
CHAPTER24 OZONETHERAPY IN VARIOUS PATHOLOGIES
83
CHAPTER24 OZONETHERAPY IN VARIOUS PATHOLOGIES "Natura inflrmttatts humana e tardiora sunt remedia quam mala " Tacitus (- 54-120 A.D.), The Life ofGn aeus Julius Agricola, Chapter 3 (From the nature ofhuman frailty, remedies work more slowly than illnesses) What Tacitus asserted remains true even today with modem medicine, although he could not know that some diseases (atherosclerosis, cancer) take years to set in. The title of the 14 th Annual Euro Meeting (March 5-8, 2002, Basel) is "The Patient is Waiting", meaning that "At the start of the 21'1 century only a relatively small proportion of all diseases can be adequately treated or even cured and only a small proportion of all patients have access to medicinal products at affordable prices". Although this seems a pretty harsh judgement, it is true that for some diseases we do not yet have a rational drug treatment, that diseases are often poorly treated, and that too many patients in poor countries do not receive any benefit or even worse are the prey of quacks. However, we can forget neither the value of antibiotics and vaccines nor the long effort to fulfil Paul Erhlich's dream of the magic bullet, which , in spite of enormous expenses, has so far yielded meagre results and remains amirage . I often complain that basic and clinical research on ozonetherapy has been too little and too slow. Yet, therapeutic progress in cancer therapy has also not been as fast and positive as had been predicted. Three decades have already passed since President Richard Nixon dec1ared war on cancer and, although knowledge about tumorigenesis has shown an incredible expansion, the mortality rate has barely decreased. I very much hope that the new generation of drugs, like the specific inhibitor 2-phenylamino pyrimidine (STI-571), which precisely targets the AbI tyrosine kinase in chronic myeloid leukemia cells, lives up to expectations and does not disappo int us as several potential miracle eures have done (Gorre et a1., 2001). Indeed there always appears to be unforeseen toxicity observed during prolonged treatment, as occurred for the HAART (Hruz et al., 2001; Fellay et a1. , 2001) which in 1996 seemed to have resolved the problem of HIV disease. All the hype during the last decade about research on gene therapy of tumours and more recently therapeutic angiogenesis (Isner et al., 1996; Patterson and Runge, 2000; Simons, 2001), once again obtained at huge cost, has indeed generated new knowledge and allowed authors to publish interesting papers in the best medical journals. Yet, all ofthis has, so far, yielded only minimal practical results and even a few deaths . Recent developments in autoimmune diseases have highlighted potentially useful new therapies with an anti- TNFa monoclonal IgG1 antibody and a protein made of two chains of p75 TNF receptor monomer fused to the Fe domain of IgG 1 (Hanauer 243 V. Bocci, Oxygen-Ozone Therapy © Springer Science+Business Media Dordrecht 2002
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of CHAPTER24 OZONETHERAPY IN VARIOUS PATHOLOGIES

CHAPTER24
OZONETHERAPY IN VARIOUS PATHOLOGIES
"Natura inflrmttatts humanae tardiora sunt remedia quam mala "Tacitus (-54-120 A.D.), The Life ofGnaeus Julius Agricola, Chapter 3(From the nature ofhuman frailty, remedies work more slowly than illnesses)
What Tacitus asserted remains true even today with modem medicine, although hecould not know that some diseases (atherosclerosis, cancer) take years to set in.
The title of the 14th Annual Euro Meeting (March 5-8, 2002, Basel) is "ThePatient is Waiting", meaning that "At the start of the 21'1 century only a relativelysmall proportion ofall diseases can be adequately treated or even cured and only asmall proportion of all patients have access to medicinal products at affordableprices" . Although this seems a pretty harsh judgement, it is true that for somediseases we do not yet have a rational drug treatment, that diseases are often poorlytreated , and that too many patients in poor countries do not receive any benefit oreven worse are the prey of quacks . However, we can forget neither the value ofantibiotics and vaccines nor the long effort to fulfil Paul Erhlich's dream of themagic bullet, which , in spite of enormous expenses, has so far yielded meagreresults and remains amirage.
I often complain that basic and clinical research on ozonetherapy has been toolittle and too slow . Yet, therapeutic progress in cancer therapy has also not been asfast and positive as had been predicted. Three decades have already passed sincePresident Richard Nixon dec1ared war on cancer and, although knowledge abouttumorigenesis has shown an incredible expansion, the mortality rate has barelydecreased. I very much hope that the new generation of drugs , like the specificinhibitor 2-phenylamino pyrimidine (STI-571), which precisely targets the AbItyrosine kinase in chronic myeloid leukemia cells , lives up to expectations and doesnot disappo int us as several potential miracle eures have done (Gorre et a1., 2001).Indeed there always appears to be unforeseen toxicity observed during prolongedtreatment, as occurred for the HAART (Hruz et al., 2001 ; Fellay et a1. , 2001) whichin 1996 seemed to have resolved the problem of HIV disease.
All the hype during the last decade about research on gene therapy of tumoursand more recently therapeutic angiogenesis (Isner et al., 1996; Patterson and Runge,2000; Simons, 2001), once again obtained at huge cost, has indeed generated newknowledge and allowed authors to publish interesting papers in the best medicaljournals. Yet, all ofthis has , so far, yielded only minimal practical results and even afew deaths .
Recent developments in autoimmune diseases have highlighted potentially usefulnew therapies with an anti-TNFa monoclonal IgG 1 antibody and a protein made oftwo chains of p75 TNF receptor monomer fused to the Fe domain of IgG 1 (Hanauer
243
V. Bocci, Oxygen-Ozone Therapy© Springer Science+Business Media Dordrecht 2002

244 CHAPTER24
and Oassopoulos, 2001). However, it remains uneertain whether they are simplyable to alleviate symptoms for a while or, more importantly, to modify the course ofthese diseases.
If I believed aneedotal results of ozonetherapy, obtained with minimal resoureesand manpower, I would say that perhaps ozonetherapy is not as bad or obsolete asorthodox medicine depiets it. Yet rather than resting on false laureIs, I would inciteozonetherapists to work hard and seriously; the sooner we clarify the validity ofozonetherapy the better it will be for everyone.
As will be discussed in this chapter, the medical applications of ozonetherapy areinnumerable (Table 19) and this fact exposes the approach to medical derision. Is itpossible that ozone acts as a panacea or the ill-famed Theriaca? Aecording totradition, Andromachus (who was Nero's quack) invented Theriaea, a very complexmixture able to neutralize poisoning and eure every illness! Indeed, he wrote a poemin 175 verses (Oe Theriaca) to describe and praise it.
Table 19. Ozonetherapy is used in thefollowing medical spectalities.
AngiologyCardiology
CosmetologyOentistry
OermatologyGastroenterology
GerontologyGynaeeologyHepatology
InfectivologyIntensive therapy
Neurology
OncologyOrthopaediesPneumology
RheumatologySurgeryUrology
The answer is a decisive NO and only a superficial observer or a sareastieskeptic would say YES : In reality, ozonetherapy seems to exert beneficial effeetsin so many, and somewhat unrelated, pathologies beeause ozone aets at abasielevel on several blood eomponents with different funetions. Moreover, thegenerated ROS and LOPs not only have the most powerful disinfeetant aetivitybut ean aet either loeally or systemieally in praetieally all eells of an organism.The most important ROS are listed in Chapter 9 (Table 6), while only the mostsignifieant LOPs (we know very little about them as ozone effeetor molecules) arementioned in Chapters 9 and 10. Target cells vary from bacteria, fungi , parasites toblood and all eells ofthe body.
The reason why I decided to continue working in this controversial field is that Ibelieve, in contrast to the erroneous (that is only my opinion!) axiom that "ozone istoxie any way you deal with it", that oxygen-ozone, if properly used, can actcontemporaneously as a disinfectant, an oxygen donor, an immunomodulator, aninducer of antioxidants (this is a real paradoxl) a metabolie enhancer and perhaps asan activator of resident stern cells . It is difficult to figure out how beneficial effectscan develop during ozonetherapy, but Figure 90 attempts to give a visual image ofhow this can happen. The centre of action is always the plasma, where ozonedissolves and generates all the effector moleeules that interaet with erythrocytes(ER), BMC, granulocytes (GRAN), platelets (PLAT) and the Endothelium. All of

OZONETHERAPY IN VARIOUS PA THOLOGIES 245
these cells will be more or less affected depending on the ozone concentrationand the ozonization modality, which in any case must be absolutely risk-free.
Figure 90. The multivaried biological response ofthe organism to ozonized blood can heenvisaged hy considering that ozonized hlood cells and compounds interact with a number oforgan s. Some ofthese represent real targets (liver in chronic hepatitis, vascular systemforvasculopathies) , while other argan s are prohahly involved in restoring normal homeostasis
This aspect is important to understand the consequent effects that will bedirected to twelve different organs or functional sectors. The plasma and theextracellular fluid are the media interconnecting the ozone generated compounds,cell released moleeules (cytokines, growth factor, autacoids, PAF, metabolites, etc.)and a multitude of target cells . Therefore, the ozonetherapeutic stimulussimultaneously triggers many functional activities, thus allowing a multivariedtherapeutic response, but also prornotes a calculated, transitory oxidative stresswhich, unlike chronic endogenous oxidative stress, has the value of atherapeutic "shock". As an exaggerated example, somewhat like the dreaded
246 CHAPTER24
e1ectroshock that we used to inf1ict on schizophrenic patients when I was a medicalstudent! In our case , the difference is substantial as we do not harm the patient andyet we induce one of the most important body responses, i.e. upregulation of theantioxidant system which is far more than the simple adaptation to COS (Fig . 88) . Ifthis is true, and we can prove or disprove it experimentally, ozone may stimulate andcorrect the natural resources gone astray, in accordance with the old saw "Medicuscurat, natura sanat" (The physician treats, nature heals) .
There is a profound difference between modern orthodox medicine andozonetherapy. On the basis ofbiochemical, physiological and pha rmacological data,the former tries to develop a specific drug able to correct the cause of the disease,and if this succeeds the result is wonderful. Unfortunately this does not alwayshappen or the success is not complete because a disease generally causes manydysfunctions and the use of a reductionist approach is inherently disadvantageous.Although ozonetherapy has limited specificity, it has the considerable advantage that"the hodgepodge of ozonized products" can mobilize natural resources thateventually may resolve the overall problem.
With this, I am not saying that ozonetherapy is preferable; my deep feeling isthat, in any circumstance, we must first offer the patient the best treatment thatorthodox medicine provides. Only ifthis does not work, or has serious side effects,or the patient does not comply with it, can we offer the option of ozonetherapy if itis applicable to the disease. I would also take this opportunity to reject the term"alternative" because ozonetherapy, as empirical as it is today, cannot be antitheticalbut only complementary. This is the correct term. It would certainly be a wonderfulachievement if, one day, official medicine would state that "for this disease.ozonetherapy is the therapy (4' choice" , This would mean that ozonetherapy hasgained respect but, I guess that plenty of water will pass under the bridge before thatday arrives.
In spite ofimportant advances, conventional medicine is still unable to provide adefinitive improvement in some pathologies. Thus it is reasonable and ethicallycorrect to take advantage of ozonetherapy when the best orthodox treatment hasfailed. As typical examples, I will report treatment of a) suppurative infectionsrefractory to all antibiotics, b) III and IV grade hind-limb ischaemia facingamputation, and c) chronic hepatitis patients either resistant to or intolerant of IFNa.Occasionally, I may only touch upon the etiopathogenesis of a disease; the readercan fare better by consulting Harrison's "Principles of Internal Medicine",
Nevertheless, the ozonetherapist must know all the pros and cons of allconventional therapeutic modalities before suggesting the use of ozonetherapy. If theyhave been unsuccessful or are unavailable, ozonetherapy can then be considered.
l. INFECTIOUS DJSEASES (BACTERIAL, VIRAL, FUNGAL, PARASITIC)
It is intuitive that ozone can have an important therapeutic role in various types ofinfections because it generates ROS (02
0
' , OH', HzOz, NO' and HOCI), also producedby granulocytes and macrophages during an infectious process (Badwey andKamowsky, 1980; Chanock et al., 1994; Anderson et al., 1997; Saran et al., 1999;

OZONETHERAPY IN VARIOUS PA THOLOGIES 247
Titheradge, 1999; Babior , 2000) . Moreover, neutrophils have a wealth of antimierobialproteins in their granules and release eytokines and autaeoids whieh, by exerting avariety of effeets , eause tissue damage as weil (Witko-Sarsat et al., 2000) .
We observe that , owing to diffuse antibiotic-resistant baeteria, rieh eountriescontinue to use often useless, expensive antibiotics, while poor countries, by sheernecessity, use ozone whieh is quite aetive and so far has hardly induced resistance.Ozone is profitably employed either as agas (02 + 0 3), which must be weilcontained in an ozone-resistant bag saturated with water vapour, or as ozonizedsaline (to be used only topieally) , or better as ozonized bidistilled water, or asozonized oils for the treatment of war wounds, anaerobie infections, trophic ulcersand bums (Miroshin and Kontorshikova, 1995). Abscesses, anal fissures, deeubitus(bed sores), fistulae, fungal diseases, furunculosis, gingivitis, inveterateosteomyelitis, peritonitis, sinusitis, stomatitis, vulvovaginitis and wound healingdisturbances have been shown to improve rapidly beeause ozonized solutionsdisplay a c1eansing effeet and act as a powerful disinfectant, whieh kills evenantibiotic-resistant or anaerobic baeteria. On the whole, ozonized solutions eontrolthe bleeding, improve the metabolism and reduee the infection (Payr, 1935;Aubourg, 1940; Rokitansky, 1982; Werkmeister, 1995; Shaschova et al., 1995;Filippi and Kirschner, 1995; Wasser, 1995; Bulinin et al., 1995; Kudravcev et al.,1995; Kasumjan et a1. , 1995; Steinhart et al., 1999).
In poor countries (I repeat), by sheer necessity, physieians have had to devise allsorts of ways to employ the gas, or more easily the ozonized water, to avoidenvironmental contamination. In Western countries, we still need to create themental attitude to profitably use ozone. Yet , I am eonvinced that, once mediealpersonnel realize the advantages, it will be put into general use, to the benefit ofpatients. Moreover , with the eurrent inerease in medieal costs, ozonetherapydeserves attention because it reduces hospital assistance and is extremely cheap.Obviously we will need to explain how ozone works and show what ozoneconcentrations are appropriate for the particular infeetion or lesion. The sehe mereported in Figure 71 (Chapter 16) shows that a concentration of 80 ug/ml (as gas)can be used only during the first phase, in which there is pus, bacteria and necrotietissue. The wound must be cleaned and exposed to the gas for only 10-15 min.Bidistilled water ozonized with 80 ug/ml has an effective content of about 20 ug/ml0 3 and is far more practieal for cleansing the wound and changing the moistedcompress throughout the day . Ozonized oil can be applied for the night. As theinfection regresses, ozone concentrations must be lowered to 2-5 ug/ml to avoidcytotoxieity and to activate local metabolism, cell proliferation and synthesis ofcytokines (POGF, bFGF, TGFß I, EGF, KOF), so as to promote synthesis of theintercellular matrix and the healing process (Beck et al., 1993; Pierce et al., 1995;Sporn and Roberts, 1993; Schmid et al., 1993; Slavin, 1996; Martin, 1997). Topicaltreatment is easy to perform because daily observation of the wound is a good guide;however, it helps to know that time , patience and complianoe are good allies .
The problem is more complex in systemic infeetions (peritonitis, large abscesses,pleural empyema), possibly complieated with toxie and septic shock. Removal ofpurulent material and rapid washing with ozonized water is useful , particularlycombined with 0 3-AHT whieh can be earried out 1-3 times a day at low 0 3

248 CHAPTER 24
concentrations (20-30 ug /ml per ml ofblood) . OJ-AHT is intended to improve tissueoxygenation and metabolism but not to increase production of pro-intlammatorycytokines, which are already superinduced by toxins. It is also not intended tosterilize blood: although bacteria and viruses suspended in water are sensitive toozone, they become fairly resistant in plasma beeause of the proteetion exerted byendogenous antioxidants .
Direet IV injeetion of gas , similar to the sterilization of drinking water in aaqueduet, is simply a mad idea and is proseribed.
OJ-AHT (2-3 sessions weekly) must eomplement topical treatment of uleers andwounds beeause the synergism leads to more rapid healing.
I will briefly deseribe three eases that have eonvineed me that ozone has greattherapeutic aetivity in suppurative infeetions :• The first ease was reported by Dr. Salvatore Mieeli, of the Hospital at Corleone
(Palermo), during the I st Ozonetherapy Meeting in Palermo (Mieeli, 1999). Thepatient was a woman, 51 years old, born with a eleft spine and sueeessiveparaplegia of the hind limbs. A previous infected deeubitus probably eausedosteomyelitis of the right coxo-femoral joint with a fistula releasing a foulsmelling seeretion (Fig . 91 a,b; Fig. 92) . For about six weeks, she was treatedintensively with several wide-spectrum antibiotics to no avail ; in the meantime,she developed septie fever (-39 Oe), progressive caehexia, lethargy and profounddebilitation. With her permission, ozonetherapy was carried by : 1) 0 3-AHT (30ug /rnl per ml of blood) every day during the first week and then onee weekl y,and, most importantly, 2) repeated direet insuftlation (via a polyethylene catheterintroduced as far as it could go) of 02-0J at a concentration of 40 ug /ml every 5min for 1 hour. After only about 12 hours, the fever receded and purulentsecret ion ceased. Loeal gas treatment was then repeated every day for one weekand then twiee weekly for three months, when total resolution of theosteomyelitis was shown radiologieally (Fig . 93). The general condition of thepatient returned almost to normal shortl y after ozonetherapy, without antibiotiesupport. After six months (Fig . 94), the patient was perfeetly healthy.
• Another ease of osteomyelitis was referred to me but this eolleague had noradiological records . It appeared in a multiple myeloma pat ient und er eytostatietherapy at the level of implantation of a eoxo-femoral prosthesis. The physieianalso used the dual approach : 0 rAHT twice weekly, but laeking a fistula herepeatedly infiltrated the area surrounding the lesion with 50 ml of gas at aconeentration of 20 ug /ml thrice weekly. He elaimed to have resolved theproblem after 5 weeks. Osteomyelitis can easily become a ehronic infeetion and Ifeel that the timely use of ozone should be weil kept in mind .
• The third ease was a 67 year-old woman in dialysis at our Hospital since 1977 .The problem started with an initial deeubitus in the eoceygeal area . In spite ofconventional therapy, the infeetion spread and she presented an extensivenecrotizing faseiitis in both legs and at the site of primary deeubitus (Fig. 95 ).Antibioties and con ventional loeal therapy carried out by a dermatologist wereineffective and the patient worsened, with septie fever and a semieomatose state .Ozonetherapy was carried out in the Nephrology Unit , using the combined

OZONETHERAPY IN VARIOUS PATHOLOGIES 249
treatment. In this case, it was the EBOO approach three times weekly inconjunction with intensive local therapy consisting in the continuous change ofcompresses soaked in freshly ozonized water during the day, substituted withozonized oil at night. The therapeutic activity of ozonized oil is simplyunbelievable. The patient returned practically to new after two months . Ipersonally followed this case and I was amazed at her rapid recovery (Di Paoloet al., manuscript in preparation).
Figure 91. (June 14. 1999). a)Radiograph ofthe rightfemoral head and iliac bone: the aspectofthefemoral neck indicates the presence ofan osteomyelitic process. b) The external aspect
ofthefistula

250 CHAPTER 24
Figure 92. (June 14. 1999) Radiographie image 0/the osteomyelitic process visualized afterinjection ofradiopaque material via a catheter. The catheter was also used to insufflate ozone
into the purulent cavity
Figure 93. (September 25. 1999) Aftertopical ozone application and OJ-ART. theradiograph shows a striking improvement
and a marked reduction ofthe abscess.There are signs ofosteoblastic
hyperactivity
Figure 94. (April 11. 20(0) Theradiograph shows an intense
osteometaplasia with disappearance ofthe abscess cavity and resolution of'the
osteomyelitis

OZONETHERAPY IN VARIOUS PATHOLOGIES 251
Figure 95. The amazing results obtained in one patient with necrotizingfasciitis treated withparenteral (EBOO) and topical (ozonized water and oil) treatments. Extensive necrotic
lesions were present between the buttocks , Oll the legs and heels. Before (left) and after (right)the treatment

252 CHAPTER24
1.1. The Special Case 0/Helicobacter Pylori (Hp)
Hp is a gram negative, microaerophilic bacterium that is acquired in childhood; itinfects the stomach of about 50-80% of children and remains for life (Rowland,2000) . In about half of subjects, Hp may cause peptic ulcer disease, chronic gastritisand possibly gastric adenocarcinoma and gastric B cell lymphoma. Hp thrives in theacid environment of the stomach by activating its own cytoplasmic urease, whichconverts urea into CO2 and ammonia (NH) . The ammonia neutralizes the gastricacid that otherwise would diffuse into the periplasm and kill the bacterium or inhibitits colonisation. A protein denominated Ure I, a member of the amidoporin family,has the crucial role of allowing up to a 300-fold passage of urea into the cytoplasmof Hp (Weeks et al. , 2000). Tombola et al., (2001) have also shown that thecytotoxin VacA increases the transepithelial flux ofurea.
There is evidence suggesting that Hp infeetion is associated with inflamedgastric mucosal epithelium accompanied by a marked local enhancement of CD4'Th I-type response. This may explain why even eradication of the infeetion does notalways improve the dyspeptic symptoms. However, the current therapeutie approachaims at eradicating the infection, which is possible in about 80% of patients aftertreatment with omeprazole (a protonic pump inhibitor) and a combination of twoantibiotics chosen among amoxicillin, clarithromycin and metronidazole (the lattertwo seem most effective). However, there are already problems of bacterialresistance, lirnited patient compliance, high costs and the Iikelihood of reinfectionabout I month after discontinuing the treatment.
It appears to me that Hp colonisation is a prototypie case in which the use ofozonetherapy would be ideal: the bacilli are localized in the deep portions of themucus gel layer and in between this layer and the apical surfaces of the gastricepithelial cells. They do not invade the mucosa and are rarely situated betweenadjacent epithelial cells . Thus , there is nothing better than ozone and the ROScaseade to transitorily create a hostile environment to Hp, since it is sensiti ve toozone . I would Iike to propose a protocol investigating the effeet of ozonized waterand ozonized oil on the model already used in experiments on Cryptosporidiosis andGiardiasis. It may be sufficient to ingest a teaspoon of ozonized oil in the momingon an empty stomaeh, followed by two-three glasses (200-300 ml) of freshlyozonized water (final 0) concentration about I0 ug/ml) I hour before breakfast. Theoil is a bit disgusting but the water is easily drinkable. I would suggest continuingthis treatment for four weeks and then repeating all the tests (Hahn et al., 2000),possibly the non-invasive ones (Hp antigens in faeces, urea breath test , whole bloodantibody tests) during the exploratory phase . A possible substitute of ozonized oil isto drink a glass of ozonized full cream milk rieh in PUFAs. It may weil have asimilar effect and it is more palatable.
Is there any danger? No adverse effects have been reported in children withGiardiasis. Moreover, ozonized water is promptly distributed over the large mucosalsurface and reacts instantaneously with mucoproteins, which at least partlyneutralize it. Hp bacilli are fully exposed to the oxidative stress and will beeliminated. Obviously the enthusiastic patient should not exceed in drinking too
OZONETHERA,PY IN VARIOUS PATHOLOGIES 253
much ozonized water to avoid the loss of cytoprotective mucus, with the risk ofinsulting epithelial cells.
There is a practical disadvantage since the patient must take freshly preparedozonized water or perhaps milk from the hospital pharrnacy at least every other day(for four weeks). Ozonized oil is quite stable in the refrigerator. I have no doubt thatan effective vaccine will eventually be developed; this mayaiso solve the problemin poor countries where Hp infection is widespread.
1.2. Viral Infections (HIV-1 Infection)
Most lipid-enveloped viruses in aqueous media are sensitive to ozone because iteasily oxidizes glycoproteins and lipoproteins of the external envelope (Akey andWalton, 1985; Shinriki et al., 1988; Vaughn et al., 1990; We11s et al., 1991;Carpendale and Freeberg, 1991). However, the virucidal activity becomes lesscertain when viruses are in biological .fluids or, even worse, when they areintracellular (hepatocytes, epithelia, CD4+ lymphocytes, monocytes, glial andneuronal cells, etc.), where the potent antioxidant system protects viral integrity.This emphasizes once again the irrationality of direct IV injection of gas. Moreover,by means of some viral components, e.g. HIV-1 trans-activator of transcription (Tatprotein) , HIV and HCV are able to inhibit or downregulate the synthesis ofantioxidant enzymes such as SOD and GSH-Px. This induces an intracellularchronic oxidative stress (increase of 0/', OHO), which favours viral replication and,by accelerating cell death, enhances expansion of the disease (Ho, 1997). There areunequivocal experimental data (Westendorp et al., 1995; Oe Maria et al., 1996;Ranjbar and Holmes, 1996; Schwarz , 1996: Akaike et al., 1998; Larrea et al., 1998;Romero et al., 1998; Rubartelli et al., 1998) that fully agree with the fact that anexcess ofNAC, GSH and cystamine suppresses in vitro HIV replication (Roederer etal., 1990; Kalebic et al., 1991; Bergamini et al., 1994), while a GSH deficiencyimpairs survival (Herzenberg et al., 1997). The increased release of extracellular Tat,associated with circulating IFNa, also suppresses immune ce11 activation and inhibitsthe production ofC-C chemokines , leading to immune co11apse (Zagury et al., 1998).
Since 1993, the mass media have misinforrned the public, boasting thatozonetherapy could eure HIV infection . I was so perplexed about these rumours thatI wrote to Dr. A. Fauci and I appreciated his concern that ozone could promotefurther oxidative stress in HIV patients (Chapter 2).
The spreading of false, sensational news is a typical but reprehensible propensityof complementary medicine, particularly ozonetherapy, favoured by quacks toexploit anguished patients and by some producers and salesmen of ozone generators.In the period 1993-95, the epidemie was mounting, AZT monotherapy was hardlyuseful and yet the wenderful results with ozone had not been published in scientificjournals, except for a pilot study of its safety and efficacy by Garber et al. (1991) .Unfortunately, this work was very badly conceived: although it showed neitherefficacy nor toxicity, it could not support any valid conclusion and I am still puzzledas to how it was accepted for publication. Can you imagine the scientific validity of

254 CHAPTER24
a test using 10 rnl ofblood (HIV infected) treated with an unknown 0 3 concentrationplus heat (?) plus irradiation with IV (?) and then reinjected IM.
In 1994, I feit as if I was between the devil and the deep blue sea : many patientsat the hospital refused AZT and other therapies and solicited me to performozonetherapy. Garber's study was uninformative but news from Germany wasc1aiming exceIlent results and I wondered what was true. I must confess that even inthese days, when I receive news that ozone (direct IV injection or hyperbaric 0 3 ! !)works weIl, I get confused and I start to wonder if I am mistaken.
I had mixed feelings when I tried to evaluate the pros and cons (Bocci , I994a, b,1996a) in order to elaborate a rational approach : I) By oxidizing the viral gp 120 orgp41 , ozone may inactivate some free viruses in plasma, but the requiredconcentration is between 40 and 80 ug/rnl gas per ml of blood. 2) If it were true thatinfected leukocytes have a decreased content of antioxidant enzymes, we might eveninduce their death, but this could lead to further viral dissemination. In any case , theozonization of 250 mI blood (about 1/20 of the blood mass) would have only anegligible impact on the total viral load. 3) It remained uncertain whether the freeinactivated viruses may either induce tolerance or may act as an endogenousimmunogen and/or as an activator of cell-rnediated immunity. While an increase ofantibodies is hardly helpful, the activation of cytotoxic T Iymphocytes (CTL) couldbe . 4) By acting on BMC, ozone may stirnulate the production of irnmunoregulatorycytokines; in 1994, we hoped that CD8 + T Iyrnphocytes present in long-termsurvivors might either release the phantom cell antiviral factor (CAF; Walker andLevy, 1989) or Th l -type cytokines, such as IFNy and IL-2, to block the shifttowards the production of Th2-type cytokines (IL-4, 5, 6, 10) (Clerici and Shearer,1993, 1994). At that time, we did not know that CTL could release ß-chemokines(MIP-Ia, MIP-Iß and Rantes) , which by binding to the second receptor (CCR5) onCD4
4
T Iymphocytes (the first receptor is known as CD4) impede the infection ofceIls by HIV-I (Cocchi et al., 1995; Feng et al., 1996; Alkhatib et al., 1996; Deng etal., 1996; Zagury et al., 1998). On the other hand, release of GM-CSF and TNF-amay have increased viral replication and accelerate the progression of the disease(Pemo et al., 1989; Mellors et al., 1991). 5) It was difficult to predict if improvedoxygenation and activation of rnetabolism could have exerted a prevalentlybeneficial or negative effect. 6) One great hope was the possibility of inducing theadaptation to COS and I don 't think that the daily oral antioxidant supplement couldinhibit the process. 7) Activation of psychosomatic factor might have been helpfulbut , at the same time, an increase of ACTH-cortisol release with a reduced DHEAsecretion may have enhanced imrnunosuppression (Clerici et al., 1994; Corley,1995). 8) A pitfall was that in 1995 we were using PVC bags for autotransfusion,which we now know may cause immunosuppression and PVC toxicity, to thepatients' disadvantage.
In July 1995, we began a trial on 10 patients (8 men, 2 wornen), aJl of them alsoHCV positive. The patients had CD4 + T cell counts of about 260 cells /ul and anaverage plasrna HIV-I RNA level of 138,000 copies per ml.
After a few sessions, the women refused to continue owing to emotional stressand one man was very depressed and gave up because his girlfriend had left hirn.

