
Changes in smoking status among substance abusers: baseline characteristics and abstinence from...
11
Changes in smoking status among substance abusers: baseline characteristics and abstinence from alcohol and drugs at 12-month follow-up Carolynn S. Kohn a,b, *, Janice Y. Tsoh a , Constance M. Weisner a,b a University of California San Francisco, 401 Parnassus Avenue, San Francisco, CA 94143-0984, USA b Division of Research at Kaiser Permanente, 2000 Broadway, 3rd Floor, Oakland, CA 94612-2304, USA Received 9 April 2002; received in revised form 19 July 2002; accepted 6 August 2002 Abstract The impact of change in smoking status on 12-month substance abuse (SA) treatment outcomes was examined among an HMO population seeking SA treatment. Of the 749 participants who entered the study at baseline, 649 (86.9%) were retained at the 12- month follow-up. At treatment entry, 395 participants were smokers and 254 were nonsmokers. At 12-month follow-up, 13% of the 395 baseline smokers reported quitting smoking and 12% of the 254 baseline nonsmokers reported starting/relapsing to smoking. Those who quit smoking were less likely to be diagnosed as alcohol dependent compared to those that remained smokers. Those who started/resumed smoking were more likely to be diagnosed as both alcohol and drug dependent at treatment entry compared to all other groups. Total days abstinent from alcohol and illicit drugs was greatest for individuals who quit smoking (adjusted M/ 310.6) or who were nonsmokers (adjusted M/294.7) and lowest for those who started/resumed smoking (adjusted M/246.6) or remained smokers (adjusted M/258.2), even after controlling for demographic (i.e. age, income), psychosocial (ASI psychiatric severity), and other treatment characteristics (length of treatment stay, prescribed bupropion) that were associated with days abstinent at 12 months. Self-initiated smoking cessation does not appear to be detrimental to SA treatment outcomes, and may be beneficial. Starting/resuming smoking after entering SA treatment may be a clinical marker for individuals at greater risk of relapse. Future studies may want to measure the smoking status of all participants at all time points in order to include this higher-risk group of substance using smokers. # 2002 Elsevier Science Ireland Ltd. All rights reserved. Keywords: Smoking; Alcohol; Drugs; Treatment outcome; Managed care; Tobacco 1. Introduction Nearly three times as many individuals with alcohol and drug problems smoke cigarettes compared to the general population, and smoking-related diseases are a leading cause of premature death among substance users (Hurt et al., 1996). Despite these statistics, few substance abuse (SA) treatment programs or providers offer structured smoking cessation services (Burling et al., 1997; Sees and Clark, 1993), even though studies suggest a substantial proportion of clients in SA treatment state a desire to quit (Ellingstad et al., 1999; Irving et al., 1994) and attempt to quit smoking and/or participate in smoking treatment during or after SA treatment (Bern- stein and Stoduto, 1999; Bobo et al., 1996b; Burling et al., 2001). Continued smoking has been linked to worse SA treatment outcomes (Frosch et al., 2000) while there is some evidence that attempting to quit smoking is not harmful to SA treatment outcomes (Lemon et al., in press), or may improve SA treatment outcomes (Bobo et al., 1998; Hughes, 1993; Shoptaw et al., 1996) and is a feasible goal (Burling et al., 2001). Barriers for imple- menting formal, standardized smoking cessation inter- ventions in SA treatment programs include beliefs that cigarette smoking is more of a ‘habit’ compared to other addictions (Karan, 1993; Sees and Clark, 1993) and a lack of information about patient populations in SA * Corresponding author. Tel.: /1-510-891-3583; fax: /1-510-891- 3606 E-mail addresses: [email protected], [email protected] (C.S. Kohn). Drug and Alcohol Dependence 69 (2003) 61 /71 www.elsevier.com/locate/drugalcdep 03765-8716/02/$ - see front matter # 2002 Elsevier Science Ireland Ltd. All rights reserved. PII:S0376-8716(02)00256-9
Transcript of Changes in smoking status among substance abusers: baseline characteristics and abstinence from...

Changes in smoking status among substance abusers: baselinecharacteristics and abstinence from alcohol and drugs at 12-month
follow-up
Carolynn S. Kohn a,b,*, Janice Y. Tsoh a, Constance M. Weisner a,b
a University of California San Francisco, 401 Parnassus Avenue, San Francisco, CA 94143-0984, USAb Division of Research at Kaiser Permanente, 2000 Broadway, 3rd Floor, Oakland, CA 94612-2304, USA
Received 9 April 2002; received in revised form 19 July 2002; accepted 6 August 2002
Abstract
The impact of change in smoking status on 12-month substance abuse (SA) treatment outcomes was examined among an HMO
population seeking SA treatment. Of the 749 participants who entered the study at baseline, 649 (86.9%) were retained at the 12-
month follow-up. At treatment entry, 395 participants were smokers and 254 were nonsmokers. At 12-month follow-up, 13% of the
395 baseline smokers reported quitting smoking and 12% of the 254 baseline nonsmokers reported starting/relapsing to smoking.
Those who quit smoking were less likely to be diagnosed as alcohol dependent compared to those that remained smokers. Those
who started/resumed smoking were more likely to be diagnosed as both alcohol and drug dependent at treatment entry compared to
all other groups. Total days abstinent from alcohol and illicit drugs was greatest for individuals who quit smoking (adjusted M�/
310.6) or who were nonsmokers (adjusted M�/294.7) and lowest for those who started/resumed smoking (adjusted M�/246.6) or
remained smokers (adjusted M�/258.2), even after controlling for demographic (i.e. age, income), psychosocial (ASI psychiatric
severity), and other treatment characteristics (length of treatment stay, prescribed bupropion) that were associated with days
abstinent at 12 months. Self-initiated smoking cessation does not appear to be detrimental to SA treatment outcomes, and may be
beneficial. Starting/resuming smoking after entering SA treatment may be a clinical marker for individuals at greater risk of relapse.
Future studies may want to measure the smoking status of all participants at all time points in order to include this higher-risk group
of substance using smokers.
# 2002 Elsevier Science Ireland Ltd. All rights reserved.
Keywords: Smoking; Alcohol; Drugs; Treatment outcome; Managed care; Tobacco
1. Introduction
Nearly three times as many individuals with alcohol
and drug problems smoke cigarettes compared to the
general population, and smoking-related diseases are a
leading cause of premature death among substance users
(Hurt et al., 1996). Despite these statistics, few substance
abuse (SA) treatment programs or providers offer
structured smoking cessation services (Burling et al.,
1997; Sees and Clark, 1993), even though studies suggest
a substantial proportion of clients in SA treatment state
a desire to quit (Ellingstad et al., 1999; Irving et al.,
1994) and attempt to quit smoking and/or participate in
smoking treatment during or after SA treatment (Bern-
stein and Stoduto, 1999; Bobo et al., 1996b; Burling et
al., 2001). Continued smoking has been linked to worse
SA treatment outcomes (Frosch et al., 2000) while there
is some evidence that attempting to quit smoking is not
harmful to SA treatment outcomes (Lemon et al., in
press), or may improve SA treatment outcomes (Bobo et
al., 1998; Hughes, 1993; Shoptaw et al., 1996) and is a
feasible goal (Burling et al., 2001). Barriers for imple-
menting formal, standardized smoking cessation inter-
ventions in SA treatment programs include beliefs that
cigarette smoking is more of a ‘habit’ compared to other
addictions (Karan, 1993; Sees and Clark, 1993) and a
lack of information about patient populations in SA
* Corresponding author. Tel.: �/1-510-891-3583; fax: �/1-510-891-
3606
E-mail addresses: [email protected],
[email protected] (C.S. Kohn).
