Chapter 1 - Basic Science of Pain - Amazon AWS
14
CHAPTER 1 Basic Science of Pain CASEY J. FISHER, MD • TONY L. YAKSH, PHD • KELLY BRUNO, MD • KELLY A. EDDINGER, BS, RVT INTRODUCTION Clinically, the most commonly referenced definition of pain initially described by Harold Merskey in 1964, and as adopted by the International Association in the Study of Pain in 1979, defines pain as “an unpleasant sensory and emotional experience associated with actual or po- tential tissue damage, or described in terms of such damage.” 1 In this chapter, we will give an overview of the pathways involved in pain processing as it occurs in both the central and peripheral nervous systems as is currently conceived. This overview will include: anat- omy involved in the processing of nociceptive stimuli; the fundamentals of systems underlying acute nocicep- tion and persistent pain states; and the linkage to chronic pain and how the immune system plays a role in this processing. PERIPHERAL ANATOMY Primary Afferents 2e4 The signal of acute nociceptive pain is propagated along sensory neurons, which have cell bodies (somas) that lie in the dorsal root ganglia (DRG) and send one of their axon projections to the periphery and the other to the dorsal horn of the spinal cord in the central nervous system. The axons of peripheral affer- ents can be classified by anatomical characteristics (Erlanger-Gasser), Conduction Velocity (Lloyd-Hunt), and by their respective thresholds for activation. Most commonly, they are known by anatomical classification into two types of A fibers (b and d) and C fibers. C fibers are small, unmyelinated, and therefore, slow conducting fibers (<2 m/s). These primary sensory afferent neurons represent the majority of afferent fibers found in the periphery and are most commonly high threshold fibers, meaning they are not activated unless the stimulus (thermal, mechanical, or chemical) is at an intensity sufficiently high enough to potentially cause tissue injury. As nociceptors, or receptors that detect noxious stimuli, they are triggered to discharge when the range of temperature or pressure corresponds to what would be considered painful. The distal termi- nals of these small C fibers display large branching den- dritic trees and are characterized as being “free” nerve endings. These nerve endings can be activated further by many specific agents in the periphery in response to tissue injury, inflammation, or infection in a concentration-dependent fashion. Table 1.1 depicts the source and nature of these agents as well as the eponymous receptor on C fibers that is activated with each agent. The fact that there are multiple stimulus modalities for these C fibers that can lead to a signal of pain is the reason they are known as C-polymodal nociceptors. In fact, C fibers can be characterized further by what provokes them to fire. There are some C fibers that do not respond to mechanical stimulation. These so-called silent nociceptors, or mechanically insensitive afferents (MIAs), only respond to very high levels of nonphysiologic mechanical stimulation and/or heat. However, they can acquire sensitivity in the face of pa- thology, such as inflammation, which leads to a sensi- tized state and activation by relatively low-intensity mechanical/thermal stimuli. Like C fibers, A-d fibers are small and can be high threshold. But, A-d fibers are myelinated, and there- fore, faster, with conduction velocity between 10 and 40 m/s. As such, A-d fibers act as nociceptors and mediate “first” or “fast” pain, whereas C fibers are responsible for “second” or “slow” pain. To put this in context, consider what happens when you touch a hot object. Your immediate reaction is to pull your hand away, which is mediated by noxious thermal sensation activating fast conducting A-v afferents. Typically, there is also a slower sensation of pain trav- eling over the slowly conducting C fibers, which relay tissue damage in the form of a burning sensation. Some populations of A-d fibers can also be lower threshold at times, meaning they begin to discharge Pain Care Essentials and Innovations. https://doi.org/10.1016/B978-0-323-72216-2.00001-6 Copyright © 2021 Elsevier Inc. All rights reserved. 1
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Chapter 1 - Basic Science of Pain - Amazon AWS

CHAPTER 1
Basic Science of PainCASEY J. FISHER, MD • TONY L. YAKSH, PHD • KELLY BRUNO, MD •
KELLY A. EDDINGER, BS, RVT
INTRODUCTIONClinically, the most commonly referenced definition ofpain initially described by Harold Merskey in 1964, andas adopted by the International Association in the Studyof Pain in 1979, defines pain as “an unpleasant sensoryand emotional experience associated with actual or po-tential tissue damage, or described in terms of suchdamage.”1 In this chapter, we will give an overview ofthe pathways involved in pain processing as it occursin both the central and peripheral nervous systems asis currently conceived. This overview will include: anat-omy involved in the processing of nociceptive stimuli;the fundamentals of systems underlying acute nocicep-tion and persistent pain states; and the linkage tochronic pain and how the immune system plays a rolein this processing.
PERIPHERAL ANATOMYPrimary Afferents2e4
The signal of acute nociceptive pain is propagatedalong sensory neurons, which have cell bodies (somas)that lie in the dorsal root ganglia (DRG) and send oneof their axon projections to the periphery and theother to the dorsal horn of the spinal cord in thecentral nervous system. The axons of peripheral affer-ents can be classified by anatomical characteristics(Erlanger-Gasser), Conduction Velocity (Lloyd-Hunt),and by their respective thresholds for activation. Mostcommonly, they are known by anatomical classificationinto two types of A fibers (b and d) and C fibers.
C fibers are small, unmyelinated, and therefore, slowconducting fibers (<2 m/s). These primary sensoryafferent neurons represent the majority of afferent fibersfound in the periphery and are most commonly highthreshold fibers, meaning they are not activated unlessthe stimulus (thermal, mechanical, or chemical) is atan intensity sufficiently high enough to potentiallycause tissue injury. As nociceptors, or receptors that
detect noxious stimuli, they are triggered to dischargewhen the range of temperature or pressure correspondsto what would be considered painful. The distal termi-nals of these small C fibers display large branching den-dritic trees and are characterized as being “free” nerveendings. These nerve endings can be activated furtherby many specific agents in the periphery in responseto tissue injury, inflammation, or infection in aconcentration-dependent fashion. Table 1.1 depictsthe source and nature of these agents as well as theeponymous receptor on C fibers that is activated witheach agent. The fact that there are multiple stimulusmodalities for these C fibers that can lead to a signalof pain is the reason they are known as C-polymodalnociceptors. In fact, C fibers can be characterized furtherby what provokes them to fire. There are some C fibersthat do not respond to mechanical stimulation. Theseso-called silent nociceptors, or mechanically insensitiveafferents (MIAs), only respond to very high levels ofnonphysiologic mechanical stimulation and/or heat.However, they can acquire sensitivity in the face of pa-thology, such as inflammation, which leads to a sensi-tized state and activation by relatively low-intensitymechanical/thermal stimuli.
