Chagas Cardiomyopathy—Where Do We Stand After a Hundred Years?
17
Chagas Cardiomyopathy—Where Do We Stand After a Hundred Years? Andréia Biolo, a Antonio L. Ribeiro, b Nadine Clausell a, ⁎ a Division of Cardiology, Hospital de Clínicas de Porto Alegre and Faculty of Medicine, Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil b Service of Cardiology, University Hospital and Faculty of Medicine, Federal University of Minas Gerais, Belo Horizonte, MG, Brazil Abstract A hundred years from its description, Chagas cardiomyopathy remains a challenging disease. Although successful vector-control strategies have decreased the incidence of Chagas disease in several Latin American countries, both migration to urban areas and immigration have spread the disease worldwide; and now, blood transfusion, organ transplantation, and vertical transmission are a concern. The pathogenesis of Chagas cardiomyopathy involves complex host-parasite interactions, where low-grade but incessant systemic infection and triggered autoimmune reaction are the main mechanisms for its development, with the contribution of autonomic damage and microvascular disturbances. Chagas cardiomyopathy is the most important clinical presentation of Chagas disease and comprises a wide range of manifestations, including heart failure, arrhythmias, heart blocks, sudden death, thromboembolism, and stroke. Recently, simple clinical prognostic scores have been developed to identify high-risk patients and help with management. The treatment of Chagas cardiomyopathy focuses mostly on managing heart failure, arrhythmias, and thromboembolism. The role of specific antiparasitic therapy in the chronic form is not yet defined, and a randomized trial is now under way to address this crucial point. In this article, we review the main clinical aspects of Chagas cardiomyopathy and underscore some upcoming challenges for the appropriate control, diagnosis, and management of this complex disease. (Prog Cardiovasc Dis 2010;52:300-316) © 2010 Elsevier Inc. All rights reserved. Keywords: Chagas disease; Cardiomyopathy; T. cruzi The year 2009 marks the 100th anniversary of the description of Chagas disease by the Brazilian physician Carlos Chagas. 1 Chagas described not only the clinical features of the disease, but also its causal agent, Trypa- nosoma cruzi, and the main mechanism of transmission, transcutaneous inoculation of the parasite by excreta of infected hematophagous insects. Infection with T cruzi is an enzootic disease, which can lead to human disease when the insect vectors—triatomine bugs—reach their domestic cycle by adapting to human dwellings. 2 A hundred years from its description, Chagas cardio- myopathy still is a challenging disease. Many questions regarding pathogenesis, clinical characteristics, and even treatment of Chagas cardiomyopathy remain unsolved. Nonetheless, increased worldwide awareness, initiatives to control dissemination, and research on mechanisms and specific therapies have brought progress into our under- standing and capacity to deal with this complex disease. Epidemiology and natural history Chagas disease has a wide distribution in Central and Latin America; epidemiologic studies carried out in 1980 to 1985 estimated a prevalence of 16 to 18 million persons infected and 100 million at risk. 3 Fortunately, successful Progress in Cardiovascular Diseases 52 (2010) 300 – 316 www.onlinepcd.com Statement of Conflict of Interest: see page 311. ⁎ Address for reprint requests to Nadine Clausell, MD, PhD, Heart Failure and Transplant Unit, Cardiology Division, Hospital de Clínicas de Porto Alegre, Rua Ramiro Barcelos 2350, Sala 2061, 90035-003 Porto Alegre, RS, Brazil. E-mail address: [email protected] (N. Clausell). 0033-0620/$ – see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.pcad.2009.11.008
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Chagas Cardiomyopathy—Where Do We Stand After a Hundred Years?

Progress in Cardiovascular Diseases 52 (2010) 300–316www.onlinepcd.com
Chagas Cardiomyopathy—Where Do We Stand After aHundred Years?
Andréia Biolo,a Antonio L. Ribeiro,b Nadine Clausella,⁎aDivision of Cardiology, Hospital de Clínicas de Porto Alegre and Faculty of Medicine, Federal University of Rio Grande do Sul,
Porto Alegre, RS, BrazilbService of Cardiology, University Hospital and Faculty of Medicine, Federal University of Minas Gerais, Belo Horizonte, MG, Brazil
Abstract A hundred years from its description, Chagas cardiomyopathy remains a challenging disease.
Statement of Conf⁎ Address for rep
Failure and TransplantPorto Alegre, Rua RaAlegre, RS, Brazil.
E-mail address: cl
0033-0620/$ – see frodoi:10.1016/j.pcad.20
Although successful vector-control strategies have decreased the incidence of Chagas disease inseveral Latin American countries, both migration to urban areas and immigration have spreadthe disease worldwide; and now, blood transfusion, organ transplantation, and verticaltransmission are a concern. The pathogenesis of Chagas cardiomyopathy involves complexhost-parasite interactions, where low-grade but incessant systemic infection and triggeredautoimmune reaction are the main mechanisms for its development, with the contribution ofautonomic damage and microvascular disturbances. Chagas cardiomyopathy is the mostimportant clinical presentation of Chagas disease and comprises a wide range of manifestations,including heart failure, arrhythmias, heart blocks, sudden death, thromboembolism, and stroke.Recently, simple clinical prognostic scores have been developed to identify high-risk patientsand help with management. The treatment of Chagas cardiomyopathy focuses mostly onmanaging heart failure, arrhythmias, and thromboembolism. The role of specific antiparasitictherapy in the chronic form is not yet defined, and a randomized trial is now under way toaddress this crucial point. In this article, we review the main clinical aspects of Chagascardiomyopathy and underscore some upcoming challenges for the appropriate control,diagnosis, and management of this complex disease. (Prog Cardiovasc Dis 2010;52:300-316)
© 2010 Elsevier Inc. All rights reserved.Keywords: Chagas disease; Cardiomyopathy; T. cruzi
The year 2009 marks the 100th anniversary of thedescription of Chagas disease by the Brazilian physicianCarlos Chagas.1 Chagas described not only the clinicalfeatures of the disease, but also its causal agent, Trypa-nosoma cruzi, and the main mechanism of transmission,transcutaneous inoculation of the parasite by excreta ofinfected hematophagous insects. Infection with T cruzi isan enzootic disease, which can lead to human diseasewhen the insect vectors—triatomine bugs—reach theirdomestic cycle by adapting to human dwellings.2
lict of Interest: see page 311.rint requests to Nadine Clausell, MD, PhD, HeartUnit, Cardiology Division, Hospital de Clínicas demiro Barcelos 2350, Sala 2061, 90035-003 Porto
[email protected] (N. Clausell).
nt matter © 2010 Elsevier Inc. All rights reserved.09.11.008
A hundred years from its description, Chagas cardio-myopathy still is a challenging disease. Many questionsregarding pathogenesis, clinical characteristics, and eventreatment of Chagas cardiomyopathy remain unsolved.Nonetheless, increased worldwide awareness, initiatives tocontrol dissemination, and research on mechanisms andspecific therapies have brought progress into our under-standing and capacity to deal with this complex disease.
Epidemiology and natural history
Chagas disease has a wide distribution in Central andLatin America; epidemiologic studies carried out in 1980 to1985 estimated a prevalence of 16 to 18 million personsinfected and 100 million at risk.3 Fortunately, successful

Abbreviations and Acronyms
ACE = angiotensin-converting enzyme
BNP = brain natriureticpeptide
ECG = electrocardiogram
ELISA = enzyme-linkedimmunosorbent assay
HRV = heart rate variability
ICD = implantablecardioverter-defibrillator
PCR = polymerase chainreaction
VPB = ventricular prematurebeat
301A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
vector-control strategiesreduced the transmissionof Chagas disease in sev-eral Latin Americancountries; and therefore,its incidence was reducedby more than 65% in2000. Initially a diseaseof rural areas in endemiccountries, the disease hasspread to cities withurban migration. Immi-gration has also spreadChagas disease to nonen-d em i c , d e v e l o p e dcountries, a process most-ly described in Australia,Canada, the UnitedStates, and Europe.4,5 In
fact, most of the estimated 100,000 infected persons in theUnited States acquired the disease while residing in endemicregions, although T cruzi–infected vectors and animals arefound in many parts of the United States and rare cases ofautochthonous transmission have been documented.6
Started in 2006, a screening program for Chagas disease inblood banks in the United States detected more than 500confirmed T cruzi–infected donations, helping preventblood-borne transmission and increase awareness of thedisease.7 In nonendemic countries, blood transfusion, organtransplantation, and vertical transmission are more likelyroutes of infection with T cruzi.2
There are 2 successive stages in Chagas disease: anacute phase and a chronic phase. In the acute phase, thereis an intense inflammatory reaction at the entry point for Tcruzi (chagoma). On conjunctiva, it may result inunilateral periorbital edema, eyelid swelling, and pre-auricular adenopathy (Romana sign). Main manifestationsinclude fever, myalgias, malaise, muscle pains, sweating,hepatosplenomegaly, heart failure from myocarditis,pericardial effusion, lymphocytosis, and, less often,meningoencephalitis. Cardiac involvement occurs inmore than 90% of cases.8 The electrocardiogram (ECG)may show low-voltage, diffuse ST-T changes andconduction abnormalities. Serologic test results for Tcruzi infection are negative during the first weeks, but thecirculating parasites can be detected by xenodiagnosis.However, diagnosis is established in few patients becauseof scarcity or absence of clinical manifestations. The acutephase lasts 6 to 8 weeks, with spontaneous recovery inmore than 95% of patients.2,9
Once the acute phase subsides, most infected patientshave no physical signs or clinical evidence of organdamage. The infection can be detected only by serologic orparasitologic tests. This form of the chronic phase ofChagas disease is called the indeterminate form and, in
most patients, persists indefinitely. Nonetheless, patientsin the indeterminate form have a subclinical degree ofcardiac involvement when tested by Holter monitoring orechocardiography, although the clinical and prognosticsignificance of those findings is not defined.2,3,10
Several years after the chronic phase has started, 10%to 40% of infected individuals will develop chronicsymptoms from involvement of various organs, mainly theheart and the digestive system. Heart involvement is themost important clinical aspect of Chagas disease becauseof its characteristics, frequency, and severity. The chronicphase lasts throughout life and results in a shortening inlife expectancy.2
Pathogenesis
The pathogenesis of Chagas cardiomyopathy is notcompletely understood, partially because disease pro-gression depends on complex host-parasite interactions.Four main pathogenetic mechanisms have been de-scribed: direct parasite damage to the myocardium,immunologic mechanisms, dysautonomia, and microvas-cular disturbances.11,12
Direct parasite damage to the myocardium
The inflammatory process that characterizes Chagascardiomyopathy is accentuated during the acute phase ofdisease; and although it may be clinically silent after that,inflammation is continuously present in patients with theindeterminate and chronic phases.13,14 Moreover, thepresence of inflammation, with consequent cell loss andfibrosis, seems to correlate with severity of heart failure.15
Parasite persistence is believed to be a trigger forlymphocytic infiltration of the myocardium, and persistentT cruzi antigens or its genomic material is found ininflammatory foci.16-20 Nonetheless, the exact mechanismwhereby parasitism causes tissue damage in the chronicphase is unclear; and a definitive cause-effect relationshipbetween progression of disease and parasite persistencehas not been conclusively demonstrated. Although directaggression by the parasite is one possibility, thestimulation of immune responses is the most likely causeof inflammation.9,11
Immunologic mechanisms
The diffuse myocarditis with myocytolysis and repar-ative fibrosis seen in chronic Chagas heart disease ischaracteristic of delayed hypersensitivity reaction, with T-cell–rich inflammatory infiltrates.21,22 However, thescarcity of T cruzi parasites and the lack of temporal andtopographic correlation with the development of myocar-dial pathology point to an autoimmunity/antigenic mimicryhypothesis, with several mechanisms implicated: antigenexposure secondary to tissue damage and environment

