Urinary cytokine profiles according to the site of blockade of ...
Upload
independentCategory
view
6download
0
Chronic Endothelin-A Receptor Blockade
in Lambs with Increased Pulmonary Blood Flow and Pressure
Sohrab Fratz1,2, Barbara Meyrick3, Boaz Ovadia2, Michael J. Johengen2, Olaf Reinhartz2,
Anthony Azakie2, Greg Ross2, Robert Fitzgerald2, Peter Oishi2, John Hess1, Stephen M. Black4,
Jeffrey R. Fineman2
1) Department of Pediatric Cardiology and Congenital Heart Disease, Deutsches Herzzentrum
München, Munich, Germany
2) Department of Pediatrics and the Cardiovascular Research Institute, University of California, San
Francisco, CA, USA
3) Departments of Pathology and Medicine Vanderbilt University, Nashville, TN, USA
4) Department of Biomedical and Pharmaceutical Sciences, University of Montana, Missoula, MT,
USA.
Running head: ETA block and increased pulmonary blood flow
Contact information: Sohrab Fratz, MD, Dept. of Pediatric Cardiology and Congenital Heart Disease,
Deutsches Herzzentrum München, Klinik an der Technischen Universität München, Lazarettstr. 36,
80636 Munich, Germany. E-mail: [email protected]; Phone: +49 89 1218 3031; Fax: +49 89 1218 3013.
Articles in PresS. Am J Physiol Lung Cell Mol Physiol (May 21, 2004). 10.1152/ajplung.00093.2004
Copyright © 2004 by the American Physiological Society.

ETA block and increased pulmonary blood flow 1
ABSTRACT
Endothelin-receptor blockade is an emerging therapy for pulmonary hypertension. However,
hemodynamic and structural effects and potential changes in endogenous NO-cGMP and endothelin-1
signalling of chronic endothelinA-receptor blockade in pulmonary hypertension secondary to congenital
heart disease are unknown. Therefore the objectives of this study were to determine hemodynamic and
structural effects and potential changes in endogenous NO-cGMP and endothelin-1 signalling of chronic
endothelinA-receptor blockade in a lamb model of increased pulmonary blood flow following in-utero
placement of an aortopulmonary shunt. Immediately after spontaneous birth shunt-lambs were treated
lifelong with either an endothelinA-receptor antagonist (PD156707) or placebo. At four weeks age,
PD156707-treated shunt-lambs (n=6) had lower pulmonary vascular resistance and right atrial pressure
than placebo-treated shunt-lambs (n=8) (p<0.05). Smooth muscle thickness or arterial number per unit
area was not different between the two groups. However, the number of alveolar profiles per unit area
was increased in the PD156707-treated shunt-lambs (190.7±5.6 vs. 132.9±10.0, p<0.05). Plasma
endothelin-1 and cGMP levels, and lung NOS activity, cGMP, eNOS, preproendothelin-1, endothelin-
converting-enzyme-1, endothelinA and endothelinB-receptors protein levels were similar in both groups.
We conclude that chronic endothelinA-receptor blockade attenuates the progression of pulmonary
hypertension and augments alveolar growth in lambs with increased pulmonary blood flow.
Key Words: Endothelin; Pulmonary Heart Disease; Congenital Heart Defect

ETA block and increased pulmonary blood flow 2
INTRODUCTION
Altered pulmonary vascular reactivity and pulmonary hypertension is a common accompaniment
of congenital heart disease with increased pulmonary blood flow1. Normal pulmonary vascular tone and
vascular smooth muscle cell proliferation is regulated by a complex interaction of vasoactive substances
that are locally produced by the vascular endothelium, such as nitric oxide (NO) and endothelin-1 (ET-
1)2-4. Endothelial injury secondary to increased pulmonary blood flow and/or pressure disrupts these
regulatory mechanisms, and is a potential factor in the development of pulmonary hypertension secondary
to congenital heart disease5,6.
ET-1 is a 21 amino acid polypeptide produced by vascular endothelial cells that has potent
vasoactive properties, and is co-mitogenic for vascular smooth muscle cells4,7. Recent data suggest a role
for ET-1 in the pathophysiology of pulmonary hypertension. For example, ET-1 concentrations are
increased in children with increased pulmonary blood flow and pulmonary hypertension, and preproET-1
gene expression is increased in adults with advanced pulmonary vascular disease6,8,9. In addition, chronic
endothelin receptor blockade has demonstrated clinical improvement in adults with advanced pulmonary
vascular disease10. However, the early role of ET-1 in the pathophysiology of pulmonary hypertension
secondary to congenital heart disease with increased pulmonary blood flow remains unclear11. In addition,
the potential effects of chronic ET receptor blockade on endogenous endothelial signaling are unknown.
To better define the role of ET-1 in the pathogenesis of pulmonary hypertension, we established a
model of pulmonary hypertension with increased pulmonary blood flow in the lamb, following in utero
placement of an aorta-to-pulmonary vascular graft. At one month of age, these lambs (shunt-lambs) have
a pulmonary to systemic blood flow ratio of approximately 2:1, a mean pulmonary arterial pressure that is
50% of mean systemic arterial pressure, and pulmonary vascular remodeling characteristic of children

