CHURACHANDPUR DISTRICT DISTRICT HEALTH ACTION ...
191
CCP PIP 2010-11 2 ND DRAFT CHURACHANDPUR DISTRICT DISTRICT HEALTH ACTION PLAN FOR THE YEAR 2010-11 PREPARED BY: DISTRICT PLANNING TEAM CHURACHANDPUR DEPARTMENT OF HEALTH & FAMILY WELFARE GOVERNMENT OF MANIPUR
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of CHURACHANDPUR DISTRICT DISTRICT HEALTH ACTION ...

CCP PIP 2010-11
2 N D D R A F T
CHURACHANDPUR DISTRICT
DISTRICT HEALTH ACTION PLAN
FOR THE YEAR 2010-11
PREPARED BY::::
DISTRICT PLANNING TEAM
CHURACHANDPUR
DEPARTMENT OF
HEALTH & FAMILY WELFARE
GOVERNMENT OF MANIPUR

CCP PIP 2010-11
P R E F A C E
The Program Implementation Plan (PIP) for the Churachandpur District is
prepared for the year 2010-11 as per the guidelines and directions from the Ministry of
Health & Family Welfare, Government of India. An elaborate exercise was undertaken
for reflecting the District needs in various Health sections. The District Planning Team
conducted Capacity Building for Health Management, Meetings with blocks level
officers, Open Sessions during ASHA training, and compilation of collected data from
ASHA and ANMs for unearthing the problems and issues in the Block level-
wise/PHCs. In addition to the District Planning Team visits various Health
Institutions to curve out the actual adverse Health situation prevailing in the District.
The District Planning Team also trained to Some Senior Medical Officers of
CHC/PHCs, BPMUs, District Health Program Officers of the various Vertical Health.
They were also involved in the making of this Integrated District Health Action Plan
2010-11. Also desk reviews, analysis of the available Block/PHCs data and indicators,
were collected for preparing this District PIP 2010-11.
The requirements of the District for NRHM initiatives are projected yearly
reasonably in the District PIP. The District will also ensure adequate monitoring and
evaluation for assessing the improvement in the progress of activities using available
data for taking corrective measures wherever necessary in the coming year 2010-11.
The District is thankful to the SHMS, Manipur officials for their directions and
help by giving us various Training relating to framing of PIP without which it would
have been difficult to frame the District PIP 2010-11 in time. Also, the DPMU, BPMU is
grateful to Jacintha Lazarus IAS, Deputy Commissioner, Churachandpur who is also
the Chairman, DHS for motivating us for the making of the Integrated District Health
Action Plan 2010-11 and hope that the impact of District PIP will enables every citizen
to benefit in the field of health and others as well “healthy Village, Healthy District,
healthy nation”.

CCP PIP 2010-11
MESSAGE
National Rural Health Mission (NRHM) was introduced in India with the
purpose of improving the health of Children, Mothers, Adolescents and others and
reaching out to meet the health needs of the people in the most remote areas of the
Nation and District. The launched of NRHM is a boon and blessing to the District.
Implementation of NRHM in the District has progressed tremendously during 2009-
10.The District Health Society, Churachandpur has accomplished many tasks through
their sincere and dedicated hard work and cooperation of the Program Management
Unit and the work teams. Further, work plans have been chalked out to improve the
health facilities in District taking into consideration the special needs of each and every
Block. The future of NRHM in District is very promising and its ultimate success lies in
the hand of the needy people through their active and sincere participation. Taking
this opportunity, I congratulate all the concerned District level Officers including the
District Mission Director and the District Program Management Unit staff, District
Family Welfare Officer, Concerned National Disease Program Officers, Senior Doctors,
Nurses, Village level workers, ASHAs, NGOs, etc. for having played crucial roles in
the making of the District PIP for the year 2010-11. Lastly but not the least, I would also
like to appreciate the District Program Management Unit in particular for their
support and hard work in planning, formulation and for their timely completion of the
District PIP for the year 2010-11.
Jacintha Lazarus, IAS
Deputy Commissioner/ Chairman District Health Mission Society,
Churachandpur

CCP PIP 2010-11
MESSAGE
I am glad that the Integrated District Health Action Plan for the year 2010-11 under National Rural Health Mission (NRHM) has been completed. The present District Health Action Plan is an outcome of great effort made by District Planning Team which constitute of different program officers headed by the Chief Medical Officer and assisted by the District Programme Management Unit
The introduction of National Rural Health Mission (NRHM) launched in the District in 2006 has brought a lot of development and change in the field of Health Sector. I take this privilege to thank all the District Planning Team members for their untiring effort in formulating the District Health Action Plan for 2010-11 and hope that their endless effort will bring changes to the entire people of the District in near future. My best wishes that all the people co-operate in smooth implementation of the programme and make the best of it.
Dr Singkhawzam Hauzel
CMO/ District Mission Director District Health Mission Society’
Churachandpur

Churachandpur District Map
II NN DD EE XX EE SS
Population: 2.50 Lacs
No of Blocks: 05
No of facility: 1 DH, 10 PHC,
66 PHSC
IMR: 12.8
TFR: 2.8

CCP PIP 2010-11
Sl. No.
Contents Page No.
1 District Background 1
2 District Profile
3 Total Budget at a Glance
a) Geographical area of the Blocks
a) Administrative Set-up of the District
b) Rural electrification status
c) District and Block Planning Process
4 Situational Analysis
a) Public Health Facilities in the District
b) Private Health facilities
c) Human Resources in the District
d) Status of Logistics
e) BCC Infrastructure
f) ICDS Programme
g) Elected representatives of Village Authorities
h) NGOs/ CBOs
i) District / Sub-district variations
j) Gender Equity
k) HMIS/ M&E ( shifted at part B )
l) Convergence/ coordination
m) Finance Utilization
n) Key RCH Indicators
o) Institutional arrangements & Organizational development: Issues and gaps
5 Lessons learned: 2009-10
6 Key issues to be addressed

CCP PIP 2010-11
Sl. No.
Contents Page No.
7 Part “A” --- RCH interventions
Vision Statement
Technical Objectives, Targets, Strategies and Activities
a) Maternal Health
b) Child Health
c) Family Planning
d) Adolescent Reproductive & Sexual Health
e) Innovations/PPP/NGO
f) Infrastructure & Institutional Strengthening
g) Strengthening Training Infrastructure
h) BCC/IEC ( budget tabulation enclosed)
i) Procurement
j) Program Management
k) Financial Management
l) Convergence/Co-ordination
m) District and Block Plans
n) Role of District, District and Block
o) Synergy with NRHM Additional ties
p) Programme Management Arrangement
q) Monitoring and Evaluation
r) Sustainability
8 Budget (3c , 3d , 3e , g)
9 Part “B” - New Interventions in NRHM
10 Part “C” - RI Strengthening
11 Part “D” - National Disease Control Program and IDSP
a) NIIDCP
b) IDSP
c) NIIDCP
d) IDSP
e) NIIDCP
12 Part “E” - Intersectoral convergence
13 Grand Total Budget of the District for the year 2010-11
CCP PIP 2010-11
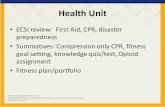
DISTRICT BACKGROUND
Churachandpur district occupies the south-west part of Manipur state. It stretches between 93° 15’E and 94° 45΄E Longitude and between 24°N and 24° 30 N Latitudes. It has 4570Sq. Km geographical area constituting 20.47% of the total geographical area of the State and it is the largest district of Manipur in terms of area. It is bounded by Jiribam Sub-Division of Imphal West, Tamenglong District on the North, Bishnupur and Chandel District on the East Myannmar (Burma) and Mizoram state on the South and Cachar largest District of Assam on the West. The District Headquarter, Churachandpur, which is the second largest town of the state, is situated at a distance of 64 kilometers from the State capital – Imphal.
It covers a geographical area spanning 4570 Sq. Km. having 10 Tribal
Development Blocks within its region viz. Lamka Block, Henglep Block, Singngat Block, Vangai Block, Samulamlan Block, Tuibuong Block, Sangaikot Block, Tipaimukh Block, Thanlon Block and Saikot Block. The District has the literary of 74.67% with the population density of 50 persons per sq km. Under these, it covers 1 District Hospital, 1 Community Health Centre, 9 Primary Health Centre and 64 Primary Health Sub Centres. The various health indicators of the District are IMR-12, Sex Ratio-996/1000, TFR-2.81, CBR-12.8, CDR-3.0 Literacy Rate (Female)-66.40)
The Integrated Program Implementation Plan (PIP) of National Rural Health
Mission is prepared with a vision to achieve the National Millennium Goals spelt out by the Government of India under H&FW and the National Population Policy Goals.
The present PIP has five parts viz.
1. Part “A” - RCH-II 2. Part “B” - New Initiatives under NRHM 3. Part “C” - Routine Immunization Strengthening 4 Part “D” - Disease Control Programs & Integrated
Surveillance and 5. Part “E” - Program Convergence
.
TOTAL BUDGET REQUIRE FOR 2010-11:
Sl. No. NRHM Component Rs. in lakhs
1 Part “A” – RCH II 127.163 2 Part “B” – New Initiatives 805.375 3 Part “C” – RI Strengthening 14.23 4 Part “D” – Disease Control Programs & Surveillance 113.28 5 Part “E” – Program Convergence 0.0
Total 1060.048

CCP PIP 2010-11
1.1 District Profile
S.No.
Background Characteristics District
1 Geographic Area (in Sq. Kms) 4570
2 Number of Tribal Development Blocks 10
3 Size of Villages ( Current Census) 641
1-500 villages 490
501-2000 villages 132
2001-5000 villages 15
5000+ villages 04
4 Number of towns 01
5 No of Police Station 01
6 No of Assembly Constituencies 05
7 Total Population (DHIS2) 2.50 Lakhs
Urban 103390 K
Rural 175317 K
Male: 144740
Female 133967
8 Sex Ratio (F/M*1000) ( as reported )
• Population Sex Ratio
• Child Sex Ratio
996/1000 967/1000
9 Decadal growth rate (DHIS2 ) 33.0%
10 Density- per sq. km. ( census 2001 ) 39
11 Literacy Rate ( statistical dept ) 74.69
-Male 84.98
-Female 64.40
12 %SC population ( DHIS2) %ST population No. of schools No. of Anganwadi Centres
387 261119
433 1010
13 Length of road per 100 sq. km. 450
14 % of villages having access to safe drinking water facility 10.5
15 % of households having electricity connection 15.11
16 % of households having sanitation facility (Specify Type –sewer, septic tank)
35.29
17 % of population below poverty line 98% (2% others)
18 Crude Birth rate ( DHIS2) 12.8
19 Crude Death rate ( DHIS2) 3.0
20 Total Fertility rate. ( DHIS2) 2.8
21 Mortality Rate: ( as per DH records) IMR
12
22 No of Village Primary schools ( census 2001) No of Village Primary school teachers No of children enrolled(Age wise)
316 350
42800
23 Health Facilities ( current) DH-1,CHC-1 PHC-10,PHSC-66 Pvt. Hospital-04
GEOGRAPHICAL AREA OF THE BLOCKS:

CCP PIP 2010-11
Churachandpur District is the largest district in terms of geographical area. It has an area of
4570 sq.kms. This constitutes 20.47% of the total area of the state (22,327 sq. km).
Geographical area of the five (5) Sub-Divisions of Churachandpur district:
Sl.No. Sub-Division Area in sq.km
1. Tipaimukh 804
2. Thanlon 1291
3. Henglep 717
4. Churachandpur 657
5. Singhat 1101
Total 4570
ADMINISTRATIVE SET-UP:
Churachandpur District has 5 (five) Sub-Divisions and 10 Tribal Development Blocks.
Each Sub-Division is under one Sub-Division Officer while each Block is under one Block
Development Office. Deputy Commissioner cum District Magistrate is the Head of Revenue
and Law & Order administration while in the capacity of Chairman DRDA, is the overall
controller and coordinator of Rural Development Schemes.
Administrative set-up of Churachandpur district
Administrative set-up of Churachandpur district
District Sub Divisions Blocks
Churachandpur
Tipaimuk Thanlon Henglep
Singngat Churachandpur
rrr
Vangai
Tipaimuk
Thanlon
Sangaikot
Henglep Singngat
Tuibuong Lamka
Saikot Samulamlan

CCP PIP 2010-11
RURAL ELECTRIFICATION IN CHURACHANDPUR AS ON 31ST MARCH, 2005:
Source: Economics survey of Manipur, 2006-2007
DEMOGRAPHY
Churachandpur District has a population of 2, 27,905 according to 2004 census of which
more than 99% of the population are Tribals belonging to Thadou, Hmar, Paite, Zou, Vaiphei,
Simte, Gangte,Lushai and Komrem. The decadal population growth of the state is 30.02%. The
total number of House hold is 46,213, out of which, 33,333 are BPL families i.e. 72.13% of the
total families live below poverty line.
Population-Male & Female
Sl.
No.
Block No. of
Household
Population
Total Male Female
1. Tipaimukh 3018 15177 7892 7285
2. Vangai 2112 13484 7090 6758
3. Thanlon 3689 14977 7673 7294
4. Henglep 6091 38428 19337 19091
5. Lamka 10590 74500 37001 37499
6. Tuibuong 7611 46388 23330 23058
7. Samulamlan 3476 20159 10054 10105
8. Saikot 2896 17431 8864 8474
9. Singhat 4099 24967 12469 12469
10. Sangaikot 2631 16036 7976 7726
Total 46213 281911 149686 139759
Source: House to house survey conducted by BDOs under NREGA
2. District Planning Process:
2.1. Process of planning:
Number of
Villages
Number of
villages
electrified
Percentage of
villages
electrified
Number of
non-electrified
villages
Percentage of non-
electrified villages
518 375 72.39 143 27.61

CCP PIP 2010-11
The District Planning process was initiated at the State level through the 3rd Round Capacity Building Management Training at Hotel Mass, Imphal during 17th to 21st Nov 2009 which was jointly organized by State Health Mission Society, Manipur in collaboration with RRC-NE and National Health Resource Centre, New Delhi. In this training, the DPMU, one PHC Medical Officer In-charge and one BPM attend the session. Subsequently, the DPMU attended the 3rd Round of HMIS Training at Classic Hotel, Imphal during 23rd & 24th November 2009
On reaching back the District, the Deputy Commissioner-cum- Chairman, District Health Society, called a meeting and constituted the District Planning Team for 2010-11, headed by DC and the members comprises of District Mission Director, District Family Welfare Officer, Medical Superintendant, ZEO, District Malaria Officer, District TB Officer, District Leprosy Officer, District AIDS Officer, DPMU, District Program Officer-ICDS, and NGOs representatives. And the District Planning Team identified District Program Manager as the District facilitator for formulating the entire District Plan.
The District Planning process kick-start after forming the District Planning Team by conducting three days Workshop for formulating Village and Block Health Action Plan 2010-11 during 30th Nov. to 2nd Dec 2009 attended by Block Level Staffs as well as four selected Sub – Centre Committee’s Chairman and ANM at CMO Conference Hall. During the workshop, the District Planning Team thoroughly gave training on how to carry out the planning at the block level as well as at the village level.
After undergoing training at the district, the entire five Block staff formed their respective Block Planning Team 2010-11, comprising of MO i/c, BPMU, AYUSH MO, CDPO, ICDS, DI, Extension Educator, MHW, LHV where-in, Block Program Manager was identified as the Block facilitator for each of the Blocks.
To formulate the BHAP, sample household survey was carried out at selected four villages under each block with the help of ASHA’s, AWW, ANM and PRI members, which was facilitated by BPMU. Apart from household sample survey, social mapping was conducted in these identified villages. The villages where sample survey was done were taken to formulate VHAP as well.
Due to constraint of time, the VHAP was formulated based on the sample survey and by interacting with the PRI/VAs members at each of the village. It should be noted here that the ANM were playing the role of a facilitator. The findings at the village level was analyzed and documented by the block planning team which was counter signed by the village chief.
After proper analysis of the findings at the village level and at the Block level, the BHAP was documented by the Block Program Manager which was counter signed by the Block MO in-charge and was submitted to the district planning team to be incorporated in the District PIP.

CCP PIP 2010-11
The District Health Action Plan again was formulated after taking inputs from the Blocks, Villages, HMIS, DLHS-3, NHFS–3, DHIS -2, facility survey report, desk review as well as from the entire district in-charge of all the health program officer in the district. Based on these indicators, District Plan was planed.
2.2 BACKGROUND AND CURRENT STATUS:
Key RCH Indicators
Past Trends Current status
Maternal Health
% of institutional deliveries
• Overall • SC/ST
41.59 (DLHS-2)
44.5 (HMIS)
% of deliveries by SBA
• Overall
• SC/ST
35 (DLHS-2)
46 (HMIS)
Child Health % of 13-24 months of age fully immunized
• Overall
• SC/ST
54 (DLHS-2)
29(HMIS)
% of children with Diarrhoea treated with ORS
36 (DLHS-2) 45 (HMIS)
% of children with pneumonia taken to health facility
46 (DLHS-2) 51 (HMIS)
Family Planning
Unmet need for spacing methods
• Overall
• SC/ST
28 (DLHS-2)
31 (HMIS)
Unmet need for terminal methods
23 (DLHS-2) 28 (HMIS)
Contraceptive prevalence rate
38 (DLHS-2)
46 (HMIS)
Regarding Maternal Health the proportion of institutional delivery and delivery conducted by SBA are 35% and 45% respectively. To improve institutional delivery, SBA training was given to 4 ANMs from various PHSC of the District. Delivery kit was also distributed to all ANMs posted at SCs level. SBA Training will be continue in the coming year so that delivery at institutional level will be achieve more higher To improve Child Health Status in the District, Training for IMNCI was conducted to 16 MOs at RIMs in the current year for 5th Batches. Training in this regard will also be continuing in the coming year too.
As drug-kits under RCH-II were also supplied containing IFA, ORS, cotton,
cipladine, condom and others to ASHA to strengthen the health result of the child at the village level in the current year

CCP PIP 2010-11
2.3. Approaches of NRHM: Communitize: The District involves the Village Authorities of all Blocks,
which helps in implementing the Program and activities under NRHM. VH & SC is form in the entire sanctioned village with additional villages included from this current year. A joint Bank Account is opened where the chairman /chiefs and ASHA are the joint signatory. Besides, this the Chairman is a signatory in PHSC Committees bank account.
Strengthening Management: For strengthening the management capacity, the DPMU attended Capacity Building training which is conducted by RRC-NE, Ghy in collaboration with PHRN and State Health Mission Society,Imphal at State Guest House in the month of June 2008.Likewise the Block Level Program Management Units are also in placed to strengthen the NRHM activities at the Block level.
Flexible financing: The District PIP is prepared based on the bottoms-up approach. Flexibility of funding is considered so as to sustain the activities under NRHM. Untied funds are placed at the Sub-centre level and are being operated with the Village Authorities representative. The Corpus Fund and Grants received by RKS are used for development activities of the concerned institutions. The Program aims for making available untied funds at different levels of health care delivery system so that service guarantees as spelled out in the “Indian Public Health Standard” can be achieved
Monitoring and evaluation: A Monitoring & Evaluation Committee needs to be set up for strengthening the program under NRHM. These Committees will monitor and evaluate the activities on a regular basis and corrective actions will be taken wherever needed. Under this the District Nodal Officer (M&E) will head the committee.
2.3.1 Management Structure at District Level
2.3.2. Sampling procedure for preparation of DPIP The District conducts simple survey to the sub centre villages of 5 to 6 per
blocks which was conducted by the block planning team of their respective blocks. Through this a representative picture of the District, Block and Village Health issues could be derived. The survey questionnaires used by the Block Planning team was elaborately designed and framed by the District Planning team in consultation with experts and state staffs. According to these findings, strategies
DC/Chairman
District Mission Director
District Fin. Manager
District Program Manager
District Program Officers
DFWO/ Member Secy
District Data Officer
CCP PIP 2010-11
and activities were chalked out and framed to achieve the goal and objective of NRHM keeping in hand the situation where they stand.
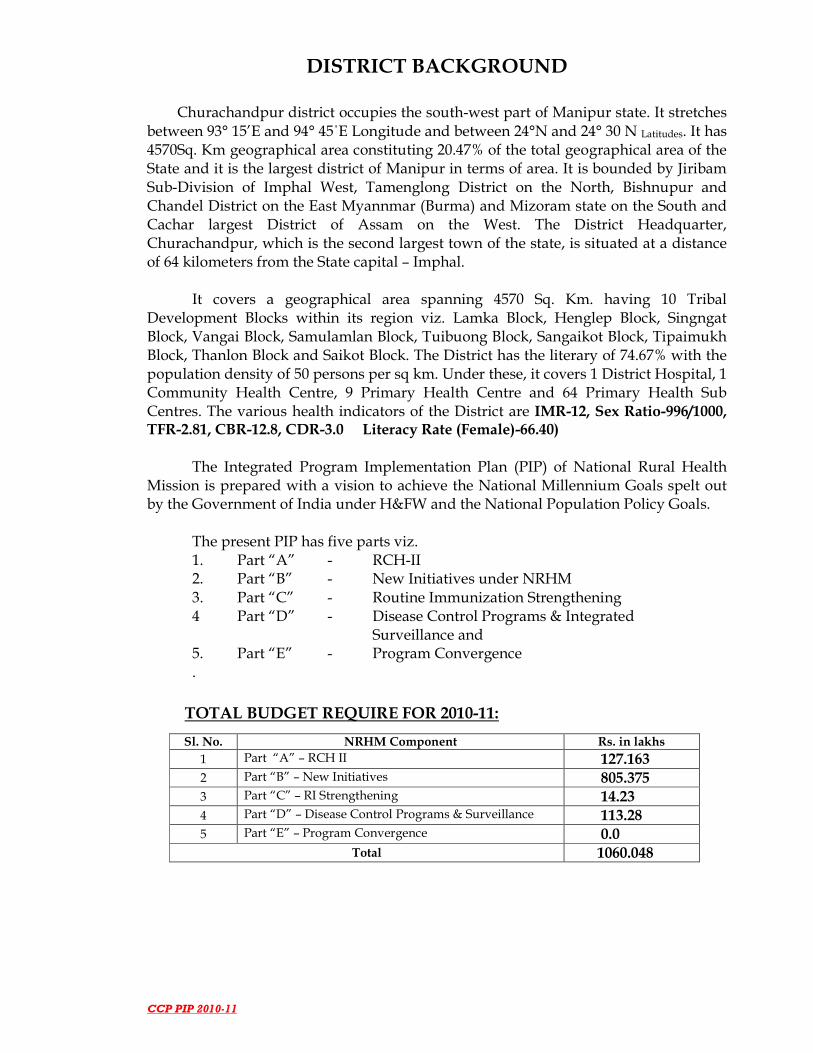
2.3.3. Management Structure at Block Level:
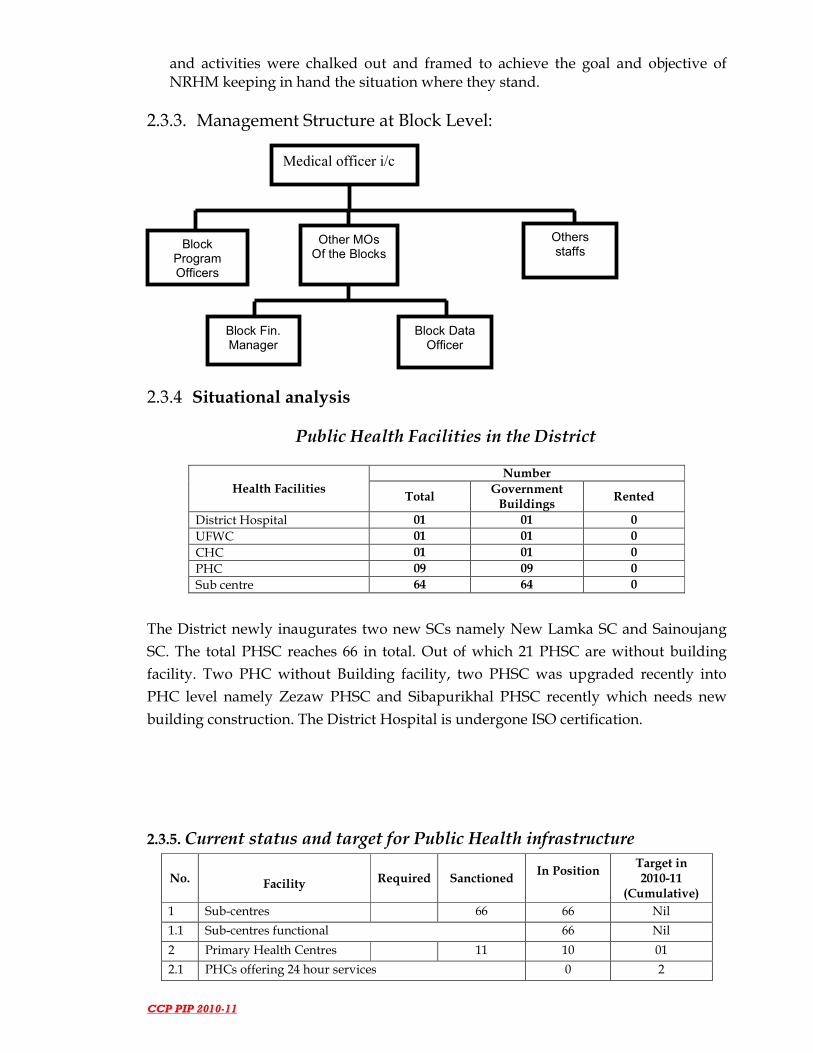
2.3.4 Situational analysis
Public Health Facilities in the District
Health Facilities Number
Total Government Buildings
Rented
District Hospital 01 01 0
UFWC 01 01 0
CHC 01 01 0
PHC 09 09 0
Sub centre 64 64 0
The District newly inaugurates two new SCs namely New Lamka SC and Sainoujang
SC. The total PHSC reaches 66 in total. Out of which 21 PHSC are without building
facility. Two PHC without Building facility, two PHSC was upgraded recently into
PHC level namely Zezaw PHSC and Sibapurikhal PHSC recently which needs new
building construction. The District Hospital is undergone ISO certification.
2.3.5. Current status and target for Public Health infrastructure
No. Facility Required Sanctioned In Position
Target in 2010-11
(Cumulative)
1 Sub-centres 66 66 Nil
1.1 Sub-centres functional 66 Nil
2 Primary Health Centres 11 10 01
2.1 PHCs offering 24 hour services 0 2
Medical officer i/c
Block Fin. Manager
Other MOs Of the Blocks
Block Program Officers
Others staffs
Block Data Officer
CCP PIP 2010-11
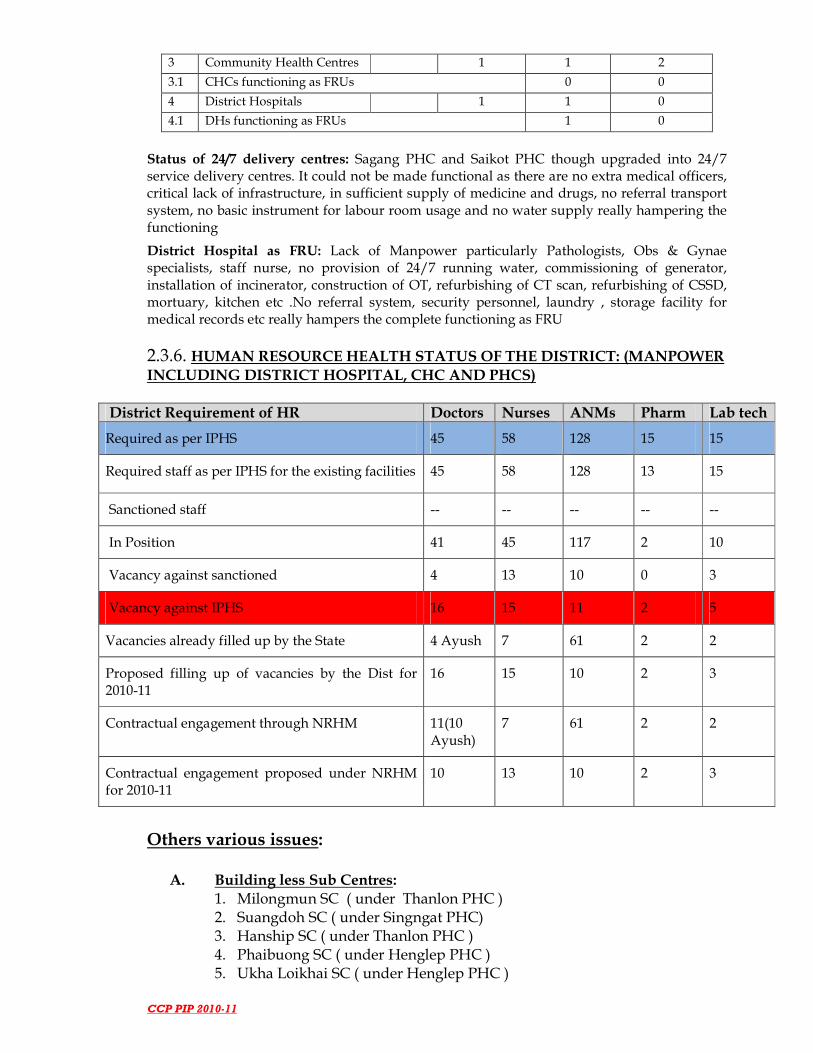
3 Community Health Centres 1 1 2
3.1 CHCs functioning as FRUs 0 0
4 District Hospitals 1 1 0
4.1 DHs functioning as FRUs 1 0
Status of 24/7 delivery centres: Sagang PHC and Saikot PHC though upgraded into 24/7 service delivery centres. It could not be made functional as there are no extra medical officers, critical lack of infrastructure, in sufficient supply of medicine and drugs, no referral transport system, no basic instrument for labour room usage and no water supply really hampering the functioning
District Hospital as FRU: Lack of Manpower particularly Pathologists, Obs & Gynae specialists, staff nurse, no provision of 24/7 running water, commissioning of generator, installation of incinerator, construction of OT, refurbishing of CT scan, refurbishing of CSSD, mortuary, kitchen etc .No referral system, security personnel, laundry , storage facility for medical records etc really hampers the complete functioning as FRU
2.3.6. HUMAN RESOURCE HEALTH STATUS OF THE DISTRICT: (MANPOWER
INCLUDING DISTRICT HOSPITAL, CHC AND PHCS)
District Requirement of HR Doctors Nurses ANMs Pharm Lab tech
Required as per IPHS 45 58 128 15 15
Required staff as per IPHS for the existing facilities 45 58 128 13 15
Sanctioned staff -- -- -- -- --
In Position 41 45 117 2 10
Vacancy against sanctioned 4 13 10 0 3
Vacancy against IPHS 16 15 11 2 5
Vacancies already filled up by the State 4 Ayush 7 61 2 2
Proposed filling up of vacancies by the Dist for 2010-11
16 15 10 2 3
Contractual engagement through NRHM 11(10 Ayush)
7 61 2 2
Contractual engagement proposed under NRHM for 2010-11
10 13 10 2 3
Others various issues:
A. Building less Sub Centres:
1. Milongmun SC ( under Thanlon PHC ) 2. Suangdoh SC ( under Singngat PHC) 3. Hanship SC ( under Thanlon PHC ) 4. Phaibuong SC ( under Henglep PHC ) 5. Ukha Loikhai SC ( under Henglep PHC )

CCP PIP 2010-11
6. Kangkap SC ( under Singngat PHC ) 7. L Khengjang SC ( under Henglep PHC ) 8. Sumtuh SC ( under Singngat PHC ) 9. Hiangtam K ( under Behiang PHC ) 10. Lungthulien SC ( under Parbung CHC ) 11. Parvachom SC ( under Senvon PHC ) 12. Sipuikon SC ( under Senvon PHC ) 13. Leisen SC( under Senvon PHC ) 14. Tuolbung SC ( under Parbung CHC ) 15. Chingmun SC( under Patpuihmun PHC ) 16. Hiangmual SC ( under Singngat PHC) 17. Khuangkhai SC ( under Saikot PHC) 18. Khaukual SC( under Saikot PHC ) 19. Kangreng SC ( under Patpuihmun PHC) 20. Ngampabung SC ( under Patpuihmun PHC) 21. Buangmun SC ( under Patpuihmun PHC ) 22. Sibapurikhal SC ( under Patpuihmun PHC ) 23. Dailon SC ( under Thanlon PHC)
B. Building less PHC: 1. Singngat PHC 2. Henglep PHC 3. Senvon PHC
C. PHC Building which need renovation:
1. Henglep PHC 2. Sinzawl PHC 3. Patpuihmun PHC
D. PHSC which need renovation 1. Bukpi SC ( under Thanlon PHC ) 2. Kaihlam SC ( under Thanlon PHC) 3. Allusingtam SC ( under Singngat PHC ) 4. Songtal SC ( under Sinzawl PHC) 5. Lungthulien SC ( under Parbung ) 6. Kangreng SC ( under Patpuihmun PHC ) 7. Sibapurikhal SC ( under Patpuihmun ) 8. Ngampabung SC ( under Patpuihmun PHC )
E. Staff Quarters which need renovation: 1. Thanlon PHC 2. Saikot PHC
F. Very difficult & Inaccessible PHSC 1. Milongmun SC under Thanlon PHC 2. Dailon SC under Thanlon PHC 3. Kaihlam SC under Thanlon PHC 4. Bungpilon SC under Thanlon PHC 5. Phaibuong SC under Henglep PHC 6. Ukha Loikhai SC under Henglep PHC 7. Kolhen SC under Henglep PHC 8. Ngarian SC under Henglep PHC 9. Nungshai under Henglep PHC 10. L Khengjang SC under Henglep PHC

CCP PIP 2010-11
11. Allusingtam under Singngat PHC 12. Hiangmual SC under Singngat PHC 13. Kangkap SC under Singngat PHC 14. Tuikuimuallum SC under Singngat PHC 15. Sumtuh SC under Sinzawl PHC 16. Aibulon SC under Sinzawl PHC 17. Hiangtam SC K under Behiang PHC 18. Parvachom SC under Senvon PHC 19. Leisen SC under Senvon PHC 20. Phailienthangpunji SC under Patpuihmun PHC 21. Kangreng SC under Patpuihmun PHC 22. Buangmun SC under Patpuihmun PHC 23. Chingmun SC under Patpuihmun PHC 24. Sibapurikhal SC under Patpuihmun PHC 25. Ngampabung SC under Patpuihmun PHC 26. Tuolbung SC under Parbung CHC
G. Institutions without Single ANM/ SN 1. Dailon SC --Thanlon PHC 2. Kaihlam SC – Thanlon PHC 3. Hiangtam (K) SC ---Behiang PHC 4. Sumtuh SC ---Sinzawl PHC 5. Aibulon SC ---Sinzawl PHC 6. Chingmun SC ---Patpuihmun PHC 7. Kharkhuplien SC –Patpuihmun PHC 8. Sumchinvum SC ---Singngat PHC 9. Hanship SC---Thanlon PHC
2.3.7 Basic Equipment Requirement at CHC/PHCs List of suggested equipments and furniture including reagents and A. Diagnostic kits
1. Equipment for assisted vacuum delivery 2. Equipment for assisted forceps delivery 3. Standard Surgical set (for minor procedures like episiotomies stitching) 4. Equipment for Manual Vacuum Aspiration 5. Equipment for New Born Care and Neonatal Resuscitation 6. IUD insertion kit 7. Equipment / reagents for essential laboratory investigations 8. Refrigerator (165 liters) 9. ILR and Deep Freezer 10. Ice box B. Requirements for a fully equipped and operational labour room A fully equipped and operational labour room must have the following: 1. A labour table 2. Suction machine 3. Facility for Oxygen administration 4. Sterilization equipment 5. 24-hour running water 6. Electricity supply with back-up facility (generator with POL)

CCP PIP 2010-11
7. Attached toilet facilities 8. An area earmarked for new-born care 9. Emergency drug tray: This must have the following drugs C. List of Furniture (including surgical) at PHC 1. Writing tables with table sheets 2. Plastic chairs (for in-patients’ attendants) 3. Armless chairs 4. Full size steel Almirah 5. Labour table 6. OT table 7. Arm board for adult and child 8. Stretcher on trolley 9. Instrument trolley 10. Wooden screen 11. Foot step 12. Coat rack 13. Bed side table 14. Bed stead iron (for in-patients) 15. Baby cot 16. Stool 17. Medicine chest 18. Solar lighting Lamp 19. Side Wooden racks 20. LPG stove 21. LPG cylinder
2.3.8. Private Health Facilities
Private Services Facilities Number and location
Approved MTP centres in Private sector 03
RMPs (Less than formal qualified practitioner) Nil
Number of nursing homes with facilities for comprehensive emergency obstetric care
04
Accredited centres for sterilization service 01
Accredited centres for IUD services 03
Training, meeting, consultation program need to be taken –up for sensitizing and awareness in achieving the goal and target being spelt out under NRHM. The HMIS report from these pvt facilities needs to be streamline so that they plays vital role in inputting their achievement.
2.4.1. Status of logistics
Logistics Elements Description
Availability of a dedicated District warehouse for health department
Warehouse at District Hospital be sanction
Stock outs of any vital supplies in last year. Procured be made by District through centre level directly. Like wise District to Block. Vit. A received but not in sufficient quantity.
Indenting Systems (from State to District) Done quarterly, except during emergencies where indent may be made at any time.
Existence of a functional system for Nil , QAC was formed but not effective due to

CCP PIP 2010-11
assessing Quality of Vaccine composition of Dist Level Officers as members who are not able to spare enough time in this connection
Procurement of medicines and drugs will be done by the District and the district will supply to the block level from this current financial year. The district also experiences frequent outbreaks of unknown diseases.
2.4.2. BCC Infrastructure in the District
• Human Resources
• Any trainings the staff in past five years
• Any functional Mass media audio- visual aids such as 16 mm projectors, Video cameras, VCD/DVD players
• 01 (DEMO)
• Yes , 2 times
• No, require-1
• Did the district prepare a BCC plan in the past year?
• BCC activities undertaken in District
• Yes
• Hoarding and wall painting for JSY and Immunization
• Village Private sector for conducting communication activities using modern media or folk media???
• No, done at state level in Radio Prog.
The essentials equipment like 16mm projector/LCD Projector is the utmost requirement of the District as lots of workshops, training are being conducted and further sought for the coming every. Others essentials media communication like digital camera, VCD needs to be procure at the District level.
2.4.3. Integrated Child Development Scheme Programme (ICDS): S. No
Name of the Block with ICDS Programme
Number of AWCs
CDPOs and ACDPOs
Supervisors AWWs AW Helpers
S F S IP S IP S IP S IP
1 Tipaimukh 107 01 Nil 107 107
2 Saikot 73 01 01 73 73
3 Sangaikot 56 01 01 56 56
4 Tuibuong 134 01 01 134 134
5 Thanlon 144 01 01 144 144
6 Singngat 128 01 01 128 128
7 Henglep 122 01 01 122 122
8 Samulamlan 65 01 01 65 65
9 Lamka 181 01 01 181 181

CCP PIP 2010-11
Total 1010 09 08 1010 1010
To co-ordinate between ICDS and DHMS in respect of programme implementation of various national activities spelt by the MoHFW, the two different departments should helps together particularly during “Village Health and Nutrition Day” where ASHA and ANM will deliver a Health talk and on that very spot the AWW will serve Hot Cook Food provided frequent meeting and consultation between the two departments. In this connection Deputy Commissioner has noted to the highest points during Governing Body meeting of the District Health Society in the current year.
2.4.4. Elected representatives to Village Authorities
S.No Name of the Block Total Village Authorities
Total VA Members
Male Female
1 Tipaimukh 58 406 Nil
2 Thanlon 62 434 Nil
3 Singngat 96 595 01
4 Henglep 130 602 Nil
5 Samulamlan 68 476 Nil
6 Lamka 232 1533 01 Total 642 4038 02
In place of PRI system which is practice in other urban areas the District have a traditional local form of governing comprising, the Village Chief and Its members. With the addition of 88 village health & sanitation committee, lots of village authorities are visible. Frequent Training, meeting, consultation with the village chairman are required for sensitization of the NRHM programme and more effective health care system in their villages.
2.4.5. NGOs & CBOs
Names of NGOs Key Activities in
Health/Nutrition/community organization
Block/Villages of NGOs operations
Sielmat Christian Hospital Curative & Maternity Health Lamka Block People Health Foundation Curative & Maternity Health Lamka Block Molvaiphei Rural Health & Research Centre
Nursing Edn & Family Planning and Community Eye Care
Saikot Block
Salom Hospice HIV AIDs Lamka Block Lamka Research & Rehabilitation Centre
HIV AIDs and Rehabilitation Lamka Block
Medicine Sans Frontiers(MSF) Holland
HIV AIDs and Others Lamka and Singngat Block

