Clinical effectiveness and quality of life of conventional haemodialysis versus short daily...
13
Nephrol Dial Transplant (2008) 23: 2634–2646 doi: 10.1093/ndt/gfn010 Advance Access publication 3 April 2008 Original Article Clinical effectiveness and quality of life of conventional haemodialysis versus short daily haemodialysis: a systematic review ∗ Jeannete Pu˜ nal 1 , Leonor Varela Lema 1 , Domingo Sanhez-Guisande 2 and Alberto Ruano-Ravina 1,3,4 1 Galician Department of Health, Galician Agency for Health Technology Assessment, Santiago de Compostela, 2 Nephrology Service, Clinic University Hospital of Santiago de Compostela, 3 Department of Preventive Medicine and Public Health, University of Santiago de Compostela and 4 CIBER de epidemiolog´ ıa y salud p ´ ublica, CIBERESP, Spain Abstract Background. End-stage renal disease is a troublesome health problem worldwide. The most usual renal replace- ment therapy is conventional haemodialysis (CHD), per- formed three times a week, 3.5–4 h per session. It has been proposed that this schedule is unphysiologic and that daily haemodialysis would be a more appropriate schedule. One of the variants of daily haemodialysis is the so-called short daily haemodialysis (SDHD), performed five to seven times per week, 1.5–3 h per session. The objective of this paper is to compare, through a systematic review, the clinical ef- fectiveness and safety of SDHD versus CHD. Methods. The following databases were searched: MED- LINE, EMBASE, NHS Centre for Reviews and Dissemina- tion (HTA, DARE and NHS EED), Cochrane, ISI Web of Knowledge, IME and IBECS. Two independent reviewers decided which papers were to be included after applying inclusion and exclusion criteria. Any discrepancy was re- solved by consensus. The quality of the included papers was measured using a quality scale developed for the purpose of this report. Results. Seventeen original articles were included. There were no randomized controlled trials. SDHD seems to be more effective than conventional dialysis. Patients on daily haemodialysis seem to present less vascular access prob- lems, better control of hypertension and in turn a reduc- tion in the antihypertensive treatment, better quality of life, lower incidence of ventricular hypertrophy, lower consump- tion of rHuEPO due to the better control of anaemia and a reduction in the use of phosphate binders as a consequence of the better control of plasmatic phosphorous. Conclusions. SDHD might result in a better clinical ef- fectiveness, mainly through a better control of the arterial Correspondence and offprint requests to: Alberto Ruano Ravi˜ na, Galician Department of Health, Galician Agency for Health Technology Assess- ment, Edif Administrativo de San L´ azaro, San L´ azaro s/n, 15781 Santiago de Compostela, Spain. Tel: +34-981-541831; Fax: +34-981-542854; E-mail: [email protected], [email protected] ∗ The full systematic review (110 pages) can be downloaded in Spanish completely free through the webpage of the Galician Agency for Health Technology Assessment (http://avalia-t.sergas.es/). tension and, therefore, a lower consumption of antihyper- tensive drugs, and a better quality of life than CHD. Keywords: end-stage renal disease; daily haemodialysis; MeSH terms: renal replacement therapy; renal dialysis; systematic review Introduction During the last decade, chronic kidney disease (CKD) de- pendent on renal replacement therapy (RRT) has increased in all countries, and despite the technological advances, there have been no significant improvements in survival [1]. Currently, it is thought that an occult renal disease ex- ists in a relatively high percentage of the population, as has been detected by the EPIRCE study in Spain [2]. This fact could also be present in other developed countries. At a world level, the highest incidence rates of end-stage renal disease (ESRD) are observed in the USA, Taiwan, Qatar and Japan. In the USA, 336 patients per million population (pmp) initiated RRT in 2003, whilst in European countries, in no case did this figure exceed 200 pmp. Survival of in- cident patients undergoing dialysis at 1, 2 and 5 years of follow-up is 85.7%, 75% and 49.4%, respectively [1]. In most countries, haemodialysis (HD) is the therapy of choice for patients with CKD [3]. Maintenance haemodial- ysis, using diffusion through hollow fibre cuprophan mem- branes can be dated back to the 1960s [4]. Since then, different HD modalities have emerged. A recent review has updated the published evidence on their effectiveness [5,6]. There is also variability in the HD frequency. While the conventional schedule is three times per week, it has been suggested that a more physiological dialysis would be a daily schedule, with six times per week during 1.5–3 h, usually called short daily haemodialysis (SDHD). There are other HD frequencies, such as long nocturnal HD, where HD is performed 8 h each night or the Tassin experience, three times per week and a duration of 8 h per session [7]. The objective of the present paper is to compare the clinical effectiveness and the quality of life of SDHD with C The Author [2008]. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved. For Permissions, please e-mail: [email protected] by guest on August 19, 2014 http://ndt.oxfordjournals.org/ Downloaded from
-
Upload
tarumanegara -
Category
Documents
-
view
0 -
download
0
Transcript of Clinical effectiveness and quality of life of conventional haemodialysis versus short daily...

Nephrol Dial Transplant (2008) 23: 2634–2646doi: 10.1093/ndt/gfn010Advance Access publication 3 April 2008
Original Article
Clinical effectiveness and quality of life of conventional haemodialysisversus short daily haemodialysis: a systematic review∗
Jeannete Punal1, Leonor Varela Lema1, Domingo Sanhez-Guisande2 and Alberto Ruano-Ravina1,3,4
1Galician Department of Health, Galician Agency for Health Technology Assessment, Santiago de Compostela, 2NephrologyService, Clinic University Hospital of Santiago de Compostela, 3Department of Preventive Medicine and Public Health,University of Santiago de Compostela and 4CIBER de epidemiologıa y salud publica, CIBERESP, Spain
AbstractBackground. End-stage renal disease is a troublesomehealth problem worldwide. The most usual renal replace-ment therapy is conventional haemodialysis (CHD), per-formed three times a week, 3.5–4 h per session. It has beenproposed that this schedule is unphysiologic and that dailyhaemodialysis would be a more appropriate schedule. Oneof the variants of daily haemodialysis is the so-called shortdaily haemodialysis (SDHD), performed five to seven timesper week, 1.5–3 h per session. The objective of this paperis to compare, through a systematic review, the clinical ef-fectiveness and safety of SDHD versus CHD.Methods. The following databases were searched: MED-LINE, EMBASE, NHS Centre for Reviews and Dissemina-tion (HTA, DARE and NHS EED), Cochrane, ISI Web ofKnowledge, IME and IBECS. Two independent reviewersdecided which papers were to be included after applyinginclusion and exclusion criteria. Any discrepancy was re-solved by consensus. The quality of the included papers wasmeasured using a quality scale developed for the purposeof this report.Results. Seventeen original articles were included. Therewere no randomized controlled trials. SDHD seems to bemore effective than conventional dialysis. Patients on dailyhaemodialysis seem to present less vascular access prob-lems, better control of hypertension and in turn a reduc-tion in the antihypertensive treatment, better quality of life,lower incidence of ventricular hypertrophy, lower consump-tion of rHuEPO due to the better control of anaemia and areduction in the use of phosphate binders as a consequenceof the better control of plasmatic phosphorous.Conclusions. SDHD might result in a better clinical ef-fectiveness, mainly through a better control of the arterial
Correspondence and offprint requests to: Alberto Ruano Ravina, GalicianDepartment of Health, Galician Agency for Health Technology Assess-ment, Edif Administrativo de San Lazaro, San Lazaro s/n, 15781 Santiagode Compostela, Spain. Tel: +34-981-541831; Fax: +34-981-542854;E-mail: [email protected], [email protected]∗The full systematic review (110 pages) can be downloaded in Spanish
completely free through the webpage of the Galician Agency for HealthTechnology Assessment (http://avalia-t.sergas.es/).
tension and, therefore, a lower consumption of antihyper-tensive drugs, and a better quality of life than CHD.
Keywords: end-stage renal disease; daily haemodialysis;MeSH terms: renal replacement therapy; renal dialysis;systematic review
Introduction
During the last decade, chronic kidney disease (CKD) de-pendent on renal replacement therapy (RRT) has increasedin all countries, and despite the technological advances,there have been no significant improvements in survival[1]. Currently, it is thought that an occult renal disease ex-ists in a relatively high percentage of the population, as hasbeen detected by the EPIRCE study in Spain [2]. This factcould also be present in other developed countries. At aworld level, the highest incidence rates of end-stage renaldisease (ESRD) are observed in the USA, Taiwan, Qatarand Japan. In the USA, 336 patients per million population(pmp) initiated RRT in 2003, whilst in European countries,in no case did this figure exceed 200 pmp. Survival of in-cident patients undergoing dialysis at 1, 2 and 5 years offollow-up is 85.7%, 75% and 49.4%, respectively [1].
In most countries, haemodialysis (HD) is the therapy ofchoice for patients with CKD [3]. Maintenance haemodial-ysis, using diffusion through hollow fibre cuprophan mem-branes can be dated back to the 1960s [4]. Since then,different HD modalities have emerged. A recent reviewhas updated the published evidence on their effectiveness[5,6]. There is also variability in the HD frequency. Whilethe conventional schedule is three times per week, it hasbeen suggested that a more physiological dialysis would bea daily schedule, with six times per week during 1.5–3 h,usually called short daily haemodialysis (SDHD). There areother HD frequencies, such as long nocturnal HD, whereHD is performed 8 h each night or the Tassin experience,three times per week and a duration of 8 h per session [7].
