Spatio-temporal motifs ‘remembered’ in neuronal networks following profound hypothermia

Vol. 81 - No. 1 MINERVA ANESTESIOLOGICA 65
R E V I E W
Anno: 2015Mese: JanuaryVolume: 81No: 1Rivista: MINERVA ANESTESIOLOGICACod Rivista: Minerva Anestesiol
Lavoro: titolo breve: COAGULOPATHY INDUCED BY ACIDOSIS, HYPOTHERMIA AND HY-POCALCAEMIA IN SEVERE BLEEDINGprimo autore: DE ROBERTISpagine: 65-75
Acidosis, hypothermia and hypocalcemia alter the process of hemostasis.1 By acting
as confounding factors, they contribute to the morbidity and mortality of bleeding patients.2-4
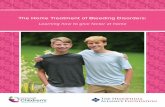
Acidosis, hypothermia and coagulopathy are known in trauma as the “triad of death” (Figure 1).5 In this combination, each factor is linked to the others in a “vicious cycle”, which exposes trauma patients to a high risk of death.6 Massive hemorrhage in patients with major trauma is re-
sponsible for over 30% of mortality and for al-most of 50% of deaths within the first 24 hours.7 Coagulation dysfunction in trauma is a complex and multifactorial process, in which acidosis and hypothermia synergistically contribute in wors-ening the outcome.2, 8
In specific population, such as patients with traumatic brain injury, the incidence of coagu-lopathy is significantly higher and its pathophys-iology remains poorly understood.9 Increasing
Coagulopathy induced by acidosis, hypothermia and hypocalcaemia in severe bleeding
E. DE ROBERTIS 1, S. A. KOZEK-LANGENECKER 2, R. TUFANO 1 G. M. ROMANO 1, O. PIAZZA 3, G. ZITO MARINOSCI 1
1Department of Neurosciences, Reproductive and Odontostomatologic Sciences, Federico II University of Naples, Naples, Italy; 2Department of Anesthesia and Intensive Care, Evangelical Hospital Vienna, Vienna, Austria; 3Department of Medicine and Surgery, University of Salerno, Salerno, Italy
A B S T R A C TAcidosis, hypothermia and hypocalcaemia are determinants for morbidity and mortality during massive hemor-rhages. However, precise pathological mechanisms of these environmental factors and their potential additive or synergistic anticoagulant and/or antiplatelet effects are not fully elucidated and are at least in part controversial. Best available evidences from experimental trials indicate that acidosis and hypothermia progressively impair platelet ag-gregability and clot formation. Considering the cell-based model of coagulation physiology, hypothermia predomi-nantly prolongs the initiation phase, while acidosis prolongs the propagation phase of thrombin generation. Acidosis increases fibrinogen breakdown while hypothermia impairs its synthesis. Acidosis and hypothermia have additive effects. The effect of hypocalcaemia on coagulopathy is less investigated but it appears that below the cut-off of 0.9 mmol/L, several enzymatic steps in the plasmatic coagulation system are blocked while above that cut-off effects remain without clinical sequalae. The impact of environmental factor on hemostasis is underestimated in clinical practice due to our current practice of using routine coagulation laboratory tests such as partial thromboplastin time or prothrombin time, which are performed at standardized test temperature, after pH correction, and upon recalcification. Temperature-adjustments are feasible in viscoelastic point-of-care tests such as thrombelastography and thromboelastometry which may permit quantification of hypothermia-induced coagulopathy. Rewarming hy-pothermic bleeding patients is highly recommended because it improves patient outcome. Despite the absence of high-quality evidence, calcium supplementation is clinical routine in bleeding management. Buffer administration may not reverse acidosis-induced coagulopathy but may be essential for the efficacy of coagulation factor concen-trates such as recombinant activated factor VII. (Minerva Anestesiol 2015;81:65-75)Key words: Acidosis - Hypothermia - Hypocalcaemia - Blood coagulation disorders - Hemmorhage - Th rombelas-Blood coagulation disorders - Hemmorhage - Th rombelas- - Hemmorhage - Thrombelas-tography.
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

DE ROBERTIS COAGULOPATHY INDUCED BY ACIDOSIS, HYPOTHERMIA AND HYPOCALCAEMIA IN SEVERE BLEEDING
66 MINERVA ANESTESIOLOGICA January 2015
evidence points to a strong interaction and exten-sive crosstalk between the inflammation and co-agulation systems.10 The brain contains all three major categories of lipids: cholesterol, sphingoli-pids and phospholipids. Injury to cerebral tissue could release a large quantity of phospholipids. The anionic phosphatidylethanolamine and the anionic phosphatidylserine have shown to bind to the coagulation factor Va and promote thrombin generation. Phospholipids released from injured neural cells are highly susceptible to oxidation but whether oxidized phospholipids are more or less active in initiating and propagat-ing coagulation remains unknown.9
Hypocalcemia, on the other hand, is frequent-ly present in patients requiring massive transfu-sions and is mostly a neglected and unrecognized condition predisposing to coagulopathy.11
The lack of the localization and control of the hemorrhagic source is the primary cause of the establishment and perpetuation of the vicious cycle. Damage control resuscitation 12 includes the immediate hemorrhage control (operative or angiographic), early initiation of blood product transfusions, appropriate fluid administration
and permissive hypotension in selected patients. Immediate rewarming, correction of coagulopa-thy and hemodynamic and metabolic stabiliza-tion should follow the appropriate procedure of control of the bleeding source.
Understanding the mechanisms of coagulopa-thy induced or aggravated by acidosis, hypother-mia and hypocalcemia might help clinicians, es-pecially anesthesiologists that often face massive bleeding in emergency 13 and in operating thea-tres settings, to adopt effective therapeutic strate-gies to counteract the impairment of hemostasis during severe uncontrolled hemorrhage. The purpose of this review was to analyze those con-founding factors and their roles in coagulopathy in various clinical settings.
Acidosis
Acidosis impairs the coagulation process in a progressive manner. Decreasing pH levels (range 7.4-6.8) were associated with a step-wise prolon-gation of clot formation time (CFT) and a re-duction in alpha-angle (AA), without significant alterations of clotting time (CT) in a thromboe-
Figure 1.—Effects of acidosis, hypothermia and hypocalcaemia on haemostasis impairment: “the vicious cycle”.
