Coal dust related lung diseases - WorkSafe QLD
63
Current and emerging occupational lung diseases Deborah H Yates Respiratory Physician St Vincent’s Hospital & Holdsworth House Medical Practice (HHMP), Darlinghurst, NSW 2010
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Coal dust related lung diseases - WorkSafe QLD
Current and emerging occupational lung diseases
Deborah H YatesRespiratory Physician
St Vincent’s Hospital & Holdsworth House Medical Practice (HHMP), Darlinghurst, NSW 2010
Introduction
• A bit of history• Old but new diseases• Some new disorders• Lessons for the
future….?
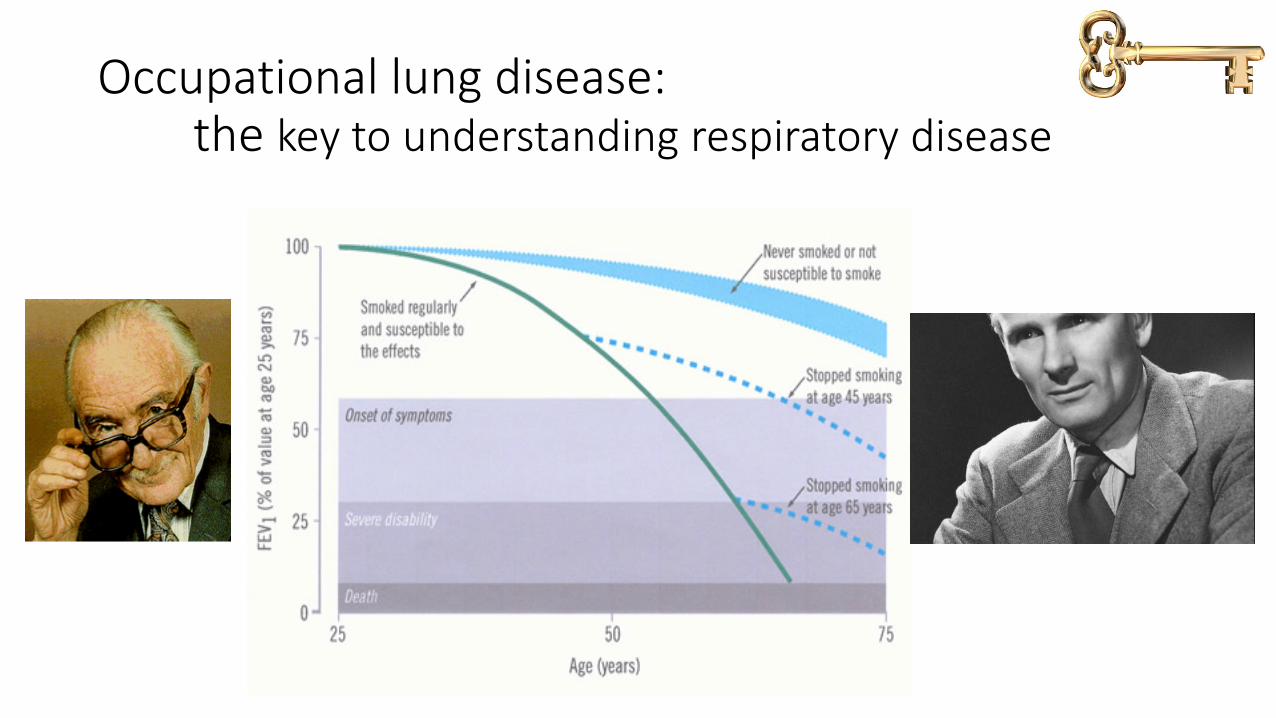
Occupational lung disease:the key to understanding respiratory disease
After WW II. Pneumoconiosis of Coal-MinersCM Fletcher. Director, Pneumoconiosis Research Unit, Medical Research CouncilBritish Medical Journal London Saturday May 29th 1948
• More than 17,000 men certified by the Silicosis Medical Board as suffering from pneumoconiosis 1932-48 & suspended from work underground
• By end of 1945, more than 12,000 men certified in South Wales
• 2/3 under age 50; 24% under 40• New cases being certified at 100/week in
1945• Two mines in South Wales where 1:3 workers
died from pneumoconiosis
• “A disastrous situation”
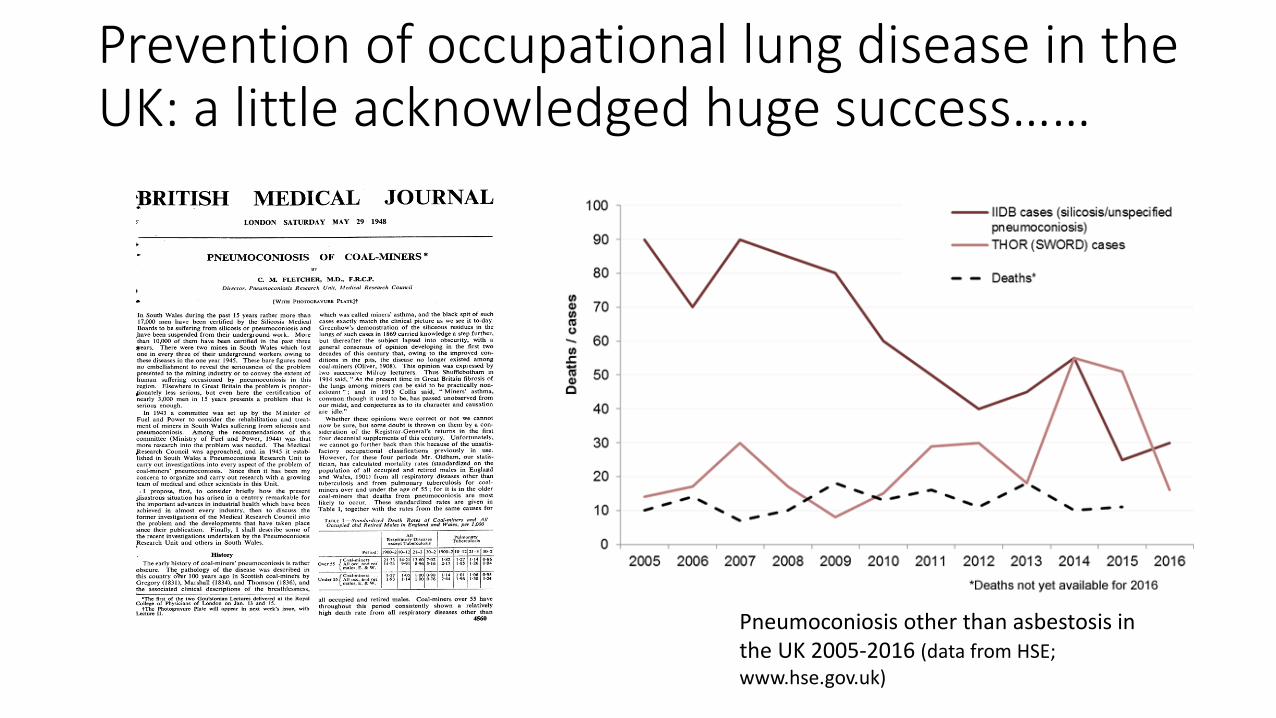
Prevention of occupational lung disease in the UK: a little acknowledged huge success……
Pneumoconiosis other than asbestosis in the UK 2005-2016 (data from HSE; www.hse.gov.uk)
The real reason that CWP no longer exists in England
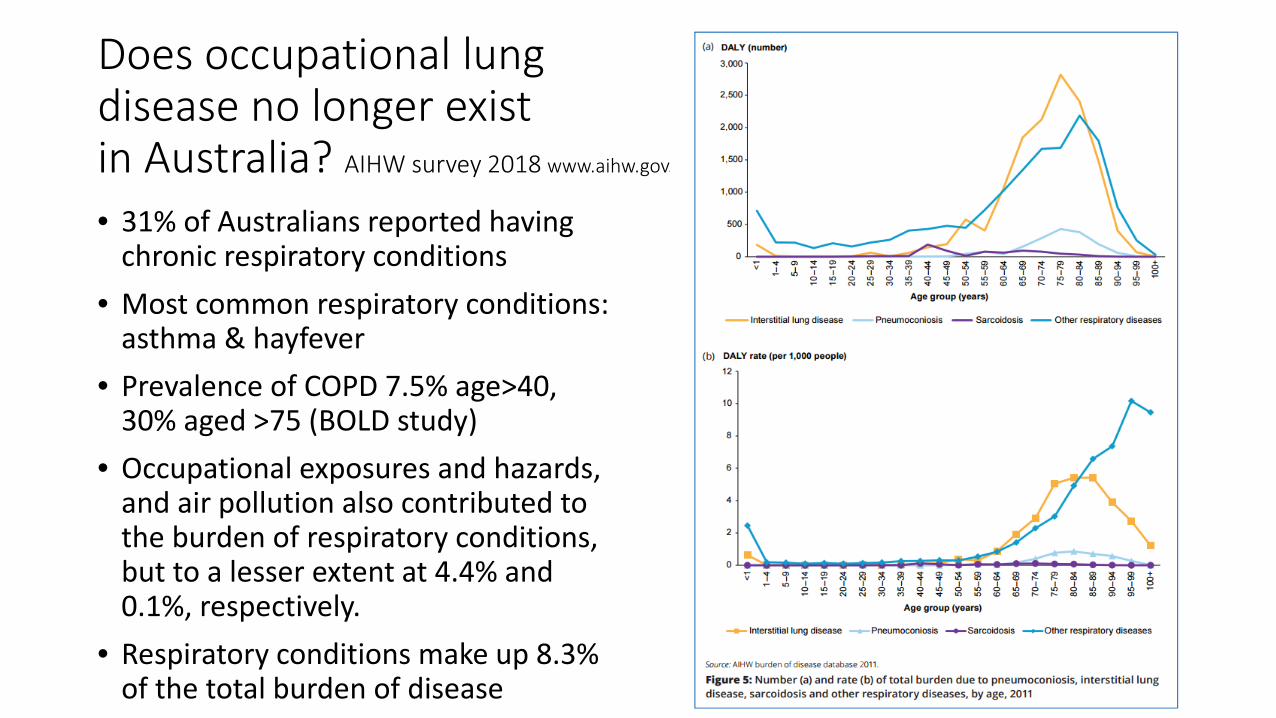
Does occupational lung disease no longer exist in Australia? AIHW survey 2018 www.aihw.gov.au
• 31% of Australians reported having chronic respiratory conditions
• Most common respiratory conditions: asthma & hayfever
• Prevalence of COPD 7.5% age>40, 30% aged >75 (BOLD study)
• Occupational exposures and hazards, and air pollution also contributed to the burden of respiratory conditions, but to a lesser extent at 4.4% and 0.1%, respectively.
• Respiratory conditions make up 8.3% of the total burden of disease
parliament.qld.gov.au/documents/committees/CWPSC/2016/CWPSC/regionalForums-Jun2017.pdf
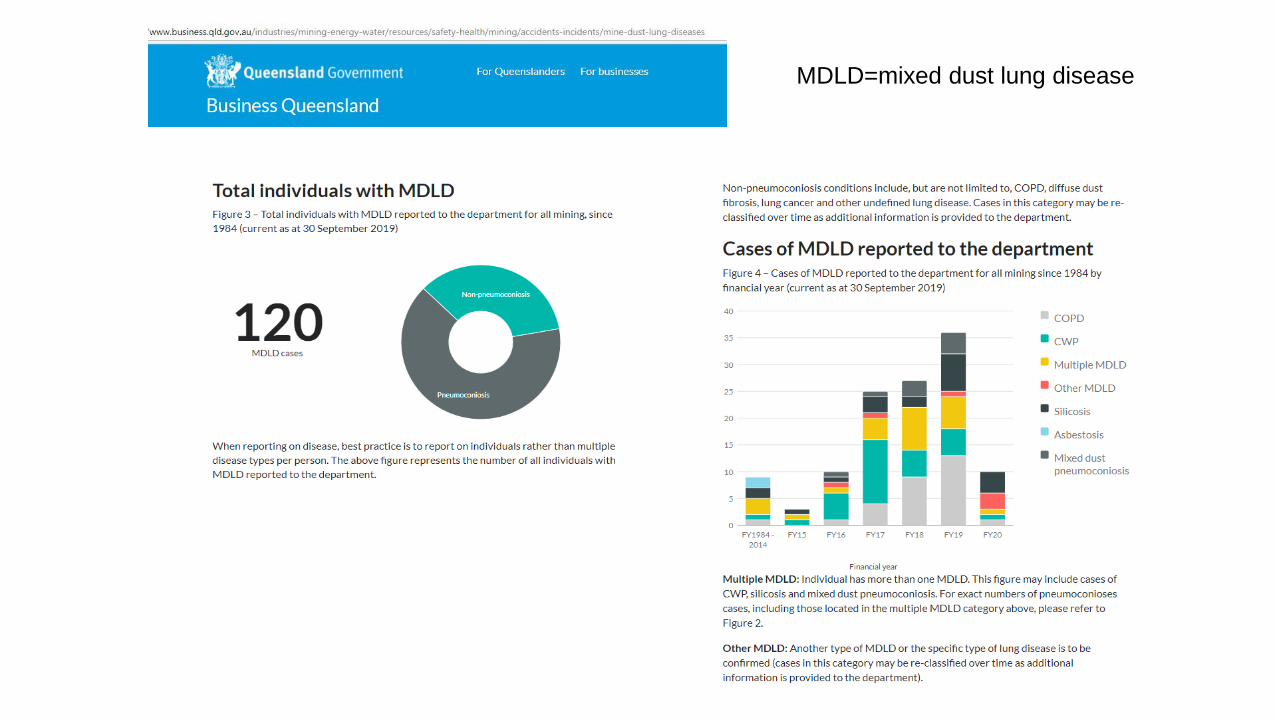
MDLD=mixed dust lung disease
www.mja.com.au/journal/.../coal-workers-pneumoconiosis-australian-perspective.