302 A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
sensitization, molecular mimicry by structurally similarepitopes between the parasite and host antigens with cross-reactive autoimmune response, and polyclonal activationwith autoantibody production.11,22 Autoantibodies specificfor various autoantigens expressed in cardiac, nervous, andother tissues have been found both in experimental modelsof T cruzi infection and in sera from infected patients.Cross-reactive antibodies between T cruzi and humanproteins, such as β-adrenergic receptors and cardiacmyosin heavy chain, have also been identified. Experi-mentally, induction of immunologic tolerance to heartantigens resulted in milder disease in a model of chronicChagas myocarditis.23-27 Therefore, Chagas cardiomyop-athy is one example of postinfectious autoimmunity, wherethe infectious agent T cruzi triggers molecular mimicry-related target organ immune damage.
Dysautonomia
There is both pathologic and functional evidence ofcardiac denervation in Chagas heart disease. Several studiesdemonstrated intense neuronal depopulation in chagasicpatients, with ganglionic damage and absolute reduction insubepicardial intramural neuronal countings.11 It is believedthat the neuronal loss in Chagas heart disease occurs mostlyduring the acute phase of infection, through directparasitism of neurons, periganglionic inflammation, andantineuronal autoimmune reaction. The observed denerva-tion, as well as the presence of autoantibodies withantagonistic effects,28 results in abnormal cardiac auto-nomic regulation, which has been demonstrated in chagasicpatients. Several studies using either pharmacologic orphysiologic stimuli demonstrated impaired parasympathet-ic heart rate regulation, with deprivation of the tonicinhibitory action normally exerted by the parasympatheticsystem on the sinus node, and lack of the vagally mediatedmechanism to respond with rapid brady- or tachycardia totransient changes in blood pressure or venous return.29-33
The parasympathetic dysautonomia is an early phenome-non; and it may be present even before left ventricularsystolic dysfunction,34 as opposed to other cardiomyopa-thies where autonomic impairment occurs as a result ofneurohumoral activation and adrenergic receptor desensi-tization. Sympathetic nervous system denervation has alsobeen described both by pathologic35 and scintigraphicstudies,36 but its the clinical meaning is controversial.Whereas it is unlikely that autonomic dysfunction plays anessential pathogenic role for the development of chagasiccardiomyopathy, all these neurogenic disturbances mayindeed contribute to the progression of Chagas heartdisease: parasympathetic impairment could be amechanismof increased vulnerability to malignant arrhythmias andsudden death37; lack of adequate heart-rate responsesincreases the dependency of cardiac output increase onvolume and shapemodifications, requiringmore ventricular
dilation and forceful contraction38; also, autonomicderangements may trigger microcirculatory vasospasm,another importantmechanism inChagas cardiomyopathy.11
Microvascular disturbances
Both functional and structural microvascular abnor-malities occur in Chagas cardiomyopathy, possiblyassociated with an underlying inflammatory processcausing perivascular inflammation of several vascularbeds.9,11 The resulting manifestations are vasospasm,decreased blood flow, focal ischemia, platelet thrombi,increased platelet aggregation, and elevated levels ofthromboxane A-2 and endothelin-1.39-42 It is believed thatmicrovascular ischemia may contribute by amplifying thechronic inflammatory aggression toward myocardialtissue. Furthermore, the focal distribution of cell necrosisand reparative fibrosis suggests a role for transientmicrovascular ischemic insults.39 Patients with Chagascardiomyopathy may have chest pain in the absence ofcoronary artery disease, segmental left ventricular dys-function, ST-T changes, and abnormal coronary flowregulation related to endothelial and nonendothelialdysfunction; and in fact, myocardial perfusion abnormal-ities have been shown in these patients.43,44 Chronicmyocardial hypoperfusion would therefore contribute toChagas cardiomyopathy as does hibernating myocardiumin chronic coronary artery disease.
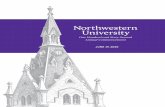
In summary, the 2 main mechanisms underlyingchronic Chagas heart disease include low-grade butincessant systemic infection and triggered autoimmunereaction, such that parasite persistence and immunologicactivity result in myocardial aggression and damage(Fig 1). Autonomic derangements and microcirculatorydisturbances are also involved and contribute to someparticular characteristics of Chagas cardiomyopathy.Once left ventricular remodeling and failure are estab-lished, neurohumoral activation and other compensatorymechanisms take place and ensure progression of thedisease, similar to what happens with other cardiomyop-athies. Nonetheless, several aspects of Chagas diseasepathogenesis are still intriguing and unsolved. Forexample, the determination of whether autoimmunity orparasite-driven damage is the predominant mechanismmay help delineate more efficacious treatment strategiessuch as immunologic interventions, trypanocidal thera-pies, and other strategies to abrogate the development andprogression of Chagas cardiomyopathy.
Etiologic diagnosis
The diagnosis of T cruzi infection is usuallyestablished by the detection of the parasite usingparasitologic tests, during acute infection, or by

Fig 1. Pathogenesis of chronic Chagas cardiomyopathy. The 2 main mechanisms of persistent parasite damage and immunologic response causemyocardial damage and fibrosis with progressive LV remodeling and failure. Nervous tissue damage and microvascular disturbances are triggered andcontribute to further LV remodeling. Cardiac arrhythmias result from LV remodeling and failure, as well as nervous tissue damage, with consequentincreased risk of sudden death (adapted from Marin-Neto et al11). Abbreviation: LV, left ventricular.
303A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
immunodiagnosis, through detection of circulating anti-bodies against T cruzi antigens, in the chronic phase ofdisease. In the acute phase of disease, laboratoryconfirmation is based on the detection of parasitesusing the fresh-blood test, the more sensitive andpreferred one, or by smear and thick drop tests.Concentration tests should be performed in highlysuspicious cases with negative fresh-blood test results.45
During the chronic phase of T cruzi infection, theconcentration of circulating parasites is too low forparasitologic detection, so that the diagnosis relies onantibody detection. Two parallel tests should be per-formed: a test with high sensitivity (enzyme-linkedimmunosorbent assay [ELISA] with total antigen orsemipurified fractions of the parasite, indirect immuno-fluorescence, or indirect hemaglutination) in combinationwith a highly specific one (ELISA using T cruzi–specificrecombinant antigens).45 If the results are inconclusive (1positive and 1 negative test result), samples must beretested; and if still inconclusive, samples should be sent toreferral laboratories to be tested using polymerase chainreaction (PCR) or Western blot methods. Recent studiesshow promising results on standardized PCR techniquesand arrays for detection of multiple recombinant proteinsthat may increase accuracy and reliability on T cruziinfection diagnosis.46,47
Clinical manifestations and clinical assessment
Chagas cardiomyopathy is the most important clinicalpresentation of Chagas disease and comprises a widerange of manifestations, including heart failure, arrhyth-mias, heart blocks, sudden death, thromboembolism, andstroke.48 Clinical presentation typically varies widelyaccording to the degree of myocardial damage; and mostpatients present a mild form of heart disease, frequentlycharacterized only by the presence of asymptomaticabnormalities on the ECG or in other complimentaryexaminations. Considering that the presence of ECGabnormalities is the most prevalent feature of Chagascardiomyopathy and that it has a definite prognosticmeaning,49-51 a Brazilian Expert Consensus definedChagas cardiomyopathy by the presence of typical ECGabnormalities (Table 1) and a positive serology result forT cruzi, independently of the presence of symptoms;those with nonspecific ECG alterations should beclassified as Chagas cardiomyopathy if they presenttypical clinical manifestations or abnormalities in otherlaboratory examinations.45
On average, cardiac involvement is fully developedaround 20 years after the primary infection, although ittakes place earlier in some subjects and later in others.52
Most untreated acute cases evolve into the so-called

Table 1Typical and nonspecific ECG abnormalities in Chagas cardiomyopathy,according to the Brazilian Expert Consensus in Chagas disease
Typical ECG Changes for Chagas DiseaseRight bundle-branch block, associated or not to left anteriorfascicular blockFrequent VPBs (N1 by ECG), polymorphous or repetitiveNonsustained ventricular tachycardia2nd- and 3rd-degree atrioventricular blockSinus bradycardia with heart rate b40 beat/minSinus node dysfunctionLeft bundle-branch blockAFElectrical inactive segmentPrimary alterations of ST-T wave
Nonspecific ECG changes observed in Chagas diseaseSinus bradycardia with heart rate ≥40 beat/minLow limb voltageNonspecific ST-T changesIncomplete right bundle-branch blockLeft anterior fascicular blockIsolated VPBs1st-degree atrioventricular block
304 A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
indeterminate form of chronic Chagas disease, defined bythe presence of infection, confirmed by either serologic orparasitologic tests, and the absence of symptoms and ofelectrocardiographic and radiologic abnormalities (com-prising heart, esophagus, and colon evaluation).49 Patientswith the indeterminate form constitute the majority ofinfected people in endemic areas, and around 40% of thesepatients may persist in this clinical situation forever.50
Patients classified as possessing the indeterminate form ofthe disease have an excellent prognosis, and deaths due tothe infection are rare.49,50 The transition from theindeterminate form to cardiomyopathy generally occursin a slow and progressive fashion, occurring in 2% to 3%of patients each year.49,50
Clinical manifestations of severe chronic Chagas heartdisease comprise 3 main syndromes: (a) heart failure, (b)cardiac arrhythmia, and (c) thromboembolism.53
Heart failure is usually biventricular, and signs andsymptoms of both left and right ventricular failure may beobserved. Left ventricular systolic dysfunction is a majorfeature of Chagas cardiomyopathy, as well as the mainpredictor of the risk of death.54 Clinical manifestations ofright ventricular failure were formerly reported as moreprevalent and more pronounced than those of left-sidedfailure55; but recently, it has been demonstrated that rightventricular dysfunction is clinically significant only whenthere is also a significant associated involvement of the leftside, especially when left ventricular filling pressure andpulmonary pressure are elevated.56 However, rightventricular involvement can occur early in the evolutionof Chagas cardiomyopathy 57,58 and is an independentpredictor of death.59 Although diastolic left ventricularabnormalities have been noted in the absence of regional
or global left ventricular systolic dysfunction, a strongcorrelation between systolic dysfunction and impairmentof left ventricular filling is usually observed in Chagasdisease.60 Left atrial volume, a marker of chronicallyelevated left ventricular filling pressures, is also a predictorof prognosis in patients with Chagas cardiomyopathy.61
Chronic Chagas cardiomyopathy is considered one ofthe most arrhythmogenic cardiomyopathies; and bothtachy- and bradyarrhythmias can occur, frequently coex-isting in the same patient. Ventricular arrhythmias,including ventricular premature beats (VPBs) and non-sustained ventricular tachycardia, are frequent in mostpatients; and malignant sustained ventricular tachycardiais not uncommon.62 Indeed, episodes of malignantventricular arrhythmia seem to be much more frequent inpatients with Chagas cardiomyopathy than those withother types of underlying heart disease.63 The severity ofventricular arrhythmias tends to correlate with the degreeof left ventricular dysfunction,64 although it is notuncommon to have patients with ventricular tachycardiaand preserved global ventricular performance.65 Thepresence of VPBs in the standard ECG is a well-knownprognostic marker, especially when associated to intra-ventricular conduction disturbances.51,66 More recently, ithas been established that the most powerful andindependent arrhythmic risk factor in Chagas cardiomy-opathy is the occurrence of nonsustained ventriculartachycardia, observed during 24-hour Holter monitoringor at the exercise testing.54,67-69
Atrial fibrillation (AF) has also been observed in 4% to12% of patients with Chagas cardiomyopathy,70 occur-ring mainly in those with advanced heart failure, relatedto large atria and reduced left ventricular systolicfunction.71 In Chagas cardiomyopathy, AF is character-ized by relatively low ventricular rate, related to thecoexistence of ventricular conduction disturbances and toan ominous prognosis. 70,72
Intraventricular and atrioventricular conduction dis-turbances are common manifestations of Chagas heartdisease and are generally related to the presence of leftventricular dysfunction and ventricular arrhythmias.51,66
Right bundle-branch block, associated or not with leftanterior fascicular block, is the most typical ECGabnormality of Chagas cardiomyopathy, although leftposterior fascicular block and left bundle-branch blockmay also occur. There is an inverse correlation betweenQRS duration and left ventricular ejection fraction73; andin a recent study, both the filtered, signal-averaged andthe standard ECGs were described as independentprognostic markers.69,74
Chagas disease is a main cause of atrioventricular blockin Latin American countries; and although functionalatrioventricular node abnormalities may occur, they aregenerally caused by widespread and distal fibrosis of theconduction system. Sinus node dysfunction is also a

