Cholestatic jaundice after hepatic transplantation☆☆☆A nonimmunologically mediated event
6
Cholestatic Jaundice After Hepatic Transplantation A Nonimmunologically Mediated Event James W. WIlllams, MD, Memphis, Tennessee Santiago Vera, MD, Memphis, Tennessee Thomas G. Peters, MD, Memphis, Tennessee Steven Van Worst, MD, hkmphis, Tennessee Louis G. Brltt, MD, Memphis, Tennessee Patrkk J. Dean, MD, Memphis, Tennessee Roger Haggitt, MD, Memphis, Tennessee James D. Made, MD, Memphis, Tennessee Hepatic transplantation exposes the liver to a num- events in the posttransplantation period, is clinical- ber of insults including hypoxia, cold temperature, ly indistinguishable from rejection, and resolves drug therapy, sepsis, general anesthesia, blood spontaneously. The recognition of this distinct enti- transfusions, and potential sepsis and immunologic ty is an important step in understanding early allo- injury. It is not surprising, then, that the allograft graft abnormalities and function and is essential for might develop cholestasis, a nonspecific manifesta- avoiding unnecessarily high and potentially lethal tion of hepatic injury. levels of immunosuppression. Jaundice after transplantation poses a significant differential diagnostic problem since it may also be produced by biliary obstruction or rejection, both of which are life-threatening complications. The abili- ty to distinguish these from other causes of jaundice and to initiate specific therapy is of central impor- tance to a successful outcome. The incidence, causes, natural history, and consequences of early cholestasis after hepatic transplantation have not been carefully defined, principally because serial hepatic biopsies have not generally been included in posttransplantation protocols. Material and Methods Utilizing close clinical and histologic monitoring in 55 consecutive hepatic allografts, we have cata- logued the incidence of cholestasis associated with several causes of hepatic dysfunction and proposed the means of distinguishing early rejection from other causes of cholestasis. Through this analysis, we have defined a syndrome of cholestasis that is apparently unrelated to immunologically mediated From May 1982 through December 1984,55 transplan- tations were performed in 50 patients. Essentially all liver donors were patients who were brain dead but had stable cardiovascular function and no evidence of hepatic dis- ease. The vascular supply of the liver in the donor was dissected, and when removal was imminent, portal vein perfusion with lactated Ringer’s solution was begun. When the liver was cooled and the hepatic artery was clamped, Collins’ solution was substituted to continue the flush. After its removal, the liver was sealed in a plastic bag containing Collins’ solution and immersed in ice. Recipient and donor procedures were coordinated to min- imize the period of cold ischemia. Cyclosporine and low dose corticosteroids were used for immunosuppression. Cyclosporine was begun at a dose of 15 to 18 mg/kg and subsequently altered to accommodate renal function. Intravenous cyclosporine was given at a third the oral dose. Methylprednisolone was begun at 1.5 mg/kg and tapered to 0.3 mg/kg by 1 week. Liver function tests performed daily included measurement of bilirubin, serum glutamic oxalacetic transaminase, y-glutamyl transpeptidase, and alkaline phosphatase levels and pro- thrombin times. Hepatic dysfunction, defined as 48 hours or more of increasing bilirubin or liver enzyme levels or failure of these levels to show progressive improvement after transplantation, was evaluated by cholangiography and biopsy. Liver biopsy was routinely performed at the time of transplantation and at 3 to 7 day intervals there- From the Departments of Surgery and Radiology, Unhwsity of Tennessee Center for the Health Sciences and Pathology, Baptist Memorial Hospital, Memphis, Tennessee. Supported in part by the Veterans Adminlstratlon, Memphis, Tennessee. Requests for reprints should be addressed to James W. Williams, MD, Department of Surgery, Rush-Presbyterian-St. Luke’s Medical Center, 1753 West Congress Parkway, Chicago, Illinois 60612. Presented at the 26th Annual Meeting of the Society for Surgery of the Alimentary Tract, New York, New York, May 14-15, 1965. Volume 151, January 1966 65
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Cholestatic jaundice after hepatic transplantation☆☆☆A nonimmunologically mediated event

Cholestatic Jaundice After Hepatic Transplantation
A Nonimmunologically Mediated Event
James W. WIlllams, MD, Memphis, Tennessee
Santiago Vera, MD, Memphis, Tennessee
Thomas G. Peters, MD, Memphis, Tennessee
Steven Van Worst, MD, hkmphis, Tennessee
Louis G. Brltt, MD, Memphis, Tennessee
Patrkk J. Dean, MD, Memphis, Tennessee
Roger Haggitt, MD, Memphis, Tennessee
James D. Made, MD, Memphis, Tennessee
Hepatic transplantation exposes the liver to a num- events in the posttransplantation period, is clinical- ber of insults including hypoxia, cold temperature, ly indistinguishable from rejection, and resolves drug therapy, sepsis, general anesthesia, blood spontaneously. The recognition of this distinct enti- transfusions, and potential sepsis and immunologic ty is an important step in understanding early allo- injury. It is not surprising, then, that the allograft graft abnormalities and function and is essential for might develop cholestasis, a nonspecific manifesta- avoiding unnecessarily high and potentially lethal tion of hepatic injury. levels of immunosuppression.