ETA block and increased pulmonary blood flow 3
with pulmonary hypertension and increased pulmonary blood flow12. Previously, we demonstrated that
shunt lambs display alterations in the ET-1 cascade at 4 weeks of age. These include increased plasma
ET-1 levels, decreased ETB receptor protein with loss of ETB receptor-mediated vasodilation, and
increased ETA receptor protein with augmentation of ETA receptor-mediated vasoconstriction, suggesting
a role for ET-1 in the pathophysiology of pulmonary hypertension secondary to increased pulmonary
blood flow13,14.
The objectives of this study were to determine the role of ETA receptor activity in the early
progression of pulmonary hypertension secondary to congenital heart disease with increased pulmonary
blood flow, and determine the potential effects of ET receptor blockade on endothelial signaling.
Therefore, we studied the effects of chronically administered PD156707 (an ETA receptor antagonist), or
placebo, in our lamb model of congenital heart disease. Four weeks after spontaneous delivery of the
lambs, hemodynamic variables, ET-1-induced vasoactive responses, and pulmonary artery morphology
were determined and compared. In addition, potential alterations in the endogenous NO-cGMP and ET-1
pathways induced by chronic ETA receptor blockade were determined by comparing plasma ET-1, plasma
and lung tissue NOx and cGMP levels, cGMP levels, tissue nitric oxide synthase [NOS] activity, and
tissue endothelial NOS, preproET-1, ECE-1, and ETA and ETB receptor protein levels in lambs with and
without ET receptor blockade.

ETA block and increased pulmonary blood flow 4
METHODS
Surgical Preparation and Care
Ewes
Twenty mixed-breed Western pregnant ewes (135-141 days gestation, term = 145 days) were operated on
as previously described12-14.
Lambs
Before spontaneous delivery, the lambs were randomly divided into a treatment and a placebo
group. The treatment group (n=12) received PD156707, an ETA receptor antagonist diluted in water (150
mg/kg/d). The placebo group (n=8) received daily water. All treatments were started within 12 hours of
spontaneous delivery, and continued for 4 weeks. The lambs were weighed daily and the respiratory rate
and heart rates were obtained weekly by a animal care nurse who was blinded to the therapy. Furosemide
(1 mg/kg IM) was administered twice daily. At 4 weeks of age, vascular pressures and flow was measured
as previously described13,14.
Experimental Protocol
After baseline measurements of the hemodynamic variables were obtained, ET-1 (250 µg/kg) was
injected into the pulmonary artery over 1 minute. The hemodynamic variables were measured
continuously.

ETA block and increased pulmonary blood flow 5
Tissue preparation
Blocks of tissue of the left lung were removed and stored for later Western Blot analysis.
Additionally, in five of the PD156707-treated shunt-lambs and five of the placebo-treated shunt-lambs,
the pulmonary arterial bed of the right lung was distended with a barium gelatin suspension and the lungs
were inflated by way of the trachea with formalin and placed in a bath of formalin for fixation.
Six random blocks for routine light microscopic examination were taken from each left lung. The
sections were then examined for the characteristic structural changes of chronic pulmonary hypertension
by the use of well-established quantitative techniques15,16. Briefly, external diameter of at least 100 arterial
profiles was measured as well as medial thickness of the muscular and partially muscular arteries. Medial
thickness was then related to arterial size using the calculation: percent medial thickness = 2 X medial
thickness/external diameter X 100. The structure of each artery was also noted -- muscular, partially
muscular, nonmuscular -- as was the structure of the accompanying airway -- bronchus, bronchiolus,
terminal bronchiolus, respiratory bronchiolus, alveolar duct, and alveolar wall. The density of the barium
filled intraacinar arteries was also assessed. Using a X 25 objective and an eyepiece reticule, the number
of barium filled arteries of less than 200 µm external diameter was counted and related to the number of
alveolar profiles in these same fields. Lastly, the number of alveolar per unit area were counted. At least
25 consecutive microscopic fields were counted for each animal.
Plasma and Tissue Determinations
Blood samples were assayed for immunoreactive endothelin (irET-1) as previously described13.
Blood samples and tissue were assayed with a cGMP [125I] assay kit (Amersham International
plc, Amersham UK) according to manufacturers instructions17.

