
Angiographic Predictors of 6Month Patency of Bypass Grafts Implanted to the Right Coronary Artery
Upload
independentCategory
view
0download
0
CLINICAL STUDIES
Cerebral Arteriovenous Malformations: Comparison of NovelMagnetic Resonance Angiographic Techniques and
Conventional Catheter Angiography
Daniel James Warren, B.Med.Sci.,Nigel Hoggard, F.R.C.R., Lee Walton, B.S.C.,
Matthias Walter Richard Radatz, F.R.C.S.,Andras A. Kemeny, F.R.C.S.,
David Martin Campbell Forster, F.R.C.S.,Iain David Wilkinson, Ph.D.,
Paul David Griffiths, F.R.C.R., Ph.D.
Section of Academic Radiology (DJW, NH, IDW, PDG), University of Sheffield, andDepartment of Stereotactic Radiosurgery (LW, MWRR, AAK, DMCF), Royal
Hallamshire Hospital, Sheffield, England
OBJECTIVE: To investigate the potential of novel magnetic resonance (MR) angiographic techniques for theassessment of cerebral arteriovenous malformations.
METHODS: Forty patients who were about to undergo stereotactic radiosurgery were prospectively recruited.Three-dimensional, sliding-slab interleaved ky (SLINKY), time-of-flight acquisition was performed, as was adynamic MR digital subtraction angiography (DSA) procedure in which single thick slices (6–10 cm) wereobtained using a radiofrequency spoiled Fourier-acquired steady-state sequence (1 image/s). Sixty images wereacquired, in two or three projections, during passage of a 6- to 10-ml bolus of gadolinium chelate. Subtractionand postprocessing were performed, and images were viewed in an inverted cine mode. SLINKY time-of-flightacquisition was repeated after the administration of gadolinium. Routine stereotactic conventional catheterangiography was performed after MR imaging. All images were assessed (in a blinded randomized manner) forSpetzler-Martin grading and determination of associated vascular pathological features.
RESULTS: Forty-one arteriovenous malformations were assessed in 40 patients. Contrast-enhanced (CE) SLINKY MRangiography was the most consistent MR imaging technique, yielding a 95% correlation with the Spetzler-Martinclassification defined by conventional catheter angiography; MR DSA exhibited 90% agreement, and SLINKY MRangiography exhibited 81% agreement. CE SLINKY MR angiography provided improved nidus delineation,compared with non-CE SLINKY MR angiography. Dynamic information from MR DSA significantly improved theobservation of early-draining veins and associated aneurysms.
CONCLUSION: CE SLINKY MR angiographic assessment of cerebral arteriovenous malformations offers significantadvantages, compared with the use of non-CE SLINKY MR angiography, including improved nidus demonstration.MR DSA shows promise as a noninvasive method for dynamic angiography but is presently restricted bylimitations in both temporal and spatial resolution. (Neurosurgery 48:973–983, 2001)
Key words: Arteriovenous malformations, Brain, Magnetic resonance angiography, Stereotactic radiosurgery
973Neurosurgery, Vol. 48, No. 5, May 2001

Cerebral arteriovenous malformations (AVMs) affect upto 0.1% of the North American population (2). Theprincipal mode of presentation for AVMs is via hem-
orrhage (30–82%), with the annual risk of hemorrhage beingreported as 2 to 4% (2, 16, 17). Other presentations includeseizure disorders, headaches, and focal, sometimes progres-sive, neurological deficits.
The goal of active management of cerebral AVMs is toeliminate the risk of future intracranial hemorrhage. Onlycomplete nidal obliteration confers total protection from therisk of further hemorrhage; there are no reported cases ofhemorrhage after angiographically confirmed nidus oblitera-tion (15). Current treatment modalities include conventionalneurosurgery, endovascular treatment, stereotactic radiosur-gery, and combinations of the three. To maximize the chanceof successful treatment, neuroimaging delineation of the ni-dus, feeding and draining vessels, and associated pathologicalfeatures of the vasculature must be of the highest possiblestandard. Conventional catheter angiography (CCA) remainsthe current reference standard for diagnosis, treatment plan-ning, and post-therapeutic follow-up monitoring of AVMs.
A high percentage of patients with AVMs present by theage of 40 years. At this age, concurrent atherosclerotic cere-brovascular disease is likely to be minimal; therefore, the riskof producing permanent neurological deficits by performingCCA in this patient population is relatively low (4, 11). How-ever, patients with AVMs often undergo multiple CCA exam-inations, and a cumulative complication rate is thus associ-ated with the CCA procedures. The development ofnoninvasive angiographic methods is a justifiable goal that isimportant for the elimination of CCA-associated complica-tions, as well as in terms of cost, radiation protection, andpatient discomfort.
This study describes our experience with the recently de-veloped magnetic resonance (MR) digital subtraction angiog-raphy (DSA) technique, which is a dynamic MR acquisitiontechnique, and with both contrast-enhanced (CE) and non-CEsliding-slab interleaved ky (SLINKY) acquisition, which is anovel three-dimensional MR angiographic technique withsuppressed slab boundary artifacts (1, 14). These techniquesare directly compared with CCA for the assessment of AVMs.
PATIENTS AND METHODS
Clinical and imaging protocol
Forty consecutive patients with cerebral AVMs were pro-spectively recruited into this study. All patients were referredto our center for stereotactic radiosurgery, with the AVMdiagnosis having been made by CCA at the referring hospital.Full approval for the study was received from the local ethicscommittee review board, and informed consent was obtainedfrom all patients.
A standard MR imaging (MRI) protocol was performed forall patients, with a 1.5-T superconducting system (Eclipse;maximal gradient strength, 27 mT/m; Marconi Medical Sys-tems, Cleveland, OH) used in conjunction with a head coil.Three fast plane pilot scans were acquired, followed by axial
dual-echo scans acquired using a fast spin echo sequence (TR,2900; TE, 12.5 and 87.5 ms, respectively; matrix, 256 [read] 3192 [phase]; flip angle, 90 degrees; field of view, 23 cm; slicethickness, 5 mm; intersection gap, 2 mm; sampling band-width, 20.83 kHz; phase sampling ratio, 0.820).
Three MR angiographic techniques were investigated. Athree-dimensional SLINKY time-of-flight data acquisitiontechnique was used, covering the whole head. The SLINKYimaging parameters used were as follows: TR, 29 ms; TE, 6.7ms; flip angle, 33 degrees; field of view, 22.0 cm; slice thick-ness, 1.0 mm; no gap (resulting in 153 axial images); resolu-tion, 512 (read) 3 256 (phase); bandwidth, 15.6 kHz; phasesampling ratio, 0.809. The total imaging time for a 153-sliceacquisition covering more than 15 cm was 579 seconds.
