
Group and Individual Cognitive-Behavioral Treatments for Youth with Anxiety Disorders: A Randomized...
28
Cognitive Therapy and Research, Vol. 24, No. 3, 2000, pp. 251–278 Group and Individual Cognitive-Behavioral Treatments for Youth with Anxiety Disorders: A Randomized Clinical Trial Ellen C. Flannery-Schroeder 1 and Philip C. Kendall 1 Children (aged 8–14 years) with anxiety disorders were randomly assigned to cogni- tive-behavioral individual treatment, cognitive-behavioral group treatment, or a wait- list control. Treatment outcome was evaluated using diagnostic status, child self- reports, and parent- and teacher-reports. Analyses of diagnostic status revealed that significantly more treated children (73% individual, 50% group) than wait-list children (8%) did not meet diagnostic criteria for their primary anxiety disorder at posttreat- ment. Other dependent measures demonstrated the superiority of both treatment conditions compared to the wait-list condition. However, a child-report of anxious distress demonstrated only the individual treatment to effect significant improvement. Measures of social functioning failed to discriminate among conditions. Analyses of clinical significance revealed that notable proportions of treated cases were returned to nondeviant limits at posttreatment. Treatment gains were maintained at a 3-month follow-up. KEY WORDS: anxiety disorders; child anxiety; group treatment; cognitive-behavioral therapy. The increasing body of research devoted to childhood anxiety disorders may well reflect the realization of the seriousness and debilitation associated with the disorders. Anxiety disorders have been demonstrated to the one of the most com- mon categories of childhood and adolescent disorders (Bernstein & Borchardt, 1991; Fergusson, Horwood, & Lynsky, 1993; Kashani & Orvaschel, 1990). This parallels the findings that anxiety disorders are the most common psychiatric disor- der in adults from the general population (Myers et al., 1984). Estimates of childhood anxiety disorders range from approximately 1% to 21% (e.g., Fergusson et al., 1993; Kashani & Orvaschel, 1990). Aside from the negative emotionality associated with the anxiety itself, childhood anxiety disorders have often been found to be comorbid with depression (Last, Hersen, Kazdin, Fin- 1 Department of Psychology, Temple University, Philadelphia, Pennsylvania. 2 Correspondence should be directed to Ellen C. Flannery-Schroeder, Department of Psychology, Temple University, Weiss Hall, Philadelphia, Pennsylvania 19122. 251 0147-5916/00/0600-0251$18.00/0 2000 Plenum Publishing Corporation
Transcript of Group and Individual Cognitive-Behavioral Treatments for Youth with Anxiety Disorders: A Randomized...
Cognitive Therapy and Research, Vol. 24, No. 3, 2000, pp. 251–278
Group and Individual Cognitive-Behavioral Treatmentsfor Youth with Anxiety Disorders: A RandomizedClinical Trial
Ellen C. Flannery-Schroeder1 and Philip C. Kendall1
Children (aged 8–14 years) with anxiety disorders were randomly assigned to cogni-tive-behavioral individual treatment, cognitive-behavioral group treatment, or a wait-list control. Treatment outcome was evaluated using diagnostic status, child self-reports, and parent- and teacher-reports. Analyses of diagnostic status revealed thatsignificantly more treated children (73% individual, 50% group) than wait-list children(8%) did not meet diagnostic criteria for their primary anxiety disorder at posttreat-ment. Other dependent measures demonstrated the superiority of both treatmentconditions compared to the wait-list condition. However, a child-report of anxiousdistress demonstrated only the individual treatment to effect significant improvement.Measures of social functioning failed to discriminate among conditions. Analyses ofclinical significance revealed that notable proportions of treated cases were returnedto nondeviant limits at posttreatment. Treatment gains were maintained at a 3-monthfollow-up.
KEY WORDS: anxiety disorders; child anxiety; group treatment; cognitive-behavioral therapy.
The increasing body of research devoted to childhood anxiety disorders maywell reflect the realization of the seriousness and debilitation associated with thedisorders. Anxiety disorders have been demonstrated to the one of the most com-mon categories of childhood and adolescent disorders (Bernstein & Borchardt,1991; Fergusson, Horwood, & Lynsky, 1993; Kashani & Orvaschel, 1990). Thisparallels the findings that anxiety disorders are the most common psychiatric disor-der in adults from the general population (Myers et al., 1984).
Estimates of childhood anxiety disorders range from approximately 1% to 21%(e.g., Fergusson et al., 1993; Kashani & Orvaschel, 1990). Aside from the negativeemotionality associated with the anxiety itself, childhood anxiety disorders haveoften been found to be comorbid with depression (Last, Hersen, Kazdin, Fin-
1Department of Psychology, Temple University, Philadelphia, Pennsylvania.2Correspondence should be directed to Ellen C. Flannery-Schroeder, Department of Psychology, TempleUniversity, Weiss Hall, Philadelphia, Pennsylvania 19122.
251
0147-5916/00/0600-0251$18.00/0 2000 Plenum Publishing Corporation

252 Flannery-Schroeder and Kendall
kelstein, & Strauss, 1987; Strauss, Lease, Last, & Francis, 1988; see Brady & Kendall,1992, for a review) and are frequently accompanied by somatic complaints (e.g.,Beidel, Christ, & Long, 1991). In addition, research suggests that anxiety disordersdo not readily remit in the absence of treatment (Kendall, 1994; Kendall et al.,1997) and are associated with negative long-term complications. Anxiety in youthhas been found to impact negatively upon children’s social adjustment (e.g., Benja-min, Costello, & Warren, 1990; Klein & Last, 1989; Rubin, 1985), academic achieve-ment (e.g., Benjamin et al., 1990; King & Ollendick, 1989), and later emotionalhealth in adolescence and adulthood (e.g., Achenbach & Edelbrock, 1981; Cant-well & Baker, 1989; Feehan, McGee, & Williams, 1993; Strain & Kerr, 1981).
Empirical studies of interventions for childhood anxiety disorders have beenincreasing over the last decade. Cognitive-behavioral interventions appreciate thecomplexities of the interactions among behavior, cognition, affect, social factors,and environmental consequences, and these procedures have been used in thetreatment of children’s fears and phobias, fears in medical and dental settings, fearsof evaluation, and anxiety disorders. Research has demonstrated their efficacy inthe treatment of anxiety-disordered children (e.g., Eisen & Silverman, 1993; Kane &Kendall, 1989; Kendall, 1994; Kendall et al., 1997; Mansdorf & Lukens, 1987; Ollen-dick, Hagopian, & Huntzinger, 1991; see also Kazdin & Weisz, 1998). Kendall andcolleagues developed and examined the efficacy of a treatment designed to reduceanxious symptomatology in children diagnosed with separation anxiety disorder,overanxious disorder/generalized anxiety disorder, and/or avoidant disorder/socialphobia. The manualized treatment (Kendall, Kane, Howard, & Siqueland, 1990)combines both training and exposure components and has demonstrated efficacyin reducing the proportion of children who are diagnosed as anxiety-disorderedat posttreatment. Maintenance of treatment gains were maintained across 1 year(Kendall, 1994; Kendall et al., 1997) and longer term (3.35 years) follow-ups (Ken-dall & Southam-Gerow, 1996).
The majority of research on childhood anxiety disorders has utilized cognitive-behavioral procedures in a child-focused individual format, with fewer being con-ducted with families (Barrett, Dadds, & Rapee, 1996; Howard & Kendall, 1996),and fewer still in groups (Albano, Marten, Holt, Heimberg, & Barlow, 1995). Severalcognitive-behavioral group treatments of anxiety in adulthood have been conducted,and all point toward their efficacy in the reduction of anxiety (e.g., Heimberg,Dodge, Hope, Kennedy, Zollo, & Becker, 1990; Renneberg, Goldstein, Phillips, &Chambless, 1990; Shaffer, Shapiro, Sank, & Coghlan, 1981). The majority of thesestudies with adults are well-controlled treatment outcome investigations, and theresults are suggestive of their utility in childhood anxiety disorders.
Although group treatments have been conducted with children for over 70years, a substantial research literature has yet to be established. The use of cognitive-behavioral procedures in a group format appears to have potential advantages overtheir use in individual formats. Groups provide opportunities for social interactions,peer mediation (e.g., peer modeling, peer and group feedback), leadership, andmultiple exposures to feared interpersonal contexts, objects, and/or situations. Also,it is likely that cognitive-behavioral groups therapies will offer some unique advan-tages (e.g., peer reinforcement, peer modeling, multiple exposures) which are diffi-
Group and Individual Cognitive-Behavioral Treatments 253
cult to implement in single-child formats. However, research is needed to determinefor whom these strategies are the most effective, and additional research is essentialin that group therapies may present some distinct disadvantages also worthy ofconsideration (Satterfield, 1994).
The use of a group format in treating children with anxiety disorders appearsto have a theortical foundation as well. Numerous research studies find socialwithdrawal and social reservedness to be correlated with anxiety (e.g., Hartup,1983; Rubin, 1985; Strauss, Forehand, Smith, & Frame, 1986). Children who didnot engage in peer interactions (versus those who did) were found to be moreanxious and depressed (Strauss et al., 1986). Although social withdrawal is onlya primary criterion in one of the three childhood anxiety disorders (i.e., socialphobia), its presence is nonetheless significant in GAD/OAD and SAD. Childrenwith OAD have been characterized as lonely, socially isolated, shy, unpopular,and socially unskilled (Strauss, 1988). SAD has been found to be associatedwith school refusal (Klein & Last, 1989); school is the location where the vastnumber of peer interactions occur. Therefore, failure to go to school indirectlyresults in a reduced number of peer social interactions. Thus, it appears thatthe implementation of a group format with anxiety-disordered children mayresult in enhanced treatment efficacy.
The purpose of the present research was to evaluate a cognitive-behavioralgroup treatment for 8- to 14-year-old children diagnosed with a childhood anxietydisorder (i.e., Generalized Anxiety Disorder, Separation Anxious Disorder, SocialPhobia). The research compared the efficacy of the cognitive-behavioral grouptreatment (GCBT) with that of individual cognitive-behavioral treatment (ICBT)and a wait-list control condition (WL). However, due to small sample sizes, thecomparison of the group and individual treatments is to be considered preliminary.The cognitive-behavioral therapy protocol that was used for both the GCBT andICBT conditions consisted of an 18-week manualized intervention. The therapyinvolved training children to use a variety of coping skills to address the somatic,emotional, cognitive, and behavioral components of anxiety. The first half of treat-ment consisted in building coping skills and strategies; the second half involvedpractice using the skills in in vivo exposures to the anxiety-producing situationsspecific to the child. The treatment also made use of relaxation, problem-solving,role plays, social reward, coping modeling, and homework assignments.
The three conditions (GCBT, ICBT, WL) were compared to assess differentialoutcome. It was expected that the GCBT would lead to equal or greater respon-siveness to treatment than the ICBT depending upon type of measure examined.It was hypothesized that the GCBT versus the ICBT would effect significant in-creases in social competence, friendships, and social activities and significant de-creases in social anxiety and loneliness posttreatment. Pre- to posttreatment compar-isons of diagnostic status, manifest anxiety, state and trait anxiety, number ofexcessive fears, internalizing behavior, and perceptions of the therapeutic relation-ship were expected to yield nonsignificant differences between the GCBT andICBT. Both treatment conditions were expected to be significantly more efficaciousthan the WL. Posttreatment gains were expected to be maintained at a 3-monthfollow-up.