ETA block and increased pulmonary blood flow 6
Utilizing a vanadium (III) and hydrochloric acid reduction, total NO, nitrite, and nitrate (NOx)
were detected by chemiluminescence (NOA 280, Sievers Instruments Inc. Boulder CO) in blood samples
and lung tissue18.
NOS activity in the lung tissue was determined by using the conversion of 3H-arginine to 3H-
citrulline as previously described19.
Western Blot Analysis
Western blot analysis (ETA and ETB receptor, prepro-Endothelin-1, ECE-1, endothelial NOS) was
performed as previously described14.
Statistical Analysis
The mean ± standard deviation was calculated for the hemodynamic variables, systemic arterial
blood gases and pH and ET-1 levels, structural changes, cGMP, NOx, and NOS activity. Comparisons
were made by the paired t-test using the Bonferroni correction, the unpaired t-test or ANOVA for
repeated measures with multiple comparison testing.
Quantitation of autoradiographic results was performed by scanning the bands of interest into an
image editing software program (Adobe Photoshop, Adobe Systems, Mt. View, CA). The means ±
standard deviation was calculated for the relative protein. Protein and structural data were compared by
the unpaired t-test. A P < 0.05 was considered statistically significant.

ETA block and increased pulmonary blood flow 7
RESULTS
Spontaneous delivery occurred 2-19 days after fetal surgery. Six of the PD156707-treated shunt-
lambs died between day 1 and 21 of life. Two lambs died from presumed sepsis, one from necrotic
enterocolitis, and one sudden death from unknown causes. Two additional lambs were sacrificed because
of respiratory distress following an aspiration event. All of the placebo-treated shunt-lambs survived the 4-
week study period. In general, we observed that the lambs in the treatment group were clinically sicker,
with increased work of breathing and decreased activity level. However, this could not be quantified and
there were no differences in body weight, respiratory rate, or heart rate between the 2 groups (data not
shown). A total of 14 lambs (n=6 treated and n=8 placebo) completed the 4-week study period, and
underwent the hemodynamic study and biochemical and morphometric analysis.
Hemodynamic Study
All lambs had an audible continuous murmur and an increase in oxygen saturation between the
right ventricle and distal pulmonary artery. The baseline systemic arterial pCO2, pO2, and hemoglobin,
were similar between the two groups and within the normal limits of the laboratory. There were no
differences in systemic arterial pH between the two groups (7.46±0.04 vs. 7.52±0.06), however both were
greater than historical controls for the laboratory13,14. Left pulmonary vascular resistance, mean right atrial
pressure, and systemic pulse pressure were decreased in PD156707-treated shunt-lambs compared to
placebo-treated shunt-lambs (p<0.05, Table 1). All other hemodynamic variables measured were not
different between the two groups. However, mean pulmonary arterial pressure in PD156707-treated shunt-
lambs was similar to values previously noted in age-matched control lambs13,14.