The objective of the present paper is to compare theclinical effectiveness and the quality of life of SDHD with
C© The Author [2008]. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved.For Permissions, please e-mail: [email protected]
by guest on August 19, 2014
http://ndt.oxfordjournals.org/D
ownloaded from

Conventional versus daily haemodialysis 2635
Table 1. Selection criteria of the studies included in the review
Aspects considered Inclusion criteria
Type of schedule Patients treated on daily HD (five to seven times per week, 1.5–3 h/session)Comparison group, patients treated on CHD (three times per week, 3–5 h/session)
Type of publication Original papers and health technology assessment reportsStudy design Systematic reviews, meta-analysis, clinical trials, cohort studies and case control studiesSetting of the dialytic treatment All or at least half of the patients were dialyzed on daily HD in dialysis centres, hospitals or self-care unitsSample size A minimum of 10 patients were treated on daily HD. The comparison group had at least 10 patientsFollow-up period A minimum of 1 month, either on daily HD or on comparison groupPatient characteristics Patients with end-stage renal diseaseOutcome variables Blood pressure control, medication requirements, vascular accesses complications, hospitalizations and quality of
life. Inclusion of studies that assessed Kt/V, clearance of different molecules and other variablesStudy starting date The dialysis treatment was performed after January 1995 in all or part of patientsOther criteria Studies excluded those conducted on animals, patients treated with daily haemofiltration, or covering dialyzers or
dialysis membranes without including patients
HD: haemodialysis; CHD: conventional haemodialysis.
conventional haemodialysis (CHD) through a systematicreview of the literature.
Methods
Literature search
A systematic search of the literature was performed. Thedatabases used were MEDLINE (Pubmed), EMBASE (Sil-ver Platter), CRD (NHS Centre for Reviews and Dissem-ination), DARE (Database of Abstracts of Reviews of Ef-fectiveness), NHS EED (Economic Evaluation Database),Cochrane Library Plus, ISI Web of Knowledge (Institutefor Scientific Information, Philadelphia), as well as othernational databases. Search strategies were created for eachdatabase using different combinations and variations ofthe following core search strategies: (‘hemodialysis’ or‘haemodialysis’ or ‘dialysis’) and (‘daily’ or ‘quotidian’or ‘frequent’ or ‘home’). The search also included otherdatabases that provided information on ongoing clinicaltrials and research projects such as ClinicalTrials.gov,Centerwatch and HSRPROJ (Health Services ResearchProjects in Progress). A fully recursive search of referencelists of relevant papers was performed to find studies notidentified by the previous search. The search was restrictedto studies published in English, Spanish, French, Italian orPortuguese, between January 1995 and January 2007.
Paper selection
Papers identified in the search were reviewed separatelyby two of the authors and those considered potentially rel-evant were selected for further analysis. The full text ofthese papers was obtained and the two reviewers indepen-dently checked each trial for fulfilment of selection criteria(Table 1). The relevant data were rigorously extracted andrecorded in evidence tables that included information onstudy type, inclusion/exclusion criteria, patient character-istics (age, sex, comorbidities and time on dialysis) andfollow-up data.
The papers were classified depending on the type ofoutcome variables evaluated: vascular accesses complica-tions, cardiovascular outcomes, anaemia and EPO dosage,
nutritional status, therapy efficiency, morbidity and qualityof life.
Study quality assessment
Study quality was assessed using a specific scale adaptedfrom a previous study on haemodialysis [6,8]. The includedpapers were assessed in a blinded way by two independentreviewers. Differences >5% in the use of the scale werenot allowed and discrepancies were resolved by consen-sus after reviewing again carefully the study assessed. Theconcordance was measured using the intraclass correlationcoefficient which is equivalent to the kappa index for con-tinuous variables [9,10].
Results
Search results
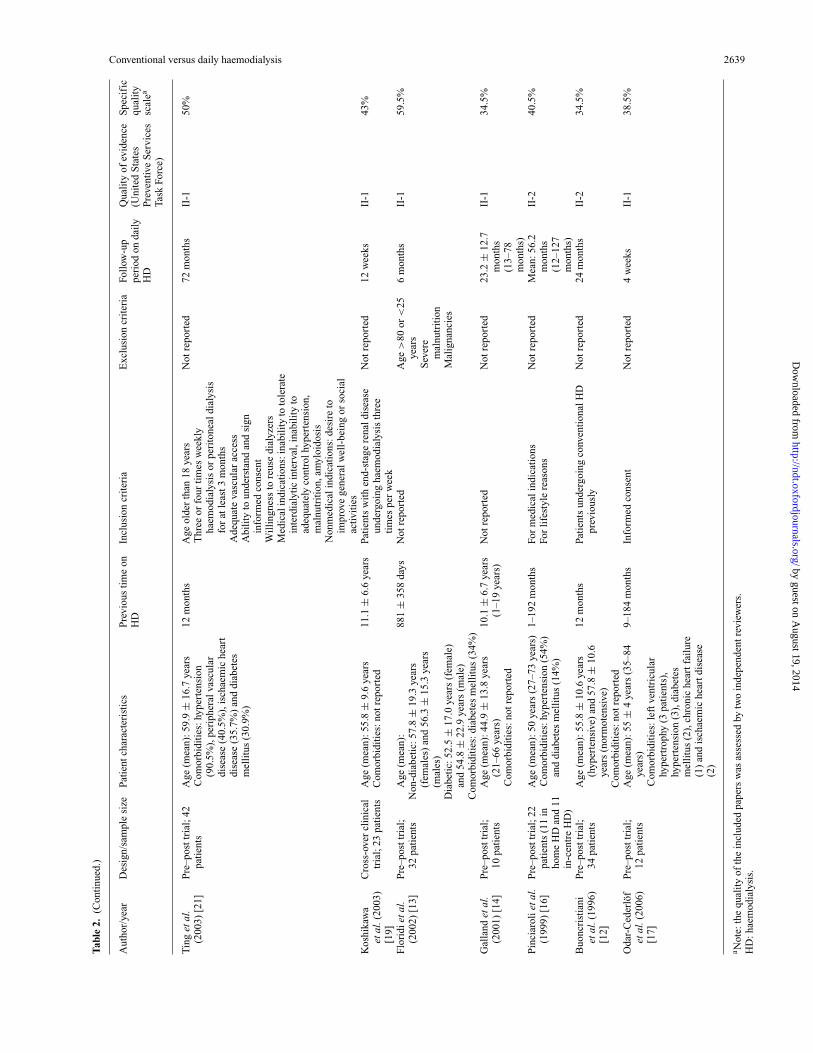
The search strategy used identified 1.673 references. Ofthese, 69 studies were considered to be potentially rele-vant and were read at full text. After applying the inclu-sion/exclusion criteria, 17 articles were included in the sys-tematic review [11–27] (Figure 1). The majority of studieswere carried out in the USA and Italy. Only two studieswere published before the year 2000, one in 1996 [12] andthe other in 1999 [16]. The details of the included studiesmay be observed in Table 2.
Effectiveness of short daily haemodialysis
Vascular access problems. Seven articles [11,18,20–24]assessed the incidence of vascular access-related compli-cations. Of these, two [22,24] showed that patients receiv-ing daily dialysis had a lower incidence of vascular accessocclusions and a higher vascular access survival in relationto patients on conventional HD. Ting et al. [21] observedan average of 0.94 problems/year on DHD versus 1.01 onconventional HD, but this difference was not statisticallysignificant. Martins Castro et al. [18] showed an elevatedvascular accesses survival and a low number of failures onSDHD, not reporting outcomes on conventional HD. Theother three studies found similar incidences of vascular ac-cess failure with both HD frequencies [11,20,23].
by guest on August 19, 2014
http://ndt.oxfordjournals.org/D
ownloaded from

2636 J. Punal et al.
Fig. 1. Identification and selection of studies.
Cardiovascular outcomes: hypertension control and leftventricular hypertrophy. Six of the eleven trials that as-sessed the effect of short daily versus conventional dialysison blood pressure control observed greater reductions inboth systolic and diastolic aortic blood pressures for pa-tients on daily dialysis [11,12,16,19,22,24]. Williams et al.[23] observed a decrease in the systolic blood pressure dur-ing SDHD only. One paper [14] showed five hypertensivepatients during conventional HD that turned normotensiveon SDHD. In three studies, the decrease in blood pressureduring daily HD was not significant [15,21,26].
In 13 papers a comparison was made of medica-tion requirements during daily and conventional dialysis.Several studies found that when patients were transferredfrom conventional to short daily dialysis they could dis-continue or reduce the doses of antihypertensive drugs[12,14,19,21,23,24] or required a lower association of dif-ferent antihypertensive drugs [21,22]. The results of thesestudies are summarized in Table 3.
Five studies observed a significant reduction in cardiachypertrophy parameters when patients were changed fromconventional to daily HD [12,14,16,24,26]. Other inves-tigations found similar values for both dialysis regimens
[11,15]. In a study carried out by Odar-Cederlof et al. [17],elevated predialysis levels of B-type natriuretic peptide de-creased when patients were transferred to daily dialysis.Floridi et al. [13] showed that an SDHD regimen couldlower the mean levels of glycation-related substances ob-served in CHD.
Anaemia and EPO dosage. The majority of trials ob-served that erythropoietin doses could be reduced duringthe SDHD period [14,15,19,21,24,26] even though somestudies reported no significant changes [11,22]. In the studycarried out by Ting et al. [21] EPO requirements were re-duced in 45% after 12 months of follow-up. Traeger et al.[24] also observed a significant reduction after 1 year butEPO requirements increased slightly with longer follow-up periods (up to 6 years). During the daily HD period,the EPO treatment could be discontinued in some patients[14,19]. For example, Koshikawa et al. [19] found that in14 patients treated with SDHD, EPO was retired in 2 anddoses reduced in 5 patients.