Drug and Alcohol Dependence 69 (2003) 61�/71
www.elsevier.com/locate/drugalcdep
03765-8716/02/$ - see front matter # 2002 Elsevier Science Ireland Ltd. All rights reserved.
PII: S 0 3 7 6 - 8 7 1 6 ( 0 2 ) 0 0 2 5 6 - 9

programs who attempt to quit smoking (Ellingstad et
al., 1999), particularly among non-community/non-re-
sidential treatment populations. In addition, limited
information exists regarding the impact of change insmoking status on SA treatment outcomes.
Currently, conflicting data exist regarding whether
smoking status is associated with worse (Toneatto et al.,
1995) or better (e.g. Bobo et al., 1998; Frosch et al.,
2000) SA treatment outcomes and may have to do with
study limitations. With few exceptions (Bobo et al.,
1998; Burling et al., 2001), previous studies have
examined only alcohol (Bobo et al., 1996a; Toneatto etal., 1995) or only drug outcomes (Frosch et al., 2000;
Shoptaw et al., 1996), but rarely both; have had limited
follow-up periods, (Bobo et al., 1996a; Frosch et al.,
2000); significant attrition (Toneatto et al., 1995) and
small samples (Shoptaw et al., 1996); and have almost
exclusively examined community or residential treat-
ment samples (Burling et al., 2001; Frosch et al., 2000).
To the best of our knowledge, no naturalisticobservational data published to date document the
change in smoking status over time among clients in
SA treatment settings. A 3-year naturalistic observation
study of 254 polydrug users who were not in SA
treatment found that a significant subsample of smokers
reported a change in smoking status despite an overall
stability in the prevalence of smoking within this sample
(McCarthy et al., 2001). This study suggests thatsubstance abusers do change their smoking statuses
over time, with shifts to both nonsmoker as well as
smoker statuses. However, the goals of this study did
not include providing descriptive characteristics of those
who change their smoking statuses, nor was it con-
ducted within the context of SA treatment, so treatment
outcomes were not reported.
Identifying characteristics of individuals whose smok-ing status changes during treatment and examining the
impact that this may have on SA outcomes are
important steps towards developing smoking cessation
interventions for this population (Ellingstad et al.,
1999). Characteristics that may be associated with
change in smoking status include demographic charac-
teristics (e.g. gender, ethnicity, income), smoking char-
acteristics (e.g. cigarettes smoked per day), SAcharacteristics (type of dependence or abuse diagnosis),
psychosocial characteristics (e.g. depression, anxiety,
problems with family or the legal system), and treatment
characteristics (e.g. length of stay (LOS) in treatment,
adjunct/self-help treatment, smoking cessation aids).
1.1. Current study
In this study, we examined demographic, smoking,substance use, psychosocial, and treatment-related char-
acteristics of individuals in SA treatment in a private
managed-care setting who at 12 months after SA
treatment admission: (a) remained smokers; (b) stopped
smoking; (c) resumed or started smoking after a period
of abstinence from smoking; or (d) remained nonsmo-
kers. We also examined the relationship of changes insmoking status to SA treatment outcomes at 12 months
(i.e. total days of abstinence). This study addresses some
of the limitations of past research studies by using a
large sample (n�/649), minimizing attrition (86.9% at
12-month follow-up), including measures of both alco-
hol and drug use, and examining how change in
smoking status is related to longer-term abstinence
from alcohol and/or drugs. Additionally, our samplewas drawn from a large, heterogeneous managed-care
SA treatment program; this program is typical of many
managed care programs in which a large segment of our
population receives treatment in that, while smoking is
not encouraged, there are few structured, formal,
standardized treatment inventions in place to assist
with smoking cessation.
2. Method
The study site was Kaiser Permanente’s Chemical
Dependency Recovery Program (CDRP) in Sacra-
mento, CA, where SA treatment services are provided
within the same health plan. The CDRP is an outpatient
treatment program, in which the first 8 weeks of
treatment are considered the ‘rehabilitation phase’ andthe following 10 months are considered the ‘aftercare
phase.’ The CDRP has both a day and an evening
program to allow flexibility for working patients. The
CDRP allows smoking in designated outside areas only.
Smoking is not allowed inside the buildings or during
treatment sessions. While smoking was not encouraged,
there were few structured, formal, standardized treat-
ment interventions in place to assist with smokingcessation. The issues of the risks of smoking were
more generally addressed in an educational group
format within the CDRP as part of a Medical Education
series. Patients had free access to nicotine replacement
products (i.e. nicotine patches and gum) and to a low
cost smoking cessation program provided off-site.
This study was part of a primary study in which
participants were randomized to receive their primaryhealth care from physicians within the CDRP or off-site
in the primary care clinics (Weisner et al., 2001).
Analyses to determine if this randomization procedure
may have had an effect on participants’ smoking
behaviors found no group differences.
2.1. Participants
Participants were 747 men and women aged 18 and
over who were admitted to the program between April
1997 and December 1998 and who met DSM-IV criteria
C.S. Kohn et al. / Drug and Alcohol Dependence 69 (2003) 61�/7162

(American Psychiatric Association, 1994) for current
drug (13 substance types) or alcohol abuse or depen-
dence at the time of intake as assessed by trained
research staff conducting the Diagnostic InterviewSchedule (DIS) for Psychoactive Substance Dependence
(Robins et al., 1989). For each substance, the ques-
tionnaire determines whether the DSM-IV diagnostic
criteria for abuse or dependence was present or absent
during the previous 30 days. Substances of dependence
for the sample as a whole, in order by most to least
prevalent, were alcohol (58.9%), stimulants (24.5%),
marijuana (16.9%), narcotic analgesics (8.9%), cocaine(8.3%), tranquilizers (3.7%), heroin (1.1%), and PCP
(0.3%). Substances of abuse (without dependence) for
the sample as a whole, in order by most to least
prevalent, were alcohol (3.5%), marijuana (2.8%), sti-
mulants (2.6%), narcotic analgesics (0.9%), cocaine
(0.8%), tranquilizers (0.3%), heroin (0%), and PCP (0%).