Thoracic Society of Australia and New Zealand

Recommendations for control of coal workers’ pneumoconiosis (CWP)
Thoracic Society of Australia and New Zealand
Zosky G, Hoy R, Silverstone E, Brims F,Miles S, Johnston A, Yates DH. Coal workers’ pneumoconiosis: an Australian perspective. Med J Aust 2016; 204 (11): 414-418.
• Goal: Eliminate CWP in Australia• 1. Exposure limits and monitoring protocols
• Standardise across Australia and harmonise to international recommendations
• 2. Screening• Develop and implement a national screening program for at-risk workers• Questionnaire, imaging, lung function testing
• 3. Medical workforce training• 4. A centralised occupational lung disease register
Non-existent diseases in a clinic in Sydney over the last two years• Silicosis & silica exposure• Coal workers pneumoconiosis• Diffuse dust fibrosis• Farmer’s lung • Hard metal lung disease• Scleroderma associated with silica exposure• Occupational asthma (glutaraldehyde, flour, isocyanates)• “Idiopathic pulmonary fibrosis” from wood dust exposure, asbestos,
silica
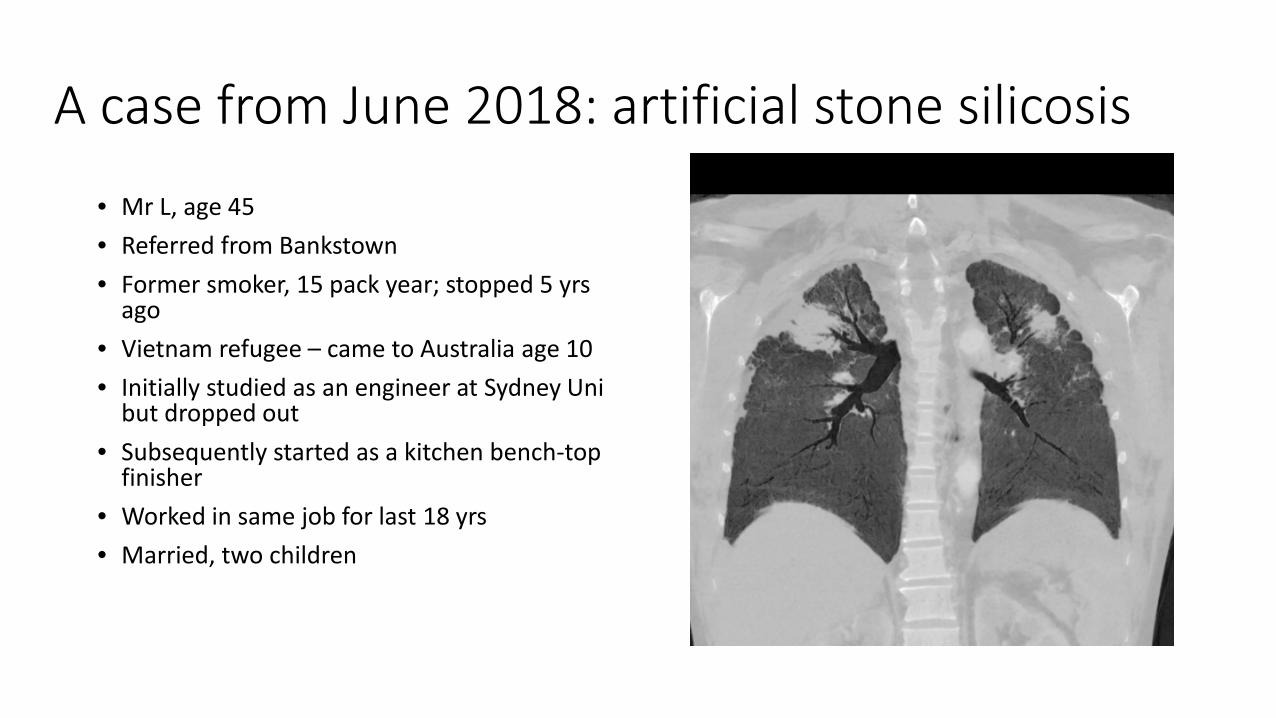
A case from June 2018: artificial stone silicosis
• Mr L, age 45• Referred from Bankstown• Former smoker, 15 pack year; stopped 5 yrs
ago• Vietnam refugee – came to Australia age 10• Initially studied as an engineer at Sydney Uni
but dropped out• Subsequently started as a kitchen bench-top
finisher• Worked in same job for last 18 yrs• Married, two children

Mr X continued
On examination:
• Raynaud’s phenomenon, arthropathy, progressive exertional dyspnoea
• Sclerodactyly, nail dystrophy, skin thickening to hands, forearms and anterior chest wall
• Bilateral upper zone crackles • Clinical features of pulmonary
hypertension
Positive ANA [titre >1/640], ENA, Scl-70
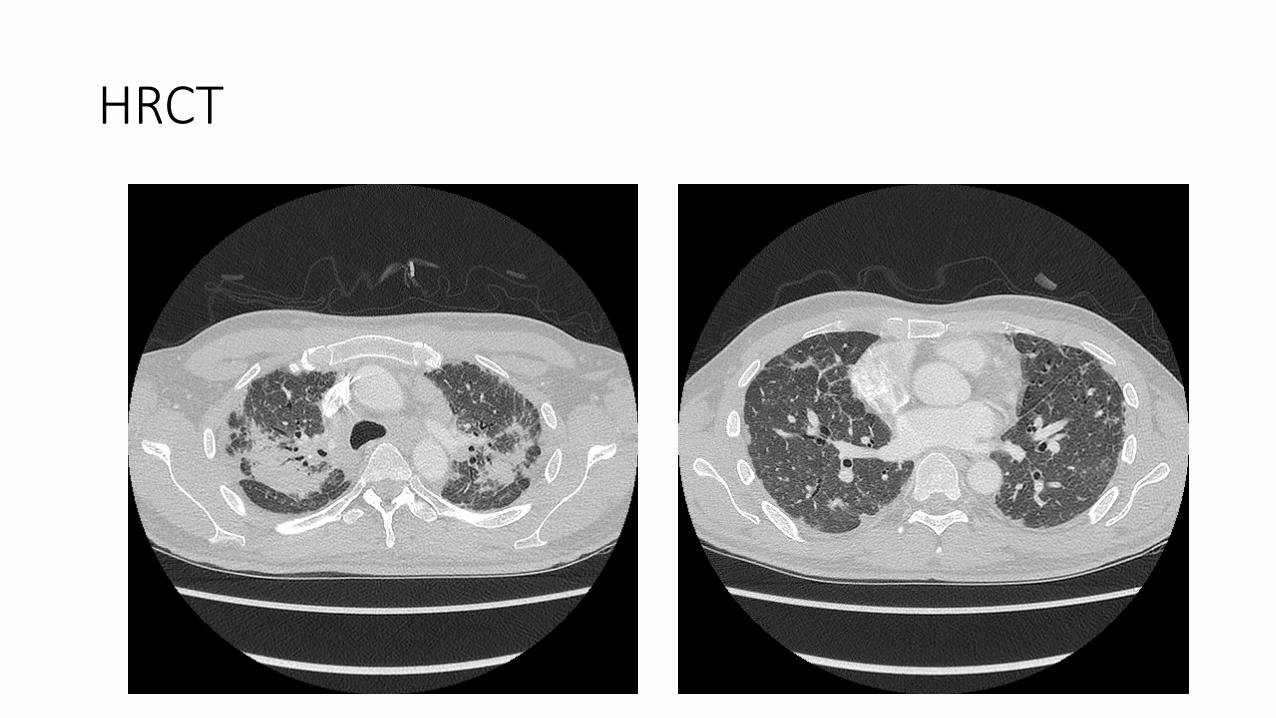
HRCT
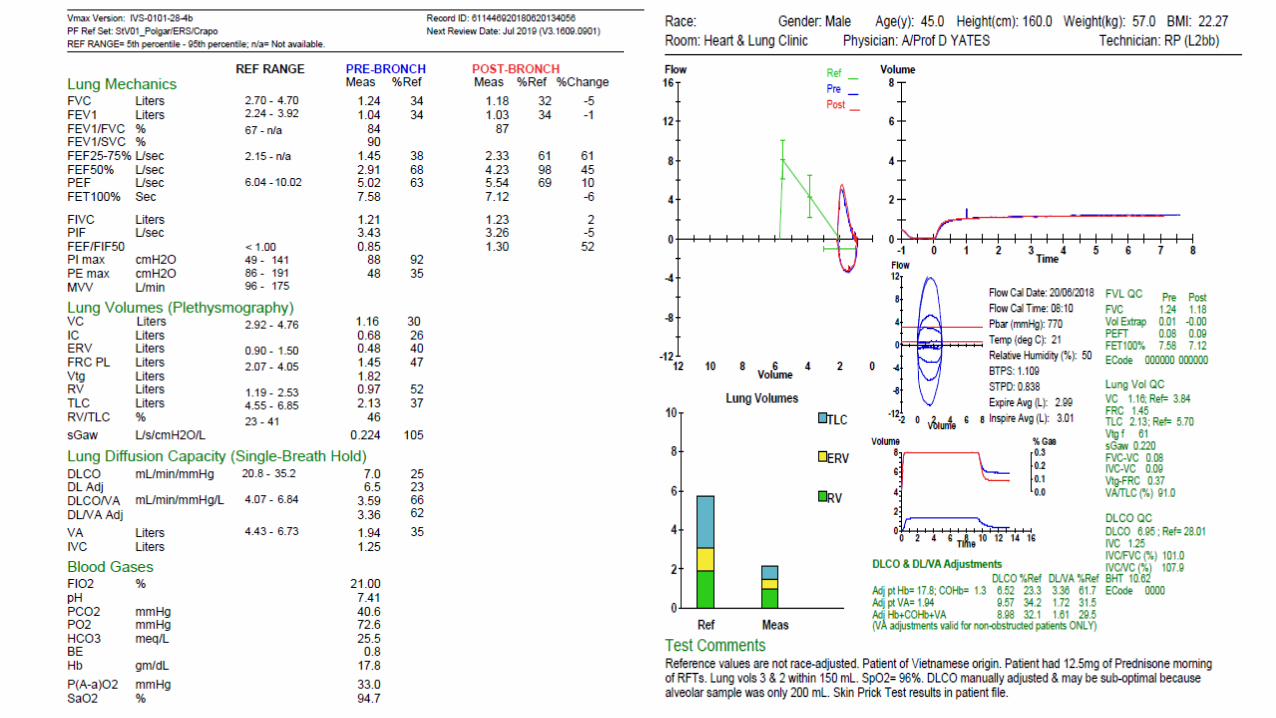
Lung function

Artificial stone silicosis
Artificial stone silicosis
• First described in Spain in 2009; 3 cases 47 cases between 2009-2012
• 3 suspected cases diagnosed in Cadiz and reported to the Andalusian Epidemiological Reporting system
• All marble workers in manufacture and home assembly of kitchen tops