Nutritional status. Ten studies reported the effects thatdaily dialysis had on various nutritional parameters.
by guest on August 19, 2014
http://ndt.oxfordjournals.org/D
ownloaded from

Conventional versus daily haemodialysis 2637
Tab
le2.
Stu
dies
com
pari
ngda
ilyha
emod
ialy
sis
(HD
)ve
rsus
conv
enti
onal
dial
ysis
(CD
)in
clud
edin
the
syst
emat
icre
view
Aut
hor/
year
Des
ign/
sam
ple
size
Pati
ents
char
acte
rist
ics
Pre
viou
sti
me
onH
DIn
clus
ion
crit
eria
Exc
lusi
oncr
iter
iaFo
llow
-up
peri
odon
daily
HD
Qua
lity
ofev
iden
ce(U
nite
dS
tate
sP
reve
ntiv
eS
ervi
ces
Task
Forc
e)
Spe
cifi
cqu
alit
ysc
alea
Fagu
glie
tal.
(200
6)[1
5]P
rosp
ectiv
eco
hort
stud
y;24
pati
ents
(12
onco
nven
tion
alH
Dan
d12
onda
ilyH
D)
Age
(mea
n):5
8.5
±16
.2ye
ars
Com
orbi
diti
es:n
otre
port
ed3
mon
ths
Pre
senc
eof
hype
rten
sion
Age
>15
and
<80
year
sC
lini
cala
ndbi
oche
mic
alst
able
cond
itio
nsat
leas
tin
the
prev
ious
mon
ths
spK
t/V
>1.
2
Lim
bam
puta
tion
Sev
ere
mal
nutr
itio
n
6m
onth
sII
-167
%
Mal
igna
ncie
s
Mar
tins
Cas
tro
etal
.(20
06)
[18]
Pre
–pos
ttri
al;2
6pa
tien
tsA
ge(m
ean)
:35.
6±
14.7
year
s(1
6–64
year
s)25
.1±
31.9
mon
ths
(1–1
59m
onth
s)In
form
edco
nsen
tM
edic
alco
ndit
ions
orpa
tien
tde
cisi
on
33.6
±18
.5m
onth
s(<
36m
onth
sin
grou
p1
and
>36
mon
ths
ingr
oup
2)
II-1
65%
Gol
dfar
b-R
umya
ntze
vet
al.(
2006
)[2
2]
Cro
ss-o
ver
clin
ical
tria
l;12
pati
ents
Age
:24–
75ye
ars
Com
orbi
diti
es:h
yper
tens
ion
(100
%),
diab
etes
(100
%),
diab
etes
mel
litu
s(8
.3%
),m
igra
ine
(8.3
%)
and
coro
nary
arte
rydi
seas
e(2
5%)
4w
eeks
Hyp
erte
nsio
n,in
trad
ialy
tic
hypo
tens
ion,
mus
cle
cram
ps,a
naem
iatr
eate
dw
ith
high
dose
sof
EP
O,l
arge
inte
rdia
lyti
cfl
uid
gain
,hyp
erka
laem
iaor
hype
rpho
spha
taem
ia
Med
ical
lyun
stab
leP
regn
antw
omen
Chi
ldre
n
8w
eeks
II-1
45%
Men
tally
disa
bled
Nes
rall
ahet
al.(
2006
)[2
5]
Pre
–pos
ttri
al;3
9pa
tien
ts(2
7on
hom
eH
Dan
d12
in-c
entr
eH
D)
Age
(mea
n):5
2.8
±15
.1ye
ars
(hom
eH
D)
and
59.2
±14
.6ye
ars
(in-
cent
reH
D)
Com
orbi
diti
es:h
yper
tens
ion
(77%
),di
abet
esm
elli
tus
(15%
)an
dhy
perp
arat
hyro
idis
m(2
7%)
6.4
–9.
9ye
ars
Not
repo
rted
Not
repo
rted
2.4
–4.
5ye
ars
II-1
45%
Com
orbi
diti
es:d
iabe
tes
mel
litu
s(2
4%on
hom
eH
Dan
d47
%in
-cen
tre
HD
),co
nges
tive
hear
tfai
lure
(29%
onho
me
HD
and
35%
in-c
entr
eH
D)
and
coro
nary
arte
rydi
seas
e(2
4%on
hom
eH
Dan
d12
%in
-cen
tre)
Ayu
set
al.
(200
5)[2
6]N
on-r
ando
miz
edcl
inic
altr
ial;
77pa
tien
ts(2
6on
daily
HD
and
51on
conv
enti
onal
HD
)
Age
(mea
n):5
1±
11.7
year
son
daily
HD
and
54±
8.5
year
son
conv
enti
onal
HD
Com
orbi
diti
es:n
otre
port
ed
3.87
±2.
97ye
ars
onco
nven
tion
alH
Dan
d2.
81±
2.98
onda
ilyH
D
Info
rmed
cons
ent
Not
repo
rted
12m
onth
sII
-171
%
by guest on August 19, 2014
http://ndt.oxfordjournals.org/D
ownloaded from

2638 J. Punal et al.
Tab
le2.
(Con
tinu
ed.)
Aut
hor/
year
Des
ign/
sam
ple
size
Pati
ents
char
acte
rist
ics
Pre
viou
sti
me
onH
DIn
clus
ion
crit
eria
Exc
lusi
oncr
iter
iaFo
llow
-up
peri
odon
daily
HD
Qua
lity
ofev
iden
ce(U
nite
dS
tate
sP
reve
ntiv
eS
ervi
ces
Task
Forc
e)
Spe
cifi
cqu
alit
ysc
alea
Yue
net
al.
(200
5)[2
7]P
re–p
ostt
rial
;21
pati
ents
Age
(mea
n):5
2±
3ye
ars
Com
orbi
diti
es:n
otre
port
ed12
mon
ths
Into
lera
nce
ofco
nven
tion
alH
D(r
efra
ctor
yin
trad
ialy
tic
hypo
tens
ion,
inte
rdia
lyti
cvo
lum
eov
erlo
ador
hype
rpho
spha
taem
ia)
Into
lera
nce
toda
ilyH
Dre
gim
en12
mon
ths
II-1
53.5
%
Am
inim
umof
6m
onth
son
conv
enti
onal
HD
Rey
nold
set
al.
(200
4)[1
1]P
re–p
ostt
rial
;39
pati
ents
(27
onho
me
HD
and
12in
-cen
tre
HD
)
Age
(mea
n):5
6±
8.6
year
s(3
6–66
year
s)C
omor
bidi
ties
:dia
bete
sm
elli
tus
(82%
),hy
pert
ensi
on(8
2%),
coro
nary
arte
rydi
seas
e(6
4%)
Mea
n:42
mon
ths
(6–2
34m
onth
s)Pa
tien
tstr
eate
dpr
evio
usly
onco
nven
tion
alH
DN
otre
port
ed2–
18m
onth
sII
-138
.5%
Wil
liam
set
al.
(200
4)[2
3]P
re–p
ostt
rial
;21
pati
ents
Age
(mea
n):5
7±13
year
s(3
5–84
year
s)C
omor
bidi
ties
:hyp
erte
nsio
n(5
7%),
diab
etes
mel
litu
s(1
4%),
left
vent
ricu
lar
hype
rtro
phy
(24%
)an
dch
roni
cob
stru
ctiv
epu
lmon
ary
dise
ase
(24%
)
75±
51m
onth
s(9
–184
mon
ths)
Pati
ents
who
had
been
stab
leon
thre
eti
mes
wee
kly
haem
odia
lysi
sth
erap
yfo
rat
leas
t3m
onth
s
Bac
tera
emia
,ps
ycho
sis,
seni
lity
His
tory
ofm
alig
nanc
yw
ithi
nth
epr
evio
us3
year
sH
isto
ryof
nonc
ompl
ianc
e
4w
eeks
II-1
42.5
%
Tra
eger
etal
.(2
004)
[24]
;G
alla
ndet
al.
(200
4)[2
8]
Pre
–pos
ttri
al;1
7pa
tien
tsA
ge:2
1–75
year
sC
omor
bidi
ties
:not
repo
rted
1–29
year
sPa
tien
tsw
ith
end-
stag
ere
nald
isea
setr
eate
dw
ith
conv
enti
onal
HD
Not
repo
rted
1–6
year
sII
-142
%
Med
ical
cond
itio
n:un
cont
roll
edbl
ood
pres
sure
left
vent
ricu
lar
hype
rtro
phy,
inab
ilit
yto
tole
rate
the
inte
rdia
lyti
cin
terv
al,m
alnu
trit
ion
Pre
scri
bed
dial
ysis
tim
eD
esir
eto
impr
ove
the
pati
ents
’sc
hedu
lefo
rw
ork
and
fam
ilyti
me
Pic
coli
etal
.(2
004)
[20]
Pro
spec
tive
coho
rtst
udy;
28on
daily
HD
(14
inho
me
HD
)an
d49
onco
nven
tion
alH
D(2
8in
hom
eH
D)
Age
:20–
77ye
ars
Com
orbi
diti
es:n
otre
port
ed65
5m
onth
sin
hom
eH
D;8
97m
onth
sin
in-c
entr
eH
D
Pati
ents
trea
ted
wit
hH
DN
otre
port
ed40
0m
onth
sin
hom
eH
Dan
d20
8m
onth
sin
-cen
tre
HD
II-2
58.5
%
by guest on August 19, 2014
http://ndt.oxfordjournals.org/D
ownloaded from
Conventional versus daily haemodialysis 2639
Tab
le2.