MR DSA was also performed. This method was fully de-scribed in a previous publication (10); briefly, it involvesacquisition of a single thick slice using a radiofrequencyspoiled Fourier-acquired steady-state technique, with acqui-sition of one image/s (TR, 7 ms; TE, 2 ms; flip angle, 40degrees; field of view, 23 cm; matrix, 256 [read] 3 150 [phase];phase sample ratio, 1.0; bandwidth, 50.0 kHz; slice thickness[single slice], 6–10 cm; 60 two-dimensional images). Sliceswere orientated to yield CCA-equivalent projections. In anygiven imaging domain (axial, lateral, or reverse Townes), oneset of 60 images was obtained as a mask. A second set wasobtained during passage of a bolus of 6 to 10 ml of 0.5 mol/Lgadolinium diethylenetriaminepenta-acetic acid (Gd-DTPA)(Magnevist; Schering AG Healthcare, Berlin, Germany), fol-lowed by a 10-ml saline flush. A separate contrast bolus wasused for each anatomic projection. The contrast agent wasadministered at a rate of 3 ml/s, via a power injector (MedradSpectris; Medrad, Inc., Pittsburgh, PA), through an 18-gaugeintravenous cannula inserted into the antecubital fossa vein.The quantity of Gd-DTPA administered was varied accordingto the nidus size, as determined from the standard fast spinecho scans, to optimize nidus observation. Ten milliliters offull-strength Gd-DTPA solution was used for small (,3-cm)AVMs, and 6 ml was used for medium-sized (3–6-cm) AVMs.A maximum of 20 ml of Gd-DTPA was administered to eachpatient (therefore, small AVMs were imaged with MR DSA intwo planes, usually the lateral and reverse Townes planes).
After imaging, the mask set for a particular image planewas subtracted from the Gd-DTPA set using proprietary soft-ware, and the resultant image was viewed using the videoreversed cine mode. After the MR DSA acquisitions (afteradministration of 20 ml of Gd-DTPA), the time-of-flightSLINKY acquisition was repeated, to yield CE SLINKY im-ages covering the whole head. The SLINKY imaging param-eters were as follows: TR, 29 ms; TE, 6.7 ms; flip angle, 33degrees; field of view, 22.0 cm; slice thickness, 1.0 mm; no gap;153 axial images; resolution, 512 (read) 3 256 (phase) (reso-lution increased acquired matrix factor 3 2); phase samplingratio, 0.809; bandwidth, 15.6 kHz.
CCA was performed under stereotactic conditions, within24 hours after MRI. A Leksell Model G stereotactic coordinateframe (Elekta Instruments, Atlanta, GA) was secured to thepatient’s head, using local anesthesia at the four sites of pininsertion. Limited selective, transfemoral, Seldinger CCA was
974 Warren et al.
Neurosurgery, Vol. 48, No. 5, May 2001

performed, appropriate to the known supply to the AVMnidus. Standard film-screen techniques and intra-arterial dig-ital subtraction were used, yielding anteroposterior, lateral,and oblique views. Images were printed with a 512 3 512matrix and a field of view of 17 cm in the anteroposteriorplane and 25 cm in the lateral plane. Computer dose-planningwas performed with GammaPlan software (Elekta Instru-ments), yielding images in which radiographic magnificationfactors were accounted for and upon which subsequent nidalsize measurements could be made.
Image analysis
Two observers, who were blinded to the results of any ofthe studies, reviewed both the CCA and MRI (non-CE and CESLINKY MR angiography and MR DSA) scans retrospectivelyand independently. Cases were reviewed randomly, and con-flicting readings were resolved by consensus. Assessment ofeach imaging technique, for all patients, consisted of the fol-lowing determinations.
Spetzler-Martin classificationThe AVM size was measured in three orthogonal dimen-
sions; the craniocaudal and anteroposterior measurementswere made in a lateral view and the mediolateral measure-ment in the anterior-posterior or reverse Townes view. Thelargest measured dimension of the nidus was used for theSpetzler-Martin classification (23). The venous drainage wasrecorded as deep or superficial. The location of the AVM, withrespect to the eloquence of adjacent brain tissue, was deter-mined by cross-sectional imaging, as is current workingpractice.
Identification of arterial feedersThe name and number of principal arterial feeders were
recorded.
Observation of associated vascular anomalies, notablyintracranial aneurysms
Intranidal aneurysms were considered to be those thatfilled early, before substantial venous filling occurred, andwere localized within the boundary of the nidus. Venouspouches, venous dilations, and simple angiomatous changeswere excluded (22).
All MRI postprocessing and review were performed usingproprietary software on a Twinstar workstation (MarconiMedical Systems). Maximal intensity projections for theSLINKY time-of-flight acquisitions (both with and withoutcontrast enhancement) were generated using standard Mar-coni algorithms. The raw data images were also scrutinized.Some cases were also reviewed after use of a surface-rendering algorithm, although measurements were not madeon these images.
CCA films were reviewed using standard methods. CCAnidal size measurements were performed on the radiosurgerydatabase using GammaPlan software (Elekta Instruments).
Patient population
Twenty male and 20 female patients, with a median age of40 years (range, 16-65 yr), were studied. Twenty-three pa-tients presented as a result of hemorrhage, eight with seizuredisorders, four with focal neurological deficits, two withheadaches, two with both a seizure disorder and a focalneurological deficit, and one with a seizure and headaches.Sixteen (40%) of the patients had undergone attempts at re-duction of the nidal size before referral for stereotactic radio-surgery. Ten patients had undergone previous endovascularembolization, and four patients had undergone previous ste-reotactic radiosurgery only. One patient had undergone bothstereotactic radiosurgery and embolization, and another pa-tient had undergone unsuccessful embolization and failedmicrosurgical resection.
RESULTS
Forty-one AVMs were assessed in the 40 patients. Two ofthe 40 patients had multiple AVMs, and one of those patientshad bilateral occipitoparietal AVMs. That patient was consid-ered for stereotactic radiosurgery for only one of the twomalformations, and the second AVM was not included in thesubsequent analysis. That patient is presented in Figure 1. Inthe other case of multiple AVMs, two small frontal AVMswere both treated using stereotactic radiosurgery; therefore,the study reports findings for 41 AVMs in 40 patients. Theanatomic locations of the 41 AVMs are presented in Table 1; 35of 41 AVMs were considered to be in eloquent areas.
Nidus size determination
Both MR DSA and CE SLINKY MR angiographic tech-niques revealed 41 of 41 nidi. Routine (non-CE) SLINKYscanning failed to reveal the nidi in 5 of 41 cases, giving thistechnique a sensitivity for nidal detection of 88%, in compar-ison with 100% for the other two methods.
