Usefulness of endoscopic band ligation for bleeding small bowel vascular lesions
6
F Junquera, E Brullet, R Campo, et al. Endoscopic band ligation for bleeding small bowel vascular lesions Table 1. Data summary for study patients No. Gender Age Disease Location Histologic results 1 M 65 Icteric hepatoma CBD, RHD Negative 2 M 75 Pancreatic head cancer CBD Positive 3 M 66 Icteric hepatoma CBD, LHD Positive 4 M 54 Gall bladder cancer CBD Negative 5 M 76 Bile duct cancer CBD, CHD Positive 6 M 64 Pancreas head cancer CBD Negative 7 M 62 PSC CHD Negative 8 M 64 Bile duct cancer CHD Positive 9 F 57 Bile duct cancer CHD Positive 10 M 65 Bile duct cancer CBD Positive 11 F 88 Bile duct cancer CBD Negative 12 M 55 Benign bile duct stricture CHD Negative 13 M 73 Bile duct cancer CHD, RHD Failure (after Billroth I) CBD, Common bile duct; RHD, right hepatic duct; LHD, left hepatic duct; CHD, common hepatic duct; PSC, primary sclerosing cholangitis. type biopsy forceps) method, care must be taken to avoid dislodging the guidewire. Prior insertion of a guidewire in the bile duct keeps the mucosal folds of the papilla1~ 11 flat and the pathway through the bile duct straight, making deep bile duct cannulation easier. The key point is to keep the duodenoscope close to the papilla, thereby allowing easy entrance into the bile duct whil e avoiding entry into the pancreatic duct. The reason for the failure of the technique in one patient was an inability to position the duo- denoscope close to the papilla, owing to anatomic changes as a result of prior surgery (partial gastrec- tomy with Billroth I anastomosis). Thus, the guidewire technique described above is a viable alternative for obtaining ETPBs without EST. REFERENCES 1. Aabakken L, Karesen R, Serck-Hansen A, Osnes M. TranspapiUary biopsies and brush cytology from the common bile duct. Endoscopy 1986;18:49-51. 2. Kubota Y, Takaoka M, Tani If, Ogura M, Kin H, Fujimura I~ et al. Endoscopic transpapiilary biopsy for diagnosis of patients with pancreaticobiliary ductal strictures. Am J Gastroenterol 1993;88:1700-4. 3. Schoefl R, Haefner M, Wrba F, Pfeffel F, Stain C, Poetzi R, et al. Forceps biopsy and brush cytology during endoscopic ret- rograde cholangiopancreatography for the diagnosis ofbiliary stenoses. Scand J Gastroenterol 1997;32:363-8. 4. Sivak MV Jr. Endoscopic management of bile duct stones. Am J Surg 1989;158:228-40. 5. Cotton PB, Lehman G, Vennes J, Geenen JE, Russell RC, Meyers WC, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc 1991;37:383-93. 6. Shields SJ, Carr-Locke DL. Sphincterotomy techniques and risks. Gastrointest Endosc Clin N Am 1996;6:17-42. 7. Freeman ML. Complications of endoscopic sphincterotomy. Endoscopy 1998;30:A216-20. 8. Sugiyama M, Atemi Y, Wada N, Kuroda A, Mute T. Endoscopic transpapillary bile duct biopsy without sphincterotomy for diagnosing biliary strictures: a prospective comparative study with bile and brush cytology. Am J Gastroenterol 1996;91: 465-7. 9. Tamada K, Higashizawa T, Tomiyama T, Wada S, Ohashi A, Sateh Y, et al. Ropeway-type bile duct biopsy forceps with a side slit for a guidewire. Gastrointest Endosc 2001;53:89-92. 10. Allescher HD. Papilla of Vater: structure and function. Endoscopy 1989;21:324-9. 11. Paulsen FP, Bobka T, Tsokos M, Folsch UR, TiUmann BN. Functional anatomy of the papilla Vateri: biomechanical aspects and impact of difficult endoscopic intubation. Surg Endosc 2002;16:296-301. Received October 31, 2002. For revision January 8, 2003. Accepted April 28, 2003. Current affiliations: Endoscopy Unit, UDIAT-CD, Corporaci5 Parc Tauli, Sabadell, Spain. Reprint requests: Enric Brullet, MD, Endoscopy Unit, UDIAT-CD, Corporaci5 Parc Tauli, Parc Tauli s / n, 08208 SabadeU, Spain. Copyright 9 2003 by the American Society for Gastrointestinal Endoscopy 0016-5107/2003/$30.00 + 0 doi:10.1067 / mge.2003.35 7 Usefulness of endoscopic band ligation for bleeding small bowel vascular lesions F~lix Junquera, MD, Enric Brullet, MD, Rafel Campo, MD, Xavier Calvet, MD, Valentf Puig-Divi, ME), Mercedes Vergara, MD Background: The optimal therapy for bleeding small bowel vascular lesions is controversial. This study investigated the efficacy and safety of endoscopic band ligation in this clinical condition. Methods: Fourteen patients bleeding from angiodyspla- sia and 4 bleeding from Dieulafoy's lesions located in the small bowel were included in this pilot study. 274 GASTROINTESTINAL ENDOSCOPY VOLUME 58, NO. 2, 2003