• Active surveillance among symptomatic peers by epidemiology unit
• Median age 33 yrs; prevalence rate among exposed workers up to 20%; mainly small family businesses; median length of employment 11 years
• Poor dust control, lack of education regarding hazards, poor PPE
Artificial stone silicosis 2012
• Israeli National Lung Transplantation service noted a dramatic increase in cases referred for LTx (15 fold increase)
• 25 cases between 1997-2010• All exposed by dry cutting of artificial
stone for kitchen & bathroom fixtures• No dust suppression; no dust sampling;
long working hours (10-12 hrs daily)• Duration of exposure: 17-22 years• Typical CT changes; restrictive changes
on lung function• 86% had tissue samples• Of the 25, 10 were transplanted• 2 had PMF; none had silicoproteinosis; 3
died
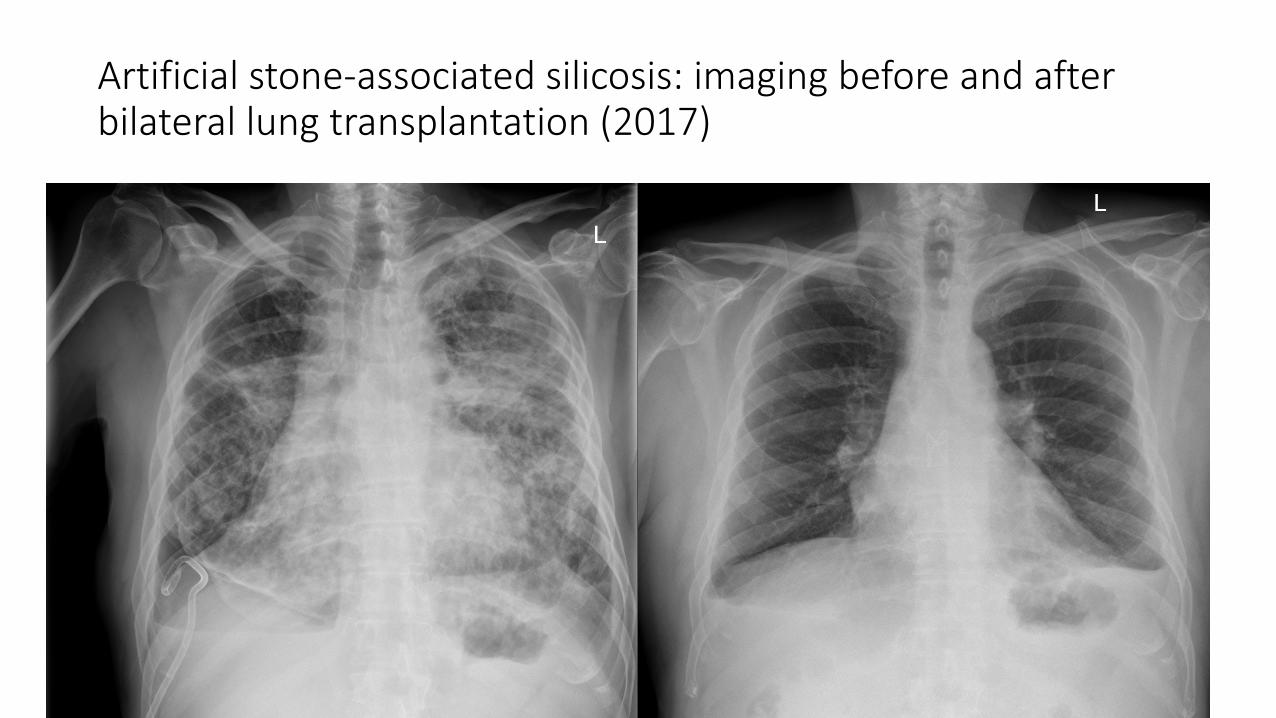
Artificial stone-associated silicosis: imaging before and after bilateral lung transplantation (2017)
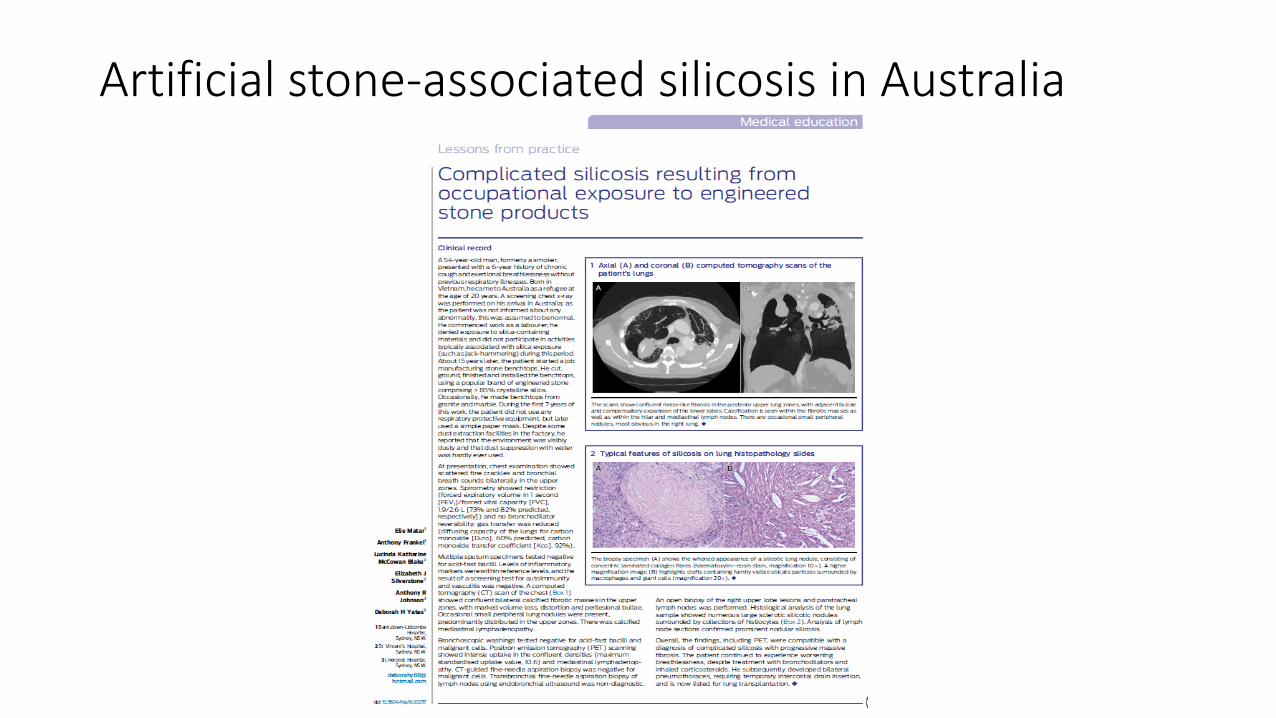
Artificial stone-associated silicosis in Australia
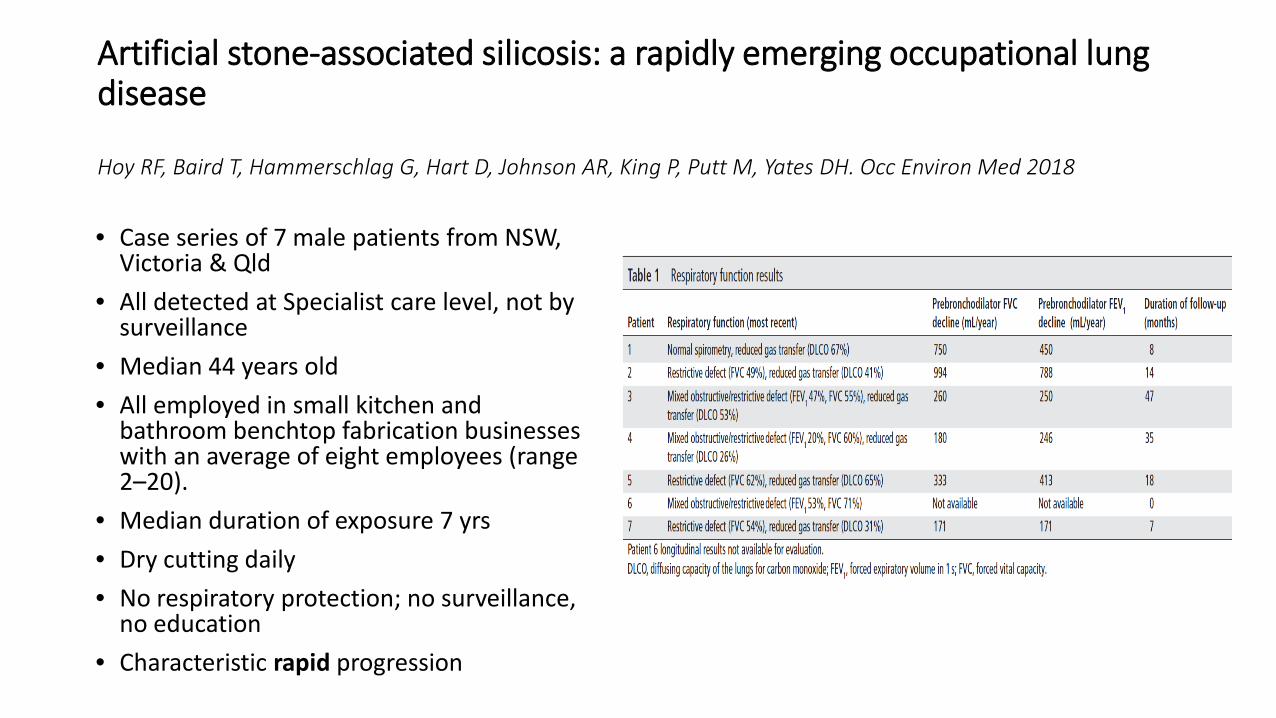
Artificial stone-associated silicosis: a rapidly emerging occupational lung disease
Hoy RF, Baird T, Hammerschlag G, Hart D, Johnson AR, King P, Putt M, Yates DH. Occ Environ Med 2018
• Case series of 7 male patients from NSW, Victoria & Qld
• All detected at Specialist care level, not by surveillance
• Median 44 years old• All employed in small kitchen and
bathroom benchtop fabrication businesses with an average of eight employees (range 2–20).
• Median duration of exposure 7 yrs• Dry cutting daily • No respiratory protection; no surveillance,
no education• Characteristic rapid progression
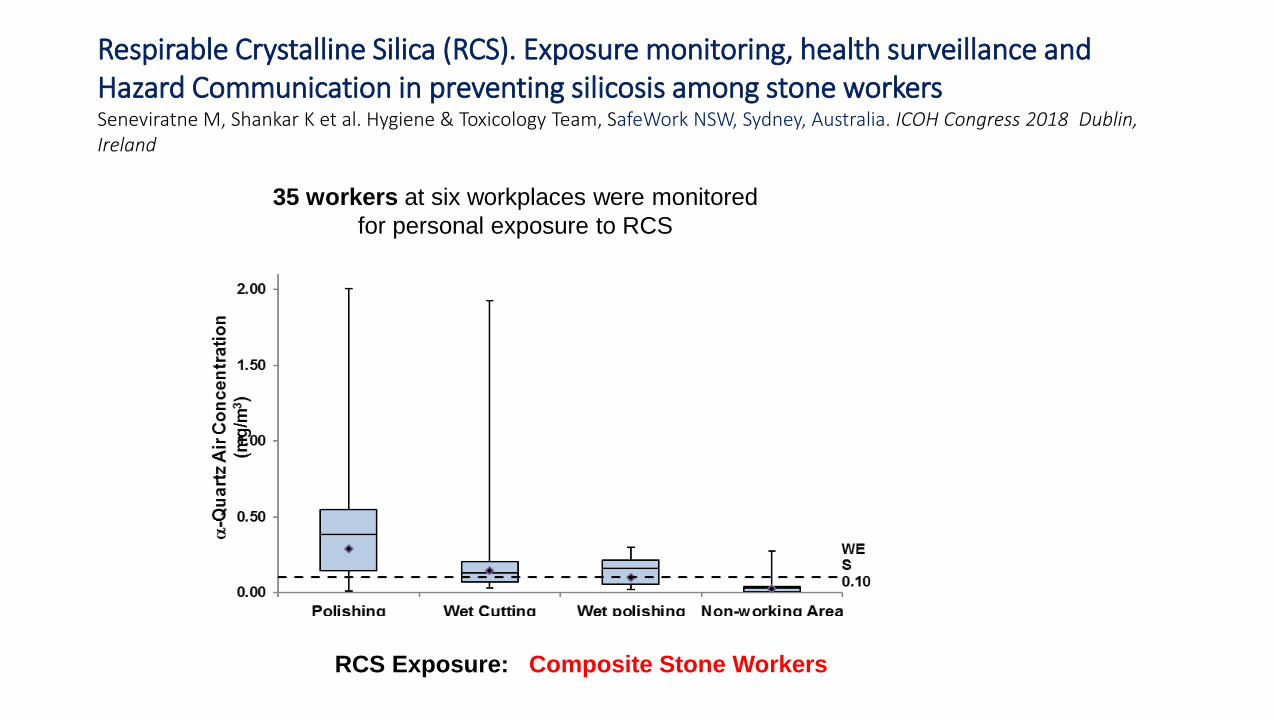
Respirable Crystalline Silica (RCS). Exposure monitoring, health surveillance and Hazard Communication in preventing silicosis among stone workersSeneviratne M, Shankar K et al. Hygiene & Toxicology Team, SafeWork NSW, Sydney, Australia. ICOH Congress 2018 Dublin, Ireland
35 workers at six workplaces were monitored for personal exposure to RCS
RCS Exposure: Composite Stone Workers
What about other disorders?