In accordance with the Spetzler-Martin classification,AVMs were awarded scores depending on their nidal size(23). CCA demonstrated 27 AVMs with maximal linear di-mensions of less than 3 cm (one point) and 14 AVMs withmaximal linear dimensions of 3 to 6 cm (two points).
CE SLINKY MR angiography proved to be the most reliableand accurate, of the three MR techniques used, for determi-nation of the AVM nidal size. The sensitivity for correctSpetzler-Martin size classification of the AVMs, comparedwith the CCA reference results, was 97.6% for CE SLINKY MRangiography, 92.7% for MR DSA, and 82.9% for non-CESLINKY MR angiography. CE SLINKY consensus results, forall dimensions measured, exhibited a mean difference fromCCA measurements of 20.5 mm (95% confidence interval),compared with MR DSA, which tended to slightly overesti-mate the nidal size (mean difference, 11.0 mm), and routineSLINKY MR angiography, which underestimated the nidalsize (mean difference, 22.0 mm).
CE SLINKY MR angiography demonstrated the best corre-lation with the CCA results (Pearson’s correlation coefficient,0.96). Although non-CE SLINKY MR angiography did not
Magnetic Resonance Angiography of Arteriovenous Malformations 975
Neurosurgery, Vol. 48, No. 5, May 2001

FIGURE 1. Images for a 49-year-old female patient with bilateral occipitoparietal AVMs, who presented with seizures. A,axial T2-weighted scan (TR, 2900 ms; TE, 87.5 ms; number of excitations, 2), showing flow voids in both AVMs. B, axialnon-CE SLINKY MR image (maximal intensity projection). Note that the left-sided AVM is identified only by an enlargeddraining vein. C, axial CE SLINKY MR image. Both right and left nidi, arterial feeders, and venous drainage systems can beclearly observed. D, surface-rendered, axial, non-CE SLINKY MR image. The left-sided AVM is identified only by the presenceof an enlarged draining vein. E, surface-rendered, axial, CE SLINKY MR image. Both AVMs can be clearly observed. F and G,axial MR DSA images obtained during passage of the contrast bolus (F, early arterial phase; G, late arterial phase). Note thatthe contours of the medial border of the AVMs are clearly demonstrated.
976 Warren et al.
Neurosurgery, Vol. 48, No. 5, May 2001

reveal five small AVMs, the correlation with CCA was stillhigh (0.94). MR DSA demonstrated a maximal linear dimen-sion correlation of 0.93. All techniques exhibited better corre-lations for size determinations for smaller (,3-cm) AVMsthan for larger (3-6-cm) AVMs. CE SLINKY MR angiographydemonstrated the best intermodality correlation for bothsmall and medium-sized AVMs (Pearson’s coefficient, 0.87and 0.86, respectively). Routine SLINKY MR angiographyexhibited correlation coefficients of 0.87 for AVMs less than 3cm in size and 0.78 for AVMs 3 to 6 cm in size, whereas MRDSA exhibited coefficients of 0.82 for AVMs less than 3 cm insize and 0.79 for AVMs 3 to 6 cm in size.
Venous drainage assessment
Venous drainage was assessed in terms of the presence orabsence of deep drainage of the AVM, as in the Spetzler-Martin classification. Of 41 AVMs in the study, 13 were re-ported to have deep elements to their drainage, with 28 thushaving superficial drainage only, as determined by CCA.
Both CE SLINKY MR angiography and MR DSA resultsagreed with the CCA results in 40 of 41 AVM cases, yieldinga sensitivity for correct venous drainage detection of 97.6%.The one spurious result involved an AVM that exhibited onlysuperficial drainage during CCA but for which both MRmethods incorrectly indicated deep venous drainage.
Routine, non-CE SLINKY MR angiography exhibited a sen-sitivity of 85.4% for correct detection of venous drainage. FiveAVMs were not detected with this technique, and it thusfollows that venous drainage of these malformations couldnot be assessed. Of the five AVMs that were not detected, fourwere superficially draining and one was a deep-draining,small, thalamic AVM. Of the 36 AVMs that were observed,correct venous drainage, in accordance with the CCA refer-ence results, was described for 35. For one additional AVM,although the nidus was observed, saturation of the venoussignal was sufficient to prevent the assessment of venousdrainage (which CCA demonstrated to be superficial only).
Spetzler-Martin classification
From the results presented above, it is possible to comparethe Spetzler-Martin classification of AVMs made on the basis
of CCA, MR DSA, CE SLINKY MR angiography, and non-CESLINKY MR angiography results. CCA graded 4 of the AVMsas Grade I, 18 as Grade II, 13 as Grade III, and 6 as Grade IV.A comparison of the various MR techniques with the CCAreference is presented in Table 2.
CE SLINKY MR angiography proved to be the most con-sistent technique in both size determination and venousdrainage assessment, and the results obtained using this tech-nique thus exhibit the highest degree of correlation with theSpetzler-Martin grades assigned to the AVMs using CCA. Ofthe 41 AVMs assessed, CE SLINKY MR angiography resultsagreed with the CCA Spetzler classification for 39 (95.1%).Two discordant results observed with CE SLINKY MR an-giography were single-point upgrades, i.e., one CCA Grade IIAVM upgraded to Grade III (because of an upgrade of venousdrainage from CCA-indicated superficial to deep) and oneCCA Grade III AVM upgraded to Grade IV (because of dis-crepancies in size measurements).
MR DSA Spetzler-Martin AVM classifications agreed in 37of 41 cases (90.2%). Four grading discrepancies were gener-
TABLE 1. Anatomic Locations of the 41 ArteriovenousMalformations, as Shown by Magnetic Resonance Imaging
Location No. of Cases
Supratentorial 36 (88%)Lobar
Frontal 8Parietal 4Temporal 4Occipital 2Multilobar 11
Basal ganglionic/thalamic 4Corpus callosum/choroidal 3
Infratentorial 5 (12%)Cerebellum 5
TABLE 2. Correlation of the Spetzler-Martin GradesAssigned to the Cerebral Arteriovenous Malformations afterConventional Catheter Angiography with the GradesDetermined Using Sliding-slab Interleaved ky MagneticResonance Contrast-enhanced Sliding-slab Interleaved ky
Magnetic Resonance, and Magnetic Resonance DigitalSubtraction Angiography Assessmentsa
No. of Cases of CCA-determined Spetzler-Martin
Grade
I II III IV
SLINKY MR Angiography-determinedSpetzler-Martin Grade
I 3 0 0 0II 0 14 1 0III 0 0 10 0IV 0 0 1 6Ungradable 1 4 1 0
CE SLINKY MR Angiography-determined Spetzler-Martin Grade
I 4 0 0 0II 0 17 0 0III 0 1 12 0IV 0 0 1 6Ungradable 0 0 0 0
MR DSA-determined Spetzler-MartinGrade
I 4 0 0 0II 0 15 0 0III 0 3 12 0IV 0 0 1 6Ungradable 0 0 0 0a CCA, conventional catheter angiography; MR, magnetic reso-
nance; SLINKY, sliding-slab interleaved ky; CE, contrast-enhanced;DSA, digital subtraction angiography.