Like C fibers, A-d fibers are small and can be highthreshold. But, A-d fibers are myelinated, and there-fore, faster, with conduction velocity between 10 and40 m/s. As such, A-d fibers act as nociceptors andmediate “first” or “fast” pain, whereas C fibers areresponsible for “second” or “slow” pain. To put thisin context, consider what happens when you touch ahot object. Your immediate reaction is to pull yourhand away, which is mediated by noxious thermalsensation activating fast conducting A-v afferents.Typically, there is also a slower sensation of pain trav-eling over the slowly conducting C fibers, which relaytissue damage in the form of a burning sensation.Some populations of A-d fibers can also be lowerthreshold at times, meaning they begin to discharge
Pain Care Essentials and Innovations. https://doi.org/10.1016/B978-0-323-72216-2.00001-6Copyright © 2021 Elsevier Inc. All rights reserved. 1

when the range of temperature or pressure correspondsto what would be nontissue damaging. In the case ofthermal stimulus, it would be considered a mildlynoxious warm/hot sensation. In the case of mechanicalstimulus, it would be considered touch or pressure thatis borderline painful. A-d fibers also differ from C fi-bers in that they express specialized nerve endingsthat serve to define their response characteristics. Thisrelationship will be delineated further in the periph-eral physiology section.
In contrast, A-b fibers are large, myelinated fiberswith the fastest conduction velocity (>40 m/s) of pri-mary afferent neurons. They are low threshold afferentfibers that fire in response to low threshold mechanicalstimulation, such as touch or pressure. Under normalphysiologic states, activation of these afferents doesnot generate a noxious sensation. However, there arecertain conditions in which these afferents initiate apain sensation, or allodynia. The definition of
allodynia is low-intensity tactile or thermal stimulicausing a pain state. This can occur in scenarios wherethere is nerve damage (for example, carpal tunnel orsciatic nerve lesions).
All of the afferent nerve fibers share the followingimportant characteristics related to the pattern in whichthey respond to a stimulus and the manner in whichthey fire:i) Afferent nerve fibers display little or no sponta-
neous firing. They do not spontaneously dischargelike other nerve cells of the brain or heart;
ii) Peripheral afferents typically display a monotonicincrease in discharge frequency that covarieswith stimulus intensity. This means that if thethermal or mechanical intensity increases, therewill be a monotonic increase in discharge fre-quency because there will be a greater depolari-zation of the terminal, which will increasefrequency of axon discharge; and
iii) Afferents serve to encode modality by being ableto transduce thermal, mechanical, and/or chemi-cal signals into a depolarization based on theirindividual nerve ending transduction properties.For the larger A-b fiber afferents, the nerve endingsare highly specialized, e.g., Pacinian corpuscle, andonly respond to specific low threshold stimuli,whereas the free nerve endings of the small C fibersrespond to a more diverse array of signals at higherthreshold.
Somatic and Visceral Afferents4,5
The location of peripheral afferents is also importantwhen it comes to the type of pain sensation. Peripheralafferent axon projections to the periphery are foundthroughout the body. The axon projections to theskin, joints, and muscles are involved in somatic pain.The axon projections to the organs are involved invisceral pain. The main functional differences betweenafferents in the viscera and somatic systems are thatthere is little distinction between nociceptive afferentsand nonnociceptive afferents, and there is significantprevalence of MIAs in the viscera. The visceral afferentsonly exist as high threshold and low threshold afferents,the latter of which responds to a range of stimulationintensities. The main anatomical difference betweenafferents in the viscera and afferents in the somatic sys-tem is that there are significantly fewer afferents in theviscera. Less than 10% of the total spinal cord afferentinput comes from the visceral afferents. This oftenmeans that visceral input travels to its more centralprojections along with somatic input. The concept ofreferred pain, whereby organ pathology causes a
TABLE 1.1Summary of Agents, Tissue Source, andReceptors Found at C Fibers12.
Agents Tissue Source Receptors
Amines Mast cells(histamine)Platelets(serotonin)
H15HT3
Bradykinin Clotting factors(bradykinin)
BK 1, BK2
Lipidic acids Prostanoids(PGE2),leukotrienes
EP
Cytokines Macrophages(interleukins,tumor necrosisfactor)
IL-1, TNFR
Primary afferentpeptides
C fibers[substance P (SP),calcitonin gene-related peptide(CGRP)]
NK1,CGRP
Proteinases Inflammatory cells(thrombin, trypsin)
PAR3,PAR1
Low pH orhyperkalemia
Tissue injury [(Hþ),(Kþ), adenosine]
ASIC3/VR1, A2
Lipopolysaccharide(LPS), formylpeptide
Bacteria (LPS,formyl peptide)
TLR4,FPR1
2 Pain Care Essentials and Innovations

concomitant dermatomal spread of pain, is thought tobe caused by convergence of somatic and visceral affer-ents onto the same wide dynamic range neurons(WDRs) at the dorsal horn level (see Fig. 1.1). This leadsto the message generated by a visceral afferent beingconflated with the input generated by a particular so-matic region, thereby accounting for the “referredpain” profile of a visceral stimulus. WDR neurons willbe discussed further in the central anatomy section.
CENTRAL ANATOMYFirst-Order Neurons: Spinal Dorsal HornProjections6,7
If the signal generated by an acute nociceptive stimulus isfollowed anatomically, from distally to proximally, theperipheral afferents extend through the DRG, where theafferent cell body lies, to the axon terminals of the spinalcord. Then, they terminate at the dorsal horn, where thedorsal root entry zone (DREZ) is found. The smaller
WDR
CoronaryIschemia
Left Arm Pain
Visceral Afferent
Somatic Afferent
FIG. 1.1 Viscerosomatic convergence. (Credit: Kelly A. Eddinger.)
CHAPTER 1 Basic Science of Pain 3
afferents tend to enter the DREZ more laterally, and thelarger afferents tend to enter the DREZ more medially.The small and large afferents collectively enter the dorsalhorn as the fascicles that make up the nerve root. Nerveroots are divided into cervical, thoracic, lumbar, andsacral segments in a rostrocaudal distribution and enteron the ipsilateral side of the dorsal horn.