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Usefulness of endoscopic band ligation for bleeding small bowel vascular lesions

F Junquera, E Brullet, R Campo, et al. Endoscopic band ligation for bleeding small bowel vascular lesions
Table 1. Data summary for study patients
No. Gender Age Disease Location Histologic results
1 M 65 Icteric hepatoma CBD, RHD Negative 2 M 75 Pancreatic head cancer CBD Positive 3 M 66 Icteric hepatoma CBD, LHD Positive 4 M 54 Gall bladder cancer CBD Negative 5 M 76 Bile duct cancer CBD, CHD Positive 6 M 64 Pancreas head cancer CBD Negative 7 M 62 PSC CHD Negative 8 M 64 Bile duct cancer CHD Positive 9 F 57 Bile duct cancer CHD Positive 10 M 65 Bile duct cancer CBD Positive 11 F 88 Bile duct cancer CBD Negative 12 M 55 Benign bile duct stricture CHD Negative 13 M 73 Bile duct cancer CHD, RHD Failure (after Billroth I)
CBD, Common bile duct; RHD, right hepatic duct; LHD, left hepatic duct; CHD, common hepatic duct; PSC, primary sclerosing cholangitis.
type biopsy forceps) method, care must be taken to avoid dislodging the guidewire.
Prior insert ion of a guidewire in the bile duct keeps the mucosal folds of the papilla1~ 11 flat and the pathway through the bile duct straight, making deep bile duct cannulation easier.
The key point is to keep the duodenoscope close to the papilla, thereby allowing easy entrance into the bile duct whil e avoiding entry into the pancreatic duct. The reason for the failure of the technique in one pat ient was an inability to position the duo- denoscope close to the papilla, owing to anatomic changes as a result of prior surgery (partial gastrec- tomy with Billroth I anastomosis). Thus, the guidewire technique described above is a viable alternative for obtaining ETPBs without EST.
REFERENCES 1. Aabakken L, Karesen R, Serck-Hansen A, Osnes M.
TranspapiUary biopsies and brush cytology from the common bile duct. Endoscopy 1986;18:49-51.
2. Kubota Y, Takaoka M, Tani If, Ogura M, Kin H, Fujimura I~ et al. Endoscopic transpapiilary biopsy for diagnosis of patients with pancreaticobiliary ductal strictures. Am J Gastroenterol 1993;88:1700-4.
3. Schoefl R, Haefner M, Wrba F, Pfeffel F, Stain C, Poetzi R, et al. Forceps biopsy and brush cytology during endoscopic ret- rograde cholangiopancreatography for the diagnosis ofbiliary stenoses. Scand J Gastroenterol 1997;32:363-8.
4. Sivak MV Jr. Endoscopic management of bile duct stones. Am J Surg 1989;158:228-40.
5. Cotton PB, Lehman G, Vennes J, Geenen JE, Russell RC, Meyers WC, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc 1991;37:383-93.
6. Shields SJ, Carr-Locke DL. Sphincterotomy techniques and risks. Gastrointest Endosc Clin N Am 1996;6:17-42.
7. Freeman ML. Complications of endoscopic sphincterotomy. Endoscopy 1998;30:A216-20.
8. Sugiyama M, Atemi Y, Wada N, Kuroda A, Mute T. Endoscopic transpapillary bile duct biopsy without sphincterotomy for diagnosing biliary strictures: a prospective comparative study with bile and brush cytology. Am J Gastroenterol 1996;91: 465-7.
9. Tamada K, Higashizawa T, Tomiyama T, Wada S, Ohashi A, Sateh Y, et al. Ropeway-type bile duct biopsy forceps with a side slit for a guidewire. Gastrointest Endosc 2001;53:89-92.
10. Allescher HD. Papilla of Vater: structure and function. Endoscopy 1989;21:324-9.
11. Paulsen FP, Bobka T, Tsokos M, Folsch UR, TiUmann BN. Functional anatomy of the papilla Vateri: biomechanical aspects and impact of difficult endoscopic intubation. Surg Endosc 2002;16:296-301.