CCP PIP 2010-11
Name of CBOs KKL YPA HYA YMA Many More Community Based Philantrophic Orgn exists
Churachandpur District
Four local NGOs were active in the District giving effective health care to the people. These four NGOs provide MCH activities and other curative Health services. Out of the 4 NGOs identified, only Lamka Nursing Home is accredited for provision of JSY Scheme currently. Beside these 4 Local NGOs, Medicine Sans Frontiers, Holland which is international NGOs plays a major role in providing Referral and Health care services to the adverse effected places
in the District. Steps initiated for accreditation of more NGOs heath organization in current year.
3.0. District / Sub-District variations:
The District has five Blocks under health organization structure whereas it has ten (10) TD Blocks out of which Henglep and Tipaimukh Block need special emphasis. The reason behind this is due to lack of good road connectivity along with approach road (difficult geographical terrain), lack of proper infrastructure (manpower, equipments, drugs & medicines, building), and huge gap of manpower. Due to all these bottlenecks, conducting and accessing health care is hampered in this two Blocks. The remaining three blocks namely Samulamlan, Singngat and Thanlon are more accessible. It is proposed that reward scheme or incentivisation of pay to the staff posted at the more far places be introduced keeping in hand based on their performance. And also reward and honorarium system be introduced for the best block and best staff amongst the NRHM staff in the District. The Village and Block had incorporated all their variations situations.
3.1 Gender Equity The District sex ratio is 993. But as far as Village Authorities is concerned female were not given preference to be their elected representatives in the District. Since the people in the District Practices patriarchal system there is no gender equity. However, there is no discrimination on the basis of gender. More or less 95% of the people belong to the same caste, creed and tribes, out of which only 5% belong to others.
3.2. HMIS/ M&E Reflected at part B
3.3. Convergence/ coordination The detailed reflected at part E Department of ICDS, Education, Village Authorities, PHED, PWD and AYUSH needs to be sensitized so that better coordination with them could be developed in 2010-11. Convergence and Co-ordination between different sections of department is a mere one since the system should be initiated from the higher level. The District level concerned is just a mere one without actual and ineffective. The Ministry take the initiative from the higher level at one hand and regular meeting of all supporting department in every quarter be introduced.
3.4. Financial Utilization

CCP PIP 2010-11
The funds are utilized as per the guidelines issued by the GoI in the District. However SoEs are not submitted in time due to lack of communication gap prevailing in most of the Blocks. From the ministry, the District Health Society received the following fund
1. 2008-09 : Rs 10.0 Crores 2. 2009-10 : Rs 7.10 Crores

CCP PIP 2010-11
4.0. Institutional arrangements and organizational development: 4.1. Issues and gaps: Even after the passage of 3 years the implementation of NRHM Programme in the district is mainly done by H&FW Dept alone with the exception of theoretical convergence of NVBDCP, RNTCP, and NLEP, IDSP etc. Others department like ICDS, PHED, PWD do not take active part in the implementation of NRHM. This is due to poor logistics program mechanism from the higher level which hampers conducting various health programmes in the blocks other than IPPI and Immunization week.
4.2. DP (donor assisted) programmes in the District: The up-gradation of District Hospital to 100 bedded is already completed. Construction works for infrastructural upgradation of the hospital building facility under process. Certification to ISO 9001 completed. Apart from Medicine Sans Frontier, Amsterdam provides required medicines, drugs and others on a need basis to the poor and needy people of the district.
5.0. Lessons learned: since 2006 to 2009:
Successes:
NRHM was launched in NE Districts on 9th Nov 2005. The actual implementation of NRHM program in the District started only on August 2006. As the Program was started late many activities could not be implemented as per the timeline given by the Govt. of India, under ministry.
NRHM implementation helped the District in decentralizing the program activities. There is a close convergence with the Village Authorities from the Sub-center level institutions to the District-level institutions. This communization has helped in making the people work with the health providers. Rogi Kalyan Samitis (RKS) are functional in all Health Institutions. Funds of RKS are utilized for development of the respective institutions and in managing crisis situation like shortage of medicine etc. apart from supply from the State Health Mission Society. There is an increase in the number of institutional deliveries. The ASHA plays as linkage between health workers and community of the villages. May health institutions had been constructed and repaired. Manpower strengthening by recruiting at the District level under the chairmanship of Deputy Commissioner had been initiated. Upgradation of infrastructure for 24/7 PHCs to four (4) PHCs had been completed. Though JSY scheme incentives could not met with the back log payments, the governments both in centre and state pump in lots of monetary assistance for payments of JSY to mothers. Additional ASHA had been in place. The performance of programme at the blocks level has been drastically improved after the introduction of DHIS2 software. Implementation of VH&SC, Committee annual untied grants is also effective as most of the villages benefit from it. Since BPMU are in placed work are carried out as per guidelines and with time bound. 8 New Construction of PHSC has been completed. Various villages carried out their sanitation programme effectively. Active participation of village authorities took place. No of sterilization rates increase.
5.1. Constraints: The District is facing many constraints too. Management capacities were found weak still in some areas like doctors particularly in District Hospital could not really understand the functioning of NRHM at the District level. They think that the NRHM programme is a short of NGOs introduce to uplift the poor section of the community and also thinks that it was totally undertaken by the family welfare department alone.
CCP PIP 2010-11
The National Disease Control Programs and Integrated Disease Surveillance Program (IDSP) activities are not converged with NRHM resulting into poor performance. As the programme implementation of IDSP and others vertical programme could not be converge as being told and promise. Inadequate infrastructure and non-availability of Specialist Doctors, SN, in district hospital and others health facilities where 24/7 delivery centres being identified. Non availability of staff quarters and bad road connectivity is still the stumbling block for program implementation effectively as most of the programs are based on specific time bound. No provision of referral system at the remote health centres, not die and hard involvement by the ICDS department, PHED, PWD also weaken the program implementation. Nevertheless, the poor concept of the existing health directorate staff about NRHM also hampers and de-motivate the contractual staff to bring out innovative and suggestive though despite of their constant negligence towards their duties. Another, constraints is that the salary of the DPMU, BPMU and all others staff under NRHM are low paid- which really could not push forwards to dedicate their works. Anti social elements interventions in any activities also make the programme in mesh as it could not be conducted as it would be. Also it delay the program output to large extent.
The difficult geographical terrains, poor transport and communication facilities, scattered nature of inhabitations and Health Institutions have hindered the program badly. Also frequent load-shedding of power, lack of safe drinking water has affected the program implementation.
5.2. Key Issues to Be Addressed
The key strategies are (i) Operationalizing Health Facilities by up-grading Infrastructure of DH to FRU and
three PHC into functional as 24/7 delivery centres ( Saikot, Sagang, Singngat, PHCs)
(ii) Capacity development
• Multi-skilling training of MBBS Doctors (CEmOC, Life Saving Anesthesia, MVA, MTP, RTI/STI, SBA, NSV, Tubectomy etc ) be a continuous process
• Other trainings (Capacity Development for VAs, DPMU,BPMU,ARSH, IUCD) (iii) Increasing awareness of the Health Facilities available to the people and motivating
them to utilize the service provisions through effective BCC.
(iv) Recommended for increase of the honorarium of all the staff under NRHM
(v) Drastically upgrade the infrastructure strengthening
(vi.) Intra/Intersectoral convergence with Health determinant Departments (vii.) Establishment of District Training Centre (viii.) Establishment of District GNM Training School (ix.) Provision FRU Services functional District Hospital
CCP PIP 2010-11
CCP PIP 2010-11
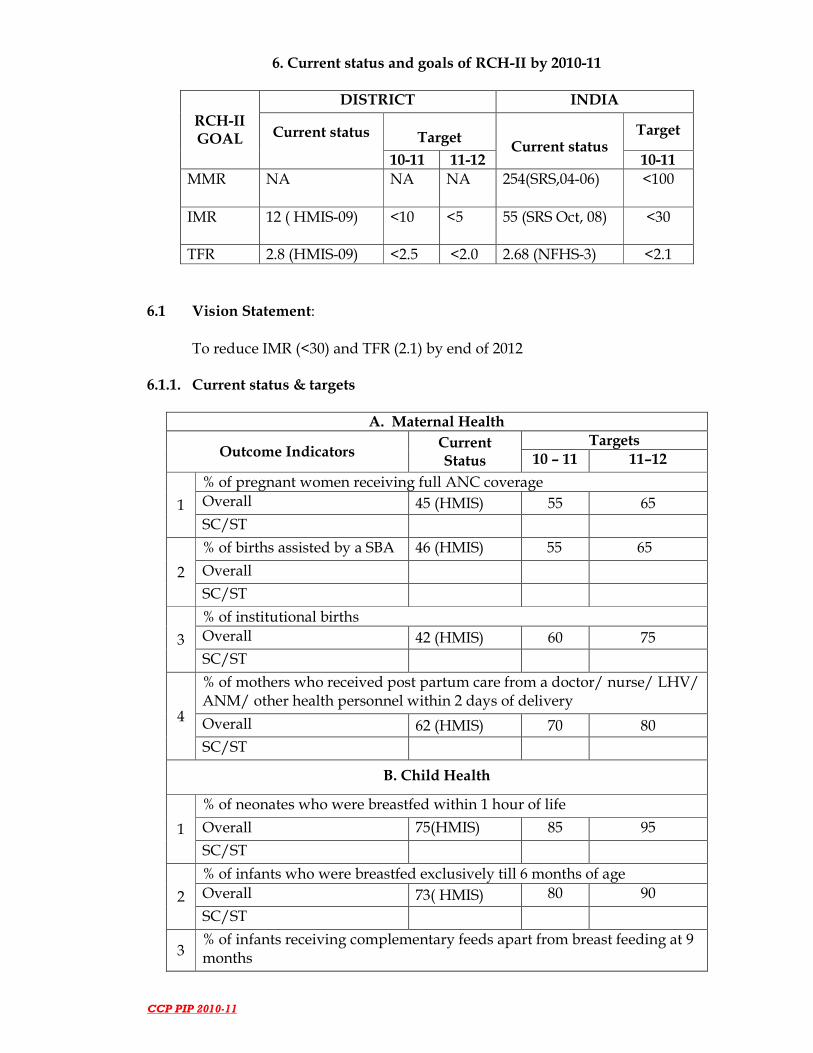
6. Current status and goals of RCH-II by 2010-11
RCH-II GOAL
DISTRICT INDIA
Current status
Target Current status
Target
10-11 11-12 10-11
MMR NA NA NA 254(SRS,04-06) <100
IMR 12 ( HMIS-09) <10 <5 55 (SRS Oct, 08)
<30
TFR 2.8 (HMIS-09) <2.5 <2.0 2.68 (NFHS-3) <2.1
6.1 Vision Statement:
To reduce IMR (<30) and TFR (2.1) by end of 2012 6.1.1. Current status & targets
A. Maternal Health
Outcome Indicators Current Status
Targets
10 – 11 11–12
1
% of pregnant women receiving full ANC coverage
Overall 45 (HMIS) 55 65
SC/ST
2
% of births assisted by a SBA 46 (HMIS) 55 65
Overall
SC/ST
3
% of institutional births
Overall 42 (HMIS) 60 75
SC/ST
4
% of mothers who received post partum care from a doctor/ nurse/ LHV/ ANM/ other health personnel within 2 days of delivery
Overall 62 (HMIS) 70 80
SC/ST
B. Child Health
1
% of neonates who were breastfed within 1 hour of life
Overall 75(HMIS) 85 95
SC/ST
2
% of infants who were breastfed exclusively till 6 months of age
Overall 73( HMIS) 80 90
SC/ST
3 % of infants receiving complementary feeds apart from breast feeding at 9 months

CCP PIP 2010-11
Overall 55 (HMIS) 60 80
SC/ST
4
% of children 12-23 months of age fully immunized
Overall 29(HMIS) 45 65
SC/ST
Outcome Indicators Current Status
Targets
10 – 11 11–12
5
% of children 6-35 months of age who are anemic
Overall 21(HMIS) 10 5
SC/ST
6
% of children under 5 years age who have received all nine doses of Vitamin A
Overall 22 (HMIS) 45 75
SC/ST
7
% of children under 3 years age with diarrhea in the last 2 weeks who received ORS
Overall 32 (HMIS) 45 65
SC/ST
% of children under 3 years age who are underweight
Overall 15 (HMIS) 10 5
SC/ST
C. Family Planning
1
Contraceptive prevalence rate (any modern method)
Overall 30 (HMIS) 40 50
SC/ST
2
Contraceptive prevalence rate (limiting methods)
Male Sterilization 0.4 (HMIS) 1.5 2.0
Female Sterilization 25(HMIS) 50 70
3
Contraceptive prevalence rate (spacing methods)
Oral Pills 5 (HMIS) 15 35
IUDs 10 (HMIS) 20 30
Condoms 15 (HMIS) 25 45
4
Unmet need for spacing methods among eligible couples
Overall 15(HMIS) 10 <5
SC/ST
5 Unmet need for terminal methods among eligible couples
Overall 20 (HMIS) 15 5
CCP PIP 2010-11
SC/ST
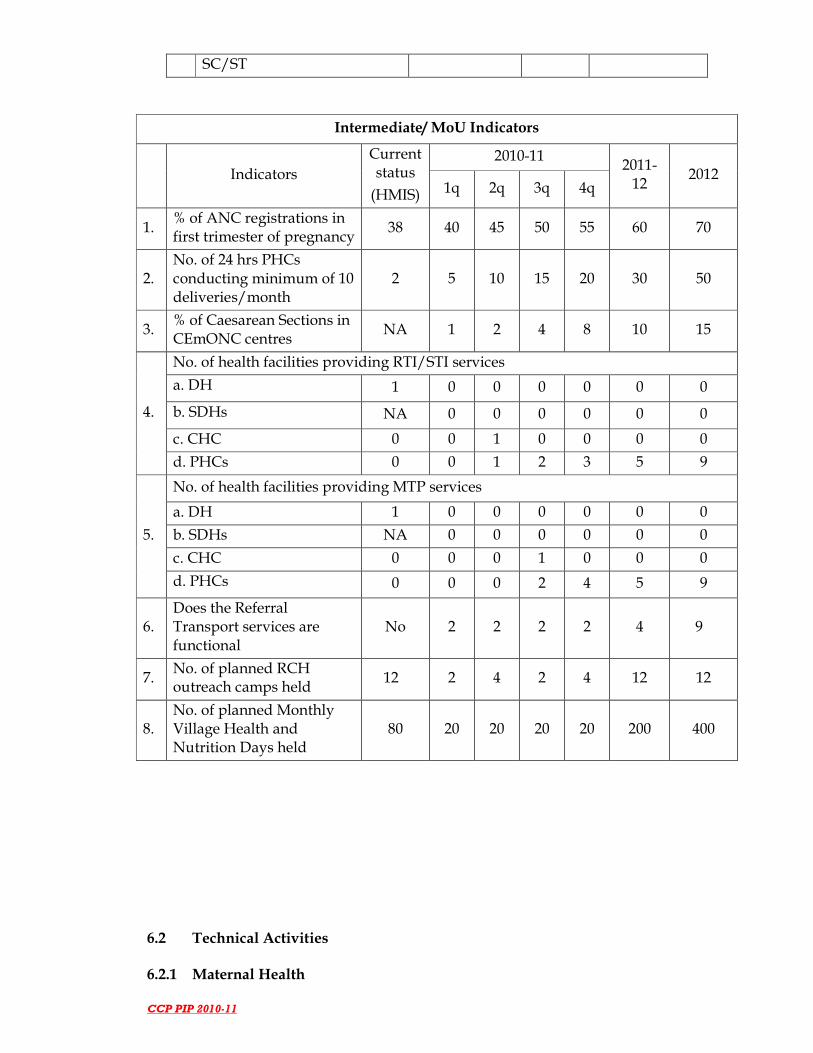
Intermediate/ MoU Indicators
Indicators
Current status
(HMIS)
2010-11 2011-
12 2012
1q 2q 3q 4q
1. % of ANC registrations in first trimester of pregnancy
38 40 45 50 55 60 70
2. No. of 24 hrs PHCs conducting minimum of 10 deliveries/month
2 5 10 15 20 30 50
3. % of Caesarean Sections in CEmONC centres
NA 1 2 4 8 10 15
4.
No. of health facilities providing RTI/STI services
a. DH 1 0 0 0 0 0 0
b. SDHs NA 0 0 0 0 0 0
c. CHC 0 0 1 0 0 0 0
d. PHCs 0 0 1 2 3 5 9
5.
No. of health facilities providing MTP services
a. DH 1 0 0 0 0 0 0
b. SDHs NA 0 0 0 0 0 0
c. CHC 0 0 0 1 0 0 0
d. PHCs 0 0 0 2 4 5 9
6. Does the Referral Transport services are functional
No 2 2 2 2 4 9
7. No. of planned RCH outreach camps held
12 2 4 2 4 12 12
8. No. of planned Monthly Village Health and Nutrition Days held
80 20 20 20 20 200 400
6.2 Technical Activities 6.2.1 Maternal Health
CCP PIP 2010-11
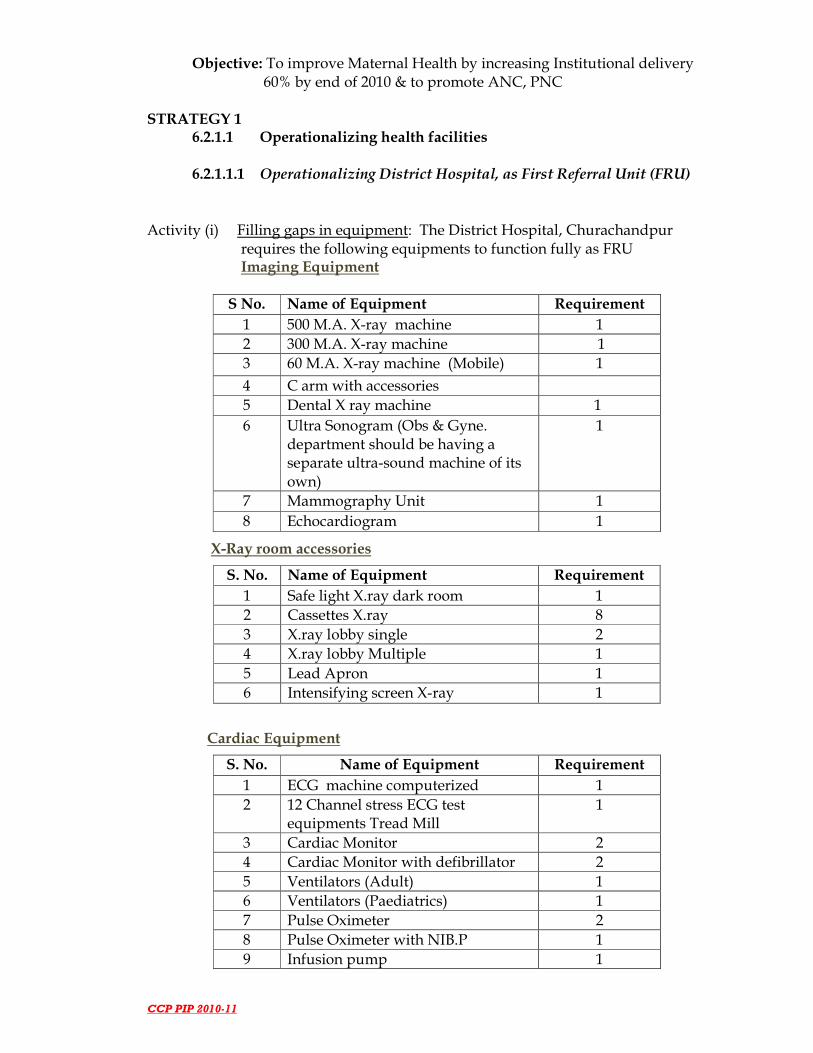
Objective: To improve Maternal Health by increasing Institutional delivery 60% by end of 2010 & to promote ANC, PNC STRATEGY 1
6.2.1.1 Operationalizing health facilities 6.2.1.1.1 Operationalizing District Hospital, as First Referral Unit (FRU)
Activity (i) Filling gaps in equipment: The District Hospital, Churachandpur requires the following equipments to function fully as FRU
Imaging Equipment
S No. Name of Equipment Requirement
1 500 M.A. X-ray machine 1
2 300 M.A. X-ray machine 1
3 60 M.A. X-ray machine (Mobile) 1
4 C arm with accessories
5 Dental X ray machine 1
6 Ultra Sonogram (Obs & Gyne. department should be having a separate ultra-sound machine of its own)
1
7 Mammography Unit 1
8 Echocardiogram 1
X-Ray room accessories
S. No. Name of Equipment Requirement
1 Safe light X.ray dark room 1
2 Cassettes X.ray 8
3 X.ray lobby single 2
4 X.ray lobby Multiple 1
5 Lead Apron 1
6 Intensifying screen X-ray 1
Cardiac Equipment
S. No. Name of Equipment Requirement
1 ECG machine computerized 1
2 12 Channel stress ECG test equipments Tread Mill
1
3 Cardiac Monitor 2
4 Cardiac Monitor with defibrillator 2
5 Ventilators (Adult) 1
6 Ventilators (Paediatrics) 1
7 Pulse Oximeter 2
8 Pulse Oximeter with NIB.P 1
9 Infusion pump 1

CCP PIP 2010-11
10 B.P.apparatus table model 6
11 B.P.apparatus stand model 3
12 Stethoscope 1
Labor ward and Neo-Natal Equipment
S. No. Name of Equipment Requirement
1 Phototherapy Unit 1
2 Emergency Resuscitation Kit-Baby 2
3 Radiant Warmer 1
4 Room Warmer 2
5 Foetal Doppler 1
6 CTG Monitor 1
7 Delivery Kit 1
8 Episiotomy kit 2
9 Forceps Delivery Kit 1
10 Crainotomy 1
11 Vacuum extractor metal 1
12 Silastic vacuum extractor 1
13 Pulse Oximeter baby & adult 1
14 Cardiac monitor baby 1
15 Nebulizer baby 1
16 Weighing machine adult 1
17 Weighing machine infant 1
ENT Equipment
S. No. Name of Equipment Requirement
1 Audiometer 1
2 Operating Microscope (ENT) 1
3 Head light (ordinary) (Boyle Davis) 1
4 ENT Operation set including headlight, Tonsils
1
5 Mastoid Set 1
6 Micro Ear Set myringoplasty 1
7 Stapedotomy Set 1
8 Stapeidoplasty 1
9 ENT Nasal Set (SMR, Septoplasty, Polypetcomy, DNS, Rhinoplasty)
1
10 Laryngoscope fibreoptic ENT 1
11 Laryngoscope indirect 1
12 Otoscope 1
13 Oesophagoscope Adult
14 Oesophagoscope Child
15 Head Light (cold light) 1
16 Tracheostomy Set 1
17 Tuning fork 1

CCP PIP 2010-11
Eye Equipment
S. No. Name of Equipment Requirement
2 Slit Lamp 1
3 Perimeter 1
4 IOL Operation set 2
5 Laser Photocoagulometer
Dental Equipment
S. No. Name of Equipment Requirement
1 Air Rotor 1
2 Dental Unit with motor for dental OP
1
3 Dental Chair 1
4 Dental Kit 1
Operation Theatre Equipment
S. No. Name of Equipment Requirement
1 Auto Clave HP Vertical (2 bin) 2
2 Operation Table Ordinary Pediatric 1
3 Operation table Hydraulic Minor 2
8 Autoclave with Burners 2 bin 1
10 Shadow less lamp ceiling type major 1
11 Shadow less lamp ceiling type minor
1
12 Shadow less Lamp stand model 1
14 Sterilizer big (Instrument) 2
15 Sterilizer Medium (Instrument) 3
16 Sterilizer Small (Instruments) 3
17 Bowl Sterilizer – big 1
18 Bowl sterilizer – Medium 1
20 Suction Apparatus - Electrical 1
21 Suction Apparatus - Foot operated 1
22 Dehumidifier 1
23 Ultra violet lamp Philips model 4 feet
2
24 Ethylene Oxide sterilizer 1
25 Microwave sterilizer 1
Laboratory Equipment
S. No. Name of Equipment Requirement

CCP PIP 2010-11
2 Balance (Electrical Monopan) 1
3 Simple balance 1
5 Semi auto analyser 1
7 Water bath 1
9 Lab Incubator 1
10 Distilled water plant 2
11 Electricentrifuge Table Top 1
12 Cell Counter Electronic 1
13 Hot plates 2
14 Rotor / Shaker 1
15 Counting chamber 2
16 PH meter 1
17 Paediatric Glucometer / Bilirubinometer
18 Glucometer 1
20 TCDC count apparatus 1
22 Test tube stands 5
23 Test tube rack 3
24 Test tube holders 3
25 Spirit lamp 5
26 Timer stop watch 2
27 Alarm clock 1
28 Lab Autoclaves 2
29 Refrigerators 2
30 Bio-safety Cabinet (Class-I) 1
Surgical Equipment set
S. No. Name of Equipment Requirement
1. MTP Set 1
2. Biopsy Cervical Set 1
3. D & C Set 1
4. I.U.C.D. Kit 1
5. LSCS set 1
6. MVA Kit 2
7. Vaginal Hysterectomy 1
8. Proctoscopy Set 1
9. P.V. Tray 1
10. Abdominal Hysterectomy set 1
11. Laparotomy Set 1
12. Formaline dispenser 2
13. Kick Bucket 6
14. General Surgical Instrument Set Piles, Fistula, Fissure
1
15. Knee hammer 2
16. Hernia, Hydrocele 1
17. Varicosevein etc 1

CCP PIP 2010-11
18. Gynaec Electric Cautery
19. Vaginal Examination set 4
20. Suturing Set 3
21. MTP suction apparatus 1
22. Thoracotomy set
23. Neuro Surgery Craniotomy Set
24. I M Nailing Kit 1
25. Dynamic Heat Nailing 1
26. Compression Plating Kit 1
27. AM Prosthesis 1
28. Dislocation Hip Screw Fixation 1
29. Fixation Fracture Hip 1
30. Spinal Column Back Operation Set 1
31. Thomas Splint 5
32. Paediatric Surgery Set
33. Mini Surgery Set 1
34. Urology Kit
35. Surgical Package for Cholecystectomy
36. Surgical package for Thyroid
37. GI Operation Set 2
38. Appendicectomy set 2
39. L.P.Tray 3
40. Uretheral Dilator Set 2
41. TURP resectoscope
42. Haemodialysis Machine
43. Amputation set 1
44. Universal Bone Drill
45. Crammer wire splints 8
46. Heamo dialysis machine
Physiotherapy equipment
S. No. Name of Equipment Requirement
1 Skeleton traction set 1
2 Interferential therapy unit 1
3 Short Wave Diathermy 1
Endoscopy Equipment
S. No. Name of Equipment Requirement
1 Endoscope fibre optic (OGD) 1
2 Laparoscope operating major with accessories
1
3 Laparoscope diagnostic and for sterilisation
1
4 Colonoscope and sigmoidoscope

CCP PIP 2010-11
5 Hysteroscope 1
6 Colposcope 1
Anesthesia Equipment
S. No. Name of Equipment Requirement
1 Anaesthetic - laryngoscope magills with four blades
1
2 Endo tracheal tubes sets 1
3 Magills forceps (two sizes) 4
4 Connector set of six for E.T.T 4
5 Tubes connecting for ETT 3
6 Air way female 4
7 Air way male 8
8 Mouth prop 6
9 Tongue depressors 8
12 CO2 cylinder for laparoscope
13 PFT machine 1
14 Boyles Apparatus with Fluotec and circle absorber
1
15 Exchange transfusion sets 1
Furniture and hospital accessories
S. No. Name of Equipment Requirement
1 Doctor's chair for OP Ward, Blood Bank, Lab etc.
15
2 Doctor's Table 4
3 Table for Sterilization use (medium)
5
4 Long Benches(6 1/2' x 1 1/2') 15
5 Stool Wooden 10
6 Stools Revolving 6
7 Steel Cup-board 9
8 Wooden Cup Board 4
9 Racks -Steel – Wooden 7
10 Patients Waiting Chairs (Moulded)
10
11 Attendants Cots 4
12 Office Chairs 2
13 Office Table 2
14 Foot Stools 7
15 Filing Cabinets (for records) 6
16 M.R.D.Requirements (record room use)
1
17 Paediatric cots with railings 5

CCP PIP 2010-11
18 Cradle 3
19 Fowler's cot 0
20 Ortho Facture Table 0
21 Hospital Cots (ISI Model ) 100
22 Hospital Cots Paediatric (ISI Model )
10
23 Wooden Blocks (Set) 2
24 Back rest 4
25 Dressing Trolley (SS) 2
26 Medicine Almairah 1
27 Bin racks (wooden or steel) 3
28 ICCU Cots 4
29 Bed Side Screen (SS-Godrej Model)
4
30 Medicine Trolley(SS) 4
31 Case Sheet Holders with clip(S.S.)
60
32 Bed Side Lockers (SS) 100
33 Examination Couch (SS) 2
34 Instrument Trolley (SS) 6
35 Instrument Trolley Mayos (SS) 4
36 Surgical Bin Assorted 25
37 Wheel Chair (SS) 4
38 Stretcher / Patience Trolley (SS)
3 each
39 Instrument Tray (SS) Assorted 30
40 Kidney Tray (SS) - Assorted 30
41 Basin Assorted (SS) 30
42 Basin Stand Assorted (SS)
43 (2 basin type ) 4
44 ( 1 basin type) 8
45 Delivery Table (SS Full) 6
46 Blood Donar Table 1
47 O2 Cylinder Trolley(SS) 8
48 Saline Stand (SS) 15
49 Waste Bucket (SS) 25
50 Dispensing Table Wooden 1
51 Bed Pan (SS) 20
52 Urinal Male and Female 20
53 Name Board for cubicals 1
54 Kitchen Utensils
55 Containers for kitchen
56 Plate, Tumblers
57 Waste Disposal - Bin / drums 8
58 Waste Disposal - Trolley (SS) 1
59 Linen Almirah 3
60 Stores Almirah 3

CCP PIP 2010-11
61 Arm Board Adult 10
62 Arm Board Child 10
63 SS Bucket with Lid 6
64 Bucket Plastic 8
65 Ambu bags 5
66 O2 Cylinder with spanner ward type
12
67 Diet trolley - stainless steel 1
68 Needle cutter and melter 15
69 Thermometer clinical 20
70 Thermometer Rectal 3
71 Torch light 10
72 Cheatles forceps assorted 8
73 Stomach wash equipment 2
74 Infra Red lamp 3
75 Wax bath 1
76 Emergency Resuscitation Kit-Adult
2
77 Enema Set 6
78 Ceiling Fan As per requirement
79 Bed Side Screen (SS-Godrej Model)
As per requirement
Post-Mortem Equipment
S. No. Name of Equipment Requirement
1 Mortuary table (Stainless steel) 2
2 P.M.equipment (list) 2
4 Measuring glasses(liquids) 2
5 Aprons 10
6 PM gloves ( Pairs ) 10
7 Rubber sheets
8 Lens 1
9 Spot lights 2
Hospital Linen
S. No. Name of Equipment Requirement
1 Bed sheets 400
2 Bedspreads 600
3 Blankets Red and blue 10
4 Patna towels 150
5 Table cloth 50
6 Draw sheet 75
7 Doctor's overcoat 30
8 Hospital worker OT coat 200
9 Patients house coat (for female) 300
10 Patients Pyjama (for male) Shirt 200

CCP PIP 2010-11
11 Over shoes pairs 60
12 Pillows 150
13 Pillows covers 300
14 Mattress (foam) Adult 50
15 Paediatric Mattress 16
16 Abdominal sheets for OT 40
17 Pereneal sheets for OT 50
18 Leggings 80
19 Mortuary sheet 30
20 Mats (Nylon) 50
21 Mackin tosh sheet (in meters) 150
Teaching Equipment
S. No. Name of Equipment Requirement
1 Slide Projector 1
2 O.H.P 1
3 Screen 1
4 White / color boards 1
5 Television color 1
7 VCD Player 1
8 Radio 1
Administrative Equipment
S. No. Name of Equipment Requirement
2 Xerox Machine 1
3 Typewriter (Electronic ) 1
4 Intercom (40 lines)
5 Fax Machine 1
7 Public Address System 1
8 Library facility
Refrigeration and AC Equipment
S. No. Name of Equipment Requirement
1 Refrigerator 165 litres 3
3 ILR 1
4 Deep Freezer 1
5 Coolers
6 Air conditioners 4
7 Central A/C for OT
Hospital Plants
S. No. Name of Equipment Requirement
1 Generator 75 KV 1
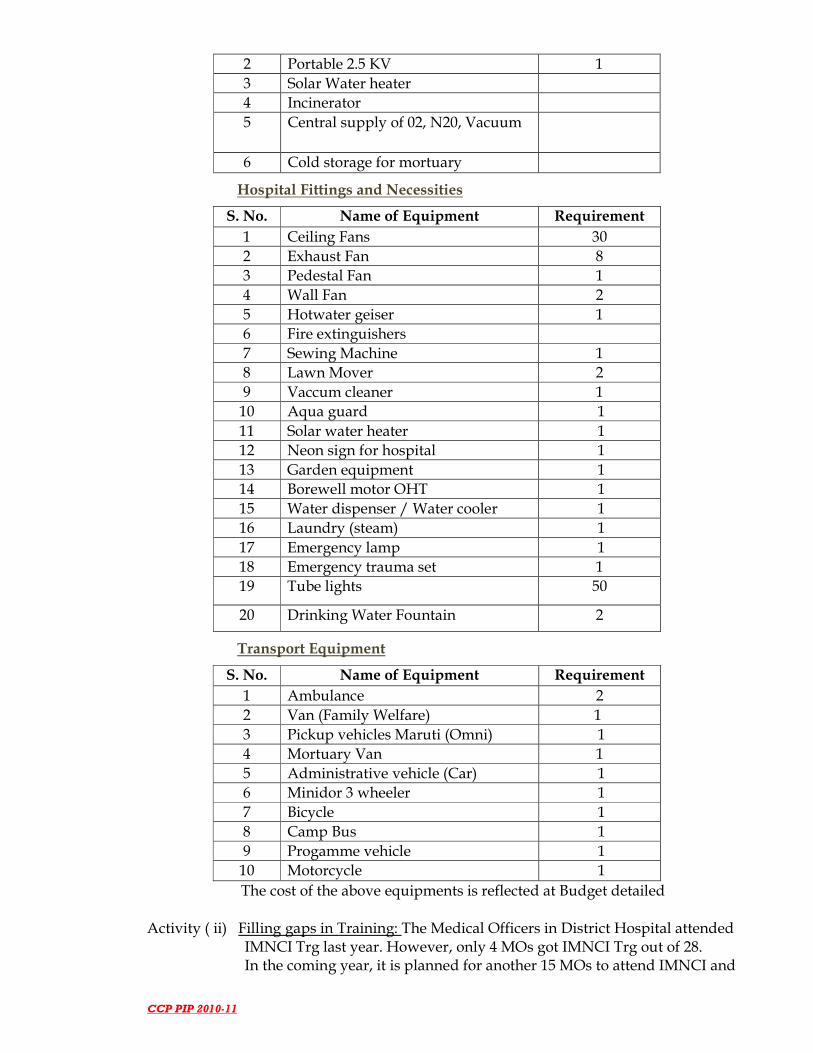
CCP PIP 2010-11
2 Portable 2.5 KV 1
3 Solar Water heater
4 Incinerator
5 Central supply of 02, N20, Vacuum
6 Cold storage for mortuary
Hospital Fittings and Necessities
S. No. Name of Equipment Requirement
1 Ceiling Fans 30
2 Exhaust Fan 8
3 Pedestal Fan 1
4 Wall Fan 2
5 Hotwater geiser 1
6 Fire extinguishers
7 Sewing Machine 1
8 Lawn Mover 2
9 Vaccum cleaner 1
10 Aqua guard 1
11 Solar water heater 1
12 Neon sign for hospital 1
13 Garden equipment 1
14 Borewell motor OHT 1
15 Water dispenser / Water cooler 1
16 Laundry (steam) 1
17 Emergency lamp 1
18 Emergency trauma set 1
19 Tube lights 50
20 Drinking Water Fountain 2
Transport Equipment
S. No. Name of Equipment Requirement
1 Ambulance 2
2 Van (Family Welfare) 1
3 Pickup vehicles Maruti (Omni) 1
4 Mortuary Van 1
5 Administrative vehicle (Car) 1
6 Minidor 3 wheeler 1
7 Bicycle 1
8 Camp Bus 1
9 Progamme vehicle 1
10 Motorcycle 1
The cost of the above equipments is reflected at Budget detailed Activity ( ii) Filling gaps in Training: The Medical Officers in District Hospital attended IMNCI Trg last year. However, only 4 MOs got IMNCI Trg out of 28. In the coming year, it is planned for another 15 MOs to attend IMNCI and

CCP PIP 2010-11
various other trainings under NRHM like LSA, RTI/STI, MVA, MTP, SBA, NSV etc. The detailed are reflected in Training Sections under Part A Activity (iii) Filling gaps in Medicines & drugs: Procurement mechanisms will be done through district level. The district will procure as per the needs of the facility. Activity (iv) Filling gaps in infrastructure: There should be provision of 24/7 running water, commissioning of generator, installation of incinerator, civil works of zoning in OT, installation of CT scan, repair of X ray dept and lead proofing as per AERB norms ,installation of automatic film processor, marking of proposed casualty space in OPD block, refurnishing of CSSD, maintenance and paintings of premises, sign postings of facilities, area lighting, re-furbishing of mortuary, laundry, kitchen, storage facility for medical records room, storage for mass casualty stores. Security personnel be in place Activity (v) Filling Gaps in Manpower: To run casualty unit, the existing MOs are engaged in various dept assisting specialists’ doctors. We need six additional 6 MOs exclusively for casualty service. We need additional 26 GNM to run the hospital efficiently. One electrician and one electric jugali under contractual basis be sanctioned. 6.2.1.1.2 For making PHCs 24/7 Service Delivery Centres Activity (i) Three PHCs namely Saikot PHC, Sagang PHC, and Singngat PHC was already identified as 24/7 services delivery centres. But due to insufficient availability of Manpower (need an additional 2 MBBS Doctors, 2 SN, 1 Lab technician in each of these 3 identified PHCs). Besides, these PHCs strongly desire dedicated Water Supply, Power supply, Ambulance Services, extra beds, Instrument for deliveries, equipments etc. without which conversion remains a mere projection. If the above mentioned facilities are provided, the delivery services could take place. Also, incentives scheme is recommended as per propose rate @ Rs 500 per delivery for a doctor & @ Rs 300 each for GNM/ANM for assisting the delivery Activity (ii) EmOC Training is strongly recommended particularly for doctors who posted at these 24/7 identified PHCs Activity (iii) SBA Training is highly recommended for SN, ANM
6.2.1.1.3 Operationalise MTP services at health facilities
Activity (i) More Training for MBBS Doctors in MTP. Activity (ii) More training for MBBS doctors in IUCD Activity (iii) Provide the facility of MTP services at 3 identified 24/7 PHCs Activity (iii) Accrediting more private clinics for MTP services Activity (v) District Quality Assurance to monitor the services effectively

CCP PIP 2010-11
6.2.1.1.4 Operationalise RTI/STI services at health facilities Activity (i) More Training for MOs posted in PHCs on management of RTI/STI. Activity (ii) Provision of RTI/STI facility in DH, and the 3 PHCs Activity (iii) Training of ASHAs to encourage referral services to health facilities Activity (iv) DMMUs to have provision of RTI/STI management facility Activity (v) Monitoring through monthly HMIS and supervision by District
6.2.1.1.5 Operationalise Sub-centres Activity (i) Construction of building for building-less Sub-Centres: The district has
currently, 21 (twenty-one) PHSCs without building. In the year 2006-07, fifteen PHSCs construction were sanctioned out of which only 10 SCs had been reported completed so far. Therefore, the district newly proposed the construction of ten 10 PHSCs for the coming year. The propose SCs to be constructed is mentioned in relevant section.
Activity (ii) Repair/renovation of Sub-Centres: 14 identified Sub-Centre buildings
were already repaired and renovated in past years. Therefore, for this coming year, the repairing and renovation of eight PHSCs are highly recommended.
Activity (iv) Training of ANMs in SBA: 40 ANMs had already completed SBA Training. Another 91 ANMs needs to be trained in the coming year. GNMs/ SN also required training in SBA. The training will be conducted at the District Hospital under the supervision of Medical Supdt. The detail reflects at Training part/section Activity (v) Additional ANMs require for Sub-Centres: There was 64 sub centres
earlier however with the newly added 2 sub centres recently, the district presently has 66 sub centres. There are 56 ANMs who are posted in all the existing Sub-Centres. Therefore, 10 additional ANMs are required to fill the unfilled gaps in 66 PHSCs. Out the existing 56 ANMs, 7 ANMs are utilized at other health centres.
The District propose the below extra incentives to ANMs as promised by
the first 100 days program execution by the UPA Govt. to those ANMs who are posted at very difficult and inaccessible areas. The District had identified 26 very difficult and in accessible PHSC coverage area under the District.
The basis of paying the extra incentives will be based on the following points: 1. Recommend an extra hardship allowance to the ANMs posted only at
the above mentioned inaccessible area be paid Rs. 3000/- per month. 2. If the above point is not suitable, we will recruit manpower from the
PHC level by the RKS Management Society to run the PHSC effectively and efficiently.