• Of the lung:• Lung cancer• Chronic obstructive pulmonary
disease (COPD)• Interstitial pulmonary fibrosis • Sarcoidosis• Obliterative bronchiolitis
Of the rest of the body:• Joint/skin disease• Kidney disease• Other cancers
Lung cancer
Sarcoidosis
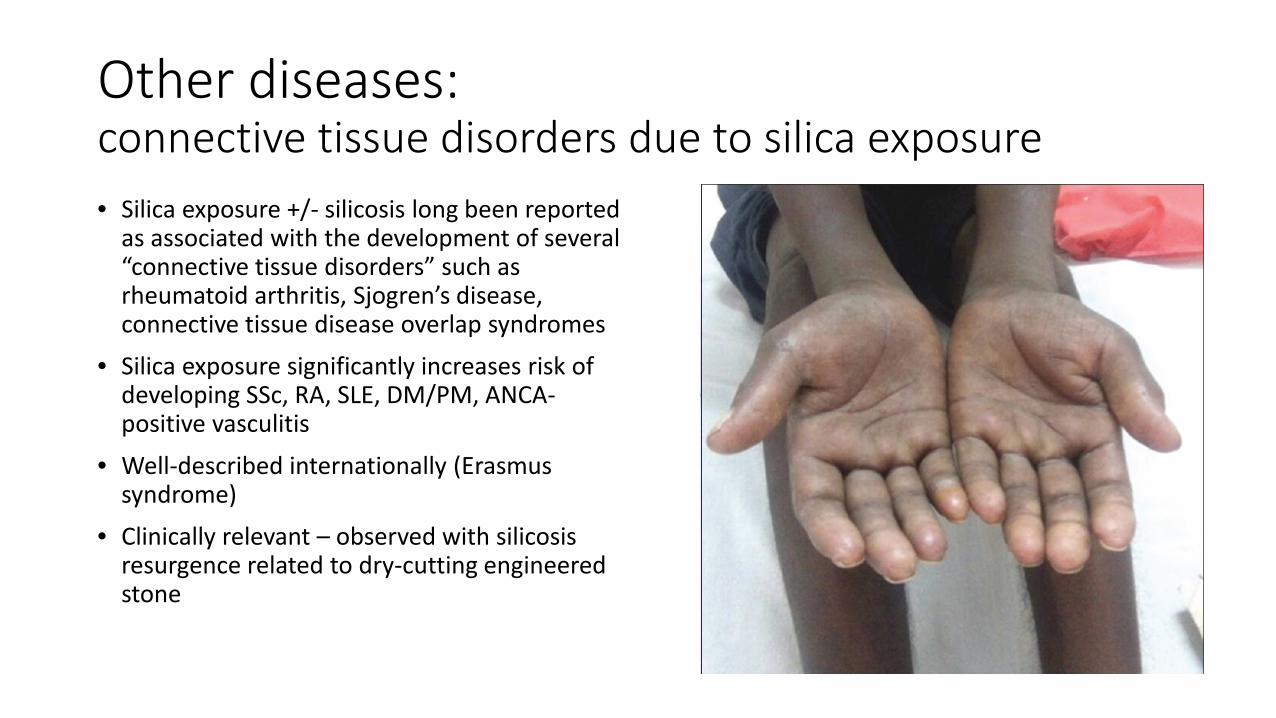
Other diseases: connective tissue disorders due to silica exposure• Silica exposure +/- silicosis long been reported
as associated with the development of several “connective tissue disorders” such as rheumatoid arthritis, Sjogren’s disease, connective tissue disease overlap syndromes
• Silica exposure significantly increases risk of developing SSc, RA, SLE, DM/PM, ANCA-positive vasculitis
• Well-described internationally (Erasmus syndrome)
• Clinically relevant – observed with silicosis resurgence related to dry-cutting engineered stone
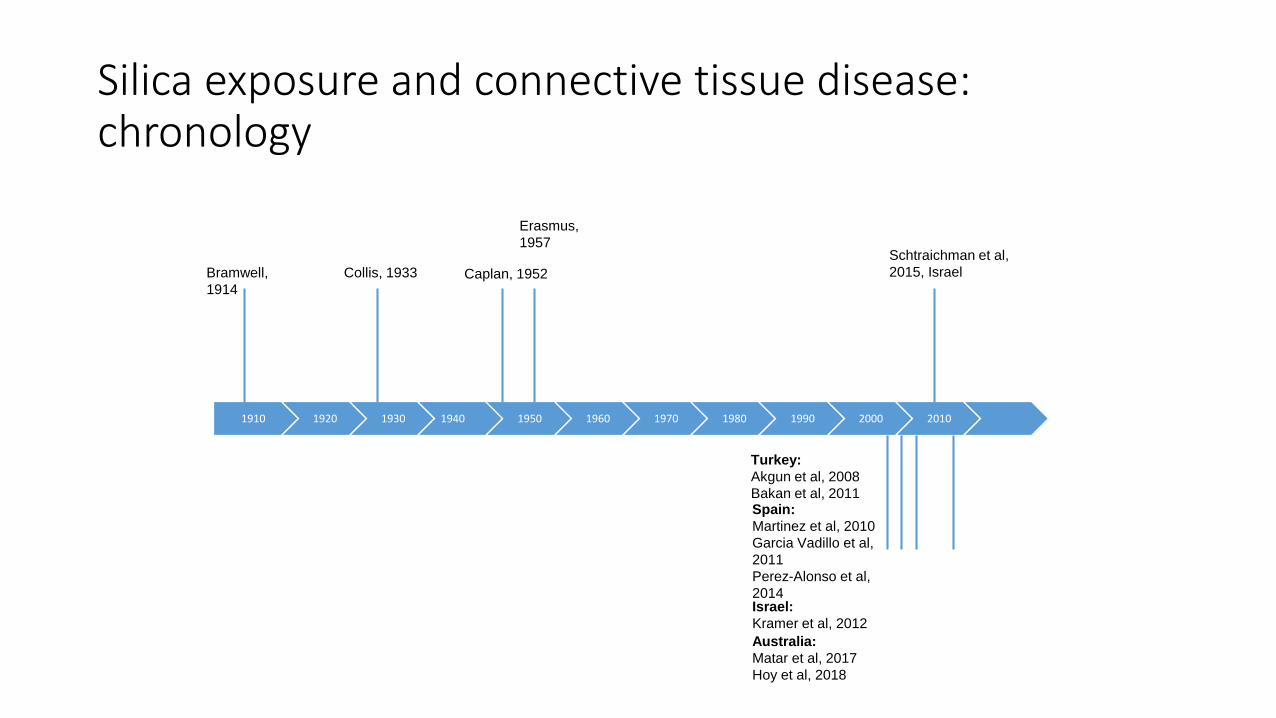
Silica exposure and connective tissue disease: chronology
1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010
Bramwell, 1914
Collis, 1933 Caplan, 1952
Erasmus, 1957
Schtraichman et al, 2015, Israel
Turkey:Akgun et al, 2008Bakan et al, 2011Spain:Martinez et al, 2010Garcia Vadillo et al, 2011Perez-Alonso et al, 2014Israel:Kramer et al, 2012Australia:Matar et al, 2017Hoy et al, 2018
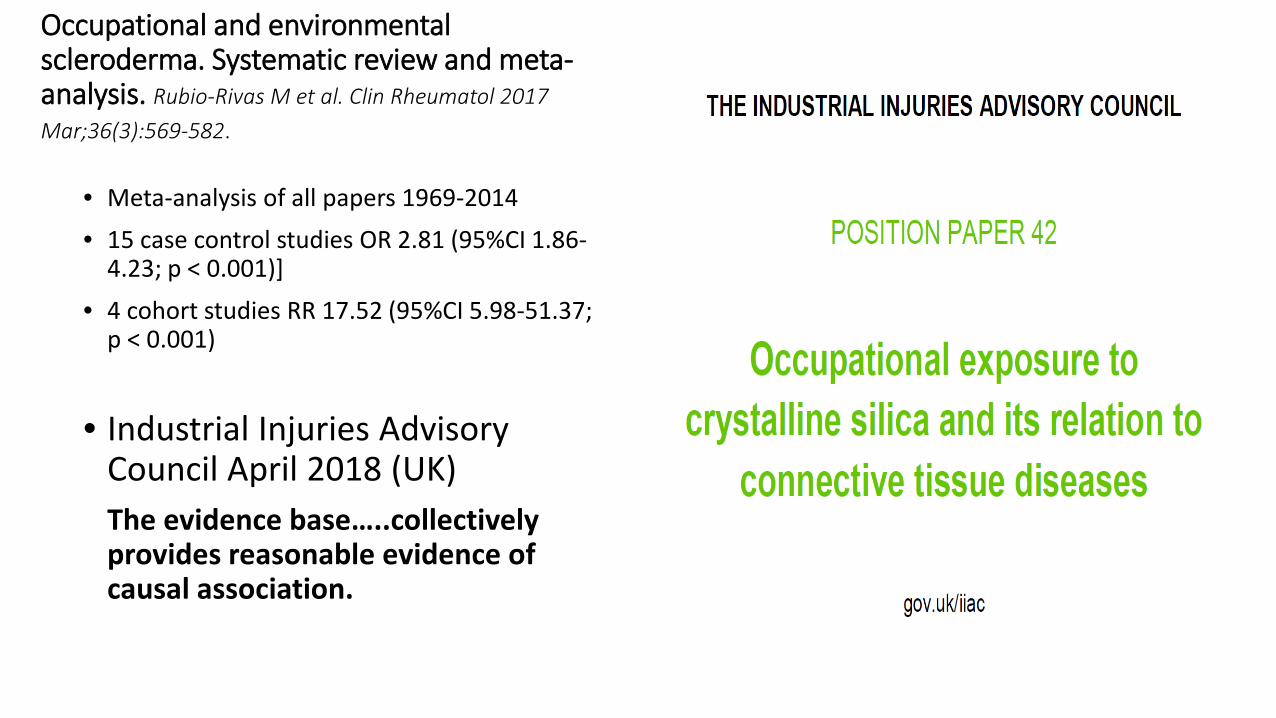
Occupational and environmentalscleroderma. Systematic review and meta-analysis. Rubio-Rivas M et al. Clin Rheumatol 2017 Mar;36(3):569-582.
• Meta-analysis of all papers 1969-2014• 15 case control studies OR 2.81 (95%CI 1.86-
4.23; p < 0.001)]
• 4 cohort studies RR 17.52 (95%CI 5.98-51.37; p < 0.001)
• Industrial Injuries Advisory Council April 2018 (UK)The evidence base…..collectively provides reasonable evidence of causal association.