Received October 31, 2002. For revision January 8, 2003. Accepted April 28, 2003. Current affiliations: Endoscopy Unit, UDIAT-CD, Corporaci5 Parc Tauli, Sabadell, Spain. Reprint requests: Enric Brullet, MD, Endoscopy Unit, UDIAT-CD, Corporaci5 Parc Tauli, Parc Tauli s / n, 08208 SabadeU, Spain.
Copyright �9 2003 by the American Society for Gastrointestinal Endoscopy 0016-5107/2003/$30.00 + 0
doi:10.1067 / mge.2003.35 7
Usefulness of endoscopic band ligation for bleeding small bowel vascular lesions
F~lix Junquera, MD, Enric Brullet, MD, Rafel Campo, MD, Xavier Calvet, MD, Valentf Puig-Divi, ME), Mercedes Vergara, MD
Background: The optimal therapy for bleeding small bowel vascular lesions is controversial. This study investigated the efficacy and safety of endoscopic band ligation in this clinical condition. Methods: Fourteen patients bleeding from angiodyspla- sia and 4 bleeding from Dieulafoy's lesions located in the small bowel were included in this pilot study.
274 GASTROINTESTINAL ENDOSCOPY VOLUME 58, NO. 2, 2003

Endoscopic band ligation for bleeding small bowel vascular lesions F Junquera, E Brullet, R Campo, et al.
Endoscopic band Iigatlon was performed by using less than 200 mBar negative pressure in suctioning the tar- get iesion into the Iigatlon cap just before band release. Mean follow-up was 18 months (range 6-31 months). Observations. Endoscopic bend Iigation achieved hemo- stasis in a single session in all patients. No adverse events occurred except for mild abdominal pain in two patients. Mortality was null, and no patient required fur- ther blood transfusion during the 40 days after endo- scopic band Iigation. No patient with Dieulafoy's lesion had further bleeding, whereas bleeding recurred in 6 of 14 (43=/@) patients with angiodyspiasla during long-term follow-up. Conclusions: Endoscopic band ligation is safe and effec- tive for treatment of acutely bieedlng small bowel vascular lesions. Although endoscopic bend Iigation is definitive therapy for Dieuiefoy's lesion, long-term efficacy in the treatment of GI bleeding from angiodysplasla is limited.
Vascula r lesions, such as ang iodysp las ia (AGD) and Dieulafoy's lesion (DL), are the cause of 10% of episodes of u p p e r GI b leeding (UGB). T h e y a re asso- c ia ted wi th s ignif icant morb id i ty and lead to signif- i c an t use of h e a l t h ca re resources . I , 2 Endoscop ic t h e r a p y now rep resen t s f i rs t l ine m a n a g e m e n t and includes mechanica l (hemoclip application), t h e r m a l ( e l ec t rocoagu la t ion , l a s e r pho tocoagu la t i on , h e a t p robe coagula t ion) , and in jec t ion t echn iques . 1-10 More recently, endoscopic band l igat ion (EBL) has ga ined i nc r ea s ing accep t ance in t he t r e a t m e n t of these lesions based on its efficacy, ease of use, and re la t ive ly low cost. 10-19 However, mos t r epor t ed da t a c o n c e r n i n g t he use of E B L p e r t a i n to v a s c u l a r les ions in t he s tomach , and t h e r e is a p a u c i t y of in fo rmat ion rega rd ing its efficacy and safe ty in the t r e a t m e n t of b leeding vascu la r lesions in the smal l bowel. 19-22 The re fo re , th i s p rospec t ive s t u d y was conduc ted to d e t e r m i n e the eff icacy and sa fe ty of E B L in the t r e a t m e n t of b leeding small bowel vas- cu la r lesions.
PATIENTS AND METHODS
This is an uncontrolled, prospective, single-center study of a cohort of patients with UGB from small bowel vascular lesions. The study was conducted in a 600-bed university hospital that is the referral hospital for a well-defined area with 350,000 inhabitants. Upper GI bleeding was defined as the presence of hematemesis and/or melena caused by lesions located proximal to the ligament of Treitz.
From June 1998 to April 2002, 1395 patients were admitted with UGB and included in a standard protocol for management of UGB. This included confirmation of UGB, a complete medical history, intravenous access, determination of hemodynamic status (pulse and blood pressure), placement of a gastric aspiration tube, and a basic diagnostic evaluation. Volume replacement was ini- tiated immediately in all patients with hemodynamically significant UGB. Comorbid disorders were treated when
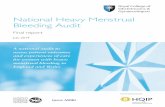
Figure 1. Endoscopic view (cap attached to endoscope) of actively bleeding Dieulafoy's lesion in second portion of duo- denum.
necessary. All patients underwent upper endoscopy with- in 12 hours of admission. Endoscopy was performed under continuous monitoring of pulse rate, oxygen saturation, and blood pressure.
