Chronic Mountain Sickness and the Heart
10
Chronic Mountain Sickness and the Heart Fabiola León-Velarde a, ⁎ , Francisco C. Villafuerte a , Jean-Paul Richalet b a Departamento de Ciencias Biológicas y Fisiológicas, Facultad de Ciencias y Filosofia, Universidad Peruana Cayetano Heredia, Lima 31, Perú b Université Paris 13, Laboratoire « Réponses cellulaires et fonctionnelles à l'hypoxie », EA 2363, ARPE, UFR SMBH, 74 rue Marcel Cachin, 93017 Bobigny, France Abstract Chronic Mountain Sickness (CMS) is an important high-altitude (HA) pathology in most mountainous regions of the world. Although its most characteristic sign is excessive erytrocytosis (EE), in the more severe stages of the disease, high-altitude pulmonary hypertension (HAPH), with remodeling of pulmonary arterioles and right ventricular enlargement is commonly found. The degree of ventricular hypertrophy depends on the vasoconstrictor pulmonary response, the intensity of vascular resistance and the level of altitude, and therefore on the degree of hypoxemia. This chapter briefly summarizes the existing data regarding the clinical and pathophysiological features of the cardiopulmonary system in CMS, with emphasis in findings from research in the Andes. The literature shows variability in cardiac output values in CMS, which might be related to the degree of EE. Recent findings have shown that cardiac output (l/min) is lower in CMS when compared with sea-level (SL) dwellers. Mean pulmonary acceleration time (ms) is significantly lower in CMS subjects than in SL and HA natives, and pulmonary vascular resistance index (Wood units) is higher in CMS and HA natives when compared with SL dwellers. Systemic blood pressure has similar values in CMS patients and healthy HA natives, but some differences arise in its control mechanisms. Although CMS individuals have a less effective vasoconstrictor reflex, their tolerance to orthostatic stress is similar to that of healthy HA natives which might be explained in terms of the larger blood volume present in CMS subjects. At present research is directed to design strategies on pharmacological intervention for CMS treatment. Recently, a clinical trial with acetazolamide, in patients with CMS has proven to be effective in increasing mean pulmonary acceleration time and decreasing pulmonary vascular resistance index, which might be indirectly due the reduction of hematocrit (Prog Cardiovasc Dis 2010;52:540-549) © 2010 Elsevier Inc. All rights reserved. Keywords: Chronic mountain sickness; Monge's disease; Heart; High-altitude pulmonary hypertension; High altitude The low barometric pressure encountered at high- altitude (HA) environments results in low O 2 partial pressure (PO 2 ) of the inspired air. This condition of hypobaric hypoxia results in decreased blood PO 2 or hypoxemia. The organism responds to this situation and attempts to keep a normal cellular oxygenation by modifying the behavior of the respiratory, cardiovascular, renal, and neuroendocrine systems. These physiologic responses are directed to normalize and maintain cellular oxygenation. Among them, the increase in hematocrit and hemoglobin concentration ([Hb]), and the elevation of pulmonary artery pressure (Ppa) represent key features in the response to HA chronic hypoxia 1-4 and are mainly directed toward increasing blood O 2 -carrying capacity and redistributing blood toward better ventilated lung areas, respectively. An excessive increase in [Hb] and/or in Ppa, however, is associated with latent lethal illnesses such as chronic mountain sickness or Monge's disease (CMS) and high-altitude pulmonary hypertension (HAPH). 5-10 The magnitude of the erythropoietic and Ppa responses, however, varies between the different HA populations. The increase in [Hb], for example, is particularly Progress in Cardiovascular Diseases 52 (2010) 540 – 549 www.onlinepcd.com Statement of Conflict of Interest: see page 547. ⁎ Corresponding author. E-mail address: [email protected] (F. León-Velarde). 0033-0620/$ – see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.pcad.2010.02.012 540
Transcript of Chronic Mountain Sickness and the Heart

Progress in Cardiovascular Diseases 52 (2010) 540ndash549wwwonlinepcdcom
Chronic Mountain Sickness and the HeartFabiola Leoacuten-Velardea Francisco C Villafuertea Jean-Paul Richaletb
aDepartamento de Ciencias Bioloacutegicas y Fisioloacutegicas Facultad de Ciencias y Filosofia Universidad Peruana Cayetano Heredia Lima 31 PeruacutebUniversiteacute Paris 13 Laboratoire laquo Reacuteponses cellulaires et fonctionnelles agrave lhypoxie raquo EA 2363 ARPE UFR SMBH 74 rue Marcel Cachin
93017 Bobigny France
Abstract Chronic Mountain Sickness (CMS) is an important high-altitude (HA) pathology in most
Statement of Conf Corresponding aE-mail address fa
0033-0620$ ndash see frodoi101016jpcad20
mountainous regions of the world Although its most characteristic sign is excessiveerytrocytosis (EE) in the more severe stages of the disease high-altitude pulmonaryhypertension (HAPH) with remodeling of pulmonary arterioles and right ventricularenlargement is commonly found The degree of ventricular hypertrophy depends on thevasoconstrictor pulmonary response the intensity of vascular resistance and the level ofaltitude and therefore on the degree of hypoxemia This chapter briefly summarizes the existingdata regarding the clinical and pathophysiological features of the cardiopulmonary system inCMS with emphasis in findings from research in the Andes The literature shows variability incardiac output values in CMS which might be related to the degree of EE Recent findings haveshown that cardiac output (lmin) is lower in CMS when compared with sea-level (SL) dwellersMean pulmonary acceleration time (ms) is significantly lower in CMS subjects than in SL andHA natives and pulmonary vascular resistance index (Wood units) is higher in CMS and HAnatives when compared with SL dwellers Systemic blood pressure has similar values in CMSpatients and healthy HA natives but some differences arise in its control mechanisms AlthoughCMS individuals have a less effective vasoconstrictor reflex their tolerance to orthostatic stressis similar to that of healthy HA natives which might be explained in terms of the larger bloodvolume present in CMS subjects At present research is directed to design strategies onpharmacological intervention for CMS treatment Recently a clinical trial with acetazolamidein patients with CMS has proven to be effective in increasing mean pulmonary acceleration timeand decreasing pulmonary vascular resistance index which might be indirectly due thereduction of hematocrit (Prog Cardiovasc Dis 201052540-549)
copy 2010 Elsevier Inc All rights reserved
Keywords Chronic mountain sickness Monges disease Heart High-altitude pulmonary hypertension High altitude
The low barometric pressure encountered at high-altitude (HA) environments results in low O2 partialpressure (PO2) of the inspired air This condition ofhypobaric hypoxia results in decreased blood PO2 orhypoxemia The organism responds to this situation andattempts to keep a normal cellular oxygenation bymodifying the behavior of the respiratory cardiovascularrenal and neuroendocrine systems These physiologicresponses are directed to normalize and maintain cellular
lict of Interest see page 547uthorbiolaleon-velardeupchpe (F Leoacuten-Velarde)
nt matter copy 2010 Elsevier Inc All rights reserved1002012
oxygenation Among them the increase in hematocrit andhemoglobin concentration ([Hb]) and the elevation ofpulmonary artery pressure (Ppa) represent key features inthe response to HA chronic hypoxia1-4 and are mainlydirected toward increasing blood O2-carrying capacity andredistributing blood toward better ventilated lung areasrespectively An excessive increase in [Hb] andor in Ppahowever is associated with latent lethal illnesses such aschronic mountain sickness or Monges disease (CMS) andhigh-altitude pulmonary hypertension (HAPH)5-10 Themagnitude of the erythropoietic and Ppa responseshowever varies between the different HA populationsThe increase in [Hb] for example is particularly
540
Abbreviations and Acronyms
AHVR = acute hypoxicventilatory response
CMS = chronic mountainsickness
Epo = erythropoietin
HA = high-altitude
HAPH = high-altitudepulmonary hypertension
[Hb] = hemoglobinconcentration
HVR = hypoxic ventilatoryresponse
Ppa = pulmonary arterypressure
PVR = pulmonary vascularresistance
SaO2 = arterial blood oxygensaturation
SL = sea-level
541F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
pronounced in AndeanHA dwellers11 whencompared with Tibetansand Ethiopians and evenmore so in those whohave CMS
Chronic mountainsickness affects peoplewho are native or long-time residents of HA loca-tions and usually beginsinsidiously in adult lifethe clinical picture disap-pears when the patientmoves to lower altitudesChronic mountain sick-ness is characterized bysevere hypoxemia exces-sive erythrocytosis for thealtitude of residence andvarious symptoms includ-ing sleep disorders head-ache dizziness tinnitusparesthesias mental and
physical fatigue and cognitive impairment612 Cyanosis isparticularly visible in the nail beds ears and lips In somecases the face is almost black and the mucosa andconjunctiva are dark red Clubbing of fingers is a frequentfinding Ultimately CMS leads to severe HAPH and couldlead to heart failure9 although to date no extensiveepidemiologic study has been performed to evaluate thelong-term deleterious effects of CMS Many of thesymptoms of CMS are thought to be caused by cerebralhypoxia1314 and this may be exacerbated by the lowcerebral blood flow caused by the high viscosity ofthe blood15
Carlos Monge-M was the first to describe a patient withCMS and presented the case at the Academy of Medicineof Lima in 19257 The patient was a native of the miningtown of Cerro de Pasco located at 4300 m in the PeruvianAndes but he was not a miner this patient was 38 age oldand showed a mean [Hb] of 211 gdL Monge-M ends hispresentation to the Academy calling the attention of thePeruvian medical community and authorities ldquoon the needto devote their medical efforts to understand thepolycythemic syndromes in order to be able to evaluatethe magnitude of impairment that these pathologies couldcause to the inhabitants of the Andesrdquo Three years laterMonge-M published an extensive article16 on cases ofCMS from Cerro de Pasco (4300 m) and Puno (3800 m)an agricultural town Monge-M considered CMS to be aldquoloss of acclimatizationrdquo because it developed only afterprolonged exposure to altitude in previously well-acclimatized subjects
Historical terms used in different mountainous regions forthis HA disease which has excessive elevation of [Hb] as acommon characteristic have been HA excessive polycythe-mia or erythrocytosis excessive erythrocytosis and HApathologic erythrocytosis A number of factors are known toinfluence the development of CMS among them altitudeage sex sleep disorders and genetic susceptibility17-19
Respiratory aspects of CMS
The primary finding in patients with CMS is excessiveerythrocytosis This excessive increase in the number ofred blood cells is caused by hypoxemia which developsmainly because differences in the respiratory pattern ofCMS individuals Compared with healthy HA natives atthe same altitude patients with CMS are relativelyhypoxic and hypercapnic2021 Alveolar hypoventilationis the main respiratory feature but also ventilation-perfusion mismatch and widened alveolar-arterial PO2gradient has been described in subjects with CMS19
Implication of the peripheral chemoreceptors as thecause of hypoxemia in CMS
The main peripheral chemoreceptors in mammals arelocated in the carotid bodies in the bifurcation of thecarotid arteries These small structures are heavilyvascularized and have an elevated blood flow for theirsize Carotid chemoreceptors stimulate ventilation inresponse to hypoxia Nevertheless in cases of prolongedresidence at high altitude this ventilatory response tohypoxia appears attenuated (ldquobluntedrdquo) in humans and insome animals
Chronic mountain sickness has been associated withpoor hypoxic ventilatory responses (HVRs)2122 but thereis no proof that changes in carotid body structure orfunction are the cause of hypoventilation in CMS20 Tobetter understand the peripheral chemoreceptor function inhypoxia short-term and sustained protocols of exposure tohypoxia have been used An acute HVR (AHVR) protocolevaluates the immediate response to a stepwise inductionof hypoxia for few minutes (6-7 minutes) A sustainedprotocol (15-20 minutes of hypoxia) determines thehypoxic ventilatory decline which is the attenuation ofthe initial ventilatory response after the first few minutesof hypoxia Acute HVR reflects peripheral control ofbreathing whereas the hypoxic ventilatory decline mayreflect attenuation of the ventilatory response by centralcontrol mechanisms although there is some debate onthis point23
When HA natives and individuals with CMS areexposed to acute hypoxia from an initial end-tidal PO2(PETO2) of 100 Torr to a final PETO2 of 45 or 34 Torr theaverage values for the slope of the AHVR for both HA
Fig 1 Arteriovenous O2 content difference (CaO2 minus CvO2) as a functionof arterial O2 saturation (SaO2) Unfilled circles represent mean data ofresidents from various altitudes and [Hb] are indicated above each circleFilled circles represent data from subjects exposed acutely to altitudes of3050 and 4570 m The (CaO2 minus CvO2) is shown as a percentage ofnormoxic values The content difference (CaO2 minus CvO2) in altituderesidents demonstrates a complex relation to SaO2 but the residents showa better sustained content difference than subjects exposed acutely toaltitude Maximal (CaO2 minus CvO2) is obtained at an [Hb] of 175 g100 mLand a SaO2 of 87 Data from Reeves and Leon-Velarde 200433
542 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
natives and subjects with CMS are around one third ofthe values for sea-level (SL) natives24 The HA nativesand subjects with CMS do not differ significantly fromeach other in their immediate response to hypoxia Inaddition when the peripheral chemoreflex contribution atPETO2 = 525 Torr is calculated from the value of AHVRmultiplied by the reduction in saturation associated withreducing PETO2 from 200 Torr to 525 Torr (AHVR times[SaO2 200] minus SaO2 525) the contribution for the SLgroup is clearly much larger than for the HA and CMSgroups and there is no difference between the HA andCMS group Overall these studies provide evidence tosupport the notion that the lower levels of ventilation inCMS subjects that is the loss of the drive to breathemay arise from mechanisms other than reductions in theperipheral chemoreflex sensitivity to hypoxia or that itscontribution is quite marginal24
Implication of central chemoreceptors as the cause ofhypoxemia in CMS
The cells of the central chemoreceptors respond mainlyto CO2 and H+ At sea level total sensitivity to CO2 innormoxia is of approximately 17 LminTorr In hyper-oxia its value ranges from 25 to 275 LminTorr and inhypoxia at a PETO2 = 50 Torr from 41 to 44 LminTorr212526 The effect of hypoxia in total sensitivity toCO2 is greater in HA natives than in natives from sea leveland than in patients with CMS The peripheral sensitivityof the chemoreceptors to CO2 (Gp) of HA natives isgreater than the Gp of SL inhabitants
The time constants for response to CO2 can beperipheral (tp) or central (tc)2728 Tp is similar betweenSL and HA natives however Tc is slower in HA nativesand even slower in subjects with CMS26 The slowness ofthe time constant in the central chemoreflex is related tothe buffer capacities of the plasma in which centralchemoreceptors are immersed The time constant dependson the cerebral flow per volume unit of cerebral tissue andon the relation between the CO2-buffering capacity of theblood and the brain29 Although cerebral blood flow hasbeen shown to be decreased in HA natives1430 thedelivery of O2 would be relatively protected due to theincreased hematocrit14 However it is not absolutelyobvious that the removal of CO2 also would be assuredAlso the increased hematocrit elevates H+ buffering butplasma flow is reduced therefore the amount ofbicarbonate in blood is reduced A quantitative analysisof these factors reveals a relative reduction of CO2
exchange in the brain in response to changes of PCO2 in thearterial blood26
Overall the interpretation of the data in peripheral andcentral chemoreflex sensitivity to CO2 is that CMSsubjects seem to have reset their central CO2 chemor-eceptors to operate around the resting PETCO2 more close
to SL standards thus around higher PETCO2 values than athigh altitude Indeed Monge-M and Monge-C3 haveshown that PETCO2 HCO3
minus and pH in CMS patients arecloser to SL values31
Excessive erythrocytosis and the heart in CMS effectof hematocrit on cardiac function
Increased [Hb] has long been considered beneficial athigh altitude because the increased oxygen-carryingcapacity of blood would compensate for decreasedarterial oxygen saturation The increase in [Hb] shouldact to maintain oxygen transport to tissues therebyreducing the need to increase cardiac output inhypoxemic subjects This concept however has beenchallenged because with a low oxygen saturation (lowPO2) increasing [Hb] would be of help up to a certainpoint and thus only a moderate increase in [Hb] wouldbenefit O2 transport When excessive however [Hb]becomes detrimental The perfect example is CMSwhere despite having a significantly higher blood O2
content32 individuals are severely hypoxemic and ill Ithas been suggested that above certain [Hb] valueerythrocytosis is no longer beneficial because of theelevated blood viscosity and increased blood volume thatleads to congestive symptoms3233 Increased bloodviscosity and blood volume which results from increas-ing [Hb] to excessive levels affects the distribution ofpulmonary blood flow and pulmonary ventilation-perfu-sion relationships resulting in impaired pulmonary gasexchange This contributes to arterial hypoxemia and
543F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
further stimulates erythropoiesis3435 Interestinglysome studies have shown that when these subjectsundergo bloodletting or hemodilution blood oxygen-ation improves and the symptoms are reduceddramatically123436 Reeves and Leon-Velarde33 havesuggested based on an analysis of arterial-venous O2
content difference at different [Hb] and SaO2 values thatup to a certain value (SaO2 of 87 and a [Hb] of 175 g100 mL) increasing [Hb] has a cardiac output-sparingeffect because of a greater oxygen extraction (Fig 1)When hypoxemia however becomes severe an elevated[Hb] no longer supports an efficient O2 transport andcardiac output has to increase yet the literature showsvariability in cardiac output values in CMS937-39
In 1959 Guyton and Richardson40 were the first tostudy experimentally the effect of hematocrit on cardiacfunction Their work showed that when hematocrit wasincreased isovolemically by 47 in dogs cardiac outputwas reduced dramatically by 51 and total peripheralresistance increased by 50 The effect on cardiac outputwas explained in the effect of increased blood viscosityon venous resistance and venous return as confirmed in alater study41
In CMS chronic hypoxemia leads to excessiveerythrocytosis accompanied by a very high bloodvolume8373842 Thus the emerging figure is somewhatdifferent to what was observed in the isovolemicexperiments in dogs Cardiac output peripheral resis-tance and systolic blood pressure in CMS patients aresimilar to those of healthy individuals at the samealtitude1037 Some recent studies however have shown
Table 1Subject characteristics in high altitude natives (HA) and chronic mountain sick
At High Altitude
HA CMS
Age (years) 393 plusmn 20 43Hematocrit () 498 plusmn 12 63O2 Saturation () 860 plusmn 10 82Orthostatic Tolerance (min) 462 plusmn 12 47SAP (mmHg) Supine 1137 plusmn 30 117Tilt 1157 plusmn 35 119DAP (mmHg) Supine 731 plusmn 23 76Tilt 764 plusmn 26 74HR (bmin) Supine 589 plusmn 20 65Tilt 706 plusmn 28 76Plasma volume (mlkg) 393 plusmn 36 34Red cell volume (mlkg) 379 plusmn 31 62Blood volume (mlkg) 772 plusmn 64 97
Subject characteristics in high altitude natives (HA) and chronic mountain sickboth high altitude groups than at SL (288 plusmn 40 P b 0001) Systolic (SAP)min) are shown in supine and tilt positions Tilt indicates values at the end obetween locations (P b 005 P b 0001 P b 00001) dagger represents sidifferences between supine and tilt There were no significant differences inwere smaller in HA and SL (275 plusmn 18 P b 0001) than in CMS Blood voCMS Values are means plusmn SE Data from Claydon et al 2004 20054254
that systemic pressure in CMS individuals is slightlyelevated when compared to healthy highlanders43
Although elevated blood viscosity would tend todecrease venous return the increased blood volumewould counteract this effect and therefore cardiac outputwould be maintained The rise in peripheral resistance dueto increased blood viscosity is most probably counteractedby the increased aortic elasticity and vasodilation in HAresidents44-46 Contrary to what is found for systolicpressure some studies have found an increased diastolicblood pressure in persons having severe CMS910 thatmight reflect an increased venous return due to increasedblood volume
Studies on the physiology of a transgenic mice line(ldquotg6rdquo mice) that overexpresses erythropoietin (Epo) haveprovided insightful information on the hypoxia-indepen-dent effects of excessive erythrocytosis on the cardio-vascular system Under normoxic conditions thisinteresting animal model exhibits a 12-fold elevation inplasma Epo concentration hematocrit values in the rangeof 85 to 90 and 75 larger blood volume comparedto its wild-type counterparts47 Despite excessive ery-throcytosis increased viscosity and elevated bloodvolume tg6 mice have normal cardiac output andblood pressure values The excessive hematocrit in tg6mice would result in elevated peripheral resistancehowever the increased sheer stress on vascular endothe-lium induces the expression of endothelial nitric oxidesynthase and an enhanced production of NO which inturn causes vasodilation and counteracts the effect ofhematocrit on peripheral resistance48 On the venous side
ness subjects (CMS)
At Sea Level
HA CMS
1 plusmn 17
8 plusmn 17
0 plusmn 12 960 plusmn 07 940 plusmn 07dagger
2 plusmn 12
2 plusmn 26 1107 plusmn 46 1151 plusmn 365 plusmn 24 1065 plusmn 28Dagger 1123 plusmn 33Dagger
4 plusmn 23 678 plusmn 42 715 plusmn 25
3 plusmn 27 758 plusmn 24 788 plusmn 30dagger
0 plusmn 20dagger 493 plusmn 22 543 plusmn 14
1 plusmn 27 554 plusmn 22 642 plusmn 28dagger
6 plusmn 18
8 plusmn 53
4 plusmn 63
ness subjects (CMS) Orthostatic tolerance was significantly greater inand diastolic (DAP) arterial blood pressures and heart rate (HR beatsf the 20 min phase of head up tilt represents a significant differencegnificant difference between HA and CMS and Dagger indicates significantplasma volumes between groups and sea level (SL) Red cell volumeslumes were smaller in HA and SL (673 plusmn 47 P b 001) compared to
544 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
due to increased blood volume tg6 mice showsignificantly elevated central venous pressure47 thatcould result in elevated diastolic pressure It is possiblethen that some of the mechanisms operating in tg6 miceare also present in CMS individuals An enhancedexpression of endothelial nitric oxide synthase in CMScould explain for example the normal peripheralresistance found in CMS patients
Systemic blood pressure control and blood flow in CMS
Although systolic blood pressure in CMS patients isoften similar to that of healthy highlanders some smalldifferences arise in the control mechanisms It has beenshown that Andean HA dwellers have a great tolerance toorthostatic stress that might be attributed to the increasedhematocrit and blood volume The CMS individuals showan exceptional tolerance to orthostatic stress but nosignificantly different from HA controls yet CMSindividuals tend to respond with smaller increases inheart rate than HA healthy subjects54 This has led tosuggest that this may reflect a smaller sympathetic responseto orthostatic stress in these individuals (Table 1) Smallresponses of vascular resistance however have beenassociated to poor orthostatic tolerance49-51 Therefore theextremely good orthostatic tolerance in CMS patientssuggests that some other mechanism is operating in theseindividuals to maintain blood pressure It is possible thatthe large blood volume occurring in these individualscompensates for the smaller sympathetic response5253
Claydon and coworkers54 have shown that at HA theperipheral vascular resistance response to orthostatic stresshad a tendency to be smaller in CMS compared to healthysubjects but after 24 hours at sea level the CMS group hada significantly smaller response This less effective reflexvasoconstriction could explain why despite a larger bloodvolume in CMS subjects their orthostatic tolerance issimilar to that of HA controls
Chronic mountain sickness subjects also show differ-ences in the autoregulation of cerebral blood flow It hasbeen shown that cerebral blood flow is slower in CMSpatients compared to healthy HA subjects55 and it hasbeen suggested that this is a consequence of the increasedblood viscosity Cerebral blood flow autoregulation issimilar in CMS and healthy highlanders at high altitudeand their values are similar to those reported in SLresidents1355 After 24 hours at sea level however CMSindividuals had a larger fall on cerebral blood flow withsmaller change in resistance when exposed to orthostaticstress55 Studies on the relationship between peripheralresistance and carotid baroreceptor function have shownthat at altitude the sensitivity of forearm vascularresistance as a function of carotid sinus pressure is similarin CMS and healthy subjects but the ldquoset-pointrdquo of the
relationship is significantly higher in the CMS group56
This difference however disappears at sea level Apossible explanation for a higher ldquoset-pointrdquo in CMSindividuals at high altitude and its normalization at sealevel could be associated to the effects of hypoxemia onsympathetic vasomotor activity It is well-known thathypoxemia increases sympathetic discharge to musclevascular beds Chronic mountain sickness subjects arenormally more hypoxemic and therefore it is likely that agreater sympathetic activation may have contributed to thealtered baroreflex function This possibility finds supportin the observation that noradrenaline and adrenaline levelsare higher in CMS patients than in healthy HA dwellers57
and that plasma catecholamines are significantly reducedin HA natives within 4 hours of descent to sea level58
Cardiac features of CMS
Thirty years ago Pentildealoza and Arias-Stella59 studiedextensively the cardiac characteristics and pulmonarycirculation of Andean dwellers and patients with severeCMS Their findings point to the presence of pulmonaryhypertension and right ventricular hypertrophy in CMSsubjects9106061 They also demonstrated a direct rela-tionship between Ppa and right ventricle size In additiona prominent main pulmonary artery was found in allpatients Clinical characteristics of pulmonary hyperten-sion were an increased pulmonary second sound oftenassociated with a soft midsystolic ejection murmur anincreased diastolic blood pressure thought to be related toexcessive polycythemia9 and an increase in heart size onchest x-ray compared to healthy highlanders a featureexplained by the increased size of the right heart chambers
In severe cases of CMS the ECG shows peaked Pwaves with increased voltage in leads II III and aVF aswell as in the right precordial leads A right QRS axisdeviation is often observed An rS pattern in the rightprecordial leads and complexes of RS or rS type in the leftprecordial leads are common findings Negative T wavesover the right precordial leads are also common Thesefindings are indicative of right ventricular hypertrophy(RVH) and overload of the right heart chambers asconsequence of pulmonary hypertension Indeed as wellas with heart size a direct relationship between Ppa andright QRS axis deviation has been demonstrated59 Whenpatients with CMS are moved to SL symptoms and signsimprove promptly and the electrocardiographic andradiographic evidence of elevated Ppa and RVH decreasesover time62
Recent echocardiographic studies of pulmonary arterypressure at high altitude support previous findings usinginvasive techniques63-65 At present Doppler echocardi-ography is preferred to evaluate accurately cardiovascular
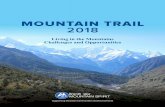
Fig 2 Cardiac output and maximal tricuspid regurgitation pressure in SL (SL control group at sea level [n = 15]) and HA (HA control group [n = 15]) andCMS groups (n = 55) at high altitude Data from Richalet et al 200968
545F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
function and cardiac morphology A recent study showedthat left atrial area was larger in SL than in HA nativesand CMS patients Right atria and ventricles were largerin CMS compared to SL and HA as shown by largerend-systolic right atria and end-diastolic right ventricularareas and a higher end-diastolic rightleft ventriculardiameter ratio This study also showed that cardiac outputis lower in CMS subjects than in SL dwellers but nodifference has been found when compared with HA
Fig 3 Pulmonary acceleration time and PVR index in SL (SL control group [n =([peak tricuspid regurgitation velocityright ventricular outflow tract time minus vel
natives (Fig 2) Left and right ventricular systolicfunctions and mitral and tricuspid inflows EA are notdifferent between SL HA and CMS Right ventricularTei index a global myocardial performance indicator(calculated as the ratio of [systolic time minus ejection time]ejection time)6667 however is increased in HA nativesand CMS patients when compared to SL controls Thesecardiac characteristics have been described in approxi-mately 50 CMS subjects the largest sample studied at
15]) HA (HA control group [n = 15]) and CMS groups (n = 55) PVR =ocity integral] times 10) + 01668
546 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
4300 m patients showed a mean [Hb] of 231 plusmn 16 gdLarterial blood oxygen saturation (SaO2) of 81 plusmn 4 andPpa of 34 plusmn 10 mm Hg68
Pulmonary hypertension in CMS
The cause of HAPH is the increase in pulmonaryvascular resistance (PVR) the underlying mechanisminvolves sustained and exaggerated pulmonary vasocon-striction and remodeling of the pulmonary vascular wall inresponse to chronic hypoxia due to proliferation anddecreased apoptosis of pulmonary artery smooth musclecells The effects of chronic hypoxia on pulmonary arterypressure are reflected in the negative correlation that existsbetween Ppa and SaO2 at high altitude596970 Arterialhypoxemia in addition to hypoxic vasoconstriction leadsto several structural changes in the pulmonary vesselsincluding an increase in the number of intimal smoothmuscle cells medial thickening in the small musculararteries and fibrinoid necrosis of the vessel walls71 Thesestructural changes in the pulmonary vessels rather thanhypoxic vasoconstriction alone are believed to beresponsible for the sustained rise in Ppa in chronichypoxia Pioneering hemodynamic invasive studies byPentildealoza and Sime910 in 10 subjects with severe CMS at4300 m showed a mean [Hb] value of 247 plusmn 24 gdL amean SaO2 of 696 plusmn 49 and a Ppa of 47 plusmn 177 mmHg values that have made the authors conclude that thesepatients have a type of hypoxic cor pulmonale in contrastto the hypertensive cor pulmonale observed in primarypulmonary hypertension However the structural changes
Fig 4 Pulmonary vascular resistance index and pulmonary acceleration time intreatment with acetazolamide (Acz) The study was organized in 2 phases (1) a ran open-label phase where all patients received acetazolamide (Acz + Acz) Theet al 200939
in the pulmonary vessels which are responsible for thesustained rise in Ppa in chronic hypoxia can have differentintensities and different onset times depending on thelength of hypoxic exposure comprising a range fromshort-term to long-term7072
Maignan and coworkers68 have described cardiachemodynamics in approximately 50 CMS cases withnoninvasive methods and found varying intensities ofPpa Although they might have been studying patients inan early disease stage they observed mean pulmonaryacceleration time and accelerationejection time ratiossignificantly lower in CMS subjects than in SL and HAnatives (Fig 3) Pulmonary vascular index was foundlower in SL than in other groups and there was nosignificant difference between HA and CMS however thenumber of patients with PVR greater than 2 Wood unitswas higher in CMS (1242) than in SL (013) and tended tobe significant when compared to HA (115) (CMS vs SLP = 003 CMS vs HA P = 008 and SL vs HA P = 034)
