
Endoscopic Band Ligation and Esophageal Stents for Acute Variceal Bleeding
18
Endoscopic Band Ligation and Esophageal Stents for Acute Variceal Bleeding Andrés Cárdenas, MD, MMSc a, *, Alejandro Fernández-Simon, MD a , Angels Escorcell b Q2 Q3 Q4 Q5 Q6 Video of Endoscopic band ligation technique accompanies this article at http:// www.liver.theclinics.com/ Acute variceal bleeding (AVB) Q9 is a dreaded complication in patients with portal hyper- tension, and the first episode in a patient with cirrhosis constitutes a significant mile- stone in the progression of the hepatic disease with important implications in prognosis. Mortality rates due to AVB have decreased in the past 30 years, from 60% to 15% to 20% at 6 weeks, thanks to improvements in general management, medical treatment, and endoscopic therapy. 1 However, there is still a significant Disclosure: None. Q8 a GI/Endoscopy Unit, Institut de Malalties Digestives i Metaboliques, Hospital Clinic, University of Barcelona, Barcelona, Spain; b Liver Unit, Institut de Malalties Digestives i Metaboliques, Hospital Clinic, University of Barcelona, Barcelona, Spain Q7 * Corresponding author. Institut de Malalties Digestives i Metaboliques, Hospital Clinic, Univer- sity of Barcelona, Villarroel 170, Esc 3-2, 08036 Barcelona, Spain. E-mail addresses: [email protected]; [email protected] KEYWORDS Cirrhosis Gastrointestinal bleeding Esophageal varices Endoscopic band ligation Esophageal stents TIPS Portal hypertension Acute variceal bleeding KEY POINTS Acute variceal bleeding (AVB) is one of the most serious and feared complications of pa- tients with portal hypertension. The management of AVB includes a stepped care approach aimed at resuscitation, restrictive transfusion policy, antibiotic prophylaxis, pharmacologic therapy with vasocon- strictors, and endoscopic therapy. The most accepted endoscopic method for treating bleeding varices is endoscopic band ligation, which is effective in approximately 90% of patients. Endoscopic sclerotherapy may be used if band ligation is not possible. Esophageal stents that cause tamponade of the esophagus are safer and more effective as a rescue therapy for AVB than balloon tamponade with Sengstaken Blakemore tubes. CLD715_proof ■ 14 August 2014 ■ 3:37 pm Clin Liver Dis - (2014) -–- http://dx.doi.org/10.1016/j.cld.2014.07.003 liver.theclinics.com 1089-3261/14/$ – see front matter Ó 2014 Published by Elsevier Inc. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Endoscopic Band Ligation and Esophageal Stents for Acute Variceal Bleeding

1
234
567
8910
11121314
151617
181920
212223
24252627
282930
313233
34353637
383940
414243
444546
4748
Endoscopic Band Ligationand Esophageal Stents for
Acute Variceal BleedingQ2 Q3Q6
Andrés Cárdenas, MD, MMSca,*, Alejandro Fernández-Simon, MDa,Angels Escorcellb
Q4 Q5
KEYWORDS
� Cirrhosis � Gastrointestinal bleeding � Esophageal varices� Endoscopic band ligation � Esophageal stents � TIPS � Portal hypertension� Acute variceal bleeding
KEY POINTS
� Acute variceal bleeding (AVB) is one of the most serious and feared complications of pa-tients with portal hypertension.
� The management of AVB includes a stepped care approach aimed at resuscitation,restrictive transfusion policy, antibiotic prophylaxis, pharmacologic therapy with vasocon-strictors, and endoscopic therapy.
� The most accepted endoscopic method for treating bleeding varices is endoscopic bandligation, which is effective in approximately 90% of patients. Endoscopic sclerotherapymay be used if band ligation is not possible.
� Esophageal stents that cause tamponade of the esophagus are safer and more effectiveas a rescue therapy for AVB than balloon tamponade with Sengstaken Blakemore tubes.
Q9
Video of Endoscopic band ligation technique accompanies this article at http://www.liver.theclinics.com/
Acute variceal bleeding (AVB) is a dreaded complication in patients with portal hyper-tension, and the first episode in a patient with cirrhosis constitutes a significant mile-stone in the progression of the hepatic disease with important implications inprognosis. Mortality rates due to AVB have decreased in the past 30 years, from60% to 15% to 20% at 6 weeks, thanks to improvements in general management,medical treatment, and endoscopic therapy.1 However, there is still a significant
Disclosure: None. Q8a GI/Endoscopy Unit, Institut de Malalties Digestives i Metaboliques, Hospital Clinic, Universityof Barcelona, Barcelona, Spain; b Liver Unit, Institut de Malalties Digestives i Metaboliques,Hospital Clinic, University of Barcelona, Barcelona, Spain Q7
* Corresponding author. Institut de Malalties Digestives i Metaboliques, Hospital Clinic, Univer-sity of Barcelona, Villarroel 170, Esc 3-2, 08036 Barcelona, Spain.E-mail addresses: [email protected]; [email protected]
CLD715_proof ■ 14 August 2014 ■ 3:37 pm
Clin Liver Dis - (2014) -–-http://dx.doi.org/10.1016/j.cld.2014.07.003 liver.theclinics.com1089-3261/14/$ – see front matter � 2014 Published by Elsevier Inc.
BOTERO MEJIA
Nota adhesiva
Angels Escorcell, MD, PhD
BOTERO MEJIA
Nota adhesiva
ICU / Liver Unit
BOTERO MEJIA
Nota adhesiva
MD, MMSc, AGAF. MMSc- stands for Masters in Medcial Science. It is a well known degree. I got this degree from Harvard Medical School
BOTERO MEJIA
Nota adhesiva
Q6-ok q2-q5- see responses in each line
BOTERO MEJIA
Nota adhesiva
AC
BOTERO MEJIA
Nota adhesiva
ok
BOTERO MEJIA
Nota adhesiva
ok, a & b have same address

web4C=FPO
Cardenas et al2
49
505152
535455
565758
59606162
636465
666768
697071
72737475
767778
798081
82838485
868788
899091
929394
95969798
99
recurrence rate and that is why after an episode of AVB patients need secondary pro-phylaxis. Endoscopy by means of using endoscopic band ligation (EBL) plays a keyrole in the management of AVB. Current available methods, combined with vasoactivedrugs, allow for the control of bleeding in approximately 90% of cases within the firstdays of the index bleed.2,3 In cases in which AVB cannot be controlled with endos-copy, balloon tamponade of the esophagus may be required; however, there aresignificant complications with this method. The recent introduction of fully coveredself-expandable metallic stents for AVB is useful in those cases in which balloon tam-ponade is considered, as it is more effective and safer for the temporary control ofbleeding. This article reviews the current management of AVB with particularemphasis on EBL and esophageal stents.
NATURAL HISTORY/DIAGNOSIS
Esophageal varices are present in nearly 30% to 40% of patients with compensatedcirrhosis and in 60% to 80% of those with decompensated cirrhosis.4 They initiallydevelop as small varices that gradually dilate at a rate of 5% per year. Varicealbleeding usually occurs late in the natural history of portal hypertension, and for vari-ces to bleed, portal pressure as measured by the hepatic venous pressure gradient(HVPG) must rise above 12 mm Hg.3,5 Certain characteristics, such as the severityof liver disease, the size of the varix, and the presence of red wale marks (especiallyon thin areas of the variceal wall), place the varices at risk of bleeding, which can occurwith an incidence of 4% to 15% per year.4,6,7 Because patients with cirrhosis with anepisode of upper gastrointestinal bleeding will have varices as the cause in 80% ofcases, bleeding in this setting should be presumed to be of variceal origin.8 Thegold standard for diagnosis of AVB is gastroscopy, which may show active bleedingor oozing from a varix (present in nearly 10%–20% of patients) (Fig. 1), signs of arecent hemostasis white nipple or adherent clot on a varix, or blood in the stomachand/or presence of varices with no other explainable sources of bleeding. Earlyrebleeding rates within the first 48 to 72 hours after the index bleed can be high(30%–40%) if patients are not properly treated.9–11 After 6 weeks, the risk of furtherbleeding is similar to that before the index bleed.11,12 Mortality rates from an episode
Fig. 1. Endoscopic view of an actively bleeding (spurting) esophageal varix in a patient withcirrhosis.