ETA block and increased pulmonary blood flow 8
In placebo-treated shunt-lambs, the intrapulmonary injection of ET-1 increased left pulmonary
vascular resistance (18.5%±26.0) and mean systemic arterial pressure (9.4% ± 5.0) (p<0.05). However, in
all PD156707-treated shunt-lambs both the pulmonary and systemic vasoconstriction to ET-1 was blocked.
Biochemical and Protein Determinations
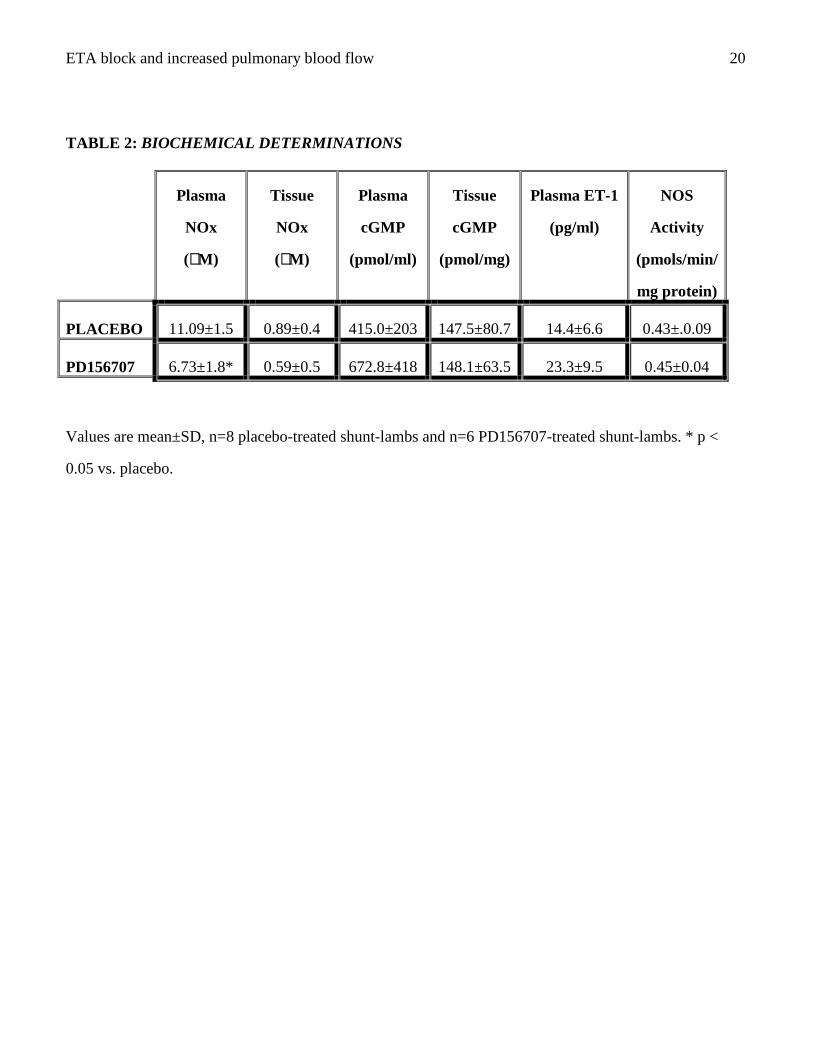
Lung tissue NOx levels, plasma and lung tissue cGMP levels, plasma ET-1 (P=0.06), and tissue
NOS activity were all similar between the two groups. Plasma NOx levels were decreased in PD156707-
treated shunt-lambs when compared to placebo-treated shunt-lambs (P<0.05, Table 2). Protein levels of
eNOS, preproET-1, ECE-1, ETA and ETB receptors were are similar between the two groups (Table 3).
Structural Studies
Morphometric analysis revealed no differences in the percent medial thickness of pulmonary
arteries between the two groups (Figure 1). However, the presence of muscular arteries appearance in the
intraacinar region at the alveolar duct and alveolar wall levels was significantly increased in the
PD156707-treated shunt-lambs compared to the placebo-treated shunt-lambs (Table 4). In addition, while
there was no difference in the number of barium-filled small arteries per unit area between the two groups
(3.8 ± 0.2, n = 5 vs. 4.0 ± 0.3, n = 5), the number of alveolar profiles per unit area was increased by 43.5%
in PD156707-treated shunt-lambs (p<0.05) (Figure 2). This led to a significant reduction in number of
small barium-filled arteries per 100 alveolar profiles in the PD156707-treated shunt-lambs (2.1 ± 0.3 vs.
2.9 ± 0.3 arteries / 100 alveoli, p = 0.002).

ETA block and increased pulmonary blood flow 9
DISCUSSION
Activation of the ET-1 cascade has been demonstrated in a variety of pulmonary hypertensive
disorders including children and animals with congenital heart disease and increased pulmonary blood
flow. The present study is the first to demonstrate that chronic endothelin receptor blockade lowers
pulmonary vascular resistance in a model of increased pulmonary blood flow secondary to congenital
heart disease, suggesting a role for ET-1 in the early pathophysiology of this disorder. Following in utero
aortopulmonary graft placement in the lamb, we found that chronic postnatal ETA receptor blockade
lowered pulmonary vascular resistance and right atrial pressure without affecting basal endogenous NO-
cGMP or ET-1 signalling. We also demonstrate the novel finding that ETA receptor blockade amplified
alveolar growth, suggesting a role for ET-1 in the regulation of postnatal alveolar development in this
setting.
Although chronic ET receptor blockade has demonstrated symptomatic improvement in adults
with advanced primary pulmonary hypertension, this would not be expected in the setting of increased
pulmonary blood flow10. Since it is well established that pulmonary vasodilator therapy in the setting of a
left-to-right shunt worsens congestive heart failure and mortality, the objective of this study was to utilize
PD156707 as a pharmacologic tool to further delineate the role of ET-1 in the pathophysiology of this
disorder, rather than a potential therapy in this setting20. As expected, PD156707-treated shunt-lambs had
increased work of breathing, decreased activity, and a greater mortality (50% vs. 0%, P<0.05) than
placebo-treated shunt-lambs. Postmortem investigation of the deaths suggested that two occurred from
aspiration events, one from an intrauterine infection, one from a postnatal urachus infection, and one
sudden death of unclear etiology. In an attempt to prevent the increased symptomatology of increased
pulmonary blood flow, both groups of lambs were treated with furosemide twice a day, beginning on the