(Con
tinu
ed.)
Aut
hor/
year
Des
ign/
sam
ple
size
Pati
entc
hara
cter
isti
csP
revi
ous
tim
eon
HD
Incl
usio
ncr
iter
iaE
xclu
sion
crit
eria
Foll
ow-u
ppe
riod
onda
ilyH
D
Qua
lity
ofev
iden
ce(U
nite
dS
tate
sP
reve
ntiv
eS
ervi
ces
Task
Forc
e)
Spe
cifi
cqu
alit
ysc
alea
Tin
get
al.
(200
3)[2
1]P
re–p
ostt
rial
;42
pati
ents
Age
(mea
n):5
9.9
±16
.7ye
ars
Com
orbi
diti
es:h
yper
tens
ion
(90.
5%),
peri
pher
alva
scul
ardi
seas
e(4
0.5%
),is
chae
mic
hear
tdi
seas
e(3
5.7%
)an
ddi
abet
esm
elli
tus
(30.
9%)
12m
onth
sA
geol
der
than
18ye
ars
Thr
eeor
four
tim
esw
eekl
yha
emod
ialy
sis
orpe
rito
neal
dial
ysis
for
atle
ast3
mon
ths
Ade
quat
eva
scul
arac
cess
Abi
lity
toun
ders
tand
and
sign
info
rmed
cons
ent
Wil
ling
ness
tore
use
dial
yzer
sM
edic
alin
dica
tion
s:in
abil
ity
toto
lera
tein
terd
ialy
tic
inte
rval
,ina
bili
tyto
adeq
uate
lyco
ntro
lhyp
erte
nsio
n,m
alnu
trit
ion,
amyl
oido
sis
Non
med
ical
indi
cati
ons:
desi
reto
impr
ove
gene
ralw
ell-
bein
gor
soci
alac
tivit
ies
Not
repo
rted
72m
onth
sII
-150
%
Kos
hika
wa
etal
.(20
03)
[19]
Cro
ss-o
ver
clin
ical
tria
l;23
pati
ents
Age
(mea
n):5
5.8
±9.
6ye
ars
Com
orbi
diti
es:n
otre
port
ed11
.1±
6.6
year
sPa
tien
tsw
ith
end-
stag
ere
nald
isea
seun
derg
oing
haem
odia
lysi
sth
ree
tim
espe
rw
eek
Not
repo
rted
12w
eeks
II-1
43%
Flo
ridi
etal
.(2
002)
[13]
Pre
–pos
ttri
al;
32pa
tien
tsA
ge(m
ean)
:N
on-d
iabe
tic:
57.8
±19
.3ye
ars
(fem
ales
)an
d56
.3±
15.3
year
s(m
ales
)D
iabe
tic:
52.5
±17
.0ye
ars
(fem
ale)
and
54.8
±22
.9ye
ars
(mal
e)C
omor
bidi
ties
:dia
bete
sm
elli
tus
(34%
)
881
±35
8da
ysN
otre
port
edA
ge>
80or
<25
year
sS
ever
em
alnu
trit
ion
Mal
igna
ncie
s
6m
onth
sII
-159
.5%
Gal
land
etal
.(2
001)
[14]
Pre
–pos
ttri
al;
10pa
tien
tsA
ge(m
ean)
:44.
9±
13.8
year
s(2
1–66
year
s)C
omor
bidi
ties
:not
repo
rted
10.1
±6.
7ye
ars
(1–1
9ye
ars)
Not
repo
rted
Not
repo
rted
23.2
±12
.7m
onth
s(1
3–78
mon
ths)
II-1
34.5
%
Pin
ciar
olie
tal.
(199
9)[1
6]P
re–p
ostt
rial
;22
pati
ents
(11
inho
me
HD
and
11in
-cen
tre
HD
)
Age
(mea
n):5
0ye
ars
(27–
73ye
ars)
Com
orbi
diti
es:h
yper
tens
ion
(54%
)an
ddi
abet
esm
elli
tus
(14%
)
1–19
2m
onth
sFo
rm
edic
alin
dica
tion
sFo
rli
fest
yle
reas
ons
Not
repo
rted
Mea
n:56
.2m
onth
s(1
2–12
7m
onth
s)
II-2
40.5
%
Buo
ncri
stia
niet
al.(
1996
)[1
2]
Pre
–pos
ttri
al;
34pa
tien
tsA
ge(m
ean)
:55.
8±
10.6
year
s(h
yper
tens
ive)
and
57.8
±10
.6ye
ars
(nor
mot
ensi
ve)
12m
onth
sPa
tien
tsun
derg
oing
conv
enti
onal
HD
prev
ious
lyN
otre
port
ed24
mon
ths
II-2
34.5
%
Com
orbi
diti
es:n
otre
port
edO
dar-
Ced
erlo
fet
al.(
2006
)[1
7]
Pre
–pos
ttri
al;
12pa
tien
tsA
ge(m
ean)
:55
±4
year
s(3
5–84
year
s)C
omor
bidi
ties
:lef
tven
tric
ular
hype
rtro
phy
(3pa
tien
ts),
hype
rten
sion
(3),
diab
etes
mel
litu
s(2
),ch
roni
che
artf
ailu
re(1
)an
dis
chae
mic
hear
tdis
ease
(2)
9–18
4m
onth
sIn
form
edco
nsen
tN
otre
port
ed4
wee
ksII
-138
.5%
a Not
e:th
equ
alit
yof
the
incl
uded
pape
rsw
asas
sess
edby
two
inde
pend
entr
evie
wer
s.H
D:h
aem
odia
lysi
s.
by guest on August 19, 2014
http://ndt.oxfordjournals.org/D
ownloaded from

2640 J. Punal et al.T
able
3.B
lood
pres
sure
and
anti
hype
rten
sive
drug
requ
irem
ents
repo
rted
inth
ein
clud
edst
udie
s
Aut
hor/
year
Foll
ow-u
ppe
riod
/sam
ple
size
(n)
Mai
nou
tcom
esR
emar
ks
Blo
odpr
essu
reA
ntih
yper
tens
ive
requ
irem
ents
Wil
liam
set
al.(
2004
)[2
3]1
mon
th/n
:21
pati
ents
Mac
hine
alar
ms
wer
e30
%le
ssfr
eque
ntdu
ring
daily
dial
ysis
than
conv
enti
onal
dial
ysis
.Mea
npr
edia
lysi
ssy
stol
icbl
ood
pres
sure
onD
HD
was
132
mm
Hg
vers
us14
0m
mH
gon
conv
enti
onal
HD
.Thi
sbl
ood
pres
sure
decr
ease
dth
roug
hout
the
foll
ow-u
ppe
riod
.The
rew
ere
nosi
gnif
ican
tdi
ffer
ence
sin
dias
toli
cbl
ood
pres
sure
Two
pati
ents
disc
onti
nued
thei
ran
tihi
yper
tens
ive
med
icat
ions
duri
ngth
eD
HD
peri
od,b
utth
ere
wer
eno
diff
eren
ces
inth
em
ean
num
ber
ofbl
ood
pres
sure
pill
sad
min
istr
ated
onD
HD
(1.9
)co
mpa
red
wit
hco
nven
tion
alH
D(1
.7)
Kos
hika
wa
etal
.(20
03)
[19]
12w
eeks
/n:2
3pa
tien
tsT
hem
ean
syst
olic
bloo
dpr
essu
reat
base
line
was
152.
3m
mH
gan
dat
the
end
offo
llow
-up
was
136.
6m
mH
g.T
hem
ean
dias
toli
cbl
ood
pres
sure
decr
ease
dfr
om84
.3du
ring
the
conv
enti
onal
HD
peri
odto
77.2
mm
Hg
duri
ngth
eD
HD
peri
od
Of
11pa
tien
tsw
how
ere
trea
ted
wit
han
tihy
pert
ensi
vedr
ugs,
5w
ithd
rew
from
the
drug
san
din
1th
edo
sew
asre
duce
d
Tra
eger
etal
.(20
04)
[24]
1ye
ar/n
:17
pati
ents
The
mea
nbl
ood
pres
sure
was
103
mm
Hg
atba
seli
nean
d91
mm
Hg
at1-
year
foll
ow-u
pon
DH
DO
fni
nepa
tien
tstr
eate
dw
ith
anti
hype
rten
sive
drug
s,th
ism
edic
atio
nw
asst
oppe
din
seve
nan
dth
edo
sere
duce
din
two
pati
ents
Buo
ncri
stia
niet
al.(
1996
)[1
2]1
year
/n:3
4pa
tien
tsA
tbas
elin
e,th
em
ean
syst
olic
bloo
dpr
essu
rew
as10
6m
mH
gan
d95
.5m
mH
gaf
ter
1ye
arof
DH
D.