Jaundice after transplantation poses a significant differential diagnostic problem since it may also be produced by biliary obstruction or rejection, both of which are life-threatening complications. The abili- ty to distinguish these from other causes of jaundice and to initiate specific therapy is of central impor- tance to a successful outcome. The incidence, causes, natural history, and consequences of early cholestasis after hepatic transplantation have not been carefully defined, principally because serial hepatic biopsies have not generally been included in posttransplantation protocols.
Material and Methods
Utilizing close clinical and histologic monitoring in 55 consecutive hepatic allografts, we have cata- logued the incidence of cholestasis associated with several causes of hepatic dysfunction and proposed the means of distinguishing early rejection from other causes of cholestasis. Through this analysis, we have defined a syndrome of cholestasis that is apparently unrelated to immunologically mediated
From May 1982 through December 1984,55 transplan- tations were performed in 50 patients. Essentially all liver donors were patients who were brain dead but had stable cardiovascular function and no evidence of hepatic dis- ease. The vascular supply of the liver in the donor was dissected, and when removal was imminent, portal vein perfusion with lactated Ringer’s solution was begun. When the liver was cooled and the hepatic artery was clamped, Collins’ solution was substituted to continue the flush. After its removal, the liver was sealed in a plastic bag containing Collins’ solution and immersed in ice. Recipient and donor procedures were coordinated to min- imize the period of cold ischemia.
Cyclosporine and low dose corticosteroids were used for immunosuppression. Cyclosporine was begun at a dose of 15 to 18 mg/kg and subsequently altered to accommodate renal function. Intravenous cyclosporine was given at a third the oral dose. Methylprednisolone was begun at 1.5 mg/kg and tapered to 0.3 mg/kg by 1 week. Liver function tests performed daily included measurement of bilirubin, serum glutamic oxalacetic transaminase, y-glutamyl transpeptidase, and alkaline phosphatase levels and pro- thrombin times. Hepatic dysfunction, defined as 48 hours or more of increasing bilirubin or liver enzyme levels or failure of these levels to show progressive improvement after transplantation, was evaluated by cholangiography and biopsy. Liver biopsy was routinely performed at the time of transplantation and at 3 to 7 day intervals there-
From the Departments of Surgery and Radiology, Unhwsity of Tennessee Center for the Health Sciences and Pathology, Baptist Memorial Hospital, Memphis, Tennessee. Supported in part by the Veterans Adminlstratlon, Memphis, Tennessee.
Requests for reprints should be addressed to James W. Williams, MD, Department of Surgery, Rush-Presbyterian-St. Luke’s Medical Center, 1753 West Congress Parkway, Chicago, Illinois 60612.
Presented at the 26th Annual Meeting of the Society for Surgery of the Alimentary Tract, New York, New York, May 14-15, 1965.