CLD715_proof ■ 14 August 2014 ■ 3:37 pm
BOTERO MEJIA
Nota adhesiva
delete comma
BOTERO MEJIA
Tachado
BOTERO MEJIA
Tachado
BOTERO MEJIA
Texto insertado
with a

Q1Esophageal Stents for Acute Variceal Bleeding 3
100
101102103
104105106
107108109
110111112113
114115116
117118119
120121122
123124125126
127128129
130131132
133134135136
137138139
140141142
143144145
146147148149
150
of variceal bleeding have significantly decreased in the past 3 decades, from 42% inthe 1980s11 to the current rates of 15% to 20%.13–17 This is largely because of theimplementation of standardized guidelines, advances in critical care, better pharma-cologic and endoscopic therapies, use of transjugular intrahepatic portosystemicshunts (TIPS), restrictive transfusion policies, and use of prophylactic antibiotics forbacterial infections. Approximately one-third of the deaths are a direct consequenceof bleeding, whereas the remaining are related to liver failure, infections, and renalfailure.8,18
GENERAL MANAGEMENT
The current recommendations for the general management of patients with anepisode of AVB have been reviewed elsewhere.19 In short, the most important aspectis providing adequate resuscitation (ie, treatment of hypovolemia), avoiding aspirationby protecting the airway and intubation in selected cases, preventing bacterial infec-tions, and stopping the hemorrhage with the use of vasoconstrictors and endoscopictherapy. Intubation always should be considered in patients with hepatic encephalop-athy and actively vomiting blood.20,21 Volume resuscitation with saline or other ex-panders should aim to keep systolic blood pressure between 90 and 100 mm Hg,which can help avoid shock and renal failure.22 Overexpansion may induce reboundincreases in portal pressure and facilitate rebleeding; therefore, a delicate fluid bal-ance is needed in these cases and adequate monitoring in the intensive care unit ishelpful. Red blood cell transfusion should aim for a hemoglobin level of 7 g/dL, exceptin patients with shock, ongoing bleeding, or ischemic heart disease.23 A trial of arestrictive transfusion policy in which patients were transfused if hemoglobin levelsdropped to lower than 7 g/dL (compared with transfusion if hemoglobin <9 g/dL)showed better survival in patients with cirrhosis (Child-Pugh A or B) transfused onlyif hemoglobin levels were lower than 7 g/dL.23 There are no data to support the routineuse of fresh frozen plasma to improve the elevated international normalized ratio in pa-tients with cirrhosis unless they are anticoagulated with warfarin or heparin or otheranticoagulants. Platelets should be transfused if they are below 50,000/mL.24 Bacterialinfections can occur in the setting of AVB, and thus all patients should receive antibi-otics. This measure decreases the risk of infection and rebleeding and improves sur-vival.25–28 In most cases, either norfloxacin 400 mg orally, twice a day for 7 days orintravenous ceftriaxone 1–2 g per day should be given. Intravenous antibiotics arepreferred in those patients with hypovolemic shock and advanced cirrhosis.29 Therapid implementation of vasoconstrictors and performance of endoscopy should beinstituted within the first 12 hours of admission.30 This interval can be shortened to6 hours in those actively vomiting blood once they are stabilized in a monitored unit.Finally, it is important to consider if the patient is a candidate for TIPS, as the earlyplacement of TIPS (within 72 hours) for patients with AVB with Child-Pugh B activelybleeding or C cirrhosis (<13 points) is associated with a significant reduction inrebleeding and mortality and thus should be considered in such cases.31
HEMOSTATIC THERAPIESSplanchnic Vasoconstrictors
There are 2 types of vasoconstrictors used in patients with AVB; the most commonlyused are terlipressin (vasopressin analogue) and somatostatin and its analogue(octreotide). These drugs with specific splanchnic vasoconstrictor activity play afundamental role in the management of AVB and need to be administered as soonas possible and before endoscopy. The early use of vasoconstrictors in most cases
CLD715_proof ■ 14 August 2014 ■ 3:37 pm

Cardenas et al4
151
152153154
155156157
158159160
161162163164
165166167
168169170
171172173
174175176177
178179180
181182183
184185186187
188189190
191192193
194195196
197198199200
201
can initially arrest bleeding, which translates into better visualization at endoscopy.These drugs also reduce rebleeding and improve survival among patients withcirrhosis and AVB.32–36 The available vasoconstrictors and their doses are shown inTable 1. A detailed analysis of the role of vasoconstrictors in AVB is out of the scopeof this review and is detailed elsewhere.36
Endoscopic Therapy
Endoscopy is one of the cornerstones of the management of AVB because it confirmsthe diagnosis and allows specific therapy during the same session. An importantconsideration before considering endoscopy is choosing the type of sedation forthe procedure, as patients need to be fully sedated for the procedure to be successful.We recommend intravenous sedation with propofol, if possible, as it is safe and bettertolerated than benzodiazepines (midazolam) plus an opiates (meperidine or fentanyl),which can trigger episodes of minimal hepatic encephalopathy.37–39 Endoscopic ther-apies for varices are effective because they cause obliteration of the varix. The 2 endo-scopic methods available for AVB are endoscopic sclerotherapy (ES) and EBL. ESconsists of the injection of a sclerosing agent (sodium morrhuate 5%, ethanolamineoleate 5%, or polidocanol 1%–2%) into the variceal lumen or adjacent to it. Thiscauses inflammation and thrombosis, creating a scar over the site of the varix.Although it is easy to perform (only need an injection catheter and the sclerosant) thereare significant side effects related to the procedure. There are a number of local andsystemic complications, which include esophageal ulcers, strictures, substernal chestpain, fever, dysphagia, and even the development of pleural effusions.40,41 Anotherproblem is the risk of bacteremia, which may arise in up to 30% to 55% of casesand can predispose to spontaneous bacterial peritonitis or distal abscesses.42,43
Other rare complications include perforation, mediastinitis, pericarditis, chylothorax,and esophageal motility disorders.40,41,44,45 Compared with EBL of varices, ES forAVB is associated with higher rebleeding rates and more side effects, such as ulcersand strictures.46 Clinical trials have shown that EBL is better than ES for all major out-comes, including initial control of bleeding, recurrent bleeding, side effects, time tovariceal eradication, and even survival.47,48
EBL
EBL was introduced an alternative with fewer complications to ES for the treatment ofesophageal varices. The concept of using EBL for esophageal varices arose in the1980s.49 Given the anatomy and zones of venous return in the gastroesophageal junc-tion Stiegmann and colleagues50 sought out a means of blocking this drainage. Theveins in the palisade zone, which extend proximal to the cardias into the lower esoph-agus, are the veins most likely to bleed because this is an area between the portal andsystemic circulation with no perforating veins from the submucosa allowing fordrainage or decompression to periesophageal veins. Thus, a way of “safely” of
Table 1Vasoconstrictors used in acute variceal bleeding
Drug Dose
Terlipressin Intravenous bolus 2 mg/4 h for 24–48 h then 1 mg/4 h
Somatostatin Intravenous bolus 250 mg followed by infusion of 250–500 mg/h
Octreotide Intravenous bolus of 50–100 mg followed by infusion of 50 mg/h
All drugs are administered for a minimum of 2 days and may be prolonged for up to 5 days.