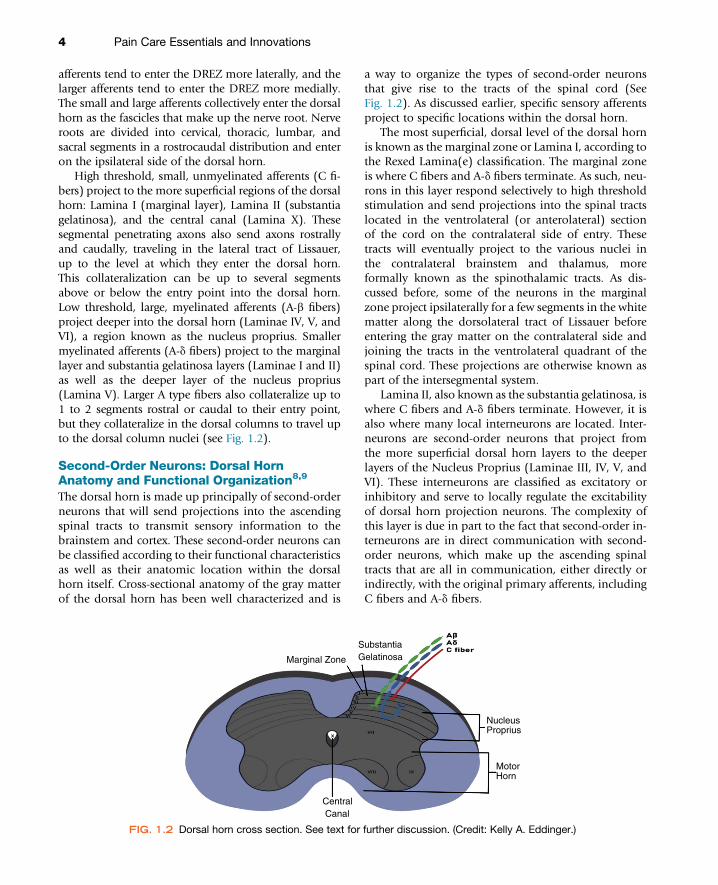
High threshold, small, unmyelinated afferents (C fi-bers) project to the more superficial regions of the dorsalhorn: Lamina I (marginal layer), Lamina II (substantiagelatinosa), and the central canal (Lamina X). Thesesegmental penetrating axons also send axons rostrallyand caudally, traveling in the lateral tract of Lissauer,up to the level at which they enter the dorsal horn.This collateralization can be up to several segmentsabove or below the entry point into the dorsal horn.Low threshold, large, myelinated afferents (A-b fibers)project deeper into the dorsal horn (Laminae IV, V, andVI), a region known as the nucleus proprius. Smallermyelinated afferents (A-d fibers) project to the marginallayer and substantia gelatinosa layers (Laminae I and II)as well as the deeper layer of the nucleus proprius(Lamina V). Larger A type fibers also collateralize up to1 to 2 segments rostral or caudal to their entry point,but they collateralize in the dorsal columns to travel upto the dorsal column nuclei (see Fig. 1.2).
Second-Order Neurons: Dorsal HornAnatomy and Functional Organization8,9
The dorsal horn is made up principally of second-orderneurons that will send projections into the ascendingspinal tracts to transmit sensory information to thebrainstem and cortex. These second-order neurons canbe classified according to their functional characteristicsas well as their anatomic location within the dorsalhorn itself. Cross-sectional anatomy of the gray matterof the dorsal horn has been well characterized and is
a way to organize the types of second-order neuronsthat give rise to the tracts of the spinal cord (SeeFig. 1.2). As discussed earlier, specific sensory afferentsproject to specific locations within the dorsal horn.
The most superficial, dorsal level of the dorsal hornis known as the marginal zone or Lamina I, according tothe Rexed Lamina(e) classification. The marginal zoneis where C fibers and A-d fibers terminate. As such, neu-rons in this layer respond selectively to high thresholdstimulation and send projections into the spinal tractslocated in the ventrolateral (or anterolateral) sectionof the cord on the contralateral side of entry. Thesetracts will eventually project to the various nuclei inthe contralateral brainstem and thalamus, moreformally known as the spinothalamic tracts. As dis-cussed before, some of the neurons in the marginalzone project ipsilaterally for a few segments in the whitematter along the dorsolateral tract of Lissauer beforeentering the gray matter on the contralateral side andjoining the tracts in the ventrolateral quadrant of thespinal cord. These projections are otherwise known aspart of the intersegmental system.
Lamina II, also known as the substantia gelatinosa, iswhere C fibers and A-d fibers terminate. However, it isalso where many local interneurons are located. Inter-neurons are second-order neurons that project fromthe more superficial dorsal horn layers to the deeperlayers of the Nucleus Proprius (Laminae III, IV, V, andVI). These interneurons are classified as excitatory orinhibitory and serve to locally regulate the excitabilityof dorsal horn projection neurons. The complexity ofthis layer is due in part to the fact that second-order in-terneurons are in direct communication with second-order neurons, which make up the ascending spinaltracts that are all in communication, either directly orindirectly, with the original primary afferents, includingC fibers and A-d fibers.
Marginal Zone
SubstantiaGelatinosa
NucleusProprius
MotorHorn
Central Canal
FIG. 1.2 Dorsal horn cross section. See text for further discussion. (Credit: Kelly A. Eddinger.)
4 Pain Care Essentials and Innovations

The nucleus proprius (Laminae III, IV, V, and VI),where large, myelinated, primary afferents (A-b fibers)terminate, has large-soma neurons, which send theirdendrites up into the upper lamina to make contactwith small, high threshold afferent input. Large, lowthreshold afferents make synaptic contact on the cellbodies and the ascending dendrites. Thus, they receiveconvergent low and high threshold input. This enablesthem to respond to low threshold and show increasingdischarge rates with increasing stimulus intensities assmall afferents are engaged. Accordingly, these cellsare referred to as WDR neurons.
The central canal (Lamina X) is the deepest layer ofthe dorsal horn. This location is where a large amountof visceral afferent input occurs and where smaller so-matic afferents (C fibers and A-d fibers) also terminate.Signals received here are high threshold temperatureand noxious mechanical stimulation. The tracts locatedhere are the second-order neurons that are crossingmidline and ascending to form the anterolateralportion of the spinothalamic tracts.