Volume 151, January 1966 65
Williams et al
TABLE I Hepatic Dysfunction: 50 Patients Receiving 55 Grafts
Cause of Dysfunction Episodes Patients
Vascular thrombosis 6 6 Biliary obstruction 4 4 Sepsis 3 2 Rejection 17 14 Cholestasis syndrome 23 16
Total 53 44
after according to a technique we have previously de- scribed [I]. Rejection when documented by histologic cri- teria was treated with bolus doses of methylprednisolone (15 mg/kg for 2 days).
Results
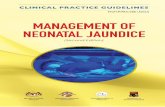
Fifty-three episodes of hepatic dysfunction oc- curred in 44 patients (Table I). The diagnoses in these patients were based on cholangiographic, his- tologic, arteriographic, and microbial culture find- ings and observations at surgical exploration. The cholestasis syndrome may have multiple causes but appears to be related to preservation injury. The histologic criteria used for diagnosing rejection were based on the examination of more than 350 biopsy specimens of patients with and without hepatic dys- function. They include mononuclear cell infiltra- tion of the portal tracts with spilling into the paren- chyma or venous subendothelial infiltration of the portal veins (each is a cardinal sign diagnostic of rejection if it occurs in more than one structure or if more than one cardinal sign is present); mononucle- ar or polymorphonuclear cholangitis; conspicuous eosinophils in the portal tracts; central subendothe- lial venous infiltration (cardinal sign); spotty necro- sis; and cholestasis which is variable in intensity. Mild mononuclear infiltration occurs in the major- ity of patients in the early postoperative period, an observation first made in sham-transplanted dogs
i %Zg
ure 1 illustrates these features in biopsy ma-
In addition to the carefully documented causes of jaundice, hepatic dysfunction developed in 18 pa- tients without any recognizable cause. The biopsy specimens of these patients with what we have termed the nonspecific cholestasis syndrome, had a characteristic histologic appearance consisting chiefly of centrilobular cholestasis and ballooning of hepatocytes (Figure 21. The cholestasis was some- times panlobular in severe cases. It was intracellu- lar, candicular, and within the interlobular ducts, with occasional marked bile plugging in the prolifer- ating ductules. Ballooning of the hepatocytes began as a microvesicular change within 48 hours going from centrilobular to panlobular. It was the first feature to resolve. Other histologic features of the nonspecific cholestasis syndrome included focal he-
Figure 1. Features of early ali~rafi re/ectlon. Top, the portal tract is expanded by a dense mononuclear cell Mltrate which extends Into the parenchyma. Bottom, endothelialltk of the central veln a8 shown here Is a hletologlc hallmark of rejectiofk (Top and bottom magnlflcatlon X 100 and X 200, reepectlvely, reduced by 30 percent.)
patocytolysis, which was usually minimal; bile duct proliferation occurring after cholestasis and hepa- tocyte ballooning, which sometimes mimicked large duct obstruction and resolved slowly but complete- ly; and cholangitis, which was uniformly present. Although these features may occur along with rejec- tion, they are clearly distinct from the early rejec- tion phenomenon which is mediated by mononucle- ar cell infiltration. Immunofluorescent stains for immunoglobulin M, immunoglobulin G, and com- plement were negative in four patients with the cholestasis syndrome.
The hepatocellular ballooning in the patients with this syndrome appeared within 5 days of diag- nosis and usually receded by 20 days. Histologic evidence of cholestasis appeared within 7 days and receded more slowly, largely disappearing by 6 weeks. Serum bilirubin levels often decreased ahead
66 The American Journal of Surgery

Cholestatic Jaundice After Hepatic Transplantation
C----W Cholestasis - Rejection
Figure 2. Features of the nonspeclfk cholestasls syndrome. Top, there Is centrllobular balhwnlng 01 the hepakcytes whkh may progress to Involve the entlre lobule. Balkoned hepatocytes obscure candllcular cholestashq and the central veln Is free of InflammaHon. Bottom, portal tracf expanslon Is caused by blle duct and duclular prollferatlon. Bile plu&tg of prollferatlng duct&es (arrows) may be promhwnt. lnflammarory cells are lnconspkuoua (Top and bottom magnlflcaUon X 200, reduced by 30 percent.)
of biopsy evidence of improvement. Unless death from some other cause superceded, the histologic characteristics and function returned to normal by 90 days in all but one of these patients without altering immunosuppressive therapy (Figure 3). The one exception was a graft with profound mal- function coming from a hemodynamically labile do- nor who experienced cardiac arrest several minutes before the liver was removed.
