A. (1958). New methods in psychotherapy: A case study. South African Medical Journal, 33, 660-663.
Lindsley, O. R. & Skinner, B. F. (1956). A method for the experimental analysis of the behaviour of psychotic patients. Am. Psych. 9, 419-420.
Moderato, P. (1997). Apprendimento e organizzazione dell'esperienza. In P. Moderato and O. Pino (Eds.) Apprendimento & organizzazione dell'esperienza. Comportamento, cogni- zione e ricordo nei bambini. Padova: Cedam.
Moderato, P., Di Benedetto, G., & Orlando, C. (1993). Dove va la psicoterapia del comportamento alle soglie del 2000? In R. Fischetti & F. Milano (Eds.), Lo psicotera- peuta e i suoi sistemi di riferimento impliciti ed espliciti. Padova: Pagus.
Moderato, P., & Chase P. N. (1995). Temi critici nell'analisi del comportamento: operanti, relazioni verbali, comportamento governato da regole. In P. Moderato & S. Sirigatti (Eds.), L'uomo che cambia. Milano: Franco Angeli.
Moderato, P., & Smith, P. (1993). Behaviour therapy up to date: the possibility of dialogue with other psychotherapies. In F. Canziani, V. Gallai, & P. Sarchielli (Eds.), Advances in
198 Paolo Moderato
neuropsychiatry. Erice: Ettore Majorana Centre for Scientific Culture, International School of Medical Sciences.
Moderato, P., & Ziino, M. L. (1994). L'evoluzione del paradigma comportamentista: dal meccanicismo al contestualismo. Archivio di Psicologia, Neurologia e Psichiatria, LV, 1-2.
Morris, R. J., & Magrah, K. H. (1983). The therapeutic relationship in behavior therapy. In M. J. Lambert (Ed.), Psychotherapy and patient relationship (pp. 154-189). Homewood, IL: Dow Jones-Irwin.
Parrott, L. J. (1987). On the distinction between setting events and stimuli. Experimental Analysis of Human Behavior Bulletin, 5, 6-11.
Rosenfarb, I. S., Hayes, S. C., & Linehan, M. M. (1989). Instructions and esperiential feedback in the treatment of social skills deficits in adults. Psychotherapy, 26, 242-251.
Sibilia, L. (1994). An etho-cognitive analysis of the patient-therapist relationship. In S. Borgo & L. Sibilia (Eds.) The patient-therapist relationship: its many dimensions. Roma: Consiglio Nazionale alelle Riazche.
Skinner, B. F. (1953). Science and human behavior. New York: Free Press. Skinner, B. F. (1964). Behaviorism at fifty. In T. W. Wan (Ed.), Behaviorism and phenom~
enology. Chicago: University of Chicago Press. Wolpe, J. (1954). Reciprocal inhibition as main basis of psychoterapeutic effects. Archives of
Neurology and Psychiatry, 72, 205-226. Watson, J. B. (1930). Behaviorism (revised edition). Chicago: The University of Chicago Press.
15
Anger Predictors of the Assaultiveness of Forensic Hospital Patients
R A Y M O N D W. N O V A C O University of California, Irvine, USA
STANLEY J. RENWICK The Duchess of Kent Hospital, UK
Introduction
Assaultive behavior by patients in psychiatric hospitals has been demon- strated to be a serious problem through a number of studies conducted in North America and in Europe (e.g. Drinkwater & Gudjonsson, 1989; Hailer & Deluty, 1988; Larkin, Murtagh, & Jones, 1988; Lion & Reed, 1983; Lucchi, Saviotti, Turrina, et al., 1993). In both public and private facilities, assaultiveness by psychiatric patients significantly impacts the therapeutic environment and presents an enormous challenge for hospital staff who must provide treatment for such behavior yet must be on guard against physical harm to themselves. That quandary is well illustrated by the staff injury data of Carmel and Hunter (1989) regarding Atascadero State Hospital, one of California's two primary forensic facilities, where, in 1986, 121 staff members sustained 135 iniuries for patient violence. This included 16% of the ward nursing staff, 5.7% of the psychiatric technicians, and 1.9% of the clinical professionals. However, in California state hospitals, civil commit- ment patients are more assaultive than are forensic patients ~ 21.5 % vs. 6.7% in a 30-day period (Novaco, 1997). Hence, assault risk is an even more serious problem for civil commitment hospitals than it is in the forensic one studied by Carmel and Hunter.
