Chronic Auditory Agnosia Following Landau-Kleffner Syndrome: A 23 Year Outcome Study
45
BRAIN AND LANGUAGE 63, 381–425 (1998) ARTICLE NO. BL981955 Chronic Auditory Agnosia Following Landau-Kleffner Syndrome: A 23 Year Outcome Study Kathleen Baynes*, Judy A. Kegl², Diane Brentari‡, Clifton Kussmaul§, and Howard Poizner² *Center for Neuroscience, University of California, Davis, ²Center for Molecular and Behavioral Neuroscience, Rutgers University, ‡Department of Audiology & Speech Sciences and Interdepartmental Program in Linguistics, Purdue University, and §Computer Science Department, Moravian College We report a 27-year-old woman with chronic auditory agnosia following Landau- Kleffner Syndrome (LKS) diagnosed at age 4 1 / 2. She grew up in the hearing/speak- ing community with some exposure to manually coded English and American Sign Language (ASL). Manually coded (signed) English is her preferred mode of commu- nication. Comprehension and production of spoken language remain severely com- promised. Disruptions in auditory processing can be observed in tests of pitch and duration, suggesting that her disorder is not specific to language. Linguistic analysis of signed, spoken, and written English indicates her language system is intact but compromised because of impoverished input during the critical period for acquisi- tion of spoken phonology. Specifically, although her sign language phonology is intact, spoken language phonology is markedly impaired. We argue that deprivation of auditory input during a period critical for the development of a phonological grammar and auditory–verbal short-term memory has limited her lexical and syntac- tic development in specific ways. 1998 Academic Press INTRODUCTION The acquisition of language depends upon adequate access to sufficiently rich linguistic input during a critical period of maturation that extends roughly from birth to puberty (Lenneberg, 1967). While language input is typically shared across the auditory–oral and visual–gestural modalities, ex- posure to a signed language via solely the visual–gestural modality will also The authors thank T.M. for the time and effort put forth doing tasks she often found unpleas- ant. We thank both her and her mother for their careful recordkeeping and willingness to share information with us. We also thank Brenda Redfern and Carl Ludy for help with data analysis. We acknowledge the support of NIDCD Research Grant R29DC1008 to K.B. and NIDCD research grant R01DC01664 to H.P. and J.K. Address correspondence and reprint requests to Kathleen Baynes, Center for Neuroscience, 1544 Newton Court, University of California, Davis, Davis, CA 95616. Fax: 530-757-8327. E-mail: [email protected]. 381 0093-934X/98 $25.00 Copyright 1998 by Academic Press All rights of reproduction in any form reserved.
Transcript of Chronic Auditory Agnosia Following Landau-Kleffner Syndrome: A 23 Year Outcome Study

BRAIN AND LANGUAGE 63, 381–425 (1998)ARTICLE NO. BL981955
Chronic Auditory Agnosia Following Landau-KleffnerSyndrome: A 23 Year Outcome Study
Kathleen Baynes*, Judy A. Kegl†, Diane Brentari‡, Clifton Kussmaul§,and Howard Poizner†
*Center for Neuroscience, University of California, Davis, †Center for Molecular andBehavioral Neuroscience, Rutgers University, ‡Department of Audiology & Speech
Sciences and Interdepartmental Program in Linguistics, Purdue University, and§Computer Science Department, Moravian College
We report a 27-year-old woman with chronic auditory agnosia following Landau-Kleffner Syndrome (LKS) diagnosed at age 41/2. She grew up in the hearing/speak-ing community with some exposure to manually coded English and American SignLanguage (ASL). Manually coded (signed) English is her preferred mode of commu-nication. Comprehension and production of spoken language remain severely com-promised. Disruptions in auditory processing can be observed in tests of pitch andduration, suggesting that her disorder is not specific to language. Linguistic analysisof signed, spoken, and written English indicates her language system is intact butcompromised because of impoverished input during the critical period for acquisi-tion of spoken phonology. Specifically, although her sign language phonology isintact, spoken language phonology is markedly impaired. We argue that deprivationof auditory input during a period critical for the development of a phonologicalgrammar and auditory–verbal short-term memory has limited her lexical and syntac-tic development in specific ways. 1998 Academic Press
INTRODUCTION
The acquisition of language depends upon adequate access to sufficientlyrich linguistic input during a critical period of maturation that extendsroughly from birth to puberty (Lenneberg, 1967). While language input istypically shared across the auditory–oral and visual–gestural modalities, ex-posure to a signed language via solely the visual–gestural modality will also
The authors thank T.M. for the time and effort put forth doing tasks she often found unpleas-ant. We thank both her and her mother for their careful recordkeeping and willingness to shareinformation with us. We also thank Brenda Redfern and Carl Ludy for help with data analysis.We acknowledge the support of NIDCD Research Grant R29DC1008 to K.B. and NIDCDresearch grant R01DC01664 to H.P. and J.K.
Address correspondence and reprint requests to Kathleen Baynes, Center for Neuroscience,1544 Newton Court, University of California, Davis, Davis, CA 95616. Fax: 530-757-8327.E-mail: [email protected].
3810093-934X/98 $25.00
Copyright 1998 by Academic PressAll rights of reproduction in any form reserved.

382 BAYNES ET AL.
yield a fully developed language system. The modality independence of lan-guage is an evolutionary advantage that ensures the full expression of thehuman language capacity, even in the absence of auditory feedback duringphonological, lexical, and syntactic development. However, this languagecapacity may be expressed differently, depending upon the modality of theexposure. The complex interplay between cognition, the innate propensityto acquire language, and adequate exposure to auditory and/or visual inputcombines to form an almost impenetrable developmental whole that makesit difficult to untangle the contributions of these factors. The case we reporthere raises some basic questions regarding the effect of deprivation of normalauditory feedback on phonological, syntactic, and lexical development in theauditory and visual modalities.
Landau-Kleffner syndrome. Since its identification as a language-specificdisorder of childhood in 1957, Landau-Kleffner Syndrome (LKS) has pre-sented a tantalizing puzzle. Landau and Kleffner (1957) reported six casesof children who had been acquiring language normally, then started to de-cline, either insidiously or abruptly. The presence of a convulsive disorderappeared to be a causal factor. Symptoms were initially reported to developover days or weeks and lasted from 2 weeks to 2 years. In the first report,improvement seemed to occur with the institution of anticonvulsive treat-ments and speech therapy. Subsequent reports of similar cases were morevariable in onset, treatment, and outcome. Chronic language impairment wasa frequent outcome, although some children appeared to recover completely.Issues of definition, pharmacological treatment, and prognosis remain unre-solved. In 1992, the apparent lack of progress prompted Landau (1992) tosay ‘‘Here is a condition of variable and really unpredictable prognosis, ofunknown cause, and for which we have no convincing evidence of empiri-cally effective treatment.’’ The rarity of the disorder and the heterogeneityof its symptoms have made systematic investigation difficult, but recent workindicates that progress is being made toward better understanding and treat-mentofLKS (Metz-Lutz,Hirsch,Maquet,de SaintMartin,Rudolf,Wioland,&Marescaux, 1997; Morrell, Whisler, Smith, Hoeppner, de Toledo-Morrell,Pierre-Louis, Kanner, Buelow, Ristanovic, Bergen, Chez & Hasegawa, 1995).
However, variations in the severity of the effect on the language develop-ment of the afflicted children remains unexplained. The onset of this disorder,usually between 3 and 7 years, with at least one case reported as early as 2years of age (Ansink, Sarphatie, & van Dongen, 1989), impacts the develop-ment of language at a time when basic language skills are emerging. Bothcomprehension and production are often severely compromised during theactive phase. Language comprehension is so severely compromised that chil-dren are sometimes thought to have become deaf, but when tested thesechildren have normal or near-normal audiograms. Soon after the onset ofcomprehension problems, expressive speech declines as well, with somechildren becoming mute or having a severely restricted vocabulary. Although

OUTCOME IN LANDAU-KLEFFNER SYNDROME 383
there are some well-documented reports of language deficits fluctuating inconcert with seizure activity (Marien, Saerens, Verslegers, Borggreve, & DeDeyn, 1993; Shoumaker, Bennett, Bray, & Curless, 1974), others report noconsistent relation (Paquier, Van Dongen, & Loonen, 1992; Rapin, Mattis,Rowan, & Golden, 1977). More importantly, when seizures are controlled,it has proven difficult to predict which children will recover completely andwhich will never reacquire normal spoken language function. Because a bet-ter understanding of the basis of the language dysfunction might serve as abasis for improved prediction and treatment, detailed language studies ofthese patients are needed.
We report here an adult female whose auditory speech and language havenever recovered after the onset of Landau-Kleffner Syndrome (LKS) at age41/2, despite seizure cessation by age 12. Our investigation of the linguisticabilities of this patient have led us to hypothesize that her language develop-ment was limited not by a language-specific disorder, but by a more generaldeficit in auditory processing that led to a failure to receive input from aspoken language. While it appears that signed language input would havebeen unhindered by her auditory processing deficit, her exposure to fluentsigned input during a period critical for language acquisition was patchy andproved inadequate to support nativelike acquisition of a signed language. Ifwe are correct, the varied prognosis for this disease indicates that early expo-sure to ASL would be beneficial for at least a subset of children and harmfulto none. Moreover, we further suggest that close observation of these caseswith their varied etiology and treatment (see Kegl, Baynes, Brentari, Kuss-maul, & Poizner, in preparation, for more detail) may help to clarify the roleof a critical period for phonology in lexical and syntactic development.
Remediation. Of particular relevance to this paper are the attempts to insti-tute some form of manual therapy after LKS has been diagnosed. Pharmaco-logical therapy is often accompanied by traditional speech therapy. In severecases, some form of manual therapy has been instituted, sometimes in theschool setting and sometimes in residential care. However, detailed descrip-tions of the therapy undertaken and its outcome are seldom available.
One early report of manual communication as an intervention in severecases demonstrated varying degrees of success (Cooper & Ferry, 1978).After reviewing the 45 cases that had been reported since 1957, they empha-sized the importance of obtaining a neurological evaluation for any childwho suddenly ceases to talk, whether or not seizures occur. However, be-cause some of these children may also have problems with gesture, theycautioned that manual communication may not always be appropriate.Tharpe and Olson (1994) noted that speech–language pathologists and audi-ologists need to be aware of the symptoms of this disorder to insure referralof these children to neurologists for diagnosis and treatment. They suggestedthat because of misdiagnosis, inappropriate treatment regimes may be uti-lized, dooming children to a lifetime of ineffective communication.

384 BAYNES ET AL.
However, given the range of symptoms and severity, diagnosis may notbe sufficient to formulate appropriate treatment. Reviewing what is knownabout language outcome, de Wijngaert and Gommers (1993) observed thatthe unique and fluctuating course of the disorder must be considered in anyrehabilitation program. Therapy will have to undergo continuous adaptationas the child moves through the course of the disorder. They do note thatvisual cues have been important in allowing children to associate the writtenword and object. They also note that some authors have found the use of amanual language to be useful, whereas others have found that exposure tosign does not prevent continuing severe problems with communication.However, the nature and extent of exposure to signed language input needsto be more rigorously reported before its contribution to circumventing lan-guage deprivation in these cases can be reasonably evaluated. Clearly, thedegree to which radically different outcomes occur with different teachingmethods further suggests that differences in the character of the languagedisruption and the degree to which nonlanguage functions are involved mustbe considered in any plan for rehabilitation.
These issues and the window that they provide into the course of languageacquisition make this disorder one of great interest in understanding the roleof auditory input on the development of language competence. In the courseof our investigation of T.M., we have concluded that, although LKS impactsmost heavily on her spoken language production and comprehension, herdisorder is not language specific, but rather represents a more general audi-tory processing dysfunction. T.M. continues to suffer from a severe chronicdeficit in both expressive and receptive spoken language. She was taught touse signed English and, unable to communicate fluently in spoken English,Pidgin Signed English (PSE) (Wilbur, 1979), remains her preferred form ofcommunication. This investigation examines the phonology, morphology,and syntax of her signed and spoken English to better understand the natureof the deficit that has limited her communication skills. We first addressthe question of whether her deficit is language specific and then attempt tounderstand what the effect has been on language development.
After reporting T.M.’s medical history and current neurological and neuro-psychological status, we will present evidence that her auditory perceptionis impaired in a way that prevented her from acquiring native competencein spoken English. We argue that T.M.’s current communicative status iscompromised as a result of deprivation of normal auditory feedback duringa period that is most critical to the development of a phonological grammar.Although there is marked variation in the linguistic outcome in Landau-Klef-fner Syndrome, we attempt to isolate the crucial factors that differentiatethe type and degree of impairment and to suggest directions for continuedresearch.
Subject. T.M. is a 26-year-old right-handed female, who was a full-terminfant, developing normally, with mildly delayed speech milestones, untilabout age 41/2. At that time, her speech deteriorated to ‘‘babble,’’ with limited