CCP PIP 2010-11
STRATEGY 2 6.2.1.2 Referral transport Activity (i) Out-sourcing Referral transport: In case of CHC Parbung, the available
outsource vehicles could not met with the little or less sanction amount. We propose for outsourcing the vehicles to all the PHCs and CHC of the District. The District had adverse geographical landscape. So it requires higher amount comparing to those in the valley districts. On an average an estimated amount of Rs 25,000/- per journey be sanction
STRATEGY 3 6.2.1.3 Integrated outreach RCH services Activity (i) Outreach RCH camps will be organized in under-served/un-served areas which will be based on the concerned PHCs whereas extra support for manpower has to be taken from District Hospitals and others PPP sections.
The District faces problems earlier years due to low sanction of money per camp. This year after we let involve the MMU vehicles and its specific manpower for operationalize, we needs an estimated amount of Rs 50,000/- per camp off 12 camps per year.
Activity (ii) It is proposed to organize Village Health & Nutrition Days at 1010
Anganwadi Centres (AWC) on Wednesdays of every months involving Village Health & Sanitation Committee members, ASHA, AWW and to be facilitate by the BPMU staff. All the activities as per the guideline of Village Health & Nutrition Days shall be implemented. Regular monitoring and reporting will be ensured by the BPMU.
STRATEGY 4 6.2.1.4. Janani Suraksha Yojana (JSY)
The objective of JSY will be to increase the current (71% to 80% ) proportion of institutional delivery. The financial assistance given to the mothers as well as the ASHAs to encourage institutional delivery will be as given below:
1. Mother’s package: (i) For institutional delivery - Rs. 700/- per case in rural areas (ii) For home delivery both - Rs. 500/- per case in rural areas 2. ASHA’s accompaniment package - Rs. 600/- per case 3. For Caesarian section - Rs. 1500/- per case in Govt. Health facilities 4. Referral package - Max of Rs. 200/- per Case

CCP PIP 2010-11
The District mostly inhabited by the ST population women having 2 live-births will get the financial assistance irrespective of their BPL status. But for home deliveries in these areas the Village Chairman has to certify that the women belong to poor family.
A. Estimated number of deliveries in 2010-11 = 4500 B. Estimated deliveries = 4000 C. Targeted number of institutional deliveries (60%) = 3200 D. Expected home deliveries = 800 E. Estimated deliveries needing C/S (2%) = 45 F. Estimated deliveries for JSY =2700 JSY budget needed (in Lakhs):
In SC/ST Population
Total
Mother’s package Urban Rural
Estimated total No. of deliveries 4000 4000
Estimated No. of deliveries in BPL/poor General families (assuming 30% in urban areas and 40% in rural areas in General population) (except for SC/ST)
3800 3800
Estimated No. of deliveries up-to the order of 2 in BPL Population (50%) (BPL status not binding for SC/ST)
2700 2700
Targeted No. of institutional deliveries (60% out of above)
2700 2700
In SC/ST Population
Total (Rs. In lakhs)
Mother’s package Urban Rural
Package for institutional delivery (@ Rs. 700/- in rural areas
2700 18.90
Estimated No. of Home deliveries in BPL/ poor families up-to Birth order of 2 (BPL status applicable to all population)
Package for Home delivery (@ Rs. 500/- per case)
800 4.0 Lacs
ASHA’s package for accompanying institutional delivery (@ Rs. 600/- per case)
1000 6.0 Lacs
Assistance for C/S @ Rs. 1500/- (Assuming 2% of all institutional deliveries)
45 0.67 Lac
Referral transport (Maximum of Rs. 200/- per case)
30 0.06 Lac
Program Management Cost including printing of JSY Card, MCH Card and Registers
0.50 0.50 Lac
Grand total Rs 30.13 Lacs

CCP PIP 2010-11
STRATEGY 5 6.2.1.5 Other strategies 6.2.1.5.1 Ensuring early registration and ANC (at least 3) for all
Pregnant women Activity (i) Ensuring that ANMs stay at their place of posting by promoting the
environment of the Sub-centres through provision of untied funds Activity (ii) Including 3 ANCs as one of the criteria for claiming financial assistance
under JSY. Activity (iii) District Mobile Medical Unit to hold ANC sessions in difficult to be
Accessed areas 6.2.1.5.2 Maternal Death Auditing: Activity (i) Formation of a District level Committee under the Chairmanship of
Deputy Commissioner to be executed at the month of April 1010 and any reported maternal deaths will be audited by using a verbal autopsy pro forma. The reason of maternal death and measures to prevent further deaths can be found out. A sum of Rs. 2.00 lakhs may be sanctioned for this.
6.2.1.5.3 Strengthening PNC Activity (i) Promoting at least 03 PNC visits through ASHAs, AWWs, ANMs. Activity (ii) Making at least one PNC visit a pre-requisite for JSY. Activity (iii) PNC through home visits by ANM before holding Monthly Village
Health Days Activity (iv) District Mobile Medical Unit be use for hard unreached areas. 6.2.1.5.4 Strengthening PPP Activity (i) MSF, Holland , and already three clinics/ nursing home/ hospital and
one additional pvt accredited hospital( Sielmat) for service coverage is already initiated. But Sielmat Hospital needs to be authenticated in current year to accomplished PPP activities at maximum inputs and output for the welfare of the people in the District. In this regard dissemination, follow up training capacity building management, monitor quality of health service between the district health society and those bodies will be develop in this year.
6.2.1.5.5 ASHA scheme: Discussed in detailed in part B 6.2.2 Child Health
Objectives: To improve health status of newborns and children
STRATEGY 1 6.2.2.1 Implementation of IMNCI Activity (I) The District identified one Obs & Gynae Specialists (Dr Paikhomba, MD) as a Child Health Nodal Officer for implementation of IMNCI effectively
CCP PIP 2010-11
in 2009-10. Also IMNCI coordination committee had already been formed. Training was also given to 16 MOs from PHC, CHC and District Hospital level at RIMS. But proper dissemination of the program could not be happen so far. Another 27 twenty seven doctors needs training. The training be organize at the District level as the district possess child specialists STRATEGY 2 6.2.2.2 Essential New-born care based on Management of Diarrhoea, ARI,
Malnutrition, Vitamin A deficiency, Activity (i) In-service re-orientation training of ANM in Facility-based and Home-
Based Newborn care (FB & HBNC): will be organize Activity (ii) Periodic training of ASHAs to include Home-based Newborn Care
(HBNC) Activity (iii) Medicines/ Drugs for Health facilities and ASHAs Activity (iv) BCC activities to strengthen the above strategy STRATEGY 3 School Health Program The formation of a District School Health Committee under the chairmanship of DC Churachandpur will be fix and accordingly the following will be executed as given below-
• Identification of District Nodal Officer (School Health)
• Preparation of dissemination of Operational Guideline for School Health
• Preparation and Printing of monthly Reporting Formats
• Preparation and printing of School Health Cards Activity (i) Training of 20 School Teachers of the District is strongly desire. Activity (ii) Quarterly visit and health check-up by PHC MO to schools along with
concerned ANM of Sub-Centre and referral of cases. Schools having more no of girls child registered will be given first most priority during implementation. Action Plan to be prepared by MO i/c PHC concerned. .
Activity (iii) Equipments and medicine to be supported by PHC concerned Activity (iv) Monthly reporting by concerned MO to District and henceforth to State. Activity (v) Monitoring by Joint Team of Education and HFW Staff STRATEGY 4 6.2.2.5 Infant and Young Child Feeding / IYCF Activity (i) BCC activities through Mass Media and IPC through ASHAs Activity (ii) Periodic training of ASHAs to include chapter on IYCF Activity (iii) Re-orientation training of Health Workers at PHC level monthly
meetings

CCP PIP 2010-11
STRATEGY 5 6.2.2.6 Care of sick children and severe malnutrition at FRUs Activity (i) Operationalization of Newborn Care Corners and Nutritional
Rehabilitation Centre in FRU and 24/7 PHCs Activity (ii) Community mobilization through ASHA for timely referral of sick
children 6.2.3 Family Planning
OBJECTIVE: To reduce the unmet needs (Terminal- from 5 to < 1; Spacing- from 7.6 to < 2) by end of 2010-11 STRATEGY 1 6.2.3.1 Terminal/limiting methods Activity (i) Observation of Sterilization Days be identified
a. Weekly at District Hospital b. Quarterly at CHC c. Monthly at identified PHCs
Activity (ii) Training of MBBS Doctors in NSV and Minilap. Activity (iii) Provision of compensation money for clients, motivation fee for ASHA
and free provision of drugs & dressing materials Activity (iv) Expanding the panel of eligible surgeons and health institutions (both
public and private) Activity (v) Quarterly NSV camps at the Blocks by using manpower from District
Hospital Activity (vi) Provision for sterilization operation in quarterly out-reach RCH camps in
Saikot PHC, Singngat PHC and Sagang PHC Activity (vii) Provision of sterilization services in District Mobile Medical Unit Activity (viii) BCC activities to make people aware of the sterilization services available
in the nearby health facilities Activity (ix) Community mobilization through ASHAs Activity (x) Quality assurance and monitoring by District Quality Assurance STRATEGY 2 6.2.3.2 Spacing methods Activity (i) BCC activities to make people aware of the spacing methods available in
the health facilities Activity (ii) Provision of IUD services at all health facilities Activity (iii) Making available ECP, Cu-T 380 in addition to OCP and Condom in all
Health Institutions i.e CHC/ PHCs Activity (iv) Motivation fee for ASHAs for Cu-T Activity (v) Performance-based honorarium for Addl. ANMs for spacing services Activity (vi) Training of newly recruited Additional ANMs on Cu-T insertion Activity (vii) Quality Assurance and monitoring
CCP PIP 2010-11
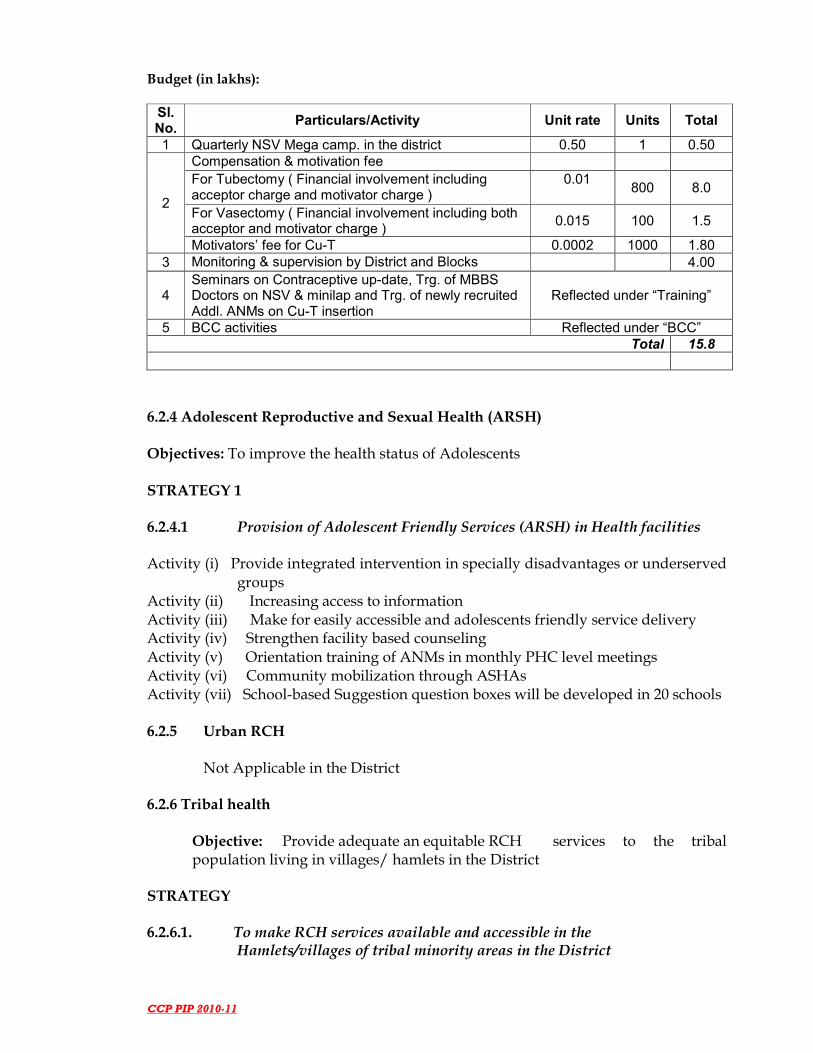
Budget (in lakhs): Sl. No.
Particulars/Activity Unit rate Units Total
1 Quarterly NSV Mega camp. in the district 0.50 1 0.50
2
Compensation & motivation fee For Tubectomy ( Financial involvement including acceptor charge and motivator charge )
0.01
800 8.0
For Vasectomy ( Financial involvement including both acceptor and motivator charge )
0.015 100 1.5
Motivators’ fee for Cu-T 0.0002 1000 1.80 3 Monitoring & supervision by District and Blocks 4.00
4 Seminars on Contraceptive up-date, Trg. of MBBS Doctors on NSV & minilap and Trg. of newly recruited Addl. ANMs on Cu-T insertion
Reflected under “Training”
5 BCC activities Reflected under “BCC” Total 15.8
6.2.4 Adolescent Reproductive and Sexual Health (ARSH)
Objectives: To improve the health status of Adolescents
STRATEGY 1 6.2.4.1 Provision of Adolescent Friendly Services (ARSH) in Health facilities Activity (i) Provide integrated intervention in specially disadvantages or underserved groups Activity (ii) Increasing access to information Activity (iii) Make for easily accessible and adolescents friendly service delivery Activity (iv) Strengthen facility based counseling Activity (v) Orientation training of ANMs in monthly PHC level meetings Activity (vi) Community mobilization through ASHAs Activity (vii) School-based Suggestion question boxes will be developed in 20 schools
6.2.5 Urban RCH
Not Applicable in the District 6.2.6 Tribal health
Objective: Provide adequate an equitable RCH services to the tribal population living in villages/ hamlets in the District
STRATEGY 6.2.6.1. To make RCH services available and accessible in the Hamlets/villages of tribal minority areas in the District

CCP PIP 2010-11
Activity (i) A mobile dispensary van fully equipped with medical facilities, and manned by doctor, an ANM and an assistant to cover the adverse block where adverse villages people inhibits especially Tipaimukh area and Vangai block needs special attention to the community as they are disconnected from the rest of the people almost all the seasons due to adverse geographical location. 6.2.7 Vulnerable groups Objective: To provide equitable RCH services to vulnerable and other marginalized
Community
STRATEGY 1 6.2.7.1. Preventive and promotive health services to marginalized
Community living Tipaimukh Block, Vangai & Henglep Block Activity (i) Provision of Extra Medicine and drugs Activity (ii) A Joint Special Monthly health check-up by staffs of PHC Parbung, Senvon PHC and Patpuihmun PHC in these Block Activity (iii) Health awareness programs with community participation including
local ASHAs Activity (iv.) Awareness program Activity (v) Effective BCC Activities in these areas
Sl. No.
Particulars Unit rate Units Total
1 Cost of Service-Type Latrine 0.0205 5 0.1025
2 Preparation of disposal area 0.12 4 0.48
3 Engaging local boats 0.12 5 0.6
4 Engaging volunteers for collection & disposal of excreta
0.36 5 1.8
5 Mobility support (hiring boats) for Health Staff on weekly basis
0.005 5 0.025
6 Procuring Plastic water filters 0.003 5 0.015
7 Purchasing alum and Chlorine tab/powder - - 0.50
8 Organizing monthly health awareness programs
0.05 10 0.5
9 Training of women on practice of chlorination in 10 batches ( each batch having 25 participants)
0.08 10 0.8
Total 26.70
6.2.8. Innovations Activity (i) Performance-based incentives for Additional ANMs posted at Sub-
Centres which were inaccessible. At present 26 sub-centres are identified as inaccessible.
Activity (ii.) Incentives be given to doctors and nurses who have conducted institutional delivery.
Activity (iii) Observation of ASHA day be observed on Mothers Day. Reward be given to the best ASHA on this day.
CCP PIP 2010-11
STRATEGY 3 6.2.8.3 NGO Program
Activity (i) Coordinating with Medicins Sans Frontier-Holland for providing RCH
services in interior parts of Churachandpur District (Singngat Block and Saikot Block) is being executed for the past three years. Their inputs for reports also play vital role.
6.2.9. Infrastructure strengthening
Objective: Provision of adequate infrastructure and Human resources for effective implementation of RCH activities in the District.
STRATEGY 1 6.2.9.1 Major Civil Works
Activity (i) PHC Construction: Construction of PHC Senvon, PHC Singngat needs to be undertaken. Presently Senvon PHC has kaccha local made building. Because of no building, various health activities and programme could not be implemented properly and executed in time. PHC Renovation: Patpuihmun PHC, Henglep PHC and Sinzawl PHC needs to be renovated along with approach road. Labour room construction: Construction of labour rooms in Sinzawl PHC and Singngat PHC needs to be undertaken as they face problems during delivery practices in a very small and congested room. PHC Staff Quarters: Repair/ Renovation of staff quarters along with compound fencing approach road in Saikot PHC and Thanlon PHC needs to be undertaken
STRATEGY 2
6.2.9.2 Minor Civil Works
Activity (i) Construction of PHSC: Twenty one identified PHSCs construction needs to be undertaken. Two new PHSC had been inaugurated in this current financial year 2009-10, but without building facility. The two PHSC are New Lamka PHSC and Sainoujang PHSC. The Total PHSC in the District after this two inclusion reaches to 66 PHSCs. The identified 10 SCs which need new construction in 2010-11:
1. Milongmun SC ( under Thanlon PHC), 2. Hanship SC ( under Thanlon PHC) 3. Phaibuong SC ( under Henglep PHC) 4. Ukha Loikhai SC ( under Henglep PHC) 5. Kangkap SC ( under Singngat PHC)

CCP PIP 2010-11
6. L Khengjang SC ( under Henglep PHC) 7. Sumtuh SC ( under Singngat PHC ) 8. Hiangtam K ( under Behiang PHC ) 9. Lungthulien SC ( under Parbung CHC ) 10. Parvachom SC ( under Senvon PHC ) 11. Sipuikon SC ( under Senvon PHC ) 12. Leisen SC( under Senvon PHC ) 13. Tuolbung SC ( under Parbung CHC )** 14. Chingmun SC( under Patpuihmun PHC ) 15. Hiangmual SC ( under Singngat PHC) 16. Khuangkhai SC ( under Saikot PHC) 17. Khaukual SC( under Saikot PHC ) 18. Kangreng SC ( under Patpuihmun PHC) 19. Ngampabung SC ( under Patpuihmun PHC) 20. Buangmun SC ( under Patpuihmun PHC ) 21. Suangdoh SC ( under Singngat PHC)
Out of the above given, PHSCs without building facilities, it is strongly desired that ten PHSCs construction be initiated this year. The 10 prioritize SC for construction – Suangdoh SC, Lungthulien SC, Kangkap SC, Sipuikon SC, Hanship SC, Hiangtam K SC, Hiangmual SC, Sumtuh SC, Milongmun SC, Khaukual SC for this year 2010-11.
Activity (ii) Repair/renovation of Subcentres: Seven identified Sub-Centre Buildings need to be renovated.
10. Bukpi SC ( under Thanlon PHC ) 11. Kaihlam SC ( under Thanlon PHC) 12. Allusingtam SC ( under Singngat PHC ) 13. Songtal SC ( under Sinzawl PHC) 14. Lungthulien SC ( under Parbung ) 15. Kangreng SC ( under Patpuihmun PHC ) 16. Ngampabung SC ( under Patpuihmun PHC )
PHSC construction of Labour room: Under DRDA, there is a provision to Construct, 64 PHSC labour rooms. So need for projection from the NRHM flexi pool budget.
PHSC upgradation to PHC: Zezaw PHSC under Singngat PHC and Sibapurikhal PHSC under Patpuihmun PHC had been up gradated to PHC where-in, it need Main Office building, Staff Quarters, Pucca compound fencing and approach road construction in 2010-11. However, it is strongly desire that Zezaw PHSC which was upgraded into PHC be constructed in this current year, leaving Sibapurikhal PHSC for the next year Additional proposal:
1. Construction of latrine/ lavatory complex for secretariat, District health society @ Rs 2 Lacs
2. Renovation of DFWO office complex @ Rs 25 Lacs

CCP PIP 2010-11
3. Construction of secretariat, district health society, complex to accommodate, DMO, DACO, DLO, DTO and DPMU @ Rs 50 Lacs
4. Construction of kitchen facilities in the District Hospital 5. Provision of bio-medical waste management pit at Singngat PHC 6. Extension for new born care corner@ Rs 0.30 lakhs at all PHC level 7. Construction of generator shed @ Rs 0.60 at those generator supplied
PHCs Activity (iii) other add-on facilities at DH, CHC and 24/7s PHCs
i.) Double telephone line for FRUs –DH be sanctioned @ Rs 0.80 ii.) Single telephone line for 2 24/7 PHCs @ Rs 0.30 An estimated amount of Rs 1.4 Lakhs will be needed in this connection iii.) Air conditioning installation at District Hospital at O.T section
@ Rs 1.0 Lac will be require. 6.2.10. Institutional Strengthening
Objective: To develop proper institutional structure for RCH service delivery STRATEGY 1 6.2.10.1 Human Resource Development Activity (i) Key persons in RCH not to be transferred before 3 years of service Activity (ii) Rationalization of posting place regular Health & FW staffs along with
formation of transparent Transfer & Posting Policy Activity (iii) Performance appraisal and reward system among Blocks and staffs Activity (iv) Developing a Transfer & Posting policy for contractual staffs Activity (v) Trainings both inside and outside District
STRATEGY 2 6.2.10.2 Logistics Management Activity (i) Additional Drugs and medicines needs to be supply Activity (ii) Monthly procurement of medicine and drugs from state authority Activity (iii) Special indent in times of necessity Activity (iv) Local purchase during calamities Activity (v) procurement of essentials drugs, medicines and others be made district level
STRATEGY 3 6.2.10.3 Monitoring and Evaluation / HMIS Activity (i) monthly, quarterly and annually reporting of Monitoring Reports Activity (ii) Installation of internet facility for web based reporting system Activity (iii) Weekly field visits by ANM/FHS Activity (iv) Forthrightly field supervision by MO PHCs. Activity (vi) Monthly field visits by DNO (ME) Activity (vi) Holding of monthly PHC level and District level review meeting

CCP PIP 2010-11
Activity (vii) Orientation of HMIS workshops for BPMU, ANMs Activity (viii) Sensitization programme for DH, FW Statistical staff 6.2.11 BCC/IEC ( Behavioral Change Communication):
• Develop a strategic media mix as per the target population and issues (Child Health, Maternal Health/ Family Planning)
a) Interpersonal communications
• Counseling at DH -FRU, 24/7 PHCs
• One to one interaction by ASHAs/ANMs/AWWs
• Group discussions at village/ block/ VAs level • Community meetings
• Workshops at blocks level
b) Community media
1. Street Plays 2. Health Mela
c) Outdoor Media:
1. Banners 2. Pamphlets 3. Posters
d) Capacity building and Training of manpower
1. Capacity building of staffs 2. Internal workshops 3. Mid term monitoring 4. Evaluation of the programme
Other systems which can be effective for BCC Talks in local cable TV on entire NRHM programme-since the district have Hornbill, ZRS, TCN, Angel Vision, and Laijom-where the scribers/ viewers are from different community background
• Lecture in Church services–during casual church services Folk artists –especially thadou kuki and Mizo dialects is popular
• Hill area: Folk-Dance Troupes ( Mizo dance and others) Equipment Requirement: LCD Projector, Digital Camera for support to Documentation. For this procurement, an estimated amount of Rs 2.0 Lacs is require Procurement of LCD Projector and its accessories Objective: To appraise the health behaviour of the people and to improve the health behaviour so that the health seeking behaviour for maternity, child and family planning
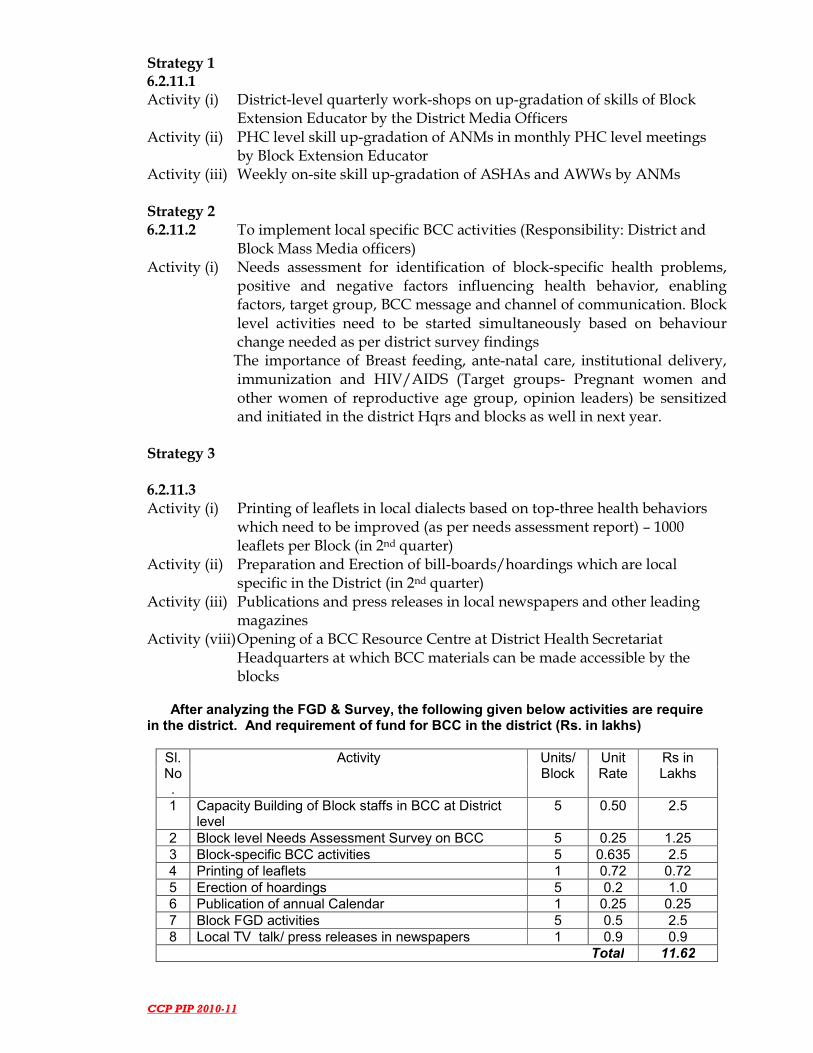
CCP PIP 2010-11
Strategy 1 6.2.11.1 Activity (i) District-level quarterly work-shops on up-gradation of skills of Block
Extension Educator by the District Media Officers Activity (ii) PHC level skill up-gradation of ANMs in monthly PHC level meetings
by Block Extension Educator Activity (iii) Weekly on-site skill up-gradation of ASHAs and AWWs by ANMs Strategy 2 6.2.11.2 To implement local specific BCC activities (Responsibility: District and
Block Mass Media officers) Activity (i) Needs assessment for identification of block-specific health problems,
positive and negative factors influencing health behavior, enabling factors, target group, BCC message and channel of communication. Block level activities need to be started simultaneously based on behaviour change needed as per district survey findings
The importance of Breast feeding, ante-natal care, institutional delivery, immunization and HIV/AIDS (Target groups- Pregnant women and other women of reproductive age group, opinion leaders) be sensitized and initiated in the district Hqrs and blocks as well in next year.
Strategy 3 6.2.11.3 Activity (i) Printing of leaflets in local dialects based on top-three health behaviors
which need to be improved (as per needs assessment report) – 1000 leaflets per Block (in 2nd quarter)
Activity (ii) Preparation and Erection of bill-boards/hoardings which are local specific in the District (in 2nd quarter)
Activity (iii) Publications and press releases in local newspapers and other leading magazines
Activity (viii) Opening of a BCC Resource Centre at District Health Secretariat Headquarters at which BCC materials can be made accessible by the blocks
After analyzing the FGD & Survey, the following given below activities are require
in the district. And requirement of fund for BCC in the district (Rs. in lakhs)
Sl. No.
Activity Units/ Block
Unit Rate
Rs in Lakhs
1 Capacity Building of Block staffs in BCC at District level
5 0.50 2.5
2 Block level Needs Assessment Survey on BCC 5 0.25 1.25 3 Block-specific BCC activities 5 0.635 2.5 4 Printing of leaflets 1 0.72 0.72 5 Erection of hoardings 5 0.2 1.0 6 Publication of annual Calendar 1 0.25 0.25 7 Block FGD activities 5 0.5 2.5 8 Local TV talk/ press releases in newspapers 1 0.9 0.9 Total 11.62

CCP PIP 2010-11
6.2.12 Procurement
The District is in needs of furniture and others essential materials for running the office of the BPMU and DPMU office smoothly. Supply of furniture and others materials for PHC and PHSCs. Even complete sets of essential furniture and chairs have not been issued to the District so far.
6.2 Program Management Objective: To strengthen the program management at District and Block levels
STRATEGY 1 6.2.14.2 District Program Management Units
Activity (i) Continuation of the contractual services of DPM, DFM and DDM Activity (ii) Procurement of Slide projector for conducting any workshop/ training Activity (iii) Allocation of separate vehicle for DPMU for M&E Activity (iv) Sanction of fund for M& E activities (detailed reflect at Part B) Activity (v) Provision of Xerox machine Activity (vi) Provision to increase Honorarium for DPMU staffs Activity (vii) Provision of LCD projector Activity (viii) Provision of Digital camera for documentation support Activity (ix) 6.2.12.3 Strengthening of Finance Management System Activity
Activity (i) Adoption of Financial delegation power at District level as per MoHFW,
GoI guidelines Activity (ii) Release of fund to Blocks within 02 weeks of receiving fund from State. Activity (iii) Ensure that FMR from Blocks to District be submitted in time. Activity (iv) Review of Physical and Financial Achievement at DC level.
6.3 Quality assurance A District Quality Assurance Committee (DQAC) is already formed under the
chairmanship of the District Deputy Commissioner strictly following the GoI guidelines. The DQAC Teams will to look after the quality of care provided for all the services provided under RCH-II.

CCP PIP 2010-11

CCP PIP 2010-11
DISTRICT TRAINING PLAN FOR 2010-11
1. SBA Training Situation:
(i) Total nurse/ANM available - 117 (ii) No. of nurse/ANM trained - 40 (iii) Number to be trained - 76 (iv.) Number to be train in 2010-11 - 76 (All) (v) SBA trainers - Available (vi.) Centres where Trg can be taken up - District Hospital, Churachandpur
SBA Trg for Nurse/ ANM in 2010-11
No. of trainees
No. of batches
Venue of training
Trainers Duration of Trg.
Time-line for Trg.
Budget requirement
76 76 nurse/ ANM having core skills
12 batches of 6 trainees
District Hospital , CCPur
4 Trainers From District doctors
Monthly April to March ( 12 batches) 1 batch for 1 month
(i) Hon for 4 trainers @ 300 per day per head = Rs. 33,600 (ii) Hon for trainees @ 200 per day per head = Rs. 4,25,600 (iii) Training material @ Rs. 300 per head (iv) Overhead Exp. / Cont. = Rs. 2,500 per batch
Rs. 3,36,000 Rs.4,25,600 Rs. 1,32,000 Rs.25,000
Total Rs.9.18 lakhs 2. Blood Storage

CCP PIP 2010-11
Situation: (i) No. of FRUs - 01 (ii) Total MO/LT trained - 01each (iii) Number not yet trained - 39 MOs & 9 LT (iv.) Number to be trained 2010-11 - 10 MOs & 4 LT
Blood storage Trg for MO & LT in 2010-11
No. of trainees
No. of batches
Venue of training
Trainers Duration of trg.
Time-line for trg.
Budget requirement
14 (MO+ LT)
14 4 batches off 5 MOs per batch & 2 LT per batch
DH-CCPur
State / District Doctors
03 days May to Aug ‘10-11
(i) Hon for 2 trainers @ 300 per day per head = Rs. 1,800 (ii) Hon for trainees @ 200 per day per head = Rs.84,00 (iii) Training material @ Rs. 300 per head = 600 (iv) Overhead Exp. /contingency = Rs. 2,000 per batch
Rs. 7,200 Rs, 84,00 Rs, 2,400 Rs, 8,000
Total 0.26 lakhs
3. RTI/STI training
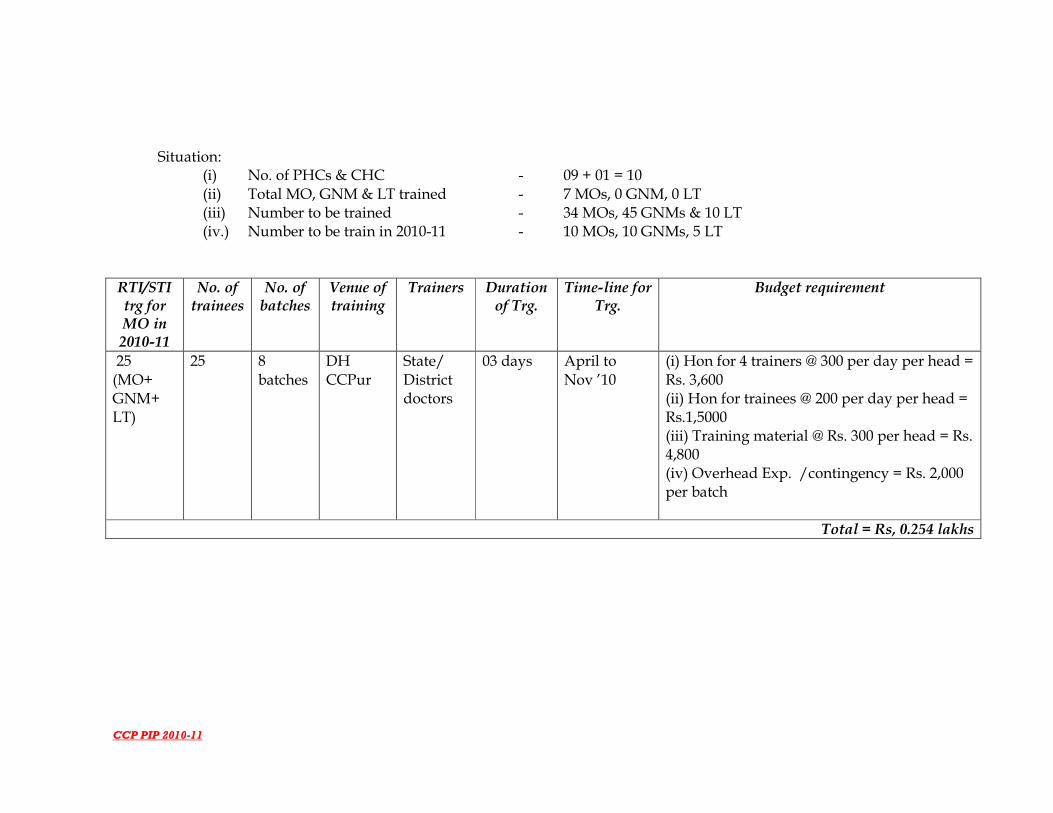
CCP PIP 2010-11
Situation: (i) No. of PHCs & CHC - 09 + 01 = 10 (ii) Total MO, GNM & LT trained - 7 MOs, 0 GNM, 0 LT (iii) Number to be trained - 34 MOs, 45 GNMs & 10 LT (iv.) Number to be train in 2010-11 - 10 MOs, 10 GNMs, 5 LT
RTI/STI trg for MO in 2010-11
No. of trainees
No. of batches
Venue of training
Trainers Duration of Trg.
Time-line for Trg.
Budget requirement
25 (MO+ GNM+ LT)
25 8 batches
DH CCPur
State/ District doctors
03 days April to Nov ’10
(i) Hon for 4 trainers @ 300 per day per head = Rs. 3,600 (ii) Hon for trainees @ 200 per day per head = Rs.1,5000 (iii) Training material @ Rs. 300 per head = Rs. 4,800 (iv) Overhead Exp. /contingency = Rs. 2,000 per batch
Total = Rs, 0.254 lakhs

CCP PIP 2010-11
4 MTP training Situation:
(i) No. of FRUs having MTP services - 01 (ii) Number of other institutions having MTP Services - 0 (iii) Number to be trained - 41 MOs, 45 GNMs (iv.) Number to be train in 2010-11 - 5 MOs, 5 GNM (v) Trainers - Available
: No. of trainees
No. of batches
Venue of training
Trainers Duration of Trg.
Time-line for Trg.
Input needed per batch Budget requirement
10 (MO + GNM)
2 batches
DH CCPur
2 District doctors
05 days
July – Aug ’10
(i) Hon for 2 trainers @ 300 per day per head = Rs. 3,000 (ii) Hon for trainees @ 200 per day per head = Rs.10,000 (iii) Training material @ Rs. 300 per head = Rs.600 (iv) Overhead Exp. /contingency = Rs. 2,000 per batch
Rs. 48,000 Rs. 10,000 Rs. 9,000 Rs. 32,000
Total 0.99 lakhs
5. Life Saving Anesthesia Skills

CCP PIP 2010-11
Situation: (i) No. of FRUs having Anesthesia facility - 01 (ii) Number to be trained - 05 MO (iii) Number to be train in 2010-11 - 05 MO (iv.) Trainers - Available
No. of trainees
No. of batches
Venue of training
Trainers Duration of trg.
Time-line for trg. Budget requirement
05 05 in 01 batches
DH CCPur
District/ State
18 weeks (126 days)
July – Nov ‘10 (i) Hon for 4 trainers @ 500 per day per head = Rs.2,56,000 (ii) Hon for trainees @ 300 per day per head = Rs.189000 (iii) Training material @ Rs. 1000 per head = Rs.1000 (iv) Overhead Exp. /contingency @ Rs. 5,000 (v) Institutional set up @ Rs. 1,00,000
Total Rs. 5.51 lakhs
6. NSV Training

CCP PIP 2010-11
Situation:
(i) Number to be trained - 4 MOs (ii) Number not yet trained - 37 MOs (iii) Number to be train in 2010-11 - 10 MOs (iv.) Trainers - Available
No. of trainees
No. of batches
Venue of training
Trainers Duration of trg.
Time-line for trg.
Budget requirement
10 MOs 02 batches of 05 trainees
DH CCPur
State/Dist 5 days July-Aug ’10
(i) Hon for 01trainers @ Rs.2000 per day per head = Rs.10,000 (ii) Hon for trainees @ 400 per day per head = Rs.20,000 (iii) Training material per batch= Rs.12,000 (iv) Overhead Exp. /contingency @ Rs. 20,000 per batch
Total 0.62 lakhs

CCP PIP 2010-11
7. IMNCI training Situation:
(i) No. of institution having neonatal care services - 01 (ii) Number to be trained - 27 MOs, 113 ANMs (iii) Number to be train in 2010-11 - 20 MOs, 15 ANMs
IMNCI Trg of MOs & ANMs
No. of trainees
No. of batches
Venue of training
Trainers Duration of Trg.
Time-line for Trg.
Budget requirement
35 (MO+ ANM)
35 02 batch DH CCPur
State/ Dist Trainers
10 days
April & May ’10
(i)Hon for 4 trainers @ 400 per day per head = Rs. 16,000 (ii) Hon for trainees @ 200 per day per head = Rs.70000 (iii) Training material @ Rs. 500 per head = Rs.10,000 (iv) Overhead Exp. /contingency = Rs. 30,000 per batch
Total=Rs. 1.26 lakhs

CCP PIP 2010-11
8. ARSH training (i) No. to be trained - 20 School teachers (ii) No of school teaches not yet trained - (iii) No of school teachers to train in 2010-11 - 20 teachers
No of
teachers to be train
No. of batches
Venue of training
Trainers Duration of Trg.
Time-line for Trg.
Budget requirement
20 01 CMO conference hall
State/ Dist Trainers
03 days
June 10 (i)Hon for 5 trainers @ 500 per day per head = Rs. 4,500 (ii) Hon for trainees @ 200 per day per head = Rs.12000 (iii) Training material @ Rs. 100 per head = Rs.3,000 (iv) Overhead Exp. /contingency = Rs. 30,000 per batch
Total = Rs.0.50 lakhs
9. Training of MOs on IMEP for 2 days