254 Flannery-Schroeder and Kendall
METHOD
Participants
Thirty-seven 8- to 14-year-old clinic-referred children, referred from multiplecommunity resources in the tri-state area (PA, NJ, DE), served as participants. The37 children came from a total sample of 45 participants (8 children failed to completethe treatment protocol). Of the 8 children who failed to complete the protocol, 2withdrew during the 9-week waiting period, 2 withdrew prior to the first treatmentsession (1 assigned to the GCBT; 1 assigned to the ICBT), and 4 withdrew duringtreatment (all 4 from the ICBT). No participants in the GCBT dropped out dur-ing treatment.
Twenty-five children were treated initially (13 ICBT; 12 GCBT) and the re-maining 12 were treated following the 9-week WL period. In the ICBT, 46% wereboys and 8% were minorities. Thirty-eight percent were age 8–10 years and 62%were 11–14 years. In the GCBT, 67% were boys and 17% were minorities. Eighty-three percent were age 8–10 years and 17% were age 11–14 years. In the WL, 42%were boys and 8% were minorities. Fifty percent were age 8–10 years and 50%were 11–14 years. All children met DSM-IV diagnostic criteria for a childhoodanxiety disorder (Generalized Anxiety Disorder, n � 21; Separation Anxious Disor-der, n � 11; Social Phobia, n � 5) and completed an 18-week, cognitive-behavioraltreatment protocol. In the ICBT, 23% were comorbid with simple phobia, 15% withADHD, and 8% with dysthymia. None was comorbid with oppositional defiantdisorder (ODD), major depression, or conduct disorder. In the GCBT, 50% werecomorbid with simple phobia, 33% with ADHD, 8% with dysthymia, 25% withODD, and 8% with major depression. None was comorbid with conduct disorder.In the WL, 17% were comorbid with simple phobia and 23% with ADHD. Nonewas comorbid with dysthymia, oppositional defiant disorder (ODD), major depres-sion, or conduct disorder.3
Exclusion criteria for participation included a disabling physical condition,psychotic symptoms, or current use of antianxiety or antidepressant medication.Children whose primary diagnosis was simple phobia were not included; childrenwho had simple phobia as secondary problems were included. Participants in theICBT and GCBT conditions who missed four or more sessions were not includedin the data analyses. Four participants (i.e., noncompleters) met criteria for thisexclusion. All noncompleters were from the ICBT condition. Due to the longitudinalnature of the study, children and their families were fully informed of the proceduresof the study, which included participating in multiple assessments (e.g., pretreat-ment, posttreatment, and 3 months following treatment).
Setting and Personnel
Therapy was provided by eight (six female; two male) doctoral candidateswithin the Child and Adolescent Anxiety Disorders Clinic (CAADC) of the Clinical
3Chi-square analyses indicated that with the exception of ODD, �2(1) � 6.80, p �.05, none of the ratesof comorbidity differed among the three conditions. Further analyses demonstrated that comorbiditywith ODD was unrelated to treatment outcome (p � .05).
Group and Individual Cognitive-Behavioral Treatments 255
Psychology Program at Temple University. The therapists underwent training in-cluding didactic presentation, role-plays, videotape observation, and discussion andparticipated in 2 h of weekly supervision. Therapists did not work with one treatmentformat (either ICBT or GCBT) exclusively. In other words, several therapiststreated both individual cases and group cases.
Measures
Children, parents, teachers, and diagnosticians completed a variety of instru-ments to provide a multimethod assessment of child functioning. This study includedchild self-report measures, parent and teacher ratings, and a structured diagnosticinterview. These assessments were completed pretreatment/pre- wait-list, post-wait-list, posttreatment, and 3 months posttreatment. All measures were administeredby a diagnostician, not the child’s therapist.
Child Measures
Several self-report measures assessed fears and anxieties in children. A measureof chronic (trait) anxiety was provided by the Revised Children’s Manifest AnxietyScale (RCMAS; Reynolds & Richmond, 1978, 1985). The 48-item scale (11 lieitems) has internal consistency (Kuder–Richardson values from .83 to .85) andadequate retest reliability (r � .68 over 9 months). Analyses of convergent validityyield correlations of .85 between the RCMAS and the STAIC A-Trait scale. Anindex of discriminant validity was provided by the measure’s low correlation (r �.35) with a state measure of anxiety (STAIC A-State) (Reynolds & Richmond, 1985).
The State-Trait Anxiety Inventory for Children (STAIC; Spielberger, 1973)includes two 20-item scales that measure the enduring tendency to experienceanxiety (A-Trait) and the situational and temporal variations in the level of per-ceived anxiety (A-State). Retest reliability over a 6-week interval ranged between.65 and .71 for the A-Trait scale and .31 and .47 for the A-State scale. Concurrentvalidity was assessed by the STAIC A-Trait’s correlations with the Children’sManifest Anxiety Scale (Castaneda, McCandless, & Palermo, 1956), r � .75, andthe General Anxiety Scale for Children (Sarason, Davidson, Lighthall, Waite, &Ruebush, 1960), r � .63. Normative data are available (Spielberger, 1973).
The Coping Questionnaire-Child (CQ-C) (Kendall, 1994) is a self-report mea-sure assessing a child’s perceived ability to cope with various anxiety-provokingsituations. In order for the situations to be relevant, situationally based, and individu-alized, three situations are chosen from information given during the diagnosticinterview. The CQ-C enables the evaluation of improvements in specific targetareas. The CQ-C has been found to be internally consistent, sensitive to treatmenteffects, and to have good retest reliability (Kendall & Marrs-Garcia, n.d.).
The Social Anxiety Scale for Children-Revised (SASC-R; La Greca & Stone,1993) consists of 22 statements which children rate on a 5-point Likert scale. TheSASC-R has adequate internal consistencies (.69–.86), and social anxiety scorescorrelate significantly with general anxiety (e.g., RCMAS). In addition, SASC scoreshave been found to correlate with self-reports of social acceptance (La Greca,Dandes, Wick, Shaw, & Stone, 1988).

256 Flannery-Schroeder and Kendall
The Children’s Depression Inventory (CDI; Kovaks, 1981) assesses the cogni-tive, affective, and behavioral symptoms of depression. The 27-item scale has highinternal consistency, moderate retest reliability, and correlates in expected direc-tions with measures of related constructs such as self-esteem, negative cognitiveattributions, and hopelessness (Kazdin, French, Unis, Esveldt-Dawson, & Sherick,1983; Kovacs, 1981). Normative data are available (Finch, Saylor, & Edwards, 1985;Saylor, Finch, Spirito, & Bennett, 1984).
The child’s perceived competence in several areas was assessed by Harter’sSelf Perception Profile for Children (SPPC; Harter, 1985). The SPPC is composedof 36 items in a structured-alternative format which asks the child to first identifywhich of two statements best describes him/her. The measure yields subscale scoresin six domains (scholastic competence, social acceptance, athletic competence, phys-ical appearance, behavioral conduct, and a general self-worth score). Internal consis-tencies of the subscales have been found to range from .73 to .86, and retestreliabilities for the subscales and general self-worth score range from .70 to .87(Harter, 1985).
A measure of children’s perceived loneliness was attained through the use ofthe Loneliness Scale (LS; Asher, Hymel, & Renshaw, 1984). The LS consists of 24items that assess children’s feelings of loneliness and social dissatisfaction. Childrenare asked to respond on a 5-point Likert scale with the degree to which they feelthe statements are true of themselves. Sixteen of the items comprise the lonelinessscore. The scale is internally consistent (Cronbach’s alpha � .90) and internallyreliable (split half correlations � .91; Spearman–Brown reliability coefficient �.91) (Asher et al., 1984). Additionally, scores have been found to be significantlynegatively correlated with friendship nominations and play ratings received fromsame-gender peers (Asher et al., 1984).
The Friendship Measure-Child (FM-C) is comprised of a subset of items fromthe Friendship Questionnaire (FQ; Bierman & McCauley, 1987). The items on theFQ fall into three distinct factors (positive interactions, negative interactions, andextensiveness of peer network). The items which comprise the positive interactionsfactor are those items included in the FM-C. Five additional questions on theFM-C assessed the number of friendships and contacts made with other childrenparticipating in the treatment program. Participants endorsed items on the FM-Cusing a 5-point Likert scale. The FQ (Bierman & McCauley, 1987) discriminatesbetween children with positive versus rejected/neglected social status and correlatessignificantly with teacher and parent reports of behavior and social competence.
The Recall of Content Questionnaire (RCQ) is comprised of five open-endedquestions that require the respondent to recall information that was presentedduring the treatment protocol. The questionnaire was developed to measure theamount of treatment content recall and to examine differences between the GCBTand ICBT conditions.
Children in the ICBT and GCBT completed the Child’s Perception of Thera-peutic Relationship (CPTR; Kendall, 1994) measure at the completion of treatment.This measure is a 10-item, 5-point scale which assesses perceptions of the qualityof the therapeutic relationship. Items include rating the therapist in terms of howmuch the child liked him/her, how close the therapist was to the child, how much
Group and Individual Cognitive-Behavioral Treatments 257
time the child would like to spend with the therapist, and to what degree the childfeels he/she can talk to the therapist. Other items assess the nature and quality ofthe therapeutic relationship. Several questions are ‘‘filler’’ items that are not scored.Children in the group condition completed the Child’s Perception of the GroupRelationship measure (CPGR) at the end of treatment. The CPGR correspondsto the CPTR with each item modified to apply to the group rather than the therapist.
A measure of group satisfaction was completed by only those children assignedto the GCBT. The measure was designed for use in the present study and is referredto as the Group Satisfaction Questionnaire (GSQ). The GSQ is comprised of ten5-point questions assessing the degree to which a child liked other group members,the therapist, the group activities, and the degree to which he/she felt a part of thegroup. The GSQ was completed at posttreatment and follow-up assessments.
Parent Measures
Parents (i.e., mothers and fathers) completed six measures concerning childfunctioning. The Child Behavior Checklist (CBCL; Achenbach, 1991a) is composedof 138 items, 20 of which assess social competencies and 118 of which assess behav-ioral problems. The behavioral items are rated on a 3-point scale. CBCL Internaliz-ing scores were used to assess change across assessment periods. The CBCL hasexhibited good retest reliability (r �.87 over 1 week, r �.62 over 1 year) andinterparent agreement (r � .65–.76). Content and criterion-related validity havebeen adequately demonstrated, as nearly all CBCL items as well as scale scores andclinical cutpoints on the scale scores discriminated between referred and nonreferredchildren. Construct validity has been assessed by the correlations between the CBCLscales and the closest counterpart scales of the Connors (1973) Parent Questionnaire(r � .56–.86) and the Quay–Peterson (1983) Revised Behavior Problem Checklist(r � .52–.88). Normative data are available for both clinical and nonclinical samples(Achenbach, 1991a).
The State-Trait Anxiety Inventory for Children-Parent version (STAIC-P;Strauss, 1987) is a modified version of the Trait scale of the STAIC and wasused to assess parents’ ratings of their children’s trait anxiety. Parents endorse thefrequency with which several statements apply to their child on a 3-point scale.
The Coping Questionnaire Parent (CQ-P) parallels the children’s version de-scribed previously. The parent rated the child’s ability to cope with the threesituations which were derived from information given during the diagnostic inter-view. The measure has been found to have good internal consistency, retest reliabil-ity, and sensitivity to treatment effects (Kendall & Marrs-Garcia, 1997).