2.2. Procedure and self-report data validity
Informed consents were obtained at baseline when the
interviews were conducted. Baseline interviews lasted
approximately 1 hour and participants did not receive
monetary reimbursement at that time. Follow-up tele-
phone interviews assessing treatment outcome took
place 12 months after intake and were conducted by
telephone interviewers located at the Division of Re-
search in Oakland, CA who were blind to participantclassification and who were not employed by the CDRP
in Sacramento. Telephone interviews lasted about 30
minute and participants were mailed a $30 reimburse-
ment check for completing the phone interview. A
validity test of self-report data using urinalysis was
conducted on-site at the CDRP at the 6-month follow-
up on all 361 randomly selected participants (55.6% of
the entire sample), each of whom received a reimburse-ment of $20 after completion of the urinalysis. The
urinalysis (using the Hitachi microparticle immuno
assay with gas chromatography mass spectrometry,
thin layer chromatography, and high pressure liquid
chromatography confirmation) tested for alcohol, bar-
biturates, benzodiazepines, cocaine, cannabis/THC, opi-
ates, phencyclidine, and amphetamines, and
comparisons yielded rates of reporting no use but testingpositive for a substance of 2.5% for alcohol, and
between 0.9% (barbiturates) and 5.8% (marijuana) for
other substances. The results for marijuana are con-
servative; it was the most commonly reported, and the
test detects tetrahydrocannabinol levels as low as 40 ng/
ml. Chronically using individuals can test positive for 30
days after use, but the self-report question asked before
the test measures use for the past 3 days. Participantswere informed that information obtained during the in-
person and telephone interviews as well as the urinalyses
results are used for research purposes only and are not
reported to the CDRP. The health plan’s automated
databases, generally an accurate measure of clinical
activities, were used to obtain information about
clinician-generated diagnoses of anxiety and depressivedisorders, LOS in treatment, and prescriptions for
nicotine replacement therapies (i.e. nicotine patch or
gum) or bupropion, and attendance to smoking cessa-
tion treatment (Selby, 1997).
2.3. Measures
2.3.1. Smoking status classification
Smoking status was determined by response to the
question ‘Are you currently smoking cigarettes?’ asked
at Baseline and at 12-month follow-up. Participants
were classified into one of four groups: SMOKERS,QUITTERS, STARTERS/RESUMERS, and NON-
SMOKERS. Participants who answered ‘yes’ at baseline
and follow-up were classified as SMOKERS (n�/342),
those who answered ‘yes’ at baseline and ‘no’ at follow-
up were classified as QUITTERS (n�/53), those who
answered ‘no’ at baseline and ‘yes’ at follow-up were
classified as STARTERS/RESUMERS (n�/30), and
those who answered ‘no’ at baseline and follow-upwere classified as current NONSMOKERS (n�/224).
Although nicotine dependence and biochemical verifica-
tion of smoking status were not assessed, self-report of
cigarette smoking has been shown to be a valid indicator
of actual use (Velicer et al., 1992).
2.3.2. Cigarette use and demographic characteristics
At baseline, participants were asked, ‘Have you ever
smoked cigarettes regularly for at least one year, meaning
at least 5 cigarettes per week, almost every week?’ and
‘How many years did you smoke before you stopped?’ At
the 12-month follow-up, they were asked how many
cigarettes per day on average they smoked in the
previous 6-month period. Age, gender, race, income,education, and marital status were obtained from the
baseline questionnaire.
2.3.3. Substance use and psychosocial characteristics at
treatment entry
The Addiction Severity Index (ASI, McLellan et al.,1992a) was used to assess severity of substance use and
psychosocial problems at admission by asking about the
number, frequency, and duration of problem symptoms
in the past 30 days. The ASI provides separate severity
composite scores from 0 to 1.0 for each of the following
seven areas, with higher scores indicative of greater
problem severity: alcohol use, drug use, employment,
medical, psychiatric, family or social, and legal pro-blems. We report means and standard deviations for all
baseline ASI composite scores (i.e. scores obtained
during baseline/treatment entry interview).
C.S. Kohn et al. / Drug and Alcohol Dependence 69 (2003) 61�/71 63

The Diagnostic Interview Schedule for Psychoactive
Substance Dependence (American Psychiatric Associa-
tion, 1994) was administered by trained research staff as
part of the baseline interview in order to obtain DSM-IV diagnoses for current (i.e. symptoms occurring within
the past 30 days) alcohol and other drug (13 substance
types) abuse and dependence diagnoses. Because the
percentage of participants that received a dependence
diagnosis for any one specific drug category was
relatively low, we examined participants based on the
following diagnoses: alcohol dependent only, drug
dependent only, both alcohol and drug dependent, andalcohol and/or drug abuse without dependence.
Baseline subscales from the shortened version of the
Symptom Checklist-90 (Alvir et al., 1988) were used as
continuous measures of anxiety and depressive symp-
toms. Subscales scores range from 0 (no symptoms) to 4
(extreme symptoms).
DSM-IV depressive and anxiety disorder diagnoses
made during the year before treatment entry (i.e. bylicensed mental health and/or primary care providers)
were identified using the health plan’s automated
diagnostic databases (Selby, 1997). These diagnoses
were based on physician and clinician assessment of
the patient. While a limitation of this method is that
structured clinical interviews and reliability checks of
diagnoses between raters are not used, a strength of this
method lies in its ‘real world’ value, in which clinicians’diagnoses are used in the manner in which they are
reported in patients’ medical charts.
2.3.4. Treatment characteristics: LOS, adjunct/self-help
SA treatment, smoking cessation aids
The health plan’s automated appointment registration
database was used to measure LOS in treatment by
calculating participants’ number of days in treatment
before being discharged or dropping out. Informationabout attendance to Alcoholics Anonymous (AA) and
Narcotics Anonymous (NA) meetings was measured
using the Treatment Services Review (TSR; McLellan et
al., 1992b). The health plan’s databases were used to
identify variables (i.e. ‘smoking cessation aids’) from
treatment entry through 12-month follow-up that might
influence the rate of smoking cessation. Smoking cessa-
tion aids included in this study were participation insmoking cessation psychoeducational groups, prescrip-
tions for nicotine replacement therapies (i.e. the patch or
gum), and prescriptions for bupropion (Jarvis and
Sutherland, 1998). We were unable to ascertain whether
bupropion was being prescribed primarily as an anti-
depressant or a smoking cessation aid. Only one person
participated in a smoking cessation group and five (2
SMOKERS and 3 QUITTERS) were prescribed nico-tine patches, likely an accurate assessment since parti-
cipants receive them free through their health plan but
must pay for them out-of-pocket if they purchase them
elsewhere. Because other smoking cessation aids were
used infrequently, only bupropion was included in the
analyses.
2.3.5. Treatment outcome: abstinence rates at 12 months
Longest period of abstinence since treatment admis-
sion was obtained from 12-month follow-up interviews
by asking participants to report in number of days theirlongest period of abstinence since beginning treatment.
Percent of individuals in each group that reported
complete abstinence during the past 30 days was also
obtained from 12-month follow-up interviews. Also, as
mentioned in Section 2.2, just over half of the partici-
pants were randomly tested using urinalysis that resulted
in a fairly high rate of corroboration between self-report
use and urinalysis results, and participants were in-formed that information provided in the context of this
study was confidential and not made available to the
CDRP or individual treatment providers.
2.4. Data analyses
Baseline demographic characteristics, psychosocial
characteristics (i.e. SCL-90 anxiety and depression
scales, ASI psychiatric and family problem severity
composite scores, and clinician generated diagnoses of
depressive and anxiety disorders), substance use char-
acteristics (i.e. age at first use, DSM-IV alcohol anddrug dependence diagnoses and ASI alcohol and drug
severity composite scores), and treatment characteristics
(i.e. LOS in treatment, adjunct/self-help SA treatment,
and smoking cessation aids) were compared across the
four groups: SMOKERS, QUITTERS, STARTERS/
RESUMERS, and NONSMOKERS using one-way
Analyses of variance (ANOVAs) for continuous vari-
ables and chi-square tests for categorical variables.Analysis of covariance (ANCOVA) was used to examine
whether number of days abstinent at 12 months differed
between the groups. Variables that were significantly
correlated with number of days abstinent at 12 months
for the whole sample were used as preliminary covari-
ates, and included age, income, ASI psychiatric severity
composite score, LOS treatment and being prescribed
bupropion. An initial ANCOVA was conducted bysimultaneously entering these covariates along with
smoking group status as potential contributors to the
outcome variable of total days abstinent at 12-month
follow-up. The initial ANCOVA was significant,
although age, income, psychiatric severity, and being
prescribed bupropion did not contribute significantly to
the model, while LOS and smoking group did contribute
significantly. Therefore, in order to present a moreparsimonious model, the final ANCOVA included only
LOS and smoking group status, which were again
entered simultaneously.