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

COAGULOPATHY INDUCED BY ACIDOSIS, HYPOTHERMIA AND HYPOCALCAEMIA IN SEVERE BLEEDING DE ROBERTIS
Vol. 81 - No. 1 MINERVA ANESTESIOLOGICA 67
the acidotic coagulopathy in animal models and accelerated the recovery of thrombin generation kinetics.21 The latter returned to baseline levels also in the acidosis group without pH neutraliza-tion, but in a delayed fashion, suggesting a possi-ble self-recovery mechanism of thrombin genera-tion from acidosis.21 The lack in improvement of acidosis-related coagulopathy after pH neutrali-zation could be attributed to the reduction of fibrinogen levels and platelet count.19, 21 In fact, acidosis seems to increase fibrinogen degrada-tion rate without affecting its synthesis; the lev-els of fibrinogen remain depleted even after pH neutralization.19, 21, 22 The reduction of platelet count may be the consequence of an accelerated removal from circulation due to the changes in the internal structure and shape when pH drops below 7.4, or due to an altered aggregation.22 Few considerations should be therefore made. Bicarbonate could not be the best therapeutic option to treat acidotic coagulopathy and may interfere with clot formation.19, 23 Coagulation function may not be restored by only pH neu-tralization, and other hemostatic factors (such as fibrinogen) could be important. On the other hand, it is worth mentioning that the use of ani-mal models, the exogenous blood acidification, the infusion of HCl instead of lactic acid, the in vitro study of postinjury acidosis effects on hemostasis, may not reflect the complex patho-physiological mechanisms which determine the coagulation impairment in severely injured and/or bleeding patient. The European Society of An-aesthesiology (ESA) guidelines 24 on severe peri-operative bleeding management suggest normal-izing pH in the context of acidotic coagulopathy even if this correction cannot completely reverse the alterations induced by acidosis.
Hypothermia
Common coagulation assays, such as PT and PTT, should be performed at the core tempera-ture of the patient inasmuch as, if performed at standard temperature (37 °C), cannot detect alterations induced by hypothermia.25-27 An in vitro study performed on whole blood found that a decrease in temperatures in the range of 37-25 °C caused a gradual impairment of
lastometric (TEM) study (in vitro acidification of blood using HCl).14 Maximum clot firm-ness (MCF) was altered only at pH<6.8 and all the coagulation impairments were reversed by restoring pH using tromethamol (THAM).14 Thus, these results suggest that during acidosis the coagulation process starts normally, but there is a delay in clot formation and a reduction in clot strength. In fact, CFT and AA measure the rapidity at which a solid clot forms, and are influ-enced by the availability of fibrinogen, platelets and coagulation factors (mostly thrombin). CT is the time until the clot starts to form, and MCF represents the maximum strength of the clot and is dependent by the contributions of fibrin and platelets.15 One study has demonstrated that the activity of factor VII (FVIIa) on a phospholipid surface was reduced by over 90%, whilst the ac-tivity of FVIIa/ tissue factor (TF) complex by 55% and the activity of prothrombinase com-plex (FXa/FVa) by approximately 70% when pH decreased from 7.4 to 7.0.16 Thrombin genera-tion occurs in two phases: the initiation phase in which the reaction is slow and the propagation phase where the greatest amount of thrombin is generated.17 Suppressing the activity of FXa/FVa complex, acidosis inhibits dramatically the prop-agation phase.18 Infusing HCl in pigs, Martini et al.19 showed that acidosis (pH 7.1) caused a significant depletion in both fibrinogen concen-tration and platelet count, and a prolongation of prothrombin time (PT), partial thrombo-plastin time (PTT), and activated clotting time (ACT). The thrombelastographic (TEG) analy-sis showed that acidosis induced impairment in AA and in maximum amplitude (MA), with a remarkable reduction of thrombin generation. Moreover, the pH normalization with bicarbo-nate did not correct the alterations of hemostasis induced by acidosis. Another study 20 found that acidosis (pH 7.1) induced in pigs by a combina-tion of a controlled hemorrhage and a decrease in respiration caused a decrease in fibrinogen concentration, platelet count and thrombin gen-eration. MA and AA were altered without com-promising PT, PTT and ACT. The coagulation impairment was not corrected after normalizing pH with bicarbonate infusion. Neutralization of pH with THAM seemed to not acutely reverse
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

DE ROBERTIS COAGULOPATHY INDUCED BY ACIDOSIS, HYPOTHERMIA AND HYPOCALCAEMIA IN SEVERE BLEEDING
68 MINERVA ANESTESIOLOGICA January 2015
the use of desmopressin only after pH correc-tion.36, 37
Desmopressin may be used as a bridge therapy to treat hypothermia-related coagulopathy during rewarming when pH is not altered.38, 39 This drug produces an increase in the plasma concentra-tions of coagulation factor VIII, von Willebrand’s Factor, tissue plasminogen activator, and an en-hancement in platelet adhesiveness.40Altough desmopressin has shown to be useful in correct-ing coagulopathy in patients with cirrhosis,41 ure-mia,42 or with either inherited (Von Willebrand disease) 43 or acquired (aspirin) 44 platelet dys-function, there is no evidence that supports the use of desmopressin in minimizing blood loss, re-ducing blood transfusion or improving outcome during massive hemorrhage in patients without pre-existing bleeding disorders.24, 45, 46
Temperature has also shown to influence the fibrinogen synthesis. In contrast to acidosis, where fibrinogen degradation is augmented, hypothermia (32 °C) seems to inhibit primarily the process of synthesis without affecting platelet counts.47 A TEG analysis performed in healthy subjects at a temperature ranging between 38-12 °C found an exponential relationship between low temperatures and increase in reaction time (R) and clotting time (K).48 The relationship among low temperatures and decrease of AA was sigmoid. Accordingly, a decrease in temperature determines a significant impairment of clot for-mation. However, the authors reported that the clot, once formed, was no longer influenced by hypothermia. Owing to the neuroprotective ef-fect resulting from the antiapoptotic activity and the decrease in the cellular metabolism, mild therapeutic hypothermia (32-34 °C) has been extensively used in cardiac surgery as well as af-ter severe brain damage.49, 50 In this particular clinical setting, the risk of severe bleeding asso-ciated to therapeutic hypothermia seems to be very low 51 and, anyway, is overcome by the ben-efits of an improved neurological outcome.52, 53 However, many concerns arise from the use of therapeutic hypothermia in major trauma pa-tients, where hypothermia could further ag-gravate the coagulopathy.54 A study involving porcine models with multiple injuries showed that therapeutic hypothermia (34 °C) did not