305A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
concern, and Chagas disease is a main underlying reasonfor implantation of pacemakers in many endemic regions.In comparison with pacemaker patients without Chagasdisease, those patients with Chagas cardiomyopathy aresignificantly younger and have lower left ventricularejection fraction and more frequent ventricular arrhythmiaduring Holter monitoring.75
Sudden cardiac death is the most frequent mechanismof death in Chagas cardiomyopathy 62 and generallyoccurs in patients with more severe disease, although itmay rarely occur in previously asymptomatic patients.65
The final event in these patients is presumed to beventricular tachycardia and fibrillation, but bradyarrhyth-mias may also occur.76
Systemic and pulmonary embolisms, arising frommural thrombi in cardiac chambers and from deep venousthrombosis due to low cardiac output, are possiblecomplications of Chagas cardiomyopathy. Stroke may beits first manifestation; and it is associated with systolicdysfunction, increased left atrial volume, apical aneurysm,intracardiac thrombi, and cardiac arrhythmias.77-79 Chagasdisease has been considered an often unrecognized causeof stroke, and it should be included in its differentialdiagnosis in patients of Latin American origin.80
Chest pain occurs in up to a quarter of patients withChagas cardiomyopathy and may be related to abnormalcoronary flow regulation, due to endothelial and none-ndothelial dysfunction, as well as to noncardiac causes,including esophagus motility disorders, typical of Chagasdisease.11 Acute myocardial infarction is not onlyuncommon in Chagas disease; but it may also presentwith atypical chest pain and, eventually, with normalcoronary arteries.81
Diagnostic evaluation
The ECG is the single most important examination inChagas cardiomyopathy. Numerous epidemiologic studieshave shown that patients with a normal ECG have anexcellent medium-term survival. 49-51 Moreover, severeglobal left ventricular dysfunction, the main prognosticmarker in Chagas disease, is rare in such patients. Thegreater the number and severity of ECG alterationsregistered in a same tracing, the more advanced themyocardial damage possibly is, and the worse theprognosis should be.62 Rarely, sudden death may occurin patients with a normal ECG as the initial manifestationof the disease.65
Echocardiography is the noninvasive technique mostoften used in the assessment of cardiac function andrepresents an important method in the evaluation of Chagascardiomyopathy, allowing the recognition of left ventric-ular systolic and diastolic dysfunction, right ventricle
involvement, and regional contractility abnormalities,including typical apical aneurysms. New echocardiogra-phy methodologies, such as tissue Doppler57,60,82-85 andstrain rate,86 may help in the evaluation of the Chagascardiomyopathy. Global systolic left ventricular dysfunc-tion is the strongest predictor of morbidity and mortality inChagas disease,59,61,69,74,87-90 and asymptomatic leftventricular systolic dysfunction is as common or evenmore prevalent than symptomatic heart failure. Identifica-tion and treatment of patients with left ventricular globalsystolic dysfunction improve survival and reduce morbid-ity. Because it is costly to submit all patients with Chagasdisease to echocardiographic evaluation, it is desirable todevelop screening methods to indicate which patientsshould be submitted to complete left ventricular evaluation.Enlarged heart silhouette at the chest x-ray, although aspecific sign for cardiac dilatation, lacks sensitivity and hasan overall poor diagnostic performance.91 The blood levelof brain natriuretic peptide (BNP), a reliable indicator ofsystolic left ventricular dysfunction in different clinicaland epidemiologic settings, is a promising screeningmethod.92-97 In patients with abnormal ECG and/or chestx-ray findings, BNP elevation has a positive predictivevalue of 80% and a negative predictive value of 97% for thedetection of patients with depressed left ventricularejection fraction.93 A diagnostic strategy including ECGand BNP performed better than the classic approach withECG and chest x-ray.95 Moreover, BNP is also a marker ofventricular arrhythmia97 and diastolic dysfunction.92,98
One of the most interesting findings in the heart inChagas cardiomyopathy is the pattern of segmentalmyocardial contractility disturbance that makes thisdisease in some way closer to ischemic rather than toidiopathic cardiomyopathy. The segments predominantlyinvolved are left ventricular apex and inferior-posteriorwall.83,84 These latter changes appear even in theindeterminate form of Chagas cardiomyopathy (about20%-30% of cases) and are universally present in cases ofsevere heart failure.83,84 Echocardiography allows theidentification of almost all apical lesions, even the smallones. It is important to note that the apical lesion inChagas disease is generally not associated with contrac-tile dysfunction in the anteroseptal segment of the leftventricle, which distinguishes Chagas disease frompatients with coronary artery disease complicated withinfarction. The involvement of other left ventricularsegments in Chagas disease does not differ from that seenin coronary artery disease, and the clinical and epidemi-ologic aspects are essential for the differential diagnosis.
The use of transesophageal echocardiography allowsthe identification of possible cardiac sources of emboliwith high accuracy.77 As Chagas disease can becomplicated by embolic events, transesophageal echocar-diography may be important in deciding the benefit ofanticoagulant therapy.

Table 2Stages of Chagas cardiomyopathy, according to the Brazilian ExpertConsensus in Chagas disease
Stage ECG Echocardiogram Heart Failure
A Abnormal Normal AbsentB1 Abnormal Abnormal
LVEF N45%Absent
B2 Abnormal AbnormalLVEF b45%
Absent
C Abnormal Abnormal TreatableD Abnormal Abnormal Refractory
Abbreviation: LVEF, left ventricular ejection fraction.
306 A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
Dynamic ECG recording (Holter monitoring) isespecially important in Chagas disease because of therelatively frequent occurrence of asymptomatic transitoryarrhythmias.99 Identificationof complex formsofventriculararrhythmias, such as couplets and nonsustained ventric-ular tachycardia, has prognostic relevance.54,68 Thedetection of potentially lethal arrhythmias, such assustained ventricular tachycardia or transient advancedheart blocks, may indicate the necessity of specificantiarrhythmic therapy or devices. Sick sinus syndrome isalso frequent in Chagas cardiomyopathy and can berecognized by Holter monitoring. The lack of significantventricular arrhythmia in 24-hour ECGdoes not, however,preclude risk of death due to arrhythmia. Ambulatorymonitoring may also be used in the investigation ofpalpitations and syncope99,100 and in the assessment of theefficacy of antiarrhythmic therapy.75 Holter monitoring isalso a valuable tool to assess heart rate variability (HRV),an indirect measure of autonomic nervous system controlof the heart. Reduced indexes of HRV could be found inChagas cardiomyopathy before the development ofovert cardiac disease,34,101 indicating mainly vagalinvolvement.102 Some HRV methods, such as heart rateturbulence,103,104 useful as prognostic markers in othercardiomyopathies may be evaluated using Holter moni-toring andmight help in the identification of patients proneto present malignant arrhythmias, an attractive hypothesisthat deserves to be tested.
In selected patients, invasive electrophysiologic studymay be useful for identifying the cause of syncope(when noninvasive test results are inconclusive)100 or forguiding the use of antiarrhythmic devices, such ascardiac pacemakers and implantable cardioverter-defi-brillators (ICDs).105 Moreover, induction of ventriculartachycardia during programmed ventricular stimulationis a predictor of cardiac death and mortality in patientswith Chagas cardiomyopathy and nonsustained ventric-ular tachycardia.106
Maximal exercise testing is usually assessed with theuse of a standard Bruce protocol and can be conductedsafely in patients with Chagas disease. Exercise testingevaluates the influence of exercise in provoking arrhyth-mias and also plays a role in defining the type of work apatient may perform. Exercise-induced ventricular tachy-cardia has the same ominous prognostic significance asthat observed in Holter monitoring.67,68 Chronotropicinsufficiency and abnormal blood pressure response aremore frequent in Chagas cardiomyopathy and may alsohamper the effort capacity of these patients.107,108
Autonomic impairment, sick sinus syndrome, and leftventricular dysfunction are putative causes of theseabnormalities; but it is also well known that somepatients with advanced cardiomyopathy may maintain anexcellent exercise capacity. Indeed, as with many otheraspects of Chagas disease physiopathology, the response
to exercise cannot be predicted by other means; and stresstesting is an essential tool in the evaluation of patientswith Chagas cardiomyopathy.
Radioisotopic techniques, such as myocardial scintig-raphy with thallium-201, have been performed in combi-nation with stress testing to study the myocardial perfusionpattern in the following clinical situations: patients with (1)chest pain, (2) left ventricular segmental abnormalities, and(3) ischemic ECG changes. Both transient and irreversibleperfusion defects may be detected by myocardial perfusionscanning in these patients. This finding may representmicrovascular abnormalities, dysautonomia, or areas ofmyocardial fibrosis.36,43 In patients who complain ofangina-like pain, perfusion disturbances may occur,usually in the presence of normal coronary arteries.Occasionally, cardiac and coronary catheterizations arerequired to exclude the presence of obstructive coronaryartery disease.109
Cardiac magnetic resonance may have a role in theevaluation of Chagas cardiomyopathy because it canoffer a wide variety of imaging tools to evaluate in detailmorphology, cardiac function, and other tissue character-istics, such as detection of edema and fat.110 Myocardialdelayed enhancement by magnetic resonance imagingcan also quantify myocardial fibrosis in patients withChagas cardiomyopathy, thus helping define severity ofthe disease.111
Staging and prognosis
Several classification systems were developed inChagas cardiomyopathy to take into account the greatclinical pleomorphism of this disease and to aid in itsclinical management. The Kuschnir et al112 and LosAndes64 classification systems are frequently used inlongitudinal studies.87,90,113,114 More recently, a Braziliancommittee of experts proposed another staging system,45
based mainly on international heart failure guidelines(Table 2).115,116 The main virtue of this new classificationsystem is that it is compatible with international standardsand, in general terms, with therapeutic recommendations