C.S. Kohn et al. / Drug and Alcohol Dependence 69 (2003) 61�/7164

3. Results
A total of 649 participants (86.9%) were retained at
12-month follow-up. Demographic differences betweenparticipants who were retained at follow-up versus those
who were not examined by one-way ANOVAs and Chi-
Square analyses and revealed that participants who were
retained at follow-up were somewhat older (M�/37.9
years, SD�/10.4) compared to those not retained at
follow-up (M�/35.6 years, SD�/9.9; F (1, 747)�/4.36,
P B/0.05). Also, participants with some post high school
education were more likely than those with none to beretained at follow-up (89.3% versus 83.9%, X2�/4.64,
P B/0.05) and participants prescribed bupropion were
more likely than those not prescribed bupropion to be
retained at follow-up (96.1% versus 85.4%, X2�/8.77,
P B/0.01). No differences were found for gender,
ethnicity, income, marital status, smoking status (i.e.
smoking at baseline versus not), diagnoses of depression
or anxiety in the past year, diagnoses of alcohol-onlydependence, drug-only dependence, or polysubstance
dependence at admission, ASI drug scores, ASI alcohol
scores, number of cigarettes smoked per day, and
depressive and anxiety symptoms at baseline. In general,
this HMO’s membership is insured primarily through
employment; income and employment levels are higher,
and addiction severity is somewhat lower than in public
populations (Weisner et al., 2000).
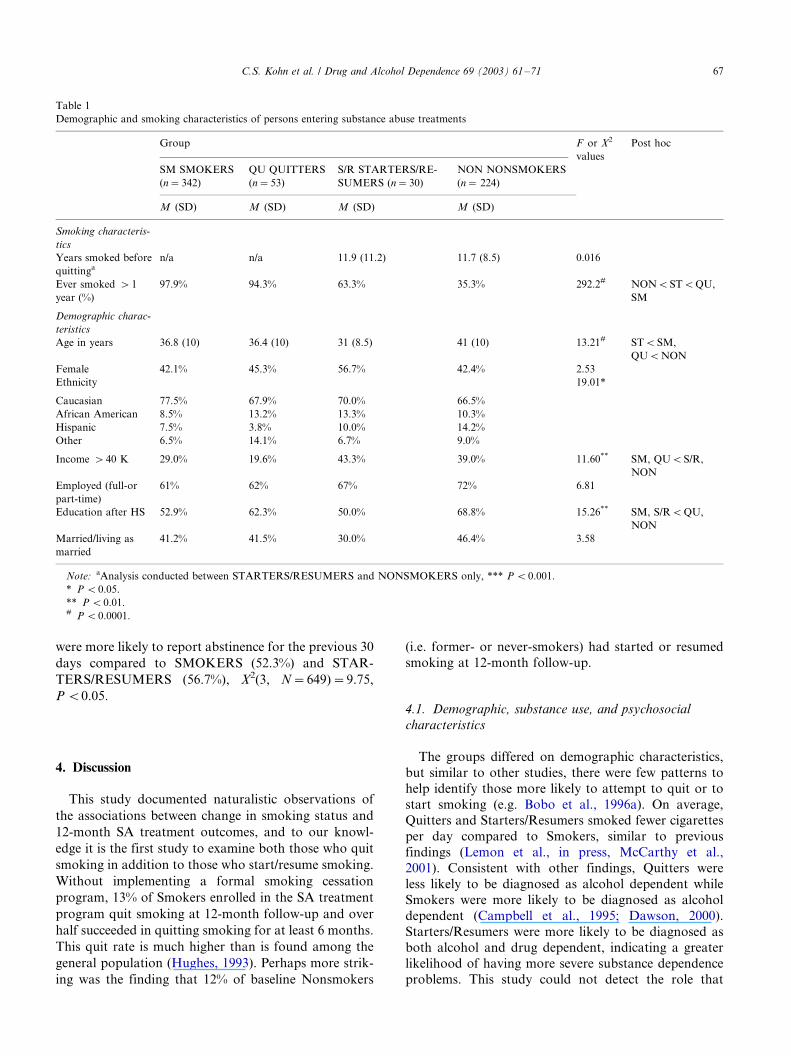
3.1. Demographic and smoking characteristics (Table 1)
Changes in smoking behaviors observed at 12-month
follow-up resulted in classifying 14% of the 395 baseline
smokers as QUITTERS and 12% of the 254 baseline
nonsmokers as STARTERS/RESUMERS. Thus, the
sample consisted of 342 (52.7%) SMOKERS, 53 (8.2%)
QUITTERS, 30 (4.6%) STARTERS/RESUMERS, and224 (34.5%) NONSMOKERS. Over half of the QUIT-
TERS (56.6%) reported having quit smoking for at least
6 months. All 30 STARTERS/RESUMERS reported
smoking during the prior 6 months. However, 36.7%
appeared to be ‘‘starters’’ as they reported never
smoking regularly for at least 1 year whereas the other
63.3% appeared to be ‘‘resumers’’ as they reported
having smoked regularly for at least 1 year and reportedsmoking an average of 11.9 years before quitting. One-
way ANOVAs revealed no differences between ‘‘star-
ters’’ and ‘‘resumers’’ on ASI composite variables and
SCL-90 measures of depression and anxiety, all P ’s�/
0.05; therefore they were combined in the STARTERS/
RESUMERS group. Of the NONSMOKERS, 35.3%
were ‘‘former smokers’’ because they reported having
previously smoked for at least 1 year and had smoked anaverage of 11.6 years prior to quitting; the remaining
64.7% were ‘‘never smokers.’’ One-way ANOVAs re-
vealed no differences between ‘‘never smokers’’ and
‘‘former smokers’’ on ASI composite variables and
SCL-90 measures of depression and anxiety, all P ’s�/
0.05; therefore they remained in the combined in the
NONSMOKERS group.At baseline, QUITTERS reported smoking fewer
cigarettes per day (M�/10.3, SD�/11.1) compared to
SMOKERS (M�/16.7, SD�/11.6), F (1, 392)�/14.22,
P B/0.0001. At follow-up, STARTERS/RESUMERS
reporting smoking fewer cigarettes (M�/9.4, SD�/8.3)
compared to SMOKERS (M�/16.9, SD�/9.3), F (1,
392)�/18.23, P B/0.0001. The groups differed to varying
degrees on the demographic variables of age, ethnicity,income, and education. NONSMOKERS were older
(M�/40.9 years, SD�/10.3) and STARTERS/RESU-
MERS were younger (M�/31.1 years, SD�/8.6) com-
pared to all other groups, F (1, 646)�/13.21, P B/0.0001.