CCP PIP 2010-11
No. already trained
No. to be trained
No. of batches
Place of training
Budget per batch
Particulars Amount (Rs. in lakhs)
09 10 02 (MOs of DHs and PHCs)
DH Hospital Honorarium for 5 trainers @ Rs. 500/- per day X2 days 0.05
Honorarium for 10 trainees @ Rs. 200 per head per day X 2 days 0.04
Training material @ Rs. 100/- per trainee for 10 trainees 0.001
Overhead expenditure, refreshment & other contingencies 0.10
Total 0.91
10. Teachers on School Health for 02 days
No. already trained
No. to be
trained
No. of batches
Place of training
Budget per batch
Particulars Amount (Rs. in lakhs)
00 20 02 (in batches of 10)
CMO conference Hall Churachandpur
Honorarium for 5 trainers @ Rs. 500/- per day X2 days 0.05
Honorarium for 20 trainees @ Rs. 200 per head per day X 2 days 0.08
Training material @ Rs. 200/- per trainee for 20 trainees 0.04
Overhead expenditure, refreshment & other contingencies 0.10
Total
0.27

CCP PIP 2010-11
CALENDAR OF TRAINING ACTIVITIES FOR 2010-11
1. April to March, 2010 : Training of ANMs in SBA, MOs in IMNCI 2. May, 2010 : Training of MOs in Blood Storage 3. June & July 2010 : Training of MOs, school teachers in ARSH 4. August, 2010 : Training of MOs in NSV 5. September, 2010 : Training of specialists in LSA 6 October, 2010 : Training of doctors in RTI/STI 6 October & November, 2010 : Training of doctors in MVA, MTP 7 November, 2010 : Training of ASHA 8 December, 2010 : Training of AYUSH doctors

CCP PIP 2010-11

CCP PIP 2010-11
6.5 Gender Equity As stated earlier 6.6 Financial management: Fund from State to the District to Blocks is already executed through e-banking system. The money need be released on time to the District so that further released to the Blocks be ensure in time for any program implementation without delay as most of the national programme are time bound activities. 6.7. Convergence/Coordination
So far convergence/coordination with WCD, Education, PRI, and AYUSH has
been established. Coordination with PHED and PWD needs to be strengthened. Activities needing intervention from the Health determinant Departments may be highlighted to the concerned Department in the Society Meetings at the District. The above mentioned Departments be members of district health society at any cost and frequent meetings be held in the district level so that convenient and understanding between the departmental could be chalked out.
6.8 District, Block and Village Health plans All the existing 5 blocks (Singngat, Tipaimukh, Thanlon, Henglep and Samulamlan) have submitted their Integrated Village, Block health Plans on 10th Dec 2009 for the year 2009-10. To enable the Integrated District Health Action Plan effective and useful, a special survey be conducted in the year to come so that the data is reliable to the nearest value. For this an amount of Rs 5 lacs will be required. The VHAP, BHAP is enclosed. 6.9 Role of District, Blocks and Villages Details reflected in Work-Plan.
6.10 Synergy with NRHM Additional ties: Construction for buildings building-less Sub-centres, Up-gradation of District Hospital and Community Health Centres to IPHS level, Decentralization of power to DH/CHC/PHCs by forming Rogi Kalyan Samitis will have synergistic effect with RCH-II.
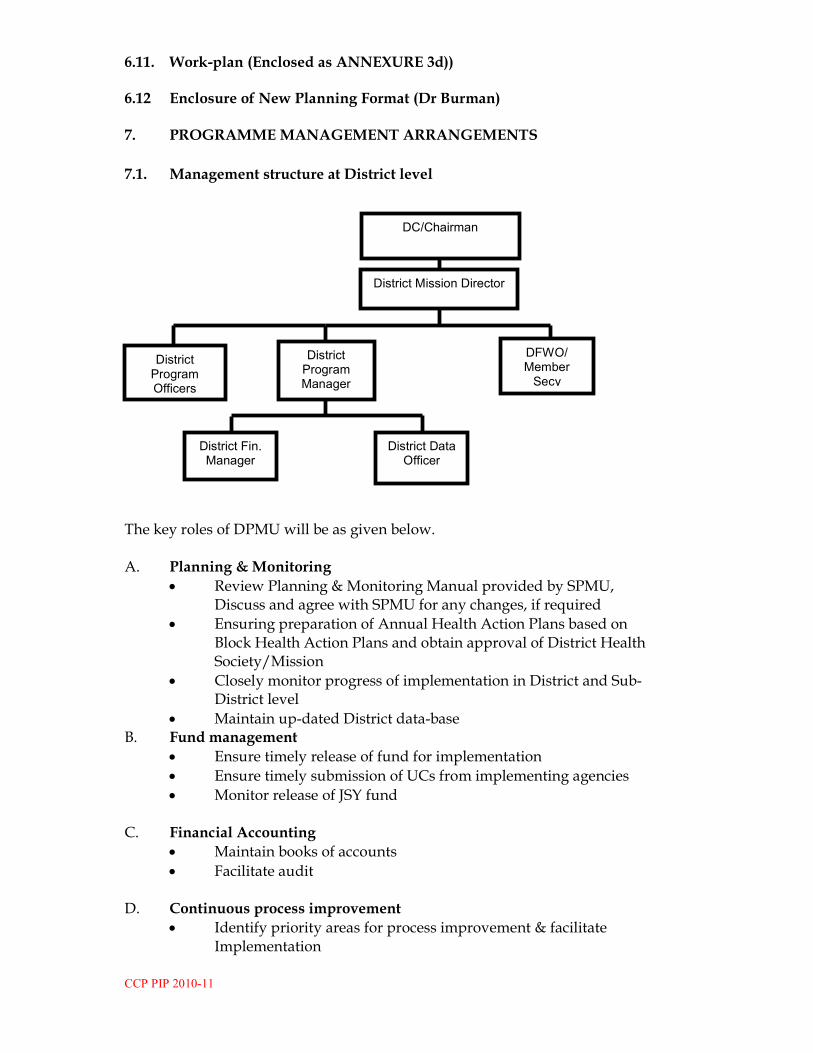
CCP PIP 2010-11
6.11. Work-plan (Enclosed as ANNEXURE 3d)) 6.12 Enclosure of New Planning Format (Dr Burman) 7. PROGRAMME MANAGEMENT ARRANGEMENTS
7.1. Management structure at District level
The key roles of DPMU will be as given below. A. Planning & Monitoring
• Review Planning & Monitoring Manual provided by SPMU, Discuss and agree with SPMU for any changes, if required
• Ensuring preparation of Annual Health Action Plans based on Block Health Action Plans and obtain approval of District Health Society/Mission
• Closely monitor progress of implementation in District and Sub- District level
• Maintain up-dated District data-base B. Fund management
• Ensure timely release of fund for implementation
• Ensure timely submission of UCs from implementing agencies
• Monitor release of JSY fund C. Financial Accounting
• Maintain books of accounts
• Facilitate audit D. Continuous process improvement
• Identify priority areas for process improvement & facilitate Implementation
DC/Chairman
District Mission Director
District Fin. Manager
District Program Manager
District Program Officers
DFWO/ Member Secy
District Data Officer

CCP PIP 2010-11
E. Administrative
• Secretariat function to District Health Society 7.2 DPM
� Planning & Monitoring � Financial management/ Accounting � District data-base maintenance � Continuous process improvement � Administrative functions � Basis for performance-appraisal
o Annual DHAP prepared on time o Monthly & quarterly Monitoring Reports prepared and analyzed before
10th of each month o Number of process improvement proposals prepared & implemented o Arrangement of meetings of State Health Mission/ Society made
including preparation of agenda notes, recording of minutes 7.3 DFM
� Ensuring timely release of funds to implementing agencies � Ensuring submission of UC/ SoE from implementing agencies � Maintain books of accounts � Facilitate audit � Basis for performance-appraisal
o Maintenance of books of accounts o Monthly/ Yearly closing of accounts in time o No outstanding UC with the District o Number of audit objections
7.4 DDM
� Maintenance of up-dated district data-base � Assist DPM in preparation of monthly progress reports, development of
DHAP, routine monitoring � Basis for performance-appraisal
• Data-base maintenance
• Physical & Financial reports compiled
8. BUDGET (Enclosed as AMMEXURES 3c, 3e and 3f)
9. MONITORING AND EVALUATION
The New MIES format prepared by GoI is already implemented in the District which is web based technique. Necessary modification in registration is done in on-line and printing of formats at various levels including the blocks of reporting is done. The M& E Section be strengthening into more accountable. Due to frequent change of reporting format, the District Nodal Officer M& E find difficult to cope with the complexity and its tedious job of reporting. In order to make the reporting and

CCP PIP 2010-11
evaluation easier, an assistant data entry be sanctioned, internet connectivity facility be sanctioned too. The detailed budget for M&E is reflected at HMIS section in Part B
10. SUSTAINABILITY
User charges are to be maintained at the health facilities wherever Rogi Kalyan
Samitis are formed under NRHM. Also, the District budget allocation is being increased from Rs 10 Crores Approx. (2008-09), Rs 8 Approx. Crores (2009-10) giving a percentage decrease from 46 %, to 36 % respectively in the last _years

CCP PIP 2010-11

CCP PIP 2010-11
Budget head 09-10 (Actual expenditu
re)
09-10 (Actual/ estimated expenditu
re)
2010-11
RCH-II NRHM
State share
Total
1Q 2Q 3Q 4Q Total
Rs. in lakhs %
1. Maternal Health
(a) JSY 7.53 7.53 7.53 7.53 30.13 30.13 30.13
(b) Others 1.11 1.56 0.62 0.63 2.57 2.57 2.57
Sub-total 9.11 9.56 8.62 8.63 34.57 34.57 34.57
2. Child Health 6.25 6.25 6.25 6.25 25.0 25.0 25.0
3. Family Planning 1.45 1.45 1.45 1.45 9.80 9.80 9.80
4. ARSH 0.06 0.023 0.10 0.10 0.58 0.58 0.58
5. Urban Health 0.0 0.0 0.0 2.37 2.37 2.37 2.37
6. Tribal Health 0.0 0.0 0.0 0.0 0.0 0.0 0.0
7. Vulnerable groups 1.0 1.0 1.0 1.0 4.0 4.0 4.0
8. Innovations 2.47 2.47 2.47 2.47 9.91 9.91 9.91
9. Infrastructure & Human resources
Reflected at part B
21.5 21.5 21.5 21.5 84.2 84.2 84.2
10. Institutional strengthening**
Reflected at part B
67.5 259.13 78.5 78.5 483.63 483.63 483.63
11. Training 4.64 4.64 4.64 4.64 18.57 18.57 18.57
12. BCC 2.905 2.905 2.905 2.905 11.62 11.62 11.62
13.PcPNDT 0.0 0.0 0.0 0.0 0.0 0.0 0.0
14. DHAP 0.0 5.0 0.0 0.0 5.0 5.0 5.0
.015. Procurement
16. Prog. Management 2.65 2.65 2.65 2.65 10.6 10.6 10.6
Total 30.065 35.478 29.625 31.995 127.163 127.163 127.163
Summary Budget
ANNEXURE 3c

CCP PIP 2010-11
ANNEXURE 3d
ANNUAL WORK PLAN 2010-11
Strategy/ Activity Timeline Responsibility (State/ Dist)
Source of fund
1. Maternal Health 1Q 2Q 3Q 4Q
1.1. Operationalize facilities
1.1.1. Operationalize DHs/ CHCs as FRUs
1.1.1.1. Organize dissemination workshops for FRU guidelines
1.1.1.2. Prepare plan for operationalization District RCH-II/ NRHM
1.1.1.3. Monitor progress against plan District RCH-II
1.1.1.4 Monitor quality of service delivery & utilization District RCH-II
1.1.2. Operationalize 24/7 PHCs
1.1.2.1 Prepare plan for operationalization of 24/7 PHCs District RCH-II/ NRHM
1.1.2.2. Monitor progress against plan District RCH-II
1.1.2.3. Monitor quality of service delivery & utilization District RCH-II
1.1.3. Operationalize safe Abortion Services
1.1.3.1. Prepare plan for operationalization RCH-II
1.1.3.2. Monitor progress against plan District RCH-II
1.1.3.3. Monitor quality of service delivery & utilization District RCH-II
1.1.4. Operationalize RTI/STI Services
1.1.4.1. Prepare plan for operationalization RCH-II
1.1.4.2. Monitor progress against plan District RCH-II
1.1.4.3. Monitor quality of service delivery & utilization District RCH-II
1.1.5. Operationalize Sub-Centres
1.1.5.1 Prepare plan for operationalization RCH-II
1.1.5.2 Monitor quality of service delivery & utilization District RCH-II

CCP PIP 2010-11
1.2. Referral transport
1.2.1. Prepare & disseminate guidelines for referral transport for PW & sick children
RCH-II
1.2.2. Implementation by Districts Dist NRHM
Strategy/ Activity Timeline Responsibility (State/ Dist)
Source of fund 1Q 2Q 3Q 4Q
1.3. Integrated outreach RCH camps
1.3.1. RCH Outreach camps in under-served areas
1.3.1.1. Implementation by Districts District RCH-II
1.3.1.2. Monitor quality of service delivery & utilization District RCH-II
1.3.2. Monthly VH & NDs at AWCs
1.3.2.1. Implementation by Districts District NRHM
1.3.2.1. Monitor quality of service delivery & utilization District RCH-II
1.4. JSY
1.4.1. Dissemination of guidelines to Sub-district level RCH-II
1.4.2. Implementation by Districts District RCH-II
1.4.3. Monitor quality & utilization State/ Dist RCH-II
1.5. Other strategies/ innovations
1.4.2. development of Incentive of doctors, SN, ANM CHC, PHC & SCs
State/ Dist RCH-II
1.4.3. Performance-based incentive for trained MBBS Drs.
State/ Dist NRHM
1.4.4. Establishment of Training Centre at District District NRHM
1.4.5 Establishment of GNM Trg School State/ District NRHM
2. Child Health
2.1. IMNCI
2.1.1. Prepare operational plan District RCH-II
2.1.2. Implementation in Districts District RCH-II
2.1.3. Monitor progress against plan District RCH-II
2.2. FBNC
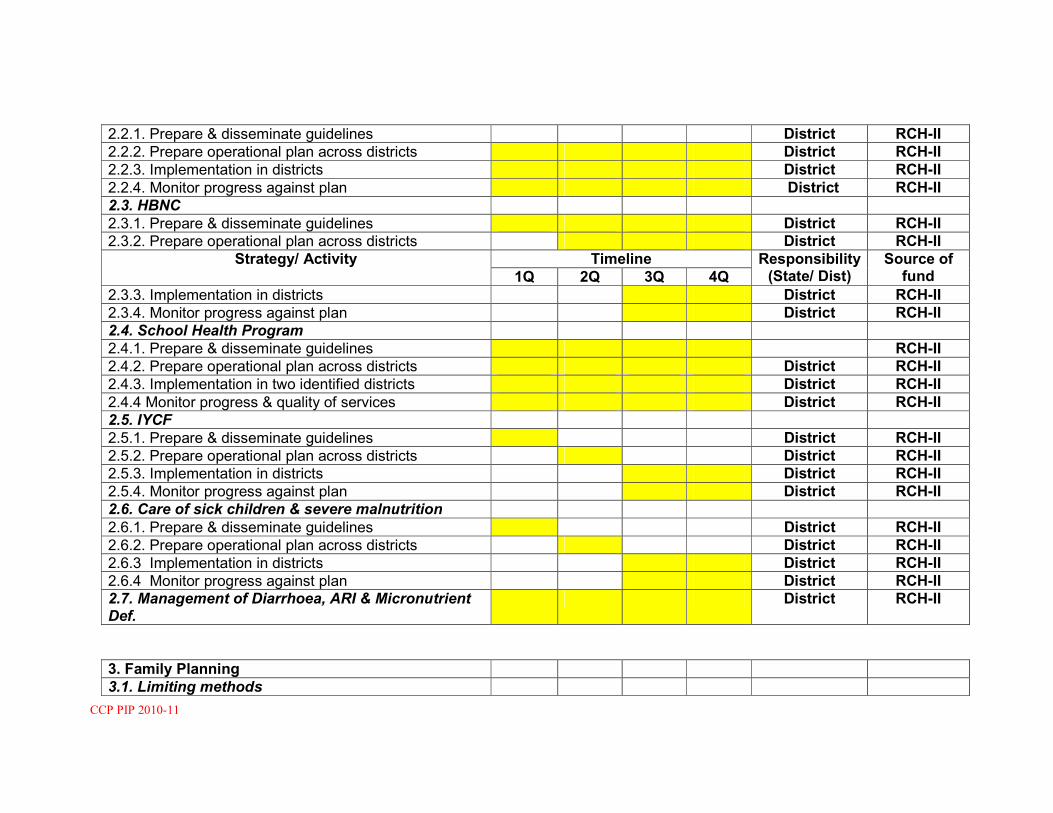
CCP PIP 2010-11
2.2.1. Prepare & disseminate guidelines District RCH-II
2.2.2. Prepare operational plan across districts District RCH-II
2.2.3. Implementation in districts District RCH-II
2.2.4. Monitor progress against plan District RCH-II
2.3. HBNC
2.3.1. Prepare & disseminate guidelines District RCH-II
2.3.2. Prepare operational plan across districts District RCH-II
Strategy/ Activity Timeline Responsibility (State/ Dist)
Source of fund 1Q 2Q 3Q 4Q
2.3.3. Implementation in districts District RCH-II
2.3.4. Monitor progress against plan District RCH-II
2.4. School Health Program
2.4.1. Prepare & disseminate guidelines RCH-II
2.4.2. Prepare operational plan across districts District RCH-II
2.4.3. Implementation in two identified districts District RCH-II
2.4.4 Monitor progress & quality of services District RCH-II
2.5. IYCF
2.5.1. Prepare & disseminate guidelines District RCH-II
2.5.2. Prepare operational plan across districts District RCH-II
2.5.3. Implementation in districts District RCH-II
2.5.4. Monitor progress against plan District RCH-II
2.6. Care of sick children & severe malnutrition
2.6.1. Prepare & disseminate guidelines District RCH-II
2.6.2. Prepare operational plan across districts District RCH-II
2.6.3 Implementation in districts District RCH-II
2.6.4 Monitor progress against plan District RCH-II
2.7. Management of Diarrhoea, ARI & Micronutrient Def.
District RCH-II
3. Family Planning
3.1. Limiting methods
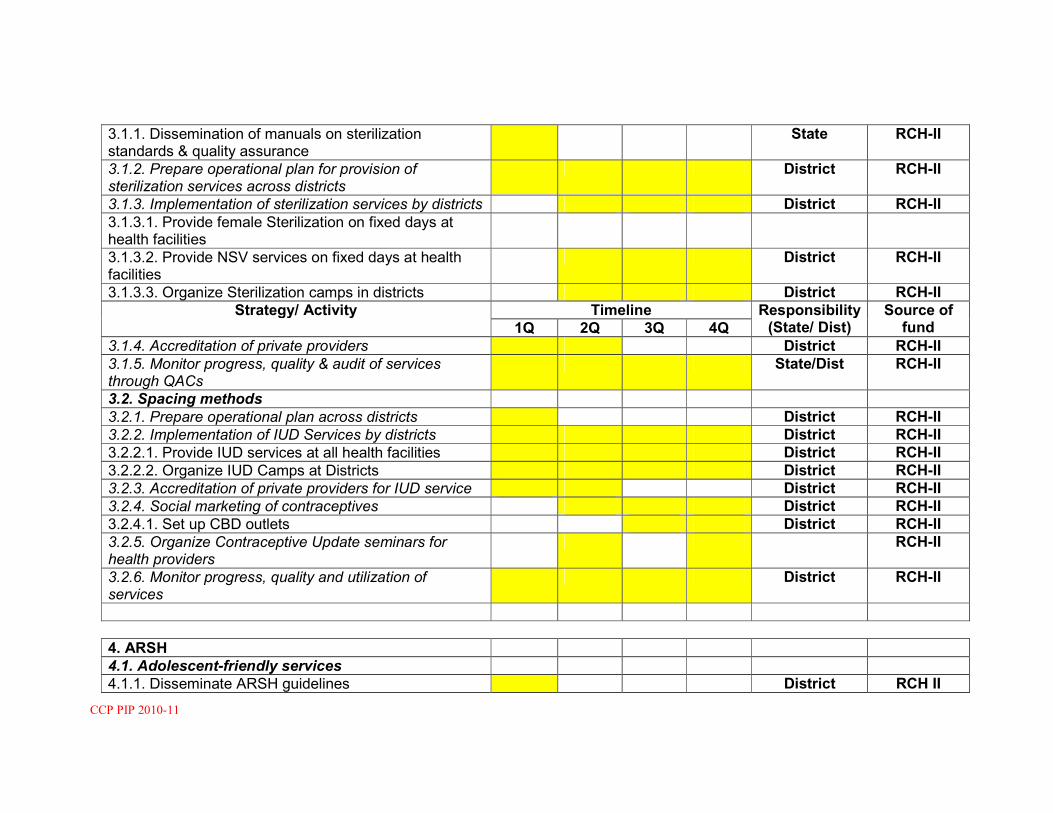
CCP PIP 2010-11
3.1.1. Dissemination of manuals on sterilization standards & quality assurance
State RCH-II
3.1.2. Prepare operational plan for provision of sterilization services across districts
District RCH-II
3.1.3. Implementation of sterilization services by districts District RCH-II
3.1.3.1. Provide female Sterilization on fixed days at health facilities
3.1.3.2. Provide NSV services on fixed days at health facilities
District RCH-II
3.1.3.3. Organize Sterilization camps in districts District RCH-II
Strategy/ Activity Timeline Responsibility (State/ Dist)
Source of fund 1Q 2Q 3Q 4Q
3.1.4. Accreditation of private providers District RCH-II
3.1.5. Monitor progress, quality & audit of services through QACs
State/Dist RCH-II
3.2. Spacing methods
3.2.1. Prepare operational plan across districts District RCH-II
3.2.2. Implementation of IUD Services by districts District RCH-II
3.2.2.1. Provide IUD services at all health facilities District RCH-II
3.2.2.2. Organize IUD Camps at Districts District RCH-II
3.2.3. Accreditation of private providers for IUD service District RCH-II
3.2.4. Social marketing of contraceptives District RCH-II
3.2.4.1. Set up CBD outlets District RCH-II
3.2.5. Organize Contraceptive Update seminars for health providers
RCH-II
3.2.6. Monitor progress, quality and utilization of services
District RCH-II
4. ARSH
4.1. Adolescent-friendly services
4.1.1. Disseminate ARSH guidelines District RCH II
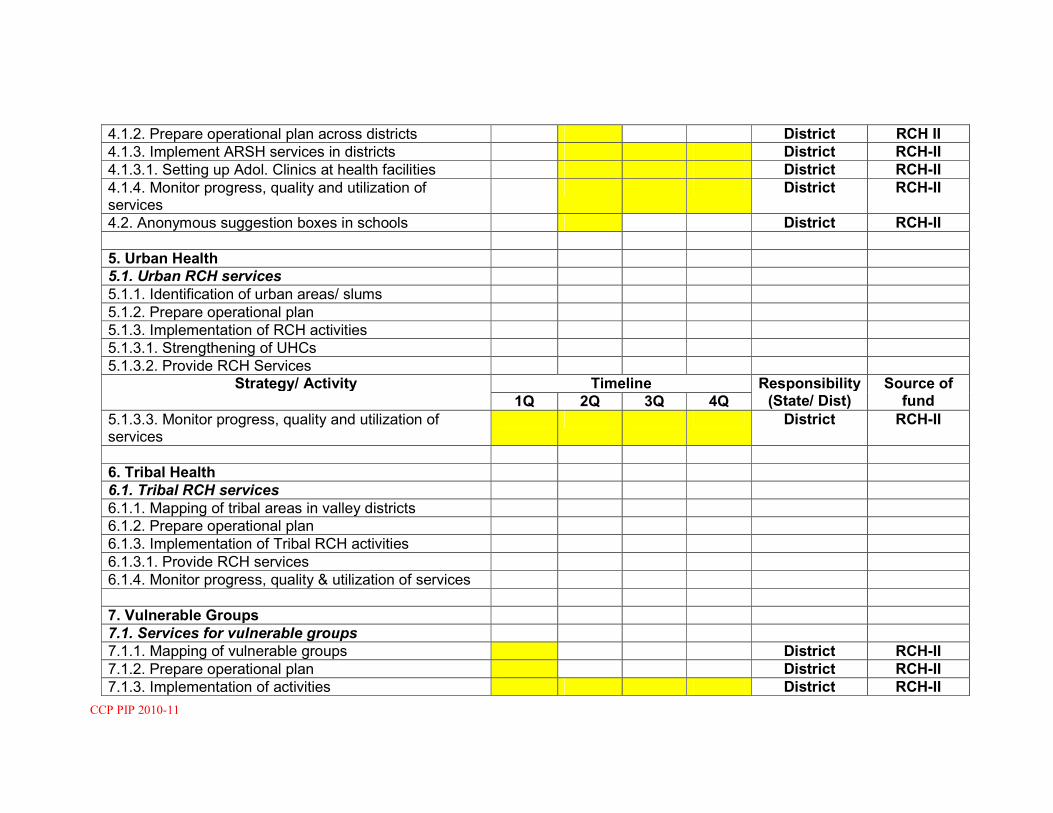
CCP PIP 2010-11
4.1.2. Prepare operational plan across districts District RCH II
4.1.3. Implement ARSH services in districts District RCH-II
4.1.3.1. Setting up Adol. Clinics at health facilities District RCH-II
4.1.4. Monitor progress, quality and utilization of services
District RCH-II
4.2. Anonymous suggestion boxes in schools District RCH-II
5. Urban Health
5.1. Urban RCH services
5.1.1. Identification of urban areas/ slums
5.1.2. Prepare operational plan
5.1.3. Implementation of RCH activities
5.1.3.1. Strengthening of UHCs
5.1.3.2. Provide RCH Services
Strategy/ Activity Timeline Responsibility (State/ Dist)
Source of fund 1Q 2Q 3Q 4Q
5.1.3.3. Monitor progress, quality and utilization of services
District RCH-II
6. Tribal Health
6.1. Tribal RCH services
6.1.1. Mapping of tribal areas in valley districts
6.1.2. Prepare operational plan
6.1.3. Implementation of Tribal RCH activities
6.1.3.1. Provide RCH services
6.1.4. Monitor progress, quality & utilization of services
7. Vulnerable Groups
7.1. Services for vulnerable groups
7.1.1. Mapping of vulnerable groups District RCH-II
7.1.2. Prepare operational plan District RCH-II
7.1.3. Implementation of activities District RCH-II

CCP PIP 2010-11
7.1.3.1. Provide RCH services District RCH-II
8. Innovations
8.1. PNDT and Sex ratio
8.1.1. Operationalize PNDT Cell
8.1.2. Orientation of Prog. Managers & service providers
8.1.3. Monitoring of sex ratio at birth
8.2. PPP
8.3. NGO Program
8.3. Weekly Radio Education Prog. For ASHAs
9. Infrastructure & human resources
9.1. Contractual staff & services
9.1.1. ANMs recruited & in position District RCH-II
9.1.2. LT recruited & in position District RCH-II
9.1.3. GNMs recruited & in position District RCH-II
Strategy/ Activity Timeline Responsibility (State/ Dist)
Source of fund 1Q 2Q 3Q 4Q
9.1.4. Specialist Doctors recruited & in position District RCH-II
9.1.5. PHNs recruited & in position
9.1.6. AYUSH Doctors recruited & in position
9.2. Major Civil Works
9.2.1. Major Civil Works for FRUs District RCH-II/NRHM
9.2.2. Major Civil Works for 24/7 PHCs District RCH-II
9.3. Minor Civil Works
9.3.1. Minor Civil Works for FRUs District RCH-II
9.3.2. Minor Civil Works for 24/7 PHCs District RCH-II
9.3.3. Minor Civil works for SCs District RCH-II
9.4. Operationalize IMEP
9.4.1. Organize IMEP workshops District RCH-II
9.4.2. Prepare operational plan across districts District RCH-II
9.4.3. Monitor progress against plan District RCH-II

CCP PIP 2010-11
10. Institutional strengthening
10.1. Human Resource Development
10.1.1. HR Consultant recruited & in position District RCH-II
10.1.2. Mapping of human resources District
10.1.3. Transfer & cadre structuring policy developed District
10.1.4. Performance appraisal & reward system developed
District RCH-II
10.1.5. Incentive policy for posting in under-served areas
District RCH-II
10.2. Logistic management
10.2.1. Identification Nodal Officer Logistic District RCH-II
10.2.2. Development of logistic plan & dissemination District RCH-II
10.3. Monitoring & Evaluation / HMIS
10.3.1. Strengthening of M & E Cell
10.3.1.1. M & E Consultant recruited & in position District RCH-II
10.3.1.2. Procurement of Computers/ Inter-net connectivity
District RCH-II
10.3.2. Operationalizing new HMIS format
10.3.2.1. Review of existing registers District RCH-II
10.3.2.2. Printing of new forms, registers District RCH-II
Strategy/ Activity Timeline Responsibility (State/ Dist)
Source of fund 1Q 2Q 3Q 4Q
10.3.2.3. Trg. of staffs State/Dist RCH-II
11. Training
11.1. Strengthening Trg. centres
11.1.1. Establishment of Trg Centre at Dist Dist RCH-II
11.2. Development of training packages
11.2.1. Translation /Development of training materials District RCH-II
11.2.2. Specialized trg equipment provide State/Dist RCH-II
11.3. Maternal Health Trg
11.3.1. SBA

CCP PIP 2010-11
11.3.1.3. Training of ANMs on SBA District RCH-II
11.3.2. EmOC Training District
11.3.2.1. Setting up of EmOC trg centre
11.3.2.2. Trg of MBBS Doctors on EmOC District RCH-II
11.3.3. Life saving Anaesthesia skills trg
11.3.3.1. Trg. Of MBBS Doctors District RCH-II
11.3.4. Trg on safe abortion services
11.3.4.1. TOT on safe abortion services District RCH-II
11.3.4.2. Trg. Of MBBS Doctors on MVA District RCH-II
11.3.5. RTI/STI Training
11.3.5.1. Trg. Of doctors on RTI/STI District RCH-II
11.3.5.2. Trg of LTs on RTI/STI District RCH-II
11.4. IMEP training
11.4.1. IMEP trg for state & district program managers District RCH-II
11.5. Child Health Training
11.5.1. IMNCI trg (pre & in-service) District RCH-II
11.5.1.1. IMNCI trg. For paramedics District RCH-II
11.5.2 FBNC
11.5.3.1. Trg. Of Doctors on FBNC District RCH-II
11.5.3.2. Trg. Of paramedics on FBNC District RCH-II
11.5.3. HBNC
Strategy/ Activity Timeline Responsibility (State/ Dist)
Source of fund 1Q 2Q 3Q 4Q
11.5.4.1. Trg of ASHAs on FBNC District RCH-II
11.6. Family Planning Training
11.6.1. Minilap training
11.6.1.1. MOs trg on minilap District RCH-II
11.6.2. NSV training District RCH-II
11.6.2.1. NSV trg for MOs
11.6.3. Contraceptive update training District RCH-II
11.7. ARSH
11.7.1 ARSH trg for MOs District RCH-II

CCP PIP 2010-11
11.7.2 ARSH trg for paramedics District RCH-II
12. BCC
12.1. Strengthening of BCC Cell at State & District
12.1.1. BCC Consultant recruited & in place District RCH-II
12.2. development of State BCC strategy State/Dist RCH-II
12.3. Implementation of BCC strategy
12.3.1. BCC activities based on DLHS-2 finding State/ Dist RCH-II
12.3.2. BCC activities based on CAN finding State/ Dist RCH-II
13. Procurement
13.1. Procurement of equipment
13.1.1. Procurement of RCH equipments
13.1.1.1. For PHCs District RCH-II/NRHM
13.1.1.2. For Sub-centres District RCH-II
13.1.1.3 For CHCs District NRHM
13.1.1.4. For District Hospitals District RCH-II
13.2. Procurement of drugs
13.2.1. Procurement from TNMSC
14. Program management
14.1. Strengthening of SPMSU
Strategy/ Activity Timeline Responsibility (State/ Dist)
Source of fund 1Q 2Q 3Q 4Q
14.1.1. SPMSU staff recruited & in position
14.1.2. Office maintenance & mobility support District RCH-II
14.2. Strengthening of DPMSU
14.2.1. DPMSU staff recruited & in position District RCH-II
14.2.2. Office maintenance & mobility support District RCH-II
14.3. Strengthening of Financial Management Systems

CCP PIP 2010-11
14.3.1. Formation of State Finance management group
14.3.2. Audits
14.3.2.1. Annual audit State RCH-II
14.3.2.2. Concurrent audit State RCH-II
ANNEXURE 3e
Detailed Budget 2010-11
Budget head Baseline/ Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual
1. Maternal health
1.1. Operationalise facilities health
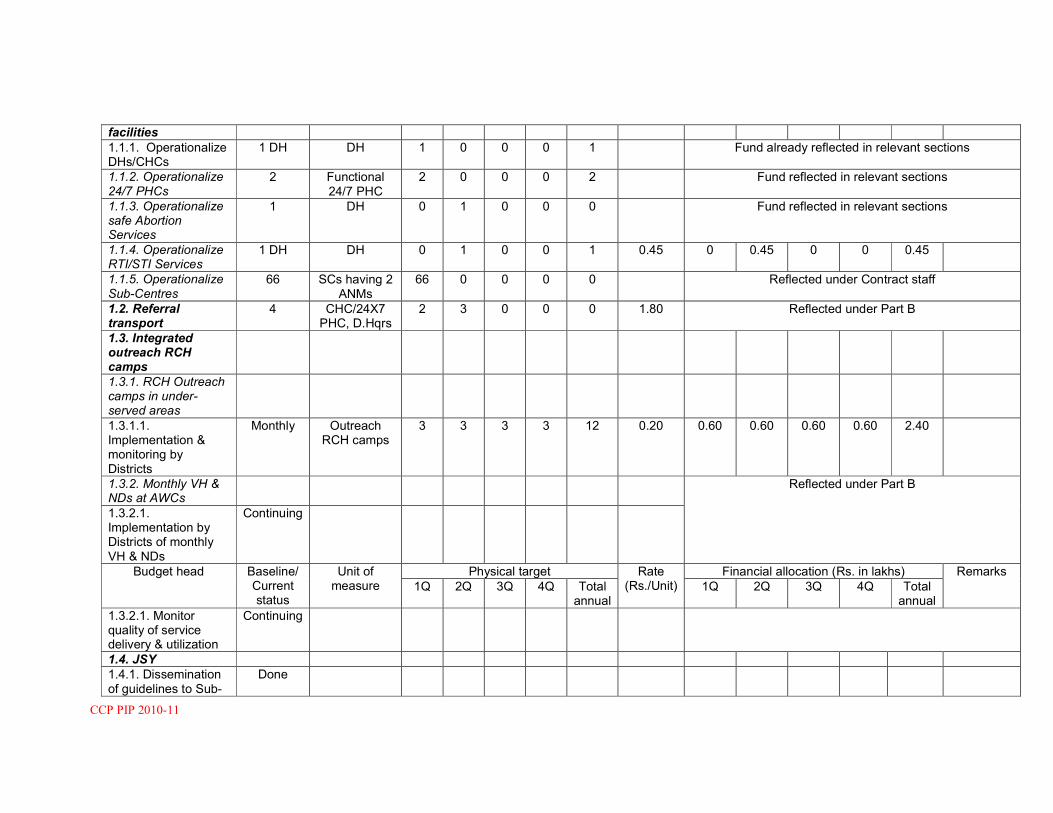
CCP PIP 2010-11
facilities
1.1.1. Operationalize DHs/CHCs
1 DH DH 1 0 0 0 1 Fund already reflected in relevant sections
1.1.2. Operationalize 24/7 PHCs
2 Functional 24/7 PHC
2 0 0 0 2 Fund reflected in relevant sections
1.1.3. Operationalize safe Abortion Services
1 DH 0 1 0 0 0 Fund reflected in relevant sections
1.1.4. Operationalize RTI/STI Services
1 DH DH 0 1 0 0 1 0.45 0 0.45 0 0 0.45
1.1.5. Operationalize Sub-Centres
66 SCs having 2 ANMs
66 0 0 0 0 Reflected under Contract staff
1.2. Referral transport
4 CHC/24X7 PHC, D.Hqrs
2 3 0 0 0 1.80 Reflected under Part B
1.3. Integrated outreach RCH camps
1.3.1. RCH Outreach camps in under-served areas
1.3.1.1. Implementation & monitoring by Districts
Monthly Outreach RCH camps
3 3 3 3 12 0.20 0.60 0.60 0.60 0.60 2.40
1.3.2. Monthly VH & NDs at AWCs
Reflected under Part B
1.3.2.1. Implementation by Districts of monthly VH & NDs
Continuing
Budget head Baseline/ Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual
1.3.2.1. Monitor quality of service delivery & utilization
Continuing
1.4. JSY
1.4.1. Dissemination of guidelines to Sub-
Done

CCP PIP 2010-11
district level
1.4.2. Implementation by Districts
1.4.2.1. Home deliveries
Home del 200 200 200 200 800 0.005 5.25 5.25 5.25 5.25 21.0
1.4.2.2. Institutional deliveries
Instl. Del 750 750 750 750 3000 0.007
1.0 1.0 1.0 1.0 4.0
1.4.2.3. ASHA packages & CS-sections
ASHA packages & CS- section
7.0
1.5. Other strategies/ innovations
1.4.2. Performance-based incentive of Addl. ANM at SCs
Reflected under Part
B
1.4.3. Performance-based incentive for trained MBBS Drs.
0 EmOC cases handled in 24/7 PHCs
5 5 10 20 40 0.01 0.05 0.05 0.01 0.02 0.13
1.4.4. Maternity Waiting Centres
1.4.5. ASHA scheme Budgeted under rel. sections
1.4.6. Maternal Death Auditing
0 Maternal deaths audited
1 1 1 1 4 0.01 0.01 0.01 0.01 0.01 0.04
Sub-total Maternal Health excluding JSY
Sub-total JSY 1.11 1.56 0.62 0.63 2.57
Budget head Baseline/
Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual
2. Child Health
2.1. IMNCI
2.1.1. Implementation in Districts
0 No. of District 1 0 0 0 1 Budget reflected in relevant sections
2.1.2. Monitor
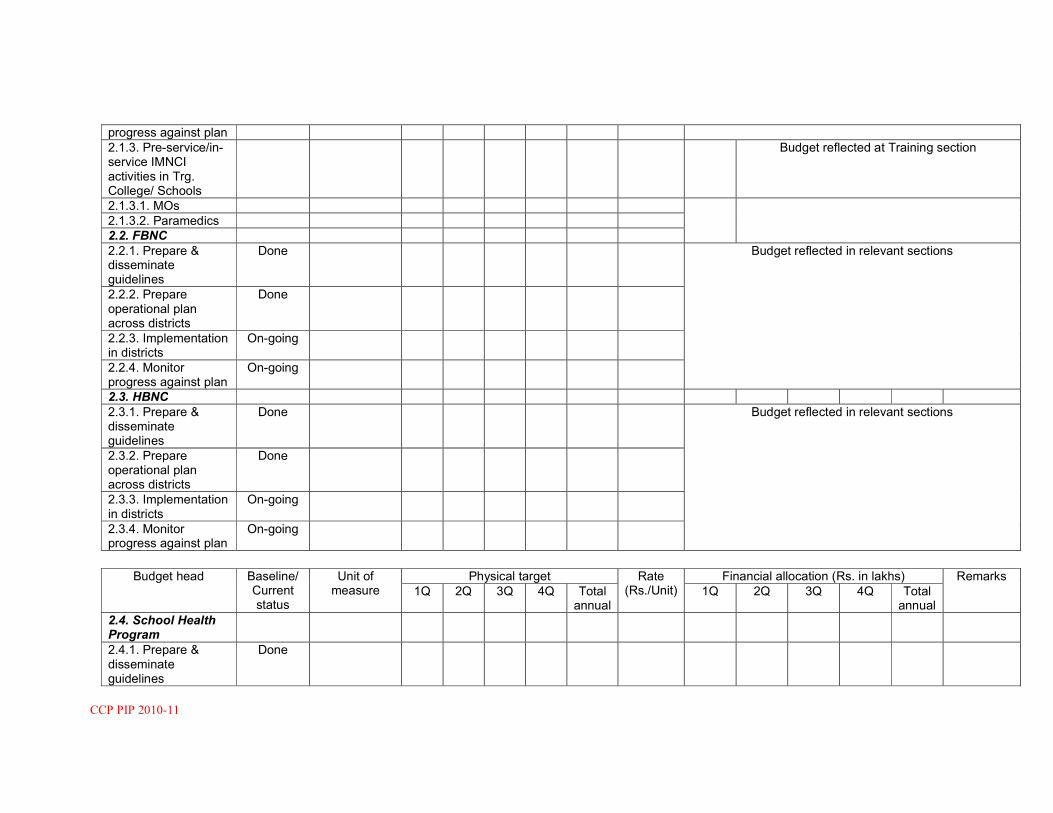
CCP PIP 2010-11
progress against plan
2.1.3. Pre-service/in-service IMNCI activities in Trg. College/ Schools
Budget reflected at Training section
2.1.3.1. MOs
2.1.3.2. Paramedics
2.2. FBNC
2.2.1. Prepare & disseminate guidelines
Done Budget reflected in relevant sections
2.2.2. Prepare operational plan across districts
Done
2.2.3. Implementation in districts
On-going
2.2.4. Monitor progress against plan
On-going
2.3. HBNC
2.3.1. Prepare & disseminate guidelines
Done Budget reflected in relevant sections
2.3.2. Prepare operational plan across districts
Done
2.3.3. Implementation in districts
On-going
2.3.4. Monitor progress against plan
On-going
Budget head Baseline/
Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual
2.4. School Health Program
2.4.1. Prepare & disseminate guidelines
Done

CCP PIP 2010-11
2.4.2. Prepare operational plan across districts
2.4.3. Implementation in two identified districts
Nil No. of operational District
5 5 5 5 20 1.25 6.25 6.25 6.25 6.25 25.0
2.4.4 Monitor progress & quality of services
2.5. IYCF
2.5.1. Prepare & disseminate guidelines
Done
2.5.2. Prepare operational plan across districts
Done
2.5.3. Implementation in districts
On-going
2.5.4. Monitor progress against plan
2.6. Care of sick children & severe malnutrition
2.6.1. Prepare & disseminate guidelines
2.6.2. Prepare operational plan across districts
2.6.3 Implementation in districts
Budget head Baseline/ Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual
2.6.4 Monitor progress against plan
2.7. Management of Diarrhoea, ARI & Micronutrient Def.