the coagulation process.28 The TEM analysis showed a prolongation of CT, CFT and a de-crease in AA. MCF was significantly impaired only at temperatures ≤28 °C. Hypothermia influences the aggregability and adhesion of platelets. Wolberg et al.29 found that for tem-peratures <33 °C both the reduced platelet func-tion and the coagulation cascade impairment contributed to the hemostasis defects. During mild hypothermia (33-37 °C) only platelet ad-hesion was found to be slightly reduced and the authors concluded that, at these temperatures, the haemostatic impairment resulted primarily from the platelet adhesion inhibition.29 Other evidences 30 demonstrated that mild hypother-mia (34 °C) had no effects on platelet function in response to collagen (activation), ristocetin (adhesion), and arachidonic acid (thrombox-ane generation). Profound hypothermia (24 °C) inhibited platelet aggregation in response to all the aforementioned molecules, but not to adenosine diphosphate (which enhanced the aggregation process).30 Results from an in vitro study 31 have shown that mild-moderate hypo-thermia (34-31 °C) potentiate platelet aggrega-tion in response to collagen, thrombin receptor activating peptide, ristocetin and adenosine di-phosphate. Hence, if platelets dysfunction is the principal mechanism of hemostasis impairment during mild-moderate hypothermia remains controversial and needs further studies.31 On the other hand, hypothermia delays the onset of thrombin generation by inhibiting the activity factor VIIa (FVIIa)/TF complex17 and slowing the initiation phase of thrombin generation.18 Meng et al. have shown that the activity of FXa/FVa and FVIIa/TF decreased progressively as the temperature was reduced, whilst the activ-ity of FVIIa alone increased.16 A computational analysis based on the Hockin-Mann kinetic model 32, 33 found that thrombin generation was delayed in a temperature-dependent fashion.34 Mild hypothermia (34-36 °C) had a little effect on thrombin generation, whilst moderate hy-pothermia (32-34 °C) delayed substantially this reaction. Acidosis interacts synergistically with hypothermia worsening the coagulopathy.35-37 Alterations induced by hypothermia could be reversed with warming 29 and improved with
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

COAGULOPATHY INDUCED BY ACIDOSIS, HYPOTHERMIA AND HYPOCALCAEMIA IN SEVERE BLEEDING DE ROBERTIS
Vol. 81 - No. 1 MINERVA ANESTESIOLOGICA 69
ing;29 routine coagulation tests may be mislead-ing and the use of point-of-care tests should be encouraged.61, 62 The ESA guidelines 24 on severe perioperative bleeding management recommend maintaining perioperative normothermia, as it reduces blood loss and transfusion requirements.
Effects of procoagulant drugs under acidosis and hypothermia
Fibrinogen, prothrombin complex concen-trates (PCC), factor VIIa (rFVIIa) and tranexamic acid should probably be part of our armamentar-ium for the treatment of life-threatening refrac-tory hemorrhage. Fibrinogen plays an important role in coagulation derangements, particularly in traumatic patients. During massive bleeding, plasma concentration of fibrinogen is reduced by hemodilution, hyperfibrinolysis, acidosis and hypothermia.63 As we have already mentioned, acidosis and hypothermia affect respectively the metabolism and synthesis of fibrinogen.47
Current guidelines recommend that a thresh-old of 150-200 mg dL-1 of plasma fibrinogen concentration should trigger the fibrinogen sub-stitution therapy.24, 64 PCC are purified coagula-tion factors produced from large plasma pools, which were initially developed for the treatment of hemophilia B.65 PCC have a concentration of coagulation factors 25 times higher than in normal plasma, and contain either tree (factors II, IX, X) or four coagulation factors (factors II, VII, IX, X).66 Some PCC also contain heparin and/or antithrombin to prevent activation, and
aggravate the coagulopathy in TEG analysis.55 Only CT and CFT were prolonged in hypother-mic animals, whilst MCF and platelet function were not altered. Therapeutic hypothermia may be safely used in trauma patients and could im-prove the survival.55, 56 Perhaps, a gradual con-trolled process of cooling does not determine the coagulation impairment seen in accidental hypothermia. On the other hand, the effect of active cooling (at 36, 34, 32 °C) on coagulation has also been studied in anesthetized patients.57 PT ratio (%) and platelet count decreased at 32 °C, whilst TEG measurements showed an in-crease in R and K parameters without alterations of MA.57 The concentration of FVII in plasma was unchanged during cooling. Short duration of mild hypothermia (≤4 hours at 32 °C) may interfere subtly with the coagulation function in healthy subjects.57 However, mild periopera-tive hypothermia (35.6 °C) was associated with a greater blood loss (16%; 95% CI 4-26%) and an increase in transfusion risk (22%; 95% CI 3-37%) compared to normothermia in a meta-analysis.58 Likewise, normothermia (core tem-perature near 36.5 °C), accomplished with active warming, reduced the blood loss by approxi-mately 500 mL compared to mild hypothermia (core temperature near 35 °C) during total hip arthroplasty.59 Summarizing, it turns out that acidosis has a more prominent effect on coagula-tion impairment compared to hypothermia (Ta-ble I);60 acidosis and hypothermia act synergisti-cally on coagulopathy;35 the alterations induced by hypothermia could be reversed with warm-
Table I.—Suggested differences among acidosis, hypothermia and hypocalcaemia on haemostasis impairment.
Acidosis Hypothermia Hypocalcaemia
Thrombin generation Inhibition of propagation phase Inhibition of initiation phase Inhibition when Ca++ is ≤0.25 mmol/L
Fibrinogen Degradation ↑ Synthesis ↓ NSPlatelet count ↓ No effect NSPlatelet function Aggregation ↓ ≤31°C: aggregation ↓*
>31°C: aggregation↑*NS
Effect of normalising pH or temperature
Coagulation remains altered Coagulation is restored NS
Effect of rFVIIa addition Efficacy reduced Efficacy not reduced NSEffect of PCC NS NS NSEffect of tranexamic acid Efficacy not reduced Efficacy not reduced NS
NS: not studied; PCC: prothrombin complex concentrates.*in response to collagen, thrombin receptor activating peptide, ristocetin but not to adenosine diphosphate.