Chronic hypoxia with appropriate acclimatization asseen in healthy HA residents induces an increase inPVR without change in pulmonary arterial systolicpressure right heart cavity dimensions or right systolicventricular function The increase in right ventricularTei index however could reflect early right ventricularimpairment68 When hypoxemia becomes severe asobserved in some patients with excessive Ppa a furtherimpairment can be found with a significant increase inpulmonary arterial systolic pressure and right cardiaccavity enlargement However contrary to the assumption59
of overt chronic cor pulmonale based on severe HAPHpatients with established HAPH did not show any
placebo and CMS patients groups before and after 3 and 6 months ofandomized double-blind placebo-controlled phase (placebo + Acz) and (2)2 phases were separated by a 4-week washout period Data from Richalet
547F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
obvious cardiac systolic dysfunction as shown byMaignan and coworkers68 This confirms the individualvariability of the severity of HAPH which is also highlydependent on risk factors and genetic susceptibilitydespite that for the moment no specific gene has beenclearly associated with the development of CMS Largeepidemiologic studies should be conducted to determinethe precise natural history prevalence and features ofheart failure in CMS
Recently an interaction between iron levels andhypoxia in the regulation of the pulmonary circulationhas been described73 The study showed that ironinfusion before an 8-hour exposure to sustained hypoxiaabolished or reduced greatly the elevation in baselinepulmonary artery systolic pressure and enhanced sensi-tivity of the pulmonary vasculature to acute hypoxia Thestudy also showed that iron chelation through deferox-amine infusion before the 8-hour hypoxia protocolelevates pulmonary artery systolic pressure significantlyThese findings led to conclude that iron availabilitymodifies pulmonary arterial pressure and pulmonaryvascular responses to hypoxia possibly through theinvolvement of the hypoxia-inducible factor hydroxyl-ation system
In a later study Smith and coworkers74 showed theeffect that iron levels could have on HA diseases thatinvolve pulmonary hypertension such as CMS This studyshowed that reduction of iron availability in CMS patientsthrough isovolemic bloodletting is associated with asubstantial increase in Ppa whereas iron supplementationis related to an attenuation of HAPH In view of the resultsthe authors suggest that this effect is consistent with thoseof acute iron chelation and thus implies that irondeficiency could exacerbate Ppa in chronic pulmonaryand cardiac disease and also that HAPH can be attenuatedby iron supplementation
It should be noted however that no long-termcontrolled studies have been carried out to evaluate allthe possible effectors related to the development ofHAPH Thus extensive research is required to determinewhich of the multiple elements that regulate Ppa at highaltitude might have a predominant role in determining thedifferent time courses and severity of HAPH
Treatment
Recently increasing attention is being drawn todifferent phenomena that may be involved in the causalchain of CMS and that were previously overlooked Theseinclude CMS risk and environmental factors such as earlyprenatal or postnatal exposure to different agents andorthe different genetic susceptibilities in different popula-tions and individuals However until having a complete
understanding of which mechanisms are better targetsfor intervention at present treatment is directed to thosecomponents of CMS pathophysiologic sequence thatare susceptible of modification through pharmacologicintervention that is on the erythropoietic response toreduce the increased red cell mass andor on the ventilatoryresponse These agents include methylxanthines adrener-gic blockers dopaminergic antagonists medroxyproges-terone peripheral ventilator stimulants such as almitrineand enalapril all of which have been tested experiment-ally75 Although phlebotomy has been shown to reducethe signs and symptoms of CMS its invasiveness andtransient effects often render it impractical
Descent to low altitudes is the ideal treatment and leadsto prompt improvement of signs and symptoms of CMSbut often patients cannot or do not want to descend tolower altitudes for economic personal andor familyreasons Recently acetazolamide has been used as animportant alternative for the treatment of CMS and itseffects have been studied in randomized placebo-controlled trials in the Peruvian Andes394376 The effectsof this carbonic anhydrase inhibitor in CMS include animprovement of ventilation through metabolic acidosisand of SaO2
76 thus causing a decrease in Epo concen-tration and excessive erythrocytosis In addition it leads toa decrease in PVR and an increase in pulmonaryacceleration time Furthermore the number of CMSpatients with pulmonary hypertension (defined by PVRN 2 Wood units) was 8 before treatment and nil aftertreatment (P = 0005) In fact the observed effect ofacetazolamide on PVR (minus17) might be indirectly due tothe decrease in blood viscosity (minus16) due to thereduction in hematocrit (Fig 4) Therefore at presentthese very encouraging results suggest that acetazolamidecould be a good alternative in the treatment of CMS3943
Statement of Conflict of Interest
All authors declare that there are no conflicts of interest
References
1 Pentildealoza D Sime F Banchero N et al Pulmonary hypertension inhealthy men born and living at high altitudes Am J Cardiol 196311150-157
2 Hurtado A Animals in high altitudes resident man In Dill DAdolph E Wilber C editors Handbook of physiology adaptation tothe environment Washington DC American Physiological Society1964 p 843-860
3 Monge-M C Monge-C C High altitude diseases mechanism andmanagement Springfield (Ill) Charles C Thomas 1966
4 Antezana G Barragaacuten L Coudert J et al The pulmonarycirculation of high altitude natives In Brendel W Zink R editorsHigh altitude physiology and medicine New York Springer-Verlag 1982 p 142-149
548 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
5 Monge C Chronic mountain sickness Physiol Rev 1943231666 Monge-M C Encinas E Heraud C et al La Enfermedad de los
Andes (Siacutendromes Eritreacutemicos) Imprenta Americana Lima1928
7 Monge-M C Sobre un caso de Enfermedad de Vaacutequez Paperpresented at Communicacioacuten presentada a la Academia Nacional deMedicina Lima Peru Academia Nacional de Medicina 1925
8 Hurtado A Chronic mountain sickness JAMA 19421201278-1282
9 Penaloza D Sime F Chronic cor pulmonale due to loss of altitudeacclimatization (chronic mountain sickness) Am J Med 197150728-743
10 Pentildealoza D Sime F Ruiz L Cor pulmonale in chronic mountainsickness present concept of Monges disease In Porter R Knight Jeditors High altitude physiology cardiac and respiratory aspectsEdinburgh Churchill Livingstone 1971 p 41-60
11 Beall CM Decker MJ Brittenham GM et al An Ethiopian pattern ofhuman adaptation to high-altitude hypoxia Proc Natl Acad Sci U S A20029917215-17218
12 Winslow RM Monge-C C Hypoxia polycythemia and chronicmountain sickness Baltimore (Md) Johns Hopkins University Press1987
13 Arregui A Cabrera J Leon-Velarde F et al High prevalence ofmigraine in a high-altitude population Neurology 1991411668-1669
14 Sorensen SC Lassen NA Severinghaus JW et al Cerebral glucosemetabolism and cerebral blood flow in high-altitude residents J ApplPhysiol 197437305-310
15 Massik J Tang YL Hudak ML et al Effect of hematocrit oncerebral blood flow with induced polycythemia J Appl Physiol1987621090-1096
16 Monge-M C La enfermedad de los Andes An Fac Med 19281-30917 Leon-Velarde F Maggiorini M Reeves JT et al Consensus
statement on chronic and subacute high altitude diseases High AltMed Biol 20056147-157
18 Leon-Velarde F Mejia O Gene expression in chronic high altitudediseases High Alt Med Biol 20089130-139
19 Monge-C C Leoacuten-Velarde F Arregui A Chronic mountain sicknessIn Lenfant C editor High altitude an exploration of humanadaptation New York Marcel Dekker Inc 2001 p 815-838
20 Kryger M McCullough R Doekel R et al Excessive polycythemiaof high altitude role of ventilatory drive and lung disease Am RevRespir Dis 1978118659-666
21 Severinghaus JW Bainton CR Carcelen A Respiratory insensitivityto hypoxia in chronically hypoxic man Respir Physiol 19661308-334
22 Vargas E Spielvogel H Chronic mountain sickness optimalhemoglobin and heart disease High Alt Med Biol 20067138-149
23 Liang PJ Bascom DA Robbins PA Extended models of theventilatory response to sustained isocapnic hypoxia in humansJ Appl Physiol 199782667-677
24 Leon-Velarde F Gamboa A Rivera-Ch M et al Selectedcontribution peripheral chemoreflex function in high-altitudenatives and patients with chronic mountain sickness J Appl Physiol2003941269-1278 discussion 1253-1264
25 Milledge JS Lahiri S Respiratory control in lowlanders and Sherpahighlanders at altitude Respir Physiol 19672310-322
26 Fatemian M Gamboa A Leon-Velarde F et al Plasticity inrespiratory motor control selected contribution ventilatory responseto CO2 in high-altitude natives and patients with chronic mountainsickness J Appl Physiol 2003941279-1287
27 Cunningham PA Wolf CB Integration of respiratory responses tochanges in alveolar partial pressures of CO2 and O2 and in arterialpH In Cherniack JG editor Handbook of physiologymdashtherespiratory system Bethesda (Md) American Physiological Society1986 p 475-528
28 Fatemian M Robbins PA Selected contribution chemoreflexresponses to CO2 before and after an 8-h exposure to hypoxia inhumans J Appl Physiol 2001901607-1614 discussion 1606
29 Robbins PA The ventilatory response of the human respiratorysystem to sine waves of alveolar carbon dioxide and hypoxiaJ Physiology 1984350461-474
30 Milledge JS Sorensen SC Cerebral arteriovenous oxygen differ-ence in man native to high altitude J Appl Physiol 197232687-689
31 Leon-Velarde F Richalet JP Respiratory control in residents at highaltitude physiology and pathophysiology High Alt Med Biol 20067125-137
32 Villafuerte FC Cardenas R Monge CC Optimal hemoglobinconcentration and high altitude a theoretical approach for Andeanmen at rest J Appl Physiol May 2004961581-1588
33 Reeves JT Leon-Velarde F Chronic mountain sickness recentstudies of the relationship between hemoglobin concentration andoxygen transport High Alt Med Biol 20045147-155
34 Winslow RM Monge CC Brown EG et al Effects of hemodilutionon O2 transport in high-altitude polycythemia J Appl Physiol 1985591495-1502
35 Cruz J Diaz C Marticorena E et al Phlebotomy improvespulmonary gas exchange in chronic mountain polycythemiaRespiration 197938305-313
36 Manier G Guenard H Castaing Y et al Pulmonary gas exchange inAndean natives with excessive polycythemiamdasheffect of hemodilu-tion J Appl Physiol 1988652107-2117
37 Ergueta J Spielvogel H Cudkowicz L Cardio-respiratory studies inchronic mountain sickness (Monges syndrome) Respiration 197128485-517
38 Rotta A Canepa A Hurtado A et al Pulmonary circulation at sealevel and at high altitude J Appl Physiol 195611143-149
39 Richalet JP Rivera-Ch M Maignan M et al Acetazolamide forMonges disease efficiency and tolerance of 6-month treatment AmJ Respir Crit Care Med 20081771370-1376
40 Richardson TQ Guyton AC Effects of polycythemia and anemia oncardiac output and other circulatory factors Am J Physiol 19591971167-1170
41 Guyton AC Richardson TQ Effect of hematocrit on venous returnCirc Res 19619157-164
42 Claydon VE Norcliffe LJ Moore JP et al Orthostatic tolerance andblood volumes in Andean high altitude dwellers Exp Physiol 200489565-571
43 Richalet JP Rivera M Bouchet P et al Acetazolamide a treatmentfor chronic mountain sickness Am J Respir Crit Care Med 20051721427-1433
44 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk III The thickness of the media of the pulmonary trunk andascending aorta in high altitude natives Circulation 1963271101-1104
45 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk II The evolution of the elastic configuration of the pulmonarytrunk in people native to high altitudes Circulation 1963271094-1100
46 Saldana M Arias-Stella J Studies on the structure of thepulmonary trunk I Normal changes in the elastic configurationof the human pulmonary trunk at different ages Circulation 1963271086-1093
47 Wagner KF Katschinski DM Hasegawa J et al Chronic inbornerythrocytosis leads to cardiac dysfunction and premature death inmice overexpressing erythropoietin Blood 200197536-542
48 Ruschitzka FT Wenger RH Stallmach T et al Nitric oxide preventscardiovascular disease and determines survival in polyglobulic miceoverexpressing erythropoietin Proc Natl Acad Sci U S A 20009711609-11613
549F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
49 Brown CM Hainsworth R Assessment of capillary fluidshifts during orthostatic stress in normal subjects andsubjects with orthostatic intolerance Clin Auton Res 1999969-73
50 Bush VE Wight VL Brown CM et al Vascular responses toorthostatic stress in patients with postural tachycardia syndrome(POTS) in patients with low orthostatic tolerance and inasymptomatic controls Clin Auton Res 200010279-284
51 Cooper VL Hainsworth R Effects of head-up tilting on baroreceptorcontrol in subjects with different tolerances to orthostatic stress ClinSci (Lond) 2002103221-226
52 Appenzeller O Thomas PK Ponsford S et al Acral paresthesias inthe Andes and neurology at sea level Neurology 2002591532-1535
53 Kwaan HC Wang J Hyperviscosity in polycythemia vera andother red cell abnormalities Semin Thromb Hemost 200329451-458
54 Claydon VE Norcliffe LJ Moore JP et al Cardiovascularresponses to orthostatic stress in healthy altitude dwellers andaltitude residents with chronic mountain sickness Exp Physiol200590103-110
55 Norcliffe LJ Rivera-Ch M Claydon VE et al Cerebrovascularresponses to hypoxia and hypocapnia in high-altitude dwellersJ Physiol 2005566(Pt 1)287-294
56 Moore JP Claydon VE Norcliffe LJ et al Carotid baroreflexregulation of vascular resistance in high-altitude Andean natives withand without chronic mountain sickness Exp Physiol 200691907-913
57 Antezana AM Richalet JP Noriega I et al Hormonal changes innormal and polycythemic high-altitude natives J Appl Physiol 199579795-800
58 Gamboa A Gamboa JL Holmes C et al Plasma catecholamines andblood volume in native Andeans during hypoxia and normoxia ClinAuton Res 20061640-45
59 Penaloza D Arias-Stella J The heart and pulmonary circulation athigh altitudes healthy highlanders and chronic mountain sicknessCirculation 20071151132-1146
60 Pei SX Chen XJ Si Ren BZ et al Chronic mountain sickness inTibet Q J Med 198971555-574
61 Wu TY Li W Li Y et al Epidemiology of chronic mountainsickness ten years study in Qinghai-Tibet In Ohno H KobayashiT Masuyama S Nakashima M editors Progress in MountainMedicine and High Altitude Physiology Matsumoto Press Com-mittee of the 3rd World Congress on Mountain Medicine and HighAltitude Physiology 1998 p 120-125
62 Sime F Penaloza D Ruiz L Bradycardia increased cardiac outputand reversal of pulmonary hypertension in altitude natives living atsea level Br Heart J 197133647-657
63 Allemann Y Sartori C Lepori M et al Echocardiographic andinvasive measurements of pulmonary artery pressure correlateclosely at high altitude Am J Physiol 2000279H2013-H2016
64 Kojonazarov BK Imanov BZ Amatov TA et al Noninvasive andinvasive evaluation of pulmonary arterial pressure in highlandersEur Respir J 200729352-356
65 Naeije R Torbicki A More on the noninvasive diagnosis ofpulmonary hypertension Doppler echocardiography revisited EurRespir J 199581445-1449
66 Tei C Dujardin KS Hodge DO et al Doppler echocardiographicindex for assessment of global right ventricular function J Am SocEchocardiogr 19969838-847
67 Harjai KJ Scott L Vivekananthan K et al The Tei index a newprognostic index for patients with symptomatic heart failure J AmSoc Echocardiogr 200215864-868
68 Maignan M Rivera-Ch M Privat C et al Pulmonary pressure andcardiac function in chronic mountain sickness patients Chest 2009135499-504
69 Cruz-Jibaja J Banchero N Sime F et al Correlation betweenpulmonary artery pressure and level of altitude Dis Chest 196446446-451
70 Wu T Chronic mountain sickness in Qinghai-Tibet China In Ge RHackett P editors Life on the Qinghai-Tibetan Plateau BeijingPekiacuten University Medical Press 2007 p 118-133
71 Arias-Stella J Saldana M The terminal portion of the pulmonaryarterial tree in people native to high altitudes Circulation 196328915-925
72 Maggiorini M Leon-Velarde F High-altitude pulmonary hyperten-sion a pathophysiological entity to different diseases Eur Respir J2003221019-1025
73 Smith T Balanos G Croft Q et al The increase in pulmonary arterialpressure caused by hypoxia depends on iron status J Physiol 20085865999-6005
74 Smith T Talbot N Privat C et al Effects of iron supplementationand depletion on hypoxic pulmonary hypertension two randomizedcontrolled trials JAMA 20093021444-1450
75 Rivera-Ch M Leon-Velarde F Huicho L Treatment of chronicmountain sickness critical reappraisal of an old problem RespirPhysiol Neurobiol 2007158251-265
76 Rivera-Ch M Huicho L Bouchet P et al Effect of acetazolamide onventilatory response in subjects with chronic mountain sicknessRespir Physiol Neurobiol 2008162184-189

Abbreviations and Acronyms
AHVR = acute hypoxicventilatory response
CMS = chronic mountainsickness
Epo = erythropoietin
HA = high-altitude
HAPH = high-altitudepulmonary hypertension
[Hb] = hemoglobinconcentration
HVR = hypoxic ventilatoryresponse
Ppa = pulmonary arterypressure
PVR = pulmonary vascularresistance
SaO2 = arterial blood oxygensaturation
SL = sea-level
541F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
pronounced in AndeanHA dwellers11 whencompared with Tibetansand Ethiopians and evenmore so in those whohave CMS
Chronic mountainsickness affects peoplewho are native or long-time residents of HA loca-tions and usually beginsinsidiously in adult lifethe clinical picture disap-pears when the patientmoves to lower altitudesChronic mountain sick-ness is characterized bysevere hypoxemia exces-sive erythrocytosis for thealtitude of residence andvarious symptoms includ-ing sleep disorders head-ache dizziness tinnitusparesthesias mental and
physical fatigue and cognitive impairment612 Cyanosis isparticularly visible in the nail beds ears and lips In somecases the face is almost black and the mucosa andconjunctiva are dark red Clubbing of fingers is a frequentfinding Ultimately CMS leads to severe HAPH and couldlead to heart failure9 although to date no extensiveepidemiologic study has been performed to evaluate thelong-term deleterious effects of CMS Many of thesymptoms of CMS are thought to be caused by cerebralhypoxia1314 and this may be exacerbated by the lowcerebral blood flow caused by the high viscosity ofthe blood15
Carlos Monge-M was the first to describe a patient withCMS and presented the case at the Academy of Medicineof Lima in 19257 The patient was a native of the miningtown of Cerro de Pasco located at 4300 m in the PeruvianAndes but he was not a miner this patient was 38 age oldand showed a mean [Hb] of 211 gdL Monge-M ends hispresentation to the Academy calling the attention of thePeruvian medical community and authorities ldquoon the needto devote their medical efforts to understand thepolycythemic syndromes in order to be able to evaluatethe magnitude of impairment that these pathologies couldcause to the inhabitants of the Andesrdquo Three years laterMonge-M published an extensive article16 on cases ofCMS from Cerro de Pasco (4300 m) and Puno (3800 m)an agricultural town Monge-M considered CMS to be aldquoloss of acclimatizationrdquo because it developed only afterprolonged exposure to altitude in previously well-acclimatized subjects
Historical terms used in different mountainous regions forthis HA disease which has excessive elevation of [Hb] as acommon characteristic have been HA excessive polycythe-mia or erythrocytosis excessive erythrocytosis and HApathologic erythrocytosis A number of factors are known toinfluence the development of CMS among them altitudeage sex sleep disorders and genetic susceptibility17-19
Respiratory aspects of CMS
The primary finding in patients with CMS is excessiveerythrocytosis This excessive increase in the number ofred blood cells is caused by hypoxemia which developsmainly because differences in the respiratory pattern ofCMS individuals Compared with healthy HA natives atthe same altitude patients with CMS are relativelyhypoxic and hypercapnic2021 Alveolar hypoventilationis the main respiratory feature but also ventilation-perfusion mismatch and widened alveolar-arterial PO2gradient has been described in subjects with CMS19
Implication of the peripheral chemoreceptors as thecause of hypoxemia in CMS
The main peripheral chemoreceptors in mammals arelocated in the carotid bodies in the bifurcation of thecarotid arteries These small structures are heavilyvascularized and have an elevated blood flow for theirsize Carotid chemoreceptors stimulate ventilation inresponse to hypoxia Nevertheless in cases of prolongedresidence at high altitude this ventilatory response tohypoxia appears attenuated (ldquobluntedrdquo) in humans and insome animals
Chronic mountain sickness has been associated withpoor hypoxic ventilatory responses (HVRs)2122 but thereis no proof that changes in carotid body structure orfunction are the cause of hypoventilation in CMS20 Tobetter understand the peripheral chemoreceptor function inhypoxia short-term and sustained protocols of exposure tohypoxia have been used An acute HVR (AHVR) protocolevaluates the immediate response to a stepwise inductionof hypoxia for few minutes (6-7 minutes) A sustainedprotocol (15-20 minutes of hypoxia) determines thehypoxic ventilatory decline which is the attenuation ofthe initial ventilatory response after the first few minutesof hypoxia Acute HVR reflects peripheral control ofbreathing whereas the hypoxic ventilatory decline mayreflect attenuation of the ventilatory response by centralcontrol mechanisms although there is some debate onthis point23
When HA natives and individuals with CMS areexposed to acute hypoxia from an initial end-tidal PO2(PETO2) of 100 Torr to a final PETO2 of 45 or 34 Torr theaverage values for the slope of the AHVR for both HA
Fig 1 Arteriovenous O2 content difference (CaO2 minus CvO2) as a functionof arterial O2 saturation (SaO2) Unfilled circles represent mean data ofresidents from various altitudes and [Hb] are indicated above each circleFilled circles represent data from subjects exposed acutely to altitudes of3050 and 4570 m The (CaO2 minus CvO2) is shown as a percentage ofnormoxic values The content difference (CaO2 minus CvO2) in altituderesidents demonstrates a complex relation to SaO2 but the residents showa better sustained content difference than subjects exposed acutely toaltitude Maximal (CaO2 minus CvO2) is obtained at an [Hb] of 175 g100 mLand a SaO2 of 87 Data from Reeves and Leon-Velarde 200433
542 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
natives and subjects with CMS are around one third ofthe values for sea-level (SL) natives24 The HA nativesand subjects with CMS do not differ significantly fromeach other in their immediate response to hypoxia Inaddition when the peripheral chemoreflex contribution atPETO2 = 525 Torr is calculated from the value of AHVRmultiplied by the reduction in saturation associated withreducing PETO2 from 200 Torr to 525 Torr (AHVR times[SaO2 200] minus SaO2 525) the contribution for the SLgroup is clearly much larger than for the HA and CMSgroups and there is no difference between the HA andCMS group Overall these studies provide evidence tosupport the notion that the lower levels of ventilation inCMS subjects that is the loss of the drive to breathemay arise from mechanisms other than reductions in theperipheral chemoreflex sensitivity to hypoxia or that itscontribution is quite marginal24
Implication of central chemoreceptors as the cause ofhypoxemia in CMS
The cells of the central chemoreceptors respond mainlyto CO2 and H+ At sea level total sensitivity to CO2 innormoxia is of approximately 17 LminTorr In hyper-oxia its value ranges from 25 to 275 LminTorr and inhypoxia at a PETO2 = 50 Torr from 41 to 44 LminTorr212526 The effect of hypoxia in total sensitivity toCO2 is greater in HA natives than in natives from sea leveland than in patients with CMS The peripheral sensitivityof the chemoreceptors to CO2 (Gp) of HA natives isgreater than the Gp of SL inhabitants
The time constants for response to CO2 can beperipheral (tp) or central (tc)2728 Tp is similar betweenSL and HA natives however Tc is slower in HA nativesand even slower in subjects with CMS26 The slowness ofthe time constant in the central chemoreflex is related tothe buffer capacities of the plasma in which centralchemoreceptors are immersed The time constant dependson the cerebral flow per volume unit of cerebral tissue andon the relation between the CO2-buffering capacity of theblood and the brain29 Although cerebral blood flow hasbeen shown to be decreased in HA natives1430 thedelivery of O2 would be relatively protected due to theincreased hematocrit14 However it is not absolutelyobvious that the removal of CO2 also would be assuredAlso the increased hematocrit elevates H+ buffering butplasma flow is reduced therefore the amount ofbicarbonate in blood is reduced A quantitative analysisof these factors reveals a relative reduction of CO2
exchange in the brain in response to changes of PCO2 in thearterial blood26
Overall the interpretation of the data in peripheral andcentral chemoreflex sensitivity to CO2 is that CMSsubjects seem to have reset their central CO2 chemor-eceptors to operate around the resting PETCO2 more close
to SL standards thus around higher PETCO2 values than athigh altitude Indeed Monge-M and Monge-C3 haveshown that PETCO2 HCO3
minus and pH in CMS patients arecloser to SL values31
Excessive erythrocytosis and the heart in CMS effectof hematocrit on cardiac function
Increased [Hb] has long been considered beneficial athigh altitude because the increased oxygen-carryingcapacity of blood would compensate for decreasedarterial oxygen saturation The increase in [Hb] shouldact to maintain oxygen transport to tissues therebyreducing the need to increase cardiac output inhypoxemic subjects This concept however has beenchallenged because with a low oxygen saturation (lowPO2) increasing [Hb] would be of help up to a certainpoint and thus only a moderate increase in [Hb] wouldbenefit O2 transport When excessive however [Hb]becomes detrimental The perfect example is CMSwhere despite having a significantly higher blood O2
content32 individuals are severely hypoxemic and ill Ithas been suggested that above certain [Hb] valueerythrocytosis is no longer beneficial because of theelevated blood viscosity and increased blood volume thatleads to congestive symptoms3233 Increased bloodviscosity and blood volume which results from increas-ing [Hb] to excessive levels affects the distribution ofpulmonary blood flow and pulmonary ventilation-perfu-sion relationships resulting in impaired pulmonary gasexchange This contributes to arterial hypoxemia and
543F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
further stimulates erythropoiesis3435 Interestinglysome studies have shown that when these subjectsundergo bloodletting or hemodilution blood oxygen-ation improves and the symptoms are reduceddramatically123436 Reeves and Leon-Velarde33 havesuggested based on an analysis of arterial-venous O2
content difference at different [Hb] and SaO2 values thatup to a certain value (SaO2 of 87 and a [Hb] of 175 g100 mL) increasing [Hb] has a cardiac output-sparingeffect because of a greater oxygen extraction (Fig 1)When hypoxemia however becomes severe an elevated[Hb] no longer supports an efficient O2 transport andcardiac output has to increase yet the literature showsvariability in cardiac output values in CMS937-39
In 1959 Guyton and Richardson40 were the first tostudy experimentally the effect of hematocrit on cardiacfunction Their work showed that when hematocrit wasincreased isovolemically by 47 in dogs cardiac outputwas reduced dramatically by 51 and total peripheralresistance increased by 50 The effect on cardiac outputwas explained in the effect of increased blood viscosityon venous resistance and venous return as confirmed in alater study41
In CMS chronic hypoxemia leads to excessiveerythrocytosis accompanied by a very high bloodvolume8373842 Thus the emerging figure is somewhatdifferent to what was observed in the isovolemicexperiments in dogs Cardiac output peripheral resis-tance and systolic blood pressure in CMS patients aresimilar to those of healthy individuals at the samealtitude1037 Some recent studies however have shown
Table 1Subject characteristics in high altitude natives (HA) and chronic mountain sick
At High Altitude
HA CMS
Age (years) 393 plusmn 20 43Hematocrit () 498 plusmn 12 63O2 Saturation () 860 plusmn 10 82Orthostatic Tolerance (min) 462 plusmn 12 47SAP (mmHg) Supine 1137 plusmn 30 117Tilt 1157 plusmn 35 119DAP (mmHg) Supine 731 plusmn 23 76Tilt 764 plusmn 26 74HR (bmin) Supine 589 plusmn 20 65Tilt 706 plusmn 28 76Plasma volume (mlkg) 393 plusmn 36 34Red cell volume (mlkg) 379 plusmn 31 62Blood volume (mlkg) 772 plusmn 64 97
Subject characteristics in high altitude natives (HA) and chronic mountain sickboth high altitude groups than at SL (288 plusmn 40 P b 0001) Systolic (SAP)min) are shown in supine and tilt positions Tilt indicates values at the end obetween locations (P b 005 P b 0001 P b 00001) dagger represents sidifferences between supine and tilt There were no significant differences inwere smaller in HA and SL (275 plusmn 18 P b 0001) than in CMS Blood voCMS Values are means plusmn SE Data from Claydon et al 2004 20054254
that systemic pressure in CMS individuals is slightlyelevated when compared to healthy highlanders43
Although elevated blood viscosity would tend todecrease venous return the increased blood volumewould counteract this effect and therefore cardiac outputwould be maintained The rise in peripheral resistance dueto increased blood viscosity is most probably counteractedby the increased aortic elasticity and vasodilation in HAresidents44-46 Contrary to what is found for systolicpressure some studies have found an increased diastolicblood pressure in persons having severe CMS910 thatmight reflect an increased venous return due to increasedblood volume
Studies on the physiology of a transgenic mice line(ldquotg6rdquo mice) that overexpresses erythropoietin (Epo) haveprovided insightful information on the hypoxia-indepen-dent effects of excessive erythrocytosis on the cardio-vascular system Under normoxic conditions thisinteresting animal model exhibits a 12-fold elevation inplasma Epo concentration hematocrit values in the rangeof 85 to 90 and 75 larger blood volume comparedto its wild-type counterparts47 Despite excessive ery-throcytosis increased viscosity and elevated bloodvolume tg6 mice have normal cardiac output andblood pressure values The excessive hematocrit in tg6mice would result in elevated peripheral resistancehowever the increased sheer stress on vascular endothe-lium induces the expression of endothelial nitric oxidesynthase and an enhanced production of NO which inturn causes vasodilation and counteracts the effect ofhematocrit on peripheral resistance48 On the venous side
ness subjects (CMS)
At Sea Level
HA CMS
1 plusmn 17
8 plusmn 17
0 plusmn 12 960 plusmn 07 940 plusmn 07dagger
2 plusmn 12
2 plusmn 26 1107 plusmn 46 1151 plusmn 365 plusmn 24 1065 plusmn 28Dagger 1123 plusmn 33Dagger
4 plusmn 23 678 plusmn 42 715 plusmn 25
3 plusmn 27 758 plusmn 24 788 plusmn 30dagger
0 plusmn 20dagger 493 plusmn 22 543 plusmn 14
1 plusmn 27 554 plusmn 22 642 plusmn 28dagger
6 plusmn 18
8 plusmn 53
4 plusmn 63
ness subjects (CMS) Orthostatic tolerance was significantly greater inand diastolic (DAP) arterial blood pressures and heart rate (HR beatsf the 20 min phase of head up tilt represents a significant differencegnificant difference between HA and CMS and Dagger indicates significantplasma volumes between groups and sea level (SL) Red cell volumeslumes were smaller in HA and SL (673 plusmn 47 P b 001) compared to
544 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
due to increased blood volume tg6 mice showsignificantly elevated central venous pressure47 thatcould result in elevated diastolic pressure It is possiblethen that some of the mechanisms operating in tg6 miceare also present in CMS individuals An enhancedexpression of endothelial nitric oxide synthase in CMScould explain for example the normal peripheralresistance found in CMS patients