OZONETHERAPY IN V ARIOUS PATHOLOGIES 255
They were between 26 and 37 years old and, after talking with them often, I realisedhow unhappy and strained they were. They were very grateful for what we weretrying to do and occasionally when I apologized for an imperfect venous puncture,they were most kind and said: don 't worry , we have been so stupid to inject anddrug ourselves so many times , throwing away our lives , that you are always perfect.Obviously I wished very much that the treatment would be beneficial, but in anycase their gratitude was so sincere that I rarely feit more rewarded.
The patients had never been treated, because they refused AZT and othercomplementary therapies, and they signed an informed consent form forozonetherapy. The trial ended in February 1996 and three patients underwent asmany as 54 OJ-AHT, receiving an overall ozone dose of 1080 mg evenly distributedin 16.2 I of blood. Although the study analysed a limited number of patients,repeated measurements of relevant virological markers indicated that ozonetherapycarried out with great care neither improves nor worsens the dynamics of HIV-1replication. CD4 + lymphocytes slightly increased (p=0.066) from 272±99 to341±133. Therapy was stopped in one patient after two months because the viralload in plasma showed a marked increase. Plasma HIV-I DNA remained stable(-57,000 copies/Iü" CD4) and HIV-I RNA levels also remained practicallyunvaried, except in one case . Serum ß2-micro-globulin increased significantly,possibly as a result of OJ-AHT-mediated immunological enhancement. Analysis ofthe three long-term ozone-treated patients at week 24 confirmed sustained CD4counts and a stable viral load . While in the lay press there have been manyundocumented claims that OJ-AHT is effective in HIV -I infection, we could notdocument any substantial advantage, even though no patient reported side effects,haematology parameters remained stable and some patients reported a feeling ofwell-being and a decreased incidence of oral candidosis and herpes labialis. The fullreport has been published (Bocci et al., 1998c) . In any event, against the mostpessimistic predictions of distinguished scientists, ozonetherapy did not harm thepatients and it is possible that the adaptation to COS induced by ozonetherapycountered the COS established by the virus . Indeed in two patients, we measured asignificant increase of erythrocytic SOD after 4 and 5 OJ-AHT (Bocci, 1996a).
Even in these days, I continue to ask myself if I was wrong in selecting the ozoneconcentration (-68 ug/ml per ml blood), or the schedule, or the use of PVC bags orwhat else? I also very much regret that I was unable to retrace these patients and seehow they fared, but the physicians in charge at the hospital did not bother to help me.
Needless to say, I have often been solicited to perform 03-AHT in the occasionalpatient, but the ID unit at the Polyclinic is not willing to perform a study. One goodreason is that HAART (no venous punctures) can be done at horne and is usuallyvery effective. This therapy has been able to inhibit HIV-1 replication, resulting inundetectable levels of free viruses in plasma in about two-thirds of patients for atleast 3 years, and thus has been a great success (Pomerantz, 1999; Gulick et al.,2000 ; Montaner and Mellors, 200 I) because it has reduced morbidity and mortality.Unfortunately, the initial hope to totally eradicate the virus has not come truebecause the virus remains hidden in resting CD4 + T cells and in sanctuaries (Chunand Fauci , 1999); as soon as HAART is stopped, plasma viremia becomes detectablein about 3 weeks (Chun et al., 1999). The benefit of complementing the therapy

256 CHAPTER24
with SC admin istration of IL-2 (Levy et al., 1999; Davey et a\., 2000) or with thepromising option of "structured intermittent therapy" (Ruiz et a\., 2001) remains tobe assessed, but it is now eertain that eontinuous HAART is toxie (Hruz et a\., 2001 ;Fellay et a\., 2001), diffieult to adhere to and very expensive, even for Amerieans(Steinbrook, 2001) .
Does it make any sense today to think that ozonetherapy eould help HIVpatients? My answer is: yes and no! No, if we want to substitute HAART withozone . The former is in eontinuous evolution and there is great hope of having evenmore potent and less toxie drugs, thus redueing treatment failures due to theinduetion of resistanee or poor eomplianee (Weller and Williams, 2001) . Despite thenews I reeeive from quaeks, I am eonvineed that ozone eannot match HAART inremoving HIV from the plasma, when we know that blocking viral replication is afundamental step . There is no need to eomment about the belief that HIV is not theerucial eulprit.
However, ozonetherapy may be useful as a eomplementary therapy for thefollowing reasons:
a) Now, with the new option of BOEX (or at least RI), we have a praetieal ,inexpensive and above all non-invasive approach (no venous puncture or risk ofinfeetion) .
b) Using a gradual increase of ozone eoneentrations (from low to medium : 20-40ug/rnl), we may aehieve:• adaptation to COS, hence a re-equilibration of the eellular redox state , which
is a fundamental proeess for inhibition of HIV replication;• eorrection of hyperlipidemia and peripheral lipodystrophy . With the EBOO
proeedure, we have already eorreeted two serious eases ofMadelung's disease;• a eorreetion of the wasting syndrome instead of administering reeombinant
GH and DHEA (Murphy and Longo, 2000) ;• a feeling ofeuphoria, counteraeting asthenia and depression.
The same objeetives can be aehieved using EBOO or OJ-AHT (in verypreearious patients, even using allogeneic AHT with LD blood), but theseapproaches are technically more eomplex , invasive and more expensive.
It is not yet elear what will be the most profieient strategy for intermittenttherapy, i.e. HAART either on a monthly or a seven-day-on-off sehedule, withozonetherapy performed during the periods ofHAART interruptions.
I would Iike to elose this section by offering my enthusiastic eollaboration toanyone seriously interested in eondueting a eontrolled study . I cannot do it herebeeause I have neither funds nor support . Yet I would bet that official medicine willdisregard my offer and eontinue to test IL-2 and hormones because , eoneeptually,the injection of drugs is preferred. Nonetheless, I insist in saying that if we want toassess whether ozonetherapy has any value, we must eonduet appropriate studies ineollaboration with expert infectivologists, virologists, pathologists and statistieians.
OZONETHER..-\PY IN VARIOUS PATHOLOGIES 257
1.3. Chronic Hepatitis (HBV, HCVand HDV)
It has been estimated that 300 million people in the world are chronically infected withHCV and about 2 million live in Italy. Chronic hepatitis diseases are somewhat lessdramatic than HIV but are certainly very serious ailments from a socio-economic pointof view. In Italy about 80% of infected people have a chronic disease but, luckilyabout 60% remain with a mild infection. On the other hand, 20% develop anaggressive disease leading to cirrhosis and liver cancer with some 20,000 deathsyearly. Current knowledge about the potential usefulness of ozonetherapy isinconclusive. In the recent past, I failed to elicit the interest of five of the best Italianhepatologists. Because of my inability to produce experimental evidence or asoundrationale , they all dedined my request to perform a RCT using OrAHT.
Is there any valid reason to justify the study?
1) The demonstration of a virucidal effect against HAV in vitro (Vaughn et al.,1990) has little relevance in vivo because hepatitis viruses are more resistant toozone than HIV and they may be protected by the plasma antioxidant capacity.
2) The oxidation ofviral particle components during blood ozonization may generate aninactivated and immunogenic vaccine, but this idea remains hypothetical.
3) The induction of cytokine synthesis (IFNß, IFNy, IL-4, IL-6, IL-8 and TNFa) inozonized blood incubated in vitro has been demonstrated (Bocci and Paulesu,1990; Paulesu et al., 1991; Bocci et al., 1993a,b, 1994b, 1998b). Yet the amountof cytokines released is small and the evidence that this happens in vivo uponreinfusion of ozonized blood is limited to the demonstration that the Mx proteinis induced in leukocytes (Bocci et al., 1994a). It is unknown whether theozonization process leads to activation of CD4+ helper T cells, (CD8 +) CTLresponses (Cemy and Chisari, 1999; Lechner et al., 2000) and NK cells . We alsodo not know whether infected hepatocytes increase the expression of MHC classII on the membrane, which is an important co-signal for their identification andsubsequent clearance. In the past, it was claimed that ozonetherapy increases IgGproduction (Washuttl et al., 1988), but there is no clear evidence of increasedantibody-dependent cellular cytotoxicity. The possible involvement of Kupfferand Ito ceIls (O'Farrelly and Crispe, 1999) with infiltrating CD4+T lymphocytesand CTL in destroying infected hepatocytes remains another possibility.Obviously, if the cellular immune response is weak because of insufficientquantities of cytokines, or because the heterogeneous viral population evolvesrapidly and becomes IFN-insensitive, or the immune system becomes tolerant toHCV antigens, the infection is not eradicated and becomes chronic (Bendinelli etal., 1999; Cemy and Chisari, 1999; Farci et al., 2000) .
4) We always say that OrOJ therapy improves oxygenation and hepatic metabolism,but this is more a cliche than a proven reality. Indirect, but rather tenuous, evidenceof this has been discussed in Chapter 19 (Rectal insufflation): after OrAHT orEBOO, fibrinogen and prothrombin plasma levels tend to normalize.
5) It is weIl documented that hepatic viral infections induce a COS, to theadvantage of the virus, and the release of cytokines (TNFa and TGFß) enhancesthe process (De Maria et al., 1996; Schwarz, 1996; Romero et al., 1998; Akaike

258 CHAPTER24
et al., 1998). In line with this ftnding is the fact that administration of NAC (plusIFN) reduces the plasma level of transaminases (Larrea et al., 1998). The localrelease of TGFß is doubly deleterious because it inhibits the synthesis ofMnSOD (while IL-I and IFNy increase it) and enhances hepatic fibrogenesis(Poynard et al., 1997; Poli and Parola, 1997). It can be hypothesized thatprolonged ozonetherapy may be able to reverse the COS by upregulatingantioxidant enzymes in the liver. This would be an interesting and positiveresult, but it remains to be demonstrated. It is also unknown whetherozonetherapy can induce the release of growth-stimulating factors (mainlyhepatocyte growth factor, HGF, and TGFo.) and/or growth- inhibitory factors toregulate liver homeostasis during infections, which implies continuous destructionand regeneration ofliver tissue (Fausto et al., 1995; Ankoma-Sey, 1999).
1.3.1. 1s There Any Clinical Evidence That Ozonetherapy is Useful in ChronicHepatitis?This is a sore point and it is shameful that neither in Germany nor in Italy have webeen able to produce serious documentation. In practice, we are still at the stage ofvague, insignificant oral communications by Dorstewitz, Konrad , Mattassi (1985)and Knock et al. (1987) who reported "more than satisfactory results" (?) in patientswith chronic HBV infection.
The only diagrammatic example of treatment, reported by Viebahn (1999) as a"diamond", is shown in Figure 96.
--- Bill.- - - - - - - GOT---y-GT
200
150
100
50
~:r! ;1t'lJj!! !~ !j1 j! 1J2 \ I I
'J r \I ,
" " '\' .,I ,
25/08 24/09 15/10 29110 04/12 04/021980/81
27/05 28/06
Figure 96. In the ozonetherapy literature, there is only this diagram showing the improvement0/three markers in a patient with chronic HB V hepatitis. 21 DrAHT were perform ed between
August 25. 1980 and June 1981. The bilirubin (BILl) level increased during theflrst monthand then declined to normal values (Viehahn. 1994) .

OZONETHERAPY IN VARIOUS PATHOLOGIES 259
Apparently after 21 0 3-AHT carried out discontinuously in about 9 months,there was normalization of the levels of two hepatic enzymes and bilirubin.Apparently two to five 0 3-AHT were already effeetive in reducing HCV RNA levelsin plasma (Yamamoto et al., 1996); these results are at variance with our data. The0 3eoneentrations used are uneertain, but a famous German ozonetherapist onee toldme that either 20 ug/ml or sometimes 100-150 (?) ug/ml produce "good results" and"patients fee! mueh better". Any eomment appears superfluous. Regretfully, we alsohave done very little. As I mentioned previously, my seminars in Rome , Florence,etc. proved useless. Eventually, I was lueky enough that Dr. Giuseppe Amato, one ofthe most re!iable ozonetherapists, who works at the hospital at Conegliano Veneto,agreed to evaluate our protoeol in the period 1996-98. We planned to evaluate thetreatment of ehronie HCV patients with 0 3-AHT: 250 rnl blood eolleeted in ACDusing at first an 0 3 eoneentration of 40 ug/ml per ml blood (total dose : 10 mg) twieeweekly for 5 months (about 40 treatments). One big problem at that time was thatwe were using PVC bags and the protoeol was stopped around Fall 1998 when werealized the risk of the release of plastic mieroparticles and phthalates. Of twe!vepatients, only nine received the full treatment while the other three reeeived between17 and 31 treatments. However, the results were very disappointing: none of thenine patients showed any normalization of hepatie transaminases, while the viralload was not measured. At least no side effeets were reeorded. It was then decided tobegin a study (June 1999) with new patients using the atoxie system (giass bottles)and testing the 0 3 eoncentration of 70 ug/ml per rnl of blood (225 ml) eollected inNa citrate (25 ml) to prevent any risk of plate!et aggregation (total 0 3 dose : 15.75mg). Fifteen patients were treated but only 14 were evaluated beeause one womanwithdrew after the third treatment. The schedule followed was somewhat unusual :three 0 3-AHT weekly for the first 3 weeks and then onee a month for a total of 2021 sessions. The sehedule had to be adjusted aecording to the hospital labour supply!In addition to the initial sampie prior to therapy, 13 sampies were colleeted perpatient (about every month) to evaluate liver enzymes, namely serum aspartateaminotransferase (SGOT), alanine aminotransferase (SGPT) and y-Glutamyltranspeptidase (GGT), and the viral pattern (anti-HCV, HCV-RNA-PCR, anti-HBs,anti-HBC, anti-Hbe, HbeAg, HbsAg) beeause four patients were also HBV positive.
Figure 97 shows that all three hepatie enzymes deereased progressive!y and wereeventually within the normal range (the statistical signifieanee between thepretreatment values and the last values was p<O.OI). However, the viral testsremained stable throughout the year . These results were reported at the I st
International Medical Ozone Society Meeting (IMOS, Siena November 2-4, 2000).On the whole, the results were promising, but the ineompleteness of the study madeit impossible to draw any conclusion.
Firstly , the schedule was not optimal, because to start abruptly with the highestconcentration is unsound and it may compromise the induetion of ozone toleranee.SecondIy, one treatment monthly is most likely insufficient; it should be performedat least onee weekly and thus a more intensive schedule must be devised. Oneproblem for patients is that they must come to the hospital for a few hours; if werequire too frequent treatments, the compliance is not so good. Then there areproblems of not having enough personnel at the hospital. Cleary the best goodwill

260 CHAPTER24
does not overcome the problem of lack of funding to pay for laboratory exams andmedical personnel and we are now at astandstill.120 .,-----------------------,
..'*
···.. ··SGOT
- ·SGPT--GGT
..'*..•&
\\
-..,.., -~,.......... "
.............., "".'.•.. '-..... -----........~ - ----
~.--~~
. . :::-....-......_-~---- "':
40
80
20
60
100
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15Sampie number
Figure 97. The pattern oftransaminase plasma levels ofpatients with chronic Hel'hepatitis treated with OrAHT throughout one year. Ordinate: lU/mi enzymes. All three
decreased levels are statistically significant (p<.O.01) (Amato et al.• 2000)
I must mention that, at the Siena congress, areport was presented by Luongo etal. (2000) regarding 0 3-AHT in 82 HCV patients. They c1aimed to have monitoredand recorded the redox potential of cell membranes (?) with a non-invasive methodfor each patient so that, on the basis of the ongoing measurements, they couldmodify and optimize the 0 3 concentration. This was not specified but presumablyranged from 0 to 60 ug/ml, according to the redox potential.
My comment was that the results sounded too good to be true, but the proof ofthe pudding is in the eating. Several types of the redox potent ial apparatus appearoften in the field of complementary medicine; while their real validity remainsquestionable, the fee of the "physician" goes up. Nonetheless, I have the duty tosummarize their data :a) 30% of patients initially presented between 250,000 and 1,000,000 HCV
copies/ml.b) 40% of patients initially presented between 1,000,000 and 5,000,000 HCV
copies/mI.c) 20% of patients initially presented between 5,000,000 and 7,000,000 HCV
copies/ml.d) 10% of patients initially presented between 7,000,000 and 10,200,000 HCV
copies /mlThe HCV-RNA was quantitatively assessed by the Reverse PCR method.

OZONETH ERAPY IN V ARIO US PA THOLOGIES 261
The amazing results are that 99% of the 82 patients treated for 3 to 6 months(schedule unknown) showed a more than 80% reduction of the viral load, with 9patients achieving negativity between 4 and 16 weeks. Biochemical and histologicalresponses were not mentioned. Patients previously pretreated with IFN or diabeticsubjects were particularly resistant to the treatment and this is not surprising.
I very much hope that this group will publish these data in an international, peerreviewedjournal, because, iftrue, they will represent a significant advancement.
In conclusion, ozonetherapy may be useful in chronic HCV hepatitis, but firmevidence ofthis is stilliacking.
Therefore, the refusal of orthodox hepatologists to test this approach iscomprehensible. It is more so because, since the 1980s, IFNs (particularly u type)have proved to be useful, although not always resolutive. Indeed even after intensive6-12 months therapy, up to 50% of patients may show a good clinical response, butabout 1/3 of them soon relapse. Particularly during the first month of therapy, mostpatients report significant and well known side effects, which partially recede lateron. Moreover, elderly patients may show a worrisome depressive state (Bocci,1988a; Spat-Schwalbe et al. , 2000; Malaguarnera et al., 200 I; Musselman et al.,2001 ). About 20% of patients do not tolerate IFN therapy, while about 70%experience acceptable side effects and a lucky 10% have no problems. Patients withextensive liver fibrosis or thrombocytopenia or anaemia have to be treated with greatcaution.
Resistance to IFN is frequent in older patients, in those with a highly chronicizeddisease or with high serum viral load or with HCV genotypes land 4 (whilegenotypes 2 and 3 are favourable), in men more than women, in black patients, inalcoholic or immunodeficient (HIV) patients, or in hepatitis complicated bycryoglobulinemia, vasculitis, membranoproliferative glomerulonephritis, arthritis,etc. (Johnson et al. , 1994).
Hundreds of good studies (Dusheiko, 1995; Hoofnagle and Bisceglie, 1997) havebeen performed, mostly using IFNu, and to make a long story short, IFN is nowconsidered the treatment of choice. The use of Peg IFNu-2a (with a very long halflife, so that only one dose per week is required to maintain effective levels in theblood) in combination with ribavirin (1 .0-1.2 g a day) for at least six months appearseffective in about 40% of patients, although half of them may continue to haveviremia once the treatment is stopped. (Heathcote et al., 2000; Zeuzem et al., 2000;Manns et al., 2001). Ribavirin, an oral purine nucleoside analogue, is modestlyeffective on its own, but it seems to develop asynergie effect with either IFNu aloneor Peg IFNu (Reichard et al., 1998; McHutchison et al., 1998; Poynard et al., 1998;Andreone et al., 1999; Cummings et al., 200 I; Younossi et al., 200 I) . Ribavirin mayinduce haemolytic anaemia, which occasionally is severe enough to require thediscontinuation oftreatment. Even though Peg IFNu-2a is a "retard" IFN, it inducesadverse effects similar to those with the unpegylated counterpart.
Chronic HBV infection affects more than 350 million people worldwide, LikeHCV infection, it carries the risk of developing cirrhosis and, once viral DNA hasbeen integrated into hepatocytes, liver cancer. The therapeutic aim is to stimulate avalid immune response, which with time may lead to viral clearance and reduce liver

262 CHAPTER24
inflammation, necrosis and cancerogenesis in vivo . Orthodox medicine is nowproviding new effective therapeutic strategies based on IFNa, whieh has anti viraland immunomodulatory properties, and several nucleoside/nucleotide analogues,name1y lami vudine, famciclovir, adefovir dipivoxil , etc ., which inhibit HBVpolymerase. Vaccines and anti sense oligonucleotides complete the armament, whiehis promising particularly because it combines drugs with different mechanisms ofaction (Boni et al., 1998; Dianzani, 1999; Pianko and McHutchison , 1999). Theoptimal dose of IFN is somewhat contentious, but usually 8-10 megaunits threetimes a week for 4-6 months e1icit a positive response in about 40% of patients, asdocumented by lack ofviral replication and improvement of liver histology.
What about the remaining 60% of patients? Clearly the remarkable scientifieprogress in this area must be translated into improved clinical praetices for allpatients, particularly those with the associated delta agent who are at a high risk. Inreality some hepatitis patients seek complementary treatments : an interesting reviewhas evaluated the effects and toxicity of frequently used herbaI produets whileozonetherapy was not even mentioned (Seeff et al., 2001)
This digression has two purposes : the first is to inform the ozonetherapist of thestate of the art, because she/he has the duty to inform the patient thoroughlyabout IFN therapy. The second is to point out that orthodox rnedicine reeeivesplenty of funding from national agencies and multinational pharmaeeuticalindustries, which are interested in developing drugs to recover their investment andmaking a profit. In comparison, ozonetherapy is like an ant to an elephant: nofunding , no laboratories, no clinics and total disorganization; the gap is too big to beclosed. Moreover, there is another huge disadvantage: IFN therapy is intrinsieallyexpensive, but the patient, once instructed, can do it casily at horne and visit thehospital every three months for acheck up. In eontrast, except for the very empiriealRI, OrAHT, EBOO and BOEX requ ire a day hospital and expensive (for theNational Health Service) medical assistance. Because it is performed privately, thepatient must bear the financial burden out of his own pocket. Moreover, medicalpersonnel are hostile to both ozone and the handl ing of infected blood. Thus,although it is likely that ozonetherapy represents a money-saving approach, wecannot evaluate the cos tlbenefit ratio beeause the benefits have not yet beendemonstrated.
In spite of enormous difficulties, I still believe that we should clarify whetherozonetherapy has some merits. This can only be done by RCTs , comparing OrO..therapy against O2 alone, because the relevance of spontaneous remissions must bec1arified .
The most suitable and practical methods are I) OJ-AHT; 2) RI and 3) BOEX, butwe could start with the first one and then proceed depending on the results .
Among ehronic hepatitis diseases, we eould examine hepatiti s C with definedHCV genotype, possibly without any previous treatment beeause of refusal of IFN.Patients should be of both sexes, between 30 and 50 years old . Informed eonsent isneeded.

OZONETHERAPY IN VARIOUS PATHOLOGIES 263
1.3.2. Proposal ofa ProtocolThe most practical schedule seems twice a week (M and Th or Tu and F):
225 ml blood in 3.8% Na citrate (25 ml) plus 225 ml O2alone or 02-0J.Use of citrate instead of heparin may reduce ozone's effectiveness but avoids
possible complications due to dyscoagulation and potential formation of miniclots.
ISI week : 30 ug/ml for a total OJ dose of 6.75 mg per treatment,2nd week: 40 ug/ml for a total OJ dose of9.00 mg per treatment,3rd week: 50 ug/ml for a total OJ dose of 11.25 mg per treatment,4lh week : 60 ug/ml for a total OJ dose of 13.50 mg per treatment,t h week: 70 ug/ml for a total OJ dose of 15.75 mg per treatment,
to be continued for 24 weeks (48 sessions) unless a problem arises . Therapy may becontinued once a week during the second semester depending on the results. Patientsshould take the usual daily .oral antioxidant supplement. Evaluation of therapeuticeffectiveness should consider the following end-points:
a) permanent serum HCV RNA clearance, tested with the most precise system .Viral load should be assessed before treatment, after 3 and 6 months therapy andthen after a further 3 months .
b) normalization of hepatic biochemistry (SGOT , SGPT, GGT, bilirubin levels).Test as in (a).
c) liver histological results, whenever possible before and 3 months after the 6month course . If liver biopsy is refused, a surrogate test to indirectly evaluateliver fibrosis may be used. Moreover, in addition to all the routine biochemicaltests, TAS, TBARS and PTG should be measured every 3 months. Of particularinterest is the evaluation of cholesterol, LOL, HOL, albumin, fibrinogen,prothrombin and CRP.
Patients with HIV, autoantibodies, autoimmune hepatitis, hypergammaglobulinemia,haemochromatosis, liver metastasis, incipient cirrhosis, extrahepatic manifestation ofHCV infection should be excIuded.
Treatment is obviously cost-free and control patients have the right to be treatedwith 02-0J after the first semester. This switch-over might actually be interesting toclearly demonstrate the role of ozone. It would be very important to have the resultsof this study and I would be glad to collaborate with anyone seriously interested inconducting it. If the results are clearly negative, we should forget aboutozonetherapy. If they show that at least 50% of patients are good responders,ozonetherapy could be useful in patients who do not tolerate IFN, in elderly patientsparticularly sensitive to psychotic effects, in hepatitis C patients with normal serumaminotransferase levels but with viremia (Hirsch and Wright, 2000), in patients afterliver transplantation and in patients who cannot afford the cost ofIFN.
As the current best conventional combination (Peg IFNa-2a with ribavirin) is notentirely satisfactory, it could be supplemented with one OJ-AHT treatment per week,which may reduce the severity of adverse effects and enhance immunoactivation.