Magnetic Resonance Angiography of Arteriovenous Malformations 977
Neurosurgery, Vol. 48, No. 5, May 2001

ated by the MR DSA assessment, all of which were single-point upgrades of CCA-determined AVM grades. A singleCCA-assessed Grade III lesion was upgraded to Grade IV,and an additional three Grade II AVMs (as indicated by CCA)were upgraded to Grade III. Incorrect venous drainage assess-ment (deep elements rather than superficial only) accountedfor one of the Grade II lesion upgrades; the other three wereall attributable to MR DSA classifying the nidus as medium(3–6 cm) in size, whereas CCA showed it to be small (,3 cm).
Non-CE (routine) SLINKY MR angiography Spetzler-Martin classifications of AVMs exhibited agreement withCCA results for 33 of the 41 AVMs (80.5%). No grade wasassigned in six cases (one Grade I AVM, four Grade II AVMs,and one Grade III AVM) because of nonobservation of theAVM (five cases) or nonobservation of venous drainage (onesmall Grade II AVM). Routine SLINKY MR angiography wasthe only one of the three MR techniques used to downgradean AVM. One Grade III AVM (as assessed using CCA) wasdetermined to be Grade II using SLINKY MR angiography(because of underestimation of the size as small rather thanmedium). Conversely, another Grade III AVM (as assessedusing CCA) was upgraded to Grade IV by SLINKY MR an-giography, on the basis of the reported size (medium ratherthan small). Representative examples are shown in Figures 2 to4.
Arterial feeders
There were a total of 88 arterial feeding vessels to the 41AVMs, as determined using CCA. Complete agreement wasobserved in 71 of 88 cases (80.7%) using CE SLINKY MRangiography. Fifteen vessels observed with CCA were notidentified, two vessels were misidentified, and two vesselswere incorrectly identified because they were not observedusing CCA. MR DSA demonstrated good agreement withCCA results, correctly identifying 81.8% of the arterial feed-ers. MR DSA did not record 12 vessels described by CCA asbeing nidal feeders, and MR DSA misidentified 4 additionalvessels. Three extra vessels were reported as feeders, andthese findings were not confirmed by CCA results.
Routine, non-CE SLINKY MR angiography demonstrated72.7% agreement with CCA results. Nineteen vessels ob-served with CCA were not identified by SLINKY MR angiog-raphy, five arteries were misidentified, and one extra vessel(not observed using CCA) was reported.
Associated vascular aneurysms
CCA indicated that five of the patients had aneurysms.Two patients had two or more aneurysms on enlarged feedingarteries. These were detected by all of the MRI modalities,with MR DSA being the most impressive in demonstratingthese lesions. Two unrelated aneurysms were identified byCCA; again, these were detected by all of the MR techniques,after observer consensus. CCA also demonstrated that onecase involved an intranidal aneurysm, which was not ob-served by either CE or routine SLINKY MR angiography.When this case was investigated with MR DSA, both observ-ers commented on the presence of an early-filling venous
pouch within the nidus, but this was not deemed to be anintranidal aneurysm.
DISCUSSION
Imaging that accurately defines the vascular anatomic fea-tures of AVMs is crucial for successful management. A com-mon cause of treatment failure for AVMs treated using ste-reotactic radiosurgery is incomplete nidal targeting. This isimportant because only complete, angiographically con-firmed, nidal obliteration confers to the patient total protec-tion from the risk of hemorrhage (25). Although targetingerrors may be multifactorial, imaging must be of the highestpossible standard to minimize such errors.
CCA remains the reference standard for cerebral AVMimaging. It has high spatial (approximately 0.2 mm) andtemporal (up to 24 frames/s) resolution, which is superior tothat of other imaging modalities. However, because the pro-cedure is associated with risks, it is justifiable to attempt todevelop noninvasive angiographic techniques with less asso-ciated morbidity.
A recent meta-analysis of three published prospective stud-ies concluded that the combined risk of permanent and tran-
FIGURE 2. Images for a 40-year-old male patient with aright-sided frontotemporal lobe AVM. This patient had previ-ously undergone incomplete embolization. A, axialT2-weighted scan (TR, 2900 ms; TE, 87.5 ms; number ofexcitations, 2), demonstrating the AVM. B, right carotidartery-selective CCA film, demonstrating the nidus and asso-ciated vasculature. C and D, Townes-projection MR DSAimages (C, early arterial phase; D, late arterial phase).
978 Warren et al.
Neurosurgery, Vol. 48, No. 5, May 2001
sient neurological complications resulting from CCA was0.3% for patients with AVMs (4–6, 11). Non-neurological com-plications after CCA are, however, considerably more com-mon; groin hematomas, for example, are reported to occur atrates of 6.9 to 8.1% (4). The risks are compounded for patientswith AVMs, because they are more likely to require multipleexaminations.
Numerous studies have evaluated the use of MR angiogra-phy as an adjunct for planning stereotactic radiosurgery forAVMs (3, 7, 8, 13). Both phase-contrast and time-of-flighttechniques have been demonstrated to be of value in provid-ing three-dimensional representations of AVM vascular archi-tecture, which supplement the two-dimensional projectiondata provided by CCA. However, it has also been demon-strated that both MR techniques have limited anatomic cov-erage and cannot consistently reveal small-caliber vessels andregions of slow blood flow. These factors, as well as thecomplicated multidirectional flow within the AVM nidus,represent a significant challenge for routine MR angiography(26). Multiple overlapping thin-slab acquisition, time-of-flightMR angiography allows greater coverage and producesgreater signal-to-noise contrast and higher resolution thanconventional MR angiography. However, this technique suf-
fers from slab boundary artifacts (“venetian blind artifacts”),which represent a major limitation (14). In this study, weassessed SLINKY MR angiography, which is a refinement ofmultiple overlapping thin-slab acquisition, time-of-flight MRangiography. SLINKY MR angiography eliminates the slabboundary artifacts by suppressing them as a series of ghosts.In addition, it produces flow-related signal enhancement,which is not sensitive to blood flow direction (14). Thesefeatures make SLINKY MR angiography theoretically farmore useful for the assessment of cerebral AVMs. SLINKYMR angiography has the added advantage of whole-headcoverage, permitting full cerebral AVM assessment, withoutinflow signal saturation, in reasonable scan times. Despite theobvious potential of SLINKY MR angiography to imageAVMs, to date there have been no published reports of thisapplication.