The Parent’s Rating Scale of Child’s Competence (PRSC; Harter, 1982) corre-sponds to the children’s version. It is composed of 28 items which assess the child’sspecific competencies and three items which require the parent to provide a globalrating for intellectual competence, social competence, and physical competence.
The Social Activities Scale-Parent (SAS-P) measures children’s participationin social activities and was designed to enable the measurement of potential changesin the type or amount of social activities over time. The SAS-P consists of twoquestions that ask the parents to list those group social activities in which theirchildren participate currently or participated in the past. Parents also indicate the
258 Flannery-Schroeder and Kendall
length of time the child participated in the listed activities and the age of the childwhen he/she participated.
The Friendship Measure-Parent (FM-P) corresponds to the children’s version.The parent is asked to respond on a 5-point Likert scale to 10 questions assessingtheir perceptions of their children’s peer relationships.
Teacher Measures
Teachers completed the Teacher Report Form (TRF; Achenbach, 1991b). TheTRF is similar in format to the CBCL. This measure is particularly useful in themeasurement of change in social and evaluative contexts (e.g., school). The TRFhas demonstrated high retest reliability (r � .90–.92) over an interval of 15 days.Interteacher agreements range from .54 (problem scores) to .55 (academic andadaptive scores) under different conditions and teacher–teacher’s aide agreementsrange from .55 (problem scores) to .60 (academic and adaptive scores) under similarconditions. The validity of the TRF has been supported by the ability of most itemsto discriminate successfully between referred and nonreferred children. Normativedata have been reported (Achenbach, 1991b).
Structured Diagnostic Interview
Clinical diagnosticians used the Anxiety Disorder Interview Schedule (ADIS-IV-C and ADIS-IV-P; Silverman & Albano, 1996), a structured diagnostic interviewschedule consistent with the DSM-IV criteria, to assess child functioning in separateinterviews with the child and with the parents. The ADIS-IV is geared toward thediagnosis of childhood anxiety disorders, but the inclusion of other disorders (e.g.,dysthymia, attention deficit hyperactivity disorder, panic disorder) allowed the diag-nostician to assess alternative conditions.
Procedure
Cases came from the children who were routinely referred to the CAADC bymultiple community agencies and schools. Within a week of referral, clinic staffarranged an intake evaluation (Pre 1) with the parents. Parents and the child signedinformed consent and completed the measures on site; the teacher forms were senthome with the parents to be given to the teacher within the week. Teachers wereprovided with stamped envelopes to mail forms. Children receiving a childhoodanxiety disorder diagnosis were randomly assigned to either the WL control (9-week) condition, ICBT, or GCBT (one of four single-gender groups). Those partici-pants assigned to the WL completed another assessment evaluation (Pre 2) at theend of the waiting period and prior to entering their treatment. These participantswere then randomly assigned to either group or individual treatment. A restrictedrandomization procedure was used in which participants assigned to the GCBT(either immediately or following wait-list) were assigned in blocks of four. Childrenand parents who were assigned to the GCBT signed an agreement of confidentialitywithin the group. All participants were assessed again after treatment (Post) and3 months following treatment (Follow-up). All assessments followed the same proce-dures as in the initial evaluation.

Group and Individual Cognitive-Behavioral Treatments 259
Intervention
The treatment protocol adapted the manual by Kendall et al. (1990) for usein the group condition (Flannery-Schroeder & Kendall, 1996). Treatment methodsincluded education including learning to recognize anxious feelings, physiologicalreactions to anxiety, and negative thoughts. Behavioral strategies included copingmodeling, role playing, relaxation training, contingent reinforcement, and in vivoexposures. The therapist provided each child with the Coping cat workbook (Ken-dall, 1990) as an aid in learning the coping skills presented during treatment.Children recorded their homework assignments (‘‘Show That I Can’’ or STIC tasks)in the Coping cat notebook and brought this notebook along with them to eachsession. The therapist reviewed the STIC tasks with the children at the start ofeach session.
Treated participants received the cognitive-behavioral treatment protocol ineither an individual or group format. The treatment consisted of 18 weeks of 50-to 60-min sessions for the individual treatment, 18 weeks of 90-min sessions for thegroup treatment, both typically meeting once a week. The treatment was largelychild-centered; however, several parent sessions were included in both treatmentformats. The first half of the treatment protocol involved the teaching of copingskills; the second half involved exposure to anxiety-eliciting situations and thepractice of the skills acquired in the first half of treatment. Both treatments consistedof four main components: (1) the recognition and labeling of somatic reactions andanxious feelings; (2) the recognition and modification of anxious self-talk; (3) thedevelopment of a plan to cope with the anxious situation; and (4) the evaluationof performance and provision of reward.
The treatment outline for the individual treatment was as follows: The firstsession included rapport-building, the identification of specific situations that thechild found frightening, and the normalization of anxiety and anxious reactions.The second session involved affective education and the identification of variousemotions. Session 3 included construction of a hierarchy of anxiety-provoking situa-tions and identification of individual responses to anxiety. After session 3, a parentmeeting was held to elicit more information concerning the child’s anxious behaviorand to provide additional information to the parents. Session 4 was devoted torelaxation training, and children received a personalized relaxation training audio-tape for their use at home. Session 5 focused on introducing the concept of self-talk and identifying self-talk in anxiety-provoking situations. Session 6 emphasizedthe modification of noncoping self-talk and the development of problem-solvingstrategies for anxiety management. Session 7 introduced self-evaluation and self-reward following attempts at managing anxiety. Session 8 involved a review of theskills and their use in a four-step plan for coping with anxiety. Session 9 involveda review of the material covered during the first half of the treatment. Sessions10–18 involved practicing the skills learned in the first half of the treatment. Skillswere first applied to imaginal situations with low levels of anxiety and then graduallyprogressed to in vivo exposures with increasing levels of anxiety. At the close ofthe therapy, the child was asked to make a commercial that summed up what he/she learned during the program. This provided an opportunity for consolidation of

260 Flannery-Schroeder and Kendall
skills learned during therapy, and the child was given a videotaped copy to takehome. Following the last session, a posttreatment assessment was conducted.
The treatment outline for the group treatment was as follows: The first sessionincluded rapport-building and the outlining of basic information about the program.The second session involved affective education and the identification of variousemotions. Session 3 included the identification of individual responses to anxiety.Session 4 involved the normalization of the experience of anxiety and the construc-tion of a hierarchy of anxiety-eliciting situations for both the group as a whole andfor individual members. After session 4, parent meetings were held individuallywith each group member’s parents to elicit more information concerning the child’sanxious behavior and to provide additional information to the parents. Session 5was devoted to relaxation training, and each group member received a personalizedrelaxation training audiotape for their use at home. Session 6 focused on introducingthe concept of self-talk and identifying self-talk in anxiety-provoking situations.Session 7 emphasized the modification of noncoping self-talk and the developmentof problem-solving strategies for anxiety management. Session 8 introduced self-evaluation and self-reward following attempts at managing anxiety. Session 9 in-volved a review of the skills and their use in a four-step plan for coping with anxiety.Session 10 was a group social event designed to continue to heighten group cohesionand affiliation. Sessions 11–18 involved practicing the skills learned in the first halfof the treatment. Skills were first applied to imaginal situations with low levels ofanxiety and then gradually progressed to in vivo exposures with increasing levelsof anxiety. In vivo exposures began with group participation and progressed toindividually conducted exposures. At the close of the therapy, the group made acommercial that summed up what they learned during the program. This wasintended to serve as an opportunity for consolidation of skills learned during ther-apy, and each group member was given a videotaped copy to take home. Followingthe last session, the posttreatment assessments were conducted.
RESULTS
Power Analyses
Effect sizes found by Kendall (1994) in a similar randomized clinical trial ofanxiety disorders in children were found to average greater than one standarddeviation for the treatment condition and less than 1/10 of one standard deviationfor the wait-list condition. Using Cohen’s (1977) f, estimates of effect size forsignificant interactions (condition by assessment period) averaged .47. Power esti-mates as determined from Kendall (1994) demonstrate that the power actuallyobtained averaged .83 on measures which assessed anxiety (e.g., RCMAS, STAIC-A-State, and A-Trait) and internalized distress (Internalizing score on the CBCLand TRF).
Using Cohen’s (1977) guidelines, with 12 ICBT, 12 GCBT, and 12 controlparticipants, the power to detect a strong within-participants (assessment period)main effect is .91. Power to detect medium and small within-participant main effects
Group and Individual Cognitive-Behavioral Treatments 261
is .54 and .12, respectively. The power to detect a strong between-participants(condition) main effect is .84. Power to detect medium and small between-partici-pant main effects is .43 and .10, respectively. The power to detect a strong interaction(condition by assessment period) effect is .84. Power to detect small and mediuminteraction effects is .43 and .10, respectively.
Reliabilities
Diagnosticians were trained to use the structured interview (ADIS) via writtenand videotaped samples. A reliability criterion of 85% agreement (kappa) was setand obtained by all diagnosticians prior to the study.
Group Comparability
One-way analyses of variance (ANOVAs) and chi-square analyses were usedto assess for pretreatment differences in age, gender, race, family income, mother’slevel of education, and father’s level of education; no significant differences werefound among conditions (WL, ICBT, GCBT). In a comparison of pretreatmentdependent variable scores across conditions, some means on child-reported mea-sures were found to differ significantly. Scores on the STAIC-A-State, F(2, 34) �13.53, p � .001, and the STAIC-A-Trait, F(2, 34) � 6.81, p � .01, were significantlylower in the GCBT compared to the ICBT and WL conditions. The mean scoreson these measures did not differ significantly between ICBT and WL conditions.Additionally, mean scores in the GCBT were significantly lower than scores in theWL condition on the LS, F(2, 34) � 3.39, p � .05, and the SASC-R, F(2, 34) �5.39, p � .01. Mean scores on these two measures did not differ significantly betweenGCBT and ICBT or between ICBT and WL.4
In analyses comparing treatment completers and noncompleters, the groupsdid not differ in age, gender, race, or family income. However, the groups did differon primary diagnoses and some dependent measures. A greater percentage ofchildren who dropped out had social phobia as their primary diagnosis, �2(2) �9.13, p � .01. Additionally, noncompleters reported significantly less depressivesymptoms (CDI) at the pretreatment assessment, t(26) � 2.85, p � .01. Mothersof noncompleters reported significantly less child anxiety on the STAIC-P, t(42) �2.25, p � .05; fathers of noncompleters reported significantly higher coping scoreson the CQ-C, t(43) � 2.13, p � .05. The remaining dependent measures yieldednonsignificant differences between completers and noncompleters.
Therapist Comparability
An examination of therapist effects revealed nonsignificant relationships withtreatment gains or maintenance of treatment gains. In other words, individualtherapists (therapist a, b, c, . . . , k) and therapist’s experience (number of times
4Analyses of covariance were considered, but deemed inappropriate in this instance due to the lack ofindependence between the covariates (e.g., pretreatment scores) and the independent variable (con-dition).
