
Prevalence and clinical correlates of pathological affective ...
Upload
independentCategory
view
0download
0
Chemotherapy-related bilateral dermatitis associatedwith eccrine squamous syringometaplasia: Reappraisalof epidemiological, clinical, and pathological features
Antonio Martorell-Calatayud, MD,a Onofre Sanmartın, MD,a Rafael Botella-Estrada, MD,a
Nicole N. Balmer, MD,b Carlos Serra-Guillen, MD,a Elisabeth Gomez-Moyano, MD,c Victor Traves-Zapata, MD,a
Celia Requena, MD,a Eduardo Nagore, MD,a Beatriz Llombart-Cussac, MD,a
and Carlos Guillen-Barona, MDa
Valencia and Malaga, Spain; and Birmingham, Alabama
From
O
A
ta
Fund
Conf
This
M
Acce
109
Background: A characteristic cutaneous eruption related to the use of cytostatic chemotherapeutic drugshas been described in the literature. This condition appears to be characterized by an erythematous eruption,primarily affecting the intertriginous areas bilaterally, together with eccrine squamous syringometaplasia asthe main histologic feature.
Objective: We sought to establish the epidemiologic, clinical, and histologic characteristics of this poorlydefined chemotherapy drug-related eruption.
Methods: Retrospective data were collected from 21 consecutive patients with this clinical and histopath-ologic pattern who attended an oncology center between January 1999 and September 2009. Two skin biopsyspecimens were obtained from all patients, with the first being taken within 24 hours of onset, and the second72 to 96 hours after onset.
Results: The patients analyzed were predominantly female (72%), with a mean age of 52 years (range10-69 years). The lesions presented clinically as bilateral erythematous plaques affecting both axillae (95%),groin (88%), and side aspects of the neck (48%). The main histologic feature in all cases was eccrinesquamous syringometaplasia, characterized by the transformation of the eccrine cuboidal epithelium intotwo or more layers of squamous cells with intercellular bridges. The onset of the eruption appeared within30 days (range 2-30 days) after the initiation of the cytostatic agent infusion. The lesions resolved withdesquamation and postinflammatory hyperpigmentation. The same cutaneous pattern recurred in up to50% of patients in whom the oncologist reintroduced the cytostatic treatment.
Limitations: Small sample size was a limitation.
Conclusions: We suggest the term ‘‘chemotherapy-related bilateral dermatitis associated with eccrinesquamous syringometaplasia’’ to describe this distinctive entity, which is primarily associated with pegylatedliposomal doxorubicin infusions and chemotherapeutic regimens used in autologous bone-marrowtransplantation. ( J Am Acad Dermatol 2011;64:1092-103.)
Key words: cytostatic agent; drug reaction; eccrine squamous syringometaplasia; intertriginous rash;oncology; pegylated liposomal doxorubicin.
the Dermatology Department, Instituto Valenciano de
ncologia, Valenciaa; Department of Pathology, University of
labama, Birminghamb; and Dermatology Department, Hospi-
l Carlos Haya, Malaga.c
ing sources: None.
licts of interest: None declared.
study has been accepted to be presented at a past American
eeting of Dermatology (Miami, 2010).
pted for publication April 12, 2010.
Reprint requests: Antonio Martorell-Calatayud, MD, Dermatology
Department, Instituto Valenciano de Oncologia, San Jose de la
Montana Street, 14, 46008, Valencia, Spain. E-mail: antmarto@
hotmail.com.
Published online April 14, 2011.
0190-9622/$36.00
ª 2010 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2010.04.021
2

J AM ACAD DERMATOL
VOLUME 64, NUMBER 6
Martorell-Calatayud et al 1093
Eccrine squamous syringometaplasia (ESS) ishistologically defined as the transformation ofthe normal eccrine duct epithelium into two ormore layers of squamous epithelial cells withintercellular bridges similar to the stratumspinosum.1-4
It has been described in association with multiple
CAPSULE SUMMARY
d We establish the epidemiologic, clinical,and pathological data along with themanagement of a previously suggestedbut not well-defined distinctivechemotherapy-related rash, reported inthe past through isolated cases or smallseries,29 analyzing a total of 21 cases.
d This is, to our knowledge, the largestseries published in the literature to date.
d We suggest the term ‘‘chemotherapy-related bilateral dermatitis associatedwith eccrine squamoussyringometaplasia’’ to describe thisdistinctive subtype of chemotherapeuticdrug reaction, related in our studymainly with pegylated liposomaldoxorubicin infusions andchemotherapeutic regimens used inautologous bone-marrowtransplantation.
well-defined entities as an in-cidental finding, and it is par-ticularly seen in patientsreceiving chemotherapy forvarious malignant neoplasms(Table I).5
In 1997 and 1996, Valkset al6 and Prussick7 respec-tively suggested the existenceof a characteristic clinical pat-tern exclusively affecting theintertriginous areas, togetherwith the presence of ESS asthe main histologic feature.This pattern appeared specif-ically as a drug reaction sec-ondary to cytostatic agents.To date, there have beenonly a few cases reported inthe literature, and thus theclinical and morphologicdata on this variant of cutane-ous drug eruptions are notwell established.