CLD715_proof ■ 14 August 2014 ■ 3:37 pm
BOTERO MEJIA
Tachado
BOTERO MEJIA
Tachado

Q10
web4C=FPO
Esophageal Stents for Acute Variceal Bleeding 5
202
203204205
206207208
209210211
212213214215
216217218
219220221
222223224
225226227228
229230231
232233234
235236237238
239240241
242243244
245246247
248249250251
252
obliterating these vessels was that of placing rubber bands on the varices in the distalesophagus similar to what surgeons use for treating hemorrhoids. The rest is history,and currently EBL is considered the endoscopic treatment of choice for AVB. In brief,EBL consists of the placement of several elastic bands (range between 4–10) on thevarices so as to occlude the varix and cause thrombosis. The technique is shown inVideo 1. Ligation of the varix and surrounding mucosa eventually leads necrosis ofthe mucosa. The bands fall off within 5 to 7 days, leaving a shallow ulcer that healsand subsequently scars. After the index treatment of an episode of AVB, scheduledrepeat sessions need to be performed at 3-week to 4-week intervals to completelyobliterate the varices and reduce the risk of rebleeding.51
There are several commercially availablemultiband devices. In Europe and the UnitedStates themost common are the SaeedMultiple Ligator (Wilson-CookMedical, Inc) andthe Speedband (Microvasive Boston Scientific Corporation). They have between 4 and10 preloaded bands. We prefer to always start the procedure with a 6-band or 7-banddevice. This allows for enough bands to be placed in a single session without havingto repeatedly intubate thepatientwith thegastroscope.Band ligators haveoneprinciple:placement of elastic bands on a varix after it is sucked into a clear plastic cylinderattached to the tip of the endoscope (Fig. 2). After the indexdiagnostic endoscopy isper-formed in a patientwith AVBand the suspected varix is identified, the endoscope iswith-drawnand the ligationdevice is loaded. Thedeviceneeds tobe firmly attached to shaft ofthe scope near the knobs (Fig. 3). At this point, the patient needs to be reintubated andthis sometimes can be difficult because the cap of the ligator makes the distal tip of thescope thicker and there is limited vision. It is better to perform a slight flexion of the pa-tient’s neck and then push very gently with slight torque to the left or right, always withdirect visualization of the pharynx.Once the esophagus is intubated, the knob on the de-vice needs to be on “forward-only”mode. After the varix is identified, the tip of the scopeis pushed toward it and continuous suction applied so the mucosa of the varix fills thecap and causes a “red-out” sign; at this point, the band can be fired and a click mustbe felt (see Fig. 3, Video 1). Afterward, the scope should not be advanced distally soas to prevent dislodgement of band. This is the reason why ligation should alwayscommence in the most distal portion of the esophagus near the gastroesophageal(GE) junction. Bands are applied in a spiral pattern, progressing up the esophagus untilall major columns of varices of the lower third of the esophagus (no more than 8–10 cmabove theGE junction) are banded. If there is a limited viewbecauseofongoingbleeding,an option is to aggressively flush with water, perform suction, and start placing bands at
Fig. 2. Endoscopic view of large varices (left) and endoscopic view of successfully placedbands in the distal esophagus (right).
CLD715_proof ■ 14 August 2014 ■ 3:37 pm
BOTERO MEJIA
Texto insertado
with endoscopy
BOTERO MEJIA
Texto insertado
to
BOTERO MEJIA
Nota adhesiva
Unmarked definida por BOTERO MEJIA
BOTERO MEJIA
Texto insertado
Winston-Salem NC
BOTERO MEJIA
Tachado
BOTERO MEJIA
Texto insertado
Natick, MA
BOTERO MEJIA
Nota adhesiva
ok, see responses
BOTERO MEJIA
Texto insertado

Q11
web4C=FPO
Fig. 3. (A) Band ligator placed on the shaft of the endoscope, the knob is attached to theworking channel. (B) The proximal end of the endoscope has a cap with premounted bandsthat allows for suction of the varix (in this case a glove is used). (C) Once the varix is suc-tioned into the cap, the band is fired and the varix is ligated.
Cardenas et al6
253
254255256
257258259
260261262
263264265266
267268269
270271272
273274275
276277278279
280281282
283284285
286287288289
290291292
293294295
296297298
299300301302
303
the GE junction. This reduces the heavy bleeding and further bands can be firedafterward.The procedure is not exempt from complications either, and these include transient
dysphagia and chest pain, which respond well to liquid analgesics (ie, acetamino-phen), as well as an oral suspension of antacids. A liquid diet should be started thesame day and soft foods the next day. Shallow ulcers at the site of bands are frequentand can bleed in up to 4% of cases.52 The use of a proton pump inhibitor (ie, panto-prazole 40 mg per day for 10 days) decreases the size of ulcers but does not preventthem from bleeding.53 Severe and rare complications, such as massive bleeding fromulcers or rarely from variceal rupture, esophageal perforation, esophageal strictures,or altered esophageal motility, may occur with EBL.54 If a patient bleeds due to an ul-cer after EBL, ES may be performed. Another option is applying Hemospray (a hemo-static powder) to the bleeding site. This powder, which is used for nonvaricealgastrointestinal bleeding, seems to be promising as a hemostatic technique for pa-tients with portal gastropathy, variceal bleeding, and bleeding after EBL ulcers.55–57