OUTCOME IN LANDAU-KLEFFNER SYNDROME 385
single word utterances (drink, hot, mama, baby, milk) and the use of initialconsonant sounds for words (/k-k-k/ for cake, /b-b-b/ for bathroom). Audi-tory language comprehension was poor, although audiological examinationon 09/13/74 indicated ‘‘at least near normal’’ hearing. Psychological exami-nation suggested normal intelligence. Neurological examination was normalexcept for an EEG done in April of 1974, which was severely abnormalbilaterally. Continuous high amplitude spikes and slow wave activity andpolyspike and wave activity were present in approximately 80% of the rec-ord. A single bolus of Valium abolished the spike and polywave dischargesand the record became ‘‘almost normal in appearance.’’ As the effect of theinjection diminished, ‘‘isolated spike activity emanating from the left tempo-ral region’’ was observed. T.M. was treated with Dilantin, Zarontin, andValium and placed in speech therapy and a class for aphasic children. Byage 7, she was enrolled in a program designed to teach sign language forprimary communication and was learning to sight read. At about age 12,T.M. discontinued her own anticonvulsants without experiencing subsequentclinical seizures.
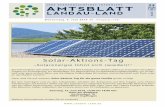
She graduated from high school and attended about two years of college,studying accounting. T.M. is currently working full-time in a clerical posi-tion. At present, her hearing is normal in her right ear and normal to border-line in her left. Her neurological examination is normal. Her EEG and MRIscan are normal. A PET scan demonstrates bilateral temporal lobe hypome-tabolism (Fig. 1). She continues to be seizure-free.
T.M. was exposed to Pidgin Signed English (PSE), a system of manuallycoded English, through most of her educational career. Her first exposure tosigning appears to have been in communication therapy from June to August,1974. She learned signs rapidly, but her auditory comprehension was veryimpaired. She was not able to identify environmental sounds at the initiationof therapy, but learned to identify a horn, a clacker, and a bell. Continuedtraining in manual communication was recommended. By 1977, her neurolo-gist noted that ‘‘she and her mother communicate quite handily [in signedlanguage].’’ Her family moved frequently and she spent time in a variety ofclassroom settings. We were not able to document the quality or extent ofexposure in all of these settings. In addition, she attended classes for twoyears at a state school for the Deaf, where she was exposed to AmericanSign Language (ASL). Following her graduation from high school, she spentabout four years in speech therapy, where the primary goal was to improveher intelligibility.
Neuropsychological testing. On the Wechsler Adult Intelligence Scale—Revised, T.M. demonstrates strong visual spatial skills (PIQ 110, range ofage-scaled scores from 9 on Picture Completion to 13 on Picture Arrange-ment and Object Assembly). On the Standard Progressive Matrices, herscores are in the normal range (50th percentile). Her visual memory is good(VM 112). Visual Span (from the WAIS-R NI) was 6 forward and 6 back-ward. On the Benton Facial Recognition Test, she correctly identified 47/

386 BAYNES ET AL.
FIG. 1. PET scan performed in November 1992 showing bilateral temporal lobe hypome-tabolism.
51 faces, placing her in the normal range. Motor skills were excellent (righthand 86th percentile, left hand 99th percentile), although there was about aone SD advantage for her nondominant left hand. Arithmetic skills as as-sessed by the Wide Range Achievement Test—Revised (WRAT-R) were atthe 50th percentile. Executive function was also within normal limits. Shewas able to do the difficult double tracking task on Part B of Trail Makingrapidly and easily. She also showed mental flexibility and the ability to ab-stract rules from feedback on the Wisconsin Card Sorting Test. She achievedfour categories in 64 trials and made very few preservative errors (Table 1).A striking divergence occurred when we assessed verbal skills. The resultsfrom the WAIS-R are from a nonstandardized administration translated intoAmerican Sign Language by one of the authors (D.B.), who also translatedT.M.’s responses. No norms are available from a comparable Deaf controlpopulation, who would also be expected to have differential access to aspectsof vocabulary and cultural knowledge typically transmitted via an auditorymodality, so her deficits may be exaggerated. However, in comparison withher performance scores, age-scaled scores range from 2 (Vocabulary) to 7

OUTCOME IN LANDAU-KLEFFNER SYNDROME 387
TABLE 1Results of Standardized Neuropsychological Tests with Less Dependence
on Language Abilities
WAIS Subtest Scores Age scaled scores PercentilesPicture Completion (9) 37Picture Arrangement (13) 84Block design (10) 50Object Assembly (13) 84Digit Symbol (12) 75PIQ 110 75
Raw scoresRaven Progressive Matrices 41 50WMS-R
Logical Memory Ia 23 35Logical Memory IIa 22 50Visual Reproduction I 36 74Visual Reproduction II 32 61
WRAT3Arithmetic 43 50
Finger OscillationRight hand (dominant) 53.5s 86Left hand 55.4s 99
Facial Recognition Test 47 WNLTrail Making Test
Part A 19.5s 63Part B 55.5s 45
Wisconsin Card Sorting Test (1 deck)Categories in 64 trials 4 NLPercent perseverative responses 17 87
Pyramids and Palm Trees TestAll picture version 50/52 WNL
a Nonstandard administration. One of the authors (J.A.K.) served as an interpreter for T.M.in this task.
(Digit Span, Arithmetic, and Similarities). T.M. was able to name only 28of 60 items from the Boston Naming Test in spoken English. She recognizedmost items and sometimes had alternate names for them. She had signs for30 of the items. On the Peabody Picture Vocabulary Test—Revised (PPVT-R), she scored at the level of a 6.4-year-old in the standard auditory adminis-tration. With a nonstandard written administration, T.M. scored at the 7.7-year-old level. On the Test of Written Language—2, T.M. demonstratedimpairment in the basics of written language such as vocabulary (1st percen-tile) and spelling (5th percentile), but was able to demonstrate increasingly‘‘normal’’ scores as tasks became more conceptual in nature (Logical Sen-tences 16th percentile, Sentence Combining 63rd percentile) (Table 2). Inan all-picture version of Pyramids and Palm Trees, T.M. showed normalcomprehension of conceptual–semantic relations, making only 2 errors outof 52 items. In short, at this time, T.M. is functioning in the average to

388 BAYNES ET AL.
TABLE 2Results of Standardized Tests with Greater Dependence on Language Abilities
WAIS Subtest Scores Age scaled scores PercentilesInformation (4) 2Digit Span (7) 16Vocabulary (2) 0.4Arithmetic (7) 16Comprehension (5) 5Similarities (7) 16
Raw scoresPeabody Picture Vocabulary Test-Form M
Spoken 74 1Peabody Picture Vocabulary Test-Form L
Writtena 88 1Boston Naming Test
Signed responses 30/60Test of Written Language
Vocabulary 8 1Spelling 9 5Style 8 16Logical Sentences 7 16Sentence Combining 7 63
aNonstandard administration.
superior range in a variety of nonverbal domains, but remains severely re-stricted in her ability to perform well on tasks associated with verbal intelli-gence.
Nonverbal auditory processing. A profound impairment of stress and into-nation in T.M.’s auditory language production prompted examination of herability to recognize auditory differences. Although her audiogram demon-strates that she is able to perceive sounds across a normal range of frequen-cies and amplitudes, her ability to process sounds normally was not certain.However, she reported that she enjoys listening to music, such as rap androck and roll, although she was unable to supply the names of any groupsor recordings that she particularly liked. T.M. also reported she could recog-nize other environmental sounds like telephones ringing, cars honking, anddogs barking. We initiated an investigation of her ability to perceive melodyand rhythm, but pilot testing demonstrated that our tasks were too difficult.Therefore, same/different tasks were developed to examine her ability tojudge pitch and duration.
EXPERIMENT 1—PITCH DISCRIMINATION
Materials and methods. Two 400 ms tones of roughly equal volume were generated so thatin half of the trials the tones had the same pitch and in half of trials the tones’ pitches differedby one to fifteen semi-tones. The mean pitch was 330 Hz with a range of 110 to 740 Hz.

OUTCOME IN LANDAU-KLEFFNER SYNDROME 389
TABLE 3Percentage Correct on Judgments of Pitch and Duration Demonstrating Accuracy on
‘‘Same’’ Judgments and Failure to Hear Differences Reliably
Pitch
Semi-tone Percentage Number Binomial p,difference correct of trials Z score two-tailed
0 83 185 7.14 ,.0011 21 29 22.42 ,.052 19 21 22.24 ,.053 31 35 21.65 ns4 34 35 21.37 ns5 50 18 0 ns6 64 25 1.01 ns7 71 24 1.52 ns8 57 23 0.48 ns9 67 14 0.94 ns10 83 12 1.83 ns111 100 8 2.83 ..01
Duration
Ms Percentage Number Binomial p,difference correct of trials Z score two-tailed
0 91 91 6.79 ,.001100 17 42 23.42 ,.001200 45 29 20.38 ns300 69 13 1.01 ns400 92 24 3.62 ,.001500 78 23 2.07 ,.05600 89 9 1.98 ,.05700 100 3 1.73 ns5001 83 35 3.12 ,.01
There were a total of 429 trials. One hundred and eight trials were run with an SOA of 500ms and the next 321 trials were run with an SOA of 1000 ms.
Procedure. T.M. was seated in a quiet room. She was told that she had to listen to the tonepairs and decide if they were the same or different. She had to type ‘‘S’’ or ‘‘D’’ on a computerkeyboard to indicate whether the pitches were the same or different. T.M. had no difficultyunderstanding or complying with this procedure.
Apparatus. Sounds were generated using a MIDI synthesizer (Roland D-110) controlled bysoftware on a Macintosh computer and played back over speakers at a comfortable volume.‘‘Piano’’ and ‘‘trumpet’’ timbres were used for the pitch discrimination task. An ‘‘electricorgan’’ timbre was used for the duration task described below because that task required atimbre with a continual amplitude over time.
Results. Percents correct for trials run at 500 and 1000 ms SOAs were notsignificantly different from one another and were highly correlated (R 5.77). These results were therefore combined for further analysis. T.M. wasable to perform the task only when the differences were greatly exaggerated(Table 3). Pitches that were the same were recognized as such with above

390 BAYNES ET AL.
chance frequency. However, when pitches differed by only one or two semi-tones, T.M. was more likely to judge them to be the same, not different.Only when tones were almost an octave apart was she able to reliably judgethat they were different. Normal subjects have no trouble noticing differencesan order of magnitude smaller than those which T.M. could reliably detect.(For example, Bentley’s Measures of Musical Abilities, described by Young(1973), involves a similar pitch discrimination test which ranges in difficultyfrom 1 semitone to 3/26 of a semitone between the pitches.) It is clear thatT.M. is not able to resolve differences in pitch with the accuracy of personswith normal hearing.
EXPERIMENT 2—DISCRIMINATION OF DURATION.
Materials and methods. Two tones of equal volume and 330 Hz pitch were generated suchthat in half of the trials they had the same duration and in half of the trials they had differentdurations. The difference in duration varied from 100 to 700 ms.
Procedure. As above, except that the task was to indicate whether the tone durations werethe same or different.
Apparatus. As above.
Results. The response pattern was similar to that for pitch. T.M. was sig-nificantly above chance in identifying sounds of the same duration, but con-tinued to call pairs the same until there was almost a 300 ms difference inlength (Table 3). She was above chance for same judgments, below chancefor 100 ms differences (because she consistently called tones the same atthis duration difference), then did not rise to above chance levels of discrimi-nation until tones differed by 400 ms in duration. Such differences are anorder of magnitude greater than the differences required to recognize manyphonemic contrasts. For example, recognition of voiced and unvoiced stopconsonants requires discriminations in the 20 ms range. These results indi-cate that, although T.M. may have perceived the acoustic stimuli associatedwith speech, she was unable to resolve the acoustic signals precisely enoughto recognize the differences between phonologically different sound seg-ments. Hence, we argue she could not develop a stable representation ofphonemes, the basic building blocks of speech.
EXPERIMENT 3—ENVIRONMENTAL SOUNDS
An investigation of T.M.’s ability to recognize environmental sounds wasundertaken as well. Other LKS patients have been reported to have normalrecognition of environmental sounds (Denes, Balliello, Volerra, & Pellegrin,1986). T.M. clearly was aware when people around were speaking and re-sponded to a variety of sounds in our laboratory, including the sound of thetelephone. She has pet dogs and stated that she can hear them barking. Shealso stated that she is aware of noises in the car, such as horns honking. Wewanted to know whether she was able to recognize familiar sounds without

OUTCOME IN LANDAU-KLEFFNER SYNDROME 391
visual context, or if she was supplementing her ability to hear the presenceof a sound with whatever environmental information was available.
Subjects. Besides T.M., eleven control subjects with normal hearing, agedfrom 18 to 34, participated in this experiment. Eight were native speakersof English and two had learned English as a second language but read andspoke fluently at the university level. All had normal or near-normal hearing.One subject identified her hearing level as ‘‘slightly subnormal’’ and anotheras ‘‘a minor hearing loss in one ear.’’ They were volunteers who were notpaid for their participation.
Materials and methods. Twenty sounds were selected from a compact disk of sound effectsand played by a Quadra 800 over a pair of Apple speakers. Length of the sound samplesvaried from approximately 500 ms (glass breaking) to 57 s (background noise in a cafeteria).Subjects were asked to identify the sound they had just heard. Each of the twenty sounds wasplayed once, except for one sound of very short duration (glass breaking) which was repeated.Subjects were tested in groups of three to five. They were asked to write the name of soundthey had just heard. Eight of the control subjects were also asked to rate the sound’s familiarityon a 5-point Likert scale ranging from 1 (I am very familiar with this sound and recognizedit immediately) to 5 (I have never heard this sound before).
Results. Control subjects correctly identified most of the sounds (mean91%; range 80 to 97%; standard deviation 5.9), and most errors were minor;a draining bathtub was mistaken for an aquarium, a motorboat for a lawn-mower, etc. In contrast, T.M. was able to accurately identify only 48% ofthe sounds. She easily recognized a number of the sounds, such as dogsbarking, children laughing, and an airplane. However, she was unable toeven guess at one-third of the sounds, including a toilet flushing, a typewriter,and brushing teeth. Of note, the two control subjects who specified that theyhad minor difficulty hearing had the most difficulty making the identifica-tions (both scored 80% correct), so this task is sufficiently difficult that evenrelatively minor hearing loss can interfere with it.
Besides the sounds mentioned above, T.M. had failed to recognize thesound of an electric typewriter, a bathtub filling, a fire alarm, wind chimes,a horse-drawn wagon, pool being played, footsteps, and a whistling teakettle,despite identifying breaking glass, an orchestra tuning up, a VW horn, atelephone ringing, cafeteria noise (‘‘people talking’’), footsteps, and a gun-shot. The diversity of these sounds, in both frequency and loudness, led usto suspect that familiarity of a sound might play some role in her ability toidentify it. Therefore, ratings of familiarity were collected to help determineif familiarity of the sounds was contributing to T.M.’s ability to recognizethem. Although the sounds that T.M. recognized correctly were rated morefamiliar than those she did not, the difference was not significant (1.45 vs1.85, t 5 21.42, p 5 .09, ns). However, as the range of familiarity wasnarrow (1 to 3.51) and most sounds were relatively familiar, we can not ruleout a contribution of familiarity.
These results indicate that even though T.M. can recognize many commonsounds in her environment without context, her ability to recognize soundsis not normal even with sound samples of relatively long duration.