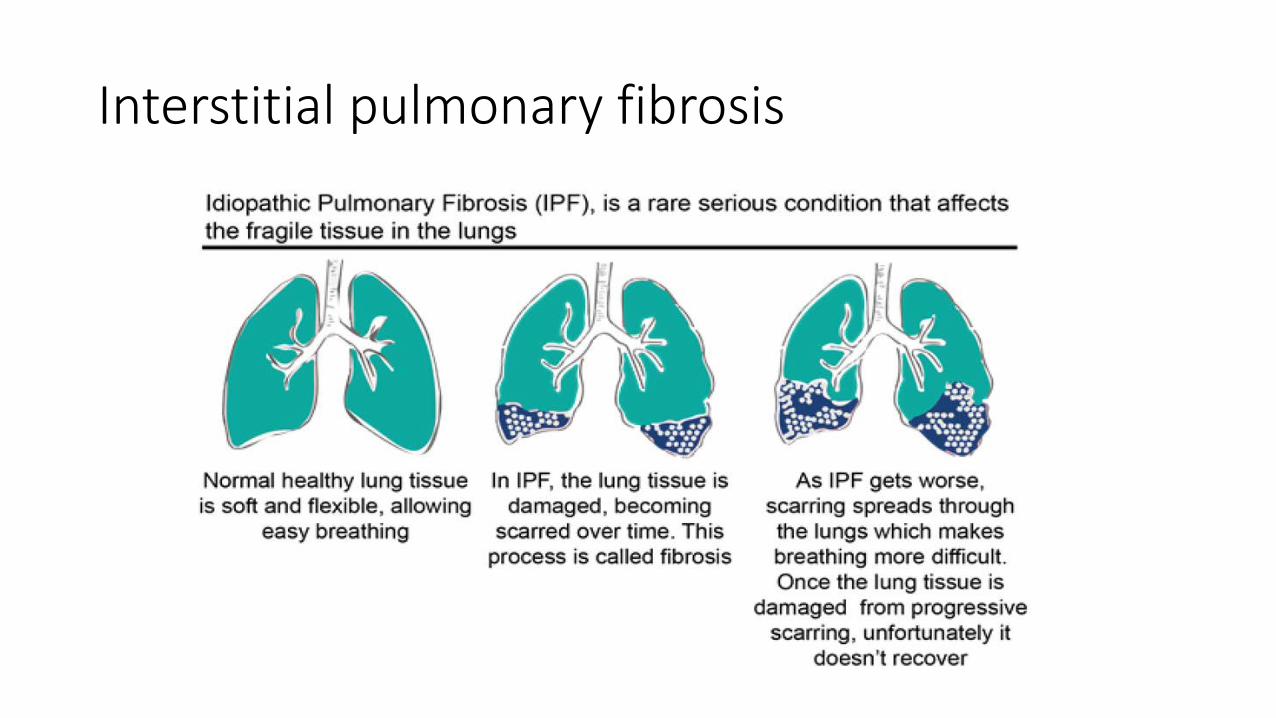
Interstitial pulmonary fibrosis
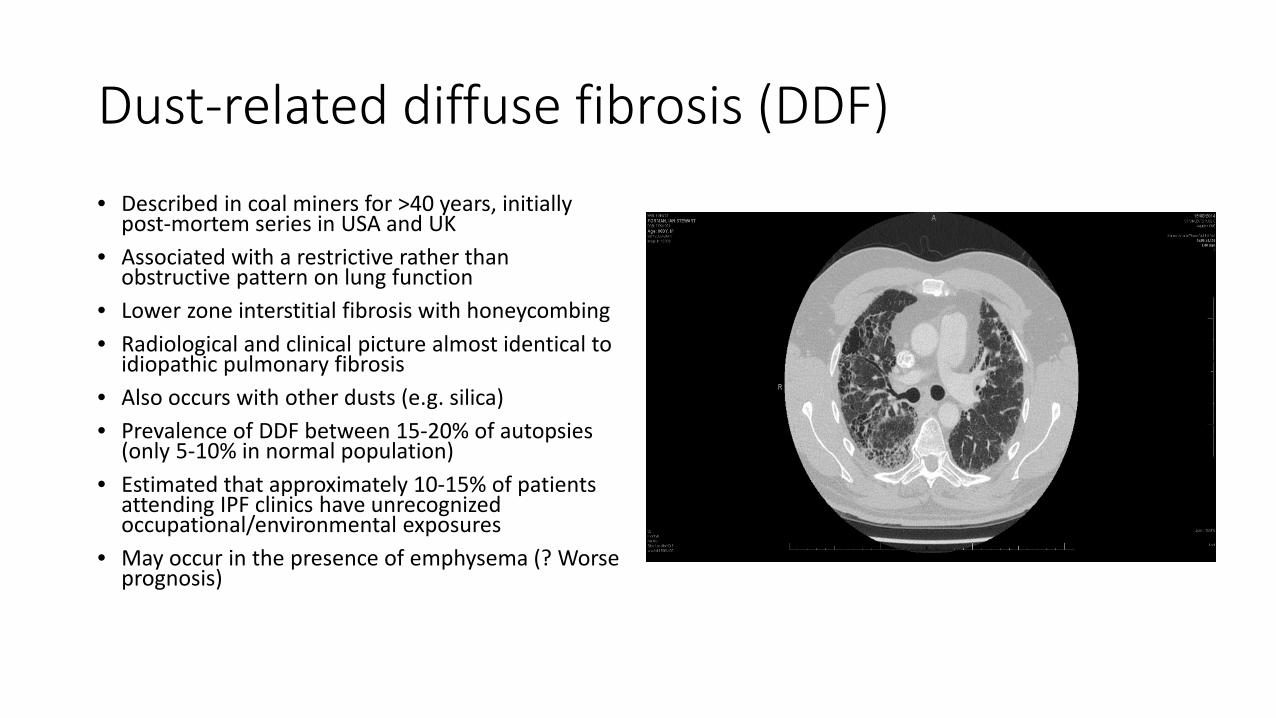
Dust-related diffuse fibrosis (DDF)• Described in coal miners for >40 years, initially
post-mortem series in USA and UK• Associated with a restrictive rather than
obstructive pattern on lung function• Lower zone interstitial fibrosis with honeycombing• Radiological and clinical picture almost identical to
idiopathic pulmonary fibrosis• Also occurs with other dusts (e.g. silica)• Prevalence of DDF between 15-20% of autopsies
(only 5-10% in normal population)• Estimated that approximately 10-15% of patients
attending IPF clinics have unrecognized occupational/environmental exposures
• May occur in the presence of emphysema (? Worse prognosis)
Interstitial pulmonary fibrosis due to silica inhalation (usual interstitial fibrosis/diffuse dust fibrosis)
• Diagnosis of IPF requires: exclusion of other known causes of ILD (e.g. domestic and occupational/environmental exposures, connective tissue disease, drug toxicity)
• Patients with ILD should be initially investigated for identifiable causes of interstitial lung disease
• Silica a well known cause of pulmonary fibrosis
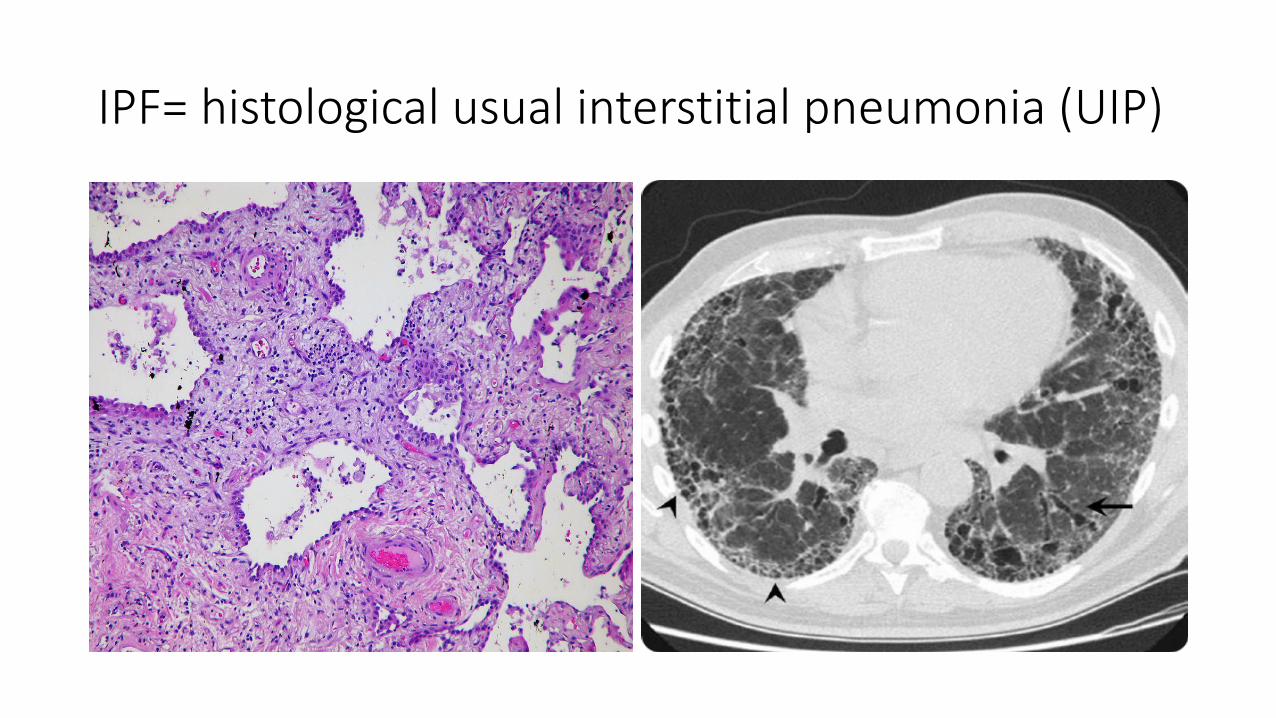
IPF= histological usual interstitial pneumonia (UIP)
Interstitial pulmonary fibrosis due to silica inhalation (usual interstitial fibrosis/diffuse dust fibrosis)
• Diagnosis of IPF requires: exclusion of other known causes of ILD (e.g. domestic and occupational/environmental exposures, connective tissue disease, drug toxicity)
• Patients with ILD should be initially investigated for identifiable causes of interstitial lung disease
Lung cancer and silica exposure: IARC Monograph – 100C 2012
Occupational exposure to silica dust and risk of lung cancer: an updated meta-analysis of epidemiological studies.
BMC Public Health 2016; 16: 1137.• Positive association of crystalline silica and
lung cancer • An exposure-response relationship between
these two, with a high degree of heterogeneity in the analyses.
• Risk tends to be more pronounced in the presence of silicosis and in the mining industry and is not significantly affected by the presence or exclusion of occupational confounding factors or by adjustment for cigarette smoking.
• A gradual reduction in the risk with time has also been noted.
Improvements in medical diagnosis and treatment
• Better imaging techniques: CT vs CXR• Lower radiation dosage• Improved understanding of biological
pathways and pathophysiology• International collaboration with global
studies providing definite answers to research questions
• Technological advances in IT allow improved and multiple analyses and “Big data”
• Huge advances in genetics• Significant advances in treatments of eg.
cancers, obstructive lung diseases
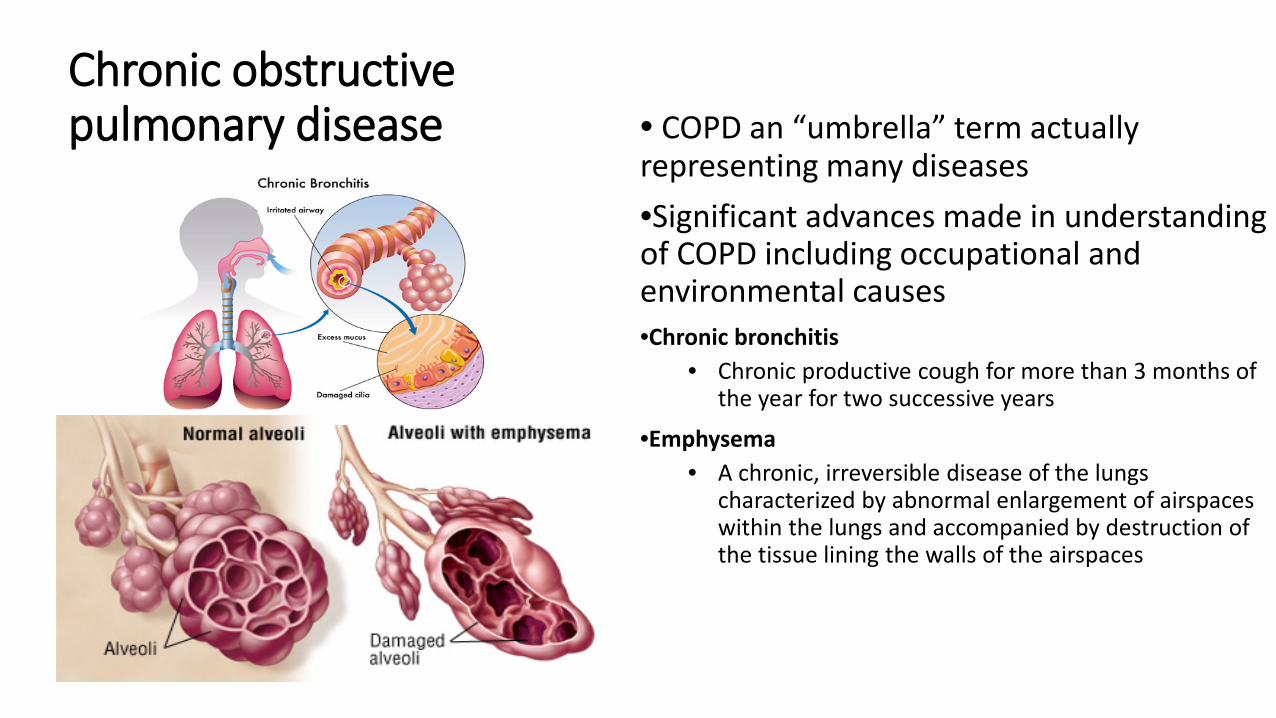
Chronic obstructive pulmonary disease • COPD an “umbrella” term actually
representing many diseases•Significant advances made in understanding of COPD including occupational and environmental causes•Chronic bronchitis
• Chronic productive cough for more than 3 months of the year for two successive years
•Emphysema• A chronic, irreversible disease of the lungs
characterized by abnormal enlargement of airspaces within the lungs and accompanied by destruction of the tissue lining the walls of the airspaces
Improved recognition of factors which produce COPD• Indoor air pollution
• Smoke from biomass fuel (wood, charcoal etc), coal
• Occupational exposures• Crop farming: grain dust, organic & inorganic dust• Animal farming: organic dust, ammonia, hydrogen sulphide• Dust exposure: coal mining, hard-rock mining, tunnelling, concrete manufacturing, gold mining, iron & steel foundries• Chemical exposures: plastic, textile, rubber, leather manufacturing industries• Transportation & trucking, automotive repair
• Treated pulmonary TB• LRTIs in childhood• Chronic asthma• Outdoor air pollution• Poor economic status• Low educational achievement• Poor nutrition
Non-smoking factors associated with chronic obstructive pulmonary disease. Salvi S, Barnes PJ. Lancet 2009;374:733-743
Occupational COPD
• COPD due to occupational dust, fume and/or vapour inhalation• Diagnosis clinically relies on the prior occupational history and also past smoking history,
therefore is inherently unreliable• Consistent evidence from population studies report that the population attributable risk is
10-15% for COPD associated with work exposures• Occupational COPD cannot be distinguished clinically from non-occupational related
COPD • Well established to be caused by silica, coal, cadmium • Many other relevant industries with vapours, gases, dusts and fumes e.g: cotton textile,
welding, grain silo workers, isocyanate workers etc etc.• Standard of care has been developed for occupational COPD (Fishwick et al.