Patients bleeding from small bowel vascular lesions were eligible for inclusion in the study. Vascular lesions comprised two conditions: AGD and DL.
Angiodysplasias were defined endoscopically as either single or multiple 2- to 5-ram diameter bright red round spots with uniform or slightly irregular margins, or lesions larger than 5 mm that appeared as raised and red- dened areas with distinctly irregular margins. 23 Angiodysplasias were classified as bleeding if ei ther active bleeding from the lesion was visualized or if fresh red blood was observed in the upper GI tract and no other potential source for bleeding was identified.
Dieulafoy's lesion was defined endoscopically as a pro- truding vessel within a minute (<3 mm) mucosal defect with normal surrounding mucosa. The DL was considered to be bleeding if any of the following were present: spurt- ing or micropulsatile streaming from a minute mucosal defect (Fig. 1), a densely adherent clot with a narrow point of a t tachment to a minute mucosal defect or normal appearing mucosa, or a non-bleeding protruding vessel (as described previously)J 0
Exclusion criteria were the following: neoplasm, severe diseases with short life expectancy, portal hypertension, pregnancy, peripapillary location of the lesion, and refusal to participate in the study.
Upper endoscopy was performed by 1 of 3 endoscopists (E.B., R.C., F.J.) without an overtube by using standard videoendoscopes (1T130, GIF-Q145; Olympus Optical Co. [Europa], Hamburg, Germany). In two patients bleeding from DL in the third part of the duodenum, I mL of ster- ile methylene blue was injected near the lesion before EBL to facilitate further identification. The endoscopic
VOLUME 58, NO. 2, 2003 GASTROINTESTINAL ENDOSCOPY 275

F Junquera, E Brullet, R Campo, et al. Endoscopic band ligation for bleeding small bowel vascular lesions
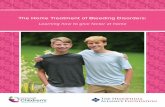
Figure 2. A, Endoscopic view (cap attached to endoscope) of banded tissue containing angiodysplastic lesion in second portion of duodenum. B, Banding-induced ulcer I week after ligation.
elastic band ligation adapter (Bard Interventional Products, Billerica, Mass.) was used for treating single AGD, whereas the multi-band ligation device (Micro- vasive Endoscopy, Boston Scientific Corp., Natick, Mass.) was used for patients bleeding from DL and those with two or more AGD. Endoscopic band ligation was per- formed with a maximum of 200 mBar negative pressure in suctioning the target lesion into the ligator cap just before band release (Fig. 2A).
After EBL, patients were treated with orally adminis- tered omeprazole (20 mg twice a day) for 14 days. Blood transfusions were given when the Hb was less than 9 g/dL (normal: 12-16 g/dL). Endoscopy was repeated 4 to 7 days al~r the initial procedure to assess the characteristics of the band-induced ulcer (Fig. 2B). All patients remained hospitalized for at least 3 days and, thereafter, were seen in the outpatient clinic every 3 months or whenever fur-
ther hemorrhage developed. In addition to a physical examination, each clinic visit included biochemical and hematologic laboratory test profiles and a fecal occult blood test.
The primary study endpoi~ts were the efficacy and safety of EBL, as measured by the rates for recurrent bleeding and morbidity. These variables were assessed during the 40 days after EBL and then during long-term follow-up. Recurrent bleeding was defined as the occur- rence of any of the following: (1) hematemesis or fresh melena during hospitalization or after discharge, or (2) melena associated with signs or symptoms of hypovolemia or a decrease in the Hb level of more than 2 g/dL relative to the most recent previous determination.
The study protocol was approved by the ethics commit- tee of our center, and written informed consent was obtained from all patients enrolled. This study was not supported financially or otherwise through any external sources.
OBSERVATIONS
During the study period, 23 patients were eligible for enrollment. Five were excluded because of the following: severe associated diseases and short life expectancy (3 patients), AGD lesion located close to the major papilla (1 patient), and refusal to partici- pate (1 patient). These pat ients were t rea ted by endoscopic injection or argon plasma coagulation. Thus, 18 patients (10 men, 8 women; mean age, 76 [6] years, range 62-89 years) bleeding from small bowel vascular lesions were included; 14 with AGD, 4 with DL. All patients presented with acute UGB, and 7 (39%) had associated chronic iron deficiency anemia (defined as Hb level <11 g/dL, plasma fer- r i t in level <15 ng/mL [30-400 ng/mL], elevated transferrin level, and serum iron <40 ~ / d L [60-158 ~tg/mL]). Other clinical and endoscopic characteris- tics are given in Table 1. Mean follow-up was 18 months (range 6-31 months).