264 CHAPTER24
Moreover, as I doubt that a brief course of ozonetherapy can reduce the viralload (as observed with HIV infect ion), we could test a hybrid approach: firstly ,knock down the viral load with a short (1-2 weeks) intensive treatment with IFNa(Neumann et al., 1998) or IFN-ß (Ikeda et al., 2000) followed by 0 3-AHT accordingto the schedule described above. ladmit that these may be hopeless speculations.Yet, for many reasons, hepatitis C is a very heterogeneous and difficult disease, forwhich ozonetherapy might be useful in complementing conventional therapies toachieve a favourable outcome.
Finally, a sort of minor plasma autotherapy can be envisaged and utilized forpriming and activating natural immunity: it may be worth while to evaluate aprotocol based on repeated, weekly IM injections of 1-2 ml autologous plasmaheavily ozonized to produce a viral immunogenic vaccine.
1.4. Herpetic 1nfections and Herpes Zoster
Herpes simplex viruses (HSV-I and HSV-2) cause human infections involvingmucocutaneous surfaces, the CNS and possibly visceral organs inimmunosuppressed patients.
HSV-I is mostly responsible for causing oral-facial herpes, but it can spread togive an herpetic eye infection that may lead to corneal blindness. HSV-2 is mostlyresponsible for lesions on the genitalia, and it recurs petiodically. HSV infection ofthe finger (herpetic whitlow) usually represents a complication of oral or genitalherpes.
Although these infections are usually limited, their frequent recurrencecompromises the patient's quality of life (Arvin and Prober, 1997). Current antiviralchemotherapy is prevalently based on systemic (oral andJor IV) administration ofnucleoside analogues: aciclovir, famciclovir and valaciclovir. These drugs are notalways effective because of aciclovir-resistant strains .
Control of HSV infection may be achieved by a vaccine, which has been late incoming and has showed effectiveness only in women not previously infected withHSV-I (Stephenson, 2000) . A promising therapy for genital herpes is the local useof a gel containing an immune response modifier called resiquimod, which is able tostimulate antibody and cytokine production (Bishop et al., 2001) .
Herpetic cheratitis can be treated with ophthalmic IFNa or IFNß plus aciclovir.Herpes zoster (HZ), or shingles, is a distressing disease affecting about 1% of theover-60 population. It is caused by the varicella-zoster virus, which remains in aquiescent state in the nerve root ganglia after recovery from chicken pox. The virusmay be reactivated during an immunosuppressive state. It causes a unilateraldermatomal, vesicular rash associated with severe pain . The frequency of locationis: trigeminal (16%), thoracic (50'%), cervical (14%) and lumbar (12%)dermatomers. If the disease goes untreated, the pain can last for months and can becomplicated by post-herpetic neuralgia (PHN). This complication is rare in youngmiddle-age patients (30-50 years) but is frequent in elderly patients. PHN should beprevented by intensive therapy as early as possible. Unfortunately, the incidence ofthis complication increases with age and with immune depression. It seems that

OZONETHERAPY IN V ARIOUS PATHOLOGIES 265
microinfusion of anaesthetics via the peridural route, initiated no later than I weekfrom the appearance of the cutaneous exanthema, may reduce the incidence andminimize the pain . By blocking the axonplasmatic transport, local anaesthetics canprevent diffusion of the HZ virus to neurones in the spinal cord, thus reducingneuronal death and the consequent allodynia and abnormal sensations. The antiepileptic, gabapentin, is widely used, but is not always effective. The sooner anappropriate treatment is started, the better. Prophylaxis in patients over 60 and atrisk has been partially accomplished by the administration of specific zoster immuneglobulin (ZIG) or by shingles vaccine (NIAID, Bethesda, USA, 1999). Antiviralchemotherapy is based on aciclovir, valaciclovir or, probably even better,famciclovir with or without prednisolone (Wood et aI., 1994, Whitley and Roizman,200 I), but they have little effect on the healing of skin lesions or pain. The use ofcorticosteroids is controversial: although they reduce inflammation, they inhibithealing and enhance immunosuppression, which is exactly what favours the virus.Administration of amitryptline (25 mg for 3 months) seems to reduce the pain(Dworkin, 1999). Taking drugs continuously can reduce or suppress herpeticinfections, but it is expensive, can cause adverse effects and induce viral resistance.
This is what official medicine offers today, but it cannot necessarily satisfy allpatients. Although these diseases are not deadly, they are serious and we must fostera sense of concern and the need ofbetter therapeutics.
As this book is aimed at critically evaluating ozonetherapy, I have the duty toreport the usual litany of wonderful results obtained with ozonetherapy. Theproblem is that these results have been reported at best in an abstract form, are verydifficult to trace and analyse, and can be considered anecdotaI. It seems thatMattassi (1981 , 1983) treated 20 patients, of which ll presented herpes simplex and9 had HZ. I believe the pat ients were treated with 5 to 12 IV injections of 02-03!After a few injections, all patients overcame the infectious episode and only a fewhad a recurrence over several years. None of the patients had side effects. Mattassi(1981) stated that results were incredibly rapid and that to be successful the therapyshould be started as soon as the lesion appears. Dr . J. Delgado, of the Center ofMedical and Surgical Research in Havana, treated 15 patients suffering from HZwith daily IM infections of Or03 and topical applications of ozonized sunflower oil.He noted a marked improvement after a few days and alI patients were cured aftertwo weeks, without showing any relapse. He concluded that "the low cost , the easyava ilability and simple application made ozonetherapy the treatment of choice". Ibelieve that Dr . H. Konrad works in Sao Paulo (Brazil); he has reported (1995,2001) that 03-AHT was effective in both herpetic infections and was able tominimize the complication of PHN evaluated in 55 patients.
I think it is important to report the experience of Dr . Giuseppe Amato, alreadycited for the study performed in chronic HCV infection. I believe that bis work intreating PHN patients is outstanding; it has been performed at the Hospital"DeGironcoli" at Conegliano Veneto in Italy during the last decade. Although this isan open study, it is praiseworthy and regards 180 patients (84 men and 96 women)between 40 and 85 years of age :

266 CHAPTER24
• age 40-50 : 30 patients (16.7%);• age 51-70: 60 patients (33.3%);• age 71-80 : 54 patients (30%) ;• age 81-85 : 36 patients (20%);
The location of HZ was as folIows:
• Ocular region: 18 patients.• Head, neck and anns: 30 patients.• Thorax : 30 patients.• Lumbar region: 48 patients.• Limbs : 54 patients.
Patients always arrived at the hospital with some delay when previous physiciansfeit unable to deal with the intense pain of acute HZ infection. Evaluation of painwas carried out with the visual analogue scale (VAS) . On the basis of previousexperience, Dr. Amato decided to abandon all conventional medication and examineozonetherapy associated with the microinfusion of anaesthetics (usually 12 ml ofmarcaine at 0.25% daily) mostly via the epidural route to block the sympatheticsystem in relation to the dennatome presenting the cutaneous rash.
The concomitant use of two therapies or the lack of a control is usually open tocriticism, but in the case of PHN it had be done for ethical reasons in order to reducethe pain.
Dr. Amato proceeded systematically to perfonn:
a) 03-AHT (150 ml of blood collected in Na citrate and a total ozone dose of 10.5mg or 70 ug/ml) every day for 4 consecutive days and then every other day for 2weeks (at least 10 treatments) .
b) Local treatment using compresses moistened with ozonized water during the day .The applicatlon of ozonized oil at night is effective and most irnportant.
c) Sympathicolysis ofthe stellate ganglion or other ganglia at various levels .
Owing to the fact that patients below 50 years rarely develop PHN, theyunderwent only ozonetherapy. Pain disappeared after 2-3 days (i.e . after 2-3 0 3AHT) and the exanthema also improved very rapidly. Three patients (out of 30)developed PHN after 2 months and they were promptly treated with anaesthetics.However, in the subjects over 50 (150 patients), Dr. Amato believed it ethicallycorrect to practise both therapies on a prophylactic basis, because they are at arealrisk of developing PHN.
Anaesthetic treatment was perfonned daily for no more than 10 days at the levelofthe stellate ganglion and for no more than 20 days in other locations .
. On average, pain disappeared after the first application:
• for about 12 hours in 36 patients.

OZONETHERAPY IN VARIOUS PATHOLOGIES
• for about 18 hours in 114 patients.• and for 24 hours in 30 patients.
267
After 3-4 days, the pain disappeared in about 90% of patients; although furthertreatment seemed unnecessary, it continued for up to 20 days in order to preventPHN later on. All patients were followed for 2 to 5 years : of 99 patients older than50 and treated as indicated above in the first week, only 12 developed mild PHN thatwas successfully treated with both therapies . Of the remaining 51 patients treatedwith a delay longer than one week, the percentage increased and was in relation tothe delay. In conclusion, it appears that the combination of ozonetherapy withanaesthetic intervention is most effective in preventing PHN in patients older than 50.
In view of the difficulty of managing PHN, the results appear impressive. Bysheer necessity, they lack controls (02 only) and, in this regard, I must report anothersurprising study. Olwin et al. (1997) found that minor AHT (10 ml of blood nottreated with O2-03 or O2) was effective in eliminating clinical sequelae in 8 of12 (66%) patients with thoracic HZ, in 9 of9 (100%) patients with ophthalmic HZand in I with lurnbar-thigh HZ. They claimed (data not presented) that IFNa., IFNßand IL-4 levels were increased in the patients within 24 hours after the IM bloodinjection . They also mentioned that another 25 cases of herpes infections of varioustypes yielded favourable results , noting that the rate of success depends on earlyintervention. A delay of 2-13 months between the first symptoms and treatmentyields negative results. As this report originates from reliable institutions (RushPresbyterian St. Luke's Medical Center and Life Seiences Department, IIT ResearchInstitute, Chicago, USA), the data ought to be true. If they are, they partly supportAmato's data; yet they totally refute the value of oxygen-ozone, Moreover, if theyare true, Health Authorities and official Medicine have the obligation to verifythem: irrespective of the skepticism toward ozone, it is outrageous that weintoxicate HZ patients with expensive, but modestly effective, pills when a fewtrivial injections of autologous blood into the patient's buttock could relieve awfulpain in 2 to 8 days. However , authoritative scientists and clinicians obviously do notbother to believe, or to read, papers published in the Journal of Alternative andComplementary Medicine and prefer to administer expensive drugs. This is evenmore reproachable because simple AHT is an old medical practice (Maddox andBack, 1935; Hardwick , 1940; Martindale and Capper, 1952); even I performed it in1953 when I was an intern in Clinical Medicine!
If dermatologists and neurologists, as weil as general practitioners, ever read thissection, they might think that everything I have written is false and it would bebetter to forget everything. I have no direct experience, but I fully trust Dr. Amatoand I am inclined to believe that, bearing in mind that orthodox medicine does notoffer much to highly distressed patients, we should attempt to prove or disprove thevalidity of either simple AHT or 0 3-AHT. As soon as I fmish writing this book, Iwill revive my proposal of a protocol evaluating herpetic infections and HZ, whichin 1999 was refused by the Professor of Dermatology . In spite of everything , I amstill optimistic that many physicians are not aware of ozonetherapy and that theymay be willing to try it. I am certainly ready to help anyone .

268 CHAPTER24
In Chapter 16, I extensively discussed the approaches of the so-called "rnajor"OrAHT and "rninor" OJ-AHT. If venous access is lacking, we can use the option ofRI or BOEX . Minor AHT, without or with 0 2-0J, is in my opinion an interestingimmunoenhancer approach and it is easy, simple, inexpensive and rapid to perform.Starting with a low dose and gradually increasing it, we can ozonize 5 ml blood (30ug /rnl and upward) followed by IM injection three times a week, and then slowdown as soon as the lesions are healed and the pain is gone . Local treatment is alsoimportant and effective when combined with OrAHT. It can be performed easily byapplying and repeatedly changing a compress moistened with ozonized water (orozonized oil at night) . Vaginal or rectal suppositories of ozonized oil can beemployed in genital-anorectal herpes . We must try to start the treatment as soon ascutaneous lesions and pain appear; the viral reactivation should be suppressed assoon as possible because it reduces the PHN complication. It appears necessary toalert all GPs to send HZ patients to the special PHN unit at the hospital as soon asthey make the diagnosis.
1.5. Papillomavirus Infections (HPV)
HPV infects the epithelium of skin or mucous membranes and may produce warts,or benign and malignant neoplasias. Common warts (Verrucae vulgaris and plana)may be present in children, while plantar warts (Verrucae plantaris) are painful andfairly common in young adults . The incidence of venereal warts (Condylomaacurninatum) has risen, particularly in women, and represents a common sexuallytransmitted disease (Cannistra and Niloff, 1996). Viral genotypes 6 and 11 carry alow risk and may cause modest dysplasia of the uterine cervical epithelium, knownas cervical intra-epithelial neoplasia (CIN I). Viral genotypes 16, 18, 31, 33 and 35are more carcinogenic and can induce a CIN II or the more severe form, CIN rn(Liaw et al., 1999). Laryngeal papillomas are typical of children and may producelife-threatening airway obstruction. Anogenital warts (venereal warts) can reachmonstrous proportions and may be associated with cervical cancer.
Effective conventional therapies include cryosurgery, surgical excision andablation with a laser. Topical treatments with antimetabolites and podophyllumpreparations are scarcely resolutive because the virus is widespread in the basal celllayer and persists if the immune system is unable to destroy infected cells . The useofboth IFNa and IFNß have been successful for laryngeal papillomatosis and partlyuseful (30-40% response) in preventing venereal HPV recurrences even afterprolonged treatment (Friedman-Kien et al., 1988; Kirby et al., 1988; Weck et al.,1988; Bocci et al., 1990). Both the cost and the adverse effects of IFNs reduce thecompliance. The fact that HPV infection is an important risk factor for carcinoma isweil known and several HPV vaccines are undergoing trials. However, ozonetherapycould be useful as a complementary therapy. To the best of my knowledge, there areno data, but it may be worthwhile evaluating a protocol in the hope of eradicatingcervical-vaginal infections. Therapy should combine parenteral approaches, such asmajor or minor OrAHT, RI or BOEX , with local treatment. After the basic surgicaltreatment, always important to remove the bulk of infected tissue, there are several

OZONETHERAPY IN VARIOUS PATHOLOGIES 269
possibilities: one is intralesional injections ofsmall volurnes ofOr03 (from 10 to 20ug/ml) . The infiltrating injections of gas must be done slowly and with great care,possibly at the base of the wart; as reported for IFNß, they are pa inful and thepatient may get discouraged. Intravaginal insufflation of Or03 (concentration: 3050 ug /ml) for a few seconds is more acceptable, as noted during treatment ofbacterial and fungal vaginitis. Instillation of ozonized water (final 0 3 concentration- 20 ug/rnl) for 5-10 min can be done at home and application of an ozonized oilpessary every night is practical and certainly far less expensive than an IFNß gel.
The benefit of ozonetherapy remains to be ascertained, but there is no risk, noside effects and certainly a low cost. The possibility of minimizing viral shedding,thus reducing the potential of transmission to sexual partners is not a trivialadvantage.
1.6. The Common Cold
The well-known manifestations of the common cold, i.e . rhinorrhea, nasalcongestion, lachrymation and sneezing, are commonly experienced each year. Sorethroat, malaise and headache are also frequently present. Although the common coldresolves without sequelae in 4 to 9 days, it is a very bothersome infection. Normalindividuals do not need particular treatment, but immunosuppressed patients are atrisk ofpulmonary infections and can be prophylactically treated with IFNa or IFNß.
Enormous funds have been spent in the hope that a few applications of IFNssprayed at the appearance of the first symptoms would abort the infection. As amatter of fact, the applications are always too late : in order to establish the antiviralstate , the IFN should bind to the cell receptors a few hours before the viral invasion.The IFN approach has been a financial blunder because the local adverse effects ofIFN are worse than the infection itself. I wish a small part of the money would bespent on evaluating the effect of ozone! I would like to give an example of theversatility of ozone, and I am not pretending to be too serious!
Ozone as agas is toxic for the nasal and respiratory mucosa and must not beused . However, in our lab, during the last five years we have prepared a lot ofozonized bidistilled water every day . It is ready after 5 min of bubbling ozone(concentration 80 ug/rnl) in water. The final 0 3 concentration is about 20 ug/ml andif it stored in a glass bottle with a tight teflon tap, it keeps for two days, even thoughthe ozone concentration progressively decreases. If anyone thinks he has caught acold, he can aspirate the ozonized water into the nostrils 3-4 times a day and cantake the bottle home for further use . Water passes into the rhinopharynx and iseliminated, but it is not harmful if swallowed. It also helps to gargle the ozonizedwater at the same time . Although nasal aspiration of ozonized water causes transientirritation (10-15 sec) , it is unbelievable how rapidly the nasal congestion, sinusaloedema and pharyngodynia disappear rapidly for 3-5 hours, after which it isnecessary to repeat the procedure. The infection resolves in 3-4 days, but it is farmore tolerable than if it went untreated. If I have time, I also perform 03-AHT onmyselfto reduce the feeling offatigue.

270 CHAPTER 24
This approach is quite empirical and it is difticult to produee praetiealapplications, so pharmaeeutieal eompanies have no reason to worry about it!
1.7. Fungal and Parasitic Infections
Most of these diseases are present in hot-humid countries and are seen lessfrequently in Europe, either as opportunistic infections or after a trip to the tropies .
Among fungal infections, those that have been treated with ozone areonychomycosis (tinea pedis or athlete's foot) and eandidiasis. Owing to the USembargo against Cuba, scientists and physieians in Havana have used ozone , asnecessity is the mother of invention. At the XII IOA Congress (LiIle 1995), it wasreported that treatment of a sick nail with 1-2 drops of ozonized sunflower oil forseveral days led to a complete eure in 69% of patients (the remaining 31'% showedmarked improvement). In contrast, in the group treated with tolnaftate solution twieea day, only 7% were eured, 25'% improved and there was no change in 68'%,probably owing to drug resistance (Menendez et al., 1995) . Using ozonized olive oiltopically, we have achieved incredible results; in fact, we now believe that thissimple preparation is really effective because it is amply disinfectant and able tostimulate the healing proeess. I predict that , as soon as prejudiees disappear andphysieians beeome aware of this fact and try ozonized oil with good results, it wiIlbecome widely used worldwide with great patient satisfaction .
Candidiasis and any other fungal infection can obviously be treated withsystemic and topical antifungals, but I can guarantee that gas insufflation (wheneverpossible), ozonized water and ozonized oil applied topically have equal , if notsuperior, effectiveness.
Giardiasis is a parasitic infeetion eaused by the protozoan Giardia lamblia,common in areas with poor sanitation and present even in the United States .
Cryptosporidiosis is also a diarrhoeal disease, caused by protozoa of the genusCryptosporidium. Good drugs Iike metronidazole are effective but have some sideeffects. In Cuba, at first they used to drink ozonized water, at least four of fiveglasses per day on an empty stornach for repeated periods of 10 days separated by aI week interval. According to Sardina et al. (1991), up to 48% of patients becameasymptomatic after the second cycle . Ingestion of ozonized oil seems moreeffective, but it is hard to swaIlow. An improved administration is represented bycapsules filled with ozonized oil. A 10-day cycle "cured" 79% of children, while theremaining 21% showed a marked improvement of symptoms but still had cysts ortrophozoites in the faeces (Menendez et al., 1995) . No side effects were reported.
There is no need to report other studies because the therapeutic modality is thesame . However, it is certainly worth keeping this approach in mind for use in poorcountries of Africa, Asia and South America affected by several fungal and parasiticdiseases. Areas lacking electricity cannot produee ozone and ozonized water . Thusthe World Health Organization (WHO) ought to promote a standard and veryeeonomical production of ozonized oil (which keeps weil) and distribute it whereneeded. I should try to promote this enterprise, although it may have little valueunless we ean reduce the rate of infection by improving sanitation in all directions.

OZONETHERAPY IN VARIOUS PATHOLOGIES 271
Just a few .words about malaria, which remains another scourge of our time,exacting atoll of I million deaths each year . Unfortunately, both the mosquitoes andthe protozoan Plasmodium falciparum have become resistant , the former toinsecticides and the latter to drugs . Almost 20 years ago, Dockrell and Playfairshowed in mice that H202 is able to kill Plasmodium yoelii. At the XV 10ACongress (London, September 10-15, 200 I), Viebahn-Hansler et al. reported thatparasite growth can be inhibited by ozone at a concentration of 80 ug/ml afterozonization of a blood cell suspension. However, in contrast to the sarcastic opinionof many scientists that ozone is a panacea, I doubt that ozonetherapy would ever beuseful because parasites are well protected by the plasma and cellular antioxidantsystem, as weil as being hidden in the spleen and other sanctuaries. Moreover, 0 3
AHT or EBOO are demanding approaches and would be difficult to organize intropical countries for the treatment of millions of people. I feel pessimistic aboutwasting our meagre resources on diseases such as HIV and malaria for which theadministration of oral drugs or a long-sought vaccine appear rational and could bemore useful on a large scale.
2. AUTOIMMUNE DISEASES
Autoimmune diseases are areal thomy problem because serious diseases such asrheumatoid arthritis (RA), Sjögren's syndrome, vaseulitis, multiple sc1erosis (MS) ,systemic lupus erythematosus (SLE), Crohn's disease, systemic sc1erosis (SSc)should have attracted our attention a long time ago, instead of treating unaesthetic,albeit very lucrative, lipodystrophy. Since 1983, this has been the almost exclus iveinterest of Italian ozonetherapists, which explains why today ozonetherapy isregarded so poorly. It is even worse that at the annual meetings, two or threeozonetherapists claim , with great rhetoric, that they are able to obtain suchwonderful results with a few OrAHT (ozone concentrations and schedule arealways uncertain) so that invalid patients are able to rise frorn the wheelchair and gobicycling or dancing . In obedience to holistic therapy and to the patient's advantage(so they say), they invariably mix ozonetherapy with magnetotherapy, phytotherapy,homeopathy, chelation therapy, etc., so that it becomes impossible to c1arify the role ofozonetherapy . Assuming that this exerts areal effect, it would be important to confirmthe results with a proper RCT in order to understand what mechanisms have beenactivated, how relevant is the placebo effect and how long the improvement lasts.
The aetiology of these diseases remains hypothetical , while the pathogeneticmechanisms are fairly common, obviously with different locations and with a strongprevalence in women. Different tissues (articular, gut mucosa, myelin, etc .) areinfiltrated by macrophages, neutrophils and CTL, responsible for an abnormalrelease of ROS and proinflammatory cytokines (IL-I ß, IL-2, IL-8, IL-12, IL-15, IL18, TNFa, IFNy), while inhibitory cytokines (lL-IO, IL- I I, TGFß 1) are largelysuppressed (Kuruvilla et al., 1991; Brandes et al., 1991; Taga et al., 1993; Akdis etal. , 1998; Letterio and Roberts , 1998; Mclnnes and Liew, 1998; Pizarro et al., 1999;Perdue, 1999; Dinarello, 1999; Herrrnann et al., 2000) .

272 CHAPTER24
Activation of enzymes, such as phospholipase A2 (PLA 2) , metalloproteinases(collagenases, elastases), cathepsins Band D, and plasminogen activators causes therelease of compounds leading to cell death and disintegration of the intercellularmatrix and/or myelin, thus perpetuating negative involution. Local release ofsubstance P, calcitonin grp (gene related peptide), bradikynin, leukotrienes, LTB4 (apotent chemotactic and hyperpermeabilizing factor) , PGE2, PGD2, PG12
(vasodilatators), TxA 2, and Frisoprostanes (both vasoconstrictors) wreak furtherhavoc and elicit oedema and pain (Cracowski et al., 2000). Interestingly, theseeicosanoids (2-series PGs and 4-series LTs) derive from AA (20:4n-6), while 5series LTs and 3-series PGs, deriving from 5, 8, 11, 14, 17 eicosapentaenoic acid(EPA, 20:5n-3) and from 4,7, 10, 13, 16, 19 docosahexaenoic acid (DHA, 22:6n-3) ,are far less phlogogenic but are practically absent (Purasiri et al., 1997). EPA andDHA competitively inhibit the conversion of AA to PGs, thus exerting usefulinhibitory effects on inflammation and inappropriate immune responses (Calder,1998). That is why a diet rich in n-3 PUFAs has been advocated for the treatment ofvarious chronic inflammatory conditions typical of autoimmune diseases (Belluzziet al., 1996; Rose and Connolly, 1999).
Throughout the years, with the progressive understanding of pathogeneticmechanisms, orthodox medicine has striven hard to offer the most effective therapy.Yet it has succeeded only in part, owing to adverse effects and unforeseencomplications. Nonetheless, the ozonetherapist has the duty to present all the possibleoptions. For the sake of space, 1can only give a few brief examples, but the reader canfind a wealth of details in Hanauer (1996) and Hanauer and Dassopoulos (2001) :
2.1. Current Therapies for Inflammatory Bowel Disease
• Sulfasalazine, oral and topical with slow release preparation.• Corticosteroids, among which budesonide is a new compound with high mucosal
potency (enema formulation) and low systemic activity. I mention these twocompounds because they are specific inhibitors of NFKB (Chapter 14,Leukocytes), which allows the synthesis of IL-113 and TNFu (Auphan et al.,1995; Wahl et al., 1998).
• Antibiotics, such as metronidazole and ciprofloxacin, used alone or in combination .• Immunomodulatory drugs: azathioprine, 6-mercaptopurine, methotrexate,
mycophenolate mofetil, cyclosporine, tacrolimus (FK 506), thalidomide. Theyhave different mechanisms of action , but substantially inhibit the production ofpro-inflammatory cytokines (lL-l, lI-2, lI-8, IL-12 , TNFu).
• Imunosuppressive cytokines to inhibit the Th I-type » Th2-type excessiveresponse. lI-IO and Il-Ll seem to suppress effector functions and Th I-typecytokine production (Taga et al ., 1993; Akdis and Blaser , 2001) . A few trialshave shown the safety and tolerance , but the ultimate efficacy remains unknown.An interesting possibility, so far evaluated in mouse colitis, is the increasedrelease of IL-lO into the gut lumen by genetically engineered bacteria. IL-IOmay be absorbed via a paracellular route and may downregulate T cell activation

OZONETHERAPY IN VARIOUS PATHOLOGIES 273
in the submucosa (Steidler et al., 2000) . TGFßl mayaiso be efficacious but hasnot yet been tested . The usefulness of IFNa remains equivocal.
• Oral tolerance. If the responsible autoantigens ean be identified , their oraladministration eould induee an immune tolerance and represent a rationaltreatment.
• Probiotics. In Chapter 19, the critical role of genetic susceptibility of the gutmieroflora and its interaction with enterocytes and the MALT was discussed .There are promising, yet unsubstantiated, results after administration oflaetobaeilli, bifidobacteria, Streptococcus thermophilus, ete. This complementaryapproach should not be disregarded, since it is non-toxie and may become moreuseful by modifying the luminal environment by intermittent hydrocolontherapy. A correet ecologieal environment can be restored by microfloraadministered via enema .
• Dietetic support. As previously mentioned, a diet enriehed with n-3 PUFAspresent in fish oil generates (via cyclooxygenase and lipoxygenase) 3-series PGsand 5-series LTs, which are anti-inflammatory and may re-equilibrate the Th lTh2 pattern (Hodgson, 1996). n-3 PUFAs can easily be taken in eapsules(Belluzzi et al., 1996) or emulsionated with milk. Although this approach isprobably not sufficient to solve the problem, it is recommended and obviouslyhas to be continued for life.
• SC administration 0/growth hormone for four months (Slonim et al., 2000) . Theoptimal dose, schedule and duration of response remain to be defined .
• The last approach regards a biotechnological "jewel", i.e. the licensing in theUSA and Europe of infliximab, an antibody against TNFa (anti-TNFa). Thischimeric antibody is about 25% mouse and 75% human and is stillimmunogenic. A humanised antibody, CDP571 (only 5% mouse and 95%human) , is probably better, but is not yet available. RCTs involving the IVinfusion of these antibodies have shown clinical benefits in about 65% ofpatients with severe Crohn's disease and fistulae. Four trials have examined atotal of 306 patients (Targan et al., 1997; Present et al., 1999) and a veryinformative commentary has been published in which Bell and Kamm (2000)conclude that "although treatment with anti-TNFa has improved the quality 0/life for some patients with Crohn's disease, knowledge ofits proper clinical rolewill come only with time". Another geneticallyengineered product is the solubleTNFa receptors consisting of two identical chains of the extracellular humanp75 TNF reeeptor monomer fused to the Fe domain of human IgG I. This isknown as etanercept and is administered SC twice a week. These new productsare now limited by their cost, not only in Europe but also in the U.S.
2.2. Current Therapies o/RA
Beeause of similarities, I will now briefly report eurrent therapies of RA (Choy andPanayi, 200 I), in whieh degenerat ion of cartilage and erosion ofjuxta-articular boneseems mainly due to the presence ofTNFa (Feldmann and Maini, 2001).