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

DE ROBERTIS COAGULOPATHY INDUCED BY ACIDOSIS, HYPOTHERMIA AND HYPOCALCAEMIA IN SEVERE BLEEDING
70 MINERVA ANESTESIOLOGICA January 2015
vitro study by Dirkmann et al.75 where coagula-tion was analysed using TEM. TXA (final con-centration, 0.33 mg/mL) abolished the effect of severe acidosis (pH, 6.91±0.02) in potentiating the fibrinolysis induced by r-tPA. Interestingly, hypothermia (33 °C) attenuated r-tPA-evoked fibrinolysis, and the addition of TXA further improved the clot stability. The use of TXA is recommended during perioperative bleeding 24 and in haemorrhagic trauma patients.64
The off-label use of factor VIIa, as a rescue ther-apy (60 �g/kg IV), was fi rst described in a trau-�g/kg IV), was fi rst described in a trau-g/kg IV), was first described in a trau-ma patient without pre-existing coagulopathies in whom surgical interventions failed to stop the bleeding.76 The treatment with rFVIIa was effec-tive in arresting the haemorrhage and improved noticeably the coagulation tests.76 The use of this drug in life-threatening refractory haemorrhage has demonstrated to be useful in enhancing hae-mostasis.77-81 In the last decade, the off-label use of rFVIIa in US hospitals has increased dramati-cally (140-fold), with cardiovascular surgery and trauma representing the most frequent fields of application, raising some concerns about this practice.82 The mechanism of action of rFVIIa is an increase of thrombin generation via factor X on the surface of activated platelet at the site of injury, independently from TF.83 The effect of acidosis and hypothermia on the rFVIIa ef-ficacy has been object of research. An in vitro study performed on whole blood of healthy volunteers found that TEG parameters (R, AA, MA) were significantly affected by acidosis (pH 6.8) but not by hypothermia (32 °C).84 Even if only acidosis showed to alter coagulation, the addition of rFVIIa substantially improved TEG parameters both in hypothermic and acidotic conditions.84 Contrarily to these findings, an-other in vitro study performed on human blood found that decrease temperatures (34 °C, 31 °C and 28 °C) proportionally prolonged PT, APTT and impaired TEG measurements (R, K, AA).85 Addition of rFVIIa improved all the aforemen-tioned parameters at every temperature tested, surmounting the modifications induced by hy-pothermia.85 Only for temperatures ≤28 °C MA (influenced by fibrin and platelets) was signifi-cantly impaired and did not improve after add-ing rFVIIa.85 Inducing lactic acidosis (pH 7.14,
proteins C, S, and Z to reduce the risk of throm-bogenesis.65 The principal indication of PCC is to reverse the coagulopathy induced by vitamin K-dependent oral anticoagulants; PCC may also be used to treat major bleeding when there is evidence of a prolonged clotting time.24, 64 Even though PCC have shown to improve haemostasis in animal models of dilutional coagulopathy,67-69 there are no in vitro or clinical data about the ef-ficacy of these concentrates during acidosis. Few studies on animals 69, 70 suggest that PCC may not be influenced by a hypothermic environ-ment, but this needs further investigation.
Tranexamic acid (TXA) is an antifibrinolytic agent used in cardiac and non-cardiac surgery to reduce the risk of blood loss and transfusion requirements.71 Most recently, some evidences pointed out a potential role of TXA in trauma. The Clinical Randomisation of an Antifibrinol-ytic in Significant Haemorrhage 2 (CRASH-2) trial 72 showed that the administration of TXA (loading dose 1 g over 10 minutes, then infu-sion of 1 g over 8 hours) within 8 h of injury significantly reduced the mortality in bleeding trauma patients without increasing the risk of adverse events. TXA could be a useful drug for bleeding trauma patients since it reduces hyper-fibrinolysis which is a direct consequence of the combination of tissue injury and shock. More-over, an exploratory analysis of the CRASH-2 trial 73 has highlighted that the most of the ben-efits from the TXA administration derive from its early use (within 3h after trauma). While we are writing, the CRASH-3 Trial (Clinicaltrials.gov NCT01402882) is in progress as an interna-tional, multicentre, randomized, double-blind, placebo-controlled trial to quantify the effects of the early administration of TXA on death and disability in patients with traumatic brain injury. But what happens when TXA is admin-istered under conditions of acidosis and/or hy-pothermia? Porta et al.74 proved the efficacy of TXA during severe metabolic acidosis. In an ex-perimental study conducted on 31 pigs in which hemorrhage and resuscitation were induced, the authors reported no difference between the in vi-tro activity of TXA at baseline pH (mean, 7.56) or acidotic pH (mean, 7.11) in reversing fibri-nolysis r-tPA-induced. These data confirm an in
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

COAGULOPATHY INDUCED BY ACIDOSIS, HYPOTHERMIA AND HYPOCALCAEMIA IN SEVERE BLEEDING DE ROBERTIS
Vol. 81 - No. 1 MINERVA ANESTESIOLOGICA 71
els of acidosis was similar,37 we can speculate that fibrinogen concentrate would likely be similarly effective under conditions of acidosis compatible with life. This feature is not evidence based, but at least there are no indirect hints in the available trials. At present, some guidelines 97 do not sup-port the off-label use of rFVIIa in massive haem-orrhage, whilst others do.24, 98 The ESA guide-lines 24 suggest that the use of rFVIIa should be restricted for life-threatening refractory hemor-rhage. In hypothermic coagulopathy rFVIIa may be used, and if acidosis is present, rFVIIa should be infused alongside pH correction.
Hypocalcemia
Acute hypocalcemia (corrected total calcium level in plasma < 2.1 mmol/L)99 is a common complications of massive transfusions.100 Cit-rate, added to stored blood, binds calcium and thereby reduces serum level of the ionized frac-tion. In fresh frozen plasma there is a greater amount of citrate then in RBCs, but citrate is rapidly metabolized by liver.3 However, a liver dysfunction caused by a pre-existing illness or
7.15) by a combination of haemorrhage and aor-tic clamp in animal models, Lesperance et al.86 found that rFVIIa was effective in reversing the acidosis-related coagulopathy by improving INR and TEM parameters (EXTEM CT). A study involving swine models also showed that pH correction was not a precondition before rFVIIa administration.87 It is worth mentioning that administration of rFVIIa in both hypothermic and acidotic conditions has shown to improve thrombin generation.87, 88 However, other find-ings suggest that whilst a hypothermic condition does not impair rFVIIa activity, acidosis reduce its effectiveness and, thus, may be not useful in acidotic patients.16, 89 Data from registries have shown an association between lower values of pH and an increased mortality in patients in whom rFVIIa was administered.90-92 Consid-ering that the rFVIIa off-label use is associated with an increased risk of arterial thromboem-bolic complication,93 its effectiveness and clini-cal benefit in bleeding patients without haemo-philia are still unproven.94-96 On the other hand, taking into account that the MCF increase upon addition of fibrinogen concentrate at various lev-
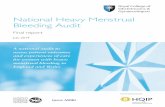
Figure 2.—Flowchart representing the correction of confounding factors (hypothermia, acidosis, hypocalcaemia) based on the European Society of Anaesthesiology (ESA) guidelines24 on severe perioperative bleeding management.
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

DE ROBERTIS COAGULOPATHY INDUCED BY ACIDOSIS, HYPOTHERMIA AND HYPOCALCAEMIA IN SEVERE BLEEDING
72 MINERVA ANESTESIOLOGICA January 2015
patients they are linked to each other, influenc-ing reciprocally and enhancing the deficit in hemostasis. Classic coagulation tests may not detect the coagulation abnormalities induced by those factors. The use of point-of-care testing performed on whole blood, such as TEG/TEM, may offer some advantages in acute severe hem-orrhages.