Inth
ehy
pert
ensi
vegr
oup
the
bloo
dpr
essu
rede
crea
sed
from
120
to10
3.4
mm
Hg
13pa
tien
tsst
oppe
dan
tihy
pert
ensi
vetr
eatm
enta
ndth
eot
hers
requ
ired
alo
wer
asso
ciat
ion
ofdi
ffer
enta
ntih
yper
tens
ive
drug
s
20pa
tien
tsw
ere
hype
rten
sive
and
14w
ere
norm
oten
sive
Ayu
set
al.(
2005
)[2
6]12
mon
ths/
n:77
pati
ents
The
rew
ere
nosi
gnif
ican
tdif
fere
nces
inbl
ood
pres
sure
at12
mon
ths
offo
llow
-up
com
pare
dw
ith
base
line
valu
es
Non
-ran
dom
ized
clin
ical
tria
lw
ith
conc
urre
ntco
ntro
ls
Gal
land
etal
.(20
01)
[14]
Mea
nfo
llow
-up:
23m
onth
s/n:
10pa
tien
tsFi
vepa
tien
tsw
ere
hype
rten
sive
duri
ngco
nven
tion
alH
Dan
dth
eyw
ere
norm
oten
sive
duri
ngth
eD
HD
regi
men
The
sepa
tien
tsst
oppe
dan
tihy
pert
ensi
vetr
eatm
ent
Tin
get
al.(
2003
)[2
1]1
year
/n:2
0pa
tien
tsT
hesy
stol
icbl
ood
pres
sure
was
eith
erst
able
orsi
gnif
ican
tlyim
prov
edon
DH
D.D
iast
olic
bloo
dpr
essu
rew
asno
rmal
onco
nven
tion
alH
D(7
9±
14m
mH
g)an
ddi
dno
tcha
nge
sign
ific
antly
onD
HD
The
num
ber
ofdi
ffer
enta
ntih
yper
tens
ive
med
icat
ions
per
pati
entd
ecre
ased
69%
from
1.3
to0.
4.T
henu
mbe
rof
anti
hype
rten
sive
pill
spe
rpa
tien
tdec
reas
ed60
%(f
rom
12.6
to5.
3pi
lls/
wee
k)R
eyno
lds
etal
.(20
04)
[11]
1ye
ar/n
:11
pati
ents
.T
hebl
ood
pres
sure
decr
ease
dto
13m
mH
gan
ddi
asto
lic
bloo
dpr
essu
reto
6m
mH
gat
the
end
offo
llow
-up
com
pare
dat
base
line
valu
es
The
mea
nan
tihy
pert
ensi
vere
quir
emen
tsde
crea
sed
from
2to
1
Gol
dfar
b-R
umya
ntze
vet
al.
(200
6)[2
2]2
mon
ths/
n:12
pati
ents
The
syst
olic
bloo
dpr
essu
rede
crea
sed
by9
mm
Hg
and
dias
toli
cbl
ood
pres
sure
by6
mm
Hg.
The
valu
esre
turn
edto
the
base
line
valu
esaf
ter
pati
ents
resu
med
conv
enti
onal
HD
The
rew
ere
nost
atis
tica
llysi
gnif
ican
tdif
fere
nces
inco
nsum
ptio
nof
anti
hype
rten
sive
drug
sbe
twee
nbo
thdi
alys
ism
odal
itie
s
Aft
er2-
mon
thD
HD
peri
od,
pati
ents
retu
rned
toco
nven
tion
alH
D
Pin
ciar
olie
tal.
(199
9)[1
6]M
ean
foll
ow-u
p:56
.2m
onth
s(1
2–12
7)/n
:22
pati
ents
Bot
hsy
stol
icbl
ood
pres
sure
(174
mm
Hg
atba
seli
ne,1
41m
mH
gat
12m
onth
san
d14
1m
mH
gat
60.7
mon
ths)
and
dias
toli
cde
crea
sed
(94
mm
Hg
atba
seli
ne,8
2m
mH
gat
12m
onth
san
d80
.9m
mH
gat
60.7
mon
ths)
duri
ngD
HD
Sys
toli
can
ddi
asto
lic
bloo
dpr
essu
rew
asas
sess
edin
hype
rten
sive
pati
ents
Fagu
glie
tal.
(200
6)[1
5]6
mon
ths/
n:24
pati
ents
The
rew
ere
nosi
gnif
ican
tdif
fere
nces
inbl
ood
pres
sure
betw
een
conv
enti
onal
HD
vers
usD
HD
No
sign
ific
antd
iffe
renc
esob
serv
edin
the
num
ber
ofan
tihy
pert
ensi
vedr
ugs
adm
inis
trat
edPa
tien
tson
DH
Dco
mpa
red
wit
han
exte
nded
form
ofco
nven
tion
alH
D(4
.5–5
h/se
ssio
n)
DH
D:d
aily
haem
odia
lysi
s.
by guest on August 19, 2014
http://ndt.oxfordjournals.org/D
ownloaded from

Conventional versus daily haemodialysis 2641
Significant improvements were observed in the majorityof the nutritional parameters studied [protein intake, nor-malized protein nitrogen appearance rate (nPNA), calorieintake, fluid intake, mean dry weight, body mass index andlean body mass] when patients were transferred from CHDto SDHD [14,16,21–24,26]. Body weight gain increased insome studies [14,19,21] but decreased [24,26–28] or re-mained unchanged in others [16].
Therapy efficiency. With the exception of one study [27],all articles showed that the daily dialysis dose (Kt/V) wasincreased in the short dialysis period [11,19–21,23,24,28].Williams et al. [23] found that with daily dialysis, phos-phorous removal per week increased by 10%. Five out ofseven studies that provided results on serum phosphate lev-els found that these were reduced during SDHD [23–26,28].Reynolds et al. [11] found no significant change for thisparameter. Another trial [27] observed that the predialysisserum phosphate concentrations decreased until 6 monthsof follow-up on SDHD and remained similar at 12 monthsof follow-up compared to 6 months.
Whilst some studies showed a reduction in phos-phate binder usage when patients were switched to dailyhaemodialysis [14,26,28], others found no significant mod-ifications [11,21,27]. Only one [24] of the three [11,22,24]studies that assessed β2-microglobulin levels during SDHDfound statistical significant differences between CHD(30.5 ± 11 mg/dl) and SDHD (24.6 ± 7.8 mg/dl).
Morbidity. The results of three studies that compared hos-pitalization rates and length of stays during the SDHD andCHD period showed opposite results. Whilst one studyfound a decrease in the number of admissions and length ofhospital stays during the SDHD therapy [21] another studyfound an increase in these events [23]. In one investiga-tion no significant differences were found between the twodialysis modalities [11].
Quality of life. Quality of life assessments were carriedout using different questionnaires, such as Kidney DiseaseQuality of Life-Short Form (KDQOL-SF) [19,21,22],SF-36 [11,24] and Alberta Quality of Life Instrument[23]. Practically all of the studies observed that the overallassessment of quality of life improved when patients wereon SDHD therapy [11,14,19,21–24]. Significant improve-ments were reported in various symptoms (cramps, chills,hypertensive episodes, itchy skin and lack of appetite),energy status, burden of kidney disease, social interaction,physical functioning and mental health status [21–23].In general, patients reported that they were feeling betterduring the daily dialysis period [21–23]. The results onquality of life are shown in Table 4.
Assessment of the quality of the included studies
The average scores awarded by the two independent inves-tigators for all the studies included in the review are pre-sented in Figure 2. The average maximum score achievedwas 71% [26] and the average minimum score 34.5% [12].The overall quality was low since the mean and medianscores were <50% (48.94% and 45%, respectively). Con-
cordance between the two independent investigators washigh. The intraclass correlation coefficient was 0.96 (IC95%, 0.89–0.98), demonstrating a high level of agreementbetween the two reviewers.
Discussion
The results of this systematic review suggest that SDHDmight offer a better clinical effectiveness than CHD interms of hypertension control and medication requirements,including EPO treatment. There does not seem to be anydifferences in vascular access related complications. A bet-ter clearance of AGE peptides, urea and phosphate has alsobeen observed. All the studies included are consistent witha better quality of life for patients treated with SDHD versusconventional HD.
It has been previously suggested that the risk of vas-cular accesses failure and the incidence of complicationssuch as stenosis could be greater in SDHD due to the fre-quent needle punctures. Despite these claims previous stud-ies did not relate the frequency of punctures with vascularaccesses dysfunction [29,30]. Some studies have shown thatother risk factors such as advanced atherosclerosis, alteredhaemostasis and metabolic abnormalities (diabetes, hyper-lipidaemia etc.) could be predictors of fistula dysfunction[31–33]. The results of this review suggest that there areno significant differences in vascular problems betweenCHD and a short daily dialysis. Some investigations haveeven reported that fistulas have better outcomes with dailyhaemodialysis compared to chronic haemodialysis [34–36].Some of the reasons that may explain this finding would bea better blood pressure control [37], improved haemostasis[38] with decreased haematoma formation at the puncturelevel [39] or reduced homocysteine levels [40].
The improvement in blood pressure control and thereduction in antihypertensive treatment has been previ-ously explained by a reduction of extracellular fluid excess[35,41,42]; these outcomes were also observed in two in-cluded papers [15,22], a better control of dry weight thatwould help attain a lower interdialytic volume [11,14] anda better control of sodium balance [12,19]. With short dailydialysis the volume status is more stable over time than withCHD. In the studies reviewing these factors were clearlycorrelated with a reduction in antihypertensive medica-tions when patients achieved better blood pressure control[11,12,14,19,23,24]. When there were no blood pressureimprovements or these were very slight, changes in theseparameters did not lead to lower medication consumption[15,22].
Another finding in relation to medication consumptionwas the reduction in phosphate binder usage in patientswho received short daily dialysis. Since these treatmentsare indicated for the control of phosphorous levels, it isindicative that SDHD provides a higher clearance of theseproducts and reduces serum phosphorus levels. Hyperphos-phataemia can induce vascular calcification [43] and prob-ably contribute to left ventricular hypertrophy [44], thussuggesting an important mechanism for the possible bene-ficial effects of SDHD.
by guest on August 19, 2014
http://ndt.oxfordjournals.org/D
ownloaded from

2642 J. Punal et al.T
able
4.Q
uali
tyof
life
resu
lts
obse
rved
inth
ein
clud
edst
udie
s
Aut
hor/
year
Foll
owup
peri
od/n
umbe
rof
pati
ents
(n)
Qua
lity
ofli
fesc
ale
empl
oyed
Mai
nou
tcom
esR
emar
ks
Gol
dfar
b-R
umya
ntze
vet
al.