274 CHAPTER 24
Orthodox therapy aims to relieve pain , reduce and possibly resolve inflammationand enhance healing.
• Non-steroidal anti-lrflammatory drugs (NSAlD) . Besides the old aspirin , theyinc1ude ibuprofen, indomethacin, naproxen, sulindac, etc . They are all associatedwith at least gastric irritation. The latest-generation cyclooxygenase I1 inhibitorsseem to be effective and have less adverse effects (Fitzgerald and Patrono,2001) .
• Glucocorticoid therapy . Except occasionally prednisone to control symptoms,this therapy is now proscribed.
• Immunosuppressive therapy. Azathioprine, cyc1ophosphamide, methotrexate at aninterrnittent low-dose may be useful, but attention must be given to adverse effects.
• Disease-modifying drugs , such as D-penicillamine, sulfasalazine, goldcompounds, are partly useful , but there is minimal evidence that they delay boneerosion or allow real healing.
• The new drugs are the previously mentioned anti-TNFa antibodies and thesoluble TNFa R fusion protein etanercept. IV administered antibodies appear toregulate the production of IL-6, IL-8, MCP-I and VEGF, reduce the influx ofinflammatory cells into joints and the blood levels of rnatrix metalloproteinases.As has been observed in Crohn's disease, in a few RCTs, about two-thirds ofRApatients have shown a c1ear beneficial response for up to 2 years (Elliott et al.,1994; Maini et al., 1999). However, in RA, infliximab has been associated withmethotrexate. Similarly, the combination of etanercept and methotrexate seemsto provide greater c1inical benefit than methotrexate alone (Lovell et al., 2000;Weinblatt et al., 2000) .
Lets us now consider the official therapeutic arsenal of Crohn's disease andRA versus ozonetherapy. Because someone may think that I am biased againstofficial medicine, I invite everyone to read Sartor's commentary (2000) about newapproaches to Crohn's disease and the commentaries ofO'Dell (1999) and Pisetsky(2000) about RA. Although all three authors agree that a new era of improvedtreatment has arrived, they caution that a multitude of bad effects may appear. Sartor(but also Bell and Kamm, 2000) is particularly critical. Possible problems include :allergic reactions and serum-sickness-like reaction, induction of antibodies todouble-stranded DNA, occurrence of lymphoma (shown already in 6 patients) anddevelopment of tubercolosis (Keane et al., 200 I) . Use of infliximab costs about12,000 pounds per year . About 33% of patients are unresponsive and some pat ientsare not suitable for immunological therapy. All previous therapies , as reviewed bySartor, are both scarcely effective and present serious adverse effects .
Regarding ozonetherapy, besides a few unbelievable anecdotes or scanty resultsby Knock and Klug (1990) , there is only the study performed at Cuba's Institute ofRheumatology in 1988 on 17 patients treated with IM injections of Os-O, (total doseof ozone : 700 ug) for 8 weeks combined with NSAID . Apparently about 25% ofozone-treated patients scored 25% better than controls (Menendez et al., 1989). It is

OZONETHERAPY IN VARIOUS PATHOLOGIES 275
reasonable to conclude that we do not know today if ozonetherapy may be useful.Nevertheless, in spite of a few charlatans' tales, we should not dismiss it a priori.
How and why could ozonetherapy be beneficial?a) Using either 03-AHT or BOEX or even the more complex EBOO approach, we
may be able to enhance immunosuppression and increase the production of IL-10,IL-II, TGFß and perhaps IL-I Receptor antagonist (IL-I Ra). The immunologicalinvestigation carried out in patients should aim at clarifying if ozonetherapyinduces anergy of the T cells that are cytotoxic. The RI approach, associated withthe parenteral ones, may be helpful in inducing immunosuppression in the gut (seeChapter 19). RI mayaiso inhibit the bacterial flora that is partly responsible forCrohn's disease . However, the possibility ofinducing immunosuppression has yetto be tested, although a hypothetical rationale and a tentative protocol have beenproposed in Chapter 14 (Leukocytes, Point 3).
b) Generalized and localized induction of antioxidant enzymes, thus eliminating theexcess of ROS production. This is a reasonable proposition, which already hasexperimental support and may be achieved by inducing the adaptation to COS.
c) Inhibition of the release of inflammatory enzymes, metalloproteinases etc ., witha progressive decrease of plasma levels of PAF, LTB4, PGE2, TxA2 andisoprostanes. The chronie inflammatory process can be slowly tumed off only ifwe can, with 6 months oftherapy, implement points a) and b).
d) Fistulae and abscesses in Crohn's diseases can be dealt with by insufflation ofozone or ozonized water and oil. An RCT could be performed in one or morehospitals, but this is beyond our means and dreams at the moment. It will beindispensable to have a control arm because the placebo effect may be relevant.
Who can pay the cost of endoscopic, radiological, histologieal, biochemical andclinical exams? We are not backed by any pharmaceutical and/or biotechnologicalfirm because ozonetherapy does not produce profits. However, if ozonetherapyproved to be useful, it would save money for the National Health Service. Yet, Idoubt that the Ministry of Health, biased and myopie as it has proved to be in thepast , will ever support this research.
2.3. Therapies ofMS
The same problems will apply to a RCT planned for MS. This is a tragic diseasebecause it very often disables young adults just when they are about to show theirmerit. I worked enthusiastically on IFN research, but in the meantime 1 was longingto evaluate if ozonetherapy would be useful for these patients. All physicians knowthat MS is a T cell-mediated autoimmune disease that can either relapse (relapsingremitting MS) or be very aggressive (progressive MS) . Good reviews of the topicare available (Rudick et al., 1997; Karp et al., 2000; Polman and Uitdehaag, 2000;Wingerchuk et al., 2001) .
Orthodox medical therapy is based on a) corticosteroids, b) immunosuppressivedrugs, namely azathioprine, methotrexate, cyclophosphamide and cyc1osporine, andmore or less c) experimental biologicals, such as IV immune globulins, copolymer I

276 CHAPTER24
(COP) 01' glatiramer acetate (Duda et al., 2000; Kipnis et al., 2000; Neuhaus et a\.,2000), which induces a shift from a Th-I to a Th-2 cytokine profile in COP-treatedpatients. The present treatment of choice (for r-rMS) is IFNß-Ia (glycosylated) andIFNß-Ib (a mutein). All of these drugs can cause immunosuppression to differentdegrees, and particularly those indicated in a) and b) may cause serious adverseeffects. Despite their biochemical difference, both fonns of IFNß (approved by USand European regulatory authorities) have a positive elinical effect, characterized bya elear reduction of both the frequency and severity of exacerbations (Amason,1993; Rudick et al., 1997; Polman and Uitdehaag, 2000). IFNßs are fairly weiltolerated. Unfortunately, owing to striking phannacokinetic and pharmaeodynamicdifferenees (Bocci, 1981b; 1987b; 1988a; 1990a; Bocci et al., 1988), IFNa-2a,which eould be therapeutically useful, causes adverse events that negatively affectthe already poor quality of life of these patients (Nortvedt et al., 1999). IFNsß arenow in wide use, but problems such as the optimal dose and sehedule, theappearance of neutralising antibodies (mostly to IFNß-I b) that may jeopardizeefficacy (AntoneIli et al., 1998), a possible relapse when stopping therapy and theeonsiderable cost, provide a glimmer of hope that a serious RCT based onozonetherapy is still meaningful. In the ease of MS, nothing serious has been doneand my attempt to interest three neurologists was in vain beeause they were weilsponsored by finns producing IFNß . Two ozonetherapists (one in Turin and anotherin Milan) reported to me that they had achieved "good rcsults" treating MS patientswith OJ-AHT eombined with either magnetotherapy 01' ehelation therapy. Nocomment!
Thus very \ittle hope remains and it also seems useless to speculate that in thesediseases, as weil as in others cited at the beginning of this section , it might havebeen useful to combine 01' to alternate cyeles of IFNß 01' anti-TNFa antibodies withozonetherapy. An old adage says: "Be not afraid of going slowly, be afraid only ofstanding still".
The problem of Raynaud's phenomenon (Block and Sequeira, 2001) inselerodenna patients will be considered in the next section .
3. ISCHAEMIC DISEASES(HlND-LIMB ISCHAEMIA, CEREBRAL AND HEART ISCHAEMIA,
VENOUS STASIS)
It appears logical to think that if blood briefly exposed to oxygen-ozone can exert abenefit, this would be best noted in isehaemic tissues . Even a partial obstruction oflimb arteries due to atheroselerosis (Lusis, 2000) 01' diabetes 01' Buerger's disease(thromboangiitis obliterans) leads to a progressive reduction of blood flow to the feet.Lack ofperfusion leads to tissue ischaemia and possibly cell death. Any minor trauma ,nonnally irrelevant, facilitates the fonnation of an ulcer, which will not heal beeauseoxygen , nutrients and soluble mediators involved in the repair process are laeking.
Aeute \imb ischaemia is frequently eaused by aeute thrombotie oeclusion of apre-existing stenosis 01' by an embolus; it requires immediate surgieal 01' medieal

OZONETHERAPY IN VARIOUS PATHOLOGIES 277
attention . Chronic limb ischaemia becomes progressively evident. In Europe, wedistinguish four stages, as classified by Fontaine:
Stage J: Feeling of cold or nurnbness in the foot and toes. Skin temperature isreduced. The foot is pale and frequently becomes cyanotic.Stage JI: Paresthesia and hypoesthesia, firstly localized and successively diffused tothe whole foot. Hyporeflexia. This is the phase with incipient neurological defect.Intermittent claudication. Pain may cease with rest.Stage IJI: Pain at rest with noctumal exacerbation. Cyanosis becomes weil evident inone or several toes , with an incipient trophic lesion or a frank uleer. (Rate ofamputation is - 15%).Stage IV: Partial or total necrosis of one or several toes. Pain often becomesunbearable (Rate of amputation is - 50%) .
The angiologist has several, precise non-invasive techniques to objectivelyassess the severity of POAD. Extensive epidemiological studies have shown thatthese patients have practically the same relative risk of death from cardiovascularcauses as do patients with a history of cerebrovascular or coronary disease. A usefulpredictive value is given by the ankle-brachial index (ABI). The normal range ofvalues is 0.91-1.30, which decreases to 0.41-0.90 in mild to moderate POAD and tobelow 0.40 in severe POAD. Patients with ABI below 0.40 are at high risk of acardiovascular event and present an annual mortality of about 25%. As I cannot gointo details, I suggest reading two excellent review articles (Dorrnandy andRutheford, 2000; Hiatt, 200 I). Each patient must be evaluated for any possiblerevascularization and there are several operative procedures with a high success rate .Lurnbar sympathectomy is no longer performed because it does not increase bloodflow to muscle. Spinal-cord stimulation also does not prevent amputation (Klomp etal., 1999). At the extreme, Taylor et al. (1999) have shown that distal venousarterialisation is a unique procedure with promising possibilities for salvage ofcritically ischaemic, inoperable limbs (stage IV). Besides surgery, orthodoxmedicine offers several therapeutic options, including useful supportive measures,such as quitting smoking, proper diet, exercise (Davies, 2000), and pharrnacologicaltreatments as folIows :
1) Vasodilatators must be able to improve collateral blood flow and avoid"stealing" blood away from underperfused muscle. Pentoxyfylline may enhanceoxygenation in ischaemic tissues by increasing blood flow to themicrocirculation. lt may improve blood rheology by decreasing blood viscosityand enhance erythrocyte flexibility . However, arecent double-blind RCTshowed no significant difference in healing rates of pure venous uleers betweenpatients taking pentoxyfilline and those taking placebo (Dale et al. , 1999). In1999, the FDA approved cilostazol, an inhibitor of phosphodiesterase type 3,which by increasing the concentration of cAMP causes vasodilatation andreduces claudication. PGE 1 and a stable prostacyclin analogue (iloprost) havebeen infused in patients with critical leg ischaemia. Both cilostazol and iloprost
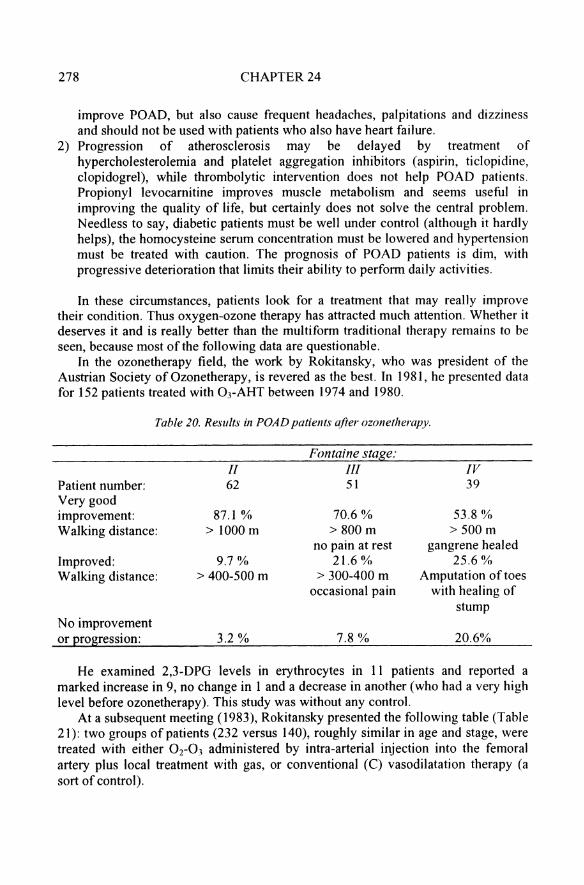
278 CHAPTER24
improve POAD, but also cause frequent headaches, palpitations and dizzinessand should not be used with patients who also have heart failure.
2) Progression of atherosclerosis may be delayed by treatment ofhypercholesterolemia and platelet aggregation inhibitors (aspirin, ticlopidine,clopidogrel), while thrombolytic intervention does not help POAD patients .Propionyl levocamitine improves muscle metabolism and seems useful inimproving the quality of life, but certainly does not solve the central problem.Needless to say, diabetic patients must be weil under control (although it hardl yhelps), the homocysteine serurn concentration must be lowered and hypertensionmust be treated with caution. The prognosis of POAD patients is dirn, withprogressive deterioration that limits their ability to perform daily activities.
In these circumstances, patients look for a treatment that may real1y improvetheir condition. Thus oxygen-ozone therapy has attracted much attention. Whether itdeserves it and is really better than the multi form traditional therapy remains to beseen, because most of the following data are questionable.
In the ozonetherapy field, the work by Rokitansky, who was president of theAustrian Society ofOzonetherapy, is revered as the best. In 1981, he presented datafor 152 patients treated with OJ-AHT between 1974 and 1980.
Table 20. Results in POAD patients after ozonetherapy .
Patient number:Very goodimprovement:Walking distance:
Improved:Walking distance:
No improvementor progression:
II62
87.1 %> 1000 m
9.7 %> 400-500 m
3.2 %
Fontaine stage:III51
70.6 %> 800 m
no pain at rest21.6 %
> 300-400 moccasional pain
7.8%
IV39
53.8 %> 500 m
gangrene healed25.6 %
Amputation oftoeswith healing of
stump
20.6%
He examined 2,3-DPG levels in erythrocytes in 11 patients and reported amarked increase in 9, no change in land a decrease in another (who had a very highlevel before ozonetherapy). This study was without any contro\.
At a subsequent meeting (1983), Rokitansky presented the following table (Table21) : two groups of patients (232 versus 140), roughly similar in age and stage, weretreated with either O2-0 3 administered by intra-arterial injection into the femoralartery plus local treatment with gas, or conventional (C) vasodilatation therapy (asort of control ).
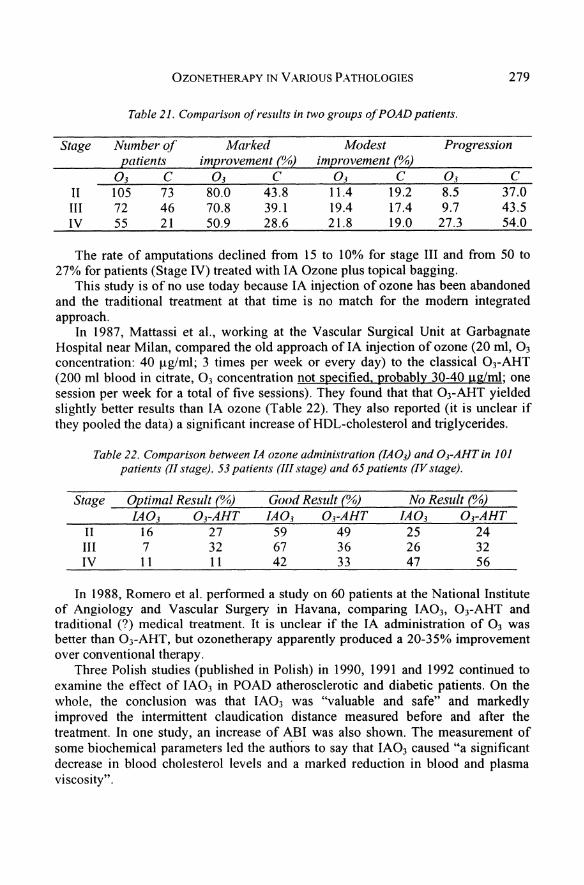
OZONETHERA.PY IN VARIOUS PATHOLOGIES
Table 21. Comparison ofresults in two groups ofPOAD patients.
279
Stage Nutnber of Marked Modest Progressionp"tients improvement (%) improvement (%)
0 3 C 0 3 C 0 3 C 0 3 C11 105 73 80.0 43.8 11.4 19.2 8.5 37.0III 72 46 70 .8 39.1 19.4 17.4 9.7 43.5IV 55 21 50.9 28.6 21.8 19.0 27 .3 54.0
The rate of amputations declined from 15 to 10% for stage III and from 50 to27% for patients (Stage IV) treated with IA Ozone plus topical bagging.
This study is of no use today because IA injection of ozone has been abandonedand the traditional treatment at that time is no match for the modern integratedapproach.
In 1987, Mattassi et al. , working at the Vascular Surgical Unit at GarbagnateHospital near Milan, compared the old approach of IA injection of ozone (20 ml, 0 3concentration: 40 ug/ml; 3 times per week or every day) to the c1assical 03-AHT(200 ml blood in citrate, 0 3 concentration not specified, probably 30-40 ug/mI; onesession per week for a total of five sessions). They found that that OrAHT yieldedslightly better results than IA ozone (Table 22). They also reported (it is unclear ifthey pooled the data) a significant increase of HDL-cholesterol and triglycerides.
Tahle 22. Comparison between IA ozone administration (IA03) and OrAHT in 101patients (II stage). 53 patients (III stage) and 65 patients (IV stage).
Stage Optimal Result (%) Good Result (%) No Result (%)/AOI DrAHT IA0 3 DrAHT IA0 3 DrAHT
11 16 27 59 49 25 24III 7 32 67 36 26 32IV 11 11 42 33 47 56
In 1988, Romero et al. perfonned a study on 60 patients at the National Instituteof Angiology and Vascular Surgery in Havana, comparing IA03, 03-AHT andtraditional (?) medical treatment. It is unclear if the IA administration of 0 3 wasbetter than O]-AHT, but ozonetherapy apparently produced a 20-35% improvementover conventional therapy.
Three Polish studies (published in Polish) in 1990, 1991 and 1992 continued toexamine the effect of IA03 in POAD atherosclerotic and diabetic patients. On thewhole, the conclusion was that IAO} was "valuable and safe" and markedlyimproved the intermittent c1audication distance measured before and after thetreatment. In one study, an increase of ABI was also shown. The measurement ofsome biochemical parameters led the authors to say that IA03 caused "a significantdecrease in blood cholesterol levels and a marked reduction in blood and plasmaviscosity".

280 CHAPTER24
After Rokitansky et al. (1981) asserted that ozone increases 2,3-DPG, lowersfibrinogen and plasma viscosity, and reduces plasma cholesterol, it has become aregular ritual to confirm these data.
The aim of orthodox therapy is to improve blood rheology by changing thelifestyle (no smoking, almost a vegetarian diet , exercise, etc.) and using severaldrugs aimed at different targets . Yet, in spite of a great effort, the success has beenmeagre . As discussed in Chapter 14 (Erythrocytes), it is hard to believe that ozonecan produce all these magie results , because during the last 6 years of c1inical work(with 0 3-AHT and EBOO) we have not been able to confirm them. We have notobserved a decrease of cholesterol plasma levels, nor a change of LDL; if anything,the fibrinogen level tends to increase slightly. In our ARMD study (about 5,000 0 3AHT) , often with 13-14 sessions , we observed a slight increase of2,3-DPG only in afew patients who had a very low level prior to therapy . This result was also obtainedby Mattassi (1985) before uso Romero et al. (1993) conducted a useful study ,comparing the relative efficacy of ozone adrninistered to POAD patients by: a) IMgas injection, b) OrAHT, c) RI, and d) standard conventional treatment. Irrespectiveof the administration route, ozonetherapy markedly improved the ABI and reducedc1audication. Thus the authors reached the conclusion that RI was as effective but fareasier to perform than 03-AHT. As I am not enthusiastic about RI, I was surprisedwhen Mattassi confirmed, at the Verona Congress (1999), that among IA, OJ-AHTand RI, the last approach is as effective as the first two and concluded that we mustbear in mind this finding because the patient who owns a generator can perform aself-administration at horne. Russian c1inicians working at the Ozonetherapy Centrein Nizhni Novgorod reported at the XII 10A Congress in Lille (1995) that ozoneadmin istered by various techniques to 132 elderly patients (IV and SC injections ofO2-03, IV infusion of ozonized rheomacrodex solution and 3-4 0 3-AHT) is "highlyeffective" and induces "significant improvement ofpatients' weil being".
Amato's observations (2000) on the effect of 03-AHT as a unique therapy forangina abdominis (AA) cannot be overlooked. AA is arare, painful abdominalsyndrome that manifests itself after a meal , probably owing to a localized transitoryischaemia of the gut. Surgical vascular correction normally solves the problern. butin the three elderly patients studied by Amato it was not feasible . A cycle of 10 OrAHT (150 ml of blood treated with 0 3: 20-40 ug/rnl per ml of blood) followed bymaintenance therapy (one treatment every month) resolved the problem very weiland patients, no Ionger afraid to have a meal , showed a marked improvementwithout any side effects. The oldest patient, a woman of 87 years, has undergonethis therapy since 1994!
Who says that ozone is toxic?A final remark can be made regarding the extraordinary capacity of combining
03-AHT with topical therapy (either gas or, better, ozonized water and oil) to allowhealing of awful decubitus or neerotie ulcers in the limbs (also see Chapter 14,Platelets, and this Chapter). It takes some time but they do heal. Figure 98, takenfrom Werkmeister's work (1995), shows that extensive lesions after X irradiationtook up to 190 days with only loeal treatment, but I believe that association withparenteral treatment would have shortened the resolution time. Regarding ulcers onlimbs, irrespective of the aetiology (atherosclerosis, Buerger's disease, diabetes,

OZONETHERAPY IN VARIOUS PATHOLOGIES 281
Raynaud's phenomenon), they do heal, even in the two exceptional cases describedby De Monte and van der Zee (2001).
160 r--------------------------,
250,
200150100,
50
40
20
oL:::::::!;s;:::;:e:~ä3I;~~A--~--_..,._--~o
140
_120N
E 100~c:: 80 o:3 60..J
Days
Figure 98. The diagram reports the time necessary/01' the healing 0/decubitus ulcers in 8patients after only topical hypobaric application o/OrOJ. according to Werkmeister (1995).
The ulcer q{153 cm' took about 190 days to heal. This time can be markedly shortened bycombining the parenteral (DrAHT) and topical (ozonized water and oil) treatments
In the first, a woman was initially treated with a percutaneous chemical (phenol)lumbar sympathectomy, supplemented with a continuous infusion (0.5 ml/hour) ofbupivacaine 0.15% via an epidural catheter; this treatment only controlled the pain.The second case was a man with painful bilateral leg ulcerations due to a vaseulitis.A lumbar epidural catheter delivering 0.5 ml/hour of bupivacaine 0.20% and 0.125mg/hour ofmorphine (3 mg/day) bare1y controlled the pain.and the ulcers worsened.In both cases, healing was achieved by removing the catheters and perfonning 40and 45 03-AHT, respectively, plus topical treatment with ozone.
Uleers from venous stasis have been treated and they also heal rapidly with thecombined treatment. However, phlebopathies have attracted less interest thanarteriopathies. If venous hypertension cannot be compensated by physiologicalmechanisms, it leads to increased penneability at the level of the microcirculation,Iymphatic hypertension, oedema and possibly torpid ulcers. I can report only oneinvestigation (Lo Prete, 2000) perfonned in patients with extended varicosity, whichexamined subjective parameters (phlebalgia, feeling of orthostatic weight or pain,fonnication and paresthesia), objective parameters (evening oedema, constantoedema, haemosiderinic dermitis, fibrous hypodennitis, eczema, skin ulcerations)and instrumental parameters (plethysmography, videocapillaroscopy and evaluationof circumference at the calf and at the ankle-malleolus) , There were 15 patients (14women and 1 man), from 20-60 years old, with marked varicosity complicated bychronic venous insufficiency. Ozonetherapy was perfonned by SC and perivenousinjection ofup to 300 ml of gas (O~ + Oj) at an ozone concentration of 8 ug/ml in 60

282 CHAPTER24
sites (5 ml per site) . There were two treatments per week, repeated for 12 weeks(total 24 sessions). The results are presented in the following tables:
Table 23a. Subjective parameters.
PhlebalgiaFeeling of orthostatic weightOrthostatic painFormicationParesthesia
Before treatment8(15) 53%15 (15) 100%15(15) 100%9 (15) 60%7 (15) 40%
Aper treatment0(15) 04 (15) 26.6%.I (15) 6.6'%0(15) 0o(15) 0
Table 23h. Objective parameters.
Evening oedemaConstant oedemaHaemosiderinic dermitisFibrous hypodermitisEczemaSkin ulcers
Before treatment15 (15) 100%4 (15) 26.6'Yo5(15) 33.3%6 (15) 40%4 (15) 26.6%2 (15) 13.3%
After treatment2 (15) 13.3%2 (15) 13.3%1 (15) 6.6%.4 (15) 26.6%.0(15) 0o(15) 0
Table 23c. Instrum ental parameter s.
Before treatmentPlethysmographyEvaluation of circumference (cm) :calfankle (malleolus)
- 18.0"
34.325.2
After treatm ent22"
33.124.5
There was a marked reduction of the peripheral venous stasis, likely due toimproved microcirculation. The SC and perivenous administration of gas causedmodest but transitory pain. No more than 5 ml per site ought to be injected. There areno other adverse effects . Simultaneous topical treatment enhances the healing oftorpidulcers. The association with OrAHT may further improve the treatment.
Let us now try to reach some conclusions. It is unfortunate that the possibility ofimproving tissue ischaemia with ozonetherapy has interested only a few vascularsurgeons. Conceptually, ozonetherapy is the warhorse of this approach and appearsto be very useful in skeletal muscle, myocardial and cerebraI ischaemia, because itmay : increase oxygen and glucose delivery by several mechanisms (Chapters 12 to14), b) enhance angiogenesis via activation of resident stern cells, c) induce thepreconditioning phenomena by upregulating the expression of antioxidant enzymesand HSPs, and d) trigger a neuro-humoral response to improve the quality of life .This is exciting, but objectively we can conclude that none of the several studies is

OZONETHERAPY IN V ARIOUS PA THOLOGIES 283
satisfactory because of inappropriate administration routes, unknown or uncertain 0 3concentrations, too brief schedules and lack of areal contro\. The only availableRCT , in line with the rules of orthodox medicine, is that perforrned by Kraft et al.(1998), who examined the effect of03-AHT on patients with mild hypertension. Theoriginal abstract folIows:
"Autohemotherapy with ozone is widely applied by German therapists who prefercomplementary medicine, in eider patients with cardiovascular problems in order toimprove various symptoms and the quality of Iife. The strong oxidant ozone may furtherincrease the already high oxidative potential of these patients and thereby counteractpositive effects of antioxidants. In the present study, the effects of autohemotherapywith ozone on cardiovascular risk factors were evaluated in 17 patients , with mildhypertension. In a randomised, double-blind, placebo-controlled crossover-study, 24 hambulatory blood pressure and blood pressure load were significantly reduced after acycle of ten autohemotherapies with ozone, but not after a cycle with placebo (oxygen)(p < 0.05) . The initial blood pressure level was restored after the end of the therapywithin 4 months. Aggregation of thrombocytes was significant and the malondialdehydeconcentration was c1early increased, serum HDL concentration was reduced, and therate of side effects was higher during the cycle with ozone . The reduction of bloodpressure may be due to an increased oxygen supply of the vascular endothelium, but anactivation of the oxidative potential of polymorphonuclear leukocytes and/ormacrophages cannot be excluded . Considering the small reduction of blood pressure,the potentially noxious oxidative mechanisms and the rather high expenses,autohemotherapy with ozone cannot be recommended as a useful alternative topharmacological treatment ofpatients with mild hypertension."
Clearly Kraft et a\. are very critical and, in my opinion, they have verified thevalidity of ozonetherapy on the wrong disease. Indeed mild hypertension is a lifelong ailment and there are optimal conventional remedies (Iow-sait diet, statins,ACE-inhibitors, etc.) to keep it under control, so that the use of ozonetherapy isunjustified. Moreover, the conclusions of these authors have been influenced byprejudice and an incomplete knowledge of the potentials of ozonetherapy.
With regard to the standard set by official Medicine, we are practically back tosquare one and if we really want to define the value of ozonetherapy in POADpatients we must first define standard conditions and then perforrn serious RCTs.The following guidelines are suggested:
I) among the four approaches, 03-AHT, RI, BOEX and EBOO, we can select thefirst or the second because they are easy to perforrn and inexpensive. IA, IV orSC injection of ozone as gas should be excluded. After a convenient wash-outperiod, patient groups may switch over to compare 0rAHT and RI in the samepatient. For OrAHT, suitable ozone concentrations may range from an initial 20ug/ml per ml of blood up to 40 ug /rnl at the beginning of the 3'd week. Twotreatments per week for a total of 16 treatments (8 weeks) . In our experience ashorter schedule is not valid. For RI, ozone concentrations may range frorn aninitial 5 J.lg up to 30 ug/rnl, increasing the gas volume progressively frorn 150 mlto 600 ml in 2 weeks. Five treatments per week for 8 weeks. This schedule is notpractical for patients.
2) Groups of POAD patients belonging to stage 11, III and IV should be ashomogeneous as possible.