Occupational Medicine 2015;65: 270-282), but not yet adopted internationally• Many large cross-sectional and now increasingly longitudinal studies

Mining dust exposure and COPD
• NHIS data 2006-2015• 1,001,559 individuals• 4.5% of miners had chronic bronchitis, 3.3% had emphysema, 6.2%
had COPD and asthma• Extraction workers had significantly increased odds ratio (OR) of
chronic bronchitis (2.18), emphysema (7.85) and COPD (2.56) compared with lower exposure occupations
Mabila SL, Almberg KS, Friedman L, Cohen R High exposure mining occupations are associated with obstructive lung disease, National Health Interview Survey (NHIS), 2006-2015. Am J Ind Med. 2018 Jul 12
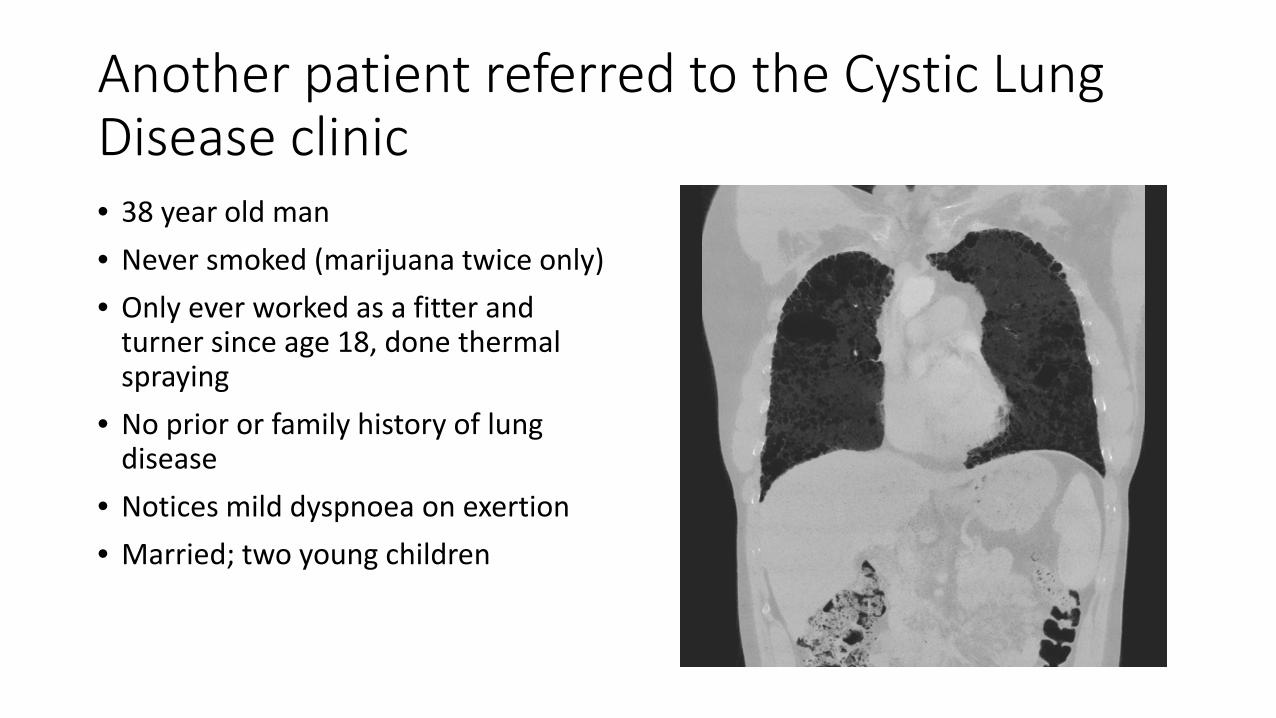
Another patient referred to the Cystic Lung Disease clinic• 38 year old man• Never smoked (marijuana twice only)• Only ever worked as a fitter and
turner since age 18, done thermal spraying
• No prior or family history of lung disease
• Notices mild dyspnoea on exertion• Married; two young children

HRCT
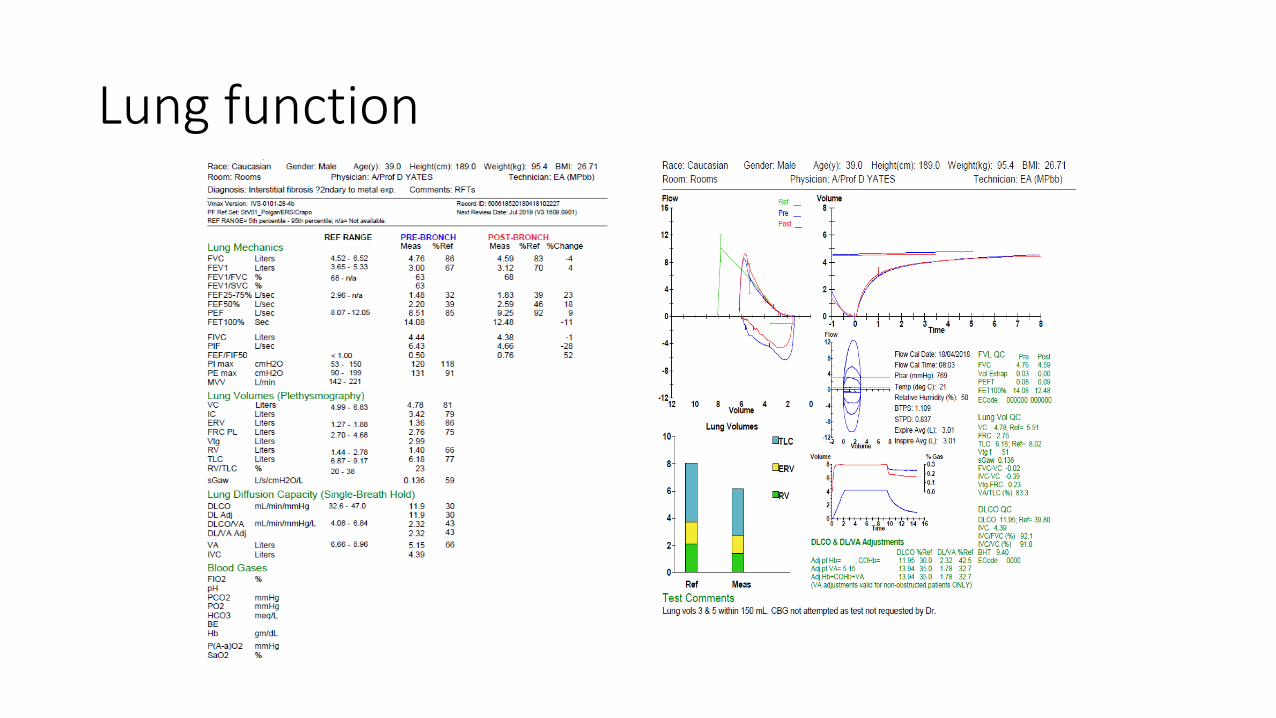
Lung function

Hard metal lung disease (with thanks to Jerry Abrahams & Sonia Sanyal, New York, USA)
Hard metal lung disease
• Disease due to exposure to hard metal (=tungsten carbide)
• Also known as hard metal pneumoconiosis, tungsten carbide pneumoconiosis, hard metal lung, giant cell interstitial pneumonitis (GIP), and cobalt lung
• Term “hard metal” NOTto do with the “heavy metals” lead, cadmium, and mercury.
• Hard metal so-called because extremely hard, approaching diamond
• Generally produced by compacting powdered tungsten carbide (WC) and cobalt (Co) (+ some other agents) into a polycrystalline material, a process called sintering, hence the term “sintered carbides” (or cemented carbides).
• Hard metal used to make or cover machine parts that require high heat resistance, or to make tools used for drilling, cutting, machining, or grinding.
• Clinical presentation of HMLD is similar HSP
• Some (but not all patients experiencing episodes of work-related subacute disease
• May evolve, variably rapidly, to lung fibrosis.
• Unique pathology: characterized, by “cannibalistic” multinucleated giant cells in airspaces (and bronchoalveolar lavage).
• First described by Liebow in 1975 but originally documented by Jobs & Ballhausen in 1940
• Process by which giant cells are produced is still largely unknown
• Case had been through two MDTs and classified as “IPF” and “unclassifiable”, without occupational exposure being recognized.