Systemic blood pressure control and blood flow in CMS
Although systolic blood pressure in CMS patients isoften similar to that of healthy highlanders some smalldifferences arise in the control mechanisms It has beenshown that Andean HA dwellers have a great tolerance toorthostatic stress that might be attributed to the increasedhematocrit and blood volume The CMS individuals showan exceptional tolerance to orthostatic stress but nosignificantly different from HA controls yet CMSindividuals tend to respond with smaller increases inheart rate than HA healthy subjects54 This has led tosuggest that this may reflect a smaller sympathetic responseto orthostatic stress in these individuals (Table 1) Smallresponses of vascular resistance however have beenassociated to poor orthostatic tolerance49-51 Therefore theextremely good orthostatic tolerance in CMS patientssuggests that some other mechanism is operating in theseindividuals to maintain blood pressure It is possible thatthe large blood volume occurring in these individualscompensates for the smaller sympathetic response5253
Claydon and coworkers54 have shown that at HA theperipheral vascular resistance response to orthostatic stresshad a tendency to be smaller in CMS compared to healthysubjects but after 24 hours at sea level the CMS group hada significantly smaller response This less effective reflexvasoconstriction could explain why despite a larger bloodvolume in CMS subjects their orthostatic tolerance issimilar to that of HA controls
Chronic mountain sickness subjects also show differ-ences in the autoregulation of cerebral blood flow It hasbeen shown that cerebral blood flow is slower in CMSpatients compared to healthy HA subjects55 and it hasbeen suggested that this is a consequence of the increasedblood viscosity Cerebral blood flow autoregulation issimilar in CMS and healthy highlanders at high altitudeand their values are similar to those reported in SLresidents1355 After 24 hours at sea level however CMSindividuals had a larger fall on cerebral blood flow withsmaller change in resistance when exposed to orthostaticstress55 Studies on the relationship between peripheralresistance and carotid baroreceptor function have shownthat at altitude the sensitivity of forearm vascularresistance as a function of carotid sinus pressure is similarin CMS and healthy subjects but the ldquoset-pointrdquo of the
relationship is significantly higher in the CMS group56
This difference however disappears at sea level Apossible explanation for a higher ldquoset-pointrdquo in CMSindividuals at high altitude and its normalization at sealevel could be associated to the effects of hypoxemia onsympathetic vasomotor activity It is well-known thathypoxemia increases sympathetic discharge to musclevascular beds Chronic mountain sickness subjects arenormally more hypoxemic and therefore it is likely that agreater sympathetic activation may have contributed to thealtered baroreflex function This possibility finds supportin the observation that noradrenaline and adrenaline levelsare higher in CMS patients than in healthy HA dwellers57
and that plasma catecholamines are significantly reducedin HA natives within 4 hours of descent to sea level58
Cardiac features of CMS
Thirty years ago Pentildealoza and Arias-Stella59 studiedextensively the cardiac characteristics and pulmonarycirculation of Andean dwellers and patients with severeCMS Their findings point to the presence of pulmonaryhypertension and right ventricular hypertrophy in CMSsubjects9106061 They also demonstrated a direct rela-tionship between Ppa and right ventricle size In additiona prominent main pulmonary artery was found in allpatients Clinical characteristics of pulmonary hyperten-sion were an increased pulmonary second sound oftenassociated with a soft midsystolic ejection murmur anincreased diastolic blood pressure thought to be related toexcessive polycythemia9 and an increase in heart size onchest x-ray compared to healthy highlanders a featureexplained by the increased size of the right heart chambers
In severe cases of CMS the ECG shows peaked Pwaves with increased voltage in leads II III and aVF aswell as in the right precordial leads A right QRS axisdeviation is often observed An rS pattern in the rightprecordial leads and complexes of RS or rS type in the leftprecordial leads are common findings Negative T wavesover the right precordial leads are also common Thesefindings are indicative of right ventricular hypertrophy(RVH) and overload of the right heart chambers asconsequence of pulmonary hypertension Indeed as wellas with heart size a direct relationship between Ppa andright QRS axis deviation has been demonstrated59 Whenpatients with CMS are moved to SL symptoms and signsimprove promptly and the electrocardiographic andradiographic evidence of elevated Ppa and RVH decreasesover time62
Recent echocardiographic studies of pulmonary arterypressure at high altitude support previous findings usinginvasive techniques63-65 At present Doppler echocardi-ography is preferred to evaluate accurately cardiovascular
Fig 2 Cardiac output and maximal tricuspid regurgitation pressure in SL (SL control group at sea level [n = 15]) and HA (HA control group [n = 15]) andCMS groups (n = 55) at high altitude Data from Richalet et al 200968
545F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
function and cardiac morphology A recent study showedthat left atrial area was larger in SL than in HA nativesand CMS patients Right atria and ventricles were largerin CMS compared to SL and HA as shown by largerend-systolic right atria and end-diastolic right ventricularareas and a higher end-diastolic rightleft ventriculardiameter ratio This study also showed that cardiac outputis lower in CMS subjects than in SL dwellers but nodifference has been found when compared with HA
Fig 3 Pulmonary acceleration time and PVR index in SL (SL control group [n =([peak tricuspid regurgitation velocityright ventricular outflow tract time minus vel
natives (Fig 2) Left and right ventricular systolicfunctions and mitral and tricuspid inflows EA are notdifferent between SL HA and CMS Right ventricularTei index a global myocardial performance indicator(calculated as the ratio of [systolic time minus ejection time]ejection time)6667 however is increased in HA nativesand CMS patients when compared to SL controls Thesecardiac characteristics have been described in approxi-mately 50 CMS subjects the largest sample studied at
15]) HA (HA control group [n = 15]) and CMS groups (n = 55) PVR =ocity integral] times 10) + 01668
546 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
4300 m patients showed a mean [Hb] of 231 plusmn 16 gdLarterial blood oxygen saturation (SaO2) of 81 plusmn 4 andPpa of 34 plusmn 10 mm Hg68
Pulmonary hypertension in CMS
The cause of HAPH is the increase in pulmonaryvascular resistance (PVR) the underlying mechanisminvolves sustained and exaggerated pulmonary vasocon-striction and remodeling of the pulmonary vascular wall inresponse to chronic hypoxia due to proliferation anddecreased apoptosis of pulmonary artery smooth musclecells The effects of chronic hypoxia on pulmonary arterypressure are reflected in the negative correlation that existsbetween Ppa and SaO2 at high altitude596970 Arterialhypoxemia in addition to hypoxic vasoconstriction leadsto several structural changes in the pulmonary vesselsincluding an increase in the number of intimal smoothmuscle cells medial thickening in the small musculararteries and fibrinoid necrosis of the vessel walls71 Thesestructural changes in the pulmonary vessels rather thanhypoxic vasoconstriction alone are believed to beresponsible for the sustained rise in Ppa in chronichypoxia Pioneering hemodynamic invasive studies byPentildealoza and Sime910 in 10 subjects with severe CMS at4300 m showed a mean [Hb] value of 247 plusmn 24 gdL amean SaO2 of 696 plusmn 49 and a Ppa of 47 plusmn 177 mmHg values that have made the authors conclude that thesepatients have a type of hypoxic cor pulmonale in contrastto the hypertensive cor pulmonale observed in primarypulmonary hypertension However the structural changes
Fig 4 Pulmonary vascular resistance index and pulmonary acceleration time intreatment with acetazolamide (Acz) The study was organized in 2 phases (1) a ran open-label phase where all patients received acetazolamide (Acz + Acz) Theet al 200939
in the pulmonary vessels which are responsible for thesustained rise in Ppa in chronic hypoxia can have differentintensities and different onset times depending on thelength of hypoxic exposure comprising a range fromshort-term to long-term7072
Maignan and coworkers68 have described cardiachemodynamics in approximately 50 CMS cases withnoninvasive methods and found varying intensities ofPpa Although they might have been studying patients inan early disease stage they observed mean pulmonaryacceleration time and accelerationejection time ratiossignificantly lower in CMS subjects than in SL and HAnatives (Fig 3) Pulmonary vascular index was foundlower in SL than in other groups and there was nosignificant difference between HA and CMS however thenumber of patients with PVR greater than 2 Wood unitswas higher in CMS (1242) than in SL (013) and tended tobe significant when compared to HA (115) (CMS vs SLP = 003 CMS vs HA P = 008 and SL vs HA P = 034)
Chronic hypoxia with appropriate acclimatization asseen in healthy HA residents induces an increase inPVR without change in pulmonary arterial systolicpressure right heart cavity dimensions or right systolicventricular function The increase in right ventricularTei index however could reflect early right ventricularimpairment68 When hypoxemia becomes severe asobserved in some patients with excessive Ppa a furtherimpairment can be found with a significant increase inpulmonary arterial systolic pressure and right cardiaccavity enlargement However contrary to the assumption59
of overt chronic cor pulmonale based on severe HAPHpatients with established HAPH did not show any
placebo and CMS patients groups before and after 3 and 6 months ofandomized double-blind placebo-controlled phase (placebo + Acz) and (2)2 phases were separated by a 4-week washout period Data from Richalet
547F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
obvious cardiac systolic dysfunction as shown byMaignan and coworkers68 This confirms the individualvariability of the severity of HAPH which is also highlydependent on risk factors and genetic susceptibilitydespite that for the moment no specific gene has beenclearly associated with the development of CMS Largeepidemiologic studies should be conducted to determinethe precise natural history prevalence and features ofheart failure in CMS
Recently an interaction between iron levels andhypoxia in the regulation of the pulmonary circulationhas been described73 The study showed that ironinfusion before an 8-hour exposure to sustained hypoxiaabolished or reduced greatly the elevation in baselinepulmonary artery systolic pressure and enhanced sensi-tivity of the pulmonary vasculature to acute hypoxia Thestudy also showed that iron chelation through deferox-amine infusion before the 8-hour hypoxia protocolelevates pulmonary artery systolic pressure significantlyThese findings led to conclude that iron availabilitymodifies pulmonary arterial pressure and pulmonaryvascular responses to hypoxia possibly through theinvolvement of the hypoxia-inducible factor hydroxyl-ation system
In a later study Smith and coworkers74 showed theeffect that iron levels could have on HA diseases thatinvolve pulmonary hypertension such as CMS This studyshowed that reduction of iron availability in CMS patientsthrough isovolemic bloodletting is associated with asubstantial increase in Ppa whereas iron supplementationis related to an attenuation of HAPH In view of the resultsthe authors suggest that this effect is consistent with thoseof acute iron chelation and thus implies that irondeficiency could exacerbate Ppa in chronic pulmonaryand cardiac disease and also that HAPH can be attenuatedby iron supplementation
It should be noted however that no long-termcontrolled studies have been carried out to evaluate allthe possible effectors related to the development ofHAPH Thus extensive research is required to determinewhich of the multiple elements that regulate Ppa at highaltitude might have a predominant role in determining thedifferent time courses and severity of HAPH
Treatment
Recently increasing attention is being drawn todifferent phenomena that may be involved in the causalchain of CMS and that were previously overlooked Theseinclude CMS risk and environmental factors such as earlyprenatal or postnatal exposure to different agents andorthe different genetic susceptibilities in different popula-tions and individuals However until having a complete
understanding of which mechanisms are better targetsfor intervention at present treatment is directed to thosecomponents of CMS pathophysiologic sequence thatare susceptible of modification through pharmacologicintervention that is on the erythropoietic response toreduce the increased red cell mass andor on the ventilatoryresponse These agents include methylxanthines adrener-gic blockers dopaminergic antagonists medroxyproges-terone peripheral ventilator stimulants such as almitrineand enalapril all of which have been tested experiment-ally75 Although phlebotomy has been shown to reducethe signs and symptoms of CMS its invasiveness andtransient effects often render it impractical
Descent to low altitudes is the ideal treatment and leadsto prompt improvement of signs and symptoms of CMSbut often patients cannot or do not want to descend tolower altitudes for economic personal andor familyreasons Recently acetazolamide has been used as animportant alternative for the treatment of CMS and itseffects have been studied in randomized placebo-controlled trials in the Peruvian Andes394376 The effectsof this carbonic anhydrase inhibitor in CMS include animprovement of ventilation through metabolic acidosisand of SaO2
76 thus causing a decrease in Epo concen-tration and excessive erythrocytosis In addition it leads toa decrease in PVR and an increase in pulmonaryacceleration time Furthermore the number of CMSpatients with pulmonary hypertension (defined by PVRN 2 Wood units) was 8 before treatment and nil aftertreatment (P = 0005) In fact the observed effect ofacetazolamide on PVR (minus17) might be indirectly due tothe decrease in blood viscosity (minus16) due to thereduction in hematocrit (Fig 4) Therefore at presentthese very encouraging results suggest that acetazolamidecould be a good alternative in the treatment of CMS3943
Statement of Conflict of Interest
All authors declare that there are no conflicts of interest
References
1 Pentildealoza D Sime F Banchero N et al Pulmonary hypertension inhealthy men born and living at high altitudes Am J Cardiol 196311150-157
2 Hurtado A Animals in high altitudes resident man In Dill DAdolph E Wilber C editors Handbook of physiology adaptation tothe environment Washington DC American Physiological Society1964 p 843-860
3 Monge-M C Monge-C C High altitude diseases mechanism andmanagement Springfield (Ill) Charles C Thomas 1966
4 Antezana G Barragaacuten L Coudert J et al The pulmonarycirculation of high altitude natives In Brendel W Zink R editorsHigh altitude physiology and medicine New York Springer-Verlag 1982 p 142-149
548 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
5 Monge C Chronic mountain sickness Physiol Rev 1943231666 Monge-M C Encinas E Heraud C et al La Enfermedad de los
Andes (Siacutendromes Eritreacutemicos) Imprenta Americana Lima1928
7 Monge-M C Sobre un caso de Enfermedad de Vaacutequez Paperpresented at Communicacioacuten presentada a la Academia Nacional deMedicina Lima Peru Academia Nacional de Medicina 1925
8 Hurtado A Chronic mountain sickness JAMA 19421201278-1282
9 Penaloza D Sime F Chronic cor pulmonale due to loss of altitudeacclimatization (chronic mountain sickness) Am J Med 197150728-743
10 Pentildealoza D Sime F Ruiz L Cor pulmonale in chronic mountainsickness present concept of Monges disease In Porter R Knight Jeditors High altitude physiology cardiac and respiratory aspectsEdinburgh Churchill Livingstone 1971 p 41-60
11 Beall CM Decker MJ Brittenham GM et al An Ethiopian pattern ofhuman adaptation to high-altitude hypoxia Proc Natl Acad Sci U S A20029917215-17218
12 Winslow RM Monge-C C Hypoxia polycythemia and chronicmountain sickness Baltimore (Md) Johns Hopkins University Press1987
13 Arregui A Cabrera J Leon-Velarde F et al High prevalence ofmigraine in a high-altitude population Neurology 1991411668-1669
14 Sorensen SC Lassen NA Severinghaus JW et al Cerebral glucosemetabolism and cerebral blood flow in high-altitude residents J ApplPhysiol 197437305-310
15 Massik J Tang YL Hudak ML et al Effect of hematocrit oncerebral blood flow with induced polycythemia J Appl Physiol1987621090-1096
16 Monge-M C La enfermedad de los Andes An Fac Med 19281-30917 Leon-Velarde F Maggiorini M Reeves JT et al Consensus
statement on chronic and subacute high altitude diseases High AltMed Biol 20056147-157
18 Leon-Velarde F Mejia O Gene expression in chronic high altitudediseases High Alt Med Biol 20089130-139
19 Monge-C C Leoacuten-Velarde F Arregui A Chronic mountain sicknessIn Lenfant C editor High altitude an exploration of humanadaptation New York Marcel Dekker Inc 2001 p 815-838
20 Kryger M McCullough R Doekel R et al Excessive polycythemiaof high altitude role of ventilatory drive and lung disease Am RevRespir Dis 1978118659-666
21 Severinghaus JW Bainton CR Carcelen A Respiratory insensitivityto hypoxia in chronically hypoxic man Respir Physiol 19661308-334
22 Vargas E Spielvogel H Chronic mountain sickness optimalhemoglobin and heart disease High Alt Med Biol 20067138-149
23 Liang PJ Bascom DA Robbins PA Extended models of theventilatory response to sustained isocapnic hypoxia in humansJ Appl Physiol 199782667-677
24 Leon-Velarde F Gamboa A Rivera-Ch M et al Selectedcontribution peripheral chemoreflex function in high-altitudenatives and patients with chronic mountain sickness J Appl Physiol2003941269-1278 discussion 1253-1264
25 Milledge JS Lahiri S Respiratory control in lowlanders and Sherpahighlanders at altitude Respir Physiol 19672310-322
26 Fatemian M Gamboa A Leon-Velarde F et al Plasticity inrespiratory motor control selected contribution ventilatory responseto CO2 in high-altitude natives and patients with chronic mountainsickness J Appl Physiol 2003941279-1287
27 Cunningham PA Wolf CB Integration of respiratory responses tochanges in alveolar partial pressures of CO2 and O2 and in arterialpH In Cherniack JG editor Handbook of physiologymdashtherespiratory system Bethesda (Md) American Physiological Society1986 p 475-528
28 Fatemian M Robbins PA Selected contribution chemoreflexresponses to CO2 before and after an 8-h exposure to hypoxia inhumans J Appl Physiol 2001901607-1614 discussion 1606
29 Robbins PA The ventilatory response of the human respiratorysystem to sine waves of alveolar carbon dioxide and hypoxiaJ Physiology 1984350461-474
30 Milledge JS Sorensen SC Cerebral arteriovenous oxygen differ-ence in man native to high altitude J Appl Physiol 197232687-689
31 Leon-Velarde F Richalet JP Respiratory control in residents at highaltitude physiology and pathophysiology High Alt Med Biol 20067125-137
32 Villafuerte FC Cardenas R Monge CC Optimal hemoglobinconcentration and high altitude a theoretical approach for Andeanmen at rest J Appl Physiol May 2004961581-1588
33 Reeves JT Leon-Velarde F Chronic mountain sickness recentstudies of the relationship between hemoglobin concentration andoxygen transport High Alt Med Biol 20045147-155
34 Winslow RM Monge CC Brown EG et al Effects of hemodilutionon O2 transport in high-altitude polycythemia J Appl Physiol 1985591495-1502
35 Cruz J Diaz C Marticorena E et al Phlebotomy improvespulmonary gas exchange in chronic mountain polycythemiaRespiration 197938305-313
36 Manier G Guenard H Castaing Y et al Pulmonary gas exchange inAndean natives with excessive polycythemiamdasheffect of hemodilu-tion J Appl Physiol 1988652107-2117
37 Ergueta J Spielvogel H Cudkowicz L Cardio-respiratory studies inchronic mountain sickness (Monges syndrome) Respiration 197128485-517
38 Rotta A Canepa A Hurtado A et al Pulmonary circulation at sealevel and at high altitude J Appl Physiol 195611143-149
39 Richalet JP Rivera-Ch M Maignan M et al Acetazolamide forMonges disease efficiency and tolerance of 6-month treatment AmJ Respir Crit Care Med 20081771370-1376
40 Richardson TQ Guyton AC Effects of polycythemia and anemia oncardiac output and other circulatory factors Am J Physiol 19591971167-1170
41 Guyton AC Richardson TQ Effect of hematocrit on venous returnCirc Res 19619157-164
42 Claydon VE Norcliffe LJ Moore JP et al Orthostatic tolerance andblood volumes in Andean high altitude dwellers Exp Physiol 200489565-571
43 Richalet JP Rivera M Bouchet P et al Acetazolamide a treatmentfor chronic mountain sickness Am J Respir Crit Care Med 20051721427-1433
44 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk III The thickness of the media of the pulmonary trunk andascending aorta in high altitude natives Circulation 1963271101-1104
45 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk II The evolution of the elastic configuration of the pulmonarytrunk in people native to high altitudes Circulation 1963271094-1100
46 Saldana M Arias-Stella J Studies on the structure of thepulmonary trunk I Normal changes in the elastic configurationof the human pulmonary trunk at different ages Circulation 1963271086-1093
47 Wagner KF Katschinski DM Hasegawa J et al Chronic inbornerythrocytosis leads to cardiac dysfunction and premature death inmice overexpressing erythropoietin Blood 200197536-542
48 Ruschitzka FT Wenger RH Stallmach T et al Nitric oxide preventscardiovascular disease and determines survival in polyglobulic miceoverexpressing erythropoietin Proc Natl Acad Sci U S A 20009711609-11613
549F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
49 Brown CM Hainsworth R Assessment of capillary fluidshifts during orthostatic stress in normal subjects andsubjects with orthostatic intolerance Clin Auton Res 1999969-73
50 Bush VE Wight VL Brown CM et al Vascular responses toorthostatic stress in patients with postural tachycardia syndrome(POTS) in patients with low orthostatic tolerance and inasymptomatic controls Clin Auton Res 200010279-284
51 Cooper VL Hainsworth R Effects of head-up tilting on baroreceptorcontrol in subjects with different tolerances to orthostatic stress ClinSci (Lond) 2002103221-226
52 Appenzeller O Thomas PK Ponsford S et al Acral paresthesias inthe Andes and neurology at sea level Neurology 2002591532-1535
53 Kwaan HC Wang J Hyperviscosity in polycythemia vera andother red cell abnormalities Semin Thromb Hemost 200329451-458
54 Claydon VE Norcliffe LJ Moore JP et al Cardiovascularresponses to orthostatic stress in healthy altitude dwellers andaltitude residents with chronic mountain sickness Exp Physiol200590103-110
55 Norcliffe LJ Rivera-Ch M Claydon VE et al Cerebrovascularresponses to hypoxia and hypocapnia in high-altitude dwellersJ Physiol 2005566(Pt 1)287-294
56 Moore JP Claydon VE Norcliffe LJ et al Carotid baroreflexregulation of vascular resistance in high-altitude Andean natives withand without chronic mountain sickness Exp Physiol 200691907-913
57 Antezana AM Richalet JP Noriega I et al Hormonal changes innormal and polycythemic high-altitude natives J Appl Physiol 199579795-800
58 Gamboa A Gamboa JL Holmes C et al Plasma catecholamines andblood volume in native Andeans during hypoxia and normoxia ClinAuton Res 20061640-45
59 Penaloza D Arias-Stella J The heart and pulmonary circulation athigh altitudes healthy highlanders and chronic mountain sicknessCirculation 20071151132-1146
60 Pei SX Chen XJ Si Ren BZ et al Chronic mountain sickness inTibet Q J Med 198971555-574
61 Wu TY Li W Li Y et al Epidemiology of chronic mountainsickness ten years study in Qinghai-Tibet In Ohno H KobayashiT Masuyama S Nakashima M editors Progress in MountainMedicine and High Altitude Physiology Matsumoto Press Com-mittee of the 3rd World Congress on Mountain Medicine and HighAltitude Physiology 1998 p 120-125
62 Sime F Penaloza D Ruiz L Bradycardia increased cardiac outputand reversal of pulmonary hypertension in altitude natives living atsea level Br Heart J 197133647-657
63 Allemann Y Sartori C Lepori M et al Echocardiographic andinvasive measurements of pulmonary artery pressure correlateclosely at high altitude Am J Physiol 2000279H2013-H2016
64 Kojonazarov BK Imanov BZ Amatov TA et al Noninvasive andinvasive evaluation of pulmonary arterial pressure in highlandersEur Respir J 200729352-356
65 Naeije R Torbicki A More on the noninvasive diagnosis ofpulmonary hypertension Doppler echocardiography revisited EurRespir J 199581445-1449
66 Tei C Dujardin KS Hodge DO et al Doppler echocardiographicindex for assessment of global right ventricular function J Am SocEchocardiogr 19969838-847
67 Harjai KJ Scott L Vivekananthan K et al The Tei index a newprognostic index for patients with symptomatic heart failure J AmSoc Echocardiogr 200215864-868
68 Maignan M Rivera-Ch M Privat C et al Pulmonary pressure andcardiac function in chronic mountain sickness patients Chest 2009135499-504
69 Cruz-Jibaja J Banchero N Sime F et al Correlation betweenpulmonary artery pressure and level of altitude Dis Chest 196446446-451
70 Wu T Chronic mountain sickness in Qinghai-Tibet China In Ge RHackett P editors Life on the Qinghai-Tibetan Plateau BeijingPekiacuten University Medical Press 2007 p 118-133
71 Arias-Stella J Saldana M The terminal portion of the pulmonaryarterial tree in people native to high altitudes Circulation 196328915-925
72 Maggiorini M Leon-Velarde F High-altitude pulmonary hyperten-sion a pathophysiological entity to different diseases Eur Respir J2003221019-1025
73 Smith T Balanos G Croft Q et al The increase in pulmonary arterialpressure caused by hypoxia depends on iron status J Physiol 20085865999-6005
74 Smith T Talbot N Privat C et al Effects of iron supplementationand depletion on hypoxic pulmonary hypertension two randomizedcontrolled trials JAMA 20093021444-1450
75 Rivera-Ch M Leon-Velarde F Huicho L Treatment of chronicmountain sickness critical reappraisal of an old problem RespirPhysiol Neurobiol 2007158251-265
76 Rivera-Ch M Huicho L Bouchet P et al Effect of acetazolamide onventilatory response in subjects with chronic mountain sicknessRespir Physiol Neurobiol 2008162184-189

Fig 1 Arteriovenous O2 content difference (CaO2 minus CvO2) as a functionof arterial O2 saturation (SaO2) Unfilled circles represent mean data ofresidents from various altitudes and [Hb] are indicated above each circleFilled circles represent data from subjects exposed acutely to altitudes of3050 and 4570 m The (CaO2 minus CvO2) is shown as a percentage ofnormoxic values The content difference (CaO2 minus CvO2) in altituderesidents demonstrates a complex relation to SaO2 but the residents showa better sustained content difference than subjects exposed acutely toaltitude Maximal (CaO2 minus CvO2) is obtained at an [Hb] of 175 g100 mLand a SaO2 of 87 Data from Reeves and Leon-Velarde 200433
542 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
natives and subjects with CMS are around one third ofthe values for sea-level (SL) natives24 The HA nativesand subjects with CMS do not differ significantly fromeach other in their immediate response to hypoxia Inaddition when the peripheral chemoreflex contribution atPETO2 = 525 Torr is calculated from the value of AHVRmultiplied by the reduction in saturation associated withreducing PETO2 from 200 Torr to 525 Torr (AHVR times[SaO2 200] minus SaO2 525) the contribution for the SLgroup is clearly much larger than for the HA and CMSgroups and there is no difference between the HA andCMS group Overall these studies provide evidence tosupport the notion that the lower levels of ventilation inCMS subjects that is the loss of the drive to breathemay arise from mechanisms other than reductions in theperipheral chemoreflex sensitivity to hypoxia or that itscontribution is quite marginal24
Implication of central chemoreceptors as the cause ofhypoxemia in CMS
The cells of the central chemoreceptors respond mainlyto CO2 and H+ At sea level total sensitivity to CO2 innormoxia is of approximately 17 LminTorr In hyper-oxia its value ranges from 25 to 275 LminTorr and inhypoxia at a PETO2 = 50 Torr from 41 to 44 LminTorr212526 The effect of hypoxia in total sensitivity toCO2 is greater in HA natives than in natives from sea leveland than in patients with CMS The peripheral sensitivityof the chemoreceptors to CO2 (Gp) of HA natives isgreater than the Gp of SL inhabitants
The time constants for response to CO2 can beperipheral (tp) or central (tc)2728 Tp is similar betweenSL and HA natives however Tc is slower in HA nativesand even slower in subjects with CMS26 The slowness ofthe time constant in the central chemoreflex is related tothe buffer capacities of the plasma in which centralchemoreceptors are immersed The time constant dependson the cerebral flow per volume unit of cerebral tissue andon the relation between the CO2-buffering capacity of theblood and the brain29 Although cerebral blood flow hasbeen shown to be decreased in HA natives1430 thedelivery of O2 would be relatively protected due to theincreased hematocrit14 However it is not absolutelyobvious that the removal of CO2 also would be assuredAlso the increased hematocrit elevates H+ buffering butplasma flow is reduced therefore the amount ofbicarbonate in blood is reduced A quantitative analysisof these factors reveals a relative reduction of CO2
exchange in the brain in response to changes of PCO2 in thearterial blood26
Overall the interpretation of the data in peripheral andcentral chemoreflex sensitivity to CO2 is that CMSsubjects seem to have reset their central CO2 chemor-eceptors to operate around the resting PETCO2 more close
to SL standards thus around higher PETCO2 values than athigh altitude Indeed Monge-M and Monge-C3 haveshown that PETCO2 HCO3
minus and pH in CMS patients arecloser to SL values31
Excessive erythrocytosis and the heart in CMS effectof hematocrit on cardiac function
Increased [Hb] has long been considered beneficial athigh altitude because the increased oxygen-carryingcapacity of blood would compensate for decreasedarterial oxygen saturation The increase in [Hb] shouldact to maintain oxygen transport to tissues therebyreducing the need to increase cardiac output inhypoxemic subjects This concept however has beenchallenged because with a low oxygen saturation (lowPO2) increasing [Hb] would be of help up to a certainpoint and thus only a moderate increase in [Hb] wouldbenefit O2 transport When excessive however [Hb]becomes detrimental The perfect example is CMSwhere despite having a significantly higher blood O2
content32 individuals are severely hypoxemic and ill Ithas been suggested that above certain [Hb] valueerythrocytosis is no longer beneficial because of theelevated blood viscosity and increased blood volume thatleads to congestive symptoms3233 Increased bloodviscosity and blood volume which results from increas-ing [Hb] to excessive levels affects the distribution ofpulmonary blood flow and pulmonary ventilation-perfu-sion relationships resulting in impaired pulmonary gasexchange This contributes to arterial hypoxemia and
543F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
further stimulates erythropoiesis3435 Interestinglysome studies have shown that when these subjectsundergo bloodletting or hemodilution blood oxygen-ation improves and the symptoms are reduceddramatically123436 Reeves and Leon-Velarde33 havesuggested based on an analysis of arterial-venous O2
content difference at different [Hb] and SaO2 values thatup to a certain value (SaO2 of 87 and a [Hb] of 175 g100 mL) increasing [Hb] has a cardiac output-sparingeffect because of a greater oxygen extraction (Fig 1)When hypoxemia however becomes severe an elevated[Hb] no longer supports an efficient O2 transport andcardiac output has to increase yet the literature showsvariability in cardiac output values in CMS937-39
In 1959 Guyton and Richardson40 were the first tostudy experimentally the effect of hematocrit on cardiacfunction Their work showed that when hematocrit wasincreased isovolemically by 47 in dogs cardiac outputwas reduced dramatically by 51 and total peripheralresistance increased by 50 The effect on cardiac outputwas explained in the effect of increased blood viscosityon venous resistance and venous return as confirmed in alater study41