Organization of the dorsal horn is not strictly basedon anatomic location of the second-order neurons.Second-order neurons can also be organized by howthey respond to stimuli and, therefore, by their func-tion. There are high threshold neurons in Lamina Iand II that are nociceptive specific and respond onlyto highly intense stimulation. The other type ofsecond-order neuron, described above, which is basedon how it responds is the WDR neuron (see Table 1.2).As the name suggests, these neurons respond to a widerange of stimulus intensities and they are able torespond with increased frequency based on how intensethe stimulation is that they are receiving. This conceptof a graded response to stimulation is how innocuouslight touch is differentiated from a noxious pinch or
squeeze. The location of these neurons is principallyin the nucleus proprius (Laminae III, IV, V, and VI).
WDR neurons are also known as modality conver-gent neurons because they do not necessarily discrimi-nate between the source of the primary afferent fromwhich they receive input. As mentioned previously,the somatic and visceral afferents can cause a referredpain due to viscerosomatic convergence. This explainswhy pain caused by coronary artery occlusion duringamyocardial infarction can cause a concomitant derma-tomal pattern of pain. This convergence can also occurbetween deeper andmore superficial somatic structures,which explains why deep muscle or bone pain can alsoshow a pattern of dermatomal spread of pain similar tothe referred pain of coronary artery ischemia.
Another characteristic of WDR neurons is that theycan be prompted to exist in a state of ongoing dischargeby low frequency, repetitive stimulation of C fiberprimary afferents. This continuous discharge has beentermed “wind-up” by Mendell and Wall in 1965.Wind up, also known now as central sensitization,will be discussed in detail later in the physiology sectionof this chapter.
Third-Order Neurons: Ascending andDescending Spinal Tracts and SupraspinalProjections9e11
In order to understand where the third-order neuronsproject, it is first necessary to understand the differentindividual ascending projections that make up theascending sensory spinal tracts. The four major projec-tions identified in the ventrolateral quadrant of the spi-nal cord are the spinothalamic, the spinoparabrachial,the spinoreticulothalamic, and the spinomesencephalicprojections. A fifth ascending projection that transmitssensory information, but not necessarily pain unless
TABLE 1.2Organization of Primary, Secondary, and Tertiary Neurons.
PrimaryAfferents Secondary Projections Tertiary Projections Results
C fibers Dorsal horndLaminae I andII
Spinothalamic tracts tomediodorsalis nucleus ofthalamus
Anterior cingulatecortexdemotional pain response
A-d fibers Dorsal horndLaminae II andV
Spinothalamic tracts toventrobasal thalamus
Somatosensorycortexdprecision mapping ofpain response
A-b fibers Dorsal columnscollateralization
Dorsal columns to mediallemniscus
Somatosensory cortexdtactilesensation and proprioception
CHAPTER 1 Basic Science of Pain 5

the system is in a state of evoked hyperpathia, is the dor-sal column medial lemniscal pathway. These projec-tions terminate in three main brainstem regions: thediencephalon, the mesencephalon, and the medulla.The third-order neurons in these regions then projectfurther to the cortex or within the diencephalon ormesencephalon.
The spinothalamic projections consist of both WDRneurons coming from the Lamina V portion of the dor-sal horn and high threshold, pain-specific Lamina Ineurons. The pain-specific, high threshold neuronsmake up the ascending tracts that will project intothe posterior ventral medial nucleus (VMpo) and themedial dorsal nucleus of the thalamus. The third-order neurons in the medial dorsal nucleus then proj-ect to the anterior cingulate cortex. The third-orderneurons in the VMpo then project to the insula. Thesepathways are both known to be less precise about theactual intensity and localization of the pain and moreinvolved in the emotional and affectual aspects ofpain. In contrast, the third-order neurons in the ven-trobasal nucleus of the thalamus, where the WDRneurons from Lamina V terminate, are more preciseabout intensity and localization of the pain (seeFig. 1.3 and 1.5). Third-order neurons in the
ventrobasal nucleus project to the somatosensorycortex and input in these areas follows a strict patternthat is consistent with the sensory homunculus in thecortex. In other words, input in this area can be inter-preted over a range of intensities with precision as towhat part of the body is affected somatotopically andwhat is the modality of the injury.
The spinoparabrachial projections start as ascendingtracts in the contralateral ventrolateral section of thedorsal horn and they terminate in the parabrachial nu-cleus of the pons (see Fig. 1.4). Third-order neurons inthis area then project to the amygdala and the VMpo. Asnoted earlier, the VMpo also projects to the insula,meaning that these projections appear to have a rolein the “affective” aspect of pain. Previous animal andhuman studies of lesions in the areas of the temporallobe and amygdala show a dysfunction in the associa-tion of the stimulus intensity of pain with its affectivecomponent (suffering).
The spinoreticulothalamic projections start asascending tracts in the ipsilateral dorsal horn just likethe WDR neurons of the spinothalamic tract, but thesetracts ascend to the reticular formation of the medulla.Here, the third-order neurons project to the intralami-nar nucleus of the thalamus that further relays
Anterior Cingulate
Somatosensory Cortex
Inferior Insula
Mediodorsalthalamic projection
VMpothalamic projection
VentrobasalThalamus
Diencephalon
Cortex
SpiniothalamicProjections
FIG. 1.3 Spinothalamic projections: see text for further discussion. (Credit: Nancy Dinh.)
6 Pain Care Essentials and Innovations

information to many areas of the cortex. The reticularformation and its projections to the cortex are a partof the reticular activating system, which is in partresponsible for regulating wakefulness and sleep-waketransition. This serves as a plausible pathway for paininterpretation to effect sleep and the sleep-wake pattern(see Fig. 1.5).
The spinomesencephalic projections start asascending tracts as a part of the anterolateral systembut terminate at the periaqueductal gray (PAG) matterand the reticular formation of the mesencephalon.From there, third-order neurons project to the lateralthalamus. The PAG is not well understood, but it doesplay a role in descending inhibition of pain throughthe bulbospinal pathway and it also causes autonomicresponses in humans when stimulated (see Fig. 1.5).
While the transmission of the pain signal is knownto be produced by the ascending tracts, there is someevidence that there are descending tracts that canfacilitate the signal. The bulbospinal projections aredescending tracts that transmit a signal in from the nu-cleus raphe magnus of the medulla to the dorsal hornthat is excitatory in nature, but it serves to modulatethe central sensitization at the WDR neuron level usingserotonergic receptors.