EBL is highly effective in the control of AVB, with an immediate efficacy in 90% ofcases.2 Two randomized controlled trials that compared EBL and ES in AVB47,48
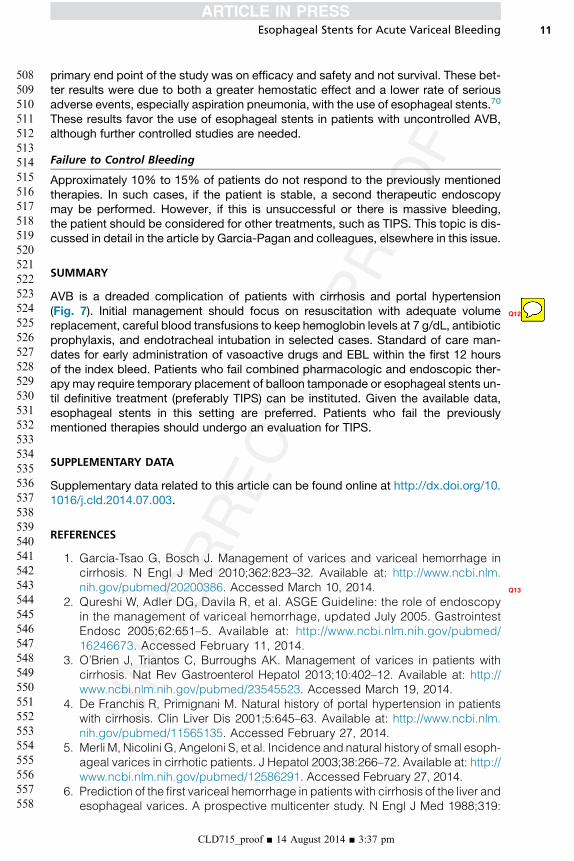
have clearly shown that treatment with EBL along with vasoconstrictors is associatedwith higher efficacy, safety, and improved mortality than ES and vasoconstrictors. Inaddition, in 8 other trials, these 2modalities also were compared in AVB and in the pre-vention of rebleeding. A meta-analysis of the 10 trials shows that EBL is better than ESin the initial control of bleeding, and is associated with fewer adverse events andimproved mortality (Fig. 4).58 Therefore, EBL is considered the endoscopic therapy
CLD715_proof ■ 14 August 2014 ■ 3:37 pm
BOTERO MEJIA
Texto insertado
or sucralfate
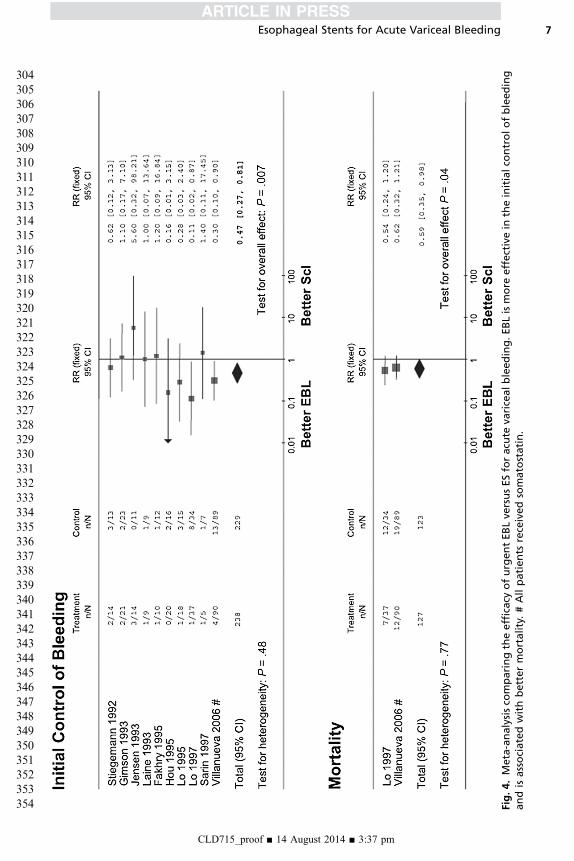
Fig.4.Meta-analysisco
mparingtheefficacy
ofurgentEBLve
rsusESforacu
teva
ricealbleeding.EBLismore
effectivein
theinitialco
ntrolofbleeding
andisassociatedwithbettermortality.#Allpatients
receivedsomatostatin.
Esophageal Stents for Acute Variceal Bleeding
CLD715_proof ■ 14 August 2014 ■ 3:37 pm
7
304
305306307
308309310
311312313
314315316317
318319320
321322323
324325326
327328329330
331332333
334335336
337338339340
341342343
344345346
347348349
350351352353
354
Cardenas et al8
355
356357358
359360361
362363364
365366367368
369370371
372373374
375376377
378379380381
382383384
385386387
388389390391
392393394
395396397
398399400
401402403404
405
of choice in AVB. Although EBL is preferred over ES for an episode of AVB, in thesetting of active hemorrhage or torrential bleeding, EBL may be sometimes difficultto perform because of lack of visibility. Therefore, both techniques are reasonable op-tions in the setting of AVB.
ESOPHAGEAL STENTS
Balloon tamponade of the esophagus is used in patients in whom endoscopic therapycannot stop the bleeding or in those patients with a known history of esophageal vari-ces in whom such profuse bleeding and hemodynamic status precludes an upperendoscopy. Current guidelines recommend using balloon tamponade only in massivebleeding, as a temporary “bridge” until definitive treatment can be instituted (for amaximum of 24 hours) in an intensive care unit.22,59 Esophageal balloon tamponade,which is typically performed with a Sengstaken-Blakemore tube, causes hemostasisby direct compression of the bleeding varices. If placed properly, tamponade mayprovide initial control of bleeding in up to 85% of cases, but recurrence is observedin 50% of the patients after deflation of the balloon.60 The most common complica-tions include aspiration pneumonia and esophageal perforation, which may occur in30% of patients, with a mortality rate of 5%mainly due to perforation.60 The incidenceof complications increases with the duration of tamponade and when tubes areinserted by inexperienced staff. Therefore, tamponade should be performed only byskilled and experienced personnel in intensive care facilities and with special cautionin patients with respiratory failure or cardiac arrhythmias. Because of the high risk ofaspiration pneumonia, tamponade should be preceded by prophylactic orotrachealintubation in most patients.An alternative to balloon tamponade is placing fully covered self-expandable metal
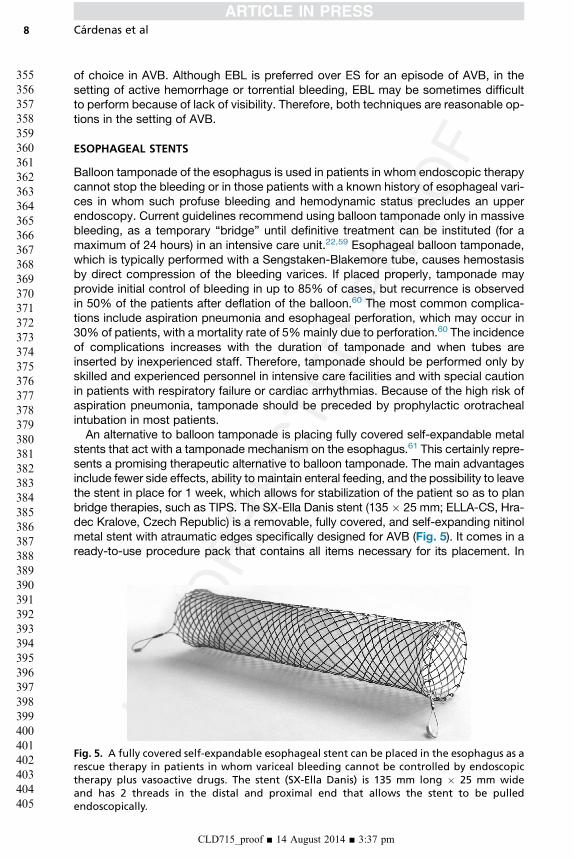
stents that act with a tamponade mechanism on the esophagus.61 This certainly repre-sents a promising therapeutic alternative to balloon tamponade. The main advantagesinclude fewer side effects, ability to maintain enteral feeding, and the possibility to leavethe stent in place for 1 week, which allows for stabilization of the patient so as to planbridge therapies, such as TIPS. The SX-Ella Danis stent (135 � 25 mm; ELLA-CS, Hra-dec Kralove, Czech Republic) is a removable, fully covered, and self-expanding nitinolmetal stent with atraumatic edges specifically designed for AVB (Fig. 5). It comes in aready-to-use procedure pack that contains all items necessary for its placement. In
Fig. 5. A fully covered self-expandable esophageal stent can be placed in the esophagus as arescue therapy in patients in whom variceal bleeding cannot be controlled by endoscopictherapy plus vasoactive drugs. The stent (SX-Ella Danis) is 135 mm long � 25 mm wideand has 2 threads in the distal and proximal end that allows the stent to be pulledendoscopically.
CLD715_proof ■ 14 August 2014 ■ 3:37 pm

web4C=FPO
Fig. 6. (A) Once the stent is advanced into the stomach, a distal balloon at the proximal endis inflated with a syringe. (B) Then the stent is pulled back until it anchors in the cardias andlower esophagus and then deployed and the introducer is withdrawn.