In CMS chronic hypoxemia leads to excessiveerythrocytosis accompanied by a very high bloodvolume8373842 Thus the emerging figure is somewhatdifferent to what was observed in the isovolemicexperiments in dogs Cardiac output peripheral resis-tance and systolic blood pressure in CMS patients aresimilar to those of healthy individuals at the samealtitude1037 Some recent studies however have shown
Table 1Subject characteristics in high altitude natives (HA) and chronic mountain sick
At High Altitude
HA CMS
Age (years) 393 plusmn 20 43Hematocrit () 498 plusmn 12 63O2 Saturation () 860 plusmn 10 82Orthostatic Tolerance (min) 462 plusmn 12 47SAP (mmHg) Supine 1137 plusmn 30 117Tilt 1157 plusmn 35 119DAP (mmHg) Supine 731 plusmn 23 76Tilt 764 plusmn 26 74HR (bmin) Supine 589 plusmn 20 65Tilt 706 plusmn 28 76Plasma volume (mlkg) 393 plusmn 36 34Red cell volume (mlkg) 379 plusmn 31 62Blood volume (mlkg) 772 plusmn 64 97
Subject characteristics in high altitude natives (HA) and chronic mountain sickboth high altitude groups than at SL (288 plusmn 40 P b 0001) Systolic (SAP)min) are shown in supine and tilt positions Tilt indicates values at the end obetween locations (P b 005 P b 0001 P b 00001) dagger represents sidifferences between supine and tilt There were no significant differences inwere smaller in HA and SL (275 plusmn 18 P b 0001) than in CMS Blood voCMS Values are means plusmn SE Data from Claydon et al 2004 20054254
that systemic pressure in CMS individuals is slightlyelevated when compared to healthy highlanders43
Although elevated blood viscosity would tend todecrease venous return the increased blood volumewould counteract this effect and therefore cardiac outputwould be maintained The rise in peripheral resistance dueto increased blood viscosity is most probably counteractedby the increased aortic elasticity and vasodilation in HAresidents44-46 Contrary to what is found for systolicpressure some studies have found an increased diastolicblood pressure in persons having severe CMS910 thatmight reflect an increased venous return due to increasedblood volume
Studies on the physiology of a transgenic mice line(ldquotg6rdquo mice) that overexpresses erythropoietin (Epo) haveprovided insightful information on the hypoxia-indepen-dent effects of excessive erythrocytosis on the cardio-vascular system Under normoxic conditions thisinteresting animal model exhibits a 12-fold elevation inplasma Epo concentration hematocrit values in the rangeof 85 to 90 and 75 larger blood volume comparedto its wild-type counterparts47 Despite excessive ery-throcytosis increased viscosity and elevated bloodvolume tg6 mice have normal cardiac output andblood pressure values The excessive hematocrit in tg6mice would result in elevated peripheral resistancehowever the increased sheer stress on vascular endothe-lium induces the expression of endothelial nitric oxidesynthase and an enhanced production of NO which inturn causes vasodilation and counteracts the effect ofhematocrit on peripheral resistance48 On the venous side
ness subjects (CMS)
At Sea Level
HA CMS
1 plusmn 17
8 plusmn 17
0 plusmn 12 960 plusmn 07 940 plusmn 07dagger
2 plusmn 12
2 plusmn 26 1107 plusmn 46 1151 plusmn 365 plusmn 24 1065 plusmn 28Dagger 1123 plusmn 33Dagger
4 plusmn 23 678 plusmn 42 715 plusmn 25
3 plusmn 27 758 plusmn 24 788 plusmn 30dagger
0 plusmn 20dagger 493 plusmn 22 543 plusmn 14
1 plusmn 27 554 plusmn 22 642 plusmn 28dagger
6 plusmn 18
8 plusmn 53
4 plusmn 63
ness subjects (CMS) Orthostatic tolerance was significantly greater inand diastolic (DAP) arterial blood pressures and heart rate (HR beatsf the 20 min phase of head up tilt represents a significant differencegnificant difference between HA and CMS and Dagger indicates significantplasma volumes between groups and sea level (SL) Red cell volumeslumes were smaller in HA and SL (673 plusmn 47 P b 001) compared to
544 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
due to increased blood volume tg6 mice showsignificantly elevated central venous pressure47 thatcould result in elevated diastolic pressure It is possiblethen that some of the mechanisms operating in tg6 miceare also present in CMS individuals An enhancedexpression of endothelial nitric oxide synthase in CMScould explain for example the normal peripheralresistance found in CMS patients
Systemic blood pressure control and blood flow in CMS
Although systolic blood pressure in CMS patients isoften similar to that of healthy highlanders some smalldifferences arise in the control mechanisms It has beenshown that Andean HA dwellers have a great tolerance toorthostatic stress that might be attributed to the increasedhematocrit and blood volume The CMS individuals showan exceptional tolerance to orthostatic stress but nosignificantly different from HA controls yet CMSindividuals tend to respond with smaller increases inheart rate than HA healthy subjects54 This has led tosuggest that this may reflect a smaller sympathetic responseto orthostatic stress in these individuals (Table 1) Smallresponses of vascular resistance however have beenassociated to poor orthostatic tolerance49-51 Therefore theextremely good orthostatic tolerance in CMS patientssuggests that some other mechanism is operating in theseindividuals to maintain blood pressure It is possible thatthe large blood volume occurring in these individualscompensates for the smaller sympathetic response5253
Claydon and coworkers54 have shown that at HA theperipheral vascular resistance response to orthostatic stresshad a tendency to be smaller in CMS compared to healthysubjects but after 24 hours at sea level the CMS group hada significantly smaller response This less effective reflexvasoconstriction could explain why despite a larger bloodvolume in CMS subjects their orthostatic tolerance issimilar to that of HA controls
Chronic mountain sickness subjects also show differ-ences in the autoregulation of cerebral blood flow It hasbeen shown that cerebral blood flow is slower in CMSpatients compared to healthy HA subjects55 and it hasbeen suggested that this is a consequence of the increasedblood viscosity Cerebral blood flow autoregulation issimilar in CMS and healthy highlanders at high altitudeand their values are similar to those reported in SLresidents1355 After 24 hours at sea level however CMSindividuals had a larger fall on cerebral blood flow withsmaller change in resistance when exposed to orthostaticstress55 Studies on the relationship between peripheralresistance and carotid baroreceptor function have shownthat at altitude the sensitivity of forearm vascularresistance as a function of carotid sinus pressure is similarin CMS and healthy subjects but the ldquoset-pointrdquo of the
relationship is significantly higher in the CMS group56
This difference however disappears at sea level Apossible explanation for a higher ldquoset-pointrdquo in CMSindividuals at high altitude and its normalization at sealevel could be associated to the effects of hypoxemia onsympathetic vasomotor activity It is well-known thathypoxemia increases sympathetic discharge to musclevascular beds Chronic mountain sickness subjects arenormally more hypoxemic and therefore it is likely that agreater sympathetic activation may have contributed to thealtered baroreflex function This possibility finds supportin the observation that noradrenaline and adrenaline levelsare higher in CMS patients than in healthy HA dwellers57
and that plasma catecholamines are significantly reducedin HA natives within 4 hours of descent to sea level58
Cardiac features of CMS
Thirty years ago Pentildealoza and Arias-Stella59 studiedextensively the cardiac characteristics and pulmonarycirculation of Andean dwellers and patients with severeCMS Their findings point to the presence of pulmonaryhypertension and right ventricular hypertrophy in CMSsubjects9106061 They also demonstrated a direct rela-tionship between Ppa and right ventricle size In additiona prominent main pulmonary artery was found in allpatients Clinical characteristics of pulmonary hyperten-sion were an increased pulmonary second sound oftenassociated with a soft midsystolic ejection murmur anincreased diastolic blood pressure thought to be related toexcessive polycythemia9 and an increase in heart size onchest x-ray compared to healthy highlanders a featureexplained by the increased size of the right heart chambers
In severe cases of CMS the ECG shows peaked Pwaves with increased voltage in leads II III and aVF aswell as in the right precordial leads A right QRS axisdeviation is often observed An rS pattern in the rightprecordial leads and complexes of RS or rS type in the leftprecordial leads are common findings Negative T wavesover the right precordial leads are also common Thesefindings are indicative of right ventricular hypertrophy(RVH) and overload of the right heart chambers asconsequence of pulmonary hypertension Indeed as wellas with heart size a direct relationship between Ppa andright QRS axis deviation has been demonstrated59 Whenpatients with CMS are moved to SL symptoms and signsimprove promptly and the electrocardiographic andradiographic evidence of elevated Ppa and RVH decreasesover time62
Recent echocardiographic studies of pulmonary arterypressure at high altitude support previous findings usinginvasive techniques63-65 At present Doppler echocardi-ography is preferred to evaluate accurately cardiovascular
Fig 2 Cardiac output and maximal tricuspid regurgitation pressure in SL (SL control group at sea level [n = 15]) and HA (HA control group [n = 15]) andCMS groups (n = 55) at high altitude Data from Richalet et al 200968
545F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
function and cardiac morphology A recent study showedthat left atrial area was larger in SL than in HA nativesand CMS patients Right atria and ventricles were largerin CMS compared to SL and HA as shown by largerend-systolic right atria and end-diastolic right ventricularareas and a higher end-diastolic rightleft ventriculardiameter ratio This study also showed that cardiac outputis lower in CMS subjects than in SL dwellers but nodifference has been found when compared with HA
Fig 3 Pulmonary acceleration time and PVR index in SL (SL control group [n =([peak tricuspid regurgitation velocityright ventricular outflow tract time minus vel
natives (Fig 2) Left and right ventricular systolicfunctions and mitral and tricuspid inflows EA are notdifferent between SL HA and CMS Right ventricularTei index a global myocardial performance indicator(calculated as the ratio of [systolic time minus ejection time]ejection time)6667 however is increased in HA nativesand CMS patients when compared to SL controls Thesecardiac characteristics have been described in approxi-mately 50 CMS subjects the largest sample studied at
15]) HA (HA control group [n = 15]) and CMS groups (n = 55) PVR =ocity integral] times 10) + 01668
546 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
4300 m patients showed a mean [Hb] of 231 plusmn 16 gdLarterial blood oxygen saturation (SaO2) of 81 plusmn 4 andPpa of 34 plusmn 10 mm Hg68
Pulmonary hypertension in CMS
The cause of HAPH is the increase in pulmonaryvascular resistance (PVR) the underlying mechanisminvolves sustained and exaggerated pulmonary vasocon-striction and remodeling of the pulmonary vascular wall inresponse to chronic hypoxia due to proliferation anddecreased apoptosis of pulmonary artery smooth musclecells The effects of chronic hypoxia on pulmonary arterypressure are reflected in the negative correlation that existsbetween Ppa and SaO2 at high altitude596970 Arterialhypoxemia in addition to hypoxic vasoconstriction leadsto several structural changes in the pulmonary vesselsincluding an increase in the number of intimal smoothmuscle cells medial thickening in the small musculararteries and fibrinoid necrosis of the vessel walls71 Thesestructural changes in the pulmonary vessels rather thanhypoxic vasoconstriction alone are believed to beresponsible for the sustained rise in Ppa in chronichypoxia Pioneering hemodynamic invasive studies byPentildealoza and Sime910 in 10 subjects with severe CMS at4300 m showed a mean [Hb] value of 247 plusmn 24 gdL amean SaO2 of 696 plusmn 49 and a Ppa of 47 plusmn 177 mmHg values that have made the authors conclude that thesepatients have a type of hypoxic cor pulmonale in contrastto the hypertensive cor pulmonale observed in primarypulmonary hypertension However the structural changes
Fig 4 Pulmonary vascular resistance index and pulmonary acceleration time intreatment with acetazolamide (Acz) The study was organized in 2 phases (1) a ran open-label phase where all patients received acetazolamide (Acz + Acz) Theet al 200939
in the pulmonary vessels which are responsible for thesustained rise in Ppa in chronic hypoxia can have differentintensities and different onset times depending on thelength of hypoxic exposure comprising a range fromshort-term to long-term7072
Maignan and coworkers68 have described cardiachemodynamics in approximately 50 CMS cases withnoninvasive methods and found varying intensities ofPpa Although they might have been studying patients inan early disease stage they observed mean pulmonaryacceleration time and accelerationejection time ratiossignificantly lower in CMS subjects than in SL and HAnatives (Fig 3) Pulmonary vascular index was foundlower in SL than in other groups and there was nosignificant difference between HA and CMS however thenumber of patients with PVR greater than 2 Wood unitswas higher in CMS (1242) than in SL (013) and tended tobe significant when compared to HA (115) (CMS vs SLP = 003 CMS vs HA P = 008 and SL vs HA P = 034)
Chronic hypoxia with appropriate acclimatization asseen in healthy HA residents induces an increase inPVR without change in pulmonary arterial systolicpressure right heart cavity dimensions or right systolicventricular function The increase in right ventricularTei index however could reflect early right ventricularimpairment68 When hypoxemia becomes severe asobserved in some patients with excessive Ppa a furtherimpairment can be found with a significant increase inpulmonary arterial systolic pressure and right cardiaccavity enlargement However contrary to the assumption59
of overt chronic cor pulmonale based on severe HAPHpatients with established HAPH did not show any
placebo and CMS patients groups before and after 3 and 6 months ofandomized double-blind placebo-controlled phase (placebo + Acz) and (2)2 phases were separated by a 4-week washout period Data from Richalet
547F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
obvious cardiac systolic dysfunction as shown byMaignan and coworkers68 This confirms the individualvariability of the severity of HAPH which is also highlydependent on risk factors and genetic susceptibilitydespite that for the moment no specific gene has beenclearly associated with the development of CMS Largeepidemiologic studies should be conducted to determinethe precise natural history prevalence and features ofheart failure in CMS
Recently an interaction between iron levels andhypoxia in the regulation of the pulmonary circulationhas been described73 The study showed that ironinfusion before an 8-hour exposure to sustained hypoxiaabolished or reduced greatly the elevation in baselinepulmonary artery systolic pressure and enhanced sensi-tivity of the pulmonary vasculature to acute hypoxia Thestudy also showed that iron chelation through deferox-amine infusion before the 8-hour hypoxia protocolelevates pulmonary artery systolic pressure significantlyThese findings led to conclude that iron availabilitymodifies pulmonary arterial pressure and pulmonaryvascular responses to hypoxia possibly through theinvolvement of the hypoxia-inducible factor hydroxyl-ation system
In a later study Smith and coworkers74 showed theeffect that iron levels could have on HA diseases thatinvolve pulmonary hypertension such as CMS This studyshowed that reduction of iron availability in CMS patientsthrough isovolemic bloodletting is associated with asubstantial increase in Ppa whereas iron supplementationis related to an attenuation of HAPH In view of the resultsthe authors suggest that this effect is consistent with thoseof acute iron chelation and thus implies that irondeficiency could exacerbate Ppa in chronic pulmonaryand cardiac disease and also that HAPH can be attenuatedby iron supplementation
It should be noted however that no long-termcontrolled studies have been carried out to evaluate allthe possible effectors related to the development ofHAPH Thus extensive research is required to determinewhich of the multiple elements that regulate Ppa at highaltitude might have a predominant role in determining thedifferent time courses and severity of HAPH
Treatment
Recently increasing attention is being drawn todifferent phenomena that may be involved in the causalchain of CMS and that were previously overlooked Theseinclude CMS risk and environmental factors such as earlyprenatal or postnatal exposure to different agents andorthe different genetic susceptibilities in different popula-tions and individuals However until having a complete
understanding of which mechanisms are better targetsfor intervention at present treatment is directed to thosecomponents of CMS pathophysiologic sequence thatare susceptible of modification through pharmacologicintervention that is on the erythropoietic response toreduce the increased red cell mass andor on the ventilatoryresponse These agents include methylxanthines adrener-gic blockers dopaminergic antagonists medroxyproges-terone peripheral ventilator stimulants such as almitrineand enalapril all of which have been tested experiment-ally75 Although phlebotomy has been shown to reducethe signs and symptoms of CMS its invasiveness andtransient effects often render it impractical
Descent to low altitudes is the ideal treatment and leadsto prompt improvement of signs and symptoms of CMSbut often patients cannot or do not want to descend tolower altitudes for economic personal andor familyreasons Recently acetazolamide has been used as animportant alternative for the treatment of CMS and itseffects have been studied in randomized placebo-controlled trials in the Peruvian Andes394376 The effectsof this carbonic anhydrase inhibitor in CMS include animprovement of ventilation through metabolic acidosisand of SaO2
76 thus causing a decrease in Epo concen-tration and excessive erythrocytosis In addition it leads toa decrease in PVR and an increase in pulmonaryacceleration time Furthermore the number of CMSpatients with pulmonary hypertension (defined by PVRN 2 Wood units) was 8 before treatment and nil aftertreatment (P = 0005) In fact the observed effect ofacetazolamide on PVR (minus17) might be indirectly due tothe decrease in blood viscosity (minus16) due to thereduction in hematocrit (Fig 4) Therefore at presentthese very encouraging results suggest that acetazolamidecould be a good alternative in the treatment of CMS3943
Statement of Conflict of Interest
All authors declare that there are no conflicts of interest
References
1 Pentildealoza D Sime F Banchero N et al Pulmonary hypertension inhealthy men born and living at high altitudes Am J Cardiol 196311150-157
2 Hurtado A Animals in high altitudes resident man In Dill DAdolph E Wilber C editors Handbook of physiology adaptation tothe environment Washington DC American Physiological Society1964 p 843-860
3 Monge-M C Monge-C C High altitude diseases mechanism andmanagement Springfield (Ill) Charles C Thomas 1966
4 Antezana G Barragaacuten L Coudert J et al The pulmonarycirculation of high altitude natives In Brendel W Zink R editorsHigh altitude physiology and medicine New York Springer-Verlag 1982 p 142-149
548 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
5 Monge C Chronic mountain sickness Physiol Rev 1943231666 Monge-M C Encinas E Heraud C et al La Enfermedad de los
Andes (Siacutendromes Eritreacutemicos) Imprenta Americana Lima1928
7 Monge-M C Sobre un caso de Enfermedad de Vaacutequez Paperpresented at Communicacioacuten presentada a la Academia Nacional deMedicina Lima Peru Academia Nacional de Medicina 1925
8 Hurtado A Chronic mountain sickness JAMA 19421201278-1282
9 Penaloza D Sime F Chronic cor pulmonale due to loss of altitudeacclimatization (chronic mountain sickness) Am J Med 197150728-743
10 Pentildealoza D Sime F Ruiz L Cor pulmonale in chronic mountainsickness present concept of Monges disease In Porter R Knight Jeditors High altitude physiology cardiac and respiratory aspectsEdinburgh Churchill Livingstone 1971 p 41-60
11 Beall CM Decker MJ Brittenham GM et al An Ethiopian pattern ofhuman adaptation to high-altitude hypoxia Proc Natl Acad Sci U S A20029917215-17218
12 Winslow RM Monge-C C Hypoxia polycythemia and chronicmountain sickness Baltimore (Md) Johns Hopkins University Press1987
13 Arregui A Cabrera J Leon-Velarde F et al High prevalence ofmigraine in a high-altitude population Neurology 1991411668-1669
14 Sorensen SC Lassen NA Severinghaus JW et al Cerebral glucosemetabolism and cerebral blood flow in high-altitude residents J ApplPhysiol 197437305-310
15 Massik J Tang YL Hudak ML et al Effect of hematocrit oncerebral blood flow with induced polycythemia J Appl Physiol1987621090-1096
16 Monge-M C La enfermedad de los Andes An Fac Med 19281-30917 Leon-Velarde F Maggiorini M Reeves JT et al Consensus
statement on chronic and subacute high altitude diseases High AltMed Biol 20056147-157
18 Leon-Velarde F Mejia O Gene expression in chronic high altitudediseases High Alt Med Biol 20089130-139
19 Monge-C C Leoacuten-Velarde F Arregui A Chronic mountain sicknessIn Lenfant C editor High altitude an exploration of humanadaptation New York Marcel Dekker Inc 2001 p 815-838
20 Kryger M McCullough R Doekel R et al Excessive polycythemiaof high altitude role of ventilatory drive and lung disease Am RevRespir Dis 1978118659-666
21 Severinghaus JW Bainton CR Carcelen A Respiratory insensitivityto hypoxia in chronically hypoxic man Respir Physiol 19661308-334
22 Vargas E Spielvogel H Chronic mountain sickness optimalhemoglobin and heart disease High Alt Med Biol 20067138-149
23 Liang PJ Bascom DA Robbins PA Extended models of theventilatory response to sustained isocapnic hypoxia in humansJ Appl Physiol 199782667-677
24 Leon-Velarde F Gamboa A Rivera-Ch M et al Selectedcontribution peripheral chemoreflex function in high-altitudenatives and patients with chronic mountain sickness J Appl Physiol2003941269-1278 discussion 1253-1264
25 Milledge JS Lahiri S Respiratory control in lowlanders and Sherpahighlanders at altitude Respir Physiol 19672310-322
26 Fatemian M Gamboa A Leon-Velarde F et al Plasticity inrespiratory motor control selected contribution ventilatory responseto CO2 in high-altitude natives and patients with chronic mountainsickness J Appl Physiol 2003941279-1287
27 Cunningham PA Wolf CB Integration of respiratory responses tochanges in alveolar partial pressures of CO2 and O2 and in arterialpH In Cherniack JG editor Handbook of physiologymdashtherespiratory system Bethesda (Md) American Physiological Society1986 p 475-528
28 Fatemian M Robbins PA Selected contribution chemoreflexresponses to CO2 before and after an 8-h exposure to hypoxia inhumans J Appl Physiol 2001901607-1614 discussion 1606
29 Robbins PA The ventilatory response of the human respiratorysystem to sine waves of alveolar carbon dioxide and hypoxiaJ Physiology 1984350461-474
30 Milledge JS Sorensen SC Cerebral arteriovenous oxygen differ-ence in man native to high altitude J Appl Physiol 197232687-689
31 Leon-Velarde F Richalet JP Respiratory control in residents at highaltitude physiology and pathophysiology High Alt Med Biol 20067125-137
32 Villafuerte FC Cardenas R Monge CC Optimal hemoglobinconcentration and high altitude a theoretical approach for Andeanmen at rest J Appl Physiol May 2004961581-1588
33 Reeves JT Leon-Velarde F Chronic mountain sickness recentstudies of the relationship between hemoglobin concentration andoxygen transport High Alt Med Biol 20045147-155
34 Winslow RM Monge CC Brown EG et al Effects of hemodilutionon O2 transport in high-altitude polycythemia J Appl Physiol 1985591495-1502
35 Cruz J Diaz C Marticorena E et al Phlebotomy improvespulmonary gas exchange in chronic mountain polycythemiaRespiration 197938305-313
36 Manier G Guenard H Castaing Y et al Pulmonary gas exchange inAndean natives with excessive polycythemiamdasheffect of hemodilu-tion J Appl Physiol 1988652107-2117
37 Ergueta J Spielvogel H Cudkowicz L Cardio-respiratory studies inchronic mountain sickness (Monges syndrome) Respiration 197128485-517
38 Rotta A Canepa A Hurtado A et al Pulmonary circulation at sealevel and at high altitude J Appl Physiol 195611143-149
39 Richalet JP Rivera-Ch M Maignan M et al Acetazolamide forMonges disease efficiency and tolerance of 6-month treatment AmJ Respir Crit Care Med 20081771370-1376
40 Richardson TQ Guyton AC Effects of polycythemia and anemia oncardiac output and other circulatory factors Am J Physiol 19591971167-1170
41 Guyton AC Richardson TQ Effect of hematocrit on venous returnCirc Res 19619157-164
42 Claydon VE Norcliffe LJ Moore JP et al Orthostatic tolerance andblood volumes in Andean high altitude dwellers Exp Physiol 200489565-571
43 Richalet JP Rivera M Bouchet P et al Acetazolamide a treatmentfor chronic mountain sickness Am J Respir Crit Care Med 20051721427-1433
44 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk III The thickness of the media of the pulmonary trunk andascending aorta in high altitude natives Circulation 1963271101-1104
45 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk II The evolution of the elastic configuration of the pulmonarytrunk in people native to high altitudes Circulation 1963271094-1100
46 Saldana M Arias-Stella J Studies on the structure of thepulmonary trunk I Normal changes in the elastic configurationof the human pulmonary trunk at different ages Circulation 1963271086-1093
47 Wagner KF Katschinski DM Hasegawa J et al Chronic inbornerythrocytosis leads to cardiac dysfunction and premature death inmice overexpressing erythropoietin Blood 200197536-542
48 Ruschitzka FT Wenger RH Stallmach T et al Nitric oxide preventscardiovascular disease and determines survival in polyglobulic miceoverexpressing erythropoietin Proc Natl Acad Sci U S A 20009711609-11613
549F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
49 Brown CM Hainsworth R Assessment of capillary fluidshifts during orthostatic stress in normal subjects andsubjects with orthostatic intolerance Clin Auton Res 1999969-73
50 Bush VE Wight VL Brown CM et al Vascular responses toorthostatic stress in patients with postural tachycardia syndrome(POTS) in patients with low orthostatic tolerance and inasymptomatic controls Clin Auton Res 200010279-284
51 Cooper VL Hainsworth R Effects of head-up tilting on baroreceptorcontrol in subjects with different tolerances to orthostatic stress ClinSci (Lond) 2002103221-226
52 Appenzeller O Thomas PK Ponsford S et al Acral paresthesias inthe Andes and neurology at sea level Neurology 2002591532-1535
53 Kwaan HC Wang J Hyperviscosity in polycythemia vera andother red cell abnormalities Semin Thromb Hemost 200329451-458
54 Claydon VE Norcliffe LJ Moore JP et al Cardiovascularresponses to orthostatic stress in healthy altitude dwellers andaltitude residents with chronic mountain sickness Exp Physiol200590103-110
55 Norcliffe LJ Rivera-Ch M Claydon VE et al Cerebrovascularresponses to hypoxia and hypocapnia in high-altitude dwellersJ Physiol 2005566(Pt 1)287-294
56 Moore JP Claydon VE Norcliffe LJ et al Carotid baroreflexregulation of vascular resistance in high-altitude Andean natives withand without chronic mountain sickness Exp Physiol 200691907-913
57 Antezana AM Richalet JP Noriega I et al Hormonal changes innormal and polycythemic high-altitude natives J Appl Physiol 199579795-800
58 Gamboa A Gamboa JL Holmes C et al Plasma catecholamines andblood volume in native Andeans during hypoxia and normoxia ClinAuton Res 20061640-45
59 Penaloza D Arias-Stella J The heart and pulmonary circulation athigh altitudes healthy highlanders and chronic mountain sicknessCirculation 20071151132-1146
60 Pei SX Chen XJ Si Ren BZ et al Chronic mountain sickness inTibet Q J Med 198971555-574
61 Wu TY Li W Li Y et al Epidemiology of chronic mountainsickness ten years study in Qinghai-Tibet In Ohno H KobayashiT Masuyama S Nakashima M editors Progress in MountainMedicine and High Altitude Physiology Matsumoto Press Com-mittee of the 3rd World Congress on Mountain Medicine and HighAltitude Physiology 1998 p 120-125
62 Sime F Penaloza D Ruiz L Bradycardia increased cardiac outputand reversal of pulmonary hypertension in altitude natives living atsea level Br Heart J 197133647-657
63 Allemann Y Sartori C Lepori M et al Echocardiographic andinvasive measurements of pulmonary artery pressure correlateclosely at high altitude Am J Physiol 2000279H2013-H2016
64 Kojonazarov BK Imanov BZ Amatov TA et al Noninvasive andinvasive evaluation of pulmonary arterial pressure in highlandersEur Respir J 200729352-356
65 Naeije R Torbicki A More on the noninvasive diagnosis ofpulmonary hypertension Doppler echocardiography revisited EurRespir J 199581445-1449
66 Tei C Dujardin KS Hodge DO et al Doppler echocardiographicindex for assessment of global right ventricular function J Am SocEchocardiogr 19969838-847
67 Harjai KJ Scott L Vivekananthan K et al The Tei index a newprognostic index for patients with symptomatic heart failure J AmSoc Echocardiogr 200215864-868
68 Maignan M Rivera-Ch M Privat C et al Pulmonary pressure andcardiac function in chronic mountain sickness patients Chest 2009135499-504
69 Cruz-Jibaja J Banchero N Sime F et al Correlation betweenpulmonary artery pressure and level of altitude Dis Chest 196446446-451
70 Wu T Chronic mountain sickness in Qinghai-Tibet China In Ge RHackett P editors Life on the Qinghai-Tibetan Plateau BeijingPekiacuten University Medical Press 2007 p 118-133
71 Arias-Stella J Saldana M The terminal portion of the pulmonaryarterial tree in people native to high altitudes Circulation 196328915-925
72 Maggiorini M Leon-Velarde F High-altitude pulmonary hyperten-sion a pathophysiological entity to different diseases Eur Respir J2003221019-1025
73 Smith T Balanos G Croft Q et al The increase in pulmonary arterialpressure caused by hypoxia depends on iron status J Physiol 20085865999-6005
74 Smith T Talbot N Privat C et al Effects of iron supplementationand depletion on hypoxic pulmonary hypertension two randomizedcontrolled trials JAMA 20093021444-1450
75 Rivera-Ch M Leon-Velarde F Huicho L Treatment of chronicmountain sickness critical reappraisal of an old problem RespirPhysiol Neurobiol 2007158251-265
76 Rivera-Ch M Huicho L Bouchet P et al Effect of acetazolamide onventilatory response in subjects with chronic mountain sicknessRespir Physiol Neurobiol 2008162184-189

543F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
further stimulates erythropoiesis3435 Interestinglysome studies have shown that when these subjectsundergo bloodletting or hemodilution blood oxygen-ation improves and the symptoms are reduceddramatically123436 Reeves and Leon-Velarde33 havesuggested based on an analysis of arterial-venous O2
content difference at different [Hb] and SaO2 values thatup to a certain value (SaO2 of 87 and a [Hb] of 175 g100 mL) increasing [Hb] has a cardiac output-sparingeffect because of a greater oxygen extraction (Fig 1)When hypoxemia however becomes severe an elevated[Hb] no longer supports an efficient O2 transport andcardiac output has to increase yet the literature showsvariability in cardiac output values in CMS937-39
In 1959 Guyton and Richardson40 were the first tostudy experimentally the effect of hematocrit on cardiacfunction Their work showed that when hematocrit wasincreased isovolemically by 47 in dogs cardiac outputwas reduced dramatically by 51 and total peripheralresistance increased by 50 The effect on cardiac outputwas explained in the effect of increased blood viscosityon venous resistance and venous return as confirmed in alater study41
In CMS chronic hypoxemia leads to excessiveerythrocytosis accompanied by a very high bloodvolume8373842 Thus the emerging figure is somewhatdifferent to what was observed in the isovolemicexperiments in dogs Cardiac output peripheral resis-tance and systolic blood pressure in CMS patients aresimilar to those of healthy individuals at the samealtitude1037 Some recent studies however have shown
Table 1Subject characteristics in high altitude natives (HA) and chronic mountain sick
At High Altitude
HA CMS