ETA block and increased pulmonary blood flow 10
first day of life. It is noteworthy that both PD156707 and placebo-treated shunt-lambs had lower
pulmonary arterial pressure, higher systemic arterial pH, and less vascular remodelling than historical
shunt controls, which only received furosemide on an intermittent basis in response to increased
symptomatology12. The effects of the aggressive diuretic regimen, in addition to the high mortality of the
treatment group were unavoidable, but significant limitations of the current study. We cannot exclude the
possibility that the high mortality selected out lambs with differential hemodynamics and vascular
morphology, and that a shorter treatment course with a less aggressive diuretic regimen may have
demonstrated greater differences between the PD156707 and placebo-treated shunt-lambs. Additionally,
we also cannot exclude the possibility that the 50% mortality has introduced other unknown serious biases
to the study. Further studies are needed to better delineate these potential factors.
In previous animal models of pulmonary hypertension, chronic ET receptor blockade attenuated
the progression of vascular smooth muscle remodeling. For example in rats exposed to either hypoxia or
monocrotaline, ET receptor blockade resulted in decreased medial thickness of the small pulmonary
arteries compared to controls21,22. Similarly, in postnatal piglets with increased pulmonary blood flow, ET
receptor blockade prevented the increase in medial thickness of the small pulmonary arteries23. However,
ETA receptor blockade did not prevent pulmonary vascular remodelling in a rat model of myocardial
infarction24. In the present study, PD156707-treated shunt-lambs displayed no differences in percent
medial thickness of the pulmonary arteries compared to controls. In fact, the abnormal presence of
muscularized pulmonary arteries in the region of the alveolar duct and wall was greater in PD156707-
treated shunt-lambs (Table 4). These surprising findings are not completely understood, but a few
potential explanations are noteworthy. First, as previously mentioned, the degree of vascular remodeling
was not generally significant in neither the PD156707-treated shunt-lambs nor the placebo-treated shunt-
lambs, and much less than historical shunt controls, which is likely due to the aggressive diuretic regimen

ETA block and increased pulmonary blood flow 11
utilized in this study. Second, the high mortality in the PD156707-treated shunt-lambs may have selected
for a group of survivors with more vascular remodelling, which could limit pulmonary blood flow and
clinical symptomatology. Lastly and most importantly, this study is unique in that the abnormal
hemodynamic state was present from birth, and treatment was started immediately following birth. Since
the early morphologic abnormalities in children with increased pulmonary blood flow are similar to the
normal fetal vascular morphology, it is likely that the early vascular changes represent a failure of the
fetal morphologic state to regress rather that remodelling. Therefore, the abnormal extension of muscle
present in the PD156707-treated shunt-lambs may represent a failure of the normal regression of fetal
morphology, and may suggest a role for ET-1 in this process.
Previously, we demonstrated that increased pulmonary blood flow induces significant alterations
in the endogenous ET-1 and NO-cGMP cascades13,14,25. In the present study, we demonstrate that chronic
ETA receptor blockade does not significantly alter these changes. For example, there were no differences
in plasma ET-1 levels, plasma and tissue cGMP levels, NOS activity, and protein levels of eNOS,
preproET-1, ECE-1, ETA and ETB receptors. Plasma NOx levels were increased in PD156707-treated
shunt-lambs. However, plasma NOx levels may be altered by differences in extracellular volume and
renal clearance26. Since lung tissue NOx levels were unchanged, differences in plasma NOx are unlikely
to represent differences in basal pulmonary NO production.
To achieve ETA receptor blockade treated lambs received 150mg/kg/dy of PD156707, an orally
active, selective ETA receptor antagonist27. The dose of PD156707 was chosen after several previous
studies showed that this dose completely blocked the vasoconstricting effects of exogenous ET-1 and
resulted in steady-state plasma concentrations that blocked ETA receptors in vivo28. To insure adequate
ETA receptor blockade with PD156707 in this study, the effect of exogenous ET-1 was studied in both
groups of lambs. Similar to our previous studies ET-1 induced both pulmonary and systemic

ETA block and increased pulmonary blood flow 12
vasoconstriction in vehicle-treated lambs13. However, in all PD156707-treated lambs, the vasoconstricting
effect of ET-1 was blocked suggesting adequate ETA receptor blockade. Interestingly, ET-1 did not elicit
pulmonary vasodilation. These physiologic data in conjunction with the protein data demonstrating no
change in ETB receptor protein, suggest that ETB receptors were not up-regulated during ETA receptor
blockade.
Lastly, this study demonstrates the novel finding that chronic ETA receptor blockade increases
alveolar, and presumably capillary, growth in lambs with increased pulmonary blood flow. As seen in
Figure 2, the number of alveolar-capillary profiles per unit area was increased by 44% in PD156707-
treated shunt-lambs (P<0.05). Although ET-1 is known to have mitogenic actions on cardiovascular
tissues, and is co-mitogenic with a variety of growth factors and vasoactive substances, there is very
limited data on the role of ET-1 in the developing lung29. However, ET-1 is expressed in the airway
epithelium of the perinatal mouse, suggesting a role for ET-1 in lung development30. In the current study,
we have uncovered a previously unknown role for ET-1 in postnatal lung development during the stimulus
of increased pulmonary blood flow. These novel observations suggest that ET-1 may play an important
role in regulating lung growth in both normal and pathologic situations. Although age-matched control
lambs with lower pulmonary arterial pressures have similar alveolar growth as vehicle-treated shunt
lambs12, our results cannot rule out that the effect on alveolarization in the ET antagonist group was not
secondary to some indirect, hemodynamic effect. Therefore, further investigations will be required to
elucidate the role of ET-1 in regulating lung development. It is likely that such studies will yield important
biologic and clinically relevant information.