As mentioned previously, the dorsal column pro-jections are made up, in large part, due to the collater-alization of the large, low threshold, primary afferents,A-b fibers (see Table 1.2). These ascending tracts stayipsilateral and ascend along the dorsal columns tothe nuclei in the medulla, where they then project tosecond-order neurons, which will cross over andcontinue to ascend as a part of the medial lemniscusto the thalamus. The third-order neurons there thenproject to the cortex. This system is not responsiblespecifically for pain, but it is responsible for tactilesensation and limb proprioception which can be pain-ful in certain pathologic states that will be consideredin the next sections (see Fig. 1.6).
PHYSIOLOGY OF NOCICEPTIONAcute Pain12,13
The initial report of pain and the physical movement toavoid a certain stimulus are responses that stem fromactivity that is initiated at the peripheral sensory termi-nal. This activity, in the form of a signal, sent via termi-nal depolarization of small unmyelinated (C fibers)and myelinated (A-d fibers) primary afferent sensoryneurons is due to the presence of potential damagingstimuli. This noxious stimulus, which can be thermal,chemical, or mechanical, creates a signal that the bodyidentifies as pain.
In most cases, acute pain is considered to be protec-tive, with the intention to remove the body fromfurther harm. The initial noxious stimulus is sensedby peripheral nociceptors that communicate with thespinal cord and ultimately send the signal to corticalregions of the brain. The most immediate and directresponse to a noxious stimulus is the flexor withdrawalreflex. When a nociceptor is activated by a noxiousstimulus, the signal travels through the primary sen-sory neuron to the dorsal horn where it synapseswith an interneuron. The interneuron synapses withan alpha motor neuron. Once the signal passes tothe motor neuron, a motor command is sent fromthe ventral horn of the spinal cord to the flexor andextensor muscles resulting in removal of the bodypart from the noxious stimulus. This reflex does notrequire processing at the cortical level, allowing for arapid response to avoid further injury.
The signal of nociception in this case is activationof C fibers. Activation of C fibers occurs with tissuepathology in the form of injury, inflammation, orinfection. These disease states cause increase ininflammatory mediators including protons, prosta-glandins (PGE2), thromboxanes, leukotrienes, growthfactors, cytokines, chemokines, and neuropeptides
VMpo
Amygdala
Dorsal Horn
Medulla
ParabrachialNucleus
SpinalCord
Pons
Cortex
Diencephalon
FIG. 1.4 Spinoparabrachial projections: see text for furtherdiscussion. (Credit: Calvin Nguyen.)
CHAPTER 1 Basic Science of Pain 7

Bulbospinal Tract
Spinoreticular Tract
Spinomesencephalic TractSpinothalamic Tract
SpinalCord
LowerMedulla
UpperMedula
Pons
Midbrain
Cortex
Thalamus
Reticular Formation
Periaqueductal gray matter
Reticular Activating System
FIG. 1.5 Spinothalamic, Spinoreticular, Spinomesencephalic, and Bulbospinal projections. See text forfurther discussion. (Credit: Nancy Dinh.)
Spinothalamic tractDorsal Column-MedialLemiscus pathway
Medulla
Thalamus
Spinal Cord
1st orderneuron
1st orderneuron
2nd orderneuron
3rd orderneuron
2nd orderneuron
3rd orderneuron
Anteriorlateralquadrant
Dorsal columnnuclei
Dorsal columns
Decussation ofmedial lemiscus
FIG. 1.6 Comparison between dorsal column and spinothalamic tracts. (Credit: Vanessa Tran.)
8 Pain Care Essentials and Innovations

(see Table 1.1). The presence of inflammatorymediators in the periphery causes sensitization of theprimary afferents and leads to hyperexcitable states.This hyperexcitable state can occur in all innervatedtissues.
Persistent Pain12
For all intents and purposes, the hyperexcitable state inthe periphery resolves when the inflammatory processresolves, except in certain cases where it does notresolve. Persistent pain states do occur due to sensitiza-tion in the periphery and at the dorsal horn, which isknown as peripheral sensitization. When the sensitiza-tion occurs at the dorsal horn level or above, it isreferred to as central sensitization.
Peripheral Sensitization12,14
In physiological states, the activation and firing ofsensory nerve endings in response to nonnoxiousstimuli occurs at a defined range. In states of chronicpain, the sensory nerve endings become sensitizedsuch that they exhibit a reduced firing threshold and/or an increased response to activation. This hyperexcit-able response to noxious and nonnoxious stimuli istermed peripheral sensitization. Following tissueinjury, cell damage occurs with activation of afferentnociceptive neurons and the aggregation of inflamma-tory cells at the site of injury. Activated nociceptorsand nonneuronal cells release chemical mediatorsincluding protons, prostaglandins (PGE2), thrombox-anes, leukotrienes, growth factors, cytokines, chemo-kines, and neuropeptides that mediate peripheralsensitization. Each of these extracellular products in-teracts with specific receptors found on the smallafferent nerve ending (see Table 1.1).
Binding of these mediators to the respective receptoron the sensory afferent terminal leads to cellular depolari-zation, increased intracellular calcium, and activation ofprotein kinases (e.g., protein kinase C and mitogen-activated protein kinases). These kinases serve to altertransducer molecules (e.g., TRPV1) and ion channels(e.g., voltage-sensitive sodiumchannels)causing increasedexcitability of the nociceptor. In some cases, the nocicep-tors are sensitized in such away to become spontaneouslyactive (as initiatedby the local chemicalmilieu).When thisoccurs, the nociceptor may be activated by a less intensephysical stimulus resulting in anallodynic state. Peripheralsensitization leads to ongoing pain and primaryhyperalgesia.
Dorsal Root Ganglia15
It has become increasingly apparent that the DRG is acomplex local neural network. Aside from the presenceof neuronal cell body of the afferent, the DRG iscomposed of astrocyte-like satellite cells that investeach cell body. The innervation provided by postgan-glionic sympathetic axons reflects the fact that theDRG lies outside the conventional blood-brain barrierand has a sympathetically innervated vasculature. Theyalso have a large population of macrophages that areactivated by neuroinflammatory stimuli, blood ves-sels, and of note, significant axon collaterals whicharise from the DRG cell body to release neurotransmit-ters in the DRG (see Fig. 1.7). The importance of thiscomplexity is that the DRG neuron can be the initiatorof ectopic activity which drives action potentials downthe glomerulus (connecting the cell body to its axon)and generate an action potential traveling bothorthodromically as well as antidromically. The DRGalso express the same receptors and channels that are
FIG. 1.7 Dorsal root ganglion structure. See text for further detail. (Credit: Kelly A. Eddinger.)