In all patients, EBL achieved hemostasis in a sin- gle endoscopic session. No patient had fur ther bleed- ing or required further blood transfusion at 40 days' follow-up. However, bleeding recurred in 6 of 14 (43%) patients with AGD during long-term follow- up. Recurrent bleeding was associated with the appearance of new AGD lesions, as demonstrated at endoscopy in 5 patients and by necropsy in 1. In con- trast , none of the 4 patients with DL had further bleeding during follow-up.
No complications were observed after the proce- dure except for mild abdominal pain tha t resolved spontaneously in two patients. No pat ient had died at 40 days after EBL. However, two patients died dur ing the long-term follow-up period of causes unre la ted to hemorrhage (bronchopneumonia and lung cancer).
276 GASTROINTESTINAL ENDOSCOPY VOLUME 58, NO. 2, 2003

Endoscopic band ligation for bleeding small bowel vascular lesions F Junquera, E Brullet, R Campo, et al.
Table 1. Demographics
Angiodysplasia Dieulafoy n=14 n=4
Associated diseases Heart disease (ischemic or valvular cardiac disease) Chronic renal failure* Cerebral vascular insufficiency Symptomatic peripheral vascular disease Diabetes mellitus Arterial hypertension
Clinical characteristics Patients with hypovolemic shockt Patients with previous episodes of UGB Use of anticoagulant drugs Use of antiplatelet drugs* Hematecrit (%) at admission, mean (SD) Transfusion requirements,w mean (SD)
Endoscopic aspects (location of lesions) Duodenal bulb 2nd Duodenum 3rd Duodenum Postanastomotic I
9 (64%) 2/4 50% 4 (28.5%) 1 (25%) 3 (21.4%) 1 (25%) 6 (43%) 1 (25%) 6 (43%) 1 (25%) 9 (64%) 2 (50%)
- - 2 ( 5 0 % )
4 (28.5%) 3 (75%) 6 (43%) 1 (25%) 1 (7%)
23 (7) 21 (3.7) 2.5 (1.7) 4.7 (1.5)
5 8 1 1 2
- - 1
UGB, Upper GI bleeding; SD, standard deviation. *Chronic renal failure: glomerular filtration rate impairment superior to 3 mo with creatinine
plasma levels higher than 1.3 mg/dL. tHypovolemic shock was defined as the presence of a systolic blood pressure less than 90 mm
Hg and pulse rate over 120 beats per minute with signs of peripheral circulatory failure. STiclopidine. w of units of packed red cells transfused during hospitalization. I]In the efferent loop (at 2 cm from Billroth II anastomoses).
DISCUSSION
Endoscopic techniques are currently considered the t rea tment of choice for patients with bleeding GI vascular lesions. 1-1~ However, the optimal endo- scopic approach, as assessed by hemostatic efficacy, ease of application, cost, and risk of complications, is not yet established.2,10-12,17, 24 Endoscopic band liga- tion is now being used for many bleeding GI disor- ders, 10-19 par t icular ly in the esophagus and the stomach, but there is a pauci ty of informat ion regarding its safety in the t r ea tmen t of bleeding lesions in the small bowel. 19-22
The resul ts of the present s tudy indicate t ha t EBL is a safe and effective t rea tment for bleeding small bowel vascular lesions. Permanent hemostasis was achieved in all cases, and no patient had recur- rent bleeding at 40 days' follow-up. With regard to AGD, these results are in agreement ~with those of previous studies in which the rate of pr imary hemo- stasis was 90% to 100% for t r e a tmen t of gastric AGD by EBL.1~ However 6 of 14 (43%) patients with AGD lesions had further bleeding dur- ing long-term follow-up, a rate similar to tha t found in other studies.6, 7 Failure of these t rea tments h a s been at tr ibuted to the difficulty of identifying and]or t reat ing all lesions, which are diffuse in nature and sometimes inaccessible, and to the appearance of
new AGD. 25 In contrast , EBL provided definitive hemostasis in all 4 patients with DL. These results are in agreement with those of other studies of EBL for t rea tment of small bowel DL; permanent hemo- stasis was achieved in 15 of the 16 patients treated (2 with DL in the first portion of duodenum; 2, the second portion; 10, Billroth II anastomoses; 2, the jejunum).19-22