(200
6)[2
2]Fo
llow
-up
to4,
8,12
and
16w
eeks
(n=
12)
KD
QO
L-S
FE
ight
of12
pati
ents
(66%
)st
ated
that
they
felt
bett
ersu
bjec
tivel
yon
DH
D.S
igni
fica
ntim
prov
emen
tin
sym
ptom
s,bu
rden
ofki
dney
dise
ase,
soci
alin
tera
ctio
nan
dfu
ncti
onin
gan
den
ergy
leve
lon
DH
D.W
hen
pati
ents
retu
rned
toco
nven
tion
alH
Dth
equ
alit
yof
life
scor
esw
ere
low
er
The
scor
esw
ere
tran
sfor
med
into
a0-
to10
0-po
ints
cale
Rey
nold
set
al.(
2004
)[1
1]Fo
llow
-up
to1,
3,6
and
12m
onth
son
DH
D(n
=12
pati
ents
)
SF
-36,
Bec
kD
epre
ssio
nIn
vent
ory,
Pati
ent-
Rat
edA
nxie
tyS
cale
(PR
AS
)an
dPa
tien
tAss
esse
dQ
uali
tyof
Lif
e(P
AQ
OL
).T
heM
enta
lCom
pone
ntS
core
and
Phy
sica
lCom
pone
ntS
core
wer
eth
epr
imar
you
tcom
esof
SF
-36
Dep
ress
ion
impr
oved
sign
ific
antly
,mea
nB
DI
scor
esfe
llfr
om15
.4at
base
line
to7.
8at
12m
onth
s.T
hePA
QO
Lin
crea
sed
from
6.4
to7.
6at
1ye
ar.N
one
ofth
edi
ffer
ence
sfo
rot
her
ques
tion
nair
esc
ores
wer
est
atis
tica
llysi
gnif
ican
t
Rep
orte
dnu
mer
ical
valu
esof
each
scal
e
All
pati
ents
repo
rted
impr
oved
soci
aliz
atio
n/re
lati
onsh
ips
and
said
they
wou
ldco
ntin
ueD
HD
Tin
get
al.(
2003
)[2
1]Fo
llow
-up
to3
mon
ths
and
each
year
(n=
42pa
tien
ts)
KD
QO
Lve
rsio
n1.
3T
here
wer
ehi
ghly
sign
ific
anti
mpr
ovem
ents
wit
hin
3m
onth
sof
star
ting
DH
Dth
erap
yin
ener
gy/f
atig
ue,s
ympt
oms/
prob
lem
sli
st,
effe
cts
ofki
dney
dise
ase,
cogn
itiv
efu
ncti
on,
qual
ity
ofso
cial
inte
ract
ion
and
sym
ptom
sdu
ring
and
afte
rdi
alys
is.A
t12
mon
ths,
wer
eim
prov
emen
tsob
serv
edin
emot
iona
lw
ell-
bein
g,so
cial
func
tion
and
sexu
alfu
ncti
on.T
here
wer
eno
sign
ific
ant
diff
eren
ces
whe
n3-
mon
thsc
ores
wer
eco
mpa
red
wit
h12
-mon
thsc
ores
Qua
lity
ofli
few
asas
sess
edin
20pa
tien
ts
Wil
liam
set
al.(
2004
)[2
3]To
star
tstu
dy,a
fter
4w
eeks
onco
nven
tion
alan
dD
HD
(n=
21pa
tien
ts)
Alb
erta
Qua
lity
ofL
ife
Inst
rum
ent
The
hype
rten
sive
epis
odes
and
cram
psw
ere
sign
ific
antly
less
freq
uent
onD
HD
.Pat
ient
sre
port
edle
ssfr
eque
nthe
adac
hes,
naus
eaan
dvo
mit
ing.
The
over
alla
sses
smen
tof
qual
ity
ofdi
alys
isim
prov
edsi
gnif
ican
tly,a
sdi
dth
eov
eral
lass
essm
ento
fqu
alit
yof
life
betw
een
dial
ysis
trea
tmen
ts
Eac
hpa
tien
tsco
red
each
ofhi
sor
her
own
dial
ysis
trea
tmen
tsus
ing
asc
ale
from
1(w
orst
)to
5(b
ette
r)
The
impr
ovem
ents
obse
rved
inA
lber
taQ
uali
tyof
Lif
esc
ore
wer
eno
tsig
nifi
cant
Sev
erit
yof
intr
adia
lyti
can
din
terd
ialy
tic
sym
ptom
sw
asgr
aded
byea
chpa
tien
t28
%th
ough
ttha
tDH
Dw
asto
oin
trus
ive
and
57%
requ
este
dto
rem
ain
onD
HD
Tra
eger
etal
.(20
04)
[24]
Thr
eeti
mes
(on
conv
enti
onal
HD
,at1
and
6ye
ars
onD
HD
)(n
=17
pati
ents
)
SF
-36
Sig
nifi
cant
impr
ovem
ents
wer
eob
serv
edin
phys
ical
scor
eco
mpo
nent
and
men
tals
core
com
pone
nt
Res
ults
wer
esh
owed
grou
ped.
No
indi
vidu
alva
lues
wer
ere
port
ed
Kos
hika
wa
etal
.(20
03)
[19]
Eac
h4
wee
ks(n
=23
pati
ents
)R
AN
D’s
Kid
ney
Dis
ease
Qua
lity
ofL
ife
shor
t-fo
rm(K
DQ
OL
-SF
)ve
rsio
n1.
2/Ja
pane
sequ
esti
onna
ire.
Qua
lity
ofli
fesc
ores
impr
oved
sign
ific
antly
aten
dof
foll
ow-u
p;43
%ho
ped
toco
ntin
ueD
HD
Rep
orte
dm
ean
scor
esof
allp
atie
nts
at5-
and
17-w
eeks
offo
llow
-up
HD
:hae
mod
ialy
sis;
DH
D:d
aily
haem
odia
lysi
s.
by guest on August 19, 2014
http://ndt.oxfordjournals.org/D
ownloaded from

Conventional versus daily haemodialysis 2643
Fig. 2. Mean quality score of the included papers.
The reduction of erythropoietin treatment observed inmany studies [14,15,19,21,22,24,26] could reflect not onlya better nutritional status but also the greatest removal ofuraemic toxins that may play a role in inhibition of ery-thropoiesis and therefore contribute to the improvementof anaemia and to the lowering of erythropoietin doses[34,45,46]. Nevertheless, some investigations have showna higher need for EPO drugs and this could be associatedwith higher blood losses [22] or increased phlebotomy orinflammation due to the more frequent dialysis sessions andconsequent exposure to the extracorporeal circuit that canenhance inflammation [11].
The results are not clear as to the improvements in hos-pital admissions rates or length of stays. Hospitalizationrates are directly associated with the number and severityof the comorbidities and also with the safety of the dial-ysis technique. Some studies suggest that SDHD causesless interdialytic fluid fluctuations and gives more freedomto the patients to elaborate their diet and this is likely tobring about a better appetite and hence a better nutritionalstatus [24,34,47–49] with the disappearance of anorexia[14], a condition very frequent in haemodialysed patients.The improvement in nutritional status, hormonal levels andother improvements associated with the greatest removalof substances related to uraemia should result in a bet-ter well-being, less complications and, as a consequence,fewer and shorter hospital admissions [16,50]. This effectwas not reflected in all of the studies analysed in this pa-per. Whilst the hospitalization days and rates decreased intwo studies [18,21], they increased [23] or remained un-
changed in other investigations [11]. This is noteworthy,since if it is expected for SDHD to have better clinicalresults this fact should be reflected in hospital admissions,which is not the case in the revised literature. SDHD seemsto contribute to a higher clearance of advanced glycationend-products (AGEs) [13]. AGE peptides derived from thecatabolism of glycated proteins accumulate in the plasmaof patients undergoing HD and may contribute to the onsetof some long-term complications such as atherosclerosis,amyloidosis and neurodigestive processes [51–55]. Reduc-tions in left ventricular hypertrophy parameters, possiblydue to better blood pressure control [12,24], decrease ininterdialytic weight gain [24,26] and decrease in predial-ysis plasma levels of natriuretic peptide [17], were otherfindings observed and these are of clinical interest becausethey are well-known risk factors for cardiovascular disease.The left ventricular hypertrophy cardiovascular disease isthe leading cause of death in patients with ESRD [56].
In comparison to CHD, short daily dialysis presenteda greater urea clearance (Kt/Vurea) [11,19–21,23,24,28]. Ithas been previously suggested that urea clearance can fluc-tuate during the dialysis session, with the dialyzer ureaclearance higher in the first hours of the session and lowerat the end [57]. The shorter duration of the dialysis sessionsin SDHD could explain the increased urea clearance.
There were no significant reductions observed in theremoval of β2-microglobulin and this could be due to thehigh molecular weight of this protein, 11 800 dalton [34,58].It has been shown that SDHD is more efficient than CHD inthe clearance of low and intermediate molecules but doesnot provide a higher removal of high weight molecules,such as β2-microglobulin [34].