Age (years) 393 plusmn 20 43Hematocrit () 498 plusmn 12 63O2 Saturation () 860 plusmn 10 82Orthostatic Tolerance (min) 462 plusmn 12 47SAP (mmHg) Supine 1137 plusmn 30 117Tilt 1157 plusmn 35 119DAP (mmHg) Supine 731 plusmn 23 76Tilt 764 plusmn 26 74HR (bmin) Supine 589 plusmn 20 65Tilt 706 plusmn 28 76Plasma volume (mlkg) 393 plusmn 36 34Red cell volume (mlkg) 379 plusmn 31 62Blood volume (mlkg) 772 plusmn 64 97
Subject characteristics in high altitude natives (HA) and chronic mountain sickboth high altitude groups than at SL (288 plusmn 40 P b 0001) Systolic (SAP)min) are shown in supine and tilt positions Tilt indicates values at the end obetween locations (P b 005 P b 0001 P b 00001) dagger represents sidifferences between supine and tilt There were no significant differences inwere smaller in HA and SL (275 plusmn 18 P b 0001) than in CMS Blood voCMS Values are means plusmn SE Data from Claydon et al 2004 20054254
that systemic pressure in CMS individuals is slightlyelevated when compared to healthy highlanders43
Although elevated blood viscosity would tend todecrease venous return the increased blood volumewould counteract this effect and therefore cardiac outputwould be maintained The rise in peripheral resistance dueto increased blood viscosity is most probably counteractedby the increased aortic elasticity and vasodilation in HAresidents44-46 Contrary to what is found for systolicpressure some studies have found an increased diastolicblood pressure in persons having severe CMS910 thatmight reflect an increased venous return due to increasedblood volume
Studies on the physiology of a transgenic mice line(ldquotg6rdquo mice) that overexpresses erythropoietin (Epo) haveprovided insightful information on the hypoxia-indepen-dent effects of excessive erythrocytosis on the cardio-vascular system Under normoxic conditions thisinteresting animal model exhibits a 12-fold elevation inplasma Epo concentration hematocrit values in the rangeof 85 to 90 and 75 larger blood volume comparedto its wild-type counterparts47 Despite excessive ery-throcytosis increased viscosity and elevated bloodvolume tg6 mice have normal cardiac output andblood pressure values The excessive hematocrit in tg6mice would result in elevated peripheral resistancehowever the increased sheer stress on vascular endothe-lium induces the expression of endothelial nitric oxidesynthase and an enhanced production of NO which inturn causes vasodilation and counteracts the effect ofhematocrit on peripheral resistance48 On the venous side
ness subjects (CMS)
At Sea Level
HA CMS
1 plusmn 17
8 plusmn 17
0 plusmn 12 960 plusmn 07 940 plusmn 07dagger
2 plusmn 12
2 plusmn 26 1107 plusmn 46 1151 plusmn 365 plusmn 24 1065 plusmn 28Dagger 1123 plusmn 33Dagger
4 plusmn 23 678 plusmn 42 715 plusmn 25
3 plusmn 27 758 plusmn 24 788 plusmn 30dagger
0 plusmn 20dagger 493 plusmn 22 543 plusmn 14
1 plusmn 27 554 plusmn 22 642 plusmn 28dagger
6 plusmn 18
8 plusmn 53
4 plusmn 63
ness subjects (CMS) Orthostatic tolerance was significantly greater inand diastolic (DAP) arterial blood pressures and heart rate (HR beatsf the 20 min phase of head up tilt represents a significant differencegnificant difference between HA and CMS and Dagger indicates significantplasma volumes between groups and sea level (SL) Red cell volumeslumes were smaller in HA and SL (673 plusmn 47 P b 001) compared to
544 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
due to increased blood volume tg6 mice showsignificantly elevated central venous pressure47 thatcould result in elevated diastolic pressure It is possiblethen that some of the mechanisms operating in tg6 miceare also present in CMS individuals An enhancedexpression of endothelial nitric oxide synthase in CMScould explain for example the normal peripheralresistance found in CMS patients
Systemic blood pressure control and blood flow in CMS
Although systolic blood pressure in CMS patients isoften similar to that of healthy highlanders some smalldifferences arise in the control mechanisms It has beenshown that Andean HA dwellers have a great tolerance toorthostatic stress that might be attributed to the increasedhematocrit and blood volume The CMS individuals showan exceptional tolerance to orthostatic stress but nosignificantly different from HA controls yet CMSindividuals tend to respond with smaller increases inheart rate than HA healthy subjects54 This has led tosuggest that this may reflect a smaller sympathetic responseto orthostatic stress in these individuals (Table 1) Smallresponses of vascular resistance however have beenassociated to poor orthostatic tolerance49-51 Therefore theextremely good orthostatic tolerance in CMS patientssuggests that some other mechanism is operating in theseindividuals to maintain blood pressure It is possible thatthe large blood volume occurring in these individualscompensates for the smaller sympathetic response5253
Claydon and coworkers54 have shown that at HA theperipheral vascular resistance response to orthostatic stresshad a tendency to be smaller in CMS compared to healthysubjects but after 24 hours at sea level the CMS group hada significantly smaller response This less effective reflexvasoconstriction could explain why despite a larger bloodvolume in CMS subjects their orthostatic tolerance issimilar to that of HA controls
Chronic mountain sickness subjects also show differ-ences in the autoregulation of cerebral blood flow It hasbeen shown that cerebral blood flow is slower in CMSpatients compared to healthy HA subjects55 and it hasbeen suggested that this is a consequence of the increasedblood viscosity Cerebral blood flow autoregulation issimilar in CMS and healthy highlanders at high altitudeand their values are similar to those reported in SLresidents1355 After 24 hours at sea level however CMSindividuals had a larger fall on cerebral blood flow withsmaller change in resistance when exposed to orthostaticstress55 Studies on the relationship between peripheralresistance and carotid baroreceptor function have shownthat at altitude the sensitivity of forearm vascularresistance as a function of carotid sinus pressure is similarin CMS and healthy subjects but the ldquoset-pointrdquo of the
relationship is significantly higher in the CMS group56
This difference however disappears at sea level Apossible explanation for a higher ldquoset-pointrdquo in CMSindividuals at high altitude and its normalization at sealevel could be associated to the effects of hypoxemia onsympathetic vasomotor activity It is well-known thathypoxemia increases sympathetic discharge to musclevascular beds Chronic mountain sickness subjects arenormally more hypoxemic and therefore it is likely that agreater sympathetic activation may have contributed to thealtered baroreflex function This possibility finds supportin the observation that noradrenaline and adrenaline levelsare higher in CMS patients than in healthy HA dwellers57
and that plasma catecholamines are significantly reducedin HA natives within 4 hours of descent to sea level58
Cardiac features of CMS
Thirty years ago Pentildealoza and Arias-Stella59 studiedextensively the cardiac characteristics and pulmonarycirculation of Andean dwellers and patients with severeCMS Their findings point to the presence of pulmonaryhypertension and right ventricular hypertrophy in CMSsubjects9106061 They also demonstrated a direct rela-tionship between Ppa and right ventricle size In additiona prominent main pulmonary artery was found in allpatients Clinical characteristics of pulmonary hyperten-sion were an increased pulmonary second sound oftenassociated with a soft midsystolic ejection murmur anincreased diastolic blood pressure thought to be related toexcessive polycythemia9 and an increase in heart size onchest x-ray compared to healthy highlanders a featureexplained by the increased size of the right heart chambers
In severe cases of CMS the ECG shows peaked Pwaves with increased voltage in leads II III and aVF aswell as in the right precordial leads A right QRS axisdeviation is often observed An rS pattern in the rightprecordial leads and complexes of RS or rS type in the leftprecordial leads are common findings Negative T wavesover the right precordial leads are also common Thesefindings are indicative of right ventricular hypertrophy(RVH) and overload of the right heart chambers asconsequence of pulmonary hypertension Indeed as wellas with heart size a direct relationship between Ppa andright QRS axis deviation has been demonstrated59 Whenpatients with CMS are moved to SL symptoms and signsimprove promptly and the electrocardiographic andradiographic evidence of elevated Ppa and RVH decreasesover time62
Recent echocardiographic studies of pulmonary arterypressure at high altitude support previous findings usinginvasive techniques63-65 At present Doppler echocardi-ography is preferred to evaluate accurately cardiovascular
Fig 2 Cardiac output and maximal tricuspid regurgitation pressure in SL (SL control group at sea level [n = 15]) and HA (HA control group [n = 15]) andCMS groups (n = 55) at high altitude Data from Richalet et al 200968
545F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
function and cardiac morphology A recent study showedthat left atrial area was larger in SL than in HA nativesand CMS patients Right atria and ventricles were largerin CMS compared to SL and HA as shown by largerend-systolic right atria and end-diastolic right ventricularareas and a higher end-diastolic rightleft ventriculardiameter ratio This study also showed that cardiac outputis lower in CMS subjects than in SL dwellers but nodifference has been found when compared with HA
Fig 3 Pulmonary acceleration time and PVR index in SL (SL control group [n =([peak tricuspid regurgitation velocityright ventricular outflow tract time minus vel
natives (Fig 2) Left and right ventricular systolicfunctions and mitral and tricuspid inflows EA are notdifferent between SL HA and CMS Right ventricularTei index a global myocardial performance indicator(calculated as the ratio of [systolic time minus ejection time]ejection time)6667 however is increased in HA nativesand CMS patients when compared to SL controls Thesecardiac characteristics have been described in approxi-mately 50 CMS subjects the largest sample studied at
15]) HA (HA control group [n = 15]) and CMS groups (n = 55) PVR =ocity integral] times 10) + 01668
546 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
4300 m patients showed a mean [Hb] of 231 plusmn 16 gdLarterial blood oxygen saturation (SaO2) of 81 plusmn 4 andPpa of 34 plusmn 10 mm Hg68
Pulmonary hypertension in CMS
The cause of HAPH is the increase in pulmonaryvascular resistance (PVR) the underlying mechanisminvolves sustained and exaggerated pulmonary vasocon-striction and remodeling of the pulmonary vascular wall inresponse to chronic hypoxia due to proliferation anddecreased apoptosis of pulmonary artery smooth musclecells The effects of chronic hypoxia on pulmonary arterypressure are reflected in the negative correlation that existsbetween Ppa and SaO2 at high altitude596970 Arterialhypoxemia in addition to hypoxic vasoconstriction leadsto several structural changes in the pulmonary vesselsincluding an increase in the number of intimal smoothmuscle cells medial thickening in the small musculararteries and fibrinoid necrosis of the vessel walls71 Thesestructural changes in the pulmonary vessels rather thanhypoxic vasoconstriction alone are believed to beresponsible for the sustained rise in Ppa in chronichypoxia Pioneering hemodynamic invasive studies byPentildealoza and Sime910 in 10 subjects with severe CMS at4300 m showed a mean [Hb] value of 247 plusmn 24 gdL amean SaO2 of 696 plusmn 49 and a Ppa of 47 plusmn 177 mmHg values that have made the authors conclude that thesepatients have a type of hypoxic cor pulmonale in contrastto the hypertensive cor pulmonale observed in primarypulmonary hypertension However the structural changes
Fig 4 Pulmonary vascular resistance index and pulmonary acceleration time intreatment with acetazolamide (Acz) The study was organized in 2 phases (1) a ran open-label phase where all patients received acetazolamide (Acz + Acz) Theet al 200939
in the pulmonary vessels which are responsible for thesustained rise in Ppa in chronic hypoxia can have differentintensities and different onset times depending on thelength of hypoxic exposure comprising a range fromshort-term to long-term7072
Maignan and coworkers68 have described cardiachemodynamics in approximately 50 CMS cases withnoninvasive methods and found varying intensities ofPpa Although they might have been studying patients inan early disease stage they observed mean pulmonaryacceleration time and accelerationejection time ratiossignificantly lower in CMS subjects than in SL and HAnatives (Fig 3) Pulmonary vascular index was foundlower in SL than in other groups and there was nosignificant difference between HA and CMS however thenumber of patients with PVR greater than 2 Wood unitswas higher in CMS (1242) than in SL (013) and tended tobe significant when compared to HA (115) (CMS vs SLP = 003 CMS vs HA P = 008 and SL vs HA P = 034)
Chronic hypoxia with appropriate acclimatization asseen in healthy HA residents induces an increase inPVR without change in pulmonary arterial systolicpressure right heart cavity dimensions or right systolicventricular function The increase in right ventricularTei index however could reflect early right ventricularimpairment68 When hypoxemia becomes severe asobserved in some patients with excessive Ppa a furtherimpairment can be found with a significant increase inpulmonary arterial systolic pressure and right cardiaccavity enlargement However contrary to the assumption59
of overt chronic cor pulmonale based on severe HAPHpatients with established HAPH did not show any
placebo and CMS patients groups before and after 3 and 6 months ofandomized double-blind placebo-controlled phase (placebo + Acz) and (2)2 phases were separated by a 4-week washout period Data from Richalet
547F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
obvious cardiac systolic dysfunction as shown byMaignan and coworkers68 This confirms the individualvariability of the severity of HAPH which is also highlydependent on risk factors and genetic susceptibilitydespite that for the moment no specific gene has beenclearly associated with the development of CMS Largeepidemiologic studies should be conducted to determinethe precise natural history prevalence and features ofheart failure in CMS
Recently an interaction between iron levels andhypoxia in the regulation of the pulmonary circulationhas been described73 The study showed that ironinfusion before an 8-hour exposure to sustained hypoxiaabolished or reduced greatly the elevation in baselinepulmonary artery systolic pressure and enhanced sensi-tivity of the pulmonary vasculature to acute hypoxia Thestudy also showed that iron chelation through deferox-amine infusion before the 8-hour hypoxia protocolelevates pulmonary artery systolic pressure significantlyThese findings led to conclude that iron availabilitymodifies pulmonary arterial pressure and pulmonaryvascular responses to hypoxia possibly through theinvolvement of the hypoxia-inducible factor hydroxyl-ation system
In a later study Smith and coworkers74 showed theeffect that iron levels could have on HA diseases thatinvolve pulmonary hypertension such as CMS This studyshowed that reduction of iron availability in CMS patientsthrough isovolemic bloodletting is associated with asubstantial increase in Ppa whereas iron supplementationis related to an attenuation of HAPH In view of the resultsthe authors suggest that this effect is consistent with thoseof acute iron chelation and thus implies that irondeficiency could exacerbate Ppa in chronic pulmonaryand cardiac disease and also that HAPH can be attenuatedby iron supplementation
It should be noted however that no long-termcontrolled studies have been carried out to evaluate allthe possible effectors related to the development ofHAPH Thus extensive research is required to determinewhich of the multiple elements that regulate Ppa at highaltitude might have a predominant role in determining thedifferent time courses and severity of HAPH
Treatment
Recently increasing attention is being drawn todifferent phenomena that may be involved in the causalchain of CMS and that were previously overlooked Theseinclude CMS risk and environmental factors such as earlyprenatal or postnatal exposure to different agents andorthe different genetic susceptibilities in different popula-tions and individuals However until having a complete
understanding of which mechanisms are better targetsfor intervention at present treatment is directed to thosecomponents of CMS pathophysiologic sequence thatare susceptible of modification through pharmacologicintervention that is on the erythropoietic response toreduce the increased red cell mass andor on the ventilatoryresponse These agents include methylxanthines adrener-gic blockers dopaminergic antagonists medroxyproges-terone peripheral ventilator stimulants such as almitrineand enalapril all of which have been tested experiment-ally75 Although phlebotomy has been shown to reducethe signs and symptoms of CMS its invasiveness andtransient effects often render it impractical
Descent to low altitudes is the ideal treatment and leadsto prompt improvement of signs and symptoms of CMSbut often patients cannot or do not want to descend tolower altitudes for economic personal andor familyreasons Recently acetazolamide has been used as animportant alternative for the treatment of CMS and itseffects have been studied in randomized placebo-controlled trials in the Peruvian Andes394376 The effectsof this carbonic anhydrase inhibitor in CMS include animprovement of ventilation through metabolic acidosisand of SaO2
76 thus causing a decrease in Epo concen-tration and excessive erythrocytosis In addition it leads toa decrease in PVR and an increase in pulmonaryacceleration time Furthermore the number of CMSpatients with pulmonary hypertension (defined by PVRN 2 Wood units) was 8 before treatment and nil aftertreatment (P = 0005) In fact the observed effect ofacetazolamide on PVR (minus17) might be indirectly due tothe decrease in blood viscosity (minus16) due to thereduction in hematocrit (Fig 4) Therefore at presentthese very encouraging results suggest that acetazolamidecould be a good alternative in the treatment of CMS3943
Statement of Conflict of Interest
All authors declare that there are no conflicts of interest
References
1 Pentildealoza D Sime F Banchero N et al Pulmonary hypertension inhealthy men born and living at high altitudes Am J Cardiol 196311150-157
2 Hurtado A Animals in high altitudes resident man In Dill DAdolph E Wilber C editors Handbook of physiology adaptation tothe environment Washington DC American Physiological Society1964 p 843-860
3 Monge-M C Monge-C C High altitude diseases mechanism andmanagement Springfield (Ill) Charles C Thomas 1966
4 Antezana G Barragaacuten L Coudert J et al The pulmonarycirculation of high altitude natives In Brendel W Zink R editorsHigh altitude physiology and medicine New York Springer-Verlag 1982 p 142-149
548 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
5 Monge C Chronic mountain sickness Physiol Rev 1943231666 Monge-M C Encinas E Heraud C et al La Enfermedad de los
Andes (Siacutendromes Eritreacutemicos) Imprenta Americana Lima1928
7 Monge-M C Sobre un caso de Enfermedad de Vaacutequez Paperpresented at Communicacioacuten presentada a la Academia Nacional deMedicina Lima Peru Academia Nacional de Medicina 1925
8 Hurtado A Chronic mountain sickness JAMA 19421201278-1282
9 Penaloza D Sime F Chronic cor pulmonale due to loss of altitudeacclimatization (chronic mountain sickness) Am J Med 197150728-743
10 Pentildealoza D Sime F Ruiz L Cor pulmonale in chronic mountainsickness present concept of Monges disease In Porter R Knight Jeditors High altitude physiology cardiac and respiratory aspectsEdinburgh Churchill Livingstone 1971 p 41-60
11 Beall CM Decker MJ Brittenham GM et al An Ethiopian pattern ofhuman adaptation to high-altitude hypoxia Proc Natl Acad Sci U S A20029917215-17218
12 Winslow RM Monge-C C Hypoxia polycythemia and chronicmountain sickness Baltimore (Md) Johns Hopkins University Press1987
13 Arregui A Cabrera J Leon-Velarde F et al High prevalence ofmigraine in a high-altitude population Neurology 1991411668-1669
14 Sorensen SC Lassen NA Severinghaus JW et al Cerebral glucosemetabolism and cerebral blood flow in high-altitude residents J ApplPhysiol 197437305-310
15 Massik J Tang YL Hudak ML et al Effect of hematocrit oncerebral blood flow with induced polycythemia J Appl Physiol1987621090-1096
16 Monge-M C La enfermedad de los Andes An Fac Med 19281-30917 Leon-Velarde F Maggiorini M Reeves JT et al Consensus
statement on chronic and subacute high altitude diseases High AltMed Biol 20056147-157
18 Leon-Velarde F Mejia O Gene expression in chronic high altitudediseases High Alt Med Biol 20089130-139
19 Monge-C C Leoacuten-Velarde F Arregui A Chronic mountain sicknessIn Lenfant C editor High altitude an exploration of humanadaptation New York Marcel Dekker Inc 2001 p 815-838
20 Kryger M McCullough R Doekel R et al Excessive polycythemiaof high altitude role of ventilatory drive and lung disease Am RevRespir Dis 1978118659-666
21 Severinghaus JW Bainton CR Carcelen A Respiratory insensitivityto hypoxia in chronically hypoxic man Respir Physiol 19661308-334
22 Vargas E Spielvogel H Chronic mountain sickness optimalhemoglobin and heart disease High Alt Med Biol 20067138-149
23 Liang PJ Bascom DA Robbins PA Extended models of theventilatory response to sustained isocapnic hypoxia in humansJ Appl Physiol 199782667-677
24 Leon-Velarde F Gamboa A Rivera-Ch M et al Selectedcontribution peripheral chemoreflex function in high-altitudenatives and patients with chronic mountain sickness J Appl Physiol2003941269-1278 discussion 1253-1264
25 Milledge JS Lahiri S Respiratory control in lowlanders and Sherpahighlanders at altitude Respir Physiol 19672310-322
26 Fatemian M Gamboa A Leon-Velarde F et al Plasticity inrespiratory motor control selected contribution ventilatory responseto CO2 in high-altitude natives and patients with chronic mountainsickness J Appl Physiol 2003941279-1287
27 Cunningham PA Wolf CB Integration of respiratory responses tochanges in alveolar partial pressures of CO2 and O2 and in arterialpH In Cherniack JG editor Handbook of physiologymdashtherespiratory system Bethesda (Md) American Physiological Society1986 p 475-528
28 Fatemian M Robbins PA Selected contribution chemoreflexresponses to CO2 before and after an 8-h exposure to hypoxia inhumans J Appl Physiol 2001901607-1614 discussion 1606
29 Robbins PA The ventilatory response of the human respiratorysystem to sine waves of alveolar carbon dioxide and hypoxiaJ Physiology 1984350461-474
30 Milledge JS Sorensen SC Cerebral arteriovenous oxygen differ-ence in man native to high altitude J Appl Physiol 197232687-689
31 Leon-Velarde F Richalet JP Respiratory control in residents at highaltitude physiology and pathophysiology High Alt Med Biol 20067125-137
32 Villafuerte FC Cardenas R Monge CC Optimal hemoglobinconcentration and high altitude a theoretical approach for Andeanmen at rest J Appl Physiol May 2004961581-1588
33 Reeves JT Leon-Velarde F Chronic mountain sickness recentstudies of the relationship between hemoglobin concentration andoxygen transport High Alt Med Biol 20045147-155
34 Winslow RM Monge CC Brown EG et al Effects of hemodilutionon O2 transport in high-altitude polycythemia J Appl Physiol 1985591495-1502
35 Cruz J Diaz C Marticorena E et al Phlebotomy improvespulmonary gas exchange in chronic mountain polycythemiaRespiration 197938305-313
36 Manier G Guenard H Castaing Y et al Pulmonary gas exchange inAndean natives with excessive polycythemiamdasheffect of hemodilu-tion J Appl Physiol 1988652107-2117
37 Ergueta J Spielvogel H Cudkowicz L Cardio-respiratory studies inchronic mountain sickness (Monges syndrome) Respiration 197128485-517
38 Rotta A Canepa A Hurtado A et al Pulmonary circulation at sealevel and at high altitude J Appl Physiol 195611143-149
39 Richalet JP Rivera-Ch M Maignan M et al Acetazolamide forMonges disease efficiency and tolerance of 6-month treatment AmJ Respir Crit Care Med 20081771370-1376
40 Richardson TQ Guyton AC Effects of polycythemia and anemia oncardiac output and other circulatory factors Am J Physiol 19591971167-1170
41 Guyton AC Richardson TQ Effect of hematocrit on venous returnCirc Res 19619157-164
42 Claydon VE Norcliffe LJ Moore JP et al Orthostatic tolerance andblood volumes in Andean high altitude dwellers Exp Physiol 200489565-571
43 Richalet JP Rivera M Bouchet P et al Acetazolamide a treatmentfor chronic mountain sickness Am J Respir Crit Care Med 20051721427-1433
44 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk III The thickness of the media of the pulmonary trunk andascending aorta in high altitude natives Circulation 1963271101-1104
45 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk II The evolution of the elastic configuration of the pulmonarytrunk in people native to high altitudes Circulation 1963271094-1100
46 Saldana M Arias-Stella J Studies on the structure of thepulmonary trunk I Normal changes in the elastic configurationof the human pulmonary trunk at different ages Circulation 1963271086-1093
47 Wagner KF Katschinski DM Hasegawa J et al Chronic inbornerythrocytosis leads to cardiac dysfunction and premature death inmice overexpressing erythropoietin Blood 200197536-542
48 Ruschitzka FT Wenger RH Stallmach T et al Nitric oxide preventscardiovascular disease and determines survival in polyglobulic miceoverexpressing erythropoietin Proc Natl Acad Sci U S A 20009711609-11613
549F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
49 Brown CM Hainsworth R Assessment of capillary fluidshifts during orthostatic stress in normal subjects andsubjects with orthostatic intolerance Clin Auton Res 1999969-73
50 Bush VE Wight VL Brown CM et al Vascular responses toorthostatic stress in patients with postural tachycardia syndrome(POTS) in patients with low orthostatic tolerance and inasymptomatic controls Clin Auton Res 200010279-284
51 Cooper VL Hainsworth R Effects of head-up tilting on baroreceptorcontrol in subjects with different tolerances to orthostatic stress ClinSci (Lond) 2002103221-226
52 Appenzeller O Thomas PK Ponsford S et al Acral paresthesias inthe Andes and neurology at sea level Neurology 2002591532-1535
53 Kwaan HC Wang J Hyperviscosity in polycythemia vera andother red cell abnormalities Semin Thromb Hemost 200329451-458
54 Claydon VE Norcliffe LJ Moore JP et al Cardiovascularresponses to orthostatic stress in healthy altitude dwellers andaltitude residents with chronic mountain sickness Exp Physiol200590103-110
55 Norcliffe LJ Rivera-Ch M Claydon VE et al Cerebrovascularresponses to hypoxia and hypocapnia in high-altitude dwellersJ Physiol 2005566(Pt 1)287-294
56 Moore JP Claydon VE Norcliffe LJ et al Carotid baroreflexregulation of vascular resistance in high-altitude Andean natives withand without chronic mountain sickness Exp Physiol 200691907-913
57 Antezana AM Richalet JP Noriega I et al Hormonal changes innormal and polycythemic high-altitude natives J Appl Physiol 199579795-800
58 Gamboa A Gamboa JL Holmes C et al Plasma catecholamines andblood volume in native Andeans during hypoxia and normoxia ClinAuton Res 20061640-45
59 Penaloza D Arias-Stella J The heart and pulmonary circulation athigh altitudes healthy highlanders and chronic mountain sicknessCirculation 20071151132-1146
60 Pei SX Chen XJ Si Ren BZ et al Chronic mountain sickness inTibet Q J Med 198971555-574
61 Wu TY Li W Li Y et al Epidemiology of chronic mountainsickness ten years study in Qinghai-Tibet In Ohno H KobayashiT Masuyama S Nakashima M editors Progress in MountainMedicine and High Altitude Physiology Matsumoto Press Com-mittee of the 3rd World Congress on Mountain Medicine and HighAltitude Physiology 1998 p 120-125
62 Sime F Penaloza D Ruiz L Bradycardia increased cardiac outputand reversal of pulmonary hypertension in altitude natives living atsea level Br Heart J 197133647-657
63 Allemann Y Sartori C Lepori M et al Echocardiographic andinvasive measurements of pulmonary artery pressure correlateclosely at high altitude Am J Physiol 2000279H2013-H2016
64 Kojonazarov BK Imanov BZ Amatov TA et al Noninvasive andinvasive evaluation of pulmonary arterial pressure in highlandersEur Respir J 200729352-356
65 Naeije R Torbicki A More on the noninvasive diagnosis ofpulmonary hypertension Doppler echocardiography revisited EurRespir J 199581445-1449
66 Tei C Dujardin KS Hodge DO et al Doppler echocardiographicindex for assessment of global right ventricular function J Am SocEchocardiogr 19969838-847
67 Harjai KJ Scott L Vivekananthan K et al The Tei index a newprognostic index for patients with symptomatic heart failure J AmSoc Echocardiogr 200215864-868
68 Maignan M Rivera-Ch M Privat C et al Pulmonary pressure andcardiac function in chronic mountain sickness patients Chest 2009135499-504
69 Cruz-Jibaja J Banchero N Sime F et al Correlation betweenpulmonary artery pressure and level of altitude Dis Chest 196446446-451
70 Wu T Chronic mountain sickness in Qinghai-Tibet China In Ge RHackett P editors Life on the Qinghai-Tibetan Plateau BeijingPekiacuten University Medical Press 2007 p 118-133
71 Arias-Stella J Saldana M The terminal portion of the pulmonaryarterial tree in people native to high altitudes Circulation 196328915-925
72 Maggiorini M Leon-Velarde F High-altitude pulmonary hyperten-sion a pathophysiological entity to different diseases Eur Respir J2003221019-1025
73 Smith T Balanos G Croft Q et al The increase in pulmonary arterialpressure caused by hypoxia depends on iron status J Physiol 20085865999-6005
74 Smith T Talbot N Privat C et al Effects of iron supplementationand depletion on hypoxic pulmonary hypertension two randomizedcontrolled trials JAMA 20093021444-1450
75 Rivera-Ch M Leon-Velarde F Huicho L Treatment of chronicmountain sickness critical reappraisal of an old problem RespirPhysiol Neurobiol 2007158251-265
76 Rivera-Ch M Huicho L Bouchet P et al Effect of acetazolamide onventilatory response in subjects with chronic mountain sicknessRespir Physiol Neurobiol 2008162184-189

544 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
due to increased blood volume tg6 mice showsignificantly elevated central venous pressure47 thatcould result in elevated diastolic pressure It is possiblethen that some of the mechanisms operating in tg6 miceare also present in CMS individuals An enhancedexpression of endothelial nitric oxide synthase in CMScould explain for example the normal peripheralresistance found in CMS patients
Systemic blood pressure control and blood flow in CMS
Although systolic blood pressure in CMS patients isoften similar to that of healthy highlanders some smalldifferences arise in the control mechanisms It has beenshown that Andean HA dwellers have a great tolerance toorthostatic stress that might be attributed to the increasedhematocrit and blood volume The CMS individuals showan exceptional tolerance to orthostatic stress but nosignificantly different from HA controls yet CMSindividuals tend to respond with smaller increases inheart rate than HA healthy subjects54 This has led tosuggest that this may reflect a smaller sympathetic responseto orthostatic stress in these individuals (Table 1) Smallresponses of vascular resistance however have beenassociated to poor orthostatic tolerance49-51 Therefore theextremely good orthostatic tolerance in CMS patientssuggests that some other mechanism is operating in theseindividuals to maintain blood pressure It is possible thatthe large blood volume occurring in these individualscompensates for the smaller sympathetic response5253
Claydon and coworkers54 have shown that at HA theperipheral vascular resistance response to orthostatic stresshad a tendency to be smaller in CMS compared to healthysubjects but after 24 hours at sea level the CMS group hada significantly smaller response This less effective reflexvasoconstriction could explain why despite a larger bloodvolume in CMS subjects their orthostatic tolerance issimilar to that of HA controls
Chronic mountain sickness subjects also show differ-ences in the autoregulation of cerebral blood flow It hasbeen shown that cerebral blood flow is slower in CMSpatients compared to healthy HA subjects55 and it hasbeen suggested that this is a consequence of the increasedblood viscosity Cerebral blood flow autoregulation issimilar in CMS and healthy highlanders at high altitudeand their values are similar to those reported in SLresidents1355 After 24 hours at sea level however CMSindividuals had a larger fall on cerebral blood flow withsmaller change in resistance when exposed to orthostaticstress55 Studies on the relationship between peripheralresistance and carotid baroreceptor function have shownthat at altitude the sensitivity of forearm vascularresistance as a function of carotid sinus pressure is similarin CMS and healthy subjects but the ldquoset-pointrdquo of the