Our aim in this study wasto establish the features of
this last poorly defined entity, by describing theclinical features of a series of patients undergoingcytostatic therapy who developed bilateral intertrig-inous lesions associated with the chemotherapeuticdrug administration, and to document the histo-pathologic evolutions of this cutaneous eruptionthrough the light microscopic evaluation of biopsyspecimens taken on each patient at different pointsin time.Table I. Conditions and drugs associated with eccrine squ
Condition
Infection Cytomegalovirus; herpes virusPhototoxic effect Tetrachlorodibenzeno-p-dioxin; beTumor Squamous cell carcinoma; keratoaInflammatory disease Pyoderma gangrenosum; lobular p
erythematosusChemotherapy drug Cytarabine; mitoxantrone; fluorour
methotrexate; busulfan; melphaOther Chronic ulcers; scars; dermatitis ar
METHODSPatients
Patients who presented with intertriginousdermatitis shortly after treatment with a chemother-apeutic agent and were assessed in our dermatologydepartment between January 1, 1999, and September1, 2009, were analyzed; all patients were from
amous syringometapla
Characteristics/examples
noxaprofen; phytophotodcanthomaanniculitis; annular elasto
acil; cisplatin; doxorubicinlan; carmustine; thiotepa;tefacta
the Instituto Valenciano deOncologia, an oncology cen-ter in Valencia, Spain. Thestudy was approved by thecenter’s ethics committee.
The following clinicaldata were recorded for eachpatient: age, sex, location ofthe lesion, interval betweenthe beginning of treatmentand onset of the disease,length of the eruption, andchemotherapy agents used.
The intertriginous patternrelated with ESS was de-fined as asymptomatic oritching/burning erythema-tous papules, plaques, orvesicles, usually symmetri-cally affecting both axillae,groin, and side aspects ofthe neck.6,7
Tissue examinationFor conventional light mi-
croscopy, tissue specimens
from the patients were bisected and fixed in 4%buffered formalin, embedded in paraffin wax, andstained with hematoxylin-eosin. Two 4-mm punchbiopsy samples were obtained from each patient.The first biopsy specimen was taken within the first24 hours after the onset of the cutaneous eruptionand the second was obtained in the interval between72 and 96 hours after the onset of clinicalmanifestations.sia10-32
ermatosis
lytic granuloma; systemic lupus
; cyclophosphamide; etoposide;pegylated liposomal doxorubicin

Table II. Characteristics of patients with chemotherapy-related bilateral dermatitis associated with eccrine squamous syringometaplasia
Case/age,
y/sex
Neoplastic
disease
Elemental
lesion(s)
Distribution
pattern
Days from end
of infusion to
rash onset
Length of
eruption, d
Drug(s) used
and dose Management
1/48/Male Hematologic
neoplasm
Erythema and edema Symmetric, groin 7 14 ABMT (cyclophosphamide,
thiotepa, carboplatin)
Prednicarbate
ointment bid
Single infusion
2/52/Female Hematologic
neoplasm
Erythema, edema,
and vesicles/erosions
Symmetric, axillae,
groin, and side
aspects of neck
4 12 ABMT (cyclophosphamide,
thiotepa, carboplatin)
Prednicarbate
ointment bid
Single infusion
3/55/Female Hematologic
neoplasm
Erythema, edema Symmetric, axillae,
groin, and side
aspects of neck
10 15 ABMT (cyclophosphamide,
thiotepa, carboplatin)
Prednicarbate
ointment bid
Single infusion
4/57/Female Hematologic
neoplasm
Erythema, edema,
and purple
patches
Symmetric, axillae,
groin, and side
aspects of neck
20 20 ABMT (cyclophosphamide,
thiotepa, carmustine)
Prednicarbate
ointment bid
Single infusion
5/51/Female Metastatic
breast
cancer
Erythema, edema,
and vesicles/
erosions
Symmetric, axillae,
groin, and side
aspects of neck
8 15 Taxotere Oral prednisone
(30 mg/d, 7 d) plus
prednicarbate
ointment bid
No recurrence in
subsequent infusions
at same dose
6/56/Female Hematologic
neoplasm
Erythema Symmetric, axillae,
groin
10 18 ABMT (cyclophosphamide,
thiotepa, carmustine)
Oral prednisone
(30 mg/d, 7 d) plus
prednicarbate
ointment bid
Single infusion
7/50/Female Metastatic
breast cancer
Purpuric and
erythematous
patches
Symmetric, axillae,
groin
2 21 Gemcitabine Prednicarbate
ointment bid
No recurrence
in subsequent
infusions at
same dose
8/53/Male Hematologic
neoplasm
Erythema, edema,
and erosion
Symmetric, axillae,
groin
30 15 ABMT (cyclophosphamide,
thiotepa, carboplatin)
Prednicarbate
ointment bid
Single infusion
9/60/Female
(Fig 5, A)
Metastatic
breast cancer
Erythema, edema,
and vesicles
Symmetric, axillae,
groin, and lower
eyelids
10 20 Liposomal
doxorubicin
Oral prednisone
(30 mg/d, 7 d) plus
prednicarbate
ointment bid
15% Reduction
in subsequent doses
JA
MA
CA
DD
ER
MA
TO
L
JU
NE
20
11
1094
Ma
rtorell-C
ala
tayu
det
al
10/59/Male
(Fig 5, B and C )
Metastatic
non-small
cell lung cancer
Erythema,
edema
Symmetric, axillae,
groin, and lower eyelids
6 15 iposomal