Whilst the majority of studies show a greater clearanceof phosphorous in short daily dialysis [23–26,28], othersdo not find significant changes [11,27]. Buoncristiani et al.[59] have pointed out that SDHD sessions >2 h do not leadto an increased removal of uraemic substances, suggestingthat 2 h is the ideal scheme and differences in the sessionduration cannot explain the observed discrepancies. It hasbeen indicated that clearance of phosphorous can depend onthe predialysis levels of phosphorous, this clearance beinghigher when these levels are >5 mg/dl [60–63]. Ayus et al.[64] have suggested that SDHD is not very efficient whenserum phosphorous levels are between 4 and 4.5 mg/dl.
The studies reflected that the quality of life improvedwhen patients were transferred from conventional dialysisto SDHD [11,14,19,21–24]. Similar results have also beenobserved in the London Study (Ontario, Canada), wherepatients reported a better quality of life in both SDHDand nocturnal haemodialysis when compared with CHD[65,66]. The studies included in the present review reportedreductions in the incidence of symptoms such as nausea,vomiting, itchy skin, cramps, chills, hypertensive episodesand dizziness during daily dialysis treatment, which reflectsa better dialysis tolerance. Improvements were also reportedin physical and mental health status. Results were consis-tent even though different questionnaires and instrumentswere used to measure quality of life, some specific to renaldisease and others to general health survey questionnairessuch as SF-36. Although results suggest that quality of lifeis improved for SDHD versus CHD, it cannot be ruled out
by guest on August 19, 2014
http://ndt.oxfordjournals.org/D
ownloaded from

2644 J. Punal et al.
that this improvement could be simply due to the change toa new procedure, since in these cases there is frequently anincrease in the attention paid to a patient. Furthermore, re-searchers involved in studies assessing the effectiveness ofa new therapy tend to be enthusiastic about on its results andthere exists the possibility of transmitting this enthusiasmto the patients included, influencing the results. It is impor-tant to note that two studies that have not been included inthis review because they did not comply with the inclusion/exclusion criteria, have found that some patients were notwilling to change from a CHD to an SDHD schedule[67,68]. These two studies found that 44% [67] and 59% ofthe patients [68] were reticent to start short daily dialysis forvarious reasons, such as a greater dependence on a dialysismachine and a worsening in their quality of life regard-ing social relationships, and this aspect must be taken intoaccount when deciding to implement a SDHD schedule.
There are certain limitations in this systematic review.Since there is no MeSH term for haemodialysis nor forthe different dialysis modalities, it complicates the searchquery in the PubMed (Medline) database. We had to use asearch strategy with free text words to find the bibliographyso we cannot exclude having missed some articles, eventhough we feel this is highly improbable since we hand-searched references lists of all articles retrieved and foundno additional articles.
This systematic review did not consider all daily dialysistreatment schedules, but considered only those frequentlydefined as short daily dialysis schedules: five to seven timesper week sessions with lengths ranging from 1.5 to 3 h. Thefindings of this review cannot, therefore, be generalized toother daily schedules such as long nocturnal haemodialy-sis or schedules with much longer durations. Two studies[36,69] were excluded from the present analysis becausedaily dialysis was performed at home in the majority ofpatients (70% and 80% were treated at home, respectively).The decision to exclude these studies was taken after con-sulting with various nephrologists, since it was consideredthat these patients could present a better compliance withthe dialysis schedule, better haemodynamic profiles andless comorbidities.
The different prescribed dialysis doses among studies,and even within the same study, greatly limit the drawingup of conclusions. When comparing both haemodialysisfrequencies, the ideal situation would be one where thedialysis doses were the same for both. Nevertheless, insome of the assessed studies Ting et al. [21] and Ayuset al. [26], the weekly time on dialysis was longer in SDHDthan in CHD (13–18 h versus 12 h) while in others [12,27]the CHD weekly time was fixed at 12 h and the SDHD washighly variable (9–22 h/week). Four of the included papers[11,16,20,25] did not show the total duration of dialysissessions at least in one of the frequencies assessed. Thesedifferences in the Kt/V achieved could affect the overallresults, the clearance of phosphorus and also the patient’squality of life. Our report strongly supports the need forbetter quality studies to assess the effectiveness of SDHD.
Another important shortcoming is the low overall meanand medium quality scores achieved by the studies, whichwere <50%. Concordance between the two independentreviewers was high, indicating that the scale specifically
designed for this review was easy to use and can clearlydifferentiate low- from high-quality studies. The mostimportant shortcomings found were small sample size,short follow-up periods and restrictive inclusion/exclusioncriteria that do not allow for a generalization of the resultsto all of the dialyzed population.
It has to be kept in mind that in the present systematicreview there are some decisive aspects that are not discussedbecause they were not the objective of this work. Theseaspects would be related to daily haemodialysis such astransportation to the facility (entailing higher costs), higherperceived burden of disease and higher consumption ofconsumables. A higher dropout of patients in the SDHDarms of the included studies cannot, therefore, be dismissed,perhaps overestimating the positive results.
In conclusion, the literature analysis indicates that in gen-eral terms, clinical outcomes might be better with shortdaily dialysis than with CHD. The main findings wereimprovements in blood pressure control and medicationrequirements. There were no differences found regardingmorbidity or mortality and this is noteworthy since it isthe ultimate expected result of SDHD versus CHD. Theevidence supports the hypothesis that quality of life im-proves when patients are transferred from a conventional toa SDHD regimen although neither of the quality of life stud-ies surpassed 50 patients. The randomized clinical studiesthat are currently underway will provide good quality andvaluable information to determine the real effectiveness ofdaily dialysis in comparison to CHD.
Acknowledgements. The authors wish to thank Dr Maduell from theHospital Clinic of Barcelona for the critical review of an extended ver-sion of this manuscript. This study was funded by the Health ResearchFund (Fondo de Investigaciones Sanitarias–FIS) grant PI05/90003 fromthe Spanish Ministry of Health & Consumer Affairs as part of a re-search project entitled ‘Clinical effectiveness of two frequencies of chronichemodialysis: conventional versus short daily hemodialysis.’
Conflict of interest statement. None declared.
References
1. National Kidney Foundation. K/DOQI clinical guidelines forhemodialysis adequacy. Am J Kidney Dis 2000; 37(Suppl 1): S7–S64
2. Otero A, Gayoso P, Garcıa F et al. Epidemiology of chronic renaldisease in the Galician population: results of the pilot Spanish EPIRCEStudy. Kidney Int 2005; 68(Suppl 99): S1–S4
3. ERA-EDTA Registry: ERA-EDTA Registry 2003 Annual DataReport Internet. Academic Medical Center, Amsterdam, May 2005.Available from http://www.era-edta-reg.org/files/annualreports/pdf/AnnRep2003.pdf
4. Shinaberger JH. Quantification of dialysis: historical perspective.Semin Dial 2001; 14: 238–245
5. Varela Lema L, Ruano-Ravina A. Effectiveness and safety of differenthemodialysis modalities: a review. J Nephrol 2007; 20: 525–542
6. Varela Lema L, Ruano Ravina A. Efectividad y seguridad de lasdiferentes variantes de hemodialisis y hemofiltracion. Santiago deCompostela: Servicio Galego de Saude, Axencia de Avaliacion deTecnoloxıas Sanitarias de Galicia, avalia-t, 2005. Series Avaliacion deTecnoloxıas. Informe de avaliacion: INF2005/03
7. Charra B, Chazot C, Jean G et al. Long, slow dialysis. Miner Elec-trolyte Metab 1999; 25: 391–396
8. Varela Lema L, Ruano Ravina A. Desarrollo y utilizacion de una es-cala de valoracion de calidad construida especıficamente para evaluar
by guest on August 19, 2014
http://ndt.oxfordjournals.org/D
ownloaded from
Conventional versus daily haemodialysis 2645
estudios que comparen modalidades de hemodialisis. Nefrologıa 2006;26: 98–107
9. Fleiss JL. The Design and Analysis of Clinical Experiments. NewYork: Wiley, 1986
10. Wiley J, Fleiss JL. The equivalence of weighted kappa and the intra-class correlation coefficient as measures of reliability. Educ PsycholMeas 1973; 33: 613–619
11. Reynolds JT, Homel P, Cantey L et al. A one-year trial of in-centerdaily hemodialysis with an emphasis on quality of life. Blood Purif2004; 22: 320–328
12. Buoncristiani U, Fagugli RM, Pinciaroli MR et al. Reversal of left-ventricular hypertrophy in uremic patients by treatment with dailyhemodialysis (DHD). Contrib Nephrol 1996; 119: 152–156