Regarding prevalence, a review by Davis (1991) concluded that rates for psychiatric inpatient violence may be increasing and that they are higher in
200 Raymond W. Novaco and Stanley J. Renwick
the United States than in Europe. It is too early for international compar- isons, especially without standardized criteria, but a very high prevalence was reported by Larkin, Murtagh, and Jones (1988) for one of the British Special Hospitals (Rampton), where 36.6% of the patients were found to be assaultive in a 6-month interval. Clearly, patient violence is not solely a U.S. problem, and there is considerable violence risk in psychiatric institu- tions, both public and private, forensic and non-forensic.
The assessment of risk is integral to risk management, as well as to the treatment of clinical problems that can predispose someone to be violent. However, the prediction of institutional violence has struggled with some of the same difficulties as has the prediction of community violence (cf. Monahan & Steadman, 1994). Advances are being made with actuarial and clinical approaches in improving predictive accuracy for in-patients (e.g., Apperson, Mulvey, & Lidz, 1993; McNeil & Binder, 1991; McNeil, Binder, & Greenfield, 1988) and for discharged patients in the community (Harris, Rice, & Quinsey, 1993; Lidz, Mulvey, & Gardner, 1993; Rice, 1997), buta theoretically important dispositional variable, namely, anger, has been neglected.
Anger has been generally ignored as a predictor of violence among hospital patients ~ for example in the early studies on this topic by Ekblom (1970), Depp (1976), and Fottrell (1980) and in most contemporary prediction studies, such as those cited above. However, Craig (1982) examined 1033 psychiatric admission cases and found that 11% had been assaultive before admission and that anger was the factor most strongly associated with assaultiveness. More incisively, Kay, Wolkenfeld, and Murrill (1988) found anger to be the strongest predictor of physical aggression in the clinical and diagnostic profiles of 208 psychiatric in-patients. They assessed these predic- tive effects for anger on physical aggression in a 3-month follow-up analysis of behavior on psychiatric wards, using clinician ratings as the outcome measure. Focusing on anger, Novaco (1994) found that clinicians' rating of anger (on a seven-item index with high reliability) were significantly related to patients being physically assaultive in analyses of concurrent data on assault and prospectively for assault data in the following year. This latter study more generally sought to develop self-report anger assessment proce- dures for psychiatric populations, and the present study is an effort to extend this line of research on anger as an assaultiveness predictor assessed by patient self-report and by clinical staff ratings.
Our theoretical position is that anger, while being neither necessary nor sufficient for aggression, is a significant activator of aggression, which is otherwise regulated by inhibitory controls. This is generally agreed among a number of theorists (Bandura, 1973; Konecni, 1975; Novaco, 1986; Zillmann, 1983). Thus, from a general theoretical standpoint, as well as from the domain-specific research on hospitalized patients cited above, our

Anger Predictors of Assaultiveness of Forensic Hospital Patients 201
expectation is that high-anger patients will be more assaultive than low-anger patients. Because assaultiveness militates against hospital discharge, we also hypothesized that anger disposition would be significantly predictive of discharge status. Importantly, we sought to examine these hypotheses in prospective analyses.
Method
Setting. Carstairs State Hospital, located between Glasgow and Edinburgh, is the only maximum and medium security forensic institution serving the whole of Scotland and Northern Ireland. Patients are referred to the hospital from the Health Boards, the prisons, and the courts. The patient population is around 225 at any one time, approximately 10% of whom are female. The hospital has ten wards, one of which is entirely female, and there are three mixed wards.