ETA block and increased pulmonary blood flow 13
GRANTS
This research was supported by grants HL61284 (JRF), HL48536 (BM), HL60190, and HL67841 (SMB)
from the National Institutes of Health and grant S/05/01 (SF) from the Deutsche Herzstiftung.
DISCLOSURES
There are no potential conflict of interests.

ETA block and increased pulmonary blood flow 14
REFERENCES
1. Hoffman JI, Rudolph AM, Heymann MA. Pulmonary vascular disease with congenital heart lesions: pathologic features and causes. Circulation. 1981;64:873-7.
2. Furchgott RF, Vanhoutte PM. Endothelium-derived relaxing and contracting factors. Faseb J. 1989;3:2007-18.
3. Fineman JR, Soifer SJ, Heymann MA. Regulation of pulmonary vascular tone in the perinatal period. Annu Rev Physiol. 1995;57:115-34.
4. Yanagisawa M, Kurihara H, Kimura S, Tomobe Y, Kobayashi M, Mitsui Y, Yazaki Y, Goto K, Masaki T. A novel potent vasoconstrictor peptide produced by vascular endothelial cells. Nature. 1988;332:411-5.
5. Giaid A, Saleh D. Reduced expression of endothelial nitric oxide synthase in the lungs of patients with pulmonary hypertension. N Engl J Med. 1995;333:214-21.
6. Giaid A, Yanagisawa M, Langleben D, Michel RP, Levy R, Shennib H, Kimura S, Masaki T, Duguid WP, Stewart DJ. Expression of endothelin-1 in the lungs of patients with pulmonary hypertension. N Engl J Med. 1993;328:1732-9.
7. Hassoun PM, Thappa V, Landman MJ, Fanburg BL. Endothelin 1: mitogenic activity on pulmonary artery smooth muscle cells and release from hypoxic endothelial cells. Proc Soc Exp Biol Med. 1992;199:165-70.
8. Vincent JA, Ross RD, Kassab J, Hsu JM, Pinsky WW. Relation of elevated plasma endothelin in congenital heart disease to increased pulmonary blood flow. Am J Cardiol. 1993;71:1204-7.
9. Yoshibayashi M, Nishioka K, Nakao K, Saito Y, Matsumura M, Ueda T, Temma S, Shirakami G, Imura H, Mikawa H. Plasma endothelin concentrations in patients with pulmonary hypertension associated with congenital heart defects. Evidence for increased production of endothelin in pulmonary circulation. Circulation. 1991;84:2280-5.
10. Rubin LJ, Badesch DB, Barst RJ, Galie N, Black CM, Keogh A, Pulido T, Frost A, Roux S, Leconte I, Landzberg M, Simonneau G. Bosentan therapy for pulmonary arterial hypertension. N Engl J Med. 2002;346:896-903.
11. Fratz S, Geiger R, Kresse H, Roemer G, Hennig M, Sebening W, Hess J. Pulmonary blood pressure, not flow, is associated with net endothelin-1 production in the lungs of patients with congenital heart disease and normal pulmonary vascular resistance. J Thorac Cardiovasc Surg. 2003;126:1724-29.
12. Reddy VM, Meyrick B, Wong J, Khoor A, Liddicoat JR, Hanley FL, Fineman JR. In utero placement of aortopulmonary shunts. A model of postnatal pulmonary hypertension with increased pulmonary blood flow in lambs. Circulation. 1995;92:606-13.
13. Wong J, Reddy VM, Hendricks-Munoz K, Liddicoat JR, Gerrets R, Fineman JR. Endothelin-1 vasoactive responses in lambs with pulmonary hypertension and increased pulmonary blood flow. Am J Physiol. 1995;269:H1965-72.
14. Black SM, Bekker JM, Johengen MJ, Parry AJ, Soifer SJ, Fineman JR. Altered regulation of the ET-1 cascade in lambs with increased pulmonary blood flow and pulmonary hypertension. Pediatr Res. 2000;47:97-106.
15. Rabinovitch M, Haworth SG, Castaneda AR, Nadas AS, Reid LM. Lung biopsy in congenital heart disease: a morphometric approach to pulmonary vascular disease. Circulation. 1978;58:1107-22.