No significant complication was observed in the 18 treated patients. Two complained of mild abdom- inal pain t ha t resolved spontaneously. This good result with respect to the safety of EBL is, in our opinion, related to the use of low negative pressure (a maximum of 200 mBar) in suctioning the target lesion into the ligation cap jus t before band release. As described in a previous report, the risk of com- plications increases when higher pressures (>400 mBar) are used, which results in peritoneal entrap- ment and a risk of delayed perforation. 26 With the use of low negative pressure, there is only mucosal and submucosal entrapment, giving EBL an advan- tage over other endoscopic techniques, including injection and thermal methods.24, 26 This technique may permit the use of EBL in other segments of the gut where the wall is relatively thin, such as the small bowel and colon, 27-29 and the risk of perfora- tion higher. Moreover, EBL may be safer than injec-
VOLUME 58, NO. 2, 2003 GASTROINTESTINAL ENDOSCOPY 2 7 7

F Junquera, E Brullet, R Campo, et al. Endoscopic band ligation for bleeding small bowel vascular lesions
tion or thermal endoscopic methods in patients with coagulopathies and those being treated with antico- agulant drugs. The mechanical hemostatic effect of EBL, which involves ischemic necrosis of the mucosa and submucosa, may be superior to other endoscopic modalities, both in terms of control of active bleeding, as well as in reducing the risk of delayed hemorrhage. In fact, it has been suggested that the hemostatic capacity of EBL in patients with altered coagulation is less dependent on the ability of the patient to form a coagulum than any other endoscopic technique. 29 This is especially noteworthy because many patients bleeding from vascular lesions have associated disor- ders requiring the use of anticoagulant medications (57% of patients in the present study). Additional advantages of EBL include simplicity, availability, and its relatively low cost.12"22,24, 29
However, EBL has several technical limitations. Both, the need for a second intubation, as well as the difficulty in identifying small lesions (resulting from the reduced endoscopic view because of the EBL cap) may. significantly prolong the procedure. Likewise, the rate of bleeding, when massive, makes identification of the bleeding point and band appli- cation difficult. Prior tattooing of these lesions, as in two cases in the present study, could minimize these drawbacks, 30 and even be of assistance at surgery if the hemostatic endoscopic procedure is unsuccess- ful. Lesions located within fibrotic tissue, or only accessible by retroflexion, can be difficult or impos- sible to band. 16-22 Identification of the major duode- nal papilla is essential because its inclusion in the banded tissue can result in biliary obstruction and cholangitis. 31 Therefore, EBL may not be appropri- ate for treating lesions near the papilla.
In conclusion, the results of the present study support the efficacy and safety of EBL in the treat- ment of acutely bleeding small bowel vascular lesions. Endoscopic band ligation is definitive in patients bleeding from DL; however, the high rate of recurrent bleeding during long-term follow-up in patients with AGD constitutes a therapeutic chal- lenge that warrants further investigation.
ACKNOWLEDGMENTS
We thank John Giba for the Engl ish correction of this manuscript.
REFERENCES
1. Foutch PG. Angiodysplasia of the gastrointestinal tract. Am J Gastroenterol 1993;88:807-18.
2. Schmulewitz N, Baillie J. Dieulafoy lesions: a review of 6 years of experience at a tertiary referral center. Am J Gastro- enterol 2001;96:1688-94.
3. Rogers BHG. Endoscopic diagnosis and therapy of mucosal vascular abnormalities of the gastrointestinal tract occurring
in elderly patients and associated with cardiac, vascular and pulmonary diseases. Gastrointest Endosc 1980;26:134-8.
4. Parra-Blanco A, Takahashi H, Mendez-Jerez PV, Kojima T, Aksoz K, Kirihara K, et al. Endoscopic management of Dieulafoy lesions of the stomach: a case study of 26 patients. Endoscopy 1997;29:834-9.
5. Brown SG, Swain CP, Storey DW, Collins C, Matthewson K, Salmon PR, et al. Endoscopic laser t reatment of vascular anomalities of the upper gastrointestinal tract. Gut 1985;26: 1338-48.
6. Rutgeerts P, Van Gompel F, Geboes K, Vantrappen G, Broeckaert L, Coremans G. Long term results of treatment of vascular malformations of the gastrointestinal tract by neodymium YAG laser photocoagulation. Gut 1985;26:586- 93.
7. Gostout CJ, Bowyer BA, Ahlquist DA, Viggiano TR, Balm RI~ Mucosal vascular malformations of the gastrointestinal tract: clinical observations and results of endoscopic neodymium: yttrium-aluminum-garnet laser therapy. Mayo Clin Proc 1988;63:993-1003.