relationship is significantly higher in the CMS group56
This difference however disappears at sea level Apossible explanation for a higher ldquoset-pointrdquo in CMSindividuals at high altitude and its normalization at sealevel could be associated to the effects of hypoxemia onsympathetic vasomotor activity It is well-known thathypoxemia increases sympathetic discharge to musclevascular beds Chronic mountain sickness subjects arenormally more hypoxemic and therefore it is likely that agreater sympathetic activation may have contributed to thealtered baroreflex function This possibility finds supportin the observation that noradrenaline and adrenaline levelsare higher in CMS patients than in healthy HA dwellers57
and that plasma catecholamines are significantly reducedin HA natives within 4 hours of descent to sea level58
Cardiac features of CMS
Thirty years ago Pentildealoza and Arias-Stella59 studiedextensively the cardiac characteristics and pulmonarycirculation of Andean dwellers and patients with severeCMS Their findings point to the presence of pulmonaryhypertension and right ventricular hypertrophy in CMSsubjects9106061 They also demonstrated a direct rela-tionship between Ppa and right ventricle size In additiona prominent main pulmonary artery was found in allpatients Clinical characteristics of pulmonary hyperten-sion were an increased pulmonary second sound oftenassociated with a soft midsystolic ejection murmur anincreased diastolic blood pressure thought to be related toexcessive polycythemia9 and an increase in heart size onchest x-ray compared to healthy highlanders a featureexplained by the increased size of the right heart chambers
In severe cases of CMS the ECG shows peaked Pwaves with increased voltage in leads II III and aVF aswell as in the right precordial leads A right QRS axisdeviation is often observed An rS pattern in the rightprecordial leads and complexes of RS or rS type in the leftprecordial leads are common findings Negative T wavesover the right precordial leads are also common Thesefindings are indicative of right ventricular hypertrophy(RVH) and overload of the right heart chambers asconsequence of pulmonary hypertension Indeed as wellas with heart size a direct relationship between Ppa andright QRS axis deviation has been demonstrated59 Whenpatients with CMS are moved to SL symptoms and signsimprove promptly and the electrocardiographic andradiographic evidence of elevated Ppa and RVH decreasesover time62
Recent echocardiographic studies of pulmonary arterypressure at high altitude support previous findings usinginvasive techniques63-65 At present Doppler echocardi-ography is preferred to evaluate accurately cardiovascular
Fig 2 Cardiac output and maximal tricuspid regurgitation pressure in SL (SL control group at sea level [n = 15]) and HA (HA control group [n = 15]) andCMS groups (n = 55) at high altitude Data from Richalet et al 200968
545F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
function and cardiac morphology A recent study showedthat left atrial area was larger in SL than in HA nativesand CMS patients Right atria and ventricles were largerin CMS compared to SL and HA as shown by largerend-systolic right atria and end-diastolic right ventricularareas and a higher end-diastolic rightleft ventriculardiameter ratio This study also showed that cardiac outputis lower in CMS subjects than in SL dwellers but nodifference has been found when compared with HA
Fig 3 Pulmonary acceleration time and PVR index in SL (SL control group [n =([peak tricuspid regurgitation velocityright ventricular outflow tract time minus vel
natives (Fig 2) Left and right ventricular systolicfunctions and mitral and tricuspid inflows EA are notdifferent between SL HA and CMS Right ventricularTei index a global myocardial performance indicator(calculated as the ratio of [systolic time minus ejection time]ejection time)6667 however is increased in HA nativesand CMS patients when compared to SL controls Thesecardiac characteristics have been described in approxi-mately 50 CMS subjects the largest sample studied at
15]) HA (HA control group [n = 15]) and CMS groups (n = 55) PVR =ocity integral] times 10) + 01668
546 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
4300 m patients showed a mean [Hb] of 231 plusmn 16 gdLarterial blood oxygen saturation (SaO2) of 81 plusmn 4 andPpa of 34 plusmn 10 mm Hg68
Pulmonary hypertension in CMS
The cause of HAPH is the increase in pulmonaryvascular resistance (PVR) the underlying mechanisminvolves sustained and exaggerated pulmonary vasocon-striction and remodeling of the pulmonary vascular wall inresponse to chronic hypoxia due to proliferation anddecreased apoptosis of pulmonary artery smooth musclecells The effects of chronic hypoxia on pulmonary arterypressure are reflected in the negative correlation that existsbetween Ppa and SaO2 at high altitude596970 Arterialhypoxemia in addition to hypoxic vasoconstriction leadsto several structural changes in the pulmonary vesselsincluding an increase in the number of intimal smoothmuscle cells medial thickening in the small musculararteries and fibrinoid necrosis of the vessel walls71 Thesestructural changes in the pulmonary vessels rather thanhypoxic vasoconstriction alone are believed to beresponsible for the sustained rise in Ppa in chronichypoxia Pioneering hemodynamic invasive studies byPentildealoza and Sime910 in 10 subjects with severe CMS at4300 m showed a mean [Hb] value of 247 plusmn 24 gdL amean SaO2 of 696 plusmn 49 and a Ppa of 47 plusmn 177 mmHg values that have made the authors conclude that thesepatients have a type of hypoxic cor pulmonale in contrastto the hypertensive cor pulmonale observed in primarypulmonary hypertension However the structural changes
Fig 4 Pulmonary vascular resistance index and pulmonary acceleration time intreatment with acetazolamide (Acz) The study was organized in 2 phases (1) a ran open-label phase where all patients received acetazolamide (Acz + Acz) Theet al 200939
in the pulmonary vessels which are responsible for thesustained rise in Ppa in chronic hypoxia can have differentintensities and different onset times depending on thelength of hypoxic exposure comprising a range fromshort-term to long-term7072
Maignan and coworkers68 have described cardiachemodynamics in approximately 50 CMS cases withnoninvasive methods and found varying intensities ofPpa Although they might have been studying patients inan early disease stage they observed mean pulmonaryacceleration time and accelerationejection time ratiossignificantly lower in CMS subjects than in SL and HAnatives (Fig 3) Pulmonary vascular index was foundlower in SL than in other groups and there was nosignificant difference between HA and CMS however thenumber of patients with PVR greater than 2 Wood unitswas higher in CMS (1242) than in SL (013) and tended tobe significant when compared to HA (115) (CMS vs SLP = 003 CMS vs HA P = 008 and SL vs HA P = 034)
Chronic hypoxia with appropriate acclimatization asseen in healthy HA residents induces an increase inPVR without change in pulmonary arterial systolicpressure right heart cavity dimensions or right systolicventricular function The increase in right ventricularTei index however could reflect early right ventricularimpairment68 When hypoxemia becomes severe asobserved in some patients with excessive Ppa a furtherimpairment can be found with a significant increase inpulmonary arterial systolic pressure and right cardiaccavity enlargement However contrary to the assumption59
of overt chronic cor pulmonale based on severe HAPHpatients with established HAPH did not show any
placebo and CMS patients groups before and after 3 and 6 months ofandomized double-blind placebo-controlled phase (placebo + Acz) and (2)2 phases were separated by a 4-week washout period Data from Richalet
547F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
obvious cardiac systolic dysfunction as shown byMaignan and coworkers68 This confirms the individualvariability of the severity of HAPH which is also highlydependent on risk factors and genetic susceptibilitydespite that for the moment no specific gene has beenclearly associated with the development of CMS Largeepidemiologic studies should be conducted to determinethe precise natural history prevalence and features ofheart failure in CMS
Recently an interaction between iron levels andhypoxia in the regulation of the pulmonary circulationhas been described73 The study showed that ironinfusion before an 8-hour exposure to sustained hypoxiaabolished or reduced greatly the elevation in baselinepulmonary artery systolic pressure and enhanced sensi-tivity of the pulmonary vasculature to acute hypoxia Thestudy also showed that iron chelation through deferox-amine infusion before the 8-hour hypoxia protocolelevates pulmonary artery systolic pressure significantlyThese findings led to conclude that iron availabilitymodifies pulmonary arterial pressure and pulmonaryvascular responses to hypoxia possibly through theinvolvement of the hypoxia-inducible factor hydroxyl-ation system
In a later study Smith and coworkers74 showed theeffect that iron levels could have on HA diseases thatinvolve pulmonary hypertension such as CMS This studyshowed that reduction of iron availability in CMS patientsthrough isovolemic bloodletting is associated with asubstantial increase in Ppa whereas iron supplementationis related to an attenuation of HAPH In view of the resultsthe authors suggest that this effect is consistent with thoseof acute iron chelation and thus implies that irondeficiency could exacerbate Ppa in chronic pulmonaryand cardiac disease and also that HAPH can be attenuatedby iron supplementation
It should be noted however that no long-termcontrolled studies have been carried out to evaluate allthe possible effectors related to the development ofHAPH Thus extensive research is required to determinewhich of the multiple elements that regulate Ppa at highaltitude might have a predominant role in determining thedifferent time courses and severity of HAPH
Treatment
Recently increasing attention is being drawn todifferent phenomena that may be involved in the causalchain of CMS and that were previously overlooked Theseinclude CMS risk and environmental factors such as earlyprenatal or postnatal exposure to different agents andorthe different genetic susceptibilities in different popula-tions and individuals However until having a complete
understanding of which mechanisms are better targetsfor intervention at present treatment is directed to thosecomponents of CMS pathophysiologic sequence thatare susceptible of modification through pharmacologicintervention that is on the erythropoietic response toreduce the increased red cell mass andor on the ventilatoryresponse These agents include methylxanthines adrener-gic blockers dopaminergic antagonists medroxyproges-terone peripheral ventilator stimulants such as almitrineand enalapril all of which have been tested experiment-ally75 Although phlebotomy has been shown to reducethe signs and symptoms of CMS its invasiveness andtransient effects often render it impractical
Descent to low altitudes is the ideal treatment and leadsto prompt improvement of signs and symptoms of CMSbut often patients cannot or do not want to descend tolower altitudes for economic personal andor familyreasons Recently acetazolamide has been used as animportant alternative for the treatment of CMS and itseffects have been studied in randomized placebo-controlled trials in the Peruvian Andes394376 The effectsof this carbonic anhydrase inhibitor in CMS include animprovement of ventilation through metabolic acidosisand of SaO2
76 thus causing a decrease in Epo concen-tration and excessive erythrocytosis In addition it leads toa decrease in PVR and an increase in pulmonaryacceleration time Furthermore the number of CMSpatients with pulmonary hypertension (defined by PVRN 2 Wood units) was 8 before treatment and nil aftertreatment (P = 0005) In fact the observed effect ofacetazolamide on PVR (minus17) might be indirectly due tothe decrease in blood viscosity (minus16) due to thereduction in hematocrit (Fig 4) Therefore at presentthese very encouraging results suggest that acetazolamidecould be a good alternative in the treatment of CMS3943
Statement of Conflict of Interest
All authors declare that there are no conflicts of interest
References
1 Pentildealoza D Sime F Banchero N et al Pulmonary hypertension inhealthy men born and living at high altitudes Am J Cardiol 196311150-157
2 Hurtado A Animals in high altitudes resident man In Dill DAdolph E Wilber C editors Handbook of physiology adaptation tothe environment Washington DC American Physiological Society1964 p 843-860
3 Monge-M C Monge-C C High altitude diseases mechanism andmanagement Springfield (Ill) Charles C Thomas 1966
4 Antezana G Barragaacuten L Coudert J et al The pulmonarycirculation of high altitude natives In Brendel W Zink R editorsHigh altitude physiology and medicine New York Springer-Verlag 1982 p 142-149
548 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
5 Monge C Chronic mountain sickness Physiol Rev 1943231666 Monge-M C Encinas E Heraud C et al La Enfermedad de los
Andes (Siacutendromes Eritreacutemicos) Imprenta Americana Lima1928
7 Monge-M C Sobre un caso de Enfermedad de Vaacutequez Paperpresented at Communicacioacuten presentada a la Academia Nacional deMedicina Lima Peru Academia Nacional de Medicina 1925
8 Hurtado A Chronic mountain sickness JAMA 19421201278-1282
9 Penaloza D Sime F Chronic cor pulmonale due to loss of altitudeacclimatization (chronic mountain sickness) Am J Med 197150728-743
10 Pentildealoza D Sime F Ruiz L Cor pulmonale in chronic mountainsickness present concept of Monges disease In Porter R Knight Jeditors High altitude physiology cardiac and respiratory aspectsEdinburgh Churchill Livingstone 1971 p 41-60
11 Beall CM Decker MJ Brittenham GM et al An Ethiopian pattern ofhuman adaptation to high-altitude hypoxia Proc Natl Acad Sci U S A20029917215-17218
12 Winslow RM Monge-C C Hypoxia polycythemia and chronicmountain sickness Baltimore (Md) Johns Hopkins University Press1987
13 Arregui A Cabrera J Leon-Velarde F et al High prevalence ofmigraine in a high-altitude population Neurology 1991411668-1669
14 Sorensen SC Lassen NA Severinghaus JW et al Cerebral glucosemetabolism and cerebral blood flow in high-altitude residents J ApplPhysiol 197437305-310
15 Massik J Tang YL Hudak ML et al Effect of hematocrit oncerebral blood flow with induced polycythemia J Appl Physiol1987621090-1096
16 Monge-M C La enfermedad de los Andes An Fac Med 19281-30917 Leon-Velarde F Maggiorini M Reeves JT et al Consensus
statement on chronic and subacute high altitude diseases High AltMed Biol 20056147-157
18 Leon-Velarde F Mejia O Gene expression in chronic high altitudediseases High Alt Med Biol 20089130-139
19 Monge-C C Leoacuten-Velarde F Arregui A Chronic mountain sicknessIn Lenfant C editor High altitude an exploration of humanadaptation New York Marcel Dekker Inc 2001 p 815-838
20 Kryger M McCullough R Doekel R et al Excessive polycythemiaof high altitude role of ventilatory drive and lung disease Am RevRespir Dis 1978118659-666
21 Severinghaus JW Bainton CR Carcelen A Respiratory insensitivityto hypoxia in chronically hypoxic man Respir Physiol 19661308-334
22 Vargas E Spielvogel H Chronic mountain sickness optimalhemoglobin and heart disease High Alt Med Biol 20067138-149
23 Liang PJ Bascom DA Robbins PA Extended models of theventilatory response to sustained isocapnic hypoxia in humansJ Appl Physiol 199782667-677
24 Leon-Velarde F Gamboa A Rivera-Ch M et al Selectedcontribution peripheral chemoreflex function in high-altitudenatives and patients with chronic mountain sickness J Appl Physiol2003941269-1278 discussion 1253-1264
25 Milledge JS Lahiri S Respiratory control in lowlanders and Sherpahighlanders at altitude Respir Physiol 19672310-322
26 Fatemian M Gamboa A Leon-Velarde F et al Plasticity inrespiratory motor control selected contribution ventilatory responseto CO2 in high-altitude natives and patients with chronic mountainsickness J Appl Physiol 2003941279-1287
27 Cunningham PA Wolf CB Integration of respiratory responses tochanges in alveolar partial pressures of CO2 and O2 and in arterialpH In Cherniack JG editor Handbook of physiologymdashtherespiratory system Bethesda (Md) American Physiological Society1986 p 475-528
28 Fatemian M Robbins PA Selected contribution chemoreflexresponses to CO2 before and after an 8-h exposure to hypoxia inhumans J Appl Physiol 2001901607-1614 discussion 1606
29 Robbins PA The ventilatory response of the human respiratorysystem to sine waves of alveolar carbon dioxide and hypoxiaJ Physiology 1984350461-474
30 Milledge JS Sorensen SC Cerebral arteriovenous oxygen differ-ence in man native to high altitude J Appl Physiol 197232687-689
31 Leon-Velarde F Richalet JP Respiratory control in residents at highaltitude physiology and pathophysiology High Alt Med Biol 20067125-137
32 Villafuerte FC Cardenas R Monge CC Optimal hemoglobinconcentration and high altitude a theoretical approach for Andeanmen at rest J Appl Physiol May 2004961581-1588
33 Reeves JT Leon-Velarde F Chronic mountain sickness recentstudies of the relationship between hemoglobin concentration andoxygen transport High Alt Med Biol 20045147-155
34 Winslow RM Monge CC Brown EG et al Effects of hemodilutionon O2 transport in high-altitude polycythemia J Appl Physiol 1985591495-1502
35 Cruz J Diaz C Marticorena E et al Phlebotomy improvespulmonary gas exchange in chronic mountain polycythemiaRespiration 197938305-313
36 Manier G Guenard H Castaing Y et al Pulmonary gas exchange inAndean natives with excessive polycythemiamdasheffect of hemodilu-tion J Appl Physiol 1988652107-2117
37 Ergueta J Spielvogel H Cudkowicz L Cardio-respiratory studies inchronic mountain sickness (Monges syndrome) Respiration 197128485-517
38 Rotta A Canepa A Hurtado A et al Pulmonary circulation at sealevel and at high altitude J Appl Physiol 195611143-149
39 Richalet JP Rivera-Ch M Maignan M et al Acetazolamide forMonges disease efficiency and tolerance of 6-month treatment AmJ Respir Crit Care Med 20081771370-1376
40 Richardson TQ Guyton AC Effects of polycythemia and anemia oncardiac output and other circulatory factors Am J Physiol 19591971167-1170
41 Guyton AC Richardson TQ Effect of hematocrit on venous returnCirc Res 19619157-164
42 Claydon VE Norcliffe LJ Moore JP et al Orthostatic tolerance andblood volumes in Andean high altitude dwellers Exp Physiol 200489565-571
43 Richalet JP Rivera M Bouchet P et al Acetazolamide a treatmentfor chronic mountain sickness Am J Respir Crit Care Med 20051721427-1433
44 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk III The thickness of the media of the pulmonary trunk andascending aorta in high altitude natives Circulation 1963271101-1104
45 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk II The evolution of the elastic configuration of the pulmonarytrunk in people native to high altitudes Circulation 1963271094-1100
46 Saldana M Arias-Stella J Studies on the structure of thepulmonary trunk I Normal changes in the elastic configurationof the human pulmonary trunk at different ages Circulation 1963271086-1093
47 Wagner KF Katschinski DM Hasegawa J et al Chronic inbornerythrocytosis leads to cardiac dysfunction and premature death inmice overexpressing erythropoietin Blood 200197536-542
48 Ruschitzka FT Wenger RH Stallmach T et al Nitric oxide preventscardiovascular disease and determines survival in polyglobulic miceoverexpressing erythropoietin Proc Natl Acad Sci U S A 20009711609-11613
549F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
49 Brown CM Hainsworth R Assessment of capillary fluidshifts during orthostatic stress in normal subjects andsubjects with orthostatic intolerance Clin Auton Res 1999969-73
50 Bush VE Wight VL Brown CM et al Vascular responses toorthostatic stress in patients with postural tachycardia syndrome(POTS) in patients with low orthostatic tolerance and inasymptomatic controls Clin Auton Res 200010279-284
51 Cooper VL Hainsworth R Effects of head-up tilting on baroreceptorcontrol in subjects with different tolerances to orthostatic stress ClinSci (Lond) 2002103221-226
52 Appenzeller O Thomas PK Ponsford S et al Acral paresthesias inthe Andes and neurology at sea level Neurology 2002591532-1535
53 Kwaan HC Wang J Hyperviscosity in polycythemia vera andother red cell abnormalities Semin Thromb Hemost 200329451-458
54 Claydon VE Norcliffe LJ Moore JP et al Cardiovascularresponses to orthostatic stress in healthy altitude dwellers andaltitude residents with chronic mountain sickness Exp Physiol200590103-110
55 Norcliffe LJ Rivera-Ch M Claydon VE et al Cerebrovascularresponses to hypoxia and hypocapnia in high-altitude dwellersJ Physiol 2005566(Pt 1)287-294
56 Moore JP Claydon VE Norcliffe LJ et al Carotid baroreflexregulation of vascular resistance in high-altitude Andean natives withand without chronic mountain sickness Exp Physiol 200691907-913
57 Antezana AM Richalet JP Noriega I et al Hormonal changes innormal and polycythemic high-altitude natives J Appl Physiol 199579795-800
58 Gamboa A Gamboa JL Holmes C et al Plasma catecholamines andblood volume in native Andeans during hypoxia and normoxia ClinAuton Res 20061640-45
59 Penaloza D Arias-Stella J The heart and pulmonary circulation athigh altitudes healthy highlanders and chronic mountain sicknessCirculation 20071151132-1146
60 Pei SX Chen XJ Si Ren BZ et al Chronic mountain sickness inTibet Q J Med 198971555-574
61 Wu TY Li W Li Y et al Epidemiology of chronic mountainsickness ten years study in Qinghai-Tibet In Ohno H KobayashiT Masuyama S Nakashima M editors Progress in MountainMedicine and High Altitude Physiology Matsumoto Press Com-mittee of the 3rd World Congress on Mountain Medicine and HighAltitude Physiology 1998 p 120-125
62 Sime F Penaloza D Ruiz L Bradycardia increased cardiac outputand reversal of pulmonary hypertension in altitude natives living atsea level Br Heart J 197133647-657
63 Allemann Y Sartori C Lepori M et al Echocardiographic andinvasive measurements of pulmonary artery pressure correlateclosely at high altitude Am J Physiol 2000279H2013-H2016
64 Kojonazarov BK Imanov BZ Amatov TA et al Noninvasive andinvasive evaluation of pulmonary arterial pressure in highlandersEur Respir J 200729352-356
65 Naeije R Torbicki A More on the noninvasive diagnosis ofpulmonary hypertension Doppler echocardiography revisited EurRespir J 199581445-1449
66 Tei C Dujardin KS Hodge DO et al Doppler echocardiographicindex for assessment of global right ventricular function J Am SocEchocardiogr 19969838-847
67 Harjai KJ Scott L Vivekananthan K et al The Tei index a newprognostic index for patients with symptomatic heart failure J AmSoc Echocardiogr 200215864-868
68 Maignan M Rivera-Ch M Privat C et al Pulmonary pressure andcardiac function in chronic mountain sickness patients Chest 2009135499-504
69 Cruz-Jibaja J Banchero N Sime F et al Correlation betweenpulmonary artery pressure and level of altitude Dis Chest 196446446-451
70 Wu T Chronic mountain sickness in Qinghai-Tibet China In Ge RHackett P editors Life on the Qinghai-Tibetan Plateau BeijingPekiacuten University Medical Press 2007 p 118-133
71 Arias-Stella J Saldana M The terminal portion of the pulmonaryarterial tree in people native to high altitudes Circulation 196328915-925
72 Maggiorini M Leon-Velarde F High-altitude pulmonary hyperten-sion a pathophysiological entity to different diseases Eur Respir J2003221019-1025
73 Smith T Balanos G Croft Q et al The increase in pulmonary arterialpressure caused by hypoxia depends on iron status J Physiol 20085865999-6005
74 Smith T Talbot N Privat C et al Effects of iron supplementationand depletion on hypoxic pulmonary hypertension two randomizedcontrolled trials JAMA 20093021444-1450
75 Rivera-Ch M Leon-Velarde F Huicho L Treatment of chronicmountain sickness critical reappraisal of an old problem RespirPhysiol Neurobiol 2007158251-265
76 Rivera-Ch M Huicho L Bouchet P et al Effect of acetazolamide onventilatory response in subjects with chronic mountain sicknessRespir Physiol Neurobiol 2008162184-189

Fig 2 Cardiac output and maximal tricuspid regurgitation pressure in SL (SL control group at sea level [n = 15]) and HA (HA control group [n = 15]) andCMS groups (n = 55) at high altitude Data from Richalet et al 200968
545F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
function and cardiac morphology A recent study showedthat left atrial area was larger in SL than in HA nativesand CMS patients Right atria and ventricles were largerin CMS compared to SL and HA as shown by largerend-systolic right atria and end-diastolic right ventricularareas and a higher end-diastolic rightleft ventriculardiameter ratio This study also showed that cardiac outputis lower in CMS subjects than in SL dwellers but nodifference has been found when compared with HA
Fig 3 Pulmonary acceleration time and PVR index in SL (SL control group [n =([peak tricuspid regurgitation velocityright ventricular outflow tract time minus vel
natives (Fig 2) Left and right ventricular systolicfunctions and mitral and tricuspid inflows EA are notdifferent between SL HA and CMS Right ventricularTei index a global myocardial performance indicator(calculated as the ratio of [systolic time minus ejection time]ejection time)6667 however is increased in HA nativesand CMS patients when compared to SL controls Thesecardiac characteristics have been described in approxi-mately 50 CMS subjects the largest sample studied at
15]) HA (HA control group [n = 15]) and CMS groups (n = 55) PVR =ocity integral] times 10) + 01668
546 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
4300 m patients showed a mean [Hb] of 231 plusmn 16 gdLarterial blood oxygen saturation (SaO2) of 81 plusmn 4 andPpa of 34 plusmn 10 mm Hg68
Pulmonary hypertension in CMS
The cause of HAPH is the increase in pulmonaryvascular resistance (PVR) the underlying mechanisminvolves sustained and exaggerated pulmonary vasocon-striction and remodeling of the pulmonary vascular wall inresponse to chronic hypoxia due to proliferation anddecreased apoptosis of pulmonary artery smooth musclecells The effects of chronic hypoxia on pulmonary arterypressure are reflected in the negative correlation that existsbetween Ppa and SaO2 at high altitude596970 Arterialhypoxemia in addition to hypoxic vasoconstriction leadsto several structural changes in the pulmonary vesselsincluding an increase in the number of intimal smoothmuscle cells medial thickening in the small musculararteries and fibrinoid necrosis of the vessel walls71 Thesestructural changes in the pulmonary vessels rather thanhypoxic vasoconstriction alone are believed to beresponsible for the sustained rise in Ppa in chronichypoxia Pioneering hemodynamic invasive studies byPentildealoza and Sime910 in 10 subjects with severe CMS at4300 m showed a mean [Hb] value of 247 plusmn 24 gdL amean SaO2 of 696 plusmn 49 and a Ppa of 47 plusmn 177 mmHg values that have made the authors conclude that thesepatients have a type of hypoxic cor pulmonale in contrastto the hypertensive cor pulmonale observed in primarypulmonary hypertension However the structural changes
Fig 4 Pulmonary vascular resistance index and pulmonary acceleration time intreatment with acetazolamide (Acz) The study was organized in 2 phases (1) a ran open-label phase where all patients received acetazolamide (Acz + Acz) Theet al 200939
in the pulmonary vessels which are responsible for thesustained rise in Ppa in chronic hypoxia can have differentintensities and different onset times depending on thelength of hypoxic exposure comprising a range fromshort-term to long-term7072
Maignan and coworkers68 have described cardiachemodynamics in approximately 50 CMS cases withnoninvasive methods and found varying intensities ofPpa Although they might have been studying patients inan early disease stage they observed mean pulmonaryacceleration time and accelerationejection time ratiossignificantly lower in CMS subjects than in SL and HAnatives (Fig 3) Pulmonary vascular index was foundlower in SL than in other groups and there was nosignificant difference between HA and CMS however thenumber of patients with PVR greater than 2 Wood unitswas higher in CMS (1242) than in SL (013) and tended tobe significant when compared to HA (115) (CMS vs SLP = 003 CMS vs HA P = 008 and SL vs HA P = 034)
Chronic hypoxia with appropriate acclimatization asseen in healthy HA residents induces an increase inPVR without change in pulmonary arterial systolicpressure right heart cavity dimensions or right systolicventricular function The increase in right ventricularTei index however could reflect early right ventricularimpairment68 When hypoxemia becomes severe asobserved in some patients with excessive Ppa a furtherimpairment can be found with a significant increase inpulmonary arterial systolic pressure and right cardiaccavity enlargement However contrary to the assumption59
of overt chronic cor pulmonale based on severe HAPHpatients with established HAPH did not show any
placebo and CMS patients groups before and after 3 and 6 months ofandomized double-blind placebo-controlled phase (placebo + Acz) and (2)2 phases were separated by a 4-week washout period Data from Richalet
547F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
obvious cardiac systolic dysfunction as shown byMaignan and coworkers68 This confirms the individualvariability of the severity of HAPH which is also highlydependent on risk factors and genetic susceptibilitydespite that for the moment no specific gene has beenclearly associated with the development of CMS Largeepidemiologic studies should be conducted to determinethe precise natural history prevalence and features ofheart failure in CMS
Recently an interaction between iron levels andhypoxia in the regulation of the pulmonary circulationhas been described73 The study showed that ironinfusion before an 8-hour exposure to sustained hypoxiaabolished or reduced greatly the elevation in baselinepulmonary artery systolic pressure and enhanced sensi-tivity of the pulmonary vasculature to acute hypoxia Thestudy also showed that iron chelation through deferox-amine infusion before the 8-hour hypoxia protocolelevates pulmonary artery systolic pressure significantlyThese findings led to conclude that iron availabilitymodifies pulmonary arterial pressure and pulmonaryvascular responses to hypoxia possibly through theinvolvement of the hypoxia-inducible factor hydroxyl-ation system
In a later study Smith and coworkers74 showed theeffect that iron levels could have on HA diseases thatinvolve pulmonary hypertension such as CMS This studyshowed that reduction of iron availability in CMS patientsthrough isovolemic bloodletting is associated with asubstantial increase in Ppa whereas iron supplementationis related to an attenuation of HAPH In view of the resultsthe authors suggest that this effect is consistent with thoseof acute iron chelation and thus implies that irondeficiency could exacerbate Ppa in chronic pulmonaryand cardiac disease and also that HAPH can be attenuatedby iron supplementation
It should be noted however that no long-termcontrolled studies have been carried out to evaluate allthe possible effectors related to the development ofHAPH Thus extensive research is required to determinewhich of the multiple elements that regulate Ppa at highaltitude might have a predominant role in determining thedifferent time courses and severity of HAPH
Treatment
Recently increasing attention is being drawn todifferent phenomena that may be involved in the causalchain of CMS and that were previously overlooked Theseinclude CMS risk and environmental factors such as earlyprenatal or postnatal exposure to different agents andorthe different genetic susceptibilities in different popula-tions and individuals However until having a complete
understanding of which mechanisms are better targetsfor intervention at present treatment is directed to thosecomponents of CMS pathophysiologic sequence thatare susceptible of modification through pharmacologicintervention that is on the erythropoietic response toreduce the increased red cell mass andor on the ventilatoryresponse These agents include methylxanthines adrener-gic blockers dopaminergic antagonists medroxyproges-terone peripheral ventilator stimulants such as almitrineand enalapril all of which have been tested experiment-ally75 Although phlebotomy has been shown to reducethe signs and symptoms of CMS its invasiveness andtransient effects often render it impractical