Groups differed in their proportion of Caucasians, X2(3,
N�/649)�/8.29, P B/0.05, and Hispanics, X2(3, N�/
649)�/10.54, P B/0.05. Groups differed in their income
level, such that NONSMOKERS (39.0%) and STAR-TERS/RESUMERS (43.3%) were more likely to report
a yearly income level above $40 000 compared to
SMOKERS (29.0%) and QUITTERS (19.6%), X2(3,
N�/649)�/11.60, P B/0.01. Lastly, groups differed in
their education level such that NONSMOKERS (68.8%)
and QUITTERS (62.3%) were more likely than SMO-
KERS (52.9%) and STARTERS (50.0%) to report
having obtained education beyond a high schooldiploma or diploma equivalent, X2(3, N�/649)�/
15.26, P B/0.01. No group differences were found for
gender, employment status, or marital status. After
examining all demographic and smoking variables,
only age, r�/0.10, P B/0.01, and income, t(632)�/
�/2.16, P B/0.05, were significantly associated with the
outcome variable of total days of abstinence. Thus,
these two variables were included as covariates in theinitial ANCOVA analysis described below.
3.2. Substance use and psychosocial characteristics at
treatment entry (Table 2)
NONSMOKERS reported being older at time of first
drug use compared to all other groups, X2(3, N�/
649)�/13.10, P B/0.001. At baseline, there were no
differences between the groups for ASI alcohol scores;although NONSMOKERS had lower ASI drug scores
compared to the other groups, F (1, 648)�/3.42, P B/
0.05. QUITTERS and STARTERS/RESUMERS were
less likely to be diagnosed as Alcohol Dependent-only
compared to the other three groups, X2(3, N�/649)�/
11.34, P B/0.01. STARTERS/RESUMERS were more
likely to be diagnosed as both Alcohol and Drug
Dependent compared to the other three groups, X2(3,N�/649)�/14.57, P B/0.001. However, none of these
substance use variables were significantly associated
with the outcome measure of total days abstinent at
C.S. Kohn et al. / Drug and Alcohol Dependence 69 (2003) 61�/71 65

12-month follow-up (all P ’s�/0.05) and thus they were
not included as covariates in the ANCOVA analysis
described below.
STARTERS/RESUMERS appeared to have thepoorest overall baseline psychosocial functioning com-
pared to SMOKERS and NONSMOKERS, including
higher SCL-90 depression scores, F (1, 648)�/6.64, P B/
0.001, higher SCL-90 anxiety scores, F (1, 648)�/7.59,
P B/0.001, higher ASI psychiatric severity composite
scores, F (1, 648)�/3.71, P B/0.05, and a greater like-
lihood of being diagnosed with a depressive disorder
during the year prior to treatment entry, X2(3, N�/
649)�/9.45, P B/0.05. QUITTERS also reported rela-
tively higher SCL-90 depression scores compared to
NONSMOKERS, F (1, 648)�/6.64, P B/0.001, and
higher anxiety scores compared to both SMOKERS
and NONSMOKERS, F (1, 648)�/7.59, P B/0.001. The
groups did not differ on the ASI family or social,
employment, legal, or medical problem severity scores,
or on the likelihood of having received an anxietydisorder diagnosis during the year prior to treatment
entry, all P ’s�/0.05. Only ASI psychiatric severity at
treatment entry was significantly associated with the
outcome measure of total days abstinent at 12-month
follow-up, r�/�/0.08, P B/0.05, and therefore this vari-
able was included as a covariate in the ANCOVA
analysis described below.
3.3. Treatment characteristics: LOS, adjunct/self-help
SA treatment, smoking cessation aids
The four groups were similar in their LOS in SA
treatment, M�/80.9 days, SD�/104.6, Range�/0�/428
days, for all participants. At 12-month follow-up, no
group differences were found for percent of participants
who attended the CDRP during the previous 6 months,
or for percent who attend AA or NA meetings duringthe previous 30 days; therefore all percentages and
means reported are for the whole sample. Twenty-seven
percent of participants reported they had attended the
CDRP during the previous 6 months and 62.9%
reported they had attended an AA or NA meeting
during the previous 30 days, M�/5.8 days of atten-
dance, SD�/7.7, Range�/0�/30 days. Because other
smoking cessation aids were used infrequently (i.e.nicotine replacement therapies), only bupropion was
examined for its potential role as a smoking cessation
aid. QUITTERS (35.8%) were more likely to have been
prescribed bupropion compared to SMOKERS (14.0%),
STARTERS/RESUMERS (16.7%), and NONSMO-
KERS (11.6%), X2(3, N�/649)�/20.29, P B/0.001.
However, days of bupropion use, milligrams prescribed,
and percent prescribed bupropion who were diagnosedwith Depressive Disorder did not differ by groups.
Overall participants used bupropion (n�/98) an average
of 3.5 months, SD�/3.6, Range�/0�/11.5 months, and
were prescribed an average of 210.7 mg, SD�/87.2,
Range�/75�/600 mg. Of those already diagnosed with a
Depressive Disorder (n�/192), 19% were prescribed
bupropion. Only being prescribed bupropion was sig-nificantly associated with the outcome measure of total
days abstinent at 12-month follow-up, t (647)�/�/2.03,
P B/0.05, and therefore this variable was included as a
covariate in the ANCOVA analysis described below.
3.4. Treatment outcome: abstinence at 12 months (Table
3)
Although the groups differed on a number of vari-ables (Tables 1 and 2), most were not used as covariates
because they were not significantly correlated with the
treatment outcome variable of days abstinent at 12-
month follow-up (all P ’s�/0.05), with the exception of
age, income, ASI psychiatric severity composite score,
and being prescribed bupropion. In addition to these
covariates, LOS in SA treatment was included as a
covariate because it is consistently highly correlated withabstinence outcome (e.g. Goldstein et al., 2000), as was
the case in this study, r�/0.42, P B/0.0001. Initially
entering LOS, age, income, ASI psychiatric severity, and
being prescribed bupropion as covariates allowed for a
more accurate examination of the variance in abstinence
rates accounted for by changes in smoking status.
An initial ANCOVA was conducted with age, income,
psychiatric severity, LOS and prescribed bupropion ascovariates along with smoking group as potential
contributors to the outcome variable of total days
abstinent at 12-month follow-up. Although the overall
ANCOVA was significant, F (3, 625)�/3.75, P B/0.05,
age, income, ASI psychiatric severity, and being pre-
scribed bupropion did not significantly contribute to the
model, F (3, 644)�/0.173, F (3, 644)�/0.752, F (3, 644)�/
2.42, F (3, 644)�/0.306, respectively, all P ’s�/0.05, whileLOS, F (1, 634)�/120.55, P B/0.0001 and smoking
group, F (3, 634)�/3.75, P B/0.05 did significantly con-
tribute to it. Therefore, in order to obtain a more
parsimonious model, we re-ran the model to include
only LOS as the covariate and smoking group as the
independent variable. The final overall ANCOVA was
significant, F (3, 644)�/4.03, P B/0.01, and total days
abstinent differed significantly by smoking group, F (3,644)�/4.03, P B/0.01, above and beyond the variance
contributed by LOS, F (3, 644)�/134.3, P B/0.0001. The
adjusted and unadjusted marginal means (Table 3) show
that at 12 months QUITTERS and NONSMOKERS
had the greatest number of days abstinent and SMO-
KERS and STARTERS/RESUMERS had the fewest
days abstinent. This finding also corresponds with the
group differences in the percent of participants atfollow-up who reported being abstinent from alcohol
and (non-nicotine) drugs at 12 months. At follow-up,
QUITTERS (69.8%) and NONSMOKERS (62.9%)
C.S. Kohn et al. / Drug and Alcohol Dependence 69 (2003) 61�/7166
were more likely to report abstinence for the previous 30
days compared to SMOKERS (52.3%) and STAR-
TERS/RESUMERS (56.7%), X2(3, N�/649)�/9.75,
P B/0.05.