CHAPTER 1 Basic Science of Pain 9

expressed on the afferent neuron terminals and corre-spondingly respond to the same mediators that acton these terminals. Following peripheral tissue injury,the DRGmay initiate upregulation of voltage-gated Naand Ca channels as well as an increase in macrophagesthat release proinflammatory mediators that driveectopic DRG activity.
Central Sensitization12,16,17
Central sensitization is the amplification and/or main-tenance of peripheral nociceptive input at the spinaland supraspinal levels. Sensitization occurs due toincreased excitation or reduced inhibition of excitatoryprimary afferent neurons. This occurs in response topersistent nociceptive input resulting in increasedrelease of glutamate, calcitonin gene-related peptide(CGRP), brain-derived growth factor (BDGF), and sub-stance P from primary afferent terminals in the spinalcord and trigeminal nucleus that results in activity-dependent changes in dorsal horn spinal function.
Second-order neurons receive input from both lowand high threshold primary afferents. The input isreceived in a stimulus intensity-dependent manner sothat an increase in discharge of WDR neurons resultsin an increase in output frequency. Repetitive stimula-tion of C fibers causes progressive and sustained partialdepolarization of the cell making it more susceptible tofuture afferent input. Under normal conditions, theWDR neuron may be activated by a natural stimulusat a discrete location. After C fiber conditioning, anatural stimulus applied over a larger area nowdisplays the ability to activate the same WDR neuron.As previously mentioned, this exaggerated dischargeof WDR neurons evoked by repetitive stimulation ofprimary afferent neurons was termed “wind-up” byMendell and Wall.
The result of central sensitization is an increasedreceptive field of the second-order neuron known assecondary hyperpathia by which pain can be evokedby a nonnoxious stimulus in adjacent noninjured tis-sue. Two mechanisms contribute to the increase inreceptive field:i) As reviewed above, primary sensory afferent neu-
rons collateralize upon entering the spinal cord,sending segments rostrally and caudally up toseveral segments; and
ii) The facilitation of central sensitization is greatlydependent on phosphorylation of the glutamate-activated n-methyl-D-aspartate (NMDA) receptor.In physiological conditions, the NMDA channel re-mains quiescent due to continuous blockage bymagnesium (Mg). However, when the membrane
undergoes progressive depolarization as producedin response to repetitive stimulation via activationof AMPA and neurokinin 1 (NK1) receptors byglutamate and substance P, respectively, the Mgblockade is removed, and glutamate is able to acti-vate the receptor. In response, there is an influx of Cathat activates voltage-gated Ca channels and phos-phorylating enzymes including protein kinases Aand C (PKA, PKC) and mitogen-activated proteinkinases (MAPK). Thus, excitation of afferent inputalong the collaterals of distal segments is insufficientto cause the neuron to fire, but once neurons in thatdistal segment become sensitized (as with “wind-up”) after injury, the input is sufficient to allowthat distant segmental neuron to fire.Specifically, PKC activates the NMDA receptor and
Na channels, causing further depolarization contrib-uting to “wind up.” P38 MAPK phosphorylates en-zymes including phospholipase A2, which initiatesrelease of arachidonic acid and provides the substratefor cyclooxygenase (COX) to synthesize prostaglandins(PGE). PGE acts presynaptically to enhance opening ofvoltage-gated Ca channels and postsynaptically to blockglycinergic inhibition at the interneuron level. The acti-vation of afferent input and second-order neurons isregulated by local inhibitory interneurons containinginhibitory amino acids including GABA and glycine.When high frequency afferent input occurs, inhibitionis reduced leading to increased response of WDR neu-rons. The loss of inhibition via GABA or glycine inputaugments the response of WDR neurons leading tofacilitation of dorsal horn excitability (see Fig. 1.8).
Neuropathic Pain18e21
Neuropathic pain, defined as damage to the peripheralafferent nerve axon itself as opposed to other structuresin the periphery around the primary afferent, causesan initial retrograde degeneration of the nerve axonin a process called Wallerian degeneration. This degen-eration leads to axon sprouting, whereby the axons willattempt to reconnect causing a neuroma formation.This injury can cause peripheral and central sensitiza-tion just like injury in other areas, but it also causes areorganization in the central processing of pain whichshould be differentiated from central or peripheralsensitization because it is specific to nerve cell damage.
The reorganization of central processing thatoccurs with neuropathic injury and pain is seen clini-cally with the phenomenon of tactile allodynia. Thisanomaly whereby large, low threshold, sensory primaryafferents (A-b fibers) that are normally only activatedcausing a sensation of light touch can produce a
10 Pain Care Essentials and Innovations

nociceptive signal giving the sensation of pain reflectsseveral events in two main areas of pain transmission:i) Injured afferent axons will develop spontaneous
activity. This ectopic activity arises both at the site ofinjury and from the DRG of the injured afferentneuron.
ii) The dorsal horn, following injury, will also showreorganization through multiple mechanismsincluding spinal glutamate release, microglia andastrocyte activity increase, loss of GABAergic andglycinergic control, and increased sympathetic
input. As discussed earlier, glutamate is responsiblefor increased NMDA activation causing neuronalexcitability. Astrocyte and microglia activation leadto increased COX, NOS, and glutamate, whichcontribute to a hyperexcitable state.Normally, glycine agonism and GABA antagonism
serve to regulate the excitatory potential of A-b fibersin the dorsal horn. Loss of that regulatory inhibitioncauses A-b fibers to produce an aggressive depolariza-tion of the WDR neurons. Of note, after nerve injury,there does not appear to be a loss of GABA/glycine
FIG. 1.8 Central Sensitization: Excitation of primary afferents produces glutamate and substance P release,which acts post synaptically on second-order neurons and excitation increases intracellular Calcium andactivates a myriad of protein kinases. See text for further discussion. Sp, substance P; MAPK, mitogen-activated protein kinase; PLA2, phospholipase A2; PGE2, prostaglandin E2; Gs, stimulatory signaling protein;NA, noradrenalin, Caþþ, calcium; 5-HT, serotonin; Naþ, sodium; COX, cyclooxygenase; PKA, protein kinase A;PKC, protein kinase C; EP, prostaglandin receptor; CaV, voltage-gated calcium channel; NaV, voltage-gatedsodium channel; NK-1, Neurokinin 1 receptor; AMPA receptor, a-amino-3-hydroxy-5methyl-4-isoxazolepropionic acid receptor; CP-AMPA, calcium permeable AMPA receptor; NMDA, N-methyl-D-aspartate receptor; WDR, wide dynamic range neuron. (Credit: Vanessa Tran.)