Key messages
— Acidosis, hypothermia and hypocal-cemia alter the process of haemostasis and contribute to the morbidity and mortality of bleeding patients.
— The lack of control of the hemorrhagic source causes and exacerbates the lethal triad.
— In the context of acidotic coagulopa-thy pH should be normalized even if this correction cannot completely reverse the al-terations induced by acidosis.
— Normothermia reduces blood loss and transfusion requirements.
— Acidosis and hypothermia affect fi-brinogen blood concentration but not tran-examic acid antifibrinolytic activity.
— Use of rFVIIa should be restricted for life-threatening refractory haemorrhage. In hypothermic coagulopathy rFVIIa may be used, and if acidosis is present, rFVIIa should be infused alongside pH correction.
— Calcium should be administered dur-ing massive transfusion to preserve normo-calcaemia.
— Point of care testing better evaluates the haemostatic impairment in hypothermic patients.
References
1. Lier H, Krep H, Schroeder S, Stuber F. Preconditions of hemostasis in trauma: a review. The influence of acidosis, hypocalcemia, anemia, and hypothermia on functional he-mostasis in trauma. J Trauma 2008;65:951-60.
2. Ferrara A, MacArthur JD, Wright HK, Modlin IM, Mc-Millen MA. Hypothermia and acidosis worsen coagulopa-thy in the patient requiring massive transfusion. Am J Surg 1990;160:515-8.
3. Spahn DR, Rossaint R. Coagulopathy and blood compo-nent transfusion in trauma. Br J Anaesth 2005;95:130-9.
4. Ho KM, Leonard AD. Concentration-dependent effect of
by hypothermia, could lead to ionized hypoc-alcaemia due to citrate chelation.100, 101 Moreo-ver, hemodilution, severe shock and ischemia may cause hypocalcaemia in trauma patients.102 Hypocalcemia (<0.8 mmol/L) in massive bleed-ing patients was strongly associated with an in-creased mortality in a cohort study.4 The pres-ence of acidosis and the amount of fresh frozen plasma transfused were major risk factors cor-related to the occurrence of severe ionized hy-pocalcaemia.4 Calcium (factor IV) anchors the side chains of coagulation factors to the phos-pholipids of the platelet membrane and plays an important role in the conversion of fibrinogen to fibrin.1, 103 Deficits in coagulation attributable to hypocalcaemia are seldom identified by com-mon coagulation tests.11 The minimum thresh-old of calcium concentration to enable a normal clot formation has been analyzed. Data from in vitro studies 104, 105 suggest that thrombin gen-eration does not occur when ionized calcium concentration is ≤0.25 mmol/L, whilst this re-action is not further promoted when calcium is ≥0.5 mmol/L. James et al.106 have shown that a normal clot formation occurred when the ion-ized calcium concentration was ≥0.56 mmol/L. The use heparin may have altered the measure of calcium concentration,106 and a threshold of 0.6-0.7≥mmol/L is considered adequate for the clot formation.1 However these in vitro results may not be extrapolated to clinical situations in which hypocalcaemia amplifies the effect on coagulopathy induced by acidosis, hypother-mia and haemodilution. Monitoring calcium concentration in such clinical situations is war-ranted. As matter of fact, the ESA guidelines 24 on severe perioperative bleeding management recommend maintaining ionized calcium con-centration at least ≥0.9 mmol/L during massive transfusion.
Conclusions
Acidosis, hypothermia and hypocalcemia induce coagulopathy via different pathomech-anisms. The algorithm for correction of con-founding factors (hypothermia, acidosis, hy-pocalcaemia) based on the ESA guidelines 24 is presented in Figure 2. In severely bleeding
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

COAGULOPATHY INDUCED BY ACIDOSIS, HYPOTHERMIA AND HYPOCALCAEMIA IN SEVERE BLEEDING DE ROBERTIS
Vol. 81 - No. 1 MINERVA ANESTESIOLOGICA 73
25. Kettner SC, Kozek SA, Groetzner JP, Gonano C, Schel-longowski A, Kucera M et al. Effects of hypothermia on thrombelastography in patients undergoing cardiopulmo-nary bypass. Br J Anaesth 1998;80:313-7.
26. Reed RL, 2nd, Johnson TD, Hudson JD, Fischer RP. The disparity between hypothermic coagulopathy and clotting studies. J Trauma 1992;33:465-70.
27. Rohrer MJ, Natale AM. Effect of hypothermia on the co-agulation cascade. Crit Care Med 1992;20:1402-5.
28. Rundgren M, Engström M. A thromboelastometric evalu-ation of the effects of hypothermia on the coagulation sys-tem. Anesth Analg 2008;107:1465-8.
29. Wolberg AS, Meng ZH, Monroe DM, 3rd, Hoffman M. A systematic evaluation of the effect of temperature on co-agulation enzyme activity and platelet function. J Trauma 2004;56:1221-8.
30. Scharbert G, Kalb M, Marschalek C, Kozek-Langenecker SA. The effects of test temperature and storage temperature on platelet aggregation: a whole blood in vitro study. An-esth Analg 2006;102:1280-4.
31. Scharbert G, Kalb ML, Essmeister R, Kozek-Langenecker SA. Mild and moderate hypothermia increases platelet ag-gregation induced by various agonists: a whole blood in vitro study. Platelets 2010;21:44-8.
32. Danforth CM, Orfeo T, Mann KG, Brummel-Ziedins KE, Everse SJ. The impact of uncertainty in a blood coagula-tion model. Math Med Biol 2009;26:323-36.
33. Hockin MF, Jones KC, Everse SJ, Mann KG. A model for the stoichiometric regulation of blood coagulation. J Biol Chem 2002;277:18322-33.
34. Mitrophanov AY, Rosendaal FR, Reifman J. Computa-tional analysis of the effects of reduced temperature on thrombin generation: the contributions of hypothermia to coagulopathy. Anesth Analg 2013;117:565-74.
35. Dirkmann D, Hanke AA, Görlinger K, Peters J. Hypo-thermia and acidosis synergistically impair coagulation in human whole blood. Anesth Analg 2008;106:1627-32.
36. Hanke AA, Dellweg C, Kienbaum P, Weber CF, Görlin-ger K, Rahe-Meyer N. Effects of desmopressin on platelet function under conditions of hypothermia and acidosis: an in vitro study using multiple electrode aggregometry*. An-aesthesia 2010;65:688-91.
37. Hanke AA, Dellweg C, Schöchl H, Weber CF, Jüttner B, Johanning K, et al. Potential of whole blood coagulation reconstitution by desmopressin and fibrinogen under con-ditions of hypothermia and acidosis--an in vitro study us-ing rotation thrombelastometry. Scand J Clin Lab Invest 2011;71:292-8.