13. Floridi A, Antolini F, Galli F et al. Daily haemodialysis improvesindices of protein glycation. Nephrol Dial Transplant 2002; 17: 871–878
14. Galland R, Traeger J, Arkouche W et al. Short daily hemodialysis andnutritional status. Am J Kidney Dis 2001; 37(Suppl. 2): S95–S98
15. Fagugli R, Pasini P, Pasticci F et al. Effects of short daily hemodial-ysis and extend standard hemodialysis on blood pressure and cardiachypertrophy: a comparative study. J Nephrol 2006; 19: 77–83
16. Pinciaroli AR. Hormonal changes in daily hemodialysis. Semin Dial1999; 12: 455–461
17. Odar-Cederlof I, Bjerllerup P, Williams A et al. Daily dialyses de-crease plasma levels of brain natriuretic peptide (BNP), a biomarkerof left ventricular dysfunction. Hemodial Int 2006; 10: 394–398
18. Martins Castro MC, Luders C, Motta Elias R et al. High-efficiencyshort daily haemodialysis. Morbidity and mortalityrate in a long-termstudy. Nephrol Dial Transplant 2006; 21: 2232–2238
19. Koshikawa S, Akizawa T, Saito A et al. Clinical effect of short dailyin-center hemodialysis. Nephron Clin Pract 2003; 95: c23–30
20. Piccoli GB, Bermond F, Mezza E et al. Vascular access survivaland morbidity on daily dialysis: a comparative analysis of home andlimited care haemodialysis. Nephrol Dial Transplant 2004; 19: 2084–2094
21. Ting G, Kjellstrand C, Freitas T et al. Long-term study of high-comorbidity ESRD patients converted From conventional to shortdaily hemodialysis. Am J Kidney Dis 2003; 42: 1020–1035
22. Goldfarb-Rumyantzev AS, Leypoldt JK, Nelson N et al. A crossoverstudy of short daily haemodialysis. Nephrol Dial Transplant 2006; 21:166–175
23. Williams AW, Chebrolu SB, Ing TS et al. Early clinical, quality-of-life, and biochemical changes of “Daily hemodialysis” (6 dialyses perweek). Am J Kidney Dis 2004; 43: 90–102
24. Traeger J, Galland R, Delawari E et al. Six years’ experience withshort daily hemodialysis: Do the early improvements persist in themid and long term? Hemodial Int 2004; 8: 151–158
25. Nesrallah G, Suri R, Zoller R et al. The international quotidian dialysisregistry: annual report 2006. Hemodial Int 2006; 10: 219–224
26. Ayus JC, Mizani MR, Achinger SG et al. Effects of short daily versusconventional hemodialysis on left ventricular hypertrophy and inflam-matory markers: a prospective, controlled study. J Am Soc Nephrol2005; 16: 2778–2788
27. Yuen D, Richardson RMA, Chan CT. Improvements in phosphatecontrol with short daily in-center hemodialysis. Clin Nephrol 2005;64: 364–370
28. Galland R, Traeger J. Short daily hemodialysis and nutritional statusin patients with chronic renal failure. Semin Dial 2004; 17: 104–108
29. Churchill DN, Taylor DW, Cook RJ et al. Canadian HemodialysisMorbidity Study. Am J Kidney Dis 1992; 19: 214–234
30. De Marchi S, Falleti E, Giacomello R et al. Risk factor for vasculardisease and arteriovenous fistula dysfunction in hemodialysis patients.J Am Soc Nephrol 1996; 7: 1169–1177
31. Feldman HI, Held PJ, Hutchinson JT et al. Hemodialysis vascularaccess morbidity in the United States. Kidney Int 1993; 43: 1091–1096
32. Goldwasser P, Michel MA, Collier J et al. Prealbumin and lipoprotein(a) in hemodialysis: relationships with patient and vascular accesssurvival. Am J Kidney Dis 1993; 22: 215–225
33. Windus DW, Jendrisak MD, Delmez J. Prosthetic fistula survival andcomplications in hemodialysis patients: effects of diabetes and age.Am J Kidney Dis 1992; 19: 448–452
34. Buoncristiani U. Fifteen years of clinical experience with dailyhaemodialysis. Nephrol Dial Transplant 1998; 13(Suppl 6): 148–151
35. Woods JD, Port FK, Orzol S et al. Clinical and biochemical correlatesof starting ‘daily’ hemodialysis. Kidney Int 1999; 55: 2467–2476
36. Quintaliani G, Buoncristiani U, Fagugli R et al. Survival of vascularaccess during daily and three times a week hemodialysis. Clin Nephrol2000; 53: 372–377
37. Fagugli RM, Vanholder R, De Smet R et al. Advanced glycationend products: specific fluorescence changes of pentosidine-like com-pounds during short daily hemodialysis. Int J Artif Organs 2001; 24:256–262
38. Lai K, Yin J, Yuen P et al. Effect of hemodialysis on protein C,protein S, and antithrombin III levels. Am J Kidney Dis 1991; 17:38–42
39. Twardowski Z, Lebek R, Kubara H. 6-Year experience with thecreation and use of internal arteriovenous fistulae in patients treatedwith repeated hemodialysis. Pol Arch Med Wewn 1977; 57: 205–214
40. Friedman AN, Bostom AG, Levey AS et al. Plasma total homocysteinelevels among patients undergoing nocturnal versus standard hemodial-ysis. J Am Soc Nephrol 2002; 13: 265–268
41. Fagugli R, Reboldi G, Quintaliani G et al. Short daily hemodialysis:blood pressure control and left ventricular mass reduction hypertensivehemodialysis patients. Am J Kidney Dis 2001; 38: 371–376
42. Nesrallah G, Suri R, Moist L et al. Volume control and blood pressuremanagement in patients undergoing quotidian hemodialysis. Am JKidney Dis 2003; 42(Suppl 1): S13–S17
43. Jono S, McKee MD, Murry CE et al. Phosphate regulation of vascularsmooth muscle cell calcification. Circ Res 2000; 87: E10–E17
44. Ishimura E, Taniwaki H, Tabata T et al. Cross-sectional association ofserum phosphate with carotid intima-medial thickness in hemodialysispatients. Am J Kidney Dis 2005; 45: 859–865
45. Galland R, Traeger J, Delawari E et al. Daily hemodialysis versus stan-dard hemodialysis: TAC, TAD, weekly eKt/V, std(Kt/V), and nPCR.Home Hemodial Int 1999; 3: 33–36
46. Fagugli RM, Buoncristiani U, Ciao G. Anemia and blood pressurecorrection obtained by daily hemodialysis induce a reduction of leftventricular hypertrophy in dialysed patients. Int J Artif Organs 1998;21: 429–431
47. Spanner E, Suri R, Heidenheim AP. The impact of quotidianhemodialysis on nutrition. Am J Kidney Dis 2003; 2: 30–35
48. Galland R, Traeger J, Arkouche W et al. Short daily hemodialysisrapidly improves nutritional status in hemodialysis patients. KidneyInt 2001; 60: 1555–1560
49. Traeger J, Galland R, Arkouche W et al. Short daily hemodialysis:a four-year experience. Nephrol Dial Transplant 2001; 30: 78–86
50. Pinciaroli AR. Results of daily hemodialysis in Cantarazo: 12 yearsexperience with 22 patients treated for more than one year. HomeHemodial Int 1998; 2: 12–17
51. Makita Z, Bucala R, Rayfield EJ. Reactive glycosylation endproductsin diabetic uremia and treatment of renal failure. Lancet 1994; 343:1519–1522
52. Miyata T, Iada Y, Horie K et al. Pathophysiology of advanced glyca-tion end-products in renal failure. Nephrol Dial Transplant 1996; 11:23–30
53. Bucala R. Site-specific modification of apolipoprotein B by advancedglycosylation end-products: implication for lipoprotein clearance anda atherogenesis. Nephrol Dial Transplant 1996; 11: 17–19
54. Brownlee M. Advanced protein glycosylation in diabetes and aging.Annu Rev Med 1995; 46: 223–234
55. Vlassara H. Advanced glycation end-products and atherosclerosis.Ann Med 1996; 28: 419–426
56. Morbidity and mortality: USRDS 2005. Annual data report. Am JKidney Dis 2006; 47(Suppl 1): S121–144
57. Depner T. Why daily hemodialysis is better: solute kinetics. SeminDial 1999; 12: 462–471
by guest on August 19, 2014
http://ndt.oxfordjournals.org/D
ownloaded from

2646 J. Punal et al.
58. Pierratos A. Nocturnal hemodialysis: an update on a five year experi-ence. Nephrol Dial Transplant 1999; 14: 2835–2840
59. Buoncristiani E. Dialisis diaria ultracorta: el mejor sistema paradisfrutar ventajosamente de altos aclaramientos. Nefrologıa 1999;19(Suppl 4): 49–50
60. Harris DCH, Yuill EJ, Chester DW. Correcting acidosis in hemodial-ysis: effect on phosphate clearance and calcification risk. J Am SocNephrol 1995; 6: 1067–1612
61. Al-Hejaili F, Kortas C, Leitch R. Nocturnal but not short hours quotid-ian hemodialysis requires an elevated dialysate calcium concentration.J Am Soc Nephrol 2003; 14: 2322–2328
62. Hou SH, Zhao J, Ellman CF. Calcium and phosphorus fluxes duringhemodialysis with low calcium dialysate. Am J Kidney Dis 1991; 18:217–224
63. Albalate M, De la Piedra C, Fernandez C. Association between phos-phate removal and markers of bone turnover in haemodialysis patients.Nephrol Dial Transplant 2006; 21: 1626–1632
64. Ayus JC, Achinger SG, Mizani MR et al. Phosphorus balance andmineral metabolism with 3 h daily hemodialysis. Kidney Int 2006; 27:1–7
65. Lindsay RM. The London, Ontario, Daily/Nocturnal HemodialysisStudy. Semin Dial 2004; 17: 85–91
66. Heidenheim AP, Muirhead N, Moist L et al. Patient quality of lifeon quotidian hemodialysis. Am J Kidney Dis 2003; 42(Suppl 1): 36–41
67. Halpern SD, Berns JS, Israni AK. Willingness of patients to switchfrom conventional to daily hemodialysis: looking before we leap. AmJ Med 2004; 116: 606–612
68. Israni AK, Halpern SD, McFadden C et al. Willingness of dialysispatients to participate in a randomized controlled trial of daily dialysis.Kidney Int 2004; 65: 990–998
69. Piccoli GB, Ladarola AM, Bechis F et al. La dialisi quotidi-ana:valutazione del primo anno di esperienza a domocilio ed in unhcentro ad assistenza limitata. Minerva Urol Nefrol 2002; 54: 1–7
Received for publication: 5.9.07Accepted in revised form: 7.1.08
by guest on August 19, 2014
http://ndt.oxfordjournals.org/D
ownloaded from