8. Schneider DM, Bourke MJ, Ghanbari A, Kandel G, Kortan P, Markon N, Haber GB. Dieulafoy's disease: clinical features and endoscopic predictors of rebleeding [abstract]. Gastro- intest Endosc 1995;41:297A.
9. Jaspersen D, Korner T, Schorr W, Hammar CH. Diagnosis and treatment control of bleeding colorectal angiodysplasias by endoscopic Doppler sonography: a preliminary study. Gastro- intest Endosc 1994;40:40-4.
10. Dy NM, Gostout CJ, Balm RK. Bleeding from the endoscopi- cally-identified Dieulafoy lesion of the proximal small intes- tine and colon. Am J Gastroenterol 1995;90:108-11.
11. Norton ID, Petersen BT, Sorbi D, Balm RK, Alexander GL, Gostout CJ. Management and long-term prognosis of Dieulafoy lesion. Gastrointest Endosc 1999;50:762-7.
12. Tseng C, Burke S, Connors P, Green R, Carr-Locke DSL. Endoscopic band ligation for treatment of non-variceal upper gastrointestinal bleeding. Endoscopy 1991;23:297-8.
13. Brown G, Harford W, Jones W. Endoscopic band ligation for an actively bleeding Dieulafoy's lesion. Gastrointest Endosc 1994;40:501-3.
14. Campo R, BruUet E. Endoscopic treatment of gastric angio- dysplasia with elastic band ligation. Gastrointest Endosc 1998;48:510-4.
15. Wong RM, Ota S, Katoh A, Yamauchi A, Arai K, Kaneko K, et al. Endoscopic ligation for non-esophageal variceal upper gas- trointostinal hemorrhage. Endoscopy 1998;30:774-7.
16. Gerson L, Yap E, Slosberg E, Soetikno R. Endoscopic band ligation for actively bleeding Dieulafoy's lesions. Gastrointest Endosc 1999;50:454-5.
17. McGrath K, Mergener K, Branch S. Endoscopic band ligation of Dieulafoy's lesions: report of two cases and review of the lit- erature. Am J Gatroentrol 1999;94:1087-90.
18. Myung SJ, Kim JW, Moon YS. Endoscopic band ligation of Dieulafoy's lesion. Gastrointest Endosc 2000;51:192.
19. Abi-Hanna D, Williams SJ, Gillespie PE, Bourke MJ. Endoscopic band ligation for non-variceal non-ulcer gastroin- testinal hemorrhage. Gastrointest Endosc 1996;43:502-4.
20. Murray KF, Jennings RW, Fox VL. Endoscopic band ligation of a Dieulafoy lesion in the small intestine of a child. Gastrointest Endosc 1996;44:336-9.
21. Nikolaidis N, Zezos P, Giouleme O, Budas K, Marakis G, Paroutoglou G, Eugenidis N. Endoscopic band ligation of Dieulafoy-like lesions in the upper gastrointestinal tract. Endoscopy 2001;33:754-60.
22. Hurlstone DP. Successful endoscopic band ligation of duode-
278 GASTROINTESTINAL ENDOSCOPY VOLUME 58, NO. 2, 2003

Endoscopic intervention for hepatolithiasis S Mahadeva, R Prabakharan, K-L Goh
nal Dieulafoy's lesions. Further large controlled studies a r e
required [letter]. Scand J Gastroenterol 2002;37:620. 23. Howard OM, Buchanan JD, Hunt RH. Angiedysplasia of the
colon. Experience of 26 cases. Lancet 1982;II:16-9. 24. Chung IK, Kim EJ, Lee MS, Kim HS, Park SH, Lee MH, et al.
Bleeding Dieulafoy's lesions and the choice of endoscopic method: comparing the hemostatic efficacy of mechanical and injection methods. Gastrointest Endosc 2000;52:721-4.
25. Marshall JK, Hunt RH. Hormonal therapy for bleeding gas- trointestinal mucosal vascular abnormalities: a promising alternative. Eur J Gastroenterol Hepatol 1997;9:521-5.
26. Campo R, Brullet E, Montane JM, Bombardo J, Sanfeliu J. Elastic band ligation in the bowel: is it really safe? Gastro- intest Endosc 1998;47:105-6.
27. witte JT, Bohlman T. Endoscopic band ligation of colonic bleeding. Gastrointest Endosc 1999;49:392-4.