Occupational hypersensitivity pneumonitis• 59 year old man• Works as an engineer
• Noticed an unusual smell when working in an office on Garden Island
• Developed cough, wheeze and dyspnoea gradually over a period of 2 years
• Abnormal CT scan
• Antibodies to Farmer’s lung antigens positive (M. faeni, T. vulgaris)
• Most of symptoms resolved after removed from exposure and given oral glucocorticosteroids
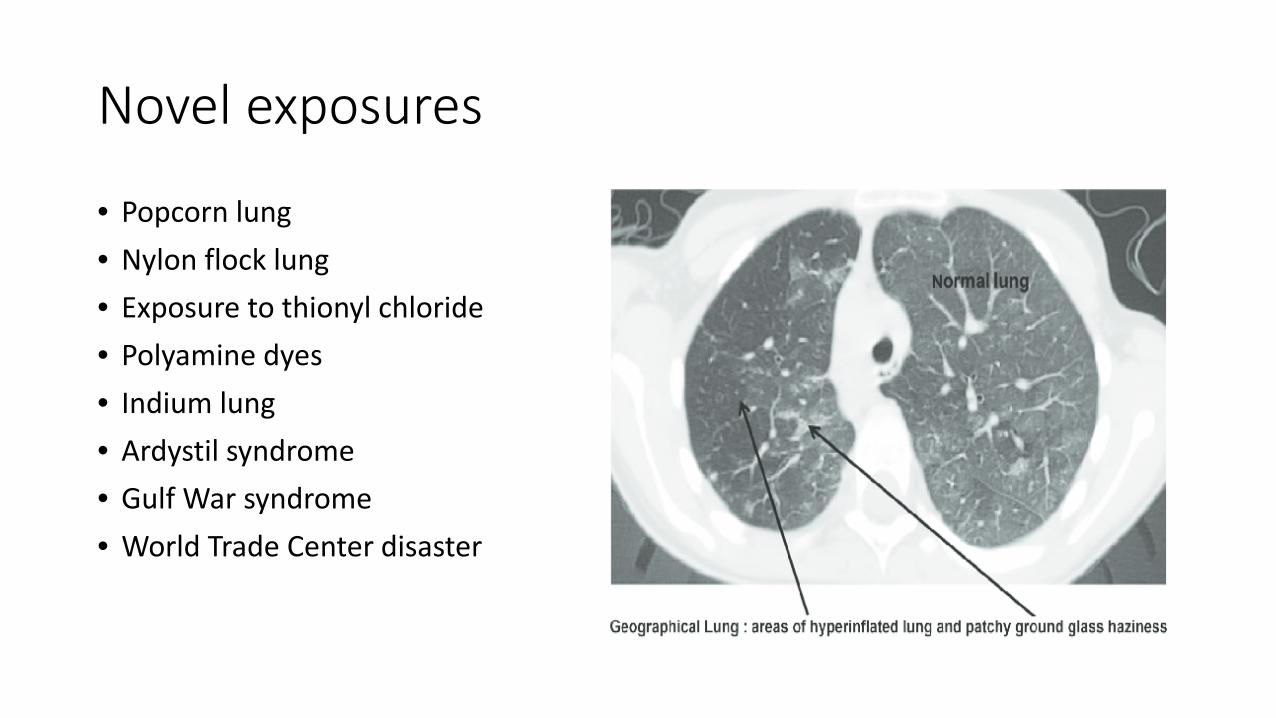
Novel exposures
• Popcorn lung• Nylon flock lung• Exposure to thionyl chloride• Polyamine dyes• Indium lung• Ardystil syndrome• Gulf War syndrome• World Trade Center disaster
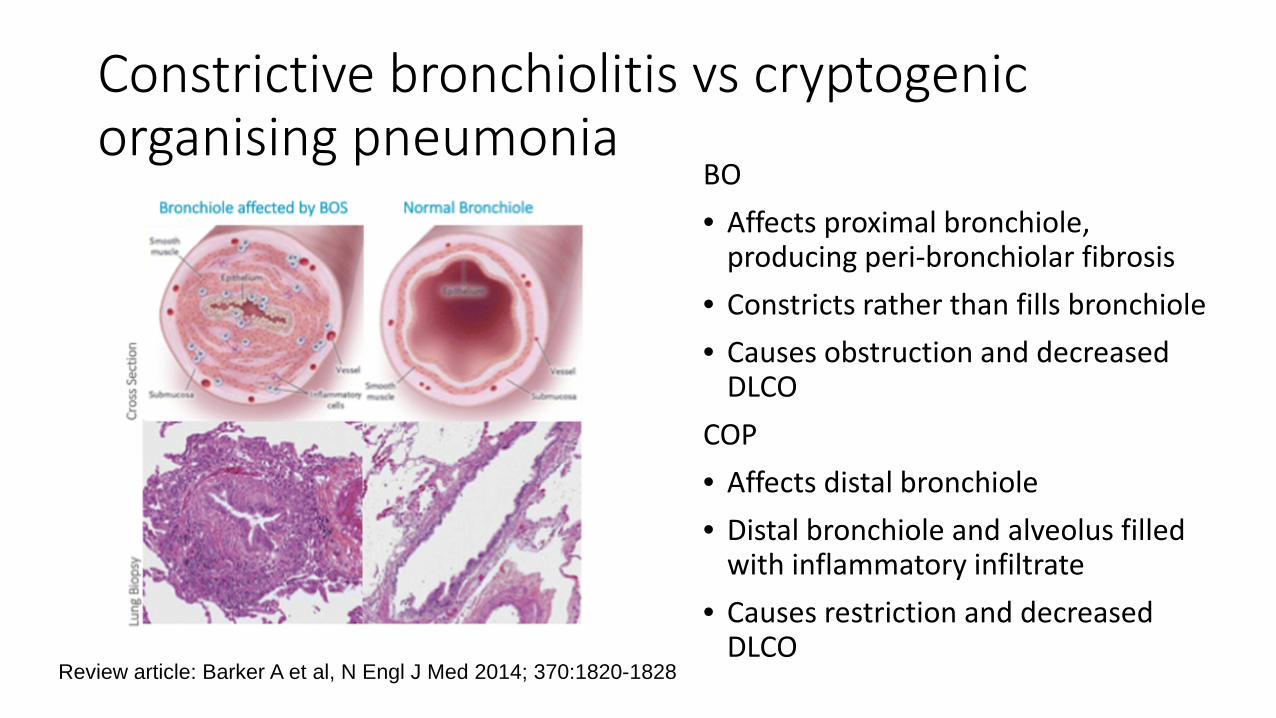
Constrictive bronchiolitis vs cryptogenic organising pneumonia
BO• Affects proximal bronchiole,
producing peri-bronchiolar fibrosis• Constricts rather than fills bronchiole• Causes obstruction and decreased
DLCOCOP• Affects distal bronchiole• Distal bronchiole and alveolus filled
with inflammatory infiltrate• Causes restriction and decreased
DLCOReview article: Barker A et al, N Engl J Med 2014; 370:1820-1828
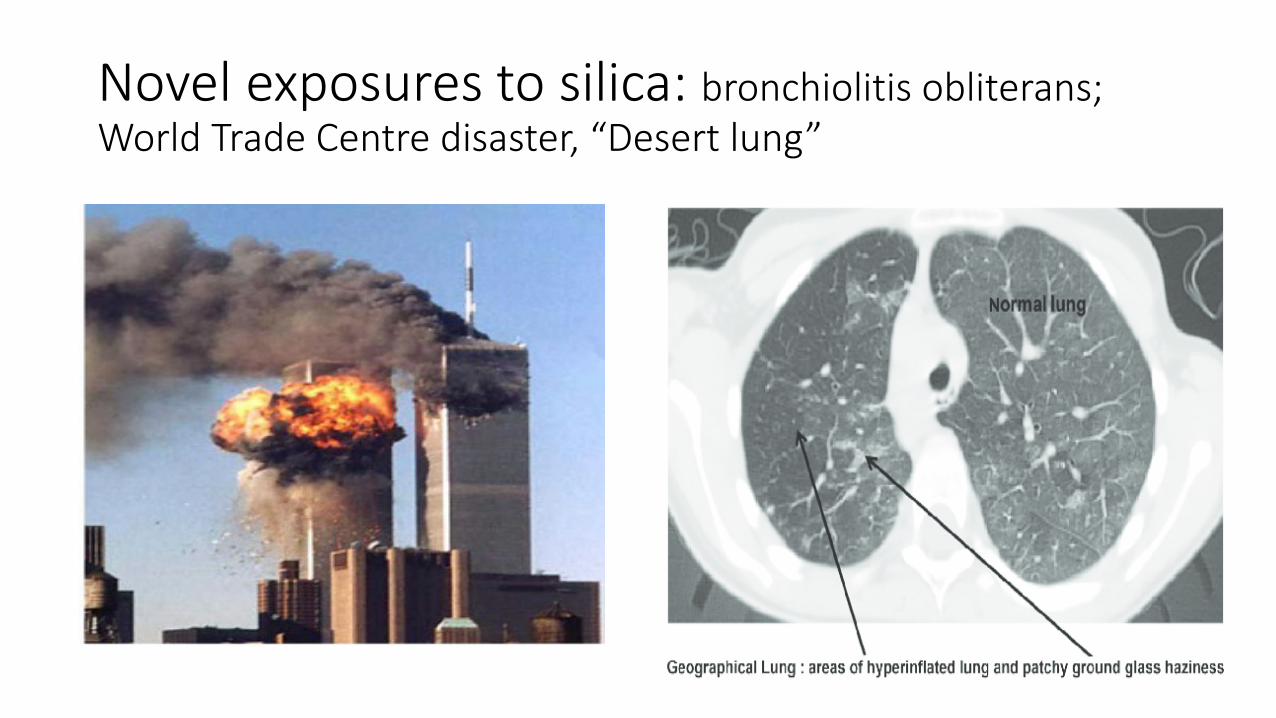
Novel exposures to silica: bronchiolitis obliterans; World Trade Centre disaster, “Desert lung”
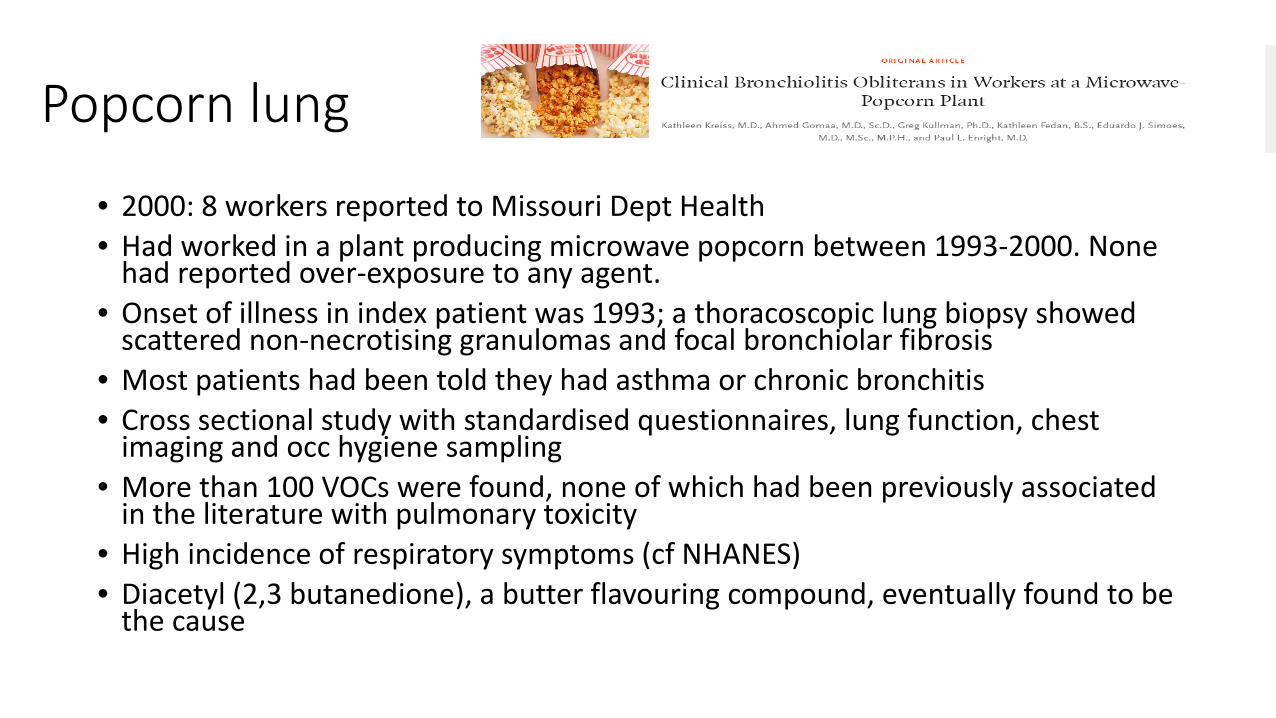
Popcorn lung
• 2000: 8 workers reported to Missouri Dept Health• Had worked in a plant producing microwave popcorn between 1993-2000. None
had reported over-exposure to any agent.• Onset of illness in index patient was 1993; a thoracoscopic lung biopsy showed
scattered non-necrotising granulomas and focal bronchiolar fibrosis• Most patients had been told they had asthma or chronic bronchitis• Cross sectional study with standardised questionnaires, lung function, chest
imaging and occ hygiene sampling• More than 100 VOCs were found, none of which had been previously associated
in the literature with pulmonary toxicity• High incidence of respiratory symptoms (cf NHANES)• Diacetyl (2,3 butanedione), a butter flavouring compound, eventually found to be
the cause
Popcorn workers’ lung

Gulf war: Constrictive Bronchiolitis
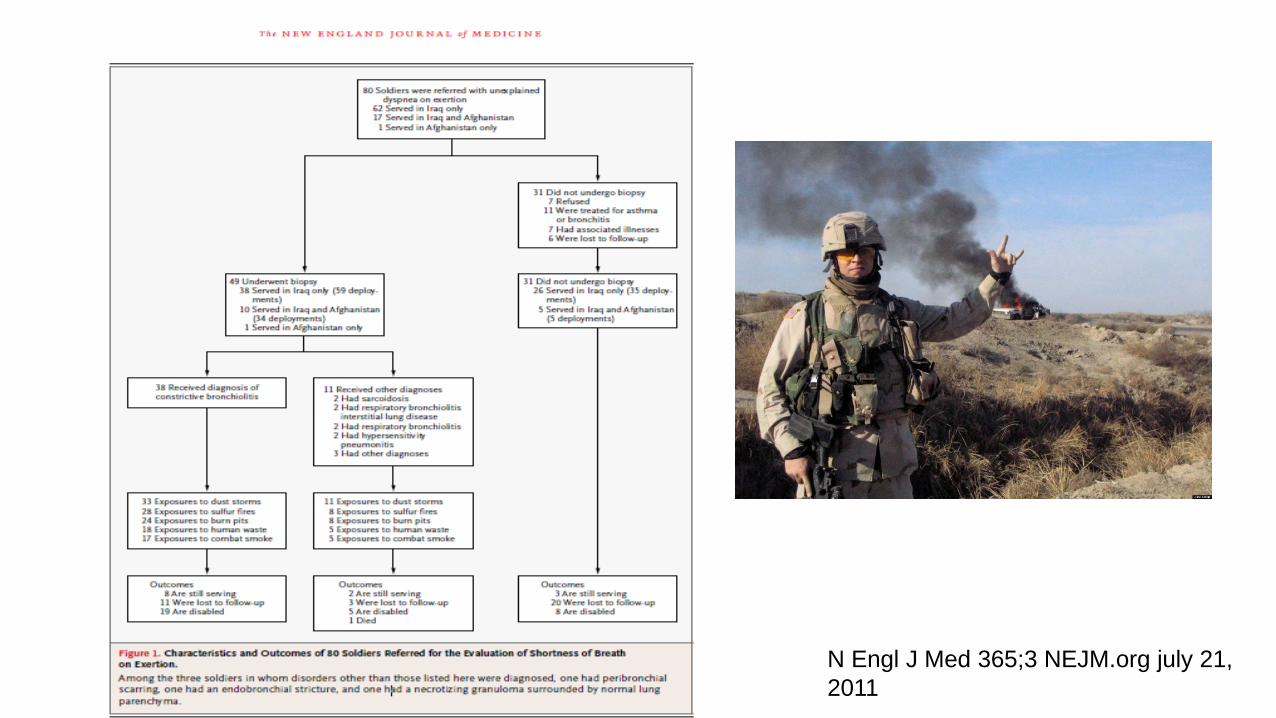
N Engl J Med 365;3 NEJM.org july 21, 2011
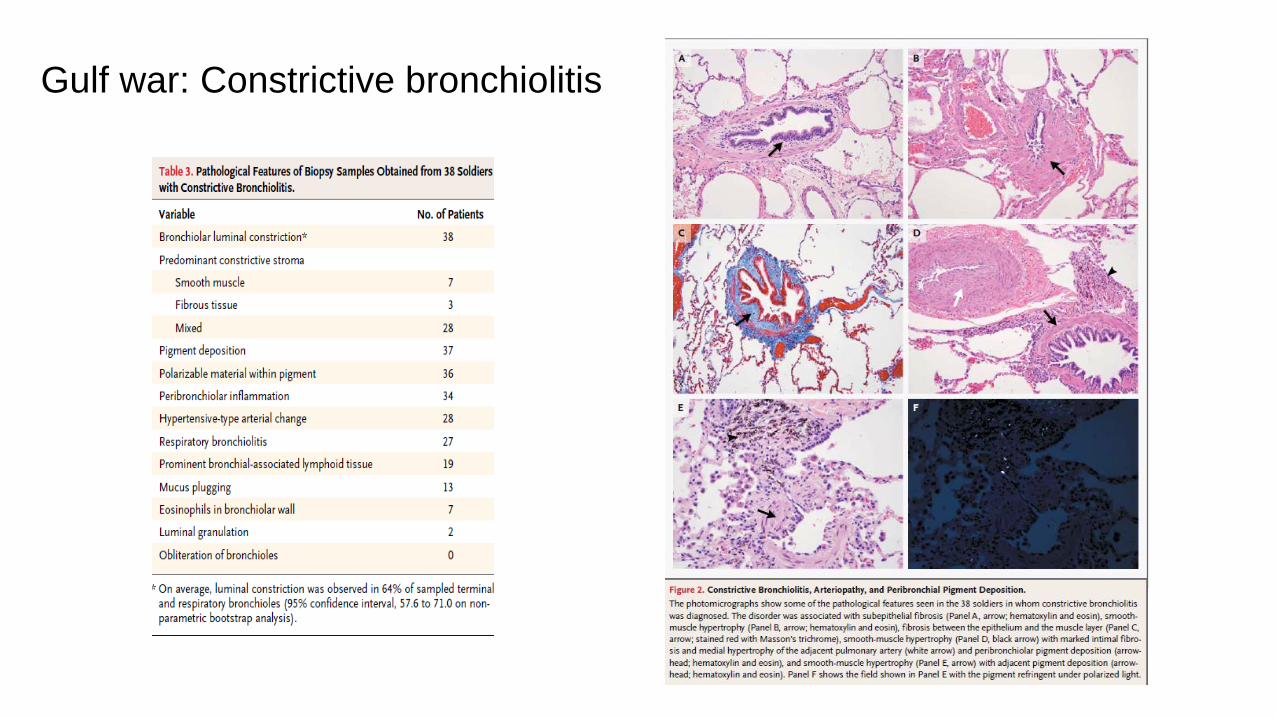
Gulf war: Constrictive bronchiolitis
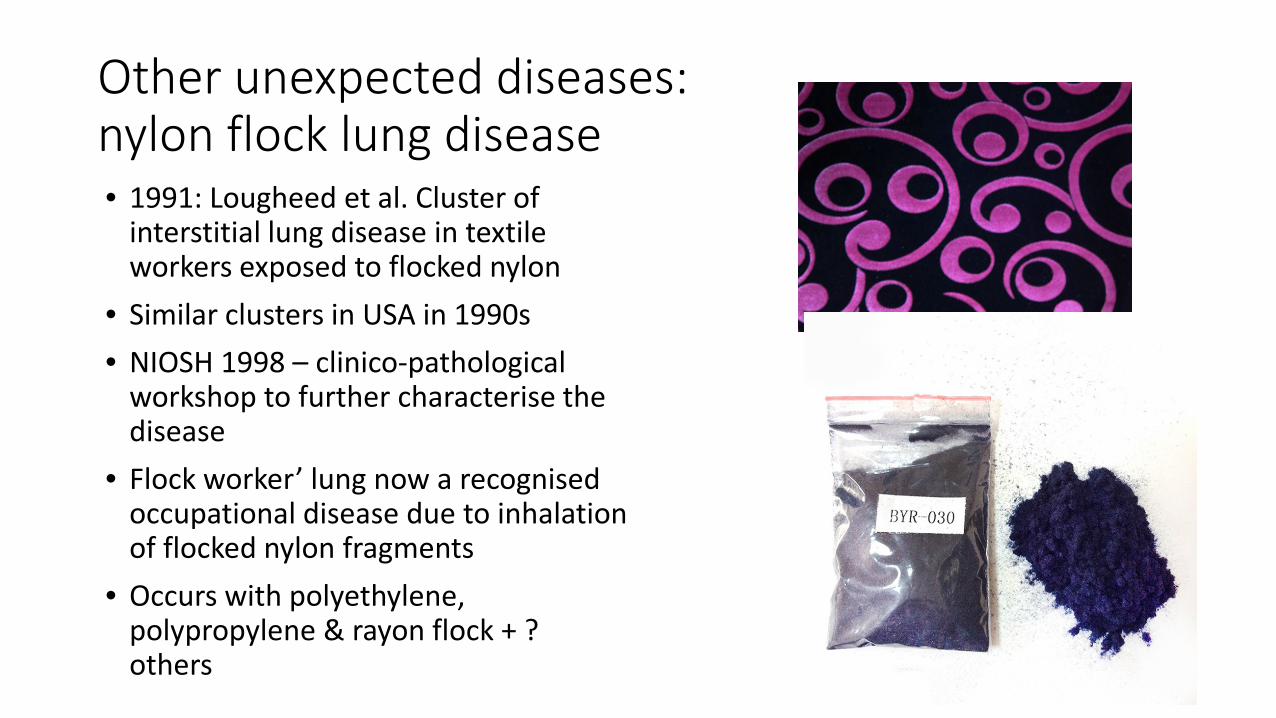
Other unexpected diseases: nylon flock lung disease• 1991: Lougheed et al. Cluster of
interstitial lung disease in textile workers exposed to flocked nylon
• Similar clusters in USA in 1990s• NIOSH 1998 – clinico-pathological
workshop to further characterise the disease
• Flock worker’ lung now a recognised occupational disease due to inhalation of flocked nylon fragments
• Occurs with polyethylene, polypropylene & rayon flock + ? others

Clinical characteristics
• Progressive breathlessness, cough without sputum
• Variable patterns seen on spirometry
• Peripheral and basal ground glass opacities
• Histology: lymphocytic bronchiolitis and peribronchiolitis with lymphoid hyperplasia
Kern DC et al. Flock Worker’s Lung. Chest 2000; 117:251-259
Novel exposures: inhaled nanoparticlese.g. Song Y, Li X, Du X. Exposure to nanoparticles is related to pleural effusion, pulmonary fibrosis andgranuloma. Eur Respir J 2009; 34: 559–567
• Some case reports now emerging where nanoparticles associated with human respiratory disease
• 7 young women admitted to hospital from the same dept of a print plant in China with rapid onset pleural effusions, mean age 29; 3 died
• Exposed to engineered polyacrylate nanoparticles in spray paint
• Used a paste of ivory white soft coating mixture of polyacrylic ester to an open bottomed pan of a machine which was used to air-spray coating material onto polystyrene boards.