284 CHAPTER24
3) Objective assessment of the stage and severity of the disease should bedetennined by the best and most precise non-invasive techn iques beforetreatment, after 8 weeks and again two months thereafter. Evaluation should beperfonned by independent c1inicians.
4) Patients should be randomized into two groups: one receiving O2-03 and one O2
only, with the same technical modalities. A third group treated with the bestconventional treatment could be included for a comparison of the efficacy . If thetreatment is valid, the control group has the right to be switched over and receivethe ozonized treatment. These data may strengthen the results .
5) A specialized statistician should evaluate all the data .6) The same protocol can be tentatively explored in patients with Raynaud's
phenomenon secondary to systemic sclerosis. A comparison can be made with anhistoricalor a new control with infusion of iloprost, which has proved to beeffective for short-tenn palliation (Wigley et al., 1994; Block and Sequeira, 2001) .
Two RCTs, one dealing with POAD and another with terminal cardiopathicpatients, will evaluate the toxicity and efficacy of EBOO according to the optimizedmethodology (reported in Chapter 17) at the Siena and Modena University clinics.We hope to be able to report the results within 2003 .
Owing to the systemic nature of atherosclerosis, both the heart and CNS are athigh risk in POAD, and there is a rather high incidence of myocardial infarction orischaemic stroke and/or terminal stage lirnb ischaemia. That is why we are testingthe validity of EBOO in end-stage cardiopathic patients when either transplantationor surgical revascularization is not feasible . Our preliminary study (Di Paolo et al.,2000) on three patients yielded results that are encouraging but regarded asanecdotal because angiocardiographic examination could not be repeated after thetreatment. This project is ongoing and we have already treated 15 patients(manuscript in preparation). For the time being, there are two studies: the Russiantrial was carried out in 39 patients with advanced coronary atherosclerosis . Theyunderwent five daily infusions (for 20 days) of ozonized saline solution. I believethat ozonization was carried out at a very low ozone concentration (perhaps 2-3ug /rnl), so the levels of HOCI were not too high and thus not too caustic! I must saythat I am dead against this procedure. However, Zhulina et al. (1993) concluded thatthe treatment was effective because angina attacks decreased from an average of 6 toabout 2 per day . There were no controls with either oxygenated saline or simplesaline, which may have shown a significant placebo effect.
The second study is one ofthe best reported in the field and I am glad to say thatthe editor of "Free Radicals in Biology and Medicine", who strongly opposes ozonein Medicine (Chapter 2), decided to publish this paper. Hemandez et al. (1995) quitecorrectly performed 03-AHT, five days per week for a total of 15 treatments, in 22cardiopathic patients. They found a significant decrease in plasma cholesterol andLDL levels (we shall see ifwe can confinn this finding after EBOO) and an increaseof erythrocytic GSH-Px and G-6PD , which is in line with the phenomenon ofadaptation to COS paradoxically induced by ozone.
It is fair to mention that the great hope of modem medicine is to use genetherapy to elicit therapeutic angiogenesis in patients with chronic myocardial

OZONETHERAPY IN VARIOUS PATHOLOGIES 285
ischaemia (Patterson and Runge, 2000 ; Jackson et al., 2001) . However, while thisnew approach matures, I do not see anything wrong in evaluating ozonetherapy.
In about 80% of patients, ischaemic stroke results from atherothrombotic orthromboembolic processes. Stroke can strike relatively young persons at the peak oftheir intellectual activity and, if not fatal, can be highly debilitating. Fortunately,Handel, Pasteur and Roosevelt, to cite a few, were able to make great contributionsto music, science and politics in spite of suffering a stroke .
Modem medicine has developed prophylactic measures able to reduce the risk oftransient ischaemic attacks (TIAs) or of stroke in prone individuals by 20-30%(Gubitz and Sandercock, 2000). Moreover, anti-atherosclerotic drugs and, ifnecessary, carotid endarcterectomy appear beneficial. In case of an acute stroke,therapy must begun within the shortest possible time (from 0.5 to 2-3 hours) toreperfuse the ischaemic penumbra surrounding the core of a cerebral infarction .Time deIays are predominantly in the pre-hospital phase and can be fatal. Hypoxiainduces a cascade of metabolic disorders, such as tissue acidosis, reduction of ATPlevels, Ca2
+ overload, activation of glutamate receptors, N-methyl-D-aspartate(NMDA) channel opening and release ofproteinases, leading to neuronal death . Theinterested reader will appreciate the complex sequence of events carefully analyzedby Besson and Bogousslavsky (1995) , Back (1998), Small et al. (1999) andRosenberg (1999) . Since the 1990s, IV thrombolysis using recombinant tissueplasminogen activator (Tpa), with due caution to avoid cerebral haemorrhage, hasbeen applied to reduce the time of reperfusion and neuronal damage . In Cuba, wherethere is a lack of Tpa (owing to the embargo), many hospital emergency units haveozone generators at hand and patients with stroke are luckily treated as soon aspossible with oxygen-ozone therapy . Thus, we again face the old dilemma, whichneed not exist if we have been able to weigh the risks and advantages of the twoapproaches.
To my knowledge, only a preliminary study has been reported by Wasser, aGerman ozonetherapist, who has treated stroke patients privately, with all possibleinherent disadvantages. He reported at the XII IOA Congress (Lilie, 1995) that he hadtreated several patients some time after they suffered an acute stroke. In spite of thislimitation, the use of 0 3-AHT every day seems to have improved the outcome, in thesense that no patient died and they apparently recovered very rapidly. A1though thestudy has obvious limitations, Dr. Wasser (1995b) has to be congratulated for hisadventurous enterprise, which deserves to be pursued. At my University, I have foundgreat disinterest; neurologists do not want to risk what they consider a reasonably validtreatment (thrombolysis) for the uncertainty of ozonetherapy .
For what it is worth, my opinion is that a controlled study using either Tpa orozonetherapy, or a combination of the two, performed at the earliest possible timeafter a stroke would be very informative. Indeed it would probably save lives orreduce the disability.
On the basis of some experimental findings and on the uncertain validity of the citedc1inical open studies, I believe that ozonetherapy could be useful in vascular diseases,particularly in poor countries. However, it must be validated by RCTs in developedcountries. Regretfully, no support from Health Authorities or private organizations isforeseeable and thus we have to continue the struggle and try to do our best.

286 CHAPTER24
4. RETINAL DEGENERATIVE DISORDERSA. Diadori and V. Bocci
4.1. Retina: Anatomical Aspects
The retina, a thin transparent membrane lining the interior of the eye , is theinitial receptor for visual stimuli . Its outer face is in contact with Bruch'smembrane of the vascular choroid; its inner surface is in contact with thevitreous body (Fig . 99) .
Sclera
Choroid
Pholo receplo rs
Relinal vessels
.'=~~'t's membrane
Figure 99. Image ofthe ocularfundus (left side) with the macula lutea at the centre.Schematic drawing (right side) 0/the several retinal layers, from the internal limiting
membrane to the sclera . RPE: retinal pigment epithelium
The neurosensorial retina is separated into 10 layers, with the photoreceptors(rods and cones) located in the outer layer and the axons of the ganglion cells(second-order neurons) collecting on the inner layer to form the optic nerve . At theextreme outer layer of the retina, there is the retinal pigment epithelium (RPE), amonolayer of cells resting on Bruchs membrane (which separates the RPE fromthe choriocapillaris), ftmctionally connected to the photoreceptors. The RPE hasseveral important functions : it phagocytoses and processes the tips of the outersegment of the photoreceptors, recycles vitamin A, transmits oxygen and othernutrients from the choroid to the photoreceptors and outer retina, and differentiatesinto macrophages and other types ofcells in response to various stimuli .
The central area of the retina (c1inically defined as the area within thetemporal vascular arcade) is referred to as the macula; the highest visual acuity(ability to see fine details) resides in the cone-rich centre of the macula, thefovea. Retina! vesse!s are absent in the fovea, rendering the fovea criticallydependent on the choriocapillaris for its metabolic requirements.

OZONETHERAPY IN VARIOUS PATHOLOGIES
Several ophthalmologie disorders of the retina and the optie nerve, ofmultifactorial aetiology, lead inevitably to peripheral and/or eentral loss ofvision by degeneration ofthe neurosensorial eells (0'Amico , 1994).
Reeent studies on the meehanisms mediating neuronal damage suggest thatapoptosis might be implieated in the death of neurosensorial eells in the retinaand optie nerve (Xu et al., 1996; Gregory and Bird, 1995; Lo et al., 1995; Adler1996; Fraser et al., 1996). In partieular, advanees in the understanding ofeellular meehanisms of retinal ganglion eell and nerve axonal damage inisehaemie injury suggest an isehaemie eomponent; seeondary effeets (seeondaryneuronal degeneration) are eaused by a toxie environment produeed by thedying eells, resuIting in free radical produetion and further tissue damage .
There is an inereasing amount of experimental evidenee that neuronaldegeneration is mediated by numerous processes, including exeitatory aminoacid (espeeially glutamate) toxieity , bursts of reactive oxygen species (freeradicaJ damage, oxidative stress), nitric oxide perturbation and Ca2+-indueeddamage (intracellular calcium influx), whieh interact to provide a fmal commonpathway for eell vulnerability. By intervening in such processes, neuroprotectiveagents have produced beneficial effeets in animal models of retinaI ganglion celldamage and optic neuropathy.
These data open a novel pathway toward really innovative pharmacologiealresearch , aimed at protecting the retina and optie nerve from neurotoxic injury(Steinberg, 1994; Orago et al., 1993; Nayak et al., 1993; La Vail et al., 1992).
In such an effort, ozonetherapy eould play a role, as a new, reliable,eomplementary treatment for the management of several neurodegenerativedisorders . Indeed there is experimental evidenee that ozone ean have importantbiological effeets (Coppola et al., 1992; Romero Valdes et al., 1993; Hernandezet al., 1995; Bocci, 1996), such as:
• improvedperfusionand eellular oxygenation(aetivationof erythrocytefimction)• vasodilatation by release ofNO and CO;• upregulation of the enzymatic antioxidant system;• induetion and release of cytokines and growth factors.
These effects eould eooperate beneficially in an attempt to increase thedefence meehanisms of eells against isehaemie and neurotoxic injury, thuspreventing eell death or reducing tissue injury in reversibly damaged cells .
It has been speculated that several irreversible degenerative disorders of theretina and optie nerve, for which no therapy has proven effective, could benefitfrom ozonetherapy (Riva Sanseverino et al., 1990; Moraleda, 1995; Marmer andParker 1998; Diadori et al., 1996, 2000) :
• age-related maeular degeneration,• degenerative myopia,• retinal vascular disorders (such as diabetes) ,• retinal inherited-degenerative disorders (such as retinitis pigmentosa),
287

288 CHAPTER 24
• ischaemic optic neuropathies,• glaucoma.
We report our experience on the efficacy of OJ-AHT in the treatment of agerelated macular degeneration (ARMD). Other disorders are still under investigation.
4.2. Age-Related Macular Degeneration
ARMD is a progressive disabling bilateral condition affecting central vision. Indeveloped countries, it is the leading cause of irreversible loss of vision inpeople over 50 years of age (Bressler et al. , 1988); its incidence increases withage, varying from 1.6% in patients 50 to 60 years of age to 20-30 % of peopleover the age of 65 (Framingham Eye Study, 1980; Pauleikoff and Koch, 1995).
Since this sector of the population is expected to increase during the nextcentury, the social and economic consequences of ARMD-related visualimpairment and blindness are destined to increase unless successful means ofprevention and treatment can be found . Therefore, ARMD is a public healthproblem of severe and growing proportions (Evans and Wormald, 1996).
4.2.1. Clinieal Presentation
The most frequent signs of ARMD are:
I) drusen . These lesions are ophthalmoscopically visible as pale yellow spotsthat may occur individually or in clusters throughout the macula. Theyconsist of an accumulation of amorphous material between the RPE andBruch's membrane, resulting in a microscopic elevation of the RPE.Although their exact origin remains unknown, current theories favour theaccumulation of lipofuscin and other cellular debris derived from cells of theRPE that are compromised by age or other factors.
2) disturban ee ur the RPE, which may appear disrupted into small areas ofhypo- and hyperpigmentation (pigmentary changes) or may become absent,forming large areas of atrophy (areolar [geographi e) atrophy).
3) ehuroidal neovascularization. In response to as yet undefined stimuli ,choroidal vessels proli ferate across Bruch's membrane under the RPE and, incertain cases, continue their extension into the subretinal space .
According to recent studies, neovascularization could be stimulated andmediated by VEGF , produced by the RPE cells under hypoxic conditions(Frank, 1997; Pournaras et al., 1997).
Copious leakage from these neovascular membranes may result in exudativedetachment of the RPE or haemorrhages, which may be confined to the areaunder the RPE or may extend under the retina. The natural course of this processis fibrotic evolution, with formation of a disciform sear.
Clinically, two forms or stages of ARMD are usually described :

OZONETHERAPY IN VARIOUS PATHOLOGIES
• "dry" or atrophie form (the most eommon, aeeounting for 80-95% of eases),eharaeterized by disturbanee of the RPE with varying degrees of drusen(hard, soft, mixed) and areolar (geographie) atrophy, in whieh loss of theRPE is aeeompanied by fallout of photoreeeptors and ehorioeapillaris. Thevisual deterioration is usually slow and gradual, and beeomes reallyimportant only in 5-10% of eases, depending on the extent and loeation ofthe area of atrophy.
• "Wet" or exudative-neovaseular form, eharaeterized by detaehment of the RPE(serous or haemorrhagic), subretinal neovaseularization, and flbrovasculardisciform searring. It is less eommon (5-20% ofeases), but is associated with aneven worse visual prognosis(severe loss of eentral vision in 70-80% of eases).
The most frequent symptoms ofthese alterations ofthe maeula are:
deereased visual aeuity (loss of eentral vision, eolour vision, ability to seefine details)metamorphopsia (distortion ofthe shape ofobjeets in view)paraeentral-central seotoma
Loss ofvision in ARMD is the result ofphotoreeeptor death, oeeurring whenRPE eells, with whieh they are assoeiated, deteriorate and die.
The loss of vision resulting from drusen and pigmentary ehanges (earlystages of the disease) is highly variable: most patients are asymptomatic orexperienee only a small visual loss or metamorphopsia . With the progressivedevelopment of larger areas of atrophy of the RPE involving the fovea, visualaeuity deereases abruptly and relative or absolute seotomas appear within theeentral 10 degrees of the visual field.
Sudden substantial loss of eentral vision, over a larger area and often at anearlier age, is generally the result of ehoroidal neovaseularization, with serous orhaemorrhagie detaehment ofthe RPE.
The natural elinieal eourse of ARMD is progressive and the final visualaeuity is usually < 20/200 (Piguet et al., 1992; Sarks et al., 1988; Barondes etal., 1990; Klein et al., 1993, 1997).
4.2.2. Pathophysiology and Risk Faetors
The eauses and faetors related to the onset and progression of ARMD remainunknown, but it now appears likely that ARMD is a multifaetorial disease,triggered by environmental faetors in those who are genetieally predisposed .
Although multiple possible riskfactors for ARMD have been identified, theimportanee of eaeh remains uncertain . Those thought to be important include:
ageing (> 55 years);genetic predisposition [familial trait], (Silvestri et al., 1994; Silvestri, 1997;Allikmets et al., 1997);
289

290 CHAPTER24
smoking (Vingerling et al., 1996);exposure to sunlight [photo-oxidative stress], (Cruickshanks et al., 1993;Darzins et al., 1997);blue iris (Sandberg et al., 1994);hyperopia (Broker et al., 1993);systemic hypertension, cardiovascular disease, and vasculopathic trait(Vingerling et al., 1995);nutritional factors, such as a low zinc and antioxidants intake (Newsome et al.,1988; Sperduto et al., 1990; Seddon et al., 1994; West et al., 1994;Chew, 1995).
The cause and pathogenesis of ARMD is unclear (Young, 1987), but anensemble of nutritional, degenerative, oxidative (phototoxic), haemodynamicand genetic factors, appear responsible and are being actively investigated.
Three main theories can be distinguished:
• primary dysfunction of the RPE (genetic predisposition or environmentalexposure).There is a consensus that the crucial lesion in ARMD involves the RPE cells.Light damage, ageing and a variety of dietary deficiencies have beeninvoked as possible primary causes of RPE failure in ARMD , withsecondary atrophy of the choroid.There are data suggesting that the outer retina, in particular photoreceptorsand RPE cells, may be particularly susceptible to the oxidation process,which leads to the formation of free radicals and highly reactive singletoxygen within the cells, causing cell death .Animal studies suggest that exposure to intense sunlight or UV radiationmay cause changes in the RPE similar to those seen in ARMD . The highmetabolic rate of the outer retina and chronic exposure to light(photochemical damage) may contribute to an underlying oxidative stress(Organisciak et al., 1997; Rapp et al., 1997, Tate et al., 1995).The retina contains a wide variety ofprotective mechanisms (e.g. antioxidants)against such damage under normal conditions, but these natural defences maydecrease with age, or may be inadequate if environmental exposure to oxidantsincreases, or if there is a genetic deficiency of such enzymes.
• Haemodynamic dysfunction in the choriocapillaris.The vascular theory (Friedman, 1997) postulates that ARMD is caused by aprogressive decrease in the compliance of the sclera (a higher coefficient ofscleral rigidity was found in patients with ARMD) and choroidal vessels,leading to an increase in the resistance of the choroid to the flow of blood .This process initiates with the deposition of lipids in the sclera and Bruch'smembrane, and results in decreased choroidal perfusion, with reducedsupply of oxygen and glucose to the retina (ischaemic damage) , and higherpressure in the choroidal vessels . According to this haemodynamic model,the decompensation of the RPE is the result of its incapacity to transport

OZONETHERAPY IN VARIOUS PATHOLOGIES
debris and metabolites against progressively unfavourable hydrostatic andosmotic gradients.
• Primary dysfunction ofphotoreceptors (ABCR mutation).ABCR mutation was found in patients with ARMD, especially in thoseaffected by the "dry" form. Since the ABCR protein is a transporter proteinfound in the outer segment of rod cells, its mutation could cause degradedmaterial to accumulate, thus interfering with retinal cell function.
4.2.3. Prevention and Treatment
At present useful therapy to prevent the natural history of ARMD remainscontroversial. On the basis of the role of oxidative stress in the pathogenesis ofthe disease, the protective effect of several food supplements (minerals andantioxidant vitamins) have been investigated, but conflicting results haveemerged (Newsome et al., 1988; Sperduto et al., 1990; Prashar et al., 1993;Cohen et al., 1994; West et al., 1994; De La Paz et al., 1996; Larkin, 2001) .
There is no known treatment for the "atrophic" form of ARMD, whichaccounts for most cases of ARMD .
Most potential therapies are addressed to the wet form of ARMD, with the aimof reducing the neovascularization . However, these treatments do not improvesight; they only help to slow visual deterioration, so they are unlikely to have animportant impact on the blindness caused by ARMD. Laser photocoagulation(Macular photocoagulation group, 1986, 1991) is indicated only for selectedpatients with well defined extrafoveal and juxtafoveal neovascular membranes,but it is often followed by a decrease in visual acuity and it does not prevent thelong-term recurrence of neovascularization (Lambert et al., 1992; Thomas et al.,1992). Photodynarnic therapy looks more promising, since it is more selective (itdoes not affect the RPE, photoreceptors and choriocapillaris), but it is onlysuitable for 10-15% ofpatients with wet ARMD and it is expensive.
Low-dose radiation therapy (teletherapy) has been proposed for thetreatment of subfoveal neovascular membranes that are unsuitable for lasertreatment, but its effectiveness has not been demonstrated.
Despite initial enthusiasm about their potential angiogenetic inhibitoryeffects, antivasoproliferative substances, such as IFNo. (Fung, 1991; Ezekowitzet al., 1992), have shown little benefit in the treatment of age-related subretinalneovascularization. There are now far more prornising anti-angiogeneticcompounds under investigation (O'Reilly et al., 1994; Aiello et al., 1995;Robinson et al., 1996).
Subretinal surgery, aiming to directly remove the offending neovascularmembrane, is very appealing, but not free from risks; moreover, in ARMD thedisturbances of the RPE make the process more complicated, and the resultsmay be disappointing.
291

292 CHAPTER24
4.3. ARMD: Personal Experience with Ozonetherapy
Owing to the lack of an effective therapy, it was decided to conduct apreliminary investigation of the efficacy of 0 3-AHT in the dry form of ARMD;this was carried out in the Department of Ophthalmology and Neurosurgery, incooperation with the Institute ofGeneral Physiology, University ofSiena.
0 3-AHT is a safe complementary approach widely used in the treatment ofischaemic vascular disorders , such as peripheral chronic arterial occlusive disease.It has been shown to activate erythrocytic metabolism and oxygen delivery tohypoxic tissues and to upregulate the expression of antioxidant enzymes, possiblyleading to the correction of an endogenous oxidative stress (Bocci 1996a,c,d).
The purpose of our study was to check its c1inical efficacy in patients withdry ARMD, compared with an age-matched control group (prospective RCT) .
The study population consisted of patients referred to the outpatient c1inic ofthe Department of Ophthalmology and Neurosurgery of the University of Siena.All patients signed an informed consent statement prior to inclusion in the study.
All patients were affected by the "dry" form of ARMD, documented byfluorescein angiography, and had at least 10 ophthalmoscopically visiblemacular drusen, characteristic pigmentary alterations, or geographic atrophy ;one eye was considered for each patient, the functionally best one in the bilateralforms . Subjects whose visual loss may have been secondary to media opacitiesor any other ocular disease besides ARMD were excluded.
The following were carried out before the first treatment, after the lasttreatment, and then every 3 months for up to I year : a fully corrected near anddistance visual acuity (V .A.) measurement; a complete biomicroscopic andophthalmoscopic examination, in which the refractive error, iris colour, lensstatus (aphakia, pseudophakia or initial cataract), disc and macula morphology,and intra-ocular pressure values (measured by applanation tonometry) werespecifieally reeorded for eaeh eye.
The experimental group consisted of 50 "dry" ARMD patients, whounderwent 12-13 sessions of OrAHT within 6.5-7 .5 weeks.
Standardized 03-AHT was carried out by exposing about 250 g blood ineitrate-phosphate-dextrose (CPD) to agas mixture eomposed of about 96% O2
and 4% 0 3, with a final 0 3 concentration of 40-70 ug/rnl gas per g of blood
(starting with 40 Ilg/m1 and gradually increasing by 5 ug/ml each session toreach 70 ug/ml by the 7th treatment). After about 5 min of thorough mixing,eaeh blood sampIe was reinfused into the donor. This procedure was repeatedtwiee a week for 12-13 times .
As a "control" group, we treated 30 "dry" ARMD patients by exposing thesame amount ofblood to O2 alone (the same number ofsessions twice a week).
Funetional ophthalmologie examination included:Mean distance visual acuity (ETDRS charts).Macula threshold test (Humphrey automated perimeter).Self-assessment test of the quality ofvision (Carta et al. , 1998).

OZONETHERAPY IN VARIOUS PATHOLOGIES
General examination included:
Blood pressure.Haematochemical data (blood cell count, plasma proteins, plasma lipids,coagulation and fibrinolysis tests) .
These data were recorded at the baseline time (before starting the therapy), atthe end of the last 03-AHT sessions, and then every 3 months for up to 1 year.In all the follow-up examinations, the examiners were blind to the results ofeach patient's initial examination.
293
4.4. Results
4.4.1. Ophthalmologie Results
Change in visual acuity from baseline at each examination was the primaryparameter used to verify the response, if any, to 03-AHT.
Mean distance visual acuity (ETDRS charts) was significantly improved in ARMDpatients (p<0.05), while no significant improvement was observed in the controlgroup. This data was confirmed by the results of the visual field (increased meansensitivity and foveal threshold in 54% oftreated patients and in 18% ofcontrols) andthe self-assessment test of quality of vision (improved quality of vision in 60% of thetreated patients and 23% ofcontrols) .
In the treatment group, the improvement rema ined stable in the first quarterand declined slightly in the next six months after the treatment (Fig . 100); at 12months, up to 41.6% showed either a regression to their pre-treatment values(33.3%) or had worse V.A. (8 .3%).
0.30
2000,25
• • 175
ä 0,20 '"'":; ~ 150 .
0,15 12S
100
0,10Pr. Post 6 9 12Pr. Post 6 9 12
Months
Figure 100. Modifications ofvisual acuity before, during and after (3, 6, 9 and 12 months)one cycle 0/ /3-14 OrAHT sessions. The left diagram reports the actual change, expressed as
a percentage ofthe right diagram.
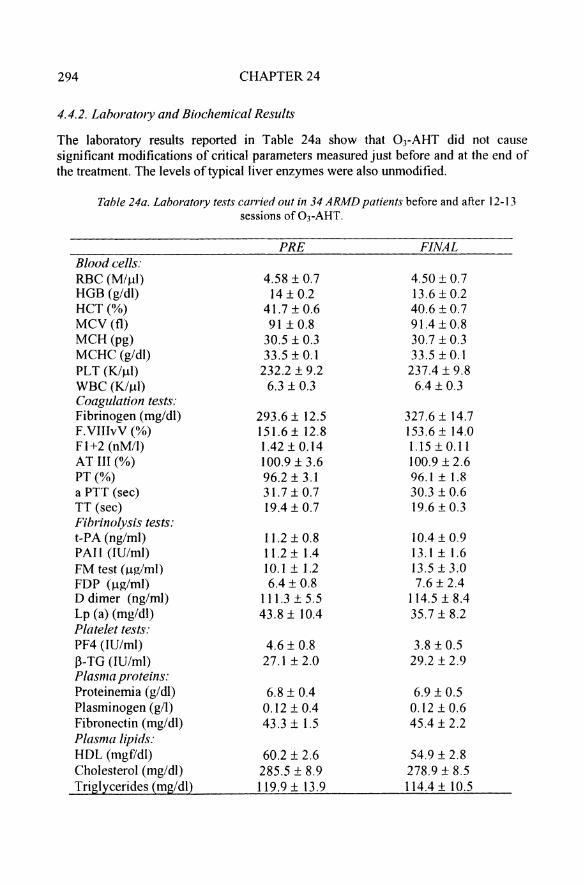
294 CHAPTER24
4.4.2. Laboratory and Biochemical Results
The laboratory resuIts reported in Table 24a show that OrAHT did not causesignificant modifications of critical parameters measured just before and at the end ofthe treatment. The levels oftypicalliver enzymes were also unmodified.
Tahle 24a. Laboratory tests carried out in 34 ARAfD patients before and after 12-13sessions ofOJ-AHT.
PRE FINALBlood cells:RBC (M/~I) 4.58 ± 0.7 4.50 ± 0.7HGB (g/dl) 14± 0.2 13.6 ± 0.2HCT (%) 41.7 ± 0.6 40.6 ± 0.7MCV (0) 91 ± 0.8 9 1.4 ± 0.8MCH (pg) 30.5 ± 0.3 30.7 ± 0.3MCHC (g/dl) 33.5 ± 0.1 33.5 ± 0.1PLT (K1~1) 232.2 ± 9.2 237.4 ± 9.8WBC (KfI.,t1) 6.3 ± 0.3 6.4 ± 0.3Coagulation tests:Fibrinogen (rng/dl) 293 .6± 12.5 327.6 ± 14.7F.VIIIvV (%) 151.6±12.8 153.6± 14.0F l+2 (nM/I) 1.42±0.14 1.15 ± 0.11AT III (%) 100.9 ± 3.6 100.9 ± 2.6PT(%) 96.2 ± 3.1 96.1 ± 1.8a PTT (sec) 31.7 ± 0.7 30.3 ± 0.6TT (sec) 19.4±0.7 19.6 ± 0.3Fibrinolysis tests:t-PA (ng/ml) 11.2 ± 0.8 10.4 ± 0.9PAli (IU/ml) 11.2 ± 1.4 13.1±1.6FM test (uz/ml) lO.1 ± 1.2 13.5 ± 3.0FDP (ug/ml) 6.4 ± 0.8 7.6 ± 2.4D dimer (ng/ml) 111.3 ± 5.5 114.5 ± 8.4Lp (a) (rng/dl) 43.8± 10.4 35.7 ± 8.2Plate/et tests :PF4 (lU/mi) 4.6 ± 0.8 3.8 ± 0.5ß-TG (IU/ml) 27.1 ±2.0 29 .2 ± 2.9Plasma proteins:Proteinemia (g/dl) 6.8 ± 0.4 6.9 ± 0.5Plasminogen (g/l) 0.12 ± 0.4 0.12 ± 0.6Fibronectin (mg/dl) 43 .3 ± 1.5 45.4 ± 2.2Plasma lipids:HOL (mgf/dl) 60.2 ± 2.6 54.9 ± 2.8Cholesterol (mg/dl) 285 .5 ± 8.9 278.9 ± 8.5Triglycerides (mg/dl) 119.9 ± 13.9 114.4± 10.5
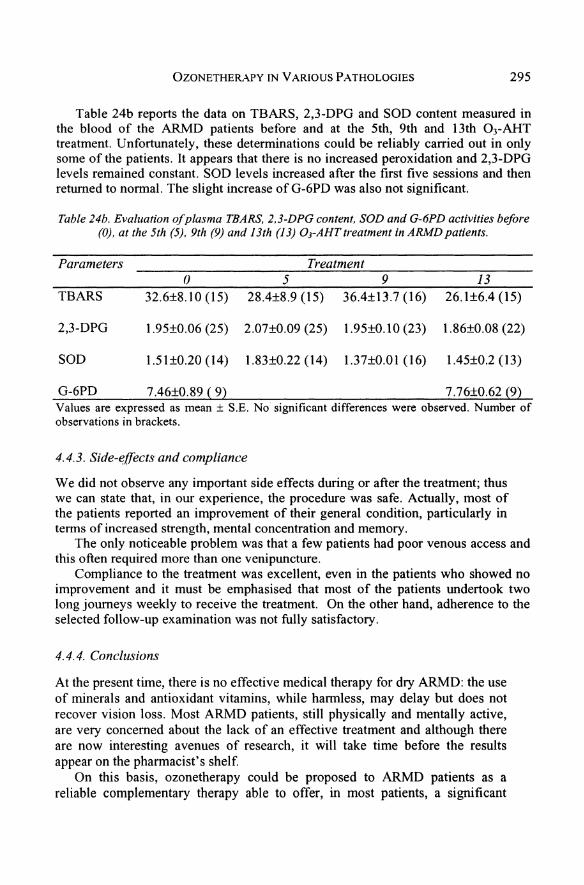
ÜZONETHERAPY IN VARIOUS PATHOLOGIES 295
Table 24b reports the data on TBARS, 2,3-DPG and SüD content measured inthe blood of the ARMD patients before and at the 5th, 9th and 13th Ü3-AHTtreatment. Unfortunately, these determinations could be reliably carried out in onlysome of the patients. It appears that there is no increased peroxidation and 2,3-DPGlevels remained constant. SüD levels increased after the first five sessions and thenretumed to normal. The slight increase of G-6PD was also not significant.
Table 24b. Evaluation ofplasma TBARS, 2.3-DPG content, SOD and G-6PD activities before(0), at the 5th (5), 9th (9) and 13th (13) OrAHT treatment in ARMD patients.
Parameters Treatment() 5 9 13
TBARS 32.6±8 .10 (15) 28.4±8.9 (15) 36.4±13.7 (16) 26 .1±6.4 (15)
2,3-DPG 1.95±O.06 (25) 2.07±O.09 (25) 1.95±O.10 (23) 1.86±O.08 (22)
SüD 1.51±0.20 (14) 1.83±O.22 (14) 1.37±O.Ol (16) 1.45±0.2 (13)
G-6PD 7.46±O.89 (9) 7.76±O.62 (9)Values are expressed as mean ± S.E. No significant differences were observed . Number ofobservations in brackets .
4.4.3. Side-effects and compliance
We did not observe any important side effects during or after the treatment; thuswe can state that, in our experience, the procedure was safe . Actually, most ofthe patients reported an improvement of their general condition, particularly interms of increased strength, mental concentration and memory.
The on1y noticeable problem was that a few patients had poor venous access andthis often required more than one venipuncture.
Compliance to the treatment was excellent, even in the patients who showed noimprovement and it must be emphasised that most of the patients undertook twolong journeys week1y to receive the treatment. On the other hand, adherence to these1ected follow-up examination was not fully satisfactory.
4.4.4. Conclusions
At the present time, there is no effective medical therapy for dry ARMD: the useof minerals and antioxidant vitamins, while harmless, may delay but does notrecover vision loss. Most ARMD patients, still physically and mentally active,are very concemed about the lack of an effective treatment and although thereare now interesting avenues of research, it will take time before the resultsappear on the pharmacist's shelf.
On this basis, ozonetherapy could be proposed to ARMD patients as areliable cornplementary therapy able to offer, in most patients, a significant