We demonstrated that SLINKY MR angiography had areasonable sensitivity for AVM nidus detection without en-hancement with gadolinium (88%). Of the five AVMs that
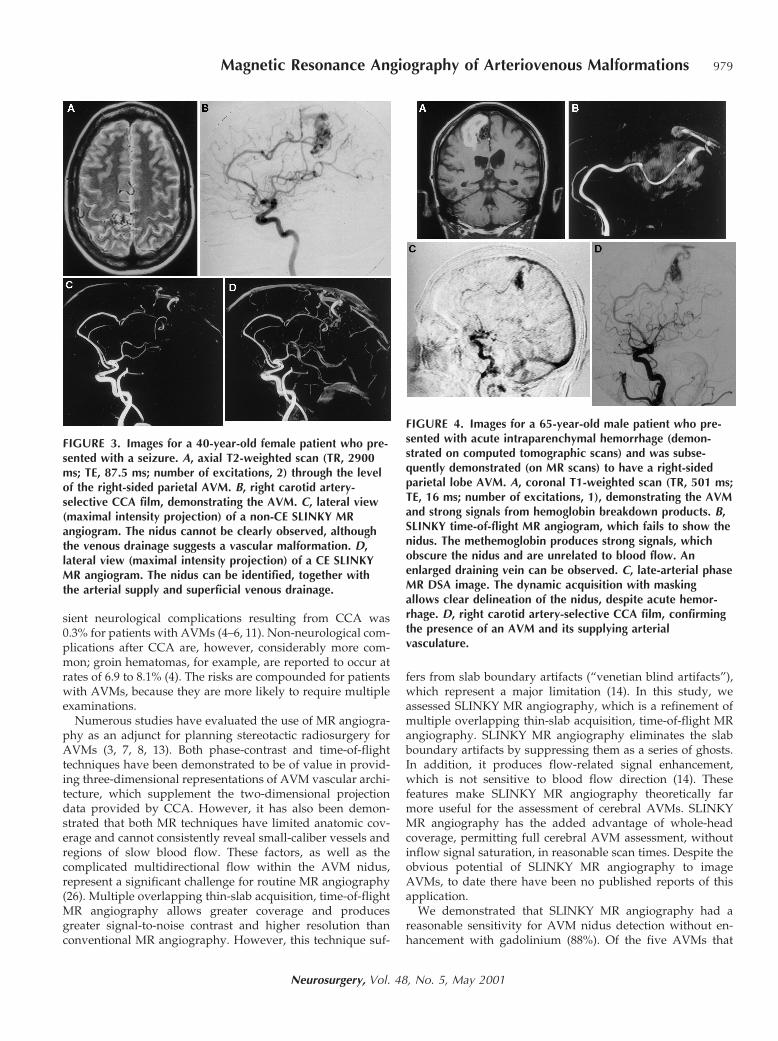
FIGURE 3. Images for a 40-year-old female patient who pre-sented with a seizure. A, axial T2-weighted scan (TR, 2900ms; TE, 87.5 ms; number of excitations, 2) through the levelof the right-sided parietal AVM. B, right carotid artery-selective CCA film, demonstrating the AVM. C, lateral view(maximal intensity projection) of a non-CE SLINKY MRangiogram. The nidus cannot be clearly observed, althoughthe venous drainage suggests a vascular malformation. D,lateral view (maximal intensity projection) of a CE SLINKYMR angiogram. The nidus can be identified, together withthe arterial supply and superficial venous drainage.
FIGURE 4. Images for a 65-year-old male patient who pre-sented with acute intraparenchymal hemorrhage (demon-strated on computed tomographic scans) and was subse-quently demonstrated (on MR scans) to have a right-sidedparietal lobe AVM. A, coronal T1-weighted scan (TR, 501 ms;TE, 16 ms; number of excitations, 1), demonstrating the AVMand strong signals from hemoglobin breakdown products. B,SLINKY time-of-flight MR angiogram, which fails to show thenidus. The methemoglobin produces strong signals, whichobscure the nidus and are unrelated to blood flow. Anenlarged draining vein can be observed. C, late-arterial phaseMR DSA image. The dynamic acquisition with maskingallows clear delineation of the nidus, despite acute hemor-rhage. D, right carotid artery-selective CCA film, confirmingthe presence of an AVM and its supplying arterialvasculature.
Magnetic Resonance Angiography of Arteriovenous Malformations 979
Neurosurgery, Vol. 48, No. 5, May 2001

were not detected, all were small; the largest of the five had amaximal linear dimension of only 15 mm, and four of theAVMs were smaller than 9 mm.
The technique tended to underestimate the nidal size, com-pared with CCA (mean size difference, 22.0 mm). Signalsaturation may have been the reason for the nonidentificationof 19 (of 88) feeding vessels supplying the nidus. Overall, theSpetzler-Martin classification of AVMs imaged using routineSLINKY MR angiography demonstrated a relative sensitivityof 80.5% for agreement with CCA results.
The use of paramagnetic contrast agents with SLINKY MRangiography has not been previously described for AVMassessment. Our results demonstrate improvement ofAVM assessment with CE SLINKY MR angiography, com-pared with non-CE SLINKY MR angiography. All 41 AVMswere observed using this technique. Figure 3 clearly demon-strates the failure of routine SLINKY MR angiography todelineate a right-sided, parietal, parasagittal lobe AVM,whereas the use of contrast enhancement permitted clearvisual assessment of the nidus, along with its feeding arteryand superficial venous drainage.
The perfect sensitivity of CE SLINKY MR angiography forAVM detection was a significant improvement, comparedwith the 88% achieved with routine, non-CE SLINKY MRangiography. The 97.6% relative sensitivity for correct nidalsize and venous drainage classifications yielded an impres-sive correlation of CE SLINKY MR angiography results withthe CCA Spetzler-Martin grading (95%). An improvementwas also observed with respect to the detection of arterialfeeders, with CE SLINKY MR angiography detecting morethan 80%. Both techniques permitted good observation offlow and unrelated aneurysms, confirming the status of MRangiography as a promising technique for cerebral aneurysmevaluation.
A single intranidal aneurysm demonstrated by CCA wasnot observed by SLINKY MR angiography, with or withoutcontrast enhancement, and review of the source images didnot aid in the observation of that lesion. The interpretation ofintranidal aneurysms is highly subjective and viewer depen-dent, and any comparison of imaging methods for such an-eurysms is also necessarily highly subjective. Flow and unre-lated aneurysms were consistently demonstrated by SLINKYMR angiography for the four patients with such lesions. Theability of SLINKY MR angiography to demonstrate aneu-rysms is evidence of its ability to reduce signal voids incomplex flow regions, which is further aided by the adjunc-tive usage of T1-shortening contrast agents.