Participants. Excluded from the project were all female patients, male patients on the mental handicap ward, and male patients on the admissions ward. We sought to include in the study all other male patients in the hospital (n= 154). Of this eligible population, 29 refused to participate or were judged by ward staff to have a severely impaired mental status. A second effort was made to test these patients the following week, but this was unsuccessful in each case. Thus, 125 male patients participated in the study, which represented 65.5% of the total male population in the hospital (n = 191) and 81.2% of those males who were eligible for the study. There were no significant differences between participating patients and excluded patients in age or length of stay in the state hospital.
Procedure. The anger self-report testing of patients was coordinated through the ward managers. It was conducted by three research assistants who consulted with the nurse in charge about which patients could be tested that day. Patients were tested individually in a private room, escorted there by a member of the ward staff, who introduced the research assistant. In all cases, the patient's responses were confidential and could not be seen or heard by ward staff.
The assistant described the purpose of the project as being an effort to study anger among patients in the hospital ~ what they got angry about, how angry they got, and how they coped with i t ~ a n d that we were hoping to establish anger treatment in the future (which has now happened). They were asked if they would be willing to complete some questionnaires about anger and were given a chance to look at them. After informed consent was obtained by signature, the testing session began, lasting approximately 30 minutes. Most of the patients preferred to have the scales read to them, with

202 Raymond W. Novaco and Stanley J. Renwick
the assistant recording the responses. It was explained to the patients that there were no right or wrong answers, that they could ask questions at any time, and that they could discontinue responding at any time. The staff observational ratings, described below, were obtained in the week following the anger self-report testing.
The following background data were obtained from hospital records: age, date of birth, legal status (penal code vs. civil commitment), number of times in prison, number of admissions to the hospital, dates of admission, reason for admission, and diagnosis. Owing to space limitations for the present article, we do not here report on these covariates, but we note that only age was found to be significantly related to assaultiveness. Central to the present study, we also obtained prospective data on assaultiveness and hospital discharge from hospital records. The discharge data pertained to whether or not the patient was discharged from the hospital during a period of 30 months after the anger measures were obtained. The assaultiveness data came from incident reports over an 18-month period, which began one year after the anger testing. This one-year delay occurred because there was not until that time a systematized incident reporting procedure.
Measures. Anger was assessed by patient self-report and by clinical staff ratings. Patient self-report of anger was assessed by two psychometric instruments: (1) The Spielberger State-Trait Anger Expression Inventory (STAXI) (Spielberger, 1991) and (2) the Novaco Anger Scale (NAS) (Novaco, 1994). The STAXI includes measures of State Anger, Trait Anger, and Anger Expression. The Anger Expression scale has subscales of Anger-In, Anger-Out, and Anger Control. The STAXI has had extensive development and validation with adolescent and adult samples, from both normal populations and clinical populations with physical health problems (Spielberger, 1991 ).
We also used a second anger measure, the NAS, which has Cognitive, Arousal, and Behavioral domain scales as components of anger disposition. It was developed and validated for use with mentally disordered as well as normal populations. In studies with psychiatric patients in California state hospitals (Novaco, 1994), it was found to have an internal reliability of .95 and a test-retest reliability of .84 and to be significantly related to a number of anger and aggressive behavior criteria, evaluated in concurrent, retro- spective, and prospective analyses, which also included comparative measures. In the validation studies, the NAS correlated .84 with the Spiel- berger Trait Anger, administered concurrently, and its predictive correlation with Spielberger State Anger was .36 at 2 weeks, .43 at I month, and .46 at 2 months with 151 patients in the analyses (Novaco, 1994).
To test the hypothesized effect of anger disposition on assaultiveness, "low anger" and "high anger" patients were compared for their assaultive

Anger Predictors of Assaultiveness of Forensic Hospital Patients 203
behavior in the follow-up interval described above. To construct these groups, patients were selected on the basis of being in the lower and upper quartiles of the STAXI Trait Anger subscale, which is a well-known anger disposition measure. Alternatively, we also used the NAS Behavioral domain as a grouping factor, as scores on that subscale reflect aggressive anger reactions. As these are alternative indices of the anger construct, we expect their effects to be redundant or convergent. For the analyses of anger predictors of hospital discharge status, we tested all STAXI and NAS scales, as well as the clinical staff rating measures described below.