4. Discussion
This study documented naturalistic observations of
the associations between change in smoking status and
12-month SA treatment outcomes, and to our knowl-
edge it is the first study to examine both those who quit
smoking in addition to those who start/resume smoking.
Without implementing a formal smoking cessation
program, 13% of Smokers enrolled in the SA treatment
program quit smoking at 12-month follow-up and over
half succeeded in quitting smoking for at least 6 months.
This quit rate is much higher than is found among the
general population (Hughes, 1993). Perhaps more strik-
ing was the finding that 12% of baseline Nonsmokers
(i.e. former- or never-smokers) had started or resumed
smoking at 12-month follow-up.
4.1. Demographic, substance use, and psychosocial
characteristics
The groups differed on demographic characteristics,
but similar to other studies, there were few patterns to
help identify those more likely to attempt to quit or to
start smoking (e.g. Bobo et al., 1996a). On average,Quitters and Starters/Resumers smoked fewer cigarettes
per day compared to Smokers, similar to previous
findings (Lemon et al., in press, McCarthy et al.,
2001). Consistent with other findings, Quitters were
less likely to be diagnosed as alcohol dependent while
Smokers were more likely to be diagnosed as alcohol
dependent (Campbell et al., 1995; Dawson, 2000).
Starters/Resumers were more likely to be diagnosed asboth alcohol and drug dependent, indicating a greater
likelihood of having more severe substance dependence
problems. This study could not detect the role that
Table 1
Demographic and smoking characteristics of persons entering substance abuse treatments
Group F or X2
values
Post hoc
SM SMOKERS
(n�342)
QU QUITTERS
(n�53)
S/R STARTERS/RE-
SUMERS (n�30)
NON NONSMOKERS
(n� 224)
M (SD) M (SD) M (SD) M (SD)
Smoking characteris-
tics
Years smoked before
quittinga
n/a n/a 11.9 (11.2) 11.7 (8.5) 0.016
Ever smoked �1
year (%)
97.9% 94.3% 63.3% 35.3% 292.2# NONBSTBQU,
SM
Demographic charac-
teristics
Age in years 36.8 (10) 36.4 (10) 31 (8.5) 41 (10) 13.21# STBSM,
QUBNON
Female 42.1% 45.3% 56.7% 42.4% 2.53
Ethnicity 19.01*
Caucasian 77.5% 67.9% 70.0% 66.5%
African American 8.5% 13.2% 13.3% 10.3%
Hispanic 7.5% 3.8% 10.0% 14.2%
Other 6.5% 14.1% 6.7% 9.0%
Income �40 K 29.0% 19.6% 43.3% 39.0% 11.60** SM, QUBS/R,
NON
Employed (full-or
part-time)
61% 62% 67% 72% 6.81
Education after HS 52.9% 62.3% 50.0% 68.8% 15.26** SM, S/RBQU,
NON
Married/living as
married
41.2% 41.5% 30.0% 46.4% 3.58
Note: aAnalysis conducted between STARTERS/RESUMERS and NONSMOKERS only, *** P B0.001.
* P B0.05.
** P B0.01.# P B0.0001.
C.S. Kohn et al. / Drug and Alcohol Dependence 69 (2003) 61�/71 67

alcohol dependence played in the changes in smoking,
but one speculation is that continued alcohol (and other
drug) use may lower inhibitions to smoke or provide
environmental, social, or physiological cues that rein-
force smoking (Dawson, 2000; Gulliver et al., 1995).
Alternatively individuals may continue to smoke in
order to decrease the sedating effects of continued
alcohol use, or conversely they may continue to use
alcohol in order to moderate the stimulant affects of
smoking (Friday’s Progress Notes, 2001). Among Star-
ters/Resumers, smoking prior to substance use may have
served as a cue that led to substance use relapse;
Table 2
Substance use and psychosocial characteristics at treatment entry
Group F or X2
values
Post hoc
SM SMOKERS
(n�342)
QU QUITTERS
(n�53)
S/R STARTERS/RE-
SUMERS (n�30)
NON NONSMO-
KERS (n�224)
M (SD) M (SD) M (SD) M (SD)
Substance use characteris-
tics
Age first used any drug 13.2 (4.4) 13.9 (2.8) 12.9 (2.7) 15.8 (6.6) 13.10*** SM, QU, S/
RBNON
DSM-IV substance use di-
agnoses
Drug dependence only 30.4% 41.5% 23.3% 26.3% 5.42
Alcohol dependence only 39.8% 24.5% 26.7% 46.4% 11.34** QU, S/RBSM,
NON
Alcohol and drug depen-
dence
20.5% 18.9% 40.0% 12.9% 14.57** NON, SM,
QUBS/R
Substance abuse only 8.3% 15.1% 10.0% 14.4% 4.24
ASI scores (range)
Alcohol (0�/0.97) 0.38 (0.31) 0.30 (0.30) 0.37 (0.31) 0.37 (0.29) 1.11
Drug (0�/0.55) 0.14 (0.13) 0.14 (0.13) 0.17 (0.14) 0.11 (0.13) 3.42* NONBSM, QU,
S/R
Psychosocial characteristics
DSM-IV depressive disor-
der and anxiety diagnosesa
Depressive disorder 27.5% 34.0% 53.3% 28.6% 9.45* SM, NONBS/R
Anxiety disorder 16.1% 18.9% 23.3% 18.3% 1.35
SCL-90 scores (range)
Depression (0�/4) 1.7 (1.1) 2.0 (1.3) 2.4 (1.1) 1.5 (1.1) 6.64*** SM, NONBS/R
NONBQU
Anxiety (0�/4) 1.3 (1.0) 1.8 (1.2) 1.9 (1.1) 1.2 (1.1) 7.59*** SM, NONBQU,
S/R
ASI scores (range)
Psychiatric (0�/1.0) 0.39 (0.26) 0.44 (0.27) 0.53 (0.25) 0.37 (0.27) 3.71* SM, NONBS/R
Social/Family (0�/1.0) 0.35 (0.27) 0.35 (0.27) 0.42 (0.28) 0.32 (0.27) 1.66
Employment (0�/1.0) 0.41 (0.24) 0.40 (0.23) 0.42 (0.23) 0.37 (0.22) 1.21
Legal (0�/0.84) 0.09 (0.18) 0.08 (0.17) 0.09 (0.19) 0.07 (0.17) 0.906
Medical (0�/1.0) 0.20 (0.32) 0.22 (0.31) 0.25 (0.36) 0.22 (0.32) 0.233
Note: aInformation about other DSM-IV diagnoses is available from the first author, but is not reported because occurrences averaged less than
4%.# P B0.0001.
* P B0.05.