Esophageal Stents for Acute Variceal Bleeding 9
406
407408409
410411412
413414415
416417418419
420421422
423424425
426427428
429430431432
433434435
436437438
439440441442
443444445
446447448
449450451
452453454455
456
addition, it has radiopaque markers at both ends and midportion for monitoring withplain chest radiographs. The stent can be deployed in the lower esophagus withoutradiological or endoscopic assistance; however, in some cases, a prior endoscopy isuseful as a means to leave a rigid guidewire in the stomach, which later aids in placing
Table 2Case series reporting the efficacy of esophageal stents as a rescue therapy for the treatmentof acute variceal bleeding Q15
No.Patients
SEMSDeployed,%
InitialHemostasis,%
Rebleed,%
Migration,%
MortalityFollow-Up, d
Hubmannet al,66
2006
15 100 100 0 13 20% 60 d
Zehetneret al,67
2008
34 100 100 0 18 29% 60 d
Wrightet al,65
2010
10 90 70 14 NR 50% 42 d
Decheneet al,63
2012
8 100 100 38 0 75% 60 d
Holsteret al,68
2013
5 100 100 20 20 40% 180 d
Zakariaet al,69
2013
16 94 88 0 38 25% NR
Fierzet al,62
2013
7 100 89 0 0 77% 42 d
CLD715_proof ■ 14 August 2014 ■ 3:37 pm
BOTERO MEJIA
Nota adhesiva
footnote- SEMS- self-expandable metal stents NR- not reported

Cardenas et al10
457
458459460
461462463
464465466
467468469470
471472473
474475476
477478479
480481482483
484485486
487488489
490491492493
494495496
497498499
500501502
503504505506
507
the premounted stent. The procedure is relatively easy to perform but basic training isneeded to understand how it is placed. Once the stent has been advanced to the stom-ach, a distal balloon at the proximal end is inflated with a syringe and then the stent ispulled back until it anchors in the cardias and lower esophagus. This then allows itsdeployment, thus no fluoroscopy is needed (Fig. 6). The stent can be removed 7 dayslater endoscopically using an overtube system (Extractor for SX-ELLA stent Danis)without causing trauma to the esophagus. Several case series have demonstrated itsafety and efficacy in AVB (Table 2).62–69 In most published cases, the stents havebeen successfully deployed inmore than 90%of patients. The results on immediate he-mostasis range between 70% and 100%. In most cases, patients can be offered abridge therapy, such as TIPS or repeat endoscopic treatment with EBL or ES. A draw-back of using the stent is migration, which can occur in 20% of cases.61,65,66
We recently performed a multicenter randomized controlled trial (published in ab-stract form) comparing esophageal stenting versus balloon tamponade in 28 patientswith AVB refractory to medical and endoscopic treatment and/or with massivebleeding precluding endoscopy.70 Fifteen patients were randomized to balloon tam-ponade and 13 to stent placement. Primary outcome measure was success of ther-apy, defined as survival at day 15 with control of bleeding and without seriousadverse events. Our results showed that esophageal stents were more effectivethan balloon tamponade for the temporary control of bleeding in those patients withabsence of rebleeding at 15 days in 77% in the stent group versus 47% in the balloontamponade group. Side effects occurred in 8% of patients in the stent group versus52% in the balloon tamponade group. There were no differences in survival, but the
Suspected variceal bleeding
Vasoactive drugs
Antibiotics, volume restitution
Endoscopy – Confirms diagnosis and can implement EBLa
control
Drugs 2-5 days
Start secondary prophylaxis
mild
Repeat endoscopic Tx
severe
TIPSfailure
failure
bConsider temporary measures
Fig. 7. Recommended algorithm for the treatment of an episode of acute variceal bleeding.a Placement of TIPS (within 72 hours) for patients AVB with Child B actively bleeding or Ccirrhosis (<13 points) is associated with a significant reduction in rebleeding and mortalityand can be considered in such cases. b Temporary measures include placement of an esoph-ageal stent or balloon tamponade. Esophageal stents are preferred, as they are safer andmore effective. The use of the balloon is associated with potentially lethal complications,such as aspiration and perforation of the esophagus. Tx, treatment.
CLD715_proof ■ 14 August 2014 ■ 3:37 pm
BOTERO MEJIA
Tachado
BOTERO MEJIA
Texto insertado
its
BOTERO MEJIA
Tachado
BOTERO MEJIA
Tachado
Esophageal Stents for Acute Variceal Bleeding 11
508
509510511
512513514
515516517
518519520521
522523524
525526527
528529530
531532533534
535536537
538539540
541542543544
545546547
548549550
551552553
554555556557
558
primary end point of the study was on efficacy and safety and not survival. These bet-ter results were due to both a greater hemostatic effect and a lower rate of seriousadverse events, especially aspiration pneumonia, with the use of esophageal stents.70
These results favor the use of esophageal stents in patients with uncontrolled AVB,although further controlled studies are needed.
Failure to Control Bleeding
Approximately 10% to 15% of patients do not respond to the previously mentionedtherapies. In such cases, if the patient is stable, a second therapeutic endoscopymay be performed. However, if this is unsuccessful or there is massive bleeding,the patient should be considered for other treatments, such as TIPS. This topic is dis-cussed in detail in the article by Garcia-Pagan and colleagues, elsewhere in this issue.
Q12
SUMMARY
AVB is a dreaded complication of patients with cirrhosis and portal hypertension(Fig. 7). Initial management should focus on resuscitation with adequate volumereplacement, careful blood transfusions to keep hemoglobin levels at 7 g/dL, antibioticprophylaxis, and endotracheal intubation in selected cases. Standard of care man-dates for early administration of vasoactive drugs and EBL within the first 12 hoursof the index bleed. Patients who fail combined pharmacologic and endoscopic ther-apy may require temporary placement of balloon tamponade or esophageal stents un-til definitive treatment (preferably TIPS) can be instituted. Given the available data,esophageal stents in this setting are preferred. Patients who fail the previouslymentioned therapies should undergo an evaluation for TIPS.
SUPPLEMENTARY DATA
Supplementary data related to this article can be found online at http://dx.doi.org/10.1016/j.cld.2014.07.003.
Q13
REFERENCES
1. Garcia-Tsao G, Bosch J. Management of varices and variceal hemorrhage incirrhosis. N Engl J Med 2010;362:823–32. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20200386. Accessed March 10, 2014.
2. Qureshi W, Adler DG, Davila R, et al. ASGE Guideline: the role of endoscopyin the management of variceal hemorrhage, updated July 2005. GastrointestEndosc 2005;62:651–5. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16246673. Accessed February 11, 2014.
3. O’Brien J, Triantos C, Burroughs AK. Management of varices in patients withcirrhosis. Nat Rev Gastroenterol Hepatol 2013;10:402–12. Available at: http://www.ncbi.nlm.nih.gov/pubmed/23545523. Accessed March 19, 2014.
4. De Franchis R, Primignani M. Natural history of portal hypertension in patientswith cirrhosis. Clin Liver Dis 2001;5:645–63. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11565135. Accessed February 27, 2014.
5. Merli M, Nicolini G, Angeloni S, et al. Incidence and natural history of small esoph-ageal varices in cirrhotic patients. J Hepatol 2003;38:266–72. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12586291. Accessed February 27, 2014.
6. Prediction of the first variceal hemorrhage in patients with cirrhosis of the liver andesophageal varices. A prospective multicenter study. N Engl J Med 1988;319:
CLD715_proof ■ 14 August 2014 ■ 3:37 pm
BOTERO MEJIA
Nota adhesiva
ok

Cardenas et al12
559
560561562
563564565
566567568
569570571572
573574575
576577578
579580581
582583584585
586587588
589590591
592593594595
596597598
599600601
602603604
605606607608
609
983–9. Available at: http://www.ncbi.nlm.nih.gov/pubmed/3262200. AccessedFebruary 27, 2014.