ETA block and increased pulmonary blood flow 15
16. Reid LM. The pulmonary circulation: remodeling in growth and disease. The 1978 J. Burns Amberson lecture. Am Rev Respir Dis. 1979;119:531-46.
17. Black SM, Sanchez LS, Mata-Greenwood E, Bekker JM, Steinhorn RH, Fineman JR. sGC and PDE5 are elevated in lambs with increased pulmonary blood flow and pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol. 2001;281:L1051-7.
18. Black SM, Bekker JM, McMullan DM, Parry AJ, Ovadia B, Reinhartz O, Lakshminrushimha S, Mata-Greenwood E, Steinhorn RH, Fineman JR. Alterations in nitric oxide production in 8-week-old lambs with increased pulmonary blood flow. Pediatr Res. 2002;52:233-44.
19. Bush PA, Gonzalez NE, Ignarro LJ. Biosynthesis of nitric oxide and citrulline from L-arginine by constitutive nitric oxide synthase present in rabbit corpus cavernosum. Biochem Biophys Res Commun. 1992;186:308-14.
20. Wessel A, Buchhorn R, Bursch J. Circulatory failure in children with left-to-right shunt in the framework of congenital heart defects: pathophysiology and therapeutic results. Klin Padiatr. 2000;212:53-9.
21. Hill NS, Warburton RR, Pietras L, Klinger JR. Nonspecific endothelin-receptor antagonist blunts monocrotaline-induced pulmonary hypertension in rats. J Appl Physiol. 1997;83:1209-15.
22. DiCarlo VS, Chen SJ, Meng QC, Durand J, Yano M, Chen YF, Oparil S. ETA-receptor antagonist prevents and reverses chronic hypoxia-induced pulmonary hypertension in rat. Am J Physiol. 1995;269:L690-7.
23. Rondelet B, Kerbaul F, Motte S, van Beneden R, Remmelink M, Brimioulle S, McEntee K, Wauthy P, Salmon I, Ketelslegers JM, Naeije R. Bosentan for the prevention of overcirculation-induced experimental pulmonary arterial hypertension. Circulation. 2003;107:1329-35.
24. Nguyen QT, Colombo F, Rouleau JL, Dupuis J, Calderone A. LU135252, an endothelin(A) receptor antagonist did not prevent pulmonary vascular remodelling or lung fibrosis in a rat model of myocardial infarction. Br J Pharmacol. 2000;130:1525-30.
25. Black SM, Fineman JR, Steinhorn RH, Bristow J, Soifer SJ. Increased endothelial NOS in lambs with increased pulmonary blood flow and pulmonary hypertension. Am J Physiol. 1998;275:H1643-51.
26. Zeballos GA, Bernstein RD, Thompson CI, Forfia PR, Seyedi N, Shen W, Kaminski PM, Wolin MS, Hintze TH. Pharmacodynamics of Plasma Nitrate/Nitrite as an Indication of Nitric Oxide Formation in Conscious Dogs. Circulation. 1995;91:2982-2988.
27. Reynolds EE, Keiser JA, Haleen SJ, Walker DM, Olszewski B, Schroeder RL, Taylor DG, Hwang O, Welch KM, Flynn MA, et al. Pharmacological characterization of PD 156707, an orally active ETA receptor antagonist. J Pharmacol Exp Ther. 1995;273:1410-7.
28. Ignasiak DP, McClanahan TB, Saganek LJ, Potoczak RE, Hallak H, Gallagher KP. Effects of endothelin ETA receptor antagonism with PD 156707 on hemodynamics and renal vascular resistance in rabbits. Eur J Pharmacol. 1997;321:295-300.
29. Goto K. Basic and therapeutic relevance of endothelin-mediated regulation. Biol Pharm Bull. 2001;24:1219-30.
30. Guembe L, Villaro AC. Immunohistochemical mapping of endothelin in the developing and adult mouse lung. J Histochem Cytochem. 2001;49:1301-9.

ETA block and increased pulmonary blood flow 16
FIGURE LEGENDS
Figure 1:
PD156707 treatment has little effect on percent medial thickness of pulmonary arteries up to >
10,000 um external diameter. Values are mean±SD, n=5 placebo-treated shunt-lambs and n=5 PD156707-
treated shunt-lambs.
Figure 2:
TOP: Light micrographs showing an increase in alveolar profiles in PD156707-treated shunt-lambs
(right) as compared to placebo-treated shunt-lambs (left). Verhoeff’s elastin stain/ Van Gieson.
BOTTOM: Bar graph showing that the number of alveolar profiles per unit area in increased in PD
156707-treated shunt lambs compared to placebo-treated shunt lambs. Values are Mean±SD, n=8 placebo-
treated shunt-lambs and 6 PD156707-treated shunt-lambs. *p = 0.002 vs. placebo.