296 CHAPTER24
general improvement of the quality of vision, so that they can experience abetter lifestyle.
5. DERMATOLOGICAL DISEASES
In 1989, the Director of the Institute of Dermatology of Siena Universitysurprisingly asked me to help study the value of O)-AHT in psoriasis, because oneof his colleagues was privately performing this therapy and c1aiming great success.Unfortunately, at that time I had no practical experience. Firstly , I noted that anassistant 'collected ozone in a syringe and, without closing the tip,' walked a longcorridor before insufflating it into the blood bottle. Secondly, they assured me thatthe ozone concentration must be very 10w (probably 2-5 ug /ml) and it was not reallyvery important because blood would become "very red" in any case . The surprisingresult was that after 7-10 treatments, one patient showed extraordinaryimprovement, another was slightly better and three patients remained the same.They tried to publish a paper but it was rejected because there were no controls.Thus my first c1inical experience was very disconcerting. Since then , I have heardseveral other anecdotes of splendid results and 11eave the judgement to the readers.
In spite of this puzzling story, it seems that Russian dermatologists and aGerman ozonetherapist (Kief, 1993b) also succeeded in treating various forms ofeczema and atopic dermatitis (AD) , which, to my knowledge, is challenging andfrustrating to treat. I had been interested in this disease from an immunological pointof view : the hallmark of AD is a Th l/Th2 imbalance (Bohn and Bauer, 1997;Campbell et al., 1999) with a reduced production of IFNy and an elevated release ofIL-4 and IL-5, which favours IgE production and eosinophilia, a typical disorder ofatopic diathesis (Beltrani , 1999; Leung, 1999) .
Prophylactic measures such as avoidance of irritants, allergic food (eggs, soy,peanuts, etc .), contact with house-dust mites or other aeroallergens, are helpful butthe mainstays of therapy have been and still are topical corticosteroids. Morerecently, in severe forms , phototherapy, cyclosporin A, azathioprine and tacrol imusointment appear to be effective but with some side effects (Rudikoff and Lebwohl ,1998; Hanifin and Tofte, 1999; Fleischer Jr., 1999).
Does ozonetherapy have any future in dermatology? If seriously performed, 0 )AHT may be useful and my "gut feeling" is that we should progressively try frommedium (40-50 ug/ml) to high ozone concentrations (80 ug/ml), as discussed inChapter 14 (Leukocytes), to readjust the Thl/Th2 balance. However, it should beremembered that this is a proposal that may not be effective.
The BOEX procedure, combining systemic and cutaneous treatment, may be anideal approach. However, patients with these diseases are often very distressed andunderstandably anxious to receive the most effective treatment immediately .Therefore, they are not interested in our controversies and this rnakes it awkward torecruit patients for a RCT . Ozonetherapy may yield some benefit at a slow pace andpatients will accept it only if, at least in the initial period, they are assisted with theproven topical anti-inflammatory options.

OZONETHERAPY IN VARIOUS PATHOLOGIES 297
6. PULMONARY DISEASES (EMPHYSEMA, ASTHMA, COPD AND ARDS)
This secnon is dedicated 10 the memory ofDr. Maria Trusso.
Ozonetherapy has not yet been tested in pulmonary disease, probably becauseeverybody knows that breathing air polluted with ozone is toxic to the respiratorysystem (Kelly et al., 1995). Two or three papers on this topic are published everyweek in international journals and this problem has been discussed in Chapters 3 and5. However, an almost irrelevant episode that occurred about four years aga suggeststhat this fact has misled us. Among our numerous ARMD patients treated with 0 3
AHT, one, with emphysema, told us that after about fourteen sessions his dyspnea wasalleviated and he could walk up to the third floor of his apartment with little effort. Isensed that he had given us a good tip and I took him to the Pneumology Unit wherethe specialist, Dr. Maria Trusso, was bewildered by the result. Actually, at first sheimagined that the treatment for ARMD was based on breathing ozone and the proposalto continue this sort of treatment appeared crazy to her. After 1 explained that wesimply ozonized and reinfused the patient's blood, she became interested and correctlyasked how ozonized blood eould improve lung funetion. That was a good question andI had to use the best of my imagination to provide a few answers:
the simple one was improved blood oxygenation. Yet this is not quite validbecause , although we reinfuse hyperoxygenated blood (p02 is easily at 500 mmHg),the infusion rate is so small (about 15 ml per minute, compared with a cardiae outputof about 5 L) that the p02 of venous blood reaehing the lungs is hardly modified.However, if ozonetherapy enhanees the delivery of oxygen at the tissue level,metabolie conditions may improve, even though ideas such as decreased bloodviscosity and increased 2,3-DPG levels in erythrocytes have not been definitivelydemonstrated. I advaneed the hypothesis that perhaps ozonized blood acting onendothelium could aetivate the release of prostacyclin. Only last year, we deteetedan enhanced release of NO in HUVECs in vitro, but we have not yet evaluatedprostaeyclin. It appears that release of NO and NOthiols may represent a mechanismfor vasodilatation, although NO could also be a double-edged sword (Barnes andLiew, 1995; Warren and Higenbottam, 1996; Jindal and Dellinger, 2000) .
A eommon denominator of asthma, emphysema, chronie obstructive pulmonarydisease (COPD) and aeute respiratory distress syndrome (ARDS) is oxidative stress. Itis demonstrated by an increase ofROS (H202)and 8-isoprostane, activation ofNF-KBwith inereased synthesis ofTNF-a, IL-6, IL-8, and inaetivation (by oxidative damage)of o l-antitrypsin and leukoproteinase inhibitor, unable to counteraet elastase,cathepsins and matrix metalloproteinases (Smith et al., 1997; Barnes, 2000). In 1996,we postulated that the paradoxieal action of ozone in inducing an adaptation to COScould be critical in readjusting the oxidant-antioxidant balance.
Finally, we searehed for other eases of emphysema and COPD . We found twopatients, a man and a woman, who after two eycles of therapy had noticed animprovement in their performance of daily activities . This response was subjectiveand could have been due to a placebo effect, but it encouraged us to make aprotocol. The Director of the Pneumology Unit agreed although he was somewhatskeptical, but not so much as the University's Professor of Pneumology, who was

298 CHAPTER24
absolutely antagonistic. The protocol was then prepared, submitted to the EthicalCommittee and, after revision, approved after about seven months . Unfortunately,the health of Dr. Trusso deteriorated (she had a metastatie breast tumour) and shedied shortly afterward, leaving four young children practically alone . We lost a verynice, energetic woman, who after accepting the idea became very enthusiastic to trythis unusual therapy .
I hoped that one of her colleagues would accept the challenge, but he thoughtthat the project was too laborious to develop and uncertain, so I found myself backwhere I started . Nothing has been done, but luckily there has been some progress inconventional Medicine , since COPD morbidity and mortality is increasing due to theuse oftobacco. Indeed it may soon become the third most common cause of death .
In addition to rehabilitation with exercise training, anti-smoking measures anddomiciliary oxygen therapy, new bronchodilators and appropriate antibiotics cancontrol acute exacerbations. After a long incubation (1957), surgical removal of themost emphysematous parts of the lung has come of age; when the operation issuccessful, short-term results are good, with marked improvement of the quality oflife (Hillerdal 1997; Bames, 2000) .
However, some of the patients do not benefit from surgery (NationalEmphysema Treatment Trial Research Group , 2001) and the value and costeffectiveness of the volume reduction surgery remain uncertain in the long run ,Moreover, medieal expenditures to treat COPD, associated with invalidity , representa significant economic and social burden for Health Authorities and society ingeneral. I believe that these are sufficiently good reasons to justify serious and wideranging experimentation with ozonetherapy. We can take advantage of OJ-AHT andeven more of BaEX and RI (non-invasive procedures), always starting with a lowdose (20 ug/rnl) with gradual dose escalation up to 35-40 ug/rnl. Needless to say,supporting measures, particularly oxygen therapy, remain available to the patient.
7. RENAL DISEASES
Prof. N. Di Paolo is the head physician of the Nephrology and Dialysis Unit at theSiena Polyclinic. He is a good friend of mine and his role in developing EBOO hasbeen crucial . However, when I proposed to evaluate ozonetherapy in not tooadvanced dialysis patients, he answered that the kidney does not have theregenerative ability of liver and there is no hope to improve the function of asclerotic kidney . He may weil be right in regard to terminal patients but my idea wasto limit progression, possibly achieving regression of initial chronic diseases . A fewrecent reports have further convinced me that during infective glomerulo-nephritisor at the initial stage ofrenal failure, ozonetherapy could have a beneficial influence .It is not worth repeating the usual mechanisms, but I wish to re-emphasize thepossibility of adaptation to COS, typically present in chronic renal failure (CeballosPicot et al., 1996b; Witko-Sarsat et al., 1998). It is weil established thathaemodialysis in itself generates RaS and consequently enhances oxidative stress . Ifeel that it is wrong to passively accept the concept of unavoidable irreversibilitybecause, in addition to potentiating the antioxidant system, ozonetherapy may switchon angiogenesis or favour the release of unknown nephropoietins. Unscientifically,

OZONETHERAPY IN VARIOUS PATHOLOGIES 299
I believe that ozone is a stimulator of untapped natural resources and we knowthat if we can just give a little help to Nature, she may respond in ways that arewonderful and unsuspected by our little minds. Einstein used to say that"imagination is more important than knowledge".
Ruggenenti et al. (200 I) have given a moral boost to my belief because theyexpertly say that today "nephropathies lack a specific treatment and progressrelentlessly to end-stage renal disease". In order to delay or avoid dialysis (whichwould be a great success), nephrologists should develop a combined approach torenal diseases by pharmacologically controlling blood pressure and loss of proteins.I now like the idea of adding ozonetherapy performed at low-rnedium ozoneconcentrations for long periods. Selected patients could undergo 1-2 EBOOtreatments every week during the final hour of dialysis. The ozonizer could besimply placed after the dialysis filter with blood exposed to very low ozoneconcentration (1-2 ug/ml).
The lack of side effects, the modest adjunctive cost, the control ofhyperoxidative state and the feeling of wellness are the most obvious and eloquentadvantages. I agree that the study of gene and stem-cell biology will favour theadvancement of science and produce important therapeutic innovations, but commonsense also suggests that the possibility of stimulating natural resources should not beneglected. Moreover , we should keep in mind that a combination of therapeuticapproaches, and not the reductionist simplification of substituting a gene, is mostlikely the best way to effectively treat the multiform manifestations of a chroniedisease.
8. HAEMATOLOGICAL DISEASES
ß thalassaemia major, fairly frequent in Italy, and sickle cell anaemia (SCA),affecting black populations, are genetic diseases leading to oxygen blood deficiencyand other serious manifestations. Ozonetherapy cannot correct the gene alterationbut in SCA it can apparently reduce the frequency of vessel occ1usive crises withrelated infarctions. SCA involves a modified Hb (Hbs), which tends to crystallizeduring deoxygenation ; this leads to a change in the shape of the erythrocytes , whichaggregate and cause vessel occ1usion. At least conceptually , ozonetherapy mayincrease oxygenation and, as often c1aimed, may improve cell pliability, although Iam not convinced about this change. A RCT, which must be reported because theyare so rare in this field, was performed in 55 SCA patients (25 control and 30experimental) at the National Center for Scientific Research at Havana. Ozone wasadministered daily (5 days per week) for 3 weeks in 30 patients via the rectal route.The control group received only analgesics, vasodilatators and IV saline infusion.The results showed that the ozone-treated group displayed a rise in arterial bloodpOz, the frequency and severity of painful crises was significantly reduced (by about50%) and there were no adverse reactions (Gomez et al., 1995). This work wassupported by a firm producing ozone generators and it is surprising that no furtherexperimentation has been reported.

300 CHAPTER24
SCA is a serious disease and it suffices to say that only 2% of about 120,000affected babies born in Africa survive to the age of five . What can official Medicinedo to help patients in poor countries? Practically nothing, because transplantationcan only be perfonned in about 1% of patients: in 1999, the number of bone marrowtransplants was only 100 and 800 for SCA and ß-thalassaemia, respectively .Moreover, 10-15% of patients do not survive.
For SCA, it would be important to have an effective and atoxic oral drug that couldbe widely and easily used . So far, hydroxyurea appears useful as it reduces Hbs andincreases the percentage of HbF, but the drug is mutagenic and somewhat toxic(Steinberg, 1999) . Clotrimazole, a specific Ca2+-activated K-I- channel (Gardoschannel) inhibitor able to reduce the deleterious dehydration of sickle erythrocytes, isbeing tested and seems promising (Brugnara et al., 1996) . Morris et al. (2000) havereported that oral arginine administration may benefit SCA patients by increasing NOproduction during a vaso-occlusive crisis. Clearly, these approaches are experimentaland only partly satisfactory and the promise of gene therapy is far from beingmaterialized. Thus, I do not see anything wrong in using ozone; with small generators,patients (after careful instruction) could do horne autotreatment using RI. However,ozonetherapy has the serious drawback that ozone must be generated and usedextempore. The unavailability of generators, medical oxygen, electricity and the needof an almost daily use for life makes ozonetherapy a solution that cannot be practicallyproposed in poor countries for SCA, malaria and HIV infection.
As always, the possibility of ozonetherapy is never mentioned by officialMedicine and 1 must presume that it is unknown. This is one of our weak points,which can only be overcome by presenting good controlled results to peer-reviewedinternational journals. However, someone has written that hydroxyurea advocatesare covering up its long-term carcinogenic potential, but I want to think that thiscannot be true . I hope that this book will serve to make this topic known andpromote unbiased clinical trials to evaluate the validity of ozonetherapy.
Finally, I must mention that I often receive calls frorn desperate people because arelative is affected by a haematological malignancy. I have great respect for whathaematologists are able to achieve in these diseases and unless we can produce goodexperimental evidence, I am not certain that the addition of ozonetherapy would beuseful. This aspect will be discussed further in the section "Cancer", although thepathophysiology of solid tumours is immensely different from haematological ones.For the inexpert ozonetherapist, I would like to remark that ozone cannot displayadirect cytotoxic effect on malignant cells .
9. NEURODEGENERATIVE DISEASES
The progressive prolongation of the human life-span is accompanied by anincrease of degenerative diseases, and those of the CNS are very crippling. There issubstantial evidenee that the combination of genetie predisposition, life-Iongoxidative damage, an excessive or poorly balanced diet , exposure to transition metalions, alcohol and tobaceo smoke intoxieation, lack of physical exercise and diabetesmay be responsible for neurodegenerative disorders such as Parkinson ', Menkes '

OZONETHERAPY IN VARIOUS PATHOLOGIES 301
and Wilson's disease, senile dementia, amyotrophic lateral sclerosis , optic nervedysfunction, primary open angle glaueoma, neurosensorial bilateral hypoacusia andmaeulopathies (Halliwell et al., 1992; Halliwell, 2001; Yu, 1994; Ames et al., 1993;Cohen et al., 1994; Jenner, 1994; Bondy, 1995; Carlsson et al., 1995; Jaeschke,1995; Pardo et al., 1995; Yoritaka et al., 1996; Simonian and Coyle, 1996; Rotilio etal., 2000; Poli and Schaur, 2000; Rotilio, 2001). Authoritative scientists, such asAmes, Halliwell, Gutteridge, Pryor, Cross, Packer, Rotilio, ete., have suggested thatneurodegenerative diseases triggered by an uneertain primary eause are perpetuated asthe cellular redox system goes awry. The pathophysiology is quite variable: in somecases, there is ehronic inflammation with the release of ROS and pro-inflammatorycytokines; in other cases, we ean observe a biochemical defect such as low GSHcontent or a deerease of antioxidant enzymes (GSH-Pxs, SOD, catalase) associatedwith improper metal binding; in other cases, there is an excessive release of NO'(hence ONOO) or of noradrenaline from presynaptic terminals or of glutamate withCa2
+ influx and activation of protein kinases, phospholipases, ete. (Pardo et al., 1995;Nakao et al., 1995; Ceballos-Picot et al., 1996a; Markesbery 1997; Aejmelaeus et al.,1997; Sagara et al., 1998; Floyd 1999; Li et al., 1999; Perry et a\., 2000; Rotilio,2001).
Ozonetherapists must know that there is intense research activity trying to finddrugs able to delay or block the neuronal degeneration and death: the usualhydrophilie and lipophilie antioxidants taken in appropriate amounts via os are notharmful but are minimally effeetive (McCall and Frei, 1999), also because only asmall percentage reach the CNS. Metal chelators may help by reducing freetransition metals and OH' formation, but one must pay attention not to exceed withthe dose. Moreover, several inhibitors of the reuptake of doparnine, of NO' synthesisand of ionotropic reeeptors to block glutamate neurotoxicity are being tested. Themore biologically oriented approaches are attempting to use neurotrophic factors orto transplant dopaminergic foetal cells (or, probably very soon, stern cells) intoseleeted areas (Weber and Buteher, 2001). Among neurodegenerative diseases,Parkinson's disease is the ideal one, because the degeneration is fairly restricted topartieular areas of dopaminergic neurons (Lang and Lozano, 1998a,b).
In spite of all this tremendous effort and biIlions of dollars spent in basic andclinieal research, we can eonc1ude that pharmaeologicaI therapy is certainly useful(levodopa is still the most effective therapy after three decades !) but only for alimited time and it does not arrest progression of the disease. The combination ofseveral experimental therapies promises to improve on the present limitations, butstill we are fighting a virtually lost war beeause neurodegenerative diseases areprojected to surpass even cancer as the second eause of death by the year 2040(Lilienfeld and Perl, 1993).
Can ozonetherapy be of any use?At first glance, it seems irrational to propose a treatment of neurodegenerative
diseases based on aseries of brief and ealculated oxidative stress (therapeutie"shock"). However, this approach (which is not a panacea) may paradoxically breakand stabilize an otherwise irreversible situation. The idea (already discussed inChapter 22) is that a gradual escalation ofthe ozone dose (from 15 to 40 ug/ml) may

302 CHAPTER24
be able to induce adaptation to COS, which in practical tenns means that, bygradually receiving trace amounts of LOPs, neuronal cells under oxidative stressmay reactivate the depressed synthesis of antioxidant enzymes. Today there is nophannacological approach able to achieve this objective, which instead can berealized, without any biotechnological trick, simply by ozonizing blood for a fewminutes. More than ever, I persevere in my idea that if neurodegeneration is not dueto an irreversible genetic defect (like amyotrophic lateral sclerosis (ALS) or LouGehrig's disease, for example), judicious administration of ozone can be helpful. InChapter 2, I related the awful story I had with the Editor of FRBM, who refused tosend me the offensive referees' comments on my minireview proposing the conceptof adaptation to COS . More than ever, I am convinced that excessive dogmatism inbiology and medicine can be very dull. While I am aware, and I repeat to everyone,that ozone is intrinsically toxic and must be used with care, I do not see any risk inevaluating this problem with 0 3-AHT, or RI, or BOEX. At worst, we will not obtainany positive result but patients will not be harmed.
Actually, if it can be believed and in support of my stubbomness, as early as1993 in Cuba , Rodriguez et al. performed a double blind RCT on 60 patientsaffected by senile dementias: group A (30 patients) was treated with O2-03 by dailyRI (50 ug /ml) for 21 days and group B with O2 only . This was an importantpioneering study . Using several psychometric tests (mental condition, capacity forself-administered medication and evaluation of daily activities), it demonstrated that73-90% of ozone-treated patients showed marked improvement without anyadverse effect. In 1995, at the XII IOA Congress in Lilie, Gomez Moraledasummarized several studies carried out in Cuba since 1990. Use of OrAHT in opticnerve dysfunction, primary open angle glaucoma, cochleo-vestibular syndrome andischaemic cerebro-vascular disease yielded an improvement ranging frorn 50 to 100%.
Therefore, in Europe and the USA, we are already a decade too late and ifozonetherapy is really useful , to how many patients have we denied this possibility?Our inadequacy and short-sightedness is unforgivable!
If we are ever able to perform a study , it will be important not only to evaluatethe clinical effects but also to c1arify the mechanism of action. At the moment, I canonly advance a few speculations: ozonetherapy can simultaneously improve bloodflow and oxygen supply to hypoxie tissue, thus stimulating aerobic glycolysis inhypofunctional cells, which by resuming normal metabolism might restore thenormal ATP content and GSH /GSSG ratio . LOPs generated during lipoperoxidationof plasma or absorbed from the rectal mucosa (R!) or the skin (BOEX) will bediluted in the plasma pool and in part can pass through the blood-brain barrier toreach the sites of neurodegeneration and upregulate the cellular synthesis ofantioxidant enzymes, which is the crucial step to readjust the impaired cell redoxsystem. The release of neuronal growth honnones and the activation of resident sterncells remain speculative, but they are not too far-fetched ideas . The possibility thatAlzheimer's disease, associated with adeposition of insoluble ß-amyloidaggregates, reflects an NO· /superoxide imbalance has been entertained by Thomaset al. (1996) . The therapeutic implication is that a prevalence of NO· oversuperoxide is advantageous and may inhibit aggregation. This may be achieved by

OZONETHERAPY IN VARIOUS PATHOLOGIES 303
the administration of exogenous SOD mimetics andJor antioxidants but,interestingly, 0 3-AHT could correct the imbalance by inducing SOD and theproduction of NO' at the same time . Two cautionary annotations appear to be inorder : the first is that functional recovery may be achieved only in initial or not tooadvanced patients, and secondly an optimal 03-AHT schedule has not yet beenworked out, although it appears reasonable to start with a low 0 3 concentration (1520 ug/rnl) and slowly raise it (in 3-4 weeks) to 35-40 ug/ml per ml ofblood. For RI,I would suggest beginning with 5 ug/ml and proceed to a maximum of 30 ug/ml anda volume of 600 ml gas . In this case, I think that the concentration (50 ug/ml) usedconstantly by Rodriguez et al. (1993) is excessive and frequently causes intestinalcramps . If an improvement really occurs, it may be necessary to continue thetreatment (once weekly or biweekly?) for life. It must be explained and understoodthat one cycle of ozonetherapy cannot be the "eure": all cells have a more or lesslong biochemical memory and must be stimulated by LOPs at intervals of 1-2weeks . Our study on ARMD has been very instructive in this sense. Retinalmaculopathies deserve a short discussion on their own. Open studies carried outusing OrAHT in both ARMD and retinitis pigmentosa showed an improvement ofvisual activity in about 2/3 of patients (Gomez Moraleda, 1995; Diadori et al,unpublished). Our study is described in a previous section. However, arecentevaluation of 10 patients with retinitis pigmentosa performed in Cuba with aregimen of electrical stimulation, 0 3-AHT and ocular surgery has not validated thismulti-technique approach. Actually it suggested that, in comparison to simplevitamin A supplementation, this complex intervention may worsen the course of thedisease (Berson et al., 1996; Weleber , 1996). Thus , this problem remains open , sincethe study examined a genetic disease and used a too complex protocol, in which itwas not possible to clarify the exclusive role of03-AHT.
Patients with neurodegenerative diseases undergoing ozonetherapy must receiveoral ant ioxidant supplementation (as has been specified in Chapter 22) because theyare frequently undernourished and may have a low TAS.
10. CANCER
Although a number of haematological cancers are now being treated successfully,the common solid cancers, which are the great majority, continue to be a problemfor mankind (Bailar III and Gornik, 1997). Owing to earlier diagnoses and sometherapeutic advances, for the first time in western European countries, the totalcancer mortality was moderate1y reduced for both sexes in the period 1990-1994(Levi et al., 1999) . However, due to prolongation of the life-span, the figures foroverall mortality from cancer (in Italy about 160,000 and in the USA about 520,000in 1993) are still dramatic. Moreover, in the same period, cancer mortality was stillincreasing in eastern European countries. This is not likely to change ovemightbecause a highly desirable improvement of chemotherapeutic compounds, so farrather unspecific and toxic , may come too slowly . An appropriate cancer preventioncampaign, aimed at early detection and the use of an appropriate diet rich in fibreand antioxidants (Dreher and Junod , 1996; Bailar III and Gamick, 1997; Kramer and