doxorubicin
Oral prednisone
(30 mg/d, 7 d) plus
prednicarbate
ointment bid
No recurrence in
subsequent infusions
at same dose
11/47/Female Metastatic breast
cancer
Erythema, edema,
and vesicles
Symmetric, axillae,
groin, and side
aspects of neck
4 14 axotere Oral prednisone
(30 mg/d, 7 d) plus
prednicarbate
ointment bid
15% Reduction
in subsequent
doses
12/53/Female Metastatic
breast cancer
Erythema, edema Symmetric,
axillae, groin
15 15 iposomal
doxorubicin
Prednicarbate
ointment bid
No recurrence
in subsequent
infusions
at same dose
13/48/Female Metastatic breast
cancer
Erythema, edema Symmetric, axillae,
groin, and side
aspects of neck
10 15 iposomal
doxorubicin
Prednicarbate
ointment bid
15% Reduction
in subsequent doses
14/63/Female Metastatic breast
cancer
Erythema and
desquamation
Symmetric, axillae,
inframammary areas
7 14 iposomal
doxorubicin
Prednicarbate
ointment bid
No recurrence
in subsequent
infusions at
same dose
15/51/Female
(Fig 1)
Metastatic breast
cancer
Erythema, edema,
and vesicles
Symmetric, axillae,
groin, and side
aspects of neck
2 18 emsirolimus Prednicarbate
ointment bid
15% Reduction
in subsequent doses
16/66/Male
(Fig 2)
Metastatic renal
cancer
Erythema
and edema
Symmetric, axillae,
and side aspects
of neck
2 13 emsirolimus Prednicarbate
ointment bid
15% Reduction in
subsequent doses
17/65/Female
(Fig 3)
Metastatic
breast cancer
Erythematous
papules
Symmetric, axillae,
and groin
3 14 iposomal
doxorubicin
Prednicarbate
ointment bid
15% Reduction
in subsequent doses
Continued
JA
MA
CA
DD
ER
MA
TO
L
VO
LU
ME
64,N
UM
BER
6
Ma
rtorell-C
ala
tayu
det
al
1095
L
T
L
L
L
T
T
L
Table II. Cont’d
Case/age,
y/sex
Neoplastic
disease
Elemental
lesion(s)
Distribution
pattern
Days from end
of infusion to
rash onset
Length of
eruption, d
Drug(s) used
and dose Management
18/37/Female Metastatic
breast cancer
Erythematodesquamative
plaques
Symmetric, axillae,
groin, and side
aspects of neck
2 12 Cyclophosphamide*
plus Adriamycin
Oral prednisone,
20 mg/d 10 d
No recurrence in
subsequent infusions
at same dose
19/69/Female
(Fig 4)
Metastatic
endometrial cancer
Erythematodesquamative
plaques
Symmetric,
axillae
10 14 Pegylated liposomal
doxorubicin
Prednicarbate
ointment bid
15% Reduction in
subsequent doses
20/50/Male Hematologic neoplasm Erythema and erosion Symmetric,
axillae
4 10 Prednisone, vincristine,
L-asparaginase,
pegylated
liposomal
doxorubiciny
Prednicarbate
ointment bid
Single infusion
21/10/Male Hematologic neoplasm Erythema, edema, and
vesicles/erosions
Symmetric, axillae,
groin, and side
aspects of neck
5 12 Prednisone,
vincristine,
L-asparaginase,
pegylated liposomal
doxorubiciny
Oral prednisone
(30 mg/d, 7 d) plus
prednicarbate
ointment bid
Single infusion
ABMT, Autologous bone-marrow transplantation; bid, twice a day.
All cytostatic drugs were administered at standard doses depending on tumor treated.
*Cyclophosphamide as drug most probably related with intertriginous dermatitis.yPegylated liposomal doxorubicin as most probable causal agent of intertriginous dermatitis.
JA
MA
CA
DD
ER
MA
TO
L
JU
NE
20
11
1096
Ma
rtorell-C
ala
tayu
det
al

Fig 1. A 51-year-old woman after 2 days of temsirolimus infusion (case 15 in Table II).Erythematous plaques localized in side aspects of neck (A and B), axillae (C), and groin (D).
J AM ACAD DERMATOL
VOLUME 64, NUMBER 6
Martorell-Calatayud et al 1097
ESS was defined histologically as the transforma-tion of the normal eccrine duct epithelium into twoor more layers of squamous epithelial cells withintercellular bridges similar to the stratum spinosum.
RESULTSA total of 21 patients were evaluated. The clinical
data are summarized in Table II. Six male (28%) and15 female (72%) patients had the intertriginouspattern. The mean patient age was 52 years (range10-69 years). Clinical findings included pruritus orburning in 14 patients (66%), whereas 7 patientsreported no symptoms (34%). The clinical morphol-ogy of the cutaneous eruptions included erythema-tous and desquamative patches, papules, plaques, orvesicles. The distribution was bilateral in all cases.The axilla was the most common site, being involvedin 20 patients (95%), with the groin also being acommon site of involvement as seen in 19 patients
(88%). Ten patients had involvement of the sideaspects of the neck (48%) (Figs 1 to 4), and twopatients had lower eyelid involvement (9.5%) (Fig 5).Inframammary folds were symmetrically involved ina single case. Two patients with associated throm-bocytopenia developed purpuric lesions accompa-nying the typical eczematous lesions of theintertriginous pattern. Palms and soles were notinvolved in any case. The eruption resolved withan intense, fine desquamation in all cases. Fourpatients also developed postinflammatory hyperpig-mentation. None of the patients developed second-ary scars.