262 Flannery-Schroeder and Kendall
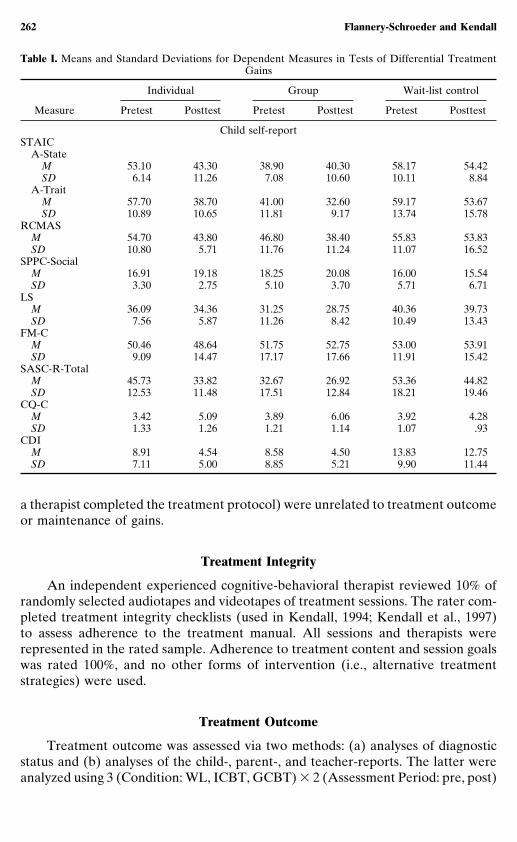
Table I. Means and Standard Deviations for Dependent Measures in Tests of Differential TreatmentGains
Individual Group Wait-list control
Measure Pretest Posttest Pretest Posttest Pretest Posttest
Child self-reportSTAIC
A-StateM 53.10 43.30 38.90 40.30 58.17 54.42SD 6.14 11.26 7.08 10.60 10.11 8.84
A-TraitM 57.70 38.70 41.00 32.60 59.17 53.67SD 10.89 10.65 11.81 9.17 13.74 15.78
RCMASM 54.70 43.80 46.80 38.40 55.83 53.83SD 10.80 5.71 11.76 11.24 11.07 16.52
SPPC-SocialM 16.91 19.18 18.25 20.08 16.00 15.54SD 3.30 2.75 5.10 3.70 5.71 6.71
LSM 36.09 34.36 31.25 28.75 40.36 39.73SD 7.56 5.87 11.26 8.42 10.49 13.43
FM-CM 50.46 48.64 51.75 52.75 53.00 53.91SD 9.09 14.47 17.17 17.66 11.91 15.42
SASC-R-TotalM 45.73 33.82 32.67 26.92 53.36 44.82SD 12.53 11.48 17.51 12.84 18.21 19.46
CQ-CM 3.42 5.09 3.89 6.06 3.92 4.28SD 1.33 1.26 1.21 1.14 1.07 .93
CDIM 8.91 4.54 8.58 4.50 13.83 12.75SD 7.11 5.00 8.85 5.21 9.90 11.44
a therapist completed the treatment protocol) were unrelated to treatment outcomeor maintenance of gains.
Treatment Integrity
An independent experienced cognitive-behavioral therapist reviewed 10% ofrandomly selected audiotapes and videotapes of treatment sessions. The rater com-pleted treatment integrity checklists (used in Kendall, 1994; Kendall et al., 1997)to assess adherence to the treatment manual. All sessions and therapists wererepresented in the rated sample. Adherence to treatment content and session goalswas rated 100%, and no other forms of intervention (i.e., alternative treatmentstrategies) were used.
Treatment Outcome
Treatment outcome was assessed via two methods: (a) analyses of diagnosticstatus and (b) analyses of the child-, parent-, and teacher-reports. The latter wereanalyzed using 3 (Condition: WL, ICBT, GCBT) � 2 (Assessment Period: pre, post)
Group and Individual Cognitive-Behavioral Treatments 263
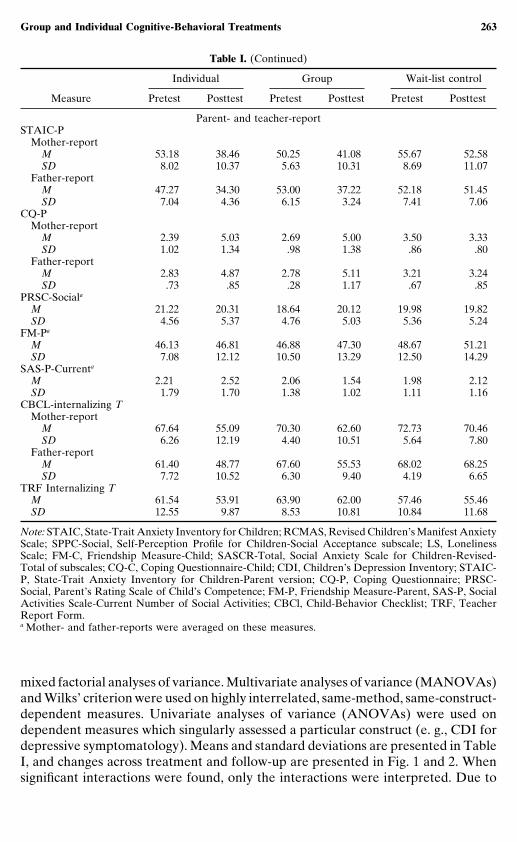
Table I. (Continued)
Individual Group Wait-list control
Measure Pretest Posttest Pretest Posttest Pretest Posttest
Parent- and teacher-reportSTAIC-P
Mother-reportM 53.18 38.46 50.25 41.08 55.67 52.58SD 8.02 10.37 5.63 10.31 8.69 11.07
Father-reportM 47.27 34.30 53.00 37.22 52.18 51.45SD 7.04 4.36 6.15 3.24 7.41 7.06
CQ-PMother-report
M 2.39 5.03 2.69 5.00 3.50 3.33SD 1.02 1.34 .98 1.38 .86 .80
Father-reportM 2.83 4.87 2.78 5.11 3.21 3.24SD .73 .85 .28 1.17 .67 .85
PRSC-Sociala
M 21.22 20.31 18.64 20.12 19.98 19.82SD 4.56 5.37 4.76 5.03 5.36 5.24
FM-Pa
M 46.13 46.81 46.88 47.30 48.67 51.21SD 7.08 12.12 10.50 13.29 12.50 14.29
SAS-P-Currenta
M 2.21 2.52 2.06 1.54 1.98 2.12SD 1.79 1.70 1.38 1.02 1.11 1.16
CBCL-internalizing TMother-report
M 67.64 55.09 70.30 62.60 72.73 70.46SD 6.26 12.19 4.40 10.51 5.64 7.80
Father-reportM 61.40 48.77 67.60 55.53 68.02 68.25SD 7.72 10.52 6.30 9.40 4.19 6.65
TRF Internalizing TM 61.54 53.91 63.90 62.00 57.46 55.46SD 12.55 9.87 8.53 10.81 10.84 11.68
Note: STAIC, State-Trait Anxiety Inventory for Children; RCMAS, Revised Children’s Manifest AnxietyScale; SPPC-Social, Self-Perception Profile for Children-Social Acceptance subscale; LS, LonelinessScale; FM-C, Friendship Measure-Child; SASCR-Total, Social Anxiety Scale for Children-Revised-Total of subscales; CQ-C, Coping Questionnaire-Child; CDI, Children’s Depression Inventory; STAIC-P, State-Trait Anxiety Inventory for Children-Parent version; CQ-P, Coping Questionnaire; PRSC-Social, Parent’s Rating Scale of Child’s Competence; FM-P, Friendship Measure-Parent, SAS-P, SocialActivities Scale-Current Number of Social Activities; CBCl, Child-Behavior Checklist; TRF, TeacherReport Form.a Mother- and father-reports were averaged on these measures.
mixed factorial analyses of variance. Multivariate analyses of variance (MANOVAs)and Wilks’ criterion were used on highly interrelated, same-method, same-construct-dependent measures. Univariate analyses of variance (ANOVAs) were used ondependent measures which singularly assessed a particular construct (e. g., CDI fordepressive symptomatology). Means and standard deviations are presented in TableI, and changes across treatment and follow-up are presented in Fig. 1 and 2. Whensignificant interactions were found, only the interactions were interpreted. Due to
264 Flannery-Schroeder and Kendall
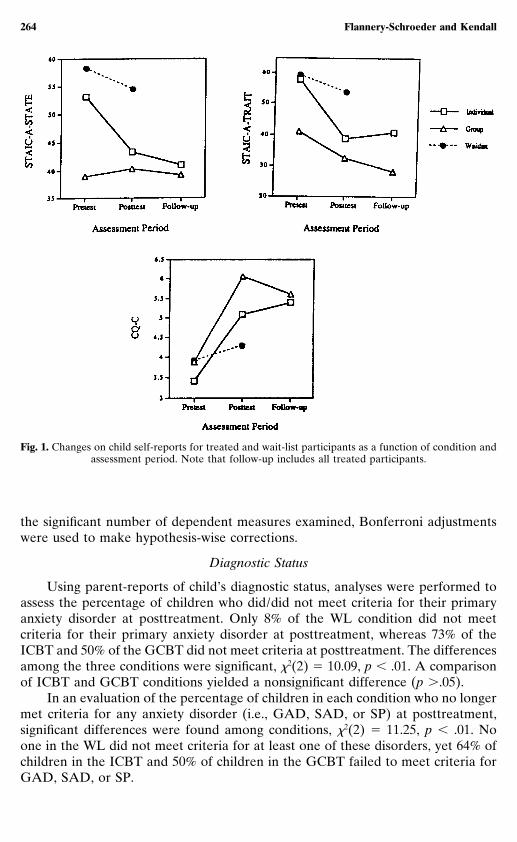
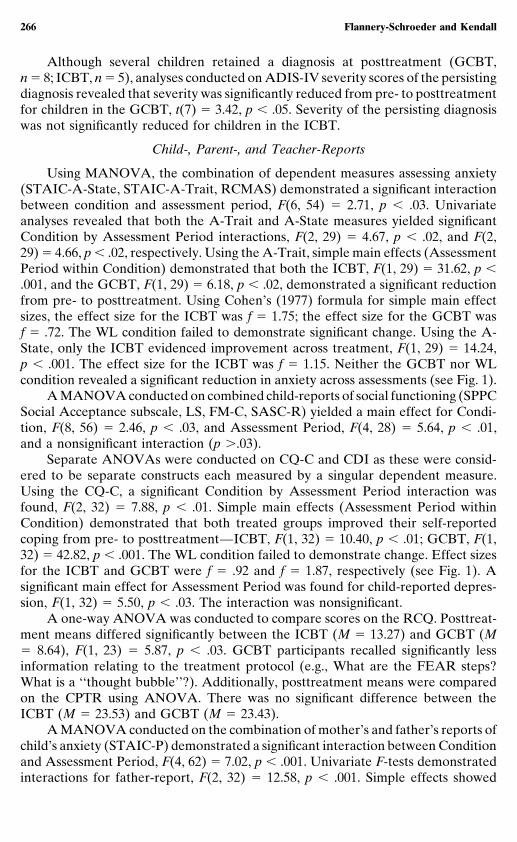
Fig. 1. Changes on child self-reports for treated and wait-list participants as a function of condition andassessment period. Note that follow-up includes all treated participants.
the significant number of dependent measures examined, Bonferroni adjustmentswere used to make hypothesis-wise corrections.
Diagnostic Status
Using parent-reports of child’s diagnostic status, analyses were performed toassess the percentage of children who did/did not meet criteria for their primaryanxiety disorder at posttreatment. Only 8% of the WL condition did not meetcriteria for their primary anxiety disorder at posttreatment, whereas 73% of theICBT and 50% of the GCBT did not meet criteria at posttreatment. The differencesamong the three conditions were significant, �2(2) � 10.09, p � .01. A comparisonof ICBT and GCBT conditions yielded a nonsignificant difference (p �.05).