28. Rivera Vaquerizo PA, Barajas Martinez JM, Blasco Colmenarejo M, Viconte Gutierrez M, Garcia Garcia V, Perez Floros R. Lower gastrointestinal bleeding due to Dieulafoy's in the upper colon. Gastreenterol Hepato12001;24:343-5.
29. Slivka A, Parsons WG, Carr-Locke DSL. Endoscopic band ligation for treatment of post-polypectomy hemorrhage. Gastrointest Endosc 1994;40:230-2.
30. Ponsky d-L, King JF. Endoscopic marking of colonic lesions. Gastrointest Endosc 1975;22:42-3.
31. Silberzweig JE, Atillasoy EO, Sheiner PA, Mitty HA. Biliary obstruction caused by endoscopic band ligation of a duodenal varix. Am J Gastroenterol 1997;92:1060-2.
Endoscopic intervention for hepatolithia- sis associated with sharp angulation of right intrahepatic ducts
Sanjiv Mahadeva, MRCP, Ranjeev Prabakharan, MRCP, Khean-Lee Goh, MD, FRCP
Background: Hepatolithlasis (intrahepatic stones) is common in Asian patients. Hepatollthlasis with intra- hepatic strictures and sharp ductsl angulation poses a particularly difficult management problem. Methods: Cases of hepatolithissis with sharp angulation of right intrahepstlc ducts were retrospectively reviewed. Observations: Five patients with hepatolithissis and right sharp intrahepatic ductal anguIstion were treated endo- scopically via ERCP.Two patients died soon after the pro- cedure. In the remaining 3 patients, treatment by dilation of the intrehepstic strictures and stent placement was only partially successful. Attempts to access the sharply angulated intrahepatic duct were unsuccessful. Conclusions: Endoscopic management of hepstolithissis associated with sharp angulation of a right intrahepatic duct is difficult and is generally managed best with percu- taneous treatment modalitles or surgery, where possible.
Hepa to l i th i a s i s , which is p r e v a l e n t in E a s t Asia, is a d i f f icu l t m a n a g e m e n t p r o b l e m . 1 A g g r e s s i v e t r e a t m e n t is r e q u i r e d to p r e v e n t t h e d e v a s t a t i n g compl ica t ions of th is d isease , which r a n g e f rom sup- p u r a t i v e cho langi t i s to s e c o n d a r y b i l i a ry c i r rhos i s a n d e v e n cho l ang ioca rc inoma . 2 However , i n t r a h e - pa t i c duc t ( IHD) s t r ic tures , p r e s e n t in up to 75% of cases in Asia, r e m a i n a l imi t ing fac tor for comple te s t one c l e a r a n c e a n d b i l i a r y d r a i n a g e . 3 A s h a r p l y
Received August 20, 2002. For revision October 15, 2002. Accepted March 19, 2003. Current affiliations: Division of Gastroenterology, Department of Medicine, University of Malaya, Kuala Lumpur, Malaysia. Reprint requests: K-L Goh, MD, Department of Medicine, Faculty of Medicine, University of Malaya, 50603 Kuala Lumpur, Malaysia. Copyright �9 2003 by the American Society for Gastrointestinal Endoscopy 0016-5107/2003/$30.00 + 0
doi:10.1067 / mge.2003.325
Figure 1. Retrograde cholangiogram showing sharply angu- lated, dilated right intrahepatic duct (arrow) containing stones (arrowheads).
a n g u l a t e d i n t r a h e p a t i c bile duct p rox ima l to a str ic- t u r e h a s been no ted as a n addi t iona l fac tor t h a t con- t r i bu t e s to t r e a t m e n t failure.4, 5 Five such cases a r e
r e p o r t e d , a n d t h e r e l a t i v e m e r i t s o f endoscop ic t r e a t m e n t a lone for m a n a g e m e n t a re discussed.
PATIENTS AND METHODS Case 1
A 78-year-old Indian woman presented with suppura- tive cholecystitis and underwent cholecystectomy, at which operation, the liver was noted to be cirrhotic. Screening studies ruled out viral causes, and there was no history of alcoholism. Thereafter, she was asymptomatic for 16 years but was then hospitalized with acute gall- stone-induced pancreatitis. ERCP revealed hepatolithia- sis with filling defects proximal to a sharply angulated right IHD (Fig. 1). Endoscopic sphincterotomy (ES) was performed, followed by extraction of stones from the extrahepatic duct and insertion of a 10F, 12-cm-long poly- ethylene, Amsterdam-type s tent into the right hepatic duct but not into the angulated duct. The s tent was changed on two further occasions (4-month intervals). The
VOLUME 58, NO. 2, 2003 GASTROINTESTINAL ENDOSCOPY 2 7 9