Staff ratings of anger variables were obtained regarding observed ward behavior using two instruments: (1) The Ward Anger Rating Scale (WARS) and (2) the Psychotic Inpatient Profile (PIP). The WARS was developed as part of a larger project on anger assessment for psychiatric patients (Novaco, 1994). This rating scale is a two-part instrument completed by the patient's ward staff key worker or primary clinician, who records judgments of the patient's behavior over the past week. Part A consists of dichotomous ratings of verbal and physical behaviors pertaining to anger and aggression: expressed suspicion, blaming, acting impulsively, having a temper tantrum, shouting, verbal abuse, verbal threats to attack (staff/patient), physical attack (staff/patient), displaced aggression, suicidal talk, suicide attempt, self-injury talk, self-injury attempt, expressed delusions, and expressed hallucinations. The staff member is instructed to record whether or not these have occurred according to the patient's actual behavior in the previous week. Part B of the instrument involves ratings on four-point scales (very little, sometimes, fairly often, very often) regarding seven affective-behavioral attributes semantically related to anger, such as "angry or annoyed," "irritable or grouchy," and "bitter or resentful."
In the present study, inter-rater reliability for the WARS Part A dichot- omous ratings was quite good, as reflected in an average percentage of agreement of 94.7% between two raters across the behavioral items for 29 patients on one ward. The "Anger Attributes" component of the scale was found to have high internal consistency, as the Cronbach alpha for the set of rated attributes was r = . 8 8 for all 154 patients. Thus, it is meaningful to consider the total score of these rated attributes as a measure of clinician judgments of patient anger. Pertinent to the patient's self-reported STAXI State Anger the previous week, the staff-rated "Anger Attributes" are significantly correlated (r-- .29, p < .001) to that criterion.
Several component indices are generated from the WARS dichotomous ratings, and two are utilized here: (1) An "Assaultiveness" index is computed by summing the recordings for "was verbally abusive to someone," "verbally threatened to attack a patient," "verbally threatened to attack a staff member," "physically attacked a patient," and "physically attacked a staff member." These items refer to overt verbal and physical aggression that is
204 Raymond W. Novaco and Stanley J. Renwick
explicitly directed at someone; (2) An "Emotional Lability" index is computed by summing the recordings for "having a temper tantrum," "shouting or yelling," and "slammed, threw, or deliberately broke some- thing" which are displays of anger but are not intended as antagonism toward another person nor explicitly to put them at risk of being harmed.
Ward behavior ratings were also obtained by the Psychotic Inpatient Profile (PIP), which is also a staff-completed inventory designed by Lorr and Vestre (1968) to examine the behavior and self-reported symptomatol- ogy of hospitalized psychotic in-patients. Twelve syndromes are derived from the inventory items addressing aspects of both positive and negative symp- toms; however, we here exclusively report on the Hostile Belligerence (HOS) scale. Supporting evidence regarding the scale reliability and validity can be found in Vestre and Zimmerman (1970) and Knight and Blaney (1977). Staff complete the PIP on the basis of their observation of the patient during the preceeding three days. In the present study, the HOS scale was found to correlate significantly (p < .0001) with the WARS indices of Assaultiveness (.65), Emotional Lability (.61), and Anger Attributes (.61).
Patient assaultiveness data were obtained from hospital incident report records. For each patient in the study, record data were examined to determine the frequency of documented physical assault, serious verbal aggression, and self-harm incidents involving the patient. Since verbal aggression incidents are rarely documented, we do not separately analyse them. Because incidents of physical assault may involve the patient as perpetrator or as victim, we separately analyse the perpetrator incidents. We thus utilize three central indices: overall incidents, physical assault incidents, and perpetrator of physical assault incidents. These data were obtained for an 18-month period beginning 12 months after the anger testing and staff ratings, as explained above. Hospital discharge data were obtained for this entire 30-month posttest period.