In an evaluation of the percentage of children in each condition who no longermet criteria for any anxiety disorder (i.e., GAD, SAD, or SP) at posttreatment,significant differences were found among conditions, �2(2) � 11.25, p � .01. Noone in the WL did not meet criteria for at least one of these disorders, yet 64% ofchildren in the ICBT and 50% of children in the GCBT failed to meet criteria forGAD, SAD, or SP.
Group and Individual Cognitive-Behavioral Treatments 265
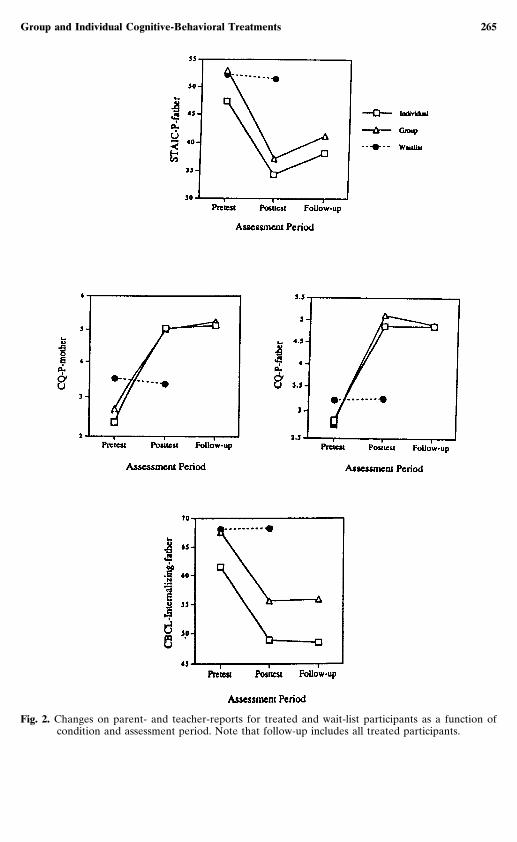
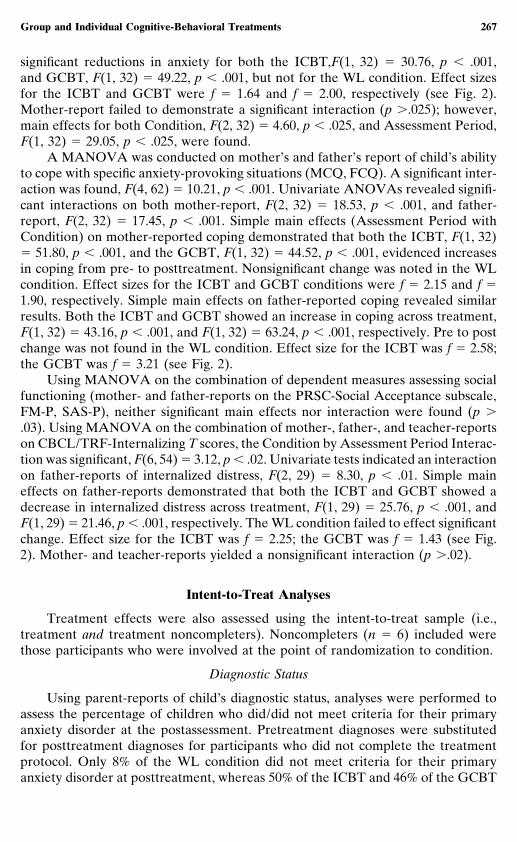
Fig. 2. Changes on parent- and teacher-reports for treated and wait-list participants as a function ofcondition and assessment period. Note that follow-up includes all treated participants.
266 Flannery-Schroeder and Kendall
Although several children retained a diagnosis at posttreatment (GCBT,n � 8; ICBT, n � 5), analyses conducted on ADIS-IV severity scores of the persistingdiagnosis revealed that severity was significantly reduced from pre- to posttreatmentfor children in the GCBT, t(7) � 3.42, p � .05. Severity of the persisting diagnosiswas not significantly reduced for children in the ICBT.
Child-, Parent-, and Teacher-Reports
Using MANOVA, the combination of dependent measures assessing anxiety(STAIC-A-State, STAIC-A-Trait, RCMAS) demonstrated a significant interactionbetween condition and assessment period, F(6, 54) � 2.71, p � .03. Univariateanalyses revealed that both the A-Trait and A-State measures yielded significantCondition by Assessment Period interactions, F(2, 29) � 4.67, p � .02, and F(2,29) � 4.66, p � .02, respectively. Using the A-Trait, simple main effects (AssessmentPeriod within Condition) demonstrated that both the ICBT, F(1, 29) � 31.62, p �.001, and the GCBT, F(1, 29) � 6.18, p � .02, demonstrated a significant reductionfrom pre- to posttreatment. Using Cohen’s (1977) formula for simple main effectsizes, the effect size for the ICBT was f � 1.75; the effect size for the GCBT wasf � .72. The WL condition failed to demonstrate significant change. Using the A-State, only the ICBT evidenced improvement across treatment, F(1, 29) � 14.24,p � .001. The effect size for the ICBT was f � 1.15. Neither the GCBT nor WLcondition revealed a significant reduction in anxiety across assessments (see Fig. 1).
A MANOVA conducted on combined child-reports of social functioning (SPPCSocial Acceptance subscale, LS, FM-C, SASC-R) yielded a main effect for Condi-tion, F(8, 56) � 2.46, p � .03, and Assessment Period, F(4, 28) � 5.64, p � .01,and a nonsignificant interaction (p �.03).
Separate ANOVAs were conducted on CQ-C and CDI as these were consid-ered to be separate constructs each measured by a singular dependent measure.Using the CQ-C, a significant Condition by Assessment Period interaction wasfound, F(2, 32) � 7.88, p � .01. Simple main effects (Assessment Period withinCondition) demonstrated that both treated groups improved their self-reportedcoping from pre- to posttreatment—ICBT, F(1, 32) � 10.40, p � .01; GCBT, F(1,32) � 42.82, p � .001. The WL condition failed to demonstrate change. Effect sizesfor the ICBT and GCBT were f � .92 and f � 1.87, respectively (see Fig. 1). Asignificant main effect for Assessment Period was found for child-reported depres-sion, F(1, 32) � 5.50, p � .03. The interaction was nonsignificant.
A one-way ANOVA was conducted to compare scores on the RCQ. Posttreat-ment means differed significantly between the ICBT (M � 13.27) and GCBT (M� 8.64), F(1, 23) � 5.87, p � .03. GCBT participants recalled significantly lessinformation relating to the treatment protocol (e.g., What are the FEAR steps?What is a ‘‘thought bubble’’?). Additionally, posttreatment means were comparedon the CPTR using ANOVA. There was no significant difference between theICBT (M � 23.53) and GCBT (M � 23.43).
A MANOVA conducted on the combination of mother’s and father’s reports ofchild’s anxiety (STAIC-P) demonstrated a significant interaction between Conditionand Assessment Period, F(4, 62) � 7.02, p � .001. Univariate F-tests demonstratedinteractions for father-report, F(2, 32) � 12.58, p � .001. Simple effects showed
Group and Individual Cognitive-Behavioral Treatments 267
significant reductions in anxiety for both the ICBT,F(1, 32) � 30.76, p � .001,and GCBT, F(1, 32) � 49.22, p � .001, but not for the WL condition. Effect sizesfor the ICBT and GCBT were f � 1.64 and f � 2.00, respectively (see Fig. 2).Mother-report failed to demonstrate a significant interaction (p �.025); however,main effects for both Condition, F(2, 32) � 4.60, p � .025, and Assessment Period,F(1, 32) � 29.05, p � .025, were found.
A MANOVA was conducted on mother’s and father’s report of child’s abilityto cope with specific anxiety-provoking situations (MCQ, FCQ). A significant inter-action was found, F(4, 62) � 10.21, p � .001. Univariate ANOVAs revealed signifi-cant interactions on both mother-report, F(2, 32) � 18.53, p � .001, and father-report, F(2, 32) � 17.45, p � .001. Simple main effects (Assessment Period withCondition) on mother-reported coping demonstrated that both the ICBT, F(1, 32)� 51.80, p � .001, and the GCBT, F(1, 32) � 44.52, p � .001, evidenced increasesin coping from pre- to posttreatment. Nonsignificant change was noted in the WLcondition. Effect sizes for the ICBT and GCBT conditions were f � 2.15 and f �1.90, respectively. Simple main effects on father-reported coping revealed similarresults. Both the ICBT and GCBT showed an increase in coping across treatment,F(1, 32) � 43.16, p � .001, and F(1, 32) � 63.24, p � .001, respectively. Pre to postchange was not found in the WL condition. Effect size for the ICBT was f � 2.58;the GCBT was f � 3.21 (see Fig. 2).
Using MANOVA on the combination of dependent measures assessing socialfunctioning (mother- and father-reports on the PRSC-Social Acceptance subscale,FM-P, SAS-P), neither significant main effects nor interaction were found (p �.03). Using MANOVA on the combination of mother-, father-, and teacher-reportson CBCL/TRF-Internalizing T scores, the Condition by Assessment Period Interac-tion was significant, F(6, 54) � 3.12, p � .02. Univariate tests indicated an interactionon father-reports of internalized distress, F(2, 29) � 8.30, p � .01. Simple maineffects on father-reports demonstrated that both the ICBT and GCBT showed adecrease in internalized distress across treatment, F(1, 29) � 25.76, p � .001, andF(1, 29) � 21.46, p � .001, respectively. The WL condition failed to effect significantchange. Effect size for the ICBT was f � 2.25; the GCBT was f � 1.43 (see Fig.2). Mother- and teacher-reports yielded a nonsignificant interaction (p �.02).
Intent-to-Treat Analyses
Treatment effects were also assessed using the intent-to-treat sample (i.e.,treatment and treatment noncompleters). Noncompleters (n � 6) included werethose participants who were involved at the point of randomization to condition.
Diagnostic Status
Using parent-reports of child’s diagnostic status, analyses were performed toassess the percentage of children who did/did not meet criteria for their primaryanxiety disorder at the postassessment. Pretreatment diagnoses were substitutedfor posttreatment diagnoses for participants who did not complete the treatmentprotocol. Only 8% of the WL condition did not meet criteria for their primaryanxiety disorder at posttreatment, whereas 50% of the ICBT and 46% of the GCBT

268 Flannery-Schroeder and Kendall
did not meet criteria at posttreatment. These differences among conditions weresignificant, �2(2) � 5.82, p � .05.
In an evaluation of the percentage of children in each condition who no longermet criteria for any anxiety disorder (i.e., GAD, SAD, or SP), significant differenceswere found among conditions, �2(2) � 7.90, p � .01. Although no one in the WLdid not meet criteria for at least one of these disorders, 44% of children in theICBT and 46% of children in the GCBT failed to meet criteria for GAD, SAD, or SP.
Child-, Parent-, and Teacher-Reports
Analyses of the intent-to-treat sample paralleled those used in analyses involv-ing treatment completers (i.e., 3 � 2 Condition by Assessment Period mixed factorialanalyses of variance). Pretreatment scores were substituted for posttreatment scoresfor participants who did not complete the treatment.