CE SLINKY MR angiography demonstrated consistentlysuperior AVM size correlations with CCA results, comparedwith routine SLINKY MR angiography. The measurement ofthe nidus is subjective, and separation of the nidus fromangiomatous changes is difficult without dynamic informa-tion. The AVMs in this study were preselected, in that thepatients had all been referred for stereotactic radiosurgery,and the majority of AVMs were small, with consequently fewangiomatous changes. This may be one of the reasons why,overall, such good correlation was observed between CESLINKY MR angiography and CCA results.
We have demonstrated that MR angiographic techniqueshave great value for the assessment of cerebral AVMs, byproviding results with high anatomic resolution; however,such techniques are limited by a lack of dynamic information,which is important for diagnosing small AVMs and distin-guishing nidi from draining veins. This has implications fordiagnosis and follow-up assessment.
Recent reports demonstrated that MR DSA can providedynamic angiographic images, with short acquisition times.Wang et al. (27) studied the somatic vasculature of 28 patients,using dynamic MR DSA and contrast enhancement. Hennig etal. (12) used a similar technique in 24 cases. Aoki et al. (1)demonstrated clear arterial and venous phase separation in 35cases of cerebrovascular disease, including three cerebralAVMs. Our group also reported early experience with thetechnique in 20 AVM cases (9). The results presented here areencouraging. The sensitivity of 100% for nidus detection is thesame as that for CE SLINKY MR angiography and is superiorto sensitivities reported in the literature for three-dimensionaltime-of-flight MR angiography (20). The present limitationsare the lack of in-plane anatomic resolution and poor tempo-ral resolution, compared with CCA. The intracranial circula-tion has a short interval between the arterial and venousphases, and small early-draining veins and simple small ar-teriovenous shunts may be overlooked.
MR DSA demonstrated a 90% relative sensitivity with re-spect to CCA-determined Spetzler-Martin classifications ofAVMs. However, nidus measurements are highly subjective;therefore, analysis beyond Spetzler-Martin classification is oflimited value. It must be accepted that there is a degree ofmeasurement variability, not only because of the subjectivityof measurements but also because of the in-plane resolution of256 3 150 (used to increase temporal resolution) for MR DSA,compared with the resolution of at least 152 3 512 for CCA.
MR DSA has a major advantage over CCA. MR DSA canimage the medial contour of AVMs with axial views, which isnot possible with CCA. Unless standard MRI/computed to-mographic scans are available for planning purposes, stereo-tactic radiosurgery cannot be accurately planned for the me-dial contour of AVMs, and the AVMs are often equated toprolate ellipsoids, which may yield suboptimal treatments.
Dynamic MR DSA was of value for the identification ofvenous drainage, correctly identifying the drainage for 40 ofthe 41 AVMs studied. The single discordant case was a su-perficially draining AVM (as assessed using CCA) that MRDSA seemed to indicate as having deep drainage.
MR DSA was the most sensitive of the MRI modalities forcorrect identification of arterial feeders (82%). SLINKY MRangiography possesses the benefit of postprocessing and ofyielding three-dimensional data sets, whereas MR DSA hasthe advantage of providing data sets with dynamic informa-tion, showing the progression from arterial filling to venousdrainage. A technique that provides three-dimensional dy-namic data sets would be ideal but is not presently available.
Although gadolinium is safe to use in high doses, large vol-umes have not been noted to be advantageous with the MR DSAtechnique. Presently, the dose for each procedure is empiricallybased on the size of the nidus, as determined from cross-
980 Warren et al.
Neurosurgery, Vol. 48, No. 5, May 2001

sectional imaging. The comparatively small volumes of gadolin-ium that we used led to better delineation of arterial, nidal, andvenous anatomic features, because of the compactness of thebolus. An additional benefit of using smaller volumes of gado-linium is the minimization of image degradation after repeatedinjections of gadolinium for different projections. The combina-tion of low-volume gadolinium administration and a maskmethod results in little discernible loss of image quality in thesecond and third angiographic procedures.
The work presented here provides a significant body ofinformation regarding the value of modern MRI techniquesfor the characterization of cerebral AVMs. Additional work byour group, using these techniques to assess the effects ofstereotactic radiosurgery, is under way. If it could be demon-strated that these MR methods are as good as CCA in deter-mining residual flow in AVMs, it would be possible to mon-itor patients with a noninvasive, non-ionizing radiationtechnique. Because of these advantages, it would be possibleto obtain more accurate information regarding the time courseof AVM obliteration, because MR examinations could be re-peated at reasonably frequent intervals.
Another important application of these MR methods, partic-ularly MR DSA, is for the assessment of patients with acuteintraparenchymal hematomas. Time-of-flight methods have sig-nificant limitations in these situations because of the early de-velopment of hemoglobin breakdown products, which impairobservation of the vascular anatomic features. Methemoglobinhas a very short T1 value (strong signals on T1-weighted imag-es); because time-of-flight angiography effectively produces T1-weighted images, early subacute hematomas produce strongsignals that are not related to flow. This produces significantnumbers of false-positive and false-negative results. MR DSAdoes not have these disadvantages, because it involves subtrac-tion of a mask and dynamic acquisition. In Figure 4, we presenta recent case of intraparenchymal hemorrhage that was investi-gated using this technique. This is very early work, and therelative sensitivity and specificity of this technique, comparedwith those of CCA, remain to be evaluated.
CONCLUSION
A noninvasive imaging method that reliably demonstratesthe presence or absence of flow in AVMs would have practicalbenefits for both patients and departments, by allowing cere-bral angiography to be avoided or expedited. Radiosurgerymay require 2 to 3 years to completely obliterate cerebralAVMs, with success rates, according to the definition pro-vided by Steinberg et al. (24), being reported to be 80% aftersuch latency periods (18, 19, 21). Within the stated latencyperiods, there remains a potential risk for hemorrhage, andthe recognition of complete obliteration is critical for subse-quent patient treatment (9, 19, 25). There are presently nopublished data regarding optimal follow-up monitoring afterradiotherapy, with most institutions offering follow-up CCA2 years after treatment (18). This approach involves a mini-mum of three (diagnostic, preplanning, and follow-up) angio-graphic assessments. Furthermore, it has been suggested thatthe outcome of stereotactic radiosurgery can be predicted on
the basis of the early CCA appearance (18). Such resultsencourage the development of noninvasive angiographictechniques for the evaluation of AVMs, to be used in sequen-tial neuroimaging of the AVMs (to monitor their resolution)and to aid in the development of tailored follow-up protocols.