7. Groszmann RJ, Bosch J, Grace ND, et al. Hemodynamic events in a prospec-tive randomized trial of propranolol versus placebo in the prevention of a firstvariceal hemorrhage. Gastroenterology 1990;99:1401–7. Available at: http://www.ncbi.nlm.nih.gov/pubmed/2210246. Accessed February 27, 2014.
8. D’AmicoG,DeFranchisR.Upperdigestivebleeding in cirrhosis. Post-therapeuticoutcome and prognostic indicators. Hepatology 2003;38:599–612. Available at:http://www.ncbi.nlm.nih.gov/pubmed/12939586. Accessed February 7, 2014.
9. Bosch J, Garcıa-Pagan JC. Prevention of variceal rebleeding. Lancet 2003;361:952–4. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12648985. AccessedFebruary 27, 2014.
10. D’Amico G, Pagliaro L, Bosch J. Pharmacological treatment of portal hyperten-sion: an evidence-based approach. Semin Liver Dis 1999;19:475–505. Avail-able at: http://www.ncbi.nlm.nih.gov/pubmed/10643630. Accessed February27, 2014.
11. Graham DY, Smith JL. The course of patients after variceal hemorrhage. Gastro-enterology 1981;80:800–9. Available at: http://www.ncbi.nlm.nih.gov/pubmed/6970703. Accessed February 27, 2014.
12. BoschJ,Garcia-Pagan JC,Berzigotti A, et al.Measurement of portal pressureandits role in the management of chronic liver disease. Semin Liver Dis 2006;26:348–62. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17051449. AccessedFebruary 27, 2014.
13. ChalasaniN, Kahi C, Francois F, et al. Improvedpatient survival after acute varicealbleeding: amulticenter, cohort study. AmJGastroenterol 2003;98:653–9. Availableat: http://www.ncbi.nlm.nih.gov/pubmed/12650802. Accessed February 27, 2014.
14. Carbonell N, Pauwels A, Serfaty L, et al. Improved survival after varicealbleeding in patients with cirrhosis over the past two decades. Hepatology2004;40:652–9. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15349904.Accessed February 27, 2014.
15. Stokkeland K, Brandt L, Ekbom A, et al. Improved prognosis for patients hospi-talized with esophageal varices in Sweden 1969–2002. Hepatology 2006;43:500–5. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16496319. AccessedMarch 6, 2014.
16. Bambha K, Kim WR, Pedersen R, et al. Predictors of early re-bleeding and mor-tality after acute variceal haemorrhage in patients with cirrhosis. Gut 2008;57:814–20. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18250126. Ac-cessed January 21, 2014.
17. Reverter E, Tandon P, Augustin S, et al. A MELD-basedmodel to determine risk ofmortality among patients with acute variceal bleeding. Gastroenterology 2014;146:412–9.e3. Available at: http://www.ncbi.nlm.nih.gov/pubmed/24148622. Ac-cessed March 11, 2014.
18. Cardenas A, Gines P, Uriz J, et al. Renal failure after upper gastrointestinalbleeding in cirrhosis: incidence, clinical course, predictive factors, and short-term prognosis. Hepatology 2001;34:671–6. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11584362. Accessed February 25, 2014.
19. Fortune B, Garcia-Tsao G. Current management strategies for acute esopha-geal variceal hemorrhage. Curr Hepatol Rep 2014;13:35–42. Available at:http://www.ncbi.nlm.nih.gov/pubmed/24955303. Accessed July 9, 2014.
20. Koch DG, Arguedas MR, Fallon MB. Risk of aspiration pneumonia in suspectedvariceal hemorrhage: the value of prophylactic endotracheal intubation prior to
CLD715_proof ■ 14 August 2014 ■ 3:37 pm

Esophageal Stents for Acute Variceal Bleeding 13
610
611612613
614615616
617618619
620621622623
624625626
627628629
630631632
633634635636
637638639
640641642
643644645646
647648649
650651652
653654655
656657658659
660
endoscopy. Dig Dis Sci 2007;52:2225–8. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17385037. Accessed March 6, 2014.
21. Rudolph SJ, Landsverk BK, Freeman ML. Endotracheal intubation for airwayprotection during endoscopy for severe upper GI hemorrhage. Gastrointest En-dosc 2003;57:58–61. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12518132. Accessed March 6, 2014.
22. De Franchis R. Revising consensus in portal hypertension: report of the Baveno Vconsensus workshop on methodology of diagnosis and therapy in portal hyper-tension. J Hepatol 2010;53:762–8. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20638742. Accessed February 24, 2014.
23. Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute uppergastrointestinal bleeding. N Engl J Med 2013;368:11–21. Available at: http://www.ncbi.nlm.nih.gov/pubmed/23281973. Accessed February 19, 2014.
24. Caldwell SH, Hoffman M, Lisman T, et al. Coagulation disorders and hemostasisin liver disease: pathophysiology and critical assessment of current manage-ment. Hepatology 2006;44:1039–46. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17006940. Accessed June 3, 2014.
25. Hou MC, Lin HC, Liu TT, et al. Antibiotic prophylaxis after endoscopic therapyprevents rebleeding in acute variceal hemorrhage: a randomized trial. Hepa-tology 2004;39:746–53. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14999693. Accessed March 6, 2014.
26. Soares-Weiser K, Brezis M, Tur-Kaspa R, et al. Antibiotic prophylaxis of bacte-rial infections in cirrhotic inpatients: a meta-analysis of randomized controlledtrials. Scand J Gastroenterol 2003;38:193–200. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12678337. Accessed March 6, 2014.
27. Fernandez J, Ruiz del Arbol L, Gomez C, et al. Norfloxacin vs ceftriaxone in theprophylaxis of infections in patients with advanced cirrhosis and hemorrhage.Gastroenterology 2006;131:1049–56 [quiz: 1285]. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17030175. Accessed February 4, 2014.
28. Chavez-Tapia NC, Barrientos-Gutierrez T, Tellez-Avila F, et al. Meta-analysis: anti-biotic prophylaxis for cirrhotic patients with upper gastrointestinal bleeding—anupdated Cochrane review. Aliment Pharmacol Ther 2011;34:509–18. Availableat: http://www.ncbi.nlm.nih.gov/pubmed/21707680. Accessed July 9, 2014.
29. Rimola A, Garcıa-Tsao G, Navasa M, et al. Diagnosis, treatment and prophylaxisof spontaneous bacterial peritonitis: a consensus document. International Asci-tes Club. J Hepatol 2000;32:142–53. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10673079. Accessed April 10, 2014.
30. Chen PH, Chen WC, Hou MC, et al. Delayed endoscopy increases re-bleedingand mortality in patients with hematemesis and active esophageal varicealbleeding: a cohort study. J Hepatol 2012;57:1207–13. Available at: http://www.ncbi.nlm.nih.gov/pubmed/22885718. Accessed July 9, 2014.
31. Garcıa-Pagan JC, Caca K, Bureau C, et al. Early use of TIPS in patients withcirrhosis and variceal bleeding. N Engl J Med 2010;362:2370–9. Available at:http://www.ncbi.nlm.nih.gov/pubmed/20573925. Accessed March 11, 2014.
32. Ioannou G, Doust J, Rockey DC. Terlipressin for acute esophageal varicealhemorrhage. Cochrane Database Syst Rev 2003;(1). CD002147. Available at:http://www.ncbi.nlm.nih.gov/pubmed/12535432. Accessed March 6, 2014.
33. Gøtzsche PC, Hrobjartsson A. Somatostatin analogues for acute bleeding oe-sophageal varices. Cochrane Database Syst Rev 2008;(3). CD000193. Avail-able at: http://www.ncbi.nlm.nih.gov/pubmed/18677774. Accessed March10, 2014.