CHAPTER 1 Basic Science of Pain 11

content release of receptors. However, it is now appreci-ated that after nerve injury, the chloride (Cl) gradient isaltered due to the loss of cellular chloride transporters.As a result, at this point, GABA or glycine receptoractivation results in an increased permeability to Cl,and in contrast to the normal state, Cl in the nerveinjury animal will flow out carrying negative chargeand resulting in a paradoxical depolarization. Hence,GABA and glycine release become an excitatory linkagerather that an inhibitory linkage.
Additionally, the presence of a neuroma will causesympathetic postganglionic afferents to sprout and bepresent at the neuroma site and in the DRG. Stimula-tion of these sympathetics will drive ectopic activity atboth the neuroma and at the DRG at that level.
Immune and InflammatoryMechanisms12,22e24
It has been well established that the process of neuro-pathic and inflammatory pain not only involvesneuronal pathways that transmit signals from peripheraltissue via the spinal cord to the brain but also immunecells that release and modulate a range of inflammatorymediators. Interestingly, evidence suggests that proin-flammatory cytokines are able to act directly on nocicep-tors in the periphery as well as the dorsal horn of thespinal cord resulting in increased afferent input and sub-sequent peripheral and central sensitization, respectively.The immune system is comprised of two independent,but intricately connected systemsdthe innate immunesystem and the adaptive immune system. The innate im-mune system is continuously active and monitoring forforeign pathogens or injury to which it mounts a gener-alized response. Alternatively, the adaptive immune sys-tem is an acquired and specific immunity that retainsmemory from prior exposures. Emerging evidence hasimplicated both of these systems in the developmentof and maintenance of chronic pain.
Injury and inflammation give rise to the release of avariety of products that can activate sensory compo-nents of the innate immune system, through recogni-tion sites such as the Toll-like receptors (TLRs). Whileclassically expressed on inflammatory cells (macro-phages), it became appreciated that they were also pre-sent on microglia and astrocytes in the neuraxis.Further, these signaling receptors are present on DRGneurons and of course on macrophages that are widelyexpressed in the DRG. Activated macrophages releaseinflammatory mediators, most notably tumor necrosisfactor-a (TNF-a), interleukin-1b (IL-1b), nerve growthfactor (NGF), nitric oxide (NO), and prostanoids aswell as complement proteins that initiate the innate
inflammatory cascade. Neutrophils are the predomi-nant recruited cell type in an acute and early inflamma-tory response causing proinflammatory effects throughthe release of lipoxygenase products, prostaglandins,NO, cytokines, and chemokines as well as possible anti-nociceptive effects through the expression of opioids.The inflammatory mediators released by innate im-mune cells modulate peripheral and central sensitiza-tion that contributes to pain hypersensitivity.
Recent evidence suggests that adaptive immunitymay also play a role in chronic pain; however, thisrole is less clear. The adaptive immune system iscomprised of B and T cells. Although some recentdata suggest that B cells may play a role through anti-body production, the majority of recent literature hasfocused on the involvement of T cells in the produc-tion and resolution of chronic pain. Studies havefound that infiltration of T cells occurs days to weekspostinjury, first at the site of injury and distal end ofthe nerve, then within the DRG, and last within thedorsal horn of the spinal cord. T cells have been foundto both suppress and promote pain via multiplemechanisms and variations in expression. T cellsmay indirectly modulate neuroinflammation via theantiinflammatory reflex. In response to norepineph-rine, b2-adrenergic receptor-expressing T cells releaseacetylcholine, which signals macrophages to switchfrom producing proinflammatory to antiinflammatoryproducts causing dampening of the immune system.T cells present in the periphery also express receptorsfor glutamate, substance P, and CGRP, which regulateT-cell adhesion, migration, and immunologicalphenotype that drives neuroinflammation.
Transition of Acute to Chronic Pain12,25e28
Normally, pain resolves with termination of the acutenoxious stimulus and resolution of tissue injury. Insome cases, pain persists after the resolution of the acuteinflammatory response. There is increased appreciationthat development of persistent pain after an acute injuryor inflammation may reflect a mechanistic transitionfrom an acute to a chronic pain state reflecting long-term changes that sustain and amplify pain signaling.The mechanisms underlying this transition arecomplex and at present poorly understood. However,this process has been demonstrated in a variety ofclinical pain states including after tissue injury, nervedamage, and inflammatory pain. Studies performedusing experimental pain models such as K/BxNserum-transfer arthritis and collagen antibody-inducedarthritis (CAIA) have found that the animals experiencetactile allodynia that persists long after the localized
12 Pain Care Essentials and Innovations

swelling and inflammation has resolved. This processappears to involve discrete pathophysiological changesthat are mediated by a combination of localized inflam-matory mediators that drive peripheral and centralsensitization and neuroimmune mechanisms.
As mentioned earlier, following tissue injury,damaged cells release factors that attract mast cells, mac-rophages, and neutrophils that release proinflammatorymediators and NGF. Proinflammatory molecules acti-vate primary afferent neurons, including A-b fibersand C fibers, that initiate a process resulting inincreased expression of Na channels that are thoughtto play a key role in spontaneous ectopic activity andincreased peripheral sensitization. NGF, a neurotrophicfactor that promotes the growth of damaged neurons, isalso thought to play a role in sensitizing peripheralnociceptors through activation of TrkA receptors.
Meanwhile, similar changes occur in dorsal hornneurons with upregulation of Na and TRPV1 receptorscontributing to a hyperexcitable state. Continuousstimulation also results in prolonged slow depolariza-tion and activation of NMDA receptors that drive“wind-up” and neuroplastic changes that enhancesignal transduction. Activation of intracellular signaltransduction cascades lead to posttranslationalchanges of receptors and ion channels present onprimary sensory and central neurons.