392 BAYNES ET AL.
Discussion. The results of these three experiments support the view thatT.M.’s auditory processing system, not just her language processing, is ab-normal. She can resolve neither pitch nor duration with normal precision.Although the most devastating effect of this problem is seen in her ability touse spoken language, it is also apparent in her ability to recognize everydayenvironmental sounds.
The 3001 ms boundary for discrimination of duration is compatible withthe view that there is a division within the auditory system for the perceptionof fast and slow temporal sequences. Tallal and Piercy (1973) reported thataphasic patients were able to discriminate two-tone sequences at normal lev-els when separated by an interval of 300 ms, but were markedly impairedat shorter intervals. Tallal, Miller, and Fitch (1993) subsequently suggestedthat a variety of language deficits may be related to temporal processingdeficiencies. Pardo, Makela, Sams, and Hari (1994) have used magnet-oencephalography (MEG) to examine rapid acoustic changes in nonspeechstimuli and also support the hemispheric differences in processing of fast (3and 30 ms changes) and slow (300 ms changes) acoustic stimuli. These re-sults suggest it may be possible to damage the fast but not the slow auditoryprocessing system. Such damage might have a more devastating effect onthe ability to process speech sounds than other environmental stimuli. In ourpatient, there also appears to be a deficit in the processing of pitch informa-tion. We cannot determine from our results whether the problem with pitchis secondary to a temporal processing deficit or represents the involvementof a separate system.
Although we can not document the stability of the deficit we have mea-sured, there is no reason to presume that T.M.’s auditory perception hasdeclined as she has matured. It seems more likely that there might have beenadditional problems that interfered with her speech processing during theperiod of her childhood when she had an active seizure disorder. However,we do know that her audiogram was always near normal and we can specu-late that there has been little change in her ability to resolve auditory signalssince the onset of Landau-Kleffner Syndrome when she was four. To demon-strate how this deficit has impacted her language development, we will nowpresent our assessment of her spoken and signed phonology and her spoken,signed, and written grammar. We defend the following points.
1. T.M. has chronic difficulty with auditory processing.2. Production and comprehension of written and spoken lexical items are
at the level of a 6- to 7-year-old.3. Production and comprehension of signed phonology are within normal
limits for a nonnative signer.4. Production and comprehension of spoken English phonology are pro-
foundly impaired.5a. Production of spoken morphosyntax demonstrates intact argument
structure with an impaired lexicon.

OUTCOME IN LANDAU-KLEFFNER SYNDROME 393
5b. Comprehension of spoken morphosyntax cannot be tested, but compre-hension of written grammar is relatively good, although flawed in a waytypical of certain deaf signers.
5c. Production and comprehension of signed morphosyntax are within nor-mal limits for a late learner.
Broadly speaking T.M.’s manually coded English is phonologically (for-mationally) normal, whereas both comprehension and production of spokenEnglish phonology is impaired. By ‘‘phonologically normal,’’ we mean thather articulation of the formational aspects of signed items falls within therange of fluent signers of ASL and manually coded English. We present datademonstrating a normal distribution and frequency of occurrence of argu-ment structure types in her spoken and written, as well as in her signed,English narrative production. In this paper, we argue that the failure to de-velop adequate spoken English is a result of the distorted auditory input thatshe received during a period critical for the consolidation of auditory lan-guage, but that there is no evidence that her ‘‘language system’’ per se wasfaulty. Further, we will argue that (1) a developmental failure to establish aproductive phonological grammar impedes development of a full lexicon(Brentari et al., in preparation) and (2) lack of some grammatical devicesmay be the result of acquiring a visual or gestural rather than an auditorylanguage (Bishop, 1982a) and/or a deficit in auditory–verbal short-termmemory.
Relationship between Manually Coded English and AmericanSign Language
To clarify our analysis of T.M.’s language use for the reader, we firstpresent a brief explanation of the differences between ASL (a typologicallydistinct language) and manually coded forms of English. As we have previ-ously stated, T.M.’s most comfortable means of communication is a type ofmanually coded English, commonly referred to as Signed English and notAmerican Sign Language (ASL). There are many differences betweenSigned English and ASL; here we will present a few of the distinguishingfeatures that are most relevant to our discussion.
ASL is a natural sign language used by the Deaf community in the UnitedStates and in portions of Canada and Mexico. In the U.S., there are upwardsof 500,000 users of ASL. While most users of ASL are to varying degreesbilingual, with English as their second language, American Sign Language istypologically very distinct from English. If one were forced to typologicallyclassify this language on the basis of both linguistic features and historicalcontact with spoken languages, ASL would fall more appropriately into thefamily of Romance languages (French, Spanish, Italian, Portuguese, etc.).Like many Romance languages, ASL allows null subjects, subject inversionto sentence final position, verb fronting, grammatical object clitics, postnom-inal adjectives (in older dialects), richer inflectional morphology on the verb,

394 BAYNES ET AL.
and canonical SVO (subject verb object) ordering. Within a typology thatincludes signed language families, ASL also patterns with those signed lan-guages that coexist with spoken Romance languages (e.g., Quebec SignLanguage, Brazilian Sign Language, Spanish Sign Language, Mexican SignLanguage) but this set extends to include Russian Sign Language as well,since all these signed language families can trace their roots back to influencefrom French Sign Language in the 1800s. However, such classification is lessmotivated than classification based upon modality influences, implicationaluniversals that follow from the fact that ASL is produced and processed inthe visual–gestural as opposed to the oral–auditory modalities.
Likewise, brain organization for ASL parallels that for spoken languagesin a crucial way: lesions in the left cerebral hemisphere, but not in the right,produce aphasias for ASL (Hickok, Bellugi, & Klima, 1996; Poizner,Klima, & Bellugi, 1987). However, the anatomical structures within the lefthemisphere that mediate signed languages are likely not to be isomorphicwith those that mediate spoken languages. There is mounting evidence fromlesion studies that the posterior parietal cortex, important for higher-ordervisual processing and visuomotor integration, may play a more importantrole in networks that mediate signed, as opposed to spoken, language (Cor-ina, Poizner, Bellugi, Feinberg, Dowd, & O’Grady-Batch, 1992; Poizner etal., 1987). Furthermore, speech and sign have been found to be differentiallydisrupted within one and the same deaf signer/speaker during intracranialcortical stimulation performed prior to resective surgery (Gilmore, Kegl,Bowers, Leonard, Roper, Fennell, Poizner, & Heilman, 1994; Kegl, Gilmore,Fennell, Bowers, Poizner, & Heilman, 1997). Thus, these data suggest thatthe left cerebral hemisphere is innately predisposed for language irrespectiveof modality, and that those anatomical structures mediating language withinthe left hemisphere may well be linked to the modality in which languagehas developed.
In contrast to ASL, Signed English is one of a set of manually codedEnglish (MCE) systems, which have either been invented by educators forthe purpose of teaching English to the Deaf, or function as a type of contactsigning between Deaf community members who know ASL and signers (of-ten hearing) who have some command of the ASL lexicon, but not its gram-mar (Lucas and Valli, 1992). These systems all follow the morphosyntacticrules of English to a greater extent (as in Signing Exact English (SEE)) orlesser extent (as in Pidgin Sign English (PSE), a contact form between MCEand ASL). In the more extreme case of SEE, signed affixes have been in-vented to correspond to English affixes, while ASL has a different mecha-nism for expressing the same structure. In the less extreme case, PSE, theword-order of English is followed, but some of the grammatical structuresof ASL are employed where appropriate (Supalla, 1986). Because of thisfundamental difference between the system T.M. prefers to use and ASL,only some of the tests normally given to assess grammatical competence inASL were appropriate.

OUTCOME IN LANDAU-KLEFFNER SYNDROME 395
There is a large overlap in the basic lexicon of the PSE and ASL (i.e.,nouns, verb stems, adjectives, adverbs, and the fingerspelled alphabet). Be-cause of this overlap, most aspects of T.M.’s phonological skills could betested using materials developed for ASL. The phonological parameters ofhandshape, movement, orientation, and place of articulation were testable inT.M., since the sublexical distinctive features of these parameters are as-sumed to be at work in both systems; therefore, T.M. could be expected torecognize differences presented in minimal pairs containing only one dif-fering feature of these parameters. Also, many articulatory phonetic proper-ties of PSE and ASL are the same, and so some aspects of T.M.’s sign fluidityand coordination could be analyzed. In addition, T.M.’s ability to read fin-gerspelling could be tested. Aspects of T.M.’s signing that could not be testedusing ASL materials are the phonological operations of ASL, such as Move-ment Insertion (Brentari, 1990), Handshape Assimilation in compounds(Sandler, 1989), or Phrase-Final Lengthening (Perlmutter, 1992), since thephonological operations of ASL do not carry over into manually coded En-glish systems. Naturally, because these systems are visual–gestural, ratherthan auditory–vocal, the phonology of English is irrelevant to an analysisof PSE.
The grammar of English (and hence that of manually coded English) andthat of ASL are different in a number of important respects, two of whichwe will elaborate on here. ASL, like many Athapaskan languages, has anelaborate system of grammatical aspect (Klima & Bellugi, 1979; Liddell,1984) that is morphologically realized on the verb. These aspectual modula-tions express the manner in which actions are executed with respect to eachother, both temporally and spatially. On the other hand, tense, which ex-presses the temporal sequence of actions with respect to each other, althoughsometimes marked in idiosyncratic lexical forms (Jacobowitz & Stokoe,1988), is not consistently present as a verbal inflection on ASL verbs. Tensein ASL is typically expressed via independent lexical tense markers (Aarons,Bahan, Kegl, & Neidle, 1995; Jacobowitz & Stokoe, 1988). English, in con-trast, has an elaborated system of inflectional tense marking, but little expres-sion of grammatical aspect. English, for example, expresses aspect usingindependent lexical items or periphrastic expressions rather than by boundmorphology. This is illustrated by the sentences in (1).
(1) Expressions of verb aspecta. Spatial aspect (distributive aspect)
I give books [to the whole class].I give books [to each student in the class].I give books [to students who are members of this internal group].
b. Temporal aspectI wait [for a long time; one event].I wait every day [for a long time; successive events].I wait often [no mention of duration of wait; successive events].

396 BAYNES ET AL.
In ASL, the portion of the sentence in square brackets is a bound, discontinu-ous morpheme associated to the verb as a type of movement of the armthrough specific paths, in specific planes in three-dimensional space. Suchspatial contrasts as trajectory shape and planar locus are key formationalbuilding blocks of ASL’s morphology. Figure 2 illustrates the structured useof spatial contrasts within ASL’s rich morphological system. Figure 2 pre-sents three morphological processes which convey different class member-ship distinctions. In form, the Apportionative Internal inflection (conveyingthe meaning, ‘‘actions distributed all over, within a single whole’’) contrastsminimally in trajectory shape with the Seriated Internal inflection (conveyingthe meaning ‘‘actions distributed with respect to internal features or typicalparts of an object’’): the former inflection is made with a circular path shapein the vertical plane of signing space, whereas the latter inflection is madewith a linear path shape. However, the Seriated Internal inflection contrastsminimally with the Seriated External inflection (conveying the meaning ‘‘ac-tions distributed over a series of objects in the same general class’’), not intrajectory shape, but in planar locus (Fig. 2). In manually coded Englishsystems, the portion of each sentence in square brackets is expressed just asit is in English, using prepositional phrases. It is this latter type of structurethat is used most often by T.M. in her signing.
A second major difference between English and ASL involves the use ofclassifiers (e.g., a grain of {sand, salt, truth}, a piece of {pie, paper, candy},a slice of {pizza, bacon, life}, a stick of {butter, dynamite, gum}). ASL hasa much more elaborate system of classifiers than does English, and theyfunction as part of the verbal as opposed to the nominal system. The set ofASL classifiers includes the following.
(2) Type of classifiers in ASLa. semantic classifiers: those that encode a whole class of object(e.g., vehicle, upright being, small animal, round solid object)b. size and shape specifiers: those that encode the size and shapeof an object (e.g., flat, disc-shaped, cylindrical, rectangular)c. instrumental (handling) classifiers: those that encode the wayan instrument or object is grasped or handled (e.g., handle cylindri-cal grip {hammer, baseball bat, motorcycle}; handle rectangularobject {book, videocassette, stack of paper}; handle writing imple-ment {pen, pencil, paintbrush})d. body part classifiers: those that encode the salient body part in-volved in a movement (e.g., legs, head, feet, eyes, hands)
Each group of ASL classifiers has combinatorial restrictions with respect tosemantics and morphosyntactic structure of the verb (Kegl, 1985; Supalla,1990). Classifiers are often a part of polymorphemic verb structures express-ing change in state or location (Supalla, 1982), containing as many as ninemorphemes, similar to such systems in Athapaskan languages. In English,

OUTCOME IN LANDAU-KLEFFNER SYNDROME 397
FIG
.2.
The
stic
kfig
ure
repr
esen
tatio
nsar
eth
ree-
dim
ensi
onal
com
pute
rgr
aphi
cre
cons
truc
tions
ofth
ese
quen
ceof
arm
posi
tions
for
the
ASL
sign
sfo
rL
OO
K-A
Tun
der
thre
ein
flect
ions
.Po
sitio
nsof
the
shou
lder
,el
bow
,w
rist
,an
dha
ndov
erth
eco
urse
ofth
em
ovem
ent
are
show
n.Su
cces
sive
arm
posi
tions
are
sepa
rate
dby
10m
sin
time.
(Rep
rodu
ced
from
Poiz
ner,
Bel
lugi
,an
dK
lima,
1991
)