CLD715_proof ■ 14 August 2014 ■ 3:37 pm

Cardenas et al14
661
662663664
665666667
668669670
671672673674
675676677
678679680
681682683
684685686687
688689690
691692693
694695696697
698699700
701702703
704705706
707708709710
711
34. Escorsell A, Ruiz del Arbol L, Planas R, et al. Multicenter randomized controlledtrial of terlipressin versus sclerotherapy in the treatment of acute varicealbleeding: the TEST study. Hepatology 2000;32:471–6. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10960437. Accessed March 10, 2014.
35. Corley DA, Cello JP, Adkisson W, et al. Octreotide for acute esophageal varicealbleeding: a meta-analysis. Gastroenterology 2001;120:946–54. Available at:http://www.ncbi.nlm.nih.gov/pubmed/11231948. Accessed March 10, 2014.
36. Wells M, Chande N, Adams P, et al. Meta-analysis: vasoactivemedications for themanagement of acute variceal bleeds. Aliment Pharmacol Ther 2012;35:1267–78. Available at: http://www.ncbi.nlm.nih.gov/pubmed/22486630. Ac-cessed July 9, 2014.
37. Riphaus A, Lechowicz I, Frenz MB, et al. Propofol sedation for upper gastrointes-tinal endoscopy in patients with liver cirrhosis as an alternative to midazolam toavoid acute deterioration of minimal encephalopathy: a randomized, controlledstudy. Scand J Gastroenterol 2009;44:1244–51. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19811337. Accessed July 9, 2014.
38. Khamaysi I, William N, Olga A, et al. Sub-clinical hepatic encephalopathy incirrhotic patients is not aggravated by sedation with propofol compared to mid-azolam: a randomized controlled study. J Hepatol 2011;54:72–7. Available at:http://www.ncbi.nlm.nih.gov/pubmed/20934771. Accessed July 9, 2014.
39. Bamji N, Cohen LB. Endoscopic sedation of patients with chronic liver dis-ease. Clin Liver Dis 2010;14:185–94. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20682228. Accessed March 12, 2014.
40. Baillie J, Yudelman P. Complications of endoscopic sclerotherapy of esopha-geal varices. Endoscopy 1992;24:284–91. Available at: http://www.ncbi.nlm.nih.gov/pubmed/1612042. Accessed March 10, 2014.
41. Lee JG, Lieberman DA. Complications related to endoscopic hemostasis tech-niques. Gastrointest Endosc Clin N Am 1996;6:305–21. Available at: http://www.ncbi.nlm.nih.gov/pubmed/8673330. Accessed March 10, 2014.
42. Rolando N, Gimson A, Philpott-Howard J, et al. Infectious sequelae afterendoscopic sclerotherapy of oesophageal varices: role of antibiotic prophy-laxis. J Hepatol 1993;18:290–4. Available at: http://www.ncbi.nlm.nih.gov/pubmed/8228122. Accessed March 10, 2014.
43. Selby WS, Norton ID, Pokorny CS, et al. Bacteremia and bacterascites afterendoscopic sclerotherapy for bleeding esophageal varices and prevention byintravenous cefotaxime: a randomized trial. Gastrointest Endosc 1994;40:680–4. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7859964. AccessedMarch 10, 2014.
44. Villanueva C, Colomo A, Aracil C, et al. Current endoscopic therapy of varicealbleeding. Best Pract Res Clin Gastroenterol 2008;22:261–78. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18346683. Accessed March 10, 2014.
45. Park WG, Yeh RW, Triadafilopoulos G. Injection therapies for variceal bleedingdisorders of the GI tract. Gastrointest Endosc 2008;67:313–23. Available at:http://www.ncbi.nlm.nih.gov/pubmed/18226695. Accessed March 10, 2014.
46. Laine L, el-Newihi HM, Migikovsky B, et al. Endoscopic ligation compared withsclerotherapy for the treatment of bleeding esophageal varices. Ann Intern Med1993;119:1–7. Available at: http://www.ncbi.nlm.nih.gov/pubmed/8498757. Ac-cessed March 10, 2014.
47. Villanueva C, Piqueras M, Aracil C, et al. A randomized controlled trialcomparing ligation and sclerotherapy as emergency endoscopic treatmentadded to somatostatin in acute variceal bleeding. J Hepatol 2006;45:560–7.
CLD715_proof ■ 14 August 2014 ■ 3:37 pm

Esophageal Stents for Acute Variceal Bleeding 15
712
713714715
716717718
719720721
722723724725
726727728
729730731
732733734
735736737738
739740741
742743744
745746747748
749750751
752753754
755756757
758759760761
762
Available at: http://www.ncbi.nlm.nih.gov/pubmed/16904224. Accessed July9, 2014.
48. Lo GH, Lai KH, Cheng JS, et al. Emergency banding ligation versus sclerother-apy for the control of active bleeding from esophageal varices. Hepatology1997;25:1101–4. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9141424.Accessed March 11, 2014.
49. Dzeletovic I, Baron TH. History of portal hypertension and endoscopic treatmentof esophageal varices. Gastrointest Endosc 2012;75:1244–9. Available at:http://www.ncbi.nlm.nih.gov/pubmed/22624813. Accessed July 9, 2014.
50. Stiegmann GV, Goff JS, Michaletz-Onody PA, et al. Endoscopic sclerotherapyas compared with endoscopic ligation for bleeding esophageal varices.N Engl J Med 1992;326:1527–32. Available at: http://www.ncbi.nlm.nih.gov/pubmed/1579136. Accessed July 9, 2014.
51. Lo GH. The role of endoscopy in secondary prophylaxis of esophageal varices.Clin Liver Dis 2010;14:307–23. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20682237. Accessed March 11, 2014.
52. Baron TH, Wong Kee Song LM. Endoscopic variceal band ligation. Am J Gastro-enterol 2009;104:1083–5. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19417747. Accessed March 10, 2014.
53. Shaheen NJ, Stuart E, Schmitz SM, et al. Pantoprazole reduces the size of post-banding ulcers after variceal band ligation: a randomized, controlled trial. Hep-atology 2005;41:588–94. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15726658. Accessed March 10, 2014.
54. Garcia-Pagan JC, Bosch J. Endoscopic band ligation in the treatment of portalhypertension. Nat Clin Pract Gastroenterol Hepatol 2005;2:526–35. Available at:http://www.ncbi.nlm.nih.gov/pubmed/16355158. Accessed March 10, 2014.
55. Ibrahim M, Lemmers A, Deviere J. Novel application of Hemospray to achievehemostasis in post-variceal banding esophageal ulcers that are activelybleeding. Endoscopy 2014;46(Suppl 1):E263. Available at: http://www.ncbi.nlm.nih.gov/pubmed/24906091. Accessed July 9, 2014.
56. Ibrahim M, El-Mikkawy A, Mostafa I, et al. Endoscopic treatment of acute vari-ceal hemorrhage by using hemostatic powder TC-325: a prospective pilot study.Gastrointest Endosc 2013;78:769–73. Available at: http://www.ncbi.nlm.nih.gov/pubmed/24120338. Accessed March 19, 2014.
57. Holster IL, Poley JW, Kuipers EJ, et al. Controlling gastric variceal bleeding withendoscopically applied hemostatic powder (Hemospray). J Hepatol 2012;57:1397–8. Available at: http://www.ncbi.nlm.nih.gov/pubmed/22864337. AccessedJuly 9, 2014.