Physical examination and review of systemsrevealed no abnormal signs or symptoms in any ofthe patients. Laboratory tests reviewed includedcomplete blood cell count, liver enzymes, urea,and creatinine levels, which showed typical changesattributable to systemic chemotherapy in all patients.
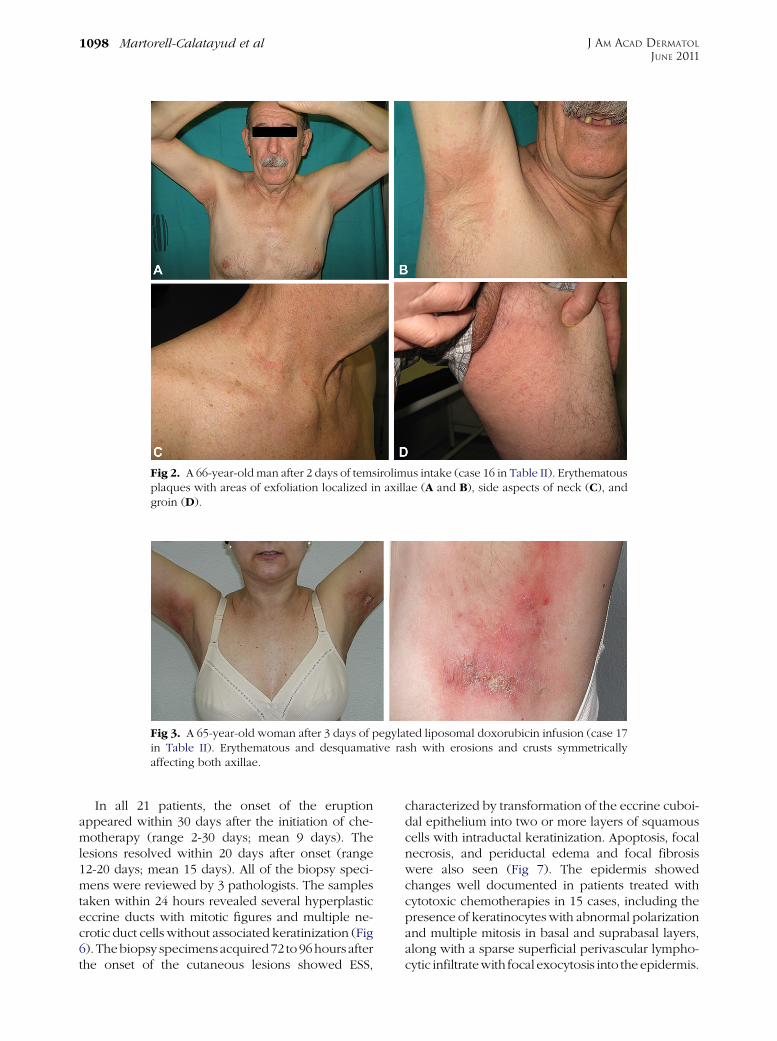
Fig 2. A 66-year-old man after 2 days of temsirolimus intake (case 16 in Table II). Erythematousplaques with areas of exfoliation localized in axillae (A and B), side aspects of neck (C), andgroin (D).
Fig 3. A 65-year-old woman after 3 days of pegylated liposomal doxorubicin infusion (case 17in Table II). Erythematous and desquamative rash with erosions and crusts symmetricallyaffecting both axillae.
J AM ACAD DERMATOL
JUNE 2011
1098 Martorell-Calatayud et al
In all 21 patients, the onset of the eruptionappeared within 30 days after the initiation of che-motherapy (range 2-30 days; mean 9 days). Thelesions resolved within 20 days after onset (range12-20 days; mean 15 days). All of the biopsy speci-mens were reviewed by 3 pathologists. The samplestaken within 24 hours revealed several hyperplasticeccrine ducts with mitotic figures and multiple ne-crotic duct cells without associated keratinization (Fig6). Thebiopsy specimensacquired72 to 96hours afterthe onset of the cutaneous lesions showed ESS,
characterized by transformation of the eccrine cuboi-dal epithelium into two or more layers of squamouscells with intraductal keratinization. Apoptosis, focalnecrosis, and periductal edema and focal fibrosiswere also seen (Fig 7). The epidermis showedchanges well documented in patients treated withcytotoxic chemotherapies in 15 cases, including thepresence of keratinocytes with abnormal polarizationand multiple mitosis in basal and suprabasal layers,along with a sparse superficial perivascular lympho-cytic infiltratewith focal exocytosis into the epidermis.