307A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
for each stage of heart failure. A comprehensive andcomparative evaluation of all these classification systemshas not been performed yet.
It must be stressed that, in any given group of patients,regardless how strict the classification is, remarkablefunctional individual differences among the constituentsof the same clinical group will be found. Chagas disease isa notable entity not only for its clinical variety, but also forthe striking individual variability, making it essential thatpatients should be stratified and followed up carefully.48
There are several potential prognostic markers in Chagasdisease, and this issue has been recently reviewed.54 Asstated above, impaired left ventricular function by echo-cardiogram or ventriculography was found to be the mostcommon and consistent independent predictor ofdeath.59,61,69,74,87-90 New York Heart Association func-tional class III/IV, cardiomegaly on the chest radiography,and nonsustained ventricular tachycardia on 24-hour Holtermonitoring or stress testing were also independentlyassociated with higher mortality. Typical ECG69,74,90,117
and echocardiographic abnormalities59 may show addi-tional prognostic value, although their practical use remainscontroversial.54 Electrophysiologic variables, obtained byinvasive study105,106 or evaluated by ECG analysis, such asQT dispersion and duration,89 were shown to haveadditional prognostic value in selected studies.
A potentially helpful simple risk score was developedto predict death in Chagas heart disease68; moreover,the score was successfully validated in independentcohorts.68,118 Six independent prognostic factors wereidentified, and each was assigned a number of points: NewYork Heart Association class III or IV (5 points), evidenceof cardiomegaly on radiography (5 points), left ventricularsystolic dysfunction on echocardiography (3 points),nonsustained ventricular tachycardia on 24-hour Holtermonitoring or stress testing (3 points), low QRS voltage onelectrocardiography (2 points), and male sex (2 points).68
Patients were classified in 3 risk groups according to thefinal score: low risk (0-6 points), intermediate risk (7-11points), and high risk (12-20 points). In the original study,the 5-year mortality rates for these 3 groups were 2%,18%, and 63%, respectively68; and in an externalvalidation sample, rates were 3%, 10%, and 67%.118
More recently, an alternative approach was pro-posed,69,74 considering only 3 risk factors: left ventricularejection fraction less than 50%, ventricular tachycardia ateither stress testing or Holter monitoring, and QRS greaterthan 133 milliseconds at ECG (or filtered QRS N150milliseconds at signal-averaged ECG).69,74 Low-risk grouphas 0 or 1 risk factor (5-year mortality, 1%); intermediaterisk, 2 factors (20% mortality); and high risk, all 3 factors(50% mortality). This simplified prognostic score had anexcellent performance in predicting death in a study with 74months of follow-up (c statistic, 0.92), and it may be anattractive alternative to the established 6-factor score.
Treatment of Chagas cardiomyopathy
The main focus of the management of Chagascardiomyopathy relies on the treatment of the 3 mainsyndromes: heart failure, arrhythmias, and thromboem-bolism. There are, however, clinical features characteris-tically Chagas related that deserve special attention inregard to therapeutic approaches. At the present time,there is limited evidence-based clinical data to supportspecific antiparasitic therapy; but few data and anincreasingly comprehensive understanding of physiopath-ologic aspects support the development of a much-awaited ongoing large clinical trial that will likely answerimportant questions.
Specific antiparasitic therapy
The benefits of antitrypanosomal therapy are clear inthe acute phase of Chagas disease. However, in thechronic form of the disease, where the role of the parasiteis less understood, it is controversial whether itseradication is beneficial.11 Nonetheless, pathogenic hy-potheses supporting the rationale for a specific antiparasitetherapy include vestiges of parasites identified by moresensitive techniques (PCR) in inflamed cardiac tissue inthe chronic phase and evidence that antitrypanosomaltherapy reduces the inflammatory burden in cardiac tissueat least experimentally.119-121
Two nitroheterocyclic drugs described in the 1960s and1970s, nifurtimox and benznidazole, showed clear anti-parasitic effects in the acute phase of Chagas disease,acting at both the circulating and tissular forms of theparasite.122,123 Currently, only benznidazole is commer-cially available for the treatment of the disease. Data from 2trials with benznidazole in the early phase of the chronicform showed encouraging results, as negative seroconver-sion was achieved in 58% to 62% of the cases after 3 to 4years of follow-up in children with Chagas disease.122,124
In addition, a small nonrandomized, nonblinded studyshowed slower progression to severe cardiomyopathy inadults receiving benznidazole.113 Finally, a systematicreview of 5 clinical trials that have studied 756 patientssuggests that the use of benznidazole can be beneficial toimprove parasite-related outcomes in Chagas cardiomy-opathy, such as negativation of xenodiagnosis and highernegative seroconversion rates.125
The efficacy and tolerance of benznidazole areinversely related to the age of the patients, with adverseeffects occurring in 30% to 50% of adult patients,including dermatitis and, more rarely, polyneuritis anddepression of the bone marrow.126,127 The absence ofrobust evidence to support the universal treatment of allChagas disease patients with benznidazole brought thequestion of the specific treatment of Chagas disease to the

308 A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
global public health agenda, with a plea for developingand testing more efficacious and safer drugs, as well as thecurrent available ones, in patients with indeterminate andchronic forms of the disease.128,129
These observations set the stage of the rationale for theBenznidazole Evaluation for Interrupting Trypanosomiasistrial (ClinicalTrials.gov identifier: NCT00123916), whichis the largest effort to appropriately address the question ofwhether the use of benznidazole will in fact influencepositively clinically relevant outcomes in Chagas cardio-myopathy. The study consists of an international LatinAmerican collaborative initiative including 2 phases: apilot study addressing safety and tolerability issues as wellas the efficacy of benznidazole on the burden of parasite-related outcomes and the full-scale program addressingclinical outcomes associated with the progression ofChagas disease in patients with established cardiac disease.The study plans to enroll 3,000 patients, with a follow-upof 5 years; and its primary outcome is a composite of death,resuscitated cardiac arrest, need of pacemaker or cardiodefibrillator implantation, new onset of heart failure,thromboembolism, sustained ventricular tachycardia, andstroke.130 As of June 18, 2009, more than 1,600 patientshave been enrolled.131
Treatment of cardiomyopathy (heart failure,arrhythmias, thromboembolism)
Traditional therapeutic strategies for heart failure suchas angiotensin-converting enzyme (ACE) inhibitors and β-blockers are likely as important in Chagas cardiomyopathyas in other heart failure syndromes. However, there arevery poor evidence-based strategies focusing on Chagasdisease specifically. Small studies have pointed similarbeneficial effects of ACE inhibitors in Chagas cardiomy-opathy. In fact, both captopril and enalapril have beenshown to improve functional class and left ventricularejection fraction, and reduce catecholamine and cytokinelevels when used in patients with chronic heart failure dueto Chagas.132,133
Similarly, the use of β-blockers is encouraged in Chagascardiomyopathy. However, its use is based on data fromlarge clinical trials that included few or no patients withChagas etiology. Nonetheless, there are specific data fromstudies dealing with Chagas disease that reinforce theimportance of β-blockade in this setting. Davila andcolleagues134 have shown that the use of metoprololimproved functional capacity, left ventricular function, andblood pressure in patients with heart failure secondary toChagas disease. In a subsequent study, Botoni andcolleagues135 demonstrated a trend toward an increase inleft ventricular ejection fraction when carvedilol was addedafter using ACE inhibitors as a first drug, showing that the
addition of carvedilol was safe, hemodynamically welltolerated, and not associated with symptomatic bradycar-dia. On the other hand, Braga and colleagues136 showedthat in less that 40% of patients already on enalapril orcaptopril was it possible to proceed to full doses ofmetoprolol, limited mainly by postural hypotension andexcessive bradycardia. In fact, it has been shown thatpatients with Chagas cardiomyopathy have a tendency tolower blood pressure levels when compared with non-Chagas heart failure, possibly limiting the progression tofull doses of ACE inhibitors as well.136,137 On the otherhand, experimental studies indicate that metoprolol wasable to reduce the ECG changes induced by thetrypanosome, suggesting that β-blockers may have a rolemodulating the proarrhythmogenic status associated toChagas cardiomyopathy.138 Putting all these piecestogether, one should start patients first on β-blockersfollowed by ACE inhibitors to prioritize the highlyproarrhythmogenic environment associated with Chagasphysiopathology where blockade of the adrenergic systemmight be an attractive strategy to prevent sudden cardiacdeath.139,140
Similarly to ACE inhibitors, aldosterone blockade inChagas cardiomyopathy has little specific evidence fromclinical trials. However, one study has shown that itmay be beneficial to add spironolactone to patientsalready using ACE inhibitors with heart failuresecondary to Chagas disease, as decreased neurohumoralactivation was seen.135 Hence, it is reasonable to usespironolactone for patients with Chagas once they fulfillclinical and laboratory criteria as considered for non-Chagas patients.
Digoxin
Digoxin is an important drug used in heart failure toameliorate symptoms and quality of life. In Chagascardiomyopathy, it has also a number of salutary effectsthat make its use almost universal, unless adverse eventsoccur or are anticipated. In fact, use of digoxin modulatessympathetic drive and rennin and aldosterone release aswell as improves several hemodynamic parameters whenadministered acutely.141 On the other hand, because of theextensive myocardial tissue fibrosis/damage and conse-quent highly arrhythmogenic milieu seen in Chagascardiomyopathy, use of digoxin should be strictlymonitored to avoid potential toxicity related to distur-bances in the conduction system.142
Thromboembolism
Oral anticoagulation is controversial in Chagasdisease. Patients with Chagas cardiomyopathy tradi-tionally come from low socioeconomic and educationalstrata, configuring a challenging scenario to manage