The volume of bile collected from the T tube during the cholestatic episode was decreased and the color of the bile was often pale. With recovery, however, the volume of the bile increased followed by return toward a normal color.
Neither the absolute values nor the changes in serum concentration of bilirubin and liver enzymes
; lb 1; ;o 2; 3b --
1 90 Days Post Transplant
Flgure 3. The flme course of serum blllrubln values In paflenk with reiecUon, cholestasls syndrome, or nelfher condition.
TABLE Ii Comparlson of Serum Liver Enzymes and Bllirubln In Patients Wlth ReJectlon and Cholestasls Syndrome
Time Bilirubin Alk Phos GGTP SGOT
n (~mol/liter) (Wliter) (U/ml) (U/ml)
Rejection
Before rejection
During rejection
17 9.1 242 296 171
17 17.5 283 332 72
Cholestasis Syndrome
Before 23 16.1 155 128 160 syndrome
During 23 22.3 219 177 192 syndrome
GGTP = y-glutamyl transpeptidase; SGOT = serum glutamic oxalacetic transaminase.
during the period of hepatic dysfunction distin- guished these patients from those undergoing dys- function caused by rejection (Table II). All parame- ters of liver function except serum glutamic oxalacetic transaminase increased significantly during dysfunction; however, the change in these parameters did not distinguish rejection from the cholestasis syndrome (p >0.05, as analyzed by anal- ysis of covariance). The timing of the peak bilirubin level in both the rejection and the cholestasis syn- drome overlap, which adds to the difficulty in dis- tinguishing these two conditions (Figure 3).
Features in the donor and recipient associated with the cholestasis syndrome are shown in Table III. Although the mean cold ischemia time was simi- lar in those with and without the cholestasis syn- drome, the liver from the unstable donor seemed more severely involved. The posttransplant serum glutamic oxalacetic transaminase levels were higher in those with the syndrome, which suggests a gener-
Volume 151, January 1986 67
Williams et al
TABLE III Features Associated Wlth Cholestasls Syndrome
With Without Features* Syndrome Syndrome
Bilirubin 23.5 f 11.7 7.7 f 4.1 (pmollliter)
SGOT 1,929 f 334+ 801 l 526 (U/ml)
GGTP (u/ml)
Cold ischemia time (min)
334 f 398 329 f 180
374 f 54 397 f 80
l Mean peak values f standard deviation occurring in the first 3 weeks after transplantation.
+ p <O.Ol.
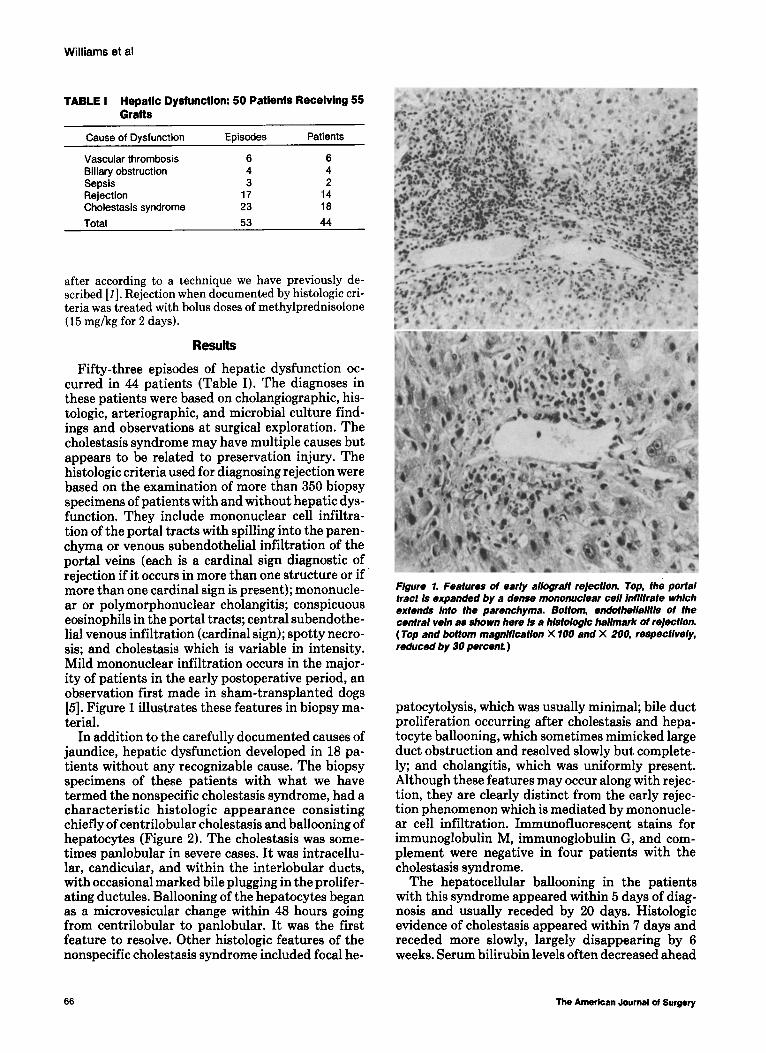
Figure 4. These three hepatobttlary radlonuclide scans (D/S/DA) were obtalned 24 hours, 5 days, and 1 month atter transplanta- tion In a patlent with profound early cholestask The f/rst study (S- 76-84) shows good uptake but no excretion of the tracer 30 minutes after rejection. Five days after transplantation, the up take Is much poorer and excretion Is stilt absent at 30 minutes. Afthough liver function appeared to be more Impalre& the pa tlent’s cttnical course was Improving, and 25 days later, the scan returned to normal. This early worsening of the radlonucllde scan has been seen in other stmtlar patients and does not portend a poor outcome.