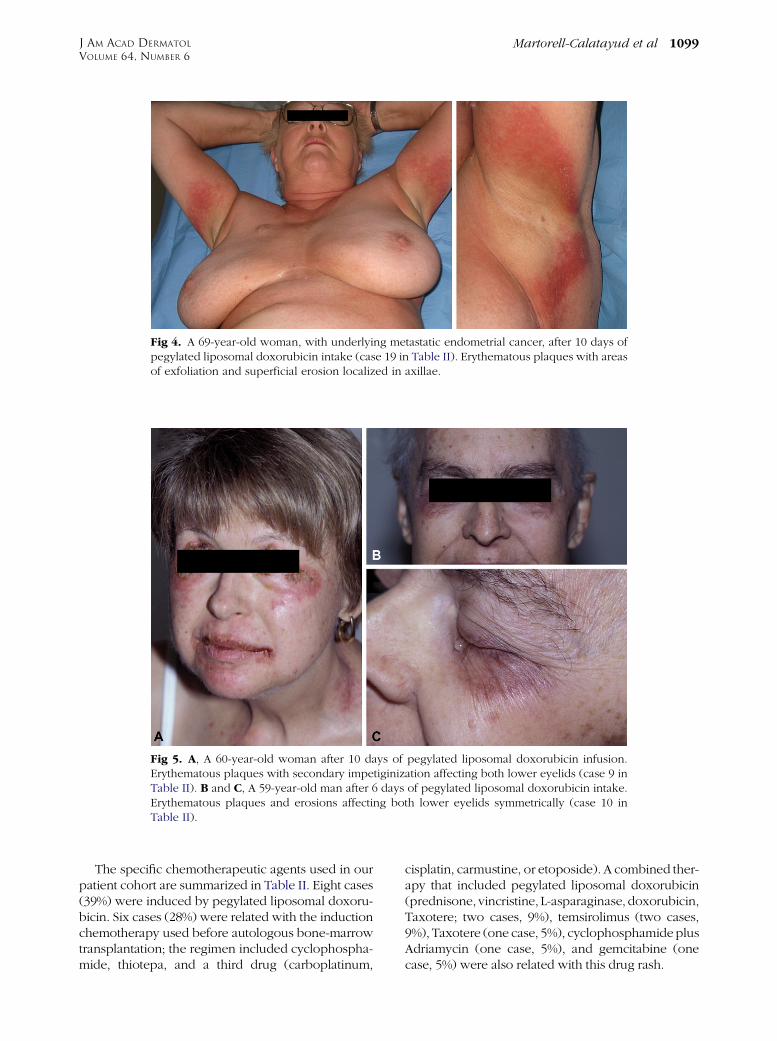
Fig 4. A 69-year-old woman, with underlying metastatic endometrial cancer, after 10 days ofpegylated liposomal doxorubicin intake (case 19 in Table II). Erythematous plaques with areasof exfoliation and superficial erosion localized in axillae.
Fig 5. A, A 60-year-old woman after 10 days of pegylated liposomal doxorubicin infusion.Erythematous plaques with secondary impetiginization affecting both lower eyelids (case 9 inTable II). B and C, A 59-year-old man after 6 days of pegylated liposomal doxorubicin intake.Erythematous plaques and erosions affecting both lower eyelids symmetrically (case 10 inTable II).
J AM ACAD DERMATOL
VOLUME 64, NUMBER 6
Martorell-Calatayud et al 1099
The specific chemotherapeutic agents used in ourpatient cohort are summarized in Table II. Eight cases(39%) were induced by pegylated liposomal doxoru-bicin. Six cases (28%) were related with the inductionchemotherapy used before autologous bone-marrowtransplantation; the regimen included cyclophospha-mide, thiotepa, and a third drug (carboplatinum,
cisplatin, carmustine, or etoposide). A combined ther-apy that included pegylated liposomal doxorubicin(prednisone, vincristine, L-asparaginase, doxorubicin,Taxotere; two cases, 9%), temsirolimus (two cases,9%), Taxotere (one case, 5%), cyclophosphamideplusAdriamycin (one case, 5%), and gemcitabine (onecase, 5%) were also related with this drug rash.
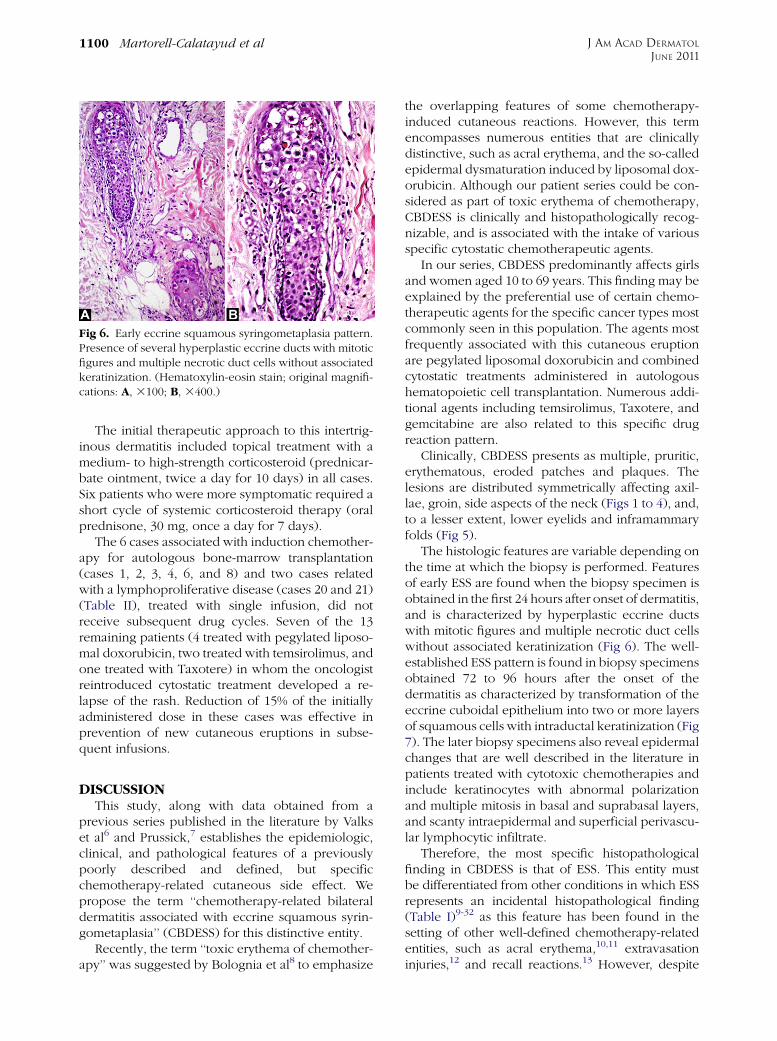
Fig 6. Early eccrine squamous syringometaplasia pattern.Presence of several hyperplastic eccrine ducts with mitoticfigures and multiple necrotic duct cells without associatedkeratinization. (Hematoxylin-eosin stain; original magnifi-cations: A, 3100; B, 3400.)