Although peripheral and central sensitization ap-pears necessary for the transition from acute to chronicpain, recent studies suggest that immune mechanismslikely also play a role.
As reviewed above, small afferent input due to localinjury produces ongoing molecule changes. Suchchanges occur at two levels. First, at the terminal (acti-vation of kinases, increased expression of channels andreceptors) leading to sensitization. Second in modelsof chronic inflammation, early inflammation leads toa postinflammation pain state where the animal dis-plays enhanced peripheral afferent and postganglionicsympathetic sprouting in the joint and the DRG. It isinteresting that many of these changes observed inchronic inflammatory states develop a phenotype(sprouting, glia activation) which resembles that of anerve injury. Microglia provide the primary neuroim-mune response and migrate to the central terminalsof afferent peripheral nerves where they undergo acti-vation in response to pain signals. Activated microgliasignal the secretion of cytokines, chemokines, andneurotrophic factors that contribute to the develop-ment and maintenance of central sensitization.Notably, proliferation of microglia has been found inthe ipsilateral dorsal horn after injury.
Recent studies have also identified Toll-like receptor4 (TLR4) as a potential driver of the transition fromacute to chronic pain. Using the K/BxN model ofarthritis, researchers found that TLR4 knockout miceshowed a resolution in pain that corresponded withthe resolution of inflammation. Further work hasdemonstrated that administration of a TLR4 antagonistcan prevent the development of persistent pain state inwild-type mice suggesting that spinal TLR4 signalingplays a significant role in mediating the transition fromacute to chronic pain. There are undoubtably otherregulatory systems that may have a similar impact.
REFERENCES1. Cohen M, Quintner J, van Rysewyk S. Reconsidering the
IASP definition of pain. Pain Rep. 2018;3.2. Raja SN, Meyer RA, Campbell JN. Peripheral mechanisms
of somatic pain. Anesthesiology. 1988;68:571.3. Koltzenburg M. Neural mechanisms of cutaneous nocicep-
tive pain. Clin J Pain. 2000;16(Suppl 3):S131.4. Weidner C, Schmelz M, Schmidt R, Hansson B,
Handwerker HO, Torebjörk HE. Functional attributesdiscriminating mechano-insensitive and mechano-responsive C nociceptors in human skin. J Neurosci.1999;19(22):10184e10190.
5. Sikandar S, Dickenson AH. Visceral pain: the ins and outs,the ups and downs. Curr Opin Support Palliat Care. 2012;6(1):17e26.
6. Willis Jr WD, Westlund KN. The role of the dorsal columnpathway in visceral nociception. Curr Pain Headache Rep.2001;5:20.
7. Ralston HJ. Pain and the primate thalamus. Prog Brain Res.2005;1(49):1e10.
8. Willis WD. The somatosensory system, with emphasis onstructures important for pain. Brian Res Rev. 2007;55:297e313.
9. Central pain pathways: the spinothalamic tract. In:Purves D, Augustine GJ, Fitzpatrick D, et al., eds. Neuro-science. 2nd ed. Sunderland (MA): Sinauer Associates;2001. Available from: https://www.ncbi.nlm.nih.gov/books/NBK10967/.
10. Price DD. Psychological and neural mechanisms of theaffective dimension of pain. Science. 2000;288(5472):1769e1772.
11. Dostrovsky J. Role of thalamus in pain. Prog Brain Res.2000;129:245.
12. Woller S, Eddinger K, Corr M, Yaksh T. An overview ofpathways encoding nociception. Clin Exp Rheumatol.2017;35(Suppl. 107):S40eS46.
13. Brennan T, Zahn P, Pogatzki-Zahn E. Mechanisms of inci-sional pain. Anesthesiol Clin North Am. 2005;23(1).
14. Gangadharan V, Kuner R. Pain hypersensitivity mecha-nisms at a glance. Dis Model Mech. 2013;6(4):889e895.
15. Ahimsadasan N, Kumar A. Neuroanatomy, DorsalRoot Ganglion [Updated October 27, 2018]. In:
CHAPTER 1 Basic Science of Pain 13

StatPearls. Treasure Island (FL): StatPearls Publishing;January 2019.
16. Woolf C. Central sensitization: implications for thediagnosis and treatment of pain. Pain. 2011;152(Suppl.3):S2eS15.
17. Harte S, Harris R, Clauw D. The neurobiology of centralsensitization. J Appl Behav Res. 2018;23:e12137.
18. Woolf C, Mannion R. Neuropathic pain: aetiology,symptoms, mechanisms, and management. Lancet. 1999;353.
19. Costigan M, Scholz J, Woolf CJ. Neuropathic pain: a mal-adaptive response of the nervous system to damage. AnnuRev Neurosci. 2009;32:1e32.
20. Zeilhofer HU. Cell Mol Life Sci. 2005;62:2027.21. Tsuda M, Masuda T, Tozaki-Saitoh H, Inoue K. Microglial
regulation of neuropathic pain. J Pharmacol Sci. 2013;121(2):89e94.
22. Totsch S, Sorge R. Immune system involvement in specificpain conditions. Mol Pain. 2018;13:1e17.
23. Laumet G, Ma J, Robison A, Kumari S, Heijnen C,Kavelaar A. T cells as an emerging target for chronic paintherapy. Front Mol Neurosci. 2019;12:216.
24. Bruno K, Woller S, Miller Y, et al. Targeting toll-like recep-tor -4 (TLR-4)-an emerging therapeutic target for persistentpain states. Pain. 2018:1e8.
25. Feizerfan A, Sheh G. Transition from acute to chronic pain.Continuing education in anaesthesia. Criti Care Pain.2015;15:98e102.
26. Vallejo R, Tilley D, Vogel L, Benyamin R. The role of gliaand immune system in the development and maintenanceof neuropathic pain. Pain Pract. 2010;10:167e184.
27. Chapman R, Vierck C. The transition of acute postopera-tive to chronic pain: an integrative overview of researchon mechanisms. J Pain. 2017;18:359e1e359e38.
28. Peng J, Gu N, Zhou L, et al. Microglia and monocytes syn-ergistically promote the transition from acute to chronicpain after nerve injury. Nat Commun. 2016;7.
14 Pain Care Essentials and Innovations