Using MANOVA on the combination of child self-report measures assessinganxiety (STAIC-A-State, STAIC-A-Trait, RCMAS), main effects for Condition,F(6, 66) � 3.99, p � .01, and Assessment Period, F(3, 33) � 7.53, p � .001, werefound. The interaction was nonsignificant (p �.03). Similarly, only main effects forCondition, F(8, 66) � 2.74, p � .02, and Assessment Period, F(4, 33) � 4.40, p �.01, were found on the combination of dependent measures of child-reported socialfunctioning (SPPC Social Acceptance subscale, LS, FM-C, SASC-R).
Using ANOVA on the CQ-C, a Condition by Assessment Period interactionwas noted, F(2, 36) � 5.69, p � .01. Simple main effects tests (Assessment Periodwithin Condition) revealed that both the ICBT, F(1, 36) � 14.20, p � .001, Cohen’sf � .91, and GCBT, F(1, 36) � 35.14, p � .001, Cohen’s f � 1.62, showed significantimprovement in child coping. The WL failed to demonstrate pre- to posttreatmentgains. An ANOVA on the CDI indicated main effects for Condition, F(2, 38) �4.30, p � .05, and Assessment Period, F(1, 38) � 4.93, p � .05. The interaction wasnonsignificant.
An interaction between Condition and Assessment Period was found on aMANOVA using parents’ reports of child anxiety (STAIC-P), F(4, 72) � 5.33,p �.01. Univariate analyses revealed only the fathers’ reports to be significant, F(2,37) � 8.45, p � .01. Simple main effects (Assessment Period within Condition)demonstrate, according to father-reports, that both the ICBT, F(1, 37) � 18.84,p � .001, Cohen’s f � 1.09, and GCBT, F(1, 37) � 38.26, p � .001, Cohen’s f �1.69, effected significant pre- to posttreatment improvements. The WL did not elicitsignificant change across assessments.
A significant Condition by Assessment Period interaction was found for moth-er- and father-reports on the CQ-P, F(4, 72) � 5.57, p � .001. Univariate testsindicated improvements on both mother-reports, F(2, 37) � 10.29, p � .001, andfather-reports, F(2, 37) � 9.00, p � .001. Using mother-reports, simple main effects(Assessment Period within Condition) demonstrated significant improvementsacross assessments for only the treated groups, ICBT: F(1, 37) � 28.43, p � .001,Cohen’s f � 1.35; GCBT: F(1, 37) � 29.89, p � .001, Cohen’s f � 1.49. Father-reports revealed similar findings, ICBT: F(1, 37) � 25.09, p � .001, Cohen’s f �1.27; GCBT: F(1, 37) � 34.84, p � .001, Cohen’s f � 1.61.
A MANOVA on the combination of parent-report measures assessing child

Group and Individual Cognitive-Behavioral Treatments 269
social functioning (PRSC-Social Acceptance subscale, FM-P, SAS-P) demonstratednonsignificant main effects and a nonsignificant interaction (p � .03). A nonsignifi-cant interaction was found using MANOVA on parent- and teacher-reports ofchildren’s internalized distress (CBCL and TRF Internalizing T scores), p � .03;however, a main effect for Assessment Period was found, F(3, 32) � 7.41, p � .001.
Clinical Significance
Assurances of clinically significant improvement cannot be derived from statisti-cally significant improvement. To assess the former, defined as changes that returndeviant participants to within nondeviant limits, normative comparisons were used(Kendall & Grove, 1988). Specific criteria were set to define clinically significantimprovement. On the CBCL/TRF, the clinical cutoff score of 65 was used. Ofchildren whose initial CBCL Internalizing T score was above 65 (parent-reportsare averaged, n � 28), 20.5% of participants in the WL condition, 85.5% in theICBT, and 69.5% in the GCBT were returned to within the normative range (CBCLT score � 65) at posttreatment. A chi-square analysis demonstrated a significantdifference among these three groups, 2(2) � 10.79, p � .01. Using TRF Internalizingscores initially above 65 (n � 12), no WL participants were returned to within thenormative range. Fully 80% of participants in the ICBT and 40% of participants inthe GCBT were returned to within normative levels. These differences among thethree conditions were not statistically significant.
Maintenance: 3-Month Follow-Up
Maintenance was assessed via two methods: (a) evaluation of diagnostic statusat the 3-month follow-up and (b) change in dependent measures from posttreatmentto follow-up. Maintenance analyses include all treated participants (i.e., childrentreated at completion of the waiting period are included with those in the ICBTand GCBT).
Diagnostic Status
Using parent-reports of child’s diagnostic status, analyses were performed toassess the percentage of children who did/did not meet criteria for their primaryanxiety disorder at 3-month follow-up. Fully 79% of the ICBT and 53% of theGCBT did not meet criteria for their primary anxiety disorder at follow-up. Thesepercentages did not differ significantly from one another. In an evaluation of thepercentage of children in each condition who no longer met criteria for any of thethree anxiety disorders (GAD, SAD, SP) at follow-up, conditions (ICBT andGCBT) were not statistically different from one another—50% of children in theICBT and 53% of children in the GCBT had neither GAD, SAD, nor SP at follow-up.
Child-, Parent-, and Teacher-Reports
Maintenance for 29 (14 ICBT; 15 GCBT) of the 37 treated participants wasexamined using 2 (Condition: ICBT, GCBT) � 2 (Assessment Period: post, follow-up) analyses. Eight participants were not available for the 3-month follow-up.

270 Flannery-Schroeder and Kendall
Table II. Means and Standard Deviations for Dependent Measures in Tests of Maintenance of TreatmentGains
Condition
Individual Group
Measure Posttest Follow-up Posttest Follow-up
Child self-reportSTAIC-A-State
M 43.54 40.91 40.18 39.18SD 11.29 13.63 10.34 11.70
STAIC-A-TraitM 37.54 40.91 33.00 28.18SD 10.59 13.80 9.86 9.98
RCMASM 44.82 34.64 38.91 29.46SD 6.52 18.50 10.74 15.23
SPPC-SocialM 18.62 17.23 19.43 19.64SD 2.87 2.98 4.18 4.67
LSM 34.92 36.69 29.64 29.21SD 5.59 7.23 8.31 8.43
FM-CM 47.54 48.54 53.29 57.07SD 15.85 13.85 17.32 16.31
SASC-R-TotalM 34.62 37.92 28.71 27.50SD 14.41 14.82 12.76 13.22
CQ-CM 5.21 5.38 5.69 5.60SD 1.16 1.08 1.39 1.49
CDIM 4.77 5.77 4.00 3.67SD 4.60 4.15 4.84 5.88
Dependent variables included in the MANOVAs and ANOVAs parallel thoseconducted in the treatment outcome section. See Table II for means and standarddeviations and Figs. 1 and 2. Nonsignificant interactions or main effects were notedon all dependent variables.
DISCUSSION
These results replicate and extend research on the efficacy of a cognitive-behavioral treatment for anxiety-disordered youth. Several randomized clinicaltrials (e.g., Kendall, 1994; Kendall et al., 1997) have, according to Kazdin andWeisz (1998), established the individual treatment as ‘‘probably efficacious’’ usingAmerican Psychological Association Task Force (1995)/Chambless and Hollon(1998) criteria. In the present study, anxiety-disordered children in both an individ-ual treatment and a group treatment demonstrated meaningful rates of posttreat-ment improvement—73% of children in the ICBT and 50% in the GCBT did notmeet criteria for their primary anxiety disorder (compared to 8% in the WL condi-

Group and Individual Cognitive-Behavioral Treatments 271
Table II. (Continued)
Condition
Individual Group
Measure Posttest Follow-up Posttest Follow-up
Parent- and teacher-reportSTAIC-P
Mother-reportM 40.50 35.79 43.07 41.00SD 11.20 8.85 11.63 10.48
Father-reportM 36.66 38.24 40.26 41.14SD 6.79 10.36 14.17 7.42
CQ-PMother-report
M 4.93 5.12 4.87 5.24SD 1.45 1.17 1.28 1.00
Father-reportM 4.86 4.86 5.24 4.90SD 1.24 1.14 1.32 1.05
PRSC-Sociala
M 19.24 19.27 22.03 20.24SD 4.61 4.47 9.18 5.50
FM-Pa
M 45.78 47.17 49.23 49.77SD 10.89 10.71 15.32 14.05
SAS-P-Currenta
M 2.59 2.36 1.93 2.15SD 1.58 1.47 1.43 .77
CBCL-Internalizing TMother-report
M 56.91 52.18 65.22 64.22SD 13.26 11.12 11.32 10.02
Father-reportM 47.23 48.48 55.95 55.83SD 9.32 10.66 9.58 6.83
TRF Internalizing TM 54.09 54.27 61.44 57.89SD 9.98 5.90 11.74 10.53
Note: STAIC, State-Trait Anxiety Inventory for Children; RCMAS, Revised Children’s Manifest AnxietyScale; SPPC-Social, Self-Perception Profile for Children-Social Acceptance subscale; LS, LonelinessScale; FM-C, Friendship Measure-Child; SASCR-Total, Social Anxiety Scale for Children-Revised-Total of subscales; CQ-C, Coping Questionnaire-Child; CDI, Children’s Depression Inventory; STAIC-P, State-Trait Anxiety Inventory for Children-Parent version; CQ-P, Coping Questionnaire, PRSC-Social, Parent’s Rating Scale of Child’s Competence; FM-P, Friendship Measure-Parent; SAS-P, SocialActivities Scale-Current Number of Social Activities; CBCL, Child-Behavior Checklist; TRF, TeacherReport Form.a Mother- and father-reports were averaged on these measures.
tion). Furthermore, 64% of children in the ICBT and 50% in the GCBT (none ofthe WL children) did not meet criteria at posttreatment for any of the three anxietydisorders (GAD, SAD, SP) targeted by the treatment protocol.
Significant improvements were found in multiple child- and parent-reports ofanxious distress and coping for both ICBT and GCBT relative to the WL controlcondition. Child-reports of trait anxiety and coping demonstrated both the ICBT and
272 Flannery-Schroeder and Kendall
GCBT to effect significant improvements from pre- to posttreatment. Additionally,father-reports of anxious symptomatology and parent-reports of coping evidencedsignificant treatment gains for children in both treatment conditions. Therefore, itappears that children and parents generally agree in their perceptions of improve-ments in anxious distress and coping as a function of the format of therapy (e.g.,individual, group). Children, however, perceived improvement in state anxiety onlywhen treated in the ICBT. However, this may be a byproduct of a floor effectproduced by significantly lower scores on child-reported state anxiety in the GCBT(versus ICBT and WL). The pretreatment differences on the STAIC-A-State andSTAIC-A-Trait occurred despite random assignment to condition. As was notedfor state anxiety, pretreatment scores on trait anxiety were significantly lower for theGCBT than for the ICBT and the WL (ICBT and WL means were not significantlydifferent). Some caution is warranted in the interpretation of these results giventhe pretreatment differences on these measures. An alternative hypothesis to atreatment-related reduction in anxious symptomatology is regression to the mean.However, evidence exists which casts some doubt upon the likelihood of this inter-pretation. If regression to the mean were a viable explanation, one would expectto find significant reductions in both the ICBT and WL conditions across treat-ment—this did not occur in the present study for either trait or state anxiety.5
The lack of pre- to posttreatment improvement in social functioning (e.g.,social anxiety, friendships, loneliness, social activities) was reflected in both child-and parent-reports. It had been hypothesized that children in the GCBT wouldevidence significantly more improvement on these variables than the ICBT, andboth treatment conditions were expected to effect significantly more improvementthan the WL condition. The absence of significant effects may be due to severalreasons. First, it may be that treatment, as applied herein, does not impact onchildren’s social functioning. Although children in the GCBT did interact with theirpeers as dictated by the treatment manual (e.g., group feedback, group role plays),their social skills were not a target of treatment. Social functioning was a target intreatment only when children’s fears involved social anxiety. Second, it may be thatthe children in this sample did not have significant social concerns. This hypothesisis buttressed by the fact that only 5 children in the entire sample (3 in the GCBT,1 in the ICBT, 1 in the WL condition) were diagnosed with social phobia as aprimary disorder. Thus, it may be that the absence of gain relates more to theabsence of this type of problem at the outset. Children with difficulties in socialfunctioning might show improvements in functioning in either the ICBT or GCBTcondition or both, but only when the sample includes the targeted problems (Beidel,1994). Third, it may be that the measures used to assess changes in social functioningare either lacking in sensitivity or may suffer from other threats to their reliabilityor validity. This possibility is unlikely, however, because previous studies conducted
5The mean scores for both trait and state anxiety in the ICBT and WL conditions parallel those meanpretreatment scores found in similar studies of anxious children (e.g., Kendall, 1994; Kendall et al.,1997). Thus, it appears that the mean pretreatment scores for the GCBT condition are somewhat lowfor an anxious sample. This difference was likely to have occurred due to small within-condition samplesizes and despite random assignment to condition.