Received, November 9, 2000.Accepted, December 22, 2000.Reprint requests: Paul D. Griffiths, F.R.C.R., Ph.D., Section of Aca-demic Radiology, Floor C, Royal Hallamshire Hospital, GlossopRoad, Sheffield, England S10 2JF. Email: [email protected]
REFERENCES
1. Aoki S, Nanbu A, Yoshikawa T, Hori M, Kurnagai H, Araki T: 2Dthick-slice MR digital subtraction angiography with one-secondtemporal resolution: Assessment of cerebrovascular disorders, inProceedings of the American Society of Neuroradiology, 1999, p122 (abstr).
2. Arteriovenous Malformation Study Group: Arteriovenous malforma-tions of the brain in adults. N Engl J Med 340:1812–1818, 1999.
3. Bednarz G, Downes B, Werner-Wasik M, Rosenwasser RH: Com-bining stereotactic angiography and 3D time-of-flight magneticresonance angiography in treatment planning for arteriovenousmalformation radiosurgery. Int J Radiat Oncol Biol Phys 46:1149–1154, 2000.
4. Cloft HJ, Joseph GJ, Dion JE: Risk of cerebral angiography in patientswith subarachnoid hemorrhage, cerebral aneurysm, and arterio-venous malformation: A meta-analysis. Stroke 30:317–320, 1999.
5. Dion JE, Gates PC, Fox AJ, Barnett HJ, Blom RJ: Clinical eventsfollowing neuroangiography: A prospective study. Stroke 18:997–1004, 1987.
6. Earnest F IV, Forbes G, Sandok BA, Piepgras DG, Faust RJ, IlstrupDM, Arndt LJ: Complications of cerebral angiography: Prospec-tive assessment of risk. AJR Am J Roentgenol 142:247–253, 1984.
7. Ehricke HH, Schad LR, Gademann G, Wowra B, Engenhart R,Lorenz WJ: Use of MR angiography for stereotactic planning.J Comput Assist Tomogr 16:35–40, 1992.
8. Essig M, Engenhart R, Knopp MV, Bock M, Scharf J, Debus J,Wenz F, Hawighorst H, Schad LR, van Kaick G: Cerebral arterio-venous malformations: Improved nidus demarcation by means ofdynamic tagging MR-angiography. Magn Reson Imaging 14:227–233, 1996.
9. Friedman WA, Blatt DL, Bova FJ, Buatti JM, Mendenhall WM,Kubilis PS: The risk of hemorrhage after radiosurgery for arterio-venous malformations. J Neurosurg 84:912–919, 1996.
10. Griffiths PD, Hoggard N, Warren DJ, Wilkinson ID, Anderson B,Romanowski CAJ: Brain arteriovenous malformations: Assess-ment with dynamic MR digital subtraction angiography. AJNRAm J Neuroradiol 21:1892–1899, 2000.
11. Heiserman JE, Dean BL, Hodak JA, Flom RA, Bird CR, Drayer BP,Fram EK: Neurologic complications of cerebral angiography.AJNR Am J Neuroradiol 15:1401–1411, 1994.
12. Hennig J, Scheffler K, Laubenberger J, Strecker R: Time-resolvedprojection angiography after bolus injection of contrast agent.Magn Reson Med 37:341–345, 1997.
13. Kondziolka D, Lunsford LD, Kanal E, Talagala L: Stereotacticmagnetic resonance angiography for targeting in arteriovenousmalformation radiosurgery. Neurosurgery 35:585–591, 1994.
14. Liu K, Rutt BK: Sliding interleaved kY (SLINKY) acquisition: Anovel 3D MRA technique with suppressed slab boundary artifact.J Magn Reson Imaging 8:903–911, 1998.
Magnetic Resonance Angiography of Arteriovenous Malformations 981
Neurosurgery, Vol. 48, No. 5, May 2001

15. Maesawa S, Flickinger JC, Kondziolka D, Lunsford LD: Repeatedradiosurgery for incompletely obliterated arteriovenous malfor-mations. J Neurosurg 92:961–970, 2000.
16. Mast H, Mohr JP, Osipov A, Pile-Spellman J, Marshall RS, LazarRM, Stein BM, Young WL: “Steal” is an unestablished mechanismfor the clinical presentation of cerebral arteriovenous malforma-tions. Stroke 26:1215–1220, 1995.
17. Ondra SL, Troupp H, George ED, Schwab K: The natural historyof symptomatic arteriovenous malformations of the brain: A 24-year follow-up assessment. J Neurosurg 73:387–391, 1990.
18. Oppenheim C, Meder JF, Trystram D, Nataf F, Godon-Hardy S,Blustajn J, Merienne L, Schlienger M, Fredy D: Radiosurgery ofcerebral arteriovenous malformations: Is an early angiogramneeded? AJNR Am J Neuroradiol 20:475–481, 1999.
19. Pollock BE, Flickinger JC, Lunsford LD, Bissonette DJ, KondziolkaD: Hemorrhage risk after stereotactic radiosurgery of cerebralarteriovenous malformations. Neurosurgery 38:652–661, 1996.
20. Pollock BE, Kondziolka D, Flickinger JC, Patel AK, Bissonette DJ,Lunsford LD: Magnetic resonance imaging: An accurate methodto evaluate arteriovenous malformations after stereotactic radio-surgery. J Neurosurg 85:1044–1049, 1996.
21. Pollock BE, Lunsford LD, Kondziolka D, Maitz A, Flickinger JC:Patient outcomes after stereotactic radiosurgery for “operable”arteriovenous malformations. Neurosurgery 35:1–8, 1994.
22. Redekop G, TerBrugge K, Montanera W, Willinsky R: Arterialaneurysms associated with cerebral arteriovenous malformations:Classification, incidence, and risk of hemorrhage. J Neurosurg89:539–546, 1998.
23. Spetzler RF, Martin NA: A proposed grading system for arterio-venous malformations. J Neurosurg 65:476–483, 1986.
24. Steinberg GK, Fabrikant JI, Marks MP, Levy RP, Frankel KA,Phillips MH, Shuer LM, Silverberg GD: Stereotactic heavy-charged-particle Bragg-peak radiation for intracranial arterio-venous malformations. N Engl J Med 323:96–101, 1990.
25. Steiner L, Lindquist C, Adler JR, Torner JC, Alves W, Steiner M:Clinical outcome of radiosurgery for cerebral arteriovenous mal-formations. J Neurosurg 77:1–8, 1992.