CCP PIP 2010-11
Sub-total Child Health
3. Family Planning
3.1. Limiting methods
3.1.1. Dissemination of manuals on sterilization standards & quality assurance
3.1.2. Prepare operational plan for provision of sterilization services across districts
3.1.3. Implementation of sterilization services by districts
Procurement of lap part printing,
Supervision,
1.00 1.00 1.00 1.00 4.00
3.1.3.1. Provide female Sterilization on fixed days at health facilities
M-10, F-300
No. of beneficiary
M-5; F-125
M-5; F-125
M-5; F-125
M-5; F-125
M-20; F-500
Budget reflected separately
3.1.3.2. Provide NSV services on fixed days at health facilities
3.1.3.3. Organize Sterilization camps in districts
Reflected separately
3.1.4. Accreditation of private providers
5 Accr. Pvt. providers
Subject to availability
Budget head Baseline/ Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual
3.1.5. Monitor progress, quality & audit of services through QACs

CCP PIP 2010-11
3.2. Spacing methods
3.2.1. Prepare operational plan across districts
3.2.2. Implementation of IUD Services by districts
3.2.2.1. Provide IUD services at all health facilities
1 1DH 1 CHC 11 PHC
No. of beneficiaries
500 500 500 500 2000 Motiv fee-
0.0002; Proc IUD set- 0.01
0.45 0.45 0.45 0.45 5.80
3.2.2.2. Organize IUD Camps at Districts
3.2.3. Accreditation of private providers for IUD service
4 Accr. Pvt. providers
Subject to availability
3.2.4. Social marketing of contraceptives
3.2.4.1. Set up CBD outlets
3.2.5. Organize Contraceptive Update seminars for health providers
1 Seminars 0 1 0 1 2 Budget reflected under Training
3.2.6. Monitor progress, quality and utilization of services
Budget head Baseline/ Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual
Sub-total Family Planning excluding Sterilization Compensation & NSV Camps

CCP PIP 2010-11
4. ARSH
4.1. Adolescent-friendly services
4.1.1. Disseminate ARSH guidelines
4.1.2. Prepare operational plan across districts
4.1.3. Implement ARSH services in districts
IUD kits 5 8 0 0 13 0.01 0.05 0.08 0 0 0.13
4.1.3.1. Setting up Adol. Clinics at health facilities
1 DH No. of health facilities having
weekly ARSH Clinics
1 1 1 1 4 Drugs @ 0.10
0.1 0.1 0.1 0.1 0.4
4.1.4. Monitor progress, quality and utilization of services
4.2. Anonymous Question boxes in schools
0 Schools having
operational Q. boxes
0 10 0 0 0 0.005 0 0.05 0 0 0.05
Sub-total ARSH
5. Urban Health
5.1. Urban RCH services
5.1.1. Identification of urban areas/ slums
Done
Budget head Baseline/ Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual
5.1.2. Prepare operational plan
Done
5.1.3. Implementation of RCH activities
5.1.3.1. Selection &

CCP PIP 2010-11
training of urban LWs
5.1.3.2. Strengthening of UHCs
5.1.3.3. Provide RCH Services
1 Functional UHC
0 0 0 1 1 2.37 0 0 0 2.37 2.37
5.1.3.4. Monitor progress, quality and utilization of services
6. Tribal Health
6.1. Tribal RCH services
6.1.1. Mapping of tribal areas in valley districts
6.1.2. Prepare operational plan
6.1.3. Implementation of Tribal RCH activities
6.1.3.1. Provide RCH services
6.1.4. Monitor progress, quality & utilization of services
Sub-total Tribal Health
Budget head Baseline/ Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual
7. Vulnerable Groups
7.1. Services for vulnerable groups
7.1.1. Mapping of vulnerable groups
Done
7.1.2. Prepare
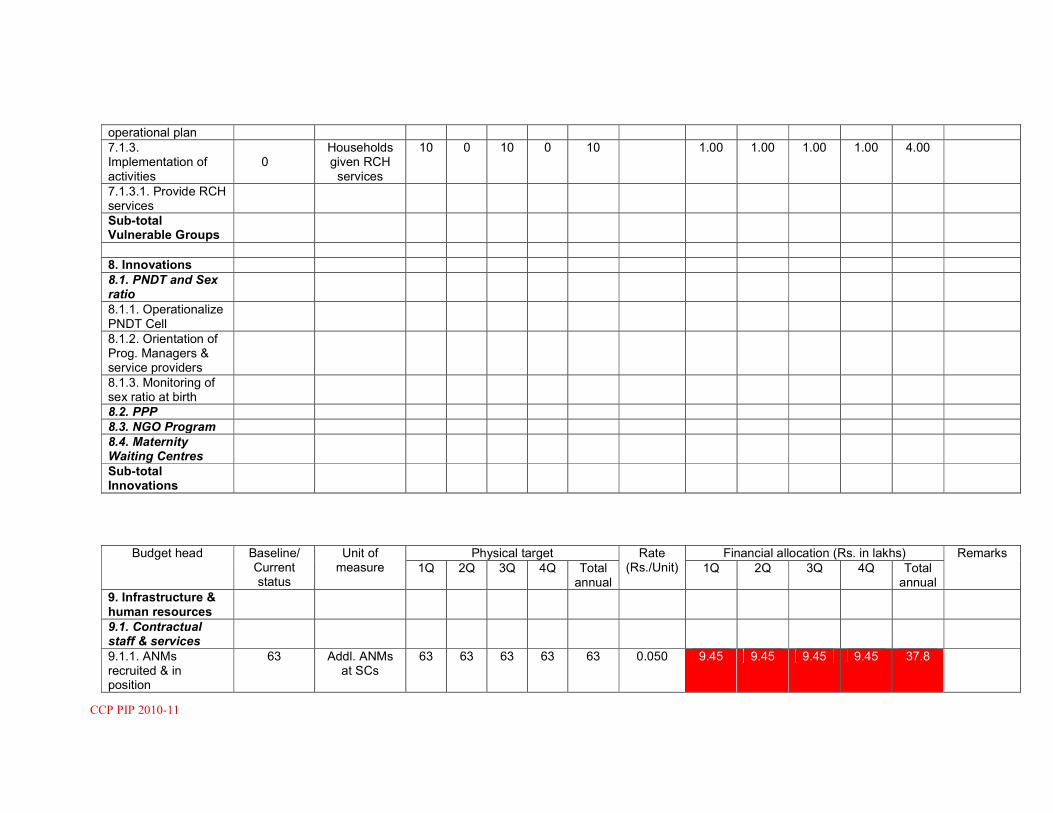
CCP PIP 2010-11
operational plan
7.1.3. Implementation of activities
0
Households given RCH services
10 0 10 0 10 1.00 1.00 1.00 1.00 4.00
7.1.3.1. Provide RCH services
Sub-total Vulnerable Groups
8. Innovations
8.1. PNDT and Sex ratio
8.1.1. Operationalize PNDT Cell
8.1.2. Orientation of Prog. Managers & service providers
8.1.3. Monitoring of sex ratio at birth
8.2. PPP
8.3. NGO Program
8.4. Maternity Waiting Centres
Sub-total Innovations
Budget head Baseline/
Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual
9. Infrastructure & human resources
9.1. Contractual staff & services
9.1.1. ANMs recruited & in position
63 Addl. ANMs at SCs
63 63 63 63 63 0.050 9.45 9.45 9.45 9.45 37.8

CCP PIP 2010-11
9.1.2. GNMs recruited & in position
12 Addl. GNMs at 24/7 PHCs
12 12 12 12 12 0.060 2.16 2.16 2.16 2.16 8.64
9.1.3.BPMU staffs 20 BPMU 20 20 20 20 20 0.075 4.5 4.5 4.5 4.5 18.0
9.1.4. Doctors recruited & in position
9 MOs (8 Ayush, 1 MBBS)
MOs 9 9 9 9 9 0.15 4.05 4.05 4.05 4.05 16.20
9.1.5. PHNs recruited & in position
9.1.6. Pharma 2 Phrama at CHCs
2 2 2 2 2 0.06 0.36 0.36 0.36 0.36 1.44
9.1.7. X-Ray Tech 1 X-Ray Tech for MMU
1 1 1 1 11 0.04 0.04 0.04 0.04 0.04 0.04
9.1.8 Lab tech 3 LT at CHC, 24/7 PHC
3 3 3 3 3 0.05 0.36 0.36 0.36 0.36 1.44
9.1.9 Drivers for MMUs
2 Drivers for MMUs
2 2 2 2 2 0.03 0.18 0.18 0.18 0.18 0.72
9.2. Major Civil Works
9.2.1. Major Civil Works for FRUs
Building construction of building-less
0 1 0 0 1 0 180.13 0 0 180.13
9.2.2. Major Civil Works for 24/7 PHCs
9.2.3 Major civil works for SCs
SCs construction
New construction for building less
SCs
23 23 23 23 23 9.0 50.0 Lacs
50.0 Lacs
50.0 Lacs
50.0 Lacs
2.0 Crores
9.2.3. Upgradation of SC to PHCs
2 SC 2 SC to upgrade to 2 PHC
2 2 2 2 2 20.0 10 10 10 10 40.0
9.3. Minor Civil Works
9.3.1. Minor Civil Works for FRUs
1 DH 1 1 1 1 1 Budget reflected at relevant section
9.3.2. Minor Civil Works for 24/7 PHCs
2 24/7 PHCs 2 0 0 0 0 Budget reflected at relevant section
9.3.3. PHC staff 2 PHC staff 2 PHC staff 2 2 2 2 2 5.0 Budget reflected at relevant section

CCP PIP 2010-11
quarters Qtrs Qtrs
9.3.4. Minor Civil works for SCs
8 Sub-Centres repair
0 23 22 0 45 0.50 0 11.50 11.00 0 22.50
9.3.5. Other facilities 7.5 7.5 7.5 7.5 30.0
Budget head Baseline/ Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual
9.4. Operationalize IMEP
9.4.1. Organize IMEP workshops
Budget reflected under relevant headings
9.4.2. Prepare operational plan across districts
9.4.3. Monitor progress against plan
Sub-total Infrastructure & Human resources
10. Institutional strengthening
10.1. Human Resource Development
10.1.1. Mapping of human resources
Done
10.1.2. Transfer & cadre structuring policy developed
Done
10.1.3. Performance appraisal & reward system developed
Developed
10.1.4. Incentive policy for posting in under-served areas
Budgeted under
maternal Health
10.2. Logistic management

CCP PIP 2010-11
Budget head Baseline/ Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual
10.2.1. Identification Nodal Officer Logistic
10.2.2. Development of logistic plan & dissemination
10.3. Monitoring & Evaluation / HMIS
10.3.1. Strengthening of M & E Cell
10.3.1.1. M & E Consultant recruited & in position
Done 1 DDM, 5 BDM
6 6 6 6 6 Budget reflected at relevant section
10.3.1.2. Procurement of Computers/ Inter-net connectivity
10.3.2. Operationalizing new HMIS format
10.3.2.1. Review of existing registers
10.3.2.2. Printing of new forms, registers
Done Budget reflected at relevant section
Sub-total Institutional strengthening
11. Training
11.1. Strengthening Trg. centres
11.1.1. Establishment of GNM Trg schools
Budgeted under Part
B
Budget head Baseline/ Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual

CCP PIP 2010-11
11.2. Development of training packages
All Training types are reflected at Training Section under Part A
11.2.1. Translation /Development of training materials
11.2.2. Specialized Trg equipment provide
11.3. Maternal Health Trg
11.3.1. SBA
11.3.1.3. Training of ANMs on SBA
11.3.2. EmOC Training
11.3.2.1. Setting up of EmOC trg centre
11.3.2.2. Trg of MBBS Doctors on EmOC
11.3.3. Life saving Anaesthesia skills trg
11.3.3.1. Trg. Of MBBS Doctors
11.3.4. Trg on safe abortion services
11.3.4.1. TOT on safe abortion services
11.3.4.2. Trg. Of MBBS Doctors on MVA
11.3.5. RTI/STI Training
11.3.5.1. Trg. Of doctors on RTI/STI
Budget head Baseline/ Current
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total 1Q 2Q 3Q 4Q Total

CCP PIP 2010-11
status annual annual
11.3.5.2. Trg of LTs on RTI/STI
11.3.5.3. Trg of MOs on Bl. Storage
11.3.5.4. Trg of LTs on Bl. Storage
11.4. IMEP training
11.4.1. IMEP trg for state & district program managers
11.5. Child Health Training
11.5.1. IMNCI trg (pre & in-service)
Reflected under Training Section
11.5.1.2. IMNCI trg. For paramedics
Reflected under training section
11.5.2 FBNC
11.5.3.1. Trg. Of Doctors on FBNC
Reflected under Training section
11.5.3.2. Trg. Of paramedics on FBNC
Reflected under Training section
11.5.3. HBNC
11.5.4.1. Trg of ASHAs on FBNC
Included under ASHA
11.6. Family Planning Training
11.6.1. Minilap training
11.6.1.1. MOs trg on minilap
11.6.2. NSV training
11.6.2.1. NSV trg for MOs
11.6.3. Contraceptive update training
Budget head Baseline/ Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total 1Q 2Q 3Q 4Q Total

CCP PIP 2010-11
annual annual
11.7. ARSH
11.7.1 ARSH trg for MOs
11.7.2 ARSH trg for paramedics
11.8 Teachers’ trg on schools Health
Sub-total Training
12. BCC
12.1. Strengthening of BCC Cell at State & District
12.1.1. BCC Consultant recruited & in place
12.1.2. Capacity building
12.2. development of State BCC strategy through CNA Survey
Blocks surveyed
5 0 0 0 5 0.05 0.25 0 0 0 0.25
12.3. Implementation of BCC strategy
12.3.1. BCC activities based on FGD, BCC Survey finding
Blocks 5 5 5 5 5 0.50 2.5 2.5 2.5 2.5 2.5 2.5
12.3.3. State activities
Sub-total BCC
13. Procurement
13.1. Procurement of equipment
13.1.1. Procurement of RCH equipments
Already reflected
Budget head Baseline/ Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual

CCP PIP 2010-11
13.1.1.1. For PHCs
13.1.1.2. For Sub-centres
13.1.1.3 For FRUs
13.2. Procurement of drugs
To be supplied in kind by GoI directly to district
13.2.1. Procurement from TNMSC by MoHFW, GoI
Sub-total Procurement
14. Program management
14.1. Strengthening of SPMSU
14.1.1. SPMSU staff recruited & in position
14.1.2. Office maintenance & mobility support
14.2. Strengthening of DPMSU
14.2.1. DPMSU staff recruited & in position
1 Functional DPMU
1 1 1 1 1 1.65 1.65 1.65 1.65 1.65
14.2.2. Office maintenance & mobility support
1 Functional DPMU
1 1 1 1 1 1.00 1.00 1.00 1.00 1.00
14.3. Strengthening of Financial Management Systems
14.3.1. Formation of State Finance management group
14.3.2. Audits
Budget head Baseline/ Current status
Unit of measure
Physical target Rate (Rs./Unit)
Financial allocation (Rs. in lakhs) Remarks
1Q 2Q 3Q 4Q Total annual
1Q 2Q 3Q 4Q Total annual
14.3.2.1. Annual To be borne from Program Management Head

CCP PIP 2010-11
audit
14.3.2.2. Concurrent audit
Sub-total Prog. Management
15. DHAP 1 5.00 5.00 5 5 5 5 5.00
Total RCH-II flexi pool
Total JSY 8.0 8.0 8.0 32.00
Sterilization Compensation
M-8, F-321
No. of beneficiary
M-5; F-100
M-5; F-100
M-5; F-100
M-5; F-100
M-20; F-400
M-0.015; F-0.01
7.50 7.50 7.50 7.50 30.00
Total NSV Camp 0 NSV Camp 1 0 1 0 2 0.50 0.50 0 0.50 0 1.0
GRAND TOTAL

CCP PIP 2010-11
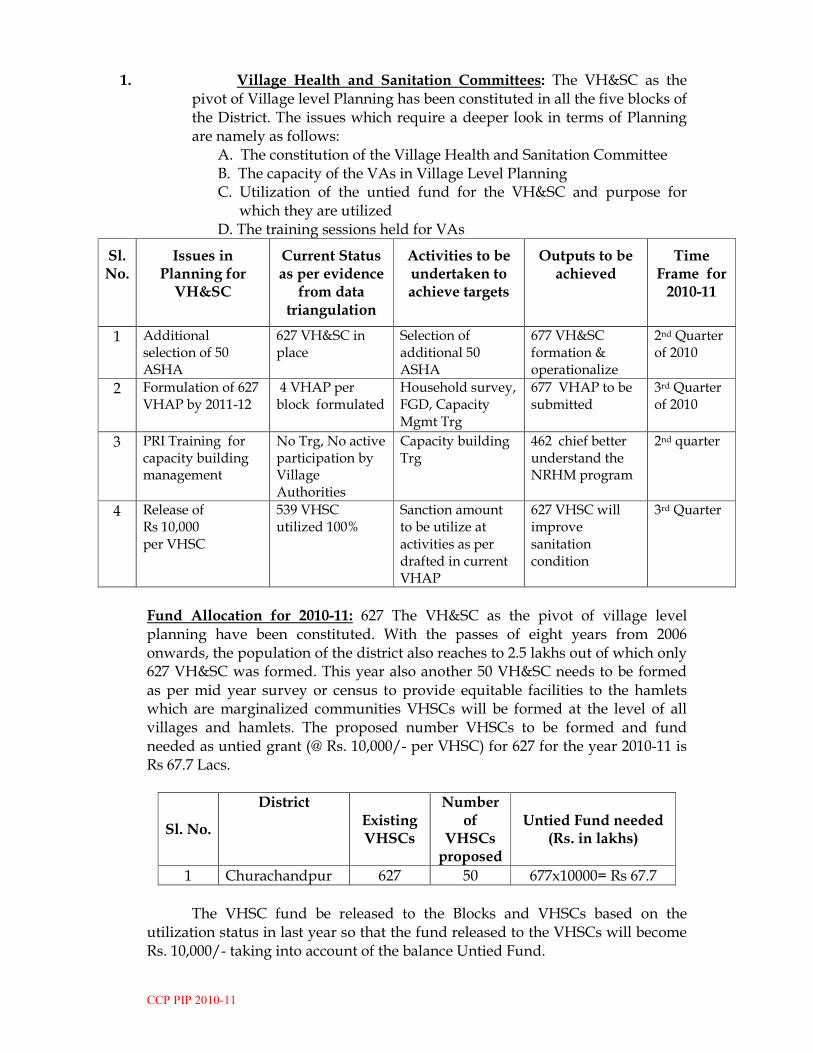
CCP PIP 2010-11
1. Village Health and Sanitation Committees: The VH&SC as the pivot of Village level Planning has been constituted in all the five blocks of the District. The issues which require a deeper look in terms of Planning are namely as follows:
A. The constitution of the Village Health and Sanitation Committee B. The capacity of the VAs in Village Level Planning C. Utilization of the untied fund for the VH&SC and purpose for
which they are utilized D. The training sessions held for VAs
Sl. No.
Issues in Planning for VH&SC
Current Status as per evidence
from data triangulation
Activities to be undertaken to achieve targets
Outputs to be achieved
Time Frame for 2010-11
1 Additional selection of 50 ASHA
627 VH&SC in place
Selection of additional 50 ASHA
677 VH&SC formation & operationalize
2nd Quarter of 2010
2 Formulation of 627 VHAP by 2011-12
4 VHAP per block formulated
Household survey, FGD, Capacity Mgmt Trg
677 VHAP to be submitted
3rd Quarter of 2010
3 PRI Training for capacity building management
No Trg, No active participation by Village Authorities
Capacity building Trg
462 chief better understand the NRHM program
2nd quarter
4 Release of Rs 10,000 per VHSC
539 VHSC utilized 100%
Sanction amount to be utilize at activities as per drafted in current VHAP
627 VHSC will improve sanitation condition
3rd Quarter
Fund Allocation for 2010-11: 627 The VH&SC as the pivot of village level planning have been constituted. With the passes of eight years from 2006 onwards, the population of the district also reaches to 2.5 lakhs out of which only 627 VH&SC was formed. This year also another 50 VH&SC needs to be formed as per mid year survey or census to provide equitable facilities to the hamlets which are marginalized communities VHSCs will be formed at the level of all villages and hamlets. The proposed number VHSCs to be formed and fund needed as untied grant (@ Rs. 10,000/- per VHSC) for 627 for the year 2010-11 is Rs 67.7 Lacs.
Sl. No.
District Existing VHSCs
Number of
VHSCs proposed
Untied Fund needed (Rs. in lakhs)
1 Churachandpur 627 50 677x10000= Rs 67.7
The VHSC fund be released to the Blocks and VHSCs based on the
utilization status in last year so that the fund released to the VHSCs will become Rs. 10,000/- taking into account of the balance Untied Fund.

CCP PIP 2010-11
2. ASHA ( Accredited Social Health’s Activist):
1. ASHA: 627 ASHAs have been selected and are actively engaged in bringing health to the community. However with these existing ASHAs the district is throwing up newer issues with clear impact on quality of services being provided by her relating to:
� Streamlining delay in payment of performance incentives to ASHAs. � Regular upgradation of skill � The timely and sustainable availability of drug kits � Supervisory structure for ASHAs
Sl. No.
Issues in Planning for VH&SC
Current Status as per evidence from data triangulation
Activities to be undertaken to achieve targets
Outputs to be achieved
Time Frame for 2010-11
1 Additional of 50 ASHA selection
627 ASHA in place
Selection of additional of 50 ASHA
677 ASHA selection
2nd Quarter
2 Training of 6th Module 627 ASHA completed 5th module Trg
6th Module Trg
Quality services
1st quarter
3 Introduction of ASHA Honorarium/incentive
No Introduction of reward to ASHA @ Rs 1000 for performance
High spirit to work culture
1st quarter
4 Separate mentoring & monitoring cell
No Separate monitoring cell/ staff to overlook ASHAs
No delay in services/ timely execution of services/program
2nd quarter
5 Procurement of ASHA drugs Kits
No Mobile Handset @ Rs 3000 per handset
627 ASHA will get connected & access to information easily
2nd quarter
3. Observation of Village Health & Nutrition Days:
It is targeted to observe Monthly Health & Nutrition Days on fixed day, fixed place basis at all the villages which will be based on the 627 existing Anganwadi Centres where the ANM of the Sub-Centre along with the local ASHA, AWW and other members of the Village Health & Sanitation Committee has to provide integrated health care services. As the VH&SC untied grant of small amount could not met with every expenses of the VHSC. Recommended separate fund amounting to Rs 12.0 lakhs especially for VHND observation, specifically for site

CCP PIP 2010-11
arrangement as well as for arranging of refreshments, a sum of Rs. 200/- per VHND may be sanctioned. Since, the fund available with the VHSC .i.e. Rs.10, 000/- only is not sufficient to cover the whole year.
Sl. No.
District
Existing AWC
Number of
proposed VHND in AWC
Budget needed (Rs. in lakhs)
1 Churachandpur 1010 500 Rs 12.0 Lacs Subcentres strengthened to IPHS:
Sub Centres: The Subcentres, is the first facility interface of community with health facility under NRHM and is the key to improving access and reach the remotest and the underserved areas. Construction, upgradation and placement of ANMs are in position in some SC. However, larger numbers of the SC are still in need of new construction and manpower, equipment etc. Taking this into serious consideration the following proposal has been made.
Sl. No.
Issues in Planning for Sub
centres
Current Status as per
evidence from data
triangulation
Activities to be undertaken to achieve targets
Outputs to be achieved
Time Frame for 2010-11
1 Recruitment of 10 ANMs in this current year
Already 2 ANM recruited at Dist level
Recruitment of 10 ANMS in 2010-11 at RKS level
71 ANMs will filled gaps
1st Qtr
2 Incentive develop for 71 ANMs
Not develop, Performance Based incentive used
Very difficult and inaccessible areas be firstly implemented
In 26 SCs coverage areas, attendance will be better
1st Qtr
3 Civil works ( new construction of SCs )
Out of already proposed 15 SCs, 10 SCs completed
Construction of 23 SCs requires in 2010-11
64 SCs will have building facilities
1Qtr-4Qtr
4 Repair/ renovation works For SCs
Already 15 SCs repaired
Repairing of 8 SCs requires in 2010-11
23 SCs already in repaired status
1Qtr- 4 Qtr
5 Procurement of equipments
Almost nil equipments in the current SCs
Basic equipments be procured through
66 SC will be operationalize
2nd Qtr

CCP PIP 2010-11
district level
6 Procurement of medicines and drugs
Same pattern undergone
To continue Adequate medicine available in stocks at PHC
1 Qtr to 4 Qtr
7 Procurement of java enabling handset with maintenance
Poor % filled data in HMIS report
Java enable handset be procure by 66 SCs ANM
Percentage of HMIS report filled will be more
1st Qtr & 2nd Qtr
8 Release of untied fund to SCs
Rs 10000/ per SCs
Rs 10000 per SC to continue
Utilize as per SCs needs
2nd Quarter
9 M &E activities Partially BPMU to execute M&E of the SCs
Better performance
Monthly
Both Regular and Contractual ANMs are not in placed in all the existing 64 Sub-Centres, an addition of another 10 ANMs are needed to be placed in the district as two SCs are being added reaching the total of 66 SCs from the previous 64 SCs. Currently in 10 SCs even single ANM are not posted. The District has a total of 102 ANMs out of which only 61 ANMs are under NRHM programme. An initiative of paying honorarium based on performance to Additional contractual ANMs posted in the Sub-Centres is proposed in 2010-11. The detailed is reflected in Part A. The budget requirement for these current 61 contractual ANMs @ Rs 5,000/- without performance scheme is given below: S.No Details No of ANMs Budget Requirement
( in lacs)
1 Fixed Basic Honorarium Annual
61 @ Rs 5000 x 12 months
Rs 36.6
2 Additional performance based incentives
61 @ Rs 3000 x 12 months
Rs 21.96
Total Rs 58.56
4. Primary Health Centres: The PHCs as the first interface of a medical
officer with the community has seen considerable progress under NRHM with many health facilities delivering 24X7 services and positioning of 3 staff nurses under NRHM. However issues which need focus in the current plan relate to:
1. Placement of human resources esp. nurses to ensure 24X7 PHC at
Saikot , Sagang & Singngat PHCs 2. Quality care 3. Parameters for monitoring & Evaluation 4. Pace of utilization of RKSs. MGs, UFs

CCP PIP 2010-11
Status of already identified 24/7 PHCs: None of the identified three PHCs could function as 24/7 Services Centre. Presently, 2 GNM is posted at Sagang PHC which is sort of one GNM. Saikot PHC had only one GNM which is sort of 2 GNM. The total requires reaches to 07 additional GNM more in the district. Another 2 GNM each is required in the current year. Moreover, due to lack of manpower, infrastructure and equipments in the said PHC, these Centres cannot be practically converted into 24/7 due to lack of staff, difficult accessibility poor infrastructure/none availability of building.
Sl. No.
Issues in Planning for
PHCs
Current Status as per
evidence from data
triangulation
Activities to be undertaken to achieve
targets
Outputs to be achieved
Time Frame for
2010-11
1 To make 2 PHCs functional
Adequate Doctors, equipment Others not in position.
Manpower recruitment Supply of equipments Manpower recruitment at RKS level
Manpower ( 3 GNMs, 2 MBBS , Lab Tech Etc) will be placed
1st Qtr
2 Construction of staff quarters of Saikot, Sinzawl PHCs along with approach road
No repairing takes place
Staff Qtrs requires repair at Saikot PHC, Sinzawl PHC
4 Type III Qtrs at 2 PHCs will be functioning
1st Qtr to 4 Qtr
3 Selection of SNM, Lab Tech, ANM, Phar, MOs etc
Lack of Manpower 1 MO each in all PHCs
Recruitment of all these concern manpower to be selected at RKS level
Adequate manpower operationalize
2nd Qtr
4 New construction of two PHCs
7 PHCs with building facility
Senvon PHC and Singngat PHC to be construct
Nine PHCs will be operationalize
2nd Qtr & 3rd Qtr
5 Develop incentive for MMBS doctors for institutional delivery conduction
No activities develop
Rs 500/ per inst. Delivery case Rs 300/ per case by GNM and ANM
No of institutional delivery will be increase
1st to 4th Quarter
6 Release of RKS maintenance & untied fund
Continue To be continue (detail reflect under relevant sections)
Norms & new innovations will be develop
1st to 4th quarter
7 New addition of one PHC- Zezaw
Nine PHCs Fund for 10 PHC be incorporated
Total of 10 PHCs will be operationalize
1Qtr to 4 Qtr

CCP PIP 2010-11
Presently there are 7 Additional GNMs exist in the District. The budget requirement for paying the honorarium of these 7 GNMs is given below for the next year 2009-10
S.No Details No of GNMs
Budget Requirement
1 Fixed Basic Honorarium Annual
7 @ Rs 6000 x 12 months
Rs 5.04 Lacs
5. Manpower strengthening of CHCs to IPHS level: The CHC currently had Two MBBS regular doctor along with one MBBS doctor under contractual. But she is utilized at District Hqrs. The requirement of manpower as per IPHS Norms are General surgeon-1, Obs & Gynae-1, Paediatrics-1, Anaesthesist-1, eye surgeon-1, GNM-4, ANM-1, dresser-1, Lab Tech-1, Radiographer-1
Sl. No.
Issues in Planning for
CHC
Current Status as per
evidence from data
triangulation
Activities to be undertaken to achieve targets
Outputs to be achieved
Time Frame for
2010-11
1 To make CHC functional as FRU
No manpower No 24 hrs emergency CS No Blood Transfusion, No referral transport
-Manpower recruitment at done at RKS/ PRI level -Supply of equipments for OT & Blood Storage -Ambulance be sanction -Impart existing manpower for Multiskilling Trg
Become FRU fully
1st Qtr to 4 Qtr
2 Construction of OT and Labour room
Not operational
-Construction of OT & Labour room
Increase in inst deliveries, and better RCH services
1st Qtr to 4Qtr
3 Recruitment of extra Manpower
2 MO 1 Lab tech 1 Phar
Recruitment of identified manpower at RKS level ( 2MO, 4 SN etc)
Adequate of manpower
1Qtr & 2nd Qtr
4 Procurement of equipments
Not sufficient as per IPHS level
Procurement of equipments at Dist level
CHC operationalize
1 Qtr & 2nd Qtr
5 Provision of 4/4 vehicle hiring
Nil Procurement of one vehicle at three(3) 24/7 PHC
RCH services more functional
1 Qtr & 2nd Qtr
6 Release of Continue To be continue As per 2nd Qtr

CCP PIP 2010-11
RKS, Maintenance, untied grant
guidelines will be implemented
7 M&E Partially done DPMU Programme implementation ensured
Monthly
6. Strengthening of District Hospital Churachandpur: The activities require in district hospital to make fully functional to FRU are sub divided into sub tasks: a) Provision of 24/7 running water (Digging tube well, inserting motor, electric panel for motor, pipe line to overhead tank, construction of OHT/ syntax tanks, connection to supply lines, provision of 10 hand wash basins), b) Commissioning of generator: financial provision of POL, construction of shelter for genset. c) Installation of incinerator: Applying for CPCB clearance, soil work, construction of shelter for incinerator, installation of weighing scale, installation of chimney stack 30 mtrs high, obtain CPCB clearance, operator for running the incinerator. D) Civil works in OT: construction of three small walls total 20 feets, fit tiles on walls up to 8 feets e) Installation of CT Scan: complete system, electric supply shelter, computer , set up as per norms f) Repair of x ray dept and lead proofing and Air conditioning of Ultra Sound room: lead proofing of doors, procurement of automatic film g) Marking propose casualty space in OPD block: erection of partition frame work hollow square, electric points two switch boards, shadow less lamp portable, h) installation of Autoclave in CSSD: provision of water supply point, provision of steam exhaust, i) Maintenance and paintings of the premises, j) sign posting of facilities area lighting j) re-furbishing mortuary, building mortuary, kitchen, storage facilities for medical records, biomedical wastes, lines bed sheets, dedicated power supply, and induction of security personnel.
Sl. No.
Issues in Planning for
DH
Current Status as per
evidence from data
triangulation
Activities to be undertaken to achieve targets
Outputs to be achieved
Time Frame for
2010-11
1 To make DH full functional as FRU
Under process ISO certification
Recruitment of specialists doctors
Services delivery will be better
1st Qtr
Procurement of equipments
It will be full functioning as FRU
1st Qtr to 4 Qtr
The detail given as below:

CCP PIP 2010-11
Works activities with Budget requirement for 2010-11: Sl. No.
Works/Activity Qty. Unit Rate in Rs.
Amount in Rs.
2. DH Churachandpur
1 Provision of 24x7 running water provision
1 Rs 5 Lacs
2 Commissioning of generator along with maintenance
1 Rs 14 Lacs
3 Installation of incinerator with maintenance
1 Rs 15 Lacs
4 Civil works in OT 1 Rs 1 Lac
5 Installation of CT Scan 1 Rs 1 Lac
6 Repair of X Ray Dept & lead proofing as per norms installation of automatic film processor
1 Rs 2 Lacs
7 Marking of propose casualty space in OPD block
1 Rs 1 Lac
8 Installation of autoclave in CSSD 1 Rs 1 Lacs
9 Maintenance and paintings of the premises
Rs 5 Lacs
10 Sign posting of facilities area lighting 5 Rs 5 lacs
11 Refurbishing mortuary 1 Rs 3 Lacs
12 Building laundry 1 Rs 10 lacs
13 Building Kitchen 1 Rs 10 Lacs
14 Storage facility for medical records room storage for mass casualty stores
1 Rs 5 lacs
15 Biomedical wastes 1 Rs 5 Lacs
16 Linens(Bed sheet, pillow cover etc) 700 Rs 3 Lacs
17 Dedicated Power supply Rs 2 Lacs
18 Security personnel induction 4 Rs 1.5 Lacs Grand Total B Rs 90 Lacs
7. Rogi Kalyan Samitis at DH, CHC, and PHCs: The Rogi Kalyan Samiti as the pivot of planning and community involvement and ownership of the health facilities has been constituted in all the 9 PHCs, 1 CHC and 1 District Hospital, Churachandpur. RKSs have contributed to local level leadership and need based decision making. The issues which needed a reflection in the planning would relate to:
• Performance and pace of utilization of funds and • Activities being under taken by RKS

CCP PIP 2010-11
Sl. No.
Issues in Planning for
RKS
Current Status as per evidence
from data triangulation
Activities to be undertaken to achieve targets
Outputs to be achieved
Time Frame for 2010-11
1 DH be made fully functional as FRU
Partial function & under ISO vigil
Recruitment of specialist, medical doctors, SN, etc
Full functioning as FRU
1st & 2nd quarters
2 2 PHCs make 24/7 delivery centres
Not functioning Recruitment of manpower, Medicines & drugs, equipments
2 PHCs namely Saikot PHC, Sagang PHC will function as 24/7 delivery centres
3rd Quarter
3 PHC Singngat 24/7 delivery centres
Functioning 24/5 without proper building
New Construction of PHC building
Fully functioning PHC
Within the current year
3 Induction of Staff Nurse at 4 identified 24/7 PHCs
2 GNMs each in 2 PHCs and 1 each in 2 PHCS
Recruitment of SN at District level
3 GNMs at each identified 4 PHCs as 24/7 delivery centres
2nd Quarter
4 Procurement of basic equipments and medicines
No basic amenities and equipments at identified 24/7 PHCs
Procurement of logistics support at District level
well equipped PHCs
3rd quarter
5 Recruitment manpower
Nil ANM shortage will be recruitment
Manpower gaps will be filled
1 Qtr
RKS Fund Allocation in 2010-11: All the existing DH, CHC Parbung and 9 PHCs have registered RKS formed with their own bank accounts opened. With the new upgradation of one SC, the total PHC reaches to 10 PHCs. The Corpus Fund/ Seed Money (Rs. in lakhs) needed for the 2010-11 is shown below. The Corpus Fund will be released to the respective health facilities taking into account the amount utilized in the previous year.
Health
Facility Unit Corpus
fund No. of units
Total amount Remarks
District Hospital 5.00 1 5.00
CHC 1.00 1 1.00
PHCs 1.00 10 10.00

CCP PIP 2010-11
Total Rs 16.0 Lacs
8. Maintenance Grant for CHC, PHCs and Sub-Centres
The budget requirement for 2010-11 will be:
Sl. No. Type of Health
Facility Untied Fund per Unit (in lakhs)
Units Total
(in lakhs)
1 CHC 1.00 1 1.00
2 PHCs 0.50 10 5.0
3 PHSCs 0.10 66 6.6 Total 12.6
9. Annual Untied Fund for CHC, PHCs and Subcentres:
The budget requirement (Rs. in lakhs) in 2010-11 will be
Sl. No. Type of Health
Facility Untied Fund per Unit (in lakhs)
Units Total
(in lakhs)
1 CHC 0.50 1 1.00
2 PHCs 0.25 10 2.50
3 PHSCs 0.10 66 6.6 Total 9.85
10. Community Monitoring:
Sensitization workshop and re-orientation on NRHM programme needs to be taken in this current year especially for representatives of Village Authorities. This would ultimately increase the level of community participation as well as community ownership in respect of health services.
Community monitoring will be started in the current year which will be based on affirming the performance of the ANMs posted in the Sub-Centres. Apart from this performance-based incentive be given to them. Also the Village level Health Committees will maintain register for observation of monthly Village Health & Nutrition Days. 11. CMO OFFICE EXTENSION FOR DPMU ROOM/OFFICE The present status of the CMO office is a barrack type building where the partition of wall is by plywood board and there is only five-rooms in which the CMO, DMO along with its staffs, and CMO administrative staffs and DPMU staffs were cramped in it. The room being very small and congested, it is therefore, propose that out of the available land, 55x17 feet in area annexed to

CCP PIP 2010-11
rear side of CMO office. As such it is strongly desired that out of the existing area, it propose to use 50x16 feet of its area to accommodate three separate rooms where-in tiles will be use in its floor and RCC roofing for further upgradation to first floor later and also to save space. The estimated cost in lump sum will be Rs 35 Lacs. This proposal is badly in need due to its situational needs. Hence, the proposal may kindly be approve in a special case. This construction works may kindly be entrusted to the District for better monitoring and supervision. 12. NEW CREATION OF VANGAI AND SAIKOT BLOCK/BPMU
A. Justification of New Block creation: Saikot PHC covering 280 numbers of villages and 35000 household with a population of 56,808 nos. It is the largest PHC in terms of population coverage. It also has 13 PHSCs. Saikot PHC is a conjunction of 4 Block namely, 1) Saikot Block (2) Sangaikot Block (30. Tuibuong Block (4). Lamka Block. In its practical point of view, it is extremely difficult to manage and monitored by Sagang PHC due to its vast geographical coverage, as such Sagang PHC comes under Samulamlan Block. Saikot PHC presently has one BFM and is without BDM and BPM which is very difficult to expedite various activities under Saikot PHC. So, it is strongly desire to create a new Block called Saikot Block or provision of full unit of BPMU.
B. VANGAI BLOCK
Patpuihmun PHC comes under Vangai TD block. It has 36 villages with seven sub-centres. It is about 336 kms from Churachandpur District Hqrs. Normally it takes three days to reach the place crossing Jiribam. One need to takes local boat to cross the Barrack River and peddle through the hill till Patpuihmun village. Communication is the biggest problem. Immunization is almost nil in this range. The PHC Patpuihmun falls under Tipaimukh Block. Practically it is extremely difficult to reach Patpuihmun from Parbung due to distance and road transportation problems, resulting in delay in programme implementation and monitoring. To remedy this problems, a new Block called Vangai Block which itself is an existing TD Block be created and which is justifiable as far as geographical demarcation of land between Parbung and Patpuihmun is concerned. The Patpuihmun PHC currently has one BAFC and requires 1 BPM and 1 BDM in Patpuihmun PHC. 12. District Mobile Medical Unit (DMMU):
Mobile Medical U nits comprising of 02 vehicles equipped with diagnostic and therapeutic accessories are in operation in the District with required manpower. It is desired that the honorarium of lab -Tech and X – Ray Technician @Rs.5000/- per month who were running the vehicles, and driver @ Rs. 4,000/- be continued. Also an annual maintenance fund including POL may be sanctioned @ Rs.2.00 Lakh for both DMMU taking into account the difficult geographical terrain of the district.