Results
Our presentation is here focused on anger predictors of assaultiveness and of discharge status in 30-month prospective analyses. First, though, it is useful to report the frequency of the anger-relevant behaviors observed by the ward staff for the one-week period following the anger testing. For the components of the WARS "Assaultiveness" index, verbal abuse was rela- tively frequent (38.7% of patients), verbal threat to attack was considerably less frequent (11.8% toward another patient, 10.9% toward staff), and physical attack was relatively infrequent (6.8% against another patient, 2.5% against staff). The WARS "Emotional Lability" behaviors, which do not directly target another person ~ namely, shouting or yelling (30.3%), "having a temper tantrum" (22.7%), and "slamming, throwing, or breaking

Anger Predictors of Assaultiveness of Forensic Hospital Patients 205
something deliberately" (6 .7%)~were varied in frequency. Behaviors related to self-harm, that is, talk of injury (4.2%), attempted injury (2.5%), talk of suicide (4.2%), and attempted suicide (0%), were not prevalent.
The hypothesis that high-anger patients would be more assaultive than low-anger patients was examined by testing for differences between these anger groups in the frequency of assaultive incidents for each patient. These patient groups were defined by the upper and lower quartiles of the STAXI Trait Anger scores and, alternatively, by NAS Behavioral scores. The outcome measures were "overall incidents" (mean = 2.5, SD = 6.0), "physi- cal incidents" (mean=2.1, SD=4.8), and "perpetrator of physical inci- dents" (mean = 1.6, SD= 4.1). Because the incident data are skewed on all three variables, the data were analyzed after being transformed to square- root scores. The results are presented in Table 15.1, with the groupings based on STAXI Trait Anger. For each critical incident variable, the mean number of incidents is significantly higher (p < .001) for the high anger group. The results for the NAS Behavioral grouping replicate these effects and are significant on all variables (p < .005). Thus, patients scoring high in anger on these psychometric tests were more likely to be involved in and to perpetrate assaultive incidents in the follow-up period, which was an 18- month period that began one year after the anger testing.
Discharge status was examined for all patients for a period of 30 months after the anger testing. Discharged versus nondischarged patients were compared on all assessed anger variables on the self-report and staff rating measures. For the self-report scales, no significant differences were found for the STAXI State Anger, Anger Out, or Anger Control scales, nor for the NAS Cognitive scale. The results for the variables found to have significant effects are presented in Table 15.2. STAXI Trait Anger and Anger-In are significant, as are the NAS Arousal and Behavior scales. The means for nondischarged patients are significantly higher in self-reported anger. For the staff rating
Table 15.1. Means and Analyses of Critical Incident Variables (Square Root) as a Function of Low Versus High Anger Disposition
Low anger High anger Incident Variable (n = 25) (n = 26) t p
Overall Incidents .42 1.54 3.49 .001 Physical Incidents (PI) .38 1.44 3.53 .001 Perpetrator of PI .28 1.27 3.65 .001
The incident data, transformed to square-root scores to reduce skewness, were obtained for an 18-month period that began one year after the anger testing. The anger groups constitute the lower and upper quartiles of patients on STAXI Trait Anger. When the groups are alternatively defined according to NAS Behavioral scores, all effects replicate (p < .005).

206 Raymond W. Novaco and Stanley J. Renwick
Table 15.2. Anger Measures Significantly Associated with Discharge Status
Patients' hospital status
Discharged Non-discharged (n=42) (n-- 78) t p
Anger self-report NAS Arousal 25.7 28.8 2.39 <.02 NAS Behavioral 25.8 28.7 2.02 <.05 STAXI Trait 15.6 19.3 2.58 <.02 STAXI Anger-In 15.1 17.5 2.57 <.02
Staff Ratings PIP Hostile Belligerence 3.5 5.8 2.47 <.02 WARS Assaultiveness 0.2 0.9 4.32 <.001 WARS Emotional Lability 0.3 1.0 3.78 <.001 WARS Anger 9.7 11.7 2.49 <.02
The self-report and staff rating data were obtained regarding 120 male patients. The hospital discharge status data pertain to a period of 30 months after the anger measures. Anger self- report measures for which there were nonsignificant effects are reported in the text.
scales, all variables were found to be significant. The nondischarged patients are significantly higher in PIP Hostile Belligerence and in the WARS measures of Assaultiveness, Emotional Lability, and Anger.