Descent to low altitudes is the ideal treatment and leadsto prompt improvement of signs and symptoms of CMSbut often patients cannot or do not want to descend tolower altitudes for economic personal andor familyreasons Recently acetazolamide has been used as animportant alternative for the treatment of CMS and itseffects have been studied in randomized placebo-controlled trials in the Peruvian Andes394376 The effectsof this carbonic anhydrase inhibitor in CMS include animprovement of ventilation through metabolic acidosisand of SaO2
76 thus causing a decrease in Epo concen-tration and excessive erythrocytosis In addition it leads toa decrease in PVR and an increase in pulmonaryacceleration time Furthermore the number of CMSpatients with pulmonary hypertension (defined by PVRN 2 Wood units) was 8 before treatment and nil aftertreatment (P = 0005) In fact the observed effect ofacetazolamide on PVR (minus17) might be indirectly due tothe decrease in blood viscosity (minus16) due to thereduction in hematocrit (Fig 4) Therefore at presentthese very encouraging results suggest that acetazolamidecould be a good alternative in the treatment of CMS3943
Statement of Conflict of Interest
All authors declare that there are no conflicts of interest
References
1 Pentildealoza D Sime F Banchero N et al Pulmonary hypertension inhealthy men born and living at high altitudes Am J Cardiol 196311150-157
2 Hurtado A Animals in high altitudes resident man In Dill DAdolph E Wilber C editors Handbook of physiology adaptation tothe environment Washington DC American Physiological Society1964 p 843-860
3 Monge-M C Monge-C C High altitude diseases mechanism andmanagement Springfield (Ill) Charles C Thomas 1966
4 Antezana G Barragaacuten L Coudert J et al The pulmonarycirculation of high altitude natives In Brendel W Zink R editorsHigh altitude physiology and medicine New York Springer-Verlag 1982 p 142-149
548 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
5 Monge C Chronic mountain sickness Physiol Rev 1943231666 Monge-M C Encinas E Heraud C et al La Enfermedad de los
Andes (Siacutendromes Eritreacutemicos) Imprenta Americana Lima1928
7 Monge-M C Sobre un caso de Enfermedad de Vaacutequez Paperpresented at Communicacioacuten presentada a la Academia Nacional deMedicina Lima Peru Academia Nacional de Medicina 1925
8 Hurtado A Chronic mountain sickness JAMA 19421201278-1282
9 Penaloza D Sime F Chronic cor pulmonale due to loss of altitudeacclimatization (chronic mountain sickness) Am J Med 197150728-743
10 Pentildealoza D Sime F Ruiz L Cor pulmonale in chronic mountainsickness present concept of Monges disease In Porter R Knight Jeditors High altitude physiology cardiac and respiratory aspectsEdinburgh Churchill Livingstone 1971 p 41-60
11 Beall CM Decker MJ Brittenham GM et al An Ethiopian pattern ofhuman adaptation to high-altitude hypoxia Proc Natl Acad Sci U S A20029917215-17218
12 Winslow RM Monge-C C Hypoxia polycythemia and chronicmountain sickness Baltimore (Md) Johns Hopkins University Press1987
13 Arregui A Cabrera J Leon-Velarde F et al High prevalence ofmigraine in a high-altitude population Neurology 1991411668-1669
14 Sorensen SC Lassen NA Severinghaus JW et al Cerebral glucosemetabolism and cerebral blood flow in high-altitude residents J ApplPhysiol 197437305-310
15 Massik J Tang YL Hudak ML et al Effect of hematocrit oncerebral blood flow with induced polycythemia J Appl Physiol1987621090-1096
16 Monge-M C La enfermedad de los Andes An Fac Med 19281-30917 Leon-Velarde F Maggiorini M Reeves JT et al Consensus
statement on chronic and subacute high altitude diseases High AltMed Biol 20056147-157
18 Leon-Velarde F Mejia O Gene expression in chronic high altitudediseases High Alt Med Biol 20089130-139
19 Monge-C C Leoacuten-Velarde F Arregui A Chronic mountain sicknessIn Lenfant C editor High altitude an exploration of humanadaptation New York Marcel Dekker Inc 2001 p 815-838
20 Kryger M McCullough R Doekel R et al Excessive polycythemiaof high altitude role of ventilatory drive and lung disease Am RevRespir Dis 1978118659-666
21 Severinghaus JW Bainton CR Carcelen A Respiratory insensitivityto hypoxia in chronically hypoxic man Respir Physiol 19661308-334
22 Vargas E Spielvogel H Chronic mountain sickness optimalhemoglobin and heart disease High Alt Med Biol 20067138-149
23 Liang PJ Bascom DA Robbins PA Extended models of theventilatory response to sustained isocapnic hypoxia in humansJ Appl Physiol 199782667-677
24 Leon-Velarde F Gamboa A Rivera-Ch M et al Selectedcontribution peripheral chemoreflex function in high-altitudenatives and patients with chronic mountain sickness J Appl Physiol2003941269-1278 discussion 1253-1264
25 Milledge JS Lahiri S Respiratory control in lowlanders and Sherpahighlanders at altitude Respir Physiol 19672310-322
26 Fatemian M Gamboa A Leon-Velarde F et al Plasticity inrespiratory motor control selected contribution ventilatory responseto CO2 in high-altitude natives and patients with chronic mountainsickness J Appl Physiol 2003941279-1287
27 Cunningham PA Wolf CB Integration of respiratory responses tochanges in alveolar partial pressures of CO2 and O2 and in arterialpH In Cherniack JG editor Handbook of physiologymdashtherespiratory system Bethesda (Md) American Physiological Society1986 p 475-528
28 Fatemian M Robbins PA Selected contribution chemoreflexresponses to CO2 before and after an 8-h exposure to hypoxia inhumans J Appl Physiol 2001901607-1614 discussion 1606
29 Robbins PA The ventilatory response of the human respiratorysystem to sine waves of alveolar carbon dioxide and hypoxiaJ Physiology 1984350461-474
30 Milledge JS Sorensen SC Cerebral arteriovenous oxygen differ-ence in man native to high altitude J Appl Physiol 197232687-689
31 Leon-Velarde F Richalet JP Respiratory control in residents at highaltitude physiology and pathophysiology High Alt Med Biol 20067125-137
32 Villafuerte FC Cardenas R Monge CC Optimal hemoglobinconcentration and high altitude a theoretical approach for Andeanmen at rest J Appl Physiol May 2004961581-1588
33 Reeves JT Leon-Velarde F Chronic mountain sickness recentstudies of the relationship between hemoglobin concentration andoxygen transport High Alt Med Biol 20045147-155
34 Winslow RM Monge CC Brown EG et al Effects of hemodilutionon O2 transport in high-altitude polycythemia J Appl Physiol 1985591495-1502
35 Cruz J Diaz C Marticorena E et al Phlebotomy improvespulmonary gas exchange in chronic mountain polycythemiaRespiration 197938305-313
36 Manier G Guenard H Castaing Y et al Pulmonary gas exchange inAndean natives with excessive polycythemiamdasheffect of hemodilu-tion J Appl Physiol 1988652107-2117
37 Ergueta J Spielvogel H Cudkowicz L Cardio-respiratory studies inchronic mountain sickness (Monges syndrome) Respiration 197128485-517
38 Rotta A Canepa A Hurtado A et al Pulmonary circulation at sealevel and at high altitude J Appl Physiol 195611143-149
39 Richalet JP Rivera-Ch M Maignan M et al Acetazolamide forMonges disease efficiency and tolerance of 6-month treatment AmJ Respir Crit Care Med 20081771370-1376
40 Richardson TQ Guyton AC Effects of polycythemia and anemia oncardiac output and other circulatory factors Am J Physiol 19591971167-1170
41 Guyton AC Richardson TQ Effect of hematocrit on venous returnCirc Res 19619157-164
42 Claydon VE Norcliffe LJ Moore JP et al Orthostatic tolerance andblood volumes in Andean high altitude dwellers Exp Physiol 200489565-571
43 Richalet JP Rivera M Bouchet P et al Acetazolamide a treatmentfor chronic mountain sickness Am J Respir Crit Care Med 20051721427-1433
44 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk III The thickness of the media of the pulmonary trunk andascending aorta in high altitude natives Circulation 1963271101-1104
45 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk II The evolution of the elastic configuration of the pulmonarytrunk in people native to high altitudes Circulation 1963271094-1100
46 Saldana M Arias-Stella J Studies on the structure of thepulmonary trunk I Normal changes in the elastic configurationof the human pulmonary trunk at different ages Circulation 1963271086-1093
47 Wagner KF Katschinski DM Hasegawa J et al Chronic inbornerythrocytosis leads to cardiac dysfunction and premature death inmice overexpressing erythropoietin Blood 200197536-542
48 Ruschitzka FT Wenger RH Stallmach T et al Nitric oxide preventscardiovascular disease and determines survival in polyglobulic miceoverexpressing erythropoietin Proc Natl Acad Sci U S A 20009711609-11613
549F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
49 Brown CM Hainsworth R Assessment of capillary fluidshifts during orthostatic stress in normal subjects andsubjects with orthostatic intolerance Clin Auton Res 1999969-73
50 Bush VE Wight VL Brown CM et al Vascular responses toorthostatic stress in patients with postural tachycardia syndrome(POTS) in patients with low orthostatic tolerance and inasymptomatic controls Clin Auton Res 200010279-284
51 Cooper VL Hainsworth R Effects of head-up tilting on baroreceptorcontrol in subjects with different tolerances to orthostatic stress ClinSci (Lond) 2002103221-226
52 Appenzeller O Thomas PK Ponsford S et al Acral paresthesias inthe Andes and neurology at sea level Neurology 2002591532-1535
53 Kwaan HC Wang J Hyperviscosity in polycythemia vera andother red cell abnormalities Semin Thromb Hemost 200329451-458
54 Claydon VE Norcliffe LJ Moore JP et al Cardiovascularresponses to orthostatic stress in healthy altitude dwellers andaltitude residents with chronic mountain sickness Exp Physiol200590103-110
55 Norcliffe LJ Rivera-Ch M Claydon VE et al Cerebrovascularresponses to hypoxia and hypocapnia in high-altitude dwellersJ Physiol 2005566(Pt 1)287-294
56 Moore JP Claydon VE Norcliffe LJ et al Carotid baroreflexregulation of vascular resistance in high-altitude Andean natives withand without chronic mountain sickness Exp Physiol 200691907-913
57 Antezana AM Richalet JP Noriega I et al Hormonal changes innormal and polycythemic high-altitude natives J Appl Physiol 199579795-800
58 Gamboa A Gamboa JL Holmes C et al Plasma catecholamines andblood volume in native Andeans during hypoxia and normoxia ClinAuton Res 20061640-45
59 Penaloza D Arias-Stella J The heart and pulmonary circulation athigh altitudes healthy highlanders and chronic mountain sicknessCirculation 20071151132-1146
60 Pei SX Chen XJ Si Ren BZ et al Chronic mountain sickness inTibet Q J Med 198971555-574
61 Wu TY Li W Li Y et al Epidemiology of chronic mountainsickness ten years study in Qinghai-Tibet In Ohno H KobayashiT Masuyama S Nakashima M editors Progress in MountainMedicine and High Altitude Physiology Matsumoto Press Com-mittee of the 3rd World Congress on Mountain Medicine and HighAltitude Physiology 1998 p 120-125
62 Sime F Penaloza D Ruiz L Bradycardia increased cardiac outputand reversal of pulmonary hypertension in altitude natives living atsea level Br Heart J 197133647-657
63 Allemann Y Sartori C Lepori M et al Echocardiographic andinvasive measurements of pulmonary artery pressure correlateclosely at high altitude Am J Physiol 2000279H2013-H2016
64 Kojonazarov BK Imanov BZ Amatov TA et al Noninvasive andinvasive evaluation of pulmonary arterial pressure in highlandersEur Respir J 200729352-356
65 Naeije R Torbicki A More on the noninvasive diagnosis ofpulmonary hypertension Doppler echocardiography revisited EurRespir J 199581445-1449
66 Tei C Dujardin KS Hodge DO et al Doppler echocardiographicindex for assessment of global right ventricular function J Am SocEchocardiogr 19969838-847
67 Harjai KJ Scott L Vivekananthan K et al The Tei index a newprognostic index for patients with symptomatic heart failure J AmSoc Echocardiogr 200215864-868
68 Maignan M Rivera-Ch M Privat C et al Pulmonary pressure andcardiac function in chronic mountain sickness patients Chest 2009135499-504
69 Cruz-Jibaja J Banchero N Sime F et al Correlation betweenpulmonary artery pressure and level of altitude Dis Chest 196446446-451
70 Wu T Chronic mountain sickness in Qinghai-Tibet China In Ge RHackett P editors Life on the Qinghai-Tibetan Plateau BeijingPekiacuten University Medical Press 2007 p 118-133
71 Arias-Stella J Saldana M The terminal portion of the pulmonaryarterial tree in people native to high altitudes Circulation 196328915-925
72 Maggiorini M Leon-Velarde F High-altitude pulmonary hyperten-sion a pathophysiological entity to different diseases Eur Respir J2003221019-1025
73 Smith T Balanos G Croft Q et al The increase in pulmonary arterialpressure caused by hypoxia depends on iron status J Physiol 20085865999-6005
74 Smith T Talbot N Privat C et al Effects of iron supplementationand depletion on hypoxic pulmonary hypertension two randomizedcontrolled trials JAMA 20093021444-1450
75 Rivera-Ch M Leon-Velarde F Huicho L Treatment of chronicmountain sickness critical reappraisal of an old problem RespirPhysiol Neurobiol 2007158251-265
76 Rivera-Ch M Huicho L Bouchet P et al Effect of acetazolamide onventilatory response in subjects with chronic mountain sicknessRespir Physiol Neurobiol 2008162184-189

546 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
4300 m patients showed a mean [Hb] of 231 plusmn 16 gdLarterial blood oxygen saturation (SaO2) of 81 plusmn 4 andPpa of 34 plusmn 10 mm Hg68
Pulmonary hypertension in CMS
The cause of HAPH is the increase in pulmonaryvascular resistance (PVR) the underlying mechanisminvolves sustained and exaggerated pulmonary vasocon-striction and remodeling of the pulmonary vascular wall inresponse to chronic hypoxia due to proliferation anddecreased apoptosis of pulmonary artery smooth musclecells The effects of chronic hypoxia on pulmonary arterypressure are reflected in the negative correlation that existsbetween Ppa and SaO2 at high altitude596970 Arterialhypoxemia in addition to hypoxic vasoconstriction leadsto several structural changes in the pulmonary vesselsincluding an increase in the number of intimal smoothmuscle cells medial thickening in the small musculararteries and fibrinoid necrosis of the vessel walls71 Thesestructural changes in the pulmonary vessels rather thanhypoxic vasoconstriction alone are believed to beresponsible for the sustained rise in Ppa in chronichypoxia Pioneering hemodynamic invasive studies byPentildealoza and Sime910 in 10 subjects with severe CMS at4300 m showed a mean [Hb] value of 247 plusmn 24 gdL amean SaO2 of 696 plusmn 49 and a Ppa of 47 plusmn 177 mmHg values that have made the authors conclude that thesepatients have a type of hypoxic cor pulmonale in contrastto the hypertensive cor pulmonale observed in primarypulmonary hypertension However the structural changes
Fig 4 Pulmonary vascular resistance index and pulmonary acceleration time intreatment with acetazolamide (Acz) The study was organized in 2 phases (1) a ran open-label phase where all patients received acetazolamide (Acz + Acz) Theet al 200939
in the pulmonary vessels which are responsible for thesustained rise in Ppa in chronic hypoxia can have differentintensities and different onset times depending on thelength of hypoxic exposure comprising a range fromshort-term to long-term7072
Maignan and coworkers68 have described cardiachemodynamics in approximately 50 CMS cases withnoninvasive methods and found varying intensities ofPpa Although they might have been studying patients inan early disease stage they observed mean pulmonaryacceleration time and accelerationejection time ratiossignificantly lower in CMS subjects than in SL and HAnatives (Fig 3) Pulmonary vascular index was foundlower in SL than in other groups and there was nosignificant difference between HA and CMS however thenumber of patients with PVR greater than 2 Wood unitswas higher in CMS (1242) than in SL (013) and tended tobe significant when compared to HA (115) (CMS vs SLP = 003 CMS vs HA P = 008 and SL vs HA P = 034)
Chronic hypoxia with appropriate acclimatization asseen in healthy HA residents induces an increase inPVR without change in pulmonary arterial systolicpressure right heart cavity dimensions or right systolicventricular function The increase in right ventricularTei index however could reflect early right ventricularimpairment68 When hypoxemia becomes severe asobserved in some patients with excessive Ppa a furtherimpairment can be found with a significant increase inpulmonary arterial systolic pressure and right cardiaccavity enlargement However contrary to the assumption59
of overt chronic cor pulmonale based on severe HAPHpatients with established HAPH did not show any
placebo and CMS patients groups before and after 3 and 6 months ofandomized double-blind placebo-controlled phase (placebo + Acz) and (2)2 phases were separated by a 4-week washout period Data from Richalet
547F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
obvious cardiac systolic dysfunction as shown byMaignan and coworkers68 This confirms the individualvariability of the severity of HAPH which is also highlydependent on risk factors and genetic susceptibilitydespite that for the moment no specific gene has beenclearly associated with the development of CMS Largeepidemiologic studies should be conducted to determinethe precise natural history prevalence and features ofheart failure in CMS
Recently an interaction between iron levels andhypoxia in the regulation of the pulmonary circulationhas been described73 The study showed that ironinfusion before an 8-hour exposure to sustained hypoxiaabolished or reduced greatly the elevation in baselinepulmonary artery systolic pressure and enhanced sensi-tivity of the pulmonary vasculature to acute hypoxia Thestudy also showed that iron chelation through deferox-amine infusion before the 8-hour hypoxia protocolelevates pulmonary artery systolic pressure significantlyThese findings led to conclude that iron availabilitymodifies pulmonary arterial pressure and pulmonaryvascular responses to hypoxia possibly through theinvolvement of the hypoxia-inducible factor hydroxyl-ation system
In a later study Smith and coworkers74 showed theeffect that iron levels could have on HA diseases thatinvolve pulmonary hypertension such as CMS This studyshowed that reduction of iron availability in CMS patientsthrough isovolemic bloodletting is associated with asubstantial increase in Ppa whereas iron supplementationis related to an attenuation of HAPH In view of the resultsthe authors suggest that this effect is consistent with thoseof acute iron chelation and thus implies that irondeficiency could exacerbate Ppa in chronic pulmonaryand cardiac disease and also that HAPH can be attenuatedby iron supplementation
It should be noted however that no long-termcontrolled studies have been carried out to evaluate allthe possible effectors related to the development ofHAPH Thus extensive research is required to determinewhich of the multiple elements that regulate Ppa at highaltitude might have a predominant role in determining thedifferent time courses and severity of HAPH
Treatment
Recently increasing attention is being drawn todifferent phenomena that may be involved in the causalchain of CMS and that were previously overlooked Theseinclude CMS risk and environmental factors such as earlyprenatal or postnatal exposure to different agents andorthe different genetic susceptibilities in different popula-tions and individuals However until having a complete
understanding of which mechanisms are better targetsfor intervention at present treatment is directed to thosecomponents of CMS pathophysiologic sequence thatare susceptible of modification through pharmacologicintervention that is on the erythropoietic response toreduce the increased red cell mass andor on the ventilatoryresponse These agents include methylxanthines adrener-gic blockers dopaminergic antagonists medroxyproges-terone peripheral ventilator stimulants such as almitrineand enalapril all of which have been tested experiment-ally75 Although phlebotomy has been shown to reducethe signs and symptoms of CMS its invasiveness andtransient effects often render it impractical
Descent to low altitudes is the ideal treatment and leadsto prompt improvement of signs and symptoms of CMSbut often patients cannot or do not want to descend tolower altitudes for economic personal andor familyreasons Recently acetazolamide has been used as animportant alternative for the treatment of CMS and itseffects have been studied in randomized placebo-controlled trials in the Peruvian Andes394376 The effectsof this carbonic anhydrase inhibitor in CMS include animprovement of ventilation through metabolic acidosisand of SaO2
76 thus causing a decrease in Epo concen-tration and excessive erythrocytosis In addition it leads toa decrease in PVR and an increase in pulmonaryacceleration time Furthermore the number of CMSpatients with pulmonary hypertension (defined by PVRN 2 Wood units) was 8 before treatment and nil aftertreatment (P = 0005) In fact the observed effect ofacetazolamide on PVR (minus17) might be indirectly due tothe decrease in blood viscosity (minus16) due to thereduction in hematocrit (Fig 4) Therefore at presentthese very encouraging results suggest that acetazolamidecould be a good alternative in the treatment of CMS3943
Statement of Conflict of Interest
All authors declare that there are no conflicts of interest
References
1 Pentildealoza D Sime F Banchero N et al Pulmonary hypertension inhealthy men born and living at high altitudes Am J Cardiol 196311150-157
2 Hurtado A Animals in high altitudes resident man In Dill DAdolph E Wilber C editors Handbook of physiology adaptation tothe environment Washington DC American Physiological Society1964 p 843-860
3 Monge-M C Monge-C C High altitude diseases mechanism andmanagement Springfield (Ill) Charles C Thomas 1966
4 Antezana G Barragaacuten L Coudert J et al The pulmonarycirculation of high altitude natives In Brendel W Zink R editorsHigh altitude physiology and medicine New York Springer-Verlag 1982 p 142-149
548 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
5 Monge C Chronic mountain sickness Physiol Rev 1943231666 Monge-M C Encinas E Heraud C et al La Enfermedad de los
Andes (Siacutendromes Eritreacutemicos) Imprenta Americana Lima1928
7 Monge-M C Sobre un caso de Enfermedad de Vaacutequez Paperpresented at Communicacioacuten presentada a la Academia Nacional deMedicina Lima Peru Academia Nacional de Medicina 1925
8 Hurtado A Chronic mountain sickness JAMA 19421201278-1282
9 Penaloza D Sime F Chronic cor pulmonale due to loss of altitudeacclimatization (chronic mountain sickness) Am J Med 197150728-743
10 Pentildealoza D Sime F Ruiz L Cor pulmonale in chronic mountainsickness present concept of Monges disease In Porter R Knight Jeditors High altitude physiology cardiac and respiratory aspectsEdinburgh Churchill Livingstone 1971 p 41-60
11 Beall CM Decker MJ Brittenham GM et al An Ethiopian pattern ofhuman adaptation to high-altitude hypoxia Proc Natl Acad Sci U S A20029917215-17218
12 Winslow RM Monge-C C Hypoxia polycythemia and chronicmountain sickness Baltimore (Md) Johns Hopkins University Press1987
13 Arregui A Cabrera J Leon-Velarde F et al High prevalence ofmigraine in a high-altitude population Neurology 1991411668-1669
14 Sorensen SC Lassen NA Severinghaus JW et al Cerebral glucosemetabolism and cerebral blood flow in high-altitude residents J ApplPhysiol 197437305-310
15 Massik J Tang YL Hudak ML et al Effect of hematocrit oncerebral blood flow with induced polycythemia J Appl Physiol1987621090-1096
16 Monge-M C La enfermedad de los Andes An Fac Med 19281-30917 Leon-Velarde F Maggiorini M Reeves JT et al Consensus
statement on chronic and subacute high altitude diseases High AltMed Biol 20056147-157
18 Leon-Velarde F Mejia O Gene expression in chronic high altitudediseases High Alt Med Biol 20089130-139
19 Monge-C C Leoacuten-Velarde F Arregui A Chronic mountain sicknessIn Lenfant C editor High altitude an exploration of humanadaptation New York Marcel Dekker Inc 2001 p 815-838
20 Kryger M McCullough R Doekel R et al Excessive polycythemiaof high altitude role of ventilatory drive and lung disease Am RevRespir Dis 1978118659-666
21 Severinghaus JW Bainton CR Carcelen A Respiratory insensitivityto hypoxia in chronically hypoxic man Respir Physiol 19661308-334
22 Vargas E Spielvogel H Chronic mountain sickness optimalhemoglobin and heart disease High Alt Med Biol 20067138-149
23 Liang PJ Bascom DA Robbins PA Extended models of theventilatory response to sustained isocapnic hypoxia in humansJ Appl Physiol 199782667-677
24 Leon-Velarde F Gamboa A Rivera-Ch M et al Selectedcontribution peripheral chemoreflex function in high-altitudenatives and patients with chronic mountain sickness J Appl Physiol2003941269-1278 discussion 1253-1264
25 Milledge JS Lahiri S Respiratory control in lowlanders and Sherpahighlanders at altitude Respir Physiol 19672310-322
26 Fatemian M Gamboa A Leon-Velarde F et al Plasticity inrespiratory motor control selected contribution ventilatory responseto CO2 in high-altitude natives and patients with chronic mountainsickness J Appl Physiol 2003941279-1287
27 Cunningham PA Wolf CB Integration of respiratory responses tochanges in alveolar partial pressures of CO2 and O2 and in arterialpH In Cherniack JG editor Handbook of physiologymdashtherespiratory system Bethesda (Md) American Physiological Society1986 p 475-528
28 Fatemian M Robbins PA Selected contribution chemoreflexresponses to CO2 before and after an 8-h exposure to hypoxia inhumans J Appl Physiol 2001901607-1614 discussion 1606
29 Robbins PA The ventilatory response of the human respiratorysystem to sine waves of alveolar carbon dioxide and hypoxiaJ Physiology 1984350461-474
30 Milledge JS Sorensen SC Cerebral arteriovenous oxygen differ-ence in man native to high altitude J Appl Physiol 197232687-689
31 Leon-Velarde F Richalet JP Respiratory control in residents at highaltitude physiology and pathophysiology High Alt Med Biol 20067125-137
32 Villafuerte FC Cardenas R Monge CC Optimal hemoglobinconcentration and high altitude a theoretical approach for Andeanmen at rest J Appl Physiol May 2004961581-1588
33 Reeves JT Leon-Velarde F Chronic mountain sickness recentstudies of the relationship between hemoglobin concentration andoxygen transport High Alt Med Biol 20045147-155
34 Winslow RM Monge CC Brown EG et al Effects of hemodilutionon O2 transport in high-altitude polycythemia J Appl Physiol 1985591495-1502
35 Cruz J Diaz C Marticorena E et al Phlebotomy improvespulmonary gas exchange in chronic mountain polycythemiaRespiration 197938305-313
36 Manier G Guenard H Castaing Y et al Pulmonary gas exchange inAndean natives with excessive polycythemiamdasheffect of hemodilu-tion J Appl Physiol 1988652107-2117
37 Ergueta J Spielvogel H Cudkowicz L Cardio-respiratory studies inchronic mountain sickness (Monges syndrome) Respiration 197128485-517
38 Rotta A Canepa A Hurtado A et al Pulmonary circulation at sealevel and at high altitude J Appl Physiol 195611143-149
39 Richalet JP Rivera-Ch M Maignan M et al Acetazolamide forMonges disease efficiency and tolerance of 6-month treatment AmJ Respir Crit Care Med 20081771370-1376
40 Richardson TQ Guyton AC Effects of polycythemia and anemia oncardiac output and other circulatory factors Am J Physiol 19591971167-1170
41 Guyton AC Richardson TQ Effect of hematocrit on venous returnCirc Res 19619157-164
42 Claydon VE Norcliffe LJ Moore JP et al Orthostatic tolerance andblood volumes in Andean high altitude dwellers Exp Physiol 200489565-571
43 Richalet JP Rivera M Bouchet P et al Acetazolamide a treatmentfor chronic mountain sickness Am J Respir Crit Care Med 20051721427-1433
44 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk III The thickness of the media of the pulmonary trunk andascending aorta in high altitude natives Circulation 1963271101-1104
45 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk II The evolution of the elastic configuration of the pulmonarytrunk in people native to high altitudes Circulation 1963271094-1100
46 Saldana M Arias-Stella J Studies on the structure of thepulmonary trunk I Normal changes in the elastic configurationof the human pulmonary trunk at different ages Circulation 1963271086-1093
47 Wagner KF Katschinski DM Hasegawa J et al Chronic inbornerythrocytosis leads to cardiac dysfunction and premature death inmice overexpressing erythropoietin Blood 200197536-542
48 Ruschitzka FT Wenger RH Stallmach T et al Nitric oxide preventscardiovascular disease and determines survival in polyglobulic miceoverexpressing erythropoietin Proc Natl Acad Sci U S A 20009711609-11613
549F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
49 Brown CM Hainsworth R Assessment of capillary fluidshifts during orthostatic stress in normal subjects andsubjects with orthostatic intolerance Clin Auton Res 1999969-73
50 Bush VE Wight VL Brown CM et al Vascular responses toorthostatic stress in patients with postural tachycardia syndrome(POTS) in patients with low orthostatic tolerance and inasymptomatic controls Clin Auton Res 200010279-284
51 Cooper VL Hainsworth R Effects of head-up tilting on baroreceptorcontrol in subjects with different tolerances to orthostatic stress ClinSci (Lond) 2002103221-226
52 Appenzeller O Thomas PK Ponsford S et al Acral paresthesias inthe Andes and neurology at sea level Neurology 2002591532-1535
53 Kwaan HC Wang J Hyperviscosity in polycythemia vera andother red cell abnormalities Semin Thromb Hemost 200329451-458
54 Claydon VE Norcliffe LJ Moore JP et al Cardiovascularresponses to orthostatic stress in healthy altitude dwellers andaltitude residents with chronic mountain sickness Exp Physiol200590103-110
55 Norcliffe LJ Rivera-Ch M Claydon VE et al Cerebrovascularresponses to hypoxia and hypocapnia in high-altitude dwellersJ Physiol 2005566(Pt 1)287-294
56 Moore JP Claydon VE Norcliffe LJ et al Carotid baroreflexregulation of vascular resistance in high-altitude Andean natives withand without chronic mountain sickness Exp Physiol 200691907-913
57 Antezana AM Richalet JP Noriega I et al Hormonal changes innormal and polycythemic high-altitude natives J Appl Physiol 199579795-800
58 Gamboa A Gamboa JL Holmes C et al Plasma catecholamines andblood volume in native Andeans during hypoxia and normoxia ClinAuton Res 20061640-45
59 Penaloza D Arias-Stella J The heart and pulmonary circulation athigh altitudes healthy highlanders and chronic mountain sicknessCirculation 20071151132-1146
60 Pei SX Chen XJ Si Ren BZ et al Chronic mountain sickness inTibet Q J Med 198971555-574
61 Wu TY Li W Li Y et al Epidemiology of chronic mountainsickness ten years study in Qinghai-Tibet In Ohno H KobayashiT Masuyama S Nakashima M editors Progress in MountainMedicine and High Altitude Physiology Matsumoto Press Com-mittee of the 3rd World Congress on Mountain Medicine and HighAltitude Physiology 1998 p 120-125
62 Sime F Penaloza D Ruiz L Bradycardia increased cardiac outputand reversal of pulmonary hypertension in altitude natives living atsea level Br Heart J 197133647-657
63 Allemann Y Sartori C Lepori M et al Echocardiographic andinvasive measurements of pulmonary artery pressure correlateclosely at high altitude Am J Physiol 2000279H2013-H2016
64 Kojonazarov BK Imanov BZ Amatov TA et al Noninvasive andinvasive evaluation of pulmonary arterial pressure in highlandersEur Respir J 200729352-356
65 Naeije R Torbicki A More on the noninvasive diagnosis ofpulmonary hypertension Doppler echocardiography revisited EurRespir J 199581445-1449
66 Tei C Dujardin KS Hodge DO et al Doppler echocardiographicindex for assessment of global right ventricular function J Am SocEchocardiogr 19969838-847
67 Harjai KJ Scott L Vivekananthan K et al The Tei index a newprognostic index for patients with symptomatic heart failure J AmSoc Echocardiogr 200215864-868
68 Maignan M Rivera-Ch M Privat C et al Pulmonary pressure andcardiac function in chronic mountain sickness patients Chest 2009135499-504
69 Cruz-Jibaja J Banchero N Sime F et al Correlation betweenpulmonary artery pressure and level of altitude Dis Chest 196446446-451
70 Wu T Chronic mountain sickness in Qinghai-Tibet China In Ge RHackett P editors Life on the Qinghai-Tibetan Plateau BeijingPekiacuten University Medical Press 2007 p 118-133
71 Arias-Stella J Saldana M The terminal portion of the pulmonaryarterial tree in people native to high altitudes Circulation 196328915-925
72 Maggiorini M Leon-Velarde F High-altitude pulmonary hyperten-sion a pathophysiological entity to different diseases Eur Respir J2003221019-1025