CCP PIP 2010-11
The detail of Budget requirement (Rs. in lakhs) for supporting the salary component of these Lab tech, X Ray Tech. and drivers is shown below.
S.No Particulars Churachandpur
Total Amount ( in lacs)
1 Salary for LT, XT & Drivers
1.2 1.2
2 POL & maintenance 2.0 2.0 3 Total 3.2 3.2
Mobile Medical Units: The provision of MMUs has greatly expanded the reach of NRHM in the underserved areas.
Sl. No.
Issues in MMUs Current Status as per
evidence from data
triangulation
No of MMUs
Activities to be undertaken to achieve targets
No of Camps held
Outputs to be achieved
Time Frame for 2010-11
1 MMUs be used Quarterly
04 camps Planned in year 2009
Planned monthly MMUs camps
Full operationalize of MMUs
Monthly
2 Monetary Rs 20000/ per camp
Rs 50000/ per camps be sanctioned
Maximum uses of resources
Monthly
3 Frequency of visit
Half yearly Quarterly Served the unnerved areas
Quarterly
4 Procurement of medicines
Adjust through camps fund
Procurement from camps fund
Served the unnerved areas
Quarterly
5 Contractual staffs honorarium sanction
Ongoing To be continue MMUs more operationalize
Monthly
13. Mainstreaming AYUSH:
Suggestions to improve the AYUSH functioning in the district- supply of essential drugs including medicinal kits. Seven Ayush pharmacist needs to be place. Propose for strongly desire for conducting Ayush Mela at blocks and village level. Establishment of Ayush Herbal garden at all PHCs. Set up of

CCP PIP 2010-11
specialized centre at PHC and sub centres once in a week. Adequate and frequent skills management training
Eight (8) AYUSH Doctors and three (3) Ayush Pharmacists are in place in
the district. All the Ayush doctors are almost in all the health institutions and the district require 8 Ayush pharmacists in 2010-11.
The Infrastructure up-gradation and drugs needed for all the AYUSH
Centres will be supported under AYUSH CSS. Currently in the District Hospital, Ayush Dept Block are under construction and in various PHCs level, construction work needs to be initiated.
The Budget requirement (Rs. in lakhs) for supporting the salary
component of these AYUSH staffs is shown below. S.No Particulars Budget ( Rs in lakhs)
1 No of Ayush Doctor 8 @ Rs 15,000 Rs 1440000
2 No of Ayush Phar 3 @Rs 5000 Rs 180000
Total Rs 16.20
14. Construction of building for building-less Subcentres:
In the year 2006-08 15 PHSCs was sanctioned for new construction but so
far ten (10) PHSCs reported its completion and 5 PHSCs still under progress. Henceforth, it is proposed that in 2010-11, 23 PHSCS new construction of be undertaken for building-less. As all these building less Subcentres are located at remote area
Sl. No.
Issues in planning in SCs
Current Status as per
evidence from data
triangulation
Activities to be undertaken to achieve targets
Outputs to be achieved
Time Frame for 2010-11
1 New construction 10 SCs completed out of 15 SCs
23 construction 66 operationalize 1 Qtr to 4 Qtr
2 Renovation of SC 15 SC renovated
8 SCs need renovation
66 operationalize 1 Qtr to 4 Qtr
3 Construction of labour room at SC
Nil To be undertaken by DRDA
66 SC will conduct delivery case
1 Qtr to 4 Qtr
The detail Budget requirement: S.No Particulars Churachandpur
CCP PIP 2010-11
1 No of Proposed construction for PHCs
2
Unit Rate 66.0
2 No. of proposed construction for PHSCs
23
Unit rate 9.00
Budget needed Rs. 339 Lacs
15. PROVISION FOR HIRING VEHICLES FOR DPMU:
The DPMU is in need of one vehicle particularly gypsy for Monitoring & Evaluation purpose. Taking into account, constraints sanctioned of Contingencies fund to the district and adverse topographical condition of the District. The DPMU could not able to visit all the blocks for Monitoring and Evaluation as the cost of hiring per vehicle reaches Rs 25000/- . So it is strongly desire that the DPMU be supplied one Gypsy or sanction hiring charge of one vehicle so that program implementation could be meted out as per spelt by the centre and state authorities. For this, an estimated amount of Rs 25000/ per visit per month be sanctioned, which will require Rs 3.0 Lacs. 16. HIRING OF VEHICLES FOR CHC&PHCs The district has already identified three PHC as 24/7 delivery centres. The real Operationazation process of these PHCs could not be carried out so far. There are many reasons for this failure, but one immediate and most important criteria for this functioning as 24/7 delivery centre is to have outsourced vehicle for the whole team of PHC including BPMU. The outsourcing vehicle scheme is already in panic degradation. So, it is strongly desire that one vehicle hiring charge for monitoring & evaluation purpose plus additional activities inspection of 3 PHCs for an estimated amount of Rs 2000/- per visit per month which will require Rs 72,000/- be sanctioned. 16. District Health Mela: It is proposed to observe District Health Mela in the District @ Rs. 5.00 Lakh per Mela. The site of Mela will be discussed in the Governing Body meeting which will be chaired by the Deputy Commissioner of the District. The District for the past two years conducted Health Mela at two blocks – Thanlon and Tipaimukh block. The same activities need to be carried out as the district covered has 60% under served areas.
17. Procurement and logistics:

CCP PIP 2010-11
The District be given empowerment for procurement of Drug/Medicine Kits for the various health institutions of the District in 2010-11. For the last two years drugs/ medicine was indent from State level which is very inconvenience for the District. The need of every district could not be the same. 18. Procurement of District Laptop, LCD projector:
Currently the District faced lots of inconvenience as there is no LCD/ Projector facility in the Secretariat. The burden of the District increased as the district conduct frequent training/ workshops/ orientation at the district level. The district proposed an estimated amount of Rs 3.00 Lakhs
19. Establishment of District Training Centre: The District has got adequate number of Manpower at present to cover the centre demand under NRHM training programme. However, there is need for establishing Training Centre in district where there is no public or private Training Centre for the District Health Society to conduct training and workshops. The District conduct frequent training and workshops and find inadequate to conduct at various public community as it is too far from the office.
Due to the long distance between the district health secretariat’s to training
Centre where training used to be held, it is proposed that the District concerned be identified as the parent institutions for training conduction for the blocks. For this activities an estimated amount of Rs 30 Lacs is require.
20. Strengthening Program Management:
Recruitment of any shortage of Manpower is done at the district level and sought to carry as it is. The segregation of BMPU staff posted at the block level currently faces problem, so bifurcate of Tipaimukh Block and Samulamlan Block is requires, as practically Tipaimukh Block covering Patpuihmun PHC is not feasible and Saikot PHC cannot function under Samulamlan Block and Tipaimukh Block respectively.
Separate BPMU staff in Patpuihmun PHC and Saikot PHC is requires. In both
the PHCs, there is one each BFM without BDM, BPM. Program implemented hampers a lots being specified by the Medical Officer in-charge of the respective PHCs. In short Block Program Manager, Block Data Manager in both these Saikot PHC and Patpuihmun PHC be recruited at the RKS/ District level. The detailed explained under Block creation section.
21. Honorarium of BPMU staffs: 19 Block Program Management Staff comprising of 4 Block Program Manager, 5 Block Data Manager and 10 Block Finance Manager are established in all existing blocks. The Monthly Honorarium of these staffs recruited on contract basis be increased from Rs 7500/- to Rs. 10,000/- for all BPM, BDM and DFM
CCP PIP 2010-11
The total budgetary support needed for supporting the BPMUs will be as given below:
Sl. No.
Particulars Units Total (in Lakhs)
1 Honorarium of BPMU 19 @ Rs 10,000x 12 months
Rs 38.0
Grand Total Rs 38.0 Lacs
22. Procurement of equipment for PHCs The numbers of requirement per PHC depends on its manpower stationed.
1. Bed sheets
2. Blankets Red and blue
3. Table cloth
4. Draw sheet
5. Doctor's overcoat
6. Hospital worker OT coat
7. Over shoes pairs
8. Pillows
9. Pillows covers
10. Mattress (foam) Adult
11. Paediatric Mattress
12. Mats (Nylon)
13. Mackin tosh sheet (in meters)
14. Doctor's Table
15. Long Benches(6 Doctor's chair for OP Ward, Lab 1/2' x 1 1/2')
16. Stool Wooden
17. Stools Revolving
18. Racks -Steel – Wooden
19. Patients Waiting Chairs (Moulded)
20. Attendants Cots
21. Office Chairs
22. Office Table
23. Foot Stools
24. Cradle
25. Fowler's cot
26. Ortho Facture Table
27. Wooden Blocks (Set)

CCP PIP 2010-11
28. Back rest
29. Dressing Trolley (SS)
30. Medicine Almairah
31. Bin racks (wooden or steel)
32. Bed Side Screen (SS-Godrej Model)
33. Medicine Trolley(SS)
34. Case Sheet Holders with clip(S.S.)
35. Bed Side Lockers (SS)
36. Examination Couch (SS)
37. Instrument Trolley (SS)
38. Instrument Trolley Mayos (SS)
39. Surgical Bin Assorted
40. Wheel Chair (SS)
41. Stretcher / Patience Trolley (SS)
42. Instrument Tray (SS) Assorted
43. Kidney Tray (SS) – Assorted
44. Basin Assorted (SS)
45. Basin Stand Assorted (SS)
46. Delivery Table (SS Full)
47. Blood Donar Table
48. O2 Cylinder Trolley(SS)
49. Saline Stand (SS)
50. Waste Bucket (SS)
51. Bed Pan (SS)
52. Dispensing Table Wooden
53. Kitchen Utensils
54. Containers for kitchen
55. Plate, Tumblers
56. Linen Almirah
57. Arm Board Adult
58. Stores Almirah
59. Arm Board Child
60. SS Bucket with Lid
61. Bucket Plastic
62. O2 Cylinder with spanner ward type
63. Diet trolley - stainless steel
64. Needle cutter and melter
65. Thermometer Rectal
66. Thermometer clinical
67. Torch light
68. Stomach wash equipment

CCP PIP 2010-11
69. Infra Red lamp
70. Wax bath
23. ASHA initiative:
S.No DISTRICT Existing Total no. of ASHA
Additional ASHA in 2010-11
New requirement for 2010-11
Total
A Churachandpur 627 50 50 677
Budget Requirement for sustainability S.No No of ASHA Rate per
VHSC Total Amount require
( in Lakhs ) B 677 Rs 0.10 Rs 67.7 Lacs
On Skills and Knowledge: Additional Interactive sessions be held every month to up-grade and refresh their knowledge, skills which will be supervised by the State Authorities. So that they can impart their skills to the fullest use for the welfare of community as whole ASHA Cell: The ASHAs are the backbone of NRHM programme. And it is well known that ASHAs active involvement is the ultimate need of the hours in order to achieve our Millennium goals and target. So in order to keep them in touch with every programme implementation in the district, a separate ASHA cell (Room) be maintained from the coming year ,so that they could update their report and discuss various programme undertaken in the district. The hiring of room charge will be @ Rs 3000 per month and separately Rs 50,000 for furniture and others essential office materials. Mentoring Group for ASHA: A District Mentoring Group for ASHA will be formed under the Chairmanship of the District Nodal Officer (ASHA). And it is propose that, separate staffs be entrusted to look after the day today activities of ASHA since it is very difficult to look after by the existing staffs. 24. Construction of PHC building for Senvon and Singngat The construction of main building and staff quarters of PHC Senvon and PHC Singngat is strongly desired. In the last year District PIP already projection were made for construction of these 2 PHCs, but it is in vain. The Staffs of these

CCP PIP 2010-11
two PHCs are function as the best in the District. Hence people from the nearby village approach the PHC. So, It is Strongly desire that a Main building along with approach road be approved for PHC Senvon and PHC Singngat. For these activities an estimated amount of Rs. 132.00 Lakhs will be needed in the current year. The budget is included in part B.
25. Establishment of GNM Training School under Public Private Partnership: Nursing Education: Bethesda school of nursing is the only Nursing school in the district and one of the best Nursing schools in Manipur. It is recognized by INC and affiliated to Manipur Nursing Council. It has the admission capacity of 30 students per year only. Since the demand of nursing education is very high in the district. It is propose that the Nursing school be run under PPP, where the District Health Mission Society, will intake fifteen 15 students and 30 students will be from Bethesda Nursing School Management side.
Manpower Requirement: The admission capacity after reaching 45 (30 from existing and 15 from DHMS) and financial assistance as salaries for two tutors@ Rs 20,000/- per month will be given. Because the require numbers of tutors for 45 students (10 students per year for three years and six months) is four as per INC guidelines. So, the two tutors will be supported by the management and the other two from the DHMS
At present the School is manage by the management board, Bethesda Nursing School and once after, the PPP agreement is initialize, there will be separate Management Board from the District Health Society Management Board.
Sl. No.
Manpower Qualification Consolidated pay per annum in lakhs
No. of personnel
Total in lakhs
A. Faculty
4. Tutors MSc Nursing or BSc Nursing (Basic)/Post basic or Diploma in Nursing Edn and Adm or its equivalent with 2 yrs experience after graduation
2.4 3 7.2
Budget Requirement will be: Sl. No.
Particulars Total in lakhs
1 Manpower ( 3 tutors ) 7.2
2 Contingency 2.0

CCP PIP 2010-11
Total Rs 9.0
26. HONORARIUM INCREMENT FOR NRHM STAFF: It is strongly desired that an increment of Honorarium for all staffs under
NRHM be made, taking into account, the rate of inflation and cost of living and workload. Moreover, for the past three years, loss of increment and hardship allowance for NRHM staff should be taken into consideration. The proposed rates of honorarium for NRHM staffs with their designation were given in the following table:
S.No Category Designation Existing Honorarium
Propose Honorarium
Remarks
CATEGORIES A District Program Management Unit 1 DPMU DPM Rs 18,000 Rs 30000 2 DPMU DDM Rs 10,000 Rs 25000 3 DPMU DFM Rs 12,000 Rs 25000 B Block Program Management Units 4 BPMU BPM Rs 7500 Rs 20000 5 BPMU BDM Rs 7500 Rs 15000 6 BPMU BFM Rs 7500 Rs 15000 C MBBS Doctors ( including Ayush) 7 Doctor MBBS Rs 15000 Rs 25000 8 Doctor Ayush Rs 15000 Rs 25000 D Staff Nurse 9 GNM GNM Rs 6000 Rs 10000 10 ANM ANM Rs 5000 Rs 80000 11 Lab Tech LT Rs 5000 Rs 7500 12 Pharmacist Phar Rs 6000 Rs 10000 13 X-Ray Tech X-Ray Tech Rs 4000 Rs 7500 14 Office Assistant OA Rs 5000 Rs 8000 15 Computer Operator CO Rs 7000 Rs 10000 16 Audiometric Asst AA Rs 7500 Rs 15000 17 DDMU Driver Drivers Rs 3100 Rs 7000
27. M&E Strategy for strengthening HMIS:
The budget allocation for Monitoring & Evaluation Officer (HMIS) of the District should be backed by an M&E strategy detailing the current status of HMIS and the proposed plan of action for taking the data capturing to the Blocks level. This should also include integration issues across health programmes and with the national HMIS. Notification of Nodal M&E Officers:

CCP PIP 2010-11
Level No of propose Nos. present Remarks
District Nil 01 DNO ( M&E)

CCP PIP 2010-11
26. Human Resource Health Status of the District : ( Manpower including District Hospital, CHC and PHCs)
State Requirement of HR Doctors Nurses ANMs Pharmacists Lab tech
Required as per IPHS 45 58 128 15 15
Required staff as per IPHS for the existing facilities 45 58 128 13 15
Sanctioned staff -- -- -- -- --
In Position 41 45 117 2 10
Vacancy against sanctioned 4 13 10 0 3
Vacancy against IPHS 16 15 11 2 5
Vacancies already filled up by the State 4 Ayush 7 61 2 2
Proposed filling up of vacancies by the Dist for 2010-11 16 15 10 2 3
Contractual engagement through NRHM 11(10 Ayush) 7 61 2 2
Contractual engagement proposed under NRHM for 2010-11
10 13 10 2 3

CCP PIP 2010-11

CCP PIP 2010-11
Budget Allocation for HMIS for 2010-11:
Major Head Minor Head Budget in Rs Details Remarks
Strengthening of M&E/HMIS
Salaries of M&E, MIS & Data Entry Consultants
1.1 Rs 15,000 per/month Rs 15,000x12x1= Rs 1.8 Lacs
Mobility for M & E Officers 1.2 Rs 2000 per/ visit Rs 2000x12 =Rs 0.24 Lac
Workshops/Training on M & E 1.3 Rs 50,000 per/ Trg Rs 50000x 5=Rs 2.5 Lacs
M&E Studies 1.4 Rs 5000/- Rs 5000/-
Others (specify) 1.5 V- SAT installation Rs 1.5 Lac
Procurement of HW/SW and
other equipments
Hardware/Software Procurement
2.1 Rs 50000/- Rs 50000/-
Rs 5000/ annual Rs 5000/- annual
Internet connectivity 2.2 Rs 5000 per month Rs 5000 x 4 x 12= Rs 2.4 Lacs
Annual Maintenance 2.3 Rs 2000 per month Rs 2000 x 12 = Rs 24,000/-
Printing & Computer Stationery 2.4 Rs 50000/- Rs 50000/-
Others
2.5
1. Procurement of LCD Projector 2. Java enabling handset @ & its maintenance @ Rs 3500
Rs 1.5 Lacs Rs 2.3 Lacs
Operationalizing
HMIS at Sub District level
Review of Existing registers – to make them compatible with
National HMIS
3.1
Rs 2000 per SC Rs 1.32 Lacs
Printing of new Registers/Forms
3.2
Training of staff 3.3 Grand Total Rs 15.35

CCP PIP 2010-11

CCP PIP 2010-11
NATIONAL RURAL HEALTH MISSION Budget Format for NRHM Mission Flexible Pool Part B
S.No. Initiative Number Proposed
Rate Proposed
Total Amount (in lakhs)
Remarks
A ASHAs
A1 Selection & Training of ASHA 50 0.0055 0.275 0
A2 VHSC Untied Grant 627 0.10 67.7 0
A3 ASHA Kit 627 0.03 18.0 0
A4 ASHA Incentives 627 0.02 12.54 0
A5 Others 0 0 0 0
TOTAL 98.515
B Infrastructure related matters
B1 New Construction of DH 0 0 0 0
B2 Renovation /Upgradation of DH 90 0 90 0
B3 New Construction of CHCs 0 0 0 0
B4 Renovation /Upgradation of CHCs 0 0 0 0
B5 New Construction of CHCs 0 0 0 0
B6 New Construction of PHCs 2 66.0 132.0 0
B7 Renovation/Upgradation of PHCs 3 3.0 9.0 0
B8 New Construction of SCs 23 9.0 207.0 0
B9 Renovation/Upgradation of SC 8 0.50 4.0 0
B10 PHC Staff Quarter 2 1.0 2.0 0
B11 DMMU 2 3.2 3.2 0
B12 Procurement of Gypsy ( 4 PHC , DHS) 0 0 0 0
B13 Construction of District training Centre 1 35 35 0
B14 Establishment of GNM Training School 1 9.0 9.0 0
B14 Any others 0 10.0 10.0 0
B14 Others 0 0 0 0
TOTAL 501.2
C Human Resources related matters
C1 Contractual Specialists 0 0 0 0
C2 Contractual Doctors 9 0.15 1.35 0
C3 Contractual Ayush doctors 8 0.15 16.2 0
C4 Contractual paramedical 20 0.75 1.8 0
C5 Contractual ANM 63 0.05 37.8 0
C6 Others 0 0 0 0
TOTAL 57.15
D Programme Management related matters
D1 District Programme Management 1 5.0 5.0 0
D2 Divisional PMSU 0 0 0 0
D3 Block PMSU 0 0 0 0
D4 District Health Action Plan 1 5 5 0
D5 Monitoring & Evaluation 1 0.05 3.0 0
D6 HMIS ( M&E) 1 15.35 15.35 0
D7 Others 0 0 0 0
TOTAL Rs 18.85
E Untied Funds, Annual Maintenance Grants and RKS funds related matters
E1 Rogi Kalyan Samiti- DH 1 5 5 0
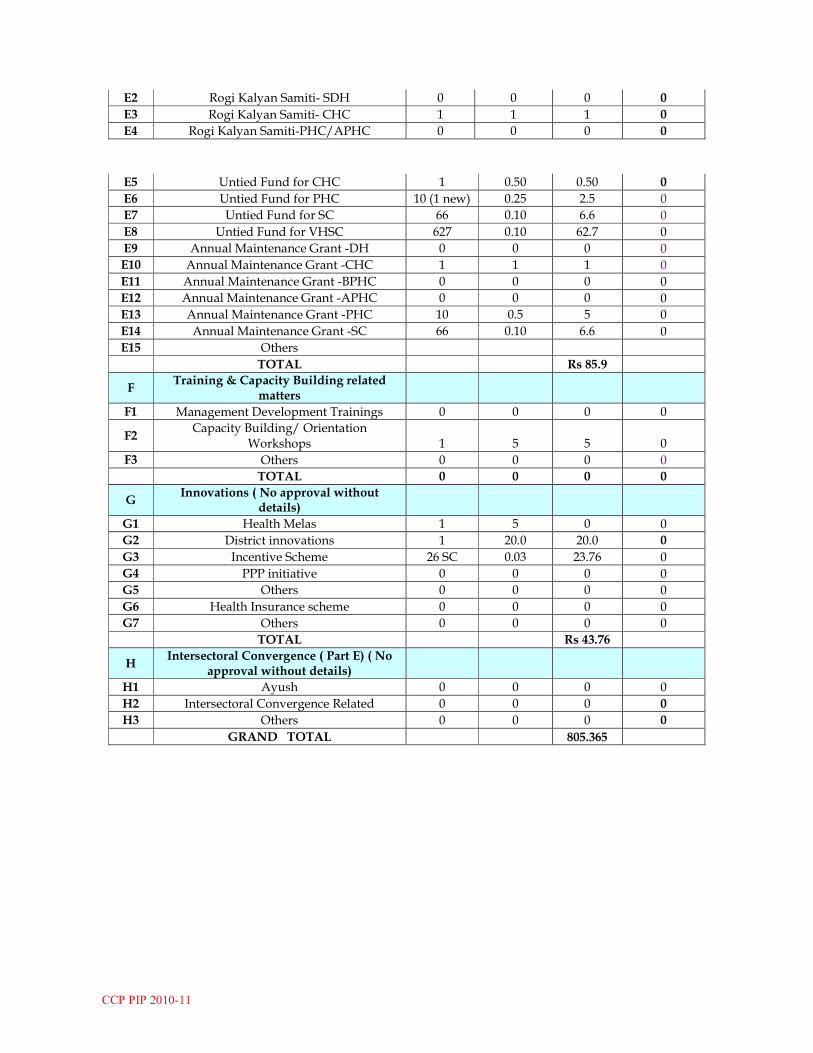
CCP PIP 2010-11
E2 Rogi Kalyan Samiti- SDH 0 0 0 0
E3 Rogi Kalyan Samiti- CHC 1 1 1 0
E4 Rogi Kalyan Samiti-PHC/APHC 0 0 0 0
E5 Untied Fund for CHC 1 0.50 0.50 0
E6 Untied Fund for PHC 10 (1 new) 0.25 2.5 0
E7 Untied Fund for SC 66 0.10 6.6 0
E8 Untied Fund for VHSC 627 0.10 62.7 0
E9 Annual Maintenance Grant -DH 0 0 0 0
E10 Annual Maintenance Grant -CHC 1 1 1 0
E11 Annual Maintenance Grant -BPHC 0 0 0 0
E12 Annual Maintenance Grant -APHC 0 0 0 0
E13 Annual Maintenance Grant -PHC 10 0.5 5 0
E14 Annual Maintenance Grant -SC 66 0.10 6.6 0
E15 Others
TOTAL Rs 85.9
F Training & Capacity Building related
matters
F1 Management Development Trainings 0 0 0 0
F2 Capacity Building/ Orientation
Workshops 1 5 5 0
F3 Others 0 0 0 0
TOTAL 0 0 0 0
G Innovations ( No approval without
details)
G1 Health Melas 1 5 0 0
G2 District innovations 1 20.0 20.0 0
G3 Incentive Scheme 26 SC 0.03 23.76 0
G4 PPP initiative 0 0 0 0
G5 Others 0 0 0 0
G6 Health Insurance scheme 0 0 0 0
G7 Others 0 0 0 0
TOTAL Rs 43.76
H Intersectoral Convergence ( Part E) ( No
approval without details)
H1 Ayush 0 0 0 0
H2 Intersectoral Convergence Related 0 0 0 0
H3 Others 0 0 0 0
GRAND TOTAL 805.365

CCP PIP 2010-11

CCP PIP 2010-11
District profile
Sl. No.
Data District
1 Blocks 5
2 Villages 627
3 Crude Birth rate ( DHIS2) 12.8
4 Crude Death rate ( DHIS2) 3.0
5 Total Fertility rate. ( DHIS2) 2.8 6 Total estimated mid-year population 2.50 Lakhs
7 Rural population (%)* 1.03 lacs 8 Urban population (%)* 1.75 lacs 9 Infant Mortality Rate
† 12
10 Below Poverty Line/Low Standards of Living Index (5)
†
95%
11 Estimated No. of Pregnant Woman 4058
Objectives: Specific objectives pertaining to the district is to have 100% beneficiaries of pregnant women be fully immunized with TT and infants be fully immunized with BCG, DPT-I, II & III, OPV-I,II & III and measles.
Goals:
1. To achieve universal immunization 2. To reduced BCG-Measles dropout 3. To sustain the Zero Polio case with adequate AFP surveillance
Reason for not achieving the target:
1. No power supply and difficult geographical terrain in Parbung CHC, Senvon PHC,
Patpuihmun PHC, Sinzawl PHC, Henglep PHC, Thanlon PHC 2. Failure to provide outreach facilities 3. Missed opportunities 4. Unreached population 5. Improved logistics leading to unmet needs 6. Poor transport mechanism making most of the hilly villages inaccessible, mainly during Rainy reason 7. Lack of residential quarters for FHWs and MOs resulting to staffs not staying at their Places of posting Suggestions:
1. Installation of Solar Operated Freezer 2. Vehicle hiring during dry season 3. Accommodation for staffs 4. Ice-line refrigerators and deep freezers
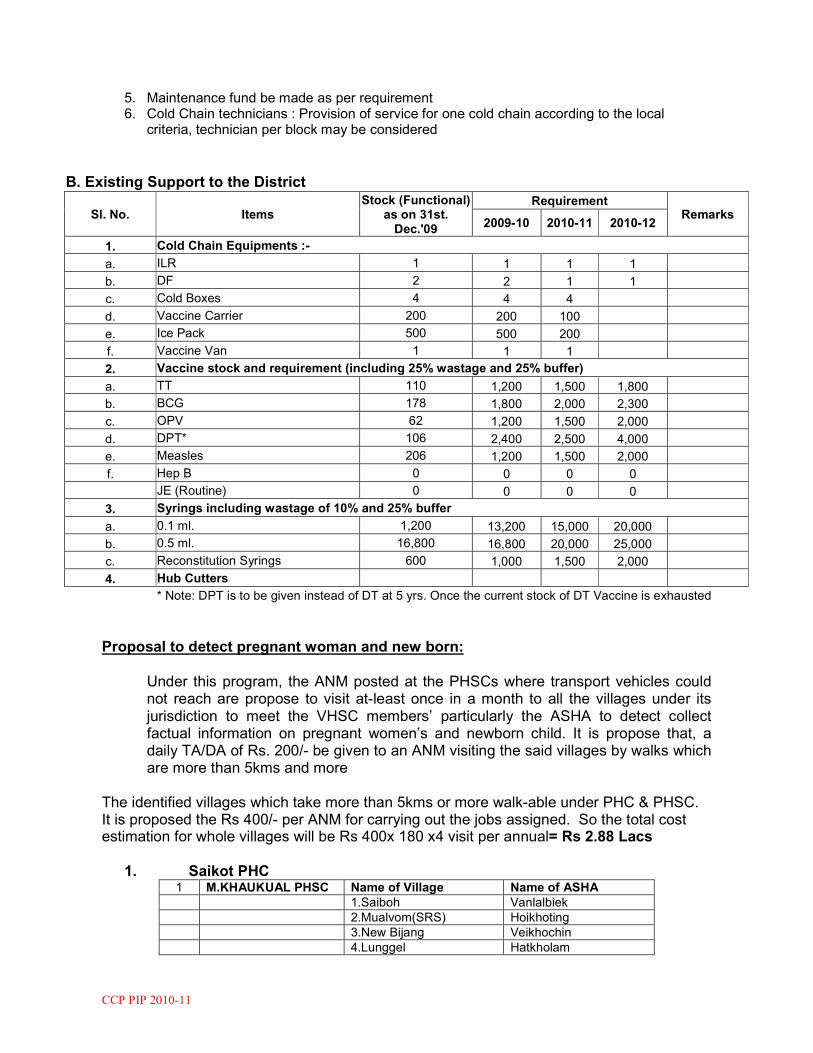
CCP PIP 2010-11
5. Maintenance fund be made as per requirement 6. Cold Chain technicians : Provision of service for one cold chain according to the local
criteria, technician per block may be considered
B. Existing Support to the District
Sl. No. Items Stock (Functional)
as on 31st. Dec.'09
Requirement Remarks
2009-10 2010-11 2010-12
1. Cold Chain Equipments :-
a. ILR 1 1 1 1
b. DF 2 2 1 1
c. Cold Boxes 4 4 4
d. Vaccine Carrier 200 200 100
e. Ice Pack 500 500 200
f. Vaccine Van 1 1 1
2. Vaccine stock and requirement (including 25% wastage and 25% buffer)
a. TT 110 1,200 1,500 1,800
b. BCG 178 1,800 2,000 2,300
c. OPV 62 1,200 1,500 2,000
d. DPT* 106 2,400 2,500 4,000
e. Measles 206 1,200 1,500 2,000
f. Hep B 0 0 0 0
JE (Routine) 0 0 0 0
3. Syrings including wastage of 10% and 25% buffer
a. 0.1 ml. 1,200 13,200 15,000 20,000
b. 0.5 ml. 16,800 16,800 20,000 25,000
c. Reconstitution Syrings 600 1,000 1,500 2,000
4. Hub Cutters
* Note: DPT is to be given instead of DT at 5 yrs. Once the current stock of DT Vaccine is exhausted
Proposal to detect pregnant woman and new born:
Under this program, the ANM posted at the PHSCs where transport vehicles could not reach are propose to visit at-least once in a month to all the villages under its jurisdiction to meet the VHSC members’ particularly the ASHA to detect collect factual information on pregnant women’s and newborn child. It is propose that, a daily TA/DA of Rs. 200/- be given to an ANM visiting the said villages by walks which are more than 5kms and more
The identified villages which take more than 5kms or more walk-able under PHC & PHSC. It is proposed the Rs 400/- per ANM for carrying out the jobs assigned. So the total cost estimation for whole villages will be Rs 400x 180 x4 visit per annual= Rs 2.88 Lacs 1. Saikot PHC
1 M.KHAUKUAL PHSC Name of Village Name of ASHA
1.Saiboh Vanlalbiek
2.Mualvom(SRS) Hoikhoting
3.New Bijang Veikhochin
4.Lunggel Hatkholam

CCP PIP 2010-11
5 Khuainuai Nianglam
6.Langvon Chinghoi
7.Hengken Nengkhotin Mate
8.Lhangnuom Kimkholhai
9. Makhau Tampak Tingneichong
10.H.Makhau Lamneichong
11.Langvom Chinhoi
12.Patjang Taineihoi
13.M.Mualhum Kimboi
14.N.Khaukual Ninglianching
15. G.Suanggel Bonny Lhungdim
16. Suangguol Nemlam
17. Khodang Hatneilhing
18. Dongjang Hoikhokim
19. L.Gangpimuol Chinneilam
20. Walkhu Ginkhochong
2 KHUANGKHAI PHSC 1.Hita Khuno Kimneichong
2.Tuisawmjang Kimsari
3.T.Khuangkhai Vungdeiching
4.Tuidam Lhingkhongai
5.Singheu Chiinngaihlian
6.Khuangkhaijang Chinthianniang
7.Leijangphai Hatneikim
8.Khengmol Thienneng
9.Gamphazol Veikholhing
10.Phaisan Lianlamniang
11.Govajang Nemkhoneng
12.K.Pangsang Khamneilhing
13.Sialsih Mangneilhng
14.Moljol Tingneineng
15. Saiboh Vanlalbiek
2. Sagang PHC
1 Name of PHSC Name of Village Name of ASHA
KOMKEIRAP PHSC 1.Louchulbung L.D.Kala
2.Gothol Vahneilhing Haokip
3.Upper Komkeirap T.Ngakpi
4.Lower Komkeirap T.Eliboi
5.Kha Aimol S.Achim
6.Keirapkhulen L.Niengboi Kom
7.Kangathel L.Nunu Kom
8.Chaiba M.K.Thuandailiu
9.Thenjang D.Tanthaului
10.Khoirentakkhuman M.Manglienchong
11.K.Paulien Lhingkhochin
2 KHOIRENTAK PHSC 1.Khoirentak Roselin
2.N.Ningthiching Nemneilhing
3.Ningthiching T.Boisi
4.Nalon Phalneiting
5.Hengkapkot Vungdeikim
6.S.Nabil Lalam
7.Leisenbung Nemjahoi
8.Teijang Mangpineng
9.Nabilkhuman Tinkhoching

CCP PIP 2010-11
10.M.Phaijang Lhaitin
11.Bungkot Thenmawi
12.Matijang Kangsi
13.Loilamkot Nemlhing
3. Sinzawl PHC
1 Name of PHSC Name of Village Name of ASHA
AIBULON PHSC 1.Phaitong Niangzanem
2.Khajang Niangkhanvung
3.Aibulon Manzaching
4. Parbung CHC 1 Name of PHSC Name of Village Name of ASHA
TUOLBUNG PHSC 1.Maulien(Thingpan) Remthangmawi
2.Tuolbung Vanzol
3.Damdeii Rourelsang
2 LEISEN PHSC 1.Leisen Zarzomawi
2.Senvon Lalengzuol
3.Senvon Rengpui
4.Senvon Zorimawi
5. Singngat PHC
1 Name of PHSC Name of Village Name of ASHA
HIANGMUAL 1.Tonglon(T) Hatpi
2.Tonglon(D) Kimpaklien
3.Buhsau Mangneiching
4.K.Tonglon Hoilalnei
5.Hiangmual Hauching
2 ALLUSINGTAM 1.Allusingtam Niangngaihman
2.L.Vokbual Donnu
3.Jabellei Nuamzahat
3 Kangkap PHSC 1. Kangkap Hoihnu
2. Tuima Khatzangai
6. Behiang PHC
1 Name of PHSC Name of Village Name of ASHA
HIANGTAM(K) PHSC 1.K.Saichang Nemkholam
2.Lancha Thenkhovah
3.Zalenphai Tingkholam
4.S.Sehken Ninghauching
5.Suangphuh Niankhoniang
6.Tonjang M.Nianching

CCP PIP 2010-11
7.Theigotang Khankim
8.Behiang(V) Vungneikim
9.Behiang M.Jubilimoi
10.Bualkot. Ngaizadim
11.Bualkot Chingngaihniang
12.Bualkot M.Vungpi
13.Hiangtam(V) Hauzaman
14.Hiangtam(K) M.Chingngaihchin
15.Tangpizol Chingngaihniang
16.Suangkuang Manngaihnuam
7. Thanlon PHC
1 Name of PHSC Name of Village Name of ASHA
MILONGMUN PHSC
1.Leijangphai Luanzakim
2.Suangsang Niengneithem
3.Sainoujang Zenzakim
4.Milongmun Vungkhanching
5.Phaijang Moinu
6.Pangen Kimkhual
2 HANSHIP PHSC 1.Hanship Manngaihching
3 KAIHLAM PHSC 1.Mualhoichiang Maman
2.Phailianbung Chingte Suantak
3.Phaipheng Luanneihoi
4.B.Munpi Mantinkhual
5.Maite Linnu
6.Mualku Dimboi
7.Umtal Nemthianlun
8.Tuilijang Ngaineikim
9.Bualtang Nianghauching
10.Thiakbung Niengthianhoih
11.Mongon Chingkhanngai
12.Pamjal Ngaineikim
13.Kaihlam Kholkhanching
14.Sinjang
4 DAILON 1.Suangpeh Dimniang
2.Thanlon Ramsan
3.Thanlon Espel
4.Thanlon Thianmoi
5.Galkapkot Khawlnu
6.Joutung Jamsei
7.Dailon Chingzakim
8. Henglep PHC
1 Name of PHSC Name of Village Name of ASHA
CHOTHEMUNPI 1.Chothemunpi Nemneichiong
2.Gouthang Nenglhing
3.Khaupijang Ngahnieng
4.Bolkot Hoinu
5.Songphu Chinkhotin

CCP PIP 2010-11
6.Songkuong Vahneilhing
7.Mamong Kimlhing
8.Mongken Lamneichin
2 L.KHENGJANG 1.L.Khengjang Hoikhochin
2.Molphei Tampak Themneilhing
3.Tonglhang Tinkholam
4.Kolchung Nemkim
5.Majuron Kuki Nenglhing
6.Napphou Kimneihoi
7.L.Phailien Chinneithiem
8.Thangsi Tinneinieng
9.L.Boljol Chinkhonem
10.Tumjangphai Lhingneihat
11.Jounoi Hoineilam
12.Zongmokot Neipi
13.K.Thenjang Ngaizalam
14.L.Thingphai Lhingneihat
15.Phoipi Nengphakim
16.M.Phaijang Lhaitin
3 SUONGDOH(CH) 1.Suongdoh (Ch) Chongzaman
2.Jikpitampak Niangtinkhol
3.Pengjang Kholkhodim
4.Kangvai Beaulalah
5.Maichammun Kimtinhat
6.Muolsang
7 Humkot
4 PHAIBUONG 1.Phaibuong Tingkhonei
2.Sanglel Hoitinniang
3.Naupanglon Boishi
4.Vantungbung Neonu
5.Khanpi Tinghoi
6.Chingmei Kuki Lhingkhonei
5 UKHA-LOIKHAI 1.Ukha-Loikhai Nengkhohoi
2.Pakol Hoicha
3.B.Mongjang
4.Bongphazol Chinnei
5. Lhanjang Nengboi
6 KOLHEN 1.Kolhen Sangkim
2.Suangpha Lynda
3.Henglep Lhingzalam
4.Nahjang Nehkhohoi
5.Mollen Veikhohoi
6.Moljen Lhaizavei
7 NUNGSHAI 1.Nungshai Vungngaihniang
2.Ainah Vahkhothem
3.Lailong(S) V.Pari
4.Lailong(L) Nenem
5.Khanpi(Kamkeilon) Neikhohat
6. Lungchuang** Jenny
7. Nahlon Neikhohoi