38. Ng KFJ, Cheung CW, Lee Y, Leung SWS. Low-dose desmopressin improves hypothermia-induced impairment of primary haemostasis in healthy volunteers. Anaesthesia 2011;66:999-1005.
39. Ying CLA, Tsang SF, Ng KFJ. The potential use of desmo-pressin to correct hypothermia-induced impairment of primary haemostasis--an in vitro study using PFA-100. Resuscitation 2008;76:129-33.
40. Lethagen S. Desmopressin (DDAVP) and hemostasis. Ann Hematol 1994;69:173-80.
41. Agnelli G, Parise P, Levi M, Cosmi B, Nenci GG. Effects of desmopressin on hemostasis in patients with liver cirrhosis. Haemostasis 1995;25:241-7.
42. Kaufmann JE, Vischer UM. Cellular mechanisms of the hemostatic effects of desmopressin (DDAVP). J Thromb Haemost 2003;1:682-9.
43. Michiels JJ, van Vliet HHDM, Berneman Z, Gadisseur A, van der Planken M, Schroyens W et al. Intravenous DDAVP and factor VIII-von Willebrand factor concen-trate for the treatment and prophylaxis of bleedings in pa-tients With von Willebrand disease type 1, 2 and 3. Clin Appl Thromb Hemost 2007;13:14-34.
44. Peter FW, Benkovic C, Muehlberger T, Vogt PM, Homann
hypocalcaemia on mortality of patients with critical bleed-ing requiring massive transfusion: a cohort study. Anaesth Intensive Care 2011;39:46-54.
5. Mikhail J. The trauma triad of death: hypothermia, acido-sis, and coagulopathy. AACN Clin Issues 1999;10:85-94.
6. Mitra B, Tullio F, Cameron PA, Fitzgerald M. Trauma pa-tients with the ‘triad of death’. Emerg Med J 2012;29:622-5.
7. Kauvar DS, Lefering R, Wade CE. Impact of hemorrhage on trauma outcome: an overview of epidemiology, clinical presentations, and therapeutic considerations. J Trauma 2006;60:S3-11.
8. Thorsen K, Ringdal KG, Strand K, Søreide E, Hagemo J, Søreide K. Clinical and cellular effects of hypother-mia, acidosis and coagulopathy in major injury. Br J Surg 2011;98:894-907.
9. Zhang J, Jiang R, Liu L, Watkins T, Zhang F, Dong J-f. Traumatic brain injury-associated coagulopathy. J Neuro-trauma 2012;29:2597-605.
10. Piazza O, Scarpati G, Cotena S, Lonardo M, Tufano R. Thrombin antithrombin complex and IL-18 serum levels in stroke patients. Neurol Int 2010;2:e1.
11. Spahn DR. Hypocalcemia in trauma: frequent but fre-quently undetected and underestimated. Crit Care Med 2005;33:2124-5.
12. Ball CG. Damage control resuscitation: history, theory and technique. Can J Surg 2014;57:55-60.
13. De Robertis E, Tomins P, Knape H. Anaesthesiologists in emergency medicine: the desirable manpower. Eur J An-aesthesiol 2010;27:223-5.
14. Engström M, Schött U, Romner B, Reinstrup P. Acidosis impairs the coagulation: A thromboelastographic study. J Trauma 2006;61:624-8.
15. Bolliger D, Seeberger MD, Tanaka KA. Principles and practice of thromboelastography in clinical coagulation management and transfusion practice. Transfus Med Rev 2012;26:1-13.
16. Meng ZH, Wolberg AS, Monroe DM, 3rd, Hoffman M. The effect of temperature and pH on the activity of fac-tor VIIa: implications for the efficacy of high-dose fac-tor VIIa in hypothermic and acidotic patients. J Trauma 2003;55:886-91.
17. Martini WZ, Pusateri AE, Uscilowicz JM, Delgado AV, Holcomb JB. Independent contributions of hypother-mia and acidosis to coagulopathy in swine. J Trauma 2005;58:1002-9.
18. Martini WZ. Coagulopathy by hypothermia and acidosis: mechanisms of thrombin generation and fibrinogen avail-ability. J Trauma 2009;67:202-8.
19. Martini WZ, Dubick MA, Pusateri AE, Park MS, Ryan KL, Holcomb JB. Does bicarbonate correct coagula-tion function impaired by acidosis in swine? J Trauma 2006;61:99-106.
20. Darlington DN, Kheirabadi BS, Delgado AV, Scherer MR, Martini WZ, Dubick MA. Coagulation changes to system-ic acidosis and bicarbonate correction in swine. J Trauma 2011;71:1271-7.
21. Martini WZ, Dubick MA, Wade CE, Holcomb JB. Evalu-ation of tris-hydroxymethylaminomethane on reversing coagulation abnormalities caused by acidosis in pigs. Crit Care Med 2007;35:1568-74.
22. Martini WZ, Holcomb JB. Acidosis and coagulopathy: the differential effects on fibrinogen synthesis and breakdown in pigs. Ann Surg 2007;246:831-5.
23. Wong DW, Mishkin FS, Tanaka TT. The effects of bicar-bonate on blood coagulation. JAMA 1980;244:61-2.
24. Kozek-Langenecker SA, Afshari A, Albaladejo P, Santul-lano CAA, De Robertis E, Filipescu DC, et al. Manage-ment of severe perioperative bleeding: guidelines from the European Society of Anaesthesiology. Eur J Anaesthesiol 2013;30:270-382.
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

DE ROBERTIS COAGULOPATHY INDUCED BY ACIDOSIS, HYPOTHERMIA AND HYPOCALCAEMIA IN SEVERE BLEEDING
74 MINERVA ANESTESIOLOGICA January 2015
Fernández-Mondéjar E et al. Management of bleeding and coagulopathy following major trauma: an updated Euro-pean guideline. Crit Care 2013;17:R76.
65. Rodgers GM. Prothrombin complex concentrates in emer-gency bleeding disorders. Am J Hematol 2012;87:898-902.
66. Franchini M, Lippi G. Prothrombin complex concen-trates: an update. Blood Transfus 2010;8:149-54.
67. Dickneite G, Doerr B, Kaspereit F. Characterization of the coagulation deficit in porcine dilutional coagulopathy and substitution with a prothrombin complex concentrate. An-esth Analg 2008;106:1070-7.
68. Dickneite G, Dörr B, Kaspereit F, Tanaka KA. Pro-thrombin complex concentrate versus recombinant factor VIIa for reversal of hemodilutional coagulopathy in a por-cine trauma model. J Trauma 2010;68:1151-7.
69. Dickneite G, Pragst I. Prothrombin complex concentrate vs fresh frozen plasma for reversal of dilutional coagulopathy in a porcine trauma model. Br J Anaesth 2009;102:345-54.