Group and Individual Cognitive-Behavioral Treatments 273
on the psychometric properties of these measures suggest adequate reliabilityand validity.
Mother- and teacher-reports of children’s internalized distress did not showtreatment effects. Mother-reports approached significance (p � .028), but wereinsufficient to exceed the adjusted probability requirements imposed by the Bonfer-roni correction. For teachers, the mean Internalizing T-scores for each condition(ICBT, GCBT, WL) fell within the normative range (�65) both before and aftertreatment. This reflects that teachers did not view the children as significantlyimpaired by anxious distress in the classroom. Although teachers, unlike parentsand children, were blind to condition (ICBT, GCBT, WL), and expectations oftreatment gains could account for treatment effects, it may also be that teachershave more difficulty in the identification of children’s internalized distress. It standsto reason that parents and children themselves would be more valid reporters.The likelihood of this explanation is underscored by the teacher-reported TRFInternalizing T-scores falling within the normative range at the pretreatment as-sessment.
Effect size calculations ( f ) on simple main effects within treatment are quitelarge and demonstrated some fluctuation among dependent measures, but, on aver-age, suggest that the treatment gains in the ICBT and GCBT are comparable.Caution is advised, however, in the interpretation of these results, as the comparisonof group and individual formats is to be considered preliminary. It is likely thatthe present study had insufficient power to detect small effects. Average effect sizef was 1.77 within the ICBT and 1.55 within the GCBT. Effect sizes calculatedbetween treatments average 1.70 for ICBT vs. WL, 1.74 for GCBT vs. WL, and.45 for ICBT vs. GCBT (using the formula [M1�M2]/ SD [controls]; Weisz, Weiss,Alicke, & Klotz, 1987; Weisz, Weiss, & Donenberg, 1992). These effect sizes exceedthose typically found in meta-analyses of child treatment outcome studies. Averageeffect sizes found in meta-analyses tend to hover around .70–.80 for treatmentversus no treatment (e.g., Casey & Berman, 1985; Kazdin, 1993, 1996; Kazdin, Bass,Ayers, & Rodgers, 1990; Weisz et al., 1987, 1992; Weisz, Weiss, Han, Granger, &Morton, 1995). According to Cohen (1977), the effect sizes found in the presentstudy are well above the threshold of .80 for a ‘‘large’’ effect and indicate thattreated children were functioning better than over 90% of wait-list children atposttreatment. However, while power analyses ensured adequate sample size todetect treatment versus wait-list effects, the present study may have had insufficientpower to discern small to moderate between-treatment differences (ICBT versusGCBT).
Analyses of the intent-to-treat sample reflect somewhat more modest indices oftreatment effects, yet the effects are noteworthy nonetheless. Analyses of diagnosticstatus reveal that 50% of participants in the ICBT and 46% in the GCBT did notmeet criteria for their primary disorder at posttreatment. Forty-three percent ofthe ICBT and 46% of the GCBT did not meet criteria for any anxiety disordertargeted by the treatment protocol (i.e., SAD, GAD, SP) at posttreatment. Severaldependent measures illustrated change across treatment (no change was foundacross the wait-list period), and all revealed both the ICBT and GCBT to be roughlycomparable in treatment effects. Effect sizes within treatment conditions were again

274 Flannery-Schroeder and Kendall
quite large (range � 0.91–1.69). Traditional outcome analyses typically include onlyparticipants who complete treatment, resulting in the least conservative estimate ofthe efficacy of outcome. Analyses of intent-to-treat samples, which are considerablymore conservative, provide indices not only of efficacy, but also effectiveness ofthe treatment. Results of both sets of analyses suggest that the present treatmentis both efficacious and effective in reducing anxious distress in children.
Normative comparisons (Kendall & Grove, 1988) reflected clinically significantimprovement defined as changes on dependent measures that return deviant partici-pants to within nondeviant limits. A significantly higher proportion of CBCL Inter-nalizing T-scores were returned to within the normative range (�65) for both treatedconditions as compared to the WL condition. However, the TRF Internalizing T-scores failed to reflect differential change among conditions. Given that meanteacher ratings of participants in all conditions (ICBT, GCBT, WL) fell within thenormative range at both pre- and posttreatment, this nonsignificant result is likelydue to a floor effect. Very few participants received TRF Internalizing T-scores of�65 at the start of treatment.
Treatment gains were evident across measures, were associated with neithertherapist nor therapist experience, and were maintained at a 3-month follow-upassessment. The rate of attrition was low (18% for the entire sample, 8 of 45participants). The rate of attrition during treatment was 31% (4 of 17 children) inthe ICBT and 0% (0 of 12 children) in the GCBT. These results concur with areview of individual and group treatments in which group treatments were foundto have fewer dropouts (Toseland & Siporin, 1986). Given comparable treatmentoutcomes, group treatment may be preferred when factors are present which corre-late with treatment attrition.
Results suggest that children in the ICBT are better at recalling what theylearned during treatment (as measured by the RCQ) than children in the GCBT.This finding is not surprising given the reductions in individual attention that arenecessitated by the group format. Although group sessions were one and one-halftimes as long as individual sessions (90 versus 50–60 min), children in the groupreceived less one-on-one instruction and attention. Time and depth apportioned tocoverage of instructional material may have been compromised by factors associatedwith groups (e.g., social distractions in the group, increased time necessary to ensurethe understanding of each group member).
Although the present study contributes to an understanding of the treatmentof anxiety disorders in childhood, it is not without limitations. As previously noted,while the power calculations reported herein are sufficient to detect differencescomparing an active treatment to a wait-list control, it is possible that there wasinsufficient power to detect differences between the two active treatment conditions(ICBT and GCBT). The present study demonstrates better the lack of sizable (i.e.,large effect size) differences between the group and individual treatment conditionsrather than the absence of any outcome differences (i.e., small or moderate effectsizes). Future research with larger sample sizes is needed to explore further thepotential for nonsignificant differences between the active treatments. Additionally,the present wait-list period was one half the length of the treatment. Several studiessuggest that anxiety disorders do not go away with time (e.g., Cantwell & Baker,

Group and Individual Cognitive-Behavioral Treatments 275
1989; Feehan et al., 1993); therefore, change without treatment (i.e., over a wait-list period) is unlikely. Furthermore, there are ethical considerations (i.e., the with-holding of treatment from clinic cases) that drive decisions about lengths of wait-list periods. Although the present study is limited by a short follow-up period (3months), research using similar samples and the same treatment protocol suggestmaintenance of gains from 1 to 5 years (e.g., Barrett et al., 1996; Kendall, 1994;Kendall et al., 1997; Kendall & Southam-Gerow, 1996).
Additional research is needed to examine the relative utility of treatmentcomponents (e.g., cognitive training, in vivo exposures) as well as the differentialutility of alternative treatments. Benefits of the latter are twofold: (a) differentialtreatment gains may be explored and (b) the effects of attention and therapeuticrelationship would be held constant across conditions. Once the utility of giveninterventions is established, researchers might systematically vary treatment factors(e.g., treatment duration, number of in vivo exposures, treatment format) to effectthe most beneficial outcomes (Kazdin, 1996). Although the present study was limitedto the group treatment of children with anxiety disorders, other childhood disorders(e.g., depression) might also be effectively treated with a cognitive-behavioral grouptherapy (Clarke et al., 1992). Group process variables (e.g., group cohesion), al-though they present possible confounds, are infrequently operationalized and shouldbe examined in terms of their independent effects.
REFERENCES
Achenbach, T. M. (1991a). Manual for the Child Behavior Checklist/4-18 and 1991 Profile. Burlington,VT: Department of Psychiatry, University of Vermont.
Achenbach, T. M. (1991b). Manual for the Teacher’s Report Form and 1991 Profile. Burlington, VT:Department of Psychiatry, University of Vermont.
Achenbach, T. M., & Edelbrock, C. S. (1981). Behavioral problems and competencies reported byparents of normal and disturbed children aged four through sixteen. Monographs of the Societyfor Research in Child Development, 46 (Serial No. 188).
Albano, A. M., Marten, P. A., Holt, C. S., Heimberg, R. G., & Barlow, D. H. (1995). Cognitive-behavioralgroup treatment for social phobia in adolescents: A preliminary study. Journal of Nervous andMental Disease, 183, 649–656.
American Psychological Association Task Force on Promotion and Dissemination of PsychologicalProcedures (1995). Training in and dissemination of empirically-validated psychological treatments:Report and recommendations. Clinical Psychologist, 48, 3–24.
Asher, S. R., Hymel, S., & Renshaw, P. D. (1984). Loneliness in children. Child Development, 55, 1456–1464.
Barrett, P., Dadds, M., & Rapee, R. (1996). Family treatment of child anxiety: A controlled trial. Journalof Consulting and Clinical Psychology, 64, 333–342.
Beidel, D. C. (1994). Anxiety disorders. In M. Hersen & S. M. Turner (Eds.), Diagnostic interviewing(pp. 55–77). New York: Plenum Press.
Beidel, D. C., Christ, M. G., & Long, P. J. (1991). Somatic complaints in anxious children. Journal ofAbnormal Child Psychology, 19, 659–670.
Benjamin, R. S., Costello, E. J., & Warren, M. (1990). Anxiety disorders in a pediatric sample. Journalof Anxiety Disorders, 4, 293–316.
Bernstein, G. A., & Borchardt, C. M. (1991). Anxiety disorders of childhood and adolescents: A criticalreview. Journal of the American Academy of Child and Adolescent Psychiatry, 30, 519–532.
Bierman, K. L., & McCauley, E. (1987). Children’s descriptions of their peer interactions: Usefulinformation for clinical child assessment. Journal of Clinical Child Psychology, 16, 9–18.
Brady, E. U., & Kendall, P. C. (1992). Comorbidity of anxiety and depression in children and adolescents.Psychological Bulletin, 111, 244–255.

276 Flannery-Schroeder and Kendall
Cantwell, D. P., & Baker, L. (1989). Stability and natural history of DSM-III childhood diagnoses.Journal of the American Academy of Child and Adolescent Psychiatry, 28, 691–700.
Casey, R. J., & Berman, J. S. (1985). The outcome of psychotherapy with children. Psychological Bulletin,98, 388–400.