Regarding discharge status, it should be noted that the only demographic or background variable in the records data that significantly related to discharge was age. The discharged patients were older (mean = 31.9 years) than the nondischarged patients (mean = 28.2 years) at the time of hospital admission. Diagnosis, previous hospital admission, index offence, and number of times in prison were not significantly related to discharge.
Discussion
Because anger is a feature of a wide range of clinical disorders, it is an important subject for mental health professionals, especially those who work in forensic institutions. Anger is a significant activator of violent behavior; however, it is also often a product of troubled life histories and part of a dysfunctional style of dealing with life's challenges. Forensic patients typi- cally have had impoverished lives, replete with trauma, abandonment, rejection, and frustration. They certainly have had agentic roles in their life tragedies, but recurrent adversity and diminished resources do induce anger as a coping response. Anger and assaultive behavior are unfortunately prevalent among patients hospitalized in psychiatric institutions, and their assaultiveness presents a serious risk to clinical staff entrusted with patient care .

Anger Predictors o f Assaultiveness o f Forensic Hospital Patients 207
The degree to which anger constitutes a risk factor for violent behavior hinges on its hypothesized role as a mediator of the relationship between aversive events and harm-doing behavior. A number of theorists concur with that proposition, although Berkowitz (1993) does not. Our study is largely a correlational analysis, but its prospective design permits inferences beyond those for associations obtained with concurrent measurement only. The results of our investigation have demonstrated that anger is significantly associated with subsequent aggressive behavior observed between 1 and 2.5 years after the anger measures were obtained. We also found that anger disposition was significantly related to whether or not the patient was discharged from the hospital. While not used as an explicit criterion for hospital discharge, problems of anger dysregulation are in some way tacitly factored into discharge decisions.
The treatment of anger and aggression among seriously violent patients is an important clinical problem. While this has been a neglected area of clinical research, we have made some important beginnings at the State Hospital where the present study was conducted. Renwick, Black, Ramm, and Novaco (1997) have demonstrated that very assaultive, high-anger patients with long histories of psychiatric institutionalization can be successfully treated for problems of anger regulation. Anger, and the treatment resistance associated with it, merits concerted clinical research attention with regard to the development of both assessment and treatment approaches.
References
Apperson, L. J., Mulvey, E., P., & Lidz, C. W. (1993). Short-term clinical prediction of assaultive behavior: Artifacts of research methods. American Journal of Psychiatry, 150, 1374-1379.
Bandura, A. (1973). Aggression: A social learning analysis. Englewood Cliffs, NJ.: Prentice- Hall.
Berkowitz, L. (1993). Aggression: Its causes, consequences, and control. New York: McGraw- Hill.
Carmel, H., & Hunter, M. (1989). Staff injuries from inpatient violence. Hospital and Community Psychiatry, 40, 41-46.
Craig, T. J. (1982). An epidemiological study of problems associated with violence among psychiatric inpatients. American Journal of Psychiatry, 139, 1262-1266.
Davis, S. (1991). Violence by psychiatric inpatients: a review. Hospital and Community Psychiatry, 42, 585-589.
Depp, F. C. (1976). Violent behavior patterns on psychiatric wards. Aggressive Behavior, 2, 295-306.
Drinkwater, J., & Gudjonsson, G. (1989). The nature of violence in psychiatric hospitals. In K. Howells & C. Hollin (Eds.), Clinical approaches to violence. London: Wiley.