** P B0.01.
*** P B0.001.
Table 3
Adjusted and unadjusted mean days abstinent from substance use at
12-month follow-up by smoking group status
Groups Adjusted mean (95% con-
fidence interval)a,b
Unadjusted
mean (SD)
QUITTERS 310.6 (270.1�/351.2) 316.9 (151.1)
NONSMOKERS 294.7 (274.9�/314.4) 297.8 (169.4)
SMOKERS 258.2 (242.3�/274.2) 257.3 (164.0)
STARTERS/RESU-
MERS
246.6 (192.6�/300.7) 223.4 (167.3)
aAdjusted means with covariate LOS, bSMOKERS, STARTERS/
RESUMERSBQUITTERS, NONSMOKERS.
C.S. Kohn et al. / Drug and Alcohol Dependence 69 (2003) 61�/7168

conversely, relapse to substance use may have provided
potent social and environmental cues that led to
resuming or starting smoking.
Examination of psychosocial factors indicated thatthe groups differed little on their family or social,
employment, legal, and medical ASI composite scores.
When prevalence of depressive and anxiety disorder
diagnoses, ASI psychiatric severity scores, and severity
of depressive and anxiety symptoms (as measured by the
SCL-90) were examined, some interesting findings
emerged. Although Starters/Resumers were most likely
to have been diagnosed with a depressive disorder in theyear prior to SA treatment entry and to report more
severe psychiatric problems on the ASI, they did not
differ from Quitters in severity of SCL-90 anxiety and
depressive symptoms reported at treatment entry. Both
Starter/Resumers and Quitters reported higher baseline
anxiety symptoms compared to Nonsmokers and Smo-
kers. Although this study can not test a causal relation-
ship between smoking status and symptoms of anxietyand depression, the relationship found indicate the
importance of examining this in future studies using a
different research design.
4.2. Treatment characteristics: LOS, adjunct/self-help
SA treatment, smoking cessation aids
The four groups did not differ on LOS in treatment,
nor in attendance to the CDRP, NA, or AA. Quittersdid not attend more treatment compared to the other
groups, which suggests that factors other than treatment
were influential on their greater days of abstinence.
Because smoking cessation aids were used infrequently
(i.e. nicotine replacement therapies), only bupropion
was examined for its potential role as a smoking
cessation aid. Quitters were more likely to be prescribed
bupropion compared to the other three groups.Although this lends some support to observations that
bupropion may aid in smoking cessation (Jarvis and
Sutherland, 1998), we cannot assess the role bupropion
may have played, particularly because it was not shown
to be significantly associated with abstinence at 12
months follow-up. Quitters’ underlying depression may
have been addressed through extra attention from their
physicians and/or clinicians in the SA treatment pro-gram, placebo effect, (Khan et al., 2001) or nicotine-like
effects (Young and Glennon, 2002), all of which tend to
increase motivation and/or ability to quit smoking.
4.3. Treatment outcome: abstinence at 12 months
Self-initiated quitting of smoking during SA treat-
ment did not appear to be detrimental to drug andalcohol abstinence among managed care recipients, a
finding similar to that found in previous research
(Burling et al., 2001; Frosch et al., 2000; Jospeh et al.,
1993; Lemon et al., in press). In fact, those who
attempted to quit smoking had more days abstinent
than those who either remained smokers or started/
resumed smoking after treatment entry, even whencontrolling for LOS in treatment. The smoking status
of substance abusers is not static (McCarthy et al.,
2001), and in fact, a fairly large minority of individuals
in SA treatment appear to successfully quit smoking
(Lemon et al., in press), suggesting that SA treatment
may present a prime opportunity to encourage smoking
cessation.
Moreover, although the findings that Smokers tend tobe more at-risk for relapse compared to Nonsmokers
and Quitters is not new (e.g. Frosch et al., 2000), this
study’s contributions to the literature include providing
corroborating evidence for this among the privately
insured managed-care population, using a large sample
size, and examining long-term drug and alcohol use
outcomes. Perhaps most unique to this study was the
examination of individuals who started or resumedsmoking after beginning SA treatment. To the best of
our knowledge, this group of Starters/Resumers has not
been discussed in the empirical literature, even though in
this study they were nearly as large a group as the
Quitters, the group that is generally examined in the
literature. By focusing on only smokers identified at
baseline measurement, we miss a potentially high-risk
group of nonsmokers or former smokers who startsmoking at a later point (e.g. after treatment initiation),
and show poorer SA treatment outcomes.
4.4. Limitations
This study was not without limitations. Although the
sample was drawn from a private, managed-care pro-
gram which is representative of a major organization of
current manner in health care, it is a sample of limitedethnic diversity and higher SES compared to commu-
nity, public, or non-insured populations. While self-
report of smoking status and smoking behavior during
the previous 6 months can generally be considered valid
(e.g. Velicer, et al., 1992), biochemical validation and a
measure of specific number of nonsmoking days at
follow-up would have provided additional independent
validation to this self-report data. Finally, although arelatively understudied group of individuals who
started/resumed smoking after treatment entry were
identified, qualitative data regarding why these indivi-
duals started/resumed smoking were not available.
4.5. Implications
This study provides additional support for researchindicating the importance of addressing and/or offering
smoking cessation within SA treatment programs
(Bernstein and Stoduto, 1999), and provides evidence
C.S. Kohn et al. / Drug and Alcohol Dependence 69 (2003) 61�/71 69

that privately insured managed-care patients appear to
have a relatively high rate of smoking cessation. These
findings highlight the clinical importance of identifying
individuals who are at-risk for starting or resumingsmoking during or after SA treatment, as they are more
likely to have difficulty remaining abstinent from illicit
drugs and alcohol. These findings also underscore the
empirical importance of measuring smoking status of all
study participants at all time points during the study.
Future smoking research should include a focus on
separating starters/resumers from continuous smokers
as this may shed some light on otherwise complex andconfusing impacts of anxiety and depression on smoking
cessation outcomes. It may also be important for future
research within substance using populations to focus on
separating starters/resumers from continuous smokers
and quitters in order to achieve a better understanding
of the relationship between smoking and SA treatment
outcomes.
Acknowledgements
This study was supported by the National Institute on
Drug Abuse (RO1 DA10572). Preparation of this
manuscript was supported by training grants from the
National Institute on Drug Abuse (T32 DA07250 and
K23 DA00468). We would like to thank Charles Moore,
MD and anonymous reviewers for reviewing earlierdrafts of this manuscript. Portions of the results were
presented at the 25th Annual Research society on
Alcoholism Scientific Meeting in San Francisco, CA in
June/July 2002. Previous studies from this database
include Weisner et al., (2001) and in Kohn et al., (2002).
This study is based on results no previously published.
References
Alvir, J.M., Schooler, N.R., Borenstein, M.T., Woerner, M.G., Kane,
J.M., 1988. The reliability of a shortened version of the SCL-90.
Psychopharmacol. Bull. 24, 242�/246.
American Psychiatric Association. 1994. Diagnostic and Statistical
Manual for Mental Disorders-IV. New York: Author.
Bernstein, S.M., Stoduto, G., 1999. Adding a choice-based program
for tobacco smoking to an abstinence-based addiction treatment
program. J. Subst. Abuse Treat. 17, 167�/173.
Bobo, J.K., Lando, H.A., Walker, R.D., McIlvain, H.E., 1996.