73 Smith T Balanos G Croft Q et al The increase in pulmonary arterialpressure caused by hypoxia depends on iron status J Physiol 20085865999-6005
74 Smith T Talbot N Privat C et al Effects of iron supplementationand depletion on hypoxic pulmonary hypertension two randomizedcontrolled trials JAMA 20093021444-1450
75 Rivera-Ch M Leon-Velarde F Huicho L Treatment of chronicmountain sickness critical reappraisal of an old problem RespirPhysiol Neurobiol 2007158251-265
76 Rivera-Ch M Huicho L Bouchet P et al Effect of acetazolamide onventilatory response in subjects with chronic mountain sicknessRespir Physiol Neurobiol 2008162184-189

547F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
obvious cardiac systolic dysfunction as shown byMaignan and coworkers68 This confirms the individualvariability of the severity of HAPH which is also highlydependent on risk factors and genetic susceptibilitydespite that for the moment no specific gene has beenclearly associated with the development of CMS Largeepidemiologic studies should be conducted to determinethe precise natural history prevalence and features ofheart failure in CMS
Recently an interaction between iron levels andhypoxia in the regulation of the pulmonary circulationhas been described73 The study showed that ironinfusion before an 8-hour exposure to sustained hypoxiaabolished or reduced greatly the elevation in baselinepulmonary artery systolic pressure and enhanced sensi-tivity of the pulmonary vasculature to acute hypoxia Thestudy also showed that iron chelation through deferox-amine infusion before the 8-hour hypoxia protocolelevates pulmonary artery systolic pressure significantlyThese findings led to conclude that iron availabilitymodifies pulmonary arterial pressure and pulmonaryvascular responses to hypoxia possibly through theinvolvement of the hypoxia-inducible factor hydroxyl-ation system
In a later study Smith and coworkers74 showed theeffect that iron levels could have on HA diseases thatinvolve pulmonary hypertension such as CMS This studyshowed that reduction of iron availability in CMS patientsthrough isovolemic bloodletting is associated with asubstantial increase in Ppa whereas iron supplementationis related to an attenuation of HAPH In view of the resultsthe authors suggest that this effect is consistent with thoseof acute iron chelation and thus implies that irondeficiency could exacerbate Ppa in chronic pulmonaryand cardiac disease and also that HAPH can be attenuatedby iron supplementation
It should be noted however that no long-termcontrolled studies have been carried out to evaluate allthe possible effectors related to the development ofHAPH Thus extensive research is required to determinewhich of the multiple elements that regulate Ppa at highaltitude might have a predominant role in determining thedifferent time courses and severity of HAPH
Treatment
Recently increasing attention is being drawn todifferent phenomena that may be involved in the causalchain of CMS and that were previously overlooked Theseinclude CMS risk and environmental factors such as earlyprenatal or postnatal exposure to different agents andorthe different genetic susceptibilities in different popula-tions and individuals However until having a complete
understanding of which mechanisms are better targetsfor intervention at present treatment is directed to thosecomponents of CMS pathophysiologic sequence thatare susceptible of modification through pharmacologicintervention that is on the erythropoietic response toreduce the increased red cell mass andor on the ventilatoryresponse These agents include methylxanthines adrener-gic blockers dopaminergic antagonists medroxyproges-terone peripheral ventilator stimulants such as almitrineand enalapril all of which have been tested experiment-ally75 Although phlebotomy has been shown to reducethe signs and symptoms of CMS its invasiveness andtransient effects often render it impractical
Descent to low altitudes is the ideal treatment and leadsto prompt improvement of signs and symptoms of CMSbut often patients cannot or do not want to descend tolower altitudes for economic personal andor familyreasons Recently acetazolamide has been used as animportant alternative for the treatment of CMS and itseffects have been studied in randomized placebo-controlled trials in the Peruvian Andes394376 The effectsof this carbonic anhydrase inhibitor in CMS include animprovement of ventilation through metabolic acidosisand of SaO2
76 thus causing a decrease in Epo concen-tration and excessive erythrocytosis In addition it leads toa decrease in PVR and an increase in pulmonaryacceleration time Furthermore the number of CMSpatients with pulmonary hypertension (defined by PVRN 2 Wood units) was 8 before treatment and nil aftertreatment (P = 0005) In fact the observed effect ofacetazolamide on PVR (minus17) might be indirectly due tothe decrease in blood viscosity (minus16) due to thereduction in hematocrit (Fig 4) Therefore at presentthese very encouraging results suggest that acetazolamidecould be a good alternative in the treatment of CMS3943
Statement of Conflict of Interest
All authors declare that there are no conflicts of interest
References
1 Pentildealoza D Sime F Banchero N et al Pulmonary hypertension inhealthy men born and living at high altitudes Am J Cardiol 196311150-157
2 Hurtado A Animals in high altitudes resident man In Dill DAdolph E Wilber C editors Handbook of physiology adaptation tothe environment Washington DC American Physiological Society1964 p 843-860
3 Monge-M C Monge-C C High altitude diseases mechanism andmanagement Springfield (Ill) Charles C Thomas 1966
4 Antezana G Barragaacuten L Coudert J et al The pulmonarycirculation of high altitude natives In Brendel W Zink R editorsHigh altitude physiology and medicine New York Springer-Verlag 1982 p 142-149
548 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
5 Monge C Chronic mountain sickness Physiol Rev 1943231666 Monge-M C Encinas E Heraud C et al La Enfermedad de los
Andes (Siacutendromes Eritreacutemicos) Imprenta Americana Lima1928
7 Monge-M C Sobre un caso de Enfermedad de Vaacutequez Paperpresented at Communicacioacuten presentada a la Academia Nacional deMedicina Lima Peru Academia Nacional de Medicina 1925
8 Hurtado A Chronic mountain sickness JAMA 19421201278-1282
9 Penaloza D Sime F Chronic cor pulmonale due to loss of altitudeacclimatization (chronic mountain sickness) Am J Med 197150728-743
10 Pentildealoza D Sime F Ruiz L Cor pulmonale in chronic mountainsickness present concept of Monges disease In Porter R Knight Jeditors High altitude physiology cardiac and respiratory aspectsEdinburgh Churchill Livingstone 1971 p 41-60
11 Beall CM Decker MJ Brittenham GM et al An Ethiopian pattern ofhuman adaptation to high-altitude hypoxia Proc Natl Acad Sci U S A20029917215-17218
12 Winslow RM Monge-C C Hypoxia polycythemia and chronicmountain sickness Baltimore (Md) Johns Hopkins University Press1987
13 Arregui A Cabrera J Leon-Velarde F et al High prevalence ofmigraine in a high-altitude population Neurology 1991411668-1669
14 Sorensen SC Lassen NA Severinghaus JW et al Cerebral glucosemetabolism and cerebral blood flow in high-altitude residents J ApplPhysiol 197437305-310
15 Massik J Tang YL Hudak ML et al Effect of hematocrit oncerebral blood flow with induced polycythemia J Appl Physiol1987621090-1096
16 Monge-M C La enfermedad de los Andes An Fac Med 19281-30917 Leon-Velarde F Maggiorini M Reeves JT et al Consensus
statement on chronic and subacute high altitude diseases High AltMed Biol 20056147-157
18 Leon-Velarde F Mejia O Gene expression in chronic high altitudediseases High Alt Med Biol 20089130-139
19 Monge-C C Leoacuten-Velarde F Arregui A Chronic mountain sicknessIn Lenfant C editor High altitude an exploration of humanadaptation New York Marcel Dekker Inc 2001 p 815-838
20 Kryger M McCullough R Doekel R et al Excessive polycythemiaof high altitude role of ventilatory drive and lung disease Am RevRespir Dis 1978118659-666
21 Severinghaus JW Bainton CR Carcelen A Respiratory insensitivityto hypoxia in chronically hypoxic man Respir Physiol 19661308-334
22 Vargas E Spielvogel H Chronic mountain sickness optimalhemoglobin and heart disease High Alt Med Biol 20067138-149
23 Liang PJ Bascom DA Robbins PA Extended models of theventilatory response to sustained isocapnic hypoxia in humansJ Appl Physiol 199782667-677
24 Leon-Velarde F Gamboa A Rivera-Ch M et al Selectedcontribution peripheral chemoreflex function in high-altitudenatives and patients with chronic mountain sickness J Appl Physiol2003941269-1278 discussion 1253-1264
25 Milledge JS Lahiri S Respiratory control in lowlanders and Sherpahighlanders at altitude Respir Physiol 19672310-322
26 Fatemian M Gamboa A Leon-Velarde F et al Plasticity inrespiratory motor control selected contribution ventilatory responseto CO2 in high-altitude natives and patients with chronic mountainsickness J Appl Physiol 2003941279-1287
27 Cunningham PA Wolf CB Integration of respiratory responses tochanges in alveolar partial pressures of CO2 and O2 and in arterialpH In Cherniack JG editor Handbook of physiologymdashtherespiratory system Bethesda (Md) American Physiological Society1986 p 475-528
28 Fatemian M Robbins PA Selected contribution chemoreflexresponses to CO2 before and after an 8-h exposure to hypoxia inhumans J Appl Physiol 2001901607-1614 discussion 1606
29 Robbins PA The ventilatory response of the human respiratorysystem to sine waves of alveolar carbon dioxide and hypoxiaJ Physiology 1984350461-474
30 Milledge JS Sorensen SC Cerebral arteriovenous oxygen differ-ence in man native to high altitude J Appl Physiol 197232687-689
31 Leon-Velarde F Richalet JP Respiratory control in residents at highaltitude physiology and pathophysiology High Alt Med Biol 20067125-137
32 Villafuerte FC Cardenas R Monge CC Optimal hemoglobinconcentration and high altitude a theoretical approach for Andeanmen at rest J Appl Physiol May 2004961581-1588
33 Reeves JT Leon-Velarde F Chronic mountain sickness recentstudies of the relationship between hemoglobin concentration andoxygen transport High Alt Med Biol 20045147-155
34 Winslow RM Monge CC Brown EG et al Effects of hemodilutionon O2 transport in high-altitude polycythemia J Appl Physiol 1985591495-1502
35 Cruz J Diaz C Marticorena E et al Phlebotomy improvespulmonary gas exchange in chronic mountain polycythemiaRespiration 197938305-313
36 Manier G Guenard H Castaing Y et al Pulmonary gas exchange inAndean natives with excessive polycythemiamdasheffect of hemodilu-tion J Appl Physiol 1988652107-2117
37 Ergueta J Spielvogel H Cudkowicz L Cardio-respiratory studies inchronic mountain sickness (Monges syndrome) Respiration 197128485-517
38 Rotta A Canepa A Hurtado A et al Pulmonary circulation at sealevel and at high altitude J Appl Physiol 195611143-149
39 Richalet JP Rivera-Ch M Maignan M et al Acetazolamide forMonges disease efficiency and tolerance of 6-month treatment AmJ Respir Crit Care Med 20081771370-1376
40 Richardson TQ Guyton AC Effects of polycythemia and anemia oncardiac output and other circulatory factors Am J Physiol 19591971167-1170
41 Guyton AC Richardson TQ Effect of hematocrit on venous returnCirc Res 19619157-164
42 Claydon VE Norcliffe LJ Moore JP et al Orthostatic tolerance andblood volumes in Andean high altitude dwellers Exp Physiol 200489565-571
43 Richalet JP Rivera M Bouchet P et al Acetazolamide a treatmentfor chronic mountain sickness Am J Respir Crit Care Med 20051721427-1433
44 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk III The thickness of the media of the pulmonary trunk andascending aorta in high altitude natives Circulation 1963271101-1104
45 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk II The evolution of the elastic configuration of the pulmonarytrunk in people native to high altitudes Circulation 1963271094-1100
46 Saldana M Arias-Stella J Studies on the structure of thepulmonary trunk I Normal changes in the elastic configurationof the human pulmonary trunk at different ages Circulation 1963271086-1093
47 Wagner KF Katschinski DM Hasegawa J et al Chronic inbornerythrocytosis leads to cardiac dysfunction and premature death inmice overexpressing erythropoietin Blood 200197536-542
48 Ruschitzka FT Wenger RH Stallmach T et al Nitric oxide preventscardiovascular disease and determines survival in polyglobulic miceoverexpressing erythropoietin Proc Natl Acad Sci U S A 20009711609-11613
549F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
49 Brown CM Hainsworth R Assessment of capillary fluidshifts during orthostatic stress in normal subjects andsubjects with orthostatic intolerance Clin Auton Res 1999969-73
50 Bush VE Wight VL Brown CM et al Vascular responses toorthostatic stress in patients with postural tachycardia syndrome(POTS) in patients with low orthostatic tolerance and inasymptomatic controls Clin Auton Res 200010279-284
51 Cooper VL Hainsworth R Effects of head-up tilting on baroreceptorcontrol in subjects with different tolerances to orthostatic stress ClinSci (Lond) 2002103221-226
52 Appenzeller O Thomas PK Ponsford S et al Acral paresthesias inthe Andes and neurology at sea level Neurology 2002591532-1535
53 Kwaan HC Wang J Hyperviscosity in polycythemia vera andother red cell abnormalities Semin Thromb Hemost 200329451-458
54 Claydon VE Norcliffe LJ Moore JP et al Cardiovascularresponses to orthostatic stress in healthy altitude dwellers andaltitude residents with chronic mountain sickness Exp Physiol200590103-110
55 Norcliffe LJ Rivera-Ch M Claydon VE et al Cerebrovascularresponses to hypoxia and hypocapnia in high-altitude dwellersJ Physiol 2005566(Pt 1)287-294
56 Moore JP Claydon VE Norcliffe LJ et al Carotid baroreflexregulation of vascular resistance in high-altitude Andean natives withand without chronic mountain sickness Exp Physiol 200691907-913
57 Antezana AM Richalet JP Noriega I et al Hormonal changes innormal and polycythemic high-altitude natives J Appl Physiol 199579795-800
58 Gamboa A Gamboa JL Holmes C et al Plasma catecholamines andblood volume in native Andeans during hypoxia and normoxia ClinAuton Res 20061640-45
59 Penaloza D Arias-Stella J The heart and pulmonary circulation athigh altitudes healthy highlanders and chronic mountain sicknessCirculation 20071151132-1146
60 Pei SX Chen XJ Si Ren BZ et al Chronic mountain sickness inTibet Q J Med 198971555-574
61 Wu TY Li W Li Y et al Epidemiology of chronic mountainsickness ten years study in Qinghai-Tibet In Ohno H KobayashiT Masuyama S Nakashima M editors Progress in MountainMedicine and High Altitude Physiology Matsumoto Press Com-mittee of the 3rd World Congress on Mountain Medicine and HighAltitude Physiology 1998 p 120-125
62 Sime F Penaloza D Ruiz L Bradycardia increased cardiac outputand reversal of pulmonary hypertension in altitude natives living atsea level Br Heart J 197133647-657
63 Allemann Y Sartori C Lepori M et al Echocardiographic andinvasive measurements of pulmonary artery pressure correlateclosely at high altitude Am J Physiol 2000279H2013-H2016
64 Kojonazarov BK Imanov BZ Amatov TA et al Noninvasive andinvasive evaluation of pulmonary arterial pressure in highlandersEur Respir J 200729352-356
65 Naeije R Torbicki A More on the noninvasive diagnosis ofpulmonary hypertension Doppler echocardiography revisited EurRespir J 199581445-1449
66 Tei C Dujardin KS Hodge DO et al Doppler echocardiographicindex for assessment of global right ventricular function J Am SocEchocardiogr 19969838-847
67 Harjai KJ Scott L Vivekananthan K et al The Tei index a newprognostic index for patients with symptomatic heart failure J AmSoc Echocardiogr 200215864-868
68 Maignan M Rivera-Ch M Privat C et al Pulmonary pressure andcardiac function in chronic mountain sickness patients Chest 2009135499-504
69 Cruz-Jibaja J Banchero N Sime F et al Correlation betweenpulmonary artery pressure and level of altitude Dis Chest 196446446-451
70 Wu T Chronic mountain sickness in Qinghai-Tibet China In Ge RHackett P editors Life on the Qinghai-Tibetan Plateau BeijingPekiacuten University Medical Press 2007 p 118-133
71 Arias-Stella J Saldana M The terminal portion of the pulmonaryarterial tree in people native to high altitudes Circulation 196328915-925
72 Maggiorini M Leon-Velarde F High-altitude pulmonary hyperten-sion a pathophysiological entity to different diseases Eur Respir J2003221019-1025
73 Smith T Balanos G Croft Q et al The increase in pulmonary arterialpressure caused by hypoxia depends on iron status J Physiol 20085865999-6005
74 Smith T Talbot N Privat C et al Effects of iron supplementationand depletion on hypoxic pulmonary hypertension two randomizedcontrolled trials JAMA 20093021444-1450
75 Rivera-Ch M Leon-Velarde F Huicho L Treatment of chronicmountain sickness critical reappraisal of an old problem RespirPhysiol Neurobiol 2007158251-265
76 Rivera-Ch M Huicho L Bouchet P et al Effect of acetazolamide onventilatory response in subjects with chronic mountain sicknessRespir Physiol Neurobiol 2008162184-189

548 F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
5 Monge C Chronic mountain sickness Physiol Rev 1943231666 Monge-M C Encinas E Heraud C et al La Enfermedad de los
Andes (Siacutendromes Eritreacutemicos) Imprenta Americana Lima1928
7 Monge-M C Sobre un caso de Enfermedad de Vaacutequez Paperpresented at Communicacioacuten presentada a la Academia Nacional deMedicina Lima Peru Academia Nacional de Medicina 1925
8 Hurtado A Chronic mountain sickness JAMA 19421201278-1282
9 Penaloza D Sime F Chronic cor pulmonale due to loss of altitudeacclimatization (chronic mountain sickness) Am J Med 197150728-743
10 Pentildealoza D Sime F Ruiz L Cor pulmonale in chronic mountainsickness present concept of Monges disease In Porter R Knight Jeditors High altitude physiology cardiac and respiratory aspectsEdinburgh Churchill Livingstone 1971 p 41-60
11 Beall CM Decker MJ Brittenham GM et al An Ethiopian pattern ofhuman adaptation to high-altitude hypoxia Proc Natl Acad Sci U S A20029917215-17218
12 Winslow RM Monge-C C Hypoxia polycythemia and chronicmountain sickness Baltimore (Md) Johns Hopkins University Press1987
13 Arregui A Cabrera J Leon-Velarde F et al High prevalence ofmigraine in a high-altitude population Neurology 1991411668-1669
14 Sorensen SC Lassen NA Severinghaus JW et al Cerebral glucosemetabolism and cerebral blood flow in high-altitude residents J ApplPhysiol 197437305-310
15 Massik J Tang YL Hudak ML et al Effect of hematocrit oncerebral blood flow with induced polycythemia J Appl Physiol1987621090-1096
16 Monge-M C La enfermedad de los Andes An Fac Med 19281-30917 Leon-Velarde F Maggiorini M Reeves JT et al Consensus
statement on chronic and subacute high altitude diseases High AltMed Biol 20056147-157
18 Leon-Velarde F Mejia O Gene expression in chronic high altitudediseases High Alt Med Biol 20089130-139
19 Monge-C C Leoacuten-Velarde F Arregui A Chronic mountain sicknessIn Lenfant C editor High altitude an exploration of humanadaptation New York Marcel Dekker Inc 2001 p 815-838
20 Kryger M McCullough R Doekel R et al Excessive polycythemiaof high altitude role of ventilatory drive and lung disease Am RevRespir Dis 1978118659-666
21 Severinghaus JW Bainton CR Carcelen A Respiratory insensitivityto hypoxia in chronically hypoxic man Respir Physiol 19661308-334
22 Vargas E Spielvogel H Chronic mountain sickness optimalhemoglobin and heart disease High Alt Med Biol 20067138-149
23 Liang PJ Bascom DA Robbins PA Extended models of theventilatory response to sustained isocapnic hypoxia in humansJ Appl Physiol 199782667-677
24 Leon-Velarde F Gamboa A Rivera-Ch M et al Selectedcontribution peripheral chemoreflex function in high-altitudenatives and patients with chronic mountain sickness J Appl Physiol2003941269-1278 discussion 1253-1264
25 Milledge JS Lahiri S Respiratory control in lowlanders and Sherpahighlanders at altitude Respir Physiol 19672310-322
26 Fatemian M Gamboa A Leon-Velarde F et al Plasticity inrespiratory motor control selected contribution ventilatory responseto CO2 in high-altitude natives and patients with chronic mountainsickness J Appl Physiol 2003941279-1287
27 Cunningham PA Wolf CB Integration of respiratory responses tochanges in alveolar partial pressures of CO2 and O2 and in arterialpH In Cherniack JG editor Handbook of physiologymdashtherespiratory system Bethesda (Md) American Physiological Society1986 p 475-528
28 Fatemian M Robbins PA Selected contribution chemoreflexresponses to CO2 before and after an 8-h exposure to hypoxia inhumans J Appl Physiol 2001901607-1614 discussion 1606
29 Robbins PA The ventilatory response of the human respiratorysystem to sine waves of alveolar carbon dioxide and hypoxiaJ Physiology 1984350461-474
30 Milledge JS Sorensen SC Cerebral arteriovenous oxygen differ-ence in man native to high altitude J Appl Physiol 197232687-689
31 Leon-Velarde F Richalet JP Respiratory control in residents at highaltitude physiology and pathophysiology High Alt Med Biol 20067125-137
32 Villafuerte FC Cardenas R Monge CC Optimal hemoglobinconcentration and high altitude a theoretical approach for Andeanmen at rest J Appl Physiol May 2004961581-1588
33 Reeves JT Leon-Velarde F Chronic mountain sickness recentstudies of the relationship between hemoglobin concentration andoxygen transport High Alt Med Biol 20045147-155
34 Winslow RM Monge CC Brown EG et al Effects of hemodilutionon O2 transport in high-altitude polycythemia J Appl Physiol 1985591495-1502
35 Cruz J Diaz C Marticorena E et al Phlebotomy improvespulmonary gas exchange in chronic mountain polycythemiaRespiration 197938305-313
36 Manier G Guenard H Castaing Y et al Pulmonary gas exchange inAndean natives with excessive polycythemiamdasheffect of hemodilu-tion J Appl Physiol 1988652107-2117
37 Ergueta J Spielvogel H Cudkowicz L Cardio-respiratory studies inchronic mountain sickness (Monges syndrome) Respiration 197128485-517
38 Rotta A Canepa A Hurtado A et al Pulmonary circulation at sealevel and at high altitude J Appl Physiol 195611143-149
39 Richalet JP Rivera-Ch M Maignan M et al Acetazolamide forMonges disease efficiency and tolerance of 6-month treatment AmJ Respir Crit Care Med 20081771370-1376
40 Richardson TQ Guyton AC Effects of polycythemia and anemia oncardiac output and other circulatory factors Am J Physiol 19591971167-1170
41 Guyton AC Richardson TQ Effect of hematocrit on venous returnCirc Res 19619157-164
42 Claydon VE Norcliffe LJ Moore JP et al Orthostatic tolerance andblood volumes in Andean high altitude dwellers Exp Physiol 200489565-571
43 Richalet JP Rivera M Bouchet P et al Acetazolamide a treatmentfor chronic mountain sickness Am J Respir Crit Care Med 20051721427-1433
44 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk III The thickness of the media of the pulmonary trunk andascending aorta in high altitude natives Circulation 1963271101-1104
45 Saldana M Arias-Stella J Studies on the structure of the pulmonarytrunk II The evolution of the elastic configuration of the pulmonarytrunk in people native to high altitudes Circulation 1963271094-1100
46 Saldana M Arias-Stella J Studies on the structure of thepulmonary trunk I Normal changes in the elastic configurationof the human pulmonary trunk at different ages Circulation 1963271086-1093
47 Wagner KF Katschinski DM Hasegawa J et al Chronic inbornerythrocytosis leads to cardiac dysfunction and premature death inmice overexpressing erythropoietin Blood 200197536-542
48 Ruschitzka FT Wenger RH Stallmach T et al Nitric oxide preventscardiovascular disease and determines survival in polyglobulic miceoverexpressing erythropoietin Proc Natl Acad Sci U S A 20009711609-11613
549F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
49 Brown CM Hainsworth R Assessment of capillary fluidshifts during orthostatic stress in normal subjects andsubjects with orthostatic intolerance Clin Auton Res 1999969-73
50 Bush VE Wight VL Brown CM et al Vascular responses toorthostatic stress in patients with postural tachycardia syndrome(POTS) in patients with low orthostatic tolerance and inasymptomatic controls Clin Auton Res 200010279-284
51 Cooper VL Hainsworth R Effects of head-up tilting on baroreceptorcontrol in subjects with different tolerances to orthostatic stress ClinSci (Lond) 2002103221-226
52 Appenzeller O Thomas PK Ponsford S et al Acral paresthesias inthe Andes and neurology at sea level Neurology 2002591532-1535
53 Kwaan HC Wang J Hyperviscosity in polycythemia vera andother red cell abnormalities Semin Thromb Hemost 200329451-458
54 Claydon VE Norcliffe LJ Moore JP et al Cardiovascularresponses to orthostatic stress in healthy altitude dwellers andaltitude residents with chronic mountain sickness Exp Physiol200590103-110
55 Norcliffe LJ Rivera-Ch M Claydon VE et al Cerebrovascularresponses to hypoxia and hypocapnia in high-altitude dwellersJ Physiol 2005566(Pt 1)287-294
56 Moore JP Claydon VE Norcliffe LJ et al Carotid baroreflexregulation of vascular resistance in high-altitude Andean natives withand without chronic mountain sickness Exp Physiol 200691907-913
57 Antezana AM Richalet JP Noriega I et al Hormonal changes innormal and polycythemic high-altitude natives J Appl Physiol 199579795-800
58 Gamboa A Gamboa JL Holmes C et al Plasma catecholamines andblood volume in native Andeans during hypoxia and normoxia ClinAuton Res 20061640-45
59 Penaloza D Arias-Stella J The heart and pulmonary circulation athigh altitudes healthy highlanders and chronic mountain sicknessCirculation 20071151132-1146
60 Pei SX Chen XJ Si Ren BZ et al Chronic mountain sickness inTibet Q J Med 198971555-574
61 Wu TY Li W Li Y et al Epidemiology of chronic mountainsickness ten years study in Qinghai-Tibet In Ohno H KobayashiT Masuyama S Nakashima M editors Progress in MountainMedicine and High Altitude Physiology Matsumoto Press Com-mittee of the 3rd World Congress on Mountain Medicine and HighAltitude Physiology 1998 p 120-125
62 Sime F Penaloza D Ruiz L Bradycardia increased cardiac outputand reversal of pulmonary hypertension in altitude natives living atsea level Br Heart J 197133647-657
63 Allemann Y Sartori C Lepori M et al Echocardiographic andinvasive measurements of pulmonary artery pressure correlateclosely at high altitude Am J Physiol 2000279H2013-H2016
64 Kojonazarov BK Imanov BZ Amatov TA et al Noninvasive andinvasive evaluation of pulmonary arterial pressure in highlandersEur Respir J 200729352-356
65 Naeije R Torbicki A More on the noninvasive diagnosis ofpulmonary hypertension Doppler echocardiography revisited EurRespir J 199581445-1449
66 Tei C Dujardin KS Hodge DO et al Doppler echocardiographicindex for assessment of global right ventricular function J Am SocEchocardiogr 19969838-847
67 Harjai KJ Scott L Vivekananthan K et al The Tei index a newprognostic index for patients with symptomatic heart failure J AmSoc Echocardiogr 200215864-868
68 Maignan M Rivera-Ch M Privat C et al Pulmonary pressure andcardiac function in chronic mountain sickness patients Chest 2009135499-504
69 Cruz-Jibaja J Banchero N Sime F et al Correlation betweenpulmonary artery pressure and level of altitude Dis Chest 196446446-451
70 Wu T Chronic mountain sickness in Qinghai-Tibet China In Ge RHackett P editors Life on the Qinghai-Tibetan Plateau BeijingPekiacuten University Medical Press 2007 p 118-133
71 Arias-Stella J Saldana M The terminal portion of the pulmonaryarterial tree in people native to high altitudes Circulation 196328915-925
72 Maggiorini M Leon-Velarde F High-altitude pulmonary hyperten-sion a pathophysiological entity to different diseases Eur Respir J2003221019-1025
73 Smith T Balanos G Croft Q et al The increase in pulmonary arterialpressure caused by hypoxia depends on iron status J Physiol 20085865999-6005
74 Smith T Talbot N Privat C et al Effects of iron supplementationand depletion on hypoxic pulmonary hypertension two randomizedcontrolled trials JAMA 20093021444-1450
75 Rivera-Ch M Leon-Velarde F Huicho L Treatment of chronicmountain sickness critical reappraisal of an old problem RespirPhysiol Neurobiol 2007158251-265
76 Rivera-Ch M Huicho L Bouchet P et al Effect of acetazolamide onventilatory response in subjects with chronic mountain sicknessRespir Physiol Neurobiol 2008162184-189

549F Leoacuten-Velarde et al Progress in Cardiovascular Diseases 52 (2010) 540ndash549
49 Brown CM Hainsworth R Assessment of capillary fluidshifts during orthostatic stress in normal subjects andsubjects with orthostatic intolerance Clin Auton Res 1999969-73
50 Bush VE Wight VL Brown CM et al Vascular responses toorthostatic stress in patients with postural tachycardia syndrome(POTS) in patients with low orthostatic tolerance and inasymptomatic controls Clin Auton Res 200010279-284
51 Cooper VL Hainsworth R Effects of head-up tilting on baroreceptorcontrol in subjects with different tolerances to orthostatic stress ClinSci (Lond) 2002103221-226
52 Appenzeller O Thomas PK Ponsford S et al Acral paresthesias inthe Andes and neurology at sea level Neurology 2002591532-1535
53 Kwaan HC Wang J Hyperviscosity in polycythemia vera andother red cell abnormalities Semin Thromb Hemost 200329451-458
54 Claydon VE Norcliffe LJ Moore JP et al Cardiovascularresponses to orthostatic stress in healthy altitude dwellers andaltitude residents with chronic mountain sickness Exp Physiol200590103-110
55 Norcliffe LJ Rivera-Ch M Claydon VE et al Cerebrovascularresponses to hypoxia and hypocapnia in high-altitude dwellersJ Physiol 2005566(Pt 1)287-294
56 Moore JP Claydon VE Norcliffe LJ et al Carotid baroreflexregulation of vascular resistance in high-altitude Andean natives withand without chronic mountain sickness Exp Physiol 200691907-913
57 Antezana AM Richalet JP Noriega I et al Hormonal changes innormal and polycythemic high-altitude natives J Appl Physiol 199579795-800
58 Gamboa A Gamboa JL Holmes C et al Plasma catecholamines andblood volume in native Andeans during hypoxia and normoxia ClinAuton Res 20061640-45
59 Penaloza D Arias-Stella J The heart and pulmonary circulation athigh altitudes healthy highlanders and chronic mountain sicknessCirculation 20071151132-1146
60 Pei SX Chen XJ Si Ren BZ et al Chronic mountain sickness inTibet Q J Med 198971555-574
61 Wu TY Li W Li Y et al Epidemiology of chronic mountainsickness ten years study in Qinghai-Tibet In Ohno H KobayashiT Masuyama S Nakashima M editors Progress in MountainMedicine and High Altitude Physiology Matsumoto Press Com-mittee of the 3rd World Congress on Mountain Medicine and HighAltitude Physiology 1998 p 120-125
62 Sime F Penaloza D Ruiz L Bradycardia increased cardiac outputand reversal of pulmonary hypertension in altitude natives living atsea level Br Heart J 197133647-657
63 Allemann Y Sartori C Lepori M et al Echocardiographic andinvasive measurements of pulmonary artery pressure correlateclosely at high altitude Am J Physiol 2000279H2013-H2016
64 Kojonazarov BK Imanov BZ Amatov TA et al Noninvasive andinvasive evaluation of pulmonary arterial pressure in highlandersEur Respir J 200729352-356
65 Naeije R Torbicki A More on the noninvasive diagnosis ofpulmonary hypertension Doppler echocardiography revisited EurRespir J 199581445-1449
66 Tei C Dujardin KS Hodge DO et al Doppler echocardiographicindex for assessment of global right ventricular function J Am SocEchocardiogr 19969838-847
67 Harjai KJ Scott L Vivekananthan K et al The Tei index a newprognostic index for patients with symptomatic heart failure J AmSoc Echocardiogr 200215864-868
68 Maignan M Rivera-Ch M Privat C et al Pulmonary pressure andcardiac function in chronic mountain sickness patients Chest 2009135499-504
69 Cruz-Jibaja J Banchero N Sime F et al Correlation betweenpulmonary artery pressure and level of altitude Dis Chest 196446446-451
70 Wu T Chronic mountain sickness in Qinghai-Tibet China In Ge RHackett P editors Life on the Qinghai-Tibetan Plateau BeijingPekiacuten University Medical Press 2007 p 118-133
71 Arias-Stella J Saldana M The terminal portion of the pulmonaryarterial tree in people native to high altitudes Circulation 196328915-925
72 Maggiorini M Leon-Velarde F High-altitude pulmonary hyperten-sion a pathophysiological entity to different diseases Eur Respir J2003221019-1025
73 Smith T Balanos G Croft Q et al The increase in pulmonary arterialpressure caused by hypoxia depends on iron status J Physiol 20085865999-6005
74 Smith T Talbot N Privat C et al Effects of iron supplementationand depletion on hypoxic pulmonary hypertension two randomizedcontrolled trials JAMA 20093021444-1450
75 Rivera-Ch M Leon-Velarde F Huicho L Treatment of chronicmountain sickness critical reappraisal of an old problem RespirPhysiol Neurobiol 2007158251-265
76 Rivera-Ch M Huicho L Bouchet P et al Effect of acetazolamide onventilatory response in subjects with chronic mountain sicknessRespir Physiol Neurobiol 2008162184-189