al hepatic injury. All but two donors had stable cardiovascular function without significant hypo- tension during or preceding donor hepatectomy. The implantation procedure was promptly per- formed in both of these cases. After transplantation, the liver in a third patient sustained warm ischemia when the supraceliac aorta was occluded for 15 min- utes to allow anastomosis of the hepatic artery to the aorta. Profound cholestasis developed in all three of these patients in the absence of signs of rejection. The duration of cold ischemia time in the remaining
patients with the cholestasis syndrome was similar to the cold ischemia time of those without develop- ment of the syndrome, and the development of cho- lestasis was not associated with identifiable donor or procurement characteristics. Posttransplant se- rum levels of cytosol enzymes (serum glutamic oxal- acetic transaminase), but not membrane-bound enzymes (y-glutamyl transpeptidase), were signifi- cantly higher (p <O.Ol) in patients with the choles- tasis syndrome.
Radionuclide hepatobiliary imaging (DISIDA) performed within 24 hours of transplantation in patients in whom cholestasis syndrome developed demonstrated a pattern of cholestasis (Figure 4). Typically, cholestasis results in prompt hepatic up- take of the radionuclide with delayed excretion into the bile. Subsequent scans, however, demonstrated decreased hepatic uptake as evidenced by contin- ued blood pool radionuclide activity and high back- ground activity. This scintigraphic finding is classi- cally representative of intrinsic hepatocyte dysfunction rather than cholestasis. These observa- tions suggest that the syndrome evolves over several days and that hepatobiliary scans that show worsen- ing hepatic function do not necessarily imply an unfavorable outcome. As recovery became apparent clinically, follow-up scans returned to a normal pat- tern.
Comments
Cholestasis is a term describing diminished or absent bile flow. Causes of cholestasis included bili- ary obstruction, chemical- or drug-associated inju- ry, sepsis, hepatitis, hormonal causes, and other as yet undefined causes. In this analysis of 55 hepatic transplant operations, we identified 18 patients in whom significant unexplained jaundice and choles- tasis developed in the immediate postoperative period. All but one of these patients had return of normal hepatic function. The one exception had profound hepatic dysfunction, probably related to severe hemodynamic instability and ultimate col- lapse in the donor before liver retrieval.