CCP PIP 2010-11
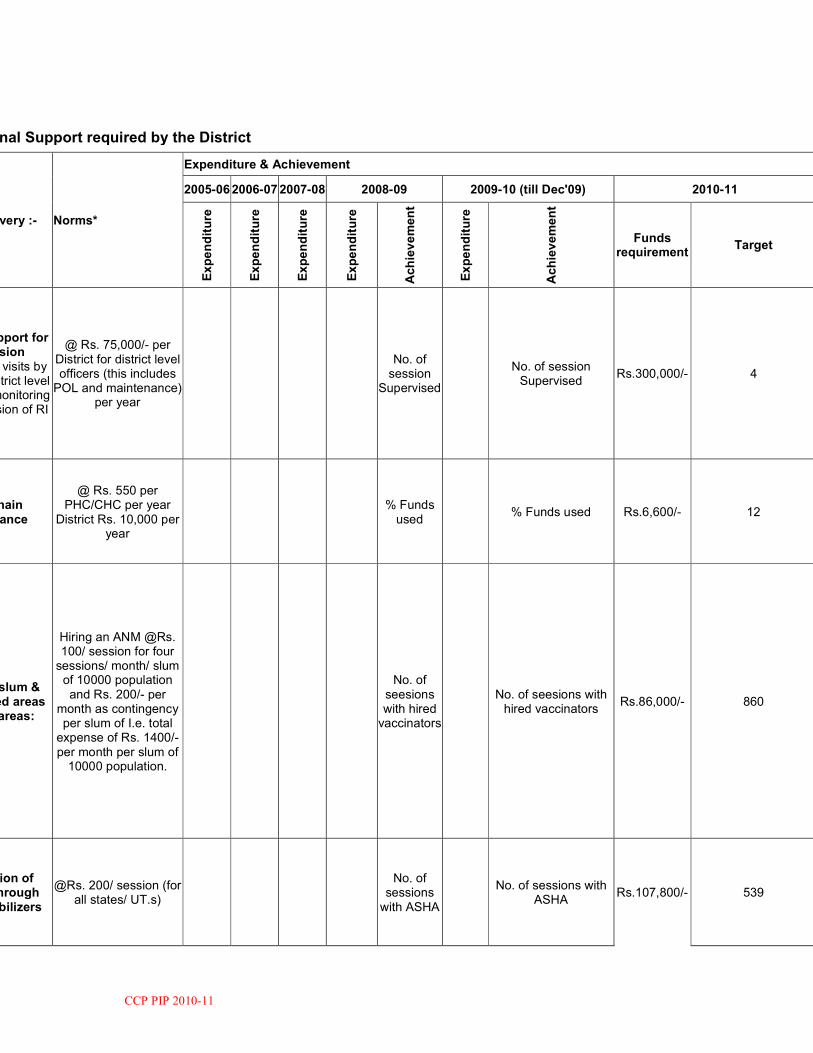
CCP PIP 2010-11
C. Additional Support required by the District
Service Delivery :- Norms*
Expenditure & Achievement
2005-06 2006-07 2007-08 2008-09 2009-10 (till Dec'09) 2010-11
Expenditure
Expenditure
Expenditure
Expenditure
Achievement
Expenditure
Achievement
Funds requirement
Target
Mobility support for supervision
Supervisory visits by state and district level officers for monitoring and supervision of RI
@ Rs. 75,000/- per District for district level officers (this includes POL and maintenance)
per year
No. of session
Supervised
No. of session Supervised
Rs.300,000/- 4
Cold Chain maintenance
@ Rs. 550 per PHC/CHC per year
District Rs. 10,000 per year
% Funds used
% Funds used Rs.6,600/- 12
Focus on slum & underserved areas in urban areas:
Hiring an ANM @Rs. 100/ session for four sessions/ month/ slum of 10000 population and Rs. 200/- per
month as contingency per slum of I.e. total expense of Rs. 1400/- per month per slum of 10000 population.
No. of seesions with hired vaccinators
No. of seesions with hired vaccinators
Rs.86,000/- 860
Mobilization of children through ASHA/ mobilizers
@Rs. 200/ session (for all states/ UT.s)
No. of
sessions with ASHA
No. of sessions with
ASHA Rs.107,800/- 539

CCP PIP 2010-11
Alternative Vaccice Delivery:
Geographically hard to reach areas (eg.
Session site>30 kms. From vaccine delivery point, river crossing etc.) Rs. 200 per RI
session
No. of
sessions with AVD
No. of sessions with
AVD Rs.160,000/- 800
For RI session in other areas @Rs. 75 per
session.
Rs.7,500/- 100
Support for Computer Assistant forRI reporting (with annual increment of 10% w.e.f. from 2010-
State @Rs. 12,000 - 15,000 p.m. Districts @Rs.12,000 p.m.
No. of C.A. in position
No. of C.A. in position Rs.144,000/- 1
Printing and dissemination of immunization cards,
tally sheets, monitoring forms, etc.
@Rs. 5 per bebeficiary
Rs.23,600/- 4720
Review Meetings
Support for Quarterly State level review meetings of district Officer @Rs. 1300/ participant/ day for three persons
(CMO/DIO/District Cold Chain Officer
No. of meetings held
No. of meetings held Rs.7,800/- 6

CCP PIP 2010-11
Quarterly Review & feedback meeting for exclusive for RI at
district level with one Block MO.s, ICDS CDPO and other stakeholders @Rs.
200 per participant for meeting expenses
(lunch, organizational expenses)
No. of
meetings held
No. of meetings held Rs.40,000/- 10
Quarterly Review meeting for exclusive for RI at block level @Rs. 75/pp as
honorarium for ASHAs (travel) and Rs. 25 per persons at the disposal of MO-I/C for meeting
expenses (refreshment,
stationary and misc. expenses)
Rs.40,775/-
Trainings District level orientation training for
ANM, Multi Purpose Health
Worker (Male), LHV, Health Assistant (Male/Female), Nurse Mid Wives, BEEs & other
specialist (as per RCH norms)
As per revised norms for trainings under
RCH
No. of persons trained
No. of persons trained 60000 No. of persons trained

CCP PIP 2010-11
Three day training of Medical Officers on
using revised MO trainging module
As per revised norms for trainings under
RCH
No. of persons trained
No. of persons trained 3500 14
One day refresher District RI
Computer Assistants on RIMS/HMIS and
Immunization formats NRHM
As per revised norms for trainings under
RCH Rs.1,200/- 6
Cold Chain handlers training for block level cold chain handlers by State and District Cold Chain
Officers and DIO for a batch of 15-20
trainees and three trainers
As per revised norms for trainings under
RCH
No. of persons trained
No. of persons trained Rs.7,600/- 76
One day Training of block level data
by DIO and District ColdChain Officer to train about the reporting formats of Immunization and
NRHM
As per revised norms for trainings under
RCH
No. of persons trained
No. of persons trained Rs.750/- 5
Microplanning To develop sub-centre ;and PHC microplans
using bottom up planning with
participation of ANM, ASHA, AWW
@Rs. Rs. 150 per sub-centre (meeting at block level, logistic)
% of SC/PHC/CHC/Dristrict
have updated microplans this year
Rs.9,900./-
% of SC/PHC/CHC/Dristrict
have updated microplans this year

CCP PIP 2010-11
For consolidation of microplan at PHC/CHC
level @Rs. 1000/- block & at district level
@Rs. 2050/- per district
Rs.3,050./-
POL for vaccine delivery from State to District and from
district to PHC/CHCs
Rs. 1,25,000/- district/year
% Funds used
% Funds used Rs.125,000./- % Funds used
Consumables for computer including provision for internet
acces for RIMS
@Rs. 600/ month/district
Rs.7,200./- 12
Injection Safety
% Funds used
% Funds used % Funds used
Red/Black Plastic bags etc.
@Rs. 2/bags/session
Bleach/Hypochlorite solution
@Rs. 550 per PHC/CHC per year
Twin bucket @Rs. 450 per
PHC/CHC per year
Any State Specific Need w;ith
justification (Please provide a separate
up on objective, strategy,
output and outcomes, basis for cost estimates etc.
10% of total amount of approved PIP
% Funds used
% Funds used % Funds used

CCP PIP 2010-11
Budget required under Immunization activities: Rs 11, 35,075 Budget requirement under propose pregnant women detection issues= Rs 2.88 Lacs Total Budget will be:- Rs 14.23 Lacs
District - wise Coverage reports (in numbers)
Sl. No.
Name of District
Yearly Target (2008-09)
Yearly Target (2009-10)
BCG Coverage (in Numbers)
OPV- 1st. Dose Coverage (in Numbers)
OPV- 3rd. Dose Coverage (in Numbers)
DPT-Coverage (in Numbers)
Infants Pregnant Women
Infants Pregnant Women
2008-09 2009-10* 2008-09 2009-10* 2008-09 2009-10* 2008-09
1. Ccpur 4728 5540 4928 5840 3847 2850 4175 3511 3395 3232 4175
Sl. No.
Name of District
Dep B - Birth Dose Coverage
Hep B - 1st. Dose Coverage
Hep B - 3rd. Dose Coverage (Wherever applicable)
Measles Coverage TT2 + Booster Coverage
JE(Wherever applicable)
2008-09 2009-10* 2008-09 2009-10* 2008-09 2009-10* 2008-09 2009-10* 2008-09 2009-10* 2008-09
1. Ccpur - - - - - - 2568 2655 - 1371 -
# Coverage for 2009-10 till Dec.'09
District - wise VPD reports in 2009-10 (in numbers)
Sl. No.
Name of District
Diptheria Whooping Cough Neonatal Tetanus Tetanus (others) Measles
Cases Deaths Cases Deaths Cases Deaths Cases Deaths Cases Deaths Cases
1. Ccpur - - - - - - - - 24 - -
Routine Immunization Monitoring System Status
Sl. No.
Name of District
RIMS Installed Computer Assistant in position
RIMS uploaded for analysis and programme monitoring
Apri.'09 May'09 June'09 July'09 Aug.'09 Sept.'09 Oct.'09
1. Ccpur - 1 - - - - 24 - -
* Write Yes/No for the month the district has uploaded RIMS data of district
CCP PIP 2010-11
NATIONAL IODINE DEFICIENCY DISORDERS CONTROL PROGRAM (NIDDCP)
Objective:
To reduce the prevalence of iodine deficiency disorder
Strategy:
Provision of making available iodated salt
Activities: 1. Checking iodine levels of iodated salt through wholesalers & retailers and household consumers in all the Blocks of the District. 2. The distribution of iodated salt in the District through open
market and Public Distribution Systems (PDS). 3. Conducting Training. 4. Dissemination of information, education and communication to
create positive consumer demand and change consumer behavior with the objective of ensuring consumption of iodated salt by the total population.
Plan of Action:
Information, Education and Communication 1. Production of booklets on iodine 2. Exhibition of IDD 3. Translation of IDD Booklets on local dialects 4. Production of booklets for school children
Survey Survey on prevalence of iodine deficiency disorders in all the blocks of the District IDD Monitoring Lab:
For quality monitoring of iodized salt sample the following reagent, glassware & equipment are needed –
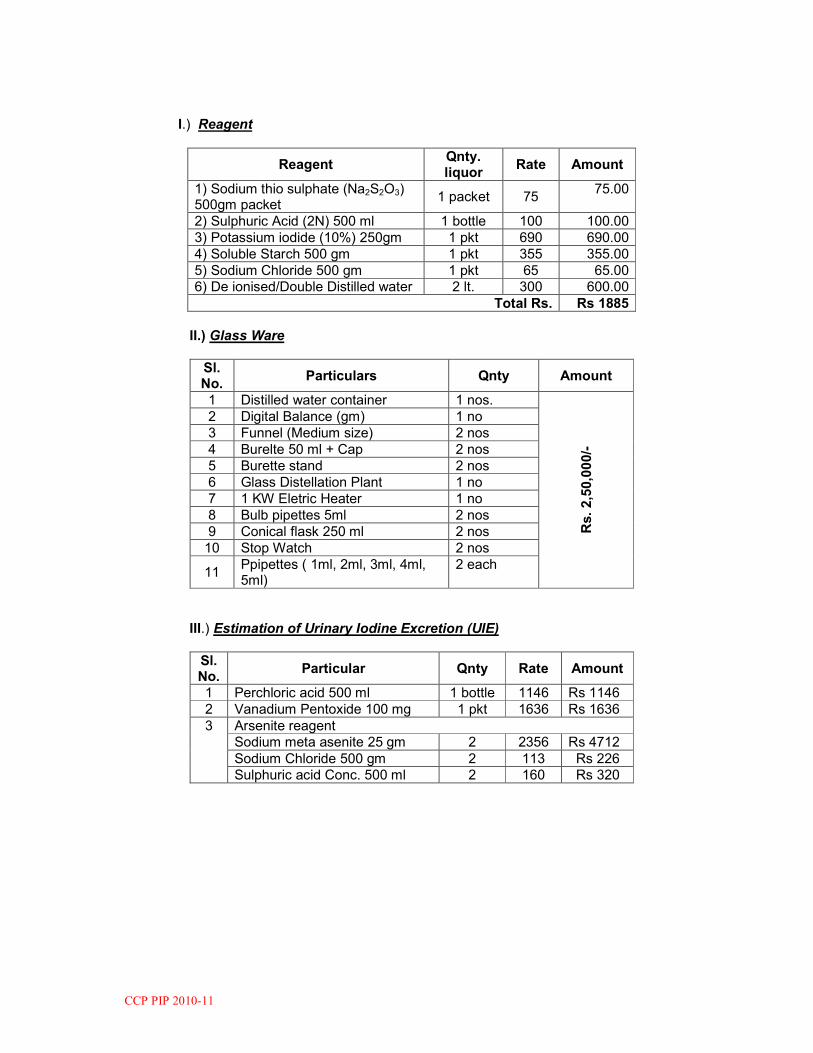
CCP PIP 2010-11
I.) Reagent
Reagent Qnty. liquor
Rate Amount
1) Sodium thio sulphate (Na2S2O3) 500gm packet
1 packet 75 75.00
2) Sulphuric Acid (2N) 500 ml 1 bottle 100 100.00 3) Potassium iodide (10%) 250gm 1 pkt 690 690.00 4) Soluble Starch 500 gm 1 pkt 355 355.00 5) Sodium Chloride 500 gm 1 pkt 65 65.00 6) De ionised/Double Distilled water 2 lt. 300 600.00
Total Rs. Rs 1885 II.) Glass Ware
Sl. No.
Particulars Qnty Amount
1 Distilled water container 1 nos.
Rs. 2,50,000/-
2 Digital Balance (gm) 1 no 3 Funnel (Medium size) 2 nos 4 Burelte 50 ml + Cap 2 nos 5 Burette stand 2 nos 6 Glass Distellation Plant 1 no 7 1 KW Eletric Heater 1 no 8 Bulb pipettes 5ml 2 nos 9 Conical flask 250 ml 2 nos 10 Stop Watch 2 nos
11 Ppipettes ( 1ml, 2ml, 3ml, 4ml, 5ml)
2 each
III.) Estimation of Urinary Iodine Excretion (UIE)
Sl. No.
Particular Qnty Rate Amount
1 Perchloric acid 500 ml 1 bottle 1146 Rs 1146 2 Vanadium Pentoxide 100 mg 1 pkt 1636 Rs 1636 3 Arsenite reagent
Sodium meta asenite 25 gm 2 2356 Rs 4712 Sodium Chloride 500 gm 2 113 Rs 226 Sulphuric acid Conc. 500 ml 2 160 Rs 320
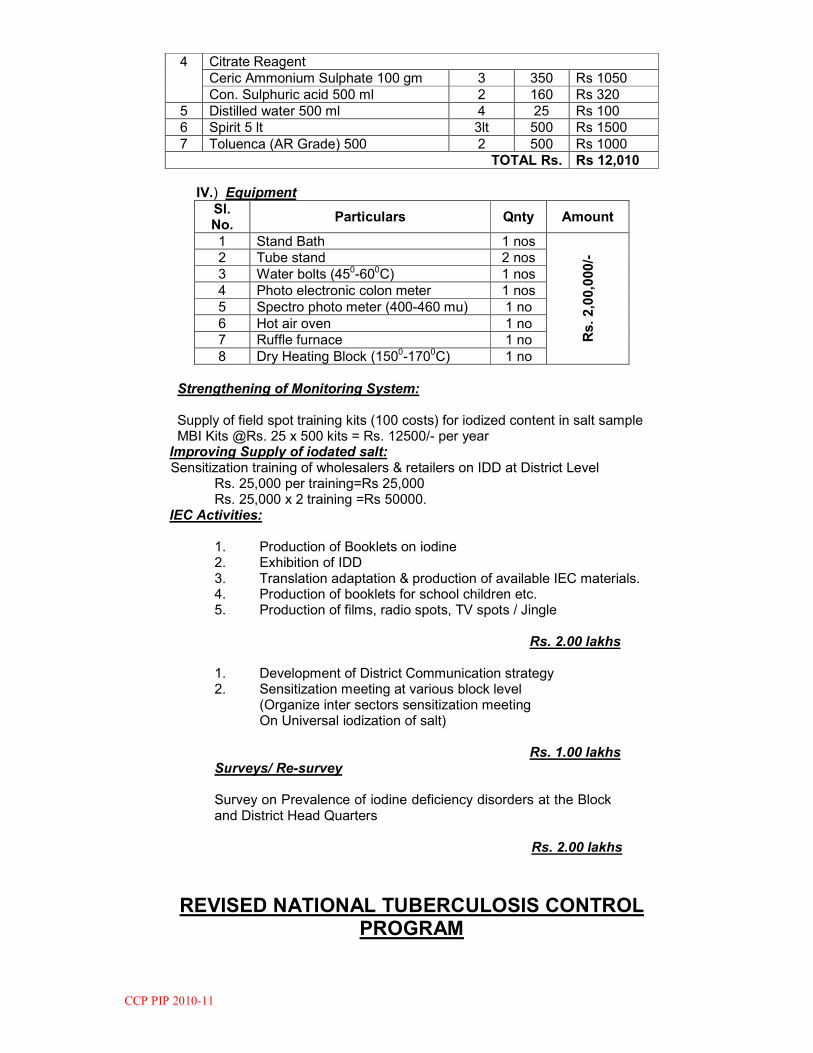
CCP PIP 2010-11
4 Citrate Reagent Ceric Ammonium Sulphate 100 gm 3 350 Rs 1050 Con. Sulphuric acid 500 ml 2 160 Rs 320
5 Distilled water 500 ml 4 25 Rs 100 6 Spirit 5 lt 3lt 500 Rs 1500 7 Toluenca (AR Grade) 500 2 500 Rs 1000
TOTAL Rs. Rs 12,010 IV.) Equipment
Sl. No.
Particulars Qnty Amount
1 Stand Bath 1 nos
Rs. 2,00,000/-
2 Tube stand 2 nos 3 Water bolts (450-600C) 1 nos 4 Photo electronic colon meter 1 nos 5 Spectro photo meter (400-460 mu) 1 no 6 Hot air oven 1 no 7 Ruffle furnace 1 no 8 Dry Heating Block (1500-1700C) 1 no
Strengthening of Monitoring System: Supply of field spot training kits (100 costs) for iodized content in salt sample MBI Kits @Rs. 25 x 500 kits = Rs. 12500/- per year Improving Supply of iodated salt:
Sensitization training of wholesalers & retailers on IDD at District Level Rs. 25,000 per training=Rs 25,000 Rs. 25,000 x 2 training =Rs 50000. IEC Activities:
1. Production of Booklets on iodine 2. Exhibition of IDD 3. Translation adaptation & production of available IEC materials. 4. Production of booklets for school children etc. 5. Production of films, radio spots, TV spots / Jingle
Rs. 2.00 lakhs 1. Development of District Communication strategy 2. Sensitization meeting at various block level (Organize inter sectors sensitization meeting
On Universal iodization of salt) Rs. 1.00 lakhs
Surveys/ Re-survey
Survey on Prevalence of iodine deficiency disorders at the Block and District Head Quarters Rs. 2.00 lakhs
REVISED NATIONAL TUBERCULOSIS CONTROL
PROGRAM
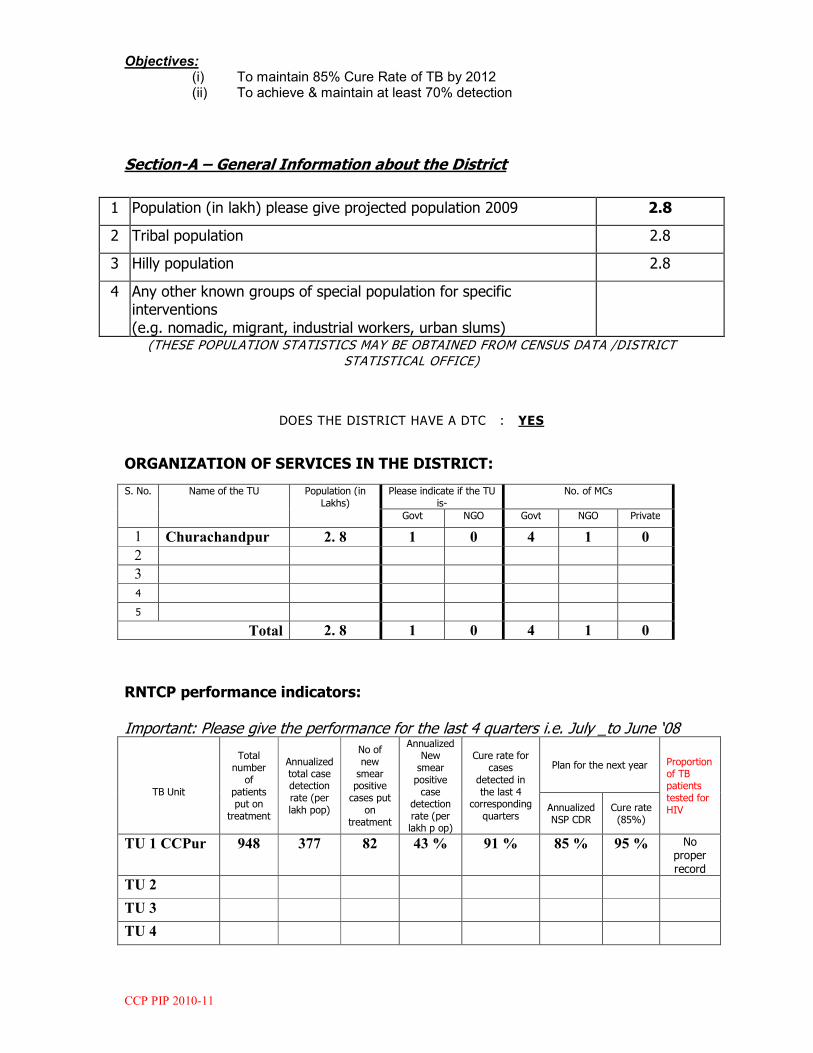
CCP PIP 2010-11
Objectives: (i) To maintain 85% Cure Rate of TB by 2012 (ii) To achieve & maintain at least 70% detection
Section-A – General Information about the District
1 Population (in lakh) please give projected population 2009 2.8
2 Tribal population 2.8
3 Hilly population 2.8
4 Any other known groups of special population for specific interventions
(e.g. nomadic, migrant, industrial workers, urban slums)
(THESE POPULATION STATISTICS MAY BE OBTAINED FROM CENSUS DATA /DISTRICT
STATISTICAL OFFICE)
DOES THE DISTRICT HAVE A DTC : YES
ORGANIZATION OF SERVICES IN THE DISTRICT:
S. No. Name of the TU Population (in Lakhs)
Please indicate if the TU is-
No. of MCs
Govt NGO Govt NGO Private
1 Churachandpur 2. 8 1 0 4 1 0
2
3
4
5
Total 2. 8 1 0 4 1 0
RNTCP performance indicators:
Important: Please give the performance for the last 4 quarters i.e. July _to June ‘08
TB Unit
Total number of
patients put on
treatment
Annualized total case detection rate (per lakh pop)
No of new smear positive cases put
on treatment
Annualized New smear positive case
detection rate (per lakh p op)
Cure rate for cases
detected in the last 4
corresponding quarters
Plan for the next year Proportion of TB patients tested for HIV Annualized
NSP CDR Cure rate (85%)
TU 1 CCPur 948 377 82 43 % 91 % 85 % 95 % No proper
record TU 2
TU 3
TU 4
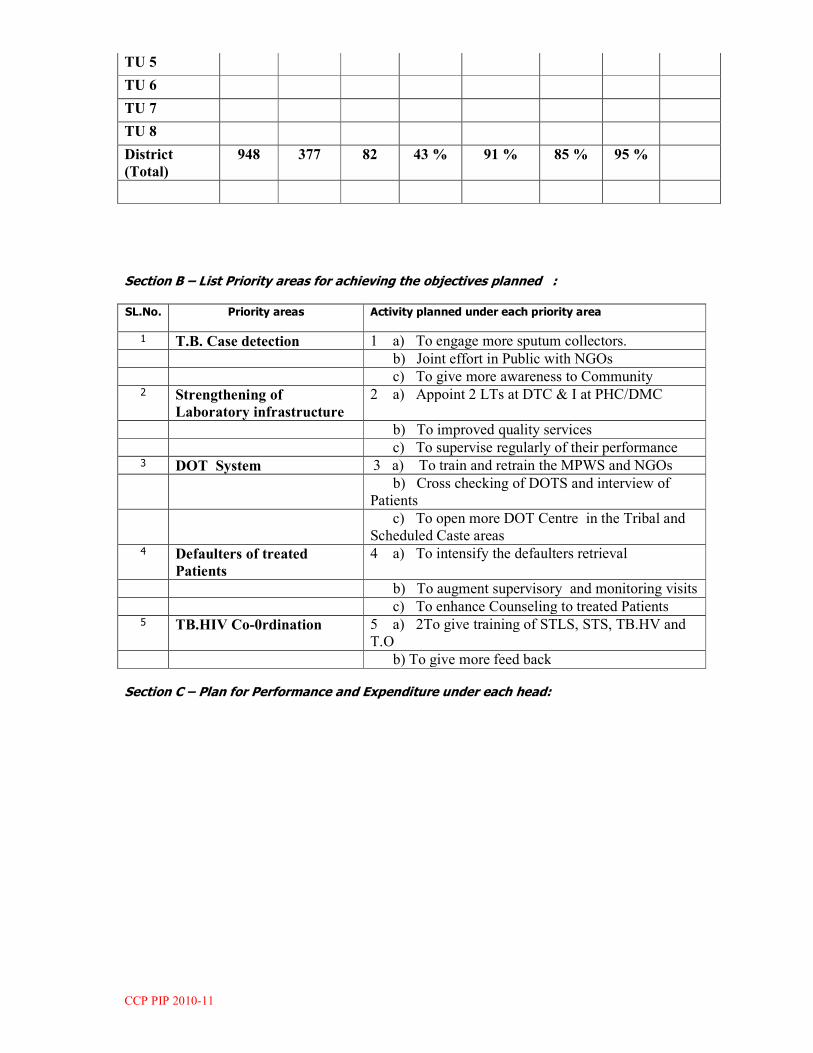
CCP PIP 2010-11
TU 5
TU 6
TU 7
TU 8
District
(Total)
948 377 82 43 % 91 % 85 % 95 %
Section B – List Priority areas for achieving the objectives planned :
SL.No. Priority areas Activity planned under each priority area
1 T.B. Case detection 1 a) To engage more sputum collectors. b) Joint effort in Public with NGOs c) To give more awareness to Community 2 Strengthening of
Laboratory infrastructure
2 a) Appoint 2 LTs at DTC & I at PHC/DMC
b) To improved quality services c) To supervise regularly of their performance 3 DOT System 3 a) To train and retrain the MPWS and NGOs b) Cross checking of DOTS and interview of
Patients c) To open more DOT Centre in the Tribal and
Scheduled Caste areas 4 Defaulters of treated
Patients
4 a) To intensify the defaulters retrieval
b) To augment supervisory and monitoring visits c) To enhance Counseling to treated Patients 5 TB.HIV Co-0rdination 5 a) 2To give training of STLS, STS, TB.HV and
T.O b) To give more feed back
Section C – Plan for Performance and Expenditure under each head:

CCP PIP 2010-11
Civil Works :
Activity No. required
as per the norms in the district
No. actually
present in the district
No. planned
for this year
Pl provide justification if an increase is planned (use separate
sheet if required)
Estimated Expenditure on the
activity
Quarter in which the
planned activity expected to be completed
(a) (b) (c) (d) (e) (f)
DTC 1 1 0 Renovation of DTC
Building and
construction of sputum
collection shed
Rs. 40,000 &
Rs. 30,000.00
= Rs.70,00.00
3rd &
Fourth Qrt.
TUs 0 0 0 0 0 DMC 5 5 1 old
DMC
By
construction/renovation
=Rs35,000.00 Second
Quarter
TOTAL Rs.
105,000.00
Laboratory Materials :
Activity Amount permissible as per the norms in the district
Amount actually spent in the last 4 quarters
Procurement planned during the current financial year (in Rupees)
Estimated Expenditure for the next financial year for which plan is being submitted
(Rs.)
Justification/ Remarks for (d)
(a) (b) (c) (d) (e)
Purchase of Lab Materials
Rs.
44,850.002
Rs.46,000.00
Rs.
60,000.00
Rs.
70,000.00
Material cost
and No. of
patients
increased
Honorarium

CCP PIP 2010-11
Activity
Amount permissible as per the norms in the district
Amount actually spent in the last 4 quarters
Expenditure (in Rs) planned for current financial
year
Estimated Expenditure for the next financial year for which plan is being submitted
(Rs.)
Justification/ Remarks for (d)
(a) (b) (c) (d) (e)
Honorarium for DOT providers (both tribal and non tribal districts)
Per
patient
500x2x12
140,000.00 Average
patient,
completed
treatment is
70/month =
70
70x250x2x12
=420,000.00
under TAP
Average
patient,
completed
treatment is
75/month =
75
73x250x2x12
= 450,000.00
under TAP
Under TAP
Rs.250/per
patient +250
per patient for
DOT provider
for average
Patient of
70/month
requirement
=(70x250x2x12
+2000)
= 422,000.00 Honorarium for DOT providers of Cat IV patients
0 0 0 0
Rs.
12,000.00
Rs.
140,000.00
Rs.
420,000.00
Rs.
450,000.00
Annual Action Plan Format Advocacy, Communication and Social Mobilization (ACSM) for
RNTCP
1) Information on previous year’s Annual Action Plan
a) Budget proposed in last Annual Action Plan: ……………….
b) Amount released by the state: …………………..
c) Amount Spent by the district- …………………
2) Permissible budget as per norm : ……………………
3) Budget for next financial year for the district as per action plan detailed below:
……………………….
Program
Challeng
es to be
tackled
by ACSM
during
the Year
20010-11
WHY
ACS
M
Objec
tive
For
WHO
M
Target
Audie
nce
WHAT
ACSM
Activities
When
Time Frame
By
WHO
M
Monitoring
and
Evaluation
Budget
Based on existing
TB
indicators
and
analysis
of
communic
ation
challenges
Desired
behavi
or or
action
(make
SMA
RT: specifi
c,
Activities
Media/ Mater
ial
Requi
red
Q1 Q2 Q3 Q4 Key
implem
enter
and
RNTC
P
officer
respons
ible for
Outputs; Evide
nce
that
the
activi
ties have
Outcomes: Evide
nce
that
it has
been
effective
Total expendit
ure for
the
activity
during
the
financial
year
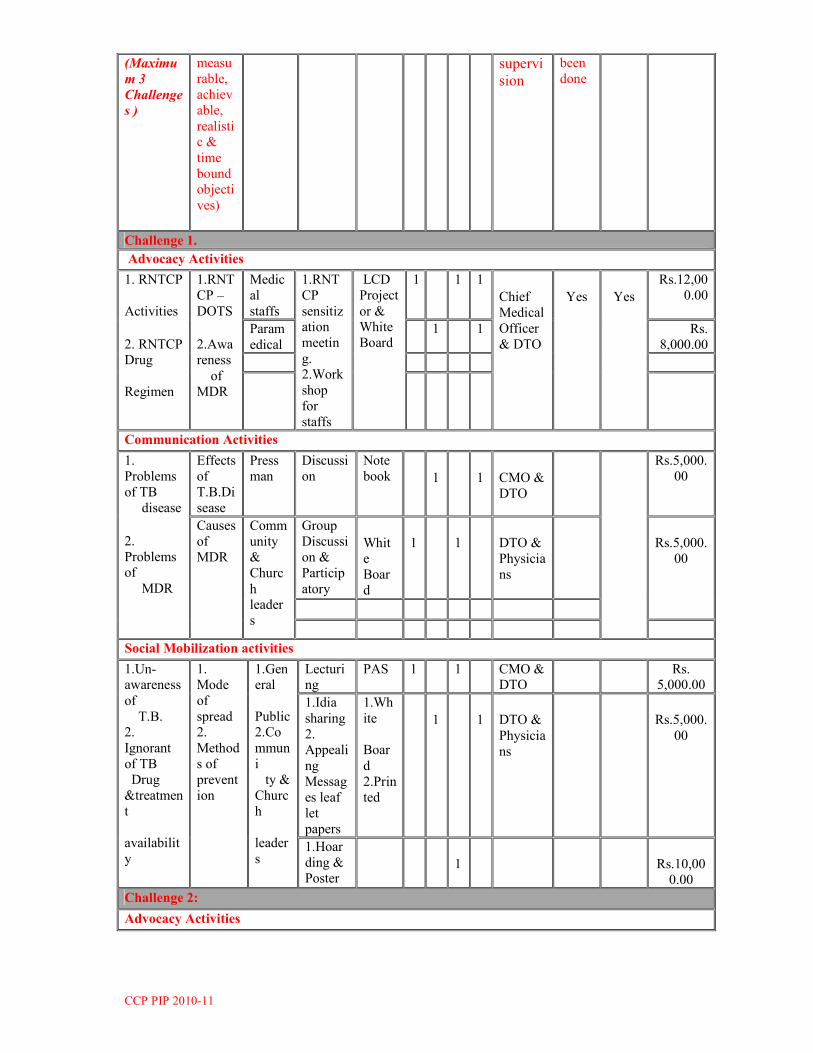
CCP PIP 2010-11
(Maximu
m 3
Challenge
s )
measu
rable,
achiev
able,
realistic &
time
bound objecti
ves)
supervi
sion
been
done
Challenge 1.
Advocacy Activities
1. RNTCP
Activities 2. RNTCP Drug
Regimen
1.RNT
CP –
DOTS 2.Awareness of
MDR
Medic
al
staffs
1.RNT
CP
sensitization
meetin
g. 2.Work
shop
for
staffs
LCD
Project
or & White
Board
1 1 1 Chief
Medical
Officer
& DTO
Yes
Yes
Rs.12,00
0.00
Param
edical 1 1 Rs.
8,000.00
Communication Activities
1.
Problems
of TB disease 2.
Problems of MDR
Effects
of
T.B.Di
sease
Press
man Discussi
on Note
book 1 1 CMO &
DTO
Rs.5,000.
00
Causes
of
MDR
Comm
unity
&
Churc
h leader
s
Group
Discussi
on &
Particip
atory
Whit
e
Boar
d
1 1 DTO &
Physicia
ns
Rs.5,000.
00
Social Mobilization activities
1.Un-awareness
of T.B. 2.
Ignorant
of TB Drug
&treatmen
t
availabilit
y
1. Mode
of
spread 2.
Method
s of
prevent
ion
1.General
Public 2.Co
mmun
i ty &
Churc
h
leader
s
Lecturing
PAS 1 1 CMO & DTO
Rs. 5,000.00
1.Idia
sharing
2. Appeali
ng
Messag
es leaf
let
papers
1.Wh
ite Boar
d 2.Prin
ted
1 1 DTO &
Physicia
ns
Rs.5,000.
00
1.Hoar
ding &
Poster
1
Rs.10,00
0.00
Challenge 2:
Advocacy Activities

CCP PIP 2010-11
Communication Activities
Social Mobilization
Challenge 3:-
Advocacy activities
Communication activities
Social Mobilization Activities
TOTAL BUDGET Rs.50,00
0.00
Equipment Maintenance:
Item
No. actually present in the district
Amount actually spent in the last 4 quarters
Amount Proposed for Maintenance during current financial yr.
Estimated Expenditure for the next financial year for which plan is being
submitted (Rs.)
Justification/ Remarks for (d)
(a) (b) (c) (d) (e)
Office Equipment (Maintenance includes computer software and hardware upgrades, repairs of photocopier,
fax, OHP etc)
1
35,000.00
45,000.00
45,000.00
Old computer
crashed and also
upgraded
Binocular Microscopes ( RNTCP)
4 5000.00 6000.00 7000.00
TOTAL Rs. 40,000.00 Rs. 51,000.00 Rs. 52,000.00
Activity No. in the district
No. already trained in RNTCP
No. planned to be trained in RNTCP during each quarter of next FY
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being submitted (Rs.)
Justification/ remarks
(a) (b) (c) (d) (e) (f)
Q1 Q2 Q3 Q4
Training of MOs 54 20
Training of LTs of DMCs- Govt + Non Govt
9 9
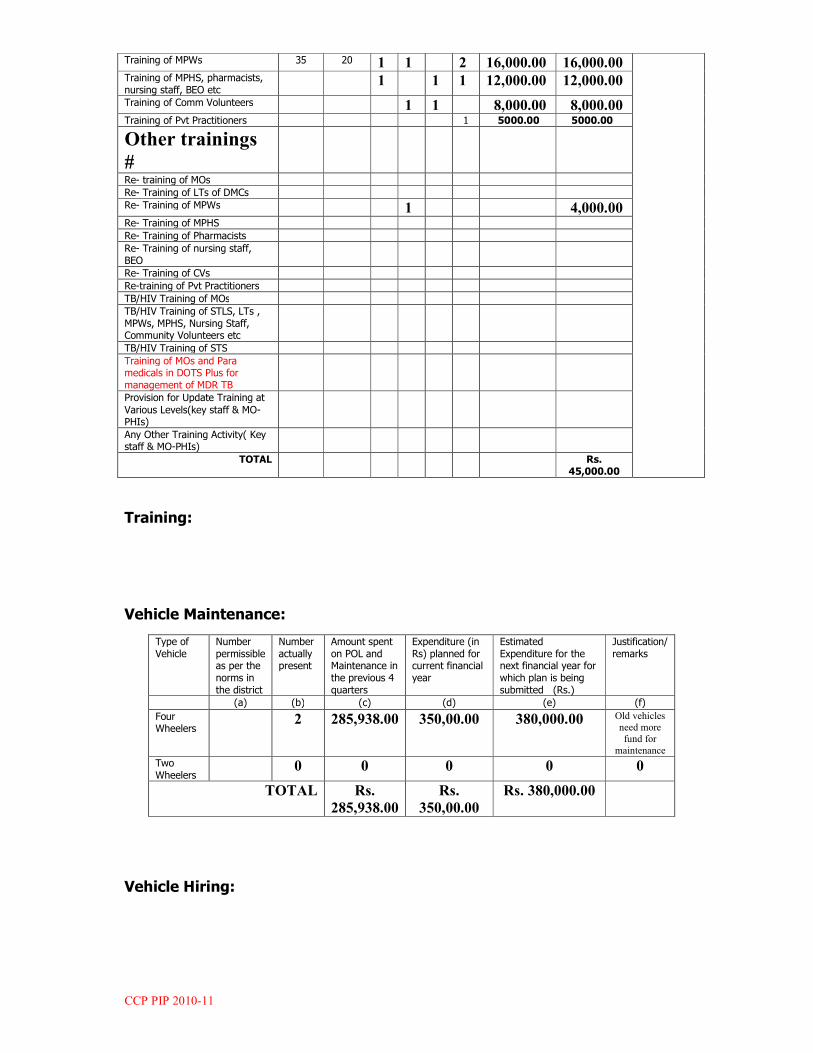
CCP PIP 2010-11
Training:
Vehicle Maintenance:
Type of Vehicle
Number permissible as per the norms in the district
Number actually present
Amount spent on POL and Maintenance in the previous 4 quarters
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being submitted (Rs.)
Justification/ remarks
(a) (b) (c) (d) (e) (f)
Four Wheelers
2 285,938.00 350,00.00 380,000.00 Old vehicles
need more
fund for
maintenance
Two Wheelers
0 0 0 0 0
TOTAL Rs.
285,938.00
Rs.
350,00.00
Rs. 380,000.00
Vehicle Hiring:
Training of MPWs 35 20 1 1 2 16,000.00 16,000.00 Training of MPHS, pharmacists, nursing staff, BEO etc
1 1 1 12,000.00 12,000.00
Training of Comm Volunteers 1 1 8,000.00 8,000.00 Training of Pvt Practitioners 1 5000.00 5000.00
Other trainings
#
Re- training of MOs
Re- Training of LTs of DMCs
Re- Training of MPWs 1 4,000.00 Re- Training of MPHS
Re- Training of Pharmacists
Re- Training of nursing staff, BEO
Re- Training of CVs
Re-training of Pvt Practitioners
TB/HIV Training of MOs
TB/HIV Training of STLS, LTs , MPWs, MPHS, Nursing Staff, Community Volunteers etc
TB/HIV Training of STS
Training of MOs and Para medicals in DOTS Plus for management of MDR TB
Provision for Update Training at
Various Levels(key staff & MO-PHIs)
Any Other Training Activity( Key staff & MO-PHIs)
TOTAL Rs. 45,000.00
CCP PIP 2010-11
Hiring of Four Wheeler
Number permissible as per the norms in the district
Number actually present
Amount spent in the previous 4 quarters
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being submitted
(Rs.)
Justification/ remarks
(a) (b) (c) (d) (e) (f)
For DTO
For MO-
TC
NGO/ PP Support: (New schemes w.e.f. 01-10-2008)