Castaneda, A., McCandless, B. R., & Palermo, D. S. (1956). The Children’s Form of the ManifestAnxiety Scale. Child Development, 27, 317–326.
Chambless, D., & Hollon, S. (1998). Defining empirically supported therapies. Journal of Consultingand Clinical Psychology, 66, 7–18.
Clarke, G., Hops, H., Lewinsohn, P. M., Andrews, J., Seeley, J. R., & Williams, J. (1992). Cognitive-behavioral group treatment of adolescent depression: Prediction of outcome. Behavior Therapy,23, 341–354.
Cohen, J. (1977). Statistical power analysis for behavioral sciences. New York: Academic Press.Connors, C. K. (1973). Rating scales for use in drug studies with children. Psychopharmacology bulletin:
Pharmacotherapy with children. Washington, DC: U.S. Government Printing Office.Eisen, A. R., & Silverman, W. K. (1993). Should I relax or change my thoughts? A preliminary examina-
tion of cognitive therapy, relaxation training, and their combination with overanxious children.Journal of Cognitive Psychotherapy, 7, 265–279.
Feehan, M., McGee, R., & Williams, S. M. (1993). Mental health disorders from age 15 to age 18 years.Journal of the American Academy of Child and Adolescent Psychiary, 32, 1118–1126.
Fergusson, D. M., Horwood, L. J., & Lynskey, M. T. (1993). Prevalence and comorbidity of DSM-III-R diagnoses in a birth cohort of 15 year olds. Journal of the American Academy of Child andAdolescent Psychiatry, 32, 1127–1134.
Finch, A. J., Saylor, C. F., & Edwards, G. (1985). Children’s Depression Inventory: Sex and grade normsfor normal children. Journal of Consulting and Clinical Psychology, 53, 424–425.
Flannery-Schroeder, E. C., & Kendall, P. C. (1996). Cognitive-behavioral therapy for anxious children:Therapist manual for group treatment. Ardmore, PA: Workbook Publishing.
Harter, S. (1982). The Perceived Competence Scale for Children. Child Development, 53, 87–97.Harter, S. (1985). Manual for the Self-Perception Profile for Children. Denver, CO: University of Denver.Hartup, W. W. (1983). Peer relations. In P. Mussen (Ed.), Handbook of child psychology (pp. 103–196).
New York: Wiley.Heimberg, R. G., Dodge, C. S., Hope, D. A., Kennedy, C. R., Zollo, L. J., & Becker, R. E. (1990).
Cognitive behavioral group treatment for social phobia: Comparison with a credible placebo control.Cognitive Therapy and Research, 14, 1–23.
Howard, B., & Kendall, P. C. (1996). Cognitive-behavioral family therapy for anxiety-disordered children:A multiple baseline evaluation. Cognitive Therapy and Research, 20, 423–443.
Kane, M. T., & Kendall, P. C. (1989). Anxiety disorders in children: A multiple-baseline evaluation ofa cognitive-behavioral treatment. Behavior Therapy, 20, 499–508.
Kashani, J. H., & Orvaschel, H. (1990). A community study of anxiety in children and adolescents.American Journal of Psychiatry, 147, 313–318.
Kazdin, A. E. (1993). Psychotherapy for children and adolescents: Current progress and future researchdirections. American Psychologist, 48, 644–657.
Kazdin, A. E. (1996). Developing effective treatments for children and adolescents. In E. D. Hibbs &P. S. Jensen (Eds.), Psychosocial treatments for child and adolescent: Empirically based strategiesfor clinical practice (pp. 9–18). Washington, DC: American Psychological Association.
Kazdin, A. E., Bass, D., Ayers, W. A., & Rodgers, A. (1990). Empirical and clinical focus of child andadolescent psychotherapy research. Journal of Consulting and Clinical Psychology, 58, 729–740.
Kazdin, A. E., French, H., Unis, A., Esveldt-Dawson, K., & Sherick, R. (1983). Hopelessness, depression,and suicidal intent among psychiatrically disturbed children. Journal of Consulting and ClinicalPsychology, 51, 504–510.
Kazdin, A. E., & Weisz, J. (1998). Treating psychological problems of youth: Status of empiricallysupported treatments. Journal of Consulting and Clinical Psychology, 66, 19–36.
Kendall, P. C. (1990). Coping cat workbook. Ardmore: PA: Workbook Publishing.Kendall, P. C. (1994). Treating anxiety disorders in children: Results of a randomized clinical trial.
Journal of Consulting and Clinical Psychology, 62, 100–110.Kendall, P. C., Flannery-Schroeder, E., Panichelli-Mindel, S., Southam-Gerow, M., Henin, A., & Warman,
M. (1997). Therapy for youths with anxiety disorders: A second randomized clinical trial. Journalof Consulting and Clinical Psychology, 65, 366–380.
Kendall, P. C., & Grove, W. (1988). Normative comparisons in therapy outcome. Behavioral Assessment,10, 147–158.
Kendall, P. C., Kane, M., Howard, B., & Siqueland, L. (1990). Cognitive-behavioral therapy for anxious
Group and Individual Cognitive-Behavioral Treatments 277
children: Treatment manual. Available from the author, Temple University, Department of Psychol-ogy, Philadelphia, PA 19122.
Kendall, P. C., & Marrs-Garcia, A. (n.d.). Development and psychometric properties of the CopingQuestionnaire. Submitted for publication.
Kendall, P. C., & Southam-Gerow, M. A. (1996). Long term follow-up of a cognitive-behavioral therapyfor anxious youth. Journal of Consulting and Clinical Psychology, 64, 724–730.
King, N. J., & Ollendick, T. H. (1989). Children’s anxiety and phobic disorders in school settings:Classification, assessment, and intervention issues. Review of Educational Research, 59, 431–470.
Klein, R. G., & Last, C. G. (1989). Anxiety disorders in children. Newbury Park, CA: Sage.Kovacs, M. (1981). Rating scales to assess depression in school aged children. Acta Paedopsychiatrica,
46, 305–315.La Greca, A. M., Dandes, S. K., Wick, P., Shaw, K., & Stone, W. L. (1988). Development of the Social
Anxiety Scale for Children: Reliability and concurrent validity. Journal of Clinical Child Psychology,17, 84–91.
La Greca, A. M., & Stone, W. (1993). Social Anxiety Scale for Children-Revised: Factor structure andconcurrent validity. Journal of Clinical Child Psychology, 22, 17–27.
Last, C. G., Hersen, M., Kazdin, A. E., Finkelstein, R., & Strauss, C. C. (1987). Comparison of DSM-III separation anxiety and overanxious disorders: Demographic characteristics and patterns ofcomorbidity. Journal of the American Academy of Child and Adolescent Psychiatry, 26, 527–531.
Mansdorf, I. J., & Lukens, E. (1987). Cognitive-behavioral psychotherapy for separation anxious childrenexhibiting school phobia. Journal of the American Academy of Child and Adolescent Psychiatry,26, 222–225.
Myers, J. K., Weissman, M. M., Tischler, G. L., Holzer, C. H., Leaf, P. J., Orvaschel, H., Anthony, J.,Boyd, J. H., Burke, J. D., Kramer, M., & Stoltzman, R. (1984). Six-month prevalence of psychiatricdisorders in three communities. Archives of General Psychiatry, 41, 959–967.
Ollendick, T. H., Hagopian, L. P., & Huntzinger, R. M. (1991). Cognitive-behavioral therapy withnighttime fearful children. Journal of Behavior Therapy and Experimental Psychiatry, 22, 113–121.
Quay, H. C., & Peterson, D. R. (1983). Interim manual for the Revised Behavior Problem Checklist.Coral Gables, FL: University of Miami, Applied Social Sciences.
Renneberg, B., Goldstein, A. J., Phillips, D., & Chambless, D. L. (1990). Intensive behavioral grouptreatment of avoidant personality disorder. Behavior Therapy, 21, 363–377.
Reynolds, C. R., & Richmond, B. O. (1978). What I Think and Feel: A revised measure of Children’sManifest Anxiety. Journal of School Psychology, 24, 313–319.
Reynolds, C. R., & Richmond, B. O. (1985). Revised Children’s Manifest Anxiety Scale (RCMAS)manual. Los Angeles, CA: Western Psychological Services.
Rubin, K. H. (1985). Socially withdrawn children: An ‘‘at risk’’ population? In B. Schneider, K. H.Rubin, & J. Ledingham (Eds.), Children’s peer relations: Issues in assessment and intervention (pp.125–140). New York: Springer-Verlag.
Sarason, S. B., Davidson, K. S., Lighthall, F. F., Waite, R. R., & Ruebush, B. K. (1960). Anxiety inelementary school children. New York: Wiley.
Satterfield, J. M. (1994). Integrating group dynamics and cognitive-behavioral groups: A hybrid model.Clinical Psychology: Science and Practice, 1, 185–196.
Saylor, C. F., Finch, A., Spirito, A., & Bennett, B. (1984). The Children’s Depression Inventory: Asystematic evaluation of psychometric properties. Journal of Consulting and Clinical Psychology,52, 955–967.
Shaffer, C. S., Shapiro, J., Sank, L. I., & Coghlan, D. J. (1981). Positive changes in depression, anxiety,and assertion following individual and group cognitive behavior therapy intervention. CognitiveTherapy and Research. 5, 149–157.
Silverman, W. K., & Albano, A. M. (1996). The Anxiety Disorders Interview Schedule for DSM-IV,child and parent versions. Albany, NY: Graywind.
Spielberger, C. (1973). Manual for the State-Trait Anxiety Inventory for Children. Palo Alto, CA: Con-sulting Psychologists Press.
Strain, P. S., & Kerr, M. M. (1981). Modifying children’s social withdrawal: Issues in assessment andclinical intervention. Progress in Behavior Modification, 11, 203–248.
Strauss, C. C. (1987). Modification of the trait portion of the State-Trait Anxiety Inventory for Children-parent form. Available from the author. Pittsburgh, PA: Western Psychiatric Institute and Clinic.
Strauss, C. C. (1988). Behavioral assessment and treatment of overanxious disorder in children andadolescents. Behavior Modification, 12, 234–251.
Strauss, C. C., Forehand, R., Smith, K., & Frame, C. L. (1986). The association between social withdrawaland internalizing problems of children. Journal of Abnormal Child Psychology, 14, 525–535.

278 Flannery-Schroeder and Kendall
Strauss, C. C., Lease, C., Last, C., & Francis, G. (1988). Overanxious disorder: An examination ofdevelopmental differences. Journal of Abnormal Child Psychology, 16, 433–443.
Toseland, R. W., & Siporin, M. (1986). When to recommend group treatment: A review of the clinicaland research literature. International Journal of Group Psychotherapy, 36, 171–201.
Weisz, J. R., Weiss, B., Alicke, M. D., & Klotz, M. L. (1987). Effectiveness of psychotherapy with childrenand adolescents: A meta-analysis for clinicians. Journal of Consulting and Clinical Psychology, 55,542–549.
Weisz, J. R., Weiss, B., & Donenberg, G. R. (1992). The lab versus the clinic: Effects of child andadolescent psychotherapy. American Psychologist, 47, 1578–1585.
Weisz, J. R., Weiss, B., Han, S. S., Granger, D. A., & Morton, T. (1995). Effects of psychotherapy withchildren and adolescents revisited: A meta-analysis of treatment outcome studies. PsychologicalBulletin, 117, 450–468.




