Cholangiography and biopsy eliminated biliary obstruction and rejection, respectively, as causes of cholestasis during the early postoperative period. These patients were not infected nor were they re- ceiving toxic doses of drugs known to produce he- patic injury. Cyclosporine itself has been reported to cause jaundice which decreases with a reduction in dosage [2]. In the patients in this study, however, the cyclosporine dosage remained constant while cholestasis and ballooning decreased, which is evi- dence against cyclosporine hepatotoxicity as an ex- planation for the jaundice. Therefore, we are left with the presumption that the injury causing cho- lestasis occurred during the preservation period. The mechanism of bile formation, still poorly un-
68 The American Journal cf Surgery

Cholestatic Jaundice After Hepatic Transplantation
derstood, appears from these observations to be particularly sensitive to cold ischemia.
Cholestasis after hepatic transplantation has been associated with late rejection in baboons and human subjects [3,4]. These observations were made in subjects treated with azathioprine rather than cyclosporine, the mainstay of therapy in this study. We have also observed cholestasis with little cellular infiltration in dogs treated with cyclospor- ine when the dose was reduced to subtherapeutic levels [5]; however, the appearance of cholestasis 3 weeks or more after transplantation is likely to be a condition different from the syndrome we are de- scribing. The cause of cholestasis in the early trans- plant period, as described herein, does not appear to be immunologically mediated. In patients with ear- ly cholestasis without histologic evidence of rejec- tion, we believe that the cholestasis is not caused by rejection for the following reasons: (1) cholestasis resolved without increasing the dose of immunosup- pressive drugs; (2) evidence of cellular infiltration in the graft is lacking; (3) negative immunofluorescent stains for immunoglobulin G, immunoglobulin M, and complement argue against the diagnosis of a humoral mechanism of hepatic allograft injury; (4) jaundice often began before typical immunologic phenomena could be generated; and (5) the degree of cholestasis tends to be exaggerated in the liver subjected to cardiovascular instability in the donor.
Although events that produce hepatic ischemia seem to exaggerate this syndrome, it nevertheless develops in livers removed from stable donors, even when the liver is subjected to less than 6 hours of cold ischemia. In the early posttransplant period, the liver appears particularly vulnerable to other causes of cholestasis as well. Sepsis, hemolysis, and hyperalimentation may be accompanied by more than the expected degree of jaundice and cholestasis in the hepatic allograft recipient.
The definition of this syndrome is important to the physician concerned with patient management after liver transplantation. The ability to distin- guish this syndrome from rejection by serial histo- logic monitoring of the allograft allows the physician to more knowledgeably manage immuno- suppression and avoid the dangers of unnecessary high dose immunosuppressive therapy.
Summary
Serial liver biopsy and close clinical monitoring in 55 consecutive hepatic allografts have disclosed a syndrome of cholestatic jaundice that simulates re- jection. This syndrome is associated with distinct histologic findings and resolves spontaneously with- out modification of immunosuppressive manage- ment. The cause of the cholestasis is probably relat- ed to subcellular organelle damage produced by cold ischemia, and its importance stems from the confu-
sion it creates with regard to rejection diagnosis. Recognition of this syndrome can result in de- creased immunosuppression in hepatic allograft re- cipients, a secondary decrease in infectious compli- cations, and improvement in the survival rate.
References
1. Williams JW, Vera S, Peters TG, et al. A technique for safe hepatic biopsy following hepatic transplantation. Surg Gyne- col Obstet 1988 (in press).
2. Starzl TE, Weil R Ill, lwatsuki S, et al. The use of cyclosporine A and prednisone in cadaver kidney transplantation. Surg Gyn- ecol Obstet 1980; 15 1: 17-28.
3. Myburg JA. Abrahams DM, Mieny CJ, Bersohn I. Choler&tic phenomenon in hepatic allograft rejection in the primate. Transplant Proc 1971;3:501-4.
4. Williams A, Smith M, Shilkin KB. et al. Liver transplantation in man: frequency of rejection, biliary tract complications and recurrence of malignancy based on an analysis of 28 cases. Gastroenterology 1973;84:1026-48.