Predictors of tobacco quit attempts among recovering alcoholics.
J Subst Abuse 8, 431�/443.
Bobo, J.K., McIlvain, H.E., Gilchrist, L.D., Bowman, A., 1996.
Nicotine dependence and intentions to quit smoking in three
samples of male and female recovering alcoholics and problem
drinkers. Subst. Use Misuse 31, 17�/33.
Bobo, J.K., McIlvain, H.E., Lando, H.A., Walker, R.D., Leed-Kelly,
A., 1998. Effect of smoking cessation counseling on recovery from
alcoholism: findings from a randomized community intervention
trial. Addiction 93, 877�/887.
Burling, T.A., Burling, A.S., Latini, D., 2001. A controlled smoking
cessation trial for substance-dependent inpatients. J. Consult. Clin.
Psychol. 69, 295�/304.
Burling, T.A., Ramsey, T.G., Seidner, A.L., Kondo, C.S., 1997. Issue
related to smoking cessation among substance abusers. J. Subst.
Abuse 9, 27�/40.
Campbell, B.K., Wander, N., Stark, M.J., Holbert, T., 1995. Treating
cigarette smoking in drug-abusing clients. J. Subst. Abuse Treat.
12, 89�/94.
Dawson, D.A., 2000. Drinking as a risk factor for sustained smoking.
Drug Alcohol Depend. 59, 235�/249.
Ellingstad, T.P., Sobell, L.C., Sobell, M.B., Cleland, P.A., Agrawal, S.,
1999. Alcohol abusers who want to quit smoking: implications for
clinical treatment. Drug Alcohol Depend. 54, 259�/264.
Friday’s Progress Notes 2001. Alcohol and Tobacco. Information
source: National Institute on Alcohol Abuse and Alcoholism,
January 1998. Retrieved March 21, 2001 from http://
www.athealth.com/practitioner/ceduc/alc_tob.html#7.
Frosch, D.L., Shoptaw, S., Nahom, D., Jarvik, M.E., 2000. Associa-
tions between tobacco smoking and illicit drug use among
methadone-maintained opiate-dependent individuals. Exp. Clin.
Psychopharmacol. 8, 97�/103.
Goldstein, M.F., Deren, S., Magura, S., Kayman, D.J., Beardsley, M.,
Tortu, S., 2000. Cessation of drug use: impact of time in treatment.
J. Psychoactive Drugs 32, 305�/310.
Gulliver, S.B., Rohsenow, D.J., Colby, S.M., Dey, A., Abrams, D.B.,
Niaura, R.S., Monti, P.M., 1995. Interrelationships of smoking
and alcohol dependence, use, and urges to use. J. Stud. Alcohol 56,
202�/206.
Hughes, J.R., 1993. Treatment of smoking cessation in smokers with
past alcohol/drug problems. J. Subst. Abuse Treat. 10, 181�/187.
Hurt, R.D., Offord, K.P., Croghan, I.T., Gomez-Dahl, L., Kottke,
T.E., Morese, R.M., et al., 1996. Mortality following inpatient
addictions treatment: role of tobacco use in a community-based
cohort. JAMA 275, 1097�/1103.
Irving, L.M., Seidner, A.L., Burling, T.A., Thomas, R.G., Brenner,
G.F., 1994. Drug and alcohol abuse inpatients’ attitudes about
smoking cessation. J. Subst. Abuse 6, 267�/278.
Jarvis, M.J., Sutherland, G., 1998. Tobacco smoking. In: Bellack, A.S.,
Hersen, M. (Eds.), Comprehensive Clinical Psychology. Elsevier
Science Ltd, United Kingdom, pp. 645�/674.
Jospeh, A.M., Nichol, K.L., Anderson, H., 1993. Effect of treatment
for nicotine dependence on alcohol and drug treatment outcomes.
Addict. Behav. 18, 635�/644.
Karan, L.D., 1993. Towards a broader view of recovery. J. Subst.
Abuse Treat. 10, 101�/105.
Khan, A., Khan, S.R., Leventhal, R.M., Brown, W.A., 2001.
Symptom reduction and suicide risk in patients treatment with
placebo in antidepressant clinical trials: a replication analysis of the
Food and Drug Administration Database. Int. J. Neuropsycho-
pharmacol. 4, 113�/118.
Kohn, C.S., Mertens, J.R., Weisner, C.M. Coping among individuals
seeking private substance abuse treatment: gender differences and
length of stay in treatment. Alcohol: Clin. Exp. Res., in press.
Lemon, S.C., Friedmann, P.D., Stein, M.D. The impact of smoking
cessation on drug abuse treatment outcome. Addict. Behav., in
press.
McCarthy, W.J., Zhou, Y., Hser, Y.-I., 2001. Individual change amid
stable smoking patterns in polydrug users over 3 years. Addict.
Behav. 26, 143�/149.
McLellan, A.T., Kushner, H., Metzger, D., Peters, R., Smith, I.,
Grissom, G., et al., 1992. The fifth edition of the Addiction Severity
Index. J. Subst. Abuse Treat. 9, 199�/213.
McLellan, A.T., Alterman, A.I., Cacciola, J., Metzger, D., O’Brien,
C.P., 1992. A new measure of substance abuse treatment: initial
studies of the Treatment Services Review. J. Nerv. Ment. Dis. 180,
101�/110.
C.S. Kohn et al. / Drug and Alcohol Dependence 69 (2003) 61�/7170

Robins, L.N., Helzer, J.E., Cottler, L., Golding, E., 1989. National
Institute of Mental Health Diagnostic Interview Schedule, version
III, revised. St. Louis, MO, Washington University, Department of
Psychiatry.
Sees, K.L., Clark, H.W., 1993. When to begin smoking cessation in
substance abusers. J. Subst. Abuse Treat. 10, 189�/195.
Selby, J.V., 1997. Linking automated databases for research in
managed care settings. Ann. Intern. Med. 127, 719�/724.
Shoptaw, S., Jarvik, M.E., Ling, W., Rawson, R.A., 1996. Con-
tingency management for tobacco smoking in methadone-main-
tained opiate addicts. Addict. Behav. 21, 409�/412.
Toneatto, A., Sobell, L.C., Sobell, M.B., Kozlowski, L.T., 1995. Effect
of cigarette smoking on alcohol treatment outcome. J. Subst.
Abuse 7, 245�/252.
Velicer, W.F., Prochaska, J.O., Rossi, J.S., Snow, M.G., 1992.
Assessing outcome in smoking cessation studies. Psychol. Bull.
111, 23�/41.
Weisner, C.M., McLellan, A.T., Hunkeler, E., 2000. Addiction
Severity Index data from general membership and treatment
samples of HMO members: one case of norming the ASI. J. Subst.
Abuse Treat. 19, 103�/109.
Weisner, C.M., Mertens, J.R., Parthasarathy, S., Moore, C., Lu, Y.,
2001. Integrating primary medical care with addiction treatment: a
randomized controlled trial. JAMA 286, 1715�/1723.
Young, R., Glennon, R.A., 2002. Nicotine and bupropion share a
similar discriminative stimulus effect. Eur. J. Pharmacol. 443, 113�/
118.
C.S. Kohn et al. / Drug and Alcohol Dependence 69 (2003) 61�/71 71




