J AM ACAD DERMATOL
JUNE 2011
1100 Martorell-Calatayud et al
The initial therapeutic approach to this intertrig-inous dermatitis included topical treatment with amedium- to high-strength corticosteroid (prednicar-bate ointment, twice a day for 10 days) in all cases.Six patients who were more symptomatic required ashort cycle of systemic corticosteroid therapy (oralprednisone, 30 mg, once a day for 7 days).
The 6 cases associated with induction chemother-apy for autologous bone-marrow transplantation(cases 1, 2, 3, 4, 6, and 8) and two cases relatedwith a lymphoproliferative disease (cases 20 and 21)(Table II), treated with single infusion, did notreceive subsequent drug cycles. Seven of the 13remaining patients (4 treated with pegylated liposo-mal doxorubicin, two treated with temsirolimus, andone treated with Taxotere) in whom the oncologistreintroduced cytostatic treatment developed a re-lapse of the rash. Reduction of 15% of the initiallyadministered dose in these cases was effective inprevention of new cutaneous eruptions in subse-quent infusions.
DISCUSSIONThis study, along with data obtained from a
previous series published in the literature by Valkset al6 and Prussick,7 establishes the epidemiologic,clinical, and pathological features of a previouslypoorly described and defined, but specificchemotherapy-related cutaneous side effect. Wepropose the term ‘‘chemotherapy-related bilateraldermatitis associated with eccrine squamous syrin-gometaplasia’’ (CBDESS) for this distinctive entity.
Recently, the term ‘‘toxic erythema of chemother-apy’’ was suggested by Bolognia et al8 to emphasize
the overlapping features of some chemotherapy-induced cutaneous reactions. However, this termencompasses numerous entities that are clinicallydistinctive, such as acral erythema, and the so-calledepidermal dysmaturation induced by liposomal dox-orubicin. Although our patient series could be con-sidered as part of toxic erythema of chemotherapy,CBDESS is clinically and histopathologically recog-nizable, and is associated with the intake of variousspecific cytostatic chemotherapeutic agents.
In our series, CBDESS predominantly affects girlsand women aged 10 to 69 years. This finding may beexplained by the preferential use of certain chemo-therapeutic agents for the specific cancer types mostcommonly seen in this population. The agents mostfrequently associated with this cutaneous eruptionare pegylated liposomal doxorubicin and combinedcytostatic treatments administered in autologoushematopoietic cell transplantation. Numerous addi-tional agents including temsirolimus, Taxotere, andgemcitabine are also related to this specific drugreaction pattern.
Clinically, CBDESS presents as multiple, pruritic,erythematous, eroded patches and plaques. Thelesions are distributed symmetrically affecting axil-lae, groin, side aspects of the neck (Figs 1 to 4), and,to a lesser extent, lower eyelids and inframammaryfolds (Fig 5).
The histologic features are variable depending onthe time at which the biopsy is performed. Featuresof early ESS are found when the biopsy specimen isobtained in the first 24 hours after onset of dermatitis,and is characterized by hyperplastic eccrine ductswith mitotic figures and multiple necrotic duct cellswithout associated keratinization (Fig 6). The well-established ESS pattern is found in biopsy specimensobtained 72 to 96 hours after the onset of thedermatitis as characterized by transformation of theeccrine cuboidal epithelium into two or more layersof squamous cells with intraductal keratinization (Fig7). The later biopsy specimens also reveal epidermalchanges that are well described in the literature inpatients treated with cytotoxic chemotherapies andinclude keratinocytes with abnormal polarizationand multiple mitosis in basal and suprabasal layers,and scanty intraepidermal and superficial perivascu-lar lymphocytic infiltrate.
Therefore, the most specific histopathologicalfinding in CBDESS is that of ESS. This entity mustbe differentiated from other conditions in which ESSrepresents an incidental histopathological finding(Table I)9-32 as this feature has been found in thesetting of other well-defined chemotherapy-relatedentities, such as acral erythema,10,11 extravasationinjuries,12 and recall reactions.13 However, despite

Fig 7. Well-established eccrine squamous syringometaplasia pattern. Transformation ofeccrine cuboidal epithelium into two or more layers of squamous cells with intraductalkeratinization. (Hematoxylin-eosin stain; original magnifications: A, 340; B, 3200.)