5. Williams JW, Peters TG, Haggitt R, et al. Cyclosporin A in orthotopic canine hepatic transplants. J Surg Res 1982;32:576-85.
Frank G. Moody (Houston, TX): Dr. Williams, did you try to correlate your cold ischemia times with the choles- tatic event? I noticed you had quite a large number of patients with chronic active hepatitis. Were they the ones who might have developed the cholestatic syndrome? I noticed you separated the variable of chronic active hepa- titis from all the other variables and events in the trans- plantation episodes.
Joaquin S. Aldrete (Birmingham, AL): Dr. Williams, have you seen this cholestasis syndrome several months after transplantation? We have one patient who present- ed with the syndrome about 7 months after transplanta- tion, and she has all the characteristics that you have shown histologically and clinically. Her bilirubin level is still elevated after 10 months. Initially I thought it was a case of rejection, but we stopped her treatment for rejec- tion after the second gram of methoprednisolone and she went on to improve. Have you noticed any changes in the prothrombin time or the platelet count? I think probably all these patients have normal prothrombin times despite the elevated enzyme levels and the hyperbilirubinemia.
James J. Reilly (Pittsburgh, PA): Dr. Williams, many candidates for liver transplantation are malnourished and often require enteral or parenteral nutrition postop- eratively. Did you find any correlation between histologic characteristics of the liver or hepatic function and any aspect of the nutritional support, specifically the amount of glucose or fat that these patients received?
Dr. Buchec (Pretoria, South Africa): I think the in- creased serum glutamic oxalacetic transaminase levels which were reported to be higher in these patients with the cholestatic syndrome is also a direct result of what you referred to as the cold ischemic phase, and probably corre- late very well with the period of hypotension.
We have been looking at these patients with jaundice in the intensive care unit, and we have noted that patients who are admitted in a very extended shock phase are the
Volume 151, January 1988 69

Williams et al
ones who are going to have jaundice, usually by the fifth to the sixth day, and the outcome depends on the presence of concurrent sepsis.
Dr. Williams, did you look at intraoperative periods of hypertension, and do these correlate in any way with the cold ischemic phase? Aren’t we just dealing with a shocked liver that is causing dysfunction of the biliary excretory mechanism?
Alfred L. Baker (Chicago, IL): Dr. Williams, is there a cutoff in terms of time of ischemia that you can give as a short-term limit beyond which this syndrome does not occur? Also, I wonder about other mechanisms that might be involved in the pathogenesis of cholestasis syndrome, such as hormonal levels, that might influence the liver. Were there any differences in the antibiotic dosages in the two groups of patients?
James W. Williems (closing): I think the importance of this paper is that the liver is subject to periods of cholestasis in the posttransplant period, and that rejec- tion can be distinguished from cholestasis by biopsy. What are the events that seem to correlate with the devel- opment of this syndrome? First, a liver subject to this syndrome is one that has come from an unstable donor
who has required high doses of vasopressor or who has had cardiovascular collapse before its retrieval. A liver sub- jected to a prolonged cold ischemic time in excess of 10 hours has an increased incidence of cholestasis. It also occurs in patients who have a completely uneventful re- trieval, a short cold ischemia time, and an uneventful implantation procedure, which I think means that there is a wide range of susceptibility to cold &hernia in the human liver. This has always been reversible in our expe- rience.
Dr. Aldrete, in regard to developments of this syndrome several weeks or months after transplantation, I think it is a different circumstance, which may be related to immu- nologic or viral damage.
Does hyperalimentation contribute to cholestasis or are there other postoperative factors? All of our patients begin parenteral hyperalimentation within a few days of transplantation so it could contribute. We have noticed that patients who have this syndrome have a higher level of jaundice associated with sepsis or drug toxicity so the liver appears to be sensitized to other causes of cholesta- sis. I think the significance of this is that cholestasis does occur, and those who are about to embark on liver trans- plant programs or participate in patient care will observe this phenomenon, particularly if you believe, as I do, in the benefits of frequent liver biopsy.
70 Tha American Journal ot Surgery