• Machine had three atomising spray nozzles and one a ventilation unit, which broke 5 months before the occurrence of the disease.
• At least 2 other case reports with nickel ENPs and titanium oxide ENPs

Occupational activities with substantial probability of worker exposure to ENPs
• Construction (e.g. products improving wear resistance and insulation materials)
• Health care (e.g. drug-delivery systems and tissue engineering)
• Energy (e.g. low-wastage storage of energy and new generation photovoltaic cells)
• Automobile and aerospace industry (e.g. reinforced and stronger materials and fuel additives
• Chemical industry (e.g. catalysts and self-cleaning surfaces)
• Electronics and communication (e.g. optical/optoelectronic components and ultra fast compact computers)
Engineered nanoparticles
Engineered nanoparticles at the workplace: current knowledge about workers’ riskA. Pietroiusti A. Magrini. Occupational Medicine, Volume 64, Issue 5, 1 July 2014, Pages 319–330,
• Nanotechnology: new technology• Engineered nanoparticles (ENPs) small: 1 - 100nm• So small that the material acquires novel physicochemical properties
useful for industrial & biomedical purposes• A growing number of workers are estimated to be involved in work
processes directly or indirectly linked with ENPs• Recent projection - 6 million workers will be potentially exposed to
ENPs in 2020
Sarcoidosis?
How to prevent such diseases? High index of suspicion• Need to believe patients! • Take a careful history – allow time• Get material safety data sheets from
patient and/or employer and/or Safework
• Look up the substances used• Exclude other explanations of disease• Get a biopsy• Ask advice (TSANZ, occ physician, occ
hygienist - nationally and internationally if need be)
• Report cases back to Safework (state and national)
• Currently, no centralized notification system exists….but in the future?
Role of surveillance: important. Has to be actually occurring!
Symptoms
• Standardized questionnaires• Many well validated respiratory
disease questionnaires now availableImaging• CT scanning clearly shown to be
superior to chest X rays but standardization of technique and interpretation not yet accepted & widely agreed
• Mobile CT scanners now available; low doses and computerized algorithms
Lung function
• Spirometry well validated but needs to be performed properly and longitudinal results are far superior to single measurements
• Measurement of DLCO the most sensitive measure of emphysema and again serial measurements preferable
• However, lung function is not specific and therefore the whole clinical picture needs to be considered
• Disruption/anxiety/cost of surveillance measures need also to be taken into account
Conclusions
• Despite excellent knowledge about preventative strategies, occupational diseases are still a huge problem worldwide
• These certainly occur in Australia and are very likely under-recognised• Australia lags behind most other developed world countries in lacking a
centralised register and a national mechanism for investigation of outbreaks of occupational lung disease
• Old diseases are making a reappearance due to traditional factors (complacency, lack of funding, carelessness, poor education of workers, management and physicians alike), and new diseases are likely to occur with new technologies producing novel exposures
• We all need to be vigilant in our clinical practice, and use global resources and expertise to diagnose these in our patients
• Such a strategy could save many lives and prevent much suffering.




