398 BAYNES ET AL.
such combinations would comprise an entire sentence, rather than be a mor-phemic part of a single word. Although T.M. used some classifier construc-tions in her spontaneous signing, she more often expressed these conceptsperiphrastically, as they are expressed in English.
Comparison of Signed and Spoken English Phonology
Signed English. T.M.’s manual articulation of Pidgin Sign English wasjudged to be normal. Her comprehension of the phonemic contrasts of ASLinvolving handshape, orientation, place of articulation, and movement wastested using a minimal pairs test developed by D.B., in which the subject isasked to identify the correct printed word (in English) when a sign is pre-sented; the foil for each test item is a sign which differs in one feature ofthe phonological parameters of ASL. Examples of minimal pairs in ASL aregiven in Fig. 3 (from Klima & Bellugi, 1979, pp. 101–103).
A phonetic measure of joint coordination while signing showed thatT.M.’s articulation of signs was phonetically like that of control signers (ofPSE or ASL). The type of measurement we did is called a handshape change-to-movement duration ratio (i.e., hs D/mov), first designed for the analysis ofParkinsonian signers (Brentari & Poizner, 1994). In the sign stream, parallelcomponents of lexical movements—handshape change, orientation change,or path movement—are synchronized with one another in time; in controlsigners, this yields a hs D/mov ratio of 1/1. In contrast, the same parallelcomponents in nonlexical movements, known as transitional movements, arenot synchronized with one another; in control signers, this yields an averagehs D/mov ratio of approximately 1/2. In Brentari and Poizner (Brentari &Poizner, 1994), it was reported that Parkinsonian signers have abnormallyhigh hs D/mov ratio in transitional movements, creating a subjective judg-ment that such signing is monotonous. T.M.’s signing patterns with controlsigners with respect to this measure.
T.M.’s ability to comprehend fingerspelled words was also tested. Whena list of semantically heterogeneous words of between 8–15 letters werepresented at a speed that allows for assimilation of letters, T.M.’s perfor-mance was excellent; she comprehended all of the words without difficultyor hesitation.
Spoken English. T.M.’s mastery of the phonology of sign far exceeds thatof the phonology of spoken English. To assess spoken English phonologicaloutput, the Assessment of Phonological Processes—Revised (Hodson, 1986)was administered. T.M. exhibited a severe articulation deficit, characterizedby a wide range of errors. Some of the most notable include the omissionof liquids, particularly post-vocalic ‘‘r’’ and some nasals. Her approach toconsonant clusters suggested a failure to apply typical processes of coarticu-lation to consonant clusters. Instead, T.M. produced the sound for each con-sonant separately, inserting an epenthetic central vowel between adjacent

OUTCOME IN LANDAU-KLEFFNER SYNDROME 399
FIG. 3. Examples of minimal signed pairs are pictured. RUBBER (top left) differs fromDOLL (top right) only in place of articulation—the chin vs the nose. CAT (middle left) differsfrom INDIAN (middle right) only in movement—two short movements away from the nosevs a single tracing movement from the nose across the cranium. CANDY (bottom left) differsfrom JEALOUS (bottom right) only in handshape—a selected index finger vs a selected pinkiefinger. (Reproduced from Klima and Bellugi, 1979)

400 BAYNES ET AL.
consonants. Vowels in general appeared to be ‘‘neutralized’’ or moved to-wards the midcentral region. Another frequent error was the prevocalic de-voicing of consonants. With the range of articulatory errors displayed, herspeech was judged to be largely unintelligible to unfamiliar listeners. Aninteresting observation was made by the transcriber, who is herself a Deaf,native signer of ASL. She noted that many individuals who are Deaf haveauditory speech that is difficult for hearing people to understand due to thevocal quality. However, their articulation is usually very clearly executed interms of visible movements of the mouth and tongue, which helps a speech-reader. In the case of T.M., her articulatory gestures were inconsistent andof little help in clarifying her phonological intentions.
Although T.M. does have some ability to lip-read and a strong desire tobe able to communicate orally, auditory communication with her was diffi-cult. Given the large differences in pitch and duration that were necessaryfor T.M. to hear sounds as different, we wanted to establish whether shecould distinguish phonemic contrasts in English.
EXPERIMENT 4—PHONEMIC DIFFERENCES IN SPOKEN SPEECH
Materials and methods. Forty-three word pairs were created from single syllable words thatdiffered only in the voicing or articulation of the initial or final consonant (deal–teal or fat–fad) or in the sound of the medial vowel (cooed–could or bit–bat). Forty-three word pairsthat were identical were also assembled from these word pairs. These two lists were combinedand randomized. The words were read aloud by one of the authors (K.B.) standing directlybehind the subject so that she was not aided by lip-reading. If T.M. was not sure of her decision,a pair could be read again at her request. The entire list was read twice in three differentsessions for a total of 258 judgments, 129 same and 129 different.
Procedures. T.M. was seated in a quiet room. She was instructed to listen carefully to eachpair of words read aloud and decide if the two words she heard were the same word or weretwo different words. She was to signal her choice by signing ‘‘same’’ or ‘‘different.’’
Results. There was no evidence of a learning effect across the three ses-sions, as overall accuracy declined (72, 70, and 66%, across sessions 1, 2,and 3, respectively). Percent correct (hits) and percent of false positive re-sponses (false alarms) were calculated. Overall, T.M. was correct 91% ofthe time in identifying two words as the same. When words were different,however, she identified them as the same 48% of the time as well (Fig. 4).A signal detection analysis using a nonparametric A′ estimate yielded an A′of .82 (Grier, 1971). These figures indicate that T.M. was indeed able tomake the discriminations with greater than chance accuracy. However, theseresults demonstrate a pattern similar to that demonstrated by her judgmentsof pitch and duration. T.M. was quite accurate in recognizing that two wordswere the same, but was frequently unable to label words as different. Shewas most accurate in the discrimination of vowel height and backness, butshowed an inability to distinguish tense from lax (e.g., [e] versus [E]; [i]versus [I]). For consonant contrasts, she was better able to make discrimina-tions in word initial as opposed to word final position (63 vs 21% correct

OUTCOME IN LANDAU-KLEFFNER SYNDROME 401
FIG. 4. The bar graph represents T.M. accuracy in recognizing that two spoken wordsare the same or different. T.M. is able to recognize that two words are the same, but falls tochance when she must recognize differences of a single phoneme. This pattern is similar tothat seen in discrimination of pitch and duration, but phonological distance was not systemati-cally varied.
on initial vs final voicing and 61 vs 28% correct on initial vs final place ofarticulation over all three administrations).
Despite the lack of precise articulation observed in her speech output,there was some consistency in her phonemic discrimination. Of the 86 pairs,she made the same judgment (all the same or all different) across all threetrials on 66% of the pairs. However, of these 15% were consistently wrong;that is, 13 pairs which were actually different were consistently judged tobe the same. Only 11 pairs (13%) were correctly and consistently judged tobe different. Of these, 7 pairs (8%) were vowel contrasts. Brentari, Kegl,Baynes, Kussmaul, and Poizner (in preparation) demonstrated that whenphonemic distance is controlled, the pattern of phonemic discrimination issimilar to that found for pitch and duration.
Discussion. Although T.M. can in some sense ‘‘hear’’ auditory phonemiccontrasts in a single word paradigm, her judgments are neither stable noraccurate enough for normal comprehension. Given the large differences nec-essary for her to be certain that two sounds differ from one another, it issurprising that she manages to distinguish these differences as well as she

402 BAYNES ET AL.
does. However, in a situation where she must decode fluent speech, her un-certainty precludes recognition of all but the most predetermined and ex-pected speech sounds. These results suggest that she needs a long soundsegment to increase her accuracy (vowel sounds generally are more staticthan the rapid format transitions required to understand consonants). It alsoappears that her processing is easily disrupted by the sound that comes beforeit, hence her poor performance on word final contrasts. Such perturbationshave made it impossible for her to identify and learn the normal phonologicalcontrasts that are the building blocks of spoken language.
As we have no reason to suspect that this degree of difficulty with auditoryprocessing represents a decline for T.M. but is more likely a stable state forher, our next goal was to try to understand how such a problem impactedher ability to learn language. For that purpose, we will compare her abilitiesto Deaf signers as well as to persons with normal hearing to try to separatethe contributions of deprivation of normal auditory stimulation from whatmight represent a more strictly language-based disorder.
Comparison of the Morphosyntax of Signed and SpokenEnglish Narratives
TM has potentially two natural languages in her repertoire, English andAmerican Sign Language. However, her exposure to both of these languageshas been less than optimal. By virtue of her auditory processing deficit, herexposure to spoken English was severely attenuated. Any input from spokenEnglish that she may have been receiving up to age 4, was severely disruptedwith the onset of LKS. In terms of American Sign Language, TM can beconsidered a late learner at best. Her first consistent exposure to ASL wouldhave occurred at a residential school for the Deaf she attended for two yearsin her teens, but by her own report, she affiliated herself with hard-of-hearing,Signed English signers rather than Deaf ASL signers.
Signed English. Signed English, TM’s self-proclaimed primary and pre-ferred mode of communication, is an artificial code for English that in itsmost consistent and elaborated form fails to achieve 100% equivalence toEnglish in terms of morpheme for morpheme correspondence and, in reality,typically manifests itself as a pidgin form between English and ASL, neitherof which serves TM as a native language.
As a child of hearing parents with a checkered educational career in termsof signed language (even Signed English) exposure, it is questionable thateven Pidgin Sign English was introduced early, intensively, and consistentlyenough to support a fully nativelike process of first language acquisition.The problem posed for us in TM’s case is how one evaluates syntactic com-petence in an individual who clearly has some language abilities, but forwhom no language (natural or artificial) may have consistently served asfirst language input throughout the critical periods for language acquisition.

OUTCOME IN LANDAU-KLEFFNER SYNDROME 403
This entails decoupling the assessment of use of clearly language-based syn-tactic and morphological operations, which can provide evidence of acquiredlinguistic competence, from nativelike mastery of all the nuances of anyspecific language, such as ASL or English.
EXPERIMENT 5—DETERMINING SYNTACTIC COMPETENCEINDEPENDENT OF LANGUAGE SPECIFIC MASTERY1
To establish that TM does indeed use syntax, independent of whether hersyntactic skills exhibit native-level mastery of English, we constructed anargument structure profile for T.M.’s spoken English narrative productionand compared it to the profiles of a Deaf, a hearing, and an aphasic subject.An argument structure profile consists of an inventory of the relative percentoccurrence of construction types produced by a given subject, where thetypes vary in terms of the number and types of noun phrases or sententialcomplements selected for by each verb.
Subjects. We compared TM’s argument structure profile with that of ahearing control, a Deaf control, and an agrammatic aphasic speaker of En-glish. The hearing control was used to provide a profile of the argumentstructure distribution of a native speaker of English. The Deaf control wasused as a more comparable profile of an individual whose auditory exposureto spoken English is compromised and for whom spoken English is not thepreferred mode of communication. Finally, we used the narrative productionof a hearing agrammatic aphasic to illustrate the profile of an individual witha frank syntactic deficit.
Materials and methods. T.M.’s spoken and signed English narrative production was evalu-ated using two 1.5-minute nonverbal cartoons viewed on videotape to elicit narratives (Mr.Koumal Flies like a Bird (Studio Animovaneho Filmu, 1969) and Mr. Koumal Battles HisConscience (Studio Animovaneho Filmu, 1973). Subjects were instructed to view each cartoonas many times as necessary (typically twice) and to recount what happened. The written narra-tives were elicited using captioned videotapes of three commercially available movies: Inter-view with a Vampire, Nell, and Moonstruck. Each videotape was watched in its entirety ondifferent evenings and subjects were asked to recount what happened in writing. They wererequired to cross out and correct the first draft of their written narratives, but erasures andsubsequent drafts were not allowed.
Using the syntactic coding system presented in Kegl, 1995, each narrative was transcribedand coded with respect to the number of words, sentences (simple vs sentential complement-taking), and construction types (based upon the number and type of NP arguments selectedfor by a given verb). Although each clause was coded for the number and type of argumentsselected by its verb, quantitative analyses focused upon clauses with verbs that either did ordid not require an external argument (a subject at d-structure). This procedure entails collectinga sufficient narrative sample identifying all verbs and coding for each clause in which theyoccur, the number and type of arguments selected for by the verb, and calculating how manyoccur in each of four categories: (1) verbs taking an external argument; (2) copular verbs
1 Preliminary results of this study were presented in Kegl, Baynes, Brentari, and Poizner(1996). A more detailed exposition of these studies appears in Kegl et al., in preparation.