70. Honickel M, Rieg A, Rossaint R, Braunschweig T, Spronk HMH, ten Cate H et al. Prothrombin complex concen-trate reduces blood loss and enhances thrombin generation in a pig model with blunt liver injury under severe hypo-thermia. Thromb Haemost 2011;106:724-33.
71. Ortmann E, Besser MW, Klein AA. Antifibrinolytic agents in current anaesthetic practice. Br J Anaesth 2013;111:549-63.
72. Shakur H, Roberts I, Bautista R, Caballero J, Coats T, De-wan Y et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet 2010;376:23-32.
73. Roberts I, Shakur H, Afolabi A, Brohi K, Coats T, Dewan Y et al. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analy-sis of the CRASH-2 randomised controlled trial. Lancet 2011;377:1096-101.
74. Porta CR, Nelson D, McVay D, Salgar S, Eckert M, Izenberg S et al. The effects of tranexamic acid and pro-thrombin complex concentrate on the coagulopathy of trauma: an in vitro analysis of the impact of severe acidosis. J Trauma Acute Care Surg 2013;75:954-60.
75. Dirkmann D, Radü-Berlemann J, Görlinger K, Peters J. Recombinant tissue-type plasminogen activator-evoked hyperfibrinolysis is enhanced by acidosis and inhibited by hypothermia but still can be blocked by tranexamic acid. J Trauma Acute Care Surg 2013;74:482-8.
76. Kenet G, Walden R, Eldad A, Martinowitz U. Treatment of traumatic bleeding with recombinant factor VIIa. Lan-cet 1999;354:1879.
77. Eikelboom JW, Bird R, Blythe D, Coyle L, Gan E, Harvey M et al. Recombinant activated factor VII for the treat-ment of life-threatening haemorrhage. Blood Coagul Fi-brinolysis 2003;14:713-7.
78. Khan AZ, Parry JM, Crowley WF, McAllen K, Davis AT, Bonnell BW et al. Recombinant factor VIIa for the treat-ment of severe postoperative and traumatic hemorrhage. Am J Surg 2005;189:331-4.
79. Mayo A, Misgav M, Kluger Y, Geenberg R, Pauzner D, Klausner J et al. Recombinant activated factor VII (NovoSeven): addition to replacement therapy in acute, uncontrolled and life-threatening bleeding. Vox Sang 2004;87:34-40.
80. O’Neill PA, Bluth M, Gloster ES, Wali D, Priovolos S, DiMaio TM et al. Successful use of recombinant activated factor VII for trauma-associated hemorrhage in a patient without preexisting coagulopathy. J Trauma 2002;52:400-5.
81. Repessé X, Au SM, Bréchot N, Trouillet J-L, Leprince P, Chastre J et al. Recombinant factor VIIa for uncontrol-
HH, Kuhnen C et al. Effects of desmopressin on thrombo-genesis in aspirin-induced platelet dysfunction. Br J Hae-matol 2002;117:658-63.
45. Ozier Y, Bellamy L. Pharmacological agents: antifibrino-lytics and desmopressin. Best Pract Res Clin Anaesthesiol 2010;24:107-19.
46. Carless PA, Henry DA, Moxey AJ, O’Connell D, McClel-land B, Henderson KM et al. Desmopressin for minimis-ing perioperative allogeneic blood transfusion. Cochrane Database Syst Rev 2004:CD001884.
47. Martini WZ. The effects of hypothermia on fibrinogen metabolism and coagulation function in swine. Metabo-lism 2007;56:214-21.
48. Ruzicka J, Stengl M, Bolek L, Benes J, Matejovic M, Krouzecky A. Hypothermic anticoagulation: testing indi-vidual responses to graded severe hypothermia with throm-boelastography. Blood Coagul Fibrinolysis 2012;23:285-9.
49. Delhaye C, Mahmoudi M, Waksman R. Hypothermia therapy: neurological and cardiac benefits. J Am Coll Car-diol 2012;59:197-210.
50. De Robertis E, Romano GM, Zito Marinosci G, Servillo G, Tufano R. Antihypertensive therapy in acute cerebral haemorrhage. Trends in Anaesthesia and Critical Care 2013;3:31-6.
51. Nielsen N, Sunde K, Hovdenes J, Riker RR, Rubertsson S, Stammet P et al. Adverse events and their relation to mor-tality in out-of-hospital cardiac arrest patients treated with therapeutic hypothermia. Crit Care Med 2011;39:57-64.
52. Polderman KH. Mechanisms of action, physiological ef-fects, and complications of hypothermia. Crit Care Med 2009;37:S186-202.
53. Piazza O, Cotena S, Esposito G, De Robertis E, Tufano R. S100B is a sensitive but not specific prognostic index in comatose patients after cardiac arrest. Minerva Chir 2005;60:477-80.
54. Tsuei BJ, Kearney PA. Hypothermia in the trauma patient. Injury 2004;35:7-15.
55. Mohr J, Ruchholtz S, Hildebrand F, Flohé S, Frink M, Witte I et al. Induced hypothermia does not impair coagu-lation system in a swine multiple trauma model. J Trauma Acute Care Surg 2013;74:1014-20.
56. Wu X, Kochanek PM, Cochran K, Nozari A, Henchir J, Stezoski SW et al. Mild hypothermia improves survival after prolonged, traumatic hemorrhagic shock in pigs. J Trauma 2005;59:291-9.
57. Kettner SC, Sitzwohl C, Zimpfer M, Kozek SA, Holzer A, Spiss CK et al. The effect of graded hypothermia (36 degrees C-32 degrees C) on hemostasis in anesthetized patients without surgical trauma. Anesth Analg 2003;96:1772-6.
58. Rajagopalan S, Mascha E, Na J, Sessler DI. The effects of mild perioperative hypothermia on blood loss and transfu-sion requirement. Anesthesiology 2008;108:71-7.
59. Schmied H, Kurz A, Sessler DI, Kozek S, Reiter A. Mild hypothermia increases blood loss and transfusion require-ments during total hip arthroplasty. Lancet 1996;347:289-92.
60. Ramaker AJDWR, Meyer P, van der Meer J, Struys MMRF, Lisman T, van Oeveren W et al. Effects of acidosis, alkalosis, hyperthermia and hypothermia on haemostasis: results of point-of-care testing with the thromboelastogra-phy analyser. Blood Coagul Fibrinolysis 2009;20:436-9.
61. Urwyler N, Theiler L, Hirschberg M, Kleine-Brueggeney M, Colucci G, Greif R. Standard vs. point-of-care meas-urement of fibrinogen: potential impact on clinical deci-sions. Minerva Anestesiol 2012;78:550-5.