26. Tsuruda J, Saloner D, Norman D: Artifacts associated with MRneuroangiography. AJNR Am J Neuroradiol 13:1411–1422, 1992.
27. Wang Y, Johnston DL, Breen JF, Huston J III, Jack CR, Julsrud PR, KielyMJ, King BF, Riederer SL, Ehman RL: Dynamic MR digital subtractionangiography using contrast enhancement, fast data acquisition, andcomplex subtraction. Magn Reson Med 36:551–556, 1996.
COMMENTS
Warren et al. present novel magnetic resonance (MR) angio-graphic techniques for the assessment of cerebral arteriovenousmalformations (AVMs) in a group of 40 patients referred forradiosurgery. In comparisons of these techniques with conven-tional transfemoral digital substraction angiography (DSA), theobjective was to elucidate the potential of the three differenttechniques. Conventional angiography is currently the standardmethod for diagnosis, treatment planning, and follow-up mon-itoring for treated AVMs, because of its very high spatial andtemporal resolution, but its invasive nature is a major problem.The radiosurgical treatment of AVMs requires a minimum of 2years for cure, making the follow-up angiographic complicationsof concern because of the multiple examinations required. Thedevelopment of noninvasive, non-ionizing radiation techniquesis therefore necessary. The MR angiographic techniques pre-sented here, especially the gadolinium-enhanced technique, ex-
hibited acceptable sensitivity for the proper diagnosis of AVMs.Treatment planning is different, because the anatomic aspectsare only a portion of the data needed to plan an appropriate safeapproach. The presence of intranidal aneurysms, perforatingartery involvement, and the precise dynamic behavior of partic-ular AVMs can be elucidated only using DSA. If embolization isrequired, DSA can be performed during the same procedure.Follow-up monitoring for radiosurgery-treated patients is antici-pated to be an area of eventual safe application of these techniques.
Jorge M. MuraEvandro de OliveiraSão Paulo, Brazil
This article reports many technical details regarding the po-tential of different MR imaging (MRI) techniques to analyze thedifferent components of AVMs. Compared with angiography,MRI provides many useful data, but no single technique is 100%reliable, even for one parameter. Contrast-enhanced (CE)sliding-slab interleaved ky (SLINKY) MR angiography detectedall AVM nidi and provided an accurate estimation of the AVMsize in 97.6% of the cases. Venous drainage was well identifiedby CE SLINKY MR angiography, as well as by MR DSA. Theweakest point is the recognition of arterial feeders, because CESLINKY MR angiography and MR DSA recognized approxi-mately 80% of the feeders but did not identify feeders, misiden-tified feeders, or even incorrectly identified feeders not revealedby angiography in 20% of the cases. In contrast, all aneurysms,except for one intranidal aneurysm, were detected, especially byMR DSA. Therefore, MR angiographic techniques are helpfulbut not completely reliable for assessment of the presence orabsence of flow in AVMs. These techniques can be used aspretherapeutic tools but cannot replace angiography. Duringfollow-up monitoring after treatment (especially radiosurgery),they may permit the avoidance of some angiographic proce-dures, which must be repeated for 2 to 3 years before success orfailure is demonstrated. This is a nice report of the technicalpossibilities of angiographic MR. These techniques are still de-veloping, and they might soon replace angiography.
Bernard GeorgeParis, France
This is a highly technical article that compares some novelMR angiographic techniques with conventional catheter an-giography (CCA) for the evaluation of AVMs. The value ofthe report is in bringing to neurosurgical attention these verysophisticated techniques. Although I am not yet convincedthat these less invasive techniques are presently able to re-place CCA, the authors’ excellent illustrations are intriguing,and CCA as we know it might soon become obsolete.
Roberto C. HerosMiami, Florida
In this article, Warren et al. describe new MR angiographictechniques, including three-dimensional SLINKY MR angiog-raphy, and compare the diagnostic sensitivity and specificityof these techniques with those of CCA for 41 patients withAVMs, using blinded observers. The CE SLINKY technique
982 Warren et al.
Neurosurgery, Vol. 48, No. 5, May 2001

exhibited 100% sensitivity for nidus detection and 95% corre-lation with Spetzler-Martin grading based on CCA results.
These results are definitely the best reported for MRI assess-ment of AVMs. The two cases of inaccurate Spetzler-Martingrading resulted from the overlooking of a deep-draining vein inone case and a discrepancy in size measurements in the other.Although these results are excellent, there are at least two majordeficits in the diagnosis of AVMs using these techniques, com-pared with CCA. As the authors note, these MRI techniquescannot currently provide the dynamic information that CCAprovides. This information is critical for the detection of smallresidual AVMs after radiosurgery or the detection of small ar-teriovenous fistulae. We question whether these MR techniquescurrently have the temporal or spatial resolution necessary foraccurate detection of these small malformations. Additionally,none of the MRI techniques exhibited more than 82% accuracy indefining the arterial supply. This poses a significant problem forsurgical planning, especially if perforator arterial feeders arepresent but not recognized. Deep perforator feeders to AVMsare considered by many experienced AVM surgeons to repre-sent a significant factor determining surgical morbidity. The MRtechniques presented in this article demonstrate how far thetechnology has developed, but significant advances must bemade before these techniques can be considered viable alterna-tives to conventional techniques.
Robert E. ReplogleDuke SamsonDallas, Texas
The authors describe novel MR angiographic techniquesthat were used to evaluate patients with AVMs who wereundergoing stereotactic radiosurgery. Until recently, CCA hasbeen the reference standard for delineating the size of AVMnidi and describing venous drainage. Any new techniquemust be at least as accurate in providing this type of informa-tion. On the basis of the description provided by the authors,it seems that the CE SLINKY MR technique comes very closeto achieving this goal. The authors report a 95% correlationbetween CE SLINKY MR angiography results and theSpetzler-Martin classification (1) defined using CCA. Both MRDSA and non-CE SLINKY have advantages and disadvan-tages; however, the overall results achieved with those tech-niques were not as good as those achieved with CE SLINKYMR angiography. It is quite possible that the CE SLINKY MRtechnique is adequate for monitoring patients who have un-dergone stereotactic radiosurgical treatment of their AVMs.CCA is associated with some risk, and this novel MR angio-graphic technique, although not perfect, provides a safe effec-tive means of monitoring these patients.
Howard A. RiinaRobert F. SpetzlerPhoenix, Arizona
1. Spetzler RF, Martin NA: A proposed grading system for arterio-venous malformations. J Neurosurg 65:476-483, 1986.
The Lee Shore (1941), by Edward Hopper. Oil on canvas. Private collection.
Magnetic Resonance Angiography of Arteriovenous Malformations 983
Copyright © 2022 FDOKUMEN




