309A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
anticoagulation protocols. Conversely, the presence ofsystolic dysfunction, increased left atrial volume, apicalaneurysm, intracardiac thrombi, and cardiac arrhyth-mias are known predictors of stroke in patients withChagas cardiomyopathy.77-79 Because specific studiesabout the efficacy and safety of anticoagulation inChagas disease are not available, management has beentraditionally adapted from international guidelines.More recently, a cardioembolic risk score for Chagasdisease patients was developed and a risk-basedstrategy was proposed.143 The risk score was calculatedadding 2 points for the presence of systolic dysfunctionand 1 point for each of the other factors: apicalaneurism, primary alteration of the ventricular repolar-ization at the ECG, and age more than 48 years. Basedon the risk-benefit analysis, warfarin prophylaxis forcardioembolic stroke in Chagas disease was recom-mended for patients with a score of 4 to 5 points, inwhom the risk of cardioembolism overweighs the riskof major bleeding. With a 3-point score, the risks ofbleeding and cardioembolism are the same; hence, themedical decision of using either warfarin or aspirin hasto be an individual one. With 2 points or less,anticoagulation is not warranted.
Antiarrhythmic strategies
Treatment of ventricular arrhythmia in Chagas cardio-myopathy is essentially empirical and not supported bylarge randomized controlled trials. This is to say that thereare no properly designed prospective trials in larger groupsof patients with Chagas disease to ascertain whetherpharmacologic or device therapy for ventricular arrhyth-mias prevents sudden cardiac death. Thus, clinicalmanagement may be subject to large variations in differentsettings; and recommendations are mainly empirical.
Patients with asymptomatic VPBs or few episodes ofnonsustained ventricular tachycardia, without significantventricular dysfunction, usually do not require anyantiarrhythmic therapy.144 At the other side of thespectrum, those patients with sustained ventriculartachycardia and those resuscitated from sudden deathmay benefit from an ICD, especially in the presence ofdepressed left ventricular function.145 Patients withchronic Chagas heart disease who have recovered fromcardiac arrest have a peculiar arrhythmogenic profilecharacterized by a high frequency of ventricularfibrillation and a short period for first shock.146 Inpatients with Chagas cardiomyopathy and ICDs, thenumber of shocks in the first 30 days is an independentpredictor of mortality.147
The main uncertainties are observed in the managementof patients with complex ventricular arrhythmias or
nonsustained ventricular tachycardia, in the presence ofabnormal left ventricular function. In those with significantarrhythmic symptoms, such as syncope and near-syncope,the electrophysiologic study may help distinguish patientswith malignant ventricular tachycardia,100,105 in whom aICD should be implanted, from those with paroxysmalatrioventricular block, with better prognosis and candidatesfor a conventional pacemaker. Asymptomatic or oligo-symptomatic patients represent a more complex challenge.Although indirect evidence had suggested that amiodaronecould reduce the risk of death in this group, such as thesubgroup analysis from the Argentinean Gesica trial,148
this benefit has never been proven. Moreover, primaryprophylaxis of sudden death with the implantation of ICDshas not been evaluated in Chagas disease and mayrepresent an unbearable financial burden for the healthsystem of Latin America countries in which the disease isendemic. Treatment of symptomatic bradyarrhythmiasdoes not differ from that recommended for othercardiomyopathies and is usually performed by permanentpacemaker insertion.
Heart transplantation
Chagas disease may account for important portions ofthe population referred for heart transplantation in areaswhere the disease is endemic. In certain parts of the world,it is the leading referring cause and in Brazil is the thirdindication for heart transplantation.149,150 A number ofuncertainties surround the context of transplanting patientswith Chagas cardiomyopathy, the important ones beingwhen to refer for transplantation, fear of reactivation of theparasitic infestation, higher degrees of rejection, andoccurrence of infections posttransplant.
Indications of heart transplantation forChagas cardiomyopathy
Although there is high individual variability regardingprognosis in Chagas cardiomyopathy, it seems that Chagasdisease is associated with poorer outcomes compared withother cardiomyopathies. In fact, Theodoropoulos andcoworkers151 found that when 5 well-accepted risk criteria(lack of β-blocker use, hyponatremia, left ventricularejection fraction b31%, New York Association class IV,and use of digoxin) are applied in Chagas, survival of lessthat 20% in 1 year was observed. Furthermore, the higherarrhythmogenic profile seen in Chagas highlights anothercharacteristic that may add to a somber outcome in thispopulation; in fact, patients using ICDs who had more than4 shocks by day 30 after device implantation had a dismalsurvival of 21% in 2 months.147 Thus, one might considerthat Chagas disease has equal or even poorer prognosis

310 A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
compared with non-Chagas heart failure and that hearttransplantation might be considered even sooner.
Outcome post–heart transplantation in Chagas diseaseis also matter of debate. However, the concerns appear tobe mostly speculative, possibly reflecting the fear of theunknown about its physiopathology. Data from centers thathave been transplanting these patients regularly and thattherefore developed sound experience are encouraging.152
Early perioperative mortality appears to be no different inChagas and non-Chagas recipients, according to dataderiving from centers that have performed this procedure inboth groups of patients.
Late follow-up data from Chagas transplant recipientsindicate that reactivation of T cruzi may occur in 27%to 90% of patients as detected by showing the mastigotein the blood or by immunohistochemistry in tissuesamples; but it seldom has major clinical impact, underthe contemporaneous immunosuppressive regimensused.153,154 Several mechanisms may account forreactivation of T cruzi infection, including use ofmycophenolate mofetil, rejection episodes, and steroidpulse therapies. However, because treatment of T cruzireactivation is easily accomplished using benznidazoleand allopurinol, mortality observed with these rareepisodes was as low as 0.7%.152
Other common concerns after heart transplant are nostrangers to Chagas transplant recipients, as the magnitudeof problems associated with rejection episodes, neoplasia,infection, and cardiac transplant vasculopathy appears tobe no different in this population. The annual rate of gradeA rejection episodes varies from 1.6 to 3.25,155,156 whereasthe reported rates of rejection episodes are not consensual—in fact, when no steroid is used, de Carvalho andcolleagues155 found less rejection in Chagas-transplantedpatients compared with non-Chagas. Immunosuppressiveregimens including steroids have shown similar or worserates of rejection in Chagas transplant recipients.157,158
Finally, analyzing data from the percentage of patients freefrom rejection episodes, it seems that rates are similar inboth Chagas and non-Chagas transplant recipients, whichis supported by the fact that death because of rejection issimilar in both patient populations.156
The incidence of neoplasia, a constant concern in longterm follow-up of transplant recipients, appears to be nodifferent in Chagas patients. The only report showing higherincidence of different tumors in these patients was laterfound to be associated with overimmunosuppresion.159
Thus, at the current status of immunosuppressive regimens,with lower levels of cyclosporine, the occurrence ofneoplasia is similar across the spectrum of etiologiesleading to cardiac transplant.155
Similarly to other transplant complications, infectionepisodes appear to be neither more frequent nor seriousin Chagas transplant recipients. Both annual rate ofinfection episodes and percentage of patients free from
infection episodes are similar in Chagas and non-Chagas recipients. It was even reported that infectioncan be less frequent in Chagas patients. Moreover,approximately 30% of these patients will experience noinfection episode in the first year posttransplantrequiring antibiotic therapy.157
Cardiac vasculopathy, a universal late complicationpost–heart transplant, remains poorly studied concerningChagas recipients exclusively. One report showed 1 in 10cases who presented with obstructive coronary lesion thatwas successfully treated with percutaneous transluminalangioplasty.157 It remains to be explored whethermeasures different from the ones recommended toprevent this complication and that are used in non-Chagas patients should be considered. At this point, useof pravastatin and strict control of traditional risk facts foratherosclerotic disease should be implemented in allpatients post–heart transplant.
Preventing disease
Prevention in Chagas disease is 3-fold. Primaryprevention aims to limit spread at the vectorial level,and blood transfusion and organ donation from infecteddonors. Secondary prevention aims to limit early andasymptomatic disease from progressing into fullydeveloped syndrome. Tertiary prevention aims tolimit, whenever possible, further organ damage andimprove clinical outcome once the complete cardiomy-opathy is established.160
Primary prevention
This strategy consists of effective chemical control ofvectors in endemic areas, stricter blood blank screening bymeans of modern serology, and screening of potentialorgan donors. These actions should be supported byhousing and epidemiologic surveillance. Preventiveactions should also involve monitoring contamination atthe laboratory and dealing with unknown infectedbiological samples. These measures have been proven toreduce markedly the number of new cases, including viacongenital route.
Secondary prevention
The strategies at this level consist of finding newlyinfected, young, yet asymptomatic cases and treatingthem with antiparasitic drugs aiming at avoidingestablished organ damage and disease spread amongfamily members and via congenital route, as welllimiting blood and organ donation from infectedindividuals. This will hopefully eradicate the parasiteand interfere with the chain of disease.160 The challengeat this level is to appropriately diagnose acute Chagas

311A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
infection and institute therapy in a timely fashion. Inmost cases, it may be totally silent; in others, itresembles nonspecific viral infection syndrome withfever and malaise. Antiparasitic therapy at this stage mayreduce significantly parasite burden and halt progressionto full disease, which was proven in children but not inadults (“specific antiparasitic therapy”). Secondary pre-vention in Chagas disease should be regarded as a keyelement to contain the development of new cases inseveral different scenarios and also limits the potentialfor establishing a severely debilitating health condition.There are potentially many aspects that should beovercome to implement efficiently secondary preventionin Chagas disease; these include (1) difficult diagnosis atthis stage (mostly silent cases); (2) misconceptionsamong physicians that antiparasitic treatment is notuseful; (3) exaggerated and unjustified fear of adverseevents with benznidazole or nifurtimox compounds; (4)lack of international guidelines on the subject; (5) limitedaccess to benznidazole or nifurtimox (low productionquantities); and (6) scarce interest from the industry todevelop new, modern antitrypanosomal compounds.161
Tertiary prevention
At this level, the remaining approach aims at improvingquality of life and morbidity and mortality from thedisease once the full spectrum of Chagas cardiomyopathyis already established. These include treating symptomsand typical clinical conditions associated with Chagasdisease (“Treatment of cardiomyopathy”).
Upcoming challenges
Globalization has made Chagas disease a less geo-graphically restricted health condition. In fact, growingmigration involving rural to urban areas in Latin Americancountries and also to large metropolitan areas outside LatinAmerica is slowly transforming the reality worldwide. It isworth noting that there has been an impressive increase inpositive test results for T cruzi in screened blood bankacross the United States in the last decade, which enhancedthe level of awareness of health authorities, calling forstricter control of blood donors. Although voluntary, at thepresent time, between 75% and 90% of blood banks in theUnited States perform routine screening for T cruzi usingthe Food and Drug Administration–approved ELISAassay.162 It is imperative that a high level of screening isimplemented targeting blood banks and organ transplan-tation protocols to avoid infected samples from spreadingthe disease. Moreover, although the number of new casesof Chagas disease has decreased in recent decades,continuous efforts in different scenarios from healthauthorities should be maintained to further reduce the
burden of Chagas worldwide and remove this conditionfrom the so-called neglected disease group from publichealth initiatives.
Future perspectives
Although the number of new cases of Chagas diseasehas dropped markedly in the last few years because ofeffective control programs, there is a large population ofindividuals who will clearly benefit from adequateclinical management. For instance, it would be desirableto have a comprehensive knowledge about someneglected clinical manifestations such as embolic strokeand chest pain. The identification of early markers ofworse prognosis would be also an important advance,helping identify a group of patients who would benefit themost from early and, perhaps, more aggressive interven-tion. More data are needed on epidemiology and specificclinical features of the disease in specific populations,such as in the elderly, as well as on the mechanismsinvolved in the progression from the indeterminate formto clinical syndromes.
At the present time, treatment of Chagas cardiomyop-athy is based on heart failure–related symptoms control.There are 2 main reasons for that: (1) there is littleevidence that, other than in small children, antiparasiticdrugs can change outcome; and (2) most diagnosis aremade in advanced stages of the disease (when reversingdamage is less likely) because for decades the Trypano-soma infection remains clinically silent. Nonetheless, asexistent drugs such as benznidazole possess numerousadverse effects, efforts should be carried to develop new,modern compounds if an effective, well-tolerated, andbeneficial therapy is to be reached. Furthermore, it isimperative that earlier diagnosis be made in potentiallyinfected individuals to limit blood, congenital, and organdonation transmissions, especially outside well-knownendemic areas. To this end, health authorities must becapable of dealing with migration from rural to urban areasin endemic regions; and nonendemic countries must setpolicies to prevent transmission efficaciously.
In summary, more sensitive and accessible diagnosticand screening tests, better-tolerated drugs, and increasedawareness regarding Chagas disease are necessary tobetter deal with a potential worldwide spread and toprovide efficacious therapy in a timely manner to a greatnumber of individuals.
Statement of Conflict of Interest
All authors declare that there are no conflicts of interest.