ETA block and increased pulmonary blood flow 17
Figure 1:
0
1
2
3
4
5
6
PercentMedial
Thickness
External Diameter (µM)
0-50 -100 -150 -200 -300 -400 -500 -1000 >1000
PlaceboPD 156707

ETA block and increased pulmonary blood flow 18
Figure 2:
Top
Bottom
0
50
100
150
200
250
# AlveolarProfiles
Per Unit Area
Placebo
PD 156707 *

ETA block and increased pulmonary blood flow 19
TABLE 1: GENERAL HEMODYNAMIC VARIABLESHemodynamic Variable Placebo (n=8) PD156707 (n=6)
mPAP (mmHg) 25.0 ± 7.4 18.3 ± 8.5
mSAP (mmHg) 55.9 ± 8.5 54.5 ± 6.5
pulse pressure SAP (mmHg) 93.1 ± 21.8 55.0 ± 17.3 *
mPAP : mSAP 0.45 ± 0.1 0.33 ± 0.1
mRAP (mmHg) 5.4 ± 0.8 4.0 ± 1.2 *
mLAP (mmHg) 9.9 ± 2.9 7.3 ± 1.9
Qlpa (ml/min/kg) 0.13 ± 0.1 0.14 ± 0.1
PVRleft (mmHg/ml/min/kg) 118.1 ± 32.0 76.5 ± 34.1 *
SVR (mmHg/ml/min/kg) 416.3 ± 229.6 450.3 ± 205.0
Qp : Qs 2.43 ± 0.8 2.85 ± 0.6
mRAP: mean right atrial pressure, mPAP: mean pulmonary arterial pressure, mLAP: mean left atrial
pressure, mSAP: mean systemic arterial pressure, Qlpa: blood flow through the left pulmonary artery,
PVRleft: left pulmonary vascular resistance, SVR: systemic vascular resistance, Qp:Qs: ratio of pulmonary
to systemic blood flow. Values are mean±S.D., * p < 0.05 vs. placebo.
ETA block and increased pulmonary blood flow 20
TABLE 2: BIOCHEMICAL DETERMINATIONS
Plasma
NOx
(µM)
Tissue
NOx
(µM)
Plasma
cGMP
(pmol/ml)
Tissue
cGMP
(pmol/mg)
Plasma ET-1
(pg/ml)
NOS
Activity
(pmols/min/
mg protein)
PLACEBO 11.09±1.5 0.89±0.4 415.0±203 147.5±80.7 14.4±6.6 0.43±.0.09
PD156707 6.73±1.8* 0.59±0.5 672.8±418 148.1±63.5 23.3±9.5 0.45±0.04
Values are mean±SD, n=8 placebo-treated shunt-lambs and n=6 PD156707-treated shunt-lambs. * p <
0.05 vs. placebo.

ETA block and increased pulmonary blood flow 21
TABLE 3: PROTEIN DETERMINATIONS (DENSITOMETRIC VALUES)
eNOS PreproET-1 ECE-1
ETA Receptor ETB Receptor
PLACEBO 63.2±15.7 21.9±9.6 4130.6±1148.0 224585.7±478183 27401.6±14094
PD 156707 52.2±11.8 30.7±14.7 3988.3±1273.8 232175.7±375440 33196.6±19536
Values are mean±SD, n=8 placebo-treated shunt-lambs and n=6 PD156707-treated shunt-lambs. * p <
0.05 vs. placebo.

ETA block and increased pulmonary blood flow 22
TABLE 4: Percentage of Fully Muscular and Nonmuscular Pulmonary Arteries Related to Intraacinar Airway Level in PD156707 and Placebo-Treated Shunt-Lambs
Respiratory Bronchiole Alveolar Duct Alveolar Wall
Degree of Muscularization
% Distribution
Degree of Muscularization
% Distribution
Degree of Muscularization
% Distribution
muscular 98 ± 5.6 muscular 48 ± 16.9* muscular 27 ± 9,1*PD156707non-muscular 2 ± 5.6 non-muscular 52 ± 16.9* non-muscular 73 ± 9.1*
muscular 85 ± 14.6 muscular 22 ± 14.4 muscular 9 ± 7.4Placebonon-muscular 15 ± 14.6 non-muscular 78 ± 14.4 non-muscular 91 ± 7.4
Values are mean ± SD, n = 5 PD156707-treated shunt-lambs and n = 5 placebo-treated shunt-lambs. *p < 0.05 vs. placebo.
Copyright © 2022 FDOKUMEN