Ekblom, B. (1970). Acts of violence by patients in psychiatric hospitals. Uppsala: Svenska Bokforlaget.
Fottrell, E. (1980). A study of violent behavior among patients in psychiatric hospitals. British Journal of Psychiatry, 136, 216-221.

208 R a y m o n d W. Novaco and Stanley J. Renwick
Hailer, R. M., & Deluty. R. H. (1988). Assaults on staff by psychiatric inpatients: A critical review. British Journal of Psychiatry, 152, 174-179.
Harris, G. T., Rice, M. E., & Quinsey, V. L. (1993). Violent recidivism of mentally disordered offenders: The development of a statistical prediction instrument. Criminal Justice and Behavior, 20, 315-335.
Kay, S. R., Wolkenfeld, F., & Murrill, L. M. (1988). Profiles of aggression among psychiatric inpatients. II: Covariates and predictors. The Journal of Nervous and Mental Disease, 176, 547-557.
Knight, R. A., & Blaney, P. H. (1977). The inter-rater reliability of the Psychotic Inpatient Profile. Journal of Clinical Psychology, 33, 647-653.
Konecni, V. J. (1975). The mediation of aggressive behavior: Arousal level versus anger and cognitive labeling. Journal of Personality and Social Psychology, 32, 706-712.
Larkin, E., Murtagh, S., & Jones, S. (1988). A preliminary study of violent incidents in a special hospital (Rampton). British Journal of Psychiatry, 153, 226-231.
Lidz, C., Mulvey, E., & Gardner, W. (1993). The accuracy of predictions of violence to others. Journal of the American Medical Association, 269, 1007-1011.
Lion, J. R., & Reid, W. H. (1983). Assaults within psychiatric facilities. New York: Grune & Stratton.
Lorr, M., & Vestre, N. D. (1968). Psychotic inpatient profile manual. Los Angeles: Western Psychological Services.
Lucci, F., Saviotti, F. M., Turrina, C., Di Fiorino, M., & Ermentini, A. (1993). La predizione del comportamento violento: Studio condotto in un ospedale psichiatrico giudiziario. Rivista di Psichiatria, 28, 212-217.
McNeil, D. E., & Binder, R. L. (1991). Clinical assessment of the risk of violence among psychiatric inpatients. American Journal of Psychiatry, 148, 1317-1321.
McNeil, D. E., Binder, R. L., & Greenfield, T. K. (1988). Predictors of violence in civilly committed acute psychiatric patients. American Journal of Psychiatry, 145, 965-970.
Monahan, J., & Steadman, H. (1994). Violence and mental disorder: Developments in risk assessment. Chicago: University of Chicago Press.
Novaco, R. W. (1986). Anger as a clinical and social problem. In R. Blanchard & C. Blanchard (Eds.), Advances in the study of aggression, (Vol. 2). New York: Academic Press.
Novaco, R. W. (1994). Anger as a risk factor for violence among the mentally disordered. In J. Monahan & H. Steadman (Eds.), Violence and mental disorder: Developments in risk assessment (pp. 21-59). Chicago: University of Chicago Press.
Novaco, R. W. (1997). Remediating anger and aggression with violent offenders. Legal and Criminological Psychology, 2, 77-88.
Renwick, S. J., Black, L., Ramm, M., & Novaco, R. W. (1997). Anger treatment with forensic hospital patients. Legal and Criminological Psychology, 2, 103-116.
Rice, M. E. (1997). Violent offender research and implications for the criminal justice system. American Psychologist, 52, 414-423.
Spielberger, C. D. (1991). State-Trait Anger Expression Inventory: Revised Research Edition. Odessa, FL- Psychological Assessment Resources, Inc.
Vestre, N. D., & Zimmerman, R. (1970). Validation study of the psychotic inpatient profile. Psychological Reports, 27, 3-7.
Zillmann, D. (1983). Arousal and aggression. In R. Geen & E. I. Donnerstein (Eds.), Aggression: Theoretical and empirical reviews. New York: Academic Press.




