312 A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
References
1. Chagas C: Uber eine neue Trypanosomiasis des Menschen. ArchSchiffs Tropenhyg 1909;13:351-353.
2. Prata A: Clinical and epidemiological aspects of Chagas disease.Lancet Infect Dis 2001;1:92-100.
3. WHO Expert Commitee: Control of Chagas disease. World HealthOrgan Tech Rep Ser 2002;905:i-109.
4. Schmunis GA: Epidemiology of Chagas disease in nonendemiccountries: the role of international migration. Mem Inst OswaldoCruz 2007;102:75-85.
5. Dobarro D, Gomez-Rubin C, Sanchez-Recalde A, et al: Chagas'heart disease in Europe: an emergent disease? J Cardiovasc Med(Hagerstown) 2008;9:1263-1267.
6. Bern C, Montgomery SP, Herwaldt BL, et al: Evaluation andtreatment of Chagas disease in the United States: a systematicreview. JAMA 2007;298:2171-2181.
7. Bern C, Montgomery SP, Katz L, et al: Chagas disease and the USblood supply. Curr Opin Infect Dis 2008;21:476-482.
8. Parada H, Carrasco HA, Anez N, et al: Cardiac involvement is aconstant finding in acute Chagas' disease: a clinical, parasitologicaland histopathological study. Int J Cardiol 1997;60:49-54.
9. Punukollu G, Gowda RM, Khan IA, et al: Clinical aspects of theChagas' heart disease. Int J Cardiol 2007;115:279-283.
10. Barretto AC, Ianni BM: The undetermined form of Chagas' heartdisease: concept and forensic implications. Sao Paulo Med J 1995;113:797-801.
11. Marin-Neto JA, Cunha-Neto E, Maciel BC, et al: Pathogenesis ofchronic Chagas heart disease. Circulation 2007;115:1109-1123.
12. Rossi MA, Bestetti RB: The challenge of chagasic cardiomyopathy.The pathologic roles of autonomic abnormalities, autoimmunemechanisms and microvascular changes, and therapeutic implica-tions. Cardiology 1995;86:1-7.
13. Pereira Barretto AC, Mady C, Arteaga-Fernandez E, et al: Rightventricular endomyocardial biopsy in chronic Chagas' disease. AmHeart J 1986;111:307-312.
14. Carrasco Guerra HA, Palacios-Pru E, Dagert de Scorza C, et al:Clinical, histochemical, and ultrastructural correlation in septalendomyocardial biopsies from chronic chagasic patients: detectionof early myocardial damage. Am Heart J 1987;113:716-724.
15. Higuchi ML, De Morais CF, Pereira Barreto AC, et al: The role ofactive myocarditis in the development of heart failure in chronicChagas' disease: a study based on endomyocardial biopsies. ClinCardiol 1987;10:665-670.
16. Tarleton RL: Parasite persistence in the aetiology of Chagasdisease. Int J Parasitol 2001;31:550-554.
17. Jones EM, Colley DG, Tostes S, et al: Amplification of a Try-panosoma cruzi DNA sequence from inflammatory lesions inhuman chagasic cardiomyopathy. Am J Trop Med Hyg 1993;48:348-357.
18. Bellotti G, Bocchi EA, de Moraes AV, et al: In vivo detection ofTrypanosoma cruzi antigens in hearts of patients with chronicChagas' heart disease. Am Heart J 1996;131:301-307.
19. Zhang L, Tarleton RL: Parasite persistence correlates with diseaseseverity and localization in chronic Chagas' disease. J Infect Dis1999;180:480-486.
20. Palomino SA, Aiello VD, Higuchi ML: Systematic mapping ofhearts from chronic chagasic patients: the association between theoccurrence of histopathological lesions and Trypanosoma cruziantigens. Ann Trop Med Parasitol 2000;94:571-579.
21. Higuchi ML, Gutierrez PS, Aiello VD, et al: Immunohistochem-ical characterization of infiltrating cells in human chronicchagasic myocarditis: comparison with myocardial rejectionprocess. Virchows Arch A Pathol Anat Histopathol 1993;423:157-160.
22. Cunha-Neto E, Bilate AM, Hyland KV, et al: Induction of cardiacautoimmunity in Chagas heart disease: a case for molecularmimicry. Autoimmunity 2006;39:41-54.
23. Ferrari I, Levin MJ, Wallukat G, et al: Molecular mimicry betweenthe immunodominant ribosomal protein P0 of Trypanosoma cruziand a functional epitope on the human beta 1-adrenergic receptor. JExp Med 1995;182:59-65.
24. Pontes-de-Carvalho L, Santana CC, Soares MB, et al: Experimentalchronic Chagas' disease myocarditis is an autoimmune diseasepreventable by induction of immunological tolerance to myocardialantigens. J Autoimmun 2002;18:131-138.
25. Cunha-Neto E, Duranti M, Gruber A, et al: Autoimmunity inChagas disease cardiopathy: biological relevance of a cardiacmyosin-specific epitope crossreactive to an immunodominant Try-panosoma cruzi antigen. Proc Natl Acad Sci USA 1995;92:3541-3545.
26. Cunha-Neto E, Coelho V, Guilherme L, et al: Autoimmunity inChagas' disease. Identification of cardiac myosin-B13 Trypano-soma cruzi protein crossreactive T cell clones in heart lesions of achronic Chagas' cardiomyopathy patient. J Clin Invest 1996;98:1709-1712.
27. Iwai LK, Juliano MA, Juliano L, et al: T-cell molecular mimicryin Chagas disease: identification and partial structural analysis ofmultiple cross-reactive epitopes between Trypanosoma cruzi B13and cardiac myosin heavy chain. J Autoimmun 2005;24:111-117.
28. Ribeiro AL, Gimenez LE, Hernandez CC, et al: Early occurrence ofanti-muscarinic autoantibodies and abnormal vagal modulation inChagas disease. Int J Cardiol 2007;117:59-63.
29. Amorim DS, Godoy RA, Manco JC, et al: Effects of acute elevationin blood pressure and of atropine on heart rate in Chagas' disease. Apreliminary report. Circulation 1968;38:289-294.
30. Manco JC, Gallo Jr L, Godoy RA, et al: Degeneration of the cardiacnerves in Chagas' disease. Further studies. Circulation 1969;40:879-885.
31. Marin-Neto JA, Gallo Jr L, Manco JC, et al: Postural reflexes inchronic Chagas's heart disease. Heart rate and arterial pressureresponses. Cardiology 1975;60:343-357.
32. Junqueira Junior LF, Gallo JL, Manco JC, et al: Subtle cardiacautonomic impairment in Chagas' disease detected by baroreflexsensitivity testing. Braz J Med Biol Res 1985;18:171-178.
33. Guzzetti S, Iosa D, Pecis M, et al: Impaired heart rate variability inpatients with chronic Chagas' disease. Am Heart J 1991;121:1727-1734.
34. Ribeiro AL, Moraes RS, Ribeiro JP, et al: Parasympatheticdysautonomia precedes left ventricular systolic dysfunction inChagas disease. Am Heart J 2001;141:260-265.
35. Machado CR, Camargos ER, Guerra LB, et al: Cardiac autonomicdenervation in congestive heart failure: comparison of Chagas'heart disease with other dilated cardiomyopathy. Hum Pathol 2000;31:3-10.
36. Simoes MV, Pintya AO, Bromberg-Marin G, et al: Relation ofregional sympathetic denervation and myocardial perfusion distur-bance to wall motion impairment in Chagas' cardiomyopathy. Am JCardiol 2000;86:975-981.
37. Baroldi G, Oliveira SJ, Silver MD: Sudden and unexpected death inclinically 'silent' Chagas' disease. A hypothesis. Int J Cardiol 1997;58:263-268.
38. Marin-Neto JA, Maciel BC, Gallo JL, et al: Effect of parasympa-thetic impairment on the haemodynamic response to handgrip inChagas's heart disease. Br Heart J 1986;55:204-210.
39. Rossi MA: Microvascular changes as a cause of chroniccardiomyopathy in Chagas' disease. Am Heart J 1990;120:233-236.
40. Rossi MA, Goncalves S, Ribeiro-dos-Santos R: ExperimentalTrypanosoma cruzi cardiomyopathy in BALB/c mice. The potential