404 BAYNES ET AL.
(don’t take an external argument); (3) other verbs not taking an external argument; and (4)uncodable utterances.
Use of this technique in aphasia studies. In prior studies of English-speaking aphasic sub-jects, Kegl (1995) used the profiles of native speakers of English as a benchmark againstwhich to measure the distribution of construction types in the narrative production of agram-matic aphasics, demonstrating that constructions lacking an external argument (and thereforerequiring various syntactic permutations of arguments to apply) were systematically avoidedor aborted by agrammatic aphasic speakers of English. Because this pattern of avoidancedistinguished even the simplest of sentences such as John slept (x⟨ ⟩, fine) versus John ar-rived (⟨ y⟩, avoided), this result was used to argue that, in English, problems in the productionof constructions lacking an external argument indicates a core syntactic deficit unconfoundedby other cognitive factors such as memory for longer sequences of words or for complexembedded sentences (typical indices of syntactic complexity).
Predicted result for subjects with a syntactic deficit. If T.M. has a syntactic deficit, wewould expect her not to produce noncopular constructions without an external argument. Thisprediction is based upon prior studies of individuals with ‘‘agrammatism.’’ They exhibit prob-lems with the syntactically triggered permutation of arguments of a verb, certain syntacticallydetermined long distance dependencies between lexical items, and syntactically conditionedmorphological agreement. In agrammatic aphasics, constructions such as those on the rightbelow are avoided in sentence production and are frequently misinterpreted in comprehension,especially when semantic strategies cannot be employed. The constructions such as those onthe left pose much less of a problem. In the examples below, x indicates the presence of anexternal argument (a d-structure subject); y indicates the presence of an internal direct argu-ment (a d-structure direct object); z indicates the presence of a d-structure indirect argument;and w indicates another phrase that, although not an argument, is obligatorily selected forby the verb. Under each sentence is a schema representing its d-structure representation (itsrepresentation prior to the application of any syntactic rules) followed by any permutation ofarguments required to yield an acceptable English sentence. The absence of an external argu-ment at d-structure is indicated by ‘‘[e].’’ In all cases where an external argument is absentat d-structure, some syntactic operation is required to assure that subject position is filled ats-structure; thus, problems with these types of sentences indicate a syntactic impairment.
Not Problematic ProblematicJohn (x) kissed Mary (y). Mary (y) was kissed by John.x kissed y [e] was kissed y → y was kissedMary (x) slept for an hour. John (y) seems to be sad (w).x slept [e] y to be wAlex (x) broke the bottle (y). The bottle (y) broke.x broke y [e] broke 7 → y brokeMary gave a book to Bill. The comedian (y) amused Bill (z).x gave y Pz [e] amused y z → y amused z
Crosslinguistic validity of argument structure profiles. Despite some variability from lan-guage to language, verbs with and without external arguments tend to exhibit the same patternsof distribution in the production profiles of fluent language users. In general, slightly overhalf the constructions produced have external arguments, while slightly under half do not.Variability exists within these two larger categories.
Predicted divergences between hearing versus Deaf speakers of English. Some crosslinguis-tic differences between English and ASL are to be expected. For example, copular sentenceswith an overt verb ‘‘to be,’’ such as the English sentences The woman is a doctor, The bookis red, or The child was frightened (⟨y⟩w) do not occur in ASL (Kegl & Poizner, 1997). Theparallel ASL construction which juxtaposes a noun phrase and a predicate nominal or adjectivewithout a linking verb is less frequent than its English counterpart:

OUTCOME IN LANDAU-KLEFFNER SYNDROME 405
hnIX WOMAN, DOCTOR‘‘The woman is a doctor’’
hnBOOK IX, RED‘‘The book there is red.’’
hnIX CHILD. FRIGHTENED‘‘The child was frightened.’’
The English of deaf individuals has been reported to exhibit problems with copular sentencesas well (Geers, Moog, & Schick 1984; McAfee, Kelly, & Samar 1990). Whereas these con-structions account for almost 25% of all sentence types produced by hearing controls, wewould expect a reduced occurrence of copular constructions in deaf subjects. This contrastswith the profile for aphasic speakers of English, who typically rely upon copular constructionsto replace those construction types that are syntactically taxing for them (e.g., adjectival pas-sive replaces verbal passive; copular measure construction (The chicken is 3 lbs.) replacesmeasure verb construction (The chicken weighs 3 lbs.), etc. While ASL signers produce fewercopular-type sentences, unaccusative constructions of the form ⟨y⟩ and ⟨yz⟩ (the common con-struction for verbs of motion/location) account for a slightly greater percentage of all utterancetypes.
If T.M. patterns with the agrammatic profile, this indicates a core syntactic deficit. If shepatterns with the Deaf, ASL-signing control in terms of an increased production of noncopularunaccusative constructions, this would indicate influence in T.M.’s English production thatfollows from exposure to ASL. If she patterns with the Deaf control in terms of reducedproduction of copular constructions, this would not necessarily demonstrate ASL influencebecause this pattern has been found more generally in the English of deaf people. Such aresult would however indicate some commonality between the language exposure history ofdeaf users of English and T.M. that may have as a basis impairment of some level of auditoryprocessing. If T.M. patterns with hearing, English-speaking controls, we would interpret thisresult as indicating the primacy of English as T.M.’s base language form.
Finally, we would expect the possibility that T.M.’s language performance in English couldvary based on the modality of input and expression. Several studies have noted that deafstudents can exhibit divergent proficiency between spoken and written English (see Loban,1974) for primary school children; and McAfee et al., 1990) for postsecondary school chil-dren). And numerous other studies have established that written and spoken language candiffer in the type and complexity of structures instantiated (Chafe, 1982; Ochs, 1979). Forexample, written languages tend to exhibit more subordination and longer mean length ofutterance.
There are drawbacks to using spoken and signed English to evaluate T.M.’s language pro-duction. The impingements of LKS on auditory processing put T.M. at a distinct disadvantagein both producing and comprehending spoken English. Signed English is an artificial codefor English and as such is not ideally adapted to the signing modality. Therefore, it is naturalfor T.M.’s Pidgin Sign English to recruit grammatical devices from ASL.
While written English is typically viewed as a secondary modality for the expression ofEnglish and cannot be assumed to parallel spoken utterances (Chafe, 1982), for T.M. it actuallyserves as her most natural form of input and production of English. This may seem counterintu-itive, because her reading of books and magazines is no more prolific than that of her peers.It may even be less. However, since the mid 1970s, television has been closed captioned, andT.M., like most Deaf people, has taken advantage of this technological innovation. An avidviewer of TV and video rentals, T.M. watches exclusively captioned material. Closed cap-tioning, in contrast with books or magazine, codes spoken English in a written modality.
Results and Discussion
Spoken narratives. Analysis of other aspects of TM’s spoken languageproduction revealed marked deficits in T.M.’s spoken output, especially withrespect to articulation, prosody, word choice, and amount of output (50% of

406 BAYNES ET AL.
that produced by her Deaf control). In addition to a marked loss of prosodyand fluency in articulation, T.M. also systematically omitted inflectional mor-phology and was limited in her vocabulary choice. Although she producedproportionally many complex sentences in her spoken English, the sententialcomplements were invariably infinitival and frequently involved subcategor-ization errors, such as using an infinitival complement when an -ing comple-ment was required by the chosen verb as in ‘‘But angel[aj] stop[sta] him tosteal[sil] ten dollar[dal]’’ for ‘‘But the angel stopped (prevented) him fromstealing the ten thousand dollars.’’ Frequently, she used a more commonword with the argument structure pattern of the more desirable target item,suggesting limited vocabulary but preserved conceptual and lexical semanticrepresentations. For example, T.M. used the word ‘‘went’’ in place of‘‘climbed’’ in her spoken English narrative, while correctly using the signCLIMB in her signed English narrative. In some cases, T.M. fell back upona less specific word in both her signed and spoken narratives. For example,she used ‘‘ask’’ in place of the more specific verb ‘‘beg’’ in both her signedand spoken versions of the same narrative.
However, only her spoken English exhibited frank semantic errors in lexi-cal choice such as ‘‘He grew up all feather from chicken’’ in place of‘‘scooped up, gathered up’’ where the superficial pattern V 1 up conditioneda substitution that yielded an anomalous sentence. Mayberry and Fischer(1989) report experiments requiring native versus nonnative speakers of bothEnglish and American Sign Language to shadow (or echo) spoken or signednarratives while they were being presented. They found that native speakerstypically substitute semantically compatible words, demonstrating their abil-ity to process and paraphrase the incoming language while nonnative speak-ers more frequently made semantically anomalous substitutions of wordsbased simply on phonological similarity, indicating that they were processingthe sound, but not the content, of the stimuli. T.M.’s word choice errors inspoken English resemble those of a nonnative speaker or second languagelearner, but her errors are based on superficial similarities at the word levelrather than the phonological level of representation.
All of these factors contributed to a marked lack of intelligibility in TM’sspoken narrative production. However, her argument structure profile, de-spite her limited vocabulary and poor pronunciation, showed her syntacticabilities to be intact. T.M.’s argument structure profile as compared with ahearing and Deaf control, as well as an agrammatic aphasic are presentedin Fig. 5. T.M. shows no evidence of a syntactic deficit. There is no decreasein the production of unaccusatives (noncopular constructions without an ex-ternal argument). She did show reduced production of copular constructions,a characteristic of the English produced by Deaf individuals (independentof signing background) that may be related to the reduced acoustic saliencyof copular verbs, which are typically contracted. She doesn’t produce anincreased percentage of unaccusatives (greater that 25%), which would be

OUTCOME IN LANDAU-KLEFFNER SYNDROME 407
FIG. 5. The production profile of T.M.’s spoken argument structure clearly contrasts withthat of an agrammatic aphasic in failing to display a drop in constructions without externalarguments, and parallels the Deaf control’s profile in exhibiting a reduced percentage of copu-lar forms. Finally, T.M.’s profile doesn’t exhibit any increase in production of noncopularconstructions without external arguments, which would be an indication of increased influenceof ASL on her production.
expected if her English was being strongly influenced by ASL grammar.Thus, in the spoken modality, her use of argument structure is typical of aDeaf user of English, not necessarily native in ASL.
Signed narratives. T.M.’s preferred mode of signing is Pidgin Sign En-glish (PSE), a pidgin incorporating some aspects of both ASL and SignedEnglish. Her version of this pidgin heavily favors Signed English in wordorder and vocabulary choice. All breakdowns in sign communication withher testers occurred when testers shifted to uniquely ASL grammatical con-structions. Although T.M. professed difficulty in reading fingerspelling, herproduction of fingerspelling was fluid, but revealed problems with the actualspelling of words (f-e-t-e-r, f-e-a-t-a-l, f-e-a-t-e-r-s, for ‘‘feathers,’’ h-u-r-t-o-p for ‘‘hilltop,’’ and in another context c-i-c-i-n-d-r-a for ‘‘Cinderella.’’
Figure 6 presents the signed narratives of TM and her Deaf control ascompared with their spoken narratives discussed earlier. While TM’s spokennarratives are half as prolific (51 utterances) as her control’s (107), indicatingan increase in difficulty with this modality of expression, her signed narra-tives are comparable in quantity of output (100 versus 97). Her signed narra-tives also exhibit more noncopular unaccusatives and an increase in the num-ber of utterances produced.
In contrast with her spoken English, T.M. showed no dysfluency in hersigning and produced almost twice as many sentences in her signed versusspoken rendition of the Koumal narratives. The increased percentage of con-structions without external arguments in TM’s signed narratives reflect an

408 BAYNES ET AL.
FIG. 6. Argument structure profiles for signed and spoken narratives for T.M. and a Deafcontrol P.T.L. are presented. The reduction in copular forms is present in both signed andspoken narratives despite T.M.’s increased fluency when signing. The increased percentageof constructions without external arguments in TM’s signed narratives reflect greater recruit-ment of ASL-like constructions in her Pidgin Sign English.
increased recruitment of ASL-like constructions in her Pidgin Sign English.A wider range of vocabulary items was available to her in her signing andshe used them in the appropriate argument structure patterns. In contrast withher spoken narratives where frequent hesitations and false starts reflectedfailure of her linguistic system to meet her communication goals, she wasable in her signed communication to express all she intended with relativeease. Still, she comes across as a late learner in her signing and it remainsto be determined whether this is attributable to the effects of her early epi-lepsy or to her patchy exposure to ASL.
Although T.M. produced a number of complex sentences in both hersigned and spoken English narratives, they all involved infinitival comple-ments (perhaps a strategy to avoid inflected forms). In both her signed andspoken English, T.M. favored constructions involving an external argument.For example, in a context where $10,000 falls unnoticed from a woman’spurse, T.M. used a form of drop that selects an agent rather than its unaccusa-tive counterpart lacking an external argument. In spoken English she misrep-resents the situation: But she drop[ped] ten thou[san]d dol[lars] (the bracketsindicate portions of the words not pronounced). In signed English shechooses an alternative transitive verb: SHE LOSE TEN THOUSAND DOL-LAR. (The lack of tense marking and plural is typical of PSE.)

OUTCOME IN LANDAU-KLEFFNER SYNDROME 409
FIG. 7. The argument structure profile for T.M.’s written narrative is identical to theargument structure profile of the hearing, native English-speaking control TM in Fig. 7. BothT.M. and P.T.L. closely approximate the distribution of spoken English, although P.T.L. showsgreater influence of her ASL exposure.
Although she favors canonical SVO order and frequently omits functionwords and inflections, T.M. does not exhibit a typical agrammatic profile interms of her use of argument structure patterns. Her sentence productiondiverges from agrammatic aphasics and from hearing, English-speaking con-trols in two distinct respects. First, copular constructions like ‘‘Mary is adoctor’’ generally make up a little under 25% of the clause types producedby controls and are even more frequent in agrammatic production. Copularconstructions are almost absent from T.M.’s narrative production in bothsigned and spoken English (a characteristic of Deaf English independent ofASL influence). Furthermore, while agrammatic speakers of English typi-cally fail to produce noncopular unaccusative constructions (the remainingargument structure patterns lacking an external argument), T.M. producesthem in the same or greater proportions as hearing, native English-speakingcontrols. Analysis of the sentences that instantiate these argument structurepatterns in T.M.’s narrative production, however, reveals a greater use ofmotion/location verbs than found with English-speaking controls and a re-duced occurrence of other unaccusative construction types such as passives,seems-type subject raising sentences, and amuse-type psychological verbs.This distribution of sentence types seems to reflect characteristics of Ameri-can Sign Language, which has a lower occurrence of copulars (Kegl &Poizner, 1997), greater representation of motion/location verbs (since loca-tives typically realized in English by prepositions function as unaccusativeverbs in ASL), reduced occurrence of passive, and no occurrences of amuse-type psychological verbs or subject raising verbs.
Written narratives. Figure 7 reveals that T.M.’s narrative production pro-file for written English is identical to the argument structure profile of thehearing, native English-speaking control in Fig. 7. We see that both T.M.and her Deaf control produce more copular constructions in their writtenEnglish, more closely approximating the distribution found in English. Fi-nally, we see that the native ASL-signing Deaf control still favors noncopular