58. Abraldes JG, Bosch J. The treatment of acute variceal bleeding. J Clin Gastro-enterol 2007;41(Suppl 3):S312–7. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17975482. Accessed July 9, 2014.
59. Garcia-Tsao G, Sanyal AJ, Grace ND, et al. Prevention and management ofgastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology2007;46:922–38. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17879356.Accessed January 21, 2014.
60. Avgerinos A, Armonis A. Balloon tamponade technique and efficacy in varicealhaemorrhage. Scand J Gastroenterol Suppl 1994;207:11–6. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7701261. Accessed March 11, 2014.
61. Escorsell A, Bosch J. Self-expandable metal stents in the treatment ofacute esophageal variceal bleeding. Gastroenterol Res Pract 2011;2011:910986. Available at: http://www.pubmedcentral.nih.gov/articlerender.
CLD715_proof ■ 14 August 2014 ■ 3:37 pm
Q14
Cardenas et al16
763764765766767768769770771772773774775776777778779780781782783784785786787788789790791792793794795796797798799800801802803804805
fcgi?artid53195306&tool5pmcentrez&rendertype5abstract. Accessed July9, 2014.
62. Fierz FC, Kistler W, Stenz V, et al. Treatment of esophageal variceal hemorrhagewith self-expanding metal stents as a rescue maneuver in a swiss multicentriccohort. Case Rep Gastroenterol 2013;7:97–105. Available at: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid53617972&tool5pmcentrez&rendertype5abstract. Accessed July 9, 2014.
63. Dechene A, El Fouly AH, Bechmann LP, et al. Acute management of refractoryvariceal bleeding in liver cirrhosis by self-expanding metal stents. Digestion2012;85:185–91. Available at: http://www.ncbi.nlm.nih.gov/pubmed/22269340.Accessed July 9, 2014.
64. Mishin I, Ghidirim G, Dolghii A, et al. Implantation of self-expanding metal stentin the treatment of severe bleeding from esophageal ulcer after endoscopicband ligation. Dis Esophagus 2010;23:E35–8. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20731698. Accessed July 9, 2014.
65. WrightG,LewisH,HoganB,et al.A self-expandingmetal stent forcomplicated var-iceal hemorrhage: experience at a single center. Gastrointest Endosc 2010;71:71–8. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19879564. AccessedMarch 11, 2014.
66. Hubmann R, Bodlaj G, Czompo M, et al. The use of self-expanding metal stentsto treat acute esophageal variceal bleeding. Endoscopy 2006;38:896–901.Available at: http://www.ncbi.nlm.nih.gov/pubmed/16981106. Accessed March10, 2014.
67. Zehetner J, Shamiyeh A, Wayand W, et al. Results of a new method to stop acutebleeding from esophageal varices: implantation of a self-expanding stent. SurgEndosc 2008;22:2149–52. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18622540. Accessed July 9, 2014.
68. Holster IL, Kuipers EJ, van Buuren HR, et al. Self-expandable metal stents asdefinitive treatment for esophageal variceal bleeding. Endoscopy 2013;45:485–8. Available at: http://www.ncbi.nlm.nih.gov/pubmed/23468191. AccessedJuly 9, 2014.
69. Zakaria MS, Hamza IM, Mohey MA, et al. The first Egyptian experience usingnew self-expandable metal stents in acute esophageal variceal bleeding: pilotstudy. Saudi J Gastroenterol 2013;19:177–81. Available at: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid53745660&tool5pmcentrez&rendertype5abstract. Accessed July 9, 2014.
70. Escorsell A, Cardenas A, Pavel O, et al. Self-expandable esophageal metalstent vs balloon tamponade in esophageal variceal bleeding refractory to med-ical and endoscopic treatment: a multicenter randomized controlled trial. Hep-atology 2013;1386A–7A.
CLD715_proof ■ 14 August 2014 ■ 3:37 pm

Our reference: CLD 715 P-authorquery-v9
AUTHOR QUERY FORM
Journal: CLD
Article Number: 715
Dear Author,
Please check your proof carefully and mark all corrections at the appropriate place in the proof (e.g., by using on-screen
annotation in the PDF file) or compile them in a separate list. Note: if you opt to annotate the file with software other than
Adobe Reader then please also highlight the appropriate place in the PDF file. To ensure fast publication of your paper please
return your corrections within 48 hours.
For correction or revision of any artwork, please consult http://www.elsevier.com/artworkinstructions.
Any queries or remarks that have arisen during the processing of your manuscript are listed below and highlighted by flags in
the proof.
Location
in articleQuery / Remark: Click on the Q link to find the query’s location in text
Please insert your reply or correction at the corresponding line in the proof
Q1 Please approve the short title to be used in the running head at the top of each right-hand page.
Q2 This is how your name will appear on the contributor's list. Please add your academic title and any other
necessary titles and professional affiliations, verify the information, and OK
ANDR�ES C�ARDENAS, MD, MMSc, AGAF, GI/Endoscopy Unit, Institut de Malalties Digestives i
Metaboliques, Hospital Clinic, University of Barcelona, Barcelona, Spain
ALEJANDRO FERN�ANDEZ-SIMON, MD, GI/Endoscopy Unit, Institut de Malalties Digestives i
Metaboliques, Hospital Clinic, University of Barcelona, Barcelona, Spain
ANGELS ESCORCELL, Liver Unit, Institut de Malalties Digestives i Metaboliques, Hospital Clinic,
University of Barcelona, Barcelona, Spain
Q3 Are author names and order of authors OK as set?
Q4 Degree abbreviations are verified against a list of known degrees. MMSc is not yet on this list. Please verify
the degree.
Q5 Please provide professional degrees (e.g., PhD, MD) for the author “Angels Escorcell.”
Q6 The following synopsis is the one that you supplied, but edited down to less than 100 words. Please confirm
OK, or submit a replacement (also less than 100 words). Please note that the synopsis will appear in
PubMed: Patients with portal hypertension and esophageal varices are at risk of bleeding due to
a progressive increase in portal pressure that may rupture the variceal wall. Appropriate treatment with
initial general measures, such as resuscitation, a restrictive transfusion policy, antibiotic prophylaxis,
pharmacologic therapy with vasoconstrictors, and endoscopic therapy with endoscopic band ligation are
mandatory. However, 10% to 15% of patients fail initial endoscopic therapy and thus rescue therapies are
needed. This article reviews the current endoscopic strategies with band ligation and esophageal stents for
patients with acute variceal bleeding.
(continued on next page)
Q7 Please verify the affiliation addresses and provide the missing information (state name, street name and zip
code for affiliation “a and b”).
Q8 As per the editorial remarks, “Please verify disclosure statement.”
Q9 If there are any drug dosages in your article, please verify them and indicate that you have done so by
initialing this query.
Q10 Please provide the city and state for Wilson-Cook Medical, Inc and Microvasive Boston Scientific
Corporation.
Q11 Please provide the name and location of the manufacturer of the Hemospray.
Q12 Figure citation were not allowed in section headings, hence Fig. 7 citation have been moved to the end of
the first sentence of subsequent paragraph. Please verify.
Q13 Please verify accessed date for all references.
Q14 Please provide volume number for Ref. 70.
Q15 Table 2: Please define SEMS and NR, and provide a heading for column 1.
Please check this box or indicate
your approval if you have no
corrections to make to the PDF file ,
Thank you for your assistance.












![[Characteristics of encrustation of ureteric stents in patients with urinary stones]](https://static.fdokumen.com/doc/165x107/633645e7cd4bf2402c0b6fc8/characteristics-of-encrustation-of-ureteric-stents-in-patients-with-urinary-stones.jpg)