Table III. Differential data between symptomatic and incidental eccrine squamous syringometaplasia
Features Symptomatic ESS Incidental ESS
Elemental lesion Erythematodesquamative and edematous papules and plaques
Location CBDESS- Intertriginous areas (axillae, groin, side
aspects of neck), inframammary folds,palms, soles, and lower eyelids
- Symmetric
Primary ESS- Trunk and intertriginous areas- Symmetric
Variable depending on specific entity
Pathogenesis CBDESS- Direct toxicity over sweat ducts as result
of concentration and secretion of drugin eccrine unit
Primary ESSExcessive sweat gland production
Indirect damage to sweat glands by nonspecificreactive change as result of concomitantinflammation
Histologic findings ESS as primary feature Changes specific to each well-defined entityESS as incidental finding
CBDESS, Chemotherapy-related bilateral dermatitis associated with eccrine squamous syringometaplasia; ESS, eccrine squamous
syringometaplasia.
J AM ACAD DERMATOL
VOLUME 64, NUMBER 6
Martorell-Calatayud et al 1101
the overlap with previously described entities, weconsider that the finding of ESS and epidermalchanges of chemotherapy, along with the clinicalpresentation of a bilateral, intertriginous cutaneouseruption exhibiting onset within 30 days of cytotoxicchemotherapy induction, denotes a specific entitythat deserves better description and clarification inthe literature.
The pathogenesis of ESS remains unclear. Basedon the hypothesis that there are different ESS sub-types depending on the cause of this histologicfinding, we suggest dividing ESS in two different
subgroups (Table III). In ‘‘symptomatic ESS,’’ ESSwould represent themain histologic feature. It shouldinclude CBDESS, and a rare entity called ‘‘primaryESS,’’ clinically defined as multiple erythematouspapules triggered by excessive sweating or exposureto heat.33,34 This variant could be explained bydamage to the eccrine ducts, by excessive sweatproduction and/or drug concentration in this secre-tion.33,34 Conversely, ‘‘incidental ESS’’ would includethe well-defined entities summarized in Table I. Inthese cases ESS findings represent an asymptomaticsecondary feature.
J AM ACAD DERMATOL
JUNE 2011
1102 Martorell-Calatayud et al
Eruption onset in CBDESS ranges between 2 and30 days after chemotherapy infusion. Lesions resolvecompletely in an average of 15 days, with intensedesquamation and postinflammatory hyperpigmen-tation in few cases.
Therapies for CBDESS have not been examinedthrough controlled trials. In our series, a combinationof topical and oral steroids were effective in mostpatients. Dose reduction of the chemotherapeuticagents (decrease of 15% of total dose) and intervalprolongation are alternative maneuvers in thosepatients whose cutaneous eruption is not controlledby corticosteroids.
In summary, we define a chemotherapy-relatedcutaneous eruption that is characterized by bilateral,intertriginous erythematous plaques, papules, andvesicles, with an onset within 30 days of the initialdrug administration, and histologically defined byESS and classic chemotherapy-related epidermalchanges. The eruption is most often seen after theuse of pegylated liposomal doxorubicin and com-bined cytostatic treatments administered in autolo-gous hematopoietic cell transplantation, althoughother cytotoxic agents are implicated as well. Mostcases of CBDESS resolve spontaneously or can betreated effectively with topical and/or oral cortico-steroids. Recurrence of the eruption with readminis-tration of the chemotherapeutic agent is notuncommon, however, which further clarifies theetiologic role of these drugs in this unusual butcharacteristic entity.
REFERENCES
1. King DT, Barr RJ. Syringometaplasia: mucinous and squamous
variants. J Cutan Pathol 1979;6:284-91.
2. Hurt MA, Halvorson RD, Petr FC Jr, Cooper JT Jr, Friedman DJ.
Eccrine squamous syringometaplasia: a cutaneous sweat
gland reaction in the histologic spectrum of ‘chemotherapy-
associated eccrine hidradenitis’ and ‘neutrophilic eccrine
hidradenitis’. Arch Dermatol 1990;126:73-7.
3. Serrano T, Saez A, Moreno A. Eccrine squamous syringometa-
plasia: a prospective clinicopathologic study. J Cutan Pathol
1993;20:61-5.
4. El Darouti MA, Marzouk SA, El Hadidi HA, Sobhi RM. Eccrine
syringosquamous metaplasia. Int J Dermatol 2001;40:777-81.
5. Garcia-Navarro X, Puig L, Fernandez-Figueras MT, Alomar A.
Eccrine squamous syringometaplasia secondary to pegylated
liposomal doxorubicin. Arch Dermatol 2008;144:1402-3.
6. Valks R, Fraga J, Porras-Luque J, Figuera A, Garcia-Diez A,
Fernandez-Herrera J. Chemotherapy-induced eccrine squa-
mous syringometaplasia: a distinctive eruption in patients
receiving hematopoietic progenitor cells. Arch Dermatol 1997;
133:873-8.
7. Prussick R. Adverse cutaneous reactions to chemotherapeutic
agents and cytokine therapy. Semin Cutan Med Surg 1996;15:
267-76.
8. Bolognia JL, Cooper DL, Glusac EJ. Toxic erythema of chemo-
therapy: a useful clinical term. J Am Acad Dermatol 2008;59:
524-9.
9. Heidary N, Naik H, Burgin S. Chemotherapeutic agents and the
skin: an update. J Am Acad Dermatol 2008;58:545-70.
10. Rongioletti F, Ballestrero A, Bogliolo F, Rebora A. Necrotizing
eccrine squamous syringometaplasia presenting as acral
erythema. J Cutan Pathol 1991;18:453-6.