62. Fries D. Coagulation monitoring under bleeding condi-tions: time to reconsider basic principles for our clinical decisions! Minerva Anestesiol 2012;78:517-8.
63. Fries D, Martini WZ. Role of fibrinogen in trauma-in-duced coagulopathy. Br J Anaesth 2010;105:116-21.
64. Spahn DR, Bouillon B, Cerny V, Coats TJ, Duranteau J,
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

COAGULOPATHY INDUCED BY ACIDOSIS, HYPOTHERMIA AND HYPOCALCAEMIA IN SEVERE BLEEDING DE ROBERTIS
Vol. 81 - No. 1 MINERVA ANESTESIOLOGICA 75
combinant activated factor VII in randomized clinical tri-als. N Engl J Med 2010;363:1791-800.
94. Lin Y, Stanworth S, Birchall J, Doree C, Hyde C. Use of recombinant factor VIIa for the prevention and treatment of bleeding in patients without hemophilia: a systematic review and meta-analysis. CMAJ 2011;183:E9-19.
95. Simpson E, Lin Y, Stanworth S, Birchall J, Doree C, Hyde C. Recombinant factor VIIa for the prevention and treat-ment of bleeding in patients without haemophilia. Co-chrane Database Syst Rev 2012;3:CD005011.
96. Yank V, Tuohy CV, Logan AC, Bravata DM, Stauden-mayer K, Eisenhut R et al. Systematic review: benefits and harms of in-hospital use of recombinant factor VIIa for off-label indications. Ann Intern Med 2011;154:529-40.
97. Lin Y, Moltzan CJ, Anderson DR, National Advisory Committee on B, Blood P. The evidence for the use of re-combinant factor VIIa in massive bleeding: revision of the transfusion policy framework. Transfus Med 2012;22:383-94.
98. Martinowitz U, Michaelson M, Israeli Multidisciplinary r FTF. Guidelines for the use of recombinant activated factor VII (rFVIIa) in uncontrolled bleeding: a report by the Israeli Multidisciplinary rFVIIa Task Force. J Thromb Haemost 2005;3:640-8.
99. Cooper MS, Gittoes NJL. Diagnosis and management of hypocalcaemia. BMJ 2008;336:1298-302.
100. Sihler KC, Napolitano LM. Complications of massive transfusion. Chest 2010;137:209-20.
101. Coté CJ, Drop LJ, Hoaglin DC, Daniels AL, Young ET. Ionized hypocalcemia after fresh frozen plasma administra-tion to thermally injured children: effects of infusion rate, duration, and treatment with calcium chloride. Anesth Analg 1988;67:152-60.
102. Vivien B, Langeron O, Morell E, Devilliers C, Carli PA, Coriat P et al. Early hypocalcemia in severe trauma. Crit Care Med 2005;33:1946-52.
103. Elödi S, Elödi P. Surface-governed molecular regulation of blood coagulation. Mol Aspects Med 1983;6:291-353.
104. Ataullakhanov FI, Pohilko AV, Sinauridze EI, Volkova RI. Calcium threshold in human plasma clotting kinetics. Thromb Res 1994;75:383-94.
105. King WH, Patten ED, Bee DE. An in vitro evaluation of ionized calcium levels and clotting in red blood cells diluted with lactated Ringer’s solution. Anesthesiology 1988;68:115-21.
106. James MFM, Roche AM. Dose-response relationship be-tween plasma ionized calcium concentration and thromb-elastography. J Cardiothorac Vasc Anesth 2004;18:581-6.
lable bleeding in patients with extracorporeal membrane oxygenation: report on 15 cases and literature review. Crit Care 2013;17:R55.
82. Logan AC, Yank V, Stafford RS. Off-label use of recom-binant factor VIIa in U.S. hospitals: analysis of hospital records. Ann Intern Med 2011;154:516-22.
83. Hedner U. Mechanism of action of factor VIIa in the treatment of coagulopathies. Semin Thromb Hemost 2006;32(Suppl 1):77-85.
84. Viuff D, Lauritzen B, Pusateri AE, Andersen S, Rojkjaer R, Johansson PI. Effect of haemodilution, acidosis, and hypothermia on the activity of recombinant factor VIIa (NovoSeven). Br J Anaesth 2008;101:324-31.
85. Kheirabadi BS, Delgado AV, Dubick MA, Scherer MR, Fedyk CG, Holcomb JB et al. In vitro effect of activated recombinant factor VII (rFVIIa) on coagulation properties of human blood at hypothermic temperatures. J Trauma 2007;63:1079-86.
86. Lesperance RN, Lehmann RK, Harold DM, Beekley AC, Sebesta JA, Martin MJ. Recombinant factor VIIa is effec-tive at reversing coagulopathy in a lactic acidosis model. J Trauma Acute Care Surg 2012;72:123-9.
87. Darlington DN, Kheirabadi BS, Scherer MR, Martini WZ, Dubick MA. Acidosis and correction of acidosis does not affect rFVIIa function in swine. Int J Burns Trauma 2012;2:145-57.
88. Darlington DN, Kremenevskiy I, Pusateri AE, Scherer MR, Fedyk CG, Kheirabaldi BS, et al. Effects of In vitro hemodilution, hypothermia and rFVIIa addition on co-agulation in human blood. Int J Burns Trauma 2012;2:42-50.
89. Hall K, Forrest P, Sawyer C. The effects of acidosis and hypothermia on blood transfusion requirements follow-ing factor VII administration. Anaesth Intensive Care 2007;35:494-7.
90. Mamtani R, Nascimento B, Rizoli S, Pinto R, Lin Y, Tien H. The utility of recombinant factor VIIa as a last resort in trauma. World J Emerg Surg 2012;7:S7.
91. Isbister J, Phillips L, Dunkley S, Jankelowitz G, McNeil J, Cameron P. Recombinant activated factor VII in criti-cal bleeding: experience from the Australian and New Zealand Haemostasis Register. Intern Med J 2008;38:156- 65.
92. Karkouti K, Beattie WS, Arellano R, Aye T, Bussieres JS, Callum JL et al. Comprehensive Canadian review of the off-label use of recombinant activated factor VII in cardiac surgery. Circulation 2008;118:331-8.
93. Levi M, Levy JH, Andersen HF, Truloff D. Safety of re-
Funding.—Sibylle A. Kozek-Langenecker received honoraria for lecturing and travel reimbursement from: CSL Behring, Biotest, Baxter, Novonordisc, Octapharma, TEM.Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Received on December 23, 2013. - Accepted for publication on March 6, 2014. - Epub ahead of print on March 7, 2014.Corresponding author: E. De Robertis, Department of Anesthesia, University of Naples Federico II, via S. Pansini 5, 80131 Naples, Italy. E-mail: [email protected]
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.
Copyright © 2022 FDOKUMEN