CCP PIP 2010-11
Activity No. of currently involved in RNTCP in the
district
Additional enrolment planned for this year
Amount spent in the previous 4 quarters
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being submitted(Rs.)
Justification/ remarks
(a) (b) (c) (d) (e) (f)
ACSM Scheme: TB advocacy, communication, and social mobilization
1 0 0
1. It is a specified
Project of EHA
for enhancing
RNTCP
2. The administration
and manpower
are very active to
enhance our
RNTCP activities
in the District.
3. It is as per the
provision of the
NGO Guide line. SC Scheme: Sputum Collection Centre/s
0 0 0 0 0
Transport Scheme: Sputum Pick-Up and Transport Service
30
0
0 =(25x2000x12 )
= Rs.600,000.00 Rs. 600,000.00
DMC Scheme: Designated Microscopy Cum Treatment Centre (A & B)
1 Rs.75,000.00 Rs.150,000.00 Rs. 150,000.00
1. It is one of the effective DMC in
the District
2. The
performance in
the past is
satisfactory
3. It is as per the
provision of the
NGO Guide line.
LT Scheme: Strengthening RNTCP diagnostic services
0 0 0 0 0
Culture and DST
Scheme: Providing Quality Assured Culture and Drug Susceptibility Testing Services
0 0 0 0 0
Adherence scheme: Promoting treatment adherence
1 0 0 =40,000/1lacx2.lac =Rs.80,000.00
=Rs. 80,000.00
1. It is a specified
Project of EHA for
enhancing RNTCP
activities
2. The
manpower
are very
active to
enhance our
RNTCP
activities
especially in
DOT
activities in

CCP PIP 2010-11
the
District 3. It is as per the provision of the
NGO Guide line. Slum Scheme: Improving TB control in Urban Slums
0 0 0 0 0
Tuberculosis Unit Model 0 0 0 0 0
TB-HIV Scheme: Delivering TB-HIV interventions to high HIV Risk groups (HRGs)
0 0 0 0 0
TOTAL Rs.75,000.00 Rs.830,000.00 Rs.830,000.00
Miscellaneous:
Activity* Amount permissible as per the norms in the district
Amount spent in the previous 4 quarters
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being submitted (Rs.)
Justification/ remarks
(a) (b) (c) (d) (e)
Stationery & Official requirement
45,000.0
0
44,536.
00
46,000.
00
60,000.00 Market rate increases day by day
TOTAL 45,000.0
0
Rs.
44,536.
00
Rs.
46,000.
00
Rs. 60,000.00
Contractual Services:

CCP PIP 2010-11
Activity No. required as per the norms in the district
No. actually present in the district
No. planned to be additionally hired during this year
Amount spent in the previous 4 quarters
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being
submitted (Rs.)
Justification/ remarks
(a) (b) (c) (d) (e) f
Medical Officer-DTC
Not to be filled It is done
as per the
District
RNTCP
Guide
line based
the
requireme
nt and the
posts
being
filled up
as per the
necessity.
STS 1 1 0 106,500
.00
111,000
.00
115,500.0
0 STLS 1 1 0 102,000
.00
111,000
.00
115,500.0
0 TBHV 1 1 0 75,600.
00
79,200.
00
85,800.00
DEO 1 1 0 75,600.
00
79,200.
00
85,800.00
Accountant – part time
1 1 0 26,400.
00
27,000.
00
33,000.00
Contractual
Drivers 2 2 0 113,400
.00
119,000
.00
125,000.0
0 Contractual LT 3 1 Rs..
281,700
.00
Rs.
480,000
.00
Rs.
550,000.0
0
Printing:
Activity Amount permissible as per the norms in the district
Amount spent in the previous 4 quarters
Expenditure (in Rs) planned for current financial year
Estimated Expenditure for the next financial year for which plan is being submitted (Rs.)
Justification/ remarks
(a) (b) (c) (d) (e)
Printing
*
Rs. 30,000.00 Rs. 40,000.00
Rs. 50,000.00 Rs. 50,000.00 Market rate & Servicing charge increases day by day.
Procurement of Vehicles:

CCP PIP 2010-11
Equipment No. actually present in the district
No. planned for this year
Estimated Expenditure for the next financial year for which plan is being submitted (Rs.)
Justification/ remarks
(a) (b) (c) (d)
4-wheeler **
2
2
0 The very old vehicles are no more function properly which hampers the routine programme works.
2-wheeler 0 0 0
Procurement of Equipment:
Equipment No. actually present in the district
No. planned for this year
Estimated Expenditure for the next financial year for which plan is being submitted (Rs.)
Justification/ remarks
(a) (b) (c) (d)
Office Equipment (computer, modem, scanner, printer, UPS etc)
0 0 0
Any Other
Section D: Summary of proposed budget for the district :
S.No. Category of Expenditure
Budget estimate for the coming FY 2010- 11
(To be based on the planned activities and expenditure in Section C)
1 Civil works 105,000.00
2 Laboratory materials 70,000.00
3 Honorarium 450,000.00
4 IEC/ Publicity 50,000.00
5 Equipment maintenance 52,000.00
6 Training 45,000.00
7 Vehicle maintenance 380,000.00
8 Vehicle hiring x
9 NGO/PP support 830,000.00
10 Miscellaneous 60,000.00
11 Contractual services 550,000.00
12 Printing 50,000.00
13 Research and studies x
14 Medical Colleges x
15 Procurement –vehicles ??
16 Procurement – equipment x
TOTAL Rs. 26,42,000.00
CCP PIP 2010-11
NATIONAL VECTOR BORNE DISEASE CONTROL PROGRAM (NVBDCP)
Objective: (i) To reduce Malaria Mortality by 30% by 2012 (ii) To reduce Malaria Morbidity by 50% by 2012
CCP PIP 2010-11
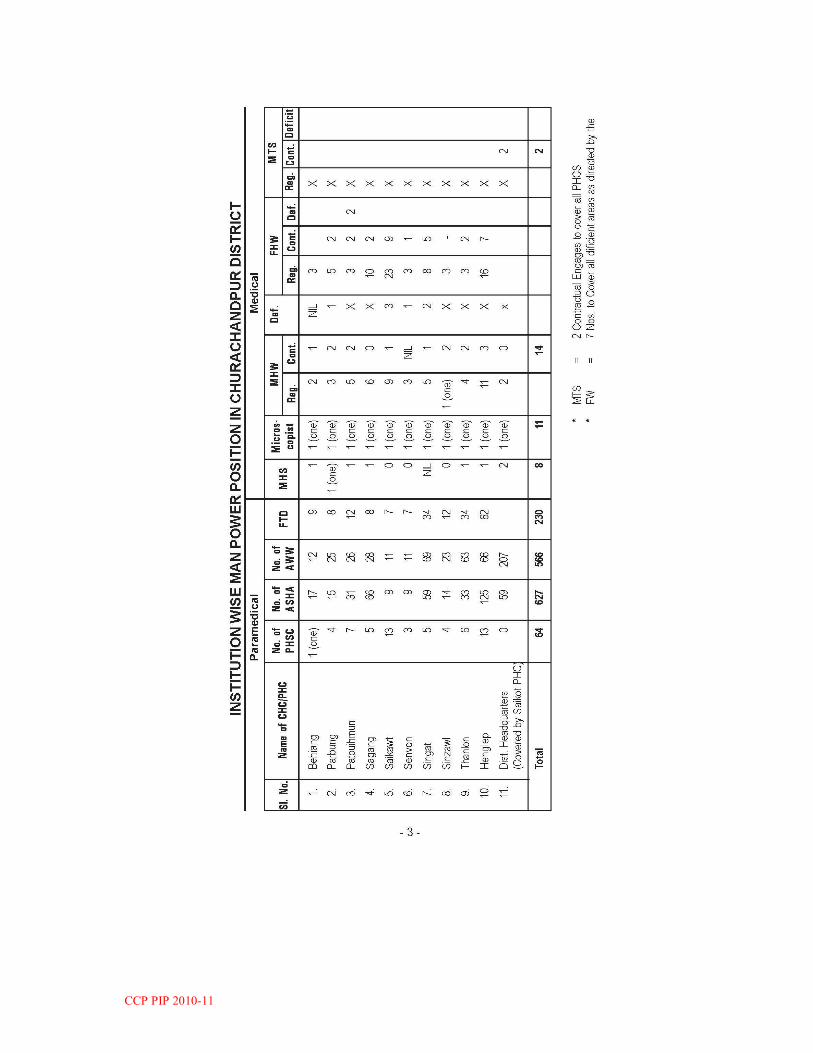
CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11
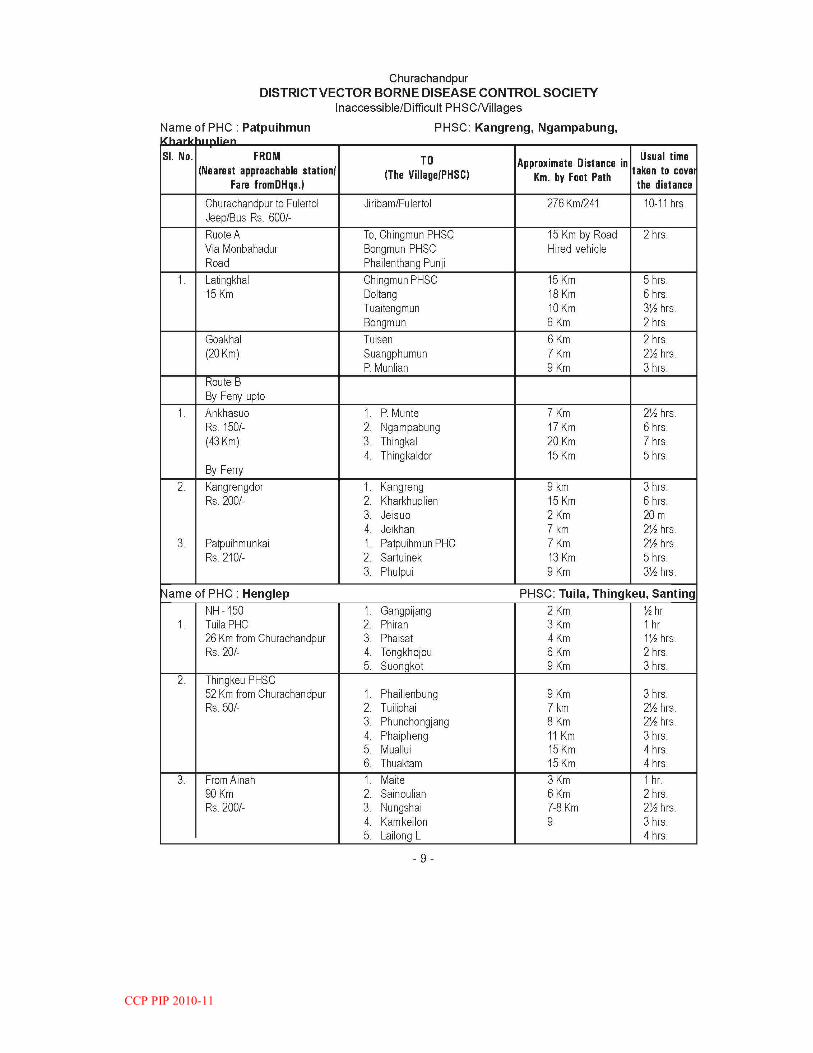
CCP PIP 2010-11
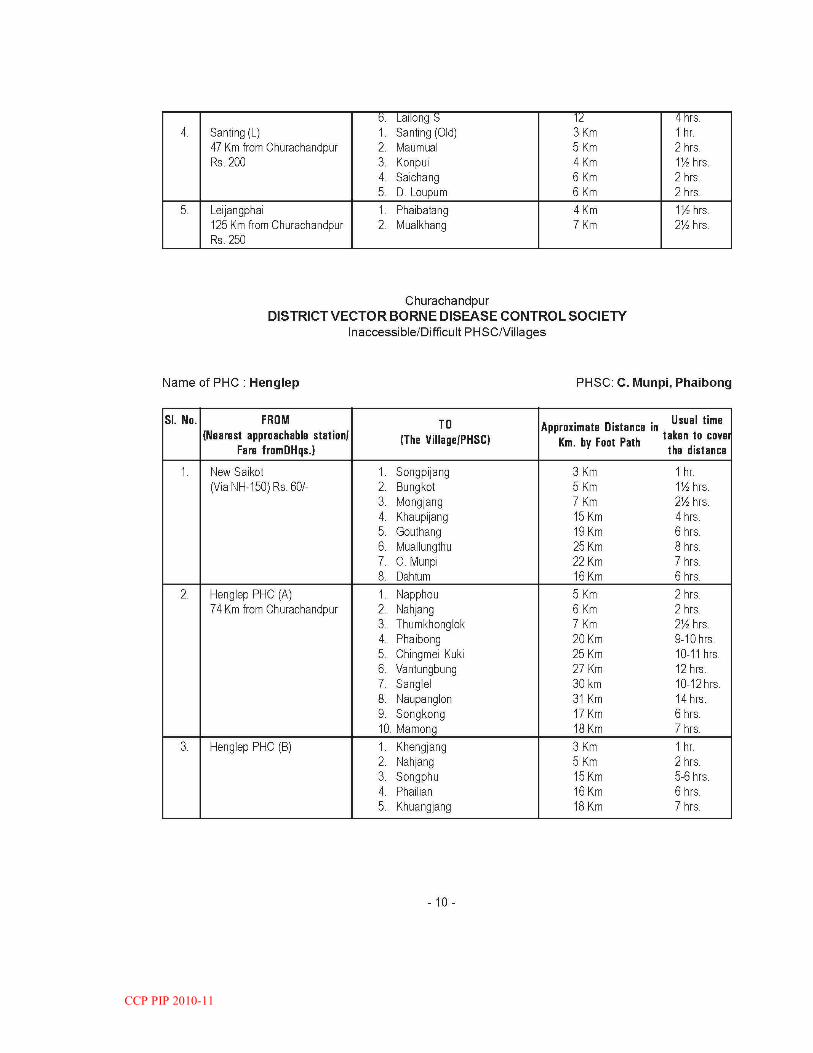
CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11

CCP PIP 2010-11
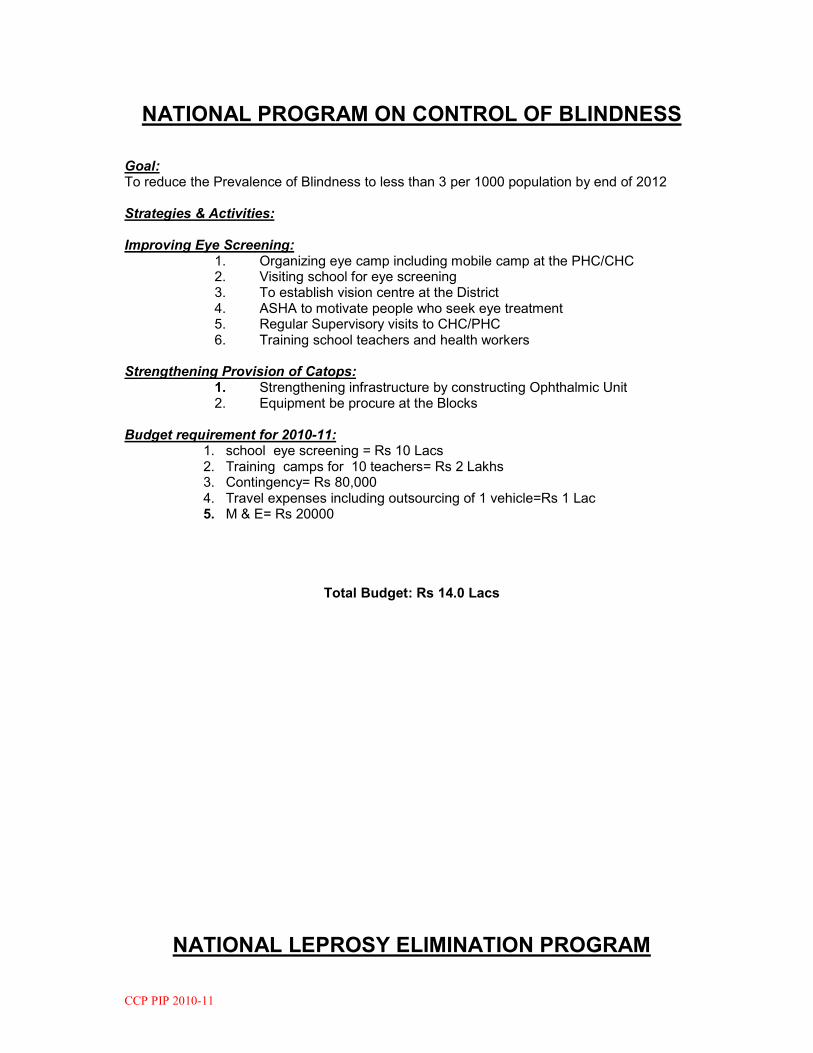
CCP PIP 2010-11
NATIONAL PROGRAM ON CONTROL OF BLINDNESS
Goal: To reduce the Prevalence of Blindness to less than 3 per 1000 population by end of 2012 Strategies & Activities: Improving Eye Screening:
1. Organizing eye camp including mobile camp at the PHC/CHC 2. Visiting school for eye screening 3. To establish vision centre at the District 4. ASHA to motivate people who seek eye treatment 5. Regular Supervisory visits to CHC/PHC 6. Training school teachers and health workers
Strengthening Provision of Catops: 1. Strengthening infrastructure by constructing Ophthalmic Unit 2. Equipment be procure at the Blocks Budget requirement for 2010-11:
1. school eye screening = Rs 10 Lacs 2. Training camps for 10 teachers= Rs 2 Lakhs 3. Contingency= Rs 80,000 4. Travel expenses including outsourcing of 1 vehicle=Rs 1 Lac 5. M & E= Rs 20000
Total Budget: Rs 14.0 Lacs
NATIONAL LEPROSY ELIMINATION PROGRAM
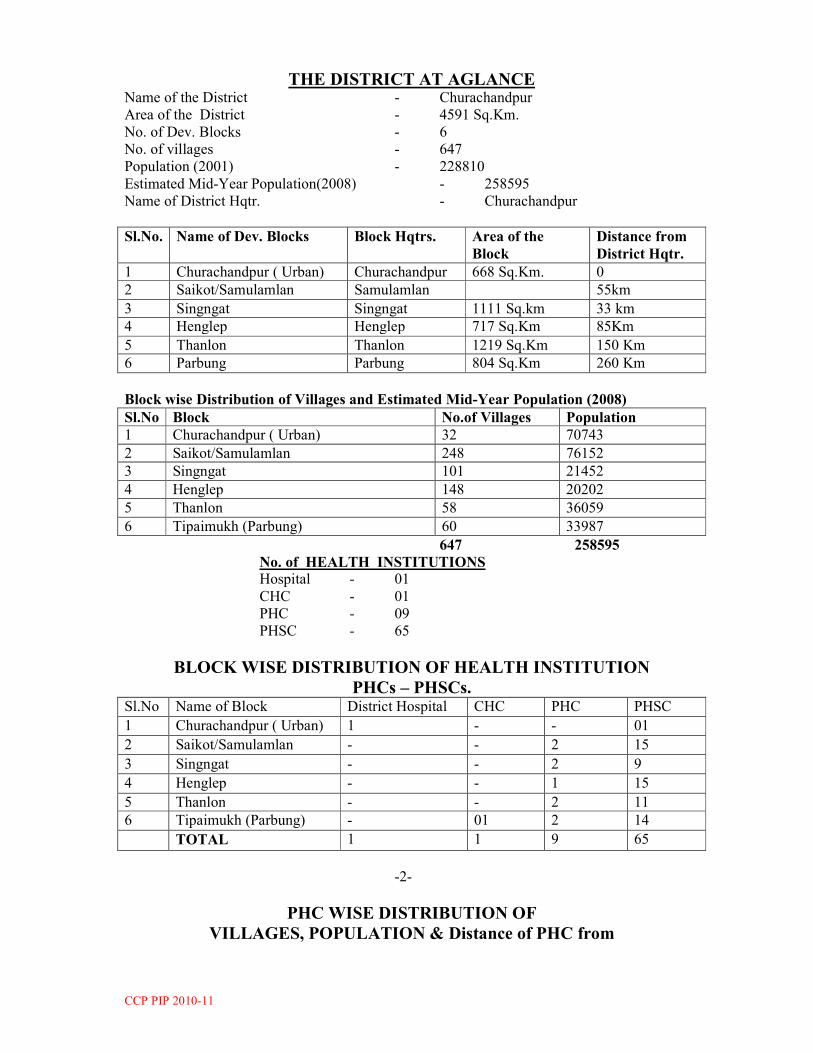
CCP PIP 2010-11
THE DISTRICT AT AGLANCE Name of the District - Churachandpur
Area of the District - 4591 Sq.Km.
No. of Dev. Blocks - 6
No. of villages - 647
Population (2001) - 228810
Estimated Mid-Year Population(2008) - 258595
Name of District Hqtr. - Churachandpur
Sl.No. Name of Dev. Blocks Block Hqtrs. Area of the
Block
Distance from
District Hqtr.
1 Churachandpur ( Urban) Churachandpur 668 Sq.Km. 0
2 Saikot/Samulamlan Samulamlan 55km
3 Singngat Singngat 1111 Sq.km 33 km
4 Henglep Henglep 717 Sq.Km 85Km
5 Thanlon Thanlon 1219 Sq.Km 150 Km
6 Parbung Parbung 804 Sq.Km 260 Km
Block wise Distribution of Villages and Estimated Mid-Year Population (2008)
Sl.No Block No.of Villages Population
1 Churachandpur ( Urban) 32 70743
2 Saikot/Samulamlan 248 76152
3 Singngat 101 21452
4 Henglep 148 20202
5 Thanlon 58 36059
6 Tipaimukh (Parbung) 60 33987
647 258595
No. of HEALTH INSTITUTIONS
Hospital - 01
CHC - 01
PHC - 09
PHSC - 65
BLOCK WISE DISTRIBUTION OF HEALTH INSTITUTION
PHCs – PHSCs. Sl.No Name of Block District Hospital CHC PHC PHSC
1 Churachandpur ( Urban) 1 - - 01
2 Saikot/Samulamlan - - 2 15
3 Singngat - - 2 9
4 Henglep - - 1 15
5 Thanlon - - 2 11
6 Tipaimukh (Parbung) - 01 2 14
TOTAL 1 1 9 65
-2-
PHC WISE DISTRIBUTION OF
VILLAGES, POPULATION & Distance of PHC from

CCP PIP 2010-11
District Headquarters.
Name of PHC No. of Villages Population Distance from
CCpur.
Saikot PHC
Sagang PHC
221
27 76152
5 kms
55 kms
Singngat PHC 78 16242 33 kms
Behiang PHC 23 5,210 68 kms
Sinjawl PHC 19 8,361 162 kms
Thanlon PHC 39 11,841 150 kms
Henglep PHC 148 36,059 85 kms
Parbung CHC 13 12,958 260 kms
Senvon PHC 13 11,781 267 kms
Patpuihmun PHC 34 9,248 260+
Churachandpur Town(Urban) 32 70743 0 km
647 258595
(Mid-Year Population -2008)
AVERAGE MAN POWER STRENGTH OF
PHC & PHSC
PHC – 2 Doctors PHSC – 1 FHW
2 Staff Nurse 1 MHW
PARA Medical Staffs 4 FHW 1 Attendant
4 MHW Total 3
1 Pharmacist
Total 11
ASHA – ( one each of 647 village = 647)
AWW = 550
AWHS = 550 -1100
No. of Doctors available for the programme = 2 / PHC x 10 = 20
Paramedical Staff ( PHC) 11 x 10 = 110
Paramedical Staff ( PHC) 64 x 2 = 130
Total = 240
Grand total - Doctors = 20
Paramedical Staff = 240
ASHA = 647
AWWs + AWHs = 1100
Grand Total = 2007
-3-
PROPOSED STRATEGY OF ACTION/OPERATION

CCP PIP 2010-11
In view of more successful implementation of the programme and for Total Elimination of
Leprosy in the District Under NRHM a new Strategy of approach with the Slogan – “EL – GROOT” –
“Eliminating Leprosy at Grass Root Level” may be implied on and Mass- Survey at Village level (
House to House Campaign) be conducted. The Prerequites of the programme are:-
(i) Orientation Training of
- Doctors and Paramedical Staffs
(ii) Awareness Campaigns – (Camps)
- District Level
- Block Level
- PHC Level.
(iii) I.E.C. - Public Meeting ( Advocacy)
- High School Children
- Quiz/Essay
(iv) Field Survey- House to House
Survey/Campaign at Village Level
(v) Planning, monitoring, Supervision & Evaluation
(vi) Monthly review meeting at District Level
1. TRAININGS
RE-ORIENTATION TRANING OF MAN POWER to be UTILISED is a must and
A. TA/DA be paid as per rules.
Health Deptt - I. Doctors - 20
DA @ Rs. 200/hd/day x 3 day x 20= Rs.12,000.00
TA @ Rs. 100/had/day x 3 day x 20= Rs 6,000.00
II. Paramedical Staff = 240
(PHC = 110+PHSC = 130)
DA @ Rs. 100/hd/day x 3 days x 240 = Rs
97,500.00
TA @ Rs. 50/hd/day x 3 days x 240 = Rs
48,750.00
III. ASHA – 647 (One each for 647 = Rs
97,050.00
DA @ Rs. 50/hd/day x 3 days x 647 = Rs
97,050.00
TA @ Rs. 50/hd/day x 3 days x 647 = Rs
97,050.00
Other Sectors – ICDS 1100
(AWW = 550 + AWH = 550)
DA @ Rs. 50/hd/day x 3 days x 550 = Rs.
82,500.00
TA @ Rs. 50/hd/day x 3 days x 550 = Rs.
82,500.00
= Rs
4,36,005.00

CCP PIP 2010-11
-4-
B. REFRESHMENT
I Tea + Snacks
(a) Rs. 40/hd x 3 days x 2007 = Rs. 2,40,840.00
(b) Lunch @ Rs. 100/had/day x 3days x 2007 = Rs. 6,02,100.00
Total = Rs. 8,42,940.00
C. TRANING MATERIALS
IEC,Banners, Poster, Leaflets, Booklets, PA Systems, Hoarding etc.
A lumpsum amount of Rs. 2,00,000.00
D. TRANSPORT (Mobility Support)
(Vehicle Hiring, Pol etc)
A Lumpsum amount of Rs. 3, 00,000/-
E. MASS SURVEY, House – to – House Survey/Campaign
@ Rs. 300/Village X 647 Village = Rs. 1,
94,100/-
F. CONTIGENCY = Rs. 50,000/-
G. MONITORING, SUPERVISION & EVALUATION = Rs.
1.00.000/-
Grand total A to G = Rs. 21,230,45.00
OTHER FINANCIAL REQUIREMENT
It is proposed that “MASS AWARENESS CAMPAIGNS” Programme be organized at
District level, Block Level and PHC level with lumpsum amounts of
i. District Level = Rs. 35,000/-
ii. Block Level @ Rs. 15,000/-
Per Block – (15,000 X 6) = Rs. 90,000/-
iii. PHC Level @5,000/-
per PHC – (5000 X 10) = Rs. 50,000/-
Total = Rs. 1, 75,000/-
-5-
PHC – WISE ESTIMATED FINANCIAL INVOLVEMENT

CCP PIP 2010-11
It is to be based on the strategy that HOUSE-to-HOUSE SURVEY (Campaign)
be Carried out in each Village and TA/DA for that Staff engaged is estimated at the
rate of Rs. 300/- per Village
1. Saikot PHC - 221 Village X 300 = Rs. 66,300/-
2. Sagang PHC - 27 Village X 300 = Rs. 8,100/-
3. Singngat PHC - 78 Village X 300 = Rs. 23,400/-
4. Behiang PHC - 23 Village X 300 = Rs. 6,900/-
5. Sinjawl PHC - 19 Village X 300 = Rs. 5,700/-
6. Thanlon PHC - 39 Village X 300 = Rs. 11,700/-
7. Parbung PHC - 13 Village X 300 = Rs. 3,900/-
8. Sencon PHC - 13 Village X 300 = Rs. 3,900/-
9. Patpuihmun PHC - 34 Village X 300 = Rs. 10,200/-
10. Henglep PHC - 148 Village X 300 = Rs. 44,400/-
11. Churachandpur (Urban) 32 Village X 300 = Rs. 9,600/-
Total Financial requirement ( To sum - up)
i. Training = Rs. 4,36,005.00
ii. Refreshment = Rs. 8,42,940.00
iii. Training Materials = Rs. 2,00,000.00
iv. Transport = Rs. 3,00,000.00
v. Mass Survey (H to H) = Rs. 1,94,100.00
vi. Contigency = Rs. 50,000.00
vii. Monitoring & Evaluation = Rs. 1,00,000.00
G.Total = Rs.21,23,045.00
NTEGRATED DISEASE SURVEILLANCE PROGRAM (IDSP)
Objectives:

CCP PIP 2010-11
(i) To establish a decentralized surveillance system for communicable and non-communicable diseases
(ii) To improve the efficiency of the existing surveillance activities of disease
control programs and facilitate sharing of relevant information with the health administration, community and other stakeholders so as to detect disease trends over time and evaluate control strategies.
Strategies: a. Decentralize and strengthen disease surveillance and response mechanisms
and facilitate sharing surveillance data for health decision making at Blocks levels.
b. Integrate private care delivery systems and medical colleges (whenever set up)
both in rural and urban areas and involve village populations and other stakeholders more effectively in the surveillance activity.
c. Integrate and strengthen an effective rural surveillance. Laboratory:
Strengthen laboratory services at the Block Level and District for more efficient performance. Mass x-ray survey be done in high risk areas in the District.
Information Technology: Facilitate use of current Information Technology for communication, data management, feedback and dissemination of reports and improving timeliness of responses.
Human Resource Development: Develop human resources so that concerned people are able to implement the
program effectively. This includes development of training curricula, training manuals and actual training of all involved parties to improve quality of data for surveillance, analysis and links to action.
Structural framework: The focal point of all surveillance related activities at the periphery will be the District Surveillance Unit (DSU). DSU will receive surveillance data from both rural and urban reporting units. There will be active involvement of NGOs, private practitioners, other Government Departments as per given guidelines.
District Surveillance Committee:
The District Surveillance Committee will be chaired by The Deputy Commissioner with the following members:
Chairperson : Deputy Commissioner Co-chairperson : Chief Medical Officer Member-Secretary : District Surveillance Officer Members : EE, PHED, Superintendent of Police IMA representative NGO representative District Health & FW Program Officers Project Director, DRDA Member, Village Authority Rep. of Pvt. Health Care Institutions Officer i/c of District Hospital District SW Officer ZEO
District Surveillance Unit (DSU):
CCP PIP 2010-11
DSU will be constituted under the chairmanship of CMO of the District with the following members:
District Surveillance Officer : District Epidemiologist Assistant Programmer : 01 (currently exist) Accountant : To be appointed on contractual basis Data entry operator : To be appointed on contractual basis 1 LDC : To be identified from existing staff
Pathologist/Biochemist/Microbiologist will be members in the DSU: The DSU will meet once a month and as often as needed during an epidemic. A routine report of this meeting should be forwarded to the District Surveillance Office once a month to give feedback on the progress and problems in various Districts. Reports of these meeting will be forwarded to the National Surveillance Cell once in three months. Laboratory strengthening: Laboratory support is essential and is the mainstay for the proper implementation for the success of the program. Therefore, there is need to update and strengthen the facilities at different Block levels in the District. As the existing facilities available at the peripheral level is very poor, it is extremely essential to renovate laboratory for which minimum amount is earmarked for each unit.
IEC, Mobilization and Community involvement: The involvement of the following organized groups having District-wide associations will be utilized effectively. The groups are NGOs, Private Hospitals, Private practitioners, Village Authorities, Community leaders, Churches, Press etc.
Social mobilization strategies:
The aim of social mobilization campaign under IDSP will be:
• To create awareness among the partners, notably the private practitioners, NGOs and the community about existing Health Programs, IDSP, the potential benefits and areas in which their participation will be solicited.
• To establish an institutional mechanism to involve the community and their leaders
• Develop a system of providing regular feedbacks to the community about disease occurrence the responses to surveillance and impact of disease control programs
• To increase the reach of the campaign through all channels of communication.
District Level and Periphery Level: Organize sensitization and mobilization meetings at District head quarters for local IMA executive members, prominent practitioners, NGOs in health, elected representatives of the local as well as District bodies, village council members, teachers, various social groups existing in the District and peripheral level.
IEC material and messages to be prepared within the local context and in the locally comprehensible language; put up hoardings, posters, distribute hand bills to create wide spread awareness. The IEC material has to be displayed in all schools all sentinel sites, prominent locations in the village and busy street crossings in urban areas, and in all places where mass human gatherings occur e.g. festivals, melas, and exhibition At village and block level : organize meetings between medical officers of the area, health workers and village health committees once in three months, with the purpose of revitalizing this institution, enhance community participation in all health related matters and identifying the community as partners in the planning and decision making process.
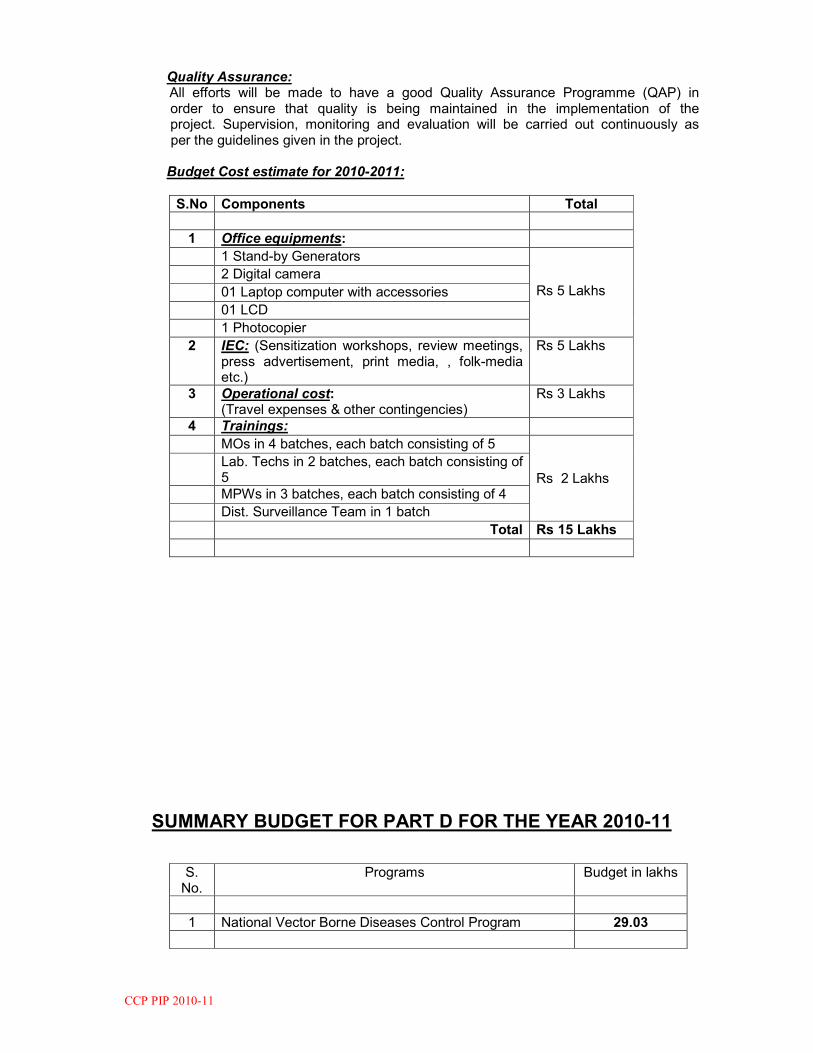
CCP PIP 2010-11
Quality Assurance: All efforts will be made to have a good Quality Assurance Programme (QAP) in order to ensure that quality is being maintained in the implementation of the project. Supervision, monitoring and evaluation will be carried out continuously as per the guidelines given in the project. Budget Cost estimate for 2010-2011:
S.No Components Total 1 Office equipments:
1 Stand-by Generators Rs 5 Lakhs
2 Digital camera
01 Laptop computer with accessories
01 LCD
1 Photocopier
2 IEC: (Sensitization workshops, review meetings, press advertisement, print media, , folk-media etc.)
Rs 5 Lakhs
3 Operational cost: (Travel expenses & other contingencies)
Rs 3 Lakhs
4 Trainings:
MOs in 4 batches, each batch consisting of 5 Rs 2 Lakhs
Lab. Techs in 2 batches, each batch consisting of 5
MPWs in 3 batches, each batch consisting of 4
Dist. Surveillance Team in 1 batch
Total Rs 15 Lakhs
SUMMARY BUDGET FOR PART D FOR THE YEAR 2010-11
S. No.
Programs Budget in lakhs
1 National Vector Borne Diseases Control Program 29.03
CCP PIP 2010-11
2 National Program on Control of Blindness 14.0 3 National Leprosy Elimination Program 21.23 4 Revised National Tuberculosis Control Program 26.42 5 National Iodine Deficiency Disorders Control Program 7.60 6 Integrated Disease Surveillance Program 15.0
Grand Total Rs 113.28

CCP PIP 2010-11
WITH DEPARTMENT OF WOMEN AND CHILD DEVELOPMENT
1. Village Health & Nutrition Day:
Anganwadi Centres (AWC) will serve as the focal point for all health and nutrition services. A Health Day (Wednesday) is fixed every month at the AWC to provide antenatal, postnatal, family planning and child health services, including immunization. On that day, an ANM and preferably an MO from the PHC will be in attendance. AWW, ASHA and other community volunteers would be responsible for ensuring that all children 0-6 years, pregnant women and lactating women, and children needing immunization and other health services are brought to the AWC on that fixed day. Monitoring of Growth Charts for U-5 Children will be done by AWW on the VHND and children needing care in addition to Supplementary Nutrition will be taken care by the MO/ ANM. 2. Coordination between AWW and ASHA:
AWWs will be mentors of ASHA and will work in tandem for counseling Pregnant Women to have institutional delivery, attend home deliveries as second attendant, motivate newly married on family planning, participate in Routine Immunization Strengthening and NIDs and facilitate referral for institutional delivery.
The compensation package for the above mentioned activities are already discussed under Part “B”. 3. Interdepartmental coordination:
Representatives from WCD are to be made members in the District Health Society and Committees starting from District level to the Village level. Monitoring and Supervision of the different activities may be facilitated through joint review meetings and common reporting formats.
WITH VILLAGE AUTHORITIES (VAs)
1. Empowerment of VAs through assured availability of adequate funds:
Untied funds may be made available to Village Health Committees and all Subcentres to be deposited in a joint Account operated by ANM and PRI representative. 2. Partnership with VAs:

CCP PIP 2010-11
VAs representatives are to be made members in all Societies and Committees viz.
District Health Mission Societies, Rogi Kalyan Samitis, Subcentres Committees and Village Health Committees. 3. Empowerment during selection of ASHA:
ASHA are to be selected by the VA after facilitating by a trained facilitator. 4. Community monitoring: VAs will be involved for monitoring the attendance and
performance of Additional ANMs. Also VA should monitor the observation of the Village Health & Nutrition Days.
WITH DEPARTMENT OF AYUSH
There is yet no separate Department of AYUSH in the District and State. An AYUSH Cell exists under the Directorate of Health Services, Manipur. The construction of Ayush Cell is under process in the campus of District Hospital, Churachandpur.
1. Mainstreaming AYUSH:
The services of the existing 7 AYUSH Doctors recruited under contractual posted at CHC and PHCs will be continued in the next year. These AYUSH staffs are to be mainstreamed into RCH services specially in providing BCC and other community mobilization activities
Civil works needed, other infrastructure up-gradation; medicine etc of the AYUSH Centres will be supported by AYUSH under CSS.
WITH MEDICINS SANS FRONTIER (MSF- HOLLAND)
The services of MSF Clinic at the District are to be utilized for the common goal of RCH & NRHM where-in they emphasized on Maternal & Child Health and other Health services. They are the boon to the District. Most of the defunct PHSCs are come into alive due to the support of MSF in medicine and staff. The DHS and the MSF signed an MoU in the year 2007. Till then they remain good health service provider to most of the underserved area in the District. Plans are sorted out to work actively together to fulfill the goal spelt by the GoI especially under RCH in the coming year.
WITH PUBLIC HEALTH ENGINEERING DEPARTMENT/ PUBLIC WORKS DEPARTMENT
To bring about better Sanitation and Safe Drinking Water Supply available to the community and also to overcome transport problems regarding approach roads to the health institutions, the PHED/PWD representatives are to be made members in all the Societies and Committees starting from District level to Village level. Thus joint planning and implementation of relevant activities will be sought.

CCP PIP 2010-11
TOTAL BUDGET REQUIRE FOR 2009-10:
Sl. No. NRHM Component Rs. in lakhs
1 Part “A” 522.35
2 Part “B” 327.15
3 Part “C” 16.10
4 Part “D” 95.65
5 Part “E” 0.0
Grand Total 961.25