410 BAYNES ET AL.
unaccusative constructions more than hearing controls, even in her writtennarratives. Despite sharing an isomorphic argument structure profile with thehearing control, T.M.’s written English is still characterized by numerousnonnativelike grammatical errors including frequent omission of agreementand tense marking, overuse of infinitival constructions, errors in verb choice,gender marking, determiner use, and a variety of biclausal raising struc-tures—all attesting to her status as a late learner of English.
Conclusions. Our analysis of argument structure distribution in T.M.’ssigned, spoken, and written narratives establishes that despite lack of na-tivelike mastery of English (or ASL for that matter), she shows no evidenceof any syntactic impairment. Furthermore, when we move away from thespoken modality (which for her is extremely compromised) and from thesigned modality (where influence from ASL grammar is unavoidable), wefind that T.M.’s production of written English confirms her own report thatEnglish (albeit preferably signed) serves as her primary, but not native, formof expression.
EXPERIMENT 6—WRITTEN GRAMMATICALITY JUDGMENTS
Although T.M.’s severe difficulty with auditory comprehension precludedassessment of her comprehension of syntax in spoken language, she has hadmuch exposure to written English and we wanted to assess her comprehen-sion of language in that modality. T.M. has studied written English in schooland is adept at a variety of recordkeeping and writing tasks. She reads booksand magazines for pleasure and watches closed caption TV. We wanted toassess her comprehension of written English to determine if she might havedeveloped a more standard English syntax through her exposure to reading.
Materials and methods. Linebarger, Schwartz, and Saffran (1983) reported on the abilityof aphasic subjects to judge the grammaticality of 351 sentences containing 10 types of gram-matical violation. These same sentences were typed and presented to T.M. in random order.
Procedures. T.M. was asked to read each sentence to herself and decide if it were grammati-cally correct or not. A short set of practice sentences was administered to her with feedbackto be certain that the task was clear.
Results. Percent of ‘‘hits’’ (correct recognition of grammatical sentences)and ‘‘false alarms’’ (ungrammatical sentences called grammatical) was cal-culated for each sentence type. An A′ statistic was calculated for each sen-tence type (Grier, 1971). T.M. was very accurate in her ability to identifygrammatical and ungrammatical sentences on the basis of a written sample(Table 4). She made no errors on tag questions and was able to recognizeviolations of phrase structure perfectly. She was least sensitive to violationsinvolving empty elements. Overall, her performance was far superior to thescores achieved by aphasic patients who have difficulty understanding gram-matical relations.
Discussion. T.M.’s performance on a written version of the Grammatical-ity Judgment task (Linebarger et al., 1983) reveals surprising syntactic com-

OUTCOME IN LANDAU-KLEFFNER SYNDROME 411
TABLE 4Examples of Violations used in Written Grammaticality
Judgments and a Nonparametric Signal Detection Measure ofAccuracy
Construction type A′ score
Strict subcategorization .86*The little boys laughed the clown.
Particle movement .89*They stood the line in very patiently.
Subject-auxiliary inversion .94*Did the old man enjoying the view?
Empty elements .73*Frank expected that they would give the job to.
Tags: Subject copying 1.00*The man is beside the truck, isn’t it?
Left branch condition .99*How many large did he order fig trees?
Gapless relatives .97*Bill found the book that the key was lost.
Phrase structure 1.00*Bill comforted the girl sad.
Reflexives .99*We myself will be on hand.
Tags: Auxiliary copying 1.00*George left the house at noon, wasn’t he?
petence in terms of sensitivity to constraints on agreement, argument selec-tion, and word order. Her errors clustered around constructions involvingempty elements, verb particle constructions with discontinuous occurrenceof the particle, passives, and subject raising constructions. Most errors wereattributable to a combination of her difficulty in processing low salienceitems such as unstressed function words and inflectional markers in conjunc-tion with the influence of ASL grammar on PSE, particularly its ability toallow null elements as the result of Topic deletion and pro-Drop in bothsubject and object position. They generally demonstrate that she is able toappreciate grammatical information in a modality to which she has normalaccess.
EXPERIMENT 7—WRITTEN COMPREHENSIONOF HIERARCHICAL STRUCTURE
Argument structure analysis focuses upon relations within the clause andnot on grammatical dependencies across clauses in embedded structures. De-spite T.M.’s demonstrated ability to appreciate a well-formed written sen-tence, it was necessary to determine if she was able to use grammatical infor-mation to guide her comprehension. Bishop (1982a) has observed in other

412 BAYNES ET AL.
Landau-Kleffner children and in deaf children who are native signers thatthere is a failure to develop this aspect of a hierarchical grammar. If thesechildren are given a sentence like ‘‘The chair that is in the hall is red’’ andhave to choose between a picture of a red chair in a white hall or a whitechair in a red hall, they will chose the picture of the white chair in the redhall. That is, they attach the sentence final verb phrase to the adjacent nounwithout appreciation of its status as an embedded phrase, whereas most na-tive speakers of English are easily able to recognize that it is the chair thatis red. They are easily able to recognize that the phrase ‘‘the chair’’ wasfollowed by the relative clause ‘‘that is in the hall’’ and when they encounterthe final phrase ‘‘is red’’ automatically associate it with ‘‘the chair.’’ Wewanted to determine whether T.M. was able to understand this relationship orif she also exhibited a problem with interpretation of this sort of grammaticalstructure.
Methods and materials. A set of twelve sentences was created. Five were taken from theTest of Receptive Grammar (Bishop, 1982b), one from Bishop (1982a), and the other sixsentences were variations on the original sentences. All sentences were seven words long andconsisted of a two-word noun phrase and a two-word verb phrase interrupted by either a three-word prepositional or gerund phrase. Four pictures were displayed for each sentence. Onewas correct, one reversed the relationship between the two actors or objects, one containedthe error described above, and one made both errors. Figure 8 illustrates the pictures displayedfor the sentence ‘‘The boy chasing the horse is fat.’’ Parsing this sentence as Bishop predictswould result in the choice of picture 3.
Procedure. The printed sentences were displayed one at a time for T.M. to read to herself.The four pictures were in view throughout this period. She was instructed to read the sentencecarefully and decide which of the pictures matched the sentence. There was no limitation onthe time she could take. She then pointed to the picture she had chosen.
Results. For all twelve sentences, T.M. systematically selected the picturewhich represented the hierarchical error (chance 5 .25, Z 5 20, binomialp , .001, two tailed). She selected these pictures confidently and was reluc-tant to believe that her responses were not correct. Her choice was clearlydictated by a grammatical analysis of the sentence and did not appear to bea default or chance selection.
Discussion. T.M.’s comprehension of grammar demonstrates the impactthat an alteration in the processing of the auditory signal can have on thedevelopment of the language system. She has experienced a profound andpersistent change in the characteristics of the linguistic system that she hasdeveloped. It appears T.M.’s grammatical system does not allow her to holdan incomplete phrase and wait for the correct grammatical structure to com-plete it. Hence, she must make the attachment of a phrase to the most imme-diately available structure. In this case, that is the noun phrase that immedi-ately precedes it. It appears that the grammar she has developed is similarto that not only of some other children with Landau-Kleffner Syndrome, butto Deaf children who have learned a signed language as their first language(Bishop, 1982a; see also Berent, 1996; McAfee et al., 1990). An attachmenterror of the type that T.M. makes is similar to an error type predicted by

OUTCOME IN LANDAU-KLEFFNER SYNDROME 413
FIG
.8.
Pict
ure
choi
ces
for
the
sent
ence
‘‘T
hebo
ych
asin
gth
eho
rse
isfa
t’’
used
inE
xper
imen
t7.
Pict
ure
1co
rres
pond
sto
inco
rrec
tas
sign
men
tof
role
sw
ithco
rrec
tas
sign
men
tof
the
adje
ctiv
e;pi
ctur
e2
toin
corr
ect
assi
gnm
ent
ofro
les
and
adje
ctiv
e;pi
ctur
e3
toin
corr
ect
assi
gnm
ent
ofth
ead
ject
ive
(the
choi
cepr
efer
red
byT
.M.a
ndob
serv
edin
othe
rL
KS
child
ren
and
nativ
esi
gner
s);
and
pict
ure
4to
the
corr
ect
choi
ce.(
Rep
rodu
ced
from
Tes
tof
Rec
eptiv
eG
ram
mar
)

414 BAYNES ET AL.
a model like that of Frazier and Fodor (1978). They suggest that certaingrammatical decisions must be made within a limited processing window.If working memory can hold only a certain number of items and decisionsmust be made without looking ahead, a number of problems arise. In normalspeakers, these factors combine to produce a limitation on the number ofembeddings that can be processed, predicting the difficulty of sentences like‘‘The boy the girl the dog bit kissed was horrified.’’ In T.M.’s case, thefailure to develop an auditory working memory may have made it impossiblefor her to form a stable representation of the phrases necessary to develophierarchical grammatical structure. It is unclear whether the failure to de-velop a phonological grammar precedes, is a result of a deficient auditory–verbal short-term memory, or if the two are only coincidentally related inour patient. Allport (1984) has suggested that phonological and short-termmemory processes are both dependent upon the same mechanisms. However,there is currently debate within the neuropsychological literature regardingthe independence of a phonological short-term store from perceptual pro-cessing in adults (see Martin & Breedin, 1992, for review). The develop-mental situation may be different (Gathercole & Baddeley, 1990) withgreater interdependence during development.
If so, other children with Landau-Kleffner Syndrome should have co-occurring problems with auditory–verbal short-term memory and the devel-opment of a productive phonological grammar. The problems with auditory–verbal short-term memory should predict grammatical impairments that willonly be apparent if specifically tested. The problems with phonological gram-mar should predict limited lexical development. Metz-Lutz et al. (1997) havereported reduced auditory short-term memory in four recovered Landau-Kleffner patients. However, children with landau-Kleffner Syndrome showdifferent levels of impact on their language development. Some children goon to develop normal or near normal auditory language after a period ofimpairment. Because this disorder strikes at such a vital period in the devel-opment of language and has such a varied outcome, it offers an unparalleledopportunity to examine in detail the consequences of the interruption of lan-guage development at different stages in the process and perhaps help us todetermine if there is a differential time course and cognitive substrate re-quired for the development of phonological and syntactic skills.
GENERAL DISCUSSION
Our dual hypotheses at this point are that (1) the disruption in auditoryprocessing secondary to Landau-Kleffner Syndrome can derail the develop-ment of a productive phonological grammar and (2) a limited auditory–ver-bal short-term memory limits the development of a hierarchical grammar.The failure to develop a phonological grammar blocks the efficient decodingand retention of the sound symbols for new objects and concepts; hence, it

OUTCOME IN LANDAU-KLEFFNER SYNDROME 415
prevents the rapid upturn in lexical acquisition seen in children learning lan-guage (Locke, 1993). We do not know if this is an all-or-none or a gradedphenomenon, i.e., whether some partial phonology may allow better lexicaldevelopment. The limitation in auditory–verbal short-term memory is a moregeneral phenomenon seen in Deaf signers as well. We suspect that it is atthe root of the unusual grammatical comprehension seen in T.M., other LKSchildren, and other Deaf signers. We do not know if the mechanism of bothof these phenomena is the same as suggested by Allport or if they are sepa-rate, as Martin’s work would suggest.
Critical Periods
The profile of T.M.’s verbal and signed languages described here we be-lieve to be a direct outcome of the deprivation of auditory input before astable phonological grammar and short-term memory have developed. Itseems likely that the disastrous consequences for T.M. occurred because thedeprivation of input intersected with a critical period in language acquisition.It is well established that there is a general critical period for language acqui-sition, based on studies showing that there is a time after which a language—even a first language—is difficult to acquire (Lenneberg, 1967) and on stud-ies showing how much of a native language a normally developing child hasmastered by age 3. In two cases of language deprivation, Genie, exposed tolanguage for the first time at age 131/2, never gained fluency in her first lan-guage (Curtiss, 1977), but Isabelle (Mason, 1942), exposed to language forthe first time at age 61/2, was evaluated as having normal language skills after18 months.
There is also evidence that there are optimal windows of acquisition forvarious aspects of grammar, which are spaced throughout the more generalcritical period. Leaving aside crosslinguistic variations in these windows ofacquisition that might reflect language-specific differences with respect togrammatical architecture, it is widely accepted that phonology is one partof grammar whose window of acquisition begins quite early (Locke, 1993)—even before birth, when French fetuses have demonstrated an ability to dis-criminate between prosodic properties of French and Russian by showingan increased level of activity when listening to French (Bertoncini, Morais,Bijeljac-Babic, McAdams, Peretz, & Mehler, 1989; Mehler, Jusczyk, Lam-bertz, Halsted, Bertoncini, & Amiel-Tison, 1988). Marcotte and Morere(1990) have suggested that the critical period in which auditory input is re-quired to establish normal language lateralization occurs before 36 monthsof age. This represents a problem for our theory, as Landau-Kleffner patientsare not usually diagnosed until at least 3 or 4 years of age. However, thissituation may indicate that the distorted feedback from this disorder is moredisruptive than complete deprivation or that these children may be linguisti-cally delayed by subclinical symptoms of the disease before it is diagnosed.

416 BAYNES ET AL.
Specifically related to this work, there is a correlation between the emer-gence of a system of phonological contrasts (i.e., a distinctive feature system)and an growth-spurt in lexical acquisition between 17 and 24 months. Thishypothesis will be developed in more detail elsewhere (Brentari et al., inpreparation). The complex interaction between the stage of language devel-opment reached when a child becomes ill, the severity of the case of LKS,and exposure to alternative communication systems offers an opportunity todocument whether or not there are separate critical periods for different as-pects of linguistic development.
Variability in outcome. Although the variable outcome following Landau-Kleffner Syndrome has made diagnosis and treatment difficult, this variabil-ity may in fact provide us with information about the developmental windowin which auditory input is most crucial. Even when seizures are successfullytreated, improvement of the language dysfunction may not follow. In fact,many cases never have a reported seizure (see Bishop, 1985, for a summary),although improved monitoring methods might have demonstrated abnormalEEG activity (Deonna, 1991; Marescaux, Hirsch, Finck, Maquet, Schlum-berger, Sellal, Metz-Lutz, Alembik, Salmon, Franck, & Kurtz, 1990). Out-come in the selected cases reviewed here varies from complete recovery ofnormal language to a persistent and severe aphasia. Mantovani and Landau(1980) followed the first six reported cases and three additional ones 24 to28 years after onset. All had maintained their recovery and graduated highschool. Of the three additional cases reported at that time, one was doingwell as a second-year college student. Two others appeared to have morechronic language difficulties. One was functioning at the 6th-grade level inspelling and arithmetic and the 9th-grade level in single word reading at age15. She used 4 to 5 word sentences with ‘‘mildly awkward syntax.’’ Thelast patient at age 17 was at the 4th-grade level in reading and spelling andrequired special education for most classes. Speech was described as ‘‘tele-graphic.’’ Overall, five of these cases could be said to have acquired normallanguage by late adolescence or adulthood, and some had college training.There did not appear to be an adequate predictor of good or bad outcomein this series. Gascon, Victor and Lombrosso (1973) reported a case withonset at age 6. The child was sent to a School for the Deaf at age 14, wherehe did slowly reacquire auditory language. He was able to complete highschool and attempted college, but dropped out. At 21, he was mildly anomicwith marked problems with reading and spelling. Likewise, Cooper andFerry (1978) reported three cases with onset before the age of 4 and severechronic language deficits who responded well to manual communication.After reviewing the 45 cases that had been reported since 1957, they empha-sized the importance of obtaining a neurological evaluation for any childwho ceases to talk suddenly, whether or not seizures occur. However, be-cause some of these children did not understand gesture, the authors cau-tioned that manual communication may not always be a useful intervention.