11. Tsuboi H, Yonemoto K, Katsuoka K. A case of bleomycin-
induced acral erythema (AE) with eccrine squamous syringo-
metaplasia (ESS) and summary of reports of AE with ESS in the
literature. J Dermatol 2005;32:921-5.
12. Bordel MT, Miranda A. Eccrine squamous syringometaplasia
from chemotherapy extravasation. Actas Dermo-Sif 2005;96:
462-4.
13. Rios-Buceta L, Penas PF, Dauden-Tello E, Fraga-Fernandez J,
Dominguez-Arciniega P, Garcia-Diez A. Recall phenomenon
with the unusual presence of eccrine squamous syringome-
taplasia. Br J Dermatol 1995;133:630-2.
14. Jerasutus S, Laohabha K, Suvanprakorn P. Primary squamous
syringometaplasia with no underlying malignancy. Int J
Dermatol 1999;38:375-6.
15. Baysse L, Boralevi F, Lepreux S, Boyer A, Morel C, Leaute-
Labreze C, et al. Eccrine squamous syringometaplasia and
cytomegalovirus infection. Rev Med Interne 2003;24:394-8.
16. Dauden E, Porras JI, Buezo GF, Garcia-Diez A. Eccrine squa-
mous syringometaplasia and cytomegalovirus. Am J Derma-
topathol 2000;22:559-61.
17. Chetty R, Bramdev A, Govender D. Cytomegalovirus-induced
syringosquamous metaplasia. Am J Dermatopathol 1999;21:
487-90.
18. Alonso V, Ramon D, Monteagudo C, Llombart B, Martin JM,
Jorda E. Eccrine squamous syringometaplasia mimicking a
herpetic infection. Int J Dermatol 2006;45:762-3.
19. Choi SW, Yang JE, Kang SJ, Lee HR, Kim CW. Herpetic infection
on the vulva associated with eccrine squamous syringometa-
plasia in malignant lymphoma. Acta Derm Venereol 1999;79:
500-1.
20. Munoz E, Valks R, Fernandez-Herrera J, Fraga J. Herpetic
syringitis associated with eccrine squamous syringometaplasia
in HIV-positive patients. J Cutan Pathol 1997;24:425-8.
21. Lerner TH, Barr RJ, Dolezal JF, Stagnone JJ. Syringomatous
hyperplasia and eccrine squamous syringometaplasia associ-
ated with benoxaprofen therapy. Arch Dermatol 1987;123:
1202-4.
22. Vargas-Diez E, Valks R, Fraga J, Fernandez-Herrera J, Garcia-
Diez A. Eccrine squamous syringometaplasia in a patient with
phytophotodermatosis. Int J Dermatol 1998;37:715-7.
23. Metcalf JS, Maize JC. Squamous syringometaplasia in lobular
panniculitis and pyoderma gangrenosum. Am J Dermatopa-
thol 1990;12:141-9.
24. Helton JL, Metcalf JS. Squamous syringometaplasia in associ-
ation with annular elastolytic granuloma. Am J Dermatopathol
1995;17:407-9.
25. Garcia-Rio I, Perez-Gala S, Fraga J, Garcia-Diez A, Fernandez-
Herrera J. Eccrine squamous syringometaplasia in a patient
with systemic lupus erythematosus. J Eur Acad Dermatol
Venereol 2006;20:608-10.
26. Sakai H, Satoh K, Manabe A, Nakane H, Ishida-Yamamoto A,
Iizuka H. Eccrine squamous syringometaplasia and syringom-
atous hyperplasia in association with linear scleroderma.
Dermatology 2002;204:136-8.
27. Sommer B, Hagedorn M, Wood F, Heenan P. Eccrine squamous
syringometaplasia in the skin of children after burns. J Cutan
Pathol 1998;25:56-8.
28. Sheen YS, Huang CL, Chu CY. Eccrine squamous syringome-
taplasia associated with sunitinib therapy. J Eur Acad Derma-
tol Venereol 2007;21:1136-7.

J AM ACAD DERMATOL
VOLUME 64, NUMBER 6
Martorell-Calatayud et al 1103
29. Van de Voorde K, De Raeve H, Van Regenmortel N, Lambert J.
Imatinib-induced eccrine squamous syringometaplasia. J Am
Acad Dermatol 2006;55(Suppl):S58-9.
30. Bhawan J, Malhotra R. Syringosquamous metaplasia: a distinc-
tive eruption in patients receiving chemotherapy. Am J
Dermatopathol 1990;12:1-6.
31. Karam A, Metges JP, Labat JP, Leroy JP, Guillet G. Squamous
syringometaplasia associated with docetaxel. Br J Dermatol
2002;146:524-5.
32. Thomas LM, Mohr M, Smith M, Boyd A. Vincristine-
induced eccrine squamous syringometaplasia 2008;25:
623-5.
33. Johnson HL, Maibach HI. Drug excretion in human eccrine
sweat. J Invest Dermatol 1971;56:182-8.
34. Jacobi U, Waibler E, Schulze P, Sehouli J, Oskay-Ozcelik G,
Schmook T, et al. Release of doxorubicin in sweat: first step to
induce the palmar-plantar erythrodysesthesia syndrome? Ann
Oncol 2005;16:1210-1.
Copyright © 2022 FDOKUMEN




