313A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
role of intravascular platelet aggregation in its genesis. Am J Pathol1984;114:209-216.
41. Tanowitz HB, Burns ER, Sinha AK, et al: Enhanced plateletadherence and aggregation in Chagas' disease: a potentialpathogenic mechanism for cardiomyopathy. Am J Trop Med Hyg1990;43:274-281.
42. Tanowitz HB, Kaul DK, Chen B, et al: Compromised microcircu-lation in acute murine Trypanosoma cruzi infection. J Parasitol1996;82:124-130.
43. Marin-Neto JA, Marzullo P, Marcassa C, et al: Myocardialperfusion abnormalities in chronic Chagas' disease as detected bythallium-201 scintigraphy. Am J Cardiol 1992;69:780-784.
44. Hammermeister KE, Caeiro T, Crespo E, et al: Left ventricularwall motion in patients with Chagas's disease. Br Heart J 1984;51:70-76.
45. Ministério da Saúde, Secretaria de Vigilancia em Saúde: BrazilianConsensus on Chagas disease. Rev Soc Bras Med Trop 2005;38(Suppl 3):7-29.
46. Deborggraeve S, Coronado X, Solari A, et al: T. cruzi OligoC-TesT: a simplified and standardized polymerase chain reactionformat for diagnosis of Chagas disease. PLoS Negl Trop Dis 2009;3:e450.
47. Cooley G, Etheridge RD, Boehlke C, et al: High throughputselection of effective serodiagnostics for Trypanosoma cruziinfection. PLoS Negl Trop Dis 2008;2:e316.
48. Rocha MO, Ribeiro AL, Teixeira MM: Clinical management ofchronic Chagas cardiomyopathy. Front Biosci 2003;8:e44-e54.
49. Ribeiro AL, Rocha MO: Indeterminate form of Chagas disease:considerations about diagnosis and prognosis. Rev Soc Bras MedTrop 1998;31:301-314.
50. Dias JC: The indeterminate form of human chronic Chagas' disease.A clinical epidemiological review. Rev Soc Bras Med Trop 1989;22:147-156.
51. Maguire JH, Hoff R, Sherlock I, et al: Cardiac morbidity andmortality due to Chagas' disease: prospective electrocardio-graphic study of a Brazilian community. Circulation 1987;75:1140-1145.
52. Rocha MO, Teixeira MM, Ribeiro AL: An update on themanagement of Chagas cardiomyopathy. Expert Rev Anti InfectTher 2007;5:727-743.
53. Rassi Jr A, Rassi A, Little WC: Chagas' heart disease. Clin Cardiol2000;23:883-889.
54. Rassi Jr A, Rassi A, Rassi SG: Predictors of mortality in chronicChagas disease: a systematic review of observational studies.Circulation 2007;115:1101-1108.
55. Marin-Neto JA, Andrade ZA: Why is there predominance ofright heart failure in Chagas' disease? Arq Bras Cardiol 1991;57:181-183.
56. Nunes MC, Barbosa MM, Brum VA, et al: Morphofunctionalcharacteristics of the right ventricle in Chagas' dilated cardiomy-opathy. Int J Cardiol 2004;94:79-85.
57. Barros MV, Machado FS, Ribeiro AL, et al: Detection of early rightventricular dysfunction in Chagas' disease using Doppler tissueimaging. J Am Soc Echocardiogr 2002;15:1197-1201.
58. Marin-Neto JA, Marzullo P, Sousa AC, et al: Radionuclideangiographic evidence for early predominant right ventricularinvolvement in patients with Chagas' disease. Can J Cardiol 1988;4:231-236.
59. Nunes MD, Rocha MO, Ribeiro AL, et al: Right ventriculardysfunction is an independent predictor of survival in patients withdilated chronic Chagas' cardiomyopathy. Int J Cardiol 2008;127:353-359.
60. Barros MV, Machado FS, Ribeiro AL, et al: Diastolic function inChagas' disease: an echo and tissue Doppler imaging study. Eur JEchocardiogr 2004;5:182-188.
61. Nunes MC, Barbosa MM, Ribeiro AL, et al: Left atrial volumeprovides independent prognostic value in patients with Chagascardiomyopathy. J Am Soc Echocardiogr 2009;22:82-88.
62. Rassi Jr A, Rassi SG, Rassi A: Sudden death in Chagas' disease.Arq Bras Cardiol 2001;76:75-96.
63. Martinelli FM, De Siqueira SF, Moreira H, et al: Probability ofoccurrence of life-threatening ventricular arrhythmias in Chagas'disease versus non-Chagas' disease. Pacing Clin Electrophysiol2000;23:1944-1946.
64. Carrasco HA, Guerrero L, Parada H, et al: Ventricular arrhythmiasand left ventricular myocardial function in chronic chagasicpatients. Int J Cardiol 1990;28:35-41.
65. Sternick EB, Martinelli M, Sampaio R, et al: Sudden cardiac deathin patients with Chagas heart disease and preserved left ventricularfunction. J Cardiovasc Electrophysiol 2006;17:113-116.
66. Mota EA, Guimaraes AC, Santana OO, et al: A nine yearprospective study of Chagas' disease in a defined rural populationin northeast Brazil. Am J Trop Med Hyg 1990;42:429-440.
67. de Paola AA, Gomes JA, Terzian AB, et al: Ventricular tachycardiaduring exercise testing as a predictor of sudden death in patientswith chronic chagasic cardiomyopathy and ventricular arrhythmias.Br Heart J 1995;74:293-295.
68. Rassi Jr A, Rassi A, Little WC, et al: Development and validation ofa risk score for predicting death in Chagas' heart disease. N Engl JMed 2006;355:799-808.
69. Ribeiro AL, Cavalvanti PS, Lombardi F, et al: Prognostic value ofsignal-averaged electrocardiogram in Chagas disease. J CardiovascElectrophysiol 2008;19:502-509.
70. Ribeiro AL: Eletrocardiografia na doença de Chagas. Rev Soc BrasMed Trop 1994;27:52-54.
71. Benchimol-Barbosa PR, Barbosa-Filho J: Atrial mechanicalremodeling and new onset atrial fibrillation in chronic Chagas'heart disease. Int J Cardiol 2007;127:e113-e115.
72. Espinosa RA, Pericchi LR, Carrasco HA, et al: Prognosticindicators of chronic chagasic cardiopathy. Int J Cardiol 1991;30:195-202.
73. Ribeiro AL, Rocha MO, Barros MV, et al: A narrow QRS does notpredict a normal left ventricular function in Chagas' disease. PacingClin Electrophysiol 2000;23:2014-2017.
74. Ribeiro AL, Lombardi F, Colosimo EA, et al: Risk stratification inChagas disease: further improvements are needed. J CardiovascElectrophysiol 2008;19:E41-E43.
75. Rincon LG, Rocha MO, Pires MT, et al: Clinical profile of Chagasand non-Chagas' disease patients with cardiac pacemaker. Rev SocBras Med Trop 2006;39:245-249.
76. Mendoza I, Moleiro F, Marques J: Sudden death in Chagas' disease.Arq Bras Cardiol 1992;59:3-4.
77. Nunes MC, Barbosa MM, Rocha MO: Peculiar aspects ofcardiogenic embolism in patients with Chagas' cardiomyopathy: atransthoracic and transesophageal echocardiographic study. J AmSoc Echocardiogr 2005;18:761-767.
78. Carod-Artal FJ, Vargas AP, Horan TA, et al: Chagasic cardiomy-opathy is independently associated with ischemic stroke in Chagasdisease. Stroke 2005;36:965-970.
79. Nunes MC, Barbosa MM, Ribeiro AL, et al: Ischemic cerebrovas-cular events in patients with Chagas cardiomyopathy: a prospectivefollow-up study. J Neurol Sci 2009;278:96-101.
80. Carod-Artal FJ, Vargas AP, Melo M, et al: American trypanoso-miasis (Chagas' disease): an unrecognised cause of stroke. J NeurolNeurosurg Psychiatry 2003;74:516-518.
81. Bestetti RB, Ariolli MT, do Carmo JL, et al: Clinical characteristicsof acute myocardial infarction in patients with Chagas' disease. Int JCardiol 1992;35:371-376.
82. Barros MV, Costa Rocha MO, Ribeiro AL, et al: Tissue Dopplerimaging enables the identification of diastolic dysfunction of

314 A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
pseudonormal pattern in Chagas' disease. J Am Soc Echocardiogr2001;14:353-359.
83. Barros MV, Rocha MO, Ribeiro AL, et al: Doppler tissue imagingto evaluate early myocardium damage in patients with undeter-mined form of Chagas' disease and normal echocardiogram.Echocardiography 2001;18:131-136.
84. Barros MV, Ribeiro AL, Machado FS, et al: Doppler tissue imagingto assess systolic function in Chagas' disease. Arq Bras Cardiol2003;80:36-40.
85. Vinicius Lins BM, Otavio Da Costa RM, Luiz Pinho RA, et al:Tissue Doppler imaging in the evaluation of the regional diastolicfunction in Chagas' disease. Eur J Echocardiogr 2001;2:94-99.
86. Silva CE, Ferreira LD, Peixoto LB, et al: Evaluation of segmentarycontractility in Chagas' disease by using the integral of themyocardial velocity gradient (myocardial strain) obtained throughtissue Doppler echocardiography. Arq Bras Cardiol 2005;84:285-291.
87. Carrasco HA, Parada H, Guerrero L, et al: Prognostic implicationsof clinical, electrocardiographic and hemodynamic findings inchronic Chagas' disease. Int J Cardiol 1994;43:27-38.
88. Mady C, Cardoso RH, Barretto AC, et al: Survival and predictors ofsurvival in patients with congestive heart failure due to Chagas'cardiomyopathy. Circulation 1994;90:3098-3102.
89. Salles G, Xavier S, Sousa A, et al: Prognostic value of QT intervalparameters for mortality risk stratification in Chagas' disease:results of a long-term follow-up study. Circulation 2003;108:305-312.
90. Viotti R, Vigliano C, Lococo B, et al: Clinical predictors of chronicchagasic myocarditis progression. Rev Esp Cardiol 2005;58:1037-1044.
91. Perez AA, Ribeiro AL, Barros MV, et al: Value of the radio-logical study of the thorax for diagnosing left ventriculardysfunction in Chagas' disease. Arq Bras Cardiol 2003;80:208-213, 202-207.
92. Barbosa MM, Nunes MD, Ribeiro AL, et al: N-terminal proBNPlevels in patients with Chagas disease: a marker of systolic anddiastolic dysfunction of the left ventricle. Eur J Echocardiogr 2006;8:204-212.
93. Ribeiro AL, dos Reis AM, Barros MV, et al: Brain natriureticpeptide and left ventricular dysfunction in Chagas' disease. Lancet2002;360:461-462.
94. Ribeiro AL, Reis AM, Teixeira MM, et al: Brain natriuretic peptidein Chagas' disease: further insights. Lancet 2003;362:333.
95. Ribeiro AL, Teixeira MM, Reis AM, et al: Brain natriuretic peptidebased strategy to detect left ventricular dysfunction in Chagasdisease: a comparison with the conventional approach. Int J Cardiol2006;109:34-40.
96. Talvani A, Rocha MO, Cogan J, et al: Brain natriuretic peptide andleft ventricular dysfunction in chagasic cardiomyopathy. Mem InstOswaldo Cruz 2004;99:645-649.
97. Talvani A, Rocha MO, Cogan J, et al: Brain natriuretic peptidemeasurement in Chagas heart disease: marker of ventriculardysfunction and arrhythmia. Int J Cardiol 2005;100:503-504.
98. Oliveira BM, Botoni FA, Ribeiro AL, et al: Correlation betweenBNP levels and Doppler echocardiographic parameters of leftventricle filling pressure in patients with chagasic cardiomyopathy.Echocardiography 2009;26:521-527.
99. Grupi CJ, Moffa PJ, Barbosa SA, et al: Holter monitoring inChagas' heart disease. Sao Paulo Med J 1995;113:835-840.
100. Martinelli FM, Sosa E, Nishioka S, et al: Clinical and electrophys-iologic features of syncope in chronic chagasic heart disease. JCardiovasc Electrophysiol 1994;5:563-570.
101. Ribeiro AL, Lombardi F, Sousa MR, et al: Power-law behavior ofheart rate variability in Chagas' disease. Am J Cardiol 2002;89:414-418.
102. Ribeiro AL, Lombardi F, Sousa MR, et al: Vagal dysfunction inChagas disease. Int J Cardiol 2005;103:225-226.
103. Ribeiro AL, Schmidt G, Sousa MR, et al: Heart rate turbulence inChagas disease. Pacing Clin Electrophysiol 2003;26:406-410.
104. Tundo F, Lombardi F, Rocha MC, et al: Heart rate turbulence andleft ventricular ejection fraction in Chagas disease. Europace 2005;7:197-203.
105. Leite LR, Fenelon G, Simoes Jr A, et al: Clinical usefulness ofelectrophysiologic testing in patients with ventricular tachycardiaand chronic chagasic cardiomyopathy treated with amiodarone orsotalol. J Cardiovasc Electrophysiol 2003;14:567-573.
106. Silva RM, Tavora MZ, Gondim FA, et al: Predictive value ofclinical and electrophysiological variables in patients with chronicchagasic cardiomyopathy and nonsustained ventricular tachycardia.Arq Bras Cardiol 2000;75:33-47.
107. Rocha AL, Rocha MO, Teixeira BO, et al: Chronotropic-metabolicindex in Chagas' disease. Rev Soc Bras Med Trop 2005;38:373-376.
108. Rocha AL, Lombardi F, Costa Rocha MO, et al: Chronotropicincompetence and abnormal autonomic modulation in ambulatoryChagas disease patients. Ann Noninvasive Electrocardiol 2006;11:3-11.
109. Simoes MV, Ayres EM, Santos JL, et al: Detection of myocardialischemia in chronic Chagas disease patients with atypic precordialpain by exercise and Holter tests. Arq Bras Cardiol 1993;60:315-319.
110. Rochitte CE, Nacif MS, Oliveira Junior AC, et al: Cardiacmagnetic resonance in Chagas' disease. Artif Organs 2007;31:259-267.
111. Rochitte CE, Oliveira PF, Andrade JM, et al: Myocardial delayedenhancement by magnetic resonance imaging in patients withChagas' disease: a marker of disease severity. J Am Coll Cardiol2005;46:1553-1558.
112. Kuschnir E, Sgammini H, Castro R, et al: Evaluation of cardiacfunction by radioisotopic angiography, in patients with chronicChagas cardiopathy. Arq Bras Cardiol 1985;45:249-256.
113. Viotti R, Vigliano C, Lococo B, et al: Long-term cardiac outcomesof treating chronic Chagas disease with benznidazole versus notreatment: a nonrandomized trial. Ann Intern Med 2006;144:724-734.
114. Benchimol Barbosa PR: Noninvasive prognostic markers forcardiac death and ventricular arrhythmia in long-term follow-upof subjects with chronic Chagas' disease. Braz J Med Biol Res2007;40:167-178.
115. Hunt SA, Abraham WT, Chin MH, et al: ACC/AHA 2005guideline update for the diagnosis and management of chronicheart failure in the adult: a report of the American College ofCardiology/American Heart Association Task Force on PracticeGuidelines (Writing Committee to Update the 2001 Guidelines forthe Evaluation and Management of Heart Failure): developed incollaboration with the American College of Chest Physicians andthe International Society for Heart and Lung Transplantation:endorsed by the Heart Rhythm Society. Circulation 2005;112:e154-e235.
116. Bocchi EA, Vilas-Boas F, Perrone S, et al: Latin Americanguidelines for the assessment and management of decompensatedheart failure. Arq Bras Cardiol 2005;85(Suppl 3):49-94.
117. Salles GF, Xavier SS, Sousa AS, et al: T-wave axis deviation as anindependent predictor of mortality in chronic Chagas' disease. Am JCardiol 2004;93:1136-1140.
118. Rocha MO, Ribeiro AL: A risk score for predicting death inChagas' heart disease. N Engl J Med 2006;355:2488-2489.
119. Kalil J, Cunha-Neto E: Autoimmunity in Chagas disease cardio-myopathy: fulfilling the criteria at last? Parasitol Today 1996;12:396-399.