OUTCOME IN LANDAU-KLEFFNER SYNDROME 417
A case study of an 11-year-old who had initial symptoms of LKS at age3 focused on the development of written language (Denes et al., 1986). At3, he had no oral language with comprehension of only a few words andexhibited some ‘‘aggressive and oppositional traits.’’ Because his audiogramwas normal, a diagnosis of infantile psychosis was considered. Although hisoral language remained impaired, his nonverbal intelligence appeared normalfor his age. His mother set out to teach him written language with sufficientsuccess that he was able to attend primary school. At the time of testing, hewas able to score 34/36 on the Colored Progressive Matrices, but he couldneither produce nor understand spoken speech. Despite his good use of writ-ten speech, he showed difficulty with tasks that required him to understand orproduce function words. The authors concluded there was a central auditorydisruption of phonological processing that interfered with his acquisition ofsyntactic processes requiring phonological mediation. However, there wasnever an attempt to teach this young man a sign language, so it is unknownhow he would have fared with that intervention. We also know little aboutthe extent of his lexical development.
Paquier and colleagues (1992) reported six cases with adult follow-up.These cases presented with fluctuating courses and with variable outcomes.Three apparently reacquired normal or nearly normal language. The otherthree cases had some degree of language involvement, with the extreme be-ing a persistent aphasia. Once again, later onset is more likely to be accompa-nied by improvement or recovery. The patient reported by Marien et al.(1993) was always mildly delayed in language milestones but was pro-gressing until his speech began to deteriorate at age 4. He continued to havefluctuating difficulties with both production and comprehension. Expressivespeech was more impaired than comprehension, causing Marien to suggestthat there was a form of LKS that had predominantly motor symptoms andto note prior cases that seemed to have predominantly motor problems. Thispatient continued to experience significantly impaired speech at the time ofthe report. Tharpe and Olson (1994) reported two cases diagnosed with LKSwith emphasis on the benefits of manual communication. One, a boy, firstexhibited some regression in language abilities at age 2.5. By 3.9, his expres-sive language was severely delayed with a severe phonological disorder. Hewas not introduced into a ‘‘total communication’’ approach until after hewas diagnosed with LKS at 4.9. He made rapid progress at that point. Asecond female patient was diagnosed at 3.5 with impairments in expressivespeech noted first. Misarticulations increased in frequency and output de-clined to only a few words. The authors stress the need for more long-termfollow-up studies to determine outcome.
The idea that Landau-Kleffner Syndrome should not be characterized asan aphasia was introduced by Rapin et al. (1977). They suggested that thesymptoms are much like those of verbal auditory agnosia or word deafness(rather than Wernicke’s aphasia) in adults, but that expressive language is

418 BAYNES ET AL.
far more disrupted in children when auditory feedback is lost or disrupted.They noted the profound loss of auditory comprehension, often mistaken fordeafness and the insidious loss of expressive speech in these patients. Fivecases were presented with careful review of language symptoms. They char-acterized the speech of their patients as being ‘‘deficient in articulation,[with] phonemic and semantic paraphasia, dysprosody and altered rhythm,and . . . [in two cases] . . . jargon.’’ Two of their cases showed apparentlynormal ability to process written language. They reported that their patientscould recognize and discriminate environmental sounds. Struck by the poorerprognosis for these children than for those with childhood aphasias due tofocal lesions, they noted that bilateral damage to auditory association areasor a subcortical lesion that isolates the dominant parietal–temporal cortexfrom the auditory association areas of both hemispheres is necessary for thissyndrome to occur. They suggest that the bilateral nature of the disruption mayblock any rehabilitative input from the right hemisphere and may explain whymany of these cases recover less well than focal childhood aphasias.
As noted previously, Bishop (1982a) investigated the grammatical com-prehension of nine children with Landau-Kleffner syndrome and comparedthem with twenty-five children with Developmental Expressive Disorder,and control groups of 4-, 6-, 7-, and 8-year-olds. Bishop concluded that lan-guage acquisition in LKS was deviant rather than delayed. Moreover, theLandau-Kleffner group patterned differently from children with develop-mental language disorders. They did not make random errors, but interpretedsentences systematically. Grammatical comprehension was compromised inthe same way for spoken English and Paget-Gorman Sign System (a manu-ally coded version of English) presentations. Further work showed that deafchildren made the same sorts of errors, indicating that the manual acquisitionof language might be the common causal factor. Both children with LKSand those that were deaf signers failed to comprehend embedded structurescorrectly. Bishop suggested that spatial and configurational information maybe easier to extract via the visual modality, but that the temporal patternswhich are the building blocks of spoken language are lacking and contributeto the failure to develop a hierarchical grammar.
Bishop (1985) subsequently reviewed the 119 published cases of LKS toexamine the variables that might help to predict outcome. Discounting sei-zure severity and remedial training as determinants of outcome, she focusedon age of onset, evidence of bilateral involvement of Wernicke’s area andits right hemisphere homologue, and finally that loss of auditory input as thechief contributors to the outcome. Of the 119 published cases, 61 had follow-up to age 12. Linguistic deficit and outcome were graded as much as possible,given sometimes scanty descriptions, and a correlational analysis was under-taken. There was a highly significant correlation between age of onset oflanguage regression and poor outcome. Children who acquired the disorderearly in childhood were less likely to have a good prognosis. When the onset

OUTCOME IN LANDAU-KLEFFNER SYNDROME 419
was later, language recovery was more likely to occur. This is compatiblewith the view of LKS as a high-level auditory processing disorder, ratherthan a unilateral insult to Wernicke’s area. We suggest this correlation isalso compatible with the view that loss or disruption of auditory input beforethe acquisition of a phonological grammar may be a key factor in predictingpoor outcome.
Metz-Lutz et al. (1997) have reported a series of four cases now recoveredfrom epilepsy. Language has recovered in concert with normalization of EEGfindings. However, careful experimental examination of these patients dem-onstrated continued disruption of dichotic listening performance in the earcontralateral to the epileptic focus. All patients continue to have deficits inauditory span tests as well. These findings support the view that a failure todevelop normal phonology may play a central role in the chronic languagestatus of these patients, as deficits in phonological processing are hypothe-sized to represent a deficit in the same mechanism that supports span tasks(Allport, 1985; Gathercole & Baddeley, 1990).
The inconsistency across these cases is clear, although early onset is usu-ally associated with poor outcome. Moreover, in studies such as that of Metz-Lutz et al., there is an implication of auditory–verbal short-term memorydeficits even in recovered cases. If our hypothesis regarding the crucial roleand restricted developmental window for phonology is correct, documenta-tion of the state of phonological development at the onset of the disease mayhelp us to better understand and predict outcomes. Likewise, we may be ableto observe whether the development of a phonological grammar and a stableauditory–verbal short-term memory are dependent upon the same mecha-nisms or can develop separately. Observations of this sort will require de-tailed work-up of patients as soon as possible after diagnosis. It is also possi-ble that different etiologies may be involved in this syndrome and differentneural loci associated with them may not have the selective impact on pho-nology that we have seen with T.M.
Summary and conclusions. T.M. may have had the capacity to acquirelanguage normally, but she did not receive auditory input during periodscritical for normal acquisition. Although her language development was byfar the most severely affected by her childhood disorder, there remain deficitsin all aspects of auditory processing that we have been able to test. Analogousto the more severe impact on language than on other areas of auditory pro-cessing, her disorder has had more severe consequences for the developmentof spoken phonology than other aspects of spoken English: i.e., both phono-logical input and output are severely disrupted. Her limited lexical develop-ment we believe may be a direct consequence of the failure to develop aproductive phonological grammar. Morphosyntactic analysis of spoken lan-guage demonstrates problems with inflectional agreement, strict subcategori-zation, and a similar poverty of embedded structures. Although T.M. demon-strates the normal range of argument structure in her speech output, her use

420 BAYNES ET AL.
of grammatical information in comprehension tasks is limited in a mannersimilar to that of native Deaf signers. The former syntactic difficulties arenot the result of a linguistic impairment, but rather an additional direct conse-quence of the failure to have adequate linguistic input when her grammarwas developing. The latter difficulty with the use of grammatical informationin comprehension tasks we suspect to be a ‘‘normal’’ variant of linguisticgrammar acquired in the absence of auditory stimulation and a possible con-sequence of a limited auditory–verbal short-term memory.
Our argument that the deprivation of auditory input during a critical periodis the key factor in her chronic impairment is dependent upon the assumptionthat T.M.’s phonological grammar had not been fully acquired when shebecame ill. We cannot know in her case if this is true. It does however posea question which can be asked as new cases arise. For this reason, we urgecareful documentation of the stage of phonological, lexical, and syntacticdevelopment in all Landau-Kleffner cases as soon as possible after diagnosis.
In contrast, T.M.’s signed phonology appears to be intact. However, mor-phosyntactic analysis of ASL demonstrates problems with inflectional agree-ment, strict subcategorization, and a poverty of embedded structures. Dothese problems reflect a deficit in her ability to acquire language as a resultof her convulsive disorder as is suggested by the identification of Landau-Kleffner as a language disorder? Or are they the result of the impoverishedexposure to ASL? Although we believe the latter view is correct, observa-tions from just one patient cannot offer definitive answers to these questions.
The opening and closing of developmental windows (see Locke, 1993,pp. 297–299) may be part of the determination of outcome in LKS. Timeof onset has been shown to be important in predicting outcome, with seizuretype and intensity less consistently related. We suggest that the stage in lan-guage development at which auditory input is disrupted rather than chro-nological age may be crucial in understanding the nature of the languagedysfunction. It will therefore be necessary to collect detailed linguistic de-scriptions of newly diagnosed children to determine at what point the acquisi-tion process has been interrupted. We recommend that as soon as possibleafter diagnosis the following minimal information regarding the stage of lan-guage and cognitive development be obtained:
Phonological development. Special attention should be given to accessingthe developing phonological grammar in young LKS patients. In Brentari etal. (in preparation), we describe in detail each of the following aspects ofphonological assessment. At the time of diagnosis, we recommend conduct-ing an interview with parents to determine the rate of phonological develop-ment prior to the discernible onset of LKS, which should include:
1. information about when the child began to babble,2. if and when formulaic expressions, such as ‘‘I’m hungry,’’ or ‘‘It’s
time for x’’ appear,

OUTCOME IN LANDAU-KLEFFNER SYNDROME 421
3. whether (and, if so, when) the child began to recognize affect in sen-tences,
4. whether (and, if so, when) the child began to use prosodic cues forappropriate sentence types.
Also, a test of the child’s ability to discriminate between the members ofminimal pairs should be tested. A phonemic distance test (Brentari et al., inpreparation; Lecours & Lhermitte, 1969) should be implemented to deter-mine when discrimination breaks down. An auditory span task like that de-scribed by Metz-Lutz et al. (1997) would also be useful.
In addition, the child’s articulatory phonology should be tested by usingan instrument such as the Hodson Assessment of Phonological Processes(Hodson, 1986) and by recording and analyzing a sample of narrative di-rected towards a known target, such as a familiar story or a short video. Atest of the child’s range of prosodic performance may also be helpful.
Lexical development. Quantitative measures of receptive and expressivelexical development will be necessary to determine whether the failure todevelop a stable phonological grammar limits lexical development. Measureswe have used such as the Peabody Picture Vocabulary Test—Revised(Dunn & Dunn, 1981) and the Expressive One Word Vocabulary Test (Gard-ner, 1990) yield information about single-word expressive and receptive vo-cabulary. Measures that require parental input such as the MacArthur Com-municative Development Inventories (Fenson, Dale, Reznick, Thal, Bates,Hartung, Pethick, & Reilly, 1993) could also provide more detailed and com-parable information about the developmental stage reached by children whendiagnosed with Landau-Kleffner Syndrome.
Syntactic development. The MacArthur Communicative Development In-ventories also provide information about syntactic development. For olderchildren, they could be supplemented with a variety of measures such asthe Test of Receptive Grammar (Bishop, 1982b). The latter test specificallyexamines some of the sentence types expected to be at risk if auditory–verbalshort-term memory is limited.
This report concerns just one subject with Landau-Kleffner Syndrome whoremains severely impaired as an adult. Other children who recover from thedisorder may have a less pervasive deficit or may have attained a more so-phisticated level of development before the onset of the disease. We thinkour results strongly suggest that T.M.’s primary impairment is in auditoryprocessing and that her ability to acquire language was indeed intact. Webelieve the chronic auditory language problems seen in this patient can betraced in large part to the failure to develop a phonological grammar. Thisdeficit has prevented her from ever entering the stage of rapid lexical expan-sion seen in children learning language and has resulted in a lifelong limita-tion on lexical development. Moreover, the accompanying deficit in audi-tory–verbal short-term memory has had specific consequences for the