304 CHAPTER24
Klausner, 1997), may help up to a point. Yet, on the whole, smoking is notdecreasing and has partly shifted from men to women and to Third World countries.
At least theoretically, immunotherapy (the fifth modality of cancer treatment)aims specifically at destroying only neoplastic cells, but unfortunately these cells arepoorly immunogenic and diabolically equipped to evade or suppress the immunesystem. In addition to showing the multiform conventional anti-neoplastic therapy,Figure 101 indicates that since 1980 a considerable effort has been made to developnew and efficient immunotherapeutic approaches, which however have failed toachieve substantial advances (Rosenberg et al., 1987; Rosenberg, 200 I ; Bocci, 1985,1987b, 1990b; Kim et al., 1996; Fenton et al., 1996; Wemer and Jolles , 1996; Reddyet al., 1997; Ernst, 1997; Motzer et al., 2001) .
SURGERY 11 RADIOTHERAPY 1 ICHEMOTHERAPY I I HORMONE THERAPY
Therapy with ribozymes
FUTURE DEVELOPMENTS
( Anliangiogenetic therapy )
1) Hlgh-Intenslty chemotherapy, regtonalRECENT DEVELOPMENTS adminIstration wlth Inhibitors ofI\~- •. I chemoreslstance and wlth granulopoletlns rescue
~ 1 2) Hyperthermla Therapy w ith anti sen seoligodeoxynucleolides
'--------- -'I 3) Photodynaml c therapy II 4) Bone marrow transplantation I
S) Immunotherapy:a) wlthlmmunomodulatory compounds (thymJc
hormones, melatonln, etc .)b) wlth Inducers or cytoklnesc) wlth exegenuus cytcklnes (lFN ,IL-2, -12, TNFa)
wlth or wlthout adoptlve Immunotherapy (LAI(, T1L)d) wlth gene therapye) wlth twnour vacctnes and dendrltlc cetls (APe)
o wlth dllTerenUaUng agents (all trans RA. tamoxlfen)g) wlth radloactlve and toxle 8I1tlbodles (the old maglc bulletI)
Figure J0J. The various aspects ofconventional antineoplastic therapy
Immunological gene therapy works weil in experimental murine tuu.ours, but sofar has been disappointing in patients (Anderson, 1992; Bubenick, 1996; Roth andCristiano, 1997; Parmiani et al., 2000) . The greatest hurdle for successful cancertherapy is a thorough understanding ofthe several mechanisms used by tumour cellsto evade the immune attack . The latest disappointment has been anti-angiogenictherapy; in spite of a perfect rationale (Carmeliet and Jain, 2000), it works very weilin mice (O'Reilly et aI., 1997; Boehm et al., 1997; Perletti et al., 2000) but not, aswe hoped, in human tumours, even though angiogenic inhibitors (Oehier andBicknell, 2000) combined with other drugs may still play an important role . Thus,after all the untimely and deleterious propaganda of the mass media, it is notsurprising that desperate patients are always looking for other possibilities,

OZONETHERAPY IN VARIOUS PATHOLOGIES 305
particularly in the vast field 'of complementary medical practices (Cassileth andChapman, 1996; Burstein et al., 1999) such as diet, nutrition and lifestyle changes,therapeutic touch (Rosa et al., 1998), mind-body control (Flach and Seachrist, 1994)and anthroposophie medicine based on the use of mistletoe lectins (Bocci, 1993b;Ernst, 2001; Steuer-Vogt et al., 2001).
In June 1995, the National Institutes of Health (NIH, Bethesda, MD, USA)included the use of oxidizing agents (ozone, hydrogen peroxide) in class 5, amongchelation and metabolie therapies, cell treatment and anti-oxidizing agents. It isnoteworthy that H20 2 has been evaluated as an anti-neoplastic agent by Zanvil Cohnat the Rockefeller University (Nathan et al., 1979; Nathan and Cohn, 1981). Otherstudies have been performed by Sasaki et al. (1967) and Samoszuk et al. (1989).
At an earlier stage, ozone was tested in cancer by Varro (1966, 1974, 1983) andZabel (1960). Thus, although ozonetherapy is more than 40 years old, it has beencarried out in a few private clinics in central Europe but it has never been acceptedby official Medicine and is currently despised in France, England, the USA andbarely tolerated in Italy. Several reasons, mostly right but partly wrong, have beendiscussed at length previously (Chapters 2 and 11).
Is ozonetherapy useful in cancer? Varro (1983) claimed that, after undergoingsurgery, chemotherapy and radiotherapy, most of his private cancer patientsbenefited from ozonetherapy, as their quality of life improved and they survived fora long period. However, these statements were not validated by statistical data andhave no scientific value. There are other anecdotal reports of major or minorautohaemotherapy having beneficial effects: for example, Beyerle (1996) treatedprostate cancer with "phenornenal" (?) results. For other types of cancer (throat,ovarian, colon and breast), he comments:
"We are seeing patients who were bedridden two years ago and sent home to die. Theyare becoming ambulatory. Their energy level is coming up. They are gaining weight.And we see these spontaneous fractures in the spine are gradually disappearing.Strength is retuming to the musculature. There is no spinal pain".
It is unclear why Dr. Beyerle has not reported the data in a peer-reviewedmedical journal, because as presented they are worthless . His comments wereactually recorded by a journalist (Null, 1996) during an interview published, fancythat!, in Penthouse, where certainly you can admire beautiful women! Anotherconfusing example was the abstract entitled "Ozonetherapy in oncology",surprisingly selected for presentation at the 12th Ozone World Congress in Lille inMay 1995 (Baltin) . If one reads the abstract, it becomes clear why ozonetherapy hassuch a low reputation in the medical field. Kief (1993a), at his clinic atLudwigshafen (Germany), has used Auto-homologous Immunetherapy (AHIT) totreat a variety of malignancies . AHIT was administered daily for aperiod of fourmonths and he claimed that it is:
"cost-effective, individually-oriented, has no-side effects, decreases pain in 70% of alI casesand increases the life-qualityand vitality in approximately 90% ofthe cancer patients",
What AHIT really was remains a mystery (apparently a mixture of the patient'sblood and urine treated with ozone!) and, to the best of my knowledge, the GermanHealth Authorities have now prohibited its use. My personal experience is very

306 CHAPTER24
limited, mostly because I have found that oncologists are very reluctant to evaluateozonetherapy. The only three cases that I had a chance to follow (two terminal lungcarcinoma and one metastatic and ulcerated breast carcinoma) did not show, asexpected, any objective improvement after repeated o.,-AHT. My feeling is that oncethe disease has reached the point ofno return, any therapy becomes practically useless .
In conclusion, today there is no evidence that ozonetherapy can be beneficial tocancer patients because:
• Randomized, double-blind clinical trials have not been performed as they shouldhave been done (Ernst and Resch, 1996).
• It is unclear whether biological and/or clinical effects, if any, are due to eitheroxygen or ozone or to both, or simply to blood retransfusion.
• The relevance ofthe placebo effect is unknown.• Too often ozonetherapy is carried out together with other conventional or natural
therapies, so that any result remains questionable.
In spite of these negative conclusions, let me enumerate (Table 25) and discusssome biological mechanisms of action that potentialIy could be activated byozonetherapy.
Tahle 25. Possible mechanisms ofaction ofozonetherapy in cancer.
I) Direct effect of oxygen-ozone on cancer cells in vitro and in vivo.2) Improved oxygenation and metabolism.3) Potential upregulation ofthe antioxidant enzymatic system with
improvement of the celIular redox potential.4) Effects on the immune system.5) Effects on the CNS and endocrine system. Therapy of cancer-related
fatigue .
I) Direct effect of oxygen-ozone on cancer cells in vitro and in vivo .Solid tumours generally tend to create an ideal microenvironment for theirgrowth, characterized by hypoxia, increased glycolysis and a high intracellularlevel of ascorbic acid . Hypoxia varies widely for different neoplasias but, onaverage, oxygen partial pressure can be between 1 and 10 mmHg (normal cellshave a p02 between 40 and 50 mmHg) depending on the distance from a nutrientvessel and the rate ofblood flow. CelIs beyond the O2 diffusion limit are anoxicand die, but hypoxic celIs remain viable, clonogenic and resistant to therapy .Indeed the rate ofmalignancy is positively corre1ated with the over-expression ofhypoxia-inducible factor l« (HIF-I) which, by upregulating the expression oftransferrin, VEGF, endothelin-I and inducible NO synthase, enhancesvasodilatation, neoangiogenesis and tumour metastasis (Brown and Giaccia,1998; Zhong et al ., 1999). Interestingly, glioblastoma multi forme, "theterminator", expresses HIF-Ia very strongly. Warburg's work in the 1920sdemonstrated that, even in hypoxia, cancer celIs intensely convert glucose to

OZONETHERAPY IN V ARIOUS PATHOLOGIES 307
lactic acid , but unless they are in anoxia their intracellular pH remains neutral(pH 7.0-7 .2) while the pH is slightly acidic (6 .8) in the interstitial fluid . It is alsonoteworthy that epithelial and haematopoietic tumour cell lines actively take upDHA and , by reductase activity, reduce it to AR (Agus et al., 1999) . Vitamin Chas many functions (Chapter 12) but the administration of megadoses, as oftendone by charlatans, may even give a metabolic advantage to malignant cells .Throughout the years, I have found reviews on tumour hypoxia very stimulating(Coleman 1988; Brown, 1999; Vaupel and Hockei , 2000; Hockel and Vaupel,2001). In conclusion, improving tumour oxygenation by significantly andconstantly increasing O2 availability and the microcirculation may slow downtumour growth and inhibit metastatization.Can ozone be of any help? It has been shown (Sweet et al., 1980; Van der Zeeet al., 1987; Washuttl et al., 1990) that the growth of human cancer is inhibitedby ozone in culture, suggesting that cancer cells have an impaired defencesystem against ozone damage. The fact that cancer cells live better in a hypoxieenvironment may imply that they have a rudimentary antioxidant system to getrid of ROS . However, it remains uncertain whether this is true for all humantumour cells in vivo , as they have high levels of AR and produce large amountsof H20 2 (Szatrowski and Nathan, 1991) . It also remains controversial whetherlipid peroxidation is low or high in tumours and when 4-HNE induces cellproliferation or cell death (Dianzani 1993; Kondo et al., 1999). This is animportant point because ozonization ofblood produces LOPs which, upon bloodreinfusion, could exert important cytotoxie effects on neoplastic cells if theyhave a poor defensive system. Zanker and Kroczek (1990) found that incubatingneoplastic cells in the continuous presence of a low dose of ozone «0.5 ppm) for24 h was distinctly cytotoxic. Moreover, ozone was able to potentiate thecytotoxicity of 5-fluorouracil (5-FU) and to increase the sensitivity in a 5-FUresistant colon carcinoma variant in vitro . However, I do not feel that the directcytotoxic action of ozone in tissue culture is important and may be misleadingbecause cancer cells never come in direct contact with ozone, not even when amad charlatan injects the gas intravenously.In practice, a cytotoxic effect could be obtained only by intratumoural injectionof 0 2-0J. Cutaneöus malignancies could be infiltrated with gas or ozonized H20or oil. Hepatic metastasis could be embolized with OrOJ via the hepatic artery(Chapter 16).
2) Improved oxygenation and metabolismThis topic received attention in Chapter 14 (Erythrocytes) and again in thischapter when we examined the problem in ischaemic tissues after reinfusion ofozonized blood. Oxygenation ofblood during ozonization has a negligible value,but the biochemical modifications induced by ozone on erythrocytes seemimportant because ischaemic muscles and perhaps hypoxie tumours will receivemore oxygen. In the case of muscles, after ozonetherapy, the venous p02decreased to 10-15 mmHg instead of 35-40, suggesting that oxygen wasdelivered to the ischaemic tissue (Rokitansky et al., 1981) .If indeed ozone is able to induce new generations of "supergifted erythrocytes",with an increased content of ATP, 2,3-DPG, antioxidant enzymes as well as an

308 CHAPTER24
elevated G6PD (Hemandez et al., 1995; Viebahn-Hansler, 1996; Bocci, 1996c),by continuing ozonetherapy for several months (actually for life), it may bepossible to profoundly modify their funct ional activities so that delivery ofoxygen increases and tumour tissues pass from a hypoxie to a normoxic state. Ifthis happens, it will dramatically change the tumour microenvironment,probably leading neoplastic cells to a dormant or a very vulnerable state,Vaupel and Hockel (2000) examined several possibilities to improve the oxygenavailability to neoplastic tissue: normobaric hyperoxia (100% O2 plus carbogen),hyperbaric hyperoxia, modification of 02-Hb affinity (shift to the right of theHb02 sigmoid curve), anaemia correction with transfusions and/or erythropoietinadministration. All of these ways are correct but more or less impractical andtransitory. Obviously, ozonetherapy was not inc1uded among these strategies,because it is a poorly known approach. It must be c1ear that a few OJ-AHTtreatments are practically useless and that we cannot permanently change thebiochemistry of mature circulating erythrocytes. I feel that this a crucial pointto keep in mind. It is only during the phase of erythroblast differentiation in thebone marrow that we can modify the cellular biochemical machinery by meansof the LOP messengers produced during ozonization of blood just beforereinfusion. Considering the erythrocyte half-life, a schedule of two sessions perweek of OJ-AHT (225 ml blood and maximum OJ concentration of 40 ug/ml perml of blood) and the dilution and catabolism of LOPs, it may be possible in 6months (48 sessions) to substitute the normal erythrocyte population with amajority of "supergifted" erythrocytes able to normalize oxygen levels inneoplastic tissues . After each 03-AHT, a new cohort of young erythrocytes willappear in the blood pool , replacing old and less effective erythrocytes.Moreover, by acting on endothelial cells, LOPs enhance NO and NOthiolformation, which may further increase the O 2 supply by improving thetumour microcirculation. The consequence of a desirable downregulation ofHIF-I will be an inhibition of angiogenesis and tumour metastasis.An additional (and not trivial) effect may be a generalized metabolic improvementinvolving the immune and neuro-endocrine system, with a tolerable quality of lifefor the patient. This is not a wild hypothesis: it already has some experimentalsupport and the possibiJity of being fully tested by measuring tissue p02 andbiochemical parameters of erythrocytes. The ideal methodological approach is OUf
EBOO and secondarily BOEX and 03-AHT (Chapter 16).3) Potential upregulation of the antioxidant enzymatic system with improvement of
the cellular redox potential.Ozone is a strong oxidizer and decomposes in a few seconds when it com es incontact with blood. Oxygen per se is practically inactive: it does saturate Hb butalthough there is an increase of solubilized O2 in the blood water, no formationof lipoperoxides has been detected. In contrast, when ozone dissolves in theplasmatic water, it gives rise immediately to a cascade of ROS and LOPs(Chapter 13). All of these compounds are unselective and in theory can damageblood cel1 components. This is probably the reason why conventional Medicineconsiders ozonetherapy a dangerous approach, more Iikely to be toxie thantherapeutical1y advantageous. However, it must be considered that if ozonization

OZONETHERAPY IN VARIOUS PATHOLOGIES 309
of blood is carried out when the ozone dose per gram of blood is preciselyknown, the reservoir of non-enzymatic and enzymatic antioxidants is capable ofminirnizing any possible damage to blood cell components. It has already beenexplained (Chapters 13 and 14) that during the ozonization procedure a"calculated" oxidative stress must occur in order to generate a certain amount ofROS and LOPs, which act as crucial signalling molecules to elicit biochemicaland immunological responses i.e. the therapeutic "shock". This means that theoxidative stress ought to be strong enough to trigger signals above the thresholdlevel (as otherwise they would be ineffective) but also be abated in a very shorttime by the antioxidant system. Thus ozonetherapy is a procedure that involves a"calculated", very transient oxidative stress capable of inducing cellularresponses without adverse effects. The exciting novelty is that ozonetherapy,cautiously carried out with a scaling-up of ozone doses, stimulates the increase ofcellular antioxidant enzymes (SOD, GSH-Pxs) capable of inhibiting chronicoxidative stress. What now seems a paradoxical effect of ozone has been describedsince 1984 as an adaptive response. Olivieri et al. (1984) were probably the first toobserve that human lymphocytes undergoing very low doses of ionizing radiationbecome resistant to a high dose of x-rays, Other studies cited in Chapter 22 clearlyshowed that animals kept in a hyperoxygenated environment could survive byupregulating the expression and activity ofantioxidant enzymes.This interesting new phenomenon of oxidative stress adaptation may explain, atleast in part, why ozonetherapy has a therapeutic activity in ischaemic,degenerative and autoimmune diseases, and possibly in cancer in which apersistent oxidative stress has been noted as a factor favouring the progression ofinvasion and metastasis (Toyokuni et al., 1995).
4) Effects on the immune system.It is obvious that, due to its strong disinfectant effect, ozone kills bacteria,viruses, fungi, etc., thus facilitating their phagocytosis by leucocytes. The nextstep was to understand how ozone activates both the humoral and cell-mediatedimmune system. We discovered that ozone acts as a mild inducer of cytokinesbecause the generated H20 2 crosses the cell membrane freely and activates thecytoplasmic NFKB, ultimately causing the transcription of mRNAs of severalcytokines (Los et al., 1995; Sen and Packer, 1996). Since the production ofseveral ILs, TNFa and IFNs is very small and transient , it appears unlikely thatinduction occurs via stimulation of a membrane lectin. In fact, in the sameexperimental conditions, the use of amitogen (PHA) that persistently activates acascade of protein kinases allows the synthesis of cytokines in amounts 1000times higher than when using ozone. Similarly, the proliferation index of BMCbarely increases after blood exposure to ozone. This interpretation is in line withthe results of Schreck et al. (1991), who found that human lymphocytes canexpress specific mRNAs after a transient exposure to 30-100 uM H20 2•
It has taken several years of research to understand how ozone works and whyeven a small activation of BMC can be useful in an immune-depressed patient. Ifozone acted as amitogen upon blood reinfusion, causing the massive release ofcytokines, we would have noted a frightening clinical response similar to thatobserved after intravenous injection of LPS, characterized by shivering,

310 CHAPTER24
hyperthennia, hypotension and malaise (Mackensen et al., 1991). Moreover, thedisadvantage of a toxic syndrome that few patients are able to tolerate is associatedwith the disruption of the cytokine network, which is usually deleterious .In contrast, ozonetherapy never causes any side effects, only very rarely atransient tiredness usually followed by a sense of well-being. Nonetheless, afterhoming in their microenvironments, activated BMC may prime or stimulateneighbouring cells, thus slowly upregulating the immune system . Obviously asingle session has no effect, and I would like to propose the same protocolsuggested previously to induce "supergifted" erythrocytes. Even a simplisticcalculation justifies this way of thinking. The immune system comprises about1012 cells dispersed in various organs . Yet for each treatment, we can at besttransiently activate only about 6 x IOR cells , for which we do not know the lifespan or the pattern of redistribution. It is useful to recall that in the course ofadoptive immunotherapy, a fairly critical number of about 1010
-11 LAK have to
be reinfused after exposure to IL-2 ex vivo (Rosenberg et al., 1987). An aspectdeserving some attention is the possibility that, during exposure of the patient'sblood ex vivo to ozone, circulating neoplastic cells (from breast , gastric, prostateand colon cancers) could undergo oxidation and become a potential autovaccine.This hypothesis is not too far-fetched because a) tumour cells have been detectedin blood (Pantel et al., 1999; Riethmuller et al., 1999); b) they are more sensitiveto ROS and LOPs than normal blood cells , and c) they could be taken up byAPe. Moreover, HSP-peptide complexes may elicit a CTL response and tumourimmunity (Tamura et al., 1997; Wells and Malkovsky, 2000) .
5) Effect on the CNS and endocrine system. Therapy of cancer-related fatigue .On the basis of casual observations, a functional interaction between the nervoussystem , the endocrine glands and the immune cells has been suspected fordecades. Immunological and neuroendocrinological studies (Blalock, 1984;Payne and Krueger, 1992; Reichlein, 1993; Jones and Kennedy, 1993) havec1early shown that these apparently distinct systems are indeed highly integrated.This topic is beyond the scope of this review, but I cannot fail to comment aboutthe pleasant feeling of euphoria and well-being reported by the majority ofpatients with chronic hepatitis and AMRD during OrAHT. This effect must bekept in mi nd because cancer patients are orten plagued by fatigue . At longlast this severe complication is receiving attention and "Cancer" has published asupplement on the topic (92, n.6, September 15, 200 I) .Would this effect also occur in cancer patients? Does ozonetherapy trigger apsychoneuroimmunological effect via the release of a cascade of endocrinesecretions, namely of CRH, ACTH, cortisol, DHEA, growth honnone,endorphins, melatonin, etc .? Could this effect be due to the withdrawal of a largeblood volume or to the reinfusion of ozonized and oxygenated blood with thestimulatory effect ofLOPs on the endothelial bed?It is not difficult to envisage that a change in the homeostatic balance is bound toevoke a multi-organ response that could positively influence the psychologicalstatus ofthe patient, hence the immune response (Fig . 102) (Flach and Seachrist,1994). How important is the placebo effect (Chapter 25) remains undetenninedbecause even a slight increase of cortisol may improve the mood of the patient

OZONETHERAPY IN VARIOUS PATHOLOGIES 311
(Coleman, 1992). Aseries of circumstances, e.g. being attentively cared for andobserving the AHT steps with "energized" blood being reinfused, compose theso-called "Hawthorne's effect", which may have a boosting effect and evoke apsycho-hormonal-immune response, the significance of which cannot be underestimated (Cassileth et a1., 1991; Cassileth and Chapman, 1996; Trussel, 1999).It is weil documented that a few cancer patients have been miraculously healedafter a pilgrimage to Lourdes!
COGNmvE STIMUlI(phys lcll , ehomlell, omDthle>
D.
Figure 102. Modern psychoneuroimmunology is based on the interactions among theCNS, endocrine system and immune system. Release ofcytokines by the immune system
influences both the CNS and endocrine system. Thus it has become possible to understandthe genesis and relevance ofthe placebo effect

312 CHAPTER24
Another important question is whether ozonetherapy should be carried out in themorning or in the aftemoon. Intuitively, I would favour the aftemoon (4-8 PM)because the normal circadian rhythm ought to be least disturbed (Bocci , 1985b).However, only experimental data can define the optimal time of the day, althoughthere is the practical problem that most ofthe work must be done in the moming .
As exemplified in Figure 103, the war on cancer is won when all cells have beenkilled. There is no doubt that tumour debulking with surgery or other therapies (Fig .10I) is essential, because a large tumour load or extensive metastasis enhances theanergie state (Elgert et al., 1998) and reduces the chance of a eure . Figure 103schematically indicates that the primary tumour could be either eradicated or moreor less extensively removed. The former case is rare because haematogenousdissemination of individual tumour cells occurs at early stages of the malignancy, ashas been clearly shown by immunocytochemical detection of epithelial tumour cellsin bone marrow (Riethmuller et al., 1999).
death
cornplete ablation and eure
minimal residual disease
..'
level
detection
relapse
.·...
· ...
..
.:-_....· .... ... ..--------_.
oTime
Figure J03. Tumoural mass reduction by cytoreductive therapy
Thus, if only about 104 neoplastic cells have been disseminated, there is hope ofeither destroying them or preventing metastatic growth if the surveillance of the immunesystem remains active. Today conventional medicine offers several approaches

OZONETHERAPY IN VARIOUS PATHOLOGIES 313
attempting to achieve this goal (Fig. 10I). The most promising appear to beimmunotherapy and the various forms of gene therapy. However, all these approachesare still experimental and it may take several years before they are validated.
If metastases are present, the problem is far more complex and chemotherapy iswidely used with mixed results; indeed the side effects frequently impoverish thequality oflife.
Can ozonetherapy be more useful than chemotherapy in metastatic cancer? It isvery difficult to answer this quest ion because the few anecdotal reports are not valid .Only unbiased, randomized, double-blind clinical studies for several cancer types,possibly carried out in several oncological institutions, can ultimately prove whetherozonetherapy can really be useful . Due to the lack of serious biological and clinicalresearch in the past , this approach remains in limbo today and is totally disregardedby conventional oncology, particularly by chemotherapists. This is veryunsatisfactory, mostly because, in spite of some progress, the death rate remainshigh and real breakthroughs are not yet in sight . Because I feel that this is one of themost important issues, I have tried to objectively review several, albeit hypothetical,reasons to pursue the evaluation of ozonetherapy, not as a procedure able to eurethe neoplasia but rather as a means to stabilize its progression, particularly inelderly patients susceptible to the serious side effects of high-dose chemotherapy.
In the last few years, I have made a useless effort to explain that this approach hasa rational basis and can be carried out in a scientific and reproducible fashion. Theozone dose can be precisely adjusted to the blood volume or patient's weight, andoptimal ozone concentrations for the proposed methods are based on experimental dataand not on homoeopathic or imaginary beliefs. Almost needless to say, a lot of basicwork remains to be done, particularly in order to define the molecular andimmunological modifications of erythrocytes and leukocytes . Analysis of theadaptation to COS may weil be able to show that ozone can profoundly modify thebiochemistry and functionality of these ceUs in order to create an environmenthostile to cancer cells. In my opinion, this a new line of thought stating that the cellmalignancy can be tamed simply through the use of a potent biological modifier .However , only reliable c1inical data can ultimately inform us about the validity of theapproach; indeed we have often observed that an improvement of immunologicalparameters is not necessarily paralleled by a complete response and prolonged survival(Bocci, 1987b; 1990b; Reddy et a1., 1997).
What will be the future of this approach? As usual, we are facing the same story .It looks unpromising unless we carry out controlled c1inical trials. At the moment,on the basis of my frustrating experience, I doubt very much that we will be able toperform them, due to the disinterest and skepticism of oncologists. Obviously thepressure of pharmaceutical companies does not allow them to experiment withanything other than cytotoxic drugs. Although I have a great admiration for thescientific strides in biology and medicine, I feet that the biased attitude of mostoncologists towards ozonetherapy is wrong and unjustified. On the other hand, mostphysicians performing ozonetherapy in private practice are unable to perform ac1inical t)-(al and the habit of mixing other therapies makes any conclusionimpossible.Donsequently, the only hope is that serious and concerted efforts will bemade in the next few years . For the moment, however, it seems that, because of the

314 CHAPTER 24
laek of dialogue and eooperation, a potential therapeutie advantage will eont inue toremain in Iimbo , perhaps to the patient's disadvantage.
11. ORTHOPAEDIC DISEASES. THE PROBLEM OF BACK-ACHE
In the last deeade, a number of orthopaedie surgeons (Riva Sanseverino, 1989;Siemsen, 1995) have begun to treat aeute and ehronie polyarthritis (osteoarthritis ofthe hip, knee, interphalangeal joints, saeroiliae joint, ete .), tendinitis, myofaseial pain,epicondilitis and earpal tunnel syndrome with intra-artieular or peri-articularinsufflation of small volumes of Or03 (5-10 ml in one or three sites with 0 3
eoneentrations from 5 to 15 ug /ml) with very eneouraging results . In Morton's disease(neurorna), up to six infiltrations of O2-03 (4 ml eaeh at 20 ug /rnl have yielded greatpain relief. In a review article , Siemsen (1995) reported that applieation of mediealozone in aeute and ehronie painful diseases ofthe joints is a eomplementary method oftreatment to obtain rapid pain relief, deeongestion, disappearanee ofoedema, reduetionof loeal temperature and inereased mobility. If performed by an expert orthopaediesurgeon, the treatment is not risky and eauses only transitory loeal pain that disappearsin 5-10 min without any other adverse effeet.
The pathophysiology of these diseases is eomplex and eharacterized by thesoftening and even destruetion of the artieular eartilage, with inereased matrixdegradation due to eollagenase and proteoglyeanases. The enzymes may be seeretedby aetivated ehondroeytes and monoeytes, whieh release IL-I and TNFo ; Synthesisof POs inereases several fold and there is a natural attempt to maintain abiomeehanieally adequate matrix. In eontrast to RA, pannus does not develop. Jointpa in may be aggravated by eoneomitant synovitis.
Drug therapy is symptomatie, aiming to reduee pain and disability . Inhibitors ofeyelooxygenase I are in wide use, with aceompanying gastritis, ete . and are beingsubstituted with inhibitors of eyclo H. Loeal injeetion of glueoeortieoids into a givenjoint ean be earried out no more than twiee per year.
Beeause eonventional medieine does not provide a "eure", patients seareh foreomplementary therapies. On the basis ofthe pathology, ozonetherapy should be the lasttreatment to perform, beeause ozone (a potent oxidant) injeeted into the synovial spaeeshould elicit further inflammation or degeneration. Therefore, it is incredible that, afterinitial but tolerable pain, ozone produees great relief for a long time. By now,innumerable patients have been treated and we eannot doubt the results . Obviouslyozone is not a "miraculous" medicine and we must try to understand how it aets.
On several oeeasions, I have asked orthopaedie surgeons to eollaborate with usbeeause I think it would be interesting to examine the synovial eontent before andafter ozonetherapy. So far, this has not been possible, either beeause most patientsare treated privately or beeause it is difficult to eolleet sampIes. Thus I can onlyadvanee a few speeulations.
Onee ozone dissolves in the synovial fluid , it reaets with free proteins, enzymes,proteoglyeans and ehondroeytes and may elicit:

OZONETHERAPY IN V ARIOUS PATHOLOGIES 315
a) Inactivation and inhibition of the release of proteolytic enzymes and ofendogenous ROS.
b) Stimulation of the proliferation of chondrocytes (probably via H202) andfibroblasts, with increased synthesis of matrix and possibly of articularcartilage. Induction of the synthesis of antioxidant enzymes (SOD, GSH-Pxsand catalase) may be a crucial event as an adaptive response to COS and toozone. That is the reason why I would start infiltrating ozone at low doses.
c) Release of bradykinin and synthesis of inflamrnatory PGs is probably inhibited,with reabsorption of oedema and pain relief.
d) An increased release of IL-I soluble receptor or of other soluble receptors andantagonists able to neutralize IL-I, IL-8, IL-12, IL-15 and TNFa.,just to name afew possible culprits.
e) Conversely the release of imrnunosuppressive cytokines, such as TGF-ßI and IL10, may inhibit inflammation. Among several growth factors, TGFß I is interestingbecause it modulates the expression of integrins and stimulates the synthesis ofmatrix proteins such as collagen and glycosaminoglycans (TrippeI, 1995; Qi andScully, 1997). 1fthis is the case, the long period ofremission can be explained.
These are just hypothetical ideas, which shouldbe verified by examining thesynovial fluid and bioptic fragments to c1arify these really paradoxical ozoneeffects. Ozone never ceases to surprise us!
In RA, the use of03-AHT at high doses has been suggested (Chapter 14). Yet itremains untested whether the association of one treatment (per week) of 03-AHT ata low-medium ozone dose would improve the outcome in osteoarthritis.
Low back pain is a very disturbing symptom that can affect , at least for a while,up to about 80% of the worId 's population. Luckily, in most cases, physicaItherap ies (exercise, manipulation therapy, etc.) can solve the problem (Cherkin etal., 1998; Samanta and Beardsley, 1999). However , if a herniated disc (protrusion ofthe nucleus puIposus through the annulus fibrosus) is present and causesconsiderable pain , it must be removed with the least invasive procedure.
Up to the I970s, the typical orthopaedic operation removed the compression butoften destabilized the mechanical and functional stability of the vertebral colurnn.Thus it has been substituted by a mini-invasive intervention. This trend wasaccentuated by chemonucleolysis, introduced by Smith in 1969. However, theintradiscal injection of chymopapain and collagenase, potent enzymes able to digestthe components of the nucleus pulposus, has been abandoned because of occasionalrisk of allergie reactions and the exorbitant cost of the pure enzymes. Subsequently,Onik et al. (1987) introduced the alternative concept of aspirating the degenerateddisc including part of the herniated material, thus reducing the abnormal pressureand relieving the nerve root compression. This technique is still in use with asuccess rate of about 75% (Bocchi et al., 1998). There are other variants of this typeof approach, the latest being nucleoplasty.
In 1988, Verga , a private ozonetherapist, noted pain relief after infiltratingtrigger points in myalgias with O2-03 and proposed to use an indireet technique byinjecting the gas into the points localizable in the paravertebral muscle (locus

316 CHAPTER24
dolendi) corresponding to the metamer of the hemiated disc , This approach is nowwidely used by many ozonetherapists in Italy and it can be defined as the indirectapproach, or as I call it: "chemical acupuncture" (Bocci, 1998a).
The "chymopapain model" probably inspired a neurosurgeon, Jucopilla et al.(1995), to test whether intradiscal injection of ozone would be nucleolytic andbeneficial. This can be defined as the direct intradiscal injection of 0 2-03' Morerecently, another indirect variant has been introduced by the epidural injection of O2
0 3 in correspondence to the lesion. This is being performed by anaesthesiologists andseems promising. The use of O2-0 3 to treat back pain syndrome is now widely used inItaly, while it is unknown abroad . As it is a minimally invasive treatment with anegligible cost and rare side effects, it is worth trying before surgical intervention . Atour University, on the basis of our protocol , over 100 patients have been treated andabout 80% have shown marked improvement (Bocchi et al., 2000) . Thus there are asmany as three technical approaches, which are exemplified in Figure 104.
EP CA IDFigure J04. Schematic viewofa transverse sectionofthe lumbarregion: NP: nucleus
pulposus. MC: medullarycana!. Thearrows indicate the three possible routes O!Or03administration. ID: intradiscal; CA: "chemical acupuncture " in theparavertebral muscle,
PM and EP: epidural injection

OZONETHERAPY IN V ARIOUS PATHOLOGIES 317
The Direct Approach
A clear view of the L4-L5 intersomatic space with the needle just before directinsufflation of O2-0 3 is shown in Figure 105 (Andreula, 2001; Simonetti et al., 2001).The direct approach is carried out under radioscopic control and an expert can do it inabout 10min. After a rest of 10-15 min, the patient can get up and often he/she isamazed by the disappearance ofthe pain, as occurs after nucleoplasty. Ifnecessary, theapplication can be repeated a.second time before changing the approach.
Figure 105. The intradiscal approachfor direct injection o/OrOJ into the nucleus pulposus.The radiograph (above) shows the correct positioning 0/the needle in a frontal scan
(Andreula , 2001). Discographie view (below) 0/a transverse lesion in the fibres oftheannulus in disc L4-L5. in continuity with ascending disc herniation (Simonetti et al.. 2001)
Good results have been obtained after either intradiscalor intraforaminalinjection of a variable volume (3-15 ml) of gas at an 0 3 concentration of 27-30

318 CHAPTER24
ug/rnl. Several thousand patients have been treated, with a success rate of 54-86'%(Alexandre and Fumo, 1998; Jucopilla et a1., 2000; Bonetti et a1., 200 I; Fabris et al.,200 I; Leonardi et al., 2001 a; Petralia et al., 200 I) . It remains unc1ear how ozoneacts . One real possibility, previously discussed at length (Bocci 1998a, 1999), is thatozone dissolves in the interstitial water and reacts immediately, generating a cascadeof ROS, among which HzOz and possibly the hydroxyl radical, OHo, whieh is mostreactive. The hydroxyl radieal appears to react with carbohydrates and amino acidscomposing proteoglycans and collagen type land 11, major components of thedegenerate nuc1eus pulposus, leading to its breakdown (MeCord, 1974; Curran et a1. ,1984; Hawkins and Davies, 1996; Bocci et al., 2001b; Leonardi et a1. , 2001b). Thesestudies, as weil as those performed on human blood, have been carried out using theElectron Paramagnetie Resonance (EPR) spin trapping technique (Ueno et al.,1998). Consequently, reabsorption of hydrolytic products and water may lead toprogressive shrinkage and disappearance of the hemiated material. Reducedmechanical irritation decreases the sensitivity of nerve axons, but nociceptors arealso excited by endogenous algesie substances released during perineural ischaemiaor neural inflammation present in the spinal ganglion and neural roots (WiIIis,1995). Thus, more than the mechanical compression as primum movens, it is theinflammatory reaction that sustains chronic pain by releasing PLAz, severalproteinases and cytokines. The continued release of ROS, PGEz, serotonin,bradykinin, cathepsins, IL-I , IL-6, substance P, etc ., causes oedema, possiblydemyelination and increased excitability of nociceptors (Fields, 1986). Indeed , it hasbeen observed that even a large hemia can be painless. Moreover, the hemia mayremain after an operation (as seen radiographically), but the pain disappears once theinflammatory disorder dies down . Interestingly, epidural injections of the antiinflammatory methylprednisolone transitorily improve leg pain and sensory deficitsin patients with sciatica due to a hemiated disc (Carette et al., 1997).
So, how does ozone act? We are again facing the ozone paradox : although OHocandegrade the degenerated material and reduce pressure, it often exerts a rapid "antiinflammatory action", partieularly because only a few ml of gas can be introducedinside the nucleus pulposus and most of the gas invades the intraforaminal space . Thismay mean that ozone rapidly blocks inflammatory reactants and stimulates therestitutio ad integrum. What is even more surprising is that this change remains stable(unlike corticosteroids) and it does not necessarily coincide with the disappearance ofthe herniated material. In fact, CAT or NMR controls in 612 patients, 5 months aftertreatment, showed that the hemia disappeared in 226 (37%), was reduced in 251 (41%)and was unmodified in 135 (22%). After another 5 months, CAT/NMR controls wereperformed again in 200 (of251) patients in whom the hernia was reduced : a furtherreduction and improvement was noted in 44 patients (22%) . In 120 patients (of 135) inwhom the hernia was unmodified, there was an improvement in 11.6'% (14 of 120)(Alexandre et al., 2000) .
Thus the ozone effect is deployed in successive phases: there is an initial rapidchange, probably with disappearance of oedema and improvement of circulatory andmetabolic conditions, followed by stasis and then a further improvement possiblydue to release of TGFß 1 and bFGF (Silver and Glasgold, 1995; TrippeI, 1995),
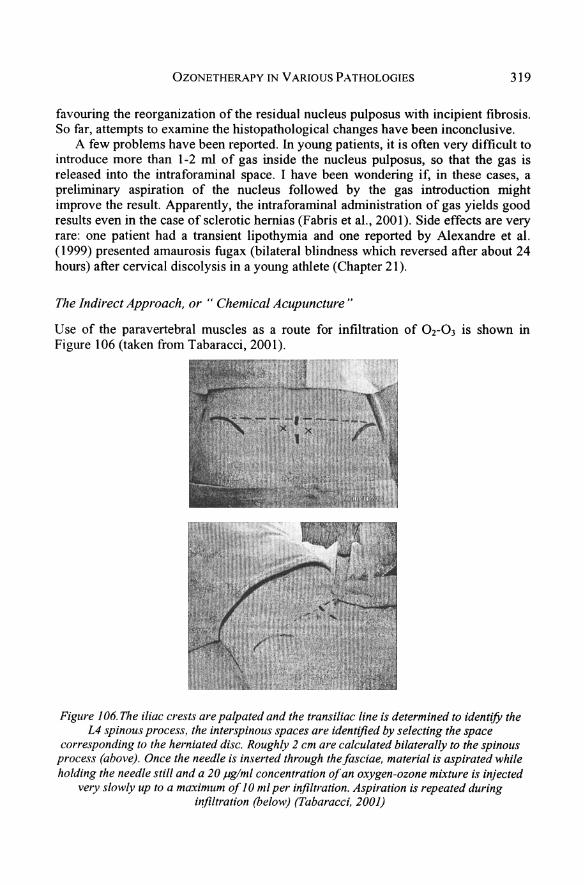
OZONETHERAPY IN V ARIOUS PATHOLOGIES 319
favouring the reorganization of the residual nucleus pulposus with incipient fibrosis.So far, attempts to examine the histopathological changes have been inconclusive .
A few problems have been reported. In young patients, it is often very difficult tointroduce more than 1-2 rnl of gas inside the nucleus pulposus, so that the gas isreleased into the intraforaminal space. I have been wondering if, in these cases, apreliminary aspiration of the nucleus followed by the gas introduction mightimprove the result. Apparently, the intraforaminal administration of gas yields goodresults even in the case of sclerotic hernias (Fabris et a1., 2001). Side effects are veryrare: one patient had a transient lipothymia and one reported by Alexandre et a1.(1999) presented amaurosis fugax (bilateral blindness which reversed after about 24hours) after cervical discolysis in a young athlete (Chapter 21).
The Indirect Approach, or " Chemical Acupuncture "
Use of the paravertebral muscles as a route for infiltration of Or03 is shown inFigure 106 (taken from Tabaracci, 2001).
Figure 106.The iliac crests are palpated and the transiliac line is determined to identify theL4 spinous process, the interspinous spaces are identified by selecting the space
corresponding 10 the herniated disc. Roughly 2 cm are calculated bilaterally to the spinousprocess (above). Once the needle is inserted througb thefasciae, material is aspirated whileholding the needle still and a 20 ug/ml concentration 0/an oxygen-ozone mixture is injected
velY slowly up to a maximum 0/10 ml per infiltration . Aspiration is repeated duringinfiltration (below) (Tabaracci, 2001)

320 CHAPTER24
This approach, which seems technically simple, has become very popular in Italy .Indeed some physicians think they can become ozonetherapists ovemight and startto inject a patient with an excessive dose of ozone, which might kill hirn owing to acomplex neurovegetative over-reaction. This has happened once and that is why it isimportant to have precise guidelines and mies for the practice of ozonetherapy.
In reality, it is an easy approach consisting in one or several (up to four)injections of 5-1 0 rn1 of O2-03 per site. The ozone concentration must not exceed15-20 IJglml because it is painful . At first, it is wise to test the patient's reactivitywith an injection of sterile saline and then start with 10 ug/ml ozone. The injectionmust be done very slowly into the trigger points corresponding to the metamers ofthe hemiated disk. The length of the needle varies (from G22 to G25) depending onthe patient's obesity. Usually two symmetrical injections (total dose 10-20 ml gaswith at most 200-400 ug ozone) repeated twice per week for about 5-6 weeks (I0-12sessions) are sufficient; ifnot, the patient is unresponsive to this approach.
I repeat that injection of O2-03 e1icits a sharp pain lasting a few minutes and theinjection must be done very slowly to avoid any risk of embolization. If we actcarefully, we can avoid serious adverse effects, such as sud den hypotension,bradycardia, mydriasis, intense perspiration and cardiac arrest (vasovagal reflex) .Any serious ozonetherapist must be prepared for this emergency, which is very rarebut can happen (see Chapter 36) .
The results of a number of studies vary somewhat (Cinnella and Brayda-Bruno,2001), but they can be summarized as : about 40% optimal, 35-40'% markedimprovement 15-25% minimal or no result. Gionovich et al. (2001) compared threeapproaches:
A) Paravertebral injection of02-03
B) Peridural injections with desamethasoneC) Paravertebral injection of'buvipicaine 0.25%
75% Satisfactory response55% Satisfactory response70% Satisfactory response
The term "chemical acupuncture" was coined (Bocci, 1998a) because we mustc1arify the role of the needle, oxygen and ozone. It was proposed to compare thisprocedure against a waiting-list control, two placebo controls (one with oxygenalone and another without any gas) and a standard-treatment control. Gionovich etal. have now shown that, as expected, even an anaesthetic has some effect. Owing toan unexpected, unintentional incorrect use of the medical generator (deliveringmedical oxygen only), we can now give a reasonable answer to the above-mentioneduncertainty. Torri et al. (1999) treated a group of 66 patients with O2-03 and a groupof 30 patients with oxygen alone. Interestingly, excellent or good responses wereobserved in 86% of patients of both groups but the O2-03 group showed astatistically significant improvement of some c1inical parameters. This suggests thatthe needle and oxygen together already have a therapeutic role, wh ich is potentiatedby the addition of ozone.
Then the question is: how does ozone injected intramuscularly work? The gasinfiltrates the musele and after 24 hours some gas bubbles move towards thevertebral canal (as seen radiologically). It was postulated that ozone will reach thesite of the hemiated material and will Iyse it. This is an untenable idea : ozone

OZONETHERAPY IN V ARIOUS PATHOLOGIES 321
dissolves rapidly into the interstitial water of the muscle and will generate H202within a few minutes; by inhibiting amyelinic fibres (C-nociceptors), the H202 willactivate the anti -nociceptive system via the descending antinociceptive system (Fig .107). As occurs during acupuncture (Ceccherelli et al., 1995), the introduction oftheneedle, reinforced by the pressure of O2-03, induces strong inhibition of nociceptors,perhaps a prolonged stunning due to H202• It is known that an algic stimulation ofthe skin and muscles can reduce pain through the mechanism of diffuse noxiousinhibitory control (DNIC) . That is why the needle + H202 + oxygen pressure can betranslated into chemical acupuncture.
Figure J07. The scheme indicates the mechanismsfor the control ofalgesie signals. Byreleasing endorphins (End.), the enkephalinergic interneuron may inhibit the presynaptic
connection ofa neurocyte (C) ofa spinal ganglion which, under compression ofa herniateddisc, stimulates the release ofsubstance P (SP). Endorphins ean inhibit the transmission of
the algesie signal to neuron D. hence to the ascending spinal-thalamicfibres. Themonoam inergic 01' serotoninergic neuron A. as a component ofantinociceptive descending
fibres , ean reinforce the analgesie effect ofneuron B

322 CHAPTER24
This mechanism is likely correct because too low 0 3 concentrations (3-10 ug/rnl)or gas volumes (1-2 ml) are ineffective, whereas too high 0 3 concentrations (above 20ug/rnl) or gas volumes can cause lipothymia . It is unclear whether pre-infiltration withan anaesthetic reduces the effect of ozone . We do not know whether the generatedH20 2 causes irreversible damage and death of the nociceptors, with a consequentincrease of the activation threshold . Furthermore, it is not known if this means ablocked release ofalgesie compounds, with a simultaneous release ofendorphins .
In conclusion, the probable mechanisms playing a role are the following :
a) release of endorphins blocks transmission of the noxious signal to the thalamusand cortex.
b) Hypostimulation (elevation of the activation threshold) linked to the oxidativedegeneration of C-nociceptors. H20 2 and LOPs may act like capsaicin.
c) Activation ofthe descending antinociceptive system.d) Simultaneous psychogenic stimulation of the central analgesie system induced
by the gas injection (elicitation of a placebo effect).e) The localized oxygenation and analgesia permit muscle relaxation and
vasodilatation, and thus a reactivation of muscle metabolism, by favouringoxidation of lactate, neutralization of acidosis, increased synthesis of ATP, Ca2
;
reuptake and reabsorption ofoedema.
Once again, by reactivating natural defence mechanisms, the use of oxygenozone surprisingly seems to solve a painful problem.
We have prepared a protocol proposing to evaluate the loeal effect (paravertebralmuscles) ofa solution ofH20 2 diluted in a 5% glucose solution. We may be able toascertain if H20 2 is the compound that acts on nociceptors and evokes the analgesieresponse. Samanta and Beardsley (1999) wondered what was the best way forwardto treat low back pain, but they did not know and eould not mention the O2-0 ,approach. If American and English orthopaedic surgeons read this book and try thisapproach, they may produce new and interesting results, useful for science andabove all for patients.
12. CHRONIC FATIGUE SYNDROME (CFS) AND FIBROMYALGIA
I am grateful to Prof. R. Mareolongo, Director of the Institute of Rheumatology,Siena University, for his broad-rnindedness and interest in evaluating ozonetherapyin RA, CFS and fibromyalgia. Some three years ago, we submitted a eomplexprotocol to the Ethical Committee, which approved it after a few revisions.However, the study on RA never took off because I was personally very doubtfulabout the ozone dose and because Prof. Marcolongo did not agree to suspendconventional medication in these patients. CFS and fibromyalgia are diseasescharaeterized by poorly understood signs and symptoms, with severe fatigue and aeontinuous flu-like syndrome that profoundly disables patients. Since 1990, I havefotlowed the abundant medicalliterature on CFS and I have realized that I could noteven attempt to give a short synthesis of an ambiguous aetiology and

OZONETHERAPY IN V ARIOUS PATHOLOGIES 323
pathophysiology. Recent papers have added some new ideas and the interestedreader may consult them (Komaroff, 2000; Manu, 2000; Reid et al., 2000; Spence etal., 2000; Natelson, 2001 ; Powell et al., 2001 ; Prins et al., 2001; Wessely, 2001).
Conventional treatment is based on antidepressants, low-dose glucocorticoids,exercise (in contrast, prolonged rest seems harmful), immunotherapy and oralnicotinamide adenine dinueleotide to increase the generation of ATP. Benefits arelimited and there are adverse effects . Cognitive behavioural therapy performed byskilled therapists appears to be an effective intervention without harmful effects . Inthis book, I have reported that 03-AHT often yields a feeling of well-being andeuphoria . This is quite true, even though we can only speculate about the reasons forthese positive effects . In search of a good therapy , CFS patients go from onephysician to another. Last year, at the hospital of Conegliano Veneto, they treatedsix patients diagnosed with CFS. 03-AHT was carried out twice per week for 8weeks and the physician in charge assured me that four patients showed a"remarkable improvement". He could not give information about the follow-up.
In our hospital, Dr. Cosentino treated one patient with a modest outcome. Iapologize for such a crude report but, given the severity of the disease, I would nothesitate one second to do 03-AHT if the patient wanted to try it. I would suspendany other drug and c1early explain that ozonetherapy may readjust the metabolie,immunological and hormonal derangements, causing only the discomfort of thevenous puncture.
Fibromyalgia is another mysterious disease . The American College ofRheumatology (ACR) has established a procedure for examining 18 tender points onthe patient. A tentative diagnosis can be made if at least 11 ofthese points elicit painwhen pressed. In Italy, fibromyalgia is considered a disease causing considerablesocio-economic problems, since it affects about 6 million people between 30 and 60years of age. The aetiology is unknown but initially seems caused by apsychosomatic factor later complicated by biochemical modifications in the musele,possibly similar to those found in CFS (Fulle et al., 2000), and neuro-psychoimmune endocrine disorder.'
Two studies have been carried out in Italy and they were reported at the IMOScongress last year at Siena University (November 2-4, 2000) . Unfortunately, theyhave not yet been published and I will give a short summary. From 1988 to 2000,Dr. Salvatore Loconte (Andria, Bari) has treated 150 patients by infiltrating 5 mI gasdirectly on the trigger points (03 concentration: 5-10 ug/ml) and perforrning a cycleof 03-AHT with about 150 ml blood and a total ozone dose of 4500 Ilg (30 ug/ml),He is a private ozonetherapist and cannot do a control but he has elaimed to achievetotal remission in about 60% of patients and partial improvement in 15%.
A RCT has been performed in the Institute of Rheurnatology of our Universityon 40 women (age 30-50) diagnosed as having fibromyalgia on the basis ofthe ACRcriteria . The scope of the study was to evaluate the effect of A) AHT with O2-03 (20patients, with 0 3 concentrations scaling up from 20 to 40 ug/ml , twice per week fora total of 16 treatments), B) AHT with O2 alone (10 patients), and C) simple AHTwithout gas (10 patients). Several standard end-points were tested before treatment,after 8 weeks and I month thereafter.
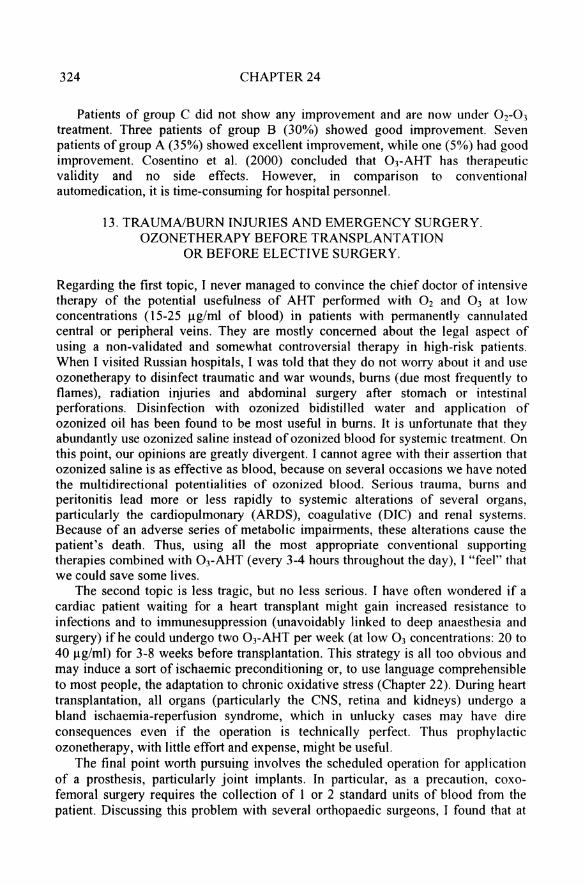
324 CHAPTER24
Patients of group C did not show any improvement and are now under Or03treatment. Three patients of group B (30%) showed good improvement. Sevenpatients of group A (35%) showed excellent improvement, while one (5%) had goodimprovement. Cosentino et al. (2000) conc1uded that 03-AHT has therapeuticvalidity and no side effects. However, in comparison to conventionalautomedication, it is time-consuming for hospital personnel.
13. TRAUMNBURN INJURIES AND EMERGENCY SURGERY.OZONETHERAPY BEFORE TRANSPLANTAnON
OR BEFORE ELECTIVE SURGERY.
Regarding the first topic, I never managed to convince the chief doctor of intensivetherapy of the potential usefulness of AHT performed with O2 and 0 3 at lowconcentrations (15-25 ug/ml of blood) in patients with permanently cannulatedcentral or peripheral veins . They are mostly concemed about the legal aspect ofusing a non -validated and somewhat controversial therapy in high-risk patients.When I visited Russian hospitals, I was told that they do not worry about it and useozonetherapy to disinfect traumatic and war wounds, bums (due most frequently toflames) , radiation injuries and abdominal surgery after stomach or intestinalperforations. Disinfection with ozonized bidistilled water and application ofozonized oil has been found to be most useful in bums. It is unfortunate that theyabundantly use ozonized saline instead of ozonized blood for systemic treatment. Onthis point, our opinions are greatly divergent. I cannot agree with their assertion thatozonized saline is as effective as blood, because on several occasions we have notedthe multidirectional potentialities of ozonized blood. Serious trauma, bums andperitonitis lead more or less rapidly to systemic alterations of several organs,particularly the cardiopulmonary (AROS), coagulative (DIC) and renal systems.Because of an adverse series of metabolic impairments, these alterations cause thepatient's death . Thus, using all the most appropriate conventional supportingtherapies combined with OrAHT (every 3-4 hours throughout the day), I "feel" thatwe could save some lives .
The second topic is less tragic, but no less serious. I have often wondered if acardiac patient waiting for a heart transplant might gain increased resistance toinfections and to immunesuppression (unavoidably linked to deep anaesthesia andsurgery) ifhe could undergo two OJ-AHT per week (at low 0J concentrations: 20 to40 ug/ml) for 3-8 weeks before transplantation. This strategy is all too obvious andmay induce a sort of ischaemic preconditioning or, to use language comprehensibleto most people, the adaptation to chronic oxidative stress (Chapter 22). During hearttransplantation, all organs (particularly the CNS, retina and kidneys) undergo abland ischaemia-reperfusion syndrome, which in unlucky cases may have direconsequences even if the operation is technically perfect. Thus prophylacticozonetherapy, with little effort and expense, might be useful.
The final point worth pursuing involves the scheduled operation for applicationof a prosthesis, particularly joint implants. In particular, as a precaution, coxofemoral surgery requires the collection of I or 2 standard units of blood from thepatient. Discussing this problem with several orthopaedic surgeons, J found that at

OZONETHERAPY IN V ARIOUS PATHOLOGIES 325
least three were interested in evaluating whether performing at least four 03-AHT(ozone at low concentrations) during the 2 weeks before the operation and thenevery day immediately after it for 4-5 days (using the predeposits as weil) wouldreduce the complications by enhancing healing and the patient's mood. I presented aprotocol to our Ethical Committee, which was approved. However, no trial hasstarted as yet because the orthopaedic surgeons do not have supporting personnel todo AHT.
In summary, I regret that this long and dreary chapter is ratherinconclusive. On the whole, I will feel great if two out of ten proposed clinical trialsbegin and if we can finish one study . The pace is too slow and I wish that we hadalready made incisive advances so that I could indicate optimal doses and schedules.Nevertheless, we have some ideas and a working hypothesis on how to proceed.
It is almost unnecessary to repeat that our good will is not sufficient and unlessthere is a concerted effort by official Medicine and govemment authorities, we willremain at the stage of "if", "perhaps" and "speculations". This is sad, not so muchfor me because I have always tried to do my best, but for the patients who will nothave the advantage of recovering more rapidly and improving their health. Nationalhealth authorities, which are always complaining about the increasing costs ofmedical assistance, could have an economical advantage if ozonetherapy waswidespread and organized in a systematic way in all public hospitals. The savingscould be dedicated to improving other areas of medical assistance. Even a childcould understand this simple reasoning. Although I have no hard data to support mycontention, I am convinced that the benefit of ozonetherapy does outweigh its cost.
Obviously pharmaceutical giants or other private organizations would make lessprofit, but they would continue to thrive just the same . An obvious comment is thatalthough the Communis' creed has failed in many ways, it has succeeded in Cuba intruly improving health assistance for everyone. A good part of the merit, however,has to be attributed to the versatility of ozone .




