315A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
120. Cunha-Neto E, Teixeira PC, Nogueira LG, et al: New concepts onthe pathogenesis of chronic Chagas cardiomyopathy: myocardialgene and protein expression profiles. Rev Soc Bras Med Trop 2006;39(Suppl 3):59-62.
121. Jones EM, Colley DG, Tostes S, et al: A Trypanosoma cruziDNA sequence amplified from inflammatory lesions in humanchagasic cardiomyopathy. Trans Assoc Am Physicians 1992;105:182-189.
122. de Andrade AL, Zicker F, de Oliveira RM, et al: Randomised trialof efficacy of benznidazole in treatment of early Trypanosoma cruziinfection. Lancet 1996;348:1407-1413.
123. Rassi A, Rassi Jr A, Rassi GG: Fase aguda. In: Brener Z, AndradeZA, Barral-Netto M, editors. Trypanosoma cruzi e doença deChagas. Brazil: Guanabara-Koogan; 2000. p. 231-245.
124. Sosa ES, Segura EL, Ruiz AM, et al: Efficacy of chemotherapy withbenznidazole in children in the indeterminate phase of Chagas'disease. Am J Trop Med Hyg 1998;59:526-529.
125. Villar JC, Marin-Neto JA, Ebrahim S, et al: Trypanocidal drugs forchronic asymptomatic Trypanosoma cruzi infection. CochraneDatabase Syst Rev 2002:CD003463.
126. Yun O, Lima MA, Ellman T, et al: Feasibility, drug safety, andeffectiveness of etiological treatment programs for Chagasdisease in Honduras, Guatemala, and Bolivia: 10-year experi-ence of Medecins Sans Frontieres. PLoS Negl Trop Dis 2009;3:e488.
127. Viotti R, Vigliano C, Lococo B, et al: Side effects of benznidazoleas treatment in chronic Chagas disease: fears and realities. ExpertRev Anti Infect Ther 2009;7:157-163.
128. Franco-Paredes C, Bottazzi ME, Hotez PJ: The unfinished publichealth agenda of Chagas disease in the era of globalization. PLoSNegl Trop Dis 2009;3:e470.
129. Ribeiro I, Sevcsik AM, Alves F, et al: New, improved treatments forChagas disease: from the r and d pipeline to the patients. PLoS NeglTrop Dis 2009;3:e484.
130. Marin-Neto JA, Rassi Jr A, Morillo CA, et al: Rationale and designof a randomized placebo-controlled trial assessing the effects ofetiologic treatment in Chagas' cardiomyopathy: the BENznidazoleEvaluation For Interrupting Trypanosomiasis (BENEFIT). AmHeart J 2008;156:37-43.
131. Marin-Neto JA, Rassi Jr A, Avezum Jr A, et al: The BENEFIT trial:testing the hypothesis that trypanocidal therapy is beneficial forpatients with chronic Chagas heart disease. Mem Inst Oswaldo Cruz2009;104:319-324.
132. Roberti RR, Martinez EE, Andrade JL, et al: Chagas cardiomyop-athy and captopril. Eur Heart J 1992;13:966-970.
133. Szajnbok FE, Barretto AC, Mady C, et al: Beneficial effects ofenalapril on the diastolic ventricular function in Chagas myocardio-pathy. Arq Bras Cardiol 1993;60:273-278.
134. Davila DF, Angel F, Arata dB, et al: Effects of metoprolol inchagasic patients with severe congestive heart failure. Int J Cardiol2002;85:255-260.
135. Botoni FA, Poole-Wilson PA, Ribeiro AL, et al: A randomizedtrial of carvedilol after renin-angiotensin system inhibitionin chronic Chagas cardiomyopathy. Am Heart J 2007;153:544-548.
136. Braga JC, Reis F, Aras R, et al: Clinical and therapeutics aspects ofheart failure due to Chagas disease. Arq Bras Cardiol 2006;86:297-302.
137. Bestetti RB, Muccillo G: Clinical course of Chagas' heart disease: acomparison with dilated cardiomyopathy. Int J Cardiol 1997;60:187-193.
138. Bestetti RB, Sales-Neto VN, Pinto LZ, et al: Effects oflong term metoprolol administration on the electrocar-diogram of rats infected with T cruzi. Cardiovasc Res 1990;24:521-527.
139. Bestetti RB, Theodoropoulos TA, Cardinalli-Neto A, et al:Treatment of chronic systolic heart failure secondary to Chagasheart disease in the current era of heart failure therapy. Am Heart J2008;156:422-430.
140. Botoni FA, Poole-Wilson PA, Ribeiro AL, et al: Treating Chagas'cardiomyopathy patients with chronic heart failure. Am Heart J2007;e33:154.
141. Khoury AM, Davila DF, Bellabarba G, et al: Acute effects ofdigitalis and enalapril on the neurohormonal profile of chagasicpatients with severe congestive heart failure. Int J Cardiol 1996;57:21-29.
142. Bestetti RB, Rossi MA: A rationale approach for mortality riskstratification in Chagas' heart disease. Int J Cardiol 1997;58:199-209.
143. de Sousa AS, Xavier SS, de Freitas GR, et al: Prevention strategiesof cardioembolic ischemic stroke in Chagas' disease. Arq BrasCardiol 2008;91:306-310.
144. Rassi JA, Gabriel RA, Gabriel RS, et al: Ventricular arrhythmia inChagas disease. Diagnostic, prognostic, and therapeutic features.Arq Bras Cardiol 1995;65:377-387.
145. Rosa RF, Neto AS, Franken RA: Chagas' disease and the use ofimplantable cardioverter-defibrillators in Brazil. Am J GeriatrCardiol 2006;15:372-376.
146. Cardinalli-Neto A, Greco OT, Bestetti RB: Automatic implantablecardioverter-defibrillators in Chagas' heart disease patients withmalignant ventricular arrhythmias. Pacing Clin Electrophysiol2006;29:467-470.
147. Cardinalli-Neto A, Bestetti RB, Cordeiro JA, et al: Predictors of all-cause mortality for patients with chronic Chagas' heart diseasereceiving implantable cardioverter defibrillator therapy. J Cardio-vasc Electrophysiol 2007;18:1236-1240.
148. Doval HC, Nul DR, Grancelli HO, et al: Randomised trial of low-dose amiodarone in severe congestive heart failure. Grupo deEstudio de la Sobrevida en la Insuficiencia Cardiaca en Argentina(GESICA). Lancet 1994;344:493-498.
149. Bocchi EA, Fiorelli A: The Brazilian experience with hearttransplantation: a multicenter report. J Heart Lung Transplant2001;20:637-645.
150. Parra AV, Rodrigues V, Cancella S, et al: Impact of socioeconomicstatus on outcome of a Brazilian heart transplant recipients cohort.Int J Cardiol 2008;125:142-143.
151. Theodoropoulos TA, Bestetti RB, Otaviano AP, et al: Predictors ofall-cause mortality in chronic Chagas' heart disease in the currentera of heart failure therapy. Int J Cardiol 2008;128:22-29.
152. Bocchi EA, Fiorelli A: The paradox of survival results afterheart transplantation for cardiomyopathy caused by Trypanosomacruzi. First Guidelines Group for Heart Transplantation of theBrazilian Society of Cardiology. Ann Thorac Surg 2001;71:1833-1838.
153. Sartori AM, Ibrahim KY, Nunes Westphalen EV, et al:Manifestations of Chagas disease (American trypanosomiasis)in patients with HIV/AIDS. Ann Trop Med Parasitol 2007;101:31-50.
154. Sartori AM, Neto JE, Nunes EV, et al: Trypanosoma cruziparasitemia in chronic Chagas disease: comparison betweenhuman immunodeficiency virus (HIV)–positive and HIV-negativepatients. J Infect Dis 2002;186:872-875.
155. de Carvalho VB, Sousa EF, Vila JH, et al: Heart transplantation inChagas' disease. 10 years after the initial experience. Circulation1996;94:1815-1817.
156. Bocchi EA, Bellotti G, Mocelin AO, et al: Heart transplantation forchronic Chagas' heart disease. Ann Thorac Surg 1996;61:1727-1733.
157. Bestetti RB, Souza TR, Lima MF, et al: Effects of amycophenolate mofetil–based immunosuppressive regimen in

316 A. Biolo et al. / Progress in Cardiovascular Diseases 52 (2010) 300–316
Chagas' heart transplant recipients. Transplantation 2007;84:441-442.
158. de Souza MM, Franco M, Almeida DR, et al: Comparativehistopathologyof endomyocardial biopsies in chagasic and non-chagasicheart transplant recipients. J Heart Lung Transplant 2001;20:534-543.
159. Fiorelli AI, Stolf NA, Honorato R, et al: Later evolution aftercardiac transplantation in Chagas' disease. Transplant Proc 2005;37:2793-2798.
160. Rassi Jr A, Dias JC, Marin-Neto JA, et al: Challenges andopportunities for primary, secondary, and tertiary prevention ofChagas disease. Heart 2009;95:524-534.
161. Senior K: Chagas disease: moving towards global elimination.Lancet Infect Dis 2007;7:572.
162. Centers for Disease Control and Prevention: Blood donor screeningfor Chagas disease: United States, 2006-2007. MMWR MorbMortal WklyRep 2007;56:141-143.