422 BAYNES ET AL.
development of a hierarchical grammatical system. Other grammatical short-comings are typical of any nonnative signer. Careful observation of newlydiagnosed cases can allow us to understand better the relationship betweenauditory–verbal short-term memory and a productive phonological systemas well as the impact of deficits in these basic linguistic processes on furtherdevelopment of the language system. Understanding of these relationshipswill provide both theoretical insight into models of language developmentand practical insight into formulation of reasonable plans for rehabilitationfor children with similar language disorders.
REFERENCES
Aarons, D., Bahan, B. J., Kegl, J., & Neidle, C. 1995. Lexical tense markers in AmericanSign Language. In K. Emmorey & J. Reilly, (Eds.), Language, gesture, and space, Hills-dale, NJ: Erlbaum.
Allport, D. A. 1984. Auditory–verbal short-term memory and conduction aphasia. In H.Bouma & D. G. Bouwhis, (Eds.), Attention and performance X: Control of languageprocesses, 313–326. Hillsdale, NJ: Erlbaum.
Allport, D. A. 1985. Distributed memory, modular systems and dysphasia. In S. K. Newman &R. Epstein, (Eds.), Current perspectives in dysphasia, Hillsdale, NJ: Churchill Living-stone.
Ansink, B. J. J., Sarphatie, H., & Van Dongen, H. R. 1989. The Landau-Kleffner Syndrome—Case report and theoretical considerations. Neuropediatrics, 20, 170–172.
Berent, G. P. 1996. Learnability constraints on deaf learners’ acquisition of English Wh- ques-tions. Journal of Speech & Hearing Research, 39(3), 625–642.
Bertoncini, J., Morais, J., Bijeljac-Babic, R., McAdams, S., Peretz, I., & Mehler, J., 1989.Dichotic perception and laterality in neonates. Brain and Language, 37, 591–605.
Bishop, D. V. M. 1982a. Comprehension of spoken, written and signed sentences in childhoodlanguage disorders. Journal of Child Psychology and Psychiatry, 23 (1), 1–29.
Bishop, D. V. M. 1982b. Test of receptive grammar. Chapel Hill.
Bishop, D. V. M. 1985. Age of onset and outcome in acquired aphasia with convulsive disorder(Landau-Kleffner Syndrome). Developmental Medicine & Child Neurology, 27, 705–712.
Brentari, D. 1990. Theoretical foundations of American Sign Language phonology. Ph.D.dissertation, University of Chicago.
Brentari, D., Kegl, J., Baynes, K., Kussmaul C., & Poizner, H. In preparation. Lexical conse-quences of the failure to develop a distinctive feature system.
Brentari, D., & H. Poizner. 1994. A phonological analysis of a deaf Parkinsonian signer.Language and Cognitive Processes, 9, 69–99.
Chafe, W. 1982. Integration and involvement in speaking, writing, and oral literature. In D.Tannen (Ed.), Exploring orality and literacy, 35–54. Norwood, NJ: Ablex.
Cooper, J. A., & Ferry, P. C. 1978. Acquired auditory verbal agnosia and seizures in childhood.Journal of Speech and Hearing Disorders, 48, 176–184.
Corina, D. P., Poizner, H., Bellugi, U., Feinberg, T., Dowd, D., & O’Grady-Batch, L. 1992.Dissociation between linguistic and nonlinguistic gestural systems: A case for composi-tionality. Brain and Language, 43 (3), 414–447.

OUTCOME IN LANDAU-KLEFFNER SYNDROME 423
Curtiss, S. 1977. Genie: A linguistic study of a modern-day ‘‘wild child.’’ New York: Aca-demic Press.
de Wijngaert, E., & Gommers, K. 1993. Language rehabilitation in the Landau-Kleffner syn-drome: Considerations and approaches. Aphasiology, 7, 475–480.
Denes, G., Balliello, S., Volerra, V., & Pellegrin, A. 1986. Oral and written language in acase of childhood phonemic deafness. Brain and Language, 29, 252–267.
Deonna, T. W. 1991. Acquired epileptiform aphasia in children (Landau-Kleffner Syndrome).Journal of Clinical Neurophysiology, 8(3), 288–298.
Dunn, L. M., & Dunn, L. M. 1981. Peabody picture vocabulary test—revised: Manual forforms L and M. Circle Pines, MN: American Guidance Service.
Fenson, L., Dale, P. S., Reznick, J. S., Thal, D., Bates, E., Hartung, J. P., Pethick, S., & Reilly,J. S. 1993. MacArthur communicative development inventories.
Frazier, L., & Fodor, J. D. 1978. The sausage machine: A new two-stage parsing model.Cognition, 13 (187–222).
Gardner, M.F. 1990. Expressive one-word picture vocabulary test—Revised. Novato, CA:Academic Therapy Publications.
Gascon, G., Victor, D., Lombroso, C. T., & Goodglass, H. 1973. Language disorder, convul-sive disorder, and electroencephalographic abnormalities. Archives of Neurology, 28 (3),156–162.
Gathercole, S. E., & Baddeley, A. D. 1990. The role of phonological memory in vocabularyacquisition: A study of young children learning new names. British Journal of Psychol-ogy, 81, 439–454.
Geers, A., Moog, J., & Schick, B. 1984. Acquisition of spoken and signed English by pro-foundly deaf children. Journal of Speech and Hearing Disorders, 49, 378–388.
Gilmore, R., Kegl, J., Bowers, C., Leonard, D., Roper, S., Fennell, E., Poizner, H., & Heilman,K. M. 1994. Functional cortical mapping of a left-handed, deaf signer of ASL, rightdominant for signed and spoken language. Cognitive Neuroscience Society Abstracts, 2,59.
Grier, J. B. 1971. Nonparametric indexes for sensitivity and bias: Computing formulas. Psy-chological Bulletin, 75, 474–479.
Hickok, G., Bellugi, U., & Klima, E. S. 1996. The neurobiology of sign language and itsimplications for the neural basis of language. Nature, 381, 699–702.
Hodson, B. W. 1986. The assessment of phonological processes—Revised. Los Angeles:Western Psychological Services.
Jacobwitz, E. L., & Stokoe, W. 1988. Signs of tense in ASL verbs. Sign Language Studies,60, 331–340.
Kegl, J. 1985. Causative marking and construal of agency in ASL. In W. Eilfort, P. Kroeber, &K. Peterson, (Eds.), Papers from the 21st annual meeting of the Chicago Linguistic Soci-ety, 120–137. Chicago, Ill.: Chicago Linguistic Society.
Kegl, J. 1995. Levels of representation and units of access relevant to agrammatism. Brainand Language, 50 (2), 151–200.
Kegl, J., Baynes, K., Brentari, D., Kussmaul, C., & Poizner, H. In preparation. Landau-KleffnerSyndrome: Modality independence of linguistic competence. In Progress in neuropsycho-pharmacology and biological psychiatry.
Kegl, J., Baynes, K., Brentari, D., & Poizner, H. 1996. Landau-Kleffner Syndrome: Modalityindependence of linguistic competence. Society for Neuroscience Abstracts, 22, 184.
Kegl, J., Gilmore, R., Fennell, E., Bowers, D., Poizner, H., & Heilman, K. M. 1997. Wada

424 BAYNES ET AL.
testing of a deaf, left-handed, ASL signer reveals right dominance for language. Journalof the International Neuropsychological Society.
Kegl, J. A., & Poizner, H. 1997. Crosslinguistic/crossmodal syntactic consequences of left-hemisphere dominance: Evidence from an aphasic signer and his identical twin. Aphasiol-ogy, 11 (1), 1–37.
Klima, E., & Bellugi, U. 1979. The signs of language. Cambridge, MA: Harvard Univ. Press.
Landau, W. M. 1992. Landau-Kleffner Syndrome: An eponymic badge of ignorance. Archivesof Neurology, 49 (4), 353.
Landau, W. M., & Kleffner, F. R. 1957. Syndrome of acquired aphasia with convulsive disor-der in children. Neurology, 7 (8), 523–530.
Lecours, A. R., & Lhermitte, F. 1969. Phonemic paraphasias: Linguistic structures and tenta-tive hypotheses. Cortex, 5, 193–228.
Lenneberg, E. 1967. Biological foundations of language. New York: Wiley and Sons.
Liddell, S. 1984. Unrealized-inceptual aspect in American Sign Language: feature insertionin syllabic frames. In Proceedings from the 20th annual meeting of the Chicago LinguisticSociety, 1. General session, 257–270. Chicago: Chicago Linguistic Society.
Linebarger, M. C., Schwartz, M. F., & Saffran, E. M. 1983. Sensitivity to grammatical structurein so-called agrammatic aphasics. Cognition, 13, 361–392.
Loban, L. 1974. Language development: Kindergarten through grade 12. Champaign-Urbana,IL: National Council of Teachers of English.
Locke, J. L. 1993. The child’s path to spoken language. Cambridge, MA.: Harvard Univ.Press.
Lucas, C., & Valli, C. 1992. Language contact in the American deaf community. San Diego:Academic Press.
Mantovani, J. F., & Landua, W. M. 1980. Acquired aphasia with convulsive disorder: Courseand prognosis. Neurology, 30, 524–529.
Marcotte, A. C., & Morere, D. A. 1990. Speech lateralization in deaf populations: Evidencefor a developmental critical period. Brain and Language, 39, 134–152.
Marescaux, C., Hirsch, E., Finck, S., Maquet, P., Schlumberger, E., Sellal, F., Metz-Lutz,M. N., Alembik, Y., Salmon, E., Franck, G., & Kurtz, D. 1990. Landau-Kleffner syn-drome: A pharmacologic study of five cases. Epilepsia, 3(6), 768–777.
Marien, P., Saerens, J., Verslegers, W., Borggreve, F., & De Deyn, P. P. 1993. Some controver-sies about type and nature of aphasic symptomatology in Landau-Kleffner’s syndrome:a case study. Acta neurologica belgica, 93, 183–203.
Martin, R. C., & Breedin, S. D. 1992. Dissociations between speech perception and phonologi-cal short-term memory deficits. Cognitive Neuropsychology, 9 (6), 509–534.
Mason, M. K. 1942. Learning to speak after six and one-half years of silence. Journal ofSpeech and Hearing Disorders, 46, 267–273.
Mayberry, R., & Fischer, S. 1989. Looking through phonological shape to lexical meaning:The bottleneck of non-native sign language processing. Memory and Cognition, 17 (6),740–754.
McAfee, M. C., Kelly, J. F., & Samar, V.J. 1990. Spoken and written English errors of postsec-ondary students with severe hearing impairments. Journal of Speech and Hearing Disor-ders, 55 (628–634).
Mehler, J., Jusczyk, P., Lambertz, G., Halsted, N., Bertoncini, J., & Amiel-Tison, C. 1988.A precursor of language acquisition in young infants. Cognition, 29, 143–178.
Metz-Lutz, M. N., Hirsch, E., Maquet, P., de Saint Martin, A., Rudolf, G., Wioland, N., &

OUTCOME IN LANDAU-KLEFFNER SYNDROME 425
Marescaux, C. 1997. Long lasting dichotic listening performances in in the follow-up ofLandau and Kleffner Syndrome. Child Neuropsychology, 3 (1), 47–60.
Morrell, F., Whisler, W. W., Smith, M. C., Hoeppner, T. J., de Toledo-Morrell L., Pierre-Louis, S. J. C., Kanner, A. M., Buelow, J. M., Ristanovic, R., Bergen, D., Chez, M., &Hasegawa, H. 1995. Landau-Kleffner Syndrome: Treatment with subpial transection.Brain, 118, 1529–1546.
Ochs, E. 1979. Planned and unplanned discourse. In T. Givon (Ed.), Syntax and Semantics.New York: Academic Press.
Paquier, P. F., Van Dongen, H. R., & Loonen, M. C. B. 1992 April. The Landau-Kleffnersyndrome or ‘‘Acquired aphasia with convulsive disorder’’: Long-term follow-up of sixchildren and a review of the recent literature. Archives of Neurology, 49, 354–359.
Pardo, P. J., Makela, J. P., Sama, M., & Hari, R. 1994. Neuromagnetic measurements ofhemispheric differences in auditory processing of frequency and amplitude modulations.Society for Neuroscience Abstracts, 20, 325.
Perlmutter, D. 1992. Sonority and syllable structure in American Sign Language. LinguisticInquiry, 23, 407–442.
Poizner, H., Bellugi, U., & Klima, E. S. 1991. Brain functions for language: Perspectives fromanother modality. In I. G. Mattingly and M. Studdert-Kennedy (Eds.), Modularity andthe motor theory of speech perception. Hillsdale, N.J.: Lawrence Erlbaum Associates.
Poizner, H., Klima, E. S., & Bellugi, U. 1987. What the hands reveal about the brain. Cam-bridge, MA: MIT Press/Bradford Books.
Rapin, I., Mattis, S., Rowan, A. J., & Golden, G. G. 1977. Verbal auditory agnosia in children.Developmental Medicine and Child Neurology, 19, 192–207.
Sandler, W. 1989. Phonological representation of the sign. Dordrecht, Netherlands: Foris.
Shoumaker, R. D., Bennett, D. R., Bray, P. F., & Curless, R. G. 1974. Clinical and EEGmanifestations of an unusual aphasic syndrome in children. Neurology, 24, 10–16.
Supalla, S. 1986. Manually coded English: The modality question in signed language develop-ment. M.A. thesis, University of Illinois.
Supalla, T. 1982. Structure and acquisition of verbs of motion and location in American SignLanguage. Ph.D. dissertation, University of California at San Diego.
Supalla, T. 1990. Serial verbs of motion in ASL. In S. Fisher and P. Siple, (Eds.) Theoreticalissues in sign language research, 2, 127–152. Chicago: Univ. of Chicago.
Tallal, P., Miller, S., & Fitch, R. H. 1993. Neurobiological basis of speech: A case for thepreeminence of temporal processing. In P. Tallal, A. M. Galaburda, R. R. Llinas, & C.Von Euler, (Eds.) Annals of the New York Academy of Science, 682, 27–47.
Tallal, P., & Piercy, M. 1973. Defects of non-verbal auditory perception in children withdevelopmental aphasia. Nature, 241, 468–469.
Tharpe, A. M., & Olson, B. J. 1994. Landau-Kleffner Syndrome: Acquired epileptic aphasiain children. Journal of the American Academy of Audiology, 5, 146–150.
Wilbur, R. B. 1979. Sign language and sign systems: Research and applications. Baltimore:University Park Press.
Young, W. T. 1973. The Bentley ‘‘measures of music abilities’’: A congruent validity report.Journal of Research in Music Education, 21, 74–79.